12 minute read
PULMONARY AND SLEEP DISORDERS


Pediatric Limb Length Discrepancies
By: Jason Malone, DO
Advertisement
Q: HOW COMMON ARE PEDIATRIC LIMB LENGTH DISCREPANCIES?
A: Limb length discrepancies are very common. Up to twothirds of the population have a leg length difference of less than 2 cm (0.79 inch). Luckily, most people do not have symptoms unless the difference is greater than 2 cm.
Q: WHAT ARE CAUSES OF LIMB LENGTH DISCREPANCIES?
A: Limb length discrepancies can be categorized into two major groups: congenital and acquired.
Congenital causes range from longitudinal deficiencies such as congenital short femurs, proximal focal femoral deficiencies, tibia hemimelia, fibular hemimelia, hemihypertrophy, unilateral clubfoot, skeletal dysplasias, and hip dysplasia. Acquired causes range from idiopathic, paralytic disorders such as cerebral palsy or polio and physeal injury from trauma, infection or tumors.
Q: WHAT TECHNIQUES DO YOU USE TO TREAT THESE PATIENTS?
A: Symptomatic leg length differences less than 1 cm can be treated with a shoe insert. A difference greater than 1 cm can be addressed with nonsurgical treatment with a customized shoe lift. However, some patients or families do not wish to use a brace or shoe insert for the rest of their life.
Leg differences can be treated with a shortening procedure on the long side or a lengthening procedure on the short side or a combination of the two. Shortening procedures are smaller surgeries that are quicker to recover from but do lead shorter stature. Lengthening procedures are classically done for differences greater than 5 cm but many deformity specialists are now treating smaller leg length differences down to 3 cm in skeletally mature patients. done for leg difference of 2-5 cm.
Q: HOW LONG DOES THE PROCESS
TAKE?
A: Distraction osteogenesis is a long process. After the initial surgery we wait about a week for the bony callus or regenerate to develop. We then lengthen 1 mm per day. Then the bone takes about 8-12 weeks to fully heal the regenerate. A large 5 cm lengthening can take about 100 days to fully heal.
Q: WHAT ARE THE POTENTIAL COMPLICATIONS INVOLVED?
A: Distraction osteogenesis is safe if performed and monitored by an experienced physician, but it can also be associated with multitude problems. The bones, tendons, muscles and neurovascular structures are growing faster than the body is used to growing, so patients can develop joint contractures, joint dislocations and nerve stretch. We combat this by using nighttime braces, starting physical therapy right away, and stopping the lengthening process if any major complication develops. We can also lengthen more in the future. You also have your standard complication that can happen with any orthopedic procedure such as infection, nonunion, malunion or hardware failure.
An epiphysiodesis can also have its complications such as fracture at the physis, continue growth, angular deformity if the entire growth plate is not fully removed and continues to grow, not timing the surgery right and not achieving the desired correction or even overcorrecting and needing to perform an epiphysiodesis on the contralateral side.
Q: WHEN SHOULD A CHILD SEE A SPECIALIST TO ADDRESS THE
DISCREPANCY?
Q: HOW DOES THE PROCESS WORK?
A: Limb Lengthening procedures were first described by Dr. Gavriil Ilizarov in the 1950s. He called the process distraction osteogenesis. The process entails making a fracture in a bone, having the patient rest for 5-7 days, then distracting the bone ends about 1 mm per day. The bones can be distracted with an external fixator, a mechanical intramedullary nail, and soon with an expanding plate. We can safely lengthen a bone about 5 cm per treatment.
External fixators are better for legs that have an associated large deformity or children with open growth plates. Intramedullary nails are better tolerated but can only be placed in the femur of children at least 8 years old once the growth plate is closed in the tibia. The new lengthening plates that should be out in the summer of 2021 will allow us to lengthen internally even when a child has an open growth plate.
Shortening procedures usually are done in growing children. This is done through a timed epiphysiodesis. I prefer to perform a percutaneous epiphysiodesis as it leaves small scars and is associated with less complications than other techniques. This is
A: A child should see a pediatric orthopedic surgeon specialized in deformity correction when they have a congenital leg length difference, when they have a physeal injury, or an idiopathic leg length difference that is symptomatic or over 2 cm.
Q: ARE YOU CURRENTLY DOING ANY RESEARCH IN THE FIELD?
A: I just finished a research paper looking through a nationwide database from 1997-2016 on trends in femoral lengthenings in pediatric patients. What we found are that most of the surgeries are performed in large urban teaching hospitals. The South does more lengthenings than any other region in the country. The surgery has become safer over the years with shorter hospital stays but like most of medicine, the costs have risen substantially through the years. We currently have the paper submit for publication.
Jason Malone, DO, is a fellowship-trained pediatric orthopedic surgeon at Nemours Children’s Health who specializes in treating limb length discrepancies and
deformities. Call (407) 650-7715 for more information.
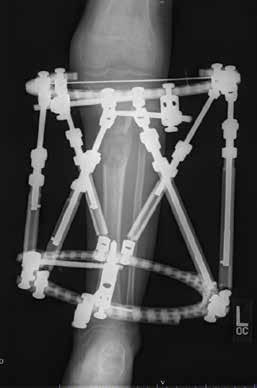
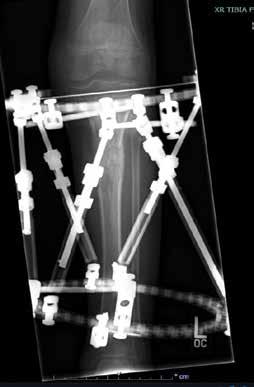
9-year-old boy had a physeal injury to his left tibia. He sustained a 5 cm leg length difference with a flexion deformity of his knee. He had a projected leg length difference 9.6 cm. He was treated with a hexapod external fixator to lengthen his leg 5 cm and correct his deformity. The tibia is now healed right before the external fixator is removed.

16-year-old boy with an idiopathic 4 cm leg length difference, right genu valgum and an osteochondroma.
He was treated with a lengthening intramedullary nail, acute correction of his knee dormity and excision of his osteochondroma.
Advancements in Digestive Health
By Shyam Varadarajulu, MD
The recently created Orlando Health Digestive Health Institute offers a comprehensive digestive disease program with areas of expertise including luminal gastroenterology, pancreatology, inflammatory bowel diseases, motility and hepatology. As president of the Orlando Health Digestive Health, I am excited about our new state-of-the-art facility in downtown Orlando, which will provide dedicated space to deliver care ranging from general GI procedures to subspecialized care for complex digestive disorders, as well as an opportunity to be at the leading edge of research with clinical trial that will bring innovation and treatment options not available elsewhere.
The new facility will house the Center for Advanced Endoscopy, Research and Education (CARE), featuring purpose-built space for advanced endoscopic services, together with the personnel and technical expertise needed for impactful clinical research and teaching. The dedicated area will be outfitted with the latest technologies to optimize clinical outcomes and maximize research productivity, including sophisticated endoscopic and fluoroscopic equipment, capability for artificial intelligence, and specific areas for observation and education.
GIFT CERTIFICATES ARE AVAILABLE
The Natural Way to Solve your Allergy, Sinus and Respiratory Discomfort.
ANTI-BACTERIAL | SIDE EFFECT FREE | ANTI-INFLAMMATORY SPECIALIZED POEM PROCEDURE
One of those advanced services is peroral endoscopic myotomy (POEM). This specialized endoscopic procedure addresses swallowing disorders such as achalasia, spastic esophageal conditions and esophagogastric junction outflow obstruction. Orlando Health is one of only five hospital systems in Florida to provide POEM treatment.
This advanced, minimally invasive therapeutic procedure to treat motility disorders of the esophagus is performed orally using high-definition upper endoscopes. This allows physicians to make mucosal incisions and subsequent submucosal tunneling to permanently relax tight esophageal muscles and open narrowed parts of the esophagus. No external cuts are required. “POEM gives us a very controlled method of cutting from inside the esophageal cavity for solving these complex disorders in a safe, effective manner,” says Ji Young Bang, MD, a boardcertified gastroenterologist and director of clinical research at the Orlando Health Digestive Health Institute Center for Advanced Endoscopy, Research & Education. An internationally recognized researcher in interventional endoscopy, Dr. Bang brings extensive experience in POEM to Orlando Health, having completed 150 of these procedures since 2017.
While POEM was developed specifically for one digestive disorder, it forms a foundation for other procedures like submucosal tunneling endoscopic resection (STER), endoscopic submucosal dissection and gastric peroral endoscopic myotomy (G-POEM). Each of these procedures differ slightly, but they are all a part of our arsenal of very advanced, complex endoscopy procedures that we can now offer to patients. A STANDARDIZED TREATMENT APPROACH
As an example of our passion for effecting meaningful contributions to research, Orlando Health Digestive Health Institute physicians are among the authors of a recently published journal article highlighting results from a study involving a new protocol to help standardize treatment options and improve clinical outcomes for patients who require endoscopic drainage of pancreatic fluid collections (PFC).1
Results from a retrospective, observational study of prospectively collected data among patients with symptomatic PFCs demonstrated significantly higher rates of endoscopic treatment success in patients treated with a combination of lumen-apposing metal stents (LAMS) and selective plastic stents (the Orlando Protocol) versus those treated with plastic stents alone. Additionally, the need for rescue surgery was significantly higher in patients treated with plastic stents alone compared with those treated using the Orlando Protocol. These results promise to bring a much-needed measure of standardization to PFC treatment.
Relieve Symptoms of: • Acne • Allergies • Asthma • Cold & Flu • Cystic Fibrosis • Dermatitis • Ear Infections • Eczema • Sinusitis
100%
NATURAL TREATMENT DRUG FREE
FUSION OF SCIENCE & NATURE
Kerri and Clay: “My son’s allergy medicines were causing terrible side effects. Now that we have been coming to The Salt Room we have been able to control his symptoms with salt therapy.”
Jessica L.: “My son looked and felt better after just one session. His cough wasn’t as bad. I felt he could breathe so much better.”
Joseph Cannizzaro, MD: “I have been recommending The Salt Room for years. It has helped my patients with respiratory nuisances and skin problems, reducing symptoms while we address the root cause to improve their long-term quality of life.”
407.862.1163 l 357 Wekiva Springs Rd., Longwood l www.SaltRoomLongwood.com ................

Traditionally, transluminal plastic stents have been placed to facilitate drainage in the endoscopic management of PFC. But today, LAMS are increasingly used instead of plastic stents, largely because of three distinct advantages LAMS offer: better drainage due to their larger diameter, less risk of peritoneal leakage and perforation due to their apposing nature, and technically easier stent deployment. Despite these advantages, there has been a lack of data validating the use of LAMS over plastic stents in patients with PFCs. By introducing a measure of standardization in PFC management, the Orlando Protocol can help to improve clinical outcomes in this complex group of patients.
Evidence supporting the Orlando Protocol is further strengthened by several additional considerations. These include significantly shorter procedural duration times for index interventions, which is an important advantage given the critically ill status of most patients, who likely cannot endure longer procedures. The Orlando Protocol also appears to be particularly useful for a subset of patients suffering from disconnected pancreatic duct syndrome, who have higher PFC recurrence rates. Utilizing the protocol can facilitate better drainage and reduce PFC recurrence in these patients, thereby reducing disease morbidity.
As one of the study authors, I can confidently state that this is the first time in the medical literature where a treatment protocol was validated prospectively for index interventions, reinterventions and follow-up, thereby standardizing the management approach outside of a clinical trial setting for patients with PFCs.
These are just two examples of the elevated level of services that the Orlando Health Digestive Institute will provide as a national and international destination for care.
References available by request
Shyam Varadarajulu, MD, is a board-certified gastroenterologist and president of the Orlando Health Digestive
Health Institute. He specializes in advanced endoscopy for the treatment of complex digestive disorders at the institute’s Center for Advanced
Endoscopy, R.esearch & Education. Dr. Varadarajulu is a sought-after researcher, educator and lecturer. He is widely published in peerreviewed journals and reference textbooks, and is currently editor of the textbook
ENDOSONOGRAPHY and a reviewer for more than 30 professional journals. After earning his medical degree at Madras Medical College in India, Dr. Varadarajulu completed his residency in internal medicine at St. Mary’s
Hospital in Rochester, New
York, followed by fellowships in gastroenterology at the
University of Connecticut and advanced endoscopy at the
Medical University of South
Carolina.
2022 EDITORIAL CALENDAR
Florida MD is a monthly medical/business digital magazine for physicians..
Florida MD is emailed directly to healthcare providers in Orange, Seminole, Flagler, Volusia, Osceola, Polk, Brevard, Lake and Indian River counties. Cover stories spotlight extraordinary physicians affiliated with local clinics and hospitals. Special feature stories focus on new hospital programs or facilities, and other professional and healthcare related business topics. Local physician specialists and other professionals, affiliated with local businesses and organizations, write all other columns or articles about their respective specialty or profession. This local informative and interesting format is the main reason physicians take the time to read Florida MD.
It is hard to be aware of everything happening in the rapidly changing medical profession and doctors want to know more about new medical developments and technology, procedures, techniques, case studies, research, etc. in the different specialties. Especially when the information comes from a local physician specialist who they can call and discuss the column with or refer a patient. They also want to read about wealth management, financial issues, healthcare law, insurance issues and real estate opportunities. Again, they prefer it when that information comes from a local professional they can call and do business with. All advertisers have the opportunity to have a column or article related to their specialty or profession. JANUARY – Digestive Disorders Diabetes
FEBRUARY – Cardiology Heart Disease & Stroke
MARCH – Orthopaedics Men’s Health
APRIL – Surgery Scoliosis
MAY – Women’s Health Advances in Cosmetic Surgery
JUNE – Allergies Pulmonary & Sleep Disorders
JULY – Neurology / Neuroscience Advances in Rehabilitation
AUGUST – Sports Medicine Robotic Surgery
SEPTEMBER – Pediatrics & Advances in NICUs Autism
OCTOBER – Cancer Dermatology
NOVEMBER – Urology Geriatric Medicine / Glaucoma
DECEMBER – Pain Management Occupational Therapy
ORTHOPEDICS CARE Just for kids.

Kids and teens need prompt and innovative care specifically designed for their growing bodies. We offer family-centered, kid-friendly care right here in Central Florida. Our expert team, including board-certified and fellowship-trained physicians, uses advanced technologies to diagnose and treat an extensive range of conditions through our highly specialized pediatric orthopedics programs.
From common to rare, we treat disorders and injuries involving bones, joints, muscles and nerves at Nemours Children’s Hospital, as well as our other specialty locations in: • Downtown Orlando • Lakeland • Lake Mary • Melbourne • Narcoosee Road • Winter Garden
Call 407.650.7715 to refer a patient. Well Beyond Medicine


