Patient-centric care: Recognising the value of non-clinical intervention
During the Society of Interventional Oncology (SIO) 2023 annual scientific meeting in Washington DC, USA, a panel of speakers delivered presentations on why patient-centred care is important, and how to provide it most effectively. The session comprised perspectives beyond interventional radiology—a nurse practitioner and a patient offered complementary and valuable insight—yet there were commonalities across the different presenters’ talks. All emphasised how crucial open communication between the patient and their family and healthcare professionals is. Only with this approach will patients receive the best care, which extends beyond clinical intervention to incorporate caring for the emotional and mental needs of the patient and their loved ones—this was a key takeaway from the session.
Physicians are co-narrators in the patient’s story
Eric Keller (Stanford University, Stanford, USA), whose presentation was delivered in his absence by Isabel Newton (University of California San Diego, San Diego, USA), underlined how “there is more to healing than what we do with our catheters and our wires”. Keller conveyed that “patients’ perspectives of the quality of our work has a lot to do with […] how nice the facility is, our body language, tone of voice and [whether] they can get hold of you for questions and concerns”. Therefore, how a patient feels their experience with a healthcare practitioner has gone is influenced by how it is framed— Keller gave the example of how it is better to tell a patient their biliary drain will be in for a year and for it to come out after six months, than it is to overpromise that it will in three months.
Keller published a study in 2018 in the Journal of Vascular and Interventional Radiology (JVIR), the presenter went on to share, which illustrated that physicians’ and patients’ perceptions of the quality of their care depend on different variables. “[Interventional radiologists] valued minimising side effects and complications,” Keller averred, whereas from the patient’s point of view it is “not so much the actual outcome as much as not being surprised [by it]”. With this in mind, Keller wished to inform delegates that a physician’s role is as a “co-narrator” who seeks to “understand [the patient’s] story” and to help them “write those next few pages”.


Keller then put forward “three important non-procedural interventions that we can do to help maximise our patients’ experiences”. The first was advanced care planning, comprising an assessment of the patient’s goals and preferences for their care. The recommendation is “to facilitate this at the beginning of serious disease”, with scope to revise in line with the patient changing their mind, the presenter relayed. “It does not have to be us [who has these conversations],” Keller continued, “but we can
Merits of splenectomy versus embolization for trauma patients up for debate

advocate for them to occur as part of the preprocedural work-up”.
The second recommendation from Keller was to share alternatives to clinical interventions, to move away from what the presenter dubbed “old-school paternalism”. He made the point that “often we do a great job at discussing our interventions but not at doing the procedure. We are also inconsistent in how we handle preprocedure [‘do not resuscitate’] DNR orders.” As a remedy, the presenter suggested that these are dealt with “well ahead of time”.
Finally, Keller emphasised that “healing is a multifactorial process—it can be easy to forget the impact of nutrition, spirituality and social determinants of health [including] the patient’s socioeconomic status, living situation, race, etc.” Detailing that physicians tend to be sceptical of alternative modes of treatment, Keller vouched for talking to patients about their use of these so as to be more “inclusive”. The concluding note was that interventional radiologists should put a greater emphasis on the precise context in which a patient is being cared for—which is shaped by the aforementioned social factors. Examples of how to maximise these contextual aspects of cancer care, according to Keller, include advanced care planning, shared decision-making, and engaging patients about other aspects of their healing to become co-narrators with patients.
Multidisciplinary interventions make a difference

The second presenter was Angela Laffan, a nurse practitioner based at the University of California San Francisco (San Francisco, USA), who runs a survivorship programme for patients who have finished treatment with curative intent. “Cancer survivorship is to help optimise patients’ overall wellness,” she outlined for the audience. She works primarily with patients with metastatic
Splenic trauma and how best to treat it was the subject of debate at the British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK). Presenting their contrasting takes on the topic were Warren Clements (The Alfred Hospital, Melbourne, Australia), who argued that “embolization is best for the patient” and Morgan McMonagle (St Mary’s Hospital and Imperial College, both London, UK), whose opinion was that “splenectomy is best for the [haemodynamically unwell] patient”.
CLEMENTS WAS UP FIRST, SETTING the scene for the debate by explaining that the spleen is a “very commonly injured organ” as it is “mobile”, and therefore susceptible to puncture, for example as a result of a rib fracture. Mortality following splenic trauma is high, Clements then noted, but embolization can allow preservation of the spleen through a simple minimally invasive pinhole treatment. The presenter outlined his preferred method for splenic artery embolization: proximally “to reduce direct flow or blood pressure at the spleen”, while allowing it to “[remain] perfused by collateral vessels”. In terms of materials, Clements put forward gel, coils, and plugs as options, but emphasised that pushable coils in particular are “nice and cheap and easy to deploy” proximally, and that this can be done effectively with three or four coils and a 5Fr catheter. “You can potentially do this in less than 15 minutes,” he added.
Clements then provided a rundown of the trials that he considered significant for their favourable findings on embolization. Firstly, he cited a study of splenic salvage and complications that he was involved in—SPLEEN-IN—which ran from 2009–2019. “We concluded that if you take the entire cohort of grades 3, 4 and 5 […] 97% of patients kept their spleen,” was his summary of the results, published in CardioVascular Interventional Radiology (CVIR) in 2020. Another Australian study that ran from 2005 to 2018 found that splenic artery embolization “reduces the length of hospital stay” in haemodynamically stable blunt splenic injuries.
Continued on page 4

www.interventionalnews.com EU Medical Device Regulation update page 4 February 2023 | Issue 89
on page 2 Profile: Aghiad Al-Kutoubi page 16
Continued
IR carpal tunnel study 19
Eric Keller
Patient-centric care: Recognising the value of non-clinical intervention
Continued from page 1
neuroendocrine tumours and used them to illustrate why survivorship matters—many live with their cancer “for years or decades” and thus “miss out on a lot of resources” by virtue of not fitting the “standard model” of a survivorship cancer patient.
Laffan explained that those who work within the programme look at patients’ individual needs, which are affected by “age, gender, stage of life, treatment, diagnosis, and goals for treatment”. Key for consideration, the presenter continued, are whether a patient prioritises quality over quantity of life, or vice versa, as well as the financial and caregiver burden that their illness is having. “This conference is looking at increasing quantity of life, but there are things we can do as healthcare providers to increase quality”.
Echoing Keller on acknowledging with patients the multiplicity of lifestyle factors that can impact their healing, Laffan cited an American College of Sports Medicine consensus paper from 2019, which recommended exercise as a means of improving cancer patients’ “quality of life, mental health, sleep”, among other factors. “Despite this, the majority of patients say healthcare providers are not routinely telling them not to exercise […] we should refer patients to exercise counselling if it is available”.
Laffan then expressed her certainty that “you all know the huge mental toll” on patients, who will often be living “from scan to scan” and footing “exorbitantly expensive” bills. Meditation can be a means of assuaging this psychological burden, and also improving symptom profile and pain levels, the presenter supplemented, recommending that physicians working with cancer patients should also offer this form of therapy where possible.
Beyond the patients themselves, Laffan then turned her focus to caregivers—a 2016 National Alliance of Caregivers study found that this group is 60% women, and 50% reported high levels of emotional stress. Half were also working in paid employment alongside their caregiving. “So, what do caregivers need from healthcare providers?” Laffan posed as a rhetorical question. “Recognition, detailed education and support with their role […] the vast majority of the time, they are not doctors or nurses,” Laffan stated, underlining that they are still “asked to perform medical tasks.”
In summary, there needs to be an “individualised approach for patients living with cancer as chronic illness,” Laffan advocated. “It is important we check in with patients and caregivers, particularly at times
of transition […] Often they smile and say they are fine but that might not be their reality.” Reiterating, Laffan’s parting note was that “extending life does not necessarily equate to living well” and therefore, the focus should also be on quality of life, intervening early with a multidisciplinary approach. An example of the success of this is Laffan’s neuroendocrine wellness clinic, where patients are referred proactively, “rather than reactively, which is what we often do”.
Patient point of view: treatment as a “miraculous” tapestry
Lynn Lazzaro (a financial advisor based in Sparks, USA) gave her patient perspective on the care that saved her life mirrored much of what Laffan’s presentation covered. Diagnosed with a 13.5cm mass on her liver in January 2016, Lazzaro told delegates how her interventional oncology (IO) team gave her a year to live, “maybe two with treatment”. Living from scan to scan as Laffan had described was Lazzaro’s reality, the presenter acknowledged. “Looking back on the journal I kept […it] almost seems to reel as if it happened to someone else”. But Lazzaro recognised her experience in the previous presenters advocating for conversations—about treatment plans, goals and how to achieve them. “My treatment team asks me these questions often,” Lazzaro affirmed, referencing Atul Gawande’s book ‘Being Mortal’, which outlines how the “ultimate goal is not a good death but living a good life all the way to the end”.

Lazzaro described her life during treatment like a “beautiful tapestry—maybe if you pulled one string the whole thing would fall apart”. However, IO, she avowed, “was the miracle that began by adding years to my life, which ultimately gave me the chance at a cure—transplant after downstaging.” Her relationship with her multidisciplinary team, as mentioned by Laffan, was instrumental in reducing hers and her family’s stress—“treating me as a whole person gave me the resilience to get up and do it all again. They kept me informed always of my prognosis—an easier conversation for some than others—but factual honesty was key for family.”
“If treatment was an art or tapestry then the outcome is really the result of the art form of your profession—your judgement, your risks, your compassion saved my life,” was Lazzaro’s thanks for the work that the IO community, drawing attention to how the clinical and non-clinical aspects of a patient’s care play complementary roles.
n INTERVIEW: SPECIALIST CLINIC BRINGS IVC FILTER INNOVATION INTO FOCUS:
William T Kuo (Stanford University, Stanford, USA), spoke to Interventional News about his work in the field of advanced inferior vena cava (IVC) filter retrieval. Recounting how he came to set up a clinic dedicated to removing these filters, he also gives aspiring physician-innovators some words of wisdom.

For more on this story go to page 7.
n SIO ANNOUNCES FIRST SITE APPROVED FOR ENROLMENT IN ACCLAIM CLINICAL TRIAL:
The Society of Interventional Oncology (SIO) has declared Mayo Clinic (Rochester, USA) the first site approved for enrolment on the society’s primary clinical trial ‘Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM) Prospective Trial for Microwave Ablation as a Local Cure.’ Constantinos T Sofocleous (Memorial Sloan Kettering Cancer Center, New York, USA) presented background to the trial, as well as its design, to delegates at the recent SIO 2023 annual scientific meeting (19–23 January, Washington DC, USA).

For more on this story go to page 13.
BSIR BUSTS MYTHS AROUND BEING A GIRL IN THE IR “GANG”:
Paula Novelli (University of Pittsburgh Medical Center, Pittsburgh, USA) brought the perspective of ‘the only girl in the gang’—the gang being her interventional radiology (IR) team at Pittsburgh—to the British Society of Interventional Radiology (BSIR) 2022 annual scientific meeting (2–4 November, Glasgow, UK) and its dedicated myth-busting session. “On all levels”, according to Novelli, women are not overinvesting in education, despite the fact that, in the USA, “women practise fewer total hours than men due to significant household responsibilities.”
For more on this story go to page 15.
Editors-in-chief: Professor Andy Adam, Dr Brian Stainken
Publisher: Roger Greenhalgh
Content director:
Urmila Kerslake
Editor: Clare Tierney
Editorial contribution:
Jocelyn Hudson, Will Date, Bryan Kay, Jamie Bell, Anthony Strzalek, Adam Pearce, Eva Malpass
Design: Terry Hawes, Wes Mitchell and David Reekie
Client relations: Michael Broughton michael@bibamedical.com
Subscriptions: subscriptions@bibamedical.com
Queries: Tel: +44 (0)20 7736 8788
Published by: BIBA Publishing, which is a subsidiary of BIBA Medical Ltd
BIBA Medical, Europe, 526 Fulham Road, Fulham, London, SW6 5NR, United Kingdom Tel: +44 (0) 20 7736 8788
BIBA Medical, North America, 155 North Wacker Drive, Suite 4250, Chicago, IL 60606, United States Tel: +1 708-770-7323
Printed by: Buxton Press
www.interventionalnews.com
Reprint requests and all correspondence regarding the newspaper should be addressed to the editor at the United Kingdom address.
© BIBA Medical Ltd, 2023. All rights reserved. Write to us!
If you have comments on this issue or suggestions for upcoming editions, write to clare@bibamedical.com
Next issue: April 2023
facebook.com/interventionalnews linkedin.com/company/interventional-news/ @in_publishing
2 February 2023 | Issue89
Putting Patients First
News in
brief The
latest stories from the interventional world
There is more to healing than what we do with our catheters and our wires.”
A specialised news source in the field of renal disease management






A trusted provider of latest news, review of cutting-edge research, congress coverage and opinion from thought leaders
Editorially independent





*Available for US and EU readers only **Available worldwide Visit renalinterventions.net and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription** Subscribe today Available in print and digital formats and through our social channels www.renalinterventions.net In this issue: Profile: Alexandros Twelve-month Wrapsody results at CIRSE 2021 Dialysis: Latest debates in Transplantation: Healthcare disparities page 20 news, insight The National Kidney Foundation (NKF) and the American Society of Nephrology (ASN) have jointly released report outlining a new race-free approach to diagnosing kidney disease. In its report, the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease recommends the adoption of the new estimated glomerular ltration rate (eGFR) 2021 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation that estimates kidney T equity,” said NKF president Paul Palevsky. “We commend the task force for the time, thought, thoroughness and e ort it took to explore this issue deeply, and recommend the best path forward for us all. The NKF and ASN urge all laboratories and healthcare systems nationwide to adopt this new approach as rapidly as possible so that we can move towards a consistent method of diagnosing kidney diseases that is independent of race. While the work of the task force is an important initial path forward, both of our organisations are committed to continuing to work to eliminate disparities in the diagnosis and treatment of kidney disease.” “As the largest organisations representing kidney patients and health professionals, NKF and ASN are committed to eliminating health disparities that harm kidney patients, and ensuring that racial bias does not ect the diagnosis Bioarti cial device receives KidneyX award after reaching preclinical testing kidney device (iBAK) has moved closer to becoming reality after being awarded US$650,000 prize from KidneyX. The device’s creator, the Kidney Project, received this award following the rst ever preclinical testing and, eventually, cliniFor the latest step forward in the development of this device, the Kidney Project team was awarded KidneyX’s Phase Articial Kidney Prize—becoming one of six winning teams selected from eld of innovators across Canada, Israel, Japan, The Netherlands, Portugal, Singapore, South Korea, the UK, and the USA. Other recipient technologies included wearable, lightweight, dialysate-free arti cial kidney (US Kidney Research Corporation) and genetically engineered pig kidneys designed to increase supplies of transplantable organs (Makana Therapeutics). Continued on page “The NKF and ASN urge all laboratories and healthcare systems nationwide to adopt this new approach as rapidly as possible so that we can move towards a consistent method of diagnosing kidney diseases that is independent of race.” Paul Palevsky Renal community reckons with removal of race variable in kidney disease diagnosis
Merits of splenectomy versus embolization for trauma patients up for debate
Continued from page 1
The SPLENIQ study group from the UK and The Netherlands found that embolization gave patients a higher life expectancy than those who had a splenectomy, Clements continued, adding that the former also proved more cost-effective.
“The most important point”, Clements underlined, is that embolization preserves function. “We do not need to think about longterm vaccination or antibiotics like we do with splenectomy patients,” he expanded, before hammering home that “no one wants a laparotomy and if we can avoid it, we are doing patients a good service.”
To conclude, Clements reiterated the speed and low cost associated with embolization for splenic trauma in stable patients, as well as the preservation of function that it facilitates. “It is quick […] effective […] has a low complication rate, fast recovery [and leaves] no visible wound,” the presenter shared, adding to his list of advantages of choosing this procedure over splenectomy.
McMonagle agreed with Clements that there is a role for embolization, but as an “adjunct” to nonoperative management which, he believes, still has a role in splenic trauma cases. “Splenectomy for trauma is one of my favourite procedures,” McMonagle then disclosed, tempering this statement by asserting that “any extreme view is bad”. For him, the choice
EU Commission proposes delay to MDR implementation

In December 2022, Europe’s health commissioner Stella Kyriakides, announced that proposals to extend the transition period for the implementation of the European Union’s (EU) Medical Device Regulation (MDR) were to be put forward in early 2023. This has now been actioned, with the EU having published a draft regulation advocating for the initial MDR implementation deadline of May 2024 to be postponed until 2027 or 2028, depending on the specific device. This measure will subsequently be voted on by the European Council and Parliament.

KYRIAKIDES INFORMED HEALTH MINISTERS
from the EU’s 27 member states of the plan at a meeting of the Employment, Social Policy, Health and Consumer Affairs Council in Brussels on 9 December, where the council members discussed the current status of the implementation of the MDR.
The regulation—which changes the way that medical devices are certified for use in the European market—first came into effect in 2021 with an initial three-year transition period, having been delayed by one year in 2020 due to the onset of the COVID-19 pandemic.
of procedure should be made in accordance with how haemodynamically well the patient is. The haemodynamically unwell “should be in the operating room,” he argued. There is also nuance in how best to treat those who are haemodynamically well, according to McMonagle, and this stems from the implications of a patient having contrast blush or not.
McMonagle then imparted his belief with regard to the use of computed tomography (CT) scanning for splenic trauma patients:


definitive”. In addition, the presenter asserted that “interventional radiology improves the chance of success of non-operative management”.
in children: in adults:
+98%
“Unless you are a surgeon planning to operate with the lights out, you do not need a CT for a haemodynamically unwell patient”.
Those who do not go to the operating room should receive non-operative management, the presenter furthered, which means chest physiotherapy, anticoagulants and “[getting] them moving”. The success rate of this he quantified as “greater than 98%” in children, and 90% for adults. “Embolization is an adjunct”.
Speaking more on embolization, McMonagle opined that “if you do not have a blush […] There is no real reason to do [one].” Moreover, he supplemented, for injuries of a low grade (1 and 2) “it is very clear now” that embolization “does not help”. Whether it does for grade 3 injuries, McMonagle said that he did not know, and that, in contrast with Clements, for grade 4s and 5s “it possibly does but it is not
Addressing Clements’ study of 232 patients, McMonagle declared it “well powered for an acute trauma study,” and acknowledged the 97% clinical success rate at discharge, but questioned why they were “embolizing everyone”. McMonagle suggested that it could have been prudent to superselect the patients for inclusion in the study based on the presence of contrast blush, as this would have shed more light on exactly whom stands to gain most from the procedure.
“The more studies that are done, the more questions they throw up,” was McMonagle’s admission that there is still more research to do on how to best treat splenic trauma injuries. In the absence of contrast blush, the presenter offered the opinion that “the jury is still out” on embolization, but acknowledged its role in improving the success of non-operative management. Splenectomy, he reiterated, is his choice for patients who are haemodynamically unwell.
Concerns have been raised over the impact of the transition to the new regulatory regime, with the European Society of Cardiology (ESC) also calling upon ministers to act to prevent a “shortfall of essential medical devices for cardiovascular patients” in December 2022, which the Society warned could include diagnostic and ablation catheters and some stents.
“Patients rightly expect to have safe and highquality medical devices,” Kyriakides told journalists at a press conference that followed the aforementioned December 2022 Council meeting, where she acknowledged it is now a “crucial time” for the transition to the new rules.
“We have been following the progress achieved towards this goal very closely in the past months and, while the number of notified bodies have increased and actions have been taken to prepare manufacturers, this is not enough,” Kyriakides added. “In addition, we are now experiencing supply shortages on the global market. We are still feeling the impacts of the pandemic, and now also the Russian war in Ukraine,
where several manufacturers of devices are located. This is creating additional complications.
“[An extension to] the transition period [will] mitigate any short-term risks. This targeted amendment will take into account the risk class of different devices and address the sell-off date. At the same time, we will work on medium- and long-term solutions to address the more structural issues that have arisen with the new rules.
“Our citizens do not only expect medical devices to be safe, they also expect them to be available. We will do everything in our power to ensure that this transition does not create any disruptions.”
Speaking to Interventional News about the position it takes, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) explained that it “welcomes the European Commission’s proposed extension of transition periods to the MDR.” Expanding upon this, the extension, according to CIRSE, is “something the society leadership also called for in a recent editorial published in CardioVascular Interventional Radiology (CVIR) in December 2022.” Moreover, for the society, “the continuous availability of safe devices for patient care, including niche indications, as well as for paediatric interventional radiology, remains the highest priority in this regard. A full statement is available at https://link.springer.com/ article/10.1007/s00270-022-03339-0”.
February 2023 | Issue89 4 Splenic Trauma Debate
No one wants a laparotomy and if we can avoid it we are doing patients a good service.”
Warren Clements
Our citizens do not only expect medical devices to be safe, they also expect them to be available.”
Stella Kyriakides
Success rate of non-operative management
+90%
Morgan McMonagle
Warren Clements
















*Available for US and EU readers only **Available worldwide A trusted provider of latest news, review of cutting-edge research, congress coverage and opinion from thought leaders A specialised news source in the cardiovascular field Editorially independent Visit cardiovascularnews.com and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription** Subscribe today Available in print and digital formats and through our social channels
Specialist clinic brings IVC filter innovation into focus
William T Kuo is an interventional radiologist based at Stanford University (Stanford, USA), where he holds a professorship. He spoke to Interventional News about his prize-winning work in the field of advanced inferior vena cava (IVC) filter retrieval— he earned the Cardiovascular and Interventional Radiological Society of Europe’s (CIRSE) Award for Excellence and Innovation in Interventional Radiology (IR) in 2022—and also took the opportunity during the interview to leave aspiring physicianinnovators with some words of wisdom.

What inspired your specialisation in advanced IVC filter retrieval and your invention of excimer laserassisted removal in particular?
I became intrigued by vena cava filters during medical school, and soon began studying everything I could about them including their creative invention, beautiful geometry, crucial function, and evolution. To me, they represented the intersection of art, science, biomedical engineering, and medicine. During my IR training, I enjoyed deploying, and especially removing, these devices which seemed straightforward at first, but I soon realised the retrieval process was not always simple.
In training, I helped develop and publish a wire-loop method to remove tilted filters, and this inventive process was something I really enjoyed. After joining my academic group, I discovered a growing number of patients suffering from problems related to indwelling filters. Although we wanted to offer more help, we soon exhausted all of our retrieval methods, and hardly anyone wanted to see these filter patients in clinic.
Traditional teaching was that filters could be left implanted as permanent devices, and I remember being advised to focus on something else, but I could not turn my back on these patients whose suffering inspired me to do better. I began to wonder if it would be possible to reverse the ‘permanent’ interactions that had formed between the organic vessel and artificial implant, perhaps on a cellular/molecular level.
The vena cava is a thin-walled vessel prone to injury, but through our early histologic analyses, we began to appreciate how a distinct layer of fibrotic tissue consistently formed along the filter attachment sites. I began searching for something that could be precise in this location, and that is when I discovered excimer laser. Rather than burning or cutting, the excimer laser adds just enough energy to disrupt the molecular bonds of surface tissue—a useful property that can remove very fine layers of organic
material without impacting underlying tissues. At 308nm wavelength, I hypothesised that excimer laser had the potential to perform 50–100 micron ablation along fibrotic tissue planes surrounding an IVC filter while sparing the native vessel wall.
Interestingly, a group in Japan had attempted excimer laser application within the canine IVC, but they quickly abandoned their experiments after noting significant vessel injury. However, I believed their results were limited due to the shorter-term dwell times (insufficient fibrotic layer) in their animal model versus the histopathology results I had observed in our human data derived from long-term filter implants. This knowledge, along with a sense of urgency in dealing with a rising epidemic of filter-related complications, gave me the confidence to bypass further animal testing and proceed with excimer laser use in humans.
Our inaugural patient travelled 2,000 miles to reach our centre in Stanford; and he became the first human to undergo successful laser-assisted filter retrieval. During the trial, which spanned nearly a decade, we accepted many high-risk cases and encountered some complications, but fortunately these were treatable. We learned from our mistakes while continuously honing our techniques to improve safety; and ultimately, we discovered that a variety of embedded filters previously considered irretrievable could now be safely removed using excimer laser, regardless of dwell time. Many patients could finally be alleviated from their filter-related morbidity or spared the risk of developing such complications.
What have been the highlights of the 10+ years since you first performed this procedure?
Looking back, the requests from our early patients to find solutions that did not yet exist was inspirational, so the main highlight has been developing a patient-inspired procedure to improve the lives of many others. Establishing a first-in-man clinical trial in conjunction with a dedicated IVC Filter Clinic has also been gratifying. It has been an honour to meet and touch the lives of so many patients from around the country and around the world. Sharing this knowledge with our trainees, clinical teams, and early adopters has been rewarding; and seeing our results eventually confirmed across multiple centres was validating. Based on our collective data, the excimer laser sheath was finally cleared by the US Food and Drug Administration (FDA) as the first ever device approved for advanced filter removal.
What led you to set up the Stanford IVC Filter Clinic?
When I began my career, patients with embedded IVC filters came to us because they had no other place to go. In 2010, filter-related complications were acknowledged as an emerging health problem when the US FDA issued a Filter Safety Alert urging all physicians caring for patients with filters to consider removing the filter as soon as protection from pulmonary embolism is no longer needed. Other health agencies and societies soon followed with similar guidelines. However, despite this heightened awareness and improving follow-up, many filters still could not be removed using standard methods, especially after prolonged implantation, subjecting patients to all the risks and anxiety of living with a permanent implant. For all these reasons, I decided to launch the Stanford IVC Filter Clinic dedicated to helping these patients.
What are the challenges and rewards associated with running a clinic of international renown?
Our early challenges were mobilising sufficient clinical resources, integrating new apparatus,training our staff, and creating protocols to safely incorporate cutting-edge techniques. We had to keep up
not only with a growing case volume but also increasing case complexity, and we wanted to achieve all of this in a timely fashion. Early on, there was so much learning from each case, and this required meticulous data recording to conduct research and a rigorous process of continuous improvement.
As we began to succeed, we attracted more referrals including more bizarre and unusual cases. From one patient to the next, we had to rapidly adapt by crafting protocols tailored to the patient. In spite of increasing case complexity over many years, the ultimate challenge was maintaining procedural success along with safety. Through these endeavours, we expanded our understanding and capability to help many patients who were previously considered untreatable. Over time, we successfully treated thousands of filter patients referred from all 50 US states and from over 10 countries.
You are currently recruiting for prospective studies evaluating filter removal— what else is on the cards over the next 10 or so years of your career?
We aim to keep studying advanced techniques and outcomes on an ever-growing variety of patients and filter scenarios referred to our centre. There will always be more to learn, and we hope our expanding data in conjunction with other centres will continue to establish new and improved protocols, guidelines, and best practices for advanced filter removal and related venous interventions. We hope to encourage all interventional radiologists to embrace data-driven methods for safer retrieval/management of embedded filters. Furthermore, by taking time to understand not just the disease but the patient with the disease, I hope more interventional radiologists will become inspired to determine further unmet needs that can spark original ideas and innovation.
What advice would you give to aspiring physician-inventors?
Question dogma, cultivate your interests, and open your mind to discover something you are truly passionate about regardless of what others may think. The possibilities are endless but your time is not, so developing intense focus and entering a flow state are essential. Along this journey, find a meaningful purpose and become dedicated to a cause greater
Issue89 | February 2023 7 Physician Innovation
INTERVIEW
Based on our collective data, the excimer laser sheath was finally cleared by the US Food and Drug Administration (FDA) as the first ever device approved for advanced filter removal.”
William T Kuo
Experts extol effective alternatives to surgery for renal cell carcinomas

The management of renal cancer patients featured prominently at the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2022 annual scientific meeting with discussions around patient selection and treatment planning preceding talks on the key therapeutic options in this space.
The first of four presentations was delivered by Rosario Grasso (Campus Biomedico University Hospital Foundation, Rome, Italy), who argued that percutaneous thermal ablation approaches like radiofrequency ablation (RFA) or cryoablation are an option for the management of patients with clinical-stage T1 renal lesions— primarily in masses <3cm in size, but potentially for larger masses in select patients too.
Grasso stated a belief that percutaneous ablation represents a safe and effective alternative to surgery in treating T1a renal cell carcinomas due to the “excellent” functional and technical outcomes seen with the procedure. The “very low” complication rate these procedures hold also compares favourably to those associated with nephrectomy, he added.
The speaker concluded that there is currently Level C evidence that, in selected patients with suspected T1a renal cell carcinoma, percutaneous thermal ablation should be offered over active surveillance owing to the “acceptable” long-term oncological and survival outcomes it has demonstrated to date. Grasso also said RFA, cryoablation and microwave ablation are all appropriate treatment modalities, and claimed that the choice of ablation method “should be left to the discretion of the operating physician”.
Treatment planning
Arian van Erkel (Leiden University Medical Center, Leiden, The Netherlands) followed this by discussing treatment planning in renal ablation—a “well-established” treatment for small T1a tumours. He posited that the first step here is to choose between surgery, ablation or active surveillance, and that this decision is an individualised one influenced by patient preference, age and life expectancy, renal function, the location and size of the tumour, and multiple other factors.
“Planning the treatment of your RFA is very important in getting complete ablation, with a sufficient margin, and in avoiding complications,” van Erkel asserted. “This planning involves
image guidance, the ablation modality and protective measures.” He further claimed that axial diameter, bowel proximity, adjacency to the ureter, and several other characteristics of the tumour, should be taken into account.
“An immediate CT [computed tomography] after ablation is, of course, important, to evaluate your complications and your ablation margins especially,” van Erkel concluded. “And, there is software on the market that can help you make these estimations in a more scientific and exact way.”
Different modalities
A closer look at the different approaches to percutaneous ablation for renal cell carcinoma was then provided by Esther Gálvez González (Hospital Severo Ochoa, Madrid, Spain). The speaker corroborated many of her colleagues’ earlier points, noting that ablative treatment is as effective as surgery in T1a tumours—adding that it can also help to preserve renal
function, and is associated with low complication rates.
Gálvez González further asserted that a key advantage held by RFA is the wealth of experience and high volume of published papers associated with the technique, but also noted two important limitations: thermal tissue conductivity and the ‘heat sink effect’. In contrast, she continued, bigger tumours can be ablated more quickly, and at higher temperatures, with microwave ablation, while its relative insensitivity to the heat sink effect allows it to be used in target areas located closer to larger blood vessels. The major limitation of microwave ablation, however, is the increased risk of complications in more central locations, which restricts its use to peripheral lesions, she added.
The speaker also touched on the various advantages and limitations of two other approaches—cryoablation, and a non-thermal technique (on which there are minimal published data) called irreversible electroporation— stating that both are essentially unaffected by impedance and the heat sink effect, but are limited by smaller ablation volumes and longer procedure times as well. Gálvez González concluded by asserting the importance of selecting the correct approach based
primarily on the size and location of the target tumour.
Combined therapies
The session’s final talk was given by Marco van Strijen (St Antonius Hospital, Nieuwegein, The Netherlands), who outlined several combined treatments in cryoablation. “Combined treatment in renal cryoablation, in my opinion, consists of either embolization—which is a safe treatment but for which scarce literature is available—or thermoprotection by liquid; air or CO ² dissection; or pyeloperfusion,” he stated. Homing in on the former technique, the speaker said that, despite the limitations around previous studies and a lack of prospective data, percutaneous embolization is considered a safe procedure that is “most effective” in reducing periprocedural blood loss, and holds potential benefits in local tumour control and procedural visibility.
Van Strijen went on to highlight two further, more recently introduced tools that he also considers among the options for combined approaches: robotic needle placement, and the use of integrated controls and augmented reality to perform ablations virtually with the aid of a HoloLens device (Microsoft). In concluding his presentation, van Strijen added: “Robotic needle placement is currently one of my favourite techniques.” Here, he cited the fact it is “very simple”, and enables steep angulations, as well as reducing radiation exposure and speeding up the procedure “considerably”.
February 2023 | Issue89 8 Renal Updates
Planning the treatment of your RFA is very important in getting complete ablation with a sufficient margin.”
Arian van Erkel
RENAL
Clockwise from top left: Rosario Grasso, Arian van Erkel, Esther Gálvez González, Marco van Strijen
MEDTRONIC HAS ANNOUNCED THE six-month results from the full cohort of the SPYRAL HTN-ON MED clinical trial. The latebreaking data were presented at the American Heart Association (AHA) Scientific Sessions 2022 (5–7 November, Chicago, USA). The study is a global, randomised, sham-controlled trial investigating the blood pressure-lowering effect and safety of RDN with the radiofrequency (RF)-based Symplicity Spyral RDN system in hypertensive patients who have been prescribed up to three antihypertensive medications, including diuretics, calcium channel blockers, ACE/ARB inhibitors or beta blockers. It met its primary safety endpoint, with a low incidence of procedure-related and clinical adverse events.
Patients who were prescribed antihypertensive medications and were treated with the Medtronic Symplicity Spyral renal denervation (RDN) system had a statistically significant and clinically meaningful reduction in office-based systolic blood pressure (OSBP), a key secondary endpoint, compared to subjects in the sham control group. However, in the primary endpoint, RDN did not demonstrate a statistically significant reduction in 24-hour ambulatory systolic blood pressure (ABPM) due to increased medications in the sham control group and the potential impacts of the COVID-19 pandemic on the clinical trial environment. The study also included win ratio, a prespecified secondary endpoint that combines reduction in blood pressure with reduction in medication burden, which enables assessment of the overall beneficial effect of RDN. The win ratio demonstrated significance in favour of RDN versus a sham procedure.
A total of 337 patients with uncontrolled hypertension were enrolled at 42 sites across the USA, Europe, Japan, Australia, and Canada, and were randomised 2:1 to RDN (n=205) versus sham control (n=132). Results were as follows:
The primary Bayesian efficacy endpoint of 24-hr systolic ABPM reduction was not met, with a 51% probability of superiority for the RDN group versus those who received a sham control procedure. However, nighttime systolic ABPM reduction was statistically significant.
6.5mmHg 24-hr systolic ABPM reduction in the RDN group versus 4.5 mmHg in the control group (treatment difference of -1.9mmHg, p=0.119)
6.7mmHg nighttime systolic ABPM reduction in the RDN group versus 3mmHg in the control group (treatment difference of -3.7 mmHg, p=0.01)
The study met the prespecified secondary endpoint, which was the change in OSBP from baseline to six-month follow-up between the RDN group (n=199) and the sham control group (n=126).
Statistically significant 9.9mmHg OSBP reductions in the RDN group versus a 4.9mmHg reduction in the sham control group (treatment difference of -4.9mmHg, p=0.001)
The study met the primary safety endpoint, evaluating major adverse events at one month postprocedure, and renal artery stenosis at six months, pooled across the SPYRAL HTN-ON and OFF MED studies (p<0.001).
For some small kidney cancers, freezing is more effective than heat treatment
For patients with early-stage renal cell carcinomas (RCCs) that measure between 3 and 4cm, cryoablation yields a lower risk of cancer-related death compared to thermal ablation, reports a preliminary study in the Journal of Urology
“In contrast, for patients with RCCs smaller than 3cm, either cold-based or heat-based therapy is just as effective in reducing cancer-specific mortality,” comments lead author Gabriele Sorce (San Raffaele Scientific Institute, Milan, Italy). “The findings may help us to better tailor the choice of ablation technique for patients with small RCCs.”
Lower risk of cancer death with cryoablation versus heating
Renal cell carcinoma is the most common type of kidney cancer. For patients with early-stage RCCs smaller than 4cm, an increasingly popular treatment option is destroying the cancer by freezing it or heating it. For these clinical stage T1a RCCs, ablation can provide high survival rates without the need for more extensive kidney surgery.
However, the outcomes of ablation appear “less favourable” for a subset of patients with clinical stage T1a RCCs: those whose tumours are between 3 and 4cm. Current European guidelines recommend cryoablation over thermal ablation for these cancers measuring 3 to 4cm, while US guidelines state that either treatment can be used. Both sets of guidelines state that freezing or heating can be used for T1a RCCs of 3cm or smaller.
To clarify the issue, an international research group analysed patients with stage T1a RCCs treated with freezing or heating between 2004 and 2018. Patients were drawn from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program. The study focused on two matched groups
of patients with cancers measuring between 3 and 4cm: 757 treated with cryoablation and 388 with thermal ablation.
Median age at treatment was 71 years. Follow-up data on cancer-specific mortality were available for 422 patients treated with freezing and 238 treated with heating.
Eight years after treatment, estimated cancerspecific mortality among patients with RCCs measuring 3 to 4cm was 8.5% for patients treated with cryoablation versus 12.9% for those undergoing heat-based thermal ablation. With both treatments, about 40% of patients died from causes other than cancer.
Implications for treatment decisions in ‘small, potentially curable’ kidney cancers
After adjustment for non-cancer-related death and other characteristics, patients undergoing thermal ablation for RCCs between 3 and 4cm were twice as likely to die of kidney cancer. In contrast, for patients with cancers smaller than 3cm, estimated cancerspecific mortality was similar between groups: 6.8% after cryoablation and 6.1% after thermal ablation.
The study is one of the first to directly compare clinical outcomes for freezing versus heating in patients with stage T1a RCCs measuring between 3 and 4cm. The results suggest that thermal ablation has “a highly statistically significant and clinically meaningful” disadvantage in terms of the long-term risk of death from kidney cancer, compared to cryoablation.
Otsuka Medical Devices and ReCor Medical submit premarket approval of Paradise ultrasound renal denervation system
Otsuka Medical Devices and ReCor Medical, a subsidiary of Otsuka, announce the filing of the premarket approval (PMA) application to the US Food and Drug Administration (FDA) for the Paradise ultrasound renal denervation (uRDN) system in the treatment of uncontrolled hypertension.

THE PARADISE URDN SYSTEM IS DESIGNED to reduce sympathetic nerve activity by denervating nerves surrounding the renal arteries to reduce blood pressure. It uses ultrasound energy to denervate the renal nerves and a water-filled balloon to protect the renal artery. The system employs an interventional procedure in which a catheter is placed in each of the main renal arteries, followed by delivery of two to three seven-second ultrasound emissions to denervate the surrounding renal nerves, thereby reducing blood pressure.

Since 2009, ReCor has been focused on developing and testing the Paradise uRDN system to treat hypertension safely and effectively. ReCor has three global, independently powered, shamcontrolled randomised clinical trials of the Paradise
uRDN system in more than 500 patients with uncontrolled hypertension: RADIANCE-HTN SOLO, RADIANCE-HTN TRIO and RADIANCE II. Each trial met its prespecified primary efficacy endpoint of blood pressure reduction, with positive safety.
RADIANCE II is the US FDA’s investigational device exemption (IDE) pivotal trial. In September 2022, ReCor and Otsuka Medical Devices announced that the trial successfully reached its primary efficacy endpoint. Results showed a reduction in daytime systolic ambulatory blood pressure of -7.9mmHg in those treated with uRDN and a difference between uRDN and sham of -6.3mmHg (p <0.0001). The results from the all three RADIANCE clinical trials have been included in the submission for approval to the US FDA.
Issue89 | February 2023 9 Renal Updates
SPYRAL HTN-ON MED study demonstrates meaningful clinical benefits consistent with other SPYRAL HTN renal denervation trials
‘Bright future’ or ‘immense loss’?
Interventionalists split over shift towards ambulatory practice
A number of speakers took to the stage at the International Symposium on Endovascular Therapies (ISET; 16–19 January 2023, Miami Beach, USA) to debate the ‘ambulatory shift’ that is currently taking place in the interventional space.
AARON MAUCK (ADVISORY BOARD, Washington DC, USA), began with a keynote lecture describing the factors driving the migration of procedures away from the hospital towards ambulatory surgery centres (ASCs) and office-based labs (OBLs)—describing this as a “seismic shift” that “everyone is preparing for”. New reimbursement policies and regulations, provider competition and innovation are among major drivers of this trend. However, Mauck stated that “the future is not etched in stone” when it comes to the ambulatory shift, adding that industry investment and purchaser/referrer steerage are among factors that could accelerate this shift, while certain data indicating poorer outcomes with peripheral vascular procedures performed in the OBL—as well as US state legislatures not being amended—constitute barriers that may slow the process.
For ambulatory practices
Several key points extoling the virtues of more ambulatory, office-based practices were delivered by Jeffrey Carr (CardiaStream, Tyler, USA). Drawing on a 15-year experience of cardiac and vascular procedures in the ambulatory environment, Carr averred that greater control of their (his team’s) schedule and patients’ clinical care was among the initial motivations behind establishing an OBL in 2008, which was then transitioned to a hybrid lab—an OBLambulatory surgery centre (ASC)—in 2014. Here, the speaker cited the possibility for diversification and optimisation of revenue, a minimised impact on reimbursement cuts, and “higher standards” for existing OBLs as among the most important benefits.
After detailing the myriad peripheral vascular, cardiac and venous interventions that can currently be performed in his centre’s office-based settings—and touching on other future possibilities, such as aortic repairs and carotid stent placements— Carr concluded that it is “vital” to follow standardised processes/protocols, while also exercising transparency and reporting outcomes accurately. He further stated that “the future is bright” for expanding procedures, reducing costs and creating high value in office-based and ASC settings.
HKUMed discovers new trimodality therapy for locally advanced liver cancer



A phase II clinical study on a trimodality therapy (START-FIT), conducted by the Departments of Surgery and Clinical Oncology, School of Clinical Medicine, University of Hong Kong (HKUMed; Hong Kong), has found that nearly 50% of patients with inoperable, locally advanced liver cancer, can be cured through this approach, which includes stereotactic body radiation therapy (SBRT) and transarterial chemoembolization (TACE). The results have been published in The Lancet Gastroenterology and Hepatology.

A TOTAL OF 33 PATIENTS WERE screened and enrolled in this treatment method from March 2019 to January 2021, for tumour diameter ranging from 5 to 17.5cm. Just under two thirds (64%) of patients had tumours with major vascular invasion that precluded them from a curative surgical procedure. The research team developed a new approach termed ‘reduce and remove’—a trimodality therapy (START-FIT)—for these 33 patients. Patients received TACE on day one for local tumour control, followed by SBRT on day 28, and then immunotherapy administered 14 days following SBRT and every two weeks thereafter. This trimodality approach is to downstage the tumour status so that it is amenable to curative surgical intervention.
After this trimodality therapy, 55% (18 patients) became suitable to receive curative surgery, of whom four patients (12%) underwent this surgery, and 14 patients (42%) had complete tumour necrosis and are receiving ongoing
monitoring with regular scans. After up to 2.5 years of follow-up, two-year survival among these patients exceeded 90%, with mild side-effects experienced throughout the treatment process. The advantages of this approach are that it is minimally invasive with a short hospital stay and a relatively high safety profile.
This treatment strategy provides the opportunity for curative surgery with promising long-term outcomes to patients who would otherwise be
This session also yielded additional tips for those wishing to establish outpatient practices—Jason Greis (Benesch, Friedlander, Coplan & Aronoff, Cleveland, USA), advised prioritising “quality of care, not volume of cases”; maximising the number of interventionalist owners and the percentage of equity they hold; and taking patient, payer and investor complaints seriously.
Against ambulatory practices
This talk was immediately followed by Dipankar Mukherjee’s (INOVA Fairfax Hospital, Falls Church, USA) presentation entitled: “Why I chose not to work in an outpatient lab”. Mukherjee noted that, since the 2011 approval of atherectomy codes for peripheral vascular interventions, migration of talent has become a problem, as “some of our best interventionalists” have moved from hospitals to OBLs. In addition to leaving some of the sickest hospitalised patients in the hands of less experienced operators, and contributing to a “serious manpower crisis” across much of the USA, the speaker stated that these interventionalists have “abandoned their responsibility” in educating future generations as well.

On top of this “immense loss” facing trainees, surgeons working exclusively in OBLs are also likely to “lose all open repair skills”, according to Mukherjee, who asked the ISET audience, ‘where would you and I be now’ if pioneering interventionalists of the past had gone to work in these ambulatory settings? He further called for the “rules of the game” in OBLs to change and for the restoration of “the values that attracted us to the profession and specialty”.
unsuitable. “This treatment strategy provides a definite treatment schedule. Most patients could have an idea on the treatment effect within six months after the start of treatment and be able to have better planning for themselves and their family. Now the team is looking forward to expanding the treatment coverage to more patients, especially those with poor liver function, to help downstage the tumour status and hence, increase the chance of fitting into the criteria for liver transplantation in the future.” This statement was shared by Albert Chan Chi-Yan, clinical professor at HKUMed’s Department of Surgery at the School of Clinical Medicine, who initiated this world-first trimodality therapy.
Speaking to Interventional News, Chan elaborated on the unique advantages of combining these three treatment modalities when treating unresectable liver cancer. “The lipiodol infusion offered by TACE provides a definite tumour staining that facilitates SBRT planning and improves the targeting and accuracy of the delivery
After up to 2.5 years of follow-up, two-year survival among these patients exceeded 90%
2.5 years up to
90% two-year survival exceeded
of SBRT. Once tumour necrosis induced by the radiation starts to occur, the host immune system [starts] to recognise their presence and the use of immunotherapy [enhances] the host immune response to recognise and to eradicate the residual tumour cells.” Chan added that the main obstacle his team encountered during this project was when seeking funding due to the novelty of the trimodal treatment, but he is now optimistic about the treatment becoming the standard of care—this will be facilitated, he conveyed, as “apart from the need to stay two to three days [in hospital] after TACE for monitoring, all the other treatments [can] be conducted in an outpatient setting.” Moreover, Chan believes that there is scope for this trimodal approach in treating other cancers—“yes, we do see the potential in lung and kidney cancer.”
February 2023 | Issue89 10 ISET Discussion
From left, Chiang Chi Leung and Albert Chan Chi Yan. Right, patient Wan Ying Keung
The future is not etched in stone.”
Jason Greis Jeffrey Carr Aaron Mauck Dipankar Mukherjee
Clinicians urge Scottish government to reverse £7 million thrombectomy funding cut
Health charities and National Health Service (NHS) clinicians have united in a call for the Scottish government to reverse a cut to the funding of stroke thrombectomy treatments.

MORE THAN 150 STROKE CLINICIANS HAVE backed a call from charities Chest, Heart and Stroke Scotland (CHSS), and the UK Stroke Association for the reinstatement of £7 million to the national thrombectomy service funding in Scotland.
An open letter to the cabinet secretary for Health and Social Care describes the 50% funding cut and recruitment freeze as a “mistake”.
The letter states that the resulting savings—which amount to less than 0.1% of Scotland’s total health budget—will create far greater costs, with Scottish patients who miss out on this “extraordinarily effective” medical treatment ending up needing longer hospital stays, community rehab and social care services, according to a CHSS media release.
Stroke physician Vera Cvoro (University of Edinburgh, Edinburgh, UK) stated: “Thrombectomy is the single most effective treatment we have for stroke. Many patients that come to our hospitals with a stroke could benefit from this treatment that prevents disability. This can mean being able to walk again, talk again and even going back to work. We have the expertise to deliver such treatment and it should be available to all people living in Scotland.”
The Scottish government had previously committed to rolling out a national thrombectomy service, which would see around 800 stroke patients receive the procedure each year, the media release notes. Such a service is expected to save the health and social care system up to £47,000 per
patient in the first five years—with a resulting total saving of £37.6 million to the NHS.
As such, CHSS and the Stroke Association are jointly calling for the Scottish government’s commitment to continuing to fund the service and recruit the staff necessary for a national rollout.
Jane-Claire Judson, CHSS chief executive, said: “CHSS and the Stroke Association are united in our plea to the Scottish government to stand by its commitment to a national thrombectomy service. It is unthinkable that the Scottish government will deny Scots a treatment we know will make a huge difference to their lives for the sake of a small, short-term budget saving. Hundreds of Scots who have a stroke each year should be able to trust they will get the best possible medical attention and chance of making a full recovery.”
John Watson, associate director Scotland at the Stroke Association, added: “Thrombectomy saves brains, money and lives. It can change the course of recovery from stroke in an instant and is one of the most effective medical interventions ever developed. We understand the financial pressure the government is under, but to cut a service that improves patients’ lives while saving money would be a serious mistake. The current resource crisis should lead to thrombectomy being prioritised, not cut.
“That is why we, alongside CHSS and clinicians at the coal face, are calling on the Scottish government to reinstate its funding for a national thrombectomy service.”.
SNIS: Physicians “should not have to choose” between family life and professional career
The Society of NeuroInterventional Surgery (SNIS) has released a position statement advocating pregnancy and parental leave policies in neurointerventional surgery, voicing support for a physician’s ambition to have a family, as well as start, develop and maintain a career in this specialty.
ACCORDING TO THE
statement, the SNIS believes that parents in the field—including those who adopt and foster—should not be penalised in any way, and legal and regulatory mandates and family friendly workplace policies should be considered when institutions and individual practitioners approach the issue of childbearing in the context of a career in neurointerventional surgery. Neurointerventionist and SNIS member Amanda Baker (University of California San Francisco [UCSF], San Francisco, USA) led a structured literature review with her peers regarding parental leave policies in neurointerventional surgery and related arenas. This involved evaluating a 2019 survey of those in the field, which included proposed
Synchron announces publication of braincomputer interface clinical trial in JAMA Neurology
SYNCHRON HAS ANNOUNCED that the medical journal JAMA Neurology has published peer-reviewed, long-term safety results from a clinical study in four patients with severe paralysis implanted with the company’s firstgeneration Stentrode neuroprosthesis device. The study found that it is possible to use the neuroprosthesis device to transmit neural signals from inside a blood vessel in the brain over a long-term period without any serious adverse events related to the device.
The SWITCH (Stentrode with thought-controlled digital switch) trial—a first-in-human study— evaluated four patients implanted with Synchron’s Stentrode. Patients completed a 12-month follow-up with no persistent neurological deficits. There were no clots or migrations of the device, a Synchron press release reports, and signal quality remained stable with no significant deterioration.
changes to reduce barriers for women and parents pursuing family life, as well as addressing concerns regarding radiation exposure.
“We are grateful to the leadership of SNIS and the Journal of NeuroInterventional Surgery (JNIS) for supporting all people—all families—in this amazing field,” said Baker. “I would like to personally thank UCSF’s Neuroendovascular Surgery programme for training me as their second female and first pregnant neurointerventionist.”
The recent position statement was developed by the SNIS’ Women in Neurointervention committee, Standards and Guidelines committee, and board of directors, and has been published in JNIS
Other recommendations made in the statement include making the use
of vacation time flexible for those undergoing family planning methods or procedures, particularly within training programmes. It also states a belief that fellowship training, career promotion and job security should be maintained during the process of starting a family.
“SNIS believes people should not have to choose between a fulfilling family life or professional career, especially when the nature and urgency of neurointerventional treatments require emotional, physical and mental demands on every person at each experience level,” added SNIS president J Mocco (Mount Sinai, New York, USA). “Things like allowing flexibility for scheduling prenatal appointments, and not penalising those who use family leave, are vital and will have lifelong benefits for those in neurointerventional surgery and their families.

“We want our practitioners to know that we do not believe taking time for family needs is a lack of commitment to the profession.”
In addition, each participant successfully controlled a personal computing device with the braincomputer interface (BCI). They were able to use the implant to generate digital switches under intentional control for routine digital activities, such as texting, emailing, and communication of care needs, the release adds.
The study was led by Peter Mitchell, the neurointerventionist who performed the procedures, and vascular neurologist Bruce Campbell (both University of Melbourne, Melbourne, Australia). The procedures were performed in a neurointerventional angiography suite.“We carefully conducted this first-in-human study with a primary focus on safety. All patients tolerated the procedure well and were typically discharged home within 48 hours,” said Mitchell.
The device is implanted in the motor cortex of the brain via the jugular vein in a minimally invasive endovascular procedure. Once implanted, it detects and transmits motor intent in order to control personal digital devices.In the trial, motor intent was detected using a robust decoder that searches for power changes in certain frequency bands. The digital switches were executed under the volitional control of frequency band shifts by the users.
Issue89 | February 2023 11 New in Neuro NEURO
J Mocco
Peter Mitchell

RCR president advocates for improved data collection and optimised training in IR
Royal College of Radiology (RCR) president Kath Halliday (Nottingham University Hospitals, Nottingham, UK) gave a presentation to the British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK) exploring how new technologies and infrastructural reforms can improve outcomes for patients under interventional radiology (IR) department care. Drawing attention to the problems with IR practice in the National Health Service (NHS), particularly with regard to capacity, she suggested harnessing artificial intelligence (AI), collecting data, and recourse to dedicated day case units and hybrid theatres could reduce waiting times and drive more effective interventions.
She drew attention to the fact that “there are no data” widely available on IR procedures. The Getting It Right First Time (GIRFT) programme reviews services and procedure outcomes across the NHS but, Halliday said, provides little in the way of information on the outcomes

of IR procedures. “We need to be able to identify IR procedures from our radiology codes,” she argued, stating that these in turn need to link to the codes used in Hospital Episode Statistics (HES), a database of NHS admissions records covering comorbidities, length of stay and outcomes.
SIO announces first site approved for enrolment in ACCLAIM clinical trial
The Society of Interventional Oncology (SIO) has declared Mayo Clinic, Rochester, USA as the first of 10 sites in the USA and Europe approved for enrolment on the society’s primary clinical trial ‘Ablation with Confirmation of Colorectal Liver Metastases (ACCLAIM), Prospective Trial for Microwave Ablation as a Local Cure.’

CONSTANTINOS T SOFOCLEOUS (MEMORIAL Sloan Kettering Cancer Center, New York, USA), the study’s global primary investigator presented the background to the trial, as well as its aims, to attendees of the SIO 2023 annual scientific meeting (19–23 January, Washington DC, USA). The Mayo Clinic site study investigators include Grant D Schmit as the principal investigator, and Matthew R Callstrom and Anil N Kurup as co-investigators (all Mayo Clinic, Rochester, USA).
ACCLAIM is the first global, prospective trial to use an objective and reproducible technical endpoint in its design, which SIO believes will drive important changes to future colorectal liver metastases (CRLM) treatment guidelines, the society announced in a press release. In this multicentre, international trial, SIO aspires to establish microwave ablation (MWA) as the preferred local curative treatment option for selected CRLM that can be ablated with sufficient margins.
According to Halliday, a similar problem exists in informing patients of their options around IR procedures, as those who present the information are often not radiologists themselves. Frequently, this is due to a lack of a dedicated area within radiology departments in which to see patients. Integrating IR procedures into a more comprehensive data management system means interventional radiologists and their patients can make more informed decisions about procedures. This will also require improvements to NHS IT infrastructure, Halliday suggests.
Capacity was another focus of Halliday’s talk. She described how “lack of capacity too often results in poor outcomes for patients,” adding that “for instance, some people wait so long for angioplasty that they end up with amputation,” then referring to the situation in some hospitals where capacity is so limited that radiologists are forced to come in to perform procedures when they are not on call. Improving
The study mandates the use of 3D software to assess the ablation zone and margins and determine if achieving complete margins during an ablation equates to procedural success, where the primary outcome is local tumour progression-free survival at two years post-ablation. This trial is funded through SIO grants from Boston Scientific, NeuWave Medical (part of Ethicon) and Varian (a Siemens Healthineers company). Participants of the trial will have a diagnosis of CRLM for which they would be offered ablation as standard of care. MWA will be performed using a combination of US Food and Drug Administration (FDA)-cleared or CE marked, commercially available MWA system and margin confirmation (visualisation) 3D software. Upon its launch, the ACCLAIM study is expected to have a three-year enrolment period of approximately 275 participants across sites in the USA and Europe.
Speaking at SIO 2023, Sofocleous began by stating his opinion that the ACCLAIM study was “way overdue” as currently, “surgery is the preferred treatment for synchronous and metachronous CRLM”. Hence, posing the rhetorical question “Why do we need the ACCLAIM?”, the presenter answered that the trial aim is “to prove that [MWA] can be the preferred treatment ahead of surgery for selected CRLM that can be ablated with margins, and to create the evidence to support the use of [MWA] for this indication.”
Furthermore, Sofocleous emphasised the importance of “standardising ablation treatment” through mandatory steps involved in image-guided thermal ablation for CRLM.
Sofocleous then referred to ablation’s recent past—when confirming the success of ablation margins was not common practice. Recent software developments,
capacity is difficult because those radiologists required to teach trainees are already overworked, she argued. It would also require creating a more hospitable workplace in terms of morale and working hours to encourage radiologists to stay in the field. For a technology-driven solution Halliday pointed to procedure simulators, which are still underused in training new radiologists. AI would also be useful for diagnostics in IR—though she said she did not believe robots would be performing procedures any time soon. concluded the question and answer that followed her presentation by advocating for expanded IR training.
namely 3D assessment software, has facilitated the confirmation of margins, the speaker noted, adding that “if we have this ability intraoperatively, as work using 3D software assessments showed, we may [be able] to retreat intraoperatively and avoid local treatment failures.”
Thanks to two National Institutes of Health (NIH) grants, Sofocleous went on to explain how he has been able to interrogate prospectively the efficacy of achieving complete tumour eradication and creating sufficient margins with tissue sampling. “You can document a minimum of 5mm margin with tissue evidence of no residual viable disease at the end of the ablation treatment,” Sofocleous clarified, furthering that this is “regardless of modality or energy” and “biopsy-proven”. Continuing, Sofocleous informed attendees that “comparisons of intraoperative assessments using contrast-enhanced CT (CECT) with the guideline standard of care—assessment at four to eight weeks post-ablation—have shown that the intraoperative CECT assessment yielding margins of less than 5mm is “the most reliable factor to predict local tumour progression”.
Sofocleous circled back to underline what “ACCLAIM is mandating to do”. Enrolment mandates “immediate 3D software assessments of the ablation zone and margins”, with a need to create an ablation margin of at least 5mm in order to avoid local tumour progression”. Once the 3D assessment has confirmed a margin greater than 5mm, Sofocleous concluded, “we believe that regardless of centre, country, operator, this unified endpoint (of ablation with minimal margin of at least 5mm) will result in high rates of sustained, long-term tumour control.”
The presenter ended by stating that the trial is anticipating opening in 10 centres, and that any FDAcleared or CE-marked 3D margin assessment software and ablation device is “acceptable” for use in the trial.
Issue89 | February 2023 13 RCR’s Perspective
[…] Some people wait so long for angioplasty that they end up with amputation.”
Kath Halliday
275
The ACCLAIM study is expected to have a three-year enrolment period of approximately 275 participants across sites in the USA and Europe
Constantinos T Sofocleous
An insight into the Middle Eastern IR landscape
Mohammad Arabi is a consultant interventional radiologist currently working at the King Abdulaziz Medical City and King Abdullah Hospitals (Riyadh, Saudi Arabia). Interventional News sat down with him to explore how interventional radiology (IR) practice varies both within the Middle East-North African (MENA) region and when compared to that of interventional radiologists worldwide. He looks ahead to the challenges this region may be up against from an IR perspective in the future, and also reflects on the advancements that have shaped how he and colleagues care for their patients today.
What are the main differences in terms of IR infrastructure/practice between the MENA region and Europe or the USA?
The practice of vascular IR (VIR) in the MENA region is substantially different when compared to the practice in Europe or North America in many ways, including clinically, academically, administratively, socioeconomically and legislatively.
Healthcare expenditure in the MENA region was estimated at 5.5% of the gross domestic product (GDP) in 2019. This is significantly lower than in Europe (9.9%) and the USA (16.3%) and varies significantly among the MENA countries. The current health expenditure per capita in the MENA region is reported at US$507 (US$275 excluding high-income countries) compared to US$3,476 in the European Union and US$10,317 in North America. This could be, in part, due to the younger and healthier population in the MENA region compared to other parts of the world. The population over 65 years is estimated at 5% of the total population, compared to 17% in North America and 21% in the European Union. This translates into differences in IR clinical practice and the nature of pathologies that prevail in the corresponding regions. The MENA region is densely populated and diabetes, end-stage renal disease, motor vehicle accidents, and some cancers are more common than in other parts of the world. The socioeconomic restraints, poor education and awareness, lack of easy access to healthcare due to limited resources and unavailability of insurance and governmental support, result in late presentations of diseases such as advanced diabetic foot or advancedstage cancer.
In countries with low incomes, governments and healthcare facilities focus on providing essential medical and surgical interventions, and access to advanced VIR procedures remains limited to few centres and those who can afford their high costs. The current economic crisis and associated inflation has made it more difficult and challenging to sustain the supply chain of the expensive IR materials. For example, the local currencies in Syria, Lebanon and Egypt reported record low exchange rates against the US dollar and euro, increasing the burden on healthcare systems.
On a positive note, the geographic location of the MENA region and existing regulations allow easier access to a wider range of supplies from both the Eastern and Western hemispheres, allowing for more flexibility in maintaining the supply chain at relatively low cost.
How does IR in Riyadh compare to elsewhere in Saudi Arabia/elsewhere in the MENA region?
The Saudi capital Riyadh has a population of nearly eight million and is served by numerous governmental healthcare facilities that provide 24/7 VIR services. While the majority of these hospitals provide essential vascular and interventional procedures, advanced VIR interventions are typically offered in tertiary care institutions. These include interventional oncology services, advanced venous and arterial procedures, hepatobiliary and transplant interventions.
In a recent presentation by Zakariya Al-Safran (King Fahad Specialist Hospital, Dammam, Saudi Arabia), former president of the Saudi Interventional Radiology Society (SIRS), the current number of interventional radiologists in Riyadh is estimated at 41% of the entire IR workforce in the kingdom (58/141). Despite the increasing number of interventional radiologists, some provinces remain devoid of IR services, and referrals to higher care centres are required for the simplest interventions.
The Saudi VIR fellowship was established in 2014 and currently, 15 graduate fellows pass through annually. This has helped in covering some of the peripheral areas that did not have access to VIR services before.
The practice of IR in Saudi Arabia is remarkably advanced compared to other parts of the Arab world and MENA region. Data from the Pan Arab Interventional Radiology Society (PAIRS) indicate that members from Saudi Arabia and Egypt constitute nearly 50% of registered interventional radiologists in the database. The available infrastructure and resources in governmental hospitals in Saudi Arabia allow offering a wide range of advanced interventions that parallel the majority of European and North American centres. The private sector, on the other hand, has also witnessed remarkable attention over the past decade due to expansion of the insurance industry and governmental support of privatisation.
How have your IR practices evolved in the last decade? What have the innovations been in terms of devices/procedures?
The increasing number of interventional radiologists in the kingdom was paralleled by expanding the services provided and the increasing complexity of the procedures. Several centres in the country offer advanced interventional oncological procedures including radioembolization and advanced ablation with microwave, cryoablation, and irreversible electroporation. The vast majority of IR services provide peripheral arterial and dialysis interventions, and have access to atherectomy, thrombectomy and intravascular lithotripsy. Recent guidelines and advances in stroke

thrombectomy added additional burden onto IR services to provide 24/7 coverage. In addition, the increasing knowledge of IR among other medical and surgical disciplines, along with increasing public awareness, resulted in higher demand on IR services. For example, more women are directly seeking uterine fibroid embolization rather than surgical treatments. Our unit performed nearly 18,000 IR procedures in 2022 compared to nearly 8,300 in 2013, adding many new procedures and techniques such as endovascular arteriovenous fistula creation, peritoneal dialysis catheter placement service, cryoablation, same-admission hepatic mapping and radioembolization, and advanced venous and arterial interventions.
What do you hope to see for IR in your region in the years to come? Do you expect the patient demographic to change in any way?
The incidence of cancer is projected to increase by 47% worldwide by 2040, and the relative magnitude of this increase will be highest in low and medium human development index (HDI) countries. The World Health Organisation reports that the prevalence of diabetes and associated complications has also been rising more rapidly in low- and middle-income countries than in high-income countries. This carries increasing burden on the healthcare systems and creates higher demand on VIR services in the region. PAIRS is working tirelessly to advance IR in the region in collaboration with other regional and global IR societies such as SIRS, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) and the Society of Interventional Radiology (SIR). Several initiatives were undertaken to further disseminate knowledge about IR among medical students and juniors, as well as several public campaigns to increase awareness about the role of IR in certain conditions such as diabetic foot, uterine fibroids and doing prostate artery embolization.
The ‘I am PAIRS’ campaign was launched in 2019 and runs in Egypt, Saudi Arabia, Morocco and Tunisia and was created by the residents/fellows/students (RFS) section under the umbrella of PAIRS. Since its inception, the RFS section has participated along with other peer societies in global events such as the
Global IR Juniors Summit organised in collaboration with CIRSE, SIR and the European trainees forum. PAIRS’s vision is to further promote and advance IR training in the region, specifically in countries where IR services are not available, scarce, or limited to basic interventions. Interventional radiologists practising in African countries such as Nigeria and Tanzania have reported their early local experience in providing VIR services such as peripheral arterial interventions, percutaneous nephrostomy placement and lung biopsy. These reports highlight the staff shortages, the challenges they have to confront and the opportunities that need to be explored. The role of IR societies such as PAIRS is to establish a network of collaboration and education to enhance local VIR practices and experiences, and provide a platform for volunteering in areas where IR services are not widely available.
February 2023 | Issue89 14 IR in the Arab World
The vast majority of [Saudi] IR services provide peripheral arterial and dialysis interventions.”
INTERVIEW
Mohammad Arabi
BSIR busts myths around being a girl in the IR “gang”
Paula Novelli, who is associate professor of interventional radiology (IR) at the University of Pittsburgh Medical Center (Pittsburgh, USA) put her own spin on a British Society of Interventional Radiology (BSIR) 2022 annual scientific meeting (2–4 November, Glasgow, UK) presentation titled ‘Women are more likely to work part-time’. The ‘myth-busting’ session as a whole saw speakers weigh in on how gendered perceptions and, in some cases, realities, can impact women interventional radiologists’ careers. Novelli in particular, bringing the perspective of ‘the only girl in the gang’—the gang being her interventional radiology (IR) team at Pittsburgh—left delegates with the salient message that “on all levels”, women are not overinvesting in education, despite the fact that, in the USA, “women practise fewer total hours than men due to significant household responsibilities.”

Novelli began her presentation
remarking that, based on a 1970s survey of 97 male and 95 female doctors, 59% of the female respondents and 87% of the men had been working full-time from graduation, with 17% of the women not working due to taking on a traditional ‘female’ role instead. The prevailing thought at the time was that medical education of women in the USA was a poor investment due to the likelihood of women practising fewer hours over their professional lifetimes. Yet, despite these figures, Novelli conveyed that the findings demonstrated “women spent 90% as much time in medical work as did men, accounting for childbearing responsibilities.” This points to the idea of the “superwoman”, the presenter elaborated—female doctors may be working fewer overall hours, but they work with increased productivity.
US $99,000
Total training cost per diagnostic radiology resident per year. On top of the half-a-million that they pay to become a physician academically
More current than the previous data, Novelli then highlighted a British Medical Journal (BMJ) op-ed from 2008, which professed the opinion that women doctors were concentrated in “family-friendly” specialties, including paediatrics, psychiatry and family medicine. This was considered to be a “ticking timebomb” since women are more likely to work part-time, and this “feminisation” of these familyfriendly specialties would mean that the specialties would disproportionately suffer the implications of part-time working and maternity leave, such as
lack of continuity of care and resource use.
However, recent data on the state of women in academic medicine from the Association of American Medical College (AAMC) Novelli countered, while “difficult to interpret” because of varying definitions of what percentage of full-time work part-time constitutes, suggests that among part-time doctors, there is an almost equal male-female split. The figures she cited were 50.1% of male part-time medical faculty, versus 49.9% women.
The “leaky pipeline” in IR
Bringing the focus to IR specifically, Novelli noted that radiology and surgery are “up there” when it comes to the specialties in which the aforementioned part-time doctors are concentrated, but that, as shown by the statistic, this is not due to a higher number of women faculty members in these specialties.
Yet, according to a Journal of the American Medical Association (JAMA)-published study of parental status among early-career physicians, the object of which was to determine which factors influence doctors’ decisions to work part-time or full-time, 75% of female participants said they were considering reducing their hours. Novelli underlined the importance of this “early gap” in hours practised between men and women, reaffirming the definite gender imbalance in this regard with anecdotal evidence: “I have never worked with another female interventional radiologist in my entire 18-year [career]”. The leaky pipeline will perpetuate the gender imbalance in medicine for the foreseeable future, Novelli posited.
The mental “toll” on women in IR
Novelli then brought burnout among interventional radiologists into the picture, flagged how, as found in a recent Society of Interventional Radiology (SIR) questionnaire, burnout was “significantly higher” than among
diagnostic radiologists, and, pertinent to the current discussion, also among women over men. Similarly, Novelli added, another JAMA study assessing depression among doctors just postmedical school found that the rate was also higher among the female respondents.
A theory Novelli brought to explain this phenomenon was that, perhaps, women need to work harder: “I do believe that we need to work harder in any academic setting just to prove ourselves.” This “toll” medicine takes on women is multifactorial, the presenter furthered, stating that female doctors are more likely to be reported, have fewer advancement opportunities, and are less likely to become full professors or academic leaders. “We are not really learning from the past,” Novelli lamented, explaining that since the seventies, there have been calls for women to receive more flexibility and respect to foster their advancement. “We need to eliminate biases and harassment,” was one of Novelli’s own calls regarding how to successfully support women in their medical careers.
Women are supported to some extent, Novelli acknowledged, mentioning the BSIR’s pamphlet that informs women of the scope for flexibility around training and provides guidance on radiation exposure for those of childbearing age who may be concerned about this aspect of an IR career.
Investment in women in medicine not misplaced
“Today, the total training cost per diagnostic radiology resident is US$99,000 a year on top of the halfa-million that they pay to become a physician academically,” was Novelli quantifying the financial extent of the commitment required to become a radiologist in the USA. Be this as it may, she opined that women are
not “overinvesting” in their medical education, as their practices, even if they do not work full-time hours, provide the same level of patient care.
Novelli’s parting words were that “as the only girl in the gang” she has been “called into the principal’s office” many times—this refers back to how it is harder to be a woman in medicine, how the standards to which women are held are higher. “But I have been able to maintain the support of family and work/life responsibilities,” she celebrated. Novelli then admitted that she is “still waiting for her ‘Me Too’ moment and is “not sure” that her 16-year-old daughter should pursue a career in medicine as “there is still a lot of work to do.”
Subsequent discussion around
the subject of Novelli’s presentation drew out the sentiment that her point about not necessarily encouraging her daughter to go into medicine was “[disheartening]”. This then raised the question of whether women could be the predominant source of negative comments dissuading their own gender from pursuing IR. Mentorship was suggested as an antidote to women’s reticence to enter a field which may have seemed, traditionally, not to be a good “fit”. “[The mentor need not] be a woman,” was Shilpi Pal’s (Ninewells Hospital, Dundee, UK) view—“[just] someone who has been in your shoes”.
Issue89 | February 2023 15 Women in IR
I have never worked with another female interventional radiologist in my entire 18-year [career].”
Paula Novelli
Aghiad Al-Kutoubi
“When I relocated to Lebanon, I was the only person with practical experience and expertise in EVAR [endovascular aneurysm repair] in the Middle East.” It was thus that Aghiad Al-Kutoubi became the first in the Arab world to perform this procedure, in doing so changing the face of interventional radiology (IR) practice in the region. Now adjunct professor of diagnostic and interventional radiology at the American University of Beirut Medical Center (AUBMC; Beirut, Lebanon), Al-Kutoubi tells Interventional News how he came to embark on his IR career; recounts the obstacles he overcame to develop an IR service in Beirut, as well as those encountered in practising IR in the country more broadly; and imparts his knowledge on how best to train interventional radiologists.
What attracted you to a career in IR?
This really happened by chance. I was attracted to radiology because of the potential of contributing to the diagnosis of disease in multiple organs and the interaction with different medical teams. My career in radiology started when I was accepted for training at St Mary’s Hospital (London, UK) in September 1977. The head of the department was David Sutton, a pioneer of angiography and its application in systems including the heart and central nervous system. I was mesmerised by the art of diagnostic angiography. Interventional procedures were only just emerging—treatment of gastrointestinal bleeding with vasoconstrictive medication, preoperative embolization of renal tumours, venous procedures, etc. I still vividly remember the first iliac angioplasty procedure that I assisted in as a registrar in 1978 and the impressive result. At the same time, ultrasound and computed tomography (CT) scanning became established tools. These modalities offered opportunities for biopsy and drainage procedures. I think I benefitted from these developments and unconsciously became an interventionalist as well as a diagnostician.
Who were your mentors?
In my earlier years, I was influenced by many people—my parents, some teachers at school and university, and close associates in my home country, Syria.
In my radiology career, I owe gratitude to David Sutton for inspiring me and Oscar Craig for his wisdom and guidance. I must also mention Averil Mansfield, who provided the best collaboration, knowledge and support.
Could you describe a particularly memorable case of yours?
There are so many, but I will mention two. The first was in the UK—a patient who developed an arteriovenous fistula between the origin of the left carotid artery and innominate vein after pinning for clavicular fracture. Suitable stent grafts were not available commercially and the case was treated with the combined efforts of IR and vascular surgery, who provided a segment of the saphenous vein that I attached to a Palmaz stent and placed it at the origin of the left carotid artery through a direct carotid approach with balloon occlusion of the innominate vein. A second similar stent was needed but we were elated that the procedure was clinically successful, and the patient avoided thoracotomy.
The second was in Lebanon, a few months after I performed the first endovascular aortic case. A
patient presented to the emergency room with type B dissection and a large leak from the distal aortic arch into the left thorax, as well as lower limb ischaemia. As luck would have had it, I had a thoracic stent graft for another elective case that was the appropriate size for sealing the point of bleeding. Balloon fenestration of the abdominal aorta treated his limb ischaemia. I saw this patient repeatedly until he passed away 20 years later from complications of lymphoma.
What were the challenges involved in building up the IR service at the AUBMC?
Although some IR procedures were being performed by colleagues, there were challenges at multiple levels. These included acceptance of new procedures; perception of competition by other specialties such as vascular surgery; acceptance of new treatment methods by insurance and third-party payers; the cost of procedures to patients; availability of appropriate equipment and paramedical staff; anaesthesia and
sedation requirements; availability of devices; and the volume of cases versus training requirements for residents. Some of these challenges required a gentle approach, with firmness and perseverance required in others. The result was of benefit not only to the AUBMC, but to the practice of IR in other centres in Lebanon and in the Middle East as experiences were exchanged and knowledge shared.
Having practised in both the UK and Lebanon, what are the main differences/ similarities associated with IR in these two geographical areas?
I think the fundamental difference is financial. In the UK, my practice was mainly in the UK’s National Health Service (NHS), where the person with the most expertise would be the one to perform the medical procedure and this was also true in the private sector. In Lebanon, the health system is spearheaded mainly
by established and respected private institutions, for example, the American University of Beirut. In contrast, the public sector provides a relatively small proportion of healthcare with limited resources and lags behind in terms of state of-the-art treatments. Private healthcare requires someone to pay for the treatment of the patient be it the patients themselves, insurance companies or other third-party payers who have to accept the value of the treatment procedure and frequently find reasons for not paying in full.
The other issue is remuneration of medical staff. Whereas in the NHS the physician is not paid per procedure, in Lebanon, the income of the physician is dependent on referral and case numbers. Therefore, a surgeon may choose not to refer the patient for an IR procedure because he would lose income. Joint arrangements for management became necessary to provide a balanced approach to the treatment of patients and to avoid ‘competition’.
16 February 2023 | Issue89 Interview
I still vividly remember the first iliac angioplasty procedure that I assisted in as a registrar in 1978 and the impressive result.”
PROFILE
Andy Watt/NB Illustration
Current appointments
2022–present: Adjunct professor, Diagnostic & Interventional Radiology (IR), American University of Beirut Medical Center (AUBMC; Beirut, Lebanon)
Past appointments
1998–2003: Honorary consultant radiologist, St Mary’s Hospital (London, UK)
1997–2021: Professor of Radiology & IR section chief, AUBMC
1997–2011: Chairman, Department of Radiology, AUBMC
1984–1998: Consultant radiologist, St Mary’s Hospital
How did you come to be the first to carry out an EVAR in the Arab world? What do you remember about how it came about, and the impact it has had since?
At St Mary’s, we had embraced this new approach to the treatment of aortic aneurysms early on, and I, with my vascular surgical colleague John Wolfe, treated a few patients with stent grafts for aortic aneurysms using the first-generation devices.
When I relocated to Lebanon, I was the only person with practical experience and expertise in this field in the Middle East. Despite this, I had a hard time convincing colleagues of the value of this method and was, in fact, the target of efforts to stop its introduction until we had a patient who developed a false aneurysm of the thoracic aorta after coarctation surgery. I had, by that time, modernised the angiography suite and was able to convince the cardiothoracic surgeon Munir Obeid that this was an ideal case for stent graft placement. With his help, and that of Ghattas Khoury, another surgical colleague, I treated this patient successfully and she went home the following day. The publicity that followed resulted in referrals and soon patients were treated by various EVAR devices— the people who had resisted were now interested! I was able to present my work at various regional fora and got colleagues in other Arab countries to pursue this approach. The rest is history!
As someone who has a passion for educating the next generation, both in the UK and in the Arab world, what would you say are the priorities when it comes to making sure interventional radiologists-in-the-making receive the highest standard of training possible?
Interesting question! I think one of most important factors is the commitment of the trainers to training! Commitment of the trainee is no less important. Secondly, establishment of a comprehensive curriculum to take into account the modern, and everchanging IR landscape—this is pivotal to ensuring the standard of training. After these first two steps, finding training centres that have the breadth of practice and case volume to meet the curriculum objectives is relatively easy. It may prove necessary for trainees to visit other centres to observe/train in procedures that are not done at their primary training centre.
What are your hobbies and interests outside of medicine?
I have pursued many sporting hobbies over the years but had to give some up after injuries. I now do scuba diving and golf, which I wish I could play better and more! Arabic calligraphy is a skill I was taught by my grandfather and I practise it occasionally, but I hope to spend more time at it. I guess grandparenting is the main ‘hobby’ now.
Society positions
Distinguished Fellow, Cardiovascular and Interventional Radiological Society of Europe (CIRSE)
First fellow, Pan Arab Interventional Radiology Society (PAIRS)
Fellow, Royal College of Radiologists (RCR)
Radiological Society of North America (RSNA)
Society of Interventional Radiology (SIR)
Medical education
1975: Medical degree, Damascus University (Damascus, Syria)
1982: Radiology specialty certification, RCR (London, UK)
17 Issue89 | February 2023 Interview
ECIO 2023
European Conference on Interventional Oncology
April 16-19 | Stockholm, Sweden

www.ecio.org
Join us for the world’s largest interdisciplinary meeting on interventional oncology!

ECIO 2023 will cover the entire spectrum of IO with all there is to know about clinical care, technical developments, and the latest data.

Register now to join colleagues from around the world in Stockholm for four days packed with informative sessions and hands-on trainings.
Browse the full programme and put together your personal itinerary.
Bring your tumour board colleague along for free !
The Collaborating Against Cancer Initiative is open to all interventional radiologists with a complete registration to take their non-radiologist MDT colleague to ECIO 2023 free of charge.

Accommodation
CIRSE’s travel partner Kuoni offers ECIO 2023 delegates an easy-to-use booking system with hand-picked quality hotels at a variety of price ranges near the congress centre.

Getting there
ECIO 2023 attendees can take advantage of reduced rates when traveling with the Lufthansa Group. Scan the code on the right to book your flight!
C RSE Cardiovascular and Interventional Radiological Society of Europe
LEADERS IN ONCOLOGIC INTERVENTIONS
Vulvar varicosities: New procedure, durable results Karim Abd El Tawab
Comment & Analysis
In the past two decades, there has been a shift in varicose vein management from conventional surgical treatments to outpatient interventional procedures. Depending on the type and site of the affected vein, patients now have many other treatment options— namely with ablation, glue, coil embolization and sclerotherapy. These minimally invasive options offer better disease control with maximal safety, less pain and less recurrence.
With increasing patient awareness, one of the common clinical scenarios interventionalists encounter now is female patients with pelvic varicosities associated with the presence of vulvar, perineal, inguinal, or gluteal varicose veins, sometimes also associated with lower-extremity varicosities.
The prevalence of vulvoperineal varices in the general population is still unknown. Yet, in a series of over 4,000 female vein clinic patients, as written
about by J T Hobbs et al in a 1990 British Journal of Hospital Medicine paper, the incidence of vulvar varices was about 4%, rising to 40% in patients with pelvic venous insufficiency. These latter patients are typically multiparous women between 20 and 40 years of age suffering from coital aches, genital heaviness, discomfort, continuous arousal, as well as lower urinary symptoms in severe cases.
Despite it being a common problem, there are few publications discussing
Non-surgical treatment found to provide long-term relief for carpal tunnel syndrome
A minimally invasive treatment for carpal tunnel syndrome provides complete and long-term relief to patients without the use of corticosteroids, according to research presented at the annual meeting of the Radiological Society of North America (RSNA; 27 November–1 December, Chicago, USA).
CARPAL TUNNEL SYNDROME IS A FORM of nerve entrapment neuropathy, involving the pressing or squeezing of a peripheral nerve. It occurs when the median nerves and tendons inside the carpal tunnel, a narrow and rigid passageway that runs from the forearm to the palm of the hand, are being pressed or squeezed at the wrist. This results in tingling, numbness and/or weakness of the fingers and hands. Carpal tunnel syndrome is the most common and widely known form of entrapment neuropathy, affecting about 3% of the US population.
Surgery is often required to treat carpal tunnel syndrome when
vulvoperineal varices management. Most of the treatment approaches are derived from case reports or very small case series. Management options include compression, ovarian and internal iliac veins embolization, surgical ligation or phlebectomy and ultrasound-guided sclerotherapy. The latter is becoming both the doctor and patient’s favourite treatment where suitable—being safe and almost painless. It involves injecting a sclerosing agent like polidocanol foam, which causes a biochemical reaction in the diseased vein that, in turn, causes the vein to collapse and harden, before it is then absorbed by the body. The use of vulvoperineal sclerotherapy has little evidence and is done under ultrasound guidance alone, which despite being sufficient for symptom improvement in most cases, does not allow full assessment of the veins going up to the pelvis.
This was our motive when developing direct fluoroscopic-guided sclerotherapy for vulvoperineal varices, which combines ultrasound guidance for vein puncture followed by contrast injection under real-time fluoroscopic guidance to assess all external genitalia veins and how they interact with pelvic and lowerlimb veins.
We published the results on our first 70 patients in the Arab Journal of Interventional Radiology (AJIR) in 2021 and we have now treated more than 160 patients using this procedure.
Varices most commonly drain into the internal iliac veins through perineal and
non-surgical methods, such as physical therapy or corticosteroid injections, are insufficient. The most common and widely used surgical method involves cutting the carpal ligament to reduce pressure on the median nerve. This method requires making an incision into the wrist.
The study’s findings show that a technique called hydrodissection effectively treats nerve entrapments without the need for surgery or corticosteroids. It involves the injection of a liquid, usually saline, into a nerve to separate it from the surrounding tissue. Ultrasound guidance is used to accurately identify nerves.
Lead author Anindita Bose (University College of Medical Sciences, Delhi, India) comments: “Previously, the studies that have been done on ultrasound-guided hydrodissection for carpal tunnel syndrome have used corticosteroids either alone or as a part of the injection, making it difficult to assess whether hydrodissection alone was beneficial, or if it was due to the effect of the steroids.”

For this randomised controlled trial, Bose and colleagues enrolled a total of 63 patients suffering from carpal tunnel syndrome. Researchers used the Tunnel Questionnaire (BCTQ), the Visual Analog Scale (VAS), and crosssectional area ultrasounds of the median nerve to assess patient pain and symptoms before and after the procedure. The 63 patients were divided into three groups. Group one received ultrasound-guided hydrodissection with just a saline injection. Group two received
internal pudendal veins, and connections with the vaginal and external iliac veins were also noted. Ovarian venous connections were not as common as most of these patients had already undergone ovarian vein embolization prior to vulvar sclerotherapy.
Technical success was achieved in all cases, with all patients showing short-term improvement in their symptoms, whether from one or two sessions of sclerotherapy. For patients who completed a one-year follow-up, recurrence was found in only 7%. The rest of the patients showed a stable therapeutic effect with no recurring varices, pain, or labial swelling.
This new procedure will be discussed at the Pan Arab Interventional Radiology Society (PAIRS) annual congress that will take place in Dubai, UAE from 11–14 February. The congress provides the opportunity for all those interested in interventional radiology (IR) to network and improve their practice by attending sessions and workshops covering all categories of IR, including like interventional oncology, venous, embolization, aortic, women’s health and musculoskeletal, as well as a dedicated track for juniors with more than 150 speakers from all over the world.
Karim Abd El Tawab is a consultant interventional radiologist at Ain Shams University Hospitals, Cairo, Egypt.

Disclosures: Abd El Tawab is a member of PAIRS 2023’s Scientific Committee.
ultrasound-guided hydrodissection with an injection mixture of saline and corticosteroid. Group three received just an ultrasound-guided corticosteroid injection with no hydrodissection.
Follow-up was done at four weeks, 12 weeks and six months. At the four-week mark, all three groups of patients showed a reduction in pain. By the 12-week and six-month mark, both groups that received ultrasound-guided hydrodissection showed further improvement while the group that received just a corticosteroid injection reported a recurrence of symptoms and an increase in BCTQ and VAS scores.
Additionally, ultrasounds showed a significant reduction of median nerve cross-sectional area in both hydrodissection groups. Group one showed a reduction of 43%, and group two showed 46%. Group three showed only an 11% reduction.
The procedure is short, requiring only 10 to 15 minutes, which can reduce costs for treatment facilities. Anupama Tandon (University College of Medical Sciences, Delhi, India) a co-author of the study, notes: “It came as a pleasant surprise when this simple procedure of ultrasound-guided hydrodissection provided patients with long-term relief.” She continues, “the patients were highly satisfied, as the cost was low, no anaesthesia or hospitalisation was needed, and they could go back in an hour and resume their routine”.
Issue89 | February 2023 19 Comment and Analysis
The patients […] could go back in an hour and resume their routine.”
Anindita Bose
SWING trial 12-month data: Novel sirolimus DCB shows “great promise” in “challenging” CLTI population
The Sundance (Surmodics) sirolimus drug-coated balloon (DCB) has an “excellent” safety profile in a “challenging, real-world, predominantly CLTI [chronic limb-threatening ischaemia] population,” and has a primary patency rate of 80% at 12 months in a per-protocol analysis population.
Ramon Varcoe (Prince of Wales Hospital, Sydney, Australia) presented these findings from the SWING first-in-human study at the VEITHsymposium 2022 (15–19 November, New York, USA).
Varcoe, who is co-lead investigator of the trial, added that the research team observed no major amputations, “very low” rates of major adverse events, and “impressive” luminal gain, which was sustained out to six-month angiogram. In addition, Varcoe reported that Rutherford category and functional outcome measures were improved. “The Sundance sirolimus-coated balloon is a novel device,” Varcoe



informed VEITH attendees. He elaborated: “It has a microcrystalline surface, but also a very sophisticated proprietary excipient, which, rather than using nanoparticles or microreservoirs uses chemistry to deliver the drug into the blood vessel wall and have it retain that much more so than the other devices on the market.”
The presenter noted that SWING is a prospective, multicentre, single-arm feasibility study that looked at patients
with stenotic or occluded lesions, and enrolled 35 patients over eight sites in Australia, New Zealand, and Europe.
The investigators performed both an intention-to-treat and a per-protocol analysis, Varcoe informed the audience. “The reason for that was because [the trial] was conducted during the COVID-19 pandemic, so we lost seven patients to the primary endpoint of angiography,” he noted, adding that there were three post-protocol deviations. Therefore, the research team focused on the 25 patients who had the per-protocol analysis.
The presenter stressed that the patients included represent a “realworld” population, including a high proportion of patients who are smokers and have diabetes, as well as a majority of patients with Rutherford category 4 or 5 disease. “They also had high proportions of moderate-to-severe calcification in excess of 18%, and around a third of these patients had total occlusions,” he added.
The first of the study’s two primary endpoints pertained to safety—freedom from major adverse limb event (MALE) and perioperative death at 30 days following the index procedure. The primary efficacy endpoint was the rate of late lumen loss at six months, as assessed by quantitative vascular angiography. Both primary endpoints were achieved, Varcoe revealed.
In the per-protocol population, there
BEST-CLI trial raises further questions over open or endovascular approach in CLTI patients
Results from the largest randomised trial comparing revascularisation strategies in patients with chronic limb-threatening ischaemia (CLTI) have ignited debate over which patients are suitable for either an open surgical or endovascular approach.
THE RESULTS FROM BEST-CLI, A MAJOR multidisciplinary trial involving investigators from the fields of vascular surgery, interventional cardiology, interventional radiology and vascular medicine, were delivered at the American Heart Association (AHA) scientific sessions (5–7 November, Chicago, USA) and published simultaneously in the New England Journal of Medicine.
Results of the trial showed that among a population of 1,830 CLTI patients deemed suitable either for an open or endovascular procedure, surgical bypass with adequate single-segment great saphenous vein (GSV) is a more effective approach. Both strategies, however, were shown to be safe and effective when it came to treating CLTI.
BEST-CLI co-principal investigators—Alik Farber (Boston Medical Center, Boston, USA), Matthew Menard (Brigham and Women’s Hospital, Boston, USA), and Kenneth Rosenfield (Massachusetts General Hospital, Boston, USA)—acknowledge that the findings will provide important information regarding their management.
But, recent discussions of the trial’s results suggest that there is still some way to go to settle the question of which strategy should be favoured in patients suitable for either approach. This was brought to the fore in a standalone BEST-CLI session at the recent 2022 VEITHsymposium (15–19 November, New York, USA), which saw commentary being led by
interventional cardiologist Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA), representing a perspective from the endovascular community, and Michael Conte (University of California, San Francisco, San Francisco, USA), providing a view from the vascular surgery sphere.
Secemsky said BEST-CLI provided robust critical evidence but bore limitations in terms of the inclusion of major reintervention in the primary endpoint, the representativeness of non-surgical specialties in the trial, as well as the “generalisability” of the patients enrolled. “Patient preference, surgical candidacy, prognosis, suitable anatomy, technical proficiency, costs and timely access to care remain important considerations when deciding whether to pursue a surgical versus endovascular strategy,” he pointed out. Conte said the trial showed that open surgery and endovascular intervention “are both safe and have
were no major amputations, no major reinterventions, and complete freedom from perioperative death, “so it was a safe device,” Varcoe reported.
The team also saw a rate of allcause death of 0%, target lesion amputations were 0%, and a “very low” rate of clinically driven target lesion revascularisation at 8%. The late lumen loss of 1mm at six months compares “very favourably” to equivalent DCB trials below the knee, Varcoe said.
At six months, the researchers observed a primary patency of 88.5%. Varcoe noted that this was consistently retained out to 12 months at 80%— which is “very good for this part of the vasculature”. Varcoe then added that, regarding quality of life, patientreported outcome measures were also consistently improved to 12 months.
In closing, Varcoe shared his belief that the Sundance device has “great promise” and “warrants evaluation in a large-scale pivotal trial” based on these findings.
complementary roles in the treatment of CLTI patients.” He said that open bypass with GSV provides more effective revascularisation in suitable candidates, and “is likely under-utilised in current practice,” adding that “an endo-first or endo-only approach to all patients with CLTI is not evidence-based care.” Centres carrying out less than 20% bypass in CLTI “should probably take stock,” he commented.
During the session, Farber delved into potential trial weaknesses. It was a pragmatically designed trial, with the possibility for selection and operator bias in enrolment and intervention, he noted. Farber also acknowledged the trial’s cohort 2—comprising patients who did not have adequate saphenous vein— as likely underpowered.
Rosenfield, meanwhile, noted the “controversy” the trial will generate: “[Amongst the BEST-CLI investigators] we have differences in the way we think it should be interpreted. My perspective is a little bit more muted than sort of the ‘Okay, this just tells the whole story about how you have to treat CLTI patients.’” His “top line,” he said, is that bypass fundamentally bears an important role in the treatment of CLTI, underscoring how the trial also showed that both procedures are safe. The lesser-discussed cohort 2, Rosenfield said, gets to one of his points of focus—that the study “raises a lot of questions that still need to be answered.”

February 2023 | Issue89 20 Peripheral News
Ramon Varcoe
Alik Farber Matthew Menard Kenneth Rosenfield
Both [are] safe and have complementary roles in the treatment of CLTI patients.”
Surmodics provides regulatory update related to its US FDA premarket approval application for SurVeil


SURMODICS RECENTLY ANNOUNCED IT HAS RECEIVED a letter from the US Food and Drug Administration (FDA) related to its premarket approval (PMA) application for the SurVeil drug-coated balloon (DCB).
In the letter, the FDA indicated that the application is not currently approvable, while providing specific guidance as to a path forward. The letter stated that certain information within two general categories— biocompatibility and labelling—must be added by an amendment to the company’s PMA application to place it in approvable form. Although the information identified by the FDA to put the PMA application in approvable form would require additional testing and analysis, the letter did not question the human clinical data submitted.

“We are disappointed by the FDA’s response to our PMA application and continue to have confidence in our SurVeil DCB including its compelling performance in the TRANSCEND clinical study,” said Gary Maharaj, CEO of Surmodics. “We are evaluating the issues raised in the FDA’s letter and plan to meet with Agency representatives regarding its contents. Based on our discussion with the Agency, our team and external advisors will determine the appropriate path forward. Concurrently, we will be evaluating options to reduce our use of cash given this development. We expect to address these topics further in connection with our upcoming first quarter fiscal 2023 earnings call.”


Surmodics notes in a press release that the SurVeil DCB is a nextgeneration device for the treatment of peripheral arterial disease and includes a proprietary drug-excipient formulation using an “innovative” process to improve coating uniformity.

Inari Medical announces first enrolment in DEFIANCE trial evaluating clinical outcomes of ClotTriever system in DVT
INARI MEDICAL HAS ANNOUNCED that the first patient has been enrolled in DEFIANCE, a prospective randomised controlled trial (RCT) comparing the clinical outcomes of patients with iliofemoral deep vein thrombosis (DVT) treated with the ClotTriever system versus anticoagulation only. The trial is led by principal investigators Xhorlina Marko, interventional radiologist at Beaumont Health (Dearborn, USA), Steven Abramowitz, chair of vascular surgery at MedStar Health (Washington DC/ Leonardtown, USA), and Stephen Black, consultant vascular surgeon, Guy’s and St Thomas’ Hospital (London, UK).


The first DEFIANCE patient was enrolled by Abdullah Shaikh, interventional radiologist at Allegheny Health Network (Pittsburgh, USA). DEFIANCE will enrol 300 DVT patients at up to 60 centres worldwide. DEFIANCE is Inari’s second RCT, enrolling in parallel to the PEERLESS pulmonary embolism trial.
“We are thrilled to enrol the first patient
and officially kick off this important clinical trial,” said Shaikh. “ClotTriever is fundamentally different to other DVT treatments. This trial is designed to produce definitive evidence to change standard of care.”
“DEFIANCE is an important step forward and will answer critical questions about how we manage DVT patients,” said Abramowitz. “Prior RCTs have focused on thrombolyticbased interventions, which have known downsides and limited effectiveness. This ClotTriever RCT is the first to compare lytic-free thrombectomy to anticoagulation for DVT.”


“With six major clinical studies, including two ongoing RCTs, Inari is wholly committed to [venous thromboembolism] patients and producing definitive evidence to support our technologies,” said Thomas Tu, Inari’s chief medical officer. “None of this is possible without the collaboration and dedication of our clinical trial investigators, who continually push the field forward in the name of better patient outcomes.”

21 Issue89 | February 2023 Peripheral News *Available for US and EU readers only **Available worldwide Subscribe today Available in print and digital formats and through our social channels Visit vascularspecialistonline.com and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription** An official publication of the Society for Vascular Surgery (SVS) A trusted provider of latest news, review of cutting-edge research, congress coverage and opinion from thought leaders Editorially independent
Steven Abramowitz
Working towards a safer IR department: “Developing common purpose and objectives”



“Concentrating on hazard identification, developing safety policies and most importantly, changing the culture in the team to engage meaningfully with these processes” was a principal message presented by Costa Tingerides (Leeds Teaching Hospitals NHS Trust, Leeds, UK) at the British Society of Interventional Radiology (BSIR) annual scientific meeting 2022 (2–4 November, Glasgow, UK), who spoke on his experience as safety lead in a teaching hospital’s interventional radiology (IR) department.
SPEAKING TO DOCTORS AND OTHER professionals, Tingerides explained how he found it difficult to get universal support on safety processes within the department as there was lack of consensus on what the priorities should be: “I propose to you that there is a spectrum of perfectly reasonable attitudes towards safety” he continued, “on one end you have got Atul Gawande and The Checklist Manifesto approach to safety and on the other end you have got the Charles Dotter approach with the core values of innovation, courage, tenacity […] I think that most IRs [interventional radiologists] if you ask them, they will place themselves towards Charles Dotter so I had my work cut out for me.”
Using examples from other safety critical industries, Tingerides emphasised the paramount importance of developing and adhering to safety policies in reducing risk in a meaningful way. He argued that healthcare is not on par with other safety critical industries in this domain. He supported this position
by outlining a recent highly publicised independent investigation led by Bill Kirkup concerning failures in East Kent Maternity Services. He pointed out that despite numerous inquiries on similar failures, the same systemic problems remain.
Tingerides expanded Kirkup’s thesis that the failures identified in East Kent were similar to those found in previous initiatives and investigations over many decades. The response to those failures were unsuccessful in preventing a “recurrence of remarkably similar sets of problems in other places”. Kirkup outlined a set of recommendations aimed at improving safety culture. These include monitoring safety performance and addressing flawed teamworking.
Concluding his report, Kirkup stated that his recommendations are not “easy or necessarily straightforward” to implement but they must be addressed “if we are to break the cycle of endlessly repeating supposedly one-off catastrophic failures.”

Pancreatic cancer patients in Ukraine treated with tumourspecific electroporation continue to improve


A team of specialists at Ulis Hospital (Ulis, Ukraine) has recently reported that the quality-of-life of the two pancreatic cancer patients treated with tumour-specific electroporation (TSE) in September 2022 continues to improve. These two unresectable, locally advanced pancreatic cancer patients had both received TSE treatments in combination with a low dose of chemotherapy, using the IQwave device (ChemoTech).
IN THE FOLLOW-UP COMPUTED tomography (CT) scans, the patients had shown almost a 50% decrease in tumour mass. Both patients are ambulatory and capable of self-care with no pain and are not on analgesics.

After seeing the promising achieved results, the Ulis Hospital team will continue to perform treatments on similar cases and has also invited cancer researchers internationally to join forces and take this treatment forward.
A press conference is planned in the coming weeks by Ulis researchers to interact with the media and attract other researchers to collaborate and explore the full potential of the TSE technology.
Alexei Kovalev of the Ulis Hospital team gave the following statement to press—“Almost five months after treatment, the response of our patients seems lasting and we are optimistic that it can sustain for many more months, with a positive impact on overall survival. We would like to invite cancer researchers internationally to join hands with us in our pursuit of exploring the TSE technology further, possibly in combination with immuno-oncology drugs.“

22 February 2023 | Issue89 Electroporation in Ukraine
*Available for US and EU readers only **Available worldwide A trusted provider of latest news, review of cutting-edge research, congress coverage and opinion from thought leaders A specialised news source in the venous arena Editorially independent Available in print and digital formats and through our social channels Visit venousnews.com and click ‘Subscriptions’ for complimentary print subscription* and e-newsletter subscription** Subscribe today
GAE’s growing evidence base broadens scope for future NICE recommendation
Mark Little (Royal Berkshire Hospital, Reading, UK) brought delegates up to speed on genicular artery embolization (GAE) for knee osteoarthritis over two sessions at the recent British Society of Interventional Radiology (BSIR) annual scientific meeting (2–4 November, Glasgow, UK). Little led audience members through the existing body of evidence for GAE’s safety and efficacy, before outlining the roadmap for growing this further in order to gain UK National Institute of Health and Care Excellence (NICE) recommendation.
“We set up the first European study [GENESIS] back in 2017 and the interim analysis was published in CVIR [CardioVascular and Interventional Radiology] last year.” Little began his presentation by offering the BSIR audience background to his research. The participants in the study, he explained, were “patients with mild-to-moderate knee osteoarthritis [OA]”, numbering 38, and who “had to have had at least an attempt at conservative treatment in the six months preceding referral.”
Regarding the method and materials used, Little shared that for GENESIS, he used 100–300-micron Embosphere particles, and “skin-to-skin”, the embolization procedure took “about an hour”.
For both GENESIS and the now-enrolling GENESIS II studies, Little stated the primary outcome as being knee pain and function, assessed according to the Knee Injury and Osteoarthritis Outcome Score (KOOS). The measure of technical success, the presenter elaborated, was carrying out the embolization, which, according to the GENESIS interim analysis, was 84%.
Posing the rhetorical question “Why was it not 100%?”, Little gave by way of an answer that they did not embolize six patients. The reasons in each case varied among a “risk of non-target embolization to the skin, anastomotic communication between the genicular and popliteal arteries posing an unacceptable risk of non-target embolization, and a lack of hyperaemia”.
Interim results show “initial improvement sustained to follow-up”, Little declared, before alluding to the fact that, for the one-year data, due for publication in 2023, “the trends are the same”.
Little then addressed the NICE appraisal for GAE that he undertook 18 months ago. NICE recommend research preferably in the form of randomised controlled trials against sham or current best practice. Patient-reported outcome data will also be key, Little reported.
Brain scans and a neuropsychometric questionnaire were also included in the GENESIS trial to evaluate the impact of chronic pain on procedure outcomes. The finding, Little relayed, was that “there is a strong signal between patient catastrophising and poor outcomes” in terms of pain.
Rounding off his coverage of GENESIS, Little concluded that the trial demonstrated that GAE for mild-tomoderate knee OA is “safe with potential efficacy” and has “good scientific rationale”.
To prove efficacy and heed NICE’s request for more data, there is GENESIS II, to which the presenter then turned.
This trial began in Autumn 2022 and is using the same KOOS primary endpoint, with a placebo comparison, the presenter outlined. Patientreported outcome data will constitute a secondary endpoint, Little added. GENESIS involved a patient questionnaire, from which the results showed that “75% [of participants] would be more than happy to have [the procedure] again”.

Session chair Robert Morgan (St George’s Hospital,
NICE publishes guidance supporting use of percutaneous ultrasound-guided microwave ablation for benign thyroid nodules
The UK National Institute for Health and Care Excellence (NICE) has published guidance stating that microwave ablation can be used “provided standard arrangements are in place for clinical governance, consent, and audit.” This has the potential to broaden access to minimally invasive alternatives to surgery available to patients with symptomatic benign thyroid nodules.

THE GUIDANCE, RELEASED mid-November 2022, describes ultrasound-guided percutaneous microwave ablation for symptomatic benign thyroid nodules as a “minimally invasive procedure that can be performed in an outpatient setting using local anaesthesia”. The aim, the document goes on to outline, is to “reduce symptoms and improve
London, UK) asked Little whether anyone in the field had gathered data over more than a year—“there are Japanese data to four years,” the presenter replied, following up by affirming that “the effects [are] maintained”.
In the second session of GAE coverage, Little spoke to deepened understanding of knee OA anatomy that has come in the last decade, citing discoveries about vessel formation as “pivotal”.
Pre-empting the question of where GAE fits into the treatment strategy, Little asserted that the majority of knee OA patients are treated by their general practitioner but that many of those will fail conservative therapy, including injections and physiotherapy. Moreover, the presenter went on, “there is a treatment gap between those [whose conservative treatment has] failed and those who are eligible for joint replacement surgery—orthopaedic surgeons do not like to operate on young patients, [for example].”
The current ideal patient, Little communicated, is one with mild-to-moderate knee OA, as these are the individuals in whom the procedure has been trialled to date. There is good data concordance despite slight differences in technique and embolic agent across various centres—“patients get better and then there is a plateau”.
Conrad von Stempel (University College London Hospitals, London, UK) put the question to Little, following his presentation, of how to convince orthopaedic colleagues to refer patients for GAE. According to Little, “these are difficult to treat patients as they will have failed conservative treatments but are not surgical candidates”. Orthopaedic colleagues “are delighted” to have another potential treatment option in the form of GAE. “It is a completely different mindset to traditional turf wars,” Little emphasised.
cosmetic appearance by making the nodule smaller while preserving thyroid function, and with fewer complications than surgery”—the “conventional treatment”.
The recommendations enumerated in the body of the document state that “patient selection should be done by a multidisciplinary team” and that the ablation procedure “should only
be done by a clinician with experience […] and specific training in thyroid ultrasound”. Moreover, it makes clear that the procedure is not suitable for patients with thyroid malignancies, and therefore assessment should be carried out before the procedure to exclude cancer.
This guidance is part of NICE’s interventional procedure programme which considers whether interventional procedures are safe and work well enough for wider use in the NHS. The committee undertook a review of the literature to evaluate the procedure’s safety and efficacy, which encompassed evidence from three systematic reviews, four non-randomised comparative studies and four case series. The committee identified the key efficacy outcomes of “symptom relief, cosmetic improvement and nodule
volume reduction”.
The safety outcomes were “pain, bleeding, damage to adjacent structures and inadvertent treatment of malignant nodules”.
Consultations with clinical experts and patient representatives also informed the recommendation decision.
This is a positive endorsement of the treatment and a complement to the 2020 European Thyroid Association clinical practice guideline for the use of image-guided ablation in benign thyroid nodules, which recommended that “Microwaves and high-intensity focused ultrasound therapy options remain to be fully evaluated”.
The NICE document also reports that “this procedure can be done with cooled and uncooled microwave ablation devices”, but that using uncooled microwave ablation devices means thinner needles can be used.
Issue89 | February 2023 23 NICE Guidance
75% [of participants] would be more than happy to have [the procedure] again.”
Mark Little
GENESIS technical success rate =
84%
Histotripsy: New technology making waves in IO
Mina S Makary & Warren A Campbell IV
Comment & Analysis
Mina S Makary, assistant professor at the Division of Vascular and Interventional Radiology/Department of Radiology at the Ohio State University Wexner Medical Center (Columbus, USA) and collaborator Warren A Campbell IV from Ohio State University’s medical scientist training programme share their take on the impact histotripsy stands to make on the ablation space within interventional oncology (IO).
Ablation techniques utilise thermal stress to induce cell death, which is accomplished using currents, cryotherapy, microwaves, lasers, or ultrasound. While effective, these ablation techniques have limitations. Transducer placement requires percutaneous or laparoscopic access. Reliance on temperature can prevent effective targeting near sensitive structures, and uniform necrosis often cannot be achieved because of the heat-sink effect near vascular structures.
The advent of histotripsy as an ablative modality has the potential to cause a shift in ablation therapies by addressing existing limitations. Histotripsy creates targeted cavitations with large amplitude pulses to mechanically disintegrate tissue—cavitations are transient steamfilled microbubbles that form when high amplitude waves travel through fluid. Rapid expansion and implosion during cavitation causes significant sheer stress to break cells into subcellular components.
Histotripsy has technical advantages over traditional ablation methods. First, renal, hepatic, and intracranial masses can be targeted transdermally. Second, the primary mechanism is mechanical tissue destruction, which improves accuracy and focus on smaller targets. Third, connective tissue is more resistant to histotripsy, reducing the likelihood of collateral damage to blood vessels or biliary structures. Lastly, the area of destruction creates hypoechogenicity which is efficient to monitor in real time. With the principles of histotripsy, there exists the potential to target any tissue in the body for ablation in a precise, rapid approach, sparing non-targeted tissue and without percutaneous incisions or forms of dangerous ionising radiation.
Histotripsy is showing promise in the treatment of cancer. Preclinical animal studies demonstrated histotripsy’s ability to treat liver, prostate, breast, kidney, oesophageal, pancreas, and brain tumours through necrosis. For metastatic tumours, data have also detected an abscopal effect, where untargeted tumours decrease in growth rate. Targeted ablation disrupts the tumour’s evasion of the immune system. Mechanical perturbation of the tumour’s microenvironment increases the exposure of immunological epitopes and removes anti-inflammatory regulatory cells, permitting immune cell infiltration and improved anti-tumour immunity. Recent developments include the phase 1 clinical trial of histotripsy on nonresectable hepatic tumours (THERESA), which was successful—all eight patients experienced no procedural complications two months after the procedure, and tissue was effectively targeted and destroyed in both primary and secondary tumours.
How to avoid (and survive) an audit
Kathy Krol is an interventional radiologist and consultant in interventional radiology practice management based in Boulder, USA. She volunteers for the Society of Interventional Radiology (SIR) Foundation and the American Medical Association.

ACCORDING TO THE AMERICAN ACADEMY of Professional Coders (AAPC), “medical auditing is a systematic assessment of performance within a healthcare organisation. Almost any element of healthcare can be audited, but most audits look at components of payer reimbursement processes to evaluate compliance with payer guidelines and federal and state regulations.”
Many of us will never be audited, but any of us could be audited. Audits may be devastating if they find significant issues. There are ways to decrease the odds of an audit of your practice. In addition, proactively protecting your practice should help you survive an audit should one occur.
Audits are mandated by law in the USA for both Medicare/Medicaid and for private carriers. Medicare estimates it paid US$27.4 billion in improper payments in 2021 alone, and estimates that 6.27% of all payments are improper. Private carriers estimate up to US$68 billion in annual losses due to improper payments. Some law firms suggest that 80% of submitted medical bills have errors. While only a small number of those represent fraud or abuse, it does show how tricky medical billing can be.
There are numerous state and federal laws that
address Medicare fraud and abuse. These laws not only define what constitutes a civil or criminal offence, but they also define the penalties for said offences.
Depending on the offence, practices may have to:
● Pay back money that the carrier finds was incorrectly paid
● Pay back money that the carrier finds was incorrectly paid, plus a penalty for every case (US$11,000 fine plus three times the government loss on each case)
● Develop and execute a corrective plan
● Be excluded from participating in the Medicare/ Medicaid programmes
● Do prison time
The penalties depend on the severity, extent, and intent of the infraction. Not knowing that one is making a mistake is not an adequate defence. Wilful intent can be determined by the law even if one does not know that what they are doing is illegal or wrong, as the law can determine that one should have known that they were making a mistake, even if they chose not to be educated on what is correct.
The future of histotripsy is currently being developed in the lab, with a focus on improving the safety, efficacy, and versatility of the procedure.
Utilisation of microbubbles and fluidfilled polymer capsules can make histotripsy safer by reducing the energy required for cavitation. Liposomes could also transport drug payloads (i.e. chemotherapies), where histotripsy initiates targeted release. Histotripsy may also permit the diffusion of larger nonpermeable biopharmaceuticals like heparin and insulin through skin via histotripsy of the stratum corneum, eliminating the need for regular injections. The debulking and tumour-targeting functions have already been proven in clinical trials, but these advancements will increase its synergistic effects with other oncological therapies.
Histotripsy is the most recent development of high-intensity focused ultrasound techniques, which have the added benefit of mechanical tissue destruction with increased precision and targeting that is less invasive than alternative techniques. Histotripsy may also have the added benefit of increasing tumour immunogenicity in metastatic disease. Preclinical models in multiple cancers have been effective, and the first human trial targeting hepatic tumours was safe and effective. The future of histotripsy includes a range of applications to treat patients increasingly safely and non-invasively.
References: See online version of the article at interventionalnews.com

Disclosures: The authors declared no relevant disclosures
There are several things that trigger audits:
● Coding errors
● Billing errors
● Incomplete or improper documentation
● Practice that is outside the norm for that patient population
● Patient complaints
● Random selection
● Whistleblowing
No one is 100% accurate on billing and coding, but careful management of your practice’s revenue cycle can help you identify coding and billing errors (both random and ongoing) and allow you to correct those. Having a compliance plan in place and adhering to that plan is the best way to protect your practice.

Documentation is critical to avoiding an audit, and can be what saves you if you are audited. Complete documentation of what was done for each patient and why is a simple requirement, but often is not performed, leaving the practice vulnerable. If this is not documented, it is considered not done! Trying to remember a specific patient months or years later is impossible without documentation to remind you what you did and why. The SIR standardised reporting templates are available to help cue you to include the appropriate information that completes the medical story for each patient encounter.
Kathy Krol
February 2023 | Issue89 24 Comment and Analysis
Cardiovascular-aortic community to come together at CX 2023
From cutting-edge aortic interventions to consensus on revascularisation strategies in the peripheral arteries, the 2023 edition of the Charing Cross (CX) Symposium comes at a crucial time in the calendar for the cardiac, aortic, vascular, and endovascular communities.


The three-day CX Symposium—taking place 25–27 April—returns to the Hilton London Metropole in central London for its second consecutive year, with attendees also tuning in virtually from across the globe. It is anticipated that the event will welcome more than 2,500 in-person attendees, with over 1,000 remote participants.
CX continues its three-year cycle of raising vascular and endovascular controversies in order to challenge the available evidence and to be able to reach a consensus after discussion with an expert audience. Sessions will explore routes to consensus in all vascular domains, spanning aortic, peripheral, venous, acute stroke and vascular access, punctuated by CX debates, live and edited cases, and workshop demonstrations.
Running over the three days, the comprehensive aortic programme opens with aortic techniques and technologies on day one, followed by a full day focused on the abdominal and juxtarenal aorta, and finishing with debate centring on the thoracic aorta.
The sessions bring together worldleading experts in management and treatment of aortic disease from the cardiovascular, vascular and endovascular worlds, with faculty including Gustavo Oderich (University of Texas Health Science Center at Houston, Houston, USA), Joseph Bavaria (University of Pennsylvania, Philadelphia, USA), Maximilian Pichlmaier (Ludwig Maximilian University Munich, Munich, Germany) and Marco
HANDSON AORTIC COURSE
Virgilio Usai (St Franziskus-Hospital Münster, Münster, Germany).
Commenting ahead of the symposium, Oderich, a member of the CX Aortic Executive Board, said: “We are all excited to see the latest advances in the arch and thoracoabdominal aorta, and for me personally, to learn from colleagues in Europe and the UK on what is going on there, and what I should change in my techniques.”
Highlights from day one include insights into advances in both open and endovascular thoracic aortic aneurysm (TAA) repair, options for the treatment of
complex aortic pathologies, and a focus on the aortic dissection toolkit.
A podium first presentation from Kevin Mani (Uppsala University, Uppsala, Sweden) is among the highlights from the abdominal aortic session at the start of day two, exploring the benefits of statin treatment after aortic repair. The following juxtarenal aortic
xxxx
consensus update session includes discussion on the impact of the ETTAA (Effective treatments for thoracic aortic aneurysms) and UK-COMPASS (UK complex aneurysm) studies’ results with reference to National Institute for Health and Care Excellence (NICE) guidelines.
On rati des experum quiam quunt offic testotaturit rem harciis int, simusam quaero beatibus ium eatempos.
Thursday’s thoracic aortic consensus sessions close off the aortic programme with a debate on the conservative management of aortic intramural haematoma, featuring Michel Makaroun (University of Pittsburgh, Pittsburgh, USA) and Jean Panneton (Eastern Virginia Medical School, Norfolk, USA).
Treatment strategies for patients with chronic limb-threatening ischaemia (CLTI) have been firmly in the spotlight following the release of the first results from BEST-CLI in November 2022. CX will provide a platform to move the conversation forward, with firstto-podium results of the BASIL 2 randomised trial—comparing a ‘vein bypass first’ or a ‘best endovascular first’ revascularisation strategy—forming the centrepiece of a peripheral trial consensus update, taking place on the first day of the CX symposium.
During the session, BASIL 2 chief investigator Andrew Bradbury (University of Birmingham, Birmingham, UK) will deliver the first results from the trial, in a session that also sees participation from BEST-CLI investigators Matthew Menard (Brigham and Women’s Hospital, Boston, USA)—providing an update on the trial—and Alik Farber (Boston Medical Center, Boston, USA), presenting BEST-CLI quality-of-life data.
In-person attendees at CX 2023 will have the opportunity to attend a hands-on aortic workshop, led by Alexander Zimmermann (University of Zürich, Zürich, Switzerland), looking at the full range of fenestrated and branched endografts, including devices that are physician-modified. The workshop will provide attendees with the opportunity to expand their knowledge and test and improve their skills in a practical session. Offering a deep dive into physician-modified stent grafts, this interactive demonstration will explore the theory behind the history and indications of these devices, and the techniques employed to create fenestrations and branches.

Issue89 | February 2023 25 CX 2023
Scan here to view SIGN UP NOW
We are all excited to see the latest advances in the arch and thoracoabdominal aorta.” Gustavo Oderich
CX 2023 will return to Hilton London Metropole
Industry News
Photon-counting CT enables lower contrast media for aortic imaging
Photon-counting detector computed tomography (CT) reduces the amount of contrast needed for CT angiography (CTA) while maintaining image quality, according to a new study published in Radiology: Cardiothoracic Imaging, a journal of the Radiological Society of North America (RSNA).
The portion of the aorta that passes through the chest and abdomen is prone to aneurysms. Risk increases with age. Doctors use CTA with contrast media to examine this region of the artery. While the iodinated contrast media used in these exams is considered very safe, there is a higher risk of adverse reactions in patients with kidney disease, or nephropathy.
“Many patients undergoing CTA of the aorta are elderly, and some may suffer from a certain degree of nephropathy,” said senior author Hatem Alkadhi from the Department of Diagnostic and Interventional Radiology at University Hospital Zürich in Zürich, Switzerland. “Thus, they might be at risk for a further reduction of their kidney function due to contrast media administration.”
Using less contrast media is also good for the environment, as iodine breakdown products have harmful environmental effects. In addition, the supply of contrast media has suffered from shortages due to COVID-19-related disruptions in the pharmaceutical supply chain.
Photon-counting detector CT is a new technology that can acquire high-quality images at lower contrast media volume than conventional CT scanners that rely on energy-integrating detectors. It also offers diagnostic quality images at lower radiation dose than those of conventional CT.
Alkadhi and University Hospital
Zurich colleague Kai Higashigaito led a study that looked at a low-volume contrast media protocol with photoncounting detector CT for CTA of the aorta in the chest and abdomen.
The study included 100 people, mean age 75. Patients underwent CTA with photon-counting detector CT of the aorta in the chest and abdomen. The patients had received a previous CTA with conventional CT at equal radiation doses.
Photon-counting CT had a higher contrast-to-noise ratio, a key measure of image quality, which translates to a lowvolume contrast media protocol. Contrast media volume was reduced by 25%.
Two independent readers rated the image quality of photon-counting CT as higher than that of conventional CT at an equal radiation dose.
“We showed that the improved image quality of CTA with photon-counting detector CT systems can be used to reduce the amount of administered
contrast media to the patients, without reducing the diagnostic yield of the examination,” Alkadhi said. “Image quality remained at the same level as that of previous CT angiography examinations in the same patients using a conventional CT, despite the fact that we reduced the contrast media volume.”
ESVS AAA guidelines alert recommends “enhanced surveillance” in patients treated with Nellix device In a newly released “focused update” to their 2019 recommendations, the European Society for Vascular Surgery (ESVS) abdominal aortic aneurysm (AAA) guidelines writing committee has published advice on the surveillance and management of patients treated with the Nellix endovascular aneurysm sealing (EVAS) system (Endologix).
Delcath Systems announces updated results from CHOPIN phase 1b trial
Delcath Systems has shared in a press release the publication of updated results from the CHOPIN phase 1b trial conducted at Leiden University Medical Center (Leiden, The Netherlands) on the use of the Delcath Chemosat hepatic delivery system with melphalan (Chemosat) in combination with the immune checkpoint inhibitors (ICI) ipilimumab and nivolumab to treat patients with metastatic uveal melanoma with liver metastases.
The publication is titled ‘Combining melphalan percutaneous hepatic perfusion with ipilimumab plus nivolumab in advanced uveal melanoma: First safety and efficacy data from the phase 1b part of the CHOPIN trial’ and was published in CardioVascular Interventional Radiology (CVIR).
The goal of the CHOPIN trial is to study the safety and potential synergistic effects of systemic ICI therapy ipilimumab plus nivolumab (IPI+NIVO) when combined with Delcath’s proprietary liver-targeted percutaneous hepatic perfusion (PHP) treatment in metastatic uveal melanoma patients. The phase 1b portion of the trial enrolled seven patients, each of whom were treated with two courses of PHP (melphalan 3mg/kg, max. 220 mg per cycle) combined with four courses IPI+NIVO escalating the dosing from 1mg/kg each IPI+NIVO (cohort 1) to IPI 1mg/kg+NIVO 3mg/kg (cohort 2).
via mobile application. We have been using the Viz software for the last several months and have seen improvements in patient care across our institution,” said Philip Batista (Cooper University Health Care, Camden, USA).
Viz.ai claims that the Viz Vascular Suite uses AI to automatically analyse an array of imaging modalities, including computerised tomography (CT), electrocardiogram (ECG), and more for suspected vascular diseases. If a suspected pathology is found, the app automatically alerts and displays high-fidelity patient scans on providers’ mobile devices. Clinicians can use Viz Vascular Suite to remotely coordinate vascular pathology care within a hospital system’s hub and spoke network and enable synchronous,communication among specialists.
Cardiovascular Systems enrols first patient in Japan for KAIZEN clinical study
Cardiovascular Systems Inc (CSI) recently announced initiation of the KAIZEN clinical study of its Diamondback 360 peripheral orbital atherectomy system (OAS) to treat calcified plaque in patients with peripheral arterial disease (PAD).

The first KAIZEN patient was enrolled by Tatsuya Nakama at Tokyo
The committee advises that all patients in whom a Nellix device has been implanted “should be identified, properly informed and enrolled in enhanced surveillance.” If device failure is detected, it states that “early elective device explant should be considered in surgically fit patients”.
The alert, authored by Jon Boyle (Cambridge University Hospitals NHS Trust and University of Cambridge, Cambridge, UK) et al, was published online ahead of print in the European Journal of Vascular and Endovascular Surgery (EJVES).
Boyle and colleagues note that they performed a scoping review of risk for late serious aortic-related adverse events in patients treated with EVAS for AAA based on a literature search in PubMed up to 7 December 2022. Following synthesis of the available evidence, the writing committee agreed on recommendations graded according to the European Society of Cardiology (ESC) grading system.
“EVAS has a very high incidence of late endograft migration resulting in proximal type 1 endoleak with risk of rupture, requiring open conversion with device implant,” the authors write, detailing their key finding from the review. They add that the reported mortality for elective explantation varies between 0% and 14%, while acute conversion for rupture has a “very dismal prognosis” with 67–75% mortality.
The determination of a safe and effective dose was a primary goal of the phase 1b portion of the CHOPIN trial. Grade 1/2 adverse events were seen in all patients and 71.4% experienced grade 3/4 toxicities. In this phase 1b dose-escalation study combining M-PHP with IPI+NIVO, the safe treatment dose was established at IPI 1mg/kg and NIVO 3mg/kg. The phase 2 part of the CHOPIN study will provide more information on both hepatic and systemic toxicity associated with the combination therapy.
The rationale for combining ICI therapy with M-PHP in metastatic uveal melanoma is based on both uveal melanoma’s specific characteristics and the unique immunomodulatory role of the liver.
Viz.ai launches AI-powered
Viz Vascular Suite
Viz.ai has announced the launch of Viz Vascular Suite—artificial intelligence (AI)-powered software enabling vascular care teams to automatically detect and triage care for suspected pulmonary embolism, right heart strain, aortic dissection, and abdominal aortic aneurysm (AAA). The company submitted a new 510(k) application to the US Food and Drug Administration (FDA) for the AAA algorithm, a press release notes.
“When Viz identifies an abnormal scan, it quickly notifies the appropriate specialists regardless of their location, facilitating seamless communication
Bay Urayasu Ichikawa Medical Center (Urayasu, Japan). Nakama said: “The Diamondback 360 peripheral OAS offered both effective treatment and ease of use. I observed significant vessel compliance change, permitting satisfactory balloon expansion at low pressure.”
CSI notes that the Diamondback 360 peripheral OAS is a minimally invasive, single-use, catheter-based device designed to differentiate between diseased plaque and healthy arterial tissue. The OAS orbiting crown reduces and modifies calcified plaque while preserving the healthy vessel wall to restore blood flow, the company claims.
KAIZEN is a prospective, singlearm, multicentre study led by Hiroyoshi Yokoi (Fukuoka Sanno Hospital, Fukuoka, Japan), and is designed to evaluate the safety and efficacy of CSI’s Diamondback 360 peripheral OAS in the treatment of de novo symptomatic calcified occlusive atherosclerotic lesions in the superficial femoral artery and/or popliteal artery. According to CSI, OAS has demonstrated safety and efficacy in the US population and this study is designed to confirm this in Japan.

26 Market Watch February 2023 | Issue89
Illustration of Nellix implantation
Diamondback 360 system
“All-purpose” drainage catheter outperforms rest in first-of-kind comparative bench test
Danial Jilani is an interventional radiologist based at Northwestern Medicine Palos Hospital (Chicago, USA), who uses the SKATER™ drainage catheter (Argon Medical) as his “go-to” catheter for a range of both “bread and butter” and more complex interventional radiology (IR) procedures. He spoke to Interventional News about why SKATER works so well for him and his patients, and the findings of a recent bench test that compared SKATER to other percutaneous drainage catheters on the market.
For Jilani, SKATER’s “all-purpose” suitability means he can use it for pneumothoraxes, chest tubes, pleural effusions, nephrostomy and biliary procedures. Moreover, SKATER works for sclerotherapy too. Ethyl alcohol and doxycycline used in this type of treatment can “break certain catheters down”, Jilani explains, however SKATER “can tolerate both these agents—having the luxury to handle both is one of the advantages of this catheter.”

There are multiple “subtle differences” that set SKATER apart, Jilani goes on to tell Interventional News. The recent findings of a bench test1, which compared a range of percutaneous drainage catheters on the points of kink resistance, flow rate and ‘pushability’ shed light on these, he reports. Among those tested, SKATER, made of a blend of durable polyurethane material, was found to be the most kinkresistant, in turn improving flow rate. Jilani notes that SKATER demonstrated a high flow rate during the bench test, with 8Fr catheters and mini pigtail catheter loops—in spite of their small size, which would typically reduce flow rate. The large, skived holes are one of the features that allow for maximal drainage.
more difficulty you have [overall] during the case, the more things can go wrong and the more time the patient spends on the table,” Jilani admits, suggesting a further reason why having a drainage catheter that can perform as SKATER did in the bench test, across all the aspects assessed, is beneficial.
Jilani goes into detail about how using SKATER can yield advantages for patients and their outcomes—“I am a firm believer that the faster you can drain an abscess, the less risk there is of recurrence.” Chronic abscesses can last for months, which, in turn, requires long-term drainage. However, with SKATER’s “large skived holes and fast flow rates”, catheter drainage is more efficient. “For the majority of patients with abscesses, we place these [SKATER] catheters and within a week, we can remove it, sometimes even faster,” Jilani relays.
Case study 1
Case study 2
Inadequate flow rate, such as seen in other types of catheters that kink more readily, means drainage takes longer, Jilani reiterates. “We follow our patients closely,” he asserts, meaning that he can say with some confidence that he has noticed “far fewer instances of kinking” compared to earlier in his career when he used other drainage catheters. Longer drainage time can lead to occlusion from bacteria and fibrin build-up and more catheter exchanges, prolonging the overall time the patient has a catheter in. Even without complications, Jilani explains that having a drainage catheter in for a long time is “very inconvenient” for patients—“they are attached to a bag […] which can make day-to-day activities hard.” The improved patient outcomes—faster drainage and therefore fewer complications related to chronic abscesses and catheterisation—that SKATER facilitates, reduce healthcare costs, Jilani is also keen to acknowledge.
To round off the discussion, Jilani summarises what it is about SKATER that makes it his “go-to” drainage catheter. “The subtle differences make an impact,” he states, referring back to SKATER’s high level of performance in the bench test: for kink resistance, flow rate and ‘pushability’. The evidence the test produced supports Jilani’s own clinical experience that “[the SKATER catheter] works well and is associated with better patient outcomes”, meaning he can continue to use it with confidence.
Case study 3
Jilani then speaks to the ‘intrinsic mechanisms’ of SKATER that, in the bench test, helped it fare more favourably than other drainage catheters. One was the “locking shoulder tip, which decreases buckling during insertion.” The hydrophilic coating also reduces friction as it is being inserted. The force required to insert the SKATER was 22% less than for some of the other catheters, and 70% less with the mini-loop catheter, Jilani relays, opining that this is an “underrated” feature of drainage catheters across the board.¹
Citing a further benefit of using SKATER, Jilani goes on to elucidate how the position markers on the SKATER are “especially helpful when doing a procedure under CT [computed tomography] guidance, as you are stepping in and out of the room and do not have your hands on the catheter the whole time”. Precision, as facilitated by these markers, is key as in a few millimetres “you can be in a structure you do not want to be in,” Jilani elaborates.
In addition, the low-profile locking system SKATER offers is, Jilani says, “so easy to use that I was able to teach myself [how to use it]”.
Providing anecdotal context for these positive data, Jilani then explains how inserting a drainage catheter into a cirrhotic liver can feel like “pushing up against a rock”, making buckling more likely. Hence, SKATER’s proven ‘pushability’ is advantageous. “The
Clinical presentation: Renal failure secondary to obstruction from bladder mass


Imaging findings: CT scan demonstrating severe hydronephrosis (top arrow) from malignant bladder mass (bottom arrows)
Clinical presentation: Shortness of breath, increasing oxygen requirement, chest pain
Imaging findings: Chest radiograph demonstrates large right pneumothorax
Clinical presentation: Right upper quadrant/epigastric pain, fever, elevated liver enzymes
Imaging findings: CT of gallbladder showing pericholecystic inflammatory changes, gallbladder wall thickening, and small gallstones consistent with acute cholecystitis
2
Imaging findings: Imageguided 8Fr percutaneous nephrostomy tube placement. Faint contrast opacifies the obstructed right kidney/renal collecting system

Imaging findings: Chest radiograph after placement of an 8Fr pigtail chest tube demonstrating resolution of pneumothorax


Imaging findings: Intraprocedural image related to 8Fr percutaneous transhepatic cholecystostomy drainage. Contrast opacifies obstructed gallbladder. Faint filling defects noted, consistent with gallstones

27 Advertorial Issue89 | February 2023 1. Data on File. Bench Testing Comparative Data Relative to Drainage Catheter Performance: An analysis of pigtail drainage catheter systems.
THIS ADVERTORIAL IS SPONSORED BY ARGON MEDICAL
tube placement for malignant obstruction Percutaneous drainage of infected bladder/acute cholecystitis
tube placement for spontaneous pneumothorax in patient with COPD
Nephrostomy
Chest
1 1 1
2
2
Danial Jilani
So easy to use that I was able to teach myself [how to use it].”

The BeBack crossing catheter: A “game-changer” in endovascular PAD practice
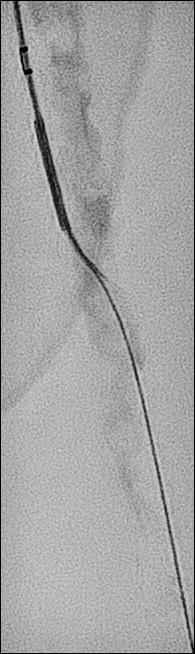


Crossing chronic total occlusion (CTO) lesions are challenging procedures. The BeBack crossing catheter—Bentley’s first product to be available in both Europe and the USA following the company’s acquisition of Upstream Peripheral Medical Technologies’ GoBack crossing catheter in September 2022—offers a new solution in this space.
Andrej Schmidt (University Hospital Leipzig, Leipzig, Germany), one of the first to use the catheter, shares his clinical experience with the BeBack, noting how it has been a “game-changer” in his endovascular peripheral arterial disease (PAD) practice.
What does your PAD practice look like, and what do you think are the most difficult aspects to overcome when treating CTO lesions?
The University Hospital Leipzig is one of the larger centres in Germany for the endovascular therapy of peripheral arterial occlusive disease, and we receive a lot of very complex cases, many of them failed in other hospitals. These are very often patients with severely calcified infrainguinal disease, but also complex iliac total occlusions.
Could you talk us through your first experience with the BeBack catheter?
We were struggling with a CTO of the common iliac artery in an abdominal aneurysm patient and failed to get through the CTO coming from retrograde, crossover and antegrade using an arm-access. Nothing worked, until eventually we used the BeBack catheter via the retrograde approach. With this, device passage through the CTO back into the aorta succeeded immediately. This experience was an eye-opener for us with regard to the success of the BeBack catheter.
Can the BeBack also be used as a support catheter?
In addition to its main purpose as a crossing catheter for complex, calcified CTOs, the BeBack indeed can be used as a support catheter since it is quite stable and stiff. This feature is very helpful in difficult total occlusions. It also can be used as a re-entry catheter, for example during a recanalisation of a CTO of the femoropopliteal segment. In the typical situation of being stuck subintimally, unable to pass the guidewire back into the true lumen distal to the CTO, the BeBack reliably helps to re-enter the distal patent segment of the artery.
How is the BeBack part of your recanalisation strategy?
This depends on the type of lesion and the problem encountered during the intervention. For example a typical femoropopliteal CTO is usually approached from antegrade. In case of inability to penetrate the
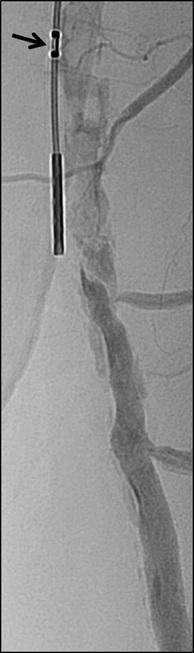
guidewire into the CTO, either due to dense fibrosis of the proximal cap or severe calcification, the BeBack catheter is used as a crossing device by pushing the adjustable needle just a little bit out of the tip of the 4Fr catheter. More frequent however is the situation that the guidewire passes the CTO subintimally and reconnection to the patent lumen distal to the CTO fails. As mentioned above, the BeBack catheter is then used as a re-entry-device by protruding the curved inner needle further out of the tip of the catheter. Different to other re-entry devices is that the BeBack is 4Fr compatible, instead of 6Fr, and introduction into calcified, tight lesions may be easier. Yet it can be used over a 0.018” guidewire, which is often the guidewire of choice in difficult CTOs, improving stability and success compared to 0.014” guidewires.
Another situation, where the BeBack is our device of choice, is a reocclusion of the femoropliteal segment with previous spot-stenting. Usually, the guidewire passes subintimally and entering into the occluded lumen of a stent within a longer CTO is not possible. In this situation the BeBack indeed reliably and fast allows the guidewire to enter into the proximal end of the occluded stent and to finalise the procedure successfully.

Below the knee we mainly use the 2.9Fr BeBack device, although also the 4Fr device is used in the proximal third of the calf for penetrating through calcific CTOs or for re-entering after subintimal guidewire passage. In some cases of severely calcified infrapopliteal lesions it can happen, that the GW passes easily intraluminally through a stenosis, but no balloon would follow due to the tightness and calcification of the lesion. In this situation, the 2.9Fr BeBack is inserted over the guidewire and, with the needle slightly protruded from the tip of the catheter, it is drilled into the problematic plaque. This technique, mimicking the Japanese technique of transcutaneous plaque-piercing, is very successful in facilitating introduction of balloons into the lesion and finalising the procedure.
Has the BeBack changed your practice and if so, how?
For many years, we and other centres have helped
Andrej Schmidt

to develop techniques to improve the success rate in difficult peripheral CTOs. The retrograde and bidirectional approach became standard in case of inability to pass a CTO from antegrade. However, in some cases it can be anticipated that establishing a retrograde access will be cumbersome or time consuming. In these cases we now prefer the BeBack to keep the intervention simple. Furthermore, a bidirectional recanalisation can be time consuming and may even fail. In this situation the BeBack helps to speed up and may even be the only way to finalise the procedure successfully.
During CTO recanalisations, do you think that sometimes physicians start too late to switch from one to another technique?
Not infrequently physicians try different guidewires and different catheters many times to pass a difficult CTO or to re-enter back into the patent distal lumen. This increases the risk of protruding the dissection distal to the CTO, destroying healthy segments which sometimes worsens the clinical situation. Furthermore radiation dose and the amount of contrast medium increases. Complications correlate with the duration of the procedure. The retrograde approach and the BeBack catheter are our technique and technology to shorten the procedure time.
How much time or how many attempts would you give yourself with conventional techniques before using the BeBack crossing catheter?
It depends on the complexity of the lesion. If we see a chance to be successful using an antegrade approach, we may proceed for some minutes. In very complex lesions, where it can be anticipated, that a conventional approach has a high risk to fail or may take time, we switch to the BeBack catheter within a minute.
If a colleague were to ask you about the BeBack, how would you describe it?
The BeBack is a reliable crossing and re-entry device. It is very slim (2.9Fr or 4Fr), yet very stable and can easily be used not only in larger diameter arteries like iliacs, but also in small arteries, even via a retrograde pedal access through a 2.9Fr sheath. Furthermore, it is possible to use it over a 0.014” and over a stable 0.018” guidewire, which is usually the wire of choice in more complex lesions. Due to its straightforward design, it is easy to position and reposition the device and control the depth and direction of the 360 degree adjustable needle from the tip of the catheter. It is helpful in quite a large variety of difficult situations and handling is easy to learn.
1. CTO of the left superficial femoral artery in a male patient suffering from severe claudication left calf.

2. After subintimal passage it was impossible to redirect the guidewire into the patent lumen distal to the CTO.
3. Positioning of the BeBack catheter to re-enter the guidewire. Arrow indicates an orientation-marker.
4. Marker appearing as a “C” indicates the direction of the needle, needle protruding maximally out of the BeBack-catheter.
5. A 0.018” guidewire passing into the patent distal lumen.
6. Result after stenting.
29 Advertorial Issue89 | February 2023 THIS ADVERTORIAL IS SPONSORED BY BENTLEY
1 2 3 4 5 6
Industry News
may be delivered through standard microcatheters (no complex mixing systems or special delivery catheters are necessary).
US Patent Office grants Notice of Allowance to IceCure for its cryogenic pump
IceCure Medical has shared in a press release that it has received a Notice of Allowance from the US Patent and Trademark Office for its patent application titled ‘Cryogen Pump’. The patent will be in effect until February 2040 and was recently granted in the European Union and allowed in Japan.
The cryogenic pump enables IceCure to bring to market a new generation of cryoablation systems with a small footprint for a wide range of clinical applications. Moreover, this pump expands IceCure’s portfolio of products with a broader range of thinner cryoprobes and catheters.
IceCure’s cryogenic pump is submersible in liquid nitrogen, works in a closed circuit, enables temperature control of the cryoprobe, improves the cooling rate during a procedure, and is designed to be used for multiple procedures or longer-duration procedures without the need to refill liquid nitrogen.
Fluidx Medical unveils new embolic for neurovascular use
Fluidx Medical has released information regarding the success of the IMPASS Embolic Device in in vivo research related to middle meningeal artery (MMA) embolizations which can be used to treat chronic subdural haematomas (CSDH) on the surface of the brain.
MMA embolization is a promising option to address CSDH and is particularly appealing for elderly patients and others who cannot undergo invasive surgical procedures. Hundreds of thousands of patients with CSDHs may benefit from this minimally invasive procedure. During the procedure, a small catheter is navigated into the MMA located within the dura mater which covers the brain, then an embolic material is delivered into the vessel to block arterial flow.
The Fluidx embolic platform is expected to bring simple preparation and controllable material delivery to a range of applications. The IMPASS device is packaged in a ready-to-use syringe, can be prepped tableside by the clinician in about 30 seconds, and
Rivermark Medical announces successful firstin-human use of its FloStent System for BPH Rivermark Medical has announced the successful first-in-human (FIH) use of its FloStent System as part of the company’s RAPID-1 FIH clinical study. The procedures were performed on 15 patients by principal investigator (PI) and urologist Ingrid Perscky Arravanti (Universidad de Panamá, Panama City, Panama) and proctored by Primary Clinical Advisor and urologist Dean Elterman (University of Toronto, Toronto, Canada) at the Pacifica Salud Hospital and the Panama Clinic in Panama City, Panama. The study evaluates the delivery, safety, and clinical effectiveness of the FloStent System for treating the symptoms of benign prostatic hyperplasia (BPH).
“This therapy is extremely
attractive as it offers patients instant improvement in BPH symptoms without the inconvenience and discomfort of traditional treatments,” stated Perscky Arravanti.
The FloStent System is intended to be the preferred first-line device treatment for BPH. The outpatient procedure involves the placement of a nitinol stent during a routine flexible cystoscopy with minimal patient recovery time and no need for a urethral catheter. The stent gently holds the prostatic urethra open to restore normal urinary function, preserve sexual function, and improve a patient’s overall quality of life. If desired, the device can be easily retrieved or repositioned after implantation.

IceCure releases preliminary data on ProSense cryoablation system

IceCure Medical, developer of the minimally-invasive ProSense system for cryoablation, which destroys tumours by freezing has announced interim results from the ICESECRET study for the treatment of patients with small renal masses (SRM) who cannot be offered kidney-preserving surgery. Data were presented at the Urological Association Conference (14 December, Eilat, Israel). The presentation, titled

“Renal Mass Cryoablation – Interim Analysis ICESECRET Study”, was delivered by Nasir Said (Bnai Zion Medical Center, Haifa, Israel).
According to the presentation, out of the 115 patients enrolled, 107 patients (112 lesions) returned for follow-up with a mean duration of 22.8 months and a range 12-60 months. In a subgroup of patients with no previous history of kidney cancer on the same kidney and a lesion ≤3cm, an 89.5% recurrence-free rate was observed at a mean follow-up time of 22.2 months when the procedure protocol was followed. The presentation concluded that, based on these interim results, cryoablation is safe and effective for treating renal masses under 5cm.
ICESECRET, a prospective, multicentre, single-arm clinical trial is being performed at Bnai-Zion Medical Center, Haifa, Israel, and Shamir Medical Center, Zerifin, Israel, and led by principal investigator Halahmi Sarel (Bnai Zion Medical Center, Haifa, Israel). The trial included 115 patients (138 lesions) with localised SRM of ≤5cm who were treated with ProSense cryoablation under computed tomography (CT) guidance. Full engulfment of the renal lesion, including a safety margin of 0.5cm was achieved in approximately 96% of the procedures where there was no anatomical limitation. Follow-up visits are performed at six weeks, six months, one year, and then annually up to five years after the procedure.
The company also announced its participation in the Society of Interventional Oncology (SIO) 2023 annual scientific meeting (19–23 January, Washington DC, USA).
Kenneth Tomkovich, diagnostic and interventional radiologist and director of breast imaging and interventions at CentraState Medical Center (Freehold, USA), is co-lead Investigator of IceCure’s ICE3 study for the treatment of small, low-risk, early-stage malignant breast tumours, and spoke at the meeting’s dedicated breast session.
Commenting on the growing interest in ProSense, Tomkovich stated: “We are seeing increasing interest from interventional radiologists and interventional oncologists, many of whom are practitioners who previously were not treating breast cancer patients. Their interest appears to be driven by the encouraging ICE3 interim results, which can drive the development of new patient markets for practitioners while making the minimally invasive procedure more accessible to patients.”
Penumbra launches Lightning Flash mechanical thrombectomy system
Penumbra announced the US Food and Drug Administration (FDA) clearance and launch of its Lightning Flash mechanical thrombectomy system.
“Lightning Flash features
Penumbra’s novel Lightning intelligent aspiration technology, now with dual clot detection algorithms,” the
company notes in a press release, adding that the system is designed to quickly remove large blood clots in the body, including venous thrombus and pulmonary emboli (PE).
The company details that Lightning
Flash, powered by the Penumbra Engine, uses both pressure and flowbased algorithms to detect blood clot and blood flow. The catheter is made with MaxID hypotube technology, allowing an inner diameter similar to large-bore catheters while maintaining a lower profile and a soft, atraumatic tip designed to help navigate the complex and delicate anatomy of the body. When used together, the device is intended to help remove blood clots quickly while minimising potential blood loss.
Lightning Flash is part of Penumbra’s Indigo system with Lightning portfolio. The company claims that Lightning products are the only computer-aided mechanical thrombectomy systems currently available in the USA and early data have shown improvement in clinical outcomes and quality of life.
Instylla announces initial enrolment in prospective, multicentre HALT Study
Instylla has announced the enrolment of the first patient in the HALT study for the treatment of peripheral arterial bleeds. The HALT study is a prospective, multicentre, singlearm study to evaluate the safety and effectiveness of the Embrace hydrogel embolic system (HES) for the embolization of arterial bleeding in solid organs and peripheral arteries.
“Embrace HES has demonstrated rapid and durable haemostasis in preclinical studies while reducing the risk of non-target embolization. I look forward to being involved with this innovative technology which will change the standard of care for future embolizations,” commented David Tahour, chief of vascular and interventional radiology at MemorialCare Long Beach Medical Center (Long Beach, USA).
The HALT study is led by Suvranu Ganguli, section chief, interventional radiology at Boston Medical Center (Boston, USA). Patients with upper gastrointestinal bleeds, kidney, liver, or spleen bleeds, spontaneous haematomas, or other peripheral arterial bleeds such as pelvic haemorrhage may be considered suitable for this study.
30 Market Watch February 2023 | Issue89
Lightning Flash system
ProSense device
Prostate anatomy without vs with BPH
Industry News
Funding secured to advance development of Pulse IVL system
AVS has announced that it raised US$20 million in Series B financing, which the company says will accelerate clinical trial timelines for its device for peripheral application in pulsatile intravascular lithotripsy (PIVL) cases, and advance development and preclinical work on a PIVL device for coronary cases.

BioStar Capital, the lead investor in the company’s Series A round, also led the Series B round.
AVS’ novel balloon-based platform, the Pulse IVL system, shatters calcium with pressure waves in frequent bursts and expands calcified arteries, all with a single device.
In September 2022, AVS announced enrolment, successful treatment, and positive 30-day follow-up data of the first patients in its POWER PAD I clinical trial, a first-in-human study. Jon George (University of Pennsylvania Health System, Philadelphia, USA) an interventional cardiologist and medical advisor to AVS, assisted in trial cases in the Dominican Republic.
“Our early trial results showed that we can successfully treat patients with multiple lesions using a single device,” said George. “We saw patients report a reduction in leg pain, increase in blood flow to the leg, and improvement in their ability to walk in our initial study. This is a patient population that needs easier access to advanced therapies and this platform has the potential to
provide that access.”
ReCor appoints Lara Barghout to lead commercialisation of Paradise renal denervation system
ReCor Medical and its parent company Otsuka Medical Devices have announced the appointment of Lara Barghout as president and chief executive officer of ReCor.

Barghout will lead the ReCor business strategy and organisation in the global commercialisation of ReCor’s Paradise ultrasound renal denervation system for the treatment of hypertension. She brings more than 20 years of experience leading global businesses in the medical device industry, joining ReCor from Siemens Healthineers, where she was senior vice president and head of advanced therapies, leading the image-guided therapy business in North America.
Prior to Siemens Healthineers, Barghout held several roles at Terumo Cardiovascular.
Barghout succeeds Andrew Weiss, who joined ReCor in 2013 and led ReCor in the development of the Paradise system from its early clinical trials, to the acquisition of ReCor by Otsuka in 2018, through the RADIANCE trial successes and the recent submission to the US Food and Drug Administration (FDA) for premarket approval.
The Paradise system bears the CE mark for the treatment of hypertension in Europe and is an investigational device in the USA and Japan.
GE Healthcare announces agreement to acquire interventional guidance innovator Imactis
guidance across an array of care areas. Imactis is a France-based company that was founded in 2009 by Stéphane Lavallée and Lionel Carrat, who created CT-Navigation, an ergonomic universal solution that provides stereotactic needle guidance, enabling intuitive pre-planning and continuous control throughout a wide range of procedures, from diagnosis to treatment.
While this innovation currently focuses on CT, GE Healthcare plans to expand the technology to its imageguided therapy (IGT) business to drive further growth.
The Imactis CT-Navigation, which
includes an integrated workstation, guidance software, and disposable procedure kit, is currently approved under the European Union’s Medical Devices Regulation (MDR) and has US Food and Drug Administration (FDA) clearance for use within the USA.
The completion of the transaction is subject to customary closing conditions, including review by the relevant governmental authorities in France. Financial details of the transaction have not been disclosed publicly.
Medtronic announces first enrolment in head-to-head randomised trial evaluating durability of EVAR
GORE Excluder AAA device family systems. The ADVANCE Trial is a global, postmarket, prospective, interventional, multicentre, randomised study that will enrol a minimum of 550 patients at up to 50 centres globally. Patients will be randomised to receive endovascular aneurysm repair (EVAR) with either the Endurant family or Excluder family grafts and will be followed at one month, one year, and annually through five years.
The first patient in the ADVANCE Trial was enrolled by the team led by Ray Workman at Novant Health Forsyth Medical Center (WinstonSalem, USA).
PRELUDE-BTK subanalysis suggests “advantage” of serration angioplasty Cagent Vascular has announced the results of a comparative subanalysis of the PRELUDE-below-the-knee (BTK) study versus plain balloon angioplasty. The study was led by Marianne Brodmann (Medical University of Graz, Graz, Austria).
Pulse IVL system
Conference calendar
4–9 March
Society of Interventional Radiology (SIR) 2023 Annual Scientific Meeting
Phoenix, USA sirmeeting.org
23–25 March
International Multidisciplinary Endovascular Forum
Florence, Italy imendoforum.com
16–19 April
European Conference on Interventional Oncology (ECIO) 2023
Stockholm, Sweden ecio.org/attend/ecio-2023
GE Healthcare announced it has entered into an agreement to acquire Imactis, an innovator in computed tomography (CT) interventional
25–27 April
Charing Cross (CX) Symposium 2023
London, UK cxsymposium.com
10–13 May
Venous Symposium 2023
New York, USA venous-symposium.com
18–21 May
Global Embolization Oncology Symposium Technologies (GEST) 2023 New York, USA annual.thegestgroup.com/GEST23
Medtronic has announced the first patient enrolment in the ADVANCE trial, a head-to-head randomised controlled trial of two leading aortic stent graft systems, the Medtronic Endurant II/IIs stent graft system and
This subanalysis compared their PRELUDE-BTK subset to a consecutive plain balloon angioplasty group. The Serranator-treated lesions had an average final residual stenosis of 17.2±8.2% vs. 33.7±15.7% in the plain balloon angioplasty group. This represents a 49% average improvement in final residual stenosis. In chronic total occlusions (CTO), there was a 62% improvement in final residual stenosis compared to the plain balloon angioplasty group. The average balloon inflation pressure was 5atm in the Serranator group vs. 9atm in the conventional balloon angioplasty group. Additionally, Serranator-treated arteries demonstrated 2.4 times greater calculated flow improvement vs. plain balloon angioplasty. These data, analysed by the same independent core lab, were recently published in the Journal of Endovascular Therapy Brodmann opined that “these results suggest an advantage for serration technology that should allow for superior wound healing and patient outcomes, while minimising the need for stent placement.”
1–3 June
International Conference on Complications in Interventional Radiology (ICCIR) 2023 Poertschach, Austria cirse.org/events/iccir
6–9 June
Leipzig Interventional Course (LINC) 2023
Leipzig, Germany leipzig-interventional-course.com
21–24 June
European Conference on Embolotherapy (ET) 2023
Valencia, Spain etconference.org/attend/et-2023
9–13 September
Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2023
Copenhagen, Denmark cirsecongress.cirse.org
8–10 November
British Society of Interventional Radiology (BSIR) 2023
Newport, UK bsir.org/meetings/bsir-asm-2023
31 Market Watch Issue89 | February 2023
Lara Barghout


