
LEADING THE WAY TOGETHER












Winter 2024 CONNECTING THRU COLLEAGUES, CAREERS, CRAFT, CALLING, AND COMMUNITY
Bringing CNS Members Together to Make Children’s Lives Better














Bringing CNS Members Together to Make Children’s Lives Better annalscns.com READ... the latest issue of ACNS For Additional Information https://www.childneurologysociety.org/ – Colleague – Annals of CNS
Annals of the Child Neurology Society ( ACNS )
CONNECTING WITH...
CNS Connections is the official news magazine of the Child Neurology Society. The title references the passionate professional interest members share in neural connections and their commitment to connecting to and staying connected with the peers, colleagues, mentors, mentees – and, above all else, friends – in the field with whom they share a career, craft, calling, and community.
Child Neurology Society
1915 West Highway 36, Suite 174 Roseville, MN 55113
Tel: 651/486-9447
Fax: 651/486-9436
nationaloffice@childneurologysociety.org
www.childneurologysociety.org
EDITOR
Daniel Bonthius, MD, PhD
MANAGING EDITOR
Monique Terrell
PROOF EDITOR
Julianne Bruce
DESIGN & LAYOUT
Kimberlea Weeks | CEVA Design Published
©2024 Child Neurology Society
COLLEAGUES 4 Letter from the President Winter Activity Highlights 6 Q&A: About the Annals of the Child Neurology Society With E. Steve Roach, MD, Immediate Past President of the Child Neurology Society CAREERS 9 Member Benefit Highlight Fellow of the Child Neurology Society Program 19 Personnel Registry COLLEAGUES 10 Research Focus Abnormal Movements in Autism: Association or Causality? CRAFT 12 Synapses HIE without the E: Babies with hypoxic-ischemic brain damage who look fine as newborns 14 Synapses What’s the wait? Delays in epilepsy surgery 16 Synapses Restoring strength and function: Nerve transfer surgery following acute flaccid myelitis COMMUNITY 18 Association of Child Neurology Nurses 2024 ACCN Award Nominations Are Now Open
MAGAZINE
CONTENTS
3 times yearly Child Neurology Society | Winter 2024 3

CNS PRESIDENT
Peter Kang, MD

Letter from the President
Dear CNS Friends,
We are closing in on the midway point between annual meetings, with a slightly longer interval due to the November timing of our 53rd Annual Meeting in San Diego. The CNS has been a hive of activity over the winter. Highlights include:
1. Completion of the merger with the Professors and Educators of Child Neurology (PECN) on January 1, and the initiation of the new Child Neurology Educators Committee, led by our thoughtful and experienced Nancy Bass.
2. New Committee appointments took effect on January 1, and committee activities are ramping up as spring begins.
3. Robust, well-attended CNS webinars, with an average of 147 registrations in 2023.
4. Several of our major 2024 CNS Awards have been announced, with an inspiring roster of awardees. More award announcements to come!


5. An enhanced partnership with the Pediatric Epilepsy Research Foundation (PERF), including a new PERF-CNS Bridge Grant program, as well as other major grant programs.
6. Our valuable partnership with the Association of Child Neurology Nurses (ACNN) continues, as their Annual Meeting will again be held in conjunction with our Annual Meeting.
7. The American Board of Psychiatry and Neurology (ABPN) has announced a new cycle of awards for 2025-2026 ABPN Awards Program. Questions may be directed to Dr. David Shin, VP of Research and Psychometrics, at dshin@abpn.org
8. We eagerly await the Child Neurology Foundation (CNF) Symposium, traditionally the first general session, setting the tone for the rest of the Annual Meeting with our closely allied partner.

COLLEAGUES
4 Child Neurology Society | Winter 2024

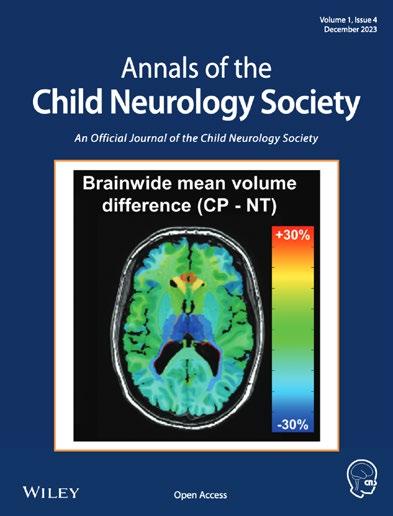
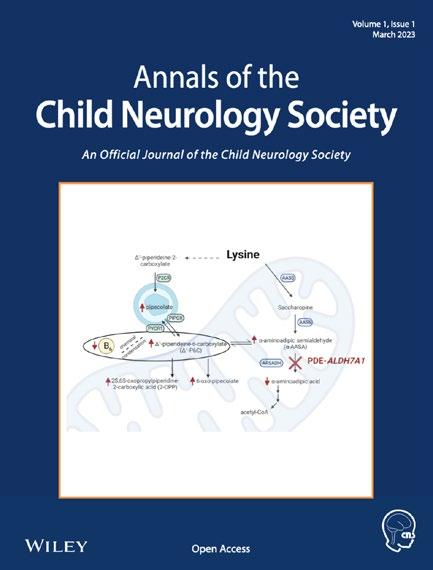
9. The Annals of the Child Neurology Society published its first four issues in 2023 and recently released its first 2024 issue. Please consider submitting your excellent work to our Society’s newest official journal!
We have been laying the foundations to ensure the long-term financial health of the CNS so that we may continue offering member services and support for many decades to come as we, our members, provide increasingly sophisticated care for our patients and make landmark discoveries in our field. In addition to a re-invention of our industry partnerships, we will be asking you periodically to help support our award programs, as we have done in the past. Donations are always welcome, and as mentioned in my Fall 2023 President’s Letter, we are making plans for a more visible fundraising campaign in the near future.
To follow up on another comment from my Fall 2023 letter, I am delighted that our 53rd CNS Annual Meeting in San Diego will feature career development and leadership development activities even more prominently than in the past. Together, we will lead the way to a better future for the children under our care. •
Your Chance to Lead the Child Neurology Society!

Are you passionate about shaping the future of child neurology?
If so, consider running for a CNS Board of Directors position! We are seeking dedicated individuals committed to advancing our mission and making a difference in child neurology. As a board member, you will help govern the CNS, ensuring that our activities align with our strategic plan and organizational priorities. Your role will also involve overseeing the society’s finances, ensuring that resources are used effectively to benefit our members.
Positions available:
• President-Elect
• Councilor for the South
• Councilor for the West

VISIT... the CNS website for position descriptions and more information on how to nominate yourself or a colleague.
https://www.childneurologysociety.org/becoming-a-cns-board-member/
Don’t miss this chance to be part of something meaningful!
Nominations open June 1, 2024
Child Neurology Society | Winter 2024 5
About the Annals of the Child Neurology Society
BY DANIEL J. BONTHIUS, MD, PHD, CNS CONNECTIONS EDITOR AND
With E. Steve Roach, MD, Immediate Past President of the Child Neurology Society
 E. Steve Roach, MD University of Texas Dell Medical School
E. Steve Roach, MD University of Texas Dell Medical School
What prompted the creation of the Annals of the Child Neurology Society?
Annals of Neurology is a terrific journal, and we should be proud of it. Annals’ articles are highly cited, and their impact factor is enviably high. On the other hand, because of its emphasis on basic science and its rigorous acceptance standards, Annals is not a reliable option for many CNS members who wish to publish. Annals of the Child Neurology Society is intended to fill that gap. We accept commentaries, clinically focused research articles, case series and case reports, and review articles. Basic science articles are welcome if they have clinical implications.
Another benefit is that the society actually owns ACNS even though it is published under contract by Wiley, the publisher of Annals of Neurology. Annals is owned by the American Neurological Association, and the other pediatric neurology journals are owned by publishing companies, so the CNS has little or no input into their operations. Ownership of ACNS allows the society to guide the journal’s editorial policies, approve its editorial staff and editorial board, and publish discipline-specific articles, such as the commentary last year about the child neurology training requirements (available at https://doi. org/10.1002/cns3.20015) or articles
derived from the award lectures at the annual meeting (see, for example, https://doi.org/10.1002/cns3.20067).
Is the ACNS now the official journal of the CNS? Or does it share this position with the Annals of Neurology?
ACNS was created to be a companion clinical journal to Annals, not to replace it. So, both journals are official CNS journals. The American Neurological Association also created a clinical journal a few years ago (Annals of Clinical and Translational Neurology, or ACTN). We have a great relationship with the editors of Annals and ACTN. Together, the three journals form an “Annals family” of journals, and manuscripts pertaining to children that are not accepted by Annals are offered a transfer to ACNS. If the manuscript has been reviewed by Annals, we can make a quick publication decision based on the existing manuscript reviews. We anticipate that these Annals referrals will generate a substantial number of articles for ACNS once it is fully established.
What were the major obstacles to overcome in order to launch this new journal?
As the CNS Board considered starting the new journal, they first
6 Child Neurology Society | Winter 2024 Q
had to determine how ACNS would relate to Annals of Neurology. Once these questions were resolved and the decision to create the journal was finalized, the real work of actually building it began.
In the span of about five months, we selected an excellent group of associate editors with expertise in the major topics of the field and assembled an impressive editorial board. We began compiling the journal’s peer reviewer database, wrote detailed instructions for authors, built the manuscript submission site, and created content for the ACNS website. In parallel, we wrote the launch editorial and began receiving and editing manuscripts even before the submission site was completed. Aside from the opening editorial, the honor of the first real ACNS article goes to Harvey Sarnat (see https://doi.org/10.1002/cns3.2).
Several obstacles remain. Articles in new journals are not automatically indexed in PubMed. A journal must first publish 25 regular articles (excluding editorials, correspondence, etc.) and meet an array of journal production standards to be eligible for indexing by PubMed. We had satisfied these requirements by last August, but PubMed has a serious approval backlog, so we are now hoping for indexing approval in another month or two. Fortunately, once approved, all the published articles are retroactively indexed.
Additionally, ACNS will not earn an impact factor for another couple of years. This delay is due solely to the way the score is calculated, so our current focus is publishing articles that will generate a decent initial impact factor.
Open-access journals have publication fees, which are a barrier for some authors. With the cratering of journal ad revenues in recent years, publication fees are likely to become widespread in the next several years. The payment models are already shifting, however, as many institutions now have agreements with major publishers to cover the fees for articles written by their faculty. In addition, the CNS supports the fees of its junior members, and Wiley offers fee waivers and discounts for individuals in resource-poor countries.
How many ACNS issues have been published so far?
Once an article is accepted and fully edited, it is promptly published on the ACNS website in its final form, aside from the pending page numbers. This process ensures very rapid publication, particularly when coupled with the journal’s expedited review option.
We periodically aggregate the recently published articles into a
CONTINUED on page 8
EDITOR’S NOTES
One of the most important and exciting new initiatives by the Child Neurology Society in recent years is the creation of the Annals of the Child Neurology Society (ACNS) ACNS published its first issue in March 2023. This is an interview with the ACNS founding Editor-inChief, Dr. E. Steve Roach. A past president of the Child Neurology Society, Dr. Roach is a Professor of Neurology at the University of Texas Dell Medical School.
Child Neurology Society | Winter 2024 7
QLooking Back and Forward
AND CONTINUED from page 7
more traditional issue. It is then that each article is assigned page numbers to accompany its existing DOI link. The issues are accessed via a small journal icon on the ACNS website (www.annalscns.com). Initially, we are compiling quarterly issues, and the fifth issue will appear in late March. As the journal grows, we anticipate that the issues will increase to bimonthly and, eventually, to monthly.
Are there certain kinds of studies or papers that are an especially good fit for ACNS?
Like other journals, we seek quality manuscripts with novel findings and new insights. Review articles are also a great fit. ACNS is a forum for child neurologists, so thoughtful commentaries about training requirements or the effect of economic or cultural developments on the field are encouraged. We have a variety of submission categories, so everyone should be able to find an appropriate format for their work.
What are the advantages to child neurologists to publishing in ACNS?
Articles in open-access journals are available to anyone with internet access, even if they cannot afford a journal subscription. These articles are read more frequently and cited more often than articles in subscriptionbased journals. Discipline-specific commentaries may also have an
easier time finding a home in ACNS than in other journals. The society benefits from having its own journal, so publishing in ACNS is also a good way to support the CNS.
The journal’s rapid review option can complete the peer review process and render an initial publication decision in ten days. If the authors speedily address any requested revisions, publication could occur in as few as four or five weeks after submission. This is a very useful option for authors wishing to quickly publish an article in preparation for a grant submission or a promotion nomination.
ACNS is also a great journal for trainees and novice writers. While our trainee mentoring program is not a back door to the publication of dreadful manuscripts, the program offers several perks designed to aid novice writers. First, each designated trainee manuscript is personally reviewed by an editor, then, in many instances, returned to the author with a list of preliminary suggestions to be addressed prior to releasing the manuscript to the regular reviewers. We try to select reviewers who have a reputation for making useful suggestions in a kindhearted way, even when they cannot recommend publication. Finally, we often allow individuals in the program additional revision opportunities, provided we can see a clear pathway to eventual publication. The CNS has budgeted a considerable annual sum to pay the publication fees for its junior members.
What can members of the CNS do to help foster the growth and strength of the ACNS?
The quality of the ACNS articles has been excellent, so read and cite the articles! Consider signing up via the website for automatic email notifications that include links to new articles. Please agree to serve as a manuscript peer reviewer when asked. Finding qualified and willing peer reviewers is the bane of most editors’ existence, so help us out. We have an informal process to guide inexperienced manuscript reviewers. Finally, you can submit your work to ACNS and encourage others to do so. If you are uncertain of the appropriateness of your manuscript, feel free to inquire (AnnalsCNS@ austin.utexas.edu).
Any final thoughts?
ACNS is progressing nicely, and it will succeed. But please be patient. Most successful journal launches take three to five years, and we are well ahead of that pace. •
8 Child Neurology Society | Winter 2024
Fellow of the Child Neurology Society Member Benefit Highlight

As the professional home of child neurologists, membership in the Child Neurology Society provides unparalleled resources and connections to hone your skills, connect with colleagues, and grow your practice. One of our newest benefits is:
Fellow of the Child Neurology Society Program (FCNS)
The FCNS program is a prestigious distinction that recognizes our most esteemed members and honors their extraordinary professional achievements and contributions.
Those earning the FCNS designation will be recognized for their dedication and accomplishments in pediatric neurology.
They will be allowed to use the FCNS credentials after their name, signifying their distinction in the field. Furthermore, their names will be featured on the CNS website as distinguished Fellows of CNS.
The FCNS program provides immense value for both academic and private practice members, including:
• Formally recognize their expertise and contribution to the field of pediatric neurology.
• Boost their reputation and raise visibility in the medical community.
• Potentially lead to promotions, greater influence, enhanced research opportunities, or increased business and patient referrals. •








Child Neurology Society | Winter 2024 9
CAREERS
Link to Fellow of the Child Neurology Society Program

CNS CONNECTIONS EDITOR
Daniel J. Bonthius, MD, PhD Medical Director, Pediatric Neurology Levine Children’s Hospital

Abnormal Movements in Autism: Association or Causality? Research Focus
BY DANIEL J. BONTHIUS, MD, PHD, CNS CONNECTIONS EDITOR
When people think of autism, they usually think only of deficits in language, social interactions, and behavior. However, motor impairments can also be present in autism. And these motor impairments may not only be associated with autism; they might also be causally linked to autism. Dr. Rujuta Wilson, an Assistant Professor of Child Psychiatry and Pediatric Neurology at UCLA, is exploring this novel concept.
The idea that abnormal movements may contribute to the development of autism stems from the recognition that exploration of the environment and the ability to socially engage with a caregiver depend upon a person’s ability to move properly. Deficits in movement may corrupt a child’s ability to explore, point, and convey thoughts, emotions, and
Dr. Rujuta Wilson, an Assistant Professor of Child Psychiatry and Pediatric Neurology at UCLA, is exploring abnormal movements in Autism.
reactions. Thus, movement abnormalities may undermine normal developmental processes and lead to precisely the types of deficits that constitute autism. Yet, there remain significant gaps in our understanding of what these motor impairments are and how they drive neurodevelopmental outcomes.
It is no accident that Dr. Rujuta Wilson’s research focuses on bodily movement. Movement has been of central importance to Dr. Wilson throughout her life. As a young child of Indian heritage, she was enthralled with dancing, learning ballet and traditional Indian dances. Continuing her interest in expressive movement, she minored in dance as an undergraduate at George Washington University, where she studied modern dance techniques. With a major in anthropology and a second
COLLEAGUES
10 Child Neurology Society | Winter 2024

minor in biology, Rujuta appreciated the interaction of culture, biology, and movement–an appreciation of interactions that paved the way for her eventual study of the role of movement in autism.
Dr. Wilson hypothesizes that impaired motor development in infancy can detrimentally impact a child’s exploration, social engagements, spatial perception, and visual coordination. She further hypothesizes that the negative cascading effect of these impairments has direct mechanistic links to the communication deficits, and repetitive and atypical motor behaviors observed in autism. To test these hypotheses, she examines a cohort of infants who are at high risk for autism (infants with an older sibling with autism).
The unique tool that Dr. Wilson uses to objectively study and quantify movements of children is the wearable movement sensor (Figure 1). These lightweight devices detect not only linear movement but also detailed aspects of infant movements, such as movement type, duration, and angular rotation. Worn on both wrists and ankles concurrently, the sensors are synchronized, thus allowing detection of movements that occur in coordination with each other. The sensors can also be deployed remotely to the home to capture movements in the child’s natural environment. Utilizing advanced signal processing and machine learning techniques, she and her team have created new measures that detect detailed characteristics of movement.
Using these methods, Dr. Wilson and her
coworkers have shown that high-risk infants with a later diagnosis of autism show lower variability in their movements compared to typically developing children. Furthermore, they found that the deficits in movement variability were more strongly correlated with autistic behaviors than with cognitive ability or adaptive skills (Reference 1). In addition, when quantitatively analyzing gait, Dr. Wilson’s team found that toddlers with autism acquire the ability to walk at a normal age but exhibit a pattern of slower pace, compared to typically developing children (Figure 2). They further found that the slower measures of pace were associated with lower scores of communication, motor skills, and adaptive function (Reference. 2).
Dr. Wilson believes that motor abnormalities may not just be a component of autism but may ultimately play a role in its diagnosis and treatment. Early motor differences could represent an endophenotype of autism. As such, detection of characteristic motor abnormalities may facilitate an earlier diagnosis of autism. Furthermore, if motor differences contribute to the language, social, and behavioral aspects of autism, then therapies for autism may need to be reconsidered and focus on remedies for the movement problems. Thus, Dr. Wilson’s ideas surrounding movement represent an important paradigm shift in the way that autism is considered and may have far-reaching consequences for the diagnosis and treatment of this important neurodevelopmental disorder. • Link to CNS Research








Focus Library Child Neurology Society | Winter 2024 11
Figure 1. Infant wearing sensors (placed in sleeves) on arms and legs to capture continuous quantitative whole-body movements.
Figure 2. Wilson RB, et al. Slower pace in early walking onset is related to communication, motor skills, and adaptive function in autistic toddlers. Autism Research 2024; 17: 27-36.
CNS CONNECTIONS EDITOR
Daniel J. Bonthius, MD, PhD Medical Director, Pediatric Neurology Levine Children’s Hospital

Child Neurology Synapses
HIE without the E: Babies with hypoxic-ischemic brain damage who look fine as newborns.
Risk factors and outcomes for cerebral palsy with hypoxic-ischemic brain injury patterns without documented neonatal encephalopathy. O. Fortin et al. Neurology 2024; 102:e208111.
What the researchers did:
As all child neurologists know, perinatal hypoxic-ischemic brain injury is a leading cause of cerebral palsy. In many cases, the infant who suffered a hypoxic-ischemic insult during labor and delivery has neonatal encephalopathy and will have characteristic abnormalities on an MRI scan of the brain. However, as all child neurologists also know, some babies are later diagnosed with cerebral palsy and have abnormal MRI scans suggestive of
a perinatal hypoxic-ischemic insult, and yet they had no evidence of neonatal encephalopathy. In fact, many of these children appeared perfectly healthy as newborns. The questions then arise: Where did this cerebral palsy come from? What proportion of children with cerebral palsy and MRI scans suggestive of a previous hypoxic-ischemic insult did not have neonatal encephalopathy? To answer these questions, a group of Canadian researchers conducted a crosssectional study in which they utilized a large national database of children at least five years old with cerebral palsy. They identified the children born at 36 weeks gestation or later whose MRI findings were typical of hypoxic-ischemic injury. They
CRAFT
12 Child Neurology Society | Winter 2024
compared the group that had neonatal encephalopathy with the group that did not. Comparisons included preconception variables, pregnancy variables, delivery variables, and postnatal variables.
What the researchers found:
Of the 169 children with cerebral palsy whose MRI findings were typical of perinatal hypoxic-ischemic injury, 140 (83%) had a history of neonatal encephalopathy, while 29 (17%) did not. Thus, about 1 in 6 children who appear to have suffered perinatal hypoxic-ischemic brain injury were not encephalopathic as neonates. The groups with and without neonatal encephalopathy differed from each other in several important and telling ways. In those born without neonatal encephalopathy, the pregnancies were more likely to have been complicated by abnormalities of amniotic fluid volume and fetal growth restriction and less likely to have been complicated by intrapartum fetal distress. Those born without neonatal encephalopathy were more likely to have higher 5-minute Apgar scores, higher cord PHs, asymmetric brain injury and hemiplegic cerebral palsy. The two groups (with and without neonatal encephalopathy) were also alike in several important ways. The severity of the cerebral palsy was equivalent in the two groups, and the patterns of brain injury observed on MRI scans were the same.
What the research means:
This research shows that a sizable proportion (1 in 6) of children whose physical exams and MRI findings suggest that they suffered a perinatal hypoxic-ischemic injury did not have
encephalopathy as neonates. Furthermore, this research sheds important light on how this phenomenon occurred. The affected children who did not have neonatal encephalopathy were more likely to have had low amniotic fluid volume, fetal growth restriction, higher cord pH, and higher Apgar scores. All these findings suggest that many of these infants without neonatal encephalopathy suffered a hypoxic-ischemic insult in utero days or weeks before birth. This injury was likely due to umbilical cord accidents, placental dysfunction, or malperfusion. By the time the babies were born, the maternal-fetal physiologic problem had corrected itself, and the encephalopathy had resolved. But the brain damage was done and would not become clinically evident for weeks, months, or years. The clinical outcomes and MRI scans of these babies without neonatal encephalopathy can be just as bad as those with neonatal encephalopathy. Thus, the absence of neonatal encephalopathy does not exclude a perinatal hypoxic-ischemic injury. It merely suggests that the insult occurred days or weeks before labor and delivery. Because these babies are not encephalopathic at birth and often appear entirely well, the diagnosis of hypoxic-ischemic brain injury is delayed by months or years. This delay may have negative implications for the child, as the opportunity for proactive rehabilitation interventions may be missed. •
to CNS Synapses Library Child Neurology Society | Winter 2024 13
Link
CNS CONNECTIONS EDITOR
Daniel J. Bonthius, MD, PhD Medical Director, Pediatric Neurology Levine Children’s Hospital

Child Neurology Synapses
What’s the wait? Delays in epilepsy surgery.
Delays in the diagnosis and surgical treatment of drug-resistant epilepsy: A cohort study. J.M. Campbell et al. Epilepsia 2024;00:1-8.
What the researchers did:
Despite the many anticonvulsants available and their diverse mechanisms of action, about 30 percent of all people with epilepsy do not experience adequate seizure control. When this group of patients has been compliant with multiple anticonvulsant trials, but continue to have seizures, they are said to have “drug resistant epilepsy” (DRE). These refractory seizure disorders are highly problematic, as they substantially diminish quality of life, drive up the healthcare costs of
epilepsy, and increase the risk of sudden unexplained death in epilepsy (SUDEP). Surgical interventions can be highly effective for many patients with DRE. Yet, despite the well-documented effectiveness of surgical interventions for DRE, delays to surgical evaluation remain an important problem. These delays further worsen quality of life, lead to higher rates of psychological and psychiatric problems, and, in adults, can diminish socioeconomic status because of ongoing disability and unemployment. In this research project, a group of investigators in the mountain west of the United States evaluated the barriers to referral to their level 4 epilepsy center. The investigators retrospectively reviewed all patients who underwent
CRAFT
14 Child Neurology Society | Winter 2024
epilepsy surgery at their center over a recent ten-year period. They measured the time from diagnosis of epilepsy to diagnosis of DRE and the time from diagnosis of DRE to epilepsy surgery. In an attempt to identify factors that underlie delays in referral to surgery, the investigators examined demographics (age, sex, and ethnicity), the type of surgery performed (neuromodulation, resection, ablation, or disconnection), health insurance status, and distance traveled to the epilepsy center.
What the researchers found:
The median interval from diagnosis of epilepsy to diagnosis of DRE was 10.1 years, from diagnosis of epilepsy to surgery was 16.7 years, and from diagnosis of DRE to surgery was 1.4 years. Insurance status played a significant role in the interval time from diagnosis of DRE to surgery. For those with private insurance, the time was 1.0 year, while those with public insurance (Medicare and Medicaid) waited almost three times longer. The type of surgery performed also influenced the time from DRE diagnosis to surgery, with those undergoing neuromodulation (e.g., vagus nerve stimulator or deep brain stimulation) surgery having a significantly longer interval time than those undergoing resection or ablation. Age of the patient also played a role, as older patients had longer intervals of diagnosis of epilepsy to diagnosis of DRE and diagnosis of epilepsy to surgery. One of the most surprising findings of the study was in regard to the relationship between distance traveled to the epilepsy center and time interval between diagnosis of epilepsy and surgery. The investigators
had originally hypothesized that a greater travel distance would lead to a greater time lag to surgery. Yet, they found the opposite. Patients who traveled more than three hours to the epilepsy center had substantially shorter lag times than those who traveled less than three hours.
What the research means:
Despite a growing body of evidence that early surgical referral is highly beneficial for patients with DRE, the lag time for these referrals remains high. The present research sheds some light on the factors underlying these delays. Lack of private insurance was identified as one important factor. Furthermore, this research study, which included mostly adult patients, found that older patients experienced greater lag times than younger patients did. Distance to the epilepsy surgery center also played a role. While the investigators expected that a greater distance would lead to greater lag times, they were surprised to find that greater distance actually reduced lag time. Why this would be so is unclear, but the authors hypothesize that it might relate to human geography. This study was conducted in the Mountain West, which means that the patients who had to travel far distances mostly came from rural areas, where physicians are likely to refer complex patients earlier. Whether the factors that delay epilepsy surgery, revealed in this study of mostly adults, also apply to children is unknown. Regardless, the important point remains that epilepsy surgery can substantially benefit patients with DRE, and child neurologists should be diligent to avoid unnecessary delays in surgical evaluation. •
Child Neurology Society | Winter 2024 15 Link to CNS Synapses Library
CNS CONNECTIONS EDITOR
Daniel J. Bonthius, MD, PhD Medical Director, Pediatric Neurology Levine Children’s Hospital

Child Neurology Synapses
Restoring strength and function: Nerve transfer surgery following acute flaccid myelitis.
Nerve transfer surgery in acute flaccid myelitis: Prognostic factors, long-term outcomes, comparison with natural history.
G.S. Rivera et al., Pediatric Neurology 150: 74-81, 2024.
What the researchers did:
Acute flaccid myelitis (AFM) is a poliolike disease that causes paralysis in children. Some patients with AFM completely recover from their weakness, but the great majority have long-term – often permanent and disabling – weakness. At present, modern medicine lacks the technology to induce the regrowth of damaged or lost motor neurons and peripheral nerves. Thus, the best intervention for AFM may be nerve
transfer surgery. Nerve transfer surgeries have been used effectively for decades for the treatment of traumatic brachial plexus injuries. However, the effectiveness of this surgery for AFM is unproven. Furthermore, even if nerve transfer surgeries can effectively reverse the weakness of AFM, many fundamentally important questions remain regarding its use and the selection of nerves and muscles. Since AFM often causes widespread injury to nerves, including potential donor nerves, the question arises to what extent can damaged donor nerves be utilized? Can EMG studies guide the selection of nerves and muscles for the transfer operation? What is the optimal timing of nerve transfer surgery in the AFM
CRAFT
16 Child Neurology Society | Winter 2024
population? To address these questions, a group of researchers in Baltimore, Maryland conducted a single center retrospective case series study in which they investigated the outcomes of 23 nerve transfer surgeries performed on 10 young children with AFM. The researchers conducted EMG/ NCV studies on the children presurgically to assess the condition of the donor nerves and recipient muscles, and they followed the patients for at least six months postoperatively to determine their outcomes. Because some of the denervated muscles in the patients did not have an available nerve to serve as a donor, these muscles were not operated upon and could serve as the internal control comparison group.
What the researchers found:
The muscles that received the nerve transfers had a substantially better outcome than the muscles that did not. The strength of the muscles that received the nerve transfers improved, while the control muscles did not. Furthermore, the recipient muscles were not only improved in raw strength, but also in function. Thus, nerve transfer following AFM can improve the strength and function of recipient muscles. Moreover, none of the donor muscles (the muscles from which the nerves for transfer were obtained) demonstrated any significant degradation in strength, thus showing that the improved strength of the recipient muscles is not at the expense of the donor muscles. When preoperative electrophysiologic studies were done to determine the health
of the donor nerves, the investigators found no difference in outcome between those nerves with evidence of denervation and those without, thus demonstrating that partially denervated nerves can be viable donors. The condition of the recipient muscles, however, was a different matter. Those muscles with the most abundant spontaneous activity on EMG, signifying chronic denervation, had the worst outcomes. The window of time in which the nerve transfer operation could be conducted successfully appeared to be quite broad. There was no correlation between time to surgery and outcome. Thus, for at least the time window utilized in this study of 6-15 months, nerve transfer for AFM remains a viable option.
What the research means:
This research examining children with AFM compared the outcome of nerve transfer surgery with the natural history of the disease. The results demonstrated that weak muscles receiving the nerve transfer surgery achieve substantially better strength than comparably weak muscles that did not receive the intervention. Thus, there is now strong evidence that nerve transfer operations truly work for AFM. Furthermore, the donor nerves can be partially injured by the AFM and still be useful to the recent muscles, and the window of time in which the operation can be conducted following AFM is broad. All of this constitutes new and exciting good news for treatment of a disease that can leave young children permanently weak and disabled. •
Child Neurology Society | Winter 2024 17 Link to CNS Synapses Library



2024 ACCN AWARDS
Please consider nominating a nurse for the Claire Chee Award or a nurse practitioner for the NP Excellence Award. We are also seeking nominations for the Innovative Clinical Practice Award.
PLANNING ON TRAVELING TO THE CNS/ACNN MEETING?
There is a travel award to help with the cost of the conference for ACNN members.



NOMINATION DEADLINE: APRIL 30 START A NOMINATION https://cvent.me/O53r3B NOMINATIONS
NOW OPEN
ARE

We look forward to seeing you...

Mark Your Calendar for Future Meetings
2025
CHILD NEUROLOGY SOCIETY
54th ANNUAL MEETING
October 8-11, 2025 • Charlotte, NC

2026
CHILD NEUROLOGY SOCIETY
55th ANNUAL MEETING
October 14-17, 2026 • Montreal, QC

