11 minute read
SafeTPen™ New Product Launch


Product launch
Since the publication of the article Phenol: past, present and future (Wooldridge, 2021) there has been a National Patient Safety Alert issued around the use of Liquid Phenol 80% (NHS 2021). The safety alert requires all bottles of multi-use Phenol with concentrations of 80% and above being removed from Podiatry clinics and safer alternatives to be sought for nail matrix ablation. The alert was published after 5 years of investigations into incidences which required some patients to be hospitalised.
Advertisement
By Michelle Gibson Training & Education Manager, Canonbury Products Ltd
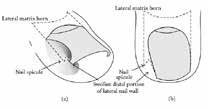
Figure 1 - Schematic illustration of the adolescent type of ingrown toe nail as cited in Haneke (2012)

Figure 2 - Stage 1 – 3 of onychocryptosis Eekhof et al., 2012) Nail pathologies make up a large part of a podiatrist’s workload, with 5% according to Moda and Latham (2016) being onychocryptosis. The requirements for the surgical removal of a toenail can have many aetiologies - shape of the nail (involution, fan shaped); poor footwear causing pressure; teenager hyperidrosis; and the most common factor being poor cutting techniques by patients or carers (Moda and Latham, 2016; Institute of Chiropodists and Podiatrists (IOCP 2022) See Figure 1
Onychocryptosis can be presented at different stages to a podiatrist:
Stage 1 often only requiring conservative treatment (e.g. packing, nail brace or gutter treatments), with
Stage 2 to 4 often requiring surgery (Martínez-Nova, SánchezRodríguez, and Alonso-Peña, 2007) and
Stage 4 is (where the skin from around the nail plate can cover the entire nail) requiring a Zadek’s procedure and referral to a Podiatric surgeon (Abbot, Maher and Wilkinson 2012). See Figure 2 Stage 2 and 3 can generally be managed with nail surgery and ablation within either NHS or private practice, as long as the suitably qualified Podiatrist has kept up to date with their local anaesthesia certificate, cardiopulmonary resuscitation and anaphylaxis training (IOCP 2022) (Royal College of Podiatrists RCoP2021).
The decision to remove the nail is often through the assessment of pain, reoccurring onychocryptosis, surgical relapse and failure of conservative treatment requiring the ablation of the nail matrix during surgery (Martínez-Nova, Sánchez-Rodríguez, Alonso-Peña 2007). This can be done as mentioned by Wooldridge (2021) and Eekhof et al., (2012) with phenolisation in conjunction with surgical removal of part or the whole nail; a Zadek’s; Vandenbos; or terminal Syme and Winograd procedures.
However Eekhof et al., (2012) concluded their report stating that phenolisation of the nail matrix combined with a surgical procedure to remove the nail was the preferred procedure, rather than purely a surgical procedure on its own. Following auditing of Phenolisation of the nail matrix it has been found that there is a minimal proportion of patients that report regrowth 1 year post op where the phenolisation has been carried out effectively (Eekhof et al., 2012; Kannegieter and Kilmartin, 2010).
Traditionally phenol has been applied through the decanting of phenol into a gallipot from a bottle, which leaves the practitioner and patient open to inhalation of the fumes, as well as possible spillage when decanting. Bottled phenol has the ability to take in the atmosphere’s moisture diluting its strength and reducing its reliability of its action as a nail ablation agent (RCoP, 2021). (RCoP 2021) T raining 30 years ago taught students to drop the phenol from an orange stick or dropper onto the blacks file within the nail sulci (IOCP 2022) and then to be rubbed in for 3 x 1 minute.

Figure 3 – Galipot containing decanted phenol
Since this time practice has been adapted into using cotton wool tipped orange sticks. However, both of these methods require a careful hand when applying across the toe / foot from a clean field or the holding of the gallipot above the area of surgery and then delivery into the sulci, ensuring that the phenol doesn’t drip onto any other skin or seep under the tourniquet. Any drips onto the surrounding skin or seepage under the tourniquet could result in other tissue damage from a phenol burn.

Figure 4 - Traditional method of phenolisation
With all of this in mind, and the only available alternative safe phenol product available on the market being the Swab-it (EZ Swab), Canonbury Products Ltd are launching a safer alternative delivery device for nail ablation combined with phenolisation. Working in collaboration with practicing podiatrists and the Institute of Chiropodists and Podiatrists (IOCP) the SafeTPen™ was conceived.


Figure 5 - SafeTPen™ logo and SafeTPen™ device
What is it?
SafeTPen™ contains blue coloured 89% Phenol USP in a 0.4ml quantity for professional use during nail matrix ablation. SafeTPen™ comes with an 18 month shelf like, is registered with the MHRA as a Medical Device and is UKCA marked – the UK equivalent of the CE mark for Europe.
SafeTPen™ contains a glass ampoule within a plastic outer coating. Use of a glass ampoule was chosen to prevent evaporation of the phenol when stored as well as prevent absorption of moisture, thereby allowing the end user to be guaranteed to have 0.4ml of phenol at 89% to use during a partial or total nail avulsion. The glass ampoule and plastic outer is designed to prevent any splash back of phenol onto the practitioner, which can happen when piercing the membrane with other devices, or spillage through decanting prior to the procedure.
The decision was made to blend a blue dye with the phenol to make it more visible to the practitioner, allowing then to easily see if the tube has been damaged prior to use; to see where the phenol has been applied correctly; and, more importantly, if any phenol has been administered by mistake to the surrounding tissue, therefore reducing the potential burning of intact skin on the patient.
Figure 4 shows leakage onto the base of the sulci during the application and figure 6 where the skin is white around the sulci post-phenol application.


Figure 8 - SafeTPen™ ready for use
Figure 6 - Post- phenolisation using the traditional method – 3 x 1minute applications
To use SafeTPen™ it is a quick “Snap, Snap and Squeeze” (figure 7) – through snapping the 2 ends of the glass ampoule (proximal to distal) and a gentle squeeze of the plastic tube phenol is loaded into the compressed polyester tip of the device ready for use. The compressed polyester was chosen for the tip so that there was no possibility of leaving cotton wool fibres within the nail matrix area, therefore reducing the chance of post-op infection due to the cotton wool fibres contributing as a foreign body. The tip is tapered and smaller overall in diameter compared to the current swabs available on the market, allowing the practitioner to have more accurate positioning and application of phenol to the site where it is needed.
Usage of SafeTPen™
Once the tip has turned blue, you know it is impregnated with phenol (see Figure 8), a further gentle squeeze will allow phenol to be dropped from the tip.
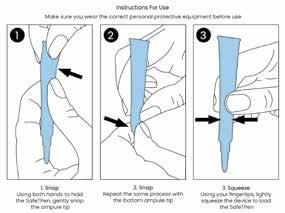
Figure 7 – How to activate the SafeTPen™
NB: Please see the bottom of page 22 for the REFERENCES for this article
SafeTPen™ doesn’t require pressure from the practitioner or aggressive rubbing into the matrix to undertake the ablation, compared to the traditional method using cotton wool or a blacks file. Excessive pressure on the SafeTPen™ tip may cause the tip to retract, at which point it is advised to discard the device to prevent excessive phenol flow rate. Recommended use of the phenol within SafeTPen™ is as per your university training or guidance through your Institute / College membership.
Gold standard practice for the use and timing of phenolisation for nail ablation is through patient assessment. Although the 3 x 1 minute application is ideal for a well perfused hallux, the actual time of the phenol applied should be related to the surface area of the nail bed that requires ablation and healing time, in which case the time should be adjusted downwards (IOCP, 2022; RCoP 2021).
Figure 9 -
SafeTPen™ in use

For each procedure undertaken, phenolisation time and amount used should be taken into consideration and recorded on the patient’s notes (IOCP, 2022 and RCoP 2021). SafeTPen™ can be used for more than 1 minute application.
Once you have applied one minute application of phenol dry if required or as per local protocol and then reapply the same SafeTPen™ into the area for the next 1 minute ablation as long as there is still phenol contained within the SafeTPen™ delivery device.
Kannegieter and Kimartin (2010) cited Giacalone (1997) in the treatment of diabetic patients with phenolisation. Giacalone (1997) is cited as saying there was no post-op infection or ischaemia from the procedure of nail surgery using phenolisation and saw an average healing time of 5 weeks. The SafeTPen™ is not contra-indicated for use in the immune-compromised patients, patients on anti-coagulants, diabetes etc., however it is the responsibility of the practitioner to have thoroughly assessed the patient’s understanding of the procedure, medical history, contra-indications to LA, tourniquet and phenol as well as the assessments of the lower limb (neurological and vascular) to ensure it is safe to proceed (IOCP, 2022; RCoP 2021) . NHS (2009) issued a National Patient Safety Alert recommending the use of CE marked, coloured and labelled tourniquets (e.g. Tournicot/Unicot from Canonbury Products Ltd.) to prevent patient injury / amputation through tourniquets being left in situ following toe and hand surgery.
The use of SafeTPen™ is required to be documented in the patient’s notes recording the batch number, the strength and the time it was applied during ablation. However, it is good practice to record the approximately volume used within the surgery e.g. using 2 x SafeTPen™ during the surgery can be recorded as 0.4ml of liquid phenol 89% (1 pen) per sulci via the SafeTPen™ delivery device or 0.8ml of liquid phenol (2 pens) via the SafeTPen™ delivery device used in total.
Following phenolisation with SafeTPen™, as with bottled phenol and the alternate swab, there is no requirement to wash the sulci out with 5% chlorhexidine spray, saline, or glycerine (RCoP 2021). It has been discussed that washing of the sulci / nail matrix areas can cause the phenol to contaminate surrounding tissue and possibly seep under the tourniquet if not protected adequately, it is also possible that the use of a post-op wash could lead to dilution and increased risk of regrowth, however this decision is the practitioner’s choice through following their training / local guidelines.
Dressing the toe on completion of the nail surgery procedure, when using SafeTPen™, doesn’t require any special dressings techniques, again the dressing choice is left to the practitioner’s knowledge / local or national guidelines.
Following the surgical procedure, the SafeTPen™ should be disposed of as medical waste, and disposed of as per clinical guidelines and the local medical waste policies.
If you have any further questions about the new alternative, safer delivery device SafeTPen™ for using phenol within surgery, please contact Canonbury Products Ltd. via info@canobury.com
Gaynor Wooldridge
There were a number of possible safe alternatives already available for chemical matrixectomy, including some well-known brands, Sodium Hydroxide or Trichloroacetic Acid.
As Chair of the Medicines and Procedures Panel (MaPP) for the IOCP, I led a team to immediately begin researching safe phenol alternatives for members and, in August 2021, we had discussions with a US provider of single-use phials. Four members trialled the new product, but we quickly decided that it was very similar to another product already available in its handling and application.
In September 2021, we began talks with Canonbury about what seemed like an exciting potential new product development, and we entered into discussions on what we, as Podiatrists, actually needed from a single-use phenol. That was incredibly easy. We all know, in our profession, what the disadvantages of the current products are:
1. The ability to access the phenol easily and safely 2. Seeing the product we’re actually using 3. Not running short of the phenol during nail surgery 4. Safely being able to apply the product with an applicator that is too large
The prototype was available at the end of November 2021, and handling it was a ‘wow’ moment. It felt so easy, safe and comfortable, and came with an applicator tip that truly suited its purpose. Yes, this was exciting!
So, here we are today with the launch of this amazing new product, that I absolutely believe will be a game-changer for the world of podiatry.






