5 minute read
Service development: POPS

| Rebecca Cole | Jason Cross | Harriet Hall | Judith Partridge |
Perioperative medicine for Older People undergoing Surgery (POPS) is a subspecialty of geriatric medicine that has evolved to address the needs of older people presenting with surgical pathology using comprehensive geriatric assessment and optimisation (CGA) with shared decision-making (SDM).
The seventh National Emergency Laparotomy Audit (NELA) report demonstrates that the proportion of older people undergoing surgery is increasing. Older people are more likely to be living with multimorbidity and frailty. The report indicates that frailty is an independent marker for poorer postoperative outcomes.1 This has been demonstrated across surgical specialities.2
CGA is a multidimensional, multidisciplinary process which identifies medical, social and functional needs, resulting in an integrated/ coordinated care plan to address those needs and is the gold-standard for the management of older people.3 Evidence supports the clinical and cost effectiveness of CGA and optimisation in the perioperative setting 4,5 . Cognisant of workforce challenges in geriatric medicine the HoW CGA study trialled delivery of perioperative CGA without a geriatrician using a ‘toolkit’ approach, concluding that geriatric medicine skills are crucial to the clinical effectiveness of the process.6
Using a CGA and optimisation approach with SDM has been endorsed through the collaborative ‘Guideline for Perioperative Care for People Living with Frailty Undergoing Elective and Emergency Surgery’. Authored jointly by the Centre for Perioperative Care (CPOC) and the British Geriatrics Society (BGS), the guideline recommends that surgical pathways for frail patients are underpinned by CGA methodology from initial assessment to discharge.7
The BGS POPS Special Interest Group provides education and training in perioperative medicine on a national level to support all members of the multidisciplinary team upskilling in management of older people undergoing surgery. This includes conferences, guidelines and an e-learning package. Curricula have been approved for both ANPs and foundation year doctors.8
Despite this evidence, guidelines and training opportunities significant variation in the perioperative care of older people remains across the UK, with the Getting It Right First Time (GIRFT) national programme aiming to standardise care through work streams in critical care, surgical specialties and geriatric medicine.9
Supporting rollout of the POPS model
Despite evidence showing the benefits of geriatrician involvement in the perioperative care of older people, few services nationally or internationally have implemented CGA-based perioperative care. In fact, a 2019 survey of acute NHS trusts revealed that only around half had such services in place.10
Following the success of other improvements networks including the Specialised Clinical Frailty Network, the NHS Elect POPS Network was established, with the aim of promoting the rollout of geriatrician-led, multidisciplinary perioperative care for older patients. To date, thirteen NHS Trusts in England and Wales have completed the six-month programme over two cohorts. The programme provides comprehensive support to adapt and implement the POPS model, ensuring it is tailored to the local context at each site. This is delivered through a trimodal approach of expert mentoring and coaching, access to a toolkit of POPS resources, and guidance in a measurement for improvement approach.
Beginning with a virtual site visit to share ideas and discuss potential barriers to change, the programme offers structured monthly core events, webinars and masterclasses. In addition to the more formal expert mentoring aspect to these virtual events, they also provide invaluable opportunities for networking between sites, building lasting links and sharing learning.
The POPS toolkit contains essential resources for establishing a local POPS service including clinical materials (such as guidelines, and letter templates), education and training materials (such as teaching programmes, slide sets), and business materials (such as core outcome sets, business plans and annual reports).
Implementation of a measurement for improvement approach is another key aspect of the programme, with sites benefitting from the support of data analysts throughout. Specific improvement measures are defined, with many sites impacting process-related measures such as length of stay and readmission rates.
These new POPS services have been established with differing initial clinical aims, including; developing pre-operative elective assessment pathways; frailty recognition; pain management in emergency general surgical patients and establishing a silver trauma service.
POPS service development: case study
The national shortage of geriatricians has required innovation to establish new POPS services. One such innovative model is the POPS service at Lewisham and Greenwich (LGT) NHS Trust in South East London. Working closely with Guy’s and St Thomas’ Trust, a senior nurse with POPS experience was identified as the lead for the POPS Network project at LGT.
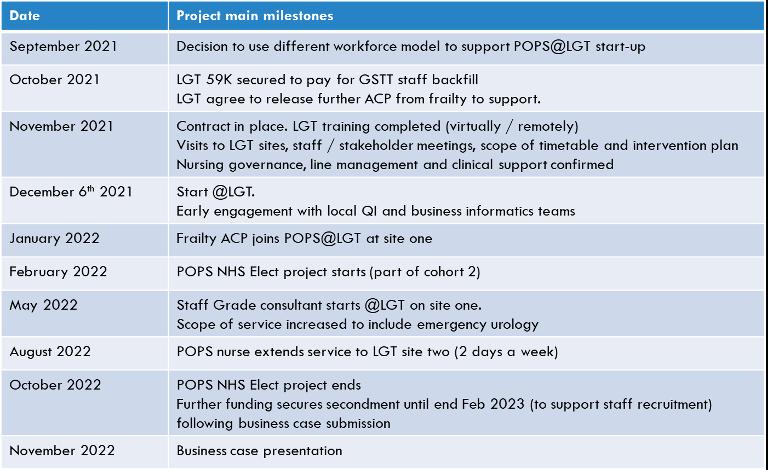
The project began in December 2021 (Table 1 timeline), focusing on emergency general surgical patients at one site in the trust. To maintain fidelity to established POPS services,
Table 1. Timeline for POPS at Lewisham and Greenwich (LGT) NHS Trust
attendance at the nursing and surgical early morning handover proactively identified patients who would benefit from CGA and optimisation.9 This was coupled with a ‘don’t wait to be asked’ style of case-finding where everyone over the age of 65 years was screened.
These methods complemented each other and allowed early input in patients who might be missed on screening by frailty score alone. In particular, it allowed inclusion of those living with mild frailty, or as highlighted in our data analysis, those where frailty had not been accurately assessed.
Once identified, each patient underwent CGA and optimisation, either in ED or when admitted to the ward. Attendance at the ward discharge MDT ensured support for the discharge planning process. The senior POPS nurse worked autonomously with clinical support from a consultant geriatrician. Prospective patient data was collected for every patient contact.
Summary of impact:
✦ Successful embedding of proactive frailty liaison service into emergency general surgery pathway
✦ >600 patients reviewed by POPS team across two sites (11 months)
✦ Length of stay reduction: two day reduction for all patients >65 years of age identified as frail (CFS 5+).
✦ Discrepancy noted between initial ‘clerking’ frailty assessment and CGA-informed clinical frailty scale score (CFS). This led to
QI-team-led, ward-based education to support accurate frailty assessment by ward teams increasing accuracy of assessment
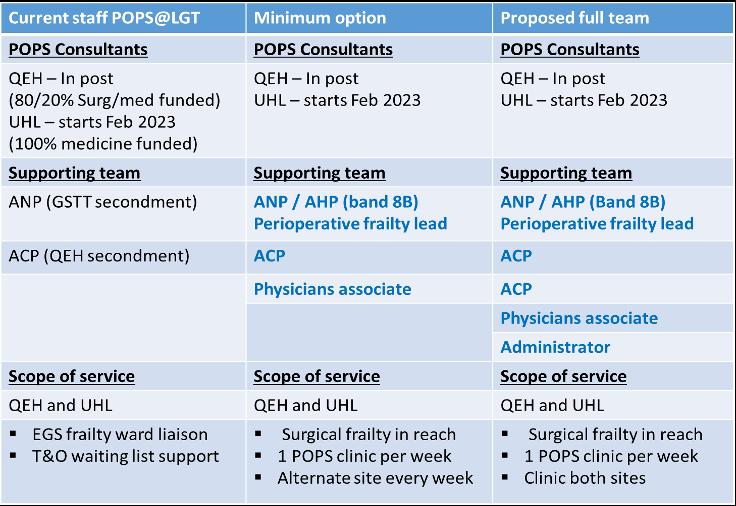
Table 2. Business case summary (text in blue denotes what is being asked for)
✦ Reduced workload for other teams, including fewer referrals to the medical frailty service
✦ NELA impact: geriatric specialist input for 70% of all appropriate NELA cases July-
August 2022 (previously 10-20%).
✦ A business case for continuation of POPS service was presented in November 2022 (Table 2).
Innovative use of the available workforce to deliver CGA and optimisation for an older surgical population living with multimorbidity and frailty is crucial to providing goldstandard perioperative care. This case study describes one example of successfully delivery in a district general hospital using the NHS Elect trimodal approach of expert mentoring, a toolkit of resources and measurement. Adapting to local challenges, innovation in the workforce model and stakeholder buy-in was key to delivering change.
Link to References







