Shared Experiences Help to Better Understand the Myeloma Journey
• Support Groups Empower Patients & Care Partners with information, insight, & hope
• The IMF provides educational support to a network of over 150 myeloma specific groups
IMF – Special Interest Virtual Groups
Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
Las Voces de Mieloma
Designed for Spanish speaking patients only
Living Solo & Strong with Myeloma
Designed for patients without a care partner
Care Partners Only
Designed to address the needs of care partners only
High Risk Multiple Myeloma
Designed to address the needs of the high-risk MM population
Smolder Bolder
Created for people living with Smoldering Multiple Myeloma
MM Families
For patients/care partners with young children
GenAI Chatbot | Welcome Myelo!
Myelo is an AI-powered chatbot serving as the International Myeloma Foundation's virtual assistant for patients, care partners, and healthcare professionals.
on Myeloma Symptoms, diagnosis, treatments, research 24/7 Availability
Symptom
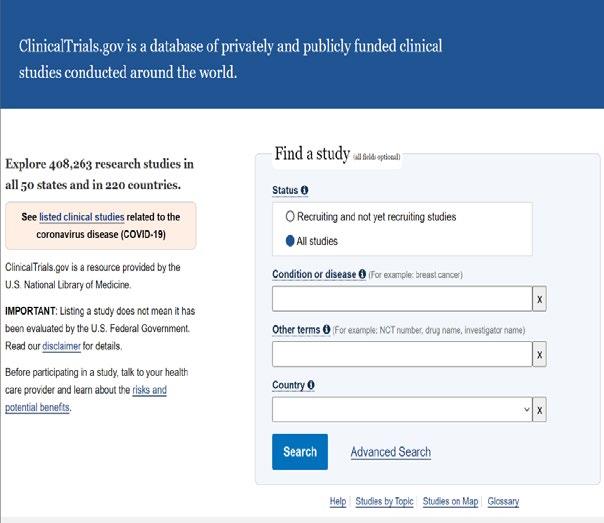
SparkCures: Clinical Trials Finder
• Online platform for cancer patients, focusing on clinical trials
• Specializes in multiple myeloma and related blood cancers
• Simplify the process of finding relevant clinical trials
• Empower patients with information about treatment options
• Features:
• Clinical trial search engine
• Personalized trial matching
• Educational resources on clinical trials
Myeloma 101
Joseph Mikhael, MD
International Myeloma Foundation
Objectives
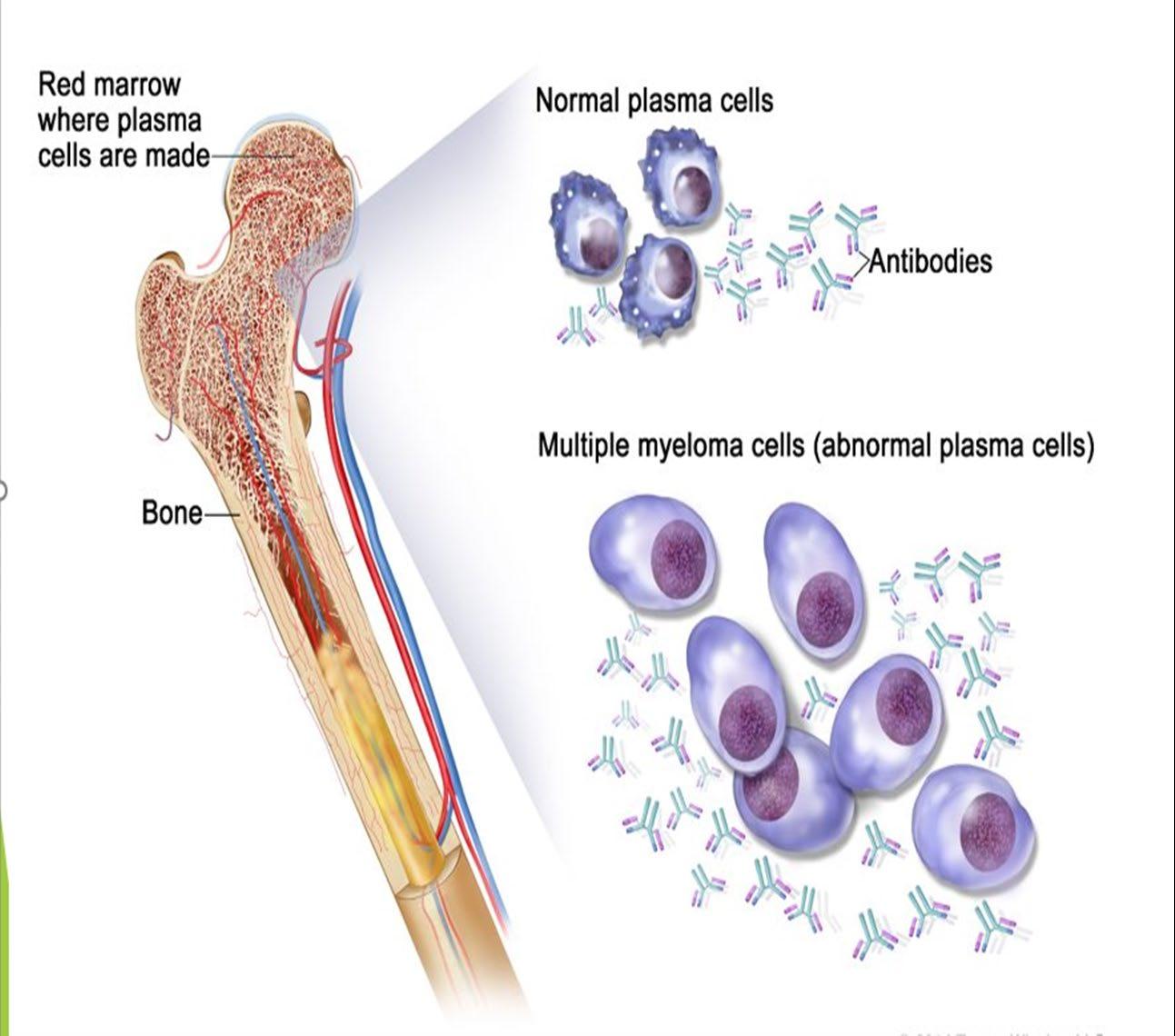
• Review the basics of blood and cancer
• Define multiple myeloma and its key features
• Discuss the staging and classification of myeloma
• Outline the approach to therapy of myeloma
• Appreciate the importance of health disparities in myeloma
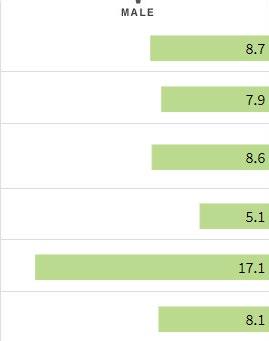
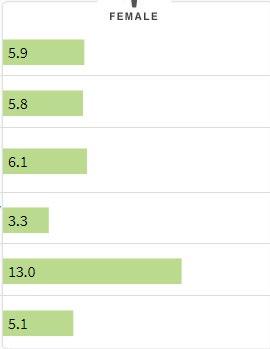
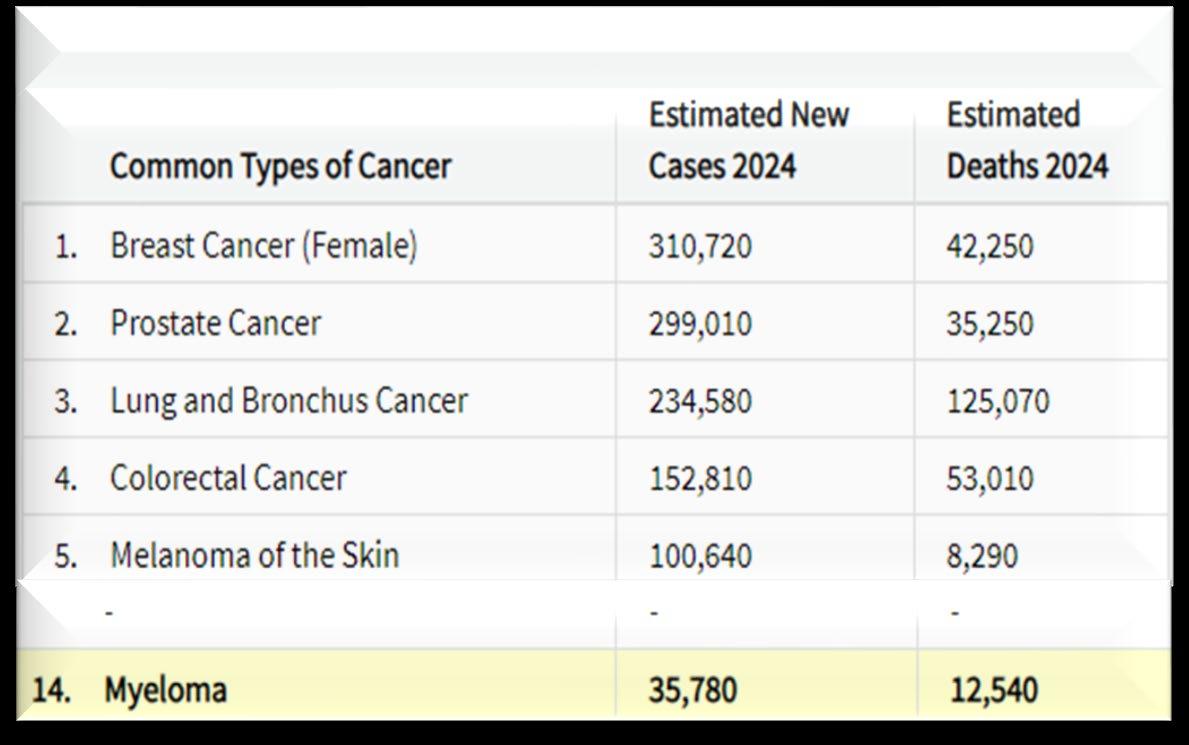
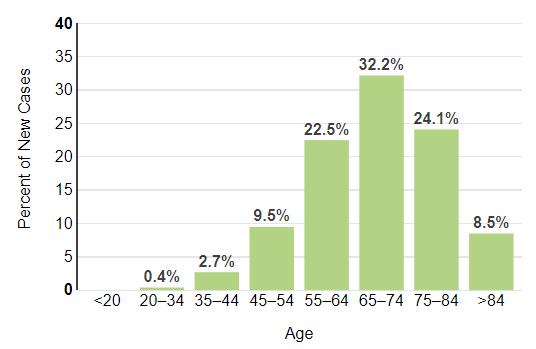
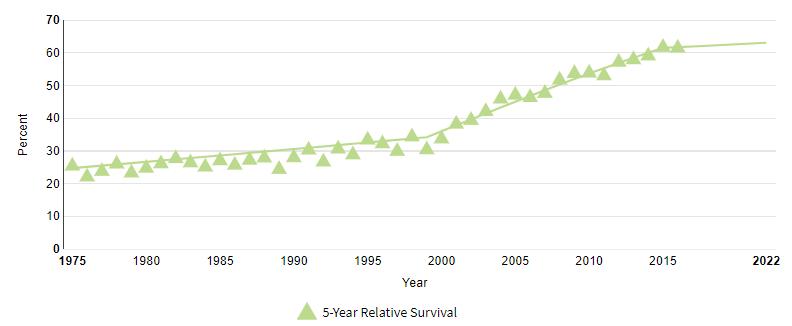
How common is Myeloma?
Rate of New Cases per 100,000 Persons by Race/Ethnicity & Sex How common is Myeloma?
Relapsed MM with 4 prior LOT CAR T therapy recommended. Insurance approved and ready to move forward.
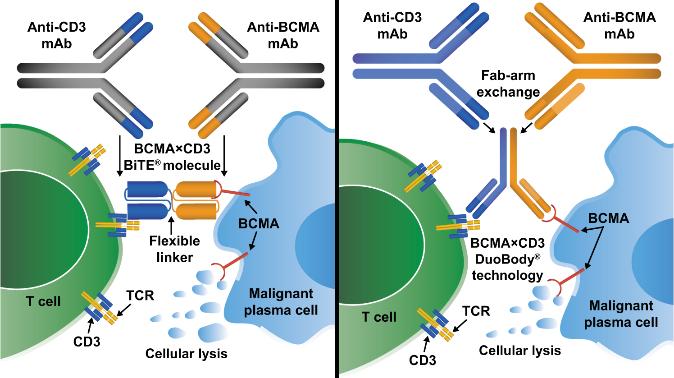
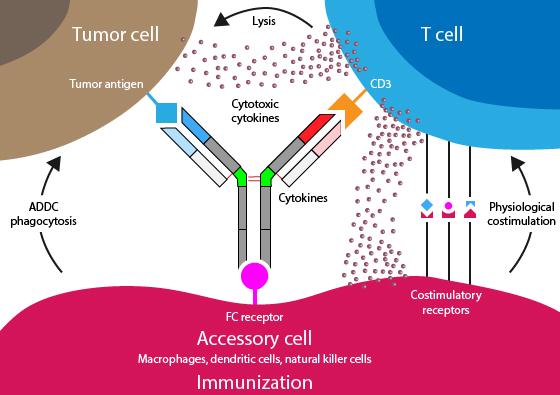
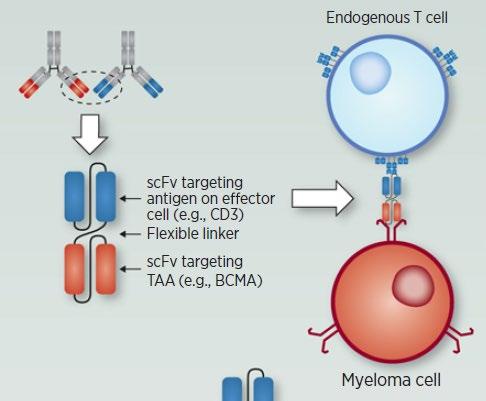
Bispecific Antibodies: Mechanism of Action
• Incorporates 2 antibody fragments to target and bind both tumor cells and T cells
• Brings target-expressing MM cells and T cells into close proximity, enabling T cells to induce tumor-cell death
Targets of Bispecific Molecule Vary
“Off the Shelf” Advantage
• No manufacturing process, unlike CAR T-cell therapy (but like ADC/belantamab therapy)
• Thus, no delay between decision to treat and administration of drug
Image Source: Shah N, et al. Leukemia. 2020;34:985–1005. Creative Commons
CC BY 4.0. Barilà G, et al. Pharmaceuticals (Basel). 2021;14(1):40.
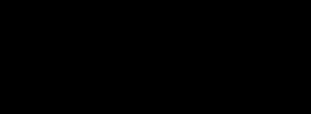
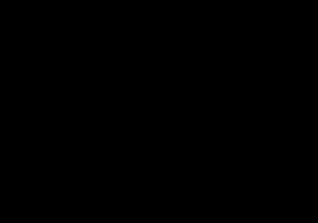
The Evolution of Myeloma Therapy
VD
Rev/Dex
CyBorD
VTD
VRD
KRD
D-VMP
DRD
Tandem ASCT (?)
Nothing
Thalidomide?
Bortezomib
Ixazomib
Lenalidomide
Combinations
D-VRD
Isa-VRD
D-KRD
Isa-VRD “More” induction?
Daratumumab?
Carfilzomib?
Lenalidomide + PI
ASCT, autologous stem cell transplant; CAR, chimeric antigen receptor; Cy, cyclophosphamide; d- daratumumab; D/dex, dexamethasone; isa, isatuximab; K, carfilzomib; M, melphalan; PD-L1, programmed death ligand-1; PI, proteasome inhibitor; Rev, lenalidomide; V, bortezomib. Speaker’s own opinions.
Bortezomib
Lenalidomide
Carfilzomib
Pomalidomide
Selinexor
Panobinostat
Daratumumab
Ixazomib
Elotuzumab
Isatuximab
Belantamab mafodotin*
Melphalan flufenamide*
Idecabtagene autoleucel
Ciltacabtagene autoleucel
Teclistamab, Talquetamab
Elranatamab
CAR T Cell Therapy
Bispecific/Tri-specific Antibodies
Cell Modifying Agents
Venetoclax
PD/PDL-1 Inhibition?
Small Molecules
* These agents are currently off the market but available through special programs
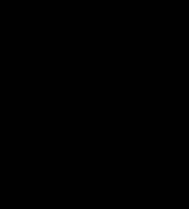
What about Disease Control and Cure in Myeloma?
Biochemical or Symptomatic Progression/Relapse
Functional Cure Unmeasurable Disease, Receiving No Treatment Active Disease Requiring Treatment Stable or Unmeasurable Disease, Receiving Treatment Control is the immediate priority with active disease Cure remains the overall goal
Defining “Cure” has many considerations:
Minimal Residual Disease Negative (MRD-)
Time Off Therapy
Second/Expert Opinion
• You have the right to get a second opinion. Insurance providers may require second opinions.
• A second opinion can help you:
– Confirm your diagnosis
– Give you more information about options
– Talk to other experts
– Introduce you to clinical trials
– Help you learn which health care team you’d like to work with, and which facility
A Call to Action – Facts About African Americans and Myeloma
The core vision of this initiative is to improve the short- and longterm outcomes of African American patients with myeloma. We want to empower patients and communities to change the course of myeloma…
IMF Nurse Leadership Board member & Cleveland Clinic Taussig Cancer Institute Cleveland, OH
OBJECTIVES
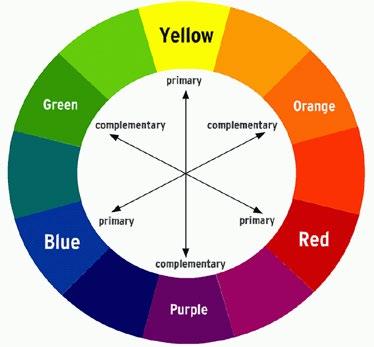
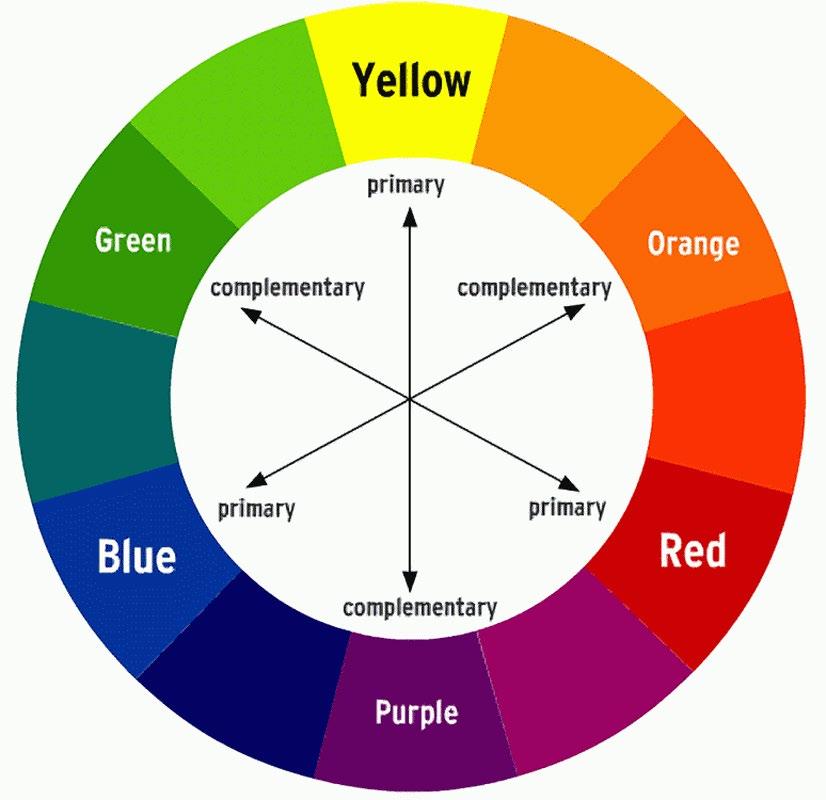
COLOR WHEEL OF TREATMENT
Myeloma and treatment side effects & symptom management
FRAMING YOUR CARE
Know your care team, Telehealth & Meeting Prep, & Shared Decision Making
LIVE LIFE IN COLOR
Healthful Living, infection prevention, renal and bone health
COLOR WHEEL OF TREATMENT
Treatment options, side effects, symptom management, & supportive care
GALLERY OF GOALS
MYELOMA TREATMENT
• Rapid and effective disease control
• Durable disease control
• Minimize side effects
• Allow for good quality of life
• Improved overall survival
SUPPORTIVE THERAPIES
• Prevent disease- and treatmentrelated side effects
• Optimize symptom management
• Allow for good quality of life
DISCUSS GOALS AND PRIORITIES
WITH YOUR HEALTHCARE TEAM
Alkylators
COLOR WHEEL OF TREATMENT OPTIONS
COMBINATIONS:
MIX, MATCH, BLEND FOR DEPTH
1
PHASE
ELIGIBILITY
Measuring Treatment Response
Determining Transplant
Eligibility
Insurance Authorization
Collecting Stem Cells
Duration: Approximately 2 weeks
Location: Transplant Center
PHASE 2
STEM CELL TRANSPLANT
TRANSPLANT
High Dose
Chemotherapy Stem Cell Infusion
Supportive Care Engraftment
Duration: Approximately 3-4 weeks
Location: Transplant Center
PHASE 3
POST-TRANSPLANT
Restrengthening
Appetite recovery
“Day 100” assessment
Begin maintenance therapy
Duration: Approximately 10-12 weeks
Location: HOME
Upfront stem cell transplant remains the standard of care for eligible patients
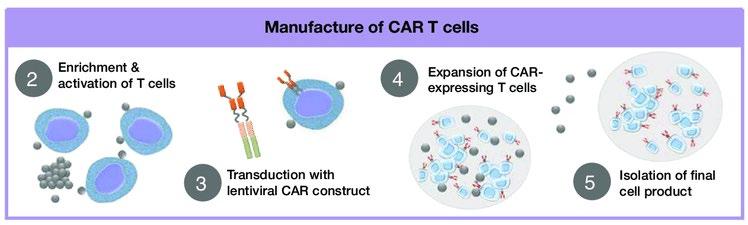
Ask for a referral to CAR Tcell center as soon as it is possible as next treatment option (ie, before relapse)
T-Cell Collection
CAR T-CELL THERAPY
No driving for 8 weeks
“One & Done” with continued monitoring
Manufacturing takes ≈ 4 to 6 weeks
Bridging therapy may be needed
• Away from home
• Often some hospital stay
• Care Partner needed
• Side effect management
• CRS, ICANS
• Low blood counts
• Fatigue and fever
• Some patients need ongoing transfusion support
BISPECIFIC ANTIBODIES
• Different bispecific antibodies have differences in efficacy, side effects
• Available after 4 prior lines of therapy (or clinical trial)
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells
• CRS and neurotoxicity
• Risk of infection
• BCMA target: greater potential for infection
• Tecvayli® (teclistamab)
BISPECIFIC ANTIBODIES
• Elrexfio (elranatamab)
• GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
• Talvey (talquetamab)
SYMPTOM MANAGEMENT
PATIENT-REPORTED SYMPTOMS
A meta-analysis identified the most common patient-reported symptoms and impact on QOL, and were present at all stages of the disease. Symptoms resulted from both myeloma disease and treatment, including transplant, and were in these categories:
Physical
• Fatigue
• Constipation
• Pain
• Neuropathy
• Impaired Physical Functioning
• Sexual Dysfunction Psychological
• Depression
• Anxiety
• Sleep Disturbance
• Decreased Cognitive Function
• Decreased Role & Social Function
Financial
• Financial burden (80%)
• Financial toxicity (43%)
IMMUNOTHERAPY SIDE EFFECTS
Cytokine Release Syndrome (CRS)
Immune effector cell–
associated neurotoxicity syndrome (ICANS)
Neuro Toxicity
Infection
IMMUNOTHERAPIES: UNIQUE SIDE EFFECTS
CRS = cytokine release syndrome. Oluwole OO, Davila ML. J Leukoc Biol . 2016;100:1265-1272. June CH, et al. Science. 2018;359:1361-1365. Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Brudno JN, Kochenderfer JN. Blood Rev. 2019:34:45-55. Shimabukuro-Vornhagen, et al. J Immunother Cancer. 2018;6:56. Lee DW, et al. Biol Blood Marrow Transplant . 2019;25:625-638.
CRS IS A COMMON BUT USUALLY MILD SIDE EFFECT WITH CAR T
IMMUNOTHERAPIES: UNIQUE SIDE EFFECTS
INFECTION CAN BE SERIOUS FOR PEOPLE WITH MYELOMA
[P]reventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Some people receiving BCMA-targeting therapies have experienced infections that are less common like CMV, PJP and fungal infections
NS, et al. Lancet Haematol.2022;9(2):143–161.
Dry Mouth
OTC dry mouth rinse, gel, spray are recommended. Advise patients to avoid hot beverages. Initiate antifungal therapy for oral thrush
MANAGEMENT OF ORAL SIDE EFFECTS
Dysphagia
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms.
Dexamethasone oral solutions “swish and spit” have been tried but with no proven benefit yet. Sour citrus or candies before meals are also recommended. Taste Changes
Dental Care
Attention to oral hygiene.
Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Weight Management
Some medications lead to weight gain, others to weight loss.
Dry mouth leads to taste changes which can lead to anorexia.
Meet with a Nutritionist
Consider diet changes, supplements
Monitor weight
Education and emotional support are key strategies to manage oral toxicities.
GI SYMPTOMS:
PREVENTION & MANAGEMENT
Diarrhea may be caused by medications and supplements
Rod NH et al 2014. PloS one. 9(4):e91965; Coleman et al. 2011. Cancer Nurs. 34(3):219-227. National Sleep Foundation. At: http://sleepfoundation.org/ask-the-expert/sleep-hygiene
• Engage in exercise but not too near bedtime
• Increase daytime natural light exposure
• Avoid Daytime napping
• Establish a bedtime routine - warm bath, cup of warm milk or tea
• Associate your bed ONLY with sleep
• Sleep aid may be needed
• Avoid before bedtime:
• Caffeine, nicotine , alcohol and sugar
• Large meals and especially spicy, greasy foods
• Computer screen time
Mustian et al. Journal of clinical Oncology. Sep 10 2013;31(26):3233-3241.
Stan DL, et al. Clin J Oncol Nurs. Apr 2012;16(2):131-141.
Zeng Y et al., Complementary therapies in medicine. Feb 2014;22(1):173-
Financial burden comes from
• Medical costs
• Premiums
• Co-payments
• Travel expenses
• Medical supplies
• Prescription costs
• Loss of income
• Time off work or loss of employment
• Caregiver time off work
Funding and assistance may be available
• Federal programs
• Pharmaceutical support
• Non-profit organizations
• Websites:
• Medicare.gov
• SSA.gov
• LLS.org
• Rxassist.org
• NeedyMeds.com
Contact the Social Services department at your hospital or clinic to talk to a social worker for assistance.
• HealthWellFoundation.org
• Company-specific website
FRAMING YOUR CARE
Know your care team, Telehealth & Meeting Prep, & Shared Decision Making
You are central to the care team
CARE TEAM COLLAGE
Be empowered
• Ask questions, learn more
• Participate in decisions
Communicate with your team
• Understand the roles of each team member and who to contact for your needs
• Participate in support network
You and Your Caregiver(s)
PREPARE FOR VISITS & CONSIDER TELEMEDICINE
Come prepared:
• Bring a list of current medications, prescribed and over the counter
• Write down your questions and concerns. Prioritize them including financial issues
• Have there been any medical or life changes since your last visit?
• Current symptoms - how have they changed (improved, worsened, stable)? Keep a symptom diary. Bring it along
• Communicate effectively: your health care team can’t help if they don’t know
Check with your healthcare team –Is telemedicine an option?
Similar planning for “in-person” appointment PLUS:
• What is the process and what technology is needed?
• Plan your labs: are they needed in advance? Do you need an order?
• Plan your location: quiet, well-lit location with strong wi-fi is best
• Plan yourself: consider if you may need to show a body part and wear accessible clothing
• Collect recent vital signs (blood pressure, temp, heart rate) self-serve blood pressure cuff is available at many pharmacies and for purchase
You are central to the care team
CARE TEAM COLLAGE
Be empowered
• Ask questions, learn more
• Participate in decisions
Communicate with your team
• Understand the roles of each team member and who to contact for your needs
• Participate in support network
LIVE LIFE IN COLOR
CARE PARTNERS ARE VITAL FOR SUCCESS
If you want to go fast, go alone, if you want to go far, go together
• Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
• Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
African Proverb
• Caring for the Care Partner
• Recognize that caregiving is difficult/stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
HEALTHY BEHAVIORS FOR PATIENTS & CARE PARTNERS
• Stress reduction, management
• Rest, relaxation, sleep hygiene
• Maintain a healthy weight, eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking
• Mental health / social engagement
• Sexual health / intimacy
• Complementary or alternative therapy
• Have a PCP for general check ups, preventative care, health screenings, vaccinations
• Have specialists for dental care, eye exams/screening, skin cancer screening
• Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
Martino J, et al. Am J of Lifestyle Med. 2015;11(6):466-475. Yang YC, et al. Proc Natl Acad Sci U S A. 2016;113(3):578-583. Pinquart M and Duberstein PR. Crit Rev Oncol Hematol. 2010;75(2):122–137.
DEVELOP A CARE NETWORK
• Strategies for enhancing social connection
• Deepen existing relationships with family, friends, and loved ones
• Build new relationships by participating in a support group, joining clubs or organizations, or volunteering
Tip: Start with small steps outside your comfort zone. Call a loved one you haven’t spoken to in a while.
Invite a person you’d like to know better for lunch, coffee, or a walk.
Hetherington C. Healthnews.
https://healthnews.com/longevity/healthspan/soci al -connection-and-
longevity/#:~:text=Research%20consistently%20de monstrates%20that%20people,of%20fulfillment%20in %20your%20life. Accessed Feb 1 2024.
YOU ARE NOT ALONE
Q&A
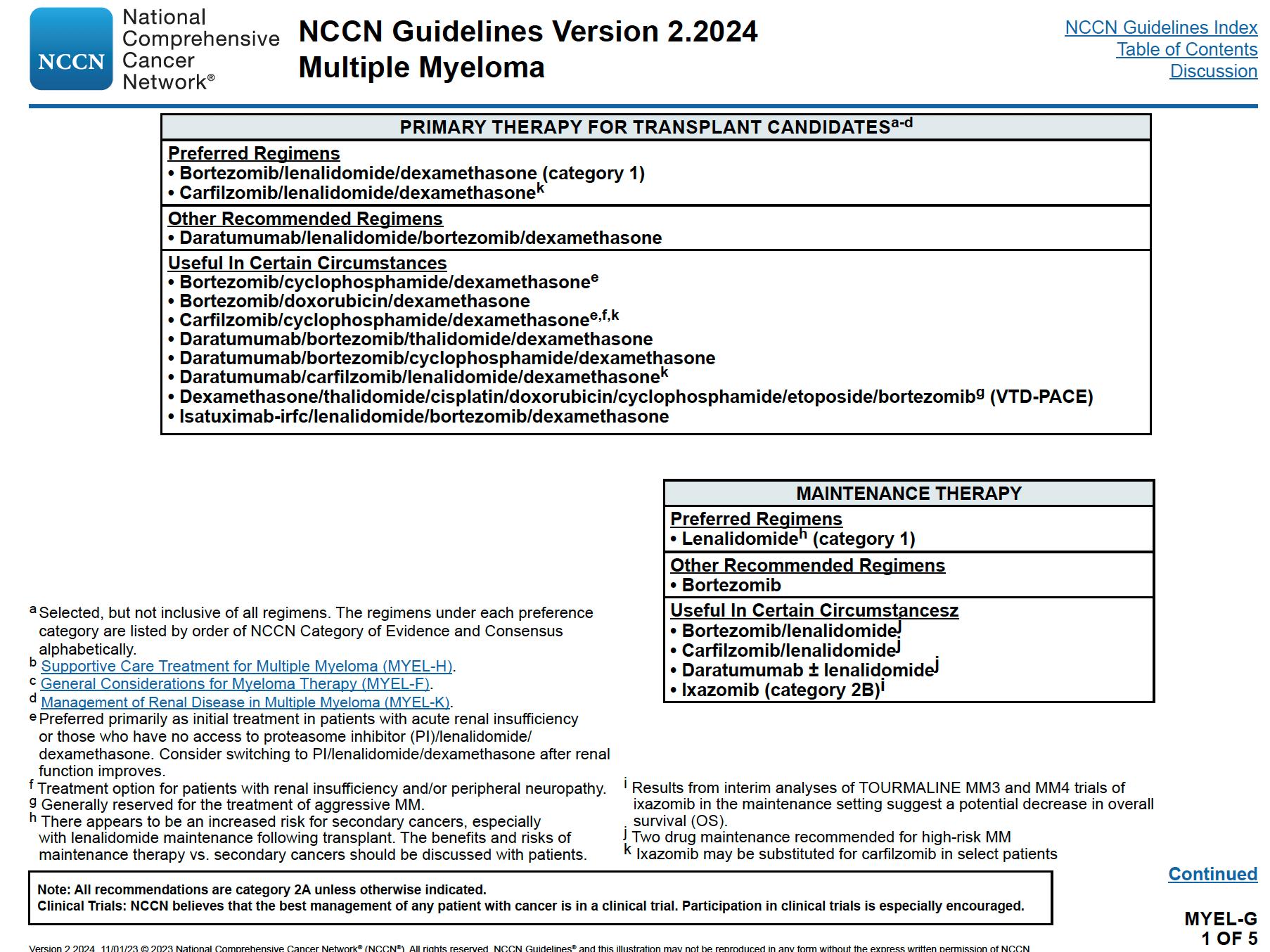
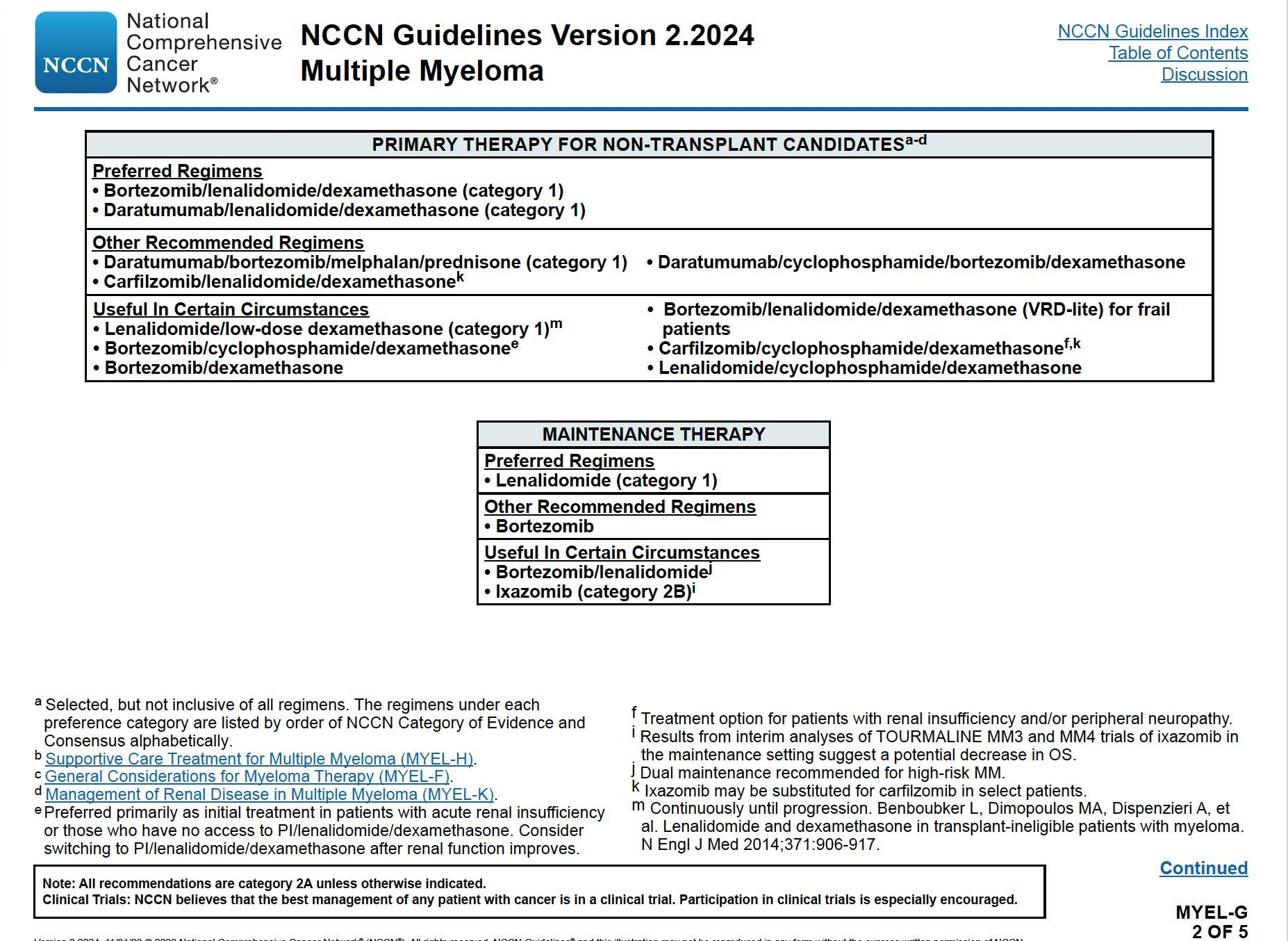
Frontline Therapy
Louis Williams, MD, MBA
Cleveland Clinic
Taussig Cancer Center, Cleveland, OH
Objectives
• Review the importance of DEPTH of response in early treatment of myeloma and the increasing use of MRD testing
• Discuss emerging approaches in transplant eligible patients, including quadruplet therapy and stem cell transplantation
• Outline the approach to a patient not going to transplant and how to optimize continuous therapy
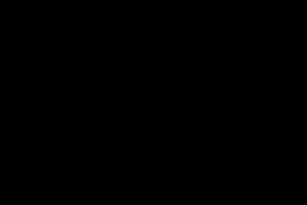
Goals of Therapy: The Iceberg Model of Myeloma
>1 Trillion
Disease Burden (# of myeloma cells)
>1 Billion
>10 Million
1 myeloma cell in 100K to 1 million normal cells
Symptomatic Myeloma
At diagnosis
Partial response
50% reduction in M protein
Very good partial response 90% reduction in M protein immunofixation positive only
Complete remission
No M-protein immunofixation negative
Minimal Residual Dis Flow Cytometry
Minimal Residual Dis Next Generation Molecular testing
Depth of response matters!
MRD refers to the persistence of residual tumor cells after treatment and is responsible for relapse1
Current techniques can detect MRD with a sensitivity of 10-6 for MM cells2
The first phase 3 study evaluating Isa + RVd for induction and maintenance in Te NDMM patients
Isa (IV) 10 mg/kg Cycle 1 Cycle 2–3
Bor (SC) 1.3 mg/m² Len (PO) 25 mg
(PO) 20 mg
Induction phase (3 x 6-week cycles)
Isa (IV) 10 mg/kg: Cycle 1
and Heidelberg University Hospital | ASH 2021
ASCT, autologous stem cell transplant; D, day; d/Dex, dexamethasone; HDT, high-dose therapy; Isa, isatuximab; IV, intravenous; NDMM, newly diagnosed multiple myeloma; PD, progressive disease; PO, oral; R/Len, lenalidomide; SC, subcutaneous; Te, transplant eligible; V/Bor, bortezomib; RVd is off label use in some countries according to the lenalidomide summary of product characteristics. 1. ClinicalTrials.gov: NCT03617731
First primary endpoint, end of induction MRD negativity by NGF (10-5), was met in ITT analysis
Patients with MRD negativity at the end of induction therapy
OR 1.83 (95% CI 1.34–2.51)
Low number of not assessable/missing† MRD status: Isa-RVd (10.6%) and RVd (15.2%)
Isa-RVd is the first regimen to demonstrate a rapid and statistically significant benefit from treatment by reaching a MRD negativity of 50.1% at the end of induction and to show superiority vs. RVd in a Phase 3 trial
IsKia EMN24 Study Design
Induction
Key eligibility criteria: TE NDMM patients aged <70 years
Stratification:
- Centralized FISH (standard risk/missing vs. high risk defined as del(17p) and/or t(4;14) and/or t(14;16); - ISS (I vs. II and III)
MOBILIZATION
Cy: 2-3 g/m2 followed by G-CSF for stem-cell collection and MEL200-ASCT MEL: 200 mg/m2 followed by ASCT
Post-ASCT consolidation
Primary Endpoint: Post-consolidation MRD
negativity (ITT analysis)
10-6
Patients
(N=151) KRd (N=151)
≥VGPR after consolidation was 94% in both arms; ≥CR 74% vs 72% and sCR 64% vs 67% in the IsaKRd vs KRd arms.
High MRD compliance and sample quality (97-100% of sample evaluable at 10-5 and 10-6 cut off.
Consistent MRD results were detected by next-generation flow
In the logistic regression analysis, ORs, 95% CIs, and p-values were adjusted for stratification factor.
MRD negativity rates improved over time (10-5)
Post-consolidation MRD negativity by NGS
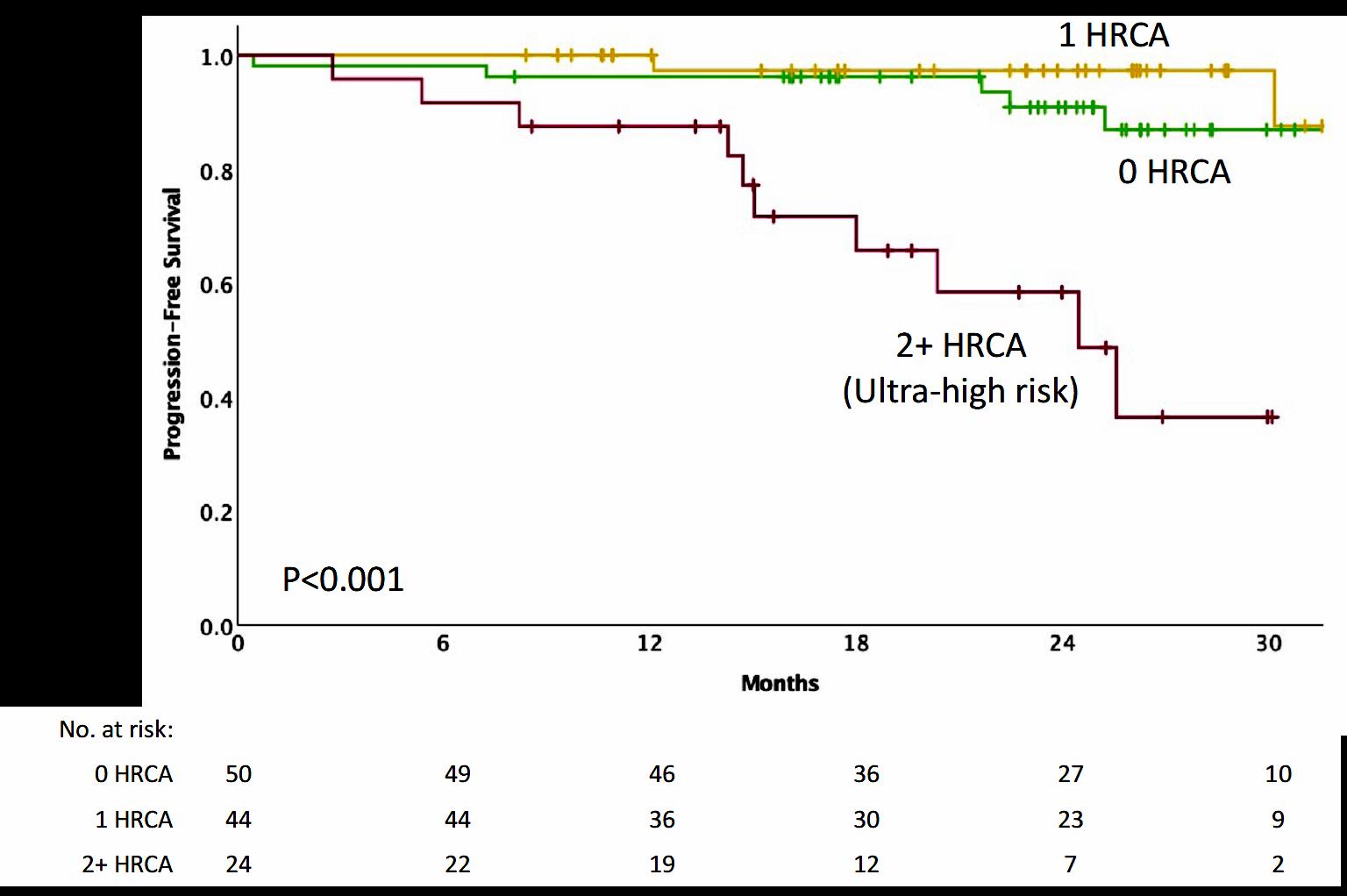
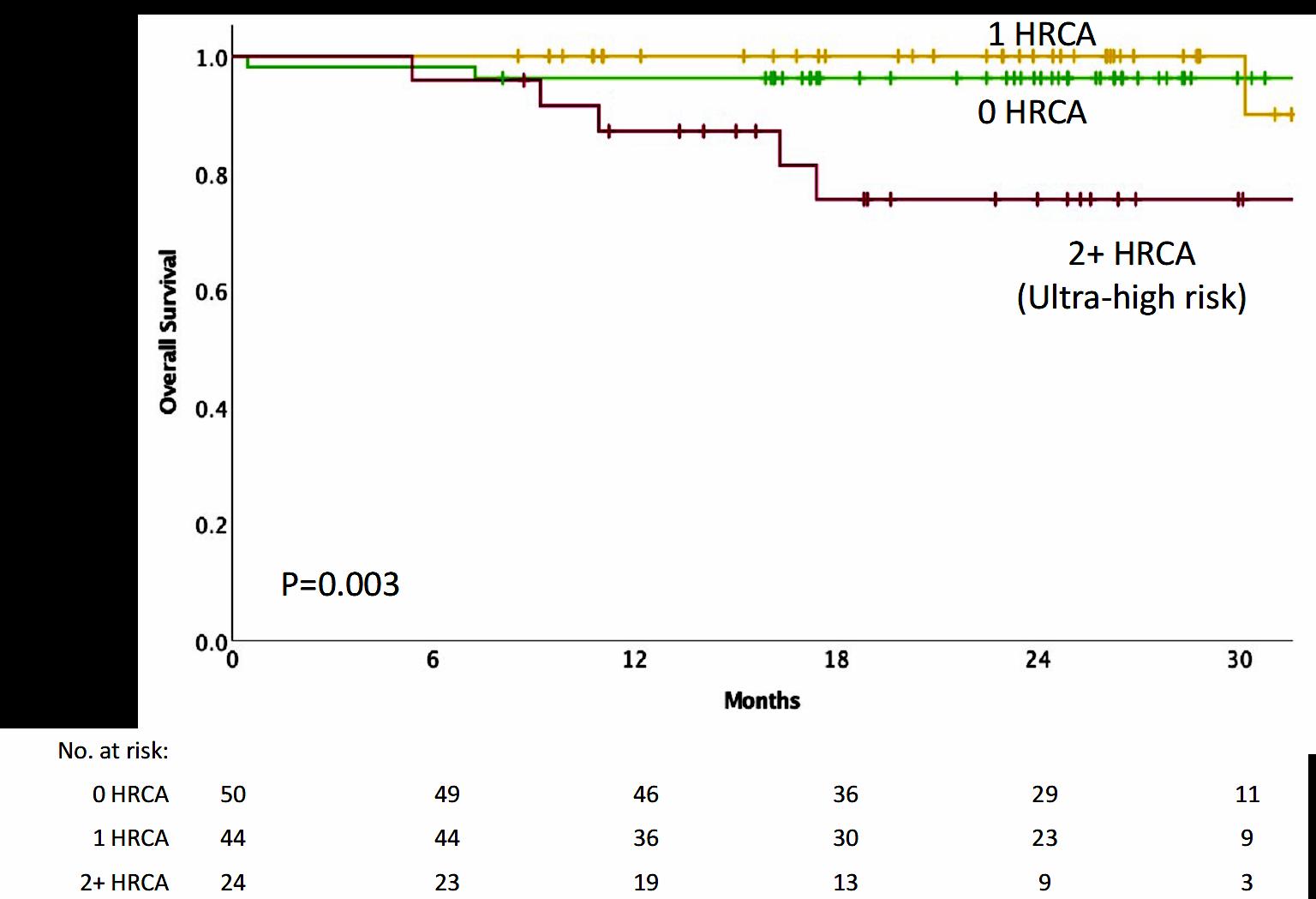
Subgroup analysis by cytogenetic risk
NGS, 10-5 NGS, 10-6
1 HRCA was defined as the presence of one of the following high-risk cytogenetic abnormalities: del(17p13.1), t(4;14) (p16.3;q32.3), t(14;16) (q32.3;q23), gain(1q21), or amp(1q21); 2+ HRCA was defined as the presence of at least two
Conclusions
• Isa-KRd significantly increased post-consolidation 10-5 and 10-6 MRD negativity, as compared with KRd
• Isa-KRd significantly increased 10-5 and 10-6 MRD negativity after each treatment phase (Induction, Transplantation, Consolidation) .
• Isa-KRd consistently increased MRD negativity at 10-5 and 10-6 in all subgroups of patients, including high-risk and very high-risk disease.
• Isa-KRd treatment was tolerable, with a toxicity profile similar to that in previous reports.
• 10-6 MRD negativity cut-off is more informative.
• 1-year sustained MRD negativity will be available in 2024
• With a longer follow-up, this trial can offer the opportunity to explore the correlation between depth of MRD negativity and PFS/OS.
Will MRD guide us to stop therapy?
MASTER Trial - Treatment
Dara-KRd
• Daratumumab 16 mg/m2 days 1,8,15,22 (days 1,15 C 3-6; day 1 C >6)
• Carfilzomib (20) 56 mg/m2 Days 1,8,15
• Lenalidomide 25 mg Days 1-21
• Dexamethasone 40mg PO Days 1,8,15,22
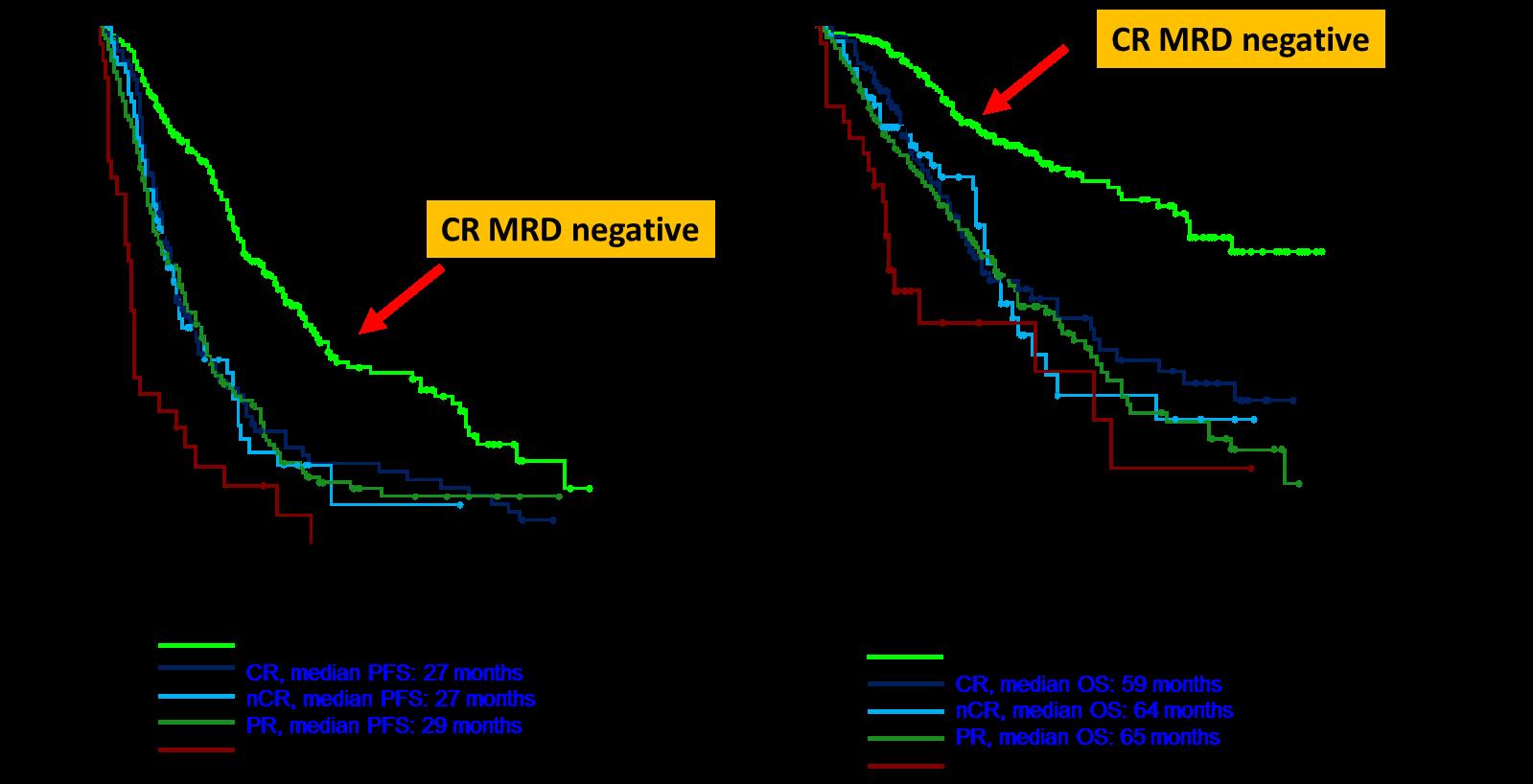
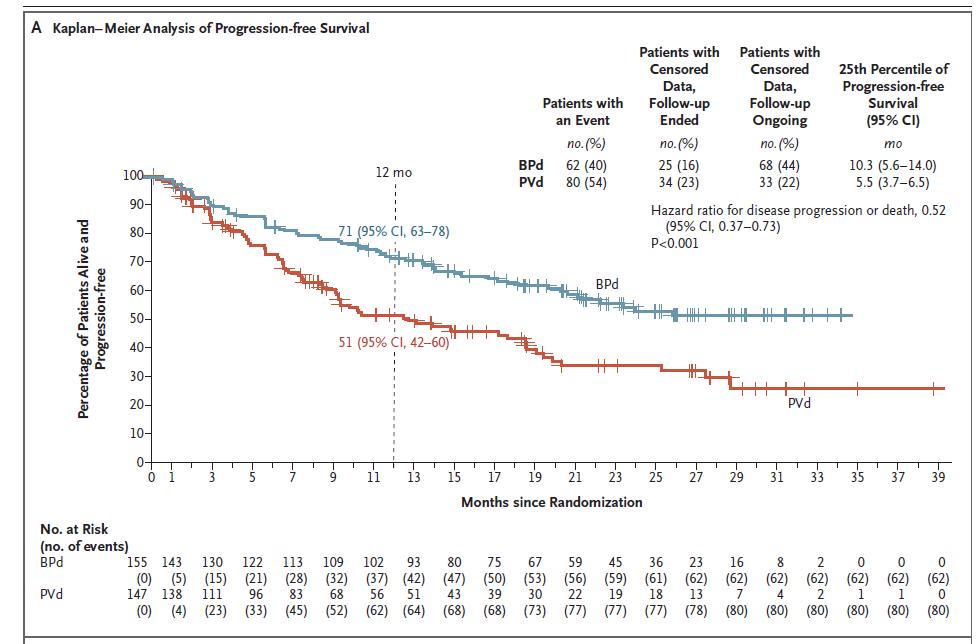
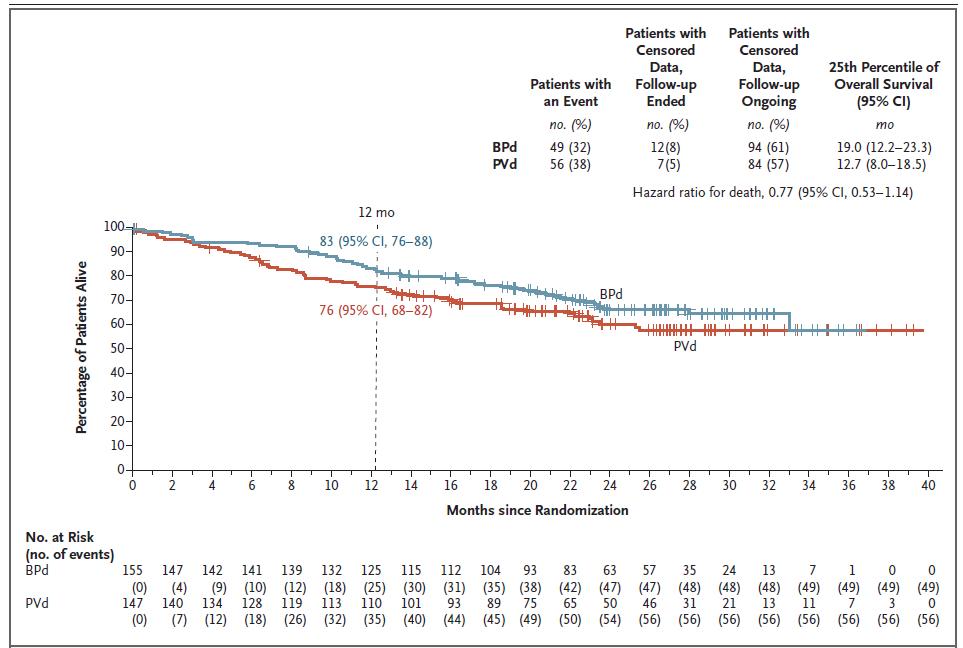
Progression-Free and Overall Survival
Frontline
Therapy and Transplant - Conclusions
• We are transitioning to quadruplets in frontline eligible patients
• BUT the optimal length of a quadruplet is still to be determined!
• Transplant still has a role in MM even with long term use of novel agents
• Consolidation therapy may deepen responses and should be considered in patients who have not achieved VGPR
• MRD guided discontinuation may be possible in lower risk groups but not high risk patients
How do we decide who is eligible for transplant?
ASCO: What criteria are used to assess eligibility for autologous stem cell transplant (SCT)?
Recommendation
Patients should be referred to a transplant center to determine transplant eligibility
• PFS 52.8 months for lenalidomide vs 23.5 in placebo
• PFS2 also prolonged 73.3 months vs 56.7 (ie not creating more aggressive clone)
• Median overall survival: 86 months v. not reached: P = 0.001
• Benefit for ≤ PR as well as VGPR/CR patients
• 29% discontinuation rate with lenalidomide
• Second primary malignancy rate higher at 6.1% vs 2.8% in placebo after PD
Induction
Treated on Myeloma XI induction protocols
N=1551 (TE=828; TNE=723)
Maintenance
10 mg/day, days 1‒21/28
Observation
Median follow-up: 27 months (IQR 13‒43)
Exclusion criteria
• Failure to respond to lenalidomide as induction IMiD, or development of PD
• Previous or concurrent active malignancies Lenalidomide
Overall PFS
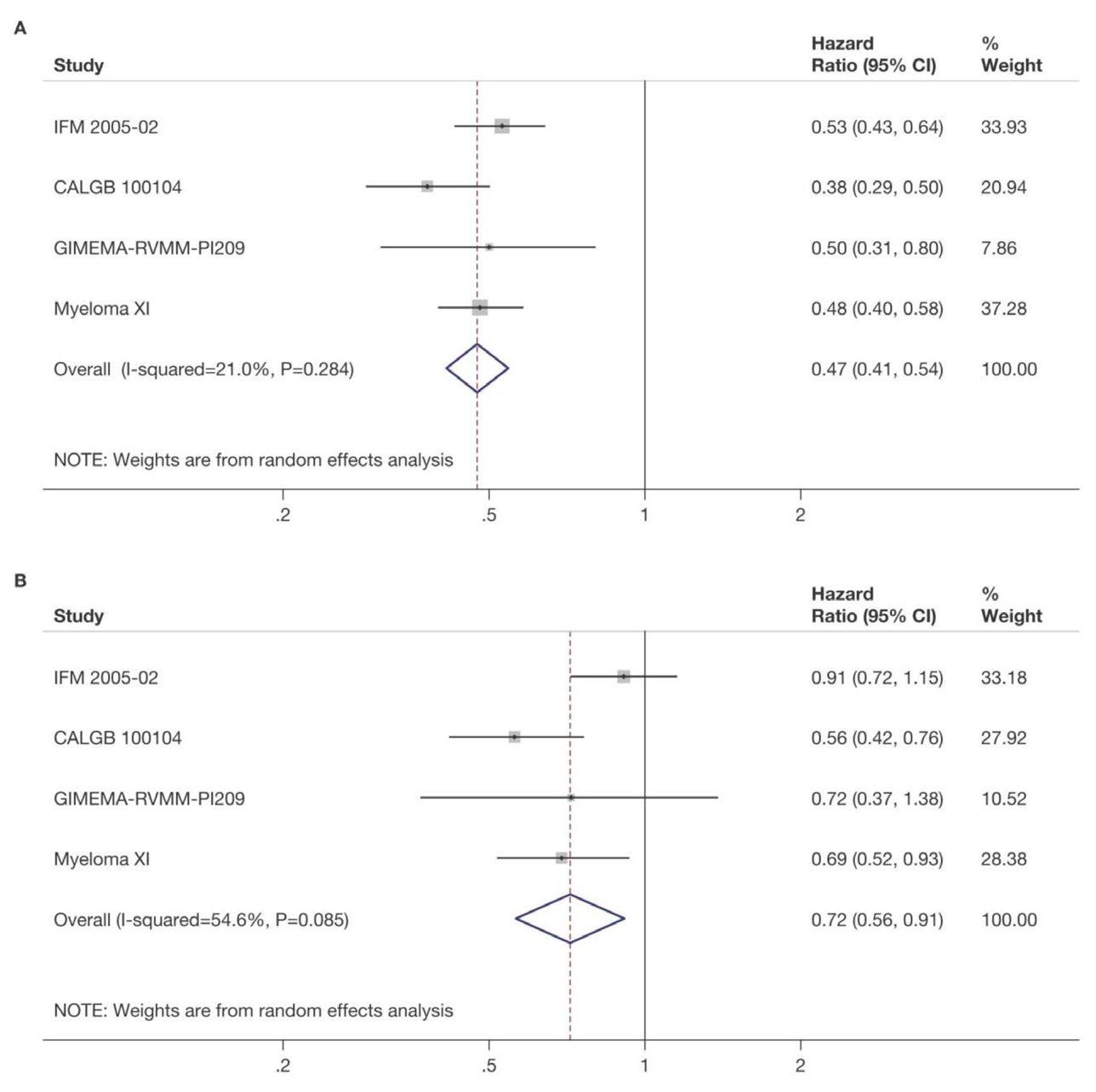
Significant improvement in PFS from 18 to 36 months, HR=0.45
Median PFS, months [95% CI]
Lenalidomide (n=857) 36 [31, 39]
Observation (n=694) 18 [16, 20]
Meta-analysis of all four randomized studies evaluating lenalidomide maintenance
But can we do better than lenalidomide alone?
FORTE Trial design
474 NDMM patients, transplant-eligible and younger than 65 years
4x KCd
K: 36^ mg/m2 d 1-2,8-9,15-16
C: 300 mg/m2 d 1,8,15
d: 20 mg. d 1-2,8-9,15-16,22-23
4x KRd
K: 36^ mg/m2 d 1-2,8-9,15-16
R: 25 mg d 1-21
d: 20 mg. d 1-2,8-9,15-16,22-23
Intensification with high-dose melphalan followed by autologous stem-cell reinfusion
4x KCd
K: 36 mg/m2 d 1-2,8-9,15-16
C: 300 mg/m2 d 1,8,15
d: 20 mg. d 1-2,8-9,15-16,22-23
R: 10 mg days 121, until progression or intolerance
4x KRd
K: 36 mg/m2 d 1-2,8-9,15-16
R: 25 mg d 1-21
d: 20 mg. d 1-2,8-9,15-16,22-23
4x KRd
K: 36^ mg/m2 d 1-2,8-9,15-16
R: 25 mg d 1-21
d: 20 mg. d 1-2,8-9,15-16,22-23
4x KRd
K: 36 mg/m2 d 1-2,8-9,15-16
R: 25 mg d 1-21
d: 20 mg. d 1-2,8-9,15-16,22-23
4x KRd
K: 36 mg/m2 d 1-2,8-9,15-16
R: 25 mg d 1-21
d: 20 mg. d 1-2,8-9,15-16,22-23
K: 36 mg/m2 d 1, 2, 15, 16 up to 2 years*
R: 10 mg days 1-21, until progression or intolerance
^20 mg/m2 on days 1-2, cycle 1 only. *Carfilzomib 70 mg/m2 days 1, 15 every 28 days up to 2 years for patients that have started the maintenance treatment from 6 months before the approval of Amendment 5.0 onwards.
Median follow-up from Random 1: 51 months (IQR 46‒55)
Median follow-up from Random 2: 37 months (IQR 33‒42)
KRd_ASCT vs. KCd_ASCT: HR 0.54, 95% CI 0.38-0.78, p<0.001
KRd_ASCT vs. KRd12: HR 0.61, 95% CI 0.43-0.88, p=0.0084 KRd12 vs. KCd_ASCT: HR 0.88, 95% CI 0.64-1.22, p=0.45 KR vs. R: HR 0.64, 95% CI 0.44-0.94, p=0.02294
3-year PFS reported in the figure. Random 1, first randomization (induction/consolidation treatment); ASCT, autologous stem-cell trasplantation; K, carfilzomib; R, lenalidomide; C, cyclophosphamide; d, dexamethasone; KCd_ASCT, KCd induction-ASCT-KCd consolidation; KRd_ASCT, KRd induction-ASCT-KRd consolidation; KRd12, 12 cycles of KRd; Random 2, second randomization (maintenance treatment); p, p-value; HR, hazard ratio; CI, confidence interval.
Progression-free survival: Random 2
KR vs. R
3-year
Conclusions about FORTE
• It appears that dual maintenance therapy prolongs PFS
• This occurs in both standard risk AND high risk patients
• It further opens the door to other dual maintenance strategies currently being used and explored:
• Lenalidomide + Bortezomib
• Lenalidomide + Ixazomib
• Lenalidomide + Daratumumab
• Others??
What about Daratumumab?
• CASSIOPEIA randomized pts to no maintenance vs dara q 8 weeks
• Overall there was a benefit to having dara maintenance vs placebo
• However, if dara had been given at induction, that benefit did not seem to continue (ie If you had dara upfront, it didn’t add more to maintenance)
• However, PERSEUS added Dara to Lenalidomide for up to 2 years based on sustained MRD status
Daratumumab (DARA) + Bortezomib/Lenalidomide/ Dexamethasone (VRd) With DARA-R (D-R)
Maintenance in Transplant-eligible Patients With Newly Diagnosed Multiple Myeloma (NDMM):
Analysis of Minimal Residual Disease (MRD) in the PERSEUS Trial*
*ClinicalTrials.gov Identifier: NCT03710603; sponsored by EMN in collaboration with Janssen Research & Development, LLC.
Paula Rodriguez-Otero1, Philippe Moreau2, Meletios A Dimopoulos3, Meral Beksac4, Aurore Perrot5, Annemiek Broijl6, Francesca Gay7, Roberto Mina7, Niels WCJ van de Donk8, Fredrik Schjesvold9, Michel Delforge10, Hermann Einsele11, Andrew Spencer12, Sarah Lonergan6, Diego Vieyra13, Anna Sitthi-Amorn13, Robin Carson13, Joan Bladé14, Mario Boccadoro15, Pieter Sonneveld6
1Department of Hematology, Cancer Center Clínica Universidad de Navarra, Pamplona, Navarra, Spain; 2Hematology Department, University Hospital Hôtel-Dieu, Nantes, France; 3National and Kapodistrian University of Athens, Athens, Greece; 4Ankara University, Ankara, Turkey; 5CHU de Toulouse, IUCT-O, Université de Toulouse, UPS, Service d’Hématologie, Toulouse, France; 6Department of Hematology, Erasmus MC Cancer Institute, Rotterdam, The Netherlands; 7Division of Hematology 1, AOU Città della Salute e della Scienza di Torino, and Department of Molecular Biotechnology and Health Sciences, University of Torino, Torino, Italy; 8Department of Hematology, Amsterdam University Medical Center, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands; 9Oslo Myeloma Center, Department of Hematology, and KG Jebsen Center for B-cell Malignancies, University of Oslo, Oslo, Norway; 10University of Leuven, Leuven, Belgium; 11Department of Internal Medicine II, University Hospital Würzburg, Würzburg, Germany; 12Malignant Haematology and Stem Cell Transplantation Service, Alfred Health-Monash University, Melbourne, Australia; 13Janssen Research & Development, LLC, Spring House, PA, USA; 14Hospital Clínic de Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), University of Barcelona, Barcelona, Spain; and GEM/PETHEMA; 15Myeloma Unit, Division of Hematology, University of Torino, Azienda Ospedaliero-Universitaria Città della Salute e della Scienza di Torino, Torino, Italy
Presented by P Rodriguez-Otero at the American Society of Clinical Oncology (ASCO) Annual Meeting; May 31-June 4, 2024; Chicago, IL, USA
R: 25 mg PO Days 1-21 d: 40 mg PO/IV Days 1-4, 9-12
R: 25 mg PO Days 1-21 d: 40 mg PO/IV Days 1-4, 9-12
DARA: 1,800 mg SCb QW Cycles 1-2 Q2W Cycles 3-4
VRd administered as in the VRd group
D-VRd
DARA: 1,800 mg SCb Q2W
VRd administered as in the VRd group
D-R
: 1,800 mg SCb Q4W R: 10 mg PO Days 1-28
Restart DARA per criteria Minimum 2 y
Primary endpoint: PFSc
Key secondary endpoints: Overall ≥CR rate,c overall MRD-negativity rate,d OS
Stop DARA therapy
after ≥24 months of D-R maintenance for patients with ≥CR and 12 months of sustained MRD negativity (10–5)
Restart DARA therapy upon confirmed loss of CR without PD or recurrence of MRD
MRD-negativity rate was defined as the proportion of patients who achieved both MRD negativity and ≥CR in the ITT population. Patients who were not evaluable or had indeterminate results were considered MRD positive.
ECOG PS, Eastern Cooperative Oncology Group performance status; V, bortezomib; SC, subcutaneous; PO, oral; d, dexamethasone; IV, intravenous; QW, weekly; Q2W, every 2 weeks; PD, progressive disease; Q4W, every 4 weeks; ISS, International Staging System; rHuPH20, recombinant human hyaluronidase PH20; IMWG, International Myeloma Working Group; VGPR, very good partial response. aStratified by ISS stage and cytogenetic risk. bDARA 1,800 mg co-formulated with rHuPH20 (2,000 U/mL; ENHANZE drug delivery technology, Halozyme, Inc., San Diego, CA, USA). cResponse and disease progression were assessed using a computerized algorithm based on IMWG response criteria. dMRD was assessed using the clonoSEQ assay (v.2.0; Adaptive Biotechnologies, Seattle, WA, USA) in patients with ≥VGPR post-consolidation and at the time of suspected ≥CR. Overall, the MRD-negativity rate was defined as the proportion of patients who achieved both MRD negativity (10–5 threshold) and ≥CR at any time.
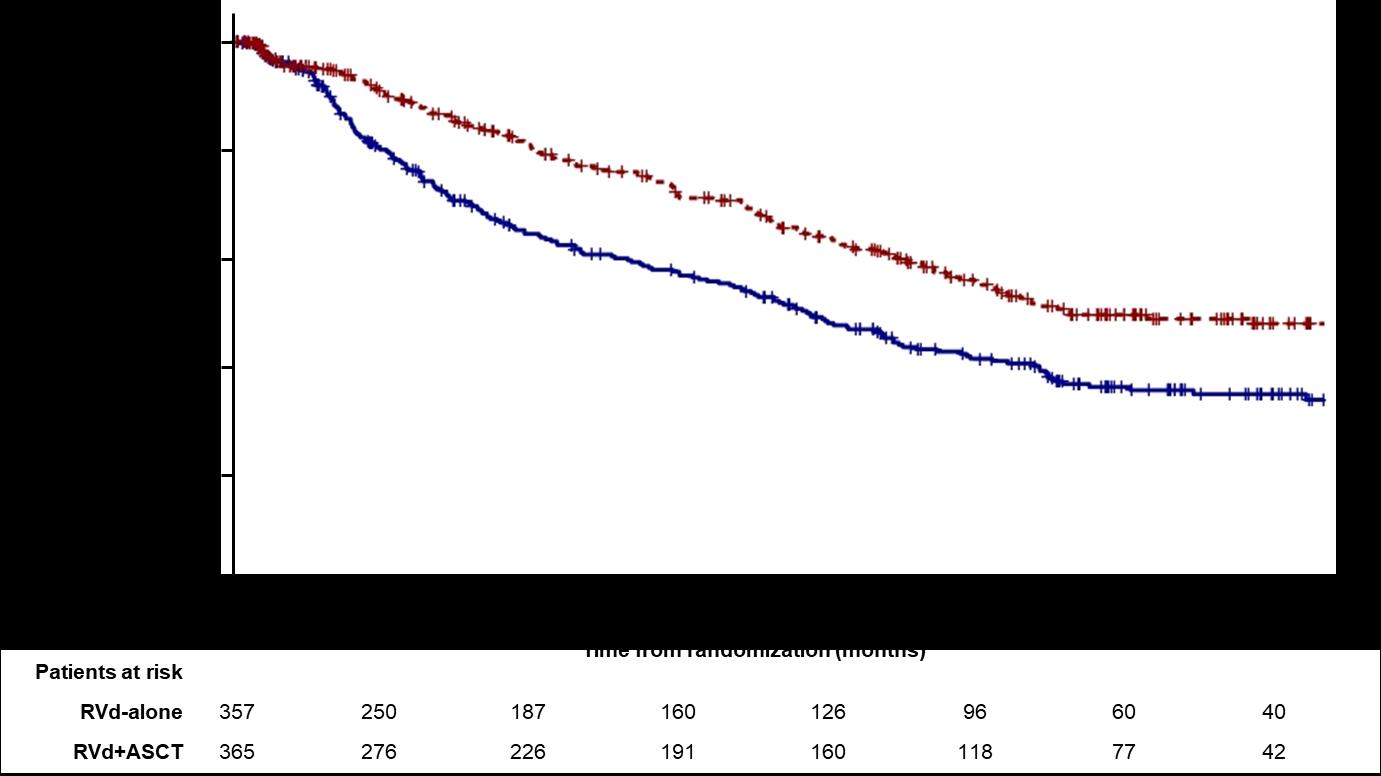
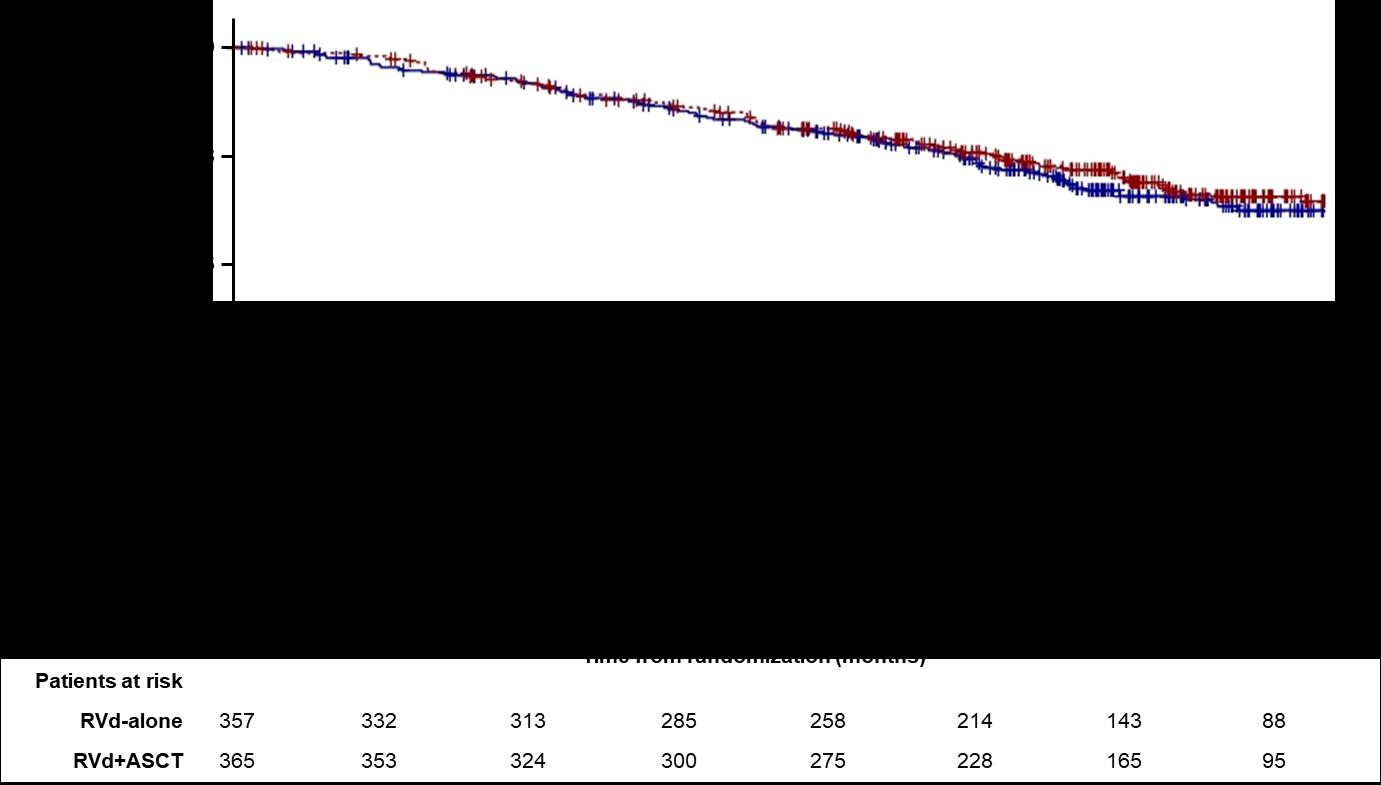
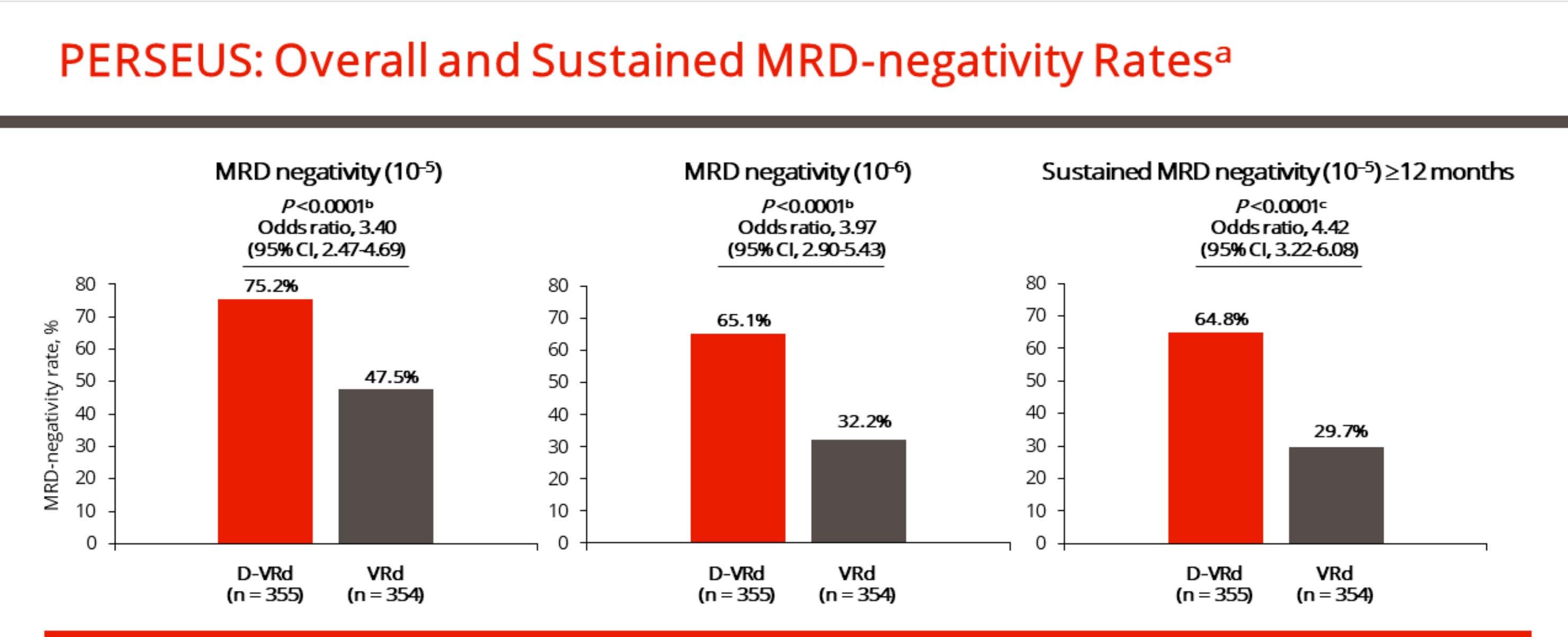
PERSEUS Primary Analysis: D-VRd Followed by D-R Maintenance Significantly Improved PFS and Depth of Response Versus VRd Followed
by R
HR, hazard ratio; CI, confidence interval. aMRD-negativity rate was defined as the proportion of patients who achieved both MRD negativity and ≥CR. MRD was assessed using bone marrow aspirates and evaluated via NGS (clonoSEQ assay, version 2.0; Adaptive Biotechnologies, Seattle, WA, USA). bP values were calculated with the use of the stratified Cochran–Mantel–Haenszel chi-square test. cP value was calculated with the use of Fisher’s exact test.
1. Sonneveld P, et al. N Engl J Med. 2024;390(4):301-313.
PERSEUS: Conclusions From Analysis of MRD
• The potential for a cure in NDMM is predicated on reaching sustained MRD negativity at 10–6
• In the PERSEUS study, for D-VRd + D-R:
– 47% of patients achieved sustained MRD negativity (10–6) for 12 months versus 19% with VRd + R
– In high-risk patients: 58% of patients achieved MRD negativity (10–6) and 30% achieved sustained MRD negativity (10–6) versus 31% and 14%, respectively, with VRd + R
• During D-R maintenance:
– The rate of MRD negativity (10–6) increased by 30% versus 15% with R alone
– 31% of MRD-positive patients converted to sustained MRD negativity (10–6) versus 10% with R alone
– 64% of patients stopped DARA after achieving sustained MRD negativity (10–5)1
These data further highlight the benefit of D-VRd and D-R maintenance as a new standard of care for transplant-eligible patients with NDMM
AURIGA: Study Design
• Objective: To determine the impact of adding DARA to R maintenance on MRD-negative conversion
Key eligibility criteria
• 18-79 years of age
• NDMM with ≥4 cycles of induction therapy and underwent ASCT within 12 months of the start of induction
• ≥VGPR at screeninga
• MRDb positive (10–5) post-ASCT
• No prior anti-CD38
• Randomization within 6 months of ASCT date
Stratification factor
• Cytogenetic riskc (standard risk/unknown vs high risk)
Maintenance: up to 36 cyclesd (28-day cycles)
1,800 mg SCe QW Cycles 1-2, Q2W Cycles 3-6, Q4W Cycles 7+ R: 10 mg PO daily Days 1-28 (after Cycle 3, 15 mg PO daily if tolerated)
Primary endpoint
• MRD-negative (10–5) conversion rate from baseline to 12 months after maintenance treatment
• N = 214 planned to achieve ≥85% power to detect 20% improvement
Secondary endpoints
10 mg PO daily Days 1-28 (after Cycle 3, 15 mg PO daily if tolerated)
VGPR, very good partial response; D, daratumumab; SC, subcutaneous; QW, weekly; Q2W, every 2 weeks; Q4W, every 4 weeks; PO, orally; CR, complete response. aAs assessed by International Myeloma Working Group 2016 criteria. bMRD based upon NGS (clonoSEQ®; Adaptive Biotechnologies). cFor stratification, cytogenetic risk was evaluated per investigator assessment, in which high risk was defined as the presence of ≥1 of the following cytogenetic abnormalities: del[17p], t[4;14], or t[14;16]. dStudy treatment continued for a planned maximum duration of 36 cycles or until progressive disease, unacceptable toxicity, or withdrawal of consent. After the end of the
AURIGA:
MRD-negative (10‒5)
Conversion
Rate From Baseline to 12 Months of Maintenance Treatmenta
• The addition of DARA to R more than doubled the MRD-negative conversion rate by 12 months • Similar benefits were seen in supplemental MRD analyses
AURIGA: Conclusions
• In TE patients with NDMM who were anti-CD38 naïve and MRD positive post-ASCT,
D-R maintenance versus R alone resulted in:
– More than doubling of the MRD-negative conversion rate by 12 months and overall at 10–5
– Improved MRD-negative conversion rates by 12 months across subgroups and disease risk status at 10–5
– More than doubling of ≥6-month sustained MRD-negative rate at 10–5
– Quadrupling of MRD-negative conversion rate by 12 months at 10–6
– Further deepening of response rates
– 47% reduction in the risk of disease progression or death, with a 30-month PFS rate of 83%
– No new safety concerns
How long should maintenance last?
Defining the optimum duration of lenalidomide maintenance after autologous stem cell transplant
data from the Myeloma XI trial.
Charlotte Pawlyn1,2, Tom Menzies3, Faith Davies4, Ruth de Tute5, Rowena Henderson3, Gordon Cook3,6, Matthew Jenner7, John Jones8, Martin Kaiser1,2, Mark Drayson9, Roger Owen8, David Cairns3, Gareth Morgan4, Graham Jackson10
1) The Institute of Cancer Research, London, UK; 2) The Royal Marsden Hospital, London, UK; 3) Clinical Trials Research Unit, Leeds Institute of Clinical Trials Research, University of Leeds, Leeds, UK; 4) Perlmutter Cancer Center, NYU Langone Health, New York, US; 5) HMDS, Leeds Cancer Centre, Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom; 6) Leeds Cancer Centre, Leeds Teaching Hospitals NHS Trust, Leeds, UK; 7) University Hospital Southampton NHS Foundation Trust, Southampton, UK; 8) Kings College Hospital NHS Foundation Trust, London, UK; 9) Institute of Immunology and Immunotherapy, University of Birmingham, Birmingham, UK; 10) Department of Haematology, University of Newcastle, Newcastle-upon-Tyne, UK
On behalf of the Myeloma XI Trial Management Group and NCRI Haem-Onc Clinical Studies Group
Multiple landmark analyses
Conclusions
• These data suggest an ongoing PFS benefit associated with continuing lenalidomide maintenance beyond at least 4-5 years in the overall patient population
• Even in patients with sustained MRD negativity, there is evidence of benefit from continuing lenalidomide maintenance for at least 3 years in total
• Randomised trials to address the impact of stopping lenalidomide maintenance in patients with sustained MRD negativity could be considered, at no earlier than 3 years
• In patients who are MRD +ve these data support continuing lenalidomide until disease progression
• No evidence of cumulative haematological toxicity was identified
• These findings emphasise the need for long term follow up of maintenance studies to enable the exploration of such questions
• There is a planned powered OS update of Myeloma XI in 2023
Commonly asked maintenance questions
• Should post-transplant maintenance therapy be recommended for all patients?
• Yes
• Which agent should be used?
• Lenalidomide remains the standard of care – we may be adding daratumumab soon
• What is the optimal duration?
• Treatment until progression remains the standard of care
• What should patients with high-risk cytogenetics receive?
• Consider lenalidomide + proteasome inhibitor or daratumumab; clinical trial
• Should MRD status dictate maintenance therapy?
• Not outside of a clinical trial
• What about Second Primary Malignancies?
• They are real, require a discussion and monitoring, but are outweighed by benefit
Relapsed Therapies & Clinical Trials
Joseph Mikhael, MD
International Myeloma Foundation
Objectives
• Discuss an approach to treating relapsed myeloma based on patient, disease and treatment characteristics
• Review the important trend of using an aggressive approach in early treatment of myeloma
• Outline the key results from recent trials in early relapse
• Discuss the approach to late relapse and the use of novel therapies such as CAR T and bispecific antibodies
Early lines treatment are important!
1st Relapse 2nd 3rd 4th 5th and beyond
Fewer patient are eligible for therapy in each subsequent line of therapy (LOT)
Figure adapted from: Yong, K et al. Br J Haematol 2016;175(2):252-264
An Approach to Relapsed MM
• It is not a simple algorithm of treatment #1 then 2 then 3…
• Leverage the benefit of multiple mechanisms of action in combination therapy
Categories:
• 1-3 prior lines
• Later Relapse
• Refractory to PI, IMiD and MoAb = Triple Class Refractory
Principles
1. Depth of Response matters…likely incorporate MRD soon 2. High risk vs standard risk…more aggressive Rx in high risk
3. Balance efficacy and toxicity…initially and constantly assess
4. Overcome drug resistance…change mechanism of action when possible
Definitions: What is relapsed/refractory disease and a line of therapy?
• Relapsed: recurrence (reappearance of disease) after a response to therapy
• Refractory: progression despite ongoing therapy
• Progression: change in M protein/light chain values
• Line of therapy: change in treatment due to either progression of disease or unmanageable side effects
• Note: initial (or induction) therapy + stem cell transplant + consolidation/ maintenance therapy = 1 line of therapy
1. Therapies change over time—clinical trials make this possible
2. Outcomes (e.g. survival) changes over time, as new therapies emerge
3. If one therapy did not work well, it doesn’t mean another won’t
4. Terms like “overall survival” and “progression free survival” typically refer to statistical probabilities for GROUPS of people and do not seal the fate of an INDIVIDUAL
5. At a given point in time, there may not be a known “right answer;” hence many opinions
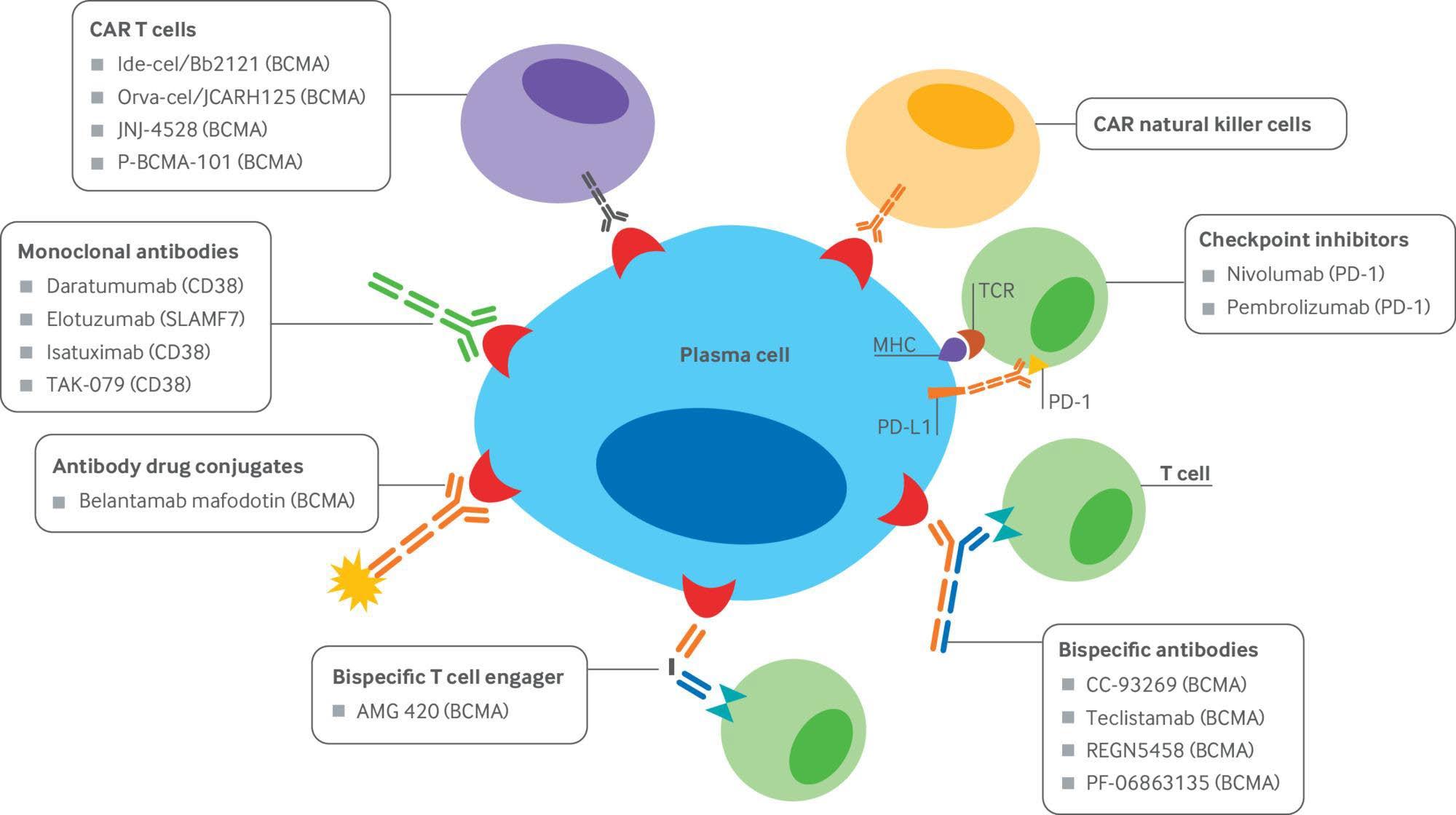
Pillars of Myeloma therapy
Emerging immunotherapies in multiple myeloma
Modified from: Shah A, Mailankody S. BMJ 2020; 370
Carvykti
Talquetamab (CPRC5D)
Cevostamab (FcRH5)
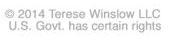
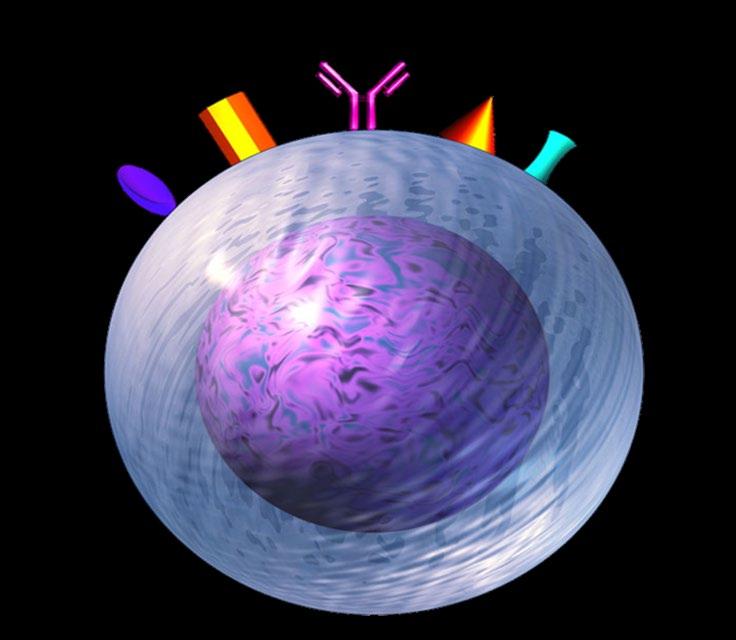
NAKED ANTIBODIES
Examples:
1. Daratumumab (Darzalex) — recognizes CD38
2. Isatuximab (Sarclisa) — recognizes CD38
3. Elotuzumab (Empliciti) — recognizes SLAMF7
Naked monoclonal antibody
Cancer cell
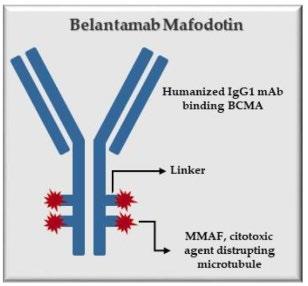
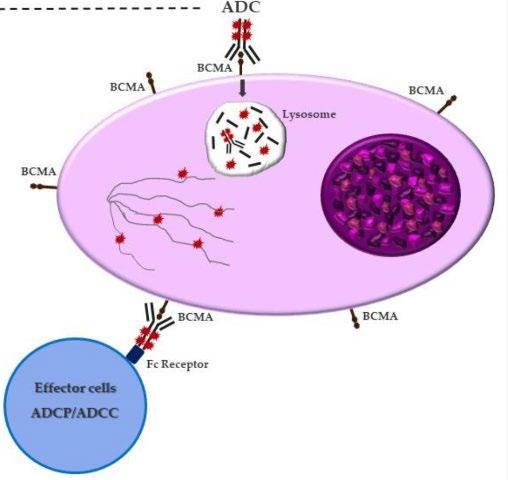
ANTIBODY DRUG CONJUGATE
Belantamab mafodotin
— recognizes
IS BLENREP (BELANTAMAB) COMING
BACK?
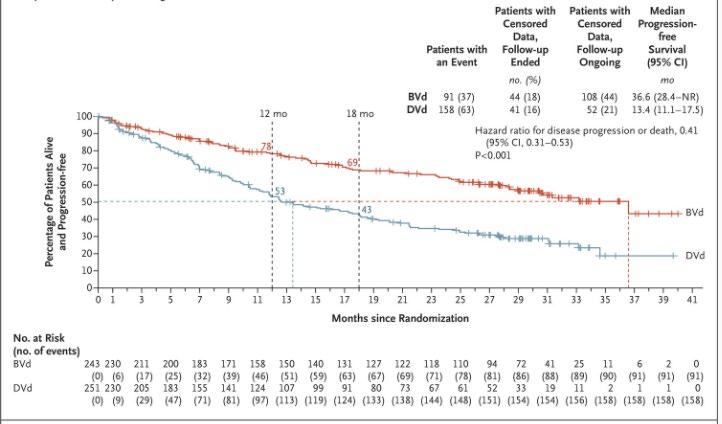
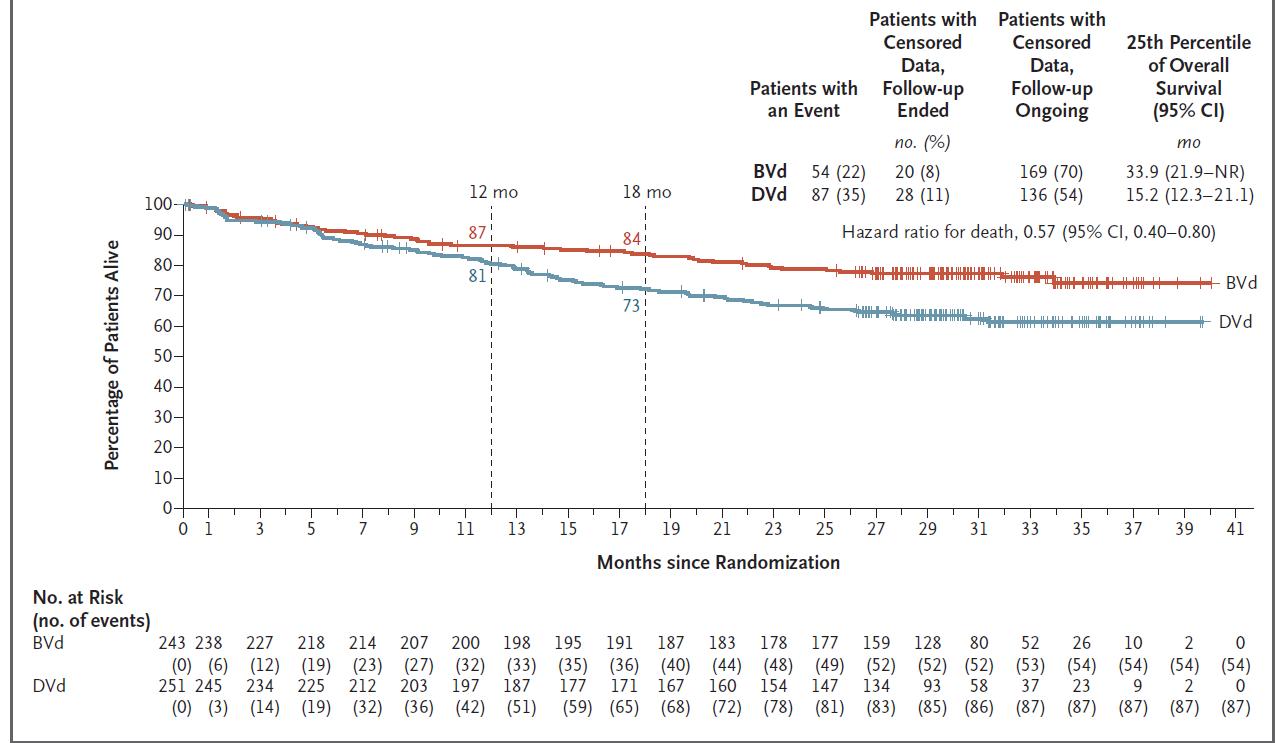
DREAMM 7: Velcade-Dex with Belantamab or daratumumab
Not Plasma Cell Leukemia (PCL) or Similar extramedullary disease (EMD)
Triple Class Refractory, Type 1*
Refractory to:
• Bortezomib
• Lenalidomide
• Anti-CD38 moAB
Off-Study Treatment Options
Triple Class Refractory, Type 2*
Refractory to:
• Bortezomib and Carfilzomib
• Lenalidomide
• Anti-CD38 moAB
Triple Class Refractory, Type 3*
Refractory to:
• Bortezomib & Carfilzomib
• Lenalidomide & Pomalidomide
• Anti-CD38 moAB
# Listed regimens are not in the order of preference
Venetoclax-based therapy if t(11;14)
Bispecific Antibody
Venetoclax-based therapy if t(11;14)
*Auto transplant is an option, if transplant candidate and feasible; **If known to be refractory to Daratumumab as single agent, use elotuzumab instead
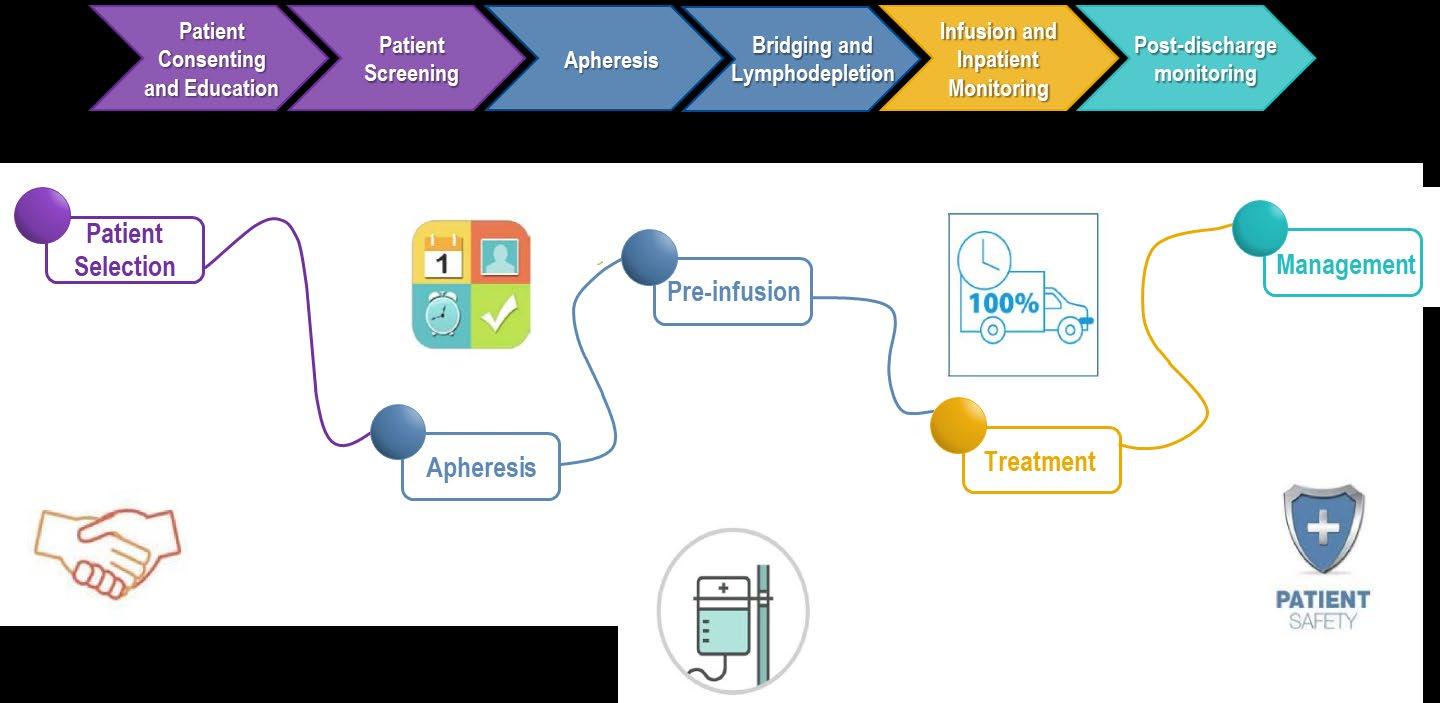
CAR T-Cell Therapy Patient Journey
Fludarabine and Cytoxan are used to create “immunologic space”
Onset 1 9 days after CAR T-cell infusion 2 9 days after CAR T-cell infusion
Duration 5 11 days 3 17 days
Symptoms
• Fever
• Difficulty breathing
• Dizziness
• Nausea
• Headache
• Rapid heartbeat
• Low blood pressure
Management
• Actemra (tocilizumab)
• Corticosteroids
• Supportive care
• Headache
• Confusion
• Language disturbance
• Seizures
• Delirium
• Cerebral edema
• Antiseizure medications
• Corticosteroids
*Based on the ASTCT consensus; †Based on vasopressor; ‡For adults and children >12 years; §For children ≤12 years; ‖Only when concurrent with CRS
Xiao X et al. J Exp Clin Cancer Res. 2021;40(1):367. Lee DW et al. Biol Blood Marrow Transplant. 2019;25:625; Shah N et al. J Immunother Cancer. 2020;8:e000734.
Bispecific and Trispecific Antibodies
There are currently 3 approved bispecific antibodies:
Teclistamab (Tecvayli)
Talquetamab (Talvey)
Elranatamab (Elrexfio)
Bispecific Antibodies
Bispecific antibodies are also referred to as dual specific antibodies, bifunctional antibodies, or T-cell engaging antibodies
Bispecific antibodies can target two cell surface molecules at the same time (one on the myeloma cell and one on a T cell)
Many different bispecific antibodies are in clinical development; none are approved for use in myeloma
Availability is off-the-shelf, allowing for immediate treatment
Cohen A et al. Clin Cancer Res. 2020;26:1541.
BCMA, GPRC5D, or FcRH5
Examples:
• Elranatamab
• Teclistamab
• TNB-303B (ABBV-383)
• REGN5458
• Cevostamab
• Talquetamab
Bispecific Antibodies: Expected Toxicities
• Cytokine release syndrome (CRS)
• Neurotoxicity (ICANS)
• Usually occurs within first 1–2 weeks
• Frequency (all grade and grade 3–5) higher with CAR T
• Cytopenias
• Target unique
• For example, rash, taste disturbance seen with GPRC5D, but not with BCMA
Similarities and Differences Between CAR T-Cell Therapy and Bispecific Antibodies
CAR T-cell therapy Bispecific antibody
Approved product
How given One-and-done
Where
Notable
IV or SC, weekly to every 3 weeks until progression
Key Points – CAR T and Bispecifics
CAR T and bispecific antibodies are very active even in heavily pretreated patients.
Side effects of CAR T cells and bispecific antibodies include cytokine release syndrome, confusion, and low blood counts, all of which are treatable.
Abecma and Carvykti are only the first-generation CAR T cells and target the same protein. Different CAR Ts and different targets are on the way.
Bispecific antibodies represent an “off-the-shelf” immunotherapy; Tecvayli was approved in October 2022, and now Talvey and Elrexfio in August 2023
Several additional bispecific antibodies are under clinical evaluation.
Refractory MM
Refractory to IMIDs (Lenalidomide and Pomalidomide), PIs
Bortezomib and Carfilzomib), Alkylators, CD38, and BCMA
Options
• Talquetamab
• Another anti-BCMA treatment approach
• Other non-BCMA immunotherapy (eg., cevostamab on clinical trial)
• Selinexor-based regimen
• VDT-PACE
• Alkylator or Bendamustine-based regimens
*CVAD or similar regimen can be used in place of VDT-PACE in older patients or patients with poor functional status
Emerging Therapies for
Relapsed/Refractory
Multiple Myeloma
Bispecific antibodies
• Cevostamab, Alnuctamab, ABBV383, and others
• Target BCMA, GPRC5D, or FcRH5 on myeloma cells and CD3 on T cells
• Redirects T cells to myeloma cells
Cereblon E3 ligase modulators (CELMoDs)
• Iberdomide
• Targets cereblon
• Enhances tumoricidal and immune-stimulatory effects compared with immunomodulatory agents
Small molecule inhibitors
• Venetoclax
• Targets Bcl-2
• Induces multiple myeloma cell apoptosis
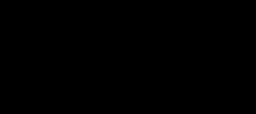
The Evolution of Myeloma Therapy
Bortezomib
Lenalidomide
Carfilzomib
VTD
VRD KRD
D-VRD
D-KRD
Isa-KRD
SCT +/- More induction
Lenalidomide
Bortezomib
Ixazomib
Lenalidomide + PI
Carfilzomib
Combinations
Pomalidomide
Selinexor
Panobinostat
Daratumumab
Ixazomib
Elotuzumab
Isatuximab
Idecabtagene autoleucel
Ciltacabtagene autoleucel
Teclistamab
Talquetamab
Elranatamab
New
Isa-VRD
D-KRD
ASCT,
CAR T or Bispecifics?
Daratumumab?
Novel CAR T Cell Therapies
Bispecific/Trispecific Antibodies
CelMod Agents
Venetoclax?
Belantamab soon?
Multiple small molecules ++++++++
autologous stem cell transplant; CAR, chimeric antigen receptor; Cy, cyclophosphamide; d- daratumumab; D/dex, dexamethasone; isa, isatuximab; K, carfilzomib; M, melphalan; PD-L1, programmed death ligand-1; PI, proteasome inhibitor; Rev, lenalidomide; V, bortezomib. Speaker’s own opinions.
Clinical Trials
Remember some of the important principles of clinical trials:
• The drive of research has brought us to where we are
Clinical TrialsOverview
• No one is expected to be a “guinea pig” with no potential benefit to them
• Research is under very tight supervision and standards
• Open, clear communication between the physician and the patient is fundamental
Clinical Trials –Why Me??
• Every patient is unique and must be viewed that way
• Benefits of trials are numerous and include:
• Early access to “new” therapy
• Delay use of standard therapy
• Contribution to myeloma world – present and future
• Financial access to certain agents
• Must be balanced with potential risks
• “Toxicity” of side effects
• Possibility of lack of efficacy
Clinical Trials Phases
ANIMAL STUDIES: Examine safety and potential for efficacy
FIRST INTRODUCTION OF AN INVESTIGATIONAL DRUG INTO HUMANS
Determine metabolism and PK/PD actions, MTD, and DLT
Identify AEs
Gain early evidence of efficacy, studied in many conditions; typically, 20 to 80 patients; everyone gets agent
EVALUATION OF EFFECTIVENESS IN A CERTAIN TUMOR TYPE
Determine short-term AEs and risks; closely monitored
Includes up to 100 patients, typically
GATHER ADDITIONAL EFFECTIVENESS AND SAFETY INFORMATION
COMPARED TO STANDARD OF CARE
Placebo may be involved if no standard of care exists; hundreds to several thousand patients
Often multiple institutions; single or double blind; sometimes open label
APPROVED AGENTS IN NEW POPULATIONS OR NEW DOSE FORMS
Why Do So Few Cancer Patients Participate in Trials?
Patients may:
• Be unaware of clinical trials
• Lack access to trials
• Fear, distrust, or be suspicious of research
• Have practical or personal obstacles
• Face insurance or cost problems
• Be unwilling to go against their physicians’ wishes
• Not have physicians who offer them trials
• Have a disconnect with their healthcare team
Diversity in Clinical Trials
There has been a lack of diverse representation in clinical trials in myeloma.
• In the U.S., approximately 20% of all myeloma patients are of African descent, but only 5%–8% of patients in myeloma clinical trials are of African descent.
This is significant for the following reasons:
• All patients of all races and ethnicities should be able to benefit from clinical trials.
• Diverse patient representation in clinical trials is required to ensure that the outcomes are applicable to all patients.
Reasons for underrepresentation in clinical trials are complex and include:
• systemic racism, accessibility of clinical trials, sensitivity to diversity by medical professionals
• misconduct in medicine in the past, the lack of trust in the system, and more.