
58 minute read
Reimbursement Page

from June July 2022 O&P Almanac
by AOPA

BUSINESS CE CREDITS
P.20
Staying Social—and Compliant
Tips for crafting a social media consent form for patients—and retaining HIPAA compliance
Editor’s Note—Readers of
Reimbursement Page are eligible to earn two CE credits. After reading this column, simply scan the QR code or use the link on page 20 to take the Reimbursement Page quiz. Receive a score of at least 80%, and AOPA will transmit the information to the certifying boards.
THE SECURITY AND PRIVACY provisions within the Health Insurance Portability and Accountability Act (HIPAA) were written and enacted long before social media sites like Facebook, Twitter, Instagram, and TikTok became popular. These social media venues have become valuable tools for reaching out to and educating patients, and for marketing your business. However, the HIPAA security and privacy rules remain relevant and must be followed; there are multiple potential areas of risk for violating the HIPAA rules and breaching a patient’s privacy on social media platforms.
How can your facility use social media without running the risk of violating HIPAA rules? This month’s Reimbursement Page examines some of the common mistakes associated with social media and HIPAA and offers tips for ensuring compliance.
Personal Health Information
When using social media platforms, or when dealing with HIPAA in general, it is never acceptable to disclose or share protected health information (PHI) outside of your normal business operations for treatment or payment. PHI is any information about a patient or the patient’s care, and any details that could expose or identify the patient’s identity. This goes beyond photographs, birthdates, health ID numbers, or telephone numbers; it also includes things like the patient’s email address or their Instagram account name.
PHI may only be included in your company’s social media posts if a patient has given their permission, in writing, to allow their PHI to be used—and then only for the purpose specifically referred to on the consent form.
Common HIPAA Violations on Social Media
Some of the more common mistakes, violations, breaches, or issues that can arise with social media and HIPAA are listed below. Remember that a breach or violation is any impermissible use or disclosure of information that compromises the security or privacy of the PHI and, ultimately, the patient. • Sharing pictures and videos of patients without their express written consent or authorization.
It is never acceptable to directly share information about your
patients outside of normal business operations, unless you have the patient’s permission. • Referring to unconfirmed news about patients, or sharing gossip about patients. • Inadvertently or accidently showing patients’ pictures or patients’ PHI. This would include posting a picture of your office where, in the background, you can see a patient or a patient chart. • Posting or sharing information to sites or groups that you thought were private. Just because a group is marked as “private” doesn’t mean that the information will not be shared with others. If you would not share it or post it in an open forum or on a public platform, then you should not share it in private. In addition, on some sites, even if they are “private,” the messages may not be encrypted and secured. Along the same lines, don’t assume that just because a post or photo has been deleted, it is no longer visible to the public.
Social Media Policy
To facilitate compliance with HIPAA and avoid potential fines, there are a few steps you can take when using social media. Most importantly, create or review your social media policy. While your policy should be tailored to fit your company’s needs, following some general rules will help protect your employees and your facility.



• For the active users with foot drop • When less support is needed during stance phase • More flexibility – greater ROM
Your social media policy should clearly define your company’s penalties for violating HIPAA on social media platforms. These could mirror your penalties or punishments for other HIPAA violations, or you may create penalties tailored specifically for social media usage. You may choose to set your policies to be strict and severe—for example, one offense is enough to fire someone. Alternatively, you may decide to give one or two warnings to an employee. Having a clear discipline policy in place will help reinforce the importance of HIPAA compliance and discourage employees from posting inappropriate information or materials.
Make sure you, your employees, and your company keep all social media accounts separate. For example, avoid using one Instagram or Facebook account for both your personal life and your facility; and try not to post work-related material on your personal account. Monitor your work accounts regularly to ensure no improper material or information has been posted. If something inappropriate does post, have protocols in place to quickly remove it. Keep in mind that improper posts may originate from people outside your company—for an example, a patient accidentally sharing some of their PHI.
Also consider including guidance on communicating with current or future patients via social media platforms. For example, if a new patient contacts you on your facility’s Facebook page asking about an appointment or treatment, you may respond to them and let them know of your office hours or how to schedule an appointment. However, you should not have the patient discuss their medical history; instead, ensure they send that information to your email or other secured means of communication.
Social Media Consent Form
The only time you or your facility may share any PHI on a social media platform is when a patient has given you express written permission. The best way to prevent most HIPAA breaches, violations, or issues with social media campaigns and posts is to have a valid authorization or consent form on file.
If you have an old photo consent or authorization form on file as part of your HIPAA intake forms, you should consider reviewing and updating the form—especially if you have not done so in a long time. Make sure new forms include information about social media usage.
Whether you are reviewing, updating, or creating a social media consent form, consider taking the following actions when preparing the document:
Explain the type of content you wish to use and share. For example, are you only asking for a photo, or are you asking the patient to share a story and provide a testimonial? This is important because each patient is different and will have varying comfort levels regarding what they may be willing to share. Specifying the type of content you will be sharing gives the patient control to choose what they are comfortable with.
Explain how the content will be used, or the purpose of the content. Do you intend to use the patient’s photo and/or story for marketing purposes or for educational purposes? Be clear on the purpose. Also consider explaining the type of information you intend to include in your posts.
If possible, specify the type of social media platforms you will be using, or where the patient’s information will end up. Perhaps allow the patient to choose which platforms they are comfortable with—and only post to those approved sites and platforms.
Explain when the information will be used and shared, and for how long you intend to share or post the information. The form should clearly identify who the patient is authorizing, so make sure your facility’s or company’s name is prominently listed. If you may authorize use by one of your agents, contractors, or businesses associates, let the patient know that—especially if you are using a third party to help with your social media campaigns and postings.
Include an age acknowledgement, or an indication that the patient is eligible to make decisions about consent and authorizations on their own. If the patient cannot make these decisions—for example, if they are a minor—then include a way to identify the legal guardian.
Include contact information. This is not always required to be directly on the consent form since contact information is usually already known. However, it is useful to include your facility’s contact information, and request the patient’s contact information, within the social media consent form.
Be clear that the patient may revoke the authorization at any time. In addition, explain what will happen if information was used or posted prior to them revoking their consent. Will you remove all previous postings, or does the revocation only apply to future postings?


Explain the patient’s rights to, or lack of, compensation if you plan to use the patient’s information and/or likeness for marketing or anything that can lead to a financial gain for you and your facility/company.
Be sure your form has a space for the patient and/or their guardian to sign and date the form.
Below is a sample consent form. Your form doesn’t have to be this long, or
SAMPLE
HIPAA: PHOTO, MEDIA, SOCIAL MEDIA RELEASE AUTHORIZATION FORM
I, (Patient or Patient Guardian Name), hereby authorize (Facility Name) and its authorized employees, agents, or contractors to publish the following personal health information (PHI) and/or story that contains my name or likeness: (Include all information that may be used).
This information, photo, and/or story may contain information relating to the diagnosis, treatment, and healthcare services provided or to be provided to me by (Facility Name) and identifies my name and other personally identifiable information. This information may be used in print media, on the radio, TV, the (Facility Name) website, blog, podcast, and on the following social media platforms: Facebook, Twitter, Instagram, and YouTube. (If you have or use other social media platforms, be sure to include them.)
The following information about me will not be disclosed if specifically stated:
I understand that I have a right to revoke this authorization by providing written notice to (Facility Name). However, this authorization may not be revoked if (Facility Name), or its employees, agents, or contractors, have taken action on this authorization prior to receiving my written notice.
I further understand that this authorization is voluntary and that I may refuse to sign this authorization. My refusal to sign will not affect my ability to seek treatment with (Facility Name), eligibility for benefits or enrollment, or payment for or coverage of services.
This authorization is valid from the date of (Date of Patient’s or Guardian’s Signature Below) and shall expire on ______________.
Lastly, I understand I will not be compensated for the use of any images or my likeness that are used in any social media platforms. I also understand that (Facility Name), and its authorized employees, agents, or contractors, are not liable to notify photographers/agencies of the use of these photos, and it is between myself and the photographer to discuss the distribution rights of any images.
Name of Patient: _________________________________________________ Signature of Patient/Guardian: _____________________________________ Guardian Relation to Patient: ______________________________________ Date: ____________ even look like this—this is just one example of how a social media consent/ authorization form could appear. The purpose of the final form is to ensure the patient has a clear understanding of exactly how their information and/or likeness will be used, and the purpose of sharing their information.
If you have any concerns about your consent forms or what should or should not be included, consider speaking with your attorney.
Protecting Your Facility
By providing a complete and thorough consent or authorization form, you will assist your patients in feeling more comfortable sharing their information, likeness, or story—especially if they can have a say and control over where it ends up and what information you use.
When you are dealing with social media, PHI, and HIPAA, caution is key. The criminal penalties for HIPAA violations could be severe, ranging from $100 to $50,000 per violation, with a maximum penalty of $1.5 million per year for each violation. A good rule of thumb is that if you would not share it or talk about in real life, then you should not share it or post it on any social media, without proper authorization and consent.
Devon Bernard is AOPA’s assistant director of coding and reimbursement services, education, and programming. Reach him at dbernard@AOPAnet.org.
This material is not intended, and should not be relied on, as legal advice. AOPA members should consult with their own legal counsel about the legal matters presented.
Take advantage of the opportunity to earn two CE credits today! Take the quiz by scanning the QR code or visit bit.ly/OPalmanacQuiz.
Earn CE credits accepted by certifying boards:
NEED TO KNOW
• O&P professionals of all ages and experience levels can embrace advocacy roles in support of patients and the profession. • Alex Gates, CPO, was spurred to advocate in Washington to support a patient seeking a policy change so she can join the military. • Chris Baschuk, MPO, CPO, FAAOP(D), attended his first AOPA
Policy Forum and has since become a vocal advocate in Utah, educating lawmakers about the profession and needed changes. • O&P student Evan Smith came to the Policy Forum without much experience—and was instrumental in convincing Rep. Pete Aguilar (D-California) to sign on to the O&P Patient-Centered Care Act. • Every voice matters—all O&P professionals can stretch out of their comfort zone and find ways to support O&P and their patients. AOPA has resources to help get started.
ACTIVISM COMES IN many forms. That was the message shared at AOPA’s Policy Forum in May, and that is the philosophy embraced by several committed O&P professionals who have found that advocating for patients on the individual level is equally important as advocating on local, state, and national levels.
The big “asks”—such as asking legislators to sign on to the Medicare O&P Patient-Centered Care Act (see sidebar on page 28)—are critical for the future of the O&P profession and the individuals requiring O&P care. But many O&P professionals also spend time and effort advocating for individual patients, and for groups of patients impacted by specific payor rules or state regulations. These individual acts of advocacy are just as important as systemic advocacy—and the two can overlap. Here’s how.
Bringing a Patient Problem to the National Spotlight
Alex Gates, CPO, a clinician and manager at Evergreen Prosthetics & Orthotics in Spokane, Washington, ramped up her involvement in national O&P advocacy this year in her quest to improve quality of life for one of her patients. Hannah Cvancara was born with fibular hemimelia that resulted in the amputation of her left foot when she was just 1. Today, the 26-year-old is a nurse and an avid athlete, using a prosthesis to surf and rock climb. She wants to serve the United States as a military nurse—but military regulations prevent individuals missing a body part, including pre-service amputations, from joining the services.
Cvancara, whose father was an Air Force flight surgeon, will not be deterred from her goal. Early this year, she approached Gates to assist her with finding a way to pursue military service. Gates began by writing a “strongly worded letter” on Cvancara’s behalf, she says—then the pair worked with AOPA to bring the issue into the national spotlight. Hannah Cvancara and Alex Gates, CPO
Cvancara hopes to one day serve in the U.S. military as a nurse.

“Hannah is a very dynamic person, so I found myself on an airplane coming to DC,” Gates says. “There are a lot of CPs and COs who don’t deal with politics”—they deal with patients. But she soon realized that advocating for policy change is an important way to improve life for individuals with limb loss and impairment. The pair traveled to AOPA Headquarters in April, where they strategized with staff members Nicole Ver Kuilen, Ashlie White, MA, Sam Miller, and others, before visiting Capitol Hill.
AOPA recently invested in enhanced legislative tracking software and used it to determine which legislators to contact for visits—those who would be most open to hearing Cvancara’s story. AOPA staff “guided us on who should speak about what at each meeting,” Gates recalls. As a prosthetist, her role at the meetings was to testify to Cvancara’s physical abilities and explain the capabilities of an individual with a prosthesis. She also spoke to the durability and stability of Cvancara’s device.
They had several successful meetings, including one “magical” visit with Rep. Cathy McMorris Rodgers (R-Washington), a representative with whom Cvancara had already established a relationship. “We discussed the barriers the disabled community faces,” says Cvancara, including her exclusion from military service as well as the need to pass the Medicare O&P Patient-Centered Care Act. Cvancara and McMorris Rodgers “share a passion for supporting disabled military,” she says. “I am so thankful for that experience and to discuss some of the changes needed in the O&P world.”
As a result of the meetings, more individuals with authority are aware of Cvancara’s situation and are working to change the rules so she— and others like her—may one day have the opportunity to join the military, according to Gates. Before visiting Washington, Gates had focused most of her energy on her patients—but she has learned that she can expand her viewpoint. “I didn’t realize I have such a powerful tool in my toolbox to advocate on each patient’s behalf,” Gates says. “It was a profound experience for me in realizing we could make our voice heard.” The experience “opened up more pathways I could take on behalf of my patients—to work with patients to push these things up higher, and to advocate.”
Keeping Patients’ Interests in Mind
Like Gates, Chris Baschuk, MPO, CPO, FAAOP(D), was recently motivated by his patients to advocate on their behalf, and for the whole profession. Formerly a regional clinical manager at Handspring, and now as the clinical director at Point Designs, Baschuk was moved to participate in his first in-person Policy Forum this year.



Levin Sliker, PhD, CEO of Point Designs, with Chris Baschuk, MPO, CPO, FAAOP(D), in front of U.S. Capitol at the AOPA 2022 Policy Forum
In addition to wanting to push the Medicare O&P Patient-Centered Care Act forward, Baschuk wants to influence policy and regulatory decisions—particularly since the durable medical equipment Medicare administrative contractors published “Upper-Limb Correct Coding Guidance” this year. The guidelines in the document, which “did not go through a proper public comment period and circumvented the appropriate Local Coverage Determination process,” according to Baschuk, limit the codes that will be covered by Medicare for upper-limb prostheses.
During the Policy Forum, Baschuk met with aides from the offices of Sens. Mitt Romney (R-Utah) and Mike Lee (R-Utah). He found Lee’s aide, Chris Medrano, to be particularly receptive to the O&P issues they discussed, including the proposed legislation.
In the weeks since the Policy Forum, Baschuk has expanded his advocacy to state legislators and is hoping that Utah lawmakers will champion the O&P cause. Several O&P Capitol Hill Club, where AOPA convened on Day Tw0 at the AOPA 2022 Policy Forum
manufacturing companies call Utah their home—the state is an “epicenter of O&P,” according to Baschuk. He has sent emails and follow-up letters to Utah’s senators and representatives to “raise awareness of issues that are a big deal” to the profession.
Baschuk encourages other O&P professionals to get involved in advocacy at whatever level they are comfortable with. “Advocacy is thinking beyond yourself; it’s about the patients,” he explains. “We need to advocate for others, but also for the profession. We all need to come together and have a common goal.
“Fundamentally, you have to find your ‘why’”—why you advocate, Baschuk says. “Then, what can you do? Inaction is action—so just try something. Send a letter to legislators. Go to the local offices of your legislators and talk to staffers. Educate yourself on the current issues and policies, and talk to AOPA staff. Be consistent—and keep going back, so they know they can’t get rid of you.”
When you are presented an opportunity to meet with a legislator—at any level—Baschuk says that it’s important to look up that individual’s voting record and identify the causes that are important to that legislator. Then find areas of overlap between the legislator’s causes and your own. “Draw parallels” to motivate legislators to sign on to your own bills, he says. Baschuk (right) at the office of Sen. Mike Lee, with Chris Medrano, legislative correspondent for Sen. Lee

Recognizing That No Experience Is Necessary
Advocacy is not solely for seasoned professionals—just ask Evan Smith. He recently learned that even O&P students like himself can make an impact. During the May Policy Forum, Smith’s participation was instrumental in convincing Rep. Pete Aguilar (D-California) to sign on to the Medicare O&P Patient-Centered Care Act.
Smith, who will graduate from the MSOP program at Loma Linda University (LLU) in 2023, traveled to the AOPA Policy Forum as the university’s student representative, sponsored by NCOPE. Smith grew up in a medical family; his father is an occupational therapist and several relatives are nurses. He originally
In 1997, the world of prosthetic knee joints was revolutionized with C-Leg,
the first microprocessor knee with both swing and stance phase control.
Since then, Ottobock has continued to build upon its success with unmatched microprocessor knees like Kenevo, Genium, X3, and now the latest iteration of C-Leg 4.
In 25 years, more than 100,000 users have walked confidently thanks to the C-Leg. Now Ottobock is taking it to the next level with over 10 feature updates drawn by feedback from both users and clinicians alike.

Here’s to 25 years of C-Leg changing lives. It’s just the beginning.
In-Person Advocacy Makes a Comeback

More than 110 AOPA members and O&P students reunited in Washington, DC, May 17-18 for the annual Policy Forum—the first time the event was held face-to-face since 2019. Attendees from across the nation convened on the Hill to take part in more than 70 congressional visits with representatives of 30-plus states.
This year, participants pushed for legislators to sign on to the Medicare O&P Patient-Centered Care Act—HR 1990 and S 2556. The congressional visits by Policy Forum attendees led to five additional co-sponsors of the legislation: Reps. Pete Aguilar (D-California), Randy Feenstra (R-Iowa), Terri Sewell (D-Alabama), and Dan Meuser (R-Pennsylvania), and Del. Eleanor Holmes Norton (D-District of Columbia).
The legislation aims to accomplish four patient-centered goals: • Distinguish O&P clinical care from the provision of durable medical equipment. • Protect patient access to necessary clinical care associated with O&P intervention, by returning the definition of “minimal self-adjustment” to its original meaning. • Protect patient access to a continuum of care by exempting appropriately credentialed clinicians from competitive bidding. • Prevent fraudulent acts targeting Medicare patients in need of O&P care by prohibiting drop shipping of custom-fit and customfabricated O&P devices.
Maggie Baumer, JD, president of NAAOP, notes that the energy at this year’s Policy Forum was high. “It was exciting to be able to go in person and visit the Hill,” says Baumer, who also is area clinic business manager for Hanger Clinic in Massachusetts.
O&P advocacy is a multilevel commitment, says Baumer, and there are many ways to get involved. When geography and expense prevent would-be advocates from traveling to the national Policy Forum, these individuals could get involved locally and at the state level, says Baumer. She encourages O&P business owners to identify employees who may be enthusiastic about advocacy, and task them with that work—perhaps allocating some of their clinical time to advocacy each month.
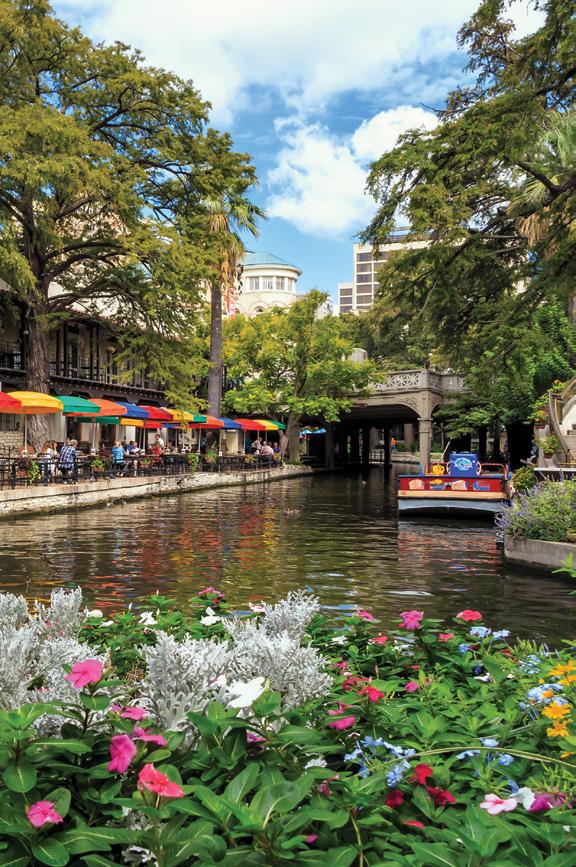
With the success of the event fresh on their minds, O&P professionals are looking forward to the next opportunity to network in person with colleagues on a national scale—at the AOPA National Assembly in San Antonio, September 28-October 1. O&P student Evan Smith met with legislators during the AOPA Policy Forum in May.


planned to become a physician—but then he “stumbled across the field of O&P” during his second year of medical school at LLU, “and it immediately piqued my interest,” he says. “It seemed like a beautiful intersection between medicine and hands-on engineering.”
Now halfway through the master’s program, he “jumped at the chance” to represent LLU at the Policy Forum. “I didn’t know a lot about it, or what to expect, but I enjoy traveling and meeting interesting, caring people in our field.” Smith says politics has never been an area of interest, but he

Smith (far right) with Policy Forum participants Debbie Hatch, Katie Devlin, and Rick Riley
“couldn’t help getting caught up in the passion that everyone had about advocacy” on Day One of the Policy Forum. “I learned that we as clinicians can make a difference for our patients in a national way, when we join together and make O&P needs known,” he says. “I also realized both how big and how small our field is. We are a relatively small group, yet we have a national presence.”
On Day Two of the Forum, he participated in congressional visits to Aguilar, Rep. Doug LaMalfa (R-California), and Sen. Dianne Feinstein (D-California). Smith and Ver Kuilen met with Aguilar himself “for about 20 seconds” before he had to rush to another meeting, then they met with one of his staffers, Elise Sugarman. “Nicole and I took turns telling Elise about the bill and how that directly impacts patients and clinicians,” Smith says.
Apparently, the pairing of a young, energetic O&P student-advocate with an O&P consumer/AOPA representative—Ver Kuilen—made quite the impression. “Two days later, on Friday, Elise emailed Nicole and I letting us know that Rep. Aguilar had agreed to co-sponsor the bill!” says Smith. “We were thrilled and quickly wrote back expressing our appreciation. We are now one step closer to getting this bill enacted.” Since then, Smith and Ver Kuilen have coordinated to send a signed thank you letter to Aguilar, along with a photo of Smith’s fellow LLU O&P students.
While Smith’s other Capitol Hill meetings have not yet yielded additional co-sponsors, Smith is still holding out hope that LaMalfa or Feinstein will sign on. Reflecting on his experience the Policy Forum, he appreciates both learning about some issues for the first time and realizing “that we are actively working to fix said issues and … that our field is just filled with amazing, caring, and intelligent people.”
As Smith discovered, anyone can make a difference, regardless of age or experience. “We need to educate our legislators about the needs and issues in our profession, and we need to educate our patients that their voice matters. Patients have the unique opportunity to tell their own stories.” He also encourages O&P professionals at all levels to “to let our legislators, patients, family, and friends know that we are invested in advocating for—and with—those who have limb loss and/ or limb impairment.”
Integrating Advocacy Into Everyday Practice
In some cases, advocating for patients can be as simple as working with patients’ insurance to ensure coverage, or Nicole Van Kuilen, AOPA manager of public helping patients without engagement; Elise Sugarman, a staffer from Rep. means to find ways to get Pete Aguilar’s office; and Smith devices.
Erik Schaffer, CP, founder and CEO of A Step Ahead the microprocessor units critical Prosthetics in New York, integrates to restoring function, causing the advocacy into each patient interaction. patient restrictions, limitations, and After each patient’s needs and goals risk of injury. Not only do they deny are established, his staff evaluates the prosthetic, but they also refuse their insurance policy for limitations to update their fee schedule, or have or exclusions that would prevent the lowered their fees, forcing the patient patient from reaching their desired or to go in-network. A prosthetic device potential functional levels. “A pros- is essential to a person’s health, and thesis is an artificial device designed our entire facility has always been to replace a missing part of the body, dedicated to advocating for our and more and more, insurance compa- patients’ needs.” nies are denying the patients their Jim Druwe, CPO, who spent eight restoration of life. So, every day, we years at Bio-Tech Prosthetics and fight against payors who deny claims Orthotics and is now with Hanger or do not want to provide the most Clinic, also believes it’s important appropriate device for their member,” to go above and beyond to help Schaffer says. “Sometimes the fight patients. In the past, he has worked lasts years—only to be denied at the with Challenged Athletes Foundation claims level.” to solicit running leg donations for
Schaffer says that some insurers are active patients. He also contacts “not following policy guidelines or the local distributors and manufacturers’ accepted standards of care outlined representatives to ask for donated by Medicare” and the Department of parts—such as liners or feet—for Veterans Affairs. Some payors “deny patients who don’t have insurance.

Ashlie White, MA, AOPA director of health policy and strategic alliances; Alex Gates, CPO; Sam Miller, AOPA manager, state and federal advocacy; Hannah Cvancara; and Kate Cvancara on their visit to Capitol Hill in April

Become an O&P Advocate
No contribution to O&P advocacy is too small. To learn how you can get involved, try the following:
■ Visit the AOPA Co-OP to view up-to-date information about what is happening in your state: www.AOPAnet.org/resources/co-op. ■ Read the State By State column in each issue of O&P Almanac for important updates. ■ Read up on the Medicare O&P Patient-Centered Care Act, and ask your members of Congress to cosponsor the bill—visit
AOPAvotes.org for details. ■ Clear your calendar for next spring and plan to attend the 2023 AOPA Policy Forum in Washington, DC. ■ If you’re encountering a policy challenge in your state, contact
Sam Miller, AOPA’s state and federal advocacy manager, at smiller@AOPAnet.org. ■ Join forces with local clinicians to share the O&P message in the community and at regional and state legislative sessions. ■ Attend the 2022 AOPA National Assembly in San Antonio,
September 28-October 1, to unite with other O&P champions and discuss top-of-mind policy issues during networking events.
“From a more local standpoint, it’s all about growing relationships,” he says. “When you show some compassion, patients will be loyal and refer others back to you.” He believes individual acts of kindness are not only good for clinicians, but good for the O&P profession—demonstrating that the profession is dedicated to its patients and their outcomes.
Calling All Advocates
As more O&P professionals recognize they, too, can play a role in advocating on behalf of the profession, O&P’s voice will get louder. “Don’t wait to be asked to advocate. Do it yourself—help your patient beyond the exam room,” says AOPA President-Elect Teri Kuffel, JD.
Even patients are beginning to recognize the power of clinician participation in advocacy initiatives. Cvancara encourages prosthetists to stretch out of their comfort zone to advocate on patients’ behalf. “Prosthetists have more power than they think in the healthcare world,” she says. “If they get to know their patients—and their hopes and dreams—they have a voice as part of their ‘continued care” for patients,” she says. “Don’t stop once the limb is done—use your voice in Congress or in the healthcare world.”
Gates, for her part, encourages other clinicians to continue advocating on behalf of patients—even if it doesn’t seem to be yielding results. “Enough people chipping away at these barriers will help break them down. It won’t happen overnight—but eventually.”
“We’re a very small profession,” adds Gates. “To make change, and to protect our field, we need to be more vocal than most—to speak out louder.”
O&P professionals will have another opportunity to make in-person visits to legislators when the Policy Forum returns in 2023. In the meantime, there are plenty of opportunities for clinicians, business owners, and students to engage in everyday activisim.
Christine Umbrell is a contributing writer to O&P Almanac. Reach her at cumbrell@contentcommunicators.com.
Tech Transitions
New materials, designs, and integration increase possibilities for O&P professionals—and patients
Interviews conducted by JOSEPHINE ROSSI
EDITOR’S NOTE: For 2022, O&P Almanac has revived the popular Leadership Series, which originally appeared in the magazine in 2015, to once again feature revealing insights and opinions from senior-level leaders on topics of critical importance to the future of the profession. To complement AOPA’s launch of a new mission and vision and emphasis on “reimagining the profession,” subsequent installments of this feature will include interviews with O&P stakeholders on topics of key importance to O&P clinicians, manufacturers, researchers, and educators.
PERSONALIZED 3D PRINTING, advanced microprocessor control, neural-machine interfaces, pressure sensor application—the world of prosthetics and orthotics has radically improved in recent years. Yet despite these and other breakthroughs, barriers exist in terms of access, affordability, functionality, and clinician know-how. With technology already so ingrained in our society, the future of balancing scientific gains with the daily needs of patients seems certain. But how do we get there as a profession?
In this third installment of the revamped Leadership Series, O&P Almanac convened four industry leaders to reflect on the significance of technology on patient care and new device development, and offer some insights for what’s next.
What technology has had the most significant impact on patients?
Russell Cannon: Thinking about it in terms of the entire length of my time in O&P, I would say the most significant technological advancement would be the advent of carbon fiber in prosthetic feet. Prior to carbon fiber being used, we were using more standard, passive materials. In fact, when I first broke into the [field], wooden feet were still being used on some patients. And certainly, plastic or nylon were rather common. Those materials don’t really provide any energy return. All of the energy, through the full gait cycle, needed to be provided by the amputee.
Once carbon fiber was introduced, it had an energy-storing rebound effect. So basically, you take a stride, you load the toe, and that puts energy into the material that springs back. The patient moves faster, more naturally. Initially, when that material was introduced, it was considered a niche product, but before too long, just about all patients were given access to carbon fiber feet, because of the energy return property. Even lower-level, what we would think of K3 or even K2, patients were getting carbon fiber feet.
Now, carbon fiber is used a lot in orthotics as well, [such as] carbon fiber AFOs. …So, both orthotics and prosthetics are benefiting from that material.
Jeff Erenstone, CPO: CAD software in combination with 3D printing. CAD technology has been slowly growing in importance, but in the past 10 years, it has really been able to jumpstart forward. ... [Meanwhile, the 3D printer has] closed the loop to go from a digital design to a physical object. That object may have some shortcomings in different ways, but it is very easy to have something in your head and, within a day or so, have that physical object in your hand.
Andreas Kannenberg, MD (GER), PhD: The development of microprocessor knees with full stance and swing control including stumble recovery has probably made the biggest impact on patients. What’s really fascinating is that [approximately] 90 to 95% of patients with knee disarticulation or above-knee amputation would benefit from the technology. There are only a few patients who are physically very fit, who prefer a non-microprocessor knee. But for most of the patients, in their daily lives, this is probably the technology that has made the biggest impact in the past 25 years.
Shane Wurdeman, PhD, CP, FAAOP(D): As a profession, we have historically interlaced our patients’ success with the advancement of technology. For example, the introduction of silicone Meet Our Contributors:
Russell Cannon is the director of sales, North America, for Lindhe Xtend, a prosthetics manufacturer based in Sweden. He has more than 30 years of experience in the O&P profession working for patient-care providers, manufacturers, and distributors. He has served as a technician and customer service representative, and held roles in sales, production, and management.
Jeff Erenstone, CPO, is founder of the nonprofit Operation Namaste and head clinician for Mountain Orthotic and Prosthetic Services. He has provided prosthetic care around the world, and has significant experience with digital technologies, especially 3D printing. He is a member of the AOPA Digital O&P Committee and Socket Guidance Workgroup.
Andreas Kannenberg, MD (GER), PhD,
graduated from Charité Medical School at Humboldt University in Berlin and worked as a physician in Germany for more than 10 years. He joined Ottobock in 2003 and has been serving as executive medical director of North America since 2013. He coordinates Ottobock’s clinical research in the Americas.
Shane Wurdeman, PhD, CP, FAAOP(D), is the director of clinical research at the Hanger Institute for Clinical Research and Education. He holds a degree in physics, a master’s degree in prosthetics and orthotics, and a doctorate in biomechanics. He also serves on the AOPA Board of Directors as the research director.




and gel liners allowed many patients who were previously limited by pain and discomfort to be able to achieve their goals with a prosthesis. The advent of the microprocessor knee in prosthetics, and now in orthotics, enhanced patient safety to the extent that patients began to recapture their lives. But, while there continues to be advances in the devices and the components that we use when caring for our patients, the advances that are dramatically impacting our patients’ lives now are related to care delivery models. We now have a process to remotely capture outcomes for our patients through their smartphone, which are then instantly fed back into the patient’s electronic health records. I then, as a clinician, can see how the patient is doing without them necessarily needing to come into the clinic. If there is a problem, it becomes easier to identify and I can bring the patient in ASAP to troubleshoot and help them get back to where they should be.
To go a step further, when the patient arrives at the clinic, the outcomes that we captured remotely through their smartphone are populated into a report that enables the patient to understand historically what their journey looks like in terms of progress—and setbacks. This has been very impactful; patients want to know how well they are doing.
What are some of the recent advances in microprocessor technology, and how are those advancements benefitting patients?
Erenstone: I think the biggest is prosthetic knee stability: The ability for the knee to sense what’s going on and prevent a fall or improve function, so that a person is able to walk around more intuitively. That’s huge because if your knee gives out, you fall to the ground.
Some of the most highly active people don’t actually need the microprocessor knees. … [O]n the other hand, someone in their 70s who is moving a little bit slower, and their coordination is not as good as it used to be, could be greatly helped by a microprocessor knee.
Kannenberg: The first patients who benefited from microprocessor technology were lower-limb amputees, with the development of microprocessor knees and then later microprocessor feet. But in the past 10 years, we’ve seen some major advancements in upperlimb prosthetics, with the development of more multiarticulating hands. What’s even more important is the development of new control mechanisms like pattern recognition and targeted muscle reinnervation.
In addition, microprocessor technology is now available to patients who are dependent on an orthosis to walk, like knee-ankle-foot orthosis (KAFO) users. As a result, patients with neurological conditions who need an orthosis to be ambulatory again have the passive devices like Ottobock C-Brace, and patients with complete paralysis have the powered exoskeletons. These developments started much earlier, but the devices have improved over time. They have become more practical to use and more viable for O&P clinicians to fit.
Wurdeman: It’s definitely an exciting time to be an O&P clinician with the integration of microprocessors making it possible to put together rehabilitation plans for patients who may not have otherwise had options for success moving forward, or perhaps their success would have been defined within a much narrower scope.
The emerging evidence on microprocessor ankle-feet is demonstrating strong clinical benefits for patients. Patients with reliance on a KAFO are starting to see new care plans that allow them to increase their activity and improve their quality of life by integrating microprocessor knees into the KAFO.
—ANDREAS KANNENBERG, MD (GER), PHD
How do you envision emerging neuroprosthetic technologies to affect your organization?
Cannon: Lindhe Xtend was founded by Christoffer Lindhe. He’s a triple amputee; he lost his left arm and both legs above the knee when he was 17. I’m close to him, and I’ve had the opportunity to see how some of the neuropathic and neuroprosthetic technologies work, both good and bad. This is a guy who’s as motivated as any amputee, and he's obviously in the industry, and he still has some issues with myo connectivity. … The technology is fantastic when it works properly and perfectly. But it’s not where it needs to be quite yet. Hopefully, in the next five to 10 years, some significant advancements will take place. …With our founder being our driving force, we are open to exploring anything that would help him, as an amputee of both upper and lower extremity. So, we would certainly see developing or partnering to develop a technology or a process that would help upper extremities, particularly with neuroprosthetic advancements, as a growth opportunity and emerging market for us down the road.
Erenstone: I foresee a lot going on in the near future with myoelectric devices and device feedback, giving patients better spatial understanding.
In 2016, I attended the Cybathlon competition in Switzerland. They had electric wheelchairs, exoskeletal suits, high-tech prosthetics [perform] in different categories. It’s not like the Paralympics where it’s all about the athlete; this was all about the technology. They called the users “pilots.” In the transradial arm category, the pilots had to do a number of tasks, like button some shirts, screw in a light bulb, do dishes—things like that. Bob Radocy of TRS won using the Grip 5 Prehensor. It was very much a John Henry moment to watch him outperform all the greatest and most expensive devices out there.
The reason that story is relevant is the feedback, not what the hands can actually do. That’s where the neural integration is huge: to be able to get that
greater input to the device and receive that feedback back from the device. There have been some interesting steps in that direction, but we need to get directly to those nerves somehow. I think that’s what’s necessary before Bob gets beat in competition.
Kannenberg: Improvements of the control for upper-limb prosthetics will have a significant impact. Many of these multi-articulating hands already offer much more function than a patient can realistically and intuitively control. The standard two-channel myoelectric control is very cumbersome to switch between the functions of the hand and the different grip types. That is not very practical. These new control mechanisms [such as pattern recognition and targeted muscle reinnervation] offer more intuitive control and more function, which is very important, but we still have a long way to go there.
Regarding orthotics, the C-Brace is a passive hydraulic microprocessorcontrolled orthosis, and the goal is to make the device ever lighter and more functional, and to improve the programming and software. Another issue [that will need to be addressed] is that the software enhancements are not considered a reason for improved reimbursement. Medicare considers all of that covered by the microprocessor codes. The [R&D work] is all included—along with all future improvements—regardless of how many man-hours or man-years you invest.
For the future, I anticipate the addition of power for prosthetic and maybe also orthotic devices. But with all of these technologies come challenges [in terms of approvals for reimbursement by payors]. Several years ago, we acquired BionX, with the only commercially available powered ankle-foot component; it is still not covered by most insurance companies. The VA covers it, but Medicare doesn’t cover it, and most private insurances don’t cover it either.
Wurdeman: Consistent with all new care options, as these new neuroprosthetic technologies become commercially available, our teams of clinical experts and scientists at Hanger Clinic will evaluate when and how leveraging such devices as part of patient-care plans can yield better outcomes. When caring for patients that need either orthotic or prosthetic care, it’s important that the approach is to find the solution for my patient’s problem, not to try to find the problem for a device to solve.
—JEFF ERENSTONE, CPO
Dr. Comfort Education
ABC approved CEU courses ABC approved CFts precertification course

For a discount use Promo Code: OPALMANAC
Visit https://www.drcomfort.com/business/resources/training
What are some of the advances in additive manufacturing that are making an impact on the design of orthoses and prostheses?
Cannon: The 3D printing revolution is here. It used to be, people were doing 3D check sockets, and that was the extent. I don’t know that there was a lot of confidence in their reliability, their durability. But with improvements in materials and the 3D printing process, [the industry has] crossed the threshold of reliability for at least check sockets going toward permanent sockets. So, I think you will see the progression on this.
One of the problems with trying to 3D print a foot—which has happened—[is] wear and tear. Three million cycles is the standard testing, and that’s a lot of steps. To have a 3D-printed foot withstand that kind of testing, and then actual realworld existence, is really difficult. I don’t think really much of anything, certainly nothing at a K3 or more level, could live up to that at this point in time. But I do think we’ll see it come within the next few years, even. If you were to tell me five years from now, there are 3D-printed feet on the market that are legitimately and commonly used, I wouldn’t be at all surprised.
Erenstone: I would say it’s definitely the Hewlett Packard MJF, multi jet fusion printer. That’s a game changer, and part of the reason is that it’s Hewlett Packard. They have 50, 60, 70 years’ worth of patents in printing technology. When 3D came around, they were able to dip into their existing pool of patents and onboard technology rather quickly—something no one else was able to do.
To go a little technical here, they’re very good at isotropic bonding, which means bonding the material evenly and without creating stress. Other technologies use lasers to bond together. As you can imagine, that heats up the material and creates some stress. Because of the chemical process that HP has, they were able to make something isotropic without creating that stress and still get consistent results.
Wurdeman: There are many potential applications for additive manufacturing in orthotics and prosthetics. However, I do see many people falling into the classic trap of trying to force a process to fix something that is not broken. The benefits of additive manufacturing, in my opinion, will ultimately be realized in areas that currently have no solution or solutions that don’t work well. One recent example was a 3D-printed partial hand for a pediatric patient. The vast array of presentations with partial hand amputation has made general solutions challenging, and those challenges expand when working with the pediatric patient. However, in this particular case, a custom 3D-printed partial hand, designed for the patient’s desired uses and encompassing the unique residual anatomy, resulted in a happy patient with improved function reflected in the patient’s outcomes report.
How does research on technologies inform your decisions for patient care, business implementation, or otherwise?
Kannenberg: Currently, we only have Class I devices. We don’t need to do regulatory research to satisfy the FDA. The research that we do is to support reimbursements of new devices by Medicare and private insurers.
For some devices, there are product categories, like microprocessor knees for above-knee amputees or knee disarticulation patients, that benefit approximately 90 to 95% of the patients [in that category of amputation]. But when we look at some other devices—for instance, the Empower powered foot—it appears that only certain patient groups really benefit from that technology.
The purpose of the research is either to better define the patient groups that are most likely to benefit from certain technologies, that is to help the clinicians match patient needs and technologies … or to improve the product or develop a training program to make more patients eligible to become responders to the technology.
…It looks like the integration of external power into neuromuscular control is not intuitive for many patients. Some patients find a way to effectively use the power, but many patients struggle with it. [We can use the research] to develop training programs to help patients better utilize the technology and broaden the indication or the patient groups that could benefit from the technology. When you look [at] studies that published the individual results of the patients, … between 40 and 50% of the patients benefited individually. … How can we help the other 50 to 60% of the patients also benefit from the technology? Maybe [we can’t], but it’s important to ask that question and look for solutions.
Wurdeman: I think the pressures of modern healthcare have made it critical that all decisions rely on research, but also recognize there is an element of experience and instinct to inform the decision. In clinical-decision making, these two
—SHANE WURDEMAN, PHD, CP, FAAOP(D)
components, research and clinical experience, combine with the patient’s personal situation to form the elements of evidence-based practice.
What one app/device/software do you rely on professionally to do your job better?
Cannon: Google Maps or whatever map feature you use on your phone. I’m a director of sales … and I’ve been on the road as far back as the late ’80s. …I look back and think, “I can’t believe how we used to do this.” I used to carry around maps and atlases, trying to figure out roads.
I realize that answer is myopic and specific to an on-the-road salesperson, but I bet some clinicians would agree with me, too. Those who have to go to various hospitals, or clinics, or patient homes. They probably feel the same way, which is, it takes a burden off your shoulders that you don’t have to worry about prepping all of that in advance—or reading a map while you’re driving.
Erenstone: I do a lot of work with nonprofits and, specifically, Operation Namaste. There, we’ve developed a software called collaborative CAD. We’re still in beta testing, but we’re providing it free to anyone in the field. We have been using it at George Brown University during the pandemic when they couldn’t have all of the students in the fabrication laboratory together. We geared our software toward helping them teach their class: Half the class would work in-person, and the other half would do it virtually in our software. They alternated weekly. Over the past two years, we have been able to improve the software and build in tools so they can somewhat compare classroom models to the digital models to ensure consistency.
This is profound because we now can teach a prosthetist how to do modern prosthetic care without physically being with them. These virtual labs allow us to improve and break down education barriers in low-income countries. Even if someone goes to school, after they finish, they’re probably not going to have the support network back at home to help them. We have the ability to go to conferences, continuing education, and so on. There, they’re isolated and on their own. Now we can continue to work with them, keep them up to speed, and easily disseminate new, modern care.
—RUSSELL CANNON


Pro Tips and Hot Topics
What’s new at the 2022 AOPA National Assembly? Almost everything
THE COUNTDOWN TO the 105th annual AOPA National Assembly is on—and with good reason. This year, more O&P professionals will be gathering in one spot than at any time in the past two-and-a-half years. AOPA is rising to the occasion, planning a dynamic educational experience featuring plenty of new content and cutting-edge presentations.
“I don’t think we have ever had such a high-level faculty or such interesting programming—such as an orthotic case study based on the treatment of former NFL quarterback Alex Smith,” says Joanna Kenton, MHA, CPO, LPO, FAAOP, co-chair of the AOPA Assembly Planning Committee. “There are so many new items this year that it is hard to cover them all!”
“I’m particularly excited about this year’s theme: The Intersection of Technology & Humanity,” says Rick Riley, co-chair of the Assembly Planning Committee. The 2022 educational content is relevant and timely, according to Riley, with many sessions focused on emerging technology, 3D printing, and new research. “Each track has a diverse range of topics, and we are excited there are more than 150 speakers scheduled to present at this year’s National Assembly.”

The Clinical Education Workgroup of the Assembly Planning Committee “has worked diligently to communicate and solidify the best speakers in the industry,” agrees Charles Kuffel MSM, CPO, LPO, FAAOP, co-chair of the workgroup. Assembly participants “will be afforded an exciting in-person opportunity to meet with peers, obtain educational and business credits, and participate in hands-on workshops,” he says.
This year’s Assembly education will bring to light new studies, concepts, and ideas that “were left virtually unknown for the past two years,” due to the COVID-19 pandemic, Kuffel adds. “Researchers, clinicians, and others have spent two years working behind doors and in lockdown on their research and clinically impactful designs.” The San Antonio conference “will allow those presenters the in-person opportunity to discuss their research and evidence-based practice models.”
These new sessions will be offered in seven distinct categories; in addition to the traditional sessions in Orthotic, Prosthetic, Pedorthic, Technical, and Business Tracks, a new Digital O&P Care Track and a new Postmastectomy Care Track will debut this year. Here’s a sneak peek at some of the buzz-worthy sessions attendees will experience this year in San Antonio. Can’t-Miss Clinical Sessions
Professional athlete Alex Smith became one of the highest profile orthosis users two years ago when he returned to quarterback for the Washington Football Team after a gruesome 2018 on-the-field leg injury that necessitated 17 surgeries. Assembly attendees will hear firsthand from Smith’s orthotist, Michael Muratore, CPO, in one of the most exciting sessions planned for San Antonio: “Orthotic Case Study Based
on the Treatment of Former NFL Quarterback Alex Smith.”
“The presentation is unique to this show. I do not recall a presentation like it in any of the shows I have attended in the past 10 years,” says Tyler Klenow, MSOP, CPO, LPO, CPT, co-chair of the Clinical Education Workgroup. Presenters—including Muratore and other members of Smith’s rehab team—will describe “the clinical details of a high-activity, highprofile user who relied on orthotic care to return him to the highest level of professional competition,” he says. Smith’s rehabilitation journey, from injury to return-to-play, will be outlined. “Rumor has it that Alex is going to record a video for attendees as well, to share his experience as a high-level end user,” Klenow adds. This session is scheduled for Thursday, September 29, at 2 p.m.
The high-profile case study is just one of many new orthotic and prosthetic clinical sessions for 2022. Another session, led by representatives from the Department of Defense (DoD), including Lee Childers, PhD, CP, and several other renowned researchers, will highlight current and future studies that are ongoing at the Center for the Intrepid, Walter Reed Military Medical Center, and Naval Medical Center San Diego. “O&P
Research Developments Across the DoD/VA Extremity Trauma and Amputation Center of Excellence,”
held Thursday, September 29, at 10:30 a.m., offers “a glimpse into the care our service members are receiving and the innovations being accomplished by the military program,” Klenow says. “The innovative mindset has always driven our profession,” he says, “and this session will reignite the imagination of attendees to create innovations in their own patient-care practices.”
Osseointegration is another hot topic and the subject of
“Osseointegration in the United States—Prosthetic Implications for
Today and Tomorrow.” This session,
i’m Going
#WeAreOandP

Alex Smith
scheduled for Thursday, September 29, at 10:30 a.m., will have a clear focus on the prosthetic approach to care. “For the right patient, osseointegration is transformative,” says Jeffrey Cain, MD, a professor at the University of Colorado School of Medicine, and one of the speakers for this session. This discussion will cover surgical considerations and procedures, rehab, potential complications, costs, and payment challenges. “We will talk about the critically important role of the prosthetist in the success of the patient after osseointegration,” adds Cain.


Two New Tracks
Looking to expand your facilities’ capabilities? Be sure to check out two new educational tracks—O&P Digital Care and Postmastectomy Care.
The O&P Digital Care Track will feature several sessions focused on digital O&P, including “Applications
and Innovations of 3D Printing in Orthotics: A Digital and Clinical
Joint Program,” set for Saturday, October 1, at 10:30 a.m. This panel discussion will be presented by experts armed with data demonstrating the durability of 3D-printed orthotic devices. Several “old school” practitioners will share their experience in taking a leap of faith into the digital manufacturing space—and will detail the results of their initial capital investment.
The new digital sessions will be capped off by an inaugural interactive experience, the Digital Care Showcase, which will take place at noon on Saturday, October 1. Participants in this hands-on event will learn about computer-based 3D design software tools utilizing a provided prosthetic or orthotic patient case, to include the patient file, a 3D scan, and positive model. Exhibitors will present a fabricated model, device, or 3D print.
AOPA expects the Digital Care Showcase to be extremely popular. “The membership has been asking for ‘hands-on’ sessions for years,” says J. Chad Duncan, PhD, CRC, CPO, who co-chairs the O&P Digital Care Committee with Jeff Erenstone, CPO. “The fact is, we are a hands-on profession—and what better way to engage membership? Additive manufacturing [is] unknown to some and very new to others. Being hands-on will allow membership to engage in a way that we hope is beneficial to their learning and allow for richer conversation about digital care.”
In one of several sessions in the all-new Postmastectomy Care Track, experts will discuss the growing need for certified mastectomy fitters. The session, “Keeping Pace With Surgical
Advancements—Partial Forms Play
a Key Role,” will take place Thursday, September 29, at 10:30 a.m. Moderated by Tanya Baer, CFom, a panel of industry experts will discuss the growing need for nontraditional breast forms, given a rise in lumpectomies in place of mastectomies. Attendees will “learn about an avenue of the postmastectomy care that is growing and not being as utilized as it could be,” says Baer, and “come away from the presentation with a better understanding on the use of partial breast prostheses and more options in the provision of care for their patients.”
“Breast cancer is a complicated disease and a complicated recovery,” adds Rebecca Weldon-Martin, CMF, CFm, who will also speak at the partial forms session. “Once the cancer is removed, there is usually a lifetime necessity for products that can improve the quality of life for the breast cancer patient. Most of these women have no idea what products are available and how they can help. … In particular, women who have had partial mastectomies or restorative surgeries are especially in need of assistance and guidance toward products that will help them.” O&P professionals “can increase your patient base and have a wider outreach in your community” by embracing postmastectomy care, Weldon-Martin says.
Fabrication Tips and Tricks
Within the Technical Education Track, a new “Fabrication Tricks & Tips” session is sure to be of interest to attendees who create orthotic and prosthetic devices. This session will showcase tips from members throughout the country, who submitted three- to five-minute videos explaining their O&P “trick or tip” to be considered for inclusion. During the Assembly, session attendees will vote for their favorite tip—and winners will be awarded cash prizes.
“The video submissions we have received focus on improving outcomes,” says Joanna Kenton, MHA, CPO, LPO, FAAOP, co-chair of the AOPA Assembly Planning Committee. “This includes materials used in fabrication, equipment, and tools for efficiency.” Attendees can expect to learn about various cosmetic finishing techniques, tips for working with black polypropylene, 3D imaging lamination, partial foot lamination using a carbon footplate, and patching holes in suspension sleeves, according to Kenton.
Better Business Practices
The Business Education Track at AOPA’s National Assembly is renowned for top-notch and futurefocused information that empowers O&P professionals to revamp and revise their business practices. This year, attendees will have several sessions with brand-new content to choose from, beginning at 2 p.m. on Thursday, September 29, when three industry experts will present Hamontree speeches on topics of critical importance to O&P businesses, and attendees will vote for their favorite presentation.
Profit-minded business owners will want to be in attendance for the first Hamontree lecture, “The Three Things You Have Control Over To Speed Up Your Cash Flow.” Stacy Toner, CBCS, will share her expertise as chief operating officer at CBS Medical & Building Consulting LLC.
Excitement Beyond Education

The 2022 AOPA National Assembly has much to offer in terms of location, exhibit hall, and networking events. Situated in downtown San Antonio, the conference center “is an impressive facility, right on the city’s River Walk—with hotels conveniently located beside the show site,” says Rick Riley, co-chair of the AOPA Assembly Planning Committee. This year’s exhibit hall will feature hundreds of cutting-edge products and technologies from worldwide manufacturers and O&P innovators. Attendees will have additional opportunities to convene and network in the exhibit hall this year. AOPA will launch the “O&P Experience Zone” on Thursday, September 29—a fun, interactive event showcasing patient success stories and their caregivers. The Experience Zone will be held in conjunction with a traditional happy hour on the exhibit hall floor.
O&P professionals will meet and greet colleagues and contacts during a new “networking icebreaker” during exhibit hall breaks, according to Joanna Kenton, MHA, CPO, LPO, FAAOP, co-chair of the Assembly Planning Committee. Friday’s lunch in the exhibit hall will have a traditional Texas barbecue theme, complete with cornhole and other games.
Assembly-goers may spy dozens of “next-generation” recruits on Thursday, September 29. “We have invited two local, health career and STEM-focused high schools to join the Assembly,” says Kenton. AOPA expects approximately 80 high school students to visit the convention center for a short presentation to learn about the O&P profession and glean insights from keynote speaker Mona Patel, who is local to San Antonio. “Then the students will break up into smaller groups” to visit the exhibit hall with tour guides, Kenton explains. They will learn about O&P products and how they assist patients, then have lunch and hear about experiences from those with limb loss. “We believe that this is a valuable opportunity to share about our amazing profession,” Kenton adds. “To hear from us and our stakeholders will be a powerful introduction to explore a career in O&P.”
Perhaps the most highly anticipated aspect of the conference is the in-person interactions. “While an online option is available and a great way to earn continuing education credits, it cannot compare to physically being at the convention center,” says Kenton. “The exhibit hall experience has an energy and a pulse that’s all its own. It allows us as professionals to network—to learn what is new and available so we can ultimately benefit the people we serve.”
AOPA members and O&P stakeholders “are ready to see each other’s faces and smiles,” says Riley. “There is pent-up demand for a big meeting that feels normal.” Riley anticipates a “great turnout” for the 2022 event. “The National Assembly is an ideal forum for gaining knowledge and building relationships,” he says. “Supporting our industry, supporting each other—that’s how we improve care and quality of life for O&P patients.”
She will inform participants of the three common causes for revenue cycles “to become disrupted and even screech to a halt.” Toner will share insights and analysis into these trends and how to identify, correct, and avoid them. “Attendees will leave with an understanding of the importance of every step of the revenue cycle,” she says, “and tools and tips on how to make their practice’s revenue cycle management strong and efficient.”
The second Hamontree presentation, headlined by Gerald Stark, MSEM, PhD, CPO, LPO, FAAOP(D), will explain the findings of a “Survey
of Emotional Burnout and Its Effects on Innovation in O&P.”
Stark will examine the definitions of “emotional intelligence” and “emotional burnout” as they relate to O&P. He will discuss findings on the levels of burnout among demographic groups, looking specifically at certification levels, experience, work context, and job function in O&P, especially during the pandemic.
O&P professionals who understand the value of outcome measures will want to stay for the final Hamontree presentation, “Using Outcome
Measures To Justify Medical Necessity, Reimbursement, and Business Development in Real-
Life Settings,” presented by Jason Kahle, MSMS, CPO, LPO, FAAOP. This presentation will discuss a novel approach to using available outcome measures to assist the clinician who is accountable for justifying medical necessity—recognizing that clinicians’ time and accountability must be considered. Kahle will “discuss outcome measures that have the best ecological validity,” he says. “These ecological outcome measures are not commonly discussed, have internal validity, are sanctioned by Health and Human Services (HHS), CMS, and Office of the National Coordinator (ONC), used every day by treating physicians, and consider medical necessity and reimbursement.” Justifying medical necessity and being accountable for patients’ needs “starts with understanding the healthcare climate for treating physicians,” says Kahle. HHS’s and ONC’s directive for quality incentive programs now dictates that physicians are paid incentives based on four considerations—quality, cost, improvement, and interoperability—so “the O&P profession must become attentive to the expectations that have been forced on physicians … and should consider these same outcome measures for our population of patients.”
Aside from the Hamontree presentations, additional business sessions touch on hot topics to help O&P businesses increase revenues and avoid claim denials. Attendees won’t want to miss the “Medicare Updates
and Comprehensive Error Rate
Testing (CERT)” session on Thursday, September 29, at 10:30 a.m. Experts on this topic—the Durable Medical Equipment Medicare Administrative Contractor (DME MAC) Outreach Team—will present an overview of recent changes and updates to the Medicare program. The DME MACs also will address the most common CERT denials for O&P claims and provide resources to help avoid and resolve common errors.


Something for Everyone
From Alex Smith, to osseointegration, to additive manufacturing and more, this year’s Assembly will feature innovative education with a great deal of never-seen-before content. The sessions highlighted above are just a small sample of the education being prepared for this year’s event. [For the full schedule of sessions planned for the conference see the Preliminary Program included with this issue, or visit www.AOPAassembly.org.]
Of course, for those who cannot attend, and for those attendees who want to see sessions they may have missed, AOPA is recording all sessions. “If an attendee would like to review or watch another session of interest, they will be able to do so through December 19,” explains Kenton. “This is especially helpful to our attendees and is unique to the Assembly since the onset of the pandemic.”







