
15 minute read
The step by step approach to marionette lines


Based on a deep understanding of facial anatomy, Simone Doreian, MD, describes her novel technique to treat marionette lines with injectables
ABSTRACT Treating the marionette folds non-surgically can be unpredictable. Non-surgical approaches include direct injection of the lines with filler, indirect approaches augmenting the mid-face or revolumising the lateral face, injection of filler along the mandible, chin augmentation, and thread lifting. A simple logical approach is needed. In the author’s experience, a direct approach to the marionette line is more effective, durable and efficient in the use of product compared to indirect approaches. The ‘Step by Step’ approach views the marionette lines as a set of two steps, an upper step lateral and a lower step medial to the fold. The goal of this approach is to minimise the height differential of the two steps and provide support, strengthening and blending of the two areas. Step 1: relax the depressor anguli oris muscle (DOA) using botulinum toxin A, responsible for constant downward tugging upon the oral commissure. Step 2: 2–3 weeks later, lift the medial lower step towards the upper step of the fold, minimising the height differential of the two areas using hyaluronic acid filler. Step 3: inject and strengthen the step edge along the labiomental crease. Total dose: 2ml hyaluronic acid filler and minimal botulinum toxin A.
SIMONE DOREIAN, MD, Cosmetic Physician, Cosmetic Physicians Society of Australasia Inc, Dr. Simone Doreian Private Clinic, 3 Harold St, Sandringham, Victoria 3191 Australia
email: simonedoreian@gmail.com
KEYWORDS Hyaluronic Acid Filler, treatment marionette lines, Filler techniques, botulinum toxin A M ARIONETTE LINES, FOLDS, OR grooves are the downward running folds of skin or wrinkles originating from the oral commissures and head inferiorly towards the mandible. They are so named after the marionette puppet, the mid-18th century puppets, which became more and more life-like with articulated chins allowing the puppet to ‘talk’. These folds of articulation in humans are perceived to create a sad, dissatisfied or tired resting appearance and are a common presentation for which patients seek cosmetic treatment. As with any cosmetic treatment, there are multiple approaches to the treatment of this region. This article describes what I believe to be a common sense approach to the non-surgical treatment of marionette lines in a step-by-step approach, described further below (Figure 1).
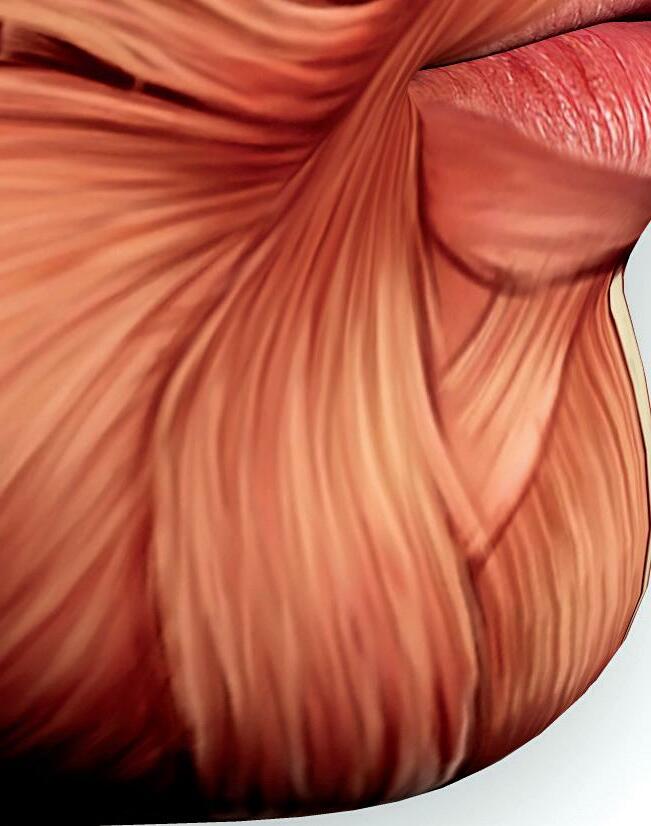
Anatomy of the marionette region The marionette lines or folds begin at the oral commissure and end in the labiomental false ligament, which is not a true ligament but rather an attachment area for muscle fibres. In a staircase analogy, the top step described is formed by the jowl fat lateral to the marionette line, hanging over and against this labiomental attachment area. The The marionette lines or folds begin at the oral bottom step, medial to the marionette fold, is perioral. The shadow cast by the top step and the height differential commissure and end in the creates the step-like appearance of the labiomental false ligament, marionettes and the impression of a which is not a true ligament but downturned mouth and visually segregated chin region. rather an attachment area for The surrounding muscles of the muscle fibres. region and their cutaneous attachments are also involved in the formation of marionette lines. As mentioned, the labiomental ligament is a site of attachment. The medial edge of the DAO attaches along the line by cutaneous ligaments, and both the depressor labii inferioris muscle (DLI) and DAO have many cutaneous ligament attachments to the overlying skin. DAO is a triangle

Figure 1 Marionette folds have a step-like formation, consisting of an upper step laterally and a lower step medially. The height differential creates a shadow and fold
Figure 2 The step of the marionette fold (white dotted line) and its relationship with the DLI medially and DAO laterally. The DAO can be remembered to lie outside and over the DLI. The mentalis muscle is a paired muscle located at the tip of the chin. These relationships are important when injecting botulinum toxin to target the downward pull of the DAO. The injections must begin lateral of the marionette fold in a lateral direction and remain superficial to avoid injecting the DLI (red dotted triangle of cross over) CONTRIBUTING FACTORS TO THE DEVELOPMENT OF MARIONETTE LINES
BONE
Hypoplastic mandible
MUSCLE
Hyperactivity and cutaneous attachments of the DAO
SOFT TISSUE
Fat loss in the lower step as well as fat descent from the top step
SKIN
Loss of elasticity and ageing
DAO

DLI
Marionette fold
DLI
Marionette fold DAO
A B

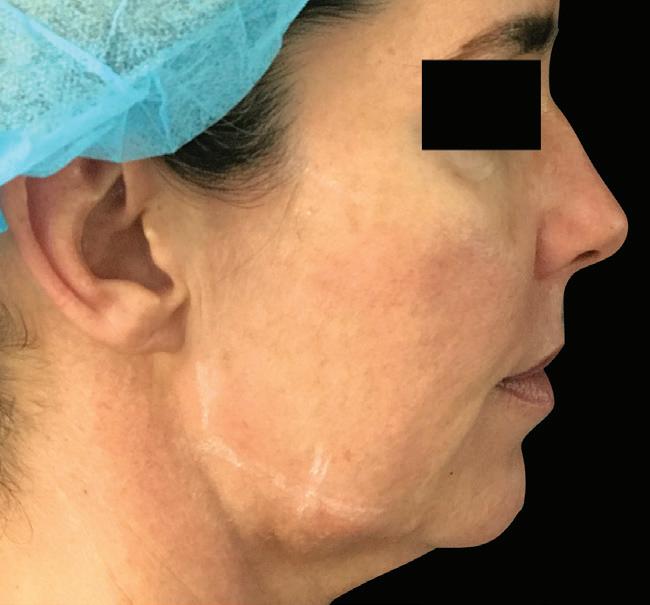
Figure 3 (A) Before and (B) immediately after jawline injection of filler along and posterior to the mandibular bone and chin; even with post procedure swelling, there is no change to the marionette line
shape, with its base originating from the mandible border and point inserting into the modiolus, tugging the corners of the mouth downward. It is situated lateral to the mandibular fold. The DLI is a parallelogram shape. It originates deep to the DAO along the mandibular border as well and inserts into the tubercle of the lip, pulling the lip down. With repeated facial movement, these cutaneous attachments contribute to the creases that develop with ageing (Figure 2).
Deep and subcutaneous fat also contributes to the step-like appearance of the marionette fold. There is a fat differential between the upper step and the lower step of the marionette region. Lateral to the marionette line, we have a large amount of fatty tissue. Medially in the perioral region, there is minimal fatty tissue. Jowl fat can increase with age. Hence the jowl fat hangs upon the ligament area, creating a step1 .
The facial artery should be avoided when injecting; running superiorly, from deep to superficial, over the mandible just anterior to the masseter muscle towards the oral commissure, sending its ILA branch across to the lower lip and deep to the muscles.
Marionette grading scale
Carruthers et al.2 developed a useful grading scale. This will help explain to the patient the severity of their problem compared to others and help us predict the likely success and amount of product necessary. For higher grades (involving more severe marionette lines), I find it useful to discuss surgical options in order to set expectations appropriately low. Fillers can only offer a partial and temporary benefit for higher grade lines, and for extremely heavy, sagging marionette lines that extend all the way to the mandible with jowls hanging laterally, surgery is likely a more reasonable suggestion.
Indirect treatments
Indirect treatments, i.e., treating other areas of the face in order to impact the marionette lines, do not tend to perform efficiently or with longevity, in my experience and opinion. These include: ■ Thread lifting: in my experience, the effect is temporary and expensive with an unacceptably high level of complications. I have formed my opinion over time from anecdotes of surgical colleagues, my own patient cases, and literature3 . ■ Indirect approaches using dermal fillers to treat the mandible body and chin. In spite of augmentation of a vertically and anteriorly deficient chin, readers can see in Figure 3 that despite improvement in the definition of the jawline and lengthening with chin and mandible augmentation, there has been little improvement in the marionette folds.
The step by step approach to marionette lines
My preferred non-surgical treatment of the marionette region is to treat the marionette fold directly using a stepby-step approach, which I will go on to describe.
The step by step approach to marionette lines addresses the causes of the step: ■ Reduce the downward tugging of the DAO upon the oral commissure using botulinum toxin ■ Elevate the lower step of the marionette line ■ Strengthen the skin across the step edge.
Step 1: Relax the muscles
To relax the DAO muscle, I use 2–3 units per side of OnabotulinumtoxinA or 5–8 units of AbobotulinumtoxinA into the belly of the DAO. Placement is essential to avoid accidentally affecting the DLI muscle. The placement of toxin in the DAO is superficial and laterally, in line with the nasolabial folds, injecting in a lateral direction slowly. The black dots in Figure 4 are placed as an injection point for the DAO. Note the relationship between the two muscles from the front view of the patient and the side profile anatomically in Figure 2. The DAO lies superficial to the deeper DLI and is more lateral to the marionette fold. A useful tool to remember this is ‘DAO lies over and outside. DLI is inside and interior.’
Step 2: Elevate the lower step upward
I use a cannula technique for marionette folds grade 2 and above, where a fold of skin creates a shadow, to elevate the sunken lower level of the marionette fold. If there is no shadow and simply a wrinkle in the skin, I skip this and simply proceed to step 3.
For grades 2 and above, I map out the area of shadowing I can see along the marionette line and across to the mental crease and prejowl sulcus. My entry point for a 50mm 25G cannula is 0.5cm above and lateral to the oral commissure or within the jowl fat on the inferior margin of the mandible. I blunt dissect space in the subcutaneous fat plane first within the shape of the shadow, aiming to temporarily detach and break some of the retinacular attachments to create a smooth injection plane. It is important that the cannula glides easily; this is how I know I am in the correct layer. Literature supports the use of volume in the subcutaneous layer to improve correction in the perioral region4. I then place a fan of filler across the marked area, approximately 0.5ml per side and massage. This lifts the lower step up toward the upper step of the jowl. See Figure 5, left image.

Product selection
I choose to use HA fillers of medium firmness and good cohesivity, for example, Restylane Volume medial to severe folds or Defyne, Teoxane’s RHA 3, or Stylage XL in less severe folds in my clinic.
Step 3: Strengthen skin at the step edge
In mild cases where only a skin crease is present with minimal shadowing, I use a direct approach with a needle. My product of choice, in this case, is Restylane. It has a high G’ and, when injected in a fern technique5, is extremely efficient and long-lasting.
Figure 4 DAO injection site: in line with nasolabial fold, lateral to marionette line. I prefer to have the patient contract the muscle by ‘looking sad’, palpate the area and inject whilst contracting. Inject in a lateral direction, superficially at 25 degree angle to avoid injecting DLI muscle.
Figure 5 (A) Step 1. Inject DAO superficially and lateral of the marionette fold. step 2: elevate the lower step by blunt dissection of the shadowed area in the lower perioral region, paying particular attention to the upper region of the marionette fold, then fill the area with HA filler 0.5-1ml with the bulk of the product placed superiorly and laterally under the oral commisure. (B) Step 3. Pull the oral commisure open, then inject a cross shape, using 2 linear retrograde injections , vertically next to the oral commisure, and obliquely , into the edge of the lower lip. This lifts the oral commisure, then proceed to use oblique V shapes down the marionette line to strengthen and blend the upper and lower steps .

In grades 2 or higher, where a fold and shadow were present, and we have detached the cutaneous attachments along the marionette region and elevated the lower perioral step area, as above, I use a direct approach with a needle again. Beginning at the oral commissure, using my non-dominant hand, I pull the skin lateral and superiorly, stretching out the marionette line. With the mouth half open, I inject a vertical line of filler from below and immediately lateral to the oral commissure in the deep dermis, as close to the corner of the mouth as possible. A second injection, to form a cross shape, injected lateral to the commissure, in an oblique direction medially into the lateral edge of the lower lip. You will see the oral commissure lifting and opening as you inject. I then perform a series of
A B
A B
V-shaped oblique injections deep along the line to blend the edge of the step, strengthening the area of cutaneous attachments, making it less likely to buckle in future. I massage using gloves from the inside and outside of the mouth, ensuring to change gloves between sides and before again touching the patient. See the right-side image in Figure 5.

Discussion
The lower face is often the region that is hardest to treat non-surgically. The result of the heaviness of tissue, the descent of soft tissue of the mid and lateral face with ageing, loss of bone support throughout the mandibular and maxillary region, increase in jowl fat, and hyperactivity of perioral muscles due to shifting mechanics as bone resorbs, is a segmented, jowly, sad or
disgruntled looking appearance. In an ideal cosmetic world, surgery would be available with no risk, cost, downtime or social stigma to correct marionette lines. However, we can make a very reasonable, cost-effective difference in the appearance of our patients, softening and reversing the downturn of the mouth and shadowing due to the stepped marionette fold, using non-surgical techniques and carefully placed dermal fillers. Many will argue that thread lifting holds a place, and it does for the physicians who have found this to be a long-lasting, lowcomplication-rated procedure; however, in my experience, this has not been the case.
We also need to remember that in treating the marionette folds, we continue to add volume to the lower face. We should only do this in areas that lack volume and be aware of when we need to offer a referral for surgery.
Figure 6 (A) Before and (B) after treatment following the Step by Step approach to marionette lines
Key points
Marionette folds are like steps: there is an upper step (jowl fat) and lower step (inferior to oral commisure and medial to marionette line)
STEP 1. DAO muscle injection with neurotoxin to reduce the dynamic component of marionette lines
STEP 2. Elevate the lower step to meet the upper step with HA filler. Use of cannula to first dissect a subcutaneous space where the greatest shadowing is in the prejowl region and placement of HA filler subcutaneously concentrating on upper third.
STEP 3. Strengthen and blend the step edge between the upper and lower steps of the marionette line. Use HA filler by needle, to elevate beneath the oral commisures, then continue with intersecting deep dermal or subcutaneous oblique V shaped injections along the step edge down the marionette lines.
Conclusion
The step by step approach to marionette folds is a logical and sequential treatment of the three contributing factors to marionette lines. It avoids unnecessary treatment of other areas that are not effective or efficient, for example, treating along the jawline, or extending the chin in the forlorn hope of providing opposite forces along the mandible, to attempt to stretch the marionette fold.
Step 1, in relaxing the input of the DAO, the recurrent downward pull upon the oral commissure is reduced, elevating the resting position of the oral commissure and sparing the HA filler from repetitive, strong sheer forces, potentially extending its duration of action.
With Step 2, in elevating the lower step, the height differential is reduced between the upper step — the jowl hanging against the labiomental cutaneous false ligament, and the lower step— the perioral tissue. This reduces shadowing and the appearance of segmentation of the lower face and the puppet-like sad appearance.
Step 3 strengthens the step edge and provides a blending and strengthening of the medial and lateral areas of the marionette line, creating a smoother contour between the lateral lower face and chin region.
The ‘Step by Step’ approach also targets deep to superficial layers in a step-by-step fashion: muscles, the subcutaneous level, and the skin.
This article is written to provide the reader with a simple direct injection approach using toxin and dermal fillers, and the writer is the first to acknowledge that surgery will, of course, deliver superior and longer lasting results in higher grade folds, but also that some patients wish to avoid the risk and down time and cost of surgical intervention. Therefore there is a great benefit to having a rational, targeted non-surgical temporary approach.
Declaration of interest Dr Doreian is a key opinion leader for Galderma, sits on a number of advisory boards, and presents at various independent conferences as an independent speaker. Dr Doreian has not been paid for this article.
References
1. Gosain AK, Klein MH, Sudhakar PV, Prost RW. A volumetric analysis of soft-tissue changes in the aging midface using high-resolution MRI: implications for facial rejuvenation. Plastic and reconstructive surgery. 2005 Apr 1;115(4):1143-52. 2. Alastair Carruthers & Jean Carruthers (2010) A validated facial grading scale: The future of facial ageing measurement tools?, Journal of Cosmetic and Laser Therapy, 12:5, 235-241, DOI: 10.3109/14764172.2010.514920 3. Gülbitti HA, Colebunders B, Pirayesh A, Bertossi D, Van Der Lei B. Thread-lift sutures: still in the lift? A systematic review of the literature. Plastic and reconstructive surgery. 2018 Mar 1;141(3):341e-7e 4. Gierloff M, Stöhring C, Buder T, Wiltfang J. The subcutaneous fat compartments in relation to aesthetically important facial folds and rhytides. Journal of plastic, reconstructive & aesthetic surgery. 2012 Oct 1;65(10):1292-7. 5. van Eijk T, Braun M. A novel method to inject hyaluronic acid: the Fern Pattern Technique. J Drugs Dermatol. 2007 Aug;6(8):805-8. PMID: 1776361





