

TheInternationalCollegeofAppliedKinesiology® USA(ICAK-USA)hasplayedacrucialrolein establishingthefoundationforclinicaland academicarenaforinvestigating,substantiating, andpropagatingAKfindingsandconcepts pertinenttotherelationshipsbetweenstructural, chemical,andmentalfactorsinhealthanddisease.
Dr.MichaelAllen
Dr.GeorgeGoodheart
Dr.DianaMladenoff
Dr.DaleSchusterman

Welcome to the third issue of our HTML publication, AK Clinical Applications Update! This is unlike our current e-newsletters With AK Clinical Applications Update, we have asked the membership to get involved by sharing their knowledge, research and demonstrations.
We are seeking doctor members and accepting submissions of their current findings (ie Research), technique articles or a video demonstrating a technique that has helped diagnose and treat your patients
Our objective is to have 4 submissions per issue that would be distributed to the full membership and archived on the website as a resource. We are now accepting submissions! Please send your article, research summary or video, to icak@dci-kansascity com for review
Please reach out to Angela Capra, 913-387-5608 or acapra@dci-kansascity.com, if you have questions or need additional information
Warm regards,
 Richard Belli, DC, DIBAK ICAK-USA Chairman
Richard Belli, DC, DIBAK ICAK-USA Chairman

A patient who has had some balance issues asked me when she can return to her usual exercise. Since starting the modified exercise program that is consistent with her postural display she has felt better, but she only wants to go back to her usual bilateral and symmetrical exercise if she is ready. “How do I know when I am ready?” she asked. I told her that we will know her status by how her nervous system responds to our provocative neurological and manual muscle testing.
One of my real concerns is watching a team of athletes all doing the same exercises to warm up. My son and I enjoy going to and watching Spring Training baseball games. We often arrive at the stadium early to watch the players go through their warmups. It strikes me that although there are six possible postures that a person can take on –seven if you count the normal posture – they can take on any one or a combination of these postures; they are all whole-body displays. However, of these six postures, four of them have to do with the cerebellum and two with the thalamus. Here is the point: If six players each with different postures do the same warmups, each of them will probably be exercising themselves right into that specific posture – their pathology –unless they know how to do things differently
The periods of warming up and cooling down are as important as the exercise itself. During warm up, blood is shunted to the muscles upon demand so it may take 10-15 minutes before a person is “warm.” It takes time for the autonomic nervous system to move blood from the internal organs to the periphery That’s what warming up is all about Once an athlete is warm it’s proper for the team to come back together again and do the same exercise because their muscles have their requisite blood supply, and their joints are ready for action
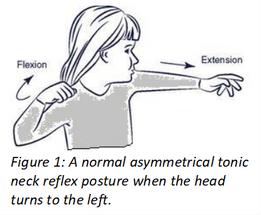
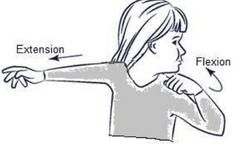
The movements caused by the asymmetrical tonic neck reflex (ATNR) are an excellent example of where blood should flow relative to warming up. It is totally within the human neurological design that turning the head to the left (Figure 1) causes an increased tone in the muscles of extension on the side toward head rotation and an increased tone in the muscles of flexion on the side opposite head rotation. This is the normal and expected posture when an “unwarm” person turns their head to the left.
We say that these normal movement patterns are reciprocal because when one muscle contracts another muscle that does the opposite function relaxes so that the first muscle can do its job of contracting. To extend your left arm, your left biceps muscle must relax so that your left triceps muscle can contract and extend your left arm. Likewise, when your right arm flexes it can only do so when the opposite activity happens: your right triceps muscle relaxes allowing your right biceps muscle to contract and your right elbow flexes.
When a person’s neck muscles turn their head to the left, for example, all the nerves from the neck muscles and their associated spinal joint motion inform the brain that the head turned left. Conversely, the neck muscle function of turning the head to the right causes other nerves to fire informing the brain that the head turned right. These incoming signals to the brain are totally unconscious. We call this “coupling.” Coupled motion informs the brain about purposeful spinal movement.
When the neck muscles turn the head to the left, properly yet reciprocally increasing the tone in the muscles of both upper extremities, as indicated in Figure 1, blood flows to the muscles according to their demand. The left extensors are nourished by the blood they need to perform useful work and the right flexors are similarly nourished. This is what warm up is all about, moving blood – with its oxygen and other nutrients – to the muscles so they can perform useful work.
However, we often find people with dysfunctional movement patterns Figure 2 shows a very common, yet pathological posture seen in clinical practice It is not unusual for a person to display an increased tone of flexor muscles on the side toward head rotation and an increased tone in the extensor muscles on the side opposite head rotation This is what I call “dysrecipria” – an “other-than-human” movement pattern Your brain instinctively knows there is something wrong, but it will not let you know it because this dysfunction is very often painless
While a dysfunctional ATNR movement will not immediately hinder a person’s activities it is nonetheless pathological; dyscoupling sends atypical signals to the brain. Since the proper neurological patterns are deeply rooted into the human neurological fabric, the dyscoupled sensory input wrongly informs the brain that the head went in the direction consistent with the muscle input when in fact the head went in the opposite direction. Over a long period, this dysrecipria causes repeated microtrauma to the muscles and joints, eventually leading to muscle fatigue, joint instability, and eventual perception of pain. Further, these abnormal signals build their own integrity while the coupled patterns – which are not being stimulated – are sacrificed, the functional design decays at the expense of disuse. This result is not healthy.
These abnormal postures must be rehabilitated to sacrifice the dyscoupling and rebuild normalcy Staying with the example of the ATNRs, the patient should start with their arms to their sides and their head straight ahead All at once – and s-l-o-w-l-y – the patient should turn their head to the left, for example, while simultaneously lifting their arms to shoulder height and extending their left upper extremity and flexing their right upper extremity. Coming back to the starting posture must be one-by-one. In other words, have the patient lower their left arm, return their head to center, and then lower their right arm. This return to neutral is just a suggestion, it can be done any way the patient likes – and since this exercise can be boring it should be done randomly – but it must be done one-by-one to discourage the pathological posture, which we are trying to erase
When a person’s joints are warm – and if their joint motion is both reciprocal and coupled – they should be able to move in any way they like and maintain their joint stability. In other words, when their joint motion has functional integrity, the pathways have their optimal stimulation, and they should move according to the original human design.
A patient should always continue their rehabilitation therapies until their movement patterns are consistent with that which would be expected for the provocation
There is much more to the rehabilitation of the ATNR than just the upper extremities, but this procedure will help develop a start for the practitioner. Insofar as my patient was concerned, I was able to release her to her normal and symmetrical exercise routine with the instructions that she warm up as directed for the time appropriate for her situation.
So often athletes over-train their muscles and end up with pathological movement patterns without even knowing it The trick is helping them understand the pitfalls of their condition and getting them to participate in their rehabilitation
The difference between gold and silver metals may depend on the functional performance of the ATNR in specific and the musculoskeletal system.
An Addendum: One of my favorite patient stories involves a six-year swimming rivalry. A few years back while teaching in England, I was asked to work on this specific swimmer to help him break his streak of stress. The frustration was tangible prior to the race. In the final race of his swimming career my patient of one visit was able to get off the starting blocks first and never look back. He easily swam away with his prized gold metal. The crowd went wild!
A follow up to the story: While the average swimmer does it in over 13.5 hours, this young athlete subsequently swam the English Channel in just over eleven hours!
by
Richard BelliDr. Goodheart had a unique way of looking at a patient´s problem and asking, “Why is that?” This allowed him to correlate many different types of examination and treatment procedures into a unified method of examining and then treating many difficult patients.
Dr Goodheart wrote many works on Applied Kinesiology, and lectured on the topic often I would like to share a paper that I thought would be fitting for this issue
Please use the link below to access one of his many papers, Innate Intelligence is the Healer.
Click here to view.



The Webster Technique was developed by Larry Webster DC over 30 years ago. The technique is defined as a specific chiropractic analysis and adjustment. The goal of the adjustment is to reduce the effects of sacral subluxation and SI joint dysfunction In so doing neuro-biomechanical function in the pelvis is improved This reduces the nervous system stress, balances pelvic bone, muscles and ligaments and optimizes the mother’s pelvic function in pregnancy and birth
The International Chiropractic Pediatric Association (ICPA) does not endorse the use of the Webster Technique as treatment for fetal malposition or in-utero constraint The technique has documented improved pregnancy and birth outcomes The technique includes a sacral analysis and correction as well as soft tissue release that can be utilized on any weight bearing individual. It is suggested that this technique is evaluated and utilized throughout pregnancy. It has also been clinically observed to help with the pain associated with menstrual cramps.
This technique is not being used to spin or turn breech babies but if you are working on pregnant women it is important to know the baby’s position.The mother will know the baby’s position from her OB or midwife evaluations. Babies are expected to move into the head down position between 28-32 weeks. If the baby’s head has been head down previously they may move back to the breech position. It is important to ask the mother about the baby’s position at each appointment.
The Webster Technique includes an osseous, muscular and ligamentous correction in the prone and supine position. The initial evaluation is:
1.
Patient is prone and check leg resistance as heels are pressed to the buttocks. The side of the greater leg resistance will be the designated the Webster side (this is the opposite of an AI sacrum).
2
The technique then calls for an adjustment to the sacrum on the Webster side with a contact at the sacral notch and a P to A thrust
3
A piriformis sweep from medial to lateral across the muscle on the ipsilateral side or bilaterally is performed.
The last prone procedure is contacting the opposite side sacrotuberous ligament and applying pressure A to P and up towards the opposite shoulder. The patient is then moved to a supine position and the pubic bone is adjusted on the opposite side of the Webster sacrum.
4. The psoas is tested for hypertonicity by stretching the arms overhead and checking the arm length The hypertonic psoas is typically the ipsilateral side as the Webster sacrum and should be released
6
5. The last treatment is on the round ligament on the contralateral side of the Webster sacrum To locate the round ligament draw an imaginary line from umbilicus 45 degrees inferior and lateral. Draw another imaginary line 45 degrees from ASIS inferior and medial to the lower quadrant. The intersection of these 2 lines is the initial place of contact. Palpate for tension and tightness. Hold I to S contact with your thumb for 1 to 3 minutes towards the opposite shoulder.
Utilizing AK and our specific muscle testing procedures we can fine tune and expand the analysis and corrections to ensure mom and baby are as balanced as they can be.
1. Patient prone test bilateral piriformis, hamstrings, and gluteus maximus for facilitation and autogenic inhibition. Correct as needed using traditional factors of the IVF.
2. Therapy localize the sacrum for subluxation and correct/adjust accordingly. May also check for sacral inspiration and expiration assisted at this time.
3 Using an indicator muscle therapy localize each sacrotuberous ligament for precise side, contact point and line of correction
4 Patient supine test bilateral psoas, iliacus, glut medius, gracilis, adductors, TFL, sartorius, diaphragm and levator ani for facilitation and autogenic inhibition. Correct as needed using traditional factors of the IVF.
5. Therapy localize the pubic bone for subluxation and correct/adjust accordingly.
6. Using an indicator muscle therapy localize the round ligament on each side for precise side, contact point and line of correction.

These steps can be checked at each visit independent of the baby position


The retina of the eye can be divided into two general areas – the area centralis and the peripheral area The area centralis is near the center of the retina in an area approximately 5 mm in diameter. It consists of the fovea, a pinhead size area of very dense packed color sensitive cone cells, surrounded by the macula, which also contains primarily cone cells. The fovea, which makes up only one thousandth of the retina, is responsible for focused vision and much research has studied the tracking movements of the eye in relation to the fovea. The macula also provides good visual input although it is not as sharp as foveal vision. The rest of the retina is the peripheral area, consisting mostly of rod cells, which are less densely packed and are more responsive to light gradients and movement. Due to the predominance of rod cells, this area is the most active in night vision. If you place both fists out in front of you with arms extended, this should cover your foveal/ macular vision and all the rest of the visual field is peripheral.
Most people rely on focused vision. Computers, television, and other screens all stimulate focused foveal vision. Few people are aware of the space around the television screen when they are watching an engaging show. Society teaches us to see and focus directly on our target of thought It is a form of tunnel vision When most people carry on a conversation, or deal with a task, they focus on the details and disregard what is going on around them
One downside to focused vision is that the subconscious mind can direct what it wants us to see as it can relegate unwanted information to the ignored periphery This is why those with great intellects sometimes lack “street smarts ” Focused vision stimulates the sympathetic nervous system and the pituitary glandular axes This can sometimes cause tension to build up in the body, as people tire with prolonged visual concentration.
Peripheral vision relies on the awareness at the edge of our focus. Peripheral vision is, therefore, less conscious, relying upon the night vision mechanism that makes us aware of subtle movements and shading. Artists naturally use their peripheral vision. They often see the world in a different way. Top performing athletes have excellent peripheral vision. Great basketball and football players see the entire court/field when playing. Children have easy access to their peripheral vision until they get hooked on screens. Anyone who has studied martial arts knows that the key to most of the maneuvers is to maintain “soft eyes.” By relaxing the eyes, which expands the visual field, it is possible to “see” the entire space with heightened alertness and readiness. If you want to see a distant star, you need to look at the area next to it instead of directly at it. Similarly, people who see auras state that you must focus beyond and to the side of a person to see an aura.
Indigenous people take nature walks using their peripheral vision They focus on a point on the distant horizon and then begin to walk Using their peripheral vision, they can avoid rocks, holes, plants, and other obstacles This allows them to blend in with their environment, to notice the subtle movements of other animals, to hear, and to feel, the voice of the earth.
Dr. Goodheart often admonished us to ‘see with eyes that see.’ He would get quite animated and repeat this phrase over and over. He had excellent powers of observation, and this included his use of peripheral vision. He would often look to the side of you as he talked and would come up with insights that were amazingly perceptive. You can’t see with ‘eyes that see’ unless you use the full visual field.
The doctor can expand his/her visual field when working with a patient. This will bring deeper resources to the doctor and allow intuitive information to flow. When you are stuck and need to get more information on how to treat someone, it can be useful to focus on the problem, then let the mind go blank while expanding the PV. This takes but a few seconds and can yield good results. A few minutes later you might have an insight on how to test things differently.
Peripheral vision activates the pineal gland as well as the parasympathetic nervous system, which tends to calm the body and mind This allows for more creativity and inspiration Most of us stay anchored in focused vision during the day, and unless we meditate, take nature walks using peripheral vision, or engage in the creative arts, this part of our awareness is relegated to sleep
Here is one possible use of peripheral vision. Locate a positive therapy localization (TL), or inhibited muscle on your patient. While maintaining the TL, have the patient lightly focus on a point straight ahead, soften her gaze and become aware of the space around her. You can place your fingers in each peripheral field and ask if she can see them without moving her focus off the area straight ahead. After a few seconds of this visual expansion the positive TL will often disappear. Now, even when the patient comes back into focused sight, the TL will no longer inhibit a facilitated muscle. This activity did not correct the problem, but it did bring in more resources to the issue. The peripheral fields carry information that we do not necessarily perceive consciously. Now when you scan the body you will find that there is another area of the spine, a muscle, an organ, an emotional issue, or nutritional need that has become the priority. When you work with this new priority you will make a deeper correction than if you had just worked on what facilitated the original TL.
When working on emotional issues, have the patient focus on the problem until you get an indicator change and then have him let go of the focus, empty his mind, and allow the PV to expand The emotional TL will disappear, but the nervous system now has more complete data to process. When you make whatever corrections that you find, the conscious and non-conscious parts will both be addressed.
Similarly, when you finish working on a person with a chronic issue, you can use PV to find new layers to correct. If you have been working on the gallbladder doing various therapies and the popliteus is now normotonic, retest it while the patient in in PV. Often you will find the muscle will inhibit. Maintain the PV until the muscle facilitates and then proceed to fix whatever new patterns emerge.
What we don’t want to ‘see’ gets relegated to the periphery, so we need to access the peripheral visual fields to obtain this information.

