BONES .
PHIII.ANGES
THH;H BONE (femur)
KNEE CAl' (pa tella)
SHiN BO NE (tiIJia)
HkOOC H RO Ng (fiIJll:a)
1\11'; 1 A'I AI<SU!>
Tre nllml. r I J, Ir I :)Int flr 1'1 .UI r I um1 I i I te 'I. - ·lk II T T \\/'01< F (I, I•• • 1", • '1/. \ I\'. A II' , J j t. I J 1114 1t ' 0_ R "lOP Al I It lr /.
ARTERIES.
FIRs rr AID TO THE I NJURED'
ARRA!,;CED ACCORDING TO TIlE RE\'ISED SYLLABUS DE T lIE FI RST AID COURSE
01' TIIE
ST. )OH1\ lJY
JA.\lE ' C_\':\,TLIE, .\LA., .\LB., F. R.C.S., HOIIOlar), Associat. rj tltt: Order oJ St joltn. l/onoJa'y LiJe .Jfeml>"r oJ: o}/d Leerurer and Examl1lcr to, tlte ASSOClalion.
\\ llh a CHAI'TER on ". tretcher Tran,p(,n," re\ i,ed from that originally WIIlten by ' ir )UH:-: Ft-kLE\. A:nll:1it o./Justlce of ti,. Order oJ St.john, In accordance with the Army tretcha Exerclst:. AI,u a CHAPTE R (being the Fifth Lecture, for Fem:d"5 o nll"), by E . .\lAcDoIIEL COSGR AVE, M.D., F.I<.C.P.I A-n ieltt oj Crace oj tlu Om'cr oJ St. jo/zn. H01Z0ralY Lij t: ,1[ember oj, a n d Lecturer and Exa lt/ut e,. to. tlze ASSoCiation.
TWELFTH EDITION, 480 ,000 to 530,000. (Tltis Edit ,OIL is sl}JIilar tv tlte .-Ito'entlt.)
Price in Cloth, IS. net: by post, IS. 2d . I n 2S 6d .; by POSt, 25. 8d.
TO liE OBTAI:-:ED AT . T. GA T E, CLERKEX\YELL, LOX DON, W. H & L. C.
qrf)t
Wriot!2 of tbe @rber of tbc of .st. lobn of .1rru5alrm in (Ji;nglanb.
4)rilb' nub' tJa tron .o f t yc @rb.c.r .
His Most Gracious Majesty Kin g Edw a rd VII., K.G. (5 ranb' t)ri.or.
His Royal Highness the Prince of Wal es , K.G.
The Most Honble . the Mar ques s of Linlithgow , K.T. .of Qtg[t
Field Ma rshal
His Royal Highness the Duke of Conn aug h t, K.G.
<0ffi.ccr 5.
Ch.ancellor-The Right Hon the \ 'iscount K:-;UTSFO[W, G C. \l.( '.
Secretary,General-Colonel Sir HERllERT JEKYLL, K..C. \1.( ; . , R.c. Rccei,/er-GclLcral-ED\\'IN FIlESHFIELD, Esq., LL.D.
AlmolLer-Tbe Rev. Canon DUCK\yOIlTH, C.Y.O., D.ll.
Registrar-i\!ajor-General the Lord CIU:VLb\[()KE, C. \-.0.
GCIll1alol{ist-Sir ALFIlED COTT SCOTT·GATTY, C Y.O. (C;::mer).
Director 0/ tILe Ambulance Depa>·tmcnt-The ;\lost Hon. the .\larquess of BIlEADALBA:-;r::. K.G.
Librarian-Lieut.·CoL RrcHAIlD HOLBECHE.
Secretary-Colonel Sir HERBERT C. PERROTT, BI., C.B.
Chainna1t 0/ the British OJ>lttltalmic Hospital, jerusalem-The RIJht Hon. the Earl of Plymoulh, C. B.
CAie/ Secreta ry 0/ l'tC Amblt/altce Department-Colonel ir HERBERT C. PERROTT , Ht •• C.B.
@ffiuu .
A ssrstalt/ Director 0/ the .-lllll'ulance Departllleltt-Lieut.-Colonel Sir RIClI.\IW CA[{:-; AC TE\IPll.:, Bt., C. r. E.
Ass is taltt Rt!a'I1"'I ,CclL''ral-r_[)II' 1:-; H. FHFSHFIEI.U, Esq . Lrb'anall-CI"RIL DAI
Assistant Surall),y alld .-icColtntaltt- '\'II .LI.\\! R. EDWARDS, Esq., A.C.A. Hon. ,\ecre/an' (1/ the 8rrti.</z Uj>lttlza!/I/ic f/ospita l jerusalcmColonel T. H. H E:-;lllEY, C. I.""
As,islant Honorary (jor Scalland) if/fte Brilisft O)'>itrllalmic f/ ospilal,JClltsrlielll- J. H UR;': E Sf!;I' E:-;SO:-;, (Unicorn P1trsuivant,) [gc Qi;olln.ciL
The CUlIn<;il con,i'l-; of the lIh. Prior, as President ex-officio , the UI1\'e UlliLt"" and the following itlcmbcrs.
Sir JUIl:-; FURl EV, C B ;\[ajor-{;cneral J. C. DALTO,', R.,\.
The Right HOIl. the Earl of RAX' Fvlll Y, G .C. ,\I.G .
Col. C. W. BUII'I'LEK nOl\ IJLEH,C. n. ir TA\!ES UICK, K.C.J:., .'Ii-R.C.P.!., H..X.
Colonel ,'ir CHAKLES .'If. \\'A1SU:>:, K C . \U;., C. B, P.K ir Dt:CKI\'ORTII, Hr., LL.D., .'I!. D.
I nspell )r·G eneral HELG RA \'E .:\IX:-'IO', .'Il.D., R.X.
Sir RICHARD DOUr-LAS POWELL, Bt., K.C.V.O., .'II.D.
The Right Hon. tbe Earl ofLATHmr. J:r )\luxu OIIEN, E'q., LL.D., F.R.C..
Lieut.·Colonel Sir RlcHM/[) C. TE\IPl.E, BI., C.LI:!.. WI LLlA:lI D. ]A\IES, I:"q., C V.O.
The Right H on. the Lord URT HCOTE, G.C . .'II.G., t;.C . l.E., C.B .
The Right Han. tht: r_arl o f BESSBUROUGH, C.\'.O , C.B.
[b C (!;;Qttt1trr.
The Chapter ton-;j,ts of the K.nights of Justice and Sub-P, dales de jure ; lhe Exe<-ulil'e ()IIi l er,; Ihe ,eleunl .'Ilembers of Council; and the following DlTirtattng
The Re\,. C.lI1on IlrI I·ARt., C. ".0 , ll. r l., lib·Dean of the Chapels Royal) 1 he Re\ . PAUL \\'. \""ATT, ANU Hrprcsrnta! I\]r l"nlrrllts of Q1irac£ gnl! Esquires.
":urg"·on·C,,,neral Sir , " 'U.L I A:l1 i Right H on . t,he Viscount L\\'LOR, K. C.Il., .'If. D. BIlACKLEY.
The H on. Lord CLAUD Colonel T. H. HENDLEY, C.l.E. HA\IIl.Tc):-;. 1 he H on . J A:lIES :\lcL-\REN TUART
The Hon. Earl CAWDOR. GRAV, .'Ila ter of Gray EU\\'I:\ FHFSIIFIEI n, E'q. C. B. HA :lIILTO:-;, E'q., C . .'If.G. Lt.-Col. fo.mlO:>:n.'l1 \\'1151):-:, e.1l., Lieut.·Colonel I1'OR PHILIPPS. C . .'If.( ;., n.s.o., R \ \I. e. D 0., ;\I.P.
Lt.·Cnl. "ir LEES K:-;OWLES. I :t. Colonel CHARLES F. ST . CLAIR
The Right Hon. the Lord 1Jr. s- .\N STRUTHER, ;\L \'.0 ,D 0. IlURLJlJeH, K.C.".O. E!1I\'IN DAWES, Esq .
Th t:! Rigbt Hon. Ihe Earl of HE:-;RY T. JOII" H OPE, Esq. KI L:lIOHEY, K.P. B :l
folioilling
art tOt of jJusticc:
H.R.H. Prin ce CHRISTIAN OF SCHLE WIG-HOLSTEIN, K.G., G.C.I3.
H.M_ KI:-IG HAAKON OF NORWAY, K.G., G.C B., G.C.V.O.
H.H. Prince ALBERT OF SCI-II.ESWIG-HOLSTEI:-I, G .C.B . , G.C.V O
H.S. H. The Duke of TECK, G.C.V.O., C.:\[.G.
H.S.H. Prince FRAXCIS OF TECK, K.C.V.O., D.:.O.
Rear-Admiral H.S. H. Prince LouIs OF BATTeXIlERI;, C.C.B., K.C. :'ILG., R .•.
H. Prince ALEXANDER GEORGE OF TECK, C.C.\'.O., D.S.O.
H.R.H. PRINCE ARTHUR OF CON:-IAUGHT, K.G., C.C. \ .. 0.
Lieut.-Col. TRF.I'ENE:-I HOLLAND, C.B.
Sir JOH 'I FURLEY, C.B. (HOlt Bailiff) .
The Right H on Loru TAN:\I0RE, C.C.M.G.
Sir NORTH DICK-LAUDER, 13t.
Maj or ir _-\RCHII3ALD Bt
Col. Sir HERBERT C. PEltROTT, Bt. C.B.
The Right Hon. Earl FERIlERS
Col. ir J. GILDEA, K.C.\'.O ., C.B.
HENRY JOH N LOFTUS, Esq
Colonel BETHEL l\IARTIN DAWES
Gen. Sir CHARLes \\' ARRE N, G.C.l\l.G., K_C.B., R.E.
Major General j CECIL DALTON, R -\.
Col. AYUIER GOULD HUNTERWESTO:-l, D.S.O., R.E.
Colonel The Right Hon. Lord \VILLI.-DI CeCIL, C.V.O.
Eml'I'I FIlESIIFII;;LD, Esq., LL.D. (flollora)), Command.:r).
Hi s Grace the DlIke of FIIF., K .T.
The Rr. H OIl. Lord BIlASSEY,G.C.B.
The RighI H on . \,iscoullt TOWN
The RighI H on . Earl
The RighI H on. Vi-collnt I';: NUTS. FORD, G.C.:\[.G. (f/t>Jt. R. l\lACLEA:>I :\lIcLF.-\:-I, E,q. FRANCIS CRESII.-\:'I LEI·E· SON GOllER, E"l.
Lieut-Col. F..-\. H U'GATE
Colonel ir CII\RLES W\'XDHA\! :\[URRAY, C. B.
The Hight HOIl . the Earl of RANFt..RI.\. G.C . :'Il.(;.
The I{i"hl HOIl. Lord. Al\DIIURST. C.C.S.I., G.C.l.E.
Sir HENRY \ RTHUR Bl.AKE, G.C .l\I.G.
The Rt. TI oll. the Earl of ::'IIE,\TH, h:..P.
A. FRASER, E"l.
The Right Hon. Lord \lllsn·N.
The :\[ost Hon. the \Jarquess of fCC;.
His Grace the J luke of PORTLAND, K.G., C.C.\'.O.
Field-;\lar,hal the Right Hon. the Earl ROBEllTS, K.G., K.P., '1T .\!:"., etc.
R OI3EllT TII/UUE. '£1 l. CARTEII, Esq.,
NOIDIA:-.' HAY FORBES, Esq., F.R.C .. (h.dill.)
Colonel C . \\'. 13,)111)1 ER BOII'DLER, C.B.
Lieut.-Col. A. C. Y .\TE. ASTI n F. TERRY.
follofuinrr atc th e
Th Lord Bi,h op of <;ALlSBURY
The in lEI/UALE.\!.
The Bishop OR:IISI3Y.
The Di,hop of The Bi"hopofflu:<FDIN. (Primal.: o./j\ ',;w Z.:ala1ld.)
£1. J'ogn
Bt<:I}lG THE DEPART')IENT OF Qiintnb- of tbe ®rber of tbe of oSt. Jlobn of ]CtIt5alem fit <Xnrr1nna.
HIS MOST GRACIOUS MAJESTY KING EDWARD VII . , KG. (50I'EREIC.N IIEAU A:-;U I'A1R')" UF THE ORUER.)
HIS ROYAL HIGHNESS THE PRINCE OF WALES , K.G . (uR\ND I'RIOR OF ntE ORDER.)
i!i:cntral \!Crrcllti\Je ([o:ntlllttee.
Consisting exclusively of ;>,Iembers and A-;sociate'i of the Order.
Dlreclor of II:e Ambulance Department an i Chair/JIa:l of Commit lu-
The :\Iost Hon. the :\Iar4ue, of BRrO:AIl uB.-\:-;E, J.;:.G.
Assislalll Dirt'cl,,, alld r>.·!,uty ,Chairll"' " - Licutenal1l·Colonel Sir RICIIIIW C. lit .. C.LE.
De/,ul),-Cltal1mfllt-Sir FURLEY, C. C. (Life :'IIemuer of the COl11lllillt!e Ifon()rtS Lilllsa). .lI';lIlb,rs.
Iajor.Gen<!ral j. C. H..A.
Colonel C. \\'. HOWllIYR Bo\\ DLER, C. C. Lieut.·Colonel \. C. V.HE .
The Rev. T. \\T. WOOD. \\'AYl':M\N DIXON. E-;lj. l\Iajor (;. E. :\IALt;T Colond'ir j. W. OTTLEY, K.C.I.E. R.E I1FI.GRAI'E NI;-';l\IS, :\1.D., R.N. GEIlHuE F"WI.ER, },s4
Surgeon.\IaJor G . H. D\RIII'I, :\ID, GEURGE ,..,sq., C Lit!ut.-Colonel . j. I'RI\IIH E, C.:--LG., L.R .C.P.
Colonel .ir CI :'II. ROIIlS, C. B.
Captain J. \\' . BIlIIER. EDMU:-;U OWEN, Esq., LL.D., F.R.C.S.
'!ttlttraI QCxccutilJ e QI:ommittcc-colltill ll ed.
Th e Lord C LAUD HAmLT0N.
A dmiral ALFRED JOHN CHATFIELD, C.13.
Sir JOHN L LANGMAN, Bt.
The Hon. ir JOHN A. COCKBURN, h..C.M.G., ilLD.
Sir ARTHUR CONAN DOYLE,
The Right non. J. L. WIlARTO'i, P.C.
Surgeon-General Sir ALFRED KEOGH, 1';:_C. n., F.R.C.S.E. &. 1.
SYDNEY \ V. _\lALh:IN, E-q.
Li<!ut.-Colonel Sir JA:lIES R. A. CLARK, Bl., C.B., F.R .C.'::; E.
Surgeon-General Sir BEN].-\:lll:-; FRA .·KLl N, K.C.LE.
JOHN SA:lIUEL GRIFFITHS, Esq .,
Lieut. -Colonel JOH:-I ARNALLT JONES. . . ir \ VILLlA:l1 THO:lIAS LEWIS, Bt., I.;:.C.\'.O.
The Hon. THo:lIAS A. BRASSEY.
The Right Hon. The Earl "r RESS BOROt:GH. C. V.O., C. B. Lieut.-Colonel GEORGE E. TWIss, F.R.C 1.
Colonel JAMES CANTLIE, F.R.C ..
Colonel T. H. HE:-.iDLEY, C LE.
urgeon-illajor G . A. HUTTO '.
Surgeon-General Sir CHARLE ilIcDO:-lO UGH CUFFE. I.;:.C B . F.R.C S.E .
Deputy- l nspector·Gener",1 :'L COATES, :.r D., R.N
F. R. CASSIDI, E q., n.
A . THEODORE BRAND, E q .. :'f.D.
J. ASTLEY BLOXA:lI, Esq., F H.C.-. FRANCIS N. ELl.lS,
Major E. \\'EST Y:lIES, M.D.
" 'ILLIA:l1 E. AUDLAND, Esq, :'II. R. C ..
J. HAMMOND ,;\lORGAN , Esq., C. '-.0., f.R.C .... Ex-Officio tlfembers 0/ COJJlJ/lltt,',·.
Colonel ir HERBERT JEKYLL, I.;:.C.l\I.G., R. E. (Secretary·General of the Order)
EDWI:-.i FRESHFIEI.D, E q., LL.D. (Rece i"er·Gelleral or the Order).
The Right Hon. I'he Earl or PLYMOUTH, C. B. (Chairman, Britis17 Ophthalmic Hospital). (!l; hicf 'srrrrt iH!?
Colonel Sir HERBERT C. PERROTT, Bt., C.B. (Se:retary of the Order).
wim tor of .s to rrg anti carc onnt<lnt.
WILLIA:'II R. EDWARDS, Esq., A.C.A. (Assistallt S ecretary and .rl.ccoltlltant 0/ flu Order). 'storritcrp cr . \VILLlAM HENRY :'IORGAN, Esq. (SujJ erintendcnt, IJwalid TrtwsjJort Corps).
REVISED 1908.
REFERENCE o 58. 1908 .
FIRST AID TO THE INJURED. SYLLABUS OF INSTRUCTION
. FIRST LECTURE.
A. Principle of First Aid.
B .. \ brief De"cription o f the IIuman Skeleton and of theMu cles.
C. Fractures-Cau"e, \'arieties, ign' and symptoms .
D. Treatment of Rule.
E. The Triangular Bandage and its application . LECTURE.
.\. Treatment of Fractures (continued). Details of treat· ment.
B. Di 'locations, prains, Strains-. igns, symptoms and treatment.
C. The IIeart anti moud Yessel-. The Circulation of theBlood.
D. and wnunds. General rules for treatment.
E. The Triangular Bandage and its application .
TIIIRD LECTURE.
A. and wounds (continued ). Details o f treatment.
B. Internal Hremorrhage-Signs, symptoms and arrest.
C. from Special Region . - igns, symptoms and arrest.
D. Scald, Bite and tings, Frost-bite.
E. ForeIgn boclJes 111 the Eye, ose and Ear.
F. The Triangular B::tndage and its application.
FOURTH LECTURE.
A. Th e K ervou Sy. tem.
B. T he Organs and of Respiration-Artificial Respiration.
C. Insensi bi lity.
D. Poiwning.
FIFTH LECTURE (for only) .
. A. Impro\"i ed method of liftin a and carrying the sick o r -injured. "'
B. Meth ods of lifting and carrying the sick or injured on stretchers .
C. Th e cOll\'eyance of such by rail o r in country carts.
FIFTH LE CTURE ( fo r Females only).
A. Preparati on for reception of accident cases.
B. Means of lifting and carrying.
·C. Preparati on of bed .
D. Removing the clothes.
E. Preparati ons for surgeon.
NOTE I.-The ubject of poisons shou ld be treated in a general manner; the common poisons cia. sified, and only their general symptoms, effects and treatment taught.
NOTE II.-The last half-hour of each lecture should be devoted to practical work, such as the app'ication o f landages and <;plint , lifting and carrying wounded on stretchers.
NOTE III.-There should be a n interval of a w eek between each lecture. A candidate for examination must attend at least fuur out of the fi,"e lectures
NOTE classes must pas in that ystem o[stretcher exercise most suitable for the locality .
NorE Y.-As liale time a'i possible is to be spent on instruction in anatomical and LJhysiological details. Lecturers and examiners are particularly requested to remember tbat it is " First "\i d' that has to be taught and tested, and not anatomy and phyiology.
Jilxed dasses q/lIlell alld wOlI/en are Oil no account permitted.
PUPILS U:-;'DER SIXTEE.'l YEARS OF AGE CA:-l O.'lLY ATTEND TlIE ,. JUNIOR" C0URSE (SECTIO:-l A, SYLLABUS 40 ).
Lecturers instructing a First Aid class , and Local Secretaries, can obtain further particulars on application to the Chief Secretary for " Paper Reference No. 80."
./\ '0 Lecturer may exallline Itis OWIl Class Jor Certificates.
9
SUMMARY OF CO ITENTS
CHAPTER I.
Principles of First Aid
Explanatory
Questions on Chapter
of the Main Arteries and Pressure
CHAPTER II.
The Human Skull, spine, ri bs and breastbon e, upper lImbs (collar-bone shoulder-blade b one bone f th £" , arnl, s o . e lorearm, carpus, meta ca r us phalanges), pelvIs, lower limbs (thigh-bone . cap, tarsus, metatarsus, phalanges) ..
Jomts ...
Muscles. Voluntary and involuntary Fractures Cause" ..' t'.
. ' -
:>, \ aIle les, sIgns and !::ympLOm">
Apparatus for treatment of Fractures .
General Rules to be observed in of Fractures
S ecial
p Fractures. Cramum, lower jaw sine ribs breast-bone, colhr-bone, shoulder-blade c,Iose .to the elbow joint, . an.' pe VIS, thIgh-bone, knee-cap, leg, crushed foot
Dtslocahons
Miscellaneous Injuries . Bruises, burns and scalds, bites of snakes and rabid animals and wounds by poisoned weapons, stings of plants and animals, frost bite, needle embedded under the skin, fish hook embedded in the skin, injuries to joints, foreign body in the eye, ear pas age and nose, wound in the front wall of the abd omen, injuries t() the organs within
Artificial Respiration . chafer'S, ilvester's, Howard's combined with ilvester', Laborde sand ::\hrshall Hall's
iO
. .
... . .. •
... .... ... ... .. . ...
Sprains . Sprains and Ruptured Muscles Questions on Chapter Page 17 20 21 22 3 1 3 2 41 1 I CHAPTER III. Page Circulation of the Blood. Organs; general (systemic) and pulmonary circulations 70 Hcemorrhage or Bleeding. Arterial, venous, capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage ... r 76 Course
Points
Aorta, arteries of the head and neck, of the upper limbs, of the lower limbs 79 Venous Hcemorrhage and Varicose Veins 93 Wounds with Venous Hcemorrhage 94 Capillary Hcemorrhage 95 Internal Hcemorrhage 95 Hcemorrhage from Special Regions 96 Questions on Chapter 99 CHAPTER
.
lY.
102 Questions on Chapter .. I 15 CHAPTER V. The Nervous
Cerebro-spinal, sympathetic... II 7 The Respiratory System 118
methods...
the abdomen and peh-is
System.
,21
Insensib ility . Causes, general rules for treatment, concus ion of the brain, compression of the brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, sunstroke and heat-stroke, convulsions in child ren, asphyxia
Electric Shock and Effects of L ightning
Questions on Chapter
CHAPTER VI.
Poisoning. General rules for treatment, special pois ons
Questions on Chapter
CHAP rER VII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three handed seats, fireman's lift, fore and aft method improvised stretchers, to cross a ditch or wall, to load or unload a wagon ..
CHAPTER IX.
Stret cher Transport. Stretchers, stretcher exercises, litters
CHAPTER X.
The F ifth Lecture (for Females only ). Preparation for reception of accident cases, choice and preparation of a room, lifting and carrying, preparation of bed, remo,ring the clothes, preparation for surgeon ...
Questions on Chapter
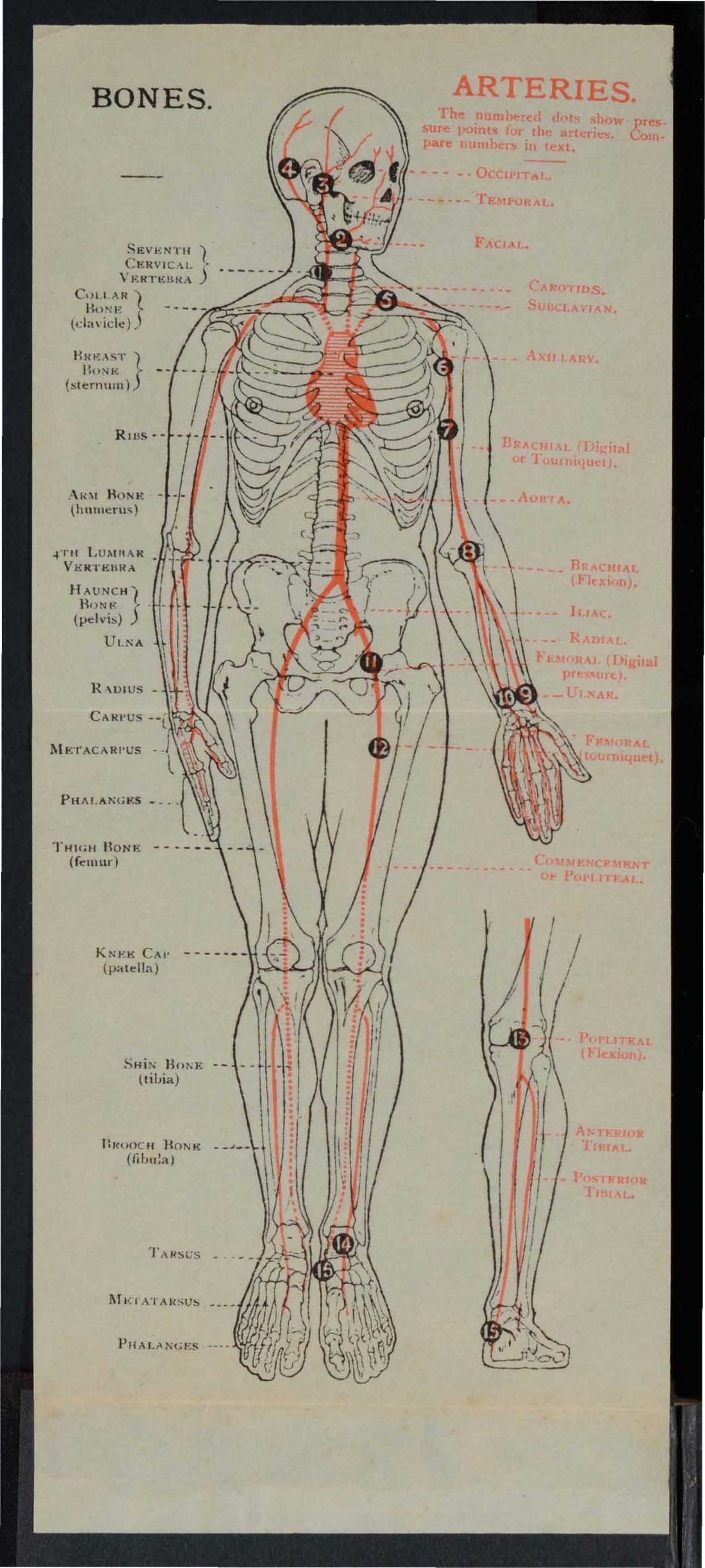
Skeleton showing position of main arteries
Skull and vertebral column
Vertebra
Bone3 of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle
Rectus
Triangular bandage spread out and folded
Large arm sling
-mall arm sling
Reef knot
Gra nny knot
knot
Bandage for fracture of lo\ver Jaw.
Bandages for simple fracture of nbs
St. John sling
for fracture o f both collar bones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint
Treatment of fracture of forearm
Treatment of cmshed hand
Treatment of fracture of thigh bone
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap ...
Treatment of fracture of leg (man and wuman)
Treatment of crushed foot...
Diagram of the heart, lungs and air passages
12
Page ISS 160 197 206 13 LI ST OF ILLU .... TRATIONS.
... .,.
... ... . ..
...
... ... .. . ..
.. . Loop
..... .
...
. . . ... .. . .
...
... . ..
...
...
... . ..
Pag-t frontispiece 2 -l 24 27 29 3 1 3 1 3 2 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 6 1 62 i J
Diagram of the circulation of the blood
Digital pressure on ca(otid artery ...
Digital pressure on facial artery '"
Digital pre ssure on temporal artery
Digital pressure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad
Digital pressure on subclavian artery '" ". "
Pad and bandages to apply pressure on axillary artery ...
Digital pressure on brachial artery (two methods)
Flexion at elbow
Digital pressure on radial and ulnar arteries " .
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery .. .
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdom en .. .
The lungs and bronchial tubes . . . .
Schafer's method of artificial respirati o n ".
Sih'ester's method of artificial respirati o n
Silvester's and Howard's methods of artificial re piration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip .. ,
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
Grip for four-handed seat
Lifting by two-handed seat. ..
Grips for two-handed seats .. ,
Cnrying by two-handed seat
Grip for seat ...
Supporting patlent .,. . , ' .
Fore and aft method of carrymg
Carrying on improvised seat
Improvised stretcher .. '
Furley stretchel:s 'T" :, Fall in"
Stretcher exerCl .e, ?\ 0: I.
Ditto, ready to lI.rt patlent
Ditto, lirting pauent. ..
Ditto, placing stretcher ... , .. .
Ditto, preparing to lo wer patient .. .
Ditto "Lowe r" . . . ... ,
Ditto' I o. II. Ready to lift patIent
Ditt o: patient lift ed . .
Ditto, O. IV. p osltlOn
Ditto second posltlOn .. ' . , ' d ' 11
Diag;ams illustrating Arm)' tr e tcher n
Ditto ...
Bed cradle ... '
Improvised bed cradle s
Pa£"c 73 RI 81 82 82 83 84 KJ. 85 6 7 7 '9 90 91 9 2 112 119 122 124 12 5 ISS 15 6 156 157 157 15 8 15 9 15Y 160 161 162 163 15
Page 1 64 165 16 7 163 168 I; 2 175 17 6 177 178 179 180 182 183 188 18 9 19 1 194 20 3 203, 204
PREFACE.
AT the request of the Central Executive Committee
I have the manual written by myself in 19 01 , as ha n dbook of the St. John Ambulance AssocIatIOn.
Throughout the revision an endeavour has been made to the study of FIrst Aid to the Injured by drawJng up. a number of general rules for the of accIdents u.nd su?den illness, and by the o mIssIon of all detaIl \,·hlch is not absolutely necessary to enable the student to acquire an intelligent knowledge of the subject.
I .. \\·ish to express my thanks to' Professor E. A. Schafer for fUl:nis.hing instructions for performing a met?o? of artIficIal respiration, to Dr. L. 1. F. for many valuable suggestions, and to the M.edlcal Members of the Central Executive CommIttee, especially G. H. Darwin, M.D . and Dr. F . R. CassIdI, for perusing the proof sheets a n d for a number of useful additions to the work.
I cannot omit also to offer my best acknow ledgm ents to Mr. \tV . R. Edwards, the Accountant and Storekeeper of the S.J.A.A., for his invaluable co-operatIO n. .
JAMES C A NTLIE.
FIRST A I D T O TH E I N J URE D.
CHAPTER 1.
T he St. John Ambulance Association has now complet ed thirty years of its existence, and during that period hundreds of thousands of men and women have been taught at it classes, in all parts of the world, how to help their injured neighbours.
First Aid to the Injured is a special branch o f practical medicine and suraery, by a knowledge of which trained persons are enabled to afford skilled assistance in cases of acciJent and sudden illness. The instruction begins and ends \yith First Aid, and the subject is taught simply but thoroughly and exhaustively. The duty of the ambulance pupils ends where the doctor 's ommences, and there ought to be no Q\'erlapping or clashing of duty or interests.
PRI TC IPLE OF FIR'T AID.
1. The First Aid student should be-
(a) Observant, that he may n ote the causes and signs* of injury.
(b) Tactful, that he may with ou t thoughtless questions learn the symptomst and history t of the case.
-
* Signs are what may be p e rceived.
t Symptoms are what the patient can tell you.
t History means the circumstances attending the accirlent or sudden illness.
(c) Resourceful, that he may use to th e b est advantage whatever is at hand to preve nt fur ther damage and to assist Nature 's efforts t o repair the mischief al ready done .
(d) Explicit, that he may give clear inst ru ctions to the patient or the bystande rs how best to assi t him .
(e) Discriminating, that he may decide which of several injuries presses most for treatment by him elf, and what can bes t be left for the patient or the bystanders to do.
2. Remove the cause of injury or danger whenever possible .
3. Severe hcemorrhage must receive the first attention , no matter what are the other injuries.
4. Air. - The patient must be in a position in . which breathing is pos ible; the air pa sages must be free from obstruction; if breathing has ceased prompt measures must be taken to restore it.
S. Rest. -A restful po ition of the body will assist the vital functions; support of the injured part \\"ill help to pre\-ent further damage, and is essential in the case of fractures of lim bs.
6. Warmth .-After e,-ery accident keep the patient warm so as to prevent the fall of temperature below the normal point.
7. When the skin is broken the wound
19
should be promptly covered with a clean absorbent d ressi ng. Should the " 'oul1d be poisoned, it is mos't impo rtant immediately to prevent the poison permeati ng the s) stem .
8. Poisons swallowed should be got rid of, or when that is inexpedient neutralised.
9. The best means of transport must be studied, and proyision made for proper care when the patient is brought to shelter. -
10. Removal of Clothing .-Clothes should not be taken off unnecessarily, but ",htn it is nEedful to remove them, the following ruies will be found of service in serious ca s:-
COAT: Remm'e from the sound side first, and, if neces ary, slit up the seam of the sleeve on the injured side.
SHIRT AKD VEST: lit down the front and remove as the coat.
TROUSERS: lit up the outer seam.
BOOT: lit the back seam and undo the laces.
SOCK: Cut off.
II . Stimulants.-It is incorrect to suppose that alcohol is the only form of stimulant, and far too frequent use of spirits is made to restore a patient after an accident often with seriou results; the safest rule, therefore, is to defer the administration of alcohol until the arrival of a doctor. 'Yhen the patient is able to swallow, strong tea or coffee, or milk, as hot as can
18
be drunk, or a small quantity of sal "olatile in water may be giyen. Sm elli ng salts may be held to nose. prinkling th e face with cold and hot water alternately, warmth applied to the pit of the stomach and over the heart, and vigorous friction of the limbs upwards haye a timulatin a e ffect.
12. Throughout his work the F irst Aid student must on no account take upon h imself the duties and respons ibilit ies of a Medical man . At times an apparently slight injury is accompanied by gra\'e danger and may actually cause loss of life. 'Wh en sending for a doctor, state the nature of the casC', and remem ber that written particulars are safer than a verbal message.
It is necessary that something should be known of the structure of the body (elementary anatomy), and of the functions o f some of the more important organs and systems (elementary physiology). A short description of the necessary anatomical and physiological points is therefore gIven as the several subjects are discussed. For purposes of description the human body is supposed to be erect, \\ith the arms hanging by the side and the pall1ls of the hands directed forwards. The" middle line" of the body runs vertically from the top of the head to a point between th e feet.
QUESTIONS ON CHAPTER 1.
The 1zume 1'a /s £Ildicate tlze ja,f{cs whe7e the answt1'S may be found.
'What is First Aid to the injured ?. ..
\Vhat qualitie s should the First Aid student po£sess?
\\'hat are signs?
\\'hat are symptoms?
\Yhat is the history of a case?
'What is often the first thing to do in an accident?
\Vhat result of injury must receiYe the nJ5t attention? , .
\\' hat three things are ab olutel), neces ar)' to an injured person? . ..
\\'hat must be done wh en the , kin is broken?
lIow must poisoning be treated? .. .
\Vhat steps mu t be taken be) o nd the actual treatment of injurie s? .. . ..
Should clothing alway be rem oyed?
How would you remove clothing when nece sar)' ?
Explain the us e and abu . e of stimulants ..
\Vhat must the First Aid tudent n o t du ?
"Vhal is element ary anatomy?
\\'hat is elementary physiology? . . ..
For purposes of descripti o n h o w is the human body supposed to be placed?
What is the middle line of the body?
20
21
PAGE 17 17 , 18 17 17 17 18 18 18 18, 19 19 19 19 19 19,20 20 20 20 20 20
CHAPTER II.
FRA C T URE S, D I LOCAT ION S, SPRAINS AND STRA I NS
.
THE KELETON.
The human body is moulded upon a bon y fra m e\yo rk (the skeleton) which sen'es-
I. - To give shape and firmness to the bod y.
2 . - To afford attachment to the muscles.
3·-To protect important organs, as in the sk ull , chest, and abdomen.
THE KULL.
The Bones of the Skull are arranged in two gro u ps, those of the brain case or cranium, and those of the face.
The Boundaries of the Cranium are the vault or dome, the rounded portion forming the top of the head; the front or brow; the back of the head , where the greatest extent of brain exists, and where t h erefore the cranium is \\'idest and deepest; the sides or temples. The base of the cranium is hidden from view by the bones of the face and of the vertebral col u mn ; in it are numerous perforations for the passage of blood \' essels and neryes; through the largest opening the brain and spinal cord are continuous.
The Bones of the Face with the exception of
t he lo we r jaw are firml): together, so mo vement bet\yeen them IS Impossible.. The cavItIes of th e n ose and of the eye sockets (orbIts) are formed by t he b ones of the and of the face co njoi ntl y. The mouth cavIty IS forn:ed between the upper a n d lower ja \\ s, the bemg the bony roo f of the which separates It from the nasal cavity a bove.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions terminating on either side at the joint between the !o\\'er jaw and the base of the cranium, situated immediately in front of the ear.
The angle of the jaw the junction of the horizontal and the vertical portIOns.
THE BACK-BOXE PINE, OR YERTEBRAL
The Vertebral Column (Fig. 1 ) i composed of bones called \'ertebrre, each of which consists ofI. -A body or bony mass in front.
2.-Processes projecting backwards, which en· close a canal for the spinal cord - the spinal canal.
3.- Two trans\'erse tweh'e pairs of which support the nbs.
22
23
Bony OF VERTEBRA. F1G. 2A. i . SURF A CES SUPPORTING HEADS OF RIBS.
Co. 4
SKULL AND VERTEBRAL
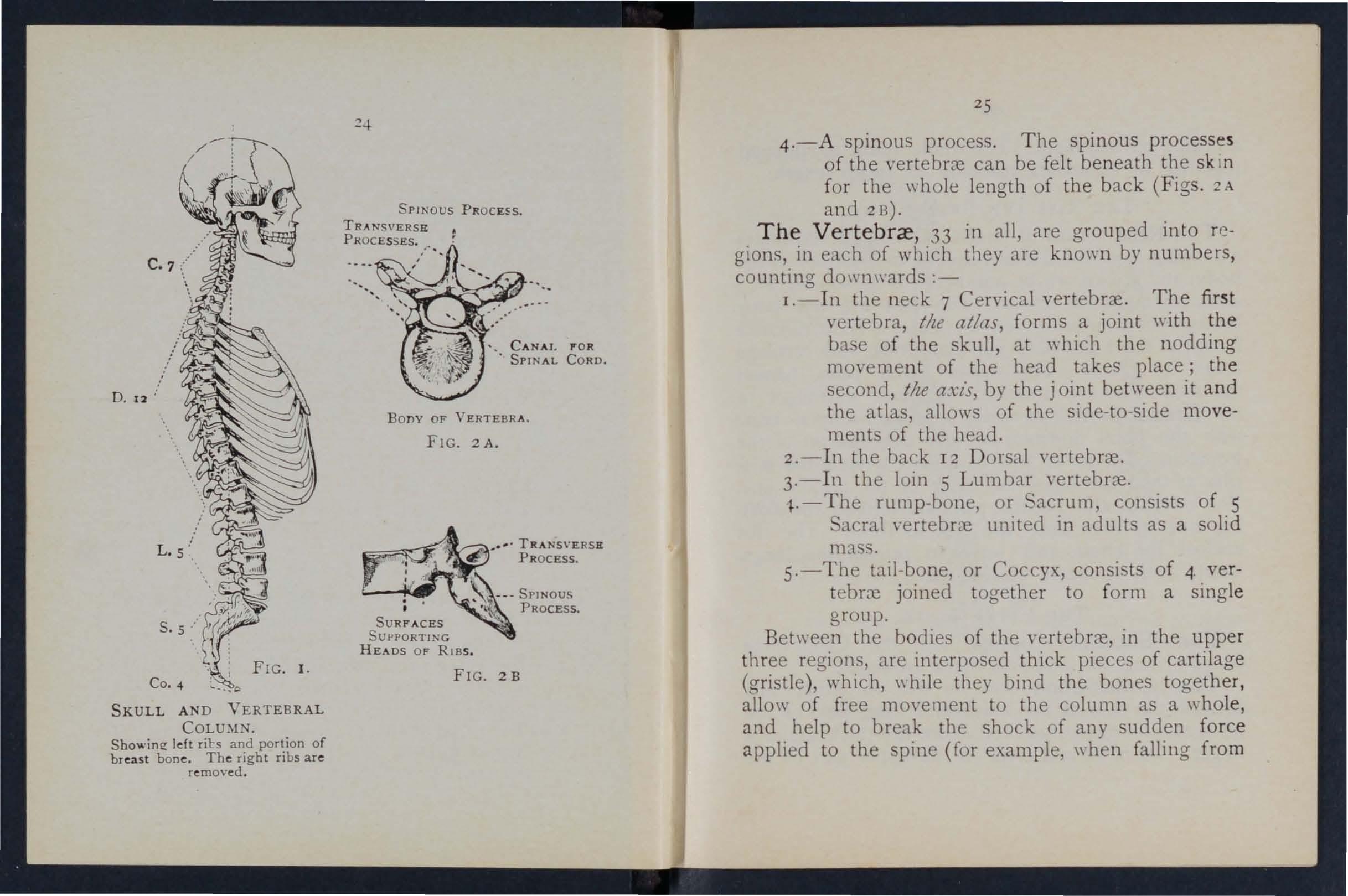
4.-A spinous process. The spinous processe s of the vertebrc:e can be felt beneath the sk In for the whole length of the back (Figs. 2 A and 213).
The Vertebrce , 33 in all, are grouped into regions, in each of which they are known by numbers, counting do\\'nwards :-
I.-In the neck 7 Cervical vertebrce. The fir st vertebra, tile atlas, forms a joint with the ba e of the skull, at which the nodding movement of the head takes place; the second, the axis, by the j oint between it and the atlas, allows of the side-to-side movements of the head.
2.-1n the back 12 Dorsal \'ertebrce.
3·-1n the loin 5 Lumbar vertebrc:e.
• • , TRANSVERSR PROCESS.
FIG. 2B
Showing left ril:s and portion of breast bone. The right ribs are removed . '. C A N A l, P'OR • SPINAL CORD.
l.- The rump-bone, or Sacrum, consists of 5 acral vertebrc:e united in adults as a solid mass.
5.-The tail -bone, or Coccyx, consists of 4- vert eb rc:e joined together to form a single group.
Between the bodies of the \'ertebrre, in the upper three region, are interposed thick pieces of cartilage (gristle), which, \\ hile they bind the bones together, allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, ",hen falling from
25
a height on the feet). The whole spi n e is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of tweh'e pairs of curved bone s extending from the dorsal vertebrre to the fr ont of the body, and are known by numbers-first, second, etc., commencing from abm·e. The ribs are not bony t hroughout their entire length, but at a short distance from the front the bony material ends, and cartilage takes its place . The upper seyen pairs, named the true ribs, are attached by their cartilages to the Breast-bone (sternum), a dagger-shaped b ne with the point downwards, just oYer the pit of the stomach . The 10\\'er fiye pairs are termed the f[llse ribs, as their cartilages fall short of the middle line. The eleventh and twelfth pairs are termed the fl ating ribs, as their ends are free in front. The ribs enclose the chest, and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder - bones are the Collar-bone (clavicle) and the houlder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part o f the neck as a narrow curved rod about the thickness of a finger. Its inner end rests on the upper part of the
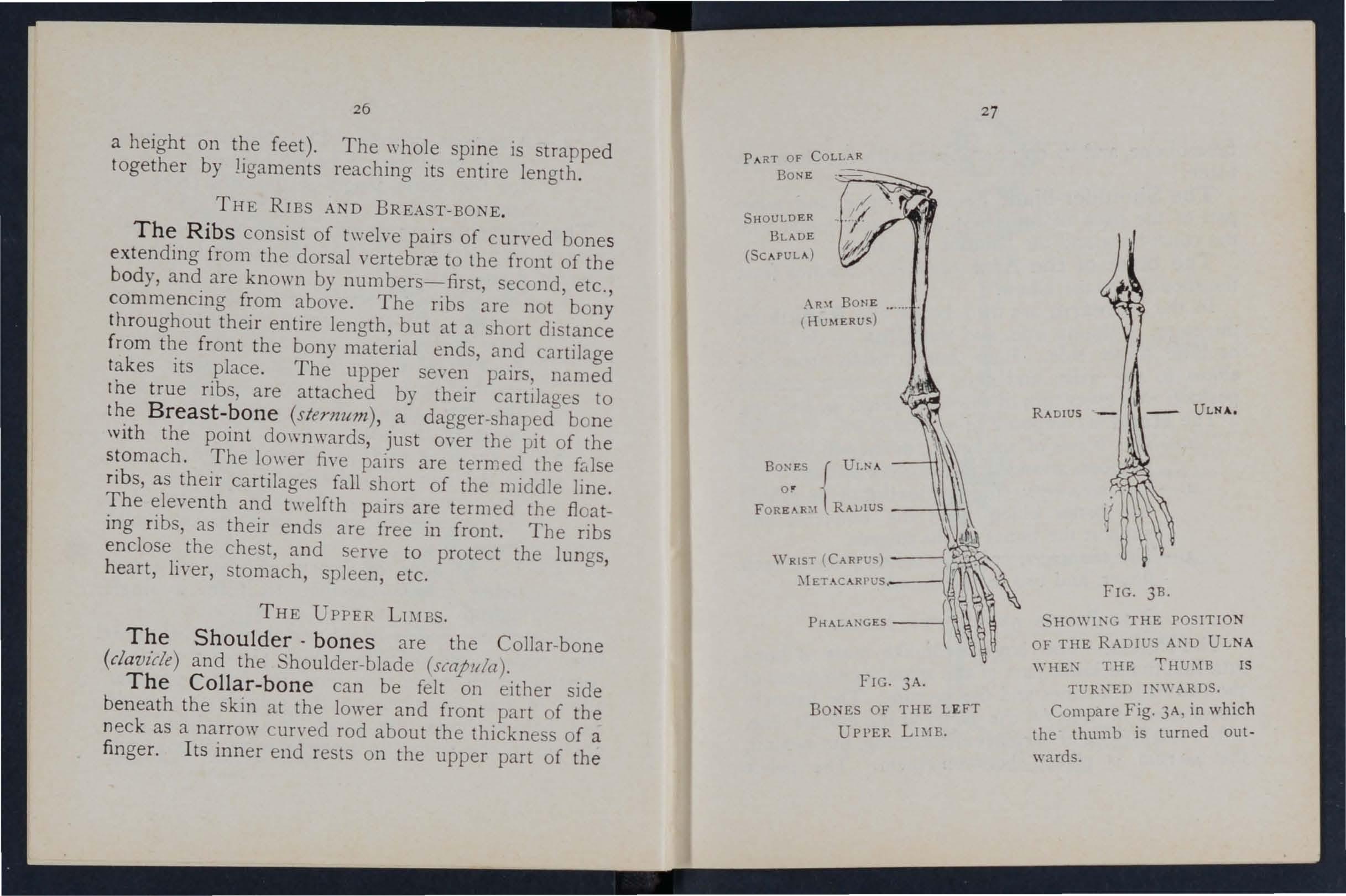
FIG. 3A.
BONES OF THE LEFT UPl'EP. LDIB.
FIG. 3B.
H0\Yl:\G THE POSITION OF THE RADIUS A"D ULNA \\' HE" THE 'THU;\IB IS TlJR"ED I"WARDS.
Co mpare Fig. 3A, in which the thumb is turned outwards.
26
PART OF R Bo N E -.....,..---,_:-. SHOULDER BLADE
BONE .•...•.
B ON ES r ULNA o r 'l RAlJlUS --+t-f-\
(SCAPULA) AR\I
( HUMERUS)
27 RADIUS
i8
br east-bone, and its outer end joins with the shoulderblade .
The Shoulder-blade lies at the upper and outer pa rt of the back of the chest, and forms joints ·with the collar-bone and the bone of the arm.
The bone of the Arm (humerus) reaches from t he shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, o r little finger side. Both bones reach from the elbow to the wrist, and they change their relative position with every turn of the hand (Figs. 3A and 3 B ).
The Hand is composed of-
I.-The bones of the wrist, or carplfS, eight in number, arranged in t\\"o ro\\ s of four.
2.- The metacarpus (the framework of the palm) ; five bones which form the knuckles and support the bones of the fina-ers.
3·-The phalanges, or finger -bones, three in each finger, and two in the thumb.
Tl:IE PELVIS AND Lo\\ ER LIMBS.
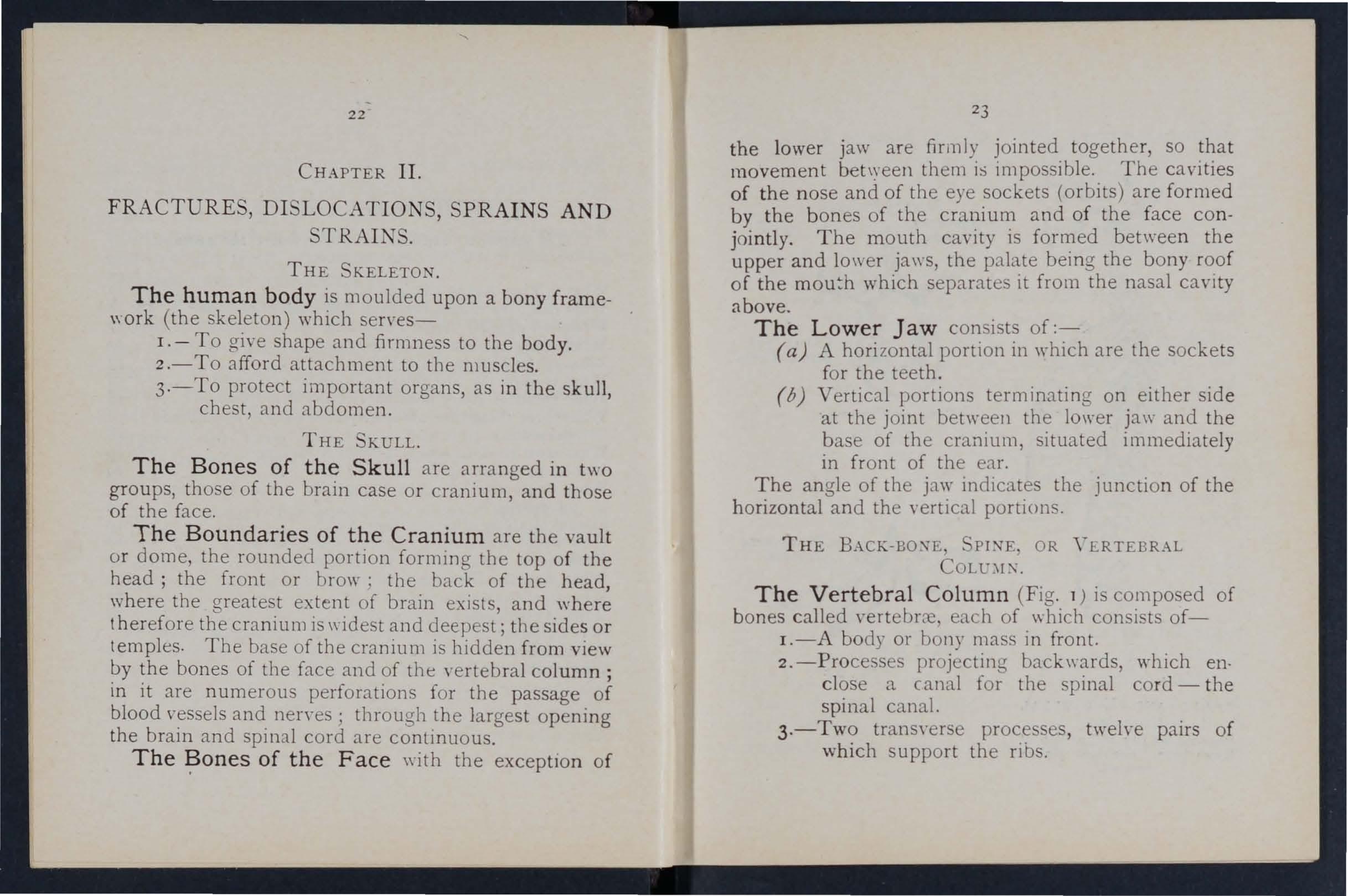
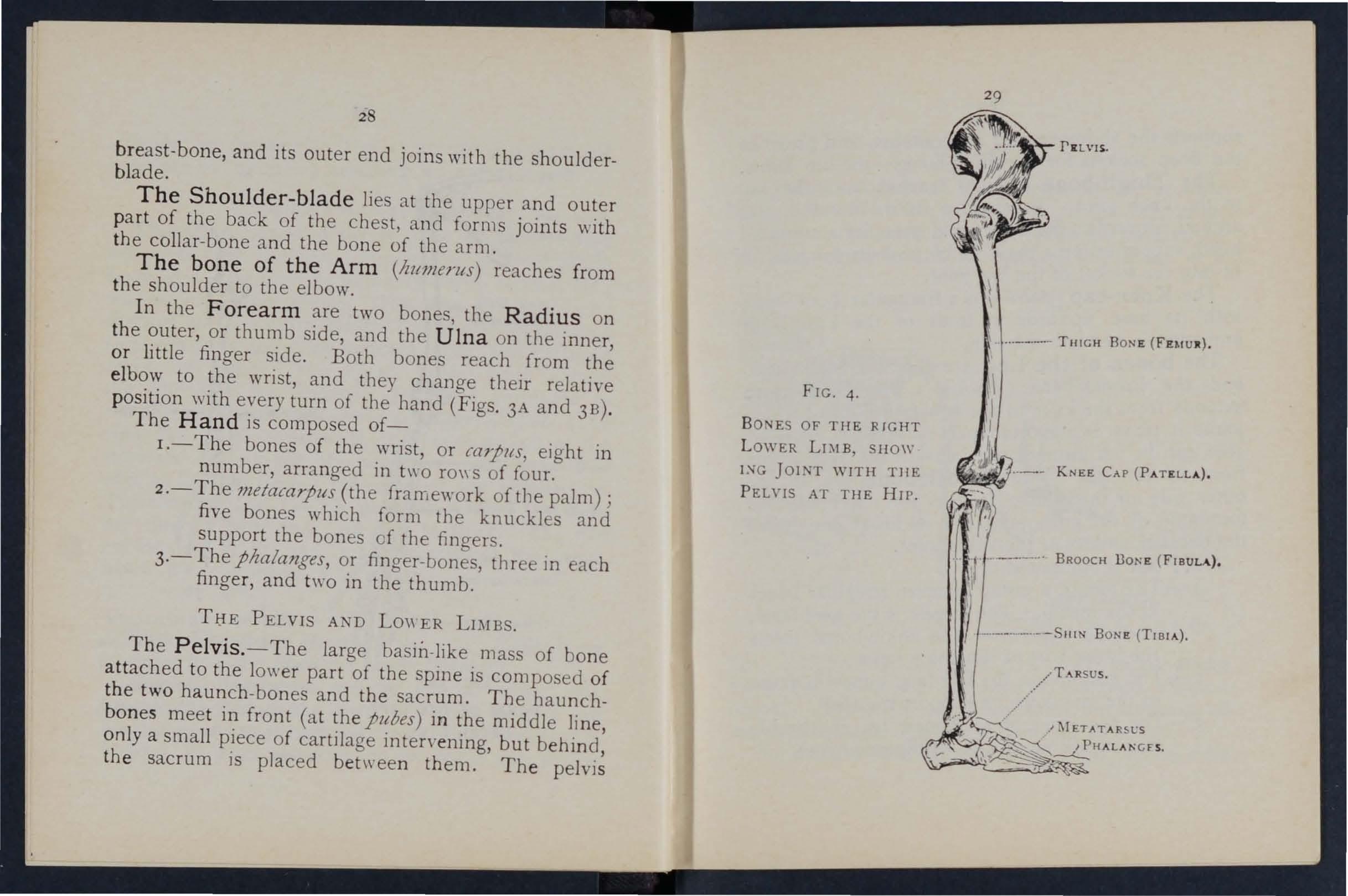
The Pelvis. - The large basin-like mass of bone attached to the lower part of the spine is composed of t h e two haunch-bones and the sacrum. The haunchbo n es meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, th e sacrum is placed between them. The pelvis
4.
BONES OF' THE RIGHT LOWER Lr;\lB, SHOW l:'-lG JOINT WlTH TlIE PEL\" IS AT THE HIP.
FIG... .. __ .--
THIGH BONE
KNEE CAP (PATELLA).
.. I ._ ....
BROOCH BONE (FIBULA).
..../
T .-\RSUS.
30
s upports the abdomen and its contents, and provides the deep sockets for the thigh-bones-the hip joints.
The Thigh-bone (femur) reaches from the hip to the k n ee joint. Its shaft is stout, rounded, and a rched forwards; the u pper end presents a rounded head, supported on a neck which projects in" ards, to fi t into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base upwards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-bone (Iibia) and the Brooch-bone (fibllla). The Shin- bone extends from the knee to the ank Ie, in both of \\ hich joints it plays an important part; its sharp edge, tilt shin, can be felt immediately beneath the skin of the front of the leg. The Brooch -bon e lies o n the outer side of the tibia. It does not enter into the formation of the knee joint, but its 10\\ er end forms the outer boundary of the ankle joint.
The Foot is composed of--
1.-The tarslls, a group of se\'en irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.-The metatarsl{s, the five long bones in front of the tarsus \\ hich support the to es .
3.- The phalanges, or toe-bones, two in the hig tOE', and three in eac h of the other toes.
3 1 JOINTS.
A Jo int is formed at the junction of two or more bones. In moveable joints such as the hip, knee, elbow, etc., the surbces of the bones are covered by cartilage, which lessens friction and the shock of a
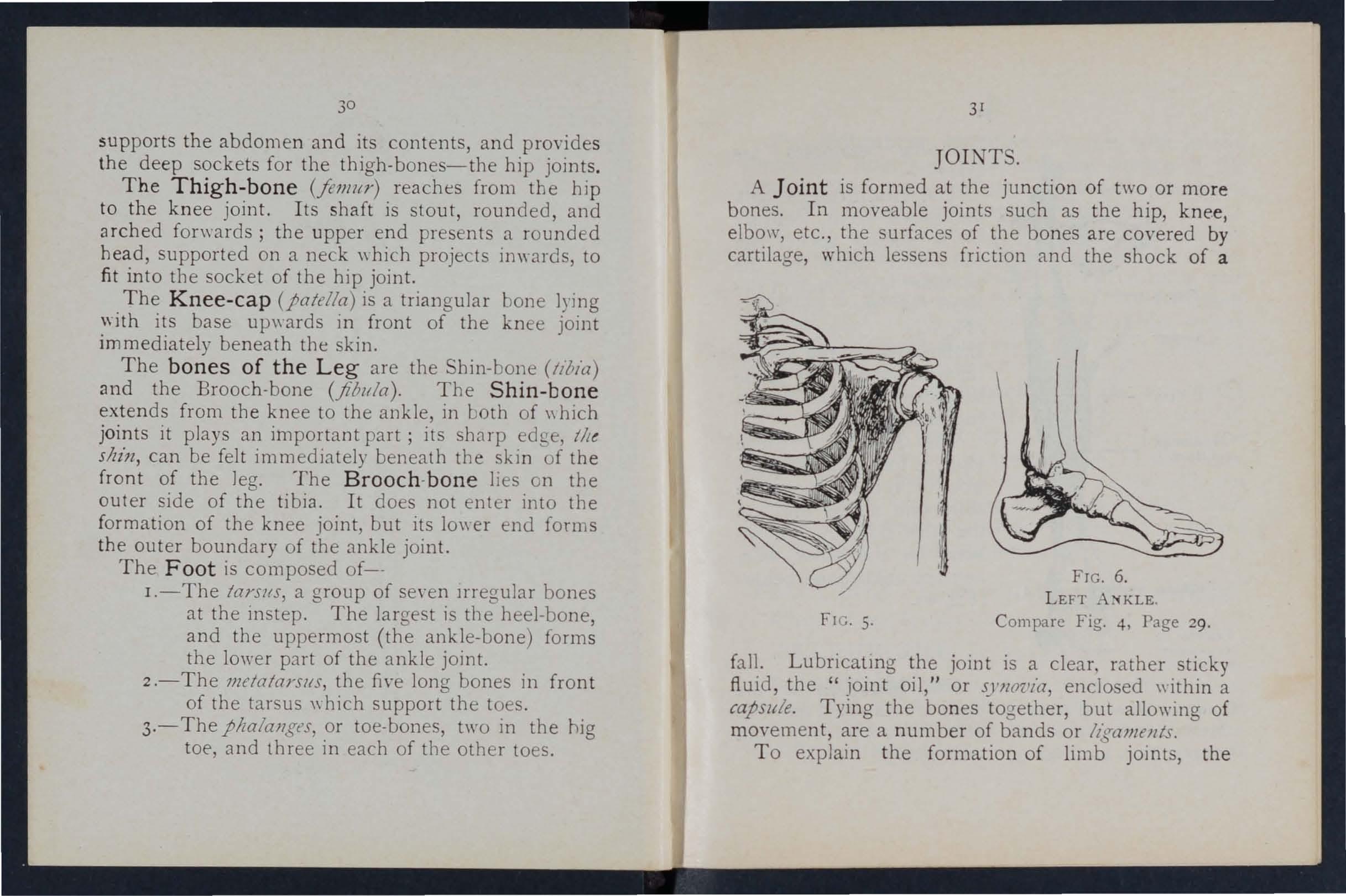
FIG. 5, FTG.6.
LEFT A:-iKLE
Compare Fig. 4, Page 29.
bll. Lubricatmg the joint is a clear, rather sticky fluid, the " joint oil," or s),JlO'l.'ia, enclosed \\ ithin a capsule. Tying the bones to -'eth er, but allo\ying of ffim'ement, are a number of bands or /i(ralllfn/s.
To explain the formation of limb joint, the
MUSCUL 1t TISSUE PATELLA
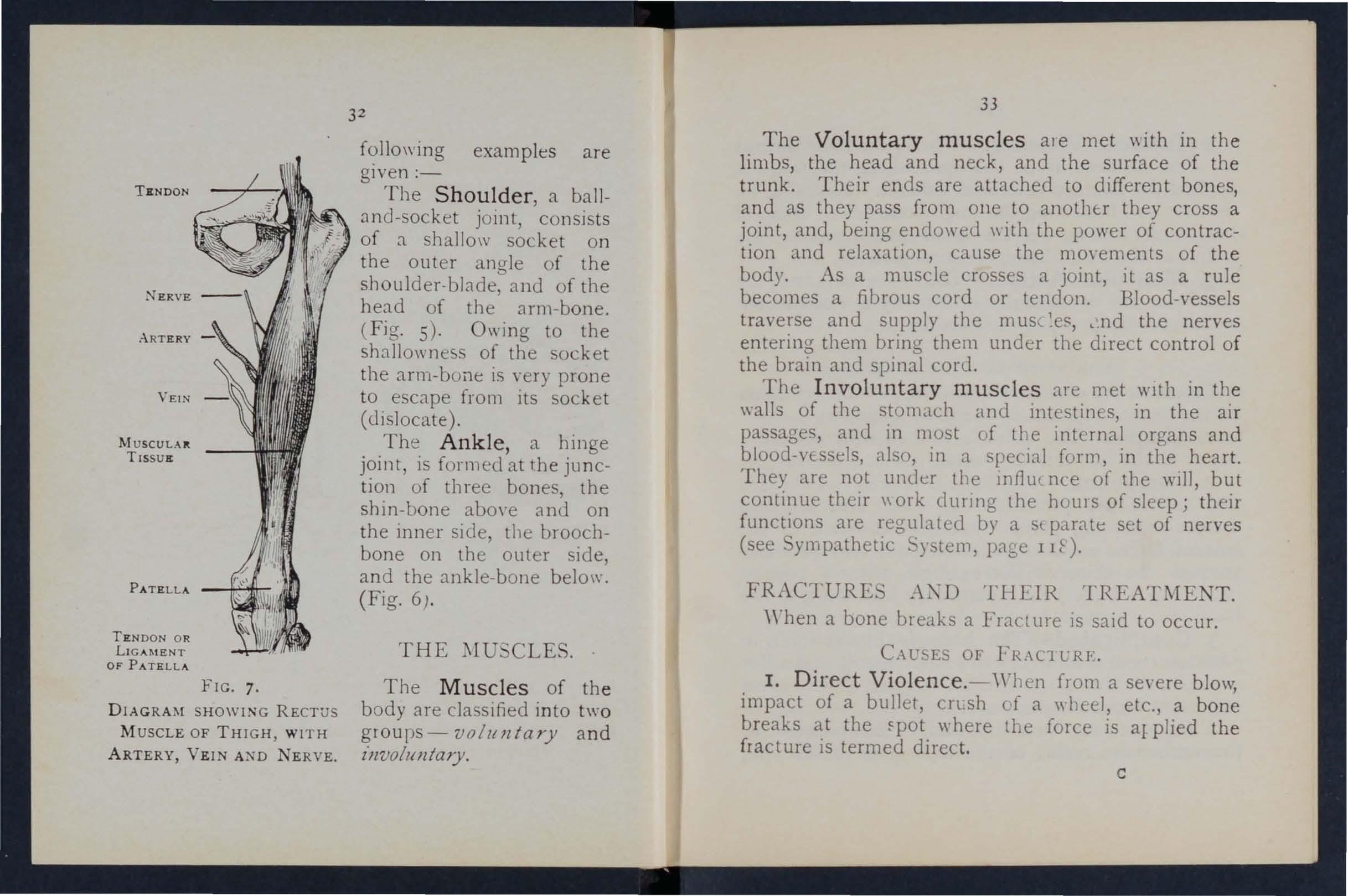
TEND ON O R LIGAMENT OF PATELLA
FIG. 7.
D IAGRAM SHOWING RECTUS
M USCLE OF THI G H , WI TH ARTER Y, VEIN Al"D NERVE.
fOllO\\ ing examples are gIven :-
The Shoulder, a balland-socket joint, consists of a shallolV socket on the outer angle of the slloulder·blade, and of the head of the arm-bone.
(Fig. 5)' Owing to the shallo\\'nes of the socket the arm-bone is very prone to escape from its socket (dislocate ) .
The Ankle, a hinge joint, is formed at the junction of three bones, the shin-bone abO\'e anu on the inner side, the broochbone on the outer side, and the ankle-bone belo\\". (Fig. 6) .
The Muscles of the body are cIa sified into two groups- voluntary and z'llvol" Jl tary.
The Voluntary muscles ale met \\ith in the limbs the head and neck, and the surface of the Their ends are attached to different bones, and as they pass frolll one to anothtr they cross a joint, and, being endoweu \\ ith the power of contraction and relaxation, cause the mO\Oe ments of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the m us,- , .nd the nerves entering them bring them under the direct control of the brain and spinal cord.
The Involuntary muscles are met wIth in thoe \\alls of the stoll1.lch and intestin s, in the air passages, and in most of the organs and blood-vessels, also, in a special form, 1I1 the heart. They are not under the lIlflmnce of the WIll, contin ue their \\ ork cl unng the haUl s of sleep; theIr functions are regulated by a Sl parate set of nenoes (see ympathettc .. y tem, page lIt).
FRACTURE .:-\{\"D THE1R TREATMENT.
When a bone breaks a Fract ure is said to occur.
Cw. ES OF FRAC1 L'RF.
I. Direct Violence. - 'Yhen from a se\'e re blo\y, impact of a bullet, cruh cf a \\ beel, etc., a bone breaks at the \rhere tbe force is a1 plied the fract ure is termed direct. c
TENDON
2
3
THE ..
33
2. Indirect Violence.- 'When the bone breaks at some distance from the spot where the force is applied the fractur e is termed indirect. Alighting 011 the feet and fracturing the thigh-bone or the bones of the leg, or falling on the hand a nd breaking the radius or the collar-bone, are examples .
3. Muscular Action. -The knee -cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them .
V ARIETlES OF
FRACTURES.
Fractures are classified according to the condition of the tissues adjacent to the bone as follows :-
I. Simple. - The bone is broken \\ ith but slight injury to the surrounding parts .
2. Compound. - The bone is broken and the skin and tissues are punctured or torn, thus allO\nng disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude through the skin, or (for example, when a bone is broken by a bullet) the wound may lead dmvn to the fracture.
3. Complicated.-The bone is broken and in addition there is an injury to some internal organ (for example, the brain, spinal cord, lung, etc.) or to some important blood-vessel or nerve.
A fracture may be compound or complicated as the immediate result of the injury; or a fracture,
35
originally sim pIe, may be converted into a compound or complicated fracture --
(a) By careless movement on the 'part of the patient.
(b) By carelessness or ignorance on the part of one rendering first aid.
pecial vari eties offmctur es may be claSSIfied according to the injury to the bone itself as follows :-
I. Comminuted. - The bone is broken into several pieces.
2. children, owing to the softe'l" state of the bony tissues, a bone may bend and crack \\ ithout breakin6 complet e ly across.
3. Impacted. - The broken ende; of the bone are driven one into the oLher.
GENERAL IGNS AND \\ HICH MAY BE
(A fracture of of the for""lrm example). FRT'. SENT.
the fem ur, humerus, or both bones or leg, affords the most complete
I. Pain at or near the seat of fracture.
2. Loss of Power in the limb.
3. Swelling about the seat of fracture. Swelling fr equently renders it difficult to perceive other signs of fracture, and care must therefore be taken not to mistake a fracture for a less serious injury.
4. Deformity of the limb -The limb assumes d.n C2
34
unnatural position, and is mis -s hapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to override, thereby prod ucing shortening.
5. Irregularity of the bone.-If the bone is close to the skin the fracture may be felt, and if compound it may be seen.
6. Unnatural Mobility. -Movement n1ay be made out at the seat of fracture.
7. Crepitus, or bony grating, may be felt or heard when the broken ends mo\'e one upon the other.
The last two signs slloltld oJ/ly be sOllglzl by a doctor.
Several of the ab0\'e signs are absent in green-stick and impacted fractures.
In addition to the signs and symptoms the patient or the bystanders may be able to gi\'e the history of the injury, and marks on the clothing or skin should be noted, as they may ser\'e to locate the fracture. The snap of the bone may haye been heard or felt.
ApPARATUS FOR TREAT\[ENT OF FRACTURES.
Splints and bandages for First Aid frequently have to be improvised.
A Splint may be impro\'ised from a walking stick, umbrella, billiard cue, broom or brush handle, policeman's truncheon, rifle, folded coat, piece of \\'ood, cardboard, paper firmly folded, a rolled-up map, or, in fact, anything that is firm and long enough to keep
the joints bmnediately above alid below the fractured bone at rest. 'When the above appliances are not available, the upper limb, if fractured, may be tied to the trunk, and in all cases a fractured lower lim b should be bandaged to its fellow.
Bandages may be irnpro\'ised from handkerchiefs, belts, straps, braces, nec kties, or any pIece of linen; calico, string or cord that COIlles to hand.
Esmarch's Triangular Bandages (Fig. 8) are made by cutting a piece of linen or calico about forty inches square diagonally into t\\O pieces.
The broad bandage is made by bringing the pomt down to the base ( Fig. 9), and then folding into h\ 0 (Fig. 10).
The narrow bandage is made by folding the bro:td I and3.ge once Ill.
The medium bandage is made by bringing the point down to the ba e, anu then foldmg into three. (Fig. I:!). This bandage may be used instead of the bro3.d or the narro\\ b.:mdage \\ hen it is better s'lited to the proportions of the 01.tient.
It is sometimes advisable to hah'e the size )1 the b3.ndage by bringing the t \\ 0 ends together before folding it into the broad, narrow, or medium bandage. When not in use, the triangular bandage should be folded narro\\'; the t\\ 0 ends should be turned to the centre, and the bandage then folded into four, reducin g it to a packet about 61 inches by inches.
Large arm-sling (Flg. I3 ).--Spread o u t a b andage, pu t one end over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang down in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm
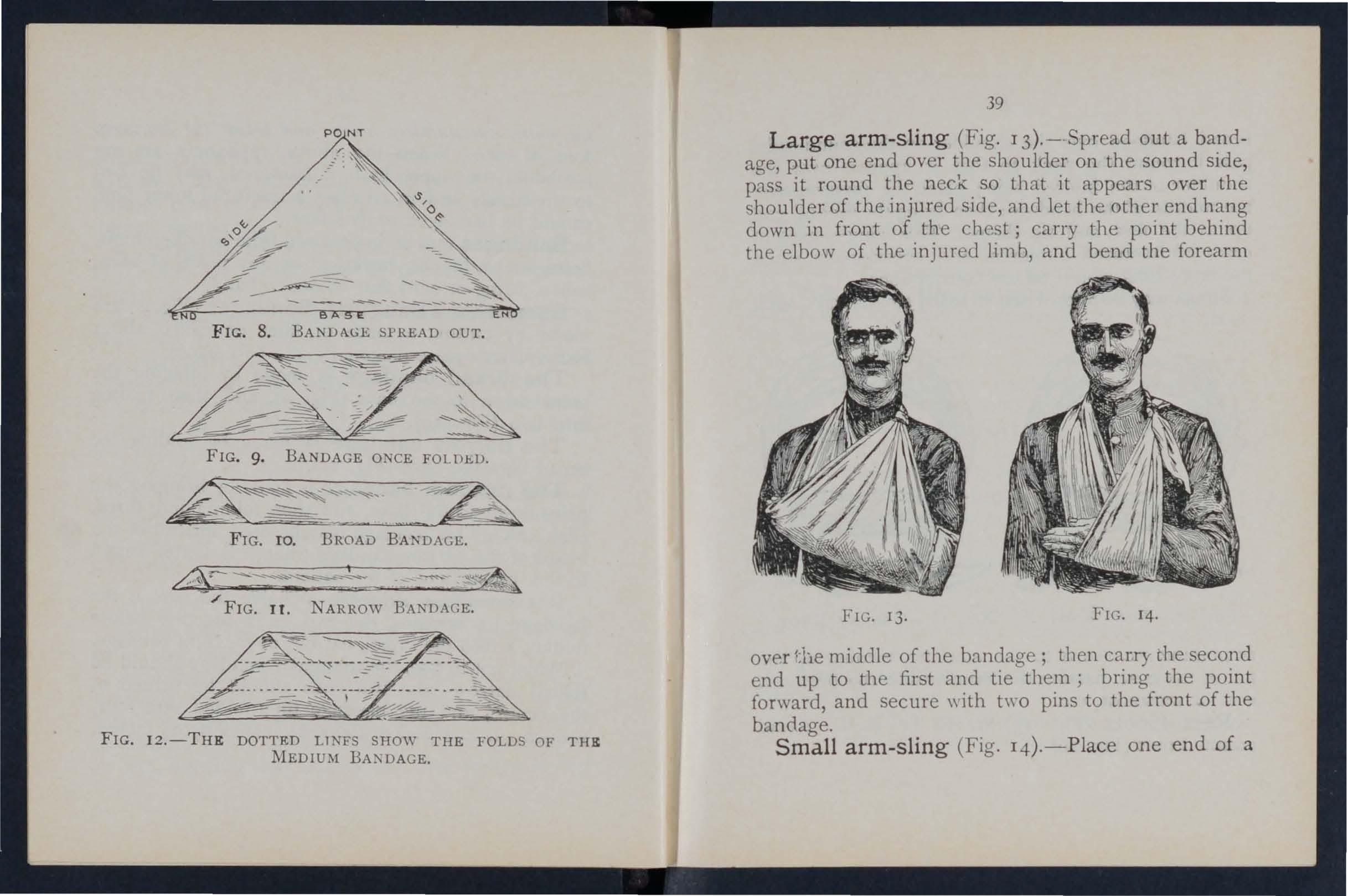
FIG. 9. BANDAGE ONCE FOLDED.
F IG. roo BROAD BANDA GE. .. /¢'\t / FIG. II . N ARROW BANDAGE.
1 2.-T H E DOTTED LlNFS SHOW THE FOLDS OF THE
ove-r the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure \\ ith h\-o pins to the front of the bandage.
Small arm-sling (Fig. I4).-P lace one end of a
FIG. MEDIUM39
Fl G. 13 .
FI G. 14.
broad bandage over the shoulder on the sound sid e, pass it round the neck so that it appears over the sho ul der of the injured side; place the forearm over the midd le of the bandage; then bring the second end up to the first, and tie them. This sling is us ed in cases of fractured humerus, and occasionally \\ hen the large sling would be too conspicuous. Slings may be improvised in many simple ways, such
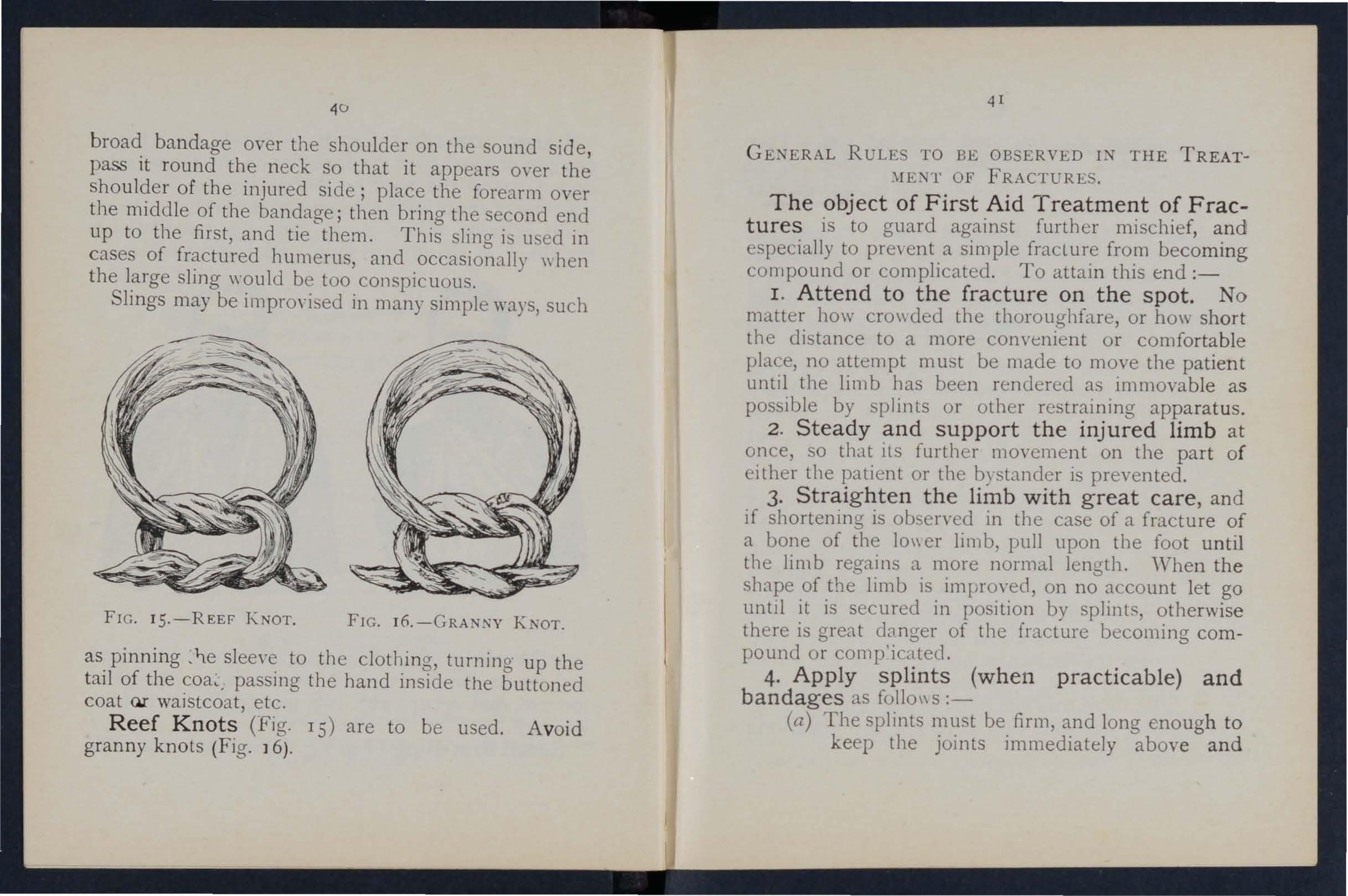
as pin n ing sleeve to the clothing, turning up the t ail of the coa< passing the hand inside the buttoned coat Qr waistcoat, etc.
Reef Knots (Fig. IS) are to be used . A void gran n y k nots (Fig. ] 6).
GE:-lERAL RULE TO BE OBSERVED I:-l THE TREATT OF FRACTURES.
The object of First Aid Treatment of Fractures is to guard against further mischief, especially to pre\ ent a simple fro.m becom m g compound or complicated. To attam thIS tnd :-
I . Attend to the fracture on the spot. No matter how cro\\ded the thoroughfare, or how sho rt the distance to a more convenient or comfortable place, no attempt must be made to mo.ve the patient untJl the limb has been rendered as Immovab le as possible by splints or otber restraining apparat us.
2. Steady and support the injured limb at once so that its furtber movement on the part of the patient or tbe bystander is prevented.
3· Straig hten the limb with great care , and if shortening is observed in the case of a fracture a bone of the 10\\ er limb, pull upon the foot untIl the limb regains a more normal length. "When the shape of the limb is improved, on no account let go untIl it is secured in position by splint., otherwise there is great danger of the fracture becoming compound or comp'icated.
4. Apply splints (whe n practicable) and b a ndag es as folIo\\ S :-
(a) The splints must be firm, and long enough to keep the joints immediately abo\'e a n d
FIG. I 5.-REEF KNOT. FIG. KNOT.42
b elow the fractured bone at rest They should, if practicable, be padded to fit accurately to the limb and be applied mer the clothing .
(b) The bandages must be applied firmly, but not so tightly as to constrict the circulation of blood in the limb. 'When the patient is in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule:-
For the trunk the broad ba;1dage should be used. Pass it once round the trunk and fasten it by tying the ends, or \\ ith hra or th rce safety pi ns on the side opposite to the fract ure, but if to secure a splint for a broken thlgh, over the splint.
For tile arm or forearm the narrow bandage should be used. Pass it twice round the limb, and tie the ends oyer the outer splint.
For tIle tlliglz or leg the narro\," or medium bandage may be used. It is frequently convenient to double the bandage at the centre, pass it under the limb, bnng the loop over the limb, pass both ends of the bandage through it in opposite directions, and tie them over the outer splint (Fig . 17).
I n ap plying bandages near a fracture the upper one should be \tecured first.
43
5. When hcemorrhage accompanies a frac dture it must be attended to firs t, and t he wou n c overed by a clean dressing.

FIG . I7.
6. No attempt must be made to remove a patient sufferin g from a f:act LIre of the spine, pelvis, or thi g h , except 1ll a recumbent po s it ion , preferably upon a stretcher. . .
7. In every case of fracture It 1.S necessary to cover the patient to keep him and so lessen the effects of the SHOCK of the aCCIdent.
8. In all doubtful cases, treat as a fracture.
PE.C1AL FRACTURES.
Fracture of the Cranium. -.\ fracture of the upper part is usually cau ed by direct yiolence-for examp1e, a blow on the head. .\ fracture of the base is caused by indirect violence, through a fall on the
4-1
head, a fall on the feet or lower part of the spine, or a severe blo\\' on the lower jaw. If tile ?I/fa part l'S fractured, the signs are s\\'ellin.g, and frequently in ensibility, either. Immediate ,or coming on gradually. If tile .IS fractured 111senslblhty may come on
FIG. 18. illllllediately, blood or a clear fluid Illay issue from the ear challnel, blood may escape from the nose, or it may pass do\\ n to the stomach, ,\ hence it may be vomited; the fracture may im'olYe the orbit, causing a blood-shot eye.
TREAT\fENT.
Injury to the brain is the great danger attending a fwcture of the cranium. For treatment see "Concussion and Compression of the Brain, " pages 13 1 , 13 2 .
Fracture of the Lower jaw. -Pain, loss of power (inability to speak and move the freely), irregularity of the teeth, crepItus and bleedmg from the gum are the usual signs and symptoms.
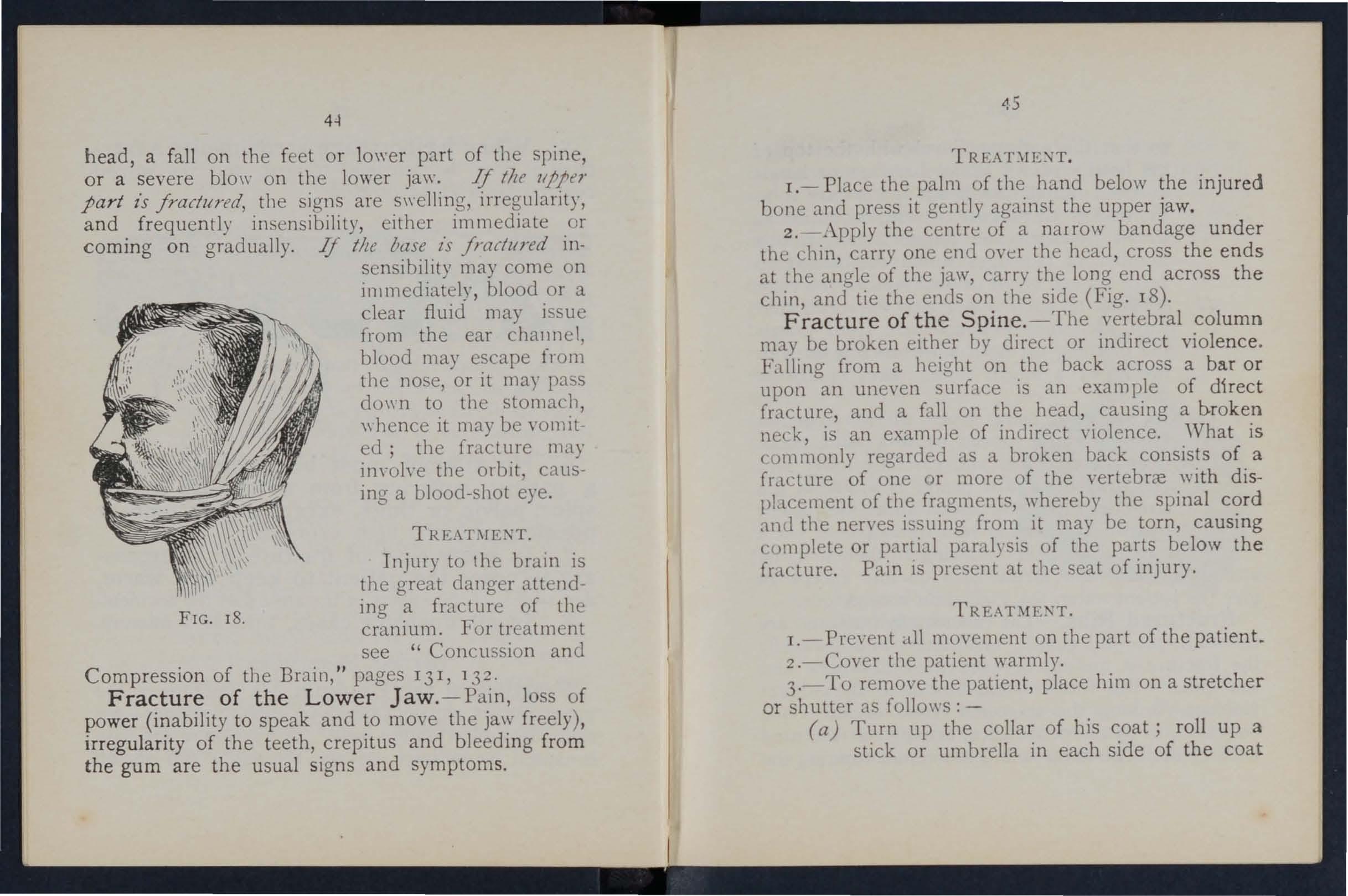
1.- Place the palm of the hand below the inju red bone and press it gently against the upper jaw.
2'4 \pply the centre of a narrow bandage under the chin, carry one end OYer the head, cross the ends at the ana-Ie of the jaw, carry the long end ac[()ss the chin anl tie the ends on the side (Fig. 18). of the Spine. -The vertebral column may be broken either hy direct or indirect violence. Falling from a height on .the back across a bar or upon an uneven surface IS an example of direct fracture, and a fall on the head, causing a b.roke? neck, is an example of indirect violence. .'Vhat IS commonly regarded as a broken back of, a f rJ.ct ure of one or more of the vertebrre \\'lth dlspbcement o[ the fragments, whereby the spinal c<;>rd and the nerves isuing [rom it may be torn, causmg complete or partial paralysis of the parts below the fracture. Pam IS present at the seat of injury.
l.-Pre,'ent all movement on the part of the patient.
2.-Cover the patient warmly .
3.-To remOl'e the patient, place him on a stretcher or shutter as fo11o\\s:-
(a) Turn up the collar of his roll up a stick or um breJla in each SIde of the coat
46
so that the ends are level \\ ith the top of his head; pass a broad bandage or handkercheif under the head and secure it to the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a num ber of bandages under the patient to sene instead of, or in addition to the coat.
(b) A bearer on each side grasps tlle rolled coat \\ ith his hands well apart; a third grasps the clothing on both sides on a level \\jth the hips; a fourth bearer takes cbarge of the legs .
(c) On the word being given, all lift together and carry the patient by short side paces oyer the stretcher and carefully lower him on to it. If a fifth bearer is a,·ailable the stretcher should be passed under the pati I1t instead of carrying 11im oyer it.
4·- O n arrival at shelter nothing further is to be attempted until the arriyal of a doctor, except to give the patient water, tea, etc., jf he is conscious.
Fractured Ribs.-The ribs usually fractured are the sixth, seventh, eighth, and ninth, and generally the fracture is midway between the breast-bone and the spine. The fracture may be caused by indirect violence, driving the fractured ends of the bone ou twards, or by direct violence, driving the fractured ends o f the bone inwards and sometimes injuring the
47
Junas or other internal organ. If the lower ribs on . the side are broken, the liver may be injured, rUle! a fracture of the lower left ribs may wound the spleen. Evidence of the fracture is afforded by pain, especially on attemptmg to take a deep breath, and by short and shallow breathmg. If the lunas are iniured blood, frothy anJ bright red, may be coughed up and ex pectomted. If the liYer or spleen is wounded intern'll hremorrhagc (. ec page 95) may occur.
TREAnIE:\,T.
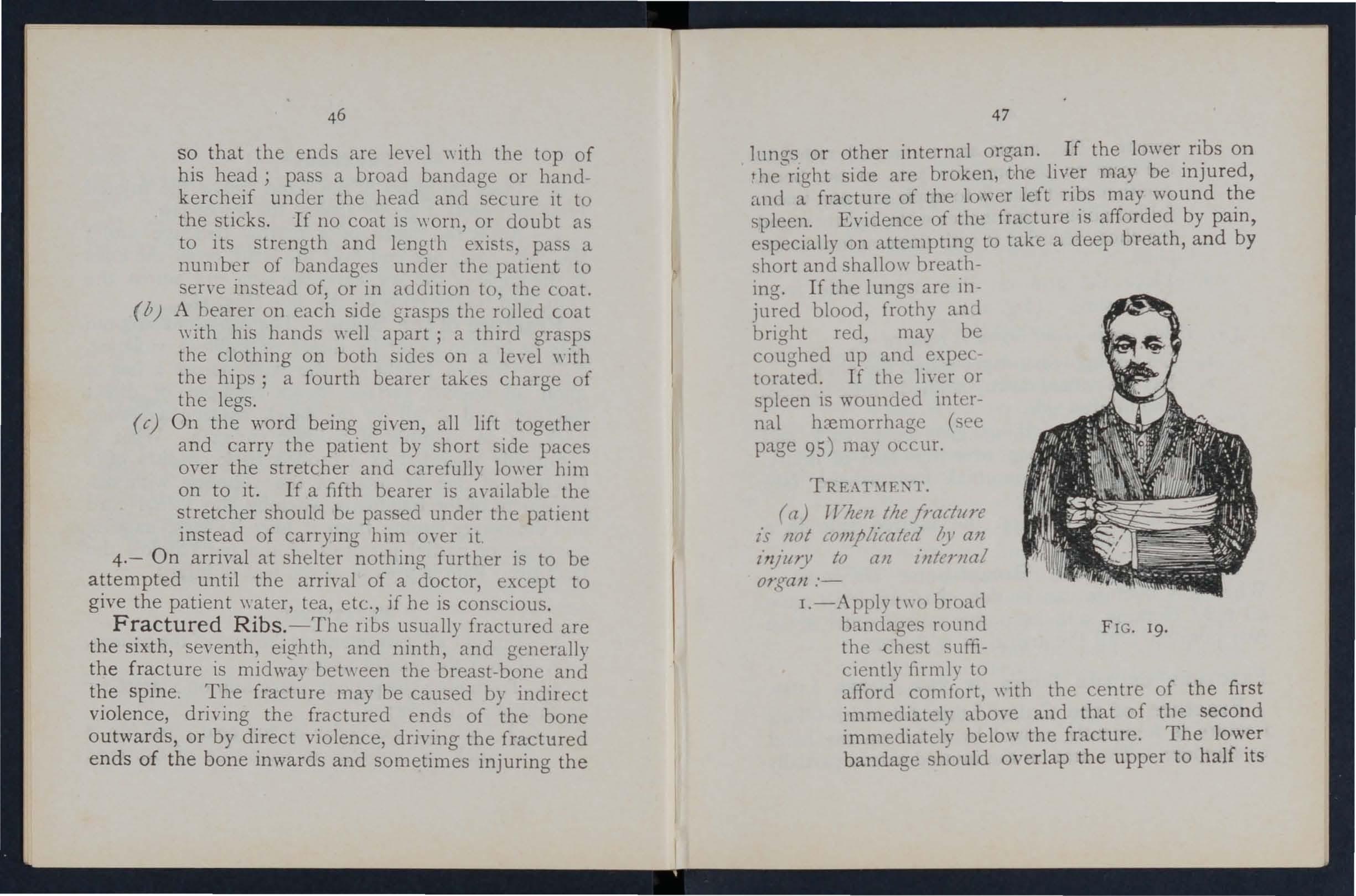
(a) TT'lZt!ll the jrarillre l·S /lot (olJljhratcd all zn/lIlY to all internal OJ:f{aJl :I.-Apply t\\'o broad b:ll1dages round FIG. 19. the .chest sufficiently firmly to afford comfort, \yith the centre of the first immediately above and that of the second immediately below the fracture. The lower bandage should overlap the upper to half its
48
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong towel, folded about eight inches wide, tightly round chest, securing it with three or four safety p111S.
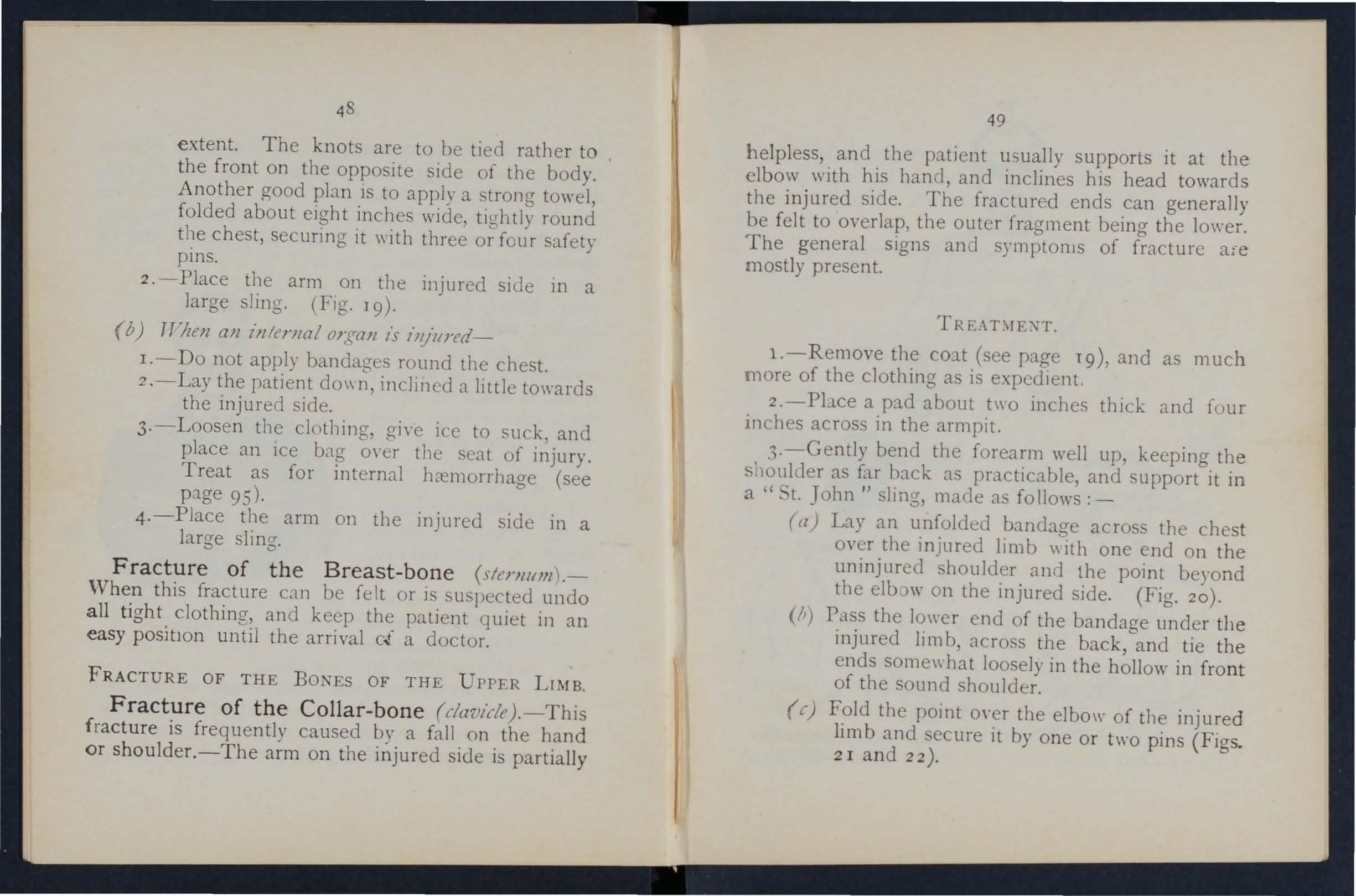
2.-Place the arm on the injured side 111 a large sling. (Fig. J 9).
(b) ,rhell all Z>llerllalorgall is illjllred-
I.-Do not apply bandages round the chest.
2.-Lay the patient do\\ n, inclined a little towards the injured side.
3·-Loosen the clothing, giYe ice to suck, and place an ice bag m 'e r the seat of injury. Treat as for internal kemorrhage (see page 95).
4·-P1ace the arm on the injured side in a large sling.
Fracture of the Breast-bone (slenWl!l l .-
\Vhen this fracture can be felt or is suspected undo all tight clothing', and keep the patient quiet in an easy positlOn until the arrival c{ a doctor.
FRACTURE OF THE Bo ES OF THE UPPER LIMB.
Fracture of the Collar-bone (dav/cZe).-This fracture is frequently caused by a fallon the hand or shouider.-The arm on the injured side is partially
49
helpless, and the patient usually supports it at the elbow with his hanel, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lower. The general signs and symptonls of fracture aie mostly present.
TR L\T)fE);,T.
l.-Remove the co::tt (see page 19), and as much more of the clothing as is expedient.
2.-Pbce a pad about two inches thick and four Inches across in tbe armpit.
,).-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a " ... t. John" sling, made as follows:-
(a) Lay an unfolded bandage across the chest over the injured limb \\ ith one end on the uninjured shoulder and the point beyond the eIb)\\' on the injured side. (Fig. 20).
(II) Pass the lower end of the bandage under the injured Ii m b, across the back, and tie the ends some"hat loosely in the hollow in front of the sound shou Ider.
(c) F?ld the POll1t O\'er the elbo\\' of the inj ured 11mb and ecure it by one or two pins (Figs. 2 I and 22).
+-Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5.-Now tighten the sling.
'Vhen both collar - bones are broken keep the
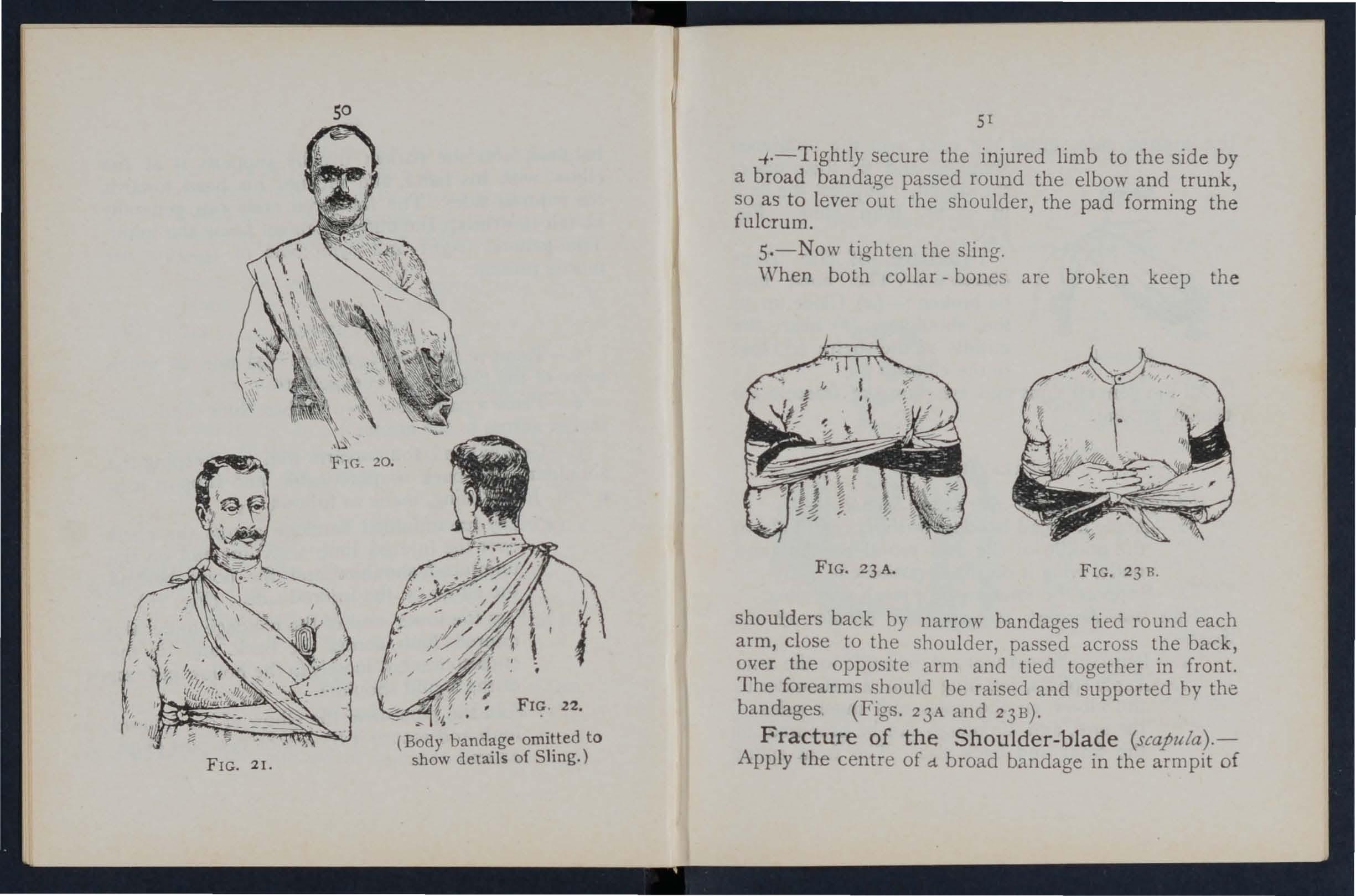
FIG. 21.
(Bod y bandage omitted to show details of Sling.)
shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported hy the bandages (FIgs. 23A and 23 B ).
Fracture of the Shoulder-blade (scapula).-
Apply the centre of d. broad bandage in the armpit of
50
51
FIG. 23A.
FIG. 23 B.
the injured side, cross the ends oyer the uninjured shoulder and tie them under
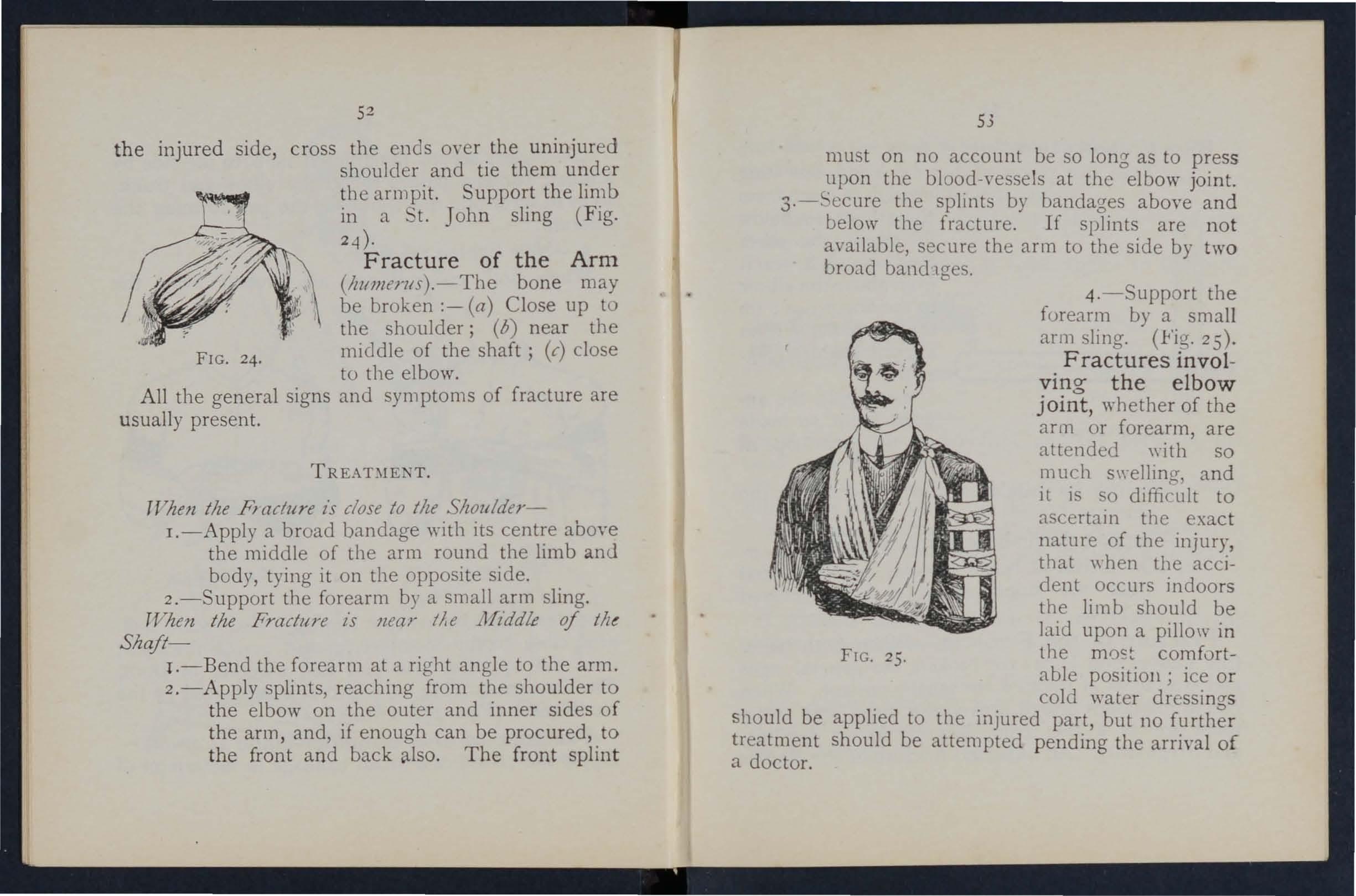
FIG. 24. the armpit. Support the limb 111 a t. John sling (Fig. 2-i ).
Fracture of the Arm (1IlI77Zerlls).- The bone may be broken :- (a) Close up to the shoulder; (b) near the middle of the shaft; (c) close to the elbow.
All the general signs and symptoms of fracture are usually present.
TREABIENT.
TVhen tlze PI aclure is close to tile ShoZllder-
I.-Apply a broad bandage with its above the middle of the arm round the lunb amI body, tying it on the opposite side. .
2.-Support the forearm by a small shng.
TVhen tlze Fracture is near I/'e l lfzddle of tht Shaft-
I.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured,. to the front and back also. The front splll1t
53
must on no account be so long as to press upon the blood -vessels at th e elbow joint. the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad bandlges.
4. -Support the forearm by a small arm sling. (.Fig. 25)'
Fractures involving the elbow joint, whether of the arm or forearm, are attended with so much s\yelling, and it is so dililrult to ascertain the exac t nature of the injury, that \\ hen the accident occurs indoors the Ii 111 b should be Jaid upon a pillow in the most comfortable positioll; ice or cold water dressings should be applied to the injured part, but no further treatment should be attempted pending the arriyal of a doctor.
FIG. 25.
lTTflen tlte acddent occurs out of doors-
1.-Take two pieces of thin flat wood, one long enough to reach from the armpit to be low
FIG . 26. the elbow, the other long enough to reach from above the elbow to the finger tips; tie them together to form a righ t angle. (Fig. 26).
'2.-Apply the angular splint so made on the inner side of the flexed limb.
3. - Secure by fracture. bandages above and below the
4·-Su pport the limb by a large arm sling.
s·-On arrival a.t remove the splint, and treat the In1Ury as if it had occurred indoors.
of the F - .-- - --m . - "Vh e n both bones (the RadlUs and Ulna) are broken, the gel1"rn.l signs and symptoms of are usually present. When one of the bones only IS the signs and symptoms are as a rnle pam, loss of pO\l,"er swelling and irregularity. An impacted fracture of the 55
just above the wrist is a common result of a fall on the hand.
TREATMENT.
This is the sam , \\ hether the fracture is of one bone or of both.
I.-Bend the forearm at right angles to the arm,
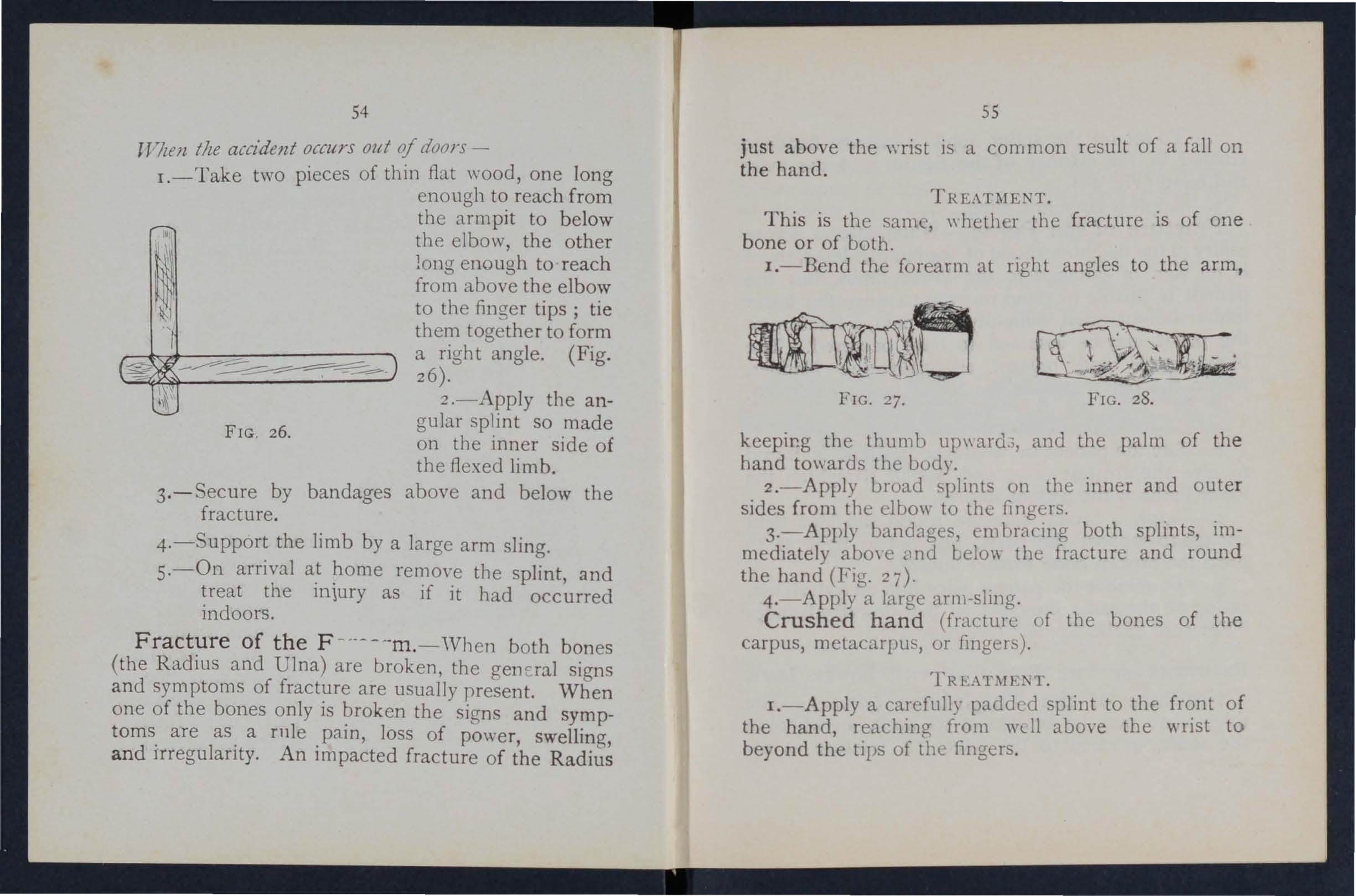
FIG. 27. FIG. 28.
kcepir.g the thumb up\\ard,:;, and the palm of the hand to\\ ards th e body.
2.-Apply broad splints on the inner and outer sides from the elbo\\ to the fingers.
3.-Apply bandages, ('111 bracing both splints, immediately above Clnd belo\\ the fracture and round the hand (Fig. '27).
4. - Apply a large arl1l-slmg.
Crushed hand (fracture of the bones of the carpus, metacarpus, or fingers).
I.-Apply a carefully padded splint to the front of the hand, reaching from wdl above the wrist to beyond the tips of tht? fingers.
54
2.-To secure the splint apply a narrow bandage crossed in the mannel of the figure 8 to the wrist and hand ( F ig . 28).
3. -Apply a large arm-sling.
Fracture of the Pelvis.- \ Vhen, after a seve re injury in the neighbourhood of the haunch-bone, there is no sign of damage to the }O\yer limbs, but the pJ.tient is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture ot th e pelvis may be assumed to have occurred . The b lood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
I.-Lay the patient in \\ hatever pOSItIOn is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further i11\\ ards.
3·-To remO\'e the patient place him on a stretcher, acting on the same principle as that described under " Fracture of the Spine " (see page 45).
FRACTURE OF THE BONES OF THE LOWER LIMB,
Frac t ure of the Thigh-bon e (femur) . - The thigh bone may be broken at its neck, anywhere in (he shaft, or close to the knee . A fracture at the 57
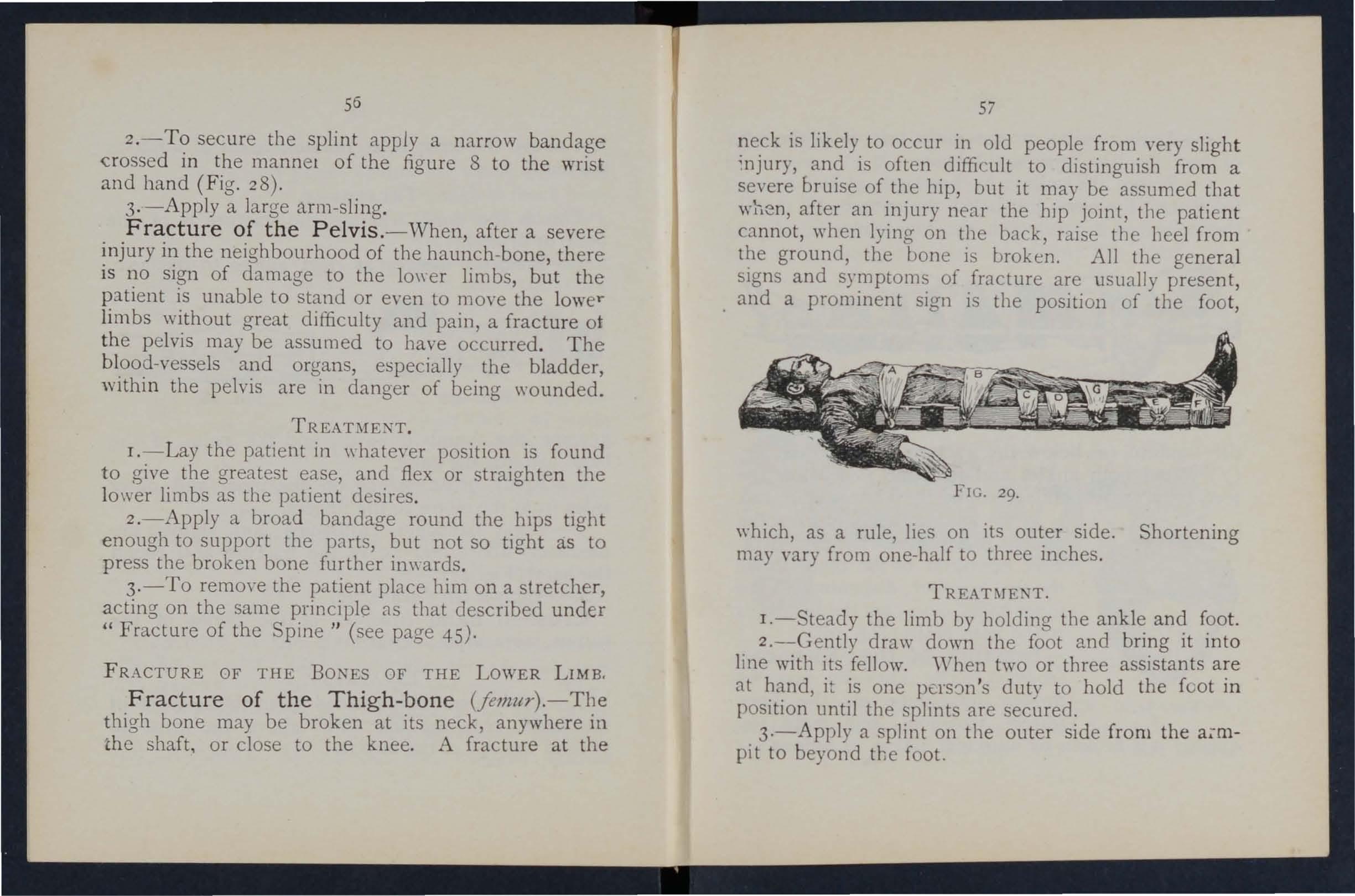
neck is likely to occur in old people from yery sligh t ;njury, and is often difficult to distinguish from a severe bruise of the bip, but it may be assumed tha t after an injury near the hip joint, tIle patie nt cannot, wben lying on the back, raise the lleel from the ground, the bone is broken. All the general sIgns and symptoms of fracture are usually present, and a prominent sign is the position of tbe foot,
FIG. 29,
\\'hich, as a rule, lies on its outer side. Shortening may vary from one-half to three inches .
TREATl\JE'T,
I.-Steady the limb by holding the ankle and foot.
2.-Gently draw down the foot and bring it int o line with its fellow. "'hen two or three assistants a re at hand, it is one duty to hold the foot in position until the splints are secured.
3·-A pply a splint on the outer side fro m the pit to beyond the foot.
56
58
4.- A pply a splint on the inner side from the top of the thigh (the fork) to the knee. .
5.-Secure the splints by bandages fo11O\\'s :(a) Round the chest just. below (b) round the pelvis on a le vel mth the hlp ]omts, (r) above
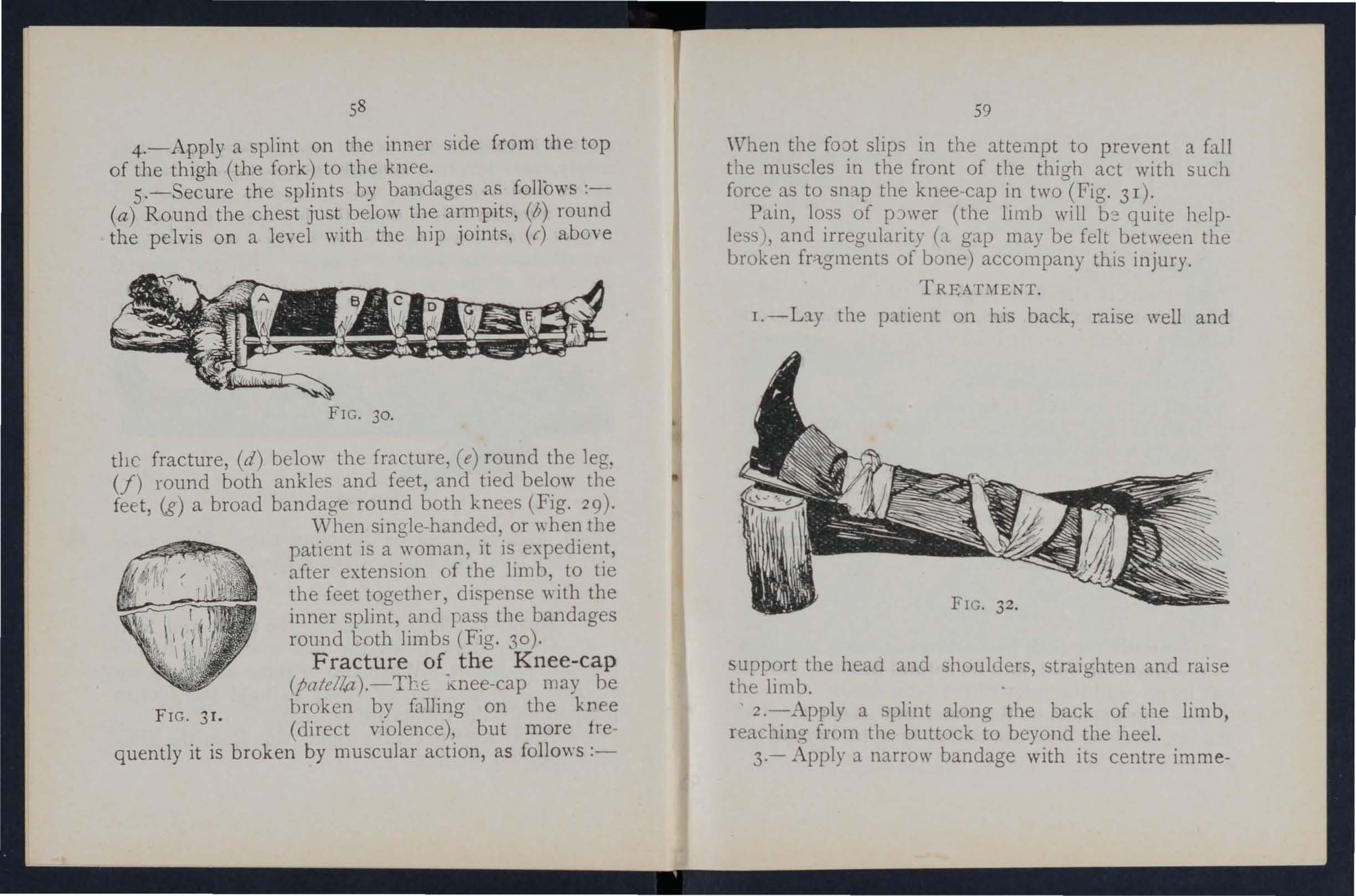
FIG. 30.
the fracture, (d) below the fracture, (e) round the leg. (f) round both ankles and feet, and tied below the feet, (g) a broad bandage round both knees (Fig. 29)·
'When single-handed, or "hen the patient is a woman, it is expedient, after extension of the limb, to tIe the feet together, dispense " 'ith the inner splint, and pass the bandages round both limbs (Fig. 30).
Fracture
of the Knee-cap
i\:nee-cap may be broken by falling on the kJ.1ee (direct violence), but more frequently it is broken by muscular action, as follows :-
FIG. 3r.
59
When the fOJt sl1ps in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee-cap in two (Fig. 3 I).
P,l.in, loss of pJwer (the limb will b2 quite helpless ), and irregularity (a gap may be felt between the broken fr>tgments of bone) accompany this injury.
r.-L::l.)' the patient on his back, raise well and support the head and shoulder, straighten and raise the limb.
, 2.-Apply a splint along the back of the limb, reaching from the buttock to beyond the heel.
3·- ...\ pply a narrow bandage with its centre imme-
-T.
the knee - :."IP, ero's the ends behind over the splint, and tie in front below the broken bone. To ensure firmn ess apply a second bandage in a similar way, but commenced belo\\' and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5. - upport the foot \\ell off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig . 3 2 ).
6.-Apply an iee bag or a cold \\ aier dr essi ng over the fracture.
Fracture of the Leg (tiNa alld jibltla).- One or both of the bones may be broken. 'Vben both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end is frequentl y mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
fo ot. If only one splint is available place it on the outer side.
4.-Secure the splints by bandages (a) above, (0) below the fracture, (i) immediately.above the knee,
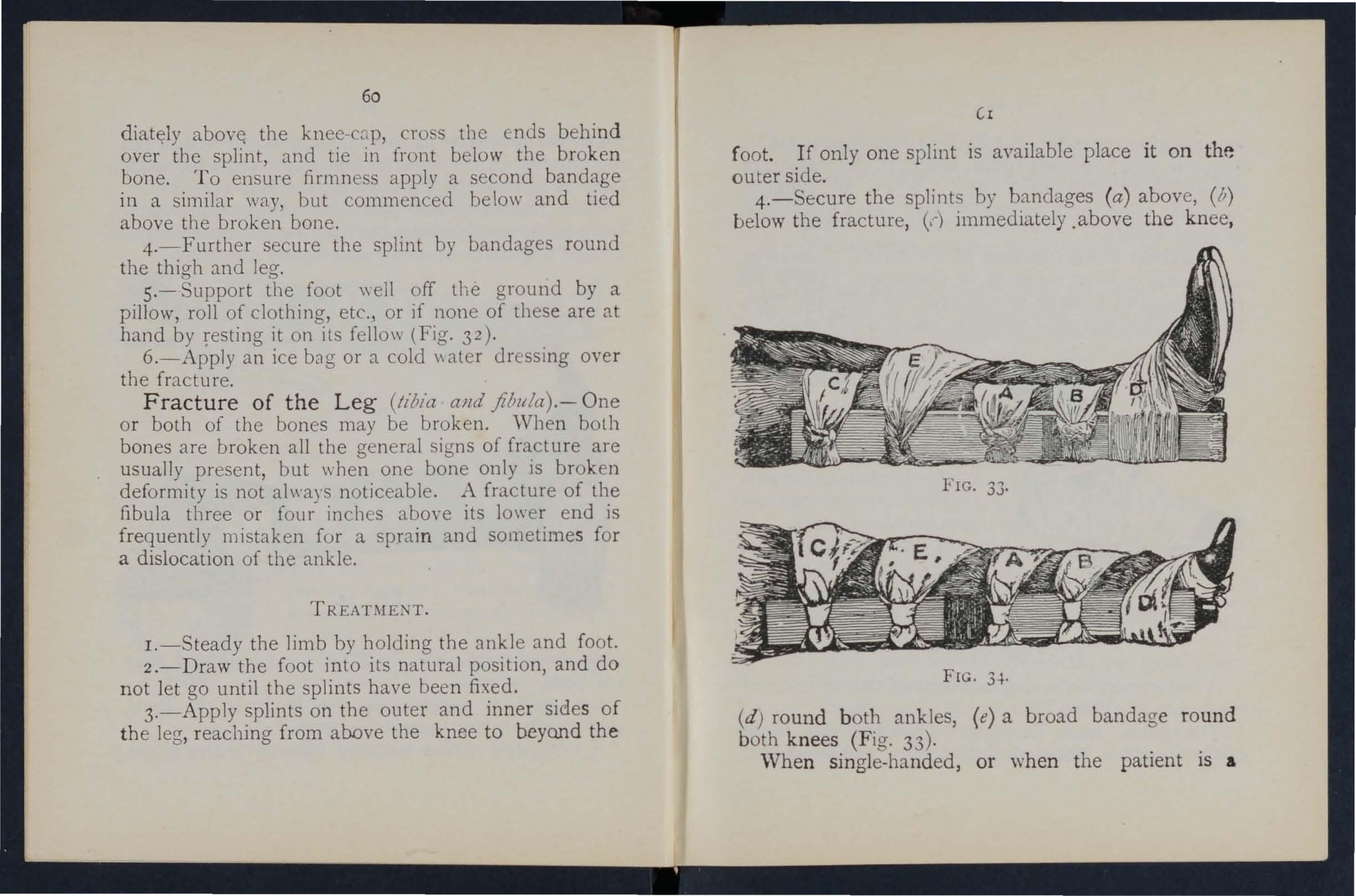
FIG. 34.
(d) round both ankles, (e) a broad bandage round b oth knees (Fi g . 33).
'When single-handed, or when the patient is a
60
C1
woman after extending the limb tie both feet together, dispende \vith the inner .s plint, and pass the round both limbs (FIg. 34). "When no spllllt available tying the legs, ank ]p.s, and knees together IS of great service. . .
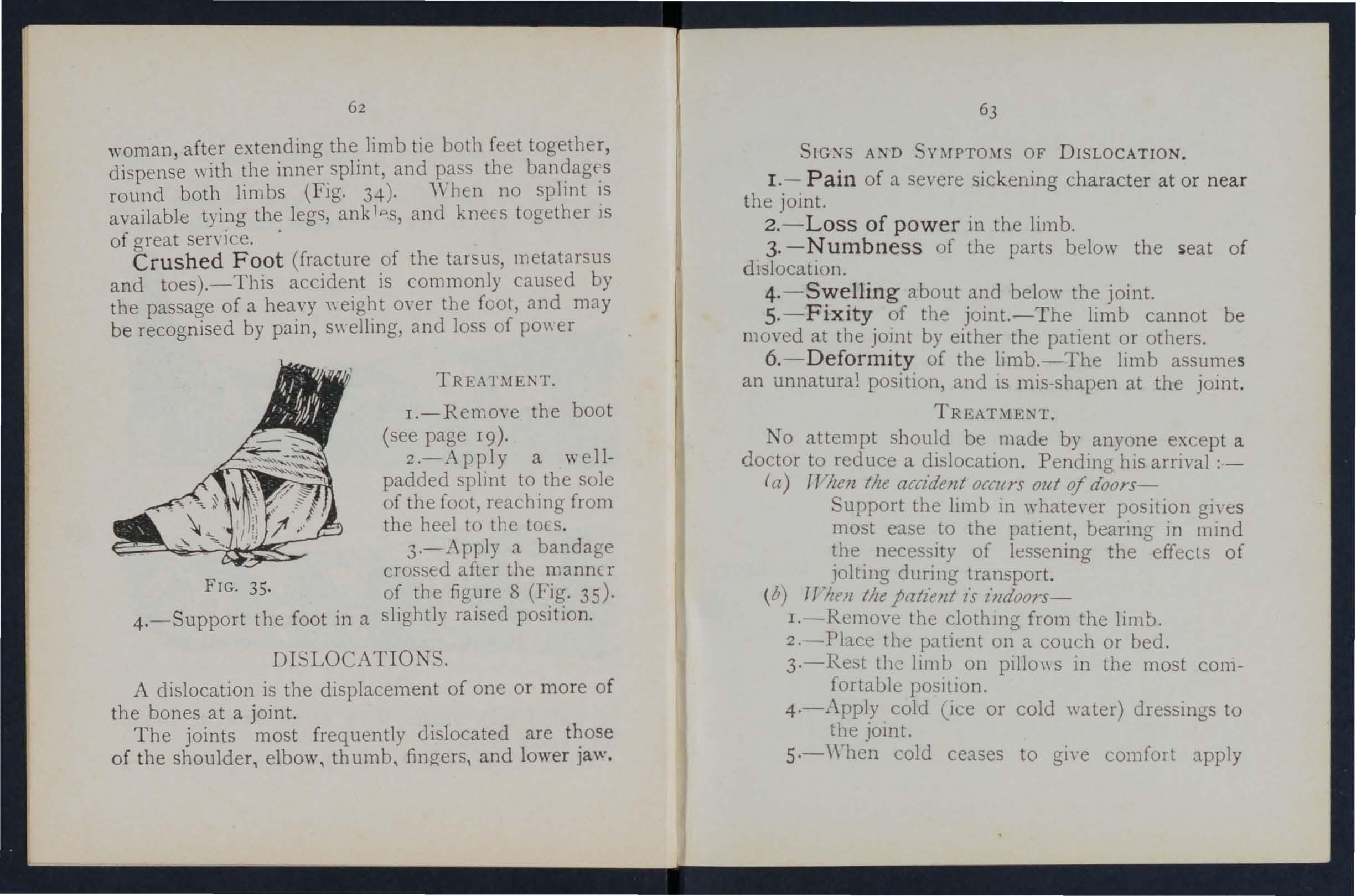
Crushed Foot (fracture of the tarsus, metatalsus a n d toes).- This accidel!t is commonly caused by the passage of a hea.vy over the foot, and may be recog n ised by pam, S\\ el1lllg, and loss of PO\\ er
FrG . 35.
4.-Support the foot in a
TREATMEI\T.
I.-Remove the boot (see page 19).
2.-Apply a wellpadded splint to the sole of the foot, reaching from the heel to the tOES.
3.-Apply a bandage crossed after the manner of the figure 8 (Fig. 35)· slightly raised position.
DISLOCATIONS.
A dislocation is the displacement of one or more of the bones at a joint.
The joints most frequently dislocated are o f the shoulder, elbow, thumb, fingers, and lower Jaw .
SIG:-fS AND OF DISLOCATION .
1. - Pain of a severe sickening character at or near the joint.
2. - Loss of power in the limb.
3. - Numbness of the parts below the seat of dislocation.
4. - Swelling about and below the joint.
s. - Fixity of the joint.-The limb cannot be moved at the joint by either the patient or others.
6.- Defo rm ity of the limb.-The limb assumes an unnatural position, a.nd 15 mis -shape n at the joint.
TREATMENT.
No attempt should be made by anyone except a doctor to red uce a di location . Pending his arrival ;-
(a) TT The n the accident OC(I( rs out of doorsupport the limb in whatever position gives most ease to the patient, bearing in l11md the neces:.ity of lessening the effects of iolting during transport.
(b) T["!tell the patiellt l'S ill doorsI.-Remove the clothmg from the limb.
2. -Pbce the patient on a cOllch or bed.
3·-Rest the limb on pillo\\ S in the most comfortable posItion.
4·-A pply cold (lee or cold water) dressll1gs to the jomt.
s·-,rhen cold ceases to give comfort apply
62
63
warmth (flannels or to\\"eI5 \nung out of hot water).
6.-Treat shock (see page 135).
SPRAINS.
'When, by a sudden wrench or t\\"ist, the ligaments and the parts around a joint are stretched and torn the joint is said to be sprained. "Going over" the ankle is a common example.
A D
1.- Pain at the joint after a t \\ ist or wrench.
2.-Inability to use the joint.
3.-S\\ elling and discoloration.
TREAnfE:'\"T OF SPRAI.Nl:D .\.-KLE.
TJ7ten Ollt of doors-
I.-Apply a bandage tightly oyer the boot, beginning on the sole at the instep, crossing it on the front of tIle ankle, and carrying it round and round the ankle, where it is to be firmly tied.
2.-\Vet the bandage after npplicaton; it is th ereby tightened.
Afler rradz/Ilg slzdlcr-
I.-Remove the boot and stocking (see pag e 19).
2.-Place the limb in the most comfortable position; usually that is well raised.
3.-Apply i e or cold water dressings to the joint as long as they relie\'e pain.
4.- " ' hen cold fatls to give comfort, apply hot fomentations.
" 'hen other joints are sprained, treat them as if dislocated.
Wb en in doubt as to the nature of the injury, treat as a fracture.
TRAIN D RUPTURED
\Vhen, during se\'ere exertion, muscle or tendocs are over-stretched they are s:lid to be strained, if thEY arc actually torn they are described as ruptured.
lG \;S A:'\"D
I.-A sudden harp pain.
2.-\\Then the muscleS of a limb are strained they may s\\ell and cause se\'erc cramp.
3·-Further exertion is diffi c ult or impossible; for e,{ll1lple, if the stram ha occurred in the back the patient may be unable to stand upright.
TRFAnfENT.
I.-Place the ratient in the most comfortable position, and afford support to the injured part.
2.-Apply hot water bottles 01 hot fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 114).
D
Q U E STION S ON CH APTER II .
Tlze num erals in dica ft fhe pages w izen t h e lIIay be fo un d
\\'hat is t h e ske l eto n , and \\ ha t p ur poses a r e sern'c1 by it?
H ow a r e th e bon es of th e sku ll a rranged?
\Vh at a re t h e b oun da ri es o f the c ranium?
D escrib e th e bo n es of th e face
D esc ri be t he l owe r jaw
Wh a t is th e a ng le of th e ja w ?
\Vh at oth e r na m es has th e back-bo n e?
\ Yh at is a vert ebra ? ...
II o w many ve rt e brre a r e th e re i n th e spine?
I'A(.P:
2J .. 22, 23 ?' -.)
\\' hat a re th e r egio ns o f th e spine, a nd ho \\ many ye rte hrre ar e t h er e in each? ..
1{ow is the spi ne endow ed wi th fr ee move ment?
Wha t is a ri b ?
H ow ma ny pa irs of ri bs a re t h ere?
What is the breast -bone? .. "
" That are t h e b o nes of t h e uppe r limb
What is th e p el vis? ...
What is th e hip join t? ... ." ...
\Vhat are th e bo n es of th e lo w er lim bs? ...
What is a joint?
Desc rib e a m oveahl e joint ...
D esc rib e th e sh oul de r j oint
D escri b e th e a nkl e joint
H ow are mu scl es cIa sin ed ?
D esc rib e volunta ry muscl es
D e scribe involunt a ry Tr'l scl es
What is a fra ct ure ? ...
\Yha t ar e
frac t ure ?
does a bone break when direct violence is
\Vhere does a bone break when indirect violence is the cause of fracture?
[row maya fracture be caused by muscular action?
In what two ways may fractures be classified?
What is a simple fracture ?...
Wbat is a compound fracture?
\ \ bat is a complicated fracture?
What i-; a comminuted fracture?
\ \ -hat is a green-stick fracture?
\\'bat fracture ' afford the most complete example of the sign.:; and symptoms? ..
In making up your mind whether a fracture had occurred or nut, \\"hat points Should you take into consideration beyond the signs and symptoms?
apparatus may be necessary for the treatment of fractures?
lTow may splints be imprm"i-;ccl ? . .. . . 36 , 37 I row may bandages be impro\'ised ?
De . cribe Esmarch's bandage 37, 3 (Fig. S)
In what ways may the triangular bandage be folded for use? 37
I r"w many kinds of arm-slings are there, and what are they called?
"'hat knot is to be tied, and \\'hat knot ayoidecl? 40 What is the object of first aiel treatment of fractures? / 4I
Give the general rules fur the treatment of fractures 41
lIov. should splints be applied? ... . ...p, 42
ITow should bandages be applied? .. ..p, 43
\ \'hat may cause a fractnre of the upper pa r t of the c ranium?
66
... ... ... ... . ..
22
causes
26 tu 2 28 30 ') 0 3 I 3 1 3 2 3 2 3 2 33 33 33 .. · 33, 34 PAGE 'Shere
the
33
the
of
cause of fracture?
\Vhat is an impacted fracture? 34 3-+ ... 34, 35 34 34 34 35 35 35 State
general signs and
that
pre el1l
case of fracture 35, 36
the
symptoms
may be
in a
35 \\'hat
36
37
39,
49
40 ,
43 2
\Vhat may cause a fracture of the base of the cranium? 43, 44
\Vhat are the signs of fracture of t he upper part of the cranium? 44
\Vhat are the signs of fracture of the base of the cranium? 44
\Vhat is the treatment for fracture of the cranium? 44
\Vhat are the signs cf fracture of the lower ja \\ ? 44
How maya fractured spine be caused? .. , 45
'Vhat is commonly regarded as a broken back? ... 45
'Vhat are the symptoms of a fractured spine? 45
How may ribs be fractured? 4 6
How maya fracture of ribs be complicated? 47
State the signs and symptoms of a simple and of a complicated fracture of ribs 47
'Vhat is a frequent cause o f fractured collar-bone? 48
'Vhat are the signs and symptoms of fractured collar,one?
... 48, 49
At points may the bone of the arm be broken? ." 52
Are the general signs and symptoms of a fracture alwa) s present in a. broken forearm? ... ... .., 54
State the cause of a common fracture of the radius 55
How would you recognise a fracture o f the pehis? 56
At what points may the thigh-bone be broken? .. , 57
'Vhat are the signs and symptoms of fracture of the thigh-bone? 57
'Vhat are the causes of fracture of the knee-cap? .. 58, 59
'Vh at are the signs and symptoms of fracture of the kneecap? 59
Are the general signs and symptom ' al \\'a) s present in a fracture of the leg? 60
'Vhat mistake may easily be made \\ hen th e fibula is broken near its lower end?
What is a dislocation?
State the signs and symptoms of dislocation
are the signs and symptoms of a sprain? 64
State the treatment of a sprained ankle .. , 64
State the trea.tment of other sprains .. 63, 65
When not sure whether the injury is a sprain or fracture how would you treat it? ... ... ... ... 65
Ihw
or ruptured?
Fir t Aid. tudent should practise impro\'i!->ing material, folding bandage, tyIng knots, making slings, and the treatment of the following injlllies.
Impr o\'i sing splints ...
Im nro\'ising bandages
Folding bandages
Large arm sling
SnuB arm sling ..
Red and granny knots
Knot for applying splint to lower limb
Fractures - Lower jaw, 44. Spine, 45, 46. Rills (simple and complicated fractures), 46to -1- Breastbone, 4. Collar-bone, 48 to 51. Both collarbones, 51. Arm, close up to shoulder 52. Arm, near middle of shaft, 52. Arm or forearm \\hen the elbow is involved, 53. Forearm, 55. Crushed hano, 55,5 6. Pelvis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single-hand ed), 5. Kneecap, 59, 60. Leg (man), 60, 61. Leg (woman or
. when single-handed), 62. Crushed foot, 6;. of door and indoors ... ... ... 63, 64
68 PAGE
... ... ... ...
...
...
60
62
63 69 PAGE
... 63 What
... ... ... ... 64 '
State the treatment of dislocation
is a ' prain?
Vhat
may muscles be strained
65 State the signs and symptoms of strains 65 t lte the treatment of strains 65
36, 37 37 37 39 39, 40 40
pratned ankle .. ... 64 Strains and ruptured muscles 65
CHAPTER III.
TH E O RGANS OF CIRCULATION.
THE organs concerned in the circulation of the blood are the Heart, the Arteries, the Veins , and the Capillaries .
The Heart is situated in the chest behind the brelst-bone and rib cartilages, between the lungs and immediately above the diaphragm; it lies obliquely with a qua r ter of its bulk to the right and the remaining three-quarters to the left of the middle of t he b ody. I ts beat may felt just below and to the inner side of the left nipple. The heart has four cavi t ies, two on either side of a central partition. The two cavities are named the right and left auricles , the two lower the right and left ventricles.
Artenes are vessels which convey blood from the heart. Veins carry blood to the heart. Capillanes connect the a r teries and veins.
In the general (systemic \ circulation arterial ulood is driven from the ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arte ries are given off to all parts of the body. These divide and sub-divide, and b ecome so small as to assume microscopic dimensions, when they are termed capillaries.
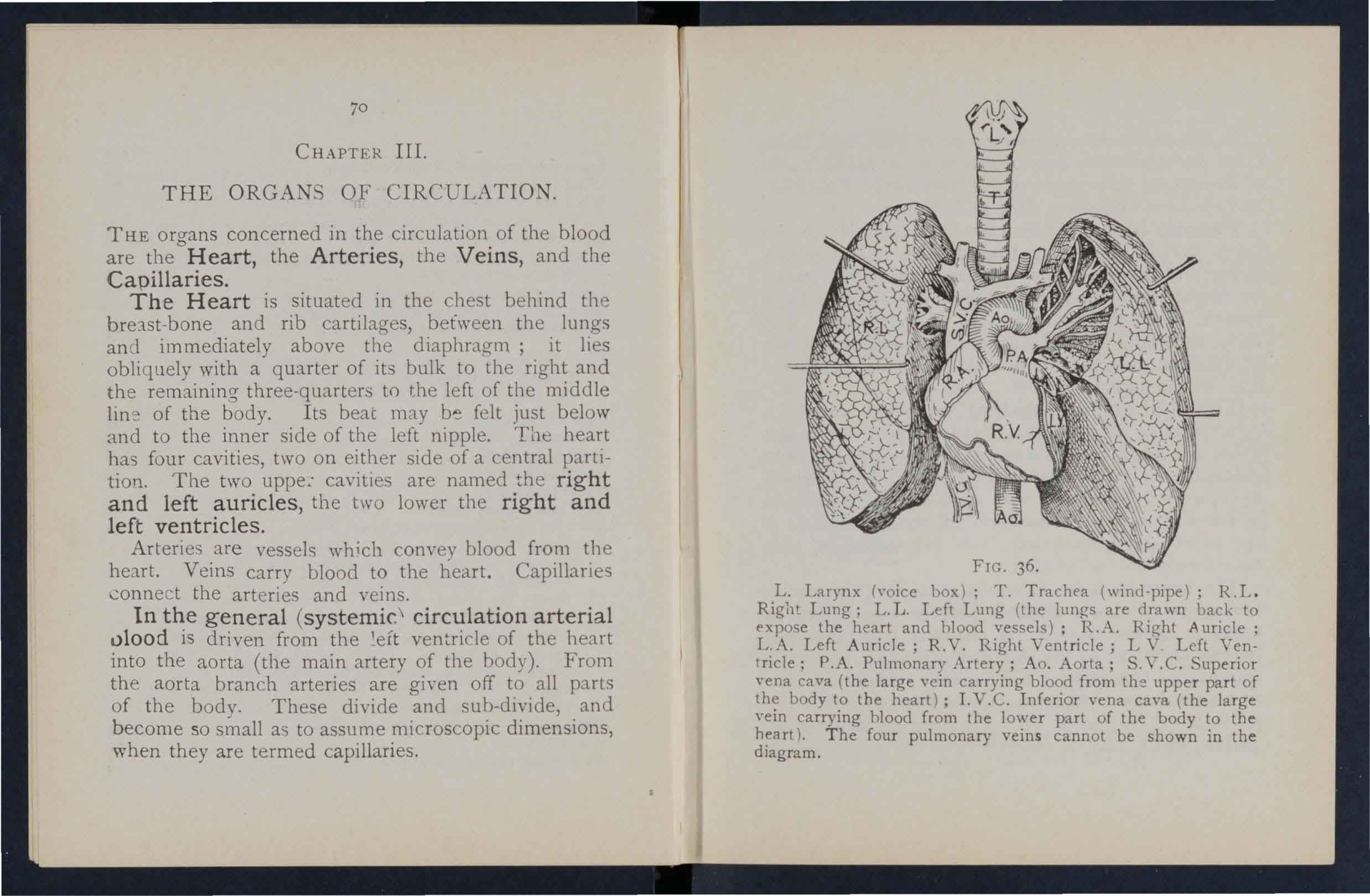
L. Larynx h'oice box); T. Trachea (wind·pipe): R.L. Right Lung; L. L. Left Lung (the lungs are drawn back to expose the heart and hlood vessels); R .A. Right Auricle; L.A. Left Auricle; R.V. Right Ventricle; L Y . Left Ventricle; P.A. Pulmonary Artery; Ao. Aorta; S.Y.C. Superior vena cava (the large yein carrying blood from the upper part of body t.o the heart): LV.C. Inferior vena cava (the large vem carrymg hlood from the lower part of the body to the heart). T he four pulmonary vein s cannot be shown in the diagram .
In the capillaries an interchange of gases and fluids takes place, wherehy the nourishment and maintenance of the tissues and organs of the body are provided for, and the blood beco mes dark and impure.
Venous blood passes from the capillaries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by neighb o urin g veins until they finally, as two large reach th e right auricle of the heart. The veins, especially in the limb . , are provided with valves at fr eq uent interval, whi ch prevent the backward fl.JW of the blood.
Th e pulmonary s ys tem of blood vessels is concerned in carrying th e blood throu gh the lungs. From the right auricle the blood pas es to the right ventricle, and is thence carried to the lungs, where it is purifi ed by contact with air, and becomes scarlet in colour; it is th en co nvey ed t o the left auricle of the heart and p1.SSe3 into the left ventr,icle, thus completing the -c irculat ion.
The heart contract in adults at an average rate of seventy-two times a minute, but the rate varies, increasing as the position is changed from the lying to the sitting or to the standing position; hence the importance of adjusting the patient's position in cases of hremorrhage. At every contraction of the left ventricle blood is forced into the arteries, causing the pulse , which may be felt wherever the finger can 1ge
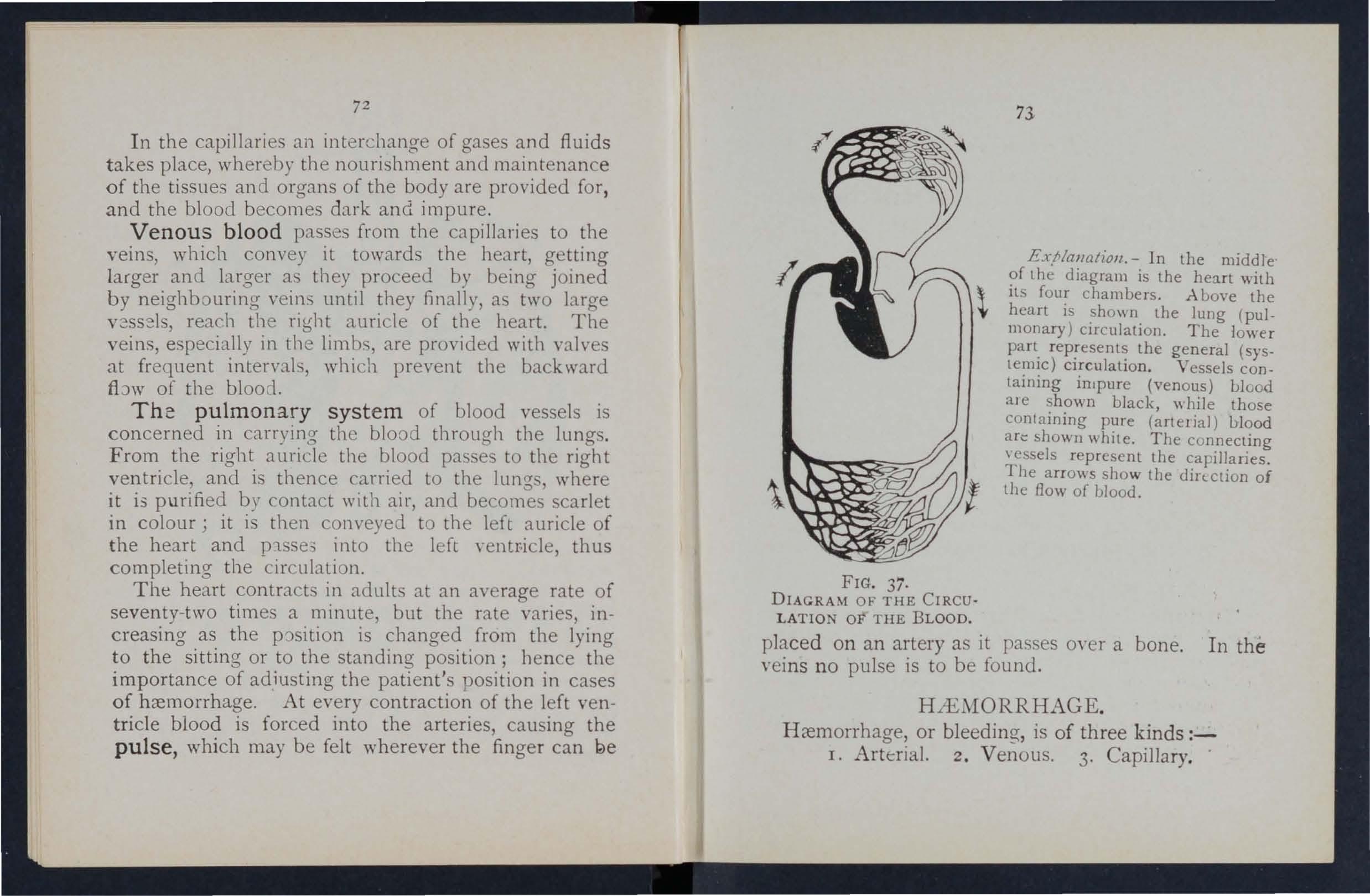
EX,NanGtioll, - In the middle of the diagram is the heart with \ its four chambe rs. .A bove the heart is shown the lung (pulmonary) circulation. The lower part represents the general (systemic) circulation. Vessels containing inJpure (venous) blood ale shown black, \\ hile those contain ing pure (a rteri a l ) blood an:: shown white. The connec ting essels represent the capillaries. The arrows sho w the dirtction of the flow of blood.
placed on an artery as it passes moer a bone. In the veins no pulse is to be found.
HiEMORRHAGE.
Hremorrhage, or bleeding, is of three kinds :I. Arterial. z. Venous. 3. Capillary. .
FIG. 37. DIAGRAM OF THE CIRCULATIO OF THE BLOOD.A RTE RIA L H fE MOR RlI AGE
I. - Blood from an artery is scarlet.
2. - lf the wounded artery is near the skin the blood spurts out in jets corres p ondin g to t h e pulsation of th e h ear t.
3. - The pressure point (see belo w) is on the heart side of the wound.
A RREST OF A R TERIAL H .tE:\lORRHAGK.
Arteri a l h ce morr hage is , whe n p rac ticable, to be arrested by pr essure , positio n of th e b ody, and eleyation of th e bleeding pa r t.
Pressure may be: -
I. - Digital-that is, app lied with the thum b or fin ge rs, a nd m ay be (a) on the wo un d ; ( b) a t a spot call ed the p ressure poi n t. T he press ur e po in ts are in dicated by nu m bered d ots o n the fr ontispiece . -
2. - Bya pad and bandage (tourniquet) (a) on the wo un d; (b) on t he point.
3. - By flexion.
To apply a pad and bandage to the wound, place a pie ce of lint o r line n or a cl ean h a n d k e rchief folded into a hard pad , o n th e bl ee d ing p o int, and secure it by a ba nd age t ightl y ti ed round th e injured part. To fold th e h an d k erchi e f, brin g the four corners to th e ce ntre, a nd rep eat th e pr oc es s until a hard pad is formed. Th e smooth surfac e is
75
placed on th e \\ ou nd, and, to prevent the pad from unfolding, the puckered surface may be stit(' h ed or fixed by a safety pin. A hard substance, s ll ch as a stone, may be enclosed in the centre of the pad.
A Tourniquet may consist of a pad to be placed on the pressure point, a straj, cord, or bandage to encircle the lim b and pad, and a tZ;f!lttmz'lll( a rrallgtmod, such as a stick or other means of twisting the band to tighten it.
To improvise and apply a tourniquet :-
1.-- Apply a firm pad on the pressure point.
2.-Encircle the 1imb by a nano\\ bandage \\ith its centre oyer the pad.
3.-Tie the end;;) of the bandage in a half knot on the oppo. ite sIde to the pad.
4.- La) the t\\ isting stick on the half knot, and 0\ er it tie a reef knot.
5.-· Twi t the stlC k to tighten the bandage, thereby prcs:;lllg the pad Uf on the artery, and am.:sting the flo\\" of blood.
6.-Lock the stIck in pOSItion by the ends of the bandage already applied, or by another bandage passed rcund the stick an-d limb.
The pad of the tourl1lquet must be accurately placed upon the pressure point so as completel) to compress the :nten·; othen\ ise arterial blood \\ill be allowed to pass alo-ng the limb, and the veins, being compressed by the tourniquet, \\ ill not allow the
74
'blood to return through them to the heart and the res ult will be d angervus swelling and conge 'tion.
Should a s u itable p ad n ot be at ha n d a knot may be .made in the cen tre of the a n d when avaIlable, a stone, cork, etc., enclosed in it to give it firmness and bulk. ee that the bula-in a and not the fLlt side of the knot is next the skin. b (:)
. An . bandage passed tightly round the lImb, ImmedIately above the seat of arterial hremorrhage, will .arrest The si m plest prepared form of thIS bandage IS a strip of elastic webbina twenty-five to thirty inche.s lona- and two inche with a piece of tap e sell n at beach end . An belt or brace the same purpose. Except ,....hen p:trt of a 11mb IS torn off it is not adyisable to use an cord or bandage 'if other apparatus can be had, as It cuts off all circulation in the limb.
Flexion of the application of a pad on the POl11t at the knee or elbow joint, flexing the lImb to make pressure, and securin a the limb in the flexed position by a bandage like the figure 8.
RULES FOR OF A
AcCmfPANIED BY ARTERIAL HiEl\IORRHAGE.
1. Stop bleeding.
II. Prevent injur ious germs from getting into the wound.
To attain these ends :--
I. Place the patient in a suitable position, bearing in mi n d that the blood escapes with less force when the patient sits, and is still more hecked \"hen he lies down.
2. Elevate the bleeding part, as thereby less blood tinds its \\ ay into it.
3. Expose the wound , removing whatever clothing is neces ary. C'ee Rule 8, a.)
4. Apply digi t al pressure . (a) If the wound IS mall on the bleeding spot. (b) If the wound is large on the pressure point next to the wound on the heart side. The nearest pl essure point is cllosen in order to ayoid utting off the circulation from as much of the part as pos. ible, but sometimes it is necessary to apply pre sure still nearer to the heart.
5. Remove foreign bodies, such as broken bits of clothing', hair, etc., een in the \\ ound; not search for foreign bodies) Oll cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boracic gauze or lint is to be preferred, but absorbent cotton wool, lint, or gauze, or a clean piece of linen will answer the purpose . hould any doubt be enter· tained as to the cleanliness of the dressing, a clean piece of unprinted paper, such as the inside of an
76
77
78 envelope, should be placed next the wound before applyi n g the pad. (Compare pages 75 and 76 .)
7. Bandage tightly over the pad unless :-
(a ) Foreign boLlies are suspected to be left '1t1see n in the wound.
(b) There is danger of causing injury to a fracture . In these cases a light dressing only should be -applied.
8. Apply a pad and banda£:e or flexion on the pressure point (see Rule 4, b ), but only in the following cases :-
(a ) As a temporary measure while the wound is being exposed, examined and covered.
(b) As a more permanent measure when bleeding cannot be stopped by the pad and bandage on the wound, or \\hen, in accordance with Rule 7, the tight bandage has not been applied.
9. Afford support to the injured part .
"Vhen part of a limb has been torn off or the \\ ound is lacerated (for example by the claw of an animal or by machinery) frequently does not come on at once, but as there is a danger of, severe h c:emorrhage later, means for its arrest should be applied. to the limb, but not tightened unless necessary. Do n ot disturb a clot of blood formed over a \\ ound . No attempt should be made to cleanse a wound except with sterilised water (that is previously boiled
79
and allowed to cool), and experience, especIally' in recent wars, has sho\\n that those wounds \\hich \\ere provisionall y treated \\ith a dry dressing a nd subdressed by a surgeon with proper app liances did best.
'tudents practising arrest of arterial should feel the pulse to see \\ hen the currpnt of blood 111 the artery has been stopped, and should then immediately relax the pressure made on the artery. In this way the importance of the accurate application of pressure will be real1 cd, and the amount of force necessary \\ill be ascertained .
THE COURSE OF 'I :MAl"\" ARTI'" RIES, AJ\D ARRF T or HlE':-'IORRHAGE.
( The numbers of the ure points refer to an ·the Frontispiece.)
THE LARGE
The .Aorta is the central or trunk a t tery of the body. Commencing at tbe left ventricle it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branches which rarry the blood to either side of the head and neck and to the upper lImbs. The Aurt:l. passes down on the Jeft of the spine to just below the na \-el, where it divides Into two great branches (t h e ilia.:::s)
\RTERJES "YlTHI"\" THE CUE T AJ\ D AlWO':-'IL'\.which convey the blood to the organs in the pelvis and to the lower limbs.
' Vounds of these arteries are one cause of internal hceJ1lorrhage (see page 96).
ARTERIES OF THE HEAD AND NECK.
The Carotid Arteries (right a n d left) the upper part of the chest and pass up on either side of the windpipe a n d, just below the le,·el of the angle of the lo\\"er jaw, divide into the Internal and External Carotid Arteries. The Internal Carotid Artery ascends deeply in the neck, and enters the cranium to supply the brain \\ iLh blood. The External Carotid Artery gives off a number of branches; to the front the artery of the tongue (Lingual), the artery to the bce (Facial); to the back the Occipital; the artery itself IS continued upwards in front of the ear, where it changes its name to the Temporal and supplies the scalp in the neighbourhood of the temples.
When a Carotid Artery is wounded , as in the case of a cut throat, apply the thumb of one hand o n the arte ry at pressure point I, pressing backwards agai nst the backbone and taking care to avoid the ·nndpipe. I t may also be necessary to apply pressure with the other thumb aboye the \\ ound for two re:l.sons: (a) To arrest the flo\\' of blood from the m ail'l (jugular) vei n in the n eck , which runs
8r
alongside of the carotid artery and is usua 11)' \\ ounded at th e same time; (0) To check the flow of blood the upper end of the carotid artery Itself, \\ hich IS ofte n considerable 0\\ ing to communication betwee n the branches of this artery and those of its
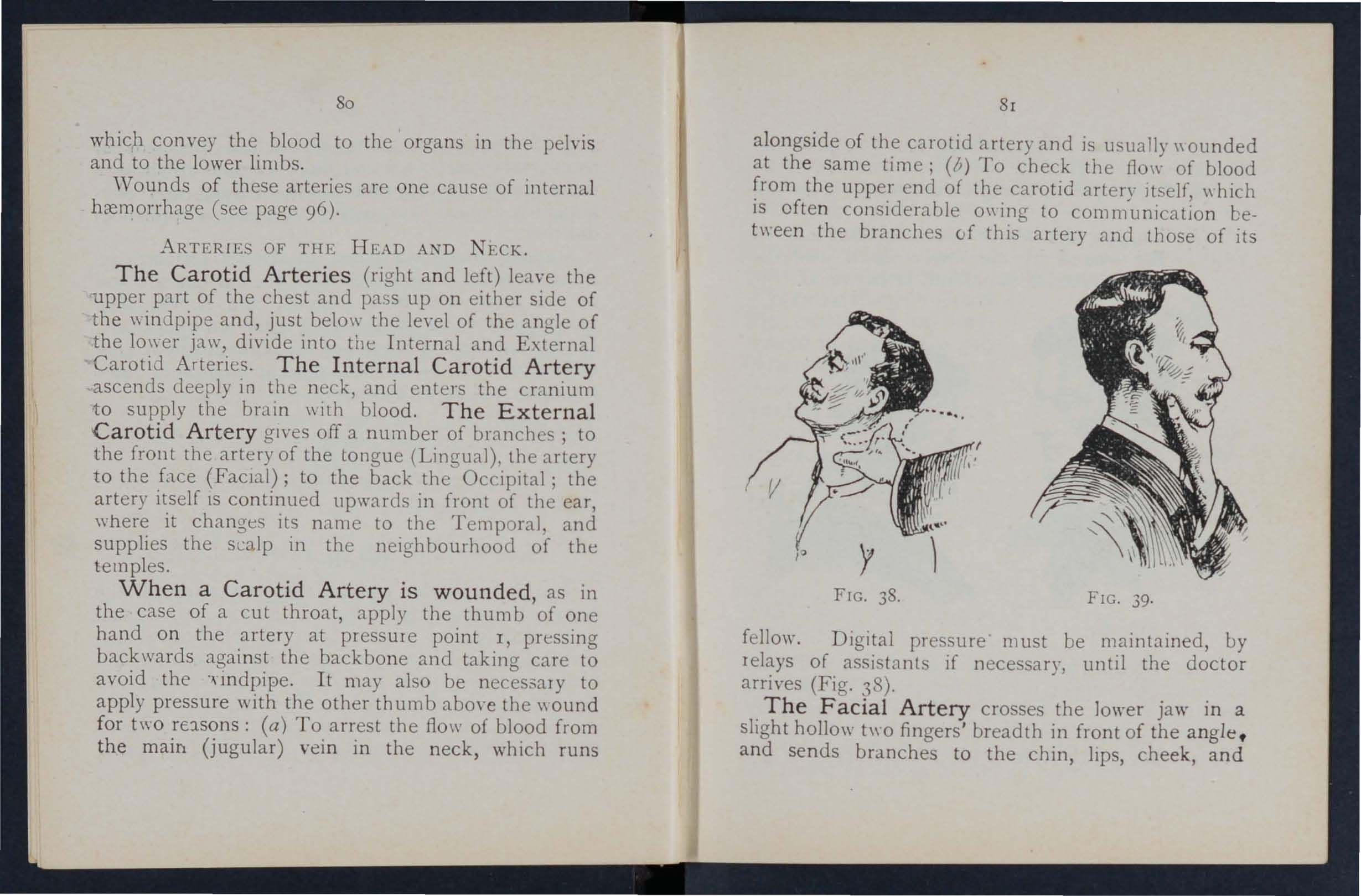
fellow. Digital pressure must be maintained, by relays of assistants if necessary, until the doctor arrives (Fig. 38).
The Facial Artery crosses the lower jaw in a slight hollo\\' t\\ 0 fingers' breadth in front of the angle . a n d sends branches to the chin, lIps, cheek, and
80
FIG. 38.
FIG. 39.
outside of the nose . Hc.emorrhage from wounds of the face below the level of the eye is to be arrested by:(a) Digita l pressur e on pressure point 2 (Fig . 39), (b ) or Gr aspi n g the lips or cheek on both sides of the wound by the finger inside -and the thum b outside the mouth or 'It/re versa.
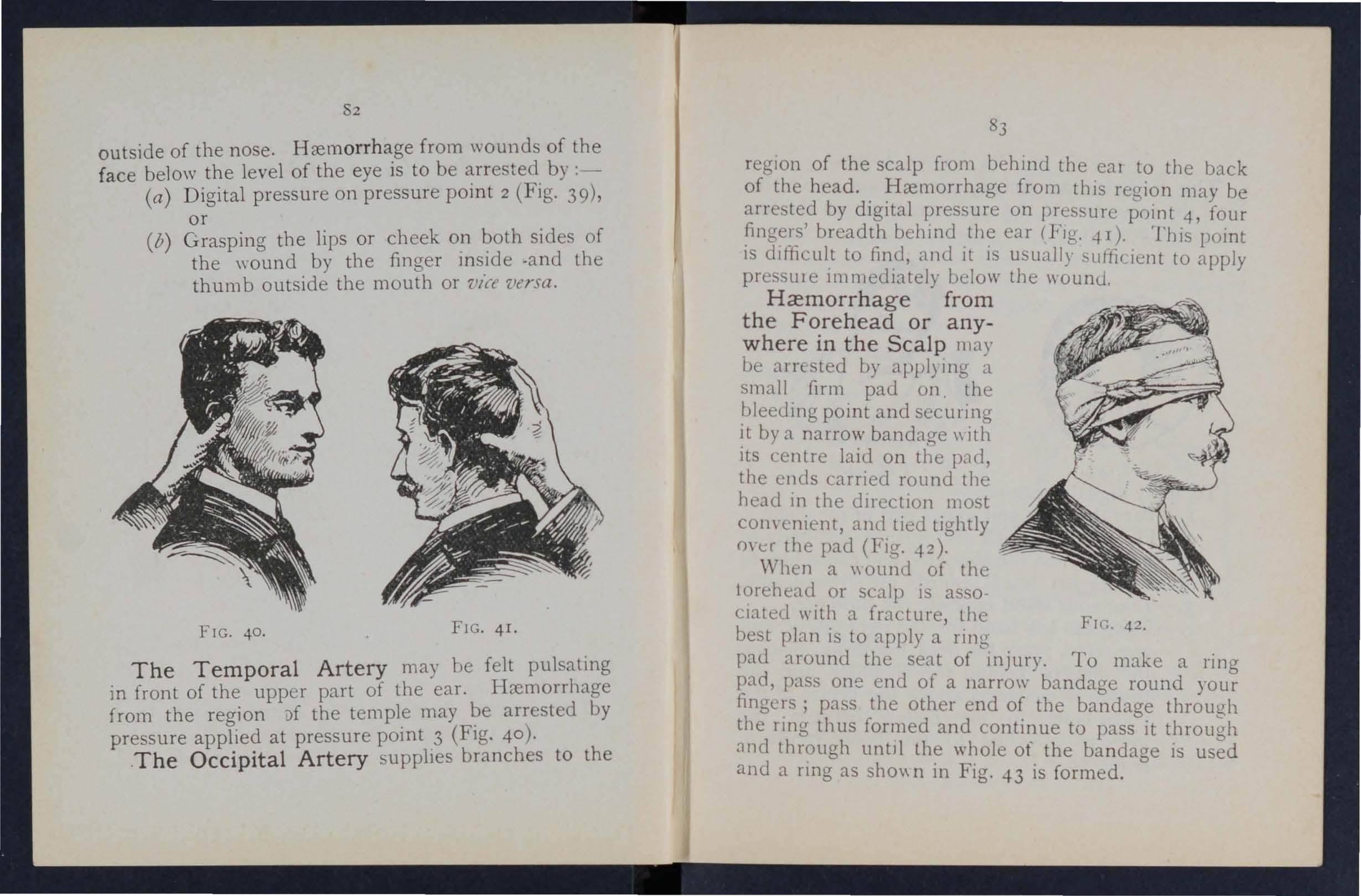
The Temporal Artery may be felt pulsating in front of the upper part of the ear. H::cmorrhage from the region i)f the temple may be arrested by pressure applied at pressure point 3 (Fig. 4 0 ).
.The Occipital Artery supplies branches to the regIon of the scalp from behind the eal to the back the head .. from this region may be by dIgItal on pressure point 4, four breadth behind .the ear (FIg ...p). This point IS dlfiicult to find, and It IS usually suftiljent to apply pre sure 1m mediately below the wound.
Hcemorrhage from the Forehead or any:vhere in the Scalp may arr sted by appl) Il1g a small firm pad on. the ?leeding point and securing by a narrow bandage \\ Ith ItS centre laid on the PJd, the ends carried round the head In the direction most convenient, and tied tightly 0\ t..:r the pad (Fig...p).
When a \\ ound of the 10rehead or scalp IS associated with a fracture, the best plan is to apply a ring pad around the sea.t of rnjury. To make a ring pad, pass one end ot a Ilarrow bandage round your fingers; pass the other end of the bandage through the rll1g thus formed and continue to pass it throu;;'h and thr?ugh unt)l the whole of the bandaae IS and a ring as sho\\ n in Fig. 4-3 is formed. 0
82
FIG. 40. FIG . 4I.
FIC. 42.
ARTERIES OF THE UPPh.R LlrIIBS.
The Subclavian Artery passes from a point behi n d the inner end of the collar-bone across the first rib to the armpit.
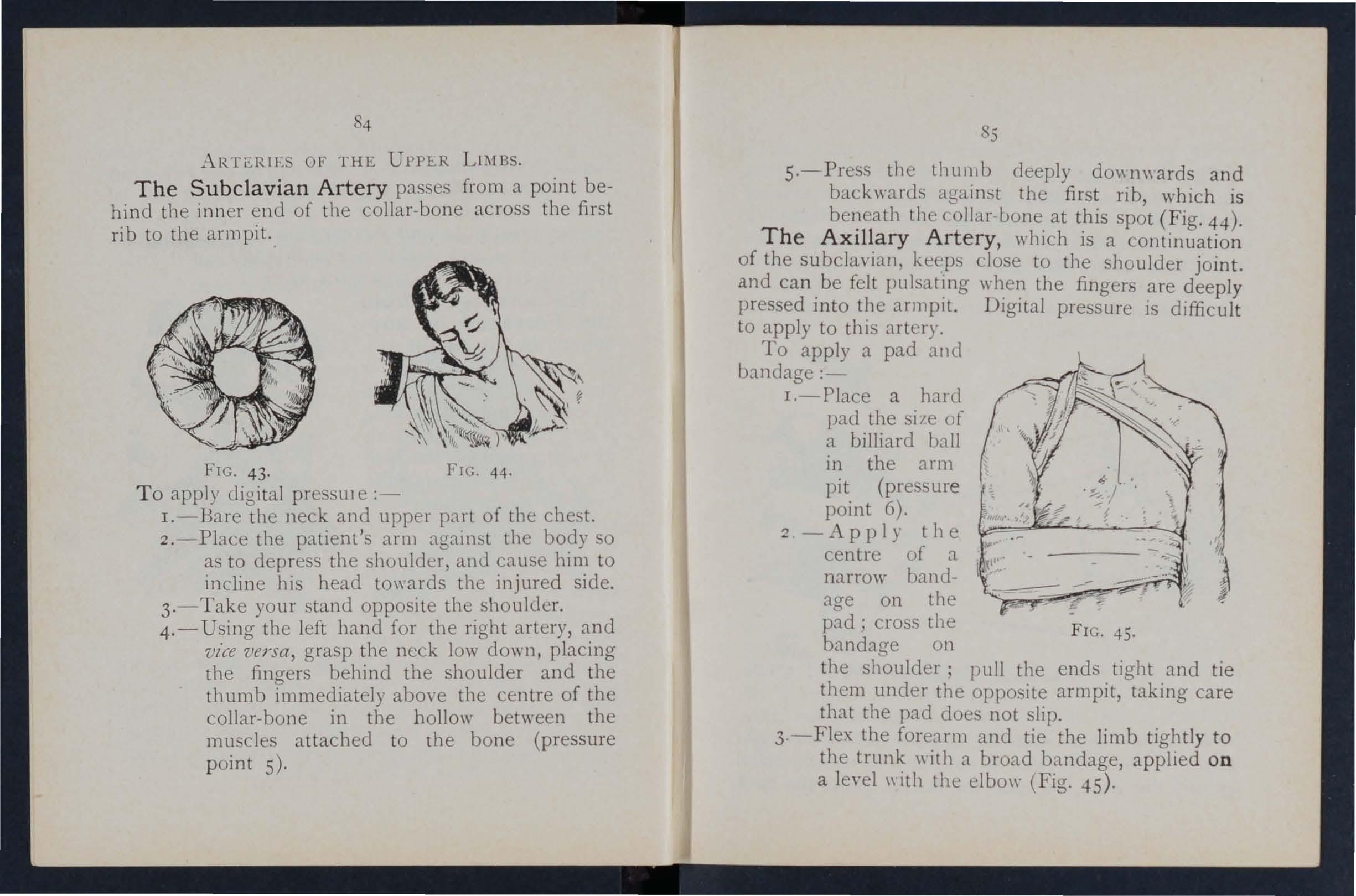
FIG. 43. FIG. 44·
T o apply digital pres Ule :-
I.-Bare the neck and upper part of the che t.
2.-Place the patient's arm against the body so as to depress the shoulder, ami cause him to incline his head towards the injured side .
3.-Take your stand opposile tIle shoulder.
4.- Using the left hand for the right artery, and vice versa, grasp the neck low down, placing the fingers behind the shoulder and the thumb immediately above the centre of the collar-bone in the hollow between the mu cles attached to the bo ne (pressure p oint 5).
85
s·-Press the lhul1lb deeply dO\\TI\\a rds and backwards agall1st the first rib, which is the collar-bone. at this spot (Fig. 44).
The AxIllary Artery, whIch is a continuation of the subclavian, keeps close to tIle shoulder joint. and can. be felt pulsat!ng the fingers are deeply pressed mto the armpit. Digital pressure IS difficult to apply to this artery.
To apply a pad and bandage:-
I.- Place a harcl pad the size of a billiard ball m the arm pit (pressure point 6).
.., -Apply the centre of a narrow bandag-e on the ; cross the bandage on
FIG. 45. the shoulder; pull the ends tight and tie them under the opposite armpit, taking care that the pad does not slip.
3·-F1ex the forearm and tie the limb tightly to the \\ ith a broad bandage, applied on a level \\ Ith the elbo\\" (Fig. 45).
4
The Brachial Ar t ery is a continu,ation (,>t the Axillary, and runs down the arm ?n the mner of the biceps muscle, gradually passmg forward until It reaches the middle of the front of the elbow, The inner seam of the coat above elbow roughly indicates its course.
Digital or pressure may be applied at or near pomt 7·
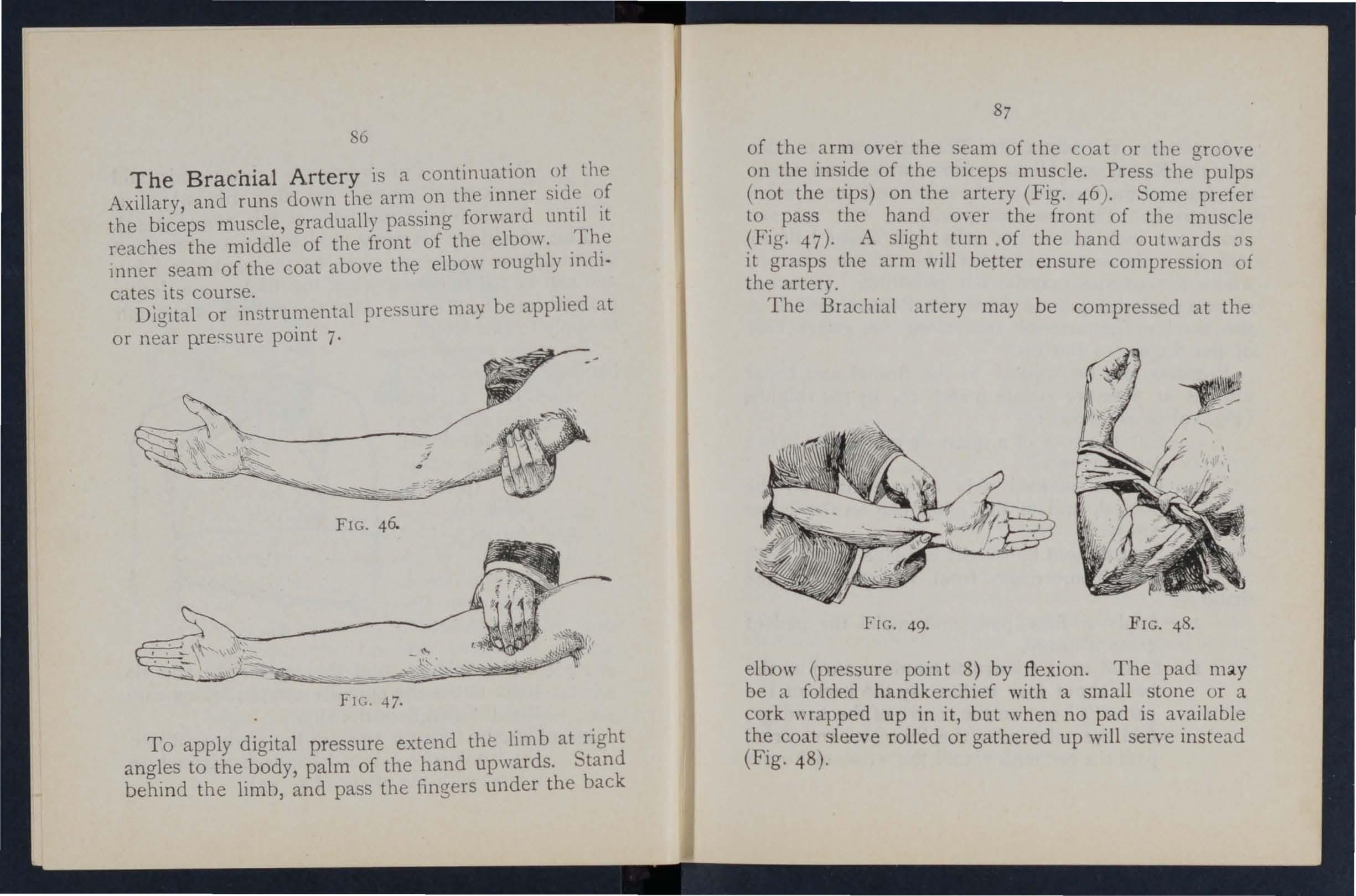
FIG, 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back
87
of the arm over the seam of the coat or the groo\'e on the inside of the biceps muscle. Press the pulps (not the tips) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47). A slight turn of the hand oUl\\ards os it grasps the arm will better ensure compression of the artery.
The Bra hlal artery may be compressed at the
elbow (pressure point 8) by fl exion. The pad be a folded handkerchief with a small stone or a cork wrapped up in it, but when no pad is ayailable the coat leeve ro ll ed or gathered up will serve instead (Fig. 48).
6
FIG. 49.
FIG 48.
88
Just below the elbo',," the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 and 10) are about one inch above wrist and about half an inch from the outer and inner sides of the forearm, where the arteries may be felt pul ating. Branches of thes = arteries join to form the Paim3.r Arches in the hand. The arteries run along on either side of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure I)Jints 9 and 10, by the thumbs (Fig. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one half on the Radi al , and of the other half on the Ulnar artery.
3·-Secure them by a tight bandage.
To arrest hremorrhage from the palm of the hand :-
I.-Appl y a firm pad, and make the patierlt grasp it firmly.
2.-Spread out a triangular bandage, turn up the base about four inches, lay the back of the patient's hand on the centre of the bandage, fold the point over the knuckles and wrist, pass the two ends round the \\ rist, make the
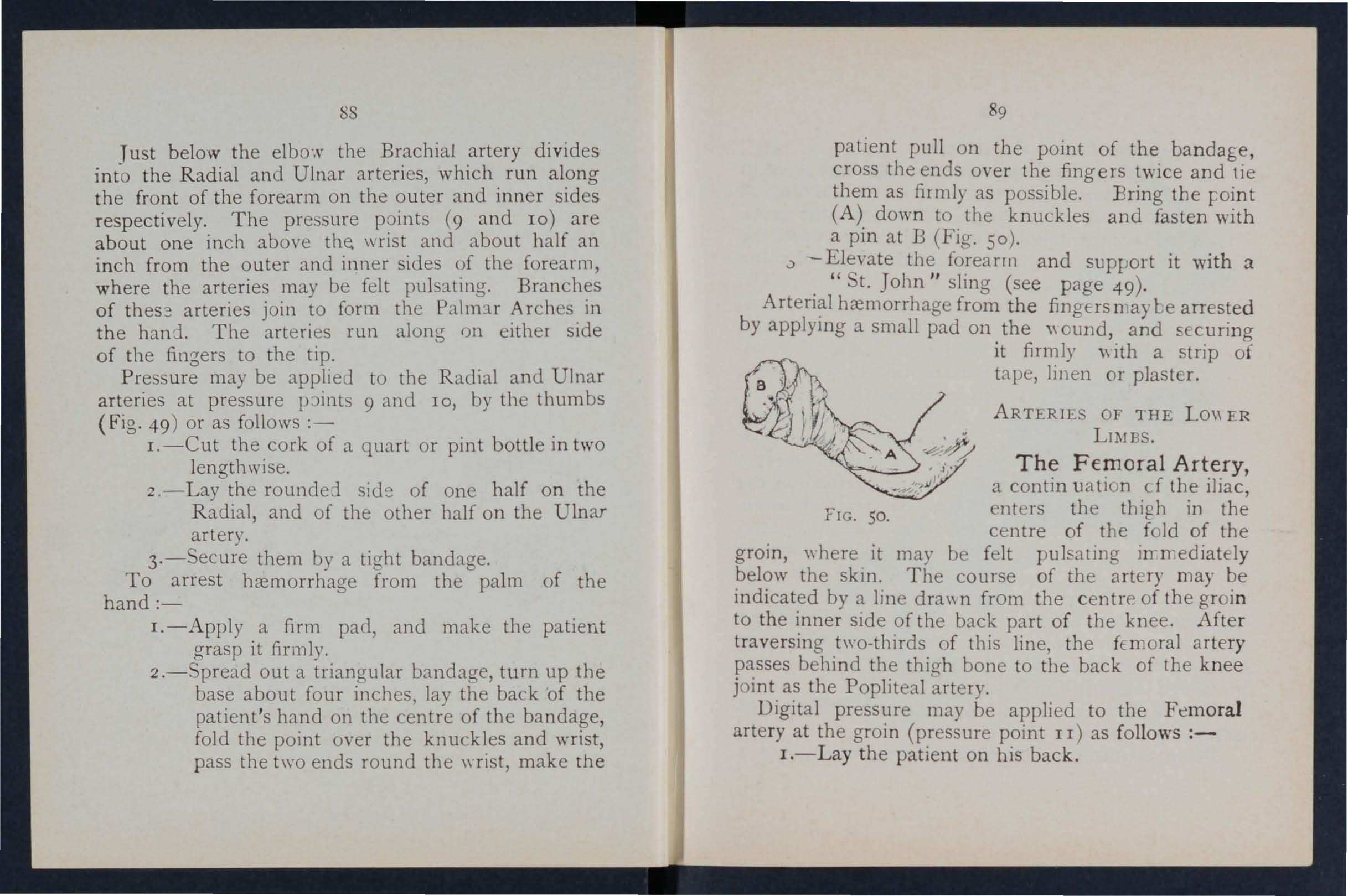
89
patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the r oint (A) down to the knuckles and fasten with a pin at B (Fig. So).
,) - Elevate the forearm and support it with a . " t. John" sling (see page 49). hremorrhage from the fingers n ,ay be arrested by applymg a small pad on. the \\ ound, and securing It firmly \\ ith a strip of tape, linen or plaster.
AR TERIES OF THE Lo" ER LU,lBS.
The Femoral Artery, a contin uation cf the iliac, FIC. 50. enters the thigh in the centre of the fold of the groin, "here it may be felt pulsating in mediat ly below the skin. The course of the artery may be indicated by a line dra\\ n from the c entre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the fEmoral artery passes behind the thio-h bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the artery at the groin (pressure point II) as follows :-
I.-Lay the patient on his back.
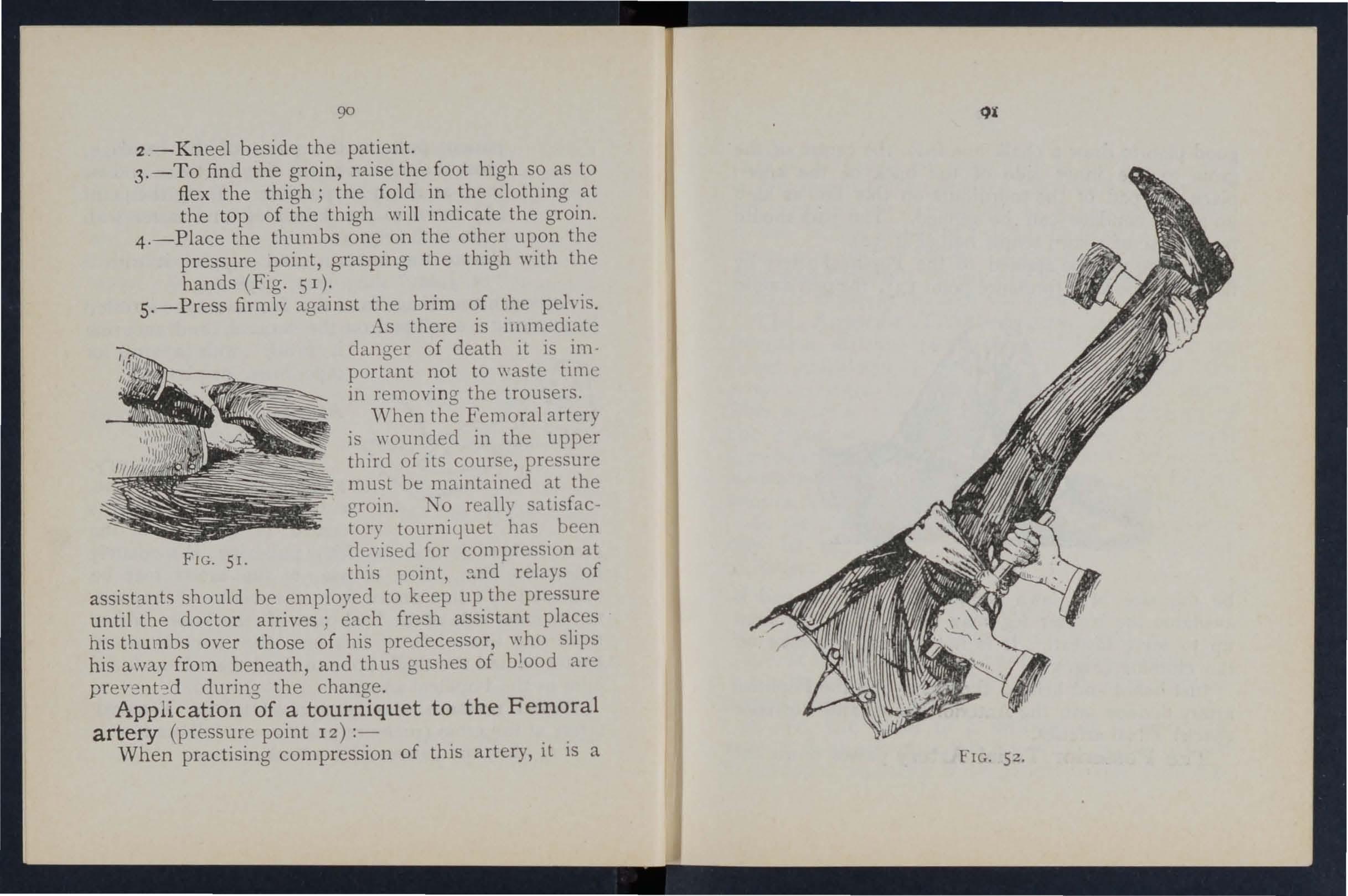
2.-Kneel beside the patient.
3.-To find the groin, raise the foot high so as to flex the thigh; the fold in the cloth ing at the top of the thigh will indicate the groin.
4.-Place the thumbs one on the other upon the pressure point, grasping the thigh with the hands (Fig. 5 I).
5.-Press firmly against the brim of the pelvis.
As there is IIllmediate danger of death it is important not to \\aste tlme in removing the trousers.
'Vhen the Femoral artery is \\"Ounded in the upper third of its course, pressure must be maintained at the groin. TO reall) satIsfactory tourniquet has been FIG. 51. d evised for compression at this point, :!.nd relays of assistants should be employed to keep up the pressure until the doctor arrives; each fresh assistant places his thumbs over those of his predecessor, who slips his away from beneath, and thus gushes of blood arc prevent od during the change.
Application of a tourniquet to the Femoral artery (pressure point 12) :-
When practising compression of this artery, it is a
90
good plan to dra w a chalk line from the centr e of th e gr oin to the in ner side of the back of t he kn ee ; place the pad of the tourniquet on this lin e a s h igh up as the ba ndage can be applied . Th e pad shoul d b e the size of a law n ten n is ball (Fig. 52) . P ressure may be applied to the P opliteal artery by flexion at the knee (pressure point 13) ; the pad should
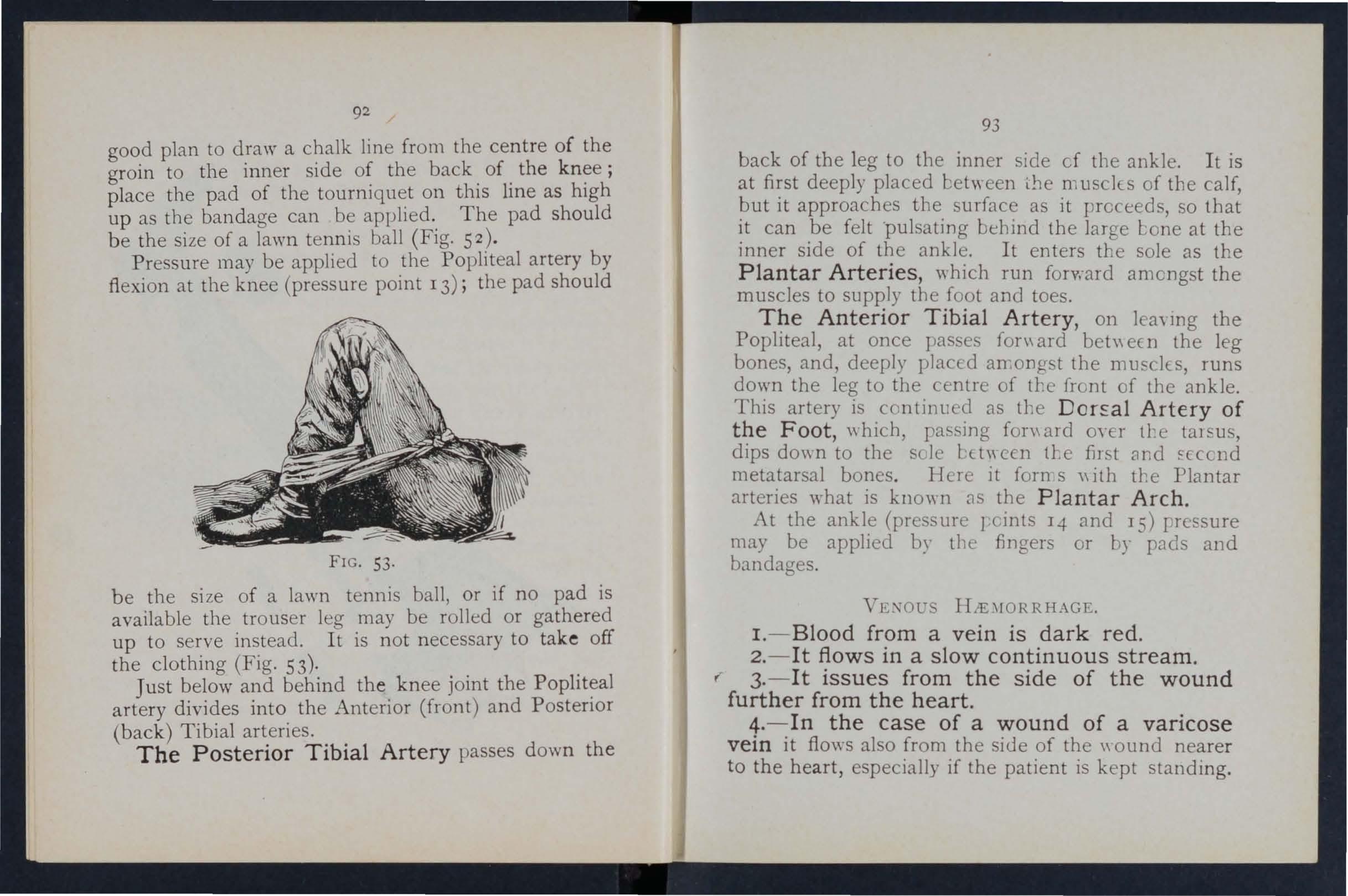
FIG. 53.
be the size of a lawn tennis ball, or if no pad is avai lable the trouser leg may be rolled or gathered u p t o serve instead. I t is no t n ecessary to ta ke off t he clothing (Fig. 53) ·
Ju st below and beh in d the k nee joint the P opliteal arter y divides int o th e Anterior (front) and Posterior ( b ack ) T ibial arteries.
The Posterior Tibial Artery passes dow n th e
93
back of the leg to the inner side cf the ankle. It is at first deeply placed bet\\ een the musclEs of the calf but it approaches tbe surface as it proceeds so it can be felt 'pulsating bebind the large at the inner side of tbe ankle. It enters tbe sole as the Plantar Arteries, which run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery on lea\ mg the Popliteal, at once pas es fon\ ard ' bet\\ ec n the leg bones, and, deeply plac ·d an,ongst the mmclcs, runs down the leg to the centre of front of the ankle
This artery is .con as tbe Artery of the Foot, whIch, passmg fon\ ard oyer tbe tal SllS, dips do\\ n to the sclc h. t \\ een fil t clnd fcccnd metatarsal bones. Here it forn s \\ ith the Plantar arteries what is known as the Plantar Arch .
At the (pressure 1 cints 14 and IS) rressure may be applJed by tIl e fingers or by pads and bandages.
VE\"OU I-I,>E\IORRHAGE.
I .- Blood from a vein is dark red .
2.-It flows in a slow continuous stream . r 3. - It issues from the side of the wound further from the heart.
4. - In the case of a wound of a varicose vein it flows also from the side of the \\ ound nearer to the he a rt, especially if the patient is kept standing.
92
Varicose Veins. - The veins of leg a.re specially apt to '" . A veIn is dibteJ, winding, and with bead-like (vancose). projections along its course. A vein becomes from several causes, such as long standing or tight garters. The first effect is. to thro.w e.-dra \\ ork upon the valves, and the bead-like projectIOns are .caused by the accumulatmg in the beh1l1d the valves. In time the vein becomes so dIlated that the valves can no longer span it.
RlTLES FOR TREATl\1E T OF A 'WOUND AccmfP.-\NIED BY HiE\lORRHAGE.
I. - Place the patient in a suitable in mind that the blood escapes WJth the patient sits and is still more checked as he lies down.
2. - Elevate the part, as thereby less blood finds its "'J.y into it.
3.-Expose the wounc1" removing \\ hatever clothinJ; is necessary. .
4. - Remove any constrictIOns, such as collar or garters, from the he ::trl side of the \\ ound ..
5. - Apply digital pressure on the ,-.Jund until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure near the wound on the side away from the heart . In the case of . a wound of a varicose vein it may also be necessary lO
apply a pad and bandage to the vein immediately above the wound, especwlly If the limb cannot be maintained in an elevated position.
6. - Treat the wound as directed by Rules 5,6 and 7, stated on pages 77 and 78.
7·- Afford support to the injured part.
CAPILLARY
HJEMORRHAGE.
1. - The blood is red.
2· . - It flows briskly in a continuous stream, or may merely ooze from the wound.
3·- It wells up from all parts of the wound.
. \. slight amount of pressure \\Ill suffice to arrest capillary bremorrhage.
L TER AL HiE:i\lORRHAGE.
'Vounds of the blood vessels \\ itbin the trunk cause bremorrhage into tbe cavity of tbe chest or of the abdomen.
SIG . s :\:-;D Y.\IPT0:\rs OF INTERNAL HiEMORRHAGE.
I.-Rapid loss of strenf!tb, giddiness and faintness, especJally wben the upright position is assumed.
2.-Pallor of the face and lips .
3·-Breathing hurned and laboured, and accompanied by yU\\ ning and sighina.
4·-T he pulse fails, and may altogetber disappear at the wrist.
94
95
5 -The p3.ti=nt throws his arms tugs at the clvt':1ing round the neck, and calls for all'. _
6.-Finally the patient may become totally uncon sci ous.
I.-Keep the p:ttient in.a recumbent posi:ion.
2 -Undo all tight clothing the r:- eck . .... -Provide for free circulation of fan the .) . p:ttient. 1 ld ll'ng
4 -Sprinkle cold water on the face; sme I t to the nostnls; avoid other forms of stlmulants, a all events until the h:emorrhage has been -Give ice to suck or coU water to drmk 1 1 t e of the h:emorrh:tge is known, apply an Ice bag over the region. f
6 -Should the patient be reduced to. a state 0 coll;pse, raise the feet and bandage the 11m bs firmly fro :n the toes to the hips and from the fingers to the shoulders.
FROM THE NOSE
I.-Place the patient in a 111 a t f·' before an open wJndow, \\"1th the head churren 0 1, Clhltrly back and the hands raised above the t rown S 19
Undo all clothing around the neck and cold (ice, a cold sponge or bunch of ')7
keys) over the no e and also the spine at the level of the collar; place the feet in hot" ater.
4·-Cause the patient to keep the mouth open, and so avoid breathing through the no e.
Blood issuing from the mouth may come hom the tongue, the gums the- socket of a tooth after extraction, the throat, the lungs, or the stomach .
H:E\[ORRHAGE FRo:-.r THE To GUE, THE GUMS, THE ,-'OCKET OF ..\ TOOTH, OR THE THROAT.
r.-Gl\·e ice to suck or cold \\ ater to hold in the mouth. If thIS IS not successful gIve \\ ater as hot as can be borne to hold in the mouth.
2.-If necessary make pressure on the carotid arterJes.
3·-If bleeding from the front part of the tongue is exee sive com pre s the part by a piece of clean lint held between the finger and thumb.
4·-If the bleedmg is from the socket of a tooth, plug the socket \nth a pIece of clean lint or cotton \\'001; over this place a small cork or other su bstance of suitable size, and in truct the patient to bite on it.
H.'E\IORRHAGE FR0:\[ THE LUXG .
Blood from the lungs lS coughed up and is scarlet and frothy 1I1 appearance.
Treat as for Internal Hcemorrh::tge (see page 95). E
96
H.t\lORRHAGE FRO:'lI THE TOMACH.
Blood from the stomach is vomited; It 1 of a c olou r a n d has the appearance of coffee grounds; It may be mix ed with food. . T reat as for Int e rnal Hcen.10 rrha ge \ -ee page 9)), exc ept that nothmg is to be gn'en by th e mouth.
Blood issuing from the Ear Channel, \\ hich enerally indicates a fractur e of. the base of the must be wip ed away a 1t 1 sues; no attempt is to be made to pI ug th e ear.
QUE ON CHAPTER III.
Th,: 1I1t llltraiS i ll dirate the pages 'wiler': the answers lIIay be foul/d.
\Yh at organs a r e concerned in the circulation of the blood?
\\ hat way ... honld arterial hxmorrhage be controlleu?
at i meant by" pres...ure point ,.?
may pressure be applied?
"hat IS a tourniquet?
\Yhy IS accuracy neCe sary in placing the pad of a tourniquet? 75
\Yh e n mayan elastic bandage be used intead of a tourniquet? 76 'Yh at i flexion? .. 76
Stale the general rules for treatment of a wound accom. panied U)' arterial hXl110rrhage ... 77, 78
If part of a limb had ueen torn off, but there \\as nct much uleeding, ho\\ wuuld you act? 78 :hould uloou clot be disturbed ?.. il:)
I it \\ i e fur an un killed pel ·on to attempt to cleanse a wound? . .. ... 78, 79 What is the ao r ta? '"
79
99
PAGE
70 the heart '" 70 Tm ce the circulation o f the blood through the body and lungs 70 to 7 2 H o\\ many time'
contract on the aye rage ? 7 2 \Yh at is the effect of
ient' po ition on the rale at \\ hich the heart contracts? 72 \Yh at t h e pul e? ... 7 2 How
73 H
? ... 74 In
74 \Yh
74 Ho\\
74
a minute doe the heart
the pat
many kind of are the re? ..
ow would you know a case of arterial hremorrhage
75
roo
De scribe the arteries of the head and neck
What i a ring pad, and what i it use?
80
\Vhy is it sometimes necessary LO com pre s the carotid artery both below anfl abo\'e the wound? 0, 8r 84 84 to 89
Describe the arteries o f the upper limbs
Describe the arteries of the lower limhs
How would you know a case of yenou hzemorrhage?.
\Yhat is a varicose vein?
How maya yein become ntricose ? 9 to 93 93 94 94
State the general rule for treatment of a wouml accompanied by , -enOl! hzem'lrrhage . 94, 95
How would you k now a ca. e of capillary hzemorrhage ? 95
How would you stop capillary hzemorrhage ? 95
\Vhat i i nternal hzemorrhage? .. 95
\Vhat would lead you to uspect internal 95, 96
State the treatment for internal hzemorrhage? ... 96
How would you arrest from the nose? ... 9 6 , 97
\ Vhere may blood issuing from the mouth come from? 97
How would you treat bleeding from the gums or throat? 97
\V hat else would you d) if the tongue ,,'ere bleeding? . 97
And if the bleeding were from the socket of the tooth? 97
H ow would you distinguish between bleeding from the lungs and from the stomach?.
And what would be the difference in the treatment? ...
Of what is bleeding from the ear channel generally a sign?
'l:'h e Student should practi e placing supposed patient'; in a proper position for the arrest of hzemorrhage (see pages 72, 77 and 94), folding firm pad (74 and 75 ), tying hard knot in bandages to form a uurniquet (7 6 ), and the application of pressure at all the pressure points shown in the frontispiece, at vanous points on the forehead and scalp, and on the palm of the hand, Pres ure should be digital, by pad and bandage, or Bell.ion, as directed in the text
101
Pressure points - Carotid artery, 80. Facial, 82. T el?1poral, 82, Occipital , 83. Subclayian, 84·
AXIllary, .5. BrachIal (by pad and bandage, pres.sure being made against the humerus and by fleXIOn at the elbow), 6. Radial and Ulnar, 87. Femoral the groin, 90.. Femoral in the thigh , 92.. Popiiteal, 92. Antenal and posterior Tiuial artene , 93.
Hremorrhage from the forehead or scalp ...
Hremorrh age from the palm of the hand.. ...
Venous hzemorrhage from a varicose or other \'ein
84 87 to 89 .. ·93, 94
PAGE
PAG II:
CHAPTER IV. BRUI ES.
A blow anywhere on the surface of the body may caus e extenslVe hGemorrhage beneath the skin, \\ ithout breakmg it-a" black eye II is an instance. The injury i accompanied by discoloration and swelling.
TREATJ\[E l T.
Apply ice or cold water dressings. A piece of lint soaked in extract of "itch hazel may be placed on the affected part.
BUR TS AKD SCALDS.
A burn is caused-
(a) By dry heat, uch as fire or a piece of hot iron.
(b) By a rail, wire or dynamo charged with a high pressur e electric current.
(c) By a corrosi ve acid, such as oil of \ itriol.
(d) By a corrosi \'e alkali, such as calIstic oda, ammonia, or quicklime.
(e) By friction, caused, for e,ample, by contact with a re \'olving wheel. (Brush burn.)
A scald is caused by moist heat, slIch as boili ng \Y ater, hot oil or tar.
TJle effect may be a mere reddening of the skin ; blisters may be formed; or even the deeper tissues
103
of the body may he charred and blackened. The cl othing may adhere to the burnt skin, and Its r emova l is impo sible without further detriment to the injured part. The great danger is hock.
I. - Carefully remove the clothing over the injured part. If stuck to the skin, the adherent clothing- mu t he cut around ",ith scissor, soaked With oIl, and left to come a\\ay subsequently.
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear pieces of lint or linen \\'ith oil, or vaseline, bnoline, or cold cream; a small quantity of boracic powd er added to the -e \\ 111 be of benefit. The in ide of a ra\\' potato scraped out and spread on 1ll1t makes a soothing- application. "When the injured surfac e is exten i,'e do not co\'er It with one large sheet of lint, but \\'ith strips about the breadth of the hand; this 1 advisable as they fit better on the part and during- . ubsequent cIre s1l1g one strip can be removed at a tllne, and a fresh dres in fT applied before the adjacent strip is taken off, The shock to the system IS thereby less than if the ",hole of the burnt surface were faid bare to the air by the removal of all the dre sinO' s at one time . 'When covered by the OIly dree; Ing em-elop the part in cotton \\001 or a pIece of flannel and apply a ba n dage.
102
\ Vhen the face is burnt, cut a mask out of lint or linen leavin a holes for the eye, I1?Se, and D ip t'his in oil or smear. it vaselllle and It t o the face and coyer It \Ylth cotton wool, Il1g o peni ngs to correspond \\"ith the hole 111 the nlas k . .
\Vhen po sible place the injured part at the temperature of the body (98 degrees) untIl Ultable d ressinas can be prepared. A de ert-spoonful of baking b soda to .a ba inful of the \\ arm water will make a soothmg lotIon.
As it is important not to lea\'e the part e\posed t o the air, it is the duty of t?e ?y ta.nders to t he dressinas while the c]othJl1g IS bemg remO\ ed.
4. - Shock. - This is partjcularly in the case of every burn or scald ot any.considelable e xtent (see page 135)' Be ,-ery apprehensIye of danger in the ca e of e,-en I igh t bu rns of the neck. .
5 - If the burn is caused by a acid bathe the part with a weak . alkalme lotio'n such as \Y3 hing soda, baki.ng so?a (Llcarbonate of magnesia, or lIme Il1 \\"arm \\ ater before applying the dressll1gs. .
6. - If the burn is caused by a alkali bathe the part with a weak lotlOn, such lemon juice or vinegm diluted wltl: all equal quantity of water. Caul/o!l.-Before USlllg water brus h off any lime that remams on the part.
7·- When a woman 's dress catches fire -
(a) Lay the \\ oman flat on the floor at once, so that the flames are uppermost; that is to say, if the front of the dress is on fire lay her on her back, and if the back of the dress is burning, place her face do\vmvards. The reason for this is that flames ascend, so that if the upright position is assumed, the flames ",ill quickly reach and burn the body, neck, and face; or if the woman lies WIth the flames undermost, they will, if unextinguished, pass over and burn the limbs, and set fire to the re t of the dress.
(b) As Soon as the ,,"oman is laid fiat, smother the flames with anything at hand, such as a rug, coat, blanket, or table cover; if made wet so much the better.
(c) A woman rendering assistance should hold a rug or blanket in front of herself when approachll1g the flames.
(
d) If a woman's dress catches fire ,,-hen nobody is by, she should lie flat, flames uppermost, smother the flames with anything handy, and call for assi tance or crawl to the bell-pull and ring; on no account should she rush into the open air.
The use of fire guards would prevent many caiamilies.
104
BI TE OF NAKE AND RABID A AND \ \, OlJNDS BY POI ONED vVEAPOKS.
Hydrophobia is caused by the bite of an animal, such as a dog, cat, fox, \\'olf, or deer from rabies. The special poisons introdu .ed Into wounds camed by yenomous and pOIsoned \\ enpons cause immediate danger to lIfe.
1. - Immediately place a constriction between the wound and the heart so as to preyent the venous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircled on the side of the wound nearest to the with the fincrer and thumb, and as soon as possIble a ligature (a piece of tape, or strip of handkerchief) should be placed tightly round the root of the finger. Compression with the finger and th um b n: ust not be relaxed until the ligature has been Additional ligatures may, with ad"antage, be applIed at intervals up the limb, . .
2. - Encourage bleedmg for a bme :-
(a) By bathing the ",!th \yarm wate r.
(b) By keeping the ll1Jured limb lo\\"; the upper limb should be allo\\'ed to hang down, and in the case of the lo\yer limb the patient should be seated \\ith the foot on the gro und.
!O7
3·- Cauterise the wound, if it is quite impossible to obtain the services of a doctor. T his is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or if these are not at hand, \\ ith a red hot wire or a fusee .
The usual solid cau tic is insufficient, as it does not reach the bottom of the wound, where the poison is.
To ensure the cau tic reaching the bottom of the wound, it should be applied on a piece of wood , such as a match cut to a point. ",Vhen the caustic ha been thoroughly applied, but not till then, the ligatures may be removed,
4·- Cover the wound, after a while, with a clean dressing.
s·- Afford support to the injured part.
6 - Treat shock if it occurs (see page 135) .
7·-In the case of a bite by a venomous snake, rub In powdered permanganate of potash and inject under the kin in the neighbourhood of the wound a solution uf permanganate of potash.
TI G OF P LANT ANI?\IAL .
These crj,'e rise to serious incOlwenience, and 111 some cases gra,'e symptoms deyelop.
TRE.-\nlE:-iT.
I .- Extract th e stin g if left in.
2.-Mop the part freely with dilute ammonia
106
108 or spirits. A paste of of soda sal yo latile is an efficient apphcatlOn. A solutlOn of washing soda or potash or the application of the b lu e bag \Yill relieve pain: , ..,
3. - Treat collapse If It occurs ( ee page 1.)5)·
FRO T BITE.
During exposure to se\'ere cold, parts of the bo?y, usually the feet, fingers, nose, or ears, lose sensatlOn a n d become fir t \\axy \\hite and after\\ards, gested and of a p,urple appearance. As lost in the part, It IS often only by tl:e remarks, , bystanders that the frost -bi tten person IS made a\\ are of his condition,
TREAT:\If.NT.
I. - Do not bring the patient into a room u n til, by friction of the ban,d by with soft snow, sensation and circula,tl0n 111 the parts are restored. Neglect of tbl . precauti o n ma) lead to death of the of the frost-f)]tlen part.
2. - When circulation is restored, keep the patient in a room at a temperature of 60 degrees,
N EEDLE E IBEDDED UNDER THE KIN,
\Vhen a needle breaks off J.fter penetrating the skin and disappears', take th,e patient to a d?ctor at once, If the wound is near a ]01l1t, keep the lllnb at rest on a splint.
F[SH-HOOK I I THE 'K I N.
D.:> not attempt to withd raw the fish-hook by the way it went in, but cut off the dressing of the hook, so that only the metal is left, and then force the point on\\'a rds through the skin until the hOJk can be pull ed out.
I.NJURIE TO JOI TT
'V ;le n a joint is injureJ by a bullet, stab, or other cau e-
I. - Wrap the part in cotton wool.
. 2. rest, support to the injured ; If the Illnb, 111 a flexed position by a sling ; If the ]o\\'e r lImb, in a straight position by a splint.
DOGY L THE EYE.
I. - Prevent t he p atient rubb ing the eye, tyll1g do\\ n a child's hands if n.=ce sar\"
2',- Pull down the lower eyel Id , \\ hen, if the lOrelgn body I seen, it can readily be removed with :1 camel's hair brush, or \\'ith co rner of a handkerchief twirled up and wetted .
3·- Wh e n the forei g n body is beneath the eyelid lift the lid fomarel, push up the lower lid beneath It and let go. The hair of the lower lid the inner surface of the upper one, and may dIslodge the body. hould the fir t attempt be un u cce 'sful, repeat it se\'eral times if neces ary . If
lIo
t he foreign body is not dislodged call the services of a d octo r as soon as possible. When, however, skilled help cannot be had, proceed as :-
(a) Seat the patient so as to face ,the lJght, stand behind him, steadying hiS head agamst your chest. ,
(
b) Place a small rod, such as a match or bodkll1, on the upper eyelid, balf-an-ihch above, the edge, pressing it bacbyards as far a y,osslble.
(c) Pull the upper eye-lashes over the rod and thereby eyert the eyelJd.
(d) the foreign .
4.-When a piece of steel is ill the eyeball drop a little olive or castor, 011 on the eyeball after pulling down the 10\\ er eyelId, 10 the lids, apply a soft pad of cotton \\001 and It by .a bandage tied sufficiently firmly to keep the e) eball -steady; take the patient to a doctor.
5. - When quick-lime is in the eye bru,sh 'away as much of it as po sible; bathe the ey:e \\Jth vinegar and \"arm \Yater, and treat as for a pIece of -steel embedded in the eyeball.
FORE I GN BODY THE EAR FA AGE.
As a rule mak e no attempt to treat a patient with a. f or eign body in the ear if the sen'ices of a doctor p ossibly be had. any attempt to remove the forelp;n body may lead to fatal consequences . If a chIld
III
cannot be induced to ke ep the fingers from the ear) tie his hands do\\'n or coyer up the ear. If an insec t IS in the ear-p:t sage, fill the ear \\' ith olive oil , when the insect will float and may be removed. Neve r syringe or probe the ear.
BODY 1.. THE NO E.
Induce sneezing by pepper or snuff. Cause the pati ent to blo\\' his nose vio!ent!y after closing the U1l'lffected nostril. Th ere is no immediate danger fro:11 a foreign body in the nose.
THE .-\BDO)IE. ,
The abdomen is bounded above by the diaphragm ; belo\\' by the pe!vis; behind by the I u m bar yertebrre; and in front and at the sides by muscular \\'alls . (Fig. 54.)
THE ORG c\)I'S C F T HE ABDO}[EN .
The Stomach lies immediately belm\' the" pit of the stomach " just belo\\' the breast-bone.
The Liver lies in the upper part of the abdomen, \\'here it is mostly cm'ered by the right lower ribs .
The Spleen lies beneath the ribs at upper part of the left side of the abdomen.
The Intestines occupy the greater part of the cavity of the abdomen.
The Kidneys lie at the back, in the r egion of t he loin.
The Bladder lies in the pelvis .
FIG. 54.
\VOUND IN THE FRONT ,,7 ALL OF THE ABDOMEN.
When tlze intestines 01 otller protrude through t h e wound, whether vertical or transYerse, bend the knees, raise the shoulders, and apply lint, a to\\el, o r
c otton wool wrapped in soft linen, a n d keep t h e
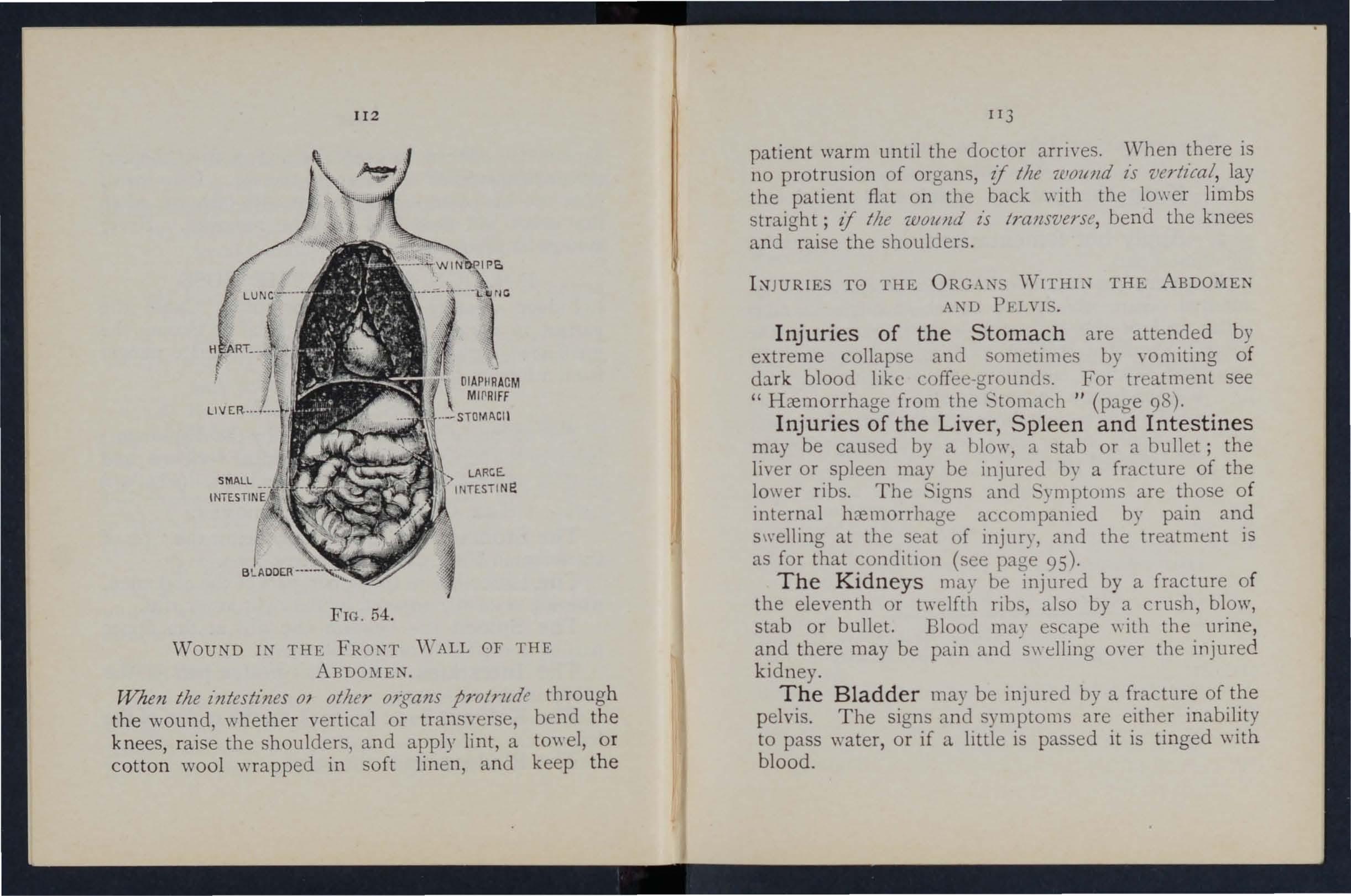
II3
patie n t warm until the doctor arrives. \Vhen there is no protrusion of organs, if tile 7.C.loltlld l'S vertical, lay the patient fiat on the back \\ ith the 10\\ er limbs straight; if the 'Woltlld £s transvers e, bend the knees and raise the shoulders .
TO THE ORG \X \ V1THL THE A'\D PELVI .
Injuries of the Stomach are attended by extreme collapse and sometimes by yomiting of dark blood like coffee-ground.. For treatment see " Hcemorrhage from the ' toma('h 1/ (page 98).
Injuries of the Liver , Spleen and Intestines may be caused by a blow, a tab or a bullet; the liyer or spleen may be injured by a fracture of the lower ribs. The igns and ymptollls are those of internal hzemorrllage accompanied by pain and swelling at the seat of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a rush, blow, stab or bullet. Blood may escape \\ ith the urine , and there may be pain and s\\elling oyer the injured kidney.
The Bladder may be injured by a fracture of the pelvis. The signs and ymptoms are either inability to pass water , or if a little is passed it is tinged with blood.
11 2
TREAT:\IE::\,T OF I NJURY TO THE KIDNEYS OR BLADDER .
Keep the patient quiet until the doctor arrIves.
2. - Apply hot fomentations oyer the painful or injured part.
Rupture (hernia) of a protrusion of an internal organ, usually the bo\yel, through the muscular wall of the abdomen, most frequently at the groin. ' hould a sudden s\yelling accompanied by pam and sickness take place in that region
1.- end for a doctor instantly.
2.-Lay the patient down \yith the buttock raised.
3·-A pply ice or cold \Yater dressings to the affected part.
QUE TrONS ON CHAPTER IV.
The 1lumerals indicate the pages 'Where tile answers may be found.
How would you treat a bruise?
How maya burn be ?
How would you t reat a burn caused by a corrosive acid?
How would you treat a burn caused by a COrro i\'e 'alkali?
\Vhat steps should be taken when a woman s dress catches fire?
tate the general rules for treatment of wounds cau ed
by poisonous biles or weu90 ns
\Vhat special treatment is required for the bite of a venomous snake?
EO\y would YOll treat a sting?
'tate the signs, symptom. and treatment of frost·bite
\Yould you attempt to remove a needle embedded under the skin?
How would you extract a fish h ook emhedded in the skin?
State the treatment for injuries to joints .
tat,,: the general rules for rem0\"ing a foreign body from
the eye...
\Yhat would you do if a piece ot .;tee1 were embedded in the eye baM ?
And when quick·lime is in the eye?
How would you try to remO\'e an insect from the ear passage ?,.
Irs
What is a bruise? PAG E 102 102 r02
r02 \Vha t is the great danger of a burn or scald? .. . 10 3 tate the general treatment for burns and scalds 103, 104
How is a scald caused?
...
r04 104 r05
106,
107
107 107, r08 108
... ... ..
. ..
108 109 r09
... .. ... ... .,
r09, IIO
rro HO III
VV Id PAGK
au yuu try to remove any othe r form of foreign body from the ear passage? ... ... ... '" 110 II I
How would you a foreign body from the nose? 'I I I
State the boundanes of the abdomen and its contents I I I
State the for of the abdomen II2, II
117 CH APTER V.
TH E NERVOU SY TEM.
. II J
How may 1l1Junes to the lIver, spleen and intestines be 3 caused? ...
What is the difference treatment of st.omach and of ll1Junes to the liver spleen and mtestll1es? ... ... '
State the treatment of injuries to th'e 0; II3
State the t r eatment of h ern ia I r 4 114
Two systems of nerves, the Cerebro-spinal and the Sympathetic, regulate the movements and functions of the body
The Cerebro-spinal System is made up of the Brain, the pinal Cord and Nerves, amI through its agency sensations are received and the \\111 causes the action of the voluntary muscles. For example , when a part is injured a sensation of p1.in is conveyed to the brain by the nerve, thus affording an indication of the seat of injury, or a warning o f a possible danger of further damage. On attentio n being directed to the injury, an attempt is instantly made to ease the pam or to move the injured part from danger.
The Brain is situated \\ithin the cranium, and is divided in the middle line, so that, \\ Ith the exception of some conn e cting bands , the right and left sides are separate.
The Spinal Cord is the long cord of nervous matter lying within the spll1al canal (see Yertebral Column, page 23)' It leaves the brain through an opening in the base of the cranium and extends to the upper lumbar vert ebrre .
116
. . . .. . . .
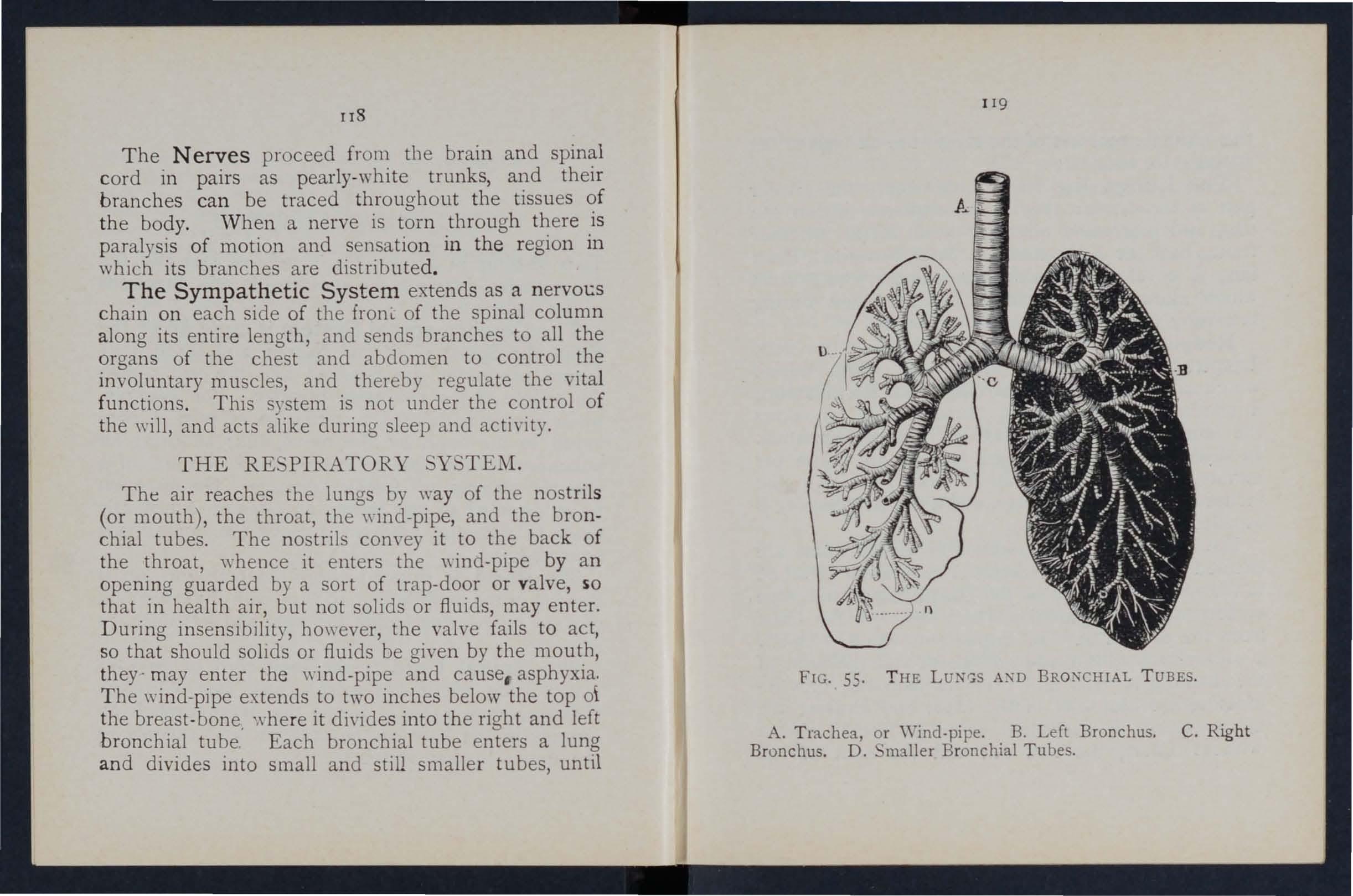
The Nerves proceed from tIle brain and spinal cord in pairs as pearly-white trunks, and their branches ca n be traced throughout the tissues of t he body. W hen a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed .
The Sympathet ic Sys t em extends as a n erVOl:S chain on each side of the fronL of tIle spinal column along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary muscles, and thereby regulate the vital functions. This system is not under the control of the will, and acts alike during sleep and activity.
THE RE PIRATORY Y TEM .
The air reaches the lungs by way of the nostrils (or mouth), the throat, the \\"ind-pipe, and the bronchial tubes. The nostrils com-ey it to the back of the throat, \\-hence it enters the wind-pipe by an opening guarded by a sort of lrap-door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, ho\\"ever, the valve fails to act, so that should sollds or fluids be given by the mouth, they- may enter the wind-pipe and cause, asphyxia. The wind-pipe extends to two inches below the top 0\ the breast -bone. '.\,he re it di,-id es into the right and left bronchial tube. Each bronchial tube enters a lung an d divides into small and still smaller tubes, until
!I8
1
19
FIG. 55. THE L UN(;S A:\D BRO:-iCHIAL TUBES.
A. Trachea, or Wind-pi pe . B. Left Bronchus. C. Right Bronchus. D. 'ma ller Bronchial Tu bes.
t he ultimate recesses of the lu n g-the air ce ll s o r aI r s paces-are reached .
The Lungs, R ight and L e ft, occu py th e g r eater pa rt of t he chest j they li e imm edi a tely wi thin the r ibs, a n d practically wherever a r ib is fel t, wh ethe r front, back or sides, there is lu n g be n eath. Each lu ng is enveloped ill a fine memb rane (the pleura ) which allows It to move within the chest during breathmg without friction .
Respiration, or b reathing, consists of two acts, Inspiration, an expansion of the chest, during whIch air .is drawn in to the lungs, and Expiration, a contrac tI on of the chest, during which ai r leaves t he l u ngs . A p.iuse follows the act of expi ration. I n healt h fi ftee n to eighteen breaths are taken per minute, and at each inspiration abou t 20 to 30 cubic inches of air e n ter the lungs, and a simila r quantity is expelled at each expiration.
The exp3.nsio n and contraction of the chest are effected partly by the muscles of respiration attached t o the ribs, but chiefly by the Diaphragm, the large arched muscuh r partition \\ hich separates the chest from the abdom en. I n inspJration, which is chIefly a muscular act, the ribs are raised, and thp arch of t he d iaphragm falls and hecomes flattened, thus inthE' capacity of the chest and causi n g the a Ir to enter. I n expiration an act performed a lmost without effort, the ribs fall and the arch of the
121
diaph ragm rises; this lessens the capacity of th e c.hes t .and fo rces air ?ut. The mechanism of respiratIo n IS so mewhat like that of ordi nary household bellows, bu t \\ ithout a valve; the rib5 may Ge compar e d to t he boards of the bello\\ s \\ hi Ie th e diaph ragm c orresponds to the leather, the air passages bei ng equivalent to the nozzle.
. As the blood depends upon the air for its purificatIOn and t he oxygen necessary to maintain life interference with breathing yery soon may produce a dangerous state called asphyxia, examples of \\ hich are afforded by drownin g, suffocation, choking, etc.
ARTIFICL \ L RE -' PIRATIOK.
PR OFESS O R CHAFER ' S METHOD.
I. - Waste no time in loosening or in removin g clothing.
2.- Lay the patient in a prone position (i. t ., back with his head turned to one s1de, so as to k eep hiS nose and mouth a\yay from the ground. No pad is to be placed under the patient, nor need the tongue be drawn out, as it \Yill fall naturally.
3. - Kneel at one side facing the patient's head, and place the palm of your hands o n h is ribs, one at each siue, the thumbs n early touchIng o ne another in the mall of the back. Leaning your body forward, slo\\ ly apply firm but
120
not violent pressure straight the back and lower part of the chest , thus dnvmg alr out and producing expiratio n (Fig. 56). D raw back
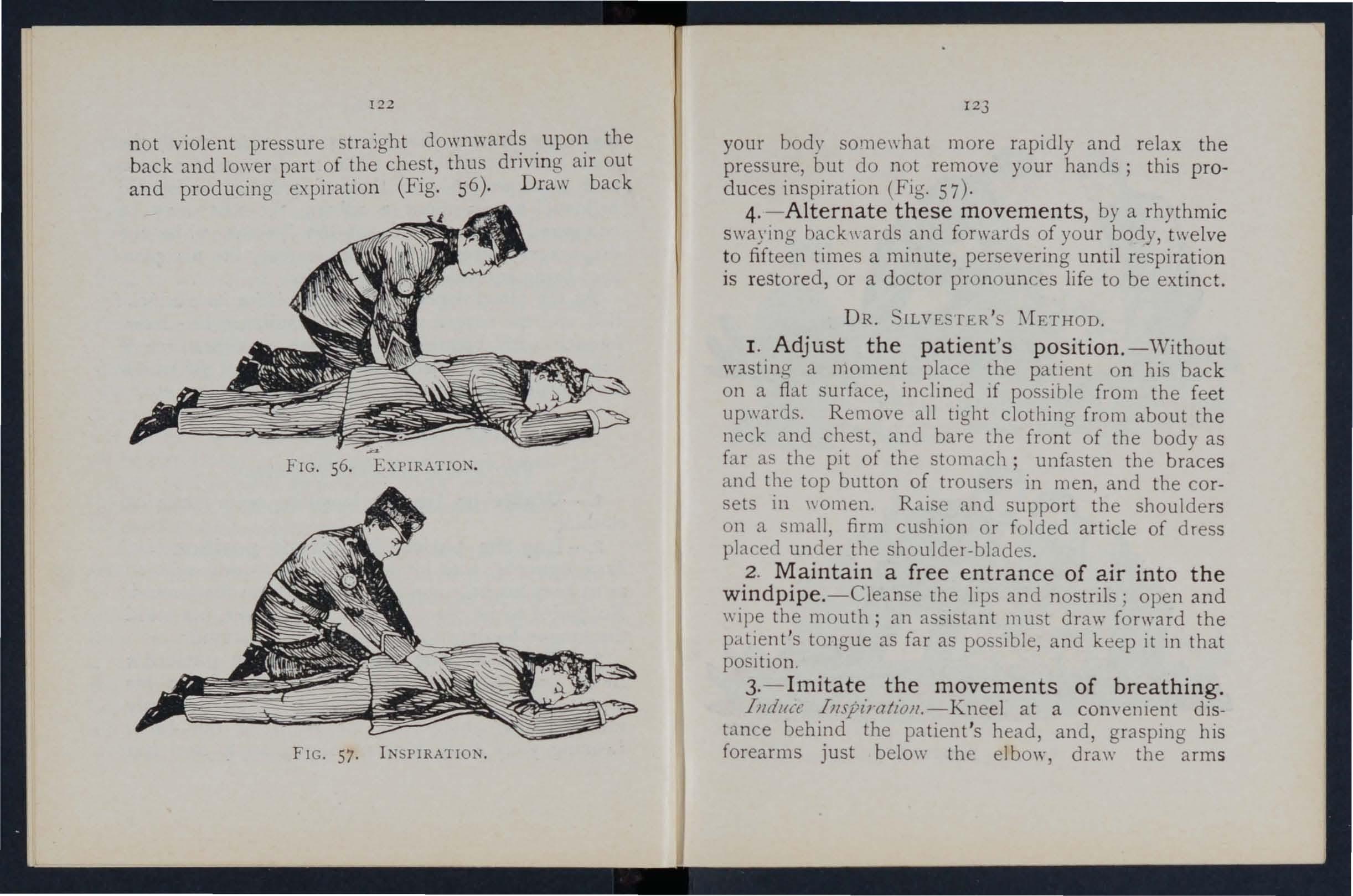
1 2 3 your body s0I11e\\hat more rapidly and relax the pressure, but do not remove your hands; this produces inspiration (Fig. 57).
4. - Alternate these movements, by a rhythmi c swayin g bacb\ ards and forwa.rds of your body, twelve to fifteen times a minute, persevering until respiration is r estored, or a doctor pronounces life to be extinct.
DR. lLVE TER'
I. Adjust the patient's position. -\Vithout W3.sting a moment pb.ce the patient on his back on a fla,t surface, inclined If possible from the fee t upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women. Raise and support the shoulders on a small firm cushion or folded article of dress pb.ced under the shouldeI-bb.des.
2 . Maintain a free entrance of air into the windpipe. -Cleanse the lip and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as pas ible, and keep it in that position.
3·- Imitate the movements of breathing.
Induct IJlSpl> ·atioll.-Kneel at a convenient distance behind the patient 's head, and, grasping his forearms just below the elbow, draw the arm s
122
FIG . 56. EXPIRATION .
FIG. 57. IN PIRATIO
58 . I SPIRATlON.
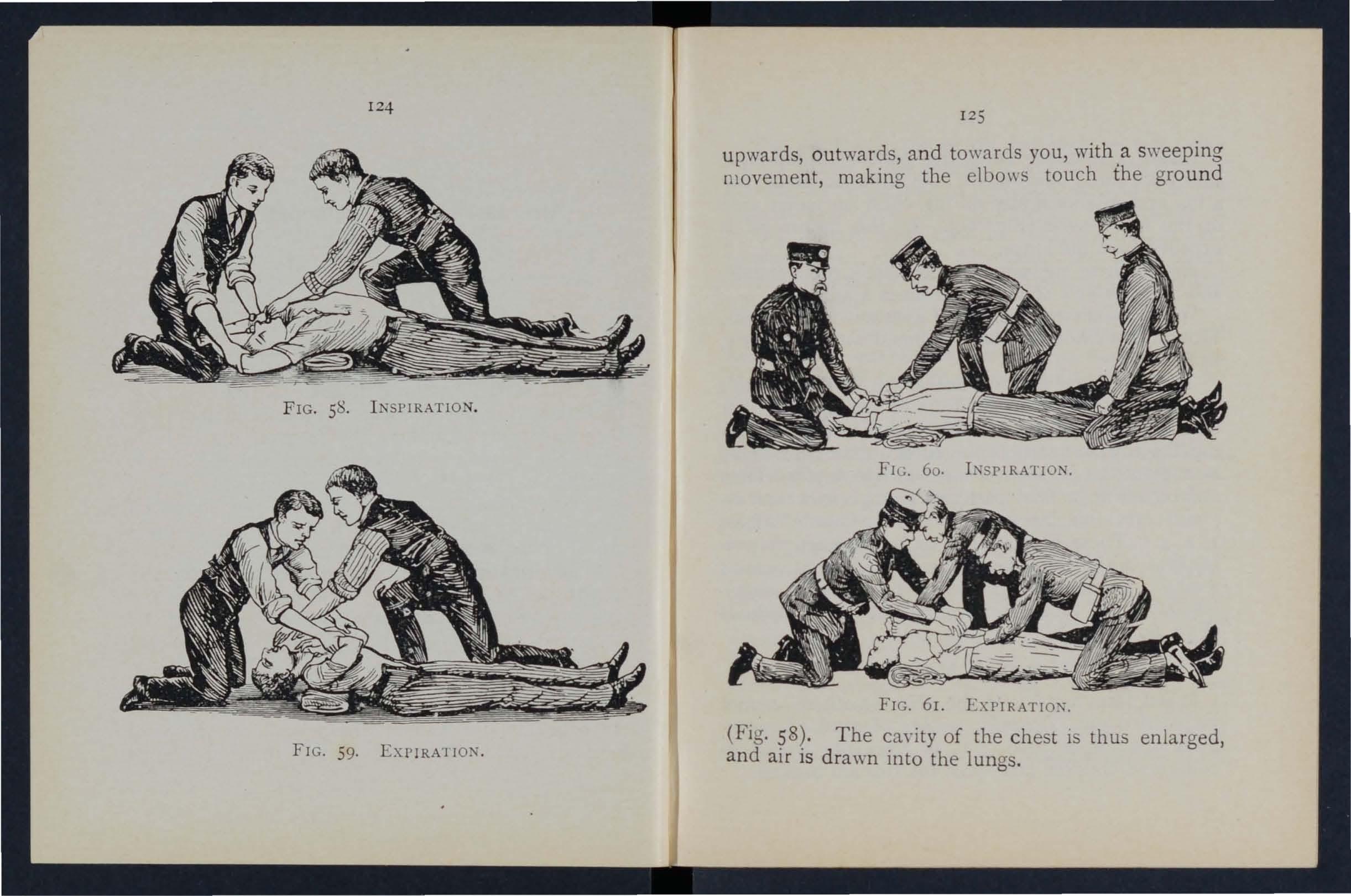
59.
upwards, outwards, and towards you, with a s\\"eeping movement, making the elbo\\!:; touch the ground
FIG. 61. EXPTRATIO,,".
(Fig. $8). The ca.\"ity of the chest is thus enlarged, and alr IS drawn into the lungs.
124
FIG
1 2
FIG.
EXPIRA1 ION.
5
Illduce explratt"oll.-Bring th e patient 's flexed arms slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (Fig. 59) . By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and pe r seyeringly about fifteen times a minute.
\Yhen a sufficient number of assi s tants are present, Howard 's method may be combined \\ ith ilYester 's, as follows ;-
The additional assistant kneels astri d e the patient 's hips with the balls of the thumbs resting on eIthe r side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Using his knees as a piYot, he presses forward on his hands . Then suddenly, with a final push, he springs back and remains erect on his knees while he 10\\ ly counts 1, 2, 3. These motions are to be repeated to correspond \vith th 06e being perfor med hy . ilvester's method, pressure on the chest being made simultaneously by those performing the t \\ 0 methods (Figs . 60 and 6 I).
LABORDE ' s METHOD
\ Yhen fr om any cau e the above methods cannot be carried out, Laborde's method of artificial respiration should be tried . It is especially u eful in s u ffocated children and when the ribs are broken. 1 2 7
T he patient is placed on his back or side; the mouth cleared; the tongue is seized-using a hand · kerchief or somethi ng to preyent it slipping from th.e fll1C1ers-the lower jaw depressed; the tongue l S pU 'Oed forward and held for t\\"o .seconds in that po ition, then allowed to recede mto the mouth, T he . e movements should be repeated about fiftee n tImes a minute.
Artificial respiration must be continued until breathll1 <T IS established, or until a doctor arm'es.
' Yhen breathing commences, regulate the artificial to corre pond with It. uccess may result eyen after t\\"o hours ' time.
Excite respiration. - 'Vhilst artificial respiration is being applied, other useful steps may be such a applying smelling salts or snuff to the nostnls, and fllCklllg the chest \\ith a damp towel.
I n duce circulat ion and warmth after natural breathing has been rest ored . '''rap the patient in dry blankets or other coyenng, and rub the limb energeticaJly towards the heart. Promote \yarmth by hot flannel', hot-\\"ater bottle,> or hot bricks ,(wrapped in flannel) applied to th e feet, the limbs and bo?), . \\'he n the po\\er of s\\'allomng has returned grve hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep Large pOUltices or fomentations applied to the
front and back of the chest 'wi ll serve to assist breathing.
. Watch the patient carefully for some time to see that the breath ing does not fail; should any signs of failure appear, at once begin artificial respiration.
IN IBILITY.
. Unconsciousness or Insensibility may arise as fo11o\\'s ;-
Injury to the Head. -Concussion and Compression of the brain.
Disease of the Brain. -Apoplexy, Epilepsy , H ysteria .
Various Causes. - hock, Fainting ( yncope), Coll apse, Alcoholic a nd other poisoning, unstroke and Heat-stroke, Infantile Conyulsions, Asphyxia.
G ENERAL RULE FOR TREATMENT OF IN SEN
I.-If a person appears about to lose consciousness, prevent hi'11 fr om falli ng, and lay him gently down.
2.-Arrest Hcemorrhage when apparent; attend ing to minor injuries is less important than tr eati ng the unconscious state.
3.-Lay the patient in the position in which breathing is most this will be on the back, or inclined to one side. As a general rule 129
raise the head and shoulders slig!ltfy when the face is flushed and keep the head low \\ hen the face is pale.
4. - Undo all tight clothing round the neck, chest and waist, unfastening the braces and top button of the trousers in men, and the corsets in women, the object being to relieve pressure on the air passnges, lungs, heart and abdominal organs. Be sur.<:; that there is no obstruction to the aIr passages by the tongue or by a foreign body in the throat. The possibilIty of false teeth obstructlllg breathing must be considered.
5. - Provide for a sufficiency of fn:.sh air by opening doors and \Y1l1dO\\"s, and by keep1l1g back a crowd.
6. - When breathing cannot be discerned apply artificial respirat i on.
7. - 0btain a doctor's help as soon as possible.
Unless unavoidable, never leave the patient until you have placed him in charge of a responsible person.
9. - Give no food or fluids by the mouth while the patient is insensIble.
IO. - Should the spine or an important bone uf the upper or of the lower limb be fractured, it must be steadied and maintained at rest as soon as possible. hould the unconsciousn ess be prolon.g.ed, the patient may be removed in a recumbent posItIOn po
128
130
to sh elter, provided t h at th e b ro k en bone is ad eq u a tely supp ort ed.
II, - When the patient is in a state of convulsion, sup port h is h ead, and a fte r wrapp in g a p iece of wood or a ny ot h er hard m aterIal in a handk e rc hief, h old it in his mouth to prev ent biti ng of th e tong u e . D o n ot forcibly restrain his limbs ; prevent him from hurti ng himself by d raggi n g hi m a\\ay f rom a so urce of danger, such as machi n ery, a wall, or fi replace; light pIeces of furniture should be pushed ou t of the way.
I2. - 0n return to consciousness water may b e given to dri n k . If the pulse is feeble give \\arm tea or coffee, provided either internal or e'{ternal, is not present. A desIre to sleep should be encouraged, except in cases of opium poisoning, a conditio:1 that may generally be recognised by the history of the case, and als ') by the pupils of the eye:; (the black opening') in the grey, blue or brown iris) minutely contracted (pin-head pupils).
.::» 13. - It must not be assumed that a person is insensible as the result of drink merely because the breath smells of alcohol ; frequently when people are feeling ill they take or are given alcoholic <;timulants, after which they may become insensible, .1)t from the drink, but from the cause that indu ced them to take it, for example. insensib ility c oming on, effects of poisoning, etc, Even if
13 1
dri,nk believed to De the actual cause of insensibIlIty, It must be borne in mind that the patient is in a very dangerous state, and he must be treated for Coll apse by being cov.ered up and kept warm.
The above general rules \\ ill enable first aid to be rendered efficiently in most cases of insensibility altho':lg h . the exact form from \\'hich the patient suffenng IS unkno\m.
COKCD 10 1 OF THE BRAIN
.
[he patient may be stunned by a blow or fall on head, or by a fall on the feet or lo\\'er part of the , . He may quickly regain consciousn ss, or insenSIbIlIty, more or less complete, may be prolonged.
TREAT;\lEi'\T.
I. - Apply the general rules for the treatment of In en lbilIty
2.- Be ye.ry apprehensive of danger in all ,cases of Injury to the head. The patient may be stunned, and after a short interval may recover some degree of or even the bram may have escaped l11jury ; yet in bol h instances IS a grave risk that a structure \\ithin the cranIum been inJured, and that a serious state of l11sens.lbIllty may de,-elop later (ee Fracture of the. ral1lum, pa&e 43 .) A cautio n should therefor e be gIven to a patIent who has lost consciousness even F2
13 2
for only a mom ent after an in j ury to th e head not to resume physi cal o r mental activity \\"ithout the consent of a doc tor.
CO MP RE. ION OF THE BRAI , APOPLEXY.
Compression of the Brain may result from the same cau ses as produce Concussion; in fact, Comp ression is frequently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no signs of injury are necessarily present..
In both conditions the face lS flushed; the brea th ing stertorous; one side of the ?ody may be more li m p t h an the other, and the pupll of one eye may be larger than that of the other j the temperature of the body is generally raised.
TREAnIENT .
I. - Apply the general rules for treatment of I nse nsibi lity.
2. - Promote warmth in the lower part of the body by the application of hot \\ a ter bottles to the a bdomen and lower limbs . C1re must be take n not t o burn the patient \\ ith the bottles, \\'hich should be wrapped in flannel, and their heat tested with the elbo w.
EPILEP Y.
:ep ilepsy may occur in persons of any age, but usually occurs in young adults. The patient falls to 133
the ground, sometimes with a scream, a n d Jnto a state of convulsion, throwing his limbs about. The treatment is according to the General especially Rule I I.
HY TERICAL FIT (BY TERIA).
Y:'IIPTO:'lS.
The patient, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and actions. he subsides on a couch or in some comfortable position, throws herself about, grinding her teeth, clenching her fists, shaking her hair loose; she clutches at anyone or anything ne:u her, kicks, cries and laughs alternately. The eyeballs may be turned up\\'ards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irreguhr symptoms may develop .
TRE ,\T\[E:\T.
I.-Avoid sympathy \\ ith the patient, and speak firmly to her.
2.-Threaten her with a cold water douche, and if she persists in her "fit, /I sprinkle her with cold water.
3·-A pply a mustard leaf at the back of the neck. treatment is necessary to cure the condition of . mind and body which gives rise to hysterical attacks.
SHOCK, FAINTING ( YNCOPE), COLLAPSE.
CAUSES.
I.- -Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and severe crush are some of the more fr equent physical causes of shock.
2.-Fright, anticipation of injury, and sudden bad news, or sometimes sudden removal of fear and anxiety after prolonged .suspense, produce shock or fainting.
3·-Some pOIsons cause shock, while others, such as alcohol, so depress the nervous system that collapse ensues.
4·-Hremv.'Ihage or heart weakness, a close or crowded room, tight clothing, fatigue, or want of food may bring on fainting or collapse.
The general condition of shock may be recognised by extreme pallor, a feeling of cold, clammy skin, pulse, and shallow breathing accompanied, If hremorrhage has been severe,. by yawning and sighing. The term "collapse /I signifies a very serious condition in \\ hich the life of the patient is in the greatest danger; the temperature of the body falls below the normal, and one great object of treatment is to prevent it sinking to a point at which life is impossible. An attendant danger of the condition of
collapse is the liability to sudden relapse after a temporary Improvement, and the utmost care and watchfulne $s must therefore be exercised to main · tain the heat of the body and to guard against failure of the heart and lungs.
I.-Remove the Cause by arresting hremorrhage, attending to injuries, loosening all tight cloth· 1I1g, especially about the chest and abdomen, remov mg from a close or crowded room, using encouraging words, etc.
2. - Lay the patient on the back, with the head low. Rais e the lower lim bs; \\ hen the patient 1 in bed this is best done by raising the foot of the bed tead.
3. - Provide for a free circulation of fresh air.
4. - If hcemorrhage has been severe and the patient is collapsed firmly bandage the limbs from the toes to the hips, alld from the fingers to the armpits.
5. - To stimulate the action of the heart, sal volatile and \\ ater may be gn'en if the J,;atient can swallow, or smelling alts may be held to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of temperature below the normal point. To accomplish this cover the patient \\ith extra clothing, or by placing
134
AND
135
136
rugs or blankets over him; get him to bed in a warm but well-ventilated rOO :11 as soon as possible. Apply warmth to the feet and to the pit of the stomach by hot water bottles or hot flannels . (T est the heat of these with the elbow before applying them.) If the pat ient can swallolV, gi"e hot d rinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the temperature of the body.
7. - If breathing cannot be discerned, apply artificial respiration.
8. - If want of nourishment has been the cause of fJ.inting or collapse, give food sparingly at first.
SUNSTROKE AND HEAT-STROKE.
"When exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weather ,,,hen heavily burdened, persons may de"elop sickness, faintness, giddiness, and difficulty in breathing. The patient complains of thirst, the skin becOlnes dry and burning, the face very flushed, the pulse quick and bounding. A very high temperature, stertorous (snoring) breathing, and insensibility may ensue.
TREADIENT.
I.-Undo all tight clothing.
2.-Remove the patient to a cool, shady spot.
137
3.- trip the patient to the \\alSt.
4·- Lay the patient do\\ n, \\ ith the head and trunk \\ell raised.
5·- Procure as free a circulation as possible of fresh air, and fan the patient vigorously.
6.-Apply ice bags or cold \\ater freely tu the head, neck, and spine, and n1 aintain this treatment until the symptoms subSide.
7·-0n return to consciousness, the patient may have \\ ater to drink. I01'\S IN
CHILDREN.
Teething or stomach tJOubles are the commonest causes of this ailment.
IG • .
pasm of the muscles of the lim bs and trunk, blueness of the face, in ensibility, more or less complete, and occasionally squinting, suspended respiratIOn, and froth at the mouth are the prominent signs.
1 . - upport the child in a \\arm rath slightly above the t(;mperature of the boely (98 degrees), so that the \\ater reaches to the middle of the trunk.
2.- Place a sponge dipped in cold water on the top of the head.
138
AS PHY X I A .
'V hen owi n a to wa n t of air, the blood is not s up p li ed ' w. th ;'{ygen the patient and is said to be asphyxiated . This condltlOn may be brought about as follows: -
1. Obstruction of the air passages.
(a) By DROWNIXG.
(b) By PRE SURE FRO.\1 OUT IDE: trangulation, hanging, smothering. .
(c) By A nODY IN THf£ l'HRO \T: hokll1g.
(d) By S \,ELLING OF '1 HE TIS OF THE THRO,\T: Inft 1.l11matIOl1, scald or the throat, poisoning by a corro Ive.
II. Inhaling poisonous gases . By coal gas (as used in the house), producer, or \Yater, gas, sl11?ke, fumes from a charcoal or coke fIre, se\\ er gas, limekiln ga , carbonic acid ga:.
III. Pressu r e on the ch est, as \\ hen crushed by sand or d t· hri . , or by a cro\\ d . . IV. Nervous a ffec ti ons, as the result of narcotic and certain oLher poisuns, cull apse, electric shock, or stroke by lightnil1lj.
TRE 1''\1.1£,\T.
In all cases of .As['ll)'xia attempts must he Illade to r emove the cause or to rUTI::>re the pn.tient from the cause. ·When flas leen done art ificial
respiration must be applied, taking c are that the au pas sages are not obstructed, and that there is abunda n ce of fresh ai r.
DRo\\ 'ING.
Persons completely immersed in \\'ater for eve!1 or fifteen minutes have been restored by artIfiCIal means. Therefore, if the body is recovered Within a rea onable time, absence of signs of lIfe is not to deter Immediate attempts to restore anImation.. . The first thing to do when the body IS to aet rid of the \\ ater and froth obstructing the alr and then mtificially to restore This is best accomplIshed either by proceedmg at once to perform artillcial respiratIOn by chafer's method or as follows :-
I.- \s quickly as possible loosen the clothing, and clear the mouth and the back of the throat.
2.-Turn the patIent face downwards, with a pad below the chest, and with the forehead upon the right forearm.
3.-"\Vhilst in this pOSItIOn apply pressure. by the hands to the patient's back oyer the lower nbs, and keep the pressure up for three seconds.
4.-Turn the patient on the right side, maintaining that position also for three seconds.
s.-Repeat these movements alternately as long as froth and \\ater issue from the mouth.
139
These opera t ions ( ?\I a r ba ll H all 's metbod) in thems elves tend t o p r omo te respi r a tion, but \\ he n the air passages a rc clea r of froth a n d wa ter ilyester ' s method of a r t ificial resp:ratio n may be u ed by itself or with H o ward 's met h od in conjunction.
\Vhile performi ng the e operation send someone t o the nearest bouse to procure blanket and dry clo thing, hot water bottl s, etc ., and to fetch a doctor.
TRAXGULATlON
Cut and r emove the band constricting the throat. Apply artifici al respiratio n .
HAKGING .
Do not wait for a policeman .: grasp the lo\\'er lim bs and raise th e body to take the tensio n off the rope; cut the rope, free -the neck; apply artificial respiratioll.
.\JOTHERl?\G.
Remove wh a t ever is smothering the patient: apply artificial respiration.
CHOKI?\G.
Open the mo uth, forcibly if need be; pass the forefinger rig ht t o the back of the throat and attempt to dislodge the foreign body; if yomiting results, so much the b etter. If unsuccessful, thump the back hard whilst th e head is bent fOr\\ard. Apply artificial respiration.
.\ OF
THf:: T l OF THE T H R OAT.
\ Vhether the swelling is caused by in ft.a mm at io n by s\\a ll owing very hot water, as no t in frequ e n tly happens to children attempting to drink fr o m t he sp out of a kettle, or by the effect of a corrosive poiso n, the treatment is as follows :-
I.-Apply a sp onge, piece of ft.annel or other clot h, ",rung out of ,'ery hot \\ at e r, to the front of the n ec k , fro 11 the chin to the top of the breast -bone .
2.-.'et the pati e nt before the fire.
3.-Gi\' e IC C to suck if it can be had ; if n o t, give cold \\'ater to drink.
-t. - Give animal or vegetable oil, a desse r tspoo nf u l at a time, to soothe the scalded throat and ease the pam.
S.-If breathing has ceased apply artifi c ial respira,tion .
By'.\JOKE O R GASES
L-Rel110\'e the patient into the fresh air. Before entering a building full of smoke tie a ha n d k e rchief. \\ et If possible, round the head 0 as t o co ver no e and mouth. I t is well to 1110ye slow ly, k eepi n g 10\\', or eyen cra\\ ling-, \\ hilst in a room full of s mo k e in sear,ch of a suff02ated pers on. Eyery op portun ity of le ttll1g m fresh air by OIJenin3 doors or windo\\s sho u ld be seized .
140
qI
2.-Apply artificial respiration.
3.-In the case of producer or ,yater gas, inhalation of oxygen will also be necessary.
ELECTRIC HOCK.
Electric current is conveyed by a cable, wire, rail, or bar, called the "Positive," and. to the source of supply by another cable, wire, rail, or bar, called the" Negative," or through the earth. In the case of an electric railway, the current is generally conveyed by an insulated rail cal;.led the third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an electrIC tramway it is frequently conveyed by an Q\'erhead conductor or trolley wire, and returned through the running rails.
Through contact with a "positive" the shock may be so severe as to cause insensibility, and the sufferer will be unable to extrIcate himself, and mU6t be liberated with all possible speed. As it is generrally impossible or inexpedient to switch off the current some other method must usually be adopted; but precautions must be taken or else the person rendering assistance will himself receive a shock.
To liberate the suff::rer from contact-
I .- Insulate yourself from the earth by standing on an "insulator" or " non-conductor," that is, a body which resists the current. Amongst such bodies
143
are indiarubber , dry glass, dry Lricks, dry silk , d ry cloth, dry wood and dry hay or straw .
2. - Protect your hands from contact with the sufferer or the electric medium by covering them with an insulator. _\.lthough indw.rubber is probably the best insulator, do 110t waste tIme in rUllning for indiarubber glQ\'es, but use dry articles of clothing; an indiarubb e r tobacco pouch or cap, or folded newspaper, \\ ould serve to protect the hands 111 an emergency. 1£ no means of insulatmg the hands are at hand an attempt may be made to drag the sufferer away by means of a loop of dry rope or a crooked stick; an umbrella is not safe because the metal ri bs would act as cond uctors-l(' of electricity, and it is not infrequently the case that the" stick" of the um brella is a metal tube.
3. - Pull the sufferer away from contact. Care should be taken to avoid touching with naked hands the sufferer 's hands, wet clothing, or boots if the soles are nailed. The armpits should be avoided as perspiration usually makes the clothing damp there.
\Vhen the suff _ er is removed from contact-
I. - Apply the general treatment for insen-
* A conductor i a body through which electricity readily passes. Amongst such bodies are copper , brass, iron, moistu r e and one's own body. ,
144
sihility (loosen clothing, procure free circulation of air and place in a recumbent position).
2. - Dip a towel in cold water and attempt to arouse him by sharply flicking the face and chest.
3·- Commence artificial respirat ion if othe-r methods fail to restore animation. "Laborde's" method (see p::tge 126) has been foupd to be very successful.
4·-Treat b urn s if there are any (see pages 103, 104).
EFFECTS OF LIGRT?\]KG.
A person struck by lightning is usually more or less deprived of consciousness. The treatment is the same as that for eJectric shock, e\:cept, of course, that the instructions for lemoyinfJ the patient from contact with the electric medium do not apply.
145
QUESTIOr ON CHAPTER V.
The Illllll cra/s indicat.: the ja,f;<'s 7.Oltere the answers may l'e (olllld.
\-Yhat are the two syst ems of nerves?
Of what is the cere bro -spinal sy stem made up? .. What is the spinal cord?
are nerves like?
In what system of artificial respirati on is the patient
. . .
.
..
... .. . ... .. '''hat
.. . PAGIt 117 117 117 1I8 Explain the sympathetic system Explain the respiratory system Explain the acts OT respiration II 118 to 120 120 How are the exp!ln io n and contraction of the chest effected? ... ... '" ... ... 120 to 121
bac·k upwards? ... ... ... .., ... .. . 121 In what systems is he laid on his back?... '" 123, 126 In what system is he laid on
back
side? ... In \\ hat system is he rolled alternately on his side and face downwards? .. .. . ... ... 139, 140 127 J I lW long should artificial r espiration be persevered \\ ilh? 12 7 \\'hat is exciting respiration? 12 7 \,"hat is inducing circulation? 127, 128 '''hy is it nece sary to watch the patient? 128 JIow may insensiiJility arise? 128 State the \'arious forms of insensibili,), ... 128 State the general rules fur treatment of insensibility 128 to 13 1 \Yould
were broken? ... \':hat wrong opinion may be
12 9
of drink? 1; collapse from drink
\"h tt is concussion of
brain? ... State the rules for treatment of concussion 130 13 1 13 1 131, 13 2
laid
his
or
you examine the patient to see if any bones
formed when the patient
smells
a serious condition?
the
What danger accompanies injury to the head?
\Vhat caution should be given to a ratient who hac; lost consciousness, even for a moment, after an injury to the head?
" 'hat are the causes of compreFsion of the brain?
In what aged people does apoplexy usually occur?
'Vhat are the signs and symptom;; of compression and apoplexy?
State the rules for treatment of the. e conditions ...
" -hat danger is there in applying hot water cottles to insensible persons, and what precautions should be taken? ... 13 2
Describe a case of epilepsy 13 2 , 133
" ' hat special care must be taken in treating a case of epilepsy? 130 ,
lIow would you treat a hysterical fit?
'''hat are the commonest physical causes of shock?
'''hat may produce shock 01 fainting?
'Yhat conditions do certain poisons bring about?
What may bring about fainling or collap e?
What two things have to be done in all cases of
asphyxia.?
What two thlllgs must be seen to before it is possible for ' respiration to do any good? ... ... 139
Is artificIal re spuat ion likely to do any good if the !!oir passages are obstructed, or if there is not abundance offresh air?
\Vh:lt is the first thing to do in a case of drowning?
By what method may artificial respiration be performed without taking any preyious steps ?
What steps must be take!} before proceeding with Silvester's method?
What should be done while artificial respiration is being performed?
State the treatment for strangulation the treatment for hanging ... the treatment for smothering
SLate the treatment for choking ...
How may a swelling of the tissues of the throat be caused?
State the treatmen t for swelling of the tissues of
How would you recognise the general condition of shod?
Describe a hysterical fit Ij2 133 133 134 134 134 134 Ij4
" ' hat special precaution must be taken in the case of 135 collapse?
State the treatment for shock, faint1I1g (syncope) aDd collapse ... 135, 13 6
How would you liberate a sufferer from contact with an electric medium?
'¥hat would you do when the sufferer wa removed from 1 contact ?
" ' hat are the causes of sunstroke and heat-stroke?
" 'hat is the effect of on the temperature of the 13 6 136 body?..
. tate the treatment for sunstroke and heat -s troke
\Vhat are the causes of convulsions in children?
\Vhat are the signs of convulsi ns in children? ...
State the treatment for convul ions in children ...
State fully the causes of asphyxia ...
What would you do in the case of a lightning ? :::
PAGE Ijl 13 2 Ij2 13 2 Ij2 13 2
... ... ... _.. . ..
136, 137 1j7 137 137 138 147
PAGE
... '"
... ...
...
138 139
... . . . ... ... .. .
...
... ... . ..
... ... . .. ... . .•
... ... . ..
... ... ... ... ... . ..
139 139 139 139 141 throat ... ... ... ... ... ... ... 141 State .the
smoke
gases 141. 142 How IS conveyed? ... ... '" ... 142
for suffocation by
or
... ... ... ... 142 143
143 144
CHAPTER V I.
PO I SONING.
Poisons may be classified according to their treatment u nder t\yO heads :-
I. - Those which do not stain the and in the treatment of which an emetIc IS to be given. Amongst these are: - " ,
(a) Arsenic, 111 ,polscn and lucifer matches\, I artar en eUc and CorrosiYe ubl1l11ate, \\ hieh a me.tall.ic tas te in the and a L Ul11111g pam III the mouth, throat and ston'acb.
(b) Strychnine, Prussic Acid, I?elladonna nightshade plant) and seyera] otber yanetIes of plants, sucb uS ; these giYe rise to cOl1YulslCnS, celmum, failure of respiration and .
(c) Poisonous meat, fish and (often mIstaken for mushrooms). usplclon of these poisons should be directed to ases \\ here se \'eral persons \\ bo haye of tbe same food develop similar signs and symptoms.
(d) Alcohol, which may cau e cc:llapse. .
(e) Opium and its preparations,
I49
Laudanum, Paregoric, Ch lo rodyne, Syrup of Poppies an 1 various soothing drinks and cordials; these cause a tendency to go to sleep, which continues until sleep becomes deep and breathing sterotorus ; the pupi ls of the eyes beco :11c minutely contracted (pinhead pupils).
2. - Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. The e are of t\\"o classes :-
(a) Acids, such a. Titric Acid (.\qua fortis), Sulphuric Acid (Oil of Vitriol), Hydrochloric, or Iuriatic, Acid ( pirits of alt), strong Carbolic Acid (Phenol) Oxalic Acid, \\ hich is contained in oxalate of potash, slIts of sorrel, salts of lei110n and some pdlishing pastes.
(/7) Alkalis, su h as Caustic Potash, Caustic oda anJ Ammonia.
OF SIl\IPLE DIRECTIO:\ FOR THE TREAT:\JE,\T OF P ';' l O:\,I:\G.
I. - Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali,
ISO
promptly give an emetic- that is, make the patient vomit as follows :-
(a) Tz"ckle tlz e back of tile tizr oat with the finger or with a feath er.
(b) NIustard- a desser t-sp oo nful in a tum blerful of luk e- wa rm wa te r.
(c ) S alt-a table-spoo nful in a tumbl erful of luk e-war m \Yate r.
(d ) IpeCadta Jllla Trine- fo r a young c hi ld, a teaspoon f ul repeated at int ervals of fift ee n mi nu tes .
3.- In all cases whe n the patie nt is n ot insensible, give M il k , Raw E gg s be a te n up w ith milk or water, Cre am and Fl our bea t e n up together, An imal or Ve g etabl e Oil (e xcep t in phosphorus poisonin g), and Te a.
Oliv e, alad, and Cod-liver oil, or o il s u ch a s that in whic h sar di n es are preserYed , may be given ; m ineral machi n e oils an d pa raffi n are u n suitabl e.
O il is so o th in rr a n d is the refo re especiall y useful in p oiso n ing by A'cids, Alk alis a n d such a s Arseni c a nd C orr osive u bli mate. D emulcent dnnks, su c h as ba rley water or t h in gru el, act in th e sam e m ann er, a nd are fr ee fr o m da n ge r in c ases of ph osph oru s poisoning .
Th ese may be give n eithe r befo re or after the em eti c if the p oison c all s for one.
,Stron g Tea acts as a n e utra li ser of many poisons,
151
and is always ss. fe. A h a ndful of tea sh o uld be thrown int o a k ettle a n d b oil ed .
4. - If the lips and mouth are stained or burned give no emetic , but -
( a) If an Acid is known to be th e po iso n g ive a n Alk al i a t o n ce . Firs t wash t he mou th out f reely with liLlle wate r or other alkaline mixture, such as soda, chalk, whiting, or magllesia or \\ all plaster in water, and afterwards let the patient sip a little of It. 'oda and potash are not to be given in the case o f pOIsoning by oxalic acid.
(b) If a strong Alkali IS kno\\'!l to be the poison give an acid at once. First \\ash the mouth out freely with lemon JUIce or vinegar diluted with an equal quantity of water, and afterwards let the patient sip a little of it.
In both cases gi,'e oil (Rule 3)'
5. - When a person has swallowed poison and to go to sleep, keep him awake by walkll1g hun about and slapping his face, neck and ches t with a wet to\\ el. trong bla ck coffee may be give n t o drink . Slapping the sol es of t he feet may also be t ried.
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7. - Apply artificial respiration if breathing cannot be discerned.
8. - Treat shock and collapse.
9. - Preserve any vomited food, or other substance, suspected of bemg the poison. Do not \\"ash yessels \\'hich may have contained the poison, and carefully guard them.
Certain poisons require special treatment, an d a f ew of the commoner of these are mentioned below 'with thei r treatment.
CARBOLIC ACID.
T he odour of the breath will aid in the detection of this poison ; the lips and mouth are usually staine d white, and several nervouS symptoms come on .
1.- Give milk, to a pint of \\'hich half an ounce of E psom Salts has been added.
2.- Treat accorJing to the general rules.
PRUSSIC J\ ClD.
T he action of this poison is extrcmely. rapId. G iddiness, stagge r ing , insensibility accomr amed . pa n ting respiration, profound. collapse .and y convu lsio ns are the general SIgns, and 111 addItIOn a sm ell of b itter almonds is often present.
I.-Place t h e pati e n t in the ope n air.
153
cold wate r on the head and SpIne contll1uously.
3.-Apply artificial respintion .
4 ·-Hold snelling salts to nostrils.
5·-Treat shock and collapse. Cec page 135. )
l\IF,\T, Fl H AXD FUi\GT.
The signs and are yomiting and purging (diarrhrea), colic, heacb.che, great weakness, raised kmpej'ature and a quick pulse.
I.-Give an emetic.
2.-\Vhen the emetic has acted, giYe castor oil.
3 -Treat collapse. (. ee page 135.)
The signs and sympto TIS are a feeling of suffocation, livid features, and COI1VUISlO:1S. The patient rests on his head and feet, and the body is arched .
TREADIEXT.
I . -Giye an emetic.
2.-Apply artificial respiration . AT COHOL.
I .- G ive an emetic if the patient can swallow.
2.-Treat colbpse by keeping the patient warm, etc. (See page 135 )
QUEST I ONS ON CHAPTER VI.
Thi! m/Jllera1s iud/cate the pager where the answers may be found.
Under what two heads m:ly poi on be cIa sifiecl ?
\Yhat are the symptoms of poisoning by arsenic?
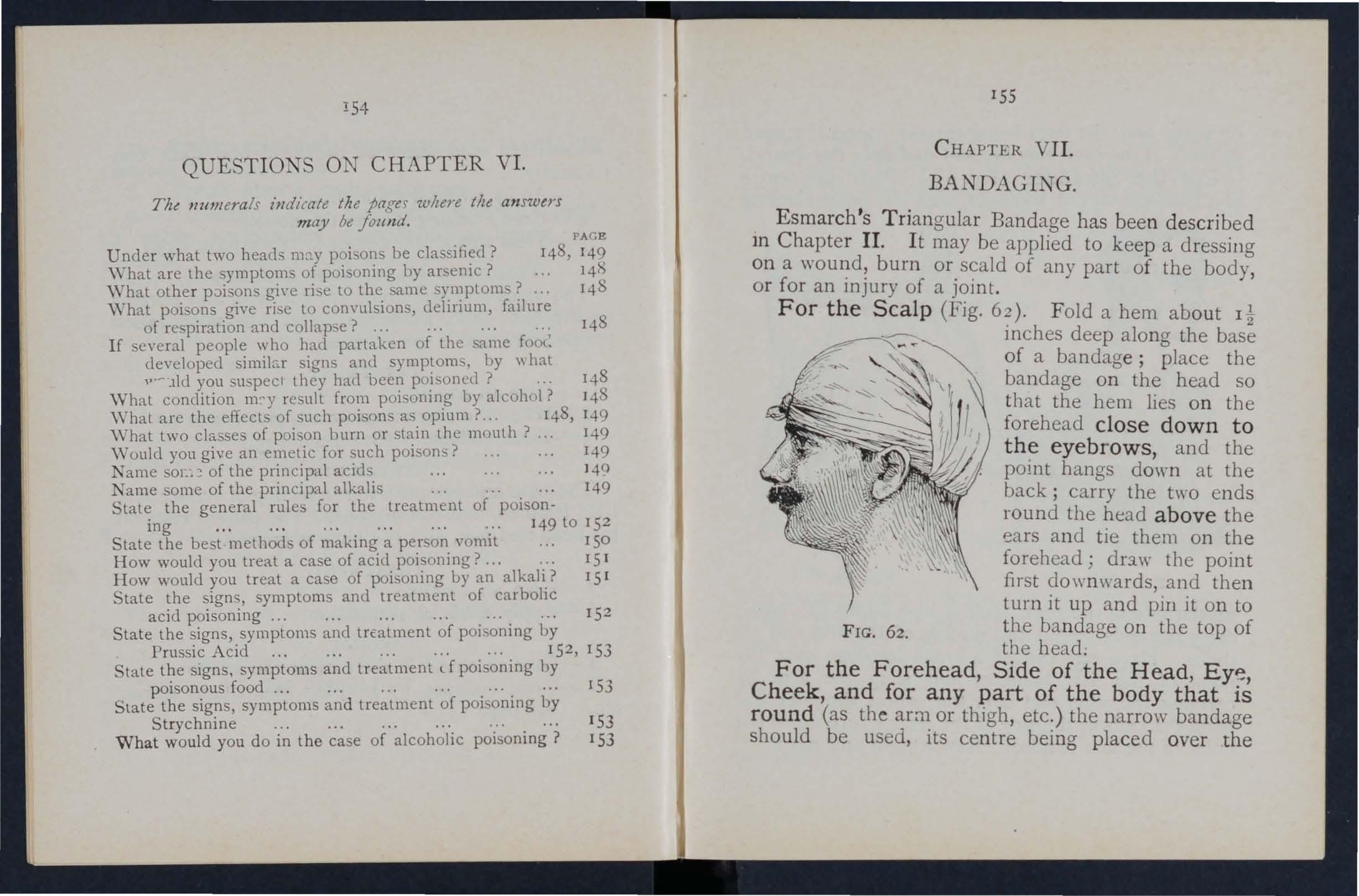
148, 149 14?)
\Vhat other p;:>isons gi\'e rise to the same symptom"? ...
\Vhat poi ons give ri e to convulsions, delirium, failure of respiration and collapse? ... 14 8 148
If everal people who had partaken of the 5..'1me foo<: developed simihr signs and symptoms, by \\ hat v·- lid you suspecl they had been poi oned ? 148
"YVhat condition m:-y re nIL from poi oning by alcohol? 14 8
\Vhat are the effects of such poi ons as opium?.. 148 , 149
\ Vhat two classes of poison burn or stain the month? ... 149
\\'ould you give an emetic for uch poisons? 149
Name oc::! of the principal acids 140
Name some of the principal alkalis 149 of poison-
State the general rules for the treatment ing 149 to 15 2
State the best methods of making a person vomit
How would you treat a case of acid poisoning? ...
How would you treat a case of poisoning by an alkali?
State the signs, symptoms and treatment of carbolic acid poisoning ...
State the signs, symptoms and trEatment of poisoning by Prussic Acid 15 2 , 153
State the signs, symptoms and treatment d poi oning by poisonous food ... ...
. . ..
C HAPTER VII. BANDAGING.
E smarch's Tri angular Bandage has bee n de scr ibed In C hapter II. I t may be applied to keep a dressing on a burn or scald of any part of the body, or for an Injury of a joint.
For the Scalp (Fig. 62). Fold a hem about Il inches deep along the of a bandage; place the bandage on the head so that the hem lies o n the forehead close down to the eyebrows, and the point hangs down at the back; carry the two ends round the head above the ears and tie them on the forehead; drs.w the point first downwards, and then turn it up and pin it on to F IG. 62. the ba n dage on the top of the head.
Slate the signs, symptoms and treatment of poi oning by Strychnine ... 153
W hat would you do in the case of alcoholic poisoning? 153 153
For the Forehead , Side of the Head Eyp Cheek, and for any part of the body that round (as the or thigh, etc.) the narrow bandage should be used., Its centre being placed over the
154
PAGE
ISO 15 1 15 1 15 2
. . .. . . .
.
155
a n d t h e e n ds bei ng carrie d round the hea d or 11mb, as the cas e may be, and tied ove r the woun d . For the Shoulder ( F ig. 63)' P lace th e c en tre of a bandage on the sho u lder, with the point running
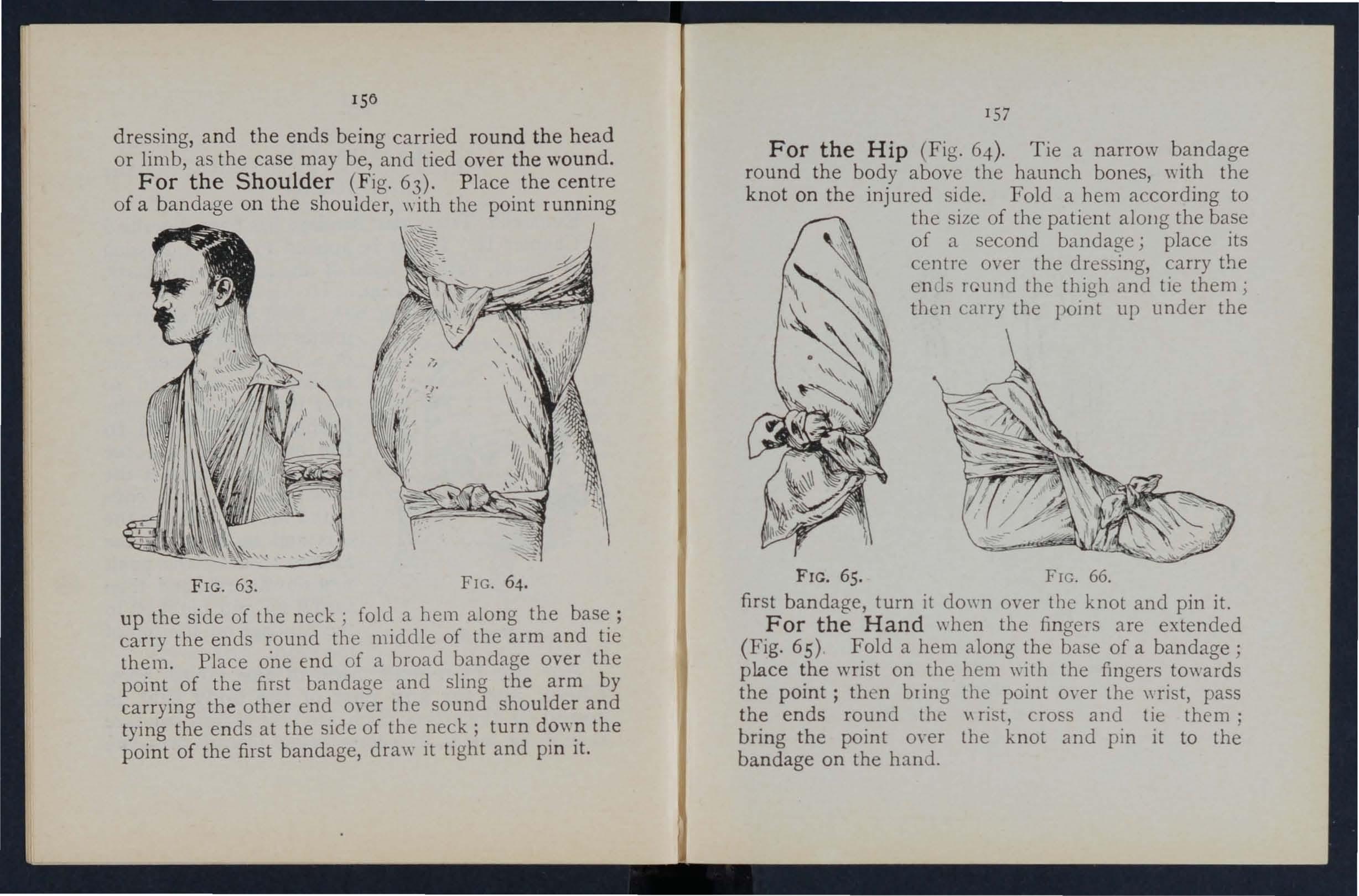
157
For the Hip (Fig. 64 ). Tie a narrow bandage round the body above the haunch bones ,,·ith the k n ot on the injured si.de. Fold a hem to the sIze of the patient alOllg the base of a second bandage j place its centre over the dressing, carry the end::. r und the thigh and tie them; then carry the point up under the
F IG . 63. FIG. 64.
u p the side of the neck; fold a hem along the base; carry the ends round the middle of the arm and tie them. Place one end of a broad bandage over the point of the first bandage and sling the arm by carrying th e other end over the sound shoulder and tying the ends at the side of the neck; turn do\yn the poi n t of the first bandage, draw it tight and pi n it.
FIG. 65. FIG. 66. first bandage, turn it down over the knot and pin it.
For the Hand ",hen the fingers are extended (Fig. 65) . a hem along the base of a bandage; place WrIst on .the hem with the fingers towards the pomt; then brIng point over the wrist, pass the ends round the \\ nst cross and tie them' bring the point over the knot and pin it to bandage on the hand.
15
5
15
8
For the Foot (Fig. 66). Place the foot on the centre of the bandage with the toes towards the point; draw up the point over th e instep, bring the ends forward and cross them; now pass the ends round
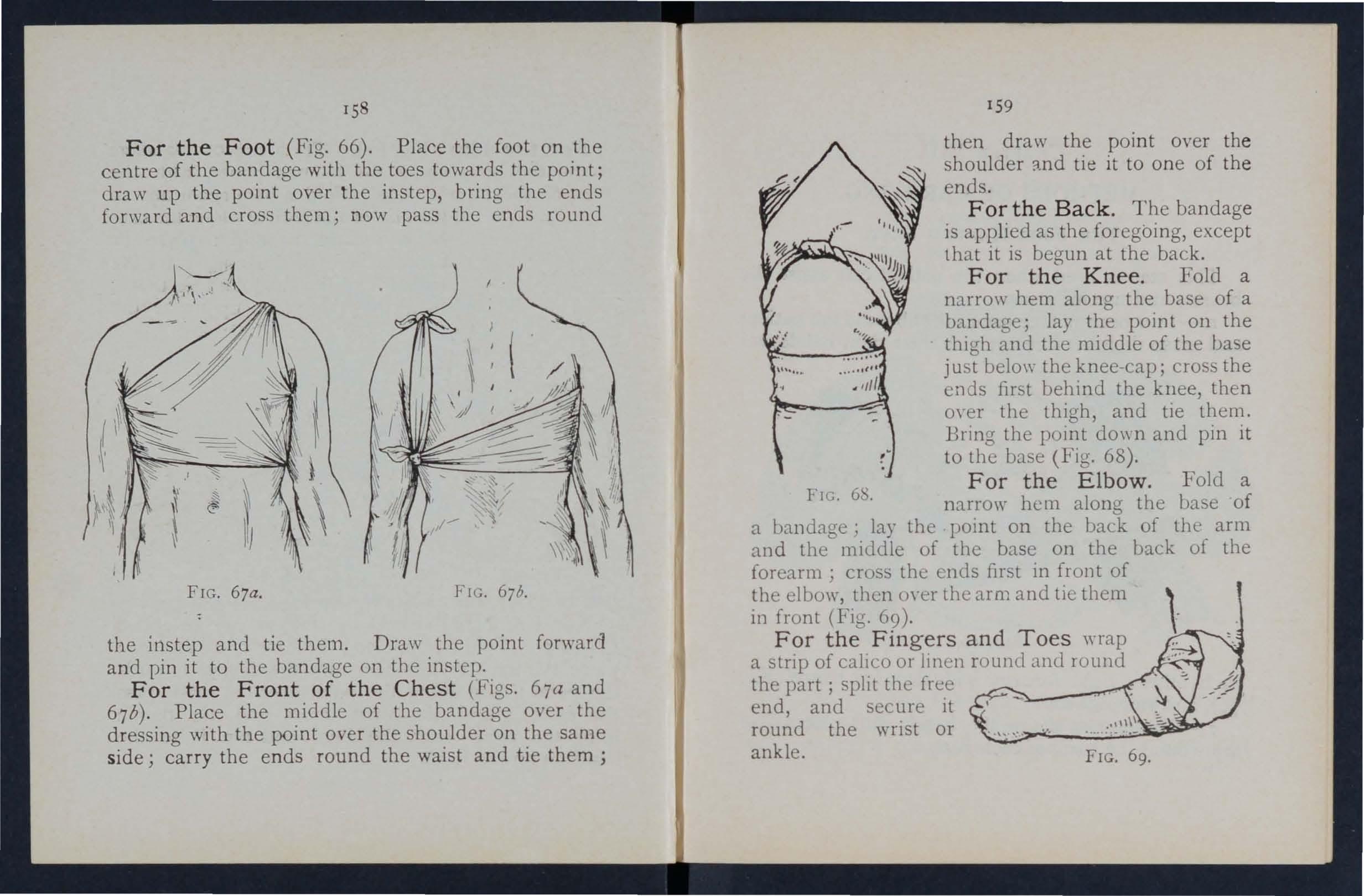
FIG . 67a. FIG. 67b.
the instep and tie them. Draw the point forward and pin it to the bandage on the instep.
For the Front of the Chest (Figs. 67a and 67 b). Place the middle of the bandage over the dressing with the point over the shoulder on the same side ; carry the e nds round the waist and tie them;
15 9
then draw the point over the shoulder :md tie it to one of the ends.
F or the Back. The bandage is applied as the foregoing, except that it is begun at the back.
For the Knee. Fold a narrow hem along the base of a bandage; lay the point on the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then oyer the thigh, and tie them. Bring the point do\\ n and pin it to the base (F ig. 68).
For the Elbow. Fold a
FIG. 6 '. narrow hem along the base of a bandage; lay the pomt on the back of the arm and the middk of the base on the back of the forearm' cross the ends first in front of the elbow, then m-er the arm and tie them in front (FIg. 69).
For the Fingers and Toes wrap a strip of calIco or 1ll1cn round and round the part; split the free end, and secure it round the wrist or ankle.
FIG. 69.
CHAPTER VIII.
METHODS OF CARRYING.
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
1.-T\\ 0 bearers face each other behind the patient and grasp their left forearm \\ ith their right hands and FIG. 70. each other's right forearm with their left hands (Fig. 70), and stoop down.
2.-The patient sits on the hands and places one arm round the neck of each bearer. 161
3·-The bearers rise together and step off, the on the right hand of the patient \\ ith the nght foot, and the left-hand bearer with the left foot.
THE EAT.
ThlS seat may be used to carry a helpless patient.
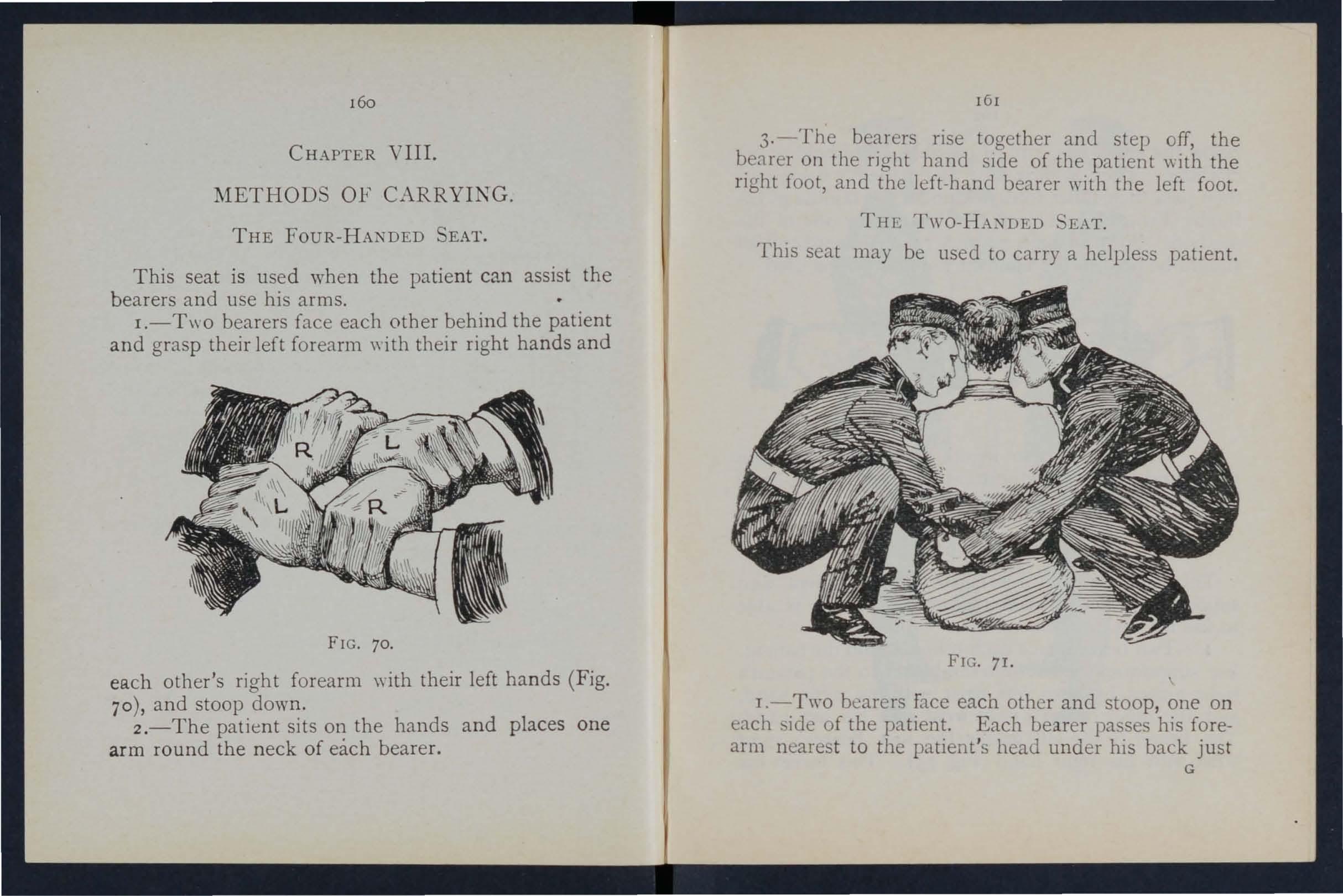
FI G 7r.
I.-Two beare rs face each other and stoop, one on each side of the patient. Each bearer pas e his forearm nearest to the patient's head under hlS back just G
160
below the shoulders, and, if possible, takes hold of hIS clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of bis thighs ( Fi g. 7 I ), and clasp th eir hands by on(; of the methods shown in Figs . 72 and 73. A handkerchief should be held in the hands if the first grip is used.
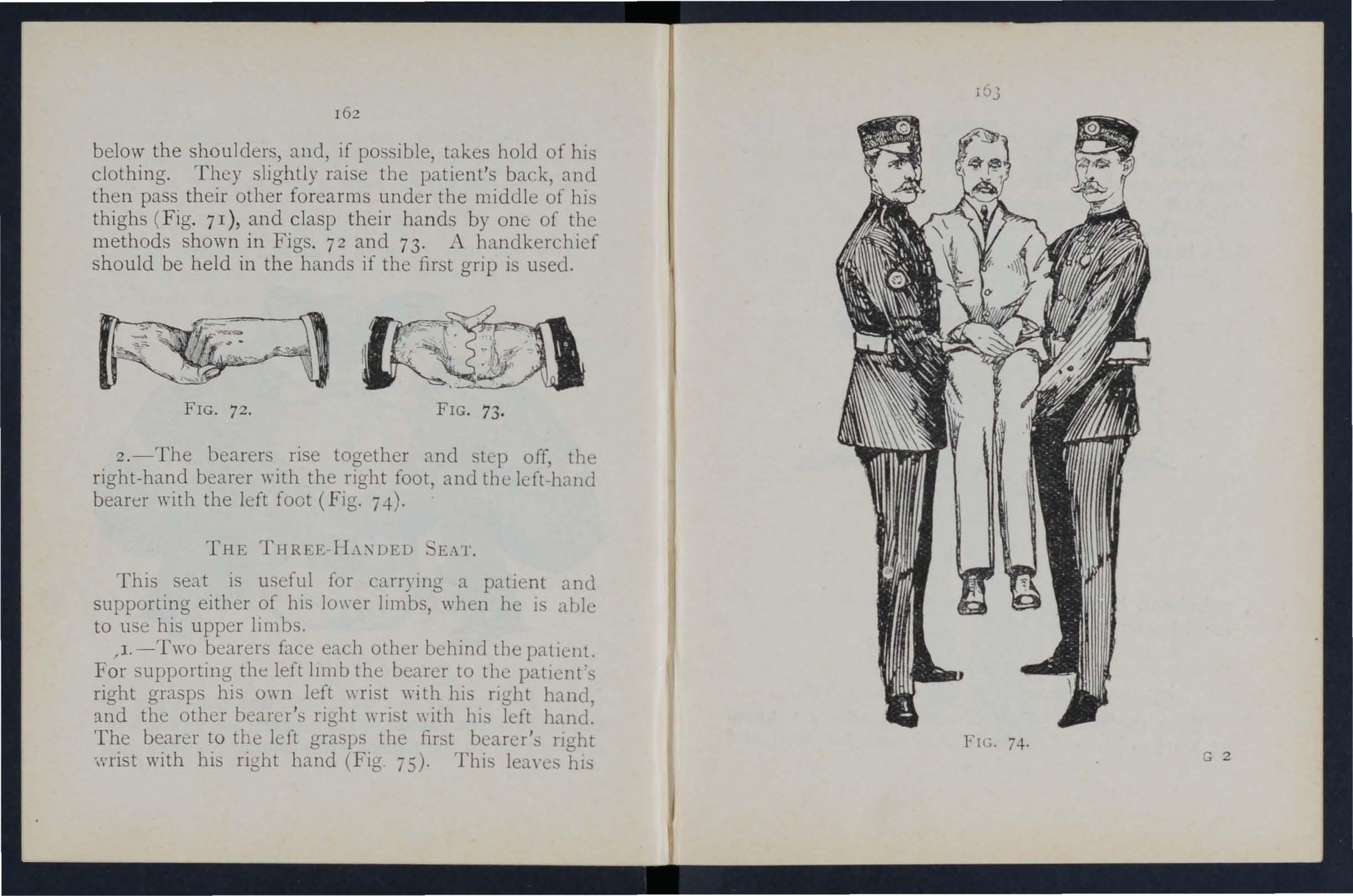
2.-The bearers rise together and step off, the right-hand bearer ,\'ith the right foot, and tbe left-band bearer with tbe left foot (Fig. 7-1-).
THE THREE-H.\:\DED K\1'.
Thi seat is useful for carryillg a patlent and supporting either of bis lo\\er limbs, when is able to use his upper limbs.
/1. -Two bearers face eacb other tbe patient. For upporting the left lJmb the bearer to the right grasps his 0'\'11 left \\'fist wi th bis righ t hanel, ::t.nd the other bearer's right \uist \\ ith his ldt hand. The bearer to the left grasps the first bearer's nght wrist with his right hand (Fig 75). This hiS
162
FIG. 72. FIG. 73.
left hand free to support the patient's left leg . For the patient's right lower limb foll o w the same directions, substituting "right" for" left" and" left" for "right." The bearers stoop do\yn.
2.-The patient places one arm round the n eck of each bearer and its on their hand.
3.-The bearers rise together and step off, the
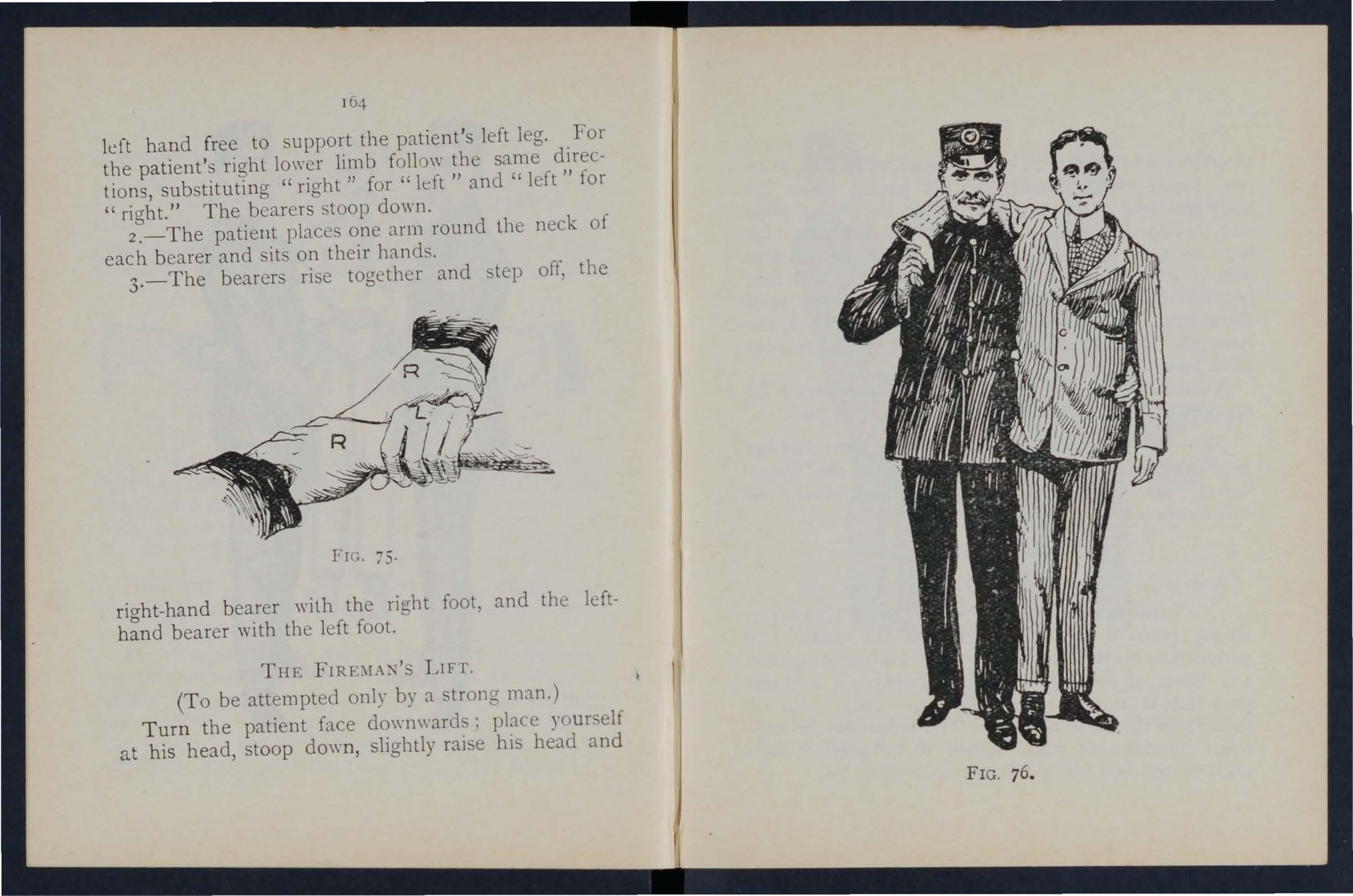
FIG. 75· right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE LIFT .
(To be attempted only by a strong man.)
Turn the patient face downwards: place yourself at his head, stoop down, slightly raise his head and
76 .
FIG.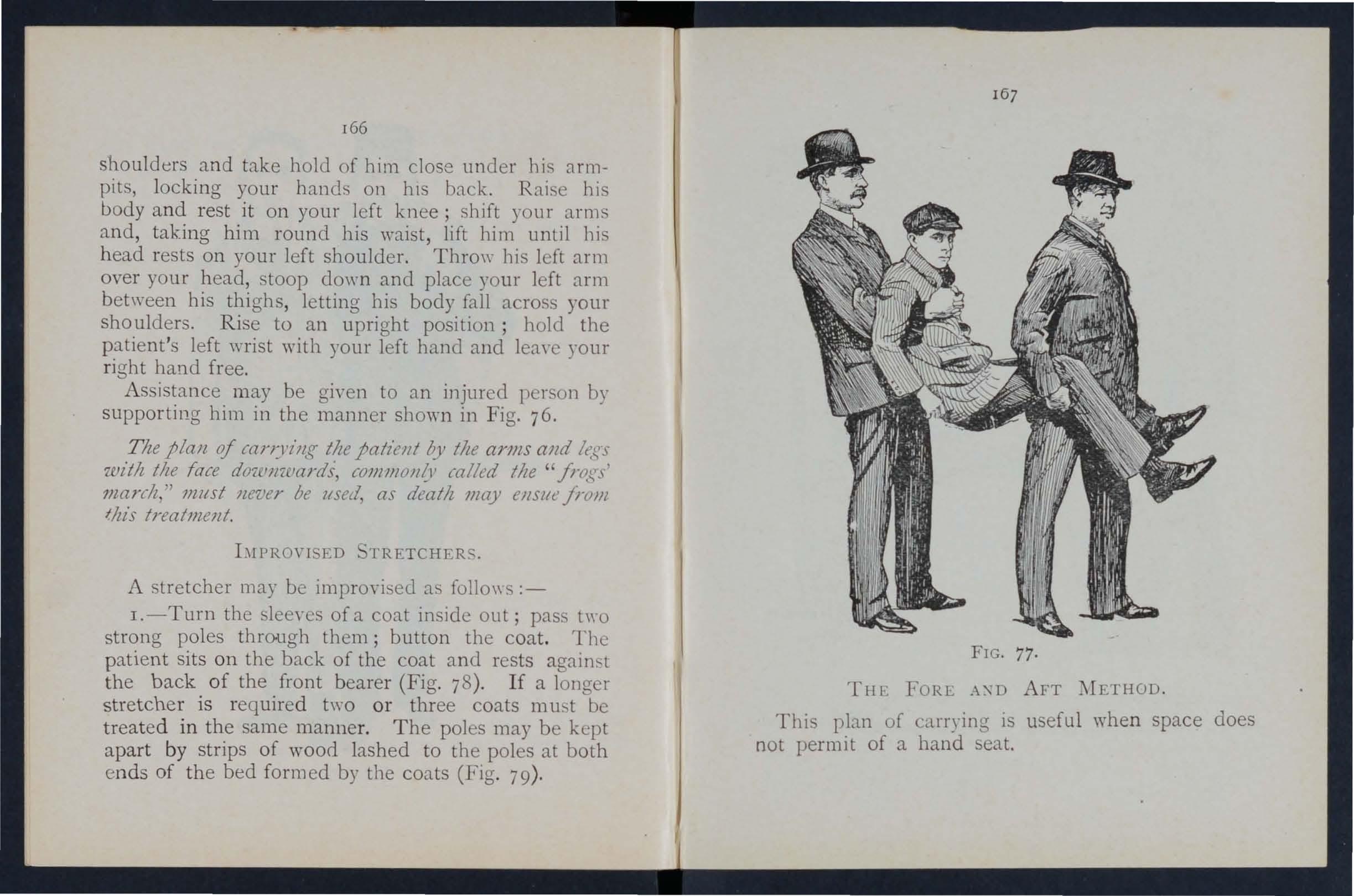
r66
shoulders and take holJ of him close under his armpit, locking your hands on hIS back. Rai. e hi body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until bis h ead rests on your left shoulder. Throw bis left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your shoulders. Rise to an upright position; hold the patient's left \\Tist with your left hand and lea,·e your ri ght hand free.
Assistance may be given to an injured person by supporting him in the manner shown in Fig. 76.
The plall of can:J'z·llg the patient by tile arms and It;!?,-s witlz tile face dowJlwards, COlllJJlOll1.1 , railed tile" frogs ' march," 7llltst never be lIsed, as deatlz may ellSll1! fr om Ihis treatmellt.
bIPRm'j ED TRETCHERC;.
A stretcher may be imprm-ised a follO\y.
1.-Turn the sleeyes of a coat inside out; pass t,\"o strong poles through them; button the coat. The patient sits on the back of the coat and rests againq the back of the front bearer (Fig. 78). If a longer stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of wood lashed to the poles at both en ds of the bed formed by the coats (Fig. 79). 167
77-
THE FORL A:;'D AFT METHOD_
Thi plan of carrying is useful when space does not permi t of a hand seat.
FIG.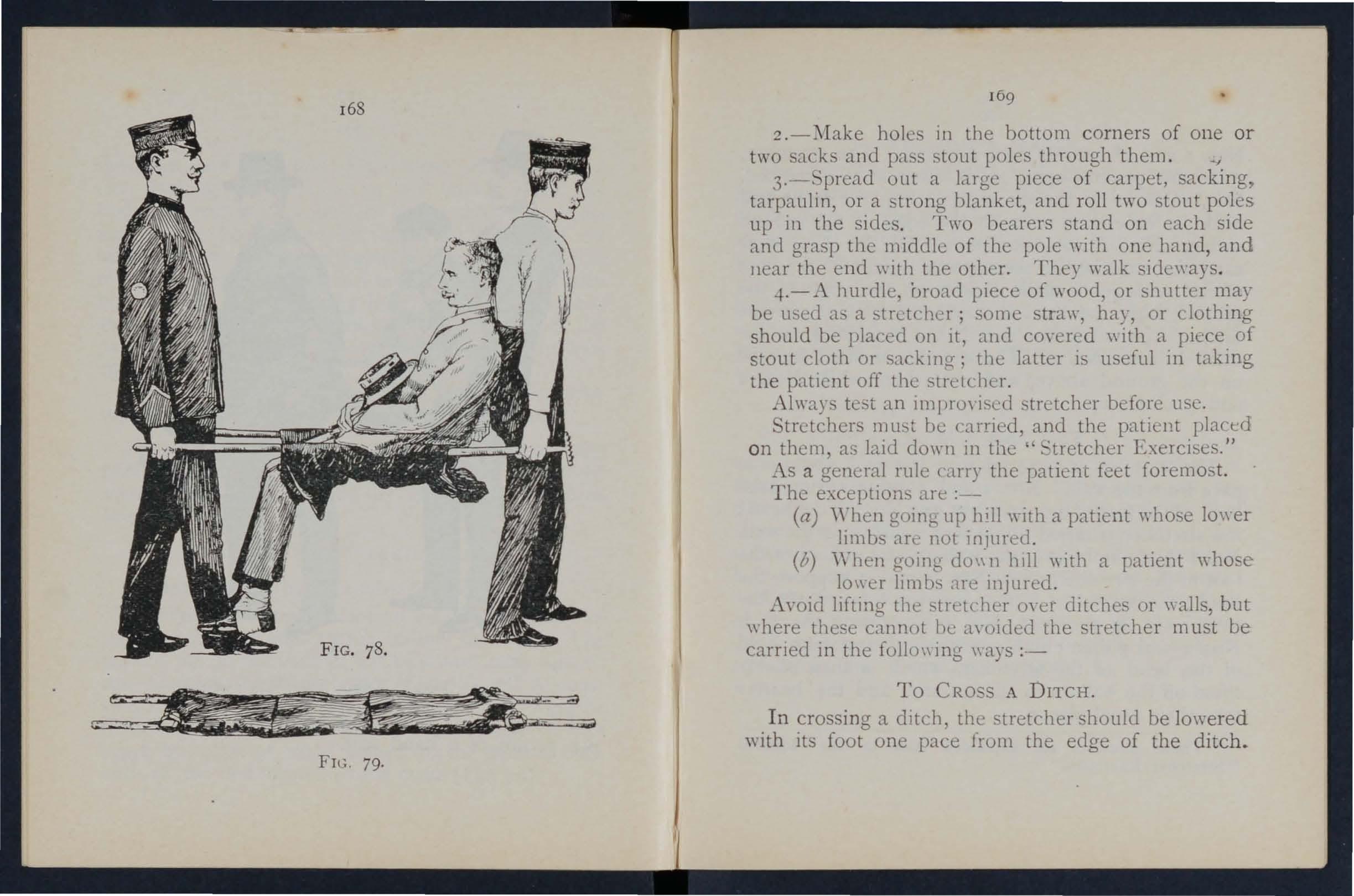
2.-Make holes in the bottom corners of one or two sack and pass stout poles throuCTh them. _/
3.-:'pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up ill the sides. Two bearers stand on each side and grasp the middle of the pole \\'ith one halld, and Ilear the end with the other. They walk idc\\'ays.
..f.-A hurdle, broad piece of wood, or shutter may be used a a streicher; some straw, hay, or clothing should be placed on it, and coyered \\ ith a piLce of stout cloth or sacking; the latter IS useful in takmg the patlcnt off the stretcher.
Always test an imprO\ lsecl stretcher before usc. tretchers be carned, and the patient placed on thcm, as laid dm\'ll in the ' Exercises."
As a general rule carry the patienc feet foremost.
The exceptions are :-
(a) \\'hen g01l1g up hill ,,-ith a patient \\-ho e 10'\ er limbs arc not injured.
(b) '\'ben going do\; 11 hill ",ith a patient lower limbs ,He injured.
the str -teher 0\ er ditches or \\a11s, but \\ here cannot I )t.; .wolded the stretcher must be carned in the follo\\ mg \\ays :-
To eRO S A DITCH.
In crossing a dItch, the stretcher should be lowered \\ ith its foot one pace from the edge of the ditch.
FIC.
169
79.
Nos. I and 2 % bearers then descend. The stretcher, with the patient upon it, is afterwards advanced, N os. I and 2 in the ditch supporting the front end whi le its other en d rests on the edge of the ground above. N o. 3 now descends . All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by TO . 3 in the ditch . No. I climbs out, TO . 2 renJaining in the ditch to assist NO . 3. The stretcher is lifted forward on the ground above, and rests there while Nos. 2 and 3 climb up.
To CROSS A 'VALL.
The stretcher is lowered \yith the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and No. 3 of the head; the stretcher is raised till the foot is placed on the wall.
o. I then climbs oyer the \Yall and takes hold of the foot of the stretcher, while Nos. 2 and 3 support the head; the stretcher is then carried forward till the head rests on the wall, TO . I supporting the foot. Nos . 2 and 3 then climb oyer the wall and take hold of the head of the stretcher, \\ hich i then slo\dy lifted off the wall on to the ground, and tht bearers take their usual places.
* These numbers are explained later in the d tatleJ "Stretcher Exercises."
T o LOAD A ' VAGON.
The stretcher is 10\\'ered with the foot one pace from the end of the \\ agon . Nos . I and 2 take hold of the foot of the stretcher, No . 3 the head . The is then raised and carried forward till the front wheels rest on the floor of the wagon . No. I then jumps into the wagon, \\hile No.2 goes to the head of the stretcber and helps NO.3 . The stretcher IS then pushed slO\rly into the wagon . If the tailboard cannot be shut, the stretcher must be lashed firmly to the sides of the \\agon.
To A
Nos. 2 and 3 take hold of the head of the stretcher, \\ bIle No. I gets into the \\agon; the stretcher is then gradually dra\\n out till the foot-wheels re t on the edge of the wagon. TO . I jumps out of the wagon, and with TO. 2 takes hold of the foot of the stretcher, 1\0. 3 supporting the head . The stretcher IS nm\/ gently dra\\n a\\ay one pace and lo\\ered.
'Vith four bearers TOS. I and 2 would lift the foot of the stretcher, while Nos. 3 and -t lift the head. This applies to eros ing a ditch or \\all, as well as to loading anu unload1l1g a wagon.
170
[7 2
CHAPTER IX.
STRETCHER TRA
The "Furley " Stre tchers (Mod el 1899) are of three viz., " O rdi nary," "Telescopic-handled, II and "PolIce." In general principle they are alike , the component parts being designated the poles,
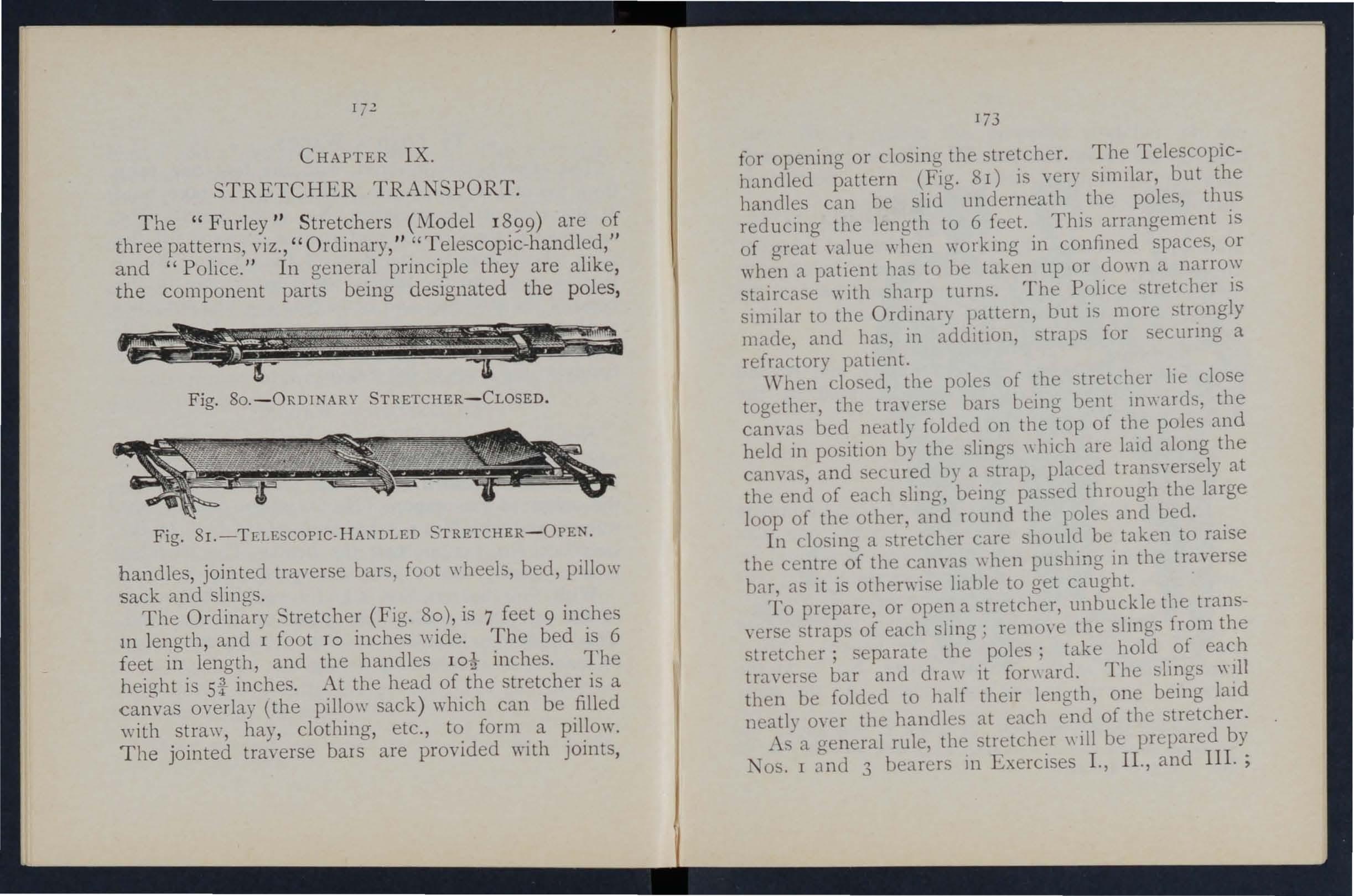
Fig. 80.-0RDINARY STRETCHER-CLOSED.
Fig. 8 I. -TELESCOP1C,HANDLED STRETCHER - OPEN handles, jointed tra\'erse bars, foot \\ heels, bed, pillow sack and slings .
The Ordinary tretcher (Fig. 80), is 7 feet 9 inches 111 length , and I foot TO inches \\"ide. The bed is 6 feet in length, and the handles inches. The height is si inches. At the head of the stretcher is a canvas o\'erlay (the pillo\\' sack ) which can be filled with straw, hay , clothing, etc., to form a pillow. The jointed traverse bars are provided with joints,
173 for opening or closing the stretcher. The TelescopicbandIed pattern (Fig. 8 I) i. very similar, but the handles can he sliJ underneath the poles, thus reducing the lellQth to 6 feet. This arrangement is of great value when \\orking in confined spaces, or when a patient bas to be taken up or do\\'l1 a narrow staircase with sharp turns. The Po!Jce stretcher is sImilar to the Ordll1ary pattern, but is more <;trongly made, and bas, in additIon, straps for secunng a refractory patient.
'Vhen closed, the poles of the stretcher lie close together, the tra, erse hal'S being bent in\\ ard'3, the canvas bed neatly folded on the top of the poles and held in position by the slings \\ bich are laid along the canvas, and secured n) a strap, placed trans,'ersely at the end of each slll1g, being pas::.ed through the large loop of the other, and round the I oles and bed.
In losing a tretcber care should be taken to raise the centre of the canvas \\ hen pushing in the traverse bar, as it is otherwise !JanIe to get caught.
To prepare, or open a stretcher, unbuckle the transverse straps of each sling; rcmO\'e the slings from the stretcher; separate the poles; take hold of each traver e bar and draw it fonmrd. The slings \\111 then be folded to half then' length, one laid neatly 0\ er the handles at each end of the stretcher.
•\ . a general rule, the trctc her \\ ill be prepared by lOS. I and 3 bearers 111 Exercises I ., II., and III. ;
174 and by TO. 2 in Exercise IV. These bearers \\ill, however, if required, assist the other bearers in attending to the patient's injuries.
lVo te.-The yarious movements detailed in the following Exercises should be carrieJ out steadily, the bearers working in unison, hurrying being carefully avoided, and eyery attention being paid to the b8arer who gives the words of command.
STRETCHER EXERCISES,
Originally drawn up by ir John I'urley, and revised in 1904 to accord \\"ith the drills adopted by the Royal Army "Medical Corp's :-
EXERCrE 1 o. 1.
FOR FOUR DEARER.
1.-The Instructor selects the bearers and numbers them-I, 2, 3, 4 at his discretion. hould one man be taller and stronger than the others, he should be styled TO. 3, as he will haye to bear the heavier part of the burden.* All orders will be given by IO. 4.
2 .-" Fall in. "-Nos. I, 2, and 3 take position on the left side of and facing the patient. 10. I places himself at the patient's knees, No. 2 at the hips, NO.3 at the patient's shoulders. At the same
* Bearers should, however, be taught to take any of the positions named in the following Exercises, whether that of No. I, 2,3, or 4 bearer.
175
ti me 1 o. 4 places the prepared stretcher on the ground by the right side of the patient about two
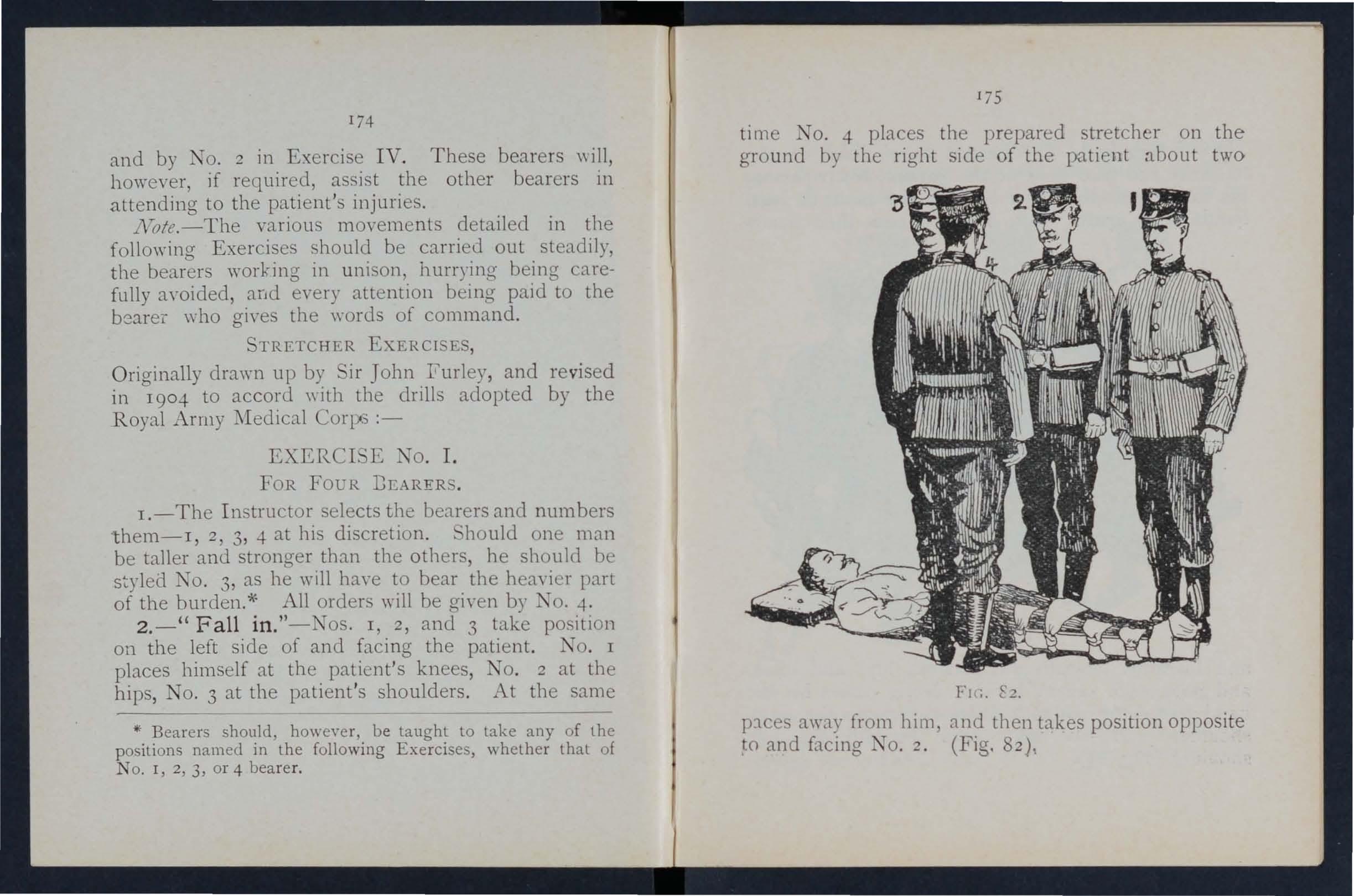
c2.
l)1ces away from him and then takes position opposite and facing TO. 2. (Fig. 82),
3.-" R ,e ady." -The bearers kneel down on the knee 2.nd take hold of the patient, No. I po. sing hIs and fore-arms beneath the patient's legs, hands wIde apart. Nos. 2 ahd 4 pass tbeir hands
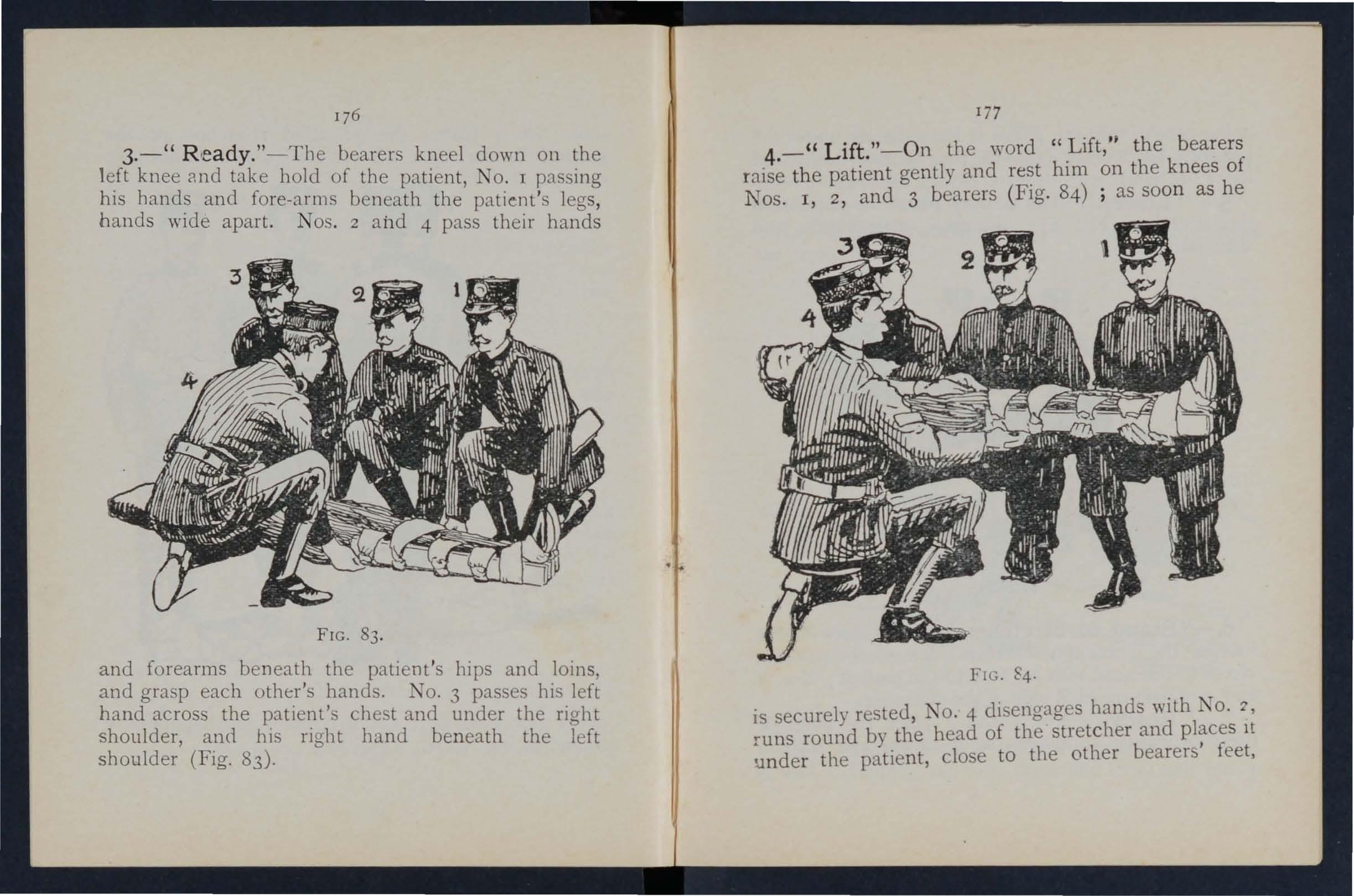
FIG. 83. and forearms beneath tbe patient's hips and 101l1s, and grasp each other's bands. NO.3 passes his left hand across the patient's chest and under tbe right shoulder, and his right band beneath the left sboulder (Fig. 83).
In
4.-" Lift." -On the word ".Lift,·' the bearers raise the patient gently and rest hIm on the knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as he
FI G 84 ·
is securely rested, NO.4 disengages hands with No. '1, runs round by the head of the stretcher and It under the patient, close to the other bearers feet,
176
being careful that th e pillow is immediately under the patient's head (Fig. 85) ' he then kneels down and locks his hands with those of No.2 (F ig. 86 ).
5. -- " Lower." -The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and th en stand up . FIC. 5.
6.-" Stand to Stretch e r. "-No. I goes to the foot of the stretcher, with his back to the patient; 3 to th e head with his face to the patient ; Nos. 2 and 4 remai n on each side of the stretcher.
7·- " Ready. "-Nos . I and' 3 place the slings (if over their shoulders, stoop down, and slip the I79
loops of the slings on to the handl es of the stretcher, \\hich they then grasp.
As soon as all is ri g ht the ,yord is given :-
8. - "Lift Stretcher. "-Nos. I and 3 bearers raise th e stretcher steadily together and stand up.
No/e.-Nos. 2 and 4 will n ow adjust the slings on the shoulder o f N os. I and 3, taking care that each is well belo\\' the le,'el of the collar and lies accurately in the hollow of the shoulder in front. Th ey will also lengthen or sho rt en the slings, haying regard to the pati ent's injuries and the relative heights of the bearers.
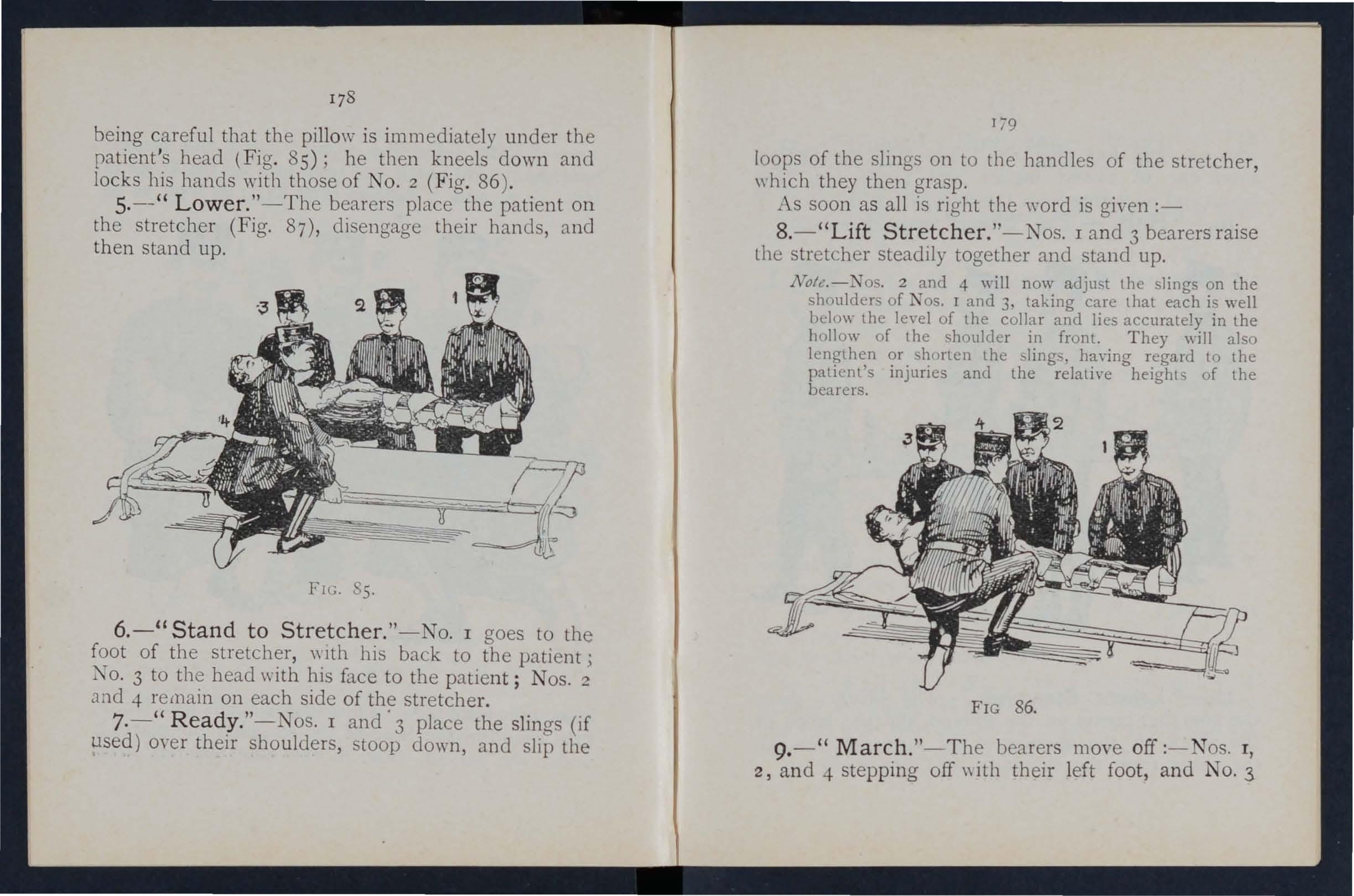
FIG 86.
9. - " March. "-The bearers move off :- N os. I , 2, a n d -t stepping off \\ ith their left foot , and NO.3
178
180
\\"ith his right foot (Fig. 87). The step should be a short one of twenty inches, and t aken with bent knees no fr 0111 the for e par t ?f the foot.
10. - Halt. -T h e b earers remam steady.
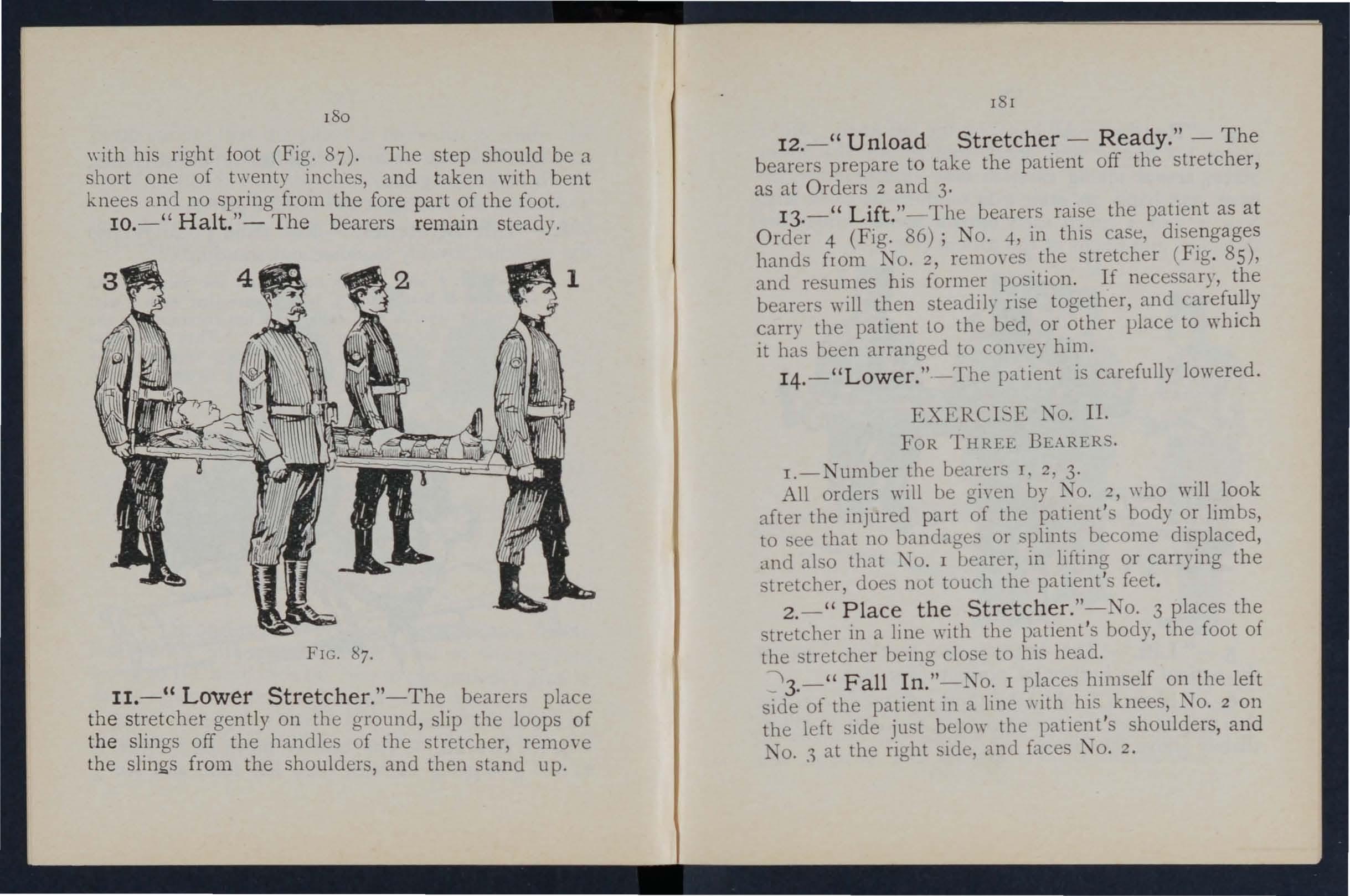
FIG. 87.
11.- " Lower Stretcher. "-The bearers place t h e gently on the ground, slip the loops of the slmgs off the handles of the stretcher remO\"e the slings fr o m the shoulders, and then up.
181
12.- " Unload Stretcher - Ready." - T he bearers prepare to take the patient off the stretcher , as at O rders 2 and 3·
13.-" Lift. "-The bearers raise the patient as a t Order 4 (Fig. 86); NO.4, in tbis case, disengages hands from J o . 2, remO\"es the stretcher (Fig . 85), and resumes his former position. If necessary, the bearers \yill then steadily ri e together, and carefully carry the patient Lo the bed, or other place to which it has been arranged to COl1\'ey him.
14. - "Lower. " - The patient is carefully lowered.
EXERCISE TO. II.
FOR THREE BEARERS.
I.-Number the bearers I, 2, 3·
All orders will be gi\'en by J O. 2, \\ ho will look after the injured part of the patient's body or limbs, to ee that no bandages or plints become displaced, and also that '0. I oearer, in lifting or carrying the stretcher, does not touch the patient 's feet.
2 .-" Place the Stretcher. "-No. 3 places the stretcher in a line "with the patient 's body, the foot of the stretcher being close to hi head .
' 3. -" Fall In. "-No. I places himself on the left side of the patient in a line with his knees, NO.2 on the left ide ju t belo\\" the patient's shoulders, a nd I o..1 at the right side, and faces TO. 2.
4.-"Ready. "-All kneel on the left knee . No. I places his ha n ds, \Yell apart , underneath the 10\\ er limb s, always taking c are, in c ase of a fracture, to have one h a nd on each side of the seat of injury. Nos. 2 and 3 grasp each other 's hands under the shoulders and thighs of the patient (Fig. 88).
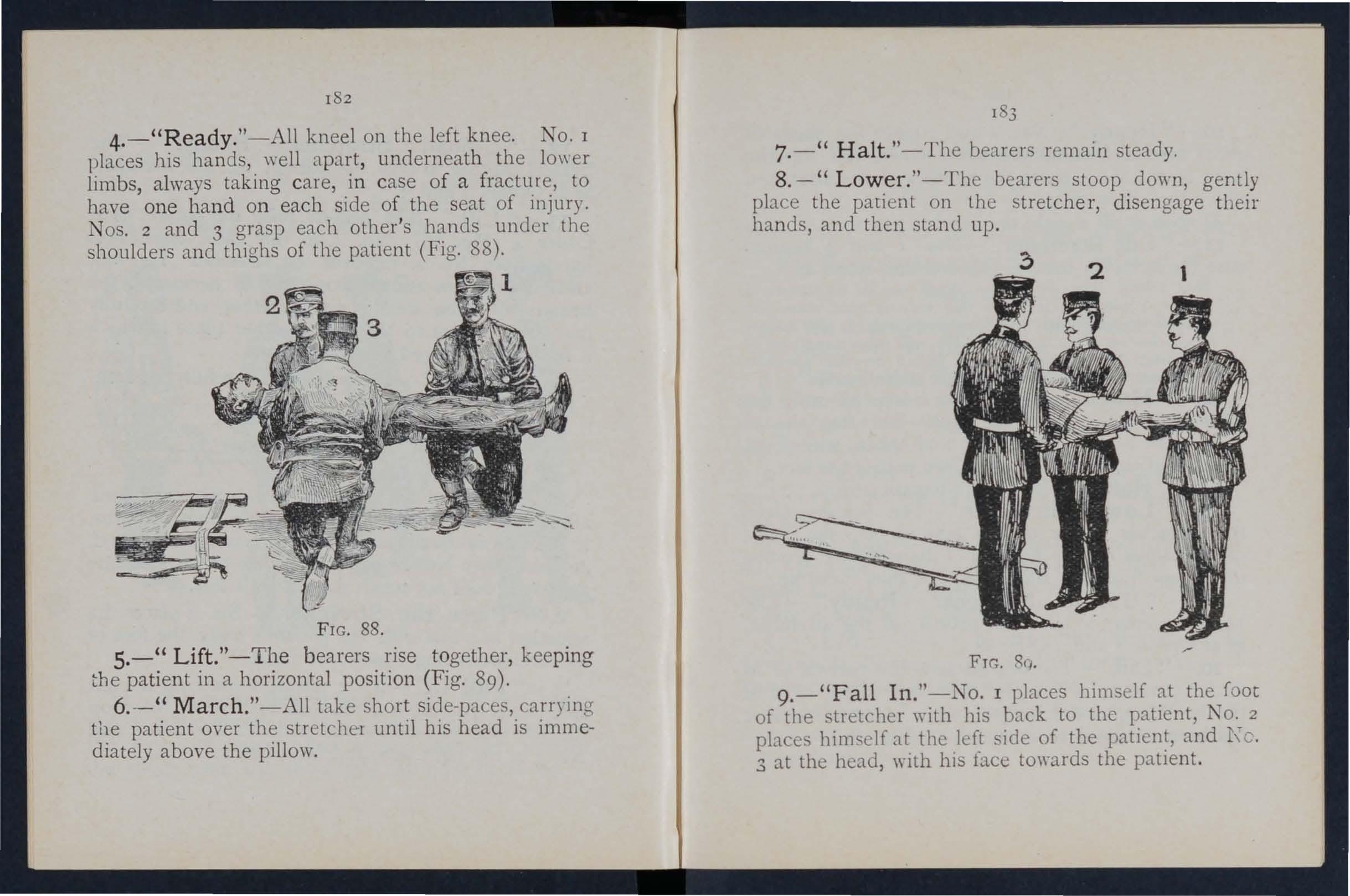
FIG. 88.
5.-" Lift."- The bearers rise t ogether, keep ing the pati en t in a horizontal positi on (Fig. 89).
6. - " March. "-All take short side-pa es, carrying the patient over the stretcher until his head is immediately above the pillow.
7. - " Halt. "- The bearers remain steady.
8. - " Low.er. "-The bearers stoop down, gently place the patIent on the stretcher, disengage their hands, and then stand up .
FTG. 8q.
9.-" Fall In ."-No. I places himself at the foot of the tretcher with his back to the patient, K o. 2 places him e lf at the left side of the patient, and [\'0. 3 at the head, with his face to\yards the patient.
r82
10. - " Ready. "-Nos. I and 3 place the slings (if used) over their shoulders, stoop down, and slip the loops of the slings on to the handles of the stretcher, whIch they then grasp.
As soon as all is right the word is gi\'cn-
11. - " Lift Stretcher."- Jos . I and 3 bearers raise the stretcher steadily together and sta nd up.
No. 2 will now adjust the 'ilings on the shoulders of K os. I and 3, taking care that each is wcll below the le\'el of the collar. and lies accurately in the hollow of the shoulder 1I1 front. Ile \\ill also lengthen or shorten the slings. ha\-ing regard to the patient's injuries and the relati\'e heights of the bcarers.
12. - " March." - TOS . I and 2 step off with the left foot, and TO. 3 with the right. The step should be a short one of 20 inches, and taken \\ ith benL knees, and no spring from the fore part of the foot.
13. - " Halt. "--The bearers remam steady .
14. -" Lower Stretcher. "--The bearers place the stretcher gently on the ground, shp the loops of the slings off the handles of the srretcher, rernO\'e the slings from the shoulders, and then stand up.
IS.'.' Unload Stretcher - Ready. " - The bearers prepare to take the patient off the stretcher, as at Ord ers 3 and 4 (Fig. 88),
16. - " Lift." - The bearers raise the patient, as at Or der 5, and carry him by short SIde steps, clear of the stretcher, to the bed, or other place to whIch It has been arranged to convey him (Fig. 89).
17. - " Lower ."- The patient is carefully lowered,
EXER I 'E III.
O.'\LY THI{EE ARE AVAILABLE AND THE , C\:-,':\,OT BE PLACED AS IN II.
r.-The In tructor numbers the bearerS-I, 2, 3. orders \\Iil be gin:n hy ;\0. 2.
2. -" Place the Stretcher. "-No. I taking the foot of the stretcher, and NO.3 the head, place it on the g-ruunu by the '>Ide of the p8.tient, and as close to him 8.5 practlc,'1ble.
3. -" Fall In." -The three hearers t8.ke the same pO:-iitlons 011 one SIde of the patient, as laid down in E-xerche o. I.
4. - " I, 2, and 3 kneel down on the left knee, pbcin,; them el\'es as clo e to the p8.tient 8.5 they com enlently ,can, and then take hold of him 8.S directed in Exercise I.
5. -" Lift. "-N"os. I, 2, and 3 raise the patient as directed in Exerci.,e I, and then move in a kneeling po itIOn up to the stretcher.
6. -" Lower. "-The hearers bend forward, carefully lower the patient 011 to the stretcher, and diseng8.ge hands.
184
I 6
7. -- " Stand to Stretcher. "-All the bearers stand up; No. I goes to the foot, No . 2 remains 111 position at the side, and No. 3 goes to the head 0\ t h e
8. - " Ready."-Nos . I and 3 place the slings (if used) over their shoulders, stoop down, an,1 slip the loops of the slings on to the handles of the stretcher, which they then grasp . '
9·-" Lift Stretcher. "-Nos. I and 3 bearers rai e the stretcher steadily together and stane! up.
No, 2 \\ ill now adjust the slings on the boulders of os.
I and 3. taking care that each is well below the len: I of the collar, and lies accurately in the hollow of the shoulder in front. IIe \\ill also lengthen or shorten the slings, haying regard to the injuries and the relati\'e heights of the hearers.
10. - " March. "-Nos. I and 2 step off with the left foot, and No . 3 with the right The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
11. - " Halt. "-The bearers remain steady.
12. - " Lower Stretcher. "-Tbe bearers place the stretcher gently on the ground, slip the loops of the ..lings off the handles of the stretcher remO\'e the slings from the shoulders, and tben stand up.
13.--" Unload Stretcher-Ready. " - '0 . r places himself on the left side of the patient, and in a lll1e with bis knees, No. 2 on the left side just below the patien t's shoulders, and NO , 3 at the right
side, and faces NO.2. All kneel on the left knee.
o. I places his hands, well apart, underneath the lower limbs, al\\ays taking care, in case of a fracture, to have one hand on each side of the seat of injury.
TOS. 2 and 3 grasp each other's hands under the shoulders and thlg-hs of the patient.
14·-" Lift ." - The bearers ri e together to their feet, keeping the patient in a horizontal position, and carry him by short ide step., clear of the stretcher, to the bed, or other place to "'hich it has been arranged to convey him.
15 ·-" Lower ."- The patient is carefully lowered .
EXERCL'E TO. IY.
FOR "C'SE
AXD NARROW
ClJTTIXGS \\ T\\ 0 ::\IJ;: x O,\LY C.\:\' BE EXGAGc.D.
T os. I and 2 " '111 carefully place the stretcher in a lmc \\ith the injured man's body, the foot of the stretcher being, if possIble';;' close to his head.
o. J straddles the patient ' s legs, placing his right Coot, \yith the toe turned outward, a little below the patient's knee . , and with the toe of the left foot clo e to the heel of i\o. 2; he then toops down, passes the left hand under the patient's thighs and
• It is not ach'isable to be too particular as to the head or foot of a. stretcher in a mine, as it would probably be quite impossible to reverse it.
I S right hand. across and under the patient's calves. No . 2 hIS feet one Oil each side of the patient between his b.ody and , the toe of each foot as near the armpIt as possIble. He then sto ops down and passes hIS hands bet\yeen the sides of the hest and the arms underneath the houlders, and locks
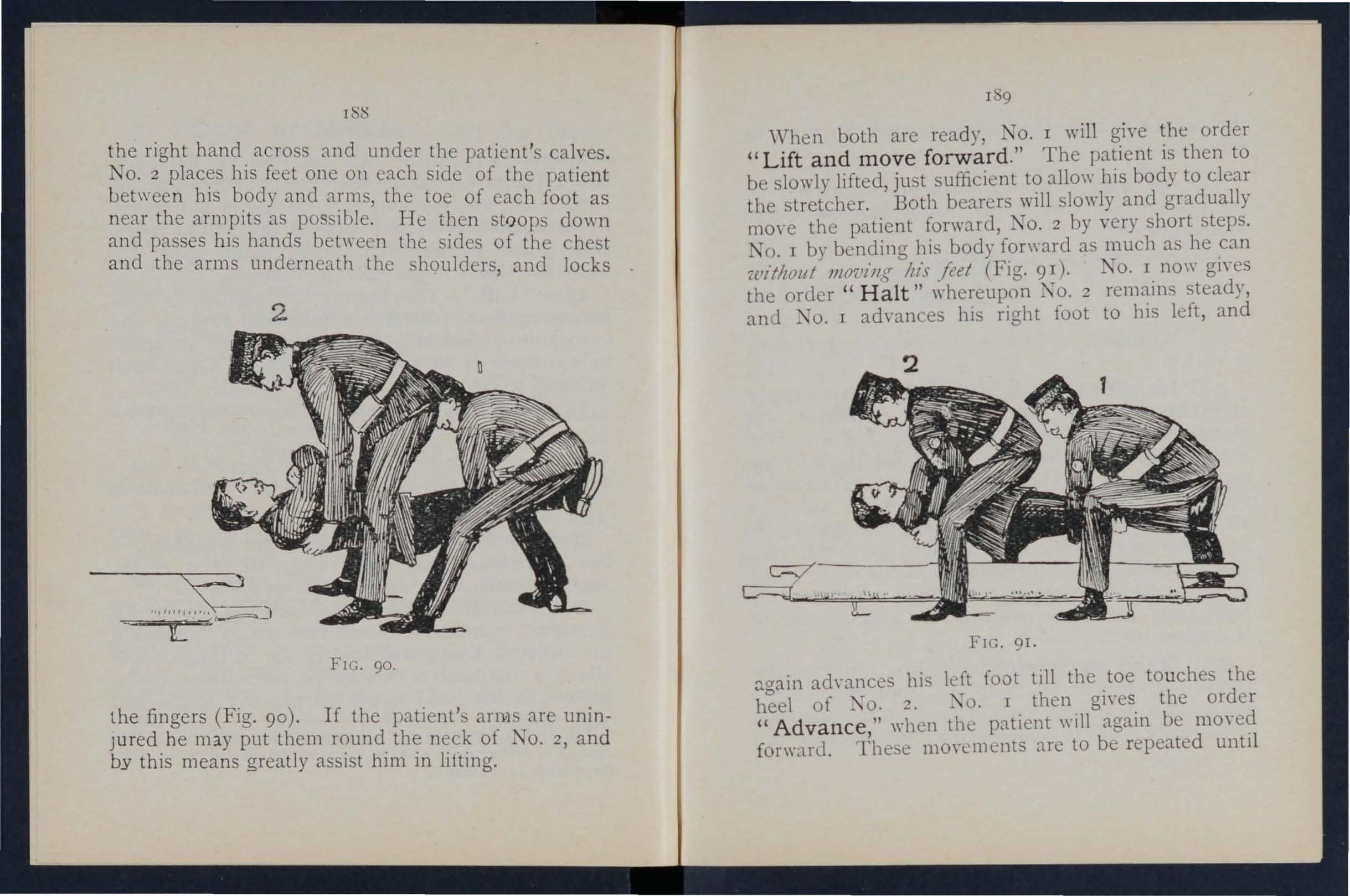
FIG. 90.
the fingers (Fig. 90). If the patient' an}1 are uninJur ed. h e m ay put them round the neck of No.2, and by thIs means greatly assist him in lifting.
I 9
'Vhen both are ready, No. I will give the order "Lift and move forward ." The patient is then to be slowly lifted, just sufficient to allo\\' his body to clear the stretcher. Both bearers will slowly and gradually move the patient forward, NO.2 by very short steps. No. I by bending his body forward as much as he can 'without JIlo7. 'iJlg Itis feet (Fig. 9 I). TO. I now gives the ordcr " Halt " whereupon NO.2 remains steady, and I advances his right foot to hIS left, and
FIG. 91.
again ad\'ances his left fo()t till the toe touches the heel of X o. ::!. J. TO. I then gives the order " Advance ," when the patient will again be moved forward. These moycments are to be repeated until
2
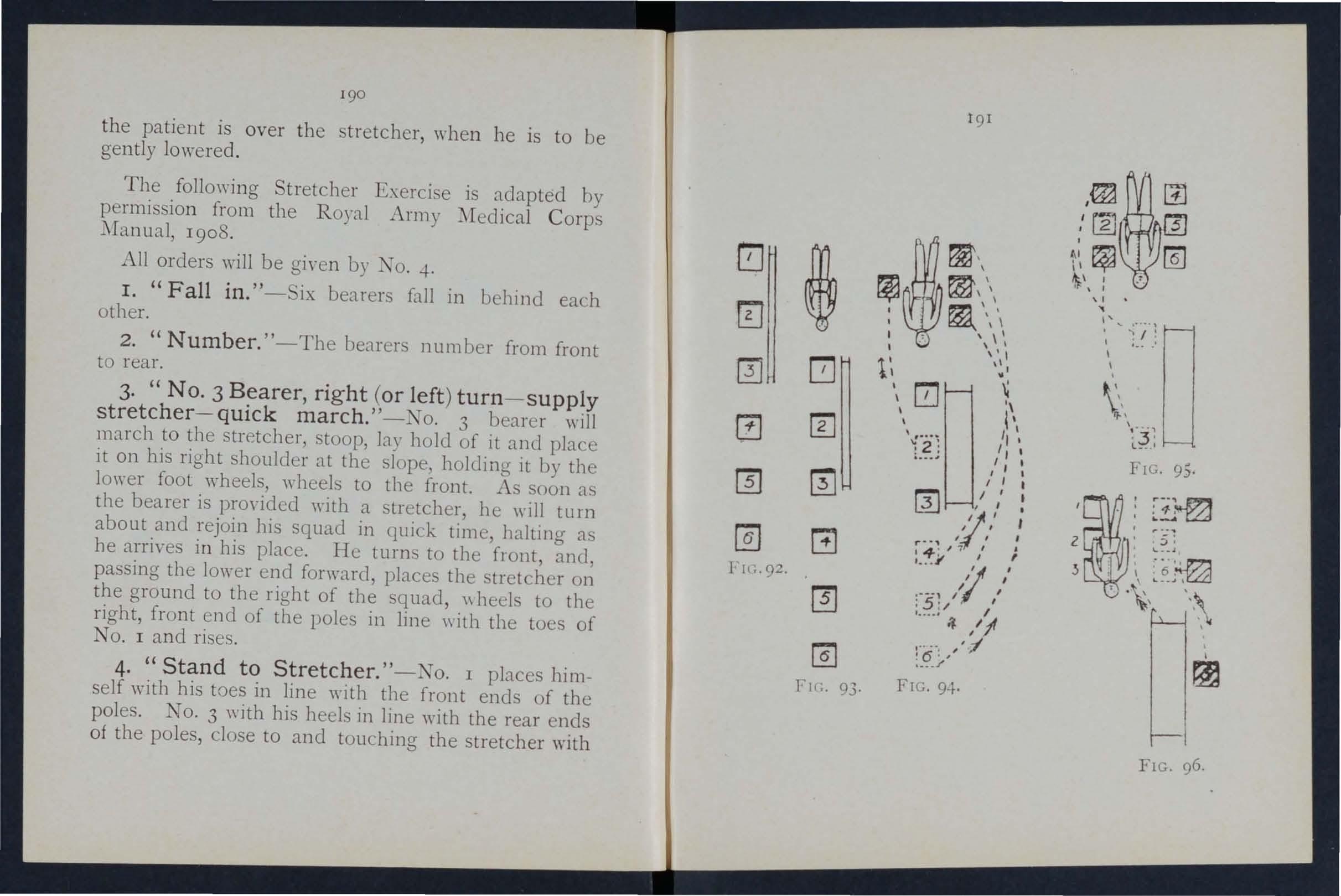
the patient is over the stretcher, when he is to be gently lowered.
The following Stretcher Exercise is adapted by permission from the Royal Army Medical C orps Manual, 19 08 .
All orders will be given by No. -to I. "Fall in. " - ix bearers fall 111 behind ea h other.
2. " Number. "-The bearers number from front to rear.
3· "No·3 Bearer, right (or left) turn - supply stretcher- quick march. " - TO. 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower foot "'heels, wheels to the front. As Soon as the bearer is prm'ide d with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place. He turns to the front, and, pa sing the lower end forward, places the tretcher on the ground to the right of the squad, \\ he 1 to the right, front end of the poles in line \\ ith the toes of No. I and rises.
4· "Stand to Stretcher. "-No. 1 places himself with his toes in line \yith the front ends of the poles. o. 3 with his heels in line with the rear ends of the poles, close to and touching the stretcher with
i tTI rn [3 m m rn @] G Il l··92 . @] rn I· ll:, 93. t9 1 I I c. \ \ '. I ' " t' ,I \ 0 u "i \ 1\ \." •• • " I l.? j /' I I I I I IT) I' I 3 , I I :/,' , ,. , I ::f:/ ) i • ___ , ,I I :.:?;/ / :t. /1 t" --. ,';1 '6 ' , .... / FIG·9-}· /rn 5 1i.1 •• , , I ".. "" 0 ' '> I ' I • •. 0' \ I \'., FIG. 95. I ! 4. I f"" 2 ' ?; , FIG. 96.
f his. I:ight foot. o. 2, 4, 5 and 6 take up their posltlO ns one pace behind and covering off the bearer in fro n t of them (Fig. 92!. -
S· "Lift Stretcher. "-lOS. I and 3 stoop, grasp both handles. of the poles \\ ith the right hand, rise together holdll1g the stretcher at the Cull extent of the arm, wheels to the ricrht.
6 "C b . ollect Wounded - Advance. " - The squad by the shortest route to the patient, and halts mthout further \Yord of command one pace from the head of and in a line with the patient (Fia.9").
7· "Lower Stretc.her. "- os. 1 and 3 .OtoC:p, place the stretcher qUIetly on the ground, and rise smartly together,
8. Stretcher. "- I and 3 turn to the nght, kneel on the left unhuckle the transyerse straps, and place the slinss on the ground besIde them, separate the poles, and traighten the tra \·erses.
. On \\ord two each take a ling, dou hIes It on Itself, slIps the loop thus formed on the near handle, and places the free ends O\'er the opposIte handle, buckle uppermost. They then rise ami turn to their left together.
'\vhile the s.tretcher is bei ng prepared by N" as. I and 3, the dIsengaged bearers \"ill adyance and render to the patient such assistance as may be required (Fig, 94),
193
The necessary assistance having be·.n rendered, NO.4 \\ill give the command-
9. "Load Stretcher. " - The bearers place themselves as f01l0\\s:- O. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; Nos. I and 4 at the knees, 2 and 5 at the hips, 3 and 6 at the shoulder, the whole kneeling on the left knee. Nos. I and 4- pa s their hands beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care be1l1g taken of the injured part, one of the bearers being detailed for purpose (Fig. 95).
10. "Lift. "-The "hole will carefully lift the patient on to the knees of os. I 2 and 3.
Two. No . . ..: 5 and 6 wIll then di engage, rise; Nos. -+ and 6 step hack one pace. X 0, 5 turn to his left, doubles to the stretch r, take hold of and ral es. it, left hand the near pole re ting on the left hlp; carrying the stretcher he returns to hiS place bet\\ een -+ and 6, and places it b neath the patIent.
Tllrce. 1\ os. -+ and 6 step fOT\\'ard one pace, and together with NO.5 kneel do\\ n on the left knee, and prepare to assi . t in lowerin,g' the patient (Fig. 96).
II. "Lower:'-The patient is lo\\ered slowly a.nd gently on to the centre of the canya.s (special c..ue being taken of the injured part).
1-'wo The bearers disengage, rise; Nos. I, 2, 3 and 6 turn to the left ; Nos. -+ and 5 to the right j H
194
No. 4 places himself three paces in front of the stretcher. No.6, having collected the kit and anns of the patient, places himself three paces in rear of the stretcher, Nos. 2 and 5 opposite the centre of the stretcher. The whole are now ready to lift stretcher and move off (Fig. 97) .
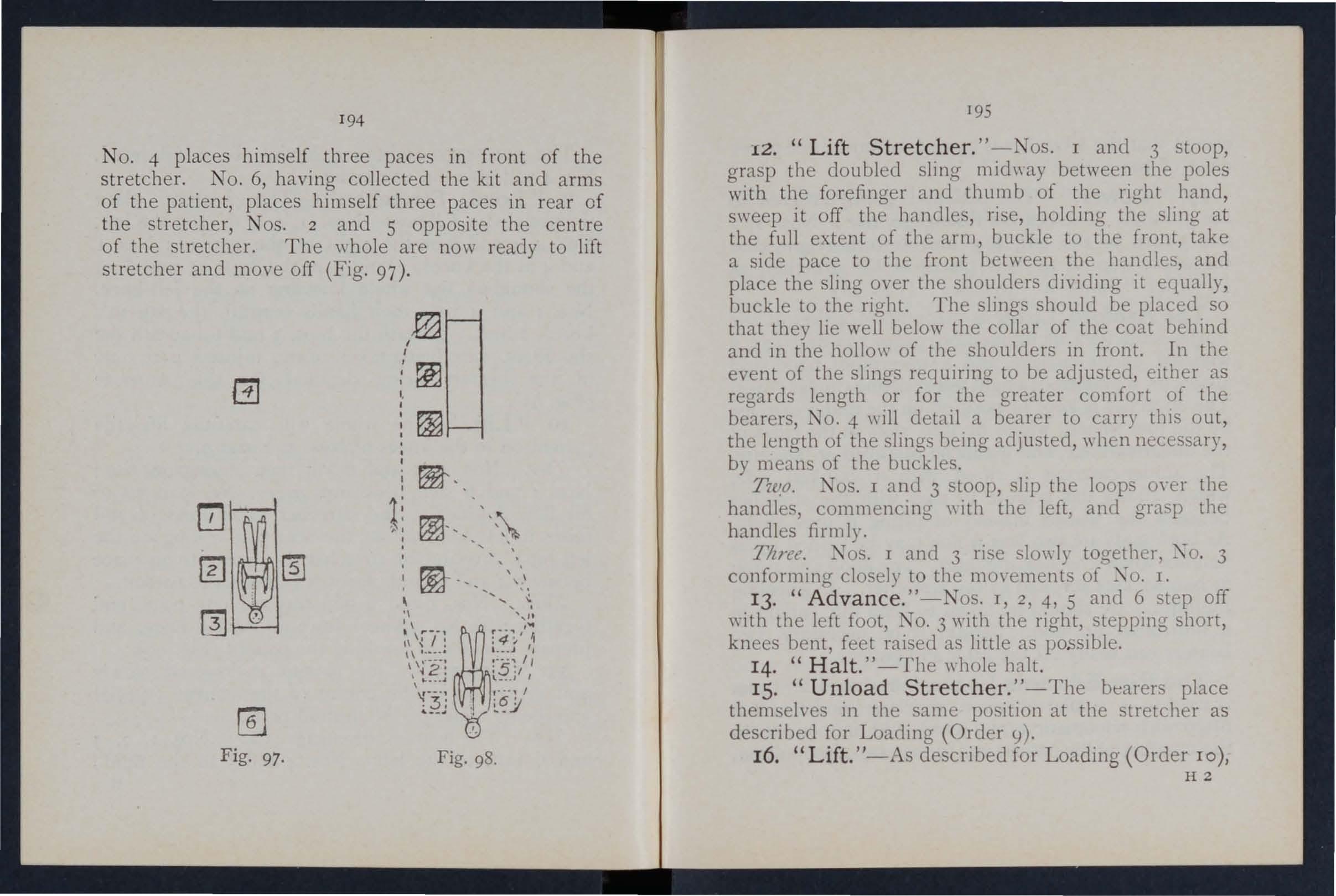
Fig. 97. Fig. 98.
195
12. "Lift Stretcher. " -Nos . I and 3 stoop, grasp the doubled sling mid\\ay between the poles with the forefinger and thumb of the nght band, sweep it off the handl es, ri se, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between the handles, a nd place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollo\\' of the shoulders in front. In the event of the slings requiring to be adjusted, either as regards length or for the greater comfort of the bearers, NO.4 \\ ill detail a bearer to carry thIS out, the length of the slings being adjusted, when necessary, by means of the buckles.
Two. os. I and 3 stoop, slip the loops m·er the handles, commencing \\ ith the left, and gra p the handles firmly.
Titre!!. I and 3 ri e lo\\"ly together, . 3 conforming closely to the mO\'e ments of X o. 1.
13. "Advance."-Nos. I, 2, 4, 5 and 6 tep off "'ith the left foot, o. 3 with the right, stepping short, knees bent, feet raisecl as little as possible.
14. "Halt." -The whole halt.
IS. "Unload Stretcher. "- The bearers place themselves in the same po ition at the stretcher as described for Loading (Order 9).
16. "Lift.'I-As described for Loading (Order 10), HZ
o
except that the stretcher is carried forward three paces clear of the pJ.tient's feet.
17. "Lower."- The patient is gently lowered to the ground. The bearers disengage, rise; os. I, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whol e step off to their places at the tretcher, as at Order "Stand to 'tretcher 1/ (Fig. 98).
The Ashford Litter is made up of either of the Furley stretchers mentioned on pages r 7 2 and 173, a wheeled under-carriage and a waterproof hood and apron, or, if preferred, a light wet-resisting canvas cover. The stretcher is kept in position on the under,carriJ.ge by the foot-wheels, ""hich fit into slots in the sides of the under-carriage, and it can be remoyed at pleasure. The under-carriage is fitted with a cranked axle, which allows the bearers to pass with the stretcher the wheels instead of lifting it O\'e r them. At both ends are two legs which may be turned up as handles when wheeling the litter. The hood and apron fit into sockets screwed to the stretcher. In wheeling the litter, care should be takell to keep the patient in a horizontal position . 'hould it be necessary, two bearers can easily lift the litter and patient.
The Rea-Edwards Litter, introduced in I9 0 4, is used in a similar manner. and one model of it is fitted with pneumatic tyres, \\hich add immensely to the comfort of the patient and to the ease of propulsion.
197
CHAPTER X.
(Be/ncr tile A/tlz Lecture Jor Females olliy, ill accordance <> 'Wdll 58.)
BV E. :'I1ACDO . ELL COSGRAVE,
WHE. ne\\ s of an accident comes, preparations hould at on e be nude so as to have everything ready before the injured person is brought in. course the preparations needful \\.ill. yary accordmg the and extent of the lI1Jury, but the follo\\'lng are the chief things whIch may have to be done.
CHOICE A:\D OF Roo:.\[.
A room must be chosen. In a bJ.d case this should be one easily reached, as it is dIfficult to carry ,an in jured person through narnw passages U'nless there is some such reason agamst It, the injured per on 's own room is best. . . The way to the room must be cleared, furniture and 100 e mats in the hall or In lobb.les should he remO\'ed. If the injured person I on a door, shutter, or stretcher, t"'? strong- chaIrs should be placed ready to support It \\ hel e\'er the bearers would be likely to reqUIre rest.
Useless furniture should be removed from the bedroom. The bed should be dra\\'n out from the \Yall
196
:,\1 D., F R C.P.I.
FOR OF ACCID:E,X I CASES.
so that both sides can be approached, and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much collapse seyeral hot bottles and hot may be required; CO\"E;r the hot bottles with flannel.
If the injury is vel")' seyere, if mud-stained clothes have to be removed, or if extensive dressinO"s have to be applied, it may be necessary to have an;ther bed, a couch or. a table placed near the bed to lay the sufferer on m the first instance. This should be so arranged that soiling may do no harm; old sheets, waterpoof materials, thin oIlcloths, or even nc\\ spaper, may be used as a protection.
LIFTIt\G AND CARRYI:\G.
If present at the place where the accident occurred it will . ?e necessary to see that the patient is fully lltted after proper "First Aiel" has been rendered.
The following rules houle! he remembered:- elect the proper num ber of persons to assist, and do not let them lift the patient until they thoroughly understand how they are to do it.
For .ordinary cases, \\here the injured person has to be. hfted a very short distance, three helpers are Two (\\'ho should be as far as of equal helght) are to bear the weight, the third is to support and take charge of the injured part. This is
best done by a person who has been through a "First /I course. If the injured person is insen Ible, another helper should support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient', back at the lower part of the shoulder-blades, and under the hips, clasping each his right hand in the other's left. The injured pat1cnt should, if practicable, place his arms round the necks of the bearers.
The thIrd helper should attend to the seat of injury; if this is a fractured limb, he should support it by placmg the palms of h1s hands under tbe limb, one above and one below the seat of the injury, grasping it firmly but avoiding unneces ary pressure.
The helpers should remain thus until the order " Lift /I is given, and then they should all lift lo\dy and steadily, avoiding jars, attempts to change position of hands, etc.
H the injured person is to be placed on a stretcher or shutter, thi should be previously placed with the bottom end at his head; the bearers should then move, one at each side of it, until the patient is oyer it. The word" Lo\\ er /I should then be given, and the injured person should then be slowly lowered. A pillow or folded-up coat hould be ready, and as the. ufferer is lowered this should be placed under his head. *
* Full directions are giyen in Chapter I\:.
198
199
lE:\.:-,r OF C.\RRYING.
Besides a stretcher, and substitutes such as a gate, a shutter, or a door, other means of carryino- can be im provised . b
I n slight injuries, where the injured person is unable t o walk, two bearers can carry him by forming a fourh anded, three-handed, or two-handed seat.
A four-handed seat is formed as described on page 160 .
A three -handed seat is made as described on page 162 .
The two -handed seat is made as described on page 161.
201 C.\RRYING UP TAlRS.
I n carrying a . lretch r up stairs the head should go fir t, and an extra helper should assist at the lower end, so as to raise it and keep the stretcher nearly horizontal.
The t\\ 0, three, or four-handed seat may be used for carr) ing up stairs; or a strong chair, the patient being carried up ba kwards. In the latter ca e cne helper 'hould walk after the cbair and help to support it, and to pre\'ent the injured person slipping out.
LIFTlXG INTO BED.
b
A single helper can lift by upporting with one arm the tlYO knee, and with the other the back. The arms mu t be pa sed well under before commencinoto lift.
A single helper can giYe support by puttino- his round the waist, grasping the hip and placing the lt1Jl1led person's arm round hi. own neck holdinothe hand ,with his o\\'n hand (FiJ. 76 , page' 16 5). b
A capItal stretcher can be improyised out of a strong sheet and two broom handles or' other hort poles , Eac,h sjde of, is \\ ounclup on a broom handle untIl tllere I Just rOOl11 for a per on to lie
Thi requires four bearers, t\\O at each sIde, to prevent t he sheet slipping .
If tbe bed is narro\\' and there IS room the tretcher should be placed on the floor \\ ith the head close to the foot of the bed. The injured person should then be lifted oyer the foot and placed on the bed. If the bed i too \\ide to admit of this, the stretcher should be placed beside it, and t\\'O helpers should stand at the far side of the stretcher. One helper passes one arm beneath the shoulders and one beneath the middle of the back, the other helper placing hIS uncler the lo\\'er part of the back and undL!' the knees. The injured person is then lifted, another helpe r pulls a\\ ay the stret her, and after a single step forward the burden is placed on the bed .
200
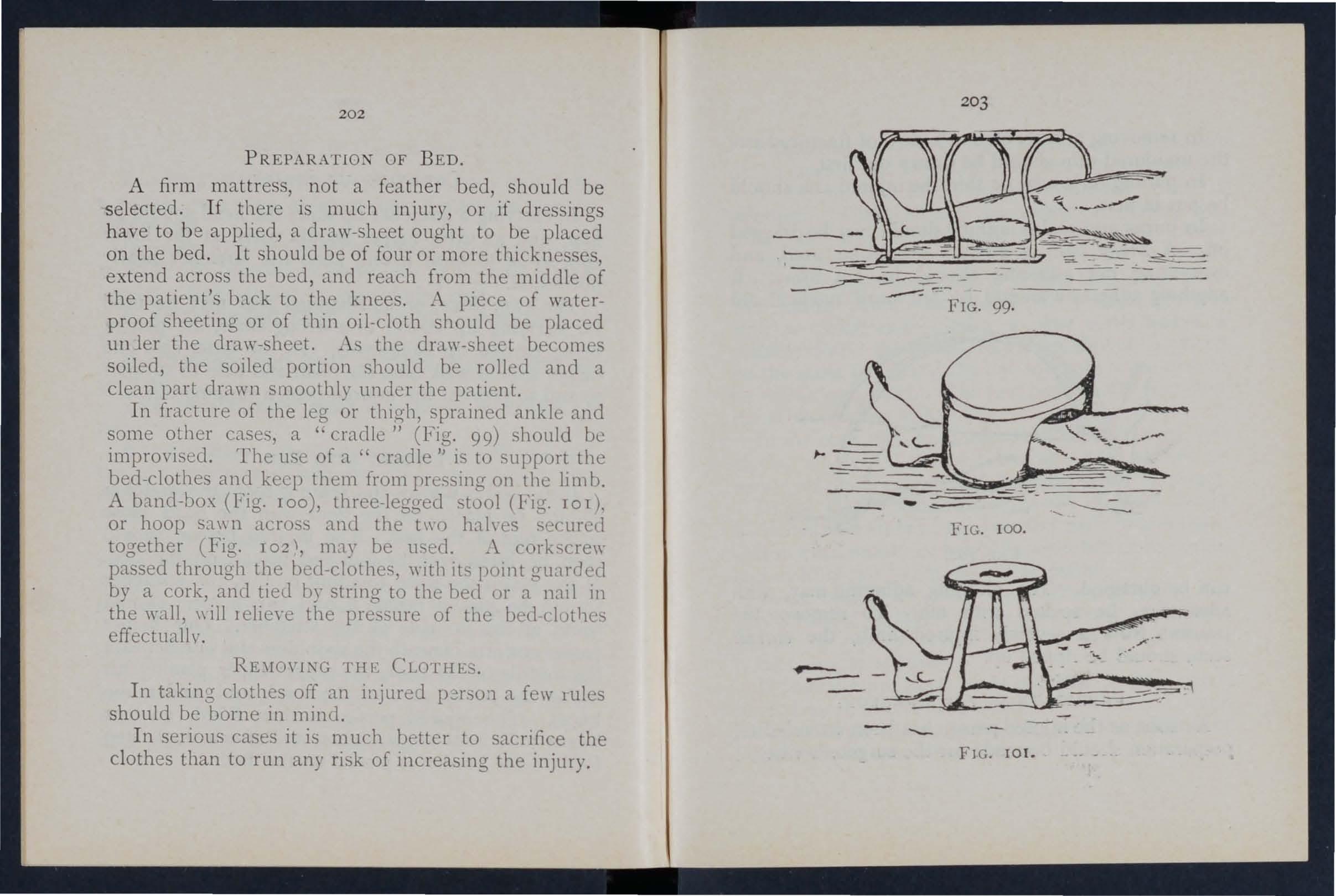
PR EP ARA TIO N O F B E D.
A firm m a ttr ess, n o t a fea th er b ed, sh o uld be s elect ed . If th e re is mu c h injury, o r if dr ess in gs have to b e ap pl ie d, a d ra w-s h ee t oug ht t o be p laced on th e be d. It sh o u ld b e of fo ur o r m ore th i kne ses, e xt e n d across t he bed , and r each from the mitldle of t he patie nt' s bac k to the knees . ...\ piece of waterproof sheeti ng or of thi n oil-cloth should be placed un ler the d raw-sheet. .As the dr.:\.\Y-sheet becomes soiled, the soiled portion shou ltl be rolled and a cl ea n part drawn smooth ly under the patient.
I n fracture of the or thigh, sprained ankle and some other cases, a "craelle" ig. 99) should be imp r ovised. The use of a " cradle II is to support the bed-clothes and keep them from pre. sing on the limb. A band-box (Fig. roo), . tool (Fig. 101), or hoop sa\\ n across and the t\\·o hahes together (Fig. 102 \, may be used . corkscrew passed through the beel-clothes, with its pomt guarded by a cork, and tied by string to tllC bed or a nail in the wall, \\illlelieye the pre ·sure of the bcLl-clothes effectuallv .
RE'IIO\'ING THE CLOTHES.
I n taking clothes off an injured p2r'3o:1 a fel\' rules sh ould be borne in mind .
I n serious cases it is m u h better to sacrifice the cl othes than to run any risk of ll1creasing the injury.
2 0 2
204
In removing a coat, etc .. in a case of fractured arm the uninjured arm should be drawn out first.
In putting on a coat or shirt the injured arm should be put in first.
In burns and scalds nothing should ever be dragged off. A slzarp pair of scissors should be used, and everything not adhering should be cut away. If anything adheres it should be left until medical aid
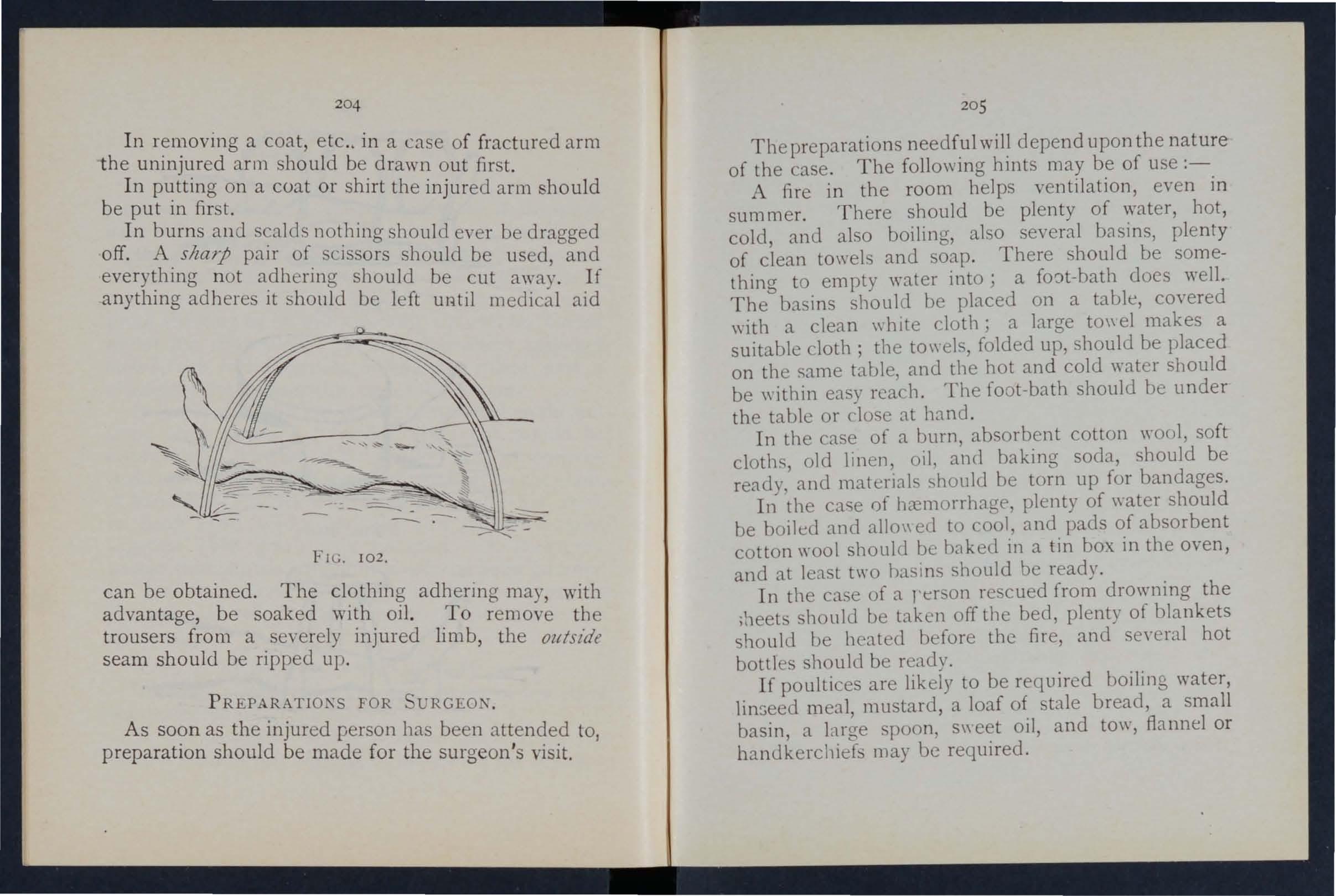
FIG. 102.
can be obtained. The clothing adhering may, with advantage, be soaked with oil. To remove the trousers from a severely injured limb, the olltszde seam should be ripped up.
PREPARATIOKS FOR URGEOK.
As soon as the injured person has been attended to, preparation should be made for the surgeon's visit.
20 5
The preparations needf.ul depend upon the nature of the case. The followlllg hlllts may be of use :-
A fire in the room helps ventilation, even in summer. There should be plenty of water, hot, cold, and also boiling, also several b8sins, plenty of clean towels and soap. There should be something to empty water into; a does well.
The basins should be placed on a table, covered "ith a clean \\ hIte cloth; a large to\\ el makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be within easy reach. The foot-bath should be under the table or dose at hand.
In the case of a burn, absorbent cotton \\'001, soft cloths, old linen, oil, ancl baking soda, hould be ready, and rnaterials should be torn up for bandages.
In the cac;e ()f hremorrhage, plenty of water should be boiled and allo\\ ed to cool, and pads of absorbent cotton \\"001 should be haked in a tin box in the oven, and at least two has1l1s should be ready.
In the case of a rer on re cued from drowning the ;11eet should be taken off the bed, plenty of blankets should be heated before the fire, and seyeral hot bottles should be ready.
If poultices are likely to be required boiling water, linseed meal, mustard, a loaf of tale bread, a small basin, a large spoon, s\\ oil, and tow, flannel or handkerchiefs may be reqUIred.
2 06
. For fomentation, have boiling water, flannel, a k itchen roller, and two Slicks, or a large lowel.
'When summoning a medical man to all accident al ways let him k now by a writte n message what ki n d of case is requi red to treat, so that he may bring whatever IS needfu l. By this means val u able time may be saved .
QUESTIONS ON CHAPTER X.
The 11Ze1Jl,,'a!s z'lldim!e the pages wlzere the G1I SWe1 s may be foulld,
vVhat points would you consider when choosing a ick roon1?
How would you clear the way to the sick room?
\ Vhat means of re ting would you provide for those carrying a patient on a stretcher?...
How would you place and arrange a bed for an accident case?
197,
Are hot bottles necessary, ami hO\l would you prepare them?
\Vhat is often necessary to lay the sufferer on in the first instance?
How would you protect this from getting soiled?
How w<')l1!d you see to the proper lifting and carrying of an In Ju.red person?
198,
\Vbat substItutes for a regular stretcher can you suggest?
How is the four-handed seat made? 160
For what cases is this seat ?... '
H ow is the three-handed seat made? 162,
For what cases is this seat useful? ..
IIow is the two-handed seat made?
For what cases is this cat useful? ...
lIow can a single helper lift?
How can a ingle helper give SUppOlt?
How would you impro\'ise a stretcher? ... . ..
How many iJearers are required for this stretcher?
H ow should a stretcher be carried upstairs?
How would you carry a patient upstairs on a chair? ..
How would you lift a patient from a 'tretcher to a hed?
lIow should a bed be prepared for an injured person? .. .
Ho\\' should a draw sheet be macle?
\Yhat would you place uncler the clraw sheet?
What should be done with the soiled part of a dra\\' sheet?
\Vhat is the use of a " cradle"? .. ,
In what" ays maya cradle be ?
lIow would you remove a coat or shIrt In the case of a fractured arill? ..
How would you put on a coal or 'hirt if the arm were injured? .. , .
In the case of a bad burn, what would you do wlLh clothing that adhered to the patient? .. .
lIow \\'ould you remove trouser from a se\'ere1y injured limb? ..
\ Vhat preparations would you make for the surgeon's "isit ? ,.. ..,
\Vhat WOUld you get ready in the case of a burn?
And \\ hal in the case of ha-morrhage?
And what in the case of a person rescued from drowning? .
\Vhat would you get ready for making poultices?
A nd for fomentations?
\ Vhat sort of a me sage would you send t e summon a doctor? ...
... ... ,.. ... ... ... . ..
... . ..
..... . ......
... ... ... ... '" ... ..
... ... ...
'" '" ...
. .. .. . .. . .. .
) .\GE 197 197 197 19 B 198 198 198 199 200 161 160
164 207
PAGE
161
162 161, 162
200 16 5 200 200 201 201 201 202 202 202 202 202 202 204 204 204 204 205 20 5 205 20 5 20 5 206 206
Abdomen FO.E;C I I I wound of 112
Accident case, preparation for 197
Acid, poisoning by 149, 151
Air, always necessal)' ... 18
Alcohol, caution a to smell of ... 130
Alcohol, poi oning by 134, 153
AI kali ,poisoni ng by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) ::0
Ankle
" sprained ...
Anterior tibial artery
Aorta
Apoplexy 30 ,3 2 64 93 79 13 2
Apparently drowned, to restore ...
Arm, bone of
" fracture of Arm-slings
Arsenic poisoning by Arterial h<emorrhage, 139 28 52 39,49 148 arre t of 74 " practising arrest of 79
" " signs of 74
Arteries
Artery, axillary ...
" course of main 70 79 85
Artery, brachial. .. " carotid .. dor al of foot facial femoral ... iliac occipital plantar '" popliteal radial ubclayian tibial temporal " ulnar ...
Artificial r e piration
Asphyxia
AlIa . 121, 129, AUli clcs ... Axillary artery
Axi '
Back, bandage for Backuone ...
Bandage, to apply to fold
Bandaging
Bed,
"
209
1'0;:;:
Bites of rabid animals 106
Bladder III, II3
Brachial artery <;6
Brain 117
COIn pression of 13 2 " concussion of 13 r
Breast-bone 26 " fracture of . . 4
Broad Landage ... 37
Broken l)oncs, see .F'rad art'.
Bronchial tuIJcs ... . IIS
Brooch-bone 30
Bruises .. 102 Burns 102
Capillaries 70 , 72
Capilku)' hn:morrhage .. 95
Capsule ,.. 3 1
Carbolic acid, poi oning by 15 2
Carotid alte:-ries ,.. :::0 " h<emorrhage from 0
Carpus...... 2
Carrying, means of 160, 200 "upstairs 201
CarLi lagc 25
Cerebro-spinal system I I 7 C er\'ical \'crte br.:c 25
Cheek, bleeding from 2
Che:-st, handage for ISS
Chlorodyne, poisoning uy 149
Choking ... £40
Circulation of the blood, organs of ... ... 70
Circulation of the blood, to induce Clayicle .. , n
62 Ditch, to cr\ s \\ ith tretcher J 69 Dorsal artery of foot 93 verteurre.. . 25
208
INDEX.
l'rge 80 93 I 9 79 2 93 9 2 88 4 93 2 8 136, 138 13 S 25 70 5 25 , to improvise ..
'" .. 159 23 42 37 37
155 201 202 14S
lifting into ...
preparation of . Belladonna, poioning by
Fag"
fracture
Clothes,
Coccyx Collape
<. ollar-bone 19, 202 25 " fracture of ... Comminuted fracture Complicated fracture , .. 13 8 26 4S 35 34 34 Compound fracture .. 'olllp ression of the brain 132 ConcLlsion of the urain 131 Conductor 143 Convulsions in children 137 Cradle, bed 202 Cranium .. , " fracture of Crepitus ... Crushed hand foot 22 43 36 55 62 Diaphragm 120 Digital pre sure
74Direct violence
33 Dislocation
(f
r emoyal t f
...
.. ,
..
2IO
Page
Dr ess, woman' s, on fire ... 105
Drowning 139
Ea r. channel, blood issuing from 98
Ear-passage, foreign body in
Page
Fireman's lift
First aid, meaning of " student
Fish-hook, embedded
Electric shock
Emetic
Epilep y ...
Elbow , bandage for joint, fracture inIIO 159 yoh'ing 53 14 2 148 149, 150 13 2
Esmarch's lliangular bandage 37
Expiration 120
External carotid arten'... 0
Eye, bandage for ' ... ) 55 foreign body in 109
Face, bones of 22
Facial artety 1
Fainting... 134
Femoral a rtery 89 " "digital pressure at groin ... 89
Femoral arte ry, tourniquet for 90
Femur 30 fr acture of 56 30 " fracture of 60
Fingers, bandage for 15 9 fracture of 55
Flexion ... at elbo\\ ". at knet.: ...
Food, poi. oning hy Fuut, bandage for bune . (Jf ... " crushed
Furearm, bones of " fracture of Forehead, bandage fur ... " h;:-emorrhage from Foreign body in thl.: larpassage ... in the eye " "in the nose
Four-handed eat
Fracture, apparatus for treatment of cau'>es of detinition of general rules for treatment involving el bow joint of arm ... of breast-bone of carpus of collar - bone of cranium of finger
Fracture of furearm of knee· cap of leg 54 5g 60 " of lower jaw ... of metacarpus of metatar:,us ... of peh'i" of ribs .. of spine of tarsu,; of thigh -b :me . .. of toes .. si6ns and symptOI11S of 44 55 62 56 46 45 62 56 6l " "arieties of 35 34 108 Frust-bite Fungi, p uisoning I)y 153
H;:-emorrhage from throat 97 from tongue 9 7 from tooth socket.. . 9 7 from upper limbs ... 84 internal 95 kinds of... 73 '-enous 93 Hand, bandage fur 157 bones of ... 2 Hanging... 140 Ilaunch-bones ... 28 } [ead and neck, arteries of 80 Head bandage fur 155 injury to... 12, 131 side of, bandage for ISS IIeart 70 " rate of contraction of 72 Heal -stroke 136 Hernia 1I4 Hi p, bandage for 15 7 History, meaning of 17 IIoward's m e lhod of artificial respiration 126 Humerus 28 fracture of 52 IIydrophobia 106 II ),slerical fits 133
Iliac arteries Impacted fracture Indirect yjolencc Insensibility 79 35, 36 .H ... 128
Gr.>neral circulali ,m 70 C;ranny knot 40 (;reen-ti c k fracture 36 Gums, h .cl11urrhage frum 97 arterial 74 capillary... 95 from gum..; 97 f(olll head and ne c k 0 frum lu\\ er limbs.. 9 from lungs 97 from nos\: 96 fr0111 stomach 98 211 Page
lIO 109 III 160 36 33 41 53 52 48 55 4g 43 55
Insensibi ity, general rules for treatment 128
Inspiration 120
Instep 30
Insulator ... 142
Internal carotid artery... fo
Internal h::emorrhage 95
Intestines, injury of I 13
In-Toluntary muscle.> 33
Jaw, angle of " lower " "fract ure uf
J oint, definition of " injuries to ...
Jugular vein
Kidneys ... " injury of
Knee, uandag€ for Knee-cap " fract ure of Knot for bandage lower limb
Knots, reef and granny
Laborde's method of artificial respiration 126
Laburnum seeds, poisoning by... 148
Lacerated wound 7-<
Large arm- ling 39
Laudanum, poisoning by 149
Leg, bones of ... ':;0
Leg, frac! ure of Lifting and carrying " into bed
Ligaments
Lightning, effects of Limbs, 10\\ er " up, er
Lime in the eye
Lip" bleeding fr(,111
Litters
Liver " injury of Luwer limus
Lumbar vertel)l;:e Lungs
arshall T1 all's met hod of artificial reo piratlon llandage :\J et acarpus fract ure of ... " fracture of '" line of body :'J outh, ulood is. ICing from ill u c1es " ruptured :-'1 u. cular action .. ,
emueddecl
rage l\' ervou sy. tern... I 17
Kose, foreign body in I II h::emorrhage from 96
Occipital artery... 2
Opi um, poisoning by 148
Pad, ring,.. 3 " to fold
Palm, hXl1lorrhage from Palmar arches .. ,
Paregoric, poisoning uy J 49
Patella 30 fracture of 5
Pel'\:is 2 " fracture of 56
Phalanges of foot 30 " of hand
Phosphoru " poisoning uy I4 , '50
Physiology (elementary) 20
Plantar arch 93 " artery 93
Plants, various, poison, ing by.,. '4
Pleura 1 20
Poi son e d we a p 0 n 5, wounds by 106
Poisoning 14
Popliteal artery... 92
Posterior tibial artery 92
Potash, caustic, poisoning by... 149
animals, uites of. ..
Radial artery Radiu " fract ure of 54
system
Rest, necessity for IS Ribs 26 " fracture of... 46 Room, choice and preparation of
Page
2) 23 44 3 1 109 80 III IT 3 15 9 )0 58 of 42 40
2112
h::emorrhagc PaKe 60 ... 198 ... 201 26, 31 144 28 26 110 2 196 III II3 28 25 120
97
from
Narrow
Needle,
Nen'e 140 37 28 55 30 62 20 97 32 65 34 37 lOS lIS 213
bandage
Page Presure, digitaL.. 74 " point.. 74 Principles of First aid
17 Prussic acid, poisoning by 152 Pubes 2S Pulmonary circulation j2 Pulse 72 Pupils of eyes 130 Questions on Chapttr I. 2 I II. 66 III. 99 IV, II5 Y. 145 VI. 154 X. 206
106
40
120
...
I\ahicl
Reef knot
P espiration
artificial 129, 138 " to excite 127 P espiratory
118
197
Pag'e
Rupture (hernia) 114
lZuptured muscles 65
Sacral yerte brre ...
Sacrum ...
Scalds 25 25, 28 102 155
Scalp, bandage for " hxmorrhage from 3 26
Scapula . ..
" fracture of .3chafer's method of artificial respiration
"'eat, four-handed three-handed " two-handed
Shin-b one
::'hock
" electric ,Shoulder, l)anclage for ... " blade ... 51 121 160 162 161 30 134 142 15 6 28
" flacture of 51 bones... 26
" joint... 32
Si ck room, choice and preparation of. ..
Signs, meaning of .
Silv ester's method of artl " ficial respiration
Simple fracture ...
Skeleton ... r Skull 197 17 1 2 3 34 22 22 43 " fracture of
Slings, arm • 39,40 , 49 214
Small arm ling ... Smothering
Snake bites
oda, caustic, poisoning by pleen " injmyof ... pinal canal cord " fracture of 23,
Spirits of salt, by
Splint, angular ..
SplinLs, rule' [or apply ing " to impro\'ise prain.
SLernum ... )) fracture of Stimulants
Slings of plants and animals
Stomach ... hreillurrhage frum " injury of .. St rains
Strangulation
Stretcher exercise Army No. I. o. II. Nu. Ill. " "No. 1\. Stretchers, Furley
PaJre
Stretchers, to ca rry ... 169 " to illl pro\'ise 166
Strychnine, poisoning by 153
Subclavian artery
Suffocation J 4 I
Sunstroke 136
Surgeon's visit, preparation for 204
Syllabus of instruction... <
Sympathetic system I I Symptoms, of... 17
Syncupe ... 134 ... 3 I
S)'stemic circulation 70
Tar,;us 3')
Temporal artery . Thigh hone 30 frac t ure of 56
Three-hand.:cl sea 162
Thrual. h.emorrhagc fr"111 97 ,. s\\dling uf tio;... ue,; of... .. 141 Tlhia 30 fracture of 60 1J:1.I1clage for . . 159
'l\lIlguc. J1:I.:1ll IlThage frum 97
TOlth socket, 11.\:111 1Irhage [rum q7 Tourniquet 75 wo,lIld "f abdomen 1'3 Two-handed . eat lOI
.
culumn 23
woune! of abel )-
\Xagon, to luad Ill' ul1Joacl I 7 I \\Tall, to cross \\ ith stretcher \Yarmth, neces"it) for ,. to prom )te ""ind-pipe \\ oman's on lire " oLlnds hy p cliSOIlCcl 1'7
,. acc. 1 mpanier1 by arterial .. 76 \Youncls accompanied hy \ C!1l0U hrem r)[rhage '\\" mnds. lacerated \Yrist 94 7
Page 39 140 lOb 149 1 I I 113 23 1I7 23 45 149 54 107 I I I 98 113 65 140 1<;0 174lSI 1 '5 IS7 172 21 5
Page Ulna 28 " fracture of .. 54 Ulnar artery 88 Unconsciousness 128 Upper limbs 26 Varico e yeins 94 Veins 70 VenOl!
blood 72 93 Ventricles
'Vertebra..
Vertebral
Vertical
men 113 Vitriol,
102
Voluntary muscles
II' 105
106
.
70
23 Vertchrx... 25
burn Il)'...
.
33
wcapons ..
GENERAL PRICE LIST . INTRODUCTION.
This Pr:ce List, which is subject to revision from time to time, has been compiled with a view to as·ist members of the Association and others in the purchase of the necessary equipment for corps and divisions of the Brigade, ambulance stations, classes and first aid and nursing work generally.
A complete and reliable Ambulance Equipment an actual necessity, and experience has proved that employers of labour and others interested in the district readily subscribe for the purchase of such appliances. Collecting cards, stating the purposes for which subscriptions are required, will be supplied gratuitously on applicalion to the II ead Office of the Association, where also any informal ion with regard to its 'work can be ubtained.
Stores of the value of lOS. or upwards will be sent carriage pa id to any part of the United Kingdom.
Owing to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhered to.
Quotations will be furnished for articles relating to Ambu lance Nursing and IIygiene, not mentioned in this list.
Orders and correspondence should be to the St. John Ambulance A sociatioI,l, St. John's Gate, Clerl.;enwell, London, E. C.
Remittances should be made payable to the St. John Ambulance Association and crossed "London and \Vestminster Ban k, Loth bury. "
HORSE CARRIAGES &. WAGO N S.
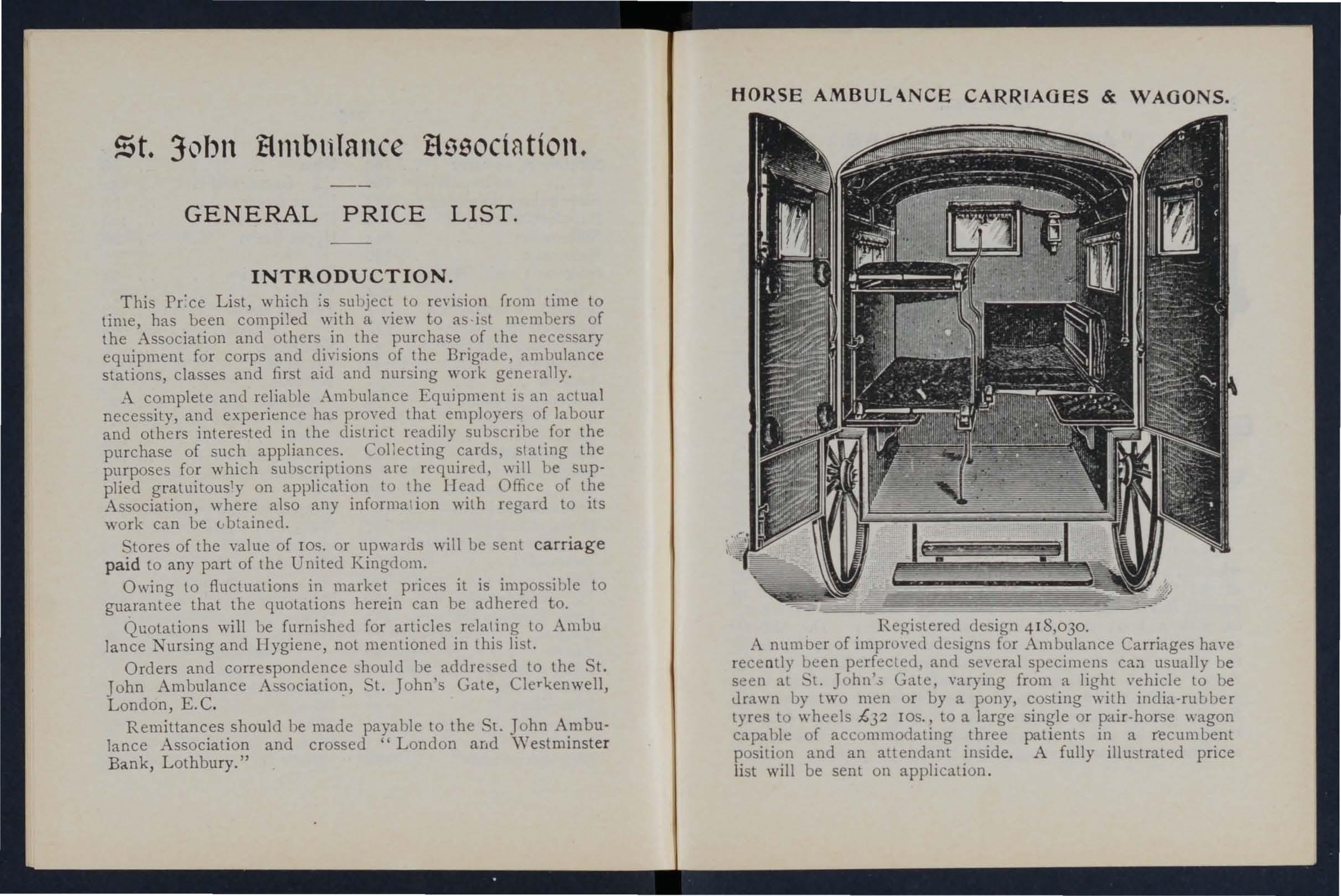
Registered design 418,030.
A number of improved designs for Ambulance Carriages ha\'e recently been perfected, and several specimens ca:! usually be seen at 't. John'.; Gate, varying from a light vehicle to be drawn by two men or by a pony, costing with india-rubber tyres to wheels £32 lOS., to a large single or pair-horse wagon capable of accummodating three patient in a recumbent position and an attendrwt inside. A fully illustrated price list will be sent on application.
st. John tltllbllTallce tl9S0CtflttOtl.
n- n- n 0 '-<. 0 ff ff .. 5': ff >-3
:1 g 3.13 [ ff ff
g. s> p,.
lI' a- ;. r» .;; g lI' Ss::;p,.",
t:l Cl> Cl>:;:;:S::r'Cl> Cl>::r' g::s r- o· 0 0'
g- ,.,. g- ,.,. 8- a. ;. lJ) ;. n no .. =. ::
Cl> Cl> O'!!. Cl> l' a 5"!!'. (') Cl>
"""g ;. ... & r» g cr' p,. r.> '" Cl> ::r' (1) X Cl> v H
o 8. '" ::r' Cl> v" ]0'-;;::- 9 lI' (D p.> .- '" Q.;::.' &'" ff""g 5. 5. ff (1) 3 .. 1f 0 p,.lI'::::8-
I-:rjoo ""::r'(1)-S::;n-g(1) s::; ;" cr'.- ;;; 0"0 9 n''::::: ::r''<::r' (b p.> rtl r.> (D '1Q ;g '< >-3 <: coo '" "0 :1 :: ::r' 0 :;:::l ;S 0 "2 Cl> g &;;::::-..-.;::; ::.?-..... ';':::;""g .Y'
Cl> n 0 g =. '" >-i ::l P 0 B -::::; r.n ::r'VlCIQ::s . 3 o"Q u' (1) 3. 0.. P ..... :; § n 0 nD:::
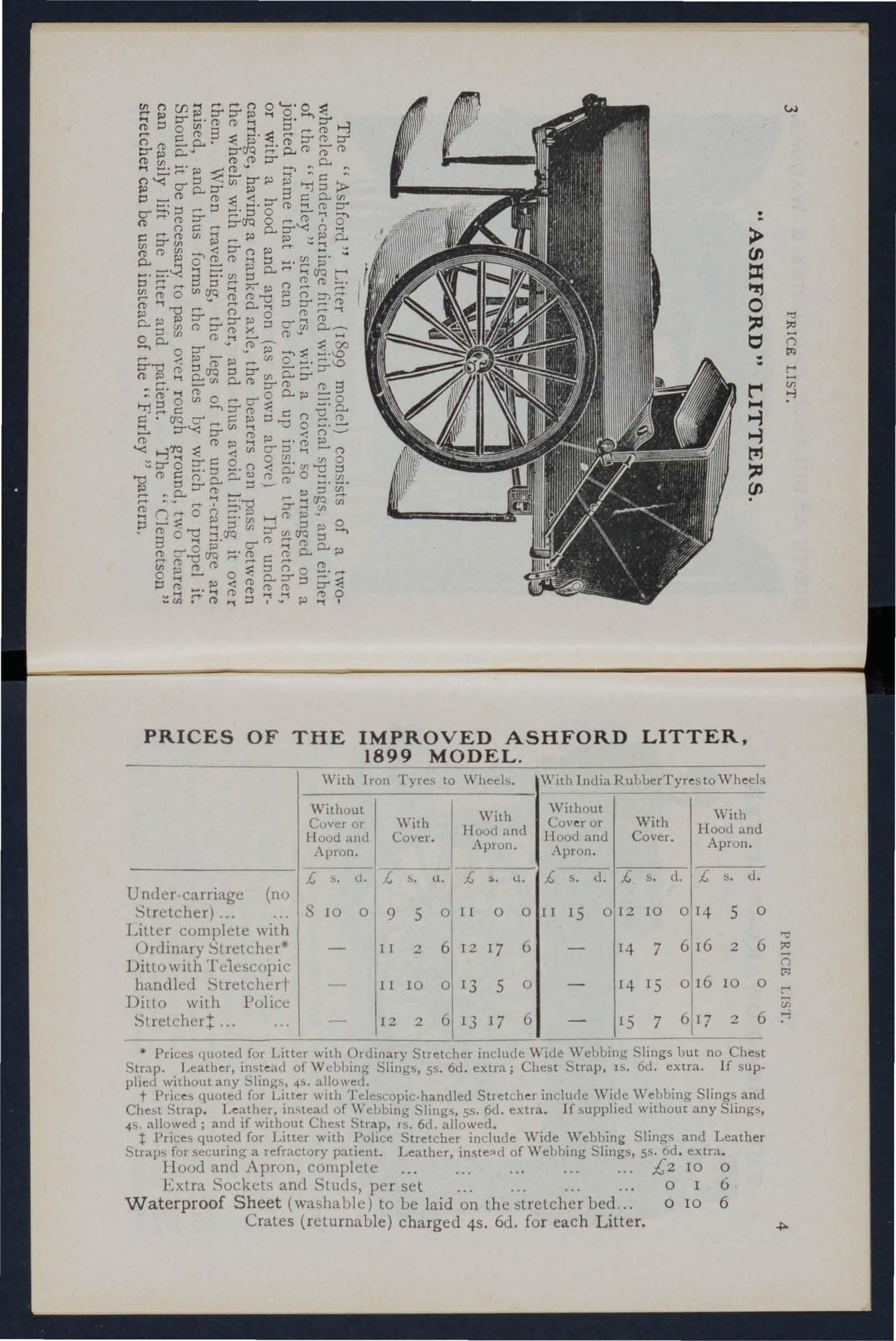
PRICES O F THE IMPROVED ASHFORD LITTER, 1899 MODEL
With Iron Tyres to Wheels. Without Whh I W;,h Cover or Ilood and CO\ er. lIood and 1\pron. AplOl1.
With India RubberTyr(!sto \Vh(!els \\'ilhout Cov(!r or Hood and ,\pron . With Cover. With Hood and Apron.
Under -ca rriage (no Stretcher)
Liller complete with Ordinary Stretchcr
Ditt o with Tc1escopic
Ditto with Police Stretcheli
Prices quoted for Litter with Ordinary Stretcher include WiLl e Wehbing Slings but no Strap. Leati1(!r, inst(!ad of Wt:bbing Slings, 5S. 6d. extra; Chest S trap, IS. ad. extra If supplied without any Slings, 4S. allowed.
t Pric(!s quoted for Litter with Telescopic-handled Stretch(!r inclu(le 'V ide \\'ebbing Slings and Chest Strap. Leather, instea(l of \Vebblllg Slings, 55. 6d. extra If supplied without any 4' allowed; and if without Chest Strap, IS. 6d. allowed
t Prices quoted for Litter with Police Stretcher include \Vide \\Tebbing Slings and Leather Straps for securing a refractory patient. Leather, of \V ebbing Slings, ss. 6d extra.
IIood and Apron, complete
£2 10 0
Extra Sockets and Studs, per set 0 I 6
Waterproof Sheet (washable) to ue laid on lhe :itrelcher bed... 0 10 6
Crates (returnaule) charged 45. 6d. for each Litter.
> (J) :J: IT! 0 ::c t!1 ::c (J)
:=;-';:; g 7' .; t
£ S. d. £ u. £ s. ll.
10 0 9 5 o II 0 0
S
£ s d.l£ I I IS 0112 IO 0 114 5 0 w "::j c=; t: Ul
r II 2
6 12 17 6 14 7 6116 2 6 n handled Stretcherl- II 10 o 13 5 0 14 IS 0 116 IO t'1 o r
12 2 6 13 17 6 IS 7 6 117 2 Vi 6 ;l
.
THE "REA =ED"v\' ARDS" LITTER. .
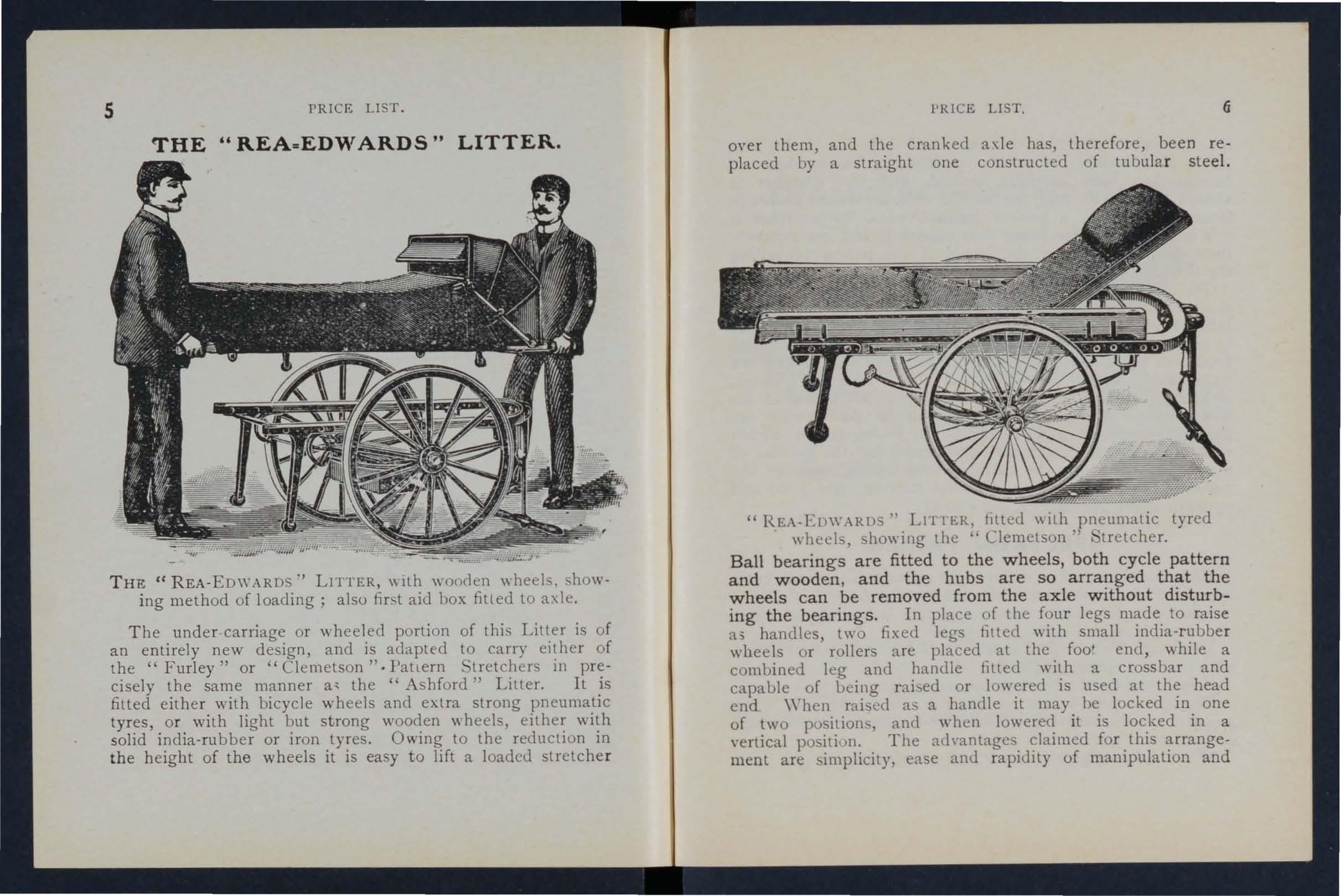
THE: "REA-E DWARDS" LITTER, \\ Ilh wooden \\ heels, showing method of loading; also first aid box fitled to axle.
Th e under-carriage or wheeled portion of this Litter is of an entirely new design, and is adapted to carry either of the "Furley" or "Clemetson". Pattern '- tretchers in precisely the same manner a, the "Ashford" Litter. It is fitted eithe r with bicycle wheels and extra strong pneumatic tyres, o r with light but strong wooden wheels, either with solid india-rubber o r iron tyres. Owing to the reduction in the h eight of the wheels it is easy to lift a 10adcLi stretche r
l'RICE LIST.
over them, and the cranked axle has, therefore, been replaced by a straight one constructed of tubu la r steel.
" REA-EDWARDS" Ll r fER, hUed \\ ith pneumatic tyred wheels, showing the' Clemetson" 'tretcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden , and the hubs are so arranged that the wheels can be removed from the axle without disturbing the bearings. In place of the fou r legs made to raise 0.3 handles, two fixed legs filted wilh small india-rubber wheels or rollers are placed at the foo' end, while a combined leg and handle fitted with a crossbar and capable of being raised or lowered is used at the head end When raised as a handle it may he locked in one of two positions, and when it is loc.ked in a \'ertical positi \) n. The ad \·anlagcs. for. thIs ment a re simplicity, ease and rapIdIty of mampulalJon and
5 PRICE LIST.
the facility afforded by the two fixed legs for raising the litter, if necessary, on to the pavement. The question of balance has been carefully studied, and the stretcher is shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is in a horizontal position being thus obtained, and consequently there is no weight on the hands of the person propelling the litter.
The pneumatic tyred wheels are strongly recommended in cas es where the small amount of care nece sary to keep them inflated can be given, as the comfort to the patient and Ease in propulsion are increased beyond all comparison with any litter yet produced. It will be noted that the prices are considerably lower than those of the "Ashford" Litter, and the following are gi\'en as examples, but owing to the vast number of combinations that can be made with the diflerent stretche rs and coverings, it is impossible within reasonable limits to set out quotations for the whole of them, but these may be calculated by adding toget her the prices of the under-carriage, stretcher selected , and hood and apron or coyer, see pages 4 and 8 to I!.
SPECIMEN PRICES.
Under-carriage only, either with pneumatic tyred cycle II'heels or solid rubber tyred wooden wheel, £10.
Litter complete with ordinary stretcher (no slings or chest strap) and hood and apron, £14 3s. 6d.
Ditto with Telescopic Handled Stretcher (with chest strap) and hood and apron, £14 I IS.
H with iron tyred wheels prices are £2 less.
The lowest priced litter complete is fitted with iron tyr eJ wooden wheels, ordinary stretcher (no slings or chest strap) and cover. Price £10 8s. Ed.
When ordering please state which wheels are required.
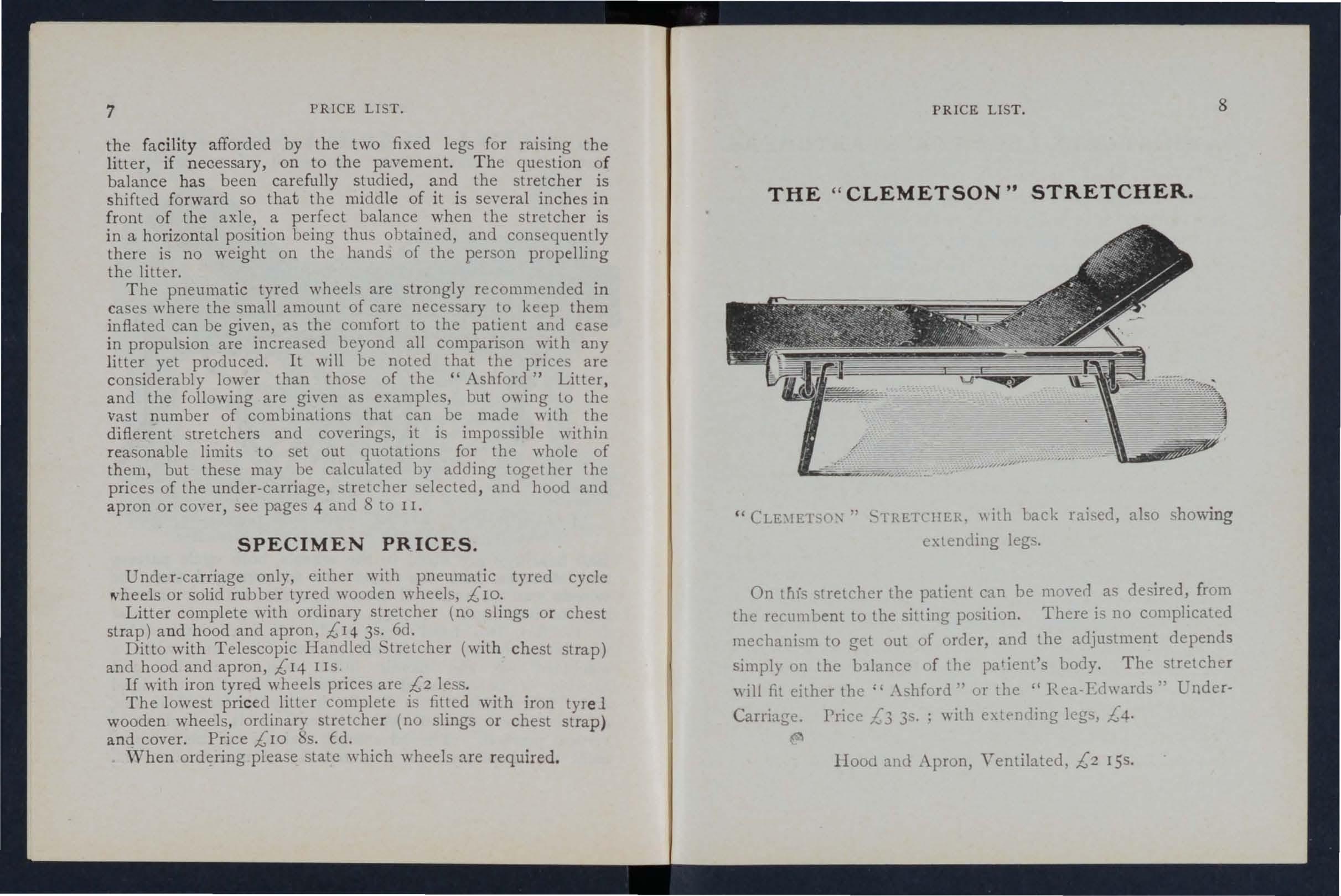
" CLE:\IETSO:,\ ,. S lRETCIIER. "ith uack raised, also showing extending legs.
On this lretcher the patient can be mo\'erl as desired, from the reCl1111 bent to the sitting position. There i no complicated mechanism to get out of order, and the adjustment depends simply on the b11ance of l he pat ient's body. The stretcher will fit either the" .\shford ., ur the "R ea-Edwards" Under-
Carriage. Price £3 3s. ; with extf'l1ding kgs, £4.
Hood anti Apron, Ventilated. £2 I5s.
7 PRICE LIST.
PRICE LIST. 8 THE"
CLEMETSON" STRETCHER.
9 PRICE LIST.
ADJUST ABLE LEGS FOR STRETCHERS .
Primarily these legs, \\ hich are independent of and rdditional to the ordinary foot are intended to f2cilitate the carriage of a stretcher in a railway compartment, in • whi ch case two on one side would be lowered and adjusted by a telescopic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the adjustable legs on the other side would rest on the floor. The four legs may be used to raise the stletcher as required. \Yhen not in use they are folded up immediately under the p oles of the stretcher.
Price per set of four, 17s.
FIRST AID BOX.
To be fixed below the axle of the " Rea-Edwards" or " Ashford» Litter.
This is intended to be kept permanently attached to the litter, and is not designed to h ng in a station or to be carried by hand.
Contents :-Set of Splints, 12 Triangular Bandages, 12 Roller Bandages, 2 t-lb . packets each Cotton \Youl Dnd Boric Lint, Adhesi\'e Plaster, Pair of Scissors, Knife, 2 oz. each Olive Oil, Tinct. Eucalyptus B.P.C., Sal Volatile, and Spirits Ether Comp., Graduated :'lea ure Glass, Kidneyshaped Dressing Basin, 6 Tampons for washing wounds, Tourniquet Pins, Safety Pin5l, X eedles, Thread and Tape. ! 'lice £2.
LIST. 10
" FURLEY" STRETCHERS WITH THE LATEST IMPROVEMENTS, 1899 MODELS .
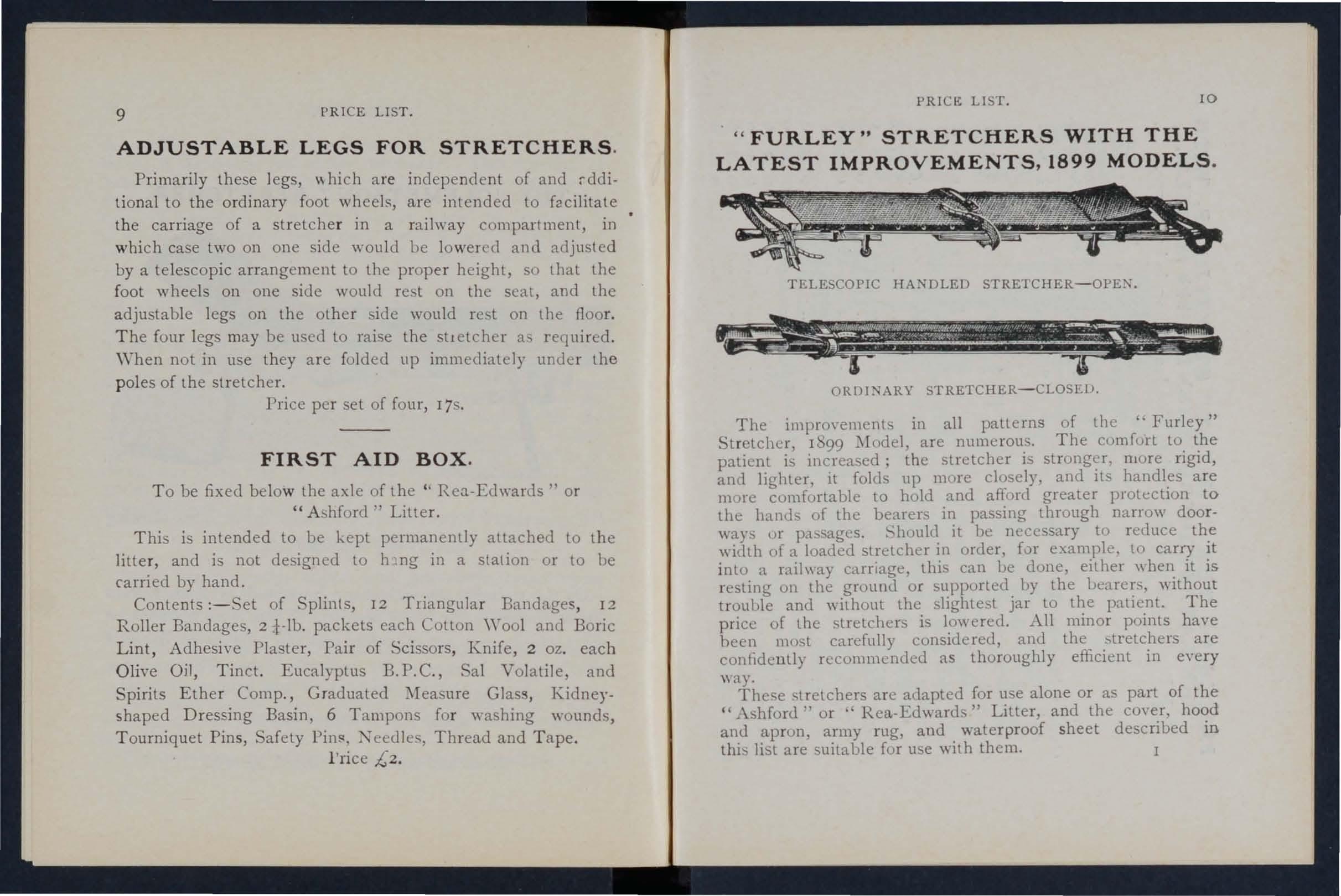
TELESCOPIC HANDLED
ORDINARY STRETCHER-CLOSElJ.
The improvement in all patterns of the c. Furley" Stretcher, 1 '99 are numerous. The comfort to the patient is increased; the stretcher is stronger, mure rigid, and lighter, It folds up more closely, and its handles are more cumfortable to hold and afford greater protection to the hands of the bearers in passing through narrow doorways ur passages. it be necessary to reduce the width of a loaded stretcher in order, fur example, to carry it into a raihmy carriage, this can he dune, either \\hen it is resting on the ground or supported II)' the bearers, \\ ithout trouhle and \\ ilhout the slightest jar to the patient. The price of the stretchers is 10\\ ered. All minor points have been most carefully considered, and the "tretchers are confidenlly recommended as thoroughly efficient in eyery way.
These stretchers are allapted for u e alone or as palt of the " Ashford" or ' Rea-Edward " Litter, and the coyer, hood and apron, army rug, and waterproof sheet described in thi list are suitable for use with them.
PRICK
PRICES OF THE "FURLEY" STRETCHERS, WITH :::: THE LATEST IMPROVEMENTS (1899 MODELS ).
N.B.- The prices of the Standard Models are shown in heavy type.
Without Slings or Chest Strap.
With Wide Webbing Slings (no Chest Strap).
With Wide With Webbing Leather Slings and Chest (no Chest Strap. Strap)
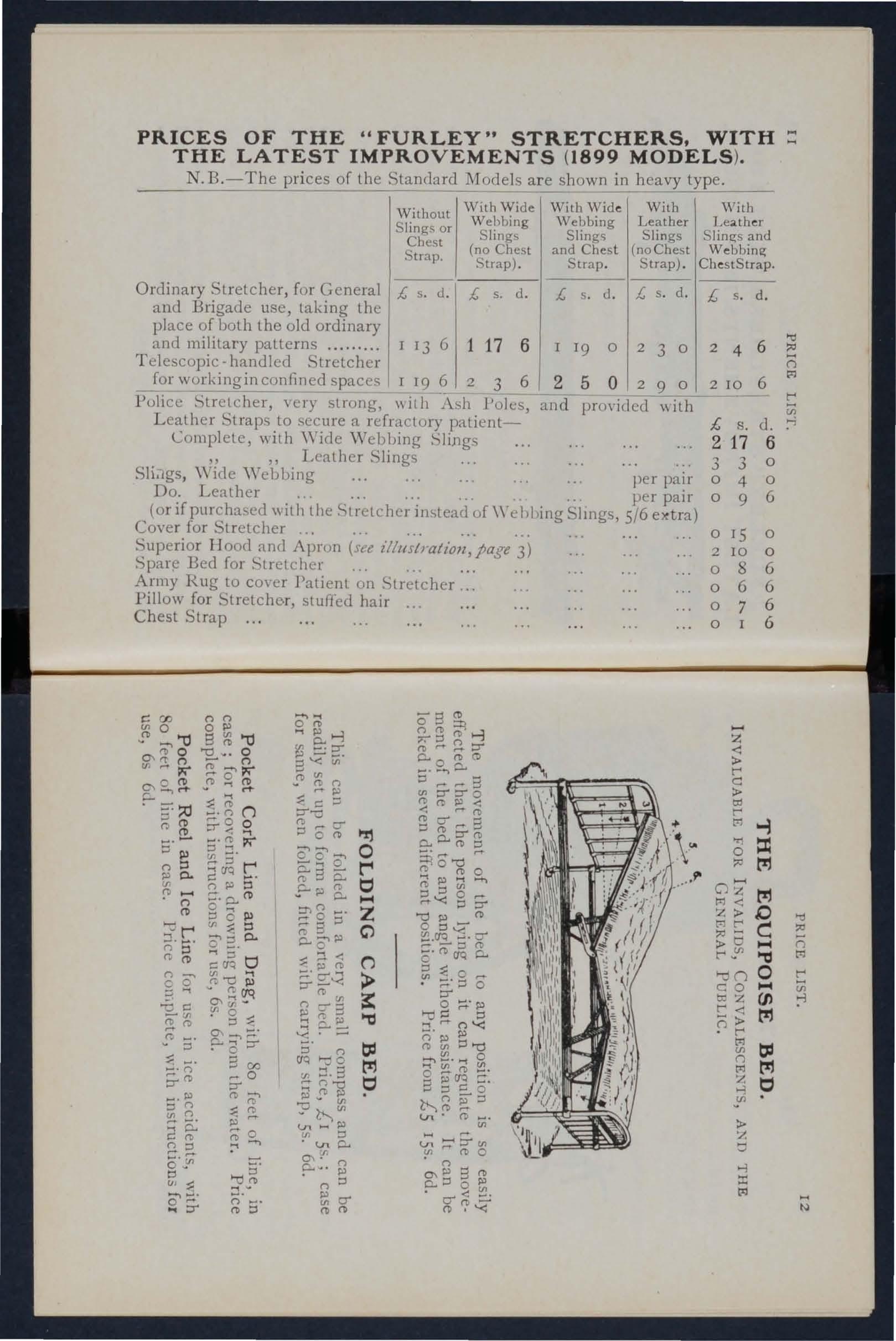
Ordinary Stretcher, for and Brigade use, tal. place of both the old a and military patterns
Telescopic-handled S for working in confined
Police Stretcher, ,ery strong, \\ it11 . \ sh Poles, and provided with Leather Straps to secure a refractory patientComplete, with Wiele Webbing Slings " "Leather Slings
SliJgs, \\ide "Webhing per pair
Do. Leather per pair (or if purchased with the Stretcher instead of\ '-L hbing Slings, 5/6 Cover for Stretcher
Superior Hood and Apron (sa z"//uslratioll,page 3)
Bed for Stretchcl Army Rug to coyer Patient on Stretcher Pillow for Stretche.r, stuffed hair
Chest Strap
£ s d. 1 13 G I 19
£ s. d. 1 17 6 2 3 6
£ s d. 1, s d. 1 19 0 2 3 0 2 5 0 2 9 0
0 v O """' '"0 ", 0 O\rt'n C/l M 5' :;0 n !!. 5' III n n n (l) r:;-:;' r. (l) n -. c 0 ::; .... -. v :l ::.;:;&0 1>' :l n C/l n 25: nO 0'(; :lV C.n ::: CY :::.' .. ::rn n o I>' 8 '"0 0 - n (\) (') c n p ::-. CL (l) o ::; 0 III V' 0' 2. 00 v r;; CTq Q'\?g ::;: 0P-'3'& 8 00 r 0 ::r0;:;' n o :;l ....., ... o (\) ..., b.--3 8"< Ul 2 c ::::; g-- """' 000' 0::::;C':o..Jo.. ..c-pg. ::t>n c... CY o r Z C) 5- n > S 6.::. y.:;. n CfQ M ir-s :» CJl lJl I>' If ::J ·lJlCL O\l'n c--. • n:l -3(1) ,.... C/l ;:r::r-o (\) 0 pl .-. '! '-(1) o c7 ::) ::) 0 & ::tlO'D o 00 g & Cl> ,- ,......... ::l (t) c·Cl> CfQ c.. 0 t:r" o >-d ::l '"'" n'< 6'"0 g. s era g-o No n j;J:;l v')Cl> V"l' (t) en" n CL:lol>' c7'-' Cl> C?.:r With Leather Slings and Webbing ChestStrap. {; s d. 2 4 6 2 10 6 £, s. d. 217 3 3 0 4 0 9 o IS 2 10 0 0 0 0 8 6 7 Iz <: » t-' c: » txl r' 6 0 0 6 0 0 6 6 6 6 t=l ...; b =: M 0 t=l r' c:: ?:! a 1-4 >-on co tcZ r' <: -» 0r' o (J) M el Q vUl » .., ::r: ttl 'tI () p:] ;; >oj i::::t ;:; p:] r' u; :-J ;:;
PRICE LIST.
" LOWMOOR JACKET ."
For use in lllines, hips' holds etc to . . . . . , ., eCUle a pallent on a st retchel (sce lllustratlOn), which can then I I d' • • • < JC pace 10 an upngh t posltlOn. P rice £1 5.
WATER BOTTLE.
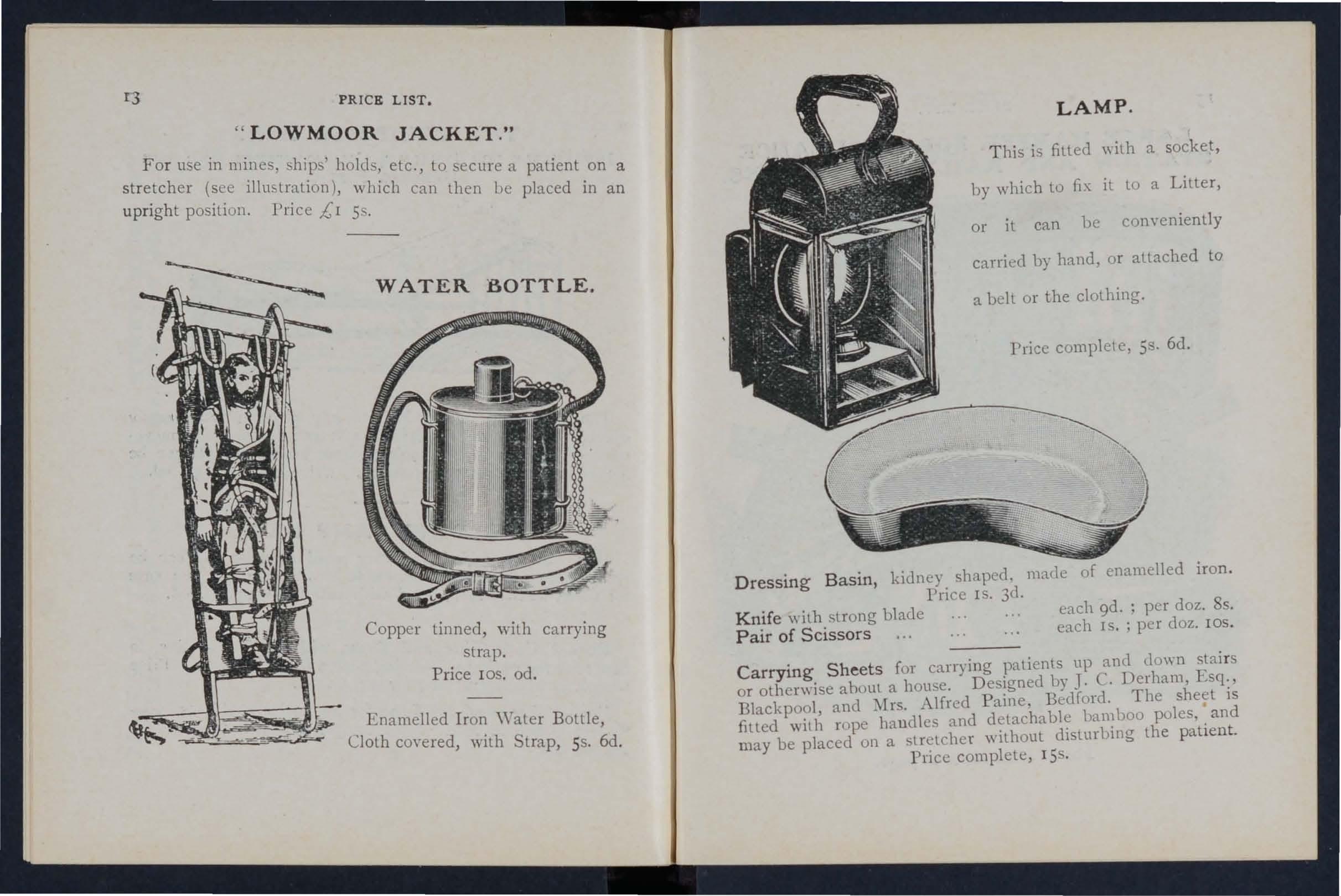
Copper tinned, with carrying strap.
P rice l OS. od .
Enamelled Iron \ Yater Bottle
Cloth coyered, with Strap, 55. 6d .
LAMP.
T his is filted with a socket, by which to fix it to a Litter, or it can he conyeniently carried by hand, or attached to a belt or the clothing.
Price complete, 55. 6d.
Dressing Basin, kidney shaped, mack of enamelled iron. Price IS. 3d .
Knife with strong blade Pair of Scissors each 9d. ; per doz. 8s. each IS. ; per doz. 105
Carrying Sheets for carrying patients up and down stai rs or otherwise abuut a house. Designed by J. C. Derham, Esq., Blackpool, and Mr. Alfred Paine. Bedford. The sheet is filled with rope handles and detachable bamboo pules, and may be placed on a stretcher \\ ithout dislurbing the patient.
Price complete, 15 .
LARGE HAMPER FOR AMBULANCE
STATION AND RAILWAY PURPOSES .
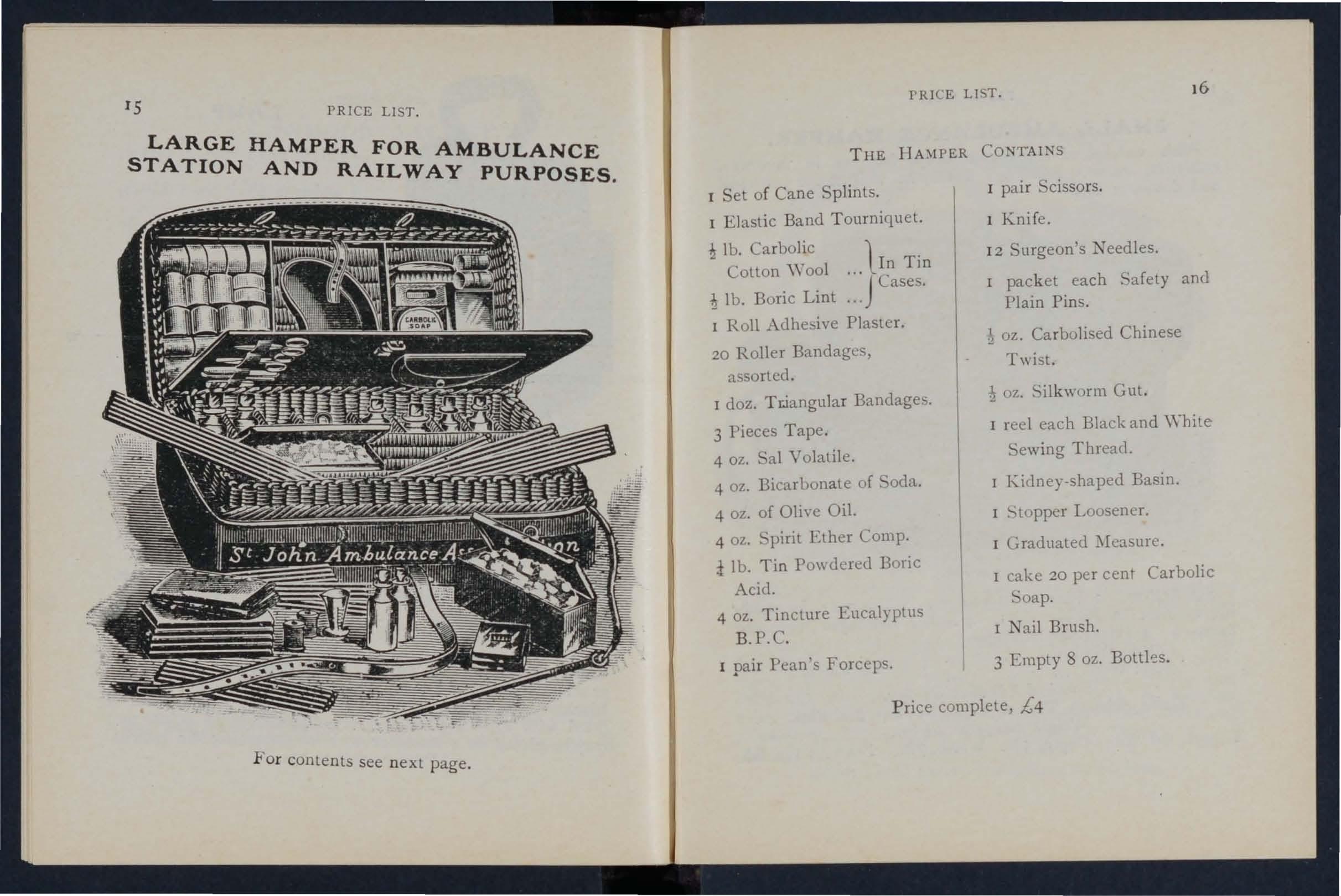
For conte n ts see n ext page .
T HE CONTAINS
I Set of Cane Splints.
I E lastic Band T ourniquet.
lb . Carbolic l T ' • I n Jll Cotton \\ 001 . . , JCase ..
lb. Boric Lint ...
I Roll Adhesive Plaster.
20 Roller Bandages, assorted .
I doz. T ciangula r Bandages.
3 Pieces Tape.
4 oz. al Volatile.
4 oz. Bicarbonate of oda.
4 oz. of Olive Oil.
4 oz. Spirit Ether Compo
i lb. Tin PO\\(lered Boric Acid.
4 oz. Tincture Eucalyptlls
B .P.C.
I pai r Fean's Forceps.
I pai r .cissors.
1 Kni fe .
I 2 Surgeon's eedles.
I pack et each 'afety and Plain Pins.
oz. Ca rbolised Chinese Twist.
1 oz. Silkworm Gut.
I reel each Black and \ Vhi te Sewing Thread.
I Kidney-shaped Basin.
I !--.topper Loosener.
I Graduated
I cake 20 per cent Carbolic oap.
I Nail Brush.
3 Empty 8 oz. Bottks.
P rice complete, £4
PRICE LIST.
PRICE LIST. 16
PRICE LIST.
SMALL AMBULANCE HAMPER .
'watel:proof co,'er and strap, for us e in factories, colhenes, and larg e works, as well as for parochial and dome tlc use.
SURGICAL HA VERSAC .
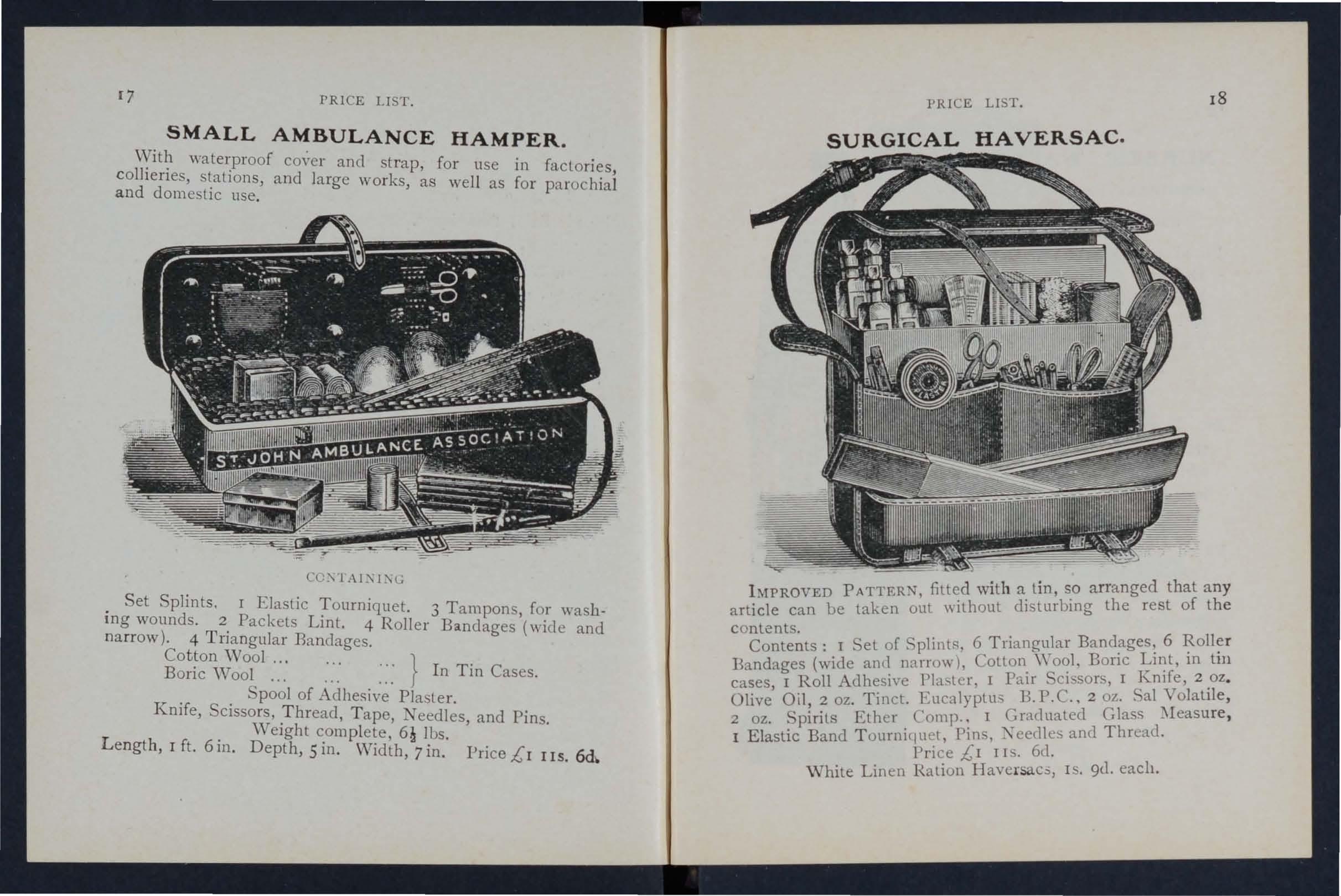
CC2\lAI:\I2\L
. Set Splints. I Elastic T ourniquet. 3 Tampons, for washll1g wounds. 2 Packets Lint. 4 R oller Bandages (wide and narrow) . 4 Tri a ngul ar Bandages.
Cotton W ool... }
Boric Wool... ...... ::: In Tin Cases.
pool of Adhe;;ive Plaster.
Knife, Scissors, .Thread, T ape, eedles , and Pins.
. \Velghl c.om pl ete, lbs.
Length, I ft. 6m. Depth, Sm. Wid th, 7 in. Pri ce £ r I IS.
IMPROVED PATTERN, filted with a tin, so arranged that any arti cle can be taken out "ithout disturbing the rest of the c ontents.
Contents: I Set of Splint!';, 6 Triangular 6 Bandages (wide anll narrow), Cotton. Bone m tlIl cases, I Roll Adhesive PIa. tel', I PaIr SCissors, I J I1lfe, 2.oZ. Olive Oil, 2 oz. Tinct. Eucalyptus B.P . C., 2 oz.• al Volatlle ,
2 oz. Spirits Ether Comp., I Gra(lualed Glass :'Ieasure, I Elastic Band T ourniquet, Pins, Xeec11 es and Thread. Price £1 II . 6d. White Linen Ration IIaversac.:;, IS. 9U. each.
PRICE LIST. 18
NURSES' WALLETS .
ORDI -ARY PADLOCK SHAPE.
\Yith out instruments, 4S- 3d.
Filled complete, containing Bow Dressing Forceps, Spalula, Probe, 2 pairs Scissors (round and sharp pointed), Clinical Thermome'.er, and Knife.
Adyanced price lOS.
ST. JOHN'S as illustraled, but imprO\'ed by the addition of flaps to protecl the inslruments.
\Yithout instruments, 7s. 9d .
Fitted complete, containing Bow Dressing Forceps, Artery Forceps (also useful for dressing), Spatula, Probe, Director with Ear Scoop, 2 pairs Scissors (round and sharp pointed), Clinic:d Thermompter (minute, r 'und), Knife, Pencil, and Safety Pins.
Price £1 IS.
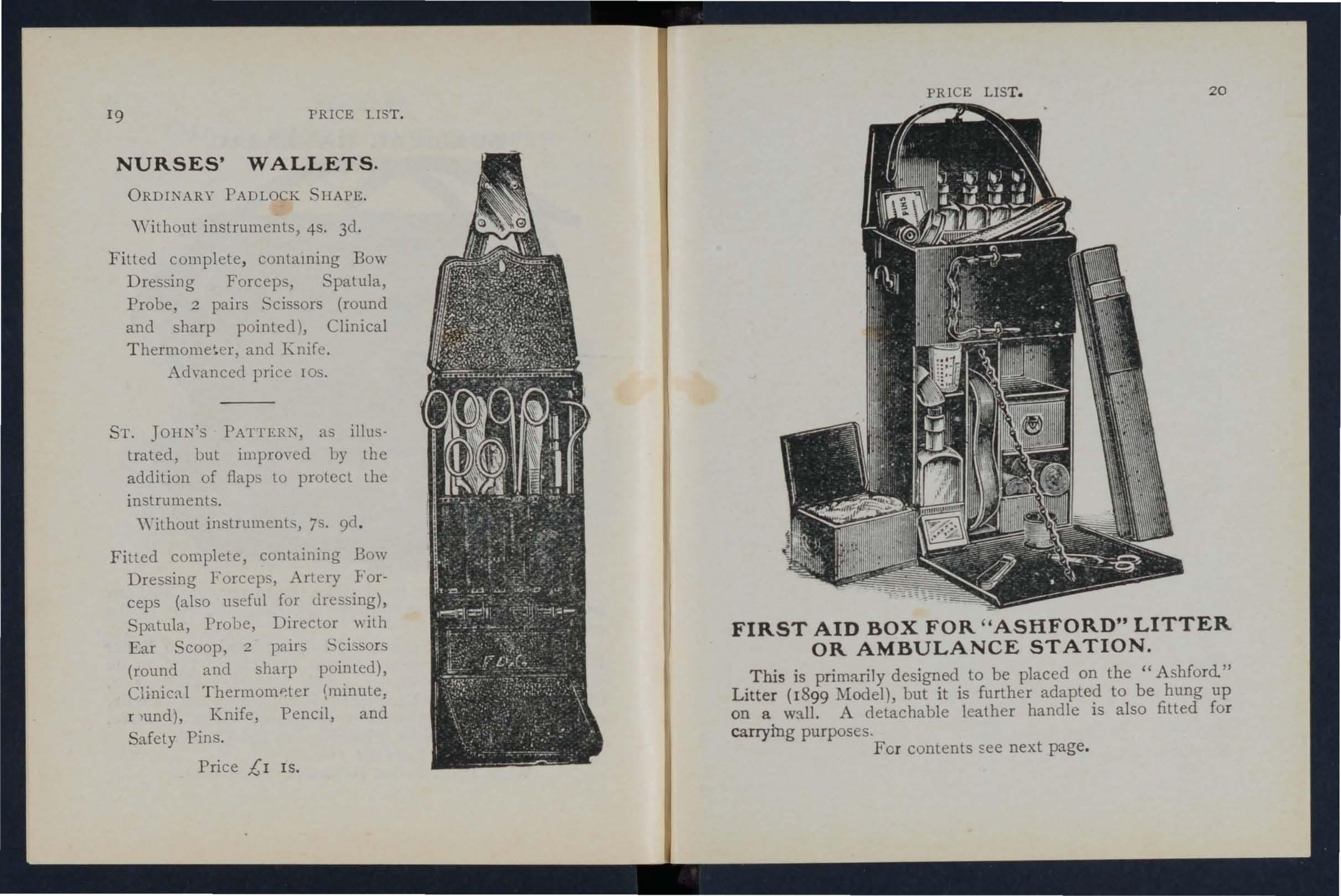
FIRST AID BOX FOR " ASHFORD" LITTER OR AMBULANCE STATION.
This is primarily designed to be placed on the "Ashford." Litter (1899 Model) but it is further adapted to be hung up on a wall. A leather handle is also fitted for carrying purposes. For contents see next page.
19
PRICE LIST.
PRICE LIST. 20
21 PRICE LIST.
COL TENT OF FIRST A I D BOX.
(Illustrated on previou, page.)
Splints j ,Elastic Tourniquet; Carbolic W ool , Bonc L1I1t, 111 cases; 1 1'-011 Adh esl.ve Plaster j 12 Roller Bandag es
6. :rnangular 3 Pieces o r Tape; Pair Scissors; I K mfe! I Kldney.shaped Basin; I Graduated ]\ To:;asure; 2 07. Ol ive Oi l;
2 oz . TlI1ct. Eucalyplu.s 2 oz. Volatile; 2 uz. Spirits Ethe r C ompo ; 8 oz. Carron Od; Pms, Safety P ms, N eedles, Thread.
PRICE COMPLETE £2 lOS .
Tourniquet, Ela tic .. .
Tourniquet, Field
\ Yooden, per set, 2/6; Cane .
per set
Greatly 11l1proyed \ Vooden plints, with gr om'ed joints and angle piece, strong ly recommended...
T?w, fO.r splint pad.ding ...
per lb.
Flrst Dressmg (Army Regulation Pattern), P nce ..
Jaconette, 44 inches \\ ide ... ... per yard 2 3
Tow, Carbolized or ;Styptic ... ... . .. per lb. 0
Waterproof Lint (in case to hang on \\all) ... ... 2
Wound Pad.- This consists of a pad of cotton wool and g::uze, to which a bandage is attached. By a cleve r conthe surface of (he pacl coming in contact with the wound IS not touched by the hand of the person app lying the pad . Price 4d . each.
SAFETY PINS.
All fasten or unfasten on either ide.
Fac ile No . S 600 or S 602 pe r 3 doz
" "S 603 ... .
D uc h ess Duplex, TO. 2 ... doz.
" Assorted
Special Blanket Safety Pins, 3 in.
" " " " in . . ..
Ambulance Station Plate, E,;amclled Iron, 3s. 6d. each.
Stretcher Depot Plate, Enamelled Iron, 3s . 6d. each.
Nursing Chart, designed l)y Miss I nc1erwick, each. Temperature Chart, each. . Registers. Class Attendance, 2S. 6cl. CertIficates, 4S. 6d. Case Repo rt, IS .
Large Physiological Diagrams. For Lecturers' usc . . Comp rising: The Uuman !-'keklon, the ;\I uscular, Artenal and Venous Systems, the Ilearl and the Blood , S imple Fracture, Compound Fracture, P ri ce per set of six, ISS. .These may be hIred a cou rse of " First Aid" lectures, gIven under the auspIces of the Association, for a fee of 5s., or \\ it h the addition of Splints, T ourniquet, ancI plain Triangular Bandages, a fee .of lOS . Boxes of Stationery for the use of Class Secretanes and others connected with the Association, containing twelve sheets of high-class paper, suitably tw::lve envelo pes beanng the device 0.[ the I nce 6d ., by post 9d . . Twice thal quantity, .pnce IS:, by post 3d . Medallions, issued in accordance wah speCial allons, .for which see lea!lct 1.C:' I:; 6")r, to be had on Co:na ge Bronze , 2S. ; Silver, 7s. 6d. ; Gold, £2 lOs. , ll1cludll1 g eng raving nam e ancl numbe r on back. velvetli ned case, 25. , Labels, to be placedaho\"c for each equentyear s ex amination issued in accordance WIth regui.1uons, as per paper rl-h . Coinage Bronze, 6d. ; Sih'er, IS. 6d. ; Gold, 12S. 6d .
NURSING INSTRUMENTS.
Bow Dressing Forceps, ful l site, IS . 3d.; small, extra we ll fini shed, I S. 6d. .. Scissors round-pointcd, IS . 3d. ; sharp-poll1ted, fo r dellcat e work , 3d . ; small rounel-pointed, blades take apa rt for cl eaning IS. 9d . Spatula, 9d . Probe , 9d. Director, with Ear Scoop, I S. 9el. Artery Forceps , 2S . 4d . Knife, ve ry thin , ivory hand le, two hl ades , IS. 9el.
. .
.
.
. .. s d 6 2 6 7 6 4 o 6 6
... ... . ..
. . .. -..
... '" each 0 9
o o o o 6 8 2 3 o 6 l'RICl£ LIST. 22
. PRICE LIST.
CLINICAL THERMOMETERS.
Rd ' Red llced Plices.
oun . Ordinary, IS .. minute IS 3d . I If . Fl t S " . ., la -mInute IS 6d a . trongly recommended as they will not roll' O' d" nary I 6cl · rapid ( . II I . r 1- Assdc' t' )" . 'h speC13. y e ectecl and reserved for the la IOn ,Wit very open scale "'s Lens Fronted. When held in' .. column of mercury is magn'fi d ed proper .posltIOn the little practice is re uir die ,a,n so easily read. A in which to hold . e to ascertam, the c?rrect position . e ll1strument. Pnce orclll1ary IS 6d . mll1ute, I . 9d.; half-minute 2S 3d ' , . . ,
K.ew Certificates (to order) d h certificates either state that 'the ' . 3 . eac . .N. B. - These point out any slight e th ll1strument IS correct or rror ere may be' the usually .con iclered necessary. ' yare Dot and half-minute instruments will only register ll1 e tuue stated under favourable circumstances.
BATH .THE1\.MOMETERS.
To Dr. Forbes' specification J d' . 2S. 3d .. Clinical Th ' . ::pan?e With Z1I1C scale, N o tiab;'fit is taken SIZe" 111 case, IS. 6d. J JOY b1 eakage 0/ Tilermollleters in tramit
TEXT BOOKs,
"FIRST Am TO TH I F E
By
C3C. .
James Cantlie, M.BC· R: C. S. The authonsed Text Book of the First A'd " ourse. IS.; by post , IS. 2d. I CATECHISM OF FIRST AID" C . Manual By J B' L' omplled from Dr. Cantlie's . . lOwn, .R C P L ReS d J
Can'ell M R C S L SAP"" . , .. , an . M . " HINTS 'AN; , . . nce 6d. ; by post 7d. B E M D LPS FOR URSING AND HYGIENE" Y , ac owell Cosgrave M D 'll t d' . -bhe application. of the
. 'b The authOrIsed Text Book for the Nursing COle, I S.; y post IS, 2d. ourse .
PRICE LIST . 24
Tl!.XT BOOKS,
h HOME HYGIENE." By John F. J. ykes, D . Sc . (Public Health), M . D., &c. Illustrated. The authorised Text Book fo r the Home Hygiene Course. IS.; by post, IS. 2d. " CATECHISM ON HOME NURSING" (based on Dr. Cosgrave's Text Book). By J. Brown, L.R,C.P., L.R.C .. " and J. M. Carvell, 1\1.R.C.S., L.S.A. Price 6d. ; by post, 7e1. " QUESTIONS AND A"SWERS UPON \YORK." By John W. :Martin, and John Martin, F.R.C.S. Ed. IS.; by po t, IS. Id. " QUESTIO -S A:-<V A;-';S\\,ERS lJl'O;-'; ;\'URSI:-;C." By John \V . Martin, l\I.D. IS. 6d. ; by post, IS. Sd.
"FIRST Am TO THE INJURElJ (:ix Ambulance Lectures)." By Profes or Frederich Esmarch. Translated from the German by H.R.II. Princess Christian. 2S.; by post, 2S. 2d . " BANDAGL G AND SURGICAL DRESSING." By Walter Pye, F.R.C.S. 2S.; by post, 2S. zd.
DR. G. H. DARWIN'S" FIRST .-\llJS," being a card to hang up, giving treatment of \'arious accidents. 2d.; by post, Sci. "To RESTORE THE ApPARENTLY DROWNED," printed in large Type with two Diagrams. Unmountecl, zd. each; by post, 3d . Mour,ted, with red border, ancl yarnished to hang up, 6d. ; post free, packed, IS.
"How TO ACT WHEN CLOTIll:-;C TAKES FIRE." By J. E. H. Mackinlay, M.R.C.S. Unmounted, 2d.; by po t, 3d . Mounted on card and yarnishecl, 4d.; by po. t, packed, 7d .
"FIRST AID PRINCIPLES." Cards of conci e directions for waistcoat !cI. each; 4d. per doz. ,'pecial quotations for large quantitie .
"SP£CI:\lEN PAPERS, First Aiel, and Hygiene Courses." 3d.; by po t -t-d.
SMALL DIAGRA:'II. Showing the human skeleton, main arteries, and points where pre sure should be applied to arrest bleeding. 2d.; by post, 3d .
PRICE LIST.
TEXT BOOKS, &c. -(contim-ted'}.
D IRECTIONS AS TO TITE RESTORATION OF PERSONS SUFFERING FROM ELECTRIC SnoCK. Large print, poster size. 3d. each; by post, 4d. ; or 2S. 6d. per dozen. AIDE MEi\IOIRE. On cardboard, in linen -l ined envelope, for the By late .Surgeon-Major P. Shepherd. Contamll1g useful Innts for FIrst Aid to the Injured. 3d.; by post 4d.
GENKRAL OTES O. FIRST Am TO BE RE DERED IN CASES OF POISONING. By Milnes Hey, M.A., l'I.R.C.S., L.R.C.P. Price 2el. ; by post, 3el. " AMBULANCE TABLETS." By Sydney Partridge, M. D. Price IS. ; by post, IS. Id.
NOTES 0 MILITARY A 'ITATION. By Lt.-Colonel H. P. G. Elkington, R.A. I.C. Price 6d. ; by post 7el. 'c B?OK," for instantaneous reference, giving concise ll1StruCtlOllS; to hang on wall. Size about one foot square. Price 2S. 6d. ; Ly post, 3s.
AIDS TO MEl\IORY. By L. 1'1. Frank Christian M.B.C.M., Eelin. 6d. per copy; by post, 7el. ' RULl!.S FoR C ORPS AND DlYISlONS, St. John Ambulance Brigade. 2d. per copy.
A History of the Order of the Hospital of St. John of Jerusalem . By the Rev. ,V. K. R. BEDFORD, 1.A., Genealogist of the Order, and Lieut.-Colonel R . H. HOLBECHE, Li b rarian of the Order. Inane Vol., Demy 8vo., 230 pp. Profusely illustrated. Price 5s.; by POSl 5s.4d . The Knights Hospitallers in Scotland and their Priory at T<:,rphichen. By GEORGE THOMAS BEATSON, M.D., C.B. With 15 pages of illustrations. Price 2s. 6d ., bound in cloth; post fre e, 2S. 8d.
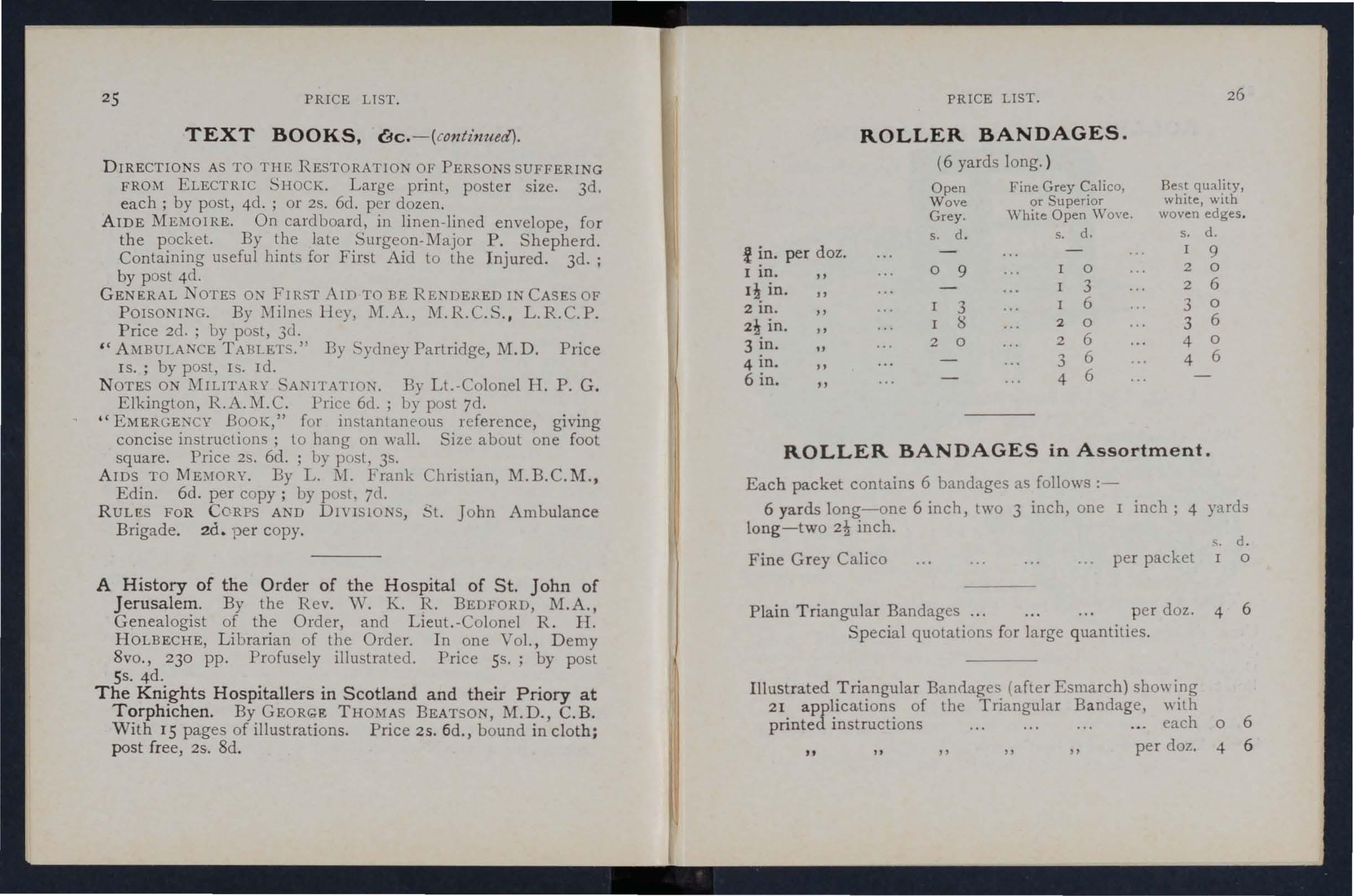
ROLLER BANDAGES in Assortment.
Each packet contains 6 bandages as follows :6 yards long-one 6 inch, two
long-two 2! inch.
Fine Grey Calico
Triangular Bandages ... per
Special quotations for large quantities.
Illustrated Triangular BanrL1.ges (after Esmarch) sbo\\ ing 21 applications of the Triangular Bandage, "ith printed instructions
PRICE LIST. ROLLER BANDAGES. (6 yards long. ) Open Fine Grey Calico, Best quality, Wo ve white, with or Superior Grey. White Open Wove. woven edges . s. d. s. d. s. d. t in. per doz. I 9 I in. 0 9 0 2 0 in. 3 2 6 2 in. 3 6 3 0 2! in. S 2 0 3 6 3 in. 2 0 2 6 4 0 4 in. 3 6 4 6 6 in. 4 6
one I inch; 4 yards
s. d.
per packet o
doz.
6
3 inch,
Plain
4
. . each 0
per doz. 4 6
.
6
PRICE LIST .
ROLLER BANDAGE MACHINE
.
De igned by D r. A. C. Tunstall. Price 25. 6d. COTTON WOOL.
\Yhite absorbent, good, I oz. packet, 2d. ; 2 oz. packet, 3d: ;
4 oz. packet, 4d. ; lb. 7d.; I lb. IS. AN l'!SErTIC-Boraclc, i lb. packet, 6d. each; perlb., IS. 6d.; CarbolIc, per Ib' 1 IS. 8d.; Alembroth, per lb., Is. 6d.; Double Cyanide, per lb., 2S. 6d. LINT.
:'IIedium quality, I oz. packet, 2d.; 2 oz. packet, 3 d .; 4 oz. packet, 6d.; lb. packet, Iod.; I lb. packet, IS. 6d. ; Boracic, I lb. packet, IS. 6d.; 4 oz. packet, 6d. GAUZES.
The-e are upplied in 6 yard lengths, \,idth about 36 inches.
• s. d .
Unmedicated white Alembroth
Double Cyanide
Boracic GAUZE TISSUE. per length 0 10 o 2
A layer of absorbent cotton wool between two sheets of gauze, good quality, per lb., IS . 6d.
PRICE LIST. PLASTERS.
Manufactured by Messrs . A. De t . Dalmas & Co. Le iceste r A dhesive Pl aste r on Cambric, in tins of yard, 6 inch es w ide 6d. T he Leiceste r Adhesive
Ribbons, in tin boxes, 6 yards long.
N ational Rubber Adhesive Plaster (Antiseptic), on spools.
D itto in card box in. widc:, yds. long .. . tin I t 3 ! S ! ,. s " " COURT PLASTER, TRICOLOR. Large Size, 9<1. ; Medium, Sd. ; Small, 3d.
2
yd
! inch wide 9d. IS. 10 yds. 1.. IS. 6d. 2 IS 9d. 2::.. 3d. inch wide
inch wide
S
.
1
6d.
Sd. rd. 3d . 3d. 6d. 9d•
Prices much Reduced
No. I . in many cases.
Arm Badges, with the device, issued unde r the autho r ity of the Central Executive Committee, having been fi rst approved by H. R. I I. the Grand Prior as the sole offi ci al and recognised Badge of the Association and Brigade.
N.B.-Tltis design is protected, and must be obtailled direct from the CwtralOffice.
No . I, fo r the use of individual c ertificated pupils- s . d.
In German Silver, Large Size
hole
I n Electro Plate, Large ize
, mall Size ditto ... ...
Small Size for button hole
I n C loth and Silk ... ... '"
I n Cloth and Silver (Registered N umbe r, 3522)
I n Cloth and \Vo rsted
Small Celluloid Badge, for button hole, a rm or brooch
White Satin Armlet, with woven Badge
Black Silk Armlet, with p rinted Badge ...
N. B.- Tltese Badges are 1£ot to be worn as decorations.
i\o. 2.
No. 2 for members of the .'t. John .\.mbulance Brigade, the name of the Corps or Division annexed on a label, oI.ly issued in <Juantilies-
In German Silver, first doz., {,r ; suusequent dozs., 12S.
In Electro Plate, first ooz., {,1 12S.; suusequent dozs., £14S.
I n Cloth and Silk, per doz., J 2S.
In Cloth and 'ih-er, per doz .. {,1 lOs.
All the above may be ,,'om by memuers of the St. John Ambulance Brigade, not \\ earing uniform, and the (;erman Silver and Electro Plated may be worn as the Arm Badge ,for alJ ranks on the B6gade Vniform.
29
... ... ' " 0
Size
... ... 0 6
0 6
mall
ditto
Small Size for button
...
. . ... ... .. .
.
... ... ...
o o 9 o 9 o 9 2 0 o 6 o 2 o o 6 PRICE LIST. 30 BADGES.
3 1 PRICE LIST.
BRIGADE UNIFORM BADGES. etc.
Officers. Collar Badges (Reg. No. 3,524) per pair " Pouch Badge ( 3,657) each Sergeants. Cap Badge ( 3.520)
" Arm Badge ( ,,3,523) "
Fatigue-"Cap Badge for Officers and Se rge ants (Reg. N o. 3 ,558 )
Corporals and Privates.
Cap Badge (Reg. N o. 3,521) ... each Arm Badge ( 3, 5.+2) .. .
Overcoat Badge ( " 1,582) .. .
Field Service Cap Badge for all ranks
Lady Officers of Nursing Divisions.
Superintendent's Cloak Badge (Reg. No. 3,658)
uperintendent's Arm Badge. ( " 3,659)
Other Nursing Officer's Cloak Badge ( " 3,555 )
Other Nursing Officer's Arm Badge (" 3,656)
Nursing Sisters. Arm Badge ( 3,522)
" Cloak Badge ( " 3,52 I)
Honorary Surgeon's Silver \Yire Cross (pattern B)
Superintendent's ilver Wire 'ta r (pattern A)
Medallion Badge (pattern D)
Nursing Badge (pattern E)
Satin Badge for Nursing SiSler's Pin Cushion
Bugler's Badge ... 4 0 Bugler's Cord
Honorary Secretary's Badge ..
Whistle and Chain each
Field Service Cap , complete ...
Private 's Brown Waist Belt and Pouch "
White Piping, per packet of yards, enough for 3 pairs of trousers (packets cannot be broken) ...
Lace, Silver per yard Black ..." (A Cap Band
BUTTONS FOR THE UNIFORM OF THE ST. JOHN AMBULANCE BRIGADE.
Issued only for the use of Officers and Members of Co rps and Divisions wearing the prescribed uniform.
ELECTROTYPES OF THE ST. JOHN AMBULANCE DEVICE.
No. I. For Cards, Tickets, &c....
2. For Tote Paper, Circulars, &c.
".). For Quarto and Foolscap Letterpaper, Circulars, &c. ... ...
4. For Small Posters...
,,5. For Large Posters...
Prints of the above Electrotypes, with the exception of No. 4A, which is shown on page 29, and No. 5B, appear on the following page.
. ..
... ... . ..
.
..
generally runs about 24 inches.) s. d. 3 0 2 6 6 0 2 0 3 9 2 3 2 3 o 6 o 8 4 6 3 9 4 0 3 3 2 0 2 3 0 8 0 8 0 I 0 8 o 3 0 0 2 0 3 9 7 8 2 II 0 I 0 I'RICE LIST. 3 2
Electro Plate, large small German Silver, large small Black Horn , large small per doz. s. d. 4 0 2 0 o o o 6 o 4
Series A. Series B for for Association Brigade use. s. d. I 0 o use . s. d. I 0 3
0 3
6
9 3 0 Complete
5 3 5 6
' eries
33 PRICE LIST. PRICE UST.
ELECTROTYPES. ELECTROTYPES.
No. I A.
For prices see NO.5 A. NO.3 A. page 32. No. I B. For prices see page 32.
NO.3 B. No.2 A.
PRICE LIST
POUCH FITTINGS.
specially selected for the.·l. John Ambulance Brigade , consisting of :-
2 Triangular Bandages, one of whi ch is sealed up in waxed paper. The other may be used fo r practice, but should be kept as clean as po sible.
2 Roller Bandages (3 in. and I in. ).
I Packet of Cyanide Gauze (I yd. compressed).
I Pair Scissors.
6 Safety Pins .
I Small Bottle of strong Smelling Salts.
I Piece of strong Cane, for tightening improyised Tourniquets .
Price, 2S. 8d. each . 6 doz. or more, 2S. 7d. each.
Packet of Cyanide Gauze (I yd. compressed). Price per doz, 2S. Sd.
mall Bottles strong. melling alts. Price per doz., 5s. 6d. pIint Ties, Webbing, and suitable Buckles. Per set of 12 yards of strong 2-inch Webbing and 15 Buckles, 2S. 6d.
T hese make "ery compact Ties fo r carrying in the Pouch.
T he \\Tebbing should be cullo meet local requirements.
Buckles only, IS. 3d. per dozen.
\Vebbing only, IS. 3d . pe r dozen yards.
I t is unnecessary to sew the Buckles. T he spikes should be passed th rough the webhing, and the short end of th e webbing should li e outwards.
These Illay l)e ohtained direct from ITebbert and Co., 35. Bethnal Green Road, E. T elep hone t\o 909, London \\'all. Telegraphic Address: "OLherwise', London. "
SW AGGER STICKS
for the use of Officers and Members of the St. John Ambulance Brigade.
Ebonised Canes, German Sih'er lounts bearing the Brigade Device.
37 l'RICE LIST . £ s. d. Flags bearing Association deyice-I2 feel by 6 feeL 6 " 5 feet by 3 feet 0 12 6 Brigade 4 ft. 1 in. by 3 ft. 0 12 0
PRICE IS. EACH. All Orders for the foregoing Stores should be given to the Local Secretary,
to
Stores Department, St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E.C. PRICE LIST . UNIFORMS.
or
the
CHIEF SURGEO"" ANI) IJO ORARY SUR(;EON. [, 5. d. Tunic (Badges extra)... 4 4 0 Trousers; Two-inch l\Iuhair Braid, side seams 5 0 Cross-uelt and Pouch : Black JIorocco 0 0 Forage Cap and Cover 9 6 Field Cap 0 12 6 Gloves ... 0 4 6 Great oat (Badges extra) 4 4- 0 'lUEF SuP r. 1\1\1J OlllER CUIE[' OFFICERS Tunic (Baclgesexlra)... 4 4 0 1'atrol Jacket (Badges exlra) 3 3 0 Fatigue J acket (Badges extra) 2 10 6 TroLlsers: Two-in ch 'Ifohair BraId clown side seams 5 0 Cross-belL, \\'h ile Patent Leather and Black ilIorocC J PUlIch (Badge extra) . 0 14 6 Forage Cap and Cover I 5 6 Field Cap (Badge extra) 0 10 0 (;IO\es ... 0 4 6 Leggings . 0 S 6 Great Coat (Badges extra) 4 4 0 SUPT. OF DIVISION A!'>D OTHER OFFICERS. Patrol Jacket (lJaclges extra). 2 6 6 Trousers : T\\ 0 inch :'II ohair Braid down side seam I 5 0 Cross-belt, \\' hitt Patent Leather and Black Murocco Pouch (B.l(lge extra) ... Fo rage Cap and Co\'er Field Cap Glo\'es .. Leggings .. Great Coat (Badges extra) o q 6 5 6 o 10 0 046 086 44 0
39
PRIC:l: LIST.
MESS DRESS FOR OFFICER.
Jackel (Badges extra)
Vest ....
1ST CLASS SERGEANT.
Patrol Jacket (Badges extra)
Chevron, 4 1Jars, Sih'er, 3s. 6d., \\'orst ed
Trousers
Forage Cap (Badge extra) ...
Cross-belt and Pouch (Badge extra)
Field Cap (Badge extra)
Buckskin Gloves
Cotton Leggings ...
Great Coat (Chevron and Badge extra)
'ERGEANTS, CORPORALS, AND RANK AND
Patrol Jacket, Tartan (Badges extra)
Trousers, Black Tartan ..
Forage Cap (Badge extra) ...
Cover for Cap
\\'aist -bel t and Pouch
Field Cap (Badge extra)
Great Coat (Badge extra)
Glo\'es (per pair) .. .
Leggings (per pair) .. .
Chenon, 3 bars, ilYer,2 6d., \\' orsted
Corporal'" 2"" IS. d.
CYCLISTS SUPERl TE:\DENT.
Patrol Jacket (Badges extra)
Cap (Badge ext ra) ...
Breeches: Grey 'e rge
Shoulder Belt and Pouch
Gloves
Gaiters
Hose ...
Great Coat
Jacket (Badges extra) ..
Cap (Badge extra)
(per pair)
Gaiters (per pair)
All Badges to he ol)lained by the Corps or Division from t. John',; Gate.
If the Corp,., or Diyi-.ion is oul of L onuon, measurements to be supplied to c()ntractor-. free of charge .
Carriage out of London extra
i, s. d. 33 6 180 2 3 6 0 4 0 o 10 9 oIl 0 0 :2 8 0 4 6 0 0 8 0 3 6 o 13 6 FILE. o II 0 0 9 6 0 3 4 0 0 0 6 6 0 :2 8 o 13 6 0 0 8 0 3 6 0 I 0 0 0 8 2 10 0 3 6 o 12 0 0 10 6 0 4 6 0 4 6 0 4 6 4 4 0 PRICE LIST. 40 CYCLISTS-RANK AND FILE. £ ". d. o 19 6 0 2 0
.
.. . Bree c hes: G l'e) -' erge .. . 0 12 () Shoulder Belt... .. . 0 lO 6 0 4 6 0 4 6 Glo\'es
IND E X TO PRI CE LI T.
Aids to M emory ." 25
Ambulance Hampers. .., IS, 17 Station l)late ... . ... 29, 31
Bandage Rolling ;,Iachine 27
Bandagt>s .. , 26
Rasin, llressing 14
Bed, Equipoise 12
" Camp 12
Books... ... ... 23, 25
Bottles (Water) 13
Buttons.. .., .. .. 32
Carriages (Horse Ambulance)
Carrying Sheet 14
Cotton \\'001.... 27
C over for tretcher or Li ller 12
Diagrams, Large "Small 24
Dressing Basin 14
Drowning Tackle 12
Electrotypes ... 33, 34. 35
Emergency Book 25
First Aid Box... ... 10, 20, 21
First Field Dressings ... 21
Flags... ...... 37
Gauzes... ... 27
Gauze Tissues .. 27
Hampers ( Ambulance) , IS, 17
Haversacs ... . ... 18
Hood and Apron for Lilter ... 4
Jaconette
Knife 14
Labels 22
Lace 3'
Lamp 14
Lint ... ... 25
L itter (Ashford)... 3, 4
Litt er (Rea.Edwards) 5· 7
L owmoor J acket 13
Medallions
urses' \ Vallets
Nursing Charts ... " Instruments .. Pillows
Plasters. . ... Pouch Fittings
Regislers , , Roller Bandage l'Iachine
Rug for Corps or Di,isions
St. Joll11 Ambulance Brigade
Safety Pins ... ... .
Scissors.. .. .
Slings, Stretcher
Splint Padding
Splint Ties Splints
Statiunery
Stretcher' Depot Plate 2:1
Stretchers ...
.. 8, 11 " Adjustable Legs for 10
S; wagger tick
Temper:uure Chart
Text Books
Thermometers Tourniquets . 1'0\\" carbolized
21 "plain
Uniform Sundries .,. 29, 31
Uniforms .. , ... 38, 39, 40 \ Vag-ons ( H orse Ambulance) 2 \ Vater Bottles ... 13
\ Vaterproof Lint
\Vaterproof. heet W histle and Chain W ool (Cotton)
PAGE.
.. , .. , .. ,
... PAGE 22 19 22 22
... 22
..
37 22 23,24 23
\'ound Pad 4 3 1 2 1
., \