
11 minute read
Understanding Glaucoma Genetics


Methods for gene discovery and implications for understanding disease mechanisms and improving patient care. Cheryl Guttman Krader reports from ARVO 2022 in Denver, Colorado, USA
Genetic investigations are providing new insights on glaucoma pathophysiology, disease risk, and therapeutic opportunities, said Janey Wiggs MD, PhD, during her Mildred Weisenfeld Award for Excellence in Ophthalmology at this year’s ARVO conference.
“Glaucoma is the leading cause of irreversible blindness throughout the world, and elevated IOP—which is commonly monitored as a sign of glaucoma—is an important risk factor. But many patients with glaucoma do not have elevated IOP,” said Dr Wiggs.
“Importantly, the disease mechanisms responsible for regulating IOP and optic nerve degeneration are poorly understood. So, our group and others have used a genetic approach to try to understand more about the pathophysiology of glaucoma: where the discovery and characterisation of genes that cause or contribute to glaucoma susceptibility can help us identify the molecular events that define disease mechanisms and, therefore, identify potential therapeutic targets that allow the development of therapies that approach the root cause of glaucoma.”
Additionally, an important part of finding genes for glaucoma is their use for genetic testing to identify people at high risk for the disease so they can have tailored surveillance and monitoring and receive timely treatment that will potentially prevent the development of irreversible blindness, she noted.
In reviewing glaucoma gene discovery research and its clinical applications, Dr Wiggs divided her talk into discussions of early- and adult-onset forms of glaucoma. The early-onset glaucomas—which include juvenile open-angle glaucoma, congenital glaucoma, and developmental glaucomas—are inherited as Mendelian autosomal recessive or dominant traits and caused by rare mutations that have very large biologic effects.
“If someone has one of these mutations, chances are the person has the disease,” she said.
Notable progress has been made in research focusing on the genetics of early-onset glaucomas. To date, 15 causative genes for early-onset glaucomas have been discovered using linkage analysis, whole exome, and whole genome sequencing, Dr Wiggs reported.
All the known genes for early-onset glaucoma can be used for genetic testing. The results can help with risk assessment, inform genetic counselling, enable tailored surveillance for at-risk persons, and identify those who can benefit from timely treatment. Researchers are also beginning to identify therapeutic targets that could spell promise for gene-based therapies, Dr Wiggs said.
However, genetic testing using the early-onset glaucoma genes discovered so far only detects a mutation in about 20% of families. Since most of the known genes were found by studying families in European Caucasian populations, research seeking to find additional genes has turned to populations with greater ethnic diversity. Dr Wiggs discussed this effort, mechanisms by which certain mutations cause early-onset glaucoma, and potential therapeutic targets that include increasing TEK signalling and knocking down myocilin expression.
ADULT-ONSET GLAUCOMAS Dr Wiggs explained adult-onset glaucomas have complex inheritance and are not caused by single mutations. Instead, DNA susceptibility variants that individually have small biological effects influence disease development.
She noted the formation of US-based and international consortiums to acquire the large data sets of cases and controls needed to give genome-wide association studies adequate statistical power for detecting the DNA susceptibility variants associated with adult-onset glaucomas. Thus far, the consortiums have identified hundreds of susceptibility genes.
Findings from the genome-wide association studies have been used to derive polygenic risk scores for risk stratification in adult populations. Such a tool has already proved important in identifying patients at the highest risk for severe disease, thereby enabling tailored surveillance and treatment.
Dr Wiggs also provided an example of how identification of genetically defined subgroups among patients with primary openangle glaucoma suggests a possible therapeutic intervention.
FUTURE GOALS “We still have so much work to do. We really need a better understanding of the genetics of early-onset open-angle glaucoma. This involves new gene discovery; but also perhaps better annotation and understanding of genes already known. For the latter reason, we have joined the ClinGen consortium,” she said.
“We are also very interested in looking at noncoding effects, whole-genome sequencing, and polygenic effects in the earlyonset glaucomas. In addition, we need a lot more research on the clinical outcomes of polygenic risk scores for primary open-angle glaucoma and other types of adult-onset glaucoma and how to implement that in our clinical design. And always, we need better and more animal and cell models to define disease mechanisms for glaucoma and test therapeutics,” she concluded.
Janey Wiggs MD, PhD is the Paul Austin Chandler Professor of Ophthalmology; Co-Director, Glaucoma Center of Excellence; Vice Chair, Clinical Research; and Associate Director, Ocular Genomics Institute at Harvard Medical School, Boston, Massachusetts, USA. janey_wiggs@meei.harvard.edu
A Vision for a New Era in Combined Glaucoma and Cataract Treatment
A Q&A with Elliot Friedman CEO, Elios Vision, Inc. and Murray Johnstone MD Clinical Professor, University of Washington
TO ELLIOT
Tell readers about Elios Vision and its background.
Elios Vision was founded in partnership with MLase, a world leader in excimer laser technology. We shared a goal to create a glaucoma procedure that was safe and effective and optimised for use during routine cataract surgery. Elios Vision was formed to drive the global clinical and regulatory strategy for the novel excimer laser platform and procedure with a dedicated team.
IOP lowering effects stable and >20% for the 8-year follow-up duration
What specific value are you hoping to bring to physicians and their patients?
Despite a decade of MIGS innovation, we are still seeking to improve surgical options to treat glaucoma at the time of cataract surgery, which affords such a perfect opportunity to access tissues implicated in glaucoma.
However, we estimate that only 15% of glaucoma patients worldwide receive a glaucoma treatment at the time of cataract surgery. Whilst access and reimbursement certainly have a role to play—especially outside of the US—we know predictable IOP and medication lowering is a must. And we have also learned that surgeons do not want to compromise cataract surgery safety and visual outcomes with glaucoma procedures that are overly complex or cause trauma. In addition, glaucoma implants during cataract surgery can be unappealing for many surgeons.
With around 6 million glaucoma and ocular hypertension patients being treated for cataract each year worldwide, we believe the ELIOS™ procedure is well placed to address these unmet needs because it is “implant free”, avoids thermal and mechanical trauma, and has a low level of intra- and postoperative complications. We’ve also observed a learning curve that can make the ELIOS procedure widely adoptable.

Figure 1: Sustained IOP lowering effect observed unto eight years.1
Figure 2: Significant reduction in medications observed at one year.2
82% of patients “meds-free” at 1 year. Mean meds reduced from 1.7 to 0.3
So what is the ELIOS procedure, and how does it work?
We know that bypassing the TM is a proven way to lower IOP. But as Murray will explain, it’s important to consider the physiology of the TM in order to restore or augment outflow predictably and with an enduring effect.
The ELIOS procedure bypasses the TM using precision laser ablation, creating ten 210-micron microchannels. This maximises the potential flow into the collector channels.
The ELIOS procedure has demonstrated strong safety and efficacy in OUS studies. Can you describe this data and how you think it differentiates your approach?
We have data on over 600 eyes from 14 studies which we find encouraging on several levels. Firstly, it appears the clinical effect is still present in more than 50% of patients assessed eight years after their procedure. Another observation is the extremely low incidence of severe complications thanks, at least in part, to the atraumatic mechanism of action of the excimer laser.
The University of Zurich just published eight-year follow-up results of ELIOS combined with cataract surgery, showing a >20% reduction in mean IOP at eight years post-operation [Figure 1]. Another study in Spain showed more than 80% of patients were “medication free” at 12 months following the ELIOS procedure [Figure 2]. Can you share your regulatory, reimbursement, and commercial plans?
The ELIOS technology is CE marked, and we have started a focused commercial rollout in Europe to generate data, establish our perprocedure fee model, expand our reimbursement coverage, and grow our key opinion leader base.
In the United States, our combination cataract ELIOS pivotal trial is well underway, and we expect to launch in 2024. We have just filed an IDE for standalone treatment and been granted our own unique reimbursement code for the ELIOS procedure.
In China and Canada, we have commenced data generation activities to support regulatory filings in the near term.
TO MURRAY
Murray, for those not familiar with your work, could you summarise your research area of expertise and share the main appeal of the ELIOS procedure?
My research focuses on aqueous outflow regulation and what goes wrong in glaucoma.
The research points to aqueous outflow regulation by a mechanical mechanism like the lymphatic and venous pumps present throughout the vascular system [Figure 3].
Studies show that SC is a collapsible chamber with inlet and outlet valves.
Pulse dependent tissue motion of the aqueous outflow system3
Figure 3

The pumping mechanism fails in glaucoma.
Ideally, we want to restore the normal pump function without causing damage.
The appeal of the ELIOS procedure is that it creates small openings in the outflow system by vaporizing tissue [Figure 4]. The procedure does not tear away or burn trabecular tissue, and does not require introducing and leaving foreign objects in the canal.
What are the main structural and functional changes that have been observed in the TM and SC in patients with glaucoma (versus non-glaucomatous eyes)?
As glaucoma progresses, there is a loss of normal trabecular tissue elastance. Because of the increased stiffness, the TM tissues can’t distend and recoil properly in response to pressure changes [Figure 5]. Loss of elastance causes the TM to lose its ability to resist pressure, and it expands outward, occluding SC and collector channels.
Is there an optimal “time” in the disease course to enhance/ restore Schlemm’s canal physiology? Is there a point beyond which the opportunity is lost?
Pulsatile flow and TM motion stop as glaucoma progresses.
The pulsatile flow and TM motion loss are associated with the TM distending into SC, closing the lumen, and preventing flow.
Early intervention is likely to be valuable in preventing chronic apposition and eventual adhesion between SC walls.
Early treatment is a likely key to preventing this cascade of negative events.
The caveat is that the benefits of earlier intervention need to outweigh the risks.
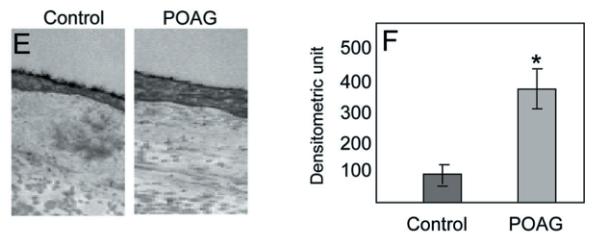
Thickening and loss of elasticity of the TM in glaucoma
Figure 5: The representative BM changes in the intra-trabecular space in transmission electron micrographs (TEM) en-bloc staining with uranyl acetate (Alcian Blue 8GX). 3 As indicated, control (55-year-old) and primary open-angle glaucoma (POAG; 55-year-old), both male cadaver donor eyes respectively. (F) Assessment of intratrabecular BM thickness from 50 locations each from individual TEM images from 6 control and POAG donors each (age 55–59, equal distribution of genders). Asterisk indicate significance (p<0.05) using two-tailed equal variance t-test.3 Some MIGS procedures rely on physical removal of the TM by excision—Is the impact of these techniques on Schlemm’s canal and the angle understood in the mid-/long-term?
SC is not a pipe but instead a delicate organ with compressible chamber containing valve-like inlet and outlet structures that can control aqueous flow.
Removal of the TM or instrumenting SC can damage structures in the distal outflow system that normally control aqueous outflow and IOP.
What has the industry learned (from MIGS?) about stenting the TM in the past 10 years, and how does ELIOS build on this?
Procedures that tear away the TM or instrument the lumen of SC can damage the physiologic regulatory structures.
Although they reduce IOP, they rely on non-physiologic mechanisms.
The ELIOS procedure creates a series of small openings into SC while leaving most of the pressure regulatory apparatus intact.
The idea that the procedure may minimise damage to the normal physiologic mechanism, combined with the fact that it is an adoptable technique, is attractive.
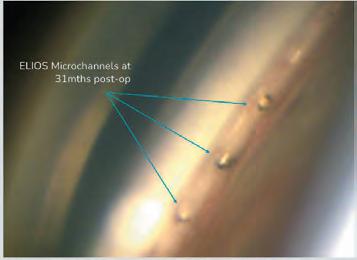
Figure 4
TO ELLIOT So in closing, how do you think glaucoma treatment will be different five years from now based on the introduction of the ELIOS procedure?
We think combining glaucoma and cataract will be the standard of care in five years, and we certainly hope the professional community will embrace these benefits of the ELIOS technology and make it the procedure of choice for their patients.
Disclaimer:
Elios Vision GmbH is the EU distributor of the ELIOS Console manufactured by MLase AG located at 82110 Germering, industriestr 17, Germany and the FIDO laser applicator manufactured byWEINERT Fiber Optics GmbH, Mittlere- Motsch-Strasse 26, 96515 Sonneberg, Germany. The ELIOS Console and FIDO Laser Applicator are CE marked and licensed for use in adult patients with glaucoma. Product feedback should be sent to productsurveillance@eliosvision.com
References:
Figure 1 Riesen M, Funk J, Töteberg-Harms M. “Long-term treatment success and safety of combined phacoemulsification plus excimer laser trabeculostomy: an 8-year followup study”. Graefes Arch Clin Exp Ophthalmol. 2022 Jan 16. Figure 2 Moreno-Valladares A, Puerto Amorós N, Mendez Llatas M, Pazos-López M, Ahmed IIK. “Combined excimer laser trabeculostomy and phacoemulsification: One year follow-up real world data of a laser-based MIGS”. Arch Soc Esp Oftalmol (Engl Ed). 2021 Dec; 96(12): 631–639. Figure 3 & 5. Carreon T, van der Merwe E, Fellman RL, Johnstone M, Bhattacharya SK. “Aqueous outflow - A continuum from trabecular meshwork to episcleral veins”. Prog Retin Eye Res. 2017 Mar; 57: 108–133.






