18 minute read
Case Study: Deprescribing to Resolve Oversedation


Deprescribing to Resolve Oversedation and Confusion in an Older Person Treated for Auditory Hallucinations and Poststroke Seizure Prophylaxis
AUTHOR
Mark Branum, PharmD, BCGP, Adjunct Assistant Professor, Drake University; Adjunct Assistant Professor, University of Iowa
This article was published in The Senior Care Pharmacist by the American Society of Consultant Pharmacists (ASCP). Doi:10.4140/TCP.n.2021.645.
INTRODUCTION
This case study reviews the pharmacotherapy of a resident in a longterm care facility being treated for poststroke seizure, hallucinations, and dementia, a geriatric syndrome that is both common in regard to its prevalence and severe in regard to its impact on the individual, families, caregivers, and health care system. This case describes the past medical history of an older resident in a skilled nursing facility that was receiving pharmacological therapy for auditory hallucinations and for poststroke seizure prophylaxis, was noted to be having side effects from drug therapy, and how the nursing staff communicated with the consultant pharmacist to resolve these issues.
KEY WORDS: Antipsychotic medication, Case study, Dementia, Geriatric syndrome, Hallucinations, Interprofessional communication, Older person, Poststroke seizure, Deprescribing, Potentially inappropriate medications.
ABBREVIATIONS: CVA = cerebrovascular accident, D2 = dopamine receptor D2, PIMs = Potentially inappropriate medications, SVA = synaptic vesicle protein type 2A, SV2A = synaptic vesicle glycoprotein 2A.
Sr Care Pharm 2021;36:645-51.
Any medication therapy can cause adverse effects, especially in older patients.
Betsy: A 91-Year-Old Female Living in a Skilled Nursing Facility Betsy is a 91-year-old resident of a skilled nursing facility where most residents are 80 years of age or older, many have significant functional limitations in terms of mobility, and most need partial or total assists with activities of daily living. The facility has an occupancy of 55 residents with a central dining room, several common areas including a sunroom, patio, activities area, chapel, and an attached clinic-run physical therapy office.
HISTORY OF PRESENT ILLNESSES
Betsy was admitted to her present nursing facility after a brief hospitalization for pneumonia. Prior to her hospitalization, she was living in a different nursing facility and was doing reasonably well. She was seen by her primary care physician every two months in that facility and was treated by a telehealth psychiatrist who diagnosed her with “major depressive disorder with psychotic features.” She had a stroke approximately two years prior to her recent hospitalization for pneumonia and had subsequent left-sided hemiplegia and hemiparesis. Progress notes from the psychiatrist prior to her hospitalization for pneumonia included “auditory hallucinations,” a “euthymic mood,” and also that she “does not hear well.” A similar note from a telehealth psychologist noted that Betsy had a “pleasant and cooperative demeanor” with some “auditory hallucinations” but no visual hallucinations noted.
Upon admission to her present nursing facility after her hospitalization, nursing staff noticed that Betsy was quite lethargic and asked if medications could be contributing. Nursing staff, including one that happened to be Betsy’s niece, reached out to the facility’s consultant pharmacist with their concerns regarding Betsy, her medications, and possible side effects. Nursing staff raised questions about her Seroquel dose at bedtime for “auditory hallucinations” and questioned whether the “man singing” that she hears might be either tinnitus or perhaps sounds overheard from another resident's television in the neighboring room. As the consultant pharmacist for the facility, you listened to the staff members’ concerns regarding Betsy’s medications, sedation, and began a thorough medication regimen review.
Past Medical History Heart failure, vascular dementia, cerebrovascular accident (CVA), hypertension, chronic atrial fibrillation, anxiety, depression, chronic obstructive pulmonary disorder, osteoarthritis, depression with psychotic features.
Social History Alcohol use: none noted; nicotine: former smoker for many years, no indication of pack/year history.
Physical Exam Height: 66”, Weight: 165 lbs, BP: 129/77, HR: 66, RR: 16, Blood sugar: 153, O2 sat: 95%, pain level: 0.
Laboratory Results RBC = 4.53 M/uL, Hgb = 14.4 g/dL, Hct = 44.4%, Na = 137 mmol/L, K = 4.2 mmol/L, Cl = 95 mmol/L, Anion Gap = 13 mmol/L, Cr = 0.70 mg/dL, eGFR = 76 mL/min/1.73 m2, glucose = 186 mg/dL.
Medications
Medication Dose
Aspirin Duloxetine Atorvastatin Lisinopril Furosemide Potassium
81 mg daily 30 mg daily 80 mg daily 2.5 mg daily 40 mg twice daily 20 mEq daily Quetiapine 12.5 mg nightly Acetaminophen 650 mg twice daily Apixaban 5 mg twice daily Levetiracetam 250 mg twice daily Metoprolol tartrate 25 mg twice daily
ASSESSMENT
The medical team ruled out other potential causes of her presenting symptom of unusual lethargy. She was not dehydrated; her electrolytes were within normal limits, and her vitals were in check. Therefore, medications were suspected to be the possible cause of her symptoms. Betsy’s clinical information provided some insight into her medication therapy. Her stroke occurred just over two years prior to her admission. The telehealth psychiatrist’s progress notes prior to her hospitalization indicated depression, anxiety, and auditory hallucinations. However, there was no indication in the progress notes as to what the auditory hallucinations were, nor if they were bothersome to Betsy.
The psychiatrist’s notes also indicated that the resident was “pleasant and cooperative,” “alert and oriented x 4,” had a euthymic mood, some avoidance and withdrawal behaviors resulting from depression, but was not agitated, delusional, or suicidal. The progress note indicated she was taking Seroquel 12.5 mg every night at bedtime and duloxetine 30 mg every morning. The psychiatrist’s progress notes indicated a plan to increase the Seroquel to 25 mg every night at bedtime, but this dose was not tolerated due to sedation and was decreased back to 12.5 mg nightly at bedtime after only four days. The final progress note from the psychiatrist before her hospitalization indicated that “Betsy does not hear well” but was “better with voices” since initiating Seroquel. Betsy had been evaluated for hearing aids and tried to adapt to using them but failed.
After her discharge from the hospital into her present facility, nursing notes indicated that Betsy was disoriented, alert only to person and had undecipherable, mumbled speech. Her respirations were easy and nonlabored at the time of admission, and she appeared to be recovering from pneumonia well. Nursing staff also affirmed that Betsy was very pleasant, cooperative, not delusional, and not at risk of harm to herself or others. She was also not complaining of hearing any voices at the time of her admission. Her niece, also a nurse in the current nursing facility, wondered if the voices she had heard were due to tinnitus or possibly from a neighbor’s loud television in the room next to hers at the prior nursing facility. Therefore, the nursing staff all affirmed that they felt Betsy would be a good candidate to taper and discontinue her Seroquel dose. Also, given that her stroke had occurred more than two years ago and she had remained seizure-free, you as the consultant pharmacist determined that her levetiracetam 250 mg twice daily for poststroke seizure prevention may no longer be necessary. It appeared as if there were at least two medications that were potentially inappropriate medications (PIMs) for Betsy that may have been contributing to her lethargy and sedation. Plan • Taper levetiracetam dose gradually over a few weeks, then discontinue entirely. • Gradual dose reduction of quetiapine to 12.5 mg every other night for three doses, then discontinue entirely. • Follow-up after discontinuation of quetiapine and levetiracetam for improvement; if not improved, next consider gradual dose reduction of duloxetine 30 mg daily.
Outcome/Follow-up Four weeks later, at the next month’s medication regimen review, Betsy was much more alert, social, and interactive. Both medications, beginning with levetiracetam, were gradually dose reduced and discontinued entirely. Nurses’ notes affirmed that Betsy seemed to be doing well, was able to speak clearly and make herself understood, and had no issues related to tapering off and discontinuing either medication. Additionally, her niece who works at the nursing facility approached the consultant pharmacist and exclaimed, “I need to thank you for helping with my aunt’s medications, she’s doing much better. It’s nice to have my aunt back.”
Sedation with quetiapine occurs mainly at lower doses because of strong histaminergic antagonism.
DISCUSSION
Betsy’s case provides an interesting example of polypharmacy, PIMs, and their consequences in an older person. Because of her stroke (CVA), she was prescribed levetiracetam to prevent poststroke seizures. CVAs are the most common cause of seizures in the older person,1 so prophylaxis after a CVA may appear warranted. However, guidelines from the American Heart Association and the American Stroke Association do not recommend prophylactic administration of antiepileptic drugs to prevent seizures in stroke patients due to a lack of data to properly guide therapy.2 Nonetheless, in this case, levetiracetam 250 mg twice daily was prescribed to prevent poststroke seizures.
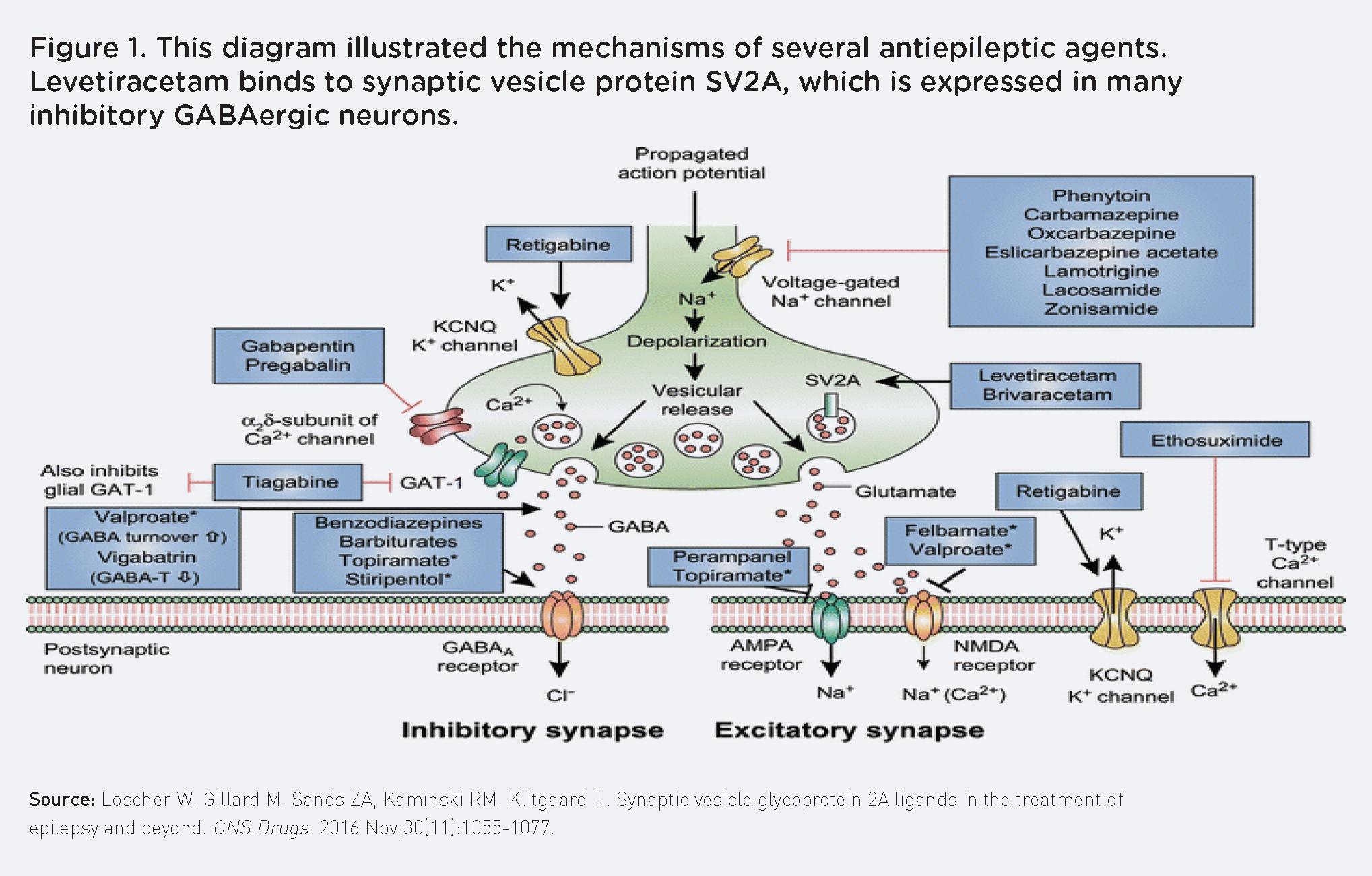
Levetiracetam is believed to exert its antiepileptic effect via binding to the synaptic vesicle protein SV2A in the brain and thereby modulating synaptic neurotransmitter release3,4 (Figure 1). SV2A is one of three isoforms of SV2, which is part of all vertebrate synaptic vesicles.5 The synaptic vesicle protein SV2A is the most common type and is found in both excitatory and inhibitory synapses of the brain.5 SV2A is also the only SV2 isoform that is expressed in many inhibitory (GABAergic) neurons.5 Levetiracetam has been shown to decrease presynaptic glutamate release in neurons with sustained and high frequency firing.5,6
While levetiracetam is generally considered to be well tolerated,7,8 older people are well-known to be more susceptible to side effects because of physiological changes related to aging. Levetiracetam can cause drowsiness and somnolence with a range between 5% and 20% in adult trials.7,9-13 However, drowsiness has been found to be more common in
older people, reported in 12% of younger patients and 24.7% of older patients.4
Quetiapine is a second-generation, atypical antipsychotic that is indicated for the treatment of bipolar disorder both as monotherapy or as an adjunct agent, major depressive disorder as adjunctive therapy, and for the treatment of schizophrenia. Despite questionable efficacy, quetiapine is frequently used for the off-label purpose of treating dementia with behavioral disturbance or behavioral and psychological symptoms of dementia. For the treatment of schizophrenia, a common dosage range of 150 mg to 750 mg is typically seen because of its low affinity for D2 receptors.14-16 At lower doses, quetiapine’s strong antagonism at histamine receptors seems to predominate,17 thereby causing sedation as the main pharmacologic effect.
In the present case, Betsy was receiving lowdose quetiapine (12.5 mg at bedtime) for auditory hallucinations. Besides the side effect of sedation at low doses, the diagnosis itself may have been suspect. Based on nursing notes and conversations with nursing staff, it was not entirely clear whether these were actual auditory hallucinations, as was diagnosed by medical staff. Nursing staff felt that it may have been caused by excess TV noise from a neighboring room, which may have resulted in confusion as to the source of the sound in an elderly patient with a diagnosis of dementia. Further, the symptom overlap between tinnitus and auditory hallucinations18,19 can lead to misdiagnosis and unnecessary treatment with medications like antipsychotics that have the potential for significant adverse effects.
Betsy’s medication regimen was adjusted by first tapering and discontinuing the levetiracetam, as she had been seizure-free for a period of longer than two years and the risk of adverse effects from medication was determined to outweigh the potential benefit. Next, her quetiapine dose was tapered and discontinued. Thankfully, the tapering and discontinuation of these two medications did significantly improve her cognition and decrease her sedation, as was verified by nursing staff, including her niece, and the attending medical provider.
GERIATRIC CLINICAL PEARLS Any medication can cause adverse effects.Any medication therapy, whether appropriately indicated or not, has the potential to cause adverse effects, especially in older patients because of their increased sensitivity to medication side effects. The use of antiepileptic drugs to decrease the risk of or to prevent further poststroke seizures is a relatively common practice. However, despite levetiracetam’s favorable mechanism of action and relative lack of drug-drug interactions, it can cause sedation in approximately 5% to 20% of patients, and this effect is more prevalent in older patients.4
Quetiapine is appropriately indicated for psychiatric disorders including treatment-refractory depression, bipolar disorder, and psychosis. At low doses, however, the effect seems to mainly be sedation, which is a function of its strong histaminergic antagonism. In clinical practice, however, medical providers often seem to overlook this fact and may be hesitant to discontinue antipsychotic medications, even at very
Tapering off low-dose, sedating, quetiapine may help clear and improve symptoms of lethargy, confusion, and sedation in older patients.
low doses for fear of treatment failure or worsening of psychiatric or behavioral symptoms. In Betsy’s case, this was not an issue as she was noted to be pleasant, had a euthymic mood, and was alert and oriented x 4. Tapering off from the quetiapine had no untoward effects, and as hoped for, also helped clear and improve her cognition.
Clinical collaboration and communication are key factors in successful medication therapy adjustment. Clinical collaboration and communication were key factors in the successful reassessment and adjustment of Betsy’s medication therapy. Consultant pharmacists are valuable members of the health care and interdisciplinary teams and are medication experts who are the most accessible health care providers. For successful collaboration, and to help ensure optimal patient outcomes, consultant pharmacists should strive to make themselves readily available and accessible by interacting with staff and by actively seeking and encouraging the routine communication of clinically useful information for their medication regimen reviews. Table 1 reviews reasons and common characteristics for good communication and successful interdisciplinary collaboration.
References: 1. Kramer G. Epilepsy in the elderly: some clinical and pharmacotherapeutic aspects. Epilepsia. 2001:4255-4259. 2. Winstein CJ, Stein J, Arena R, et al. American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and Outcomes Research. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169. doi: 10.1161/ STR.0000000000000098. Epub 2016 May 4. Erratum in: Stroke. 2017;48(2):e78. Erratum in: Stroke. 2017;48(12):e369. PMID: 27145936. 3. Abou-Khalil B. In the treatment of epilepsy levetiracetam. Neuropsychiatr Dis Treat. 2008;4(3):507-523. 4. Löscher W, Gillard M, Sands ZA, et al. Synaptic vesicle glycoprotein 2A ligands in the treatment of epilepsy and beyond. CNS Drugs. 2016;30(11):1055-1077. 5. Yang XF, Weisenfeld A, Rothman SM. Prolonged exposure to levetiracetam reveals a presynaptic effect on neurotransmission. Epilepsia. 2007;48:1861-1869. 6. Meehan AL, Yang X, McAdams BD, et al. A new mechanism for antiepileptic drug action: vesicular entry may mediate the effects of levetiracetam. J Neurophysiol. 2011;106:12271239. 7. Ben-Menachem E, Falter U. Efficacy and tolerability of levetiracetam 3000 mg/d in patients with refractory partial seizures: a multicenter, double-blind, responder-selected study evaluating monotherapy. European Levetiracetam Study Group. Epilepsia. 2000;41(10):1276-1283. 8. Alsaadi TM, Shatzel A, Marquez AV, et al. Clinical experience of levetiracetam monotherapy for adults with epilepsy: 1-year follow-up study. Seizure. 2005;14(2):139-142. 9. Cereghino JJ, Biton V, Abou-Khalil B, et al. Levetiracetam for partial seizures: results of a double-blind, randomized clinical trial. Neurology. 2000;55:36-42. 10. Shorvon SD, Lowenthal A, Janz D, et al. Multicenter double-blind, randomized, placebo-controlled trial of levetiracetam as add-on therapy in patients with refractory partial seizures. European Levetiracetam Study Group. Epilepsia. 2000;41:1179-1186. 11. Berkovic SF, Knowlton RC, Leroy RF, et al. Placebo-controlled study of levetiracetam in idiopathic generalized epilepsy. Neurology. 2007;69:1751-1760. 12. Brodie MJ, Perucca E, Ryvlin P, et al. Comparison of levetiracetam and controlled-release carbamazepine in newly diagnosed epilepsy. Neurology. 2007;68:402-408. 13. Noachtar S, Andermann E, Meyvisch P, et al. Levetiracetam for the treatment of idiopathic generalized epilepsy with myoclonic seizures. Neurology. 2008;70:607-616. 14. Richelson E, Souder T. Binding of antipsychotic drugs to human brain receptors: focus on newer generation compounds. Life Sci. 2000;68:29-39. 15. Gefvert O, Lundberg T, Wieselgren I-M, et al. D2 and 5HT2A receptor occupancy of different doses of quetiapine in schizophrenia: a PET study. Eur Neuropsychopharmacol. 2001;11:105-110. 16. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209-1223. 17. Stahl SM. Selective histamine H1 antagonism: novel hypnotic and pharmacologic actions challenge classical notions of antihistamines. CNS Spectr. 2008;13:1027-1038. 18. Santos RM, Sanchez TG, Bento RF, Lucia MC. Auditory hallucinations in tinnitus patients: emotional relationships and depression. Int Arch Otorhinolaryngol. 2012;16(3):322-327. 19. Alvarez Perez P, Garcia-Antelo MJ, Rubio-Nazabal E. “Doctor, I hear music”: a brief review about musical hallucinations. Open Neurol J. 2017;11:11-14. 20. Nancarrow SA, Booth A, Ariss S, et al. Ten principles of good interdisciplinary team work.
Hum Resour Health. 2013;11:19. doi:10.1186/1478-4491-11-19. 21. Babiker A, El Husseini M, Al Nemri A, et al. Health care professional development: working as a team to improve patient care. Sudan J Paediatr. 2014;14(2):9-16. 22. O’Daniel M, Rosenstein AH. Chapter 33: Professional communication and team collaboration. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for
Nurses. Rockville, MD: Agency for Healthcare Research and Quality (US); April 2008.
Accessed October 15, 2020. https://www.ncbi.nlm.nih.gov/books/NBK2637/.
Reasons consultant pharmacists need good communication skills20,21
• The number of geriatric patients with complex care needs is increasing
• The complexity of skills and knowledge needed to provide care is increasing
• Specialization within health care and fragmentation of disciplinary knowledge increases the number of practitioners providing care for residents
• To promote safe continuity of care with a focus on continuous quality improvement
• Ensure positive interactions with other staff members to achieve optimal patient care Common characteristics of good communicators21,22
• Promote open communication
• Help maintain a respectful environment
• Share responsibility for team success
• Regular and routine communication and sharing of information
• Ask questions to get patient-specific and actionable information
• If there is a lack of clear information, talking with several staff members to get their feedback
• Focus on what is right for the patient
PLANNING TO STOP HIV IN IOWA: HIV & HCV TESTING PROJECT
In January, the Iowa Department of Public Health’s Bureau of HIV, STD and Hepatitis hosted a meeting to kick-off their strategic planning process. IPA staff, along with representatives from local and state health agencies, community advocates, and people living with HIV attended the virtual event. IDPH outlined the planning process and focus areas of the Stop HIV Iowa plan.
While the state of Iowa has seen a nearly 30% reduction in new HIV diagnosis since 2016, ranks second in viral suppression among all states, and is within the top four states for other key measures along the HIV care continuum, challenges still remain. Health disparities and other barriers must be addressed to stop the HIV epidemic in Iowa. IDPH is asking for assistance in creating a plan to reduce new HIV Diagnoses 75 percent by 2025 and 90 percent by 2030. In 2020, the baseline was 100 HIV diagnoses among Iowans.
Increasing access to testing has been a priority for IDPH in fighting the HIV epidemic. Since 2019, IPA has been collaborating with IDPH to manage a multi-year project implementing HIV screenings in community pharmacies. There are currently twelve Iowa pharmacies offering free HIV screenings for their communities, and three of those are also offering free HCV screenings.
IPA is looking to gain more interest in the project in the following counties: Palo Alto, Pocahontas, Calhoun, Webster, Humboldt, Kossuth, Clarke, Decatur, Lucas, Monroe, and Wapello. These are areas of the state that the Iowa Department of Public Health considers focus areas based on their epidemiology reporting.
To participate or to learn more, please contact Kellie Staiert, IPA’s Lead Project Manager, at kstaiert@iarx.org. To learn more about Stop HIV Iowa, visit www.stophiviowa.org.
STOP HIV IOWA FOCUS AREAS:
Primary Prevention & Diagnosing Medical Care & Support Services Addressing Sexually Transmitted Infections Viral Hepatitis Workforce Behavioral Health Health Equity Social Determinants of Health Stigma

IPA MEMBER FORUMS
Learn, Network & Engage Independent & Community Pharmacy Practice Forum – June 21, 2022
STAY TUNED FOR 2023 DATES!
Open and FREE to ENGAGED Pharmacist, Pharmacy Technician and Student Pharmacist members.






Help Advance IPA’s Legislative Agenda... Become a Champion Advocate!

Are you interested in becoming an important partner in helping IPA advance its legislative and regulatory agenda throughout the year? IPA is looking for Champion Advocates across the state of Iowa to build relationships with their elected officials. Help us designate a Champion Advocate in every House and Senate district! Our goal is to establish trust and familiarity with legislators. As you work to educate your legislators on key issues facing pharmacy, we can help build their understanding of our concerns regarding patient care and the roles of pharmacists and pharmacy technicians.
By volunteering as a Champion Advocate, you would be kept up-to-date on the latest information relating to IPA’s advocacy agenda and would be ready to answer the call when IPA needs to make a grassroots push.
What Do Champion Advocates Do? • Build relationships outside of the legislative session by hosting pharmacy visits with legislators and delivering PAC contributions when needed • Contact legislators during session to explain how pending legislation would affect their pharmacy practice • Relay personal experiences to help legislators understand the important roles that today’s pharmacists and pharmacy technicians play in enhancing the health care of Iowans • Stay informed with bill tracking/IPA legislative priorities and participate in bi-weekly update calls