“This

“This

….
from
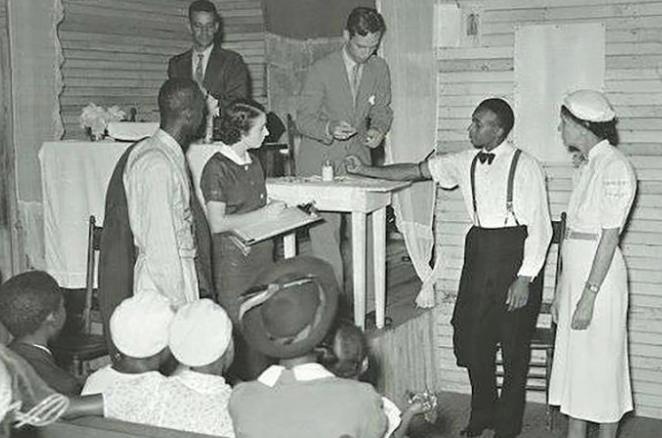
Pastor Mike McClure, Jr. is one of many individuals across the state speaking out and encouraging others to take the COVID-19 vaccination. He shares his strong feelings for his own children and family and recognizes that others need to make their own decisions to protect themselves and their community.

The Alabama Community Engagement Alliance (CEAL) Against COVID-19 Disparities is an NIH-funded, state-based outreach and engagement effort in communities that have been hardest hit by COVID-19. This team of community members and researchers; is addressing the myths, misinformation, distrust, and skepticism surrounding COVID-19. AL CEAL is removing barriers to testing and vaccination, and working to earn back the peoples’ trust of the scientific community.
Through their website, communities can access information on vaccination status, ongoing efforts and educational content about: how were the vaccines made, flu vaccines vs COVID-19 vaccines, vaccine effectiveness and safety, myths and misconceptions, and heart-felt sentiments from physicians and researchers. By educating the communities, more people are receiving up to date information and answers from healthcare professionals.
Pastor Mike is one of many individuals using the platform to share his story. He continues, “I believe this is what is necessary for us to move forward in this new normal.”



an interview with Dr. Matthew Sample
CONTRIBUTORS
Kimberly Waldrop, MA
Matthew Sample, MD, FACC
William Budd, PhD
Jelly Reese
D Kishore Yellumahanthi, MD, MPH, FAAFP
Sarah Sharman, PhD
Joanice Thompson
Bobi Jo Creel, RN, MSN, CRNP Karen Petersen
Joi Rice
Adam Reiger Carr
Carl Stephenson, MD
Winston T. Capel, MD, FACS, FAANS Tiernan O'Neill
ADVERTISING
Join our mission to establish and grow an alliance among our community and healthcare providers. Together, we can change the way healthcare information has been and will be distributed for years to come.
To reach our readers, whether through editorial contribution or advertising, please contact Kelly Reese at 256.652.8089 or kellyreese.im@gmail.com
Terrie Ledbetter, Senior VP
Leigha Parker
Kimberly Waldrop, MA
Blake Bentley, President
Kelly Reese, Founder Key Common, COO
www.insidemedicinemagazine.com
The information and opinions contained in this publication constitute general medical information only and should not be construed as medical advice. Before making important medical decisions, readers should consult with a physician or trained
their needs and concerns assessed in a clinical setting appropriate for their problem.
provider of their choice






With the dawn of a new year, many of us will make a resolution to improve our health. Three of the most common resolutions involve health improvement.
Unfortunately, the odds of keeping a resolution are not in our favor. Only 8% of people will keep their resolution for the entire year. Since many of us are looking to improve our health, it is important to discuss our resolutions with our healthcare provider. An important component to our health maintenance and improvement is the annual examination with laboratory testing. This visit sets our baseline and helps identify common physical issues prior to them manifesting themselves to us.







One of the most important laboratory tests is the Glycated Hemoglobin (HgB-A1C). This test measures the average of blood glucose over the previous 2-3 months. This laboratory test is one of the tests used to diagnose diabetes mellitus. 15% of the US population currently suffers from diabetes mellitus, sometimes referred to as sugar diabetes.










Diabetes mellitus is the result of our body’s inability to maintain a healthy blood glucose level. There are two classifications of the disease. Type I diabetes occurs when the pancreas is unable to manufacture insulin, a hormone required for our body to use glucose. Persons with this form of the disease need to inject insulin and closely monitor their intake of carbohydrates. Type II diabetes is the result of prolonged periods of elevated blood glucose levels that result from inadequate production of insulin from the pancreas or the body’s resistance to the insulin produced. Treatment of the disease varies with diabetes and severity of the condition.




Symptoms of diabetes mellitus are often subtle and can go unrecognized for prolonged periods. The most common symptoms are frequent urination, excessive thirst, hunger, and fatigue. Excessive levels of blood glucose led to long-term consequences. Complications include heart disease, stroke, nerve damage and eye damage. Once diagnosed with diabetes or pre-diabetes, it is important to maintain healthy blood glucose levels to minimize the long-term effects of the disease.



Diet and exercise are often used to halt the disease's progression from pre-diabetes to diabetes. Diet and exercise are important components of a healthy lifestyle for any diabetic patient. Most people with elevated blood glucose levels find it difficult to begin an exercise program. It is important to discuss an exercise program with your healthcare provider prior to beginning to minimize your chances of an adverse outcome. All exercise programs should start slowly and gradually increase in duration and intensity.
Metformin is often used as a first line agent in the treatment of Type II diabetes. This medication increases the sensitivity to insulin at the cellular level causing our body to utilize carbohydrates causing the level of glucose more efficiently in the blood to decrease. This medication also suppresses a person's appetite. Metformin and other related medications have been on the market for nearly 30 years. Metformin commonly causes gastrointestinal disturbances such as nausea, vomiting and diarrhea. In the initial stages of the disease, Metformin can be a successful adjunct to diet and exercise.
Glucagon-like peptide 1 (GLP1) receptor agonists are a new class of medications that have demonstrated strong results in management of Type II diabetes. These medications such as Ozempic, Mounjaro, and Wegovy when used with diet and exercise produce dramatic responses in blood glucose management and weight loss. Semaglutide (Ozempic and Wegovy) was approved by the FDA in 2019. These medications increase insulin production from the pancreas and inhibit production of glucagon. This effect improves the utilization of glucose thereby reducing overall blood glucose levels. These medicines are administered by injection into fatty tissue once per week. Side effects include delayed gastric emptying and reduced intestinal mobility leading to nausea and constipation. Person’s that take Ozempic or Wegovy as directed typically lose weight. The average person using these medications as directed will lose up to 15% of their body weight.
In 2022, Mounjaro (Tirzepatide) was approved by the FDA for treatment of Type II diabetes mellitus. This medication combines GLP-1 stimulation with a synthetic hormone gastric inhibitory polypeptide (GIP). Com-
bining these two hormones further reduces gastric emptying, causing persons to feel fuller for longer periods of time, reducing overall food consumption. In clinical trials, participants lost up to 22% of their body mass with 91% of participants reducing their A1C levels to less than 7.0 and 47% of patients reduced their A1C to non-diabetic levels. In addition to glycemic control and weight loss, Mounjaro has been shown to reduce cholesterol and triglycerides.
These classes of medications have received a lot of attention over the past few months as weight loss medications. Semaglutide (Wegovy) is approved by the FDA for persons with a body mass index greater than 30% or 27% with a health complication. Tirzepatide (Mounjaro) is not currently approved for weight loss, but the manufacturer is completing the requisite clinical trials and plans to apply for approval in 2023.
Uncontrolled blood glucose levels lead to various complications including heart disease, stroke, kidney damage, eye damage, and nerve damage. It is important to monitor blood glucose levels routinely and check your A1C level at least once per year. The variety of medications to treat diabetes has improved over the past 10 years leading to improved long-term outcomes for patients with the disease.








 by: Joanice Thompson
by: Joanice Thompson
I come from a large family. Everything we did was rooted in service to one another and as an adult, that servanthood became a large part of my life, personally and professionally. For that reason, a career in healthcare meant so much to me. I spent over 30 years at The University of Alabama at Birmingham. I served as the associate director for Community Outreach at the UAB Minority Health and Health Disparities Center and as an early figure in the development of the Cancer Center Office of Community Outreach and Engagement. During my time at UAB, I had the privilege to work on many grass-root efforts that targeted underserved communities. So, I’ve figured out a thing or two about what people need and what works to get goals accomplished.
B-INCLUDED is a community-based, digital health platform designed for Black residents of Jefferson County. When


residents sign up to use the platform, members have access to life-changing resources that can help you make informed decisions about your health. It allows you to invite family and friends so they can have the opportunity to do the same. What is so different about B-INCLUDED is that never before has a platform been created especially for local residents to address their specific needs. National and even regional platforms have made some impact but for the most part, their scope considers a broader population. B-INCLUDED on the other hand is solely focused on Birmingham’s Jefferson County residents. Most of us know the feeling of being left out or not having immediate access to some of the things we’ve most needed. This is one of the obstacles B-INCLUDED addresses. Residents won’t have to search here and there for what is needed because everything is compiled in a digital format that allows access anytime from their computers and phones.
In addition to the access, I’m also impressed with the offerings. My career in healthcare has literally taken me to the doorsteps of Jefferson County residents. I have a pretty good idea of what is needed and B-INCLUDED addresses those needs. This community engagement is a “health-first” priority, where residents can tackle some of the bigger issues that gradually and significantly impact their overall quality of life. When you start from the root, which is often diabetes, lupus, obesity, then you can see how it affects employment (can’t work if you’re sick) and finances (there’s nomoney if you’re unable to work).
B-INCLUDED is working from the root up and I look forward to seeing the short and longterm impact this campaign has on Birmingham residents. Yes, you deserve a better shot at a better quality of life. Join today!

That’s why I’m so excited about B-INCLUDED.M s W alla de a n S t r eete r , Bush H ill s Ne ig hbo r hoo d Assoc ia t i on P res i den t


Sponsorship opportunities available, contact Anna Kirkpatrick at akirkpatrick@hudsonalpha.org or visit hudsonalpha.org/double-helix-dash-sponsors-info









 by: Adam Reiger Carr
by: Adam Reiger Carr
Every commercial real estate transaction has an ideal timeframe to begin the process. Most healthcare professionals understand that opening a new office or relocating an office doesn’t happen overnight, but the majority of professionals are not aware of the ideal timeframes for each type of transaction. Different types of problems arise when starting a transaction too early or too late, and both need to be avoided.
If you start the process too early, it creates a scenario where you spend your valuable time looking at properties and evaluating options, working with lenders and other members of your team, only to find out the landlords or sellers won’t negotiate with you yet. Many landlords and sellers won’t take their spaces off the market for extended periods of time while waiting for the tenant or buyer to be ready to transact, because there is too much time before the transaction will actually take place.
Or if they do negotiate, they won’t be willing to offer you even close to their best terms since they are going to lose income on holding a space vacant for an extended period of time. On the other hand, if they will put forth reasonable terms, it is predicated upon you moving forward immediately, which can leave you stuck paying for a space you can’t occupy for a period of time or paying unnecessary rent on your former space if you leave early.
When starting a transaction too late, an entirely new set of problems arise. To start, most people underestimate how long a commercial lease or purchase transaction takes. They imagine it is similar to buying a home or leasing an apartment, which unfortunately is not the same as a commercial transaction timeline.
Simply identifying the top options and then negotiating a mutually agreeable deal can take several months. The legal process of reviewing contracts and finalizing details with lenders, architects, contractors, and equipment and technology providers comes next; this portion can also take months.
This is followed by the build out process if renovations are required. While you can build out a new space in 6 to 10 weeks depending on the size and scope of the project, you first have to design the space, then get construction documents and engineered plans created, then submit for and receive permits to start the build out. After construction, you need to leave time for installing furniture, fixtures, equipment and technology, final permitting and approvals, while also leaving room for uncontrollable delays, and change orders.
If you are relocating from a previous office and you don’t vacate your former space prior to the lease expiring, you’ll likely pay between 125 to 200% of your last month’s rent based on a provision found in most leases called “Holdover.” This allows the landlord to charge you a higher month-to-month lease rate as a penalty for not vacating or signing a new lease.
Learn about your genetic risk for certain cancers including breast, ovarian, colorectal and prostate cancer. In collaboration with your physician and a genetic counselor, use the information to plan future medical care. What you learn could potentially impact your parents, siblings, children, cousins and others.
The test is offered FREE to any woman or man between the ages of 28-30 in Madison, Jackson, Limestone, Marshall and Morgan Counties in Alabama. The test also is offered at a reduced cost of $129 to adults 19 and over in those five counties.
Our simple cheek swab can help empower you to make important healthcare decisions for you and your family.
If you only had two choices, starting too early is definitely better than starting too late but it is by no means your top option. Fortunately, there is an ideal timeframe to start each type of transaction and you don’t have to choose between the lesser of two mistakes. You can set yourself up for success by understanding the requirements of each type of transaction and how long each process takes.
Although there are many additional details needed to ensure each type of transaction is handled properly, let’s start with the correct timing for the primary types of transactions that Healthcare Professionals will engage in:
• Start-up or new office: 10 – 12 months in advance
• Relocation: 10 – 12 months in advance
• Purchasing an existing building or condo: 10 – 12 months in advance
• Buying land to develop a new building: 18 – 24 months in advance
• Buying a practice and getting a new lease or purchasing the building: 60 – 90 days
Every type of transaction starts with a specific approach and detailed game plan that is aimed at maximizing the opportunity. Getting the best possible deal and terms is extremely important, but so is making sure you don’t waste valuable time that could have been spent in your practice. If you lose the equivalent of twenty to thirty hours of your time—which is what an average commercial real estate transaction requires to be handled properly—how much money would that cost you in lost production?
Equally as important as saving time and money is avoiding costly mistakes that people make all too often when they don’t understand the nuances of healthcare real estate. The old adage, “if I knew then what I know now…” can easily be avoided by hiring licensed professionals that specialize in real estate for healthcare practices. The reason patients come to see you is because you are trained in a specific skillset that offers skill and expertise that they require and that few people have. The same is true for real estate professionals that can help you identify your top options, negotiate the most favorable terms, save you a substantial amount of time, and avoid common pitfalls.
The first step to maximizing any commercial real estate transaction: Start the process at the right time.
CARR is the nation’s leading provider of commercial real estate services for healthcare tenants and buyers. Every year, thousands of healthcare practices trust CARR to achieve the most favorable terms on their lease and purchase negotiations. CARR’s team of experts assist with start-ups, lease renewals, expansions, relocations, additional offices, purchases, and practice transitions. Healthcare practices choose CARR to save them a substantial amount of time and money; while ensuring their interests are always first.
Visit CARR.US to learn more and find an expert agent representing healthcare practices in your area.






Working in a primary care clinic as I do, it is not uncommon these days to meet with a wide range of sales representatives pitching you ideas on how to increase your revenue stream. A few years ago, I was talking with one such equipment supply representative. They were giving me all the details and attempting to sell me the latest and greatest piece of lab equipment that could provide in-depth gastrointestinal testing for patients within our primary care clinic. As they began to sense I was not willing to make the purchase, they asked me “what could be a greater asset in the care, diagnosis and treatment of our patients?” I briefly paused and replied, “sending a patient to a Gastroenterologist who has dedicated their entire education and careers to the field of this specialty.” Needless to say, having failed to make the sale, the representative was more than a little defeated and was not happy with my answer. But it was the truth. With that said, it would be misleading to believe primary care doctors have no place in the care or coordination of patient special health care concerns.
In the simplest terms there are two types of doctors a patient may interact with throughout their health care lives. There are primary care doctors and specialists. Coordinating care and assigning who is ultimately responsible for the care of patients between these two types can be tricky and a cause for great confusion; especially for patients. This article will focus on a model and expectation a patient may have as they navigate between the two.
Primary care physicians, whether family medicine or internal medicine trained, are generally the patient’s first point of contact. It is often assumed that these doctors can handle the basics such as acute illness or pains, superficial skin issues, and routine disease maintenance. Depending on the patient and the comorbid conditions they are afflicted with and the preferences of their primary care physician, it is not uncommon for them to see each other multiple times throughout the year. Thus, they form a close and intimate relationship. Naturally, most patients feel comfortable and prefer to receive as much care as possible from their primary care doctor. But these primary care doctors may not be able to or should not render care in all circumstances. That is when specialists are sought after. Whether it be resources, knowledge or expertise in handling either complex or highly sophisticated diseases, they are simply more equipped. Generally, while there are many good and highly skilled primary care physicians it is best to have the involvement and care of a specialist in certain cases.
Having said the above, many people get lost and are not sure when to use a primary care physician and when to bypass them and search out directly for a specialist. The answer is simply, never. The primary care physician plays a very important role in the whole process.
First, they help diagnose a patient with a suspected “issue” and make sure they are directed to the appropriate specialist. This can mean two things. Patients, while full of good intentions, often can’t determine which type of specialist is best for them and can often confuse one symptom when overlooking others and ultimately misdiagnose themselves. As a result, this can waste precious time and money go-
ing to the wrong type of specialist(s). These poor decisions can often be influenced by friends, family or the proliferation of direct-to-patient marketing. Many specialists, or at least good specialists, get frustrated when their schedule is full of patients who really should not be seeing them.
Additionally, even if the correct specialist is designated, sometimes the match is not a good fit for a variety of other reasons outside of medical care. Simply, it is the primary physician’s responsibility to not only send the patient to the correct specialist based on disease conditions and care but also vet that specialist as a good fit for the patient. By care, we mean more than navigating the patient away from unskilled specialists but instead certain specialists, while highly skilled, may not match and mesh well with certain patient personality types. This is often a consideration, with all things being equal in care, a primary care physician may make. They have developed a strong relationship with both specialists and patients and can understand what approach works for some while not others. In this sense, I generally see and believe a good primary care physician is playing the part of an air traffic controller. While able to care for the routine, and likely more than capable to handle more, they effectively point patients in the right direction to meet their health care needs.
Secondly, being seen as air traffic controllers may seem like a diminished role for any doctor, it is extremely important and requires a great amount of due diligence. A good primary care physician should do multiple things for their patients prior to referring to a specialist. Any diagnostic or preventative testing that is readily accessible to them which can confirm a patient’s need for a specialist should always be performed prior to a patient being sent on. This ensures the time, effort, and yes even sometimes cost for both the patient and the specialist is not wasted. Patients who are pointed in the wrong direction can often feel dejected and may simply give up and/or ignore what could be a potentially significant untreated disease. Specialists can also get unengaged when they need to start with the basics rather than hit the ground running in their field of expertise when they first see a patient. This unlikely hurts the patient directly at the time, but it can hurt the patient or other patients when their primary care physician has not developed a good referral relationship and practice with good specialists. As a result, the patients of those certain primary care physicians are not seen quickly, taken seri-
ously, or are maybe even unable to access the best specialists in the area and field.
Thirdly, as the patient’s first point of contact we can also view primary care physicians as a hub of information. A patient’s chart, a complete chart, is housed at their primary care clinic and rarely anywhere else. This record contains years and years worth of encounters, medications failed or succeeded, test results and various specialist notes and testing from the past. Seen individually or as a collection, this medical recap of a patient and their health history is crucial in managing current health concerns as well. This information can be used by your doctor to care and coordinate care for that patient effectively and wholly. To this end, there are three things a patient should always do to ensure this goal:
1) Always tell your specialists or other facilities (hospitals, surgery facilities) away from your primary care physician about who is your primary care doctor and request all notes and labs be copied to them
2) Request specialist or facility notes/test results for yourself and then provide your primary care doctor copies for your chart
3) Periodically check with your primary care physician and their office to find out if the copies were received and reviewed by your primary care doctor. If not received, press the specialist office to participate in closing the circle of care. If not reviewed, press your primary care doctor on being more involved in your care
Your chart then, a complete chart, housed at the office of your primary care physicians is quite the resource as we age and our health history and future needs building. It will also help to make sure no doctor orders testing, treatment plans or medical decision making is not unnecessarily duplicated. Furthermore, it will help your primary care doctor in communicating more effectively with any possible other specialists they need to coordinate with.
Lastly and briefly mentioned earlier, your primary care physician can help you avoid the less than credible specialists. There are doctors and other individuals (Physician Assistants, Nurse Practitioners, “Wellness Centers”….etc) that are claiming to be experts in what-

ever field they find to be either (a) an interest in or (b) a lucrative source of income. They are not board certified and rarely hold any distinction or measurable skill to make the claim they can actually help other than once again they find representing a certain field or issue as beneficial to themselves alone. These individuals or clinics are often populated as a result of patients bypassing their primary care doctor and self-referring based on advice they receive from friends, families or direct-to-patient marketing. In the end, they often unnecessarily cost the patient money and time. They can also harm the patient by missing out on or delaying legitimate care. Involving a good and interested primary care doctor throughout your specialist journey can help protect patients from themselves and others. Too often, patients keep these forays a secret because they do know any better and these potential harms could have easily been avoided.
By and large the relationship you have with your primary care doctor(s) throughout your health care life is by far the most widespread and intimate patient-doctor relationship you will experience. Having said that, it only makes sense to rely on their expertise and assistance in the referral and specialist experience as much as possible. They are best equipped to understand at a minimum the correct direction and destination for your ills. They hold a personal and vested interest in your health care like no other. Good primary care doctors are knowledgeable to both the general field of specialties and specific individual specialists that can best serve their patients unique needs. They can be relied on throughout the journey to safeguard and coordinate your medical history. Furthermore, they will protect patients from others as well as themselves. Skipping your primary care doctor as you seek assistance in your medical condition would be forgoing and ignoring the years and years of medical advice you have trusted to that point and would be terribly ill advised.
The ability to sequence and analyze an organism’s DNA has revolutionized the field of biology, allowing researchers to understand how the genome functions and how changes in the genome affect all life on earth. Careers in the fields of genetics and genomics are booming. In this new Everyday DNA blog series, Careers in Genomics, we will learn about different career paths in genetics and genomics.