15 minute read
NEWS & EVENTS


news | EVENTS Upload your videos to Dentevents.TV now and win a smartphone gimbal

Dentevents.TV has launched a brand new feature to allow anyone working in dentistry to upload and share videos that’s easier than ever. Simply login at www. dentevents.tv and click “Upload Video” to get started.
Whether you have a webinar recording, a product hack, a clinical technique, a product review or unboxing, a diatribe on difficult patients or some wisdom or humour about dentistry, you’re invited to share your video with your peers.
Plus, the author of the video that receives the most votes before August 31 will receive a DJI OM 5 Smartphone Gimbal Stabiliser (Phone not included) to help you make even better videos in the future.
“Dentevents.TV has continued to grow in popularity following its launch during the first COVID lockdown, but moving forward, we need to attract more content to take it to the next level,” said Dentevents. TV publisher Joseph Allbeury. “We have a great catalogue of dental videos available free and on demand 24/7 already, but now we’re looking for more content created by members of the dental community.
“Many people working in dentistry are already prolific content creators and we want to engage with these people and encourage them to use dentevents. tv as an additional way to share their videos with their peers. Part of this is making it far easier to load videos and part of this is incentivising videos creators to share their content.”
The latest videos added to the site appear under “Recently Added” and a new “VOTE” button has been added to enable anyone visiting the site to vote for the videos they like. “You have to login to Dentevents.TV to watch the videos and vote,” Mr Allbeury said. “Each person can only vote once for a video, but they can vote for multiple videos.
Only videos added between 1 July and 31 August 2022 can be voted for. So if you load a video onto the site, then it’s in your interests to encourage your friends to login as well and vote for it. The VOTE button activates after you have watched the video.”


For more information on the contest, visit Dentevents.TV. It’s free to login and watch any of the videos 24/7 and VOTE.
Dentevents.TV is a brand new dental video streaming service Watch a growing list of hundreds of videos related to dentistry all in one place www.dentevents.tv
news | EVENTS Proven 3-Step water treatment protocol

With increased emphasis on infection control in the current pandemic environment, there is a new focus on ensuring dental unit waterline quality is adequately maintained
A-dec Product Manager, Shal Hafiz says that together with daily waterline maintenance with a proven solution like A-dec ICX tablets, it’s important to monitor water quality and periodically shock the lines. New A-dec ICX Renew – launched in Australia in May – is the perfect complement to self-contained waterline units to ensure the highest quality water is delivered to patients.
ICX Renew is a shock treatment and part of the “A-dec 360 Maintenance” approach which includes regular waterline maintenance; waterline quality monitoring; and periodic shock treatment.
ICX Renew clears deposits and contamination which can build up over time, without harming plastic tubing or corroding dental unit components, unlike some harsh treatments.
“Contaminated water lines can cause odour and foul-tasting water that can also present a potential health risk,” Mr Hafiz said.
The latest ADA Infection Control Guidelines suggest a shock treatment if CFU (colony forming units) reach 200 CFU/mL.
“These shock treatments are required periodically to clean dental unit waterlines and more often if dental units have been left unused for any period, such as over a holiday break,” Mr Hafiz said.
He said A-dec dealers now offer a waterline testing service using a highly accurate high tech Lumitester device.
This water testing service could easily be incorporated in clinics as part of routine equipment servicing.
“It’s good practice to test microbial levels in water lines regularly – at least every six months, as this is a good protocol to ensure dental unit waterline quality is not forgotten,” Mr Hafiz said.
“In keeping with ADA Guidelines, A-dec recommends a three-step: ‘Maintain, Monitor, and Shock’ approach to keeping water lines clean.
“Monitoring requirements will depend on your water quality and the clinic’s individual requirements,” Mr Hafiz said. “Initially, test water once a month. If the results pass your specified action level for three successive months (i.e. 200 CFU/ mL), reduce the testing protocol to quarterly.”
Mr Hafix said the A-dec 360 Maintenance system took the uncertainty out of waterline maintenance, ensuring water quality and patient safety was maintained and that equipment was protected.
“Some testing systems are inaccurate and take up to 72 hours to produce a result, which could mean you are using contaminated water on patients while awaiting your test results.
“A-dec’s 2-minute Lumitester system produces an accurate result in just two minutes, without the need for cumbersome and potentially inaccurate manual counts. If your test triggers an action level, treat your dental units with ICX Renew. Best results are achieved by adding the ICX Renew Tablets to the dental unit waterline and letting it sit overnight.”
ICX Renew turns the dental unit waterline water blue, indicating the shock treatment is at work in the waterline. The next day the lines are flushed until they are clear and are then ready to be refilled with clean water and a regular ICX tablet matching the size of the water bottle.
Mr Hafiz said both ICX and ICX Renew were completely safe to use in dental units and did not cause corrosion of metals or damage to soft components. “Some other shock treatments use harsh nappy sanitiser chemicals which can harm dental tubing, diaphragms and ‘O’ rings.”
A-dec ICX, ICX Renew and the Lumitester dental unit waterline test are all available from your A-dec dealer.

Contact A-dec on 1800-225-010 or visit: australia.a-dec.com to find your nearest authorised A-dec dealer or representative.
Unwanted guests in your waterlines?

When you SHOCK, let ICX RENEW.

Unwanted visitors like bacteria love to colonise in your dental unit waterlines. A daily waterline maintenance protocol with A-dec ICX® waterline treatment tablets, along with periodic ICX Renew™ shock treatments, will help reduce
these nasty microorganisms.
For complete trademark information, visit a-dec.com/legal/trademarks. © 2021 A-dec Inc. All rights reserved.
Water Flosser compared to interdental brush on bleeding scores and gingival abrasion
Slot DE, Lyle DM, Van der Sluijs E, Hennequin-Hoenderdos N, Van der Weijden F. J Dent Res 2018; 97(Special Iss. B): Abstract #0622 (www.iadr.org). Conducted at Academic Center for Dentistry Amsterdam (ACTA), Netherlands.
Objective
To compare the effectiveness of a Waterpik Water Flosser (WF) and interdental brush (IDB) on bleeding indices and gingival abrasion.
Methodology
Seventy-eight subjects completed this 4-week, randomized controlled trial. Subjects were assigned to one of two groups; Waterpik Water Flosser (WF) plus a manual toothbrush or interdental brush (IDB) plus a manual toothbrush. Gingival inflammation was evaluated by measuring Bleeding on Pocket Probing (BOPP) and Bleeding on Marginal Probing (BOMP). Data was collected on contra-lateral quadrants. The Gingival Abrasion Score (GAS) was used to compare the incidence of abrasion between the groups.
Results
Both groups demonstrated a significant reduction in BOPP and BOMP from baseline to four weeks for all sites and interdental sites separately. The WF group was significantly more effective than the IDB group for reducing BOPP for all sites at week four (p=0.030) and BOMP for all sites and interdental sites at week four (p=0.003, p=0.019 respectively). There were no differences in gingival abrasion scores between the groups.

Plaque Removal
100
80
% R education
60
40 String Floss Water Flosser
29%
MORE EFFECTIVE*
74.4%
57.7%
29%
MORE EFFECTIVE*
81.6%
63.4%
24%
MORE EFFECTIVE*
33%
MORE EFFECTIVE* 68.2% 69.4% 85.7%
51.1%
39%
MORE EFFECTIVE*
62.9%
45.2%
20
0
Whole Mouth Approximal Marginal Facial Lingual * Statistically significant difference
Conclusion
The Waterpik Water Flosser is significantly more effective than the interdental brush for improving gingival health in this clinical study.
Want more information?
For more information or to book a free Waterpik Lunch and Learn, email professionalAU@waterpik.com
READ ME FOR CPD
Preventing needle stick injury

By Dr Greg Mahoney, BDSc, PhD, MSc (Dent), GradDipClinDent, FADI, FPFA
Sharps injuries in dental practice remain a concern today even though dentistry adopted preventive practices in the 1980s.
An Australian study found 27.7% of dentists had experienced at least one sharps injury in the previous 12 months and 16.1% of these involved a contaminated instrument that had been previously used on a patient. Furthermore, the most common devices to cause sharps injury in the previous 12 months were needles (14.4%).1 Hollow-bore needle injuries are of particular concern, since they are likely to contain residual blood and are associated with an increased risk for blood-borne virus transmission. Of the 57 documented cases of occupational HIV transmission to healthcare personnel reported to CDC from June 1995 to December 2002, 50 (88%) involved percutaneous exposure. Of these, 45 (90%) were caused by hollow-bore needles and half of these needles were used in a vein or an artery.2
The risk
Blood-borne viruses that could potentially be transmitted by a sharps injury include hepatitis B and C, as well as HIV. The risk of transmission following a skin puncture injury is dependent on: • Whether the person who previously used the object had an infection; • The level of virus in their blood; • The amount of blood involved; • The type of needle or syringe in question; • The time that has elapsed since it was used; and • The nature of the injury.
So in dentistry, the most likely source of a blood-borne virus transmission is the local anaesthetic needle, being hollow and injected into a vascular rich area. It is estimated that up to 14% of inferior dental nerve blocks result in an intravascular injection and with an infiltration may too puncture a blood vessel.3
ULTRA SAFETY PLUS TWIST
safe & easy
Protects you and your staff from needle stick injuriesFigure 1. The new Ultra Safety Plus Twist from Septodont.
Complies with latest regulations
Intuitive device > Available with either sterile single use or sterilisable handle
Passive or active aspiration:
security for the patient
Transparent barrel:
aspiration is clearly visible

Sliding protective sheath:
protection from needle stick injuries

Two different positions:
fi rst Holding Position (reversible) fi nal Locking Position (irreversible)
Figure 2. The Ultra Safety Plus from Septodont.

The risks of acquiring other bloodborne viruses from a contaminated needle are considerably higher than the 0.23% for HIV with 6-30% for hepatitis B and 1.8% for hepatitis C.4 Acquired hepatitis B and C cases have been reported in Australia.5,6
Following known exposure to blood borne virus, post-exposure prophylaxis (PEP) should be considered. PEP is known to be over 80% effective in preventing HIV from needle stick injuries and while oral health care workers are vaccinated against hepatitis B, there is no vaccination for Hepatitis C. Post exposure prophylaxis protocols are an essential part of everyday practice although are an expensive and time consuming process with a considerable emotional toll.7 It makes eminent sense for all dental operatories to adopt effective needle stick injury prevention protocols and safety equipment. The criteria for local anaesthetic delivery should be: • Compatible with the existing local anaesthetic cartridge; • Able to be used for all techniques for local anaesthesia; • Single use or autoclavable; • Proven to be effective in reducing or eliminating needle stick injury; and • Cost effective.

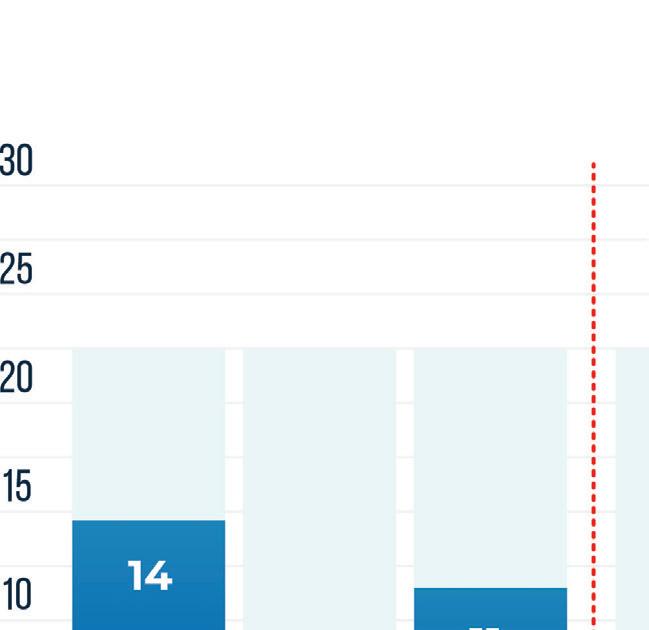
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries.
FREQUENCY OF NEEDLE STICK INJURIES
ULTRA SAFETY PLUS INTRODUCTION
YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
With Ultra Safety Plus, needle stick injuries Figure 3. Zakrzewska found that the number of avoidable needle decreased from an average of 11.8 to 0 injuries per stick injuries reduced from an average 11.8 per 1,000,000 hours 1,000,000 hours worked(1) worked to zero in UK dental schools. Consequently it has been adopted by most dental school across the UK.8-10
(1) J.M Zakrzewska et al. Introducing safety syringes into a UK dental school – a controlled study. Brit Dent J 2001 ; 190; 88-92.
Prevention
Areview of the availability of safety systems, including needleless systems, found that one system met the above criteria - the Ultra Safety Plus from Septodont. The Ultra Safety Plus™ and now the new Ultra Safety Plus Twist (also from Septodont) system – which does not require the re-sheathing or removal of a needle from its syringe – has been in my private practice for over 10 years and in that time there has been no cases of local anaesthetic needle stick injury.
Evaluating the system against the desirable criteria
Compatibility: The system uses the existing 2.2ml cartridges.
Technique: The system comes with preloaded a 27 or 30 gauge needle in short and extra short and looks, feels and acts like the traditional dental injection.
Autoclavable: It comes in single use and if desired, an autoclavable plunger.
Effectiveness at reducing needle sticks: Zakrzewska found that the number of avoidable needle stick injuries reduced from an average 11.8 per 1 million hours worked to zero in UK dental schools (Figure 3). Consequently it has been adopted by most dental school across the UK.8-10
Cost effectiveness. The University of Queensland found the cost of safety syringes was comparable to non-disposable syringes, however the reduction in the cost of managing sharps injuries was substantial.11

A INTUITIVE NEW PATENDED DESIGN
Only 2 easy steps are needed for a secure assembly
1.

A secure lock
2.
ULTRA SAFETY PLUS “The system works by sliding down a captive rigid TWIST sheath over the needle when loading up a new cartridge, exposing the needle and cap. After injection, the sheath is moved up to the first click so that the needle can be uncovered for a second injection if required. At the end of the injection, the sheath
A secure lock is slid up till the second click
ULTRA SAFETY PLUS TWIST 1 box of 100 sterile needles + 1 STERILISABLE handle 1 box of 50 sterile needles 1 box of 50 sterile SINGLE-USE handles 1 sterilisable handle length gauge color code
Introduce the pins of the handle in the notches of the barrel Twist the fi nger grip to lock it

2.
Twist the fi nger grip to lock it
x short - 10 mm 30 g short - 25 mm 30 g short - 25 mm 27 g long - 35 mm 27 g long - 35 mm 25 g
Find the relevant details in the instructions manual
Please visit our website for more information: www.septodont.com

BROCHURE 3 volets SEPTODONT v16 GAMME XL OK 23/09.indd 1-3
The system works by sliding down a captive rigid sheath over the needle when loading up a new cartridge, exposing BROCHURE 3 volets SEPTODONT v16 GAMME XL OK 23/09.indd 1-3 the needle and cap. After injection, the sheath is moved up to the first click so that the needle can be uncovered for a second injection if required. At the end of the injection, the sheath is slid up till the second click which is a one way lock to permanently lock the sheath in place over the needle, preventing sharps injuries during changeover between patients. Adopting sharp safe methods is essential in all dental practices. The Ultra Safety Plus and Ultra Safety Plus Twist provides the dental team with the necessary tool to provide safe practice. If sharp safe habits are not expected of each team member, the risk of a sharp injury increases.
References
1. Leggat PA, Smith DR. Prevalence of percutaneous exposure incidents amongst dentists in Queensland. Aust Dent J. 2006;51(2):158-61. 2. CDC. Workbook for Designing, Implementing and Evaluating a Sharps Injury Prevention Program 14 Dec 2019]. Available from: https://www.cdc.gov/ sharpssafety/part1TEXTONLY.htm. 3. Taghavi Zenouz A, Ebrahimi H, Mahdipour M, Pourshahidi S, Amini P, Vatankhah M. The Incidence of Intravascular Needle Entrance during Inferior Alveolar Nerve Block Injection. J Dent Res Dent Clin Dent Prospects. 2008;2(1):38-41. 4. CDC. Exposure to Blood :s What healthcare personnel need to know. National Center for Infectious Diseases Divison of Healthcare Quality Promotion and Division of Viral Hepatiti. 2003. 5. Haber PS, Young MM, Dorrington L, Jones A, Kaldor J, De Kanzow S, et al. Transmission of hepatitis C virus by needle-stick injury in community settings. J Gastroenterol Hepatol. 2007;22(11):1882-5. 6. Res S, Bowden FJ. Acute hepatitis B infection following a community-acquired needlestick injury. J Infect. 2011;62(6):487-9. 7. McAllister J. Literature review for the national guidelines for post-exposure prophylaxis after nonoccupational and occupational exposure to HIV (revised). National PEP Guidelines Expert Reference Group 2016;Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine. 8. Zakrzewska JM GIaJJ. Introducing safety syringes into a UK dental school – a controlled study. BrDent J 2001(190):188-92. 9. Zakrzewska JM BE. Use of dental safety syringes in British and Irishdental schools. . Br Dent J. 2003(195):207-9. 10. Oliver G, David DA, Bell C, Robb N. An Investigation into Dental Local Anaesthesia Teaching in United Kingdom Dental Schools. SAAD Dig. 2016;32:7-13. 11. Walsh L. Sharps injuries during patient changeover: Are you getting the point. Australasian Dental Practice January/February 2018:64-6.
