Download pdf Pcep book 4 specialized newborn care robert a sinkin (editor in chief) full chapter pdf
PCEP Book
4 Specialized Newborn Care Robert A Sinkin (Editor In Chief)
Visit to download the full and correct content document: https://ebookmeta.com/product/pcep-book-4-specialized-newborn-care-robert-a-sinki n-editor-in-chief/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
PCEP Book 3 Neonatal Care Robert A Sinkin (Editor In Chief)
Jason Crase, Senior Manager, Production and Editorial Services
Theresa Wiener, Production Manager, Clinical and Professional Publications
Peg Mulcahy, Manager, Art Direction and Production
Linda Smessaert, Director, Marketing
Published by the American Academy of Pediatrics
345 Park Blvd Itasca, IL 60143
Telephone: 630/626-6000
Facsimile: 847/434-8000
www.aap.org
Information about obtaining continuing medical education and continuing education credit for book study may be obtained by visiting www.cmevillage.com.
Several different approaches to specific perinatal problems may be acceptable. The PCEP books have been written to present specific recommendations rather than to include all currently acceptable options. The recommendations in these books should not be considered the only accepted standard of care. We encourage development of local standards in consultation with your regional perinatal center staff.
The American Academy of Pediatrics is an organization of 67,000 primary care pediatricians, pediatric medical subspecialists, and pediatric surgical specialists dedicated to the health, safety, and well-being of all infants, children, adolescents, and young adults.
While every effort has been made to ensure the accuracy of this publication, the American Academy of Pediatrics does not guarantee that it is accurate, complete, or without error.
The recommendations in this publication do not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be appropriate.
Statements and opinions expressed are those of the authors and not necessarily those of the American Academy of Pediatrics. Any websites, brand names, products, or manufacturers are mentioned for informational and identification purposes only and do not imply an endorsement by the American Academy of Pediatrics (AAP). The AAP is not responsible for the content of external resources. Information was current at the time of publication.
The publishers have made every effort to trace the copyright holders for borrowed materials. If they have inadvertently overlooked any, they will be pleased to make the necessary arrangements at the first opportunity.
This publication has been developed by the American Academy of Pediatrics. The contributors are expert authorities in the field of pediatrics. No commercial involvement of any kind has been solicited or accepted in the development of the content of this publication.
Every effort has been made to ensure that the drug selection and dosages set forth in this publication are in accordance with the current recommendations and practice at the time of publication. It is the responsibility of the health care professional to check the package insert of each drug for any change in indications or dosage and for added warnings and precautions.
Every effort is made to keep Perinatal Continuing Education Program consistent with the most recent advice and information available from the American Academy of Pediatrics.
Please visit www.aap.org/errata for an up-to-date list of any applicable errata for this publication.
Special discounts are available for bulk purchases of this publication. Email Special Sales at nationalaccounts@aap.org for more information.
Perinatal Continuing Education Program (PCEP), 4th Edition
Textbook Editorial Board
Editors
Editor in Chief, Neonatology
Robert A. Sinkin, MD, MPH, FAAP
Charles Fuller Professor of Neonatology
Department of Pediatrics
University of Virginia Children’s Hospital
Vice Chair for Academic Affairs
Division Head, Neonatology Charlottesville, VA
Editor in Chief, Obstetrics
Christian A. Chisholm, MD, FACOG
Medical Director for Outpatient Clinics, Labor, and Delivery
Vice Chair for Medical Education
Professor of Obstetrics and Gynecology
Division of Maternal-Fetal Medicine
Department of Obstetrics and Gynecology
University of Virginia School of Medicine
Charlottesville, VA
PCEP Editorial Board Members
Melissa F. Carmen, MD
Associate Professor of Pediatrics
Division of Neonatology
University of Rochester Rochester, NY
Susan B. Clarke, MS, NPD-BC, RNC-NIC, CNS
NRP Instructor Mentor
Master Trainer, Helping Babies Survive
Affiliate Faculty, Center for Global Health
Colorado School of Public Health
University of Colorado Anschutz Medical Campus Aurora, CO
Robert R. Fuller, MD, PhD
Associate Professor
Division of Maternal-Fetal Medicine
Department of Obstetrics and Gynecology
University of Virginia School of Medicine Charlottesville, VA
Ann Kellams, MD, FAAP
Professor, Department of Pediatrics
Vice Chair for Clinical Affairs and Director of Breastfeeding Medicine Services
University of Virginia Charlottesville, VA
Sarah Lepore, MSN, APRN, NNP-BC
University of Virginia Children’s Hospital
Neonatal Intensive Care Unit Charlottesville, VA
Peter D. Murray, MD, MSM, FAAP
Assistant Professor of Pediatrics
Division of Neonatology
University of Virginia Children’s Hospital Charlottesville, VA
Susan Niermeyer, MD, MPH, FAAP
Professor of Pediatrics
Section of Neonatology
University of Colorado School of Medicine
Colorado School of Public Health Aurora, CO
Barbara O’Brien, MS, RN Director, Oklahoma Perinatal Quality Improvement Collaborative
University of Oklahoma Health Sciences Center Oklahoma City, OK
Chad Michael Smith, MD, FACOG
Medical Director, Oklahoma Perinatal Quality Improvement Collaborative Vice President, Medical Affairs, Mercy Hospital Oklahoma City Oklahoma City, OK
Jonathan R. Swanson, MD, MSc, FAAP
Professor of Pediatrics
Chief Quality Officer for Children’s Services
Medical Director, Neonatal Intensive Care Unit
University of Virginia Children’s Hospital Charlottesville, VA
Sharon Veith, MSN, RN
Assistant Professor of Nursing School of Nursing
University of Virginia Charlottesville, VA
Santina Zanelli, MD
Associate Professor of Pediatrics Division of Neonatology
University of Virginia Children’s Hospital Charlottesville, VA
Continuing Education Credit
Accreditation and Designation Statements
In support of improving patient care, this activity has been planned and implemented by the American Academy of Pediatrics and the University of Virginia School of Medicine and School of Nursing, which is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the health care team.
AMA PRA Category 1 Credit
The University of Virginia School of Medicine and School of Nursing designates this enduring material (PI CME) for a maximum of 56.5 AMA PRA Category 1 Credits. TM Physicians should claim only the credit commensurate with the extent of their participation in the activity.
ANCC Contact Hours
The University of Virginia School of Medicine and School of Nursing awards 56.5 contact hours for nurses who participate in this educational activity and complete the post-activity evaluation.
AAPA Category 1 CME Credit
This activity is designated for 56.5 AAPA Category 1 CME credits. Approval is valid for 3 years. PAs should only claim credit commensurate with the extent of their participation.
Credit is awarded upon passing book exams, not individual educational unit posttests. Possible credits: Book 1, 14.5; Book 2, 16; Book 3, 17; Book 4, 9. To obtain credit, register online at www.cmevillage.com, choose Courses & Programs, then E-Learning, and scroll down to the PCEP program. Click on the PCEP program link and navigate to https://med.virginia.edu/cme/ learning/pcep/pcep-book-exam-certificate/ and pass the book exams.
Disclosure of Faculty Financial Affiliations
The University of Virginia School of Medicine and School of Nursing as a Joint Accreditation Provider adheres to the ACCME Standards for Integrity and Independence in Accredited Continuing Education, released in December 2020, as well as Commonwealth of Virginia statutes, University of Virginia policies and procedures, and associated federal and private regulations and guidelines. As the accredited provider for this CE/IPCE activity, we are responsible for ensuring that health care professionals have access to professional development activities that are based on best practices and scientific integrity that ultimately supports the care of patients and the public.
All individuals involved in the development and delivery of content for an accredited CE/IPCE activity are expected to disclose relevant financial relationships with ineligible companies occurring within the past 24 months (such as grants or research support, employee, consultant, stock holder, member of speakers bureau, etc). The University of Virginia School of Medicine and School of Nursing employ appropriate mechanisms to resolve potential conflicts of interest and ensure the educational design reflects content validity, scientific rigor, and balance for participants. Questions about specific strategies can be directed to the University of Virginia
School of Medicine and School of Nursing of the University of Virginia, Charlottesville, Virginia.
The faculty, staff, and planning committee engaged in the development of this CE/IPCE activity in the Joint Accreditation CE Office of the School of Medicine and School of Nursing have no financial affiliations to disclose.
Disclosure of Discussion of Non-FDA-Approved Uses for Pharmaceutical Products and/or Medical Devices
As a Joint Accreditation provider, the University of Virginia School of Medicine and School of Nursing, requires that all faculty presenters identify and disclose any off-label or experimental uses for pharmaceutical and medical device products.
It is recommended that each clinician fully review all the available data on new products or procedures prior to clinical use.
Specialized Newborn Care
For more information, see the other books in the Perinatal Continuing Education Program (PCEP) series
Book 1. Maternal and Fetal Evaluation and Immediate Newborn Care
Unit 1: Is the Mother Sick? Is the Fetus Sick?
Skill Unit: Determining Fetal Presentation With Leopold Maneuvers
Unit 2: Fetal Age, Growth, and Maturity
Unit 3: Fetal Well-being
Skill Unit: Electronic Fetal Monitoring
Unit 4: Is the Baby Sick? Recognizing and Preventing Problems in the Newborn
Skill Unit: Management of Oxygen in the Delivery Setting
Skill Unit: Free-Flow Oxygen and Positive-Pressure
Ventilation
Skill Unit: Endotracheal Intubation
Skill Unit: Chest Compressions
Skill Unit: Emergency Medications
Skill Unit: Apgar Score
Book 2. Maternal and Fetal Care
Unit 1: Hypertension in Pregnancy
Unit 2: Obstetric Hemorrhage
Unit 3: Infectious Diseases in Pregnancy
Unit 4: Other Medical Risk Factors in Pregnancy
Unit 5: Obstetric Risk Factors: Prior or Current Pregnancy
Unit 6: Psychosocial Risk Factors in Pregnancy
Unit 7: Gestational Diabetes
Unit 8: Prelabor Rupture of Membranes and Intra-amniotic Infection
Skill Unit: Sterile Speculum Examination
Skill Unit: Tests for Suspected or Proven Rupture of Membranes
Book 3. Neonatal Care
Unit 1: Oxygen
Skill Unit: Administering Oxygen
Measuring Oxygen Concentration
Blending Oxygen and Compressed Air
Heating and Humidifying an Oxygen/Air Mixture
Skill Unit: Monitoring Oxygen
Peripheral Arterial Blood Gas Sampling
Unit 2: Respiratory Distress
Skill Unit: Detecting a Pneumothorax Transillumination
Chest Radiography
Skill Unit: Treating a Pneumothorax
Needle Aspiration
Chest Tube Insertion
Unit 3: Umbilical Catheters
Skill Unit: Inserting and Managing Umbilical Catheters
Unit 4: Low Blood Pressure (Hypotension)
Skill Unit: Measuring Blood Pressure
Unit 5: Intravenous Therapy
Skill Unit: Peripheral Intravenous Infusions
Inserting and Managing Peripheral Intravenous Infusions
Unit 6: Gestational Age and Size and Associated Risk Factors
Skill Unit: Estimating Gestational Age by Examination of a Newborn
Unit 7: Thermal Environment
Skill Unit: Radiant Warmers
Skill Unit: Incubators and Neutral Thermal Environment
Unit 8: Hypoglycemia
Skill Unit: Blood Glucose Screenings
Pretest Answer Key
Glossary
Index
Unit 9: Preterm Labor
Unit 10: Inducing and Augmenting Labor
Unit 11: Abnormal Labor Progress and Difficult Deliveries
Unit 12: Imminent Delivery and Preparation for Maternal/Fetal Transport
Pretest Answer Key
Glossary
Index
Unit 6: Feeding
Part 1: Feeding Principles
Part 2: Tube Feeding
Skill Unit: Nasogastric Tube Feedings
Unit 7: Hyperbilirubinemia
Appendix: Identification and Treatment of Jaundice
During the First Week After Birth
Unit 8: Infections
Unit 9: Identifying and Caring for Sick and At-Risk Babies
Subsection: Vital Signs and Observations
Subsection: Tests and Results
Unit 10: Preparation for Neonatal Transport
Subsection: Caring for Parents of Transported Babies
Unit 11: Neonatal Abstinence Syndrome (Neonatal Opioid Withdrawal Syndrome)
Pretest Answer Key Glossary Index
Unit 1: Direct Blood Pressure
Objectives
In this unit you will learn the
A. Difference between direct and indirect blood pressure monitoring
B. Reasons for direct blood pressure monitoring
C. Equipment needed for direct blood pressure monitoring
D. Interpretation of blood pressure waveforms
Unit 1 Pretest
Before reading the unit, please answer the following questions. Select the one best answer to each question (unless otherwise instructed). Record your answers on the test and check them with the answers at the end of the book.
1. A damped pressure tracing may be caused by each of the following findings except
A. Air bubbles in the tubing
B. Hypotension
C. Severe anemia
D. A clot at the tip of the umbilical catheter
2. True False Special intravenous tubing is needed for direct blood pressure monitoring.
3. True False A narrowed pulse pressure may suggest certain congenital heart defects.
4. True False The reference range for direct blood pressure measurements is different than the reference range for indirect blood pressure measurements.
5. True False When a direct blood pressure monitoring waveform shows slow decrease in pressure during diastole, it may indicate increased systemic vascular resistance.
6. The transducer for direct blood pressure measurement should be level with the
A. Baby’s heart
B. Electronic monitor
C. Umbilical catheter
D. Intravenous infusion pump
7. Direct blood pressure measurement is used for each of the following reasons except
A. Continuous blood pressure monitoring
B. Increased accuracy of the measurements
C. Obtaining information about a baby’s cardiac status
D. Measurement of acid-base balance
1. What are the 2 general types of blood pressure monitoring?
A. Indirect blood pressure measurement
Indirect measurement is the typical way in which blood pressure is measured. An inflatable cuff is wrapped around an arm or a leg. The cuff is then inflated to a pressure somewhat higher than the anticipated blood pressure. Manual palpation or a mechanical device (oscillometric measurement) is used to detect changes in arterial flow as the cuff is deflated. (See Book 3: Neonatal Care, Unit 4, Low Blood Pressure [Hypotension].)
B. Direct blood pressure measurement
Direct blood pressure measurement occurs when the measuring device is connected to a catheter inserted directly into an artery, commonly the umbilical artery or a peripheral (eg, radial) artery.
2. How are direct blood pressure measurements obtained?
An arterial catheter is connected to special tubing that resists changes in pressure. This “high pressure” tubing is used to transmit the arterial pressure at the catheter tip to a transducer. The transducer converts the mechanical pressure of blood in an artery into an electrical signal. The electrical signal is displayed as a waveform on a screen. The resulting pattern is the blood pressure waveform.
3. Why is direct blood pressure measurement used?
Direct monitoring is used in sick babies who have an arterial catheter in place. It is especially important for unstable babies. The 3 primary advantages of direct monitoring are
• It allows continuous blood pressure monitoring.
• It gives the most accurate form of blood pressure measurement.
• The waveform shape may suggest certain clinical conditions.
4. What equipment is needed for direct blood pressure monitoring?
General points about direct blood pressure monitoring are presented here; details of the technique are covered in the Skill Unit: Transducer Blood Pressure Monitoring. The following equipment is needed for direct blood pressure monitoring:
A. Arterial catheter
In babies, an umbilical arterial catheter is most commonly used. When it is not possible to use the umbilical artery, a small catheter is placed in one of the peripheral arteries— usually a radial artery—and then connected to the appropriate monitoring equipment.
B. Electronic monitor with waveform display
This monitor has one channel that allows continuous cardiac (electrocardiographic) monitoring and another channel for blood pressure monitoring. It has a calibrated screen where the blood pressure waveform is displayed, as well as a digital readout of the systolic, diastolic, and mean blood pressures.
C. Non-distensible tubing
This connects the arterial catheter and transducer. It is made of stiff plastic and is sometimes called high-pressure tubing.
D. Transducer
Several brands of disposable transducers are available.
E. Transducer cable
This connects the transducer with the electronic monitor. Sometimes the transducer and cable are a single unit.
F. Intravenous pump
This pump should be able to deliver a low volume of fluid (,1 mL/h). It should also be able to deliver fluid continuously, rather than in pulses. With advanced technology of intravenous (IV) pumps, many are able to deliver low volumes with a syringe option to enable monitoring indirect arterial pressure. If this is not an option, a syringe pump can be used. Follow your hospital’s protocol for use of the appropriate device.
G. Intravenous solution
To obtain continuous blood pressure readings, the system must remain open between the catheter and transducer. This significantly increases the risk of clot formation within the catheter unless a continuous infusion of IV fluid is maintained.
Physiological (normal) saline will cause less sludging of blood in a catheter than a glucose solution will; however, small babies may receive excessive sodium and insufficient glucose if normal saline is used to help keep the catheter patent. Calculate the requirements of your patient. (See Book 1: Maternal and Fetal Evaluation and Immediate Newborn Care, Unit 8, Hypoglycemia, and Book 3: Neonatal Care, Unit 5, Intravenous Therapy.) Heparin should be added to the IV solution. Most experts recommend using an IV solution with 0.5 to 1.0 U of heparin per milliliter and infusing it at a rate of at least 0.5 mL/h.
H. Mechanism to hold the transducer at the level of the baby’s heart
Sometimes the transducer is mounted on an IV pole with a holder that may be raised or lowered as the baby’s position is changed. Most commonly, however, transducers are designed to rest on the bed alongside the baby.
Self-test A
Now answer these questions to test yourself on the information in the last section.
A1. Indirect blood pressure measurement uses an __________ __________ wrapped around the baby’s arm or leg, while direct blood pressure measurement uses a __________ inserted into an __________.
A2. What are the 3 primary reasons for using direct blood pressure monitoring?
A3. True False A continuous infusion should be given through an umbilical arterial catheter when it is being used for continuous blood pressure monitoring.
A4. True False Non-distensible tubing is an optional piece of equipment for continuous direct blood pressure monitoring.
A5. True False An intravenous pump that delivers fluid in regular, tiny pulses is the preferred type of pump to use with a direct blood pressure monitoring arterial catheter.
Check your answers with the list near the end of the unit. Correct any incorrect answers and review the appropriate section in the unit.
5. What are reference neonatal blood pressure ranges?
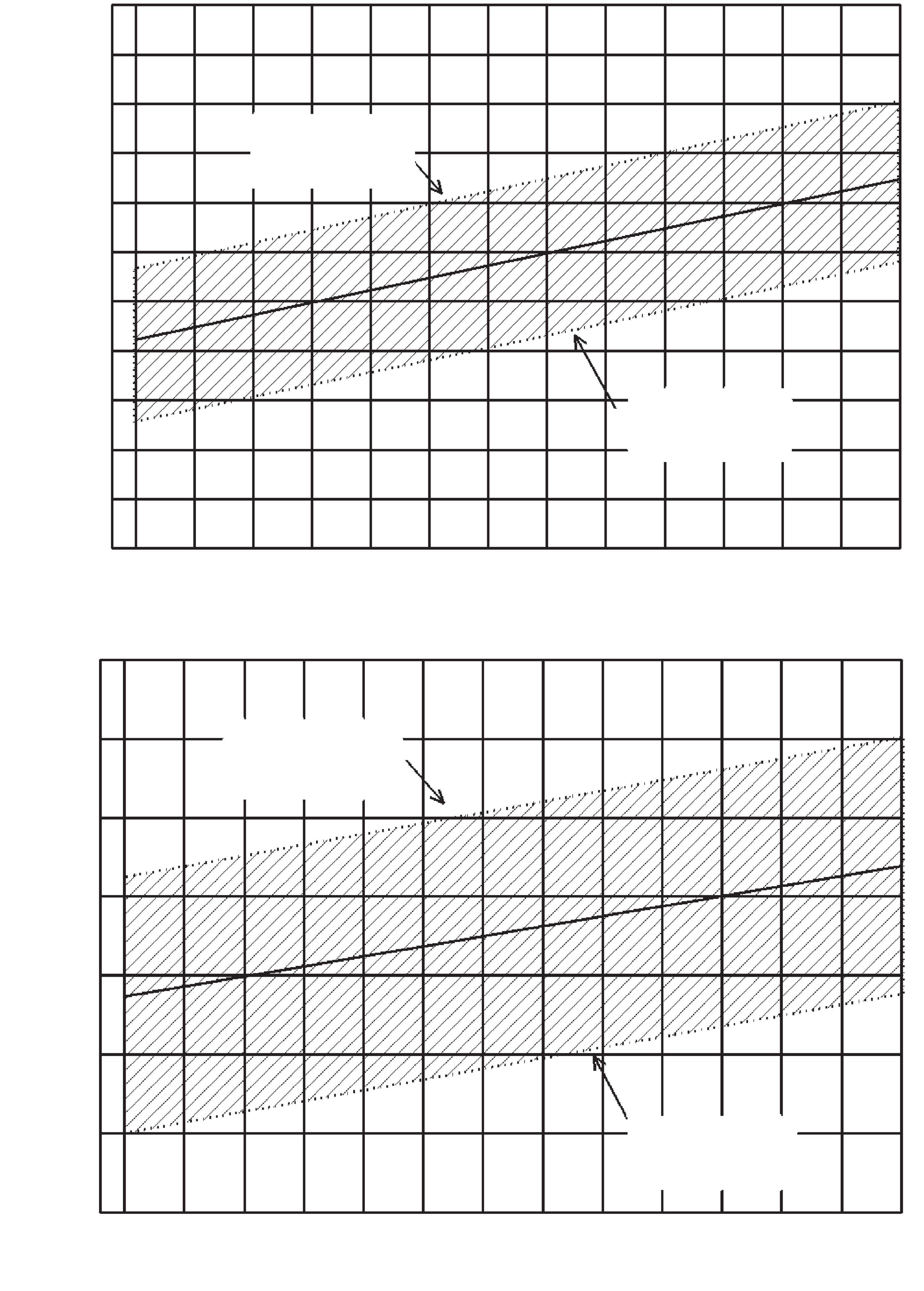
Figures 1.1, 1.2, and 1.3 show the reference ranges of blood pressure for babies of different birth weights and at different gestational and postmenstrual ages.
Birth Weight (g)
Birth Weight (g)
1.1. Systolic and Diastolic Blood Pressure During the First Day After Birth
Adapted with permission from Zubrow AB, Hulman S, Kushner H, Falkner B. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. J Perinatol 1995;15(6):470–479.
Figure
Figure 1.2. Systolic and Diastolic Blood Pressure for Babies of Different Gestational Ages During the First 5 Days After Birth
Adapted with permission from Zubrow AB, Hulman S, Kushner H, Falkner B. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. J Perinatol 1995;15(6):470–479.
Figure 1.3. Systolic Blood Pressure for Babies of Different Postmenstrual Ages
Adapted with permission from Zubrow AB, Hulman S, Kushner H, Falkner B. Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. J Perinatol 1995;15(6):470–479.
6. How do you interpret blood pressure waveforms?
A. Blood pressure waveform: normal configuration
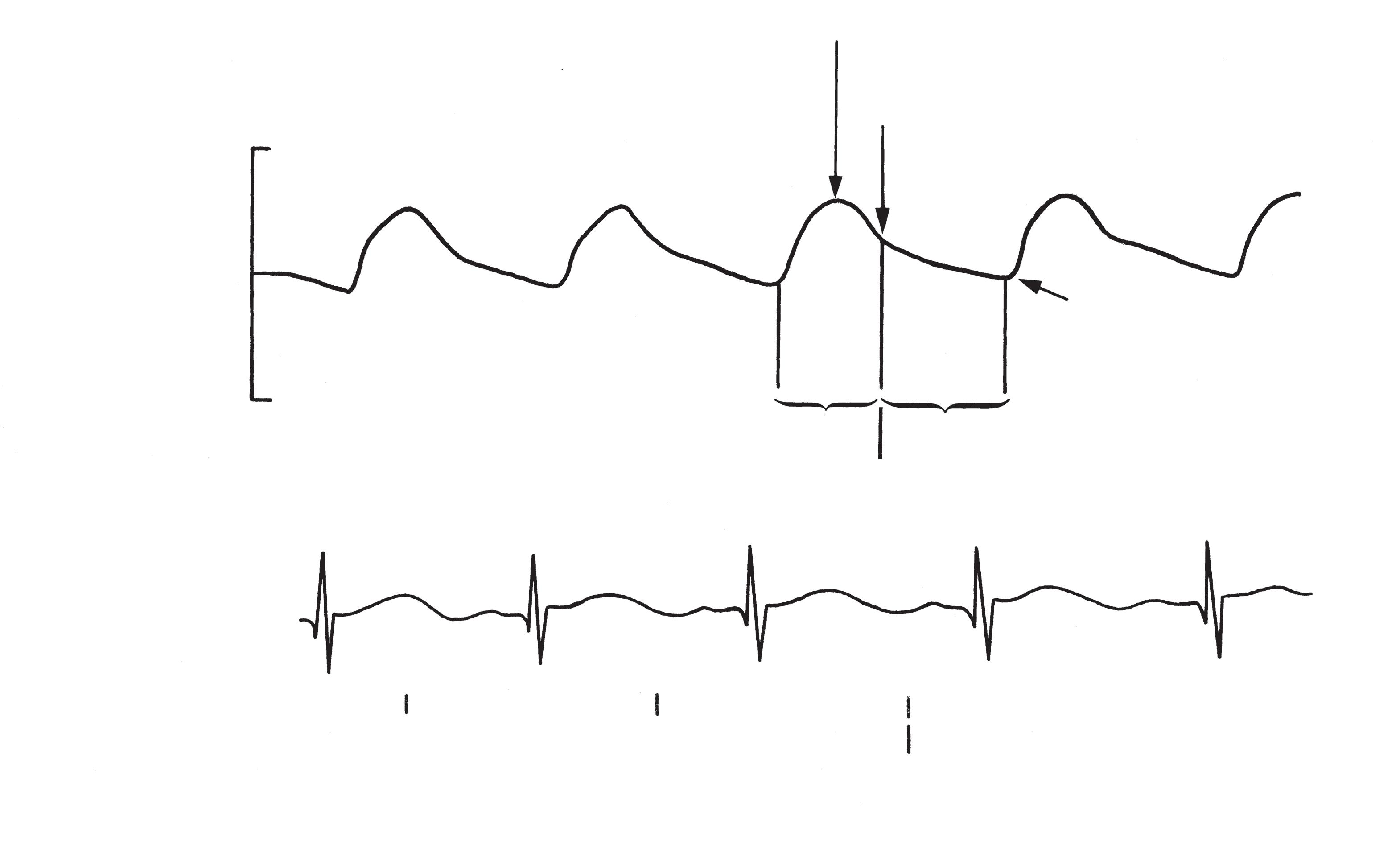
Figure 1.4 shows a normal newborn blood pressure waveform, as it appears in relation to a cardiac monitor (electrocardiogram) tracing.
The shape of the pattern corresponds with events happening within the heart. These are described as follows:
• Systolic phase: Time during which the heart is ejecting blood
• Peak pressure: The highest point during systole (systolic pressure)
• Dicrotic notch: Point of closure of the aortic valve
• Diastolic phase: Time during which the heart is filling with blood
• Minimum pressure: The lowest point during diastole (diastolic pressure)
• Pulse pressure: The difference between peak and minimum pressures
• Mean pressure: The average pressure of the complete cardiac cycle
The key segments to recognize are the sharp increase during systole, the dicrotic notch, and the slower decrease in pressure during diastole.
In addition to displaying the blood pressure waveform, nearly all monitors digitally display continuous readings of systolic, diastolic, or mean arterial pressure (or any combination of those).
B. Blood pressure waveform: abnormal configuration
1. Damped waveform
The most common cause of an abnormal pressure waveform is a damped tracing in which the waveform “flattens out.” Usually, the systolic pressure will seem to be decreased and the diastolic pressure will seem to be increased, causing little change
Figure 1.4. Arterial Waveform
Aortic Pressure (mm Hg)
Peak Pressure
Dicrotic Notch
Diastolic Phase
Systolic Phase
in the mean arterial pressure. These changes may be subtle or more dramatic, leading to an almost flat line for a pressure tracing. A damped waveform with subtle changes can be recognized by the disappearance of the dicrotic notch.
A damped tracing may be caused by
• Air bubbles within the tubing or at the transducer: These air bubbles may be very tiny. Careful inspection of the full length of the tubing and all connections is required. If air bubbles are found, they should be flushed from the system while taking care not to infuse any into the baby. Flush the tubing and transducer by
– Turning the stopcock off to the baby
– Opening the transducer to air
– Flushing the IV fluid through the transducer and out the port that is open to air
• Kink in the tubing: This is a rare occurrence but should be considered whenever a waveform is damped.
• Hypotension: A baby in shock may also seem to have a damped waveform. Always be sure to check the blood pressure values by indirect means and assess the baby’s clinical condition.
• Clot at the tip or within the lumen of the catheter: This is the most common reason for a damped tracing. If this is the suspected cause of a damped waveform, aspirate blood from the catheter. Then slowly flush the catheter with 0.5 to 1.0 mL of flush solution. Reopen the system between the catheter and the transducer. If the waveform remains damped, and no other cause for a damped tracing can be found, the catheter needs to be removed.
If a waveform is damped because of a suspected clot at the tip or within the lumen, the catheter needs to be removed and replaced with a new one.
2. Abnormally shaped waveform
Waveforms of a particular shape, or changes in a baby’s waveform, may suggest abnormal findings in cardiac status. These findings are usually subtle and should be considered only suggestive of the corresponding problem.
Finding
• Slow pressure increase during early systole
• Slow pressure decrease during diastole
• Rapid pressure decrease during diastole
C. Abnormally wide or narrow pulse pressure
Possible Cause
• Poor left ventricular contractility
• Aortic stenosis
• Increased systemic vascular resistance
• Left-to-right shunting, such as from a patent ductus arteriosus
Pulse pressure is the difference between peak systolic and minimum diastolic pressures. Wide or narrow pulse pressure may suggest certain cardiac abnormalities. A change in pulse pressure may suggest the development of certain problems, such as a pneumothorax or pneumopericardium, which may affect cardiac function.
Reliable normal values of pulse pressure in newborns have not been defined. A pulse pressure less than 10 mm Hg, however, is generally considered too narrow. A pulse pressure significantly greater than the value of the diastolic pressure is generally considered too wide. For example, a systolic pressure of 60 mm Hg and a diastolic pressure of 20 mm Hg give a pulse pressure of 40 mm Hg, which is significantly greater than the diastolic pressure.
Pulse Pressure
Narrowed
Widened
Possible Cause
• Coarctation of the aorta
• Pneumothorax
• Pneumopericardium or hemopericardium
• Aortic stenosis
• Hypoplastic left side of the heart
• Shock (cardiogenic, septic, or hemorrhagic)
• Heart failure
• Patent ductus arteriosus
• Aortopulmonary window
• Arteriovenous fistula
• Truncus arteriosus
• Hyperthyroidism
• Aortic regurgitation
These waveform findings are only suggestive of the abnormalities listed and must be considered together with other clinical and diagnostic findings. Consult your regional perinatal center if you have any questions about a baby’s cardiac status.
Self-test B
Now answer these questions to test yourself on the information in the last section.
B1. A damped waveform may be caused by Yes No
Hypotension
Air bubbles in the tubing Patent ductus arteriosus
Clot at the catheter tip
B2. True False The pulse pressure is the same as the mean pressure.
B3. True False The lowest point of the waveform indicates the diastolic pressure.
B4. List 2 possible causes of a narrowed pulse pressure.
B5. List 2 possible causes of a widened pulse pressure.
Check your answers with the list near the end of the unit. Correct any incorrect answers and review the appropriate section in the unit.
Self-test Answers
These are the answers to the Self-test questions. Please check them with the answers you gave and review the information in the unit wherever necessary.
Self-test A
A1. Indirect blood pressure measurement uses an inflatable cuff wrapped around the baby’s arm or leg, while direct blood pressure measurement uses a catheter inserted into an artery.
A2. Provides most accurate form of blood pressure measurement Allows continuous measurement of blood pressure Produces waveform shape that may aid in the diagnosis of certain clinical conditions
A3. True
A4. False. Reason: Only non-distensible tubing allows accurate transmission of pressure between the catheter and transducer without being “lost” in the elasticity of regular intravenous tubing.
A5. False. Reason: An intravenous pump that delivers a low volume of fluid continuously, rather than in pulses, is the preferred type of pump for direct blood pressure monitoring.
Self-test B
B1. Yes No
X Hypotension
X Air bubbles in the tubing
X Patent ductus arteriosus
X Clot at the catheter tip
B2. False. Reason: The pulse pressure is the difference between peak (systolic) and minimum (diastolic) pressures. Mean blood pressure is the average pressure of the complete cardiac cycle.
B3. True
B4. Any 2 of the following causes:
• Coarctation of the aorta
• Pneumothorax
• Pneumopericardium or hemopericardium
• Aortic stenosis
• Hypoplastic left side of the heart
• Shock (cardiogenic, septic, or hemorrhagic)
• Heart failure
B5. Any 2 of the following causes:
• Patent ductus arteriosus
• Aortopulmonary window
• Arteriovenous fistula
• Truncus arteriosus
• Hyperthyroidism
• Aortic regurgitation
Unit 1 Posttest
After completion of each unit there is a free online posttest available at www.cmevillage.com to test your understanding. Navigate to the PCEP pages on www.cmevillage.com and register to take the free posttests. Once registered on the website and after completing all the unit posttests, pay the book exam fee ($15) and pass the test at 80% or greater to earn continuing education credits. Only start the PCEP book exam if you have time to complete it. If you take the book exam and are not connected to a printer, either print your certificate to a .pdf file and save it to print later or return to www.cmevillage.com at any time and print a copy of your educational transcript.
Credits are only available by book, not by individual unit within the books. Available credits for completion of each book exam are as follows: Book 1: 14.5 credits; Book 2: 16 credits; Book 3: 17 credits; Book 4: 9 credits. For more details, navigate to the PCEP webpages at www.cmevillage.com.
SKILL UNIT
Transducer Blood Pressure Monitoring
This skill unit will teach you the principles of continuous electronic blood pressure monitoring. Study this skill unit, and then attend a skill practice and demonstration session. You will learn how to apply the principles studied in this unit to the specific equipment used in your hospital.
To master the skill, you will need to demonstrate each of the following steps correctly, using the specific equipment available in your hospital:
1. Assemble the equipment.
2. Set up continuous infusion.
3. Flush tubing and transducer with infusion fluid.
4. Connect tubing to “baby’s” (mannequin’s) arterial catheter.
5. Level the transducer with the baby’s heart.
6. Zero the monitor.
7. Set alarms.
8. Measure the baby’s blood pressure.
PERINATAL PERFORMANCE GUIDE
Using Transducer Blood Pressure Monitors
ACTIONS
Preparing the Equipment
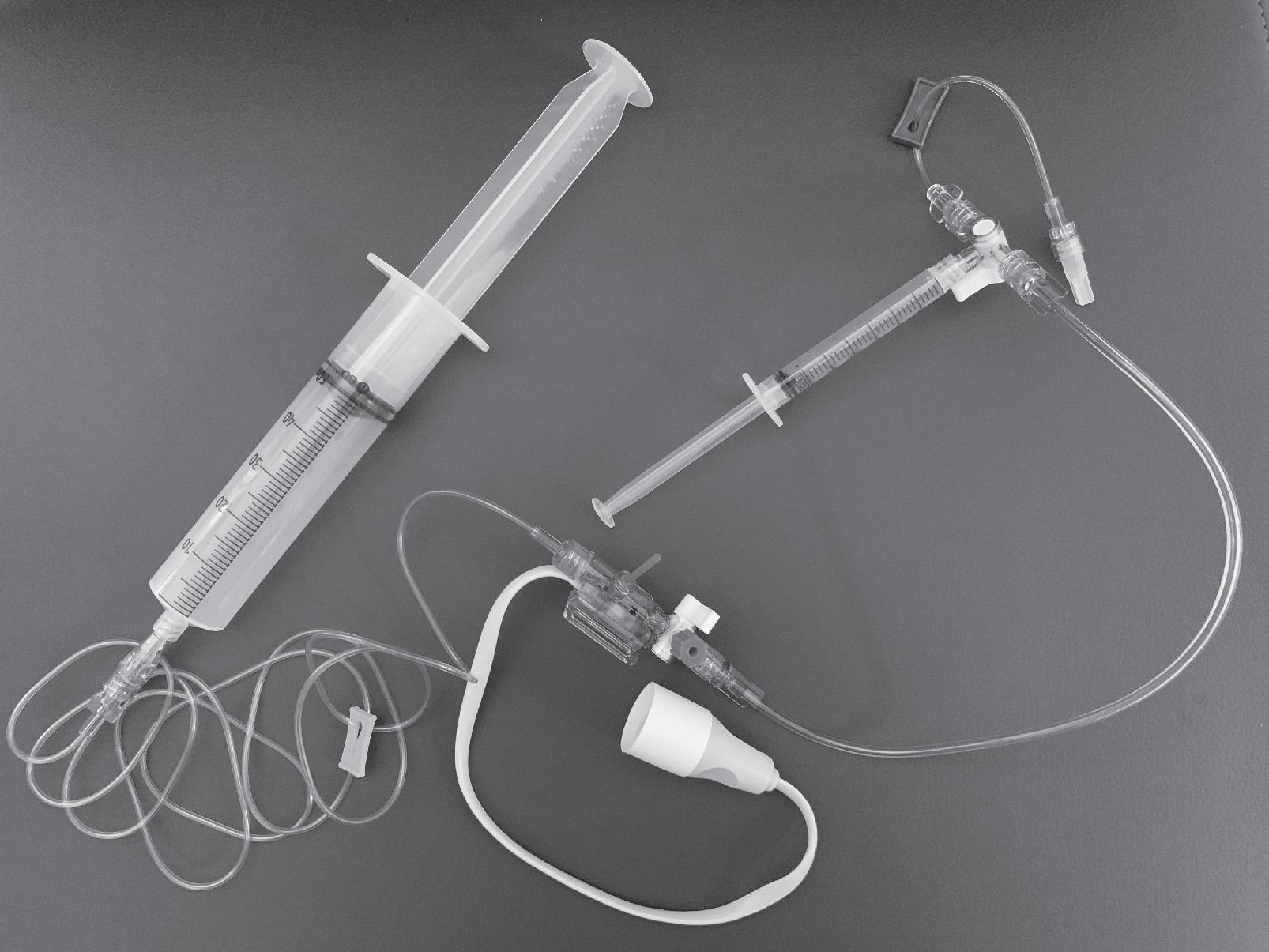
1. Collect the equipment.
• Electronic monitor
• Non-distensible (high-pressure) tubing
• Transducer with stopcock
• Transducer cable
• Infusion pump that can deliver less than 1 mL/h in continuous flow
REMARKS
The baby should have an arterial catheter already in place with extension tubing and Luer lock attached.
An infusion pump should be used to ensure that a constant, correct volume is infused. The use of an infusion pump will prevent backup of blood into the catheter and possible obstruction of the line with a thrombus.
• Heparinized intravenous (IV) solution
• Three-way stopcock
• Adjustable-height clamp to hold transducer at the level of the baby’s heart (optional)
• Sterile gloves
• Hat and mask
• Sterile field
• Sterile caps to close all open ports
2. Assemble the equipment while maintaining sterile technique.
This is usually pharmacy prepared.
Many transducers are designed to rest on the baby’s bed, next to the baby. Know the requirements of the transducer you are using.
Most transducer kits come preassembled; if not, connect infusion to tubing ➝ transducer with stopcock ➝ non-distensible tubing ➝ stopcock ➝ extension tubing ➝ arterial catheter.
Arterial setup. If your kit is not preassembled, connect the pieces in this sequence by using sterile technique.
ACTIONS
Preparing the Equipment (continued)
REMARKS
3. Set up the continuous infusion. A heparinized solution (0.5 to 1.0 U/mL) of normal saline is most commonly used. Other heparinized solutions (eg, sodium acetate or half-normal saline) may be used. See section 4.G in the unit.
4. Flush the heparinized IV solution through the IV tubing, transducer, stopcock, and non-distensible tubing.
As an additional safeguard, nondistensible tubing that has an air-bubble filter incorporated into it is available. Know the features of the tubing used in your hospital.
5. Connect the non-distensible tubing with stopcock to the extension tubing attached to the baby’s arterial catheter.
6. Use a syringe on the third port of the stopcock (the stopcock that is connected to the arterial catheter) to draw blood into the catheter, to be sure there is a brisk blood return before beginning to infuse fluid through the catheter.
7. Turn the stopcocks so they are open between the baby’s arterial catheter and the IV fluid, as shown in the figure below.
8. Begin infusion of the heparinized IV fluid. Infusion at a rate of at least 0.5 mL/h is generally recommended.
Be sure to clear the tubing of all air bubbles, including very tiny bubbles. Snapping a fingernail or tapping gently against the transducer or tubing can help dislodge stubborn bubbles.
If the tubing is flushed slowly, air bubbles are generally less of a problem. Also, hold the transducer so the exit to the non-distensible tubing is uppermost. This will help ensure that the transducer fills completely and no air bubbles are trapped in a corner of it.
There is no need to pull blood into the syringe or even fill the catheter with blood. You just need to see a flash of blood in the catheter and observe that the catheter can be aspirated easily.
Double-check to be sure no air bubbles are in the tubing.
Neither this infusion rate nor the IV fluid used is designed to fulfill a baby’s fluid requirements, but rather to keep the catheter patent. Keep track of the volume infused because even this low infusion rate can provide a significant volume for small babies.
to
Configuration During Infusion: System Open Between Intravenous Fluid and Arterial Catheter
ACTIONS
Calibrating the Blood Pressure Monitor
9. With the baby supine, level the transducer with the baby’s heart. Use the baby’s midaxillary point to approximate the level of the heart. In most cases, this may be accomplished by simply putting the transducer flat on the bed next to the baby.
Sometimes transducers are clamped to a pole beside the bed. They should be clamped at a point level with the baby’s mid-axillary area.
Arterial catheter
Extension tubing with Luer lock
REMARKS
In some cases, it may be useful to tape the transducer to a small, folded blanket that is placed next to the baby. This will keep the transducer flat and raise it slightly off the bed, to the mid-axillary level of the baby’s chest.
However the transducer is positioned, it is important that the position relative to the baby remain constant. Changing the transducer level compared to the baby will result in false readings.
Non-distensible tubing
Transducer with stopcock
Non-distensible tubing
Fluid infusion
Third port (used when blood drawn—closed)
Third port (used to zero transducer—closed)
Configuration During Calibration: System Closed to Arterial Catheter (Baby), Open Between Transducer and Air
10. Zero the monitor.
• After leveling the transducer, turn the stopcock on the transducer off to the patient and open to the air. Remove the cap to the stopcock port. Zero the transducer by following the manufacturer’s instructions for zeroing.
• Adjust the display so that the blood pressure reads zero.
Note: Some monitors need to be calibrated to both zero and a higher number, usually 100 mm Hg.
11. Begin to monitor the baby.
• Close the system to atmospheric pressure and reopen it between the IV infusion and the baby’s arterial catheter.
• Cap the port that was open to atmospheric pressure with a syringe or sterile cap.
In most cases, this is accomplished by simply pressing a “zero” button on the monitor screen.
Be sure you know the requirements of the specific equipment used in your hospital.
The system should, again, be configured the same way as shown in the figure after step 8.
Stopcock
ACTIONS
REMARKS
Calibrating the Blood Pressure Monitor (continued)
• Check again to be sure no air bubbles have entered the tubing.
• Check to be sure the monitor is set for a scale appropriate to neonatal blood pressure values.
Measuring the Baby’s Blood Pressure
12. Set the alarm limits appropriate to the baby’s blood pressure. If the baby is initially hypotensive, readjust the alarm limits as the blood pressure is corrected.
13. Observe the character of the pressure waveform. Determine if the waveform is a damped or an undamped tracing.
14. Read and record the baby’s blood pressure. This may be read from the screen or the digital readout.
Sometimes air enters the stopcock, and then the tubing, when the stopcock is opened to air during calibration.
Most monitors have 2 or 3 pressure scales that may be used. Generally, the 0 to 100 mm Hg scale is used for babies. If a different scale is used, the waveform may sometimes, depending on a baby’s blood pressure, appear to be off the screen.
Determine if the alarm limits on your monitor can be set for systolic/diastolic or mean blood pressure (or both). Then set the alarm limits 5 to 10 mm Hg higher and 5 to 10 mm Hg lower than the baby’s blood pressure reading.
If the waveform is damped, investigate the cause. Review section 6.B.1 in the unit.
Usually, the baby’s systolic, diastolic, and mean arterial pressures (MAPs) are recorded (eg, 65/45 MAP 53). If a digital readout is not available, only the systolic and diastolic pressures can be read from the waveform tracing on a calibrated monitor screen.
15. Regularly, routinely examine the tubing to be sure no air bubbles have entered the system.
16. Periodically check the baby’s blood pressure by indirect measurement with an inflatable cuff.
17. Periodically repeat steps 9 through 11 to calibrate the monitor.
If any air bubbles are found, remove them from the system.
Direct and indirect blood pressure readings should correlate very closely.
The transducer setup is commonly calibrated 2 to 3 times a day, whenever the disposable transducer and tubing are changed, and whenever there is a question about waveform quality.
Unit 2: Exchange, Reduction, and Direct Transfusions
Objectives
In this unit you will learn
A. Why exchange, reduction, and direct transfusions are performed
B. What type of donor blood is used
C. The effects of anticoagulants on donor blood
D. How to prepare donor blood
E. How exchange, reduction, and direct transfusions are performed
F. How to monitor the baby for potential complications
Unit 2 Pretest
Before reading the unit, please answer the following questions. Select the one best answer to each question (unless otherwise instructed). Record your answers on the test and check them with the answers at the end of the book.
1. True False Blood glucose screening test results should be checked immediately after any exchange transfusion.
2. True False When an umbilical arterial catheter is used in an exchange transfusion, it is used only to withdraw blood from the baby.
3. True False No baby should undergo more than one exchange transfusion.
4. True False Packed red blood cells (hematocrit level .70%) of appropriate group and type should be used for an exchange transfusion.
5. A reduction exchange transfusion is different from an exchange transfusion for hyperbilirubinemia because
A. A larger volume of blood is exchanged.
B. Infectious complications are more likely to occur.
C. Blood is not given.
D. Rebound hypoglycemia is more likely to occur.
6. What is the preferred age of donor blood used for an exchange transfusion?
A. 1 to 10 days.
B. 10 to 15 days.
C. 15 to 20 days.
D. Age of the blood is not an issue.
7. True False A term, 4,000-g (8 lb 13 oz) baby with tachypnea who has been treated for hypoglycemia and has a venous hematocrit level of 68% should be considered for a reduction exchange transfusion.
8. True False Phototherapy lights should be used after every exchange transfusion for babies with hyperbilirubinemia.
9. True False All preterm babies should be transfused with packed red blood cells if their hematocrit level is less than or equal to 25%.
10. True False Capillary blood from a heel stick sample is the preferred way to test a baby’s hematocrit level.
11. Which of the following findings is a possible sign of anemia in a stable, growing, preterm baby?