

DENTAL SOLUTIONS
Cosmetic & Restorative CONTENTS
Digital & Lab
Endodontics
Handpieces & Instruments
Orthodontics
Pain Control
Preventive
Surgical

Restoration
“Working with the AquaCare as part of my daily routine gives me the confidence that my bonding is the best it can be. Often excess hand piece oil can contaminate your cavity during preparation and if not removed can seriously compromise bond strength. Prior to bonding, decontaminating the cavity with 27μm Aluminium Oxide will help to ensure that the cavity with be clean and oil free.”
Richard Field


1: Patient presented with food trapping mesial and distal to the Upper left 5. This was stemming from a poor medial and distal contact point from the adjacent defective restorations.



to an indirect
Dr Richard Field
United Kingdom


PIc
Pic 2: Isolation was achieved with a non latex rubber dam.
Pic 3: The old restorations and caries was removed from the upper right 4 6 and 7 reviewing a carious pulp exposure on the upper right 6.
Pic 4: Cavities were cleaned with 27μm Aluminium Oxide using the AquaCare unit to ensure bonding surfaces are clear of contaminants.
Pic 5: An MTA plug was placed as a means of direct pulp capping over the exposure on the upper right 6.
Pic 6: Direct composite was used to restore the Upper right 4 and 7 with a GIC core placed as a long term provisional on the upper right 6 in order to monitor pulp vitality prior
restoration.
Performance and Practicality with PANAVIA™ Veneer LC
Since 1983 PANAVIA™ by Kuraray Noritake Dental Inc. has been the gold standard for dental cements throughout the world. Their latest cement, PANAVIA™ Veneer LC, sets a new standard for porcelain veneer cements through incredible performance and ease of use. The following clinical case demonstrates the use of PANAVIA™ Veneer LC.
A 31-year-old female (Fig 1) was referred for porcelain veneers to replace lost tooth structure and to improve aesthetics. The patient exhibited moderate attrition of her anterior and bicuspid teeth (Fig 2), the result of nocturnal bruxism and a tendency to an edge-to-edge occlusion. She had a Class I malocclusion on a Skeletal Class I tending III base with the right maxillary canine in cross-bite. The treatment plan included orthodontic treatment, porcelain veneers, and an occlusal splint.
Orthodontic treatment (by Dr Nour Tarraf) included full-fixed appliances with TADs and IPR of mandibular anteriors, and arch retractions to reduce protrusion (Fig 3, post-orthodontic treatment). A preliminary digital design (Fig 4) was performed to guide the diagnostic wax-up and a digital mock-up (Fig 5) was utilised to verify the diagnostic wax-up prior to carrying out the intra-oral mock-up. The patient was unable to afford the restoration of the maxillary bicuspids until a later stage so the reconstruction was limited to the maxillary anterior teeth.
Using the diagnostic wax-up, silicone keys were fabricated to guide tooth preparations. Orthodontic treatment allowed prosthetic treatment to be additive in design which meant that tooth preparations could be conservative. Labial reductions were limited to 0.3mm and incisal reductions were performed only where needed to create an incisal butt joint for the veneer (Fig 6). Minimal preparations allowed the veneers to be bonded almost entirely to enamel, which is important for the long-term survival of porcelain veneers (Ref 1).
There was no need to significantly mask the colour of the cervical region of the tooth and non-carious cervical lesions were absent, so fine chamfer margins were prepared at equi-gingival level.
Splinted provisional veneers (Fig 7) were fabricated using bisacryl ensuring sufficient interdental space to allow hygiene access for small interdental brushes. The labial surface of the provisional veneers were glazed with a unfilled resin and cemented using the spot-etch technique, ensuring all excess flowable composite was removed prior to curing (Fig 8). Twice daily interdental cleaning of the provisional veneers and thorough brushing of labial margins during the provisional phase maintained soft tissue health, important for the try-in and cementation of the definitive veneers.
A dry try-in of the definitive veneers was performed to check the fit of the veneers and a wet try-in was performed using try-in paste to assess aesthetics. The PANAVIA™ Try-in pastes accurately mimic the cement shades. Four useful shades are available (Fig 9). The White and Brown shades are useful to correct small discrepancies in shade requiring subtle increases or decreases in shade value respectively. Conveniently the try-in pastes are the same as the PANAVIA™ V5 range of try-in pastes (excluding opaque). Following the try-in procedure the teeth were isolated using rubber dam and the floss ligature technique. KATANA™ Cleaner (Fig 10) was used to clean the veneers prior to silanating with CLEARFIL™ CERAMIC PRIMER PLUS (Fig 11). Veneers that have not been pre-etched should be etched with hydrofluoric acid prior to silanization. The use of the ProsMate™ Baton allows the cleaning, etching and silanization of all veneers simultaneous-ly (Fig 12). The veneers are arranged systematically on the ProsMate™ Tray ready for the cementation procedure (Fig 13). Tooth surfaces were pre-treated with phosphoric acid (K-ETCHANT Syringe) and PANAVIA™ V5 Tooth Primer (Fig 14).















Fig 2
Fig 4
Fig 3
Fig 5 Fig 1
Fig 6
Fig 9
Fig 7
Fig 10
Fig 8
Fig 11
Fig 13
Fig 12
Fig 14
Fig 15
The newly designed cement applicator tip reduces air bubbles and the wide 16-gauge tip (Fig 15) allows light and easy control of cement extrusion while also providing efficient wide coverage during application. PANAVIA™ Veneer LC has excellent handling because of its ideal paste consistency. It is non-sticky and its viscosity prevents the cement from flowing beyond the veneer margins until the veneer is seated. It is not runny or stringy. Furthermore its thixotropic properties results in lower film thickness during seating of the veneer. These excellent handling properties are due to the development of new filler technology which consists of spherical silica and nano cluster fillers (Fig 16).
The “touch-cure” mechanism of PANAVIA™ V5 Tooth Primer importantly seals the bonding interface while the extended working time and stability of the cement under ambient light allows the simultaneous cementation of multiple veneers. In this case all six lithium disilicate veneers (technical work by Yugo Hatai) were cemented simultaneously with PANAVIA™ Veneer LC Paste (Clear).
Tack-curing each veneer for one second allowed smooth and easy bulk removal of excess cement with an explorer (Fig 17). Remaining excess uncured paste was removed with brushes. Final curing was performed by light curing lingual and labial surfaces. Following removal of the rubber dam residual cured cement was removed with a sickle scaler, number 12 scalpel blade, serrated ribbon, interproximal polishing strip, floss, interdental brush and a rotary brush.
The optical characteristics of PANAVIA™ Veneer LC, use of fine chamfer margins, and well-fitting translucent restorations produces a gradual and smooth transition of colour from tooth to veneer where margins disappear and soft tissues respond in a healthy way (Fig 18). The color stability, excellent abrasion resistance and high gloss durability of PANAVIA™ Veneer LC preserves integrity and aesthetics at the margins over the long term. The extraordinary bond strength of PANAVIA™ products, so familiar to our profession over the last 20 years, is still second to none (Fig 19).
References
1. Layton DM, Walton TR. The up to 21-year clinical outcome and survival of feldspathic porcelain veneers: accounting for clustering. Int J Prosthodont. 2012 Nov-Dec;25(6):604-12. PMID: 23101040.
• Before using this product, be sure to read the Instructions for Use supplied with the product.
• The specifications and appearance of the product are subject to change without notice.
• Printed color can be slightly different from actual color.
• KATANA is a registered trademark or trademark of NORITAKE CO, LIMITED
• PANAVIA and CLEARFIL are registered trademarks or trademarks of KURARAY CO, LTD.




A/Prof Alan Yap BDS (Syd), MDSc Hons (Pros)(Syd), FAANZP

Fig 18
Fig 19
Fig 17
Fig 16






CLEARFIL MAJESTY™ ES-2 Universal
Considerations on the use of a universal composite in the anterior region
Composites with a universal shade concept, a reduced number of shades that may be selected without any shade guide are a clear trend in restorative dentistry. With specific blend-in properties, these materials can help streamline restorative procedures and reduce chair time, take some pressure off the dental practitioner and contribute to potentially good outcomes. Some users, however, are skeptical about a wide-scale use of the materials, particularly when it comes to restoring teeth in the anterior region. The reasons may be a comparatively high translucency requiring the separate application of a blocker (oropacious shade) in certain situations, or a too limited shade offering.
Personal experience shows that CLEARFIL MAJESTY™ ES-2
Universal is perfectly suitable for a wide range of singleshade restorations in anterior teeth. It offers great polishability and long-term gloss retention and is available in just four
Universal light: for natural results in brighter teeth
shades: One universal shade (U) originally designed for posterior restorations, universal light (UL) and universal dark (UD) as the two major options for anterior teeth and, finally, universal white (UW) for the imitation of any bleached shade. In general, all four options may be used in the anterior and posterior region. As the blend-in ability is due to proprietary light-diffusion technology and not managed via an increased translucency, the application of a blocker is usually not necessary and even larger areas can be restored quite inconspicuously.
For those asking themselves when to select which shade in the anterior region, the following clinical case examples and comments may provide some useful guidance. The recommendations and practical tips are based on personal experience. All patients were in treatment for diastema closure or shape correction, but the selection criteria are the same for other types of anterior restorations, too.
This young patient aged 35 with microdontia presented in the dental office with the desire to have more beautifully shaped teeth. His teeth were almost free of dental caries, but with deficiencies in oral hygiene and signs of gingival inflammation. A deep bite was also evident. After professional tooth cleaning and oral hygiene advice, the teeth were restored with CLEARFIL MAJESTY™ ES-2 Universal in the shade UL.


Fig. 1: Initial situation
Fig. 2: Initial situation: Deep bite.


Reasons for selecting universal light:
• For younger patients (tooth shades A2 and lighter)
• Situations in which light easily passes through the composite (e.g., Class III, Class IV)
Universal dark: for natural results in darker teeth
Universal light properties:
• High light scattering effect
• Well-balanced translucency
Abrasion and shape correction was also the major reason for this 58-year-old female patient to ask for cosmetic dental treatment. She was unhappy with the appearance of the anterior teeth in the maxilla, which showed signs of tooth wear and discolouration. The selected treatment approach was composite veneering with CLEARFIL MAJESTY™ ES-2 Universal in the shade UD. The shade was selected based on the indication and the somewhat darker shade of the patient’s natural teeth.

Reasons
for selecting universal dark:
• For older patients (tooth shades A3 and darker)
• Situations in which light easily passes through the composite (e.g., Class III, Class IV)
Universal: whenever a high translucency is desired

Universal dark properties:
• High light scattering effect
• Well-balanced translucency
In teeth in which the areas to be restored are surrounded by a lot of non-discoloured tooth structure – as may be the case in Class I, II and Class V cavities – the use of CLEARFIL MAJESTY™ ES-2 Universal in the shade U may be an option. The 28-yearold patient, who presented for diastema closure, had teeth with a comparatively low translucency and different shades due to smoking and excessive coffee consumption. As the composite was applied in enamel areas only, the relatively high translucency of the universal shade seemed beneficial in this case.
Fig. 5: Initial clinical situation.
Fig. 6: Treatment outcome.
Fig. 3: Teeth restored with composite in the single-shade technique.
Fig. 4: Immediate treatment outcome.

Reasons for selecting universal:
• Large amounts of underlying or surrounding tooth structure present
• Medium light-scattering desired

Universal properties:
• High translucency
• Medium light-scattering effect
Universal white: for all patients asking for a bleached effect
For all cases that require a particularly bright tooth shade – e.g. children or patients with bleached teeth / asking for a bleached effect in their restorations – CLEARFIL MAJESTY™ ES-2 Universal in the shade UW is likely to be the first choice. The young patient aged 28 shown below asked for diastema closure including shape and shade correction: She wanted to have a brighter, more beautiful smile.




Fig. 9: Initial clinical situation.
Fig. 11: Treatment outcome …
Fig. 7: Initial clinical situation.
Fig. 10: Shape and shade correction were desired in this case.
Fig. 12: … leading to the beautiful smile the patient desired.
Fig. 8: New smile of the patient.
Reasons for selecting universal white:
• Cases requiring a particularly high brightness or value
• Restorations in deciduous teeth
• Restorations in bleached teeth
Conclusion
Universal white properties:
• Well-balanced translucency
• High light-scattering effect
One universal composite, four shades: In the case of CLEARFIL MAJESTY™ ES-2 Universal, this portfolio is absolutely sufficient for single-shade restorations even in the aesthetically demanding anterior region. Properties such as a nice blend-in effect, a great polishability and gloss retention over time support dental practitioners in creating beautiful restorations. As shade determination may be based on very few criteria instead of a complex shade guide, the whole restoration procedure becomes less stressful and more efficient. Furthermore, with only four shades to stock and usually no blocker needed, the number of materials on stock is reduced, leading to facilitations in stock management as well.


Dr. Jusuf Lukarcanin
Certified Dental Technician (DCT)
Optimizing intraoral and extraoral substrates
For maximal adhesive potential using a novel mdp-based surfactant solution
The everyday practice of adhesive restorative dentistry, whether utilizing direct or indirect restorations, is fraught with the need for ideal environmental conditions to generate an optimal prognosis. The bonding of composite resin is the foundation of direct and indirect restoratives, as it provides the link between restoration and tooth. As dentistry strives to be minimally invasive, the treatment of the bonding interface is reflected in this philosophy by the use of self-etching multisubstrate acidic monomers such as 10-methacryloyloxyldecyl dihydrogen phosphate (10-MDP). There are myriad opportunities for both intaglio and fitting surfaces to be contaminated with varying agents to the detriment of restoration prognosis.
Some of the contaminants to be considered are of course, moisture from exhalation, ambient humidity in the oral cavity, blood, saliva and artificial sources such as provisional cement during a two-stage indirect delivery technique. Moisture is an agent which is only welcomed via a controlled approach during the dentin penetration phase of priming the substrate for adhesion, however if excessive in quantity will compromise the hybridization of the interface. Blood and saliva are ubiquitous in restorative dentistry, and best controlled via the application of rubber dam as part of an absolute isolation philosophy. Contamination of the prepared surface can also occur through artificial cements or lubrication agents. Hemostatic agents such as ferric sulphate and aluminium chloride have the ability to deposit insoluble precipitates on the surface of the tooth in a manner that 33% orthophosphoric acid can only partially remove. Also considered is the particulate deposition of dentin and enamel as part of standard tooth preparation. This smear layer is residual on the dentin surface, often occludes dentinal tubules, and is an obstacle that must be overcome in order to bond to the hydroxyapatite and collagen fibrils of the surface.
Overall, the risks to adhesive compromise and at worst, adhesive failure are high. This report details the use of a novel solution for debriding both indirect restorative and tooth intaglio with a 10-MDP salt-based solution that has the flexibility to be used both extraorally and intraorally.
Endemic Contaminants: Moisture, Blood and Saliva
Moisture is a critical component to maximize the adhesive bond strength of certain modern universal adhesives. The presence of moisture allows for increased penetration of bonding solutions into dentinal tubules and between collagen fibrils, ultimately bolstering the resilience of the hybrid layer1. During the cementation of an indirect restoration, both salivary and blood contamination of the mating surfaces have been shown to have a deleterious effect on bond strengths, with blood contamination faring the worst in all conditions2 Van Meerbeek et al reported on technique sensitivity with one-step contemporary universal adhesives3. The basis of his findings note that these adhesives require water as an ionization medium for the self-etching reaction, with the need to evaporate water from the interfacial surfaces in order to maximize bond strengths. Despite this, these interfaces are considered semi-permeable which predisposes the hybrid layer to an increased risk of hydrolytic degradation in adhesive solutions that are not 2-hydroxyethyl methacrylatefree (HEMA-free), which has a greater affinity for water.
Periera et al tested varying degrees of wetness of dentin substrate controlled with variables such as short vs. long air blasts, wet vs. dry cotton pellets, microbrush use and an intentionally over-wet surface. In all groups, the “wettest” dentin intaglio surface resulted in the lowest shear bond strength4
The influence of saliva and blood contamination is clearly negative in situations where the bonding interface was contaminated before or after adhesive application. For saliva, this reduction is due to the deposition of salivary glycoprotein on the surface, and relative to blood, macromolecules such as fibrinogen and platelets block access to the tubules for effective bonding. Blood contamination was found consistently to be more profoundly deleterious on bond strength relative to saliva2
In general, on smear layer-affected dentin, chlorhexidine was consistently superior to other agents such as ethanol, EDTA, aloe vera in establishing the highest shear bond strength to dentin. On dentin that had previously been etched and contaminated with blood and saliva, the agent subsequently applied that showed the highest recovery of shear bond strength was 37.5% phosphoric acid5. A study on the nanomechanical and nanoroughness of etched dentin and self-etching adhesive treated dentin both contaminated with saliva revealed that KATANA™ Cleaner was capable of restoring control values of complex modulus and nanoroughness relative to control6
Synthetic Workflow Contaminants: Dental stone, Hemostatic Agents, Root Canal Sealers and Provisional Cements
A 2020 study by Marfenko et al demonstrated that salivary contamination showed significantly lower bond strengths relative to intaglio contamination by dental stone from laboratory processes. The application of a silane coupling agent to the intaglio surface has a protective effect on the bond strength7. The caveat is that lithium disilicate-based restorations are often requested pre-etched with hydrofluoric acid from the laboratory. Often, the case is returned to the clinician on the secondary or primary model. If already treated with hydrofluoric acid, the surface can now be considered recontaminated with the stone or resin model or simply skin oils from handling. The unprotected surface needs to be decontaminated in any case following the try-in procedure, which now may feature elements of dental stone, blood and saliva, not to mention hemostatic agents such as aluminium chloride and ferric sulphate. If silane coupling agents are applied prior to try-in, the question of whether the intaglio surface was truly contaminant-free after removal from the model.
Aluminium chloride is a hemostatic agent that leaves an insoluble precipitate on the surface of the dentin, that is only partially removed when treated with phosphoric acid, resulting only in a partial recovery of shear bond strength relative to control. The application of ethylene diacetyl tetrasodium acetate (EDTA) returned the bond strengths to the level of
normal dentin8
The bonding of polycrystalline ceramic restorations and metal alloys is contaminated with saliva upon try-in. This can be removed via steam cleaning and air particle abrasion set at 2.5 bar for 15 seconds9. Phosphoric acid is often mistakenly applied as a cleaning agent to the intaglio surface. In polycrystalline ceramics such as tetragonal zirconia polycrystal, this is disastrous, as phosphates will bond firmly to the free sites that the 10-MDP monomer normally bonds to as part of the APC protocol of zirconia bonding, significantly compromising bond strength (Blatz, 2016)10. A study of modern surface cleaners demonstrated successful debridement of the surface using KATANA™ Cleaner for both blood and saliva-contaminated substrates11, 12
Provisional cements are thought to have a deleterious effect on the shear bond strength of adhesively-bonded indirect ceramic restorations. Ding et al (2022) uncovered that resinbased and non-eugenol cement use in the provisional phase decreased the bond strength relative to control, whilst the use of calcium hydroxide and polycarboxylate cements exhibited acceptable metrics. Debridement of the prepared surface with air particle abrasion (APA) resulted in recovery of decreased bond values to that of control13. Equally useful was the application of Immediate Dentin Sealing (IDS)14, a technique characterized ideally by APA before adhesive bonding and the application of a resin coat, occluding both the dentin tubules as well as the oxygen inhibition layer, allowing the resin-dentin bond to mature and strengthen in the absence of stresses. This approach is effective in minimizing postoperative hypersensitivity and bacterial ingress, as well as optimizing the shear bond strength particularly when indirect ceramics are concerned15. Hardan et al found that the shear bond strength was highest when IDS was completed using a three-step etch and rinse adhesive protocol14
Hemostatic agents used in clinical dentistry exhibit a pH of 1.1 to 3.0 and are as acidic as self-etching primers16

Chaibutyr and Kois found that dentin when contaminated with 25% aluminium chloride or 13% ferric sulphate demonstrated a significantly lower shear bond strength to dentin, which was significantly recovered using the etch-and-rinse approach17 This approach albeit successful was only able to achieve partial reversal of shear bond strength deficits relative to control, with a pre-etching application of EDTA required in order for full recovery8. KATANA™ Cleaner was found to have a positive effect on the cleaning of dentin contaminated with both aluminium chloride and ferric sulphate.
The bonding of dentin substrate contaminated with root canal sealers is a concern for the integrity of core buildups postendodontic treatment. The use of KATANA™ Cleaner was found to be generally superior to the ethanol test subgroup in the removal of zinc-oxide eugenol-based sealer with equal performance to 70% ethanol for the epoxy resin-based sealer18
Clinical Case Demonstration
A 35 year old ASA 1 female patient presented to the practice with multiple failing composite restorations in the second quadrant that were planned for replacement. Prior to the delivery of topical and local anaesthesia, it is common procedure in the practice to ascertain shade specifics of planned restoratives before potential dehydration can affect the optical properties of the natural tooth. Smart monochromatic composites (Fig. 1) are a class of direct restoratives that leverages the ability of its nanofiller



composition and refractive index to mimic the structural colour of the surrounding enamel and dentin19. This typically enables a clinician to have a simplified selection of shades on hand.
Two carpules of 2% Lignocaine with 1:100,000 epinephrine were delivered via buccal infiltration before absolute isolation was achieved using a non-latex rubber dam (Isodam HD Heavy, 4D Rubber, UK) (Fig. 2). The old restorations were excavated along with caries (Fig. 3), and the dentin structure assessed for residual decay with a detector dye (Caries Detector, Kuraray Noritake Dental Inc.). The preparation cavosurface margins were gently bevelled before surface treatment with air particle abrasion (30psi, 29 micron aluminium oxide in a 17.5% ethanol carrier, Aquacare UK) (Fig. 4). The enamel margins were etched with 33% orthophosphoric acid and rinsed (Fig. 5). The preparation surfaces were decontaminated further of any residual smear or powder residue using a MDP-based surfactant (KATANA™


Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 1

Cleaner, Kuraray Noritake Dental Inc.) (Fig. 6). A single step self-etching universal adhesive was applied to the preparation as per manufacturer instructions and air thinned before light curing (Fig. 7).
A matrix-in-matrix approach was utilized for the second bicuspid as the first step to allow for simultaneous anatomic construction of the mesial and distal marginal ridges. This technique does not require the use of a wedge as the outer circumferential Tofflemire matrix (Omnimatrix, Ultradent Products) tightens cervically around the inner anatomicallycurved sectional matrix (Garrison Firm Band, Garrison Dental Solutions) allowing for a hermetic gingival seal (Fig. 8). If required, the setup may be further modified by the use of Teflon inserted between the two matrices to provide better proximofaciolingual adaptation. As a result, finishing and contour creation post-band removal is kept to a minimum.



Following this, a traditional sectional matrix system may be employed to close contacts and build marginal ridges in the conventional manner (Fig. 9).
Following marginal ridge construction, the matrix assembly was removed and with the Class II lesions converted into a Class I situation, microlayering proceeded with a high flexural strength flowable liner (CLEARFIL MAJESTY™ Flow, Kuraray Noritake Dental Inc.) prior to the application of a monochromatic composite resin (CLEARFIL MAJESTY™ ES-2 Universal U shade, Kuraray Noritake Dental Inc.). The buccal cusps were constructed first as the author considers this essential to establishing restoration lobe proportions (Fig. 10). Subsequent layers were completed in a lobe-bylobe approach to finish the occlusal anatomy (Fig. 11 and 12). The restoration was checked for occlusal functional conformativity, finished and polished to high shine (Fig. 13).


Fig. 8
Fig. 9
Fig. 10
Fig. 11
Fig. 6
Fig. 7


Discussion
Dental substrates are often contaminated in both direct and indirect restorative processes. Historically, etch-and-rinse approaches have been successful for at least the partial recovery of bond strength however it is not practical in situations where selective or self-etching is the adhesive strategy. The restorative dentist in these cases can use the 10-MDP monomer in self-etching systems to target nondemineralized dentin such as CLEARFIL™ Universal Bond Quick to establish an acid base resistance zone (ABRZ) otherwise known as Super Dentin20. The presence of the operative smear layer impedes full access of the self-etching primer to the dentin substrate in some cases. In such cases,
without KATANA™ Cleaner, APA is required to transform the substrate back to control bonding potential. APA as a modality is only utilized by a subset of dental practitioners often due to financial constraints or lack of technique experience. KATANA™ Cleaner thus represents a versatile tool for the decontamination and optimization of substrate surfaces for adhesive bonding both in intraoral and extraoral applications. Its ability to re-establish ideal bonding values in areas that are not effectively reached by APA such as endodontic canal anatomy in a non-invasive manner literally cements it as a truly indispensable tool for the modern restorative dentist.


Dr Clarence Tam HBSc, DDS, FIADFE, AAACD
Fig. 12
Fig. 13
Disclaimer: Some indications are not described in the product’s Instructions for Use and are based on published research and/or the author’s experience. Before using each product, read carefully the Instructions for Use supplied with the product for full details and workflows.
References:
1. Sugimura R, Tsujimoto A, Hosoya Y, Fischer NG, Barkmeier WW, Takamizawa T, Latta MA, Miyazaki M. Surface moisture influence on etch-and-rinse universal adhesive bonding. Am J Dent. 2019 Feb;32(1):33-38. PMID: 30834729.
2. Taneja S, Kumari M, Bansal S. Effect of saliva and blood contamination on the shear bond strength of fifth-, seventh-, and eighth-generation bonding agents: An in vitro study. J Conserv Dent. 2017 May-Jun;20(3):157-160. doi: 10.4103/0972-0707.218310. PMID: 29279617; PMCID: PMC5706314.
3. Van Meerbeek B, Van Landuyt K, De Munck J, Hashimoto M, Peumans M, Lambrechts P, Yoshida Y, Inoue S, Suzuki K. Technique-sensitivity of contemporary adhesives. Dent Mater J. 2005 Mar;24(1):1-13. doi: 10.4012/dmj.24.1. PMID: 15881200.
4. Pereira GD, Paulillo LA, De Goes MF, Dias CT. How wet should dentin be? Comparison of methods to remove excess water during moist bonding. J Adhes Dent. 2001 Fall;3(3):257-64. PMID: 11803713.
5. Haralur SB, Alharthi SM, Abohasel SA, Alqahtani KM. Effect of Decontamination Treatments on Micro-Shear Bond Strength between Blood-Saliva-Contaminated Post-Etched Dentin Substrate and Composite Resin. Healthcare (Basel). 2019 Nov 1;7(4):128. doi: 10.3390/healthcare7040128. PMID: 31683858; PMCID: PMC6956069.
6. Toledano M, Osorio E, Espigares J, González-Fernández JF, Osorio R. Effects of an MDP-based surface cleaner on dentin structure, morphology and nanomechanical properties. J Dent. 2023 Nov;138:104734. doi: 10.1016/j.jdent.2023.104734. Epub 2023 Oct 2. PMID: 37793561.
7. Marfenko S, Özcan M, Attin T, Tauböck TT. Treatment of surface contamination of lithium disilicate ceramic before adhesive luting. Am J Dent. 2020 Feb;33(1):33-38. PMID: 32056413.
8. Ajami AA, Kahnamoii MA, Kimyai S, Oskoee SS, Pournaghi-Azar F, Bahari M, Firouzmandi M. Effect of three different contamination removal methods on bond strength of a self-etching adhesive to dentin contaminated with an aluminum chloride hemostatic agent. J Contemp Dent Pract. 2013 Jan 1;14(1):26-33. doi: 10.5005/ jp-journals-10024-1264. PMID: 23579888.
9. Yang B, Lange-Jansen HC, Scharnberg M, Wolfart S, Ludwig K, Adelung R, Kern M. Influence of saliva contamination on zirconia ceramic bonding. Dent Mater. 2008 Apr;24(4):508-13. doi: 10.1016/j.dental.2007.04.013. Epub 2007 Aug 6. PMID: 17675146. 10. Blatz MB, Alvarez M, Sawyer K, Brindis M. How to Bond Zirconia: The APC Concept. Compend Contin Educ Dent. 2016 Oct;37(9):611-617; quiz 618. PMID: 27700128. (7)
11. Awad MM, Alhalabi F, Alzahrani KM, Almutiri M, Alqanawi F, Albdiri L, Alshehri A, Alrahlah A, Ahmed MH. 10-Methacryloyloxydecyl Dihydrogen Phosphate (10-MDP)-Containing Cleaner Improves Bond Strength to Contaminated Monolithic Zirconia: An In-Vitro Study. Materials (Basel). 2022 Jan 28;15(3):1023. doi: 10.3390/ma15031023. PMID: 35160968; PMCID: PMC8838745.
12. Tian F, Londono J, Villalobos V, Pan Y, Ho HX, Eshera R, Sidow SJ, Bergeron BE, Wang X, Tay FR. Effectiveness of different cleaning measures on the bonding of resin cement to salivacontaminated or blood-contaminated zirconia. J Dent. 2022 May;120:104084. doi: 10.1016/j. jdent.2022.104084. Epub 2022 Mar 3. PMID: 35248674.
13. Ding J, Jin Y, Feng S, Chen H, Hou Y, Zhu S. Effect of temporary cements and their removal methods on the bond strength of indirect restoration: a systematic review and meta-analysis. Clin Oral Investig. 2023 Jan;27(1):15-30. doi: 10.1007/s00784-022-04790-6. Epub 2022 Nov 24. PMID: 36422719; PMCID: PMC9877054. 14. Hardan L, Devoto W, Bourgi R, CuevasSuárez CE, Lukomska-Szymanska M, Fernández-Barrera MÁ, Cornejo-Ríos E, Monteiro P, Zarow M, Jakubowicz N, Mancino D, Haikel Y, Kharouf N. Immediate Dentin Sealing for Adhesive Cementation of Indirect Restorations: A Systematic Review and Meta-Analysis. Gels. 2022 Mar 11;8(3):175. doi: 10.3390/gels8030175. PMID: 35323288; PMCID: PMC8955250.
15. Samartzi TK, Papalexopoulos D, Sarafianou A, Kourtis S. Immediate Dentin Sealing: A Literature Review. Clin Cosmet Investig Dent. 2021 Jun 21;13:233-256. doi: 10.2147/CCIDE. S307939. PMID: 34188553; PMCID: PMC8232880.
16. Woody RD, Miller A, Staffanou RS. Review of the pH of hemostatic agents used in tissue displacement. J Prosthet Dent. 1993 Aug;70(2):191-2. doi: 10.1016/0022-3913(93)90018-j. PMID: 8371184.
17. Chaiyabutr Y, Kois JC. The effect of tooth-preparation cleansing protocol on the bond strength of self-adhesive resin cement to dentin contaminated with a hemostatic agent. Oper Dent. 2011 Jan-Feb;36(1):18-26. doi: 10.2341/09-308-LR1. Epub 2011 Feb 21. PMID: 21488725.
18. Tian F, Jett K, Flaugher R, Arora S, Bergeron B, Shen Y, Tay F. Effects of dentine surface cleaning on bonding of a self-etch adhesive to root canal sealer-contaminated dentine. J Dent. 2021 Sep;112:103766. doi: 10.1016/j.jdent.2021.103766. Epub 2021 Aug 5. PMID: 34363888.
19. Ahmed MA, Jouhar R, Khurshid Z. Smart Monochromatic Composite: A Literature Review. Int J Dent. 2022 Nov 8;2022:2445394. doi: 10.1155/2022/2445394. PMID: 36398065; PMCID: PMC9666026.
20. Nikaido T, Weerasinghe DD, Waidyasekera K, Inoue G, Foxton RM, Tagami J. Assessment of the nanostructure of acid-base resistant zone by the application of all-in-one adhesive systems: Super dentin formation. Biomed Mater Eng. 2009;19(2-3):163-71. doi: 10.3233/BME-2009-0576. PMID: 19581710.
Practical tips for reliable endodontic treatment
Dr Friederike Listander, Germany - HYFLEX OGSF Sequence Files
Introduction
Orifice opener, glide path file, shaping file, and finishing file—for classic endodontic treatment, a compact system of nickel–titanium (NiTi) files is often sufficient to achieve reproducible results in the preparation of the respective root canal anatomy.
The following case report illustrates how the skilful use of a fixed sequence of pre-bent files enables even dental practices with only occasional endodontic cases to develop a treatment routine in which they can have a high level of confidence. In addition, in this article, practical tips for drying and obturating root canals are provided.
The principle of maximum tooth preservation constitutes a key component of our practice philosophy. Owing to our broad range of services, we utilize state-of-the-art technology in the various indication’s areas in our daily routines to offer our patients the best possible treatment in each case. In endodontics, this means, among other things, automated preparation using a state-of-the-art motor as a navigation aid, as well as the use of an easy-to-remember NiTi file sequence. This structures workflows and ensures that the sequence of work steps becomes intuitive and quick to perform after a brief learning period. A standardized treatment protocol minimizes potential sources of error on the one hand and facilitates an effective procedure on the other hand, as reflected in the following endodontic case.


Fig. 1: Pre-op radiograph of tooth #27.
Fig. 2: Measurement radiograph for working length control.

Case presentation: Irreversible pulpitis of tooth #27
In February 2024, a 46-year-old female patient presented to our practice with severe pain in her left upper jaw. After a positive vitality test and strong response to the percussion test, a diagnosis of irreversible pulpitis of tooth #27 was confirmed radiographically (Fig. 1). The patient agreed to a two-session root canal treatment, which was started at the first appointment.
After surface anaesthesia and numbing of the affected tooth, a dental dam was placed, which is standardly done ahead of tooth preparation. Additional sealing of the dental dam with liquid dental dam effectively prevented irrigation solution from running into the patient’s throat. This was of particular advantage because treatment was made even more difficult by limited opening of the mouth.
After creating the access cavity, the individual root canals were probed and expanded under the operating microscope using a diamond-coated ultrasonic tip. The respective working lengths were determined with the aid of an apex locator. A measurement radiograph was taken as confirmation and showed that the lengths matched the electronic measurements (Fig. 2).
The affected canals were first prepared manually using a hand file to the required size 20. This was followed by the electrochemical irrigation protocol using an ultrasonic tip (Fig. 3). The classic sequence of sodium hypochlorite...
EDTA, sodium chloride, and chlorhexidine in 0.2% concentration to disinfect the canals, this supported the effective removal of tissue residue and debris. Medical calcium hydroxide was placed into the cleaned canals for

temporary sealing and ultimately fixed with PTFE tape before sealing the tooth provisionally with DUOTEMP (COLTENE). Before polishing the temporary filling, the occlusion was checked, and the patient was then discharged symptom-free until the subsequent treatment session.
Fig. 3: Ultrasonically activated irrigation.
Fig. 4: Easy-to-remember HyFlex EDM file sequence: Opener, Glider, Shaper and Finisher.


Efficient instrumentation with an easy-to-remember NiTi sequence
The actual preparation and final obturation of the root canals were performed during the second appointment. The patient was pain-free when she presented to our practice again. The dental dam placed for this treatment was again sealed with liquid dental dam after local anesthesia to provide better protection for the patient.
The user-friendly endodontic motor CanalPro X-Move (COLTENE) and the HyFlex EDM instruments in the OGSF sequence (COLTENE; Fig. 4) were chosen for straightforward preparation. The abbreviation “OGSF” stands for the first letters of the four NiTi files, which can be used to treat the majority of typical endodontic cases quickly and conveniently: the Opener (orifice opener) opens the tooth to be treated, the Glider (glide path fille) helps to create a glide path which follows the natural contour of the canal, the Shaper (shaping file) efficiently removes bacteria and infected tissue and creates the prerequisites for the canal obturation, and

Fig. 5: Preparation with the cordless CanalPro X-Move endodontic motor.
Figs. 6a-c: Master point fitting with 30/.04 HyFlex EDM gutta-percha points. Intra-oral view (a). Radiograph (b). Individual gutta-percha points (c).
Fig. 6a
Fig. 6b
Fig. 6c
the Finisher (finishing file) ensures that the apical area is sufficiently cleaned and that there is sufficient space for irrigating solutions to reach the apex.
The mesiobuccal cusp tip served as a reference point for determining the working length of the mesiobuccal canal: preparation was performed over 19mm up to size 30/04 with the finishing file. Likewise, the distobuccal canal was instrumented to the same working length (reference point: distobuccal cusp tip). In comparison, the palatal canal had a working length of 21 mm; and here, too, the natural canal contour could be replicated with the compact OGSF sequence up to size 30/04 with the finishing file.
The motion patterns programmed in the motor make handling the files extremely easy and enable the working length to be reached in just a single pass. Clamped in the cordless handpiece, the files also give one a good feel for the anatomical contour of the canal (Fig. 5).
The well-organised set of four coordinated special files with matching gutta-percha points offered the great ad- vantage that no individual files had to be preselected ahead of treatment. The prebent files moved safely in the centre of the canal, making handling extremely smooth. Furthermore, the files are highly resistant to breakage, and this ultimately benefits both the patient and the practitioner.
Sustainable drying with fewer paper points
The sequence of electrochemical irrigation followed the same protocol as in the first treatment session. After the last irrigation sequence, the canals could be dried well with a particularly narrow endodontic suction cannula, therefore requiring fewer paper points. In addition, the paper points can be tested easily on a firm surface after they have been in the canal to see whether there is any remaining liquid in the canal.
A master point fitting with 30/04 HyFlex EDM gutta-percha points was selected to match the file system (Figs. 6a-c). Here, the palatal canal length was shortened by 0.5mm.
HyFlex EDM master points of the same length were used for thermoplastic filling of the three root canals, and about the canals were filled three-dimensionally with liquid guttapercha. The AH Plus bioceramic sealer (Dentsply Sirona) provided the required sealing. Here, it is perfectly sufficient to coat only the lower part of the gutta-percha points with sealer. Furthermore, the canal entrances were covered with a flowable composite in Shade A1 in combination with a matching acid etching gel, primer and bonding agent. BRILLIANT EverGlow Flow high-performance composite (COLTENE) in the opaque version in Shade A3 was used for the final restoration. The final radiograph confirmed the reliable sealing of the three canals in tooth #27 (Fig. 7).

Conclusion
Using a standardised NiTi file sequence such as HyFlex EDM OGSF, the majority of classic root canal treatments can be prepared quickly and reliably. Owing to the structured sequence of Opener, Glider, Shaper and Finisher files, practice teams and patients benefit from efficient and safe root canal treatment. With a few simple steps, one can save both time and material in order to achieve all-round sustainable treatment.
About
Dr Friederike Listander studied dentistry at Ulm University in Germany from 2004 to 2009. She then worked from 2009 to 2012 as a dentist and research assistant at Ulm University’s dental clinic. In 2013, she specialised in endodontics and established her own practice in 2014.
Since then, she has attended numerous training courses to continue to expand her expertise in endodontics, aesthetic dentistry, periodontics, implant dentistry and microsurgery. Dr Listander is also active as a speaker in Germany and abroad.

Fig. 7: Post-op radiograph of tooth #27.

Bulk fill materials - the ideal material for small class II restorations.
A sample case with Ecosite Bulk Fill
Introduction
The common method of composite resin placement for large cavities is the technique where the restorative material is placed in subsequent increments of about 2 mm thickness in order to achieve a sufficient degree of conversion and low stress shrinkage. Recently, new resins, bulk composites, with the ability to be placed and cured in layers up to 5mm were introduced. The use of a bulk filling protocol reduces the amount of time required for the clinician to complete the restoration, which is beneficial both for practitioner and patient. In addition, bulk restorative materials demonstrate less stress at the interfaces with reduced microleakage. From a clinical point of view, they present good handling, permit the achie- vement of good contact points and some of them present good mechanical properties due to the high filler load and improved organic resin matrix. In daily restorative procedures, they seem perfect for many clinical scenarios. Most dentists only think to use of bulk fill materials when confronted with large cavities, but in fact, it can be beneficial to use them even in small to medium sized cavities. In this kind of restoration, it is not easy to use layering techniques such as the Centripetal Build Up Technique due to the reduced dimensions of the cavity. These small restorations get all the workflow advantages like the deep polymeri- sation achieved by bulk fill materials. Furthermore, due to their smaller size, they face per se even less shrinkage stress in high C factor cavities.
My favourite structural bulk material is Ecosite Bulk Fill (DMG). It presents very good physical properties such as low shrinkage stress (1.28 MPa), high compressive strength (> 300 MPa) and good flexural strength (>100 MPa). These characteristics are similar to the most common traditional
nano hybrid composite materials available in the market. Ecosite Bulk Fill (DMG) also has some clinical assets such as handling, sculptability, and mimicry. This last aspect makes it possible to restore almost all teeth with just a single universal shade. Due to all the aforementioned aspects, this restorative material was the right choice for the following clinical case.
Clinical Case
The patient, a young teenage girl, came into the office for a dental checkup (Fig. 1). After X- ray bite wing examination (Fig. 2), a medium size interproximal cavity was reported in tooth 16. After local anaesthesia and rubber dam placement (Fig. 3), an indirect occlusal access to the lesion was performed (Fig. 4) and carious tissues removed. Margins were slightly beveled (Fig. 5) and a sectional matrix with a separating ring placed in order to achieve a tight contact point (Fig. 6). After acid etching the margins (Fig. 7), all in enamel (note the ability of the DMG Etching Gel to stay in place), a dentine bonding agent, LuxaBond Universal (DMG), was applied. Then a very thin layer of flowable composite resin, Ecosite Elements High- light OA2 (DMG), was placed (Fig. 8) in order to further reduce the risk of microleakage and achieve better marginal adaptation. In addition, if there is a dischromic dentin as substrate, such as post amalgam stained dentin or tertiary dentin, this opaque flowable can reduce stain transmission through the quite translucent bulk material, improving aesthetic results.
After light curing the flowable layer, Ecosite Bulk Fill (DMG) composite resin was placed in a bulk application, carved and light cured for 20 seconds (Fig. 9). Finally the restoration was finished and polished (Fig. 10), the rubber dam was removed (Fig. 11 and 12), a radiography performed to check margins (Fig. 13) and the occlusion checked.














Fig. 1: Pre op occlusal view
Fig. 4: Occlusal access to inter proximal lesion
Fig. 7: Selective enamel etching
Fig. 10: The restoration after polishing
Fig. 13: Radiological check: note the good radiopacity of Ecosite Bulk Fill (DMG)
Fig. 2: Bite wing reporting an inter proximal mesial lesion on tooth 16
Fig. 5: Cavity cleaned and shaped
Fig. 8: Application of LuxaBond Universal (DMG) and a thin layer of Ecosite Elements Highlight OA2 (DMG)
Fig. 11: Occlusal view of the finished restoration
Fig. 3: Rubber dam in place
Fig. 6: Application of a sectional matrix and a separating ring
Fig. 9: Application of Ecosite Bulk Fill (DMG) in just one single increment.
Fig. 12: Lateral view of restoration after rubber dam removal
Conclusion
The use of Ecosite Bulk Fill (DMG) allows us to achieve good aesthetic and excellent clinical performance in a short period of time. The special characteristics of this material give the practitioner a fast and reliable composite, with low stress at the margin, minimum marginal gaps, good mechanical performances and, due to its chameleon abilities, good aesthetic. It seems only logical to also use it in little-to-medium class II cavities!

References
Dewaele M, Asmussen E, Devaux J, Leloup G. Class II restorations: influence of a liner with rubbery qualities on the occurrence and size of cervical gaps. Eur J Oral Sci. 2006 Dec;114(6):535-41.
Fabianelli A, Sgarra A, Goracci C, Cantoro A, Pollington S, Ferrari M. Microleakage in class II restorations: open vs closed centripetal build-up technique. Oper Dent. 2010 May-Jun;35(3):308-13.
Ferracane JL, Lawson NC. Probing the hierarchy of evidence to identify the best strategy for placing class II dental composite restorations using current materials. J Esthet Restor Dent. 2021 Jan;33(1):39-50. doi: 10.1111/jerd.12686. Epub 2020 Nov 18. PMID: 33206440.
Kaisarly D, Langenegger R, Litzenburger F, Heck K, El Gezawi M, Rösch P, Kunzelmann KH. Effects of application method on shrinkage vectors and volumetric shrinkage of bulkfill composites in class-II restorations. Dent Mater. 2021 Nov 23:S0109-5641(21)00307-9.
Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012 Jun;40(6):500-5.
Van Ende A, De Munck J, Lise DP, Van Meerbeek B. Bulk-Fill Composites: A Review of the Current Literature. J Adhes Dent. 2017;19(2):95-109. doi: 10.3290/j.jad.a38141. PMID: 28443833.

Dr Andrea Fabianelli, DDS, PhD, MSc


Lithium (di)silicate: Strength & aesthetics
by Dr José Ignacio Zorzin, Germany
The combination of modern nanohybrid composites and adhesive systems makes it possible to directly restore almost any tooth, preserving it with minimal invasiveness. However, if the tooth structure defect is so significant that it is not possible to establish sufficient proximal contact directly or if the functional design of the occlusal surface and cusps can only be achieved sub-optimally, a direct adhesive restoration is no longer the best treatment option. For these cases, indirect, adhesive tooth-coloured restorations such as ceramic inlays, onlays, and crowns are an ideal solution.
Lithium (di)silicate ceramics
Most dental ceramics have two phases: a glass and a crystalline phase. If the crystalline phase is produced by a thermal process (nucleation and crystallisation), these materials are called glass ceramics. The glass phase is crucial for the aesthetics of the material: it gives the material its colour and its translucency. Unfortunately, it has relatively low strength and resistance to fractures due to its amorphous structure. The strength of glass ceramics results from the crystalline phase, which gives the material the necessary toughness to withstand masticatory forces. The higher the proportion of the crystalline phase, the better the mechanical properties of the ceramic. (Serbena et al., 2015) However, the crystallites scatter the incoming light and make the material opaque. The tooth-like aesthetics and mechanical properties of a glass ceramics result from the interaction of the two phases. Dental glass ceramics, such as leucite (Initial LRF, GC Corp, IPS Empress Press or CAD, Ivoclar Vivadent) or feldspar ceramics (Vita blocs Mark II, Vita Zahnfabrik) have a crystallite content of approximately 40% by volume. (Guazzato et al., 2004) They exhibit excellent aesthetics with high translucency and show a fracture toughness of approximately 1 MPa•m1/2. (Belli et al., 2018) Reinforced
glass ceramics, such as lithium (di)silicate ceramics, have a considerably increased crystallite content of approximately 70% by volume and therefore show significantly higher fracture toughness compared to feldspar and leucite glass ceramics. (Belli et al., 2018) Due to their toughness and aesthetics, lithium (di)silicate ceramics are the material of choice for full crowns in the premolar, molar, and anterior, as well as for inlays, onlays, and overlays.
The higher mechanical properties of lithium (di)silicate ceramics rely on not only the higher crystallite content but also the microstructure of the crystallites. This glass ceramic contains crystallites of lithium silicate (Li2SiO3) and lithium disilicate (Li2SiO5), which have an elongated form (Fig. 1). These elongated crystallites form an interlocking bulk microstructure, which hinders the growth of potential cracks by deflection around the crystallites. (Belli et al., 2017) The improved mechanical properties of lithium disilicate compared to those of leucite ceramics are also reflected in everyday clinical practise: partial crowns made of milled lithium disilicate ceramics show a significantly higher survival rate than partial crowns made of milled leucite ceramics. (Belli et al., 2016)
Depending on the manufacturer, these reinforced modern glass ceramics are available as pressed ceramic (e.g., Initial LiSi Press, GC, Fig. 2a) or as CAD/ CAM blocks (Initial LiSi Block, GC, Fig. 2b). Because some lithium (di)silicate ceramics are too hard, they are milled in a pre-crystallised form (e.g., IPS e.max CAD, Ivoclar Vivadent). After milling, a crystallisation firing is performed to ensure that the restoration retains its final aesthetics and strength (“twostep-chairside”, CAD/CAM ceramics). Other variants (e.g., Initial LiSi Block, GC) do not require separate crystallisation firing (“one-step-chairside” CAD/CAM ceramics) and they
can be postprocessed immediately after milling, by painting (e.g. Initial Lustre pastes ONE, GC), micro-layering (Lustre Pastes ONE and SQIN ceramics, GC) or simply by polishing to high gloss. The latter procedure probably also has clinical advantages: In vitro studies show that pure polish leads to less abrasion of the antagonists in the area of the contact points. (Lawson et al., 2014).
Cavity design
To reach a maximum of fracture resistance and aesthetics, tooth coloured partial crowns should be adhesively attached to the tooth. If a conventional adhesive luting of the restoration is intended (acid-etching of the tooth and dentine bonding), it is recommended to check if rubber dam can be placed (e.g., for inlays and onlays). In cases where subgingival preparation margins cannot be kept dry with a rubber dam, a “proximal box elevation” can be performed. In this case, a direct adhesive filling is placed using a matrix technique, which moves the preparation margin further coronally, so that rubber dam placement is possible. (Frankenberger et al., 2013) Generally, the preparation of tooth-coloured partial crowns is based on the preparation rules for ceramic inlays and partial crowns. (Frankenberger, 2007) The most important rule is that all transitions in the cavity are rounded to minimise stress peaks. The preparation should be designed so that the restoration always has a minimum layer thickness of 1.0-1.5 (in accordance with the manufacturer’s recommendations for partial crowns) especially in the area of the central fissure, one should be aware to leave sufficient space. The residual tooth structure in the cusp area should not be less than 1.5 mm thick either. If this is not reached or if the preparation margin reaches the tip of the cusp, the cusp must be shortened. An angle of 90° should be created at the transition from the restoration to the hard tooth substance. The opening angle of
the proximal cavities should also be 90°. The opening angle of the cavity wall to the occlusal should be 6 to 10°. Adhesive luting of lithium (di) silicate ceramics.
Lithium (di)silicate glass ceramics can be relatively easily adhesively luted to the tooth. Regardless of the method for adhesive luting, the correct pre-treatment of the restoration is crucial. Lithium (di)silicate ceramics are etched with 5% hydrofluoric acid according to the respective manufacturer’s instructions and then thoroughly rinsed with water spray. Hydrofluoric acid dissolves the glass phase from the surface and creates a rough micro-retentive surface. This surface is treated with a silane containing adhesion promoter. By evaporation of the solvents in the silane primer, the silanol group of silane condenses and chemically bonds with the etched glass-ceramic surface. The methacrylate residue of the silane coupling agent points toward the adhesive joint, where it can polymerise with the luting composite. This process is called salinisation.
Pre-treatment of the tooth and luting materials
Maximum adhesion to the tooth is required for inlays, onlays, and veneers so that the lithium (di)silicate ceramic can achieve its maximum strength and aesthetics. For this purpose, the tooth should be pre-treated by enamel etching technique and dentine bonding. For these procedures, an absolute dry field technique by means of a rubber dam is indispensable. (Falacho et al., 2023) For inlays, onlays and veneers, adhesive / multistep cements (e.g., G-CEM Link Force, G-CEM Veneer, GC; Multilink Automix, Variolink Aesthetic, Ivoclar; RelyX Ultimate, 3M) and universal cements with adhesive/primer (G-CEM ONE with AEP or G-Premio Bond, GC Corp; RelyX Universal and Scotchbond Universal Plus, 3M) can be used. (Maravic et al., 2023)
When luting full crowns of lithium (di) silicate ceramics, where no enamel is left and sufficient retention is given, no pre-treatment of the tooth is required and self-adhesive/ one-step cements (RelyX Unicem Automix 2, 3M) or universal cements in self-adhesive mode (G-CEM ONE, GC; RelyX Universal, 3M) can be the materials of choice. (Maravic et al., 2023)
Polish
The fitting of the restoration to the cavity or adjustment of the occlusion after placement is often unavoidable. Studies show that this can damage the surfaces of the ceramics to such an extent that their strength is permanently reduced, and the probability of fractures increases. For this reason, the restoration should be perfectly polished after grinding, from the red band to the yellow band, and finally to the white band finishing bur. Simple polishing on a roughly ground restoration is not sufficient. Although it appears glossy to the eye, it leaves deep defects on the surface. (Lohbauer, 2018)
The Clinical Case
Inadequate restorations of teeth 46 and 47 had to be replaced (Fig. 3a). After the removal of the deficient restorations and caries, the decision was made to restore the teeth with two lithium disilicate press ceramic inlays (Initial LiSi Press, GC, Fig. 3b), due to the extent of the cavities. After try-in, the inlays were etched (Fig. 3c) with 5% hydrofluoric acid for 20 seconds and silanised (G-Multi PRIMER, GC Corp., Fig. 3d). After isolation of the teeth with rubber dam, the enamel surfaces of the cavity were selectively etched with 35% phosphoric acid gel (Fig. 3e). The cavity was pre-treated with an adhesive primer (G-CEM ONE AEP, GC, Fig. 3f) for subsequent luting with universal cement (G-CEM ONE, GC). After luting using the tack-cure technique, excesses of universal cement were removed and the teeth and restorations polished. After removal of the rubber dam, the
restoration fitted nicely in the tooth (Fig. 3g).
Conclusions
Lithium (di)silicate glass ceramics are the ideal material for indirect tooth coloured restorations like inlays, onlays, and crowns because of the gentle aesthetics paired with toughness. Knowledge of the correct cavity design and adhesive procedures is essential for the best long-term performance in clinics.
Author Bio:
Priv.-Doz. Dr José Ignacio Zorzin is a senior dentist, researcher, and lecturer at the Department for Operative Dentistry at the University Hospital of Erlangen. His research topics include adhesive luting of indirect restorative materials, ceramics, and composites. His main clinical topics are minimally invasive aesthetic restorative procedures, endodontics, and dental photography. Dr Zorzin passed his state examination with distinction in 2009, received his doctorate in 2011 on the topic of dental adhesives, and received his Venia legendi (habilitation) in 2019 on the topic of dental materials in modern dentistry. He regularly publishes in scientific journals and is a sought-after speaker at conferences and continuing education courses.
REFERENCES :
BELLI, R., PETSCHELT, A., HOFNER, B., HAJTO, J., SCHERRER, S. S. & LOHBAUER, U. 2016. Fracture Rates and Lifetime Estimations of CAD/CAM All-ceramic Restorations. Journal of Dental Research, 95, 67-73.
BELLI, R., WENDLER, M., PETSCHELT, A. & LOHBAUER, U. 2017. Mixed-mode fracture toughness of texturized LS2 glass-ceramics using the three-point bending with eccentric notch test. Dental Materials, 33, 1473-1477.
BELLI, R., WENDLER, M., PETSCHELT, A., LUBE, T. & LOHBAUER, U. 2018. Fracture toughness testing of biomedical ceramic-based materials using beams, plates and discs. Journal of the European Ceramic Society, 38, 5533-5544.
FALACHO, R. I., MELO, E. A., MARQUES, J. A., RAMOS, J. C., GUERRA, F. & BLATZ, M. B. 2023. Clinical in-situ evaluation of the effect of rubber dam isolation on bond strength to enamel. Journal of Esthetic and Restorative Dentistry, 35, 48-55.
FRANKENBERGER, R., HEHN, J., HAJTO, J., KRAMER, N., NAUMANN, M., KOCH, A. & ROGGENDORF, M. J. 2013. Effect of proximal box elevation with resin composite on marginal quality of ceramic inlays in vitro. Clinical Oral Investigations, 17, 177-83.
FRANKENBERGER, R., MÖRIG, G., BLUNCK, U., HAJTÓ, J., PRÖBSTER, L., AHLERS, M. O. 2007. Präparationsregeln für Keramikinlays und –teil- kronen unter besonderer Berücksichtigung der CAD/CAM-Technologie. teamwork Journal of Continuing Dental Education, 6, 684–690.
GUAZZATO, M., ALBAKRY, M., RINGER, S. P. & SWAIN, M. V. 2004. Strength, fracture toughness and microstructure of a selection of all-ceramic materials. Part I. Pressable and alumina glass-infiltrated ceramics. Dental Materials, 20, 441-448.
LAWSON, N. C., JANYAVULA, S., SYKLAWER, S., MCLAREN, E. A. & BURGESS, J. O. 2014. Wear of enamel opposing zirconia and lithium disilicate after adjustment, polishing and glazing. Journal of Dentistry, 42, 1586-91.
LOHBAUER, U. B., RENAN; WENDLER, MICHAEL 2018. Einfluss der Politur auf die Festigkeit zahnfarbener Dentalmaterialien. Quintessenz Zahntechnik, 44, 1546-1559.
MARAVIC, T., MAZZITELLI, C., MANCUSO, E., DEL BIANCO, F., JOSIC, U., CADENARO, M., BRESCHI, L. & MAZZONI, A. 2023. Resin composite cements: Current status and a novel classification proposal. Journal of Esthetic Restortorative Dentistry, n/a. SERBENA, F. C., MATHIAS, I., FOERSTER, C. E. & ZANOTTO, E. D. 2015. Crystallization toughening of a model glass-ceramic. Acta Materialia, 86, 216-228.



Fig. 1: SEM image of Initial LiSi Press after etching with hydrofluoric acid. The lithium disilicate crystallites were coloured orange by image post-processing, the glass phase is grey. Image: courtesy of Priv.-Doz. Dr Renan Belli.









Fig. 3f: Cavities after application of the adhesive enhancing primer (G-CEM ONE AEP, GC Corp.).
Fig. 2a: Lithium disilicate glass ceramic ingots for pressing (Initial LiSi Press ingots, GC).
Fig. 3g: Luted and polished restorations under rubber dam.
Fig. 2b: Lithium disilicate CAD/CAM Block for CEREC (Initial LiSi Block, GC).
Fig. 3h: Restorations after removal of the rubber dam. Rehydration of enamel will take place over the next days.
Fig. 3a: Inadequate restorations in teeth 46 and 47.
Fig. 3b: Inlays made from pressed lithium disilicate (Initial LiSi Press, GC Corp.) for teeth 46 and 47.
Fig. 3c: Etching of the lithium disilicate inlays with hydrofluoric acid.
Fig. 3d: Silanisation of the etched surfaces (G-Multi PRIMER, GC Corp.).
Fig. 3e: Selective acid etching of the enamel with phosphoric acid gel under a rubber dam.
Dr José Ignacio Zorzin Germany
Torqtech Red Band 1:5 Ultra Mini Handpiece Part.
02
Interview with the Developer of the Torqtech Red Band Handpiece.
Morita released the Torqtech Red Band Ultra Mini Handpiece in October 2022 in response to requests from many dentists. This product was finally developed despite many difficulties through the high technological skills and persistent creative efforts of engineers at J. MORITA MFG. CORP. 12 years after the first release of the Torqtech series. We interviewed Mr. Hitoshi Tanaka, one of the engineers at J. MORITA MFG. CORP., for his insight into the development of the Torqtech Red Band Handpiece in Part 1 and the Torqtech Red Band Ultra Mini Handpiece in Part 2.
In 2022, the Ultra Mini joined the portfolio of the Torqtech Red Band Handpiece series.
Tanaka: At the same time as the Torqtech series was released in 2010, Morita also released the TwinPower Turbine Ultra series (Powerful Micro Head). The power of a turbine decreases if its head size is reduced, due to the smaller impeller. Morita introduced a new double impeller mechanism, which achieved strong power and constant torque and was highly evaluated by dentists. We also received many requests for a smaller head size for the red band handpiece. However, to realize this, there were unique difficulties that were not present when downsizing the

turbine head. The downsizing of a turbine head is achieved by reducing the size of the impeller. In contrast, because a red band handpiece is driven by a motor, downsizing gears in the same manner would result in larger burdens on the gears and bearing, causing a problem with durability. Therefore, we needed to downsize the bearing without altering the gear system, while simultaneously increasing its durability.
There were unique difficulties that were not present when downsizing the turbine head. How did you improve the bearing?
Tanaka: A common bearing has an inner ring and an outer ring, respectively on the inside and outside of a ring-shaped groove where the balls rotate, with an inner retainer that retains the balls at equal intervals. The retainer is the most crucial element of a bearing and is also the most vulnerable to damage. Whereas metal materials are commonly used for retainers, a metal retainer rapidly wears out through fast rotation. Therefore, we use a special resin material for the Ultra Mini. Whereas resins are inferior to metals in strength, their extreme lightweight is stronger than metals against wear through fast rotation. Common resins easily deteriorate at high temperature and are therefore extremely vulnerable to sterilization, and can be damaged through repeated autoclaving. To solve this problem, we use a special resin material featuring both heat and steam resistance for the retainer part of the Ultra Mini.
Double impeller system of the TwinPower Turbine.
PART 2: Torqtech Red Band Ultra Mini Handpiece the Most Compact Size in the World
Did you also improve the structure, in addition to the material?
Tanaka: There are two structures for bearings: deep groove bearings and angular bearings. A deep groove bearing has a ball placed on a deep groove, with the retainer holding the ball from one side and capping it with the outer ring. This is the structure used for conventional red band handpieces. The Ultra Mini uses an angular bearing, which withstands a larger axial load than a deep groove bearing. An angular bearing has a groove only on one side, with a basket-shaped retainer that holds the ball from all sides. By using an angular bearing, we achieved about twice the retainer strength and reduced axial run out. Through repeated experiments and durability tests, we achieved the present bearing specification over a period of about five years. The bearing is the core of turbines and contra-angles and is the most vulnerable to damage. Because technology continuously advances over time, our development has never ceased even after the release of the Ultra Mini in 2022.
The Ultra Mini also has an improved water injection method.
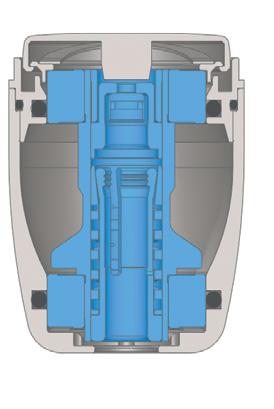
Tanaka: A conventional red band handpiece uses a threeport water irrigation system. In the case of three-port water injection, a complicated pipeline is required inside the head, which inevitably increases the head height. Therefore, we designed the Ultra Mini head to use a unique, single-port water injection system. However, with the single-port water injection used in general small heads, the water injection power is simply reduced to one-third.In the case of a red band handpiece, they are often used under higher loads than
air turbines, and cooling the bur is important because heat generated in the cutting area may have an adverse effect on the tooth pulp. In order to avoid this issue, we developed an all-new wide, single-port water irrigation system.It has a water injection port in the center and two chip air holes on each side for a total of 4. This mechanism aims the water flow at the center and spreads it out in a fan shape. This makes it possible to cool a wider area from the shank of the bur to the tip.With single-port water injection, the water could easily miss the bur, which could cause the bur to heat up and the teeth to char. Wide, single-port water irrigation is unique and is unaffected by water and chip air pressure.(The wide oneport system is patent pending.)
What ideas were used in the wide single-port system?
Tanaka: Unlike common chip air tubing, which has one tube through to the air outlet, the Ultra Mini has a tube that




Water spraying with the wide one-port system.
(The photos were taken without chip air. Due to the temperature increase of the bur, the temperature indicating material has changed its color to white to indicate high temperatures.)
(Left) Accurate water injection. (Right) Inaccurate water injection.
branches to four air outlets. The holes are so small that it is difficult to visually find them on the actual product. Each hole is only 0.2mm, about the size of hair. Specialists with long experience in processing have combined their expertise to realize this product. Engineers engaged in production upgraded their skills through in-house training to handle the extremely precise processing and complex assembling necessary to produce the Ultra Mini. The final assembling and product inspection require especially high skills that only several engineers are certified for. Although this may not be an ideal process from the viewpoint of productivity, we cannot avoid this aspect in pursuit of the most compact size and the highest durability in the world. We believe that, by going our own way to boldly challenge precise and complex processing and assembling, we can establish unique and unparalleled characteristics

We cannot afford to compromise the knowledge, skills, and passion that we have inherited from our predecessors. We realized the Ultra Mini by aiming to develop the most compact head size in the world, resolving many difficulties one after another through concerted efforts of the development and manufacturing teams. I hope that clinicians will immediately feel the difference and experience the high usability and durability achieved through all these efforts.






Hitoshi Tanaka Associate Engineer, Research and Development Group
1
J. MORITA MFG. CORP.

Unique chip air outlet of the Ultra Mini
Size comparison between Torqtech Red Band Handpiece Standard vs. Ultra Mini.
View Product

Carriere Motion 3D appliance
The sagittal First revolution
The SAGITTAL FIRST™ Philosophy is a time-tested approach that standardises, simplifies, and shortens Class II and Class III treatment times. It employs the Carriere Motion 3D Appliance to treat the AP dimension at the beginning of treatment before placing brackets or aligners. By resolving the most difficult part of treatment first, you can achieve a Class I platform in 3 to 6 months, shortening total treatment time by a minimum of 6 months 1. You know how excited patients and parents become when you mention shorter treatment times.


1 “Treatment Effects of the Carriere Distalizer (Motion 3D) Using Lingual Arch and Full Fixed Appliances”, Journal of the World Federation of Orthodontists, May 2014
CLASS III - Mark
PROVIDED BY: DR. LUIS CARRIÈRE
INITIAL - 5/22/18






PROGRESS 1 - 5/22/18 - Placement of the Motion 3D Class III Appliance
22/5/18



PROGRESS 2 -10/1/18 - Class I platform achieved in 4 ½ months, uncrowding the lower arch
1/10/18



PROGRESS 3 - 10/1/18 - Placement of the SLX 3D Clear Brackets with M-ONE .015 Cu Nitanium 27°
1/10/18



PROGRESS 4 - 10/29/18 - With M-TWO .020 x .020 Cu Nitanium 35° archwire
29/10/18




PROGRESS 5 -11/27/18


PROGRESS 6 -1/15/19 - With M-TWO.FIVE .019 x .025 Cu Nitanium 35° archwire
27/11/18 15/1/19



[CONTINUED ON NEXT PAGE]


The right pH for both the patient and the dental practitioner
A happy patient becomes a longterm patient. A painless anaesthetic injection will quickly dispel any apprehensiveness in the dental practice, and get treatment off to a good start. A 2004 study showed that patients judge their dental practitioner first and foremost on their skill in giving pain-free injections. Injections do not have to be something to fear –on the contrary, they can be the first step in a relationship of trust with the practitioner. To achieve this, the dental practitioner must be able to rely on supplies of the highest quality: not just the syringe and the needle, but also the local anaesthetic chosen. For although they may contain the same active ingredients, brands of local anaesthetic can differ considerably, depending on the manufacturing process, the way they are sterilized, the excipients they include, their pH level, and so on.
pH, an important aspect of local anaesthetics
The pH of the solution has an important place as one of the factors that distinguish between anaesthetics, as it varies from one product to another and one manufacturer to another. While human tissues are pH-neutral (7.4) under normal physiological conditions, solutions used in anaesthesia on the
other hand need to be somewhat acidic.
Each cartridge of injectable solution includes a local anaesthetic, sometimes alone and sometimes mixed with a vasoconstrictor such as adrenalin. The advantage of the vasoconstrictor is that it significantly increases the duration of anaesthesia. But the drawback is that adrenaline requires an acidic or even very acidic pH, if it is to remain stable and active throughout the product’s shelf life. A solution that contains adrenaline will therefore be more acidic than one that contains anaesthetic alone. For this reason, all manufacturers have to lower the pH of their anaesthetic solutions to prevent the vasoconstrictor degrading. Finally, the acidity level, which is set by the manufacturer, will depend on the formulation, and the excipients and preservatives included. The difficulty therefore is to offer the dental practitioner a solution that is stable and effective, but with the least-acidic pH possible.
Negative clinical consequences of an acidic pH
Unfortunately, injecting an acidic solution has clinical consequences for both patients and practitioners, which cannot be ignored. First of all, the more acidic the pH, in other words the further it is from the
neutral physiological level, the more the patient will feel the injection… meaning a more painful injection, irrespective of the practitioner’s technique and experience. This pain has to be taken into account, as it is the main determining factor in the trust between patient and his dental practitioner.
Secondly, another pH-related clinical effect is that the more acidic the solution, the longer the onset time –that unavoidable wait between the moment of the injection and the time the anaesthetic takes effect. There are actually two forms of anaesthetic compound in a solution, in an acid-base balance: ionized forms (which do not penetrate the cell) and non-ionized forms (which go to the heart of the cell, an essential stage in achieving anaesthesia). The balance between the two depends on the solution’s pH. The closer this is to physiological pH, the higher the proportion of non-ionized or “active” forms. When the solution is injected, the body buffers the solution, in other words it brings it up to physiological pH. During this process, the acidbase balance is altered and more active molecules are present. This physiological buffering process takes time, and is a major factor in the anaesthetic’s onset time. So the more

acidic the pH of the injected solution, the longer the body needs to bring the solution to 7.4, with the effect of increasing the onset time.
Tailored pH for Septodont anaesthetics
Top quality anaesthesia is the highest priority for Septodont. That’s why the company focuses on making products with the lowest possible acidity, to limit their adverse effects for both practitioners and patients. The group has spared no expense in developing solutions with higher pH levels, investing over the years in projects to constantly improve and adapt its formulations.
This has enabled Septodont research teams to gradually increase the pH of its leading products, such as Septanest, by developing unique formulations that are compatible with a standard shelf life and the least-acidic pH possible. And now Septanest is available on the market, with a level that is considered to be low-acid compared to competing equivalent forms, at a pH of 4.0–5.5.
Being totally committed to optimal quality, and making constant improvements, is of course a long-
term approach for Septodont. This commitment to excellence makes a real difference in the dental practice, and has enabled Septodont to claim its place as world leader in dental anaesthesia.
An emphasis on quality in product manufacturing
One feature of Septodont unique production process involves including a terminal sterilization stage, a gold standard for the health authorities in the manufacture of sterile pharmaceutical products. This method ensures the highest guarantee
of sterility for all the group’s local anaesthetics, including Septanest. As the world leader in dental anaesthesia, Septodont has the world’s largest production capacity: 9000 square metres over two manufacturing sites (in France and Canada). It produces over 500 million cartridges per year, all benefiting from this terminal sterilization stage.

View Product
The Magic Wand of Painless Dentistry
I have been using the STA wand for over 19 years having been introduced to the STA Wand at a course in Ballarat where I volunteered to have the STA. The only time I previously had intraoral local anaesthetic (LA) was more than ten years earlier as a third-year dental student. I did not feel the LA and subsequently bought a STA unit.
As a Specialist Periodontist, I generally see an older demographics of patients for the management of periodontitis, implant placements, extractions and periodontal surgeries. However, I treat a number of teenagers who are either undergoing or recently completed orthodontics. A local orthodontic practice sends a large number of his patients to my practice as we have the “Magic Wand”.
I most frequently do infiltrations on the buccal aspects of the teeth when I do initial stage non-surgical periodontal treatment and the occasion supportive periodontal maintenance patient. However, I also use the STA wand to do palatal injections for implants, extractions, periodontal surgeries and rarely for non-surgical root surface debridement. With the STA Wand, the palatal injections are painless unlike conventional palatal injections which can be very sore. I don’t do single-tooth anaesthesia as I do not do restorative treatment or endodontics.
On average, it takes me 2-4 minutes to use the STA Wand. I count 25 beeps when I do an infiltration and then do the next injection a few teeth away for non-surgical periodontal treatment. For implants, extractions and periodontal surgeries, I use the entire carpule of LA, giving the LA both buccally and lingually or palatally.
A couple of tips for using the STA Wand include dispensing a couple of drops of LA on the mucosa before inserting the needle, holding the Wand with a pen grip and asking your patients to count the beeps. This is a fantastic distraction.
My patients love the Wand. They ask, “aren’t you going to give me a needle” and “why don’t all dentists have the Wand?” My answer to the first question is “I already have” and the patients look at me incredulously. My answer to the second question is” I honestly don’t know but they should”. The STA Wand is an invaluable part of my practice. There are two pieces of equipment that I won’t work without – my loupes and the STA Wand.



Author:
Dr Susan Wise is a Specialist Periodontist in the South Eastern suburbs of Melbourne. Susan graduated as a dentist from the University of Melbourne in 1994 and as a periodontist at the University of Queensland in 2002.
Susan is an Australian Dental Association Board Director. She is a Past President of the Royal Australasian College of Dental Surgeons, Australian Dental Association Victorian Branch and the Australian Society of Periodontology Victorian Branch. Susan has been a demonstrator to and examined undergraduate and postgraduate students in periodontics.

Dr Susan Wise Specialist Periodontist View Product
7 Ways To Extend The Life Of Your Ageing Patient’s Smile
We are living for longer and maintaining our expectations of function and aesthetics into maturity. Ageing well is important [1] .
Many of our ageing patients are motivated to maintain long-lasting smiles that are both aesthetic and functional. But what happens to our teeth as we age? And what can you do to help your patient’s smile last the distance?
It’s (partly) about dentine and enamel.
Dentine is predominantly made of hydroxyapatite mineral and collagen. The findings from my PhD indicate that in mature teeth, dentine mineral deposits fill the tubules to span from the pulp through to the dentine-enamel junction [2, 3]. The dentine collagen weave becomes less organized because of a process known as cross-linking that results in a stiff collagen matrix [4] A combination of stiff collagen and increased minerals makes mature teeth more brittle, and prone to fracture [5]
Furthermore, the increase in tubular mineral and change in the collagen network, combined with the increased formation of new dentine around the periphery of the pulp, results in a noticeable change in light transmission through the tooth to affect aesthetics [6]
Aged enamel appears aesthetically different as well. With time, the hard enamel thins due to wear, attrition, abrasion and erosion [7]. The thinned enamel remains connected to dentine that acts to cushion the forces we place on teeth. Yet the characteristic change to aged dentine reduces the capacity to dissipate forces, to form visible crazes and cracks to develop in the enamel [5]
The food and drinks we consume fill the micro-gaps created by the crazes and cracks to discolour and stain teeth. Aesthetically, these stains are easily managed by tooth whitening using peroxide-containing products [8] such as the Colgate Optic White range. However, there are other ways we can help our patients extend the life of their teeth. Here are seven tips to prevent dental decline.
1. Avoid unnecessary forces
Counsel your patients to avoid using their teeth for nonfunctional activities [9] such as holding working tools or to open packaging.
Help your patients avoid unnecessary forces such as grinding or clenching by screen ing for Sleep Apnoea [10] and bruxism at their check-up appointments. Depending on the severity of sleep apnoea, your patients may benefit from an anterior advancement mandibular splint or a CPAP machine. For those who experience nocturnal grinding, encourage the use of an occlusal splint [11]
For patients who have large restorations [12], or root canal treated teeth [13], consider full or partial coverage indirect restorations to support the remaining tooth structure from cracking or breaking [14]
2. Share the load
Most ageing patients will have missing teeth, particularly in the posterior region of their mouth. Review your patient’s chewing capacity. Occasionally, despite having a near full complement of teeth, some patients may lack reasonable points of functional contact. Encourage your patient to consider treatment options that distribute the forces evenly, to
prevent the wear and breakdown of the limited number of teeth that are being ‘overloaded’.
Some options you may consider are bridges [15], implants [16] and well-fitted dentures [17] to support your patient’s function and occlusion. Ensure the dentures are checked regularly for fit and support, and replace these every ten years [18]
Don’t forget to educate your patients on how to care for their new fixed or removable prostheses. For those with good manual dexterity and existing oral hygiene habits such as flossing, encourage your patients to continue the process. Support your patients with additional needs, for example by encouraging the use of interdental brushes. For those who struggle to reach posterior teeth, or have issues with manual dexterity, or even floss-avoiders, a Colgate water flosser could be a good solution.
3. Preserve enamel
Enamel is the hard crystal coat that lends to aesthetics and protects dentine from acidic challenges [19]. Enamel preservation includes using appropriate toothbrushes, technique, toothpastes and avoiding erosive influences.

Counsel patients to replace hard bristled brushes with soft ones and encourage the use of electric brushes that provide additional monitoring capacity.
For instance the Colgate Pulse Series 2 connects with an app on their phone to help monitor ‘hard’ brushing with a pressure sensor, brushing times and helps patients locate
where they are missing the cleaning.
Help patients understand the nature of acids in their diet [9] . Many people believe that acids are ‘alkaline’ due to a popular health movement. Unfortunately, these patients succumb to drinking apple cider vinegar and lemon juice when their teeth are most vulnerable on awakening or consume ‘refreshing’ citrus fruits after physical exertion.
4. Enhance saliva
The buffering capacity of saliva reduces the effects of acid challenges, flushes teeth and gums, promotes soft tissue healing and prevents erosion and decay [20] . Healthy saliva flow is also significant to help patients digest

carbohydrates, swallow and speak.
As we age, saliva quality and quantity declines, often exacerbated by age-related changes to salivary glands and life-saving medications that are xerostomic. Two medications that cause significant symptoms in patients include antidepressants and antihypertensives [21]. If you are concerned about medication-related xerostomia, counsel your patients and contact their GP to advocate for substitution. Patients who suffer from reflux may benefit from medications to mitigate acid regurgitation. This is also another worthwhile reason to speak to your patient’s doctors. Many GPs welcome collaborative care of our patients [22]
5. Manage periodontal disease
Chronic periodontal disease is often a painless, occasionally asymptomatic issue that can cause significant tooth loss to affect health, function and aesthetics. Most ageing people

who suffer with periodontal disease often encounter multiple comorbidities [23], and you may be the first person to identify such issues. Encourage patients with periodontal issues to be assessed for conditions such autoimmune disorders or diabetes.
Other than tooth retention, explain the significance of maintaining gum health, including reducing the immune load to the body and reducing gingival recession to prevent exposed darker tooth roots. Root surfaces, particularly in ageing people, are more susceptible to caries and erosion [24]
6. Manage and prevent senescence
Cellular senescence is the process that changes DNA in our cells to reduce our ability to withstand physical, chemical or biological damage. Cellular senescence enhances new cancer formation, the spread of existing cancers and the onset of chronic illnesses such as Alzheimer’s disease, diabetes, osteoporosis and heart disease [25]
We can help our patients reduce cell damage by helping them manage lifestyle factors such as smoking, uncontrolled diabetes and chronic infections such as periodontal disease.
7. Help our patients to adapt and evolve with their changing needs
Ageing affects cognition, manual dexterity and eyesight to prevent your patients from practicing oral hygiene to the best of their ability [26]. Regular recalls are an opportunity for you to observe these changes in your patients. Occasionally, you may note that a previously diligent patient may have reduced
capacity or let their oral hygiene slip. In these instances, switching your patient to higher fluoride toothpastes, mouthwashes and helping them switch from practices such as flossing to interdental brushes may be helpful [27]. Increasing the regularity of their cleaning appointments may also serve to keep a check on your patients and support their needs better.
So, remember ageing teeth are prone to fracturing and breaking. You can help your patients extend the life of their smile by helping them reduce unnecessary masticatory forces on existing dentition, share the load by using removable or fixed dental prostheses, preserve enamel, enhance saliva, manage periodontitis, mitigate senescence and adapt with your patients. We are all in this together.

Dr Arosha Weerakoon
Author:
Dr Arosha Weerakoon is a Senior Lecturer at the School of Dentistry, The University of Queensland (UQ), and owner of Tewantin Family Dental.
Arosha has a Master’s in Public Health and a PhD (UQ); her thesis is titled, ‘Dentine, Adhesive Interfaces & Physiological Ageing’. She is a Fellow of the Royal Australasian College of Dental Surgeons, the International College of Dentists and the Pierre Fouchard Academy. Arosha is the Assistant Secretary for the International Dental Ethics and Law Society, and Deputy Chair and oral health representative for the Country to Coast Queensland Clinical Advisory Council.
In recognition of her commitment to professional learning and development, Arosha was awarded the 2022 BOQ Specialist Practice Bursary for Dental Excellence from the Australian Dental Association (QLD). In 2019, Arosha was awarded the Brisbane Lord Mayor’s Convention Trailblazer Grant. In the same year, Arosha won the top prize, The Vice Chancellor’s Award, for her research pitch titled, ‘It’s about bonding with fillings’ hosted by Universities Australia. As part of her prize, Arosha completed an internship at The Conversation Media Group Headquarters in Melbourne. To date, she has published eleven articles promoting oral health with The Conversation Media Group.
Arosha believes that community engagement, interdisciplinary collaboration and patient empowerment is the key to improving oral and general health for all. She hopes to use her role as a Colgate Advocate for Oral Health to create meaningful discussions with oral and general health professionals to improve health practices, patient outcomes and to encourage more clinicians to engage with research.
1. Jones, J.A., et al., Edentulism Predicts Cognitive Decline in the US Health and Retirement Cohort Study. J Dent Res, 2023. 102(8): p. 863-870.
2. Li, C., et al., Dentinal mineralization is not limited in the mineralization front but occurs along with the entire odontoblast process. International journal of biological sciences, 2018. 14(7): p. 693.
3. Weerakoon, A.T., et al., Does dentine mineral change with anatomical location, microscopic site and patient age? Journal of Structural Biology: X, 2022. 6: p. 100060.
4. Weerakoon, A.T., et al., Dynamic dentin: A quantitative microscopic assessment of age and spatial changes to matrix architecture, peritubular dentin, and collagens types I and III. Journal of Structural Biology, 2022. 214(4): p. 107899.
5. Weerakoon, A.T., et al., Coronal dentin differs between young and mature adult humans: A systematic review. Archives of Oral Biology, 2022. 144: p. 105553.
6. Miura, J., et al., Accumulation of advanced glycation end-products in human dentine. Archives of oral biology, 2014. 59(2): p. 119-124.
7. Atsu, S.S., et al., Age-related changes in tooth enamel as measured by electron microscopy: Implications for porcelain laminate veneers. The Journal of Prosthetic Dentistry, 2005. 94(4): p. 336-341.
8. Irusa, K., et al., Tooth whitening procedures: A narrative review. Dentistry Review, 2022. 2(3): p. 100055.
9. Kaidonis, J.A., Oral diagnosis and treatment planning: part 4. Non-carious tooth surface loss and assessment of risk. British Dental Journal, 2012. 213(4): p. 155-161.
10. Association., A.S. Obstructive Sleep Apnoea Assessment Questionnaires. [Webpage] 2024 [cited 2024 Octoer 20]; Available from: https://www.sleepprimarycareresources. org.au/osa/assessment-questionnaires.
11. Minakuchi, H., et al., Managements of sleep bruxism in adult: A systematic review. Japanese Dental Science Review, 2022. 58: p. 124-136.
12. Tennert, C., et al., Posterior ceramic versus metal restorations: A systematic review and meta-analysis. Dental Materials, 2022. 38(10): p. 1623-1632.
13. Dioguardi, M., et al., The influence of indirect bonded restorations on clinical prognosis of endodontically treated teeth: A systematic review and meta-analysis. Dental Materials, 2022. 38(8): p. e203-e219.
14. Kaup, M., et al., Shear bond strength of Biodentine, ProRoot MTA, glass ionomer cement and composite resin on human dentine ex vivo. Head Face Med, 2015. 11: p. 14.
15. Whang K, Resin-based Composites, in Phillips’ science of dental materials, Anusavice KJ, et al., Editors. 2013, Elsevier/Saunders: St. Louis, Mo.
16. Misch, C.E., et al., Posterior Implant Single-Tooth Replacement and Status of Adjacent Teeth During a 10-Year Period: A Retrospective Report. Journal of Periodontology, 2008. 79(12): p. 2378-2382.
17. Oki, K., et al., The Significance of Posterior Occlusal Support of Teeth and Removable Prostheses in Oral Functions and Standing Motion. International Journal of Environmental Research and Public Health, 2021. 18(13): p. 6776.
18. Taylor, M., M. Masood, and G. Mnatzaganian, Longevity of complete dentures: A systematic review and meta-analysis. The Journal of Prosthetic Dentistry, 2021. 125(4): p. 611-619.
19. Zanatta, R.F., et al., Comparison of micro-CT and conventional dye penetration for microleakage assessment after different aging conditions. International journal of adhesion and adhesives, 2019. 89: p. 161-167.
20. Xu, F., L. Laguna, and A. Sarkar, Aging-related changes in quantity and quality of saliva: Where do we stand in our understanding? Journal of Texture Studies, 2019. 50(1): p. 27-35.
21. Gueiros, L.A., M.S. Soares, and J.C. Leão, Impact of ageing and drug consumption on oral health. Gerodontology, 2009. 26(4): p. 297-301.
22. Weerakoon, A., L. Fitzgerald, and S. Porter, An Australian government dental scheme: Doctor-dentist-patient tensions in the triangle. The Journal of Forensic Odontostomatology, 2014. 32(Suppl 1): p. 9.
23. Liu, Y., et al., Does Periodontitis Affect the Association of Biological Aging with Mortality? J Dent Res, 2023. 102(8): p. 909-918.
24. Leiva-Sabadini, C., et al., Nanoscale Dynamics of Streptococcal Adhesion to AGEModified Collagen. Journal of Dental Research, 2023. 102(8): p. 957-964.
25. Aquino-Martinez, R., The Emerging Role of Accelerated Cellular Senescence in Periodontitis. J Dent Res, 2023. 102(8): p. 854-862.
26. Yang, Y., et al., Improving oral hygiene for better cognitive health: Interrelationships of oral hygiene habits, oral health status, and cognitive function in older adults. Journal of Advanced Nursing, 2024. 80(1): p. 275-286.
27. Woon, C., Improving oral care for hospitalised patients: choosing appropriate products. British Journal of Nursing, 2020. 29(9): p. 520-525.
Oral Cancer: Social Determinants in Australia
Cancer. A word we’re all familiar with, a thought not so pleasing, and a community crisis that needs greater public awareness. So, how do we achieve this?
Oral cancer has become one of the six most common cancers globally. It affects the oral cavity soft tissues, hard tissues and oropharynx4. A variety of locations are affected by what is known as Oral Squamous Cell Carcinoma (OSCC). Much thought must be given to why many individuals are vulnerable to this disease. Many risk factors for oral cancer are linked to social habits and behaviours, such as smoking and alcohol consumption. These behaviours are very common and are the two leading and most harmful factors in the risk of developing oral cancer in the Australian population². however, further consideration of secondary determinants such as age, stress, nutrition, family history of cancer and viruses with particular focus on the Human Papilloma Virus (HPV), must be borne in mind. Although contributing factors have become well established, it is with risky behaviours and poorer health literacy4 that more and more cases of oral cancer are seen today.
OSCC exhibits unpredictable signs and symptoms, and to the untrained eye, is almost always undetected until later stages of manifestation4. Non-healing ulcers are found to be the most common sign of OSCC4. Roughly 49% of Australian patients have never heard of oral cancer and the many risks that contribute to the development of this illness³. Furthermore, not only is half the population unaware, only half of the Australian community currently attend for dental checkups and oral cancer screenings each year4. This therefore limits early diagnoses and puts strain on oral care services. Many patients with oral cancer are unaware of their condition, predominantly due to the lack of early symptoms that
may be easily identified, such as a runny nose when developing the common cold. Signs and symptoms are what usually drives a person to seek healthcare, however in the instance of OSCC, this generally occurs at a late stage of development. This results in over 60% of patients being diagnosed with stage III or IV OSCC with a five-year survival rate of 15-55%³. OSCC is a serious and life-threatening disease that requires further exploration, with focus on the how and why. How are new cases being found in some populations and not others, and why is this somewhat specific to a particular group? Social determinants.
Many healthcare professionals rely on specific determinants or ‘red flags’ to understand an individual’s risk of a disease or illness. In Australia, oral cancer diagnoses are more commonly seen in those with regular use of alcohol and who smoke, with the growing population over 40 having higher risk of OSCC³. Frequent use of tobacco products is linked to oral cancer, as either smoking or chewing of tobacco directly contacts many surfaces in the oral cavity. Long-term binge drinking is another behaviour which appears to be linked to cancer formation². Oral bacteria metabolise alcohol and produce acetaldehyde, a well-known carcinogen². Alcohol consumption, even when minimal or moderate puts an individual at risk of OSCC, 30 times greater when combined with long-term smoking6. It is with limiting or removal of these two specific determinants that your oral cancer risk is vastly reduced.
Social Determinants
Many risk factors or social determinants have been identified, but who will be at greater risk of oral cancer is the question. Not everyone who has a risk factor will experience oral cancer and not everyone who has little to no risk will be in the clear,
so what makes the difference in early diagnosis? It is through regular oral health assessments and screening undertaken by a general medical practitioner or general dentist that early detection and risk status can be determined³. High-risk factors are seen as6:
• Long Term Smoking
• Heavy Alcohol Consumption
• Age of 40+
• History of Human Papilloma Virus (HPV)
• Family History of Cancer
• Poor Nutrition
• Stress
• Ultraviolet (UV) Exposure
• Patient Delay in Self-Detection of Signs & Symptoms
Additionally, many as yet unproven determinants/behaviours have been identified as potential risks for OSCC. Such as vaping, ill-fitting dentures and poor oral hygiene⁶. With a lack of evidence to suggest direct links, it may still be helpful to address factors with the potential for modification and positive health outcomes.
Early Detection
Improved public knowledge is shown to greatly decrease an individual’s risk, seeing as greater knowledge allows for greater understanding of consequences. Evidence suggests a trending decline in OSCC incidence in the Australian population as a result of lifestyle changes¹. This is supported via oral health promotion and campaigns such as graphic health warnings on cigarette packaging¹. Oral cancer has vast potential to be successfully treated when an early diagnosis is made, and it is by understanding one’s risk and maintaining oral cancer screenings that this can be better achieved³. In support of early identification, the following signs and symptoms in and around the mouth should never be overlooked4.
• Non-healing Ulcer
• Red/White Patches
• Continuous Bleeding Gums
• Difficulty moving Tongue
• Reduced Opening
• Pain on Swallowing
• Loss of Taste
• Altered Sensations
Read more
It is with modification of lifestyle factors and early detection via thorough oral cancer screenings, that greater prevention of OSCC is achievable5. Trained professionals should encourage safe alcohol consumption and endorse smoking cessation to those at high risk. By promoting healthier choices and regular dental checks, together this can positively improve an individual’s outcome and quality of life4
Author Bio
Latisha Sykora is a fourth-year student pursuing a Bachelor of Dental Surgery at the University of Adelaide. As a proud Mudburra-Jingili woman, she possesses great desire and commitment to elevate Indigenous oral health outcomes by promoting leadership and preventive measures. Latisha’s journey in dentistry began in 2012, completing a schoolbased traineeship in dental assisting, an experience that fuelled her interest in oral disease, particularly in rural and remote communities. Her determination led to becoming a graduate Oral Health Therapist in 2019. Currently, she serves as a supporting clinician at the Indigenous Oral Health Unit (IOHU) at the University of Adelaide, while also devoting time to work in private practice. For Latisha, early intervention and education hold the key to achieving excellence in oral health. She actively demonstrates this belief by mentoring Indigenous students and serving as a Director of the Indigenous Dental Association Australia (IDAA). In 2022, she was awarded the Student Leadership Award for Indigenous Allied Health Australia (IAHA). Through her inspiring work and leadership, Latisha joins the Colgate Advocates for Oral Health: Content Community ready to embody a lasting impact on Indigenous oral health and create a brighter, healthier future for her community.
REFERENCES:
1. Ramamurthy, D, Sharma, D & Thomson, P, 2022, ‘Oral cancer awareness in patients attending university dental clinics: A scoping review of Australian studies’, Australian Dental Journal, vol. 67, issue. 1, pp. 5-11, <https://onlinelibrary.wiley.com/doi/ epdf/10.1111/adj.12877>.
2. Bosetti, C, Carioli, G, Santucci, C, Bertuccio, P, Gallus, S Garavello, W, Negri, E & La Vecchia, C, 2020, ‘Global trends in oral and pharyngeal cancer incidence and mortality’, Internal Journal of Cancer, vol. 147, issue. 4, pp. 1040-1049, <https://pubmed.ncbi.nlm. nih.gov/31953840/>.
3. Webster, JD, Batsone, M & Farah, CS, 2019, ‘Missed opportunities for oral cancer screening in Australia’, Journal of Oral Pathology & Medicine, vol. 48, issue. 7, pp.. 595603, <https://pubmed.ncbi.nlm.nih.gov/31188491/>.
4. Yang, LC, Yang, A, Chen, LN, Firth, N, Prabhu, SR & Zachar, J, 2022, ‘Knowledge of Oral Cancer Amongst Dental Patients Attending Public Clinics in South East Queensland, Australia’, Journal of Cancer Education, vol 37, issue. 4, pp. 924-931, <https://pubmed. ncbi.nlm.nih.gov/33068265/>.
5. Wolfer, S, Kunzler, A, Foos, T, Ernst, C, Leha, A & Schultze-Mosgau, S, 2022, ‘Gender and risk-taking behaviours influence the clinical presentation of oral squamous cell carcinoma’, Clinical and Experimental Dental Research, vol. 8, issue. 1, pp. 141-151, <https://pubmed.ncbi.nlm.nih.gov/34989151/>.
6. American Cancer Society 2024, Can Oral Cavity and Oropharyngeal Cancers Be Prevented?, <https://www.cancer.org/cancer/types/oral-cavity-and-oropharyngeal-cancer/ causes-risks-prevention/prevention.html>.

Latisha Sykora
Bachelor of Dental Surgery at the University of Adelaide.

How to properly care for braces
Tips from a dentist
Wearing braces can be a hassle, especially when eating and cleaning them properly. We talked with TePe’s dental expert, Dr Michaela von Geijer, to understand the challenges of wearing braces. How can dental professionals make life easier for the patient, and what needs to be done to keep the teeth and gums healthy during treatment?
Many patients with braces will develop white spots during treatment; studies show a range of 2–97%. Studies also show that 1 in 2 will develop white spots on more than one tooth.1,2 The white spots develop very quickly, so it’s important to clean thoroughly right from the start of the treatment.3 As dental professionals, we have the responsibility and knowledge to guide the patient to the most suitable oral hygiene tools. We should instruct and encourage the patient and ensure that they master the technique of cleaning braces, which is quite challenging. We rely on the patient’s ability to clean thoroughly daily until the next appointment.4
What is most important to remember when you have fixed braces?
Well, patients with braces are at high risk of developing caries, and gingivitis is also common. That’s why they need to care exceptionally well for their teeth, which means cleaning them thoroughly several times daily. I usually discuss the three pillars for healthy teeth and gums while wearing braces: a healthy diet, extra fluoride and thorough cleaning.
What advice do you give to your patients when it comes to eating?
Eating hard foods, especially during the first days after the braces are fitted or tightened, can be difficult. Soft foods will be much more manageable, but one should also remember that soft, sticky foods are more difficult to remove, prolonging the acid attacks that damage the teeth. Cutting down on sugary food and avoiding sugary snacks are crucial. Saliva rinses and neutralises acids but needs time to work. Cavities form if one doesn’t give the mouth a break between meals.
Are there any concerns regarding drinks?
It’s good that you brought this up! Those with braces must avoid soft drinks or juices, as they contain too much sugar. Patients should have been informed that they must stick to water during the treatment with orthodontic appliances and drink water when thirsty.
What about zero-sugar soft drinks?
Zero-sugar soft drinks can only be consumed occasionally and together with food because they still contain acid, which can cause erosion of teeth.5 Therefore, when thirsty, I recommend water.
You mentioned extra fluoride earlier; why is it beneficial?
Yes, fluoride strengthens teeth, so your daily toothpaste should contain it. I often recommend adding a fluoride rinse during the day or whenever it is suitable. There are also additional ways to apply fluoride if needed.
The third pillar you mentioned is daily cleaning. Can you elaborate?
The dental professional recommends brushing teeth and braces at least twice daily, but even better, after every meal. Bring a toothbrush and other special devices to work or school. More than just a toothbrush for cleaning teeth and braces is required. I advise using a try-out kit, like the TePe Orthodontic kit, containing all the essential tools to let the patient discover what products they prefer and can handle.
What tools are included in TePe’s Orthodontic kit?
The Orthodontic kit is an ideal try-out kit for finding your favourites. Daily cleaning with a regular toothbrush is the cornerstone of good oral health, with or without braces. Here’s a one-by-one walkthrough of the products.




The TePe Supreme Compact™ is a two-level toothbrush, making it an ideal all-around brush for both teeth and braces. Its multi-level bristles provide improved cleaning around brackets and under wires. It is a very nice brush for cleaning along the outside and inside of the gumline, as well as chewing surfaces.
TePe Compact Tuft™ is an option to clean around the brackets and under the wire to avoid forming white spots. It is also a perfect brush for cleaning erupting teeth, molars or wisdom teeth.
TePe Interdental Brushes Original is another option for cleaning around brackets and under wire is the yellow (ISO size 4) or green (ISO size 5) interdental brush. The brush can be curved to facilitate reaching under the wire.




1. Sugarclock good
2. Sugarclock bad Tepe Orthodontic Kit
The TePe Supreme Compact™ TePe Compact Tuft™
TePe IDB Original TePe Angle™
TePe EasyPick™
TePe Implant Orthodontic Brush
TePe Interspace™
Some prefer TePe Angle™ with a pre-angled brush and long handle for cleaning around brackets and under the wire. A green brush (ISO size 5) is included.
TePe EasyPick™ is another option for cleaning between teeth, around brackets, and under wires. It’s a flexible, silicone-coated toothpick available in two sizes: orange (XS/S) and blue (M/L) for easy selection.
Orthodontic
wax to relieve soreness
The kit also includes wax that can be applied from the start of the treatment. This wax relieves discomfort and soreness from the braces. Replace the wax after eating and remove it before brushing.
Is there anything else you would like to add?
As the teeth are adjusting, different brushes might suit the patients during different times of the treatment. One might even say that you can’t have too many brushes when wearing braces.
I would like to mention two more specialty brushes. TePe Implant Orthodontic Brush is specially made for cleaning braces and can be bought separately. This brush has an extra slim brush head that allows cleaning on, above, and under the wire.
The last brush I would like to mention is TePe Interspace™, with a tapered brush tip for optimal access in difficult-toreach areas. It has a sturdy handle, which some people prefer. The brush comes with replaceable brush tips with different textures, soft and medium.
Great, a lot of helpful tools. So, how do you motivate the patient to follow through with this regimen?
Yes, it sounds like a lot, but it’s basically about spending ten more minutes daily cleaning during a limited period. As a patient, you will get the satisfaction of having healthy, straight and nice-looking teeth. Besides, the good habits formed during this time will benefit individuals for the rest of their lives. We know that good oral health also influences overall health in the long run.
Fact box
Brace-friendly eating and drinking
• Try to limit food and drink intakes to five a day (1) and avoid snacking between meals (2).
• Drink water between meals and when thirsty.
• Limit unnecessary sugar and restrict sugary snacks to one day a week.
Toothbrushing advice
• Use a regular toothbrush, such as TePe Supreme Compact, with fluoride toothpaste to strengthen your teeth. Brush all surfaces along the gumline for at least two minutes.
• Clean the brackets and wire thoroughly using an interdental brush and a specialty brush like the TePe Implant Orthodontic brush.
• Bring your oral hygiene tools with you during the day.
REFERENCES:
1. Migliorati M. et al. Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: a systematic review. Eur J Orthod 2015 Jun;37(3):297-30
2. Mummolo S. et al. Periodontal status of buccally and palatally impacted maxillary canines after surgical-orthodontic treatment with open technique. J Oral Sci. 2018 Dec 27;60(4):552-556.)
3. Lopatiene K. et al. Prevention and Treatment of White Spot Lesions During and After Treatment with Fixed Orthodontic Appliances: a Systematic Literature Review. J Oral Maxillofac Res. 2016 Apr-Jun;7(2): e1.
4. Khoroushi&Kachuie. Prevention and Treatment of White Spot Lesions in Orthodontic Patients. Contemp Clin Dent. 2017 Jan-Mar;8(1):11-19.
5. Chan A.S. et al. A systematic review of dietary acids and habits on dental erosion in adolescents. Int J Paediatr Dent. 2020 Nov;30(6):713-7332020.
About Michaela von Geijer, Doctor of Dental Surgery
Dr von Geijer works part-time at a private dental office in Sweden and TePe HQ in Malmö, Sweden. She has long clinical experience and is particularly interested in prevention and oral health. She has always placed a high value on working with preventive care. Dr von Geijer has held temporary preclinical positions as amanuensis at the University of Lund, including basic research and assistance with education/training at the medical and dental schools. She also has experience lecturing to professionals when employed by pharmaceutical companies and companies within the dental industry. Since 2015 Dr von Geijer has been employed by TePe and been a lecturer at universities worldwide.
Michaela von Geijer
Doctor of Dental Surgery

Smart scaffolds: the future of bioceramic
Guy Daculsi1
Abstract
The commercial offer for bioceramic bone substitutes is very large, however, the prerequisites for applications in bone reconstruction and tissue engineering, are most often absent. The main criteria being: on the one hand physicochemical features providing surgeons with an injectable and/ or shapeable biomaterial; on the second hand the multi-scale bioactivity leading to osteoconduction and osteoinduction properties. In order to obtain greater suitability according to the nature of the bone defect to be treated, new bone regeneration technologies, ‘‘smart scaf- folds’’ must be developed and optimize to support suitable Ortho Biology.
The related degenerative osteo-articular pathology involved by the aging population is a major societal issue. The autologous bone grafts are commonly used by clinicians in both dental and maxillofacial surgery, orthopaedic, trauma and spinal surgery. However the collection of autologous graft requires a second surgical site, and the volume of graft used is limited and of variable quality.
A new goal is to develop a bone regenerative medicine approach, where cell suspensions and/or osteoinductive agents are implanted in association with suitable advanced scaffolds to trigger endogenous regenerative processes of bone and not only to directly repair injured tissues. To successfully design a tissue repair strategy centred on the activation of endogenous regenerative mechanisms for the repair of a tissue deficit, some prerequisites should be considered. First of all, a 3-D micro-environment enhancing cell adhesion, proliferation and differentiation. Secondly, an adequate scaffold for diffusible growth factors and
modulators of cell maturation/differentiation promoting endogenous stem/progenitor cell recruitment, thus facilitating tissue regeneration.
The feasibility was demonstrated in bone tissue engineering to produce a hybrid material from an autologous bone marrow associated with synthetic matrices. All data indicated the necessity to use some specific scaffolds able to support these new and promising surgical technologies. The main goal was to develop a high potential synthetic bone substitute (‘‘smart scaffold’’) which will not only promote osteoconduction but also osteopromotion i.e. the ability to enhance of osteoinduction. This property was confirmed by the combination with human Mesenchymal Stem Cells (hMSC) suspension with ‘‘smart osteogenic scaffold’’ MBCP Technology in clinical trials from the European program (REBORNE 7th PCRD, www.reborne.org) (Fig. 1).
The smart bioceramic scaffolds will address the above prerequisites for repair and regeneration of bone. The interest of such technology is to provide to the surgeons:
1. A resorbable medical device with versatile handling properties (solid bioceramics, or injectable to mouldable),
2. Optimized presentation for combination with osteogenic suspensions,
3. A delivery system for growth factors or biomimetic peptides of bone morphogenic proteins.
Fig.1 Smartbioceramics

• Restorevolume
• Stabilize
• Regeneratebone
This smart scaffold technology platform is considered by the scientific experts, the clinical community, as part of the ‘‘Smart Biomaterials Diamond Concept’’ [1]:
• Restore volume
• Stabilize
• Regenerate bone
Recentlyseveralpublicationsdemonstrateosteoinductiveorosteostimulativeorosteogenicpropertyforsome micromacrostructuredcalciumphosphateBioceramics [2–6].Thekeypointisthenano-microscalelevel.The microporesareinvolvedintheearlyeventsofbodyfluids diffusionandphysico-chemicalinteractionbetweenproteins,biologicalionsofbodyfluidsandimplantcrystal surfaces.Theseinteractionsareconsideredosteoinductive oratleastpromoterofthemineralization.
boneremodellingandfinallycontributingtoingrowthat theexpenseofthebioceramics.TheprocessesofdissolutionofCaPandbiologicalprecipitationoccurringintothe microporesoccursimultaneouslywithosteoidandbone formationafterimplantationinbonysitesandnon-bony sites.Duetothespecificinterfaceformedbythebiological precipitation,thenewlyformedmineralizedsurfaceactsas anintelligentmatrixforundifferentiatedcells,specifics spreadinganddifferentiationinosteogeniccellslinesdue tothehighCaandPionsenvironmentcontent[7].This mustbeassociatedtothenicheconceptrequiredfordevelopingthebestscaffold.
Recently several publications demonstrate osteoinductive or osteostimulative or osteogenic property for some micro macro structured calcium phosphate Bioceramics [2–6]. The key point is the nano-microscale level. The micropores are involved in the early events of body fluids diffusion and physico-chemical interaction between pro- teins, biological ions of body fluids and implant crystal surfaces. These interactions are considered osteoinductive or at least promoter of the mineralization.
Osteoinductionistheaccelerationofnewboneformationbychemicalmeans.Thistermmeansthatprimitive, undifferentiatedandpluripotentcellsaresomehow stimulatedtodevelopintothebone-formingcelllineage. Oneproposeddefinitionistheprocessbywhichosteogenesisisinduced.Incomplement,osteoinductioncanbe alsodefinebyactiveosteoinduction(asgrowthfactors BMPactivity),orpassiveosteoinduction(orosteopromotion)ifthescaffoldswasable,byitsnano,microand macrostructure,toinduce/promotetheosteogeniccelldifferentiation.Thusthedevelopmentofa‘‘smartscaffold’’to supportnewsurgicalapproachforregenerativemedicineis achallenge.
Thespecificityofthescaffoldwasanoriginaland uniquenano-microstructureandmacrostructureinvolving incontactwithbiologicalfluids,bonemarrow,hMSC,a dynamicprocess,includingphysico-chemicalprocesses, crystal/proteinsinteractions,cellsandtissuecolonization,
Thebioceramicsgranulescanalsobecombinedwith hydrogelfor‘‘injectable-mouldablebioceramics’’.The hydrogelwillbeconsideredonlyasacarrier,giving rheologicalpropertiesforthebioceramicsgranuleshandling[8].
Themaincriteriabeingontheonehandphysico-chemicalfeaturesprovidingsurgeonswithaninjectableand/or mouldablebiomaterial;onthesecondhandthemulti-scale bioactivityleadingtoosteoconductionandosteoinduction properties.Inordertoobtaingreatersuitabilityaccording tothenatureofthebonedefecttobetreated,asocalled bioceramic‘‘smartscaffold’’,usinglatestinnovatingsynthesisprocessandknowledgetotheforefrontofthebone tissueengineeringfield,shouldindeedincorporatebellowingcharacteristics[9]:
Osteoinduction is the acceleration of new bone formation by chemical means. This term means that primitive, undifferentiated and pluripotent cells are somehow stimulated to develop into the bone-forming cell lineage. One proposed definition is the process by which osteogenesis is induced. In complement, osteoinduction can be also define by active osteoinduction (as growth factors BMP activity), or passive osteoinduction (or osteopromotion) if the scaffolds was able, by its nano, micro and macrostructure, to induce/promote the osteogenic cell differentiation. Thus the development of a ‘‘smart scaffold’’ to support new surgical approach for regenerative medicine is a challenge.
The specificity of the scaffold was an original and unique nano-microstructure and macrostructure involving in contact with biological fluids, bone marrow, hMSC, a dynamic process, including physico-chemical processes, crystal/ proteins interactions, cells and tissue colonization, bone remodelling and finally contributing to ingrowth at the expense of the bioceramics. The processes of dissolution of CaP and biological precipitation occurring into the micropores occur simultaneously with osteoid and bone formation after implantation in bony sites and non-bony sites. Due to the specific interface formed by the biological precipitation, the newly formed mineralized surface acts as an intelligent matrix for undifferentiated cells, specifics spreading and differentiation in osteogenic cells lines due to the high Ca and P ions environment content [7]. This must be associated to the niche concept required for developing the best scaffold. The bioceramics granules can also be combined with hydrogel for ‘‘injectable-mouldable bioceramics’’. The hydrogel will be considered only as a carrier, giving rheological properties for the bioceramics granules handling [8]
• Multiplewaysofbiomaterialsabsorptionbysurroundinghosttissues:
The main criteria being on the one hand physico-chemical features providing surgeons with an injectable and/or mouldable biomaterial; on the second hand the multi-scale bioactivity leading to osteoconduction and osteoinduction properties. In order to obtain greater suitability according to the nature of the bone defect to be treated, a so called bioceramic ‘‘smart scaffold’’, using latest innovating synthesis process and knowledge to the forefront of the bone tissue engineering field, should indeed incorporate below characteristics [9]:
Fig. 1 Smart bioceramics scaffold from MBCPÒ Technology used in Reborne European clinical trials
• Multiple ways of biomaterials absorption by surrounding host tissues:
1. Chemical dissolution process [10]
2. Lacunar resorption by osteoclasts thanks to biomimetic mineral phase [11, 12]
3. Macrophagic phagocytosis of bioceramics fragments [13]
• Multi-scale 3D porosity:
– Intragranular macro porosities acting as osteoconductive niches for cell adhesion, proliferation and differentiation [14]
– Intragranular microporosities for volume interconnection networks, improved specific surface area for bioactive molecules adsorption and higher dissolution rate [15, 16]
– Intergranular 3D space available to body fluids circulation for a bioactive environment favourable to cell colonization, cell signalling, protein adsorption, and ionic exchanges [17]. The combination of this triple porosity involves a very low density bioceramic with higher osteointegration capability.
Acknowledgments
• Bioactive properties:
1. ions release for bone metabolism (calcium, phosphate) [18]
2. apatitic re-precipitation and nucleation process from bioceramics crystals dissolution [19, 20]
3. body fluids interaction with biomolecules adsorption for cell adhesion, growth factors osteoinduction, integration in bone regeneration cycle etc. [21, 22]
• Biomimetic: bone-like crystallography, microstructure and chemistry [23]
• Osteoconduction and osteoinduction potential [24]
• Biocompatibility (non-immunogenic, non-cytotoxic...) [25, 26]
The research leading to these results has received funding from the European Union’s 7th Framework Programme under Grant Agreement No. FP7-HEALTH-2009-241879 (REBORNE).
Received: 17 July 2014 / Accepted: 24 February 2015 © Springer Science+Business Media New York 2015
REFERENCES:
1. Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: the diamond concept. Injury. 2007;38:S3–6.
2. Fellah BH, et al. Osteogenicity of biphasic calcium phosphate ceramics and bone autograft in a goat model. Biomaterials. 200 8;29(9):1177–88.
3. Yuan H, et al. Cross-species comparison of ectopic bone for- mation in biphasic calcium phosphate (BCP) and hydroxyapatite (HA) scaffolds. Tissue Eng. 2006;12(6):1607–15.
4. Habibovic P, de Groot K. Osteoinductive biomaterials—proper- ties and relevance in bone repair. J Tissue Eng Regener Med. 2007;1(1):25–32.
5. Daculsi G, Layrolle P. Osteoinductive properties of micro mac- roporous biphasic calcium phosphate bioceramics. Key Eng Mater. 2004;254:1005–8.
6. Le Nihouannen D, et al. Ectopic bone formation by microporous calcium phosphate ceramic particles in sheep muscles. Bone. 2005;36(6):1086–93.
7. Daculsi G, et al. Smart calcium phosphate bioceramic scaffold for bone tissue engineering. Key Eng Mater. 2013;529:19–23. 8. Daculsi G, et al. Osteoconduction, osteogenicity, osteoinduction, what are the fundamental properties for a smart bone substitutes. IRBM. 2013;34(4):346–8. 9. Zhang Y, et al. Dissolution properties of different compositions of biphasic calcium phosphate bimodal porous ceramics follow- ing immersion in simulated body fluid solution. Ceram Int. 2013;39(6):6751–62.
10. Daculsi G, Uzel AP, Weiss P, Goyenvalle E, Aguado E. Devel- opments in injectable multiphasic biomaterials. The performance of microporous biphasic calcium phosphate granules and hydro- gels. J Mater Sci Mater Med. 2010;21(3):855–61.
11. Lan Levengood SK, et al. Multiscale osteointegration as a new paradigm for the design of calcium phosphate scaffolds for bone regeneration. Biomaterials. 2010;31(13):3552–63.
12. Yamada S, et al. Osteoclastic resorption of calcium phosphate ceramics with different hydroxyapatite/b-tricalcium phosphate ratios. Biomaterials. 1997;18(15):1037–41.
13. Jensen SS, et al. Osteoclast-like cells on deproteinized bovine bone mineral and biphasic calcium phosphate: light and trans- mission electron microscopical observations. Clin Oral Implants Res. 2014. doi:10.1111/clr.12376.
14. Coathup MJ, et al. Effect of increased strut porosity of calcium phosphate bone graft substitute biomaterials on osteoinduction. J Biomed Mater Res A. 2012;100(6):1550–5.
15. Chan O, et al. The effects of microporosity on osteoinduction of calcium phosphate bone graft substitute biomaterials. Acta Bio- mater. 2012;8(7):2788–94.
16. Li X, et al. The effect of calcium phosphate microstructure on bone-related cells in vitro. Biomaterials. 2008;29(23):3306–16.
17. Hollister SJ. Porous scaffold design for tissue engineering. Nat Mater. 2005;4(7):518–24.
18. Sa ́nchez-Salcedo S, et al. In vitro structural changes in porous HA/b-TCP scaffolds in simulated body fluid. Acta Biomater. 2009;5(7):2738–51.
19. LeGeros RZ, Ben-Nissan B. Introduction to synthetic and biologic apatites. Advances in calcium phosphate biomaterials. Berlin: Springer; 2014. p. 1–17.
20. Campion CR, et al. Microstructure and chemistry affects apatite nucleation on calcium phosphate bone graft substitutes. J Mater Sci Mater Med. 2013;24(3):597–610.
21. Cao W, Hench LL. Bioactive materials. Ceram Int. 1996;22(6):493–507.
22. Vasilescu E, et al. Interactions of some new scaffolds with simulated body fluids. Rev Chim. 2011;62(2):212–5.
23. Chai YC, et al. Current views on calcium phosphate osteogenicity and the translation into effective bone regeneration strategies. Acta Biomater. 2012;8(11):3876–87.
24. LeGeros RZ. Properties of osteoconductive biomaterials: calcium phosphates. Clin Orthop Relat Res. 2002;395:81–98.
25. Legeros RZ. Biodegradation and bioresorption of calcium phos- phate ceramics. Clin Mater. 1993;14(1):65–88.
26. Lu J, et al. Comparative study of tissue reactions to calcium phosphate ceramics among cancellous, cortical, and medullar bone sites in rabbits.
J Biomed Mater Res. 1998;42(3): 357–67.
In conclusion, the future of bioceramic scaffolds supports the role of microporous and macroporous CaP bioceramics in osteoinduction. De novo bone regeneration can be achieved, with potential ‘‘superiority’’ to autograft. Although micropores and CaP absorption, in addition to the niche concept, appear to be key requisite features for efficient smart scaffolds during bone regeneration, the cascade of biological events leading to MSC differentiation and osteogenesis remains unclear. View Product