● In addition to The Technologist, DTA members can also log on to the DTA’s website –www.dta-uk.org – and access the quarterly Articulate CPD facility where they will find a host of interesting articles while also gaining CPD hours for successfully completing the multiple-choice questionnaires.
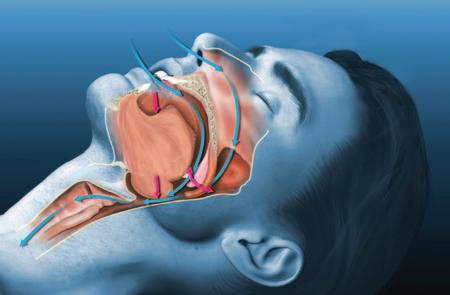
● Articulate and The Technologist are just two of the benefits of DTA membership that provide a valuable resource for GDC registered technologists. Enjoy! And, amongst other informative texts, find out why a coypu’s teeth are so brown – what causes sleep apnoea –and how to perform CPR.
Editor: Derek Pearson
t: 07866 121597
Advertising: Rebecca Kinahan
t: 01242 461 931
e: info@dta-uk.org
DTA administration: Rebecca Kinahan
Operations Coordinator
Address: PO Box 1318, Cheltenham GL50 9EA
Telephone: 01242 461 931
Email: info@dta-uk.org Web: www.dta-uk.org
Stay connected: @DentalTechnologists Association
@The_DTA @dentaltechnologists association
Dental Technologists Association (DTA)
DTA Council:
Delroy Reeves President
Joanne Stevenson
Deputy President
Tony Griffin Treasurer
Chris Fielding, David Gale, Dominika Krowiarz
Robert Leggett, Patricia MacRory and Jade Ritch.
Editorial panel: Tony Griffin Joanne Stevenson
Editorial assistant: Dr Keith Winwood
Published by: Stephen Hancocks
ISSN: 1757-4625
dta column thefuture of amalgam in dental practice – jason wong and chris mcconnell graduate reflections – eboni-rose williams audit again – crown and bridgework – dr chris turner living and working with change – part 1: technological change – kevin lewis flexible dentures: a case study – jo stevenson ‘seven steps to save UK dentistry’: – patients first report changes affecting the dental lab – ian cumberland in a Q&A mental health part 1 – tracey o’keeffe
Representing you for 35 years PPP
DTA Autumn Council Meeting
The DTA management team will convene at the Holiday Inn Birmingham Airport on November 2, 2024, to discuss key initiatives and strategic plans for the year ahead.
The meeting will focus on several important topics. Tony Griffin, the Treasurer, will present the financial report for 2023/24 and propose the budget for 2024/25. Council members will discuss proposals to maintain and enhance member benefits. The members will put forward charity recommendations for 2025. Derek Pearson will report on the activities and proposals of the Editorial Board. The Council will engage in discussions on current employment issues in the UK Dental Laboratory sector and explore ways the DTA can benefit its members, plus outline
2025 Subscription
There will be a slight increase in the 2025 subscription fee. The decision to proceed with the 2025 increase has been made by the DTA management team, setting the renewal fee at £125 for a 12-month membership. We take pride in our membership benefits package which has been specifically tailored to provide value and support for our dental technologist members. Here’s a recap of what’s included:
● Webinars! *New for 2025*
● Access to over 20 hours of free, qualityassured and verifiable CPD annually, offering lifelong learning tailored to the needs of dental technologists, covering core subjects.
updates and links with various dental professional bodies, including recent meetings with the Chief Dental Officers.
If you are interested in attending an upcoming meeting to learn more about becoming a Council member or Ambassador, kindly reach out via email to info@dta-uk.org with the subject line ‘DTA Council’. If you have any feedback you wish
to share with the team and fellow members, please complete our annual survey. We will also be celebrating 35 years since the Dental Technologists Association (DTA) was established in 1989 as the Dental Technicians Education and Training Advisory Board (DTETAB). What changes have affected the way our members work over the last 35 years? Please let us know.
DTA Annual Membership Survey
The DTA annual member survey is now open, and we highly value your input. Your feedback helps us tailor our products and services to better meet the needs of dental technologists like you. By submitting your response before the deadline on 30 January 2025, you will also have a chance to win a £100 Amazon voucher.
To participate, simply complete the survey using the provided form and return it in the enclosed pre-paid envelope. Alternatively, you can respond online by clicking the link in the DTA November e-newsletter or on the DTA website. If you are not receiving DTA emails, please update your information in the members’ area.
● A personalised Logbook that updates automatically upon completing a CPD activity, incorporating ‘reflection’ as required by GDC for ECPD.
● Cost-effective professional indemnity insurance meeting the statutory requirement for our dental technologist members.
● Immediate access to a wealth of information, advice sheets, and guidance documents on regulatory updates, technical aspects, FAQs, factsheets, templates, and business management within the members’ area of the DTA website.
● Free legal, tax, and counselling helpline available 24/7, 365 days a year.
● And there’s much more! Explore our
website for a comprehensive list of membership benefits at www.dtauk.org/membership-benefits
Additionally, we continue to offer a sixmonth trial membership for DT’s and CDT’s who have not previously been a DTA member. This trial includes all the benefits of full membership for half a year: access to over 10 hours of CPD over six months, PDP, Log Book, DTA Journals, exclusive insurance offers, 24-hour helpline, support, guidance documents, and more.
Addressing the Recruitment Crisis in Dental Technology
As the leading voice and an active association for dental technologists, we are deeply concerned about the ongoing recruitment challenges faced by dental laboratories in Northern Ireland and across the UK.
As highlighted by the Managing Director of McDowell & Service Dental Laboratory Ltd, there has been a persistent struggle to recruit appropriately trained and qualified dental technicians in the region. The demand from dental labs has significantly outpaced the number of graduates entering the field.
Many full-time BTEC graduates who have secured employment in dental labs often find it challenging to adapt to the functional and efficient demands of a commercial environment. This has led to a high turnover rate, with many graduates leaving the trade altogether.
The DTA strongly advocates for the day release/apprentice arrangement as the most effective training and recruitment model. This approach involves employing a trainee full-time while allowing them to attend college for theoretical education one day a week. This model has proven successful for McDowell & Service, which recently employed a trainee full-time and
enrolled them in a part-time Foundation Degree in Dental Technology at Cardiff University.
However, although the DTA acknowledges the financial burden this places on dental laboratories, including costs for travel and accommodation when trainees must attend college in person. the DTA believes that investing in training at all stages of a dental technician’s career is crucial for the future of the dental technology sector.
We are calling on dental laboratory owners to invest in the development of their team members, especially trainees, to ensure they gain valuable qualifications and hands-on experience. This investment is essential for both maintaining a skilled workforce and advancing the field of dental technology. We have been discussing these issues during regular meetings with Chief Dental Officers across the UK.
We report on our meeting with Tom Ferris, Scotland’s Chief Dental Officer, to discuss the future of dental technology education
The DTA recently held a productive meeting with Tom Ferris, the Chief Dental Officer (CDO) for Scotland, to discuss the current state and future of dental technology education in Scotland. The meeting was attended by key members of the DTA, including President Delroy Reeves,
Council Members Rob Leggett and Jade Ritch, and Lead DCP Elaine Hutchison. During the meeting, several critical issues were addressed:
1. Funding for Technician Training: The CDO acknowledged the lack of current funding for extending technician training in Scotland and shared that his team were working through options to improve the current position.
2. Enhancing Dental Technology
Education: Discussions were held on the challenges faced by training centres faced with the need to focus on modern as well as traditional technology methods. It was noted that the number of registered dental technicians has decreased from 7,400 in 2008 to around 5,000 today, highlighting the urgent need to prioritise the entry-level pipeline; with a particular emphasis on widening-access programmes.
3. Collaborative Support for Dental Technologists: The DTA and CDO explored ways to work collaboratively to support both qualified dental technologists and students in training. Ideas included utilising underused training lab capacity, and encouraging dental hospitals and registered labs to take on trainees.
4. Future Meetings and Broader
Representation: The group discussed the importance of ensuring a range of organisations are involved in future meetings to better represent the dental technology community. The next meeting is scheduled for February 2025, with plans to invite additional contacts.
We remain committed to advancing the field of dental technology and ensuring that dental technologists receive the support and training they need to succeed in what can be a tough working environment. We look forward to continued collaboration with the CDOs and other stakeholders to achieve these goals.
Festive Season & New Year Opening
The DTA office will close over the festive period from 1.00pm on Friday 20th December and will
Your Wellbeing
The Importance of Mental Health During Winter: Tips for Staying Well and Supporting Others
As the days grow shorter and temperatures drop, many people find their mental health taking a hit. The winter months can be particularly challenging, with the lack of sunlight and colder weather contributing to feelings of sadness, lethargy, and even depression, a condition recognised as Seasonal Affective Disorder (SAD). Understanding the importance of mental health during this time and knowing how to stay well can make a significant difference. Continue reading below for some tips to help you maintain your mental health and support others during the winter months.
● To find wellbeing resources visit the DTA Members’ area and log in with your member details.
reopen on Monday 6th January 2025 at 9.00am.
● If you’re membership renewal is due during this time and you need to make any changes, please send an email to info@dta-uk.org prior to 6th December 2024 to allow our team sufficient time to deal with your request.
● To discover more about Seasonal Affective Disorder, visit the NHS website: https://www.nhs.uk/mentalhealth/conditions/seasonal-affectivedisorder-sad/overview/
Why Mental Health Matters in Winter
Winter can exacerbate mental health issues due to several factors:
● Reduced Sunlight: Less exposure to natural light can disrupt your circadian rhythm and lower serotonin levels, leading to feelings of depression.
● Cold Weather: Colder temperatures can limit outdoor activities, reducing physical exercise and social interactions.
● Holiday Stress: The festive season can bring about financial stress, loneliness, and unrealistic expectations.
Tips for Staying Well
1. Maximize Natural Light: Try to spend time outdoors during daylight hours. Even a short walk can help boost your mood. If getting outside is difficult, consider using a light therapy lamp.
2. Stay Active: Regular physical activity can improve your mood and energy levels. Activities such as walking, running, yoga, or even cleaning at home can be beneficial.
3. Eat Well: A balanced diet rich in fruits, vegetables, and whole grains can positively impact your mental health.
Avoid excessive sugar and caffeine, which can lead to mood swings.
4. Maintain a Routine: Keeping a regular schedule for sleeping, eating, and activities can provide a sense of normalcy and control.
5. Stay Connected: Reach out to friends and family regularly. Social connections are crucial for mental well-being. If inperson meetings are not possible, use video calls or social media to stay in touch.
6. Practice Mindfulness and Relaxation: Techniques such as meditation, deep breathing, and progressive muscle relaxation can help reduce stress and anxiety.
7. Seek Professional Help: If you find it challenging to cope, don’t hesitate to seek help from a mental health professional. Therapists and counsellors can provide support and strategies to manage your mental health.
Supporting Others
1. Check-In Regularly: Make a habit of checking in on friends and family, especially those who live alone or are going through tough times.
2. Offer Practical Help: Simple gestures such as helping with groceries, gritting pathways, or running errands can make a big difference.
3. Encourage Professional Help: If someone you know is struggling, gently
Dental Technology Showcase (DTS) 2025 – Save the date!
The organisers of the Dental Technology Showcase (DTS) are planning for the event to take place on Friday 16th and Saturday 17th of May 2025 at the Birmingham NEC, for more information, visit https://www.the-dts.co.uk/
Save the date and we’ll see you there.
GDC Whistleblowing
Disclosures
encourage them to seek professional support. Offer to help them find resources or accompany them to appointments if needed.
4. Be a Good Listener: Sometimes, just being there to listen can provide immense comfort. Let them know you care and are there for them.
Charities and Resources
Several organisations offer valuable resources and support for mental health:
● Mind: Provides advice and support to empower anyone experiencing a mental health problem.
● Samaritans: Offers a safe place for you to talk any time you like, in your own way –about whatever’s getting to you.
● Mental Health Foundation: Works to prevent mental health problems and support those who need help.
● Rethink Mental Illness: Provides expert, accredited advice and information to everyone affected by mental health problems.
By taking proactive steps to care for your mental health and supporting those around you, you can help make the winter months more manageable and even enjoyable. Remember, it’s okay to ask for help and to offer it to others.
The General Dental Council (GDC), along with eight other UK healthcare regulators, has published its 2024 annual report on whistleblowing disclosures. A GDC spokesperson provides more information
Since 2018, all the healthcare regulators have jointly compiled an annual report to highlight our coordinated effort in working together to highlight and address whistleblowing concerns raised with us. The aim of the report is to be transparent about how we handle disclosures, to highlight the action taken about these issues, and to help support collaboration across the health sector. Speaking up to protect others is important, and we want to encourage this, especially when there are serious concerns regarding public safety or confidence in the dental professionals we regulate.
This year we received 79 whistleblowing disclosures, compared to 82 last year. To improve how we deal with whistleblowing concerns. we enhanced the way we review concerns when we receive them, through our initial assessment process. This has enabled us to better identify whistleblowing complaints earlier. During this period, we also reviewed and amended our processes and procedures for the identification of whistleblowers, which included moving the responsibility for whistleblower identification to our In House Legal Advisory Service as part of their role within our Initial Assessment Decision
Group. This enabled us to take an early legal review of all cases which has helped identify whistleblowers and provide better protection and support to them. In addition, work is ongoing to amend our initial concern reporting webform to allow individuals raising concerns to self-identify as whistleblowers. The report also highlights that, relative to other healthcare regulators, the GDC received a higher proportion of disclosures in relation to the size of our register. This is because most dentistry is provided in a primary care setting and outside the more robust clinical governance frameworks that characterise some other forms of healthcare and may mean that alternative disclosure routes are less present in dentistry.
This Whistleblowing disclosures report 2024 is published jointly by us with the General
Chiropractic Council, General Medical Council, General Optical Council, General Osteopathic Council, General Pharmaceutical Council, Health and Care Professions Council, Nursing and Midwifery Council and Social Work England. Our definition of a whistleblower is an employee who reports wrongdoing in the workplace that affects others.
If you want to report wrongdoing that you have seen at work, you may be protected in law as a whistleblower. The issue you are reporting needs to be in the public interest. Whistleblowing (disclosures in the public interest) and reporting a public protection concern are not always the same. Read the guidance below before identifying yourself as a whistleblower. If you are a registered dental professional, you have a responsibility to record and report any patient safety incidents as soon as you can, and to take action if patients or colleagues are at risk. We provide guidance on raising concerns in Standards for the Dental Team. We cannot resolve workplace grievances or disputes. You can blow the whistle about an incident or issue:
● That has happened in the past
● Is happening in your workplace now
● You believe will happen in the near future.
If you work in the NHS (or HSC in Northern Ireland), you should consider using the whistleblowing procedures where you work. As a whistleblower you’re protected by law. Read the UK government advice on whistleblowing before reporting. It explains who is protected by law and the types of complaints that count as whistleblowing.
● You may also be able to get advice from:
● England: Freedom to Speak Up Guardians
● England and Wales: Protect
● Scotland: Independent National Whistleblowing Officer
● Northern Ireland: NI Direct government services
Some issues or incidents that happen at work may amount to a serious concern about the behaviour of a dental professional. You should review our guidance, and if your think action is needed to protect you or others, report it to us. If you are unsure about whether the wrongdoing you have seen at work is something you should report, think about what might happen if you do not mention it. If in doubt, raise your concern. We investigate serious concerns that suggest a dental professional could be:
● Causing harm to the public, patients or colleagues
● Undermining public confidence in the dental profession.
Examples include:
● Violence, sexual assault, misconduct, and discrimination.
● Any serious criminal offence, including potential fraud or theft.
● Serious or repeated mistakes in patient care or treatment, including breaking patient confidentiality, not responding to a patient’s needs, and not referring when needed.
We can also look into people who may be practising dentistry (including tooth whitening) without being registered.
● To find out more about how to raise a concern, visit https://contactus.gdc-uk .org/Complaint/Process/1, and to download the Whistleblowing disclosures report 2024, visit https:// www.gdc-uk.org/about-us/ourorganisation/reports/whistleblowing
■ For the Love of Digital Dentures
Davide Accetto explores the benefits of CAD denture design
Over the last few years, I have travelled all over UK and Ireland to share my love for digital dentures. I am the founder and Director of Nifty Dental Solutions a cutting-edge innovative dental lab focused on Digital Dentures and CAD design outsourcing solutions for labs and dental clinics. Digital, digital, digital... I know! Sometimes hearing this word can be very annoying for dental professionals, but whether we like it or not, we are facing a new age which is completely reshaping the dental industry.
We all acknowledge that dental technology is not going to remain as the handcrafting artisanal profession it used to be. The answer is not in trying to fight against the digital workflow, but in accepting that – as much we might not like the change and love our professional roots – we must adapt to our new digital workflow if we want to succeed, and survive.
We have a real problem in our profession –put simply there are not enough technicians and this is a hard fact. But have you ever wondered why? Perhaps dental technology is a lesser-known profession? Perhaps there is a lack of appeal? We know there are problems with spaces for training and fewer dental technology students in the pipeline. We must accept that there could be any number of reasons for this drop in technologist numbers, but we need to raise our profile and focus on attracting the next generation to the dental laboratory. What is great about dental technology is that everyone can learn to do this job if they are only willing to master the skills required. I want you to picture yourself as a young person who is choosing their career
right now in 2024. Now, would your dream job be getting your hands dirty using strange materials to make teeth, with a very slow, steep learning curve using traditional methods to earn an average salary? Would you want to work long hours at the bench waxing and modelling around a dental impression as you watch the digital world advance around you? How satisfied would you feel knowing there are other, more innovative and exciting professions to choose from?
Even as new CAD-CAM and AI technology develops, analogue manufacture is slow getting out of the dental technology picture. In every field the present is digital. Your kids are experienced digital operators, and for some of you your grandchildren learned to swipe on a digital screen before getting their first milk tooth. The world is not standing still. It is predicted that AI will be thousands of times more intelligent than humanity in less than 10 years from now. Artificial intelligence is a very hot topic these days and some scientists are concerned that it might fly the human nest and start putting its own needs first. AI is building its very own conscience and emotions, and, guess what, AI is always learning from you!
Without even realising it we are creating a very close relationship with this
intelligence; we impact it at least 15 times a day using different technologies. When you drive your car, pick up your food at the grocery store, like that picture on Instagram, order your takeaway meal, AI takes note. The list of our AI interactions is very long. But what of the future?
Will AI replace some professions?
Denture demand is a huge business. In the USA alone there is a predicted growth of 200 million denture wearers over the next 15 years. And if you run a traditional prosthetic dental lab, you’re probably sitting on a gold mine without realising it.
By adopting to CAD-CAM technology you will be able to reduce the workload on your team’s shoulders, offer better salaries, manufacture more product more quickly, offer a modern alternative product, and yes, actually make more money! What a disgraceful way to behave. Or instead, you can keep on using plaster and wax, flasking, packing acrylic, and keep trying to attract staff that prefer to sit at a nice clean keyboard. I say see you on the other side of the bridge, good luck! In fact, everybody can do it with or without getting involved with the CAD-CAM knowledge.
Outsourcing your CAD design and CAM manufacture can be a very efficient way to
■ For the Love of Digital Dentures (cont...)
start increasing digital production right now, creating shortcuts and focusing on finishing rather than design and manufacturing. Without facing investment costs for equipment and going through intense training and recruitment, this will allow you to offer a modern product alongside your analogue devices.
An analogue denture should cost more than a digital version. Yes, you heard right. Reducing the analogue production will make it fall into the niche of ‘skilled bespoke manufacturing products’ that will fit with some clients’ expectations. Clients who are usually willing to pay more.
So, I hear you ask, will digital dentures replace analogue dentures? The simple answer is no, not yet. I do not think digital dentures are here to replace anything but just to provide an alternative to the traditional product. Nobody is forcing you to embrace it, as long as there is someone capable of providing a traditional product, analogue dentures will coexist with digital.
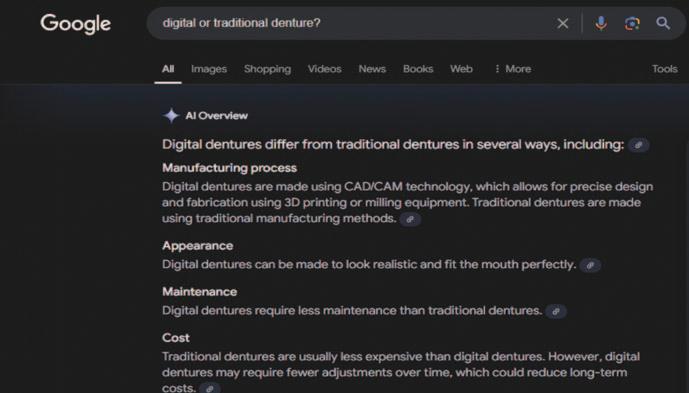
What are we all doing these days when we do not know something and need answers quickly? We all grab our fancy modern smartphone powered by AI and ask Google,
so imagine a patient needs a denture, but they do not know what to choose from traditional or digital. When they search online AI using Google, they’ll receive this answer I’ve illustrated here.
We can stand still or adapt and evolve. In the end, this is a personal call. “It is not the strongest of the species that survives, not the most intelligent that survives. It is the one that is the most adaptable to change.” This quote is often attributed to Charles Darwin, but it was actually written in 1963 by Leon C. Megginson, a Professor of Management and Marketing at Louisiana State University
at Baton Rouge. The quote may have been inspired by Darwin’s work, but I found it on Google using an AI search.
● If you would like to know more and start your journey with digital dentures you can email me:
davide@niftydentalsolutions.co.uk
Webinar
● An Introduction to Digital Dentures: Adapting to change hosted by Davide Accetto in Spring 2025. 2025 webinar dates will be announced in February with details of how to register.
Put Your Request in For Dental Technology Training UK
We are committed to supporting GDC registrable dental technologist training providers by facilitating access to various UK training resources. We encourage employers to connect with these providers. In order to explore course placements for the upcoming academic year, students and employers are advised to reach out to education providers promptly to secure a placement. With some courses filling up quickly, early contact is recommended. Dental laboratories also have the opportunity to sponsor training positions or offer work placements based on individual course provider requirements.
Spread the word among colleagues about the importance of reaching out to local Dental Technology educational providers, and supporting them. One such new provider is Yeovil College.
● Contact Adrian.Ponter@yeovil.ac.uk for more information about places on the course.
In order to be recognised and work as a Dental Technician, it is a legal requirement to be currently registered with the General Dental Council (GDC). Technicians will often begin their careers as trainees in a commercial dental laboratory, a dental
practice, or a dental hospital. They typically blend practical training with part-time education to earn an accredited qualification. Liaising directly with a course provider is essential to securing a training place.
● The GDC lists approved dental technology programmes and qualifications on its website and you can find out more about specific options such as Apprenticeships through the National Apprenticeship Service (www.apprenticeships.gov.uk) or Careers Wales (www.careerswales.gov.wales)
■ The Future of Amalgam in the Dental Practice
Amalgam fillings are a silvercoloured combination of mercury and a silver alloy (50% mercury, 35% silver, and 15% tin, copper and other metals).
Amalgam is long lasting and hard wearing and has been used in fillings for at least 150 years.
It is economical to use and it is not unusual for an amalgam filling to last 15 to 20 years.
Its use in dentistry has become something of a hot topic which is why Jason Wong, Chief Dental Officer for England, and Chris McConnell, Past President of the BACD and Director/CoFounder of Real Dentist Academy, came together to discuss the future of the material before an engaged audience during the BDIA Dental Showcase at ExCel in London.
Together, they presented ‘The Big Amalgam Debate: What is the truth currently?’ which was chaired by Edmund Proffitt, Chief Executive of the BDIA. This timely conversation followed the fifth meeting of the Conference of the Parties to the Minamata Convention (COP-5) in October/ November of 2023, where there was an agreement to phase-down the use of dental amalgam, and ban the use of mercury in cosmetics from 2025. Whether dentists are for or against the plan, there was still some uncertainty both about the requirements of dentists in England and
the UK at large, as well as some of the alternatives available to clinicians. Jason and Chris tackled these topics and more during their 45-minute session.
“Phase-down
has always been the position”
With some palpable confusion surrounding the amalgam use obligations for dentists at present, Jason set out to clarify the legal position of the UK. Amalgam was the most “controversial topic” at COP-5, with initial plans to completely cut out amalgam use by 2030. A few weeks before the conference, in a move that was declared “slightly surprising” to the Chief Dental Officer for England, a proposal was made to bring the phase-out forward, with allowances for medical exceptions based on the clinician’s judgement.
Jason made it clear that he stood by the idea of a phase-down rather than an immediate phase-out of amalgam use. He
thefuture
acknowledged previous considerations by a former Chief Dental Officer on whether a stance leaning towards phase-out should be taken, but he was adamant, “Phasedown has always been the position.” The current focus on reducing amalgam use comes following research and developments regarding amalgam’s environmental impact, and that of mercury in particular. However, Jason felt there is still a space for amalgam in dentistry.
“While the Minamata Convention was about the environmental impact of amalgam, we have very little data on the alternatives,” he said. “There is insufficient research for us to move from one material, when we have not done the research on the other.” Jason encouraged further research on the environmental impact of glass ionomers and composites as part of the UK’s move towards an amalgam phase-down. Following Brexit, Jason emphasised: “The EU position will not affect the position of England as far as dental amalgam is concerned.”
There are alternatives to amalgam available to modern dentistry, especially with regards to NHS dental care, which was clearly significant to the speakers’ audience. Chris was in favour of not using amalgam whenever possible. “No amalgam in dentistry is more about tooth preservation,” he explained to his audience. “Are there
suitable alternatives to amalgam? Yes, 100%,” he stated, “it’s called composite, and more specifically bulk fill composite.”
Chris discussed clinical studies that found a recurrent complication in some composite restorations – secondary caries. However, he insisted that this was largely preventable. “It is the skill of the clinician that is causing the issues of secondary caries,” he said, and spoke further on the ways clinicians can optimise their restoration techniques for a more effective and reliable restoration outcome.
After recalling the development of composites, he displayed the differences between each solution, see below, and explained how a dentist can make the most of what they have to hand. According to Chris one part of the restoration workflow in particular is not looked at hard enough, which is that of light curing. “When is the last time you checked the output of your light?” he asked his audience, as he highlighted the importance of consistently checking your systems.
Some clinicians, he observed, may question the potential economic ramifications of replacing amalgam with other solutions such as composite, but he was quick to warn against the way this this argument has
been framed. He cited the GDC principle 1.7.1, which states that ‘patients’ interests must be put before any financial gain’.
Towards the end of the session questions were invited from members of the audience which raised topics such as allowing medical exemptions for amalgam use and the implementation of amalgam phasedown into reform plans. Attendees left the debate with a greater understanding of the current position on amalgam. The future use of dental amalgam has yet to be definitively decided, but it’s thanks to the help of people such as Jason Wong and Chris McConnell that patients can continue to feel safe and protected in the dental practice for years to come.
Other than amalgam what types of dental fillings are currently available from the dental practice? Advice provided to patients is that there are a number of different alternative fillings, including:
● Composite fillings
● Glass ionomer
● Gold inlays and onlays
● Porcelain inlays
The advice is simple as you’ll see, but it provides a useful overview regarding restoration materials using plain English
while avoiding jargon, making it easier for the patient to understand and provide informed consent.
Amalgam fillings, as described above, are usually used on the posterior teeth. The mercury in dental amalgam is not poisonous once it has been combined with the other materials in the filling. Research into the safety of dental amalgam has been carried out for over 100 years. So far, no reputable ‘controlled’ studies have found a connection between amalgam fillings and any medical problem, however disposing of dental amalgam waste can be an issue for the environment.
Composite fillings are strong, but may not be as hard wearing as amalgam fillings. Composite fillings are tooth coloured and made from powdered glass quartz, silica or other ceramic particles added to a resin base. After the tooth is prepared, the filling is bonded onto the area and light cured. The composite chosen should match the shade of the natural dentition, although over time staining can happen.
Glass ionomer fillings, however, form a chemical link with the tooth. They may also release fluoride, which helps to prevent further tooth decay. This type of filling is fairly weak which is why they are usually only used on baby teeth and ‘non-biting’ surfaces such as around the ‘necks’ of the teeth. Little preparation is needed as the filling bonds directly to the tooth.
Gold inlays and onlays can be used in most areas of the mouth. An inlay is small and placed within the biting surface of the tooth. An onlay can cover a larger area of the tooth. Gold is the most long-lasting and hard-wearing filling material and will last for many years. It does not tarnish and has great strength.
One of the differences between gold and other filling materials is that the gold filling is manufactured in a laboratory based on an impression of the cavity supplied by the surgery while a temporary filling will be
placed in the cavity in the interim. This type of filling is more expensive.
Porcelain inlays are manufactured in the lab or in the practice using CAD/CAM or more traditional techniques. The digital
workflow can see the porcelain restoration fitted after just one or two visits. Porcelain can be hard wearing and long lasting. It can also be coloured to match the natural dentition, but it too can be the more expensive option.
Development Outcome C – 30 minutes
To complete your CPD, store your records and print a certificate, please visit www.dta-uk.org and log in using your member details.
Q1 What is the correct alloy mix for dental amalgam?
A 28% mercury, 36% silver, and 36% tin, copper and other metals
B 50% mercury, 35% silver, and 15% tin, copper and other metals
C 62% mercury, 18% silver, and 20% tin, copper and other metals
D 35% mercury, 35% silver, and 30% tin, copper and other metals
Q2 How long has amalgam been used in dental fillings?
A 200 years B 97 years C 150 years D 109 years
Q3 How long will an amalgam dental filling last?
A 10-12 years B 25-30 years C 15-18 year D 15-20 years
Q4 When was COP-5 during which the phase-down of amalgam in dental filling was put forward?
A October/November 2023 B August/September 2023
C February/March 2024 D June/July 2024
Q5 Which alternatives to amalgam are described as the more expensive options?
A Gold inlays and onlays B Glass ionomer fillings
C Porcelain inlays D a) and c) only
■ Eboni-Rose Williams: Graduate Reflections
A recent graduate from Bolton University, polymath Eboni-Rose Williams shares her thoughts about the modern dental profession and the place of the young technologist as part of the dental team.
As a recent graduate I am enthusiastic about dental technology, and I have gained realworld experience working within a private prosthetics lab where I had responsibility for both learning and training the team regarding CAD/CAM. I have also started my
own business, Digidental Technology, after winning funding from Bolton University. I 3D print educational models for dental students to help improve their dental morphology skills and knowledge. Recently I was thrilled to join the Charity Den-Tech on its Uganda Mission, where we provided dentures for 100 patients.
The Technologist editorial team invited me to write about my experiences as a dental technology student, and share my reflections on what I saw as going well and also where I believe education still needs to improve. I was asked to discuss what motivates me as a dental technician and
what I saw as my potential career path. To add depth to my discourse I was also asked share any advice that I thought might prove valuable to dental technology students and any observations that might prove useful to employers and lab owners.
I would like to start with putting forward my personal advice for my fellow dental technology students. While I was studying, I was fortunate to have had fantastic support from the teachers at Bolton University, for which I will always be grateful. They always encouraged and supported we students to do our best. They were truly inspiring due to not only their technical skills but also their passion for their disciplines and teaching style.
Having good mentors while learning makes the world of difference to your progress and opens the door to many potential opportunities. I am very lucky to have had such amazing supportive mentors; people who believed in my capabilities while also pushing me to do more. My time in university was an inspirational experience. As well as imparting knowledge and wisdom. I am so grateful to everyone that has been kind enough to support me so far, Thank you!
My advice to fellow students? Always do your best but instead of just chasing a firstclass honours make sure to establish a decent work/life balance and try to socialise. Burnout due to overwork is not fun! ABO, always be organised. Remember to be kind to yourself and when the learning curve begins to look like a cliff face take a moment to realise that everyone
Eboni-Rose Williams
started where you are now, everyone was a beginner at one point. You will get there, practice makes progress.
Make good use of work experience – where you can get it. There are lots of kind, incredible people to learn from and be inspired by but you must seek them out, even if that means contacting 50 labs until a kind few let you observe and practice your skills. I found it difficult to find placements, but I am very grateful to those professionals kind enough to let me observe, ask questions, and share their insights with me.
Don’t be disheartened if they can’t offer you the chance to visit right away, dental labs are at a premium just now and they may be too busy, but keep trying and there may be future opportunities when they have the time.
Furthermore, follow people on social media (Instagram, Facebook and LinkedIn) and you can find motivational examples of what is possible.
Top tip, practice your skills at home and keep revising your knowledge. For example, I would carve teeth in stone and soap in order to practice my anatomy and enhance my manual dexterity. I got this idea from a mentor, now I share it with you. And, this is important, always be prepared to speak to your teachers and mentors, ask questions, don’t be afraid, they are there to guide you.
Don’t be afraid to be the youngest tech or almost technician in the room. The people you look up to are supportive, especially if they see your passion for the industry. It’s a cliché but true, it’s always good to step outside of your comfort zone and important to spend time in rooms where you’re not the smartest or most skilled person. When you feel out of your depth, that’s where you start to grow.
Always take notes, be inspired and keep working hard. Some things take nine or more attempts till you get it right and will take
even longer to master it. The higher you set your bar the longer it might take to reach it, but don’t be ashamed to be a newbie. We’re so lucky, this is a fantastic time to be a dental technician. We can be digital pioneers, a source of value to laboratories.
We have so much to offer our profession, but first our profession has so much to offer us, starting with placements. How can you make the most of these opportunities? And how can you demonstrate that you were worth the effort?
Here are a few handy tips:
● Show you’re interested. Take notes, ask questions (ones that show you’re paying attention and curious to learn). If you show them you want to learn they’ll be more likely to want to teach you and give you some extra tips.
● Take notes. Recording what your tutors teach you shows you’re eager to learn, and they’ll prove a useful resource to look back on, while also helping you to avoid asking blindingly obvious questions or asking about something which has been presented to you all too recently. It builds proactivity and shows you’re interested to learn, and it tells your instructors you’ve been listening.
● Observe and ask questions about what you’ve seen. Remember, the people teaching you are experts in their field, sharing their time and skills with you is invaluable. One day you might be doing the same for a newbie just like you, and it will be a privilege to learn from you.
● Get the right mental attitude! Go with a positive attitude. More often the mentor you are observing will be taking time out of their working day to support you – and that will most likely mean their time will be less productive as a result. Be grateful and treat them all with respect, even if it’s not a department you’re most interested in pursuing in the long term.
● Say thank you and feedback what you have learned. It shows you value their time and they are more likely to want to support you in the future. It’s nice to be nice, gratitude is its own reward, that’s a simple established fact.
Use social media as a tool. I post on Instagram to share my developments through university, and demonstrating my passion for dental technology has opened up incredible opportunities. I suggest to every new technician they should do so, and I have already motivated some to walk the media path.
graduatereflections
Yes, it is daunting and scary at first, but you are doing it for you. Show your work, explain what you have learned from your mistakes and be proud to demonstrate your growth! I see my social media as a digital diary of my journey and I am excited to see how my skills have grown once I am qualified and working on real cases.
Don’t expect too much too soon. You are on a career journey and that won’t helped if you compare your year zero to someone else’s year 30. You will get there, but it will take time and hard work. The journey might not be easy but it will be even more rewarding once you get there.
If you do not feel ready to share your work, at least follow some dental pages. dentistry.co.uk is great to keep updated with dental news, as is www.dentalreview .news. Consider joining professional organisations such as the DTA or DLA. Networking with professionals can provide valuable insights and opportunities. Attending dental shows is fantastic for networking, you can get inspired by excellence, learn and get updated on dental developments. Bonuses include: they are free to attend and full of freebies. This year at DTS there were some amazing talks.
I especially loved the presentation by Deepa Bharakhda, a dental technician from Dencraft in Leicester, during which she demonstrated the fundamentals of private dentistry and touched on the importance of model analysis to help with occlusal rims,
trays and tooth set-ups. I also loved the talk by Beth Brown, The Party Enamel and Emily Pittard, CDT and from the Hive Dental Lab and Clinic, who were delving into an inspiring case study regarding the DenTech Charity supporting a domestic abuse survivor and how they transformed her life with a beautiful smile!
Furthermore, I learned lots from Timothy Jackson, CDT and Jamie Sawdon, a technician and Directors of Prime Dental Laboratory, on Digital Copy dentures using 3Shape technology, I gained extra tips and tricks. Their knowledge and precision is so inspiring and they are so kind to offer support always.
There were even more great talks too (unfortunately some I missed)! I can only suggest you attend them next year. I was asked if I had anything to say to lab managers about supporting students. First thank you for sharing time with us, but please be patient and remember your early
days at the bench. Give students a chance, we all want to do well and learn.
Finally, how might education improve?
When we leave university and walk out into the professional arena feeling like Bambi on the ice, it would help if we arrived at the workbench ‘work ready’. That means being used to strict time restraints and our skills being up-to-date. We need to be able to think for ourselves and be proactive in the workplace so that we are regarded as an asset instead of a burden.
More hours in placement would help us to improve and speed up our acceptance as a useful member of the team, and we need more support in finding placements. And our lessons should replicate time restraints and independence that we will face in the real world, so that rather than doing a Bambi and sliding hopelessly on the ice we can feel confident that we have a solid start towards gaining the skills we need to succeed.
Deepa Bharakhda
Eboni-Rose, Andrea Johnson and JB trimming dentures in Uganda
■ Audit Again: Crown and Bridgework
By Dr Chris Turner MSc, BDS, MDS, FDSRCS, FCGDent Specialist in Restorative Dentistry (Rtd)
We can now combine the two and review the quality of the impressions that you receive and those of the underlying tooth preparations.
For example:
● How many times do you struggle to trim a die and see preparation margins?
● What happens if you ask the dentist for a new impression?
● Are the preparations of a suitable standard?
● Are the impressions made in flexible plastic trays?
In previous articles I have stressed that the results patients see of crown and bridgework are yours not mine – and latterly we have considered the importance of audit, including the qualitative Likert scale. Aims:
● What actions do you take when there are problems for you?
You could use the following Likert classification:
● Unacceptable due to drags, no clear margins, air blows, impressions pulled from trays, incorrect preparation.
● Poor due to no clear margins and errors in tooth preparation.
● Average due to preparation errors that can, and should have been, overcome.
● Better as there are minor preparation errors and the die can be trimmed.
● Good as there are clear margins and the preparation is to an acceptable standard.
Earlier in my career I gave about 50 handson crown and bridge courses for eight dentist participants who were asked to bring their own preparations burs to the course. Some forgot, and some practices had only one set and would not allow a participant to borrow them for the day, and too many were worn or of poor shape.
Dentists were then asked to use their own burs, or choose from a wide selection of used burs, to prepare a central incisor tooth on a phantom head for a porcelain jacket crown. This meant that I was looking for
shoulders of 0.8 to 1.0mm width and a classic textbook coronal preparation. The results were shocking. On a typical day only one preparation might be good, sometimes better, and the remainder – the majority –generally poor or unacceptable.
The most common faults were:
a. Over reduction incisally, leaving about half of the coronal height rather than two-thirds. The reason: making the incisal reduction as the first or an early stage in the tooth preparation.
b. Inadequate occlusal clearance in both centric occlusion and especially protrusive movements. The reason: making the palatal reduction the last stage of tooth preparation rather than the first.
c. Inadequate reduction at the incisal tip. The reason: dentists start their labial reduction and are concerned about pulpal exposure, but have to create a shoulder. They rotate the handpiece through 15 degrees to create the shoulder and lose the line of insertion and withdrawal. Crowns will then always be bulky labially.
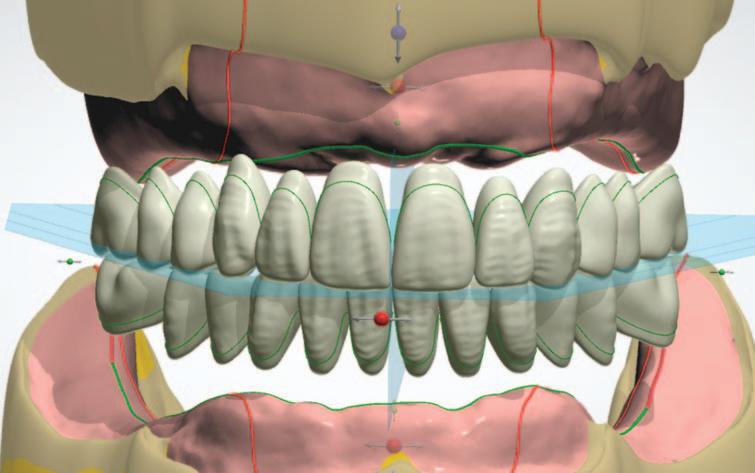
d. Shoulder width. For traditional porcelain jacket crowns this should be between 0.8 and 1.0mm around the tooth whereas when porcelain fused to metal crowns (PFM) are prescribed the labial and interproximal shoulders should be 1.5mms although the palatal reduction is significantly less. Experience suggests that
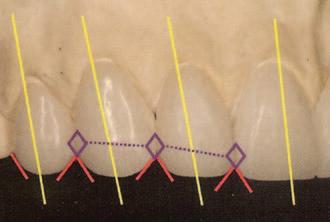
Ideal Contact Points
laboratoryaudit
1.5mm wide shoulders were rarely achieved because of potential pulpal damage either by exposure or by overheating during tooth preparation. Inevitably, these crowns can also be bulky.
One study suggested that the labio-palatal width of PFM crowns could be 1 – 2 mms greater than that of the natural tooth before preparation. Fortunately, with modern materials such as zirconium oxide reinforced crowns margins can be made smaller and chamfered rather than shouldered.
e. Inclination of the long axis of the preparation to either the right or the left. The reason: I have seen this during the courses that I have held and found that this was due to the way that dentists held their handpieces, right handers to the right and vice versa.
f. Deep subgingival preparations. Ideally preparations should be supra-gingival but pre-existing caries and aesthetics may require a sub-gingival margin. This should be limited to a depth of 0.5mm to avoid damage to the periodontal attachment and always requires a method of retraction to achieve a satisfactory impression. My tip for dentists was to use a CPITN probe, that has a 0.5mm ball end as a depth gauge.
If you have ever been told by a dentist to use an impression that is, in your judgement unsatisfactory, would you make a restoration and compromise your own training and standards? Dentists need to understand that, from time to time, even the best has an impression problem. It happens!
Your difficulty in defining margins and finishing lines on a die is a common problem. You do your best, but why does it
happen? Preparations have been taken subgingivally and the impression made without gingival retraction usually because dentists do not use, and/or do not know how to use retraction cords. The ideal impression will have an extension into the retracted pocket and a clearly defined finishing line. Have you ever considered sending back the models and asking the dentist to trim them to the margins? Have you ever asked dentists to use retraction routinely?
As always there is a fine line between keeping your customers happy and supplied with their crowns and bridges and your own professional standards as an essential member of the dental team. You are in a unique place to offer guidance to dentists who have not attended courses like mine about their crown preparations and what would help you and them obtain better results for their patients. The downside of poorly fitting, overhung or deficient crown margins is the development of periodontal disease that can lead to tooth loss later in life.
Can you meet that challenge? Why do you want to try to rescue sub-standard preparations? During my career I had the opportunity to work with outstanding technical support and learned to take advice when it was given. That helped me become a better dental professional, you, in turn can help my colleagues.
When crown and bridgework is good it is hard to identify on casual looking. Try this test. Look briefly at the people you see in the supermarket check-out queue. Can you spot if they have crowns? If you can then that has to be the result of an unsatisfactory restoration.
Development Outcome B – 30 minutes
To complete your CPD, store your records and print a certificate, please visit www.dta-uk.org and log in using your member details.
Q1 In this article which of the following has NOT been classified as making an impression ‘unacceptable’?
A Drags B Damaged in transit C No clear margins D Air blows
Q2 When preparing a central incisor tooth for a porcelain jacket crown what shoulder width is the writer looking for?
A 1.00 to 1.5mm B 0.5 to 0.8mm C 0.8 to 1.00mm D 0.75 to 0.95mm
Q3 What are the most common faults when preparing a central incisor for a porcelain jacket crown?
A Over reduction incisally B Inadequate occlusal clearance
C Inadequate reduction at the incisal tip D All of the above
Q4 When PFM crowns are prescribed what should be the labial and interproximal shoulder width?
A 1.5mm B 1.00 to 1.25mm C 0.90mm D 1.25 to 1.70mm
Q5 What does the writer say dentists do not use/do not know how to use for gingival retraction?
A Rubber dam B Bayeaux metal gingival retractor C Retraction isolator D Retraction cords
■ Living and working with change
Part 1: Technological Change
Aims:
■ To demonstrate the continuous nature of change and the accelerating pace of technological change
■ To explain how and why the law and the regulatory environment struggle to keep up with technological change
■ To provide practical illustrations of the challenges of change and how it affects both our personal and professional life
CPD Outcomes:
■ Effective communication with patients, the dental team and others across dentistry, including when obtaining consent, dealing with complaints, and raising concerns when patients are at risk;
■ Effective management of self and effective management of others or effective work with others in the dental team, in the interests of patients; providing constructive leadership where appropriate; [Effective practice and business management].
■ Maintenance and development of knowledge and skill within your field of practice; Clinical and technical areas of study: Emerging technologies and treatments:
■ Maintenance of skills, behaviours and attitudes which maintain patient confidence in you and the dental profession and put patients’ interests first. [Professional behaviours]
Development Outcomes:
by Kevin Lewis
This is the first in a series of three linked articles looking at the implications of change in our professional and personal life. These implications are often practical and/or human in nature but they may have professional, ethical and often legal consequences – many of which might not be immediately apparent. In this opening article we focus upon technological change, and the impact of various forms of technology. The two remaining articles (which will appear in following issues of this publication) will firstly cover the profound impact of generational changes, and then conclude with an exploration of how attitudes and behaviour are influenced by change – and vice versa.
This article starts from the premise that change is inevitable and continuous. This is well evidenced by the fact that the Greek philosopher Heraclitus is quoted as saying that ‘change is the only constant’. He is
reported by Plato to have said this 2,400 years ago – and no doubt in ancient Greek – but Heraclitus did have a point; every generation since the start of time, long before he came on the scene, will have experienced different things to those who preceded them and those who succeeded them. Even within a single generation, the relentless process of change continues and each new generation starts out seeing itself as being different (and perhaps ‘better’ in some way), breaking new ground,
technologicalchange
embracing and demanding change and questioning and challenging the status quo. And a few decades later, each new generation ends up tut-tutting and making despairing noises about the generations coming along behind. To add further spice, most workplaces will contain a mix of people from different generations (we will look at what this means in Part 2).
During the course of any career – especially in dynamic and fast-evolving fields like dentistry and dental technologyequipment and instrumentation, materials and work processes that are new and ‘cutting edge’ one minute are soon rejected (and sometimes ridiculed) as being oldfashioned, outdated and no longer fit for purpose. There is also a view in wider society that the pace of change has been rapidly accelerating, and the key factor that drives and supports this perspective is technological change, the pace of which is frankly breathtaking.1
Technological change is all around us and it pervades every facet of our professional and personal lives. Some people are continually fascinated and excited by this – others are challenged and confused by it, and some feel completely overwhelmed and turned off by it and would much prefer things to stay as they were. The effect that different kinds of change can have on personal (and organisational) attitudes and behaviour will be discussed in the third and final article in this trilogy which will span three consecutive issues of this publication.
Context
Technology in one form or another has been around since the dawn of time.
About 3,000 years ago, the Stone Age and the Bronze Age had both passed, and the Iron Age had dawned. But against that extended backdrop, it was not until about 500 years ago (in the middle of the reign of Henry VIII) that things started to progress a little faster – but still at a snail’s pace compared to modern times. The invention of the steam engine 300 or so years ago was a game-changer and laid the foundations for the Industrial Revolution, but the pace of technological change is perhaps best illustrated by the fact that the Wright Brothers made the world’s first manned aeroplane flight (lasting all of 12 seconds) only 120 years ago, and yet within barely half of the intervening period (55 years ago) we were witnessing the first human footsteps on the surface of the moon – a slightly longer trip. The moon landing was only made possible by the invention of computers, of course, and similarly today’s communications revolution could not have happened without the internet which for most of us was still unimaginable science fiction until the late 1980s and 1990s – just 30-40 years ago. And today we have already entered the realms of artificial intelligence (AI) and are becoming aware of its potential benefits (and risks). Not only are each of us likely to feature many times a day on CCTV and many other different kinds of 24/7 surveillance, we think nothing of being looked down upon by drones, orbiting
satellites and from a continuously-staffed international space station.
As so many of us live our lives in constant fear of being separated – even briefly –from our smartphones, it is salutary to bear in mind that photography itself is only 200 years old, domestic electricity and landline telephones only appeared in the late 19th and early 20th century (100-150 years ago) and took some time to reach most of the population. 100 years ago only 800,000 of the entire UK population had mains electricity in their homes – that’s roughly the size of the population of Leeds today.
The UK saw its first mobile phones about 40 years ago but the earliest models were so bulky that it almost took two people to lift most of them! Smartphones with their inbuilt digital cameras followed about 20 years ago and we all know how each new iteration of hand-held and hands-free devices brings yet more features in the confident hope that we will come to rely upon them. And the rest (as they say) is history….although it’s fair to say that ‘the digital revolution’ still means different things to different people.
Another salient consideration is the coming-together of different technologies, and the dangers of assuming firstly that each of them will perform as intended and secondly that someone, somewhere has
worked out and implemented all the necessary safeguards and mitigations. This confidence is understandable but often misplaced; a vivid and tragic illustration of this was the Grenfell Tower fire in June 2017 when an electrical malfunction in a reputable (Hotpoint) fridge-freezer in the kitchen of a single flat caused the appliance to catch fire. This, coupled with some flawed building design decisions made less than two years earlier, and the choice of unsuitable highly flammable materials used to insulate and externally clad the building, resulted in the catastrophic inferno which claimed the lives of more than 70 people and injured many more.
Grenfell Tower, in West London, was almost 50 years old at the time, having been built in the 1970s. However, it had undergone a major ‘face lift’ type of refurbishment during 2015–2016 using (as one might expect) more ‘modern’ materials than those used in its original construction. Had that very recent refurbishment not taken place, it is almost certain that the fire could and would have been contained within the confines of the single flat in which it originated (as intended by the compartmentalisation fire management policy widely adopted in high-rise buildings), and no loss of life would have resulted. So much for modern materials and modern technology, although the subsequent Inquiry2 has revealed that many of the limitations and dangers of the materials used in the refurbishment were already well known by the manufacturers and suppliers, but deliberately not shared with those who were commissioning the work at the relevant time. They are not alone in having being seduced by the lure of the new (and no doubt, cost considerations) and being guilty of not asking enough questions, or the right questions, when placing their trust in new technology which they do not (yet) fully understand.
The professional implications
When the General Dental Council (GDC) issues its guidance on any matter, it tends
technologicalchange
to do so in general terms rather than specifics, setting out broad principles which can then be interpreted and applied to a range of existing and new situations, rather than getting involved in the fine detail. In common with other regulators, especially in relatively conservative fields such as healthcare, developments in society and in the professional workplace tend to move a lot faster than the regulators can keep up with and this is particularly true of dentistry and dental laboratories especially where technological and scientific advances are concerned. This gap in awareness and understanding has been compounded and made worse by successive changes in the Dentists Act, because the organisation’s workforce deliberately contains no dental registrants and the governing Council itself now has only six registrants (4 dentists and 2 DCPs out of 12 Council members), regulating about 123,000 dental health professionals. When the GDC was established by the 1955 Dentists Act, an initial 50-strong Council included 41 dental health professionals bringing a wealth of first hand experience to inform Council policy and decisions.
The GDC (see Panel 1 overleaf) speaks about the need to keep one’s knowledge and skills up to date, but is silent on the question of what this might mean in
practical terms when faced with technological change on multiple fronts. Registrants are also reminded that they must work within the limits of their knowledge, skills and professional competence – and this creates a fresh challenge for us each and every time something new comes over the horizon.
Also relevant to the issue of technological change is Standard 9.1 which reminds registrants that how they behave in their personal life matters just as much as how they conduct their professional life.
But there are knock-on effects that technological change can have upon our ability to comply with other aspects of the GDC’s guidance. New techniques, new equipment and new materials are unfamiliar and relatively untried in comparison to well-established technologies in which we are well practised and experienced. As a result, neither we, nor the people who are selling it to us and/or training us in its use, have a complete understanding of the potential risks and limitations. ‘New’ is not always ‘better’ or ‘safer’, but its attraction is often that it is quicker, or more convenient…. or simply, more fun? Do your customers or patients have a right to know that you are effectively a beginner in the use of the new
technologicalchange
Panel 1: Selected paragraphs extracted from Standards for the Dental Team3
(please note that the sections quoted below have been chosen for the purpose of this article and are not comprehensive. Refer to the full text of the guidance).3
Standard 7.1: You must provide good quality care based on current evidence and authoritative guidance
7.1.1 You must find out about current evidence and best practice which affect your work, premises, equipment and business and follow them.
7.1.2 If you deviate from established practice and guidance, you should record the reasons why and be able to justify your decision.
Standard 7.2: You must work within your knowledge, skills, professional competence and abilities
7.2.1 You must only carry out a task or a type of treatment if you are appropriately trained, competent, confident and indemnified. Training can take many different forms. You must be sure that you have undertaken training which is appropriate for you and equips you with the appropriate knowledge and skills to perform a task safely.
technology? Might that affect their decision to let you go ahead? Look carefully at Paragraphs 7.2.1 and 7.2.2 (Panel 1) and think of the last time you installed some new equipment or started using a new material or technique.
But on the other hand, there are risks associated with shunning the new and sticking with your tried and tested ways of doing things. If you are a business owner, you may even be exposing your staff to risks which there are now new ways to avoid. You may wish to consider 7.1.1 and 7.1.2 (Panel 1) in that light.
Our decisions as to whether or not to embrace new technologies can be driven by many different factors whether economic, or sheer timing and practicality. How many times have we bought a new car, or home appliance, or some other device or product and are faced with a choice between a cautious like-for-like replacement or a more ambitious investment in newer technology? Once you start to appreciate the benefits of the latter, have you ever wished that you had done it sooner? Of course the GDC is looking at
7.2.2 You should only deliver treatment and care if you are confident that you have had the necessary training and are competent to do so. If you are not confident to provide treatment, you must refer the patient to an appropriately trained colleague.
Standard 7.3: You must update and develop your professional knowledge and skills throughout your working life.
7.3.1 You must make sure that you know how much continuing professional development (CPD) activity is required for you to maintain your registration and that you carry it out within the required time.
7.3.2 You should take part in activities that maintain update or develop your knowledge and skills. Your continuing professional development (CPD) activity should improve your practice. For more information, see the GDC’s advice on CPD.
Standard 9.1: You must ensure that your conduct, both at work and in your personal life, justifies patients’ trust in you and the public’s trust in the dental profession.
these decisions only through the lens of doing the best for patients and they have no interest in whether you become happier, healthier, more (or less) profitable, more (or less) efficient or productive as a result.
But another good and topical example of how the GDC’s ‘broad principles’ approach comes up against rapid technological change, is seen in terms of the exponential growth of social media. For some years since publishing its 2013 guidance, the GDC had appeared somewhat flat-footed in its understanding and approach but to its credit has updated and improved its social media guidance in January 2024.4 It places the onus squarely upon registrants to conduct themselves in this environment in the same professional way as they would if communicating face-to-face with patients, colleagues and members of the wider public. Registrants are reminded that ‘… The standards expected of dental professionals do not change because they are communicating through social media, rather than face to face or by other traditional media. You have a duty to behave professionally both online and offline’. They are further reminded that they must
● respect patient confidentiality : avoid publishing information which could identify patients on social media, without first obtaining their consent
● avoid posting any information (including personal views, photographs or videos) which could damage public confidence in the profession
● respect and maintain appropriate boundaries with patients and think very carefully before accepting ‘friend’ requests from patients
● never instigate or take part in any form of cyber bullying, intimidation or use of offensive language, including sharing inappropriate content posted by someone else
The informality and perceived freedom of social media platforms can lead to people saying or doing things with a sense of impunity or unaccountability, without fully appreciating the potential consequences. Many of the problems stem from naivety regarding privacy settings and – especially in today’s fast-moving digital and AIenhanced world – how easily things can be misinterpreted, manipulated and miscommunicated by others. More than
most other new technologies, social media has blurred the distinction between our professional and personal life and that blurring brings its own dangers for any dental registrant (ref Standard 9.1, Panel 1).
The legal implications
Having said (above) that professional regulation is notable for its tendency to be one step behind the latest developments within the environment that is being regulated, this is arguably even more true of the law.
A good recent example of this is the Digital Economy Act 20175 which with the best of intentions made various regulations relating to online services, including strict age verification rules to protect children in the fast-growing and increasingly complex online world. But before all the regulations proposed under this Act could be brought fully into force, further developments and the emergence of new threats made it necessary to introduce a new and wider-reaching Online Safety Bill which finally became the Online Safety Act 2023.6 But even that is not yet in force; public and stakeholder Consultations dealing with different aspects of the legislation and ways to implement it took place in the early months of 2024, but in the meanwhile new and even more insidious online behaviours by individuals and unfulfilled assurances from the big tech companies and their platforms, have already prompted yet more proposed legislation to further extend and strengthen this Act and its powers, and it is hoped and expected that this added protection will come into force next year (2025).
The process of creating or amending legislation is painstakingly slow and clunky, and quite properly so because it becomes quite literally ‘the law of the land’. Taking the time to get it right is ultimately in everybody’s best interests, and anticipating loopholes and potential challenges or unintended consequences can avoid everyone adopting the view of Mr Bumble (Charles Dickens’ creation in Oliver Twist)
CPD OutcomesA,B,C&D 60minutes technologicalchange
that ‘The Law is an Ass’. The downside of this is that bad things can flourish while we are all waiting for change to happen.
Every new piece of equipment and instrumentation, and every new material or product we use, arrives into a tapestry of overlapping existing legislation which we need to be aware of, to understand and comply with. Very often the risks and threats arise not only in relation to the actual item or product, but also to how we use it. Most of us will know, for example, that it is illegal to hold and use a phone, tablet, sat nav or any other device that can send or receive data, while we are driving (or riding a motorcycle).7
This applies whether the phone is online, offline or in flight mode, even if your car is stationary (eg at traffic lights or stuck in heavy traffic) and – not widely appreciatedeven when you are in the passenger seat, supervising a learner driver. This prohibition extends equally to voice calls, texts, taking and/or sharing photos or videos. Failure to comply with this legislation can result in anything from 6 penalty points, to a driving ban and the loss of your license, but that conviction must then be reported to the GDC and the professional consequences of that could be more serious in certain circumstances.
Websites
Laboratory owners and CDTs who own and operate a dental practice will often maintain and control a website to showcase their services. As soon as you do so, you plunge yourself and your business into a deep pool of compliance requirements. You may wish to use Panel 2 (overleaf) as a checklist against which to measure the current level of compliance achieved by your own website (or any website controlled by others that you happen to appear on).
Digitally speaking
Arguably the biggest recent change in the field of dental technology – and perhaps the wider dental profession too in some respects – is what has come to be known as ‘the digital revolution’. Paradoxically, digital workflows are of course a progression rather than a necessarily ‘binary’ decision. But replacing traditional impressions with digital scans opens the door to a range of other developments, and in-house milling and 3-D printing are further natural steps on that journey that can create huge opportunities for both individuals and businesses – and patients, too. Not every laboratory (nor every dentist) is quite ready to make the leap of faith (nor the capital investment) involved in throwing oneself
technologicalchange
Panel 2: Website compliance
1. Does your website contain the information listed below? Is it clearly displayed, prominent/easy to find and accessible?
a. Company name and company registration number (if applicable)
b. Country of company registration (if applicable)
c. Registered address of company, and/or business address
d. Web address, email and other (eg phone) contact details
e. VAT number if applicable
f. Name and GDC registration numbers of all registrants working in the business
g. Your privacy policy (to comply with the requirements of GDPR)8
h. Your cookie policy, explaining what cookies are used on your website and why. (to comply with the Privacy and Electronic Communications Regulations /PECR).9
i. Your accessibility statement, explaining any reasonable accommodations and special arrangements you have made to facilitate equal access to the information for all those seeking it (to comply with the Equality Act 2010).10 The Government publishes The Web Content Accessibility Guidelines (known as WCAG),11 which are an internationally recognised set of recommendations for improving web accessibility, suggesting ways to make digital services, websites and apps accessible to everyone, including users with impairments
j. Any Terms and Conditions that anyone wishing to use your website must agree to when using your website.
2. Some websites feature testimonials and/or ‘before and after’ images. You must have obtained the express consent of any person whose personal information, image(s) or any other sensitive personal information (under GDPR) appears on your website. This consent must be in place for each specific use and the person must understand how it is being used, and when. If you are using borrowed or library images, you must have the relevant consent from the owner of the intellectual property, to comply with The Copyright, Designs and Patents Act 1988.12 If you are using images that you have found and downloaded from the internet, you must similarly ensure that you have the relevant permissions for when and how you plan to use the image(s). Some image libraries will grant you a license to use one or more images in return for a subscription or one-off fee.
3. If your website provides a facility for patients/potential patients to make an enquiry and/or leave a message and their contact details for a reply, you should have security measures in place to protect against unauthorised access, alteration, disclosure or destruction of that data.
4. Other (consumer) legislation and guidelines from bodies such as the Advertising Standards Authority also apply. We have covered them in detail in earlier articles in this series13, 14,15
CPD OutcomesA,B,C&D
into the deep end of the digital pond. But experience to date suggests that there is a greater appetite to ‘go digital’ amongst younger dentists, and a greater reticence amongst older dentists who have become comfortable with (and both experienced and competent in) what they know best. We will return to this dichotomy and other aspects of the digital revolution in upcoming articles.
Summary
This article has sought to demonstrate the fast pace of change in the modern world, and the challenge of keeping up with technological and scientific developments and the skills needed to take full advantage of them. It has illustrated some of the ways in which new technology can be our friend, and also some other ways in which it can become our enemy creating unforeseen dangers for us.
technologicalchange
In the next two issues of The Technologist we will look more closely at the implications of generational change (Part 2) and finally, how technological change can impact attitudes, behaviour and risk (Part 3)
References
1 Timeline charting the fast pace of technological transformation across centuries. World Economic Forum via https://www.weforum.org/agenda/2023/02/thistimeline-charts-the-fast-pace-of-tech-transformationacross-centuries/
2 Grenfell Tower Inquiry Final Report via Statement on Publication of Phase 2 Report | Grenfell Tower Inquiry https://www.grenfelltowerinquiry.org.uk/news/ statement-publication-phase-2-report
3 Standards for the Dental Team General Dental Council https://www.gdc-uk.org/
4 Guidance on using social media General Dental Council January 2024 via Guidance on using social media (https://www.gdc-uk.org/docs/default-source/guidancedocuments/guidance-on-using-social-media)
5 Digital Economy Act 2017 via Digital Economy Act 2017 (https://www.legislation.gov.uk/ukpga/2017/ 30/contents)
7 Using a phone, sat nav or other device when drivingGOV.UK (https://www.legislation.gov.uk/ukpga/2023/50)
8 The General Data Protection Regulation (GDPR). The Data Protection Act 2018 via Data Protection Act 2018 (https://www.legislation.gov.uk/ukpga/2018/12/content s/enacted)
9 The Privacy and Electronic Communications (EC Directive) Regulations 2003 via The Privacy and Electronic Communications (EC Directive) Regulations 2003 (https://www.legislation.gov.uk/uksi/2003/ 2426/contents)
10 Equality Act 2010
11 Accessibility and assisted digital Web Content Accessibility guidelines (WCAG 2.1) October 2023, HM Government https://www.gov.uk/service-manual/ helping-people-to-use-your-service/understandingwcag
12 The Copyright, Designs and Patents Act 1988
13 Nothing but the Truth, The Technologist Vol 13 Issue 1, Feb 2020
14 Great Expectations, The Technologist Vol 13 Issue 3, August 2020,
15 Dollars and Sense, The Technologist Vol 14 Issue 3, Aug 2021
Graduated in London 1971. He spent 20 years in full time general dental practice and 10 further years practising part time. He became involved in the medico-legal field in 1989, firstly as a member of the Board of Directors of Dental Protection Limited (part of the Medical Protection Society group of companies). He became a dento-legal adviser in 1992 and from 1998 was the Dental Director of Dental Protection for 18 years and also an Executive member of the Council (Board of Directors) and Executive management team of the Medical Protection Society, roles from which he stepped down in 2016. Since 2018 he has been a Special Consultant to the British Dental Association, in relation to BDA Indemnity.
He is a Founder and Ambassador for the College of General Dentistry, and was a Trustee Board member 2017-22 Kevin has been writing a regular column in the UK dental press since 1981 –originally as the Associate Editor of Dental Practice and since 2006 as the Consultant Editor of Dentistry magazine. He still writes and lectures regularly in the UK and internationally, and has been awarded honorary membership of the British, Irish and New Zealand Dental Associations. He is also an Honorary Member of the British Society for Restorative Dentistry.
Kevin Lewis, BDS (Lond) LDSRCS (Eng) FDSRCS(Eng) FCGDent
technologicalchange
Development Outcomes A, B, C & D – 60 minutes
To complete your CPD, store your records and print a certificate, please visit www.dtauk.org and log in using your member details.
Q1 Approximately how long ago was the steam engine invented? (select the nearest)
A About 500 years ago B About 400 years ago
C About 300 years ago D About 150 years ago
Q2 What was the approximate time interval between the Wright Brothers’ first (12-second) aeroplane flight, and man’s first walk on the surface of the moon? (select the nearest)
A 125-150 years B 100-125 years
C 75-100 years D 60-70 years.
Q3 Roughly how long ago was the internet launched?
A 50-60 years ago B 30-40 years ago
C 20-30 years ago D 15-20 years ago
Q4 How did the tragic Grenfell Tower fire start in London, in June 2017?
A An electrical fault in a domestic appliance causing it to catch fire
B A computer fault in the heating and ventilation system
C A malfunction in the wiring of the building
D A combustion event involving a mobile phone battery
Q5 When did the General Dental Council publish its revised Guidance on the Use of Social Media?
A October 2018 B September 2022
C January 2024 D July 2024
Q6 In relation to the GDC’s current Guidance on the Use of Social Media, only one of the following statements is true – which one is it?
A The standards expected of dental professionals vary according to whether they are communicating face-to-face, through social media or through other media channels
B The standards expected of dental professionals depend upon whether they are communicating through social media in connection with their professional life, or in their personal life
C When communicating through social media, the standards expected of dental professionals only apply if the individual is identifiable as a registered member of the dental profession
CPD OutcomesA,B,C&D 60minutes
D The standards expected of dental professionals do not change because they are communicating through social media: they apply irrespective of whether or not the individual is identifiable as a registered member of the dental profession
Q7 When was the Digital Economy Act passed?
A 2014 B 2017 C 2020 D 2023
Q8 When was the Online Safety Act passed?
A 2020 B 2021 C 2022 D 2023
Q9 Which piece of legislation does the acronym ‘PECR’ refer to?
A Personal Expression of Choice Regulations
B Privacy and Electronic Communications Regulations
C Prevention of the Exploitation of Computerised Records Act
D Posting of Electronic Criticism Restrictions Act
Q10 Which one of the following pieces of legislation do you need to comply with when considering the accessibility requirements of a website in connection with a dental laboratory or CDT business?
A The Health and Safety at Work Act 1974
B Companies Act 2006
C Equality Act 2010 D Broadcasting Act 1990
■ Jo Stevenson : Flexible Dentures
A Case Study
Jo takes us through the process of constructing flexible dentures using Valplast nylon material
Flexible dentures can be tricky and time consuming to construct. Regular Pmma material is relatively easy to trim and polish but the nylon material of flexible dentures can take more time and effort to achieve a high polish.
I have been constructing flexible dentures for 18 years and hope sharing my technique can help technicians achieve the best outcome. There are many flexible denture materials on the market, but in this case, I am using Valplast.
Step 1: Block out and duplicate model
(Fig 1)
Any large undercuts around the teeth need to be blocked out including a small amount at the gingival margins, you don’t want the finished denture pressing on the gingival margins as it can become a gum stripper. As the denture is totally tissue bound it does move around on the soft tissues so any bulbous or bony areas on the buccal surface needs a small amount of block out to protect them.
waxed onto the teeth and will save time when trimming.
Step 2: Trimming / Setting teeth
Valplast material has no chemical bond with the acrylic so to hold the teeth in place requires mechanical retention in the form of holes drilled through the teeth. Trim and shape the teeth to ensure that no part of the tooth touches the model. this will allow the base material to surround the tooth. There can be a small amount of tooth-to-tooth contact high up on the tooth. (Fig 2+3)
■ To gain insight into the successful manufacture of flexible dentures, including the techniques and materials used
CPD Outcomes:
■ Maintenance and development of knowledge and skill within your field(s) of practice
■ CPD specific for your daily role(s).
■ Upskilling opportunities.
Outcome: C
A small post dam is scribed onto the model, it doesn’t have to be very deep as it in more a finishing line than a food trap line. On the duplicate model draw the outline of the denture. This will be a guideline when waxing to ensure that it will not be over
Retention holes need to be in a T shape drilled into the thickest area of the teeth, one each on mesial and distal sides and one through the underside of the teeth. (Fig4+5)
Figure 1
Figure 2
Figure 3
dentures
Near the bottom of the tooth where the clasp will emerge the tooth needs to be trimmed back slightly so that the Valplast material will be a little thicker where the clasp emerges giving it strength. (Fig 6) Set the tooth in place with a small amount of wax and check the bite is correct then you can wax the rest of the denture. I like to drip the wax onto the model so I can control how thick it is and it also seals the wax to
the model, it can be waxed a bit thinner than an acrylic denture. (Fig 7) You can then carve the wax back to the lines drawn on the model and carve around the acrylic teeth. (Fig 8+9)
Step 3: Flasking
The teeth on either side of the denture are trimmed flat and all access areas of the model are removed. Coat the bottom of the flask with a thick mixture of Kaffir-D plaster and place the waxed-up dentures on it making sure all the wax remains exposed. Ensure everything around the dentures is flat and smooth and there are no undercuts. Multiple dentures can be flasked together; and in this case an addition is also buried underneath the other cases. (Fig 10).
Spruing
When spruing each denture gets its own sprue attaching it to a thin area as attaching to a thick area a bubble can appear in the
Valplast material. For larger dentures two sprues can be added. Smaller sprues are also placed across the teeth to ensure the material injects quickly to all areas of the denture. (Fig 11)
Separating solution is painted on the plaster and the top of the flask is screwed down, it can then be topped over with Kaffir-D plaster mixed to the same consistency as the bottom half. Pour the plaster in the flask on a vibrating plate to eliminate bubbles. When the plaster sets the wax can be boiled out. (Fig 12)
I like to steam clean the model side of the flask to make sure all loose plaster is eliminated and it is very clean. As it is more difficult to steam the tooth side of the flask as teeth may be dislodged, I inspect it closely for loose plaster and push down firmly on each tooth to make sure it is firmly in place. This provides an excellent opportunity to make sure all teeth have retention holes in case any have been missed.
The flask is then clamped closed and it is ready to inject the Valplast material as per manufacturer’s instructions. I prefer to do this when the flask is still hot as I find it helps the material to flow better especially if you are doing multiple cases in one flask. When the flask is cool you can de-flask. If possible, keep the denture on the model as it can help with trimming later on.
Step 3: Trimming
Initial trimming can be done with a normal acrylic tungsten burr. Try to only trim in one
Figure 6
Figure 8
Figure 9
Figure 7
Figure 10
Figure 11
direction working the loose threads of material towards the edges. If it is still on the model, you can trim back to the lines that were drawn earlier and thin the flanges. The model can support the clasps but if the model isn’t there keep your finger behind the clasps to support them. (Fig 13+14).
The acrylic burr is only used for rough trimming and thinning. To smooth and shape I use a grey rubber stone that is also used for acrylic work. It is used on half speed on a hand piece because if it is too fast the friction can melt the Valplast material.
I tend to spend a lot of time using the grey stone smoothing the material and shaping the edges (Fig 15). There will be small
threads that can be worked towards the edges and then cut away using a sharp scalpel. (Fig 16) When the denture is thinned and smoothed it can be fitted to the model and you can check that the clasps sit in the gingival margin and are thin and blended into the gums. (Fig 17+18).
When you are sure the denture fits and is thin enough you need to spend more time with the grey stone to get a very smooth surface.
Very lightly rub in all directions burnishing the material smooth. It is important to get the surface as smooth as possible at this stage as polishing will not remove any trimming marks.
Step 4: Polishing. (Fig 19)
There are three stages of polishing.
1 Pumice with an acrylic polishing brush that doesn’t contain calico, this is a slightly harsher brush than the ones containing calico but I have found it gets a better result with Valplast. Do not use too much pressure when using this brush as the friction can melt the material and you will have to go back to the grey stone to smooth it again. Make sure you support the back of the clasps as any heat created can warp the clasps (Fig 20). Try to keep the denture moving in different directions and don’t hold the brush in one position too long as it can heat up quickly.
2 After the pumice is washed off you buff the denture using a dry calico mop and gold Tripoli polish. This is done on high speed on the lathe and again do not use too much pressure and keep the denture moving, polishing in different
Figure 12
Figure 13
Figure 14
Figure15
Figure 16
Figure17
Figure18
Figure19
flexibledentures
directions. Spend a lot of time at this stage as it is the stage where you slowly work the shine onto the denture and create a seal on the surface. It will take time but it should start to shine up.
3 Soft calico mop and blue shine polish. The final polishing stage should bring up the high shine on the denture, using the mop at slow speed with the blue shine polish. Buff with light pressure again working in
all different directions, a few minutes of this should bring up the high shine.
When steam cleaning the polish residue off don’t hold the nozzle too close as it a can dull the shine. There could be a few threads
Development Outcome C – 60 minutes
remaining at the edges and they can be cut off with a sharp scalpel. The denture can be fitted back on the model and checked to ensure the clasps are sitting in the correct place. It is then ready for the patient.
(Fig 21-2)
To complete your CPD, store your records and print a certificate, please visit www.dta-uk.org and log in using your member details.
Q1 Why don’t you want the finished denture pressing on the gingival margins?
A It can cause distortion in the flexible part of the denture
B It can become a ‘gum stripper’
C The denture can expand and become loose
D When biting the teeth can slide down into the uncomfortable ‘glove’ position
Q2 What is used to protect any bulbous or bony areas on the buccal surface of the patient’s oral anatomy?
A A fine layer of spongy Valplast material to the inner surface
B A flexible sheath adhered to the inner denture
C A small amount of block out D b) and c) only
Q3 Valplast has no chemical bond with acrylic, so how are the teeth retained?
A T-shaped retention holes drilled through the teeth
B A fine retention cup of the same material at the lower edge of the teeth
C A screw thread cut into the lower edge of the teeth
D The application of dental cement into the denture socket
Q4 Near the bottom of the tooth where the clasp emerges, why should the tooth be trimmed back slightly?
A To allow for thickness of the dental cement
B So that the retaining cup fits snugly
C So that the Valplast material will be a little thicker for greater strength
D The tooth settles more comfortably into the denture
Q5 When flasking what is used to coat the bottom of the flask?
A Kaffir-D plaster B The spongy separating material
C Gypsum D Heat-proof silicone
Q6 Why should the sprues be attached to a thin area?
A For easier access B To stop a bubble appearing
C It is more malleable for the technician
D Cost saving during manufacture
CPD OutcomeC 60minutes
Q7 Why are smaller sprues placed across the teeth
A For greater stability in the final denture
B To limit the chances of distortion during injection
C To ensure the material injects quickly to all areas of the denture
D To meet the material manufacturer’s recommendations for optimum denture strength
Q8 What do you do to eliminate the chances of bubbles appearing during the plaster top-up process?
A Tap the flask while pouring the plaster
B Put the flask on a vibrating plate
C Pour the plaster from the rim of the flask
D No need to do anything, bubbles are very rare
Q9 Why should the grey stone used for smoothing be kept at half speed?
A Used too fast it will melt the Valplast
B Too fast runs the risk of gouging the Valplast
C The technician retains greater control of the smoothing process
D A greater speed will make the material break down into threads that must be cut away with a very sharp scalpel
Q10 Which of the following is NOT one of the stages of polishing described by the author?
A Try to keep the denture moving in different directions while polishing
B Buff the denture using a dry calico mop and gold Tripoli polish
C Polish with an acrylic polishing brush that contains calico
D Use a soft calico mop and blue shine polish for a high shine
Figure’s 21-22
Figure 20
■ ‘Seven steps to save UK dentistry’: Patients First Report
The Technologist reports from the House of Commons
On the evening of Wednesday 11th September in the House of Commons, after a day that boasted a mixture of brilliant sunshine and drenching rain in the UK Capital, the Association of Dental Groups (ADG) launched its ‘Patients First’ report which details seven core recommendations for Government that, “if implemented will transform the experience for dental patients in every corner of the United Kingdom.” The Technologist was amongst the guests and here shares the evening’s highlights with DTA members.
At present, dental services are in abject crisis. Many pockets of the country have become ‘dental deserts,’ where low numbers of dentists mean it is near impossible for patients to access dental care.
A quarter of English children have experienced dental decay. The number of adults seen by a dentist was 17.5% lower in the 24 months up to June 2023 than the comparative period in 2019.
Too many desperate patients, sometimes waiting years for a dental appointment, resort to agonising DIY dentistry. Others turn to the GP or A&E in their droves, piling pressure on other NHS services already on their knees. A staggering 380,000 people present at their GP with a dental problem every year.
of our existing dental teams.”
CPD OutcomeB 60minutes
He explains: “Dentists are not entering the workforce at anywhere near a high enough rate, nor staying put once qualified.”
Carmichael continues: “There are too few places at UK dental schools, preventing the growth of home-grown talent, while unnecessary bureaucracy prevents hundreds of high-quality dental experts from practicing here.
Aim:
■ Better understanding of recent initiatives that support patient interests and care
CPD Outcome:
■ Effective work with others in the dental team, in the interests of patients
Development Outcome: B
Meanwhile data shows that 4.7 million people called the NHS 111 line regarding dental care from 2019 onwards, with average calls per day increasing to 3,327 in 2023/2024 compared with 2,024 in 2020/21, at the height of the pandemic.
The ADG – which presented its report in Parliament to MPs and Peers from across the political aisle including Chief Dental Officer Jason Wong (above left with Neil Carmichael) – seeks to work with the new Government to improve dental care across the board.
The member group, which represents 10,000 clinicians, and 1,800 practices, is campaigning to improve the ‘recruitment’ and ‘retention’ of the dental workforce, which it views as the twin central challenges plighting our services.
Neil Carmichael, Chair of the ADG and former MP commends: “the excellent work
“Meanwhile dental contracts are so unappealing that experienced dentists are choosing to retire early, reduce their NHS commitments, or reduce their working hours.” He observed that the UK has a dismally low number of dentists per head of population compared with other advanced European economies.
Carmichael added: “Our recommendations are centred around increasing the numbers of dentists working in order to provide better access for patients. Just 100,000 more dentists will create 750,000 more appointments, massively improving access for so many patients in dire need, and reducing pressure on NHS services
elsewhere. We stand ready to support the new Government in putting patients first.”
The ADG’s seven recommendations, most of which can be actioned in the short term, without legislative change, and with no cost to Government, are as follows:
1 Commit to support recruitment: Accelerate long-term workforce plan and unlock barriers preventing high-quality international dentists registering
2 Use commissioning solutions: To meet the needs of the population and roll out examples of successful flexible commissioning
3 Plan the workforce: Recognise the relationship between the mixed economy, skill mix and devolved nations
4 Invest in community prevention: Support water fluoridation, have policies for sugar reduction, hold Integrated Care Boards/ LA/ NHS to account for delivering community preventative schemes like supervised toothbrushing
5 Renumerate practice-based prevention: Offer realistic remuneration and promote flexible commissioning for practicebased prevention.
6 Protect the dental budget: Ringfence the budget and require ICBs to have a clear plan for dental underspend.
7 Support the retention of the workforce: Continue to reform the dental contract and ensure that pay review processes are transparent.
Tom Whiting, GDC Chief Executive and Registrar, concluded the evening’s presentations, saying: “As one of the
Jason Wong
healthcare professional regulators in the UK, our priority is public protection. Our most important responsibility is to maintain the register – a list of everyone who is allowed to practise dentistry in the UK. We regulate seven dental professions across the four nations of the UK – all the professions that make up the dental team. In total that is around 122,000 registered professionals at present.
“We grant registration only to those dental professionals who meet our requirements on education and training, health and good character. We set standards for organisations who provide dental education and training in the UK. And we quality assure and inspect UK education providers.
“We set standards of conduct, performance and ethics for the dental team, and for their continuing professional development. We investigate serious concerns raised about dental professionals. Where appropriate, we take action through our fitness to practise process.
“Patients and the public should be confident that the dental treatment they receive is provided by a dental professional who is properly trained and qualified and who meets our standards. We have an essential role in making dentistry work in the UK.”
He continued: “Our research highlights significant barriers to accessing dental services, especially within the NHS. The public report difficulties in booking regular appointments, particularly affecting younger people, those from ethnic minorities, and people living in urban areas.
“There is evidence that the recovery of dental services after the pandemic has not only stalled but may have gone into reverse. We believe that this needs urgent attention. The Health and Social Care Select Committee inquiry into NHS dentistry last year made a number of recommendations that the GDC has acted on.
“To inform the debate about the dental workforce, we gathered data about the working patterns of dental professionals, which includes where and how they work and whether they deliver NHS or private care. We shared that data gathered from dentists in March and we will publish data from dental care professionals in the Autumn. My thanks have already gone to the BDA and others for encouraging participation in gathering that information.
“There are around 45,000 dentists registered to practise in the UK. Around one third fully or predominantly deliver private care and around 42% are fully or predominantly delivering NHS care. 42% of dentists work less than 30 hours per week. The second recommendation we have acted on is to support the full use of the skills of the whole dental team, we welcomed the government’s proposals to allow dental hygienists and dental therapists across the UK to legally supply and administer specific prescription-only medicines, without the need for a dentist’s prescription.
“And thirdly, to speed up changes to the process of international registration for new applicants seeking to work in the NHS, we used legislation changes in 2023 to increase capacity in the route for overseas qualified dental professionals to register to practise in the UK. Only half of new dentists being registered last year trained in the UK. Most of the rest – 40% of the total – registered on the basis of European qualifications. And the final 10% passed our Overseas
Tom Whiting
Registration Examination – the ORE – to show that they meet the standards we require. Around two thirds of those sitting the ORE pass.
“If we want more dentists and other dental professionals, there needs to be a multipoint plan for the capacity needed to train them. The supply of UK qualified dentists is fixed in the short term – but we are receiving inquiries from those who want to set up new dental schools, in which we play a quality assurance role.”
He concluded: “And there is an important question we all need to think about – what proportion of our dental workforce needs should we be aiming to meet from people trained in the UK. We have already tripled the number of places for part 1 of the ORE and increased capacity of the Part 2 exam by a third. We very much want to increase the flexibility and capacity of the ORE and we are currently tendering for more capacity for next year.
“What is clear is that there is unprecedented demand for ORE places. So far this year, we’ve received almost 90% of the number of applications that we received in the whole of last year alone. It shows no signs of slowing down. However, there is no certainty that increasing international registration of dentists will provide a solution to the challenge of delivering care, particularly NHS care, that meets patients’ needs. Once a dentist is registered with the GDC, where and how they work and whether they provide NHS or private treatment is a matter for them.
“We know that there is active consideration of a scheme to provisionally register overseas qualified dentists – prior to them being fully registered. We also know putting such a scheme in place will take time and will need all those in the sector to work together. Furthermore, for the longer term, there’s a real need to modernise the legislation we work under – so that we can protect patients and support dental professionals effectively.”
Development Outcome B – 60 minutes
To complete your CPD, store your records and print a certificate, please visit www.dta-uk.org and log in using your member details.
Q1 How many patients present at their GP with a dental problem?
A Around half a million B 380,000 C 265,000 D 675,000
CPD OutcomeB 60minutes
Q2 During 2023-2024, on average how many people per day called the NHS 111 line regarding dental care?
A 6,283 B 1,480 C 4,928 D 3,327
Q3 According to ADG Chairman Neil Carmichael how many more dental appointments would be created by an additional 100,000 dentists?
A 500,000 B 950,000 C 750,000 D 625,000
Q4 What measure are recommended to be invested in to support community prevention (recommendation 4)?
A Water fluoridation B Sugar reduction
C Supervised toothbrushing D All of the above
Q5 According to Tom Whiting, GDC Chief Executive and Registrar, how many dental professions are regulated by the GDC across the UK?
A Four B Five C Six D Seven
Q6 How many dental professionals are registered at present?
A 122,000 B 135,000 C 112,000 D 142,000
Q7 Approximately how many dentists are registered in the UK?
A 37,000 B 52,000 C 45,000 D 40,000
Q8 Of that number, what percentage of dentists are fully or predominantly delivering NHS care?
A 29% B 42% C 37% D 53%
Q9 What percentage of new dentists last year were registered on the basis of European qualifications?
A 30% B 35% C 40% D 32%
Q10 What percentage of newly registered dentists passed the Overseas Registration Examination (ORE)?
A 10% B 15% C 8% D 12%
DLA’s President Ian Cumberland in a Q&A with The Technologist
■ Changes Affecting the Dental Lab
● What are the major changes to the dental laboratory industry that are currently affecting the DLA?
The dental laboratory industry is experiencing several significant changes that impact both the DLA and its members. One of the primary changes is the rapid advancement in digital dentistry, including the widespread adoption of digital impressions, CAD/CAM technology, and 3D printing. These technologies are reshaping how dental appliances are designed and manufactured, offering more precision and efficiency but also requiring significant investment in new equipment and training for technicians.
Additionally, regulatory changes from bodies such as the General Dental Council (GDC) and the Medicines and Healthcare products Regulatory Agency (MHRA) continue to evolve, impacting how laboratories must operate to ensure compliance. The shift towards stricter quality control, data protection measures (GDPR compliance), and the integration of digital workflows require laboratories to update their practices regularly.
Furthermore, the economic pressures stemming from increased material costs, Brexit-related supply chain disruptions, and inflation have affected operational costs and pricing strategies within the industry. The DLA is actively working to provide
guidance and support to its members to navigate these changes effectively.
● What does the DLA see as the demands of the MHRA with the progressions of digital technology within the dental team?
The DLA recognises that the MHRA’s demands are increasingly focused on ensuring that all digital dental technologies, such as CAD/CAM systems and 3D printers, meet stringent safety and efficacy standards. As digital technologies become more integral to dental laboratories, the MHRA is keen to ensure that the products used in patient care are of the highest quality and that the software and hardware involved comply with medical device regulations.
With the progression of digital technology, the MHRA expects dental laboratories to implement the same kind of standards and procedures to this technology as it has done to more traditional methods. This includes rigorous validation processes for digital workflows, and comprehensive
training for all personnel involved in using the technology.
Moreover, there is a growing emphasis on cybersecurity and data protection, particularly given the sensitivity of patient data involved in digital impressions and digital design processes. The DLA advises its members to stay updated on the latest MHRA guidelines and ensure full compliance to avoid regulatory penalties and maintain high standards of patient care.
● How does the DLA consider the major issues that will affect the industry within the next five years?
Over the next five years, the dental laboratory industry is likely to face several key challenges and opportunities. One major issue is the ongoing digital transformation. While digital dentistry offers enhanced precision, efficiency, and new capabilities, it also requires significant upfront investment in technology and ongoing training to keep up with rapid advancements. Laboratories will need to balance these investments with the practicalities of running a business, particularly smaller operations that may find it challenging to adopt new technologies.
Workforce demographics are another critical issue. The industry is seeing an ageing workforce with a concurrent shortage of new entrants, which could lead to a skills gap. The DLA is actively encouraging initiatives to attract new talent into the industry, such as partnerships with educational institutions, apprenticeships, and promoting the profession’s value and career prospects.
Increased automation may assist with the problem of workforce shortfall but new and existing workforces require agility to meet expected change and advancement.
DLA’s President Ian Cumberland
Regulatory changes and compliance will continue to be a focus, especially as new technologies emerge that may not yet be fully understood within the current regulatory framework. The DLA anticipates closer collaboration with regulatory bodies like the GDC and MHRA to ensure that new technologies are safely and effectively integrated into dental practices.
● How do you see technological advances such as AI impacting dental technicians?
Artificial Intelligence (AI) is poised to have a significant impact on the dental laboratory industry, particularly in enhancing the precision and efficiency of workflows. AI can assist in the design and planning of dental appliances by analysing digital impressions and proposing optimal treatment solutions, which can save time and reduce human error.
However, while AI can automate certain repetitive tasks, it is unlikely to replace the nuanced skill and artistry of experienced dental technicians. Instead, AI is expected to complement their work, enabling technicians to focus on more complex and bespoke cases that require human expertise. The laboratory industry has a history of embracing change and will continue to do so in my opinion.
The DLA views AI as a tool that can enhance the profession, provided that dental technicians receive proper training to integrate AI technologies into their workflows effectively. This technology also presents an opportunity for the profession to evolve, with technicians playing a critical role in overseeing and refining AI-driven processes.
● Has the shortage of student technicians and an ageing technician workforce proved a problem?
Yes, the shortage of student technicians and an ageing workforce is a significant
questionsandanswers
concern for the dental laboratory industry as it would be for any industry. This shortage has led to difficulties in succession planning and ensuring that critical skills and knowledge are passed on to the next generation of technicians. As older technicians retire, the industry faces the risk of a skills gap that could impact the quality and availability of dental laboratory services.
To address this, the DLA is focusing on several initiatives to attract more young people to the profession. These include raising awareness about the career opportunities within dental technology, developing apprenticeship schemes, and working with educational institutions to ensure that training programmes are relevant and aligned with industry needs.
● What is the main positive initiative supporting the dental profession and driving change, i.e., 3D printing and new materials?
One of the most positive initiatives currently supporting the dental profession is the integration of 3D printing technology and the development of new materials. 3D printing is revolutionising dental laboratories by enabling faster, more accurate, more predictable and more cost-effective production of dental appliances. It allows for the creation of complex structures that would be challenging or impossible to fabricate using traditional methods.
Additionally, advances in materials science have led to the development of new, more
durable, and aesthetically pleasing materials for dental prosthetics and appliances. These innovations provide better outcomes for patients and open up new possibilities for dental treatments.
The DLA is committed to supporting its members in adopting these new technologies and materials, providing training and resources to help laboratories remain at the forefront of these developments and continue to deliver high-quality dental solutions.
● What message would the DLA like to share with DTA members?
The DLA would like to convey a message of collaboration and mutual support to the DTA members. As two integral parts of the dental industry, dental laboratories and dental technicians together share a common goal of providing the best possible care and outcomes for patients.
The DLA values the skills and expertise of dental technicians and believes that by working closely together, both organisations can advocate more effectively for the profession, enhance standards, and ensure the continued growth and success of the dental sector.
The DLA encourages open communication, shared learning, and collaborative efforts between dental technicians and laboratories to navigate the challenges and opportunities ahead. Together, we can build a stronger, more innovative, and resilient dental profession.
■ Mental Health Part 1: Understanding the Mental Health Continuum
Tracey O’Keeffe, MA (Education), BSc (Critical
Care),
RN, MAFHP, MCFHP
This is the first in a series of three papers looking at mental health, with an aim to develop awareness, understanding and greater confidence in working with individuals who are affected with mental health problems.
The Department of Health (1999) suggest that one in six people will be experiencing a mental health problem at any given time and, more recently, Mental Health Matters (2022) state that one quarter of people will be affected at some point in their life. Alongside this, the figures suggest that 19.5% of men and 33.7% of women will have a confirmed mental health diagnosis (Stansfield et al. 2016). Essentially, this means that all clinicians within healthcare will come into contact with people experiencing psychological challenges and as well as physical health problems. It also fairly likely that they themselves may well be one of those statistics.
It is worth noting too, that these statistics may be underestimated due to a number of factors creating problems in measuring prevalence (Stansfield et al. 2016) (see Figure 1). Firstly, many individuals live with complex and multifactorial long term
Reacting Injured
● Experiencing temporary and reversible mental distress, eg berevenment, unemployment
● Severe and persistent distress that could impact on their life and lead to a mental disorder
● Diagnosis of mental illness which affects their daily life
conditions, and mental health issues may be hidden or not fully identified, with the physical presentation of illness taking precedence. Secondly, the funding cannot match the need, and finally, diagnostic procedures and processes can be varied with many causative factors still being explored and fully understood. All this leaves a hidden “iceberg” of unseen mental health problems.
THE MENTAL HEALTH AND MENTAL ILLNESS CONTINUUM AND TRAJECTORY
The complex picture of diagnosis has the potential to contribute to Williams’ (2003; 97) views on “diagnostic uncertainty, symptomatic uncertainty and trajectory uncertainty”. This is compounded by possible societal stigma and labelling. Taking a thoughtful and considered approach to the aetiology and management
is important and needs to be viewed as multifactorial (Gallop and Reynolds 2004, Trenoweth and Allymamod 2010).
Indeed, the term “mental health” means different things to different people. Although many people may automatically think negatively, “mental health” of course can also indicate wellness. How we view and react to these words may be symbolic of our experiences, our knowledge or, indeed, misconceptions and preconceptions. Although we can consider the two separate terms, mental health and mental illness, this still creates issues as mental health appears to be more of a moving scale or journey. Mental Health Matters (2022) discuss the Mental Health Continuum (see Figure 2). The suggestion here is that people will move and transition between wellness and illness, with or without a confirmed mental illness
Figure 1: The challenges in measuring mental health prevalence
Figure 2: The mental health continuum
Normal function
The ability to deal with everyday life and its demands
Being able to make decisions that feel right based on clear thinking and problem-solving
Understand, process and express internal emotions and feeling alongside those of others
diagnosis, with around 50% of mental health problems lasting longer than one year (Jenkins et al. 2008). The journey is not unidirectional and people will fluctuate dependant on many different factors.
Starting with the concept of “healthy” to the left of the continuum, this indicates an individual who is able to “function normally” creating by a sense of internal confidence about any challenges that may arise. They will have a sleep pattern providing rest and restoration. Activity will be appropriate to their physical ability and health. They may experience mood swings but these are not debilitating. This reflects The World Health Organisation’s definition of mental health (2018) as a “state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community”. This is echoed by Mind (2017a) who identify five focal elements of positive mental health (see Figure 3).
Next on the continuum comes “reacting” and this denotes those whose emotions may feel more volatile, with episodes of sadness, nervousness or irritability. Relaxing and sleeping may be difficult. Intrusive thoughts can affect this, as well as interfering with decision-making and productivity. Worry and anxiety can lead to less social connection. Importantly, the distress experienced here is often reversible through self-management strategies and the individual’s normal support systems. Looking at the third section, this transient unsettled state moves to a position of
Being part of the community and society as well as forming and maintaining relationships
Feeling comfortable with the purpose of life and the world
“injured” indicating significant functional impairment. Sleep becomes more disturbed, either struggling to get to sleep or feeling the need for excessive sleep as way of escaping reality. Dealing with any intrusive thoughts can become unmanageable, leaving the individual feeling preoccupied and wishing to withdraw from social interaction. Alongside anxiety, sadness, tearfulness or anger, deeper sensations and emotions surface including hopelessness and worthlessness. External intervention may need serious consideration at this point to avoid escalation and movement further along the continuum.
The final (although still resolvable) stage is termed “ill”. At this point, the person will be experiencing definite functional impairment with emotions that feel persistent, severe and disabling. A sense of overwhelm may be evident with associated high anxiety levels, panic attacks and/or depression. Connection with reality may be lost as thought processes become confused, compounded by poor sleep and subsequent fatigue. Suicidal ideations may arise, with these are either internalised as thoughts or expressed through self-destructive actions and behaviours. Professional intervention at this “ill” stage is essential and this will include exploration into cause (including a possible clinical diagnosis), treatment and management, as well as addressing any necessary safeguarding needs.
Throughout this continuous spectrum of mental wellness and illness, it is important to note that the person’s experience and journey is not reliant solely on a clinically
diagnosed mental health disorder. An individual with no official diagnosis and usually “well” could progress swiftly from “healthy” to “ill” in response to any acute threats to personal well-being. Conversely, a person with a recognised mental health disorder could live much of their life in the “healthy” state if the condition is managed well.
RISK FACTORS FOR MENTAL HEALTH PROBLEMS
It can be seen that mental health and illness is moveable and somewhat unpredictable, with people having potential to move fluidly along that continuum, whether officially diagnosed or not. Causative factors for ill health are plentiful and complex, and the aetiology can often be aligned to a composite and compound mix of elements (Mind 2017b). Figure 4 highlights the variety of risk factors associated with mental health problems.
Changes in mental health can stem from traumatic life events, even if the experience is apparently positive. An example would be childbirth where life adjustments need to be made with possible alteration to established relationships. Challenges in early life, or Adverse Childhood Experiences (ACEs), have been found to increase risk of both physical and psychological ill health in adulthood (Nelson et al. 2000). As well as life changes, environmental element can be impactful. Poverty and deprivation, including poor housing, or lack of safety can negatively affect mental health (Public Health England 2019). Abuse may be a key component regarding security and safety. However, any sort of uncontrollable factors like loss of employment can destabilise a person’s sense of security, both financially and from a societal role perspective.
The individual themselves may have genetic disposition to poor mental health and certain disorders. Family history of mental illness can create challenges to the whole family with later repercussions. Lifestyle choices, too, can influence mental wellbeing. An example would be the use of
Figure 3: Focal elements of positive mental health (based on Mind 2017a)
mentalhealth
Low self-esteem or insecurity which may increase vulnerability
Lifestyle choices, including drugs or alcohol misuse and addiction
Mental ill health within the family which may be hereditary or genetic
Family breakdown including divorce or domestic violence or abuse
Negative life experiences such as homelessness and unemployment
Experiencing or being around prejudice or discrimination, violence and crime or poor living conditions
Feeling of isolation or rejection, particularly from friends and family
Life change, positive or negative, including mattiage, job changes, relocation, etc
Environmental or community difficulties including high levels of crime or poor housing
alcohol and drugs which can result in a transition into poor mental health. This is, however, another complex situation with many individuals having experienced a clinical mental health diagnosis becoming a trigger for substance misuse with possible addiction. When an individual has two or more co-occurring conditions or disorders, with one usually being addiction, this is known as “dual diagnosis”. The order in which they manifest may vary, with one being the initiator of the other (the Dual Diagnosis Hub 2022). Furthermore, Lowe and Abou-Saleh (2014) highlight the challenge of this particular group of individuals, in that their needs are often unique and incongruent with the service provision offered, compounded further by lack of understanding and stigma. People falling into this group may also have reduced mental capacity, whether that be transitory or long-term or be suffering from life-changing events such as trauma, violent crime or post military combat. Indeed, Mind (2017b) suggest post-traumatic stress disorder can have long-term mental health effects on top of the physical experience
Traumatic life events such as berevement and sudden illness or being the victim of an attack or assault
Debt or financial worries stemming from either an acute event or long-standing economic hardship
Inadequate internal coping mechinisms of lack of external support
the individual went through.
The final noteworthy risk factor for mental health is poor physical health. The links here are well-researched, with quite startling connections between the psychological and physiological wellness of individuals.
CONNECTIONS BETWEEN PHYSICAL AND MENTAL HEALTH
There appears to be a bi-directional relationship between physical and mental health implying physical manifestations can cause poor mental health and vice versa (Glew 2016). Naylor et al. (2016) highlight further that a combination of severe mental illness and poor physical health often run concurrently, resulting in a reduced life expectancy. Statistics clearly demonstrate this link (see Figure 5). The complexity of the healthcare needs of these individuals can result in poor management from medically unexplained symptoms or from greater emotional and psychological need (Naylor et al. 2016). Ironically, a lack of appropriate and compassionate care can
encourage a reciprocal lack of engagement. This can manifest as poor attendance at appointments and poor uptake of screening services, potentially complicated even further by physical limitations. Lifestyle choices may also be implicated here in the connection (Nicolle 2022) with less favourable dietary intake, limited physical activity and smoking, thereby creating worsening of physical health. However, The Royal College of Nursing (2022) also highlight genetic changes and risk factors, as well as the impact of poor mental health on blood glucose, cholesterol levels and changes in lung function. This highlights further the many routes of connection between mind and body health.
IMPLICATIONS FOR THE CLINICIAN
Although dental services may not seem to have a direct link with mental health diagnosis, it is evident that the complex nature of poor mental health can create challenging situations for all healthcare professionals and for the individuals receiving treatment and care. Connell et al. (2012) stress the relevance of the building trust, based on acceptance free of stigma, labelling or rejection. Gaining trust and allowing the person to feel at ease can practically facilitate treatment at that moment, but it may also influence areas such as education and empowerment for better dental self-care. Furthermore, a lack of understanding and knowledge surrounding the complex interactions between mental health and physical health, alongside the myriad of risk factors, can result in inappropriate assumptions or judgements being made. Life choices made by the individual may be impacting their dental health, but the drivers for these choices are often not apparent and are frequently non-linear and influenced by many different factors.
Leading on from this and expanding further, potential challenges could arise around consent, compliance and concordance. Possible medication side effects and symptom instability can alter
Figure 4: Risk factors for mental health problems
the individual’s ability to consent to treatment and make decisions, with this capacity fluctuating at each meeting or consultation (Hoffman 2016). It is important therefore that the individual’s understanding is assessed ensuring that mental capacity has not changed. Ng et al. (2007) highlight possible lack of adherence to treatment regimes or post-treatment follow-up care required at home. Dependant on the individual, family or carer involvement may be needed, but this would only be appropriate within the context of client agreement (Hoffman 2016). Furthermore, Connell et al. (2012) discuss how control, autonomy and choice are significant factors with regard to quality of life, with those with more severe mental health conditions experiencing a loss of these elements. Clinicians, therefore, need to be measured in their approach, creating an open dialogue which strives for mutually agreeable goals and health plans. This style of interaction can maximise the chance of positive outcomes through shared understanding, concordance and cooperation.
A final consideration is that of medication contraindications or the impact on the individual’s mental health condition. Any new treatment or intervention needs to be assessed through a holistic view of the individual’s current medical regime. Indeed, it may be necessary to liaise with the individual’s General Practitioner if other medications are to be commenced, administered or invasive procedures undertaken (Hoffman 2016).
CONCLUSION
In conclusion, mental health is a complex subject. It can present challenges for both the individual experiencing it, and also for clinicians trying to negotiate through a multifaceted health history and treatment plan. Trying to isolate or compartmentalise the person to simplify this is likely only to result in more problems. Humans are biopsychosocial beings and therefore the approach needs to be holistic, based on knowledge, understanding and empathy.
Figure 5: Connections between physical and mental health problems
Depression in creases mortality by 50% and doubles risk of heart disease in adults
People with Long Term Conditions (LTC) are 2-3 x more likely to develop depression
People with three LTC’s are 7 x more likely to develop depression
People with Bipolar Disorder or Schizophrenia die on average 16-25 years earlier (CVD, infectious diseases, obesity, lipids and diabetes)
Hard to reach groups have a much lower level of accessing screening and public health programmes
Children with physical illness are 2 x more likely to suffer from emotional or conduct disorder
Working from this stance creates a more collaborative route and helps to mitigate against misconceptions, potential volatility or disengagement, ultimately enhancing the chance of positive health outcomes.
This first paper has just skimmed the surface of mental health. The subject is vast and the following two papers will expand on more specific areas. The next article will consider some of the common mental health conditions, whilst the final paper will explore the often challenging situation regarding suicide and self-harm. We will consider how we may respond appropriately and in a helpful way to ensure we are not only working within our duty of care, but also reacting in a manner that gives the individuals concerned trust and confidence in us from a professional and personal perspective.
References
– Connell, J., Brazier, J., O’Cathain, A., Lloyd-Jones, M. and Paisley, S. 2012. Quality of life of people with mental health problems: a synthesis of qualitative research, Health Qual Life Outcomes, 10, 128
– Department of Health. 1999. National Service Framework for Mental Health; Modern Standards and Service Models, available at www.dh.gov.uk (accessed 26.12.10)
– Dual Diagnosis Hub. 2022. What is dual diagnosis and how common is it? [online] [viewed 26.8.22]. Available at: www.dualdiagnosis.org.uk
– Gallop, R. and Reynolds, W., (2004), Putting It All Together: Dealing with Complexity in the Understanding of the Human Condition, Journal of Psychiatric and Mental Health Nursing, 11, 357-364
– Glew, S. 2016. Closing the gap between physical and mental health training. British Journal of General Practice. 66 (651). 506-507
– Hoffman, K. 2016. Managing Lower Extremity Conditions In Patients With Mental Illness, Podiatry Today, 29 (4), 30-40
– Jenkins, R., Meltzer, H., Jones, P., et al. 2008. Foresight Mental Capital and Wellbeing Project, Mental Health: Future Challenges, London: The Government Office for Science
– Lowe, A. L. and Abou-Saleh, M. T. 2014. The British experience of dual diagnosis in the national health service. Acta Neuropsychiatrica. 16 (1). 41-46
– Mental Health Matters. 2022. The Mental Health Continuum. [online] [viewed 25.8.22]. Available at: mental-health-matters.org
– Mind. 2017a. What are mental health problems? [online] [viewed 25.8.22]. Available at: www.mind.org.uk
– Mind. 2017b. What causes mental health problems? [online] [viewed 26.8.22]. Available at: www.mind.org.uk
– Naylor, C., Das, P., Ross, S., Honeyman, M., Thompson, J., and Gilburt, H. 2016. Bringing together physical and mental health. A new frontier for integrated care. [online] [viewed 28.8.22]. Available at: www.kingsfund .org.uk
– Nelson, C. A., Bhutta, Z. A., Burke Harris, N., Danese, A. and Samara, M. 2020. Adversity in childhood is linked to mental and physical health throughout life. BMJ. 371. Available at: DOI:https//doi.org/10.1136/bmj.m304
– Ng, K. O., To, S. B., and Shukur, H. 2007. Treating orthopaedic patients with psychiatric illness and their treatment outcomes, Journal Orthopaedics, 4 (3), 19
– Nicolle, L. 2022. How do mental and physical health interact? Geriatric Medicine Journal. [online] [viewed 25.8.22]. Available at: www.gmjournal.co.uk
– Public Health England. 2019. Mental Health: environmental factors. [online] [29.8.22]. Available at: www.gov.uk
– Stansfield, S., Clark, C., Bebbington, P., King, M., Jenkins, R. and Hinchliffe, S. 2016. Common Mental Health Disorders, in, McManus, S., Bebbington, P., Jenkins, R. and Brugha, T. (eds), Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014, Leeds: NHS Digital
– The Royal College of Nursing. 2022. Physical health in mental illness. [online] [viewed 26.8.22].
Available at: www.rcn.org.uk
– Trenoweth, S. and Allymamod, W. 2010. Mental Health, In: C. Margereson, and S. Trenoweth. (Eds), Developing Holistic Care for Long-Term Conditions, Abingdon; Routledge
– World Health Organisation. 2018. Mental health: strengthening our response. [online] [viewed 12.3.22].
Available at: Mental health: strengthening our response (who.int)
UK PROFESSIONAL DENTAL TECHNOLOGIST
● are individually registered with the GDC to be able to use the titles that relate to our role in the UK
● maintain our own lifelong learning through relevant continuous professional development (as provided free to the Dental Technologists Association [DTA] members)
● ensure that we are covered by specific indemnity insurance related to our dental laboratory custom-made dental device manufacturing work, and if necessary, related clinical work and/or extended roles
● work within the GDC Scope of Practice for our registered role, along with other extended areas as confirmed by further additional training
● are, as a current GDC registered dental technologist, able to sign-off custom-made dental devices under MHRA/MDR regulations, indicating that such appliances are fit for purpose as stated on the Statement of Manufacture
● maintain and develop our dental team networks to enhance patient care