5 minute read
The History of Prescription Drugs and Health Insurance


BY EMMA PETERS
According to a recent poll conducted by the Campaign for Sustainable Rx Pricing, 70% of voters across the political spectrum are worried about drug prices and a third of them have trouble affording their medications. To understand how this concern has become somewhat universal to the U.S. population, the history of prescription drugs and its correlation with health insurance is needed.

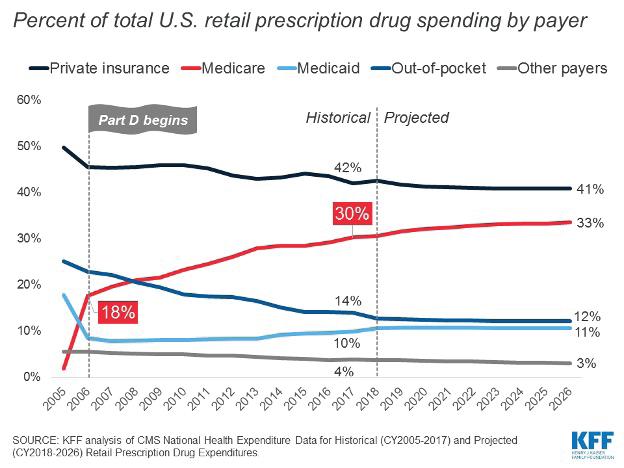
Learning this history will benefit health insurance professionals looking to better understand how health plans have evolved in the drug coverages offered. Illustrated in the first graph, the cost of retail prescription drugs has steadily increased since the early 1960s. Coincidentally, it was during the 1960s that insurance companies began offering prescription drugs as a health plan benefit, which created a new job role of pharmacy benefit managers (PBMs) who were meant to help insurers contain drug spending. Marty Mackary argues in his book “The Price We Pay” that PBMs have been one of the largest contributors to spending on retail prescription drugs because of their lack of transparency in what’s known as “the spread.” According to Mackary, “the PBM is the middleman, so if that pharmacy charges $10 for the medication, the PBM might bill the employer $50 and pocket the extra $40 — that’s the spread.”
In addition to the creation of PBMs, in the 1970s and 1980s there was also a scientific explosion which led to further transformation of the pharmaceutical industry. Scientists were able to isolate the genetic basis of certain diseases, opening a lot of therapeutic areas for new drugs. With the influx of new drugs, pharmaceutical manufacturers were eager to patent these products and create higher demand through some brand name products such as Valium and Tagamet. The 1980s also saw the rise of managed care organizations (MCOs), such as Health Maintenance Organizations (HMOs) and Preferred Provider Organizations (PPOs). These entities introduced a new approach to health insurance, emphasizing cost containment and preventive care. Many managed care plans included prescription drug coverage as part of their benefits package, making medications more accessible. Yet, studies have found that when the potential market for a type of drug grows, there is an increase in the number of new drugs developed in response to the demand. Insurance expansion has been shown to drive health spending upwards, despite its goals in increasing accessibility.
In the 1980s and 1990s, there was a growing emphasis on generic drugs as a cost-saving measure to combat the growing prices. The Hatch-Waxman Act of 1984 streamlined the approval process for generic medications, leading to increased competition and lower drug prices. Health insurance plans increasingly encouraged the use of generics through lower copayments, making prescription drugs more affordable for patients.
However, by 1992, three events impacted the number of new drugs released into the market:
1)Regulations on drug ads were relaxed
2)More rapid FDA approvals were made
3)New fees were collected from pharmaceutical manufacturers.
All of these developments caused a push of new drugs to enter to the market. These changes impacted the period from 1995 up until the mid 2000s, as spending grew rapidly and numerous “blockbuster” drugs were introduced instead of generic medications, such as Viagra, Lipitor and Celebrex.
One of the most significant milestones in the history of prescription drug coverage came in 2003 with the passage of the Medicare Modernization Act. This legislation established Medicare Part D, a program that provides prescription drug coverage to Medicare beneficiaries. Part D offered a range of private insurance plans, giving seniors and eligible individuals access to a wide array of medications.
The Medicare Part D program expanded drug accessibility and introduced a benefit structure which incentivized enrollees to choose less expensive generic drugs. Although this universal prescription drug benefit was meant to lower costs, statistics show that prices went up as more drugs were available to participants in this program.
By 2010, the Affordable Care Act (ACA) was enacted, which provided consumers with subsidies that lower costs of health insurance and expands the Medicaid program in some states. During the first 1.5 years of ACA, the number of prescriptions filled by adults using Medicaid coverage increased by 19% in states that expanded Medicaid compared to states that did not.
In the years following the ACA’s implementation, concerns about the affordability and accessibility of prescription drugs persisted. Once the new Hepatitis C drug was introduced in 2014 there was a significant spike in drug prices that mirrored that of the 1990s. A productlevel approach for measuring inflation estimated a 10% gross drug price increase from 2013 to 2020 for HCV drugs, whereas a class-level approach including the higher prices of the new drugs showed a 31% gross price increase.
Policymakers and advocacy groups pushed for measures to increase transparency and competition in the pharmaceutical industry.
In 2022, the Inflation Reduction Act was enacted to make improvements to Medicare which is expected to expand benefits, lower drug costs, keep prescription drug premiums stable and improve the strength of the Medicare program. Drug costs have been significantly affected by policies and developments within the health insurance industry. The expansion of programs such as Medicaid and Medicare Part D, development of generic drugs over the years, and the influence of PBM’s are all factors that have contributed to the increase in drug costs in the United States.
Emma Peters is a media intern at California Broker Magazine. She recently graduated from Point Loma Nazarene University summa cum laude, with a Bachelor of Arts in Literature and a minor in Humanities.