IMF Chief Medical Officer (TGen, City of Hope Phoenix, AZ)
Myeloma 101: What You Need to Know (30 minutes)
Joseph Mikhael, MD, Med, FRCPC, FACP
IMF Chief Medical Officer (TGen, City of Hope Phoenix, AZ)
Management For Newly Diagnosed, NOT Going to Transplant (20 minutes)
Marc Braunstein, MD, PhD, FACP
Fellowship Program Director (NYU Grossman Long Island School of Medicine New York, NY)
Q&A
BREAK (10 minutes)
Myeloma Management for People Newly Diagnosed: Transplant Eligibility, Logistics & Planning (25 minutes)
Noopur Raje, MD Director, Center for Multiple Myeloma (Massachusetts General Hospital Boston, MA)
Living Your Best Myeloma Life: Side Effect Management and Patient Empowerment (30 minutes)
Mary Steinbach, DNP, APRN
IMF Nurse Leadership Board Member (Huntsman Cancer Institute, University of Utah Salt Lake City, UT)
Q&A
Closing Remarks
Thank you to our sponsors!
WHAT IS #MYELOMAACTIONMONTH?
Myeloma Action Month is a global social awareness campaign that takes place every March to raise awareness of multiple myeloma. Every March, we urge you to champion Myeloma Action Month to make an impact on those living with the disease. Will you take action for the myeloma community?
Visit www.myelomaactionmonth.org to learn how you can join the movement.
Myeloma 101
Joseph Mikhael, MD MEd, FRCPC, FACP
OBJECTIVES
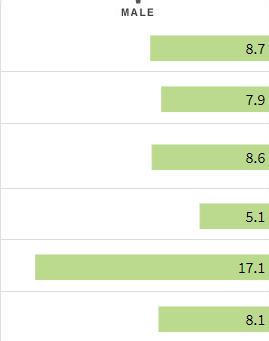
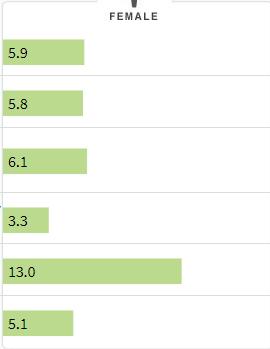
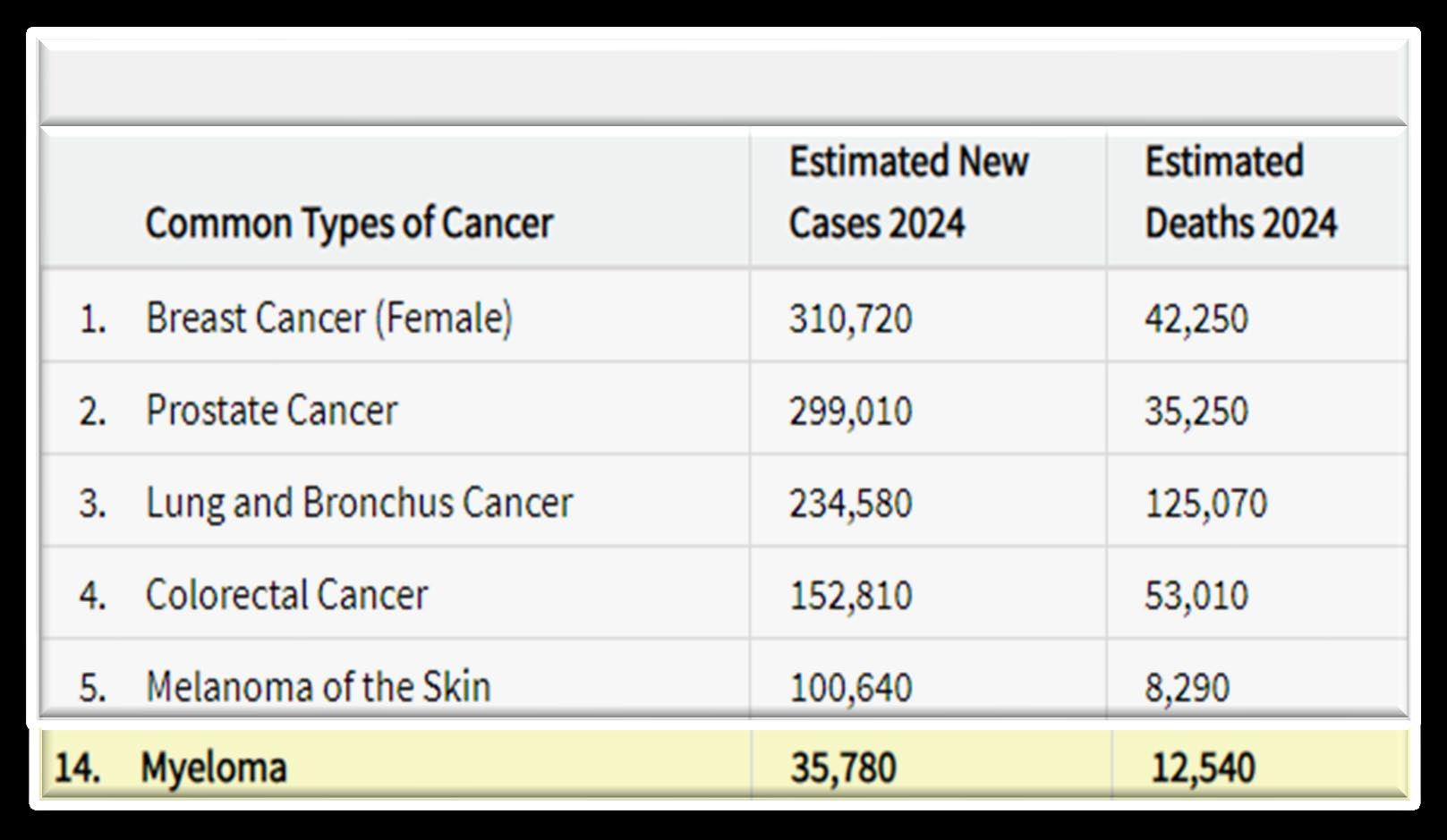
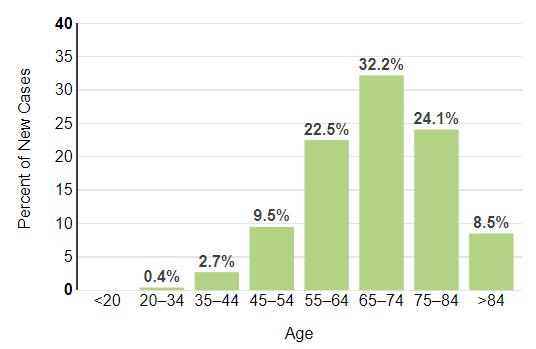
How common is Myeloma in the US?
What
Causes Myeloma? How/Why Did I Get This?
Environmental Factors:
• Exposure to some chemicals
• Radiation exposure
Examples:
Agent Orange
Burn pits
Pesticides, Herbicides
Firefighter/First Responder exposures
Individual Factors:
• Age
• Family History of related disorders
• Personal History of MGUS or SMM
• Obesity
VA Study Documents Health Risks for Burn Pit Exposures
Leukemia and Multiple Myeloma Set to Be Added to List of Conditions Linked to Burn Pits
In most cases, the honest truth
WE DON’T KNOW
Multiple Myeloma Diagnosis Can Be Challenging
Kyle RA. Mayo Clin Proc. 2003;78:21-33.
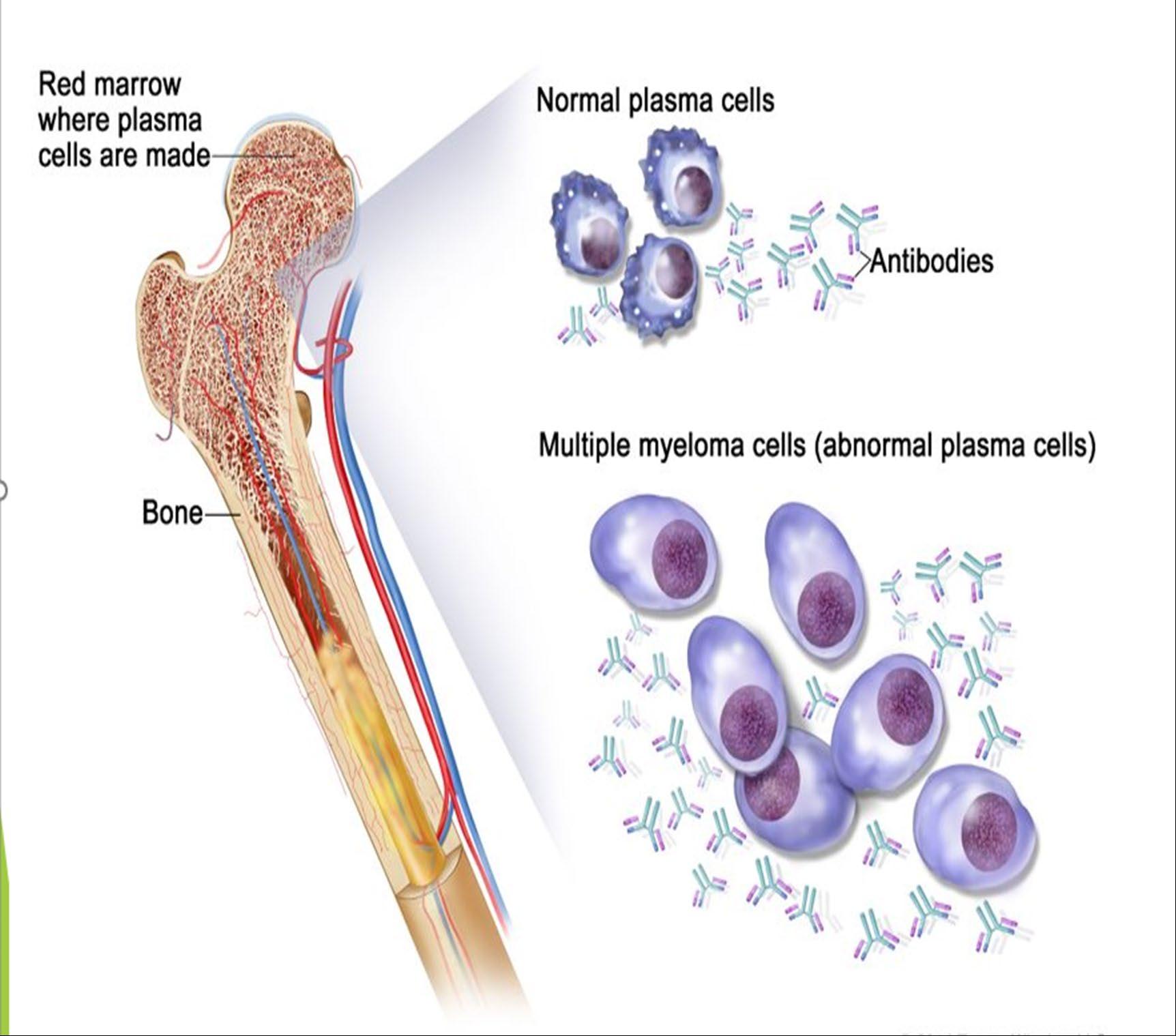
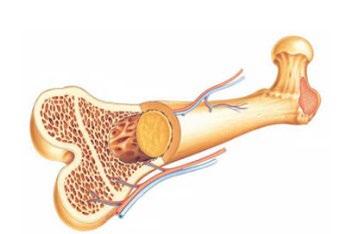
What is the Connection Between Bone Marrow & Myeloma ?
Photo Credit
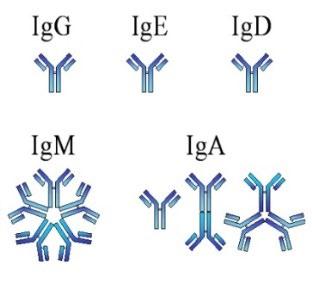
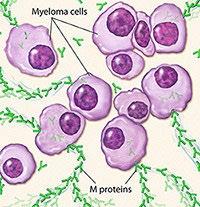
Understanding (Mono)clonal Plasma Cells
Heavy Chain: G, A, M, D, E
Heavy Chain = M-Spike
65% IgG – most common
20% IgA – associated with AL Amyloid
5% to 10% light chain-only (kappa, lambda)
Less common: IgD, IgE, IgM
Is Myeloma the Only Protein Disorder?
• AL-Amyloid
• POEMS
• Light or Heavy Chain Deposition Disease
• MGCS = Clinical
• MGRS = Renal
• MGNS = Neuro
Condition
Clonal plasma cells in bone marrow
MGUS1-4 (Monoclonal Gammopathy of Undetermined Significance)
SMM1-5,8 (Smoldering Multiple Myeloma) Active Multiple Myeloma6-8
Presence of Myeloma
Defining Events
Likelihood
* In clinical trial
Testing For Myeloma: Blood & Urine
Test Name
CBC + differential
Complete metabolic panel
Beta-2 Microglobulin (B2M)
Lactate Dehydrogenase (LDH)
What it means
Hemoglobin, WBC, Platelets
Creatinine, Calcium, Albumin, Liver function
Part of staging and risk stratification
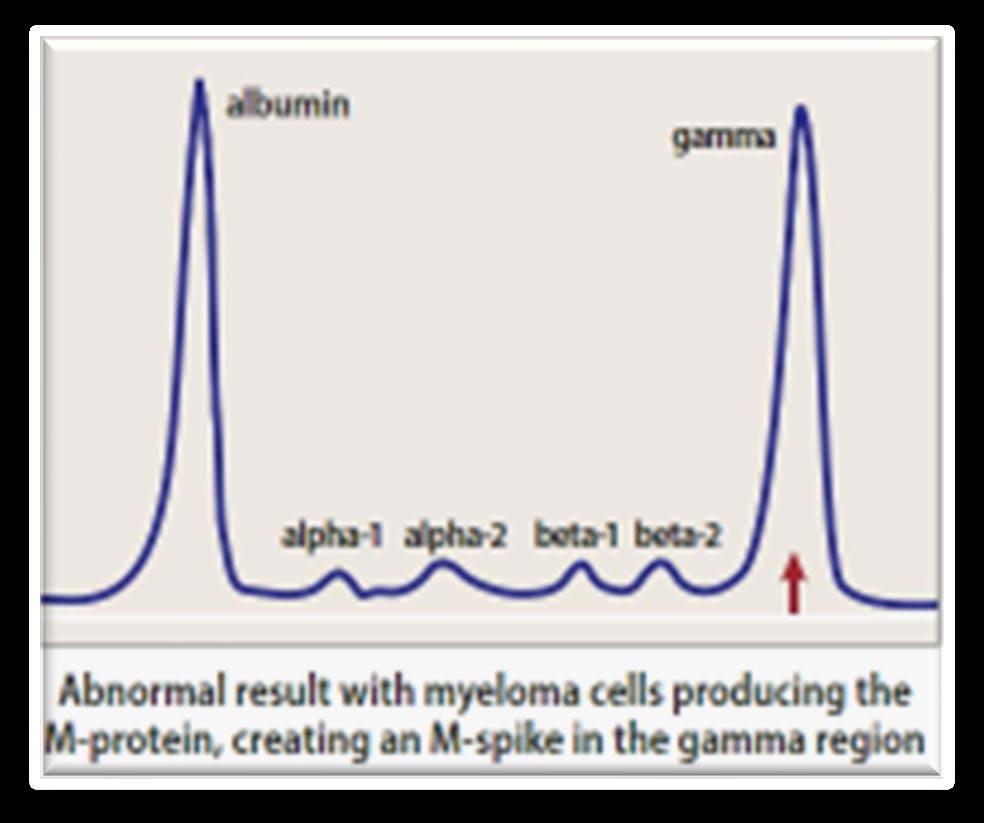
Serum Immunofixation and Protein
electrophoresis (SPEP+IFE)
Immunoglobulins (G, A, M, D, E)
Free light chain assay with kappa/lambda ratio
Urine immunofixation & protein
electrophoresis (UPEP+IFE)
Measures the level of normal and clonal protein
Identifies the type of clonal protein
Measures the level of normal and clonal protein
SV, et al. Lancet Oncol. 2014;15:e538-3548. Ghobrial IM, et al. Blood. 2014;124:3380-3388; mSMART.org; NCCN.org
Identifies the type of clonal protein
This Photo by Unknown Author is licensed under CC BY-SA-NC
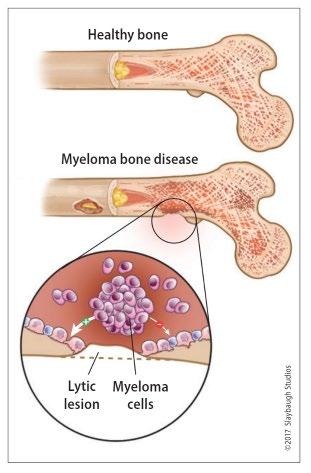
Testing For Myeloma: Imaging
Imaging:
– Skeletal survey: Series of X-rays; less sensitive than other techniques
– Whole body low dose (CTWB-LD CT )
– Positron Emission Tomography (PET/CT)
– Magnetic Resonance Imaging (MRI)
Healthy bone versus myeloma bone disease
This Photo by Unknown Author is licensed under CC BY-NC-ND
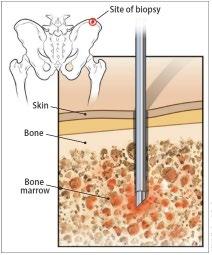
Testing For Myeloma: Bone Marrow
Bone marrow biopsy & aspirate • Bone marrow plasma cells (%) • Congo Red staining if concern
Bone marrow genetics
• Cytogenetics
• Fluorescence in situ hybridization (FISH)
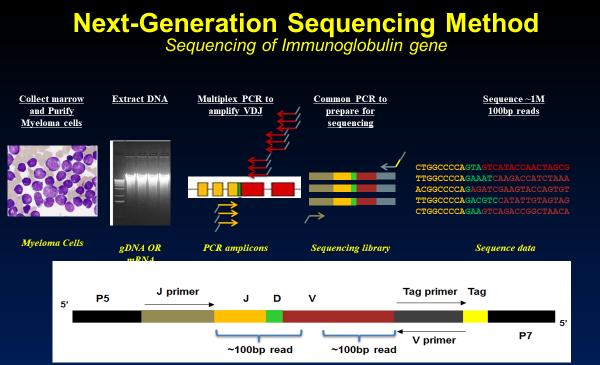
• Next generation sequencing (NGS)
This Photo by Unknown Author is licensed under CC BY-SA
What
is (the importance of) Myeloma Staging & Risk Stratification?
• Updated as new information becomes available
• Helps to guide therapy and measure response to treatment
• Provides some prognostic value
• Standardizes terminology in medical practice
High Risk FISH Results*
What is the Myeloma Treatment Landscape?
Initial Therapy (a.k.a. Frontline, Induction)
Quad Therapy (ex. CD38+ MoAb + VRd)
HD-Melphalan + Stem Cell
Transplant (ASCT)
Maintenance
Treatment for Relapse
Consolidation
Therapy
Supportive Care and Living Well
Treatment for Relapse
Treatment for Relapse
Treatment for Relapse
Treatment for Relapse
Drug Class Overview
(thalidomide)
(lenalidomide)
(pomalidomide)
Rev, Len
or Pom
(daratumumab)
(isatuximab)
Drug Class Overview
Peptide Drug Conjugate* Pepaxto (Melphalan Flufenamide)
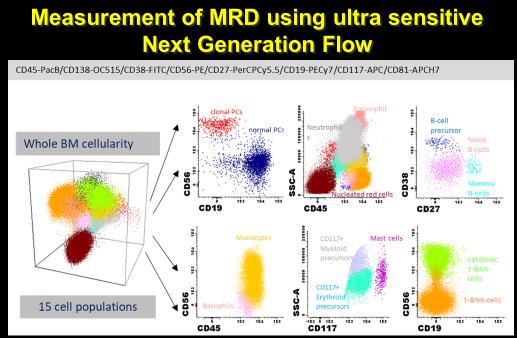
Negative by next generation flow (NGF) (minimum sensitivity 1 in 10-5 nucleated cells or higher)*
mCR AND normal Free Light Chain ratio, Bone Marrow negative by flow, 2 measures
CR AND negative PCR
Complete Response: Negative immunofixation (IFE); no more than 5% plasma cells in BM; 2 measures
Very Good Partial Response: 90% reduction in myeloma protein
Partial Response: at least 50% reduction in myeloma protein
Minimal Response
Stable Disease: Not meeting above criteria
Progressive Disease: At least 25% increase in identified myeloma protein from lowest level
MRD = Minimal Residual Disease
sCR = Stringent Complete Response; BM = Bone Marrow
Kumar, S., Paiva, B., Anderson, K. C., Durie, B., Landgren, O., Moreau, P., ... & Dimopoulos, M. (2016). International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. The lancet oncology, 17(8), e328-e346.
When Do I Need A New Treatment?
• Not every relapse requires immediate therapy
• Each case is different
Symptomatic or extramedullary disease
Asymptomatic biochemical relapse on 2 consecutive assessments
Asymptomatic high-risk disease or rapid doubling time or extensive marrow involvement Consider Observation Monitor Carefully Consider Treatment
Patient-/Disease-Specific Monitor Carefully
Initiate Treatment
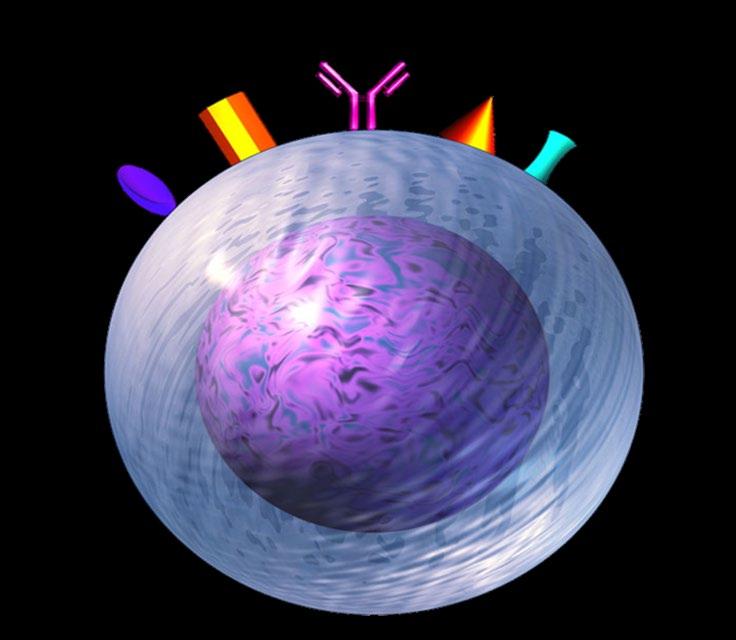
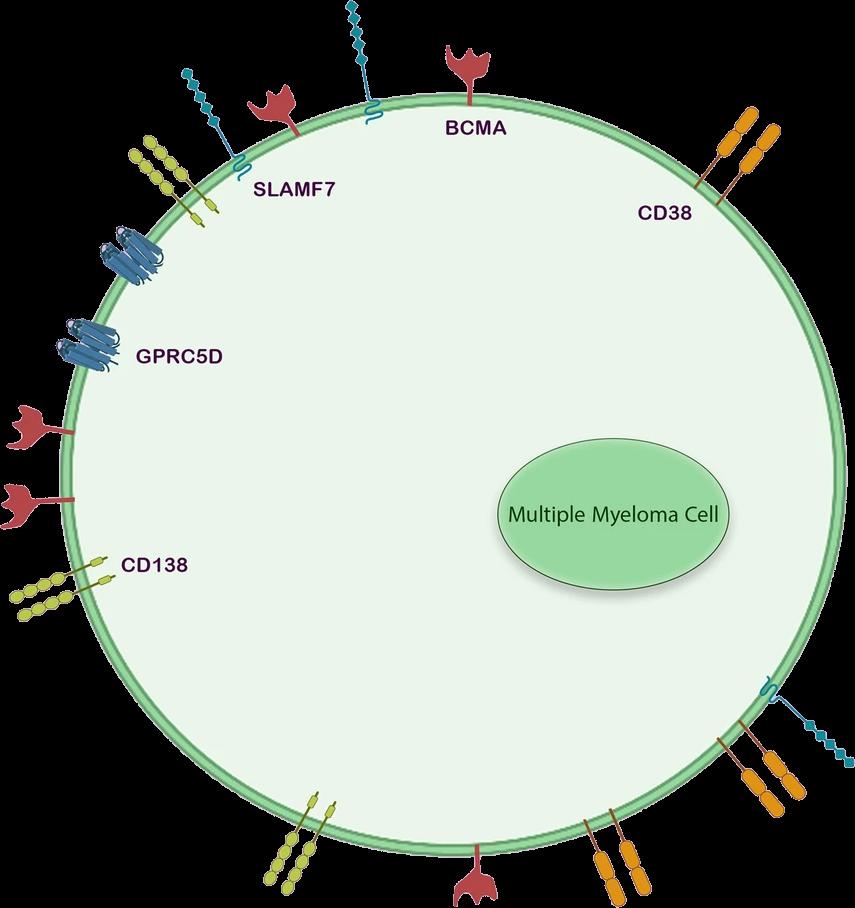
Targets on the Myeloma Cell Surface and Therapeutic Antibodies
Bi-Specific Antibodies
Talvey (Talquetamab) CAR-T
Antibody Drug
Empliciti (Elotuzumab)
Bi-Specific Antibodies
Bi-Specific Antibodies
CAR-T
Monoclonal Antibodies
Daratumumab and Darzalex Faspro
Sarclisa (Isatuximab)
TAK-079 MOR202
Immune Therapies
Abecma (Ide-cel CAR-T)
Carvykti (Cilta-cel CAR-T)
Tecvayli (Teclistamab)
Elrexfio (Elranatamab)
Other CAR Ts
Other Bi Specific Antibodies
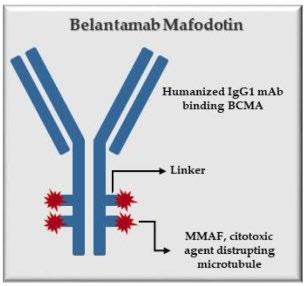
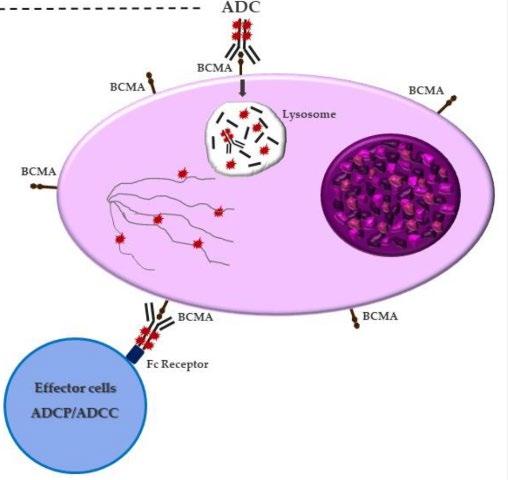
Antibody Drug Conjugates
How it works:
An antibody directed at a target (BCMA) combined with a cytotoxic agent (chemotherapy)
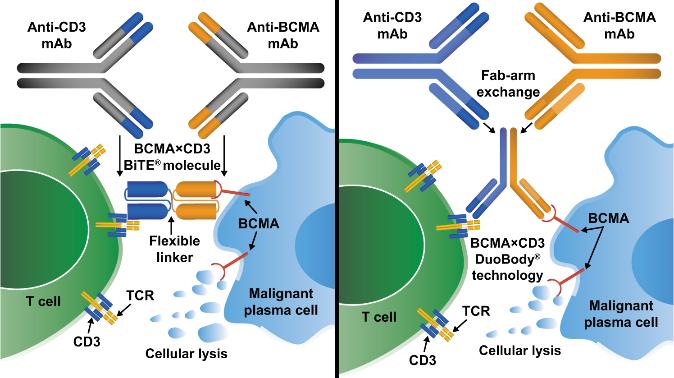
• Incorporates 2 antibody fragments to target and bind both tumor cells and T cells
• Brings target-expressing MM cells and T cells into close proximity, enabling T cells to induce tumor-cell death
Targets of Bispecific Molecule Vary
FcRH5
“Off the Shelf” Advantage
• No manufacturing process, unlike CAR T-cell therapy (but like ADC/belantamab therapy)
• Thus, no delay between decision to treat and administration of drug ADC = Antibody-Drug Conjugate; BCMA = B-Cell Maturation Antigen; CD3 = Cluster of Differentiation 3; FcRH5 = Fc receptor-homolog 5; GPRC5D = G-protein coupled receptor family C group 5 member D
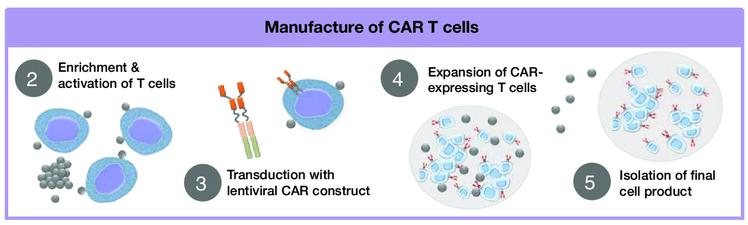
The Process of CAR T Cell Therapy
CAR T therapy recommended. Insurance approved and ready to move forward.
* These agents are currently off the market but available through special programs
Anito-cel
Cevostomab
Linvoseltamab
Iberdomide, Mezigdomide
Sonrotoclax
Second/Expert Opinion
• You have the right to get a second opinion. Insurance providers may require second opinions.
• A second opinion can help you:
– Confirm your diagnosis
– Give you more information about options
– Talk to other experts
– Introduce you to clinical trials
– Help you learn which health care team you’d like to work with, and which facility
Management for Newly Diagnosed, NOT Going to Transplant
Marc Braunstein, MD, PhD, FACP
Management for Newly Diagnosed Myeloma,
NOT Going to Transplant
Marc Braunstein, MD, PhD, FACP
Associate Professor of Medicine
Fellowship Program Director
NYU Grossman Long Island School of Medicine
Perlmutter Cancer Center at NYU Langone Hospital—Long Island
@docbraunstein
@Perlmutter_CC
Objectives
• Discuss the evolving treatment strategies
• Understand different combination regimens
• Highlight the importance of individualized approaches
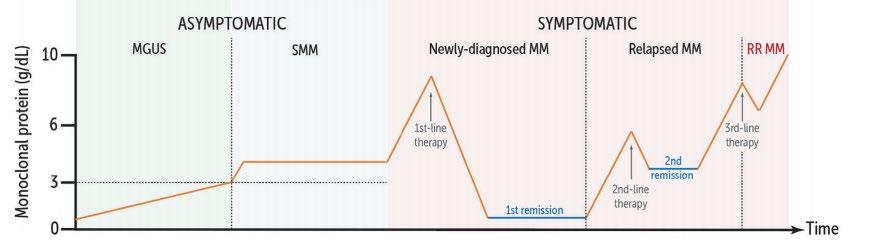
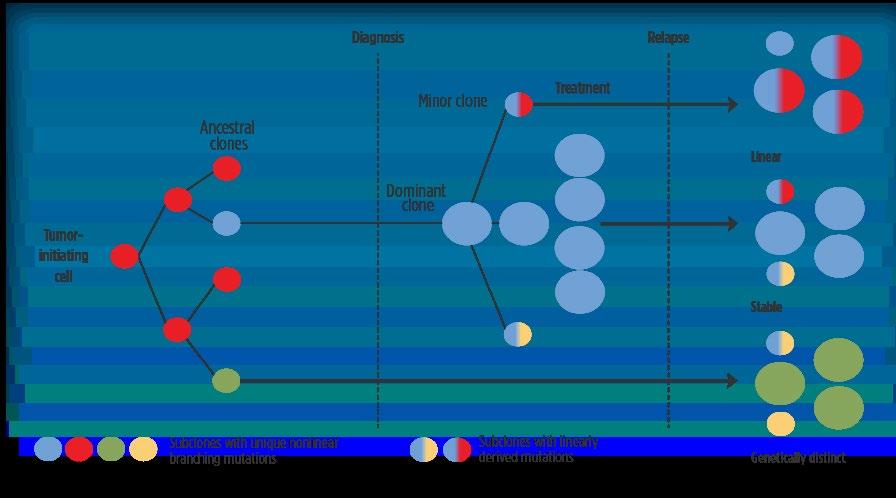
The Myeloma Journey
Reference: Ho et al. Leukemia 2020
Goals!
#1: identify myeloma as early as possible, limit organ damage
#2: delay progression, increase survival, improve quality of life
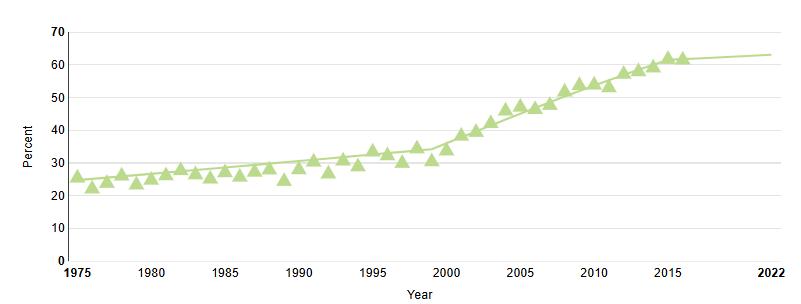
Advances in Treatment Have Doubled MM Survival
Therapeutic advances:
High dose melphalan and ASCT Lenalidomide, Bortezomib Next gen IMiDs and PIs CAR-T cells Bispecific abs Monoclonal antibodies
61% 5-year survival
Reference: http://seer.cancer.gov
Increasing Use of Antibody Therapies in MM
PIs and IMiDs
Monoclonal Abs T cell Redirection 2024)
New MM Diagnosis
Many Ways to Get to the Destination
Choosing the Best Treatment for You
Individual Myeloma Treatments
Overall fitness
Comorbidities
Fitness for transplant Caregiver support Preferences
o Disease burden
o Organ dysfunction
o Stage/genetic risk
o Emergency situations
Treatment plan
Bone support
Infection prevention
Diet and exercise
Emotional support
New MM Diagnosis
Typical Approach for Newly Diagnosed MM
Transplant
Multi-drug Combination (Induction)
*No transplant
High dose melphalan and stem cell transplant (Consolidation)
Maintenance
Consolidation with additional cycles
*Transplant eligibility best assessed by expert in transplantation
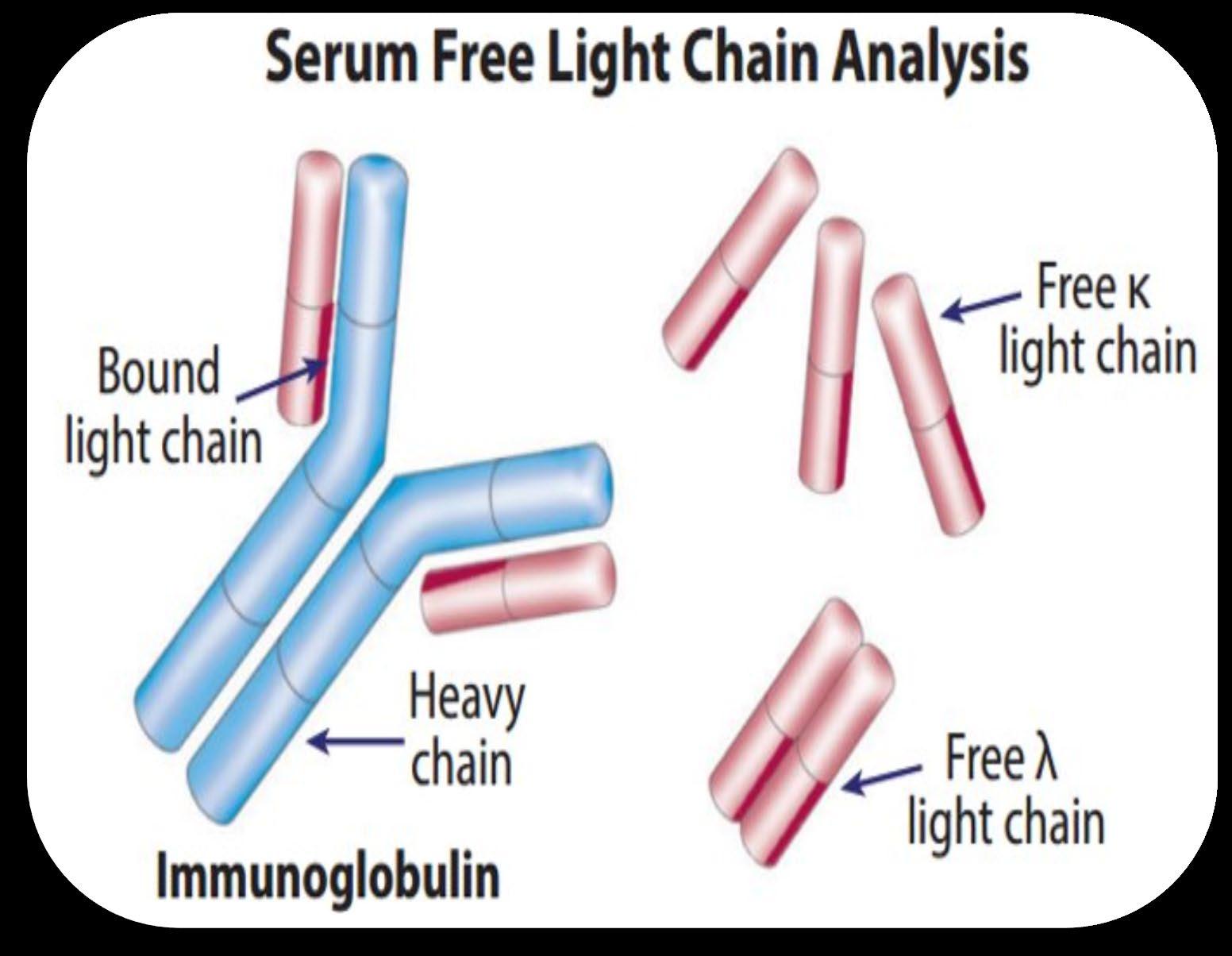
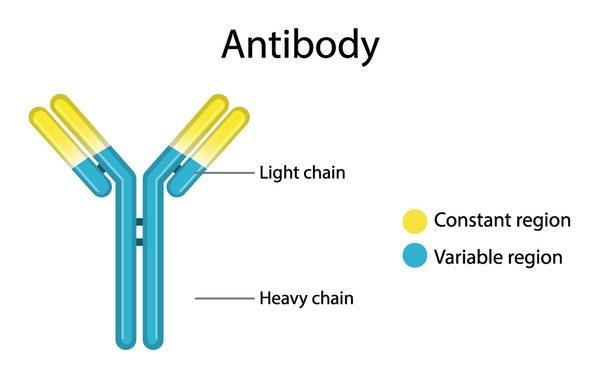
Monoclonal Antibodies (Immunoglobulins)
Target binding region
(kappa or lambda)
Monoclonal-spike in Myeloma
IgG: 50%
IgA: 20%
Light chain only: 15%
IgM and non-secretory: <5%
(IgG, IgA, IgM, IgD, IgE)
Prior to Monoclonal Antibodies:
Proteasome Inhibitors + Immunomodulators
Reference: Durie et al. Lancet 2017
Antibody Drugs Targeting Myeloma Plasma Cells
Teclistamab, Elranatamab (bispecifics) Elotuzumab
Talquetamab (bispecific)
References: Sheykhhasan et al. Nature 2024
Daratumumab
Isatuximab
Belantamab
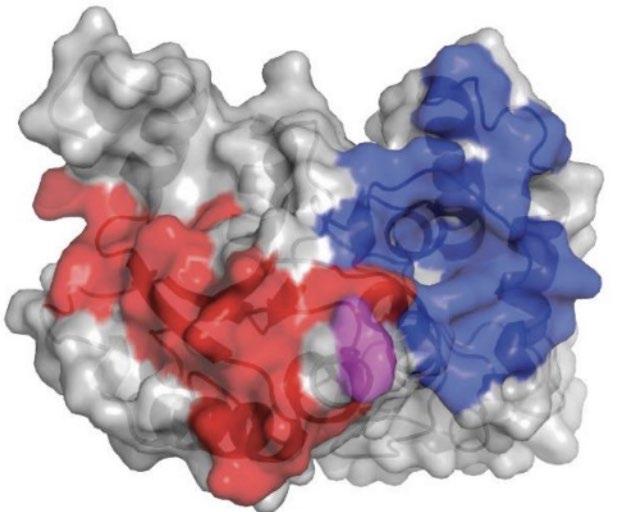
Monoclonal Antibody Drugs Targeting CD38
• CD38 is present on the surface of MM plasma cells
• Daratumumab (Dara) and Isatuximab (Isa) target different parts of CD38
• This leads to plasma cell destruction
• Both can be given IV, only daratumumab is available subcutaneously
• Both have shown efficacy in newly diagnosed and relapsed MM when combined with other agents
• Side effects are similar: primarily reduced blood counts and infections
CD38 on MM cell surface
Using Antibodies in Newly Diagnosed MM
Phase 3 Randomized Controlled Studies All Positive!
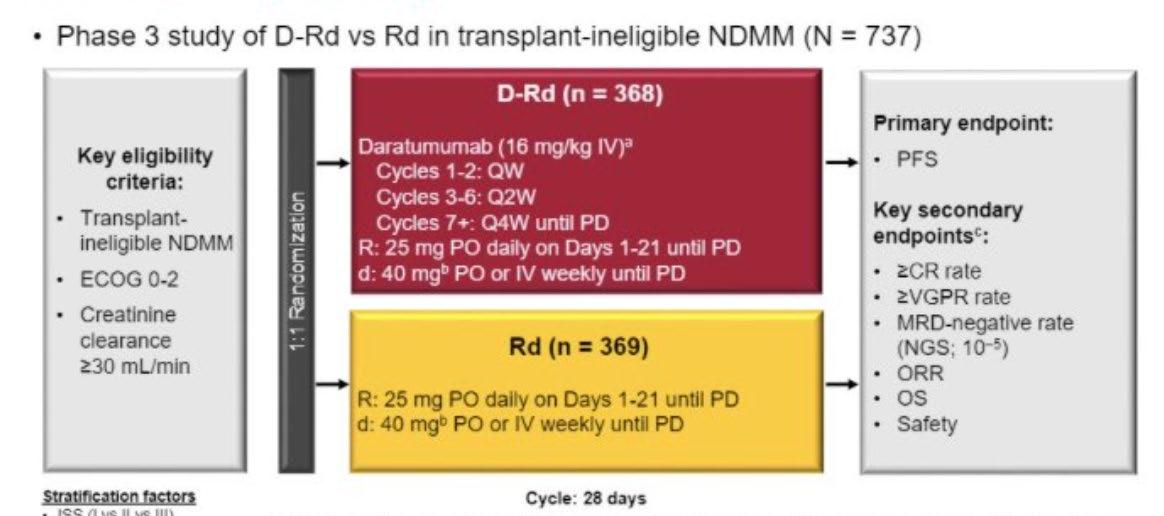
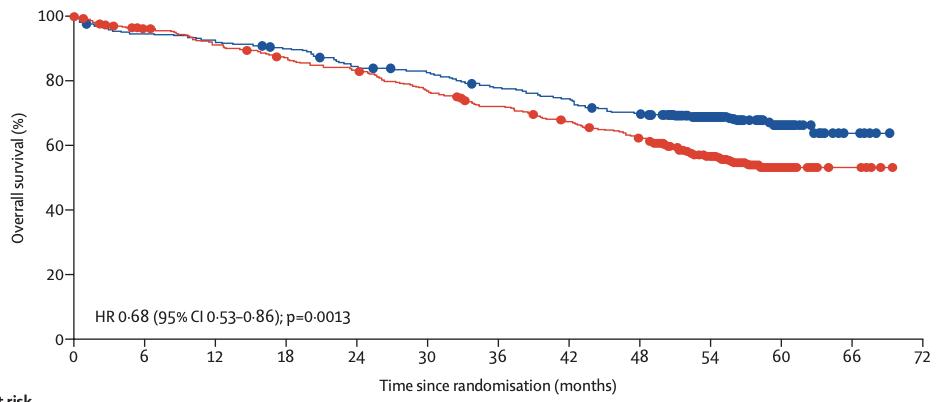
MAIA Study: Dara-Rd vs Rd
31% (DRd) vs 10% (Rd) became MRD negative
References: Facon et al . Lancet Oncol. 2021
Facon et al. N Engl J Med. 2019
San-Miguel et al. Blood Jan 2022
93% vs 82% progression free at 5 years
66% vs 53% overall survival
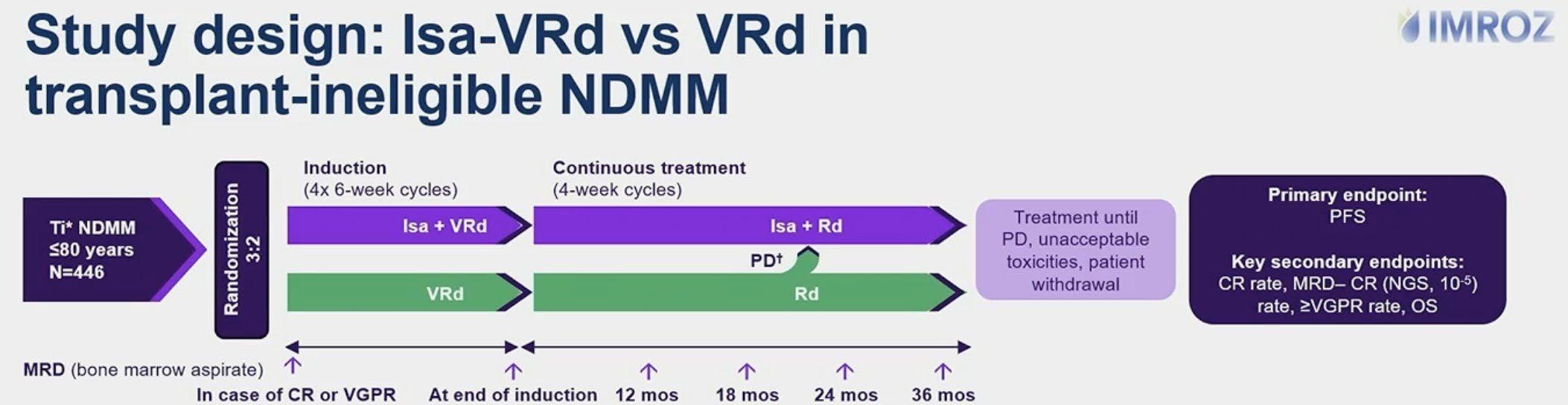
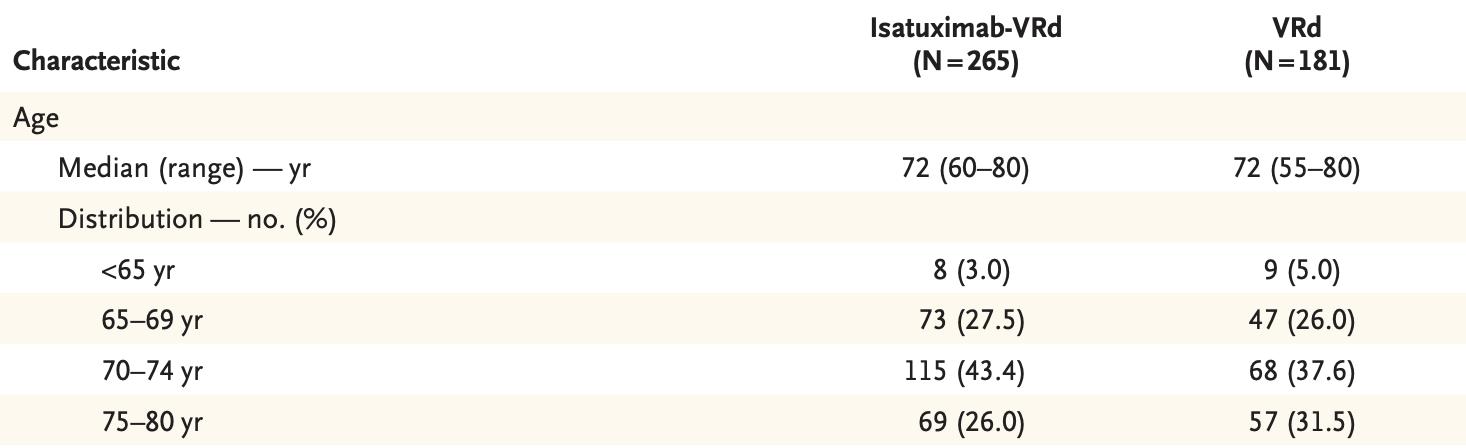
IMROZ: Isa-VRd vs VRd (now FDA approved)
Median age: 72 (range 55-80)
Transplant ineligibility was related to either age over 65 or other medical conditions
References: Facon et al. ASCO 2024
Facon et al. NEJM 2024
IMROZ: Study Population
References: Facon et al. ASCO 2024
Facon et al. NEJM 2024
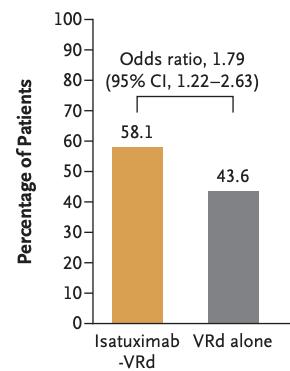
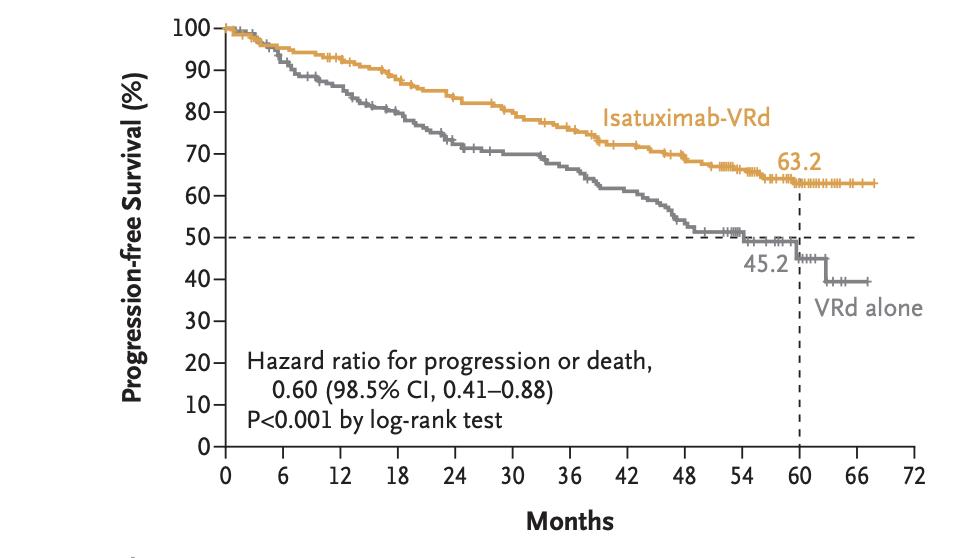
Isa-VRd:
MRD negativity and Delayed Progression
MRD Negativity Progression Free Survival
References: Facon et al. ASCO 2024
Facon et al. NEJM 2024
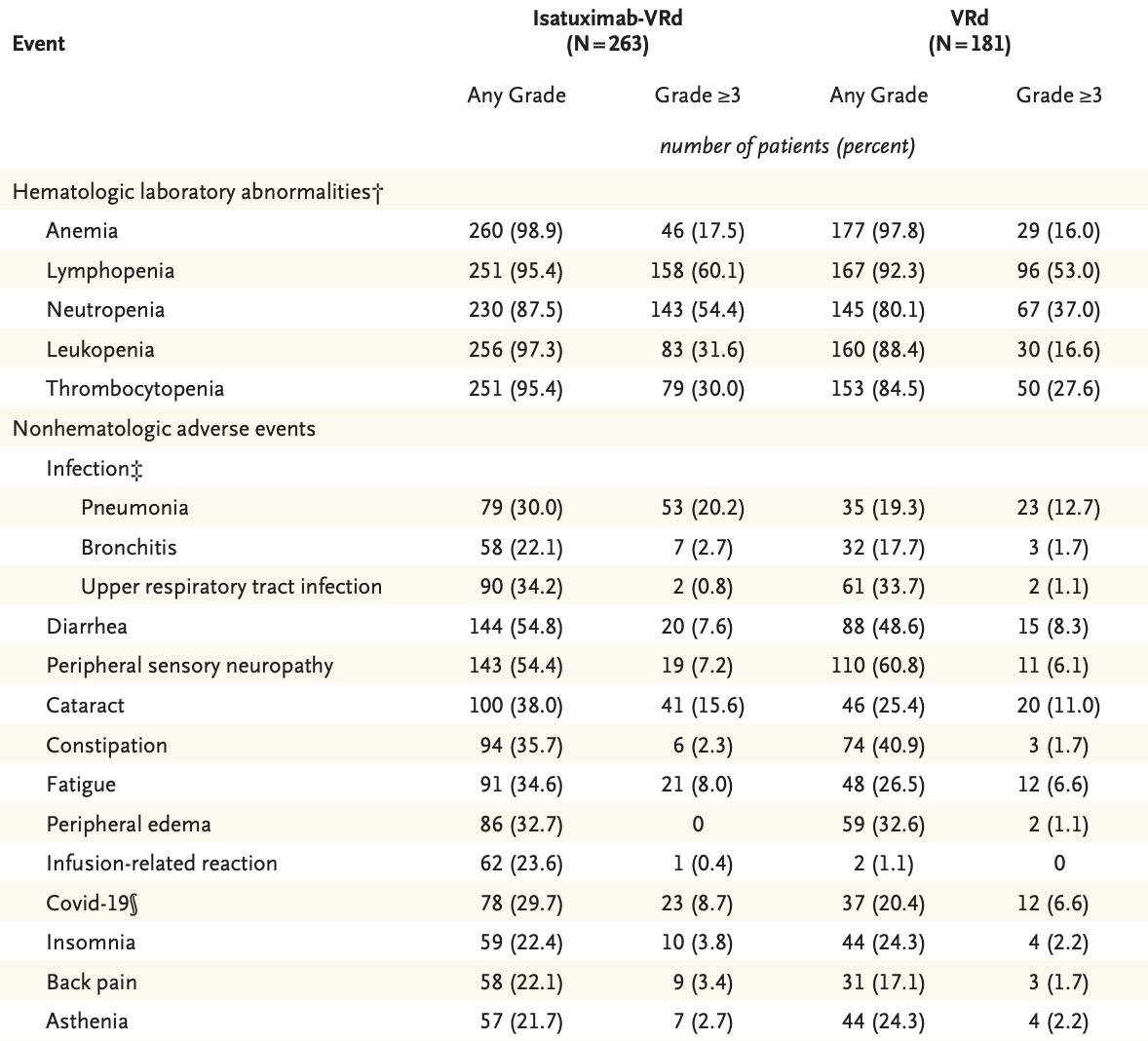
Side
Effects were Associated with the Drug Classes
References: Facon et al. ASCO 2024
Facon et al. NEJM 2024
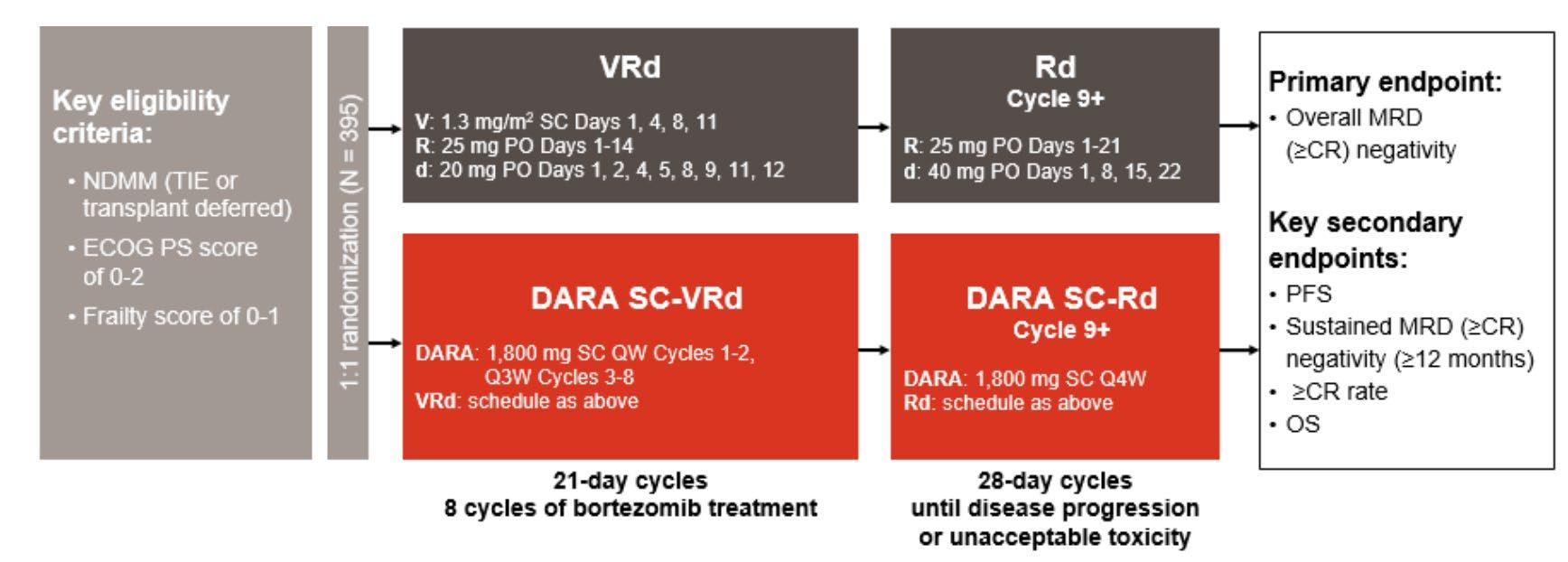
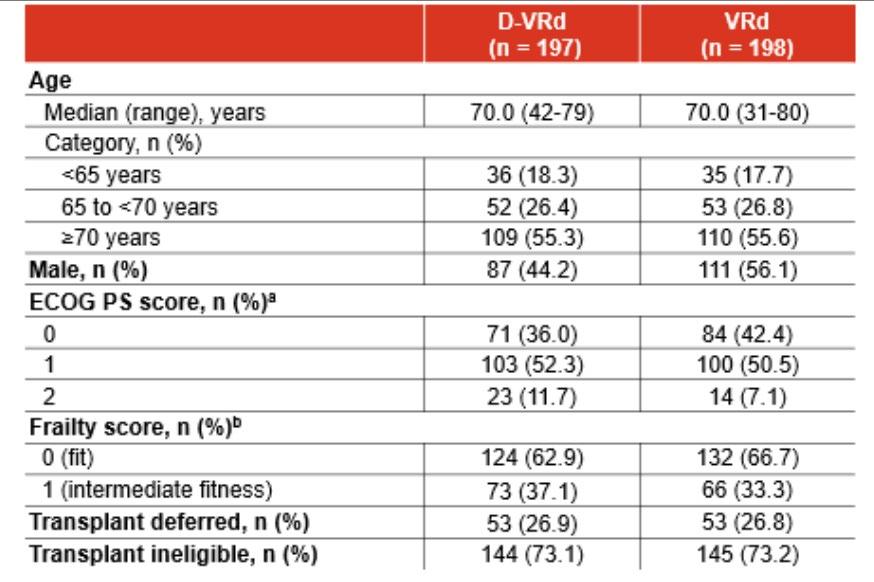
CEPHEUS: Dara-VRd vs VRd
Median age: 70 (range 31-80)
Transplant ineligibility was related to either age over 65 or other medical conditions
References: Zweegman et al. ASH 2024
Usmani et al. Nat Med 2025
CEPHEUS: Study Population
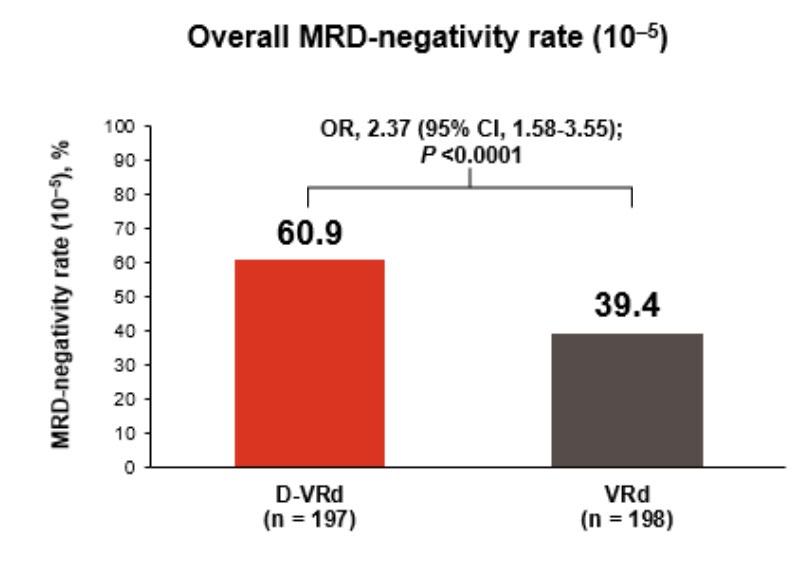
Dara-VRd:
MRD negativity and Delayed Progression
References: Zweegman et al. ASH 2024 Usmani et al. Nat Med 2025
Established Safety was Consistent with the Drug Classes
References: Zweegman et al. ASH 2024
Usmani et al. Nat Med 2025
• Belantamab is an antibody drug conjugate targeting BCMA
• Teclistamab and Elranatamab are bispecific antibodies targeting BCMA
• Talquetamab is a bispecific antibody targeting GPRC5D
• Abecma and Carvykti are CAR T-cells that target BCMA
Treatment of Newly Diagnosed MM without Transplant
• We are witnessing an immunotherapy revolution in MM!
• Adding either daratumumab and isatuximab to VRd improves outcomes in newly diagnosed MM patients with or without stem cell transplant
• Isatuximab-VRd is now approved in transplant ineligible patients
• While transplant remains a standard of care for eligible patients, no study has compared quadruplet regimens with or without transplant
• Studies of bispecific antibodies and CAR T-cells in the first line setting may facilitate novel immunotherapy approaches used earlier in the disease course
• Regardless of the regimen used, the goals remain the same to prolong survival, prevent organ damage, and improve quality of life
Thank you!
NYU Perlmutter Cancer Center Myeloma Team:
Dr. Faith Davies
Dr. Gareth Morgan
Dr. David Kaminetzky
Dr. Marc Braunstein
Stem Cell Transplant Team:
Dr. Maher Abdul Hay
Dr. Jingmei Hsu
Dr. Oscar Lahoud
Dr. Anne Renteria
Dr. John Vaughn
Staff, Fellows, and our Patients and their Caregivers
Q&A
10 - Minute BREAK
STILL TO COME…
Myeloma Management for People Newly Diagnosed: Transplant Eligibility, Logistics & Planning (25 minutes)
Noopur Raje, MD
Director, Center for Multiple Myeloma (Massachusetts General Hospital Boston, MA)
Living Your Best Myeloma Life: Side Effect Management and Patient Empowerment (30 minutes)
Mary Steinbach, DNP, APRN
IMF Nurse Leadership Board Member (Huntsman Cancer Institute, University of Utah Salt Lake City, UT)
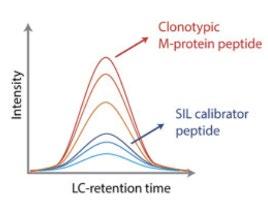
Determine clonotypic peptide by RNA sequencing of bone marrow aspirate or by analysis of serum M protein
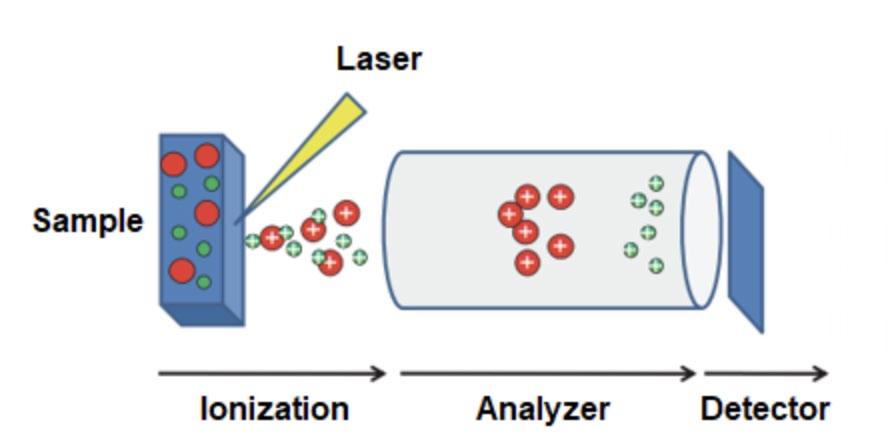
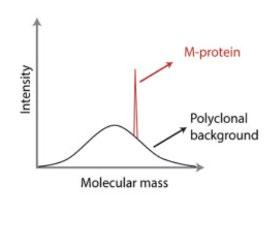
Mass spectrometry is more sensitive than SPEP/IFX (100 mg/L)
Speed of assay depends on modality: MALDI-TOF faster than LC-MS
Allows detection of therapeutic monoclonal antibodies
LC-MS more sensitive than MALDI-TOF
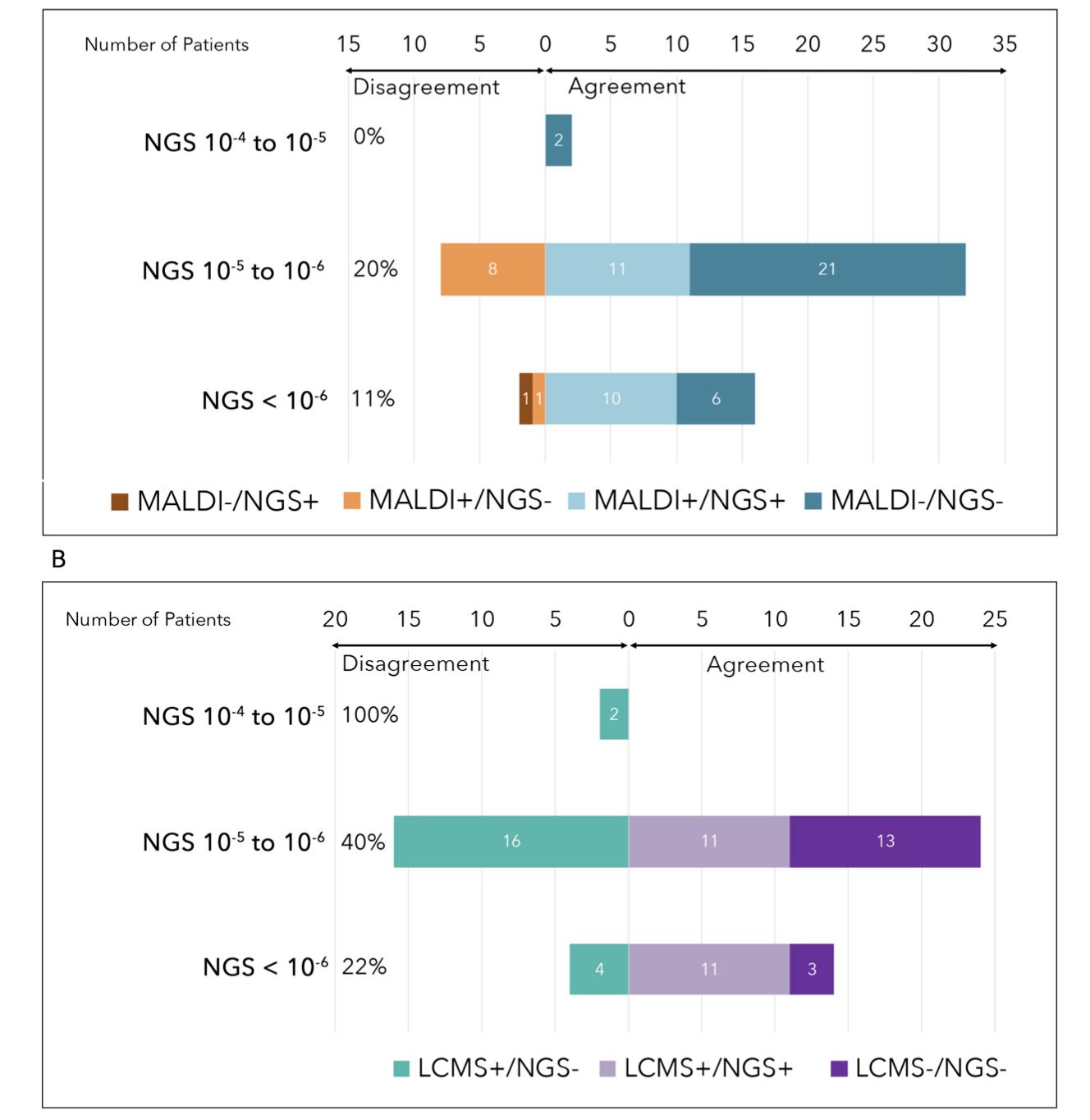
Comparison of Binding Site Mass Spec to NGS
Compared NGS to two Binding Site mass spectrometry methods (MALDI TOF and LC-MS) in 36 patients with newly diagnosed multiple myeloma who completed KRd × 18 cycles.
Binding Site MALDI TOF comparable to NGS at 10−5 to 10−6
Binding Site MALDI TOF is being developed as EXENT assay
LC-MS (related to miRAMM) comparable to NGS at 10−6 or better
Derman BA et al., Blood Cancer
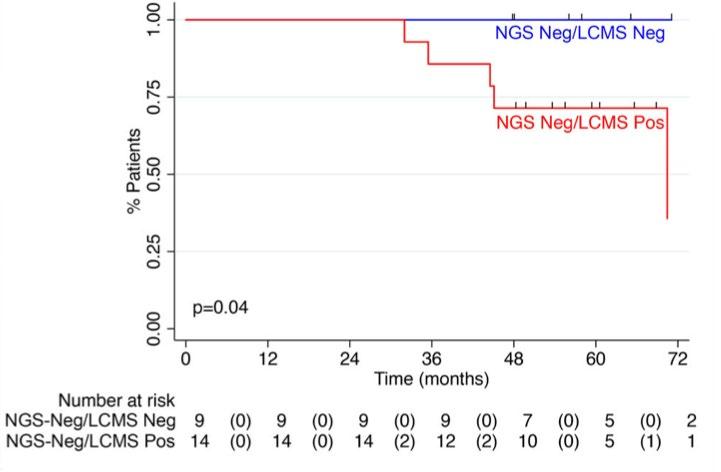
MRD Assessment by LC-MS May Be Superior To NGS
Progressionfree survival
Progression-free survival by MRD status after 18 cycles of KRd
LC-MS can stratify outcomes among NGS negative patients
NGS at 10−5
Derman BA et al., Blood Cancer
Treatment
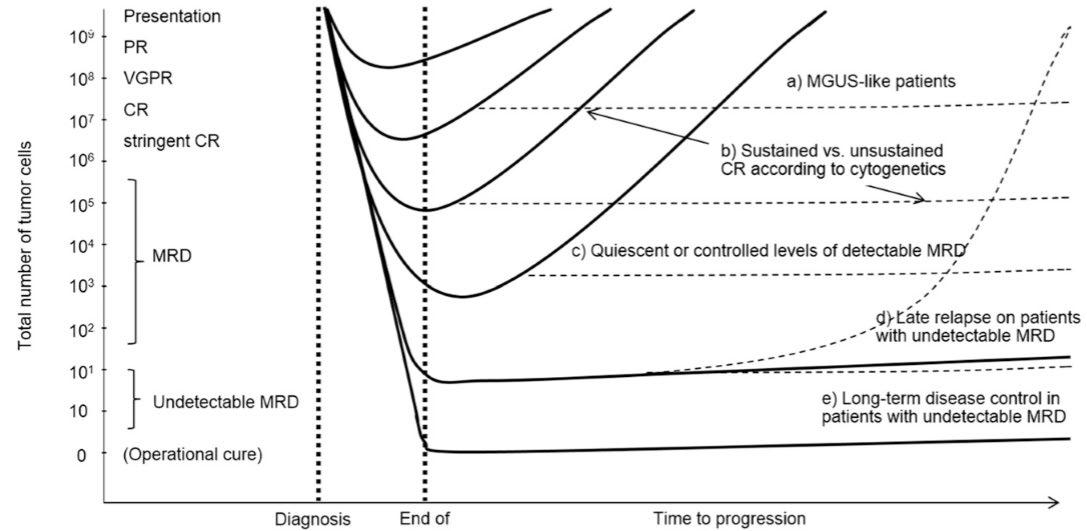
Goals of Treatment in Multiple Myeloma
Bonello F, et al. Cancers (Basel). 2019;12(1):15. Munshi NC, et al. JAMA Oncol. 2017;3:28–35.
Depth of Response
Duration of Response
Quality of Life
Long Term Survival
Amelioration of symptom burden?
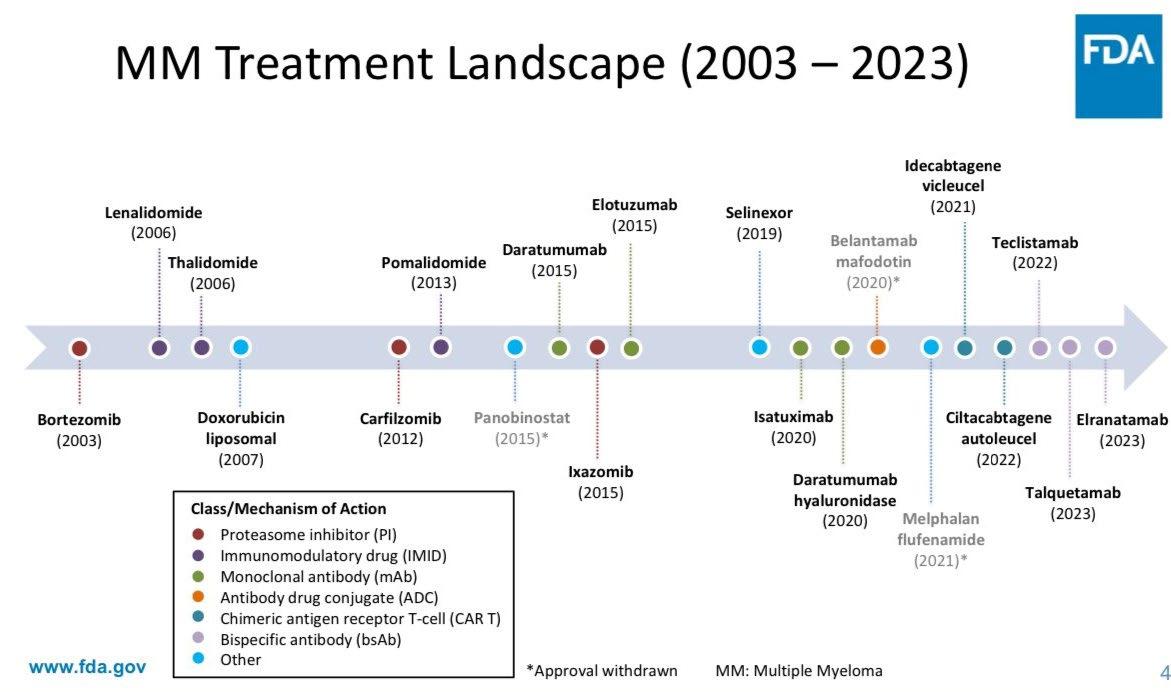
Drugs Approved For Multiple Myeloma Since 2000
Proteasome inhibitor
Immunomodulatory drug
Target CD38
Target BCMA
bortezomib
zoledronic acid
doxorubicin liposome (Doxil)
thalidomide
lenalidomide
pomalidomide daratumumab ixazomib elotuzumab
carfilzomib panobinostat†
idecabtagene vicleucel ciltacabtagene autoleucel
belantamab mafodotin melflufen*
selinexor isatuximab
denosumab
Initial FDA approval date in multiple myeloma
*Withdrawal from US market in October 2021 withdrawn in January 2022 †Withdrawn from US market in November 2021
aConsolidation initiated 60–100 days post transplant; bPatients who complete maintenance cycles 7–32 may continue single-agent lenalidomide thereafter; cProtocol amendment allowed q4w dosing option. Phase 2 trial – patient enrollment between December 2016 and April 2018.
Transplant-Eligible NDMM – 24 Months of Maintenance
Laubach JP et al. ASH 2021, Virtual Meeting. Abstract 79.
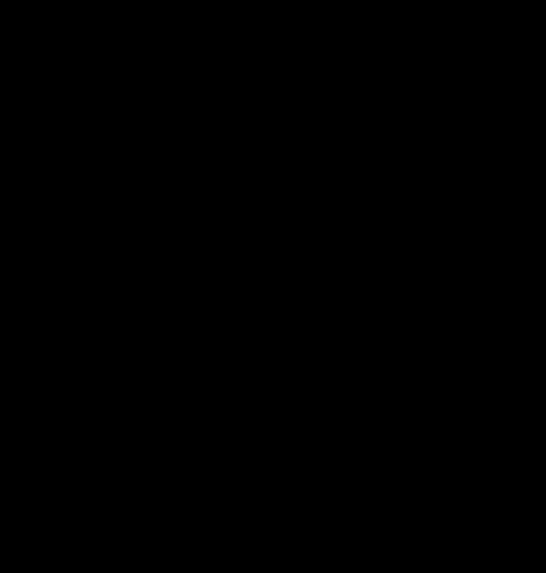
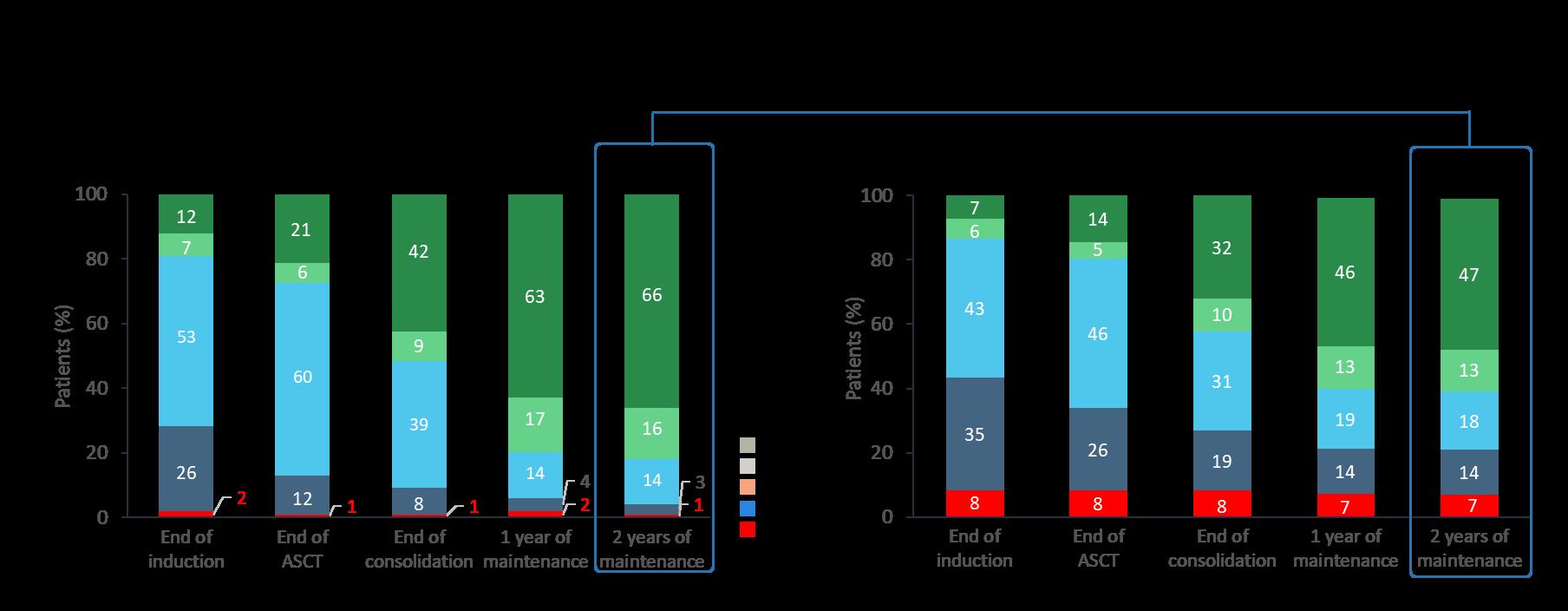
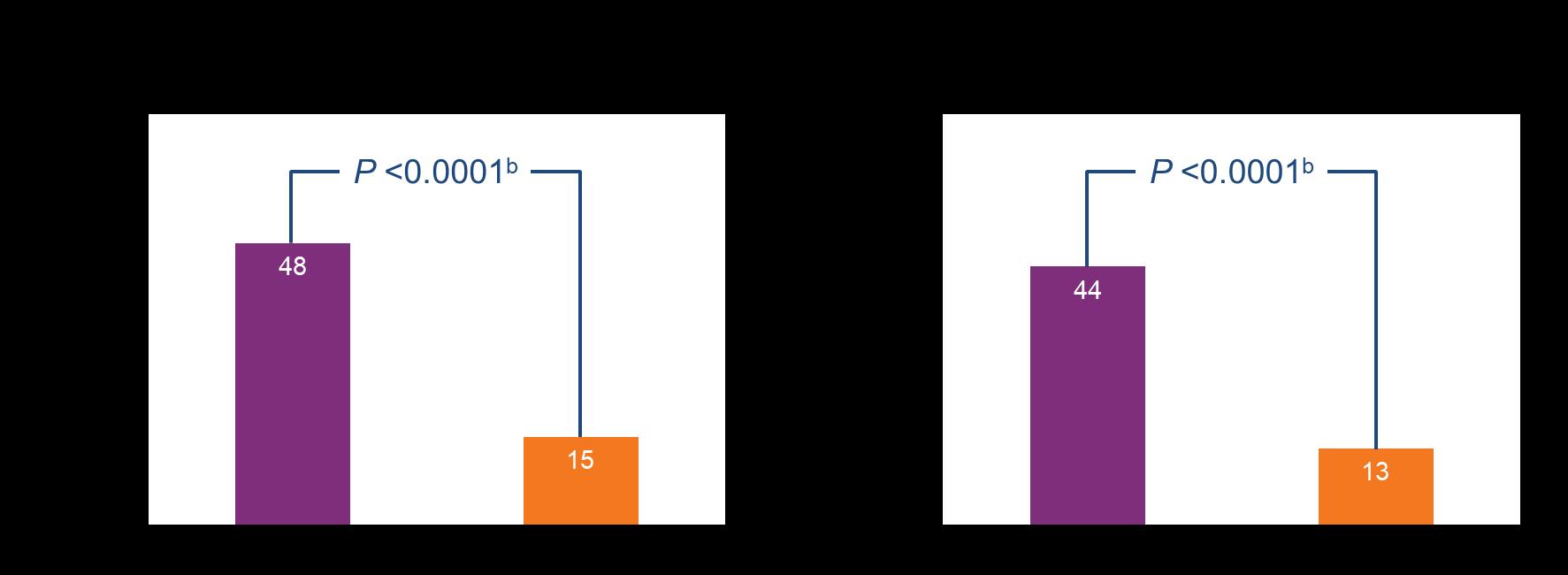
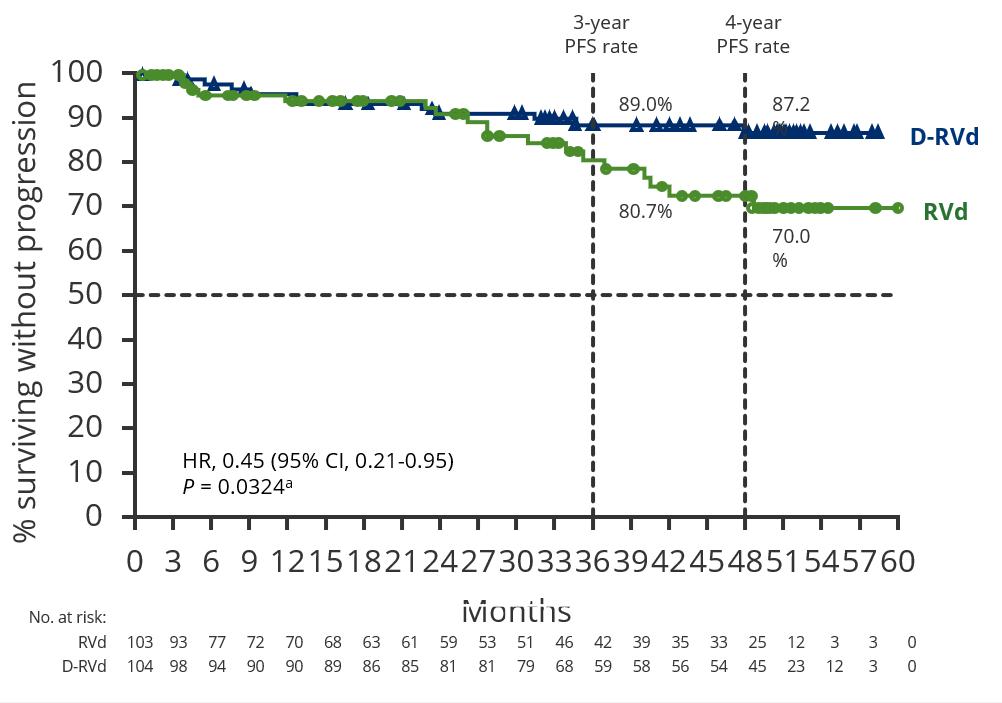
GRIFFIN: Updated MRD and PFS Data
D-RVd Improved Rates of Durable MRD Negativitya (10–5) Lasting ≥6 Months or ≥12 Months Versus RVd
aThe threshold of MRD negativity was defined as 1 tumor cell per 105 white cells. MRD status was based on BM aspirates by NGS per IMWG. bP values calculated by Fisher’s exact test.
• Median follow-up: 49.6 months
• Median PFS was not reached in either group
• The separation of the PFS curves begins beyond 1 year of maintenance and suggests a benefit of prolonged DR therapy
Frontline for TE: Quads vs Triplets
Sonneveld P et al. EHA 2024. Abstract S201. Raab M et al. EHA 2024. Abstract S202. Gay F et al. ASH 2023. Abstract 4. Leypoldt LB et al. IMS 2023. Abstract OA-43.
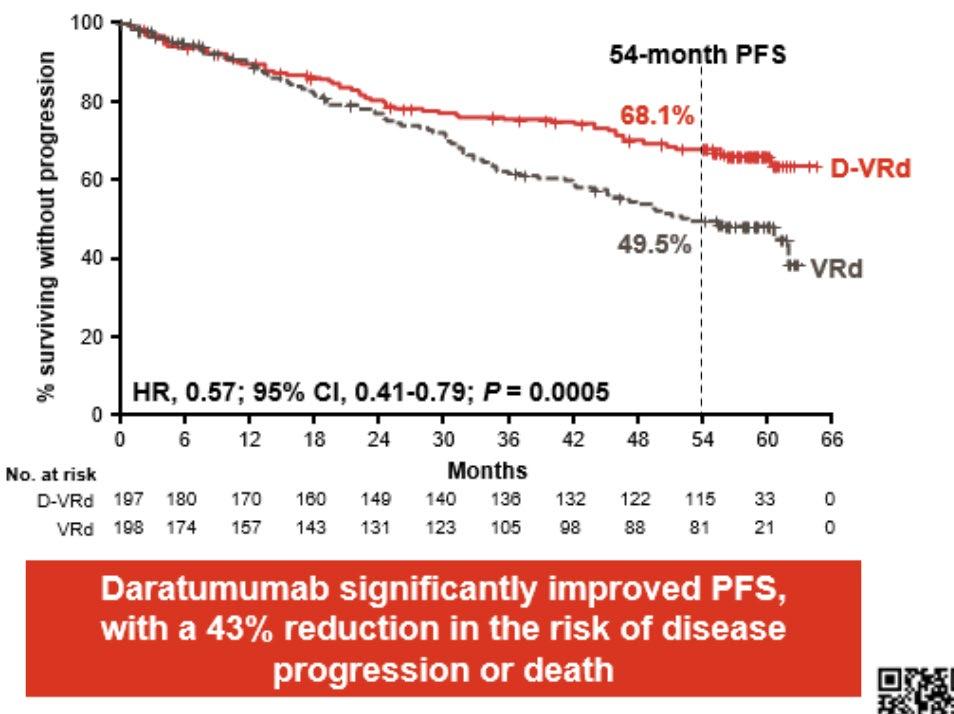
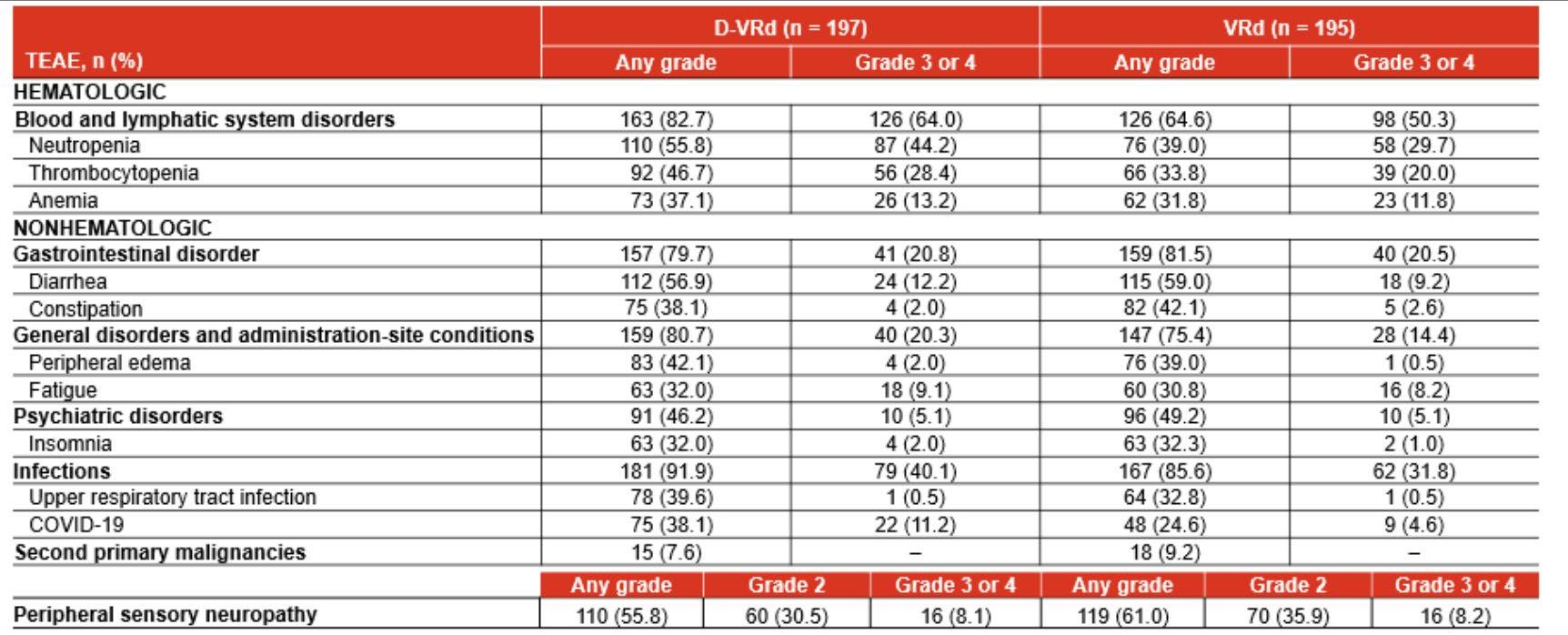
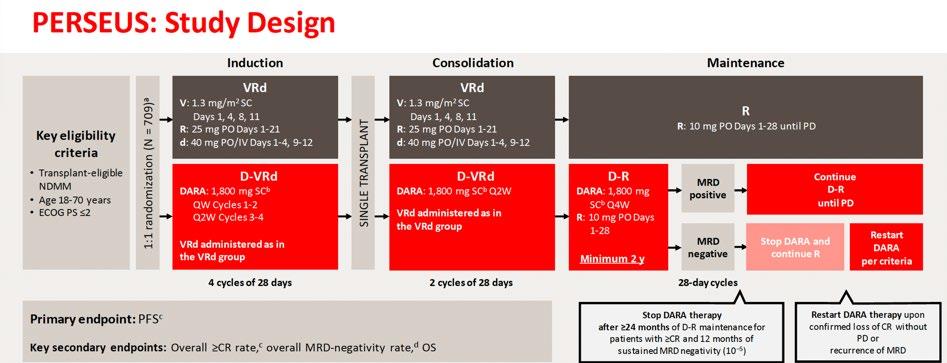
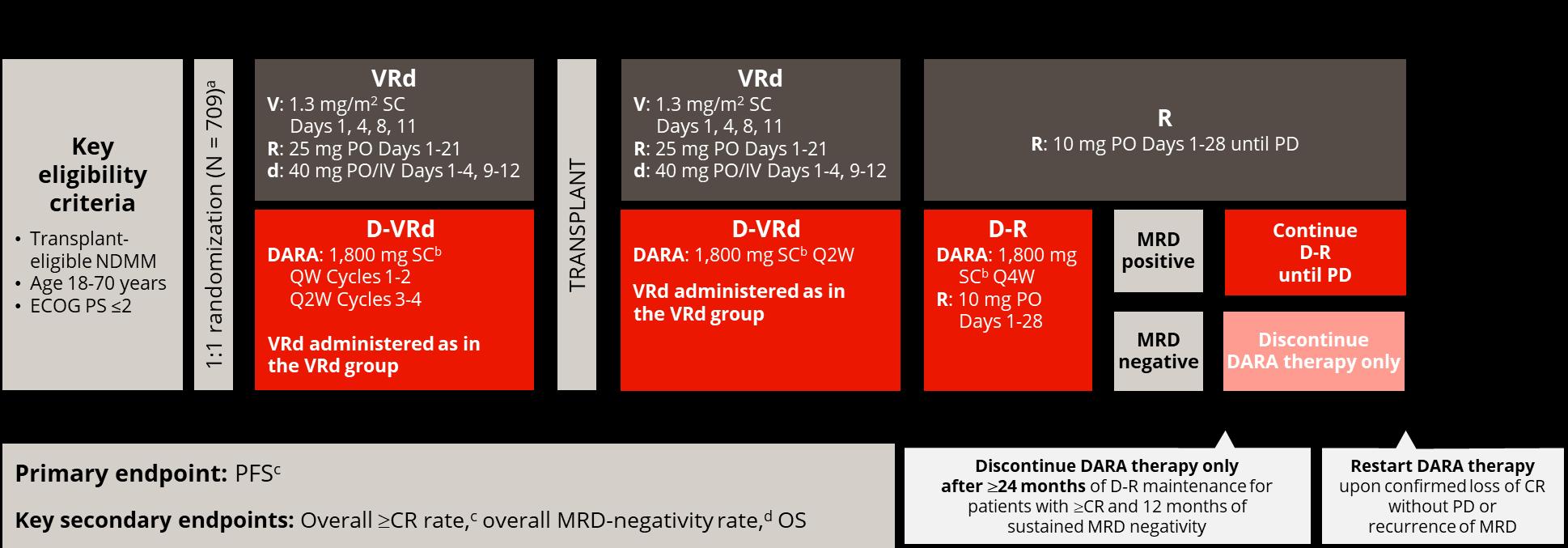
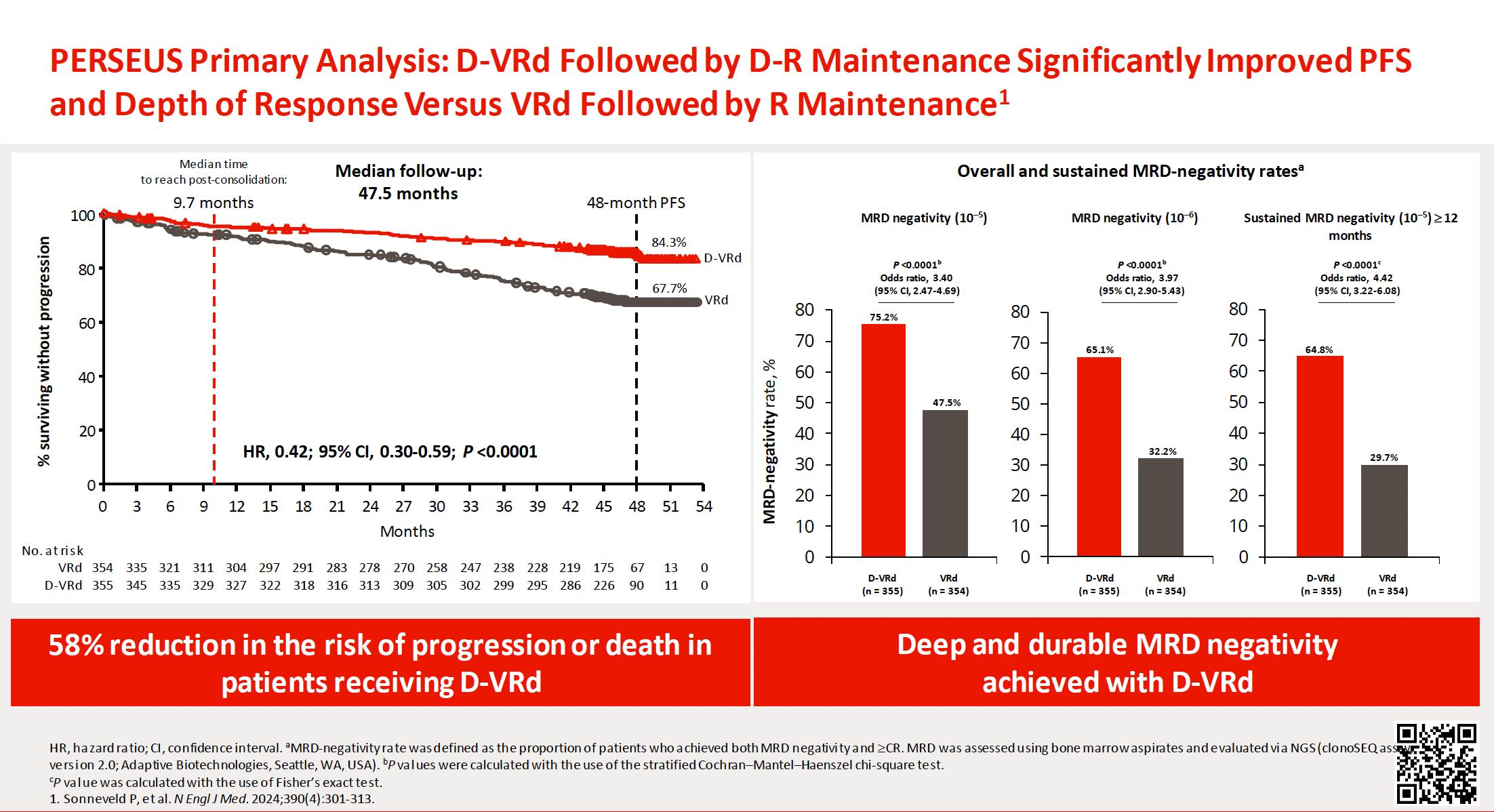
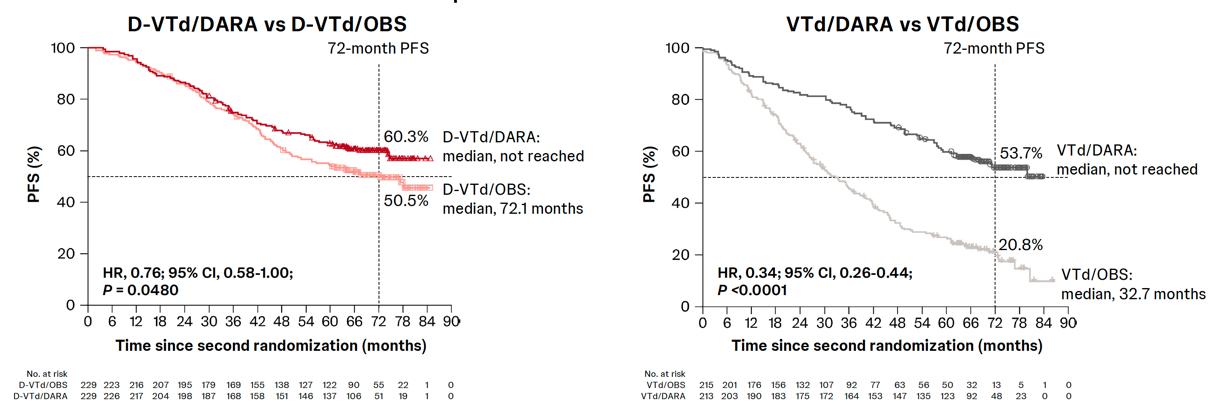
Phase 3 PERSEUS: D-VRd vs VRd
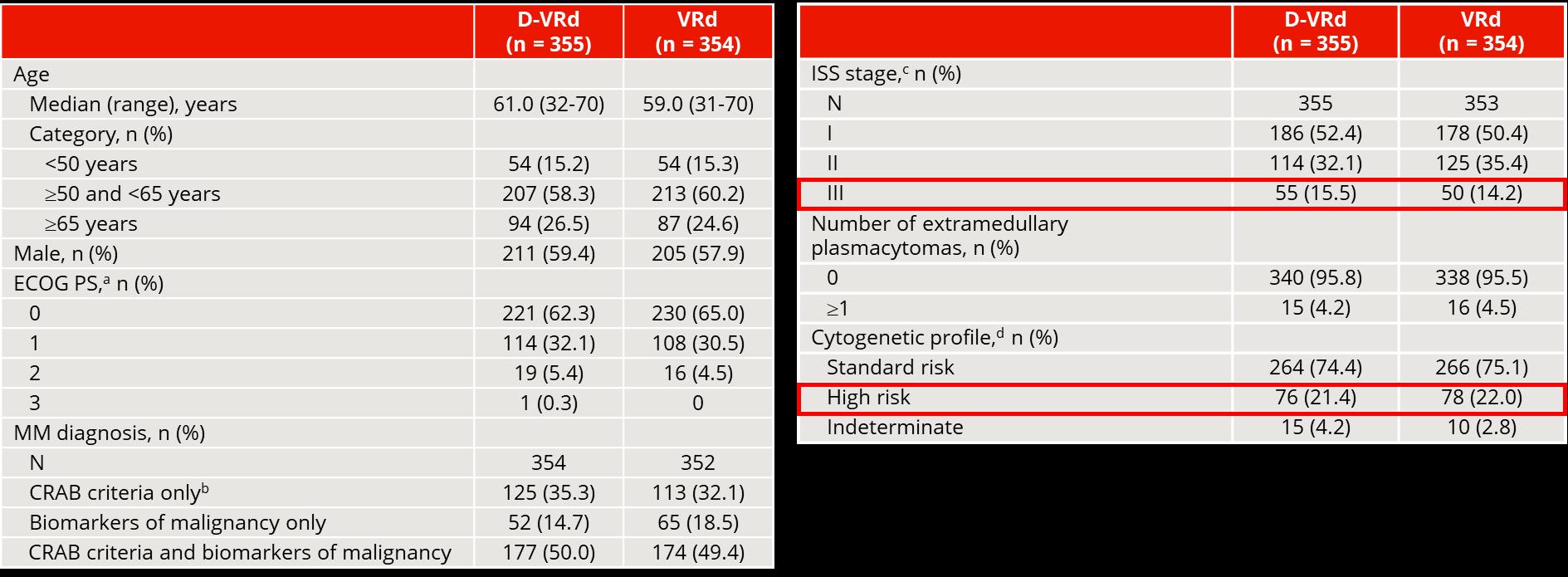
PERSEUS: Patient Characteristics
Sonneveld P et al. ASH 2023. Abstract LBA1.
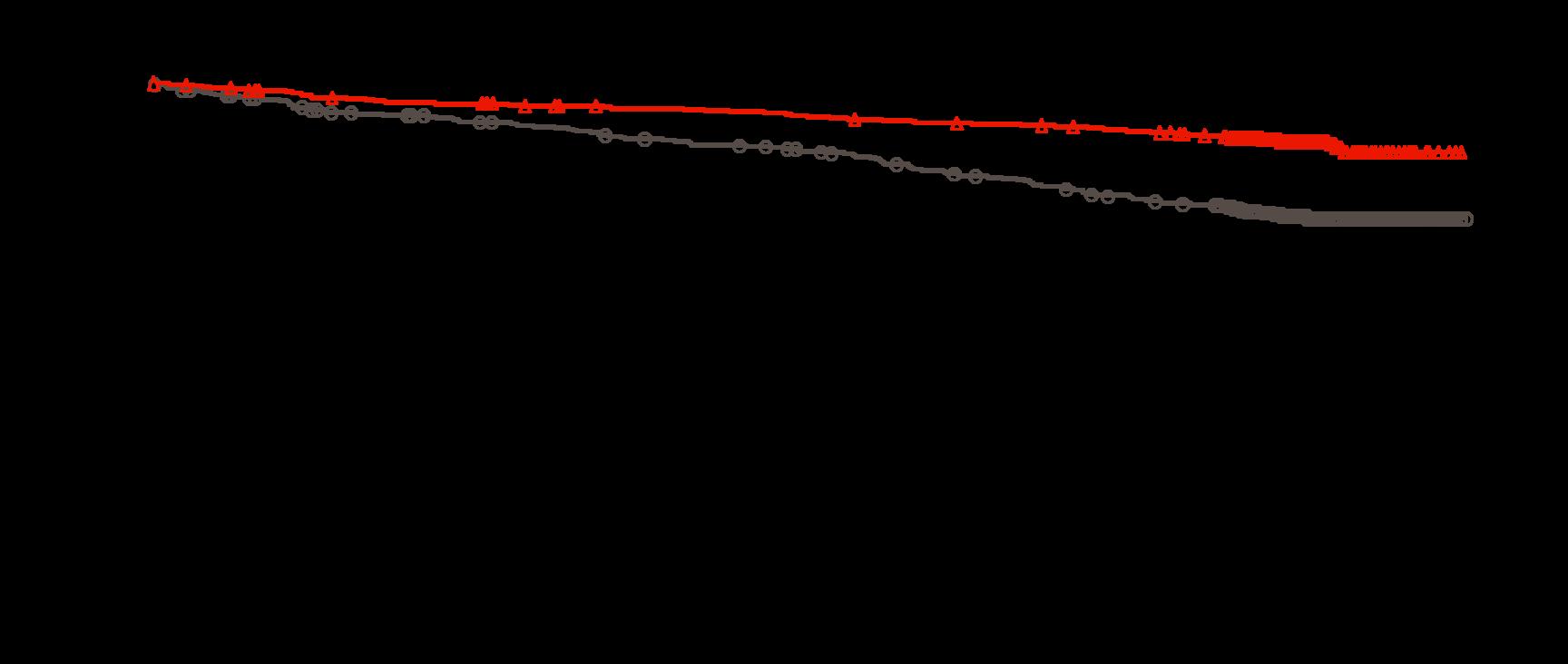
PERSEUS: Primary Endpoint – PFS
PERSEUS: Sustained MRD-Negativity Rates
64% (207/322) of patients receiving maintenance in the DVRd group discontinued daratumumab maintenance after achieving sustained MRD negativity (lenalidomide maintenance continued).
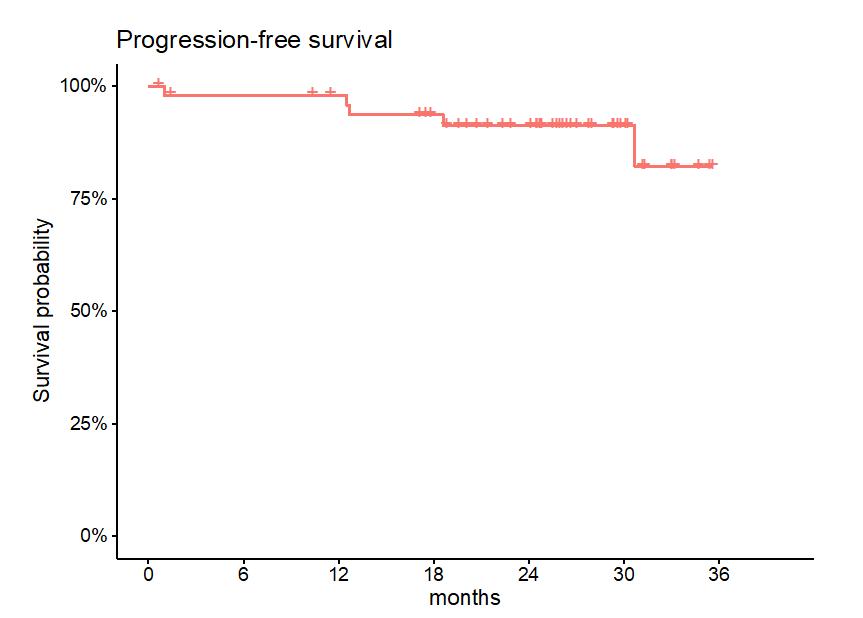
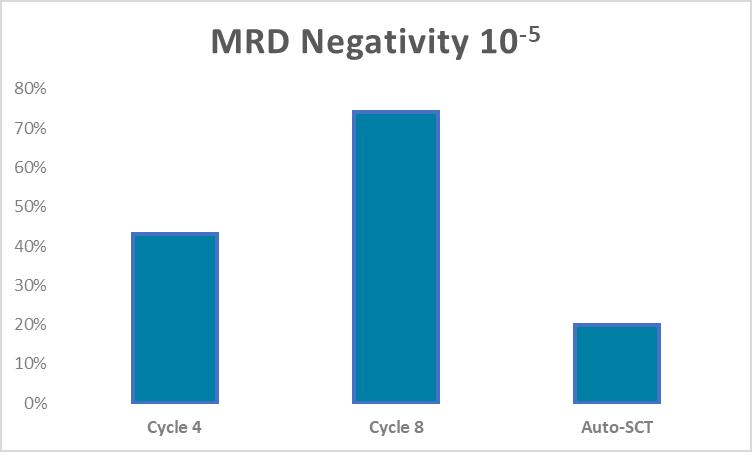
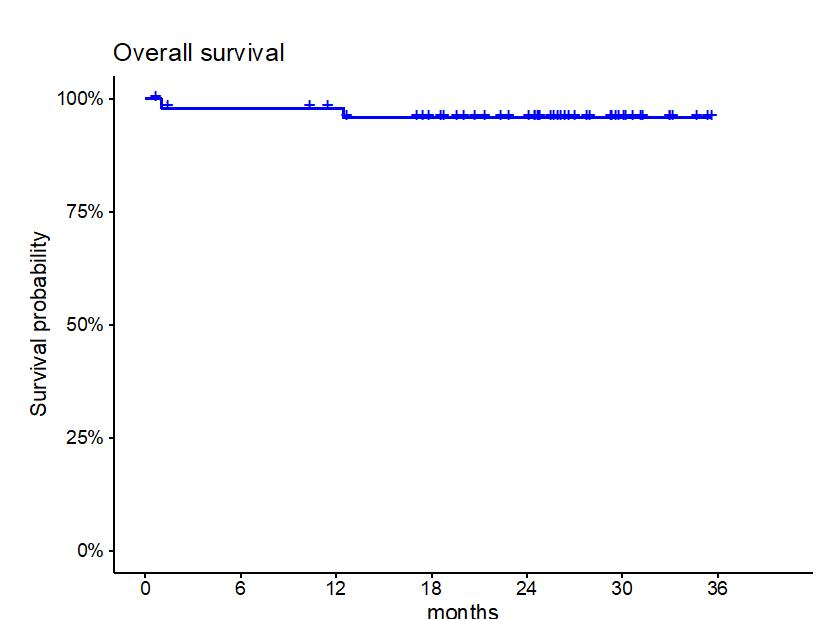
The SKylaRk Trial:
Isatuximab, Once Weekly Carfilzomib, Lenalidomide, and Dexamethasone in TE NDMM
Screening
Enrollment
Induction (C1-4)
• Lenalidomide 25 mg po Days 1-21
• Carfilzomib 56 mg/m2 IV Days 1, 8, 15
• Dexamethasone 20 mg po Days 1, 2, 8, 9, 15, 16
• Isatuximab 10 mg IV Q1 week for 8 weeks, then Q2 weeks for 16 weeks, thereafter Q4 weeks
Stem cell collection (SCT)
Autologous SCT
Consolidation (C5-6)
• Lenalidomide 25 mg po Days 1-21
• Carfilzomib 56 mg/m2 IV Days 1, 8, 15
• Dexamethasone 20 mg po Days 1, 2, 8, 9, 15, 16
• Isatuximab 10 mg IV Day 1
Transplant-Deferred
Induction (C5-8)
• Lenalidomide 25 mg po Days 1-21
• Carfilzomib 56 mg/m2 IV Days 1, 8, 16
• Dexamethasone 20 mg po Days 1, 2, 8, 9, 15, 16
• Isatuximab 10 mg IV Day 1
Maintenance (stratified based on cytogenetics and MRD status)
Standard-risk and/or MRD negative:
• Lenalidomide 10 mg po Days 1-21
High-risk and/or MRD positive:
• Lenalidomide 10 mg po Days 1-21
• Carfilzomib 56 mg/m2 IV Days 1, 8, 15
• Isatuximab 10 mg IV Day 1
The SKylaRk Trial: Isatuximab, Once Weekly Carfilzomib, Lenalidomide, and Dexamethasone in TE NDMM
Response to Therapy
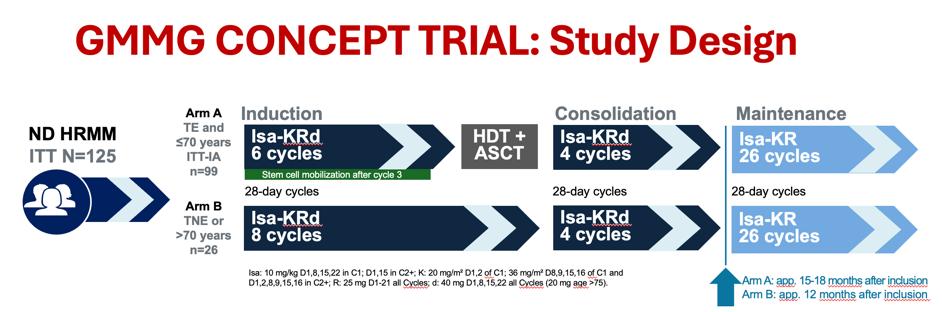
GMMG CONCEPT TRIAL: Study Design
Induction Maintenance Consolidation
Isa: 10 mg/kg D1,8,15,22 in C1; D1,15 in C2+; K: 20 mg/m² D1,2 of C1; 36 mg/m² D8,9,15,16 of C1 and D1,2,8,9,15,16 in C2+; R: 25 mg D1-21 all Cycles; d: 40 mg D1,8,15,22 all Cycles (20 mg age >75).
HRMM criteria: ISS stage II or III PLUS ≥1 of: del(17p), t(4;14), t(14;16) and/or >3 copies 1q21 (amp1q21)
Primary objective: MRD negativity after consolidation (NGF, 10-5)
Secondary objective: PFS
Key tertiary objectives: ORR, OS, safety
IMS 2023. Abstract OA-43.
Maintenance
• What to use for maintenance??
• SR
– Lenalidomide is SOC
• HR
– Doublet or triplet?
– IMiD + PI or CD38
– PI + IMiD + CD38
• How long to give maintenance?
• SR
– 3yr/until prog/based on MRD
• HR
– Until progression
SR=Standard Risk; HR=High Risk; SOC=Standard of Care
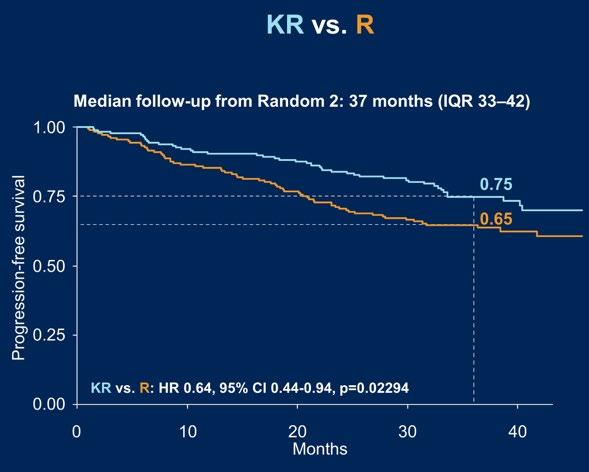
FORTE Trial
CASSIOPIEA
Questions over the next 5 years
• Can we use fixed duration treatment based on MRD
• Can we use immunotherapy early and replace transplant with immunotherapies?
• Can we use risk adapted approaches?
• Can we combine with TCRs?
• Where will belamaf fit?
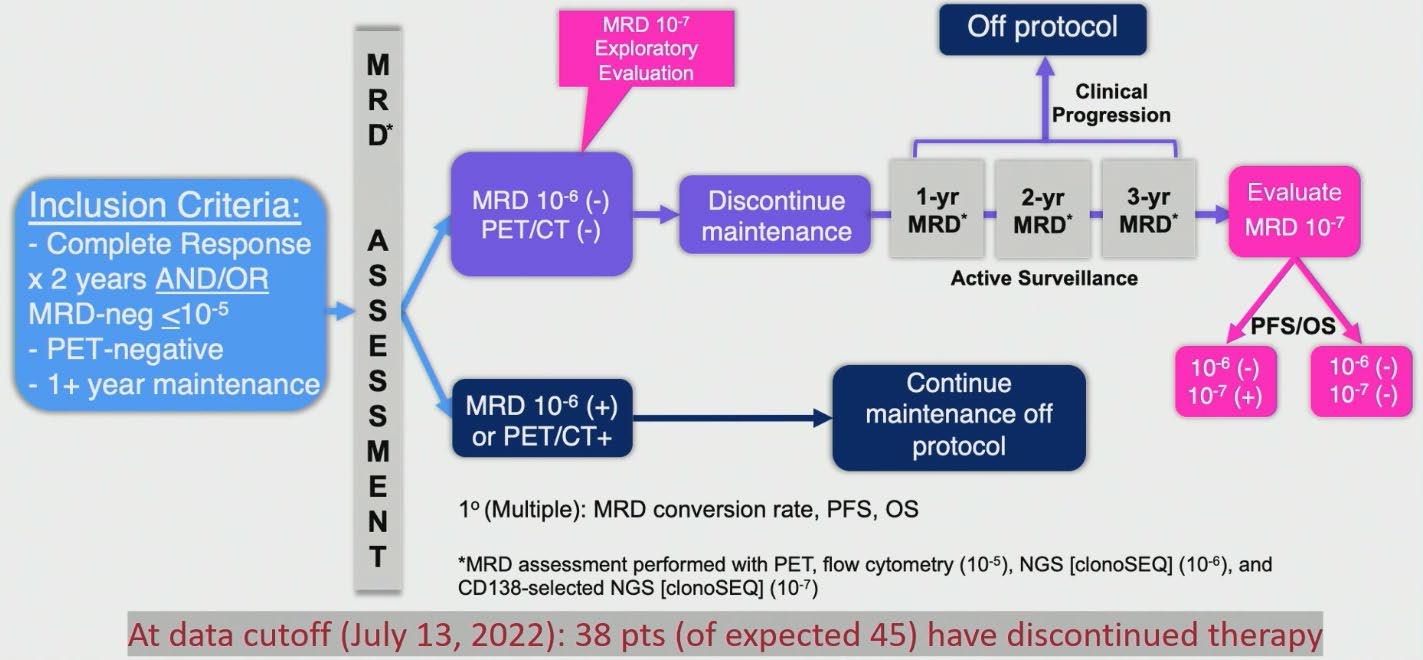
MRD2STOP: Prospective Trial using MRD(-) to Guide Discontinuing Maintenance
Therapy in MM
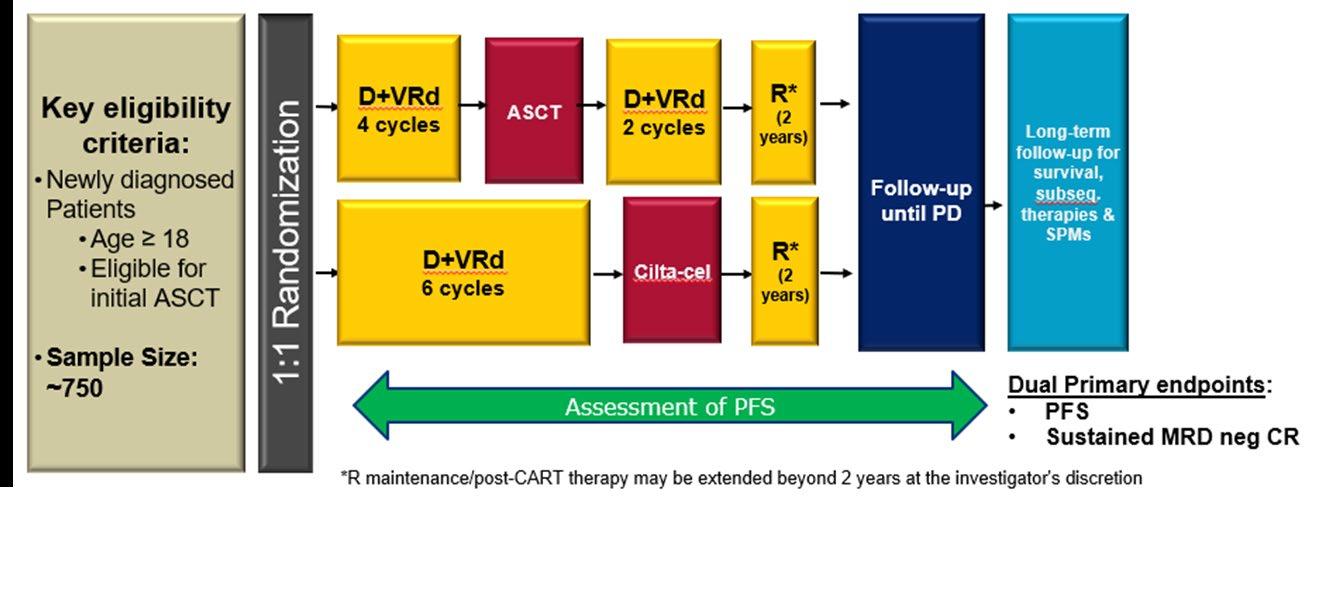
CARTITUDE - 6:
Randomized, phase 3 in NDMM, transplant eligible
Lenalidomide (oral) (Revlimid)
Rash
Thrombosis (DVT)
Second malignancy (<5%)
Diarrhea (longer term)
Myelosuppression
Congenital limb shortening
Ixazomib (oral) (Ninlaro)
Nausea
Diarrhea
Rash
Dexamethasone (Decadron)
Mood changes
Insomnia
Hyperglycemia
Fatigue
Side effects (not an exhaustive list)
Pomalidomide (oral) (Pomalyst)
Myelosuppression
Second malignancy (<5%)
Thrombosis (DVT)
Congenital limb shortening
Bortezomib (sc, IV) (Velcade)
Peripheral neuropathy
Shingles
Blepharitis
Hypotension
Carfilzomib (IV) (Kyprolis)
Hypertension
Heart failure
Shortness of breath
Thrombotic events
Daratumumab (sc, iv) (Darzalex)
Myelosuppression
Infection
Infusion-related reactions
Diarrhea
Elotuzumab (IV) (Empliciti)
Infusion-related reactions
Prophylaxis
Aspirin for thrombotic risk related to IMiDs
Acyclovir for risk of shingles with proteasome inhibitors, anti-CD38 monoclonal antibodies
• IVIG if recurrent life-threatening infections or IgG<400
• Social Work
• Palliative Care
• Physical Therapy & Rehabilitative Medicine
Future for MM
• Continued search for novel targets
• The power of immune strategies remains to be harnessed: sequencing CARs/BiTEs/ Dual targeting strategies
• Transform chronicity into CURE
Living Your Best Myeloma Life: Side Effect Management and Patient Empowerment
Mary Steinbach, DNP, APRN
Seasons of Multiple Myeloma
Mary Steinbach, DNP, APRN
Huntsman Cancer Institute
University of Utah & IMF Nurse Leadership Board
Understanding Multiple Myeloma Spring into Treatment Enjoy Life’s
Summer of Success
Understanding Multiple Myeloma
Don’t be Left in the Cold…Understand Myeloma
MYELOMA
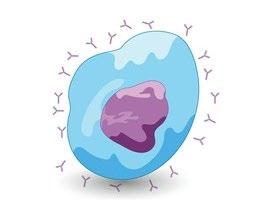
Plasma Cells come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).
In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).
Bone marrow
Don’t be Left in the Cold…Understand Myeloma
Bone marrow
Anxiety
Stress
Depression
Decreased red blood cells
Decreased white blood cells
Myeloma protein in blood and urine
• Clonal myeloma plasma cells can cause many symptoms
– Crowd out normal bone marrow cells
– Produce myeloma protein
– Can cause kidney dysfunction
– Affect bone cells (balance of osteoclasts & osteoblasts)
Changes in bone remodeling
Infections Are Serious for People with Myeloma
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma.
Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
• Bone-strengthening agents (prescribed by your healthcare team)
Report any new or worsening bone pain to your healthcare provider
Spring into Treatment
Treatment of Newly Diagnosed Myeloma
Induction
Consolidation
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients)
Maintenance
Prolonged lower-intensity treatment designed to sustain remission
National Comprehensive Cancer Network® (NCCN®) NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) for Multiple Myeloma. Version 1.2025. To view the most recent or complete version of the guideline, go online to NCCN.org; Rajkumar et al, 2014. Rajkumar SV. Am J of hematology. 2022;97(8):1086–1107. https://doi.org/10.1002/ajh.26590; Faiman et al, 2016.
Induction Standard of Care: Frontline Quadruplet
Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma
Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
• Sarclisa (isatuximab)
Proteosome Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
At infusion clinic. Subcutaneous injection or infusion
Supportive Medication:
Immunomodulatory drug (IMID)
• Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
• Decadron (dexamethasone)
Oral medication taken at home
• Antiviral prophylaxis (i.e. acyclovir or valacyclovir) to prevent viral infections particularly shingles.
• Antibacterial agents (i.e. Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs .
• Bone-strengthening agents (i.e. zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Are Steroids Messing With Your Sunny Disposition?
Steroids enhance the effectiveness of other myeloma therapies
Your provider may adjust your dose. Do not stop or alter your dose of steroids without discussing it with your provider
Managing Steroid Side Effects
• Consistent schedule (AM vs. PM)
• Take with food
• Stomach discomfort: Over-the-counter or prescription medications
• Medications to prevent shingles, thrush, or other infections
Steroid Side Effects
• Irritability, mood swings, depression
• Difficulty sleeping (insomnia), fatigue
• Blurred vision, cataracts
• Flushing/sweating
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
Peripheral Neuropathy Management
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e. diabetes).
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy. Other medications and supplements
• Hydration is very important
• Electrolyte replacement is common
• Good skin care will help prevent irritation
• Stool exam may be needed to rule-out infection
• If no infection, anti-diarrheal medication may be prescribed
Discuss GI issues with healthcare providers to identify causes and make adjustments to medications and supplements
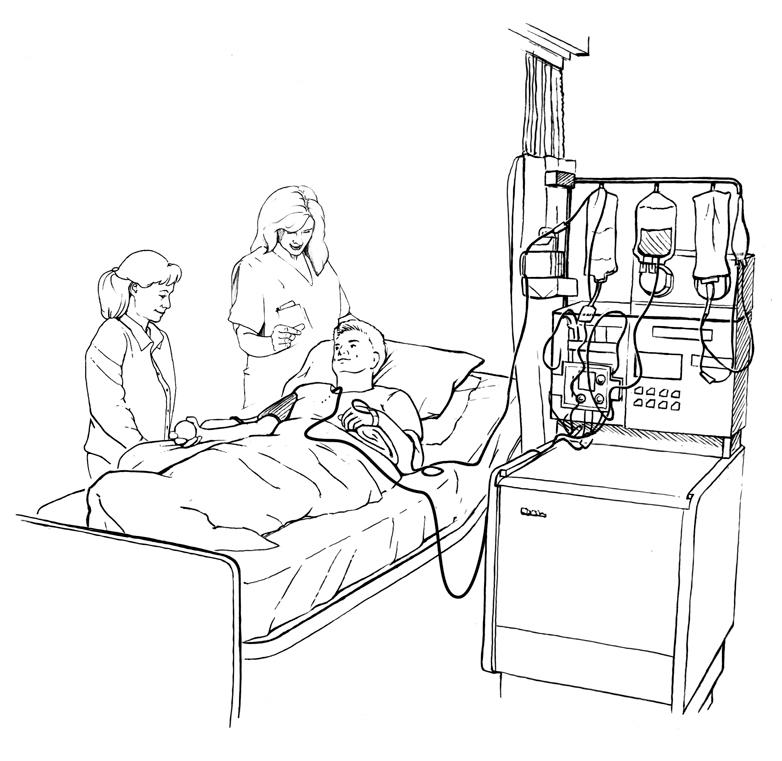
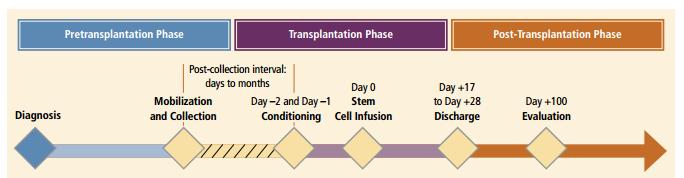
Post Transplant
Phase 3: Post Transplant
Marked by engraftment and a transition to home care and recovery
Time is needed for full recovery. This will vary from one person to another.
Care partner support will still be needed in the early days after returning home.
Day +21: APPROXIMATE time when people will transition to home. Restrengthening, regaining energy
Appetite recovery
Day +60 to Day +100: anticipate start of maintenance therapy
Near 6 months: Begin post-transplant immunizations
Care Partner Support during ASCT
• Care partner support is essential for the entire transplant process.
• Phase 1: Sedated procedures; Education sessions
• Phase 2: Some transplant centers allow for outpatient transplant management if a care partner is present to assist with daily activities, medication management and alert the medical team of changes
• Phase 3: Continued support and assistance is often needed in the early days after returning home. Less assistance will be needed as time and healing go on.
• Care partner(s) can be one person or a rotation of many people.
Maintenance Therapy Is Recommended for All
• Maintenance therapy is recommended for patients with myeloma
– After transplant (ASCT)
– In transplant-ineligible or those with deferred transplant after induction/consolidation
Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression 98.8% >35% of patients ≈25% of patients
Often, people do not share these symptoms with their providers. Talk to your provider about symptoms that are not well controlled or if you have thoughts of self-harm.
Cultivate A Care Network
• Multiple studies demonstrate that strong social ties are associated with
– Increased longevity including people with cancer
– Improved adherence to medical treatment leading to improved health outcomes
– Lower risk of cardiovascular diseases
– Increased sense of purpose & life satisfaction
– Improved mood and happiness
– Reduced stress and anxiety
– Enhanced resilience
Martino J, et al. Am J of Lifestyle Med. 2015;11(6):466-475.
Yang YC, et al. Proc Natl Acad Sci U S A. 2016;113(3):578-583.
Pinquart M and Duberstein PR. Crit Rev Oncol Hematol. 2010; 75(2):122–137. Hetherington C. Healthnews.
https://healthnews.com/longevity/healthspan/social-connection-andlongevity/#:~:text=Research%20consistently%20demonstrates%20that%20pe ople,of%20fulfillment%20in%20your%20life. Accessed Feb 1 2024.
Strategies for enhancing social connection
– Deepen existing relationships with family, friends, and loved ones
– Build new relationships by participating in a support group, joining clubs or organizations, or volunteering
Tip: Start with small steps outside your comfort zone. Call a loved one you haven’t spoken to in a while.
Invite a person you’d like to know better for lunch, coffee, or a walk.
Enjoy Life’s Bounty
Harvest Good Health
Have a primary care provider & have recommended health screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Diabetes
• Colonoscopy
• Women specific: mammography, pap smear
• Men specific: prostate
• Vision
• Hearing
• Dermatologic evaluation
• Dental checkups & cleaning
Develop & maintain healthy behaviors
• Good nutrition
• Regular activity
• Quit tobacco use
• Sufficient sleep (next slide)
An ounce of prevention is worth a pound of cure. Benjamin Franklin
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56. Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
Plentiful Sleep: Important for Good Health
• Adequate rest and sleep are essential to a healthful lifestyle
• Sleep hygiene is necessary for quality nighttime sleep and daytime alertness
– Engage in exercise but not too near bedtime
– Increase daytime natural light exposure
– Avoid daytime napping
– Establish a bedtime routine - warm bath, cup of warm milk or tea
• Associate your bed ONLY with sleep
– Avoid before bedtime:
• Caffeine, nicotine, alcohol and sugar
• Large meals and especially spicy, greasy foods
• Computer screen time
• Sleep aid may be needed
Rod NH et al 2014. PloS one. 9(4):e91965; Coleman et al. 2011. Cancer Nurs. 34(3):219-227.National Sleep Foundation. At: http://sleepfoundation.org/ask-the-expert/sleep-hygiene Mustian et al. Journal of clinical Oncology. Sep 10 2013;31(26):3233-3241; Stan DL, et al. Clin J Oncol Nurs. Apr 2012;16(2):131-141; Zeng Y et al., Complementary therapies in medicine. Feb 2014;22(1):173-186.
#MyelomaActionMonth: Take Action During March!
WHAT IS #MYELOMAACTIONMONTH?
Myeloma Action Month is a global social awareness campaign that takes place every March to raise awareness of multiple myeloma. Every March, we urge you to champion Myeloma Action Month to make an impact on those living with the disease. Will you take action for the myeloma community?
Visit www.myelomaactionmonth.org to learn how you can join the movement. Will you take action for
Thank you to our
sponsors!
OUR VISION: A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values :
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.