1
CONTENIDO B O DY TO M 5 B O DY TO M , D E SA M S U N G DELEC CIENTÍFICA
7 9
A B O C A D O S A L A I N N O VA C I Ó N
10
C O N S U LT O R Í A E S P E C I A L I Z A D A
15
SERVICIO TÉCNICO EXPERTO
16
¿POR QUÉ ELEGIRLO?
17
S O B R E N E U RO LÓ G I C A Y B O DY TO M
18
C A R A C T E R Í S T I C A S P R I N C I PA L E S
20
BENEFICIOS 22 SEGURIDAD 23 C O M P AT I B I L I D A D 2 4 ÁREAS DE APLICACIÓN
28
FOLLETOS 31
Esta carpeta fue generada por el equipo de consultores de DeLeC Científica. Buenos Aires, Argentina. 2019. DeLeC Científica Uruguaya - Representante Regional Exclusivo Fco. García Corina 2357 – Piso 1. Montevideo - Uruguay DeLeC Científica Argentina – Agente Comercial Local Aráoz 821 -C1414DPQ - Buenos Aires – Argentina. Tel: (+54-11) 4775 5844
2
L
a cirugía robótica ya es una realidad. Aunque la historia de la cirugía se remonta a más de 2000 años; las últimas dos décadas del siglo XX han mostrado una marcada revolución en la medicina, debido a todos los cambios que ha provocado en la manera de hacer, enseñar y practicar la cirugía. Los sistemas de cirugía guiada por imagen proveen información preoperatoria e intraoperatoria a los cirujanos, mediante la proyección de imágenes obtenidas por un sistema de navegación, en relación con la anatomía del paciente. Este sistema crea un plan quirúrgico y una guía interactiva, utilizando modalidades de imágenes diagnósticas, como tomografía computarizada. Este nuevo paradigma, ofrece un adecuado tratamiento y resultados muy satisfactorios a los pacientes. Garantiza un riesgo de intervención mucho menor y una óptima recuperación en el menor tiempo posible. BodyTom es el primer tomógrafo móvil de 32 cortes capaz de trasformar cualquier habitación en una sala de imagenología avanzada. Permite realizar angiografías con bolus tracking, visualizando el flujo sanguíneo en venas y arterias y tiene un sistema avanzado de visualización con perfusión, que ofrece un estudio preciso en situaciones de stroke. Diseñado para ser utilizado en pacientes de cualquier peso y tamaño, BodyTom provee imágenes de alta calidad en cualquier sitio donde se lo solicite (ver página 20). Su software de tecnología avanzada permite visualizaciones 2D, 3D y MPR. Tiene la posibilidad de comunicarse vía WiFi, lo que le permite integrarse fácilmente con los sistemas de información de las instituciones de salud, la navegación quirúrgica, y otras plataformas tecnológicas (ver página 24). Posee ventajas que lo transforman en un equipo versátil, útil para muchas áreas de atención de la salud: es un equipo autoblindado, no requiere un búnker y puede trasladarse a todas las instalaciones. Es compatible con todos los neuronavegadores que trabajen con el formato DICOM, funciona con baterías externas que se cargan en la red normal de 220V, está diseñado para llegar donde se lo necesite (ver página 28). En DeLeC Científica seleccionamos este equipo para los sistemas de salud de Argentina, Uruguay, Bolivia y Paraguay porque estamos seguros que ayudará a mejorar la calidad de atención, disminuir los riesgos de vida y mejorar los tiempos y resultados de la rehabilitación.
3
4
BODYTOM
5
Evita traslados de riesgo.
6
BODYTOM, DE SAMSUNG
¿Qué es el sistema BodyTom? BodyTom™ es más que un equipo de imágenes, es una solución multidepartamental, porque ofrece la posibilidad de realizar tomografías en todos los servicios evitando la complicación y el costo de trasladar los pacientes. Permite acercar el tomógrafo a la terapia para evaluar pacientes riesgosos de mover. Con BodyTom™ en la guardia, se puede realizar una rápida evaluación de las personas que ingresan con síntomas de stroke o con politraumatismos, ganando tiempo en situaciones donde cada segundo cuenta. Ofrece la capacidad de tomar imágenes en cirugías de columna, trauma, ortopédicas o neurocirugías, dentro del mismo quirófano, antes, durante y después de la cirugía. Esto brinda mayor seguridad y calidad de atención. Incluso puede ser utilizado para diagnóstico como un tomógrafo fijo convencional. BodyTom™ es una solución flexible para todo el hospital.
7
8
DELEC CIENTÍFICA
9
¿Quiénes somos?
ABOCADOS A LA
DeLeC Científica es una empresa exitosa, en constante crecimiento, líder en innovación tecnológica aplicada a la medicina que fue fundada en el año 2003 por un grupo empresario de capitales nacionales, con vocación de servicio y alto grado de Responsabilidad Social.
“Si en el futuro somos lo que proyectamos, en el presente somos lo que hacemos en virtud de aquella decisión y proyecto”. José Ortega y Gasset
¿Cuál es nuestra misión y concepto de negocio? Nuestra misión es impulsar la mejora continua de nuestro sistema de salud regional, ofreciendo para ello los mejores productos de la revolución tecnológica del siglo XXI. A tal fin, nos hemos propuesto hacer foco en lo especial y proveer soluciones a problemas de los que nadie se ha ocupado, teniendo en cuenta que hay muchas empresas de electromedicina, de todo tipo y tamaño, que se dedican a atender el mercado de volumen con soluciones estandarizadas que dejan afuera a mucha gente.
¿A quiénes servimos y con qué tipo de productos? Servimos a las comunidades científicas y médicas proveyéndoles productos y servicios de última generación y alto valor agregado. Nos concentramos exclusivamente en aquellos que son seguros y están debidamente certificados y aprobados por los organismos internacionales de control - FDA y CE - y también los nacionales - ANMAT y ARN –; todo en el marco de un soporte pre y post venta de excelencia.
¿En qué nos especializamos? Somos consultores altamente especializados en el desarrollo e implementación de programas médicos de excelencia soportados por equipos y sistemas de real innovación tecnológica.
10
INNOVACIÓN
¿Cómo estamos organizados? La firma cuenta con seis áreas de trabajo con roles bien definidos. • División de Sistemas Médicos: Se distingue por proveer la mejor tecnología de punta disponible, a partir de la revolución tecnológica del siglo XXI, para cubrir necesidades de equipamiento de diagnóstico y también de tratamiento. Busca optimizar resultados clínicos y al mismo tiempo mejorar la calidad de la experiencia vivida por los pacientes antes, durante y después del proceso de tratamiento. • División de Cirugía Robótica y Simulación: pone a disposición de la comunidad médica la posibilidad inigualable de asistencia robótica a la cirugía mínimamente invasiva y también los únicos simuladores quirúrgicos verdaderamente realísticos; considerados los mejores del mundo en cirugía virtual. • División de Radioterapia y Radiocirugía: Ofrece la trilogía ideal de equipos para tratamiento de tumores malignos y benignos. • División de Ingeniería, Soporte Técnico y Aplicaciones Clínicas: Asegura el correcto funcionamiento de la base de equipos de innovación tecnológica instalada, incluyendo su actualización continua, y brinda servicio docente a los usuarios para asegurar su correcta utilización y las buenas prácticas. • División de Comunicación y Marketing: Área en constante crecimiento que busca llegar estratégicamente a los públicos de relevancia para la empresa y trasmitir un mensaje claro sobre su misión y objetivos. Para que “las cosas sean” es necesario comunicar que existen. “No se desea lo que no se conoce”. • División de Administración, Personal y Finanzas: Optimiza los resultados económicos de la empresa, cuidando que haya una distribución equitativa de los recursos entre los seis grupos de interés: proveedores, clientes, personal, accionistas, bancos/inversores y el fisco. Su objetivo principal es velar por una gestión eficiente y ecuánime al momento de crear valor económico produciendo, al mismo tiempo, valor social.
11
Precisión submilimétrica e innovación en tratamientos de radioterapia y radiocirugía.
Radioterapia intraoperatoria, Pequeño, ligero, móvil, autoblindado y efectivo.
Tomógrafo de mamas con imágenes 3D realmente isotrópicas.
Hospitales móviles diseñados a la necesidad del cliente.
Tomógrafos móviles autoblindados de uso en clínicas y ambulancias.
Adquisición continua de imagen en bipedestación 2D y 3D con baja dosis.
Simuladores de alta y mediana fidelidad y sistema audiovisual con herramientas de gestión.
Cabezas para intubación, torso para trauma y monitor multiparamétrico simulado.
Tecnología no invasiva que ayuda a visualizar venas no visibles a simple vista.
Sistema de adquisición de señales biológicas y software para educación e investigación.
12
¿Cuál es nuestra filosofía? Nuestro lema es ganar cuando el cliente también gana, cumplir con lo prometido y hacerlo a tiempo.
¿Qué nos diferencia del resto de las empresas del rubro? Nuestro diferencial es que no sólo proveemos equipos, sino que desarrollamos programas médicos de excelencia, acompañando al cliente desde la etapa embrionaria del proyecto hasta su optimización operativa. • Seleccionamos el equipamiento necesario y lo instalamos. • Brindamos soporte técnico con garantía oficial. • Nos encargamos del entrenamiento de los médicos y del personal de la institución local. • Una vez que llegamos a una institución, nunca nos vamos.
¿Cuál es nuestra modalidad de trabajo? Trabajamos en equipo con proveedores y clientes a través de una continua actividad de docencia. No tenemos vendedores, pero nos atenemos al perfil y la descripción habitual de las tareas de un vendedor técnico. Nuestro equipo se compone de profesionales universitarios, frecuentemente con posgrado que, a poco de ingresar a la compañía, son enviados a las distintas fábricas representadas para capacitarse de la mejor forma para ofrecer cada producto con solvencia técnica y científica.
¿Contra quiénes competimos? No poseemos competidores, ya que vamos en una dirección distinta al resto, usualmente: cambiando paradigmas.
13
¿Dónde comercializamos y soportamos nuestros productos? La firma comercializa la mayoría de sus productos en Argentina, Uruguay, Paraguay y Bolivia. Sin embargo, muchas veces, a pedido de distintos fabricantes, extendemos nuestro radio de acción llegando a otros países de América del Sur. En el 2010 introdujimos la cirugía robótica en Colombia, preparando el terreno para que luego se nombrara un distribuidor local. Antes, en el 2008, habíamos instalado las dos primeras unidades da Vinci que hubo en Brasil. Lo hicimos en el Hospital Albert Einstein y en el Sirio Libanes, ambos de Sao Paulo. Cabe destacar que también en este país existe actualmente un distribuidor local para esta tecnología.
¿Cuál es nuestra visión de futuro? En el mediano plazo esperamos ser líderes regionales y referentes indiscutidos en innovación tecnológica aplicada a la medicina. Esto lo lograremos gracias a nuestro comportamiento empresarial, calidad de relaciones que establezcamos, eficiencia y efectividad de nuestros productos y servicios. Apostamos a ser una organización de renombre y prestigio regional, comprometiéndonos con la comunidad y ayudando para la construcción de un mundo mejor a través de la mejora continua del servicio de salud.
Oficinas de DeLeC Científica
14
C O N S U LT O R Í A
Nuestra experiencia en el ámbito de la innovación tecnológica en salud nos dice
ESPECIALIZADA
que el mejor equipo de diagnósitico por imagenes no hace una intervención de calidad por sí mismo. Tan importante como la herramienta son la formación, la comprensión de la tecnología, el buen uso, el asesoramiento y los objetivos que orientan la práctica. Por eso en DeLeC Científica acompañamos a las instituciones desde el desarrollo de los proyectos, el diseño de nuevas áreas o servicios de salud, el asesoramiento en la adquisición de nuevas tecnologías, los requerimientos normativos y legales, la diagramación logística, el mantenimiento y el monitoreo del uso. Un asesoramiento adecuado es clave para: - obtener planificaciones que permitan optimizar el tiempo de los proyectos, - prever los riesgos potenciales para garantizar la viabilidad en el mediano y largo plazo, - identificar todos los stakeholders alrededor del proyecto y prever cuál será el impacto en ellos, - conseguir una mirada profunda sobre la inversión, el retorno y reconocer oportunidades que no están a la vista. Con el fin de asesorar tomando como referencia los máximos estándares de calidad, los consultores de DeLeC nos actualizamos de acuerdo a los programas de formación de las firmas que representamos y participamos de forma activa en la agenda más relevante de la innovación tecnológica médica en Occidente.
15
Ofrecer un servicio técnico de alta performance, alineado tanto a las exigencias y
SERVICIO TÉCNICO
estándares de las marcas con las que trabajamos, como a los requerimientos de
EXPERTO
nuestros clientes es un punto destacado en nuestra empresa. El equipo técnico asiste en la interpretación de los requerimientos previos (condiciones eléctricas, infraestructura, etc.), se ocupa de la instalación, cuando el equipo lo requiere, y luego monitorea el funcionamiento y el uso para garantizar el desempeño óptimo de la tecnología. El servicio de instalación de DeLeC Científica para el equipo Radixact cumple con todos los procesos recomendados por la fábrica. Nuestros técnicos deben cumplir con un cronograma de formación y capacitación anual, en las casas matrices de las firmas que representamos. Por lo tanto, desde DeLeC Científica ofrecemos una asistencia de instalación y posventa certificada por fábrica.
16
¿POR QUÉ ELEGIRLO?
17
Cuando se le pregunta a Eric Bailey, presidente de NeuroLogica, acerca de
SOBRE
su motivación para comenzar con la compañía, recuerda dos hechos que lo
NEUROLÓGICA Y
marcaron para siempre.
BODYTOM
El primero, cuando un ataque cerebrovascular dejó a su abuelo en un estado muy débil durante diez años. Y el segundo, cuando su hermano murió debido a una lesión en la cabeza que sufrió en un accidente automovilístico. De allí la idea de fundar NeuroLogica. Una tomografía computarizada podría haber salvado a su hermano y quizá mejorado la calidad de vida de su abuelo. En el año 2004, la empresa norteamericana NeuroLógica desarrolló y comenzó a comercializar el CereTom®, primer tomógrafo portátil del mundo para tomar imágenes de cabeza y cuello. Su compacto diseño y software de avanzada permiten trasladar este equipo por todas las áreas de un hospital. Al estar autoblindado, no existe la necesidad de un búnker o la asignación de protección radiológica en el sector donde se deba realizar la tomografía. Luego de las excelentes repercusiones y muy buenos resultados, la compañía creó el BodyTom™, equipo que mantiene las mismas ventajas, pero permite realizar tomografías de cuerpo entero. BodyTom™ es una solución flexible para todo el hospital.
18
19
CARACTERÍSTICAS PRINCIPALES
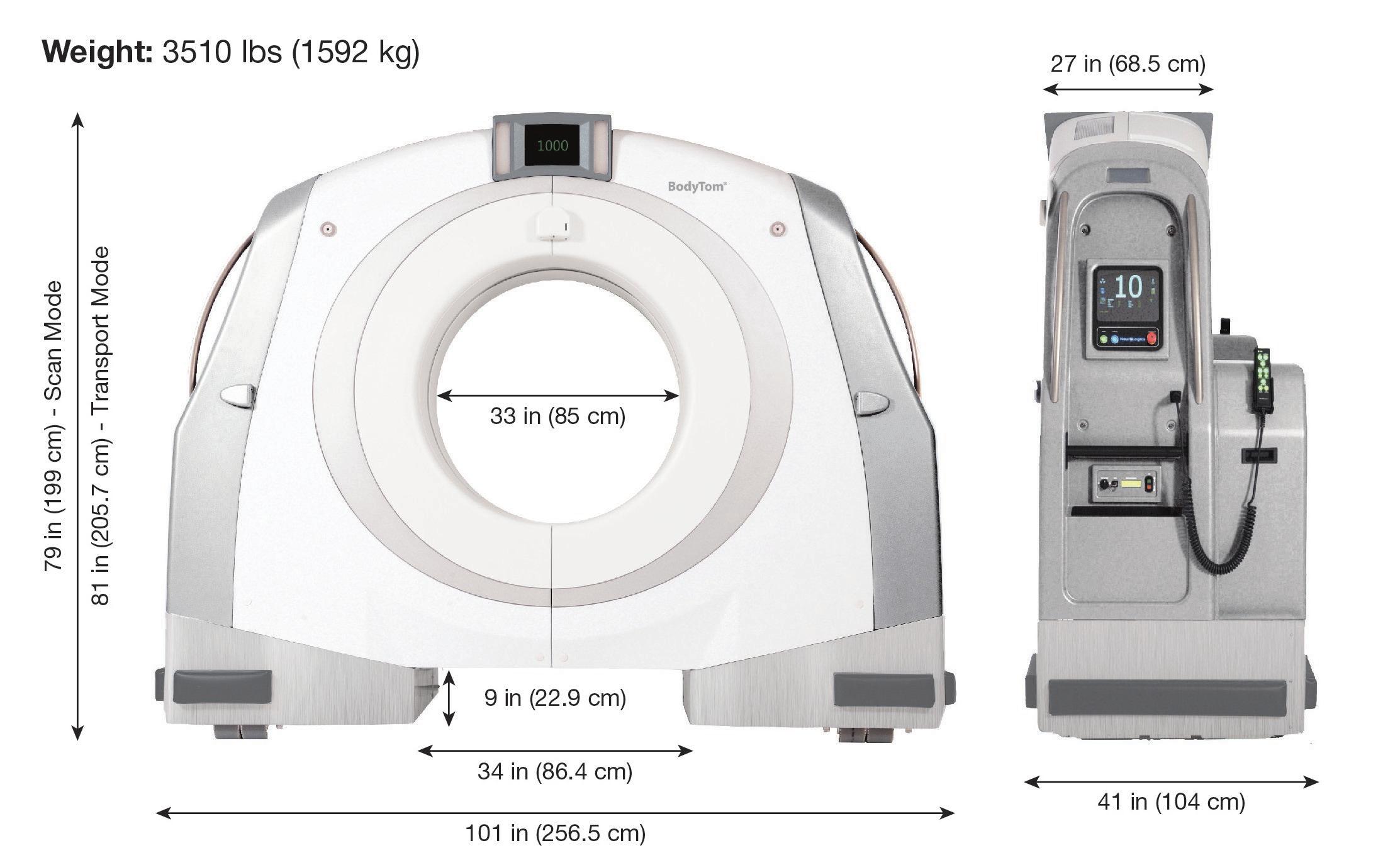
BodyTom™ permite llevar el valor de las imágenes médicas a la cama del paciente. Es el primer tomógrafo portátil de 32 cortes del mundo para tomar imágenes de cuerpo entero. Está diseñado especialmente para escanear pacientes de todos los tamaños, ya que su gantry es uno de los más amplios del mercado, con un diámetro interno de 85 cm. BodyTom™ es un equipo capaz de transformar cualquier habitación en una sala de imágenes de avanzada. Las capacidades de software de la Workstation permiten visualización 2D, 3D y reconstrucción multiplanar, y las imágenes producidas tienen compatibilidad DICOM 3.1. Estas características, sumadas a la comunicación wireless con la que cuenta el equipo, permiten total integración con cualquier sistema de PACS con el que se trabaje en la institución.
Dimensiones:
Peso: 1592kg.
20
Cabe destacar que el sistema de conducción de BodyTom™ permite que un solo operador pueda transportar y preparar el tomógrafo en cualquier servicio o sala de la institución en que sea requerido. Durante el transporte, la pantalla de estado del BodyTom™ muestra automáticamente la imagen que obtiene una cámara en el lado contrario, para observar el camino. Características técnicas principales: • Parámetros de escaneo
- Tomógrafo multislice de 32 cortes de 1,25mm.
- 85 cm de diámetro interno de gantry.
- 60 cm de campo de visión (FOV).
- 2 metros de rango total de escaneo (de pies a cabeza).
- Capacidades de escaneo: scout, helicoidal, axial y dinámico.
- Posibilidad de realizar angiotomografías y estudios de perfusión.
- 4 láseres de posicionamiento.
• Especificaciones del tubo de rayos-x
- Ánodo rotatorio, refrigerado por aceite.
- Voltaje: 80, 100, 120, 140kV.
- Corriente máxima: 300mA.
- Tubo de 3,5MHU.
- Potencia: 42kW.
• Imagen
- Equivalente a la de los mejores tomógrafos del mercado.
- Máxima resolución: 17 pares de líneas por centímetro.
- Matriz de imagen de 512 x 512.
- Compatibilidad DICOM 3.1.
- Compatible con todos los sistemas de navegación quirúrgica, PACS, HIS, RIS.
- Reconstrucción de 32 imágenes por segundo.
• Alimentación
- De pared:
- Voltaje: 100-120 / 208-240 VAC ± 10%
- Corriente: 20-30A
- Frecuencia: 50/60Hz
- Batería de duración aproximada de 12 horas en standby.
21
BENEFICIOS
BodyTom™ presenta diferentes beneficios y características que engloban una idea principal: poder acercar el
tomógrafo al paciente y ofrecer la más alta calidad de imagen, sin riesgos asociados. Esto implica mayor calidad de atención para los pacientes, mayor eficiencia en el funcionamiento de los servicios, y beneficios económicos para la institución en general.
BodyTom™ es tecnología de punta, primer tomógrafo portátil de cuerpo entero de 32 cortes. Esta portabilidad se logra, por un lado, gracias a su sistema de conducción y fácil maniobrabilidad. Por el otro, gracias a que el equipo está autoblindado para proteger tanto a los pacientes como al personal de la radiación dispersa. Esto también implica que no requiere de la construcción de un búnker y sus costos asociados. Para utilizarlo en cualquier sala simplemente se conecta a 220V, y a su vez posee un sistema de baterías que le dan una autonomía de hasta 12 horas en stand-by, o un promedio de 6 tomografías. A diferencia de otros tomógrafos, BodyTom™ es de fácil instalación: en cuanto se desembala, está listo para calibrar y usar. Además, su uso está simplificado porque cuenta con protocolos preconfigurados. Igualmente, durante la primera semana un especialista en aplicaciones clínicas lleva a cabo el entrenamiento necesario para los usuarios del equipo. Luego, el Departamento de Aplicaciones Clínicas de la empresa mantiene contacto regular con el cliente, para asegurar eficiencia en el funcionamiento del sistema. BodyTom™ puede ser aplicado en muchas áreas y servicios de la institución. Al ser utilizado en el quirófano, permite realizar exploración preoperatoria, intraoperatoria y postoperatoria de los pacientes, brindado mayor seguridad y precisión durante los procedimientos, y por lo tanto mejores resultados. BodyTom™ es compatible con todos los navegadores quirúrgicos, por lo tanto, las imágenes cargadas en estos sistemas pueden ser obtenidas inmediatamente antes de la cirugía, o incluso durante la misma. Para mayor información, ver la sección de Compatibilidad.
El uso de BodyTom™ en terapias permite evitar el traslado de pacientes delicados por grandes distancias, desde la unidad de terapia intensiva hasta el tomógrafo fijo para control. De esta manera, se puede realizar un mejor seguimiento de la evolución del paciente, sin riesgos. Además, brinda mayor disponibilidad de tiempo a los intensivistas para cubrir otras necesidades. Por otro lado, esto también libera el uso del tomógrafo fijo para diagnóstico de otros pacientes, por lo que permite un manejo más eficiente de los recursos de la institución. En la guardia, BodyTom™ permite una rápida evaluación de los pacientes que ingresan con síntomas de ACV o con politraumatismos, mejorando los tiempos de tratamiento. En los pacientes que sufren un ACV, el tiempo es un factor fundamental, porque con cada segundo ganado se evita la pérdida de millones de neuronas: tiempo es cerebro. Para mayor información sobre las aplicaciones clínicas del equipo y las ventajas que ofrece en las distintas especialidades, ver la sección de Áreas de Aplicación.
22
SEGURIDAD
BodyTom™ presenta distintas características de diseño y de uso pensadas para minimizar el riesgo de radiación: - Blindaje interno de plomo de 0,75 mm de espesor. - Protocolos de escaneo predefinidos, basados en edad y peso, modificables sólo por el usuario administrador. - Posibilidad de adquirir un software de reducción de ruido que permite trabajar con la mitad de la dosis, sin resignar calidad de imagen: Software RadRedux. - Chequeo y verificación de dosis (FDA / Iniciativa MITA) - La dosis se indica en pantalla previo a cada escaneo. - Un informe de dosis se genera para cada serie DICOM. - Mensajes de alerta. - Seguimiento de auditoría. - De manera opcional se puede incluir blindaje adicional contra la radiación en la Workstation, para mayor protección de los operarios. NeuroLogica también realizó estudios de la radiación dispersa emitida, utilizando un fantoma de cuerpo entero adulto y una camilla radiolúcida. Los resultados indican que BodyTom™ cumple con las recomendaciones de la ACR para dosis en tomografía (CTDI). Además, cabe destacar que BodyTom™ cuenta con la aprobación de la FDA, el marcado CE, y está habilitado por ANMAT. Es tecnología de punta que está siendo utilizada en más de 50 hospitales en el mundo.
23
CO M PAT I B I L I DA D
• Integración con los sistemas de comunicación BodyTom™ tiene compatibilidad DICOM 3.1 y por lo tanto se puede integrar completamente a los sistemas de PACS, HIS, RIS y otros con los que cuente la institución. La comunicación con los PACS se da de la siguiente manera: • Desde el escáner se pasa la información a la Workstation del BodyTom™ y finalmente a los PACS del sanatorio u hospital. • Estos tres elementos se pueden comunicar vía wireless o por cable. Como se puede observar en el gráfico existen cinco combinaciones posibles que dependerán de las necesidades y posibilidades de cada institución.
24
• Fijaciones radiolúcidas para el cráneo Para las aplicaciones clínicas de BodyTom™ en cirugía de columna o en neurocirugías, existen distintos tipos de fijaciones que se pueden utilizar diseñadas especialmente por NeuroLogica: - Abrazadera para el cráneo (skull clamp). - Herradura (horseshoe) para posición boca abajo. - Scanboard, que permite adaptar cualquier cama para realizar tomografías de cabeza. BodyTom™ también posee completa compatibilidad con todos los tipos de marcos estereotáxicos del mercado:
MAYFIELD
DORO
MIZUHO
25
• Camillas para cirugía BodyTom™ es compatible con una gran variedad de camas para cirugía, ya sea de columna, trauma, ortopédica o neurocirugía. Las principales características a tener en cuenta son: - La camilla debe ser radiolúcida. - La apertura del gantry es de 85 cm, por lo que el ancho de la cama debe ser menor. - La apertura en la base del tomógrafo tiene 22,9 cm de altura, y por lo tanto la base de la camilla debe ser menor. - El rango máximo de escaneo del BodyTom™ es de 2 metros, con lo cual también es ideal utilizar camas expandibles, para aprovechar toda la funcionalidad del tomógrafo. Algunos ejemplos de camas son:
Camilla Insite (Mizuho OSI) Allen Spine Table (Hill – Rom)
Jackson Spine Table (Mizuho OSI)
26
• Navegación Quirúrgica - Total compatibilidad con los sistemas de navegación con tecnología DICOM Ready. - BodyTom™ permite exploración preoperatoria directamente en la camilla del quirófano. Estas imágenes instantáneas luego se transfieren al sistema de navegación para la planificación del procedimiento. - Con BodyTom™ es posible tomar imágenes intraoperatorias para actualizar la navegación y, de ser necesario, realizar correcciones en el tratamiento, sin la necesidad de que el paciente salga del quirófano ni modifique su posición. - La exploración postoperatoria, finalmente, permite confirmar que se hayan alcanzado los objetivos del procedimiento.
BRAINLAB
STRYKER
MEDTRONIC
27
ÁREAS DE APLICACIÓN
28
29
• Neurocirugía Utilizando el BodyTom™ con cualquier sistema de fijación de cráneo radiolúcido se pueden obtener imágenes intraoperatorias de alta calidad. Esto potencia la utilidad de los neuronavegadores, con los que el tomógrafo tiene compatibilidad total, mejorando los resultados quirúrgicos. Según el Dr. Brad Mullin, director de neurocirugía en Mt. Carmel East Hospital, la diferencia de trabajar con BodyTom™ en quirófano “es como la diferencia entre la televisión y la televisión en alta definición.” • Cirugía de Columna Con BodyTom™ es posible transformar el quirófano en una sala de imágenes para columna, gracias a su gantry de 85 cm de apertura y al campo de visión (FOV) de 60 cm. BodyTom™ es compatible con todos los sistemas de navegación quirúrgica, y permite tomar imágenes desde C1 hasta S5 en una sola pasada. Ofrece alta calidad de imagen tanto para hueso como para tejido blando. • Cirugía Ortopédica La capacidad de realizar tomografías de alta calidad en un quirófano puede mejorar significativamente la eficiencia en el tratamiento y el cuidado de los pacientes. Por su portabilidad, BodyTom™ puede ser llevado de un quirófano a otro para realizar escaneos de pacientes críticos, convirtiéndolos así en salas de imágenes sin los costos asociados a la instalación de tomógrafos fijos. • Terapia Con BodyTom™ es posible realizar imágenes tomográficas de los pacientes complejos en la terapia sin correr el riesgo asociado a su traslado. Esto no solo brinda mayor seguridad y mejor cuidado a los pacientes, sino que también permite mejorar la eficiencia y disponibilidad de tiempos de los intensivistas. • Diagnóstico por Imágenes BodyTom™ entrega imágenes de alta calidad diagnóstica tanto para hueso como para tejido blando. Tiene compatibilidad DICOM 3.1, por lo que las imágenes pueden ser compartidas en los sistemas de información de las instituciones para su posterior evaluación. • Guardia El diagnóstico rápido y manejo eficiente de los pacientes críticos en la guardia son elementos clave para su cuidado, donde el tiempo es un factor de suma importancia. Al estar autoblindado, BodyTom™ permite realizar tomografías dentro de esta misma sala, evitando traslados y mejorando los tiempos de tratamiento.
1 “Interventional Radiologists use Minimally Invasive Methods to Speed Surgery Recovery.” Mike Mahoney. Revista Columbus CEO, abril 2015.
30
FOLLETOS
31
ImĂĄgenes intraoperatorias sin posponer decisiones crĂticas.
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
BodyTom
®
Portable, full body 32-slice CT scanner
Image Gallery
EC/ICA bypass
Contrasted body scan
3D full spine scan
CT angiography
Scan of healthy brain
3D full body contrast
3D contrasted spine scan
Lung scan
3D spine
Cervical spine
53
Image Gallery
AP scout after scoliosis correction
Urogram contrasted scan
Vascular abdominal scan
Kidney detail
2D MIP, lung scan, vascular detail
Liver detail
Pedicle screw placement confirmation
DBS placement, pre-op CT scan
DBS placement, intra-op confirmation
Low dose scout scan
Lateral scout after scoliosis correction
14 Electronics Avenue | Danvers, MA 01923 | Telephone: 1 (978) 564-8500 | Email: info@neurologica.com BodyTom is a registered trademark of NeuroLogica Corporation. Š2015 NeuroLogica Corporation. All rights reserved.
54
1-NL4000-120 rev01
PUBLICACIONES ACADÉMICAS
1
Contenido DEEP BRAIN STIMULATION FOR REFRACTORY TOURETTE SYNDROME: ANALYSIS OF CENTROMEDIAN/ PARAFASICULAR TARGET WITH SYMPTOM IMPROVEMENT 4 VALIDATION ON INTRAOPERATIVE 32-SLICE COMPUTED TOMOGRAPHY AS A USEFUL ADJUNCTTO MR -AND MER- GUIDED DBS IMPLATANTION IN STNTARGETED PARKINSON’S DISEASE: EXCITING PROSPECTS ON THE HORIZON
4
INTRAOPERATIVE PORTABLE CT-SCANNER BASED SPINAL NAVIGATION - A FEASIBILITY AND SAFETY STUDY
5
THE INTRAOPERATIVE PORTABLE CT SCANNER-BASED SPINAL NAVIGATION: A VIABLE OPTION FOR INSTRUMENTATION IN THE REGION OF CERVICOTHORACIC JUNCTION
11
HEAD INJURY
19
INTERVENTIONAL RADIOLOGISTS USE MINIMALLY INVASIVE METHODS TO SPEED SURGERY RECOVERY
2
27
A continuación se pone a disposición una selección de publicaciones científicas que avalan las características y beneficios del sistema Radixact, de BodyTom. En la selección de estos papers se dio prioridad a los contenidos más recientes y pertinentes, teniendo en cuenta la presentación que se ofrece en la carpeta Radixact confeccionada por DeLeC Científica. Si el lector desea ampliar la información científica sobre los usos del Radixact puede consultar a los sitios www.delec.com.ar, o bien al correo: comunicaciones@delec.com.ar.
3
Deep brain stimulation for refractory tourette syndrome: Analysis of centromedian/ parafasicular target with symptom improvement
4
Validation on intraoperative 32-slice computed tomography as a useful adjunctto MR -and MER- guided DBS implatantion in STN-targeted Parkinson’s disease: exciting prospects on the horizon
Acta Neurochir DOI 10.1007/s00701-014-2184-8
CLINICAL ARTICLE - SPINE
Intraoperative portable CTscanner based spinal navigation Intraoperative portable CT-scanner based spinal - a feasibility and study navigation - asafety feasibility and safety study Pavel Barsa & Robert Frőhlich & Vladimír Beneš III & Petr Suchomel
Received: 5 May 2014 / Accepted: 14 July 2014 # Springer-Verlag Wien 2014
Abstract Background Navigation based on an intraoperative CT scan is not a new approach to spinal instrumentation. Innovative intraoperative imaging technology, however, opens new horizons to more precise image acquisition as well as to further workflow. Planning of screw entry-points and trajectories in this study had been based on intraoperative imaging obtained by a portable 32-slice CT scanner. This prospective study evaluates feasibility, accuracy, and safety of this novel approach in an initial series of 85 surgeries. Method Medical records and radiological materials of 82 patients who underwent the first 85 consecutive stabilisations were analysed. Incorrect screw position, medical and technical complications as well as availability of this procedure in particular spinal levels were the subject of evaluation. Results Out of 571 implants inserted in all spinal levels, only five screws (0.87 %) did not meet the criteria for correct implant position. These screw misplacements had not been complicated by neural, vascular or visceral injury and the surgeon was not forced to change the position intraoperatively or during the postoperative period. The quality of intraoperative CT imaging sufficient for navigation was obtained at all spinal segments regardless of a patient’s habitus or positioning or comorbidity. Conclusion Intraoperative portable CT scanner-based navigation seems to be an effective way of doing spinal instrumentation guidance. High precision of implant insertion confirms the preconditions of navigation usage during more complex surgeries at any level of the spine.
P. Barsa (*) : R. Frőhlich : V. Beneš III : P. Suchomel Department of Neurosurgery, Regional Hospital of Liberec, Husova str. 10, 460 63 Liberec, Czech Republic e-mail: pavel.barsa@nemlib.cz
Keywords Spinal instrumentation . Surgical navigation . Intraoperative imaging . Computed tomography . Portable CT scanner Abbreviations CT computed tomography LED light emitting diode 3D three-dimensional CTDI computed tomography dose index DLP dose length product
Introduction In the field of neurosurgery, new frameless stereotactic navigation systems have been reported since the 1990s [1]. Their function is based on highly precise monitoring of labeled instruments positioned in the registered surgical field. Even if this procedure is associated with a certain degree of inaccuracy, mainly due to the movement of brain structures during retraction and resection of brain tissue (brain shift); this method has been widely clinically adopted and has become a standard in intracranial surgery [2]. Applying the same principle to spinal surgeries was more complicated. The problems are caused by changes in the alignment of individual vertebrae compared to intracranial structures where the anatomical position is relatively constant. Anatomical interpretation of the position in a moving spine, as acquired during preoperative imaging, is virtually impossible to predict over time. With the exception of individual vertebrae and static spinal segments (ankylosis), it is not possible to register anatomic spinal sections in a way corresponding with the preoperative scan. Despite these problems, navigation techniques appeared in spinal surgery in the 1990s. A spinal navigation system based on thke optoelectronic principle was
5
Acta Neurochir
designed by Nolte et al., based on laboratory work in 1995 [3]. Its function and safety in clinical practice was described in a comparative study with fluoroscopy guided surgeries five years later by Laine et al. [4]. Recently, the methods of navigated procedures have been developing. A breakthrough was the recent introduction of intraoperative 3D fluoroscopy [5] and much more precise intraoperative CT [6–8] as the initial imaging for the navigated spinal procedures. Intraoperative imaging will capture the spinal segment of interest in the anatomical position the surgeon will instrument. This way, precision and security of individual steps can be ensured [9]. The authors of the presented paper analyzed prospectively collected data in the series of first 85 consecutive surgeries where navigated spinal instrumentation had been based on intraoperative portable CT-scanner imaging. They analyzed technical feasibility of the navigation and CT scan acquisition in all spinal levels. This study further evaluated the accuracy of screw insertion and safety of the procedure for the patient.
Methods Surgical technique Not less than 12 h before the surgery, a competent patient was given all the relevant information about the treatment and voluntarily gave the consent not only with the stabilization but also with the intraoperative portable CT scanner-based navigation. The informed consent included discussion of the nature of the procedure, reasonable alternatives to the proposed intervention, and the relevant risks and benefits associated with the procedure, including a possible higher radiation dose from the portable scanner. The patient position as in in classical fluoroscopy guided surgeries should be simultaneously chosen so that the vertical axis of the instrumented segment corresponds, if possible, with the axis of the portable CT scanner gantry (Body Tom TM ®, NeuroLogical, Danvers, USA) (Fig. 1). In the area of the median skin incision, ten fiducial markers provided by the manufacturer of the navigation system (Stealth™, Medtronic, Minneapolis, USA) were placed. They were used for surgical field registration after the skeletization. A further feature in the surgical field registration is the Stealth navigation tracking device attached to a not moving spinous process of one of the instrumented vertebrae (Fig. 2). A portable full body 32slice CT scanner acquires images of the selected spinal section including the registration markers. It is automatically sent (in the DICOM format) to the navigation system using a direct Ethernet connection. In spinal fixation, we use helical scanning to produce a 1.25 mm slice thickness. The picture is reconstructed into a three-dimensional volume by the Stealth navigation system that will render the skin surface (in the soft tissue display mode) including the fiducial markers. In the 3D
6
Fig. 1 The portable CT scanner in working position
calcified tissue display mode, we will identify the spinal surface structures and insert virtual implant trajectories in this view. The navigation system also facilitates eventual visualization of the screw trajectory course in sagittal, coronary, and transversal planes. In addition, the navigation system offers “probe view” software, which displays the transition of a virtual implant through a bony structure, similarly to an endosonography examination (Fig. 3). This way, we can define the length and diameter of the intended implant. All the steps of instrumentation are made by the prepared navigation plan. The exact position of the screw entry-point may be determined using a navigated probe and may be marked with a burr on the surface of the vertebra. The dip should be deep enough to provide support for a technical punch. We will use it to drill the trajectory to the specified depth and orientation. After drilling the passage for the screwwe may predrill the thread to bone or we may insert the implant directly (self-tapping screws). In multiple stage instrumentations a tracking device is attached to a spinous process as close to the middle parts of the instrumented section as possible. Instrumentation in this case starts from the peripheral part (e.g., in L3-L5 stabilization, we attach the frame
Fig. 2 The navigation tracking device attached to the spinous process of one of the instrumented vertebra at cervical level
Acta Neurochir
Fig. 3 Plan for pedicular screw insertion in the cervical spine
to L4 and instrumentation starts from L3 and L5). This way navigation inaccuracy due to deflection of the tracking device during the instrumentation may be minimized. After implant insertion, we finish the decompression or reconstruction and secure the individual segments of the internal fixator. The correct implants position is confirmed before the end of procedure with a portable CT scanner (Fig. 4). Patients During the first 18 months of portable CT scanner usage in our department (October 2012–April 2014), the technology of
Fig. 4 Correct anatomical position of pedicle screws inserted at the level of C5
navigated spinal procedures based on intraoperative CT imaging was used in the initial series of 85 consecutive surgeries performed in 82 patients, where we inserted a total of 571 screws. The patient group consisted of 43 men and 39 women of mean age of 54.1 years (range 25–79 years, median 56 years) with the majority of patients being operated for a degenerative condition in the lumbar spine. Exact information about the indication for the surgical procedure is shown in Graph 1; anatomic distribution of the implants is depicted in Graph 2. Evaluation of accuracy of the screw placement For the purpose of this study, the correct screw position is defined as the positioning of the screw where no part of the
Graph 1 Indications for spinal stabilizations
7
Acta Neurochir
Graph 2 The anatomic distribution of implants
screw shaft or tip penetrates the surface of the instrumented bony structure. In this aspect, not only breeching of the pedicle cortex but also perforation of the cortical bone covering the surface of the vertebral body or surface of the vertebral foramen is defined as incorrect screw insertion [10].
Results Altogether five screws out of 571 inserted spinal implants (0.87 %) did not meet the criteria for correct position: in a single L5 pedicle screw, the threads penetrated through the caudal cortex of the pedicle; one thoracic screw in the T5 and one in the T8 were found to perforate through the ventral vertebral cortex less than 3 mm and a single screw inserted into the T6 vertebra breached the medial pedicle cortex (Fig. 5). The incorrect insertion in ventrally perforating thoracic screws had been adjusted before closing. In instrumented cervical segments, one C3 pedicle screw perforated the cranial end-plate due to rostral orientation of the screw. In our series, there was no neurovascular structure or visceral injury or dural sac laceration observed. Correct screw insertion prevented breaking of the instrumented pedicle, and there were no clinical consequences that would necessitate a reoperation to optimize the implant position or decompression of neural structures. During the intraoperative CT based surgeries, we did not have a single case of wrong level surgery or a case where the
8
surgical field lucidity was disrupted due to obesity of the patient or anatomical localization with poor radiological visibility or due to radiological artifacts of metal instruments. After the registration of the surgical field was completed, the navigation system analyzed the precision of the registration process. Average value in our operated patients was 0.44 mm (range of 0.2–1.0 mm), and all calculated values were sufficient to confidently perform instrumentation. In general, higher precision was reached over a larger registered field. This method of navigated screw insertion based on intraoperative portable CT scanner imaging was applicable in all anatomical levels throughout the spine. In no case we were forced to convert navigated screw insertion into a fluoroscopically guided procedure. The Body Tom TMŽ gantry diameter (85 cm) allowed us to perform image acquisition even in obese patients. In specific anatomical situations, like in the lumbo-sacral junction, the relatively broad angular scatter requires changing the camera position so that it is able to capture the position of passive reflectors in navigated instruments. The change of camera position assumes the operating theater staff cooperation. There is only a few seconds delay in the overall time to complete the surgical procedure. Inclusion of the intraoperative CT-based navigation is associated with an increased number of surgical steps. New operation actions include: acquisition of the initial scan, processing of the CT image, trajectory planning, and surgical field registration. In our setting, the completion of these steps
Acta Neurochir Fig. 5 The CT scan obtained after T6 pedicle screws insertion had identified a medial cortical breach of 2 mm in the left site. This situation was considered to be acceptable without the need for replacement and uncomplicated postoperative course confirmed the consideration
resulted in an 18–40 min increase in the operation time, according to the extent of the instrumented area and complexity of anatomy. Using the intraoperative CT imaging navigation eliminates the irradiation of the operating theatre staff during the insertion of screws , as the surgical and anesthesia teams are out of the irradiated area during the scanning. CT image acquisition is associated with a higher radiation load for the patient. In our patients, this radiation load is characterized by average values of CTDI at vol 63.8 mGy and DLP 1,660.3 mGy.cm (median 65.6 mGy and 1,619 mGy.cm).
Discussion Navigated spinal instrumentation in 571 inserted implants series proved its precision and safety with an error rate of 0.87 %. It was a series of 85 instrumented spinal procedures in 82 consecutive patients in whom we decided to test the functionality of the new system to reveal eventual complication. In the group of the very first patients, we used anatomical and even fluoroscopy control during implants insertion for additional verification. After getting used to the system (five to eight surgeries), we completely relied on the virtual reality of the navigation system. As we concentrated on gaining the maximum experience, the navigation had been used even in the lumbar instrumentation, i.e., in situations, where we would reach comparable results as measured by the insertion precision and clinical safety We even used standard fluoroscopic guidance during the surgery. This step has significantly helped in gaining early clinical experience that allowed us operate with higher confidence even in anatomically more complex areas of the upper cervical spine and the cervico-thoracic junction. Simultaneously, we gained experience with instrument navigation of high angular range during lumbar stabilizations. Intersegmental angles in lumbar lordosis may reach tens of degrees. In this situation, the optoelectronic camera system may not be able to
read the position of the registered instrument in the field and requires a change of camera position. It is a situation showing a weak point of the optoelectronic navigation system, and we may presume that an electromagnetic navigation system independent on visibility of the surgical field registration points can solve these problems in the future [11–13]. Other issues to discuss are higher time demands and the patient’s radiation exposure. The duration of surgery is prolonged by acquiring the initial scan, processing of the CT image, trajectory planning, and surgical field registration. Increasing the operation time, measured from the skin incision to wound closure, was associated with increasing the anesthesia duration and prolonging the period when the surgical wound was open. About a half an hour delay found during our procedures is significant in short stabilization [14]. With the increasing number of instrumented segments, the time difference decreases when compared to fluoroscopically guided surgeries. We suppose, particularly in large surgeries of spinal deformities, that the time difference will not be significant [15]. Theoretically, the time delay in navigated procedures may be shortened using methods of automatic registration. The CT scan acquisition is associated with higher radiation exposition of the patient compared to standard fluoroscopy; however, it eliminates the operating theatre staff irradiation being out of the irradiated part of the operating theatre [16]. Both of these moments, prolonging the surgery duration and higher irradiation of the patient, should be counterbalanced by the safety of the surgery itself. Despite the increased number of surgical steps, the learning curve is relatively less steep when both the surgeon and the OT staff become proficient with a minimum amount of effort/ time during the series of the first five to eight procedures. Further technological development in this area may focus on possible automatic registration and on improving the visibility of marked instruments in the surgical field. Both aims may be reached by changing the parameters of the electrooptic system or via the stated replacement for another navigation modality. All the progress in this area may lead to further
9
Acta Neurochir
minimization of the surgical approach and to the utilization of robotic placement for all spinal instrumentation [17]. The clinical experience of the surgeon supported by anatomical and biomechanical knowledge, in combination with the professional approach of the full team, will still be a prerequisite for optimal surgical results.
Conclusion
5.
6.
7. 8.
Navigation based on intraoperative portable CT-scanner imaging is one of the future paths leading to more precise implant insertion into spinal structures. Our initial experience has proven the performance of the system in the spinal surgery field and has confirmed its usability in all the anatomical levels of the spine. High precision of implant insertion confirms the preconditions of navigation usage during surgeries of deformities in congenital or dysplastic or post-traumatic situations as well as in anatomically complex areas of the cervical spine and cervical-thoracic junction. Previous clinical experience with a responsible team approach is a prerequisite of good morphological and clinical results.
10.
Conflicts of interest None.
13.
References 1. Golfinos JG, Fitzpatrick BC, Smith LR, Spetzler RF (1995) Clinical use of a frameless stereotactic arm: results of 325 cases. J Neurosurg 83:197–205 2. Willems PW, van der Sprenkel JW, Tulleken CA, Viergever MA, Taphoorn MJ (2006) Neuronavigation and surgery of intracerebral tumours. J Neurol 253:1123–1136 3. Nolte LP, Zamorano LJ, Jiang Z, Wang Q, Langlotz F, Berlemann U (1995) Image-guided insertion of transpedicular screws. A laboratory set-up Spine 20:497–500 4. Laine T, Lund T, Ylikoski M, Lohikoski J, Schlenzka D (2000) Accuracy of pedicle screw insertion with and without computer
10
9.
11.
12.
14. 15. 16.
17.
assistance: a randomized controlled clinical study in 100 consecutive patients. Eur Spine J 9:235–240 Waschke A, Walter J, Duenisch P, Reichart R, Kalff R, Ewald C (2013) CT-navigation versus fluoroscopy-guided placement of pedicle screws at the thoracolumbar spine: single center experience of 4, 500 screws. Eur Spine J 22:654–660 Fan Chiang CY, Tsai TT, Chen LH, Lai PL, Fu TS, Niu CC, Chen WJ (2012) Computed tomography-based navigation-assisted pedicle screw insertion for thoracic and lumbar spine fractures. Chang Gung Med J 35:332–338 Steudel WI, Nabhan A, Shariat K (2011) Intraoperative CT in spine surgery. Acta Neurochir (Wien) Suppl 109:169–174 Tonn JC, Schichor C, Schnell O, Zausinger S, Uhl E, Morhard D, Reiser M (2011) Intraoperative computer tomography. Acta Neurochir (Wien) Suppl 109:163–167 Costa F, Cardia A, Ortolina A, Fabio G, Zerbi A, Fornari M (2011) Spinal navigation: standard preoperative versus intraoperative computed tomography data set acquisition for computer-guidance system: radiological and clinical study in 100 consecutive patients. Spine 36:2094–2098 Kosmopoulos V, Theumann N, Binaghi S, Schizas C (2007) Observer reliability in evaluating pedicle screw placement using computed tomography. Int Orthop 31:531–536 Amiot LP, Lang K, Putzier M, Zippel H, Labelle H (2000) Comparative results between conventional and computer-assisted pedicle screw installation in the thoracic, lumbar and sacral spine. Spine 25:606–614 Fraser J, von Jako R, Carrino J, Härtl R (2008) Electromagnetic navigation in minimally invasive spine surgery: results of a cadaveric study to evaluate percutaneous pedicle screw insertion. SAS J 2:43–47 von Jako R, Finn MA, Yonemura KS, Araghi A, Khoo LT, PerezCruet M (2011) Minimally invasive percutaneous transpedicular screw fixation: increased accuracy and reduced radiation exposure by means of a novel electromagnetic navigation system. Acta Nerochir (Wien) 153:589–596 Sasso RC, Garrido BJ (2007) Computer-assisted spinal navigation versus serial radiography and operative time for posterior spinal fusion at L5-S1. J Spinal Disord Tech 20:118–122 Papadopoulos EC, Girardi FP, Sama A, Sandhu HS, Cammisa FP Jr (2005) Accuracy of single-time, multilevel registration in imageguided spinal surgery. Spine J 5:263–267 Bandela JR, Jacob RP, Arreola M, Griglock TM, Bova F, Yang M (2013) Use of CT-based intraoperative spinal navigation: management of radiation exposure to operator, staff, and patients. World Neurosurg 79:390–394 Ringel F, Villard J, Ryang YM, Meyer B (2014) Navigation, robotics and intraoperative imaging in spinal surgery. Adv Tech Stand Neurosurg 41:3–22
Eur Spine J DOI 10.1007/s00586-016-4476-6
HEALTH TECHNOLOGY ASSESSMENT & TRANSFER
The intraoperative portable CT scanner-based spinal navigation: a viable option for instrumentation in the region of cervico-thoracic junction Pavel Barsa1 • Robert Fr} ohlich1 • Miroslav Šercl2 • Pavel Buchvald1 • 1 Petr TheSuchomel intraoperative portable CT scanner-based spinal navigation:
a viable option for
instrumentation in the region of cervico-thoracic junction Received: 10 November 2015 / Revised: 22 February 2016 / Accepted: 23 February 2016 Springer-Verlag Berlin Heidelberg 2016
Abstract Purpose Innovative intraoperative imaging modalities open new horizons to more precise image acquisition and possibly to better results of spinal navigation. Planning of screw entry points and trajectories in this prospective study had been based on intraoperative imaging obtained by a portable 32-slice CT scanner. The authors evaluated accuracy and safety of this novel approach in the initial series of 18 instrumented surgeries in anatomically complex segment of cervico-thoracic junction. Methods We report on the single-institution results of assessment of anatomical accuracy of C5–T3 pedicle screw insertion as well as its clinical safety. The evaluation of total radiation dose and of time demands was secondary endpoint of the study. Results Out of 129 pedicle screws inserted in the segment of C5–T3, only 5 screws (3.9 %) did not meet the criteria for correct implant positioning. These screw misplacements had not been complicated by neural, vascular or visceral injury and surgeon was not forced to change the position intraoperatively or during the postoperative period. Quality of intraoperative CT imaging sufficient for navigation was obtained at all spinal segments regardless of patient́s habitus, positioning or comorbidity. A higher radiation exposition of the patient and 27 min longer operative time are consequences of this technique.
& Pavel Barsa pavel.barsa@nemlib.cz 1
Department of Neurosurgery, Regional Hospital of Liberec, Husova Str. 10, 460 63 Liberec I, Czech Republic
2
Department of Radiodiagnostics, Regional Hospital of Liberec, Liberec, Czech Republic
Conclusions The intraoperative portable CT scannerbased spinal navigation is a reliable and safe method of pedicle screw insertion in cervico-thoracic junction. Keywords Spinal instrumentation Intraoperative imaging Computer tomography Pedicle screw Cervical and thoracic vertebrae Abbreviations C-Th Cervico-thoracic CT Computed tomography LED Light emitting diode 3D Three dimensional CTDI Computed tomography dose index DLP Dose length product
Introduction Recent advances in technology of intraoperative imaging have widened possibilities of image guidance in several surgical techniques. The introduction of navigation technique based on intraoperative imaging improved clinical results with reduced complication rate in various fields including hip, knee, as well as spine surgery. In the field of spine surgery, incorrect pedicle screw placement may result in permanent neurological damage, vascular or visceral injury with persistent pain that may in many cases further lead to reinterventions, claims and increased costs. Areas of particularly high risk of pedicle screw malpositioning are also anatomical regions of lower cervical spine and upper thoracic segments not only because of difficulties in obtaining adequate intraoperative
123 11
Eur Spine J
lateral skiascopy view but also because of decreased pedicle dimensions, lack of anatomical landmarks as well as relatively frequent anatomical variations of this junctional segment [1–4]. These unique characteristics of cervico-thoracic junction have highlighted the value of precision in pedicle screw placement. Previous studies evaluating the accuracy of cervical and upper thoracic pedicle screw placement have shown high variability in malposition rate, ranging from 6 to 41 % [5– 7] according to surgeońs clinical experience and modality of intraoperative imaging used. The advent of frameless stereotactic navigation principles [6] into the spinal surgery has further increased the potential of accurate screw insertion. A breakthrough was the recent introduction of 3D fluoroscopy [7–9] and even more precise portable CT scanner [10] as a tool of intraoperative imaging later used in 3D anatomy planning and navigated screw insertion. The intraoperative image acquisition is of particular interest as it captures the entire spinal segment in the anatomical position the surgeon will instrument. The following clinical study aimed at evaluation of feasibility and accuracy of intraoperative portable CT scanner-based spinal navigation for the segment of cervicothoracic junction. The three primary endpoints of this prospective study included evaluation of the number of misplaced screws, the number screw revisions during the same surgical session and incidence of malposition-related clinical complications. The secondary endpoint of the study aimed at evaluation of total radiation dose and the time necessary for CT scanning, planning the screw trajectory and navigated screw insertion.
Materials and methods Surgical procedure Not less than 12 h before the surgery a competent patient was given all relevant information about the treatment and gave the voluntary consent not only with the stabilization but also with the intraoperative portable CT scanner-based navigation. The informed consent included discussion on the nature of the procedure, reasonable alternatives to the proposed intervention, and the relevant risks and benefits associated with the procedure, including possible higher radiation dose from the portable scanner. The patient position alike in classical fluoroscopy guided surgeries should be simultaneously chosen so that the vertical axis of the instrumented segment corresponds, if possible, with the axis of portable CT scanner gantry (Body TomTM , NeuroLogical, Danvers, USA) (Fig. 1). In the area of median skin incision, 10 fiducial markers provided by the manufacturer of the navigation system (StealthTM,
123 12
Fig. 1 The 32-slice portable CT scanner and workstation of surgical navigation system
Medtronic, Minneapolis, USA) were placed. They were used for surgical field registration after the skeletization. Further feature in the surgical field registration is the Stealth navigation tracking device attached to a non-moving spinous process of one of the instrumented vertebrae. Portable full body 32-slice CT scanner acquires images of the selected spinal section including the registration markers. It is automatically sent (in the DICOM format) to the navigation system using a direct Ethernet connection. In spinal fixation, we use helical scanning producing a 1.25 mm slice thickness. Picture is reconstructed into a three-dimensional volume by the Stealth navigation system that will render skin surface (in the soft tissue display mode) including the fiducial markers. In the 3D calcified tissue display mode, we identify the vertebral surface structures and insert virtual implant trajectories in this view. The navigation system also facilitates eventual visualization of screw trajectory course in sagittal, coronary and transversal plane. In addition, the navigation system offers ‘‘probe view’’ software which displays the transition of a virtual implant through a bony structure, similarly to an endosonography examination. This way, we can define not only precise position but also the length and diameter of the intended screw (Fig. 2). All the steps of further instrumentation are led by the prepared navigation plan. The exact position of the screw entry point may be determined using a navigated probe and may be marked with a burr on the surface of the vertebra. The dip should be deep enough to provide support for technical punch—we will use it to drill the trajectory of the specified depth and orientation. After drilling the passage for the screw we may pre-drill the thread to bone. In multiple-stage instrumentations, typical for the cervicalthoracic junction pathologies a tracking device is attached to a spinous process as close to the middle parts of the
Eur Spine J Fig. 2 Pre-op planning of left C5 pedicle screw insertion as shown by navigation workstation
instrumented section as possible. Instrumentation in this case starts from the peripheral part (e.g. in C5–T2 stabilization, we attach the frame to C7 and instrumentation starts from C5 or T2 leaving C7 vertebra as the last instrumented structure). This way navigation inaccuracy due to deflection of the tracking device during the instrumentation may be minimized. After implant insertion, we finish the decompression or reconstruction and secure the individual segments of the internal fixator. The correct implants position is confirmed before the end of procedure again with a portable CT scanner. Evaluation of accuracy of pedicle screw placement Intraoperative multi-detector row CT scans were acquired in helical mode for all patients to assess implant position. The series consisted of 1.25-mm-thick CT sections reconstructed at 1 mm intervals. The raw data were used to reconstruct transverse 1.25-mm-thick CT sections every 1 mm with a field of view adequate for visualization of the section of spine, as well as coronal and parallel to the screw axis reformats. The reformatting and interpretation of CT images in multiple planes was performed postoperatively on CT scanner monitor by two observers (a spinal surgeon-PB and independent senior radiologist-MS). A consensus interpretation was obtained for each screw. Evaluation of screw placement was performed according to the criteria published by Learch modified to include also assessment in the coronal and sagittal reformatted images [11]. A screw was classified as cortical encroachment if the pedicle cortex could not be visualized and if bone in excess of 2-mm was visible on the opposite direction (Grade 0). Frank screw
penetration was defined when not only the cortex was invisible but also when the screw trajectory was outside the pedicular and vertebral body boundaries. Frank penetration was further subdivided according to Wiesner and defined as minor—Grade 1 (\2 mm), moderate—Grade 2 (2–4 mm) and severe—Grade 3 ([4 mm) [12]. Finally we looked for possible disc penetration on the sagittal reconstructions. Evaluation of intraoperative clinical adverse events and postoperative clinical complications All patients had been closely followed throughout their hospital stays and during an initial 6-month postoperative period. To capture any perioperative or post-discharge complications, all postoperative care and patient follow-up appointments were completed at a single point in our clinical service. Demographic information, diagnosis, instrumented levels, time of surgery and radiation exposure, accuracy of screw insertion, percentage of pedicle screw revision, type and number of clinical complication were entered prospectively into a central database. Prior to initiation of the study, a list of possible clinical complications was compiled and used for prospective identification (Table 1). Major and minor complications were defined based on widely accepted methodology. The definition of a complication used in this study was broad and included all perioperative instrumentation related adverse events. Major complications were defined as events responsible for permanent sequela(e) or requiring further intervention, such as reoperation. All events with transient detrimental effect (including medical adverse events) or surgical complications with limited need for further intervention (puncture,
123 13
Eur Spine J Table 1 List of possible clinical complications related to pedicle screw insertion Major clinical complication
Minor clinical complication
Screw insertion-related event producing a detrimental effect or requiring significant further intervention including reoperation
Screw insertion-related event producing only transient detrimental effect not requiring further intervention
Permanent spinal cord dysfunction
Transient spinal cord dysfunction
Permanent nerve root dysfunction
Transient nerve root dysfunction
Durotomy requiring surgical revision
Durotomy successfully managed during index op.
Vertebral artery injury causing stroke
Asymptomatic vertebral artery injury
Visceral/pleural injury requiring surgery
Visceral/pleural injury not requiring op. revision
Hemodynamically significant blood loss
Blood loss requiring aggressive intravenous fluids/blood administration
Screw loosening or avulsion
re-suturing) were deemed minor. Results were prospectively recorded and maintained in the prospective protocol. Evaluation of radiation exposure and time necessary for navigated screw insertion CT scanner effective dose was recorded from console displayed dose length product (DLP), which is a product of CTDI (Computed Tomography Dose Index) and scan length—the dose in a single slice multiplied by scan length. This is an estimate of the energy from radiation absorbed per unit mass. New operation actions associated with the intraoperative CT-based spinal navigation include acquisition of the initial scan, processing of the CT image, trajectory planning and surgical field registration. The time required for completion of the sequence of these steps was subject of measuring and recording as a part of our prospective protocol. Statistical evaluation A cohort́s characteristic was described using summary statistics (continuous data with mean, standard deviation, median, minimum and maximum; binary and categorical data with number and percentage).
Results From July 1st 2013 through July 31st 2015, 18 patients (10 men, 8 women; mean age of 49.6 years, range 31–75) who needed reconstructive surgery in cervico-thoracic junction were treated by pedicle screw stabilization guided by intraoperative CT-based computer navigation at the authoŕs institution. Surgically treated disorders in the cervico-thoracic junction included spinal injury in ten patients, spinal metastatic tumour in 4 cases, cervical degenerative instability in 3 subjects and 1 case of failed previous surgery. The mean operative time was 238 min (range
123 14
129–352 min) and the mean estimated blood loss was 568 ml (range 200–1450 ml). After the registration of the surgical field was completed, the navigation system analysed the precision of registration process in every surgery. The average value in our group of operated patients was 0.41 mm (range of 0.20–0.90 mm) and all calculated values were sufficient to perform instrumentation confidently. In general, higher precision was reached over a larger registered field. Accuracy of C-Th junction pedicle screw placement One hundred and twenty-nine pedicle screws were inserted in the region of C-Th junction. The number of implants inserted at each level was following: C5–28; C6–25; C7–22; T1–24; T2–18; T3–12. Results of evaluation of screw insertion accuracy are featured in Table 1. Of the 129 pedicle screws, 124 screws (96.1 %) were fully contained inside the pedicle and vertebral body or maximally encroached the cortex (insertion accuracy Grade 0) (Figs. 3, 4). Next 4 pedicle screws (3.1 %) penetrated pedicle or vertebral body boundaries less than 2 mm (Grade 1) (Fig. 5) and a single screw (0.8 %) inserted at the level of C6 had been introduced completely outside the pedicle boundaries (Grade 3). The latter was the case, where intraoperative finding of very narrow and completely sclerotic pedicle in the end-vertebra of the construct (C6) precluded drilling the passage for pedicle screw. In this situation we had to decide for an alternative extrapedicular trajectory via upper medial quadrant (safe zone) with penetration of cranial vertebral body end plate (Fig. 6). In this aspect, this is rather the case of ‘‘intentional screw malposition’’ than true malposition. Despite this fact we are including this situation into the category of frank penetrations as similar situation may distort results as unrecognized cause of malposition also in other insertion techniques. Also the breach of ventral wall of vertebral body up to 2 mm found in 2 pedicle screws may be considered by many authors as optimal bicortical screw
Eur Spine J
Fig. 3 Intraoperative transverse CT scan verifying T3 screws fully contained inside pedicles and vertebral body (Grade 0)
Fig. 5 Left pedicle screw penetrates ventral boundaries of the T1 vertebral body less than 2 mm (Grade 1)
Clinical complications
Fig. 4 Sagittal reconstruction of intraoperative CT image depicting an anatomically correct position of left-side pedicle screws after the instrumentation of segment C5–T2 (Grade 0)
There were no intraoperative or postoperative complications directly related to pedicle screw insertion such as an injury to vertebral artery, spinal cord, nerve root or an injury to adjacent organs. Thus, no pedicle screws were removed as a result of neurovascular or splanchnic complication. Postoperatively, one patient developed painful transient unilateral C8 radiculopathy. That was a case of high-energy trauma patient operated on for unilateral C7/ T1 traumatic subluxation that had been completely reduced by an intraoperative distraction–translation manoeuvre using pedicle screws. The postoperative clinical condition has been treated conservatively and radicular pain disappeared within 4 postoperative days. A delayed superficial wound healing with temporal secretion but without local or global inflammatory response has been noted in two other postoperatively bedridden patients. Also this clinical situation had been treated conservatively and did not require surgical re-intervention. Radiation exposure and duration of CT scan and screw navigation
insertion. This situation, however, did not meet our criteria defining correct screw placement (full containment of the screw inside the bone distal to the entry point) and is therefore included in the category of malpositioned implants. A final incidence of screw misplacement in our study was 5 out of 129 (3.9 %) and the precise analysis is depicted in Table 2.
The use of the intraoperative CT-based imaging navigation eliminates the irradiation of the operating theatre staff during screws insertion, as the surgical and anaesthesia team is out of the irradiated area during the scanning. CT image acquisition is associated with higher radiation load for the patient. In our group of patients, this radiation load
123 15
Eur Spine J
Fig. 6 Extrapedicular trajectory and penetration of cranial end plate in the left C6 pedicle screw (Grade 3)
Table 2 Anatomical characteristics of misplaced pedicle screws Level
No. of screws
Misplacement (% per level)
Misplacement grade I
II
III
Medial
Lateral
Ventral breach
C5
28
0
0
0
0
0
0
0
C6
25
2 (8 %)
1
0
1
1
1
0
C7
22
0
0
0
0
0
0
0
T1
24
0
0
0
0
0
0
0
T2
18
2 (11.1 %)
2
0
0
0
0
2
T3
12
1 (8.3 %)
1
0
0
1
0
0
129
5 (3.9 %)
4 (3.1 %)
0 (0 %)
1 (0.8 %)
2
1
2
Total
has been characterized by average values of CTDI vol 60.8 mGy and DLP 1620.3 mGy cm (median 62.6 mGy and 1614 mGy cm). Inclusion of the intraoperative CT-based navigation is associated with an increased number of surgical steps. New operation actions include: acquisition of the initial scan, processing of the CT image, trajectory planning and surgical field registration. In our setting, the completion of these steps resulted in a 27.4 min increase in the operation time (range 19–38 min), according to the extent of the instrumented area. All the remaining surgical steps run, compared to the skiaskopy-guided insertion, faster because the need for the C-arm positioning is eliminated.
123 16
Direction of malposition
Discussion This study reports encouraging morphological as well as clinical results for pedicle screw placement in the cervicothoracic junction using computer navigation based on intraoperative portable CT scanner imaging. This is the first report of similar type of intraoperative imaging used during the instrumentation in this junctional region. The question, however is, whether these results are comparable to results reported in navigated instrumentations based on other imaging modalities. Lee et al. in their study compared 2D fluoroscopy and 3D isofluoroscopy-guided placement of pedicle screws in
Eur Spine J
C7, T1 and T2 vertebrae against screw insertion from laminoforaminotomy. The accuracy of pedicle screw placement was significantly improved with computer-assisted techniques (81 % of screws completely within the pedicle in 2D fluoroscopy, 89 % in 3D isofluoroscopy against 70.9 % of screws in laminoforaminotomy). Majority of navigated screws (17 of 108) breached the pedicle by a margin of less than 2 mm and 1 screw by 2–4 mm. All breaches were in a lateral direction and none of the perforations required revision [13]. Sugimoto et al. reported 3.6 % (4/110) penetration rate in pedicle screws inserted under the 3D isofluoroscopybased navigation in the segment of C7–T3. All the misplaced screws penetrated pedicle cortex \2 mm and the study did not specified the direction of penetration [14]. Bledsoe et al. evaluated accuracy of pedicle screw insertion into T1-T3 under 3D isofluoroscopy-based navigation. This study reported 6.7 % (10/150) rate of pedicle violations, all of them being Grade 1 (B2 mm). The direction of violation included three medial, four inferior, two superior, and one minor anterolateral vertebral body perforation. No patient experienced complications associated directly with the placement of the screws or the use of intraoperative image guidance [8]. In multicenter study focused on assessment of subaxial pedicle screw placement accuracy published by Nakashima et al., in subgroup of 3D isofluoroscopy-based navigation, the incidence of 15.4 % of Grade I and 4.1 % of Grade II maplosition has been calculated [15]. Tian et al. assessed the accuracy of pedicle screw placement assisted by different navigation systems in human cadaver model of lower cervical spine. The placement accuracy was estimated by gross view during postsurgical dissection. The 2D fluoroscopy navigation screw placement was associated with 45 % rate of Grade 1 and 12.5 % of Grade 2 penetrations, in preoperative CT-based navigation subgroup 12.5 % incidence of Grade 1 malposition was recorded and finally in the Iso-C 3D navigation screw placement 10 % incidence of Grade 1 penetration was described [16]. All above-mentioned reports using technologies of intraopertive imaging for spinal navigation have been very positive, and most authors who use them regularly consider them a step up in accuracy and, hence, safety. The grade of pedicle screw penetration in our prospective study was classified into four groups: screws fully contained into the pedicle, perforated screws up to 2 mm, displacement 2–4 mm and malpositioning exceeding 4 mm. It has been shown that medial pedicle penetration of more than 4 mm may endanger neural elements causing the neurological deficit. Although there is no strong literature evidence ensuring that pedicle breaching less than 2 mm is
safe, most surgeons consider it as safe zone for eventual pedicle perforation [6, 17]. Possible criticisms of the pedicle screw navigation based on intraoperative portable CT scanner images may be addressed on higher time demands and increased patient́s radiation exposure. The procedural time in this technique is highly dependent on the experience of the entire surgical team. The duration of surgery itself is prolonged by acquiring the initial scan, processing of the CT image, trajectory planning and surgical field registration. Increasing of the operation time, measured from the skin incision to wound closure, is inevitably associated with increasing the anaesthesia duration and prolonging the period when the surgical wound is open. About 27 min delay found during our procedures is significant in short segment stabilization. In longer stabilization the time difference compared to fluoroscopically guided surgeries decreases as all instrumented segments are registered during this time period. We suppose, particularly in large surgeries of spinal deformities, that the time difference will not be significant. The time delay in navigated procedures may be theoretically shortened using methods of automatic registration. The CT scan acquisition is associated with higher radiation exposition of the patient compared to standard fluoroscopy; however, it eliminates the operating theatre staff irradiation being out of the irradiated part of the operating theatre. The impact of the radiation dose for patient raises questions and considerations especially from ethical point as it is difficult to define the limits between the effectiveness of the insertion technique and the stochastic risk related to radiation exposure. Both the moments, prolonging the surgery duration and higher irradiation of the patient, should be counterbalanced by the safety of the surgery itself. Some limitations of the present study should be acknowledged. Mainly, we had to deal with remarkable heterogeneity of the study population, including age and gender, the indication of surgery and the difference between the anatomy and size of pedicles in lower cervical and upper thoracic spine both being evaluated together. Furthermore, a single-institution experience of highly dedicated staff familiar with spinal navigation techniques may positively bias results of this study compared to ordinary user accuracy. In conclusion, the navigation based on intraoperative CT scans exhibits high accuracy in cervico-thoracic junction pedicle screw placement and eliminates the risk of wrong level surgery. We believe this study functions as a useful feasibility study and larger multi-institutional comparative investigations are needed to more clearly define the reliability, potential complications as well as advantages of intraoperative CT-based navigation during pedicle screw
123 17
Eur Spine J
placement in the cervico-thoracic region. We should also emphasize that despite this technology is proving to be a useful adjunct to spinal instrumentation, it should not completely replace spine surgeońs knowledge of pedicle anatomy and technical experience during pedicle screw placement. Compliance with ethical standards Conflict of interest
None.
References 1. Panjabi MM, O’Holleran JD, Crisco JJ 3rd, Kothe R (1997) Complexity of the thoracic spine pedicle anatomy. Eur Spine J 6:19–24 2. Ugur HC, Attar A, Uz A, Tekdemir I, Egemen N, Genc Y (2001) Thoracic pedicle: surgical anatomic evaluation and relations. J Spinal Disord 14:39–45 3. Vaccaro AR, Rizzolo SJ, Allardyce TJ, Ramsey M, Solvo J, Balderston RA, Cotler JM (1995) Placement of pedicle screws in the thoracic spine. Part I: morphometric analysis of the thoracic vertebrae. J Bone Joint Surg Am 77:1193–1199 4. Vaccaro AR, Rizzolo SJ, Balderston RA, Allardyce TJ, Garfin SR, Dolinskas C, An HS (1995) Placement of pedicle screws in the thoracic spine. Part II: an anatomical and radiopgraphic assessment. J Bone Joint Surg Am 77:1200–1206 5. Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew D (2004) Free hand pedicle screw placement in the thoracic spine: is it safe? Spine 29:333–342 6. Zhao LJ, Xu RM, Ma WH, Jiang WY (2010) Evaluation of the value of pedicle screws for cervicothoracic fracture-dislocation. Orthop Surg 2:27–31 7. Reinhold M, Bach C, Audigé L, Blauth M, Magerl F (2008) Comparison of two novel fluoroscopy-based stereotactic methods for cervical pedicle screw placement and review of the literature. Eur Spine J 17:564–575 8. Bladsoe JM, Fenton D, Fogelson JL, Nottmeier EW (2009) Accuracy of upper thoracic pedicle screw placement using threedimensional image guidance. Spine J 9:817–821
123 18
9. Tabaraee E, Gibson AG, Karahalios DG, Potts EA, Mobasser JP, Burch S (2013) Intraoperative cone beam-computed tomography with navigation (O-ARM) versus conventional fluoroscopy (CARM): a cadaveric study comparing accuracy, efficiency, and safety for spinal instrumentation. Spine 38:1953–1958 10. Hecht H, Kamphuis M, Czabanka M, Hamm B, König S, Woitzik J, Synowitz M, Vajkoczy P (2016) Accuracy and workflow of navigated spinal instrumentation with the mobile AIRO CT scanner. Eur Spine J 25:716–723 11. Learch TJ, Massie JB, Pathria MN, Ahlgren BA, Garfin SR (2004) Assessment of pedicle screw placement utilizing conventional radiography and computer tomography: a proposed systematic approach to improve accuracy of interpretation. Spine 29:767–773 12. Wiesner L, Kothe R, Schulitz KP, R} uther W (2000) Clinical evaluation and computer tomography scan analysis of screw tracts after percutaneous insertion of pedicle screws in the lumbar spine. Spine 25:615–621 13. Lee GY, Massicotte EM, Rampersaud YR (2007) Clinical accuracy of cervicothoracic pedicle screw placement: a comparison of the ‘open’ lamino-foraminotomy and computer-assisted techniques. J Spinal Disord Tech 20:25–32 14. Sugimoto Y, Ito Y, Tomioka M, Shimokawa T, Shiozaki Y, Mazaki T, Tanaka M (2010) Clinical accuracy of three-dimensional fluoroscopy (IsoC-3D)-assisted upper thoracic screw insertion. Acta Med Okayama 64:209–212 15. Nakashima H, Yukawa Y, Imagama S, Kanemura T, Kamiya M, Yanese M, Ito K, Machino M, Yoshida G, Ishikawa Y, Matsuyama Y, Ishiguro N, Kato F (2012) Complications of cervical pedicle screw fixation for nontraumatic lesions: a multicenter study of 84 patients. Clinical article. J Neurosurg Spine 16:238–247 16. Tian W, Liu Y, Zheng S, Lv Y (2013) Accuracy of lower cervical pedicle screw placement with assistance of distinct navigation systems: a human cadaveric study. Eur Spine J 22:148–155 17. Fisher CG, Sahajpal V, Keynan O, Boyd M, Graeb D, Bailey C, Panagiotopoulos K, Dvorak M (2006) Accuracy of thoracic vertebral body screw placement using standard fluoroscopy, fluoroscopic image guidance and computer tomographic image guidance. J Neurosurg Spine 5:520–526
7
Head Injury James M. Schuster and Philip F. Stahel
Head injury
The management of a head-injured patient with multiple other injuries presents one of the most challenging and difficult clinical scenarios in trauma critical care. This is due in part to the fact that the treatment of other injuries, such as orthopedic, spine, and craniofacial fractures, has the potential for worsening the neurologic outcome. This potential worsening is not necessarily directly related to the primary repair or the timing of surgery, but more to the fact that additional surgery with potential blood loss and possible resultant hypotension or hypoxia can adversely affect an injured brain. It has been shown that a single episode of hypotension or hypoxia can adversely affect outcome of all severities of head injury [1–6]. Management of polytrauma patients with head injuries requires strict adherence to ACLS principles, close coordination, and communication between all involved surgical specialties, including simultaneous procedures when appropriate. Decision making is all about assessing relative risk with priority initially given to lifeJ.M. Schuster, MD, PhD Department of Neurosurgery, University of Pennsylvania, Philadelphia, PA, USA P.F. Stahel, MD (*) Department of Orthopaedics and Department of Neurosurgery, University of Colorado School of Medicine, Denver Health Medical Center, Denver, Colorado, USA e-mail: philip.stahel@dhha.org
threatening and neurologic injuries, but with a simultaneous evaluation and possible management of orthopedic, spine, and craniofacial injuries. This often requires flexibility on the part of the involved services as surgical decisions should not be based on convenience. This approach provides an opportunity for imaginative and innovative surgical management. Definitive repair procedures are not always possible or appropriate because of the length of the case, inability to appropriately provide neurologic monitoring, and the potential for significant blood loss and massive fluid administration. Other options include placement of external fixation, choosing a surgical approach based on reduced operative time and reduced blood loss, or staged procedures. The trauma surgery team often serves as the coordinator of care for multiple injured patients, as each involved service can be somewhat myopic in their approach to the patient. However, once the life-threatening hemodynamic injuries are stabilized, the neurosurgery consultant feels the obligation to protect the brain and spinal cord at all costs. While the neurosurgeons are usually very involved with the simultaneous management of spine injuries, they also have to be well informed about the effects of delayed treatment of orthopedic or craniofacial injuries. Again, this very often comes down to an assessment of relative risk. This is because ultimately, while patients with lost or suboptimally functioning
Š Springer International Publishing AG 2017 H.-C. Pape et al. (eds.), Damage Control Management in the Polytrauma Patient, DOI 10.1007/978-3-319-52429-0_7
71
19
J.M. Schuster and P.F. Stahel
72
Polytrauma patient with head injury ACLS Head CT Neuro exam
Operative head injury (emergent) Craniotomy/ craniectomy
Yes
No Other operative injuries
Other operative injuries Yes No
No
Simultaneous/sequential procedures if possible Yes
(Consider timing)
ICU Spine Facial fractures
Spine
Early stabilization With least Time and Blood loss
Pelvis/ Long bone
Cervical
Thoracolumbar
Reduction/ stabilization
Repair CSF leak at craniotomy Delay primary repair
Facial fracture
Ortho
Ext-fix washout
Ext-fix washout
Delayed Repair Unless CSFleak
Decompression/ stabilization
Fig. 7.1 Decision-making flow sheet for polytrauma patient with associated head injury
limbs or craniofacial defects can return to independent functioning, this is less often the case in patients with significant brain injuries. Again an overall concern for avoiding secondary injury must be paramount. The intent of this chapter is to provide a template for rapidly managing
20
head injuries in polytrauma patients including an initial assessment paradigm (Fig. 7.1) to aid in making decisions about the need for emergent neurosurgical intervention, as well as a system for prioritizing and coordinating the treatment of other injuries.
7
Head Injury
7.1
Initial Assessment
The overall approach to a head-injured patient should be aggressive and timely treatment of the primary injury and avoidance of secondary injury. The basic underlying questions that need to be addressed early in the assessment are as follows: “Does this problem need immediate surgical intervention? Is the injury likely to require intervention in the near future? Or is this an injury unlikely to need surgical intervention?” This decision is based on a clinical and radiographic assessment of the patient. Injuries such as epidural hematomas (EDH), subdural hematomas (SDH), intraparenchymal hemorrhages, contusions, or penetrating injuries with altered neurologic status (especially pupillary abnormalities and lateralizing motor finding) often require emergent surgical intervention. The question of salvageability often arises especially in patients with fixed, dilated pupils and Glasgow Coma Score of 3 [7, 8]. While the decision should be individualized, the survivability of such injuries is debatable. However, it is imperative that the clinical assessment is not altered by pharmacologic muscle paralysis and/or injuries/medications that can alter pupillary function. There is also a danger of being too reassured by a patient’s initial clinical assessment such as in patients with the “talk and die syndrome.” This is generally seen in a young patient with bifrontal and/or subfrontal injuries (often contusions) who initially
Fig. 7.2 Patient at risk for “talk and die syndrome.” (a) CT scan showing frontal contusions. (b) CT scan showing right hemicraniectomy (arrow) after progressive neuro-
73
may be awake and talking (Fig. 7.2). Because of basal-frontal swelling near the brainstem, any perturbation such as a seizure or hypoxemia can set in motion a rapidly progressive clinical spiral leading to fixed dilated pupils which then requires emergent surgery to avoid poor outcome [9]. Once the decision is made that a patient needs an operation, the question then arises: What operation? The operative plan must take into account the presence of intracranial hematomas, overall brain swelling, intracranial foreign bodies, involvement of major vascular structures, and the involvement of air sinuses that need to be addressed to avoid CSF leak. The general approach is to evacuate hematomas, debride devitalized tissue, remove accessible foreign bodies, and repair CSF leaks. The other decision is whether the patient is likely to have significant problems with raised intracranial pressure postoperatively. Concerns for postoperative management often lead the decision to perform a craniectomy with storage of the bone subcutaneously in the abdomen or in the freezer until which time the brain swelling has subsided and the bone can be replaced. This procedure also requires dural augmentation with pericranium, or a dural substitute to allow swelling of the brain out of the bone defect, thus decompressing the brain. The procedure can be performed unilaterally, bifrontally, or bihemispheric depending on the pattern of injury [10–14] (Fig. 7.2b,c). The removal of bone must be adequate to ensure that as the brain swells out
logic decline. (c) CT showing replacement of bone at 8 weeks after patient made excellent neurologic recovery
21
J.M. Schuster and P.F. Stahel
74
of the defect, it is not lacerated or contused against a bone edge. Craniectomy, if performed adequately, is the most effective and durable way to reduce intracranial pressure. While ultimate outcome is still heavily tied to the severity of the initial injury and neurologic status, there is evidence that hemicraniectomy can reduce intracranial pressure and improve brain oxygenation as measured by invasive monitoring in head-injured patients [15, 16]. The other advantage of hemicraniectomy and the subsequent improvement in ICP and brain oxygenation is it often makes postoperative management less physiologically stressful to the patients as they are less likely to require osmotic diuretics, blood pressure support, and heavy sedation. In patients with less severe injuries but labile intracranial pressure, the placement of a ventriculostomy for CSF diversion can be an extremely effective and less physiologically stressful way of treating raised intracranial pressure. After aggressive surgical treatment of the primary intracranial injury, the introduction of aggressive neurocritical care has been shown to positively impact brain-injured patients [17–19]. Using monitoring to measure brain oxygenation and intracranial pressure, the use of continuous EEG to detect seizures and ischemia, and protocol-driven approaches to glycemic control and hyperthermia are now routinely implemented [20–22]. Early tracheostomy and enteral access are now initiated to facilitate patient care [23, 24]. Finally, consulting services such as orthopedics often enquire about when a patient is stable enough to allow further surgery. This decision needs to be individualized for each patient based on injury severity, clinical exam, neurophysiologic stability based on monitoring, the perceived urgency of the proposed surgery, and the potential physiologic stress of the surgery including length, risk of large blood loss, or large fluid volume administration. Physiologic monitoring is also recommended during the case (ICP, brain oxygenation) which may affect positioning and the potential of aborting the procedure if a problem arises. Essentially, management in the OR must be an extension of the management in the
22
ICU with the same vigilance with regard to monitoring and proactive intervention [25]. As can be seen from the above discussion, there is an apparent paradox in the treatment approach to a patient with a head injury and other associated injuries. We aggressively and definitively treat the primary CNS injury to help avoid secondary injury while treating other associated injuries in a damage control fashion. This is due in part to the fragile nature of CNS structures with little reparative capability, little function reserve, and a narrow timing window with regard to salvageability after injury. We will discuss this approach in the subsequent sections. Finally, by definition, surgical decision making involves relative risk assessment, and therefore it is imperative that patients and families understand the complexity of these interactions and have realistic expectations for outcome and recovery.
7.2
Head Injury Associated with Major Chest/Abdominal Injury
Stabilizing a patient’s cardiopulmonary status must always be the highest priority in dealing with a trauma patient. However, there are clinical scenarios in which a patient is taken emergently to the operating room to deal with life-threatening thoracoabdominal trauma with a suspected brain injury and no confirmatory neuroimaging. There is traditional support for placing burr holes on the side of a “blown” pupil in the ED or in the OR during thoracoabdominal surgery. While if performed correctly there is the potential to relieve pressure from an evolving EDH or SDH, this may not be the definitive procedure and a craniotomy may also be required [26, 27]. This in theory could follow after cardiopulmonary stabilization. In the case of bilateral “blown” pupils, practitioners must keep in mind that hypoxia/ hypotension can cause pupillary abnormalities that do not indicate an intracranial spaceoccupying mass [28]. As neurosurgeons, we are sometimes asked to place intracranial monitors in patients undergoing “crash” thoracotomies or exploratory laparotomies with suspected
7
Head Injury
intracranial pathology. However, elevated ICP is difficult to interpret in a patient lying flat or head down and receiving massive fluid resuscitation. Additionally, therapeutic interventions such as mannitol would not be indicated in a hypotensive patient. The key is early cranial imaging. A rapid helical CT scan preoperatively if possible, or utilization of portable CT scanners interoperatively, would obviate this problem.
7.3
Head Injury Associated with Cranial Facial Injury
Head injuries from blunt force trauma or penetrating injuries have the potential for involvement of the air sinuses such as the frontal sinus as well as cranial facial structures [29, 30]. While not absolute indications for surgical intervention, the presence of pneumocephalus and/or a CSF leak must be closely monitored. Increasing pneumocephalus or rhinorrhea/otorrhea that does not resolve spontaneously may require surgical intervention. The goal of surgery in a patient with significant intracranial pathology (hematoma, contusion) associated with pneumocephalus/CSF leak (for instance, from an anterior skull base fracture/frontal sinus fracture) is to adequately deal with the intracranial pathology and stop the CSF leak: essentially isolating the brain from the nose [31, 32]. There is often input from multiple services including neurosurgery and ENT, OMFS, or plastics, but it is generally in the patient’s better interest to delay the definitive repair of facial fractures because of the overall extension of the operative time [33]. If CSF diversion is required to protect the repair, a ventriculostomy is preferred to a lumbar drain in a patient with suspected intracranial swelling. Compression of the optic nerve could also be addressed by this approach if indicated [34]. Skull base fractures can also cause damage to carotid arteries. There should be a high index of suspicion with these types of fractures. Treatment options include medical management, or more invasive surgical or endovascular therapy. Therapy depends on the risk-benefit ratio of each option considering the natural history of each
75
injury type including mild intimal irregularities, intimal flaps, pseudoaneurysms, fistulas, and occlusions. The need for treatment is determined in part by the collateral circulation to the brain and the degree to which the lesion is thrombogenic [35]. It is beyond the scope of this chapter to discuss the management of traumatic carotid injury, but the risk of anticoagulation would have to be considered in a patient with significant intracranial injury [36].
7.4
Head Injury with Spine Injury
There is a high incidence of associated spine fracture with head injury especially with falls and motor vehicle accidents [37]. It is often difficult to clinically clear the cervical spine in a patient with a significant head injury even without obvious radiographic abnormalities. But the more pressing difficulty occurs with the combination of an operative head injury and an operative spine injury. In the case of spine fracture/dislocation with a spinal cord injury such as with bilateral jumped facets and burst fractures, early decompression and stabilization is optimal [38, 39]. While these injuries can be decompressed in traction, this delays mobilization which has been shown to negatively impact outcome secondary to pulmonary issues [40–43]. With simultaneous operative injuries, the cranial portion could be completed, and the cervical spine reduced and stabilized through an anterior approach if possible. In critically ill patients with unstable thoracolumbar fractures, a posterior approach can be utilized in a time-efficient and less physiologically stressful manner for decompression/stabilization even if an anterior approach will subsequently be required. This staged stabilization/decompression allows mobilization and thus helps avoid life-threatening pulmonary complications [42, 43]. These stabilization procedures can sometimes be performed in a percutaneous/ minimally invasive method, significantly reducing blood loss [44]. Blunt vertebral artery injury is associated with complex cervical spine fractures involving sub-
23
J.M. Schuster and P.F. Stahel
76
luxation, extension into the foramen transversarium, or upper C1 to C3 fractures [45]. The posterior circulation stroke rate has been reported as high as 12–24% after traumatic vertebral artery injury [46, 47]. Treatment of vertebral artery injuries such as dissections, pseudoaneurysms, fistulas, and occlusions must be individualized with regard to the use of anticoagulation and/or endovascular treatment based on the patients’ clinical status, risk of ischemic/thrombotic potential for the individual lesions, and the suitability of the patient for anticoagulation based on their intracranial pathology and other injuries [46–48].
7.5
Head Injury with Orthopedic Injury
The combination of head injuries and significant orthopedic injuries are relatively common with motor vehicle accidents and falls. Major orthopedic trauma can be both life threatening (pelvic fractures with vascular injuries) and limb threatening especially with open and potentially contaminated extremity injuries. Ideally, head injuries and orthopedic injuries can be assessed and if possible treated simultaneously. If the patient is going to the OR for an operative head injury, every effort should be made to treat orthopedic injuries in a damage control fashion. Any open fracture or other critical musculoskeletal injury that can realistically be splinted or casted and treated definitively in a delayed fashion should be. Any injury that can be treated with external fixation or washed out and closed when the patient initially goes to the OR for a head injury should be treated simultaneously. This damage control method has been shown to be both safe and effective [49–55]. The problem often arises when these injuries are not dealt with simultaneously and early. Once the patient is in the ICU, there is generally resistance to allow the patient to go to the OR if they have labile vital signs especially brain oxygenation and intracranial pressure difficulties. In this case, these decisions need to be made in a coordinated fashion between the involved services. This often results in a compromise in which the patient is allowed
24
to go to the OR for a less time-consuming and less physiologically stressful procedure. While this is an area of discussion, there is growing evidence to support this approach [51–53, 56].
7.6
Summary
The management of a polytrauma patient with a significant head injury represents one of the most complicated clinical scenarios encountered by the trauma team. However, it provides an opportunity to implement innovative and imaginative management strategies that require communication, coordination, and flexibility among the involved subspecialties. Primary intracranial pathologies need to be treated aggressively and secondary injuries avoided at all costs. Head injuries, spine injuries, orthopedic injuries, and craniofacial injuries with CSF leaks need to be assessed and treated simultaneously if possible. The definitive treatment of the noncranial injuries can often be delayed with the initial therapies designed to stabilize spine, pelvis, and long bone injuries as well as repairing CSF leaks associated with cranial facial injuries. This facilitates management in the ICU and helps prevent pulmonary complications, which are a major source of morbidity and mortality. Additionally, neurocritical care, provided in the ICU, needs to be extended to the OR to avoid secondary brain injury. Subsequently, with stabilization and improvement of the head injury, the noncranial injuries can be readdressed.
References 1. Chesnut RM. Secondary brain insults after head injury: clinical perspectives. New Horiz. 1995;3(3):366–75. 2. Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993;34(2):216–22. 3. Chesnut RM, Marshall SB, Piek J, et al. Early and late systemic hypotension as a frequent and fundamental source of cerebral ischemia following severe brain injury in the Traumatic Coma Data Bank. Acta Neurochir Suppl (Wien). 1993;59:121–5. 4. Chi JH, Knudson MM, Vassar MJ, et al. Prehospital hypoxia affects outcome in patients with traumatic
7
Head Injury
5.
6.
7.
8. 9. 10.
11.
12.
13.
14. 15.
16.
17.
18.
19.
brain injury: a prospective multicenter study. J Trauma. 2006;61(5):1134–41. Jeremitsky E, Omert L, Dunham CM, et al. Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion. J Trauma. 2003;54(2):312–9. Manley G, Knudson MM, Morabito D, et al. Hypotension, hypoxia, and head injury: frequency, duration, and consequences. Arch Surg. 2001;136(10):1118–23. Tien HC, Cunha JR, Wu SN, et al. Do trauma patients with a Glasgow Coma Scale score of 3 and bilateral fixed and dilated pupils have any chance of survival? J Trauma. 2006;60(2):274–8. Udekwu P, Kromhout-Schiro S, Vaslef S, et al. Glasgow Coma Scale score, mortality, and functional outcome in head-injured patients. J Trauma. 2004;56(5):1084–9. Reilly PL. Brain injury: the pathophysiology of the first hours. ‘Talk and Die revisited’. J Clin Neurosci. 2001;8(5):398–403. Hutchinson PJ, Corteen E, Czosnyka M, et al. Decompressive craniectomy in traumatic brain injury: the randomized multicenter RESCUEicp study (www. RESCUEicp.com). Acta Neurochir Suppl. 2006;96:17–20. Jagannathan J, Okonkwo DO, Dumont AS, et al. Outcome following decompressive craniectomy in children with severe traumatic brain injury: a 10-year single-center experience with long-term follow up. J Neurosurg. 2007;106(4 Suppl):268–75. Munch E, Horn P, Schurer L, et al. Management of severe traumatic brain injury by decompressive craniectomy. Neurosurgery. 2000;47(2):315–22; discussion 322–3. Polin RS, Shaffrey ME, Bogaev CA, et al. Decompressive bifrontal craniectomy in the treatment of severe refractory posttraumatic cerebral edema. Neurosurgery. 1997;41(1):84–92; discussion 92–4. Shaffrey M, Farace E. Decompressive craniectomy. Crit Care Med. 2003;31(10):2560–1. Stiefel MF, Heuer GG, Smith MJ, et al. Cerebral oxygenation following decompressive hemicraniectomy for the treatment of refractory intracranial hypertension. J Neurosurg. 2004;101(2):241–7. Timofeev I, Kirkpatrick PJ, Corteen E, et al. Decompressive craniectomy in traumatic brain injury: outcome following protocol-driven therapy. Acta Neurochir Suppl. 2006;96:11–6. Diringer MN, Edwards DF. Admission to a neurologic/neurosurgical intensive care unit is associated with reduced mortality rate after intracerebral hemorrhage. Crit Care Med. 2001;29(3):635–40. Fakhry SM, Trask AL, Waller MA, et al. Management of brain-injured patients by an evidence-based medicine protocol improves outcomes and decreases hospital charges. J Trauma. 2004;56(3):492–9; discussion 499–500. Hyman SA, Williams V, Maciunas RJ. Neurosurgical intensive care unit organization and function: an
77
20. 21. 22.
23. 24. 25. 26.
27. 28.
29. 30. 31.
32.
33. 34.
35. 36.
American experience. J Neurosurg Anesthesiol. 1993;5(2):71–80. Jordan KG, et al. J Clin Neurophysiol. 1999;16(1):14–39. Kilpatrick MM, Lowry DW, Firlik AD et al. Hyperthermia in the neurosurgical intensive care unit. Neurosurgery. 2000;47(4):850–5; discussion 855–6. Van den Berghe G, Wouters PJ, Bouillon R, et al. Outcome benefit of intensive insulin therapy in the critically ill: Insulin dose versus glycemic control. Crit Care Med. 2003;31(2):359–66. Bouderka MA, Fakhir B, Bouaggad A, et al. Early tracheostomy versus prolonged endotracheal intubation in severe head injury. J Trauma. 2004;57(2):251–4. Perel P, Yanagawa T, Bunn F, et al. Nutritional support for head-injured patients. Cochrane Database Syst Rev. 2006;(4):CD001530. Grotz MR, Giannoudis PV, Pape HC, et al. Traumatic brain injury and stabilisation of long bone fractures: an update. Injury. 2004;35(11):1077–86. Liu JT, Tyan YS, Lee YK, et al. Emergency management of epidural haematoma through burr hole evacuation and drainage. A preliminary report. Acta Neurochir. 2006;148(3):313–7; discussion 317. Springer MF, Baker FJ. Cranial burr hole decompression in the emergency department. Am J Emerg Med. 1988;6(6):640–6. Andrews BT, Levy ML, Pitts LH. Implications of systemic hypotension for the neurological examination in patients with severe head injury. Surg Neurol. 1987;28(6):419–22. Alvi A, Doherty T, Lewen G. Facial fractures and concomitant injuries in trauma patients. Laryngoscope. 2003;113(1):102–6. Martin 2nd RC, Spain DA, Richardson JD. Do facial fractures protect the brain or are they a marker for severe head injury? Am Surg. 2002;68(5):477–81. Rocchi G, Caroli E, Belli E, et al. Severe craniofacial fractures with frontobasal involvement and cerebrospinal fluid fistula: indications for surgical repair. Surg Neurol. 2005;63(6):559–63; discussion 563–4. Bell RB, Dierks EJ, Homer L, et al. Management of cerebrospinal fluid leak associated with craniomaxillofacial trauma. J Oral Maxillofac Surg. 2004;62(6):676–84. Weider L, Hughes K, Ciarochi J, et al. Early versus delayed repair of facial fractures in the multiply injured patient. Am Surg. 1999;65(8):790–3. Levin LA, Beck RW, Joseph MP, et al. The treatment of traumatic optic neuropathy: the International Optic Nerve Trauma Study. Ophthalmology. 1999;106(7):1268–77. Larsen DW. Traumatic vascular injuries and their management. Neuroimaging Clin N Am. 2002;12(2):249–69. Cothren CC, Moore EE, Biffl WL, et al. Anticoagulation is the gold standard therapy for blunt carotid injuries to reduce stroke rate. Arch Surg. 2004;139(5):540–5; discussion 545–6.
25
78 37. Holly LT, Kelly DF, Counelis GJ, et al. Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors, and injury characteristics. J Neurosurg. 2002;96(3 Suppl):285–91. 38. Fehlings MG, Perrin RG. The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine. 2006;31(11 Suppl):S28–35; discussion S36. 39. Fehlings MG, Perrin RG. The role and timing of early decompression for cervical spinal cord injury: update with a review of recent clinical evidence. Injury. 2005;36(Suppl 2):B13–26. 40. Chipman JG, Deuser WE, Beilman GJ. Early surgery for thoracolumbar spine injuries decreases complications. J Trauma. 2004;56(1):52–7. 41. Holland MC, Mackersie RC, Morabito D, et al. The development of acute lung injury is associated with worse neurologic outcome in patients with severe traumatic brain injury. J Trauma. 2003;55(1):106–11. 42. McHenry TP, Mirza SK, Wang J, et al. Risk factors for respiratory failure following operative stabilization of thoracic and lumbar spine fractures. J Bone Joint Surg Am. 2006;88(5):997–1005. 43. McLain RF, Benson DR. Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine. 1999;24(16):1646–54. 44. Rampersaud YR, Annand N, Dekutoski MB. Use of minimally invasive surgical techniques in the management of thoracolumbar trauma: current concepts. Spine. 2006;31(11 Suppl):S96–102; discussion S104. 45. Cothren CC, Moore EE, Biffl WL, et al. Cervical spine fracture patterns predictive of blunt vertebral artery injury. J Trauma. 2003;55(5):811–3. 46. Biffl WL, Moore EE, Elliott JP, et al. The devastating potential of blunt vertebral arterial injuries. Ann Surg. 2000;231(5):672–81.
26
J.M. Schuster and P.F. Stahel 47. Miller PR, Fabian TC, Bee TK, et al. Blunt cerebrovascular injuries: diagnosis and treatment. J Trauma. 2001;51(2):279–85; discussion 285–6. 48. Lee YJ, Ahn JY, Han IB, et al. Therapeutic endovascular treatments for traumatic vertebral artery injuries. J Trauma. 2007;62(4):886–91. 49. Giannoudis PV, Pape HC. Damage control orthopaedics in unstable pelvic ring injuries. Injury. 2004;35(7):671–7. 50. Harwood PJ, Giannoudis PV, Probst C, et al. The risk of local infective complications after damage control procedures for femoral shaft fracture. J Orthop Trauma. 2006;20(3):181–9. 51. Pape HC, Giannoudis P, Krettek C. The timing of fracture treatment in polytrauma patients: relevance of damage control orthopedic surgery. Am J Surg. 2002;183(6):622–9. 52. Pape HC, Grimme K, Van Griensven M, et al. Impact of intramedullary instrumentation versus damage control for femoral fractures on immunoinflammatory parameters: prospective randomized analysis by the EPOFF Study Group. J Trauma. 2003;55(1):7–13. 53. Pape HC, Hildebrand F, Pertschy S, et al. Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 2002;53(3):452–61; discussion 461–2. 54. Renaldo N, Egol K. Damage-control orthopedics: evolution and practical applications. Am J Orthop. 2006;35(6):285–91; discussion 291. 55. Taeger G, Ruchholtz S, Waydhas C, et al. Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma. 2005;59(2):409–16; discussion 417. 56. Brundage SI, McGhan R, Jurkovich GJ, et al. Timing of femur fracture fixation: effect on outcome in patients with thoracic and head injuries. J Trauma. 2002;52(2):299–307.
Health Watch
INTERVENTIONAL RADIOLOGISTS USE MINIMALLY INVASIVE METHODS TO SPEED SURGERY RECOVERY Interventional radiologists
use minimally invasive
methods to
speed surgery recovery
27
PHOTO COURTESY OF MOUNT CARMEL HEALTH SYSTEM PHOTO COURTESY OF MOUNT CARMEL HEALTH SYSTEM By Mike Mahoney By Mike Mahoney From the April 2015 issue of Columbus CEO From the April 2015 issue of Columbus CEO Key procedures in interventional radiology generally involve delivering therapies via Key procedures in interventional radiology generally involve delivering therapies via small catheters and radiological probes. small catheters and radiological probes.
IR procedures typically add precision to stentsthat open up blood vessels and balloon IR procedures typically add precision to stentsthat open up blood vessels and balloon angioplasty, originally a radiological innovation that now is a standard procedure for angioplasty, originally a radiological innovation that now is a standard procedure for cardiac surgeons. cardiac surgeons. Embolization cuts off the blood supply to malignant or malfunctioning cells, tumors or Embolization cuts off the blood supply to malignant or malfunctioning cells, tumors or organs, minimizing damage to the rest of the body, often an alternative to amputation or organs, minimizing damage to the rest of the body, often an alternative to amputation or organ extraction or to address uterine fibroids and arrest post-partum uterine bleeding. IR organ extraction or to address uterine fibroids and arrest post-partum uterine bleeding. IR specialists use small catheters to deliver chemoembolization agents, microscopic specialists use small catheters to deliver chemoembolization agents, microscopic radioactive isotopes, tiny coils or microscopic particles as precision-aimed clotting agents. radioactive isotopes, tiny coils or microscopic particles as precision-aimed clotting agents. Thrombolysis, on the other hand, opens up blood vessels through precision delivery of Thrombolysis, on the other hand, opens up blood vessels through precision delivery of clot-busting drugs and/or chemicals to a blockage site, such as a brain clot that produces clot-busting drugs and/or chemicals to a blockage site, such as a brain clot that produces stroke. Again, the key instruments include small catheters guided by radiologists. stroke. Again, the key instruments include small catheters guided by radiologists.
28
Cryoablation kills cancer cells by freezing them. Today's smaller catheters avoid frostbite complications as the cryo probe enters the surface of the skin. Radiofrequency Ablation uses RF energy to kill malignant or malfunctioning cells. In vertebroplasty/ osteoplasty, surgeons use image-guided catheters to deliver medical-grade bone cement to reinforce deteriorated or damaged spinal tissue and discs. Angiographyemploys a catheter to enter the blood vessel and inject dye to make arteries or veins visible by X-ray.
Interventional radiologists have emerged from X-ray labs into operating rooms, using minimally invasive techniques to treat hard-to-reach parts of the body and turning a lowprofile specialty into a burgeoning surgical field with its own clinical and outpatient services. In the process, they're reducing costs, shortening recovery times and easing pain. "Interventional radiology is perhaps the most interesting medical field that a lot of folks haven't heard about," says Dr. James Spain, chief of interventional radiology at The Ohio State University Wexner Medical Center. "We invented minimally invasive. We rarely make an incision over a quarter of an inch—just a nick in the skin—and we put a Band-Aid on at the end." "If you think of the human body as a complex geography of tissue, blood vessels, neurons and bones, the equipment of today's interventional radiologists acts like the body's GPS system," says Dr. Brad Mullin, director of neurosurgery at Mt. Carmel East Hospital and adjunct assistant professor of neurosurgery at Ohio State. Interventional radiology specialists are opening outpatient clinics to see patients and provide radiation, chemo, burn and cryo therapies. "Our direct interaction and treatment of patients has evolved quickly," said Dr. John Lippert, an interventional radiology and vascular specialist at Riverside Radiology and Interventional Associates, closely affiliated with OhioHealth. This transformation follows the development of ever-smaller probes, catheters and instruments, with a breakthrough in reducing probe size in 2011. "We had been freezing tumors since the '60s, but the probe was as big as my finger. Now the technology means probes just a little bigger than an IV needle," Lippert says.
29
Significant dividends have been realized. The field has expanded the range of minimally invasive surgery now available, minimizing risks of infection from open surgery and limiting damage to healthy tissues surrounding a tumor, blockage or fragmented bone. That means many interventional radiology procedures are available on an outpatient basis and typically don't involve general anesthesia. Those factors hasten recovery time, helping patients return to work and home. It yields productivity benefits for employers and savings for the healthcare system. "We're talking about recovery times that in some cases are down to days and weeks instead of weeks and months," Lippert says. "Patients are surviving conditions once thought to be life-ending and going back to their jobs, their families and a better quality of life." For cancer patients, miniature probes and catheters deliver radiation or chemotherapy, or alternatively provide precision burning or freezing of tumors to destroy malignant cells, avoiding nearby muscles, blood vessels and nerves. Specialists recently introduced TARE (trans-arterial radioembolization) via TheraSphere, a branded process of delivering microscopic glass particles filled with yttrium-90 directly to liver tumors, Spain says. "In many cancers, particularly renal carcinoma where the kidney can get very large, there would be substantial blood loss if they take the kidney out, but not so much if we embolize it," says Spain. "So we release things into the artery feeding the kidney to cause it to be blocked. It could be a coil or small particles, each smaller than a grain of sand, and ultimately they stop the flow of blood to the capillaries." For spinal injuries and disk deterioration procedures, Mullin now uses a fully portable BodyTom (a CT scanner) in the operating room at Mt. Carmel East, the only one in central Ohio to do so. The BodyTom feeds real-time information to a new spine mask by Stryker— another first—that displays detailed LED images of the spine, surrounding tissue and surgical instruments. Pairing the devices in the operating room eliminates inaccuracies as patients change position from X-ray table to the OR. "It's like the difference between television and highdefinition television," Mullin says.
30
Not all interventional radiology specialists work directly in the operating room. At the new James Cancer Hospital, IR specialists work close at hand in three new interventional radiology suites just down the hall from the fourth floor oncology surgical suites. The Riverside group IR specialists offer both clinical/outpatient treatment and in-hospital care. In the future, new techniques will deliver microwave therapy by catheter, as well as minimally invasive techniques to treat benign prostate tumors while preserving sexual response, Spain says. And interventional radiologists hope to guide connections between the brain and artificial limbs. "You need to do that minimally invasively, with computer technology and scans that are four generations from what we have today," Mullin says. Mike Mahoney is a freelance writer.
31
Consultoría integral, la mejor capacitación y entrenamiento para el profesional de la salud y el servicio postventa más completo.
D E LE C C I E NTÍ FI CA U R U G UAYA
DELEC CIENTÍFICA ARGENTINA
www.delec.com.uy
www.delec.com.ar
Fco. García Cor na 2357 - Piso 1 Montevideo, Uruguay. Tel. (+598) 2711 4466 Cel. (+598) (0) 93 507 500 delecuruguay@delec.com.uy
Aráoz 821 - C1414DPQ C.A.B.A - Argen na Tel. (54-11) 4775 - 5844 Fax. (54-11) 4803 - 2505 consultas@delec.com.ar
DELEC CIENTÍFICA