9 minute read
Unraveling the Mysteries of Dead Bag Syndrome

By Liliana Werner, MD, PhD, and Nick Mamalis, MD
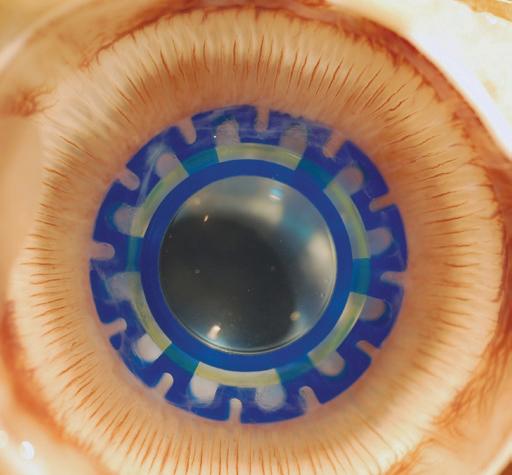
Since the early 2000s, ophthalmologists have been reporting something mysterious in their practices: patients—years after their routine cataract surgeries—presenting with dislocated intraocular lenses (IOLs). In these cases, the capsular bag appeared to be clear and had become diaphanous and floppy—unable to support the IOL within it.
Samuel Masket, MD, a surgeon and clinical researcher in Los Angeles, first observed the condition and coined the term “dead bag syndrome” to describe it.
Until then, pseudoexfoliation syndrome, uveitis, myopia, and pars plana vitrectomy were the main conditions associated with progressive zonular weakening and late postoperative in-the-bag IOL dislocation.1 These conditions did not appear to be a factor in the patients with suspected dead bag syndrome.
At the Intermountain Ocular Research Center at the Moran Eye Center, we have dedicated significant resources to studying dead bag syndrome, including a collaboration with Dr. Masket and others in 2022 to publish the first formal, peer-reviewed study of the condition.2

Landmark Findings
In this first study, published in the Journal of Cataract & Refractive Surgery, we included 10 suspected dead bag syndrome cases in patients 65 and older, with a mean time between implantation and explantation (when performed) of 10.6 ± 5.6 years. It is noteworthy that no signs of zonular instability were reported during the implantation surgeries, which were all uneventful. Eight IOLs and seven capsular bags were removed because of subluxation or dislocation.
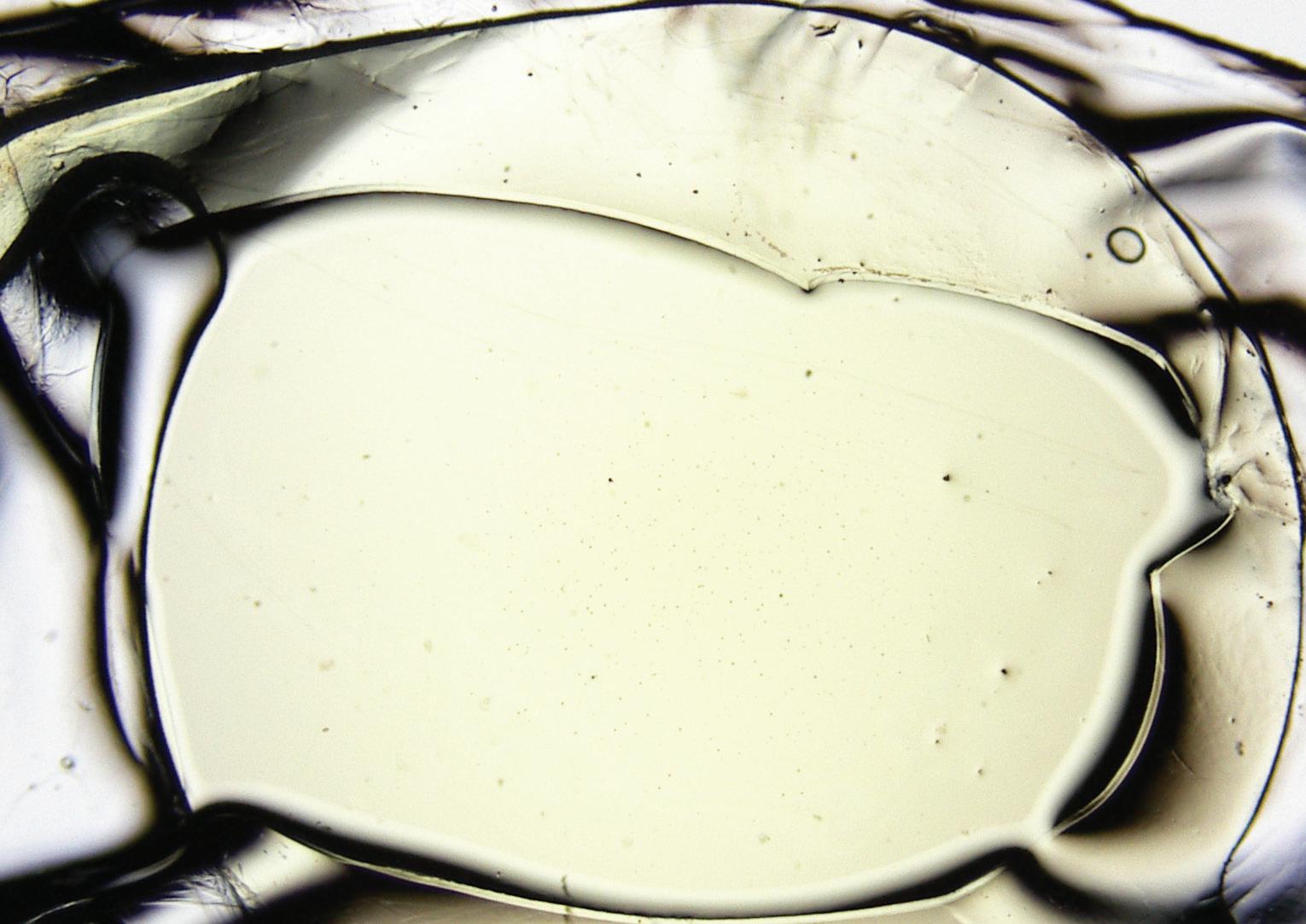
Findings from the histopathologic examination of the capsular bags included:
• The capsule showed signs of degradation, such as thinning or splitting, or both.
• Lens epithelial cells (LECs)—the parental cells responsible for growth and development of the transparent ocular lens— were completely absent in two specimens, while the other specimens had rare LECS on the inner surface of the capsule.
• Explanted IOLs were three-piece silicone IOLs or single-piece hydrophobic acrylic IOLs. One IOL optic showed a small amount of granular pigment deposition, but the optics of the other IOLs were unremarkable.
• We believe splitting of the capsule occurring at the level of the zonular attachments led to subsequent in-the-bag IOL dislocation.
As part of the same study, we compared the dead bag syndrome histopathological findings with those of capsules from 40 cases of in-the-bag IOL dislocation, including 26 cases with evident pseudoexfoliation material.3
We observed LECs and Soemmerring’s ring formation in all 40 cases. Capsulorhexis phimosis was also a relatively common finding, while capsular splitting/delamination was only found in one specimen. A review of the literature indicates there is also capsular splitting/delamination in true exfoliation syndrome.4 However, in this condition, which can be associated with chronic exposure to intense heat or infrared radiation, there is usually a thin membrane of delaminated capsule on the anterior surface of the crystalline lens before cataract surgery. These differences added to evidence that dead bag syndrome is a distinct entity.

Continuing Research
In a presentation at the 2023 American Academy of Ophthalmology annual meeting, we described the results from the review of another 14 cases of suspected dead bag syndrome.
Of these cases, nine IOLs and 11 capsular bags were removed due to subluxation/ decentration.
In another study presented at the American Society of Cataract and Refractive Surgery 2023 meeting, we examined the nature of capsular bag tissues obtained from dead bag syndrome patients by using immunohistochemistry in collaboration with a Japanese group.
Capsular bags from nine patients were obtained after IOL explantation, with capsular bag removal and processing for light microscopic immunohistochemical analysis for collagen type I (fibrous tissue marker), collagen type IV and laminin (both components of basement membrane or lens capsule), vimentin (lens epithelial cell cytoskeleton), and fibronectin (wound healing-related matrix component). The capsular tissue in dead bag syndrome cases showed traces of activity in a small number of LECs in postoperative wound healing and pro-fibrotic reactions, suggesting that LECs were present in the capsule in the postoperative early phase, followed by death and detachment.
Discussion
There are a lot of unknowns in the etiology of dead bag syndrome, but we hypothesize that late postoperative zonular failure is related to capsule splitting/delamination occurring at the level of zonular attachments.
It is important to note that this syndrome does not have any association with a particular IOL design or material. We’ve also considered other possible associations. Many surgeons wondered if our findings regarding the scarcity of LECs could be related to capsular polishing, a widely used technique during cataract surgery to prevent capsular bag fibrosis and opacification, especially in association with premium IOLs.5-9
It is, indeed, described that cortical lens fibers and LECs continue to deposit extracellular matrix and lens capsule components at their basal ends. This process contributes to the thickening and structural integrity of the capsule throughout life. However, even extensive polishing cannot completely remove all LECs, and polishing is usually not performed at the capsular bag equator, as this region is not readily visible. Therefore, to date, there is no established association between capsular polishing and this condition.
We also explored Dr. Masket’s observation of cases involving white, intumescent cataracts that evolved into dead bag syndrome, suggesting oncotic pressure within the capsular bag may play a role in killing LECs. However, many dead bag cases are not related to this type of cataract, and other factors are likely involved in its origin.
There have been numerous informal discussions about dead bag syndrome in the field, and surgeons have described many suspected cases that involved less severe signs, such as capsules that were floppy and delicate but still exhibited a certain amount of proliferative material within, including abnormal gel-like Soemmerring’s ring formation. It is possible that the findings described in our first study may represent the severe end of a spectrum.
In discussions with researchers focused on the crystalline lens, it becomes evident there are still unknowns in the relationship between LECs and the capsule, especially in postcataract surgery cases. Although LECs are important for the formation of the capsule, this structure represents an anchor point for the basal surfaces of epithelial and fiber cells and provides necessary signals for proper lens cell proliferation, migration, and differentiation.10
In dead bag syndrome, another possibility is that the initial problem is in the capsule itself, which would initiate a cycle of LEC damage, with further damage to the capsule.
Next Steps
Our first study represented an initial formal assessment of dead bag syndrome, raising awareness of this condition and establishing a basis for further discussions and much-needed additional formal studies. We certainly hope it accomplished its goal.
Our laboratory will continue addressing the many unanswered questions about the syndrome, not only about its etiology but also its manifestations.
As the research continues, we advise management on a case-by-case basis, depending on presentation and status of the zonular support.
About the Authors
Dr. Werner is co-director of the Intermountain Ocular Research Center and Moran’s vice-chair for equity, diversity, and inclusion. She is recognized as a foremost authority in the IOL field and was the first woman to receive the prestigious American Academy of Ophthalmology’s Charles D. Kelman Award and Lecture. She is also the first woman and the first Latina to hold the position of U.S. Associate Editor for the Journal of Cataract & Refractive Surgery. Dr. Werner holds the Ralph and Mary Tuck Presidential Endowed Chair at the University of Utah Department of Ophthalmology and Visual Sciences.
Dr. Mamalis directs Moran’s Ophthalmic Pathology Laboratory and is a renowned expert on intraocular lenses as co-director of the Intermountain Ocular Research Center. He is a past president of the American Society of Cataract and Refractive Surgery (ASCRS) and has received the American Academy of Ophthalmology Life Achievement Honor Award, among others. He is the holder of the Calvin S. and JeNeal N. Hatch Presidential Endowed Chair at the University of Utah Department of Ophthalmology and Visual Sciences. In his clinical practice, Dr. Mamalis specializes in cataract and other anterior ocular surgeries.
REFERENCES
1. Late In-the-Bag Intraocular Lens Dislocation: Incidence, Prevention, and Management. Gimbel HV, Condon GP, Kohnen T, Olson RJ, Halkiadakis I. Journal of Cataract & Refractive Surgery. 2005;31:2193–2204.
2. Clinical and Histopathological Findings in the Dead Bag Syndrome. Culp C, Qu P, Jones J, Fram N, Ogawa G, Masket S, Mamalis N, Werner L. Journal of Cataract & Refractive Surgery. 2022;48:177–184.
3. Pathologic Evidence of Pseudoexfoliation in Cases of In-the-Bag Intraocular Lens Subluxation or Dislocation. Liu E, Cole S, Werner L, Hengerer F, Mamalis N, Kohnen T. Journal of Cataract & Refractive Surgery. 2015;41:929–935.
4. Surgical Approach, Histopathology, and Pathogenesis in Cataract Associated with True Lens Exfoliation. Journal of Cataract & Refractive Surgery. Cooke CA, Lum DJ, Wheeldon CE, Teoh H, McGhee CN. 2007;33:735–738.
5. The Lens Capsule. Danysh BP, Duncan MK. Experimental Eye Research. 2009;88:151–164.
6. Hydropolish: A Controlled Trial on a Technique to Eradicate Residual Cortical Lens Fibers in Phacoemulsification Cataract Surgery. Wang SB, Quah XM, Amjadi S, Tong J, Francis IC. European Journal of Ophthalmology. 2015;25:571–574.
7. Fluid-Jet Technique to Polish the Posterior Capsule for Phacoemulsification Surgeries: Efficacy and Safety Evaluation. Liu Z, Cao Q, Qu B, Wang W, Ruan X, Zheng D, Jin G, Tan X, Jin L, He M, Congdon N, Lin H, Luo L, Liu Y. Journal of Cataract & Refractive Surgery. 2020;46:1508–1514.
8. Evaluation of Laser Capsule Polishing for Prevention of Posterior Capsule Opacification in a Human Ex Vivo Model. Luft N, Kreutzer TC, Dirisamer M, Priglinger CS, Burger J, Findl O, Priglinger SG. Journal of Cataract & Refractive Surgery. 2015;41:2739–2745.
9. Aspiration Curette for Anterior Capsule Polishing: Laboratory and Clinical Evaluation. Menapace R, Di Nardo S. Journal of Cataract & Refractive Surgery. 2006;32:1997–2003.
10. The Effects of Extracellular Matrix on Cell Attachment, Proliferation and Migration in a Human Lens Epithelial Cell Line. Oharazawa H, Ibaraki N, Lin LR, Reddy VN. Experimental Eye Research. 1999;69:603–610.
LEARN MORE

About the Intermountain Ocular Research Center
Established in 1982 and currently directed by Liliana Werner, MD, PhD, and Nick Mamalis, MD, this nonprofit, independent laboratory based at the Moran Eye Center performs basic, in-depth research on intraocular lenses. The center provides services and education for surgeons, clinical ophthalmologists, their patients, and manufacturers. More than 1,000 peer-reviewed publications from the center guide companies and physicians worldwide as the center vets new lens technology. The center also is involved in the analysis of Toxic Anterior Segment Syndrome (TASS) and other causes of postoperative inflammation following cataract surgery.