4 minute read
Case report IVL: A paradigm shift in the treatment of common femoral artery lesions


Raphaël Coscas (Ambroise Paré Hospital, AP-HP and Paris-Saclay University, Paris, France) illustrates the use and benefits of Shockwave Intravascular Lithotripsy (IVL; Shockwave Medical) in a common femoral artery (CFA) case. Owing in large part to the therapy’s ability to modify vessel compliance, Coscas believes endovascular repair of the CFA using IVL as the main preparation tool for calcified lesions “should be discussed routinely”.

ENDOVASCULAR REPAIR OF THE CFA is subject to controversy. Open surgery remains considered the ‘gold standard’ due to its excellent long-term patency,1 but early local complications (wound dehiscence, infection, crural nerve injuries) are frequent drawbacks that can impair the comfort and the walking capability of the patient for several weeks.2 Endovascular repair is a compelling approach in CFA lesions, especially when they do not involve the bifurcation. The French randomised TECCO trial demonstrated that endovascular repair was associated with fewer early complications and similar patency rates at 24 months when compared to open surgery.3 However, many physicians are still reluctant to use endovascular repair for CFA lesions since these lesions are generally highly calcified and endovascular repair is fraught with technical failures. Implanting a stent in the CFA is possible but it could create challenges for future femoral access. These points highlight the need for specific preparation tools for CFA lesions.
Over several years, endovascular repair of the CFA in an outpatient setting has become a first-line approach in our centre. IVL totally changed our perception of endovascular repair of the CFA as it allows better preparation of heavily calcified lesions. IVL improves the luminal gain and decreases the rates of dissections and stent placement as demonstrated by the Disrupt PAD III trial.4
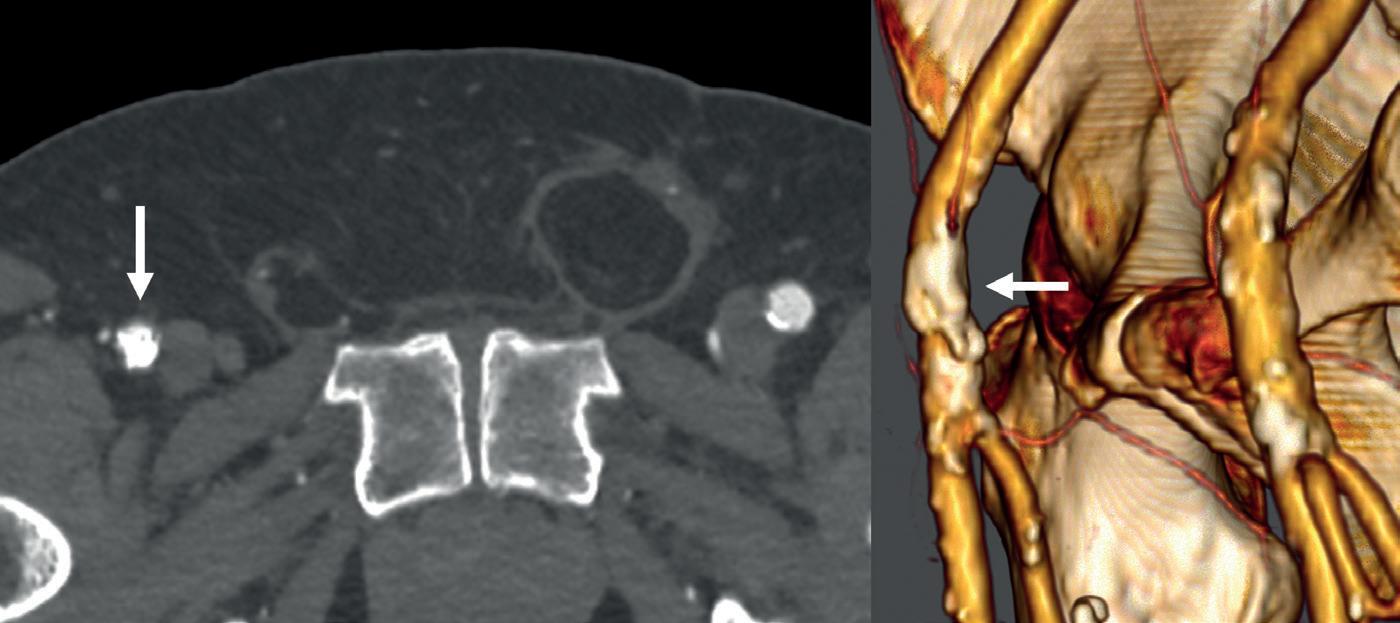
Here we present the case of an 84-year- old man with severe disabling claudication of the right lower limb due to a highly calcified stenosis of the CFA. He has no major comorbidities and lives alone at home. Duplex scan evaluation revealed a tight stenosis of the common femoral artery with a heavily calcified circumferential lesion and a peak systolic velocity of 380cm/s. The duplex waveform was monophasic below the lesion. A non-significant iliac stenosis and severe lesions of the distal arteries were also evident. A computed tomography angiography (CTA) scan confirmed a highly calcified stenosis of the CFA sparing the bifurcation (Figure 1). The CFA diameter was measured as 7.4mm. The contralateral CFA presented as calcified but not stenosed and thus suitable for puncture. An endovascular repair of the CFA using an IVL preparation was decided as our preferred strategy.
The procedure was scheduled as a sameday discharge intervention and performed under local anaesthesia with sedation in an operating room using standard fluoroscopic guidance with a mobile C-arm. A 7Fr 45cm sheath was brought from the contralateral femoral artery with a crossover technique. The initial angiography showed the lesion, which appeared to be a near occlusion of the CFA (Figure 2), with a low flow in the profunda femoris artery (PFA). A 0.014” wire was positioned antegrade in the PFA due to lesion morphology to preserve the bifurcation. An 8x60mm M5+ IVL catheter

(Shockwave Medical) was selected to prepare the lesion. The use of a slightly oversized balloon allows a perfect apposition to the lesion to deliver the sonic pressure waves. Care was given to deliver the pulses using an overlap strategy to bring the sonic waves at different levels of the lesion to fracture the plaque (Figure 3). The fact that the balloon is inflated at a low pressure (four atmospheres) allowed for inflation in the distal portion of the PFA without having the fear of damaging it. A total of 300 pulses was delivered on the lesion to optimise the effect of IVL. The postpreparation angiography was performed with two different incidences (anterior and oblique view) showing a successful preparation. The luminal gain was satisfactory without significant residual stenosis or dissection. An 8x60mm drug-coated balloon was inflated at eight atmospheres for three minutes as the anti-restenotic therapy. Completion angiography showed a successful procedure with good flow in the CFA, the PFA and the superficial femoral artery (SFA; Figure 4). The patient was discharged home the same day with dual antiplatelet therapy. At six-month follow-up, the patient presented as healthy and could walk without any limitation. Duplex scan evaluation confirmed a satisfactory mid-term result of the procedure without any significant restenosis and a triphasic flow at the level of and below the lesion.


This case illustrates the use and benefits of IVL in CFA lesions. The availability of an 8mm M5+ facilitates optimal sizing for most CFA lesions. IVL therapy expands the endovascular treatment opportunities for CFA lesions. It modifies the compliance of the vessel by creating microfractures in the plaque, allowing for a controlled expansion with limited complications. In cases where a stent may finally be needed, this ‘leave nothing behind’ approach is usually viable, and maintains options for future procedures. Sufficient preparation using IVL allows for better stent deployment and apposition. Recent data from various centres and registries support the use of IVL in CFA lesions.5–7 In today’s practice, endovascular repair of the CFA using IVL as the main preparation tool for calcified lesions should be discussed routinely.
References
1. Aboyans V, Ricco JB, Bartelink MEL, et al. Editor's choice - 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(3):305–68.
2. Halpin D, Erben Y, Jayasuriya S, et al. Management of isolated atherosclerotic stenosis of the common femoral artery: a review of the literature. Vasc Endovascular Surg 2017;51(4):220–7.
3. Goueffic Y, Della Schiava N, Thaveau F, et al. Stenting or surgery for de novo common femoral artery stenosis. JACC Cardiovasc Interv. 2017;10(13):1344–54.
4. Tepe G, Brodmann M, Werner M, et al. Intravascular lithotripsy for peripheral artery calcification: 30-day outcomes from the randomized Disrupt PAD III trial. JACC Cardiovasc Interv. 2021;14(12):1352–61.
5. Colacchio EC, Salcuni M, Gasparre A, et al. Midterm results of intravascular lithotripsy for severely calcified common femoral artery occlusive disease: a single-center experience. J Endovasc Ther. 2022:15266028221105188.
6. Baig M, Kwok M, Aldairi A, et al. Endovascular intravascular lithotripsy in the treatment of calcific common femoral artery disease: a case series with an 18-month follow-up. Cardiovasc Revasc Med. 2022;43:80–4.
7. Brodmann M, Schwindt A, Argyriou A, Gammon R. Safety and feasibility of intravascular lithotripsy for treatment of common femoral artery stenoses. J Endovasc Ther. 2019;26(3):283–7.
Raphaël Coscas is a professor of vascular surgery at Ambroise Paré Hospital, AP-HP and Paris-Saclay University in Paris, France.



