
Welcome!

Thank you for joining us today for the March 2nd, 2024,
International Myeloma Foundation’s Regional Community Workshop –San Diego

Welcome!
Thank you for joining us today for the March 2nd, 2024,
International Myeloma Foundation’s Regional Community Workshop –San Diego







IMF Regional Community Workshop
March 2nd, 2024 - Agenda
9:00 – 9:15 AM
9:15 – 9:45 AM
Welcome & Introductions, Robin Tuohy
Myeloma 101, Autumn Jeong, MD
9:45 – 9:55 AM Q&A
9:55 – 10:40 AM
Taking the Reins of Your Multiple Myeloma Care, Sandra Rome,
RN, MN, AOCN, CNS
10:40 – 10:50 AM Q&A
10:50 – 11:00 AM
Coffee Break
11:00 – 11:45 AM Frontline Therapy, Rahul Banerjee, MD, FACP
11:45 – 11:55 AM Q&A
11:55 AM – 12:40 PM LUNCH
12:40 – 1:00 PM
1:00 – 1:10 PM
1:10 – 1:30 PM
1:30 – 1:40 PM
1:40 – 2:25 PM
2:25 – 2:35 PM
2:35 – 2:45 PM
2:45 – 3:00 PM
IMF Regional Community Workshop
March 2nd, 2024 – Agenda after lunch
Local Patient & Care Partner Panel, Becky Elliot, Patient & Doug Elliot, Care Partner
Q&A
Maintenance Therapy, Rahul Banerjee, MD, FACP
Q&A
Relapsed Therapies & Clinical Trials, Autumn Jeong, MD
Q&A
Closing Remarks
Coffee / Network
Multiple Myeloma affects patients and families. The IMF provides FREE resources to help both patients and families.
Established in 1990, the IMF’s InfoLine assists over 4600 callers annually and answers questions across a wide variety of topics including:

Frequent topics:
Treatment questions along the spectrum of care
Clinical Trial access and understanding
Side effect management and health issues
Financial resources for myeloma-related expenses
Myeloma Specialist Referral contact information
Support group information
Caregiver Support




A core mission of the IMF is to provide thorough and cutting-edge education to the New publications

The IMF Support Group Team is Here For You!
Shared Experiences Help to Better Understand the Myeloma Journey
• Support Groups Empower Patients & Care Partners with information, insight, & hope
• The IMF provides educational support to a network of over 150 myeloma specific groups

Support.myeloma.org

We are happy to help connect you with an existing support group or help form a new one! We assist with virtual, in-person, and hybrid options for meetings. Reach out to us at SGTeam@myeloma.org

Local Support Groups: You Are Not Alone!
San Diego Multiple Myeloma Support Group
Meets hybrid on the 2nd Monday of each month at 6:30PM
Inland Empire, CA
Myeloma Support Group
Meets hybrid on the 3rd Saturday of each month at 10:30AM
Orange County Myeloma Support Group
Meets in-person every other month & virtually the alternate months on the 1st Thursday of each month
Los Angeles Multiple Myeloma Support Group
Meets virtually on the 3rd Saturday of each month at 10:30AM

Santa Cruz Multiple Myeloma Support Group
Meets virtually on the 1st Monday of each month at 4:30PM
Rancho Mirage, CAEisenhower Lucy Curci Cancer Center
Myeloma Support Group
Meets virtually on the 1st Thursday of each month at 3PM
Local Support Groups: You Are Not Alone!
Myeloma Stompers (Napa/Sonoma)
Meets virtually on the 2nd Friday of each month at 10AM
San Gabriel Valley Myeloma Support Group
Meets in-person on the 1st Monday of each month at 6:30PM
San Francisco Bay Area Myeloma Support Group
Meets virtually on the 3rd Saturday of each month at 10AM

Upland, CA Myeloma Support Group
Meets hybrid on the 1st Friday of each month at 10AM
Sacramento Area Myeloma Support Group
Meets virtually on the 1st Saturday of each month at 10AM
San Fernando Valley Myeloma Support Group
Westlake Myeloma Support Group
Meets virtually on the 2nd Saturday of each month at 11AM
Meets in person on the 3rd Wednesday of each month at 7PM
Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
Las Voces de Mieloma
Designed for Spanish speaking patients
Living Solo & Strong with Myeloma
Designed for patients without a care partner

Coming Soon!
Care Partners Only
Designed to address the needs of care partners

Smolder Bolder
Created for people living with Smoldering Multiple Myeloma
MM Families

High Risk Multiple Myeloma
Designed to address the needs of the high-risk MM population
MGUS 4 Us
Created for people living with MGUS
For patients/care partners with young children



Autumn (Ah-Reum) Jeong, MD
Assistant Professor of Clinical Medicine
Division of Blood and Marrow Transplantation
UCSD Health

•Research funding from GPCR Therapeutics and Pfizer.
•Introduction to multiple myeloma (MM)
•Epidemiology
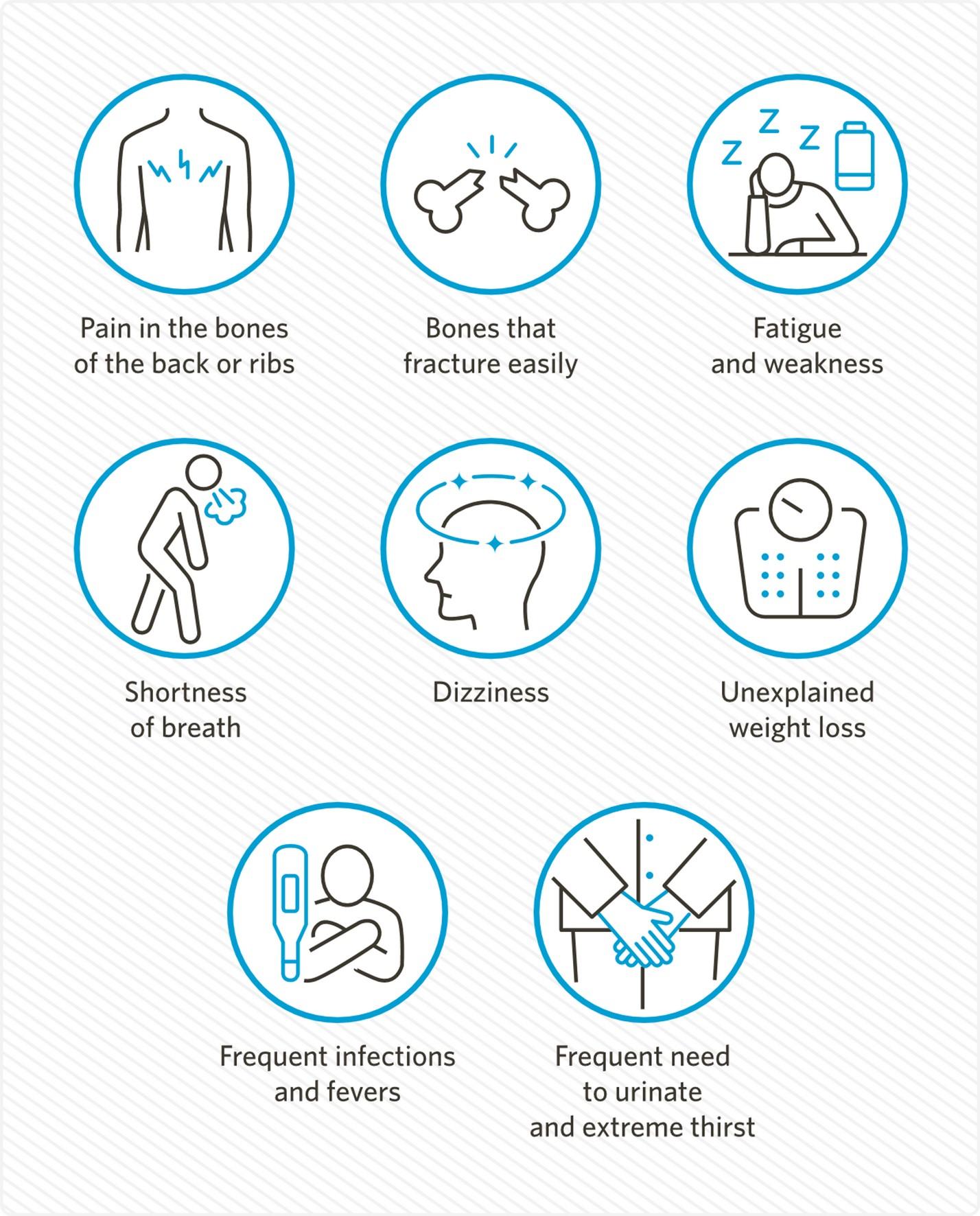
•Symptoms
•Diagnosis
•Prognosis
How are blood cells made? crab/
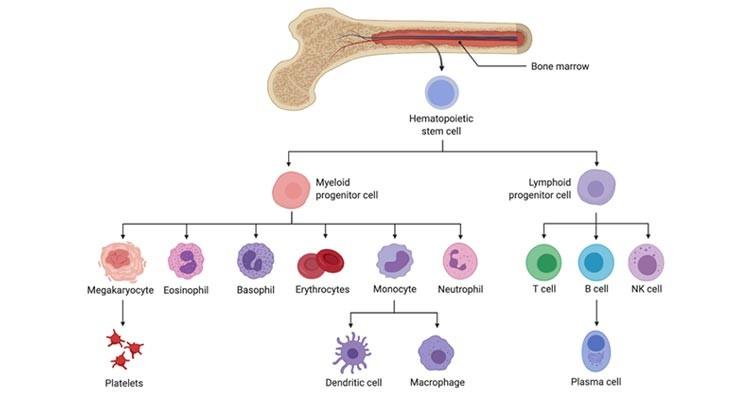


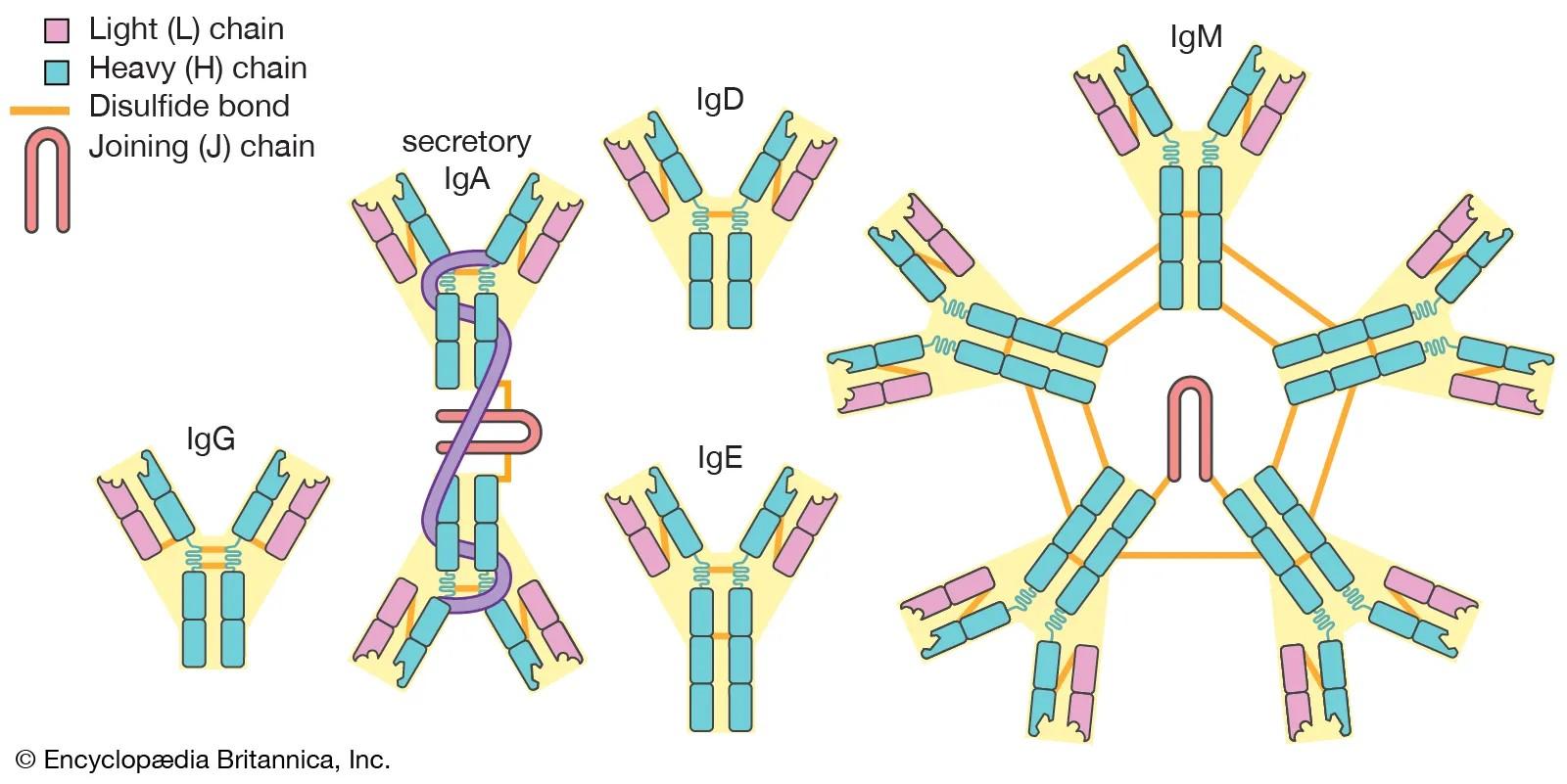
Plasma cells help fight infection by making antibodies (proteins)
https://badmanstropicalfish.com/arrowcrab/
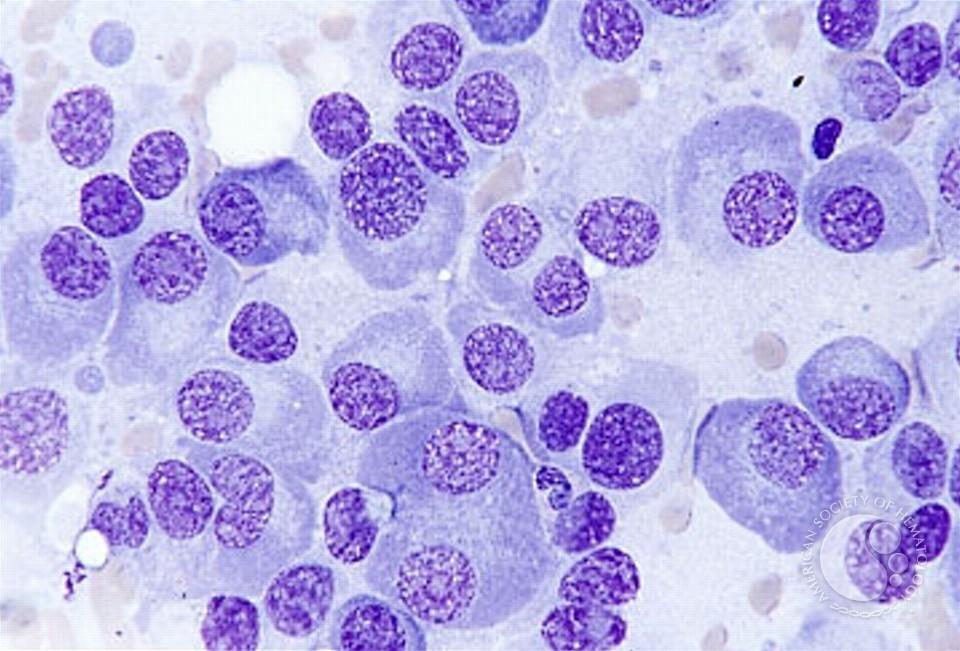
Multiple myeloma (MM) is a cancer of the plasma cells
Mutation

Lung cancer
Also called:
https://badmanstropicalfish.com/arrow-
Lung Cell Plasma Cell
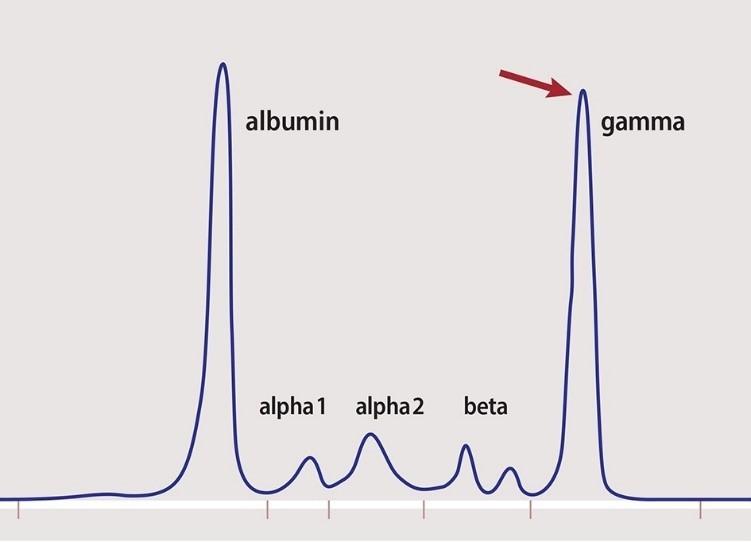
Immunoglobulins
M-spike
M-protein
Paraprotein
Multiple myeloma
•According to American Cancer Society,
• About 35,780 new cases will be diagnosed (19,520 in men and 16,260 in women) in the US in 2024
• In the United States, the average lifetime risk of getting multiple myeloma is about 1 in 103 for men and about 1 in 131 for women
https://badmanstropicalfish.com/arrowcrab/
Causes, risk factors, and prevention
•Cause of MM is still not fully understood
•Risk factors include:
• Older age
• Male sex
• African American race (twice as high as White Americans)
• Family members with MM
•Because above risk factors are unavoidable, there is no known way to prevent MM
https://badmanstropicalfish.com/arrowcrab/
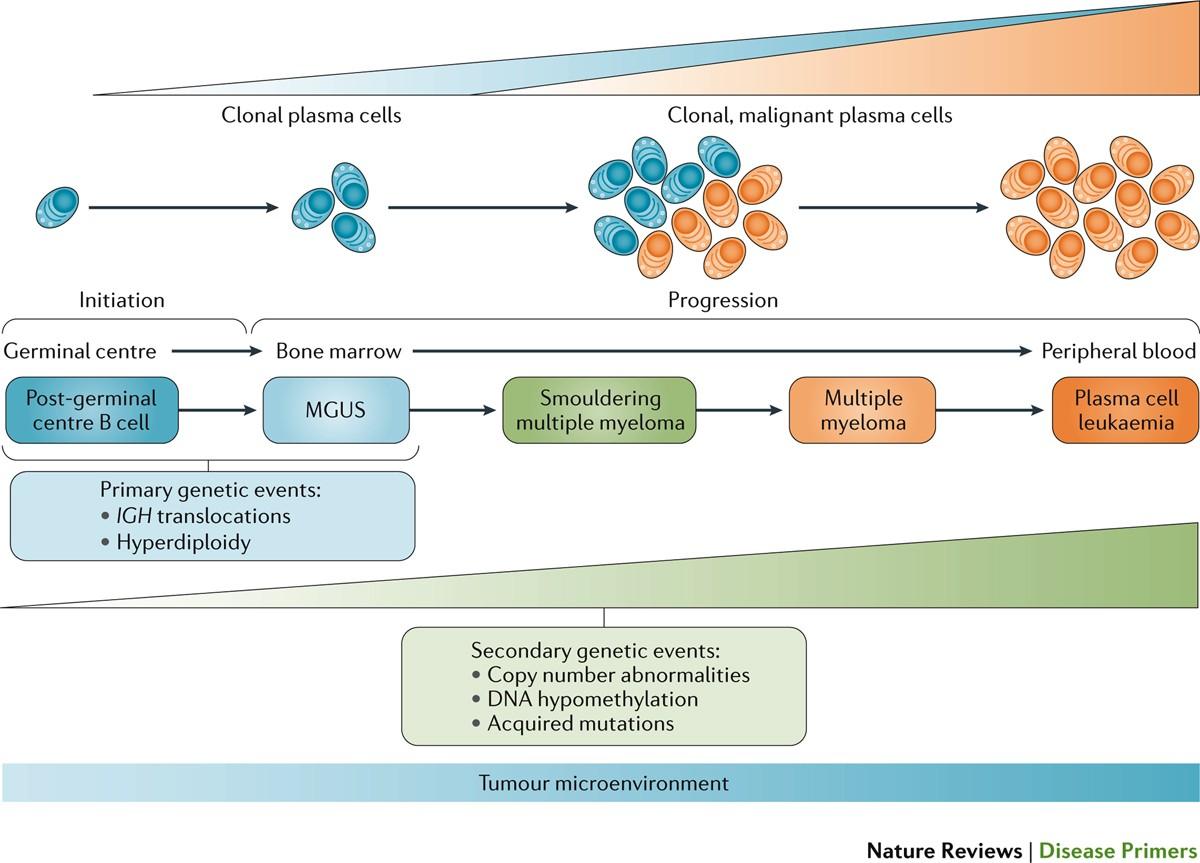
Monoclonal gammopathy of unknown significance
Kumar, S. et al., Nat Rev Dis Primers 3, 17046 (2017).
MRI bone lesion

https://badmanstropicalfish.com/arrow-crab/
Calcium
Renal impairment
Anemia
Bony lesion
•Bone marrow biopsy: to determine how much plasma cells there are in the bone marrow
•Laboratory evaluation: to determine the amount of paraprotein (antibody) made by the plasma cells
•Urine evaluation: to determine if any paraprotein (antibody) are spilled into the urine
•Bone imaging (CT, MRI, PET/CT, X-ray): to determine if any bone lesions from plasma cells
https://badmanstropicalfish.com/arrowcrab/
Understanding the labs
•Serum protein electrophoresis (SPEP) and serum immunofixation (sIFE)
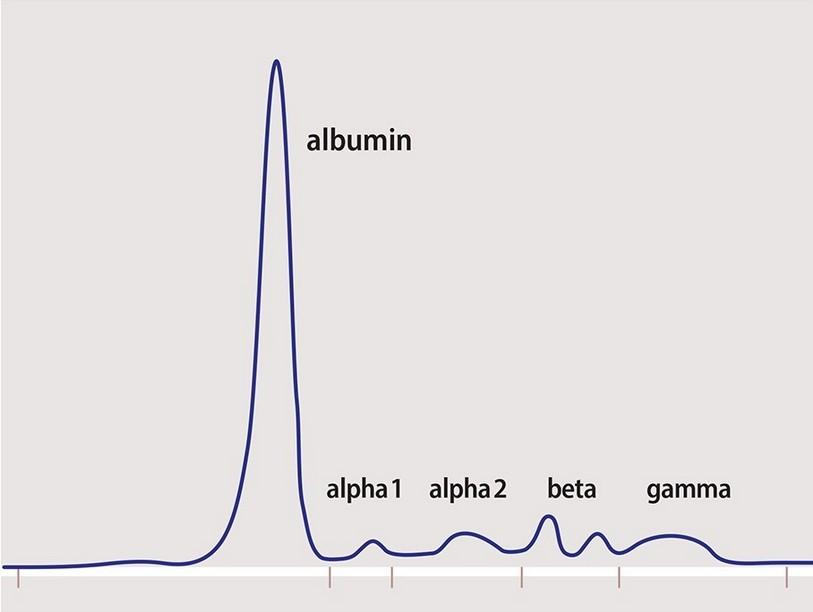
•Quantitative immunoglobulins
• IgG
• IgA
• IgM
•Kappa, lambda, and K/L
• Kappa
• Lambda
• Kappa/Lambda ratio
Thank you!
Questions?
Autumn (Ah-Reum) Jeong, MD
UC San Diego Health
Moores Cancer Center
•Introduction to multiple myeloma (MM)
•Epidemiology
•Symptoms
•Diagnosis
•Prognosis
Sandra Rome, RN, MN, AOCN, CNS
Cedars-Sinai, IMF Nurse Leadership Board Member
Today’s Topics

Myeloma and treatment options, side effects, symptom management, & supportive care

Know your care team & be an empowered patient

GOING THE DISTANCE
Healthful and meaningful living
Treatment options, side effects, symptom management, and supportive care


Rapid and effective disease control
Durable disease control
Improved overall survival
Minimize side effects
Promote good quality of life
Prevent disease- and treatment-related side effects
Optimize symptom management
Promote quality of life
Discuss your goals and priorities with your healthcare team.

FRONTLINE
MAINTENANCE
Velcade® (bortezomib)
Darzalex® (daratumumab)
Velcade® (bortezomib)
Ninlaro® (ixazomib)
Kyprolis® (carfilzomib)
RELAPSE
PENDING FDA
APPROVAL
Ninlaro® (ixazomib)
Darzalex® (daratumumab) in clinical trial
Darzalex® (daratumumab)
Empliciti® (elotuzumab)
Sarclisa® (Isatuximab)
Revlimid® (lenalidomide)
Thalomid® (thalidomide)
Revlimid® (lenalidomide)
Thalomid® (thalidomide)
Revlimid® (lenalidomide)
Pomalyst® (pomalidomide)
• CelMods
‒ Iberdomide
‒ Mezigdomide
Dexamethasone
Prednisone
Prednisolone
SoluMedrol
Dexamethasone
Prednisone
Prednisolone
SoluMedrol
Melphalan Cyclophosphamide
Melphalan + ASCT
Melphalan
Cyclophosphamide
Bendamustine
Elrexfio™ (elranatamab)
Tecvayli® (teclistamab)
Talvey™ (talquetamab)
Other Bispecific Antibodies
‒ Cevostamab
Melphalan + ASCT
CAR-T
− Ide-Cel
− Cilta-Cel
Xpovio® (Selinexor)
Doxil (liposomal doxorubicin)
Other CAR-T Venclexta® (venetoclax):BCL2 inhibitor for t(11;14) Blenrep (belantamab mafodotin)*: antibody drug conjugate
NOTED SIDE
EFFECTS Neuropathy
Carfilzomib: Cardiac
Infusion reaction
DVT/PE
See steroid slide
Myelosuppression
CRS and neurotoxicity; infection risk
Talvey: skin/nail/GI Infection risk
CAR-T: CRS and neurotoxicity
Myelosuppression, GI Xpovio: low sodium Blenrep: eye-related
Measuring treatment response
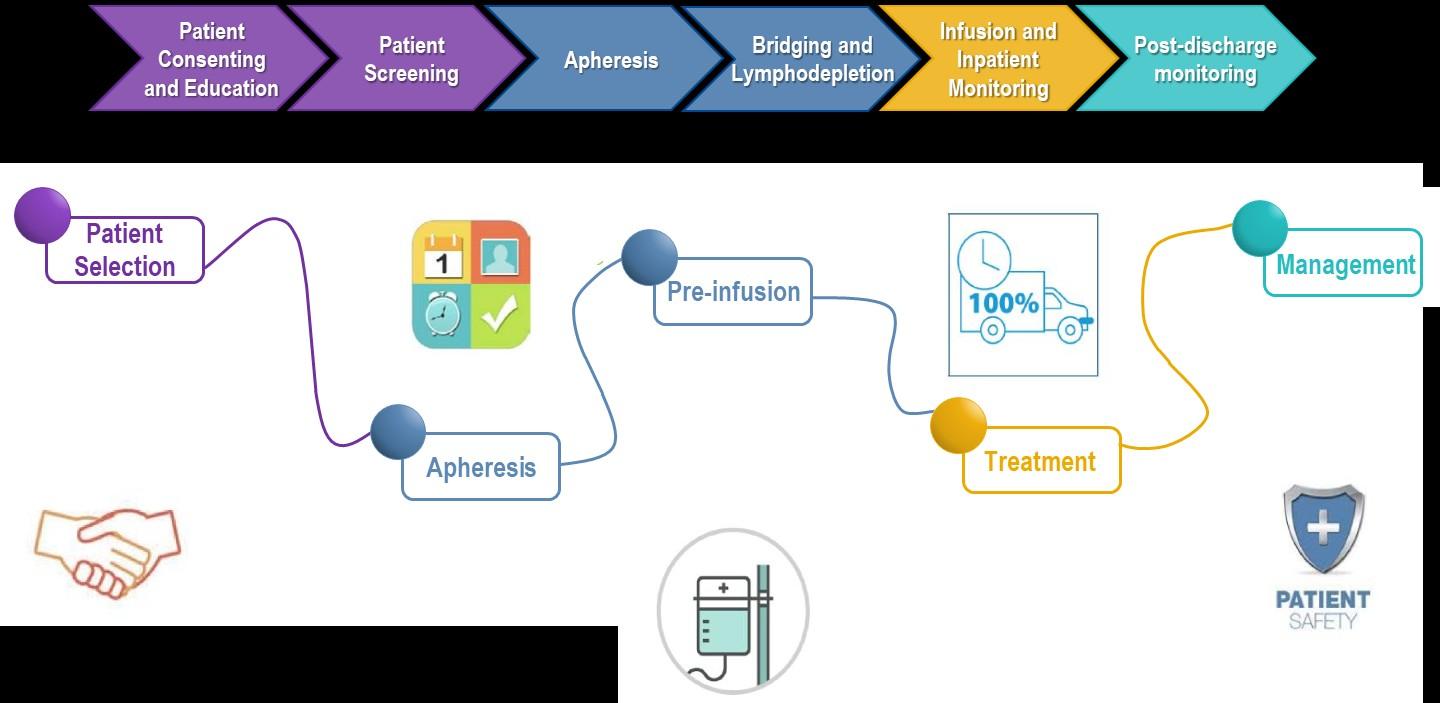
Determining Transplant Eligibility
Insurance authorization
Collecting stem cells
High Dose Chemotherapy, stem cell infusion
Supportive Care Engraftment
Duration:
Approximately 2 weeks
Duration: Approximately 3-4 weeks
Location: Transplant Center POSTTRANSPLANT
Location: Transplant Center
Restrengthening
Appetite recovery
“Day 100” assessment
Begin maintenance therapy
Duration: Approximately 10-12 weeks
Location: HOME
Upfront stem cell transplant remains the standard of care for eligible patients
Ask for a referral to CAR Tcell center as soon as it is possible as next treatment option (ie, before relapse)
No driving for 8 weeks
“One & Done” with continued monitoring
T-Cell Collection
Manufacturing takes ≈ 4 to 6 weeks
Bridging therapy may be needed
• Away from home
• Often some hospital stay
• Care Partner needed
• Side effect management
• CRS, ICANS
• Low blood counts
• Fatigue and fever
• Some patients need ongoing transfusion support
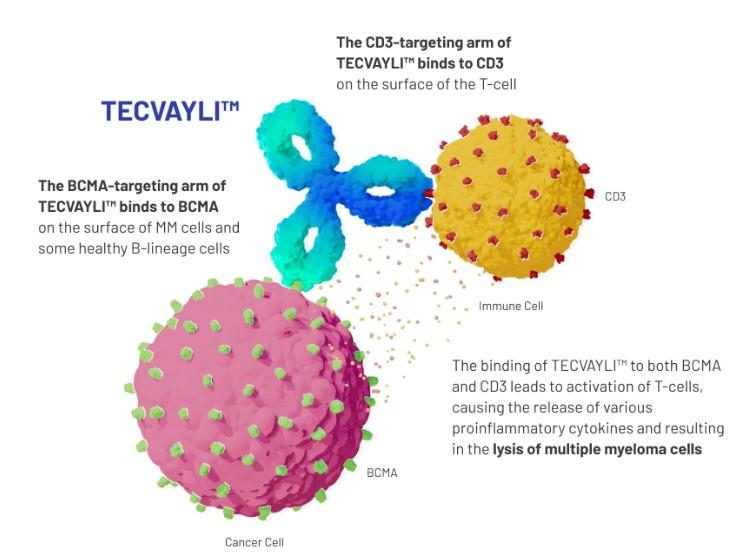
Horse of Another Breed:
Antibodies
•Different bispecific antibodies have differences in efficacy, side effects
– Available after 4 prior lines of therapy (or clinical trial)
– About 7 in 10 patients respond
– Off-the-shelf treatment; no waiting for engineering cells
– CRS and neurotoxicity
– Risk of infection
•BCMA target: greater potential for infection
– Tecvayli® (teclistamab)
– Elrexfio™ (elranatamab)
BISPECIFIC ANTIBODIES
•GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
– Talvey™ (talquetamab)


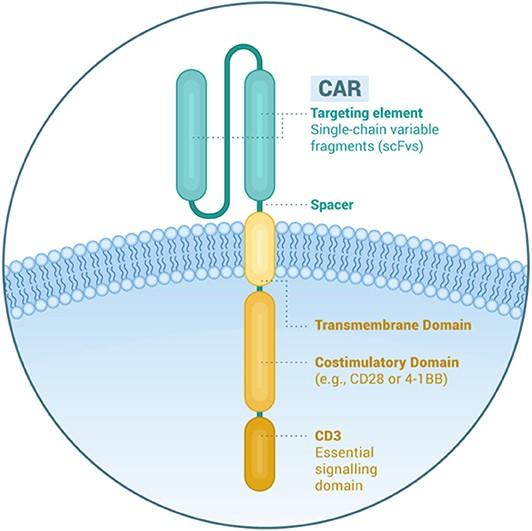
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; MM = multiple myeloma; scFV = single chain fragment variable; CRS = cytokine release syndrome. Shah N, et al. Leukemia. 2020;34(4):985-1005. Yu B, et al. J Hematol Oncol. 2020;13:125.
Confusion
CAR T and Bispecific Antibodies: Unique Side Effects CRS
Weakness
Fever Fatigue
Shortness of Breath Diarrhea
Headache
Nausea / vomiting
CRS is a common but often a mild & manageable side effect
CAR = chimeric antigen receptor; CRS = cytokine release syndrome. Oluwole OO, Davila ML. J Leukoc Biol. 2016;100:1265-1272. June CH, et al. Science. 2018;359:1361-1365. Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Brudno JN, Kochenderfer JN. Blood Rev. 2019:34:45-55. Shimabukuro-Vornhagen, et al. J Immunother Cancer. 2018;6:56. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638.
CAR T and Bi-specific Antibodies: Unique Side Effects
Infection Can Be Serious for People With Myeloma
[P]reventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.


Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team: Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
IMWG = International Myeloma Working Group; HCP = healthcare provider.
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Preventative and/or supportive medications (next slide)
Medications Can Reduce Infection Risk
Type of Infection Risk
Herpes virus reactivation (HSV/VZV); CMV reactivation
Bacteremia, pneumonia, and urinary tract infection
PJP (P jirovecii pneumonia)
Fungal infections (aspergillus)
IgG < 400 mg/dL or recurrent infections
ANC < 500 cells/μL
COVID-19
Medication Recommendation(s) for Healthcare Team
Consideration
Acyclovir prophylaxis
Consider prophylaxis with levofloxacin
Consider prophylaxis with trimethoprim-sulfamethoxazole
Consider prophylaxis with fluconazole
IVIg
GCSF 2 or 3 times/wk (or as frequently as needed) to maintain
ANC > 1000 cells/μL and maintain treatment dose intensity
Antiviral therapy if exposed or positive for covid per institution
recommendations
Some people receiving BCMA-targeting therapies have experienced infections that are less common like CMV, PJP and fungal infections
ANC = absolute neutrophil count; BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; CMV, cytomegalovirus; GCSF = granulocyte colony-stimulating factor; HSV = herpes simplex virus; IVIg = intravenous immunoglobulin; PJP = Pneumocystis jirovecii pneumonia; VZV = varicella zoster virus.
RAJE NS, et al.
Lancet Haematol
.2022;9(2):143–161.
Talvey™ (talquetamab): Common But Generally Mild and Painless Derm AEs
Dry skin and exfoliation


FINDING YOUR GAIT
GOING THE DISTANCE
Nail thinning and pealing


Steroids: The Good, The Bad, The Ugly

Steroids enhance the effectiveness of other myeloma therapies
Do not stop or alter your dose of steroids without discussing it with your provider
• Irritability, mood swings, depression
• Difficulty sleeping (insomnia), fatigue
•Consistent schedule (AM vs. PM)
•Take with food
•Stomach discomfort: Over-the-counter or prescription medications
•Medications to prevent shingles, thrush, or other infections
• Blurred vision, cataracts
• Flushing/sweating
• Increased risk of infections, heart disease
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Muscle weakness, cramping
• Weight gain, hair thinning/loss, skin rashes
• Increased blood pressure, water retention
• Increased blood sugar levels, diabetes
GI Symptoms:
Prevention & Management
Diarrhea may be caused by medications and supplements
– Laxatives, antacids with magnesium
– Antibiotics, antidepressants, other (check with provider, pharmacist)
– Supplements: milk thistle, aloe, cayenne, saw palmetto, ginseng
Avoid caffeinated, carbonated, or heavily sugared beverages
Take anti-diarrheal medication if recommended
Discuss GI issues with health care providers to identify causes and make adjustments to medications and supplements
Constipation may be caused by medications and supplements
–
Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
– Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency
Increase fiber
•Fruits, vegetables, high fiber whole grain foods
•Fiber binding agents – Metamucil®, Citrucel®, Benefiber®

Fluid intake can help with both diarrhea and constipation and helps kidney function


Weight Management
Anorexia (difficulty eating) Weight loss; Steroids Weight gain
– Monitor weight for significant loss or gain
– Adjust diet (reduce calories or add supplements )
Pain can significantly compromise quality of life
Sources of pain include bone disease, neuropathy and medical procedures
•Management
– Prevent pain when possible
• Bone strengtheners to decrease fracture risk
• Antiviral to prevent shingles
• Sedation before procedures
– Interventions depend on source of pain
Tell your healthcare provider about any new bone or chronic pain that is not adequately controlled
• May include medications, activity, surgical intervention, radiation therapy, etc
• Complementary therapies (Mind-body, medication, yoga, supplements, acupuncture, etc)
• Scrambler therapy for neuropathy
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e. diabetes).
Symptoms:
•Numbness
•Tingling
•Prickling sensations
•Sensitivity to touch
•Burning and/or cold sensation
•Muscle weakness
Prevention / management:
•Bortezomib once-weekly or subcutaneous administration
•Massage area with cocoa butter regularly
•Neuroprotective Supplements:
– B-complex vitamins (B1, B6, B12)
– Green tea
•Safe environment: rugs, furnishings, shoes
Report symptoms of peripheral neuropathy early to your health care provider; nerve damage from neuropathy can be permanent if unaddressed
If neuropathy worsens, your provider may:
•Adjust your treatment plan
•Prescribe oral or topical pain medication
•Suggest physical therapy
•Risk Factors
– Active multiple myeloma (light chains, high calcium)
– Other medical issues (ex: Diabetes, dehydration, infection)
– Medications (MM treatment, antibiotics, contrast dye)
•Prevention
– Stay hydrated – drink water
– Avoid certain medications when possible (eg, NSAIDs), dose adjust as needed
•Treatment
– Treatment for myeloma
– Hydration
– Dialysis

Many myeloma patients will experience kidney issues at some point; protecting your kidney function early and over time is important

98.8%
Fatigue is the most commonly reported symptom.
Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression
>35% of patients
≈25% of patients
Often, people do not share these symptoms with their provider. Talk to your provider about symptoms that are not well controlled or if you have thoughts of self harm. Help is available.
Financial burden comes from
•Medical costs
– Premiums
– Co-payments
– Travel expenses
– Medical supplies
•Prescription costs
•Loss of income
– Time off work or loss of employment
– Caregiver time off work

•Funding and assistance may be available
– Federal programs, IRA & Medicare “Extra Help”
– Pharmaceutical support
– Non-profit organizations
– Websites:
• Medicare.gov
• SSA.gov
• LLS.org
• Rxassist.org
• NeedyMeds.com
• HealthWellFoundation.org
• Company-specific website
Contact the Social Services department at your hospital or clinic to talk to a social worker for assistance.
Be an empowered patient; engage in your care
Be empowered
Ask questions, learn more
Express your goals/values/preferences


Ask for time to consider options
Communicate with your team
Understand the roles of each team member and who to contact for your needs
Arrive at a treatment decision together
Create a support network







Don’t Get Left in the Dust:
Communicate How You Feel With Your Team
Unmanaged Myeloma can cause:
Calcium elevation
Renal dysfunction
Low blood counts
Infection Risk
Blood clots
Bone pain
Neuropathy
Fatigue
Your team may be able to help, but only if they know how you feel.
Side Effects of Treatment can cause:
GI symptoms
Renal dysfunction
Low blood counts
Infection Risk
Blood clots
Neuropathy
Fatigue

If you want to go fast, go alone, if you want to go far, go together African Proverb
•Care partners may help in many ways including medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
•Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)


•Caring for the Care Partner
– Recognize that caregiving is difficult/stressful
– Encourage care partners to maintain their health, interests, and friendships
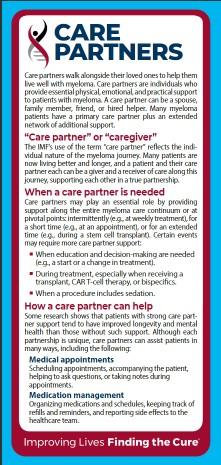
– The IMF has information and resources to help care partners


Form A Posse: Build Strong Social Ties & Cultivate a Sense of Belonging
•Multiple studies demonstrate that strong social ties are associated with
– Increased longevity including people with cancer
– Improved adherence to medical treatment leading to improved health outcomes
– Lower risk of developing cardiovascular diseases
– Increased sense of purpose and life satisfaction
– Reduced stress and anxiety
– Improved mood and happiness
– Enhanced resilience
Martino J, et al. Am J of Lifestyle Med. 2015;11(6):466-475.
Yang YC, et al. Proc Natl Acad Sci U S A. 2016;113(3):578-583.
Pinquart M and Duberstein PR. Crit Rev Oncol Hematol. 2010; 75(2):122–137.
•Strategies for enhancing social connection
– Deepen existing relationships with family, friends, and loved ones
– Build new relationships by participating in a support group, joining clubs or organizations, or volunteering
Tip: Start with small steps outside your comfort zone. Call a loved one you haven’t spoken to in a while. Invite a person you’d like to know better for lunch, coffee, or a walk.

Hetherington C. Healthnews.
https://healthnews.com/longevity/healthspan/social-connection-andlongevity/#:~:text=Research%20consistently%20demonstrates %20that%20people,of%20fulfillment%20in%20your%20life. Accessed Feb 1 2024.
Important for Good Health
•Adequate rest and sleep are essential to a healthful lifestyle
•Shortened and disturbed sleep cause
– Increased heart-related death
– Increased anxiety
– Weakened immune system
– Worsened pain
– Increased falls and personal injury
•Things that can interfere with sleep
– Medications: steroids, stimulants, herbal supplements
– Psychologic: fear, anxiety, stress
– Physiologic: sleep apnea, heart issues, pain
• Sleep hygiene is necessary for quality nighttime sleep and daytime alertness
– Engage in exercise but not too near bedtime
– Increase daytime natural light exposure
– Avoid daytime napping
– Establish a bedtime routine - warm bath, cup of warm milk or tea
•Associate your bed ONLY with sleep
– Avoid before bedtime:
• Caffeine, nicotine, alcohol and sugar
• Large meals and especially spicy, greasy foods
• Computer screen time
•Sleep aid may be needed
Maintain Good Health
Have a Primary Care Doctor
Have Recommended Health Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Diabetes
• Colonoscopy
• Vision
• Hearing
• Dental checkups & cleaning
• Women specific: mammography, pap smear
• Men specific: prostate
Maintain a healthy weight
Good nutrition
Activity or exercise
Sufficient sleep
An ounce of prevention is worth a pound of cure.
 Benjamin Franklin
Benjamin Franklin
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.

Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.

Seattle, WA
Rahul Banerjee, MD, FACP Fred Hutchinson Cancer Center
Rahul Banerjee, MD, FACP
Assistant Professor, Division of Hematology & Oncology
University of Washington / Fred Hutchinson Cancer Center
IMF Regional Community Workshop (San Diego)
March 2, 2024 – 11:00am
Fred Hutchinson Cancer Center

•Consulting: BMS/Celgene, Caribou Biosciences, Genentech/Roche, Legend Biotech, Janssen Oncology, Pfizer, Sanofi Pasteur, SparkCures
•Research funding: Novartis, Pack Health
•I generally use generic drug names, but – given this audience – I’ll try to mention brand names each time as well. No endorsements intended.
Fred Hutchinson Cancer Center
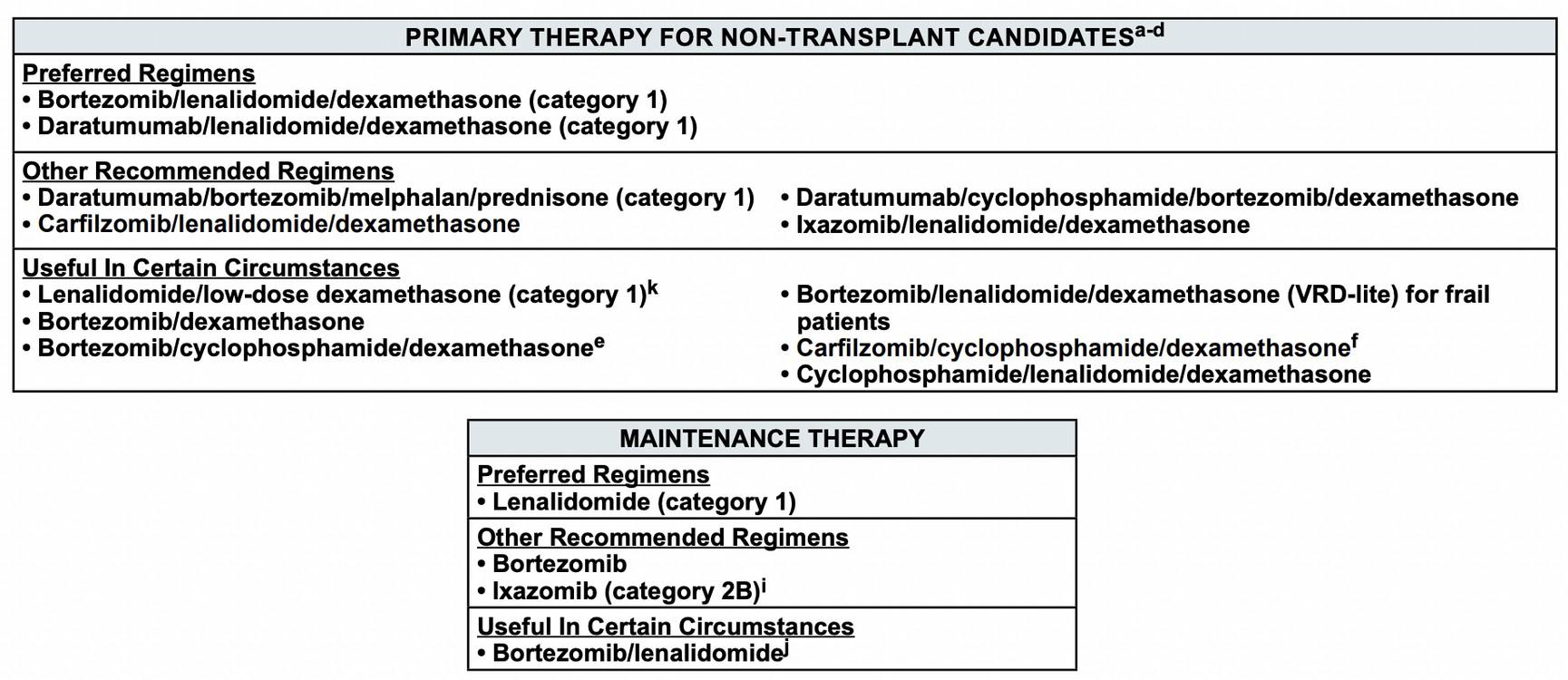
Here are the options for frontline therapy
•We don’t make this easy for anyone, including doctors…

Questions
1. Should I prescribe a triplet or a quadruplet?
• Triplet: Two active anti-myeloma drugs, plus dexamethasone
• Quadruplet: Three active anti-myeloma drugs, plus dexamethasone
2. How can I tailor the doses for you?
• Rationale: Better-tolerated myeloma treatment means more time on treatment, which can mean longer lengths of remission
3. Should I refer you to a transplant center?
• Or, if no transplant, should we collect and store stem cells?
4. What type of maintenance should I start?
• For example, just lenalidomide (Revlimid®) by itself.
• OR, Revlimid® plus another drug like bortezomib (Velcade®).
1. Should I prescribe a triplet or a quadruplet?
• Triplet: Two active anti-myeloma drugs, plus dexamethasone
• Quadruplet: Three active anti-myeloma drugs, plus dexamethasone
2. How can I tailor the doses for you?
• Rationale: Better-tolerated myeloma treatment means more time on treatment, which can mean longer lengths of remission
3. Should I refer you to a transplant center?
• Or, if no transplant, should we collect and store stem cells?
4. What type of maintenance should I prescribe?
• For example, just lenalidomide (Revlimid®) by itself.
• OR, Revlimid® plus another drug like bortezomib (Velcade®).
•Triplets include:
• CyBorD: Cyclophosphamide (Cytoxan®), bortezomib (Velcade®)
• VRd: Bortezomib (Velcade®), lenalidomide (Revlimid®)
• KRd: Carfilzomib (Kyprolis®), lenalidomide (Revlimid®)
• Dara-Rd: Daratumumab (Darzalex®), lenalidomide (Revlimid®)
•Quadruplets (Dara = Darzalex®, isa = Sarclisa®)
• Dara-CyBorD
• Dara-VRd or Isa-VRd
• Dara-KRd or Isa-KRd
Fred Hutchinson Cancer Center
•Daratumumab (Darzalex®) and isatuximab (Sarclisa®) are both CD38 monoclonal antibodies, meaning they attack CD38 on the surface of myeloma cells. Either direct or immune-mediated cell death follows.
•Most centers use dara, while Kaiser typically uses isa.
• From studies to date, both drugs perform about the same. However, isa isn’t yet FDAapproved for frontline treatment.
•In short, the benefits of adding dara or isa are profound:
• Deeper remissions: Higher rates of complete response (M-spike gone) and MRD negativity (we can talk about this in Q&A)
• Faster remissions: This may mean better patient quality of life
• Longer remissions: In other words, longer “progression-free survival”
Fred Hutchinson Cancer Center
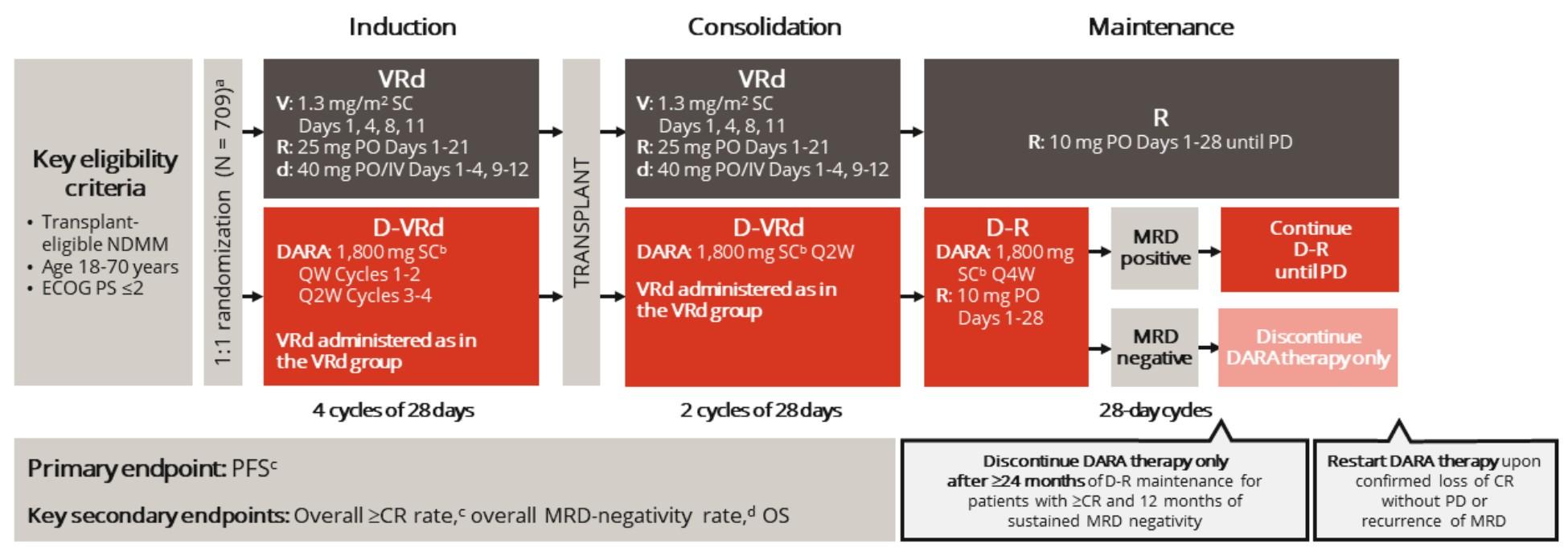
Wait, I thought this trial had another name?
•Yes, a year ago I would have presented GRIFFIN!
Greek claim to fame
Phase and location
Lion-eagle hybrid Slayer of Medusa
American Phase 2 trial powered for depth of response
Daratumumab
details
Sample
Dara-len maintenance?*
IV infusion given in complicated 3-week cycles
European Phase 3 trial powered for duration of response
Abdominal injections given in normal 4-week cycles
Continued until progression in DVRd group (not typically done in US)
Same, but could drop dara if sustained MRD-neg (10-5)
* Meaning both Darzalex® and Revlimid® after transplantation, with the Darzalex® every 4 weeks.
Fred Hutchinson Cancer Center
Practice-changing? Was for most US myeloma experts
Hopefully for the rest of the US…
4-year PFS: 84% with D-VRd versus 68% with VRd. PFS means alive and disease-free.
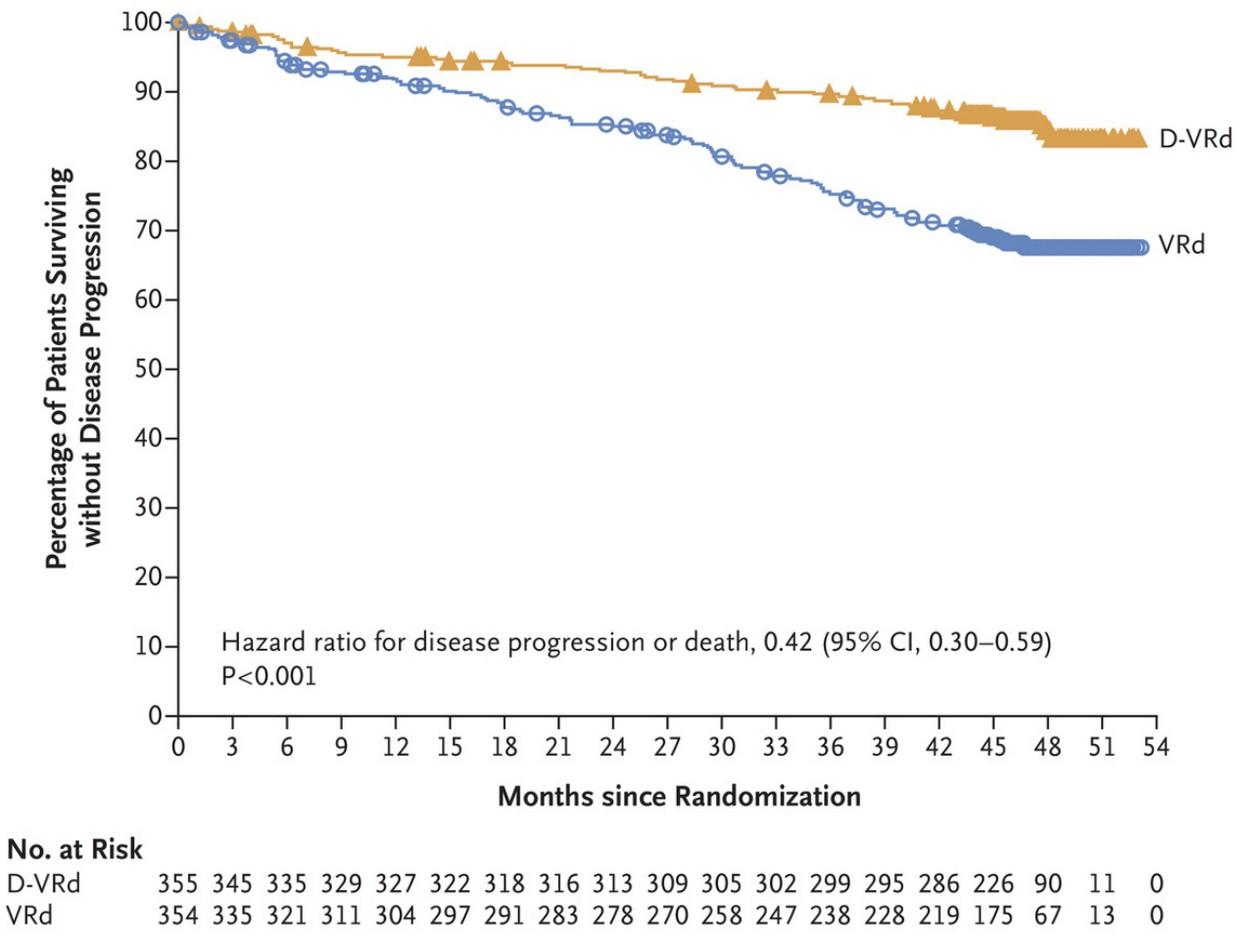
In D-VRd arm, 64% of pts stopped dara maintenance after 2 years.
•No! Many permutations exist.
• MASTER study (Costa et al): High rates of MRD negativity and safe ability to stop all maintenance with Dara-KRd + ASCT + Dara-KRd
• ASH 2023 (Gay et al): Isa-KRd + ASCT outperformed KRd + ASCT in terms of MRD negativity (45% vs 26% after induction at 10-5)
• Press release around ASH: IMROZ (Isa-VRd vs VRd) met its PFS endpoint among ASCT-ineligible patients
•In real life, I’d say any CD38 quadruplet is fine
• Kaiser patients often receive Sarclisa® (isatuximab) first-line
• Kyprolis® (carfilzomib) might be better than Velcade® (bortezomib) for the patient with neuropathic pain at baseline
•Many of you have wrestled with this decision after meeting with a transplant expert: Should I stay or should I go?
•My practice is still to use 4 drugs in this setting.
• Quadruplets have been studied before in patients who don’t go onto transplantation (ALCYONE, GMMG-CONCEPT)
• “Dynamic frailty” is real in MM: for some patients, rapid disease control means their pain is better and they’re no longer “frail.”
• ASH 2023 (Smits et al): Patients who become less frail with therapy have similar PFS to counterparts who were more fit all along.
• Many times, 4 drugs become 3 drugs anyways (more on this soon…)
Fred Hutchinson Cancer Center
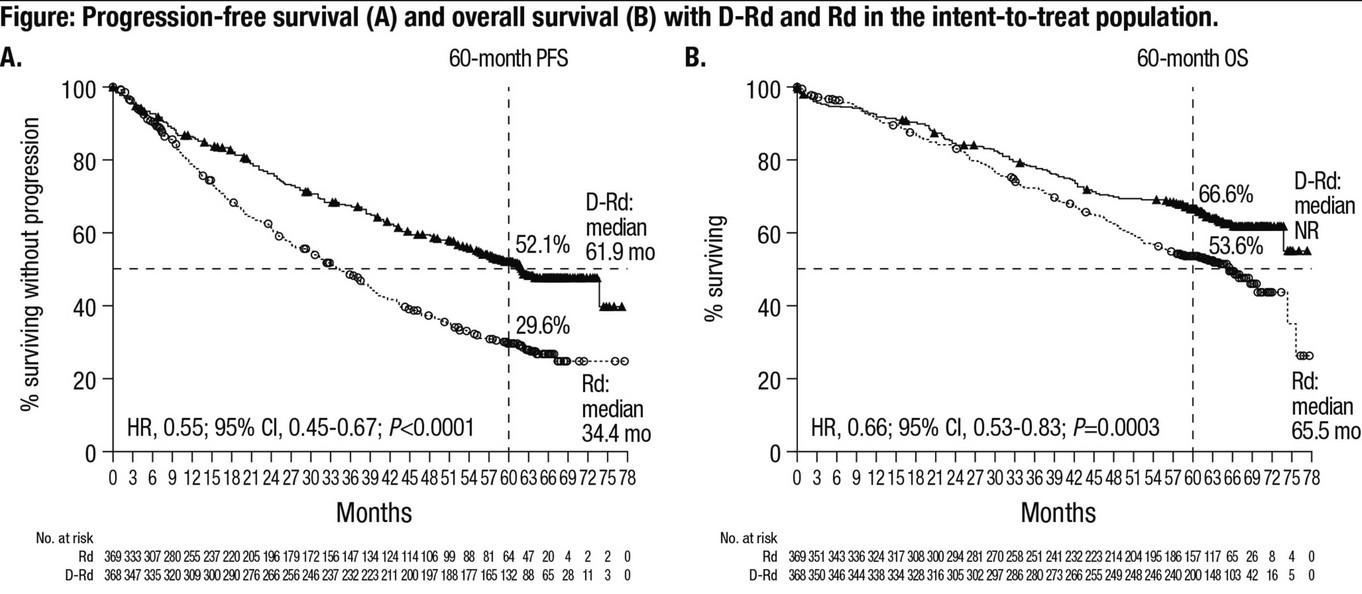
•A dara-containing triplet (Dara-Rd) was better than a doublet containing lenalidomide (Revlimid®) and dexamethasone
• Median PFS (length of remission) > 5 years!!
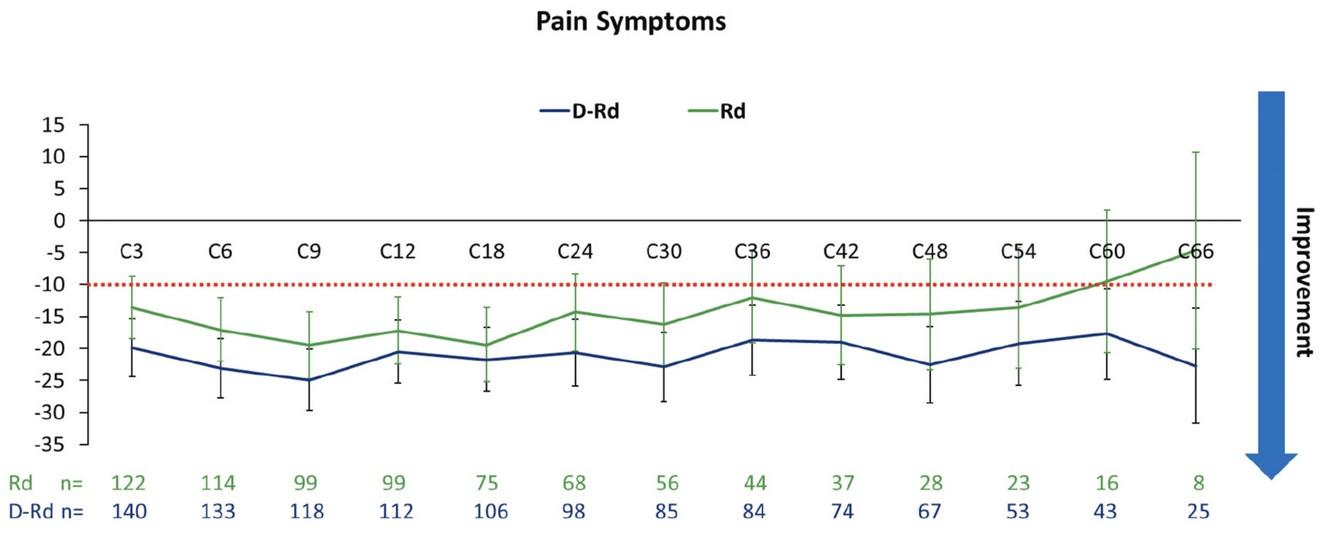
•At 2022 ASH meeting, shown to benefit quality of life as well:
• Pain scores were lower and remained lower with dara
Fred Hutchinson Cancer Center
Are there other options for ASCT-ineligible?
•Two main treatment options for “transplant-ineligible patients” with newly diagnosed myeloma:
•Dara-Rd: Daratumumab (Darzalex®) & lenalidomide (Revlimid®) from the previous slide.
• In brief, no bortezomib (Velcade®) which has a neuropathy risk.
•VRd-lite: Bortezomib (Velcade®) & lenalidomide
• “Lite” = not as many toxicities as the VRd of 20 years ago.
• In brief, no daratumumab here.
Fred Hutchinson Cancer Center
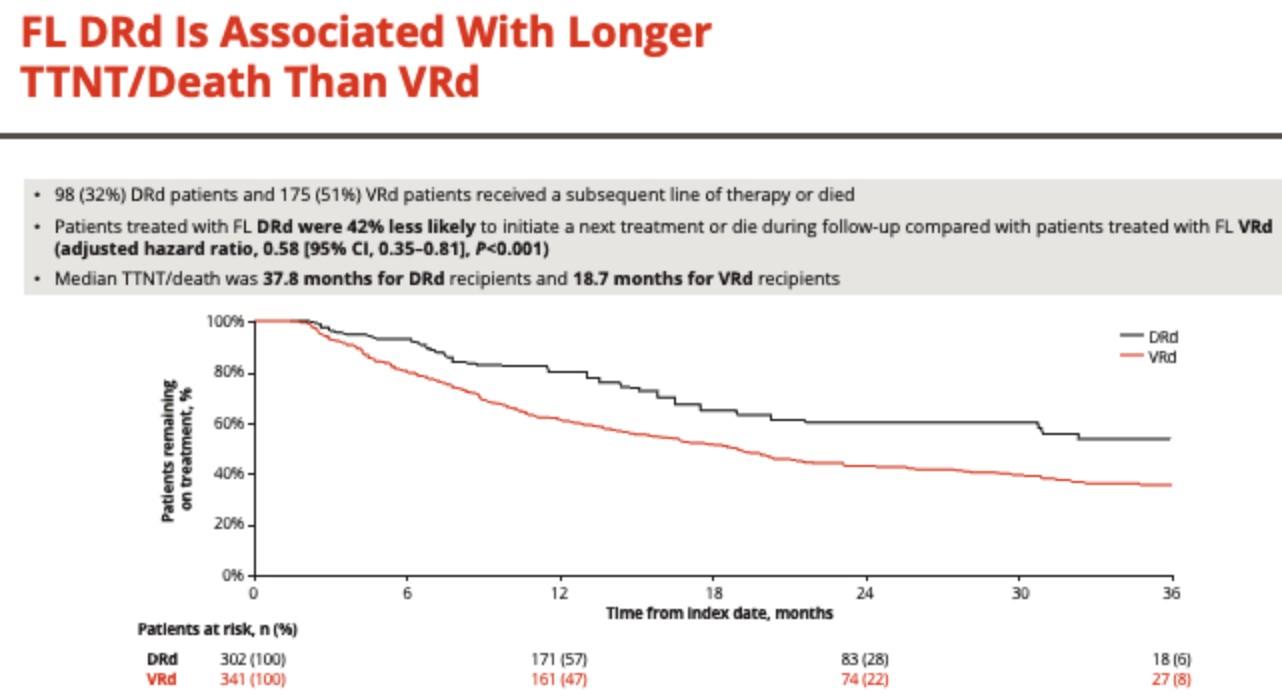
•In a real-world analysis presented last year (here) at our big ASH 2023 meeting, Dara-Rd seems to be better
• “Time to next treatment,” meaning until the doctor switched treatments due to relapse or side effects, was longer:
Median TTNT/death was 37.8 months for DRd versus 18.7 months for VRd-lite.
Fred Hutchinson Cancer Center
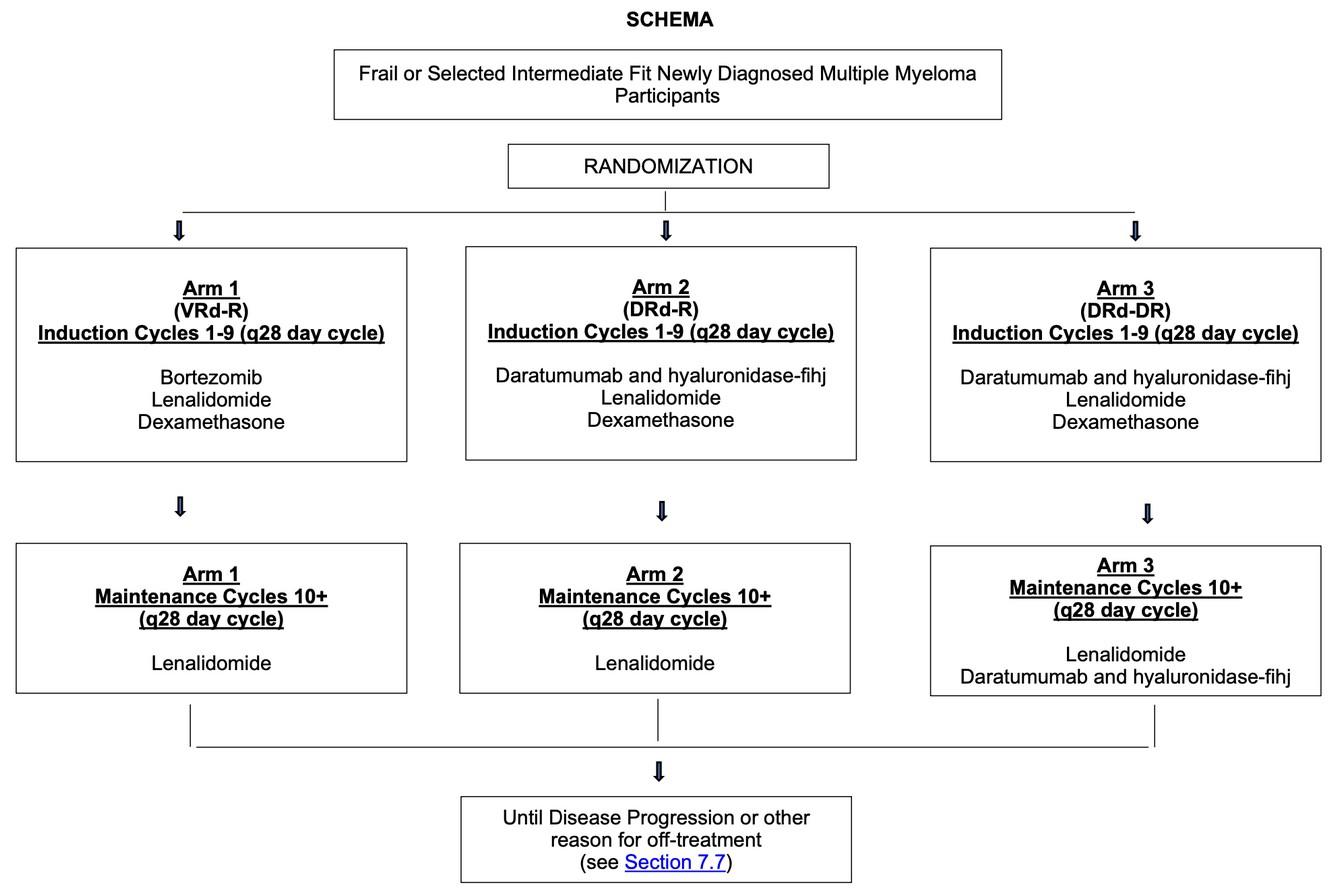
•We have an ongoing study (SWOG S2209) run by academic investigators hoping to answer this question:
•For patients <75 who are relatively healthy, I tend to favor a quadruplet containing daratumumab. For example, Dara-VRd.
• For high-risk features, I think about Dara-KRd or Isa-KRd.
•For patients who are older or less healthy, I am comfortable with a triplet and generally prefer that it includes Dara, e.g. Dara-Rd.
•I am 100% fine if a quadruplet becomes a triplet with time due to toxicities. We treat our patients, not numbers.
• For example: Velcade® causing neuropathy
• For example: Revlimid® too expensive
• Dropping the dex doesn’t even count as “losing” a quadruplet
Fred Hutchinson Cancer Center
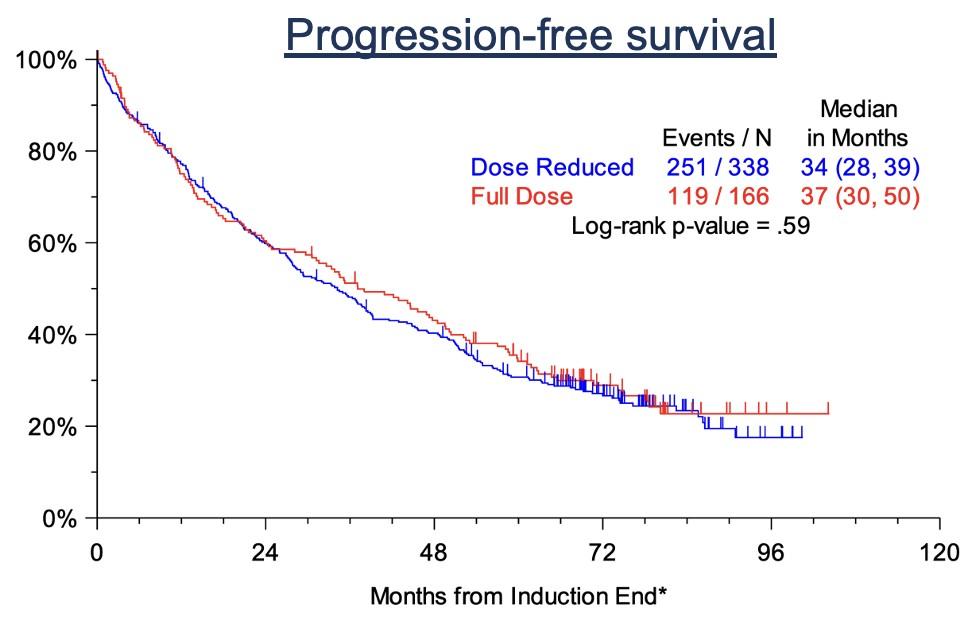
•Down with dex!
• In a pooled analysis of two large trials, >50% of patients (even on trials!) had dex dose reductions
• These patients did just fine compared to patients who stayed on full-dose dex (and probably had fewer side effects)
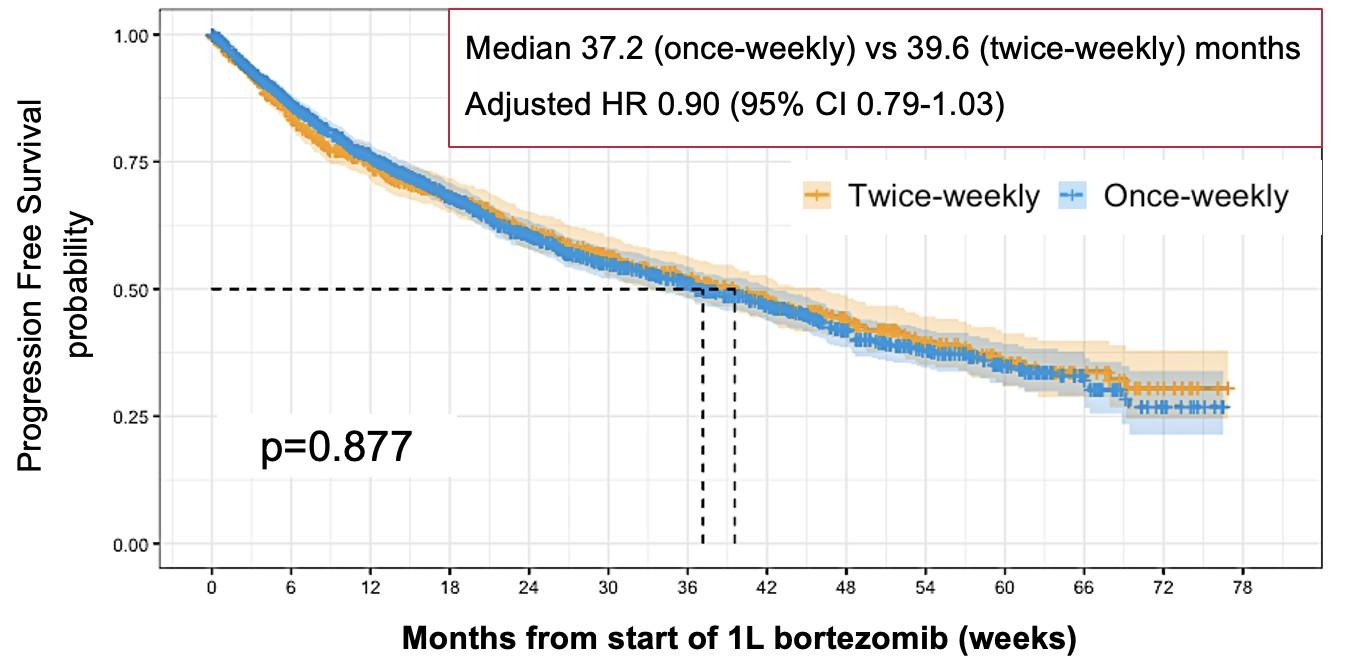
•Once-weekly bortezomib
• Some of you likely received bortezomib (Velcade®) injections twice per week
• The trials still do these unfortunately, but we really shouldn’t.
• More “time toxicity”
• More neuropathy
• Same efficacy
•Side effects of dara (Darzalex®) or isa (Sarclisa®):
• Frequent infections, prolonged COVID shedding. Okay to skip a dose if infections occur. Can consider antibiotics or IVIG if infections keep happening.
•Side effects of bortezomib (Velcade®):
• Neuropathy: Velcade should generally only be dosed once per week, not twice per week. Tell your physician to call me if they disagree.
• Blepharitis (eye styes): Stay tuned for a survey about this, as we’re trying to understand more about how to prevent this.
•Side effects of lenalidomide (Revlimid®):
• Fatigue, rash, joint pains: We can go as low as 2.5mg 21/28 days
• Financial toxicity ($$$ co-pays): Pharmacy assistance programs
Fred Hutchinson Cancer Center
•TONS of side effects, and often not needed.
•What most trials use:
• Dex 40mg weekly for most patients
• Dex 20mg weekly for patients aged ≥ 75
•My personal style:
• Start with the above, and counsel my patients carefully
• Any issues with 40mg? Drop to 20mg immediately.
• Any issues with 20mg? Drop to 12mg immediately, or stop.
•Talk to your doctor if you’re having side effects. More often than not, you can probably stop the dexamethasone!*
Fred Hutchinson Cancer Center
* You can probably also stop Tylenol and Benadryl as pre-medications with daratumumab / Darzalex® or isatuximab / Sarclisa® as well after the first month. Talk to your doctor.

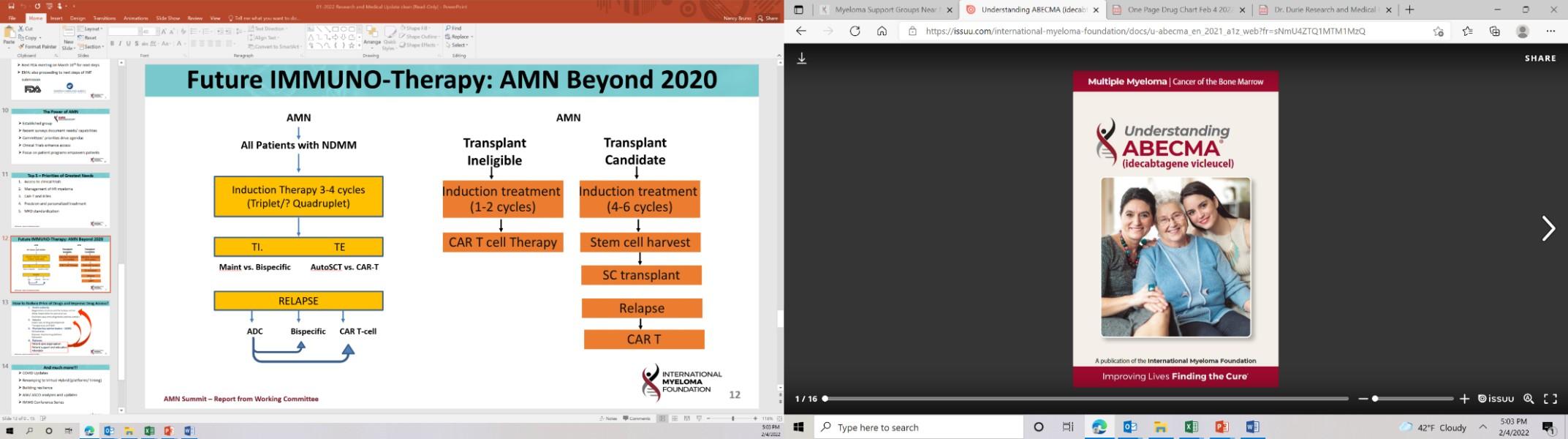
•In other words, after 4-6 months of initial therapy, should we move to:
• Autologous stem cell transplantation, also known as
• High-dose melphalan followed by stem cell rescue, also known as
• BMT (but with your own cells, not that of a donor)
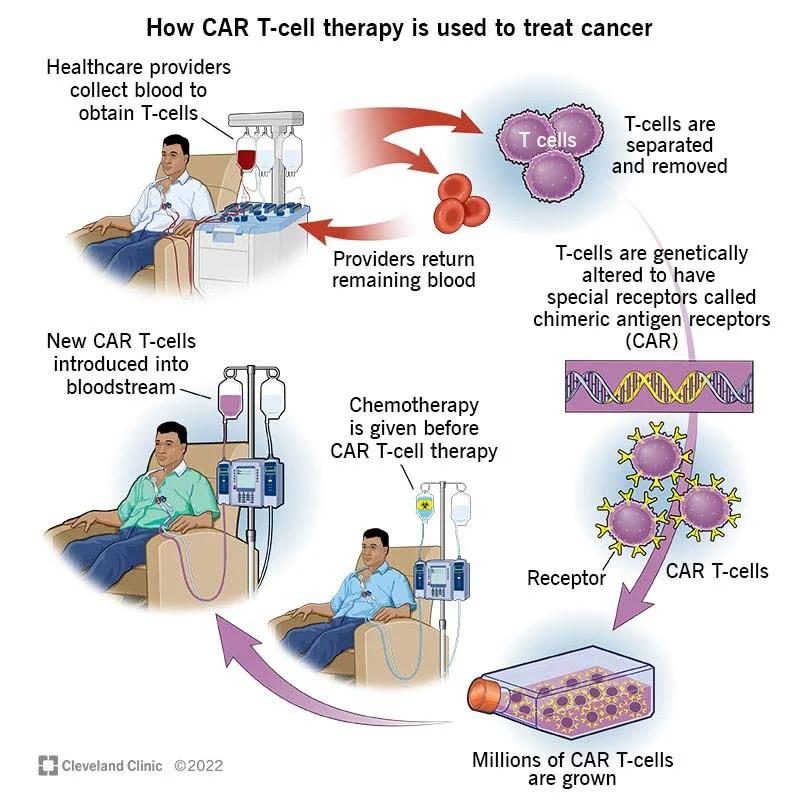
•How transplant works, in a nutshell:
• Single high dose of chemo obliterates the bone marrow, killing 99.999% of what it sees there (both bad cells and good cells).
• Normally, a patient’s good marrow (stem cells to make RBCs, WBCs, and platelets) could never recover from this. So, we pre-collect patient’s own stem cells beforehand.
• Once the chemo is given, we give back the stem cells and they find their way home! The chemo does the “heavy lifting” here, not the transplanted cells themselves.
Fred Hutchinson Cancer Center
•I’m intentionally going to focus on a high level here, since every patient’s case is so unique. Talk to your doctor if this applies to you.
•DETERMINATION study looked at transplant versus no transplant in patients aged 65 or younger who were receiving a triplet (VRd) as induction.
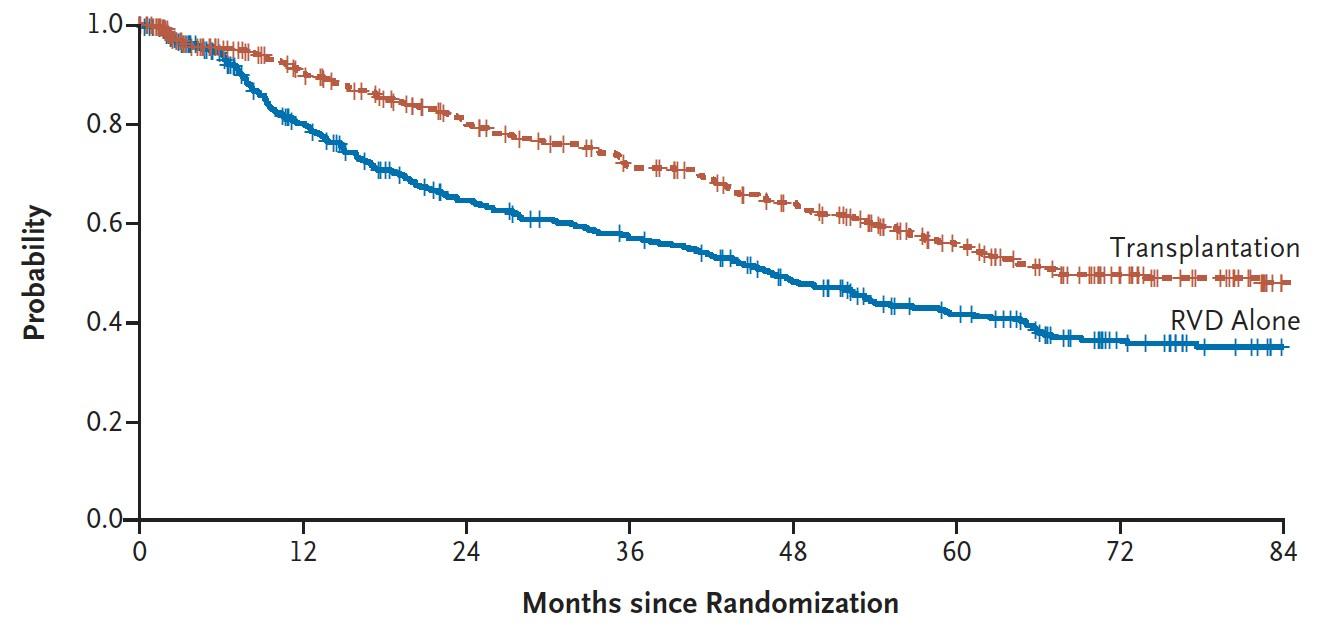
PFS: Patients stay in remission for longer (average 68 months versus 46 months)…
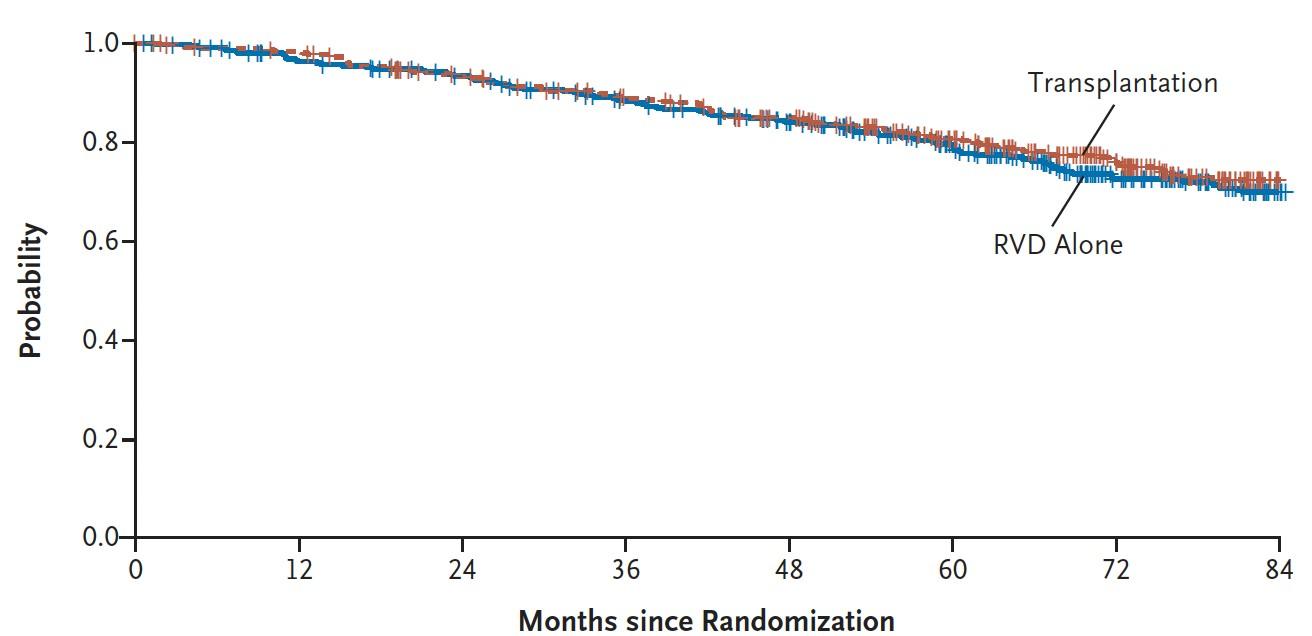
OS: Despite collecting data for more than 6 years, no evidence that transplant helps patients live longer.
Fred Hutchinson Cancer Center
•What other health conditions do you have?
• For patients with recent heart attacks or significant lung disease, the risks of transplant may outweigh the benefits. For patients with AL amyloidosis, the risks of transplant generally outweigh the benefits if Dara-based treatment working.
• FYI: Transplant has never been studied in randomized trials for adults ≥65 years old. We typically wouldn’t plan to offer transplant if someone is well into their 70s.
•What are your preferences regarding quality of life & logistics?
• Would you be willing to relocate to the big city for ~2 months?
• Do you have a caregiver who could come with you?
• Would you want to take a ~3-month dip in quality of life if it had the potential benefits from the previous slide.
•No right answer, and this is often a tough decision for patients.
Fred Hutchinson Cancer Center
•What’s the rationale for this?
• Some patients are not interested in upfront transplantation itself
• Collecting stem cells via the blood gets quite tricky after ~6 months of exposure to lenalidomide (Revlimid®).
•Most important question: could I collect & store stem cells?
• Some insurance companies won’t pay for this
•If I collect stem cells, am I obligated to do a transplant later?
• Not necessarily. Second transplants are getting rare in myeloma.
• The stem cells may be used for other reasons, e.g. peri-CAR-T to help with side effects like low blood counts from marrow inflammation.
Fred Hutchinson Cancer Center
•Goal: Prevent future “lytic lesions” or fractures in bones
• How? Bisphosphonates (zoledronic acid, Zometa®) or denosumab (Xgeva®)
• Caveats: Impaired jaw healing, potential for low blood calcium
•Goal: Prevent infections
• Strategy #1: Acyclovir or valacyclovir (Valtrex®) to prevent shingles
• Strategy #2: Vaccinations, including “childhood vaccines” after transplant
• Strategy #3: [Less common] Antibacterial medications, including Bactrim® (sulfamethoxazole/trimethoprim) or Levaquin® (levofloxacin)
•Goal: Improve pain control as soon as possible
• Radiation therapy definitely helps for painful bone fractures
• Kyphoplasty (cement in spine) has a more mixed history here
Fred Hutchinson Cancer Center
Questions your doctor should think about:
1. Should I prescribe a triplet or a quadruplet?
• If at all considering transplant: Use a quadruplet.
• If not transplant-eligible: Consider Dara-Rd with daratumumab
2. How can I tailor the doses for you?
• You don’t get extra points for unneeded side effects.
• Dexamethasone in particular is likely overused after the first month.
3. Should I refer you to a transplant center?
• When in doubt, always worth it to at least have a consultation
4. What type of maintenance should I prescribe?
• Coming up in the next talk!
Myeloma Action Month is a global social awareness campaign that takes place every March to raise awareness of multiple myeloma. We urge the community to champion Myeloma Action Month to help make a positive impact on those suffering from this blood cancer.
Will you take action for the myeloma community?
Myeloma Action Month: Last Years Impact!


Fred Hutchinson Cancer Center
Global Campaign. Join the Movement!
• Myelomaactionmonth.org:
o Over 45 Participating Countries
o Photo Uploader to share on social
o Social Media Toolkit
o Social Action Aggregator
• FB Lives:
o Beth Faiman: Myeloma Q&A
o Dr. Joe & Dr. Saad Usmani: Live from Boca PFS!
o Dr. Urvi A. Shah: Insights on Nutrition
• Like, comment, and share your insights and hashtag
#MyelomaActionMonth across IMF social channels







Myeloma Action Month: Other ways to Take Action
March for Myeloma ACTION Month
•Join Us In Person or Virtually for the March for Myeloma 5k Run/Walk.
•Taking place in Boca Raton, Florida, March 15 before the PFS!
 Fred Hutchinson Cancer Center
Fred Hutchinson Cancer Center
Raise awareness on a global scale by answering the question: What do you wish people knew about myeloma?
•Be part of our Global Action “Pass the Paper” Video.
•Watch the “how to” video and visit myelomaactionmonth.org to find out more!

Rahul Banerjee, MD, FACP
Assistant Professor, Division of Hematology & Oncology
University of Washington / Fred Hutchinson Cancer Center
IMF Regional Community Workshop (San Diego)
March 2, 2024 – 1:10pm
Fred Hutchinson Cancer Center
•Consulting: BMS/Celgene, Caribou Biosciences, Genentech/Roche, Legend Biotech, Janssen Oncology, Pfizer, Sanofi Pasteur, SparkCures
•Research funding: Novartis, Pack Health
•I generally use generic drug names, but – given this audience – I’ll try to mention brand names each time as well. No endorsements intended.
Fred Hutchinson Cancer Center
1. Should I prescribe a triplet or a quadruplet?
• Triplet: Two active anti-myeloma drugs, plus dexamethasone
• Quadruplet: Three active anti-myeloma drugs, plus dexamethasone
2. How can I tailor the doses for you?
• Rationale: Better-tolerated myeloma treatment means more time on treatment, which can mean longer lengths of remission
3. Should I refer you to a transplant center?
• Or, if no transplant, should we collect and store stem cells?
4. What type of maintenance should I start?
• For example, just lenalidomide (Revlimid®) by itself.
• OR, Revlimid® plus another drug like bortezomib (Velcade®).
1. Should I prescribe a triplet or a quadruplet?
• Triplet: Two active anti-myeloma drugs, plus dexamethasone
• Quadruplet: Three active anti-myeloma drugs, plus dexamethasone
2. How can I tailor the doses for you?
• Rationale: Better-tolerated myeloma treatment means more time on treatment, which can mean longer lengths of remission
3. Should I refer you to a transplant center?
• Or, if no transplant, should we collect and store stem cells?
4. What type of maintenance should I start?
• For example, just lenalidomide (Revlimid®) by itself.
• OR, Revlimid® plus another drug like bortezomib (Velcade®).
•What is maintenance therapy in myeloma?
• Milder version of induction, used indefinitely:
• Fewer medications
• Lower doses & frequencies
• Generally continued until progression (myeloma numbers rising)
•Goal: Maintain remission for longer without unduly worsening quality of life
Fred Hutchinson Cancer Center
Daratumumab (Darzalex®)
Bortezomib
Lenalidomide (Revlimid®)
Dexamethason e (“Dex”)
Zoledronic acid or denosumab (bone strength)
Yes, often monthly
Often every 3 months (stop after 2 years)
•Advantages of lenalidomide:
• It’s a once-a-day pill (plus aspirin), so no extra clinic visits
• Very adjustable dose, down to 2.5mg
• It works! In a pooled “meta-analysis,” proven to help patients live longer
•Disadvantages of lenalidomide:
• Expensive!!!
• Annoying pregnancy-related requirements
• Many side effects, including rash, fatigue, and low blood counts
• Difficult to dose in kidney disease
Fred Hutchinson Cancer Center
At 7 years, 62% survival with lenalidomide versus 50% otherwise.
•It didn’t used to be.
• In the big French study (IFM 2009) showing that transplant lengthened remissions, lenalidomide was only continued for 1 year.
• However, in the more recent American trial (DETERMINATION), lenalidomide was continued until progression or toxicities.
•Why did this shift happen?
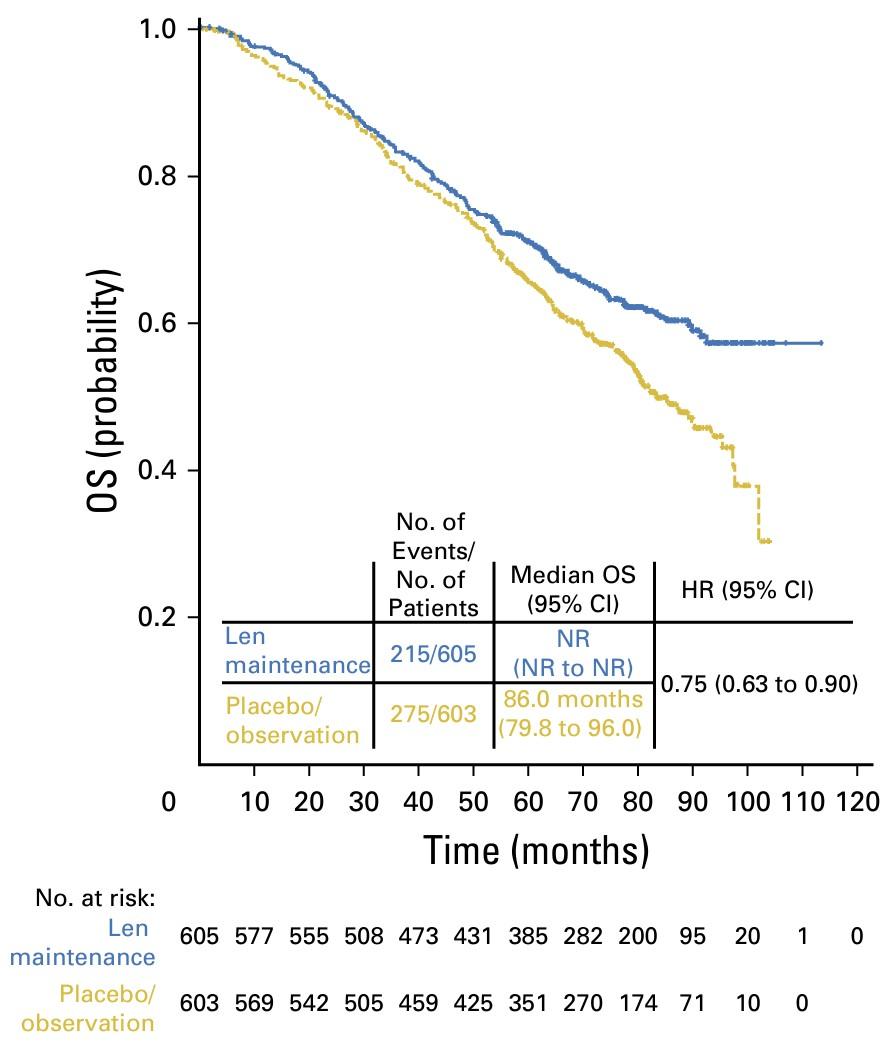
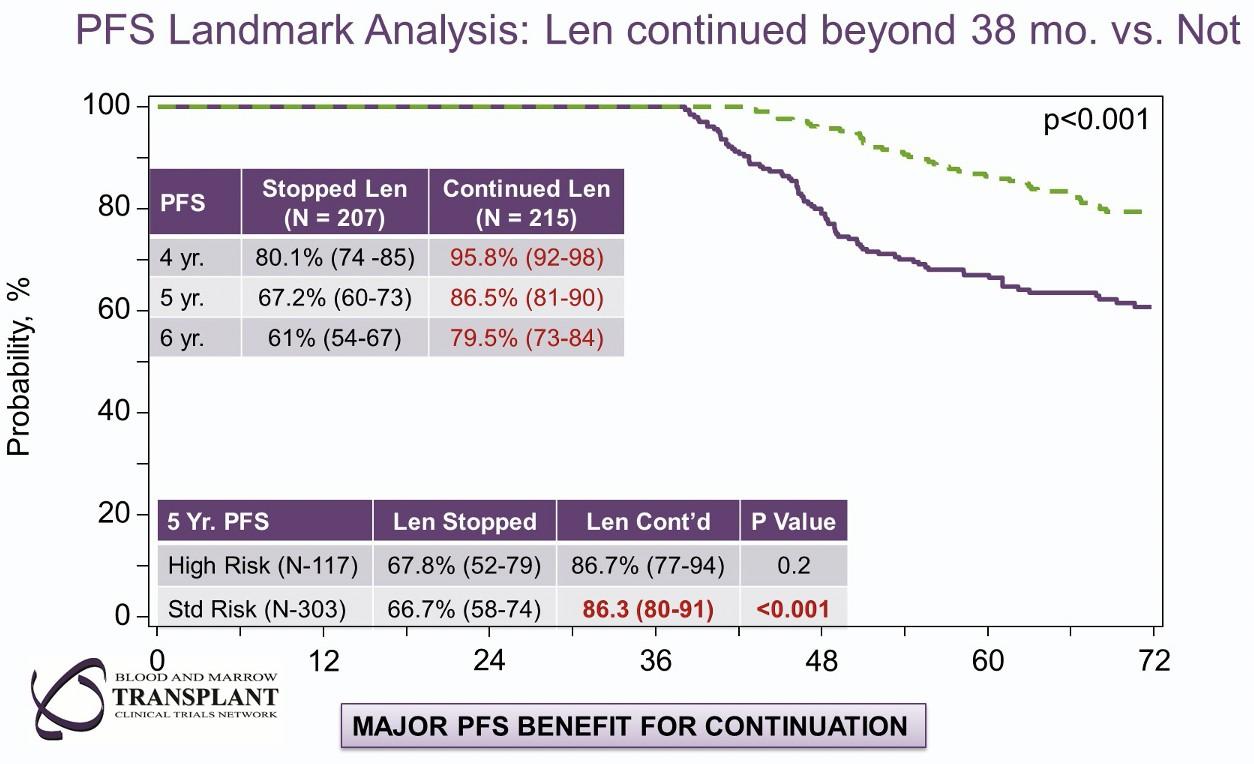
• Several studies, including this BMT-CTN 0702 study. Relapses can begin as soon as the lenalidomide is stopped.
Fred Hutchinson Cancer Center
Len until progression (50% pts)*
Len stopped @ 3 years (48% pts)*
* Balanced but not randomized.
•You don’t get extra points for unneeded side effects
• I always prescribe “off weeks,” which can help us figure out any subtle side effects (or low blood counts) as a reason to lower dose.
• Even on trials, dose goes down with time.
•Don’t cancel your vacation tickets because the len didn’t come on time!
• With maintenance, a few missed doses here and there are totally fine.
• HOWEVER: Keep moving your legs! DVT risk is very real even during maintenance.
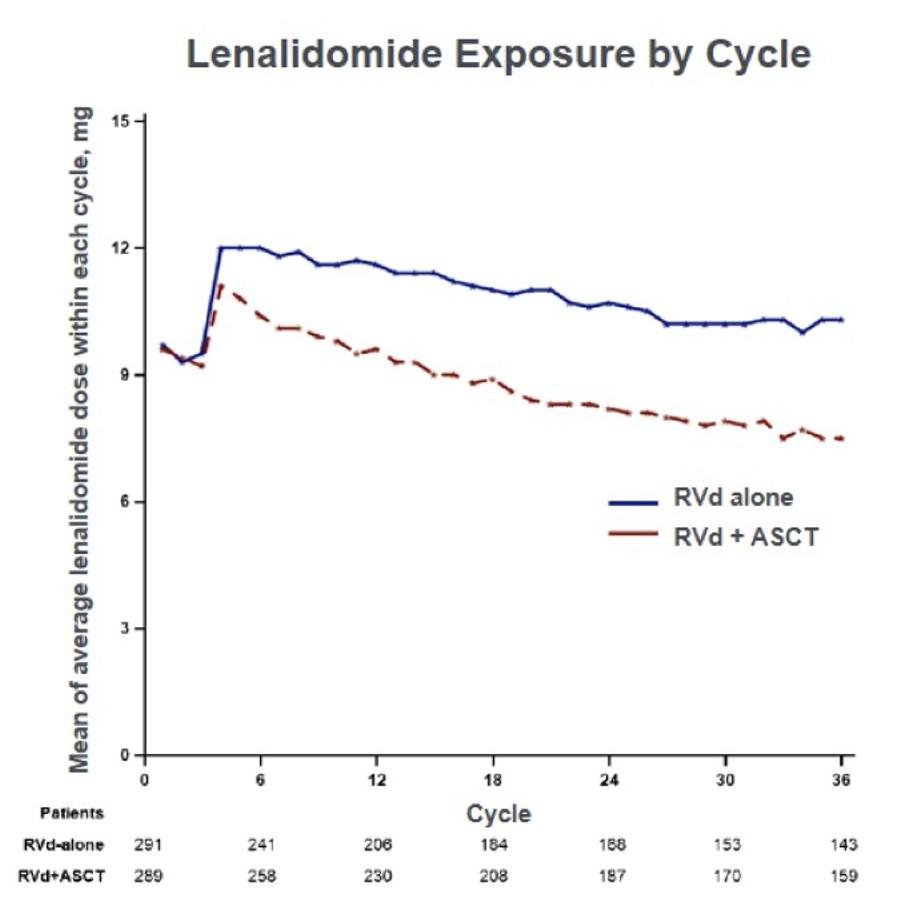
Even on clinical trials like DETERMINATION where our hands are somewhat tied, patients rarely remain on lenalidomide 15mg.
•Doublet maintenance typically includes lenalidomide plus:
• Bortezomib (Velcade®) injections every two weeks, what I typically use; OR:
• Daratumumab (Darzalex®). We’re awaiting the results of a study called AURIGA to tell us whether Dara + Revlimid is better than Revlimid, so I’m waiting for those results.
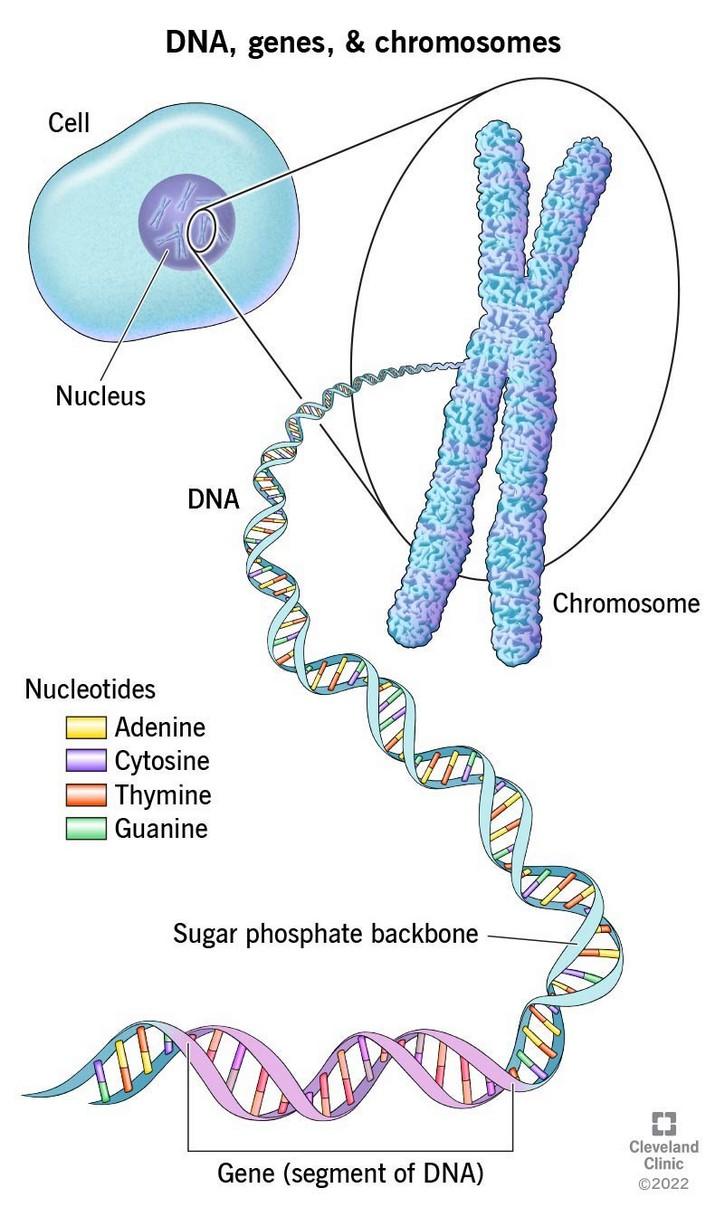
•When would I use doublet maintenance?
• For patients with high-risk cytogenetics, meaning DNA / chromosome features of the myeloma cells that suggest that transplant won’t last for as long.
• For patients who didn’t achieve a full remission with frontline therapy or transplant.
•Why would I use doublet maintenance?
• Helps counteract high-risk cytogenetics or inadequate response.
•As before, dexamethasone really shouldn’t be a part of maintenance.
Fred Hutchinson Cancer Center
•If you’re having symptoms, absolutely!
• For patients being observed, I absolutely recommend monthly labs and potentially annual scans to ensure there are no early signs of the myeloma returning.
•What if I achieve MRD negativity?
• MRD (measurable residual disease) typically refers to the bone marrow biopsy having fewer than 10 out of a million cells left that are myeloma cells.
• VERY complicated topic that we can discuss further in the Q&A. MRD-negative doesn’t mean cure, and MRD-positive can be totally fine in some cases.
• Growing research around “sustained” MRD negativity, i.e. no sign of disease on repeated bone marrow biopsies at least several months apart.
•So what if I achieve sustained MRD negativity?
Fred Hutchinson Cancer Center
•Single-arm MASTER Phase 2 trial of Dara-KRd & transplant:
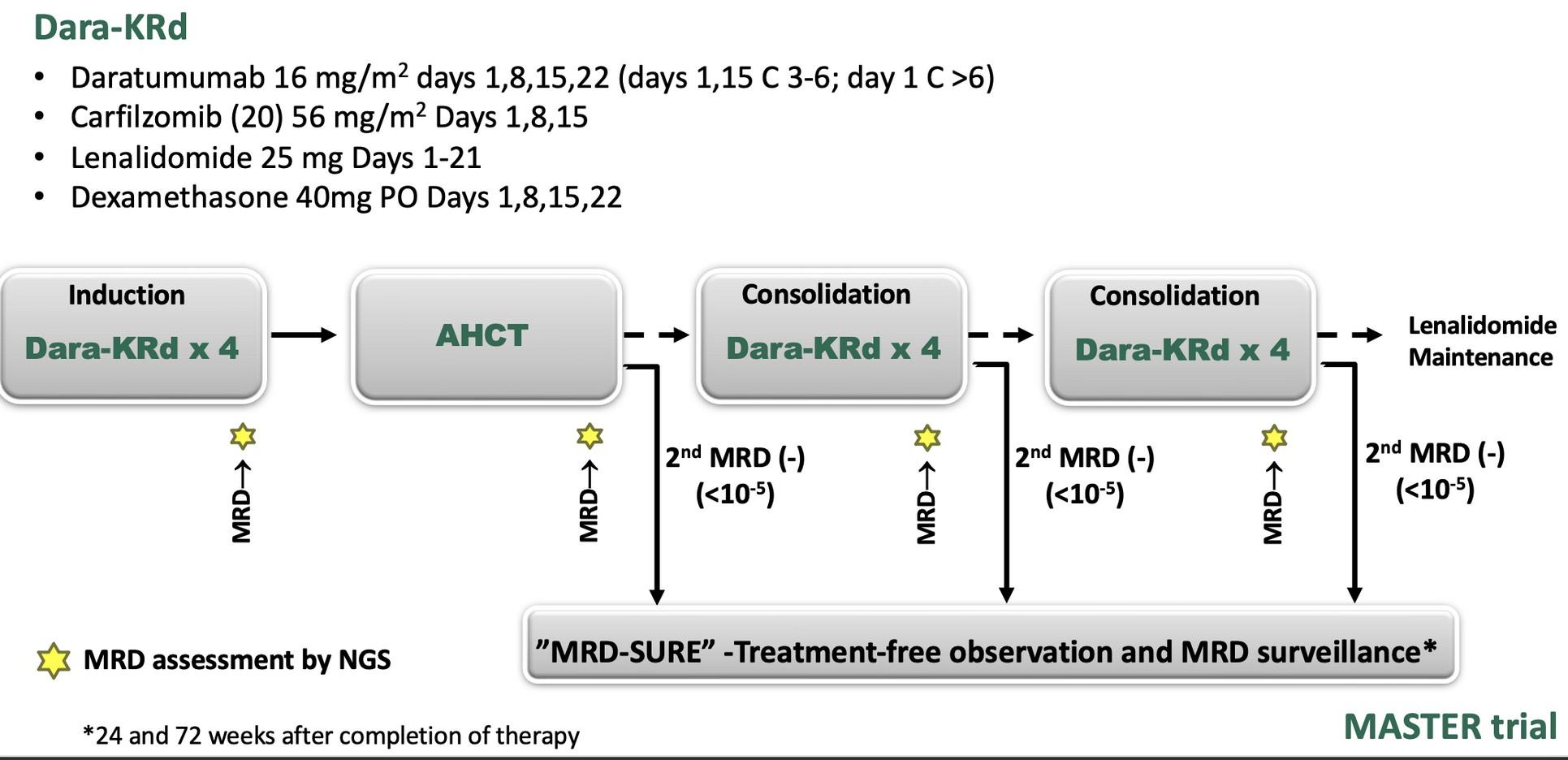
Compared to what we typically do:
• Dara-VRd more typically used at most US centers
• Typically quad x4-6 before ASCT, not quad sandwich
• No defined “MRD sure” treatment-free observation period
•HRCA = High-risk cytogenetic abnormality on bone marrow biopsy, including del(17p), t(4;14), t(14;16), gain(1q), or amp(1q)
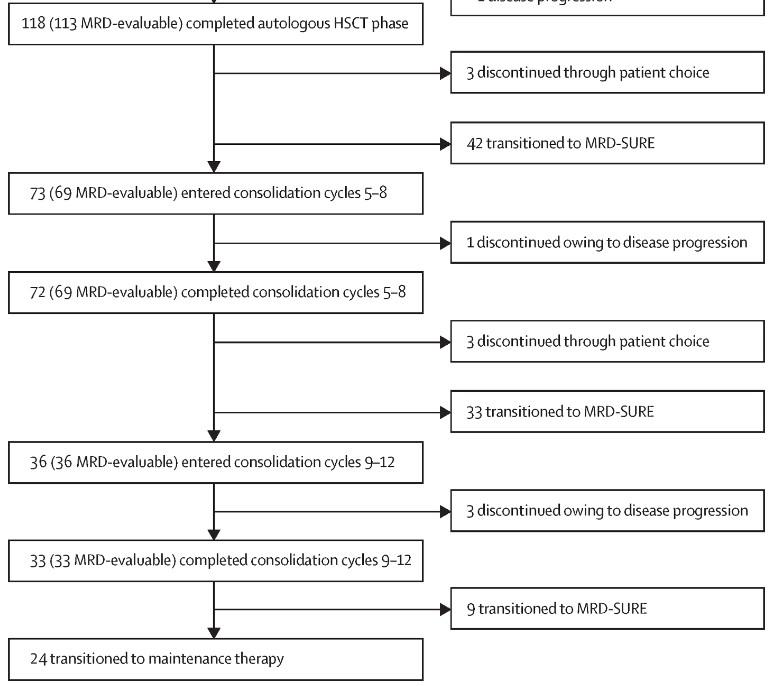
•71% (n = 84) of enrolled patients entered MRD-sure (stopped all treatment), including:
• 78% of patients with 1 HRCA
• 63% of patients with 2 HRCAs
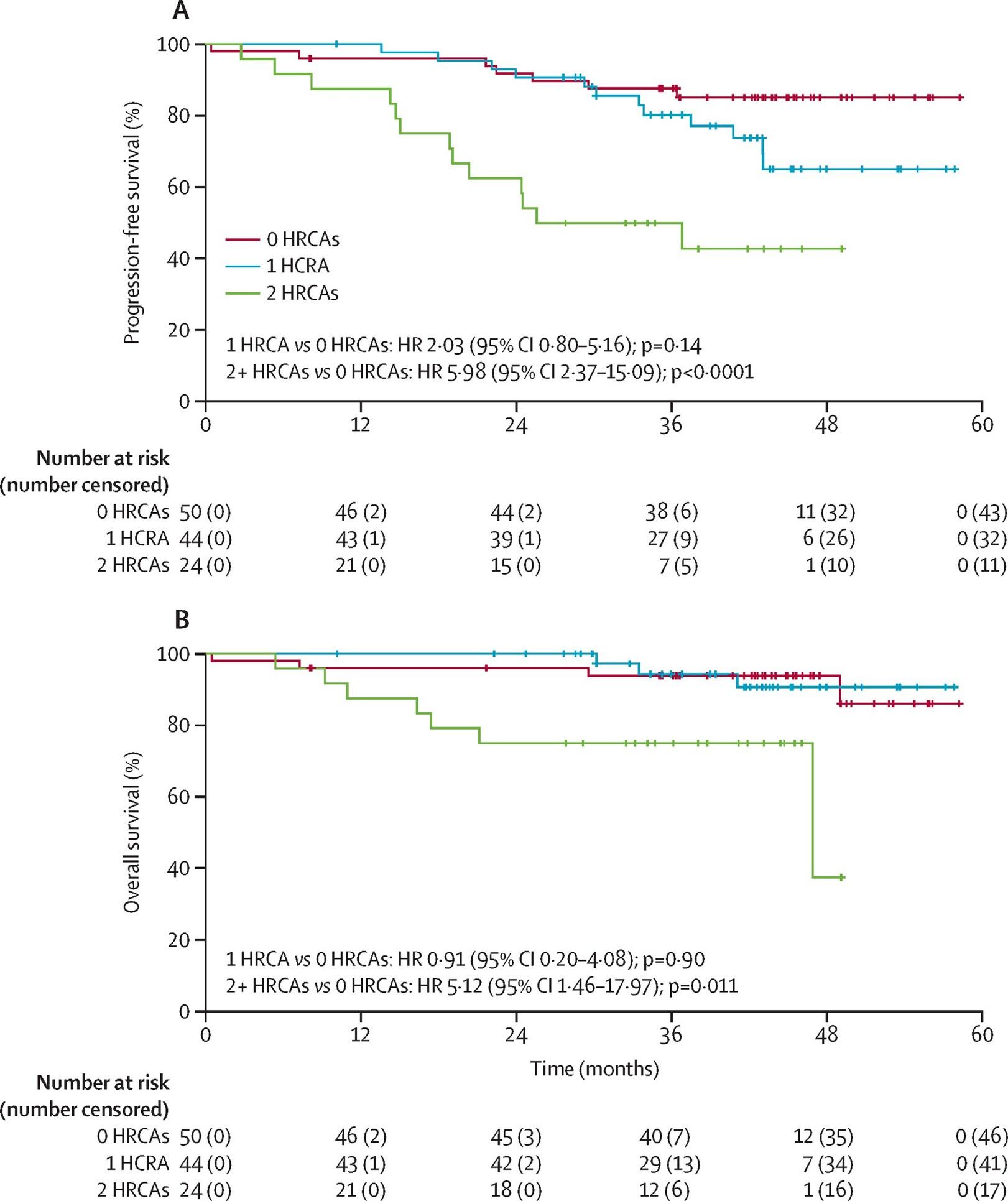
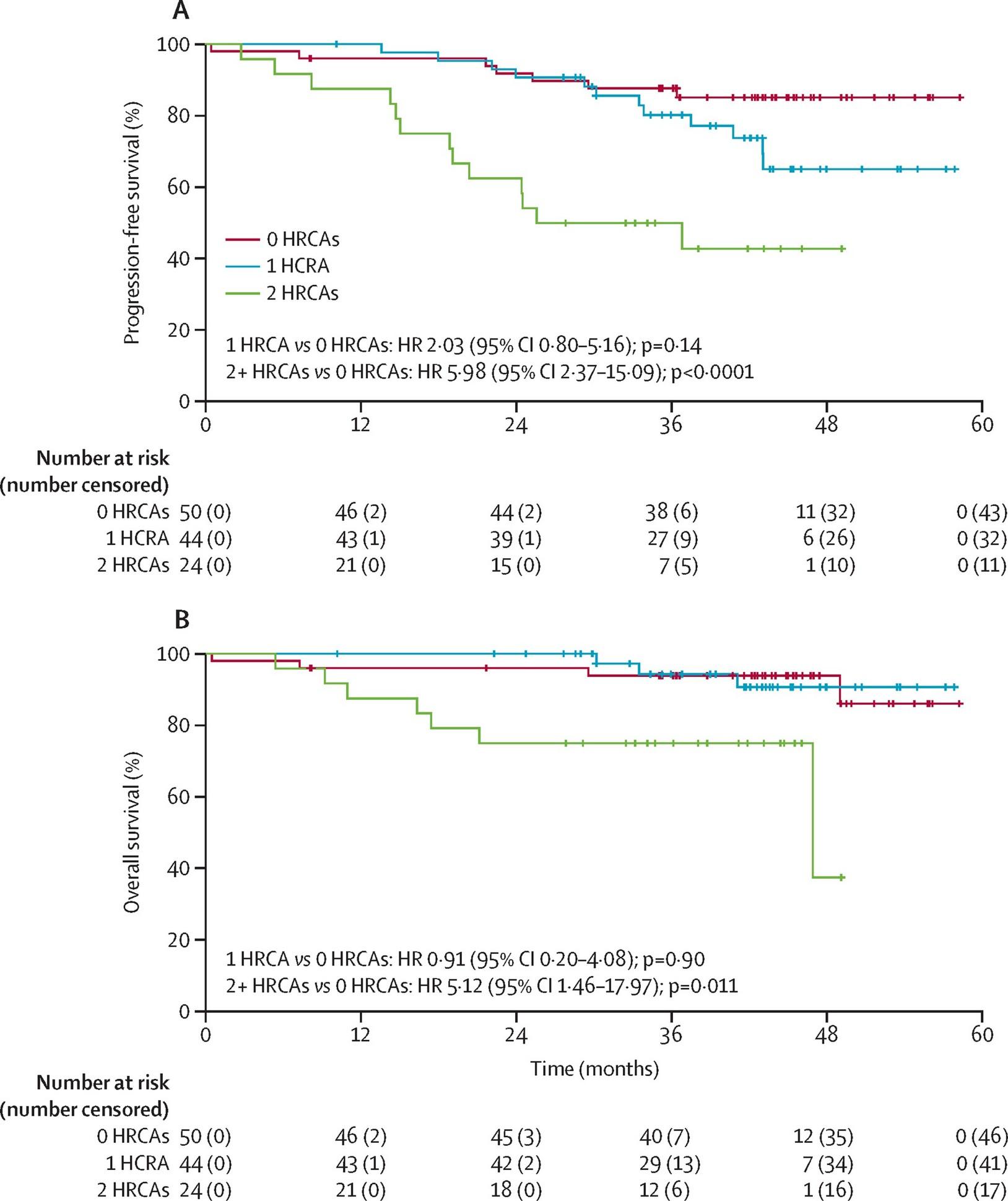
•Some patients with MM do great with stopping all maintenance therapy and just observing
• However, for patients who have 2 or more “high-risk” features, this might not be as good of an option as just waiting.
• “Sustained” MRD negativity, including negative imaging like a PET-CT or MRI, is better than a one-time negative reading
•For now, continued lenalidomide maintenance should still be the standard of care for most patients
• Technically, “MRD-sure” patients should continue to get bone marrow biopsies to evaluate for MRD resurgence…
• It’s unclear whether MASTER still applies to other treatment paradigms with MRD negativity, e.g. Dara-VRd or single-agent len maintenance
For now, MRD is not the end-all-be-all
•Some MRD-positive patients have an “MGUS-like” phenotype with excellent long-term outcomes
•Current real-time MRD assessments are based on serial bone marrow biopsies, which aren’t ideal.
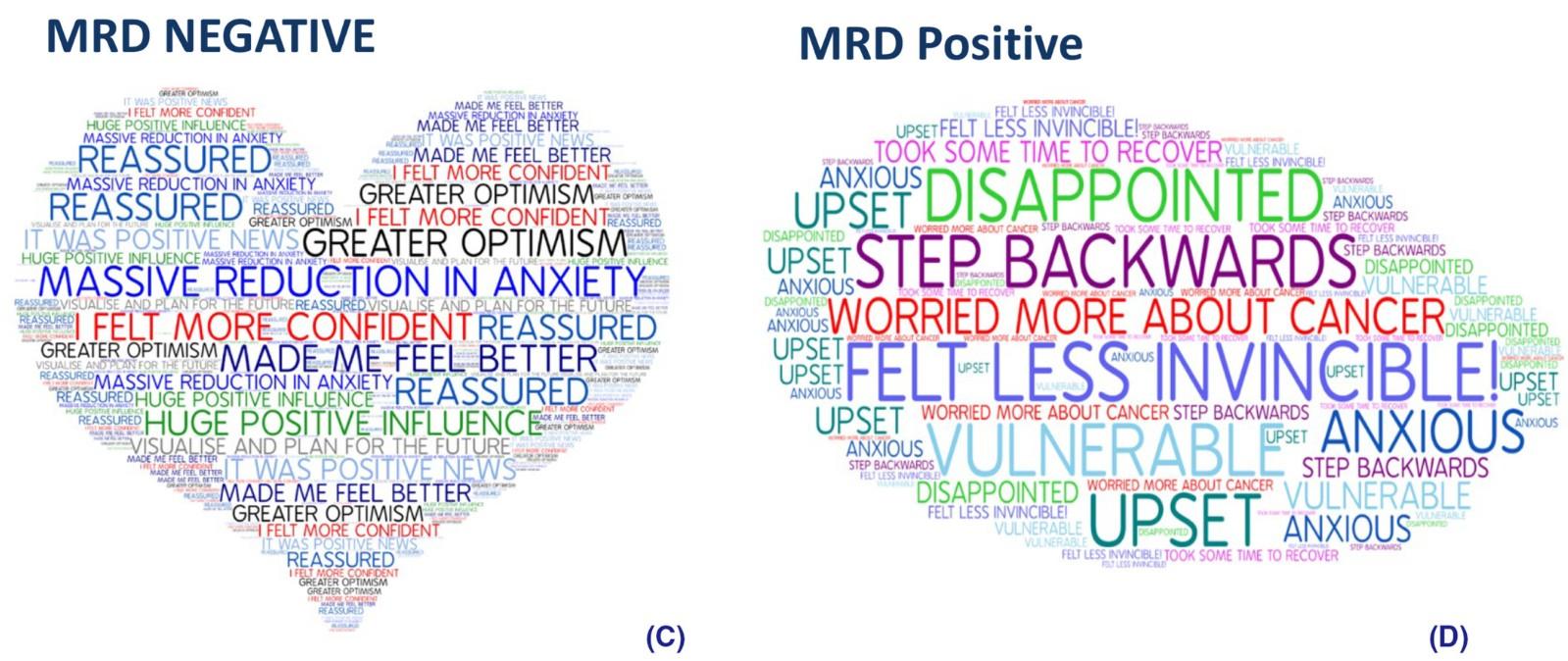
Unfortunately, we have hyped up MRD negativity a bit too much as a field – I will openly admit that.
•For patients who underwent transplantation:
• Lenalidomide by itself if no high-risk features
• Lenalidomide plus bortezomib (Velcade®) or plus carfilzomib (Kyprolis®) [no dex] if any high-risk features
•For patients who didn’t undergo transplantation:
• I generally get to the above (or lenalidomide + daratumumab) depending on both patient and disease-related factors
•For patients interested in MRD-guided decision-making:
• We have a very careful discussion about the knowns and unknowns so far. Every year I tweak the discussion we have about this.
Fred Hutchinson Cancer Center
Autumn Jeong, MD
University of California San Diego
Relapsed Multiple Myeloma
Autumn (Ah-Reum) Jeong, MD
Assistant Professor of Clinical Medicine
Division of Blood and Marrow Transplantation
UCSD Health
•Research funding from GPCR Therapeutics and Pfizer.
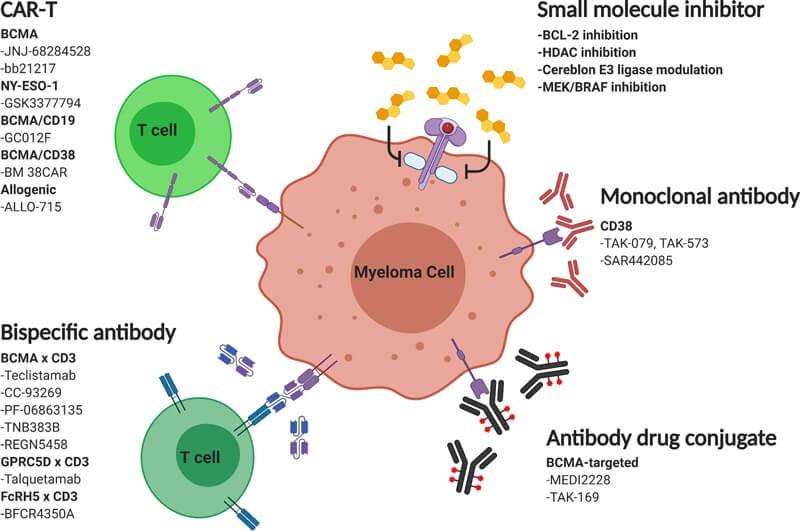
•Anti-myeloma therapies
•CAR T-cell therapy
•Bispecific antibody therapy
•Clinical Trials
Approved Myeloma Therapies
Proteosome Inhibitor
Bortezomib (Velcade)
Carfilzomib (Kyprolis)
Ixazomib (Ninlaro)
Immunomodulatory drug
Lenalidomide (Revlimid)
Pomalidomide (Pomalyst)
Anti-CD38 Antibody Alkylator
Daratumumab (Darzalex)
Isatuximab (Sarclisa)
Cyclophosphamide (Cytoxan)
Melphalan
Other
Selinexor (Xpovio)
Elotuzumab (Emplicti)
Venetoclax (Venclexa)
Steroid
Mix and match the above options based on side effects
Approved Myeloma Medications
Proteosome Inhibitor
Bortezomib (Velcade)
Carfilzomib (Kyprolis)
Ixazomib (Ninlaro)
Immunomodulatory drug
Lenalidomide (Revlimid)
Pomalidomide (Pomalyst)
Anti-CD38 Antibody Alkylator
Daratumumab (Darzalex)
Isatuximab (Sarclisa)
Cyclophosphamide (Cytoxan)
Melphalan
Other
Selinexor (Xpovio)
Elotuzumab (Emplicti)
Venetoclax (Venclexa)
Steroid
Mix and match the above options based on side effects
Approved Myeloma Medications
Proteosome Inhibitor
Bortezomib (Velcade)
Carfilzomib (Kyprolis)
Ixazomib (Ninlaro)
Immunomodulatory drug
Lenalidomide (Revlimid)
Pomalidomide (Pomalyst)
Anti-CD38 Antibody Alkylator
Daratumumab (Darzalex)
Isatuximab (Sarclisa)
Cyclophosphamide (Cytoxan)
Melphalan
Other
Selinexor (Xpovio)
Elotuzumab (Emplicti)
Venetoclax (Venclexa)
Steroid
Mix and match the above options based on side effects
Approved Myeloma Medications (Used Alone)
BCMA CAR-T
Ide-Cel (Abecma)
Cilta-Cel (Carvykti)
BCMA Bispecific Antibody
Teclistamab (Tecvayli)
Elranatamab (Elrexfio)
Approved to use after failing 4 different lines of therapies
GPRC5D Bispecific Antibody
Talquetamab (Talvey)
Formulation/Administration
•Intravenous (IV)
•Subcutaneous (SQ)
•Starts weekly and may eventually extend to monthly
Side effects
•Infusion reactions (rash, shortness of breath, swelling, low blood pressure)
•Skin reaction
•Cold-like symptoms
•Decreased blood cell count
Formulation/Administration
•Intravenous (IV)
•Weekly
Side effects
•Cold-like symptoms
•Decreased blood cell count
•High blood pressure
•Diarrhea
•Tiredness
•Fever
•Shortness of breath
•Kidney and liver injury
Pomalidomide (Pomalyst)
Formulation/Administration
•Oral (PO)
•Daily, with a week break
Side effects
•Decreased blood cell count
•Diarrhea
•Tiredness
•Infection
•Nausea
•Birth defects
•Blood clots
•Liver injury
•New cancers
Different target for different cancers
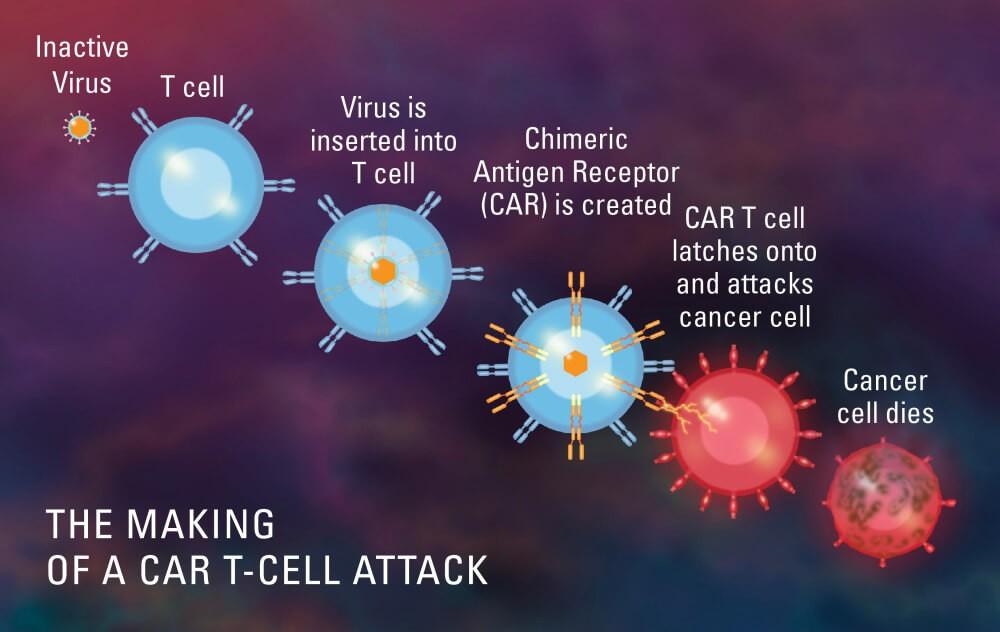
CAR T-Cell Therapy
Idecabtagene
vicleucel (Abecma)
Binds 1 epitope of BCMA
Ciltacabtagene
autoleucel (Carvykti)
Binds 2 epitopes of BCMA
CAR T-Cells: currently approved after receiving 4 prior therapies
Cytokine release syndrome (CRS)
Immune-effector cell associated neurotoxicity syndrome (ICANS)
https://www.tecvaylihcp.com/dosing-andadministration
Bispecific antibodies: currently approved after receiving 4 prior therapies
Notable side effects
Skin, nail, taste changes
•One time treatment
•More intense treatment, requires chemotherapy
•Long manufacturing time
•Single target (BCMA)
Bispecific Abs
•Ongoing treatment
•Less intense treatment
•Off-the-shelf (immediate treatment)
•Multiple targets (BCMA and GPRC5D)
CAR T-Cells for earlier treatment
Other clinical trials
•CAR T-Cells with different targets (GPRC5D) / multiple targets (CD19 and BCMA)
•Allogeneic CAR T-Cells
•Bispecific antibodies with different targets (FcRH5)
•Bispecific antibodies as earlier line of treatment
•Bispecific antibodies with different combinations
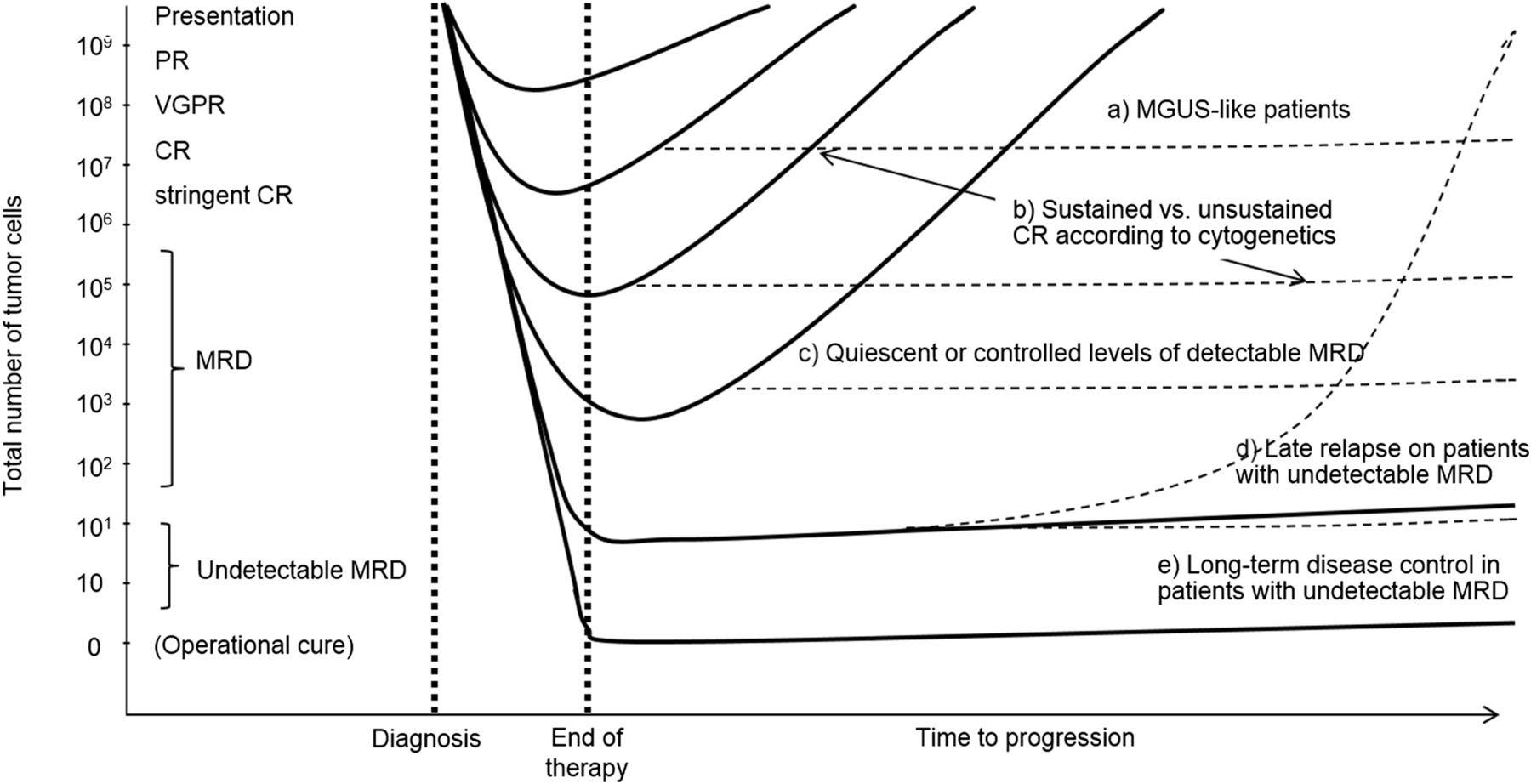
Bruno Paiva et al., Blood, 2015;125(20):3059–3068.
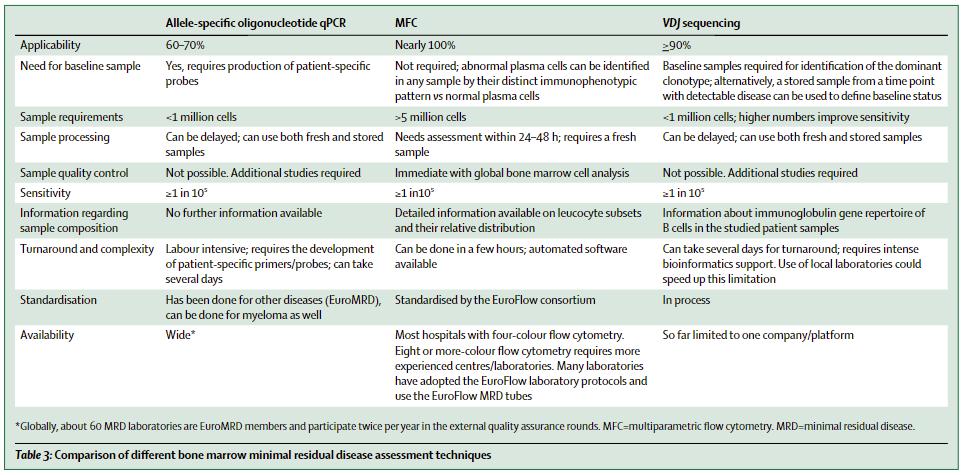
146 MRD is prognostic
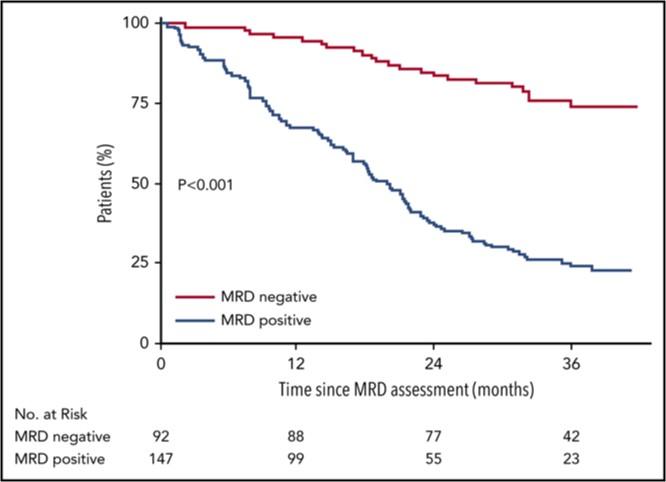
Perrot et al., Blood (2018) 132 (23): 2456–2464.
•Achieving MRD negativity predicts better outcomes.
• Patients who achieve MRD have a longer remission and longer survival
Many unanswered questions with MRD monitoring
•Limitations of MRD monitoring
• Spatial heterogeneity and extramedullary disease
• Bone marrow biopsy is needed
•MRD adoptive treatment algorithm?
• Should we intensify treatment if MRD negativity is not achieved?
• Should we stop treatment if MRD negativity is achieved?
• How long of a MRD negativity is sufficient?
Thank you!
Questions?