The President's Line
Fellow practitioners,
It was great seeing so many of you at PES! I am excited to announce registration for Ocala Equine Conference (OEC) 2023 is open! We’re proud to bring OEC 2023 to the new, state-of-the-art World Equestrian Center (WEC) from Jan. 20-22, 2023. One of the world’s most expansive, climatecontrolled indoor and outdoor equestrian sports facilities, WEC will serve as the stage for our dynamic, equine-exclusive continuing education.

I want to personally thank all the veterinary professionals who volunteered to assist in Hurricane Ian relief efforts. The devasting storm left many on the coast reeling, but the FVMA/FAEP in conjunction with the Florida Veterinary Corps offered boots-on-the-ground assistance. With the assistance of Dr. Terry Clekis, FVMA disaster response committee chair, the Florida Veterinary Corps deployed 86 individuals across impacted regions.
ADAM CAYOT DVM adamcayot@hotmail.com
SALLY A. L. DENOTTA DVM, PhD s.denotta@ufl.edu
The FVMA has also established the FVMA Foundation Hurricane Ian Relief & Recovery Fund. Powered by nearly $30,000 in donations, the fund is dedicated to assisting veterinarians who incurred out-of-pocket expenses due to storm-induced clinic damage or from providing medical care, food, or shelter to animals affected by the storm. All Florida veterinarians can apply for Hurricane Ian aid via the FVMA’s online form at fvma.org. If you are able, please consider donating to the fund through our website and assisting our fellow practitioners.
As the Florida legislative session (April 10 – June 8, 2023) begins gearing up, we ask that you pay special attention to your emails as we fight to protect veterinary medicine and animals in Florida. Your voice matters – we can’t win without you.
COREY MILLER DVM, MS, DACT cmiller@emcocala.com



ANNE L. MORETTA

VMD, MS, CVSMT, CVA maroche1@aol.com
JACQUELINE S. SHELLOW DVM, MS






FVMA PRESIDENT-ELECT jackie@shellow.com
Finally, enjoy the fall weather and holidays with your people. We hope to see you at OEC 2023!
Armon Blair, DVM
Ocala Equine Hospital
FAEP Council President
If anyone is struggling with mental wellness, please do not hesitate to reach out to colleagues, friends, or the FAEP (call 800.992.3862).
Our Membership Assistance Program (MAP), which is free for all members, offers personal and professional consultation to help you be your best. More information and wellness resources can be found at fvma.org
Opinions and statements expressed in The Practitioner reflect the views of the contributors and do not represent the official policy of the Florida Association of Equine Practitioners (FAEP) or the Florida Veterinary Medical Association (FVMA), unless so stated. Placement of an advertisement does not represent the FAEP’s or FVMA’s endorsement of the product or service.

2 The Practitioner Issue 3 • 2022
FAEP | 7207 MONETARY DRIVE, ORLANDO, FL 32809 | PH:
| FAX:
EMAIL:
800.992.3862
407.240.3710 |
INFO@FVMA.ORG | WEBSITE: WWW.FVMA.ORG


















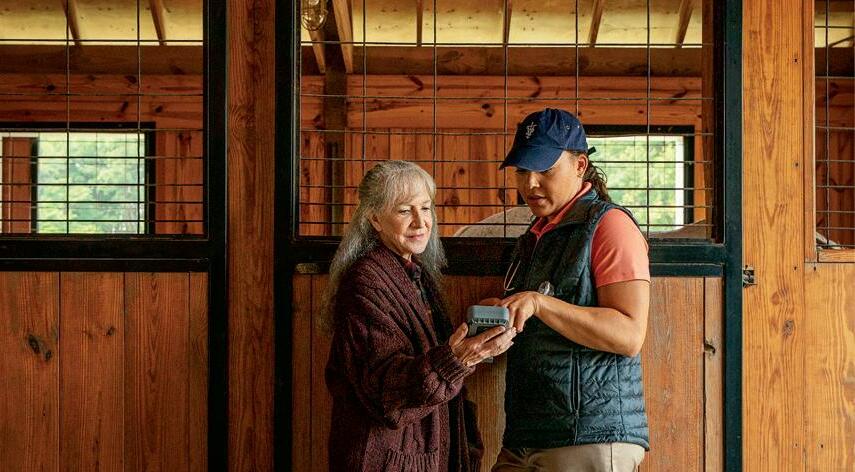
| The Practitioner 3 www.fvma.org | thefaep | @thefvma Visit WedgewoodPharmacy.com to view pricing and details. Mary, Account Manager, with Calvin MISOPROSTOL 1400mcg Apple-Molasses Flavored Gourmeds ® Wedgewood Pharmacy is now compounding: NEW! View Pricing FAEP Practitioner Ad 0822.indd 1 8/22/2022 2:23:38 PM Accidents happen. Learn how the AVMA Trust can shield your practice from devastating financial consequences. Is your workers’ compensation insurance provider well-versed in these common and costly accidents? Learn how insurance coverage through the AVMA Trust can meet the needs of a modern practice at avmaplit.com/WCadvantage. Exposure to Toxins and Chemicals Average Cost: $2,825 Employee Strains, Sprains, Trips and Slips Average Cost: $8,591 Animal Bites and Attacks Average Cost: $1,585
Huber, FVMA Industry Relations
It is with considerable pleasure and gratitude that we welcome our 2022-2023 educational partners. The FAEP established the educational partnership in 2012 and has enjoyed industry membership and support ever since. Some of these partners have been with us from the beginning, and all are key contributors to our successful equine outreach in Florida and beyond.

The importance of our educational partners cannot be overstated. Their support helps to fi nance the activities of the FAEP including the following key programs, events, and activities:
•The FAEP’s two annual conferences
∙
Ocala Equine Conference (OEC)
∙ Promoting Excellence Symposium (PES)
• Conference speaker programs
•Event activities and continued growth
•The FAEP’s equine journal, The Practitioner
• Emergency response initiatives throughout the U. S.

•Legislative advocacy in Tallahassee to promote healthy veterinary-related lawmaking by supporting key lobbyists and legislators who support our mission
Je Queen | 561-215-7089 jqueen@americanregent.com
Boehringer-


Stacie Sink | 484-467-1140 (North Florida) stacie.sink@boehringer-ingelheim.com
Heather Walston | 252-205-7372 (South Florida) heather.walsron@boehringer-ingelheim.com
Arenus
Brady Karren | 630-283-2158 brady.k@arenus.com
BiMeda Booth 57
Ed Howard | 630-828-1006 ehoward@BiMeda.com
Covetrus
Lynn Fedash | 954-614-2476 (South Florida)
Michaela Arcaro | 970-819-8909 michaela.arcaro@conturavet.com

lynn.fedash@covetrus.com
Kaylynne Brennan | 352-286-1567 (Central Florida) kaylynne.brennan@covetrus.com

4 The Practitioner Issue 3 • 2022
Ralph
WELCOMING OUR 2022-2023 FAEP EDUCATIONAL PARTNERS OUR 2022-2023 EDUCATIONAL PARTNERS
American Regent Booth 58
Animal Health Booth 55
Ingelheim Booth 59
Booth 51
ConturaVet Booth 54
The commitment from our educational partners is key to the success of our association’s mission. Our mutual support contributes to our partners’ sustained engagement in our programs and events.
Dechra Animal Health Booth 61
Shelly Derks | 913-302-0239 shelly.derks@dechra.com
Diedra de Bruin | 727-366-7462 diedre.debruin@dechra.com
Patterson Veterinary (Equine)

Booth 60
Gretchen Hill | 352-843-8822 (North and Central Florida)
Gretchen.hill@pattersonvet.com
Brian Conner | 315-335-0003 (South Florida) brian.conner@pattersonvet.com
Amber Moore | 386-689-9543 (North Florida, GA, AL) amber.moore@pattersonvet.com
Kentucky Performance Products Booth 50
Delia Nash | 859-361-2575 dnash@kppusa.com
Wedgewood Pharmacy Booth 53

Jenn Horner | 856-832-2336 (Headquarters) jhibbard@wedgewoodpharmacy.com
Merck Animal Health Booth 56
Steve Montemarano | 740-972-6554 steve.montemarano@merck.com
Zoetis Booth 52
Courtney VanDerbeck | 352-239-2039 (north Florida and south Georgia) courtney.vanderbeck@zoetis.com Barbara Lanigan | 561-309-7473 (South Florida) barbara.lanigan@zoetis.com
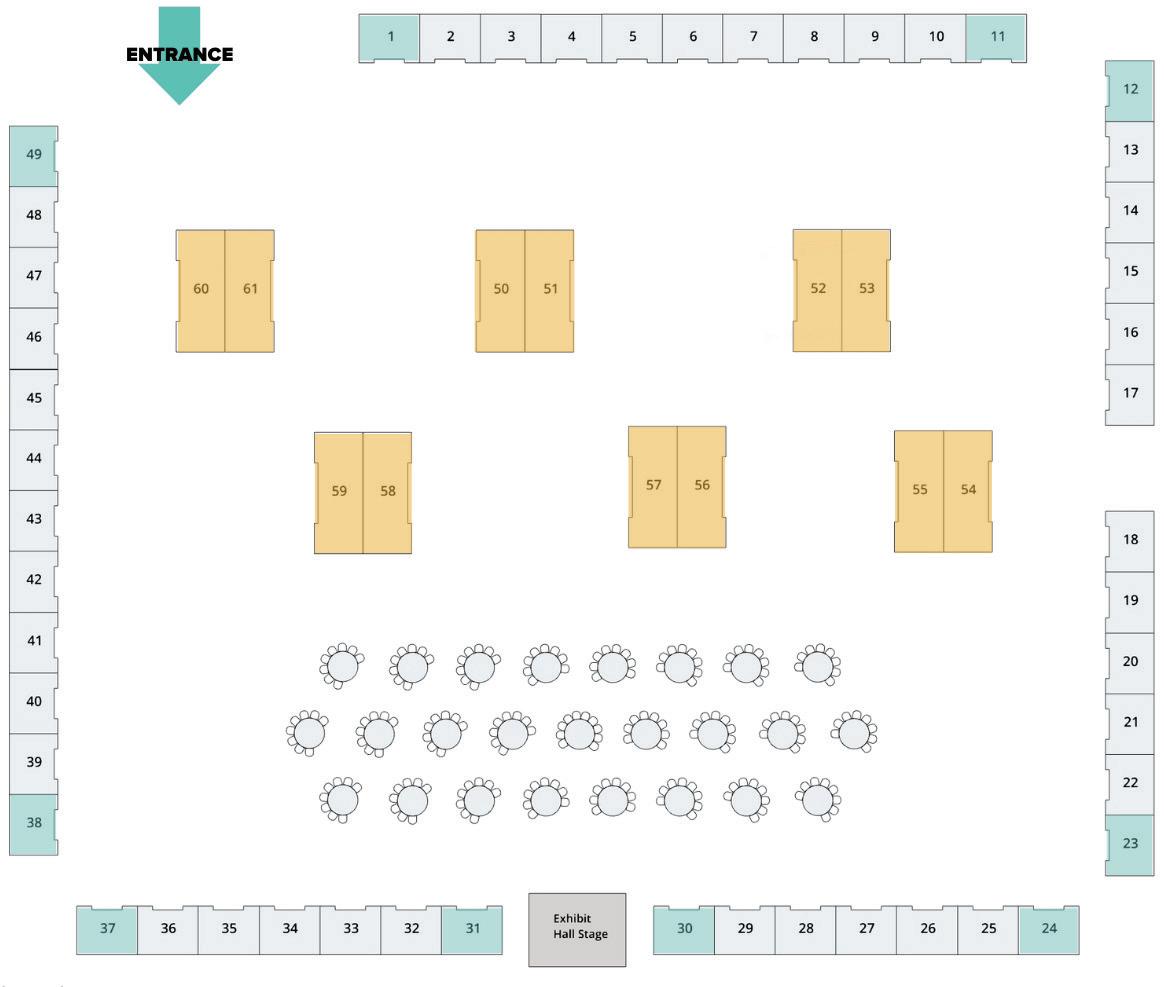
OUR EDUCATIONAL PARTNERS WILL BE AT OCALA EQUINE CONFERENCE THIS JAN. 20-22, 2023. WE ENCOURAGE YOU TO STOP BY THEIR BOOTHS TO SAY HELLO AND THANK THEM FOR THEIR CONTINUED SUPPORT.
By understanding your business, we can offer you the right resources and solutions to help your practice succeed. We are a full-service equine partner committed to helping you stay on top of industry advancements that impact the health of your practice and patients.
Through our continuing education, products, software, equipment and unrivaled service, we are here to help you keep your patients healthy and performing at their highest level. 800.279.6452 | pattersonvet.com/equine

5
EQUINE DIVISIO N
| The Practitioner
www.fvma.org | thefaep | @thefvma PARTNERSHIP.
20PE0003m (10/19)
OUR 2022-2023 EDUCATIONAL PARTNERS (CONT.)
Dr. Jacqueline S. Shellow DVM, MS

MEMBER SPOTLIGHT:
Dr. Jacqueline S. Shellow holds many titles: past president of the Florida Association of Equine Practitioners (FAEP) (2010), FAEP council member (2006-present), FAEP representative to the Executive Board of the Florida Veterinary Medical Association (FVMA) (2017-2022), FVMA Legislative Committee member (2008-present) and more, including president-elect of the FVMA. Despite her many hats, she never planned to be so involved.
“I don’t think anyone plans to become involved in organized veterinary medicine; it just happens!” she said. “Of course, I was a student member of all of them in veterinary school and then continued on after I started practicing; and then someone asks you to get more involved. I have a hard time saying no, and still do!”
First, it was being on committees for the American Association of Equine Practitioners (AAEP) and then the FAEP, which was founded to offer high-quality, equine-exclusive continuing education for Florida veterinarians. She became a board member of the FAEP, was heavily involved with the merging of the FAEP with the FVMA, and since then has only become more committed to organized veterinary medicine.
Growing up in South Florida in a house in an avocado grove, Dr. Shellow’s family and neighbors had lots of animals. She started caring for and riding horses at an early age and joined the Saddle Tramps 4-H Club in Miami, where she met key mentors who are still her good friends today. Around that time, she also met equine veterinarian, Dr. Tom Brokken, who she ended up working with after graduating from the University of Florida College of Veterinary Medicine (UFCVM) in 1987.
“Back then, besides racetrack work, Teigland, Franklin, Brokken (TFB Equine) did farm work in South Florida,” Dr. Shellow said. “In 1990, when Dr. Teigland retired, I became a partner, and they became primarily a Thoroughbred racetrack practice. I practiced equine racetrack medicine with TFB Equine and traveled with my clients and their horses for over 30 years.”
Prior to veterinary school at the University of Florida, Dr. Shellow attended Stephens College and then the University of Kentucky, where she obtained a master’s degree in equine nutrition. In 1994, she was certified in veterinary acupuncture by the International Veterinary Acupuncture Society, and in 1998, certified in animal chiropractic by the American Veterinary Chiropractic Association. Dr. Shellow continued her work with TFB Equine until 2019. She now works part time at the Embassy Lakes

Animal Hospital, a small animal hospital in Cooper City, Fla. and also fills in as an examining track veterinarian at Gulfstream Park – a role she also filled for Hollywood Greyhounds and Palm Beach Kennel Club until Greyhound racing ended in Florida.
“It has been wonderful,” Dr. Shellow said of her experience in the profession. “I love working on racehorses. I love working on athletes. I’ve worked on some awesome horses over the years and had some great clients. I worked with racing Greyhounds and fell in love with them also.”
Besides adopting one and then fostering a few more, she has been involved with a Greyhound adoption group that works tirelessly finding these retired racers good forever homes, in addition to training some to become service dogs for veterans.
Her work and commitment to veterinary medicine has earned her much recognition over the years. In 2010, the FVMA named
| The Practitioner 7 www.fvma.org | thefaep | @thefvma
Dr. Shellow with her horse, Boots. Image courtesy of Joanna Jodko.
Dr. Shellow as a Gold Star Award winner for her work as liaison between the FVMA and the FAEP, and in 2014 she was the FVMA’s Veterinarian of the Year.
Outside of veterinary medicine, Dr. Shellow likes to spend time with her family, her animals, and traveling, especially on her bike. She enjoys being outside biking, running, hiking, and practicing yoga.


Her best advice to new veterinarians is to find good mentors.
“I have had some great mentors throughout my career and am very grateful. Many were also involved in their professional associations or in organized veterinary medicine and encouraged me to be involved and give back to my profession – and, of course, the animals.”

8 The Practitioner Issue 3 • 2022
Dr. Shellow with her beloved Romeo, a retired racing Greyhound that she adopted. Image courtesy of Dr. Jacqueline S. Shellow.
Dr. Shellow with friend and mentor, Dr. Tom Brokken of TFB Equine, who was also past president of the AAEP and is pictured here receiving the FAEP Lifetime Achievement Award.
Image courtesy of Dr. Jacqueline S. Shellow.
Dr. Shellow with her dogs. Image courtesy of Dr. Jacqueline S. Shellow.

| The Practitioner 9 www.fvma.org | thefaep | @thefvma
Dr. Shellow with her late husband, Barry Faske, who sadly passed away this year.
Images courtesy of Dr. Jacqueline S. Shellow.



 Image courtesy of Canva
Image courtesy of Canva
ALTERNATIVE IMAGING TECHNIQUES FOR EVALUATION OF THE PURCHASE EXAMINATION
RICHARD D. MITCHELL | DVM, MRCVS, DIPL. ACVSMR
Take Home Message








The examination for purchase may present issues that are difficult to interpret, complicating the ability to provide the client with practical advice. The use of multiple imaging modalities may clarify issues that arise. Radiography has been the gold standard for imaging in the purchase examination process, but ultrasound, thermography, nuclear scintigraphy, MRI, and CT may enhance the veterinarian’s ability to give good advice to the client. Newer imaging technologies may be integrated to offer a more complete assessment.
Digital Radiography
The decision of what to image radiographically can be the subject of much debate.
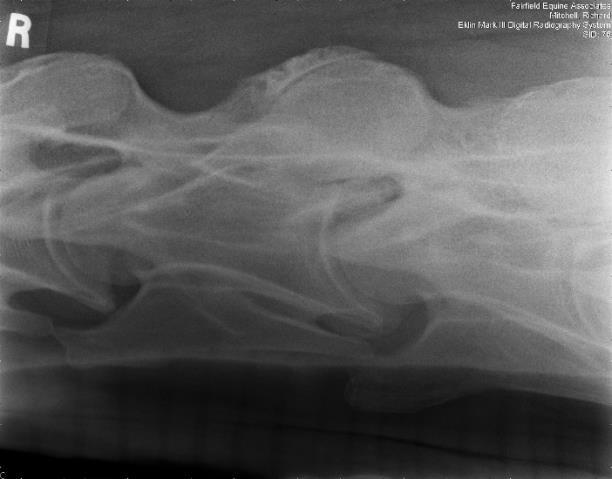
Knowledge of the discipline in which the horse is to function is essential in order to make appropriate decisions related to imaging. With the English sport horse or Western performance horse, certain common lameness issues are known to occur more frequently, and the choice of what regions to radiograph should be based on likely probability. Additionally, any other skeletal fi ndings that raise concern during the resting physical and exercise examinations should also be evaluated. Good positioning and technique are critical for consistent evaluations.1 Radiographic examination may expose old problems that have since resolved. Some injuries, such as suspensory enthesopathies, will remain radiographically evident but may predispose to injury in the future. Having access to previous radiographs can be extremely valuable in the assessment of the significance of abnormal fi ndings. For example, a proximal plantar P1 fragment in a hind fetlock may not represent as much risk for future hind limb lameness when found in a 10-year-old jumper if it was known to be there when the horse was four years old (Figure 1.). Comparison to previous radiographs may also help predict the long term significance and progression of some lesions as well. For example, moderate osteoarthritic changes associated with a pastern joint in a warmblood found in today’s examination may carry less significance if known to have been there on radiographs two years prior.

The radiographic examination may produce results that seem inconsistent with the physical examination. Bony lesions may be identified that one would expect to be related to lameness, yet the horse is sound. Further radiographic images using less routine projections may be necessary for a more complete evaluation. Other imaging techniques, such as ultrasound or scintigraphy, can be employed in order to yield more information about the significance of a radiographic fi nding. A subsequent second physical examination on a different day may also be of
benefit. As mentioned previously, previous images of the horse that demonstrate the existence of a lesion for several years are important for interpreting current clinical significance.

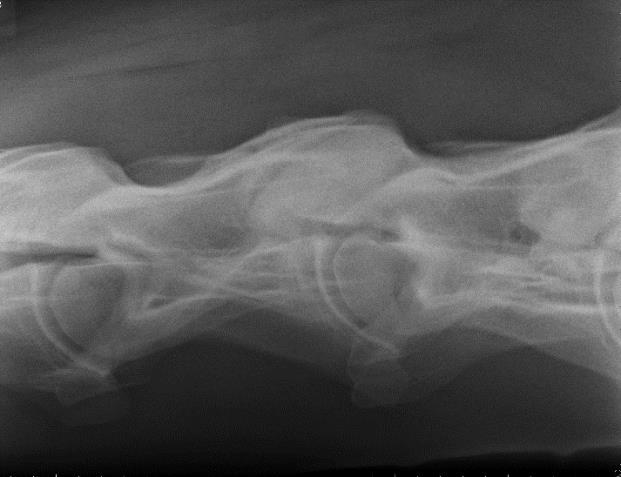
The development and advancement of digital radiography has allowed for diagnostic field radiographs of the neck and some parts of the thoracolumbar spine. Lateral images of the cervical spine may demonstrate the presence of osteoarthritis, vertebral anomalies, and abnormalities of the vertebral canal, such as stenosis. One can also acquire very diagnostic oblique images of the cervical articular processes with practice (Figures 2A and 2B).
Portable generators in the 80 to 90 kVp range enable one to acquire diagnostic images of some thoracic vertebral bodies and articular process joints in the field. Care needs to be taken to minimize radiation exposure for the operators.
| The Practitioner 11 www.fvma.org |
thefaep | @thefvma
Figure 1: A proximal plantar P1 fragment in an eight-year-old warmblood presented for purchase examination, demonstrating no effusion or lameness.
Image courtesy of Dr. Richard D. Mitchell.
Portable generators in the 80 to 90 kVp range enable one to acquire diagnostic
abnormalities of the vertebral canal, such as stenosis. One can also acquire very diagnostic
oblique images of the cervical articular processes with practice.(Figs. 2A and 2B).
abnormalities of the vertebral canal, such as stenosis. One can also acquire very diagnostic oblique images of the cervical articular processes with practice.(Figs. 2A and 2B).
some thoracic vertebral bodies and articular process joints in the field. Care needs minimize radiation exposure for the operators.
RFigure 2A: Field radiograph using portable machine and DR technology demonstrating enlargement of an articular process joint. Cranial is to the left.
Fig. 2A: Field radiograph using portable machine and DR technology demonstrating enlargement of an articular process joint. Cranial is to the left.
Fig. 3 Oblique thoracic image of a 16.2 hand Warmblood, 84 KVP/.18 sec generator, demonstrating marked, multifocal, ventral spondylosis. Such lesions associated with stiffness and poor performance, in the author’s experience
Fig. 2A: Field radiograph using portable machine and DR technology demonstrating enlargement of an articular process joint. Cranial is to the left.
Image courtesy of Dr. Richard D. Mitchell.
Thermography
Figure 3: Oblique thoracic image of a 16.2 hand Warmblood, 84 KVP/.18 sec with a portable generator, demonstrating marked, multifocal, ventral spondylosis. In the author’s experience, such lesions may be associated with stiffness and poor performance. Image courtesy of Dr. Richard D. Mitchell.
indicate deviations in expected patterns that may be further evaluated by other means. Muscle pathology in various regions may be detectable using thermal imaging. Such tools may also be used to monitor resolution of inflammation on subsequent examinations.3
Thermal imaging can be a useful screening tool for the purchase examination. horse, scanning the limbs and back in general with a modern infrared camera can and reasonably quick to perform. Early pathology in the distal limb may be detectable foot balance issues that are producing subtle inflammatory changes. Thermographs may indicate deviations in expected patterns that may be further evaluated by other as?. Muscle pathology in various regions (examples?) may be detectable using Such tools may also be used to monitor resolution of inflammation on subsequent
Fig. 2B: Field radiograph using portable machine and DR technology demonstrating articular process osteoarthritis (oblique view). Cranial is to the left
Figure 2B: Field radiograph using portable machine and DR technology demonstrating articular process osteoarthritis (oblique view). Cranial is to the left.
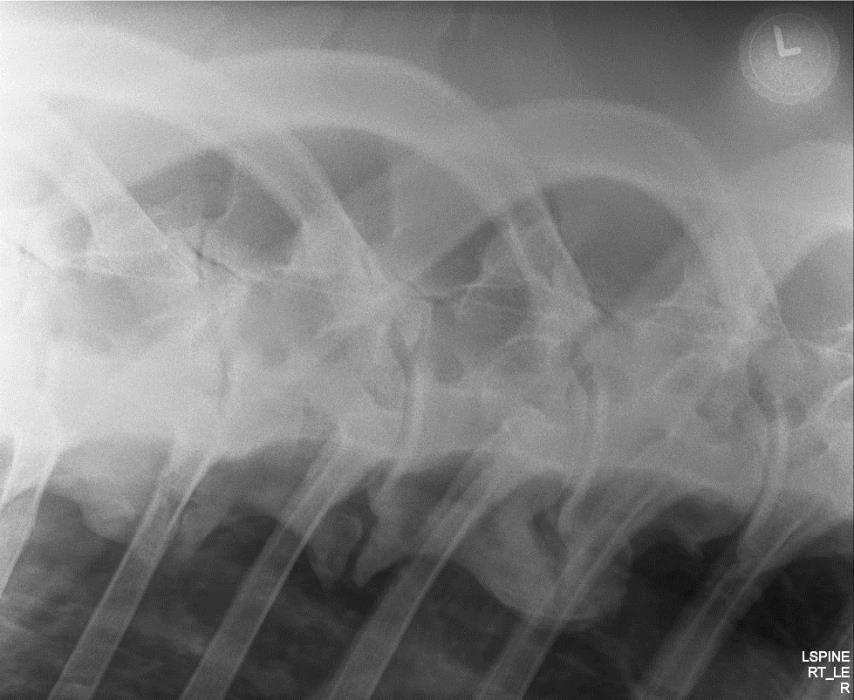
Fig. 2B: Field radiograph using portable machine and DR technology demonstrating articular process osteoarthritis (oblique view). Cranial is to the left
Image courtesy of Dr. Richard D. Mitchell.
Thermography
Thermal imaging can be a useful screening tool for the purchase examination. For the sport horse, scanning the limbs and back in general with a modern infrared camera can be beneficial and reasonably quick to perform. Early pathology in the distal limb may be detectable as well as foot balance issues that are producing subtle inflammatory changes. 2 Thermographs of the back may
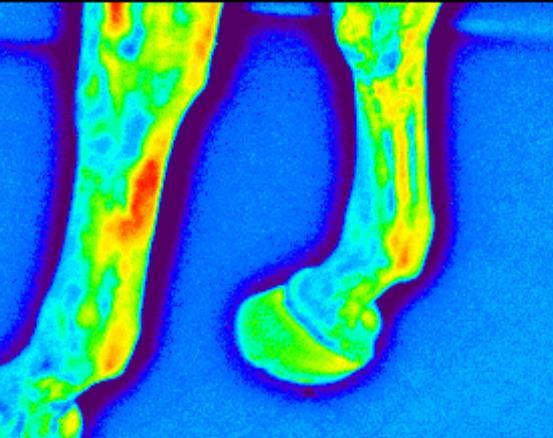
Fig. 4: The above image indicates an area of possible inflammation metacarpal region that may justify a closer look with ultrasound
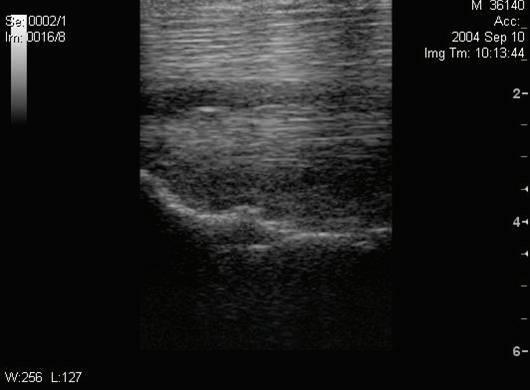
Figure 4: The above image indicates an area of possible inflammation in the left palmar metacarpal region that may justify a closer look with ultrasound imaging.
Ultrasonography
Image courtesy of Dr. Richard D. Mitchell.
The soft tissue structures of the metacarpal and metatarsal regions examined with ultrasound during purchase examinations. Previous screening may have suggested soft tissue inflammation in a specific
12 The Practitioner Issue 3 • 2022
R
significant DFTS effusion is noted. The palmar fetlock and pastern, dorsal and dorsal coronet may also be examined if indicated
Ultrasonography

The soft tissue structures of the metacarpal and metatarsal regions are most commonly examined with ultrasound during purchase examinations. Previous palpation or thermography screening may have suggested soft tissue inflammation in a specific region that may be more completely evaluated with ultrasound.
There is a high incidence of suspensory ligament injury in jumper, dressage, and event horses.4 Similarly, injury to the flexor tendons and digital flexor tendon sheath (DFTS) is not infrequent with varying distribution of affected structures between the fore and hindlimbs.5 The tendinous and ligamentous structures of the pastern can also be injured and ultrasonographic assessment of this region should be included if physical examination fi ndings, such as swelling and sensitivity, sufficiently raise suspicion about these areas. The size, shape, and fiber pattern of the distal sesamoidean ligaments and flexor tendons should be compared between affected and non-affected limbs. The degree of DFTS eff usion and synovial proliferation as well as the thickness of the annular ligaments can also be evaluated.
Knowledge of the complicated anatomy of the lower limb is required for proper evaluation, but the majority of the tendinous and ligamentous structures proximal to the distal sesamoidean (navicular) region can be readily imaged. 6 Good preparation of the site to be examined is essential. Clipping is not always an option in a horse offered for sale, and if the horse’s hair coat is such that diagnostic images are not possible one can ask the seller or the agent for permission to clip. If done, this should be in a careful and symmetrical manner so as not to “label” the horse. Many show horses have very short hair coats that do not present an issue for ultrasound examination while others may be more challeng ing. If the examination will be compromised by hair coat such that the images are non-diagnostic, the client should be so informed.
Fig. 6: Ultrasound images of a right fore palmar pastern that was palpation demonstrating a lesion in the right straight distal sesamoidean normal left pastern is on the left.
Figure 6: Ultrasound images of a right fore palmar pastern that was mildly thickened on palpation demonstrating a lesion in the right straight distal sesamoidean ligament. The normal left pastern is on the left.
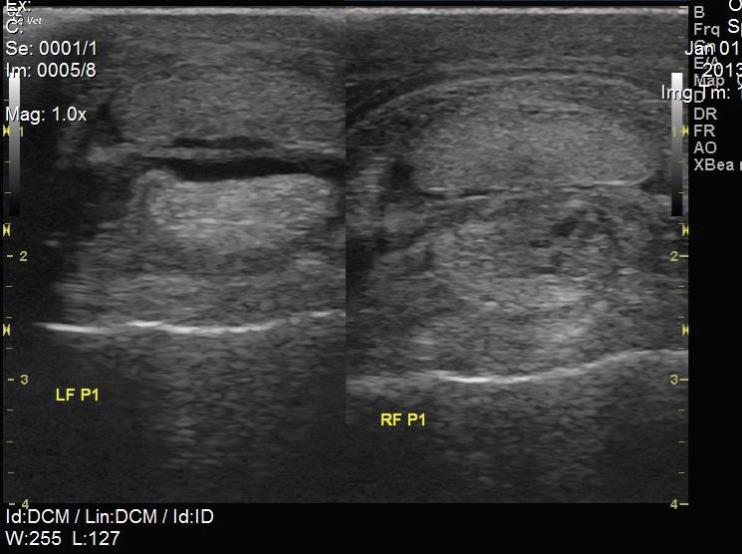
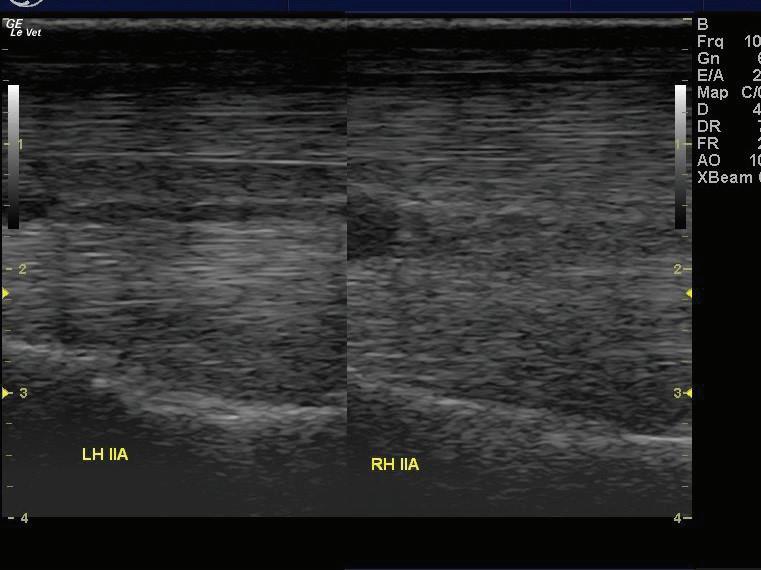
Image courtesy of Dr. Richard D. Mitchell.
Knowledge of the complicated anatomy of the lower limb is required for proper evaluation, but the majority of the tendinous and ligamentous structures proximal to the distal sesamoidean (navicular) region can be readily imaged.6 Good preparation of the site to be examined is essential. Clipping is not always an option in a horse offered for sale, and if the horse’s hair coat is such that diagnostic images are not possible one can ask the
seller or the agent for permission to clip. If done, this should be completed in a careful and symmetrical manner so as not to “label” the horse. Many show horses have very short hair coats that do not present an issue for for ultrasound examination, while others may be more challenging. If the examination will be compromised by hair coat such that the images are nondiagnostic, the client should be so informed.
The solar aspect of the foot, with some trimming and soaking preparation examined by a transcuneal approach to visualize the distal deep digital the navicular bone and the insertion of the DDFT on P3. 7 This technique utilized when there was a high suspicion of palmar foot pain and may (This technique may prove difficult in hot, dry climates without extensive soaking.) A 7.5-8 MHz linear probe works well for this view. The proximal navicular bone, the navicular bursa, deep digital flexor tendon, and collateral
As for the distal limb, the proximal third of the collateral ligaments of the distal interphalangeal joint (DIPJ) may be evaluated with a 7.5-10 MgHz linear transducer on the medial and lateral aspects of the coronet band. Significant response to distal limb flexion and evidence of DIPJ eff usion might suggest looking at these structures. Th is technique requires special preparation of the coronet with clipping (in some cases) and thorough hydration of the skin along with some practical experience. The middle and distal thirds of the DIPJ collateral ligaments cannot be visualized due to acoustic impedance from the hoof wall.
As previously mentioned, the palmar or plantar pastern should be examined if thickening or significant DFTS eff usion is noted. The palmar fetlock and pastern, dorsal fetlocks and pastern, and dorsal coronet may also be examined if indicated.
Fig. 5: Left hind suspensory origin is thickened with an inhomogeneous fiber pattern. The origin enthesis is irregular compared to the right hind. The horse demonstrated a mild left hind lameness but no obvious enlargement on palpation.
Figure 5: Left hind suspensory origin is thickened with an inhomogeneous fiber pattern. The origin enthesis is irregular compared to the right hind. The horse demonstrated a mild left hind lameness but no obvious enlargement on palpation. Image courtesy of Dr. Richard D. Mitchell.
As for the distal limb, the proximal third of the collateral ligaments of the distal interphalangeal joint (DIPJ) may be evaluated with a 7.5-10 MgHz linear transducer on the medial and lateral aspects of the coronet band. Significant response to distal limb flexion and evidence of DIPJ effusion might suggest looking at these structures. This technique requires
The solar aspect of the foot, with some trimming and soaking preparation of the frog, may be examined by a transcuneal approach to visualize the distal deep digital flexor tendon (DDFT), the navicular bone, and the insertion of the DDFT on
| The Practitioner 13 www.fvma.org | thefaep | @thefvma
P3.7 Th is technique would likely only be utilized when there was a high suspicion of palmar foot pain and may require a followup visit. (Th is technique may prove difficult in hot, dry climates without extensive poulticing and soaking.) A 7.5-8 MHz linear probe works well for this view. The proximal aspect of the navicular bone, the navicular bursa, deep digital flexor tendon, and collateral sesamoidean ligaments may be visualized with an 8 MHz microconvex probe placed between the bulbs of the heel. A limited view is available but may demonstrate evidence of distal deep digital flexor abnormalities, navicular bursal eff usion, and thickening of the collateral sesamoidean ligaments. Again,
this is a technique that requires some practical experience and good anatomical knowledge.
If, in the course of the examination, local pain or stiffness in the neck is noted, ultrasound examination may be very helpful in evaluating the cranial and dorsal margins of the articular processes and the degree of eff usion and capsular thickening/ capsulitis. Back pain may be further evaluated with ultrasound by evaluating structures such as the spinous processes, supraspinous ligament, and thoracolumbar articular process joints.
If in the course of the examination, local pain or stiffness in the neck is noted, ultrasound examination may be very helpful in evaluating the cranial and dorsal margins of the articular processes and the degree of effusion and capsular thick ening/capsulitis. Back pain may be further evaluated with ultrasound by evaluating structures such as the spinous processes , supraspinous
Nuclear Scintigraphy
Often a horse may demonstrate a faint lameness or radiographic findings of the feet and navicul ar bone that are suspicious of pathology. Many exceptional equine athletes may exhibit


14 The Practitioner Issue 3 • 2022
Figure 8: Illustration of probe position across a cervical facet and resultant image demonstrating an osteophyte and fluid within the joint capsule.
Image courtesy of Dr. Richard D. Mitchell.
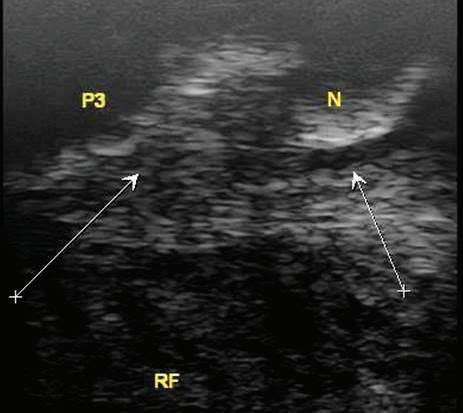
Fig. 7: Transcuneal ultrasound image and corresponding anatomy of the navicular bone and distal deep digital flexor tendon viewed with 8 MHz linear probe.
thoracolumbar articular process joints
Figure 7: Transcuneal ultrasound image and corresponding anatomy of the navicular bone and distal deep digital flexor tendon viewed with 8 MHz linear probe.
Image courtesy of Dr. Richard D. Mitchell.
Fig. 8: Illustration of probe position across a cervical facet and resultant image demonstrating an osteophyte and fluid within the joint ca psule.
Nuclear Scintigraphy
Often, a horse may demonstrate a faint lameness or radiographic fi ndings of the feet and navicular bone that are suspicious of pathology. Many exceptional equine athletes may exhibit mild issues in various areas, and clients are still interested in purchasing them. If additional radiographic images are not conclusive or not possible, nuclear scintigraphy may aid the decision process, if available. Th is is the buyer’s choice and fi nancial responsibility, but the seller must be willing to allow this semi-invasive procedure. Areas of increased radiopharmaceutical uptake (IRU) are characteristic of some structures in working horses and knowledge of this is required, 8 but this imaging modality can be extremely helpful in evaluating the significance of the fi ndings of other modalities such as radiography and ultrasound.


Radiographically abnormal navicular bones can sometimes be attributable to individual variation, and comparison between contralateral limbs is vital. However, a radiographically abnormal navicular bone that demonstrates intense IRU on scintigraphy is more likely to be indicative of inflammation and is of greater clinical significance than one with a normal uptake pattern.

Fig
Figure
image of the left proximal metatarsus demonstrating lysis and sclerosis at the suspensory ligament origin. Ultrasound indicates abnormal dorsal fiber pattern and an irregular bony origin.
Image
Figure 9: Abnormally shaped navicular bone with proximal enthesophyte formation in a horse with faint lameness that subsequently demonstrated intense radiopharmaceutical uptake on scintigraphic imaging.

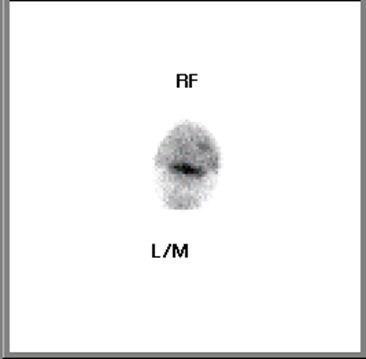
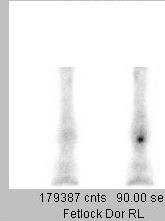
Figure 11: Nuclear scintigraphic images of the left hind limb of the same horse in Figure 10, demonstrating IRU at the origin of the left hind suspensory ligament. The right hind by comparison, in the image on the right, appears to be within normal limits.
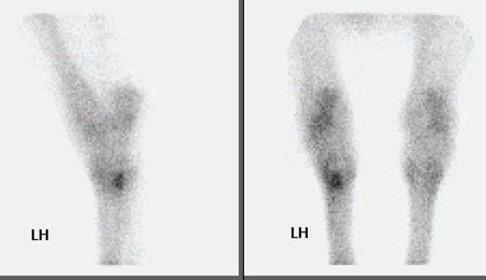
Image courtesy of Dr. Richard D. Mitchell.
Fig 11: Nuclear scintigraphic images of the left hind limb of the same horse in Fig 10 demonstrating IRU at the origin of the left hind suspensory ligament. The right hind comparison, in the image on the right, appears to be within normal limits. Variations of normal anatomy may be innocent but can in some cases be the tell-tale signs developing pathology. Investigating such findings with a combination of imaging techniques may prevent unfortunate consequences later. An example follows in Fig.12-14
Fig.9: Abnormally shaped navicular bone with proximal enthesophyte formation in a horse with faint lameness that subsequently demonstrated intense radiopharmaceutical uptake on scintigraphic imaging.
Image courtesy of Dr. Richard D. Mitchell.
Variations of normal anatomy may be innocent but can in some cases be the tell-tale signs of developing pathology. Investigating such fi ndings with a combination of imaging techniques may prevent unfortunate consequences later. An example follows in Figures 12, 13, and 14.
Radiographic and ultrasonographic findings may be concerning for origin lesion. Nuclear scintigraphy can be useful in assessing the current state of in the proximal palmar/plantar metacarpus/tarsus and therefore providing valuable information by which the clinician may predict outcomes. An example follows in Fig.
Radiographic and ultrasonographic fi ndings may be concerning for a possible suspensory origin lesion. Nuclear scintigraphy can be useful in assessing the current state of activity in the proximal palmar/plantar metacarpus/tarsus and therefore providing valuable information by which the clinician may predict outcomes. An example follows in Figures 10 and 11.
Fig 12: Purchase examination image on the left and lameness examination image on right 6 months post-purchase that blocked to an abaxial sesamoid block. Area of sclerosis and region of subchondral injury of the sagittal groove of the proximal first phalanx which may be enhanced by a slightly flatter beam angle.
| The Practitioner 15
|
www.fvma.org
thefaep | @thefvma
10: Radiographic image of the left proximal metatarsus demonstrating lysis and sclerosis at the suspensory ligament origin. Ultrasound indicates abnormal dorsal fiber pattern and an irregular bony origin.
courtesy of Dr. Richard D. Mitchell.
on scintigraphic imaging
Radiographic and ultrasonographic findings may be concerning for a possible suspensory origin lesion. Nuclear scintigraphy can be useful in assessing the current state of activity in the proximal palmar/plantar metacarpus/tarsus and therefore providing valuable information by which the clinician may predict outcomes. An example follows in Fig. 10&11
10: Radiographic
Variations of normal anatomy may be innocent but can in some cases be the tell-tale signs of developing pathology. Investigating such findings with a combination of imaging techniques may prevent unfortunate consequences later. An example follows in Fig.12-14
demonstrating subchondral osseous fluid associated was associated with an incomplete sagittal sulcus
Fig 12: Purchase examination image on the left and lameness examination image on the right 6 months post-purchase that blocked to an abaxial sesamoid block. Area of sclerosis and region of subchondral injury of the sagittal groove of the proximal first phalanx (P1) which may be enhanced by a slightly flatter beam angle.
Figure 12: Purchase examination image on the left and lameness examination image on the right six months post-purchase that blocked to an abaxial sesamoid block. Area of sclerosis and region of subchondral injury of the sagittal groove of the proximal first phalanx (P1) which may be enhanced by a slightly flatter beam angle.
Image courtesy of Dr. Richard D. Mitchell.
Figure
Fig. 14: Post-surgical image of the previously noted placement. The patient was responding favorably.
Image
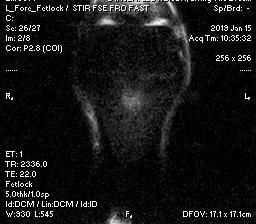
Fig. 13: Nuclear scintigraphic image(left) showing focal zone of IRU on the proximal aspect of the left front first phalanx (P1) and corresponding dorsal plane MRI STIR image demonstrating subchondral osseous fluid associated with subchondral bone injury which was associated with an incomplete sagittal sulcus fracture.
Figure 13: Nuclear scintigraphic image (left) showing focal zone of IRU on the proximal aspect of the left front first phalanx (P1) and corresponding dorsal plane MRI STIR image demonstrating subchondral osseous fluid associated with subchondral bone injury which was associated with an incomplete sagittal sulcus fracture.
Image courtesy of Dr. Richard D. Mitchell.
The previous set of figures illustrate a subtle lesion examination that in retrospect led to a problem that certainly can be rewarding to identify an issue that should be taken not to overinterpret the significance
The previous set of figures illustrate a subtle lesion that went unrecognized in the purchase examination that in retrospect led to a problem that was fortunately successfully resolved. It certainly can be rewarding to identify an issue that might lead to subsequent problems, but care should be taken not to overinterpret the significance of radiographic findings and excessively negatively prognosticate, particularly when the horse is not currently exhibiting signs of lameness. Litigation has been pursued in cases for failure to identify abnormalities during a prepurchase examination and also in cases in which the veterinarian assigned unfounded, excessive risk to the purchase of a horse. Seeking a second opinion on peculiar findings, especially for the less experienced clinician, is often much appreciated by the buyer and seller alike.
Magnetic Resonance Imaging (MRI)
The advent of standing MRI has made this imaging technique much more practical and available for the further investigation of suspected problems discovered in the purchase examination. Advances in technology have made good-quality images possible in the standing horse, reducing the need for general anesthesia in many cases involving the distal limb. A seller may find this
Fig. 14: Post-surgical image of the previously noted left front fetlock six months after screw placement. The patient was responding favorably. The previous set of figures illustrate a subtle lesion that went unrecognized in the purchase examination that in retrospect led to a problem that was fortunately successfully resolved. It certainly can be rewarding to identify an issue that might lead to subsequent problems, but care should be taken not to overinterpret the significance of radiographic findings and excessively



16 The Practitioner Issue 3 • 2022
14: Post-surgical image of the previously noted left front fetlock six months after screw placement. The patient was responding favorably.
courtesy of Dr. Richard D. Mitchell.
is a more acceptable way to allow the horse to be imaged. The modality is especially useful for the evaluation of suspected issues in the distal limb and within the hoof capsule.9 MRI is not a screening tool but is very useful for examining structural details and detecting inflammation in specifically targeted areas. Examples would be suspected subchondral cyst-like structures, an abnormal navicular bone found on routine radiography, or suspected tendon or ligament pathology on ultrasound.
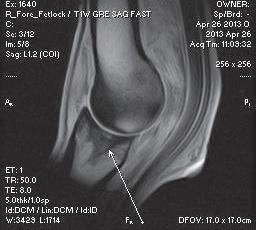
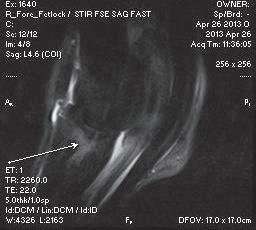

An example of a purchase examination where MRI was very helpful follows: The horse in question was a 12-year-old Grand Prix Dressage horse that had been successfully competing in FEI classes in Europe. Physical examination was unremarkable except for positive distal limb flexion tests in both forelimbs. There was no apparent lameness working on a lunge or under saddle. Radiographs indicated some varying bone densities in the subchondral bone of proximal P1in both forelimbs, suggestive of subchondral bone injury. An MRI unit was conveniently located nearby and an examination was recommended. A standing MRI examination of both fore fetlock regions was performed. Radiographic and MRI images are shown in Figure 16 and 17. Significant pathology was identified in the subchondral bone of proximal P1 in both forelimbs on radiography that appeared to be active on MRI (bone fluid or edema) (Figure 15). The horse was also discovered to have similar radiographic lesions in the RH fetlock.
The right fore fetlock appeared to have a more distinct area of intraosseous fluid signal and subchondral defects that presented a high risk for affecting future soundness (Figure 17). Th is information resulted in the buyer declining the purchase of the horse.
fetlock regions was performed Radiographic and MRI images are shown in Fig. 16 & 17. Significant pathology was identified in the subchondral bone of proximal P1 in both fore limbs on radiography that appeared to be active on MRI (bone fluid or edema) (Fig 15?). The horse was also discovered to have similar radiographic lesions in the RH fetlock.
The right fore fetlock appeared to have a more distinct area of intraosseous fluid signal and subchondral defects that presented a high risk for affecting future soundness (Fig 17) This information resulted in the buyer declining the purchase of the horse.
MRI provides a means by which to evaluate the current activity of bone lesions and accompanying soft tissue changes. While nuclear scintigraphy may give some idea of local bone activity or increased blood flow, MRI adds the benefit of providing information regarding osseous structure as well.
MRI provides a means by which to evaluate the current activity of bone lesions and accompanying soft tissue changes. While nuclear scintigraphy may give some idea of local bone activity or increased blood flow, MRI adds the benefit of providing information regarding osseous structure as well.

Computed Tomography (CT)
Recent developments in in computed tomography are increasing the availability of this technology for the equine patient.8 Standing units (Fig 18) have been developed which allow for imaging of the head, neck, and distal limbs.a As standing units become more available, this modality can be used to further interrogate questionable osseous radiographic findings in the purchase examination process. Utilization of standing units requires less sedation and
Computed Tomography (CT)
Recent developments in computed tomography are increasing the availability of this technology for the equine patient. 8 Standing units (Figure 18) have been developed which allow for imaging of the head, neck, and distal limbs.a As standing units become more available, this modality can be used to further interrogate
a Asto CT LLC 3300 Commercial Avenue Madison, WI 53714
a Asto CT LLC 3300 Commercial Avenue Madison, WI 53714
| The Practitioner 17 www.fvma.org |
thefaep | @thefvma
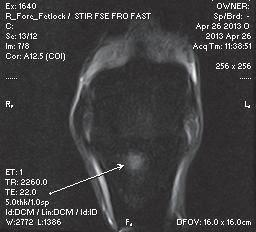
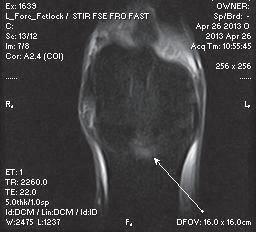
Figure 15: Radiographic images of both fore fetlocks demonstrating subchondral sclerosis and focal lucent areas bilaterally.
Image courtesy of Dr. Richard D. Mitchell.
Fig. 15: Radiographic images of both fore fetlocks demonstrating subchondral sclerosis and focal lucent areas bilaterally.
Fig. 16: Dorsal plane MRI STIR images of both fore fetlocks demonstrate focal zones of hyperintense signal indicative of osseous fluid in proximal P1.
Figure 16: Dorsal plane MRI STIR images of both fore fetlocks demonstrate focal zones of hyperintense signal indicative of osseous fluid in proximal P1. Image courtesy of Dr. Richard D. Mitchell.
Fig. 15: Radiographic images of both fore fetlocks demonstrating subchondral sclerosis and focal lucent areas bilaterally.
Fig. 16: Dorsal plane MRI STIR images of both fore fetlocks demonstrate focal zones of hyperintense signal indicative of osseous fluid in proximal P1.
Figure 17: Sagittal MRI images of the right fore fetlock (STIR on the left and T1 on the right) demonstrate an extensive lesion associated with the sagittal groove that is indicative of subchondral bone injury or possibly incomplete fracture.
Image courtesy of Dr. Richard D. Mitchell.
Fig. 17: Sagittal MRI images of the right fore fetlock (STIR on the left and T1 on the right demonstrate an extensive lesion associated with the sagittal groove that is indicative of subchondral bone injury or possibly incomplete fracture.
prospective purchase.
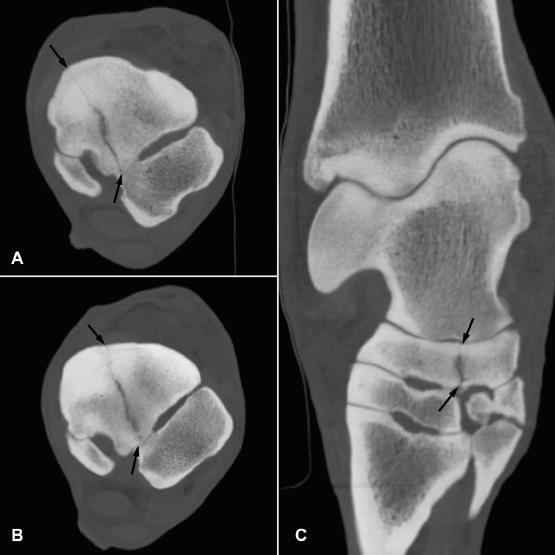
Figure 18: On the left is an image of a standing CT unit capable of imaging the lower limbs. The middle radiographic image demonstrates a possible central tarsal bone fracture. The CT image on the right confirms the presence of the central tarsal bone fracture which was captured by the unit pictured on the left.

Image courtesy of Dr. Richard D. Mitchell.
Fig. 18: On the left is an image of a standing CT unit capable of imaging the lower limbs. The middle radiographic image demonstrates a possible central tarsal bone fracture and the CT image on the right confirms the presence of the central tarsal bone fracture which was captured by the unit pictured on the left.
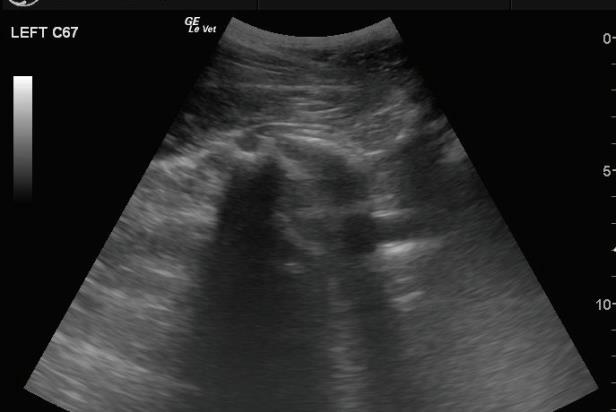
questionable osseous radiographic fi ndings in the purchase examination process. Utilization of standing units requires less sedation and significantly shorter scanning time compared to MRI. While CT is not ideal for soft tissue structures when compared to MRI, the superior bone resolution of CT allows excellent visualization of subchondral bone lesions.7 Some units can even evaluate the cervical spine to C7-T1 if there is concern about the degree and distribution of osteoarthritis identified on survey images.
Conclusion
Multiple alternative techniques for imaging are available to the equine practitioner for the complete and accurate evaluation of the horse presented for purchase. In addition to an initial thorough physical examination, the integration of multiple imaging techniques and modalities will provide the necessary information for the client to make an informed decision regarding the prospective purchase.

Dr. Mitchell is originally from North Carolina, where he participated in foxhunting and hunter/jumper competitions from his childhood to his adult years. He is currently a senior partner of Fairfield Equine Associates in Newtown, Conn., practicing equine veterinary medicine and surgery with an emphasis on lameness and imaging. Dr. Mitchell has served as an official veterinarian for the US Equestrian Team at six Olympic Games as well as multiple Pan American and World Games. He has been internationally certified in veterinary acupuncture and equine locomotor pathology and is a diplomate of the American College of Veterinary Sports Medicine and Rehabilitation. Dr. Mitchell has authored many nationally and internationally published articles and textbook chapters on equine healthcare and welfare. He has served on multiple boards of directors including USEF, the Connecticut Veterinary Medical Association, the American Association of Equine Practitioners, and the EQUUS Foundation as well as serving currently as a Trustee for the American Horse Council. He is the current Chair of the AAEP Foundation Advisory Council. He was a founding board member of the International Society of Equine Locomotor Pathology (ISELP).
18 The Practitioner Issue 3 • 2022
will provide the necessary information for the client to make an informed decision regarding the
Richard D. Mitchell, DVM, MRCVS, Dipl. ACVSMR
Acknowledgements
The author has no fi nancial interests or conflicts of interest relative to commercial items mentioned or the contents of this paper.
References
1. Dyson S, Radiography and Radiology, In: Diagnosis and Management of Lameness in the Horse, Eds, Ross M and Dyson SJ, Saunders, Philadelphia, pp. 153-166.
2. Turner TA. Evaluating the sore performance horse, in Proceedings, Compendium Equine Seminars from October–December 2001;8–13.
3. Soroko, M and Howell, K, Infrared Thermography: Current Applications in Equine Medicine, JEVS, Sept. 2018, pp 90-96
4. Murray RC, Dyson SJ, Tranquille C, et al. (2006) Association of type of sport and performance level with anatomical site of orthopaedic injury diagnosis. Equine Vet J (Suppl); 36:411-416.
5. Boswell RP, Mitchell RD, Dyson SJ (2003) Lameness in the Show Hunter and Show Jumper. In: Diagnosis and Management of Lameness in the Horse, Eds, Ross M and Dyson SJ, Saunders, Philadelphia, pp 951-975
6. Denoix, JM, The Equine Distal Limb, Jul 2000, CRC Press
7. Jacquet S and Denoix, JM, Ultrasonographic examination of the distal podotrochlear apparatus of the horse: A transcuneal approach, EVE, Feb 2012, pp. 90-96
8. Dyson SJ, Martinelli MJ, (2003) Image description and interpretation in musculoskeletal scintigraphy. In: Equine Scintigraphy, Eds: SJ Dyson, RC Pilsworth, AR Twardock, M Martinelli, EVJ, Newmarket, Suffolk, pp.89-91
9. Redding R, Anatomy and Imaging of the Equine Foot and Digit, Proceedings of the Ocala Equine Conference, Jan 25, 2020, Ocala, FL
10. Alexandra LC, Wulster, KB, Darko, S, Richardson, DW, Validation of standing cone beam computed tomography (CT) for diagnosing subchondral fetlock pathology in the Thoroughbred racehorse, 2018 ACVR IVRA Joint Scientific Conference, Fort Worth, TX, USA Oct 14–19, 2018

Horses make us better. Together, we make them better, too.
ASERVO ® and EQUIHALER ® are registered trademarks of Boehringer Ingelheim Vetmedica GmbH, used under license. GASTROGARD ®, EQUIOXX®, MARQUIS ® and SURPASS ® are registered trademarks, and the Horse Head logo™ is a trademark of Boehringer Ingelheim Animal Health USA Inc. PRASCEND ® and VETERA ® are registered trademarks of Boehringer Ingelheim Vetmedica GmbH, used under license. ZIMECTERIN ® is a registered trademark of the Boehringer Ingelheim Group.
©
2021 Boehringer Ingelheim Animal Health USA Inc., Duluth, GA. All rights reserved. US-EQU-0199-2021
• Aric Adams, DVM, DACVS
• Robin Bell, BVSc, MVSc, DipVetClinStud, DECVS, DACVSMR


• Tiffany Hall, DVM, DACVIM, DACVECC



• Sara Lyle, DVM, PhD, Dip. ACT
• Martha Mallicote, DVM, MBA, DACVIM


• Brittany Martabano, DVM, MS, DACVO
• Melissa Restifo, DVM, DACVIM
• Lisa Fultz, DVM, MS, DACVIM


• Jose Garcia-Lopez, MD, DACVS, DACVSMR

YOU ARE INVITED TO OCALA, FLA. “The Horse Capital of the World” FOR OUR WORLD-CLASS PROGRAM OF CUTTING- EDGE LECTURES AND HANDS-ON INSTRUCTION.
of Maven
&
Offering world-class, equine-exclusive continuing education
Photo courtesy
Photo
Film
SPEAKERS INCLUDE:
CONTINUING EDUCATION CREDITS AAVSB RACE This program
AAVSB RACE, CE Broker Provider #50-27127 Sponsor of Continuing Education in New York State Florida Board of Veterinary Medicine, DBPR FVMA Provider #0001682 • Surgery/Lameness • Internal Medicine • Reproduction • Business • Wellness • Ophthalmology TOPICS INCLUDE: Fun In Florida! 2023 OCALA EQUINE CONFERENCE Register now for big savings on your conference pass. Don’t be late! Early bird discount ends Dec. 21, 2022. Register online: Scan QR code
#20-961414 is pending approval for 24 continuing education credits. Veterinarians and veterinary technicians may earn up to 16 hours from continuing education sessions. Veterinarians that attend the comprehensive equine ultrasound wet lab may earn an additional 8 hours of continuing education credit for a total of 24 hours of continuing education credits.













SPONSORED BY: WET LAB FEES INCLUDE: • Expert instruction • Rotation through all stations • Breakfast and lunch • Round-trip transportation between Hilton Ocala and the Equine Medical Center of Ocala COMPREHENSIVE EQUINE ULTRASOUND WET LAB FRIDAY, JAN. 20 | 8:15 A.M. – 4 P.M. Sharpen your imaging skills! Our ultrasound wet lab will include various imaging stations led by renowned veterinary instructors. World-class, equine-exclusive continuing education THANKyou! JAN. 20-22, 2023 | OCALA, FLA. WORLD EQUESTRIAN CENTER $895 WET LAB ONLY $695 WET LAB WITH CONF. REGISTRATION