26 minute read
Peer Mediated Groups Nonpharmacologic Management of Pain for and By Those with Sickle Cell Disease

from DJPH - Minority Health - from Disparities to Equity
by Delaware Academy of Medicine and the Delaware Public Health Association

Stephanie Guarino, M.D., M.S.H.P.
Internal Medicine and Pediatric Hematology/Oncology Physician, Nemours Children’s Health;
Director, Adult Sickle Cell Program, Center for Special Health Care Needs, ChristianaCare Charmaine S. Wright, M.D., M.S.H.P.
Medical Director, Center for Special Health Care Needs, ChristianaCare Lee M. Pachter, D.O.
Institute for Research on Equity & Community Health (iREACH), ChristianaCare;
Professor, Pediatrics & Population Health, Thomas Jefferson University Sophie M. Lanzkron, M.D., M.H.S.
Johns Hopkins University
BACKGROUND
Sickle cell disease (SCD) is a genetic disorder that causes red blood cells to become misshapen and break down. Affecting 90,000 Black and Brown people in the US, the disease causes decreased blood flow resulting in pain, fatigue, and infection. SCD causes significant morbidity across the lifespan, affecting all aspects of patients’ daily functioning. Finding ways to manage the most common and debilitating complications, including chronic pain, is of utmost importance to restoring quality of life and decreasing health care utilization in this population. Several studies have estimated that chronic daily pain affects 30-50% of adult patients with SCD.1,2 Furthermore, in both pediatric and adult patients with SCD, those with more frequent chronic pain report more frequent depressive symptoms, more frequent hospital admission, and more significant functional disability.2,3 Those patients on chronic opioid therapy report poorer health-related quality of life (HRQL) outcomes as well as higher symptom burden and more somatic symptoms including depression and anxiety.4,5 Racism and stigma provide further barriers in the appropriate management of sickle cell disease.
RACIAL DISPARITIES
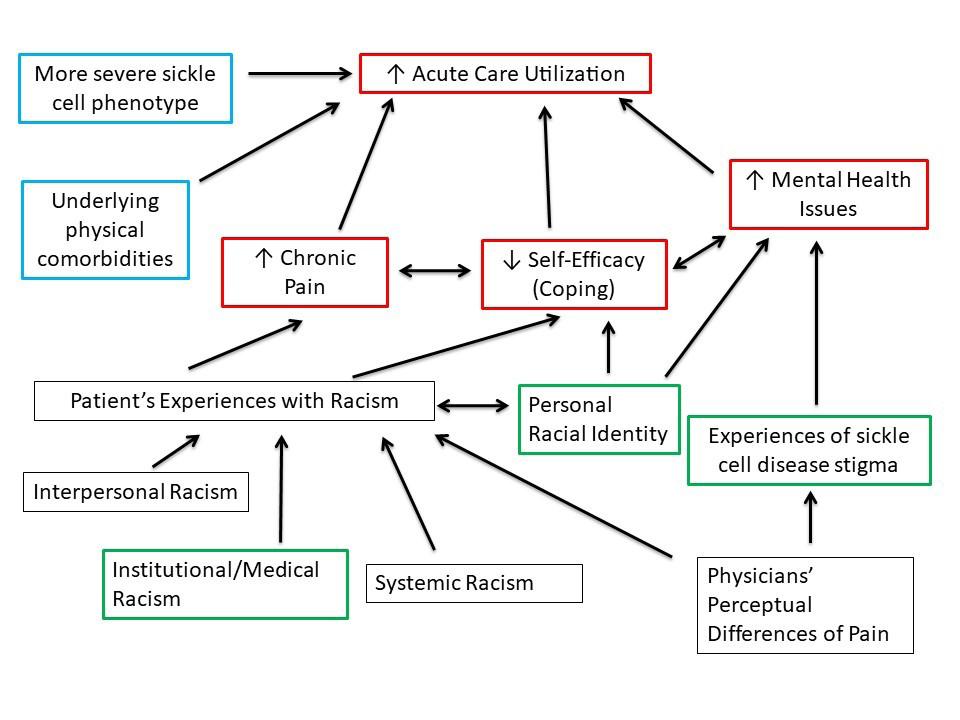
Racial disparities in pain care appear to stem, in part, from a perceptual source. Previous psychological research in this domain has focused on high-level social cognitive processes. For example, volunteer adult participants, registered nurses, and nursing students attribute higher thresholds for pain to Blacks vs. Whites6,7 as a function of stereotypes regarding social status8 and false beliefs about racial biological differences.9 Beyond these factors, other work links reduced care for racial minorities’ pain to implicit racial bias10 and beliefs regarding substance abuse.11 Notably, studies of experimental pain suggest that Black participants exhibit lower pain tolerance and thresholds for pain12,13 stemming from cultural and neurobiological differences in pain beliefs, experiences, and coping.14 However, other work demonstrates a separate, potentially more tractable source of disparities in pain care: Biases in the visual perception of painful facial expressions. Specifically, White perceivers consistently demonstrate more conservative thresholds for seeing pain on Black (vs. White) faces.15 This perceptual bias stems from disruptions in configural processing: racial bias in pain perception was intact for upright faces, but significantly reduced when faces were inverted. Critically, racial bias in pain perception was still present when equating stimuli on skin tone, luminance, contrast, structure, and expression, and this bias in pain perception positively predicted racial bias in treatment independent of explicit prejudice and stereotypes. In sum, we suggest that disparities in pain care stem, in part, from a perceptual source. Disrupted configural processing of Black faces yields more stringent thresholds for the interpretation of perceived pain in Black patients, triggering a cascade of biased processing and behavior fueling societal-level racial inequity in care. It is unclear how experiences of bias and discrimination affect health outcomes such as SCD pain. Discrimination is associated with decreased self-efficacy and poor mental health outcomes (see Figure 1). The Improving Patient Outcomes with Respect and Trust (IMPORT) study demonstrates that patients with SCD report higher rates of race-based discrimination compared to other Black patients.16 Disease-based discrimination was associated with more significant self-reported pain. Previous research has shown that patients with SCD report experiences of poorer interpersonal care when hospitalized than other patient groups (9). Furthermore, these patients report poor communication with medical personnel, which has been associated with lower trust and higher rates of discharge against medical advice (10). Because virtually all patients with SCD identify as Black or other racial and ethnic minorities, it is important to understand how experiences of racism and stigma interact to affect a patient’s health and functioning. It is unclear how physical, psychosocial, and other drivers influence pain, self-efficacy at managing SCD and care utilization in patients with SCD and chronic pain.
THE IMPORT STUDY
The IMPORT study demonstrated important relationships between experiences of SCD-related stigma and increased acute care utilization.6 The IMPORT study was an NHLBIfunded observational cohort study of SCD patient experiences with health care. Participants were recruited at two academic medical centers in the Baltimore/Washington, DC Metro area. To be eligible for participation, clinic attendees needed to be over 15 years of age, with HbSS, HbSC, Hb SB-thalassemia, or Hb SS/α-thalassemia and no plans to move within three years. Participants completed a battery of surveys including the SelfCare Self-Efficacy Scale (SCSES) upon enrollment and every six months across three years. A total of 291 subjects were enrolled.
Red boxes: outcomes of interest Blue boxes: physical drivers Green boxes: psychosocial drivers Black boxes: additional drivers
Dr. Lanzkron is a co-investigator on this project and maintains IRB approval for the study at Johns Hopkins (IRB00234974). Patients with SCD report greater burden of disease-based discrimination that is associated with higher self-reported pain measures.7,16 Racism can be experienced at many levels; health care settings are certainly not immune and have been sources of some of the most egregious examples in our history. Since SCD is predominantly seen in Black patients, experiences of racism are a key contributor to their health.12–14
EXPERIENCES OF RACISM
Experiences of racism have negative effects on chronic pain and depressive symptoms in SCD. Previous research noted that higher levels of perceived racism predicted more depressive symptoms in adolescents with SCD.15 An additional study found that in adolescent patients with SCD, greater experiences of racism were associated with greater pain burden and greater perceived health-related stigma was associated with lower health-related quality of life.17 Although a systematic review demonstrated an association between pain and depressive or anxiety symptoms in pediatric SCD, they noted the need for ongoing research to better understand the relationship and to extend the research to adult patients.18 Furthermore, ways to intervene to moderate these effects have not yet been studied.
SELF-MANAGEMENT PROGRAMS
Self-management programs may be efficacious for treatment of chronic pain. Though not yet tested for patients with SCD, peer-led self-management groups as an alternative to those facilitated by experts have been trialed in other patient populations with positive results. For example, in other chronic diseases such as diabetes and HIV, selfmanagement programs have been shown to improve health outcomes and patient self-efficacy.5,8 Research has shown feasibility and effectiveness in pain management for elderly nursing home patients and women living with HIV/AIDS.9,10 In these studies, there was a significant reduction in daily pain scores as well as an improvement in patient-reported mood measures; sample sizes were small and did not include SCD patients. Our preliminary data also showed that most respondents felt that peers or people living with SCD should be involved in leading the groups. This finding reinforces the importance of using a community-engaged research (CEnR) approach to developing such a programmatic intervention. Additionally, mental health literature demonstrates that group interventions can be used to decrease disease-specific stigma; this has not yet been studied in SCD.19
ChristianaCare’s Sickle Cell Program cares for almost half of the 400 adult patients with SCD who reside in Delaware. In a pilot funded by the Delaware Center for Translational Research ACCEL program, we are adapting the general curriculum of a peer-mediated pain group specifically for use in SCD using key informant interviews with patients with SCD and family members. The general six-week curriculum for a peer mediated group intervention helps patients with a range of chronic illnesses decrease pain levels and develop coping skills. Patientreported outcomes are measured and monitored via PROMIS-29 scale at the beginning and end of the program, as well as through the Global Impression Scale at the end and the PHQ9 and GAD7, measures of depression and anxiety, throughout. This program provides a supportive platform for patients to share their narrative and struggles. During individual meetings prior to group sessions, the patient and physician identify challenges and begin to work on solving problems. The course teaches skills that help manage pain through relaxation, visualization, and guided imagery exercises. Participants set realistic goals that are congruent with their morals and values and create a paced, modified, or replacement approach to accomplish those goals. Adding the perspective and curricular items important to those patients with SCD, specifically addressing racism and stigma, we hypothesize will enhance the effectiveness of the intervention. The next steps in this work are funded through a COBRE grant supporting the Delaware Comprehensive Sickle Cell Research Network of which ChristianaCare is a member. We plan to examine the complex interplay between experiences of racism at many levels, disease-related stigma, and racial identity on chronic pain. First, we will analyze the landmark IMPORT dataset to evaluate the relationship between SCDrelated stigma and self-efficacy in the management of SCD. Next, we will explore the themes of racism in a medical setting, SCD-related stigma, and self-efficacy in disease management in order to incorporate them into the curriculum. Finally, we will demonstrate feasibility of the SCD-specific chronic pain curriculum we have created through extensive community engagement. While group interventions have demonstrated effectiveness in improving outcomes for other chronic diseases, they have not yet been studied in SCD. The use of peermediators is also novel in SCD. Once these relationships are better understood and the curriculum has been proven feasible, we can pilot the intervention and evaluate its impact on the experience of chronic pain and effective self-management of disease in adult patients with SCD.
INNOVATION
Previous research has begun to evaluate the relationship between experiences of racism, stigma, and chronic pain in SCD, yet significant gaps in our understanding of these interactions remain. Furthermore, the way that patients’ self- perception of race influences these experiences is also unclear. As the mental health literature demonstrates, one way to effectively fight stigma is through group interventions. This evaluation of the IMPORT dataset will be the first analysis of the associations between experiences of stigma and self-efficacy at managing SCD. These data were collected from a large group of adult patients with SCD in a longitudinal cohort at two major institutions and demonstrate important interactions between SCD-related stigma, worsening pain, trust, and communication in healthcare.6 This innovative study was the first to specifically examine these factors in SCD and demonstrated a greater burden of race-based discrimination than was previously reported in other Black cohorts, indicating the unique barriers faced by patients with SCD. Additionally, the study validated a SCD-specific tool to evaluate stigma and collected data on ratings of self-efficacy. However, the relationship between these two factors has not yet been explored. This project will be the first to look at how racial identity relates to experiences of stigma and discrimination and ratings of self-efficacy at managing SCD. The interaction between these factors have not been explored, particularly through a qualitative methodology. An improved understanding of these relationships, particularly in adult patients with SCD, will better inform our intervention to address the drivers of chronic pain and acute care utilization. Patients with SCD may experience both race-based discrimination and SCD-related stigma, both of which are influenced by a patient’s own racial identity. This will be the first peer-mediated intervention that specifically targets chronic pain in SCD. Group programs have documented efficacy in general chronic pain management, but this will be the first study to examine peer-led groups to improve self-efficacy in SCD. Ultimately, having an effective non-pharmacologic approach to chronic pain would be a ground-breaking intervention that addresses an outcome that patients have expressed is important to them. The intervention will be developed based on specific needs identified by the community of patients with SCD. Any treatment modality must address not only the physical manifestations and chronic pain, but also the patients’ psychosocial experiences of racism and stigma. Our proposed project is driven by strong interest from our patients with SCD based on preliminary data. We will build on the work accomplished during the first year of our CTR Pilot Project into this COBRE2 target project, to adapt the current chronic pain curriculum for use in SCD. The intervention will be led by peer leaders with SCD in collaboration with clinicians, representing a paradigm-shift in the approach to patient education and care delivery. By involving patients with SCD in community-engaged research to evaluate and adapt materials, the curriculum and peer leaders produced by this project will be unique. We will be the first research group to create an intervention that addresses how bias and discrimination affect health outcomes in SCD pain, led by the very patients who experience it. The relationship of these drivers, especially as they relate to chronic pain in SCD, will give patients a nonpharmacological treatment option and a new approach to hopeful self-care. Dr. Guarino may be contacted at:
1. Smith, W. R., Penberthy, L. T., Bovbjerg, V. E., McClish, D.
K., Roberts, J. D., Dahman, B., . . . Roseff, S. D. (2008, January 15). Daily assessment of pain in adults with sickle cell disease.
Annals of Internal Medicine, 148(2), 94–101. https://doi.org/10.7326/0003-4819-148-2-200801150-00004 2. Sil, S., Cohen, L. L., & Dampier, C. (2016, June). Psychosocial and functional outcomes in youth with chronic sickle cell pain. The Clinical Journal of Pain, 32(6), 527–533. https://doi.org/10.1097/AJP.0000000000000289 3. Lee, S., Vania, D. K., Bhor, M., Revicki, D., Abogunrin, S., & Sarri, G. (2020, July 7). Patient-reported outcomes and economic burden of adults with sickle cell disease in the
United States: A systematic review. International Journal of
General Medicine, 13, 361–377. https://doi.org/10.2147/IJGM.S257340 4. Adam, S. S., Telen, M. J., Jonassaint, C. R., de Castro, L. M., & Jonassaint, J. C. (2010, July). The relationship of opioid analgesia to quality of life in an adult sickle cell population.
Health Outcomes Research in Medicine, 1(1), e29–e37. https://doi.org/10.1016/j.ehrm.2010.04.002 5. Sogutlu, A., Levenson, J. L., McClish, D. K., Rosef, S.
D., & Smith, W. R. (2011, May-June). Somatic symptom burden in adults with sickle cell disease predicts pain, depression, anxiety, health care utilization, and quality of life: The PiSCES project. Psychosomatics, 52(3), 272–279. https://doi.org/10.1016/j.psym.2011.01.010 6. Bediako, S. M., Lanzkron, S., Diener-West, M., Onojobi,
G., Beach, M. C., & Haywood, C., Jr. (2016, May). The measure of sickle cell stigma: Initial findings from the
Improving Patient Outcomes through Respect and Trust study. Journal of Health Psychology, 21(5), 808–820. https://doi.org/10.1177/1359105314539530 7. Haywood, C., Lanzkron, S., Bediako, S., Strouse, J.J.,
Haythornthwaite, J., Carroll, C.P., …, & Beach, M.C. (2014,
Dec). Perceived discrimination, patient trust, and adherence to medical recommendations among persons with sickle cell disease. J Gen Intern Med, 29(12) 1657-1662. doi: https://doi.org/10.1007/s11606-014-2986-7 8. Trawalter, S., Hoffman, K. M., & Waytz, A. (2012). Racial bias in perceptions of others’ pain. PLoS One, 7(11), e48546. https://doi.org/10.1371/journal.pone.0048546 9. Hoffman, K. M., Trawalter, S., Axt, J. R., & Oliver, M.
N. (2016, April 19). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the
National Academy of Sciences of the United States of America, 113(16), 4296–4301. https://doi.org/10.1073/pnas.1516047113 10. Sabin, J. A., & Greenwald, A. G. (2012, May). The influence of implicit bias on treatment recommendations for 4 common pediatric conditions: Pain, urinary tract infection, attention deficit hyperactivity disorder, and asthma. American Journal of Public Health, 102(5), 988–995. https://doi.org/10.2105/AJPH.2011.300621 11. Hausmann, L. R. M., Gao, S., Lee, E. S., & Kwoh, K. C. (2013, January). Racial disparities in the monitoring of patients on chronic opioid therapy. Pain, 154(1), 46–52. https://doi.org/10.1016/j.pain.2012.07.034 12. Bailey, Z. D., Krieger, N., Agénor, M., Graves, J.,
Linos, N., & Bassett, M. T. (2017, April 8). Structural racism and health inequities in the USA: Evidence and interventions. Lancet, 389(10077), 1453–1463. https://doi.org/10.1016/S0140-6736(17)30569-X 13. Trent, M., Dooley, D. G., Dougé, J., Cavanaugh, R. M., Lacroix,
A. E., Fanburg, J., . . . Wallace, S. B., (2019, August). The impact of racism on child and adolescent health. Pediatrics, 144(2), e20191765. https://doi.org/10.1542/peds.2019-1765 14. Power-Hays, A., & McGann, P. T. (2020, November 12).
When actions speak louder than words – racism and sickle cell disease. The New England Journal of Medicine, 383(20), 1902–1903. https://doi.org/10.1056/NEJMp2022125 15. Mougianis, I., Cohen, L. L., Martin, S., Shneider, C., & Bishop,
M. (2020, September 1). Racism and health-related quality of life in pediatric sickle cell disease: Roles of depression and support. Journal of Pediatric Psychology, 45(8), 858–866. https://doi.org/10.1093/jpepsy/jsaa035 16. Haywood, C., Jr., Diener-West, M., Strouse, J., Carroll,
C. P., Bediako, S., Lanzkron, S., . . . Beach, M. C., & the
IMPORT Investigators, & the IMPORT Investigators. (2014,
November). Perceived discrimination in health care is associated with a greater burden of pain in sickle cell disease.
Journal of Pain and Symptom Management, 48(5), 934–943. https://doi.org/10.1016/j.jpainsymman.2014.02.002 17. Wakefield, E. O., Popp, J. M., Dale, L. P., Santanelli, J. P.,
Pantaleao, A., & Zempsky, W. T. (2017, February/March).
Perceived racial bias and health-related stigma among youth with sickle cell disease. J Dev Behav Pediatr, 38(2), 129–134. https://doi.org/10.1097/DBP.0000000000000381 18. Reader, S. K., Rockman, L. M., Okonak, K. M., Ruppe,
N. M., Keeler, C. N., & Kazak, A. E. (2020, June).
Systematic review: Pain and emotional functioning in pediatric sickle cell disease. Journal of Clinical
Psychology in Medical Settings, 27(2), 343–365. https://doi.org/10.1007/s10880-019-09647-x 19. Schomerus, G., Angermeyer, M. C., Baumeister,
S. E., Stolzenburg, S., Link, B. G., & Phelan, J. C. (2016, February). An online intervention using information on the mental health-mental illness continuum to reduce stigma. Eur Psychiatry, 32, 21–27. https://doi.org/10.1016/j.eurpsy.2015.11.006
From the Delaware Division of Public Health Public Health Alert Web portal provides COVID-19, monkeypox, and flu updates
To provide information about current public health issues of elevated concern, the Division of Public Health (DPH) launched a Public Health Alert web portal, de.gov/PublicHealthAlerts, on September 1. The user-friendly central landing page provides access to the COVID-19, monkeypox, and flu web pages. COVID-19 information can still be found at de.gov/coronavirus, monkeypox information can still be found at de.gov/monkeypox, and flu information can still be found at flu.delaware.gov. A new webpage to provide information about monkeypox was also unveiled at the same time. As of September 13, 34 cases of monkeypox were reported to DPH. The cases are among 33 men and one woman and range in age from 18 to 64. The Centers for Disease Control and Prevention reported 21,985 monkeypox cases in the U.S. as of September 12, with Maryland, Pennsylvania, New Jersey, and Washington, D.C. each having between 457 and 649 cases. The JYENNOS vaccine, approved by the Food & Drug Administration for use against smallpox, is authorized for use with monkeypox in high-risk and immunocompromised individuals. Nearly 1,000 individuals in Delaware had received one dose of the two-dose series as of September 13. Vaccine appointments can be scheduled at NewarkUrgentCare.org and beebehealthcare.org/online-scheduling. To schedule a vaccine appointment at a DPH clinic, call the monkeypox hotline at 866-408-1899. A screening evaluation will be conducted first. Visit de.gov/monkeypox for vaccine eligibility requirements, vaccine clinic locations, a medical providers section, and flyers in English and Spanish. For more information, call the monkeypox hotline at 866-408-1899 Monday through Friday from 8:30 a.m. to 4:30 p.m. or email questions to DPHCall@delaware.gov.


September 2022

Bivalent COVID-19 booster vaccine now available in Delaware
Updated COVID-19 vaccine booster doses, called bivalent boosters, are now available to individuals who completed their primary vaccination series (two doses of Pfizer, Moderna or Novovax, or one dose of Johnson & Johnson) two months earlier. The Moderna and Pfizer bivalent boosters target two strains of COVID-19 – the original strain of the virus and two of the Omicron variants (BA.4 and BA.5), the current most widespread variants in the world. Individuals may choose either the Pfizer or Moderna bivalent booster, regardless of which primary series vaccine or original booster dose they had previously. The Pfizer bivalent booster is currently authorized for ages 12 and older; while Moderna’s is currently authorized for 18 years of age and older. With back to school and other group activities now occurring, DPH asks parents of children under age 12 to have their children complete the primary COVID-19 vaccine series and get the original monovalent booster to protect them. At a minimum, completing a child’s primary series now will make children eligible for the bivalent booster when it is approved for younger children. Since the Omicron variants are widely circulating, DPH encourages eligible Delawareans to get the bivalent boosters to protect against severe illness, hospitalization, and death. Bivalent boosters are currently available at DPH clinics. Visit de.gov/getmyvaccine or vaccines.gov for other locations. For more information, visit de.gov/boosters, email questions to DPHCall@delaware.gov, or call 866408-1899 Monday through Friday from 8:30 a.m. to 4:30 p.m. Those who are deaf, hard of hearing, Deaf-Blind or speech disabled can contact DPH by dialing 711 first using specialized devices (i.e. TTY, TeleBraille, voice devices).

DPH re-accredited as nationally accredited public health agency
The Division of Public Health (DPH) is among only 22 percent of the accredited public health departments in the country to earn continued accreditation this year. The national Public Health Accreditation Board (PHAB) reaccredited DPH on August 18. To maintain its accreditation status, DPH demonstrated that it meets PHAB’s quality standards and measures. The Centers for Disease Control and Prevention identifies accreditation as a critical strategy for strengthening public health infrastructure. “After 2½ years of the COVID-19 pandemic, Delawareans have learned how important it is to have a strong public health response in our state,” said Delaware Department of Health and Social Services (DHSS) Secretary Molly Magarik. “I am grateful to the Public Health Accreditation Board for this re-accreditation, but I am especially grateful to the employees of the Division of Public Health for the work they have done and continue to do during the pandemic, and the work they do every day to evolve, improve and advance the health of Delawareans. This is another way we are building a healthier and stronger Delaware.” DPH Interim Director Dr. Rick Hong expressed gratitude to outgoing Associate Deputy Director Cassandra Codes-Johnson and Office of Performance Management Director Matthew Whitman for their dedication and tireless work in spearheading the re-accreditation process. Additionally, he recognized the work of former DPH Director Dr. Karyl Rattay in building a strong foundation within the Division which led to DPH’s initial accreditation in June 2016. For more information, read the press release at https://www.dhss.delaware.gov/dhss/pressreleases/ 2016/dphaccreditation-060816.html. Household emergency kits should be refreshed once or twice per year. Fall is a good time to undertake that task, beginning with canned goods. PrepareDE.org recommends that kits have at least a three-day supply of non-perishable food and a can opener. As temperatures cool, stores typically offer sales on canned soup, tomato sauce, and canned meats. Pre-Thanksgiving sales feature canned vegetables and evaporated and condensed milk. Every week, buy a few extra cans, reaching to the back of the store shelf for cans with the longest expiration dates. Pop-top cans do not require a can opener. Put those cans aside, using a dedicated indoor shelf. Place items with the nearest expiration date at the front and use them first. Begin your household emergency kit with the following items: • One gallon of drinking water per person per day • Food – non-perishable, three-day supply • Can opener, mess kits, paper cups, plates, paper towels, plastic utensils, and garbage bags • Battery-powered or hand crank radio, flashlight, battery-powered lantern, extra batteries, heavy work gloves, and a whistle • First aid kit and personal items, such as medications, glasses, dentures and cleaner, and hearing aids. • Toilet paper, feminine supplies, and diapers • Disinfecting wipes and disposable face masks • Soap, shampoo, hand sanitizer, moist towelettes, toothbrush and toothpaste • Cash because ATM machines may not work • Cell phone power bank or car charger • Copy of important documents in waterproof portable container or sealed Ziploc bags • Recent photos of family members in waterproof portable container or sealed Ziploc bags • For each person, a seasonally appropriate change of clothing and rain gear • Fire extinguisher. Read the complete checklist at https://www.preparede.org/make-a-kit/.


The Angle Measuring Tool uses visual, sound, and vibration cues to set an extension ladder at the proper angle. For the free app, visit the App Store, Google Play, or www.cdc.gov/niosh/topics/falls/mobileapp.html.
Preventing falls eliminates traumatic injuries, lost work, and health care costs
Falls can result in broken bones, head injuries, and temporary or permanent disabilities leading to major life changes for the individual and their families. Governor John Carney and Lieutenant Governor Bethany Hall-Long have proclaimed September 18-24, 2022, as Falls Prevention Awareness Week. Falls are the leading cause of trauma-related hospitalizations in U.S. adults aged 65 and older, with one in four in that age group falling every year, according to the Centers for Disease Control and Prevention (CDC). In 2021, 1,833 seniors over the age of 64 fell and were seen at a Delaware trauma center, according to the Delaware Trauma Registry. The Delaware Coalition for Injury Prevention’s (DCIP) Falls Prevention Team recommends older adults reduce their risk of falling by engaging in consistent physical activity and balance exercises, getting regular hearing and vision exams, receiving appropriate nutrition and sleep, having medication reviews with their doctor or pharmacist, and keeping homes and yards clutter-free, well-lit, and modified as needed. In the community, ramps and walkways should be maintained and well-lit. To improve coordination and balance, older Delawareans can enroll in A Matter of Balance© classes. For a schedule, call Volunteer Delaware 50+ at 302-515-3020. To schedule the fall prevention programs BingoCize and ThinkFirst to Prevent Falls© , send an email to Christiana Care at injuryprevention@christianacare.org. For free family and provider resources, visit the CDC at https://www.cdc.gov/steadi/index.html.
Household upgrades can reduce falls
Making small household upgrades can benefit all household members, especially seniors and those at risk of falling. Use these suggestions: • Change faucets and doorknobs to levers, which individuals with arthritis or less dexterity can grasp more easily. • Make flooring transitions seamless by eliminating door thresholds. Flush entryways accommodate those with mobility challenges. • Remove unnecessary furniture, rugs, and clutter to widen walkable corridors and lessen the risk of falling. • Install grab rails and supports in showers, near toilets, and close to kitchen seating. Hire a professional to install grab bars properly. • Use smart lighting that is activated by motion or darkness. Rocker light switches are easier to push than smaller toggle switches. • Install a stair-lift for individuals with fall risks who are advised not to use stairs.
Falls Prevention Team hosts free movie and health fair September 20
On September 20, the Falls Prevention Team and the Modern Maturity Center (MMC) will show the movie “Denying Gravity.” The movie highlights in a relatable, good-humored approach the benefits of fall prevention activities for seniors. A small health fair with information on preventing falls precedes the movie. The entire event is free and open to the public and runs from 11:00 a.m. to 1:00 p.m. at the MMC, located at 1121 Forrest Avenue in Dover, Delaware. Registration is not required. Should movie-goers choose to stay for lunch in the Longwood Dining Room, the cost is $6 for ages 60+ and $9 for ages 59 and younger. Visit www.modern-maturity.org for more information.

The DPH Bulletin – Special flu edition



It’s time to get your 2022 flu vaccine

The 2022-23 influenza season begins October 3, 2022. The Division of Public Health (DPH) reminds Delawareans 6 months of age and older to get their annual flu vaccine for protection against flu illness, hospitalization, and death. Being vaccinated protects you and those at risk of flu complications. Those at higher risk of becoming ill from the flu should closely manage their health. Individuals at higher risk are children younger than 5 years old (especially children younger than 2 years), adults 65 years and older, pregnant people, and those with chronic underlying medical conditions. Chronic conditions include asthma, Chronic Obstructive Pulmonary Disease and other lung diseases, heart disease, diabetes, neurologic conditions, blood disorders, obesity, and weakened immune systems. DPH urges flu vaccinations for those who live or work with infants under 6 months of age and those who live or work in congregant settings such as long-term care and correctional facilities. For more information about flu, visit flu.delaware.gov and cdc.gov/flu, or call 1-800-282-8672. Click here for the difference between cold and flu.

Tips to prevent flu
• Get your flu vaccine every year. • Avoid close contact with sick people. • Cover coughs and sneezes with a tissue, or cough or sneeze into your inner elbow. • Wash hands often with soap and water for 20 seconds or use hand sanitizer. • Do not touch your eyes, nose, and mouth. • Clean and disinfect frequently touched surfaces. • If sick with flu-like illness, stay home for 24 hours until fever-free (temperature less than 100 degrees Fahrenheit) without fever-reducing medication. If symptoms worsen, call your doctor.
Preliminary 2021-2022 U.S. Flu Season Burden Estimates, October 1, 2021 through June 11, 2022, as of June 17, 2022

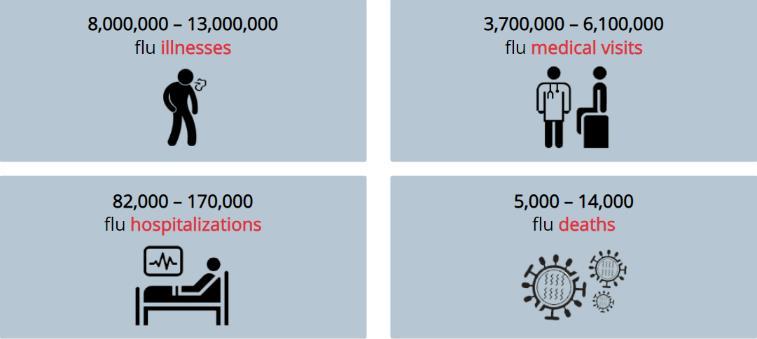
Source: CDC, www.cdc.gov/flu/about/burden
Stay well to help our health care system
Delawareans who are vaccinated against the flu reduce the burden of flu illness on health care providers, emergency departments, and hospitals. They avoid unnecessary sick visits to providers, trips to the emergency department, and hospitalizations due to flu. Providers can concentrate on assisting the sick and keeping healthy individuals well. Hospitals beds can be for those needing them most.
Seek flu vaccine at numerous places
Flu vaccines are available to the public from health care provider offices, pharmacies (including grocery store pharmacies), DPH clinics, health centers, urgent care clinics, and community vaccination events. Many employers and schools offer the flu vaccine on site. Visit flu.delaware.gov for locations. The flu vaccine is free to most Delawareans, even if you do not have insurance. Individuals without insurance or covered by Medicaid or Medicare may receive vaccines for flu and COVID-19 at Public Health clinics and community Visit the CDC at vaccination events. Flu www.vaccines.gov/ vaccines may be given at the same time as other vaccines, including the COVID-19 and monkeypox vaccines. Discuss concerns with your health care provider. For more information about flu vaccines in Delaware, visit flu.delaware.gov or call 1-800-282-8672.
The Centers for Disease Control and Prevention now recommend that adults 65 years and older get higher dose or adjuvanted flu vaccines over standard-dose unadjuvanted flu vaccines. Visit https://www.cdc.gov/flu/highrisk/65over.htm.




