Milestones - the magazine of the Royal College of Paediatrics and Child Health - autumn 2024
The Clean Air Fund has made a great poster, Display it and share it, be a climate change co-star.
‘Twas the Milestones before Christmas and all through the edition, Members are stirring and sharing their missions. Young people the heart and focus throughout, Nothing without them, if it’s them it’s about.
Young people Bite Back for food that is healthy, And not disadvantage the children less wealthy.
The Powering Up team share their journey of creation, A health movement that's sure to inspire the nation. The real-life insight of personal costs to driving this feat, Aligned working to one’s values; less bitter, more sweet.
Transforming child health services won’t be an easy task, Alongside the Darzi Review, the blueprint lays down the ask. It’s time CYP stopped being at the back of the queue, Prioritising and advocating is what we still need to do.
SPA time is essential for building the skillset, Of resident doctors whose needs have been unmet. The Rota Gaps Survey results won’t be a huge surprise, But to rota coordinators might acknowledge their cries.
Our regular features are far from plain, Taking a trip down ADC memory lane.
Ash’s Baking School has a festive twist, And a game review for the Christmas list.
on a creative project
battling junk food advertising
more
There’s a lot more inside, too much to mention, But if you want to write for us, pay close attention. Give us an email any time; day or night, And to all who say yes, good luck and good write!
Dr Seb Gray
Contact
on the blueprint for change
General Paediatric Consultant
Salisbury NHS Foundation Trust
We’d love to hear from you – get in touch at milestones@ rcpch.ac.uk
Copyright of the Royal College of Paediatrics and Child Health. All rights reserved; no part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical, photocopying, recording, or otherwise – without prior permission of the publishers. The views, opinions and policies expressed in Milestones do not necessarily reflect those of the College. While all reasonable efforts have been made to ensure the accuracy of the contents of this publication, no responsibility can be accepted for any error, inconsistency or omission. Products and services advertised in Milestones are also not recommended or endorsed by the College. Readers should exercise their own discretion and, where necessary, obtain appropriate independent advice about their suitability. Royal College of Paediatrics and Child Health is a registered
The latest news and views
President’s update
Professor Steve Turner RCPCH President
Articles like this bring the challenge of a sixweek interval between me writing it and you reading it. Having digested the autumn budget – you can read the College’s response below – our thoughts turn to winter and I imagine there’s a good chance you plan to mark some events(s) in this season of festivities. Christmas gifts are exchanged between 6 December and 5 January. Buddhists celebrate Bodhi Day on 8 December. The Jewish festival of Chanukah starts on 25 December and ends on 2 January, and the Muslim celebration of Lailat al Miraj falls on 27 January.
Asian communities will mark the Lunar New Year with fireworks, feasts and time
The budget: our response
The budget shows the government is serious about raising the bar when it comes to prevention of ill health in children.
The College welcomes the announcement that the Soft Drinks Industry Levy will be extended and further funding for breakfast clubs, which will support a generation of children to lead healthy, happy and productive lives.
Important steps have also been taken that should help to address child poverty. However,
spent with family. And while this time of year is traditionally cold and dark for many of us, when we lived in Australia, the long school holidays saw searing heat, blinding sun and reindeer-suited water-skiers.
There are many ways to end one year and begin another, however, many of us will find ourselves working. Serious illnesses do not respect dates and there will no doubt be di cult clinical experiences, so look out for your teammates.
That said, less serious illnesses seem to take a short break – every paediatric ward I’ve worked on has been amazingly empty for a few days over Christmas. The eye of the storm. I’m sure there’s some learning in this. But enjoy it if you are working.
The festive season should be an opportunity for rest, however short. I hope you and your family and friends can spend quality time together in the coming weeks.
it is disappointing to see the two-child benefit limit remains, keeping over a million children in poverty and driving health inequalities. It is not clear how the government plans to address the specific pressure child health services are under. The Darzi Review was clear – our children are sicker than ever. Announcements on the NHS are positive, but it remains to be seen how child health services are considered as part of these. Unless children
and child health services receive specific attention, they are forgotten.
As the Health Secretary sets out his plans to deliver 40,000 extra NHS appointments and wider reforms, we urge him to remember the words of Lord Darzi, and to set out specifically how the government will address the unacceptable state of child health services today. Our blueprint for health services is clear in the steps the government can take to recover child health services, and go from left behind to leading the way.
RCPCH Annual Conference 2025
Dr Jonathan Darling RCPCH Vice-President for Education and Professional Development Annual Conference Chair
How is your paediatric ‘battery level’? Do you want an energy boost for the next leg of your journey? Let me introduce you to the ultimate paediatric charging station: the RCPCH Annual Conference! Enjoy inspirational content and a range of CPD to keep up to date – plus fun, friendly networking and socialising opportunities – to inspire and energise you for the year ahead! Whether you’re a regular or a newcomer, join us in Glasgow on 26-28 March to celebrate our specialty. Our programme includes plenaries by: Nitin Kapur (RACP Australia) reflecting on Ryan’s rule; Peter Lachman on patient safety; Monica Lakhanpaul bringing insights for child health from the Covid-legacy; and Steve Tomlin on sustainable medicines for children. We’ll have the usual amazing range of special interest groups and workshops with plenty of clinical content. And watch this space for our social programme.
Early bird bookings are now open: www.rcpch. ac.uk/news-events/rcpchconference/book-your-place
RCPCH College
Strategy 2024-27
Our new Strategy has launched outlining the first phase of a 10year strategic outlook. Our four goals focus on:
(1) The size, skill and welfare of the UK child health workforce are prioritised by senior NHS decision-makers to meet the needs of children and young people across the four nations;
(2) Child health is at the centre of decision-making across the four nations;
(3) Research, evidence and clinical standards improve safety and child health outcomes; and
(4) RCPCH has an international impact in paediatrics and child health.
These goals were developed in partnership with members and children and young people because they are practical, progressive and have distinct outcomes. They will guide the College throughout the next 10 years.
During the first three-year phase, these three enablers will run through our four strategic goals. They are:
(1) Improving the membership experience;
(2) Improving the offer for our members with College roles and staff; and
(3) Enabling efficiencies and diversifying our income. Together these enablers will help us work smarter to create greater impact for our members and for child health.
Visit www.rcpch.ac.uk/ work-we-do/rcpchstrategy-2024-27 to download our strategy and learn more about our strategic goals.
Government announces ban on disposable vapes
Dr Mike McKean RCPCH Vice-President for Policy
Great North Children’s Hospital in Newcastle
In October, the College achieved a significant victory in its campaign to ban disposable vapes in the UK, with governments across the UK announcing a ban would come into e ect from June 2025. This marks a pivotal moment for child health and environmental protection.
The College first called for this ban in June 2023, highlighting the disproportionate use of disposable vapes among children and young people, as well as their detrimental impact on the environment.
With research indicating a quarter of 11- to 15-year-olds had used a vape in the previous year, the campaign by the RCPCH was driven by growing concerns over the risks posed by disposable vapes to young people’s health, potentially leading to nicotine addiction and respiratory issues. The campaign captured the attention of the press, politicians and other organisations in the sector.
As Vice-President for Policy, I have regularly been called upon to emphasise the urgent need for bold action, as has the College President. In Westminster, Dr Helen Stewart, O cer for Health Improvement, went before a committee of MPs to detail the impact of youth vaping, which led to them urging the government to act.
In addition to the ban on disposable vapes, the RCPCH has advocated for broader measures to regulate the sale and marketing of e-cigarettes. These include restricting e-cigarette flavours that appeal to children, implementing
plain packaging for devices and liquids, and limiting marketing strategies that target young people. The environmental benefits of the ban are also significant. An estimated five million disposable vapes are discarded each week, contributing substantial waste.
Our successful campaign is a testament to the power of advocacy and the importance of prioritising children’s health and environmental sustainability. We urge the government to implement robust plans for enforcement and monitoring to ensure the ban’s e ectiveness and to protect future generations from the harms of vaping. We are also very mindful that a generation of young people who were not cigarette smokers may now be addicted to nicotine, so our advocacy work in this area is not over.
For now, we should celebrate this win, what it means for child health, and the precedent it sets for other countries. We very much hope that when this edition of Milestones reaches you, the Tobacco and Vapes Bill will be well on its way to becoming law.
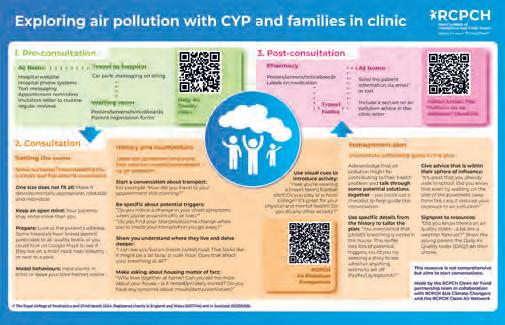
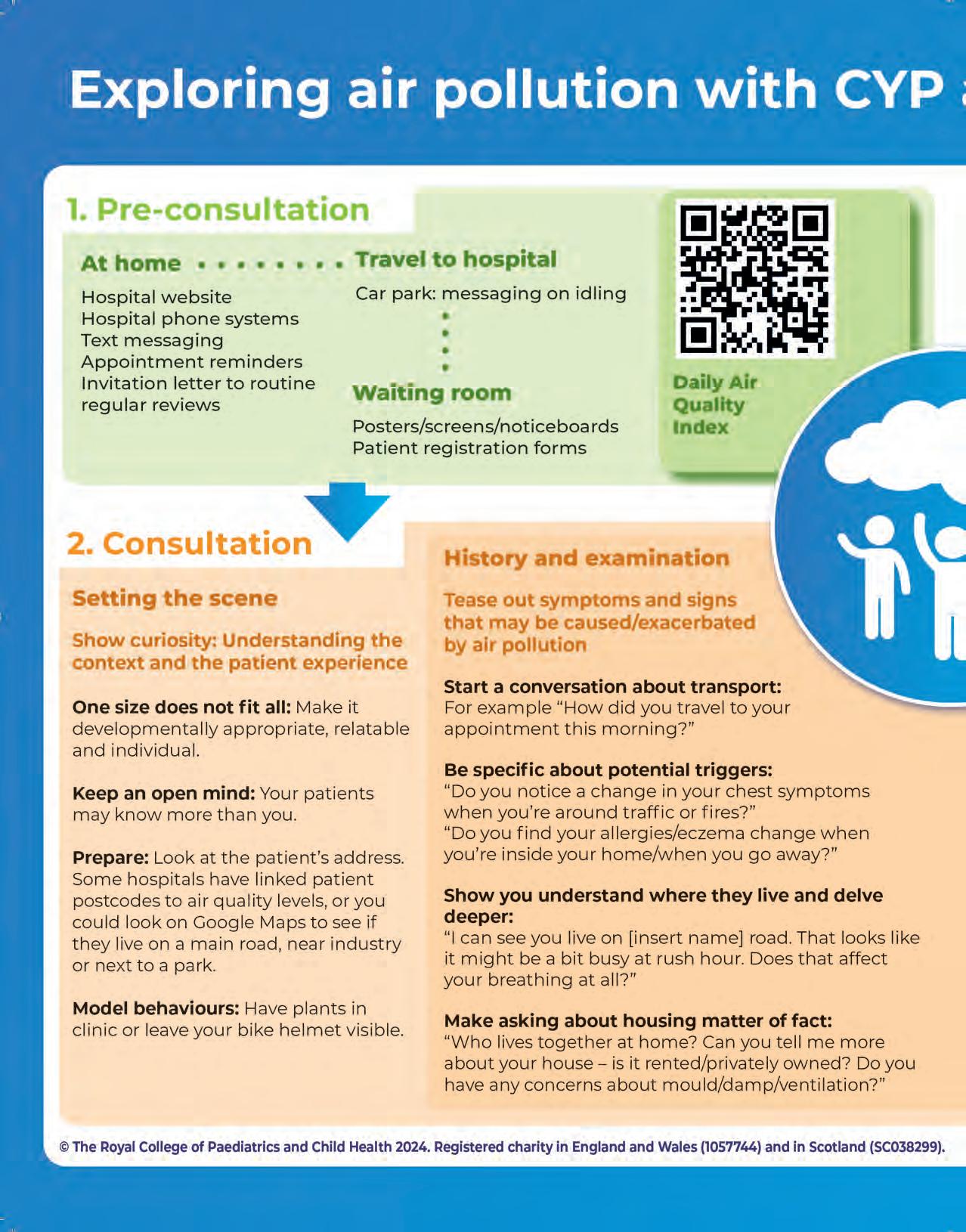
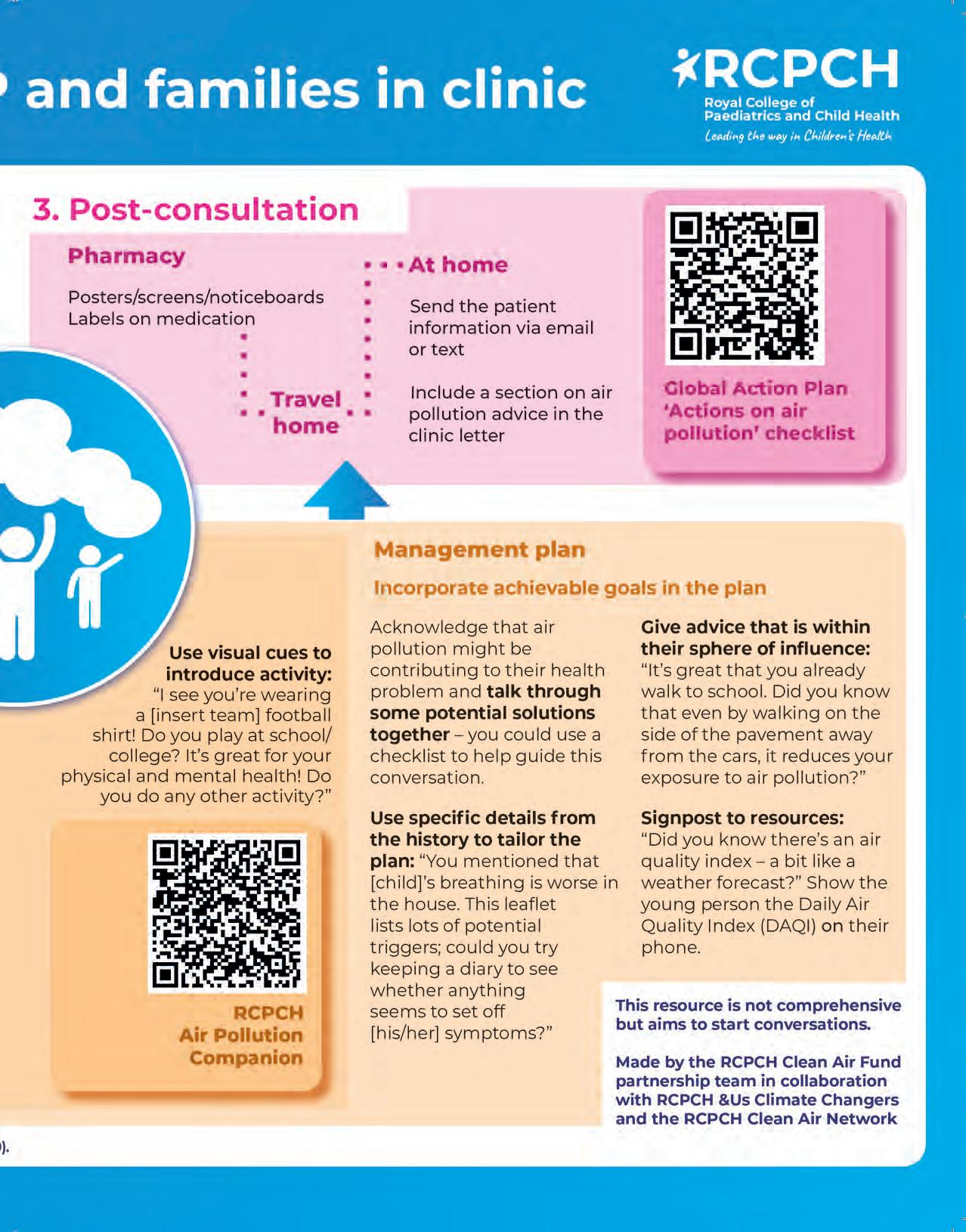
Introducing the Clean Air Fund poster
We are excited to share our poster ‘Exploring air pollution with CYP and families in clinic’ in the middle of this issue – pull it out and stick it on a hospital wall near you! Maybe you could organise a teaching session around it, or send us a photo of it in your workplace?
Produced in collaboration with the RCPCH &Us Climate Changers and members of the RCPCH Clean Air Network, this poster aims to illustrate opportunities for introducing air pollution into the patient pathway through secondary care. This work has been produced as part of the RCPCH Clean Air Fund Partnership programme, which is currently
part of the College’s policy team.
Air pollution is the second biggest risk factor for death in under-fives globally. In the form of tiny particles (eg PM2.5) and gases (eg NO2) air pollution is breathed in, absorbed into the bloodstream, and causes pathology throughout the body. As well as exacerbating respiratory diseases such as asthma, we know it has effects across the life course: preterm births; cardiovascular disease in adolescence; and mental health impacts.
Child health professionals are uniquely placed to advocate about air pollution – we are trusted by society and encounter many people in our
Find your pull-out poster on page 16
day jobs. Yet members have told us they struggle because of a lack of time, knowledge or resources.
We have released a new website, the ‘Air Pollution Companion’, which has lots of information and support for learning and talking about air pollution. We hope by
Staff spotlight
Henna Davé Workforce and Careers Team
I’m incredibly proud to work for the College and contribute to the development of future paediatricians. A key part of my role is leading the #ChoosePaediatrics programme, designed to highlight the specialty and offer essential support to those aspiring to join the field.
One of the many highlights of my role is managing the annual #ChoosePaediatrics
prize awards for medical students and foundation doctors at the RCPCH Conference. It’s fulfilling watching these talented individuals receive welldeserved recognition. This reminds me of the powerful impact we have in fostering and celebrating paediatricians of the future.
Having been at the College for a few years, it’s truly rewarding to see past prize award winners come full circle – from attending the prize awards as medical students to returning as paediatric trainees, even taking on leadership roles and volunteering roles within the College. Seeing
sharing this poster and signposting to the website we can start to overcome some of these barriers together. If you have any feedback, contact us at cleanair@rcpch.ac.uk
Find out more: www.rcpch.ac.uk/keytopics/air-pollution
them flourish in a field they love fills me with a sense of pride.
I couldn’t have done this without the support of my incredible colleagues and senior clinicians over the years, which has been equally inspiring, and it’s that unity and shared mission that make each conference so special. With our upcoming conference on the horizon, I can’t wait to welcome the new aspiring paediatricians and reconnect with those continuing to flourish in the wonderful world of paediatrics. Because #ChoosePaediatrics –there’s no job quite like it!
Journal: ADC update
Nick Brown Archives of Disease in Childhood Editor-in-Chief
@ADC_BMJ
I was recently asked to see an ostensibly well two year old child with an ‘unusual heart murmur’. For some reason, the way it was described gave me a strong gut feeling that ‘this might be something’, the extreme right axis deviation on the ECG only enhancing that conviction. What clinched it, though, even before ‘properly examining’, was the clubbing –
visible from a good metre away – a sign transporting me back to training days.
This was a while ago (although, in reality, we never stop training), when there was no warning on antenatal scans of congenital cyanotic heart disease (no regional cardiothoracic teams now lined up for delivery, no cystic fibrosis transmembrane regulators) and post-pertussis or measles bronchiectasis all so common that eyelids remained conspicuously un-batted at the sight of clubbing – almost to the extent that it would have been considered ‘too easy’ a case for the Membership clinical.
Journal: BMJ Paediatrics Open update
BMJ Paediatrics
Shanti Raman
BMJ Paediatrics Open Editor-inChief
@BMJ_PO
Open has continued to publish interesting papers throughout 2024. As a mark of how busy we are, as of 14 October, 552 papers have been received, which almost exceeds the total for the whole of 2023 (557). The journal is receiving almost 60 submissions per month, 219 papers have been published so far this year, compared with 136 last year. Some of this growth is thanks to the topic collections, which we are very committed to:
bmjpaedsopen.bmj.com/pages/ topic-collections
Our ‘Health and Wellbeing of Street and Working Children’ topic collection call has drawn to a close and, with many papers already published, we will soon have available online a truly thoughtprovoking set of articles.
Our new collection, ‘Disability and Development in Early Childhood’ (see below) is open for submissions until March 2025 and the call for submissions for ‘Preventing and Mitigating the Impact of the Climate Crisis on Child Health’ will continue for the rest of 2024.
Watch a recording of our webinar The Climate Crisis and Child Health: A Sustainable
So what does this tell you other than my ballpark training epoch? To me, it illustrates the need to stay open-minded – even if this means rethinking an approach – staying hungry for knowledge and making the most of the breadth and depth of writing in archives (adc.bmj.com) – of course! You might even want to become reviewers yourselves. Various presentations will soon hit the site –and we’d love to have you involved.
Find out more: Bradford J, Connett GJ. Clubbing and hypoxia in an adolescent male. Archives of Disease in Childhood 2024;109:482
Agenda for Future Generations (a collaboration of BMJPO and ISSOP) here: bit.ly/4fPhgm8. Our panel discussed the crisis and outlined the necessary steps to shape a future agenda for protecting child health.
Remember, as RCPCH members you benefit from a 25% APC discount when you submit to BMJPO – reviewers also receive a 25% discount if they submit a paper within 12 months of reviewing for the journal (and we always need reviewers).
Our Digital Growth Charts win another prestigious award
RCPCH’s Digital Growth Charts – in partnership with Digital Health and Care Wales (DHCW) – won the HTN Health Tech 2024 Award for ‘Best Solution for Clinicians’. The RCPCH has been working with DHCW since 2022 to introduce the RCPCH’s Digital
Growth Charts into their flagship national integrated care system – the Welsh Clinical Portal. They believe it will significantly improve data sharing and continuity of care throughout Wales and in various care settings. Look out for further updates in the next issue.
The College has called for a pause in physician associate appointments, find out more at www.rcpch.ac.uk/PA-recruitment-pause
Diary dates
Events are online unless otherwise stated. We will add to this list over the coming months, so keep an eye on our website
Safeguarding, neurodevelopmental disorders and neurodisability, Level 3 (27 January)
How to Manage: Adolescent Health (4 February)
Effective Educational Supervision (11 February)
Read more
Find more dates at www.rcpch.ac.uk/courses www.rcpch.ac.uk/events
How to Manage: Childhood Poverty (12 February)
How to Manage: When a child dies – the role of the paediatrician (London, 26 February)
Statement and report writing – Scotland, Level 3 (5 March)
RCPCH Learning
RCPCH webinar: Upskilling child health professionals to talk about air pollution
RCPCH webinar: Whooping cough (pertussis) – an update
Applications of Genomics in Paediatrics (online learning) learning.rcpch.ac.uk
Podcasts
Measles in 2024: what paediatricians need to know
What you can do for sustainable healthcare learning.rcpch.ac.uk/home/ podcasts
Meet our new Registrar and Assistant Registrar
I’m a practising consultant paediatric nephrologist in Bristol – appointed in 2002, having trained in London, Bristol and Paris. From a clinical perspective, I have a particular interest and expertise in kidney transplantation in CYP and did my PhD in this area. I am clinical co-lead for transplantation in Bristol and was chair of the NHSBT paediatric subgroup of the UK Kidney Transplant Advisory Group until 2022.
Away from the ward, my focus for many years has been on quality improvement and risk management (including clinical standards/guidelines, patient safety and patient information) and I’ve held many management and leadership roles, including president of the British Association for Paediatric Nephrolo until September 2024.
As Registrar, I work closely with the President, senior o cers and College sta to oversee governance, and develop and implement an overarching strate to support our workforce. As chair of the Membership Committee and Ethics and Law Committee and vicechair of the Invited Reviews Programme Board (IRPB), I’m very keen that ‘the voice of the paediatrician’ is heard at all levels of the College, so that we may best understand the challenges and share the achievements in the delivery of paediatric healthcare.
As a consultant in paediatric infectious diseases at Northwick Park Hospital, London, my acute work is in the paediatric emergency department, while my outpatient clinic focuses on the care of unaccompanied asylum-seeking children.
I’m the Associate Medical Director for Education, Research and Innovation for London North West Healthcare NHS Trust, which involves having strategic oversight of the quality of education across the Trust.
In my capacity as South West London System Dean, I’m seconded for some of my time to NHS England. I’m lucky to have such varied roles and privileged to work with brilliant colleagues.
At RCPCH, I was the Global O cer between 2015 and 2020 –working to design and deliver programmes to improve the quality of care and reduce mortality in district general hospitals in several lower-income countries – and have been a Trustee since 2020, with a particular focus on equity, diversity and inclusion.
Becoming Assistant Registrar in August has been a steep learning curve! One main area of responsibility is the Invited Reviews Service, which helps organisations address issues with models of care, safety, quality of services or team communication. I encourage colleagues to get involved in voluntary roles at RCPCH – I have learned so much.
Dr Bhanu Williams RCPCH Assistant Registrar
Dr Jan Dudley RCPCH Registrar
Service development
The service journey: what I’ve learned along the way
Dr Lisa Bray Paediatric Consultant and Rheumatology Consultant
– Lead for Paediatric Rheumatology University Hospital Sussex NHS Foundation Trust
Navigating the service development
road is not always easy. Having spent my first four consultant years developing my subspecialty service, I wanted to share some top tips.
Dream big – aim for your vision of the best possible service
Imagine what that service would look like. What would make it the best? This is also a great consultant question for those with interviews coming up.
Think about how your patients access your service
Consider the stepping stones your patients have crossed to get to you. Mapping patient journeys over the first year of my job helped me understand the referral processes. This information is excellent evidence for planning business cases and making change.
Consider what patients within the service already receive Services can vary greatly, even between subspecialties within the same setting. Discuss with colleagues what their services look like. Do they o er something that could be utilised by your service, or vice versa? This could be as simple as sharing a piece of equipment with another service on your site or inspiring a more complex business case for a larger service development.
Listen to your patients
How do the people using the service think it could be improved? Ask patients informally in clinics or on the ward and more formally in surveys, and take
information from any feedback and thank you cards. These are all wonderful opportunities to understand what patients feel and need. In my service, the patients wanted a contact point, so I made cards, and a new email address for my subspecialty was created which has been well used and brings mutual benefit.
Identify and mitigate the risks that exist within your service
What risks still need mitigating, and how might that be done? In my service, this meant creating e-safety alerts on patient electronic records with care plans for those immune-modulated, ensuring open access was available. Writing guidelines at local and national levels helps improve patient safety and gives consistency in healthcare, helping to remove inequality for patients. Consider utilising and providing guidance on what ‘gold standard’ care can be provided to patients in your service.
Optimise the onward patient journey
Whether they are being discharged or transitioned to adult care, when the patient leaves your service do they have all they need? Is there anything more that can be done to prepare our young people for the next step in their healthcare journey? I created a transition survey to try and analyse transitions to adult care, which is ongoing work. Ensuring other teams providing care to our patients are copied into letters is a basic, but sadly all too readily forgotten, step that improves patient care.
Ensure all your skills are utilised How can you introduce those to your setting? This may mean putting together business cases, finding and funding new equipment, and building a team around you to bring to the service all it needs to be its best.
“Ask patients informally in clinics or on the ward and more formally in surveys, and take information from any feedback and thank you cards”
Service development doesn’t need to involve groundbreaking equipment, medications or research. It is generated by seeing what the service needs, bringing your positive experiences gained through training and pulling all the best bits into your day-to-day practice.
I hope these tips help you create an ambitious to-do list for your service development. Consider who can help you – from colleagues partaking in audits to meeting with charity boards and putting together business plans with colleagues and managers, it takes time and dedication to make and sustain positive change. What you want to achieve may not always be possible, but put the patient at the heart of all you do, keep your service improvement to-do list refreshed and aim to create your vision of the best possible service for your patients.
Leading the way
An update on RCPCH’s blueprint for transformational change
Dr Ronny Cheung RCPCH Officer for Health Services
Evelina London Children’s Hospital
In September, the College launched From left behind to leading the way: a blueprint for transforming child health services in England, a document highlighting the increasing challenges paediatricians working in child health services – and the children and young people (CYP) we serve – face today that sets out a comprehensive plan for change.
It’s no secret that child health services have not only become more stretched over the past decade, but also deprioritised in national health policy and decision-making. Children are waiting longer than adults to access healthcare and paediatric services aren’t recovering at the same rates as adult services. This disparity has coincided with an unprecedented increase in demand for children’s health services, which is forecast to grow further due to both preventable (eg childhood obesity) and non-preventable (eg increased medical complexity) rises in childhood illness.
“Children are waiting longer than adults to access healthcare and paediatric services aren’t recovering at the same rates as adult services”
This is why I’ve been working (in collaboration with members of our Health Services Committee, College sta and our President and Senior O cers, as well as with decision-makers in government) to better enable the College to use its voice
– to raise these challenges and call for greater support for paediatricians at both a national and local level.
Across seven central themes, we set out a series of evidence-based, practical and immediate solutions. These are intended to act as a guide to the transformational change that is needed across child health services in England.
1. Fair funding for children
2. Children prioritised by Integrated Care Systems
3. A sustainable child health workforce
4. Data and digital innovation
5. Reduce pressure on urgent and emergency care
6. Reinvest in community health services
7. Improve the interface between primary and secondary care
Looking ahead, the College will continue our overarching call for the UK Government, Department for Health and Social Care (DHSC) and NHS England to restore and prioritise health services for children. In the immediate term, we are engaging with the development of the NHS 10-year plan. This is likely to be framed around three shifts: hospital to community; treatment to prevention; and analogue to digital. Our blueprint aligns well with these shifts and has provided a useful basis for conversations with the relevant teams at DHSC.
Child health services are our focus with this report, but we recognise meaningful change must go beyond this. We call for ambitious action to prevent illness and address the wider determinants of health through a ‘child health in all policies’ approach. And as CYP have highlighted through RCPCH &Us, all of this should be set in the context of two fundamental principles: listening to children’s voices and respecting children’s rights.
The blueprint was well-timed. A week after publication, we saw the governmentcommissioned Lord Darzi’s Independent Review into NHS performance. This confirmed many of the concerns we had already highlighted – that our child health services are in crisis, and this is having an impact on child health outcomes. It referenced our evidence submission and the blueprint itself.
We also continue to build consensus around priority recommendations in the blueprint, including: our calls for fair funding and a Children’s Heath Investment Standard; for Integrated Care Systems to prioritise children and be more clearly held accountable for meeting their needs; and to ensure the proposed ‘left shift’ from hospital to community care works for all children. Underpinning all of this are our calls to support paediatricians and develop a child health workforce strate , which is particularly important with a refresh to the Long Term Workforce Plan due in summer 2025.
As paediatricians, we too must do our bit. Examples of excellence in paediatric services abound across the country, where, despite resource constraints and workforce pressures, waiting times are coming down and the quality of care is improving. This is happening through collaborative working, embracing new models of care and innovative approaches to traditional problems. As such, I was pleased to support the College’s submission to the 10-year plan consultation and encourage members to do the same.
Throughout our work on the blueprint, the College continues to remind the government that investing in – and reforming – paediatric services and the workforce is fundamental to the future health and economic wellbeing of the UK.
Our perspective on the blueprint for transforming child health services
Toby, age 19
Maryam, age 23
We are the future. But if we are the future, we need to be looked after now. We have the right to the best possible healthcare and for the government to provide quality health services for all children (Article 24 of the United Nations Convention on the Rights of a Child). Having good health and access to good health services matters to us, our families and our communities – so we can contribute fully in the future.
In summer we were involved in reviewing a draft of RCPCH’s blueprint – Transforming child health services in England – bringing a fresh view on the priorities being discussed by the College. Now that the report has been published, we’ve been looking again at the recommendations and thinking about the ones that feel most important to us, as children and young people, right now.
Reinvesting in community health services is essential for improving the care and support available to children and young people. Long waiting lists for appointments, such as asthma reviews, often leave us without timely access to healthcare. By investing in community child health services and expanding the workforce, these delays would be reduced, and providing continuous support
outside of traditional GP hours would ensure children and young people have a constant point of contact for managing symptoms at home or asking health-related questions.
Reinvestment benefits other areas such as education and local authorities. For example, having a school nurse available means children and young people receive immediate care if symptoms worsen during the school day. This support must be needs-led, allowing access without requiring a formal diagnosis, thus promoting quicker intervention and reducing the strain on overstretched services. The recommendation to invest in community health services ensures that children and young people have access to care when and where they need it most.
The report’s recommendations around improved data and digital solutions are very important and could be very useful if implemented. Standardising the use of an NHS number for children and young people would not only help clinicians, but also impact how data is shared between services, allowing a young person to access their own files quickly and easily online, as well as use any service that has access to their digital records. Transitioning to a digital red book is also important. Physical copies of patient records are now no longer as useful – a digital copy would give ease of access for clinicians, patients and families. However, implementation could be tricky, as the practical issues of building a system to support this may present some challenges.
RCPCH &Us: The Children and Young People’s Engagement Team delivers projects and programmes across the UK to support patients, siblings, families and under 25s, and gives them a voice in shaping services, health policy and practice. RCPCH &Us is a network of young voices who work with the College, providing information and advice on children’s rights and engagement.
SPA time
The importance of Supporting Professional Activities (SPA)
Dr Sarah Hallett
Paediatric
ST5 (C4)
East Midlands School of Paediatrics
RCPCH
Assessments
Trainee Representative
Jess Groucutt
ST8 Paediatric
Registrar Sandwell and West Birmingham
NHS Trust
Trainee Representative for the West Midlands
The Training Charter has been in place since March 2019, when a College surveyfound inconsistencies in the training experience across the UK. It describes seven domains that training units should be striving towards to achieve high-quality training, with the sixth speci cally talking about Supporting Professional Activities (SPA). In summer 2022, the Charter was updated to bring SPA time in line with other College recommendations, with eight hours per month for tier one trainees and 16 for tier two trainees. A key aim of the RCPCH trainee committee is to ensure that the standards of the Training Charter are upheld and regularly updated. From our individual experiences and feedback from regional representatives, we found SPA time in particular was poorly adhered to, so a SPA working group was formed to tackle this issue.
What is SPA time?
SPA time is vital, as postgraduate doctors in training (PGDiT) undertake a wide range of non-clinical activities required by the curriculum, and o en due to clinical pressures, these activities take place in personal time. Adequate rostered SPA time ensures that these activities can be accessed and completed by trainees equitably. SPA synonyms include
continuing professional development (CPD), self-development time (SDT), educational development time (EDT) and care days. The following are examples of what SPA time may be used for, but this is not an exhaustive list:
Quality improvement projects and audit
Guideline development
Research
Publications
Preparation for regional/national presentations
Management activity
Preparing teaching sessions
SPA time should not be used for: private study leave (eg exam preparation); completing mandatory training or clinic administration; performing audits required for service delivery; attending regional or departmental teaching nor attending clinical situations such as GRID or SPIN-speci c clinics.
Placement units must enable trainees to meet all requirements within paid time, while the English junior doctor contract (NHS Doctors and Dentists in Training contract 2016, version 11, schedule 4) details two clauses that support SPA time: Work schedules should be designed to meet the service delivery needs of the organisation and the education and training needs of the doctor.
The generic work schedule will list and identify the intended learning outcomes (mapped to the educational curriculum), the scheduled duties of the doctor, time for quality improvement and patient safety activities, periods of formal study (other than study leave), and the number and distribution of hours for which the doctor is contracted.
SPA time is integral to each consultant’s job plan. When the new consultant contract evolved in 2003, a suggested
breakdown of the week was 7.5 sessions for direct clinical care (DCC) and 2.5 sessions for SPA. The Academy of Medical Royal Colleges estimates that 1-1.5 SPA per week are the minimum for a consultant’s CPD for revalidation.
How much SPA time should paediatric trainees have?
SPA time is not unique to paediatric trainees, and the table highlights recommendations and requirements across di erent specialties. It demonstrates that the Training Charter recommendations for SPA time are lower than many others. There has been a general growing recognition of the importance of this time (eg following the Health Education England Foundation Programme Review) and it was agreed with NHS Employers in England that Foundation Doctors should be given time in the working week for nonclinical professional activities. An FY1 should receive an average of one hour per week and three hours per week for FY2 doctors (~12 hours per month). This means that when an ST1 commences paediatric training their minimum SPA time recommendation is less at only eight hours per month.
Unfortunately, despite the recommendations for paediatric trainee SPA time being relatively lower, a recent trainee survey conducted by the RCPCH trainee committee revealed very low compliance – 287 responses from across the UK with a range of departments covered revealed 75.6% of ST1-3 trainees and 76.3% of ST4-8 trainees did not get rostered SPA time.
For those who did have rostered SPA time, access was an issue – 44% of trainees felt they were unable to take it more than half of the time or not at all and only 25.8% were able to take their SPA time as per rota. The main reasons for being unable to take their SPA time were
Speciality
rota gaps, staff sickness and the inability otherwise to take their annual leave days if SPA days were not used.
The same survey revealed that trainees were unaware they could exception report for lost rostered SPA or having to spend time outside their scheduled working hours to complete necessary activities for the curriculum, so we have been encouraging PGDiT to exception report. This enables rotas to be adjusted, hospitals to apply for more funding and doctors to get either time back or financial recourse. Other nations may pursue a similar structural change via diary card monitoring systems. Unfortunately the survey found that many doctors have never exception reported and have often never been able to do so.
Positive SPA experiences
By giving trainees enough SPA time, we create a fairer system, including a level playing field for job applications. We discriminate less against people who may find it challenging to complete all the
“I do get some limited aspirational study leave time (five hours in six months) but having SPA time has made it so much easier to keep up and ensure everything else portfolio-wise is done without eating into my own time”
Katie, studying for a masters in paediatric palliative care
curricula-required non-clinical activities in their own time, such as those with caring responsibilities. The benefits go beyond individual trainees too – better prepared newly qualified consultants, superior quality improvement projects, audits and research, and more availability for teaching will advantage departments
and the treatment of young people.
Receiving adequate SPA time may also have a positive impact on rotas, as we know of multiple trainees who opted to work LTFT to have more time for ePortfolio and other activities required for training, while maintaining a work-life balance. PGDiT are likely to feel less burnt out, with improved staff morale having a knock-on effect throughout the paediatric community, therefore potentially improving paediatric trainee retention.
The Training Charter has been updated to reflect the importance of SPA time, the national survey has been presented to regional heads of schools and a Beginners Guide to SPA circulated to trainees. Trainees should be encouraged to escalate to college tutors and rota coordinators if SPA time is not reflected in their work schedule and exception report when doing SPA-related activities in their own time.
The Training Charter can be found at www.rcpch.ac.uk/ resources/training-charter
Examples of Postgraduate Doctors in Training (PGDiT) SPA time recommendations
Feeling heard
Youth ambassadors report from International Adolescent Health Week
WIAHW UK Lead
ith the theme of Thriving not just surviving: Building adolescents’ resilience, this year’s International Adolescent Health Week (IAHW) took place from 7-13 October with youth ambassadors and professionals from around the world helping to raise awareness about adolescent health and educate young people on resources and support available to them.
The issues surrounding young people today
Amelia, age 24
I’ve seen the devastating e ects that mental health challenges can have on young people and, as they continue to rise, we must understand them not just from a clinical perspective, but also from a more holistic viewpoint that takes in shared lived experiences. And while funding is limited and appointment times
can feel restricted, we must position the patient at the heart of each interaction and allow young people to feel heard and seen. Organisations like the International Association of Adolescent Health (IAAH), which hosts IAHW, o er a chance for young people to be seen, raise awareness of adolescent health and teach others how best to interact with them. To better understand the challenges young people face, let’s explore the key areas that shape their world today.
1. Social media
Young people can experience high levels of FOMO (fear of missing out) due to social media. They see continuous updates of their peers’ lives and meet-ups and – if they’re not included – it can leave them questioning why they weren’t invited or why their life might be perceived di erently from someone else’s. This can bruise a young person’s selfesteem and confidence.
2. Educational settings
High expectations and exam pressure can see young people compare their
Amelia’s advice to healthcare professionals
Empathy and active listening: It’s about listening – not just to respond, but to truly understand. Keep an open mind to whatever the young person is experiencing. This allows them to feel heard and supported, meeting them wherever they are on their journey.
Be present in their spaces: Meeting young people where they are and being fully present with them makes a real difference. It’s not always about fixing things, but about accepting
them. If talking is difficult, be open to alternative ways of communication, like writing things down.
Offer choice and flexibility: Giving young people options helps them feel empowered. Whether it’s a face-toface chat, a virtual check-in, support by email, or using physical objects to help express feelings when things become overwhelming, offering flexible ways to connect can make reaching out feel easier and more accessible.
successes. Burnout among young people is a critical issue and perhaps not as recognised as it is among adults.
3. Geopolitical situation
Exposure to conflict and global crisis can be incredibly anxietyinducing. Navigating this is tricky with information (as well as disinformation and misinformation) and conversations bombarding young people both online and o ine. It can be tricky to ‘switch o ’ from constant negative exposure.
4. Post-pandemic
Since the pandemic, there’s been a rise in health anxiety, the number of people dealing with long-term conditions and concerns about potential future pandemics. Young people are concerned for the health and safety of themselves and family members.
5. Cultural shifts
Peer pressure and a need to ‘fit in’ can impact young people. Self-exploration and discovery are key to navigating identity struggles. Young people today are more likely to explore things such as gender fluidity, along with challenging modern values and cultural expectations.
Seyi Adeleye
Healthcare professionals can play a vital role in helping young people to get support
Young people and abuse – how healthcare professionals can help Sophie, age 17
I grew up in an abusive household and having the chance to voice my experience is something many don’t get the opportunity to do. Abuse is a topic that I was taught was taboo. Understandably, it’s not a nice thing to talk about, but interventions on child abuse often rely on the child speaking up – so how can we expect them to speak up when we avoid the topic?
Identifying abuse in a 15-minute appointment, particularly when the abuse is emotional or sexual as opposed
“An adolescent facing abuse should not be judged on the abuse they face but met with an understanding of their experience”
to physical abuse or neglect, can be difficult and emphasises the need for all organisations that provide care (such as the NHS, schools and social services) to effectively communicate between each other so that even the smallest of signs aren’t missed.
In addition to some types of abuse being more difficult to identify, they can come with stigmas attached. One stigma I find particularly damaging is that emotional abuse isn’t as valid as other types of abuse as it doesn’t leave visible injuries. An adolescent facing abuse should not be judged on what kind of abuse they face but should be met with an understanding of their experience.
Another stigma I have seen is around the type of adult who can be an abuser and how an adolescent who has experienced abuse behaves. As a child I was taught by outdated videos from the school’s health and wellbeing curriculum what abuse was. It depicted white middle/lower class males drinking from bottles, but not a single female, someone dressed in business attire or a person from an ethnic minority. This idea is very misleading and can lead to bias in reporting abuse. An abuser can appear polite, the characteristics are not mutually exclusive.
Sophie’s advice to healthcare professionals
Communicate with other care organisations: Signs of abuse are less likely to go unnoticed if they have been reported through multiple systems like the NHS, the police and schools. Reporting signs of abuse, no matter how minor, is vital to provide support to vulnerable adolescents.
Ensure young people feel acknowledged: Speaking up as an adolescent takes a lot of confidence, so validate their mental health difficulties.
Consider how your words are perceived: Saying ‘things will get better’ could be seen as dismissive. You could add ‘…despite how hard it is now’.
It’s good to talk
IAHW is a timely reminder of the 1.8 billion young people living in our world who require healthcare just as much as newborns, toddlers and the elderly. What can we do to support them? Because, more than ever, young people rely on us to give them the chance to speak and we must listen to them, respond to them and address their concerns. This isn’t something we can achieve alone. For our adolescents to truly thrive, we need to ensure that they not only have structures around them in which they feel safe, but structures in which effective crossprofessionality communication takes place so their issues are fully addressed.
Similarly, the child being abused was always shown as being quiet and not disruptive. Being abused has a massive effect on behaviour and children experiencing abuse can express antisocial, aggressive and disruptive behaviour. The behaviour of a young person should not affect the support they receive. We mustn’t dismiss all poor behaviour as ‘teens just being teens’.
For more information on how to support young people, to find out what we got up to in IAHW 2024 and to find out how to get involved in 2025, visit iaah.org/iahw or contact IAHW on social media.
Rota Gaps Survey 2024
A window into the state of our workforce
Kay Tyerman Consultant Paediatric Nephrologist, Leeds Children’s Hospital Officer for Workforce and Careers, RCPCH
Paediatric Head of School, NHSE
Yorkshire & Humber
Rota gaps have a detrimental impact on the wellbeing, morale and training of resident doctors, ultimately a ecting the delivery of patient care. In 2018, the BMA’s ‘Medical rota gaps in England’ survey found that 80% of respondents had been ‘encouraged to take on the workload of multiple sta ’ and 65% said ‘medical trainees are pressured to take on extra shifts’. The following year, as part of a snapshot survey in collaboration with Getting it Right First Time, the RCPCH Workforce team showed on average 10% of sta missing on weekday rotas in general paediatrics and 10% of neonatal units reporting gaps.
The post-pandemic workforce landscape
Paediatrics has welcomed the ability for doctors to take Out of Programme Opportunities and train flexibly – the percentage of Post-Graduate Doctors in Training (PGDiT) working Less Than Full Time (LTFT) having increased from 27.6% in 2018 to over 56% now. Furthermore, following the transition to Progress+, indicative training time has been reduced from eight to seven years with an earlier transition to Tier 2 duties necessitating greater protection for clinical training. This has all added to rostering complexity to balance e ective sta ng needed to deliver high-quality acute care alongside protecting daytime training opportunities.
Given these changes, the Workforce team conducted a survey to explore frequency and duration of Tier 1 and 2 rota gaps in multiple settings (District General Hospitals (DGH), Tertiary/Teaching Hospitals,
Foundation Trusts) and across general paediatrics, neonatolo , subspecialty plus combined general/neonates and combined general/subspecialty rotas. The survey was distributed through College tutors across all four UK nations and open from AprilJune 2024.
All respondents described the number of Full Time Equivalent (FTE) individuals required to sta a rota and gaps were quantified as a percentage of this FTE. Respondents were also asked to specify the reason for and duration of gaps, the use of locums, and to provide feedback on perceived barriers and facilitators for rota improvement.
Of 204 Trust or Health Boards (THB), 97 (47.5%) provided data for at least one rota – 110 units/hospitals and 153 rotas in total; 13 rotas showed no gaps. While the total number of UK paediatric rotas is unknown, the response rate was comparable across seven NHS England regions and each devolved nation.
Rota gaps across the UK
Although a snapshot survey and not without limitations, the key findings make stark reading:
Overall rota gaps across England, Scotland and Northern Ireland were consistent at 20-23.5%; Wales experienced considerably lower gaps at 11.3% (this latter finding should be treated with caution due to the low response rate).
Across all nations, Tier 2 gaps were higher compared to Tier 1 except Northern Ireland where Tier 1 gaps exceeded those of Tier 2. There was regional variation in rota gap frequency with the lowest in Wales, London and East of England and the highest in the Midlands, South East, North East & Yorkshire comparable with that of Scotland and Northern Ireland.
Rota gaps by region and rota tier
Combined general paediatric/neonatal rotas experienced the highest rota gaps (23.4%) which were greater for Tier 1 (25%) than Tier 2 (22.1%); all other rota types showed the reverse. Perhaps it’s unsurprising that Tier 2 gaps are generally higher than Tier 1 given the trend of moving to LTFT as PGDiT progress through training. However, it is concerning that there are higher rates of Tier 1 gaps in Northern Ireland, which may reflect recruitment di culty. An increasing number of PGDiT are also choosing to train flexibly from entry (ST1), which needs to be factored into recruitment numbers.
Other findings
Combined general paediatric/neonatal rotas are most likely in a DGH setting, where the relatively small workforce is more vulnerable to changes including parental leave and early training completion. DGHs may also lack financial ability to mitigate for gaps, particularly given the potential unpredictability of those between rotations. Rota gap duration was most commonly three to six months with the leading cause
The new survey has highlighted some of the reasons for rota gaps
Rota gaps across the UK – by region and rota tier
THB = Trust or Health Boards
Note on data: Some trusts submitted information from multiple units and/or multiple rotas for individual units; percentage = proportion of rota gaps by FTE
being LTFT working (32.4%) and ‘lack of Deanery allocation’ (26%) while use/nonuse of locums was evenly split, potentially reflecting local workforce availability or variation in locum rates.
LTFT working was the most common reason for lack of improvement in gaps, followed by the ability to recruit appropriately-skilled individuals and lack of financial support to fill parental leave. The unpredictability of rotational gaps with late notification of ‘Deanery’ allocation and Occupational Health restrictions on working patterns were also barriers. Conversely, employment of Locally Employed Doctors, who are often International Medical Graduates, improved rotas as did improved PGDiT allocation and use of slot shares. A few units also
“LTFT working was the most common reason for lack of improvement in gaps”
reported the benefits of e-rostering in utilising the workforce and improving PGDiT satisfaction.
So, what do these survey results mean for us? Although just a snapshot of workforce capacity to staff acute rotas, it doesn’t bode well for resident doctor training or wellbeing. Our survey results are in line with the GMC National Training Survey, which showed an increasing percentage of paediatric PGDiT disagreeing/strongly disagreeing that
‘educational/training opportunities are rarely lost due to gaps in rota’ (30.5% in 2024 v 25.8% in 2021) with an increase in self-rated high risk of burnout postpandemic (16.4% in 2024 v 9.3% in 2019). This is a worrying trend that ultimately will affect the ability to recruit and retain our paediatric workforce.
Wherever you work, I encourage you to read the Rota Gaps Survey report and consider what this means for your unit and team. It does not provide solutions, but awareness of the data is the first step to understanding the issues and working towards improving a concerning situation for the paediatric workforce.
The full report will be published on the RCPCH website
Outpatient clinics
An opportunity for professional development
Dr Maria Gogou
Consultant
PaediatricianPaediatric Neurologist, University General Hospital of Alexandroupolis, Greece
Honorary Fellow, Department of Neurology, Great Ormond Street Hospital for Children, London, UK
As consultants, we spend most of our working time seeing patients in outpatient settings. Nevertheless, during training our work is mainly focused on inward patient care or support of the emergency department. The time dedicated to formal training in clinics is not guaranteed, and may even be inadequate, and resident doctors may be underrepresented. Could this gap have an impact on their preparedness to run outpatient services safely and e ciently in future?
What can resident doctors learn from outpatient clinics?
The outpatient setting reflects a more personalised service where a resident doctor can develop and expedite their communication skills. Outpatient clinics are the places where we build therapeutic relationships with attention to the child’s and family’s/carers’ concerns and establish rapport. In a more protected environment, children and their parents/ carers are more open to sharing worries and concerns, sharing with residents their perspective of living with a chronic disease and discussing possible solutions to their problems, a fact which improves trainees’ understanding of what shared decision-making means.
Similarly, the setting of an outpatient clinic permits a paediatrician to meet and observe a child outside the context of an acute illness, think over their broader needs, estimate the dynamics of family relationships and educate them on how to cope with complex situations. Even
in a video appointment, we have the unique opportunity to observe the home environment and get an idea of the living conditions of our patients. The clinic is the place where we can communicate all the nuances of a diagnosis and cope with questions of long-term treatment planning and questions of uncertainty. In other words, we develop our personal style as consultants.
In parallel, the presence and guidance of the attending consultant can serve as an excellent role model, generate supportive discussions, inspire professional values and attitudes, and allow resident doctors to develop their autonomy in a gradual, competencybased way.
Outpatient clinics often have a considerable administrative workload, including clinic letters, essential referrals and the involvement of multiple stakeholders. However, those duties help a trainee develop accountability, navigate through healthcare services and boost their interprofessional relationships.
A tool for teaching medical students
In fact, outpatient clinics incorporate elements both from everyday wardbased activities (history taking, physical examination, diagnostic investigations, therapy strategies) and from ambulatory care (continuity, responsibility, economics). This combination can o er unique opportunities for case-based teaching for students in a less pressing environment using real-world data. Students can be taught and supervised to perform clinical examinations and receive feedback from residents and consultants. This also represents a promising perspective for resident doctors, enabling them to step up, see themselves apart from trainees as instructors, share their learning experiences and provide constructive
Outpatient clinics are where we build therapeutic relationships
“Students can be taught and supervised to perform clinical examinations and receive feedback from residents and consultants”
feedback to colleagues. This reflects an example of how ordinary care provision can trigger the transgenerational transmission of knowledge and values.
Challenges for resident doctors
Active participation in outpatient clinics and learning opportunities can frequently
be missed due to time constraints and interruptions, understaffed medical teams and last-minute changes in rotas. The unpredictable nature of our work often impacts scheduled activities and trainees are pulled out of clinics to support ‘first-line’ posts, while the lack of protected time for administrative work makes them sacrifice their personal time to keep up with jobs and deadlines related to clinics. At the same time, over the past few years, the COVID-19 pandemic has impacted attendance in clinics, while the introduction of telemedicine and virtual appointments has increased the complexity of the interaction between patient and doctor, and generated new challenges.
How resident doctors can benefit most from their exposure to outpatient clinics
Before the clinic
Make sure you have protected time for the clinic; ask colleagues to keep the bleep while you’re in the clinic and update your availability in your email accounts. Find out which patients you’re allocated to see and read over their conditions. This will empower you during consultation.
Review results from previous investigations; do not stick to reports but chase raw data as well (eg X-rays) and liaise with doctors from other specialties to discuss them. This will broaden your knowledge horizons and increase your interprofessional relationships.
During the clinic
Clarify your role from the very beginning and explain who is the consultant leading the clinic. This is reassuring for the family if they expected to see someone else. Be open-minded and do not stick to information provided in previous letters. Do not hesitate to double-check and confirm information and do re-examine the patient.
If you are joined by other healthcare professionals (eg nurse practitioners, therapists, social workers) or students, make sure everyone is engaged and given the opportunity to ask questions. You can learn a lot from listening to others’ perspective and comments. Start dictating the clinic letters before the family leaves and use your notes to confirm and summarise the main discussion points and the agreed management plan.
When summarising the case to the supervising consultant, encourage the patient/family to correct any information that’s not
precise. This empowers them and increases participation.
After the clinic
Discuss with the consultant the need for follow-up as soon as possible and use these letters as a means of reflection through your consultation.
Find time to discuss with the supervising consultant differential diagnosis and the rationale of investigations requested or treatments started.
Actively seek feedback from the supervising consultant. This can be in the form of an informal discussion or an arranged postclinic meeting. Actively ask them what you can improve and adjust to maximise your performance.
Keep a log of the cases you encounter (whether you are in a formal training system or not) and make sure you see a reasonable variety of cases.
Try to monitor the progress of the patients you see, chase results and liaise with families to learn about outcomes.
Read over the conditions you have encountered; this will maximise learning and increase your recall in similar situations in the future.
Ask parents/carers to complete GMC feedback forms. This is an efficient way of keeping up with professional requirements (eg appraisal, revalidation).
In general, outpatient clinics can offer a holistic view of what care of a paediatric patient means and become a thriving place for practising paediatrics, allowing resident doctors to develop the mindset of a consultant. Let’s try to add more educational value to everyday clinical activities!
Powering Up: a creative journey
One version of this story ends with sunshine and rainbows. The other is the truth
Dr Guddi Singh Consultant Paediatrician Founder & Director of WHAM (Wellbeing & Health Action Movement)
@DrGuddiSingh
The characters
Let me back up. A year ago, Milestones kindly o ered WHAM (Wellbeing & Health Action Movement) a platform to share our creative co-production journey to tackle health inequalities with young people (YP). Our project, Powering Up, backed by Health Foundation seed funding, explored the art and science of meaningful coproduction and empowerment in health. We joined forces with Dr Mary Salama’s Canal Project and Judi Alston’s One to One Development Trust to engage underrepresented YP in ‘creative, patient-led system redesign’. This tale unfolded across three issues of Milestones, with you, dear reader, as our companion.
The plot
Co-led by YP, Powering Up tested two complementary community-based, participatory methods: we used citizen science in Birmingham and the arts in London. Creativity infused everything – from concept to content, national dissemination (remember the pink hats and tote bags at #RCPCH24?) and even propelled our diverse young team to the HSJ Awards final.
In recent decades, the creative health movement has surged, backed by mounting evidence. The WHO endorses artistic media in healthcare and communities for diverse health benefits: promotion, condition management and disease prevention. The biggest secret in healthcare is the power of creative health for change. I know it works, because I’ve seen it for myself.
Powering Up ignited the 3 Es of empowerment – education, empathy, expression – through creativity. We’ve connected 100+ YP from the UK’s poorest boroughs with local clinicians. Both groups report Powering Up as:
1. Therapy: Creativity speaks without words, feeling like home. The increased sense of agency helped mental health.
2. Prevention: Education boosts patient adherence and reshapes clinicians’ perspectives for better long-term outcomes.
3. Intelligence: Creative methods catalyse genuine co-production by breaking down barriers, fostering vulnerable exchanges that reveal possible system improvements.
Powering Up’s greatest impact was on clinicians: in a matter of days, 10 young
“The creative health movement has surged, backed by mounting evidence”
diverse women (no men applied) went from believing they had little agency or power to confidently taking centre stage to speak up for their patients. Formative experiences like this have ripple e ects well beyond the walls of a room; these clinicians are transformed. In time, what hope – and change – will they bring to the NHS?
Which now leaves me to be creative. When health systems are slow to adopt creative approaches, how can we fund and sustain such initiatives?
Creative health is proven to have value – both worldwide and locally – but our systems lack the coordinated and
The Powering Up team and chosen YP took part in Show Up! in summer 2024
Creative co-production can tackle health inequalities
Bethany Gabriel
Final year medical student
King’s College London
What was Show Up!?
Performed in front of a live audience at the Science Gallery London on 19 July 2024, Show Up! involved 14 young people aged 14-17 years old, 11 clinicians and one week of creative arts workshops, which took place in a south London school. The aim was to utilise creative approaches – music, dance, poetry and theatre – to understand health inequalities experienced by YP.
First impressions
At first, I was apprehensive. I had no idea what I was getting into. Using creative methods in healthcare research had never occurred to me, so when Dr Guddi Singh asked, I responded: “But I’m not creative!”
The reality
This wasn’t a typical research project trawling through endless anonymised data. We got to know participants as they shared personal experiences through discussions and creative activities. No artistic background
concerted policies that could make it a reality. Medicine still excludes certain ways of knowing and being. Healthcare and medical funding continue to privilege quantitative and biomedical methods, and health professional cultures curtail how we behave. I was humbled and inspired by the courageous young clinicians who took part in Powering Up, even in cases where they didn’t have the support of their supervisors.
By some measures, Powering Up was a success. I should have been riding high. Instead, I broke down. Sleepless nights,
was required, and I admired the participants’ enthusiasm to try new things and embrace the project’s spirit. Creative methods broke down barriers – YP felt confident to ask the clinicians challenging and probing questions and vice versa, leading to meaningful insights that are often left unsaid. In just five days, Show Up! used arts-based methods to help YP and clinicians produce one music video, two new tracks, three choreographed dances, four drama sketches and 12 poems exploring the experience of health inequality. The final performance was amazing, delivering a strong message about the challenges faced by young men of colour, cultural misunderstandings in health systems and gaps in mental health services.
After-show thoughts
Show Up! demonstrated how diverse groups can co-produce something meaningful and completely changed my view on the value of creative arts and co-production in healthcare research. I feel creative co-production is underutilised and underappreciated in healthcare. Clinicians should be exposed to and educated about creative methods, along with raising patient awareness of ‘fun’ research they can get involved with.
gastric ulcers and cracked teeth – the signs and symptoms of someone trying too hard on too little. As so many of us know, trying to improve services and mentor a team with integrity, care and intention is hard. I didn’t want to fail those around me: honouring hard-earned bonds with YP and clinician participants, serving yet empowering my team, and staying true to co-production at every stage – all despite lacking institutional backing and resources. But anything less means settling for the status quo; we can all testify to how maddening it can be to
“I was humbled and inspired by the courageous young clinicians who took part in Powering Up, even in cases where they didn’t have the support of their supervisors”
work in systems that fail to properly serve patients and healthcare workers.
Leaders puzzle over our workforce crisis, but it goes far beyond fair pay. Powering Up showed job satisfaction stems from meaning, morals and community – not just career advancement. It’s about aligning work with our values and fostering the conditions to creatively and radically reimagine health.
The end?
Life is too complicated for happy endings. I share my story to show that success, however small, comes at a cost. Powering Up was always about more than achievements and accolades. In our first piece for Milestones, I wrote: “...much more important than outputs or products for me is the ‘how’.”
Show Up! used the arts to explore health inequalities
Showing up – even when it’s tough
Karelle Evans Lecturer in children’s nursing
What was your role in Powering Up?
I’m a lecturer in higher education, specifically a nurse who educates other nurses at a university. In Show Up!, I was the ‘youth link’, bridging the gap between YP and clinicians and helping both sides share their vulnerabilities.
Why did you want to get involved with something like this?
As a black woman with chronic illness, I can empathise with young people’s experiences, particularly regarding health inequalities. I aim to encourage YP to defy societal expectations and pursue their dreams, despite the barriers they might face. In Show Up!, I rediscovered my joy for creative arts – particularly dance which has been limited by pain – and this inspired the young participants to express their creativity, too.
People say that the arts are a waste of money. What’s your take? Joy in the NHS is hard to find because we’re overworked, understaffed and often unable to provide holistic care.
It feels like a conveyor belt, where patients are just numbers and there’s little time for meaningful interaction. I became a nurse to help people, not just treat symptoms, and it’s frustrating that so many colleagues feel the same but are limited by the system. The arts are often dismissed, but they’re essential, especially for YP who lack proper health education. If we invested in creative methods alongside traditional medicine, we’d have a more well-rounded, healthier society. The young people I spoke to lacked confidence in areas like sexual health and that education gap is concerning.
Tell the truth: what is it like to work with doctors? What needs to change?
Let’s just say that working with doctors has been mixed! But this project showed me their vulnerabilities too, which helped bridge the gap between nurses and doctors. We should normalise collaboration and friendship between healthcare professionals. I’d like to see healthcare embrace creative methods, involve YP more and prioritise the wellbeing of both patients and staff. The NHS is being run into the ground and we need to rebuild it with a focus on mental health, work-life balance and compassion for each other.
at the heart of both nursing and medical history, and it’s only fitting that tackling it is a joint venture. As such, my friend and queen of all trades Karelle Evans closes us out with her insights as a nurse in our team (left).
Powering Up’s journey revealed a profound truth: being myself is enough. Like you, what matters is doing good work aligned with one’s values. In a world of challenges, that’s not just enough – it’s everything.
Join WHAM, a movement to inform, empower and unite clinicians who fight health inequality, at www.whamproject. co.uk, and visit the Powering Up website at www.whamproject. co.uk/powering-up/home
Further reading and resources:
● Lessons in hiking: the ups and downs of making change: q.health.org.uk/blog-post/ lessons-in-hiking-the-ups-anddowns-of-making-change
One might read this as a story of me losing my sparkle, falling for self-blame over system critique. Nearly trading pink hats for pink prescriptions. But it’s also a recovery tale. In the end, my younger teammates (some half my age), who embody authenticity and love, helped me rediscover joy and laughter. They’re teaching me leadership through self-care –echoing the black intersectional feminist, poet and civil rights activist Audre Lorde’s wisdom that self-preservation is ‘political
warfare’. By mirroring my HOW, they’ve reignited my spark. I’m not sure that was the intention of Powering Up, but I’m glad it’s the result.
Thanks for joining our year-long journey. The story’s not over. The next chapter is still a work in progress but, rest assured, we’ll keep seeking ways to brighten healthcare while illuminating inequality.
For now, medical student Bethany Gabriel reports on our London arts pilot Show Up! (see page 23). Social justice lies
● Power to change: a 21stcentury paediatrician and their patient in conversation: bmjpaedsopen.bmj.com/ content/8/1/e002972
● Teach children so they can teach their families: bmj.com/ content/386/bmj.q1925/rr
● Health Foundation podcast: nhsconfed.org/podcast/equity
● The Creative Health Toolkit: creativehealthtoolkit.org.uk
● National Centre for Creative Health: ncch.org.uk
The Show Up! performance in London
Biting back
Youth activist movement takes aim at junk food advertising
Whether on bus stops, billboards or social media, it’s hard to miss the constant bombardment of junk food adverts aimed at young people – and the impact on my generation’s health is undeniable. That’s why at Bite Back we’re pushing back – and we’re making progress.
Our mission? A fairer food system
Bite Back was founded to fight for a fairer food system, one where young people aren’t pressured into unhealthy food choices by a relentless tide of junk food marketing. We believe every child deserves access to healthy, a ordable food. This year marks Bite Back’s fifth anniversary, and I’m proud to be part of a youth-led movement that’s making real change happen. We’ve mobilised thousands of young people to raise their voices and demand healthier food environments. From challenging major corporations to holding the government to account, we’re proving that young people can lead the charge in transforming the food system. And our e orts are paying o .
Celebrating a major win
This year, the Advertising Standards Authority (ASA) banned a Just Eat advert that was irresponsibly targeting under16s. This ruling came after a complaint made by a 15-year-old Bite Back activist, highlighting the power of youth activism. The advert promoted McDonald’s products that are high in fat, salt and sugar (HFSS) directly to children. This was a clear violation of ASA regulations, which are designed to protect young people from harmful food marketing, and the decision sent a strong message that brands can no longer get away with
ignoring them. It’s a win not just for us at Bite Back, but for every young person who’s tired of being targeted by unhealthy food ads.
Launching bold campaigns in 2024
In summer 2024, we launched our bold anti-junk food campaign at the Bullring in Birmingham and Westfield London, two of the busiest shopping centres in Europe. Our billboards replaced fast-food adverts with powerful messages calling out the junk food industry. As I walked past these billboards, I felt a sense of pride knowing that our voices were finally being heard in spaces usually dominated by companies with endless marketing budgets. But that’s not all. In 2024, Bite Back launched three pivotal reports addressing critical issues in the food system:
1. Are Food Giants Rigging the System Against Children’s Health? exposes how major food manufacturers use tactics that undermine children’s health, particularly in vulnerable communities.
2. Sweet Deception: Are Food Giants Using Child-Appealing Tactics Responsibly? reveals the manipulative strategies used in junk food marketing to target children and calls for stricter regulations.
3. How Far Can We Trust the Food Giants with Planetary Health? explores the connection between the food industry, climate change and young people’s futures, advocating for a more sustainable food system that prioritises both health and the environment.
Building a healthier future
There’s still so much more to do. Junk food companies aren’t going to give up easily. But at Bite Back, we’re determined to keep pushing for a food system that puts health before profit. Our generation is at a turning point. The choices we make
Want to support Bite Back’s mission?
One impactful step is to advocate for healthier food environments within the communities you serve. By raising awareness among parents, schools and local councils about the risks of junk food advertising and the importance of accessible, nutritious food options, paediatricians can help build momentum for change. Additionally, partnering with Bite Back on educational initiatives or sharing Bite Back’s research and resources with families can empower young people to make informed choices. Together, we can create a united front, pressing policymakers and food companies to prioritise child health. Visit biteback2030.com for more information.
now, and the environment we grow up in, will shape our futures. That’s why we’re calling on the UK government to continue taking bold steps to regulate junk food marketing and support healthier communities. It’s not just about removing junk food ads from our high streets, it’s about creating spaces where healthier food options are always available.
We’d love to hear from you, get in touch through our channels
@RCPCHTweets
The latest member news and views
Updates in Paediatric Emergency Medicine
Insights from the APEM Conference, October 2024
Dr Katherine (Katie) Keaney
Specialty Registrar in Emergency Medicine (PEM subspecialty) RCEM representative on the APEM committee
In a world of rota pressures and rush it can be easy to lose sight of why we choose to work in paediatrics. Especially in the trenches of A&E. What better remedy than gathering with a group of enthusiastic, knowledgeable and inspiring professionals at the APEM conference?
So I headed up north to Newcastle excited and a little daunted by the impressive programme, which ranged from lightning presentations to lively panel discussions and an interactive adventure! Highlights included results from the much-anticipated FIDO (Febrile Infant Diagnostic Assessment and Outcome) study that’s being published soon and looks into how we can better spot infants with serious infections. There was some stimulating discussion around investigation strategies and our perception and communication of risk. Do we practise shared decision-making with a reliable evidence base? The treatment of this group can vary hugely between practitioners and
Nathaniel age 13
PowerWash
Simulator is a fun yet calming online game. You play as a company that has to clean up ash from a volcano. There are multiple tools that you can use to help you clean while you look at the scenery of a small
across emergency and inpatient services. Regarding results, I won’t spoil the surprise! But I’ll be looking out for data on patients presenting early (under six hours) and following immunisation.
Dr Samantha Jones led a panel discussion on collaborative management of the abandoned child. We’ve all felt sad and frustrated when a child with complex mental health and behavioural needs gets stuck in hospital, sometimes for days, due to breakdown in social care and increasingly stretched mental health services. This puts pressure on emergency departments and paediatric wards. The team in Leicester attacked this problem, developing an inspiring pathway linking ED, paediatrics, mental health, the integrated care board and social care from the front door. What did I take away? This issue can be tackled if services cooperate early. If in doubt escalate, then escalate again!
There was also sobering data presented by Dr Liz Herrieven from the NCMD (National Child Mortality Database) report on deaths in children with learning disabilities and autism, which found that 31% of children who died from 2019-21 had a learning disability. Diagnostic overshadowing delaying
town, ironically called Muckingham. This is a game for those who want to relax while having fun. You can play on your own or with someone on a separate device in co-op mode. You can wash vehicles like vans, dirt bikes and antique cars as well as clean playgrounds, houses
Facebook @RCPCH
Instagram @RCPCH
milestones@rcpch.ac.uk
diagnosis and treatment may contribute to mortality. Do we factor this increased risk into our practice? As a paediatric community, this is an issue we can and must address.
And who would believe that a simulation session would be the highlight of the day? The PEM Adventures team led a fantastic interactive simulation of a child presenting with severe sepsis. It was fascinating to watch research being brought to life – proof that teaching can be engaging if you get creative!
As a tired trainee, this conference updated my knowledge and rekindled my passion for paediatrics. Our community is dedicated to improving children’s lives and I’ve been inspired to give myself some homework and further reading:
RCEM’s Learning Disabilities Toolkit, September 2024
We Can Talk (www.wecantalk.online) for evidence-based mental health e-learning
FIDO study (www.fidostudy.co.uk)
If you’re keen to get involved or need help getting started, you can now apply for a bursary to fund your PEM project. Go to apem.org.uk to find out more.
and skate parks. Some extras add more things to clean, like the Mars rover, and on that level, there are mysterious footprints that lead to a hatch.
I enjoy how it is so satisfying that it can make you forget about your troubles. This is a great game for all ages with its simple-to-master controls. Available on PC, PlayStation, Xbox, Meta Quest and Switch.
Find your Clean Air Fund poster on page 16
Starter for ten
We put 10 questions to a consultant paediatrician and their paediatric trainee
Dr Emma Blake
Child Mental Health Paediatric Consultant
Isle of Wight NHS Trust, HIOW Healthcare Foundation Trust, HIOW ICB @EmmaBla55820253
1. Describe your job in three words Hectic, complex, fascinating.
2. After a hard day at work, what’s your guilty pleasure? I am part of a community choir, excellent end-of-week therapy.
3. What do you find challenging about your time in academia? Breaking down medical segregations. Siloed working. People thinking about a patient in terms of organs and diseases. The split between mental and physical health.
4. What is the best part of your working day? I have been really inspired by our NHS Youth Forum. Young people impress me with their ideas, ener , compassion and kindness.
5. What was the best advice you received as a trainee? As a registrar in Melbourne, I spent time with a range of mental health specialists. They brought a di erent approach to problems than the traditional model I had been taught.
6. Who is the best fictional character of all time and why? Sherlock Holmes. Power of observation, deduction and reasoning. Passion for justice. Blunt. I love a neurodiverse mind.
7. What three medications would you like with you if you were marooned on a desert island filled with paediatric patients? Cefotaxime, salbutamol and adrenaline.
Dr Shayna Swaine
Resident Doctor (FY1)
Paediatrics – Conquest Hospital (ESHT)
Paediatrics Medical Elective – St Mary’s Hospital (IOW) @ShaynaSwaine
1. Describe your job in three words Inspiring, lively, challenging.
2. After a hard day at work, what’s your guilty pleasure? Watching my latest Netflix pick with a bag of crisps.
3. What do you find challenging about your time in academia? The biggest transition from a student to a doctor was the shift in responsibility. I’m still learning to feel more confident in myself. The best aspect of paediatrics is there is always a supportive team around.
4. What is the best part of your working day? Walking onto the ward and exchanging smiles and ‘good mornings’ with the team, or the interesting conversations with patients!
5. What was the best advice you received as a trainee? Work within your limits, but always seek out new opportunities. Never be afraid to ask for help.
6. Who is the best fictional character of all time and why? Scooby-Doo. I am a total dog-lover! Although he feels nervous, he always finds it within himself to push his limits, be brave and solve mysteries. He does this with love and joy – and with his friends (and a snack!) by his side.
8. What would you like your superpower to be and why? To be able to stretch time, to spend more time with patients to help them work through a problem.
8. What would you like your superpower to be and why? To be able to stretch time, to spend more time with patients to help them work through a problem.
7. What three medications would you like with you if you were marooned on a desert island filled with paediatric patients? Salbutamol, co-amoxiclav and Calpol.
9. What would you say to yourself as a medical student? I was once asked in a student interview why I didn’t want to be a social worker. It seemed like a stupid question. But now my work is so aligned with social workers that it doesn’t seem so crazy.
8. What would you like your superpower to be and why? Teleportation! To be able to travel everywhere in the world would be amazing and the greatest gift.
inspire the next generation of academic (Paediatric Mental Health Association) and in
10. How can you and your colleagues inspire the next generation of academic paediatricians? Working with the PMHA (Paediatric Mental Health Association) and RCPCH Mental Health Advisory Committee – we aim to train paediatricians to consider mental health as their core business and think of young people holistically.
9. What would you say to yourself as a medical student? Learn to trust your instincts and know that leading with kindness will always make your day brighter. Medicine is the most rewarding feeling in the world and the hard work will absolutely pay o .
10. How can you and your colleagues inspire the next generation of academic paediatricians? Working with paediatric patients is the best job – you get to have fun, play and feel the ener of bravery all day. The team is full of engaging, kind people who push me to be a better doctor.
Course review: How to manage childhood poverty
Dr Dita
Aswani
Consultant
Paediatrician
Sheffield
Children’s Hospital
National GIRFT
Clinical Advisor for Children and Young Adults
Diabetes
Asst Officer for Nutrition and Obesity, Health Improvement Committee, RCPCH
@DrDita
Childhood poverty affects 4.3 million children in the UK, meaning 30% of children and young people live below the poverty line. This is a significant number of the children we see in clinic and, more importantly, a greater proportion of those who are not brought to elective appointments and who end up accessing urgent care.
There is a lot we can do as paediatricians to minimise the impact of poverty on healthcare provision, by raising our understanding and awareness, developing the confidence to ask questions by sensitive and compassionate enquiry, and by challenging our own bias. We need to develop a universal approach to supporting all families, rather than targeting individuals. How often have you had an opinion on someone’s socioeconomic context based on their appearance or employment? Most children in poverty have at least one parent in paid work.
We can give excellent clinical advice, but this is of limited value if the recipient can’t afford to travel to an appointment, doesn’t have the technology or understanding to navigate a complex appointment system, can’t afford healthy food, or may not have the confidence or selfadvocacy to live well with a condition. By looking at our services through the lens of poverty, we can make changes that will result in less exclusion and more equity and accessibility.
This brand new course – a collaboration between the Children North East (CNE) charity and RCPCH – arises from impactful work with paediatric diabetes teams in the
Northeast and Yorkshire, where there are pockets of particularly deep deprivation.
CNE has worked in schools and arts and health spaces with the ethos that any planned activity should not identify, exclude, treat differently or make assumptions about those whose household income or resources are lower than others.
National Paediatric Diabetes Audit data has demonstrated a disparity in access to diabetes technologies (continuous glucose monitors, pumps and hybrid closed-loop systems) between those living in the most and least deprived postcodes. These devices improve quality of life and long-term outcomes. NICE technology appraisals have recommended these advanced therapies for all children, and although overall uptake is increasing, inequity in access has worsened over time. It is convenient to put this disparity down to personal patient choice rather than examining systemic barriers that result in healthcare system discrimination or the unconscious bias we might hold as healthcare professionals.
CNE studied three paediatric diabetes services in the Northeast and Yorkshire and identified common themes leading to inequalities in healthcare that disadvantage those living in poverty. Supporting NHS England’s focus on the Core20PLUS5 framework, funding from the Children and Young Adults Diabetes Programme gave 31 diabetes teams and three complications from excess weight services in the region the opportunity of childhood poverty training and strategies to povertyproof their services in 2023.
Learning was published in a Common Themes report and a Workforce Guide to help teams with practical changes in five broad areas:
Further reading and resources:
Scan the QR codes to access: ● Common Themes report
● Workforce Guide
travel, appointments, education, financial guidance and technology. The desire to instil a critical lens into every speciality and improve healthcare by considering the wider determinants led to the development of How to Manage: Childhood Poverty, which launched in July 2024. It was highly evaluated and will continue to run biannually. This course is suitable for all paediatric healthcare professionals at any stage in their career, as well as their service managers. Where possible, it is recommended that delegates attend with at least one other colleague from their team or organisation, as this will strengthen their ability to make a tangible difference in the workplace.
Treat your colleagues to a batch of Christmas biscuits
It’s the time of year when I struggle to decide what to get my department and ward team for Christmas to thank them for their hard work. Instead of buying chocolates, I often give out a selection of baked goodies, like these shortbreads. Simply add orange and chocolate to crumbly, buttery shortbread and you have the perfect Christmas treat!
Ingredients
• 100g caster sugar
• 200g unsalted butter, soft and cubed
• 300g plain flour
• 1 large orange, zest only
• 100g dark chocolate chips, plus a bit extra for drizzle (optional)
Instructions
1. Add the sugar to a large mixing bowl. Zest the orange directly into the bowl and use an electric hand mixer to quickly combine.
2. Add the butter into the bowl and beat the mixture together with the mixer until softened and slightly flu y.
3. Sift in the plain flour and add the chocolate chips. Beat again until combined and the mixture starts to form clumps.
4. Bring the mixture together with your hands until the dough has combined (do not overwork) and tip out onto your work surface.
5. Lightly flour your work surface and the top of the dough. Using a rolling pin, flatten out the dough, turning regularly and keeping it together, until it is roughly 1cm in thickness.
Using a cookie cutter (around 7.5cm in diameter) press out circles and place them onto a lined baking tray. Bring the remaining dough back together and repeat the process until you have around 12 shortbread biscuits. Place the baking tray into the fridge for an hour to allow the dough to rest.
7. Preheat your oven to 160°C (fanassisted). Sprinkle a little extra sugar over each shortbread biscuit before baking. Bake the biscuits for 13-15 minutes until the edges are firm, and the biscuits are lightly browned. Allow the biscuits to cool on the tray before transferring them to a cooling rack to allow them to cool completely.
8. Finish with an optional drizzle of melted chocolate and grated orange zest.
History taking: The flexibility of being categorical
Dr Richard Daniels
Paediatric registrar
St Mary’s Hospital
@DrRDaniels
In evidencebased practice, we often start with a question. This mental training has bled over into my column. Often, I will ponder something and, via historical tangents, arrive at my chosen topic. In this case, I was clearing out back issues of ADC after my wife’s patience had been exhausted. It got me thinking about how big the ADC archive is, and what
the first issue looked like. Fortunately, it’s all online –so I travelled back in time to January 1926.
Rickets was the theme of the first issue and it included a piece by Donald Paterson, a newly minted registrar at the time and someone I’ve written about previously. There were also pieces on pes cavus, inconsistencies in infant feeding formulas, the relationship between ketonuria and urine pH, and a case series on a cuttingedge therapy involving injecting a child’s father
with his son’s infected blood, before drawing the father’s blood and transfusing the antibodyfilled serum back into the child. He survived. The three other case studies did not.
My favourite part, however, came in the introduction by Sir Thomas Barlow, another Victorian polymath physician whose career highlights included discovering the pathology of infantile scurvy and being a Royal Physician to three monarchs. He posited that one difference
between the ‘study of child diseases’ and their matured specialities was the presence of generalists. He then suggests that specialisation should occur, not by organ, as with adult medicine, but by age, and suggests three cohorts until puberty is reached. Add that to the movement for adolescents to be recognised as a subspeciality and there’s a manifesto for a revamp of how child health is delivered – maybe something to consider for the 100-year anniversary!
A day in the life
“Child protection can be lifesaving”
Dr Alison McLuckie
Consultant
Acute and Community Paediatrician
Lead Paediatrician for Care Experienced Children and Young People (NHS Lothian)
Lead
Paediatrician for Child Protection (Edinburgh)
My typical day starts with a dog walk. Living in Scotland means this often happens in the rain and results in a very muddy spaniel by 8am. Like lots of us, mornings require military precision, so the workday often feels like relative relaxation by the time it gets started. I have been lucky enough to have the support of my parents, particularly my mum, which has been indescribably important and has allowed me to do much more than I could have achieved on my own.
I’m fortunate to have a varied clinical job, partly by design and partly due to being in the right place at the right time. I was keen when I became a consultant (with my subspecialty recognition being in Community Child Health) to continue to practise acute paediatrics. So, for four daytime weeks and 12 evenings a year, I contribute to the acute paediatric consultant rota: assessing new admissions, leading ward rounds and working in the acute receiving unit at the Royal Hospital for Children & Young People (RHCYP) in Edinburgh. This is a tertiary teaching hospital in Scotland’s second largest health board and, although it’s tiring, I love it.
This part of my job provides a welcome balance to my community paediatric workload as Child Protection and Care Experienced Lead Paediatrician for Edinburgh City and NHS Lothian respectively. I still find it amazing how quickly children get better with salbutamol, prednisolone and the right amount of clinical acumen. Maintaining relationships with my acute and
When I finish work
I try to sit still, but invariably do not manage this. I run a charity redistributing used children’s books so I’m often found surrounded by books or bits of recycled plywood (which we use to make little libraries). I also took up horse riding and climbing with my children this summer. Learning new skills together has been brilliant and riding and climbing are now a fun and challenging way for us to carve out time together in a busy world.
subspecialty colleagues also means that I understand the different pressures facing paediatrics services and I think that helps collaboration when needed from my child protection and community caseload. I also enjoy my neurodevelopmental work. I like getting to know families and being able to help with things that are not typically ‘medical’. I am a clinical contact for the CHAI (Community Help and
Advice Initiative) Welfare Advice service in RHCYP, which has been very important in supporting families. Although it can be challenging at times, all the parts of my job complement each other and I don’t think I would practise in the same way without all the components working together.
Many people think child protection must be the most difficult part of my job, but I don’t think it is. There are definitely vicariously traumatic situations – which can sit with me for some time – but they serve as a reminder that child protection is vital work and can be lifesaving in the same way that acute paediatrics is.
I have just finished a Masters in Public Health and my dissertation was on children’s rights. Approaching this topic academically and now being able to apply it to healthcare systems, particularly for care experienced children as we work to keep Scotland’s promise (www. thepromise.scot), is very rewarding.
Launching the Youth Navigator service in July 2021 was a memorable moment. It started as a collaboration with – and is run by – Medics Against Violence (www.mav.scot) in three hospitals in Scotland, and provides a youth work-based approach to helping adolescents aged 12-16 who present to healthcare services. One of the things that stuck with me about this piece of work was the support, which was given freely by colleagues already doing similar work. Being able to reach out to teams such as those at King’s Adolescent Outreach Service (KAOS), the Redthread charity and the existing Navigator team was incredible.