Nationwide, patients are languishing on waiting lists. Dartmouth devised a solution.
In just a single week, the Department of Dermatology cleared almost its entire waiting list of nearly 4,000 patients, some of whom had been longing to get an appointment for months. The schedules-cleared, allhands-on-deck approach to improving new patient access—aptly named Patient Access Week—was the first of its kind in the nation.
The problem of unwieldy waiting lists isn’t exclusive to Dartmouth Health: Dermatology clinics across the country are experiencing huge referral backlogs, particularly in academic medical centers. Among the many contributing reasons is the concern that physicians will not have enough appointments available
Continued on page 3
Alicia Dagrosa, MD, MBA, RES ’21, MED ’17, TU ’16, examines a patient during Patient Access Week in April.
We believe this approach will become a sustainable solution to creating access for all patients.
M.
Our goal in the Department of Dermatology is to provide excellent patient care, which includes expanding access to care. In December, we embarked on a massive undertaking to reduce our referral backlog of nearly 4,000 patients who had been waiting for appointments, sometimes for months.
Our department isn’t alone in this problem, but we are the first to try a new approach to creating access, which we dubbed Patient Access Week. I am thrilled to tell you about its huge success, both for patients and providers alike.
In fact, everyone in our entire department—and even a few in other departments—devoted much time and energy to this endeavor. We believe this approach will become a sustainable solution to creating access for all patients.
In this newsletter, you’ll read about some of our recent achievements, both in terms of patient care and innovative research. I also want to share a sneak peek into our future vision. We are investigating the potential
to expand our residency program. Although I cannot share all the details yet, I’m excited about everything I see on the horizon for our department. Stay tuned.
Please also join me in congratulating Jillian Rork, MD, on receiving a grant of more than $300,000 from the National Institutes of Health to study whether psoriasis increases cardiometabolic risk for people with Down syndrome. We also have plans for expanding our basic research efforts with additional scientists whose labs can collaborate with researchers in other disciplines, such as immunology, oncology, and microbiology.
Thank you for joining me in supporting our department, our patients, our residents, and our staff.
M. Shane Chapman, MD, MBA, RES ’99
Chair and Professor, Department of Dermatology, Dartmouth Hitchcock Medical Center and the Geisel School of Medicine
Shane Chapman, MD, MBA, RES ’99
Continued from page 1
Pioneering Patient Access to Care
for established patients who need follow-up care. In addition, academic medical centers typically have a smaller number of dermatologists on staff but receive referrals from outside clinics to handle more complex presentations. For certain conditions, patients might have to wait six months for an appointment simply because there are fewer subspecialty providers.
Shane Chapman, MD, MBA, RES ’99, chair of the Department of Dermatology, couldn’t accept that these patients had to wait so long for the care they needed. So, Chapman; Caitlin Yazel, APRN, Dermatology nurse manager; and other department leadership worked to create a plan to solve the backlog, which they first implemented December 11-15, 2023.
The Countdown Begins
“Shane had the idea for a new patient access week, and we started planning in April 2023,” Yazel says. “We pulled our thoughts together to consider all the potential problems, like how would patients move
Kristan Schiele, MD, a second-year resident, with patient David Davison during the second Patient Access Week in April 2024. “I couldn’t believe I got in so quickly,” Davison says.
through the clinic? And are we going to have enough space in the parking lot?”
With so many patients to see, the entire department, including physicians, nurses, medical assistants, residents, administrative assistants, the research team—literally everyone—came to clinic all day every day. As a testament to the thoughtful planning, no one in the Department of Dermatology called in sick or took vacation that week.
“A key cultural point was asking faculty regularly for their input,” Yazel says. “We gave updates at faculty meetings and asked, ‘What makes you nervous about this? What aren’t we thinking of?’”
Yazel also brought the plan to the nursing team for input. Everyone brought up different potential obstacles, so by the time the big week arrived, nearly all the kinks had been worked out. “That was our strategy to address concerns that might make this plan unsuccessful,” she says. “People had opportunities to think this through.”
Making the Most of Every Appointment
Among the concerns were logistics—getting so many patients in the door for appointments would not be easy. To make it happen, visits were limited to about 10 to 15 minutes to discuss the patient’s main concern. If a patient had a complex issue, Chapman or Yazel would handle the case, so the faculty could keep the flow of patients moving smoothly.
Cheyanne Jones, RN, felt apprehensive about how to handle the sheer volume of patients. The answer was to change the normal appointment model.
“We weren’t on a specific provider schedule. It was more like first come, first served,” Jones says. “There were a certain number of patients scheduled at 9:00 am, a certain number at 10:00 am, and so on. Whichever provider was ready for another patient would come out to get someone.”
Julianne Mann, MD, MED ’07, section chief of Pediatric Dermatology, says it felt exhilarating to serve so many patients that week. She recalled one of her patients who had a large melanoma on the back. “It’s so rewarding to see someone like that patient and think, ‘Wow, if this melanoma had progressed, this patient’s journey could have been very different.’
“We chose medicine as a profession because we want to make a difference in people’s lives. One way to do that is to create access for patients who are waiting to be seen,” Mann says. “With this new model, we can reach patients who need us. That’s very rewarding and makes the extra effort well worth it.”
Residents in the Mix
Residents also contributed to the week’s success, forgoing surgeries and didactic learning in order to spend all their time in clinic. In addition to the positive feeling of helping so many patients, residents also enjoyed the sense of teamwork.
“It was cool to come together as a team and see all the energy throughout the week,” says Matthew Davis, MD, a fourthyear resident. “We all had the same mindset and same goal of seeing as many new patients as possible. It was a lot of work, but a great solution to a complex problem.”
“We were tired but satisfied,” says Dylan Badin, MD, a third-year resident. “We’ve been through a tough challenge together. As residents, we’ve been studying it, and now we can see it, diagnose it, and treat it. The things we’ve been learning correlates with good patient care.”
Quality care for patients and staff alike
As Department of Dermatology’s vice chair of quality improvement, Julianne Mann, MD, MED ’07, felt excited about caring for more patients during Patient Access Week, but she also wanted to make sure the physicians, nurses, residents, and others were cared for in the process.
“It’s powerful to join together as colleagues to address the problem of patient access that we’re each individually struggling to respond to,” says
Alicia Dagrosa, MD, MBA, RES ’21, MED ’17, TU ’16, (right) and James Feng, a third-year medical student at Geisel School of Medicine, examine patient Sandra Button during Patient Access Week in April.
A Model for Success
The department held more patient access weeks in February, April, and June. Most of these were follow-up appointments, and since then, the department’s schedules have returned to normal. The fears that faculty might become overwhelmed with new patient follow-ups, thankfully, didn’t come to bear.
Even though appointments were brief, the high ratings on the department’s patient survey revealed that patients were pleased with their care and appreciated that providers took time to connect with them on a personal level.
Newport, Vermont, residents Daniel Cordeau and Ann AzurCordeau were among the patients seen in April—though only Ann had an appointment. But Daniel had recently been referred to a dermatologist for a concerning spot on his back and wondered whether Brian Simmons, MD, RES ’20, would mind taking a look after he finished with Ann’s examination.
“I just mentioned it to him; I didn’t think he’d do anything. But he looked at it and said, ‘We can take care of that,’” says Dan, who had the concerning spot removed the same day, thanks to a cancelation in Simmons’ schedule. “I’ve never been in a hospital like this where a doctor will say, ‘I’ll do it now.’”
Yazel, Jones, the residents, and others all said the model was a huge success and that it could be applied to other departments dealing with patient backlogs.
“It might look different because patient needs in other departments are different,” Yazel says, “but the concept can be applied across the spectrum.”
We chose medicine as a profession because we want to make a difference in people’s lives. One way to do that is to create access for patients who are waiting to be seen. With this new model, we can reach patients who need us. That’s very rewarding and makes the extra effort well worth it.
Mann, the section chief of Pediatric Dermatology. “But this kind of innovation must also be sensitive to the needs of the human beings on the health care team. We could roll out a new care delivery model that’s great for patients, but if doctors and nurses and secretaries are overworked, stressed out, and miserable, then it’s not a good model.”
In addition to the department providing lunch and snacks for clinical teams every day that week, Mann
also helped create a staff experience survey. This helped doctors, nurses, technicians, and secretaries feel that they had a voice and an opportunity to share ideas for improvement. The survey results mirrored her own feelings: “We learned our clinical teams loved it. The fact that we focused not only on excellent patient care but also looking after doctors and nurses makes this model really exceptional. It’s a signal to them that their needs matter, too, and it motivates people to work hard and be at their very best.”
Julianne Mann, MD, MED ’07 Section Chief, Pediatric Dermatology
AI at the Cutting Edge of Surgery
Algorithm analyzes surgical margins of cancerous tissue in real time
Surgeons face a delicate balance when removing a cancerous tumor: They need to extract all of the cancer while leaving as much healthy tissue intact as possible.
But figuring out exactly where that line lies can be tricky. So Matt LeBoeuf, MD, PhD, section chief and director of Mohs Micrographic Surgery, and his colleagues are investigating how artificial intelligence (AI) and machine learning could help surgeons make the most precise excisions possible in real time.
Most surgeries require removing the tumor and sending the tissue to a lab for analysis of the margins, which could take days and can delay fixing the site. The dilemma lies in the question of how much tissue to remove—the larger the margin, the better the chance that all the cancer is
removed, but it’s also more likely that too much healthy tissue goes with it. On the other hand, if the margin is too small, some cancerous tissue might remain, resulting in the need for another surgery.
Currently, even without AI, LeBoeuf can make these kinds of decisions in real time during surgery, but this approach is largely limited to skin cancers treated within the Dermatology Department at Dartmouth Hitchcock Medical Center (DHMC). That’s because there’s a pathology lab onsite and LeBoeuf has specialty training to analyze and precisely map any remaining tumor—but not all surgeons have that training. Typically, LeBoeuf uses a 1- to 2-millimeter margin of tissue during surgery, and then analyzes the margin within 15 to 30 minutes. He can easily return to surgery and excise more tissue if needed.
Matt LeBoeuf, MD, PhD,
section chief and director of Mohs Micrographic Surgery (right), is investigating how artificial intelligence (AI) and machine learning could help surgeons make the most precise excisions possible in real time.
“It’s an iterative process of removing tumors, and doing it this way results in less than 0.5% recurrence,” LeBoeuf says. It also helps him spare surrounding healthy tissue. With confidence that the tumor is completely removed, he can fix the surgical site the same day. LeBoeuf wants to make this procedure seamless in other departments at DHMC and at other institutions, and one way of making that possible, he says, is using AI.
In his research, LeBoeuf is working to use AI to combine the logistical processes of analyzing tissue. “AI takes all of these skillsets and puts them into one virtual platform, which automates these decisions,” he says. No longer would a pathologist have to be onsite for real-time analysis—they could analyze the tissue digitally from anywhere in the world.
“We’ve started thinking about how this can be applied to nonskin cancers, too, specifically oral and airway cancers,” LeBoeuf says. “Those types of tumors have high rates of positive margins and the tumor coming back.”
Yet, particularly with oral and airway cancers, excising more tissue might mean that surrounding anatomic structures are affected, maybe unnecessarily. AI could help minimize this possibility all over the body.
“This has a great potential to change the way we do surgery in the future, and we’re moving forward in a thoughtful, deliberate manner,” says LeBoeuf, who is collaborating with others, including Louis Vaickus, MD, PhD, medical director of pathology informatics at DHMC, and Joshua Levy, PhD ’21, assistant professor of dermatology at the Geisel School of Medicine at Dartmouth. LeBoeuf notes, “We must be skeptical of anything that’s new. With AI, you’re assuming the computer will do the job as well as human surgeons do currently, and that’s a lot to ask right now. We must make sure patients are protected.”
Although this technology won’t be ready for implementation for many years, LeBoeuf says the AI algorithm already is highly effective at detecting and mapping tumors; however, the research so far has focused on only one tumor type and only at DHMC. LeBoeuf says the algorithm will need to be adjusted for other types of tumors and different analysis equipment at other clinics.
“The biggest challenge with AI is ensuring the algorithms used with internal data can be applied to external data, such as slides from other medical centers. Slide variations make a big difference with algorithms,” LeBoeuf says. “This is a reasonable next step for future grant funding; we would do multi-institutional collaborations. The algorithm is performing extremely well here, and we want to make sure it can be broadly applied anywhere in the country and hopefully even beyond.”
Coming Soon: Insights about psoriasis in people with Down syndrome
Psoriasis is associated with increased cardiometabolic risk factors and cardiovascular disease in the general population, resulting in a higher incidence of heart attack and stroke. But this association has not yet been explored in people with Down syndrome, a population that has been considered protected against cardiovascular disease. As a result, dermatologists have often found it difficult to know how to appropriately screen for cardiovascular risk in patients with Down syndrome and psoriasis.
That may soon change, as Dartmouth Health pediatric dermatologist Jillian Rork, MD, recently received a two-year grant of more than $300,000 from the National Institutes of Health for a new research study titled, “Down Syndrome and Psoriasis: An Investigation of Cardiometabolic Risk.”
This study will use a population-level database to enhance the understanding of psoriasis in people with Down syndrome and to explore whether psoriasis could present an exception to their presumed cardiovascular disease resilience.
“With improved life expectancy for people with Down syndrome, understanding how common chronic medical conditions, such as cardiovascular disease, affect this population is crucial,” Rork says. “This research could significantly affect patient care.”
What role does the skin microbiome play in cancer progression?
Prouty grant funding puts tiny suspects under the microscope
The death of singer/songwriter Jimmy Buffett from Merkel cell carcinoma thrust this rare and aggressive form of skin cancer into the spotlight. Lurking in its shadows is a common (and typically harmless) virus that lives on the skin, which appears to be the leading cause of the disease.
“That’s one of the few skin cancers linked specifically to a virus, but other viruses are living on the skin all the time. Other shifts in the skin microbiome might relate to other types of skin cancer,” says Dorothea Barton, MD, FEL ’13, RES ’11, MED ’07, section chief of Complex Medical Dermatology.
Barton and her colleagues in dermatology, epidemiology, pathology, and bioinformatics are building a database to categorize the skin microbiome and see
which bacteria, fungi, and viruses live on the skin, and what amounts are normal versus harmful.
Her new study focuses on developing reliable methods to categorize this data and investigate the skin microbiome’s role in cancer development and progression. This study focuses on certain non-melanoma skin cancers, which are the most common skin cancer types in New Hampshire and Vermont.
Barton’s research was recently selected as a Prouty Pilot Project, receiving a grant of $110,000 in a philanthropically supported program aimed at supporting preliminary cancer studies. She hopes the preliminary data from this study will help her secure larger grants for further investigation.
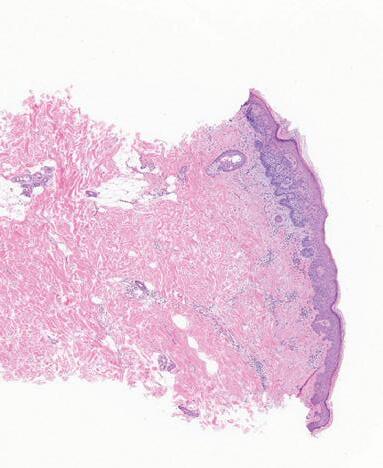
A punch biopsy (above) from the left shoulder showing skin cancer, illuminated in purple, at a magnification of 100x. The image shows well circumscribed, superficially located basaloid cell tumor with hyperchromatic, pleomorphic nuclei and mitoses consistent with basal cell carcinoma, superficial type.
Produced by:
Viruses are living on the skin all the time. Other shifts in the skin microbiome might relate to other types of skin cancer.
Dorothea Barton, MD, FEL ’13, RES ’11, MED ’07 Section Chief, Complex Medical Dermatology