
25 minute read
The foot in psychology, body language, and social life

2 A short history of ankle fractures
3 Development of radiological classifications
Although the first attempts at classifying ankle fractures date back to the preradiological era, these classification schemes were based exclusively on experiments. Only after the introduction of radiological examination was it possible to open a clinically relevant debate about this issue.
3.1 Chaput classification The first classification of ankle fractures reflecting radiographic findings was published by Chaput in 1907 [13]. He based it on experimental studies of his predecessors, particularly Tillaux, and distinguished between four basic groups of fractures: • Abduction fractures • Adduction fractures • Supramalleolar fractures caused by adduction or abduction • Comminuted fractures
The first two groups are fracture dislocations, while the third and fourth groups include pilon fractures. Ample drawings used in the text show that Chaput had a good knowledge of all types of fibular fractures in terms of the level of fracture line. He described in great detail the fractures of the medial malleolus and fractures of the posterior rim of the distal tibia, distinguishing between different sizes of the avulsed fragment. He repeatedly mentioned Tillaux experimental studies and the fragment of anterior tubercle of the distal tibia described by him (Tillaux’s fragment externe) known today as the Tillaux-Chaput tubercle or fragment.
3.2 Destot classification In 1911, Destot [14] introduced a concept which remains relevant today, consisting in division of ankle fractures into those compromising the stability of fracture dislocations, ie, fractures which involve only the mortise and disturb the equilibrium of the foot, versus those involving the “pilon tibial” or the tibial “pestle”, ie, the support of the body. Both groups were subdivided into individual patterns (Fig 2-5).
3.3 Tanton classification Another classification of ankle fractures was published in 1916 by Tanton [10] who based it on the Destot’s concept, ie, distinguishing between malleolar and pilon fractures.
Malleolar fractures were subdivided into the isolated (medial or lateral malleolus) and the associated ones. The latter group included four fracture patterns, according to the level of the fibular fracture in relation to the syndesmosis (Fig 2-6): • Fractures bi-malléolaires basses (Weber A type) • Fractures de Dupuytren basses (Weber B type) • Fractures de Dupuytren types (low Weber C type) • Fractures de Maisonneuve (high Weber C type)
Pilon fractures were divided into total and partial ones. In the latter group, he distinguished between isolated fractures and fractures combined with malleolar fractures. Therefore, pilon fractures included also fractures of both malleoli with
26
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek

a
b


Fig 2-6a–c Tanton classification of fibular fractures. a Fractures bi-malléolaires basses. b Fractures de Dupuytren basses. c Fractures de Dupuytren types [10]. Fig 2-5 Destot classification of malleolar fractures [14].

c
27
2 A short history of ankle fractures
a fracture of the posterior rim of the distal tibia (fracture of posterior malleolus). Medial malleolar fractures were in Tanton classification divided into vertical and horizontal ones, and horizontal fractures into the following types (Fig 2-7): • Fractures de la pointe (fractures of the apex) • Fractures de la partie moyenne (fractures of the middle part) • Fractures de la base (fractures of the base, transverse, or vertical)
3.4 Lane contribution In 1921 Lane [24] published an interesting article on ankle fractures in which he distinguished between abduction and adduction fractures. According to Lane, with the foot in adduction there first occurs a vertical medial malleolar fracture and then a transverse lateral malleolar fracture (Fig 2-8). Lane distinguished between three phases of an abduction fracture. He proposed that with abduction and external rotation of the foot, it is the fibula that is fractured first, followed by a medial malleolar fracture, or rupture of the deltoid ligament, and finally avulsion of a posterior tibial fragment of variable size. Although Lane was wrong regarding the sequence of lesions in adduction and abduction fractures, he was the first in the radiological era to present a categorization of ankle fractures based on the mechanism of injury. “ According to Lane, with the foot in adduction there first occurs a vertical medial malleolar fracture and then a transverse lateral malleolar fracture.”


28


a b
a b c Fig 2-7a–c Tanton classification of fractures of medial malleolus. a Fractures de la pointe. b Fractures de la partie moyenne. c Fractures de la base [10].

Fig 2-8a–b Lane grading of adduction fracture [24].
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek
3.5 Ashhurst-Bromer classification Chaput, Destot, and Tanton died almost at the same time, at the end of World War I. Their premature deaths were probably caused also by personal suffering and tragedies they experienced during the war and in the case of Destot also by the radiation syndrome.
Fortunately, they had a worthy successor on the other side of the Atlantic, namely the American surgeon Astley Paston Cooper Ashhurst (1876–1932). His father, a prominent American surgeon John Ashhurst (1839–1900), named him after the famous English surgeon sir Astley Paston Cooper (1768–1841). During World War I, APC Ashhurst served in France where he cooperated with the French physicians and thus got acquainted also with publications by Chaput, Destot, Tanton, and others.
In 1922, Ashhurst together with Bromer published a remarkable radiological study developed on the basis of a thorough review of the literature and of 300 ankle fractures [1]. Fractures were divided according to the mechanism of injury into: • Fractures by external rotation • Fractures by abduction • Fractures by adduction • Fractures by compression in long axis of leg • Fractures by direct violence (supramalleolar types)
From the anatomical-pathological viewpoint, Ashhurst and Bromer distinguished five fracture patterns, namely a fracture of: • Fibula below the inferior tibiofibular joint • Fibula obliquely through the inferior tibiofibular joint • Fibula above the inferior tibiofibular joint • Tibia, involving the ankle joint • Supramalleolar fractures, not involving the ankle joint directly
3.6 Henderson classification In 1932, the American orthopedic surgeon Melvin Starkey Henderson (1883–1954) published an ankle fracture classification based on Tanton’s concept [25]. Using the term trimalleolar fractures that he introduced before, he divided the fractures into three groups: • Isolated malleolar fractures (including posterior malleolus) • Bimalleolar fractures (without and with displacement) • Trimalleolar fractures (medial, lateral, posterior)
In this way, Henderson resolved the drawback of the Tanton classification that included malleolar fractures combined with a posterior malleolar fracture into the group of pilon fractures. One year later in 1934 Henderson [26] slightly modified his classification scheme. “ During World War I, APC Ashhurst served in France where he cooperated with the French physicians and thus got acquainted also with publications by Chaput, Destot, Tanton, and others.”
29
2 A short history of ankle fractures
3.7 Danis classification In 1949, Robert Danis (1880–1862) published an extraordinary book on internal fixation “Théorie et Pratique de l’Ostéosynthèse” [27], part of which dealt with the surgical treatment of ankle fractures. Danis divided ankle fractures according to the level of the fibular fracture in relation to the syndesmosis into four groups (Fig 2-9):
• A transverse fibular fracture below the insertion of both tibiofibular ligaments, caused most probably by adduction (fracture sous-ligamentaire).
• An oblique interligamentous fracture caused by torsion, where the anterior tibiofibular ligament is intact and the posterior tibiofibular ligament is torn or avulsed together with a tibial bone fragment (fracture inter-ligamentaire).
• An oblique fracture above the insertion of the tibiofibular ligaments onto the fibula caused by torsion where the anterior tibiofibular ligament is torn and the posterior tibiofibular ligament is also torn or avulsed together with a tibial bone fragment (fracture sus-ligamentaire basse).
• A transverse fracture of the fibula caused by abduction of the foot, located several centimeters above the insertion of tibiofibular ligaments on the fibula. Both ligaments are injured, including the interosseous membrane that is ruptured up to the level of the fracture of the fibula (fracture sus-ligamentaire haute).
Medial malleolar fractures were divided into transverse and vertical ones, a concept that may also be found in Malgaigne’s textbook. The above-mentioned overview shows that the Danis classification scheme of ankle fractures according to the course of the fracture line on the fibula was not original. The first to introduce such a scheme was Tanton [10], followed by Ashhurst and Bromer [1]. Danis’ contribution consists in associating the level of the fibular fracture with a certain type of lesion of tibiofibular ligaments, even if incorrect from the viewpoint of current knowledge. “ Danis’ contribution consists in associating the level of the fibular fracture with a certain type of lesion of tibiofibular ligaments, even if incorrect from the viewpoint of current knowledge.”


30
a b
Fig 2-9a–d Danis classification of fibular fractures [27]. c d
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek
4 Posterior fragment of distal tibia
Fracture of the posterior rim of the distal tibia in ankle fracture dislocations is a subject of continuing interest. In the German-language literature, this fragment is commonly referred to as “Volkmann’sches Dreieck” [28], while English-language authors prefer the term “posterior malleolus” or “posterior rim (edge) of distal tibia” [1, 29, 30].
4.1 The first description Sir Astley Paston Cooper (1768–1841) is sometimes presented as the first author to describe avulsion of the posterior rim of the tibia, namely in 1819 in Surgical Essays [31] and later in 1822 in A Treatise on Dislocations [32]. However, the description and drawings show that it was a fracture of the tibial pilon rather than a fracture dislocation of the ankle (Fig 2-10). Thus, the first to describe this injury was probably Henry Earle (1879–1838), grandson of Percival Pott, in 1828, namely on the basis of autopsy findings [33].
4.2 Volkmann’s triangle In the German-language literature, the separated posterior rim of tibia is referred to as “Volkmann’sches Dreieck” (Volkmann’s triangle) [28]. However, this term is not correct, as repeatedly pointed out by some authors [2–6]. The drawings and description suggest that Richard von Volkmann (1810–1885) described avulsion “ Sir Astley Paston Cooper (1768–1841) is sometimes presented as the first author to describe avulsion of the posterior rim of tibia.”

Fig 2-10 Cooper’s drawings of ankle fractures [32].
31
2 A short history of ankle fractures
of the lateral part of the distal tibia in the sagittal plane, apparently a compression fracture, ie, a tibial pilon fracture, as shown also by his original drawings (Fig 2-11). In no case did he describe avulsion of the posterior fragment of the distal tibia, and avulsion of the anterior tibial fragment was mentioned only marginally [34]. Thus, Volkmann’s is the first known description of a successful operative treatment of an open fracture of the tibial pilon (resection of the distal tibia), rather than avulsion of a posterior tibial fragment.
The term “Volkmann’sches Dreieck” appeared in the German-language literature in the 1920s. One of the first surgeons to use it was probably Karl Ludloff (1864–1945) [35, 36] in 1926 who was followed in 1931 by Fritz König (1866–1952) [37] and Fritz Felsenreich [38, 39]. After World War II, the term “Volkmann’sches Dreieck” was adopted by a number of German surgeons [28]. In the first AO textbook from 1963, Willenegger and Weber used the term Earle-Volkmann type [40]; however, in the last issue of the AO manual from 1991 [41] it is referred only as the Volkmann triangle. Weber in his textbook from 1966 [9] used Earle’s name for the avulsed posterior tibial fragment, and he associated avulsion of the anterior tibial fragment with the Volkmann name. “ Volkmann’s is the first known description of a successful operative treatment of an open fracture of the tibial pilon.”
4.2.1 Posterior malleolus The term “malléole postérieure” (posterior malleolus) was introduced by Destot [14] in 1911. In his view, fractures of the posterior malleolus may occur either in a combined or an isolated form. In 1912, Birscher [42] suggested the term “malleolus lateralis posterior” which, however, has not been accepted.
4.2.2 Cotton fracture In 1915, Frederic Jay Cotton (1869–1938) described a “new type” of ankle fracture that was later associated with his name [43]. It was a fracture of both malleoli in conjunction with a fracture of the posterior rim of the distal tibia (Fig 2-12). Cotton, however, was wrong. The same fracture was described by Robert Adams (1795–1871) as early as in 1836 [44] in a 53-year-old woman who sustained “…the partial dislocation forwards of the tibia, combined with a simple fracture of the fibula.” The woman subsequently died and the autopsy revealed that “…the internal malleolus itself had been broken, and small portion of the back part of the edge of the articular cavity of the tibia was avulsed.” Description of this case is highly valuable as it was illustrated by two drawings of the affected limb (lateral and medial) and two drawings of the joint skeleton.
32
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek
a b Fig 2-11a–b Drawing of Volkmann’s cases. a Scheme of fracture lines. b Line R marks the level of resection [34].



Fig 2-12 Cotton’s drawings of “Cotton fracture” [43].
33
2 A short history of ankle fractures
4.2.3 Classification The efforts to classify fractures of the posterior rim of the distal tibia appeared soon after this fracture was first described on a radiograph by Chaput [13] in 1907. In 1913 Grondahl [45] divided this fracture pattern into three groups, namely “proper fractures of posterior lip, fractures of posterolateral corner of distal tibia, and fractures consisting of cortical avulsion from the dorsal surface of the tibia.”
Souligoux [46] in his classification that was published in 1913 also distinguished between three types of injury to the posterior rim. In the first pattern only “the posterior tubercle” was avulsed, and the rest of the posterior rim remained intact. In the second pattern the entire posterior rim (lip or edge) was avulsed as “a thin bone lamella.” The third pattern included also fractures of the entire rim, namely in the form of “a conical fragment on wider base carrying a piece of articular surface of varying size.” In 1922 Ashhurst and Bromer [1] introduced a classification of the avulsed posterior fragments according to their size into “small, medium and large fragments.”
In 1940 Nelson and Jensen [47] divided fractures of the posterior rim of the distal tibia into “classic fractures” involving more than one third, and “minimal fractures” involving less than one third of the articular surface (Fig 2-13). In the classic type the authors’ recommended internal fixation by a screw via a posteromedial approach. The recommendation to reduce and fix operatively any posterior rim fragment bearing at least one third of the articular surface was accepted by a number of other authors and is, in fact, generally respected even now. “ In 1922 Ashhurst and Bromer [1] introduced a classification of the avulsed posterior fragments according to their size into small, medium and large fragments.”
4.2.4 Operative treatment The first authors who focused in detail on ankle fractures with a separated posterior fragment at the beginning of 20th century, eg, Meissner [21], Birscher [42], Sussman König [22], Hilgenreiner [23] and others were aware of instability of this type of fracture. They recommended foot traction, or even tenotomy of the Achilles tendon. Poor maintenance of ankle joint reduction in this way rather than the joint incongruence led to the first attempts at operative treatment of these fractures.

Fig 2-13 Nelson and Jensen classification of fracture of posterior fragment [47].
34
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek
5 Beginnings of operative treatment A powerful impulse for the development of classification and operative treatment of ankle fractures was given only after it was possible to establish an exact diagnosis, ie, identify individual fragments and the degree of their displacement. It is no wonder that the first radiologically documented cases of internal fixation of ankle fractures appeared in the same period as the above-mentioned radiological studies [4].
Operative treatment of ankle fractures was launched simultaneously by William Arbuthnot Lane (1856–1943) and Albin Lambotte (1866–1955) as early as the first decade of the 20th century [17–20]. Within the period 1905–1914, they described technical principles that are still observed today. Lane preferred plate osteosynthesis, which he applied primarily in the fibular fractures, including suprasyndesmotic fractures and vertical fractures of the medial malleolus (Fig 2-14). Lane fixed transverse fractures of the medial malleolus with a screw. Lambotte, on the other hand, never used a plate and preferred screws or nails in the internal fixation of both malleoli (Fig 2-15). “ Operative treatment of ankle fractures was launched simultaneously by William Arbuthnot Lane (1856–1943) and Albin Lambotte (1866–1955) as early as the first decade of 20th century.”

a b

Fig 2-14a–c Lane technique of fixation of fibular fractures by plate. a Fibular fracture. b Medial malleolus fracture. c “Antiglide” technique [17, 18].

Fig 2-15 Lambotte screw technique [20]. c
35
2 A short history of ankle fractures
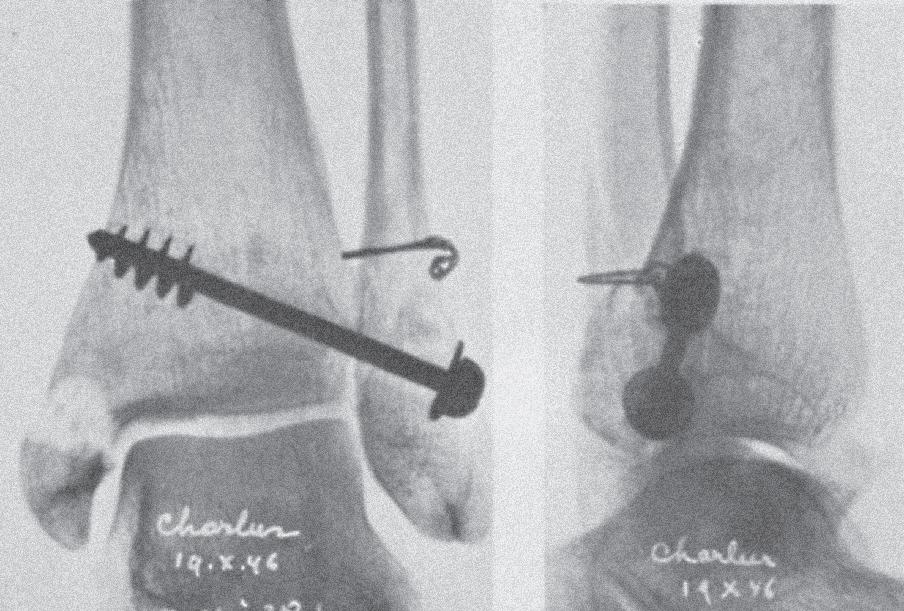
These two authors presented the technique of wire cerclage and also of tibiofibular (“syndesmotic”) screws used to fix both a fractured fibula (fibula pro tibia) and tibiofibular diastasis (Fig 2-16). It is difficult to state which of the two authors was the first in this respect. Lambotte’s first case dates back to 1903 but was published as late as 1907 (Fig 2-17) [19]. Lane’s cases may be found without specification of the date in his 1905 book [17].
In 1912 Emil H Beckman (1872–1916) from the Mayo Clinic in Rochester was probably the first who published in United States [48] a radiograph of a fracture of the medial malleolus fixed with a plate.
Another prominent advocate of internal fixation of fractures was Ernst William Hey Groves (1872–1944) but he mentioned internal fixation of ankle fractures only briefly [49, 50]. In 1918, he described a technique of so-called bolted plates, ie, internal fixation of both malleoli by plates fixed together with a bolt, which he was most probably the first to use [49].
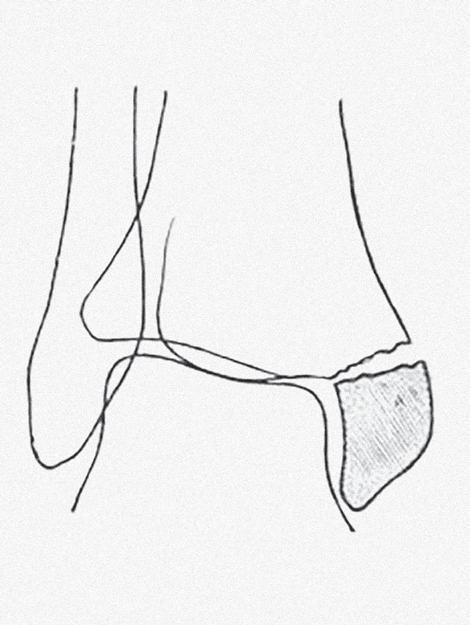
Internal fixation of the ankle was covered in great detail by Jacques Leveuf (1885–1948) in 1925 [51]. He used various techniques for internal fixation of the fibula, ie, wire cerclage, a tibiofibular screw, or a plate. He was the first to describe a combination of a plate and a tibiofibular screw (Fig 2-18).
In 1930, Karl Ludloff (1864–1945) [52] performed the first tibiofibular syndesmosplasty, using a tendon graft (Fig 2-19). In 1940, Philip Lewin [53] recommended stabilizing the tibiofibular mortise with a wire loop (Fig 2-20).
The contribution of Robert Danis, considered as one of the fathers of modern internal fixation, to the operative treatment of ankle fractures is somewhat controversial. In both his books published in 1932 [54] and 1949 [27], he completely ignored the medial malleolus. He fixed lateral malleolar fractures with wire cerclage, a short “intramedullary” nail, or a combination of both or with a cancellous screw inserted through the distal fibula into the tibia (Fig 2-21). Rather questionable was also the quality of reduction of fragments of the fibular malleolus. He used a bolt for stabilization of the tibiofibular mortise.
Operative treatment of posterior malleolar fractures lagged behind the operative treatment of fractures of the lateral and medial malleoli. The first attempts were reported in the early 1920s. Internal fixation of a fracture of the posterior rim of the distal tibia was first published in 1922 most probably by Lounsbury and Metz [29]. They used the posteromedial approach to perform open reduction of the
36
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek

Fig 2-16 Lambotte technique of stabilization of tibiofibular syndesmosis [20]. Fig 2-17 Lambotte case of ankle fracture treated by “syndesmotic” screw [19].

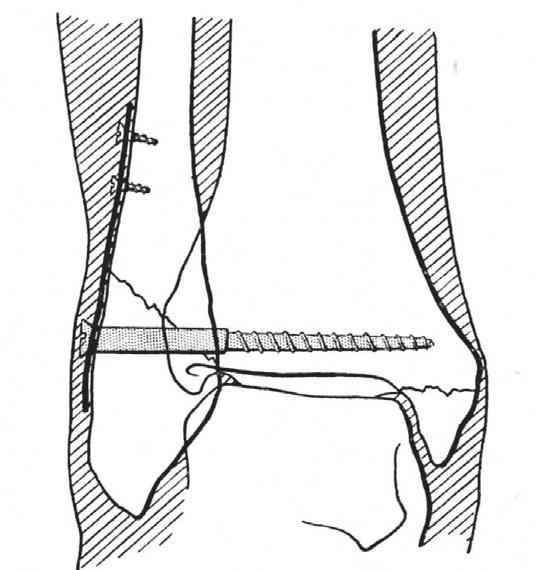
Fig 2-18 Leveuf technique of combination of fibular plate and “syndesmotic” screw [51]. Fig 2-19 Ludloff technique of syndesmoplasty by tendon graft [52].
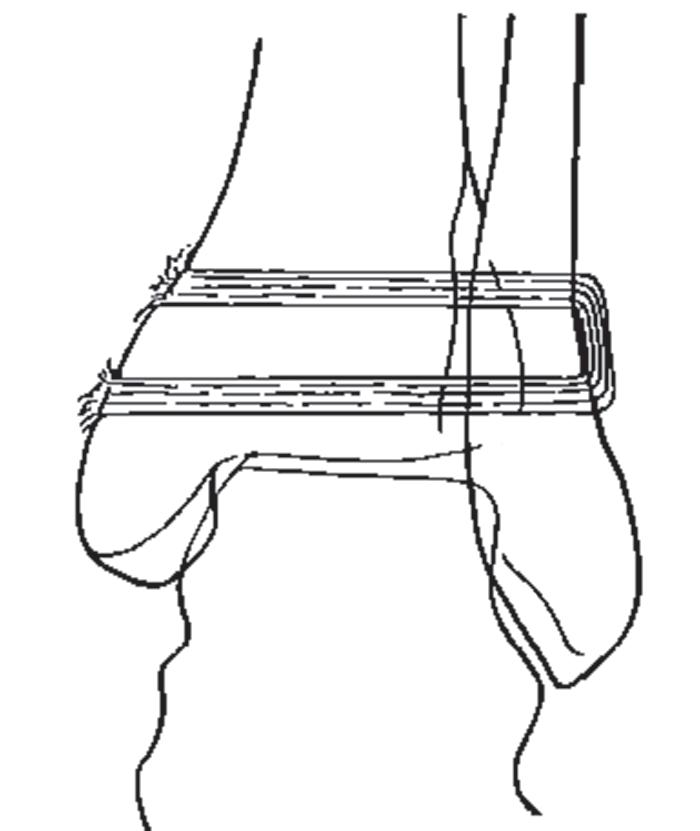

Fig 2-20 Lewin technique of stabilization of tibiofibularis mortise by wire loop [53]. Fig 2-21 Danis technique of fixation of bimalleolar fracture by wire loop and transsyndesmotic cancellous screw. The fracture of the medial malleolus was neglected [27].
37
2 A short history of ankle fractures
posterior fragment and fixed it with a bone peg inserted in the anteroposterior direction (Fig 2-22). In 1925, Leveuf [51] described reduction of the posterior malleolar fragment via a posterior Delbet transachillary approach, its fixation with a screw inserted in a posteroanterior direction, and a simultaneous internal fixation of the distal fibula, also with a screw (Fig 2-23). In 1926 [36] and 1927 [37] Ludloff published reports of open reduction and internal fixation of an irreducible fracture of the posterior malleolus via the posterolateral approach (Fig 2-24).
The use of operative treatment was significantly promoted by the above-mentioned study published by Nelson and Jensen [47] in 1940. In 1942, Rostock [55] recommended, after open reduction and internal fixation of the posterior fragment of the distal tibia, to check the accuracy of reduction by a radiograph taken before closure of the surgical wound. In 1947, Venable and Stuck [30] described anatomical reduction and fixation of the posterior fragment with screws via the posterolateral approach, in combination with internal fixation of the lateral malleolus using a plate. In 1949, Danis [27] recommended internal fixation of the posterior malleolar fragment with a screw also via the posterolateral approach. “ Internal fixation of a fracture of the posterior rim of the distal tibia was first published in 1922 most probably by Lounsbury and Metz.”
All the above-mentioned techniques were adopted by AO/ASIF and included into its armamentarium at the beginning of the 1960s [40, 41]. Its protagonists modified individual implants and added wire tension loop to this repertoire but no substantial change was made in the operative technique until the end of the 20th century.
6 Conclusion
The above-mentioned overview shows that the foundations of radiological examination, classification, and operative treatment of ankle fractures were laid in the first quarter of the 20th century. The most important role in this process was played by the French surgical school and authors publishing in French. Danis’ contribution to classification as well as to operative treatment of ankle fractures is largely overestimated, while those of Tanton, Lane, and Lambotte remain rather underappreciated.
Acknowledgments
This study could not have been possible without the extraordinary help in collecting original sources by Ludmila Frajerová from the Klementinum (Czech National Library) and Mirka Plecitá from the 3rd Faculty of Medicine, Charles University, Prague. I also extend appreciation to Ludmila Bébarová and Professor Chris Colton, MD, FRCS, for editing the English version of this chapter.
This chapter was supported under the grant AZV CˇR 16-28458A: Trimalleolar fractures of the ankle-CT diagnostics of fractures of posterior malleolus, their CT classification, operative treatment.
38
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek

Fig 2-22 The open reduction and fixation of fracture of the posterior fragment performed by Lounsbury and Metz [29].

Fig 2-24 Ludloff technique of fixation of fracture of posterior malleolus [52]. Fig 2-23 Internal fixation of fracture of the posterior malleolus and distal fibula via transachillary approach after Leveuf [51].
39
2 A short history of ankle fractures
References
1. Ashhurst APC, Bromer RS. Classification and mechanism of fractures of the leg bones involving the ankle. Arch Surg. 1922;4:51–129. 2. Bartoní ˇ cek J. Avulsed posterior edge of tibia: Earle’s or Volkmann’s triangle? J Bone
Joint Surg. 2004 Jul;86(5):746–750. 3. Bartoní ˇ cek J. Early history of operative treatment of fractures. Arch Orthop Trauma Surg. 2010 Nov;130(11):1385–1396. 4. Bartoní ˇ cek J, Kostlivý K. [The history of fractures of the posterior lip of the tibia in fracture-dislocations of the ankle.] Ortopedie. 2014;8:132–136. Czech. 5. Lauge N. Fractures of the ankle. Arch Surg. 1948;56:259–317. 6. Serfling HJ, Brückner R, Flemming F [A historical study on the concept of Volkmann‘s triangle]. Zentralbl Chir. 1966 Oct 1;91(40):1457–1466. German. 7. Somford MP, Wiegerinck JI, Hoornenborg D, et al. Ankle fracture eponyms. J Bone Joint
Surg Am. 2013 Dec;95(24):e198(1–7). 8. Bonnin JG. Injuries to the Ankle. London, Heinemann; 1950. 9. Weber BG. Die Verletzungen des oberen Sprunggelenkes. Bern, Huber; 1966. German. 10. Tanton J. Fractures en Général: Fractures des Membres—Membres Inférieurs. Paris: JB
Bailliere; 1916. French. 11. Hönigschmied J. Leichenexperimente über die Zereissungen der Bänder im
Sprunggelenk mit Rücksicht auf Enstehung der indirecten Knöchelfracturen. Dtsch Z
Chir. 1877;8:237–259. German. 12. Malgaigne JF. Traité des Fractures et des Luxations. Paris, JB Baillère: 1847. French. 13. Chaput VAH. Les Fractures Malléolaires du Cou-de-pieds et les Accidents du Travail. Paris:
Masson; 1907. French. 14. Destot E. Traumatismes du Pied et Rayons X. Paris: Masson; 1911. French. 15. Helferich H. Atlas und Grundriss der traumatischen Frakturen und Luxationen. 7. Auflage.
Munich: Lehmann; 1906. German. 16. Cotton FJ. Dislocation and Joint Fractures. Philadelphia: Saunders; 1910. 17. Lane WA. The Operative Treatment of Fractures. London: Medical Publishing Co; 1905. 18. Lane WA. The Operative Treatment of Fractures. London: Medical Publishing Co; 1914. 19. Lambotte A. L’Intervention Opératoire Dans les Fractures Récentes et Anciennes Envisageé
Particulièrement au Point de Vue de L’Osteo-synthese. Brussels: Lambertin; 1907. French. 20. Lambotte A. Chirurgie Opératoire des Fractures. Paris: Masson; 1913. French. 21. Meissner. Eine typische Fraktur der Tibia in Talocruralgelenk. Beitr Klin Chir. 1908;61:136–149. German. 22. König S. Über Absprengungsfrakturen am vorderen und hinteren Abschnitt des distalen Endes der Tibia mit Berücksichtigung der Rissfrakturen. Inaugral-Dissertation.
Würzburg, Königl Bayer Julius-Maximilians-Universität; 1912. German. 23. Hilgenreiner H. Die Extensions- und Flexionsfraktur am unteren Ende der Tibia und
Fibula. Bruns Beitr. 1913;87:384–412. German. 24. Lane WA. The disastrous results of certain abduction fractures of the ankle-joint. Rev
London. 1921;34:309–311. 25. Henderson MS. Trimalleolar fractures of the ankle. Surg Clin N Am. 1932;12:867–872. 26. Henderson MS, Stuck WG. Fractures of the ankle: recent and old. J Bone Joint Surg. 1933;15:882–888. 27. Danis R. Théorie et Pratique de l'Ostéosynthèse. Paris: Masson; 1949. French. 28. Hansen H. Über die Fraktur des Volkmann‘schen Dreiecks. Dissertation. Hamburg; 1950.
German. 29. Lounsbury BF, Metz AR. Lipping fracture of lower articular end of tibia. Arch Surg. 1922;5:678–690.
40
The Foot: Arts, Myths, and Secrets Stefan Rammelt, Hans Zwipp
Jan Bartoníˇcek
30. Venable CS, Stuck WG. The Internal Fixation of Fractures. Springfield: Thomas; 1947. 31. Cooper AP, Travers B. Surgical Essays. Part II. London: Longman & Hurst; 1819:95–181, 234–235. 32. Cooper AP. A Treatise on Dislocations and on Fractures of the Joint. London: Longman et al; 1822. 33. Earle H. Simple succeeded by compound dislocation forwards, of the inferior extremity of the tibia, with fracture of its posterior edge, comminuted fracture of the fibula, amputation of the leg, and death. Lancet. 1828–29;II/6:346–348. 34. Volkmann R. Beiträge zur Chirurgie anschliessend an einen Bericht über die Thätigkeit der chirurgischen Universitäts-klinik zu Halle im Jahre 1873. Leipzig: Breitkopf und Härtel; 1875:104–109. German. 35. Ludloff K. Zur Frage der Knöchelbrüche mit Herausprengung eines hinteren
Volkmann‘schen Dreiecks. Zbl Chir. 1926;53:390–391. German. 36. Ludloff K. Weitere Erfahrungen mit der Verschraubung des Volkmann‘schen Dreiecks.
Zentralbl Chir. 1927;54:1002–1003. German. 37. König F. Operative Chirurgie der Knochenbrüche. Band I: Operationen am frischen und verschleppten Knochenbruch. Berlin: Springer; 1931:186. German. 38. Felsenreich F. Untersuchung über die Pathologie des sogenannten Volkmannschen
Dreiecks neben Richtlinien moderner Behandlung schwerer Luxationsfrakturen des oberen Sprunggelenkes. Arch Orthop Unfall Chir. 1931;29:491–529. German. 39. Felsenreich F. Deuerresultat nach “percutaner Nagelung” von Verrenkungsbrüchen des oberen Knöchelgelenkes mit Abbruch dritter Fragmente. Arch Orthop Unfall Chir. 1936;37:166–178. German. 40. Müller ME, Allgöver M, Willeneger H, eds. Technik der operativen Frakturbehandlung.
Berlin: Springer; 1963:123–124. German. 41. Müller ME, Allgöwer M, Schneider R, Willneger H, eds. Manual der Osteosynthese. 3. Aufl.
Berlin: Springer; 1991:595–612. German. 42. Bircher E. Abrissfaktur am malleolus lateralis posterior. Centralbl Chir. 1912;39:171–173.
German. 43. Cotton FJ. A new type of ankle fracture. JAMA. 1915;64:318–321. 44. Adams R. Ankle joint, abnormal conditions. In: Todd RB, ed. The Cyclopaedia of Anatomy and Physiology of Man. London: Longman; 1835–1836(vol II):154–164. 45. Grondahl NB. Fractura marginalis posterior tibiae og andre bruddkomplikationer ved ankelbrudd. Norsk Mag F Laegevidensk. 1013;11:737 (quoted from Lauge – 5). Norwegian. 46. Souligoux E. Des fractures du cou-de-pied. Tribune Med. 1913;47:1 (quoted according to
Lauge - 5). French. 47. Nelson MC, Jensen NK. The treatment of trimalleolar fractures of the ankle. Surg Gynec
Obst. 1940;71:509–514. 48. Beckman EH. Repair of fractures with steel splints. Surg Gyn Obst. 1912;14:71–76. 49. Hey Groves EW. On Modern Methods of Treating Fractures. New York: Wood & Co; 1916. 50. Hey Groves EW. On Modern Methods of Treating Fractures. New York/Bristol: Wood & Co/
Wright; 1921. 51. Leveuf J. Traitement des Fractures et Luxations des Membres. Paris: Masson: 1925:430–436.
French. 52. Ludloff K. Die Wiederherstellung der normalen Knöchelgabel. Dtsch Z Chir. 1930;225:321–338. German. 53. Lewin P. The Foot and Ankle: Their Injuries, Diseases, Deformities and Disabilities.
Philadelphia: Lea & Febiger; 1940. 54. Danis R. Technique de l'Ostéosynthèse. Paris: Masson; 1932. French. 55. Rostock P. Erkennung und Behandlung der Knochenbrüche und Verletzungen. Leipzig:
Barth; 1942:336. German.
41
