5 minute read
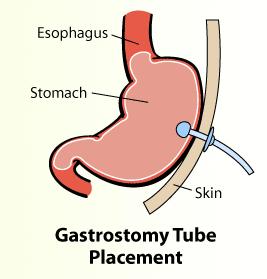
Pre-procedure Preparation for Gastrostomy Tube Placement


Cindy Ward, DNP, RN-BC, CMSRN, ACNS-BC - CRMH Clinical Nurse Specialist
Advertisement
Gastrostomy tubes are placed for those patients unable to take nutrition orally. Gastrostomy tubes may be placed surgically, endoscopically, or radiologically. Surgical placement may be done laparoscopically or as an open procedure. Endoscopic placement is generally less expensive and takes less time. Radiologic placement is done with fluoroscopic or CT guidance and requires that the stomach be insufflated with air1,2. No difference in morbidity or mortality has been found between surgical gastrostomy and percutaneous endoscopic gastrostomy1,3,4. A practice question arose regarding pre-procedure preparation/fasting for gastrostomy placement. The purpose of this review is to identify best practice related to fasting prior to gastrostomy tube placement.
When to Use Gastrostomy Tubes
Gastrostomy tubes are recommended for medium or long-term enteral feeding. Patients receiving feedings via gastrostomy may have less occurrences of missed feedings and increased weight gain compared to those receiving feeding via nasogastric tube5. More permanent feeding tubes should be considered if feeding is expected to be needed for longer than four weeks2,6,7,8 .
Search Strategy
Resources searched included UpToDate, Health and Education Research Online (HERO), American College of Gastroenterology, American Gastroenterological Association, American Society for Gastrointestinal Endoscopy, World Gastroenterology Organization, British Society of Gastroenterology, North American Society for Pediatric Gastroenterology, Hepatology & Nutrition, European Society of Gastrointestinal Endoscopy, Society of Interventional Radiology, American Society of Anesthesiologists, American College of Surgeons, Royal College of Surgeons of England, and the National Institute for Health Care and Excellence. The search term used was pre-procedure preparation for PEG placement. A total of 18 articles or guidelines were reviewed with 14 included in this review. Three of the articles found were systematic reviews of descriptive or qualitative studies. The other 11 were literature reviews or clinical practice guidelines.
Pre-procedure Fasting
There is no universally accepted standard for pre-procedure fasting9. The American Society of Anesthesiologists recommend the following guidelines for patients having procedures requiring general anesthesia, regional anesthesia, or procedural sedation and analgesia: clear liquids up to two hours before procedures; light meal, nonhuman milk, or infant formula up to six hours before procedures; additional fasting time of eight hours or more for meals with fried foods, fatty foods, or meat10,11,12. The Society of Interventional Radiology also recommends allowing clear liquids up to two hours before the procedure.
When to Begin Tube Feeding
Tube feeding may begin four hours or less post-procedure5,6,13. Early initiation of feeding following gastrostomy tube placement may potentially decrease hospital length of stay by achieving tube feeding goal rates earlier8. The European Society for Paediatric Gastroenterology, Hepatology, and Nutrition recommends initiating feeding as early as three hours post-procedure in stable children with no complications14 .
Implications for Practice
When preparing a patient for gastrostomy tube placement, the provider typically orders the patient to remain fasting after midnight regardless of the procedure time, and to keep the patient fasting after the procedure until the following morning before resuming or starting tube feeding. Based on the evidence found in this review, tube feeding could be continued up until six hours prior to the
gastrostomy tube placement and feedings resumed four hours after placement. This would improve patient outcomes, resulting in less time without nutrition and could result in earlier achievement of goal tube feeding rate and decreased length of stay.
Resources
1. DeLegge MH. Gastrostomy tubes: Placement and routine care. UpToDate. 2022. Retrieved October 12, 2022 from https://www.uptodate.com/contents/gastrostomy-tubes-placement-and-routine-care?search=peg% 20placement&source=search_result&selectedTitle=1~89&usage_type=default&display_rank=1#H59179605 2. Long S, Fernando D, Boyd C, Katrivesis J, Park H. Interventional techniques to support enteral nutrition. Dig Dis
Interv. 2022; 6(1), 52 – 60. doi: 10.1055/s-0042-1742295 3. Herb J, Rodriguez-Ormaza N, Cunningham C, Bartl N, Jadi J, Charles A, Reid T. Gastrostomy tube outcomes among surgical and non-surgical services: A retrospective review. Am Sur. 2021 Advance online publication. Doi: 10.1177/00031348211047173 4. Varone A, Stephen A, Kheirbek T, Adams C, Cioffi W. Outcomes of PEG placement by acute care surgeons compared to those placed by gastroenterology. Surg Endosc. 2022. Advance online publication. doi: 10.1007/ s00464-002-09262-2 5. Boullata JI, Carrera AL, Harvey L, et al. ASPEN Safe Practices for Enteral Nutrition Therapy Task Force. ASPEN
Safe Practices for Enteral Nutrition Therapy. J Parenter Enteral Nutr. 2017; 41(1), 15-103. doi:10.1177/0148607116673053 6. NICE. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. CG32. 2017. https://www.nice.org.uk/guidance/cg32/chapter/1-Guidance#enteral-tube-feeding-in-hospital-and-thecommunity 7. Rajan A, Wangrattanapranee P, Kessler J, Kidambi TD, Tabibian JH. Gastrostomy tubes: Fundamentals, periprocedural considerations, and best practices. World J Gastrointest Surg. 2022; 14(4), 286 – 303. Doi: 10.4240/wjgs.v14.i4.286 8. Wei M, Ho E, Hegde P. (2020). An overview of percutaneous endoscopic gastrostomy tube placement in the intensive care unit. J Thorac Dis. 2020; 13(8), 5277 – 5296. doi: 10.21037/jtd-19-3728 9. Early DS, Lightdale JR, Vargo JJ, et al. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest
Endosc. 2018; 87(2). 327 – 337. doi: 10.1016/j.gie.2017.07.018 10. American Society of Anesthesiologists Task Force on Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: Application to health patients undergoing elective procedures. Anesthesiology, 2017; 126(3), 376 – 393. doi: 10.1097/ALN.0000000000001452 11. American Society of Anesthesiologists Committee on Standards and Practice Parameters. Practice guidelines for moderate procedural sedation and analgesia 2018. Anesthesiology, 2018; 128, 437 – 479. Doi: 10.1097/
ALN.0000000000002043 12. Tam AL, Heran MKS, Sangha BS, et al. Society of Interventional Radiology standards division 2019 document review. J Interv Radiol, 2020; 31, 282 – 283. doi: 10.1016/j.jvir.2019.10.007 13. Roveron G, Antonini M, Barbierato M, et al. (2018). Clinical practice guidelines for the nursing management of percutaneous endoscopic gastrostomy and jejunostomy (PEG/PEJ) in adult patients: An executive summary. J
Wound Ostomy Continence Nurs, 2018;45(4), 326 – 334. doi: 10.1097/WON.0000000000000442 14. Homan M, Hauser B, Romano C, et al. Percutaneous endoscopic gastrostomy in children: An update to the
ESPGHAN position paper. J Pediatr Gastroenterol Nutr, 2021;73(3), 415 – 426. doi: 10.1097/
MPG.0000000000003207






