20 minute read
Bovine Reproductive Problems for the Mixed Animal Practitioner

from 2023 MVMA Proceedings Book
by movma

Missouri Veterinary Medical Association Convention January 27, 2023
Celeste Morris, DVM, MBA, MPVM Assistant Professor, Food Animal Ambulatory Service University of Missouri College of Veterinary Medicine c.morris@missouri.edu
Abstract
Beyond dystocia, there are many other reproductive challenges that can present to veterinarians for treatment. This talk will discuss management of other common reproductive disorders in the bovine, such as freemartins, twins, retained fetal membranes, metritis, pyometra, cystic ovaries, and vaginal and uterine prolapse. It will attempt to propose practical, summary notes on these conditions and the most common and/or easiest routes to diagnosis and treatment.
Key Words: Cystic ovarian disease (COD), twin management, freemartins, uterine prolapse, vaginal prolapse, metritis, pyometra, retained fetal membranes (RFM)
Normal Bovine Reproduction Review
¥ Reproductive anatomy: Bicornuate uterus with a very small uterine body ¥ Estrous cycle o Non-seasonal, polyestrous o 21 day cycle (17-24 day range) o 2-3 waves of follicles o Estrus length: ~12-18 hour average o Ovulation 24-30 hours after the onset of estrus (after they go out of estrus, usually) ¥ Gestation: ~280 days (270-292 day range), cotyledonary placentation (convex placentomes) ¥ Normal uterine involution: ~35-45 days
Cystic Ovarian Disease (COD)
¥ Synonymous terminology: Cystic ovaries, cystic ovarian disease, ovarian cysts, cystic ovarian degeneration ¥ Follicular Cyst Definition (COD): “Presence of a follicle(s) with a diameter of at least 20 mm, present on one or both ovaries in the absence of any active luteal tissue, which clearly interferes with normal ovarian cyclicity” (Hopper, 2021) o Older definitions require 10 days – not easily known in routine reproductive examinations o Cystic ovaries can be present with luteal tissue if the cyst is not steroidogenic ¥ Luteal Cyst: Luteal structure that is >20 mm and persistent, interfering with normal cyclicity or known progression of a previously diagnosed follicular cyst o Differentiation between large/cavitated CL and luteal cyst in one visit can be challenging (based on clinical signs and history, not just presence of a large luteal structure), keep in mind that cavitated CLs are normal o Often has irregularly filled luteal tissue with cavities or strands (trabeculae) which can help differentiate luteal cyst versus CL ¥ Etiology o Multifactorial condition o Individual genetic factors, phenotypic traits, environmental factors, metabolic and cellular factors, and management factors o Most widely accepted theory is related to LH surge (absent, insufficient, or improperly timed) o Other likely related factors: Breakdown in estradiol positive feedback loop, loss of progesterone negative feedback, protracted estradiol secretion by the dominant follicle, heat shock protein, high NEFAs o Leads to follicles that continue to grow and become anovulatory o Can resolve on their own or continue to re-grow in the same spot even after resolution
¥ Risk factors: High milk production, calving in summer months, increased parity/age, overconditioning precalving, increased NEFAs, genetics (low heritability, 0.07-0.12), MGA use in beef heifers, genetics ¥ Classification of cysts o Most common: follicular vs luteal o Differentiation can be based on degree of luteinization or hormones produced o Thought to be different phases of the same process: follicular cyst à luteinization à luteal cyst o Differentiation can require combination of history and physical examination, +/-ultrasound, +/serum progesterone levels ¥ Clinical signs: Anestrus > persistent estrus (nymphomania) ¥ Diagnosis o Clinical signs o Transrectal palpation o Transrectal ultrasound o +/- serum progesterone levels (uncommon in routine practice) ¥ Treatment o Non-hormonal therapies (not recommended) § Ovariectomy § Manual crushing o Hormonal therapy § Follicular cyst ¥ GnRH – First line, most common, usually works o Mechanism: Cause an LH surge exogenously within 2 hours o Causes luteinization of the follicular cyst and ovulation of a dominant follicle if present o Resumption of normal cyclicity in 72-85% of cows and return to estrus within 3 weeks if a dominant follicle was present o Can also follow with prostaglandin in 7-10 days following GnRH to speed up the process
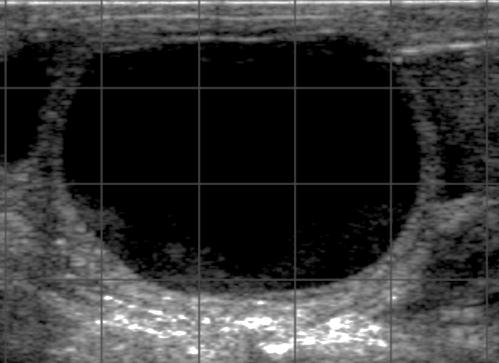
Follicular Cyst (<3 mm rim, anechoic center)
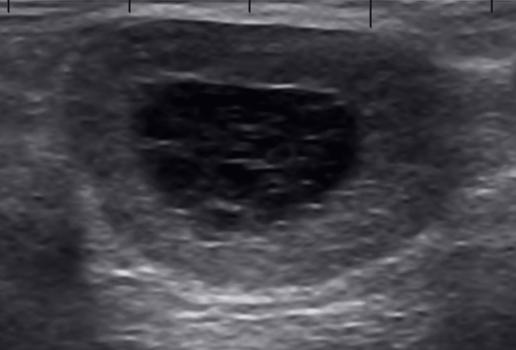
§ Luteal cyst ¥ Prostaglandin o Mechanism: regression of luteal tissue o Estrus in 90% of cows by 8 days following treatment § Undetermined type of cyst (unable to determine if luteal or follicular, may be transitional): Concurrent GnRH + prostaglandin treatment can be used to elicit response § Additional treatments for refractory cysts Luteal Cyst (>3 mm rim, hyperechoic strands) ¥ hCG o Mechanism: Should be used only if cyst is refractory to GnRH treatment o LH like properties cause the cyst to luteinize o Can also follow with prostaglandin in 7-10 days o Dose: 10,000 IU IM o More costly than GnRH, can cause immune reaction, legality?
¥ Progesterone (CIDR Device) +/- prostaglandin +/- ovsynch o Mechanism: § Progesterone “resets” the hypothalamic-pituitary-ovarian axis § Reduced LH secretion § Regression of the cystic structure § New follicular wave after removal o Dose: One cattle CIDR contains 1.38 g progesterone
Cyst Classification Rim Width Ultrasound Appearance Primary Hormone Secreted Most common treatment
Follicular Thin (£3 mm) Luteal Thick (>3 mm) Anechoic fluid Estradiol GnRH – synthetic or analog (100 µg IM)
Variable - more hyperechoic (luteal tissue), often have trabeculae or echogenic strands Progesterone Prostaglandin (25 mg dinoprost or 500 µg cloprostenol IM)
Twins & Twin Management
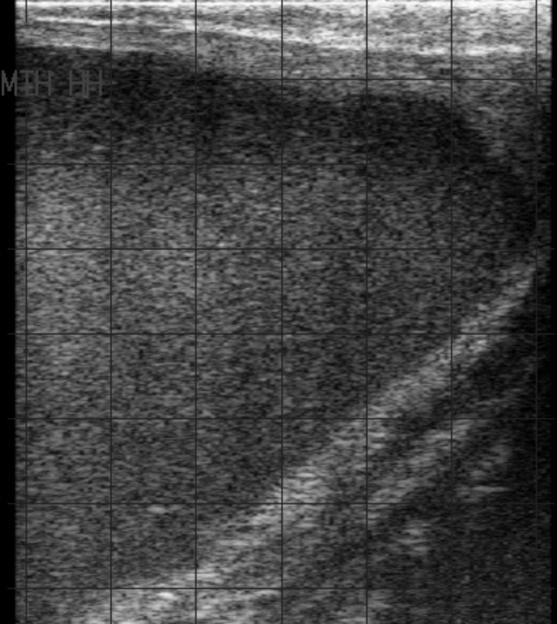
¥ Risk Factors: High producing dairy cows, genetic propensity, more common in dairy than beef ¥ Associated challenges: Increased pregnancy loss, especially <60 days. Dystocia, periparturient disease, freemartinism, spontaneous regression (may occur without consequences) ¥ Diagnosis o Suggestive § Transrectal palpation: Enlarged horn for stage of pregnancy § >95% of twins are dizygotic – examine for 2 corpora lutea ¥ Recommendation to make ovarian examination part of normal pregnancy diagnosis if performed when twin diagnosis is possible to complete examination § Ultrasound visualization of “Twin line” (apposing chorioallantoic membranes) o Definitive § Palpation of 2 fetuses § Ultrasound visualization of 2 fetuses ¥ Treatment: Current standard is not to reduce twins - no treatment recommended (risks outweigh benefits) ¥ Management recommendations o Monitor more closely for potential pregnancy loss and dystocia o Likely will calve early (a few days) § If dairy, dry off early to compensate o Can increase energy in the diet in late gestation o Monitor for metabolic disease
Freemartins
¥ Definition: Sterile female produced from a twin (male/female) pregnancy ¥ Etiology o XX/XY chimera produced as a result of anastomosis of placental vessels (day 28-30) before sexual differentiation (mixing of hematopoietic stem cells) o Female is exposed to AMH and testosterone during sexual differentiation, which results in abnormalities of the normal female reproductive tract (often partial regression of paramesonephric duct products) ¥ Risk Factors: All breeds of cattle are affected o Remember: If the male twin dies after sexual differentiation, freemartin heifers can appear to be born as singles ¥ Clinical signs o Enlarged or prominent clitoris o Elongated clitoral hairs o Shallow vagina
o Small or incomplete cervix o Small, incomplete, or absent uterus o Small or hypoplastic ovaries o Otherwise systemically healthy ¥ Presentation o Heifers that were born co-twin to a male and/or are hard breeders, don’t stand for a bull, or that are open at the end of an appropriate breeding season where others are pregnant o Abnormal external genitalia ¥ Diagnosis o Clinical signs and history o Absence of normal, functional reproductive tract (transrectal palpation and/or ultrasound) o Measurement of vaginal depth: <1/3 depth of heifers the same age o Karyotyping (XX/XY Chimera), PCR testing – unusual ¥ Treatment – none, cull if breeding stock
Vaginal Prolapse
¥ Etiology o Can be vaginal or vaginal and cervical o More common in bovine than in many other species o Not related to uterine prolapse o Usually occurs in late gestation and with increased intra-abdominal pressure ¥ Risk Factors: Genetics (especially Herefords, Charolais, limousine, shorthorns and bos indicus breeds), increased intra-abdominal pressure in late pregnancy, extreme cold weather, overconditioning (perivaginal fat), intake of large volumes of poorly digestible roughage, poor vaginal conformation, increased estrogen influence (late pregnancy, estrus) ¥ Guidelines: o Retain vaginal and cervical tissue in order to allow delivery and weaning of live offspring o Perform retention procedure as soon as possible to decrease tissue damage and exposure (try to go within a few hours) o Cull after job is finished (likely to recur at next gestation/parturition) and do not keep female offspring ¥ Classifications o Grade I: Intermittent (usually present when animal is laying down) o Grade II: Tissue prolapsed and continuously visible o Grade III: Prolapse of the vagina along with cervix (tissue all visible but still healthy/intact), bladder may be involved o Grade IV: Vaginal mucosa appears necrotic, is fibrosed, or is damaged (with or without cervical involvement) ¥ Short term treatment o Carefully replace the tissue § Apply gentle pressure until replacement can be completed – use palms or fists, not fingers, to avoid traumatizing the tissue § Be patient and don’t force it! Finding the location with give is key § Hypertonic saline and/or water with sugar can make a hypertonic paste that is easily applied § If very edematous, can wrap in a towel and squeeze to attempt to decrease the size of the tissue mass § If not making progress with pressure, an occasional twist of the tissue 15-30 degrees can help facilitate slipping back inward o Buhner Stitch (most common) § Supplies: ¥ Caudal epidural anesthesia (2% Lidocaine, 5-10 ml syringe, 18 ga 1.5” needle) ¥ Water ¥ ~2 feet of 3/8” umbilical tape ¥ Gerlach (Buhner) needle
¥ Optional: #10 blade, betadine solution for soaking umbilical tape, antiseptic solution if needed, obstetrical lubricant ¥ If severe or chronic, can use hypertonic solutions to aid in replacement – see Uterine Eversion (Prolapse) Section for details § Directions ¥ Caudal epidural anesthesia ¥ Clean the vulva and surrounding 2-3 inches of tissue with water and/or dilute antiseptic solution if needed ¥ Optional: o 1 cm stab incision made on midline below the vulva o 1 cm stab incision midway between anus and top of vulva o Presenter’s preference is not to do stab incisions and use the needle to make the holes for passage of the umbilical tape – 1 cm apart on midline below the vulva (horizontally) and 1 cm apart on midline above the vulva (horizontally) halfway between the anus and the vulva ¥ Gerlach (Buhner) needle passed starting ventrally below the vulva (if stab incision was made, insert through stab incision) and driven dorsally in the deep musculature lateral to the vulva, exiting the skin halfway between the vulva and the anus (through stab incision if one was made) o Place non-dominant hand inside the vagina to ensure the needle doesn’t exit through the vaginal mucosa ¥ Thread needle with umbilical tape o 1/3 on one side, 2/3 on other side (leave a long enough tail that one end can reach along the whole track of the needle) ¥ Pull needle down and out, drawing umbilical tape through track just made lateral to the vulva ¥ Unthread umbilical tape and repeat placement of needle on the opposite side of the vulva ¥ Thread umbilical tape from the dorsal exit of the other incision through the eye of the needle and pull down, threading the same piece of umbilical tape down through the opposite side ¥ Tie ends below the vulva together and tighten until the opening of the vulva is ~2 fingers in width o Bow +/- knot for late gestation/impending calving § Can be opened and retied if necessary, depending on the amount of owner observation that is possible o Square knot for open animals ¥ The tie should be tucked under the ventral, haired portion of the vulva as not to cause irritation to the opening of the vulva ¥ Need close observation once Buhner stitch is placed if calving! o Caslick’s – not recommended, often insufficient o Bootlace technique § Directions: ¥ Caudal epidural anesthesia ¥ Eyelets are placed on either side of the vulva in dorsal to ventral line ¥ Umbilical or Buhner tape is used to lace up the vulva (like boot laces) § Stronger than a caslick’s § Undesirable due to vulvar inversion and extra time and supplies for suture placement § Must be loosened prior to calving, need close observation o Horizontal or vertical mattress § Directions ¥ Caudal epidural anesthesia ¥ Needle passed across the top of the vulvar lips in a horizontal line, then repeated from the same side back across with spacing of about 2-3 cm between bites § Undesirable due to vulvar edema that frequently develops
§ Recommend placement with stents or buttons to decrease edema formation § Must be loosened prior to calving, need close observation ¥ Long term treatments, secondary methods o Minchev or modified minchev vaginopexy o Winkler Cervicopexy ¥ Supportive care o Antibiotics: only in cases of severe trauma (usually Grade IV) o Anti-inflammatories: As needed basis o Steroids: Avoid in late gestation, can induce parturition ¥ Directions following placement o Monitor animals carefully § Untie if signs of calving are seen § Retie after calving § Monitor for normal urination and defecation
Uterine Eversion (Prolapse)
¥ Etiology o Usually occurs within 24 hours after calving o Not related to vaginal or cervical prolapse ¥ Risk Factors: Multifactorial condition o Reduced uterine contractility following primary or secondary uterine inertia § Primary uterine inertia: hypocalcemia, reduced prostaglandin and oxytocin receptors, myometrial defects § Secondary uterine inertia: exhaustion, dystocia o Prolonged recumbency following paralysis or hypocalcemia § Increased intra-abdominal pressure o Extreme weather changes ¥ Guidelines o True emergency! Uterus becomes quickly traumatized, contaminated, and edematous! o Do not transport animals if possible o Handle animals carefully and slowly if they are mobile o Unlikely to recur, do not need to cull based on occurrence of uterine prolapse ¥ Treatment – Replace! o Contraindications for replacement § Significant trauma § Obvious prolapse of abdominal organs o Cow positioning § Cow standing or down depending on the circumstances, experience, or preference § If down, legs straight behind the animal can help significantly to open space in the caudal abdomen § If standing, can use a towel or a sheet to help support the weight of the uterus § Can lift the hind end of the cow if necessary or indicated, but recommended only if absolutely necessary due to potential trauma o Supplies § Caudal epidural anesthesia (2% Lidocaine, 5-10 ml syringe, 18 ga 1.5” needle) § Water +/- dilute cleaning solution § Obstetrical lubricant § Optional: Plastic bag for uterus, hypertonic saline, sugar, towels, dextrose o Epidural anesthesia o Clean uterus o Remove any easily removable fetal membranes (do not tear) o Large and unruly uterus tips § Can place in or on a plastic bag to help with cleanliness and weight/edema § If the cow is standing, can “sling” the uterus with a towel or a sheet to decrease worsening dependent edema and help reduce the weight burden
§ If the cow is down, resting the uterus on your abdomen/chest can be helpful for support § If needed, hypertonic solutions (hypertonic saline, sugar, dextrose) can be applied to help decrease edema and facilitate replacement ¥ Use of sugar or other hypertonic solutions can be irritating to the endometrium and are not uniformly supported, but can help in cases of severe edema – they should only be used if replacement without is not possible ¥ Hypertonic saline and/or water with sugar can make a hypertonic paste that is easily applied o Use gentle, steady pressure (fists or palms only, fingers are likely to puncture the uterus) to gently apply pressure and feel for which part of the uterus has any give toward the vulvar opening § If identifiable, try to find the non-gravid horn (slit or small opening) with smaller placentomes to start with steady pressure o Continue with gentle pressure until replacement can be completed § Be patient and don’t force it! Finding the location with give is key o Fully invert the uterine horns § If the end of the uterine horns cannot be reached by hand, the practitioner can use a large bottle (presenter’s preference is plastic, like a soda bottle or hypertonic bottle) in the hand to gently invert the horns inside the cow ¥ Treatment – Amputation – only if no other options (significant trauma to the uterus, untenable size/inability to replace) o Open § Incision in the uterine body to explore contents of the uterus (return any exposed viscera to the abdominal cavity) § Fan out the broad ligament on each side and individually double ligate and cut visible vessels § Place overlapping mattress sutures across the uterine body and amputate just distal § Suture over stump with simple continuous sutures and return the stump o Closed § Salvage procedure and doesn’t take into consideration trapped viscera § Ligate the entire organ and leave it to slough ¥ Supportive care o Anti-inflammatories o Systemic antibiotics o Oxytocin (20-30 IU IM, repeat in 30-60 min or 40-100 IU IM or IV once) o Retention (Buhner) suture? § Controversial § If the cow is standing and responds to therapy (oxytocin) well, unlikely the uterus will evert again § If the cow is down, unable to stand, is still showing significant tenesmus, has other complicating conditions, the uterus may be more likely to re-prolapse o +/- Calcium therapy (Calcium Gluconate, CMPK) ¥ Directions following replacement o 18-20% mortality rate after replacement (usually internal hemorrhage from uterine artery) –communicate with clients o Prognosis for future fertility is usually acceptable as long as replacement was successful and the animal is systemically healthy afterward o No known heritable component, minimal chance of recurrence
Retained Fetal Membranes (RFM)
¥ Definition: Retention of allantochorion and/or amnion for > 12 hours after calving ¥ Etiology: Abnormal or incomplete placental maturation preventing the usual easy separation and expulsion of fetal membranes ¥ Direct risk factors: Induction of parturition, dystocia, uterine torsion, cesarean section, abortion/uterine infection ¥ Indirect risk factors: intensive stress, twinning, subclinical hypocalcemia, fetal dropsy
¥ Clinical signs o Usually visible tissue hanging from vulva >12 hours after calving o If still present at 36 hours, likely to stay for 6-10 days o Without smell to malodorous (big range) ¥ Diagnosis o History, clinical signs o Visual and physical examination ¥ Treatment o Condition contained within the uterus (no signs of systemic illness) § Monitoring for development of systemic signs (inappetence, lethargy) § If the membranes are long, damaged, or dirty, tie them in a knot to prevent further contamination but still allow the weight of the membranes to apply consistent tension to the remaining parts § If the membranes are malodorous, but she is otherwise well, no systemic treatment is necessary o Systemic illness (lethargy, inappetence, fever, etc) § Systemic antibiotics (not intrauterine) +/- anti-inflammatories +/- fluid therapy o Summary § Hormonal therapies not shown to help § Only treat if systemically affected § Do not flush the uterus, administer intrauterine antibiotics, intrauterine antiseptics, or attempt to manually remove the membranes ¥ Can apply light traction in case the membranes are “floating” but do not attempt manual removal § Do not manually dilate the cervix ¥ Long term complications o Delayed uterine involution à increased number of days from calving to first estrus o Loss of milk production o Predisposes to metritis (dairy > beef)
Metritis
¥ Definition: inflammation of all of the layers of the uterus (endometrium, myometrium, serosa) ¥ Etiology o Usually seen within the first 2 weeks (can be diagnosed up to 3 weeks) o Repeated or overwhelming bacterial contamination of the uterus post-calving resulting in infection o Organisms: E. coli (early/first week) à Truperella pyogenes (later) § Can be complicated by Fusobacterium necrophorum ¥ Risk Factors: Dairy > Beef, dystocia, twins, stillbirth/abortion, retained fetal membranes, negative energy balance (elevated NEFAs), ketosis, immunosuppression ¥ Clinical signs
Color Consistency Smell Time
Lochia Bloody to reddish-brown Mucoid Odorless Normal up to 3 weeks
Metritis Usually brown Watery Fetid <21 days o Localized infection (contained within the uterus) § Fetid discharge § May not have any other outward clinical signs o Acute puerperal metritis/Systemic metritis/Toxic septic metritis § Fever, inappetence, lethargy, tachycardia, and/or dehydration § Enlarged, fluid filled, flaccid uterus § Brown, watery, fetid discharge
¥ Diagnosis o History and clinical signs o Physical examination - Uterus may expel fetid fluid upon palpation ¥ Treatment
o Localized: Monitoring § No treatment if not systemically ill o Acute puerperal metritis/Systemic metritis/Toxic septic metritis § Anti-inflammatories § Systemic antibiotics § +/- fluid therapy, electrolytes (Ca2+), ketosis treatment o Summary § Only treat if systemically affected § Do not flush the uterus, administer intrauterine antibiotics or intrauterine antiseptics § No known benefits associated with treating with oxytocin or prostaglandin
Pyometra
¥ Definition: accumulation of pus in the uterus in the presence of a CL and a closed cervix ¥ Etiology o Dairy: Early ovulation when the uterus is still clearing post-calving resulting in a closed cervix and trapping of bacteria within the lumen à results in increased CL lifespan due to increased concentrations of PGE2 o Beef: Tritrichomonas foetus >>> other ¥ Risk factors: Previous diagnosis of reproductive disease (RFM, metritis) ¥ Clinical signs o Anestrus (no vaginal discharge) o Not systemically affected otherwise ¥ Diagnosis o Palpation: Fluid filled uterus in the presence of a CL and no positive signs of pregnancy § Wall of the uterus is often thickened § Variable in size, can be in one horn or both § Can confirm with ultrasound – variable echogenicity, from anechoic with speckles to highly cellular ¥ Treatment o Dairy or non-infectious: Most cows will respond to a single dose of prostaglandin § Can treat twice 14 days apart if non-responsive § Will need at least one heat cycle following luteolysis to increase the chances of successful conception after complete uterine clearance of debris o Beef or suspected infectious: If CL present, can still treat with prostaglandin, BUT consider below § If several cows present with pyometras and the herd also has low pregnancy rates overall, suggest testing the pyometra fluid and/or bull for Tritrichomonas foetus § Recommend culling these animals due to overall disease risk and decreased reproductive efficiency for this season § Tritrichomonas regulations (State of Missouri): https://agriculture.mo.gov/animals/health/disease/trich.php § 2021 Disease Map: https://agriculture.mo.gov/animals/pdf/PositiveTrichomoniasisMap2021.pdf
General Reminders
¥ Epidural anesthesia: o Dose: ~1 ml 2% Lidocaine/200 lbs (Adult bovine rule of thumb: 4-8 ml) o Caudal epidural (Sacral/coccygeal space) o 18 ga 1.5” needle
Pyometra
¥ Estradiol prohibited for use in food animal practice (If not sure about legalities of medications, submit a
FARAD request or visit the site for guidance) ¥ Oral progestogens not for use in livestock species ¥ Consider the job of the animal you’re treating and let that help you make treatment decisions o Don’t forget withdrawal periods, even on pets ¥ Antimicrobials approved for use in adult lactating dairy cattle (also for lactating goats, sheep where there is human consumption of dairy products): o Oxytetracycline (LA200) - Follow labeled route, dose, frequency (ELDU Permitted) o Penicillin (PPG) - Can dose at 3-5 ml/100 lbs (label dose is 1 ml/100 lbs) (ELDU Permitted) o Ampicillin (Polyflex or ampicillin sodium) - Follow labeled route, dose, frequency (ELDU Permitted) o Ceftiofur (Naxcel, Excenel, Excede) - Follow labeled dose, route, frequency, duration (Can change indication but nothing else, ELDU Restricted) ¥ Always educate and include the producer ¥ Call us if you have questions!
Bovine Medication Table
Anti-Inflammatories
Trade Name Drug Name Route Dose+ Meat
withdrawal*
Milk Withdrawal* Special Notes
Banamine Flunixin meglumine IV 1.1-2.2 mg/kg or 1-2 ml/100 lb
4 days 36 hours q24 hr, consult FARAD if multiple doses Topical 3 ml/100 lbs 8 days N/A Not for dairy - Meloxicam PO 0.5-2 mg/kg Approx. 30 days, consult FARAD Approx. 14 days, consult FARAD q24 hr
- Dexamethasone IM or IV 0.1-0.15 mg/kg Approx 6 days, consult FARAD Approx 3 days, consult FARAD Avoid in pregnant animals
Reproductive Hormones
Trade Name Example
Drug Name Route Dose+
Meat withdrawal*
Milk Withdrawal* Special Notes
Lutalyse Dinoprost IM 25 mg (5 ml) 0 days 0 days Pyometra, Estrumate Cloprostenol IM 500 µg 0 days 0 days luteal cysts; caution with Lutalyse HC (half dose) Cystorelin Gonadorelin IM 100 µg IM 0 days 0 days Follicular cysts - Oxytocin IM or IV 20-100 IU 0 days 0 days Can repeat if given smaller doses or just give once
*If going off label or giving multiple doses, always extend your withdrawals and submit a FARAD request + Always refer to medication label for dosing information
Sources
¥ Bovine Reproduction; Hopper, R.M., Ed.; 2nd Edition.; Wiley & Sons, Inc: Hoboken, NJ; ISBN 9781119602361. ¥ Current Therapy in Large Animal Theriogenology; Elsevier, 2007; ISBN 9780721693231. ¥ Veterinary Reproduction and Obstetrics; Elsevier, 2019; ISBN 9780702072338.



