9 minute read
Mechanical thrombectomy: ClotTriever offers “extended window” for DVT treatment


During a recent webinar hosted by Inari Medical, a multidisciplinary group of physicians focused in on how to select eligible patients for the endovascular treatment of deep vein thrombosis (DVT). Three presenters highlighted why endovascular intervention should be considered in certain patients, the gaps in the guidelines, and the benefits of mechanical thrombectomy for improved DVT outcomes.
Vascular surgeon Marie Josee van Rijn (Erasmus MC Rotterdam, Rotterdam, The Netherlands) shared her opinion that endovascular intervention should be a “no-brainer” in patients who present with sensory or motor loss. In cases such as this, she explained: “The patient will lose their leg if you are not going to intervene.” Timely intervention in these patients, however, “can result in good outcomes within one to two hours,” the presenter emphasised.
Other patients might not present with sensory or motor loss, but still with severe symptoms, van Rijn said. At this point, the presenter referenced a patient who had leg swelling and pain, but whose leg was not immediately threatened. In this case, van Rijn outlined that early restoration of vein patency would result in symptom relief in the short term and that preserving valvular function would result in longerterm benefits. She added that—in order to try and prevent pulmonary embolism and limit the risk of recurrent DVT and post-thrombotic syndrome (PTS) in this patient—the clot should be removed from the vein in the legs.
The presenter then considered what the future of this patient, who was diagnosed with iliofemoral DVT, might look like. Van Rijn stated that up to 50% of patients with DVT are expected to develop PTS, with highest risk after iliofemoral DVT; around 90% of PTS patients are unable to work 10 years after iliofemoral DVT; and over 10% of PTS patients develop venous leg ulcers.
Van Rijn showed an image of what the patient’s leg might look like in a couple of years’ time, pointing out hyperpigmentation at the medial side of the ankle. “There has been an ulcer that has now healed but is very disabling,” the presenter explained. “We want to prevent [similar patients] from getting into a situation like this,” van Rijn stressed.
Conservative therapy, the presenter pointed out, often leaves residual clot behind, which can lead to adverse events and is associated with a higher risk of death. Van Rijn noted that, while all DVT patients at her centre receive compression therapy and anticoagulation, a multidisciplinary team discusses those patients with an iliofemoral DVT to decide whether endovascular treatment would be appropriate. This depends on the severity of symptoms, she explained, but also other patient factors including life expectancy, mobility and comorbidities, as well as the he said presently recommend treatments ranging from anticoagulation and/or compression to newer technologies like catheter-directed thrombolysis (CDT) and mechanical thrombectomy. This “broad range” of recommendations makes decision-making “very complex,” he remarked.
“evolution” of thrombus, Wilton stressed that the timing of DVT intervention is key. “Ideally, we want to treat [these patients] in the early, fibrin-rich phase [of thrombus development],” she said. Unfortunately, however, the speaker noted that a significant proportion of patients will present outside of this time period for a number of reasons, including “suboptimal referral pathways”.
The onset of clinical symptoms of DVT is often used to estimate thrombus composition—and thus age—in order to determine effective treatment, Wilton informed webinar viewers. However, clinical symptoms can vary “significantly,” she said, and are “not particularly good” at informing interventionists of thrombus age. Imaging, on the other hand, can be an important tool in determining the age of thrombus, Wilton stated.
Lichtenberg explained that the latest guideline statement on the topic comes from the Society of Interventional Radiology (SIR), which advocates a thrombus removal strategy. It does not, however, recommend mechanical thrombectomy, Lichtenberg told delegates. Instead, the society recommends CDT or pharmacomechanical therapy. The reason given is that the evidence on mechanical thrombectomy is lacking, the presenter noted.
According to Lichtenberg, however, the time is now to implement the data that are available on mechanical thrombectomy in routine practice, also pointing out that more data are in the pipeline.
The presenter mentioned that the European Society for Vascular Surgery (ESVS) 2021 guidelines on the management of venous thrombosis, in comparison to the update from SIR, state that early thrombus removal strategies should be considered in selected patients with symptomatic iliofemoral DVT.
Sharing some data of his own, Lichtenberg conveyed that he and colleagues recently published a systematic review and meta-analysis on endovascular mechanical thrombectomy versus thrombolysis in patients with iliofemoral DVT.
Among the results from this study, the researchers found a “highly significant difference” between CDT and mechanical thrombectomy for the endpoint of major bleeding complications. “This is the argument to stop CDT therapy and to change to mechanical thrombectomy,” Lichtenberg averred. “Efficacy was the same [between the two groups], but the major bleeding complication rate was significantly higher in the CDT arm. That means the safety endpoint is the argument to stop CDT therapy.”
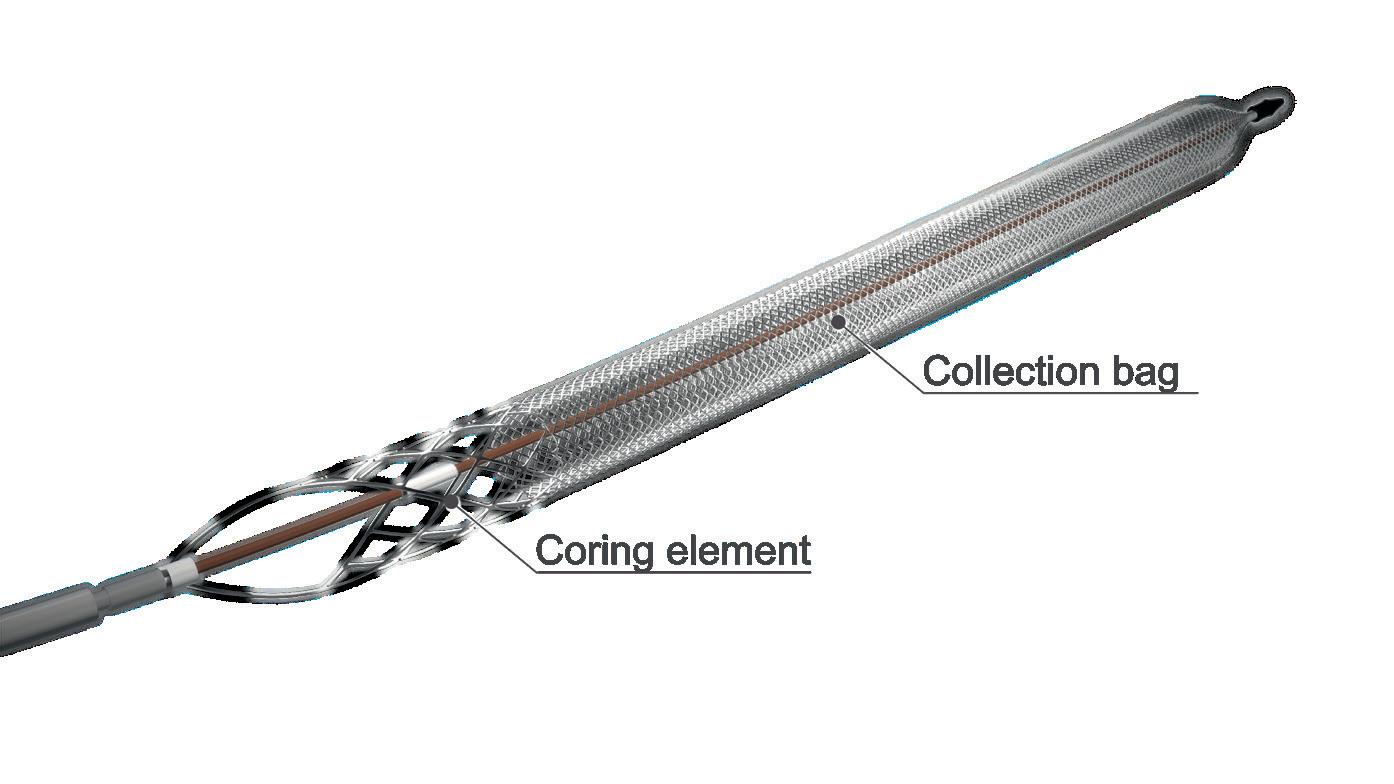
At this point, Wilton turned to the data on treatment options. One study the presenter cited showed that more than 70% of clot removed at the time of DVT treatment was resistant to lysis.1 Turning the audience’s attention to mechanical thrombectomy, Wilton referenced the CLOUT registry which, she summarised, demonstrated the safety and effectiveness of the ClotTriever (Inari Medical) across acute, subacute and chronic thrombus subgroups. “[The device] achieved successful thrombus removal in more than 90% of patients and with low devicerelated significant outcome problems,” she reported.2
“In summary,” Wilton relayed, “the age of thrombus is difficult to ascertain from history alone.” Imaging, she reiterated, is a helpful tool in determining the age of thrombus, and technique and device selection are “absolutely key”. She continued that the majority of venous clot is resistant to lysis at the time of treatment. The ClotTriever “is effective in acute, subacute and chronic thrombus as it can deal with clot of different ages, including in patients who may have had a previous DVT”.
“Time to update” guidelines
Finally, angiologist Michael Lichtenberg (Klinikum Hochsauerland, Arnsberg, Germany) addressed gaps and limitations in the DVT guidelines, which
Lichtenberg also referenced the CLOUT registry, which he said showed mechanical thrombectomy to be a “highly efficient option”. As a result, he expressed his belief that “it is time to update many of these guidelines now”. “We should implement mechanical thrombectomy as a first-line strategy for patients with acute iliofemoral DVT,” he argued in closing. In light of these results, van Rijn stressed that “we are not going to treat every single DVT invasively, but there is this option, and we should at least consider it and discuss it”.
Wilton remarked that the choice between conservative treatment and intervention is frequently a “difficult” one. While there are some patients “you are clearly going to treat,” she said, deciding on the best course of treatment for the “more borderline cases” is often a challenge. The ClotTriever, according to Wilton, has been “excellent” in this regard. She explained: “I think [the ClotTriever] has really enabled us to treat those patients in whom you are not sure whether intervention will significantly benefit them—is the right thing to do—but actually when you review them again in a week or so, you are still able to make a decision to intervene if appropriate. If they have gotten completely better after a week or two of conservative therapy, fine, they do not need any treatment. The ClotTriever enables us to have that extended window to offer intervention to appropriately selected patients.”
Handheld ECG device scoops CX 2023 Innovation
Showcase prize
Judges of the CX 2023 Dragon’s Den-style contest—the finale of the 2023 Charing Cross (CX) International Symposium (25–27 April, London, UK) Innovation Showcase programme— described the field of entrants to this year’s edition of the competition as the strongest line-up in its history.
THE JUDGING PANEL OF physician-innovators selected HeartEye, a Netherlandsbased developer of handheld electrocardiogram (ECG) devices, as the overall winner of the innovation prize, which comes with a £1,000 award. Honourable mention was given to four other entrants.

Peter Doevendans (UMC Utrecht, Utrecht, The Netherlands) gave an overview of the HeartEye technology in a short presentation entitled
‘ECG anytime, anywhere in 60 seconds’, describing it as a “digital transformation” for ECG acquisition. HeartEye is a pocket-sized device that can take clinical-standard ECG readings wirelessly, negating the need for a large, stationary ECG unit. The technology, which has been developed with the support of an Innovative Medical Devices Initiative (IMDI) grant from the Netherlands Organisation for Health Research and Development (ZonMw) is patented,
Detecting, predicting and preventing aortic ruptures with computational modelling
IN PHYSICS OF FLUIDS, BY American Institute of Physics (AIP) Publishing, researchers from the Indian Institute of Technology (BHU) Varanasi and Indian Institute of Technology Kanpur made a computational model of the cardiovascular system in order to predict early abdominal aortic aneurysm (AAA) rupture and monitor patients’ blood vessel conditions. The team investigated the effect of realistic, patient-specific AAA shapes on the haemodynamics of pulsatile Newtonian fluids in an aortofemoral artery under normal and diseased conditions.
Predicting the risk of AAA rupture involves a combination of imaging studies, such as ultrasound, computed tomography (CT) scans, magnetic resonance imaging (MRI), and haemodynamics, as well as clinical factors such as age, sex, smoking history, and family history of AAA.
“If an AAA is detected early, treatment options such as surgical repair or endovascular stent grafting are available to prevent rupture,” said the authors. “These treatments are both effective at reducing the risk of rupture and improving survival rates.” and could be marketed to healthcare providers or direct to consumers within two years, Doevendans noted.
Using image-based computational blood dynamics, the researchers mimicked specific health conditions and investigated various hemodynamic parameters. Their patient-specific geometric models of a human aortofemoral artery were constructed from 3D medical imaging data.
To solve the blood flow governing equations under the pulsating conditions caused by the heart’s beating, they used finite elementbased simulations. The team found that aneurysm size alters the blood flow velocity distribution. In addition, flow separation occurs during systolic deceleration, and the vortex begins to travel in the aneurysm sac. Among other complex dynamics, this may influence the blood circulation of lower extremities.
“In the future, such computational work will help in development of digital twins of the cardiovascular system,” said first author Sumit Kumar (BHU, Varanasi, India). Digital twins are virtual patient representations that receive real-time updates on a variety of data variables, an AIP press release explains.
“We have been doing this for a number of years, and this was the toughest by far,” said judging panellist Robert Mitchell (Park City, USA), before the announcement of HeartEye as the winner of the prize.
Euphrates Vascular, the developer a nano-scale endovascular system to address microvascular occlusion and no reflow, was among those singled out by the judges as being of particular interest. Presenter David Deaton (Medstar Georgetown University Hospital, Washington, DC, USA) told the judges that the Pulse NanoMed device extends the reach of current therapies, and has been given approval to begin a US Food and Drug Administration (FDA) investigational device exemption (IDE) trial in patients with acute ischaemic stroke.
Tilo Kölbel (University of Hamburg, Hamburg, Germany) introduced Mokita Medical, which has developed a technology to address air embolisation during procedures such as thoracic endovascular aneurysm repair (TEVAR) and transcatheter aortic valve implantation (TAVI), a cause of stroke and cognitive decline. The Mokita technology uses a gas-soluble fluid to eliminate air from devices, and is being developed into a disposable device that can be connected to the delivery system for a transcatheter procedure.
The company is planning a first-inman study for 2024, and anticipates commercialisation from 2026 onwards.
Mitchell praised Kölbel’s work in this area as being “really important and impactful”, and said that the entry had been one of the options strongly considered for the prize.
Another technology featured in the session included a non-invasive, wearable monitoring system for arteriovenous fistulas (AVFs), intended to aid early identification of failing AVFs. The innovation, presented by Ali Kordzadeh (Anglia Ruskin University, Braintree, UK) is worn like a wristwatch by patients to monitor venous outflow. Novel device coating materials were also exhibited, with Tony Simula (Mawson Lakes, Australia) detailing Bioinvisible, a drug-free polymer coating that could replace existing drug coatings in devices such as stents, vascular grafts and heart valves.
Amsterdam UMC leads an AI-powered hunt for high-risk vascular patients
A new study will focus on using artificial intelligence (AI) to predict the worsening of vascular disease in people with an aortic aneurysm or peripheral arterial disease (PAD), a press release reports. VASCUL-AID is a large European study led by Amsterdam UMC, and recently launched thanks to a Horizon grant worth €6.4 million.
KAK KHEE YEUNG (Amsterdam UMC, Amsterdam, The Netherlands) comments: “Our vessels are an important part of the cardiovascular system that keeps people alive. Once you have a vascular disorder such as an aneurysm, we see that the aggravation of these diseases also increases the chance that you will eventually die from another cardiovascular disease. This indicates to us that we also need to investigate how we can stop these conditions that seem to occur outside the heart, but that do affect the functioning of the cardiovascular system. At the moment it is not possible to predict the course of aneurysm or of PAD. People live in uncertainty about how their disease will develop and this results in many hospital visits and treatments. We would like to identify and isolate people with a high risk of their condition worsening from the large group in order to develop a more specific treatment plan. VASCULAID should make this possible.”
The press release states that VASCUL-AID will unite partners across Europe to develop infrastructure in which data from patients with aneurysms and PAD can be monitored. Six clinics across Europe, including Oxford University, will actively collect data from these patients. Using genetic data and imaging studies, as well as looking at protein profiles in blood and medication use. This will then be combined with existing databases and biobanks. Patients will also gather their own data. An app has been developed that will gather data from telephones and wearable device relating to, for example, daily activity and quality of life as well as their heart rate.







