
57 minute read
Analyze

Case study 1
Biological Rhythms during Residence in Polar Regions by Josephine Arendt
Advertisement
Living in polar regions, you have to adapt to certain circumstances such as: extreme cold, day length and sometimes isolation for long amounts of time. The weather during polar winter has a huge effect on the residents. Transportation is often restricted in the winter due to the weather and distance. Satellite communication can also be affected due to the weather, it can make it hard to communicate with external contacts. These factors can lead the residents to feel isolated. The physiology of people and over-wintering have been studied; studying this they found out that it was the lack of natural light was the biggest problem. The evidence showed that the circadian system is disrupted by the polar winter due to the lack of natural light. The latitudes of 66.33’, north and south above the Polar Circle, the sun is above the horizon for 24 hours for at least one day out of the year (midnight sun) and it also goes below the horizon for 24 hours for at least one day out of the year (polar night). When you increase the latitude there will be more days where you either see no sunlight or constant sunlight. A study done at Halley Bay, where the sun doesn’t rise for 100 days in the winter and doesn’t set for 100 days in the summer, showed during the winter with only artificial light and minimal natural light, the maximum light exposure was 500-700 lux (which is a measurement of illumination). During the summer when the sun doesn’t set, the light exposure got up to around 40,000 lux. You can generate a light-dark cycle in summer, in the conditions of the sun not setting by using window treatments at certain time, keeping a normal sleep schedule and wearing night masks if needed. In the winter, the light-dark cycle depends on artificial light in order to increase the maximum light exposure. Actually in most work environments the artificial light barley exceeds 300-500 lux. To maintain the circadian rhythm you need 200-1000 lux of white light. A number of studies show that morning light of sufficient intensity which would be 10,000 lux for 30 minutes; was enough to put people in remission of SAD (Seasonal Affective Disorder). A delay in circadian phase is the root of SAD. Data shows that women have a greater chance of getting SAD and have more sleep and mood problems than men. Based on a questionnaire, women suffer more from prolonged Antarctic residence than men.
In a typical working polar environment, a problem reported frequently during the winter is sleep. “Mid-winter insomnia” is known by the difficulty of falling asleep in the region or northern Europe. Treatments were designed to advance circadian phase by using bright white light early in the morning for 30min-1hour, it was successful. It also succeeded in making the subjects fall asleep faster and reducing morning tiredness. In the summer, bright daylight during the night for night workers, will evidently help shift the circadian system to the night mode during the hours of sleep and artificial darkness. From a few small studies, the data suggests that delayed circadian phase in winter is due to lack of bright white light in the morning, and for the summer it is due to exposure to bright white light on the delayed part of the light phase, if the daylight is not artificially taken away in the evening and if work/sleep periods are not scheduled.
Furthering the study on white light, they found that short-wave length light (blue light) is the best type of light to use with regarding shifting the circadian system. Blue light proved to be better than the white light in the following categories; sleep timing, latency and length of sleep. Internal desynchrony (loss of synchrony between two or more circadian rhythms) of sleep impairs cognitive performance along with associating to developing heart disease and possibly cancer. Conclusion: The lack of natural light or bright light during the polar night means that the time which the circadian rhythm starts is diminished. In the summer during midnight sun, light exposure can hurt the circadian system by forcing phase shift. There are ways to treat both of these; during the polar night the use of white or blue light at an intensity of 200-1000 lux for 30 minutes can improve sleep and morning tiredness while also helping advance the circadian phase. In the summer exposure to bright white light during the delayed phase; to help delay the advance of the circadian phase you have to set work/ sleep schedules and during the night use black out blinds or an eye mask to block out the light. All of the data in this case study showed me some aspects I need to include. In the center I need to provide black out blinds during midnight sun and in polar night I need to include a certain intensity of white and blue light throughout. This case study also showed me I should include some type of light therapy as well, for the women who suffer from SAD; it also supported the fact that I am focusing on women for my center because women are more likely to develop SAD, sleep and mood disorders than men.

Case study 2
Seasonal Affective Disorder: An Overview of Assessment and Treatment Approaches by Sherri Melrose
Seasonal Affective Disorder, also known as SAD, is a type of recurring major depression with a seasonal pattern; most commonly it is the beginning of fall into the winter months. People with SAD overly produce melatonin, which is a hormone that responds to darkness casing sleepiness. As the day gets darker sooner, your body produces melatonin causing people with SAD to feel sleepy and lethargic. Also, people with this disorder have problems regulating their serotonin, which is responsible for mood balancing. Lower levels of serotonin can cause depression. The combination of both low serotonin and increased melatonin impacts the circadian rhythm. The circadian signal that indicates a seasonal change in day length has been found to be timed different in people with SAD; which means it is harder for their bodies to adjust to the seasonal change. Seasonal Affective Disorder occurs four times more in women than men and the age of onset is between 18 and 35. People who live further from the equator in the northern regions are most susceptible; 10% of the population in Alaska experiences SAD compared to the 1% in southern states. There are a few treatment options for people with this disorder such as: antidepressants, light therapy, vitamin D, counseling or combinations of these. Light boxes as light therapy that emit full spectrum light similar to sunlight are a good option. Symptoms of SAD may diminish by sitting in front of a light box first thing in the morning for 20-60 minutes with exposure of 10,000 lux. This amount of bright white light is actually 20 times greater than ordinary indoor lighting. Conclusion: The ages 18-35 are at high risk for Seasonal Affective Disorder which is also the age range and demographic I was aiming towards; this case study helped support that decision. It also supported my decision for creating this center in Alaska because as stated in the case study northern regions are more susceptible and 10% or Alaska’s population experience SAD. I wasn’t entirely sure from my first case study on how bright 10,000 lux really was but this study showed me that it is actually 20 times brighter than average indoor lighting which is a lot. That statement made me rethink on my previous statement on wanting to incorporate that bright white light thought the building but instead make light therapy rooms or a light therapy group area.

Case study 3
Understanding Controls, Behaviors and Satisfaction in the Daylit Perimeter Office: A Daylight Design Case Study by Julia Day M.A. , Judy Theodorson M.Arch., Kevin Van Den Wymelenberg M.Arch.
Daylight can positively impact occupants if done the right way. Some benefits of natural daylight are: increased occupant satisfaction, psychological and physiology health benefits and increased productivity in the workplace. Even though daylight has many benefits, it is important to allow the user of the space control or manipulate the daylight within their environment because it can lead to increased energy from electric light and can take away the benefits from natural daylight. Illuminance can be described the total amount of light falling on a given surface. Illuminance is often measured horizontally at desk height, as it is the height where occupants normally work. Luminance is defined as the photometric quantity most closely associated with ones perception of brightness. In simpler terms; it usually refers to the amount of light that reaches the eye. Materials, reflectance of materials and colors can all affect the Illuminance value of a space. If there is high contrast of luminance values in a space there can be glare problems which is not ideal for people who work with computers. Glare or high brightness contrast can cause discomfort to the occupants. The location, latitude and climate should also be thought of when designing an interior space. The northern sky provides dim, diffused and bluish light. North or South facing windows are recommended with the use of overhangs to block out the direct sunlight. Blinds are a much need aspect to control glare, sunlight and overheating. They allow the occupants to control their environment as well. Horizontal blinds are used for high sun in the south and vertical blinds are used to intercept the low sun angles in the North, to intercept the low sun angles in the North, East or West. Full spectrum light from daylight has both psychological and physiological effects as previously stated. People in daylight offices continuously report that they have a better well-being than being in the common florescent light. Daylight has been proven to have the potential to decrease headaches, Seasonal Affective Disorder (SAD), reduce stress and eyestrain. This also applies to the windows having a view or landscape and nature.


Conclusion: This case study informed me on how I should be thinking about the interior space especially in the Northern region, which is where my center will be located. It brought to my attention that I should definitely provide vertical window blinds due to the region and the fact that occupants prefer to control their personal environment. Having my center located in Alaska it is important to utilize all the day light in the winter months and also be able to shut it out during the 24hour light periods. In this case study they explained why it is better to have North or South facing buildings or windows because that it where you can get the most daylight; with that they suggest putting overhangs on the windows to cut out direct sunlight but In my case I think direct sunlight might be beneficial. There are also many health benefits for having daylight and a view in office or any spaces for that matter, which in my center I think is crucial to provide easy and minimal health benefits such as: reducing stress, increasing well-being, decreasing headaches and decreasing SAD.
Case study 4
Sexual assault and posttraumatic stress disorder: A review of the biological, psychological and sociological factors and treatments by Kaitlin A. Chivers-Wilson.
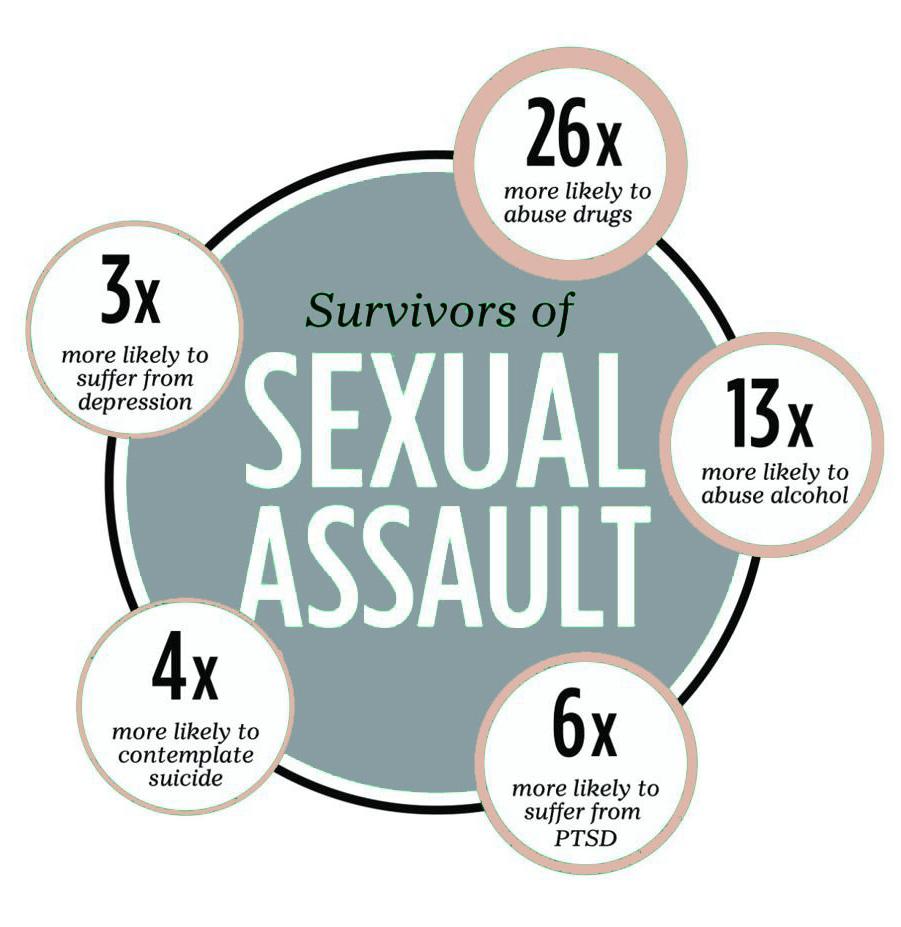
Post-Traumatic Stress Disorder (PTSD) in sexual assault survivors is extremely higher than the national prevalence of PTSD. Sexual assault is any form of sexual contact without consent. Healing from this trauma doesn’t mean the survivor will forget what happened or not have any symptoms. Recovering and healing is subjective meaning it is not linear and there are many paths; it is measured by whether the survivor acquires skills, attitude, and involvement in order to get their life back on track. There are many factors when on the road to recovery, including, support from others, previous self-concept, mental strength and professional treatment. The life time prevalence in women who have been sexual assaulted is 50%. Sexual assault is the most frequent cause of PTSD in women; 94% experience PTSD the first two weeks after the assault. There is no perfect treatment for everyone who experiences PTSD. When thinking of treatments you have to think about the biological, psychological and sociological impacts. Intervention also needs to be considered. After an assault, survivors experience something called “The Rape Syndrome” (RTS), this can affect all survivors of sexual violence, not just rape. There are three phases to RTS. The first is “The Acute Phase”, it occurs righter after the assault and the survivors experiences a wide range of emotions; shaking, crying, yelling or the opposite being calm and subdued. Secondly is, “Outward Adjustment”, it is when the survivor focuses on the assault, often high level of denial, and goes about their normal day to day. The final one being “Long Term Reorganization”, in which the survivor integrates the assault into their view of themselves and resolves their feeling about the perpetrator. Cognitive factors play a huge part on the outcome of PTSD after sexual assault; these include, mental defeat and confusion, negative appraisal of emotions, avoidance and perceived negative responses from others. When a survivor of sexual assault thinks that there’s have failed to bring positivity and support, there is a greater risk of PTSD. Sexual assault is categorized as an uncontrolled event and is more distressing than a controlled event. Survivors will often attempt to blame themselves as they believe that negative outcomes can be avoided. To improve PTSD, treatments should emphasize on controlling the present situation and hat can be done about the impact of the event, rather than how it could’ve been avoided. Control over the recovery results in lowered distress levels. Group therapy can be very effective when helping survivors. They get the opportunity to share their experiences in a safe and understanding environment. According to a survey, over half the women who went through sexual assault never told anyone about their trauma. There are also many types of individual therapy including PTSD specific that can also really help these survivors as well.
Conclusion: This case study gave me an idea of how sexual assault really affects the female survivors. PTSD is a serious mental illness that 94% of women experience after sexual assault. Many people can act out in yelling, crying and shaking or the complete opposite and be calm and subdued. This information showed me I need to design psychologically safe for those people who experience a wide range of emotions; this will help keep them and everyone around them safe. The case study also explained the many treatments for people with PTSD and sexual assault; there were at least 4 types of individual types of therapy (one included medication). It will be crucial to include multiple individual therapy rooms for all types of therapy and have a medication closet in the medical center. Group therapy is very effective when helping these survivors and making sure it is a safe environment. Since it is so effective I should include multiple group therapy areas for different sizes of groups.

Case study 5
Supporting survivors of sexual violence: protocol for a mixedmethods, co-research study of the role, funding and commissioning of specialist services provided by the voluntary sector in England
Sexual violence is one of the most pervasive forms of violence that effects women, men and children. Sexual violence can occur in family and intimate relationships. These survivors of sexual violence can and do recover but unfortunately there can be long term effects on health, well-being and social life. Rates of PTSD are the highest in people who have experienced sexual violence compared to all other forms of traumatic experiences. Depression, anxiety, suicide, self-harm, alcohol/drug abuse and sexually transmitted infections are also all higher in those who have experienced sexual violence. It also affects relationships with family members, friends and intimate partners and their ability to participate in community life. A company called Voluntary Sector Specialist (VSS) has helped in providing services to sexual violence survivors including; crisis and long term counseling/ therapy, telephone helplines, play therapy, support in accessing other services and support groups and social activities. They enable survivors to increase confidence and to thrive long-term. Based on a survey with 395 adults’ survivors and 175 child survivors; based on the survivor’s responses, they typically want timely, locally available services, a chance of therapy and long-term support from the agencies. They need to feel safe, believed and respected. Also counseling and psychotherapy were shown to be the most helpful sources. VSS did encounter the issue of waiting lists and a limited amount of time for a therapy session.
analysis
Conclusion: This case study also showed me the severity that sexual assault can have. People may attempt self-harm or suicide and those are very serious and dangerous acts. It will be important for me to include safety in every aspect of my design, from the housing to the therapy and medical clinic. Something that supported the medical clinic aspect that STI’s were the highest in sexual assault survivors and to include that into my center would make it safer and easier for these women to seek the medical treatment. It was also said based on a survey that the survivors wanted support from the agency long term and I think that can be implemented thought the transitional housing especially but also through all other aspects.
Case study 6
Transitional Housing for Victims of Intimate Partner Violence
Many survivors of intimate partner violence (IPV) find themselves homeless in effort to escape the violence. Leaving intimate partner violence is the leading cause of homelessness in the United States, especially for low income women and children. 92% of women who are homeless have experienced severe physical or sexual abuse in their struggle to find housing. Women who experience IPV and housing instability also report poor health outcomes, including depression, stress and worse self-care. Domestic violence shelters offer great needs for these survivors such as; confidential location and 30-60 days of stay but they often do having waiting lists. Transitional housing programs offer survivors long term suitable housing and often include additional services. The typical period of stay is 6 months-2 years and includes relevant support programming (counseling, employment assistance and case management. There are issues found with some transitional housing: cultural sensitivity and gender inclusion. Transitional housing can help these survivors move successfully to permanent housing.
analysis
Conclusion: This case study focused on women and children who have been physically abused in an intimate partnership. This many not directly apply to sexual assault, but sexual abuse is still considered abused and it does happen with people in IPV. I think this case study helped me decide on whether or not I needed transitional housing for a shelter and it showed me transitional housing would be a better option because of the benefits it has. No matter the violence these women experience it is important that if it is done by their partner or family member that they have somewhere safe to live and figure out their next moves. Housing instability as stated in the study can cause poor health including depression. Stress and loss of self-care. For my center it is important that these women have some sort of stable housing if needed and this can help their overall health. One thing they said that stood out to me was cultural inclusion; my center being based in Alaska I should somehow address the indigenous culture of Alaska into the design as well.
Case study 7
The Perils of Institutionalization in Neoliberal Times: Results of a National Survey of Canadian Sexual Assault and Rape Crisis Centres by Melanie A. Beres, Barbara Crow and Lise Gotell
This article reports on a national survey of Canadian rape crisis and sexual assault centers in 2005. There have been pressures to redefine these women focused centers as “Victim Centers” to dismantle the gender specific centers but these Canadian Centers continue in social change activism and define themselves specifically as feminist/pro-women/equality seeking organizations. Early centers worked to organize support for raped women and to create a social change center embraced by womenfocused organizational forms, such as Take Back the Night marches, and supporting survivors helped create empowerment and political resistance. The goals of these centers was to challenge the system that enable sexual violence and women oppression and to provide places where women would be believed and would be strengthened both individually and collectively. Many centers grew and developed from that to employ staff and develop programs for crisis intervention; individual counseling and support; group counseling; advocacy; accompaniment to the police, courts and hospitals; public education and prevention; keeping records; and raising awareness about sexual violence. 15% of respondents from the survey of 135 centers in Canada, reported that transinclusion was actively being debated within their center; suggesting that the presence of transgender women would take away from the possible education on anti-rape activism for radical feminist. Conclusion: This case study was what I had in mind for my centers goals and view from the community. I want this center to be women’s focused and not all genders, as I feel violence against women is a very big issue as also stated in this study. This study also showed all the aspects that’s these centers included and brought support for my decisions. One part that was brought was the inclusion of transgender women and whether or not they should be included and in my center they will absolutely be included as they ARE women. This made me think how I can be more inclusive in design for the transgender women; I could include transgender women signage and art to showcase transgender women inclusion.

Site Visit 1
Central Minnesota Sexual Assault Center
DATE + TIME - Thursday, October 29th, 1PM DEMOGRAPHICS – There were no people in the center except the staff that were all women; two being in their 20’s and the other in her 40’s. They also accept all genders and ages. Also they expect all genders. ACTIVITIES – Since there weren’t any people seeking the help of the sexual assault center at the time I went I didn’t get to see any activities going on. They provide many services such as: 24-hour crisis hotline, safety planning, one to one support counseling, harassment and restraining orders, Criminal Justice Advocacy, Professional + Community training/education, etc. CIRCULATION – One entrance from the main road which had an ADA compliable ramp. To the right of the entrance they had group therapy rooms and a kitchen. There were some stairs that lead to six private offices and a bathroom. On the left of the entrance there was a bathroom and a small library which was also the Childrens therapy room. Down the hall further there was a room for staff and extra storage for donations. They didn’t have much signage so it was a bit confusing on where to go. ACOUSTIC CONDITIONS- Thin walls. Wood floors. Some carpeted areas. Staff member said they did have some sound proofing insulation but wasn’t working well. Space echoed a lot. I could hear sounds/ voices through other rooms. LIGHTING CONDITIONS – There were many windows for natural light. Had bright ceiling lights and white walls to brighten the space. Every space had one window or more. FF&E CONDITIONS – They had an abundance of furniture due to remodeling. Entry had four waiting chairs but a little further by the reception desk there was a pile of chairs and tables. Hallway had about 10 chairs. Group therapy rooms had couches, chairs, table and a rug. Offices had a desk, file cabinets and a couch. Staff room had a dining table and some couches along with a small TV area. AIR QUALITY – Seemed well ventilated as the average house would. TEMPERATURE - Comfortable.
analysis
DESIGN CONCLUSION - I would say this space was an example of something I would not like to do. The acoustics were not good and in a space where people are sharing intimate moments or scenarios they wish not to share with others sound proofing is key and much needed. Also universal design is something I am going to design with and this space didn’t have any elevators for people in wheel chairs, no railings, but did have ADA bathroom and door way sizes. There was also no signage except for the bathrooms, so I found it very confusing on where to go or where things were. I did however like how the individual therapy and offices were upstairs and the more group activity based aspects were on the first floor.

Site Visit 2
Middle Way Housing
DATE + TIME - Thursday, November 5th, 10AM DEMOGRAPHICS – Seem to have a very diverse staff. They focus on women and children. ACTIVITIES – I did a virtual tour for their transitional housing and emergency shelter so I physically did not see an activity but they proved a 24 hr- crisis hotline, counseling, resident advocacy, crisis intervention and more. CIRCULATION – From a virtual tour it was a bit hard to see how well the place did circulate but it seemed it floor had a main square space with a long hallway to another main square space. Also each building has a vestibule with a locked door before entering the reception area. SPACES- In the shelter building they have 11 and 6 bathrooms including an ADA one. For the transitional housing they have 28 units with 2-3 bedrooms each. Each building has its own kitchen, pantry, laundry and donation room. They provide locked storage separate from the rooms because they do not lock the bedrooms. The shelter had around 15 offices and 2 meeting rooms. In the transitional housing it seemed they had maybe 4 office space behind the reception area. Also both seemed to have multi purpose rooms and children areas. LIGHTING CONDITIONS – Since I was not physically in the space it was a little bit hard to tell how good the lighting was. They used troffer lights in almost every single area and some space seemed darker than others, especially the hall ways. It seemed unevenly lit in both buildings. FF&E CONDITIONS – Nothing seemed to be physiological safe furniture.
analysis
DESIGN CONCLUSION- The emergency shelter virtual tour showed the most and both building were very similar from what I gathered. I liked on the outside of the shelter they used frosted like glass that was very thick so people could not see into the shelter. In order to get into either buildings you had to buzz in and have someone come let you in. Right away each building had a small vestibule (with a locked door) but the shelter included some seating in theirs. The shelters reception desk had an all glass front with a small opening at the bottom for safety and the transitional housing had some hanging glass with a huge opening and didn’t seem very safe. In my center I would include these aspect of safety: including an buzz in system with locked door vestibule, and a reception desk that is both safe for the staff and clientele to make sure the entire process is safe. I didn’t really like how all units had more than one bedroom. In my center I would include options of, single and double just because my demographic is not families. It did bring to my attention of how many bathrooms I may need, the shelter had 6 bathrooms on the housing floor. Also these types building need quite a bit of storage for donations and supplies. One thing this site visit really helped me with was how many offices and staff space is needed, I thought open office space would be okay but from this site visit I realized that most staff with offices are staff that need to talk privately with a client.




Site Visit 3
Domestic Violence Solution
DATE + TIME – Thursday, November 5, 11PM DEMOGRAPHICS – They had a very diverse staff. They welcome mainly families and children and also include the LGBT+ community. CIRCULATION – Since this was a virtual tour it was hard to tell how good the circulation was and they only showed the bedroom units and not the entire building. Based on what the rooms seem very spacious, there is extra room for a play area and dining area. SPACES- It seemed there was a huge entry that could act as a living or dining area, another living area, small play room, bedroom and small kitchen. LIGHTING CONDITIONS – Based on the pictures it looked very well lit and had a lot of windows. FF&E CONDITIONS – All of the furniture was very updated but still not physiologically safe. They had tons of seating options and a coffee table. There were also some storage shelves for toys and personal belongings.
analysis
DESIGN CONCLUSION- This site visit showed me how nicely designed these units can be and that they can be spacious. It was well lit, had nice furniture and enough space for a family. They did although include a small kitchen in the units and for my project I do not think that would be safe option for my users. In these units it also seemed like the windows were openable and again I don’t think that would be safe for people going through trauma. Considering the furniture was moveable and that there were some art work on the walls, they did not consider physiological safe furniture which is needed in these types of centers. I am going to make sure I include many safety aspects that they did not consider when designing these units.




Site Visit 4
Casa Youth Shelter
DATE + TIME – Thursday, November 5, 1PM DEMOGRAPHICS – Staff seemed somewhat diverse. They accept people from the ages of 12-17 and families are welcome to do counseling with their child. CIRCULATION – It was a bit hard to tell how good the circulation was due to it being a virtual tour. Based on what I could gather their public/office spaces seem very small and cluttered. The bedrooms however seemed very spacious. SPACES- There was a dining/TV room, kitchen + pantry, bedrooms, care closets, recreational room, minimal office space, multi-purpose/ therapy room, community room and a outdoor court yard LIGHTING CONDITIONS – Lighting seemed uneven. They used troffer lighting in all of the main space except the bedrooms which were well lit.
analysis
DESIGN CONCLUSION- I would say their main public spaces are a good example of what not to do, but on the other hand their bedroom units were very well done. I liked how bright and open the bed rooms were, they also included a desk area in the bedroom and a big closet. I think having a desk space included is a very good idea that I will need to incoporate because some of these women may work or go to school. Even though their public spaces where cluttered and small they did at least provide room dividers for those spaces which I wish to utilize in my center as well. The lighting in this building was uneven and I think it is very important to have a well-lit setting because an uneven lit space can have negative effects on health and in these types of spaces we should be focusing on improving health.




Survey 1
General Sexual Assualt Survey
10% 7.5%

80%
15%

82%
10% 5%

82%
12.5%
17.5%
70%
25%

7.5% 67.5%
45%

55% 20%
7.5%
72.5%

Survey 2
General Sexual Assualt Survey







For part of my research on designing a type of sexual assault healing center, I conducted two surveys. The first survey was a general survey to see how much sexual violence and assault affects the community. Both surveys included three questions; age, race and gender. I included these to show that sexual assault can happen to all ages, races and genders. In the first survey I included some gender based questions to see if including men in this type of center would be a good idea. The two gender based questions showed that men were the cause of the sexual violence and that most people wouldn’t feel comfortable having men in this type of center.
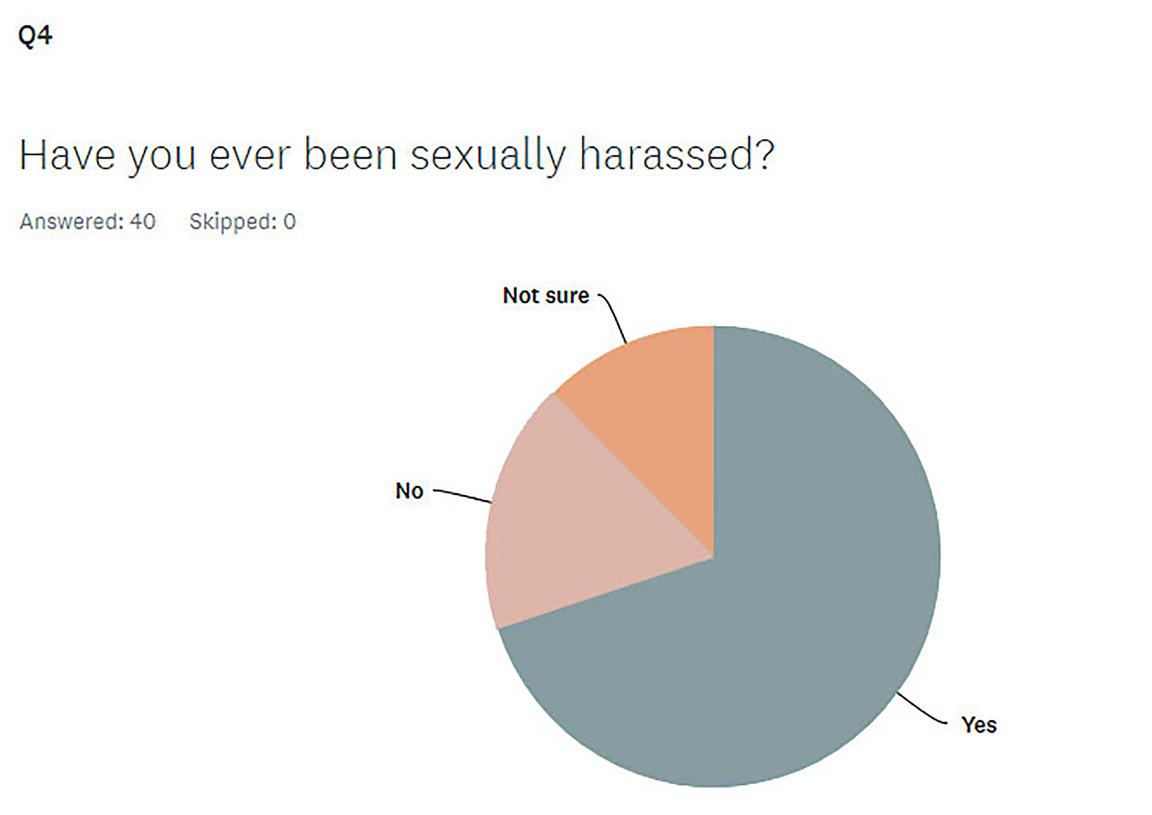
From the first survey I did not get the results I was hoping for. Around 82% of females and 15% of males took my survey; the question asking, if the user had been sexually assaulted, 55% said yes and 45% said no. This led me to conclude that maybe sexual violence/assault isn’t as big of an issue or that the people taking my survey weren’t sure what sexual assault entailed. My next move was to send out a second survey. I sent out this survey on the exact same platforms and had very different results. This survey showed that I had significantly less males take this survey; there were 90% females and 5% males, the remaining percentage were non-binary. From this data led me to believe even more that I should not include men in this type of center. The question that gave me the results that I was looking for was, “Below are examples of sexual assault: If you, someone you know, or have witnessed any of the acts below; please check which ones.” I then provided examples of sexual assault. Almost all of the participants checked more than one act of sexual assault; only 15% said they couldn’t relate to the question. That data showed me that sexual violence/assault is indeed an issue. I then asked the question of “How problematic is sexual assault in your opinion?” and 95% said that it was either very or extremely problematic. This shows that it is a problem in many people’s communities and society as a whole.
My last question was, “Would you know how to defend yourself in a situation of sexual assault?” The results were about half yes and half no. The reason I asked this question was because for my center I wanted to include self-defense classes to help engage and make the community safe from sexual assaults happening. A participant of my survey brought up to me, that even if people think they know how to defend themselves, many people freeze in the moment or their attacker may be stronger than they are. That statement showed me it would be necessary to incorporate a self-defense aspect so these people can get back out into society safely.
Interview 1
Sexual Assualt Survivor Megan Muras

1. What was your age
when your sexual assault happened? How old are you now?
There was a couple, child molestation, and then most recent I was 23 years old. Now I am now 26.
2. Did you know the perpetrator? If so what were they to you?
Yes, I knew the first man well because he was friends with my grandparents, so I would see him often. The most recent man I only knew from one date, I wouldn’t say he was trusted.
3. What was the perpetrators race and age?
I think he was in his early 30’s and he was white.
4. What type of sexual
assault occurred? Rape and molestation.
5. What setting did the assault occur? At his house.
6. What did you do
after the assault? Did you seek out the police? Did you receive medical
treatment? I went home and took a shower. I did not seek medical treatment, but did end up getting an STD test done a little later.
7. After the assault did you reach out to anyone and tell them about what happened (friend or
family)? I didn’t tell anyone on the first day but a couple days later I did tell my mom and got a restraining order on the man from the most recent rape.
8. Did you go to therapy? If so how long after? If not,
why? Yes I went to therapy, and treid out different therapy strategies; a Somatic therapist and did EMDR. Which is body healing like soul healing and then a specific kind of PTSD therapy.
9. 94% of women experience PTSD after sexual assault. Do you think you are part of
that percent? Yes, I would hyperventilate. I was nervous to go anywhere and that if I did I would run into him. I couldn’t be hugged, cry for an hour almost every day, couldn’t sleep, and stopped partying. I was always anxious and didn’t want to go out. Felt like any made make me jump.
10. Did you ever consider suicide do to your assault?
No, there were times I thought about but wouldn’t go through with it.
11. Do you find anything more difficult after your
assault? Dating, being alone, being around some of my guy friends, and opening up to people; because the man seemed really put together. I am still not good with hugging people, and don’t like to party or drink anymore.
12. Do you feel safe going
out in public alone? No
13. Would you know how to defend yourself in a situation where a sexual assault would occur again? Do you think you could actually act upon
the situation? She thinks now she wouldn’t freeze up. Megan said she’s not a violent person but she thinks she might be able too but it would be really hard. She carries pepper spray and a tazer.
14. Did your assault affect home/work/school life?
School was a mess, and I couldn’t concentrate and got bad grades, but my teachers were somewhat understanding. I lost motivation. and was depressed. My sister had a baby, but it was hard for me to be happy about it. But my mom is a therapist so she was helpful.
15. If there were a place like the one I wish to create, would you have gone?
Would you go now? I am very introverted, but I would really like group therapy and not to have any men around and just to have women to talk too about what happened to one another. Having a safe place with people that know what you’re feeling would be very helpful.
16. How beneficial do you think this would be for sexual assault survivors?
Very helpful because not everyone has parents or friends like mine or has opportunity’s to go therapy or get help.
17. Do you think men who have been sexually assaulted should be able to attend? Or do think that could make some women
uncomfortable? No, because I would think that it could trigger PTSD in some women and make them uncomfortable, unless flamboyantly gay.
INterview analysis
I did an in person interview with a sexual assault survivor named Megan Muras. I chose to interview her because I wanted her story and her insight on the overall process and how it affected her. I had done some previous research on sexual assault statics, which helped me ask the right questions. Megan had gone through multiple cases of sexual assault from the time she was a child and up until three years ago when she was 23. Based on some research, 93% of sexual violence survivors knew their perpetrator and so did Megan. When she was a child she was molested by her grandparent’s friend who was a man and when she was 23 she was raped by a man she had been on one date with; she knew her perpetrators. Having someone you knew or wanted to get to know and having them commit an act of sexual assault against you has many negative effects. I had told her that 94% of women experience PTSD after sexual assault and asked if she felt like she contributed to that 94%; without hesitation she said yes and that she experiences multiple symptoms of PTSD still to this day. She would hyperventilate, have constant anxiety and fear that she would run into them, couldn’t go out with her friends, would cry every day, couldn’t sleep and more. I then asked her if she had found anything more difficult after her assault and again without hesitation she said yes. Megan stated that she has a hard time dating, being hugged, being alone, and opening up to people. She said she had a hard time opening up how they dress, what their job is, or what kind of car they drive, any type of man can. That wasn’t all she felt was difficult, she said it really affected her friendship with her guy friends and that she had a hard time being around them. Also, going out and partying or being drunk she felt she couldn’t do anymore. School, work and home life were also affected. She said her school life was a mess, she lost motivation and her grades were falling. As for home life she said her sister had a baby and she struggled to feel happy about because of what she was going through. On a positive note, Megan’s mother is a therapist and her family was
very comforting and understanding. There are some aspects I wish to include in my center. I want to include some form of medical center for the sexual assault victims to come and seek out after their assault. A recent study showed that only 21% of rape victims seek out medical help so I wanted to ask Megan if she was part of that 21% or not. What Megan did after her assault was, she went home and took a shower which many do because it helps them feel as if they washed away what happened. She did get an STD test a couple days later but no rape kit or immediate medical examination was done after her assault. The other aspect I wish to include is community self-defense classes for women. Even if people think they know how to defend themselves, many people freeze
up but it would be hard for her to fight back because she is not a violent person.
Megan did seek out therapy and is still currently going. I asked her if there were a center out there like the one I wish to create would she have gone. Would she go now? She stated that she is very introverted, but thinks that she could benefit now from group therapy and having a safe place where people are going through what you’re going through would be really nice. I then asked how beneficial she thought my type of center would be for sexual assault survivors; she said, very helpful because not everyone has parents like hers or has the same opportunity to go seek therapy or medical treatment.
Interview 2

Planned Parenthood Employee Jenny Mattifs
1. Which Planned Parenthood do you work
for? I work at the Boise Planned Parenthood.
2. Planned Parenthood for women and men or just
women? Planned Parenthood offers services to both men and women.
3. What services are provided?
We offer many services: - Periodic Well Visits/Pap Smears/Breast Checks - STI testing/treatment - Cancer Screening/Colposcopies/LEEPs - Medication abortions - Pregnancy Evaluations/Gestational Ultrasounds - Birth Control Services (pills, IUD, implant, rings, depo shot) - Immunizations (Gardasil series) - Gender Affirming Hormone Care (available to 18+) - Vasectomies - PrEP - Ectopic pregnancy/PUL oversight, care, and referral.
4. What would you say your most used service is?
Our most used services, by far, are our birth control services. On an average day, I would be comfortable saying we see about 40% birth control related visits.
5. Does your location provide services for sexual assault survivors? If not do you think all locations should? If so what are they?
Currently, we do not have services dedicated to sexual assault survivors that visit us. We have select referrals that we partner with closely in the community to assist our patients in their recovery. I believe it would be beneficial for us to have a social worker on site; available for our patients, with a follow up plan if necessary.
6. How many doctors/ nurses do you have on staff
on a normal day? On a normal day, we have 1-2 PA-C’s/RN’s on staff. We have our doctors on staff only for visits that require oversight. Doctors are on site 1-2 times per week.
7. How many exam rooms
do you have? We have 7 exam rooms.
8. How many clients would you say come in, in a
day? We see on average 35 patients per day.
9. Are there any spots where you think Planned Parenthood is lacking?
Operationally, I believe PP is an example of medical integrity, respect, and body autonomy. That being said, I believe PP could flourish by offering more volunteering opportunities. We currently have a teen-run group, and I see amazing things that come from that team. That opportunity being opened to the general community could really help us echo our message: care. No matter what.
10. For my type of center what services would you
recommend? First off, super cool that you’re doing this project. Secondly, I would recommend seamless integration for the client. Things like having insurance completely handled, or simply offering cash only visits. A large portion of anxiousness or hesitation to go through with visits are cost related. If these services are going to be offered via community support or grants, even better. Sound-proofed exam rooms. High-security, locks on exam room doors. Services I would recommend that you offer for your center: - Trauma processing - Home relocation services - Welfare application/review services - Access to local women’s center for additional home/vocational/meal needs - Opportunity for gatherings of fellow survivors to share, if they would like.
INterview analysis
I interviewed a Planned Parenthood employee, Jenny Mattefs. She currently works at the Boise, Idaho Planned Parenthood. I interviewed her because Planned Parenthood has many medical services for both women and men; I was not aware they also catered towards men. I wanted to know what kind of services they offered as it may apply to my type of center. Their services include: Periodic Well Visits/Pap Smears/ Breast Checks, STI testing/treatment, Cancer Screening/Colposcopies/ LEEPs, medication abortions, Pregnancy Evaluations/Gestational Ultrasounds, Birth Control Services (pills, IUD, implant, rings, depo shot), Immunizations (Gardasil series), Gender Affirming Hormone Care (available to 18+), Vasectomies, PrEP and, Ectopic pregnancy/PUL oversight, care, and referral. She said they currently do not have services dedicated to sexual assault survivors that visit them. They have select referrals that they partner with closely in the community to assist their patients in their recovery. Jenny believes it would be beneficial for the Planned Parenthood she works at to have a social worker on site: available for their patients, with a follow up plan if necessary. I then asked her what type of services she would recommend for my type if center she responded with, “Services I would recommend that you offer for your center: trauma processing, home relocation services, welfare application/review services, access to local women’s center for additional home/ vocational/meal needs, opportunity for gatherings of fellow survivors to share, if they would like”. This answer showed me that I should include the transitional housing aspect. Instead of home relocation services, I would like my center to be one of those services along with additional/ vocational/meal needs.
I also asked some questions to help give me an idea how big this medical aspect should be in my center. At Jenny’s place of work they have seven exam rooms and see around 35 patients per day in Boise, Idaho has around the same population as my location in Anchorage, Alaska. I then needed got know about how many doctors/nurses they have on staff for some space requirements. Jenny said, on a normal day, they have 1-2 PA-C’s/RN’s on staff. They have their doctors on staff only for visits that require oversight. Doctors are on site 1-2 times per week. This helped me gather I won’t need many individual offices in the medical area.
Experiment
Plant Growth
For my experiment I chose to take clippings from a Pothos plant. I chose to do this experiment to simulate that the effects of Polar Night and Midnight Sun would have on human beings and how a good night and day cycle would. These plant clippings can regrown in water or soil. I did not have any soil so I chose to put 3 clippings into 3 separate jars of water. I then put the first jar up by the window here it would get direct sunlight and also experience a normal night and day cycle. The second plant I put under a constant white light lamp; the reason for this is I wanted the plant to experience what Midnight Sun would be like and they said artificial light for this type of plant would work. Lastly I put the third plant in a kitchen cabinet that my family never opens, this was to simulate Polar Night. I let these clippings sit in their environment for a week as it said it usually take 7-14 days to show any major growth; as I was not looking for any major growth I ended it at 7 days.
The plant that grew the biggest root was the plant by the window as it had the perfect setting for growth. Coming in second was the one in constant light, which surprised me a little because we would feel the plant would be overwhelmed by all the light and would die but that was not the case. Lastly the one in the dark barely grew at all because it got no light during the 7 days. This plant can grow roots in water in artificial light and darkness. I decided I needed three environments based on some research about mental health, Seasonal Effective Disorder, Midnight Sun, and Polar night. The first environment I set up a simulation of constant light by using a white light lamp. I didn’t know what to expect since it was still able to grow in artificial light. After 7 days it ended up with a medium sized root coming out. The second environment I set up was a normal environment for a plant to grow; the normal day to day cycle of sunlight and then darkness. I put this clipping in a window that faces the sunrise and also gets the angle of the afternoon sunlight. This clipping ended up having a large root in a short amount of time, I was impressed. Lastly I put a plant clipping in space of constant darkness. As I suspected it did grow a small root. This experiment showed me that plant life is greatly effected by its environment just as people are. Plants need a stable environment to fully flourish as people do as well. It was clear that plants could still grow in the non-ideal environment but not much, they struggled more than the plant in the stable environment. People in Alaska experience extreme light and dark seasons and that can affect how someone functions both mentally and physically. The experiment showed how these environments effect life physically. In the center it will be crucial to really build that stable environment through design for each season.



Day 1 Root Growth Environments Day 7 Root Growth







Observation of Behavior
I arrived at Mocha Monkey in Waconia Minnesota at around 2:50 pm on a Friday. Mocha Monkey is a coffee shop that has two levels; the first level has a few high-top tables, two regular tables with four chairs and then there are two plush leather chairs with a coffee table by the fireplace. I decided to go two the second floor as there are many more options for seating that I could observe. Walking up the stairs to the right they have some lounge seating, one high-top table and two tables with four chairs. To the left of the staircase there are multiple rooms, the first room has a booth and table arrangement (this is where I sat), two seat table and then a one chair desk by the railing. Into the middle room there is a rather large table with four chairs and a rocking chair in the corner. In the last room it is split into like two separate spaces; one half has a long table with six chairs and then another small table with one chair. On the other half there is also a long table with five chairs, one big plush leather chair and then a high-top table with the wrong heighted chairs. When I first walked in there were 3 women using the high-top tables and two women using one of the regular tables and no one was using the plush leather chairs by the fireplace, which I was surprised about because normally when I go there they are normally used. Moving on up to the second floor I sat in the wooden booth seating. To the left of the staircase there were some women around the age of 18-22 and seemed to be doing homework as they had laptops and books. I do not know how long they were there before but from the time I got up there at 2:55, they left at 3:15. There were also two women kind of across from me talking and drinking a beverage; again they were there before me so I don’t know the exact time they stayed there but they ended up leaving at 4:20. I check to see if there were any people in the back rooms and there was one lady around the age of 40-50 and one other around the age of 13-15 maybe and they seemed to be doing work at the individual seated tables. I did not end up seeing them leave before me and I left at 5:30 pm. At around 4:30 two women around the age of 50-60 came in and one sat in the big plush leather chair while the other turned a chair around to talk and they only stayed for about 30 minutes. Another group of about four women around the age of 60-65 came in and they sat in the middle room with the long table that had six chairs; they stayed for about 20 minutes. A family of six ended up coming in and they practical used the whole left side of the stair case and ended up using the floor for sitting as well. The family stayed for about an hour. About 20 minutes after they left a group of five boys and two girls around the age 15-17 came in and used the lounge space and moved some of the tables and chairs around so they could all talk in a circle. The boys ended up going down stairs and used the two chairs by the fireplace while some of the others stood around them.
analysis
I chose to do an observation of what types of seating people preferred and how long they stayed in the seating arrangement they chose. Mocha Monkey has always had so many types of seating so I chose to go there. Normally my friend and I go there to work on homework as so do many other people. Since I went on a Friday I didn’t see many people working on homework probably due to the fact it was the end of the week and most people just seemed to be hanging out having a beverage. Once upon a time before Covid-19 happened they used to have a group of couches and they were always full, but sadly they changed them to individual chairs for the lounge area. Normally I would choose a high-top, but I chose to sit in the booth because it gave me the most range to observe most of the seating. Overall I would say many people if they are doing some sort of work prefer to use a regular height table with a bigger table for some work space. The people who just came with one other person almost always chose to sit at a table made for two and seemed to stay a while. The women who were older seemed to seek out a more comfortable place to sit and when the lounge area was a taken they went to a table but neither groups of the older women stayed very long and it had me thinking maybe it was because the chairs were wooden and not very comfortable for someone in that age range. The family of six was very interesting to watch. They used the entire left side so anyone that same upstairs during that time did not use that side. The kids ended up using every lounge chair and table space. Something that surprised me is after they used all seating types they ended up moving to the floor to sit and even the mom joined in. This made me think for my center I should include some comfortable floor like seating for those who prefer not to use a table, couch or chair. Overall this observation showed me I need to include private work spaces along with group workspaces for those people who may be brining school or work with them to this center. For the people coming and possibly making friends and talking with to others and hanging out might need some lounging options instead of tables and chairs. I noticed the group of teenagers made a circular like layout with the furniture and this made me think I should provide circular layouts of future so people can talk face to face with everyone they are talking too. Places to put your things was a big thing I noticed that people needed. A lot of people were not sure where to put their belongings so they would set them on the ground or in the chair next to them. There were some coat racks on the first floor but nothing on the second floor and I think maybe each setting area should have a place to set your things.
Design Theory 1
Comfort Theory
Based on the Comfort Theory and Practice book by Katharine Kolcaba there were three types of comfort to begin with: relief, ease and renewal which later got changed to transcend. Relief is the experience of a patient who has had a specific comfort need met. Ease is a state of calm or achievement. Transcendence is the state in which one rises above problems or pain. Katharine began to research more on comfort theories, holism, and human experience. At first she just focused on the physical and mental aspect, but her researched pushed further into that there are actually four types of comfort when thinking about human experiences: physical comfort, psychospiritual comfort, environmental comfort and sociocultural comfort. The physical comfort aspect really focuses on patients in pain and being able to ease that pain. Some examples on how to achieve that are: homeostatic mechanisms such as fluid/electrolyte balance, stable blood chemistry, adequate oxygen saturation and other metabolic indications of health. In addition to physical comfort, positioning was very important. This means sitting correctly, having freedom to move independently, and well-fitting furniture need to be included to enhance physical comfort. Doing this can lead to increased function and activity. Onto physhospiritual comfort which is the combination of physiological health and spiritual health. It includes: self-esteem, faith in a higher being or order, being independent, feeling relaxed, being informed and feeling useful. Psychospiritual comfort is basically whatever gives life meaning for someone and gives them self-esteem, self-concept, sexuality, and a relationship to a higher being or order. Environmental comfort is a key aspect when creating a design and is used to promote physical and cognitive functions. Some examples of environmental aides for comfort are: hand rails, non-glare lighting, grab bars in restrooms, calendars and clocks, minimal noise and ADA accessible furniture; which all contribute to better comfort and function. There are also some other things to think about when it comes to environmental comfort as a designer such as designing with external surroundings, conditions and influences in mind. Color, light, noise, ambience, temperature, window views access to nature and use of natural elements are all aspect we as designers have control over to make the space more comfortable. Lastly there is sociocultural comfort. A study found the friendliness and caring staff members was essential in achieving social comfort. The patients of this study stated that they looked to their nurses and other staff members for social comfort rather than their families but family was still important. Making the user feel at home, important, intelligent, supported and valued is also important. Culture has made its way into this context of comfort. When designing it is important to think about other cultures besides your own and some things to think about are: traditions, language, clothes and customs.
analysis
This design theory implements the well-being and comfort of the user. For physical comfort as a designer I think physical comfort is really important in a center focused on healing. Some aspects I will be including for physical comfort are: well fitted furniture for all body types, ergonomically correct furniture and designing a space where the disabled feel abled. Physhospiritual comfort I don’t necessarily think can be designed but it more can be achieved through the staff and personal but I think there are some ways to achieve it in design. First off, I think creating the space for the self-defense classes can indeed bring up someone’s selfesteem and self-concept. Including many different types of therapy and transitional housing can also contribute to physhospiritual comfort because it can bring independence, relaxation and the feeling of being useful. The environmental comfort aspect spoke to me the most as a designer and how it promotes physical and cognitive function. I will be including hand rails, non-glare lighting, grab bars in restrooms, calendars and clocks, minimal noise and ADA accessible furniture; which will all contribute to better comfort and function for the users in my center. Thinking about: color, light, noise, ambience, temperature, window views access to nature and use of natural elements are all things I have thought about and will continue to think about when designing to make sure these women are comfortable in this healing environment. Lastly, in sociocultural comfort I felt it was again more of the staff that can achieve this, but the study did say that culture was included in this. I will need to take in account, language and customs when designing this center especially the native culture. I want all users to feel comfortable and included while making a unique and functional design.
Design Theory 2
Place Attatchment Theory
Interior design influences the atmosphere and experiences created in spaces. When interior designing you want to be able to create a space were people have good place attachment so the users will keep coming back. Users from three different coffee shops were surveyed about some of the key characteristics and design elements that cause them to feel an attachment to their specific coffee shop. The top five design elements were: cleanliness, aroma, adequate lighting, comfortable furniture and a view of the outdoors. The survey also showed that seating by windows, walls or partial walls were most popular. The reason for this is because the people were drawn to elements of physical structure as it seems to provide protection and they can watch the people around them. Based on another study place attachment is an important concept for designers because it effects both functional and meaningful aspects of space. People create a strong sense of place attachment when they are satisfied with the environment, which supports both mental and physical health. The sense of belonging contributes to a person’s ability to experience attachment to a place. Place attachment involves different social relationships including individuals, groups, and cultures. When designing a space to create this sense of place attachment there are few things to consider:
• Include access to natural areas such as gardens or walking trails to increase mood, increase satisfaction, encourage communication and provide refuge for users.
• Design space to create a sense of community to encourage place attachment through socialization.
• Allow for spontaneous social interaction by crossing circulation paths.
Use a variety of unique materials.
• Include areas for public display of achievement for the users to make them feel more connected to the space.
analysis
For this women’s focused sexual assault center I am designing it is definitely important to create a positive place attachment so these women will come back and continue to heal, while having a positive experience in the healing process. As stated in the research there are ways as a designer to help create positive place attachments to the space. Including adequate lighting will be very important for the space I am designing; based on previous research lighting will be key in this environment. It will help to have god lighting during both the long dark season and long light season. Some sort of connection to the outdoors can influence a positive effect on a person. Including large windows with a view to the outdoors I think would be the most beneficial for this center as it will allow for lots of daylight to come in as well as bring the positive influence with a view to the outdoors. Comfortable furniture is important as well you want the user to feel comfortable especially in a place where women have experienced trauma and are there to heal. Having comfortable lounge areas to encourage socialization could help these women during their process of healing. Making sure there is a comfortable layout of furniture by having seating by windows and walls will make the users feel safe and in a sexual assault center the biggest aspect is safety. Something I found interesting was to increase socialization and community among users, as a designer you can design circulation paths to cross and I think doing this will be very helpful in the center. Increasing the sense of community can help a person feel they belong and for my center community, socialization and feeling belonged are all important aspects when healing to get back out into society.
