
16 minute read
grade 3: score = 8

from Breast Pathology
by IHC001

Degree of differentiation of the tumour tissue. Applicable to all the cases Good specimen preparation – a prerequisite! - Thickness of tissue - Volume of fixative - Time - Needle cores 5-6 hours - Larger specimens 12 hours or more
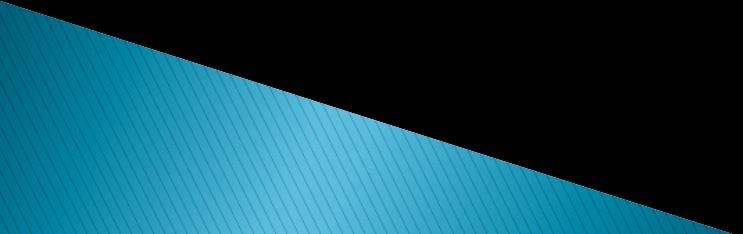
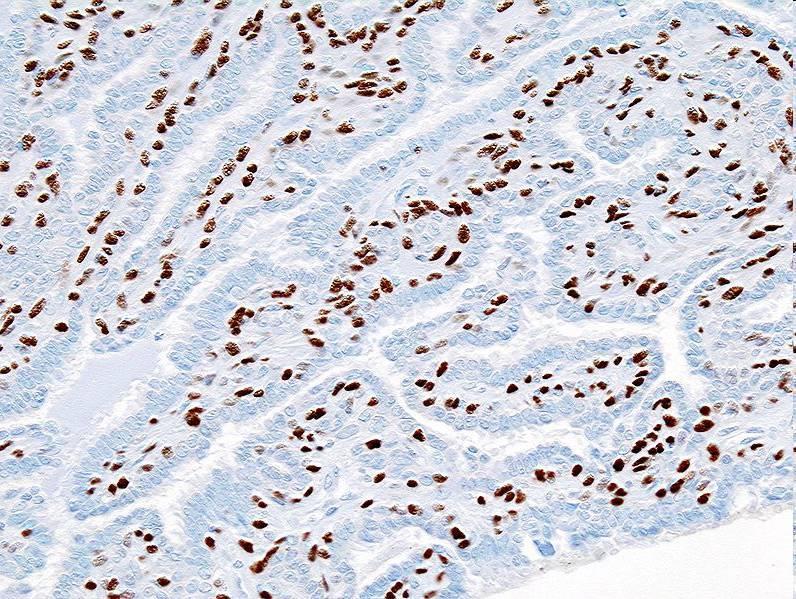
All parts of the tumour are scanned. Clear acinar or gland formation or defined tubular structures with a central luminal space are assessed semi-quantitatively.
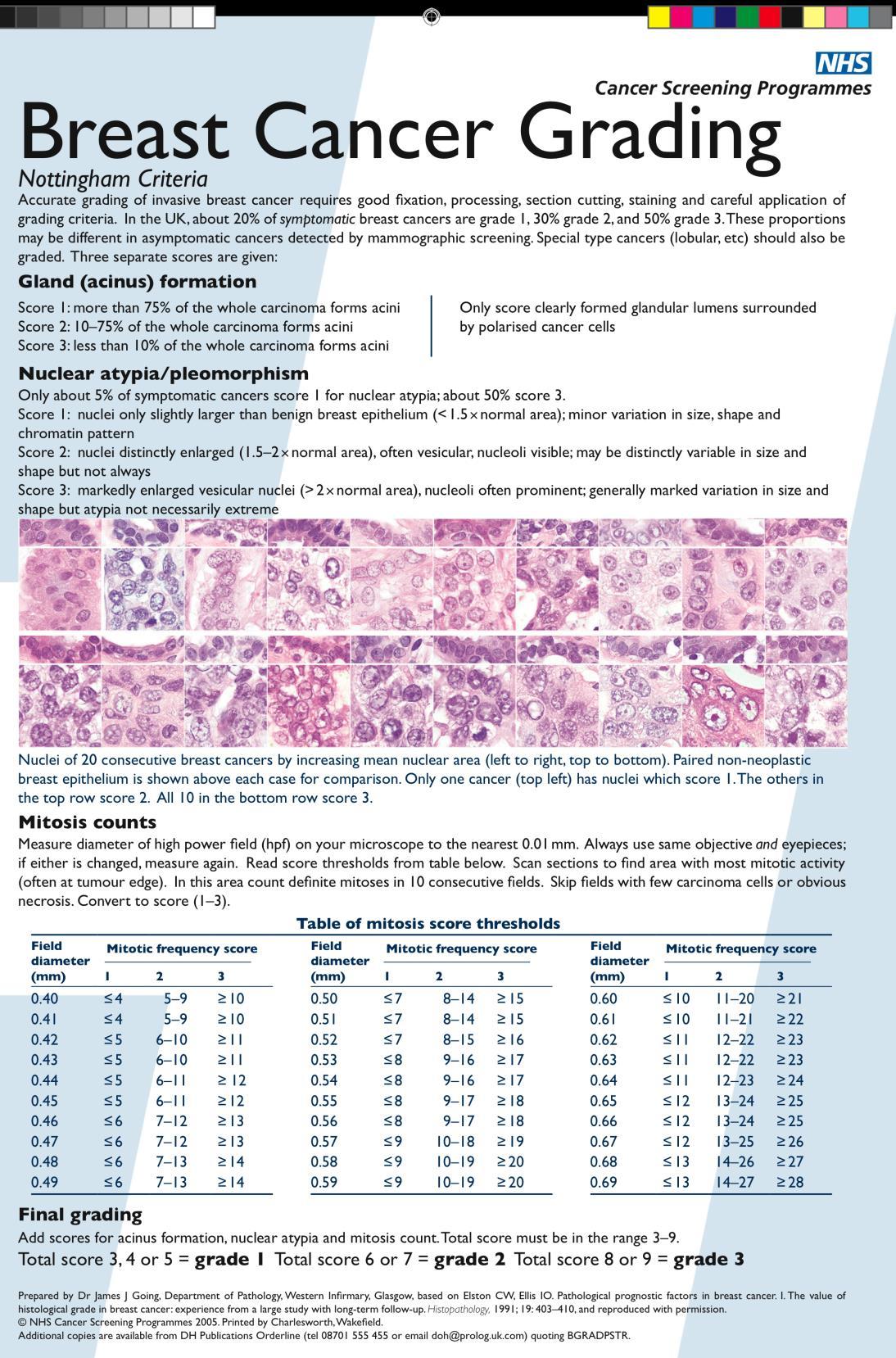
Score 1

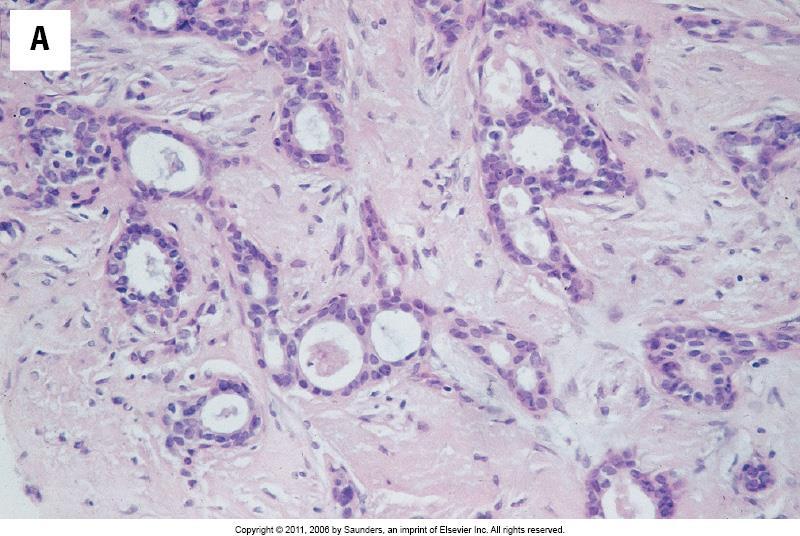
Score 2

Score 3

1: Nuclei small in size with little increase in size in comparison with normal breast epithelial cells, regular outlines, uniform nuclear chromatin. 2: Cells larger, open vesicular nuclei, visible nucleoli, moderate variation in both size and shape. 3: Vesicular nuclei, prominent nucleoli, marked variation, large bizzare forms.




Mitotic counts


In unselected breast cancer series, the overall survival has been shown to be significantly better in patients with grade I tumours than in those with grade 2/3 tumours. Histological grade has a prognostic value that is equivalent to that of LN status and greater than that of tumour size.



In a sentinel lymph node, a single metastasis measuring 0.3mm is classified as:
◦ A - isolated tumour cells ◦ B - micrometastasis ◦ C - metastasis ◦ D - none of the above

B
Reference TNM classification 6th edition
Single sentinel node metastasis is classified as Individual Tumour Cells (ITCs) ≤0.2mm Micrometastasis >0.2mm to ≤2mm Metastasis >2mm
ITCs pN0 Micrometastasis pN1(mic)
Identification of more LNs in the specimen Examining the entire node thoroughly - levels - slicing node thinly IHC RT-PCR
ITCs should not be used in decisions about adjuvant treatment. Micromets: ANS, axillary clearance. Local protocols. Radiotherapy.
Topic 3

pN0 (i+) isolated tumour cells
pN0 no metastasis
pN1mi, >0.2 mm, none >2.0 mm
pN1 Macrometastasis >2.0 mm

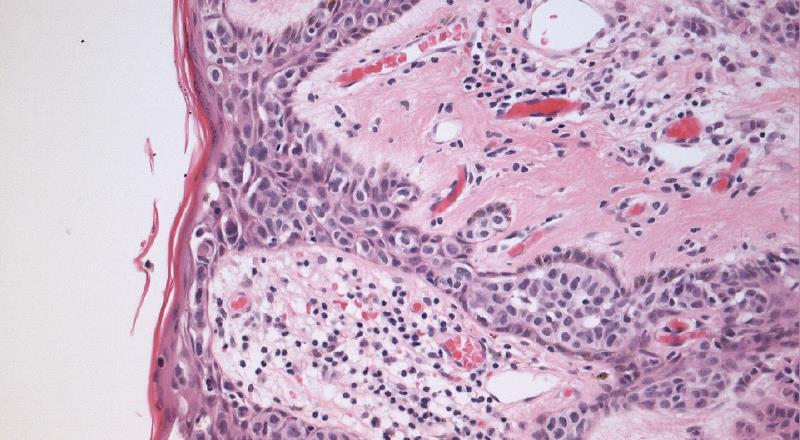
A 63 year old lady presents with nipple erythema and ulceration. A nipple biopsy reveals large round cells with large nuclei, prominent nucleoli and abundant vacuolated cytoplasm within the epidermis. The cells are positive for CK7 and negative for S100. What is the most likely diagnosis?
◦ A – Malignant melanoma ◦ B - Paget’s disease ◦ C - Bowen’s disease ◦ D - Phyllodes tumour
B
More frequent in post-menopausal women 1 – 4.3% of all breast cancers Associated invasive carcinoma almost always seen, but rarely (<5%) no carcinoma is found in mastectomy specimens
Defining histologic feature is the presence of malignant glandular epithelial cells within the squamous epithelium of the nipple.
Malignant melanoma Bowen’s disease Clear cell change Toker cell hyperplasia Exclude epidermal infiltration by underlying tumour invading skin
Paget’ s – LMWCK (Cam5.2), CK7, EMA, CEA,
Her2 positive, GCDFP-15, PAS+
Melanoma - S100, melanA, HMB45, SOX-10 positive
Bowen’ s – HMWCK, p63 positive



A HER2 immunohistochemistry score 2+ breast carcinoma means that:
◦ A - The tumour should be regarded as negative for
HER2 overexpression ◦ B - The HER2 gene is amplified ◦ C - The HER2 gene is not amplified ◦ D - The tumour should be regarded as positive for
HER2 overexpression ◦ E - FISH testing should be performed
E
Reference Walker et al., Clin Pathol. 2008:818-24.
Her2 immunohistochemistry assesses HER2 protein overexpression. A 2+ score requires further testing by FISH for gene amplification.

0/1+: Negative for HER2 overexpression
2+: Borderline
Test for gene amplification (FISH)
No – Negative Yes - Positive
3+: Positive for HER2 overexpression
Only membrane staining of the invasive tumour should be considered when scoring the IHC tests. If a commercial kit assay system is used, it is recommended that laboratories adhere strictly to the kit assay protocol and scoring methodology. Local modifications of techniques can lead to false positive and negative assay results.
0 Negative No staining/incomplete membrane staining in < 10% cells 1+ Negative Faint/barely perceptible incomplete membrane staining in >10% cells 2+ Borderline weak to moderate complete membrane staining in >10% cells 3+ POSITIVE Strong and complete membrane staining in more than 30% tumour cells.

1+ 2+

HER2 positive breast carcinomas more aggressive
Establishing the tumour HER-2 status is a prerequisite for the use of targeted therapy with Trastuzumab (Herceptin)

A 47 year old lady presents with a left breast lump.
Examination reveals a cyst, which partially resolves on aspiration. There is general bilateral breast nodularity. Core biopsy of the area of concern shows breast tissue with ducts lined by large cells with abundant eosinophilic cytoplasm, stromal fibrosis, cyst formation and sclerosing adenosis.
Assuming the biopsy is representative, what is the correct biopsy code?
◦ A - B2 ◦ B - B3 ◦ C - B4 ◦ D - B5a ◦ E - B5b
A


B1 - Inadequate/normal tissue B2 – Benign
◦ Fibroadenoma, fibrocystic change, sclerosing adenosis, duct ectasia, abscess, fat necrosis B3 - Atypical lesion, probably benign
◦ ADH, lobular neoplasia, phyllodes, papillary lesions,
RS/CSL, columnar cell lesions with atypia B4 - Suspicious for malignancy
◦ Tiny foci, technical problems e.g. crushing B5a - In-situ carcinoma B5b - Invasive carcinoma B5c – uncertain in-situ/invasive B5d- other cancers eg lymphoma

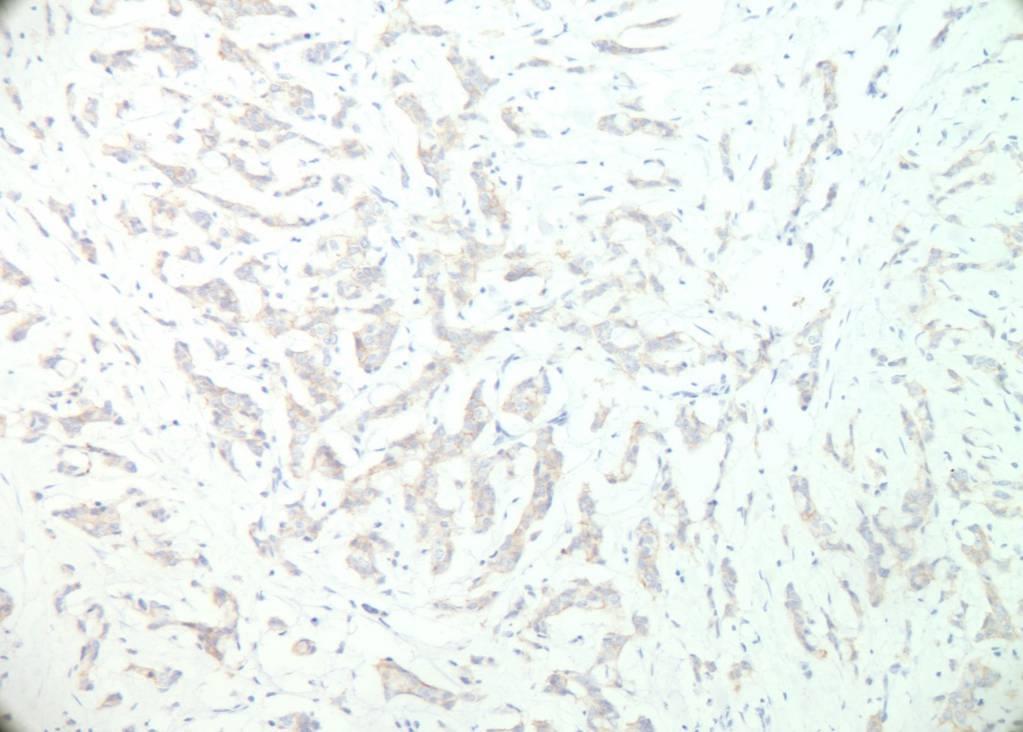
A 43 year old woman, previously treated for invasive ductal carcinoma, presents with a breast lump and blue discolouration of the overlying skin. Biopsy shows a tumour composed of irregular spaces lined by pleomorphic cells, abnormal mitoses and infiltration into the surrounding tissue. The tumour cells are negative for AE1/AE3 and positive for CD31 and CD34.
What is the most likely diagnosis?
◦ A - Recurrent ductal carcinoma ◦ B - Malignant phyllodes tumour ◦ C - Spindle cell carcinoma ◦ D - Lobular carcinoma ◦ E - Angiosarcoma
E

Overall rare breast tumour Known to be associated with previous radiotherapy Irregular vascular spaces, variably pleomorphic cells. Positive for vascular markers CD31 and CD34 and usually negative for epithelial markers
Atypical vascular proliferation after radiotherapy Other haemangiomas

Low High

High
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
Each of the following patients had a breast biopsy. For each one select the most likely condition from the list of options. Each option may be used once, more than once or not at all.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma
F Phyllodes tumour J Intraductal papilloma
G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma
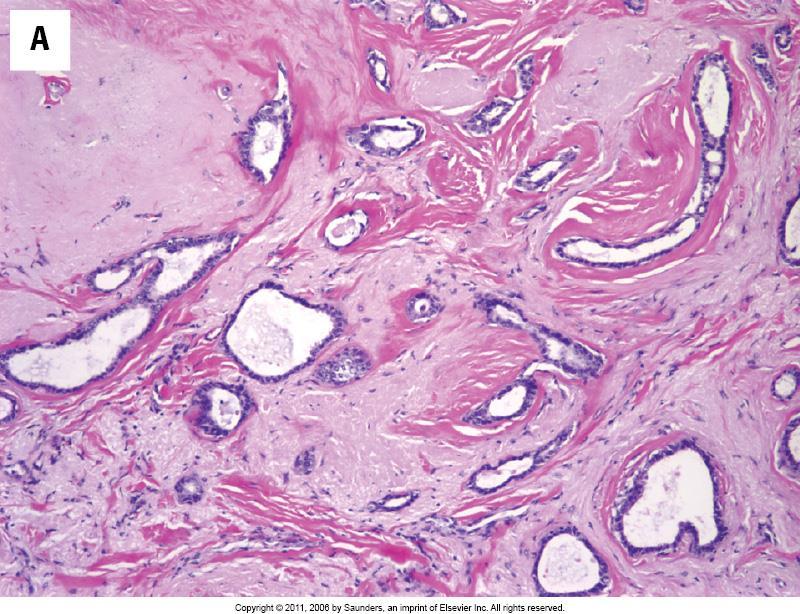
A 45 year old female with a firm lump in the outer quadrant of the breast. The biopsy shows a stellate lesion with 95% angulated tubules, apical snouts and stromal desmoplasia.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
Pure tubular carcinomas ± 5% of all invasive breast carcinomas Bland tubules with angulated outline and open lumen Haphazard tubular arrangement in a desmoplastic stroma SMM and p63 negative Good prognosis compared to other invasive ductal carcinoma
ΔΔ Sclerosing adenosis


Tubular ca SMM
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
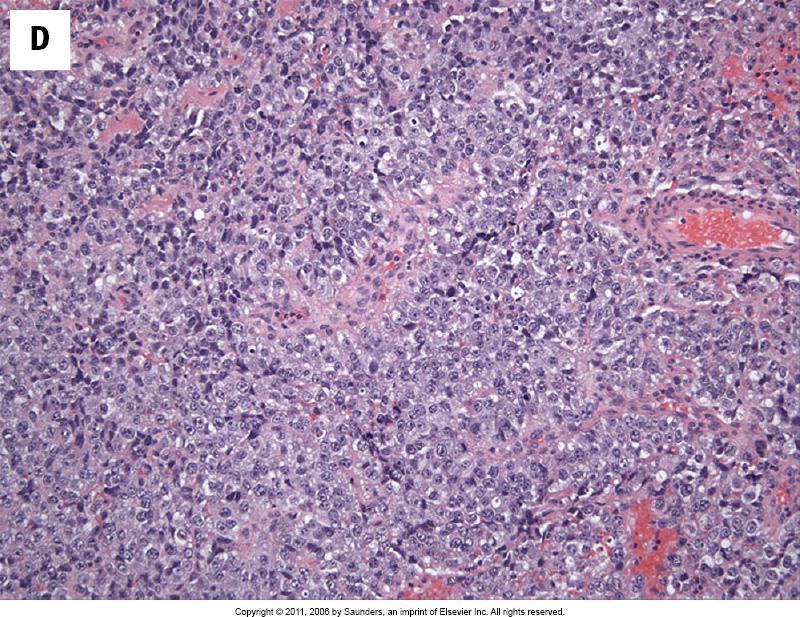
A 65 year old female with bilateral breast lesions. A biopsy of one shows single file cords of tumour cells with intracytoplasmic spaces.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
5-14% of breast carcinomas High incidence of multifocal and bilateral disease Tumour cells may show mucin filled vacuoles E-cadherin negative
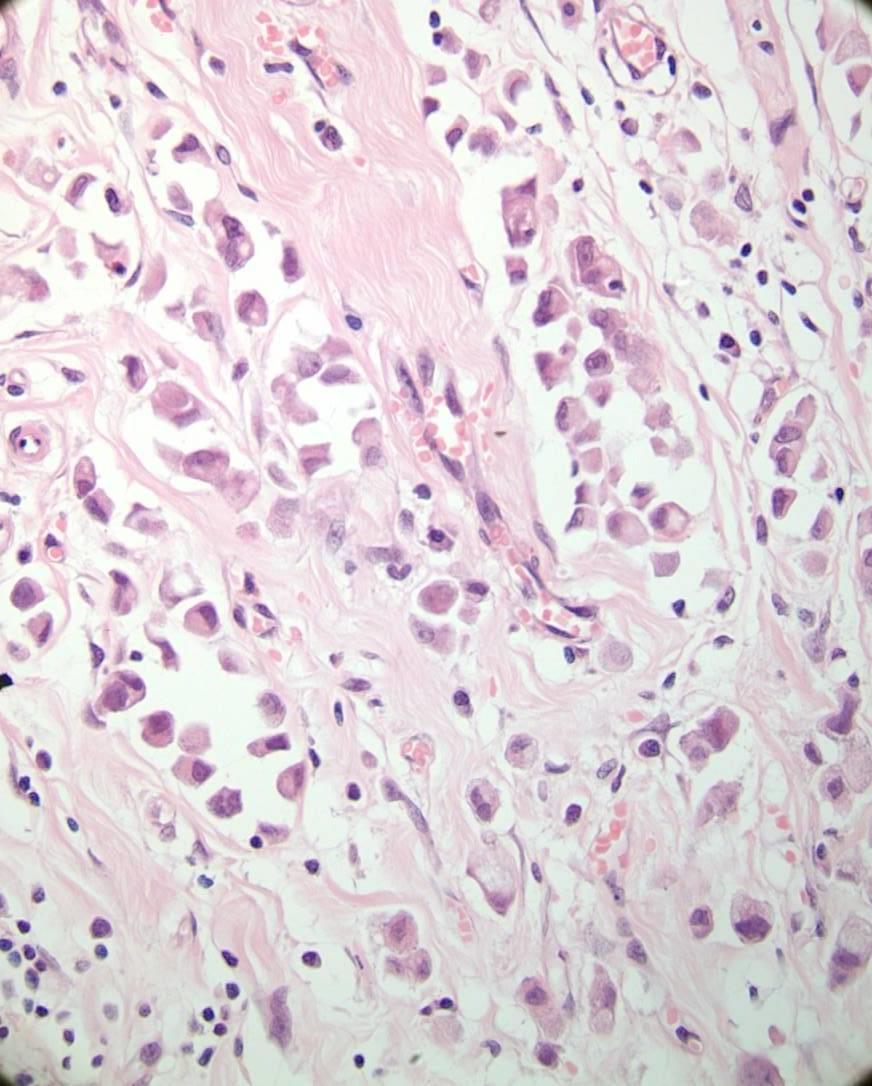

E-cadherin
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosinglLesion K Fibroadenoma J Intraductal papilloma
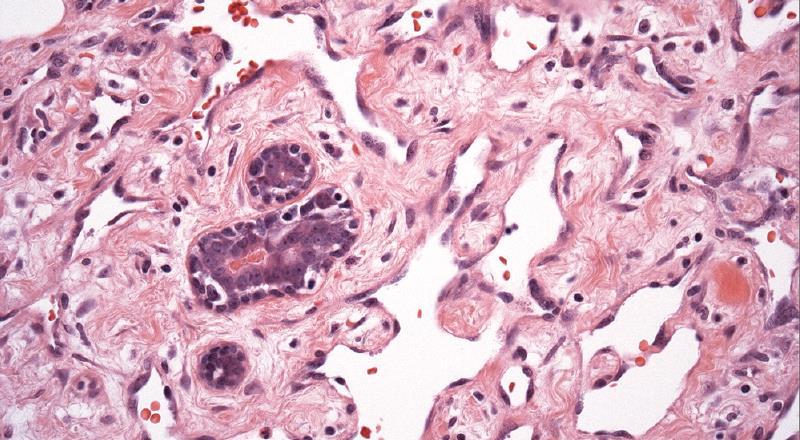
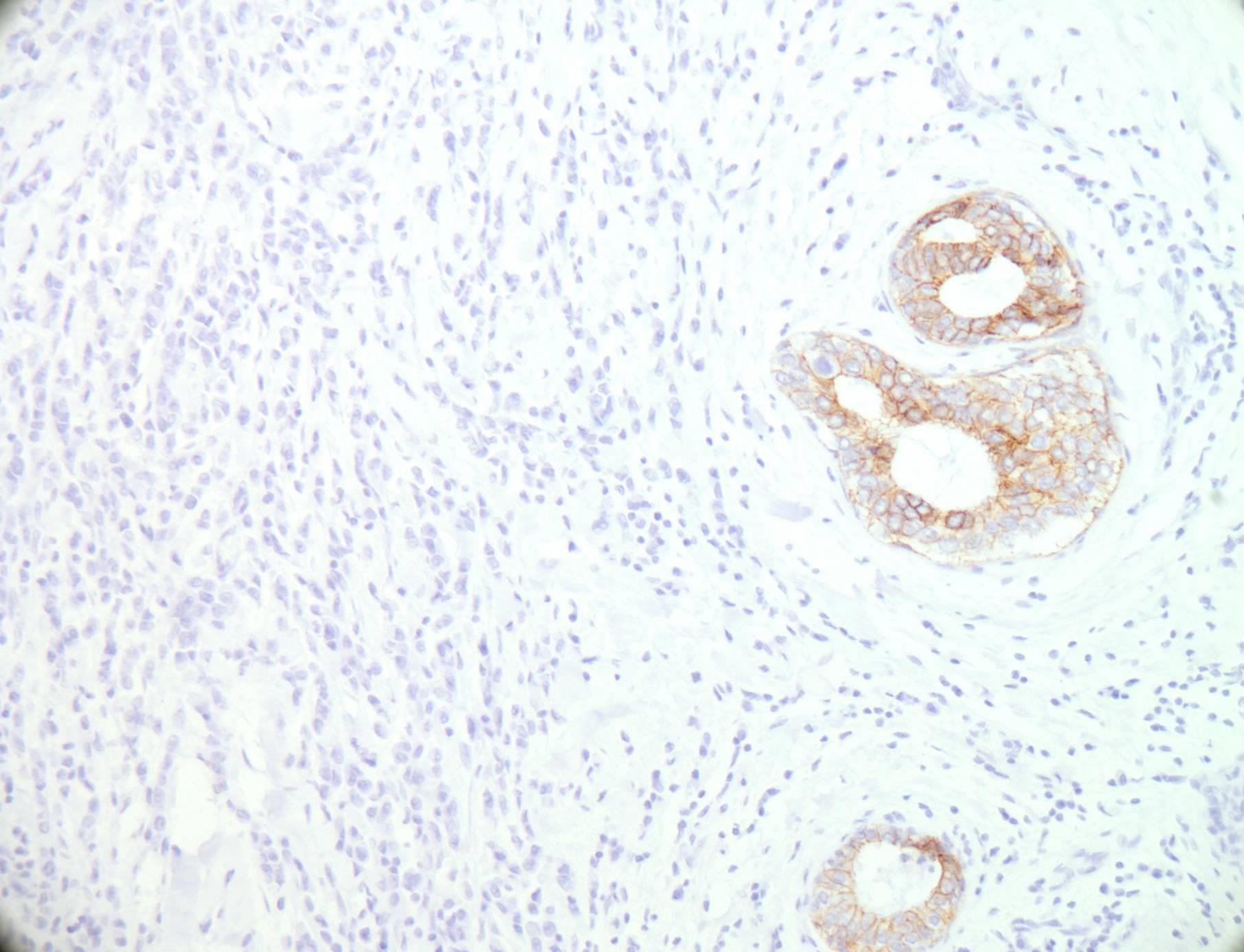
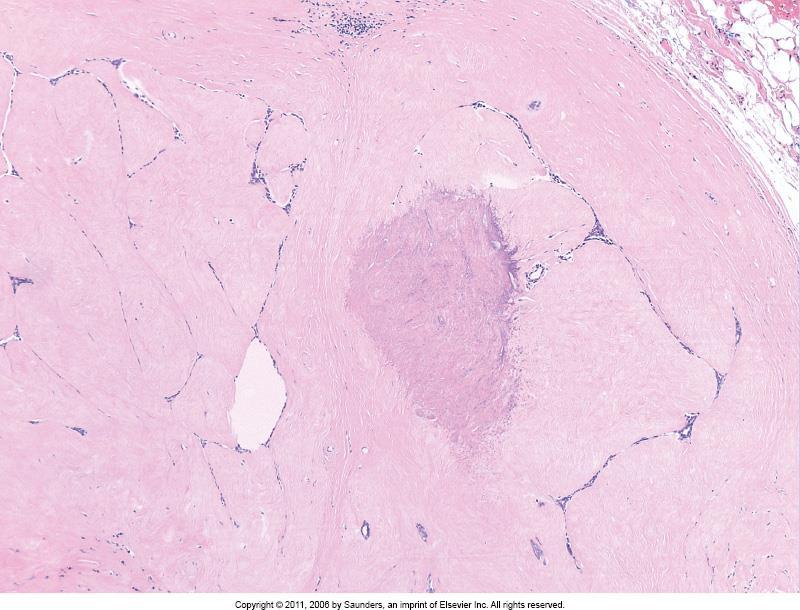
A 43 year old female has a mammographically detected stellate lesion with dense central fibrosis. Histology shows central fibrosis and elastosis from which ducts radiate out. The ducts are positive for p63 and SMM.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma


Central fibroelastosis Entrapped benign ducts Associated epithelial hyperplasia <1cm radial scar >1cm complex sclerosing lesion Increased risk for subsequent breast cancer development
ΔΔ Tubular carcinoma (myoepithelial markers are helpful)
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
A 25 year old female with a circumscribed, encapsulated 2 cm breast lump showing an intracanalicular growth pattern.
There is no stromal atypia.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
Most common breast tumour in young women Discrete palpable mass Benign tumour Biphasic pattern- stroma and ducts Intracanalicular/pericanalicular patterns- no clinical significance ΔΔ Phyllodes tumour- stromal overgrowth, cytological atypia, increased mitosis

FIBROADENOMA
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
A 52 year old female has bloody nipple discharge. Biopsy reveals a localised papillary proliferation of hyperplastic ductal cells on fibrovascular cores within a dilated duct.
A Tubular carcinoma
B DCIS C LCIS D Atypical hyperplasia E Ductal carcinoma F Phyllodes tumour G Benign ductal hyperplasia H Atypical ductal hyperplasia I Lobular carcinoma J Radial scar/Complex sclerosing lesion K Fibroadenoma J Intraductal papilloma
Most common cause of spontaneous nipple discharge from a single duct Typical age 35-55 years Benign intraductal papillary lesion Fibrovascular cores lined by dual population of ductal and myoepithelial cells


NHS Breast Screening Programme Publication 58, Pathology Reporting of Breast Disease
Histopathology Annual Review Issue January 2008
http://www.breastpathology.info/index.html
