2 minute read
Micromonovision with Non-Diffractive Enhanced Monofocal IOL


Lens using positive spherical aberration yields spectacle independence for some.
HOWARD LARKIN REPORTS
Most patients implanted bilaterally with a new non-diffractive enhanced monofocal intraocular lens targeting micromonovision ended up with good distance and intermediate vision, and many achieved spectacle independence.
The results came from a retrospective study of the first 30 patients bilaterally implanted with the Rayner RayOne EMV IOL, which uses positive spherical aberration to stretch the focal distance. Patients were assessed 12 to 15 months postoperatively. Mean age was 69 years, reported Elizabeth Law PhD, MSc, MCOptom.
Dominant eyes were targeted for emmetropia, and non-dominant eyes for -0.75 D to -1.25 D. Patients’ previous experience with monovision determined the myopia level targeted in the non-dominant eye. Those without monovision experience were targeted closer to -0.75 D, while those with experience closer to -1.25 D, Dr Law said.
Good distance vision
In the dominant eye, mean uncorrected distance visual acuity was 0.12 ± 0.10 logMAR (or about 20/25), while it was a little better than 0.30 (0.28 ± 0.14, or about 20/40) in the non-dominant eye. Binocular uncorrected distance vision was 0.07 ± 0.06 logMAR. Mean corrected distance vision was better than 0.0 (or 20/20) monocularly and binocularly, Dr Law reported. However, “nobody wore spectacles for distance vision even though it was slightly better corrected, and none were unsatisfied.”
The study allowed patients with up to 1.0 D corneal astigmatism to be implanted, which may explain why mean distance vision improved with correction, Dr Law said.
“Perhaps we were not quite stringent enough in treating astigmatism in these patients.”
69 years
Patients were assessed 12 to 15 months postoperatively. Mean age was 69 years, reported Elizabeth Law PhD, MSc, MCOptom.
Intermediate and near vision
Not surprisingly, mean uncorrected intermediate vision was significantly better in the non-dominant eye and binocularly than in the dominant eye, coming in at better than 0.2 (0.18 ± 0.14) in the non-dominant eye and binocularly (0.15 ± 0.12), and a little better than 0.4 in the dominant eye. As expected with micromonovision approach, near performance was slightly less than intermediate, with a mean of about 0.3 (0.32 ± 0.16) in the non-dominant eye and binocularly (0.28 ± 0.16), and about 0.5 for the dominant eye (0.53 ± 0.10).
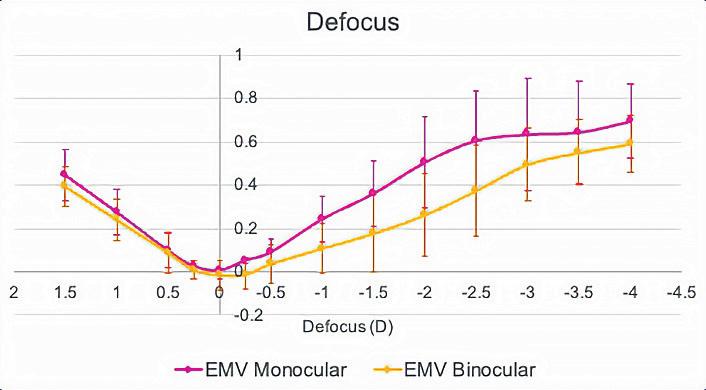
The binocular defocus curve was also better than monocular performance, yielding a mean uncorrected visual acuity of better than 0.2 from +0.75 D to -1.50 D for the micromonovision approach, Dr Law said. There were no reports of dysphotopsias in the group.
“We certainly have achieved an extended range of focus,” she said. “A lot of our patients are spectacle independent.” She disclosed she is doing a longer-term study of the same lens, sponsored by Rayner.
Dr Law presented her findings at the 40th Congress of the ESCRS in Milan.
Elizabeth M Law PhD, MSc, MCOptom, is lead optometrist and researcher at Southend University Hospital, Mid and South Essex NHS Trust, and BMI Southend Private Hospital, both in the United Kingdom. elizabeth.law6@nhs.net
Learn more at ESCRS.org




