Staff Information Folder Care After Death


NHS Harrogate and District NHS Foundation Trust
Introduction.......................................................................................................................................................... 1 Care after death 2 Breaking bad news .................................................................................................................................. 3 Good practice guidelines 3 Breaking bad news face to face 3 Breaking bad news by phone 4 Spiritual care & religious practices 7 Resources in meeting spiritual and religious needs ..................... 8 Common themes in meeting religious or cultural needs ....... 9 Modesty & gender issues 9 Supportive community 9 Drugs and treatments 9 Spiritual pain/distress 10 Care after death 10 Communication skills around individuals’ spiritual and religious needs 11 Organ and tissue donation 13 Organ donation 13 Tissue donation 13 Referrals for potential donors within Harrogate 14 Body donation to medical science 15 Contents
Care after death: practical procedures 16 What to do after a patient has died 16 Removal of lines / drains 16 Implantable Cardioverter Defibrillator 17 Personal cares after death 18 Transfer of the deceased to the Mortuary ........................................................ 19 Mortuary identification requirements 19 Viewing of the deceased 20 Viewing in the Mortuary 20 Early release of a body ..................................................................................................................... 22 Information to provide family/friends 24 Someone I care about has died in hospital. What do I do next? booklet 24 What do I do next 25 What delays may a staff member face around completion of MCCD 26 How to register the death 27 What information do I need to register a death? 28 Staff support and development 29 Personal support 29 Staff development and training 29 End of life care training 30
You matter most
Caring for people and those important to them at the end of life, and after death, is a privilege. There is only one chance to get it right and the care given will leave a lasting memory with loved ones.

The role of the healthcare staff at the end of life extends beyond death to provide care for the deceased person and support to their family and carers. The physical care given by healthcare staff following death in all care settings has traditionally been referred to as ‘last offices’. However in this guide we refer to ‘care after death’. The new terminology is intended to reflect the on-going support offered to families and carers and the physical preparation of the body called ‘personal care after death’.
Caring for people who are close to death demands compassion, kindness and skilled application of knowledge. This guide is a tool to equip staff with the practical knowledge they need to deliver high quality care with compassion and empathy to the dying patient and their family, and to run alongside Trust policies and procedures.
1
Introduction
Care after death is:
• Honouring the spiritual or cultural wishes of the deceased person and their family/carers while ensuring legal obligations are met.
• Preparing the body for transfer to the mortuary or funeral directors’ premises.
• Offering family and carers present the opportunity to participate in care after death and supporting them to do so.
• Ensuring the privacy and dignity of the deceased person is maintained.
• Ensuring that the health and safety of everyone who comes into contact with the body is protected. It is important to adhere to infection prevention precautions. The nature of the death and the context in which it has occurred may affect the level of support needed by those who have been bereaved. For example, some deaths are expected and peaceful while others may be sudden or traumatic. As a result, families and carers are likely to have a range of responses and needs and they may also have differing views about how the person should be cared for after death.
Care after death requires sensitive and skilled communication, addressing the needs of the family and carers and respecting the integrity of the person who has died. It is a very difficult time for those who have been bereaved and can be emotionally challenging for healthcare staff.
2
Breaking bad news
Good practice guidelines
Breaking bad news may be one of the most difficult tasks faced by health care professionals. It is hard to predict how a person will react when receiving bad news. The way in which we present bad news is an important factor in how it is received, understood and dealt with. Breaking bad news is a complex skill, requiring us to impart the information clearly and sensitively, as well as recognising and responding to emotions. You may not be involved in breaking bad news regularly and may not feel confident, even with years of experience. We advise people to always seek support from others if necessary.
Ideally, news regarding the death of a loved one should be delivered in person and not over the telephone. However, for guidance if news does have to be given by telephone, see page 4.
Breaking bad news face to face
• Choose a suitable environment and ensure that the room is free from interruptions.
• Ensure you have protected time. This may mean turning off bleeps or mobile phones.
• Identify who the family members are and what relationship they have to the patient. They may wish to call other family members to support them.
• Speak simply and honestly and try to avoid jargon and euphemisms, e.g. passed away, departed. Although difficult, it is best to say the person has died.
• Avoid overwhelming the family with too much information.
• Be aware of your own body language and reactions.
3
•
Ensure the family knows what will happen next.
• Be sure to offer support and treat people with empathy and sensitivity.
Breaking bad news by phone
It may be necessary to deliver bad news over the telephone, where this absolutely cannot be avoided, please see the guidance below.
Step 1: Prepare
• Take a moment to compose yourself. A few slow deep breaths will help you focus.
• Check patient’s information: name, relevant background and current status. Check the name of the person you are ringing and their connection to the patient. Ensure you have the patient’s permission to speak to the person, or are acting in their best interests when discussing clinical information.
• Consider rehearsing or discussing what you are going to say with a colleague.
• Find a space where you won’t be interrupted. Pass your bleep or phone to a colleague.
Step 2: Starting off
• Introduce yourself by name. Clearly explain which team and hospital you are calling from.
• Establish who you are speaking to. Check they are free to talk and can talk privately. Ask if there is anyone else they want to be in on the call too.
• Speak slowly with pauses between sentences. Counting to 3 in your head can help slow you down, particularly if you’re feeling nervous.
4
•
If the person does not answer the phone, don’t divulge any details about the patient’s condition, but leave a message asking them to call the ward back.
Step 3: Setting up the conversation
• Set the context e.g. ‘I’m calling about your dad who has been with us on X Ward for a few days now’.
• Check their understanding of the situation e.g. ‘What was the last update you had from the medical team?’ or ‘Would you mind telling me what you have been told about their condition?’
• Give them a warning shot e.g. ‘I’m afraid that things are changing with your dad and I need to update you about what is happening. I am sorry that we have to have this conversation on the phone, but I want to make sure you know what is happening’.
Step 4: Giving knowledge & information
• Talk VERY slowly, honestly and realistically. If the patient is sick enough that they might die or that they have died, explain this.
• Avoid euphemisms and technical jargon. You may need to talk about de-escalation from ICU or respiratory support, stopping all active management, or you may have to break the news of someone’s death.
• Listen for reactions to gauge when they are ready for more information. Remember pauses are important as you can’t see the other person’s reaction to what you are saying.
• Check they are following e.g. ‘This must be very difficult to hear. Would you like me to repeat anything?’
5
Step 5: Managing the response
• Distress may limit the person’s capacity to absorb information. Acknowledge how upsetting this is e.g. ‘I can only imagine how hard this is for you. I am so sorry.’
• Silences can feel uncomfortable and longer than they actually are on the telephone. It is difficult to know how a person is reacting when you can’t see them; there may be other people in earshot including children.
• Using sounds and words, e.g. ‘uh-huh’, ‘mmm’, ‘take your time, I’m still here’ replaces eye contact or touch, and confirms your presence.
Step 6: Make a plan
• Finish by explaining what will happen next: either the management plan, or, if the patient has died, practical steps.
• Reassure the person that all patients are regularly reviewed and cared for, and that there are always staff around to ensure the patient is not in distress, and to provide human contact.
• Check their understanding: ‘I realise this has been an extremely difficult conversation. There has been such a lot to take in; is there anything you would like me to go over?’
• Establish a plan for further phone conversations if needed. Leave contact details in case the person has more questions or concerns.
• Record the conversation in the notes.
These are emotionally exhausting conversations. Take a 5 minute break and have a cup of tea. Talk to your team.
6
Spiritual care and religious practices
Good spiritual care responds to the hopes, concerns and faith of an individual without judgement or imposing any beliefs. Often by effectively meeting spiritual needs a person feels more hopeful, reassured and peaceful. This positive effect also can benefit family and other carers too.
An important part of spiritual care for many includes meeting their religious needs. Responding to religious needs of people will include recognising issues that may be important especially towards the end of life.
Understanding a patient’s spiritual needs is about having compassionate communication and giving those under our care the time to express what is important to them. This will be unique to each patient and may include both religious needs and other requests for personalised supportive care. There are some notes on communication skills and asking the right questions at the end of this chapter.
For specific information about the different religious approaches to end of life care and death: HDFT Spiritual, Religious and Pastoral care policy on the intranet.
Alternatively, the Chaplaincy Team are available 24 hours a day and can be contacted on (55)3045 or via switchboard.
7
Resources
in meeting spiritual and religious needs
A member of the healthcare team dealing directly with the patient or carers is the most important resource as they can identify that someone has spiritual needs to be met. These needs should be recorded and planned for.
The family, friend or carers in attendance with a dying patient may be able to give advice regarding the specific spiritual or religious needs of a patient when that individual is unable to communicate. They may also have needs of their own.
The Chaplaincy Team is based at Harrogate and District NHS Foundation Trust and is available to provide advice, training and direct support where appropriate. They provide a 24/7 on-call service to help support patients, carers and staff. Local faith groups may be able to provide support when the patient already has that supportive connection. The Chaplaincy Team have a directory of contact details for the Harrogate and District.
The Chaplaincy Team are on-call 24 hours a day. Please contact via the hospital switchboard.
8
Common themes in meeting religious or cultural needs
Modesty & gender issues
Modesty in dress and a requirement to be treated by a healthcare professional of the same sex is important in some religions. Staff should consider these requirements in order to preserve the dignity of the patient.
However, it is not always possible or feasible to provide same sex attendance, particularly without adequate notice that this might be an issue.
Supportive community
An essential part of a patient’s religious and spiritual care may involve the support of family and/or their particular community. This is applicable across the different healthcare settings.
A faith leader visiting them may also be important. If appropriate this may be facilitated outside of normal visiting hours with permission from the senior nurse on duty. Chaplaincy can be helpful in a number of ways both for the patient/family and staff either by providing direct care or advice to staff as needed.
Drugs and treatments
For religious reasons some patients may raise issues with prescribed medicines or treatments that involve porcine-based drugs or alcohol-based drugs/treatments.
However, if there is no ready alternative the patient may be happy to take the prescribed medicine as allowances in their religious observance may be made for the sake of their physical health.
9
Spiritual pain/distress
This may present as: Fear of death or abandonment - Unresolved anger - spiritual emptiness, hopelessness - unresolved past experiencesconfusion or doubt about beliefs - need for reconciliation, comfort, peace – The why questions: why me? why God? why now? why this? - Feelings of guilt - inability to trust
“The realisation that life is likely to end soon may well stimulate a desire to put things first and to reach out to what is seen as true and valuable – and to give rise to feelings of the unfairness of what is happening, and at much of what has gone on before, and above all a desolate feeling of meaninglessness. Here is, I believe, the essence of ‘spiritual pain’.”
- Dame Cicely Saunders
Care after death
Many religions and beliefs include in their teachings views on dying, death and the afterlife. For many religions, life does not end with death.
In the event of a death, staff should consult the patient’s relatives to determine their preferences with regard to preparation of the body and other religious requirements. It is important to remember that early burial is a requirement in some religions. The early release of a deceased patient is explained on page 22.
Seek to understand the family and don’t make assumptions based on what you may know about a religion. The family may practice differently/not practice what their named religion is.
10
Communication skills around individuals’ spiritual and religious needs
• Vocabulary can be difficult; words do not always have the same meaning for different people.
• Always ask the person about himself or herself.
• Religious needs are individual to each patient and family.
• Question your own assumptions e.g.: I understand that some people of your faith like to… how about you?
• Choose words and phrases that are comfortable for you.
• Ask open questions where possible.
• Do not be tempted to answer unanswerable questions.
• Learn to live with unanswered questions and respect them.
• How is what you are dealing with affecting you as a person?
• What does all this mean for you?
• You seem thoughtful; tell me what’s going through your mind?
• How does what’s happening to you fit with your expectations of life?
• How do you feel things are going?
• How do you feel you are coping?
• How does this make you feel?
• How important is your faith to this situation?
11
How does your faith or religious belief support you or cause difficulties?
• If prayer is part of your life, how well is it supporting you just now?
• How can we help you to continue to practice your faith whilst unwell?
• Suggestions to responding to questions about your own faith or beliefs:
• Tell me what made you ask me that?
• It seems this is an important area for you. Tell me more about it.
• Some questions are unanswerable. I’m interested to know how you feel about it/how would you answer that question?
•
12
Organ and tissue donation
Organ donation
Donation of organs from the body can only be considered before death occurs and is only possible when a patient is in certain hospital areas such as the Intensive Care Unit or the Emergency Department.
For more information on Organ and Tissue donation:
www.organdonation.nhs.uk 0800 432 0559
Tissue donation
When a relative/friend dies at home or in hospital it may be possible for them to donate tissues for transplant or research. Donated tissues such as skin, bone, tendons and heart valves can dramatically improve people’s lives and eye donation can restore sight.
Most people can be considered for tissue donation after death. There are some age limitations for some tissues and some medical exclusion criteria.
Donation can take place within 24 hours after someone dies and donation is subject to Coroner’s consent in relevant cases.
If the patient had expressed a wish to donate or they or their family would like to discuss this further, please provide the leaflet available on the ward or call NHS Blood and Transplant Tissue
Donation on 0800 432 0559 to speak to a specialist nurse.
www.nhsbt.nhs.uk
13
Referrals for potential donors within Harrogate and District Hospital
As Harrogate & District is an alliance referrer, a referral should be made for all patients directly after the patient has died, by contacting the telephone below. A specialist nurse may then contact the family to explore options and discuss content before any donation takes place.
For more information on Organ and Tissue donation: www.organdonation.nhs.uk
www.nhsbt.nhs.uk
0800 432 0559
14
Body donations to medical science
Under the Human Tissue Act, written consent must be given from the deceased before death. Consent cannot be given by anyone else after their death.
Human Tissue Authority www.hta.gov.uk
There are a number of establishments across the UK who accept body donations for medical science.
The family are responsible for contacting the agreed medical school to inform them of the patient’s death as soon as possible so that arrangements can be made by the school to collect the deceased. If a body is donated to medical science then no funeral arrangements will be necessary though registration and collection of the death certificate takes place in the normal way.
www.nhsbt.nhs.uk
15
Care after death: practical procedures
No treatments should be stopped until the person has been verified by a doctor or competently trained registered nurse / advanced clinical practitioner.
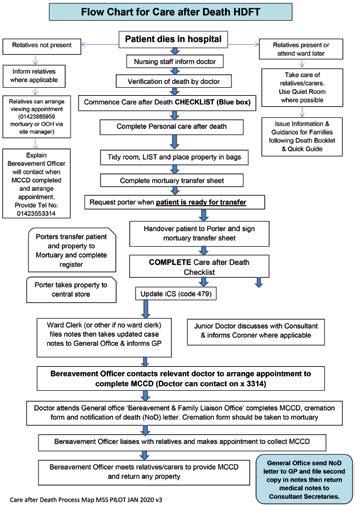
What to do after a patient has died: standard operating procedure for care after death
The flow chart to guide practice is available in the blue ‘Care after Death’ box on every adult ward including the emergency department.
What to do after a patient has died, out of the ward area in hospital
The site co-ordinator and mortuary can be contacted for advice. It may be more appropriate and dignified for the deceased person to be transferred directky to the mortuary viewing room to perform personal cares.
Removal of lines/drains
If a death is sudden or unexpected or you are made aware by medical staff that referral to the Coroner is likely:
• Invasive lines and drains should be left in situ, but must be capped or clamped off and catheters should be spigotted.
• Endotracheal (ET) tubes should be left in situ.
If the death was expected then it is acceptable to remove invasive lines and drains.
16
What to do after a patient has died with an Implantable Cardioverter Defibrillator (ICD) in situ
Ideally, the ICD should have been switched off when it was recognised that the person was dying. However, if due to unforeseen circumstances this is not the case or if this occurs out of normal working hours, please seek further advice as below:
If a patient dies with a functioning ICD in situ, it needs to be turned off before it is removed. If urgent and out of hours the use of a magnet to deactivate the ICD can be considered. Magnets are available on ICU and in the Emergency department.
Refer to HDFT policies on the intranet: “ICD deactivation at end of life” and “Magnet application in patients with ICD’s”.
It is necessary for the device to be removed after death regardless of how the body is to be disposed of. It is essential that the funeral directors are informed if a device is STILL in situ when the body is moved. It is essential that the device is removed if the body is cremated.
For further advice:
Office Hours: Cardiac Physiologist: 01423 553323
Resuscitation Department: 01423 555601
Out of Hours: LGI switch: 0113 243 2799 ask for the On-call Cardiac Physiologist covering pacing or Cardiology Registrar
17
Personal cares after death
Some family members/carers may wish to assist with the personal care in acknowledgment of individual wishes, religious or cultural requirements. Prepare them sensitively for changes to the body after death and be aware of manual handling and infection control guidance.
A Standard Operating Procedure for Personal Cares after Death is in place across the organisation.
The most up-to-date flow chart to guide practice is available in the blue ‘Care after Death’ box on every adult ward or on the intranet under Palliative and End of Life Care:
nww.htft.nhs.uk/trust-wide/palliative-and-end-of-life-care
18
Transfer of the deceased to the Mortuary
Mortuary identification requirements
• Death must have been verified in writing in the patient’s notes and the Care after Death checklist by either a doctor or a registered nurse competent in Verification of Expected Death prior to transfer to the Mortuary Department.
• Two ID bands.
• Complete Mortuary Transfer Sheet (attached to the deceased prior to removing the body from the clinical area).
• Any remaining jewellery must be noted on the transfer sheet.
• The nurse who signs the transfer sheet is responsible for ensuring that the two ID bands and the transfer sheet are correct.
• The porters collecting the deceased should check the details of the wristbands and sign the transfer sheet before removing the body from the ward.
• A body bag (available through the porters) should be used if the patient has a notifiable disease or fluid leakage not managed by padding. Attach ‘high risk’ label, PPE requirements should be followed.
• When a deceased patient is being transferred to the Mortuary, it must be done discreetly, in a respectful manner, maintaining privacy and dignity at all times.
19
Viewing of the deceased
Please speak with Clinical Site Manager, Matron or Mortuary Team if unsure.
It is preferable for the bereaved relatives to view the deceased on the ward (where possible). Viewing in the mortuary is also possible, however families may prefer to view once the person has been transferred to the funeral directors.
Viewing in the Mortuary
Please refer to the flow chart on next page, 21.
20
Procedure for the viewing of a deceased in Harrogate District Hospital Mortuary
Family or Police contact the Hospital
Members of staff must not inform relatives they can ‘view whenever they want’ as they could be required to wait, or even be turned away.
Out of hours’ viewings should only be for exceptional circumstances. These may include sudden deaths requiring police identification. Any relative requesting a viewing out of hours should be informed of the appointment system and given details of how to contact the Mortuary during the mortuary opening hours. In the event of a necessary out of hours viewing, then the Clinical Site Manager must be contacted in the first instance.
There are specific arrangements for deaths in Emergency Department, and for stillbirths, intrauterine deaths and miscarriages defined in the Procedure for the viewing of a deceased in Harrogate District Hospital Mortuary
If relatives have physical contact with the deceased, they should be advised to use the hand sanitiser on leaving the department
Monday–Friday 8am- 4pm Mortuary Staff via 01423 553391
Out of hours
Clinical Site Manager via switchboard
• Clinical Site Manager to request the Charge Hand Porter goes and checks the deceased is suitable and without a coroner/police viewing restriction and reports any issues and then makes appointment
• To consider if the family might want support from Chaplains
• On call mortuary staff c an be contacted via switchboard for advice
• Might ask a nurse from the ward, or the duty Matron, to accompany the bereaved relatives for the viewing.
Appointment time made with family or police Name, Address. DOD and DOB must be taken to confirm identity of deceased Request they report to the hospital main reception on arrival
Preparation for Viewing
Mortuary Staff or Charge hand Porter
• Identify the correct deceased from the Mortuary Register, white board and on fridge door.
• Check the details for any known risk of infection that might render viewing hazardous.
• Remove the deceased from the fridge, CHECK IDENTITY TAG against details given and place the tray on the viewing trolley.
• Move the trolley into position in the viewing room and drape with the covers provided.
Mortuary Staff
• When informed meet the family at main reception and escort them to the waiting area of the viewing room
• Request family complete Viewing Identification Form unless Police ID. Using this form confirm the identification of the deceased for viewing against the ID band and mortuary transfer sheet of the deceased.
• Allow the relatives to enter the viewing room and provide support and assistance
• Escort the family back to main entrance.
Clinical Site Manager Nurse / Duty Matron
• When informed, to meet the family at main reception and escort them to the waiting area of the viewing room. Charge Hand Porter will be present to admit in to the area.
• Request family complete Viewing Identification Form unless police ID. Using this form confirm the identification of the deceased for viewing against the ID band and mortuary transfer sheet of the deceased.
• Allow the relatives to enter the viewing room and provide support and assistance.
• Escort the family back to main entrance.
Conclusion of Viewing
Mortuary Staff or Charge hand Porter
• Return the deceased immediately to its place in the refrigerator located by white board and fridge door.
• Record the date and time of the viewing in the appropriate section of the mortuary register.
• Ensure the department is secure.
The complete policy, Procedure for the viewing of a deceased in Harrogate District Hospital Mortuary can be found on the intranet

POLICY ON A PAGE. REFER TO THE ACTUAL POLICY FOR FULL DETAILS Policy version 6.2



21
Early release of a body
Harrogate Hospital
If the patient is to be referred as a Coroner’s case, early release may not be possible.
In hours
• Follow usual procedures, contact Medical Examiner’s Office and Mortuary as soon as aware
Out of hours (OOH)
Please note: Registration of death can only take place at the Register Office within office working hours, Monday - Friday. Rather than providing incorrect paperwork, it may be more appropriate to consider raising as urgent case for the Medical Examiner’s Office to progress on the next working day.
If early release is to go ahead:
• Inform the Clinical Site Manager.
• Inform mortuary staff via switchboard.
• Verify the death.
• Complete personal care of deceased.
• Doctor to complete Medical Certificate of Cause of Death (MCCD) and cremation form. OOH MCCD book and cremation forms are kept in Site Co-ordinators Office.
• Hospital release form to give family. This must be completed by the family and handed to their funeral director. If OOH, these are available from the Clinical Site Manager.
• Transfer deceased to Mortuary.
• Release deceased from Mortuary.
22
Ripon Hospital
In hours
• Follow usual procedures for Ripon Hospital
Out of hours (OOH)
Please note: Registration of death can only take place at the Register Office within office working hours, Monday - Friday. Rather than providing incorrect paperwork, it may be more appropriate to raise as urgent case for the Medical Examiner’s Team/GP to progress on the next working day.
• Contact OOH GP to discuss
23
Information to provide to families/those important to the patient
‘Someone I care about has died (Hospital or Community). What do I do next?’
• The staff members’ role is ensuring that written information is given in a supportive way.
• Provide families/carers with the appropriate bereavement information pack, ‘Someone I care about has died: What do I do next?’. In Hospital, a quiet space should be located to allow the family to receive information and ask appropriate questions.
• Point out relevant numbers where appropriate e.g. Medical Examiners and/or General Office
• Ensure the correct nominated next of kin details are documented on the electronic patient record
24
Medical Certificate of Cause of Death (MCCD)
The Medical Examiner Officer will contact the nominated point of contact directly by phone after the death has occurred (usually within 72 working hours). They will advise when the MCCD has been completed and electronically sent to the Registry office. The Medical Examiner will advise when a face to face appointment with the Registrar can be arranged.
Medical Examiners are senior NHS doctors who, after completing specialist training, work part-time in this role. Their job is to give an independent view of causes of death and the care provided (except which have to be investigated by a coroner).
Medical Examiners and Medical Examiners Officers offer families and carers of the person who died an opportunity to ask questions or raise any concerns about the causes of death or about the care the person received before their death.
Please note, if the death is referred to the Coroner there will be a delay in the certificate being issued. The Medical Examiner will guide the bereaved families through this process.
Medical Examiner Office
01423 559274 (during office hours only excluding Bank Holidays).
25
What delays may a staff member face around completion of MCCD?
Sometimes there are unavoidable delays in the issuing of the MCCD. In these circumstances the person’s body cannot be released immediately and a delay may be expected.
The main causes of such delays are:
• When the death takes place at the weekend or a public holiday. Staff will endevour at all times to assist in the fulfilling of any particular religious requirements families or carers may have in relation to funeral practices. If families or carers need to proceed quickly in the hospital, ward staff should contact the clinical site manager to seek further assistance.
• When the death is reported to the Coroner
• When the funeral is to take place out of England or Wales. An ‘Out of England’ order will need to be issued to you by the Coroner before proceeding. A ‘Free from Infection’ Certificate must be issued by the hospital prior to transportation. The funeral director can arrange this.
26
How to register the death:
Death can only be registered by the following people:
• A relative.
• Someone who was present at the death.
• An occupier of the house where the death occurred or official from the public building where the death occurred eg. the hospital.
• The person making the arrangements with the funeral director.
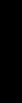
Harrogate Register Office
Bilton House
31 Park Parade
Harrogate HG1 5AG
Book an appointment once the MCCD has been completed. 01609 780 780
www.northyorks.gov.uk/death
27
LANCASTER PARK ROAD KNARESBOROUGH ROAD KNARESBOROUGHROAD A59 A6040 SKIPTONROAD A59 SKIPTONROAD A59 HARROGATE REGISTER OFFICE A661 WETHERBYROAD A661 STWINIFRED’SAVENUE ROSLYNROAD STCLEMENT’SROAD STWINIFRED’SROAD L A N C A S T E R P KRA DAOR WILLASTON CRESCENT SlingbyWalk SlingbyWalk COACH ROAD HARROGATE AND DISTRICT NHS FOUNDATION TRUST NORTH PARK ROAD PARKCHASE REGENT PARADE DEVONSHIREPLACE CLARO ROAD COACH ROAD PARK PARADE HURSTLEIGH TERRACE LYNTON GARDENS TORRS ROAD BIRSTWITH ROAD ROSEVILLE ROAD ROSEVILLE AVE SILVERFIELDSROAD HIGHGATE P A R K GRANBYROAD The Stray HarrogateKNARESBOROUGHROAD The Empress N EMPR SSE ADNUOR BOUT Copyright © 2023 RNS Publications
What information do bereaved relatives need to register the death?
In addition to the Medical Certificate of Cause of Death, the registrar will ask about:
• Dates and places of birth and death.
• Full name and marital status.
• Home address.
• Last occupation (even if retired).
• If married – the date of birth of the surviving partner.
• If female – maiden name, husband’s full name and occupation. The Registrar will then issue two forms:
• A green form for the Funeral Director
• A white form for the Department of Work and Pensions (if needed)
There is no charge for registering a death however there is a charge for additional certified copies of the death certificate. Certified copies will be needed to send to banks, building societies, insurance companies etc. as most organisations will not accept photocopies.
28
Staff support and development
Personal Support
Bereavement affects those around you in different ways.
• Offer support to other patients as necessary.
• Be aware of your own reaction to death.
• Find time to debrief with colleagues, seek support as appropriate.
• Consider clinical supervision session if felt necessary.
Staff can also access further support including:
• Staff counselling service
• Occupational health
• Chaplain department
• Line managers
• Peers
Staff development and training
All staff who are involved in the care of dying patients and in supporting family, carers and/or others at the time of a death and afterwards, should participate in appropriate training and development. The Trust has a responsibility to provide training opportunities, and it is the responsibility of the Line Manager in conjunction with the staff member to identify and meet training needs.
29
End of life care training
End of life care training can be accessed via the links below.
Local:
Information on training can be accessed via intranet

nww.htft.nhs.uk/trust-wide/palliative-and-end-of-life-care
National:
There are e-learning programmes that have been developed nationally and are available via OLM or Health Education
England website www.e-lfh.org.uk/programmes/end-of-life-care
30

