
6 minute read
Endovascular treatment of aortoiliac aneurysms: What


about the hypogastric artery?
In this case report, Ozan Yazar and Lee Bouwman (Zuyderland Medical Center, Heerlen, The Netherlands) outline the successful endovascular treatment of an aortoiliac aneurysm in the hypogastric artery—an anatomy which they stress poses various technical challenges for iliac branch endografts.



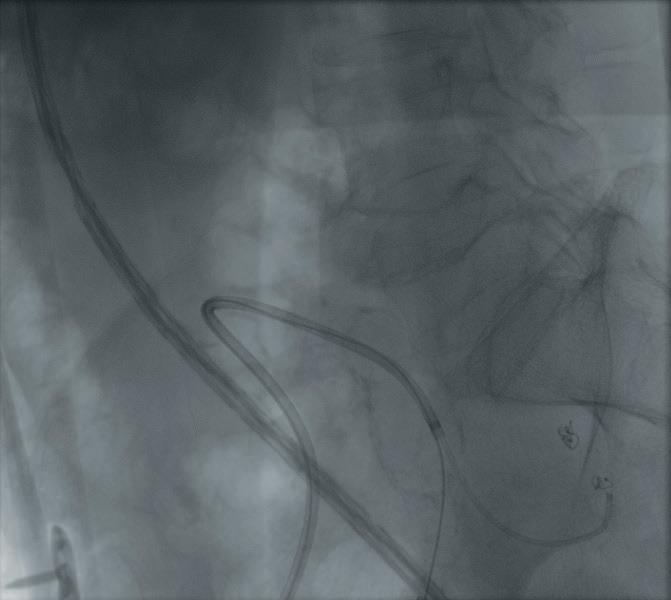
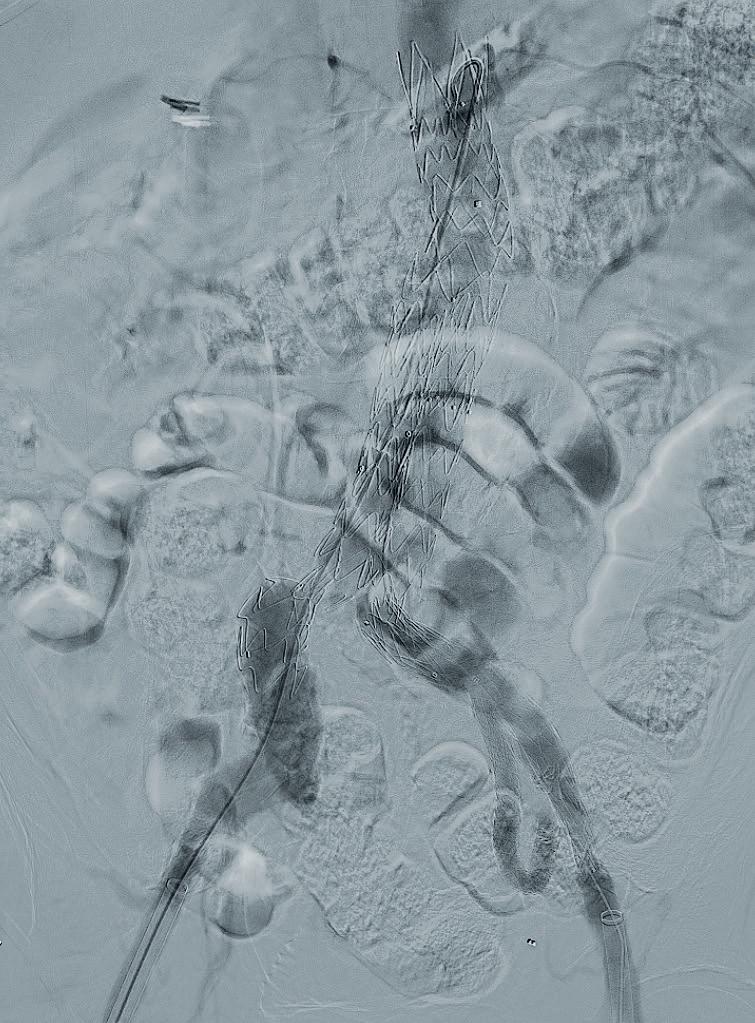
CONCOMITANT COMMON ILIAC artery (CIA) ectasia or aneurysm is revealed in up to 40% of patients with abdominal aortic aneurysm (AAA).1 Different techniques have been described to treat these patients with a diseased distal landing zone.2,3 One of the major disadvantages in placing stent grafts in these unfit zones is the hazard of type 1b endoleaks, resulting in higher reintervention rates.4 The endovascular repair of aortoiliac aneurysms has advanced to the use of iliac branch devices, resulting in patency of the hypogastric artery and a suitable landing zone in the external iliac artery (EIA). Clinical and technical success rates are high.5 Since 2014, the E-liac stent graft system (Artivion/Jotec) has been CE marked for the treatment of iliac artery aneurysms. This system shows promising results at 12-month follow-up in the PLIANT registry with a device-related reintervention rate of 5% and a primary hypogastric artery patency rate of 98%.6 In a systematic review, Dube et al describe the natural progression of CIA diameter following AAA repair. They show that the growth rate is higher in large CIA (1.5mm growth in 16mm iliac arteries vs. 2.7mm growth in 20mm iliac arteries).7 Our strategy in the treatment of aortoiliac aneurysm is to perform a regular endovascular aneurysm repair (EVAR) when the CIA is 14mm or less, a flared limb when the CIA is between 15 and 20mm and if the CIA is larger than 20mm to use an iliac branch device. However, we take several factors into consideration, such as the comorbidity and life expectancy of the patient, history of intestinal surgery or thoracic EVAR, chronic hypogastric occlusion, and the sexual and daily activity of the patient. With regards to the hypogastric artery, if the diameter is more than 10mm, we prefer a healthy landing zone more distally in the superior gluteal artery (SGA). We describe the case of a 70-year-old male patient who was admitted to our outpatient clinic due to pneumonia. The chest computed tomography (CT) scan revealed a pneumonia as well as an AAA. An additional CT angiography (CTA) was performed to view the entire aorta. CTA showed an AAA of 71mm, bilateral CIA aneurysms of 23mm and a left hypogastric aneurysm of 39mm (Figures 1a, 1b and 1c). His relevant medical history included hypertension and chronic pulmonary disease. The patient was asymptomatic, however, due to the large AAA we decided to treat the patient within four weeks as per society guidelines. We planned a percutaneous endovascular treatment (EVAR plus left iliac branch device plus right flared limb) under local anaesthesia. Due to the large hypogastric aneurysm we decided to land in the SGA (Figure 2). We first performed a coiling embolisation of the side branch to create a safe distal sealing zone (Figure 3a) Then we deployed the iliac branch device the traditional way. Three balloon-expandable covered stents (E-ventus; Artivion/Jotec) were placed in the SGA (Figure 3b). Further deployment of the iliac branch device was performed and subsequently the E-tegra (Artivion/Jotec) EVAR procedure was performed. The completion angiography showed patency of the renal arteries, bilateral EIA, right hypogastric artery and left SGA without any endoleak (Figures 4a and 4b)
References
1. Armon MP, Wenham PW, Whitaker SC, et al. Common iliac artery aneurysms in patients with abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 1998;15(3):255–7.
2. McDonnell CO, Semmens JB, Allen YB, et al. Large iliac arteries: a high-risk group for endovascular aortic aneurysm repair. J Endovasc Ther. 2007;14(5):625–9.
Lee Bouwman
3. Kalteis M, Gangl O, Huber F, et al. Clinical impact of hypogastric artery occlusion in endovascular aneurysm repair. Vascular. 2015;23(6):575–9.
4. Duvnjak S, Balezantis T. Endovascular treatment of aortoiliac aneurysms with a flared iliac limb. Int J Angiol. 2019;28(1):57–63.


5. Kouvelos GN, Katsargyris A, Antoniou GA, et al. Outcome after interruption or preservation of internal iliac artery flow during endovascular repair of abdominal aortoiliac aneurysms. Eur J Vasc Endovasc Surg. 2016;52(5):621–634.
6. Brunkwall JS, Vaquero-Puerta C, Heckenkamp J, et al. Prospective study of the iliac branch device E-liac in patients with common iliac artery aneurysms: 12-month results. Eur J Vasc Endovasc Surg. 2019;58(6):831–838.
7. Dube B, Ünlü C, de Vries JPPM. Fate of enlarged iliac arteries after endovascular or open abdominal aortic aneurysm repair. J Endovasc Ther 2016 Oct;23(5):803–8.
Lee Bouwman is a vascular and endovascular surgeon at the Zuyderland Medical Center in Heerlen, The Netherlands
Ozan Yazar is a vascular and endovascular surgeon at the Zuyderland Medical Center.
Figure 3a. Coiling of a branch of the SGA
Figure 3b. Covered stents (E-ventus)
Figure 4a. Completion angiography
Figure 4b. Patency of the left SGA
Bilateral iliac side branch device implantation for complex aneurysms
Theodosios Bisdas (Athens Medical Center, Athens, Greece) shares a case report highlighting the benefits of the E-liac and E-tegra devices (Artivion/Jotec) for the treatment of complex abdominal aortoiliac and hypogastric artery aneurysms.
I PRESENT THE CASE OF A 72-year-old male undergoing total endovascular repair of a complex bilateral aortoiliac abdominal aortic aneurysm (AAA). The most relevant comorbidities of the patient included arterial hypertension, severe coronary artery disease, previous coronary artery bypass grafting with occluded venous bypasses, hypercholesterolaemia, chronic obstructive pulmonary disease and ongoing smoking. The aneurysm was found in the framework of a routine duplex ultrasound due to an asymptomatic pulsatile mass in the abdomen. The computed tomography angiography (CTA) revealed an extensive aortoiliac AAA with maximum diameter of the infrarenal aorta of 7cm and of the right and left common iliac arteries of 5cm and 6cm, respectively. In addition, a 4cm aneurysm of both hypogastric arteries was observed (Figure 1).

Considering the fragile cardiovascular profile of the patient and the risk of an open surgical repair, the patient was scheduled for an endovascular repair. The main technical challenges were the angulated and short proximal neck, the absence of thrombus in the large aneurysm sac, which would complicate the cannulation of the contralateral gate, the large aneurysms of the iliac bifurcation and finally the embolisation of the branches of the aneurysmatic hypogastric arteries in order to prevent future type 2 endoleak.

The E-tegra bifurcated endograft and the E-liac side-branched device were selected as the devices of choice for this case. After percutaneous access from both common femoral arteries, the E-liac device was placed first in the left iliac bifurcation. A contralateral 12Fr sheath was used to gain access in the hypogastric arteries through the side branch. An 8Fr, 90cm sheath was inserted via a Rosenwire (Cook Medical) into the left gluteal artery. A second puncture of the 8Fr sheath was used to insert a Berenstein catheter (Merit Medical) into the aneurysm sac of the hypogastric artery. A 2.7Fr Progreat microcatheter (Terumo Europe) was used to navigate the integrated wire into the patent branches of the sac in order to embolise them. The embolisation was done using standard Ruby coils (Penumbra). After the embolisation, the bridging between the gluteal artery and the iliac side branch was performed by implanting an 8mm E-ventus balloon-expandable stent (Artivion/Jotec) and a 100mm Viabahn endograft (W L Gore). The same procedure was followed for the contralateral iliac and hypogastric artery aneurysm. The AAA was finally excluded via implantation of the bifurcated main body and connecting it to both iliac side branch devices with the iliac limbs. The final angiogram revealed a successful exclusion of this complex aortobi-iliac aneurysm (Figure 3) The main challenges of such “large” aortoiliac aneurysms with concomitant hypogastric artery aneurysm consist of: (1) the stability of the iliac side branch device during the cannulation of the side branch and the delivery of the different endografts, (2) the challenging cannulation and embolisation of the side branches of the aneurysmatic hypogastric artery and (3) the stability of the stents between the target branch of the hypogastric artery and the side branch of the iliac side-branched device. Both the E-liac device and the E-tegra bifurcated endograft remain user-friendly and trusted devices for such challenging anatomies with proved efficacy.1 The implantation and the behaviour of the endograft as concerns flexibility and stability were excellent in our case. The embolisation of the branches was done using the Progreat microcatheter with the integrated guidewire. In order to facilitate the navigation of the microcatheter and to avoid any accidental closure of the target artery, we prefer to first cannulate the gluteal artery and to secure it via a Rosenwire and an 8Fr sheath and then to double puncture the sheath for the delivery of the microcatheter in the rest of the branches. Finally, the bridging between the iliac side branch and the gluteal artery was performed via the combination of balloon-expandable stent grafts and the self-expandable Viabahn endograft. This technique has been reported to be effective and durable for concomitant hypogastric aneurysms.2

References
1. Mylonas SN, Ruemenapf G, Schelzig H, et al. A multicenter 12-month experience with a new iliac side-branched device for revascularization of hypogastric arteries. J Vasc Surg 2016;64(6):1652–1659.
2. Bosiers MJ, Panuccio G, Bisdas T, et al. Longer bridging stent grafts in iliac branch endografting does not worsen outcome and expands its applicability, even in concomitant diseased hypogastric arteries. J Cardiovasc Surg (Tor) 2020;61(2):191–195.
Theodosios Bisdas is head of the Clinic of Vascular Surgery at Athens Medical Center in Athens, Greece.


