
24 minute read
Viewpoints


Should autism diagnoses be prevented early in development?
By Iciar Iturmendi Sabater
Advertisement
Autism is characterised by social and communication differences relative to the normative standards of the general population. It is considered a neurodevelopmental disorder since its neurobiological determinants are present very early in development, with the mean age of diagnosis being three and a half years for children who start showing early signs of autism before ten years of age.¹ As autistic* people usually claim their diagnosis as a critical part of their identity since childhood² the question arises: should research efforts aim at preventing or curing this neurodevelopmental condition?
This question has sparked debate after the recent publication of a randomised controlled trial in JAMA Pediatrics.³
A positive parenting intervention to decrease autism symptomatology Controversy arises: should autism be prevented or ‘cured’?
The JAMA Pediatrics study, carried out in Australia, tested the efficacy of a social skills training for caregivers of infants at risk of autism called the iBASIS Video Interaction for Positive Parenting (iBASISVIPP). The researchers hypothesized that the training would decrease autism diagnoses and symptom severity in children by the age of three.
A team of specialised therapists (psychologists or speech pathologists) implemented the iBASIS-VIPP training among 45 caregivers of infants at risk, while 44 caregivers received the traditional training (a two-hour information workshop on autism which is considered the current best practice on caregiver training). Both interventions had been piloted in previous studies and showed to produce no harm. Throughout the ten home-sessions over five months of iBASISVIPP intervention, specialised therapists guided caregivers in understanding the potential of their infants’ interaction styles while going over previously filmed caregiver-infant interactions. Its main objective was to achieve optimal interaction between infants and caregivers.
Dr. Andrew Whitehouse’s research team found that, by three years of age, autism was diagnosed in 21% of infants whose parents did not receive the iBASISVIPP training, compared to only 7% of infants whose caregivers participated in the training. The iBASIS-VIPP positive parenting intervention lowered the odds of infants at risk of autism being diagnosed with the condition at three years of age. The severity of future autistic symptomatology was also significantly smaller among the children whose parents participated in the iBASIS-VIPP training.
An important question that this study left unanswered was: might the effectiveness of the iBASIS-VIPP intervention in reducing the odds of autism diagnoses extend beyond childrens’ three years of age? Future research might aim to answer this question by performing a longitudinal study. Soon after publication, these findings became a controversial topic among researchers and autistic individuals on Twitter, as different newspapers (e.g.: The Guardian5, The Telegraph6) cited the results of the study as potential evidence that the iBASIS-VIPP can ‘cure’ autism.
In fact, The Guardian rectified its wording and now states at the bottom of the publication:
“This article was amended on 1 October 2021 to remove a reference to the therapy not being “a cure” for autism, as this term is not appropriate within the context of reporting on autism”.
But why is the term ‘cure’ problematic to describe the findings of this investigation and in the context of autism research in general?
The aim of the iBASIS-VIPP intervention is not to change the interaction style of the infant at risk of autism to accommodate the ‘normative’ expectations of their caregivers and societal norms. Instead, the intervention seeks to help caregivers adapt to their infant’s communication styles and change their attitudes towards their autistic child. To that extent, the intervention does not aim to prevent or cure autism, but rather to construct a more understanding social environment that welcomes neurodiversity.

‘cure’ or prevention of autism when the iBASIS-VIPP intervention actually changes expectations and behaviours in the social context of the child, but not in the child at risk of autism.
This iBASIS-VIPP approach attempts to battle medical accounts of autism by considering the ‘double empathy problem’ of autism. Medical explanations characterise autism by individual’s deficits in the capacity to understand the mental states and intentions of others. This psychological ability is known as theory of mind. However, more sociologicallyoriented researchers and autistic individuals themselves have emphasized that it is not only autistic individuals who struggle to understand their nonautistic counterparts, but also non-autistic persons who have trouble interpreting the intentions of autistic individuals. This is known as the double empathy problem, which proposes that the social and communication difficulties that define autism in medical diagnostic manuals like the International Classification of Diseases (ICD) or Diagnostic and Statistical Manual of Mental Disorders (DSM) are not within the autistic individual, but rather the result of interactions between two or more people who struggle to understand each other’s states of mind.⁴ Dr. Whitehouse released a Twitter statement7 addressing the debate his paper had given rise to, insisting:
“Autism can’t be prevented, this is not an aim the study authors believe in. The babies remain neurodivergent, but they are not showing the same degree of developmental barriers that lead them to meet ‘deficit-focused’ DSM-5 diagnostic criteria of autism”.
What Dr. Whitehouse means is that the findings of his research seem to show that infants whose caregivers are helped to better understand their interactional needs, grow in such a way that they are less likely to meet the deficit-focused medical definition of autism, which locates the social and communication problems within the autistic individual. Interventions such as the iBASIS-VIPP may in fact importantly shift the focus of autistic social and communication difficulties from the individual onto the social context, and thus make communities, not individuals, responsible for their remediation.
Autistic individuals will remain autistic, but their autism may not result to be an impairment in their daily lives if their environment is understanding of the way they socially interact differently from others. Under this paradigm, autistic individuals may thrive as their differences become valuable sources of diversity in our communities. As Durkheim (1895) put it, deviance in society challenges standard norms and promotes social change. *Identity-first language has been used throughout this article to fit the evidence available on the language preferences of the autism community8
Moving beyond medical accounts of autism
References
1. Hof MV, Tisseur C, Berckelear-Onnes IV, et al. Age at autism spectrum disorder diagnosis: A systematic review and meta-analysis from 2012 to 2019 National Autistic Society [Internet]2020 [cited 2021 Oct 7];25(4):862–73. Available from: https://journals.sagepub. com/doi/full/10.1177/1362361320971107 2. Milton D, Sims T. How is a sense of well-being and belonging constructed in the accounts of autistic adults? Disability & Society [Internet]. 2016 [cited 2021 Oct 4];31(4):520–34. Available from: https://www.tandfonline.com/doi/abs/10.1080/09687599.2016.1 186529 3. Whitehouse AJO, Varcin KJ, Pillar S, et al. Effect of Preemptive
Intervention on Developmental Outcomes Among Infants Showing
Early Signs of Autism: A Randomized Clinical Trial of Outcomes to Diagnosis. JAMA Pediatr [Internet]. 2021 [cited 2021 Oct 5];e213298–e213298. Available from: https://jamanetwork.com/ journals/jamapediatrics/fullarticle/2784066 4. Milton D. On the ontological status of autism: the ‘double empathy problem.’ Disability & Society [Internet]. 2012 [cited 2021 Oct 4];27(6):883–7. Available from: https://www.tandfonline.com/doi/ abs/10.1080/09687599.2012.710008 5. Sample I. Autism therapy aimed at infants may reduce likelihood of later diagnosis [Internet]. The Guardian. Guardian News and
Media; 2021 Sept 20 [cited 2021 Oct 17]. Available from: https:// www.theguardian.com/society/2021/sep/20/autism-therapy-infants-study-social-development 6. Knapton S. ‘Coaching’ parents found to reduce autism diagnosis by two-thirds [Internet]. The Telegraph. Telegraph Media Group; 2021
Sept 20 [cited 2021 Oct 17]. Available from: https://www.telegraph. co.uk/news/2021/09/20/two-thirds-autism-cases-could-prevented-baby-video-intervention/ 7. Whitehouse, A. Comment on JAMA Pediatrics paper: https:// twitter.com/AJOWhitehouse/status/1441709985763713031 2021
September 25th [cited 2021 Oct 18[Tweet]. Available from: @
AJOWhitehouse 8. Kenny L, Hattersley C, Molins B, Buckley C, Povey C, Pellicano E.
Which terms should be used to describe autism? Perspectives from the UK autism community [Internet]. 2015 Jul 1 [cited 2021 Oct 17];20(4):442–62. Available from: https://journals.sagepub.com/ doi/full/10.1177/1362361315588200?casa_token=3HaB8RzSKmcAAAAA%3A2x7-glkC3anF3vr4z6gK8--gpbFFg2Ke8_OmivjZ_MKhxFatf3H8zoaTmPwg-VsrqeYoRz62nt9z
FROM PAST TO FUTURE: AI AND ITS APPLICATIONS

IN MEDICINE
By Madhumitha Rabindranath
Artificial intelligence (AI), machine learning, and big data are predominantly associated with tech industries; however, these tools are becoming increasingly applicable to other disciplines, especially medicine. Institutions are offering workshops and courses about AI and the University of Toronto recently founded the Temerty Center for AI Research and Education in Medicine (T-CAIREM) to drive AI innovation in healthcare.1 For individuals who are removed from the world of computer science, AI concepts can be overwhelming.
What is AI?
According to IBM, AI “leverages computers and machines to mimic the problem-solving and decision-making capabilities of the human mind”.2 To put it simply, companies continually mine for large datasets that AI can use to parse and make meaningful decisions, solving more complex and interesting problems.
There are two forms of AI – narrow and general AI.2 Most applications use narrow AI where models perform specific tasks with high accuracy. For example, virtual chatbots are algorithms used to resolve routine issues. Conversely, general AI works to mimic the human mind such as achieving self-awareness. Examples of these are found in science-fiction such as in the film, I, Robot but have not been achieved in the real world. datasets and testing the model on a novel cohort, validating its performance against gold standards. The process is long as models require continuous fine-tuning; thus, most medical applications are still in development. The following are some clinical applications of AI.
Within AI exists different subclasses that are implemented for specific functions. Machine learning (ML) is a set of algorithms that are trained to analyze large datasets and create predictive models. Deep learning (DL) has a similar function to ML but is useful for unstructured data such as imaging and requires less human input for training. Other types include natural language processing and robotics. With diverse functionalities, AI is a promising tool that has the potential to revolutionize our world.
Why is it a big deal now?
Although the buzz around AI is recent, its concept was first envisioned in the 1950s. John McCarthy and Alan Turing, two of the founding fathers of AI, coined the term at a Dartmouth summer conference, spearheading AI research.3,4 While many scientists tried to build complex machines, there were limitations to their implementation such as cost and low computational power.5,6 As technology improved, the gains in computational power and data storage were matched with lower costs, making AI models more attainable.
What are some clinical applications of AI?
AI applications in medicine are endless, ranging from diagnostic and predictive models to assistive therapies. The general principle of building AI models requires training algorithms with large, labeled Electronic Patient Records
Electronic patient records (EPRs) have large amounts of clinical information which can be useful for research and clinical decision-making. However, EPRs are rarely structured and are difficult to parse through. One way to tackle this issue is to use natural language processing algorithms that flag keywords during patient-physician conversations and automatically fill in relevant EPR sections.7 This would facilitate standardized record-keeping and better patient-clinician interactions, reducing the burden of maintaining records on clinicians. Intelligent record-keeping systems can also assist clinicians in flagging patients for review and potentially interact with wearable technology to enable constant patient management.
Histopathology and Medical Imaging
To improve diagnostic workflows, DL can be used to learn specific features of medical imaging or pathology slides which can assist clinicians in providing diagnoses. Several studies have shown that using DL to diagnose various pathologies such as cancer type and fibrosis is comparable to clinicians.8–10 Some tools are also

undergoing approval for clinical use. For example, Medo.AI recently received FDA approval for their AI platform that detects hip dysplasia, common in infants, using ultrasound images.11
What are some issues with AI?
Despite its advantages, there are some challenges to implementing AI in clinical settings. Many clinicians are enthusiastic about the implications of using AI, but its integration is stalled by the limitations of translating these models to the clinic. The following are some issues of AI in healthcare and how they can be overcome.
The “Black Box” Problem
The flexibility of using AI for diverse problems comes at a cost. Dubbed the “black box” problem, we are unable to explain AI decision-making as we can only make educated inferences, despite many AI models’ outputs matching clinical expertise. Without the means to understand AI decision-making, it is risky to use these tools in the clinic especially concerning patients’ lives. Fortunately, efforts to create more explainable AI models are underway but there are concerns about affecting AI performance.12 Another way to tackle this issue is to have domain-specific guidelines for interpretability.13 For example, in computer vision (a subclass of DL for image analysis), models can learn specific prototypes for parts of the image that are important for classification, and new images testing the model are classified based on learned prototypes.13 These prototypes can provide more interpretability of its learning process, increasing our confidence in AI decision-making.
Data Security and Safety
Another concern stems from data security issues and biases in AI models. For generalizable and successful modeling, AI tools require large amounts of data, requiring researchers to use open-source datasets. However, in clinical applications, hospitals will need to make EPRs widely available and share data across institutions, posing serious data security concerns. Many private companies are also interested in healthcare applications of AI and can receive access to EPRs, infringing on patients’ privacy rights.14 Hence, anonymized data may be useful in these situations; however, reidentification is possible using these algorithms.14 To ensure ethical compliance, regulatory bodies can provide oversight. For example, the FDA is recently providing a new framework to regulate clinical applications of AI models.12
Final verdict?
Despite these challenges, AI is a promising tool that has the capacity to transform medicine, both in research and clinic. Extensive validation studies are required before these algorithms are deployed to the clinic. With increasing innovation in this field, AI will help tackle complex clinical problems and provide decisions that consider this complexity. AI, ML, and its variants will truly bring medicine to the digital era and provide opportunities to revolutionize healthcare.
References
1. U of T launches new Temerty Centre for AI Research and Education in Medicine [Internet]. [cited 2021 Sep 27]. Available from: https:// tcairem.utoronto.ca/news/u-t-launches-new-temerty-centre-ai-research-and-education-medicine 2. What is Artificial Intelligence (AI)? [Internet]. 2021 [cited 2021 Sep 28]. Available from: https://www.ibm.com/cloud/learn/what-is-artificial-intelligence 3. Amisha, Malik P, Pathania M, et al. Overview of artificial intelligence in medicine. J Fam Med Prim Care. 2019;8:2328–31. 4. Artificial Intelligence (AI) Coined at Dartmouth [Internet].
Celebrate Our 250th. 2018 [cited 2021 Sep 28]. Available from: https://250.dartmouth.edu/highlights/artificial-intelligence-ai-coined-dartmouth 5. The History of Artificial Intelligence [Internet]. Science in the News. 2017 [cited 2021 Sep 28]. Available from: https://sitn.hms.harvard. edu/flash/2017/history-artificial-intelligence/ 6. Early Popular Computers, 1950 - 1970 - Engineering and Technology History Wiki [Internet]. [cited 2021 Sep 28]. Available from: http://ethw.org/Early_Popular_Computers,_1950_-_1970 7. Willyard C. Can AI Fix Medical Records? Nature. 2019;576:S59–62. 8. Ghahremani P, Li Y, Kaufman A, et al. DeepLIIF: Deep Learning-Inferred Multiplex ImmunoFluorescence for IHC Quantification [Internet]. 2021 May [cited 2021 Sep 24] p. 2021.05.01.442219.
Available from: https://www.biorxiv.org/content/10.1101/2021.05. 01.442219v1 9. Yu Y, Wang J, Ng CW, et al. Deep learning enables automated scoring of liver fibrosis stages. Sci Rep. 2018;8:16016. 10. Dermatologist-level classification of skin cancer with deep neural networks | Nature [Internet]. [cited 2021 Jan 23]. Available from: https://www.nature.com/articles/nature21056 11. MEDO.AI. MEDO.ai receives FDA approval to automatically detect hip dysplasia, preventing the leading cause of early hip osteoarthritis and hip replacement surgery. GlobeNewswire News Room. 2020. 12. Kelly CJ, Karthikesalingam A, Suleyman M, et al. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019;17:195. 13. Rudin C. Stop explaining black box machine learning models for high stakes decisions and use interpretable models instead. Nat
Mach Intell. 2019;1:206–15. 14. Murdoch B. Privacy and artificial intelligence: challenges for protecting health information in a new era. BMC Med Ethics. 2021;22:122.
Vaccine Passports: The Current Controversy

By Archita Srinath
It has been almost two years since the COVID-19 pandemic shook up the world in ways we never knew possible. Phrases like “social distancing” and “work from home” are now in our everyday vocabulary and checking to see if you have your mask before leaving the house is as normal as checking for your phone, wallet, and keys. Moreover, people are dealing with the unimaginable trauma of losing their loved ones and livelihoods whilst unable to engage with their social support systems. With the constant fear of contracting this virus anytime we step out of our homes, it has made the last two years one of the most challenging times in our lifetime. So, when the scientific community ran shouting “help is on the way dear” like a vaccine wielding Mrs. Doubtfire, most of us breathed a sigh of relief. However, when the Ontario government mandated “vaccine passports” for entry into public spaces, concerns over safety, privacy and equitable access to the vaccine were raised. So, let me pose these questions: are these fears valid? And if they are, how can we work to resolve them?
Many people view the implementation of vaccine passports as a way to coerce them into getting a vaccine that they feel is unsafe. Making vaccination mandatory to hold certain jobs or attend social events impedes people’s financial and mental state, therefore, making them more likely to get the shot even if they do not want to. Although it is true that these mandates are warranted given the risk that COVID-19 poses on human health, safety concerns are valid. We need to acknowledge the fact that many people fear long-term effects. Medical research has failed countless times in the past which has resulted in the harm and death of numerous people. Therefore, the lack of trust in the medical system is understandable, especially in marginalized populations that have historically been the victims of medical malpractice. Even though clinical trials and public health data support the safety and efficacy of the COVID-19 vaccines, it is vital that efforts to communicate this are inclusive and comprehensive.1 Theref ore, combating misinformation on social media should be prioritized and the media should avoid sensationalizing rare side effects by carefully presenting them with context.
Most vaccine passport opposers feel that the government is overstepping its boundaries by limiting the free will we expect in a democratic society. However, this argument is trite since proof of immunization for free movement in public spaces is not a new concept in Canadian society. One major system that requires proof of immunization against infectious diseases for entry are schools.2 Hospitals and other health care settings require their staff to show proof of vaccination before working on the premises. These requirements have been around for ages but has never seen the pushback that the COVID-19 vaccines have received. According to Dr. Raywat Deonandan, an epidemiologist from the University of Ottawa, labeling proof of immunization as “vaccine passports” contributes in part to this resistance as it reminds people of restrictive border security.3 Therefore, changing the way in which vaccine passports are referred to can also be helpful to reduce this anxiety.
Another commonly cited reason against vaccine passports is loss of privacy. However, privacy concerns can be dispelled if the government takes measures to protect the app against security breaches and ensures that they are only tracking

relevant personal information. According to the Ontario Government, the app never stores personal information and does not display your health card number to the person checking your passport.⁴ Additionally, Ontario allows for proof of vaccination to be shown through a printed copy. So, if you have privacy concerns with the app, printing out a certificate or asking the Provincial Vaccine Contact Centre to mail you a copy is an ideal solution.⁴ With these provisions, vaccine passports are no more intrusive on personal privacy than verifying your identification at a local bar.
There are also concerns from the Ontario Human Rights Commission over barriers to equitable vaccine access for everyone.⁵ People who are not able to get vaccinated even if they wanted could therefore face discrimination based on their immunization status. However, there are resources available to help combat many barriers for marginalized communities. The National Newcomer Network offers support in many languages to undocumented and migrant workers to get their vaccines without the need for government identification.⁶ The Accessible Drive to Vaccines program will ensure that anyone who needs help getting to a clinic will be able to get a ride.⁷ This is meant to help individuals with disability and older people with mobility issues to get their shots. However, a major gap in the aid available does exist for people experiencing homelessness. Although there are avenues to get a vaccine without the need for a health card, showing proof of vaccination still proves to be difficult as they may not have a cell phone or be able to keep a printed copy safe from theft.
Finally, according to the Centre for Disease Control, vaccinated individuals are much less likely to become seriously ill and spread the disease than unvaccinated people.1 Therefore, ensuring that everyone in a poorly ventilated public space like a gym or restaurant is vaccinated is helpful to slow down the spread of COVID19. As long as we continue to work at making vaccines more accessible to every single Canadian, curb the spread of misinformation on the internet, and protect everyone’s reasonable right to privacy, vaccine passport is a great new method to get us back to normal life. And who does not miss that? References
1. Coronavirus Disease 2019 (COVID-19) [homepage on the
Internet]. Centers for Disease Control and Prevention. 2021 [cited 2021 Oct 18]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/fully-vaccinated-people.html 2. Vaccines for children at school [homepage on the Internet]. ontario. ca. 2021 [cited 2021 Oct 18]. Available from: https://www.ontario. ca/page/vaccines-children-school#exemptions 3. Bensadoun E. ‘Vaccine passport’ or ‘immunization record’? Why experts say there’s power in words - National | Globalnews.ca [homepage on the Internet]. Global News. 2021 [cited 2021 Oct 18].
Available from: https://globalnews.ca/news/8171936/vaccine-passport-language-concerns/ 4. Ontario Newsroom [homepage on the Internet]. News.ontario.ca. 2021 [cited cited 2021 Oct 18]. Available from: https://news.ontario. ca/en/backgrounder/1000980/using-your-enhanced-vaccine-certificate-frequently-asked-questions 5. OHRC policy statement on COVID-19 vaccine mandates and proof of vaccine certificates | Ontario Human Rights Commission [homepage on the Internet]. Ohrc.on.ca. 2021 [cited 2021 Oct 18]. Available from: http://www.ohrc.on.ca/en/news_centre/ohrcpolicy-statement-covid-19-vaccine-mandates-and-proof-vaccinecertificates 6. Covid-19: Vaccination for undocumented and migrant workers in Ontario [homepage on the Internet]. National Newcomer
Navigation Network. 2021 [cited 2021 Oct 18]. Available from: https://www.newcomernavigation.ca/en/news/covid-19-vaccination-for-ontario-undocumented-and-migrant-workers.aspx 7. Ontario Newsroom [homepage on the Internet]. News.ontario. ca. 2021 [cited 2021 Oct 18]. Available from: https://news. ontario.ca/en/release/1000389/ontario-providing-accessible-rides-to-covid-19-vaccination-sites

The Pros of Probiotics
By Kyla Trkulja

The human microbiome is estimated to contain about 100 trillion bacteria consisting of over 1000 species.1 Over the past few decades, the importance of this group of organisms has become abundantly clear, as these microbes act as their own organ system with many metabolic, immunological, and endocrine-like functions that influence human health.2 For example, microbes in the gut synthesize vitamins, amino acids, and important metabolic byproducts for the human host.3 These include vitamin K for blood clotting and short chain fatty acids (SCFAs) for energy.3 Other benefits include the breakdown of dietary toxins, nutrients, and carcinogens, conversion of cholesterol into other essential fats, assisting in the maturation of the immune system, and protecting humans from harmful bacteria that could otherwise invade the gut.2 This wide variety of health benefits is due to the gut microbiota consisting of organisms that have specialized enzymes and abilities that differ from us humans, allowing them to live in our bodies and thrive without causing us harm while actually promoting health and preventing disease.
How does the microbiome influence health?
An imbalance in the microbiome, known as dysbiosis, has been associated with immune disorders, susceptibility to infections, and pathologies such as cardiovascular disease, obesity, diabetes, liver and brain disease, autism, and mood disorders.2,3 Various studies have examined the composition of the gut microbiome and its associations with conditions including inflammatory bowel disease (IBD), inflammatory skin diseases such as psoriasis and dermatitis, arthritis, diabetes, obesity, and atherosclerosis.3 In addition, recent research has found that our lifestyle and diet choices influence the microbiome of the gut; for example, high intake of red meat increases the abundance of bacteria that produce trimethylamine-N-oxide (TMAO), a compound that increases the risk of cardiovascular disease.3 Findings such as these have demonstrated that we as humans have the ability to influence our own microbiomes, which can improve our health if done strategically.
Manipulating the microbiome with probiotics
Various foods such as cultured milk products and yogurts contain lactic acid bacteria, a source of consumable microbes that can promote a healthy gut microbiome.3 Commonly referred to as “probiotics”, these foods enriched in beneficial bacteria can have a positive impact on our health. In fact, companies even sell probiotic supplements that can be taken as capsules, tablets, packets, or powders so the benefits can be obtained without necessarily consuming the appropriate foods.⁴ The most widely used probiotics are the beneficial Lactobacillus and Bifidobacterium groups, which may have health benefits such as reducing body fat mass, improving glucose and lipid balance, and regulating the immune system.2, ⁴-⁵
Some of the health benefits of probiotics have been validated through randomized controlled trials and extensive research, but others are only supported by inconsistent evidence.4 There is strong
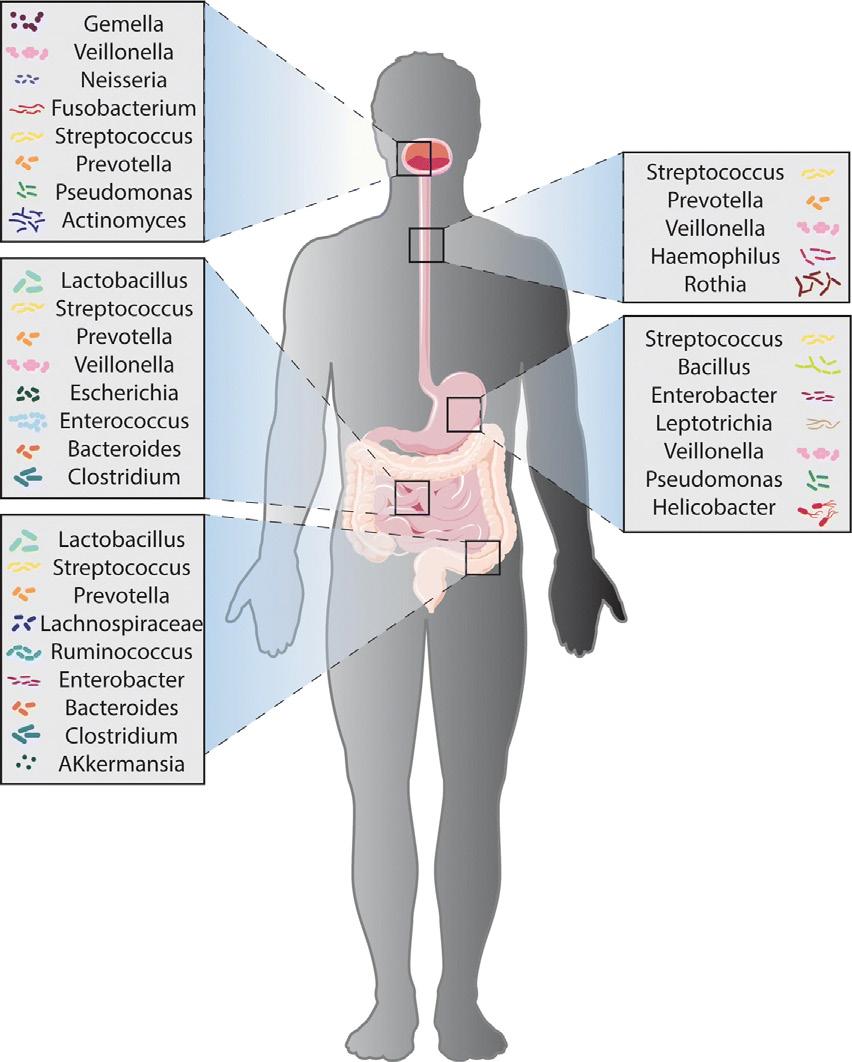
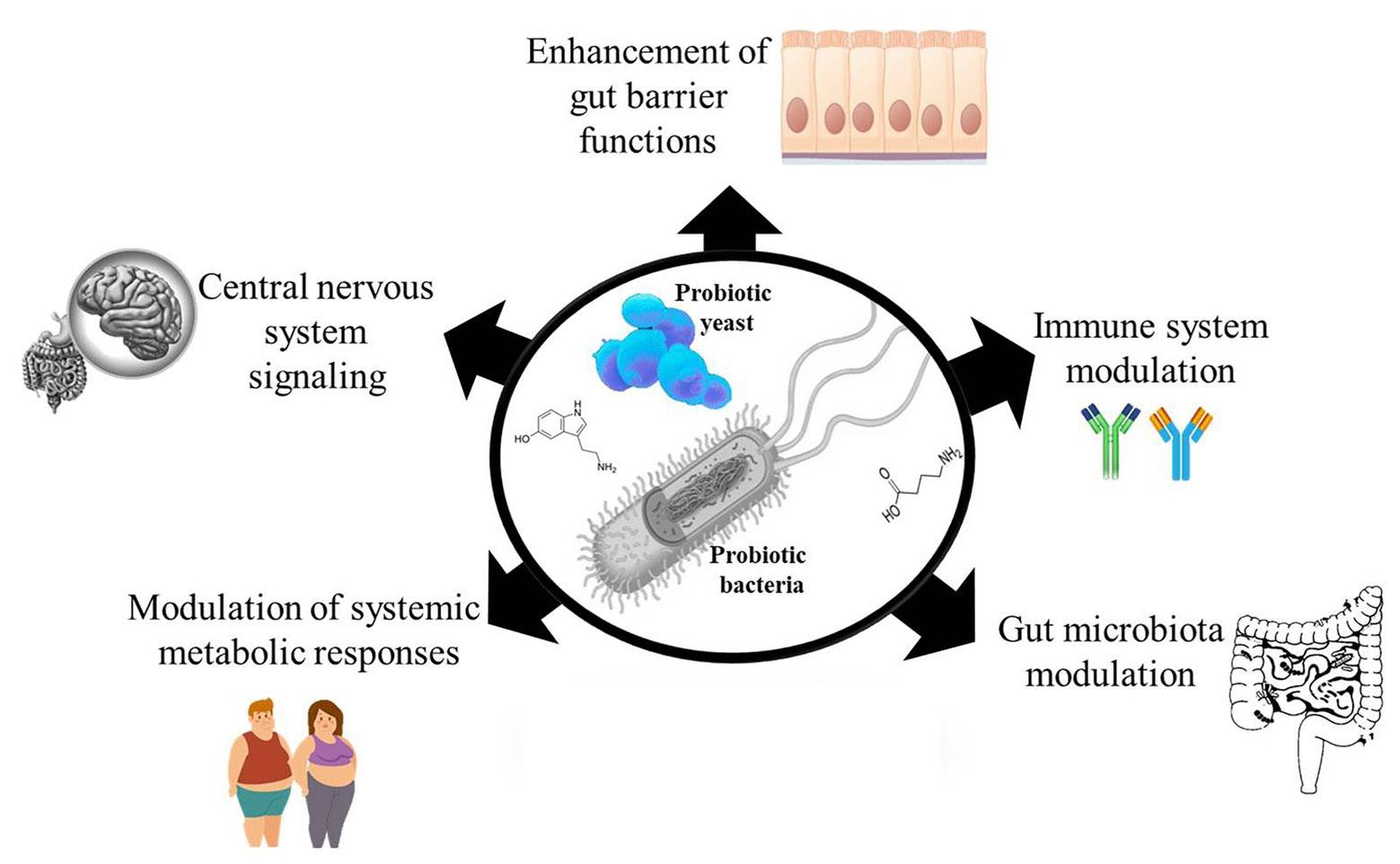
Figure 1 (left). The composition of the human gut microbiome, estimated to contain over 1000 species. Figure 2 (right). The widespread benefits of regular probiotic consumption extend far beyond the microbiome.
evidence supporting the use of probiotics to improve stool consistency, regulate bowel movements, reduce abdominal bloating, prevent vaginal, E. coli, and H. pylori infections, and reduce the incidence and symptoms of the common cold.⁶ Other less supported benefits may include improvement of mood, reduction of depression and anxiety symptoms, weight loss, and balancing of metabolic markers of health such as cholesterol and proinflammatory cytokines.2-3, ⁵-⁶ Furthermore, probiotics have been found to potentially aid in weight loss and have maximum health benefits when combined with diet and exercise. This is due to the bacteria breaking down metabolic byproducts like fermented proteins that are produced when exercising.⁷ Future research will hopefully be able to decipher which benefits are reliable, but even with our limited knowledge, the potential pros of consuming probiotics outweigh the cons.
Nonetheless, it is important to note a few other considerations before taking probiotics. Most importantly, everyone’s body is different, and their age, gender, co-morbidities, genetics, and body environment may result in a different outcome when taking probiotics; as a result, probiotics might not benefit everyone, and may even be harmful for some.1,⁸ Similarly, since probiotics contain live microorganisms, there is the risk of infections, side effects, and complications in some individuals.1,⁴ Those who are most at risk are immunocompromised individuals or people with immunological disorders; however, everyone should talk to their doctor before taking probiotic supplements, just like they would with any medication.⁸
The gut microbiota also depends on other factors such as genetics and diet; therefore, taking probiotic supplements will not result in benefits without taking this into consideration.⁶ Finally, it’s important to remember that the gut microbiome can change quickly, returning back to baseline within 1-3 weeks after ceasing probiotics.⁶ This emphasizes the fact that probiotics should be combined with a healthy lifestyle for maximum benefits, and that they are not a permanent solution to wellness.
However, despite the considerations, probiotics are generally considered a safe, accessible, and well-tolerated way to balance the gut microbiome and improve health. Talk to your doctor to determine which type of probiotics you should take, since they aren’t all created equal, and combine them with healthy living to let you and your microbiome thrive.
References
1. Lordan, C., Thapa, D., Ross, R. P., et al (2020) Potential for enriching next-generation health-promoting gut bacteria through prebiotics and other dietary components. Gut Microbes, 11:1, 1-20, DOI: 10.1080/19490976.2019.1613124 2. Gérard, P. (2016) Gut microbiota and obesity. Cellular and Molecular Life Sciences, 73, 147–162. https://doiorg/10.1007/s00018-015-2061-5 3. Singh, R.K., Chang, HW., Yan, D. et al. (2017) Influence of diet on the gut microbiome and implications for human health. Journal of Translational Medicine, 15, 73. https:// doi.org/10.1186/s12967-017-1175-y 4. Williams, N. T. (2010) Probiotics. American Journal of
Health-System Pharmacy, 67(6), 449–458. https://doi. org/10.2146/ajhp090168 5. Mueller, M., Ganesh, R. & Bonnes, S. (2020) Gut Health = Mental Health? The Impact of Diet and Dietary Supplements on Mood Disorders. Current Nutrition Reports, 9, 361–368. https://doi.org/10.1007/s13668-020-00340-2 6. Khalesi, S., Bellissimo, N., Vandelanotte, C. et al. (2019)
A review of probiotic supplementation in healthy adults: helpful or hype? European Journal of Clinical Nutrition, 73, 24–37. https://doi.org/10.1038/s41430-018-0135-9 7. Sergeev, I. N., Aljutaily, T., Walton, G., et al (2020) Effects of Synbiotic Supplement on Human Gut Microbiota,
Body Composition and Weight Loss in Obesity. Nutrients, 12(1), 222. https://doi.org/10.3390/nu12010222 8. Kothari, D., Patel, S., Kim, S. K. (2019) Probiotic supplements might not be universally-effective and safe: A review. Biomedical Pharmacotherapy, 111, 537-547. doi: 10.1016/j.biopha.2018.12.104.








