3 minute read
High-quality imaging has taken the accuracy


Advancing biometry
High-quality imaging has taken the accuracy and precision of modern biometry to new heights. Dermot McGrath reports
Recent advances in anterior segment biometry devices in combination with the latest IOL formulas have greatly improved the accuracy of IOL power calculations for today’s patients, according to Jaime Aramberri MD.
“The latest generation of measuring devices have helped to improve accuracy in IOL calculations thanks to the ability to precisely measure both anterior and posterior corneal curvatures and take account of other relevant parameters that may affect the final outcome,” he said at the 25th ESCRS Winter Meeting.
Dr Aramberri noted that the development of high-quality swept-source OCT imaging has taken the accuracy and precision of modern biometry to new heights and made it easier to test eyes such as those with dense cataracts that were difficult to scan with traditional optical biometry devices.
Comparing the features of SS-OCT to optical biometers and Scheimpflug tomography devices, Dr Aramberri said that the difference is not flagrant when it comes to axial length measurements.
“Axial length measurements have been very accurate and precise since the first IOLMaster back in 1999. Many tests have been conducted showing excellent agreement and precision of most instruments with a high level of repeatability between devices,” he said.
The real advantage of being able to obtain a B-scan with SS-OCT, he explained, is the more precise measurement of anterior chamber depth (ACD) and lens thickness (LT) as the boundaries where the peaks are generated can be anatomically identified
“This all-surface detection makes it very useful in dense cataracts and abnormal eyes with modern power formulas for more accurate IOL position estimation. We can also clearly identify the pseudophakic boundaries with the B-scan in order to check and optimise the performance of the IOL predicting algorithm,” he said.
Another useful advantage of the B-scan’s cross-sectional image of the entire eye is the ability to check fixation in patients using the foveal pit scan, he added.
Calculating corneal power using only anterior surface measurements is a frequent source of error in IOL power calculations, said Dr Aramberri. Current biometric devices typically measure corneal power using a standardised keratometric index of refraction – usually 1.3375 – to convert the measured radius of the anterior corneal surface into keratometric dioptres.
This standard keratometric index of refraction assumes a constant ratio of anterior-to-posterior corneal curvature, which works well for normal eyes, but not with aberrated corneas or those treated with LASIK or other procedures that alter the anterior corneal curvature.
“To avoid this error in a particular eye, the total corneal power should be calculated from anterior and posterior measurements as well as corneal pachymetry,” he said.
A total corneal power parameter that can be input in regular formulas without IOL constant adjustment started years ago with the Equivalent K reading in Pentacam (Oculus), and later in Cassini (i-Optics). The new Total Keratometry (TK) value measured by the IOL Master 700 (Carl Zeiss Meditec) takes advantage of the high accuracy of SS-OCT in imaging the posterior cornea, pointed out Dr Aramberri.
Some recent studies indicate that higher prediction accuracy can be obtained using TK values along with some of the newly-
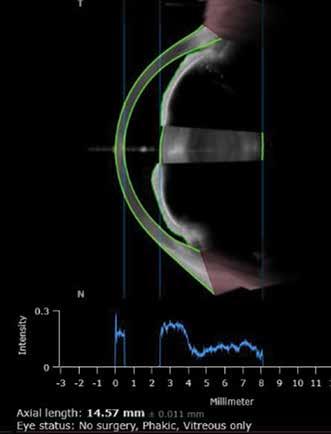
Very short AXL (14.57mm) and cataract with Anterion SS-OCT (Heidelberg) Courtesy of Jaime Aramberri MD
developed IOL calculation formulas. Fabian et al demonstrated that in comparison to conventional keratometry, a notable trend in lowering the absolute prediction errors was observed by applying TK input into the Haigis and the Barrett Universal II/Toric TK formulas in normal eyes (J Refract Surg. 2019;35(6):362‐368). For cases after laser refractive surgery, a study by Lawless et al showed that best results were obtained using TK together with Barrett True-K and Haigis formulas (Clin Exp Ophthalmol. 2020;10).
With a myriad of calculation formulas now available, Dr Aramberri said that studies have shown that more recent formulas such as Kane, Olsen and Barrett Universal II offer a greater degree of accuracy compared to older formulas such as Hoffer Q, Holladay 2 or SRK/T.
“There are a few reasons for this improvement. Firstly, the high quality of data in terms of measurements and refractions with optical biometry. Secondly, the improvement of IOL position estimation, and empirical fits to correct bias in extremes of ranges for axial length and keratometry. Finally, taking account of the role of the posterior cornea in the calculation has helped to improve our results,” he said.
Dr Aramberri stressed the importance, however, of intelligent use of the available formulas and methods.
“The key point is that the more regular the cornea is, the less it matters which regular formula we use, whereas thick lens models require adapted formulas and for extreme cases we need to use exact ray-tracing methods,” he said.






