BELRA to Lepra – A century at the forefront of leprosy care
Introduction
This is the story of a non-governmental organisation that set itself the task of fighting a (then) incurable disease – that of leprosy. Three men, influential in their work in India, decided that instead of just looking after those who had been affected by this disease, they would find a cure, and so the ‘British Empire Leprosy Relief Association’ (BELRA) came into being in 1924, and for a century has been fighting this most misunderstood of diseases.
I joined LEPRA in September 1981, and remained with the charity until November 2018. During these years I became fascinated by its history, and the fact that it so nearly didn’t happen in the first place, but belief and trust in providence, and a righteous cause, ensured that it did. Because of this I wanted to make certain that its history was written down – warts and all. I was privileged, during my time with the charity, to meet and interview many of its layworkers and doctors, and this has also led me to write their history as well so that that, too, is not forgotten. Many gave their lives in the cause of leprosy, and I have felt it incumbent on me to speak for them. As I had worked for LEPRA for so long, and knew its history so well, I was the one who usually attended the funerals of ex-BELRA/LEPRA workers – a priest at one of these joked that I was probably ‘LEPRA’s memory’ as I had worked for the charity for so long, and he was possibly right.
About the Author
Born in 1952, in Edinburgh to an English Naval Petty Officer and a Scottish mother, we moved to England in 1956 when I was four. I went to Heybridge Primary School, and Maldon Grammar School, and then entered the Royal Navy as a Radio Operator in 1969. I have a BA (Hons) in History and a Diploma in European Humanities.
My first contact with LEPRA was when I applied for the job of computer operator which had been advertised in the local press, but when I arrived, I discovered that the job was actually for someone to set up and run a computer system, not just someone who could use the machine. However, the Director’s Secretary at that time, was just about to emigrate to New Zealand, and I was asked if I would consider that post instead – I agreed. I joined LEPRA in September 1981 and worked for the charity until November 2018 when I left to look after my partner who was terminally ill.
I started my career with LEPRA as Secretary to the Director, Francis Harris, and then became the Research and Projects Officer, Assistant Editor to our medical journal Leprosy Review, and then, because of my long association – longer even than that of Miss Wallich! ( all will become clear as you read on) – became its historian. I set up and ran displays for various meetings, set up the little museum with items that I had rescued from imminent destruction by various Chief Executives (usually locking them away in filing cabinets when I went on leave and taking the key with me –the items, not the Chief Executives!) and I set up the library.
My work with LEPRA has enabled me to travel extensively to leprosy-endemic countries for field visits or to attend congresses in India, Bangladesh, Nigeria, the Netherlands, Belgium, Mexico, China, Japan and Nepal.
Life was not always easy during my 37 years with the charity – what relationship lasting that long doesn’t have its up and downs? – but an experience during my first visit to India ensured that,
whatever happened, I would stay with them. This was when I visited Dr. Desikan and his wife at Wardha in India in 1989. He was undertaking reconstructive surgery on the hands of a young woman who had been thrown out by her husband because she had leprosy, and had taken their two small children away as well. She sat on the bed looking really unhappy, with her fingers bandaged. I felt so sorry for her – she could have been my daughter – so I went across and put my arms around her to give her a hug. She gasped, and I thought “My God, Allen, what have you done?” I asked Dr. Desikan to apologise to the girl if I had offended her in any way. His answer was “No, Irene, it’s just that people don’t normally hug people with leprosy.” From that day I was dedicated to the cause and the people we served.
On 7th January 1997, a debate on ‘The Monarchy’ was held at the National Exhibition Centre in Birmingham, and I was privileged to be asked to represent LEPRA, and speak of the incredible support that the Royal Family had given us since our inception, and are still giving us to this day
I have had the honour of being Secretary to the Medical Advisory Board, and to the Editorial Board of Leprosy Review (as well as being the journal’s Assistant Editor), and have been privileged to meet and work with so many incredible people.
I have a deep and abiding admiration for all that BELRA/LEPRA/Lepra has done, and for all that LEPRA India has achieved since its inception, and I will always support them in whatever capacity I can.
BELRA to Lepra – A century at the forefront of leprosy care
Use of the word ‘leper’ was banned at the International Leprosy Congress in Havana in 1948, and quite rightly so, as it merely perpetuates the stigma and fear of this completely curable disease. BELRA fought hard for this ban, and we are justly proud of this. However, it will be used in this publication in its historical context, and no disrespect to anyone with, or affected by leprosy is intended, or implied, and is only used where in documents, letters, and the parlance of the day it appears.
Prologue
Before 1915 the outlook for those with leprosy was little better than in Biblical times or in the Middle Ages. Despite the discovery of the leprosy bacillus, Mycobacterium leprae by GerhardHenrik Armauer Hansen, a Norwegian scientist, in 1873, little effort had been made to control leprosy, and it remained very much the feared disease that it had always been. The only measure commonly used was compulsory segregation or, as it usually turned out, life imprisonment with no hope of recovery. Such a drastic and cruel measure, unknown in the case of any other disease at the time except, perhaps, the plague, was based on ignorance resulting in the unreasoning, and largely unfounded, dread of leprosy. This arose from the great disfigurement and crippling deformities that developed at a time when no cure was available, and the only ‘treatment’ was to isolate those affected ‘without the camp’ 1 i.e. away from normal habitation. Even in the early years of the 20th century in what was then the British Empire, the doors of the prison-like ‘leper’ asylums might well have been surmounted by the dreaded words: Abandon hope all ye who enter here! 2
1 The Bible: Leviticus 14:3
2 Taken from Dante’s 14th century epic poem ‘Divine Comedy’ as the words over the entrance to Hell
One of the most important names in the fight against leprosy was that of Sir Leonard Rogers. Born on 18th January, 1868, in Compton Gifford, Devon, the son of a Captain in the Royal Navy, on leaving school he trained in medicine at St. Mary’s Hospital, in London, and took the Fellowship in February 1893 at the minimum age of 25. He joined the Indian Medical Service, as he said long afterwards, “…solely in the hope of finding better opportunities for research, when there were few openings in Great Britain.” In the years of military duty in India he gave all his spare time to pathologic research and applied, as the occasion arose, for special appointments to study epidemics. He was not merely interested in scientific discovery, but passionately dedicated to the promotion of preventive measures. About the turn of the century, he made a pioneer study of the febrile illness known as kala-azar 3 in Assam where it was causing depopulation and threatening the tea industry, and though forestalled by Leishman and Donovan, who identified the causative parasite in 1903, he followed up this work for many years and introduced the employment of antimony 4 for kala-azar in 1915.
In 1910 he was appointed Professor of Pathology at the Calcutta Medical School, and shortly afterwards began working towards the setting up of a specialist teaching unit for tropical diseases. Meanwhile, he simplified and improved treatment of snake-bite, and proved that the mortality of cholera could be checked by intravenous injections of hypertonic salt solution combined with the oral use of potassium permanganate. He also introduced emetine for the cure of amoebic dysentery, and for his pioneering research work he was knighted in 1914.
In an article in Leprosy Review in April 1934, Sir Leonard wrote of the events that led to the formation of the British Empire Leprosy Relief Association, using a curiously detached form of speaking of himself:
“…the innumerable remedies advised in the treatment of leprosy bore witness to their small value, and none of them had ever sufficed to clear up the symptoms and remove the infectivity of any appreciable number of cases.
The most generally used of these methods was the old Indian remedy, chaulmoogra oil, which Ralph Hopkins of Louisiana showed to have some power of retarding the progress of the disease, but it was too nauseating to be curative. In the first decade of the present century [20th] the writer, working in Calcutta, had found gynocardic acid, the lower melting point fatty acids of chaulmoogra oil, to be less nauseating and more effective orally than the whole oil, and a medical colleague of his was cleared of a widespread leprosy rash by it. After demonstrating the great value of injections of emetine, the active principle of the ancient remedy ipecacuanha, he wrote in 1912 to a firm of manufacturing chemists, who had previously done valuable research in showing that chaulmoogra and hydnocarpus oils consisted mainly of chaulmoogric, hydnocarpic acids, and so-called gynocardic acid, to ask if they could prepare soluble products of these fatty acids suitable for injection, but a reply in the negative was received.
3 Also known as Visceral leishmaniasis (VL), it is fatal if left untreated in over 95% of cases. It is characterised by irregular bouts of fever, weight loss, enlargement of the spleen and liver, and anaemia.
4 The chemical element of atomic number 51, a brittle silvery-white metalloid
In the meantime, Dr. Victor G. Heiser, the founder of the great Culion leprosy segregation settlement of the Philippines, had been using very painful intramuscular injections of chaulmoogra oil with beneficial results, apparently of a temporary nature, as Dr. Wade 5 later could find no evidence of any of the patients having been discharged recovered. In the middle of 1915, while on a visit to Calcutta, Dr. Heiser urged Sir Leonard to undertake further work on the subject, with the result that soluble gynocardate of soda was made. This was reported by Sir Leonard in February, 1916, to be of greater value by injection than by the fatty acid orally. Later in the same year, he showed that it could safely be given, with still better results, intravenously, and that it thus might produce reactions in the leprous lesions with actual breaking up of the causative acid-fast bacilli in the human tissues. A year later, he was able to record, with photos and coloured plates, a series of 26 cases with complete disappearance of all the leprous lesions in 50% of cases of not more than three years duration, and in 25 per cent. of those of three to five years duration before treatment. Thus, the important principle was established, that the injection of soluble preparations of the active principles of chaulmoogra and hydnocarpates constituted an effective treatment more especially of early cases of leprosy.
Subsequent improvements in the technical application of this principle may be briefly mentioned. During his four and a half years’ investigations in Calcutta, Rogers showed that Hydnocarpus Wightiana oil from Western India was better than the chaulmoogra oil of Burma. After his return to England in 1920, he obtained a less irritating form of sodium hydnocarpate in the form of Alepol…” 6
In the BELRA Report for 1928 it was noted:
Sodium hydnocarpate is now being largely distributed in the form of ‘Alepol’ of Burroughs Wellcome & Co., and a Fraction C. of Martindale & Co. The former has been very favourably reported on by Dr. Rose of British Guiana, Dr. R.G. Cochrane, and others, but a few samples have caused much pain so could not be used. Martindale’s C fraction of hydnocarpus oil is both painless and even cheaper than ‘Alepol,’ and it has been found most effective by Dr. Neff in Fiji, so large quantities have been sent out during the last few months for a full trial and it promises very well. Yet a third preparation on similar lines is also being tested, so this very cheap and effective drug enables the large number of lepers now coming forward to be treated within the limits of our resources, which would have been impossible if the ethyl esters, costing twenty times as much, had to be relied on… 7
5 Herbert Windsor Wade, was an American medical doctor notable for his work on leprosy. He served as Medical Director of the Culion leprosy colony from 1922 to 1959.
6 Leprosy Review Vol. V. No. 2, April, 1934 pp. 54-55
7 Annual Report for 1928, p. 15
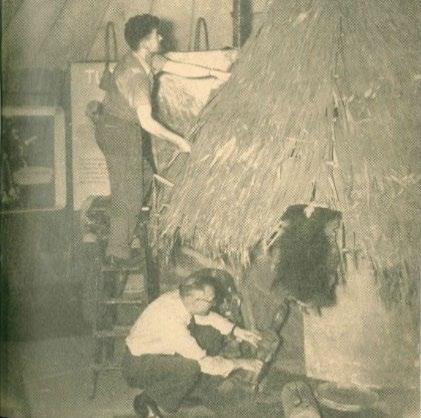
As mentioned, Dr. Victor Heiser, had urged Sir Leonard to use his incredible powers of research to find a cure for the disease based on the use of chaulmoogra oil – the then legendary folk cure for leprosy The problem was that the oil had such a nauseating effect that patients generally were unable to take sufficient doses for it to have any noticeable effect. Sir Leonard was very near to retirement from the Indian Medical Service at this point, and was busily engaged in raising funds for, and organising the work of, the Calcutta School of Tropical Medicine, which he had established in 1914 whilst he was Professor of Pathology at the Calcutta Medical College. This was to become a unique and very personal humanitarian
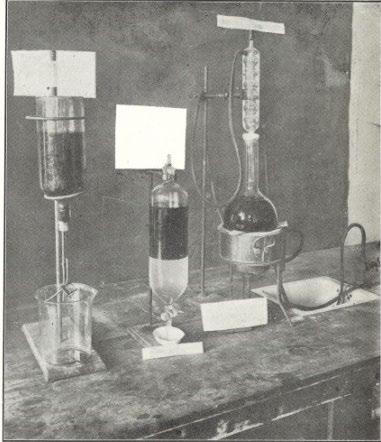
But, as the author of LEPRA’s 50th Anniversary booklet noted: “…Heiser knew Rogers to be a great investigator, and he struck him at his weakest point. His curiosity aroused, Rogers cancelled his intended departure for England in order to conduct his own experiments separating the ‘lower melting point fatty acids’ from the oil of the crushed plant, or, as his colleague Dr. Ernest Muir was later to describe the process more comprehensibly, ‘making a soap out of the oil, and injecting a solution of the soap into the veins.’” 8
(Right: purifying the oil)
Treatment with this new preparation met with some success and, encouraged by this, Sir Leonard pressed for the non-segregation of those with the disease. He was certain that outpatient treatment of sufferers would reduce the fear and stigmatisation of leprosy. He was president of the 1919 Session of the Indian Science Congress, and at an International Conference in Calcutta, which ran from the 3rd to the 6th February, 1920, on ‘The Leper
8 LEPRA: An Historical Sketch 1924-1974, p. 2
The Calcutta School of Medicine
Problem,’ organised by the Mission to Lepers, Sir Leonard and Dr. Muir participated in order to learn the extent of the spread of the disease.
In 1920, satisfied that the results of this treatment were convincing, and having seen to it that his School was well and truly founded, Sir Leonard made good his plans for official retirement and returned to England the following year. Dr. Ernest Muir took charge of the school’s leprosy department, the first to be opened – and was to continue and perfect the treatment, while Sir Leonard studied everything he could lay his hands on about every aspect of leprosy. He pleaded for a variation on the traditional segregatory methods, but the existing Mission to Lepers (what is now The Leprosy Mission), who looked after those afflicted, would not entertain such an idea.
In India at that time, the Rev. Frank Oldrieve, Secretary for India of the Mission to Lepers, a dynamic and enterprising man, had conceived a plan to spread leprosy control work throughout Bengal, based on the new treatment worked out by Sir Leonard, and he sought to leave the Mission. He appreciated that missionaries had done excellent humanitarian work amongst those with leprosy for many years, but he saw the need for a medical organisation to spearhead outpatient work and to foster research into all aspects of the disease.
(Frank with his wife and daughters)
Missionary work, which laid emphasis on care, had expanded, but the resistance of the bacillus to a number of treatments put on the market had restored the label ‘incurable’ to the disease, and nowhere were services organised to combat or control it. Frank Oldrieve’s task was to initiate such services, based on the conviction that a cure was possible.
He had enlisted support from government and business circles; as a friend of the Viceroy (at that time, Lord Chelmsford), he moved easily among influential people, and counted Sir Leonard, Dr. Muir and their friend Sir Frank Carter, a well-known philanthropist, Member of the Legislative Council of Bengal, and Sheriff of Calcutta, among his personal friends, and he already had a great deal of knowledge about leprosy It was written of him:
“…Oldrieve’s personality was legendary, but he also had a considerable acquaintance with anti-leprosy work, having served a term in the Belgian Congo prior to undertaking the organisation of the work of the Mission to Lepers in New Zealand. It was from there that his career had taken him to India. His fitness for tropical work had been in doubt since Blackwater Fever had forced him to give up his work in the Congo, but his energy repeatedly saw him through the hazards that ill-health put in his way. His journeys, both within and outside India, made him a noticeable, if perhaps slightly difficult
member of the Mission’s team, and their willingness to release him was probably not untinged with relief.” 9
9 LEPRA: An Historical Sketch 1924-1974, pp. 3-4
CHAPTER ONE
“…To rid the Empire of Leprosy” - The founding of The British Empire Leprosy Relief Association (BELRA)
As mentioned, at the beginning of the 20th century there was no cure for leprosy. Missionary organisations were in the forefront of looking after those who were affected by it, but no attempt had been made to investigate what caused it, or how it could be cured. But three pioneering men felt that this had to be tackled, and decided to act decisively to find one.
On 29th March, 1923, the problem of leprosy in the British Empire was discussed by Sir Frank Carter, Sir Leonard Rogers and the Rev. Frank Oldrieve, the last of whom, as noted earlier, was about to relinquish his appointment as Secretary in India of The Mission to Lepers. At a later meeting on 6th June, 1923, Sir Frank – a benefactor of many of Frank Oldrieve’s schemes in Calcutta – promised to provide the funds necessary to put his plans into action as, like Sir Leonard, he had retired to England and found himself ideally placed to support the proposals. Strengthened by this assurance of funding, Sir Leonard called a meeting on 12th July, 1923, when a number of influential supporters met at the India Office, with Lord Chelmsford in the chair, to inaugurate the work of a new Association, known as the British Empire Leprosy Relief Association (BELRA), who’s boldly stated aim was “…to rid the Empire of leprosy.” BELRA’s first logo was the Cross of St. George, with the implication of ‘fighting the dragon of leprosy.’
This new Association was formed with the following as officers:
Lord Chelmsford (formerly Viceroy of India)
Sir Edward Gait (ex-Governor of Bihar and Orissa), Chairman of the Executive Committee
Sir Frank Carter, Hon. Treasurer
Sir Leonard Rogers, Hon. Medical Secretary
Rev. Frank Oldrieve, Secretary
It is to the credit of those last three men named, that no single eminent person, invited to serve, on this or future committees, refused.
The reason that the founding date of BELRA is 1924 rather than 1923, is because a series of events, quite beyond the control of the trio of founders, postponed the public launching until 31st January of the later year.
The Executive Committee was constituted to complete the organisation, and to arrange for a public appeal to be made later at the Mansion House, London - permission for which had already been obtained. The Mansion House appeal had been fixed for December, 1923, but had to be postponed to 31st January, 1924, on account of the worsening health of the Prime Minister, Bonar Law, which precipitated an unexpected general election. BELRA was duly inaugurated on this day. The inaugural meeting at the Mansion House was presided over by the Lord Mayor of London and addressed by the Duke of Devonshire and by Lord Chelmsford who, as mentioned, subsequently became its first President. Sir Frank Carter most generously gave the necessary financial aid to set the Association on its feet.
It was later noted:
“The eminent, who had so whole-heartedly responded to Sir Leonard’s invitation covered a wide range of notable and interested people, including the popular, and, happily for the Association, vocal Prince of Wales (later to become Edward VIII) Consenting to become the Patron of the Association, the Prince established a status for its work that was to prove immeasurably important to Frank Oldrieve when he began his task as Secretary. Lord Chelmsford, now succeeded by Lord Reading as Viceroy in India, became the Chairman of the General Committee, a title later changed to that of President, while Sir Edward Gait, former Governor of Bihar and Orissa, headed the new Executive Committee.” 10
At this inaugural meeting, a message from H.R.H. The Prince of Wales was read out:
“…The elimination of leprosy from the British Empire is a wonderful ideal alike for British Medical Science and for British Administration. His Royal Highness is confident that this ideal can be realised if the Association is accorded the support it merits.”
The office for BELRA was set up in Sir Leonard’s consulting rooms at 24 Cavendish Square, London, and the three founders began to enlist supporters – not so much to promote a possible cure, as to take on a new sense of obligation towards those suffering from leprosy throughout the British Empire. Substantial connections were made, helped to a very large extent by the Prince of Wales becoming the first patron of the new Association. The Lord Mayor of London gave an inaugural dinner at the Mansion House where an appeal was made for ‘ a considerable capital sum to enable the work of the Association to make a good start.’ However, an unfortunate combination of adverse circumstances, including the fact that the City of London had just made a subscription of a quarter of a million pounds for the Japanese Earthquake Relief Fund to help survivors of the devastation of Tokyo and Yokahama which had occurred the previous September, and the taking of office by the first Socialist Government, headed by Ramsey MacDonald, 11 with the resultant fear of increased taxation, this appeal brought in very little money and was most disappointing. Clearly, funds had to be raised by other means Only £4,000 (instead of the hoped for £250,000) was raised from dinner subscriptions – a mere drop in the financial ocean deemed necessary to set the Association ‘afloat.’ The founders might
10 LEPRA: An Historical Sketch 1924-1974, p. 4
11 Interestingly his precarious government did not survive the year
have been forgiven had they judged that things were set against them; instead, they took emergency measures which fairly reflect their zeal and seriousness of purpose.
Sir Leonard, as mentioned, had cleared space in his consulting rooms to house the immediate trappings of the new Association’s administration, while Sir Frank made good his promise to underwrite the initial expenditure, but it was plain that some stable system of producing funds was needed. But the time could not have been worse for trying to engage the public’s imagination and persuading individuals and organisations to loosen their purse-strings. The uncertainty of the times brought caution first in financial matters, and although a start had been made, it was a rather shaky organisation that took on its first secretarial employee in the person of Helen Wallich when her agency sent her along to Sir Leonard’s consulting rooms. Knowing nothing about leprosy, and by no means committed to humanitarian work, Miss Wallich unknowingly embarked on a career that was to last for 34 years, during which she was to play a larger part than she imagined in the Association’s progress.
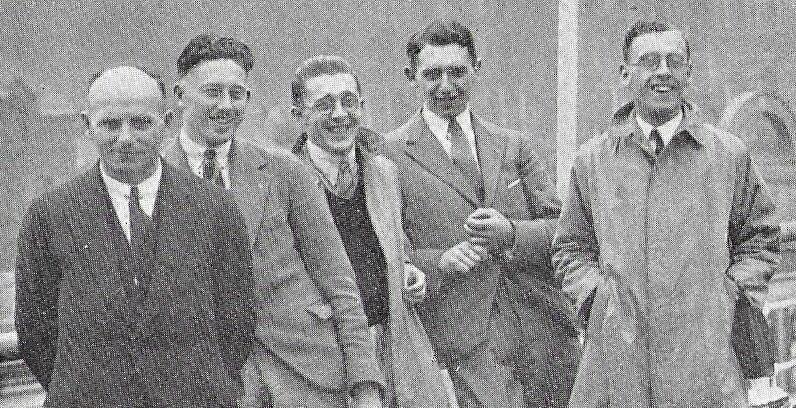
As it had not been possible to raise any substantial financial aid in the capital city, the founders turned to the provinces with happier results. From January to June 1924, Frank Oldrieve organised meetings at which both he and Sir Leonard spoke: Rotary Clubs, and in Municipal Offices, etc. in Bristol, Glasgow, Liverpool, Birmingham, Dublin, Manchester and Edinburgh. Sir Leonard had hoped to get the support of particular cities for leprosy work in some part of the Empire overseas with which they traded, such as Liverpool to finance work in West Africa, but owing to a slump in trade the appeal there failed too. Active branches were, however, formed in Edinburgh, Glasgow and Bristol.
Despite not raising the quarter of a million pounds felt necessary to begin the campaign, Frank Oldrieve was confident that the funds would be forthcoming, and so, undaunted, he set off for India to set up new branches of the Association there. Travelling with letters of recommendation, and largely at the expense of shipping lines and railway companies, his purpose was to establish a branch of the Association in India, and in 1925 the BELRA Indian Council was formed. Lord Reading, as the Viceroy, appealed to the people of India on 27th January:
“I make an appeal today to India on behalf of the Leprosy Relief Association. I am confident that the object of my appeal cannot fail to commend itself to the sympathy both of the rich and the poor and to all classes and creeds without distinction in India. None, I feel, can be insensible to the terrible sufferings of those afflicted by this disease, or blind to the danger of the spread of this dreadful malady already so widely diffused in India. I have convinced myself by personal observation that wonderful work is already being done in India on behalf of the lepers, and for the prevention and cure of the disease. The new methods of treatment hold out great hope of alleviation and even of cure; but the work is limited in scope because it is cramped for want of funds. Contributions are urgently needed for the extension and support of institutions for the treatment of lepers and for further research connected with the disease.
I ask all classes to join me now in an earnest campaign to combat this dreadful disease. In the name of humanity, I appeal to all thoughtful and sympathetic men and women in India to help this labour of mercy and to contribute funds for the consummation of this noble purpose.”
There was, of course, only one class that could respond. Maharajah vied with Maharajah to contribute to the Viceroy’s personal appeal. By the closing date of 27th January 1926, the Viceroy’s appeal had brought in a sum of over twenty lakhs of rupees (£150,000), the income that resulted from the investment of the appeal fund was disbursed to the Indian Council branches in the States, and it maintained the Association’s work in India independently of contributions from the UK until it was supplemented by a grant of £23,500 from King George V’s Silver Jubilee Indian Fund some ten years later. As BELRA’s professional fundraiser noted some years later:
“Detractors of charity who are wont to ask ‘why these people don’t help themselves’, might ponder on the fact that the Association’s work in India flourished for thirty years as a result of local generosity, while it took over forty years to raise a similar sum in a single year at home.” 12
The reason India was chosen as the first overseas branch of BELRA was obvious: the infrastructure of the British Raj was in place; chaulmoogra trees grew in abundance and there were more than enough ‘lepers’ to cure.
Frank Oldrieve had met the Prince of Wales in India in 1922, when he had been summoned to comment on the leprosy problem, and the prince sent for him again when he learned of his intended departure for West Africa in 1926. The success in India, and the formation of the Association’s Indian Council, had been personal triumphs for Frank, and he had found a formula to apply in other colonies. In the first report since its inception, BELRA noted:
Leprosy is the most terrible of all the diseases which afflict humanity. There are at the lowest computation 300,000 lepers in India and other British possessions, and the real number is probably far greater. Leprosy was formerly regarded as incurable, but recent researches have led to the discovery of methods of treatment which, if given at a sufficiently early stage, cause the disappearance of all the signs of the disease. It is now certain that leprosy can be eradicated from any country where adequate arrangements are made for the proper treatment of all persons contracting the disease.
FORMATION OF THE ASSOCIATION
This being the case, it was clearly incumbent on us in Great Britain to do all in our power to get rid of leprosy in all countries over which the British flag flies. The British Empire Leprosy Relief Association has been formed with this object, and it has received support from the highest quarters. H.R.H. the Prince of Wales has graciously accepted the office of Patron. The Vice-Presidents include the Secretaries of State for Foreign Affairs, India, and the Colonies, the Viceroy of India, and the Governors-General of Canada, South Africa, Australia, and New Zealand. Viscount Chelmsford, late Viceroy of India, is
12 LEPRA: An Historical Sketch 1924-1974, p. 8
Chairman of the General Committee, which includes amongst other influential persons some of the prominent members of the medical profession…
WORK OF THE MEDICAL COMMITTEE
Detailed information has been collected regarding the prevalence of leprosy in all parts of the Empire, and the Medical Committee of the Association has approved a memorandum drafted by Sir Leonard Rogers, the Medical Secretary, indicating the best way of dealing with the leprosy problem, having regard to varying local conditions in the countries affected. This memorandum has been widely circulated by the Colonial Office and also in India. In addition, pamphlets dealing with the latest methods of treatment have been distributed freely, together with summaries of the latest literature on the subject, which have been reprinted from the Tropical Diseases Bulletin. A very important treatise on ‘Leprosy’ has been published by Sir Leonard Rogers and Dr. Muir, and a more popular book, ‘India’s Lepers,’ by Mr. Oldrieve, the Secretary of the Association. 13
PROGRESS IN TREATMENT
Favourable reports continue to be received of the beneficial results of the new treatment. The largest number of recoveries have been obtained by the Americans. Thus, several hundred lepers have recently been discharged recovered from the great Culion settlement in the Philippines, and a number more are awaiting the completion of the rigid tests which are made before they are released. At Honolulu during the last four years over 50 per cent of the cases admitted to the asylum have been discharged recovered, and at the present rate there will be a reduction of over 40 per cent in the total number of lepers in Hawaii in a single decade. Although in our own vast Empire we cannot yet report as extensive good results, yet, with the spread of knowledge regarding the cases suitable for treatment, increasingly favourable reports are being received from many parts, including areas which formerly recorded want of success. Dr. E. Muir, of the Calcutta School of Tropical Medicine, has made a further important practical advance by showing that the pure oil from the ripe seeds of the Southern Indian Hydnocarpus Wightiana is as efficacious as the ethyl esters now used, which cost at least ten times as much. The tree in question should grow well in all tropical colonies; and as it fruits in five years, the remedy could then be obtained at very little cost. Arrangements are being made to distribute supplies of its seed wherever required.
Everything is ready for a successful campaign against leprosy in the British Empire as soon as the requisite funds are available, and it is earnestly hoped that we shall soon be able to wipe out the reproach of being so far behind the Americans in applying the new treatment in our colonies.
COMMITTEE
13 This is available in Lepra’s Head Office
The Committee greatly regret that they have lost Sir Clifford Albutt 14 and Sir Malcolm Morris 15 by death. On the other hand, the Executive Committee have gained a valuable colleague in Viscountess Willingdon, 16 who has always taken very great interest in the cause of the lepers and founded a highly successful leper colony at Chingleput in Madras. Lord Lloyd 17 accepted an invitation to join the Committee, but was prevented from taking an active part owing to his leaving for Egypt to take up his appointment as High Commissioner. The Executive Committee has held regular meetings. In addition to preparing the memorandum already mentioned, the Medical Committee had a meeting with some twenty men connected with the Colonial Medical Service, and discussed with them the best means of dealing with leprosy in various parts of the Empire.
FORMATION OF THE BRANCHES OVERSEAS
The Association is doing all in its power to encourage the formation of local branches in all parts of the Empire where leprosy is prevalent. The Earl of Reading, Viceroy of India, has already formed an Indian Branch of the Association. The Governors of Provinces and leading Indian Princes accepted his invitation to become Vice-Presidents, and influential committees were constituted in various parts of the country. Mr. Oldrieve was deputed to India to assist in the arrangements for the formation of this branch. Its appeal for funds was issued in January of this year, and already a sum of over £140,000 has been collected for the work in India.
Arrangements have been made for Mr. Oldrieve to visit the colonies in West Africa and the West Indies and British Guiana during the early part of 1926, and there is reason to hope that branches will then be established in most of these colonies. Many of them, however, are comparatively poor, while in some of them leprosy is far more widespread in proportion to the population, than it is in India. It will therefore be necessary, if the campaign is to succeed, for a larger measure of financial assistance to be given by the parent association than in the case of India, where a very great deal can be done with the funds raised locally. The same remark applies to the colonies and mandated territories of East Africa 18, where it is hoped that branches will also be formed later on.
PUBLICITY
To make known the needs of the situation as regards the prevalence of leprosy in the Empire, and the work of the Association, numerous addresses and lectures have been given by the Chairman of the Executive Committee, Dr. T. Cochrane, the Hon. Medical Secretary, and the Secretary. Addresses have been broadcast at Edinburgh, Glasgow,
14 Sir Thomas Clifford Allbutt (1836-1925) was an English physician best known for his role as president of the British Medical Association 1920, for inventing the clinical thermometer, and co-founder of the History of Medicine Society
15 Sir Malcolm Morris (1849-1924) was an English surgeon specialising in skin diseases.
16 Marie Adelaide Freeman-Thomas (1875-1960)
17 George Ambrose Lloyd, 1st Baron Lloyd, GCSI, GCIE, DSO, PC (1879 - 1941) was a British Conservative politician and colonial administrator
18 An authorization granted by the League of Nations to a member nation to govern a former German or Turkish colony. The territory was called a mandated territory, or mandate.
and Cardiff. Addresses have been given to Rotary Clubs at London (2), Belfast (2), Bexhill, Birmingham, Bournemouth, Bradford, Bristol, Cambridge, Colchester, Croydon, Dublin (2), Edinburgh (2), Glasgow, Harrogate, Leicester, Liverpool, Manchester, Torquay, Wolverhampton, Worthing and York. The Luncheon Clubs at Glasgow and Leeds have been addressed, public lectures have been delivered, and the film ‘Leprosy’ has been shown, while some sermons and addresses have been given in churches. Articles have been contributed to quarterly and monthly magazines, and a very large number of articles, notes, and interviews have appeared in the daily press. Lady Willingdon organized a dinner at the Savoy Hotel, at which Prince and Princess Arthur of Connaught were to be present, and Earl Balfour, Viscountess Chelmsford, the Earl of Clarendon, and Sir Johnstone Forbes-Robertson were to speak. This function, unfortunately, had to be abandoned owing to the death of Queen Alexandra. Most of the guests, however, kindly gave their dinner subscriptions to the fund, which thus benefited to the extent of £186 10s. A small exhibit was shown at the British Empire Exhibition at Wembley.
As it was found that these steps were not by themselves sufficient to bring in the requisite funds, supplementary methods were considered. Extensive advertising was thought inadvisable owing to its costliness, and it was agreed that the most hopeful means of bringing the facts home to people in all parts of the country was by the establishment of provincial branches of the Association. In furtherance of this policy branches have already been formed in Edinburgh, Glasgow, and Bristol, and a number of the most prominent people in these cities have kindly joined the local committees, which are already doing excellent work. The Central Committee takes this opportunity to express its grateful thanks to them for their most welcome assistance in this great humanitarian crusade. It is hoped that similar branches will shortly be formed at Manchester and other important centres.
H.R.H. THE PRINCE OF WALES
The Prince of Wales, the Patron of the Association, is taking the greatest interest in the campaign against leprosy. His Royal Highness sent most encouraging messages on the occasion of the inaugural meeting, and again when the Indian branch was formed. A further message which he sent to be read at the dinner at the Savoy Hotel, which was abandoned in the circumstances already described, is printed inside the cover of this report [given below this full report]. When His Royal Highness visited India in 1922, he sent for Mr. Oldrieve in order that he might have first-hand information regarding leper relief work in that great country. During his recent tour in West Africa, one of the first questions he put to the Governor of one of the colonies was “What are you doing for the lepers here?” In South Africa the Prince spent a considerable time on a personal visit to a leper asylum. And on learning that Mr. Oldrieve is shortly going to West Africa and the West Indies, he again sent for him, on 14th December, to learn what it is hoped to do there. 19
19 First Report, 1925, pp. 3-9
The first report also gave a list of those who had agreed to become members of the various Committees:
Patron:
H.R.H. The Prince of Wales, KG 20
Vice-Presidents:
The Secretary of State for Foreign Affairs
The Secretary of State for the Colonies
The Secretary of State for India
H.E. The Viceroy of India
H.E. The Governor-General of Canada
H.E. The Governor-General of South Africa
H.E. The Governor-General of New Zealand
Chairman of General Committee:
*The Rt. Hon. Viscount Chelmsford, GCSI, GCIE, GCMG, GBE, late Viceroy of India 21
Chairman of Executive Committee:
*Sir Edward Gait, KCSI, CIE, Member of the India Council 22
Chairman of Medical Committee:
*Sir J. Rose Bradford, KCMG, CB, CBE, FRS 23
Hon. Medical Secretary:
*Sir Leonard Rogers, CIE, MD, FRS, IMS (retd.) 24
Hon. Treasurer
*Sir Frank Carter, CIE, CBE 25
Secretary
*Rev. Frank Oldrieve
Executive Committee
Those marked with an asterisk and the following:
The Viscountess Willingdon, CI, GBE 26
Sir Charles MacLeod, Bart 27
Dr. Andrew Balfour, CB, CMG 28
F.H. Brown, Esq., CIE 29
Dr. Thomas Cochrane
Lt.-Col. F.E. Fremantle, MP, FRCP 30
Dr. A.E. Horn, CMG 31
20 Knight Companion of the Order of the Garter
21 Knight Grand Commander of the Order of the Star of India, Knight Grand Commander of the Order of the Indian Empire, Knight Grand Cross of the Order of St. Michael and St. George, Knight Grand Cross of the Order of the British Empire
22 Knight Commander of the Order of the Star of India, Companion of the Order of the Indian Empire
23 Knight Commander of the Order of St. Michael and St. George, Companion of the Order of the Bath, Commander of the Order of the British Empire, Fellow of the Royal Society
24 Companion of the Order of the Indian Empire, Medical Doctor, Fellow of the Royal Society, Indian Medical Service
25 Companion of the Order of the Indian Empire, Commander of the Order of the British Empire
26 Companion of the Order of the Crown of India, Dame Grand Cross of the Order of the British Empire
27 Baronet
28 Companion of the Order of the Bath, Companion of the Order of St. Michael and St. George
29 Companion of the Order of the Indian Empire
30 Member of Parliament, Fellow of the Royal College of Physicians
31 Companion of the Order of St. Michael and St. George
Between 1923 and 1925 both the Prince of Wales and, later, King George V, gave £100 each to BELRA.
On 10th October, 1925, the new Rajah Sir Charles Brooke Memorial Leprosy Settlement was opened at 13th Mile, Penrissen Road, Kuching, Sarawak. (The old ‘Leper Settlement’ was at the 5th Milestone Rock Road and it accommodated about 70 patients). This was one of the first of the ‘new’ leprosy settlements to embrace BELRA’s vision for the control of the disease.
The message from the Prince of Wales, alluded to earlier, to be read at the dinner at the Savoy Hotel on 25th November, 1925, but which had to be abandoned, is given below:
“As Patron of the British Empire Leprosy Relief Association, I am glad to hear that so much has been accomplished during the past year.
The thanks of all of us who are interested in the Association, are due to H.E. the Viceroy of India, and to the members of the Indian Branch of the Association, for the extremely generous support they have accorded the movement.
I sincerely hope that it may arouse equal interest at home, to enable a practical use to be made throughout the Empire of the mass of valuable information which has been collected by the efforts of the Medical Committee.
It will indeed be a splendid achievement on the part of this generation, if the terrible scourge of leprosy can be stamped out in the British Empire for ever.” 32
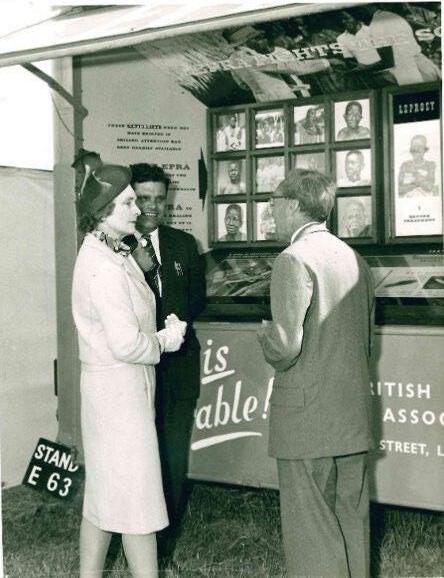
As mentioned, in South Africa, the prince spent a considerable amount of time on a personal visit to a leprosy asylum, pre-dating Her Majesty, Queen Elizabeth II and, later, Princess Diana, in being the first member of the British Royal Family to visit a leprosy centre.
32 First Report, 1925, inside front cover
BELRA’s first collecting tin
CHAPTER TWO
Spreading the word – calculating the true number of those with leprosy in the Empire - 1926-1930
Having set up the new organisation, the next challenge was getting the word out to people that something was actually being done to combat the disease. At that time of course, it could really only be tackled in the areas where it was prevalent, and local branches of BELRA were set up to spread the word that something was being done about it, and that people could hope again that a cure might be found.
The expansion of the number of local branches which would undertake eradication programmes became Frank Oldrieve’s continuous objective, to be accompanied by the spreading of Sir Leonard’s policy of anti-segregation. On this basis, Frank set sail for Africa on 6th January, 1926 to set up BELRA Branches in Nigeria, the Gold Coast [Ghana] and Sierra Leone. The Governors of these colonies showed great interest in his visit, and did everything they could to make it a success. In each case Frank prepared a report on the situation and made various suggestions for dealing with local conditions and establishing branches of the Association; he persuaded local Governments to pay the salaries of Medical Secretaries, while funds from the United Kingdom enabled the London headquarters to send out doctors.
After his tour in West Africa, Frank proceeded to the West Indies, where he visited Barbados, Trinidad, and Jamaica. He also went to British Guiana. In each place he visited the existing institutions for those with leprosy, including the very good and up-to-date settlement on the island of Chacachacare, Trinidad. Rigorous compulsory segregation had been the rule in the islands, but in spite of this, the early cases were not found in institutions, and it was clear that if real progress was to be made in reducing the incidence of leprosy, there had to be some relaxation in compulsory segregation and bringing treatment of early cases at dispensaries, or by private practitioners – to take treatment to the people rather than the people to treatment. Hopes were high that in Barbados and British Guiana, the leprosy problem was so slight that the disease would be eradicated within 15 years and, significantly, Frank pressed for a relaxation of the segregation laws which, even in those early days, it was felt, inhibited early cases from coming forward for treatment. The policy remained characteristic of BELRA/LEPRA’s work over the years.
In the 1926 Annual Report the list of estimated sufferers was repeated with the caption “…the above figures represent a very conservative estimate made several years ago. They are now known to be far too low. In India alone there are thought to be at least one million lepers.” (Later, in 1927, the estimates were again revised with Africa now thought to have 158,000 patients, 90,000 of whom were in Nigeria.)
Literature on leprosy was sent to all parts of the Empire, including reprints of pamphlets by Dr. Muir, and Sir Leonard, copies of the reports on the Secretary’s tours to British Colonies in West Africa, the West Indies and Malta. Supplies of the seeds of Hydnocarpus Wightiana were sent, at BELRA’s cost, to every colony where leprosy was prevalent, in order that the plants might be grown on the spot, where, it was hoped, that within five or six years the oil would
thereby be available locally. In addition, supplies of chaulmoogra oil were sent out to many places where treatment was given. Special dispensaries were opened for ‘lepers’, doctors were trained in the diagnosis and treatment of leprosy, and research work was undertaken; 67 doctors from various provinces in India were trained in Calcutta, and these, in turn, would train local doctors. £5,920 13s. 1d was received in donations and subscriptions towards this work. However, treatment by chaulmoogra oil produced its own problems, as noted earlier, as they were painful, and often caused unwonted side effects.
The 1926 Annual Report noted:
…Recent opinions of some of the most experienced workers in the endemic areas indicate that Rogers’ original method of injecting both subcutaneously and intravenously the sodium salts of the more soluble low-melting point fatty acids of hydnocarpus oils is still the most active method of treatment. Although this has been, of late, largely replaced by ethyl esters, on account of blocking of the veins induced by the hydnocarpates, rendering it difficult and often impossible to continue the injections for long, it is believed that this difficulty has now been overcome, and a painless, almost unirritating, and very cheap preparation has already been issued to a number of reliable workers for trial in the endemic areas. If their reports are favourable a more simple and economical treatment will then be available, and this will result in increased efficiency, and there will follow a more rapid diminution of the disease. 33
The Indian Council of BELRA was now actively at work. An anti-leprosy campaign was launched under its auspices in all parts of India. In each Province a local committee was formed, with a strong medical element, to deal with questions relating to the campaign, and to administer its share of the funds. But it appeared that the disease was even more prevalent in India than was at first thought, according to the Indian Council. A medical man (sadly unnamed) was appointed as Secretary of the Indian branch, and worked in close co-operation with Dr. Muir, the Leprosy Research Worker at the Calcutta School of Medicine. A very valuable booklet by Dr. Muir on the ‘Diagnosis, Treatment and Prevention of Leprosy’ was published and widely circulated to aid the cause. Illustrated booklets entitled “What the Public should know about Leprosy”, and “A Popular Lecture on Leprosy” were also published, while sets of coloured lantern slides, to illustrate the lecture, were prepared. 34 Work was now underway to educate the public on the disease of leprosy, and what they could do to help eradicate it.
Great help and encouragement had been given by the Secretary of State for the Colonies, who wrote a letter to each of the Governors of British colonies in East Africa inviting their assistance in connection with Frank Oldrieve’s visits. Great help was also afforded by various authorities who provided travelling facilities for Frank during his tours, and to Messrs. Elders & Fyffes & Co., of London; the United Fruit Company of New York; Messrs. the P. & O. S.N. Co.; and Messrs. Elder Dempster & Co.; the Union Castle Steamship Co.; the Sudan Government Railways, the Kenya and Uganda Railways, the Rhodesian Railways, and the South African Railways, for the help that they gave in the way of free or aided passages on their lines.
33 Annual Report 1926, pp. 6-7
34 These are housed in Lepra’s archive in the Indian Council Pamphlets, ‘Leprosy in India’ Vol. 1 1929
In October, the Medical Sub-Committee of the Association, invited doctors connected with the Colonial Service, who were then home on leave, to meet at BELRA’s office, and a number availed themselves of the invitation, which resulted in a useful conference.
A year later, Frank Oldrieve undertook a monumental journey, calling in on Mediterranean pockets of leprosy and then moving southwards through every country on the path from the Sudan to South Africa. He visited Uganda, Kenya, Zanzibar, Tanganyika (Tanzania), Nyasaland (Malawi) and Southern and Northern Rhodesia, (later to become Zimbabwe and Zambia respectively) and branches were set up there. Addressing parliamentary assemblies, visiting palaces and ‘leper’ colonies, he called in on Egypt on his return journey and had covered 16,000 miles by the time he reached home, having set up schemes for anti-leprosy work in four countries. In Uganda he was received by the King of Buganda, and addressed the Native Parliament; in Zanzibar he was received by His Highness the Sultan. Where it could be arranged, Frank gave a public lecture, and between Cairo and Cape Town he delivered 18 lantern lectures (an early form of image projection), and the film ‘Leprosy’ was used eight times. He also addressed Rotary Clubs in Pretoria and Cape Town, preached in seven churches, and was broadcast from Durban. Articles and interviews on the countries comprising the tour were given Altogether Frank Oldrieve covered some 9,500 miles by train, 3,600 miles by motor, and 2,800 miles by steamer, as mentioned, a total of over 16,000 miles in this one tour in and around East and Central Africa.
In East Africa, the Governments of Kenya, Tanganyika and Nyasaland made definite proposals and outlined schemes for the organisation of leprosy work in their territories. Governments proposed to set apart special funds for developing leprosy work, and asked for close cooperation of the missionary bodies in their territories in carrying out the schemes suggested. But not all governments were in a strong position financially, and looked to BELRA for help.
In Nigeria and the Gold Coast, the Governors appointed whole-time medical men as Honorary Secretaries of the respective local branches, and they devoted all their time to developing leprosy work in these colonies. In India a doctor was appointed as Research Worker in connection with the Indian Council, as the branch in India was called by the Viceroy. BELRA’s committee felt that it would be helpful if a branch of the Association could be formed in every part of the Empire where those with leprosy were found but, it was noted, there was no idea of the local branches being controlled from the UK as the Association only existed ‘to be of service to those who are carrying on the work.’ 35
1927 became a very significant year for the Association. A new preparation of chaulmoogra oil came into use for the treatment of leprosy and was sent out by BELRA to all parts of the Empire, both to Government Medical Officers and missionaries. Dr. Muir had found a simple way of giving the oil without blocking the veins of patients, based on Sir Leonard’s idea, but less painful to deliver. Messrs. Burroughs, Wellcome and Co. put the new formula on the market under the name of ‘Alepol’ at a cost that allowed of solutions being made up for two full doses twice a week for a year at less than 2s. 6d. per case. Further large supplies of the seed of the chaulmoogra tree were also being sent out to the Empire to be planted where needed. But there was an enormous amount of hard work to be done. The new treatment depended on supplies of chaulmoogra oil and the transportation of the necessary seeds
35 Leprosy Notes, No. 1 March 1928 p. 2
provided an immediate and practical task. It would take five years for the planted seeds to bear fruit and it was confidently – if naively – hoped that 30 years would be a long enough period for leprosy to be eradicated.
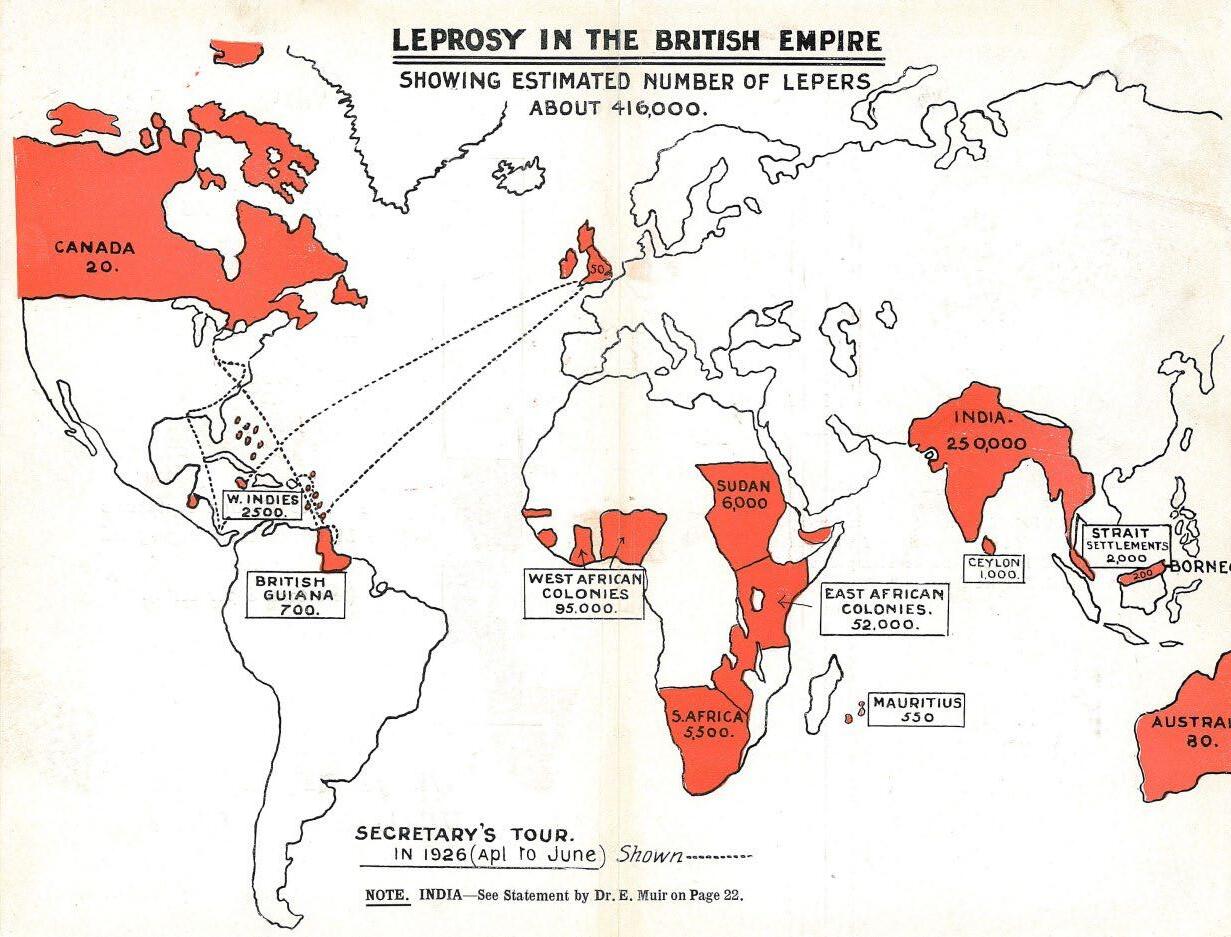
In February 1927 a joint discussion on the subject of leprosy at the Tropical Diseases, Dermatological and Therapeutical sections of the Royal Society of Medicine, brought great advances. It was estimated that there were 416,000 people with leprosy in the British Empire (only 31,000 of those were segregated or treated – less than 8%). The numbers were: Canada – 20; w. Indies – 2,500; British Guiana – 700; UK-50; West African Colonies – 95,000; Sudan –6,000; S. Africa – 5,500; East African Colonies – 52,000; India – 250,000; Ceylon – 1,000; Mauritius – 550; Straits Settlements – 2,000; Borneo – 200; Australia – 80.
With the exception of India, all the countries visited by Frank Oldrieve drew on funds raised at home, but these were modest enough. At the end of 1928, the Association’s assets stood at just over £7,000 – a small sum with which to take on a barely understood disease. The Government of Kenya asked BELRA to help financially to carry out the establishment of Treatment Centres and Leprosy Settlements in the Colony. In some places, Nigeria for instance (the Emirs in the north), in Uganda, Kenya, Tanganyika and in Southern Rhodesia, the Governments provided housing and food for a few leprosy sufferers, but much remained to be done. There were 52 ‘lepers’ at Likwenu in Nyasaland, and Southern Nigeria had 484 in May and 700 in July, and the use of potassium iodide which had been considered too dangerous for use in the treatment of leprosy as it produced very severe reactions, had proved very effective after a new batch had been developed which made the patient feel much stronger and had fewer side effects.
Financially, too, 1927 was a stable year - £6,472.7s.11d was received in donations and subscriptions, and £5,968.2s.11d was spent.
Work on expanding leprosy work came in June 1928 when the Itu Leprosy Settlement was founded in Nigeria, by Dr. A.B. Macdonald as an out-patient camp, but, according to one of his letters home soon became inadequate to “…deal successfully with the hundreds of people who came, grasping at even the slenderest hope of recovery.” 36
By the end of 1928 there were twelve countries, including Malta and Cyprus, where a branch of BELRA was to be found, and the idea of working throughout the Empire had changed from a pipe-dream into reality. Also, a preparation known as ‘Martindale’s C Fraction’ of hydnocarpus oil was discovered to be painless, effective and even cheaper than ‘Alepol’ so large quantities were sent out for trial purposes to British Colonies in Africa. Spreading its influence further into Africa, a treatment centre was built at Malamulo, Nyasaland with money provided by BELRA.
In 1928, Frank Oldrieve resigned for “…personal and domestic reasons” (which included his indifferent health at the time). It is often overlooked that in resigning, he revealed a humility which might otherwise have remained hidden behind the glare of his distinctive character, for he stressed the need for a ‘medical man’ to lead the Association’s now extensive forces as his replacement. His immense contribution to the welfare of leprosy sufferers in all the countries he brought into the Association’s field of activities was justly praised. BELRA’s Fundraising Officer in the 1950s, noted:
“It seems incredible that one man, acting entirely alone, could have achieved so much in such a comparatively short space of time, and the record of Oldrieve’s achievements should not preclude a reminder of his problems. Even now, anti-leprosy work is not everywhere conducted in the most accessible places. For Oldrieve, the comparative comfort of an official residence gave way to the makeshift, camp-bed village stop-over. Cabin gave way to railway compartment, and in turn to horse-back. Native parliament changed to village meeting and lantern-slide lecture to interpreted pep-talk. To say that Oldrieve became all things to all men is to commit a grave error of understatement. He had to adjust, too, to all circumstances, often with alarming rapidity.” 37
When he could, Frank Oldrieve journeyed about the British Isles as well, expanding the branches at home. But his major domestic contribution was not in the fundraising field. The ignorance of the public was a barrier to increasing the income; but the ignorance of those placed in the forefront of the anti-leprosy struggle was more serious still. To counteract this, Frank began to compose Leprosy Notes, a distillation of the findings of leprosy workers around the world, 5,000 copies going to those who were in need of up-to-date information. Less colourful as a contribution to the leprosy sufferer’s well-being than his energetic travels, nevertheless Leprosy Notes, and what was made of the publication, may still be fairly regarded as among the Association’s major steps towards the achievement of its aims.
36 Dr. Macdonald’s Personnel File
37 LEPRA: An Historical Sketch 1924-1974, pp.8-9
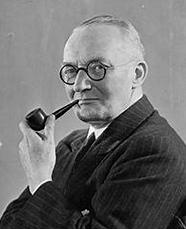
In 1928, Frank had found, not surprisingly, that he had set himself too strong a pace. If his path was smoothed by the colonial administration, it had never been less than arduous and uphill. Clearly there would have been times on his travels when he was urged, and perhaps expected, to take an expert stance on matters about which there was probably no definitive opinion. Misunderstanding of leprosy is, even today, so profound that the merest smattering of knowledge converts an interested layman into an apparently erudite authority. His 14 years’ experience probably enabled him to know more than many who were better qualified scientifically, about leprosy as a medical and social problem. His work had helped to show, even in such a brief period, that leprosy had been underrated. In 1925, the Association had announced boldly that ‘300,000 at the lowest computation’ was the alarming number of those with leprosy in the Empire. This sat rather uncomfortably beside estimates of those in India alone. By 1928, the figure had risen to over 400,000, qualified by the cryptic addition that ‘there are between a half a million lepers in India;’ clearly there were certainly a lot more people affected than had been bargained for, and identified cases increased by the day. As the estimates of the number of leprosy cases expanded, so the absolute faith in the new treatment came into question. In Calcutta, Dr. Muir had developed the cure to a stage where the early difficulties of giving the treatment by injection, which Sir Leonard had found caused blocking of the veins, had been largely overcome, but the injections were still complicated and painful. On a journey to Kerala in South India, Dr. Muir, in the company of Dr. Robert Cochrane (right) of the Mission to Lepers, had found a variety of the chaulmoogra plant whose fruit needed a less costly processing than the variety Sir Leonard had been using, and the treatment was soon to be in commercial production Supplies had been sent to every country in the Empire where leprosy was to be found, and in Fiji alone over a thousand trees had been planted, but other problems were beginning to emerge. For the leprosy sufferer there was a cure that was more painful than the disease; for the scientist, a baffling and unyielding disease, ill-documented and, until now, largely swept under the carpet.
With the appointment of Dr. Cochrane, the ‘medical man’ that Frank Oldrieve had requested in 1928 as the new Medical Secretary, BELRA took on a more formal medical role, and interestingly from another Mission to Lepers man. Dr. Cochrane, son of a famous father, Dr. Thomas Cochrane, had already distinguished himself in the leprosy field by producing a number of useful and informative pamphlets explaining the disease and its treatment in clear and decisive terms. He was a considerable acquisition, and together with his father, who served on BELRA’s Medical Committee, and Sir Leonard, he now headed a formidable medical team. Termed the ‘Medical Secretary,’ he was obliged to spend some of his time on nonmedical matters, but Miss Wallich, BELRA’s secretary, had already gained a great deal both in capability and commitment in the time she had been working for the Association, and dealt with a lot of these
By now there was a sufficient weight of records and correspondence to make life in Sir Leonard’s consulting rooms less than comfortable so, late in 1928, the Association’s goods and chattels were moved to 29 Dorset Square, with the telephone number of Paddington
7832. By then, the income had settled at about £7,000 a year, still a long way short of the immense sums necessary, despite the growth of local branches in the UK.
Dr. Cochrane, who had been brought in precisely because of his medical qualifications, sought to upgrade Frank Oldrieve’s new and still embryonic, Leprosy Notes, to the status of an authoritative medical journal. The quality of the contributions being received was sufficient to warrant this, and he felt that BELRA’s status would be enhanced. Although Sir Leonard was initially against this idea (“We are not in a position to start a scientific journal,”) it was decided that from there on Leprosy Notes would be published as Leprosy Review and subtitled ‘The Journal of the British Empire Leprosy Relief Association,’ and if papers were considered too scientific or technical, they would be offered to the emerging International Journal of Leprosy which was in the pipeline from the newly-established ‘Leonard Wood Memorial’ in America. Since Dr. Cochrane, as Editor of Leprosy Review could decide himself what was or was not ‘too technical,’ it is not surprising that he agreed to the restriction.
However, deciding whether chaulmoogra could cure leprosy was easier said than done. Firstly, exactly what was meant by the term ‘chaulmoogra’ differed from place to place. For some, chaulmoogra meant crushed seeds from the Hydnocarpus family, for others it was the fruit, or distilled oils mixed with chemical compounds, particularly salts and disinfectants. Secondly, how the treatment should be applied also differed. Should it be rubbed on the skin, taken orally, or through injections under the skin or directly into the veins? At what doses, and for how long? Thirdly, there were no global standards for classifying cases. When proponents of chaulmoogra produced statistics showing up to 60% cure rates, opponents argued that those listed as ‘cured’ had never had the disease in the first place, or that the disease inevitably would reappear.
In South Africa, the English-born South African doctor and bacteriologist Sir Spencer Lister expressed the opinion that while hydnocarpus oil was useful in treatment in the early stages of leprosy, this did not mean that it was a definite cure. Speaking with some trepidation as a layman, he said, he wished to point out that when they spoke of a disease as curable, this did not mean that in all circumstances and under every condition leprosy could be cured. Mankind died of curable diseases every day, but that fact did not impair their faith in those diseases being curable if they were treated in proper time and under proper conditions. The Association had a remarkable record to show, but he trusted that their supporters would not think that they were yet in a position to relax their efforts. Sir Leonard said that he did not think that the criticism made by Sir Spencer would have been forthcoming if the full details given in his (Sir Leonard’s) report had reached him. There was the most complete evidence that the early cases of leprosy could be cured! Sir Leonard went on to say that the leading authorities in Calcutta (where Dr. Muir had been doing nothing but leprosy work for the past seven years), and at the great leprosy settlement at Culion in the Philippines, were agreed that nearly every early case of leprosy was curable. At Culion, he insisted, no fewer than 1,000 patients had been released on parole as recovered within the last few years. The South African reports showed that, although segregation was compulsory, the settlements had very little practical experience of early
cases. This was ‘…owing to the tendency to concealment which was so unhappy a feature of enforced segregation unalleviated by outdoor treatment in the early non-infective stage.’ 38
Modern advances in leprosy treatment bring both the ‘cure’ and the methods into question, but in the 1920s chaulmoogra oil remained the only generally used treatment for leprosy up to the time of the development of Dapsone in the late 1940s, although expert opinions vary greatly as to its effectiveness. Statistical information was sparse. The number of leprosy sufferers in the British Empire was originally quoted as 300,000. By 1929, this figure was considerably increased to over 500,000, while reports from India alone suggested that many more than even this figure were to be found in the sub-continent. We must remember that the concept of the British Empire was still strong enough to suggest considerable ease in implementing a concerted plan over very widespread territories. 39
At the Annual General Meeting of BELRA on 24th February 1928, Sir Leonard presented his report, noting that the past year, the fourth of the active work of the Association, had been one of remarkable progress in several directions. He highlighted the interesting tour of Frank Oldrieve, from Cairo to the Cape, through the whole of British East and South Africa, which completed his visits of the last three years ‘…to nearly all the leprosy-ridden portions of our Empire, except Oceania.’ He noted:
“…we are now in touch with 62 medical men and women, many of them missionaries, who are actively engaged in treating some of the 158,000 lepers in our African possessions, and during last year we gave grants for hutting accommodation for leper patients and other buildings to 25 centres, including eight out-stations in Uganda. We have also distributed over 100,000 doses of our improved preparation, Alepol…and expect to send out over a quarter of a million doses this year…
Whole time medical men have been trained in Calcutta by Dr. Muir for Nigeria and the Gold Coast, and two more will be sent shortly, all of whom are being financed by the Provincial Governments with the approval of the Colonial Office, with whom we are working closely, and who are represented on our Executive and General Committees.
In India some 60 medical men are being trained each year under Dr. Muir in the Calcutta School of Tropical Medicine, and many clinics and dispensaries are being opened by them all over India with the help of our flourishing India branch. Recent surveys by Dr. Muir’s assistants in the worst affected districts of Bengal and Bihar, has revealed the presence of one to three or four early cases of leprosy for each advanced one returned in the census, and several dispensaries opened there by the local authorities have each attracted 200 to 500 early cases for treatment within a few months. This will result in many early cases being cleared up and prevented from going on to the later infective stages, and is thus striking at the root of the problem, as it must lead in a decade or two to a material reduction in the lepers in this important centre, from which Calcutta and many other towns and pilgrim places derive many of their cases.”
40
38 Leprosy Notes, No. 1 March 1928, p. 5
39 LEPRA News No. 11 Autumn 1972 p.2
40 Leprosy Notes No. 1, March 1928, p. 6
At the end of the 1920s the dominant approach to leprosy prevention around the world was still segregation. The recommendation from the Third International Leprosy Conference in Strasbourg in 1923 had insisted that those isolated should be treated humanely, but otherwise reaffirmed the policy advice first advocated by the Norwegian leprologist (and identifier of the leprosy bacillus), Gerhard Armauer Hansen at the first International Leprosy Conferences in Berlin (1897) and Bergen (1909). Leprosy was contagious, and therefore the best way for society to defend itself was through isolating those affected.
According to the proponents of chaulmoogra, such as Sir Leonard and Dr. Muir, having a cure changed everything. First, segregation and leprosy laws should be abandoned. As long as the disease was seen as a crime and detection meant lifelong segregation, people would do their best to hide their disease for as long as possible. This increased the risk of contagion, and the risk of missing the window of opportunity for the chaulmoogra treatment to work. Secondly, the expensive isolationist institutions should be replaced by cheap outpatient clinics and treatment in the patient’s own home. It also meant that treatments should be voluntary in the belief that once former patients could return to their communities cured, they would spread the word and encourage others to seek help. Always an opponent of segregation, Sir Leonard noted:
“In New South Wales compulsory segregation costs £200 per leper per annum, or enough to supply drugs for treating 1,600 cases in dispensaries, and even in India 60 out-patients could be treated for the cost of maintaining one advanced case in an asylum. A decade ago, only segregation was available but, in addition to being infinitely more expensive than our present dispensary system, it inevitably resulted in the poor lepers hiding themselves until too advanced to profit much by treatment, and in their infecting others before they were discovered and isolated, so it may possibly do more harm than good now an effective treatment for early cases is available. Where compulsory segregation is already in force, we do not advise its immediate abolition, but that all newly discovered lepers should be examined by a small board of expert medical men, with power to permit early uninfective cases to be treated as outpatients at dispensaries instead of being segregated, so as to attract for treatment the early amenable cases. This plan is being adopted in some of our colonies with great advantage, and in proportion to the success of such early treatment the necessity for segregation will be reduced until it reaches the vanishing point with great saving in cost, and the eventual disappearance of this middle-age approach to humane medical science of today.” 41
In the House of Commons on 27th February, 1928, Mr. Harry Day asked the Secretary of State for the Colonies if any new stations were being built within the Empire for the treatment of leprosy by the hydnocarpus oil remedy, and whether he could make a full statement on the subject. Mr. Amery, Secretary of State for the Colonies, replied:
“In those parts of the Empire where leprosy exists active measures are being taken by the medical departments for its control, in many cases in co-operation with the British
41 Leprosy Notes No. 1, March 1928 p. 7
Empire Leprosy Relief Association and other agencies. Medical Officers trained in recent methods have been detailed for special duty in Nigeria, the Gold Coast, Fiji, and other Colonies, while in all areas attention is being given to the possibility of the eradication of the disease by the establishment of treatment stations, as in Tanganyika, Nyasaland, Uganda, or by such other means as the situation appears to demand.” 42
BELRA was now officially recognised by the British Government as being a ‘player’ in the eradication of leprosy.
In his last ‘Editorial Note’ in July 1929, Frank Oldrieve wrote:
“It is with very sincere regret that for the last time I write as Editor of LEPROSY NOTES. Since the formation of The British Empire Leprosy Relief Association, six years ago, it has been my privilege to be the Secretary, and the work has gradually developed until there are branches of the Association, with influential Committees, or representatives of the Association, in almost all parts of the Empire where leprosy is at all prevalent.
The work has been made very much easier by the help that has always been given by those whom, whether connected with the Government or Missionary Societies, I have met or with whom I have corresponded, in all parts of the Empire. I take this opportunity of very warmly thanking all those who have helped me, in ways too innumerable to mention. I shall never forget the many kindnesses I have received from leprosy workers in every part of the Empire that I have visited.
LEPROSY NOTES will in future be edited by Dr. R.G. Cochrane, who succeeds me as Secretary of the Association, and while expressing my great indebtedness to all those who have been my helpers in commencing the publication, and I am very grateful indeed to those who have contributed articles, I should especially like to mention Mr. F.H. Brown, CIE, a member of the Executive Committee of the Association, and on the staff of The Times, for his invaluable advice, and kindly criticism.
I think it should be clearly stated that my interest in the work of the Association has not in any way diminished, indeed it is only because I feel that it is in the highest interests of the work of the Association that a medical man should be the Secretary, that I have felt impelled to resign. I am more than ever convinced that the object of the Association can be achieved if those who are able to do anything will wholeheartedly tackle the part of the work that lies in their hand.” 43
A primary effect of the formation and the early work of BELRA was the awakening of both official and medical minds to the needs of those suffering from leprosy. The disease had previously been a curiosity, and an almost wilfully misunderstood curiosity at that. The fact of throwing the spotlight onto the actual disease, and not just its consequences, was something of an achievement in itself. From the first few years of its activity, BELRA saw a world-wide campaign to reduce leprosy to numerical proportions at which it could be regarded, if only in
42 Leprosy Notes, No. 1 March 1928, p.7
43 Leprosy Notes, No. 6, July 1929 p. 1
lay terms, as having been eradicated. However, as surveys progressed it became clear that the number of cases of leprosy had been grossly underestimated, and as these expanded, so the absolute faith in the new treatment came into question. In 1928 in Calcutta, Dr. Muir had developed the cure to a stage where the early difficulties of giving the treatment by injection, which Sir Leonard had found caused blocking of the veins, had been largely overcome, but the injections were still complicated and painful.
But BELRA was not alone in its concern. The Mission to Lepers had been working for 50 years; medical congresses, which followed the first one on a regular basis, had repeatedly called together the world’s most expert minds. What distinguished BELRA was its non-alignment with any cause except that of the physical and social wellbeing of the leprosy sufferer. Its attitude was summed up by Sir Leonard who did not pull his punches on the subject:
The organisation of the great humanitarian work of caring for the leper, which is so largely in the hands of the Christian missions of various denominations, requires to be remodelled in the light of the new situation, for it is evident that a greater service is rendered by curing the leper in the early stages of the disease than in providing a home for him after the affection has reduced him to a hopeless wreck. 44
Strangely enough, his zeal to promote out-patient treatment did not put Sir Leonard at loggerheads with the Mission (to which BELRA had made small grants from its own modest funds). Moreover, it was through the Mission that Frank Oldrieve had come to learn of the leprosy sufferer’s needs, and it was through the same door that his successor, no less a missionary for being the medical man that Frank had recommended, entered into a long career with the Association.
The first flush of success at achieving three branches of BELRA in 1924 had subsided into a pallor of patient optimism. However, this was reborn when new branches in Dundee, Aberdeen, Plymouth, Brighton and Hove, Cheltenham, Hull, Rugby and Worcester, were all officially set up in 1928 but, sadly, the income did not, materially, improve. A doggedness replaced the urgency of the first days:
“The period of surveying the needs of our Empire is past. The active work of healing our very numerous lepers has been entered upon and this will become increasingly effective in exact proportion to the funds entrusted to us for carrying out our great task.” 45
Interestingly, the work of the Association was kept in the mind of the British Parliament, as in the House of Commons on 25th March, 1929, Sir Robert Thomas asked the Under-Secretary of State for India approximately the present number of ‘lepers’ in India; how many treatment centres were now open; to what extent those centres were State supported as regards initial establishment, maintenance and payment of their medical staffs; and whether The British Leprosy Relief Association received any financial aid from public funds? The Under-Secretary of State for India (Earl Winterton) advised him that the number of those with leprosy in India
44 LEPRA: An Historical Sketch 1924-1974, pp.12-13
45 LEPRA: An Historical Sketch 1924-1974, p.13
as identified by the census of 1921, was 102,513, but that it was very probable that the number was considerably in excess of that returned. An interesting exchange then ensued:
Sir Robert Thomas: Is the Noble Lord aware that there are more lepers under the British flag than under any other flag?
Earl Winterton: That is exceedingly probable, in view of the fact that one-fifth of the whole population of the world is under the British flag.
Mr. Day: Is it not the fact that the latest remedy for leprosy is greatly alleviating that disease?
Earl Winterton: Yes, I believe that is so. My noble friend has a very distinguished medical adviser at the India Office, who was closely associated with the discovery of that particular remedy. 46
Another boost to BELRA’s status came in a Report by the ‘League of Nations’ in 1930 which stated:
In some quarters, there may be an impression that the work of the British Empire Leprosy Relief Association is conducted in an essentially missionary spirit – that is to say, that religious aims take precedence over medical and scientific aims. That is not the case. The Association is not a charitable institution. It is a health organisation on a grand scale, which endeavours to exercise international action on scientific lines. The British Empire Leprosy Relief Association certainly deserves a high place among institutions for international action against leprosy.
Surveys were undertaken in Uganda in the Western and Buganda Provinces as the numbers of people with leprosy there were, as yet, unknown, but it was estimated that there were at least 20,000 in Uganda. To combat this, BELRA completed five out-patient dispensaries in this area. Also, a new settlement at Kakamega, in Kenya was built, and at other stations in Kavirondo district, drugs were sent and those with leprosy were treated as out-patients.
In the Tanga District of Tanganyika in the north, and along the central railway line, particularly at Shinyanga, leprosy work was being undertaken, and BELRA provided £500 towards this. In Nyasaland and Northern Rhodesia there were probably more centres for leprosy treatment than in any other colony in East or Central Africa at this time. There were 59 centres to which BELRA sent drugs, and grants to these centres amounted to over £1,300.
Southern Rhodesia, the latest of the colonies to attain full Dominion status, 47 had a great deal of leprosy. A Medical Officer and Superintendent of the Central Leprosy Institution at Gomohuru was appointed. It was also noted that there were more than 5,000 ‘lepers’ in the
46 Leprosy Notes, No. 6, July 1929, p. 3
47 A Dominion was one of several self-governing nations of the British Empire. With the evolution of the British Empire into the Commonwealth of Nations, there are no longer any dominions.
Union of South Africa, and Dr. Muir was invited to discuss the leprosy problem with the Union authorities.
However, at this point in history, the great world depression broke at a time when the United Kingdom had still not fully recovered from the effects of the Great War more than a decade earlier. The world financial crisis began to overwhelm Britain in 1931; investors across the world started withdrawing their gold from London at the rate of £2½ million a day, and Britain was driven off the gold standard. The financial crisis now caused a major political crisis in Britain in August 1931. With deficits mounting, the bankers demanded a balanced budget; the divided cabinet of Prime Minister Ramsay MacDonald’s Labour government agreed; it proposed to raise taxes, cut spending and, most controversially, to cut unemployment benefits by 20%. The attack on welfare was totally unacceptable to the Labour movement. MacDonald wanted to resign, but King George V insisted he remain and form an all-party coalition ‘National Government.’ The Conservative and Liberal parties signed up, along with a small cadre of Labour, but the vast majority of Labour leaders denounced MacDonald as a traitor for leading the new government. Although, as noted, Britain went off the gold standard, it suffered relatively less than other major countries in the Great Depression. In the 1931 British election, the Labour Party was virtually destroyed, leaving MacDonald as Prime Minister for a largely Conservative coalition. All of this had a dramatic effect on BELRA.
CHAPTER THREE
Depression, the overseas workers and ‘The First Leprosy Prevention Organisation’ – 1931-1939
To give an illustration of the crisis, the effects on the northern industrial areas of Britain were immediate and devastating, as demand for traditional industrial products collapsed. By the end of 1930 unemployment had more than doubled from 1 million to 2.5 million (20% of the insured workforce), and exports had fallen in value by 50%. In 1933, 30% of Glaswegians were unemployed due to the severe decline in heavy industry. In some towns and cities in the north east, unemployment reached as high as 70% as shipbuilding fell by 90%. The National Hunger March of September - October 1932 was the largest of a series of hunger marches in Britain in the 1920s and 1930s. About 200,000 unemployed men were sent to the work camps, which continued in operation until 1939. In the less industrial Midlands and Southern England, the effects were short-lived and the later 1930s were a prosperous time which was a boost to BELRA, and during the depression, Rev. ‘Tubby’ Clayton helped the Association develop fundraising strategies, but more of him later.
BELRA’s Annual Report for 1931 – entitled ‘The Empire’s Open Sore’ – noted:
…Not many years ago it was considered that India, China, and the Far East generally was the home of this dread malady, but recent investigations have shown that Africa is as heavily, if not more heavily, infected with this scourge than India. Further, if one had been asked the number of sufferers in the world some five or six years ago the reply would have been two to three million. A statement recently made by Sir Leonard Rogers, the Hon. Medical Adviser to the Association, and one of the leading authorities on the disease, shows this to be inadequate: -
Two decades ago, Dr. Heiser estimated the world’s lepers at 2,000,000 at a time when the prevalence in Africa was not known. More recently as a result of three years study of the literature the estimate was not less than three million. Since then, the leprosy surveys of Dr. Muir, recently confirmed in British Guiana by Dr. Rose, showed that for each typical advanced case there are anything from two to three early cases in existence, so the world’s lepers may very easily number 10,000,000. I will place the number at the very conservative estimate of 5,000,000.
The Report went on to state:
…These figures are placed in the forefront of the report on the work of the Association for 1931 because it is obvious that the magnitude of the task which is before us is not realised by the general public. As has often been stated, leprosy is the ‘Cinderella’ of tropical diseases…When one contemplates the immensity of the task there is a temptation to throw one’s hands up in despair and exclaim that it is beyond accomplishment, but man has faced as hard tasks as this before. When the Empire is up against depression and difficulties it is good to be able to raise a clarion note to our fellow citizens of the Empire to take vigorous action in the endeavour to deal this open sore of the Empire…
The work of the British Empire Leprosy Relief Association is divided into four sections, from the practical side: - (1) there is the direct giving of grants to institutions in the field where definite preventive and curative work is being done; (2) there is the supplying of drugs and instruments for treatment; (3) there is the distribution of literature which helps to keep workers up to date in all aspects of the subject, and (4) there is research work which must be continually pursued. The Association is a clearing house for receiving and disseminating information, so that successful methods adopted in one place may be quickly made known in other places.
In the early 1930s, the dominant approach to leprosy prevention around the world was still segregation. The recommendations from the Third International Leprosy Congress, held in Strasbourg, France from 28th - 31st July 1923 had been that “…the segregation of patients has to be humanitarian and has to allow the leprosy sufferer to be near their families, if this is compatible with an efficient treatment.” Sadly, all too often that recommendation was overlooked or simply ignored.
In 1931 the newly formed Leonard Wood Memorial in America called an International Conference in Manila and the International Leprosy Association came into existence; its objectives were purely scientific. At this Conference BELRA was recognised as the ‘first leprosy prevention organisation’ and thereafter its position in the world as an extremely important organisation was established.
This was a time of further expansion. A new treatment centre at Kilimatinde, Tanganyika was completed by the Church Missionary Society (CMS) with funds that BELRA had given them in 1929, and a further grant of £500 was made by BELRA for the work of the Africa Inland Mission at Shinyanaga in Tanganyika, and a new leprosy settlement at Msambweni, on the Kenyan coast, was completed and occupied. On the other side of the world, Dr. F.G. Rose, from Georgetown, Guiana, reported that more than half the cases in the settlement were voluntary admissions, which was seen as a great advance, and that word was reaching those with the disease that there was hope.
By 1932 it was noted that there were now 17 provincial branches of BELRA in India: Assam, Baluchistan, Bengal, Bangalore, Bihar and Orissa, Bombay, Burma, Central India, Central Provinces and Berar, Hyderabad, Madras, Mysore, North-West Frontier Province, Punjab, Rajputana, United Provinces of Agra and Oudh and Western India States. It was also noted that the settlement at Sungei Buloh in Malaya was working well under the direction of BELRA’s Dr. Gordon Ryrie, and treating over 1,000 patients.
In 1933 the Rev. ‘Tubby’ Clayton, Vicar of All Hallows by the Tower, and founder padre of Toc H, began his historic connection with BELRA. 48 During the Great War, Tubby ensured that Talbot House, a soldier’s rest and recreation centre which he founded in 1915 in Poperinghe, Belgium was open to men and officers alike and, with a
48 Toc H is an international Christian movement. The name is an abbreviation for Talbot House
nod to Dante, he put up a notice over the entrance door which read ‘Abandon rank all who enter here.’ 49
Tubby’s first encounter with leprosy had been in 1931, when he was visiting the little groups of Toc H members in West Africa. In Nigeria he came face to face for the first time with the disease and the misery it created. He saw small, dilapidated colonies in which only the most hopeless cases congregated, living in decaying huts in squalor, colonies to which a minimum of medical skill and attention was given. A chance meeting with Dr. Alastair Macdonald, who ran the Itu Leprosy Settlement in Nigeria, on the boat going home, fired his enthusiasm and zeal for tackling the disease. Dr. Macdonald had told him that doctors working in the leprosy field could not cope with the administrative and technical calls on their time as well as their medical duties, and appealed for help.
It was through the Colonial Secretary, Philip Cunliffe-Lister, a member of Toc H, that Tubby first became aware of the work of BELRA, which he described as “…a great cause starving in the midst of plenty,” so he called for volunteers amongst his Toc H members to help with the general running of leprosy settlements. Over 300 people volunteered, and since Toc H had no overseas organisation of its own, Tubby offered their services to BELRA which agreed to pay them ‘…enough to keep body and soul together, but not enough to make them rich,’ and indeed it was barely enough to live on. Tubby’s experience of leprosy had been with advanced cases, and it is understandable that his sympathy should have been aroused. However, even Tubby’s own account of his original involvement leaves out two significant factors. First, although BELRA had sent people overseas before, they were either its own officers or doctors, whose salaries were paid by way of a grant to the settlement at which they were employed. Secondly, it is probable that Tubby Clayton himself was never completely aware of having made a particular contribution to the overall work of the Association, without which its survival is at least open to question; for it was he who introduced fundraising as a consistent and routine part of BELRA’s work which hadn’t existed before. The idea of sending out layworkers was revolutionary, but it was also something of a reversal of policy.
It was decided to employ a full-time person to build up BELRA’s subscription list, and to orchestrate appeals to possible subscribers for money, and send these donors human literature designed to maintain their interest. In December 1933, a Special Committee was to become effectively the fundraising arm of the Association, since it had no counterpart working body of its own. It consisted of members of Toc H, BELRA, and ad hoc members, and indeed with Sir Frank Carter and Dr. Cochrane representing the Association, it would have been a lavish duplication of time and effort if the eventual amalgamation had not taken place. Tubby Clayton did not serve on the Committee – a fact which may at once be regretted and applauded. An Organising Secretary, Mr. Fellowes-Farrow, was appointed, but the public appeal was put off, first to permit the proper planning of the work ahead, and then to await
49 Taken from Dante’s 14th century epic poem ‘Divine Comedy’ as the words over the entrance to Hell.
the arrival of volunteers in the field so that the publicity would have something tangible on which to hang.
In July 1934, Dr. H.C. Armstrong took up his duties in the Behwai Station, Ho, in the Gold Coast and began surveying the lake villages in that area. Ten villages were surveyed with a total population of 2,651 and 84 people were found to have leprosy – a rate of 31.69 per mile! The Buluba Leprosy Settlement in Uganda was founded by Sisters of the Irish Order of St. Francis, and BELRA provided funding for this.
Further efforts were made to interest the public in the work. A special campaign was launched in Sussex. The Prince of Wales assisted in fundraising efforts by sending the following message:
“…we are fortunate in this country in that the horrors of leprosy have never gained a hold over our own people, but in many parts of the Empire this immemorial scourge still claims a terrible number of victims. The British Empire Leprosy Relief Association, of which I am Patron, is performing a very vital task in combating leprosy in India, Africa, the Levant and the West Indies. I hope the public will recognise the importance of their work, and will respond generously to their appeal.” 50
Arrangements proceeded for getting the first volunteers trained and allocated to overseas posts. The five men chosen from the Toc H volunteers for leprosy work began to study at the Livingstone College for Tropical Diseases in Leytonstone prior to being sent out for in-field training in Nigeria.
The course members at Livingstone College in 1934 Len Parker is in the middle of the back row, on his left is Pete Pedrick, and then Hamish Macgregor. Norman Crayford is on the far right of the second row, and Will Lambert is seated in the front row far left. The principal is shown in the front row with his dog (sadly the names of the other course and staff members are not known, but one could be Herbert Spencer)
50 BELRA Annual Report for 1935, p.2
It was felt at that time, of course, that it was the duty of everyone to ‘…free our brothers in the Empire from leprosy,’ and with that in mind, on 28th December, 1934, the first Toc H worker, Herbert Spencer, sailed for Dichpalli in India.
Dr. Robert Cochrane was awarded the Kaisar-i-Hind Gold Medal, First Class, in March 1935 for his outstanding work with those affected by leprosy in India, and in June five more Toc H workers completed their training and sailed for Nigeria to establish a reputation and a way of life for the Association.
They were (l-r: Will Lambert, Pete Pedrick, Hamish MacGregor, Leonard Parker and Norman Crayford. All five were presented to Her Majesty Queen Mary at the Rev. Tubby Clayton’s house in London before they left for Africa.
In India, Mahatma Gandhi (pictured below) gave a boost to those working in leprosy by personally nursing Parchure Shastri, the great Sanskrit scholar, who suffered from leprosy. Greatly admired for his devotion to the Indian cause, Gandhi epitomised the philanthropic worker, and his words greatly assisted the cause:
“…leprosy work is not merely medical relief; it is transforming frustration of life into joy of dedication, personal ambition into selfless service…”
The Indian work continued to flourish. Well formed in its two-year gestation, the overseas staff began to grow, as replacements were found to enable the first men to take home leave after two years. Soon an ever-changing pattern took shape, in which a man would finish a tour in Africa to find himself in the West Indies or a remote Pacific Island. The demands for lay staff soon became so numerous that the separation of the two anti-leprosy interests became redundant. Now moved to 131 Baker Street, BELRA took stock of its administration and moved to rule out duplication. Almost as if the arrival overseas of the first volunteer had ended its labour, the Special Committee rested. It held its last meeting on 5th March, 1936, scheduling its next one for 2nd July. By that date, however, the Association had incorporated under the Companies Act and its purposes and those of the Committee were so manifestly the same that amalgamation was logical. Thereafter, the role of Toc H would be maintained by service on the Executive Committee of three Toc H members, one of whom, until his death in 1972, was the Rev. Tubby Clayton.
The five Toc H men who left for Africa in June 1935 (and landed in Lagos on 4th July) for their 5-year stint in leprosy work, were not alone in their desire for the more active side of the campaign. Dr. Cochrane also felt the call to practice his by now renowned stills where they could be of most direct benefit to the leprosy sufferer. He had become the Association’s
Medical Secretary through the processes of reorganisation that characterise this period of BELRA’s history. A few weeks after the first volunteers’ departure for Nigeria, he accepted the post of Superintendent at the Lady Willingdon Leprosy Settlement in Madras. He had more than justified Frank Oldrieve’s opinion that a medical man was required at the helm, and his achievements and stature, both personal and professional, happily reflected on BELRA during his initial tenure of office and throughout the remainder of its history.
While serving on the Special Committee, Dr. Cochrane also followed the pattern established by Frank Oldrieve of touring the places where leprosy was a problem. His journeys were necessarily follow-ups to Frank’s, and much of the pioneering work had already been done, but Dr. Cochrane built up a repository of information which established BELRA as a knowledgeable source of factual material. He did this through the Leprosy Study Centre - the only library of histopathological slides of the disease available at that time. (This was eventually transferred to the Department of Human Anatomy at Oxford).
In January 1930, he had toured Egypt, the Sudan and the Eastern States of Africa. In 1932-33 he was away for a record nine months visiting India and Ceylon [Sri Lanka]. In India he consulted with Dr. Muir who was also conducting survey work, and who was to build on Dr. Cochrane’s mass of information. His report on the situation in Ceylon which Dr. Cochrane prepared, drew effusive thanks from the Government, and within two years had become the basis of the campaign towards leprosy control on the island. In 1934 Dr. Cochrane went to the West Indies and was able to pay a visit to ‘…the best organised leprosarium in the world’ at Carville, in the U.S.A. In Jamaica he established that leprosy was on the decline; in Barbados and Trinidad, however, it still presented a large problem, as it did in British Guiana.
True to his faith in Leprosy Review, Dr. Cochrane had raised it to its scientific status, notwithstanding the appearance of the International Journal of Leprosy in 1931. Also, as Medical Secretary, he changed a well-meaning, rather ill-informed effort to influence progress, into an objective analysis of the problem. However, with his departure back to the field, a gap was left and, retiring from India, Dr. Ernest Muir, foremost investigator into leprosy with 15 years’ research already to his credit, followed Dr. Cochrane as Medical Secretary. Leaving his assistant and disciple, Dr. John Lowe, in India, Dr. Muir inherited a more mature organisation than had been Dr. Cochrane’s lot.
No longer required to turn his hand to everything, the Medical Secretary could rely on a continuous programme of public appeal, the centre of which in 1935 had come to be a travelling exhibition. This consisted of a static model of an outpatients’ department; illuminated panels of ‘Leprosy through the Ages’, and ‘Landmarks of the Past’ depicting churches, lazar houses and other buildings involved in medieval leprosy. There was a ‘talkie’ film entitled ‘A stain on the Empire’s flag’, produced by the Organising Secretary which gave an insight into the modern (at that time) methods of dealing with the leprosy problem. 51 There was also an ‘oriental market’ stocked with an assortment of goods from the Far East which was a great attraction and proved a valuable source of revenue for BELRA.
The colourful and very useful career of Mr. Fellowes-Farrow came to an end soon after Dr. Muir’s arrival. In his stead a Business Secretary, Mr. J.A. Gilbert, was appointed, and the
51 Sadly, to date we have not been able to locate a copy of this
separation of medical and administrative duties began. Dr. Muir still held the titles of General and Medical Secretary, but as time went on, he turned his attention more and more to tours and medical matters. Mr. Gilbert was to become the founder of the line of administrative descent that leads to the present Chief Executive Officer.
On 20th January, 1936, King George V died, and the Prince of Wales, BELRA’s Patron, was hailed as King Edward VIII. But in early December, a constitutional crisis in the British Empire arose when King Edward indicated his intention to marry Wallis Simpson, an American socialite who was divorced from her first husband and was in the process of divorcing her second. The marriage was opposed by the governments of the United Kingdom and the Dominions of the British Commonwealth. Religious, legal, political, and moral objections were raised.
As the British monarch, Edward was the nominal head of the Church of England, which at this time did not allow divorced people to remarry in church if their ex-spouses were still alive. For this reason, it was widely believed that Edward could not marry Mrs. Simpson and remain on the throne. As a twice-divorced woman, Mrs. Simpson was perceived to be politically, morally and socially unsuitable as a prospective queen consort. It was widely assumed (although not proven) by the Establishment that she was driven by love of money or position rather than love for the King. Despite the opposition, Edward declared that he loved Mrs. Simpson and intended to marry her as soon as her second divorce was finalised. The widespread unwillingness to accept Mrs. Simpson as the King’s consort, and Edward’s refusal to give her up, led to his abdication on 11th December 1936, and his brother, Albert, who became King George VI, took over as BELRA’s Patron.
King George warmed to his role as Patron by noting “The real greatness of a Nation is often shown by its regard for the weaker brethren, the poor, the afflicted, the blind, the deaf, the maimed.”
A further innovative fundraising vehicle during this year had been launched in the form of the Child Adoption Scheme, which raised funds for the treatment of children as in-patients of leprosy hospitals. This proved most successful and brought healing and happiness to many a child. It was known that leprosy attacked young children most easily, but if the disease could be caught at an early stage, the chances of a cure were very great. It was of the highest importance to separate infants from infected parents at the very earliest moment, for it was believed that the disease was not hereditary, and if they were taken away in time, they would remain uninfected. It was also considered desirable to bring children who had already contracted the disease under treatment as soon as they were found. There were, of course, many infected children who had no adult relations to look after them or who, through their relations’ fears of the disease, had been turned out from their families and were outcasts. It was with these things in mind that the scheme for the sponsoring or adopting of such a child by someone at home was started. The sponsor would make him/herself responsible for an annual payment of £5 which would be sufficient to maintain and educate the child while under treatment, until he or she became self-supporting. 52 Fortunately for BELRA, members of the 52 BELRA Quarterly Magazine, October-December 1962, p. 103
Royal Family were among the first to sponsor children in this way, and this gave great impetus to the scheme.
As Medical Secretary, Dr. Muir, began a further series of visits to Africa. On 14th April, 1936, he visited the Azare Leprosy Settlement in Nigeria, and suggested that they be amalgamated into the nearby Somaila Settlement. On 20th April, he visited the Garkida Leprosarium, which at that time was run by the Brethren of Christ Mission, and on 23rd April, he went to the Bauchi ‘Leper’ Camp. From 8th -14th May, he was at the Itu ‘Leper’ Colony and met the five Toc H men who had now completed their in-field training and were about to go to their individual postings. Will Lambert went to Somaila, working with recently found cases of leprosy who were physically capable of being directed into agricultural work and house building. Pete Pedrick went to Maiduguri, where life was a good deal tougher. Like Norman Crayford at Katsina, he worked with advanced cases, originally gathered in off the streets, less in an act of kindness than to remove a distasteful sight from the public gaze. Hamish MacGregor went to Itu, a town rather than a leprosy settlement, with its own school, church, law court and police force; and Len Parker was sent to Onitsha, a new settlement being started by Dr. T.D.F. Money. At the end of the year BELRA Layworkers John Stacey and Mr. Hockley, were sent out to Somaila to relieve the Toc H workers there for home leave, and in January 1937, BELRA Layworkers Norman Sced, of Dovercourt, and Fred Tuck, of East Dereham, sailed for Nigeria and more Toc H men went into training.
On 1st March 1937, Dr. Muir was formally appointed General and Medical Secretary at a salary of £700 p.a. and a Travelling Allowance of £50 p.a. – riches indeed.
On 10th March, 1937, whilst on leave, BELRA Layworkers Norman Crayford, Will Lambert and Pete Pedrick were again presented to H.M. Queen Mary at 42 Trinity Square, London, (right) the Headquarters of Toc H in the UK and, in the evening, they were welcomed by members of the House of Commons.
In May 1937 BELRA Layworker, John Stacey, handed over the settlement at Somaila in Northern Nigeria, to the Sudan Interior Mission, and he moved in July to Ogbomosho in the Oyo Province of Southern Nigeria to take charge of the ‘leper’ camp under the American Baptist Mission there.
Great news was announced in September 1937 when 87 patients were discharged from the Itu Leprosy Settlement. Amongst these were the head nurse of the hospital, and two of his staff. They went on to assist the mission in running a dispensary, and a baby and general welfare centre in their own town, which further helped to lessen the stigma of the disease.
On 9th October, 1937, a joint BELRA/Toc H training day on leprosy was held. Dr. Muir was the coordinator, and Len Parker, the Toc H layworker from Nigeria, and Mr. A.J. Cowell from BELRA, took the sessions. Ten days later, a new innovation came in the form of the BELRA Quarterly Magazine, which was introduced as a means of reaching far more potential supporters, and as a way of educating the general public about the work the Association was doing in the field of leprosy, and
about the disease itself. The first edition noted proudly that ‘The Governor-General of the Commonwealth of Australia had honoured the Association by becoming one of its VicePresidents.’ But part of BELRA’s function was to promote educational propaganda in the British Isles, in order to arouse the public conscience to a full understanding of leprosy. The new BELRA Quarterly Magazine of January 1938 noted:
Now it is well known that things learned through the medium of ‘eye-gate’ are much more thoroughly absorbed than facts obtained in other ways, so BELRA has produced a colourful and fascinating Educational Exhibition.
This Exhibition is called “The Shadow on the Orient,” and is a vivid attempt to portray one of the greatest stains on our civilization, and it has been planned to bring home to every patriotic citizen his duty towards that vast mass of suffering humanity throughout the British Empire.
Already the Exhibition has met with instant success in the towns it has visited. A successful effort, of course, needs the full co-operation of all local Churches, Rotary Clubs, Toc H, L.W.H, [League of Women Helpers] Inner Wheel, Y.M.C.A., etc., and enquiries will be welcomed by the Secretary at 131 Baker Street, W.1, from whom all details and literature can be obtained.
A very successful Exhibition was held at Bristol in September last, and over 3,000 people attended. It was opened by the Duchess of Beaufort. Equally successful showings were at Sheffield and Huddersfield in November and December. 53
Again, BELRA’s offices proved too small for the wealth of medical and administrative material, and the Association moved into larger premises just down the road at 115 Baker Street in September 1938 (at the time of the Munich crisis) 54
The year saw a flurry of new layworkers travelling to leprosy settlements, and in March 1938 Dr. James Ross Innes and Sir Alexander Waddell, KCMG, 55 56 undertook a leprosy survey of the British Solomon Islands. Sadly Dr. Ross Innes was forced to end his survey in April due to contracting malaria. One of the many perils faced by doctors and workers overseas.
A new and innovative fundraising source was discovered by means of radio, and in June, 1938 a broadcast appeal by the BBC Broadcaster Christopher Stone dramatically raised the annual income from £7,000 to £20,000. The appeal received support from all quarters of the Empire; even from Kashmir and Assam, and Yatung in Tibet – from the British Trade Agent there. 57 An editorial on the appeal noted:
53 BELRA Quarterly Magazine, January 1938, p.9
54 September 29th–30th, 1938: Germany, Italy, Great Britain, and France sign the Munich agreement, by which Czechoslovakia had to surrender its border regions and defences (the so-called Sudeten region) to Nazi Germany. German troops occupied these regions between October 1st and 10th 1938.
55 (1913-1999) Colonial Secretary in Gambia (1952-1956) and Sierra Leone (1956-1960)
56 KCMG – Knight Commander of the Order of St. Michael and St. George
57 BELRA Quarterly October 1938, p. 43
On Sunday, June 19th, through the courtesy of the BBC, Christopher Stone made a very moving appeal on behalf of the BELRA. In his speech Mr. Stone begged for the help of all his listeners in the great crusade for eradicating leprosy from the British Empire. He said “Father Damien was not the only martyr…At this moment there is a big organization ready and able to abolish leprosy from the face of the earth, if the funds are forthcoming; men and women devoting their lives to it; that great brotherhood, Toc H, has twelve young men – heroes – out there now in the jungle settlements, and dozens more waiting eagerly to volunteer if the money to send them out can be raised. It’s a noble crusade and a winning cause.”
Mr. Stone then explained how BELRA, supported by Colonial Governments and Medical Authorities, with H.M. the King at its head, exists to co-ordinate efforts, organize research, and collect funds. “Toc H,” he said, “works with it wholeheartedly. Last year 208,000 doses of life-saving anti-leprotic drugs were sent, and that’s something – but awfully little, really, when you know that there are three million lepers, at least, and that each one needs two injections per week for several years, and when you know that at last, after all these centuries of horror, lepers can be cured, and leprosy stamped out; this is a holy war if ever there was one.”
The response to this appeal was overwhelming. Mailbags packed full of letters arrived by every post, until the office staff found themselves quite unable to cope with it alone, and friends were hastily called in to open envelopes and count money – the work went on from early in the morning until late at night in an endeavour to keep pace with the incoming sea of letters. Deeply touching was the spirit of sacrifice with which men and women of small means showed their wish to help those so much poorer than themselves. It could not have been easy for many people who sent us stamps and postal orders to have spared what they did, and we can only say, as Christopher Stone did, “All that we send into the lives of others comes back into our own.”
It was also very gratifying to receive the messages of friendliness and goodwill which so often accompanied the money, and to know that as a result of the appeal a far wider section of the public has become acquainted with the work which is being done by BELRA in the campaign against leprosy. The sum received amounted to just under £9,000, and we shall now be able to send six more lay workers “into the field” on their errand of mercy. 58
But June was not good for everyone. Torrential rain flooded Southern Rhodesia and severely disrupted the work at the Ngomahuru Leprosarium where BELRA Layworker, William Densham was working. He wrote home:
“At the moment we are in rather a nasty plight in Southern Rhodesia owing to the worst rains for many years. The whole country is flooded. The pump, by which we get out water from the river, was completely smashed - £600 worth under water. The railway is washed out, and we have no food for the patients. I expect some will desert soon. The lorry, trying to bring the meal from Fort Victoria, turned on its side in a bog, and the mealies are now all in the water. Our runner brought the post through today, although
58 BELRA Quarterly October 1938, pp. 37-38
I don’t know how he did it. I spent three hours yesterday endeavouring to get an engineer across two flooded rivers, so that he might repair the pump. We managed it, but it was hard, wet work.” 59
In July Dr. Frank Davey and BELRA Layworker, Albert Sowden, visited four ‘leper’ villages in Uzuakoli. Dr. Davey noted:
“The Chief told us there were 113 lepers, but, as we saw many more than that, he was obviously lying. We discovered that they had been cast out and allotted land on which to build and farm, but nothing had been done as regards treating them. When we asked what happened to those too ill or incapable of working, the Chief replied with a shrug of his shoulders, ‘Many die’!” 60
However, on a happier note, BELRA Layworker, John Stacey wrote home to say he had shown films to his ‘leper’ inmates, most of whom had never seen a film before, and they were thrilled by the experience.
Celyn Evans, Local Secretary for BELRA in North Wales, sailed for Zaria, Nigeria, to take over from Will Lambert, and new recruit William Walter went to Uzuakoli where he was in charge of the dispensary, Scouting and experimental agriculture – layworkers were men ‘of many parts,’ and did so much to ease the burden carried by the doctors.
By the end of 1938 BELRA had one nurse and 19 lay-workers in the field, at a total outlay of £12,280. 61 (Ten years later the cost had risen to £15,250 for one doctor, three nurses and 17 others; while BELRA’s total overseas expenditure (including research and child adoptions) reached £25,300, compared with £13,670 in 1938. 62) All seemed in place for the Association to flourish as never before. At home, order and efficiency reigned in the new offices and funds were at a record high. A new General Secretary, Mr. J.R. Martin, was appointed in 1939.
However, on 3rd March, 1939, a tornado wreaked havoc in the Itu Leprosarium. Frank Bye, BELRA Layworker wrote:
The other evening a heavy tornado did considerable damage to the colony, which met the full force of the wind. A block of new patients’ quarters that I have just completed were rather badly knocked about. The roof was torn solidly from the joists and timbers, and was hurled into the bush. Much of the corrugated iron roofing was completely destroyed. When I tell you that the roof, nearly 80 feet long, was wrecked like this, you can imagine that the tornado was no summer breeze! Several of the banana, orange, and papaw plantations were levelled, with not a tree left standing. It was as though a tank had passed that way. The main administration building, containing the offices, dispensary, and stores, lost its roof, and was lifted clean, with pillars, from the concrete bases, and heeled over at an angle of about 60 degrees. The
59 BELRA Quarterly July 1939, pp. 8-9
60 BELRA Quarterly July 1938, p.28
61 BELRA Quarterly, January 1950, p. 1
62 BELRA Quarterly, January 1950, p. 1
roof of a small brick-built produce store was hurled in one piece for nearly 20 yards! I am now trying to clear up the mess, and what a mess! 63
On a less dramatic note, the question of compulsory segregation of those with leprosy was prominent again at BELRA’s Annual General Meeting in 1939:
Two things, both in the Annual Report and in Dr. Muir’s more detailed reports of his various visits, stand out and are emphasized – the futility of compulsory segregation, and the value of social work. Such experience as I have had bears out these two theories. Voluntary segregation is far more effective than coercion, and unless you keep the patients happy and contented with occupation, recreation, nutrition, and decent conditions of life generally you will not be very successful with your injections. Only this year I saw a remarkable example of that at Ngomahuru, an ideal leprosarium in Southern Rhodesia, where, over a period of the last 10 years, the number of patients discharged reached the almost incredible annual average of fifty per cent. This very week I had a letter from the Superintendent there in which he said, ‘It is believed at Ngomahuru that no case can be considered as incurable until it has been given a good trial. It is quite impossible to say beforehand whether a case will react to treatment or not. Some of the apparently hopeless cases have got well.’ (Sadly, the writer was unnamed).
However, the leprosy sufferer’s ‘Dawn of Hope’, the period of BELRA’s consolidation, was soon to be threatened by the gathering clouds of another war, but the worldwide upheaval was also to coincide with the most significant advance in the history of leprosy treatment. 64
63 BELRA Quarterly, April 1939 p.7
64 LEPRA News No. 13, Spring 1974 p. 2
CHAPTER FOUR
War – a ‘Wonder Drug’ – and “the greatest step that has ever been taken in the history of colonial medicine” - 1939-1945
The onset of war in 1939 curbed the progress of anti-leprosy work in the field. Territories in which programmes of treatment and research were going on fell into enemy hands – some staff returned home to join the forces. The structure of the work was therefore severely shaken, and became a casualty of the hostilities far away from the firing line. Many volunteers did remain at their posts, but the emotional conflict was great. Many felt that unless the war was won, the work of the Association would inevitably end. Others tried to enlist locally, to be turned down on the grounds that they were too useful where they were. Staff in the UK were reduced to almost half in the last four months of the year as a measure of war economy, and those who were left worked harder than ever for the cause.
In February 1940 Dr. James Logan arrived in Uburu, Nigeria, after sailing from Liverpool during that period of the Second World War designated the ‘war of nerves ’ The MV Accra on which he sailed was torpedoed and sunk not long afterwards. Dr. Charles Ross sailed for Uzuakoli on 19th March, to take up his post as the second BELRA doctor there, and in May, Celyn Evans, the BELRA worker at Zaria, in Nigeria, joined the R.N.V.R. as a sub-Lieutenant, where his previous service in the Mercantile Marine proved very useful. In August, the entry of Italy into the war brought Cyprus into the centre of active operations in the Eastern Mediterranean, and John Stacey joined the local forces there.
Back at home, ideas to spread the Child Adoption Scheme appeared in the April 1940 issue of the BELRA Quarterly Magazine:
Would you like to give a child health and happiness? Would you like to play fairy godfather or godmother to some small child who might otherwise grow up maimed and despondent? BELRA has arranged an adoption scheme whereby the admission to, and keep and treatment of a leper boy or girl in a Nigerian settlement can be secured for the sum of £2/10/0 a year, and the child thus rescued from what might be a living death. Sunday Schools, The League of Women Helpers, and other groups, as well as generous individuals, have taken up the idea with enthusiasm. The illustrations…show some of the adopted children, and are good proof that these little ones can be made strong and well with your help. 65
Surprisingly, income increased during the war years, helped by the Adoption Scheme; by the end of the war annual income had reached over £38,000.
On 28th September, 1940, a bomb in Baker Street made the office unsafe for occupation and it therefore had to be evacuated. All the belongings of the Association were moved to a room
65 BELRA Quarterly Magazine, April 1940, p. 11
in 25 Kidderpore Avenue, Hampstead, the home of the General Secretary, Mr. Martin, which became, for a while, the official headquarters. The BELRA Quarterly carried details of the event:
“…two days before the last number of the BELRA Magazine was due to appear, the office in Baker Street was bombed, and a direct hit, by what was evidently a heavy bomb, completely demolished an extension of the building at the back. The adjacent wall of the main structure and its windows were wrecked, and debris crashed into and littered the rear rooms of the office. Fortunately, the incident took place at night when there was no one in the premises so there were no casualties, and fortunately also, the damage to our office equipment and other property was very slight. The work was transferred to, and quickly resumed, at our new temporary address given on the cover [25 Kidderpore Avenue] and will be continued there for the present. It is regretted that the last issue of the Magazine reached readers rather late owing to this unfortunate happening.” 66
In October 1940, the BELRA Quarterly carried the following Editorial:
We write on the anniversary of the outbreak of the war. The year that has passed has brought with it many trials of faith and endurance, but has not been without its triumphs. Looking back on it, BELRA, and the cause for which it strives have much to be thankful for. At its outset the Association determined that as far as lay in its power the struggle against disease and distress which it conducts should go on. It pledged itself to do its utmost to maintain the fight against leprosy, and to continue to help our fellow subjects in the colonies afflicted with this disease.
With the loyal support of its friends, this pledge has been kept, and not a single worker has been withdrawn from the field because of financial necessity. It is unfortunately true that contemplated extensions of work abroad have had to be postponed, in some cases because other authorities concerned were not in a position to undertake their share of responsibility, or because trained workers were not forthcoming. Nevertheless, in the current year three new doctors have been sent out and one Toc H lay-worker recruit is at present preparing to proceed to Nigeria. On the other hand, some lay-workers have felt that their duty lay, for the time being, in the armed forces which are contending against the moral and physical dangers which threaten to overwhelm the world. These workers the Association readily released, feeling, as one of them said, that unless the war was won its work would inevitably end. This work goes on in the spirit described by the Chairman of the Executive Committee of the Association at its Annual General Meeting: “We treat the victims as human beings, and not as mere economic chattels, we endeavour to convince them that we do not regard them as outcasts, and we ever maintain that spirit of freedom which is the essence of our Empire and which has contributed so much to the united front which our Empire shows today.”
67
Also in 1940, Dr. Muir, the Medical Secretary, departed for the West Indies. The war had prevented his undertaking a tour of the colonies in that part of the world which had been
66 BELRA Quarterly Magazine, January 1941 p. 1
67 BELRA Quarterly Magazine, October 1940, p. 1
planned to start in the spring or early summer. Dr. Muir went, at the request of the Colonial Office, to take charge of the important leprosy settlement at Chacachacare in Trinidad, with permission to carry on, at the same time, his usual work of leprosy inspection, survey and advice, in the West Indies and the British colonies in South America. It was hoped that he would be able to visit some other countries in that continent, from which invitations had reached him with a view to securing the benefit of his experienced help and counsel. As this work was due to keep him away for 18 months. Sir Leonard, the Honorary Medical Adviser, kindly agreed to carry on the Medical Secretary’s work at headquarters for this period. 68
But it was not only the war that took its toll. In October 1940 a group of 50 women, fearing the establishment of a clinic at Orifite, in Nigeria, knocked down the walls and destroyed the thatch. Dr. Money, the Superintendent of the area, took the opportunity to deliver a lecture on leprosy control. The offending women were dealt with by a native court (although we were not told what happened to them.)
There were celebrations when BELRA’s Nursing Sister, Miss Dorothy (‘Dotty’) Jordan, Nurse at Kumi in Uganda, was awarded the MBE 69 in the New Year’s Honours List. This was presented to her by Sir Charles Dundas, Governor of Uganda. The following year Dr. F.G. Rose, of Georgetown, Guiana, was awarded the OBE 70 in recognition of his leprosy work at the Mahaica Leprosy Centre there.
But sadness was never far away, and whilst returning home on leave from Nigeria in 1941, Frank Bye (left), who had been sent out as a Toc H volunteer in 1937, and had been working at Zaria, was killed by enemy action on 18th April, 1941, when his ship was sunk. Work in the Owerri Province of Nigeria had to be halted as there were insufficient staff to undertake it; there were 43 clinics and 11,500 registered patients, and the number was rising steadily. Then, on 8th January 1942, Japanese troops invaded and occupied the Sungei Buloh ‘Leper’ Hospital in the Federated Malay States. Dr. Gordon Ryrie (right), the Superintendent there, refused to leave his patients, and was later transferred to a concentration camp Dr. Muir also lost his son through enemy action at sea in 1943.
An article in the Western Australian of 23rd June, 1945, declared:
Recently in a list of some of those civilians reported in an Internee camp in Singapore appeared the name of Dr Gordon Ryrie, medical superintendent of the leper settlement at Sungei Buloh, FMS 71 It seems Scots have always figured prominently as Britain’s ‘unofficial ambassadors.’ Here was another of them doing a really grand job.
68 BELRA Quarterly Magazine, January 1941 pp.1-2
Years of devoted service among those afflicted with the scourge of leprosy had made Gordon Ryrie a combination of guide, philosopher, friend and ‘family’ physician to thousands of unfortunate people. When the Japs invaded Malaya, it was soon evident that certain institutions could not be evacuated further south. The leprosarium at Sungei Buloh was one of these.
As the tide of battle flowed against us those Europeans not in the services or in some administrative positions moved back to Singapore Island. Dr Ryrie did not come with them. Perhaps he hoped to be allowed by the Japanese to carry on his good work among those to whom his guidance meant so much. An interesting feature of Sungei Buloh is that despite the fact that it is only twelve miles from the capital of the FMS, Kuala Lumpur, its only walls are the densely forested hills and ravines one finds in this part of the peninsula. The model settlement for such it is provided a home for approximately two thousand lepers, a small fraction of the three million said to inhabit the globe. This large family of Chinese, Indians, Malays, Javanese, Thai, Eurasians and others was able to live in complete harmony, despite differences in language, religion and customs. Their common bond was the fetter of leprosy which forced them to a period of isolation in a number of cases whole life.
Prior to the completion of the settlement which brought with it a great improvement in conditions, quite a number of lepers contrived to escape from the old leprosarium. Many of these lapsed into a life of crime, or else spent what little money they had on useless quack remedies. Later the leper began to realise he was better able to prepare for his reception into society again by remaining with those who had his welfare so much at heart. Attempted escape became a rare occurrence. Along with his drug therapy, Dr Ryrie knew it was necessary to secure a genuine understanding of the psychology of the leper. His special gifts of enthusiasm and sympathy enabled him to have his patients fight their disabilities, and look forward to the day of their possible release. The leper was made to realise he was the victim of a serious disease, not a horrible unclean animal to be shunned by his fellow men. The order was “don’t cringe!”
The leprosarium had its township centrally situated amidst farm lands, where lepers were encouraged to cultivate fruit trees and vegetables, and breed pigs and poultry. There were sports grounds for those able to participate, clubs and reading rooms, and a number of schools for the children. To minimise the likelihood of the disease spreading outside as a result of handling paper money used in the settlement, special currency notes were placed in circulation. Besides being taught elementary hygiene, the lepers were informed what symptoms of their disease to watch for, and the degree of relief they might expect from treatment. The education programme was designed to fit the leper to take his place in the world outside when and if he was pronounced cured with the least possible embarrassment.
A number of cases of early leprosy were discovered in routine examination of schoolchildren of nearby towns and villages. By isolating and treating the sufferers of the disease in its early stages quite a high percentage of cures were recorded. Besides being medical superintendent, Gordon Ryrie was registrar of births, deaths and marriages, a judge of the divorce court, and chief police officer of the small but efficient police force recruited from among those lepers of good physique.
Roll on an invasion of Malaya. May Dr Ryrie be released soon to carry on his merciful work. 72
But, undeterred by all this, or perhaps even inspired by it, on 4th October, 1942, work began on the Makete Leprosarium in Tanganyika, and it was officially opened by Miss Joan Whittington, OBE, Overseas Director of the British Red Cross Society and a member of the BELRA Executive Committee, in the presence of Lady Twining, Dr. Liston, the new Director of Medical Services for Tanganyika, and Sir Charles Matthew, Chief Justice of Malaya who, as Chairman of the Tanganyika Red Cross four years previously, had been, with Lady Twining, most active in forwarding the project.
In April 1943, Dr. Cyril Wallace (right with his wife Linda) took over the Makutupora Leprosarium in Tanganyika
In his book The Flags Changed at Midnight, Michael Longford gave an insight into the problems of racial prejudice that Cyril and Linda Wallace faced in their work:
…One of the other medical establishments in Rungwe District was [also] run by a person of mixed race. Cyril Wallace was a fully qualified doctor who was also an ordained Anglican priest. He was in charge of a large and well-managed leprosarium at Makete. Cyril and his assistants gave loving care to a few hundred lepers, many of whom were disfigured and evil-smelling. Cyril’s father had been a doctor working in the Caribbean, and had there married a black woman. Cyril had graduated at a British university and qualified as a doctor. His wife Linda was Egyptian by birth, and a Coptic Christian. They had no children. Cyril had the rank of Medical Officer and was on a much higher salary scale than William Manning [another mixed-race doctor], but he was not eligible for membership of the Rungwe Club. Like William Manning, Cyril Wallace was also awarded the MBE for his exceptional work, but he died of cancer soon after the award was made.
The Wallaces were on home leave in Britain when I first arrived in Tukuyu, but I met them both soon after they returned. They were very hospitable people, and we often visited each other’s houses. One Sunday, I was having lunch with them at Makete when
72 From the Western Australian, 23rd June, 1945, entitled ‘Man Against Death’
Linda started to talk about the suffering that the colour of their skin had caused them. She gave as an example the air journey that they had recently made from Britain to Dar es Salaam. The plane had developed a fault in Nairobi, and the aircrew had told all the passengers that they would not be able to continue the journey until the next day, but that accommodation had been booked at the airline’s expenses in one of the best hotels in Nairobi. When Cyril and Linda reached the hotel, however, the white girl at the reception desk absolutely refused to admit them. Linda and Cyril had called the girl’s attention to a blackboard behind the reception desk, where the names of guests were entered beside the appropriate bedroom numbers. The notice-board indicated that room 23 had been reserved in the name ‘Dr. and Mrs. Wallace’, but that made no difference to the hotel’s policy. After trying unsuccessfully at a number of other hotels, the Wallaces had eventually spent the night in the airport waiting-room.
I expressed my horror at the way they had been treated, and Cyril said then that they were both devoted to children, but had decided before they got married that they would never have a family of their own, as they did not want to bring children into the world to suffer in the way that they themselves had suffered. I should have expressed myself more diplomatically, but I told them that I thought it would be a privilege for any child to have parents like them, and that I felt their decision had been understandable but misguided. Linda then began to cry gently, and Cyril put his arms round her and kissed her. I too found this visit a very painful one, but it did not harm our friendship. 73
It is almost unthinkable today, that because he was of West Indian blood, Dr. Wallace was not allowed to stay in the hotel in Dar es Salaam, when he and his wife first arrived in the country, especially since he was there to help those inhabitants who were suffering from leprosy.
In May, BELRA Layworker, Fred Tuck, informed Head Office that the 100,000th patient had been enrolled. However, war conditions meant that a brake had to be put on developments due to petrol rationing.
On 23rd April, St. George’s Day, a broadcast appeal in the ‘Week’s Good Cause’ series was made by Dr. Macdonald from Itu Leprosarium. It was only a five-minute appeal, but it had a great impact on its listeners:
73 Longford, 2001, pp. 36-37
Good evening! Leprosy is not a pleasant word. To most of us it suggests something ugly and fearful but, thank goodness, remote. In Eastern Nigeria, where I live, leprosy is by no means something remote; in fact, more than a thousand lepers are living less than a mile from my home.
Don’t think that a modern Leper Settlement is a place of hopelessness and despair. It is very different from that. Just try and picture our Settlement. Come with me on any morning and you will be impressed by the atmosphere of cheerfulness. If you look at the crowds waiting their turn at the treatment building you will find little evidence that they are lepers, beyond of course, the sad signs of the disease on their bodies. Patience and good humour abound. It is the same wherever you go. Even the hospital, reserved for the worst cases, looks a place of hope with its white walls in their setting of lawns and flowerbeds.
From the hill on which it stands you can get some idea of the size and the scope of the Settlement. Before you is the Church, beyond it the infant and primary schools, then the ulcer treatment building and finally the communal feeding centre. Away to the left you see the sports field and the roofs of the industrial buildings. To the right there are separate homes for children, old people and cripples. Flanking all these are the model towns where able-bodied patients live a normal and busy life. Now for the other side of the picture. In my corner of Nigeria, for every patient in the Settlement there are seventy outside. Think of it! 75,000 lepers. I know many African villages where one person in every twenty is a leper. It is impossible for me to describe to you the misery and degradation of these unfortunate people who, in their neighbours’ eyes are outcasts both from society and religion.
During recent years it has been possible to help some of them. In our Province alone, 14,000 are being treated every week at out-patient clinics and many are willingly isolating themselves in model leper village communities. Every year hundreds are being discharged, free from all signs of the disease. The Native Administration does what it can and Governments are sympathetic, but Nigeria and most parts of the Empire where leprosy prevails are very poor. What we have done would have been impossible were it not for the British Empire Leprosy Relief Association (BELRA for short) which works with Toc H, and has sent us a doctor, a nursing sister and four Toc H lay workers to assist at our settlement.
All that I have said so far relates to one corner of Nigeria. In other parts the same sort of thing is going on. Look wider afield. There are over two million lepers in the British Empire today. Many of them could be useful citizens if given the chance. Sufferers are clamouring for help and have to be refused it. Volunteers are eagerly awaiting the opportunity to give it. BELRA needs the funds with which to send them.
Money goes a long way when dealing with leprosy. From five to ten shillings will cover the cost of essential drugs for treating a patient for a year. In Nigeria £3 will give a leper a chance of a lifetime and keep him in a settlement for a year.
However much or little you can send it will all help. Won’t you have a hand in this work? It stands for a world of new hope for somebody. 74
On 25th June, 1943, the ‘lepers’ at Sungei Buloh, Malaya, now prisoners of the Japanese, listened to the BBC on their forbidden radio – a lifeline. Whether they heard the appeal by Dr. Macdonald is not known, but we know from Dr. Ryrie that the radio was extremely important to them. If they had been caught with it, it would have meant instant death for them, but their need to keep in contact with the outside world was paramount, something we today take for granted.
In the spring of 1944 BELRA again moved offices, this time to 167 Victoria Street, London. There were further staff movements too. Dr. Bob Cochrane was appointed the first Honorary Director of the Leprosy Campaign in the Madras Presidency, in India, and in November 1944 BELRA Layworker Albert Sowden was transferred from Lui in the Sudan to Mbabane in Swaziland to establish and supervise a new settlement there, and Dr. Charles Ross took over the running of the Uzuakoli Leprosy Centre in Nigeria. Things were beginning to move to establish more centres to tackle the disease.
Leprosy Elimination? Dapsone – the ‘wonder’ drug
In Nigeria in 1944 “…the greatest step that has ever been taken in the history of colonial medicine” was announced. That step was the implementation of Dr. Muir’s programme of leprosy control which had been postponed due to the war. The Colonial Development and Welfare Fund granted a quarter of a million pounds for a 5-year programme, which dove-tailed nicely onto the work of the Nigerian branch that Frank Oldrieve had established on his first visit there. Dr. Frank Davey, introduced by Dr. Muir to the new drugs, was to head the scheme, but it was the research aspect that BELRA was asked to finance, and for which it was necessary to find the right man. Dr. John Lowe, (right), who had succeeded Dr. Muir when he took office as General and Medical Secretary in 1935, had left India and BELRA’s service in 1943. The fact that he was available in 1944 was sheer good fortune, not only for BELRA, but for the leprosy world as a whole
BELRA Layworker Will Lambert was awarded the MBE 75 in the 1945 New Year’s Honours list, but sadly on 31st January, Sir Frank Carter, one of BELRA’s founding members, died at Wargrave in Berkshire aged 80. He had been Treasurer of the Association for over 20 years. His funeral was held on 5th February at Stubbings Church, Pinkney’s Green, Maidenhead. The notice read ‘No flowers, but donations to BELRA, 167 Victoria Street, SW1 (Indian papers please copy.)’
74 BELRA Quarterly Magazine, May 1944 pp.5-6 – This appeal raised £599 10s 2d
75 Member of the Order of the British Empire
In 1945, as in the five years of war which preceded it, the conditions made progress in antileprosy work difficult, both at home and abroad, but a vigorous 21st Birthday Campaign, designed to publicise BELRA’s work and raise funds, gave a new impetus to staff. The campaign was launched at a Mansion House meeting on 26th April, entitled ‘The Coming of Age Campaign.’ Financially the results of this were disappointing, but much valuable work was done in making the situation with regard to leprosy in the Empire generally known in Britain.
At this time, Dr. Muir was still in the West Indies, working on ‘A 5-year Plan for the Control of Leprosy in the Colonies,’ and learned of the developments with a new drug – Diacetyl Diaminodipenyl Sulphone (DDS) or Dapsone. He reported to the Committee that “…there seem to be good grounds to hope that it may prove a valuable addition to the weapons available against leprosy and be effective in advanced cases which chaulmoogra oil fails to improve.” He returned to England in the same year, and met with Dr. Frank Davey on leave from Uzuakoli, in Nigeria, and showed him the Dapsone samples he had brought with him, which Dr. Davey took back to Africa to try on his patients there. He found the sulphone derivative useful and ordered more, receiving supplies of the sister drug sulphetrone. Frank Davey later became the Medical Secretary of the Methodist Society, but was also an active member of the BELRA Medical Committee.
1945 was also a busy year for Dr. Cochrane who was now working in the Christian Medical College in Vellore, South India, but on a fundraising visit to Belfast he made an important discovery. In a public meeting, where he was describing the dazzling array of drugs now available to the medical world, he fell into discussion with a member of the audience who was familiar with Dapsone, but not in its application to leprosy – he knew it as a treatment for mastitis in cows. Dr. Cochrane noted that the cows, who appeared very healthy indeed, were being treated with pure Dapsone and not one of the derivatives. He returned to India impatient to try out this new possibility.
Of all the methods of application available to him, he chose the injection, and was delighted to find that the reduction in the number of bacilli in the patients was dramatic. Eagerly he published his findings, faithfully recording the problems as well as the achievements. He sent a sample of Dapsone to Dr. David Molesworth, who had taken over at the Sungei Buloh settlement in Malaya after Dr. Ryrie’s release. Dr. Molesworth had been given no indication of the dosage, but in his desire to spread any possible benefits amongst the largest number of patients, he selected a hundred and divided the available supply so as to maintain them on a course of injections. As a result, each patient received very little Dapsone. This time though, the results were even more interesting, because due to the lower dosage, Dr. Molesworth noted benefits without harmful effects. Publishing his findings, he set off a chain reaction of research into Dapsone to find the correct dosage that would give no side-effects at all.
On 11th November, 1945, Dr. Gordon Ryrie, late of Sungei Buloh Leper Hospital in Malaya, who had suffered so much at the hands of the Japanese, arrived in Southampton from Colombo on the Athlone Castle; his wife, who had gone to meet him, did not recognise him as he had changed so much.
CHAPTER FIVE
New developments, but crumbling Empire, 1946-1956
At the end of the Second World War, attitudes and priorities changed dramatically in the world. Countries formerly under British control were agitating for independence, rival factions in various countries were jostling for control as Britain began to step back from its former colonial approach. However, its concern for its colonies didn’t waver, and BELRA stood staunchly by those who needed its help.
The year 1946 found BELRA with new requests for help. The BELRA Research Unit began working alongside the Government Medical Department in Nigeria. In March, Nursing Sister Rose Stinton joined BELRA and sailed for Nigeria, going into leprosy work through the Colonial Development and Welfare Scheme. BELRA was also requested to provide a doctor and two Layworkers for Sierra Leone and Nigeria, and surveys were carried out in the Gold Coast, Gambia and Nigeria. Celyn Evans, now returned to leprosy work after the war, was appointed Government Leprosy Officer in Cyprus, and Nurse Gladys Tarling sailed for Oji River in Nigeria.
On March 25th, 1946, the Leper Colony Sub-Committee of the Lagos Council of Social Service in Nigeria, met Michael Smith, a member of BELRA, who was passing through Lagos at the time, and discussed with him the possibility of forming a local Branch. Later permission to do so was received from the Director of Medical Services and the first meeting of the Lagos branch of BELRA took place on Monday, June 24th, 1946. That September, the foundations for a welfare policy were designed at the Uzuakoli Leprosy Settlement in Nigeria with especial notice of physiotherapy for patients. Mr. Stanley Alderson, another BELRA Layworker, evolved a series of exercises for those with clawed hands, and in December, BELRA Layworker Leslie Corbridge, was sent to Luapula, Northern Rhodesia to assist William Densham.
At the end of the war, the Association opened its new office at 176 Victoria Street, and the following year, the General Secretary, Mr. J.R. Martin, resigned, and took his place on the Executive Committee like his predecessor. Mr. A.C. Edgar took over in what was to be a difficult and stormy tenure and, at the same time, Dr. Muir, returning from the West Indies, approached Dr. Gordon Ryrie to be Assistant Medical Secretary.
The Spring of 1947 was a busy one with romance firmly in the air. On 10th April BELRA Layworker, Lawrence Birnbaum, married BELRA Nurse Grace Tarling at Zaria, in Nigeria, and on 24th May BELRA Layworker Michael Smith (Biochemist at Uzuakoli, Nigeria) married Edna Manchée of BELRA Headquarters staff in London.
Robin Dunford was sent out for training as a BELRA Layworker to Itu, Nigeria, on 11th June, and on the same day, Mr. & Mrs. Fred Newton, BELRA Layworkers, sailed for their first tour of duty and joined the team at Uzuakoli, Nigeria, as permanent Welfare Workers, following the foundation laid by Stanley Alderson. Also in this year, Dr. John Lowe was appointed head of the BELRA Research Unit, joining Dr. Davey, who had established the overall project Dr. Lowe set to work, initially on the whole range of the new drugs, considering the methods of application and their effect. When Dr. Molesworth’s findings had pinpointed low dosage as
being the most effective method, research at Uzuakoli moved on to it and for the next year intensive work was done on refining the process. Unlike its derivatives, DDS in its pure form cost a trifling sum to produce. The prospects of finding a new drug for use against leprosy had been considered thin, and one that was cheap had been thought almost impossible. However, in 1949, BELRA’s 25th year, Dr. Gordon Ryrie, as the new Medical Secretary, announced that Dapsone was the new cheap and effective cure for leprosy, and optimism was running high in the UK that if only sufficient funds could be found to provide the drug to all sufferers, elimination of leprosy within the Empire was feasible, and within sight.
But the Empire was not in a happy situation. On 14th August, 1947, the independent state of Pakistan was founded and, the following day, India gained its independence and became a Sovereign Nation. But the process of partition led to immense loss of life.
‘Partition’ – the division of British India into the two separate states of India and Pakistan –was the ‘last-minute’ mechanism by which the British were able to secure agreement over how independence would take place. At the time, few people understood what Partition would entail or what its results would be, and the migration on the enormous scale that followed took the vast majority of contemporaries by surprise. Partition triggered riots, mass casualties, and a colossal wave of migration. Millions of people moved to what they hoped would be safer territory, with Muslims heading towards Pakistan, and Hindus and Sikhs in the direction of India. As many as 14-16 million people may have been eventually displaced, travelling on foot, in bullock carts and by train. Estimates of the death toll post-Partition range from 200,000 to two million. Many were killed by members of other communities and sometimes their own families, as well as by the contagious diseases which swept through refugee camps. Women were often targeted as symbols of community honour, with up to 100,000 raped or abducted. What can explain this intensely violent reaction? Many of the people concerned were very deeply attached not just to religious identity, but to territory, and Britain was reluctant to use its troops to maintain law and order. The situation was especially dangerous in the Punjab, where weapons and demobilized soldiers were abundant.
On the other side of the world, in relative peace, Dr. Gordon Ryrie was officially appointed Medical Director of BELRA in 1947, and on 24th September he left for a tour of the Nigerian leprosy work. BELRA Layworker, Walter (Wally) Leach, went with him to support and help him as he was still so weak after his time in the Japanese concentration camp. Dr. Charles Ross was appointed Medical Superintendent of the Rivers Area of the Nigeria Leprosy Service.
Following India’s independence, it was felt, politically, that a new regime was necessary which would reflect not only in name, but also in spirit, the changes that had come over the country With this in mind, a Resolution was passed at the first All-Indian Leprosy Workers’ Conference in Wardha in November 1947 as follows:
While appreciating the work done by the Indian Council of the British Empire Leprosy Relief Association, this Conference is of the opinion that in view of the present political developments in that country, the title and the constitution of the Association should be suitably changed.
Therefore, the Indian Council of BELRA handed over its assets to the newly established Association, known as Akhil Bharat Kushta Smitit. This Association was to carry on and consolidate the new spirit generated at the Wardha Conference and to prepare for the transformation of the Indian Council of BELRA into a new body.
Another new initiative at this time was the introduction of the ‘BELRA Exhibition’ – a set of moveable artefacts that could illustrate the work that the Association carried out in Africa. Thatched huts could be re-created, and with photographs from the field, it gave the British public an insight into what BELRA was doing, and the challenging conditions in which they worked. As an artist of some note, Wally Leach took charge of this new venture, and painted many of the backdrops that were used.
1948 broke with more sadness for BELRA. After his departure, from the organisation in 1928, Rev. Frank Oldrieve had had no formal connection with BELRA, although their paths occasionally crossed, so he had returned to missionary work in South Africa. Going back to Swaziland, he stayed for three days at Bremersdorp. On March 17th he set off for his headquarters in Pretoria, calling in to have a final talk with Mr. Sowden, a former BELRA employee. On arrival there he complained of feeling ill and went to bed; the following morning paralysis, after a stroke, had set in. He was taken to Mbabane Hospital by ambulance, where he became progressively worse, and passed away on the afternoon of Sunday March 21st. He was laid to rest in a little graveyard at Mbabane. Heads of Government departments, missionaries, Mr. and Mrs. Sowden, Dr. Flack and a few others joined with Mrs. Oldrieve and her daughters to mourn his loss. The BELRA Quarterly magazine noted:
He died as he had lived – thinking, planning and praying for those ‘without the camp.’ His remains rest on a lonely hillside, but it is our hope and belief that the seed planted in Swaziland will bear an abundant fruit, and that the plans he had for spiritual and physical relief to Swazi sufferers will be implemented by those who, with him, have been carrying the torch of hope to the sufferers in all lands. 76
In 1948 it was officially recognised that Dapsone, the sulphone drug in use for many years, was indeed effective against the bacillus which causes leprosy. Moreover, there were two advantages: it was cheap, and it could be taken easily by the patient in pill form. There was great confidence in Dapsone, and because treatment could be just as effective if carried out at home, and the Association decided to change from giving grants for buildings to money for Landrovers, whose quality and uniqueness at the time were universally appreciated.
Fundraising efforts were renewed with Sir Malcolm Sargent conducting the London Symphony Orchestra at a concert in the Albert Hall. The ‘BELRA Players,’ an enthusiastic group of Gilbert and Sullivan devotees, was formed under the Presidency of the Marchioness of Willingdon, with the objective of presenting a high standard of light opera and raising funds for BELRA. There was also a new hope that those suffering from leprosy would become more acceptable as the word ‘leper’ was banned at the International Leprosy Congress in Havana in April –something that BELRA had been calling for for many years. 76 BELRA Quarterly Magazine, July 1948 pp. 28-29 [Article by D. Hynd]
Dr. Gordon Ryrie, now returned from his overseas travel, became Editor of Leprosy Review. Dr. Cyril Wallace, was transferred to the Makete Leprosarium in Tanganyika where again, he pioneered its development into one of the best institutions in the country. But a record flood in the Itu Leprosarium led to the destruction of 45 houses, causing 250 ‘displaced persons,’ who were taken in by other ‘lepers’ in the settlement.
In its Silver Jubilee year in 1949, BELRA’s income totalled over £30,000, which was just as well, as on Monday 21st February the hospital at Itu Leprosarium in Nigeria, burnt to the ground due to an electrical fault, possibly because of a short in the electric wiring system above the ceiling in the upstairs ward. But despite this setback, the first group of patients were started on Dapsone here this year. A great boost for those with leprosy came on 9th June, when the Girl Guides of Mbabane, Swaziland, were invited to attend the King’s Birthday Parade – no ‘lepers’ had ever been invited to anything like this before, and this gave further proof that those with leprosy were the same as everyone else.
Sir Leonard Rogers, never entirely away from the Association’s affairs, and not at all from those of the Medical Committee, had not accepted the claims of Dapsone. He began a long campaign to establish a widespread control scheme based on chaulmoogra oil which he still believed to be the answer, going so far as to consult forestry experts on massive tree-planting schemes. When Dr. Lowe submitted his report on the first year’s work in Nigeria to the Medical Committee, Sir Leonard felt it was inadequate, and declared that the laboratory at Uzuakoli was not of primary importance in the fight against leprosy. This attitude set the work back in Nigeria quite considerably. The biochemist working with Dr. Lowe, found the atmosphere too strained and went to work for Dr. Cochrane in India. Dr. Lowe himself resigned in June 1949, and the Association’s Research Unit, where work had been completed to the point of establishing the method for using Dapsone, was taken over by the Nigerian Leprosy Service, for which Dr. Lowe continued to work.
Writing at the time of the 25th Anniversary in 1949, Dr. Cochrane entitled his notes on the period ‘The Dawn of Hope’:
“…if the formation of the Association had been the first glimmering of daylight on leprosy treatment and control, certainly the spirited activity of BELRA’s first ten years evened out onto a hopeful, if greyish, dawn. The chaulmoogra seeds which were the basis of Sir Leonard Rogers’ treatment had been sent to every country within the British Empire where leprosy was to be found. Further researches were afoot, particularly under Dr. Muir in India, and ‘leprosy control’ became a more current phrase in describing the day-to-day task of leprosy workers. But the medical advances, overshadowed by the ‘dapsone era’ may prove to have been incidental to the awakening of a new determination to deal with leprosy – a concentration of energies and skills which was a necessary forerunner of modern successes and achievements.”
Lady Willingdon, never far from the fundraising side of things, organised a Silver Jubilee sale and meeting at the Overseas League, Park Place, St. James’ Street, London on 8th November, and she organised several other events during the year.
Before the war, treatment relied almost wholly on hydnocarpus oil, which cost 10/- a year for each patient. By 1950 the use of sulphones, requiring £6 to £7, was widely extended.
The BBC ‘Week’s Good Cause’ appeal on the 15th January, 1950 was given by a ‘cured leper’. For several weeks the whole staff were engaged in dealing with the thousands of letters it evoked, and bringing to account the £12,918 12s. 0d. collected up to the end of March, when the fund was closed. This appeal was significant, in that it was the first time that the voice of someone who had had the disease was heard, and his story touched the hearts of so many, although, sadly, the public was not told his name. However, hearing the voice of someone who had leprosy ‘humanised’ him, and people could associate with the problems and trials that he was enduring, and feel great sympathy for his situation. He said:
You probably don’t know much about leprosy, and whatever knowledge of the disease you have was perhaps learned in childhood through Bible stories, or tales of the Middle Ages. Well, I was in exactly the same position, so you can imagine the shock when, three years ago, just after my demobilisation, I learnt that somehow or other I had contracted leprosy. How, will always remain a mystery.
Unfortunately, it is not a disease that you can discuss with others, and very soon I found that unconsciously I was cutting myself off from my friends. I had visions of being sent to some leprosy settlement and cut off from the world. I broke off my engagement, and all my future hopes and plans were shattered.
But very shortly after this I was put into the hands of the British Empire Leprosy Relief Association (known as BELRA); and it was there that I met doctors who had spent a lifetime in work among lepers. Here, at last, I was able to discuss my illness quite openly, and from them I regained confidence in the future.
The treatment in my case was very short – in fact, it was only a matter of a year before I was completely cured: and all the experiences of that period are today something like a bad dream. I can now again live a full and natural life. The girl I was to marry, after being told of my illness, has been fine enough to come back, so it is for her sake, more than my own, that I must remain nameless.
But I was one of the lucky ones. As a matter of fact, there are not very many lepers in this country: but in the British Empire there are some three million, of whom only one in ten can so far get any treatment.
BELRA and others are doing their best; they are providing doctors to supervise the leprosy settlements and the research work; they are sending out nurses to give hospital treatment and train local staff. Special welfare workers from this country are also provided to help the patients in their buildings, farms and handicrafts; to run the Scouts and Guides; and to take care of the children. For it is the children that leprosy attacks first; many tonight, from pain and misery, will fall asleep only when they have cried themselves into exhaustion. Without proper care they will grow up hideous and deformed.
Yet today none of this misery need exist, for with the latest drugs no case is hopeless. The cures are mounting, but are limited by the lack of resources. This means that many have to be denied the latest treatment, and doctors are forced to choose which patients shall be given a real hope of recovery. In one African settlement hundreds of children will very shortly have to be sent away unless further funds are available to cover their cost. We cannot, and will not let this happen. Many of them might be completely cured this year; and the cost is so small – only £10 a year is needed for the care and treatment of each child.
I am asking you to help save these children, and all those who depend on us. Won’t you put your hand in your pocket? Won’t you sit down and write a cheque or go out and buy a postal order or a book of stamps, and send along to BELRA (that is the British Empire Leprosy Relief Association, 167 Victoria Street, London, S.W.1). And thank you on behalf of us all. [Reproduced by courtesy of the British Broadcasting Corporation]
On 2nd February, 1950, Mrs. Marjorie Savory began work in the Oji River Leprosy Settlement, Nigeria, where her husband, Tarka, was the doctor. The Savory’s were devoted to Nigeria, but were ultimately to die there under tragic circumstances during the civil war.
On 13th February BELRA Layworker, George McKay, gave a talk after the Annual General Meeting in London, on work at the Ho Leprosy Settlement in the Gold Coast (formerly German Togoland) where he was currently working. This was something of a departure from the normal end of meeting speaker, and this was warmly welcomed as it informed participants of what was actually happening in the field.
In the April 1950 BELRA Quarterly Magazine it was noted:
Discharges from Uzuakoli exceeded one thousand last year, including ‘a significant number of sulphone patients who represent the first trickle of what will become a mighty flood.’ In parts of the Province Dr. Davey reports that leprosy is showing signs of dying out. He adds: “Times change. Until recently leprosy was such a social disaster that the very name of it was not spoken among our people unless absolutely necessary. They simply said that the patient was ‘sick’ without specifying the illness. This week the schools in the Settlement gave a breaking up concert, the major item of which was entitled ‘Leprosy – old and new’. It took the form of an impromptu play, lasting for about an hour, in which the children showed what happened to a person affected with leprosy in the past and in the present. It gave a wonderful opportunity for acting, and all the aspects of the Settlement were represented humorously, including treatment, and including Dr. Lowe and myself. Five years ago, such a thing would have been unheard of. Now they can laugh at it. The concert spoke volumes regarding the whole change in outlook that is coming over the people. There is no doubt that sulphone has contributed quite a lot to this, for one sees no despondent patients nowadays, except where sulphone treatment is impossible. 77
77 BELRA Quarterly Magazine, April 1950, p.29. Sadly the ‘myself’ in the article wasn’t named.
Dr. Harold Wheate, in East Africa, told the same story:
The results of modern leprosy treatment are most encouraging, and fully confirm the recent statement in the BELRA Quarterly that no case can now be considered incurable. The tragedy is that so few are sent here in the earliest stages of the disease, and some not until they have developed a permanent deformity of the hands and feet. I admitted a little girl the other day who had lost the sight of one eye – if her parents had sent her in a few years ago this could have been saved. It will take a long time to break through this barrier of ignorance but, as one of our African assistants always tells me, “Sir, they will learn.” Twenty children with the nodular type of leprosy are being treated with sulphetrone and all have shown dramatic improvement. Most of them have been here a number of years, and were going steadily downhill with little chance of cure. Now this new drug is no ‘lightning cure’; we expect that at least two years’ treatment will be necessary, and in some of these children probably more. But the extraordinary thing is that we can look forward confidently to the day when they will be cured. Only a few years ago such a thing was unknown. 78
On 28th April, 1950, the Governor-General and Lady Arden-Clarke visited Ankaful Leprosarium in Ghana to see the work of Dr. Alasdair McKelvie. Also, the research side of the work at Sungei Buloh Leprosy Settlement in Malaya, was strengthened by the arrival of Dr. F.S. Airey, an established dermatologist, under the Colonial Development and Welfare Fund.
In August, Lady Baden Powell, Head of the Girl Guides Association, on an overseas tour, visited the Guides from Oji River and Uzuakoli, in Nigeria. She later visited Mbuluzi ‘Leper’ Hospital in Swaziland and met Guides there – an unprecedented event, and still at Oji River, Janet, the Girls’ Compound Mistress, was discharged, symptom free but, because of the support and help given to her by the settlement, she chose to return to become Head of the Feeding Centre there, although she could have stayed ‘outside ’
It took about two years to fulfil the formalities involved in closing the BELRA India Office and to form the new Association called the Hind Kusht Nivaran Sangh (The Indian Leprosy Association). Appreciation of the work of BELRA in India was voiced at the All-India Leprosy Conference in Madras during October 1950 in a report presented by Sardar Bahadur Balwat Singh Puri, Hon. Secretary of the Hind Kusht Nivaran Sangh. The activities of BELRA had included research, surveys, propaganda, post-graduate instruction in leprosy, the publication of the quarterly journal Leprosy in India, and assistance in laying down policies for anti-leprosy work in the country. These had resulted in an increased knowledge of the incidence of the disease 79 and of its diagnosis and treatment. The Hind Kusht Nivaran Sangh, which had taken over the functions of the BELRA Indian Council would, no doubt, it was felt, be instrumental in further stimulating anti-leprosy work in the country. The HKNS began to function in earnest from 1950, with the President of India as its first President. BELRA’s association with India was now at an end…for the time being.
A survey of Kochirira in Nyasaland revealed some 30,000 cases of leprosy among a population of two and a half million, and with BELRA’s withdrawal from India, this seemed an important
78 BELRA Quarterly Magazine, April 1950 p.30
79 Estimated at the time to be one million
place in which to put its energies now. Taking stock of the situation, BELRA felt that they could regard the last five post-war years as a period of satisfactory consolidation and rehabilitation in areas already occupied before 1939. But, it concluded, this was not enough, and the hope and intention now was to advance the frontiers and outposts from which the campaign against leprosy in the Empire might be fought and won. 80
His Majesty King George VI, now Patron of BELRA, learned that the Nigerian boy adopted by him in 1948 had been discharged in 1950 symptom-free, and immediately agreed to sponsor another boy. Shortly after this, Her Royal Highness, Princess Elizabeth adopted a second girl after the discharge of her first BELRA child, and Her Majesty Queen Mary joined in the scheme with the first Royal Adoptee to come from East Africa. Meanwhile, the General Secretary, Mr. Edgar, despite his long association with the work, came under heavy criticism, for some of his views and actions, and he resigned. Dr. Ryrie, who had taken over from Dr. Muir as General Secretary, was forced by ill-health to resign as well, which necessitated a complete replacement of key staff. With the confusion about the role of General and Medical Secretaries, the loss of the Research Unit in Nigeria, and the increasing emphasis on outpatient treatment that Dapsone made possible, BELRA lost its firm overseas policy and seemed to be floundering about. This reign of confusion came to a temporary halt with the appointment of Mr. H.S.M. Hoare as General Secretary, and the return of Dr. Cochrane as Medical Secretary. However, being pre-eminent as an authority on all aspects of leprosy, Dr. Cochrane was sought after by many other organisations, and within a year, he had become Leprosy Adviser to the Ministry of Health, coupling his duties with those of BELRA. The following year again found him undertaking assignments on behalf of the emerging World Health Organisation of the United Nations, and ultimately his tours abroad increasingly represented many organisations other than BELRA. However, in his capacity as Adviser to the Ministry, Dr. Cochrane was charged with the task of making recommendations concerning leprosy in the British Isles, and as a result of these, leprosy was made a notifiable disease in 1951, a move for which BELRA had striven since wartime.
1951 also saw divisions in the Medical Committee over the idea to open up a new leprosarium. However, since Dr. Cochrane saw such an institution as necessary, and since the report which he freely circulated was to the Ministry from their own adviser, he felt it would be accepted. Unfortunately, in that document he had also, without recourse to the Medical Committee, made several statements concerning the policy of BELRA and that brought angry criticism from members. It was disappointing that things had come to such a state.
The death of King George VI, on 6th February, 1952, the first Sovereign to be Patron of BELRA came as a great shock to everyone He had sponsored two Nigerian boys under the adoption scheme, both of whom were discharged cured. Shortly before his death, His Majesty had directed that his latest contribution should be towards the cost of building further BELRA children’s homes required for the extension of the adoption scheme to areas in East Africa which had not yet been able to benefit from it. 80 BELRA Quarterly Magazine, July 1951, p. 50
In 1952, the new Queen Elizabeth II, now Patron of BELRA (which she took on after her father’s death), on a visit to South Africa, demonstrated her genuine sympathy in the unhappy plight of the victims of leprosy when she and Princess Margaret left the Royal Party at a Jamboree to walk over to speak to a group of ‘leper’ guides who were not allowed to take part, but only to watch the display in isolation. This striking incident, which reflected the Queen’s great compassion for those less fortunate than herself, is recorded in the picture on the right which was used on the front cover of the BELRA Quarterly of July, 1952. In this issue a report on the BELRA Exhibition noted:
The BELRA Exhibition had a flying start to its 1952 season with visits to Coventry, Portsmouth and Oxford. The Mayor of Coventry, the Lord Mayor of Portsmouth and Doctor Gilbert Murray. OM 81 at Oxford, gave powerful support with notable speeches praising the work and aims of BELRA and stressing the need for every help, in which they set a fine example by generous personal donations. Altogether £840 was collected on this first tour of the season and many offers of further help were made, as a result of which we expect to establish new Branches at each of the three centres.
The Exhibition will hardly seem the same this year, as Mr. Walter Leach, who has been its backbone for five years, has at last fulfilled his hope of working among the patients whose cause he has so long devotedly served, and flew out in May to Kumi in Uganda, where he will join the other BELRA staff of Dr. Wheate, Mr. Dick Boteler, and Miss Dorothy Jordan. He enjoyed every moment of the flight which he says was “most thrilling all the way: the passing over the Alps, the landing at Rome with just time to see the most important sights of this great city and the flight over the Mediterranean and landing in the darkness at Cairo. The sunrise at Khartoum and then following the course of the mighty River Nile. Then over the jagged peaks of the mountains of Ethiopia and now over those vast inland seas or lakes at the source of the Nile.”
We have also had the pleasure of personal news from Mr. John Cocks, the last Exhibition Secretary, who has visited us during a short furlough from Hong Kong. Readers will remember how he and his assistant, Mr. Dennis Wright, set off by jeep for Australia with two friends. The successful conclusion of the trip was celebrated by the presentation of £100 by Mr. H. Barnes of the National Travel Agency, Tividale, who had promised this sum if they reached their goal. This we duly passed on, but the adventurers tore up our cheque – although for much of the journey they had been penniless but for any money they could earn by broadcasts of press articles en route. So we are deeply grateful for their generous gesture through which our cause benefits by £100.
We have been lucky to find Mr. Stanley Wilce a man of wide business experience and tireless enthusiasm to maintain the tradition as Exhibition Manager. With regular help from Mr. Norman Crayford, during the interval between his assignments in Cyprus and the Gold Coast, and from Mr. George Cooper, pending his posting to Newala in South Tanganyika, he has seen that “the show goes on,” sometimes late into the night, so as
not to turn away any of the thousands who have queued to see it. For the rest of the year he will have a permanent helper in Mr. Thomas Noade, whom we recruited at Oxford, with casual assistance from overseas workers home on leave. 82
The January 1953 issue of the BELRA Quarterly reported:
For the first time the BELRA Exhibition has this year had a nonstop tour, from its opening at Coventry on April 12th to the end of the Leicester showing on November 15th Between those places it has visited Portsmouth, Oxford, Hull, York, Harrogate, Gainsborough, Sheffield, Bradford, Bristol, Bath, Peterborough and Northampton. Twice flooded, blown down once, and subjected to all the usual hazards, it has always opened on time and remained open throughout its advertised run. For this we owe a great debt to the toughness and enthusiasm of the new Manager, Mr. S. Wilce, and his assistant, Mr. T. Noade, whose picture appears on our cover. [Shown above] 83 The exhibition was made up of artefacts and reconstructions of housing at it appeared in the countries in which BELRA worked.
The Coronation year of 1953, which opened so well for BELRA, was historical in many ways. At the Annual General Meeting, Rev. ‘Tubby’ Clayton read the speech in the absence of the Rt. Hon. Oliver Lyttleton:
“We meet this year almost on the eve of the Coronation of our young Queen, whom we are thankful and proud to have as Patron of the British Empire Leprosy Relief Association. This is no mere formal title, as Her Majesty has long taken a genuine personal interest in the welfare of leprosy victims. In 1947, the Princess Elizabeth was one of the first Royal sponsors to adopt a child patient under the BELRA scheme. Since then both the two girls whom she sponsored at Itu in Nigeria have in turn been cured, and Her Majesty has, since she came to the throne, graciously provided to continue her support and agreed that it be used this year towards the building of new children’s homes in places where the BELRA Adoption scheme is
82 BELRA Quarterly Magazine, July 1952, p. 57
83 BELRA Quarterly Magazine, January 1953, pp. 92-93
The ‘Medical Stand’ at the Exhibition
now being introduced. This special Royal help where the need is greatest will, with her Majesty’s assent, be commemorated by tablets on the walls of two such homes at Makete in Tanganyika, with the words:
This cottage was built in the year of the Coronation of Her Majesty
QUEEN ELIZABETH II
Patron and Benefactress of BELRA and
This cottage was built in thankful and humble memory of His Majesty
KING GEORGE VI
Patron and Benefactor of BELRA
Lest these tokens of our Queen and Patron’s interest be deemed less than personal, we gratefully recall other yet happier touches. The Girl Guides at Itu Leper Colony were favoured with a portion of Her Majesty’s wedding cake: they also received signed portraits of the Princess Elizabeth and the Princess Margaret, whose statues (by a patient sculptor) as young children in Guide and Brownie uniforms overlook the settlement playground Such memories will surely enhance the pride and devotion with which all members of the Association and all the patients whom we strive to help will wish to serve and uphold our gracious Queen during her Coronation and throughout her reign. So, I sincerely hope that all our well-wishers will be moved to make a special response, as their own Coronation Tribute, to the cause of leprosy relief in which Her Majesty has herself shown such personal interest.
This year has also brought sadness. The death of Her Majesty Queen Mary removes another of our Royal sponsors, who – like her granddaughter – took a close interest in the BELRA girl she had adopted at Kumi in Uganda. It is worthy of record that Queen Mary herself made the approach to BELRA after reading of the cure of the first boy adopted by King George VI; and that once more, only a few weeks before her death, she recalled that the original period of the adoption was completed and not only paid for another two years’ care and treatment but sent a personal gift of an embroidery set to the child herself. Such thoughtfulness would be remarkable in any lady of over 80 years; in a Queen it is superb.”
Queen Elizabeth II had always maintained a close personal interest in Itu Colony and, in her first Birthday Honours, awarded the CBE 84 to its founder and superintendent, Dr. A.B. Macdonald. (Her father had awarded him the MBE 85 in 1934).
Other surprises, not quite so pleasant, were Dr. Cochrane’s acceptance of the post of Technical Medical Adviser to the American Leprosy Missions, and the non-renewal of BELRA’s lease on the premises at 167 Victoria Street, where they had become so well known. Although BELRA appreciated the sincerity which prompted Dr. Cochrane to renew his long association with the missionary side of leprosy relief, his tireless and restless devotion to all that might serve the needs, physical as well as spiritual, of leprosy patients throughout the world would be sadly missed. It was characteristic that he should have undertaken to act as Medical Secretary of BELRA for as long as required, in addition to his work for the Leprosy Mission. Most fortunately at this time, Dr. John Lowe, CBE, felt able to accept the Committee’s invitation to become Medical Secretary as soon as he was released from the Nigerian Leprosy Service in which he had so notably crowned the work he had begun as BELRA Director of Research at Uzuakoli.
As far as office accommodation was concerned, BELRA had never really dared to hope for an extension of its stay in the old offices at the wartime rental, which was only a fraction of what was normal for office premises in Victoria Street. The landlords were most generous in accommodating themselves over the move, and BELRA thought itself very fortunate to find new premises at 8 Portman Street on a long-term lease and at an ultimate cost which could hardly be expected within several miles of Central London.
On Saturday 20th June, 1953, the BBC’s radio broadcast on the Home Service, ‘In Town Tonight.’ featured BELRA’s former layworker, Robin Dunford, now a Regional Fundraiser in the UK. This half-hour programme, introduced by the well-known tune, ‘Knightsbridge March,’ by Eric Coates, was one of the first of the ‘chat shows,’ presented by Eric Maschwitz, and brought interviews of topical interest to its listeners, and this in turn brought BELRA to a wider audience. In July 1953 the BELRA Quarterly Magazine reported:
The BELRA Exhibition opened its Coronation season in the City on June 19th and has a continuous programme up to October 10th, during which it hopes to visit Kensington, Chelsea, Folkestone, Horse Guards Parade, Southwark, Stepney, Woolwich, Finsbury Health Centre, Islington, and St. Marylebone. 86
Further exhibitions followed in 1953, with the one in Manchester being opened by the actor Sir Lawrence Olivier, and on 22nd August it opened on Horse Guards Parade with addresses given by Mr. Tom O’Brien, MP 87, and close friend of the Trade Unions (who raised some £5,000 for BELRA) and H.E. Shri B.E. Kher.
84 Commander of the Order of the British Empire
85 Member of the Order of the British Empire
86 BELRA Quarterly Magazine, July 1953, p. 137
87 Member of Parliament
In the October 1953 issue of the BELRA Quarterly Magazine, a note about the St. Paul’s Cathedral exhibition reported:
We were privileged to open our Coronation season on a bombed site in the City of London, beside St. Paul’s Cathedral, and received a wonderful send-off from a highly distinguished ‘platform,’ with the Rev. P.B. Clayton, Vicar of All Hallows, Barking-by-the-Tower and FounderPadre of Toc H in the Chair, Sir Frederick Wells, Bt., Alderman of Bread Street Ward as opener, and our own founder, Sir Leonard Rogers, to speak for BELRA. 88
In October 1953 the International Leprosy Association held its Sixth Congress in Madrid, where Dr. Bob Cochrane, Dr. John Lowe, Dr. Ernest Muir and Dr. James Ross Innes all played prominent parts, and the redoubtable Miss Wallich of BELRA Head Office dealt almost unaided with the whole secretarial administration. On Dr. Muir’s resignation after 18 years from the post of Hon. Secretary and Treasurer, Dr. Lowe, Medical Secretary designate of BELRA, was invited to succeed him. The following month, the Mission to Lepers held its first world-wide conference in India, with Drs. Cochrane and Muir again present. Dr. James Ross Innes, BELRA and E.A.H.C. [East Africa High Commission] Inter-territorial Leprologist, and newly created a member of H.M. Colonial Research Service was made Director of the new BELRA-E.A.H.C. Research Centre. Speaking at the BELRA Exhibition in Limehouse, he gave the association a new motto: ‘Mercy and Judgement –or Welfare founded in Knowledge.” 89
Mr. Hoare, who had taken over as the new General Secretary in 1950, brought a new order to the office, and established the precedent of lay General Secretaries visiting the work in the field. After the demise of the Nigerian Research Unit, the need for an alternative centre in Africa was strongly felt, and Mr. Hoare went round the favoured areas with the leprosy expert Dr. Muir had recommended, Dr. James Ross Innes, who had previously made a survey of the Solomon Islands on behalf of the Association. East Africa now replaced West Africa as the centre of BELRA’s concentration, but the new research unit that was eventually established at Itesio (later renamed Alupe), never quite became what Uzuakoli had been, and BELRA’s interest in its work gradually waned over the next ten years.
In 1953 too, the World Health Organisation published the first report of the Expert Committee on Leprosy covering the proceedings at its first session in November, at which Dr. John Lowe attended as a member and Dr. Ernest Muir as consultant, and both were nominated as special rapporteurs.
88 BELRA Quarterly Magazine, October 1953, p.146
89 BELRA Quarterly Magazine, January 1954 pp. 2-3
On 18th November, 1953, Her Royal Highness the Duchess of Gloucester, made a personal visit to the BELRA Exhibition in Charing Cross Underground Station. His Worship the Mayor of Westminster received her and introduced Sir Shenton Thomas, BELRA’s Chairman, who then presented Mr. and Mrs. E.B. Alexander, Commander J.H. Carrow, Dr. A.M. Wilson Rae, Lady Thomas and Mrs. J. Twinch, representing the Executive Committee, Mr. D. McKenna of the Transport Executive, and Mr. W. Berry, Mr. R. Dunford, Mr. R. Heald, Mr. H.S.M. Hoare, Mr. C. Mead, Miss H.M. Wallich and Mr. S. Wilce, of the BELRA staff, home and overseas. Her Royal Highness, who had been sponsor in turn to two BELRA adopted girls in Nigeria, both cured, and a boy in Tanganyika, still under treatment, gave much time to hearing the story behind each display, and on leaving, kindly signed the Visitor’s Book. 90
As mentioned, Dr. Cochrane’s second period in office came to an end in 1953, when he accepted an offer to join the American Leprosy Missions. Sadly, Dr. John Lowe, who had rejoined BELRA to take over this post, was already ill, and died in May 1955. Another blow to BELRA’s self-esteem was the wrecking, by a gang of hooligans, of the Mobile Exhibition. Despite the sadness of these years, a system of regional fundraising was set up, and in 1954, 17 new committees were formed. Appeals to Trade Unions were sustained throughout the year and increased by the extension of the Tanner Appeal, 91 which produced over £2,500 and brought receipts for 1954 to £81,514.
In an article by a News of the World reporter, BELRA’s Exhibition was described in the January 1954 edition under the heading “This Exhibition is a Shocker – with a Purpose”:
Yesterday there opened in London for a week an exhibition which will enable the British Public to see for themselves the work of men and women who have silently led the revolt against leprosy and are winning a great battle against the earth’s most dreaded scourge.
With many of us the disease is associated only with the past, with Biblical stories and the poor unfortunate creatures who carried with them a bell and cried “Unclean ” Yet there are in the world today seven million victims, three million of whom are in the Commonwealth and a few hundred here in Britain.
What is being done to fight such a disease? Is there a cure?
Just a stone’s throw from Whitehall, in Horse Guards Parade to be exact, startling facts and statistics are presented which will make the man-in-the-street sit up and take notice. For the British Empire Leprosy Relief Association prove at their exhibition that the disease once known as the ‘living death’ no longer means imprisonment for life with
90 BELRA Quarterly Magazine, January 1954, p. 5
91 Jack Tanner, C.B.E., was the former President of the Trades Union Congress
little hope of recovery. It shows how it can be treated, and in time be cured by the use of new and powerful drugs.
I, with many other people was able to see how the hideous appearance of a young leper boy’s face had been transformed into a joyous picture of a smiling lad.
I was able to see victims undergoing treatment and a realistic diorama of the famous Itu Colony in Nigeria with its patients at work.
I learned of the two leprosy hospitals in England, and was appalled to find that the disease had increased in Britain since the war as a result of soldiers returning from overseas.
I was able to see, too, men and women and children of the Commonwealth ravaged by the disease.
This might be called a ‘Shock the Public’ exhibition for it surely does that. It shocks them into the realisation that leprosy is not a disease of thousands of years ago, and that it lays claim to millions of their fellows. And with that shock should also come the realisation that the public, in no matter how small a way, can help to eradicate this scourge from the face of the earth.
Of the 3,000,000 Commonwealth victims only some 10 per cent are within the realms of treatment. This is considered by the Association as a great tragedy. But perhaps the greatest tragedy of all is that eight out of every 10 of those victims contract the disease in early infancy.
While at the Exhibition I learned of the Association’s child adoption scheme and of the shining example set by our own Royal Family. Under the plan some 1,750 infected children are provided with care and treatment at an annual cost of £5 a head. Already one child is cured of the disease each day of the year. The ‘Parent’ who adopts a child is sent the name and photograph of the protégé. Then follows three times a year a medical report on the child’s progress. Such is the work of BELRA.
A special panel on display shows how members of the Royal Family have maintained their interest in sufferers and contains photographs of ‘adopted’ children cured as a result of the help given by the Queen, the Duke of Edinburgh, the Queen Mother, the Duke and Duchess of Gloucester, and by the late Queen Mary, and King George VI.
Mr. Tom O’Brien, M.P., Chairman of the TUC 92 General Council, presided when Shri B.G. Kher, High Commissioner for India, opened the exhibition. The usual crowd to be seen gazing at the Horse Guards was much larger yesterday as notable personalities began to arrive for the opening ceremony. I admired those people who, having read the announcement outside the large white marquee in Horse Guards Parade, had sufficient
courage to go inside and learn about a serious and mutilating disease – and how they could help in the war against it. 93
Her Majesty the Queen visited the Oji River Settlement in Nigeria on 16th February, 1956. Mrs. Marjorie Savoury (right), of the Church Missionary Society, who with her husband Tarka, ran the settlement, wrote about the Girl Guides’ Guard of Honour, and how all the patients were thrilled to think that they had really met the Queen, and all thought that she looked ‘very beautiful.’ Her Majesty, ever mindful of the close association between BELRA and Toc H (many of whose layworkers were stationed at Oji River), sent a message of greeting to all staff following her visit.
The July 1954 issue of the BELRA Quarterly noted that at the Annual General Meeting on May 6th ‘…the climax of a joyful meeting was the announcement of the ‘adoption’ by Her Majesty the Queen of a girl at Kumi,’ following the discharge, cured, of her previous adoptee.
On 1st July, 1956, BELRA’s Appeals Secretary, Bill Berry, made the Association’s first television appeal. This raised £22,000, taking the annual income over £100,000 for the first time. There were 2,134 children registered in the Child Adoption Scheme, and there were 29 BELRA workers overseas in this year – two doctors, seven nurses (two male), one biochemist, one laboratory technician, 18 layworkers and one clerk.
93 Reprinted from the News of the World, August 23rd, 1953.
CHAPTER SIX
Loss of Empire, turmoil, and a change of name and logo – 1957 - 1975
With the colonial map of the world changing very rapidly, BELRA moved to keep up with these events, and its support, and even its name was to change to reflect these momentous variations. The map of the world may have been changing, but the challenge of leprosy was not, and it was imperative that BELRA kept up its fight against the disease.
On 1st March 1957. Dr. James Ross-Innes was appointed BELRA’s new Medical Secretary, and in April, the Association extended its field of operations to Northern Ireland and Mr. G. Allport was appointed its first Organising Secretary. Fundraising was becoming a more prominent part of BELRA’s work at home to raise the necessary funds for its overseas projects.
Ghana was the first of the African countries to gain its independence from Britain on 6th March, 1957, but it was not the last and, due to this, BELRA felt it had to change its name to reflect the current world situation.
At its 33rd Annual General Meeting on 4th June 1957, Sir Alan Burns, Chairman of the Executive Committee, announced a change in the Association’s title. The ties with the Empire, so strong at the time of formation, were publicly relaxed and the word was taken out of the title, although the territorial restrictions on giving aid were not changed, and the abbreviation ‘BELRA’ was retained for the time being. Also, as the new Medical Secretary, Dr. James Ross Innes, gave an impassioned plea for the retention of leprosaria in BELRA’s work:
“In former times leprosy control rested almost entirely on the leprosarium, and every country but Norway relied on it. In former days cures of leprosy were few, but by the long residence of patients in a leprosarium, some degree of segregation was achieved. Nowadays, the public health control picture has become wider and more flexible. The dispensary, and various forms of village and home segregation and treatment of patients are being brought into wider and wider use. Also, the sulphone drugs are being used widely by such means, and in every country more and more people are being brought under treatment.
Coming to you, as I do, from active work abroad, I wish, however, to sound a note of warning, namely that we keep a balance and use all methods in co-ordination. An idea has grown up that the leprosarium must be abolished, and that we should turn our backs on it
and put all our efforts into out-patients and home segregation work. I wish to state from my experience abroad that this is nonsense.
The leprosarium must not be abolished nor pruned, but must remain and be strengthened, for necessary control segregation of those who need it, for necessary hospital care for those who need it, for necessary preventive and curative orthopaedic care, and above all for the necessary training of nationals of the country concerned to act as leprosy medical assistants and secure the success of the wider district work which should be based on a good regional leprosarium. One can never forget the care of children, those born of leprosy patients and those who have been contacts of leprosy cases. Also, one should not forget the search for registry of all contacts, the carrying out of frequent surveys and resurveys for leprosy, the founding of rehabilitation centres for arrested cases with deformity, the establishment of social assistance programmes, and finally, the possible use of BCG 94 as a preventive inoculation against leprosy.
The modern tendency seems to rely a little too much on the sulphone drugs. If we get these into the patients all will be well, or so the thought seems to run. This is a mistake. Leprosy is too tough a disease to be conquered by using only a part of the armament, and I insist on the integrated use of all public health measures from leprosarium to teaching and propaganda…” 95
The financial picture for 1957 was good. It was the first time that the total receipts from all sources exceeded £100,000, but it was recognised that with no television appeal for several years, this figure would not be regularly maintained without increased activity on the part of all concerned. 96
BELRA’s work was extended to three more countries in 1957: Nyasaland, Sierra Leone and the Cameroons under British Administration. A BELRA Appeal was successfully launched in Canada too, and through this appeal contact was made with Mr. G.A. Hansen, the grandson of the famous Norwegian Dr. Hansen who discovered the leprosy bacillus. 97 Mr. Hansen visited London the following year and called at the BELRA Office.
1957 was also a most stimulating and hopeful year in regard to advances in knowledge about leprosy: the bacillus was studied by electron-microscopy which made magnifications of 100,000 possible, and it began to yield some of its secrets; tissue culture of the rat leprosy bacillus was partially successful, and gave promise that it would be possible in time to successfully culture the human leprosy bacillus.
In December, 1957, BELRA was represented at a Biennial Meeting of the Association of Leprologists in Gorakhpur, Uttar Pradesh, India, by Dr. Ross-Innes.
In the 1958 Birthday Honours, Dr. Alisdair McKelvie, Specialist Leprologist in Ghana, sponsored by BELRA, was appointed OBE, and his wife was awarded the Royal African
94 The Bacillus Calmette–Guérin (BCG) vaccine is a vaccine primarily used against tuberculosis.
95 BELRA Quarterly Magazine, July-September 1957, pp. 35-36
96 BELRA Quarterly Magazine, July-September 1957, p. 37
97 BELRA Quarterly Magazine, July-September 1958, p. 41-42
Society’s Bronze Medal for services to education in Africa; Dr. Arthur Garrett, Area Superintendent of the Eastern Nigerian Leprosy Service, received an MBE. 98
The inaugural meeting of the new Belfast BELRA Committee took place in May, and at the Annual General Meeting on 5th June in London, BELRA layworker, George Cooper, gave an address to members, and Dr. Ernest Muir took over as Chairman of the Medical Committee. In an article entitled ‘The Cost of Caring’ in the BELRA Quarterly Magazine of July-September 1958 the Child Adoption Scheme was outlined:
For quite some time BELRA has been concerned with the rising cost of caring for children under the Adoption Scheme. The present subscription of £5 5s. per annum for two years does not meet the requirements of the settlements who are co-operating in the scheme. After giving earnest and thoughtful consideration, the committee has decided to increase the child adoption subscription to £10 per annum for all new adoptions entered into on and after the 1st September, 1958. The emphasis is on new adoptions, existing ones to remain at £5 5s. until the present two-yearly agreement has been fulfilled. It is hoped that sponsors will continue to support this vital part of our work on behalf of child leprosy sufferers throughout the Commonwealth.
So that as many people as possible may be able to share in caring for these poor sufferers, it is suggested that two or more friends may like to share in the adoption of a child if the increased adoption fee is too much for an individual to undertake.
Of course, there is nothing to prevent groups of people banding together to form an adoption syndicate as suggested in the last issue of the BELRA Quarterly by the Harpenden Committee.
The cost of caring may mean some sacrifice, but the joy of caring can be shared by all.
The Association is pleased to announce that Her Majesty the Queen, who has been a sponsor now for many years, has graciously consented to make the increased adoption payment of £10 on her adoptee. 99
Therefore, on 1st September, 1958, in line with the rising costs of maintaining the projects, the Child Adoption Scheme raised its subscription to £10 per child which boosted funds.
On 24th October, 1958, Dr. Gordon Ellard joined BELRA as a laboratory technician and went to the newly established East African Leprosy Research Centre at Alupe on the border of Kenya and Uganda to research into new drugs for leprosy which would combat resistance.
On 12th July, 1959, St. Martin’s Settlement Church, Ongino, Uganda, was dedicated and on 15th November, Robin Dunford, Regional Fundraiser and former BELRA Overseas layworker, made another appeal for BELRA, this time on the ‘Week’s Good Cause’ on the BBC which raised £5,640.
98 Member of the Order of the British Empire
99 BELRA Quarterly, July-September 1958, pp. 48-49
The Earl of Halifax, President of BELRA died on 23rd December, 1959. His place was taken by the Rt. Hon. Alan T. Lennox-Boyd, CH, MP, 100 who took a very keen interest in the Association’s affairs.
Keeping the Association in the public’s eye, Dr. A.B. Macdonald, CBE 101, of Itu Leprosarium, was the subject of BBC Television’s ‘This is Your Life’ programme, when the ‘big red book’ was presented by the programme’s host, Eamonn Andrews. The photo shows Mr. & Mrs. Macdonald, Hamish Macgregor and Eamonn Andrews. Other members of BELRA’s overseas workers, as well as Hamish Macgregor, who had worked most closely with him, gave testimonies to his work.
In January, 1960, vandals broke into BELRA’s exhibition warehouse and demolished the entire exhibition. The miscreants were subsequently apprehended and punished by the law. The April-June 1960 issue of the BELRA Quarterly Magazine noted:
BELRA regrets to announce that the exhibition arranged for 1960 has had to be abandoned. During January a band of hooligan teenagers broke into the exhibition warehouse and proceeded systematically to demolish the whole of our exhibition. This was a very sad blow to BELRA but the Committee felt that in the circumstances it would be difficult to build and organise a new exhibition in time to complete an effective programme during 1960. Arising out of the acts of sabotage that took place at the exhibition, the miscreants were subsequently apprehended and punished by the law. 102
However, Dame Anna Neagle, the English actress and singer, came to the rescue and signed autographs in aid of BELRA to help raise funds to replace the exhibition.
On 1st October, 1960, Nigeria gained its independence from Britain, and 27th April, 1961, Sierra Leone did the same, and there was much rejoicing and many celebrations in these countries. In May the following year, Sierra Leone held its first general elections as an independent nation.
Many celebrities have assisted the Association over its history, and on 17th June, 1961, the singer Matt Munro opened the 9th Annual Garden Fete in Rushden (Eastern Region) on behalf of BELRA. The net profit was £548.
On 30th July the school building at the Morogoro-Litisha Leprosy Settlement in Tanganyika, supported by BELRA funds, was opened
100 Member of the Order of the Companions of Honour, Member of Parliament
101 Commander of the Order of the British Empire
102 BELRA Quarterly Magazine, April-June 1960, p. 22 (although we are not told what that punishment was).
In 1961 BELRA unveiled its new Exhibition Van. This was contained in a four-ton Morris vehicle with a 30 horse power diesel engine. The vehicle was 28 feet, 3 inches long, 7 feet, 9 inches wide with an overall height of 10 feet. It was painted pale blue with white lettering and the BELRA badge (the red cross on a white shield with the word ‘BELRA’ over the top). 103
The new Mobile Exhibition Unit began its life of service in the Sanctuary outside Westminster Abbey on Monday, 14th August, 1961. The opening ceremony was performed by the Deputy-Mayor of Westminster, Councillor R.L.
Everest. The Sub-Dean, Canon A. Fox, attended and welcomed the opener into the Abbey precincts. Some viewers remarked that the Exhibition was most attractive and instructive.
In 1961 in Uzuakoli, Dr. Stanley Browne was undertaking pioneering studies on B663, one of the newly synthesised rimino-phenazine compounds. From his carefully conducted pilot, and extended trials in lepromatous leprosy, B663 (later re-named Clofazimine) proved to be a powerful anti-leprosy drug and was also found to have anti-inflammatory activity. Clofazimine, (often sold under the brand name Lamprene), is a medication used together with rifampicin and dapsone to treat leprosy, specifically for multibacillary (MB) leprosy and ENL (Erythema Nodosum Leprosum), an inflammatory condition which produces painful nodules below the skin’s surface.
Tanganyika gained its independence from Britain on 9th December, 1961, and Mr. Allan Chapman, BELRA’s General Secretary, sent a cablegram to the new Prime Minister, conveying BELRA’s best wishes. Allan Chapman himself retired as General Secretary in 1962, and Air Vice-Marshal W.J. (Bill) Crisham, CB, CBE, 104 R.A.F. (Ret’d) was appointed as his successor. Dr. Muir resigned as Chairman of the Medical Committee, and Dr. R.J.W. (Dick) Rees, of the National Institute for Medical Research in Mill Hill, London, succeeded him.
Another momentous moment came with the adoption of the logo of the ‘shattered head,’ which depicted the world of leprosy inside the head of an African child. The red of the world indicated the greatest prevalence of the disease, and kept where BELRA worked in the forefront of its fundraising schemes.
On 15th April, a BBC Television appeal by Dr. T.F. Davey, CBE (formerly at Uzuakoli Research Centre in Eastern Nigeria, and now a member of BELRA’s Executive Committee), raised £8,458.
103 BELRA Quarterly, July-September 1961, p. 60
104 Companion of the Order of the Bath, Companion of the Order of the British Empire
Sir Leonard Rogers, one of the founders of BELRA, died on 16th September, 1962. Many in the Association believed that despite his wonderful early work, his reluctance to ‘move with the times’ had held back the work that BELRA could have achieved, especially regarding the Nigerian Research Centre. Under the direction of a new General Secretary and a new Chairman of the Executive Committee (Sir George Seel), the Association re-thought its future role.
Despite its break with India following independence, contact was maintained through the new Secretary of the Hind Kusht Nivaran Sangh –Professor T.N. Jagadisan - but BELRA had withdrawn its support, except for minor grants, notably from the new Children’s Fund, in favour of working more in Africa. As BELRA’s work was expanding rapidly now, a new post was created of Assistant General Secretary, and Francis Harris, MC, 105 was appointed to fulfil this role.
The Children’s Fund started treating children on an outpatient basis in November 1962, which was a departure from the established ‘in-house’ work undertaken previously.
The months of January and February 1963 in the UK, will long be remembered for the severity of the winter. Snowstorms, blizzards, very severe frosts, snowdrifts, blocked roads – not to mention the discomforts caused by frozen pipes, electricity cuts and shortage of fuel – played havoc with the ordinary routine of life. Several weather records were broken, for all the wrong reasons, during those two months, and many of BELRA’s normal fundraising and educational activities had to be cancelled or severely curtailed, but many went ahead due to the enthusiasm and determination of the band of loyal helpers and friends that were the ‘BELRA supporters ’ However, one bright spot in these cold and miserable days, was the appointment, on 31st January, of Dr. Charles Ross as Director of the East African Leprosy Research Centre in Alupe, Kenya, which BELRA supported.
An ITV appeal on 3rd March by John Lakin, BELRA’s overseas worker from Abeokuta, Western Nigeria, raised £8,392, and on 19th July, the actor, Jack Warner, well known as ‘Dixon of Dock Green’ in the television police series of the same name, made an appeal on behalf of LEPRA which raised £2,477.11.3d.
On 18th July, 1963 the General Secretary wrote to all Leprosy Settlements about the Child Adoption Scheme:
As you may know, the Association’s Child Adoption Scheme in which your settlement participates has been in operation since 1937. As a result of the advances made in the treatment of leprosy over the years, the Scheme has naturally become somewhat outdated in certain aspects. In particular, the more effective and rapid treatment of children has, in many cases, reduced the period of in-patient treatment, with the result that the rules applicable to the Child Adoption Scheme exclude many children needing only shorter-term in-patient treatment, or just out-patient treatment. Also, this tends to encourage the retention of children in leprosaria who should rightly be treated on an out-patient basis, possibly some from their homes.
105 Military Cross
There is a further point in regard to the working of the Child Adoption Scheme that some settlements seem to expect this Association to maintain children in leprosaria after the age of 16 for reasons other than medical e.g. education. Such grounds for support are unacceptable. The Association is, of course, prepared to consider supporting special cases of children in need of continued in-patient anti-leprosy treatment after the age of 16, where there is need for this, until the age of 17.
In the light of the above, our committee have considered means of providing help to settlements for the treatment of child leprosy sufferers who are ineligible for inclusion in the Child Adoption Scheme. It was decided that a ‘Children’s Leprosy Treatment Fund’ be introduced to run parallel with the existing Child Adoption Scheme, but quite separately. The British public will be invited to subscribe to the fund which will be allocated at the discretion of the Committee.
In order to stimulate public interest, group photographs of children are needed. I would be most grateful therefore, if you would be kind enough to send me some good negatives of child groups, suitable for enlargement, at your earliest convenience. As many children as possible, especially small children, should be included in the groups, the idea being to show pictures of typical children being supported by the Scheme. It is of course not necessary to include only the most serious cases – the well-looking ones are just as important. In order to ensure good results, I suggest that, if possible, a professional photographer be employed. Two or three negatives would be ample. Would it also be too much to ask that new negatives be forwarded, say every six months, so that we shall always have a fresh supply of up-to-date publicity material? This is absolutely essential to the success of the new scheme. I shall, of course, be glad to arrange for the reimbursement of reasonable costs in respect of the photography, postage, etc.
I would also greatly appreciate it if you would let me have your suggestions for a scale of donations to the fund which you consider would be suitable, and appeal to the public, e.g. 5/- will provide something for so long etc. in about 8-10 steps upwards to, say £50.
With my apologies for giving you so much trouble. 106
Therefore, a new fund – known as the Children’s Welfare Fund was set up. Its name was then changed to the Children’s Leprosy Treatment Fund in November 1963, with the object of enabling help to be given to settlements in respect of children suffering as the result of leprosy but who were not eligible for inclusion in the Child Adoption Scheme. Children undergoing inor out-patient treatment were eligible for help on a per capita basis as appropriate to the situation. The scheme was meant to operate in parallel with the Child Adoption Scheme, and grants were made at the discretion of the Committee. 107
In the first issue of the new LEPRA Magazine (the updated version of the BELRA Quarterly) for March 1964 the Editorial noted:
106 Loose paper.
107 LEPRA Magazine, No 1 1964, p. 4
While an effective vaccine has not yet been developed which will prevent people from getting leprosy, a considerable advance in the treatment of the disease has been achieved in recent years with the introduction of new drugs, with the result that young children in particular can normally be cured of the disease quite quickly, and before the onset of deformity. The Medical Committee of the Association has reported that eradication of the disease is now possible, depending on the availability of adequate resources. The Committee considered that a pilot eradication scheme could be applied to an area with a high incidence of leprosy, probably in Africa, where there are some eight to ten thousand patients needing treatment, and where Government support and co-operation would be forthcoming. It is estimated that, for all practical purposes, the area could be cleared of leprosy in seven to ten years. The project envisages a small high-grade staff in the field under the direction of an experienced leprologist. The project is now in the advanced planning stage and it is hoped that a reconnaissance team will soon visit certain countries in Africa to select a suitable area.
The pilot scheme will cost about £150,000 in the first year and thereafter about £50,000 per annum. It is anticipated that substantial financial support for the very realistic project will be forthcoming from foundations and other organizations, as well as from the Association. 108
Dr. R.J.W. Rees, Chairman of the Medical Committee, and Air Vice Marshal W.J. Crisham, General Secretary of LEPRA, visited Kenya and Nyasaland 109 during April, 1964, at the invitation of the governments concerned, to decide which country offered the most favourable conditions for the Pilot Leprosy Control Project. In Kenya leprosy was most prevalent in the Nyanza Province which included the areas bordering on Lake Victoria. Following an aerial survey of the relevant areas to give the team an idea of general conditions and the distribution of population, a visit was paid to the East African Leprosy Research Centre – Director, Dr. C.M. Ross. The Research Centre was adjacent to the Government Leprosarium at Alupe. The latter had received considerable support from LEPRA over the years. After visiting many clinics with Dr. Ross in the Alupe district, the remainder of the ground survey was carried out from Kisumu, the provincial capital. The team then returned to Nairobi for discussions with the Ministry of Health and then flew on to Blantyre, Malawi.
After consideration of the report by the visiting team, the Executive Committee of LEPRA decided that the Southern Province of Malawi offered the most favourable conditions for the project. Accordingly, a formal offer of the project to the new Malawian Government was made, subject to certain basic conditions, including the proviso that the main programme could not be started unless appropriate financial support was assured. This offer was accepted by the Malawi Government. Detailed plans and estimates were made and the raising of the necessary financial support was actively pursued. The estimated capital costs were £100,000 and the recurring costs £40,000 per annum for 7-10 years. The project received the approval of the World Health Organization. 110
108 LEPRA Magazine, No. 1 1964, p. 1
109 Nyasaland formally became Malawi on Monday 6th July 1964
110 LEPRA Magazine No. 2 1964, pp. 6-7
Again, in Malawi an aerial survey of the endemic areas was followed by a ground survey, including visits to the Government Leprosarium at Kochira, two leprosaria run by the White Sisters at Mua and Utale in the Central Province of Malawi, the Adventist Leprosy Hospital at Malamulo, and Likwenu Leprosy Settlement (UMCA) 111 in the Southern Province. The team also visited various general hospitals throughout the country. They were accompanied throughout by Dr. Gordon Currie, the Government Leprologist, who had a thorough understanding of the country and its people. Before leaving the country, the team – Dr. Rees and Air Vice Marshal Crisham – had interviews with Dr. Banda, the Prime Minister, and Sir Glyn Jones, the Governor.
H.R.H. the Duchess of Gloucester, always a great supporter of BELRA, came to view the mobile exhibition van at the Royal Show in Birmingham in 1964. She is shown with Mr. Robin Dunford, Regional Organising Secretary (behind H.R.H.), and Mr. Wally Leach, Exhibition Manager. Both Robin and Wally had been BELRA overseas workers and so had many tales to tell.
On 24th October, 1964, Northern Rhodesia also gained independence from Britain. Southern Rhodesia had been granted self-government in 1923, and after negotiations, the administration of Northern Rhodesia had been transferred to the British Colonial Office in 1924 as a Protectorate, with Livingstone as its capital (this moved to the more central Lusaka in 1935). Politically, in 1953 both Rhodesia’s (North and South) were joined with Nyasaland (now Malawi) to form the Central African Federation. Northern Rhodesia was the centre of much of the turmoil and crises that afflicted the federation in its last years. At the centre of the controversy were insistent African demands for greater participation in government, and European fears of losing political control. On 31st December, 1963, the Federation was dissolved, and Northern Rhodesia became the Republic of Zambia. However, at independence, despite its considerable mineral wealth, Zambia faced major challenges. Domestically, there were few trained and educated Zambians capable of running the government, and the economy was very largely dependent on foreign expertise, with most of Zambia’s neighbouring countries still colonies or under white minority rule. Leprosy work suffered as a result.
But the future of the fight against the disease could not be written off and, following discussions which had been taking place for over a year, it was decided to demonstrate, on a worthwhile scale if, as the doctors were now saying, leprosy could be cured with DDS (Dapsone) monotherapy provided adequate dosages were applied. The parameters provided by the Medical Committee were 10,000 untreated leprosy patients in an area with good internal and external communications, and a stable government for at least 10 years. Malawi was officially chosen, and this project not only rejuvenated the Association, which had been close to collapse for lack of positive direction, but gave it new life, especially in its fundraising field. The Malawi Leprosy Control Project was duly set up. The project was endorsed by the World Health Organization. It provided a small, fully staffed and equipped unit, capable of dealing with 10,000 leprosy sufferers and of clearing the disease from a selected area in 10
111 Universities Mission to Central Africa
years. Mobile teams operating on regular schedules identified and treated all ‘open’ infectious cases, aiming to treat all early cases before the onset of deformity, and to maintain a close surveillance of ‘contacts,’ especially children. In this way it was felt that treatment could be brought within easy reach of all sufferers from their own homes, and do away with the need for segregated ‘colonies.’
For an association which had not committed itself to expenditure for more than three years at a time, the prospect of setting up and running a mobile treatment scheme for a 7–10-year period was quite new. LEPRA expanded this so that eventually the whole country was covered by a network of local people giving out treatment on a regular basis. Foundations were laid for the project by Dr. Gordon Currie, with the help of Mr. John Eldon and Mr. Tony Drake, two of the long-term members of the overseas staff and, as the formal agreement was signed in London on 25th May, 1965, by the Association’s President, Alan Lennox-Boyd (now Viscount Boyd of Merton) (left), and the High Commissioner for Malawi, H.E. Dr. N.W. Mbekeani; Dr. David Molesworth stepped in as the Project’s leader on 1st January 1966.
After considerable discussion a site was found to hold a territorially limited and finite project that would test all the easy assertions that leprosy could be controlled. A small area around Blantyre, which held a population of about 1,250,000, with an estimated 10,000 leprosy sufferers was ideal to become the site of the Control Project. The plan was to bring all leprosy cases, registered and yet to be found, under treatment within 10 years. President Hastings Kamuzu Banda officially opened the new Control Centre on 20th October 1966.
There were control schemes elsewhere, and there was mobile treatment, but the clear declaration of a time limit was original and courageous. The project was based on a centre that was to be built in the grounds of the Queen Elizabeth Hospital in Blantyre, and would be provided with enough vehicles and staff to make treatment available at points within three miles of access to all patients. The vehicles would distribute Dapsone at weekly intervals to patients at home or at work. Funds were available from the Brown Memorial Trust in Malawi to augment the £500,000 that LEPRA would have to raise for the project.
The arrival of the first landrovers heralded the beginning of the mobile treatment and of a new and bold way of putting the disease into its proper social perspective, as they were decorated with LEPRA’s name in large red letters, avoiding the alternative of operating surreptitiously in response to leprosy’s ill-founded traditions. This new idea was to pay off handsomely, as villagers delighted in being associated with the weekly event of a landrover’s arrival. Long before the end of its 10-year period, the project had found and brought under treatment a greater number of patients than that originally estimated for the area. The
project discovered practical weaknesses in the theoretical ideal, and moved to provide equally practical solutions to them.
The project area covered some 2,000 square miles, equivalent to the size of Norfolk, and had a population of well over one million people, including an estimated 12,000-15,000 leprosy sufferers. A start was made in May 1965, but only small-scale operations were possible until 1966, when the new permanent Director, Dr. David Molesworth, took over. The training of Medical Assistants, who had been seconded from the Government Medical Service, was a first priority; also, the arrangement of intensive publicity on a national scale. The project centre buildings were completed and taken into use by May 1967. By the end of that year there were 6,266 registered patients, including 3,600 new cases. BCG vaccination had been given to 3,500 young contacts. During 1968 the number of registered patients rose to 8,752 including a further 1,500 new cases. Four mobile (Landrover) teams were operating in conjunction with two bicycle circuits and one case finding team.
The aim of the project was two-fold: firstly, to demonstrate that leprosy could be wiped out in an endemic area, and secondly, to demonstrate the most effective and economical way of doing so. The first mobile team went into action on May 25th 1965 and assumed responsibility for over 2,700 registered cases in Malawi. Intensive surveys went ahead progressively to find and treat all other cases in the area. After negotiations with the government there, on 8th August, 1966, work began on the site of the LEPRA Headquarters (above) in the grounds of the Queen Elizabeth Hospital, Blantyre, and a block of flats were obtained, at a very reasonable rate, in Blantyre for the senior members of the staff. Dr. Gordon Currie, the Acting Director of the Project, had provided invaluable, indeed brilliant help in setting this project up. His services had been very generously made available by the Government of Malawi. Because of his special experience and sense of practical realities, this was one of the many ways in which the Government of Malawi gave practical help and co-operation at every stage.
The Malawi Leprosy Control Project became LEPRA’s flagship project, and their Landrovers, with their distinctive logo and red name, became a very familiar sight in the countryside. With the regularity of a bus timetable, they set up a treatment delivery system that was soon replicated by other NGOs throughout the world, and the LEPRA logo became synonymous with hope and treatment.
In neighbouring Zambia, Dr. Colin McDougall, the Government’s Leprosy Specialist, heard about the project and went to see for himself. He was so impressed that he returned to
inaugurate a similar scheme, for which LEPRA readily supplied vehicles and staff, and for the first time supplied a launch to facilitate mobile treatment, using the Zambezi as a highway. In Sierra Leone, LEPRA was able to capitalise on its provision of lay staff, by means of Mr. Bob Lowes and Mr. Frank Mead, by joining a nation-wide campaign based on the Malawi model. Treatment was taken to an estimated 66,000 leprosy sufferers, adding more staff, vehicles and equipment to those provided by other agencies and the Sierra Leone Government.
In 1965 the film The Name of the Cloud is Ignorance, made free of charge for LEPRA by the Hon. Richard Bigham (later to become Viscount Mersey), about its work in India, was presented at the Venice Film Festival and won two awards; the next year it was entered for the XIX International Film Festival at Salerno where it won an award for the best documentary film.
LEPRA had now entered a new era of positive action, and ways of reaching the public. Its aid to India, which had fallen off after the formation of the Hind Kusht Nivaran Sangh, now strangely, surpassed that to any other country, with the exception of Malawi, with grants mainly for the treatment of children, which was shown to be so effective with the new drug regimens. But the new emphasis was on the growing LEPRA Control Project in Malawi
On 11th November 1965, Southern Rhodesia’s prime minister, Ian Smith, unilaterally declared his territory’s independence from Britain. Not since the United States in 1776 had a British colony declared itself independent, and the Rhodesian declaration was not dissimilar in language and structure of sentences to its American forerunner
On 19th November, the actor Jack Warner (now an OBE.) gave another moving and effective appeal for LEPRA on the BBC ‘Week’s Good Cause’ on Radio 4. Donations amounted to £2,151.
LEPRA moved headquarters yet again into its last headquarters in London, on 25th November, to the freehold premises at 50 Fitzroy Street, W1.
In 1967 the emphasis had been placed on fundraising as an entity of LEPRA. Now that the Malawi Control Project had taken off, there was something positive to raise funds for, and a new position of Fundraising Officer was created; this was filled by Mr. T.A. Stringer, MA 112 ‘Bertie,’ as he was called, was the first ‘professional’ fundraiser that LEPRA had employed, and pointed the way to the more concentrated effort that was to follow. He was keen to engage supporters on a very personal level, showing that they could personally make a difference to someone’s life. One of his initiatives was the production of the ‘Dapsone Card’ which encouraged supporters to ‘buy’ a tablet to help fight the disease.
In Sierra Leone, the main opposition leader Siaka Stevens’ All People’s Congress defeated the ruling Sierra Leone People’s Party (SLPP) under Sir Albert Margai’s leadership in the closely contested 1967 Sierra Leone parliamentary election. Stevens ruled Sierra Leone from 1968, and while in office, he suppressed oppositions and critics of his government, making life in the country uncomfortable for many expatriates, and certainly for those working in the leprosy field
John Lakin, Layworker at the Abeokute Leprosy Settlement in Nigeria, was awarded the OBE 113 in the New Year’s Honours list in 1968 in recognition of his outstanding services to leprosy. But in the world, great problems were looming.
The Nigerian Civil War, also known as the Nigerian - Biafran War, began with the secession of the southeastern region of the nation on 30 th May, 1967, when it declared itself the independent Republic of Biafra. The ensuing battles and well-publicised human suffering prompted international outrage and intervention Biafra represented the nationalist aspirations of the Igbo ethnic group, whose leadership felt they could no longer coexist with the federal government dominated by the interests of the Muslim Hausa-Fulanis of Northern Nigeria. The conflict ultimately resulted from political, ethnic, cultural and religious tensions which preceded the UK’s formal decolonisation of Nigeria from 1960 to 1963, which led to a military coup, a counter-coup, and anti-Igbo pogroms in Northern Nigeria. Within a year, Nigerian government troops surrounded Biafra, and captured coastal oil facilities and the city of Port Harcourt. A blockade was imposed as a deliberate policy during the ensuing stalemate which led to the mass starvation of Biafran civilians. During the 21⁄2 years of the war, there were about 100,000 military casualties, and between 500,000 and 2 million Biafran civilians died of starvation. This and the concurrent Vietnam War, was one of the first wars in human history to be televised to a global audience.
The plight of those starving in the area was brought to the fore in human publicity but, inevitably, the plight of those with leprosy and those working to help them, was less prominent, and the fighting caused great problems for LEPRA.
In February 1968 there was trouble in the Gambia, as there had been in many other African countries following independence. On 20th February LEPRA Layworker Frank Mead, was taken before the Magistrates Court on a ‘charge’ of non-payment of taxes and sentenced to 14 days hard labour. His cause was, naturally, taken up by the District Medical Supervisor and the First Secretary of the British High Commission. The charge was dropped, but just a week later Frank advised LEPRA Head Office that a senior African official told him that it was time he ‘got out’ so that his job could be ‘Gambianised ’ Frank complained that the official had also interfered with his work, which had not in any way helped with staff discipline.
There were no better tidings from Nigeria, as on 6th March, 1968, news came through that the Eja Memorial Hospital, 20 miles from Uburu, where LEPRA Layworker, Harry Smith, was working, was bombed and destroyed by rebel Nigerian forces.
In April, 1968, LEPRA Layworker, Frank Mead, and his wife Jenny, left the Gambia and moved to Sierra Leone to work with Bob Lowes. Frank was finally cleared of all charges of tax
113 Officer of the Order of the British Empire
avoidance. LEPRA Layworker, Tony Drake, was sent to Chipata in the Eastern Province of Zambia to set up and supervise a leprosy control scheme jointly with the Government, based on the Malawi pattern.
There was sadness too as on 2nd May, Dr. James Ross Innes, the former Medical and General Secretary, died aged 65. His widow, Elizabeth kept up the running of Leprosy Review until arrangements could be made for it to be taken over by the publishers, Academic Press. In the meantime, Dr. Stanley Browne (left) took over as Editor. Also known as ‘Bonganga’ by the community members with whom he worked, Stanley was a British Baptist medical missionary and leprologist known for his work and his many research achievements throughout the 20th century in the Belgian Congo, Nigeria, and India including his early use of Dapsone. He received numerous awards throughout his academic and professional career. He is also known as an academic for his early publications surrounding his findings of leprosy of which he published about 150 articles and five books. His acquisition to LEPRA was immense, and under his editorship Leprosy Review went from strength to strength.
A more ‘diplomatic’ presence was brought to LEPRA’s hierarchy when at the AGM on Wednesday 5th June, Mr. Philip Knights, Crown Agents, joined the Executive Committee. 114
The 1968 Annual Report made comment on the Malawi project:
A year of consolidation and continued expansion. The Project has now been running three years. The Centre, virtually completed by the end of 1967, has been in action for 18 months and continues to prove satisfactory.
Four mobile teams have been giving treatment in addition to two bicycle runs in areas where motoring is not practicable. One small area still remains to be brought in. A case finding unit has completed a satisfactory coverage of Chief Nkalo’s area and has now moved on to a second area. The total number of registered patients is 8,752. During the year 1,500 new cases were seen and charted as well as 835 PTUs. [sadly, who these were was not given] Total 2,335.
LEPRA Centre. The siting of the Centre within the Queen Elizabeth Hospital grounds has proved wholly successful and there has been no further unreasoning fear of contagion – we are now accepted! The Centre was described in last year’s report. This year the work in the operating theatre was completed with the installation and wiring of the sterilizers so it is now complete and has been in use throughout the year.
Since more men and women seek admission to the wards, we have taken the two large wards for the men giving 28 beds, and the two side wards with four beds each for the women – this works well in practice.
114 The Crown Agents began life in the 1700s, when colonial administrations employed agents to recruit people and procure and ship supplies to the colonies. Some agents had been authorised to manage British Treasury grants and they had become known (unofficially) as crown agents.
Training. Apart from our own staff, the Ministry of Health has sent doctors joining the service to us as part of their introduction to Malawi. Apart from these we have had batches of nurses in training, Health Assistants in training, Staff Nurses returning from overseas and the new draft of Peace Corps Volunteers. There was a Seminar on children’s diseases when Dr. Molesworth read a paper on Leprosy in Children, and a Medical Conference where Dr. Clegg read a paper on Leprosy Facts and Figures in Malawi and The Possibilities of Treatment in District Hospitals.
Lectures have been given to various groups, either at our request when we need help such as to the Directors of the Tea Association and then to the Dispensers on their estates at Cholo and Mlanje; or a group has asked for a lecture and if possible, we have given this. We cannot afford to miss any chance of getting our message across. We have had a leprosy control officer from Zambia who came for a week to see the Project at work.
Case Finding. As reported in 1967 attempts to survey whole villages by gathering them together at a given moment failed, and the examination of contacts proved too wasteful of time and energy for the results achieved. A new approach was therefore tried with the team living in the particular area, moving from village to village and house to house. The Native Authority of Chief Nkalo was selected as Mr. Mkango, the Medical Assistant in Charge, belonged to this area.
Preliminary work consisted of a visit first to the District Commissioner and then, together with him and Mr. Mkango to meet Chief Nkalo and his headmen to explain our purpose and what help we would need. Thereafter the team moved in, and with only one exception co-operation was full and the work went smoothly forward. BCG 115 being given to all under 15 years.
In all 19,581 people were examined, and BCG given to 11,899; 59 new cases and 4 PTU were found which, added to known cases, 119 in the area plus 14 doubtfuls, gives a prevalence of 10 per 1,000. This is in an area which has been relatively well provided with Medical Services and leprosy treatment has been available for some years.
In August 1968 Miss Dawn Smith, a Laboratory Assistant, took over the laboratory at the LEPRA Centre in the Queen Elizabeth Hospital grounds in Blantyre. She received a Zeiss Research Microscope through the generosity of the Wenela African Interest Fund. 116
Also in August, the Hon. Richard Bigham made a second film for LEPRA, about their work in Malawi this time, entitled Outpatients not Outcasts, which was in colour and ran for 30 minutes. The film had its premiere before a distinguished audience on 14th December at Unilever House cinema through the kindness of Mess. Unilever Ltd. and the United Africa Company.
On 6th September, 1968, Swaziland also gained its independence from Britain, and the pattern of leprosy work there changed under the new regime.
115 Bacillus Calmette-Guerin is a vaccine usually given to fight TB
116 Wenela was the Witwatersrand Native Labour Association
London was chosen from 16th-21st September, 1968, as the venue for the International Leprosy Congress – the first time it had been held in the UK.
On 28th September 1968, John Lakin, (now OBE), LEPRA Layworker at the Abeokute Leprosy Settlement in Nigeria, had a further award placed on him when he was installed as an Egba Chief by the Alake of Abeokuta, in recognition of his outstanding services for leprosy sufferers in Egbaland. But on 30th September, Mrs. Marjorie Savory and her husband (who had been at Oji River Settlement in 1956 when Her Majesty the Queen had visited) were killed by Federal Troops during the capture of Okigwe on 30th September 1968 – a great shock to all working in the country.
The LEPRA team in Malawi was strengthened when in September, Geoff Bulley and Iorweth Rogers, LEPRA Layworkers, took up appointments in Malawi as Field Officers. Another boost to the work was when the Leprosy Craft Shop was set up in the town to sell baskets made by leprosy patients. Despite the ‘brazen’ use of the word ‘Leprosy’ outside the shop, buyers were not deterred and patients received not only a monetary, but a psychological boost to be perceived as ‘normal’ people. The following year it was noted that the project had begun to fulfil its wider purpose by arousing considerable outside interest, especially in Africa, in its policy and methods. The LEPRA Annual Report for 1969 noted:
The world problem of leprosy, far from diminishing following the introduction of the sulphone curative drugs, continues to be aggravated by rising world populations, bringing reduced standards of hygiene and living conditions which are conducive to the spread of the disease.
The work of treating cases has continued. In addition to the four Mobile Units with Landrovers there are now three cycle units, the third of these closing the gap that existed between the southern edge of the Zomba run and the adjacent parts of the Blantyre and Mlanje circuits. This now produces full coverage on the ground. Rains were very heavy and hampered the runs for the first part of the year and in August political unrest made things very difficult particularly in Mlanje where our case-finding team had to be withdrawn and the treatment run limited.
At the end of the year, it was possible to begin discharging those no longer in need of treatment. Chief Nkhumba’s area was covered by the case finding team and proved very much more difficult than Nkalo.
The total number of registered patients is now 10,019. During the year we found 1,001 new cases and 242 PTUs, a total of 1,243.
Celebrities have always helped the cause, and in November the actress Hayley Mills (daughter of actor Sir John Mills) opened the Christmas Fair of the Harpenden Branch of LEPRA. Another celebrity joined the fray when the comedian and actor, Norman Wisdom (1915-2010), headed a cricket team for LEPRA in Blackpool’s Stanley Park and raised £350.
In 1970 LEPRA Layworker, Doug Coffin, was awarded an MBE in the Queen’s Birthday honours for his work with leprosy, and Dr. Frank Davey was awarded the CBE for his ‘services to leprosy treatment.’
January was a very significant month, for another Mobile Unit for leprosy treatment was started from Utale, Malawi, on a very small scale, by means of one bicycle tour visiting villages at monthly intervals, but it was a start, and on 1st June BBC 1’s ‘Troubleshooter’ series featured leprosy in Africa – LEPRA helped the production team with photographs.
The hospital complex at Balaka, Malawi was completed in December 1970, and 10,000 cases of leprosy were registered in the country as Dr. David Molesworth took complete charge of the project. The project area covered 250,000 people with an estimated prevalence rate of 2% leprosy. As the project reached its climax, requests for extensions to cover the whole country were being met in a concerted operation, but worrying reports from the field told of the spectre of drug resistance looming on the horizon. Such a threat could be positively proved thanks to the work of Dr. Dick Rees of the National Institute for Medical Research in London through his work on leprosy bacilli in the footpad of the nude mouse. Undaunted, however, LEPRA provided aid in 1971 in Cameroon, Gambia, Sierra Leone, Tanzania, Uganda and Zambia, and funds were provided for leprosy research in the UK.
But in 1971, Siaka Stevens, the controversial Prime Minister, abolished Sierra Leone’s parliamentary government system and declared Sierra Leone a presidential republic. Despite this, on 24th July, 1971, LEPRA Layworker, Bob Lowes, applied for and received funds from LEPRA to convert the redundant Railway Station at Magburaka, Sierre Leone, into a Laboratory and records office, and a LEPRA centre for the whole of the work in the country, and the Northern Provinces in particular.
On 28th July, 1971, celebrities Jimmy Tarbuck (a comedianright) and Freddie of Freddie and the Dreamers’ (a pop groupleft) headed teams in the LEPRA North West Region’s charity football match. Not to be outdone, 16 blind Cub Scouts from the Royal London Society School climbed Mount Snowdon and raised over £8,000 for LEPRA.
But it was with great regret that the news came through on 28th September, 1971, that Dr. James Arthur Kinnear Brown CMG, MD, BSc, DTM & H, 117 the great researcher into the BCG
117 Companion of the Order of St. Michael and St. George, Medical Doctor, Bachelor of Science, Diploma in Tropical Medicine and Health
vaccine against leprosy, died in Hale, Cheshire aged 69. He was an English surgeon who carried out outstanding work for leprosy patients in Uganda. In 1932 he developed the Uzuakoli Settlement for leprosy patients and inaugurated a mass treatment campaign for leprosy patients throughout Uganda, backed by the Uganda Government. He undertook extensive surveys on leprosy in Uganda and Kenya and made preliminary investigations into the possible value of BCG vaccination in the prevention of leprosy. He was the principal author of the First and Second Reports on the BCG vaccination investigation. In 1951 he had been elected a Fellow of the Royal Society of Tropical Medicine and Hygiene and in 1957 he became a member of the WHO Expert Committee on Leprosy. In 1967 he received the honour of the CMG for his outstanding work in Uganda. He was a member of the International Leprosy Association and author of over 60 publications on leprosy – his death meant a great loss to the field of leprosy.
With the retirement of Bill Crisham as General Secretary in November 1971, Francis Harris, MC took over, and shortly thereafter the title of General Secretary was replaced with that of Director.
1972 started well with an ATV television appeal on 31st January, by the star of the ‘soap opera’ Crossroads, Noele Gordon, raising £6,600 for the Emene Leprosy Village in Nigeria. This was renamed the ‘Crossroads Village’ in her honour. Also, on that day, a radio appeal broadcast in Scotland by Mr. English, the Scottish organiser (!) raised £1,200 with a script that he had written himself.
However, in Zambia, it became clear that the political situation was becoming increasingly tense. In a letter to head office of 5th February, 1972, LEPRA Layworker, Iori Rogers noted that “A tin of dried milk has gone in a single leap from K3.05n to K4.80n – an increase of K1.75n or almost £1 – and this on an essential commodity.” 118 Less than two weeks later, on 22nd February, field workers learned that the Ministry of Health in Zambia had reversed its policy of outpatient treatment and integration, returning to inpatient care. By 5th June economic measures in Zambia were getting much tighter. In light of this, Dr. Jogan, the Medical Officer for the area, felt that it wasn’t worth opening up any new work if there was no money to maintain it. The Zambian government of the time seemed more interested in buying Mercedes cars for their officials and commandeering leprosy workers’ houses.
Things were no better in Uganda however, as it was learned that LEPRA mail was being intercepted, and staff were advised to ‘keep a low profile ’ However, H.R.H. The Duke of Gloucester, visited the Kumi Leprosy Settlement in the country and encountered no problems, although in December Uganda’s President, Idi Amin, restricted the movement of ‘foreign’ workers in the area, and this had a tremendous effect on LEPRA staff there.
Over the next few years, the work extended to Colombia, Ethiopia, Peru, Togo and Zaire under the Children’s Fund, and in 1972 research began into a new antibiotic drug, Rifampicin. Sadly, Rev. Tubby Clayton never saw the outcome of the Rifampicin trials as he died on 16th December, but in grateful memory of his magnificent contribution to LEPRA’s work, the Clayton Memorial Lecture was established to encourage medical staff to take an interest in leprosy.
118 Iori Rogers’ personnel file 351, p.42
Fundraising priorities for the next five years were decided in 1973. The income at the end of 1972 had reached £286,600 and a major expansion drive was planned to coincide with LEPRA’s 50th anniversary in 1974. Research, training of indigenous staff, involvement in and support of the leprosy aspect of multi-purpose rural health projects, extension of children’s work and a wider distribution of the medical journal Leprosy Review were accepted as the most important priorities.
There was more acclaim in the New Year’s honours List for 1973 with LEPRA Layworkers Ronald Heald and Bob Lowes each being awarded the MBE for their contribution to leprosy work.
On 8th January, 1973, despite the Sierra Leone government’s restrictions, the Leprosy Control Programme in Freetown, was launched. But in March prices were continuing to rise in Zambia and there were severe shortages with queues for cooking oil as supplies could not get through from Rhodesia, and on 23rd May a drunken driver crashed the new LEPRA Mansa Landrover on the Kabalenge Road putting it completely out of commission. Worse was to come when in June, due to severe shortages, LEPRA staff houses became victims of burglary.
In July 1973 Dr. Gjalt Boerrigter, a Dutch doctor, was appointed Leprologist in charge of the Northern Region Project in Malawi, and throughout the project disposable syringes and needles came into use in place of the old glass ones which had to be sterilized, thereby making treatment easier. On 27th August, 1973, Malawi’s President for Life, Dr. Hastings Kamuzu Banda, officially opened the Chilumba Jetty in Northern Malawi, and invited LEPRA to assume nation-wide responsibility for the Leprosy Control Project, and this was a most welcome sign of LEPRA’s status in the world of leprosy at that time.
But there was more trouble in Africa. In August, 1973, Fr. Serra, the Director of leprosy work in Sierra Leone, upset many in the Ministry of Health, and put LEPRA’s work there in jeopardy. At the same time, the government of Zambia voted K1.5 million to the United National Independence Party (the only political party allowed) for transport, K1.2 million to the police for transport, but would not allow LEPRA Landrovers to have petrol for their work. But despite all the problems and political concerns, this was also a year of records. The amount of money spent by LEPRA on grants and services was twice that spent ten years earlier, and £25,000 more than ever before in the history of the Association. The ordinary income was up £60,000 on 1972 which in itself had been a record year.
An appeal by the actor Gerald Harper (left) on 13th January, 1974, raised £19,332, and on 27th January another appeal by presenter Michael Barratt (right) raised £9,409. A host of celebrities of stage, screen, radio and television, pledged their support for LEPRA in its Golden Jubilee year.
In March, Nigel Evans, the film maker, went to Sierra Leone to make the film ‘Mariama’ for LEPRA. However, the Ministry of Information there was, for some unknown reason, very uncooperative, and the film was eventually made in Liberia. But LEPRA still provided layworker support for the country in the form of Pieter Shipster, who went out to help Bob Lowes. Later in the year Pieter started work on his own in the Pujehun District, in an area covering 1,500
square miles, which had never had a leprosy programme before. The 143 patients registered since he arrived had all self-presented, which was a wonderful thing; by the end of the year, he had a total of 68 clinics with an average of two patients per clinic.
LEPRA began its Medical Elective Scheme for medical students to encourage them to undertake their compulsory elective period of study in leprosy, and this became a very successful project, which brought many excellent doctors into this field (including Dr. Diana Lockwood, a future editor of Leprosy Review.)
Problems arose in Uganda in May when President El Haddji Idi Amin took control of the country, and layworkers and doctors alike had their mail censored, and petrol was in very short supply. Problems increased in Zambia too, as on 24th September, Dr. Jogan and other LEPRA staff were turned out of their houses so they could be ‘beautified’ to house the Heads of State and VIPs that were arriving for the Independence celebrations. But, loyal to his patients, and despite all the political interference, Dr. Jogan gave permission for Ridafin 119 to be used for dapsone-resistant patients in the country.
LEPRA moved its headquarters in November from London to Fairfax House in Colchester, as it was felt that it was less expensive than London, and there was an easy direct rail link with the capital. However, the London office remained a foothold in the capital for fundraising. But the Association noted, sadly, that Dr. Ernest Muir had died on 1st November, aged 94.
By December things had deteriorated in Zambia to the extent that Dr. Jogan was ‘chastised’ by the Principal Secretary, Ministry of Health, for writing to LEPRA for help, as all requests ‘have to be passed through the Ministry of Health ’ On 4th January 1975, James Callaghan, Foreign Secretary to the Labour Government in the UK, visited Zambia for an official reception in Lusaka, and he met Dr. Jogan, but in Dr. Jogan’s words he was “…hauled away before I could protest about the situation.” 120
On 16th January, 1975, the old Medical Committee was replaced by the Medical Advisory Board, and Dr. Dick Rees was invited to become its first Chairman.
By February, crime in Zambia had soared due to shortages, yet in April the Zambian government announced that they would spend 1 million Kwacha on twelve VIP houses for members of the government, but there would be no money for leprosy work. Things became worse for leprosy workers as the Zambian army took control of the transport department in August, to ‘stamp out expatriate corruption and for the sake of efficiency’!
In Sierra Leone in July 1975, over a dozen senior military and government officials convicted of planning to overthrow President Stevens, were executed. Sierra Leone became a one party state after that, in which Stevens’ All People’s Congress (APC) was the only legal political party in the country.
119 It worked by stopping the growth of bacteria, but only worked for bacterial infections. It didn’t work for viral infections such as the common cold, or flu
120 Dr. Jogan’s Personnel File
Back home on 25th September the London Soft Toy Fair was held at the Chenil Galleries, Kings Road, Chelsea when H.R.H. The Duchess of Gloucester attended. She is shown with Francis Harris, Director of LEPRA.
The boat ‘Bill Crisham’ (named for the former General Secretary of LEPRA) was launched on Lake Malawi in October to be used as a mobile clinic visiting villages along the shoreline which were inaccessible by road, as had been done in Zambia on the Zambezi River. More troubles in Zambia were reported in November when the Government cancelled all import permits ‘because of the foreign exchange problems.’
Due to the ever-changing situation in the field of leprosy, the highly successful Child Adoption Scheme was wound up at the end of the year, as it was based on in-patient treatment and emphasis was now on out-patient treatment, letting patients lead as normal a life as possible. The remaining children not ready for discharge were transferred to the newly established Children’s Fund Scheme.
LEPRA became one of the first associations to introduce multi-drug therapy (MDT) at field level for all patients with lepromatous leprosy in 1975 The drugs used in WHO-MDT were a combination of rifampicin, clofazimine and dapsone for multibacillary leprosy patients (i.e. more bacilli) and rifampicin and dapsone for paucibacillary patients (i.e. less bacilli). Among these, rifampicin was the most important anti-leprosy drug and therefore was included in the treatment of both types of leprosy. For multibacillary (MB) leprosy, the standard adult regimen was: rifampicin: 600mg once a month; dapsone: 100mg daily; clofazimine: 300mg once a month and 50mg daily for a duration of 12 months. For paucibacillary (PB) leprosy, the standard adult regime was: rifampicin: 600mg once a month; dapsone 100mg daily for a duration of six months. Ideally, patients were expected to go to the leprosy clinic once a month so that clinic personnel could supervise administration of the drugs prescribed. However, many countries with leprosy had poor coverage of health services and monthly supervision of drug administration by health care workers was not always possible. In those cases, it was necessary to designate a responsible third party, such as a family member or a person in the community, to supervise the monthly drug administration. Where health care service coverage was poor and supervision of the monthly administration of drugs by health workers was not possible, the patient could be given more than the 28 days’ supply of multidrug therapy blister packs. This tactic helped make multidrug therapy easily available, even to those patients who lived under difficult conditions or in remote areas. Patients who asked for diagnosis and treatment were often sufficiently motivated to take full responsibility for their own treatment of leprosy. In this situation, it was important to educate the patient regarding the importance of compliance with the regimen and to give the patient responsibility for taking his or her medication correctly and for reporting any untoward signs and symptoms promptly. The patient was also warned about possible reactions.
The project of developing a vaccine was given official backing by WHO, which had chosen leprosy as one of the six diseases to be give special attention under its Programme for Research and Training in Tropical Diseases. Dr. Rees and his colleagues in the National Institute for Medical Research in London, made great strides with funding from LEPRA,
developing methods of extracting and purifying high yields of bacilli, and studies began on humans. Dual drug therapy was also introduced into Malawi to counteract the threat of dapsone resistance in this year
CHAPTER SEVEN
LEPRA becomes ‘International’ – and drug delivery easier - 1976-1991
LEPRA consolidated its international work in 1976 by becoming a full member of the International Federation of Anti-leprosy Organisations (ILEP) – a relationship it still maintains today. This organisation ensured that leprosy control work was shared amongst its members throughout the world, and thereby avoided duplication of work in the same country. LEPRA was duly invited, as it was already in charge of leprosy work there, to co-ordinate on its behalf leprosy work in Malawi. John Eldon’s outstanding administrative work in Malawi was rewarded by an MBE in the Birthday Honours List.
Also in January, a new rehabilitation project in Mayoso, Sierre Leone, began to take shape, and ten patients were started on home industries. One was set up as a petty trader, and a gardening project was launched, enabling patients to grow vegetables both for their own use and for sale. In March an offer of seeds from Messrs. Thomson and Morgan was gratefully received by Bob Lowes for the gardening project. Sadly, it later transpired that they were not a great success due to the damp climate – only the radishes thrived! However, more serious trouble was brewing in Sierra Leone as on 25th April, 1976, a spate of burglaries in Magburaka of ‘important’ houses (the Medical Officer, Chief of Police, Russian Embassy, etc.) led to the culprits being arrested and severely beaten at the Police Station.
Things were no better in Nigeria, for LEPRA Layworker, John Lakin, experienced difficulties in expanding the Emene (‘Crossroads’) village due to illegal land encroachment, and to address this he called a meeting of the Military Governor, the Army, Police, TV and Press to put forward his complaints.
“…at the land palaver 121 I explained, people were encroaching all round us and every farming season stopped us from expanding and that the DO of Nkanu Division had given me the go-ahead at the end of 1972. He asked me to put all into writing so that he could study it. I explained that I had done this first of all for Asika and then Col. Ochefu so he asked for copies to photostat.
He was full of praise for our achievements, asked many questions, visited the patients, shook hands with many of them and they were full of praise, due to the fact that that very day they had received one huge pig, 20 doz. eggs, and a cockerel each. He then asked so many questions about leprosy, I was able to tell him what LEPRA was doing in research and finance and the inevitable question “What is the government doing to help?” and the answer only promises as yet. I quoted a MOH letter to the Immigration Department which stated that there was no place for the ‘burnt out’ cases other than this Centre and there was a need for such as the government was unable to provide one. He said that he would support such a venture continuing and after the settling of the land dispute the Welfare Department should be contacted to continue the good
121 A long discussion
work. I had asked him to pay a private visit and reminded him of it before he left, he replied “I promise to do so, this is indeed a lovely site, so quiet.” 122
A terrific thunderstorm in Magburaka, Sierra Leone, caused severe damage to Bob Lowes’ house as he wrote to Head Office:
“…there was a blinding flash and a noise like fifty steamrollers crunching up together. All the electric light bulbs went off like grenades and many of the wall fittings and switches were ripped off and sent flying across the room. The fuse box was completely disintegrated. A goat and two chickens died of shock across the road, but luckily no human was injured.” 123
The Seychelles became an independent republic within the Commonwealth on 29th June, 1976, and although LEPRA had not had a layworker there since Mr. Penrose in 1965, they maintained good relations with the new authorities. However, things had become so bad in Zambia, that on 31st July, LEPRA severed all aid to the country, and Iorwerth Rogers, its layworker there, was offered a post in Malawi instead. Also, in September in Uganda, mail from LEPRA staff was being censored, and rationing was now common for foodstuffs.
In November, LEPRA layworker, David Brooks, left Sierra Leone and handed over the work to Mr. Sesay, a Sierra Leonean, in accordance with LEPRA’s policy of handing over work as soon as possible to indigenous staff. But in Malawi, on 1st December, LEPRA received a formal request from the Bishop of Mangochi, to undertake the running of the Balaka Leprosy Hospital, ‘in its entirety.’ However, at a meeting with the Secretary of Health in January 1977, the Ministry was of the opinion that the Hospital at Balaka should be donated to the Government of Malawi who would request LEPRA to run it. The following month LEPRA applied to the Medical Missionaries of Mary in Drogheda, Ireland, for staff to run the hospital.
For the Christmas appeal in 1976, LEPRA adopted a novel idea of posting an airmail letter, written by Dr. David Molesworth, from Malawi. This proved to be extremely successful, and was a contributing factor in LEPRA’s income reaching half a million pounds the following year A 16-sheet poster about LEPRA, designed by Mr. Tom Eckersley, won the Design Council Award, and an appeal by Robert Robinson, Chairman of BBC Radio’s ‘Brain of Britain’ raised over £8,000.
A LEPRA supporter, Mr. J.G. Stacey, wrote to Head Office at the end of 1976 to offer his collection of woodworking tools, both hand and electric, for use in leprosy work. These were offered to Bob Lowes, in Sierra Leone, and he was very glad of them for his rehabilitation project. But in February 1977 there were student riots in Freetown, and John Lakin in Emene, Nigeria handover his work to the Marist Brothers, a Roman Catholic Organisation. He then retired from leprosy work. 1977 was, of course, the Queen’s Silver Jubilee and many events were held to signify her support for LEPRA and the charity’s work in the 25 years since she had acceded to the throne.
122 John Lakin’s Personnel File
123 Bob Lowes’ Personnel file
June 1977 saw LEPRA’s familiar blue transparent static collecting boxes being replaced by more noticeable ones, bearing an attractive showcard in the LEPRA colours of red, white and black.
In 1977 concern over the incidence of Dapsone resistance rose sharply as there was worldwide mounting evidence that strains of M. leprae were resistant to Dapsone. In an effort to find an answer to the problem, following an idea from Francis Harris, its Director, LEPRA arranged what became known as the ‘Heathrow Meeting’ in London on 16th August 1977 under the Chairmanship of Dr. Dick Rees, the Chairman of LEPRA’s Medical Advisory Board, which included scientists from France, Belgium, Holland, Germany and the UK. This meeting was held in a room at Heathrow Airport to define the seriousness of Dapsone resistance and to draw up guidelines to its prevention and treatment in the field and, during one intensive, but highly successful day (perhaps unique amongst medical meetings for its level of friendliness and unanimity), thrashed out a series of definitions, priorities and practical recommendations. The ‘Heathrow Report’ (known as ‘ILEP No. 1’) was accepted by the ILEP Medical Commission at their meeting in December 1977. This coincided with LEPRA becoming the ILEP Co-ordinator in Malawi.
In November, 1977 the American singer, Sammy Davis Jnr. opened his week at the London Palladium with a Royal Gala Performance in aid of LEPRA. H.R.H. Princess Alexandra attended, and several members of LEPRA’s staff were presented to her.
In 1978 a dramatic increase brought the Association’s income to over £800,000 – the Easter Appeal, signed by Dr. Rees, raising over £28,000. He was awarded the CMG in the New Year’s Honours List, and his elevation reflected well upon LEPRA and our association with him and the National Institute for Medical Research, at Mill Hill in London
Dr. Gjalt Boerrigter took over total responsibility for the project in Malawi on the retirement of Dr. David Molesworth in July 1978, and Dr. Colin McDougall (right) became Editor of Leprosy Review.
In October 1978, in view of his outstanding contribution to the fight against leprosy, Dr. Frank Davey was appointed a VicePresident of LEPRA.
The Christmas Appeal, in the form of another airletter, was signed by Bob Lowes from the Magburaka Leprosy Settlement in Sierra Leone. This was also very successful and passed the £30,000 mark in donations
As a result of a brilliantly successful idea of Mrs. Valerie Profumo (the former actress Valerie Hobson) in 1978, of asking women in the UK for a ring so that operations could be funded on patients with hands clawed by leprosy, the Ring Appeal was launched on 13th June 1979 at Sothebys. The slogan was ‘A ring for a hand’ and the public gave with their usual generosity. A large book with the names of all those who donated rings was
made up and included Royalty, and commoners alike. The Ring Appeal, which raised £38,000, enabled medical teams engaged in surgery and physiotherapy to remobilise the hands of patients crippled by leprosy. The majority of grants from this fund went to centres in India
It was also decided in 1979 that our outstanding medical journal, Leprosy Review, should be sent free of charge to those members of the medical profession working in the leprosy field who were unable to afford the subscription (£11 per annum).
In June 1979, petrol shortages hit LEPRA’s work in Malawi, but despite this, the organisation set up a scientific research centre, home to the Karonga Prevention Study (KPS) in the country.
In April, 1980, LEPRA’s Director, Francis Harris, M.C., who had converted to Catholicism, had an audience with The Pope, John Paul II, in Rome, and a second auction of rings, this time in Glasgow, raised a further £22,745 for reconstructive surgery.
Following a successful feasibility study, LEPRA began the Evaluation Project in Karonga District, Northern Malawi with a view to finding answers to how people became infected with leprosy and why some developed the disease and some did not. It was felt that by studying an entire population over several years, rather than individual patients, common denominators might be found which could point to the sources of infection, how it was transmitted and the risk factors for acquiring the disease. The objectives of this study were:
• To gain further knowledge concerning the natural history of leprosy and its spread in that community in northern Malawi;
• To identify risk factors and their role and relative importance for the transmission of leprosy in the area;
• To evaluate the case findings and treatment programme in the Leprosy Control Project; and
• To evaluate the impact of the past and present BCG programme on leprosy in the area.
Karonga District was deemed an ideal site for the project, and Professor Paul Fine (left), of the London School of Hygiene and Tropical Medicine, and the German doctor, Jőrg Pőnnighaus (right), formerly a Medical Officer in Zambia, set themselves the task, backed by LEPRA funding. The study was undertaken for six years, during which time all participants were examined and questioned in detail
Between 1980 and 1984 the population of the entire district (approximately 112,000 people) was visited, interviewed and physically examined by four teams that systematically covered the district on foot, by bicycle, and later by motor cycle from mobile camps. Each individual, each household, and each building within a household was numbered. For every individual a questionnaire was completed giving information about age, sex, parents, village of birth, level
of education, occupation, hygiene and many other items. All buildings were measured and construction materials noted. This was to see whether the bacilli could possibly exist in the soil or in the buildings. It was recorded which people within a household slept in which building. Each household was located within ten square metres on specially developed aerial photographs. Finally, each individual was examined from head to foot for signs of leprosy and for characteristics which would help in identification (such as scars or birthmarks); anyone found to have leprosy was registered and treated.
Once the population had been covered, it was studied in detail again for any new developments. It was hoped that data from these surveys, once analysed, would be able to discover what made some people more susceptible than others to contracting leprosy. The data gathered was processed by computers in the London School of Hygiene & Tropical Medicine. The Government of Malawi provided excellent support – the 1978 census details were made available to LEPRA’s teams, and aerial photographs were taken to make identification of houses easier.
On 18th April, 1980, Southern Rhodesia formally gained its independence from Britain and became known as Zimbabwe. The government held independence celebrations in Rufaro stadium in the capital, Salisbury. Lord Christopher Soames, the last Governor of Southern Rhodesia, watched as Charles, Prince of Wales, gave a farewell salute and the Rhodesian Signal Corps played “God Save the Queen.” Many foreign dignitaries also attended, including Prime Minister Indira Gandhi of India, President Shehu Shagari of Nigeria, President Kenneth Kaunda of Zambia, President Seretse Khama of Botswana, and Prime Minister Malcolm Fraser of Australia, representing the Commonwealth of Nations. The Rastafarian singer, Bob Marley, sang ‘Zimbabwe’, a song he wrote, at the government’s invitation in a concert at the country’s independence festivities. President Shagari pledged $15 million at the celebration to train Zimbabweans in Zimbabwe, and expatriates in Nigeria.
Zimbabwean President Robert Mugabe’s government used part of the money to buy newspaper companies owned by South Africans, increasing the government’s control over the media. The rest went to training students in Nigerian universities, government workers in the Administrative Staff College of Nigeria in Badagry, and soldiers in the Nigerian Defence Academy in Kaduna. Later that year, President Mugabe commissioned a report by the BBC on press freedom in Zimbabwe. The BBC issued its report on 26th June, recommending the privatization of the Zimbabwe Broadcasting Corporation and its independence from political interests. This, for some reason, was not taken up.
In 1981 the World Health Organization (WHO) recommended Multidrug Therapy as an effective treatment for leprosy. LEPRA had, of course, been using this for some time.
Keeping up with fundraising in the UK, the Easter Appeal was signed by Chris Bonington, LEPRA’s new President, and in October LEPRA was due to hold a Toy Fair at the New Century House in Manchester, but sadly the venue burnt down beforehand!
LEPRA’s annual income topped the £1 million mark in 1982, due in part to Radio and TV personality, David Jacobs making a radio appeal, athlete Sebastian Coe signing the Easter Appeal, and doctors John Stanford, of the Middlesex Hospital in London, and Gjalt Boerrigter, of the Malawi project, signing two separate Christmas appeals.
By October 1982, Sierra Leone was in a bad state economically, and in most other ways. ExLEPRA Layworker, Bob Lowes, now retired and setting up a Nature Reserve near Magburaka, noted:
“…there is no foreign exchange and consequently very few imports. This makes it very difficult to obtain even basic necessities. Medical stores are empty…there is no law and order…paraffin is hard to come by…every sort of crime is rampant, especially in Freetown, where gangs of armed thugs openly break into properties in the daytime, let alone at night…” 124
On 29th October, 1982, H.R.H. The Duke of Gloucester, Vice-President, of LEPRA, (centre in the picture), visited the Colchester Office in Fairfax House, Causton Road. In an incredible logistical nightmare, no cars were allowed from any of the offices in the block to park in the extensive car park around the building, so space was found for them in the grounds of the Castle Park. This was to ensure that the duke could land in his helicopter without there being any chance of bombs in cars.
In 1982, a new form of fundraising was born in the first Edinburgh to St. Andrews Bike ride. This was very well supported and extremely successful and, due to this initiative, sponsored overseas bike rides took place in India, Malawi and later in Brazil.
In 1983 LEPRA introduced the WHO-recommended multi-drug treatment for all leprosy patients throughout Malawi and its medical teams treated over 15,000 patients, which was a great achievement, reducing the duration of treatment for tuberculoid (non-infectious) leprosy from three years to six months, and for the lepromatous (infectious) leprosy from life to a minimum of two years. 125 Sadly in that year LEPRA’s President, Lord Boyd, was killed in a road accident in London. He was an inspiring and greatly admired President of the Association who held office for 23 years. He once told the House of Commons, and was applauded from both sides of the house “…discrimination on the ground of colour is quite deplorable and, like all rudeness, is both stupid and offensive.” Since most of LEPRA’s work was, and is, amongst
124 Bob Lowes’ Personnel file
125 LEPRA News No. 51, Autumn 1984, p.3
people of colour, it was particularly dear to his heart. Shortly before his death, however, Lord Boyd learned of the exciting developments in the introduction of the new short-term treatment for leprosy patients with multi-drug therapy (MDT) and the development of a possible vaccine. The role of President was assumed by the mountaineer, Chris Bonington.
Ever keen to engage in new ideas for fundraising, and to tackle the increasing problem of blindness associated with leprosy, a £100,000 appeal was launched by LEPRA on 10th January, 1984, to establish a special fund for the prevention of blindness. This jewellery appeal had for its slogan ‘An Eye for a Gem; a Gem for an Eye.’
In February 1984, members of LEPRA’s Medical Advisory Board discussed the possibility of a return to working in India by the setting up a new project in Orissa. Dr. Penelope Key, a member of LEPRA’s Executive Committee at the time, who worked in Orissa for the Overseas Development Administration, had been having discussions on LEPRA’s behalf with members of the Government. After two years of negotiations, LEPRA’s application to set up an MDT control programme in the State of Orissa was rejected by the Government on the grounds that Orissa was a ‘highly sensitive’ area. It was thought this was due to a military base for rocket launchers being located in the vicinity. However, LEPRA was advised to re-apply requesting districts proposed by the Government. LEPRA’s film A Disease Called Leprosy was made in India during this year and was to become an excellent fundraising and educational tool. LEPRA also took over the Presidency of ILEP for two years which greatly enhanced its status.
Also in 1984, the first survey of the Evaluation Project in Karonga came to an end, and all the data collected was coded and shipped to the London School of Hygiene & Tropical Medicine for analysis. During this first survey it had been noted that scars from BCG (a vaccine against TB) were more common in those who didn’t have leprosy than in those who did, suggesting BCG gave possible protection against leprosy. Meanwhile, a new leprosy vaccine had been developed, but not yet tested
As 1984 was LEPRA’s Diamond Jubilee year, the event was celebrated with a Service of Thanksgiving at All Hallows Church in London, on Thursday 16th February, attended by Her Majesty the Queen as Patron, and taken by the Archbishop of Canterbury, Dr. Robert Runcie. This was a fitting location for the event as, of course, All Hallows had been Tubby Clayton’s church. Chris Bonington, LEPRA’s new President, was also present. It is interesting to recall that when invitations were sent out, many people pleaded an earlier engagement, but the moment it was announced that Her Majesty would be there, it was astonishing how many of these
‘prior engagements’ were cast aside or suddenly disappeared (left: the procession down the aisle).
But there was great sadness in the loss of three great leprosy workers. On 3rd August, 1985, Dr. Robert Greenhill Cochrane, so long the Medical and General Secretary of BELRA, died aged 86, and on 25th January, 1986, (coincidentally World Leprosy Day), Dr. Stanley Browne, died aged 79, and Dr. Alasdair McKelvie, former Superintendent of the Ho Leprosarium in the Gold Coast (Ghana) and later Leprosy Secretary in Malawi, also died aged 81. The loss of so many great leprosy workers in so short a time came as a severe blow to the work, as their combined knowledge and expertise was incalculable.
A second survey of the Karonga Prevention Trial (KPT) was begun in 1985 to identify those who had developed leprosy since their previous examination. Information from the first survey was compared for common factors and contrasted with information on those not infected. To make the exercise more worthwhile, a vaccine trial was mooted. A new leprosy vaccine had been developed, but not yet tested in large numbers of people. Approximately 120,000 people agreed to take part in the vaccine trial. The aim was to examine for both leprosy and TB and find whether the protection offered by BCG could be improved by adding either a repeat BCG or the new leprosy vaccine. The trial was ‘double-blind,’ i.e. neither the vaccinator nor the person being vaccinated knew which vaccine was being given. The code for each vaccine was kept by a third party in the UK. Early in 1986, LEPRA began the Karonga Vaccine Trial in Malawi. The study was based on the LEPRA Evaluation Project population, and was chosen by WHO for a leprosy vaccine trial in Africa because of the unique and extensive epidemiological data available. The new President, Chris Bonington, visited Malawi to see for himself the work on the ground (and to climb Mount Mulanje).
On 4th May, 1986, Ashley Cooper from Clitheroe, began his attempt to scale the Munros – all 277 mountains in Scotland over 3,000 feet in height. LEPRA’s President, Chris Bonington, hoped to join him ‘for a mountain or two.’ The trek raised over £7,000 for LEPRA.
In June 1986, the second survey of the Evaluation Project in Karonga, Malawi, began and by the end of the month, 17,700 had been vaccinated by four LEPRA field teams under the vaccine trial. However, the HIV epidemic in Karonga district in the mid-1980s caused great concern. Since the depressed immunity characteristic of HIV infection could interfere with the effects of the various vaccines used, the project embarked on a separate study, comparing the HIV status of leprosy and TB cases with adequate controls – individuals not known to have leprosy or TB or otherwise were at a similar risk to being infected with HIV – so the effect of HIV on leprosy and TB could be assessed.
At the end of the second survey, new cases of leprosy and TB were detected by field staff posted to all health units in the district. Everyone visiting these centres, regardless of the reason for attendance, were interviewed to establish their identity number (with the aid of enormous computer listings containing the entire population) and subsequently examined. In addition, a sample survey of 5,000-6,000 individuals was held annually in different parts of the district to validate the method of case finding at health centres. All project data was entered onto computers and shipped to the London School of Hygiene and Tropical Medicine. As there were more than 200,000 people on the database, there were inevitable clerical
errors, and it took almost five years to ‘clean’ the data. Given that in Karonga district most people didn’t know their date of birth, names were commonly changed, and the various languages spoken were strictly oral thus permitting various spellings of names, it was a formidable task to keep track of so large a number of people over so many years. Credit is due to the very hardworking, dedicated local staff of the project.
Encouraged by this, LEPRA ran a ‘Leprosy Awareness Week’ from 1st-6th July, and at the end of this, Sunday 6th July, a television appeal by BBC Broadcaster, Julian Pettifer brought in £40,000. LEPRA’s film A Disease Called Leprosy was honoured in this year with a commendation by the British Medical Association. The BMA, in association with the British Life Assurance Trust, awarded the certificate in recognition of the film’s educational objectives, which was a great achievement.
When the first Leprosy Symposium was held in China from 25th-29th November, 1986, LEPRA’s Director, Francis Harris, addressed the meeting.
Sadly Dr. David Molesworth, the former Director of the Malawi Project, died on 15th December aged 73, and another stalwart of the fight against leprosy was lost.
A great achievement, however, was the hosting of the SADCC (Southern African Development Coordination Conference) Seminar on leprosy control work in Malawi in May 1986 for neighbouring African countries. Senior leprosy workers from Lesotho, Mozambique, Swaziland, Tanzania, Zambia and Zimbabwe attended and shared experiences of leprosy control work in their countries. The Seminar was held in order to try and standardise the quality of leprosy control work in central and southern Africa through assistance with staff training, advising on leprosy control and sharing recent developments in research and treatment.
In May, ‘Fair Shares’, a consortium of eight Third World charities, including LEPRA, had a press launch at the House of Commons. The group was formed to maximise upon the benefits of the Payroll Giving scheme introduced by the Chancellor in March 1986.
LEPRA Layworker, Ben Hopper, was awarded the MBE in the New Year’s honours list for 1987 in recognition of his services to leprosy care and control in Africa, and later that year Air ViceMarshal Bill Crisham, the former General Secretary of BELRA, died aged 81, and Dr. Dick Rees retired as Chairman of LEPRA’s Medical Advisory Board.
Dr. Hastings Banda, President for Life of Malawi, recognised the help LEPRA had given to Malawi in its fight against leprosy, by awarding its Director, Francis Harris the ‘Order of the Lion of Malawi’ in recognition of ‘…outstanding services to humanity.’ The insignia were presented to him by the Malawi High Commissioner, His Excellency, Mr. Mtawali, at the Annual General Meeting held on 29th June, 1987, and on 23rd September, Mr. Mtawali, visited LEPRA’s office at Fairfax House in Colchester. 126
126 The insignia now has pride of place in the association’s museum
The CYCAL Rickshaw Ride from John O’Groats to Lands End was undertaken by two young men – Justin Busbridge (22) & Johnny Hooper (26) – from 30th August to 13th September, 1987. The two students, from Manchester University, pedalled an amazing 3,500 miles during 1988, first touring and working in leprosy clinics in Nepal and Bangladesh, and then racing down Britain in a colourful rickshaw that they brought back from Bombay (now Mumbai). During the final leg of their journey, they received valuable newspaper, radio and television coverage, projecting LEPRA’s name and cause in front of a significant audience. For the two men though, the highlight of their winding journey down from John O’Groats to Lands End came on Saturday, 3rd September when they were presented to Her Majesty the Queen at the Braemar Games. Her Majesty showed great interest in their efforts and jokingly remarked of the rickshaw, “Is it road worthy?”
Francis Harris retired in 1987 after 25 years’ service, just as the three years of hard and frustrating negotiations with the Government of India resulted in the re-establishment of firm links with the sub-continent. He was succeeded by Neil Winship, late of the Tank Regiment. He came to LEPRA from World Vision, for whom he worked out a successful mission to bring emergency food supplies through to Southern Sudan.
At that time, Dr. K.V. Desikan, the Director of the Central JALMA Institute for Leprosy in Agra, had built up the clinical department and the number of registered patients quickly rose from 7,000 to 25,000 under his gentle and caring leadership. At Agra, he started a home for disabled and destitute patients with a school for their children as, having contracted leprosy himself at the age of 14 (although it was not formally diagnosed until nearly 20 years later) and having come from a very poor family, this helped him to understand the troubles and frustrations of the poor and under-privileged, and cemented his desire to help deserving people. When LEPRA decided to try to have a more ‘hands on’ approach to work in India, it was, naturally, to Dr. Desikan that they turned, and he became LEPRA’s Clinical Consultant on leprosy in India in April 1987.
Discussions were held with the Government of India about setting up a sister organisation to LEPRA, and it was natural that this organisation should be headed by Dr. Desikan. He and LEPRA’s new Director, Neil Winship, drafted the Memorandum of Articles of Association. Following on from this, in September of that year the Leprosy Histopathology Centre in Wardha was established.
In February 1988, the Government of India Ministry of Health and Family Welfare signed an agreement with LEPRA covering additional support under the National Leprosy Eradication Programme for the MDT work in Bidar District, Karnataka State - LEPRA’s first project in India since 1947. LEPRA also offered support for Medak and Karimnagar, all with Dr. Desikan’s guiding hand behind it. However, it was obvious that the smooth movement of funds between UK and India would require the setting up of a registered society to accept foreign contributions as legally required under the Foreign Contributions (Regulations) Act (India) 1976. Therefore, on 3rd August 1989, the LEPRA Society of India was officially inaugurated as a separate sister organisation working in partnership with LEPRA UK although being, for the time being, financially dependent. Founder members of the Association were:
Dr. K.V. Desikan (Chairman)
Dr. D.D. Palande (Vice-Chairman)
Mr. B.M. Kothadiya
Mr. R.S. Mani
Mr. Bhogishayana
Mr. E.A.N. Winship (Director, LEPRA)
Sadly, Francis Harris, who had done all the groundwork to make this happen, wasn’t there. The headquarters was set up in Secunderabad, with premises located in Vikrampuri, and an immediate effort was made to identify administrative and medical staff to undertake the necessary expanding work.
A new innovation for LEPRA-supported projects was the introduction of Blister Calendar Packs in 1988. These packs were designed to make distribution of the drugs and patient compliance easier (a pill was pressed out each day), and they did not become contaminated as they used to do when kept in jars, as each pill was sealed and dated. This prevented the wastage normally encountered with the use of loose drugs ruined by exposure to moisture, and it meant that a whole course of treatment could be delivered in one package. LEPRA also backed crucial research at the Royal College of Surgeons of England, in London, to understand nerve damage in leprosy – something that plagued patients throughout the world.
September was a busy month as far as staff matters were concerned.
LEPRA’s Clinical Consultant in the UK, and Editor of Leprosy Review, Dr. Colin McDougall, retired. Professor John Turk (right), of the Royal College of Surgeons, took over as Editor of the journal, and became the new Chairman of the Medical Advisory Board, and Dr. Sebastian Lucas (left), of the London School of Hygiene & Tropical Medicine, and University College, London, took over the histopathology work from Dr. McDougall.
In October, the Bidar, Medak and Karimnagar MDT projects were launched in India, and LEPRA’s influence in the sub-continent spread.
The Christmas appeal was signed by LEPRA’s President, Chris Bonington and brought in record returns of over £125,000 which enabled the total income to reach an impressive £2.3 million, which was a great help when LEPRA began its first ‘own’ Indian project in Hyderabad called
‘HYLEP’. There were three Easter appeals in 1989 – signed by Joy Maitland (Director of Fundraising), Dr. Colin McDougall, of Oxford, and Irene Allen (LEPRA).
The number of leprosy sufferers receiving treatment through programmes supported by LEPRA rose from 10,000 at the end of 1988 to 27,500 at the end of 1989, with 7,000 patients cured and released from treatment. The second survey for the Karonga Prevention Trial came to an end in 1989, but work in Malawi was made more difficult by the influx of one million Mozambiquan refugees pouring into the country to escape the civil war. This had begun when Mozambique won independence in 1975, after a decade of fighting its colonial master Portugal; the country was plunged into a civil war in 1977. As civilians lost homes and land, their only recourse was to flee to a safer country, and Malawi was seen as that option.
Malawi had had a complicated relationship with both FRELIMO (the Marxist Mozambique Liberation Front, and RENAMO (the anti-communist insurgent forces of the Mozambican National Resistance). During the mid-1980s, FRELIMO repeatedly accused Malawian President Hastings Banda of providing sanctuary for RENAMO insurgents. Mozambiquan security forces occasionally carried out raids into Malawi to strike at suspected RENAMO base camps there –a practice which brought them into direct confrontation with the Malawian Defence Force.
In 1990, with the Cold War in its closing days, apartheid crumbling in South Africa, and support for RENAMO drying up in South Africa, the first direct talks between FRELIMO and RENAMO were held, which ultimately paved the way for a multiparty system, and a new constitution was adopted in November 1990, when Mozambique became a multi-party state, with periodic elections and ‘guaranteed’ democratic rights. However, the war claimed a million lives, decimated the economy and left the nation littered with landmines, and the influx of refugees into Malawi hardly diminished.
Back in the UK, a new innovation in 1990 was the introduction of the Christmas catalogue as part of fundraising efforts; 1,500 orders were received, worth almost £24,000 and £6,000 was received in donations; the annual income reached the £3 million mark. Almost 20,000 patients were released from treatment as cured in 1990, and LEPRA set up new projects in Nigeria and in Orissa (the BOLEP Project), where the prevalence rate for leprosy was a staggering 228 cases per 10,000 population. Throughout the year in Hyderabad, cinemas showed slides on leprosy at all five daily shows (at the request of the Police Commissioner!) and the city corporation’s 2,000 buses each carried a sticker saying ‘Leprosy is Curable.’
The following year, World Leprosy Day was celebrated by a Commemoration Service held at St. Paul’s Cathedral on Friday 25th January, 1991, with H.R.H. The Duke of Gloucester and the High Commissioner for Malawi being present. However, reports from LEPRA’s new project launched in rural areas of Orissa indicated the discovery of one of the worst leprosy rates in the world. Initial reports suggested that the estimated prevalence rate for leprosy in the BOLEP project could be as high as 35 cases per 1,000 of population. In what could, ultimately, be an antidote to such finds, trials began on a new drug (Ofloxacin) 127 which, it was hoped, would drastically reduce the length of time taken to cure patients, and would be especially
127 Ofloxacin is a quinolone antibiotic useful for the treatment of a number of bacterial infections. When taken by mouth or injected into a vein, these include pneumonia, cellulitis, urinary tract infections, prostatitis, plague, and certain types of other infectious diseases.
appropriate for patients living in outlying communities for whom compliance with months or years of MDT was a problem.
The UK recession of 1991 hit many businesses, and LEPRA too found itself in financial difficulties. The recession was primarily caused by high-interest rates, falling house prices and an overvalued exchange rate. Membership of the Exchange Rate Mechanism (1990-1992) was a key factor in keeping interest rates higher than desirable. The recession also came after the late 1980s economic boom – a period of high economic growth and rising inflation. It was decided, therefore, to reorganise the working practices of LEPRA’s fundraising staff which proved to be expensive and somewhat controversial, involving the closure of regional offices and fundraising staff working from home. As a result, a substantial operating deficit was incurred, and reserves were drawn upon to counteract this, but at the end of the year the final deficit was £77,564. Fundraising did not pick up as had been expected, so the Director and Head of Fundraising resigned, and LEPRA struggled to make up the shortfall by cutting back on programme spending. It was a very anxious time for all concerned. However, amidst all the gloom of that dismal year, a breakthrough came in leprosy surgery with the autogenous muscle graft technique which could restore sensation to limbs. 128 LEPRA began supporting work on this exciting technique in India at the Sacred Heart Centre in Kumbakonam, in Ethiopia at the All Africa Leprosy Research and Training Centre (ALERT), and in Brazil at the Institutio Lauro de Souza Lima in Bauru.
LEPRA had also cooperated with a film unit from the BBC History Unit for a programme on leprosy which was being made as part of a series on the social history of medicine. This was broadcast in a four-part series in late September as the BBC Television programme ‘Pestilence and Punishment’ – leprosy was the subject in the second episode entitled ‘The Dreaded Lurgi.’
The KORALEP Project was launched in Koraput, India on 2nd October 1992, and a new video was made entitled ‘Something to Smile About ’ But it was also learned with great sadness that Bob Lowes, ex-LEPRA Layworker, had died aged 76. There was also little to smile about on the financial front.
It was reluctantly accepted that due to severe administrative difficulties and a shortfall in income during the recession, LEPRA would have to withdraw from Nigeria. This was a severe blow, exacerbated by the Nigerian Government’s refusal to release LEPRA’s equipment that was being held up at the port, until a huge sum had been paid – money that LEPRA simply did not have, and should not have been asked to pay considering that the object was to help the people of Nigeria with their leprosy problem. This was particularly galling as LEPRA had spent the last two years building up connections with staff and patients alike.
128 The autogenous nerve graft serves as a conduit pairing an innervated, normally functioning muscle with a denervated muscle. After interposing the harvested graft between the muscles, axonal sprouting is induced in the normal muscle and traverses the graft to innervate the denervated muscle.
The shortfall in income was eased slightly by Chris Bonington’s appeal on Radio Four’s ‘Week’s Good Cause’ which raised almost £40,000 and an Emergency Appeal put out later in the year raised £99,000. However, distrust of the Nigerian Government meant that LEPRA did not pay to have their equipment released, and this was handed over to another charity working there. Terry Vasey was officially appointed as Director in 1992 having served as Acting Director during the months of turmoil.
Hampshire Medical Student, John Gilbody, won the LEPRA Essay Competition for an unprecedented third successive year in 1992
LEPRA was requested to take responsibility for a leprosy project in Ceará State in Brazil in 1992 and also completed the handover of the Malawi National Leprosy Control Programme to the Malawi Ministry of Health. LEPRA continued to work in Malawi though, undertaking prevention of disability programmes where necessary. Results from the vaccine trial that had been going on in Venezuela since 1983 proved to be inconclusive, which was disheartening especially given LEPRA’s own vaccine trial which was coming to an end. However, the ending of the Civil War in Mozambique brought some peace and sanity to the continent of Africa, but sadly LEPRA’s Medical Director in Malawi, Dr. Gjalt Boerrigter, retired.
It is wonderful to note that in these years, that members of BELRA/LEPRA staff were awarded between them seven country medals, eight OBEs and 14 MBEs – I don’t think many other associations could boast this.
CHAPTER EIGHT
Another change of leadership and logo, and a major breakthrough…Oh, and ‘Blue Peter’ 1992-2011,
Moving back into India was a great time for LEPRA, but it also caused some problems with regards to its public image and the way it was presented. The current logo image of the ‘shattered head’ – a very African image – was unhelpful and frankly unacceptable when fundraising in India.
Therefore, it was decided in 1992 that LEPRA’s logo should be replaced by the logo of the hand with the words ‘heal me…hear me…touch me…see me.’ This logo was designed by Sarah Crosby and given free of charge to LEPRA – although the words were incredibly similar to those used in a song from the 1969 hit rock opera ‘Tommy,’ by the pop group ‘The Who.’ The name of the charity was also changed to ‘LEPRA Health in Action’ which was easier to translate for the new Brazilian project.
In February 1993, the new LEPRA India office building in Secunderabad was inaugurated by Mrs. Nancy Trenaman, Chairman of LEPRA’s Executive Committee, attended by the Chief Minister, Mr. Vijayabhaskara Reddy, and Terry Vasey, the new Director of LEPRA UK. This new purpose-built, air-conditioned headquarters had ample room beneath for the jeeps, and also in the upper floors for offices and conference requirements.
The Northern Ireland Premiere of the film ‘City of Joy’ raised £3,000 for LEPRA’s funds. The film was based upon the novel of the same name by Dominique Lapierre, and looked at poverty in modern India, specifically life in the slums. The film starred Patrick Swayze, Pauline Collins, Om Puri and Shabana Azmi, and brought the plight of those in poverty-stricken areas of India to a wider public.
But this was also a very sad year due to the untimely death of John Kelson, the fundraising consultant and trainer, on his way home from the LEPRA Staff Conference in Lincolnshire. It was also sad in the retirement from the Editorship of Leprosy Review, of Professor John Turk. This was also a somewhat traumatic time for LEPRA in other ways, as the decision was taken to install a new computerised donor base, and the disruption of installing equipment and training staff inevitably took its toll. Also, it was unfortunate that having given all Regional Organisers a direct link to the Head Office computer system, it was decided to make them all redundant, and introduce a whole new fundraising system of Community Co-ordinators and volunteers. By losing all the regional organisers it was felt by the management that funds could be raised more cost-effectively, although staff feared that contact with donors and the goodwill created through personal contact with a regional organiser would be lost. However, LEPRA staff, with their usual dedication to duty, rallied round and kept the impetus going and eventually a more settled atmosphere returned to the offices.
Better news came in 1994 when on 18th February, the Leprosy Reconstructive Surgical Hospital, at the Hoina Leprosy Research Trust, Muniguda, India, was inaugurated for reconstructive surgery on clawed hands. Funded by the States of Jersey, this new unit offered hope and cosmetic surgery in a remote part of Orissa and provided a facility much needed in the area. A new pre- and post-operative physiotherapy unit and additional patient housing was also built for the Reconstructive Surgery Unit in Hoina, Orissa. To aid rehabilitation of those with leprosy, a new agricultural programme was funded in Uttar Pradesh, and a community farm was funded as part of the new Prevention of Disability Programme in Hoina. Forty-eight staff from LEPRA India and Government programmes were trained in TB control and HIV awareness raising, making them one of the most highly trained workers in India.
At LEPRA’s 70th AGM in 1994, H.R.H. The Duke of Gloucester addressed supporters and staff. In continuance of the celebrations, a concert was held in St. Marylebone Parish Church, a Garden Party was held in Lambeth Palace, and the Commonwealth Carol Service was held in aid of LEPRA. The Carol Service, on 7th December, 1994, was held in St. Martin-in-the-Fields, London, and recorded by the BBC World Service for transmission on Christmas Day. The address, written by the writer P.D. James, The Baroness James of Holland Park, was powerfully delivered by one of our greatest actors, and a long-term LEPRA supporter, having himself fronted appeals on our behalf – Paul Scofield.
In 1995 LEPRA India celebrated the fact that they had cured more than 100,000 patients, and Malawi was celebrating that they were down to just 1,000. Mrs. Nancy Trenaman retired as Chairman of the Executive Committee, and Mrs. Prunella Scarlett of the Commonwealth Trust took over at the Annual General Meeting. Sir Gawain Bell, former Chairman of the Executive Committee, died at the age of 86.
1996 was a remarkable year for LEPRA and significant new sources of funding were found which enabled it to substantially expand its activities, including investigating new programme areas in Brazil and India.
The codes were broken on the Malawi vaccine trial in late summer, and the data analysed. It was hoped that the mass of information gathered over the years would produce something of great interest once the analysis had been completed. The vaccine trial – the largest ever carried out in Africa, the first trial ever carried out of repeat BCG vaccinations, and the only combined leprosy/TB vaccine trial in the world - having been broken, the results were published on 5th July in The Lancet. The research showed that a second vaccination with BCG reduced the risk of leprosy infection by a significant amount over and above the first vaccination which was routinely given – indeed it showed that a repeated BCG vaccination could provide up to 85% protection against leprosy infection – a great step forward in the fight against the disease. BCG vaccination has long been used against TB and against leprosy in regions where leprosy is endemic, such as India, Africa and South America. But there had never been a detailed study made of its effect, and this ten-year project which combined a trial of a second BCG vaccination with other vaccines, proved a major breakthrough. The success of LEPRA’s work was reiterated in September 1996 when it handed over responsibility for the National Leprosy Control Programme in Malawi to the Government as there were insufficient cases of leprosy to warrant our remaining in the country any more.
Also in 1996, a successful application for funding was made to Glaxo Wellcome for research into leprosy reactions. The application to the Overseas Development Administration (ODA) for funding a joint leprosy/TB/HIV Awareness Programme in Koraput was approved in this year.
But perhaps the most exciting of all, was the fact that a successful application was made to the BBC Television’s Blue Peter programme, and LEPRA became the partner charity for their 1996 ‘Bring and Buy Sale for Leprosy’ appeal. This appeal was launched in November to raise funds for the expansion of work in India and Brazil over a 5-year period, and by the end of the year had raised almost £1m. LEPRA was chosen as the partner charity for the appeal because in April and May of 1996 it had run a ‘Leaping for LEPRA’ appeal in schools, asking children to be sponsored for the triple jump in their sports day events. This appeal was supported by Jonathan Edwards, the world triple jump record holder and Olympic record holder and gold medallist. The BBC were interested, and ran a short item on Blue Peter showing Jonathan at a school in Newcastle talking to children about leprosy. Some months later LEPRA was asked by the BBC to submit an application for the Blue Peter Appeal. A meeting took place at the beginning of August, and what seemed like an eternity passed before LEPRA was told at the end of September that they had been chosen. The launch date was 8th November, which gave just six weeks to organise the biggest appeal that LEPRA, or any other charity, is likely to have in its history. Some £2,800,000 was raised from this appeal – the largest sum ever raised from a Blue Peter Appeal in its history.
The response was so great that LEPRA had to take over part of the army barracks in Colchester to be able to deal with the volume of mail. All staff, no matter their given role in the organisation, took part in opening the thousands of letters from the children (l-r Maureen Rose, Director’s Secretary; Annette Bull, Finance; Irene Allen, Leprosy Review; Mavis Belcher, Receptionist). The appeal not only brought in a much-needed boost to funds, but also brought LEPRA into the limelight and introduced the disease of leprosy to a whole new generation. As Stuart Miles, presenter of Blue Peter at the time said on his visit to the Blue Peter Research Centre in Hyderabad in 1999:
“Filming the appeal was emotional, shocking and life affirming all at the same time. The people we met, including many children who were living with leprosy, had a huge impact on me and their stories and images were so powerful. We knew this was a message we had to get out there and that the children of the UK would respond to it, which they did in their thousands. The Bring and Buy kits were being sent out in their hundreds, so we knew it was going to be a large total, but I don’t think anyone could have predicted the final amount, £2.8 million. I felt so emotional and proud to have been a small part of something which engaged children and young people to make a difference to the lives of people with leprosy around the world.” 129
LEPRA was elected to the Standing Committee of ILEP in 1996, and appointed to hold the Chair of TALMilep (ILEP action group on Teaching and Learning Materials in Leprosy ) This was a cause dear to LEPRA’s heart as it had always been in the forefront of educational materials, not only for the general public, but also for those in teaching and medical establishments.
In India, a new temporary hospitalisation ward was built and opened in LEPRA’s BOLEP programme in Orissa and ambulances were provided for this unit, and also for the unit in LEPRA’s KORALEP programme.
In Brazil in 1996, 1,000 health agents were trained in Ceará, and the renovation of the Dona Libania Reference Centre in the State was started with funding from the Blue Peter Appeal, and it was refurbished and expanded in 1997. The new money from the Blue Peter Appeal also enabled new projects to be started – JUNLEP in India and Rio Grande do Norte and Paraíba in Brazil. Also, additional funding not only from Blue Peter but also from DFID (the Government’s Department of International Development) meant that TB control work and initiatives to increase awareness of HIV/AIDS were supported in this year.
In Malawi the Chairman and the Director had meetings with the President to discuss the handing over of the National Leprosy Control Programme to Government.
The highly successful sponsored cycle rides through India, Malawi and Brazil attracted a large number of entrants, and raised a considerable amount of money. Where LEPRA was unique in this was that they asked participants to raise their own costs and also £1,575 in sponsorship money (enough to cure 75 people from leprosy). The new Lunch for LEPRA
129 Lepra News, Autumn 2018
initiative was also launched this year on World Leprosy Day, and was fronted by the ‘Crafty Cook’, Michael Barry.
LEPRA was also asked to be represented with a stand at the exhibition which accompanied the Commonwealth Heads of Government Meeting (CHOGM) in Edinburgh in October 1997. A ‘Commonwealth Centre’ was set up in the Assembly Rooms in George Street with a series of seminars and exhibitions involving non-government organisations, all of whom had connections with the Commonwealth. LEPRA was fortunate enough to secure a stand in a prime location at the exhibition, and was even more fortunate in being visited by the Princess Royal (seen above with Ros Kerry, Regional Fundraising Manager for Scotland).
In 1998 LEPRA moved back into work with TB control and began raising awareness of HIV/AIDS with the ‘Healthy Highways’ project which targeted long-distance lorry drivers in India. In October of that year LEPRA opened a new project in Bangladesh. It was also another year of expansion of work with new programmes starting up in Orissa and Mozambique, and LEPRA extending financial help to other organisations working in Nepal and Madagascar. A lot of the funding for these projects came from the European Union and the National Lottery Charities Board towards specific projects in India.
On the personal fundraising side things improved. ‘Mr. Motivator,’ the fitness guru, who sprang to fame on British television, fronted a sponsored aerobics event at Spitalfields Market in London. This led to schools taking up the challenge and doing sponsored workouts. Also, following on from the success of the Blue Peter Appeal, a rose, named after the young Brazilian girl featured in the appeal (Adriana) was developed by Fryers Roses of Knutsford. Further, as success breeds success, The National Lottery Board, who previously had only given money to UK institutions, awarded £226,000 to LEPRA for its work. LEPRA’s Director, Terry Vasey, became President of ILEP for four years –the second time LEPRA had been honoured with the Presidency, and LEPRA was also awarded ‘Investors in People’ status
In readiness for the expansion of work in Brazil, LEPRA appointed Dr. Mauricio Lisboa Nobre as the Field Representative. At Giselda Trigueiro Hospital in Natal, he ran a state reference outpatient clinic for leprosy where doctors in medical residence were trained. Additionally, his main activities included the training of doctors and nurses from the Family Health Programme for leprosy management and support for field researches conducted by the Tropical Medicine Institute of Rio Grande do Norte Federal University, especially on leprosy epidemiology and contact tracing.
Three new custom-built mobile leprosy education vans were provided for India in an effort to raise awareness that leprosy can be cured. These vehicles were used to great effect in hardto-reach areas as they had their own generator and could show films – something had worked very successfully.
1999 was LEPRA’s 75th anniversary, and one of the events to celebrate this was a function at the Royal Geographical Society in London in February when Her Majesty the Queen and His Royal Highness the Duke of Edinburgh presented the prizes for the ‘Quest for Dignity’ art competition. Entrants had to communicate, through either a painting or a sculpture, a sense of victory not just over the disease of leprosy, but also over the stigma and prejudice that has been associated with it in the past. This competition was run in both the UK and India. Neelima Reddy, who came up with the winning picture, received her award from The Queen. Part of her winning picture is reproduced here. Former BELRA workers and others associated with LEPRA were present, along with the prize-winners, for what was a memorable evening.
The number of entries for the competition was very high, both from the United Kingdom and from India, and the standard of work in each of the categories was excellent. The depictions given by the students of the isolation that those with leprosy feel was very imaginative and their interpretations were as individual as they were. LEPRA also had a large display of where it had worked over the years, and many of the former overseas workers, in conversation with the Royal party, told of their experiences in the field – right: Mr. Terry Vasey, H.M. The Queen, visitor and Mrs. Irene Allen, display organiser.
Following his participation in the ‘Quest for Dignity’ competition and reception, Colchester MP Bob Russell tabled an Early Day Motion in the House of Commons congratulating LEPRA on its 75th anniversary.
Sadly, in that year LEPRA lost two of its Vice-Presidents – Sir Ian Fraser and Dr. Dick Rees. Sir Ian had been a highly respected and much decorated physician, and Dr. Rees had been the first Chairman of the Medical Advisory Board and a tireless worker for leprosy. A research fund was established in Dick Rees’s memory to encourage others to research into the disease.
The LEPRA rose ‘Adriana’ was launched at the Chelsea Flower Show, and much acclaimed by celebrities such as (the now disgraced) Rolf Harris, Christopher Biggins and Jane Asher. LEPRA also took possession of a new computer system to improve the speed of handling donations.
In September 1999, the National Lotteries Charities Board awarded LEPRA a grant of £275,563 to start work in Mayurbanjh, India. The grant funded vehicles, medical equipment, a revolving loan fund, salaries, running costs, information materials etc.
A State of Emergency
A devastating cyclone hit the State of Orissa in October 1999 and caused destruction on a vast scale. Many of LEPRA’s projects were destroyed, and the plight of those with leprosy was dire. LEPRA Field staff were greatly moved by what they saw and, although already stretched to the limit, redoubled their efforts to help. Still in India, a site for the proposed Blue Peter funded laboratory in Hyderabad was bought, and building work began.
On the 14th December, 1999 the Blue Peter Research Centre, built from the proceeds of the Blue Peter Appeal, was inaugurated by Dr. Michael J. Herridge, Deputy British High Commissioner. The centre is now an excellent training and treatment centre for those with leprosy, and high-quality research work is continually carried out on the disease.
LEPRA also undertook new work in Brazil and after much negotiation with its government, and new work was also supported in Nepal, China, Mozambique and Madagascar. LEPRA India was set to begin work in New Delhi after extensive discussions with the Indian Government, and a Medical Officer was finally selected for the new programme in Zambezia Province, in Mozambique, and work began at last. In an extraordinary spirit of international co-operation, LEPRA joined the Global Alliance for the Elimination of Leprosy in 1999. This alliance, consisting of the World Health Organisation (WHO), ILEP, governments of the major endemic countries and other large organisations, and the drug companies Novartis and the Nippon Foundation, set itself the task of eliminating leprosy as a public health problem in each country of the world by the year 2005. LEPRA also took the initiative to work with other allied diseases.
In 2000, LEPRA also helped in the aftermath of the devastation of Cyclone Eline which hit Mozambique, causing horrendous floods. But it was not all bad news. LEPRA India’s Chairman, Dr. Desikan, was awarded the prestigious Damien-Dutton Award in recognition of his lifetime contribution to the care of those affected by leprosy, thereby encouraging others to follow his fine example. The World Bank also extended their support in India for a further three years which enabled LEPRA to initiate a new series of health education vans in the country. It also meant that LEPRA could expand its ‘Healthy Highways’ project – a national programme which aimed to reduce the level of sexually transmitted diseases, thereby controlling the spread of HIV infection by targeting truck drivers. After a lengthy application process, LEPRA was invited by the government through the National Leprosy Programme, to undertake leprosy work in two districts of Rajshahi Division: Sirajganj and Pabna. However, devastating Monsoon floods brought chaos and disrupted the work. But despite this, the new project began at once to make a significant impact. LEPRA awaited the possibility of funding prevention of disability work in China.
The Asian Leprosy Congress was held in Agra, India from 9th to 13th November 2000, and over 1,300 delegates, including representatives from LEPRA, attended. This Regional Congress was brought about to promote more frequent interaction among participants of the International Leprosy Congress, held every five years, and to highlight regional issues, problems and achievements. It had been decided that Asia would be the most appropriate area for the first Regional Congress to take place, in view of the tremendous leprosy problem which the continent was still facing in spite of the enormous progress which had been made in combating the disease over the past 10-15 years. Even though the focus was on Asia, the Congress welcomed delegates from all over the world to share their experiences. Field-based staff were particularly encouraged to attend, to allow them access to training workshops and to contribute their own experiences to this process. LEPRA India was extremely well represented on this count with a total of 19 oral presentations and eight poster presentations. These were extremely well received by colleagues from other organisations, and were a very positive indicator, not only of LEPRA India’s wealth of experience, but also of the interest and motivation of some of the younger members of its growing team of field workers.
2001 was a significant year for LEPRA as a breakthrough in the understanding of leprosy was achieved when the genome of Mycobacterium leprae was sequenced, thereby enabling the understanding of the molecular basis of drug resistance, and the identification of potential new targets for drug development. An international team of scientists led by Stewart Cole’s laboratory at EPFL’s Global Health Institute (École Polytechnique Fédérale de Lausanne) isolated, sequenced and analysed the genomes of 154 strains of M. leprae from around the world. The study found several genes associated with resistance to antibiotics, including new genes that might point to previously unknown mechanisms of drug resistance. The results afford new and refined insights into the genome. The availability of the complete M. lepromatosis genome may prove to be useful for future research and care for the infection. The new Regional Office in Bhubaneshwar, Orissa, in India was opened in 2001, and the project in Brazil trialled new health education kits, and support was provided to MORHAN, the patient advocacy group there, in line with LEPRA’s policy of support and help with local groups.
Health Education vans in India played a major role in spreading the message that leprosy is curable. Each van cost £20,000; but can reach as many as 100,000 people every year. In 2001 there were nine vans based in Mayurbhanj, in the north east corner of Orissa. The team in each van consisted of a health educator, two paramedics and the driver. The van set up in market places, or other areas where crowds gather, and the staff gave a talk on the signs and symptoms of leprosy and encouraged people to come forward for examination. A giant screen set up behind the rear doors of the vehicle, showed films (with a very loud sound system) interspersed with snippets of the latest Bollywood blockbusters to attract attention. The leprosy films were translated into the local language (Oriya) to ensure that everyone understood what the teams were telling them. Other films were often shown on lymphatic filariasis (elephantiasis) and HIV/AIDS to help answer some of the other local concerns.
The ever-irrepressible Dr. Desikan, in India (left in the picture) was honoured with the International Gandhi Award for his outstanding work in leprosy, and tireless UK fundraiser, and former overseas worker, Wally Leach, 100 years old, was made MBE in the 2001 New Years Honours List. Both men, in very different ways, were incredible ambassadors for LEPRA and its pioneering work.
Another initiative in 2001 was an Eye Care Workshop, hosted in the UK, where eye care specialists worked together to produce a guideline that could be used internationally when dealing with leprosy-related eye problems.
2002 was a momentous year in many ways. Firstly, LEPRA began a 3-year project on the molecular epidemiology of M. leprae. This study looked to further understand the causes of leprosy transmission and why some people are more susceptible to the disease than others. Secondly, support from the London School of Hygiene & Tropical Medicine, together with funding from the Wellcome Trust, enabled LEPRA to continue further studies into the immunology of leprosy, TB, and HIV/AIDS in Malawi, and trials for TB vaccines showed that the vaccine has protective effects against leprosy among the local population.
LEPRA India also had a remarkable year in that the International HIV/AIDS Alliance chose it to be the lead agency in HIV/AIDS protection work in Andhra Pradesh, thereby increasing LEPRA’s involvement with the management of this disease. In another show of its growing importance, the Head of Finance and Administration for LEPRA India was requested by the Institute of Chartered Accountants for India to produce accounting and auditing guidelines to be used by all Non-Profit Organisations in India. This was an extremely important assignment, and reflected the high regard in which LEPRA was held in India. LEPRA India also set up its own fundraising operation to increase the contribution to its local programmes from in-country fundraising activities. An important new working partnership was also established with Sight Savers International to provide eye care and sight-saving surgery in three districts of Orissa. Work on a new surgical unit was also begun in this year, and India appointed 40 new counsellors to help in the fight against HIV/AIDS in Andhra Pradesh, in partnership with the Andhra Pradesh AIDS Control Society, UNICEF, and the District Co-ordinator of Health Services. LEPRA India staff were also honoured in August 2002 when two of its female workers received the State Award for the ‘Best Placement Officer of Persons with Disabilities’.
LEPRA’s work in Angola grew in 2002 as LEPRA joined forces with the Angolan Government and the American Leprosy Missions to fight leprosy and tackle more general health issues now that some order had been restored after years of civil war.
In February 2003 LEPRA’s international contribution to the fight against leprosy was recognised at the Third Meeting of the Global Alliance for the Elimination of Leprosy (GAEL) in Yangon, Myanmar. In Brazil, LEPRA undertook a Strategic Review, and operational research was
identified as an urgent requirement to enable the charity to identify the most effective way to address the priority needs. The Department for International Development (DFID) and Civil Society Challenge Fund also co-funded a project to provide support to five local leprosy groups in Ceará State.
2003 was a year of fundraising initiatives: An appeal on Radio 4 by LEPRA’s President, Sir Chris Bonington, C.B.E., raised over £37,000; the Celebrity Shoe Auction raised £10,000, another Celebrity Jewellery Appeal was launched, and the cruise specialist, Swan Hellenic, chose LEPRA to be its partner charity until the end of 2004.
But, as always, there was sadness too. Dr. Jo Colston, Chairman of the Medical Advisory Board and long-time friend and supporter of LEPRA died suddenly aged only 54. Among his earliest achievements were the development of methods to determine the number of viable cells of the leprosy bacillus, an uncultivable pathogen, and their susceptibility to drugs. As an adviser to the World Health Organisation (WHO), he was instrumental in devising the multi-drug therapy that has brought leprosy to the verge of elimination. He then turned his attention to tuberculosis, and made seminal contributions to the microbiology, immunology and prevention of the disease while leading the division of mycobacterial research at the National Institute for Medical Research (NIMR) in Mill Hill, north London. Dr. Desikan also retired as the Chairman of LEPRA India – another incalculable loss. But highlights included Sir Chris Bonington receiving ‘The Big Red Book’ in BBC Television’s ‘This is Your Life’ programme, and women achievers in LEPRA India being rewarded for their tireless efforts.
In May 2004, LEPRA’s prestigious medical journal, Leprosy Review, was cited as one of the top five tropical medicine journals as referenced by the Institute of Scientific Information, and on 1st December, a special Thanksgiving Service was held at St. Martin in the Fields, London, to mark LEPRA’s 80th Anniversary. Also, the new Reconstructive Surgery Unit at St. Joseph’s Leprosy Centre in Madhya Pradesh, became operational, and was formally opened in December. The unit carried out about 12 operations per month to help those with deformities caused by leprosy, and meant that those requiring leprosy-related surgery would not have to travel several days to have their operations. Reconstructive surgery was one of the main ways of helping those with obvious physical disabilities (like clawed hands) reverse the outward signs, although most of these surgeries were not able to reverse the damage already done. The autogenous muscle-graft study of 1991, although successful in a small number of cases, had proved too costly and too ‘random’ to be of universal use, but at least reconstructive surgery could take away the stigma of perceived disability in most cases.
In 2005 LEPRA’s Executive Committee approved £18,750 for a new project in Orissa. This was an exciting new initiative looking at addressing the health needs of a migrant population in respect of HIV/AIDS transmission. The project aimed to improve the deplorably poor health and living conditions in Ganjam and Gajapati districts for migrant workers. The growth of LEPRA’s work in India also meant that some staff formerly based in the LEPRA India Office, were re-located to a new office in Hyderabad. Those staff involved with overseeing LEPRA India’s projects in Andhra Pradesh, Bihar and Madhya Pradesh were given their own Regional Office.
Growth and development were central to discussions about LEPRA’s work in Bangladesh, and it was recognised that to take this development forward, it would be necessary to establish an office and country representative in Dhaka, and £40,000 was earmarked for this. LEPRA was also successful in attracting funding for work to improve awareness of Lymphatic Filariasis (LF) in five districts of Bangladesh. £59,000 was made available for LEPRA to work with a partner organisation in each of those areas where training on the disease was provided through the partners to volunteers, local workers and leaders. Communities were informed through a series of health education activities such as visits to schools and colleges, film shows to villages, group meetings, distribution of leaflets and posters and broadcasting a short film for television. Villagers were encouraged to take part in the drug administration programme provided by the government health department of Bangladesh. This mass drug administration programme aimed to eliminate LF over a five-year period.
Work also started this year in Guatemala to prevent malaria and improve access to health services. This work reduced infant mortality by the provision of mosquito nets, draining mosquito breeding areas, and strengthening the network of anti-malaria volunteers. LEPRA focused on this area because the community included isolated and vulnerable people who lived in the most malaria-endemic areas of the country. There were many changes in LEPRA’s work in Mozambique in the early 2000s, with Dr. Wolfgang Hippke, LEPRA’s Representative, formerly based in Zambezia Province, and his wife Jane, moving to the capital Maputo to work for the Ministry of Health. Dr. Hippke still oversaw LEPRA’s leprosy and TB work in Zambezia while the charity identified a new person to continue and further develop the work there. The Mozambican Government also asked LEPRA to become involved in other activities. 2005 saw a considerable expansion of LEPRA’s work in Angola. Following the departure of its Representative, Mary Stewart, at the end of her contract in 2004, LEPRA began the search for appropriate people to take the work forward. In order to strengthen the sustainability of its support, LEPRA focussed on local recruitment as well as identifying support mechanisms in Luanda which would allow for better support to, and development of, its work in Moxico Province.
In 2005 LEPRA moved to its new offices at 28 Middleborough, Colchester – a self-contained octagonal building which had formerly been part of a large insurance company. Also in that year, the prestigious American Centers for Disease Control and Prevention (CDC) awarded LEPRA India a $340,000 grant to set up an HIV care and support programme in Andhra Pradesh, and The Big Lottery Fund approved a five-year grant to help them work with largely tribal communities in Mayurbhanj, Orissa. They contributed £560,000 of the £746,000 needed.
In January, 2006, the novelist, Victoria Hislop’s debut novel The Island won the Galaxy British Book Awards prize of ‘Newcomer of the Year.’ The Island told the story of someone who discovered that her relatives had once been on the island of Spinalonga, which was, for a large part of the 20th century, Greece’s colony for those with leprosy. Victoria made mention of LEPRA’s work at the end of her book, and royalties from this come to us. She is now an ambassador for the charity.
The Government of the State of Andhra Pradesh commissioned LEPRA India to place Counsellors in each of its HIV testing centres. These centres directly benefitted 258,817 who walked in to be voluntarily tested; 31,993 of these were found to be positive; and the BBC Medical Correspondent, Fergus Walsh, visited India and worked closely with LEPRA staff for a film.
New ways of fighting leprosy came in 2007 when the use of Global Position System (GPS) technology to identify potential leprosy cases was brought in to find ‘hidden’ cases. This successful system was trialled in other parts of LEPRA’s work. GPS is a satellite-based radio navigation system owned by the United States government, and is one of the global navigation satellite systems that provide geolocation and time information to a GPS receiver anywhere on or near the Earth where there is an unobstructed line of sight to four or more GPS satellites. It does not require the user to transmit any data, and operates independently of any telephonic or internet reception, though these technologies can enhance the usefulness of the GPS positioning information. It provides critical positioning capabilities to military, civil, and commercial users around the world. Although the United States government created, controls and maintains the GPS system, it is freely accessible to anyone with a GPS receiver, which is of immense benefit to those needing to find particular settlements, especially in isolated rural locations.
The rise of TB in India in 2007 was also noted, and LEPRA teams were attacked with stones by tribal villagers who thought their sputum collections were to be used for witchcraft! But it wasn’t only TB that was on the rise – LEPRA joined the Global Alliance to Eliminate Lymphatic Filariasis (GAELF) to give support to the Global Programme, primarily in Bangladesh, and the success of this is testament to the collaboration between partners that LEPRA promotes. Lymphatic Filariasis causes swelling of the legs and genitals and is not only debilitating but stigmatising, and causes great distress.
Former leprosy patients in the Alto Molocue district of Mozambique started their own self-help group in this year. Sixty members, of whom 31 were former leprosy patients, participated in shared farming activities according to their skills and remaining physical capabilities. LEPRA supported and encouraged this group to include non-leprosy patients so as to lessen the stigma surrounding their efforts. They also helped provide tools and seeds, and ran training courses in organisational development and project design and management so that these projects could become better developed and sustainable for the long-term.
A request was made in 2008 by the LF Programme Manager of Nepal for LEPRA to assist in mass drug administration and self-care management because of its successful work in Bangladesh and
India. At this time LEPRA was the only organisation with field staff dedicated to address LF and soil transmitted helminthes (parasitic worms) in Asia; because of this massive commitment to neglected tropical diseases, LEPRA was voted vice chair of the group by the members of the network.
Devastating floods hit India’s north-eastern state of Bihar in May 2008, but LEPRA managed to continue its work, and mobile clinics were launched in response to the most common health issues affecting isolated and hard-to-reach communities.
Wonderful news from Malawi in 2008 that there were NO reported cases of leprosy in the district was greeted with great satisfaction, but notification that HIV was spreading rapidly dampened this down. Later, news that funding promised from major donors would not be forthcoming forced LEPRA to close its programme in Angola, but the work in Guatemala on preventing malaria and improving access to health services was expanded.
The following year, a key emerging challenge for LEPRA India was the increased failure of government healthcare systems to diagnose leprosy at an early stage. In April of that year 40 National Leprosy Programme Managers from around the world, and members of the World Health Organization (WHO) met in New Delhi, to discuss the next global strategy to combat the disease.
But at the Blue Peter Research Centre (BPRC) in Hyderabad, research work pressed ahead, and a small multi-centre study project on TB looked at factors responsible for infection, and also the diagnosis and epidemiological features of multidrug-resistant TB which was causing so many problems. The immunological and molecular aspects of leprosy, TB and HIV-TB co-infection were also studied, developing molecular techniques to detect the presence of Mycobacterium leprae and drug-resistant mycobacterium in clinical and environmental samples – a vast undertaking. But that was not all; BPRC also undertook to study TB and HIV co-infection in patients who were already HIV positive, to determine the rate of progression to full-blown AIDS and, keeping with the TB theme, the molecular epidemiology of TB and lymphatic filariasis. It was also carrying out drug sensitivity tests on behalf of the National TB Programme to detect TB multidrug resistance in four districts in Andhra Pradesh, and processing, analysing and reporting on tests for those with HIV.
In Malawi, 2009 marked the third year of a 5-year research programme being undertaken by the Karonga Prevention Study, which covered HIV and demography, and TB and pneumococcal diseases, looking at the consequences of antiretroviral therapy (ART), and the resulting improved life expectancy, and prevention of HIV infection.
A ‘Global Appeal’ was initiated on 25th January, 2010 by Yohei Sasakawa, WHO Goodwill Ambassador for leprosy, in Mumbai, India. Fifteen world business leaders signed the Global Appeal in support. According to WHO there were 133,717 new leprosy cases registered in India, which accounted for more than 65% of leprosy cases worldwide.
In May, Tata Steel teamed up with LEPRA India to launch LEPRA Sparsh, a hospital/referral centre project aimed at providing treatment to those affected by leprosy in the state of
Jharkhand. LEPRA continued its focus on fighting leprosy stigma in Colombia, and it trained volunteers in TB recognition in Mozambique, but the charity was in dire financial straits and its Chief Executive, Terry Vasey, resigned.
A new phase in LEPRA’s life began when Sarah Nancollas, the first female CEO, took over control on 1st September 2010, working to fight disease, poverty and prejudice, and she transitioned it from being a medically-focused to a people-focused development charity. Sarah was also Chief Executive of Canon Collins Trust, a southern African education charity where she introduced a number of activities to specifically empower women and girls.
It was clear that having drawn on reserves for some time to maintain its projects, this level of output was not sustainable, and finances were in a dire state, so far-reaching, and very difficult decisions had to be taken on its work. LEPRA sought to reduce the number of programmes it supported, and many of the South American projects were handed over to other ILEP NGOs to cover. This was a depressing time when many programmes were closed down due to lack of funds, and several good and dedicated staff members, both in the UK and abroad, were made redundant through no fault of their own. However, Sarah, with her pragmatic approach, managed to obtain loans from ILEP members to enable LEPRA to continue work until restructuring had been achieved.
On 31st October, 2010, the BBC’s Medical Correspondent, Fergus Walsh, presented the Radio 4 Appeal on behalf of LEPRA on the subject of lymphatic filariasis. This appeal was repeated on 4th November and the two raised over £40,000.
In January 2011 screening camps in three areas of Madhya Pradesh, India, led to 117 people coming forward, and of these, 43 underwent surgery for leprosy-related conditions, and in line with the trend of more people coming forward, leprosy was declared ‘de-eliminated’ in Orissa, with the prevalence rate moving from 0.6 to 1.09 people per 10,000 population. Also, a new study from the Blue Peter Public Health Research Centre in Hyderabad identified new biomarkers to detect TB early in HIV positive people.
In January 2012 Dr. Paul Saunderson took over as Editor of Leprosy Review from Dr. Diana Lockwood, who had been Editor since 1996. He has been a member of the WHO Technical Advisory Groups for both leprosy and Buruli ulcer. Having gained his medical degree at Cambridge in 1976, he had worked in the field of leprosy since 1981. He started his career at a mission hospital in western Uganda, and in 1994 was appointed Director of the Leprosy Control Division of ALERT in Ethiopia.
In addition to providing direct services through referral centres, technical resource units and laboratories, LEPRA trained 2,272 community volunteers in India, as well as 13,000 government health staff and 2,928 unregulated and undertrained private health practitioners and village doctors – no mean feat. In May, Bihar reported around 20,000 new cases of leprosy – the highest new case detection rate in India. There were also 30,000 new cases of kala-azar in Bihar, and the districts in North and East Bihar were especially prone to malaria and kalaazar as they were hit by floods every year. It was also noted that an astonishing 25 out of 38 District Leprosy Officer posts were vacant in Bihar. However, 300 women were trained in
tailoring and embroidery in LEPRA’s Cairn sponsored community health project in Arogya Disha in India. LEPRA also increased its awareness campaign on Lymphatic filariasis which gave renewed hope to ‘hidden’ women in India
Sadness came with the news that ex-LEPRA Administrator in Malawi, John Eldon, MBE and Dr. Arthur Garrett, late of Oji River Leprosarium in Nigeria, died in 2012.
The LEPRA Blue Peter Public Health Research Centre continued researching and developing new diagnostic tests for MDR TB in an effort to find a cheap and effective way of diagnosing its strains earlier and increasing patients’ chances of survival. Also, a victory was won when LEPRA took the film maker Aardman to task over their proposed animated film ‘Pirates! In adventures with Scientists.’ They were persuaded to remove an objectionable ‘joke’ concerning leprosy, and this was a considerable achievement.
CHAPTER NINE
Another ‘beginning’ and a re-brand 2012-2023
Another considerable achievement in 2012 was the fact that LEPRA was able to repay all the outstanding loans that were taken out to keep it afloat, and the charity became debt-free. To celebrate this, and to enter into a new phase of its work, the London-based branding and creative agency called ‘Industry’ began work on LEPRA’s rebranding, giving their expertise free of charge, and on 1st June 2013, LEPRA in the UK became Lepra (although LEPRA India retained its capital lettered title), exchanging the ‘hand’ for the ‘speech bubble’ as its logo.
In 2013, a new project in Bangladesh began to work with more than 22,000 people affected by physical disability to improve livelihood opportunities by skills training and business grants. As the responsibility for diagnosing and treating leprosy with MDT moved progressively to governments, Lepra focused increasingly on working to mitigate the impact of the disease, through community health education, treatment of reactions, prevention of disability and supporting groups of people affected by leprosy to access appropriate services and support.
Research to date has still been unable to determine fully how leprosy is incubated and transmitted. Until more is understood it was felt inappropriate to commit to ending the fight against this disease within a defined period of time. Lepra’s focus was to make leprosy of little consequence to the person contracting it, easily diagnosed and treated, causing no residual disability and attracting no stigma. At the same time, it sought to change the lives of children, women and men that were living with the consequences of untreated leprosy, supporting them to improve their lives.
With its many years of expertise, Lepra demonstrated that it could use the experience it had developed in leprosy to address other neglected diseases, in particular to address disability management and stigma reduction in lymphatic filariasis (LF). Given the scale of LF (120 million cases worldwide with 40 million living with an LF disability) and a strong overlap in endemic areas, Lepra felt it had a real opportunity to rebuild leprosy knowledge and skills, and access new sources of funding through working in combination with LF.
The global annual incidence estimate of visceral leishmaniasis (VL) at this time was between 201,500 and 378,500 cases. Over 90% of such cases occurring in six countries – Bangladesh, Brazil, Ethiopia, India, Nepal and Sudan – with India accounting for about 50% of the global burden. Lepra had some limited experience of successfully applying its community-based approaches to tackle VL and wanted to demonstrate this on a larger scale.
In 2015 LEPRA re-evaluated its goals, and recognised that it was values led, driven by the needs of the individual rather than limited to the treatment of a disease. With its values as its compass, Lepra felt it could be agile and ambitious in the future whilst responding to need. To that end its new values were sharpened up to meet the needs of the 21st century, and in pursuit of its vision it would be, as it always had been:
• People centred, together with the people it works with and for, acknowledging the world from their perspective
• Transparent and accountable to the people it works with, its staff, supporters, and stakeholders;
• Innovative and demonstrating bold leadership at all levels;
• Effective and efficient;
• Collaborative, working together to achieve the benefits of synergy
Its vision was to be a leader in reducing the incidence and impact of leprosy and other neglected diseases. Driven by its focus on leprosy, its purpose, therefore, was to enable children, women and men affected by neglected diseases to transform their lives and overcome poverty and prejudice. To this end, three new projects were begun in April 2015: ‘Restoring Lives of Forgotten People’ in Samastipur, Bihar, India, which was funded by the Big Lottery Fund, and ‘Combined Approaches to Tackle Leprosy and Lymphatic Filariasis (Sankalp)’ in both Andhra Pradesh and Odisha which was funded by Effect Hope, which tackles leprosy and LF. A baseline study of all blocks of the district was undertaken by the block coordinators using the Knowledge, Attitude and Practice (KAP) tool. This data provided details on the case loads of leprosy, LF and hydrocele in the district. The long-term aim was to improve health education, self-help and self-care, training, and introducing, where appropriate, mobile technology.
A mobile footcare van - a unique initiative of LEPRA Society - with the support of Pavers Shoes, UK was also started in April 2015 to provide protective footwear to the people affected by leprosy and LF in 63 colonies of Bihar. The van moved around in hard-to-reach areas distributing footwear made from Micro-Cellular Rubber to men and women affected by leprosy. A protective footwear unit was also established at Hasanpur by LEPRA Society. Sankalp – a holistic project to tackle LF and leprosy, and this was launched in Odisha on 23rd November 2015. It was implemented in collaboration with the Department of Health, Government of Odisha in 1,272 villages of seven blocks of Puri district and two blocks of Nayagarh district with the goal of breaking transmission, preventing disability and addressing issues of dignity and poverty of those affected by lymphatic filariasis and leprosy.
In 2015, Lepra also started to fund work delivered by Netherlands Leprosy Relief (NLR) in the Zambezi province of Mozambique.
A referral centre is a one-stop hub and the fulcrum of the activities in leprosy. The old Centre at Dhoolpet in Hyderabad, was relocated to Mahaboobnagar in Telangana, and inaugurated in January 2016, as nearly 12 per cent of leprosy Grade 2 disability and 1,001 LF cases were reported from here. Also, the health infrastructure in terms of expertise for leprosy and LF services was inadequate in Mahaboobnagar district. The purpose of the centre was, and is, to
promote early case detection among women and children and prevent disability as well as to halt the worsening of existing disabilities among people affected by LF and leprosy. It also empowers these people and their forums to claim their rights and entitlements. People living in the town and district can now easily access the services there.
In Madhya Pradesh, LEPRA leveraged State NLEP funds to conduct Prevention of Disability (PoD) camps and facilitated provision of footwear. The Government provided entire budgets for organising camps in all districts of the state. LEPRA Society’s Technical Resource Units contributed to the improvement in case detection and management of leprosy cases and also the implementation of Leprosy Case Detection Campaign and Intensive Case Detection Drive in endemic blocks. As part of its advocacy, LEPRA Society has been taking up the rights of people affected by leprosy particularly on the issues of stigma, discrimination and human rights. LEPRA Society continues to work in partnership with other organisations such as the Association of People Affected by Leprosy (APAL), the Society for Leprosy Affected People (SLAP) in Andhra Pradesh and Telangana, APAL in Odisha, and Sam Utthan in Bihar to support existing advocacy initiatives. It also helps build the capacity of these organisations and links them to state administrative machinery to access welfare schemes.
India carries 55 per cent of the global burden of LF, which is not curable, but can certainly be contained. LEPRA Society is currently the forerunner among NGOs in developing an integrated approach for disability care in leprosy and LF. Disabilities in LF have been addressed through home-based and community-based approaches. Self-care advocated by LEPRA Society has helped in morbidity management through which people have found relief. Three new projects were begun by LEPRA Society in this year: Sankalp in Odisha and Andhra Pradesh (with support from Lepra in the UK) and the Munger Project. The organisation also took part in the Neglected Tropical Disease NGDO network where it contributed to discussions to WASH (Water Sanitation and Hygiene) and NTDs (Neglected Tropical Diseases), particularly leprosy. LEPRA was nominated in the Morbidity Management and Disability Prevention working group. Restoring Lives of Forgotten People in Bihar (funded by the Big Lottery Fund) adopt this integrated approach to treat people affected by leprosy and LF. KoBo mobile Technology is being used for Knowledge, Attitudes and Practices (KAP) study and data collection in Sankalp projects. LEPRA Society supported the State Filariasis Programme Unit in the MDA in Bihar and Madhya Pradesh. It also participated in a national level consultation meeting on Innovative Approaches in Prevention of Disability (PoD) programmes organised by ILEP and the Government of India.
The five-year strategy which was begun in 2016 renewed Lepra’s efforts to make leprosy a disease of little consequence; easily diagnosed and treated, leaving no obvious disability and attracting no stigma. This compelled us to support children, women and men to live healthily and economically secure lives, participating and contributing to their communities.
In 2017 a new Chief Executive was appointed. Geoff Prescott had worked for many years overseas in medical humanitarian aid. With a background in business strategy and disaster response, operations management, and non-profit management, he had worked as a freelance consultant before joining the Lepra team.
2018 saw the return of Blue Peter presenter, Stuart Miles to the Blue Peter Public Health Research Centre, which he had officially opened in 1996. As a result of this return trip, Stuart became a Lepra Ambassador, helping to launch the successful ‘£1 from you’ appeal, and making numerous media appearances to raise awareness.
On Wednesday 30th January 2019, Lepra partnered with Cantata Dramatica to bring together an evening of contemporary choral music hosted by London’s St. Stephen Walbrook Church for World Leprosy Day. A sold-out crowd witnessed the performance, which featured the world premiere of Nick Bicat’s ‘Akathistos’, a dramatic retelling of the famous Orthodox Hymn that saved Byzantium from the Persian Siege in 626AD. In attendance was guest speaker Roger Right, CEO of Snape Maltings and the Aldeburgh Music Festival who spoke about his experience with leprosy. This event raised over £2,500. A petition, entitled “I am not my disease, don’t call me a ‘leper’!” collected over 748 signatures during the evening. It was sent to the UN Secretary General to highlight the discrimination and prejudice those with leprosy still face, and to bring about important changes to the language used about leprosy.
2019 also saw a Memorandum of Understanding signed with the John Bradburne Memorial Society in Zimbabwe. John Randal Bradburne, (1921 – 1979) was an English lay member of the Third Order of Saint Francis, a poet, and warden of the Mutemwa ‘leper’ colony at Mutoko, Rhodesia (now Zimbabwe). He was killed by nationalist guerrillas and he is a candidate for canonisation. On 15 July 2019, the Holy See gave the nihil obstat for the start of the cause of canonisation by giving Bradburne the title of ‘Servant of God’. In the same year Lepra began working in an advisory capacity in the Mutemwa Leprosy Care Centre, providing essential skills and training for those helping people affected by leprosy in Zimbabwe. Following a visit by Lepra staff, a shipment of specialist sandals was sent to the centre, providing tailor-made protective footwear for those affected by leprosy. Training for local cobblers was also provided.
Lepra India colleague, Rajni Kant Singh was awarded the Mphasis Universal Design Award in late 2019 at the India International Centre in New Delhi. Rajni had developed a ‘Mobile Foot Care Unit’, which delivered protective footwear to those in remote and isolated regions of India. His work allows for those in these remote areas to access the necessary lifesaving treatment and care they need. In his capacity as Bihar State Coordinator for Lepra India, Rajni has dedicated 20 years of his life to helping those affected by leprosy and LF. He also champions those with Hydrocele, a symptom often linked to LF, as he himself was affected by this, and undertook surgery. Since then, he was made Lepra’s State Coordinator for Bihar, and now helps other men in a similar situation to know that there are options for them. Following this, Lepra teamed up with the Vodafone Foundation on an exciting new project called Mobilising Men’s Health. The project helps men to overcome hydrocele by funding surgery and offering a bursary to cover lost wages during their recovery. Unfortunately, at the moment, LF and hydrocele do not qualify as disabilities in much of India, so a big part of Lepra’s work is to lobby governments at the state and national level to change this, as the effects of LF and hydrocele can be debilitating.
On 21st October, 2019, Lepra signed a historic Memorandum of Understanding with the rotary clubs of Delhi South, Delhi Southend and New Delhi. These clubs are members of Rotary
International, an organisation that boasts more than 35,000 clubs in over 200 countries. The Memorandum of Understanding is focused on working in partnership to establish the ‘Control of Leprosy in India.’ A pilot project was developed to create a showcase of a model leprosy awareness and case detection campaign.
On 30th October 2019 Lepra said farewell to its esteemed colleague, Dr. Aprue Mong, who had served as the Country Director in Bangladesh since 2007. Qualified in medicine and surgery, Dr. Mong was an invaluable asset to Leprosy Bangladesh. His passion for those affected by leprosy allowed him to drive for changes to government health policies. Dr. Mong said, “When I came to work with Lepra, I knew we needed to do something big. The Bangladesh health system was not responding to the leprosy problem in the country and the government were not helping those in need.” Dr. Mong continued to work with Lepra Bangladesh in an advisory capacity, and was succeeded by Dr. David Pahan.
In December 2019, Lepra staff attended the National Conference on Leprosy in Dhaka, Bangladesh, along with its in-country team. Lepra, with The Leprosy Mission, supported by the Sasakawa Foundation of Japan, was instrumental in organising this event following a study it conducted, where it discovered that 75% of doctors and health care staff received no training at all on leprosy. This conference aimed to change that, and was, in fact, a wonderful show of progress and momentum in this. The Prime Minister of Bangladesh, Sheikh Hasina, reaffirmed the Bangladeshi government’s commitment to tackling leprosy and making it a national health priority.
The celebrations for World Leprosy Day on 28th January, 2020, took the form of an event in the House of Lords. The evening focused on the Mental Motivators project in Bangladesh. The event was attended by H.R.H. The Duke of Gloucester, Chair of the Trustees, Charles Bland, and hosted by The Lord Gadhia. LEPRA India marked the occasion by embarking on a Leprosy Fortnight! An ambitious appeal was launched in India ‘Mission One Crore (M1C)’ (the equivalent of £100,000) to raise these substantial funds through various sponsored charity walks, in five different states across India. The Head of Resource Mobilisation with LEPRA India, Kasturi Kilaru, said of the event, “M1C as a fundraising event is unique, because it is the first time in the history of LEPRA Society that all the staff (over 500 people) are involved directly in fundraising…M1C is not only an attempt to raise one Crore Indian rupees, but is also an opportunity journey to reach out to one Crore people with our message.”
Also on 28th January, Lepra launched its ‘New Faces of Leprosy’ gallery exhibition at the House of Lords. This travelling exhibition, shot by professional photographer, Tom Bradley, and curated by Professor Diana Lockwood, travelled around the UK during 2020 to highlight the stories and lives of some of those affected by leprosy. The object of the exhibition was to show leprosy patients having a normal life, working and having a family, and intended to show that those affected by this disease are strong and can overcome anything.
In the aftermath of World Leprosy Day, and with a renewed global commitment to fighting leprosy and making it a priority throughout 2020, Lepra once again quantified its stance on key areas in leprosy care. The global leprosy community had now found itself at a crossroads with regard to care and management of those affected. The World Health Organisation was
committed to introducing two measures against leprosy, Single Dose Rifampicin Post-Exposure Prophylaxis (SDR-PEP) and the addition of Clofazimine to the existing 6-month paucibacillary (PB) antibiotic treatment regime. Lepra, as an evidence-led organisation, therefore were opposed to WHO’s SDR-PEP protocol because it believed that there was not enough statistical evidence of benefit from these protocols to justify deflecting attention from active-case-finding (ACF). Evidence suggested that 57% of the milder PB cases would not contract leprosy over two years (The COLEP study) if given SDR-PEP. Multibacillary (MB) cases, immediate family and 43% of others would Another piece of research showed that SDR-PEP could actually lead to more cases of MB leprosy i.e. the type that leads to serious disability and is infectious for others if the recipient has had a BCG vaccination, which most do in Bangladesh and India (The Maltalep study). Secondly, contact screening calls for people affected by leprosy to disclose their status to friends, neighbours and colleagues. People affected by leprosy suffer great prejudice, discrimination and unfairness in both their personal and professional lives.
Lepra is, and always has been, against any method of screening that jeopardises a person’s safety, and inclusion in society, and thirdly, during a time of tremendous concern throughout the medical community with regard to antibiotic resistance, the introduction of single-dose Rifampicin as a means of combatting leprosy increases the risk of drug resistance. Rifampicin is the most potent and widely used antibiotic used for TB and occurs in approx. 2.8 million people in India, so the concern is significant for TB as well as leprosy. Currently, the antibiotic Clofazimine is not included in the 6-month paucibacillary (PB) leprosy treatment regime. The WHO recommended that this be added to existing treatment for those with PB leprosy. Lepra opposed this for several key reasons:
1. Clofazimine’s side effects can lead to lower overall treatment compliance. It can cause severe skin pigmentation, something directly related to social and inclusion issues in many countries.
2. There is no clinical evidence to suggest that this has a positive impact on the treatment of those affected by PB leprosy.
3. The use of this unnecessary extra antibiotic increases the risk of antibiotic resistance.
But in early 2020 the Covid-19 pandemic which had begun in China in December 2019, proved to be a significant social and economic global catastrophe, which systematically exposed and exacerbated the exclusion of the under-privileged and marginalised communities in the leprosyendemic world. India’s second wave of Covid caused a massive surge in infections and deaths. The unprecedented public health emergency and subsequent lock-downs disproportionately impacted people affected by leprosy and LF. Covid-19 vaccinations became a major humanitarian priority for both the public and private health sectors. However, people affected by leprosy often faced delays in receiving the vaccine, with the pandemic only adding to the neglect and exclusion already faced by so many. The emergency vaccination programme, funded by Lepra and Effect Hope provided vaccinations across six states in India (Andhra Pradesh, Bihar, Jharkhand, Madhya Pradesh, Odisha and Telangana) for over 17,987 people. During the pandemic, many people were hesitant and had concerns about the safety and efficacy of vaccination, and Lepra’s intervention helped people affected by leprosy make informed choices about the vaccination programme, and provided transport to the vaccination centre for those unable to make the long journey because of their disabilities.
The emotional impact of a leprosy or LF diagnosis can be severe, and the problems due to the endemic all add up to great concern among patients. In addition to the physical implications, prejudice, fear and a lack of knowledge can lead to further secondary harms such as social exclusion, the loss of income, employment, and the breakdown of family life. As a result, over 50% of people with newly diagnosed cases of leprosy and LF will develop anxiety and/or depression. In Bangladesh, Lepra’s Mental Motivators project was developed to create an inclusive and sustainable, community-led support mechanism designed to improve the mental health and quality of life for families. Following Lepra’s person-centred, holistic approach, the project aimed to enhance self-esteem, status, social interaction and inclusion within people’s immediate community and wider society, to help them gain access to public and private opportunities and services. Initially, Lepra Bangladesh recruited 30 Mental Motivators from existing self-support groups from four district. They were provided with mental health training including stress management, listening skills and low-level support for managing depression and anxiety. In April 2020, this project was extended, with three new districts and 20 additional Mental Motivators trained to provide support within their communities. The project took on a new significance throughout the Covid-19 pandemic, with Lepra’s community-led support offering the most vulnerable members of society vital emotional help and support at this difficult time. The project was re-named ‘Proshanti,’ meaning ‘tranquillity’ and was further extended in April 2021 into three more districts with an additional 20 Mental Motivators recruited in those areas. In its third phase, 1,100 counselling sessions were provided, with 40 new self-care groups established, and the programme was able to act as an important touch point for those needing additional support such as food aid, additional income and Covid-19 vaccinations.
For those at Lepra, as with most other organisations, 2021-2022 was another year dominated by Covid-19. Everything that they did was framed by the constant backdrop of this pandemic, as they kept on pushing through its various waves and lockdowns. This meant doing all they could to support those affected by leprosy and LF, and great tribute must be paid to the incredible work of LEPRA teams in India, Bangladesh and the UK. Their hard work ranged from providing Protective Personal Equipment (PPE), to ensuring access to Covid-19 testing and vaccinations, supplying oxygen cylinders, or providing food and financial aid for those affected by leprosy and LF. During this time, the World Health Organisation estimated that there was a 41% reduction in new leprosy cases detected due to Covid-19 in 2020, but Lepra’s own experience from India and Bangladesh suggested that this figure could be even higher. This being the case, LEPRA India increased referral centre services in rural India that were previously scaled back due to the lockdowns, and in Bangladesh they formed more self-support groups and federations so that they could advocate for full inclusion in society of those with leprosy and LF.
The start of 2022 brought another change of leadership in the shape of Jimmy Innes, the current (2024) Chief Executive Officer, effective from 10th January. Prior to his appointment at Lepra, Jimmy was CEO at ADD International since 2017, working for disability rights and inclusion in Africa and Asia. Before that, he was responsible for programme delivery in the fields of maternal, reproductive and newborn health at Options Consultancy Services. Keen to continue the holistic, person-centred care that Lepra’s healthcare experts on the ground provide for those who need it most, Jimmy identified new commitments for the 2022 Global Disability Summit, which most closely resonate with Lepra’s own organisational aims and which are within its means to deliver.
8th September, 2022 was a very sad day when our patron of almost 70 years, Her Majesty Queen Elizabeth II died in Balmoral, in Scotland. She had been a staunch and loyal supporter of Lepra ever since she acceded to the throne, and gave a great boost to leprosy work by her compassion and care. All staff who had had the privilege of meeting Her Majesty through their work with Lepra, spoke of her great understanding and compassion for the disease and those it affected.
On 20th September 2022, a travelling photographic exhibition by Tom Bradley, showing the ‘true’ face of leprosy opened in Edinburgh at The Pavilion at Myreside, then on 23rd September it travelled to Glasgow and the Trades Hall, and then to Ripon Cathedral on 29th November (which coincided with ‘Giving Tuesday’). The exhibition sought to break down the barriers of prejudice that surround people with leprosy. In the spring of 2023, Tom and Professor Diana Lockwood travelled to Bangladesh, to continue the landmark documentary series, telling the story of real people affected by leprosy and changing perceptions of this widely misunderstood disease.
As the centenary of this incredible charity loomed, an ‘End of Century Celebration’ was held at the Athenaeum Club, in Pall Mall, London, on 28th October, 2023, for valued champions and supporters, to celebrate the difference Lepra, with their contribution, has made over 99 years to the lives of people with leprosy and allied diseases. This event launched the ‘New Faces of Leprosy Bangladesh Exhibition’ with photographer Tom Bradley, and was hosted by Mrs. Suzanne McCarthy, Chair of Lepra, Jimmy Innes, CEO of Lepra, H.R.H. The Duke of Gloucester, VicePresident of the Charity, and Professor Diana Lockwood, as part of the photographic exhibition.
To celebrate our centenary, an event was held at the House of Commons on 31st January 2024, where the Chair of Lepra, its CEO and its historian, Irene Allen, all gave short presentations on the charity, its history and its aims for the future.
CHAPTER 10
The next Century - What will the future Hold?
Given the problems that were thrown in our way even before we were officially ‘up and running’ back in 1924, it is amazing that the charity ever existed in the first place. But belief in what we were aiming to do, and trust in the general good nature of people, ensured that we went on to become one of the most trusted organisations working in leprosy and its allied diseases, and we are confident that our standing in the future will not decrease.
Our founding principles remain true today, and we will continue to take a pioneering, personcentred approach, advocating for early case detection building and strengthening community-led healthcare, fighting leprosy-related discrimination and providing a voice for some of the world’s most vulnerable people; those who are still experiencing the physical, social, economic and emotional impact of leprosy, LF, and other stigmatising diseases. We are also part of the History of Leprosy Project, which aims to ensure that the history of those with leprosy, and the people that cared for them, is not forgotten.
We have had many ups and downs – like any other organisation – but we have overcome them through hard work, dedication, belief in our cause and, of course, love. King George VI set out his ideas of the ‘greatness of a nation’ when he became our Patron, and we hope and believe that we have lived up to his expectations – and we always will.
On 7th May 2024, we received a letter from Buckingham Palace, informing us that King Charles III was to continue our Royal patronage. To receive such news, particularly in our centenary year was not only an incredible honour for the organisation, but also a direct and potent message of hope and solidarity for the people we support. One hundred years on, we are thankful that the Royal Family continue to shine the brightest of lights on leprosy and LF, and will continue to until we are needed no more.
A 3-year partnership with the Asian Media Group, a publisher of some of the country’s most iconic and trusted media was signed on 3rd July 2024. This partnership will help raise the profile of our cause to new audiences who share our vision of health inclusion and innovation for those affected by leprosy and LF.
It has been a wonderful Centenary year for Lepra so far, punctuated by some great events and activities to mark our milestone. We have been reflecting and celebrating our long and rich history at the forefront of care, treatment and support for thousands upon thousands of people
in the world affected by leprosy and LF. We take pride in Lepra’s heritage, but we are also acutely aware of how much more needs to be done.
Leprosy still exists. LF still exists. Millions of people still live with the lifelong impacts of both.
So, as we look back over our one hundred years, 2024 is also a time for us to take stock of where we are going as well as where we have come from. We are determined to build on the successes of the past, and further our work in the years ahead. We know we have more to give to support people affected by leprosy and LF in the world.
Over the past months we have been planning for the future and are delighted to have developed our new six-year strategy for 2024-2030. The strategy is all about health, inclusion and innovation for people affected by leprosy and LF.
The health focus builds on what we already do well. We have a long track record in healthcare service provision for people affected by leprosy and LF and it will continue to be a cornerstone of our work.
The inclusion focus accelerates our work on addressing stigma and discrimination, as well as supporting empowerment, quality of life and wellbeing for people affected by leprosy and LF –placing them at the forefront, and amplifying their voice and agency to realise full inclusion and equality in society.
The innovation focus enables us to test and trial new ways of caring, treating and supporting people affected by leprosy and LF. There has been so much progress in care and treatment for people affected by leprosy and LF over the past decades, but more needs to be done to support the millions of people still affected.
Our renewed focus on innovation and research also reconnects us with our past, and our proud history of research and innovating for better care and treatment.
Our new Global Strategy will ensure that we stay true to Lepra’s roots and heritage. We will always place the needs of people affected by leprosy and LF at the forefront of all that we do –as we have always done. And as we celebrate our hundred years, we know that we would be doing something wrong if Lepra was still around for anything like a hundred more. Our Global Strategy helps us to look ahead with clarity of purpose, and keep working towards a world where we are needed no more.
Bibliography
Allen, I, A Labour of Love – The History of BELRA/LEPRA’s Overseas Workers, Manuscript in progress, 2023
BELRA Annual Reports
BELRA Quarterly Magazines
Kerslake, R.T., Time and The Hour; Nigeria, East Africa and the Second World War, The Radcliffe Press, London, 1997
Leprosy Review
Longford, Michael, The flags changed at midnight, Gracewing, 2001
MacDonald, A.B, In His Name - The Story of a Doctor in Nigeria, Oldbourne Book Co. Ltd, London, 1964
Overseas workers’ personnel files
Stringer, T.A., LEPRA: An Historical Sketch 1924-1974, The British Leprosy Relief Association, 50 Fitzroy Street, London W1P 6AL, 1974