
34 minute read
Reimbursement Page

from May 2022 O&P Almanac
by AOPA

Managing Reimbursement Pain Points DENIED
Tips for maneuvering same or similar denials, RAC audits, and more
DENIED
EARN 2 QUIZ ME!
BUSINESS CE CREDITS
P.18
Editor’s Note—Readers of
Reimbursement Page are eligible to earn two CE credits. After reading this column, simply scan the QR code or use the link on page 18 to take the Reimbursement Page quiz. Receive a score of at least 80%, and AOPA will transmit the information to the certifying boards.
“THESE ARE THE TIMES that try men’s souls.” This quote, attributed to Thomas Paine in his 1776 publication, “The American Crisis,” was written during a time when General George Washington’s Continental Army was suffering through several demoralizing defeats and the bitter Valley Forge winter. While a comparison of the daily struggles that O&P businesses face due to reimbursement challenges to those of the Continental Army during the early stages of the American Revolution might seem a bit dramatic, the struggle is real.
In today’s O&P climate, reimbursement challenges continue to grow, and they are becoming more difficult to manage. This month’s Reimbursement Page examines some of the more common situations that frustrate O&P providers and offers strategies to help manage the pain points and improve the success of O&P businesses.
Same or Similar Denials
When it comes to O&P pain points, same or similar denials are consistently at the top of the list of AOPA member frustrations. Medicare policy does not allow for the provision of replacement items within the items’ defined “reasonable useful lifetime.” In addition to not covering replacement of identical items, Medicare also will not cover items that are considered “same or similar” to items that were previously provided to the patient.
Unfortunately, Medicare’s definition of same or similar is rather broad and often creates significant coverage challenges involving treatment methodologies that are considered clinically appropriate. A common example of a frustrating same or similar denial occurs when a Medicare beneficiary is treated with a prefabricated walking boot to stabilize an acute injury and, after a more comprehensive evaluation, it is determined that the patient requires additional treatment with a custom-fitted or custom-fabricated ankle-foot orthosis. Another common example occurs when a patient receives an orthosis to treat an orthopedic condition and several years later is prescribed another orthosis that Medicare considers “same or similar” to treat a new and different condition. In both of these scenarios, the Medicare claim for the second orthosis will almost certainly be denied as a same or similar item.
While same or similar denials cause tremendous frustration, the Medicare appeals process can be used effectively if there is proper documentation in the patient’s medical record that discusses either the need for advanced treatment beyond acute stabilization or the independent nature of the orthopedic conditions that warrant coverage of a second orthosis within reasonable useful lifetime timeframes. AOPA continues to address concerns regarding the overbroad interpretation of same or similar classifications with the durable medical equipment Medicare administrative contractors (DME MACs) and CMS to ensure that Medicare beneficiaries continue to have access to medically necessary, clinically appropriate care.
Reasonable Useful Lifetime Denials
Reasonable useful lifetime restrictions are another source of frustration for O&P providers. While often part of the process that results in a same or similar denial, Medicare claim denials caused solely by useful lifetime restrictions are often a result of unreasonable requirements that an O&P item or component last for at least five years. The Social Security Act states that in absence of guidance from the Secretary of Health and Human Services, the reasonable useful lifetime of an item designated as durable medical equipment, prosthetics, orthotics, and supplies is no less than five years.
The Medicare Improvements for Patients and Providers Act established that prostheses can be replaced without regard to useful lifetime restrictions. However, the Medicare Knee Orthosis Policy established a reasonable useful lifetime of one to three years for knee orthoses, and other orthoses fall under the five-year minimum useful lifetime requirements. Claims for replacement orthoses that are identical to the original orthosis will be denied if the orthosis is less than five years old regardless of the condition of the orthosis.
Exceptions to these restrictions include replacements due to a change in patient condition and replacements due to loss, theft, or irreparable damage of the original orthosis. Replacement due to irreparable damage must be supported by documentation that identifies a specific incident that caused the damage and does not include damage due to wear.
When appealing claim denials involving replacement orthoses, it is important that your documentation is specific as to why replacement is necessary outside of reasonable useful lifetime restrictions.
RAC Audits
The Medicare Recovery Audit Program is not a new process. It began in 2005 as a limited demonstration project that was quickly expanded into a permanent part of Medicare Program Integrity Operations. Recovery audit contractor (RAC) audits continue to be a significant pain point for O&P providers.
RAC auditors are highly incentivized to identify Medicare overpayments, collecting contingency fees between 9% and 12% for every overpayment that is ultimately recovered. Since O&P claims represent relatively high costs per claim, they are an attractive target for RAC audits. The fact that RAC audits can review claims that were paid up to three years in the past often creates accounting challenges for O&P businesses when RAC audits result in significant overpayment requests.
While RAC audits are an established process, certain rules may protect you when building strategy on how to deal with them. RAC contractors are limited to performing complex audits on a maximum of 10 O&P claims per tax ID every 45 days. Complex audits are those that are based on medical necessity and include the issuance of an additional documentation request (ADR). Automated RAC reviews, which are based on coverage restrictions based in policy (e.g., no acrylic on preparatory base codes), are not subject to the 10-claim limit. O&P providers should challenge RAC auditors if they issue more than 10 ADRs within a 45-day period.
In addition to ADR limits, RAC contractors must publish and maintain lists of audit issues that have been approved by CMS. RAC contractors may not perform audits on claims that do not include CMS-approved issues. Providers should verify that any RAC audits involve approved issues before responding.
Finally, RAC contractors must return any contingency fees if a provider successfully appeals the RAC determination. This is not profitable for the RAC and may make you a less attractive target for future audits.
Medicare Policy Coverage Gaps
AOPA members often express frustration with out-of-date Medicare medical policies or policies that have obvious gaps in coverage. While AOPA continues to work with the DME MAC contractors to ensure that Medicare Local Coverage Determinations (LCDs) and Policy Articles offer appropriate access to medically necessary, clinically appropriate care, there are certain situations where an item or service is simply not a Medicare benefit or there is medical policy that restricts coverage regardless of its clinical effectiveness.
A recent example involves Medicare coverage of knee orthoses used to treat osteoarthritis. While there is significant evidence of the benefits of treating knee osteoarthritis using unloader-style knee orthoses, the current Medicare Knee Orthosis LCD requires objective documentation of joint laxity in order for certain knee orthoses to be considered medically necessary. While an unloader brace may be effective in relieving pain associated with osteoarthritis, it may be difficult to objectively identify joint weakness or laxity—creating a coverage quandary. Make sure that you fully understand all of the medical necessity and other coverage requirements before providing a service to a Medicare beneficiary. If you believe there is insufficient documentation to support a service prescribed by a physician, you may want to consider obtaining an advance beneficiary notice from the patient.
Relieving the Pain
The pain points discussed above represent a sample of the challenges that O&P providers face on a daily basis. AOPA’s reimbursement staff will continue to work with our contacts at CMS and the DME MACs to help ease O&P administrative challenges and allow you to focus on providing Medicare beneficiaries with the best O&P care available.
Joe McTernan is director of coding and reimbursement services, education, and programming at AOPA. Reach him at jmcternan@AOPAnet.org.
Take advantage of the opportunity to earn two CE credits today! Take the quiz by scanning the QR code or visit bit.ly/OPalmanacQuiz.
Earn CE credits accepted by certifying boards:
This Just In
Reunited in Advocacy

O&P stakeholders take part in AOPA’s 30th Policy Forum


MORE THAN 110 AOPA MEMBERS and O&P students reunited in Washington, DC, May 17-18 for the annual AOPA Policy Forum—the first time the event was held in-person since 2019. O&P business owners, managers, clinicians, educators, and students joined forces to learn about advocacy strategies, game-plan for one-on-one congressional visits, and meet up with legislators and their staff.
The first day of the Policy Forum, participants learned “Advocacy 101,” discussed the “why” of advocacy, discovered how outcomes help elevate the role of O&P professionals as clinical care providers, heard successful advocacy stories, learned expert tips on communicating with legislators, and participated in breakout sessions to prepare for their Capitol Hill visits.
The second day, attendees split up into small groups to meet with individual senators and representatives or staff members to share their stories and deliver their “ask”: that the legislators sign on to cosponsor the Medicare O&P Patient-Centered Care Act—HR 1990 and S 2556. Participants completed more than 70 congressional visits with representatives of 30-plus states. They used the opportunity to connect with lawmakers, explain the value of O&P clinicians as care providers, and increase awareness of the Medicare O&P PatientCentered Care Act.
Look for details about the event and a discussion of the importance of advocating both in Washington and in daily O&P practice in the June/July O&P Almanac.

AOPA President Dave McGill welcomed participants during the Opening Luncheon.
AOPA Board Member Shane Wurdeman, PhD, CP, FAAOP(D), discussed the importance of outcome measures during the session on “Defining Today’s O&P Care Provider.”
Participants met in breakout sessions Tuesday afternoon to game-plan for congressional visits.
Attendees enjoyed the opportunity to discuss O&P advocacy in-person.
Sam Miller, AOPA manager of state and federal advocacy; Nicole Ver Kuilen, AOPA manager of public engagement; Alex Gates, CPO, a clinician at Evergreen P&O; Jane Lucas, counsel at Alston & Bird; and Ashlie White, AOPA director of health policy and strategic alliances, led a discussion on “The Advocate Experience.”


Participants were encouraged to ask questions and share their viewpoints during this year’s interactive Policy Forum. Dozens of O&P professionals chose to attend the optional “Advocacy 101” session prior to the Opening Luncheon.



White shared why it’s important for O&P stakeholders to advocate for both their patients and the profession.
Attendees appreciated the opportunity to access advocacy strategies and details about the Medicare O&P Patient-Centered Care Act prior to their legislative visits.
Keynote Speaker Candace Doby motivated participants to find their “courage” when meeting with legislators.


A Therapeutic Touchfor

UPPER LIMB
The benefits of and strategies for collaborating with occupational therapists for improved outcomes
By CHRISTINE UMBRELL
NEED TO KNOW:
• For prosthetists who treat patients with upper-limb loss, working closely with occupational therapists (OTs) is key to successful patient outcomes.
• Not only do OTs help train patients in using their new devices, they also help them to integrate the prosthesis into their life, and teach them to perform increasingly complex tasks that will aid them in carrying out activities of daily living.
• In addition to teaching “skills drills,” OTs consider the environments in which clients will be using their devices and help them translate the skills they learn in therapy into meaningful activities.
• OT-prosthetist partnerships add value when treating limb loss patients who experience pain—whether residual limb pain, phantom pain, or general body pain that may have been preexisting.
• More training is needed to educate more OTs on working specifically with limb loss patients, and prosthetists can help fill the void by raising awareness of the profession and offering training courses to area OT professionals.
Lucas learned to pick up blocks and complete other new tasks after hours of occupational therapy and prosthetic training. AFTER YEARS OF failures in finding a prosthesis that would assist their son in using his left arm, Lucas’s parents turned to the team at Handspring in Salt Lake City. Months of virtual preparation involving prosthetic evaluation and occupational therapy—Lucas lives in Hawaii—resulted in the 8-yearold finally receiving a well-fitting and functional device during a three-day visit to the Utah facility.
When Lucas tried out his prosthesis, comprising a self-suspending socket, a prosthetic forearm and wrist, cable and harness, and multiple terminal devices, he was able to stack blocks, grasp a snowball, and play alongside his twin sister. “It was the first time he was able to reliably hold things with that side of his body,” explains prosthetist Chris Baschuk, MPO, CPO, FAAOP(D), a regional clinic manager at Handspring. “Lucas asked me, ‘Do I get to take this home?’ When I said ‘yes,’ I got the biggest hug!” This success would not have been possible without a team approach to care that prioritized both occupational therapy (OT) and prosthetic innovation. Baschuk worked closely with Debra Latour, OTD, MEd,
OTR/L, as well as prosthetist Amy
Ginsburg, CPO, to design an appropriate solution. “Debi spent a lot of time evaluating him and establishing his needs,” then preparing him for the prosthesis. “It was critical to have her input” to understand what Lucas needed in a prosthesis to function in his natural environment. During OT evaluations, Latour “sees things I don’t necessarily see,” Baschuk says. Lucas’s positive outcome came about “because we were all working as a team.”


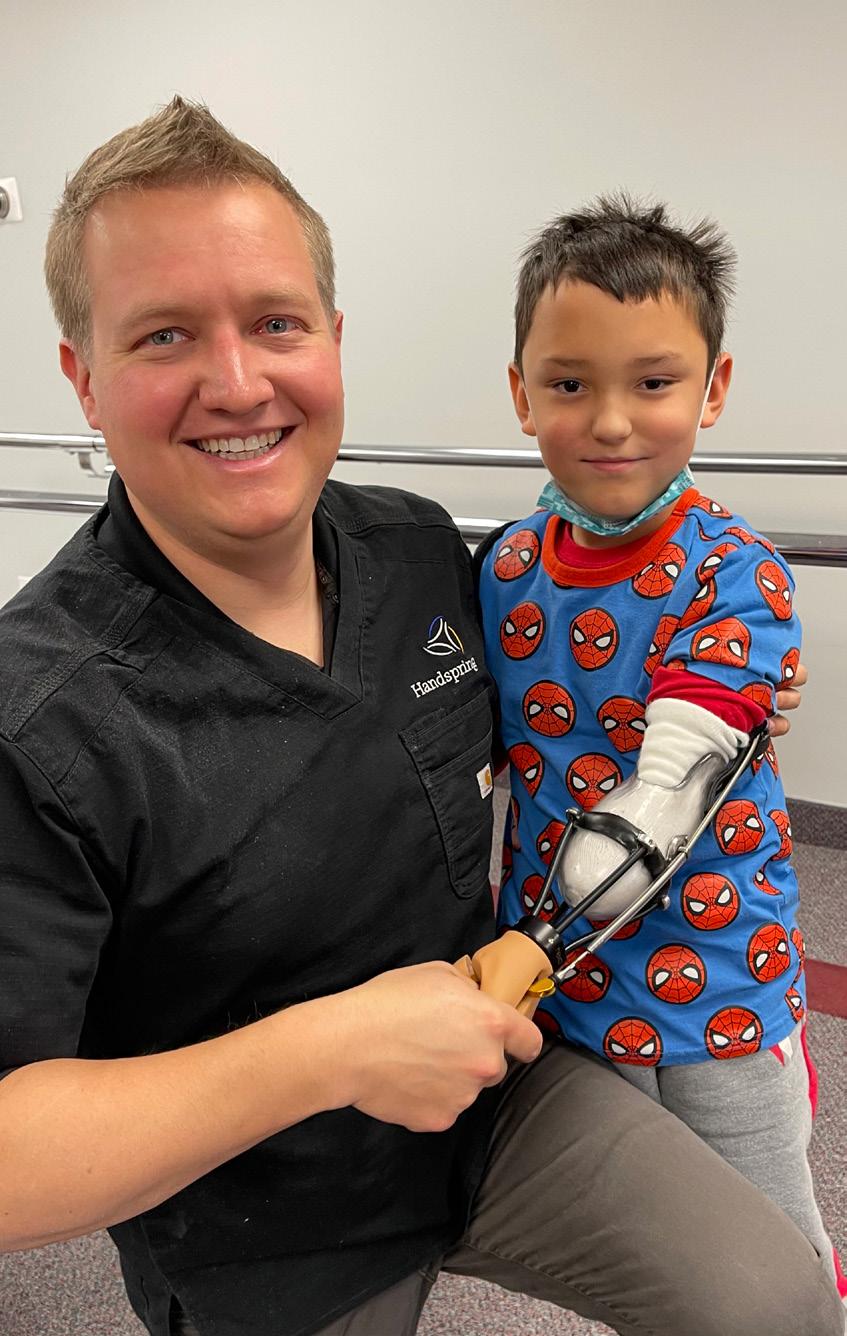
Chris Baschuk, MPO, CPO, FAAOP(D), fit 8-year-old Lucas with a prosthesis after multiple sessions with an occupational therapist.
Early Intervention
Upper-limb prosthetists say that working closely with occupational therapists is key to successful patient outcomes. Baschuk notes that such cooperation is necessary to validate the functionality and design of the prosthesis.
An effective OT who is experienced in amputation teaches patients not only how and when to use a prosthesis, but also which device is appropriate for specific tasks. “The OT helps them learn to integrate the prosthesis into their life, and works closely with the prosthetist to explain areas of deficit so that the prosthetist can properly adjust the device,” Baschuk says.
Rob Wagner, CP, an upper-extremity specialist at Wright & Filippis, emphasizes the value of OT intervention both prior to and after a patient receives a prosthesis. Whether a patient is fit with a body- or electric-powered upper-extremity prosthesis, “we want the OT to work with the patient before receiving the device so they can improve their range of motion, to strengthen the flexors and extensors, so they’ll be able to use the device” once it is delivered, says Wagner.
At Arm Dynamics centers, the prosthetist-OT collaboration “happens right at the beginning, and goes right to the end—lifelong care,” says Kerstin Baun, MPH, OTR/L, national director of therapeutic services. “It’s so important that the initial evaluation is collaborative because you’re really getting at: What is important to this person? What will matter to them at the end?” The answers to those questions will enable the team to select and fit an optimal prosthetic solution, and develop a plan of care that facilitates the patient to succeed in using the device.
John Miguelez, CP, FAAOP(D), president and senior clinical director at Arm Dynamics, equates collaborative care between a prosthetist and an OT with a relay race: “There are times when we’re both holding onto the baton, and there are times when we’re passing it back and forth,” he explains. “You’re maximizing the patient’s time and making sure that you identify potential barriers that could arise, and dealing with those proactively so there aren’t delays in the rehabilitation of the patient.” The initial evaluations enable the prosthetist and OT to assess the patient’s physical limitations and capabilities and assess range of motion, strength, edema, scar management, and other factors that inform a successful fitting process, according to Baun. Arm Dynamics OTs also assess the patient’s social and psychosocial needs—“the mental health and well-being,” she says. “You’re dealing with the physical pieces, but you’re also paying attention to what’s going on for them socially—do they have the resources they need, and if not, can I help facilitate getting those in place? The same goes for mental health needs.” Individualized Care After initial evaluations, individualized OT sessions prepare the patient for successful use with the prosthesis, according to Baun. OTs usually start with education—about the prosthesis, how to care for it, and how to care for the residual limb—before moving on to the basics of component operation, and donning and doffing independently.
As a next step, therapists may ask patients to perform rote, simple actions. “We start with a simple task, and as the individual shows control and skill, we can grade to more complex activities,” explains Baun. Early tasks may include holding a
water bottle and learning to drink from it, or cutting food with a fork and knife. “Once those skills are mastered, we can shift to more complex activities— preparing a meal, or looking at tasks to enable return to work.” Teaching patients to perform increasingly complex tasks can help prevent prosthesis abandonment, according to Wagner. “You can make a great prosthesis, but if the patient doesn’t understand how to functionally use it, they won’t use it,” he says. “When OT shows them how to carry out daily activities using a prosthesis— like folding clothes or opening a bag of chips—they want to use their devices.” The type of upper-extremity device a patient receives affects the amount and the type of therapy needed, according to Baun. Even patients with less complex devices, such as custom silicone restorations, benefit from working with an OT, but therapy will be more intense for individuals with more advanced components. “A fully electric prosthesis is going to require programming; it’s going to require learning to control the various components of the device, learning how to preposition it, and how to optimize the function of it. That often requires collaborative problem-solving and lots of practice.” The patient and their demeanor also influence the therapy plan. “We could have two patients with the same level of amputation, being fit with essenKerstin Baun, MPH, OTR/L tially the same prosthetic device, that need two completely different amounts and types of therapy,” Miguelez explains. “Part of the art is to understand what will work best for each patient’s personality and preferred learning mechanism.” Many prosthetists attend some OT appointments to get a better understanding of the patient and their needs, says Baschuk. “I like to get involved in at least one or two OT appointments, both before and after delivery, to
Rob Wagner, CP John Miguelez, CP, FAAOP(D)
validate that the design of the prosthesis is meeting the functional needs of the patient,” he says. “Sometimes the initial plan you thought would work” for a particular patient doesn’t progress as hoped. “It’s an iterative process. You use the device in training sessions with the OT, then deliver the prosthesis, then transition into the maintenance phase,” he says. “The patient may come back as they get used to the device and try to do more with their prosthesis than they originally

Debra Latour, OTD, MEd, OTR thought they could,” which may require device adjustments and well as more therapy.
For O&P facilities that don’t have OTs on staff, prosthetists may need to travel to participate in OT sessions with patients. At Wright & Filippis, Wagner travels throughout the state of Michigan to treat patients, and he has developed relationships with OTs in different regions. “There are not a lot of upper-limb patients, so it’s good to stick with one OT [in an area] so they can build up their experience” working with this select patient base, he says.
Wagner also lends equipment to OTs to facilitate more productive therapy sessions. For example, for myoelectric devices, he loans a tester, or he sets up a hand (without a socket) with a few electrodes so the patient can practice before prosthesis delivery. Working with feedback machines allows the OT and patient to see EMG signals as the patient moves. For some myoelectric devices, he introduces
What an Experienced Occupational Therapist Wants You To Know
Debra Latour, OTD, MEd, OTR, is an occupational therapist, the doctoral capstone coordinator and a professor of occupational therapy (OT) at Western New England University, and a consumer of upper-limb prosthetics. Born with right upper-limb absence in 1956, Latour became a prosthesis user at 14 months old in an innovative program at Shriners Hospitals for Children in Springfield, Massachusetts. As a trailblazer, she became a prolific prosthesis user—despite having never participated in OT herself.
In high school, she learned about the OT profession and decided to pursue a career in the field. She earned a bachelor’s degree in occupational therapy, embraced clinical roles, and eventually earned master’s and doctorate degrees and university positions. In addition to serving as a clinical therapy consultant at Handspring, she also teaches upper-extremity courses for OTs and physical therapists, has authored multiple textbook chapters, and consults to Fillauer-TRS Inc.
Given her experience, Latour offers the following advice to prosthetists who treat upperlimb patients: • Embrace collaborative care. Prosthetists should work with OTs and other members of the rehab team to share knowledge and provide overlapping—rather than siloed–patient care. • Ensure that all persons with upper-extremity absence have access to OT care. Even individuals using passive and body-powered components can improve their outcomes when they take part in OT. • Encourage clients to participate in preprosthetic training. Individuals can get started using simulators and other training devices when working with OTs, even before their prostheses are ready. “They’ll start to train their minds on
how to use their prostheses, and will be more comfortable once they get their devices,” Latour says. • Focus on communication skills. Recognize that other members of the healthcare team—and the device users themselves—may not understand or feel comfortable with some of the terminology prosthetists use. Embrace person-first language, and avoid technical terms. • Help train OTs in prosthetic subspecialties.
There are more than 80,000 OTs in the United
States, but specialized training specific to limb loss is hard to access, says Latour. Prosthetists can raise awareness of the profession and the need for OTs with expertise in upper-limb loss/ absence, and offer training courses to area OT professionals.
software that trains the patient via video games—directing cars through a maze, or opening and closing a hand. “Then they’re more prepared to practice ADLs after they receive their device,” Wagner says.
Taking Field Trips
In addition to teaching “skills drills,” OTs consider the environments in which clients will be using their devices. “An OT will take the time to figure out specific activities—those most meaningful—they want to be able to accomplish,” says Latour.
Occupational therapy plays an important role in ensuring the prosthesis design and rehabilitation plan addresses patient’s individual concerns, says Latour. “OT looks beyond limb loss to the total person, and helps people find their voice,” she explains. “We can learn what is troubling them, and in what environments they find themselves. We discuss intimate topics such as how they dress, grooming, toileting, and relationships with spouses. They are much more open to talking to OT about these topics—and we can bring back the relevant information to the prosthetist.”
At Arm Dynamics, OTs work with patients at locations where they will most benefit from using their devices. “It’s one thing to be successful in the clinic, but when you add the physical uniqueness of different environments, and the social challenges of having people look at you, it really changes the demands of the task,” explains Baun. “It adds psychosocial layers, and complexity.”
Home visits, for instance, can yield positive results. In addition to evaluating how the patient can use their device and how much support they have at home, the OT can recommend modifications to the patient’s home or specific external devices to accomplish different tasks, “well beyond the scope of the prosthetist,” says Baschuk.
Many OTs also accompany patients as they engage in community activities, according to Miguelez—for example, visiting the grocery store to teach patients how to grab items to place in their carts and pay for purchases. The OT’s role is “to be there and support them, and note the things they did really well, and the activities that were more difficult—then spend more time perfecting control through training, so the patient feels confident in any environment,” he says.
In-person worksite evaluations also can be informative. Baun frequently goes with patients to their workplaces—offices, factories, and even construction sites—to understand the physical tasks involved in their jobs. “Helping them problem-solve in the ‘here and now’ is hugely beneficial. It helps them get to that next level, and helps them problem-solve through challenges.” She also accompanies patients to physical activities, such as going to the gym, paddle-boarding, or rock-climbing—where she can assess whether they have appropriate activity-specific componentry. “We can take that information back to the prosthetist,” who can make changes and adjustments, Baun explains.
All of these field visits help boost patients’ confidence—which can prevent prosthesis abandonment, according to Miguelez. “We want our patients to continue to wear their prostheses, so anything we can do to lower or eliminate the potential for abandonment is really important,” he explains.
Even after patients have received their definitive devices and are satisfied with their function, collaborative follow-up is beneficial. Patients at Arm Dynamics complete a short survey every three months to ensure they are still on track in their rehabilitation journey. The data they provide helps identify lapses or reduced prosthesis use—“we can ask them to come in so we can talk about it and address any issues,” says Miguelez. “Sometimes it’s as simple as they’ve taken up a new hobby, and they were never trained with their prosthesis in that activity— so we have them come in and work with their therapist. That can mean a huge change in quality of life.”

John Miguelez, CP, FAAOP(D), works with a patient on activating grip patterns with his multiarticulating hand.
Measurement Tools Inform Upper-Limb Care Plans

Kerstin Baun, MPH, OTR/L, guides a patient through a series of basic functional tasks.
Outcome measures can be just as important for upper-limb patients as they are for lowerlimb patients. At Arm Dynamics, occupational therapists and prosthetists work closely to capture and analyze patient data. For example, the team leverages the Wellness Inventory during patients’ initial evaluations, explains Kerstin Baun, MPH, OTR/L, national director of therapeutic services.
The Wellness Inventory is a patient screening tool that helps identify psychosocial changes that could have a negative impact on rehabilitation or success with the prosthesis, and screens for issues such as substance use, pain, PTSD, depression, and other quality-of-life issues. “A lot of these patients sustain their amputations as a result of an accident, so many have post-traumatic anxiety or depression,” says Baun. In fact, Arm Dynamics’ research in studying Wellness Inventory responses has found that 58% of patients screen positive for depression and/or post-traumatic anxiety.
Baun says it’s also common for patients to screen positive for substance use, which can be a coping mechanism postamputation. “We want to make sure they’re shifting to positive coping mechanisms” by helping to find and put in place the support and resources they need, Baun says.
“The Wellness Inventory informs our whole approach” and is given to patients more than once, Baun says. After patients become comfortable with their prostheses, “we touch base with them again, using that exact same inventory, to learn what’s changed, what’s been resolved, and what may still need attention.”
Clinicians at Arm Dynamics also leverage other measurement tools, such as a performance measure called the Capacity Assessment of Prosthetic Performance for the Upper Limb (CAPPFULTM) and Comprehensive Arm Prosthesis and Rehabilitation Outcomes Questionnaire (CAPROQTM), a patient-reported outcome measure. “We use these at multiple time points to tap into both objective and subjective data; how well they are able to use their prosthesis, as well as their perceived function and satisfaction with their device, along with various elements of pain,” says Baun. “It’s so critical to look at it long-term, to ensure they’re successful not only in the clinic, but in real life settings—that is the essence of lifelong care and the goal of occupational therapy.”
Treating Pain
Collaborating with OTs adds value when working with limb loss patients who experience pain, according to Baschuk. “If they say their shoulder, or arm, or other side of their body hurts, the OT can usually watch and figure out why” the pain is occurring, then assist in devising a plan to prevent or reduce that pain.
Latour says OTs also may uncover information that patients did not realize was relevant to share with their prosthetists—such as previous sound-side injuries that still bother them. Sometimes OTs can help explain problems patients encounter with new devices: “Prosthetists take pride in their end product,” she explains, “so some people are afraid to speak up if there is a problem.” But they may feel comfortable sharing that information during therapy—and OTs can serve as a bridge to the prosthetist. “We teach our clients self-advocacy.”
At Arm Dynamics, clinicians screen patients for pain at initial evaluations and periodically thereafter, says Baun. Pain can run the gamut from residual limb pain, to phantom pain, to general body pain that may have been preexisting or was caused by the accident that resulted in the amputation. How the care team proceeds with patients who screen positive depends on the etiology. “For someone who has phantom limb pain, we would want to work collaboratively with their physician to make sure they have the medication they need, and may connect them with a counselor to help deal with trauma,” Baun explains.
OTs also may implement pain management strategies, such as graded motor imagery—therapy using specific imagery to train the brain away from pain—and mirror therapy, or other pain management techniques, according to Baun. “It depends on the individual therapist and their training,” she says. “Arm Dynamics therapists are trained in using modalities, which usually focus on residual limb pain, and pain that’s more peripheral. Regardless of etiology, they may be helping the patient consider a lifestyle approach to pain management,” which could involve nutrition, exercise, meditation, and even sleep hygiene.
“Sometimes, as people become more functional with their prosthesis, and as the rehabilitation process continues, pain diminishes over time as life normalizes for them,” adds Baun. But for others, consultation with a surgeon may be advised. “If pain persists, we can speak to patients about the potential of surgery—for example, targeted muscle reinnervation for treatment of neuromas. OTs can facilitate a team approach to find solutions to persistent pain problems.”
Expanding Partnerships
To provide optimal patient care, prosthetists work not only with OTs but also with other members of a rehabilitation team, which may include a surgeon, physiatrist, case worker, psychologist, physical therapist, and massage therapist, says Baschuk. “For upper-limb care, it’s a multifaceted challenge,” he explains. “Everyone on the team needs to know the goal and consider the ramifications across those specialties.”
Ultimately, collaborative care will help ensure patients’ needs are met. With a team approach, “the patient feels they have people in their corner who will go to bat for them,” Baschuk adds. “Each of us on the rehab team can help empower them from a different angle. It’s a really rewarding experience when we all work together.”
Christine Umbrell is a contributing writer to O&P Almanac. Reach her at cumbrell@contentcommunicators.com.

Rob Wagner, CP, visits OT facilities to work with the therapist and patient together, and sometimes lends equipment to OTs to facilitate more productive therapy sessions.
TexasSome Things New in
Mark your calendar for the AOPA National Assembly in September

REGISTRATION OPEN SOON! WE CAN’T WAIT TO SEE YOU!
O&P PROFESSIONALS ACROSS the country are already gearing up for the 105th AOPA National Assembly, which will feature brand-new content and top-class speakers. This year’s conference will explore the “Intersection of Technology + Humanity” and will take place September 28 through October 1 at the Henry B. Gonzalez Convention Center in San Antonio.
Future-Focused Education
The in-person Assembly, co-sponsored by the Texas Society of Orthotic and Prosthetic Professionals, will launch several “new” features—including a Postmastectomy Care Track and an O&P Digital Care Track.
The Postmastectomy Care Track was added due to overwhelming feedback from the community on the need for information, as well as the need to maintain the CFm credential, according to Joanna Kenton, MHA, CPO, LPO, FAAOP, co-chair of the AOPA 2022 National Assembly Planning Committee. This track also aligns with AOPA’s focus on diversity, equity, and inclusion, and supports the drive to ensure equitable access to diverse patients.
Over the past few years, the number of sessions addressing digital technology have increased. “Digital fabrication has traditionally been a part of the Technology Track,” Kenton explains, but “we felt that the digital world has evolved into its own category.”

The O&P Digital Care Track will include a new interactive experience during a breakout session, where companies can consider two case studies—one in prosthetics or one in orthotics—and share with participants how they would handle the cases leveraging their technologies, according to J. Chad Duncan, PhD, CRC, CPO, who co-chairs the O&P Digital Care Committee with Jeff Erenstone, CPO. “This will be a more immersive experience and informative for Assembly-goers,” he says.
Duncan also encourages attendees to consider the content on additive manufacturing within the Digital Care track, which will touch on the many ways 3D-printing technologies can be integrated into O&P facilities.
The Technical Education Track will debut a new “Fabrication Tricks & Tips” session, which will showcase tips from members throughout the country, who previously submitted three- to five-minute videos explaining their O&P “trick or tip” to be considered for inclusion. During the Assembly, participants in this session will vote for their favorite tip—and winners will be awarded cash prizes.
The range of sessions to be offered in San Antonio are intended to target the interests and needs of today’s clinicians and business owners. “The Assembly Planning Committee has
AOPA will launch the “O&P Experience Zone” during the Assembly on Thursday, September 29—a fun, interactive event showcasing patient success stories and their caregivers. The Experience Zone will be held in conjunction with a traditional happy hour on the exhibit hall floor. This year’s exhibit hall will feature hundreds of cuttingedge products and technologies from worldwide manufacturers and O&P innovators.
Sports enthusiasts won’t want to miss a cool new fundraising event at Top Golf San Antonio—details to come.
done a wonderful job identifying great presentations,” says Duncan. “I’ve been impressed with the quality of the submitted presentations. All the committees involved are dedicated to a great learning experience for the attendees. There is something for everyone who comes—that being front office, technician, clinician, to the owners.”
Fresh Experiences
Inspiring keynote speakers and new trade show experiences headline this year’s event.
Mona Patel, a licensed clinical social worker who founded and leads the San Antonio Amputee Foundation (SAAF), will deliver one of the keynote presentations. At the age of 17, Patel was struck by a drunk driver and underwent more than 20 limb salvage surgeries before deciding on an elective right below-knee amputation. In addition to her role as executive director of SAAF, Patel has contributed to the advancement of individuals with limb loss in many ways, including serving on the board of the Amputee Coalition of America, leading a successful grassroots legislative effort for a bill that now mandates fair insurance coverage for prosthetic limbs, and supporting individuals with new amputations. Patel is excited to share her story and the work of SAAF during the Assembly.
CHOOSE FROM 7
EDUCATIONAL TRACKS
IN SAN ANTONIO
• Prosthetic • Orthotic • Pedorthic • Technical • Business • NEW: Postmastectomy Care • NEW: O&P Digital Care
Fostering a Sense of Community
The National Assembly will offer numerous opportunities for attendees to network and make connections with other O&P stakeholders from all realms of the O&P profession— including clinicians and business owners, suppliers and manufacturers, and educators and researchers.
Taking part in the AOPA Assembly, which offers the unique blending of the business and clinical sides of O&P, is a great way to get involved in the greater O&P profession, says Duncan. “You’ll feel a greater sense of belonging within the profession,” he says.
San Antonio Can’t-Miss Attractions in
This year, why not extend your visit, and bring the family, to take advantage of the many cultural and historical attractions in and around San Antonio? Below are just a few of the many places of interest—and don’t forget the Alamo!

The River Walk: This 15-mile urban walkway is the No. 1 attraction in Texas and runs through downtown San Antonio. Lined by restaurants, shops, and bars, the River Walk is open 24/7. Visit www.thesanantonio riverwalk.com.
Go Rio Electric Barges: These barges offer narrated river cruises and run along the San Antonio River Walk. Learn about the city’s culture, history, and architecture while taking in the view. Visit www.goriocruises.com.
Tower of the Americas:
This 750-foottall downtown landmark was built for the 1968 World’s Fair and offers a panoramic view of the Alamo City. Don’t miss the Observation Deck, a 4D theater ride, or the revolving Chart House Restaurant. Visit www.towerof theamericas.com. The Pearl: This 22-acre mixed-use space is a restored and repurposed former brewery and is committed to “craft, quality, and hard work.” Attractions include restaurants, retailers, and one of three campuses of the Culinary Institute of America. Visit https://atpearl.com.
Witte Museum:
This famous space features the nature, science, and culture of the region. Visit www. wittemuseum.org. “You can get involved to make a difference and to make sure the profession is relevant.” In addition, “you get to meet so many people at the Assembly,” and then bring back what you learn to share with your co-workers, colleagues, or students.
And although there is a virtual option for the Assembly this year, those that make it to San Antonio will benefit from the renewed sense of community, according to Duncan. “The fact we are coming together is important. Our profession is built on relationships and engaging with others,” he says. “Virtual is nice, but it does not provide you with that side conversation or continued discussion after hearing a really good or thought-provoking presentation.”
For those who are unable to travel to San Antonio this year, full conference registration grants virtual access; a virtual-only option also is available. The virtual sessions will be offered for 60 days, starting two weeks after the in-person Assembly.
Duncan encourages in-person Assembly-goers to take advantage of nearby attractions in Texas. “AOPA has done a wonderful job in locating the conference in the heart of San Antonio,” he says. “This allows Assembly-goers great eating options and fun areas to investigate along the River Walk. Just walking along Texas’s No. 1 attraction is worth it.
“A lot is changing in our profession, and the personal connections will keep us moving forward,” adds Duncan. “The welcoming atmosphere of San Antonio will definitely encourage and support people connecting, especially if they take a boat ride on the river.”
The 2022 AOPA National Assembly will open for registration in June. Be on the lookout for registration and hotel information, as well as details on additional special events planned for San Antonio. Visit www.AOPAassembly.org for details, and contact Assembly@AOPAnet.org with questions.








