18 minute read
The Important Pelvic Floor – Jaki Nett

from Yoga Samachar FW2016
by IYNAUS

BY JAKI NETT
The pelvic floor is a topic that is approached very gingerly when discussed in a yoga classroom setting. It is not an
Advertisement
area that we talk openly about like we do our back, legs, arms, or chest. As teachers, we tend to be cautious
about how we include the subject—especially in a general yoga class. But it’s important nonetheless.
The pelvic floor is referred to in two ways: the pelvic floor as an area or the pelvic floor as an anatomical structure. It is important to understand the anatomical pelvic floor and its accessory muscles to be able to work with the pelvic floor area in your yoga practice.
The Anatomical Pelvic Floor Pelvic floor muscles are postural muscles—slow twitch muscles, endurance muscles. Pelvic floor muscle dysfunction affects muscle fiber length and contractile force. Stretched and stiff muscle fibers have a decreased ability to generate power for support.
The anatomical pelvic floor has many functions. First, the muscles of the pelvic floor connect the front body to the back body. Second, they close off the bottom of the pelvic outlet. Third, they are responsible for the support of the abdominal viscera. And forth, they resist the internal downward force called the “Valsalva maneuver,” which is a silent wrecker of the pelvic floor muscles.
What is the Valsalva maneuver? It is a natural force that increases interabdominal pressure—the internal force we use to stabilize the core of the body when any form of elimination is needed; it helps force things out.
The dynamic, anatomical/mechanical chain reaction of Valsalva is the sequential inhalation and retention of the breath, which flattens out the diaphragm, blocks the throat, contracts the abdominal muscles, and constricts the sphincters in the pelvic floor and anus. It can have a different result depending on which valve or sphincter is open or weak when Valsalva is expressed.
We experience Valsalva when we laugh hard and loud, sneeze, cough, vomit, defecate, lift a heavy weight, or when we do Paripurna Navasana. These actions can set fear into a woman with weakness of the urethra sphincter, also known as “incontinence.” The push during childbirth is Valsalva to the 100th power.
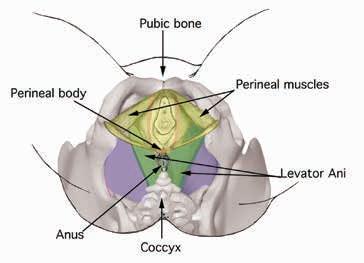
Pelvic Floor Area The boney boundary of the pelvic outlet is created by the pubic bone, the ischial tuberosities or sitting bones, and the inferior sacrum or coccyx. Two muscle layers close off the pelvic outlet: These two layers are the perineal and the levator ani muscle groups, collectively called the perineum or pelvic floor. The levator ani is referred to as the true pelvic diaphragm or true pelvic floor. The perineal muscles are known as the urogenital diaphragm. The levator ani is the deeper of the two layers. The perineal muscle group is more superficial and comprises the perineal body, which is often referred to as the “perineum.” The perineal body is the strong center-supporting member that supports the pelvic floor muscles. When there is damage to the perineal body it weakens this important support.
Pelvic outlet with perineal muscle groups transparency overlaying levator ani muscle groups
Pelvic Floor Dysfunction There are three pelvic floor dysfunctions that can occur separately or together: • Incontinence • Vaginal laxity • Overstretched levator ani and perineal muscle groups, i.e. weak pelvic floor
Incontinence can occur in two basic forms: stress and urge. Stress incontinence is when there is a sudden build up of Valsalva and the pressure forces urine out. Urge incontinence is when the bladder has lost its ability to feel the slow filling-up of urine, creating the sudden urgent need to get to a toilet.
Vaginal laxity is when the vagina has become stretched and has lost its ability to contract. In yoga, when a student inverts, air sometimes enters the vagina, and when the student comes down, it expels with a sound. The ability to consciously contract the vagina along with correct alignment will help control this issue.
Overstretched pelvic floor muscles can be caused by Valsalva, being overweight, strain from constipation, pregnancy, bad posture, pelvic floor operations, sedentary life, menopause, aging, and other issues.
Often people confuse a prolapsed uterus with pelvic floor muscle weakness, but it’s not weakness in that area per se. Prolapse is the result of overstretched ligaments that need to suspend and hold the uterus in its proper place. When these ligaments become stretched and lose their ability to keep the uterus properly aligned, the uterus can slip and turn itself to align with the vaginal canal and move down. And the unconscious pressure of Valsalva can further assist the uterus in moving downward. Contracting of the vaginal muscles will not stop the the uterus from descending. But when the prolapse is at “first stage,” inversions can help manage it.
When working with the pelvic floor muscles, understand that the collective area of the pelvic floor can present different dysfunctions. There can be weakness of the urethra sphincter but no other weakness, laxity of the vaginal canal but no incontinence—or a person can have both.
Muscle Groups Obviously, the external manifestation of the female and male genitalia is quite different, but the musculature and their actions are basically the same in both sexes.
The perineal muscle group contains the superficial pelvic floor muscles that are shaped like a triangle—the urogenital triangle. These muscles take their origins from the pubis and ischial tuberosities and form the perineal body. The perineal muscle group includes: • Ischiocavernosus • Bulbospongiosus • Transverse perineal • Perineal body
The perineal muscles are concerned with urination in both sexes, and in the male, with ejaculation.
The levator ani is supported by the perineal muscle group. The levator ani is a wide, thin muscular sheet that is actually made up of three muscle sets. Together, these muscles form an efficient muscular sling that resists the rise of intrapelvic pressure and supports and maintains the pelvic viscera in position. In women, the levator ani is open in front to allow for the passage of the vagina and urethra, which structurally predisposes a weaker foundation. In men, it is not open in front, which allows for a more stable pelvic floor with only the urethra passing through. An interesting note about the levator ani is that the majority of its fibers are mostly associated with the anus, i.e. levator, “lifting” and ani, “anus.” The levator ani, which takes it origins from the pubic bone, illium, and coccyx, includes the following muscles: • Bulbospongiosus • Puborectalis • Pubococcygeus
Because the perineal muscles and levator ani muscles are very close together, it is impossible to precisely neutralize one and activate the other, but with a little understanding and sensitive work, localized contraction can be achieved.
In addition, there are two vaginal muscles that run in opposition to each other. The deeper layer, the stronger of the two layers, runs lengthwise along the canal. When it contracts, it pulls the vaginal canal upward. The inner layer, which can be felt with the fingers, has fibers that run in a circle around the canal. When they contract they close the circumference of the vaginal canal. These muscles together are known as the “vaginal coat” and can be contracted to counteract vaginal laxity.
When doing pelvic floor work, contractions are kept between the perineal body forward toward the pubic bone. Because the anal sphincter and buttock muscles are stronger than the weakened pelvic floor muscles, they should be negated as much as possible so their contraction does not override the weaker muscles.
Working With—or against—Valsalva Remember, Valsalva is downward pressure. Become aware of how much Valsalva is unconsciously being produced in everyday life. Learning how to reverse this pressure is paramount. In most articles about the shape of the pelvic floor, it is described as having the shape of a basin or hammock. In 1976, a study by Hjartardottir, Nilsson, Peterson, and Lingman in Sweden used MRI to reveal that the pelvic floor is actually a dome shape when muscular tone is present. They concluded that the idea of the basin or hammock shape came from early dissections done on older women who had had many babies.
When practicing the lift of the pelvic floor or reversing Valsalva, visualize a dome and try to make the lifting dome-shaped. Be sure to make the lift conscious and soft.
In Muscles: Testing and Function, Kendall, McCreary, and Provance state that “without minimizing the importance of proper foot position that establishes the base of support, it may be said that the position of the pelvis is the key to good or faulty postural alignment.”
A Yoga Sequence for the Pelvic Floor? I do not give a set pelvic floor sequence. Any asana is an opportunity to bring awareness and health to the pelvic floor muscles. Pelvic floor muscle work can be very tiring—so selected asanas should be interspersed thoughout the sequence of your choice. Again “a set yoga sequence” is not the way, but keeping certain concepts in mind while practicing is the key: • Keep the pelvis correctly aligned at all times. • Use a strong external rotation at the hip joint when the pose demands it. • Lift the pelvic floor softly to reverse Valsalva. • Make pelvic floor contractions soft and site-specific.
Remember: Contractions are made from the perineal body forward. • Do not contract the buttock area; this area should be kept as inactive as possible.
External rotation at the hip joint is important when it comes to yoga asana. External rotation action in asana gives an unexpected bonus: the lifting and strengthening of the levator ani. There are six deep muscles in the pelvis that produce external rotation. Two external hip joint rotator muscles are especially important in pelvic floor work: the obturator internus and piriformis. The obturator internus takes its origin from the inner surface of the pelvic bone; the piriformis takes its origin from the inner surface of the sacrum. Both muscles insert on the grater trochanter. Because of their location and lines of pull, the pelvic floor diaphragm is affected because of the communication between their fascial connections to the levator ani.
For a yoga practitioner, poses such as Trikonasana, Vrksasana, Baddha Konasana, Supta Baddha Konasana, Upavistha Konasana/Sama Konasana, and contralateral rotation of the hip joint as with Ardha Chandrasana are a boon to the pelvic floor muscles.
Three poses address the pelvic floor directly: Tadasana, Baddha Konasana, and Bakasana. Each of these asanas teaches us the basic actions to support the pelvic floor muscles.
TADASANA
Tadasana teaches how to align our posture to stand up correctly. When the body is aligned in its evolutionary upright alignment, muscles work the way they are suppose to. When standing in Tadasana, the pelvis must keep its anatomical neutral position (i.e., not in an anterior tilt or sway back, which dumps the abdominal contents forward and shifts the pelvic floor backward, or in a posterior tilt or tucking of the tailbone, which grips the anus and buttock muscles and moves the pelvic floor forward). No matter what configuration an asana takes, it is about balance, and Tadasana is the first teacher of pelvic floor balance and placement.
When the pelvis is in its natural upright position, the abdominal contents are kept in place with the aid of the abdominal muscles, which lift the pubis from the front, as well as the hamstrings, which pull down the sitting bones in the back. The body knows what to do, and when it is put into alignment, it will do its job. Asana evolved from the spiritual man. So when we work with asana, keep in mind the anatomical body.
BADDHA KONASANA
Baddha Konasana teaches external rotation at the hip joint. Baddha Konasana action at the hip joint can be found in many asanas. Remember, external rotation at the hip joint also activates the muscles of the levator ani to contract and bring lift. Just think how many opportunities asana offers for this action. Parvatasana in Baddha Konasana

BAKASANA
Bakasana teaches how to balance on the arms and hands. Bakasana is very powerful because in it, Valsalva is reversed and lifted up. The abdominal muscles contract and are pulled back to the spine, and the urogenital triangle is pulled forward and upward. The open Tadasana and compacted Bakasana, if done correctly, will put you on the fast track to strengthening the pelvic
floor muscles.

Bakasana
PRICKING ATTENTION
Mr. Iyengar once instructed to teach an asana or an action inherent in an asana in order to “prick” the attention, to develop sensitivity. I use the following asanas to prick the attention toward the pelvic floor area:
Keep the feet, ankles, and legs together and bring the arms overhead; lift the heels up high and stand on the toes.
Align the pelvic floor and vaginal canal and lift them up as you balance on the toes.
Make a connection between the pelvic floor and the lifting arms and interlaced fingers. Let the lifting of the arms lift the pelvic floor.
The toe stand teaches how to reverse Valsalva and how to lift the pelvic floor.
Vrksasana (phasic leg position)
Toe stand in Urdhva Baddhangulyasana
Stand with the left side toward a wall and the left hand at the wall for balance.
Keep the pelvis stationed as the right leg moves and rotates at the hip joint.
Rotate the right leg out strongly, bend the right leg and hold it about 12 inches off the floor.
Vrksasana
Keeping the left side and pelvis in place, contract the deep hip rotators at the right hip joint to bring the right thigh/leg back in line with the left.
The effect on the pelvic floor can be felt when the obturator internus of the lifted leg is first put into contraction and then required to become a supportive and stabilizing muscle.
Ardha Chandrasana (from Tadasana)
Turn the right leg out. Place your right hand on the floor and lift the left leg to a right angle to the floor.

Keep the right leg in strong external rotation (the action you learned from the phasic leg in Vrksasana).
Keep the right leg stable as the pelvis and left leg rotates.
Rotate the pelvis into vertical alignment. The left leg and pelvic bone are positioned and held up by the deep rotators of both hip joints.
Utkatasana
Lift the arms and align the pelvis as in toe stand Urdhva Baddhangulyasana.
Slowly bend the knees. Lift the pubis upward and slide the urogenital triangle forward.
Descend the sacrum downward and allow the lumbar spine to move a little backward and lengthen.
Keep the sitting bones and vaginal canal pointing straight down. Do not grip the anal sphincter.
Utkatasana
Bend the knees only as far as the alignment of the pelvis and torso is maintained in the upright position.
Do not go to the deepest knee flexion because the action of the pelvic floor will be lost as the buttocks begin to stick out.
This asana teaches the movements of the pelvis and brings sensitivity to the pelvic floor.
Inversions
Pelvic alignment in inversions is important. While in Tadasana, the vagina points directly downward; in inverted asanas such as Sirsasana and Adho Mukha Vrksasana, it should point upward.
The Pelvic Floor After Pregnancy Pelvic floor work should be practiced before becoming pregnant because it will familiarize a woman with how these muscles can be strengthened. With the growth of gestation and hormonal changes, muscles and ligaments of the abdomen and pelvis relax. It becomes futile to try to strengthen the pelvic floor muscles during pregnancy because nature is going to win. Even if delivery is through a C-section, the pelvic floor muscles will have become relaxed just the same. Understand, the body is getting ready for the big “Valsalva” of childbirth.
After giving birth, a woman should take time to rest. When she is ready to start her asana practice, she should begin with a restorative sequence. Pelvic floor work should be interspersed throughout the chosen sequence. After delivering a baby, a woman’s pelvic floor is in its weakest state, and trying to contact those muscles can produce stress and a feeling of failure, which could cause her to stop trying.
First practice asanas to start lifting the pelvic floor and to strengthen the vaginal canal. Start in a supine position because this takes stress off of the internal organs, which have been stretched from pregnancy and delivery.
Supta Baddha Konasana with toes to the wall.
Make sure the lumbar spine is elongated and the broadest part of the sacrum is flat on the floor.

Supta Baddha Konasana
Place the hands on the top of the thighs at the hip joint.
Contract the outer hips to take the thighs toward the floor as in Baddha Konasana and, at the same time, push the top of the thighs toward the feet. Remember not to arch the lumbar spine.
Now softly lift the pubic plate and abdominal area in and up.
Lift the muscles of the pelvic floor into the shape of a dome and softly contract the vaginal canal upward.
Supta Baddha Konasana (variation)
Fold a blanket into a narrow width to support the spine.
Place two blocks at the wall about two feet apart.
Recline on the blanket with the lower end of the blanket at the floating ribs and your buttocks on the floor. Place your feet on the blocks and rotate the feet to place the outer edge of the feet flat on the blocks—this moves the thighs into Baddha Konasana position.
Keep the pelvis level and hold the lift to feel as though it is levitating. Now add the pelvic floor action you have learned.
This variation helps strengthen the muscles of the pelvic floor and vagina and also supports the sacroiliac joint. The ligaments in this area are also often stretched during pregnancy and delivery.
Upavistha Konasana (variation)
Sit on the floor and spread your legs as wide apart as you can.
Place your hands on the floor behind you. Lean back, laterally rotate your legs, and bring the outer legs and little toe side of the feet to the floor.

Lift the pelvis just a
Upavistha Konasana little, then the pubic
plate, and then softly lift the vaginal area into a dome shape.
Now move to the classic position and align your pelvis in its vertical position with your torso perpendicular to the floor. Do not tilt the pelvis forward and project the lower belly out or round the spine back.
Lift the pubic plate up; lift the vaginal area into a dome shape. Interlace the fingers and place the hands on top of the head or bring them into Namaskarasana. Press the legs down firmly and balance on the sitting bones.
Once control for lifting the pelvic floor has been gained, standing poses can be introduced. But gravity is not your friend: It is paramount to keep the pelvis from tilting forward.
Utkatasana is also important after giving birth because it teaches a woman to put the abdominal contents, which were pushed outward during pregnancy, back into the pelvis.
Supported inverted poses use gravity to assist in pelvic-floor conditioning. During pregnancy, the pelvic floor muscles are slowly stretched, and during delivery, Valsalva and hormones cause the pelvic-floor muscles to relax and be easily stretched to the maximum. The vaginal canal is also stretched considerably during delivery.
Supported Salamba Sarvangasana with wall or chair
• From your choice of prop set up, bring your feet to the wall or backrest of the chair.
• Keep the legs hip-width apart and allow gravity to assist in dropping the pelvic floor inward. Bring the pelvis forward to align the pelvis perpendicularly. Now slowly start closing the vaginal canal. Remember, do not make your contraction hard and try to relax around the anal sphincter.
Tight Pelvic Floor Muscles The pelvic floor muscles must have tone to maintain support. They must be able to contract to maintain continence, and they must be able to relax to allow for urination and bowel movements, and in women, sexual intercourse. When these muscles have too much tension, they will often cause pelvic pain, lower back pain, or urgency and frequency of the bladder and bowels. Tight and painful pelvic floor muscles can be stressful especially when it comes to intercourse.
When addressing tight pelvic floor muscles, put the pelvis in a position where those muscles are not needed for support—such as in supported inverted asanas. When the pelvic floor is engaged, it will interfere with the relaxation of the vaginal muscles, and it is important to learn to totally relax the pelvic floor.
Wall rope Baddha Konasana
• Once into position, the feet and legs of Baddha Konasana aid in relaxing the pelvic floor.
• Because of the position of the legs, the vaginal muscles are opened and with the assistance of gravity and time, the pelvic floor muscles will relax. Chair Sarvangasana
• Once the shoulders are on the support, place the soles of the feet at the top of the backrest, and slip one arm at a time under the chair and hold the back legs of the chair.
• Arch the lumbar spine and let the buttocks become relaxed and allow the sacrum to drop toward the seat of the chair.
• Keeping the feet on the backrest, bring the bottoms of the feet together and let the legs fall apart into Baddha
Konasana.
• Allow the lower abdominals, inner groin, and pelvic floor to relax and consciously let the vaginal canal open and relax.
Unsupported asanas will not relax tight pelvic floor muscles because in order to hold asanas such as Sirsasana and Sarvangasana in correct balanced alignment, there must be contractions at the pelvic floor.
A 3-D Look at the Pelvic Floor To get a good visual understanding of the pelvic floor muscles, look at AnatomyZone’s “Pelvic Floor Part 1: The Pelvic Diaphragm—3D Anatomy Tutorial,” https://www.youtube.com/ watch?v=P3BBAMWm2Eo, and “Pelvic Floor Part 2: The Perineal Membrane and Deep Perineal Pouch—3D Anatomy Tutorial,” https://www.youtube.com/watch?v=q0Ax3rLFc6M on YouTube.
Jaki Nett (Intermediate Senior I) is the co-owner of Iyengar Yoga Napa Valley and is on the faculty at the Iyengar Yoga Institute of San Francisco. She authored A Crack in the Mask: A Humanistic Approach to Managing Incontinence and Iyengar Yoga: An At-Home Practice. Jaki’s teaching style is anatomy-centric.
Baddha Konasana in sling Sirsasana





