7 minute read
Wide awake local anaesthetic no tourniquet (WALANT) hand surgery in a community setting eight years experience

Ashita Paul, Jagannath Chakravarthy, Martin White and John Harrison
The WALANT (Wide awake local anaesthetic no tourniquet) technique is an alternative to the regular surgical pathways, and bypasses the need for traditional theatre working with high staffing levels, and complex hospital pathways. The technique has been implemented for many distal extremity surgeries including in the hand, carpal tunnel decompression, Dupuytren’s contracture release, trigger finger release, ganglion excision, tendon repair and transfers, and distal radius fracture fixation.
The WALANT technique uses large volume local anaesthetic and local vasoconstrictive agents to attain a good field block and relatively bloodless surgical field. The technique avoids tourniquet pain, long fasting periods, and the need for peri-operative cannulation and monitoring. The patient can continue to be on their regular medicines and continue their day-to-day life without much disruption as the recovery time is often shorter than with traditional anaesthetic techniques. The technique is cost-effective and inexpensive in comparison with traditional surgery with studies suggesting similar outcomes and complication rates [1].
Inception
The Cumbria Hand Surgery Service was setup in 2016 as a collaboration between the Gateshead Health NHS Trust and Cumbria Medical Services. The aim was to provide a patient centred service outside of a hospital setting. Cumbria has a large geographical area with patients often travelling long distances, and significant pressures on local hospitals with long waiting times for assessment and treatment of hand conditions.
Referrals into the clinic are screened and limited to five conditions: Dupuytren’s contracture, trigger finger release, cubital tunnel syndrome, finger ganglia / swellings, and De Quervain’s tenosynovitis. The WALANT technique has a significant learning curve. We visited Probus Surgical Centre in Cornwall (www.probussurgicalcentre.co.uk ) who at that time were doing WALANT Dupuytren’s surgery. We then practised the technique on elective lists in the hospital setting and once confident started in the community.
The referrals received are from the local MSK service and direct from GPs. A good working relationship with these services, including the provision of education sessions, has meant high quality referrals to the clinic. A healthcare centre setting helps avoid a lot of the logistical issues seen with hospitals such as poor parking provision, confusing signage for departments and having to speak to several different staff as part of each visit who are often not directly part of the patient’s care. The clinic is based in South Carlisle with good access to major roads.
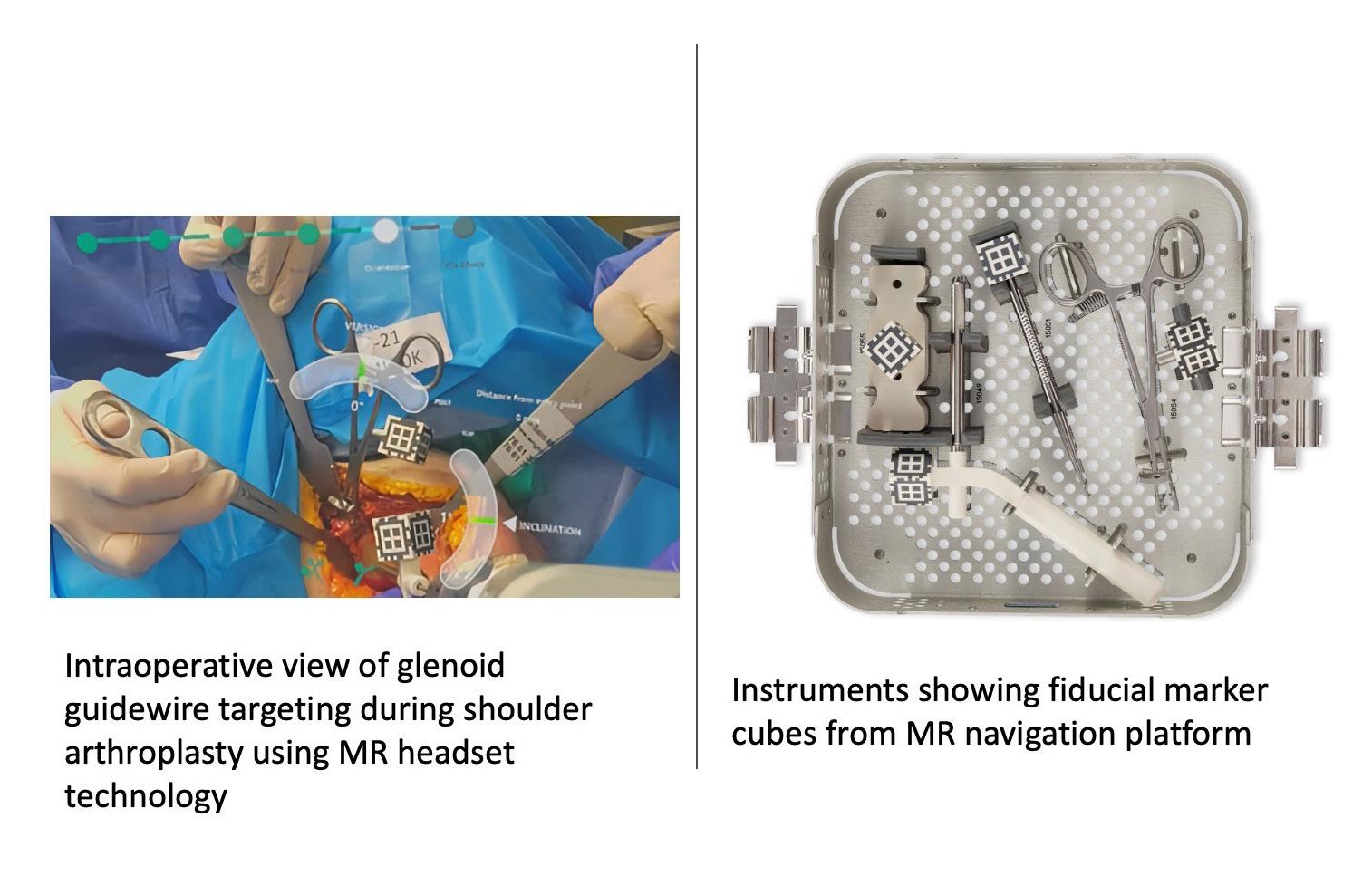
There are three staff (surgeon and two scrub), and patients meet the same team at each visit. We use 1% lignocaine and 1:200000 adrenaline +- 0.084% bicarbonate (1ml per 10mls LA). Antibiotics are not used. Single gloves are worn, with gowns only for more complex Dupuytren’s cases (Figure 1). There are 5-7 cases per list and the majority are Dupuytren’s surgeries.
The afternoon clinic will typically have 10 new patients at 10-minute intervals. Routine investigations such as X-ray and ultrasound imaging, and nerve conduction studies are usually requested as part of the screening of referrals, and available for the clinic visit. If a surgery is agreed, they are given a date before leaving the clinic, so they can plan work, etc. The peri-operative management of any anticoagulant medication is arranged, and any allergies confirmed.

More recently, guidelines have been produced by the British Society for Surgery of the Hand (BSSH) for wide-awake surgery [2]. We generally follow these apart from their recommendations for theatre staffing as our theatre staff admit and discharge patients. The increased interest in WALANT surgery has been at least partly due to COVID-19.
Present review
The hand surgery clinic currently runs two to three sessions every month with a theatre list in the morning followed by an afternoon clinic session. 1,691 new patients have been seen, and 1,046 operations performed (see Table 1).

In 2016, we had a conversion rate of 59.85%, which has now increased to 76.39% in 2023. The service remains efficient with a four week waiting time for the clinic appointment, and four to six-weeks for the surgery. This efficient process was maintained through the COVID-19 period and could be expected to do so in any further events. We have had few complications such as wound healing delay, and incomplete correction of contractures, but no deep infections.
Our cost analysis of 30 consecutive fasciectomy patients in 20203 demonstrated that we were able to save over £900 per Dupuytren’s case when we compared the costs for the same surgery being performed in community vs. hospital (£184.97 vs. £1052.74). It should be noted the main savings highlighted were theatre cost (£722), and staffing (£244.79), and these figures do not include the cost of the anaesthetic consumables. Healthcare generates a huge quantity of landfill waste, and by the use of smaller drapes, no gowns, and no anaesthetic equipment, drugs or monitoring, we generated significantly less waste per case (Figure 2). Patients do not change into a hospital gown and stay in their own clothing during the procedure. We e-consent so no paper consenting forms are generated.
Post-operatively the majority of patients are managed with an advice leaflet and GP practice nurse for suture removal. Physiotherapy is not routinely organised but does occur if it is felt necessary at the time of surgery or if the patient re-contacts the team with movement difficulties. As a result of the low follow-up appointment rate, we achieve a high new patient to follow-up ratio.
Patient satisfaction has been high agreeing with published studies [4]. We have received an average of 33 feedback questionnaires annually (range 17-65). These generally demonstrate excellent feedback.
Future plans
We have carried out new patient video clinics using Accurx Software (www.accurx.com). Our patients are often older and have restricted mobility and this decreases the travel time and inconvenience related to traditional hospital consultations. One-stop clinics for carpal tunnel surgery occur in a pathway separate to our clinic, and we aim to achieve a similar pathway for pre-tendinous cord Dupuytren’s patients.
Conclusions
The Cumbria Hand Surgery service has run successfully for eight years and serves a large geographical area. We manage a high volume of work with a small team of three. We have had no serious complications or deep infection. There is a significant cost saving and this model of working may help to reduce waiting times for hand surgery nationally. We have adapted our working to reduce waste with measures such as no patient gowns, a gownless scrub team, small drape packs, and paper-light with electronic notes and e-consenting.
Embracing new ways of working out of secondary care may lead to more simplified and economical pathways being developed, both to the benefit of patients and to help reduce the strain on valuable healthcare resources.
References
1. Steiner MM, Calandruccio JH. Use of Wideawake Local Anesthesia No Tourniquet in Hand and Wrist Surgery. Orthop Clin North Am. 2018;49(1):63-8.
2. British Society for Surgery of the Hand (BSSH). Hand surgery: Guidelines for operating outside of main theatres. Available at: www.bssh.ac.uk/_userfiles/pages/files/ professionals/girft/girft-operating_outside_ theatres.pdf
3. Noureddine H, Vejsbjerg K, Harrop JE, White MJ, Chakravarthy J, Harrison JWK. Fasciectomy under local anaesthetic and adrenaline for Dupuytren’s contracture in a community setting in the UK with a cost analysis. Bone Joint J. 2020;102-B(10):1354-8.
4. Tan E, Bamberger HB, Saucedo J. Incorporating Office-Based Surgery Into Your Practice With WALANT. J Hand Surg Am 2020;45(10):977-81.