Caring for people and those important to them at the end of life, and after death, is a privilege. There is only one chance to get it right and the care given will leave a lasting memory with loved ones.
The role of the healthcare staff at the end of life extends beyond death to provide care for the deceased person and support to their family and carers. The physical care given by healthcare staff following death in all care settings has traditionally been referred to as ‘last offices’. However in this guide we refer to ‘care after death’. The new terminology is intended to reflect the on-going support offered to families and carers and the physical preparation of the body called ‘personal care after death’.
Caring for people who are close to death demands compassion, kindness and skilled application of knowledge. This guide is a tool to equip staff with the practical knowledge they need to deliver high quality care with compassion and empathy to the dying patient and their family, and to run alongside Trust policies and procedures.
Bereavement Officer contact numbers:
Doncaster
Bereavement Tel: 01302 642516
Medical Examiner Officer Tel: 01302 644748
Bassetlaw
Bereavement Tel: 01709 572567
Medical Examiner Officer Tel: 01909 572568
Mortuary
Doncaster Tel: 01302 642861
Bassetlaw Tel: 01909 572814
Useful contact numbers:
End of Life Team
Doncaster Tel: 01302 642182
Bassetlaw Tel: 01909 572678
Chaplaincy
Doncaster Tel: 01302 642237
Bassetlaw Tel: 01909 572846
Where is the Bereavement Office located?
Doncaster Royal Infirmary - basement corridor
Bassetlaw - back corridor
Recognising Dying
It can be challenging to recognise when a patient is entering their last hours and days of life, and at times that uncertainty may act as a barrier to communication with the dying person and their loved ones.
However, these uncertainties can often be shared as part of an open and honest conversation acknowledging that someone is deteriorating.
Who can recognise that a patient is dying?
Each member of a multidisciplinary team can help recognise a deteriorating patient, and often observations from the patient’s family or the patient themselves are invaluable. A doctor of ST3 level or above should be involved to evaluate whether reversible causes have been excluded, and the patient should be reviewed by a consultant within 24 hours.
When we recognise someone is dying:
• An individualised plan of care is made with the input of the patient and those important to them.
• Symptoms can be monitored, managed and medicated.
• The patient and family can be supported appropriately through a pivotal time.
• Unnecessary investigations and interventions can be discontinued.
• It gives the patient and their family time to prepare, both emotionally and practically.
• It allows spiritual needs to be addressed.
• It improves the chance of people dying in the place of their choosing.
How do you recognise dying?
We have the opportunity to recognise dying in a patient with:
• A potentially reversible illness that has reached their ceiling of appropriate treatment and continues to deteriorate.
• A progressive, incurable illness that is deteriorating without reversible factors.
Factors to be taken into consideration include:
• The person’s underlying condition(s)
• Whether reversible causes of deterioration have been ruled out or treated
• Their ceiling of treatment
• The rate of their deterioration
What are some signs of deterioration?
• Increasing physiological dysfunction recognised by increasing Early Warning Score
• A progressive deterioration in function and reliance on assistance
• Increasing fatigue, spending more time asleep
• A lack of interest in food and drink
• Weakness and swallowing difficulties, including an inability to swallow secretions
• Changes in breathing pattern or skin colour
Communication
When a patient is dying it is important that they are given the opportunity to be included in conversations and to have open and honest discussions about their care.
It can be good to start by exploring what the person already understands about their condition, if there is anything they want to discuss and anyone else they want to include in conversations.
If the patient is likely to die soon then it is important to communicate this sensitively to them or to their family, if they are unable to take part in conversations.
The level of detail you go into will vary from person to person. Some people like to have all information available and others will find it burdensome or confusing.
Generally, people are far more likely to be distressed by lack of information than by open, honest discussions.
• Who is present – does the patient want people they are close to present for support?
• Know the patient’s history and information
• Ensure that your communication is clear, compassionate, open and honest
Language is important – it is much clearer to use the words ‘dying’ and ‘last few days of life’ than ‘poorly’ or ‘for TLC’, for example use:
• ‘Plan of Care’ NOT ‘pathway’
• ‘Review medication’ NOT ‘stop treatment’
• ‘Died’ NOT ‘passed away’
A model to support you in Breaking Bad News
Breaking Bad News
You cannot soften the impact of bad news. However, delivering this news will not only ensure the message is clear and understood but also helps the person adjust to the consequences of the news.
PREPARE
• Find out what the patient already knows and find out how much the patient wants to know. Give a warning signal. Break the news using simple but clear language.
PAUSE
• Wait for a response.
ASSESS
• Focus on the patient’s feelings. Encourage the patient to express their concerns. Check the patient understands. Make a plan of action with the person, including positive practical support but not false reassurance.
• Ensure a follow-up appointment is available. Give written information as appropriate. Check your own state of mind before seeing the next patient.
Setting up the conversation:
Gather relevant information and think about the terminology you will be using (it must be understandable by all involved), privacy and who needs to be there (staff, significant others). Consider how to open this conversation.
Perception:
Find out what the patient knows and how serious they think it is. Use open ended questions to ensure you get the information needed.
- What is your understanding of your illness?
- What did Dr X tell you when they sent you here?
Invitation:
Patients have the right to hear every detail but they also have a right not to hear or want to know every detail. Unless you ask, you will never know how much information they need.
- Offer to answer any questions they may have.
Knowledge:
Having found out what the patient already understands – clarify this and use this as your starting point. Build the conversation.
Give information in small chunks and check that it has been understood. Simplify if needed. Listen to the person’s agenda, not just your own!
Emotions:
Respond to the person’s emotions – people react in different ways. Acknowledge what you see and ask about it – ‘what are you thinking’ – explore further if you need to.
Empathy will offer support and allow the person to express their feelings and worries.
Summary and Strategy:
People will look to health professionals for help in making sense of confusion and offering plans for the future. Make a plan or strategy and explain it, for example preparing for the worst and hoping for the best. Help identify their coping strategies, other sources of support and incorporate them.
DOCUMENT the conversation clearly in the notes!
Talking to relatives
A guide t o compassionate phone communication during COVID-19
Introduce SPEAK SLOWLY OPEN WITH A QUESTION ESTABLISH WHAT THEY KNOW
GRACE WARD SISTER
I’m calling to give you an update on your brother, Frank
Are you OK to talk right now?
Helpful concepts
Honesty with uncertainty
Can you tell me what you know about his condition?
There are treatments that might help Frank get better, such as giving him oxygen to help with his breathing But if his heart stopped, we wouldn’t try to restart it, as this wouldn’t work
We hope Frank improves with these treatments, Hope for the best, plan for the worst but we’re worried he may not recover
Sick enough to die
Comfort and reassure
Frank is very sick and his body is getting tired Unfortunately he’s now so unwell that he could die in the next hours to days
I’m so sorry to tell you this over the phone, but sadly Frank died a few minutes ago
Is there anything you can tell me about Frank to help us look after him? What matters to him?
I am so sorry Please, take your time
We’ve been looking after him and making sure he’s comfortable
It must be very hard to take this in, especially over the phone
I can hear how upset you are This is an awful situation
Ending the call
Before I say goodbye, do you have any other questions about Frank? Chat with a colleague
Do you need any further information or support?
Developed by Dr Antonia Field-Smith and Dr Louise Robinson, Palliative Care Team, West Middlesex Hospital
REMEMBER
Children are in families too – it may be a parent, a grandparent or another family member who is in hospital – they are never too young to grieve and the way that they experience events around a death, particularly whether they are included, involved and listened to, can have a great impact on their bereavement journey.
Research has demonstrated that early truthful conversations, using simple language and giving information in small amounts, are very important for children and young people. You can find more information:
www.childbereavementuk.org
www.winstonswish.org
Both organisations have Freephone Helplines that can advise parents and carers or professionals about supporting bereaved children.
“I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.”
- Maya Angelou
The End of Life Care team does have a number of children’s books to support young people.
Individual Plan of Care
Planning for the last days of life
When a patient is dying it is important to discuss their needs and wishes for the last days of life. Some patients will be able to discuss this themselves, but others may be too unwell or not have the capacity to do so.
If the patient lacks capacity and is unable to participate in conversations then those people close to them should be involved in discussions and if appropriate, in making decisions in their best interests. It is important to ask if the patient has made or recorded any decisions in advance. They may have an advance decision to refuse treatment in place or may have appointed a lasting power of attorney. Some patients may previously have expressed wishes about where they would prefer to die. All decisions should be made in accordance with the principles of the Mental Capacity Act (2005).
An individual plan of care
Each patient who is recognised to be dying must have a plan for their care that considers their individual needs. The plan should be discussed openly with the person and those identified as important to them. The plan must be reviewed on a daily basis and altered if the patient’s needs have changed.
Documenting the plan of care
The ‘Individual Plan of Care for the Last Days and Hours of Life’ supports the documentation of care provided for a person in the last days and hours of life. It also contains a lot of useful guidance about things to consider when caring for a dying person.
Important things to consider within the plan
• Preferred place of death
• Symptom management
• Nutrition and hydration
• Practical needs
• Social needs
• Psychological support
• Family involvement and support
• Spiritual needs
• Cultural needs
• Religious beliefs
• Individualise care to the patients/those important to their wishes.
Does the patient have a ReSPECT form in place?
The ReSPECT process creates personalised recommendations for a person’s clinical care and treatment in a future emergency in which they are unable to make or express choices. These recommendations are created through conversations between a person, their families, and their health and care professionals to understand what matters to them and what is realistic in terms of their care and treatment.
Is it Valid?
If not what are the patient’s wishes and ensure these are documented on a ReSPECT form by the treating team.
Support for patients and families
Practical Support:
Guest beds
We have guest beds that can be put next to the patient’s bed if they need someone to stay with them or if they are in the last days of life. They give relatives a chance to spend those precious last days or hours next to their loved one.
Pets
As a general rule animals will not be allowed in clinical areas within the Trust; with the exception of trained and assessed therapy dogs and assistance dogs.
In specialised circumstances (the dying patient) a pet may be permitted to visit if it is beneficial to the emotional and physical needs of the patient. This must be discussed with the Infection Control team and patient safety issues of the individual and other patients within the area fully considered prior to permitting the visit.
Parking vouchers
Parking vouchers are available to allow family members to park free of charge. Please contact EOL team who will ensure this is done on our electronic system on the Hive.
Nutrition and hydration
Reduced oral intake is part of the dying process. This can be an emotive topic and should be discussed routinely with patients (where possible) and their families.
Simple measures to support nutrition and hydration when someone is dying
When a person is able to eat and drink, they should always be supported to do so as they desire. When someone is dying, the purpose of nutrition and hydration should be patient comfort and enjoyment.
If the person has swallowing problems, discuss the benefits and risks of continuing to eat and drink. When someone only has a short time to live it may still be appropriate for them to eat and drink even if there is a risk of aspiration.
All patients should be offered frequent mouth care. Consider using a patient’s preferred drink in place of water during mouth care.
Oral thrush is common – assess all patients and treat as necessary.
Thirst or dry mouth can also be relieved by simple measures such as:
• Sucking on ice lollies or small chips of ice
• Assistance with brushing teeth or cleaning dentures
• Application of lip balm
Clinically assisted hydration for dying patients
Clinically assisted hydration, for example intravenous or subcutaneous fluids, may be of benefit for patients who are dying but whose condition is deteriorating slowly, or for those who are experiencing:
• Thirst not manageable by oral measures
• Nausea and vomiting
• Confusion and restlessness due to delirium
There are some risks associated with clinically assisted hydration in the last days of life, which must be balanced against potential benefits:
• Increased pulmonary or peripheral oedema
• Increased chest secretions
• Increased frequency of urination, which may be distressing for some patients.
• Local discomfort from insertion of intravenous cannulas or subcutaneous infusions.
There is no clear evidence that either providing or withholding clinically assisted hydration has any effect on how long a patient will live.
The decision to trial clinically assisted hydration in a dying patient must be individualised to the patient’s circumstances. Trials should be reviewed every 12 hours to assess for benefits and adverse effects.
Patients who wish to die at home and require clinically assisted hydration can be supported with subcutaneous fluids in the community.
For further details please see NICE Guidance NG31 – Care of dying adults in the last days of life.
Symptom management
Anticipatory medication
Why should anticipatory medication be prescribed?
NICE guidelines recommend we pro-actively manage symptoms in the last days of life, by prescribing medication in advance, so that if the patient develops a symptom, it can be managed promptly.
There are five symptoms which occur most commonly in the last days of life, whatever the cause of the patient’s deterioration is:
• Pain
• Agitation
• Nausea and/or vomiting
• Excess respiratory secretions
• Breathlessness
Explain to the patient and family why the medications have been prescribed and the indications.
Prescribing guidance is given on page 18.
Care of the dying – symptom observation chart and guidelines
This chart assists healthcare professionals in assessing and managing symptoms in patients who are in the last days and hours of life. The chart should be completed by trained nurses.
• It aims to support high quality care to patients.
The chart should be used in conjunction with the Individualised Plan of Care and Support for the Dying Person in the Last Days and Hours of Life.
Please refer to the Symptom Control guidance for more information.
Spiritual Care
The chaplaincy department is here to support all patients during their time in hospital and provides 24/7 cover for urgent call outs via Switchboard.
As chaplains we seek to:
• Listen and be alongside patients
• Provide patients with the space where they can be truly honest if they wish, about how it really feels right now.
• Show empathy and kindness
• Help the patient draw strength from the things that matter to them
• Assist with religious needs, when asked to
As chaplains we do not:
• Preach or be judgemental
• Push religion onto people
• Visit for long periods of time
Please do offer the chaplaincy service to patients, perhaps simply saying:
‘If you need someone to talk to, our chaplains are good at listening’
If the person has a faith, perhaps ask:
‘Would you like one of our chaplains to say a prayer with you, or to give you a short blessing?’
Common themes in meeting religious
Modesty & gender issues
Modesty in dress and a requirement to be treated by a healthcare professional of the same sex is important in some religions. Staff should consider these requirements in order to preserve the dignity of the patient.
However, it is not always possible or feasible to provide same sex attendance, particularly without adequate notice that this might be an issue.
Supportive community
An essential part of a patient’s religious and spiritual care may involve the support of family and/or their particular community. This is applicable across the different healthcare settings.
A faith leader visiting them may also be important. If appropriate this may be facilitated outside of normal visiting hours with permission from the senior nurse on duty. Chaplaincy can be helpful in a number of ways both for the patient/family and staff either by providing direct care or advice to staff as needed.
Drugs and treatments
For religious reasons some patients may raise issues with prescribed medicines or treatments that involve porcine-based drugs or alcohol-based drugs/treatments.
However, if there is no ready alternative the patient may be happy to take the prescribed medicine as allowances in their religious observance may be made for the sake of their physical health.
Spiritual pain/distress
This may present as:
Fear of death or abandonment - Unresolved anger - spiritual emptiness, hopelessness - unresolved past experiencesconfusion or doubt about beliefs - need for reconciliation, comfort, peace – The why questions: why me? why God? why now? why this? - Feelings of guilt - inability to trust
“The realisation that life is likely to end soon may well stimulate a desire to put things first and to reach out to what is seen as true and valuable – and to give rise to feelings of the unfairness of what is happening, and at much of what has gone on before, and above all a desolate feeling of meaninglessness. Here is, I believe, the essence of ‘spiritual pain’.”
- Dame Cicely Saunders
Care after death
Many religions and beliefs include in their teachings views on dying, death and the afterlife. For many religions, life does not end with death.
In the event of a death, staff should consult the patient’s relatives to determine their preferences with regard to preparation of the body and other religious requirements. It is important to remember that early burial is a requirement in some religions. The early release of a deceased patient is explained on page 34.
Seek to understand the family and don’t make assumptions based on what you may know about a religion. The family may practice differently/not practice what their named religion is.
Communication skills around individuals’ spiritual and religious needs
• Vocabulary can be difficult; words do not always have the same meaning for different people.
• Always ask the person about himself or herself.
• Religious needs are individual to each patient and family.
• Question your own assumptions e.g.: I understand that some people of your faith like to… how about you?
• Choose words and phrases that are comfortable for you.
• Ask open questions where possible.
• Do not be tempted to answer unanswerable questions.
• Learn to live with unanswered questions and respect them.
• How is what you are dealing with affecting you as a person?
• What does all this mean for you?
• You seem thoughtful; tell me what’s going through your mind?
• How does what’s happening to you fit with your expectations of life?
• How do you feel things are going?
• How do you feel you are coping?
• How does this make you feel?
• How important is your faith to this situation?
• How does your faith or religious belief support you or cause difficulties?
• If prayer is part of your life, how well is it supporting you just now?
• How can we help you to continue to practice your faith whilst unwell?
• Suggestions to responding to questions about your own faith or beliefs:
• Tell me what made you ask me that?
• It seems this is an important area for you. Tell me more about it.
• Some questions are unanswerable. I’m interested to know how you feel about it/how would you answer that question?
Care after death
Care after death requires sensitive and skilled communication, addressing the needs of the family and carers and respecting the integrity of the person who has died. It is a very difficult time for those who have been bereaved and can be emotionally challenging for healthcare staff.
There is only one opportunity to get this right. People may not remember what you said, however they will always remember how you made them feel.
What to tell bereaved relatives
Give them a bereavement pack and tell them that the bereavement officer will contact them in the next 24 hours.
What to do during your bereavement
Doncaster and Bassetlaw Teaching Hospitals
Foundation Trust
Doncaster Royal Infirmary
Important information for all ward staff
• Please inform the Bereavement Office of the death straight away. We need to be aware of this so that we have the information to hand when the family contact us. Also please ensure the Ward Clerk emails the notification of death.
• We contact the wards each morning to request the deceased’s hospital notes. The reason we need them as soon as possible is because the MEDICAL EXAMINER must scrutinise the notes of every patient who has died and talk to the attending doctor(s) before the death certificate can be issued. The notes must be correctly filed in line with Trust requirements.
• Please do not send the family directly to the Bereavement Office. Please give them a Bereavement pack and ask them to call us later that day or preferably the next working day.
• Do not tell families the certificate will be ready immediately. It can take time for the doctor to complete the medical certificate of cause of death & all the other required forms. The coroner may be involved which often creates a delay of 2–3 working days.
• If you are unsure of what to do next, please call us. We will be happy to help you and answer any queries you may have.
IMPORTANT: If you do not know the answer to a relative’s question about our service, please ask them to call us. We understand it can be difficult and you wish to help, but providing the wrong information to families at this time can be damaging.
Good practice guidelines
Care after death is….
• Preparing the body for transfer to the mortuary (last offices/ care after death) as soon as possible after the death has occurred.
• Providing the family with practical, yet compassionate support and advice on the next steps.
• Offer family and carers who are present the opportunity to participate in care after death and supporting them to do so.
• Ensuring the privacy and dignity of the deceased person is maintained.
• Honouring the spiritual or cultural wishes of the deceased person and their family/carers.
• Ensuring that the health and safety of everyone who comes into contact with the body is protected. It is important to adhere to infection prevention precautions and to highlight where there is a risk of communicable infection.
The nature of the death and the context in which it has occurred may affect the level of support needed by those who have been bereaved. For example, some deaths are expected or peaceful while others may be sudden or traumatic. As a result, families and carers are likely to have a range of responses and needs and each may also have differing views about how the person should be cared for after death.
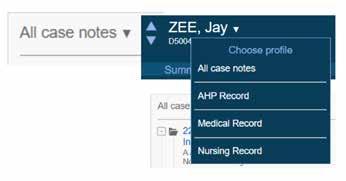
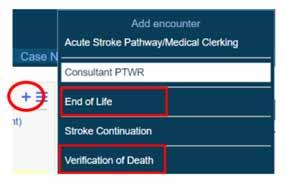
Verification of Death goes DIGITAL
The Verification of Death is going digital. We are getting an increase in incidents where Verification of Death is either not completed correctly or even at all. From now on there is a form to be completed for all inpatient deaths and this can be accessed as below.
Instructions for Doctors
1. Select patient and click ‘Case Notes’
2. Click ‘All case notes’ and select ‘Medical record’
3. Click ‘+’ sign and select Verification of Death
4. Open the Verification of Death form and complete. Nurses can complete elements of this form but not all. Once completed please press SUBMIT!
For queries please contact the EOL Team 642182 or the Digital Team 644445
Last Offices
Preparing the body for transfer to the mortuary (personal care after death/last offices)
• Close the mouth and eyes as soon as possible after death. To further assist with closing the mouth, a rolled up towel or sheet can be placed beneath the chin.
• Lines & drains: Leave cannulas, endotracheal (ET) tubes and lines in place. Spigot nasogastric tubes, remove catheter bags and clamp the urethral catheter. Removal of these can cause excessive leaking of bodily fluids.
• Affix identification tags around the wrist(s) and ankle(s) – not too tightly - always double-check the ID bands are correct!
• Dentures: If dentures cannot be put in, place them in a labelled denture pot and put next to the deceased. Do not put dentures in the patient’s property bag.
• Dress the deceased in a shroud or a hospital gown or the patient’s own nightwear (if requested by the family).
• Use a clean sheet to wrap around the deceased. Use a small amount of micropore tape to secure the sheet. Do not apply tape across the head as this can distort the facial features. Never tie the sheet with bandages.
• High risk/infection risk including Covid-19 infection: If the deceased is known to be high risk ie: blood borne/ airborne infection please place them in a body bag and write “HIGH RISK” on the body bag. Ensure the zip is at the head of the body bag so that mortuary staff can quickly identify the deceased.
• Use of body bags: If purging (leakage) does occur, place the deceased in a body bag. Each ward orders its own supply of body bags.
• Complete the notification of death form - in full (SEE BELOW).
• DO NOT remove jewellery – it is safer left on the body and unless the family specifically request for you to remove it, there is no reason to do so. Please record on notification of death form.
• Document the valuable items which are left on the body on the mortuary admission form (see below).
NHS Number:
District Number:
and Bassetlaw
NOTIFICATION OF THE DEATH OF A PATIENT
Surname:
Forename(s):
Address: D.o.B.:
Please complete in BLOCK CAPITALS and ensure a label is on all sheets.
Ward/Department: Male Female
Occupation (if RETIRED, please state previous occupation):
Patient’s identification verified by (PRINT NAME):
DO NOT REMOVE existing ID bands – see policy for further details
Does the deceased pose a high risk of infection (refer to Last Offices Policy PAT/T30) Yes No
If ‘Yes’, please complete below:
Danger of infection sticker applied to outside of body bag? Yes No
The Service Assistant has been informed that the body is a potential infection risk Yes No
Date of Death: Time of Death:
(Maintain patient confidentiality)
Doctor to be contacted for Death Certificate: Mobile: Bleep: (doctor who last saw patient alive)
Consultant’s name:
Surgery:
GP Telephone Number:
GP Name:
Valuables left on the patient at request of family / next of kin (Further information must be recorded in Nursing Notes):
Other property given to family:
(Details also to be recorded in property book)
Property Located: On ward In Finance Department In General Office
Next of Kin:
Address:
Contacted by (Print Name):
Relationship to the deceased:
Telephone number:
Designation:
Prosthesis: Dentures False limb(s) Hearing aid Pacemaker Other:
List medical devices left in-situ:
Form completed by:
Signature: Print name:
Transfered to Mortuary by: (Print Name):
Designation:
Designation:
I have confirmed and checked the Patient ID (form and ID wristband match) on the ward area at handover: Yes No
Personal property
• If the family members are present at the time of death, it is advisable for them to take their relative’s personal belongings home with them.
• Personal property items should always be neatly packed with clothes folded.
• Valuable items (such as jewellery, loose cash, key etc) must be listed in the valuables property book and placed safely in a sealed, clearly labelled envelope. Do not leave them loose in the property bag amongst clothes and toiletries etc.
• Do not put the following items in the patients’ property bags:
- Open packets of biscuits/confectionery/open bottles of drink
- Cardboard receivers, urine bottles, vomit bowls
- Perishable food (meat, dairy, fruit etc)
- Dentures (these should be placed in a labelled container and placed with the deceased before they are transferred to the Mortuary.
Always consider how you’d wish to receive your loved one’s personal belongings under these circumstances
Transfer of the deceased to the Mortuary
Mortuary identification requirements
• Death must have been verified in writing in the patient’s notes or on the Nerve Centre and the Care after Death checklist by either a doctor or a registered nurse competent in Verification of Expected Death prior to transfer to the Mortuary Department.
• Two ID bands - one on admission, one on death.
• Complete Notification of Death form (attached to the deceased prior to removing the body from the clinical area).
• Any remaining jewellery must be noted on the Notification of Death form.
• The nurse who signs the N.O.D. sheet is responsible for ensuring that the two ID bands and the N.O.D. are correct.
• The porters collecting the deceased should check the details of the wristbands and sign the transfer sheet before removing the body from the ward.
• A body bag (available from mortuary) should be used if the patient has a notifiable disease or fluid leakage not managed by padding. Where the deceased was known or suspected to have been infected, there is no requirement for a body bag unless fluid leakage is present. Attach ‘high risk’ label and should be written on the transfer sheet.
• When a deceased patient is being transferred to the Mortuary, it must be done discreetly, in a respectful manner, maintaining privacy and dignity at all times.
Viewings
Viewings are by exception only and always by appointment only
This is an additional service and cannot be extended to every family as we do not have the capacity for this.
Very often, we advise families that it may be best to view their loved one at the funeral home. Sometimes people prefer to remember them as they were in life – it is a very personal choice and no one should feel obligated to do this if they are unsure.
Never tell a family they can have a viewing “at any time” or “whenever they want”. We run an appointment system which is essential for the smooth running of the department to ensure families are given dedicated time to visit.
Please bear in mind that we have ONE non-denominational viewing room: it is no longer referred to as the Chapel of Rest.
We can provide a limited viewing service during office hours only (8am – 4pm Monday to Friday)
The only exceptions to this are police identifications for sudden deaths and paediatric deaths, where the on call mortuary senior member of staff will attend on these occasions.
Spiritual & pastoral care - chaplaincy
The Spiritual and Pastoral Care Team is there for everyone (patients, families and staff) whatever their beliefs and needs.
They provide care for all those living with caring, dying, death and grief. They offer empathy, compassion, a listening ear and support for all.
“We respond with sensitivity to the needs of the individual, recognising that spirituality is unique for each person. So the support we offer is person-led, and may or may not involve religious beliefs.
We can help people to be in touch with their own sources of strength, comfort and peace. If requested we can offer rituals and prayers of a religious nature, or humanist words of committal for the person who has died.
We are a team from a range of faith and belief communities, including Christian, Muslim, Hindu, Buddhist, Sikh, Jewish and Humanist (non-religious) – and we can put people in touch with their own faith leaders if these are not represented within our team.
Faith deaths out of hours
If a faith death occurs out of usual daytime working hours and the family requires urgent registration of death and removal of the deceased for burial, contact the duty matron who will initiate the Out Of Hours Faith Death Procedure (See Trust SOP BO 18) Hive.
If it is expected that there may be a faith death out of hours, please alert the Bereavement Office (by 4pm) and we can provide advice and support to family and staff.
How to register the death
Death can only be registered by the following people:
• A relative.
• Someone who was present at the death.
• An occupier of the house where the death occurred or official from the public building where the death occurred eg. the hospital.
• The person making the arrangements with the funeral director.
What information do bereaved relatives need to register the death?
In addition to the Medical Certificate of Cause of Death, the registrar will ask about:
• Dates and places of birth and death.
• Full name and marital status.
• Home address.
• Last occupation (even if retired).
• If married – the date of birth of the surviving partner.
• If female – maiden name, husband’s full name and occupation.
The Registrar will then issue two forms:
• A green form for the Funeral Director
• A white form for the Department of Work and Pensions (if needed)
There is no charge for registering a death however there is a charge for additional certified copies of the death certificate. Certified copies will be needed to send to banks, building societies, insurance companies etc. as most organisations will not accept photocopies.
Early release of a body
In hours
• Follow usual procedures and contact Bereavement Team and Mortuary as soon as aware
Out of hours (OOH)
If early release is to go ahead:
• Verify the death.
• Complete personal care of deceased.
• Doctor to complete Medical Certificate of Cause of Death (MCCD) and cremation form.
• Transfer deceased to Mortuary.
• Release deceased from Mortuary.
What to do after a patient has died with
an Implantable Cardioverter Defibrillator (ICD) in situ
It is the legal responsibility of the doctor completing the death certificate to inform the Mortuary of the presence of an implantable cardiac device, by completing a ‘Deceased Details and Mortuary Transfer Document’ stating that a Defibrillator (ICD/ CRT-D) is in situ.
Mortuary to confirm presence of ICD/CRT-D.
Mortuary staff to source manufacturer of implanted device where possible.
• Each patient should carry their ICD Identification Card.
• Contact ICD clinic at Sheffield Northern General Hospital or ICD Clinic at Leeds General Infirmary.
Mortuary staff to contact pacing physiologists to request deactivation.
• Contact Cardio-Respiratory Department on ext. 642456.
• Mortuary to state make/model of device.
Pacing physiologist to disable ALL TACHYARRHYTHMIA THERAPIES/or DETECTION on device, which is verbally communicated with mortuary staff, with a copy of new device parameters stored in Mortuary to confirm device status.
• Wherever possible, diagnostics data to be stored electronically or printed.
• Where necessary, send data to ICD Centre for review.
• Copies of data to be stored in Departmental Records within the Cardio-Respiratory Dept.
Organ and Tissue Donation
Organ Donation
Donation of organs from the body can only be considered before death occurs and is only possible when a patient is in certain hospital areas such as the intensive care or critical care unit.
Tissue Donation
When a relative or friend dies at home or in hospital, it may be possible for them to donate tissues for transplant or research. Donated tissues such as skin, bones, tendons and heart valves can dramatically improve people’s lives and eye donation can restore sight.
Most people can be considered for tissue donation after death. There are some age limitations for some tissues and there are some medical exclusions.
Donation must usually happen within 24 hours of death (sometimes up to 48 hours) and this is sometimes subject to Coroner’s consent. Check with the Mortuary and Bereavement Office first. The NHS Blood and Transplant Tissue Donation service can be contacted on 0800 432 0559/0300 123 23 23
Body Donations (To Medical Science)
Under the Human Tissue Act (HTA) written consent must be given before death. Consent cannot be given by anyone else after their death.
There are a number of establishments across the UK who accept body donations for medical science (see hta.gov.uk for the full list).
The family are responsible for contacting the agreed medical school to inform them of the patient’s death as soon as possible so that the arrangements can be made to transfer the body.
It is important you inform the Bereavement Office immediately of proposed body donations because there are strict time pressures from the medical school for the body to be accepted. The family will still need to obtain the death certificate and register the death in the normal way beforehand.
Tissue Donation
TISSUE
DONATION ASSESSMENT PRIOR
TO REFERRAL –A GUIDE FOR HEALTH PROFESSIONALS
The criteria below are to help staff carry out an initial assessment of the deceased to see if they might be a suitable donor. If you require further assistance please call:
National Referral Centre (NRC) on 0800 432 0559 (opening times 08.00-20.00).
MAIN CONTRAINDICATIONS TO ALL TISSUE DONATION:
• Dementia, Alzheimer’s, Parkinson’s - Neurodegenerative disease of unknown aetiology
• Progressive memory loss of unknown origin - Risk factors for CJD or its variant dementia
• SARS-CoV-2 (Covid 19)
• History of haematological cancer (Lymphoma, leukaemia, myeloma).
• Thrombocytopenia of unknown cause
• History of malignant melanoma
• History of chronic viral hepatitis or HIV infection
• Diseases of unknown aetiology if cause unclear e.g. Multiple Sclerosis
• Previous Organ or Tissue Transplant
• Some behavioural/Lifestyle risks (e.g. current IV drug use)
SPECIFIC CONTRAINDICATIONS TO EYE DONATION:
• Primary and metastatic eye cancer
• Intrinsic Eye disease: e.g., active eye inflammation or infection.
• Sepsis due to a viral or fungal infection (NB. bacterial sepsis not a contraindication for eye only donation)
SPECIFIC CONTRAINDICATIONS TO MULTI TISSUE DONATION (EYE DONATION STILL POSSIBLE):
• Any Sepsis/systemic infection
• Cancer – exceptions are: basal cell carcinoma, non-haematological pre-cancerous diseases e.g. Barretts oesophagus and cancer in situ fully excised.
Following review of the above contraindications your patient is a potential tissue donor:-
Following patient’s death please ask the Next of Kin/family if they would like more information about the possibility of tissue donation. This is something positive for the family and can give them comfort and pride in helping others. If the family agree to this obtain a contact number from Next of Kin and refer the patient to the National Referral Centre on the contact number above. Tell the family to expect a call from the National Referral Centre (in daytime hours) but if they do not receive a call it means that the patient has been assessed further and are not suitable for tissue donation. The National Referral Centre will also check the Organ Donation register to check if any known decision is registered by the patient.
They will require some information about the patient’s hospital stay. If the patient dies between 20.00-08.00 you can still call the National Referral Centre and leave a message. A Tissue Coordinator will contact the ward after 08.00 the following day for the required information. Please ensure the notes are available for this on the ward however if not, they will call General Office. If the patient is not suitable the NRC will inform you and will not contact the family.
• One chance to get it right: Duties & Responsibilities of Health Care Staff, LACDP, June 2014
• Leadership Alliance for the Care of Dying People via NHS England website
• NICE Guideline NG31 “Care of dying adults in the last days of life” Dec 2015
Additional Resources for Those Important to the Patient
Please speak to the nurse in charge to identify the location of the below resources on your ward:
• End of Life and Bereavement Resource Box: containing memory boxes, comfort packs, car parking voucher, memento resources, tissue donation information etc.
• Care and Support in the Last Days of Life leaflet
• Eating and Drinking with Risk of Aspiration Information leaflet
• Hospital Chaplaincy and Spiritual Care Services leaflet
Staff support and development
Personal Support
Bereavement affects those around you in different ways.
• Offer support to other patients as necessary.
• Be aware of your own reaction to death.
• Find time to debrief with colleagues, seek support as appropriate.
• Consider clinical supervision session if felt necessary.
Staff can also access further support including:
• Staff counselling service
• Occupational health
• Chaplain department
• Line managers
• Peers
Staff development and training
All staff who are involved in the care of dying patients and in supporting family, carers and/or others at the time of a death and afterwards, should participate in appropriate training and development. The Trust has a responsibility to provide training opportunities, and it is the responsibility of the Line Manager in conjunction with the staff member to identify and meet training needs.
End of life care training
End of life care training can be accessed via the links below.
National:
There are e-learning programmes that have been developed nationally and are available via OLM or Health Education England website www.e-lfh.org.uk/programmes/end-of-life-care
Bereavement Care
Good bereavement care is really important for both the patient and their loved ones when someone has died or is dying. Bereavement is everybody’s business – we can ALL make a difference. Often relatives say they remember the little things that staff did for them that made them feel cared for … very often we worry about ‘saying the right thing’ and that fear can stop us saying anything!
It is important to listen to patients and families about what they want, involve them in discussions and offer choices.
When health services get it right, showing empathy and providing good quality care, bereaved people are supported to accept the death and to move into the grieving process as a natural progression. However if we get it wrong, this can cause additional distress which can affect how someone grieves for a long time after a death.
For example, families tell us they appreciate being offered the opportunity to care for their loved one after death – ask if they want to comb their hair or help to wash and dress them – and support them to do so. They might not want to, but it means a lot to relatives if they are asked.