

BONES .

}\I<'I HO'IE(hlllll<:nl')
41'11 (pehi!» J
UI:,\A
HAlJlUS -
l\J RI'US •
PHAI.ANr.FS - •..
THIGH BONE (femur)
CAl' (p<ltella) BPNf:;: (tibia)
Jll{ CltlCH BONE (fibula) .:'II'.• rAJAR!.US
ARTERIES.
'u The .numbered dOIS show res. e POint for. the arleri,'. t.m • ) re numbers III text._. • FAC.IAL.
C"Alwr/J s.
AXIIIAI:V.
'\Of
BRACHIAl (Flexion).
hl"(.. RAIJIAl. ORAl (D'gilal -,ressurt:).
I {,I PUI' rFAI.
FIRsrr AID TO THE INJURED·
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF TIlE FIRST AID COURSE OF THE T.
JOIIN

A.:)SOCIATION.
M.A., :'1.B., F .R .C.S., HOllolary Associate r/ tile Order n/ St. Jolm. Ilonola'y Lift Jlemba' oJ; and Lecturer and EXallll1lcr to, tlze hssociatioll.
\\,ith a CHAPTER on " Stretcher reyised from that originally written by ' ir ]<JH:>; FURLEV, A'II/Kltt 0./ /usilce 0/ tlte Order 0/ St. jo ltn , in accordance with the Army Stretcher Exercises. Also a CHAPTER (being the Fifth Lecture, for 1 em;des onl}), by E. ;\IACDO\\EL COSGR AVE, M.D., F.R.C.P.I., o..J (,,1 au 0./ tlu O,,:cr 0/ St. jolm, Honoral:), Lije J/ember oJ; and Lecturer and Exami1Zt:r to, the Association.
THIRTKENTH EDITION, 530,000 to 580,000 (This Ed, lien is similar to tlu: e/e,;cntlt alld twcifrlt.)
Price in Cloth, IS. net; by post, IS. 2d In i.lorocco, 25. 6d.; b) POSt, 25. Sd. TO BE OBTAll':ED AT
ST. JOlIN'S GATE, CLERKE TWE LL, LOKDON, E.C.
\\'. H. & L. C. 50,ooo-9/Ofj.
ny
q[l)t of tbe ®rber of tbe of .$t. .3Jobn of lrnl%alcm tn
allb' Va twn .O'f ®rh tr.
His Most Gracious Majesty King Edward VI!., K.G.
(5ra n1l- t}ri.or .
His Royal Highness the Prince of Wa l es, K.G.
The Most Honble . t he Marques3 of Linlith g o w, K.T . .of
Field Marshal
His Royal Highne ss the Duke of Conn a u ght, K.G.
(!;;*e.cntibc @ffi.af S.
Chancellor-The Right Hon . the Viscount G.C::\LG.,
Secretary-Gmeral-Colonel Sir HERBERT JEKYLL, K.C.:\l.G., R.E.
Receiver-General-EDWIN FI{ESHFIELD, Esq., LL.D.
Almoner-The Rev Canon DUCKWORTH, C.V.O., D.D.
Registrar-Major-General the Lord C. V _O.
Genl!alo!{ist-Sir ALFRED SCOTT SCOl'r-GATTv, C.V.O. (Garter).
Director 0/ the Ambula'u:,.e D.parlmcnt-The 1\Iost Hon. the Marquess of BI/EADALBANE, h.G.
Librarian-Lieut -Col. RICHARD HOLBECHE
S ecretary-Colonel Sir HERBERT C. PERROTT, Bt., C.B.
Chairman 0/ the B,itislt OphtILalmic Hos/,ital , Jerusalem-The Righ t Hon. the Earl of Plymou th, C . B.
Chie/ S ec,-eta ry oj tlte Ambulance Dr:pa'tm en t- C olonel Sir HERBERT C . PERROTT. St. , C B. ';; ssisbllt (!i;xt.Clltibt @ai.cms.
A s sI sta n t Director if tlte A mb li lan ce D epartmen t-Lieu t.-Colo ne l Sir RICHARD CARNAC E, Bt., C.l.E.
Assistan t Recei71cr-Geltcral-F.IlWIN H FRESIlFIEI.D, Esq
Assista n t LlbraYia n -CvRII. DAVENI'OllT. EsC].
Assistant .scC1·etaryand R. EDWARDS, Esq , A.C.A
Holt. Secretary 0/ tile Britislt GpMlt a 1111 ic //ospital , Colonel T. H. HENOLI!Y, C.l.E.
As,isttlltt Honorary Sl!crctary (fir Scotland) 0/ tlte Britislt O/>Itlltalm ic flospilal,jerusalem- j. H OI/NESr EVENso N, Esq. (UnicornPursllivant. ) 4tO ltll .cir.
The Coun c il consists of the Sub-Prior, as President ex-officio. th e Executive Officers, and the fo!lowlI1g itl ctnbrrs.
Sir JOlIN FURIEY, C . B.
Major-General J. C. DALTOI', R.A.
The Right 11 011. the Earl of R .\KFURIY, G.C.:\l.G.
Col.C W. BO\\I>LFR BO\\,DLER,C.B.
Sir jAMFC; DICK, h.C.B., :\I.R.C.P l., R.N.
Colonel Sir CHARLI!S :'If. \\'A1S0:-l , K C.:\I.G., C. B., R.F<:.
Sir DYCE DUCK\\'olnH, Bt., LL.D., :'I1.D.
Inspe c tor -Gen eral BELGRAI'E :'II D., R.:\'.
[I1C

Sir RICHARD DOUr.LAS POWELL, Ht., K.C. V.O., 1\1.V.
The Right £I on . the Earl ofLATHOJ\l • E"q., LL.D" F.R.C.S.
Lieut. -Colonel Sir RICHARD C . TEilIPLE, Bt., C.LE D. jMtES, Esq . , C.V.O .
The Right Hon. the Lord NORTHCOTE, G.c.:'II.(;., G.C . I.E., C . B .
The Right Hon. the Earl of BEssBOROUGH, C.\'.O, C.B.
The consists of the Knights of justice and S';Jb-Preb.tes de fur t; ; tbe ]:,xecull\,e Officers; the seleu"d :'Ilembers of CouncIl; and the following ®moatllllJ
The Rev. Canon SHEPPARD, C. \-.0 ., D.D., (, ub-Dean of the Chapels Royal)
The Re\,. PAUL W. WYATT, AND <as l \'llirrIJIS of (!jirace ant JEsq uires .
Surgeon-General ir \\ ILL! AM Thp. Right Hon . the Viscount TAYLOR, K.C. n., ill. D. BRACKLEY, The Right Hon. Lord CUUD Colonel T. H. HENDLEY, C.I.E. The Hon. JAMES McLAREN STUART Right Hon. CAWDOR. GRAY, Master of Gray. EUWI:-I HANSON F RESHFIELD, [sq. C. B H .UIlLTON, Esq., C. LG. Lt.-Col. EmlO:-lD 1\1. \VII.SON, C. B., Lieut.-Colonel IVOR PHILII"'S, C.1\f.G., D.S.O., R.A.:O-LC, D.S.O" ?>LP, Lt.-Col. _ ir LEES KNOWLES, lit. Colonel CHARI_ES F . ST. CLAIR
The Right H o n. the Lord DES- ..\N STRUT IIER, :-'f.\'.0 ,D.S.O. BOROUr.H, h.C.V.O. EDWIN DAWES, E q.
The Rigl-tt Hon. the Earl of HENRY T JOHN H01'E, Esq. KIUI OREY, K.P. B 2

forowing are iitnigl)ts of .5Iusiicc:
H .R. H. Prince CHRISTIAN 01" SCIII.ESWIG-HoLSTEIN, KG, G.C.B.
R.M. KI'IG H o\A 1{0'l 01" :-.rORIVAY, K .G., G.C.B., G.C.V.O.
H. H. Prince ALilEilT 01" SCIII.r:C;WIG-HoLSTEIN, G.C.ll., G.C.V.O.
H.S.H. The nuke of TECK, G.C.V.O,
H.S.H. Prince FRA;o.:CIS 01" TECK, K C. V.O., D.S.O.
R ear-Admiral H . S . H Prince LouIs 01" Ih TTE'IIU;;R'; , G.c. B., K.C. \I.G .,
H.S.H . Prince ALI'XA'IDEll GE'IRGE 01" TECK, G.C.V.O., D.S.O.
R.R.H. PIUNCE ARTIIUR 01" CONNAUGHT, K.G., G.C.V.O .
Lieut.-Col. TRF.VENEN J HOI.LAND, C. B.
Sir JOH'I FURLEY, C.B. (lIellL. Bailiff)·
The Lord STAN;'IORF.,
Sir THO;l!AS NORTH DICK-LAUDER, Bt.
Major Sir ARCHIB\LD 1.A\18, Bt
Col. Sir HERBERT C. PEIWOTT, Bt C.B.
The Right Hon . Earl FERRERS.
Col. Sir J. GIJ.DEA, K.C.V .O., C.B.
HENRY JOH N LOP'Tu s, Esq.
Colonel BETHEL ;\ I ARTIN DAWES
Gen. Sir CHARLES \V .o\RIlEN, G.C.l\ 1. G., K..C.B., R.E.
Major General J AJlIES CECIL DALTON, R A.
Col. AYLMER GOULD HUNTERWESTON, D.S.O., R.E.
Colonel The Right I ron. Lord C"ClL, C.V.O.
EDWIN FllI;;SI IP'II".Il, LL.D. (!{eI/Lora})' CIJlIIJllfllldcr).
!Tis Grace the I )ukt! or FII-'F., K .T . rile Rt. H on. Lord BIlASSgY ,G.C.B
The Ric;ht [l on Viscount TE\lPLETO\\tN.
The TI on. Earl A\IIlERST.
The Right lion. \'iscollnt KNUTS· FOIlD, G C. \[ .(;. (1!1111. Blti/ijj) R. \fAcl JEo\:-I 1\1 \CI.F.AN, ,\IlTIl UR Vln:-lCIS GIO;;SIL\M LEvESO'l GOII'ER,
Lieut-Col. v.A. H EV';ATR LA\TnERT. Colonel ir CH \llI.ES WY NDIIA\ I C. B.
The Ric-ht J[ on the Earl of RAN· P'uRI,Y, G.c.i\U;.
The l<i::;hl Hon Lord SANDIIURST, G.C.S.I., G.C.I.E.
Sir IIE :-IRY AI<THUR DI.AK!!:, G.C .\l.G.
The Rt. HOIl. LIlt! Earl of MEATH, K.P.
A. ELl\!U:-ID FllASI"'l, Es'1
The Right Hon. Lord
The :'Irost Hon. the \larquess o f eRE·\ Il ,\ 1.11,,\:>' E, lZ.t;. Grace the iJukt! or PORTl.AND, K. G., G.C.V O.
Fieltl- 'f arsh,,11 the Hon. lhe Earl ROBERTS, IZ.(";., K. P., 1' .11:'., etc.
ROI3EllT BIWIJENEI.L Esq., F R.C.". NOIOI \'1 IT,\y FORBES, Esq., F.R.C.S. (I·:dill.l
Colonel C. W. B )IVDI.ER BOWDLER, C.B.
Lieut.·Co\. A. C. Y \ TE. ASTI.EY F. TERRY. folloming ute tilt
The in JEIWSALE:lI. I The Bishop of DUNE[)I:-l.
Loro Bi"hop of C:\USIlUIlY. I The Bishop of GIIlR.\lTAR.
The Bishop 0 ( Primate 0/ Ncw Zealatui.)
J'OgH
Till!: \. 'ICE OF QJimnl:r lOtiO!Q of tbe @rbet of tbe of .%t. Jlobn 0 f ](rmmleIH itt QFIt!Jlana.
F'ntro '.
HIS MOST GRACIOUS MAJESTY KING EDWARD VII . , KG. ilEAl> \:-':D l'ATR'):>' 01" TilE ORDER.)
HIS ROYAL HIGHNESS THE PRINCE OF WALES , K.G. ((,II I'RI()I< 01' TilE ORDEII.)
\[mtrlll Q:Crrclltibc r-O nn1l ttcC. exclu,i\'cly or :'.Ielllbers ami AssoLiate'i of the Order.
DIJ'/:ctor 0/ tl:e AIII/>U/,lJlC£ D.,/,arilllcilt alli Chairlllllll 01 COllllllittu-
The Hon. the ;\I.lrquess or BllEADAl.BANE, K.G.
Assist,lIIt Direct,,,, (lild f),,/,u<,' Cllllirllla ll - Lieutenant·Colonel Sir RICII.\IW C. TE\II'1 E, Hr., C.l.E:.
De/'lItr·Cllilir/llfw-Sir JOItN FURLEY, C. B. (Life Member of the Commiltee //lllLllris Calls.i).
.I/(mbcrs.
i\fajor.\'.:neral J C. nIl 10:-':, R,,\. C. \\'. 1:)\\I>I.I-1{ IlolI'l>LER, C.B. Lieut.,Colond A. C. \'\ rEo
The ReI. l. W. \\'''"l>. \N f)1,\O:-':, J ,q.
Major G. F. \\'Y:-':DIlA\l :'If \LET.
Colclnd Sir J. \\'. OrTl.hY, K.C.I.E. R.E. Inspt!':lOr.t;cnt!ral l:gl.l;RAI'E )fI:-l:-lIS, M.D., R.N.
GEORGI!: F .. w 1.I;;1{, Surgenn-:'Ibjor l:. H. n.\l<\\,l:-l, :\LD. .'. EI 1.1"'0'1, Esq., :'If. R C.S. Lit!ut.·Cnlonel C. J. C.:'II.G., L.R.C.P.
Colonel Sir C!.F:\!F'IT :'II. RI)YIIS, C.B.
Captain J. \\'. :\ClIT HU\\'EIL
ED\!U!'Ill OIlEN, l:..q., LL.D., F.R.C.S.
qtrntraI Qtommittu-co1ltinued.
The Lord CLAUD HAMILTON.
A dmiral ALFRED J OHN CHATFIELD, C. n.
Sir J OHN L LAN GMAN, Bt.
The Hon Sir J OHN A. COCKBURN, K .C.M .G., M.D.
Sir AR THUR C ONAN DOYLE, M.D
The Right non. J. L. WHARTON, P.C.
Surgeon -General Sir AI.FRElJ KEOGH, K.C.B., F.R.C.S.E. & 1.
SYDNEY \V. MALKIN, E<q.
Lieut.-Colonel Sir R. A. CLARK, Bt., c.n ., F.R.C.S.E.
Surgeon-General ir FRA 'KLlN, K.C.I.E.
J OH:-I SAMUEL GRIFFITHS, Esq., 1\1. R.C
Lieut. -Colonel JOHN AR'IALLT JONES, M D.
Sir \S LEWIS, Ht., K.C. V.O .
The H()n. A. BRASSEY.
The Right Hon. The Earl of liESSllOROUGH. C.V.O , C B.
Lieut.-Colonel GEORGE E. TII'ISS, F . R.C.S .I.
Colonel JAMES CANTLIE, F.R.C.S.
C olonel T. H. HE:-10LEY, C . I.E.
Surgeon-illajor G. A. HUTTON.
Surgeon-General Sir CHARLES 1\IcDONOUGH CUFFE, K.C.B . , F.R.C S.E.
Deputy- rnspector-General ::\1. COATES, M D., R. N.
F. R. CASS!l)I, Esq., M.D.
A. THEODORE BRAZ'O. Esq., M.D.
J. ASTLEY BI-OleA)I, F R.C.S.
FRANCIS N. ELLIS, E 'Q
M ajor E. WEST ilI.D.
\V ILLl.UI 1<:. A UDI. .u:n, Esq, :\LR.C. S.
J. HAMMOND ::\I ORG\N, Esq., C.V.O., F.R.C.S. Ex·Officio Ilfelllbers 0./ COJIIJllitlt:e.
C olonel Sir HERBERT JEKYLL, K.C.l\I.G., R E. (Secretary -General o f the Order).
EDWIN FRESHFIEI.D, Esq., LL.D. (Receiver-General of the Order). The Right H on. The Earl of PLY.\IOUT!I, C. B. (Chairll1.ln , Britisl7 Ophthalmic Hospital). ([hicE .sCmtllf!) .
Colonel Sir HERBERT C. PERROTT, Bt., c.n. (Se : relary of the Order).
UJirrctor of anb C!rcotlntant.
WILLIA::\I R. EDWARDS, A.C.A. (Ass is tant S ecretary and Accou ntant o..f tlze Order ) . .$lordtceper.
HE NRY M ORGAN, Esq. ()ujer i n tutdcnt , I ,tva/id Tra ll sjort Coris).

REVISED I 908.
FIRST AID TO THE INJURED.
SYLLABUS OF INSTRUCTION.
FIRST LECTURE.
A. Principles of First Aid.
B. A brief Description of the Human Skeleton and of the Muscles.
C . Fractures-Causes, varieties, signs and symptom s.
D. Treatment of Fracture General Rules.
E. The Triangular Bandage anti its application.
ECO:'-ll) LECTURE.
A. Treatme nt of Fractures (continued) . Details of treatment.
B. Dislocations, prains, Slrains-. ign, symptoms and treatment.
C. The H ea rt and Blood Ve sels. Th e Ci rculatio n of the Bl ood.
D. H remo rrhage ann woun ds. General rules fo r treatme nt .
E. The Triangular Bandage and its a pplicati on .
RHF ERENCF. No. 58. 1908T IIlRD LE TU RE.
A. H ::e morrhage anu wJunus (conti nued) . De tai ls o f tre atme n t.
B. I nternal I-Iremo rr hage-Signs, symptoms and a rrest.
C. IT ;:emorr hage from Special Regions.-Signs, symptoms and a rrest.
D . Bru ises, Burns and calds, Bites and Stings, Frost-bite.
E . Foreign bodies in the Eye, Nose and Ear.
F . The Triangular Bandage and its application.
FOURTH LECTURE.
A. Th e Tervous Sy. tem.
B . T he O rgan and Mechanism of Respiration - Artificial R esp iration.
C . I nsensibility.
D. Poironing .
FIFTH LECTURE ((or ;,Iales only).
I mprovised methods of lifting and carrying the sick or in ju red .
B. of lifting and c Hrying the sick or injured on stretche rs.
C. T he conveyance of such hy rail or in country carts .
FIFTH LFCTURE (for Females only'.
A. Preparation fo r reception of accident cases.
B. M eans of lifting and carrying.
C. P r eparat ion of bed .
D. Removing the clothes.
E. Prepa rations for surgeon .

N OTE I. -The subject of poisons should be t r eated in a gene ral manne r ; the common poisons cia sitied, a nd on ly t h eir gene ral symptoms, effects and treatment taught.
aTE H .-The last half-hour of each lecture should be devoted to practical work, such as the 1:Ipp'ication of uandages a ld splir.ts, lifting and carrying wounded on stretchers
aTE III. -There should be an inte r val of a week betwee n each lecture. A candidate for examination must attend at least fuu r out of the lIve lectures .
NOTE IV.-;'Iale must passin that sy tem of stretc her exercise most suilaule for the locality
NOTE V.-As little time as possible is to be spent o n instruction in anatomical andL.hysiological details. Lectu re rs and examiners are particularly requestld to rememuer tllat it is " First Aid" that has to be taught and tested, and not anatomy and phy iology.
lI.Iixed classes 0/ //len and w.Jmen are on no a((Oltll! permitted.
PUPILS U:-mER SIX IEE:-.I YEARS OF AGE CA. O.\:LY ATTE D THE" JUNIOR" CuURSE A, SYLLABUS 40).
Lecture r5 instructing a Fir s t Aid clas s , and Local Secretarlea, can obtain further particulars on application to the Chief Secretary for .. Paper R.eference No. 80."
No Lectu r er m ay exami1U hir Class for Cerfijicillu.
9
SUJ\ll\I

II.
The Human SkeletorJ. Skull, spin e, ri bs an d breastb one, upp er limbs (co lla r- bone , shoulder- blade, a r mb one, b ones of the forearm, carpus , metaca rpus, pha lang es), p elvis, lower li mb s (thigh-bone , kn eecap, ta rsus, metatarsus, phalanges) ...
for treatment of Fractures.
the treatment of
Special Fractures. Cran ium, lower jaw, spine , ribs, b reast-bone, collar-bone, shoulde r -blade, a r m-bone or bones close to the el bow j lint, fo rea rm, crushed ha nd, pelvis, thigh-bone, knee-cap, leg, cr ushed foot
Miscellan eous Injuries . Bruises, bums and scalds, hites of snakes and rabid animals and by poisoned weapons, Slings of plants and animals, frost bite, needle embedded undtr the skin, fish hook err.beclded in the skin, injuries to joints, fo reign body in the eye, ea r passage and nose, wound in the fmnt wall of the
the orga
Schiife r's, Sil ve ste r's, H oward 's
10
ENTS CHAPTER I. Principles of First Aid 17 Explanatory 20 Questions on Chapter 2 1 CHAPTER
A R Y OF C O NT
22 Joints .. . 3 1 Muscles. Voluntary and involuntary 32 Fractures. Cause.>,
33 Apparatus
36
Fractures 4 1
43 Dislocations 62 Sprains 64 Sprains and Ruptured Muscles .. . 65 Q uestions on Chapter 66 1 I C H APTE R III. Pag t Circulation of the Blood . O rga ns; ge n era l (system ic ) a nd pul mona ry circulations 70 Hcemorrhage
Bleeding. Arterial, venous, capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage ... ' 76 Course of the Main A r teries and Pressure Points . Aorta, a r teJies of the head and neck, of the upper limbs, of the lower limbs 79 Venous Hcemorrhage and Varicose Veins 93 Wounds wit11 V eno us Hcemorrhage 94 Capillary Ha:!morrhage 95 Internal Hccmo r rhage 95 Hcemorrha :;-e from S pecial Regions 96 Questions o n Chapter 99 CHAPTER IY.
...
\'arieties, signs and
..
General Rules to be observed in
or
injuries
ns \, ilhin the abdomen and pel\'i, 102 Questi ons on Chapter ... ... 1 15 CrrAPTER Th e N ervous System. Cerebro-spi nal , .. . II7 T he R es piratory System 11 8 Artificial Respiration.
combine d with
Ha ll' s me thods .. . 121
abdomen,
t::>
Silvester's, L1.bo rde's a nd Ma rshall
Insensibility. ('"auses, general rules for treatment, concussion of the brain, compression of !.he brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, unstroke and heat-struke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPTER VI.
Poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages fur the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. FOLir, two, and three handed seats, fireman's lift, fore and aft method, improvistd stretchers, to cross a ditch or wall, to load or unload a wagon ..
CHAPTER IX.
Stretcher Transport. Stretchers, stretcher exercis ns, litters
CHAPTER X.
The Fifth Lecture (for Females only ). Preparation for reception of accident cases, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparation for surgeon ... uestions on Chapter

Skeleton showing positi on o f main arteries
Skull and vertebral column
Vertebra
Bones of the left uppt:r limb
Bones of the right lower limb
Shoulder Joint
Ankle ...
Rectus Muscle
Triangular bandage spread out and fuld cd
Large arm !;Iing
Small arm sling
Reef knot
Granny knot... , .. .
Loop knot
Bandage for fracture of lower jaw
Bandages for simple fracture of rib
St. John sling
Band ges for fracture of b o th co llar bones
Bandage for fracture of sh o ulder Glade
Treatment of fracture of arm
Angular splint
Treatment o f fracture of forearm
Treatmtnt of crush ed hand ...
Treatment of fracture of thigh bone
Treatment of fracture of thigh b o ne (woman)
Fracture of knee cap
Treatment of fracture of knee cap
Treatment of fracture of leg (man and wuman)
Treatment of crushed foot ...
Diagram of the heart, lungs and air pa-sages
12
Page 128 142 145 155 160 197 206 13 LIST OF ILLU":TRA IrONS.
. . . .. . .. . . ..
.. .
... . .. . .. . .
... . ..
Pare .frontispiece 2-424 27 29 31 3 1 32 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 71
Diagram of the circulation of the blood
Digital pressure on carotid artery ...
Digital pre:.sure on facial artery
Digital pressure on temporal artery
Digital pres,ure on occipital artery
Pad and b a ndage to arrest haemorrhage from temple
Ring pad
Digital pressure on subclavian artery '" '" '"
Pad and bandage, to ap?ly pressure on axillary artery ...
Digital pressure on brachial artery (two methods)
Flexion at elbow
Digital pressure on radial and ulnar a rteries .. ,
Pad and bandage to arrest hremorrhage from palm
Digital pressure on fem ora l artery .. ,
Tourniquet on femoral artery
Flexi on at knee
Organs of the chest and abdomen",
The lungs and bronchial tubes
Schafer's method of anificia l r espiration" ,
Silvester's method of a rtificial respirati on
Silvester's and Howard 's methods of artifici ..tl respirati on combi ned
Bandage for the head
Bandage for the shoulder
Bandage for the hip, ..
Bandage for the hand
Bandage for the foot
Band age for the chest
Bandage for the knee
Bandage for the elbow
Grip for fou r-handed seat
Lifting by two-handed seat. ..
Grips for two-handed seats, . .
Carrying by two-handed seat

Grip for three-handed seat .. ,
Supporting patient ... ' ..,
Fore and aft method of ca rrywg
Carrying on improvised seat
Improvised stretcher '"
Furley ,.,
Stretcher exerCIse, o. 1. ' c Fall in "
Ditto, ready to ]i.ft patient
Ditto, lifting patlent."
Ditto, placing stretcher ,
Ditto, to lower patient.. ,
Ditto "Lowe r ... .., ...
Ditto: No . II. Ready to lift Fatient
Ditto, patient .,' "
Ditto, No. IV. FIrst pOSItIOn
Ditto, second position .,' '" . , ..
Diagrams illustrating Army stretcher drill
Ditto .. ,
Bed c radle
Improvised bed cradles
Pa£,c 73 81 81 82 82 83 84 84 85 86 7 7 89 90 9 1 112 11 9 122 124 12 5 ISS 156 156 157 157 15 8 159 159 160 161 162 163 15
Page 1 64 165 1 6 7 168 168 17 2 175 17 6 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
PREFACE.
AT t he request of the Central Executive Commi ttee
I h ave the manual written by myself in 1901 , as the offiClal handbook of the St. John Ambulance Association.
T hroughout the revision an endeavour has been m ade to simplify the study of Fnst Aid to the Injured by drawing up a number of general rules for the of accidents and sudden illness, and by the om ISSIon of all detail \\ hich is not absolutely n ecessary to enable the student to acquire an intellig e n t knowledge of the subject.
I wish to express my thanks to Professor E. A . S chafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. 1. F. for many valuable sugge tions, and to the M edIcal Members of the Central Executive Commi ttee, especially Surgeon-Major G. H. Darwin, M.D . an d Dr. F. R. Cassidi, for perusing the proof sheets an d for a number of useful additions to the ·work.
I cannot omit also to offer my best acknowledgm en ts to .1r. VV. R. Edwards, the Accountant and Sto r ekeeper of the S .J.A.A., for his invaluabl e co-operatio n.
J C A TLlE .

FIRST AID TO THE I N J U RED.
CHAPTER 1.
T he St. John Ambulance Asso iation has now completed thirty years of its existence, and duri ng that period hundreds of thousands of men and women have been taught at its classes, in all parts of the world , how to help their injured neighbours.
First Aid to the Injured is a special branch of pra.ctical I?edicine and surgery, by a kno\\ledge of whIch tra1l1ed persons are enabled to afford skilled assistance in cases of accident and sudden illness. The instruction begins and ends; with First Aid and the is taught simply but thoroughly' and exhaustlvely. The duty of the ambulance pupils ends where the commences, and there ought to be no overlapp1l1g or cbshing of duty or interests.
PRINCIPLE OF FIR T AID.
I. The First Aid student should be-
(a) Observant, that he may note the causes and signs * of injury.
(b) that he may without thoughtles s questlOns learn the symptoms t and history t of the case.
• Signs are what may be percei\·ed.
t are what .the patient can tell you.
t Hlst.Ory means the cIrcumstances attending the accioe n t or sudden
(c) Resourceful , that he may use to the best advantaae whatever is at hand to prevent further damage and to assist Nature's efforts to repair the mischief already done.
(d) Explicit, that he may give clear instructions to the patient or the bystanders how best to assist him.
(e) Discriminating, that he may decide which of several injuries presses most for treatment by himself, and ",hat can best be left for the patient or the bystanders to do.
2 . Remove the cause of injury or danger whene\'er possible.
3. Severe hcemorrhage must receive the first attention , no matter what are the other injuries.
4. Air. - The patient must be in a position in which breathing is possible; the air passages must be free from obstruction; if breathing has ceased prompt measures must be taken to restore it.
. 5. Rest. -A restful position of the body will assist t he vital functions; support of the injured part will hel p to p re\'ent further damage, and is essential 111 the case of fractures of limbs.
6. Warmth .-After every accident keep the patient warm so as to prevent the fall of temperatur e belo w the normal point .
7. When the skin is broken the wound

should be promptly covered with.a clean dressi ng. Should the wound be pOIsoned, lS most important immediately to prevent the pOIson permeating the S) stem. .
8. Poisons S\\ allowed should be got nd of, or when that is inexpedi nt. neutralised.
9. The O(; st means of transport must be studied and provision made for proper care when , , the patient is brought to shelter.
10. Removal of Clothing.-Clothes should not be taken off unnecessarily, but ",h(n it is needful to remove them, the following rules will be found of service in serious cases :-
COAT: RemO\'e from the sound side first, and, if necessary, slit lip the seam of the sleeve on the injured side.
SHIRT AND VEST: lit down the front and remove as the coat.
TROUSERS: lit up the outer seam.
BOOT: lit the back seam and undo the laces.
SOCK: Cut off.
II. Stimulants.-I t is incorrect to suppose tha t alcohol is the only form of stimulant, and far too frequent use of spirits is made to restore a patient after an accident, often with serious results; the safest rule therefore is to defer the administration of alcohol untii the of a doctor. \Vhen the patient is able to swallow, strong tea or coffee, or milk, as hot as can
18
19
2 0
b e dru n k , or a small quantity of sal rolatile i n water may be given . Smelling sa.lts may be held to the n ose . Sp r in k lin g the face with colu and ho t wa ter a lte rnately, warmth <1ppli e d to the pit of tbe stomach and o yer the h eart, and \ igor o us fricti o n of the limbs u p wards haye a stimulating e ffect.
12. Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an appa re ntly sli g ht injury is accompai1ied by graye d a nge r anu may actually caus e loss of life . ' Vb en sending for a doctor, state the nat ur e of the casC', and re member that \\ritten pa rt ic ula rs are safer than a verbal message.
I t is ne cessary that something shou ld be known of the structure of the body (elementary anatomy) , and o f the functions o f some of the more important o rga n s and systems (elementary physiology). A sho rt descriptio n of the neces ary anatomica l and physiological poin ts is therefore give n as the several su bjects are d iscussed . For purposes of des cription th e h u man body is s u pposed to be er ect, \\it h the a r ms h a n gi n g by t h e side and the palms of the ha n ds directed forwa r ds. T he" middle li n e " of the body runs vertica lly from the top of the head to a poi n t betwee n the feet.
'he pages wh e7e 'h e
What is F irst A id to the injured ? .. ..
What qualities should the First Aid student pc£sess?
What a re signs? ... ...
Aid
\Vhat is ele mentary anatomy?
What is elementar y physiology?
Fo r p urposes of
on h(;w is the human body supposed to be ced ?
21 QUESTIONS ON CHAPTER 1.
Th e lIu mer a ls indicate
ans wers 17.ay be found.
.. . . .. . .. \\'hat are symptoms? What is t he history o f a cas e ? ... . ,. What is ofte n
fi rst
to d o in an :o ccident? . . . \Vhat
. . .
P.AG 17 17, 18 17 17 17 18 18 pe rson? .. . . . .
must be done
skin is broken? How must poisoning b e treated? .. . 18 ... 18, 19 19 What steps must be taken be) o nd the actual treatment of injuries? . . . ... . .. .. . . . . Should clothing always be rem oyed? . . . . . . 19 19 19 How would you remove clothing
? Explain the use
ahu e of
timulal ts ...
no t d v ? . .. 1 9,2 0 2 0
the
thing
r esult of injury must receiye the first attention?
What t hr ee things are abs o lutely nec essary to an injured
What
" hen the
" hen n e ces ar)"
and
s
What must the First
stud e nt
descripti
What is the middle line of the
20 20 20 20
...
body?
= 2

CHAPTER II .
FR ACTURE S, D I SL OCA TION S, SPRAIN S AND STRA I NS.
THE SKELETON.
The human body is moulded upon a bony fram ewo rk (the skeleton) which ser\'es-
1.- To give shape and firmness to the body.
2 - To afford attachment to the muscles.
3 . - To protect important organs, as in the skull, chest, and abdomen .
THE SKULL .
The Bones of the Skull are arranged in bm gr oups, those of the brain case or cranium, and those o f the face.
The Boundaries of the Cranium are the vault o r dome, the rounded portion forming the top of the h ead; the front or brow j the back of the head, wh ere the g reatest extent of brain exists, and where ther efo re the cra n ium is widest and deep st; the side s or temples. The base of the cranium is hidden from view by the bo n es of the face and of the vertebral col u mn ; in it are nu merous perforations for the passage of blood vessels and nerves j through the largest opening th e b rai n and spinal cord are continuous. "
The Bones of the Face with the exception of
the lower jaw are firmly jointed together, so tha t movement between them is impossible. The ca\' lties of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face co njointly. The mouth cavity is formed between the upper and lower jaws, the palate bei ng the bony roo f of the which separates it from the nasal cavIty above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions term inati ng on ei ther side at the Joint between the lower jaw and the base of the cranium, situated immediately in f ron t of the ear. angle of the j lW indicates the junction of the honzontal and the \'e rlical portions.
THE B.-\CK -BO :\TE, SPI:\lE, OR YERTEBRAL
The Vertebral Column (Fig. ]) is composed of bones called , ' ertebrce, each of which consists of-
r.-A body or bony mass in front .
2.-Process_s projecting backwards, which en. close a canal for the spinal cord - th e spinal canal.
3·-Tw? transyerse processes , twelve pairs of whIch support the ribs.
23
D.12

FIG . I.
Co. <4-
SKULL AN D VERTEBRAL COLU:'1N.
Showing left rics and portion of breast bone. The right riLs ar e removed.
SPINOUS PROCESS.
BODY OF VERTEBR A
FIG. 2A.
SUR FACES SUPPORTING HEADS OF RIBS.
4.-A spinous process. The spinous processes of the vertebr<e can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B) .
The 33 in all, are grouped into regions, in each of which they are known by numbers , counting downwards :-
I.-In the neck 7 Cervical vertebr::e. The first vertebra, tile atlas, forms a joint with the base of the skull, at which the nodding moven'1ent of the head takes place; the second, tile a:c/s by the j oint between it a nd the atlas, allows of the side-to-side movements of the head.
2.-In the back 12 Dors:ll \'ertebr<e.
3.-111 the loin 5 Lum bar \'ertebr<e.
1·-The rump-bone, or '- :lcrum, consists of 5 acral vertebr<e uniteu in adults as a solid nuss .
5·-Th e tail-bone, or Coc yx, consists of 4 verkbr,'e joineu together to form a singl e group.
Between the bodies of the vertebr::e, in the upper region, are interposed thick pieces of cartilage (gristle), which, \\hile they bind the bones together , allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, \\hen falling from
.
25
, .
a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
Th e Ribs consist of tweh'e pairs of curved bones extending from the dorsal vertebrre to the front of the body, and are known by numbers-first, second, etc., commencing from above. The ribs are not bony t hroughout their entire length, but at a short distance f rom the front the bony material ends, and cartilage takes its place. The upper se,'e n pairs, named the true ribs, are attached by their cartllages to the Breast-bone (sternum), a dagger-s haped bone with the point downwards, just oyer the pit of the stomach. The lower fiye pairs are terrred the false ribs, as their cartilages fall short of the n Jiddle line. The eleventh and twelfth pairs are termed tIle floating ribs, as their ends are free in front. The ribs enclose the chest, and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LnIBs.
The Shoulder · bones are the Collar-bon e (clavicle) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the n eck as a narrow curved rod about the thickness of a fi nger. Its inner end rests on the upper part of th e

BONE
RADIUS ' - I -- Ul.N A .
BOlo1ES { ULNA Of' RAlJiUS --+t-'t'-\
,WRIST (C ARP US) -i £.1 ETACARPUS.----i
PHALANGES --i
FlG. 3A.
BO:-<ES OF THE LEFT UPPEP. LDIE.
FIG. 3B.
HO\\'JN G THE POSiTIO N OF THE RADIUS AND ULNA
WHE:-I TH& THUMB IS TUR:-IED Ir\WARDS. Compare Fig. 3A, in which the thumb is turned outwards.
26
PART OF COLLAR BONE SHOULDER BLADE (SCAPULA)
ARM
••...•. (HUMERU S)
breast-bone, and its outer end joins with the shoulderblade.
The Shoulder-blade lies at tbe upper and outer part of the back of the chest, and forms joints with the collar-bone and the bone of the arm.
The bone of the Arm (lllI?1lCrlls) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their relative position with every turn of the hand (Figs. 3A and 3 B ).
The Hand is composed of-
r.- The bones of the wrist, or carp"s, eight in numb er, arranged in t\\O ro\\ s of four.
2.- The metacarpus (the fran,ework 0f the palm) ; five bones which form the knuckleS and support the bones d the fingers.
3.- Th e phalanges, or finaer-bones, three in each finger, and two in the th umbo
THE PELVIS AND Lo ·.. ER LIM! s.
The Pelvis. - The large basin-like mass of co ne attached to the lower part of the spine is composed of the two haunch-bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed betwe e n them. The pelvis

BOJ';ES OF THE RIGHT LOWER LIMB, SHOW. ING JOINT WITH THE PELVIS AT THE HIP.
28
FIG. 4.
.....__•
THIGH BONE (FEMU R). .- KNEE CAP (PATUL A).
BROOCH BONK (FIBuLA)o
/ ........
/TA RSUS.
30
su pports the abdomen and its contents, and th e deep sockets fo r the thigh-bones-tlle hlp Jomt.s.
The Thigh-bone (femur). reaches from tte hlp to t h e k n ee joint. Its shaft lS stout, rounded, and arched forwards; the u pper .a rounded head, supported on a neck. "!ll.ch projects mwards, to fi t into the socket of the hlp Jomt.
The Knee-cap (fatella) is a triangular cone lying \vith its base up" ards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-bone (tiNa) a nd the Breech-cone (fibula). Shin-b o.ne extends from the knee to the ankle, m loth of \\hlch jo ints it plays an important part; its sharp .edt;e, shz'" can be felt immediately beneath the skm of the fro n't of the leg. The Brooch-bone lies. on the outer side of the tibia. It does not enter mto the formation of the knee joint, but its 10\\ er end th e outer boundary of the ankle joint.
The Foot is composed of-- .
1.-The tarsus, a group of se\"en Irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lo\yer part of the ankle joint.
2 ,-The meta ta rSlfS, the five long bones in front of the tarsus" hich support the toes.
3·-The }halanges, or toe-bones, two in the hig tOE', and three in each of the other toes.
3 1 JOINTS.
A Joint is formed at the junction of two or more bones. I n moveable joints such as the hip, kne e , elbow, etc., the surfaces of the bones are covered by cartilage, which friction and the shock of a

FIG. 6.
LEFT A!,(KLE.
FJG·5· Compare Fig. 4. Page
fall. Lubricating the joint is a clear, rather sticky fluid, the" joint oil," or synovia, enclosed within a capsuk Tying the bones together, but allowing of movement, are a number of bands or
To exp'ain the formation of limb joints, the
TENDON

MUSCUL A It TISSUE PATELLA
TENDON OR LIGAMI!:NT OF PATRLLA
FIG. 7.
D IA G RAM SHOWDIG RECTUS MUSCLE OF TH1GH, W1TH ARTERY, VX1N A ND NERVE.
32 following examples are given :-
The Shoulder, a balland-socket joint, consists of a shallow socket on the outer angle of the shoulder-blade, and of the head of the arm-bone. (Fig. 5). Owing to the shallown ess of the socket the arm-bone is yery prone to escape from its socket (dislocate).
The Ankle, a hinge joint, is formed at the junction of tbree bones, the shin-bone abO\'e and on the inner side, the broochbone on the outer side, and the ankle-bone below. (Fig. 6).
THE MU CLES.
The Muscles of the body are classified into two groups-voluntary and t"nvoluntary.
33
The Voluntary muscles are met with in the limbs, the head and neck, and the surface of the trunk. Their ends are attached to different bones, and as they pass from one to anothe r they cros s a joint, and, being endowed \\ ith the power of contraction and relaxation, cause the moyements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the mus the nerves entering them bring them under the direct control of the brain and spinal cord .
The Involuntary muscles are met with in the \\alls of the stomach and intestines, in the ai r passages, and in most of the internal organs and blood-vessels, also, in a special form, in tbe heart. They are not under the mflu(nce of the wlll, but contin ue their \\ ork d uri ng tbe hours of sleep; their functIons are regulated by a separate set of nerves (see Sympathetic \stem, page IlS).
FRACTURES A l TD THEIR TREATMEN T
.
When a bone breaks a Fract ure is said to occur.
CAU ES OF FR,\CTURE.
I. Direct Violence. - '.\ 'hen from a severe blow, impact of a bullet, cn.. sh of a wheel, etc., a bone breaks at the !=pot where the force is applied the fracture is termed direct. c

2. Indirect Violence. - "When the bone at some distance from the spot where the force IS applied the fracture is termed. indirect. Ali ghti ng on the feet and fracturing the thIgh-bone or the of the leg, or falling on the hand a nd breakIng the radius or the collar-bone, are examples.
3. Muscular Action. - The and the arm-bone are occasionally broken by a vlOlent contraction of the muscles attached to them.
VARIETI ES OF FRACTURES.
Fractur es are classified according to the condition of the tissues adjacent to the bone as .
I. Simple. - The bone is broken \\Ith but slIght injury to the surrounding parts.
2. Compound. - The bone is broken and the and tissu es are punctured or t?rn, thus allO\\lng disease-produ cing germs to obtaIn entrance to the sea t of fract ure The fractured ends may protrude through the skin, or (for example, when a bone is broken by a bullet) the wound may lead do\\ 11 to the fracture . .
3. Complicated.-The bone is broken and In addition there is an injury to some internal organ (for example, the brain, spinal cor d, lung, etc.) or to some important bloo d-vessel or nerve.
A fracture may be compound or com plic.... ted as the immedi2.te reslllt of the injury; or a fracture, 35
originally simple, may be converted into a compound or complicated fracture-
( a) By .careless movement on the part of the patIent.
(b) By carelessness or ignorance on the part of one rendering first aid.
. Special \'ari etles of fractures may be classIfied accord mg to the injury to the bone itself as follo\\ s ;_
I . Comminuted. - The bone is broken into severJ.l pieces.
2. Green-stick. - In children, owing to the softer of the bony tissues, a bone may bend and crack WIthout breaking cornpletely across,
.3. Impacted. - The bruken end" of the bone are drIven one into the oiher.
GENERAL SIG. S AND \\ HICH MAY BE PRI '.
(A fracture of the fem ur humerus, or both bones of the forl"'qrm or leg, affords the most complete example),
I. Pain at or near the seat of fracture
2. Loss of Power in the limb.
3· Swelling ab?ut .the seat of fracture. Swelling frequently renders It dIfficult to perceive other signs of fracture, and care must therefore be taken not to mistake a a less serious injury,
4· DeformIty of the hmb . - The limb assumes an
34
unnatural and is mis-shapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to override, thereby producing shortening.
5. Irregularity of the bone.-If the bone is close to the skin the fracture may be felt, and if compound it may be seen.
6. Unnatural Mobility.-Movement may be made out at the seat of fracture.
7. Crepitus, or bony grating, may be felt or heard when the broken ends moYe one upon the other.
The last two signs s!lOuld on!)' be SOl{gilt bJ I a doctor.
Several of the above signs are abscnt in green-stic k and impacted fractur es .
In addition to the signs and symptoms the patient or the bystanders may be able to giYe the history of the injury, and marks on the clothing or skin should be n oted, as they may serye to locate the fracture. The snap of the bone may nave been heard or felt.
A pPA RATUS FOR 'fREATl\[ENT OF FRACTURES.
Splints and band 2.ges for First Aid frequently have to be improvised.
A Splint may be impro\"ised from a walking stick, umbrella, billiard cue, broom or brush handl e, policeman's truncheon, rifl e, folded coat, piece of wood , cardboard, paper firmly fol ded, a rolled-up map, or in fact, anyth z'7tg that is firm and long enouglz to keep

th e joiJlts z'mtllf'diate£v above and below the fracturecl bone at rest. When the above appliances are not available, the upper limb, if fractured, may be tied to the trunk, and in all ca es a fractured lower limb should be bandaged to its fellow .
Bandages may be impro\'ised fro m handkerchiefs, belts, straps, braces, n eckties, or any piece of calico, string or cord that comes to hand .
Esmarch's Triangular Bandages (Fig. 8) are made by CUlling a piece of linen or calico about forty inches squarE: Jlagonally into two pieces.
The broad bandage is made by bringing the pomt down to the base (Fig. 9), and then folding into t\\ 0 (fig. 10).
The narrow bandage is made by folding the bro:l.d I a 11dage once I r).
The medium bandage i made by bringi ng the point down to the basp, and then folding into three. (Fi g. 1.2). 1'l1is may be used instead of the broad or the narro\\' ba ndage \\ hen it is better sllited to the proportions of the patient.
I t is sometimes advisable to halve the size .)1 the banda ge by bringing the t \\ 0 ends togethe r before foldin g it into the broad, narrow, or medium bandage.
Nhcn not in use, the triangular bandage should be folded narro\\'; the h\ 0 ('nds should be turned to the ce ntre, and the bandage then folded into four, redu cing it to a packet about 61 inche> by inches.
37
FIG. 9. BANDAGE ONCE FOLDED.
FIG. 10. BROAD BANDAGE. 4r:-
FIG. It. NARROW BANDAGE.

39
Large arm-sling (Fig . 13).- Spread out a bandage, put one end over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang down in front of the che t; carry the point behind the elbow of the injured limb, and bend the forearm
DOTTRD LINFS SHOW THE FOLDS OF THa MEDIUM BANDAGE.
FIG. 13. FIG. 14. over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure \\ith two pins to the front of the bandage.
Small arm-sling (Fig. q.).-Place one end of a
--7;;a
.
broad bandage over the shou lder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side; place tIle forearm over the middle of the bandage; then bring the seco nd end up to the first, and tie them. This sling is used in cases of fractured humerus, and occasionally \\ hen the large sling \YOU Id be too conspicuous. Slings may be in,pro\'ised in many simple ways, such

as pinning the sleeve to the clothing, turning up the tail of the coat, passing the hand inside the buttoned coat or waistcoat, etc.
Reef Knots (Fig. IS) are to be used. Avoid gran ny knots (Fi g . 16).
GENERAL RULES TO BE OBSERVED IN THE TREAT:'IIENT OF FRACTURES.
The object of First Aid Treatment of Fractures is to guard against further mischief, and especially to preyent a simple fracLure from becoming compound or complicated. To attain this E:nd :-
1. Attend to the fracture on the spot. No matter ho\\' cro\\'ded the thoroughfare, or ho\\' short the ditance to a more convenient or comfortable place, no attempt mu s t be made to mm'e the patient until the limb has b ee n re nd e red as immovable as possible by splints or other restraining apparatus.
2. Steady and support the injured limb at once, so that its furth e r movem ent on the part of eIther the pati ent or th e by stander is pre\' ented.
3. Straighten the limb with great care , and if shortenll1 g is obs c rn' d in the case of a fracture of a bone of the 10\\ er limb, pull upon the foot until the limb regains a more normal length. ,Vhen the shape of tIle limb is imrJro\'ed, on no account let go until it is secured in position by splints, otherwise there is great (lan geI' of the fracture becoming compound or comp ' icated.
4. Apply splints (when practicab le) and bandages as folIo\\s :-
(a) The splints must be firm, and long enough t o keep the joints immediately above and
40
FIG. IS.-REE F KNOT. FIG. I6. -GRANNY KNOT
below the fractured bone at rest They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The bandages must be applied firmry, but not so tightly as to constrict the circulation of blood in the lim b. 'When the patient is in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a I',eneral rule:-
For the trunk the broad should be used. Pass it once round the trunk and fasten it by tying the ends, or \\ ith two or tbree safety pins on the side opposite to tIle fraet me, but if to secure a splint for a broken thigh, oyer the splint.
For the arm or forearm the narrow bandage should be used. Pass it twice round the limb, and tie the ends oyer the outer splint.
For the tltiglz or leg the narrow or medium bandage may be used. It is frequently convenient to double the bandage at the centre, pass it under the limb, brll1g the loop over the limb, pass both ends of the bandage through it in opposite dIrections, and tie them over the outer splint (Fig. 17)·
In applying bandages near a fr acture the uppe r one should be secured first.
5· .When hcemorrhage accompanies a ture It must be attended to first, and the wound covered by a clean dressing.

FIG . 17 .
6. attempt must be made t& remove a .patIent . sufferin.g from a fract ure of the pelVIS, or thIgh, except in a recumbent posItion, preferably UpO!l a stretcher.
7· In every case of fracture it is necessary to cover the patient to keep him warm and so lessen the effects of the SHOCK of the 8. In all doubtful cases, treat as a fracture.
PECL\L FRACTURES.
of the Cranium. -A fracture of the upper part IS usually cau. eel by direct violence-for a ?n the head. A fracture of the ba se IS caused by ll1duect violence, through a fall on the
42
,n
head, a fall on the feet or lower part of the spine, ()r a sev ere blow on th e lower jaw. If tlze upper part is fractured, the signs are S\\ elli n g, irre&ularity, and frequ e ntly insensibility, either immediate or commg on gradually. If tlte base z's fractured in· sensibility may come on
FIG. 18_ immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass down to the stomacll, \\ hence it may be vomited ; the fracture may invoh-e the orbit, causing a blood-shot eye .
TREi\T:'ITEI'\T.
Injur y to the brain is the great danger attending a fracture of the cranium. Fur treatment see "Concussion and Compression of the Brain," pages 13 1 , 13 2
Fracture of the Lower Jaw. - Pain, loss of power (inability to speak and to move the jaw freely), uregularity of the teeth, crepitus and bleeding from the gum are the usual signs and symptoms.

45
TREATME.\TT.
1.- Place the. palm of the hand below the injured bon e and press It gently against the upper jaw.
2. ---:Apply the centre of a narrow bandage under the chm , carry one end over the head cross the end at .the of the jaw, carry the lono-' end across th! Chill, and tie the ends on the side (Fig. IS).
Fracture of Spine. - The vertebral column may_ be broken either by direct or indirect violence. Fa1l1l1g from a heil1-ht on the back across a bar or upon an uneven surface is an example of direct and a fallon the head, causing a b.roken neck, IS an example of indirect violence. I\That is commonly reo-arded as a broken back consists of a fracture of one or morc of the yertebrce \\ Ith diS. pLlcement of th.e fragments, whereby the spinal cord and the nen-es from it may be torn, causing complete or paral) sis of the parts below the fracture. Pam IS present at the seat of injury.
TREAT:'I1E . -T.
I.-Pr event all m?"ement on the part of the patient.
2.- ,over the patlcnt warmly.
3.-10 remove the patIent, place him on a stretcher or shutter as follo\\'s :-
(a) up the collar of his coat; roll up a stIck or umbrella in each side of the coat
so that the ends are len;l ,,-ith the top of his head ; pass a broad bandage or handkerchief u nder the head and secure it to t he sticks . If no coat is worn, or doubt as to its strength and length exists, pass a num ber of bandages under the patient to sen-e in tead of, or in addition to, the coat.
(b) A bea rer on each side grasps the wlled coat with his hands well apart; a third grasps the clothing on both sides on a leyel with the hips; a fourth bearer takes charge of the legs .
(() On the word being gi,-en, a1l lift together and carry the patient by short side paces O\-er the stretcher and carefully lo\\er him on to it. If a fifth bearer is ayailable the stretcher should be passed under the patient instead of carrying him oyer it.
4.-0n arrival at shelter nothing further is to be attempted until the arriYal of a doctor, except to gi,-e the patient water, tea, etc_, if he is conscious.
Fractured Ribs. - The ribs usually fractured are the sixth, seyenth, eighth, and ninth, and aenerally the fracture is midway bet\\"een the and the spine. The fracture may be caused by indirect vi')lence, driving the fractured ends of the bone outwards, or by direct violence . driying the fractured e n ds of the bone inwards and sometimes injuring the

47
lungs. or o.ther internal organ . If the lower nbs on the nght slde broken, the liver may be injured and a ot lower left ribs may wound spleet:. EVldence ot the fracture is afforded by pain, espectally on atte11lpttn'T to take a deep breath and by short and shallo\\" breath- '
If the lungs are inJured blood, frothy an 1 bright red, may be coubhed up and expectorated. If the li,-cr or spleen is wounuecI intcr(Sll,; page 95) may occur.
TR EAT'\lEXT.
. (£7) JJ Ilcll the fradure tS not complicated /1\' an in/lilY to all z"nt:rllal organ :-
I.-Apply t\\"o broad bandages round the chest sufficiently firml\" to .comfort. with the centre of the first aboye and that of the second ImmedIately below the fracture. The lower bandage should overlap t he upper to hal f its
FIG. 19.
48
extent. The knots are to be tied rather to the front on the opposite side of the body.
Another good plan is to apply a strong towel, folded about eight inches wide, ti g htly round chest, securing it with three or four safety pms .
2.-Place the arm on the injured side m a large sling. (Fig. 19).
(b) Jrhen an infernal organ is z'Jljllred-
I.-Do not apply bandages round the chest.
2.-Lay the patient do\\'n, inclined a little toward s the injured side.
3.-Loosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Treat as for internal h<emorrhage (see page 95).
4.-Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (sferJlltm).-
When this fracture can be felt or is suspected undo all ti ght clothing, and keep th e patient quiet in an easy positIon until the arrival d a doctor.
FRACTURE OF THE BONES OF THE UPPER LIMB. of the Collar-bone (da7)lde ) .-This fracture is frequ ently caused by a fall on the hand or shoulder.-Th e arm on the injured side is partially
49
helpless, and the patient usually supports it at the elbow with his hand, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the 10\\ er The general sIgns and symptol1ls of fracture are mostly present.

l.-R emove the coat (see page 19), and as much more of the clothing as is expedient.
2.-PLlc e a p:td about t\\'o inches thick and four inches across in the armpit.
3.-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a" t. John" sling, made as fo 110ws : -
(a) Lay an unfolded b:ll1dage across the chest over the injured limb \\ ith one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fig. 20).
(/J) the end of the bandage under the tnJured hm b, across the back, and tie the ends some\\ hat loosely in the hollow in front of the sound shoulder.
(c) F?ld the point over the eloo\\' of the injured 11mb and secure it by one or t'v\' O pin::. (Figs 21 and 22).
4.-Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5.-Now tighten the sling.
'Yhen both collar - bones are broken keep the

FIG. 2I.
(Body bandage omitted to show details of Sling.)
shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by the bandages. (Figs. 23A and 23B).
Fracture of the Shoulder-blade (scapula).-
Apply the centre of a broad bandage in the armpit of
51
FIG. 23A.
FIG. 23 B.
52
t he injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. J ohn sling (Fig. :14)·
Fracture of the Arm
(hume77(s).- The bone may be broken :-(a) Close up to the shoulder; (b) near the FIC. 24. middle of the shaft; (c) close to the elbow.
All the general signs and symptoms of fracture are usuall y present.
TREATMENT.
lVhen the Fracture is close to the Shollider-
I.-Apply a broad bandage with its centre above the middle of the arm round the limb and body, tying it on the opposite side.
2.-Support the forearm by a small arm sling
When the Fracture is near tAe 11liddle of Shaft-
1.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reachin a from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
must on no account be so long as to press. upon the blood-vessels at the elbow joint.
3.-Secure the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad FTC . 25.
4.-SUPP )rt the furea rm by a small anl sli ng. (Fig. 25)
Fractures involving the elbow joint, whether of the arm or forearm, are attended with so much swellin g, and it is so dIfficult to ascertain the exact nature of the mjury, that when the accident occurs indoors the limb should be hid upon a pillo\\ in the most comf0rtable positioll; ice or cold water dressings should be applied to the injured part, but no further treatment should be attempted pending the arrival of a doctor.
TVhen the accident occurs out of doors-
1.-T ake two pieces of thin flat wood, one long enough to reach from the armpit to below the elbow, the other long enough to reach jl from above the elbow I to the finger tips ; tie 'I them together to form ____ a right angle. (Fig. 26).
FIG . 26.

3.- Secure by fracture .
2.-Apply the angular splint so made on the inner side of the flexed limb. bandages above and below the the limb by a large arm sling.
5·-0 n arnval at home remoye the splint d t h · . , an . reat t e Injury as if it had occurred Indoors.
Fract:ure of the Forearm.' Vhen both bones (the RadIus and Ulna) are broken the I' d ' genera a n symptoms of fracture are usually present. ' Vhen o ne of the bones only is ?roken the signs and sympto ms. a re as. a rnle pam, loss of power, sweiling and Irr egu lanty. An impacted frac t ure of the
just above the \uist is a common result of a fall on the hand .
TREATMENT.
This is the same, \\ hether the fracture is of on e bone or of both.
I .-Bend the forearm at right angles to the arm ,
FIe. 27. FIG. 28.
keepir.g the thumb up\\ard3, and the palm of th e hand to\\ards the body.
2.-Apply broad splints on the inner and oute r sIdes from the elbow to the fingers.
3.-Apply bandages, em bracing both splints, immediately abo\'e Clnd below the fracture and round the hand (Fig. 27).
4.-Apply a large arm-sling.
Crushed hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREATME T.
I. - A pply a carefully padded splint to the f ront of the hand, reaching from well above the wrist to beyon d the tips of the fingers .
54
55
2.- To sectlre the splint apply a narrow bandage crossed in the mannel of the figure 8 to the wrist and hand (Fig. 28).
3.-Apply a lar ge arm-sling.
Fracture of the Pelvis.-"Th en, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lo\\"er lirnbs, but the patient is unable to stand or even to move the lower Fmbs without great difficulty and pain, a fracture ot the pelvis may be assumed to ha\'e occurred . The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
TREA
I. -Lay the patient in \\ hate\'er pOSltlon is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further il1\\arc1s.
3.-To remove the patient place him on a stretcher, acting on the same principle as that described under " Fractur e of the Spine" (see page 45)·
FRACTURE OF THE BONES OF THE LOWER LIMB.
Fracture of the Thigh-bone (femur).- The thigh bone may be broken at its neck, anywhere in the shaft, or close to the knee. A fracture at the 57
neck is likely to occur in old people from very slight and is often difficult to distinauish from a severe bruise of the hip, but it may be bassumed that when, after an near the hip joint, the patient cannot, when lYll1g on the back, raise the heel from ground, the bone is broken. All tbe general sIgns and of .fracture :ll:e usually present, and a promll1ent sIgn IS the position of the foot,

which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TRE.-\T\JENT.
I.-Steady the limb by holding the ankle and foot.
2. -Gently draw down the foot and bring it into line with its fellow. "When hyo or three assistants are at hand, it is one ptXs')l1'S duty to hold the foot in position until the splints are secured .
3·-Apply a splint on the outer side from the armpit to beyond the foot.
56
58
4.-A ppl y a splint on the inner side from the top of the thigh (the fork) to the knee.
5.-Secure the splints by bandages as follows :(a) Round the chest just. below (b) round the pelvis on a level mth the hlp JOInts, (c) above

FIG. 30.
the fracture, (d) below the fracture, (e) round the leg, (/) round both ankles and feet, and tied below tIle feet, (g) a broad bandage round both knees (Fi a 29).
·When single-handed, or" hen the patient is a woman, it is expE!'di nt, after extension f tbe lin b, to tie the feet together, dispense with the inner splint, and r ass tIle bandages round both limbs (Fig. 30).
Fracture of the Knee-cap
(patella).-The knee-cap 11 ay be broken by falling on tbe Imee (direct violence), but more frequently it is broken by muscular action, as follows :-
FIG. 3I.
59
When the foot slips in the attc to prevent a fall the muscles in the front of the thi gh act with such force as to snap the knee-cap in two (Fig . 3 I).
Pain, loss of pJwer (the limb will b= quite helpless), and irregularity (a gap may be felt between the broken frJ:tgments of bone) accompany this injury.
TREAnrE T.
1. -L:ly the patient on his back, raise well and support the head and shoulders, straighten and raise the limb.
2.-Apply a splint along the back of the limb, r eachin a from the buttock to beyond the heel.
3.- Apply a narrow bandage with its centre imme-

diately abm-e the knee-c["tp, cross the e nds behind over the splint, and tie in front below the broken bon e . T o ensure firmness app ly a second bandage in a similar \yay, but commenced below and tied abov e the broken bone.
4. -Further secure the splint by bandages round the thigh and leg.
5.- S u pport the foot \\ell off tbe ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fello\\ (Fig. 3 2 ).
6.-A pply a n ice bag or a cold \\ater (Jressing ove r the fr acture.
Fracture of the Leg (tt'Na alld fibula).- One or both of the bones may be broken. 'When both bones are broken all the general signs of fracture are usu ally present, but \\ llen one bone only is broken deformity is not ah\ ays noticeable. A fracture of the fibula three or four inches abm-e its low e r end is frequ ently mistaken for a sprair. sometimes for a dislo cation of the ankle.
TREAT:\IE:\,T.
I.-S teady the limb by holding the nnkle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-A pply splints on the outer and inner sides of th e leg, reaching from aoo\'e the knee to beyond the (r
foot. If only one splmt IS available place it on the outer side.
4·-Secure the by bandages (a) above, (b) below the fracture, (c) Immediately above the knee,
Fcc. 3+.
(d) round b oth ankles, (e) a broad bandage round both knees (Fi g. 33).
When single-hand ed , or when the patient 15 a
60
62 woman, after extending the limb tie both feet together, dispense \\'ith the inner splint, and pass the bandages round both limbs (Fig. 34) . \V hen no splint is availabl.e tying the legs, ankles, and kne s together is of great service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).- This accident is commonly caused by the passage of a heavy \\ elgh t over the fcot, and may be recognised by s\yelling, and loss d Po\\ er.
TREATMEi\T.
I.-Ren ,oyc the boot (see page 19).
2.-"\pply a \\"ellpadded splll1t to the sole of the foot, reach1l1g from the heel to tIle tOtS.
FIG. 35.
4.-SuPPort the foot in a
3·-Apply a bandage aftt.r the manner cf the figure 8 (FiR· 35). slIghtly raIsed po ilion.
DISLOCATIONS.
A dislocation is the displacement of one or more of the bones at a joint.
The joints most frequently dislocated are those of the shoulder, elbow, thumb, fingers, and lower jay.: ,

OF DISLOCATION.
1.- Pain of a severe sickening character at or near the joint.
2. - Loss of power in the limb.
3. -Numbness of the parts below the s; eat of dislocation.
4. - Swelling about and below the joint.
S. - Fixity of the joint.-The limb cannot be moved at the jO)Jlt by either the patient or others.
6. - Deformity of the limb.-The limb assume s an unnatural position, and IS mis-shapen at the joint.
TREATME T.
No attempt should be made by anyone except a doctor to reduce a di location. Pending his arrival ;--
(a) JJ7JleJl the accident oCClIrs out of doorsSupport the limb in whatever position gives most ease to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) TVllen the patient is z'lldoors-
I.-Remove the clothing from the limb.
2.-PLl.ce the patient on a couch or bed.
3·-Rest the limb on pillows in the most comfortable position.
4 ·-A pply cold (ice or cold water) dressings to the jomt.
s·-\Vhen cold ceases to give comfort appl y
warmth (flannels or to\\"els wrung out of hot ·water).
6.-Treat shock (see page 135).
SPRAINS.
When, by a sudden wrench or b\'ist, the ligament s and the parts around a joint are stretched and torn the joint is said to be sprained. "Going over /I the ankle is a common example.
SIGNS AND
I.-Pain at the joint after a twist or wrench.
2.-In a bility to use the joint.
3.-S\Yelling and discoloration.
TREAT;\fEXT OF AXKLE.
T,[Then out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing it on the front of the ankle, and carrying it round and round the ankle, where it is to be firmly tied.
2.-,Ye t the bandage after applicaton; it is thereby tightened.
After rradzz'Jlg slzdter-
I.-Remove the boot and stocking (see page 19).
2.-Place the limb in the most comfortable position j usually that is well raised.

3·-A pply ice or cold water dressings to the joint as long as they relieve pain.
4·-,,\'hen cold falls to give comfort, apply hot fomen tati ons.
When other joints are sprained, treat tbem as if dl located.
"Yh en in doubt as to the nature of the injury, treat as a fracture.
TRAIN RUPTGRED
"Yh en, during severe exertIOn , muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured.
IGXS .\XD L\fPTmrs.
I.-A sudden sharp pain.
2.-\\Tben the mu cles of a limb are strained they may swell and cau e se\'erc cramp. is diffi cul t or impossible; for example, If the strall1 has occurred in the back the patient may be unable to tand upright.
TRFAT'IE 1 T.
I.-Place the patient in the most comfortable po Ition, and afford support to the injured part.
2.-Apply hot water bottles 01 hot fomentations when the pain is very se \·ere.
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 114 ) .
QUESTIONS ON CHAPTER II.
The numerals indicate the pages where the allSWt'rs uta)' be found.
What i - the skeleton, and \\hat purposes are sen'cd by it?
II ow are the bones of the skull arrangcd ?
\Vhat are the boundaries of the cranium?
Describe the bones of the face
Describe the lower jaw '"
What is the angle of the jaw? ...
\Vhat other names has the back-bone?
\\'hat is a vertebra?...
lI ow many \'ertebrrc are there in the spine?
\ \'hat are the regi ons of the spine, and ho\\ many vertebrre are there in each?
I fow is the spine endowed \\ ith free movement?
\"hat is a rib?
How many pairs of ribs are' 't'here?"
'Vhat is the breast-bone?
\Vhat are the bones of the upper liml)s?
What is the pelvis?
What is the hip juint ?
\Vhat are the bone of the lower lim bs ?
What is a joint?
Describe a mO\'ealJle joint .. .
Describe the shoulder joint
Describe the ankle joint ...
ITow are muscles classified?
Describe voluntary muscles
Describe involuntary n"'scles
\Vhat is a fracture? ... .-
'Vhat are the causes of fracture?

doe a bone break when indirect
TI ow maya fracture be caused by muscular action?
In what two ways may fractures be cia,> ified ?
What is a simple fracture ? ..
\\'hat is a compound fracture?
What is a complicated fracture?
\\'hat i' a comminuted fra cture?
\Vhat is a green- tick fracture?
is an
fractures afford the most complete example o f the signs and symptoms?
In making up your mind \\hether a fracture had occurreu or not, what point· should you lake into consiuera· tion beyond the .;;igns and symptoms? 35
\\'hat apparatus may be neces_ary for the treatment uf fractures? ... 36 How may splints be improvi<;ed ? ... ... 36 , 37
ow may bandages be impw\'i"ecl? .. , .. . 37 Describe Esmarch's triRngular bandage .. 37.3 (Fig. 8)
In "hat ways may the triangular bandage be folded for llse? 37
II!"'w many kinds of arm-slings an.: and what are they called? .. ... 39, 40 , 49
\\'hat knot is to be tied, and what knot avoided? ... 40
What is the object of first aid treatment of fractures? 4I Give the general rules fur the treatment of fractures 4 I H ow should splints be applied? ... . .. 41, 42
H ow should bandages be applied? ... 4 2 , 43
\Vhat may cause a fracture of the upper part of the cranium? 43
66
PACE
.......
... ... ... 22 22 22 22,2] 23 23 23 23 25
.. ...
... ... .. .
.. .
... ... ... ..,
...
... .. .
25 25 26 26 26 to 2' 28 30 ')0 3 I 3 I 3 2 3 2 32 33 33 33 ... 33· 34 PACK "'here does a bone break when direct violence is the cause of fracture? ........ . 33
the cause
fracture?
"There
violence is
of
....... ..
\\'hat
fracture? ... 34 34 .. 34, 35 34 34 3435 35 35 State the general signs anu symptoms that may be present in a case o f fmcture ... ... .. 35, 36
... ... ... ... . ..
impacted
\Vhat
Ir
\Vhat may cause a fracture of the base of the cranium? 43, 44
\Vhat are the signs of fracture of t he upper part of the cranium? 44
'What are the signs of fracture of the base of the cranium? 44
\Vh at is the treatment for fracture of the clanium ? 44
\Vhat are the signs cf fracture of the luwer ja\\ ? 44
How maya fractured spine be caused? 45
\Yhat is commonly regarded a a hruken back? ... 45
\Vhat are the symptoms of a fracturul . pine? 45
How may ribs be fractured? 46
How maya fracture o f ribs be cUJ1lplicatnl? 47
State the signs and symptums of a simple and of a cumplicated fmct ure 01 ri bs 47
\Vhat is a frequent cause of fractl1led culbr-bune? 48
\Yhat are the signs and symptoms of fractured c ullar'" 48,49
At points may the bone of the arm he hroken? '" 52
Are the general signs and sympt o ms of a fracture al\\ ays present in a hroken forearm? ", 54-
State the cause of a c o mmon fracture of the radius 55
lIow would you recogni se a fracture of the peh'is? 56
At what points may the thigh-bone be brukell? '" 57
"That are the "igns and symptoms of fracture uf the thigh-bone? '" ,.. '" ", ". 57
\Yh at are the causes of fracture of the knee-cap? ., 58, 59
'vVhat are the si.;ns and symptoms of fracturc of the kneecap?
Are the general signs and symptom always present in a fracture of the leg?
\Vhat mistake may ea. ily be made when the filmla is broken near its lower end?
What is a dislocation?
State the si gns and symptoms of dislocation

the treatment of a sprained
First Airl . tudent should practise material, folding bandage.:;, tying knots, makillg lings, and the trcatment of the follo\\ ing injul ies.
Fractures - Lower jaw, 44. 45. 46. Ribs (C;iI11ple and complicated fractures), 46t) 4. Brea.tbone, 4. Collar-bone, 48 to 51. Both collarbones, 51. Ann, close up to shoulder, 52. Ann, near mIddle of shaft, 52. .Arm or forearm \\ hen the elbow is il1\'oh'ecl, 53. Forearm, 55. Crushed hanel, 55, 56. Pelvis, 56. Thigh (man). 57, 5S. Thigh (woman, or man when single-handec1), 58. ](neecap, 59, 60. Leg (man). 60, 6I. Leg (woman or man when "ingle-handed), 62. Cru hed foot, 62. of doors and indoors
63, 64
68 PAGE
59
60
60
63 69 PAGE State the
... 63 What is a sp rain? 64 \Vh
64 State
ankle ", 64 State the treatment of other sprains 63, 65 \\'hen not sure whether the injury is a sprain or f ract ure how would you treat it? 65 Ihw m:ty muscles be strained
65 State the signs and symptoms of strains 65 St
tht: treatment of strains 65
62
treatment of dislocation
at are the signs and symptoms of a sprain?
or ruptured?
,lte
Improvising sp'ints 1m )royi ing bandages Folding bandages 36,37 37 37 39 Large arm sling Snull arm sling Reef and granny knots .. 39,40 40 Knut for applying splint to lower limh
pramed ankle .. 64 Strains and ruptured muscles 65
...
CHAPTER III.
THE ORGANS OF CIRCULATION.
THE organs concerned in the circulation of th;: blood are the Heart, the Arteries, the Veins, and th e Capillaries.
The Heart is situated in the chest behind the bre.1st-b:me and rib cartilages, between the lungs and immediately above the diaphragm; it lies obliquely with a quarter of its bulk to the right and the remaining three-quart er to the left of the middle of the b ody. I ts beat m ay be felt just below and to the inn er side of the left nipple. Th e heart has bur cavities, two on either side of a central partition. The two upper cavities are named the right and left auricles, the two lower the right and left ventricles.
Arteries are \'ess2ls which convey blood from the heart. Veins carry blood to the heart. Capillaries conne ct the arteries and veins.
In general (systemic ) circulation arterial blood IS driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all parts of the body. Th ese divide and sub-divide, and become so small as to aSS'lme mic roscopic dimensions, when they are term ed capillaries.

L. Larynx (voice box); T. Trach ea (wind·pipe); R.L. Right Lung; L. L. L eft Lung (the lungs are d.rawn to expose the heart and hlood vessels); R A. A uncle; L.A . Left Auricle; R.V. Right Yentric1e; L V Left tric1e; P. A. Pulmonary Arte ry; Ao. A o rta ; S. V.C. upenor vena cava (the large vein carrying blood from the upper part of the body to the heart); LV.C. Inferior vena cava (the large vein ca rrying blood from the part of the body the heart). The four pulmonary vems cannot be shown 10 the d iag ram .
70
I n the capillaries an interchange of gases and fluids t a k es place, whereby the nourishment and maintenance of the tissues and organs of the body are provided for , and the blood becomes dark and impure.
Venous blood passes from the capillaries to the veins, which convey it towards the heart, <Yetting larger and larger as they proceed by being joined by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with vah-es at frequent interv::1.ls, which prevent the backward flow of the blooJ.
The pulmonary system of blood vessels is concerned in carrying th,- blood through the lungs . From the right auricle the blood passes to the right ventricle, and is thence carried to the lung, where it i5 purified by contact with air, and becomes scarlet in colour; it is then conveyed to the left auricle of the heart and passes into the left ventFicle, thus completing the circulation .
The heart contracts in adults at an average rate of seventy- t wo times a minute, but the rate varies, inc reasing as the position is changed from the lying t o t he sitting or to the standing position; hence the importance of ad,iusting the patient's position in cases of hoemorrhage. At every contraction of the left ventr icle blood is forced into the arteries, causing the pulse, which may be felt wherever the finge r can I!> e
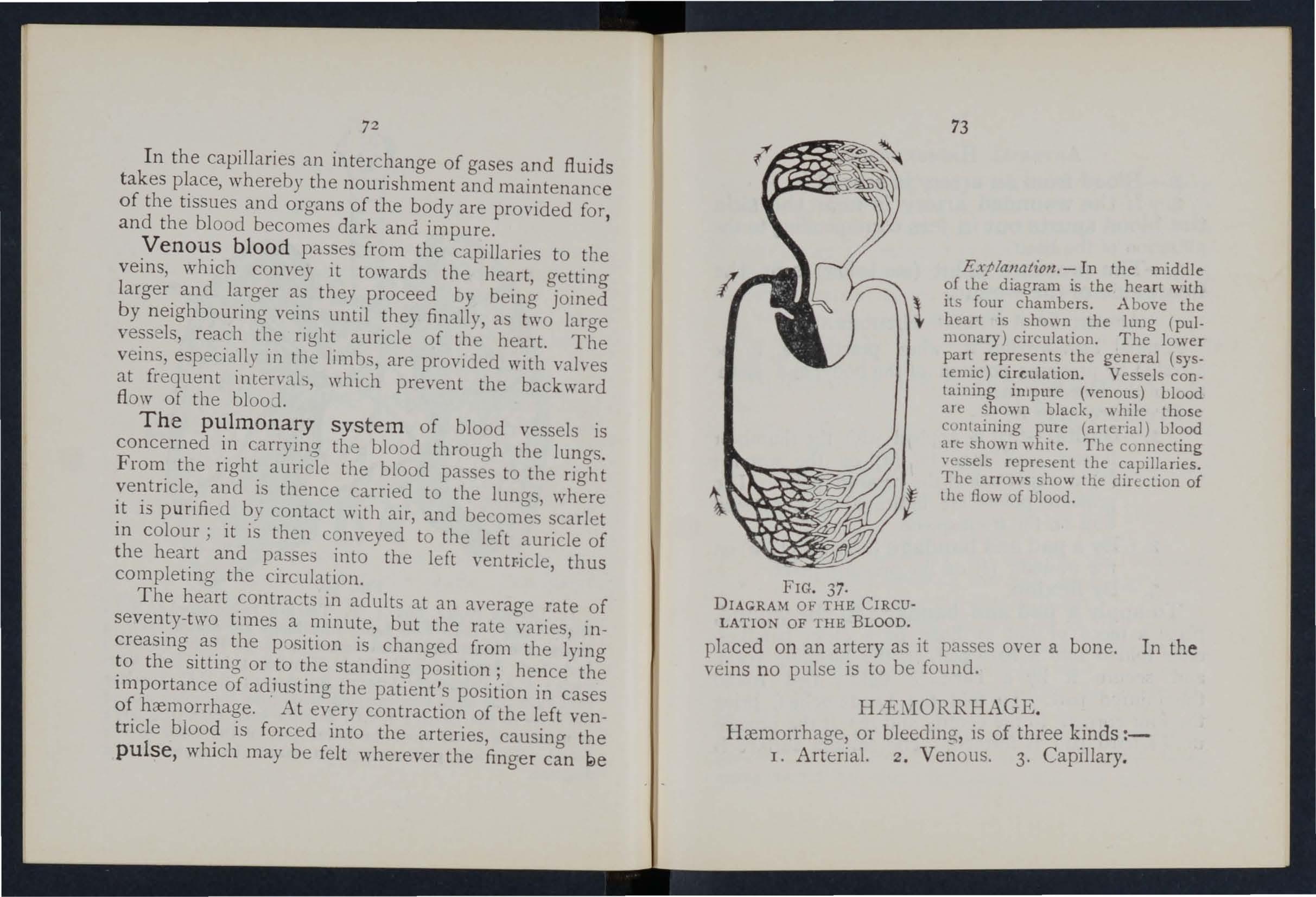
Explalla/£oll. - In the middle of the diagram is the heart with \ its four chambers. .A hove the " heart is shown the lung (pul. monary) circulation. The lower part represents the general (systemic) circulation. Vessels CODtaining impure (venous) blood al e sho,"\- n black, "hile those
DIACRAM OF THE CIRCULATION OF THE BLOOD. containing pure (arterial) blood art: shown white. The c o nnecting vessels represent the capillaries. The arrows show the din.ction of the flow of blood.
37·
placed on an artery as it passes over a veins no pulse is to be found. bone. In th e
H::emorrhage, or bleeding, is of three k.inds :1. Arterial. 2. Venous, 3. CapIllary.
72
73
FIG.
A RTERIAL HIE \WRRHAGE .
I. - Blood from an artery is scarlet. .
2. - If the wounded artery is near the skIn the blood spurts out in jets corresponding to the p ulsation of the heart.
3.-The pressure po i nt (see below) is on the heart side of t he wound.
ARREST OF ARTERIAL HIE.:\IORRHAGE.
Arterial hc:emorrhage is, when practicable, to be arrested by pressure, position of the body, and elevation of the bleeding part.
Pressure may be :-
I. - Digital -that is, applied with tIle thumb or and may be (a) on the wound; (l,.) at a spot called the pressure point The pressure points are indicated by numbered dots on the fronti piece.
2 .- Bya pad a nd ba n da g e (tourniquet) (a) on the wound; (b) on the point.
3 . - By fl exi o n .
To apply a pad and bandage to t he wound, place a piece of lint or linen or a clean handkerchief fo lded into a hard pad, on the bleeding !Joint, and secure it by a bandage tightlY tied round the injured part. To fold the handkerchi e f, bring the four corners to the centre, and the process until a hard pad is formed. The smooth surface is

75
placed on the \yound, and, to prevent the pad from unfolding, the puckered surface may be stItched or fixed by a safety pin. A hard su bstance, such as a stone, may be enclosed in the centre of the pad.
A Tourn iquet may consist of a pad to be placed on the pressure point, a slrai' , [O:d, or. bandage to en ircle the limb and pad, and a tighlewJlg arrangement such as a stit k or other means of t\\ isting the band to tighten it. .
T o impro vise and apply a tourmquet.:-
I.-Apply a firm pad on the pressme romt. .
2.-Encircle the lin ·b by a narro\\ b. ndage \\Hh its centre oyer the pad.
3.-Tie the ends of the bandnge in a half knot on the oppcsite side to the pad.
4.-Lay the t\\ isting stick on the half knot, and oYer it tie a reef knot.
5.-Twist the stIck to the bandage, thereby pressing tbe pad UI n the artery, and arresting the flo\\ of blood.
6.-Lock the stick in pOSItion by the ends of the bandacye nlready applied, or by another bandage passed round the stick and limb.
The pad of the tournIquet must be accurately placed upon the pressure point so as completely to compress the artery; othen\ ise arterial blood \\ ill be allowed to pass along the limb, and the veins, bing by the tourniquet, \\ ill not allow the
74
blood to return t h ro u gh the m to th e h ea r t, a n d the r es ult will b e d a n geruus swell ing a ntI co ngestion.
S houl d a s u itab le pa d n o t be a t h a n d, a k n ot ma y b e made i n the c e n tre o f the ba n dage, and when a vailable, a stone, cork , etc ., enclosed in it to giye i t fi r m n ess and bulk . ee that the bulgi n g and n ot the filt side of the knot is next the skin.
An elastic bandag e passeJ tightly round the limb, immediately abm'e the seat of arterial hremorrhage, will arrest bleeJing . The simplest prep:ued form of this bandage IS a strip of elastic \\ ebbing, twenty-five to th irt)' inches long and t\\ 0 inches wide, with a piece of tape se\\ n at each en l. An clastic belt or brace will serve the S:lmc purpose. E'\cept when p:ut of a limb is tOln off, It IS not achisable to use an elastic cord or bandage if other C:1n be had, as it cuts off all circulation in the limb.
Flex io n consists of the applic:1tion of a pad on the pressure point at the knee or elbo\\ joint, flexll1g the limb to make pressure , and securing the limb in t he flexed p')sition by a bandage crossed like the fi gure 8.
RULES FOR T REAT)1E;-;T OF A ,VODXD
AC COMPANIED BY ARTERL\L I-LEl\IORRHAGE.
1. Stop bleeJing.
II. P revent injur io us germs from getting into the wound.

To a ttain t hese e n ds :-
1. . .the patient in a suitable position, bea nn g 111 mmd th a t t he b lo o d escapes wit h less force whe n th e patie nt si t s, a n d is till mo r e checked when he lies down.
2. Eleva.te the . bleeding part, as thereby less blood finds Its \\ ay 1I1to it.
3. Expose the wound, remoyin a \\hateve r clothing is nece ar)' . (ee Rule 8, a.) b
4. Apply digital pressure.
(a) If the wound IS small on the bleeding spot. (b) If the wound is large on the pressure poin t next to the wound on the heart side. The nearest pI essure point is chosen in order to a\oicl utting orr the circulation from as much of the part as pos,i ble, but sometim s it is neces 'ary to apply pressure still nearer to the heart.
5. Remo'.'e fore.ign bod ies, such as broken glass , bits of clothing, hair, etc., ern in the \\ ound; do not Search for foreign bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. 1\ hard dry pad of boracic puze or lint is to be preferred, but absorbent cotton \\'001, lint, or gauze, or a clean piece of linen will answer the purpose. ... hould a n y doubt be enter· tamed as to the cleanliness of the dressin a a clean piece of unprinted paper, such as the inside o f a n
76
77
78 envelope, should be pbced next the wound before applyi n g tIle pad. (Compare pages 75 and 76.)
7. Bandage tightly over the pad unless :-
(a ) Foreign bodies are suspected to be left unsee n in the wound.
(b) T here is danger of causing injury to a fracture. I n these cases a light dressing only should be applied .
8. Apply a pad and bandag e or fl e xion on th e pressure point (see Rul e 4, b ), but only in the following cases :-
(a) As a. temporary m eas ure while the wound is being exposed, examined and covered.
(b) As a more pernunent measure \vh e n bleeding cannot be stopped by th e pad and bandage on the wound, or when, in arcord,lllCC \\ itb Rule 7, the tight bandage has not becn applied.
9. Afford support t o th e inj u red pa rt.

"Wben p:ut of a limb has been torn off o r th e \\ ound is bcerated (for example by the claw of an animal or by machinery) hremorrhage frequently does not come on at once, but as there is a dangcr of seyere h::emorrhage later, means for its arrest should be applied to the limb, but not tight e ned unless n ecessary. Do not disturb a clot of blooJ formed O\'cr a wound. No attempt should be made to cleans e a wound except with sterilised water (that is previously boiled 79
and alloyred to cool), and experience, especially in r ecent wars, has sho\\ n that those wounds \\ hich \\ ere provisionally treated \\ith a dry dressing a n d subsequ ently dressed by a surgeon \\ith proper appliances did best.
tudents practising arrest of arterial hremorrhage should feel the pulse to see \\ hen tI'e currpnt of blood in the artery has been stopped, a nd should then immediately relax the pressure mac:e on the artery. In this way the importance of the accurate application of pressure \\ ill be realised, and tIle amount of forc.e necessary \\ ill be ascertained.
THE COURSE OF THE ARTF RIl S, A!\ D THE ARRE T OF H .'E:"I IORRH.\GE
( The numbers of the pres'ure points rt.fer to tho"e on the Frontispiece)
THE LARGE ARTERIES THE. CHEST Ai'I D AllD O:"lIE 'l'.
The Aorta is the central or trunk al tery of the body. Commencing at tbe left ventriclc it forms an arch behind the upper part of the breast-bone. From the arch are gi\'en off the large branches \\ hich carry the blood to cither side of the head and neck and to the upper limbs. The /\crtn passes down on the left of the spine to just below the navel , where it divides into two great branches (the ilia;:s)
wh ic h convey the blood to the organs m the pelvis and to the lower limbs.
owounds of these arteries are one cause of internal hremorrhage (see page 96).
ARTER rES OF THE HEAD AND NECK.
The Carotid Arteries (right a n d left) leave the upper part of the chest and pass up on either side of th e windpipe and, just below the level of the angle of the lo\yer jaw, divide into the Internal and External Carotid Arteries. The Int e rnal Carotid Artery ascends deeply in the neck, and enter the cranium to supply the brain with blood. The Ext e rn al Caro t id Artery gIves off a number of branches; to the front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the Occipital; the artery itself IS continued upwards in front of the ear, where it changes its name to the Temporal, and supplies the scalp in the neighbourhood of the temples.
When a Caro t i d Art ery is wounded , as in the case of a cut throat, apply the thumb of one hand o n the artery at pressure point I, pressing backwards agai nst the backbone and taking care to avoid the 1, indpipe. It may also be necessary to apply pressure with the other thumb above the \\ound for two reasons: (a) To arrest the flow of blood from th e main. (jugular) vein in the neck, which runs
81
a longside of the carotid artery and is usually \\ ounded at the same time; (/I) To check the flow of f rom the upper end of the carotid artery itself, \\ hich is ofte n considerable 0\\ ing to communication between the branches of this artery and those of its

38, FIG. 39·
fellow. Digital pressure must be m,aintained, by relays of assistants if necessary, untIl the docto r arrives (Fig. 38). . .
The Facial Ar t ery crosses the lower FW III a slight hollow t\\ 0 fingers' breadth in front of the an gle . and sends branches to the chin, lrps, cheek, an d
80
FIG.
outs id e of the nose. H rem orrh age from wounds of the fac e below level of the eye is to be arrested by:-
(a ) D IgItal pressure on pressure poi n t 2 ,Fig. 39), or
(b ) Grasping the lips or cheek on both sides of the wound by the finger inside -and the thumb outside the mouth or v/ce versa.

FIG. 40. FIG . 4I.
The Temporal A rtery may be felt pulsating in front of the upper part of the ear . Hremorrhage from the region !)f the temple may be arrested by pressure applied at pressure point 3 (Fig. 4 0 ).
The Occipital Art e ry supplies branches to the
region o f th e scalp from beh ind the ear t o the bac k of the hea d. H remorrhage from this region may be arrested by d igital pressure on pressure point 4 , four fingers' breadth behind the ear (Fig. 41). This point is difficult to find, and it is usually sufficient to apply pressure immediately below the wound.
Hcemorrhage from the Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the bleeding point and securing it by a narrow bandage \\'ith its centre laid on the pad, the ends carried round the held III the direction most cOlwenient, and tied tightly OYer the p .td (FIg. 42)
When a \\'ound of the torehead or scalp is associated with a fraclure, the best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fingers; pass the other end of tbe bandage tbrough the ring thus formed and continue to pass it tbrough and through until the whole of the bandage is used and a ring as sho\\ n in Fig. 43 is formed.
FIG. 42.
82
ARTERIES OF THE UPPER LIJ\IBS.
The Subclavian Artery passes frorn a poi n t behin d t h e in ner end of the co ll a r-bone across the firs t rib t o the armpit.

FIG. 43· FIG. 44.
T o apply digital pressUl e :-
I.-Bare the neck and upper part of the chest.
z .-Place the patient's arm against the body so as to depress the shoulder, amI cause him to mcline his head to\\ards the injured side.
3·-Take your stand opposite tIle shoulJer.
4· - Using the left hand for the right artery, and vice versa, grasp the neck low down, placing the fingers behind the shouJJer and the thumb immediately above the centre of the collar-bone in the hollow between the muscles attached to the bone (pressure p oint 5) . 85
5.- P ress the thumb deeply do\\ n \\'a r ds a nd back wards agamst the fi rst rib, wh ich is beneath th collar-bone at this spot (Fig. 44).
The Axill a ry Art e ry , which is a continuation of the subclavian, keeps close to the shoulder joint. and can be felt pulsating when the fingers are deeply pressed into the armpit. Digital pressure is difficult to apply to thiS artery.
To apply a pad and bandage:-
I.-Place a hard pad the size of a billiard ball 111 the arm pit (pressure point 6).
2.-Apply the centre of a narrow bandage on the pad; cross the FIG. 45 . bandage on .. the shoulder; pull the ends tight and tIe them under the opposite armpit, taking care that the pad does not slip.
3.-Flex the forearm and tie the limb to the trunk \\ ith a hroad bandage, applIed o n a level \\ ith the elbow (Fig. 45 ) ·
84
The Brachial Artery is a continuation of the Axillary, and runs down the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The inner seam of the coat above the elbow roughly indicates its course.
Digital or instrumental pressure may be applied at or near Jlfessure point 7.

FIG. 46.
FI G. -1-7.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back
87
of the arm over the s am of the coat or the groove on the insi.de of the biceps muscle. Press the pulps (not the tIpS) on the artery (Fig. 46). orne prefer to pass the hand oyer the front of the muscle (Fig. 47). A slight turn of the hand out\\ards as it grasps the arm will better ensure compression of the artery.
The Brachia l artery may be compressed at the
FIG. 49.
elbow (pressure point 8) by flexion. The pad may oe a folded handkerc hief with a small stone or a c o rk wrapped up in it, but when no pad is a\'ailable coat sleeve rolled or gathered up will serve instead (Fig. 48).
86
88
. Just below. the elbow the Brachial artery di yides mto the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pr e sure points (9 and 10) are about one inch abov e the wrist and about half an inch from the <?uter and inner sides of the forearm, where the artenes may be felt pul atinO'. Branches of thes e arteries join to form the Ar ches in the hand. The arteries run along on either side of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and la, by the thumbs (Fi g. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3·-Secure them by a tight bandnge.
To arrest hremorrhage from the palm of the hand :-
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, turn up the base about four inches, lay the back of the patient's ha.nd on the centre of the bandage, fold the POll1t over the knuckles and wrist pass the two ends round the wrist, make

89
patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the point (.-\.) dow n to the knuckles and fasten with a pin at B (Fig. So ).
3·- Elevate the forearm and support it with a . " t. John" sling (see page 49).
hremorrhage from the fingers nay be arreste d by applymg a small pad on the" ound, and securing it firmly \\ lth a strip of tape, linen or plaster.
AR TERIES OF THE LO\'. ER LDIBs.
The Femoral Artery, a con tin un tion of the iliac, FIG. 50. enters the thigh in the centre of the fold of the groin, \\ here it may be felt pulsating immediately below the skm. The course of the 3.rtery may be indicated by a line dra \\ n from the cen trf' of the groin to the inner Side of the back part of the knee. After traversing t\yo-thirds of this line, the femo ral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groi n (pressure point I I) as follows ;I.-Lay th e patient on his back .

2.-Kneel beside the patient.
3.-To find the groin, raise the foot high so as to flex the thigh; the fold in the c10thing at the top of the thigh will indicate the groin.
4.-Place the thumbs one on the other upon tIle pressure point, grasping the thigh with the hands (Fig. 5 I).
s.-Press firmly against the brim of the pelvis.
As there is illlmediate danger of death it is important not to \\ aste time in removing the trousers.
"When the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been FIG. 51. devised for compression at this point, :?.nd relays of should be employed to keep up the pressure until the doctor arrives; each fresh assistant places his thumbs over those of his predecessor, who slips his away from beneath, and thus gushes of blood are prevented during the change.
Application of a tourniquet to the Femoral artery (pressure point 12) :-
When practising compression of this artery, it is a
92
good plan to draw a chalk line from the centre of the groin to the inner side of the back of the knee; place the pad of the tourniquet on this line as high up as the bandage can be applied. Th e pad should be the size of a lawn te nnis ball (Fig. 52 ).
Pressure may be applied t o th e Popliteal artery by fl exion at the knee (pressure point 13); th e pad should

FIG . 53.
be the size of a lawn tennis ball, or if n o pad IS avail able the trouser leg may be rolled or gathe red up to serve instead. It is not n ecessary to take off the cl o thing (Fig. 53).
Just below and b ehind the kn ee joint the Poplit eal artery divides into the Anterior (front) P os terior (back ) Tibi al arteries.
The Posterior Tibial Artery passe s down the
93
back of th e leg to th e inner side of the ankle. It is at first deeply placed b tw ee n lhe muscles of th e calf, but it approaches the surface as it r ro eeds, so that it can be felt pulsating behind the large cone a t the inner side of the ankle . It enters the sole as the Plantar Arteries, "hich run fory, ard amongs t the muscles to supply the foot and toes.
The Anterior Tibial Artery, on I aymg the Popliteal, at once passes for\\ard bet" e(n the leg bones, and, deeply placed amongst the runs down the leg to the centre of tl' e [rent f the ankle. This artery IS continued as tLe Dorsal Artery of the Foot, "hich, passing fen\ ard on:r the tarsus, dips do\\ n to the S( Je t l t\\ ern t1 e fiLt and metatarsal bones . Hue It fcrn s \\ith the Plantar arteries what IS kno" n as the Plantar Arch. At the ankle (pressure points LJ- and IS) pressure may be applied by the fingers or by pads and bandages.
H.'E\IORRHAGE.
I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3. - It issues from the side of the wound further from the heart.
4.-In the case of a wound of a varicose vein it flows also from the side of the \\ ound nearer to the heart, especially if the patient is kept standing.
Varicose Veins .-The veins of the leg are specially apt to beco :n;; varicose. A varicose vein is dilateJ, win:iing, and with bead-like (varicose) . projections along its courSe. A vein becomes from several causes, such as long standing or tight garters. The first effect is to throw e'\tra work upon the valves, and the bead-like projections are cau ed by the blo ::)] accumula.tll1g in the pockets behind the valves. In time the vein becomes so dilated that the vah'es can no longer span it.
RULES FOR OF A
ACCO:\IP.\,:·HED BY H :E \IORRH,\.GE.
I. - Place th e patien t in a suitab le position , beanns in mind that the blood escapes with forc e when the patient sits and is still morc checkcu as he lies down.
2. - Elevate the part, as thereby less blood finds its way into it.
3.-Expose th e wound , remoying \\ clothin:; is necessary.
4.- Remove any constrictions , such as l.he collar or garters, from the he1.rt ide of the \\ ound.
5. - Apply digital pressure on the \yound until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure near the \,"ound on the side away from the heart. In the case of a wound of a varicose vein it may also be necessary to

apply a pad and bandage to the vein immediate ly above the wound, esp clally if the limb cannot be maintained in an elevat d position.
6. - Treat the wound as directed by Rules 5, 6 and 7, stated on pages 77 and 78.
7. - Afford support to the injured part.
CAP1LL.\RY
I. - The blood is red .
2. - It flows brisk ly in a cont inuous stream, or may merely ooze from the wound.
3·- It wells up from all parts of the wound. A slight amount of pressure "ill suffice to arrest capillary hcemorrhage.
INTERNAL H.iEl\IORRHACE.
\Vounds of the blood vessels \\ithin the trunk (J.use hcemorrhage into the ca\'ity of the chest or of tje abdomen.
Src. s Y:\fPTO:-'fS OF INTER AL
I.-Rapid 10 s of strene:th, giddiness and faintness, espeCIally \\ hen the upright position is assumed.
2.-Pallor of the face and lips .
3·-Breathing hurned and laboured, and accompanied by ya\\ ning and sighing.
4·-The pulse fails, and may altogether disappear at the wrist .
94
95

5.-The patient throws hi arms about, tltss at the clothing round the neck, and calls for air.
6.-Finally the patient may become totally unconscious.
I.-Keep the patient in a recumbent position.
2.-Undo all tight clothing about the neck.
3.-Provide for free circulation of air; fan the patient.
4.-Sprinkle cold water on the hce; hold smelling salts to the n ostnls; avoid other forms of stim ulants, at all events until the hzemorrhage has been controlled.
s.-Give ice to suck or coU water to drink; if the seat of the hremorrhage is known, apply an ice bag Jver the region.
6.-Should the patient be reduced to a state of collapse, raise the feet and bandacre the limbs firmly from the toes to the hips and from the fingers to the shoulders.
HALVIORRHAGE FRO:\I THE NOSE (NOSTRfLS) .
I.-Place the patient in a sitting position in a curre nt of air before an open window, \\ ith the head thro\Vn slightly back and the hands raised above the head.
2.-Undo all clothing around the neck and chest.
3.-Apply cold (ice, a cold sponge or bunch of 97
keys ) over the nose and also the spine at the level of the collar; place the feet in hot \\ ater.
4.-Cause the patient to keep the mouth open, and so avoid breathing through the nose.
Blood issuino- from the mouth may come hom the tongue,Othe gums, the socket of a tooth after extrac!ion, the throat, the lungs, or the stomach.
HIE:\IORRHAGE FRO:\T THE TONGUE, THE GUMS, THE OCKET OF A TOOTH, OR THE THROAT.
r.-G1\'e ice to suck or cold \\ ater to hold in the mouth. If thIS IS not successful gIve \\ater as hot as can be borne to hold in the mouth.
2. If necessary make pressure on the carotid arteries .
3. If bleeding from the front part of the tongue is exces Ive compress the part by a piece of clean lint held bet\\'een the finger and thumb.
4.-If the bleedmg is the socket of a tooth, plug the socket with a piece of clean lint or cotton wool; over this place a small cork or other substa nce of suitable size, and instruct the patient to bIte on it.
HIE:\IORRHAGE FRQ:\! THE LU);'Gs.
Blood from the lungs is coughed up and is scarlet and frothy in appearance.
Treat as for Internal Hremorrhage (see page 95).
96
E

HlE:\[ORRHAGE FRO [ THE STOMACH.
Blood from the stomach is vomited; it IS of a dark colour and has the appearance of coffee grounds; it may be mixed with food.
Treat as for Internal Hremorrhage (see page 95), except that nothing is to be giyen by the mouth.
Blood issuing from the Ear Channe l, which generally indicates a fracture of the base of the cranium, must be wiped away as it issues; no attempt is to be made to pI ug the ear. 99
QUESTIONS ON CHAPTER III.
Tile numerals z'ndicate the pages where the allsweJ s may be found.
\Vhat organs are concerned in the circulation of the
blood?
Describe the heart ... 70 Trace the circulation of the blood through the bed)' and lungs 70 to 72
How many times a minute does the heart contract on the average? ... ... 72 'What is the effect of the patient' position on the rate at which the heart contracts? 72
would you know a case of arterial h::emorrhage
In what way should arterial hremorrhage be controliLd?
is meant by " pre sure point"?
may pre ure be applied?
is a tuurniquet ?
is accuracy necessary in placing the pad of a tourniquet?
When mayan elastic bandage be used inst ead of a tourniquet? 76 What is flexi on?
State the general rules fo r treatment of a wound accompanied by arterial h::emorrhage ..... . 77, 78
If part of a limb had been torn off, hut there was nd m uch bleeding, how would you act? 78
Should blood clot be di turbed ?... ... . . ...
I s it \\ ise for an un killed person to attempt to cleanse a wound?
98
PAG K
... 70
What
... 72 How
... ...
... 74
..
... ... ... ...
is the pulse?
many kinds of hremorrhage are there?
73 How
?
74 \Vhat
74 How
74 What
75 Why
... 75
'" ... 76
. ., ... ... ... ... ... ...
W
. .. 79
78, 79
hat is the aona?
roo
Describe the arter:ies of the head and neck 80
Why is it sometimes neces a ry to compress the carotid artery both below and above the wound? ... 80, 8r
'What is a ring pad, and what is its u e ? 84
Describe the arteries of the upper lim bs 84 to 89
Describe the arteries of the lower limbs 89 to 93
How would you know a case of venous hremorrhage ? .. 93
What is a varicose vein? 94
How maya vein become varicose? ... 94
State the general rule for treatment of a wound accompanied by venou ... 94, 95
How would you k now a case of capillary hremorrhage ? 95
How would you stop capillary hremorrhage ? 95
'What is internal hremorrhage? 95
'\That would lead you to suspect internal hremorrhage? 95, 96
State the treatment for internal hremorrhage? .,. ... 96
How would you arre t ha::morrhage from the nose? '" 96, 97
vVhere may blood is uing from the mouth come from?.. 97
How would you treat bleeding from the gum or throat? 97
What else would you do if the tongue were bleeding?.. 97
And if the bleeding were from the socket of the tooth? 97
How would you distinguish between bleeJing from the lungs and from the tomach ?.. ... 97
And what would be the difference in the treatment? .. 97
Of what is bleeding from the ear channel generally:1. >.ign ? 98
The Student should practise placing suppo ed patients in a proper position for the arrest of hremorrhage (see pages 72, 77 and 94), f()lding firm pads (74 and 75), tying hard knots in bandages to form a t·;)Urniquet (76), and the application of pres ure at all the pre ure point!. shown in the frontispiece, at vanous points on the for ehead and scalp, and on the palm of the hand. Pressure shou ld be digital, by pad and handage, or flexion, as directed in the text.

Pressure points - Carotid ..artery, 80. Fac.ial, 82. T emporal, 82. OccIpItal , 83. SubclaVian, 84·
Axillary, 85. BrachIal (by pad and bandage, pressure being made humerus and by flexion at the elbow), 86. Rachal and Ulnar, 87· Femoral at the groin, 90. Femoral in .the 9 2 • Popliteal, 92. Anlcrial and postenor Tlblal a rterie , 93, Hremorrhage from the forehead or scalp ...
IIremorrhage from the palm of hand.. .:.
Yen ous hremorrhage from a \'ancose or other \'em 84 87 to 89 ,·,93,94
PACE
lOI PAC.
CHAPTER IV. BRUISES.
A blow anywhere on the surface of the body may cause hcemorrhage beneath the skIn, \\'ithIt-a" black eye II is an instance. The Injury IS accompanied by discoloration and swelling.
TREATMENT.
Apply ice or cold \Yater dressings. A piece of lint soaked in extract of \\ itch hazel may be placed on the affected part.
BURN AND SCALDS.
A burn is caused-
(a) By dry heat, such as fire or a piece of hot iron.
(b) By a rail, wire or dynamo charged with a high pressure electric current.
(c) By a corrosive acid, such as oil of vitriol.
(d) By a corrosive alkali, such as caustic soda, ammonia, or quicklime .
. (e) By friction, caused, for example, by contact wIth a revoI.ving wheel. (Brush burn.)
A scald IS caused by moist heat such as boiling water, hot oil or tar. '
.The effect may be a mere reddening of the skin ; bhsters may be formed ; or even the deeper tissues

103
of the body may be charred and blackened . The clothing may adhere to the burnt skin, and its removal is impossible without further detriment to the injured part. The great danger is Shock.
TREAT:'IfENT.
I .-Carefully remove the cloth i ng over the inj ured part . If stuck to the skin, the adherent clothing must be cut around with scissors, soaked with oil, and left to come away subsequently.
2 . - Do not break blisters.
3. - Immediately cover up the part . Soak or smear pieces of lint or linen \\'ith oil, or vaseline, lanoline, or cold cream; a small quantity of boracic powder added to the e \\ill be of benefit. The inside of a raw potato scraped out and spread on lInt makes a soothing application. \Vhen the injured surface is extensive do not cover it with one large sheet of lint, but with strips about the breadth of the hand; this IS advisable as they fit better on the part, and during subsequent dr eSS Ings one strip can be removed at a time, and a fresh dressing applied before the adjacent strip is taken off. The shock to the system is thereby less than if the whole of the burnt surface were laid bare to the air by the removal of all the dressings at one time. When covered by the oily dressing envelop the part in cotton wool or a piece of flannel and apply a ba n dage.
102
When the face is burnt, cut a mask out of lint or linen, leaving holes for the eyes, nose, and mouth. Dip this in oil or smear it \\ith vaseline and apply it to the face and cover it with cotton wool, leaving op enings to correspond \\ ith the holes in the mask.
vVhen possible place the injured part in water at the temperature of the body (98 degrees) until suitable dressings can be prepared. A dessert- poonful of baking soda added to a basinful of the \\ arm water will make a soothing lotion.
As it is important not to lea\'e the part exposed to the air, it is the duty of the bystanders to prepare th e dressings while the clothing is being remO\ ed.
4·-Treat Shock. -Thi. is particularly ne c sary in the case of e\'ery burn or scald of any con iderable extent (see page I35). Be yery apprehensi\'e of danger in the case of even sligh t burns of the ne k.
5·- If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bi arbonate of soda), magnesia, or slaked lime Ln \\ arm \\ ater before applying the dressings.
6. - If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion, such as lemon juice or vinegal diluted with all equal quantity of water. Cautz'oll.-Before using water brush off any lime that remains on the part.

105
7
- When a woman's dress catches fire -
.
(a) Lay the woman flat on the floor at once., so that the flames are uppermost; that IS to say, if the front of the dress is on fire lay her on her back, and if the back of the dress is burning, place her face downwards. The reason for this is that flames ascend, so that if the upriaht position is assumed, the flames \\ ill q uic k Iy reach and b urn the body, neck, and face; or if the lies with the flames undermost, they WIll, if unextinguished, pass over and burn the limbs and set fire to the rest of the dress.
{b) As so;n 3.S the woman is laid flat, smother the flame \\ith anything at hand, as a ru a coat blanket, or table coyer; If made 0' wet so much the better.
(
c) A woman rendering assistance should hold a ru a or blanket in front of herself when b approaching the flames.
(
d) If a woman's dress catches fire when nobody is by, she should lie flat, uppermost, smother the flames with anythIng handy, and call for assistance, or crawl to the bell-pull and ring; on no account should she rush into the open air.
Th e use of fire guards would prevent many calam ilies.
104
BI TES OF SNA K E AND R AB ID AN I MALS , AN D \ VO U ND S BY P OI O NED "WEAPONS .
Hy drop hobia is caused by the bite of an animal, as a dog, cat, fox, \\'olf, or dee r su ffering from rabIes . T he special poisons in troduced into wounds caused by venomous snakes and poisoned \\ en pons cause immediate danger to life.
TREAT:\IE T.
I. - Immediatelyplace a constriction between the wound and the heart so as to preyen t the venous blood from carrying the poison through th e body. If, fo r example, a finger is bitten it should be enci r cled on the side of the wound nearest to the heart with the finger and thumb, and as soon as po sible ligature (a string, piece of tape, or strip of handkerchief) should be placed tightly round the root of the finger. Compression with the finger and thumb must not be relaxed until the ligature has been applied . Additional ligatures may, with adyantage, be applie d at inte r vals up the limb.
2. - Encourage bleeding for a time :-
( a) By bathing the wound with v,'arm wate r .
(b) By keeping the injured limb low; the uppe r should be allowed to hang down, and 111 the case of the lo\\"er limb the patient should be seated with the foot on th e grou n d.

3. - Cauterise the wound, if it is quite impossible to obtain the services of a doctor. Thi s is best done by burning with a fl uid caust ic , suc h as ca u s tic potash, pure carbolic acid, or nitric acid, o r if th ese a re not at hand, with a red hot wire or a f use e.
T he u sual slid cau tic is insufficient, as it does not r each the bottom of the wound, where the poison is.
T o ensure the caustic reaching the bottom of the wound, it should be applied on a piece of wood, su ch as a match cut to a point. \Vhen the caustic has been thoroughly applied, but not till then, the ligatures may be removed.
4. - Cover the wound, afte r a while, with a clean dr essin3
5.-Afford support to the injured part.
6 - Treat shock if it occurs (see page 135).
7. - In the case of a bite by a venomous snake, rub in powdered permanganate of potash and inject under the skin in the neighbourhood of the wound a solution of permanganate of potash.
ST IN GS O F P L ANT AN D AN I MALS.
These give rise to serious inconvenience, and In s ome cases grave symptoms develop.
TREATl\IEr T.
I. - Extract the sting if left in .
2.- Mop the part freely with dilute ammonia
I06
108 or spirits. A paste o f bicarbo n ate of soda and sal volatile is an efficient application. A solution o f wash in g so d a or potash or the application of the b lue bag will relieve pain.
3. - Treat collapse if it occurs (see page 135 ) .
FRO T BITE.
Durin g exposure to seYere cold, parts of the body, usu ally t he feet, fingers, nose, or ears, lose sensation a nd become first \\ axy white and afterwards congested and of a purple appearance . As sensation is los t in the part, it is often only by the remarks of bystanders that the frost-bitlen person is made awar e of his condition.
TREATME TT.
I. - Do not bring the patient into a warm r<?om u n til , by frict!on of the hand or hy rubbing wIth soft snow, sensatIOn and circulation in the affected par ts are restored. Neglect of this precaution may lead to death of the of the frost-bitten part.
2. - When circulation is restored, keep the pa tient in a room at a tem perature of 60 degreec;.
N EEDLE EMBEDDED UNDER THE SKIN.
\tVhen a needle breaks off :::.fter penetrating the skin a nd disappears, take the patient to a doctor at once. If the wound is near a joint, keep the limb at rest on a splint.

FISH-HOOK EMBEDDED IN THE SKIN .
Do not attempt to withdraw the fish-hook by th e way it went in, but cut off the dressing of the hook, so that only the metal is left, and then force the point onwards through the skin until the hook can be pulled out.
INJURIE TO JOINTS.
\Vhen a joint is injured by a bullet, stab, or other cause-
r. - W r a p t h e p art in cotton w ool.
2. - Afford r est an d s upport to the injured li mb ; if the upper limb, in a flexed position by a sling; If the lo\\'er limb, in a straight position by a splint.
FOREIG BODY L - THE EYE.
I. - Prev ent th e p atient rub bi ng the eye, t) ing down a child's hands If necessary.
2.- Pull d own t h e lowe r eyelid, when, if the foreign body is seen, it can readily be removed with a camel's hair brush, or with the corner of a handker· chief twirled up and wetted.
3. - W he n t he forei gn body is b e neath the upper ey eli d lift the lid fOf\\ard, push up the lower lid beneath it and let go. The hair of the lower lid brushes the inner surface of the upper one, and may dislodge the body. hould the first attempt be unsuccessful, repeat it se\'eral times if necessary . If
the foreign body is not dislodged call the services of a .docto r as soon as possible. When, however, skilled help cannot be had , proceed as follows ;-
(a) Seat the .so as to face the light, and stand behmd hIm, steadying his bead against your chest.
(b) Place a small rod, such as a match or bodkin on the upper eyelid, half-an-inch aboye edge, pressing it backwards as far as It0ssible.
(c) Pull the upper eye-lashes UP\\ ards oyer the rod, and thereby evert the eyelid.
(d) Remove the foreign tody.
4.-When a piece of steel is em be dd e d in the eyeball drop a little olive or castor oil n the after pulling down the 10\\ er eyeJid, close the hds, apply a soft pad of cotton \\ 001 and recure it by a bandage tied sufficiently firmly to keep the eyeball steady; take the patient to a doctor.
5. - When qu.ick-lime is in the eye brush as much of It as possible; bathe the eye \\ ith vmegar and warm water, and treat as for a piece of steel embedded in the eyeball.
F O REIGN BODY IN THE EAR PASSAGE.
A.s a rule n:a k e no to treat a patient with forel.gn body m the ear If the services of a doctor can possIbly be had) any attempts to remove the foreig n b ody may lead to fatal consequences. If a child

III
cannJt be induced to keep the fingers from the ear, tie his hands down or cover up the ear. If an insect is in the ear-p:1ss:1ge, fill the ear \\'ith olive oil, when the insect will R.nt and may be removed. Never syringe or probe the ear.
FOREIGN BODY I:.f THE NO E.
Induce sneezing by pepper or snuff. Cause the patient to blow his nose after the um.ffected nostril. There IS no ImmedIate danger fro:11 a foreign body in the nose.
THE ABDO)lEN.
The abdomen is bounJed above by the diaphragm; below by the pelvi ; behind by the lumbar vertebrre; and in front and at the sides by muscular \Yalls. (Fig. 54·)
THE ORGANS GF THE
Th e Stomach lies immediately below the" pit of the to n:1ch " just belo\\' the breast-bone.
Th e L iver lies in the upper part of the abdomen, where it is mostly covered by the right lower ribs.
Th e Spleen lies beneath the ribs at upper part of the left side of the abdomen.
Th e Intest ines occupy the greater part of the cavity of the ab30l11cn.
Th e Kidn e ys lie at the back, in r egion of th e loin.
The Bladder lies in the peh·is.
110
FIG. 54.
W OUND IN THE FRONT , VALL OF THE ABDO:\IEN .
Wh en the intestines 0 7" other organs p r otrude throu g h the woun d, wheth er vertical o r t ransverse be nd the kne es, ra ise the sh ou lders, a n d app ly lint , to we l, or cotton wool wra p ped in soft lin en, a n d k eep the

II J
pati e nt war m un til the doctor arrives. is no pro tru sion of or gans, if tile zs lay the pat ien t fi at on the back WIth the 10\\ er lImbs straight ; if tlze wound z·s Iransverse , bend the knees and raise the shoulders.
I NJURIES TO THE O RG.\NS 'VITHIN THE ABD011EN AND PELVIS .
Injuries of the Stomach are attended by extreme collapse anJ sometimes by yomiting of dark blood like coffee ·grounds. For treatment see " Hremorrhage fro:11 the "'tomach /I ( page 98). .
Injuries of the Liver, Spleen and I nt e stmes may be caused by a blow, a stab or a bullet; the liver or spleen may be injured by a fracture of the lower ribs. The igns and Symptoms are those of internal hremorrhage accompanied by pain and swelling at the scat of injury, and the trc.atment is as for that condition (see page 95)'
The Kidneys may be injured by a fracture of t he eleventh or twelfth ribs, also by a crush, blow, s tab or bullet. Blood may escape with the urine , and there may be pain and s\\ elling oyer the injure d k idney .
The Bladder may be injured by a fracture of the p elvis . T he signs and symptoms are inabil:ty t o pass water , o r if a little is passed it is tmged wlt h blo od .
112
-TREATMENT OF INJURY TO THE KIDNEYS OR BLADDER.
1.- Keep the patient qu iet until the d.octor arrives.
2.-Apply hot fomentations over the painful or inj ured part.
Rupture (hernia) consists of a protrusion of an -internal organ, usually the bo\\-el, through the lllUS, cular wall of th e abdomen, most fr eq uently at the gr?in. a sudden s\yelling accompanied by pam and sickness take place in that region
I.-Send for a doctor instantly.
2.-Lay the patient down with the buttocks raised.
3·-A pply ice or cold water dressings to the affected part.

QUESTIONS ON CHAPTER I
114
V. TIle numerals indicate tile pages where the answers may be found. rAG E What is a bruise? 102 lIow would you treat a bruise? IOZ How maya burn be ca.used ? 102 lIow is a scald caused? 102 What is the great danger of a burn or scald? .. , 1 0 3 State the general treatment for burns and scalds 103, 104 How would you treat a burn caused by a corrosive acid? ... 104 lIow would you treat a burn caused by a corrosive 'alkali ? 104 \Vhat steps should be taken when a woman's dress catches fire? 105 State the general rul es for treatment of wound s caused by poisonou bites or weapons .. , . _. 106, 107 \Vhat special treatment is required for the bite of a venomous snake? ... 107 lIow would you treat a sting? 107, 108 tate the signs, symptoms and treatment of fr ost-bite ... 108 Would you attempt to remove a needle embedded under the skin? . _ ... .. , ... 108 How would you extract a fish hook em bedded in the skin? 109 State the treatment for injuries to joints . , ... ... 10 9 Stat"! the general rules for rem0ving a foreign body from the eye... ._. .., ... ... ... 1 0 9, 110 What would you do if a piece ot ;teel were embedded in the 110 And when quick-lime is in the eye? \10 How would you try to remove an insect from the ear passage? .. , I II
\ Vould yuu try to remove any other form of fo reign body from the ear pasE;age ? ... ... ... .. . 1 10, II I
How would you remove a foreign body from the nose? I I I tate the boundaries or the abdomen and its contents I I I
State the treatment ror \\ounds or the abdomen lIZ 113
How may injuries to the lin:r, pleen and intestines be ' caused?
. II 3
'Vhat is the difference between treatment of injuries to st.omach and or injuries to the liver, spleen and lI1teslll1es?

II3
State the treatment ()f injuries to the kidneys or bladder 11 4
State the treatment of hernia .. . '" ... ... 114 I 1
C HAPTER V .
T HE NERVOUS SYST EM .
T wo systems of nerves, the Cerebro-spinal and th e. Sympathetic, regulate the moveme n ts and functions of the body
The Cerebro-spinal System is made up of the Brain, the Spinal Cord and rerves, and through it!t age n cy sensations are received and the \\ ill causes the actio n of the voluntary muscles. For example, when a part is injured a sensation of plin is veyed to the brain by the nerve, t hus affording an indIcatio n of the seat of injury, or a warning of a possible danger of further damage. On attentio n being directed to the injury, an attempt is instantly made to ease the pain or to move the injured part from danger.
The Brain is situated \\ithin the cranium, and is divided in the middle line, so that, with the e-xception of so;ne conne cting bands , the right and left sides are separate.
The Spinal Cord is the long cord of nervous matter lying within the spinal canal (see Vertebral Colum n, page 23) . I t leaves the brain through an o pe ning in t he base of the cranium and extends to t he upper lumba r verteblze.
lIb !'''GIr
... .. . ..
... ... ... ... ..
7

The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissues of the body. When a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nervo\:s chain on each side of the froni: of the spinal column along its entire length, and sends branches to all the organs of the chest and ahdomen to control the involuntary muscles, and thereby regulate the vital functions. This system is not under the control of the will, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air reaches the lungs by way of the nostrils (or mouth), the throat, the wind -pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind-pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they; may enter the - wind-pipe and causer asphyxia. The wind-pipe extends to two inches below the top 0\ the breast-bone, where it divides into the right and left bronchial tube. Each bronchial tube enters a lung at!d divides into small and still smaller tubes,
FIG. 55. THE LUN':;S A:-ID BRONCHIAL TUBES. A. Trachea, or Wind-pipe. B. Left Bronchus. C. Right Bronchus. D. Sm3.11er Bronchial Tubes.121

the ultimate recesses of the lung-the air cells or air spac es-are reached.
The Lungs, Right and Left, occupy the greater part of the chest; they lie immedIately within the ribs, and practically wherever a rib is felt, whether fr ont , back or sides, there is lung beneath. Each Jung is em'eloped in a fine membrane (the pleura) which allows It to move within the chest durinO' breathlllg witho ut friction.
diaphragm rises;. this lessens the capacity of the c.hest .and forces air ?ut. The mechanism of respiratIOn IS somewhat hke that of ordinary household bellows, but \\ ithout a valve; the ribs may be compared to the boards of the bellows \\ hile the diaphragm corresp onds to the leather, the air passages being equivalent to the nozzle.
b
Respiration, or breathing, consists of two acts, Inspiration, an expansion of the chest, during which air ,is drawn into the lungs, and Expiration, a contraction of the chest, during which air leaves t:le lungs. A p3.use follow,; the act of expiration. In health fifteen to eighteen breaths are taken per minute, and at each inspiration about 20 to 30 cubic inches of air enter the lungs, and a similar quantity is at each expiration.
The expansion and contraction of the chest are effcctej partly by the muscles of r espi ration attached to ribs, but chiefly by the Diaphragm, the large arched muscuhr partition which separates the chest from th e abdom en. In inspiration, which is chlefly a muscular act, the ribs are raised, and thp arch of the diaphragm falls and becomes flatt ene d, thus inc:easin g the capaciLy of the chest and causing the aIr to enter. In expiration, an act performed almost without effort, the ribs fall and the arch of the
. As the blood depends upon the air fo r its purificatIOn and the oxy gen n ecessary to maintain life interference with breathing "ery soon may prod'uce a dangerous stat e called asphyxia, examples of which are afforded by dr owning, suffocation, choking, etc.
ARTIFI CL \L RE -' PIRATIO .
PROFESS OR CH;\FER 'S METHOD.
I.-Waste no time in loosening or in removing clothing.
2.-Lay the patient in a prone position (i. t., back upwards ) with his head turned to one SIde so as to keep his no se and mouth away from the No pad IS to be placed under the patient, nor need the tongue be dra\\ n out, as it ",i1\ fall naturally.
3.-Kneel at one side facing the patient's head, and place the palm o f your hands on his ribs, one at each side, the thumbs nearly touchmg one another in the small of the back. Leaning your body forward, slo\\ 11' apply firm but
120
n ot viole nt p ressure st raight the bac k an d lower par t of th e ches t, thus d rlv m g air out and p ro d u cing expiratio n (Fig . 56). D raw bac k

FIG. 56. EXPIRATION.
1 2 3 your body some\Vhat more rapidly and relax the pre ssure, but do not remove your hands; this p rodu ces inspiration (Fig. 57)·
4. - Alternate these movements , by a rhythmi c s waying backwards and forwards of your body, twelve t o fifteen times a minute, persevering until respiration is restored , or a doctor pronounces life to be extinct.
DR. SILVESTER ' S "METHOD.
I . Adjust the patient 's position .-\Vithout wasting a moment place the patient on his back on a fiat surface, incli ned if possible from the feet up\Vards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in \\ omen. Raise and support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades.
2 . Maintain a free entrance of air into the windpipe. -Cleanse the lips and nostrils; open a n d wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that positio n .
3. - Imitate the movements of breathing. Induce Inspz"rat/on.-Kne el a t a convenient di sta n c e beh ind the patient 's head , and, grasping his fo re a r ms j us t below the elbow , draw the arm s
122
F IG. 57. I NSPIR ATION.
FIG. 58. INSPIRATION.

FIG. 59. EXPIRATIOX.
upwards, outwards, and towards you, with a sweeping movement, making the elbo\\ s touch the ground
FIG. 61. EXPIRATIOX.
(Fig. 58). The cavity of the chest is thus enlarged, and air is dra"wn into the lungs.
124
1 2 5

Induce expzratt'o1l.-Bring the patient's flexed arms slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (Fig. 59)' By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and perseveringly about fifteen times a minute.
When a sufficient number of assistants are present, Howard's method may be combined with ilvester's, as follo\\'s :- J.,..
The additional assistant kneels astride the patient's hips with the balls of the thumbs restin3 on either side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Using his knees as a pivot, he presses forward on his hands. Then suddenl)" with a final push, he springs back and remains erect on his knees while he slowly counts I, 2, 3. These motions are to be repeated to correspond with those being performed by 'ilves ter's method, pressure on the chest being made simultaneously by those performing the two methods (Figs. 60 and ,6 I).
LABORDE's METHOD.
'When from any cause the above methods cannot be carried out, Laborde's method of artificial respiration should be tried. It is especially useful in suffocated children and when the ribs are broken. 1
The patient is placed on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from th.e fino-ers-the lower jaw depressed; the tongue IS pulled forward and h eld for two. seconds in that position, then allowed to recede mto the mouth. Thes e movements should be repeated about fifteen times a minute.
Artincial respir ation must be continued breathin g is established, or until a doctor arnves.
'When natural breathing co 111 mences, regulate the artificial respiration to correspond with It. Success may result even after two hours' time.
Excite respiration.- 'Vhilst artificial respiration is being applied, other useful steps may be employed, such as applying smelling salts or snuff to the nostnls, and flIcking the chest" ith a dam} to\yel.
Induce circulation and warmth after natural breathing has been restored. 'Vrap the patient in dry blankets or other covering, and rub the limbs ene rgetica lly towards the heart. Promote warmth by h?t flannels, hot-water bottles. or hot bricks ,( wrapped m flannel) applied to the feet, the limbs and bo?y.
'Vhen the power of swallo\\,ll1g has returned gJve hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep . Large poultices or fomentations applied to the
126
2 7

f ront a n d back of the chest will serve to assist breathing.
Watch the patient carefully for some time to see that the breath ing does not fail; sho uld a ny sign s of failure appear, at once begin artificial respiration.
I N " E IBILITY.
Unconsciousness or Insensibility may arise as follows :-
Injury to the Head. -Concussion and Compression of the brain.
Disease of the Brain. -Apoplexy, Epilepsy, Hysteria.
Various Causes. -Shock, Fainting ( yncope), Collapse, Alcoholic and oth er poisoning, Sunstroke and Heat-stroke, Infantile Convulsions, Asphyxia .
G ENERAL RULE FOR TREATMENT OF I
NSE
J ·IBILITY .
I.-- If a person appears about to lose consciousness, prevent hi'11 from falling, and lay him gently down .
2. - Arrest Hcemorrhage when apparent; attending to minor in juries is less important than tr eati ng the unconscious state.
3. - Lay the patient in the position in which breathing is most easy-usually t h is will be on t he back, o r in cli n ed to one sid e. As a gene ral rule I29
raise the hea.d and shoulders slightly whe n the fac e is flushed, and keep the head lo\V "hen the face is pale.
4. - Undo all tight clothing round the neck, chest and waist, unfasteni ng the brace s a nd top butto n of the trous ers in me n, a n d the corse ts in women, the object bei ng to relieve pressure on the air passages , lungs, heart and abdomi n al organs. Be sur.c that there is no obstruction to the air passages by the tongue or by a forei g n body in the throat . The possibility of false teeth obstructmg breathing must be considered.
s. - Provide for a sufficiency of fresh air b y opening doors Cl nd wind ows, and by keeping bac k. a crowd.
6. - When breathin g cannot be discerned apply artificial respirat io n.
7. - 0b tain a doctor 's h e lp as soon as possible.
unavoida bl e, never le ave the patien t until you have placed him in charge of a re sp o n sible p e rson .
9. - G iv e no foo d or fluids whatever by t he mouth while th e patient is ins e nsible .
IO. - Should the sp i ne or an important: Do ne uf the upper or of th e lo w e r limb be fractured , it must be st eadied and ma intain ed at rest as soon possible. hould th e uncon ciousness be prolo nged. the patient may be removed m a recumbent pOSitIOn
128
to shelter, provided that the brok e n b one is ad eq uate ly supported.
11.-When the patient is in a state of consupp o rt his h ea d, a nd a ft er wr a p p in g a pIece of wood or a ny o th er h a r d m a terI a l in a h a ndkerch ie f, h o ld it in h is to prev ent bitin g of th e to n.g ue. Do r est ra in hi s li m bs; p revent hIm from hurtm g hIm se lf by draggi n g hi m a\\ay from a o f d a n ge r, s uc h as m achi n e r y, a wa ll , o r fir e pl a ce; li g ht pI e c es of f urni ture sho u ld be pu she d out of th e way .
12: - 0n to consciousness wate r ma y b e gIve n to d n n k . . If the pulse is feoble give warm tea or co ffee , prOVIded hremorrhage, internal o r exte rn al , is n ot presen t. A desIre to sleep sho u ld be except in cases of opium poisoning, a . c o n d itIon th at may ge n erally be r ecog n is e d by the hI sto ry o f t h e case, a nd also b y th e p u pil of the bla.c k open in gs in t h e grey, blue or b ro wn Ins ) be m g mmut ely co ntracted (pi n -h ead p u pils) .
. - It not be assumed that a person 1S insensIble as the result of drink merely because the breath smells of alcohol' fr eq uently p e ople are fee l ing i ll th ey ta k e or' a re g iven c:.tlmula nts, afte r whi c h may become insensIble, .1 0t from the drink, but from the cause induc.ed them to take it, for example, insensibIlIty commg on, effects of poisoning, etc . Even If

13 I
dr in k is be lieved to De t h e ac tu al cause of i nsensibili ty, it mus t be bo rn e in mind that the patient is in a ve ry dangercus state , ar,d he m ust be tr eated for Collapse by being covered up and kept \\arm.
The abo\'e general ru les \\ il1 enable first aid to be rendered efficiently in most cases of insensibili t y, although the exact form from \\ hich the patient is sufferi ng is unknown.
C O TCU 10 OF THE BRAI :i\l" .
[ he patient may be stunned by a blow or fall o n t he head, or by a fall on the feet o r lower part of the spine. He may qui kly regain consciousness, or insensibility, more or less complete, may be prolonged.
I. - Apply the general rules for the treatmen t of Insen Ibtlity
2. - Be very apprehensive of danger in all cases of injury to the head. patient may be stunned, and after a short interyal may recove r some degree of consciousness or even the Dral11 may apparently have escaped injury; yet in both instance s there is a gra,-e risk that a structure \\ ithin the craniul1l has been injured, and that a serious state of insensibility may de\'elop bter (ee Fracture of the Cranium, page 43.) A cautio n should therefore be given to a patient \\'ho has lost consciousness even
130
13 2
for only a mo me n t after an injur y to th e head not to r esume phys ica l or m e ntal activit y without the con:,ent of a do c t or.
C O MPRESS I ON OF THE BRAIN, APOPLEXY .
Compression of the Brain may result from the same c a uses as produce Concussion; in fact, Compressi o n is fr equently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no sign s of injury are neces arily present.
In both conditions the face is flu hed; the br eathi n g s tertorous; one side of the body may be m ore l imp than the other: and the pupil of one eye may b e larger t han that of the other; the temperature of the b ody is generally raised.
TREATMEN T
I. - Apply the general rules for treatment of Insensibility.
2. - Promote warmth i n the lowe r part of the body by th e application of hot \\ater bottles to the a bdomen and lower lim bs. Care must be taken not t o burn the patient \\ ith the bottles, which should be wrapped in flannel, and their heat tested wIth t h e elbow.
EPILEP Y.
c:.pilepsy may occur in persons of any age, but us ually occ urs in young adults. The patient falls to

I33
the ground, sometimes with a scream, a n d Jn to a state of convulsion, throwing his limbs abo ut. The treatment is according to the Genera l especially Rule 11.
HYSTERICAL FITS (HY TER I A).
SIGJ. S AND
The patient, usually a young gir l, in co n sequer.cf of mental excitement, suddenly loses command of her feelings and actions. he subsides on a couch or in some comfortable position, thrO\\'s herself about, grinding her teet h, clenching h e r fists, shaking her hair loose; she clutches at anyone or anything ne :tr her, kicks, cries and laughs alternately The eyeballs may be turned up\\'ards, and the eyelid s opened and shut rapidly. At times froth appears at the lips, and othel' symptoms may develop.
I.-Avoid sympathy \\ ith the patient, and speak firmly to her.
2.-Threaten her with a cold \Yater douche and if she persists in her "fit," sprinkle her with' cold water.
j.-Apply a mustard leaf at the back of the neck . :\ledical treatment is necessary to cure the co nd ition of mind and body which gives rise to hysterical attacks.
[34
SH OCK, F AI NT I NG ( YNCOPE), COLLAPSE.
CAUSES .
I.-·I njury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and severe crush are some of the more frequent physical causes of shock.
2.-Fright, anticipation of injury, and sudden bad news , or sometimes sudd n removal of fear and anxiety after 'prolo nged suspense, produce shock or faintmg.
3.-Some poi sons cause shock, \\ hile others, such as alcohol, so depress the nervous system that collapse ensues.
4.-Hcemorrhage or heart \\'eakn ss, a close or c rowded room, tight clothing, fatigue, or \\ ant of food may bring on fa1l1ting or colbpsc.
IGNS A D Y'!PTO:'l!S.
The general condition of shock may be by extreme pallor, a feeling of clammy feeble pulse, and shallow breatn1l1g if hcemorrhaae has been severe, by yawnmg and sighing. The term "colb.pse" signiiies. a .ve:y serious; condition in which the life of the patJent IS m the greatest danger; the tem perature of the body falls below the normal, and one great object of is to prevent it sinking to a point at "'hich. I.Ife IS impossible. An attendant danger of the condItIOn of
c ollapse is the liability t o sudden relapse a fter a temporary Improvement , a nd the utmost ca re a nd watchfulne ss must therefore be exercised t o mai n · tain the heat of the body and to guard against fa il ur e of the heart and lungs.
T REA L\IENT.
I. - Remove the Cause by arresting hcemo rrhage, attending to in juries, loosening all tight clo th . especially abo u t the chest and abdomen, remo v ' m g from a close or crowded room, using encouragi n g words, etc.
2. - Lay the patient on the back with the low. the lower limbs; the patient IS m b ed thIS IS b est do n e by raising the foot of t he bedstead.
.3. - Provide for a free circulation of fresh aIr.
4:. - I.f has been severe and the p atIent IS col!apsed, firmly bandage the limbs from the t oes to t he hIps, alld from th e fingers to the a r mpit s.
5. --:-To stimulate the action of the heart, sal volatIle and water may be gIven if the ):,atient ca n swall ow, 0: sm"l1ing salts may be held to the nostrils.
6. - It IS of the utmost importance to use every means of preventing a fall of temperature below nor.mal poi n t. To accomplish thi s cove r t he pa t Ient Wl t h extra clothing, or by p la c ing
I35
13 6
rugs or blankets over him j get him to in a warm but well-ventilat ed room as soon as possible. Apply warmth to the fe et and to the pit of the stomach by hot water bottles or hot flannels. (Test the heat of these with the elbow before applying them.) If the patient can swallow, give hot d rinks, such. as . (ea or coffee. It is well to add sugar, as It aids rn raising the temperature of the body.
7. - If breathing cannot be discerned, appl y artificial respiration.
8. - If want of nourishment has been the cause of fainting or collapse, give food sparingly at first.
SUNSTROKE AND HEAT-STROK-E.
vVhen exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weathe.r when he::tvily burdened, persox:s may. develop. sickness, faintness, giddiness, and difficulty m breathmg. The patient complains of thirst, the skin becomes and hurning, the face very flushed, the pulse qUIck and buunding. A very high temperature, stertorous (snoring) breathing, and ins e nsibility may ensue.
TRE ATMENT
I.-Undo all tight clothing.
2.-Remove the patient to a cool, shady spot .

137
3·- trip the patient to the \\alSt.
4·- L a y the patient do\\n, \\ith the head and trunk well raIs ed.
5·- Proc ur e as free a circulation as possible of fresh air, and fan the patIent vigorously.
6.-Apply ice bags or cold water freely tu the head, neck, and spine, and maintain this treatment until the symptoms subSIde.
7·-0n return to consciousness, the patient may have \\ ater to drink.
IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
.IG.·S.
pasm of the muscles of the limbs and trunk., blueness of the face, In e nsibil ity, more or less complete, and occaSIOnally ,q uinting, suspended respiration, and froth at the mouth are the promine nt signs .
TREAT\rE:,\T.
1.- upport the child in a warm bath slightly above the temperature of the body (98 degrees), so that the water reaches to the middle of the trunk.
2..-Place a sponge dipped in cold \Yater on the top of the head.
13 8
ASPHYXIA.
-When, owing to want of air, the bIo?d IS . not supplied with oxygen the patient bIe, and is said to be asphyxiated. Thls conditIOn may be brought about as follows: -
I. Obstruction of the air passages.
(a) By DROWNING. ,
(b) By PRE SURE FRQ:\1 OUTSIDE: tranguiatlOn, hanging, smothering.
(c) By A FOREIG. BODY IN THE THROAT: Choking.
(d) By SWELLING OF THE TISSUES OF THE THROAT: InflammatIOn, scald of the throat, poisonin g by a corrOSI\'e.
II. Inhaling poisonous g ase s. By coal gas (as used in the house), producer, or water, gas, smoke, fumes fr om a charcoal or coke fire, sewer gas, limekiln gas, carbonic acid gas.
III. Pressure on the chest, as when crushed by sand or debris, o r by a crowd.
IV. Nervous affections , as the result of narcotic and certain other poisons, collapse, electric shock, or stroke by lightning.
GEKERAL TREATMENT.
I n all cases of Asphyxia attempts must be made to remove the cause, or to remJve the patient from the c aus e . When this has been done artificial
139
respiration must be applied, taking c are that the air passages are not obstructed, anJ that there is abundance of fresh ai r.

Persons completely immersed in \\ aler for even ten or fifteen minutes have been restored by artificial means. Th erefore, if the body is recovered WIthin a reasonable tim e, absence of signs of bfe is not to deter immediate attempts to restore animation,
The first thmg to do wh e n the body is recovered is to ge l rid of the \\ ater and froth obstructing the , air pa ssages , and th en artificially to restore This is best accompbshed either by proceedll1g at once La perform artificial respiration by chafer's m ethod, o r as follo\\ S :- .
I.--As qUickly as possible l oosen the clothmg, and clear the mouth and the back of the throat.
Z.- Turn the pati nt face downwards, with a pad below the chest, and with the forehead upon the right forearm.
3.-"\Vhilst in this pOSitIOn apply pressure by the hands to the patient's back o\'er the 10\\ er ribs, and keep the pressure up [or three seconds .
4. - Turn the patient on the right side, mamtaining that position also for three second, .
5.- Rep eat these movement alternately as long as troth and \\at e r issue from the mouth.

These operations ( farshall Hall's method) in themselves tend to promote respiration, but \\ hen the air passages are clear of froth and water ilvester's method of artificial respIration may be used by itself or with Howard's method in conjunction.
'While performing these operations send someone to the nearest house to procure blanket and dry clothing, hot water bottles, etc., and to fe tch a doctor.
STRANGULATION.
Cut and remove the band constricting the throat. Apply artificial respiration.
HA 'GIN G.
Do not wait for a policeman: grasp the 100\'er limbs and raise the body to take the tension off th e rope; cut the rope, free the neck; apply artificial respiratioll.
::\J OTHERIl\'G .
Remove whateyer is smothering th€" patient: apply artificial respiration.
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to the back of the throat and attempt to dislodge the foreign body; if vomiting results, so much the better. If unsuccessful, thump the back hard whilst the head is bent forward. Apply artifi ial respiration. 141
S \\,ELLING OF THE Tl SSUES OF THE THROAT.
'Whether the swelling is caused by inflammation by swallowing very hot water, as not infrequently happens to children attempting to drink from the spout of a k ettle, or by the effect of a corrosive poison, the treatment is as follows :-
I.-Apply a sponge, piece of flannel or other cloth, wrung out of very hot water, to the front of the neck t from the chin to the top of the breast-bone.
2.- et the patient before the fire.
3.-Give Ice to suck if it can be had; if not, give c old \\'ater to drink.
4.-Give animal or vegetable oil, a dessertspoonful at a tIme, to soothe the scalded throat and ease the pain.
5.-If breathing has ceased apply artificial respiration.
UFFOCATION BY ':\IOKE OR GASES.
I.-R emove the patient into the fresh air. Before entering a building full of smoke tie a handkerchief, \\ et if possible, round the head 0 as to cover the nose and mouth. It is well to 1110\'e lowly, keeping low, or e"en era\\ ling, whilst in a room full of smoke in search of a suffocated person. Eyeryopportunity of Iettin a in fresh air by openi ng doors or windows should be seized.
2.-Apply artificial respiration.
3.- In the case of producer or water gas, inhalation of oxygen will also be necessary.
ELECTRIC SHOCK.
Electric current is cOlweyed by a cable, wire, rail, or bar, called the "Positive," and returns to the source of supply by another cable, \yire, rail, or bar, called the" Negative," or through the earth. In the case of an electric railway, th.e current is generally conveyed by an insulated rail the third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an electric tramway it is frequently conveyed by an overhead conductor or trolley wire, and returned through the running rails.
Through contact \\ ith a " positive" the shock may be so severe as to cau e insensibility, and the sufferer will be unable to extncate himself, and must be liberated with all possible speed. As it is generr..Jly impossible or inexpedient to S\\ itch off the urrent some other method must usually be adopted; but precautions must be taken or else the person rendering assistance will himself receiYe a shock.
To liberate the sufferer from contact-
I. - Insul a t e y o urself fr o m th e earth by standing on an "insulator" or " non-conductor," that is a body which resists the current. Amongst such bodies

143
are indiarubber , dry glass, dry bricks, dry silk , dry cloth, dry wood and dry hay or straw.
2. - Protect your hands from contact with the the electric medium by covering them wlth an msulator. Although indiarubber is the best insulator, do not waste time in runnmg. for indi.aru.bber gloves, but use dry articles of clothmg ; an mdJarubber tobacco pouch or cap or newspaper, would serve to protect the m an emergency. If no means of insulating the hands are at hand an attempt may be made to drag the away by means of a loop of dry rope or a crooked stIck; an umbrella is not safe the meta.l w.ould act as conductors* of electricity, and It IS not mfrequently the case that the" stick " of t he umbrella is a metal tube.
3. - Pull the sufferer away from contact. Care should be taken to avoid touching with naked ha n ds the sufferer 's hands, wet clothing, or boots if t h e soles .are. nailed . The armpits should be avoide d as perspIratIOn usually makes the clothing dam p there.
' Vhen the suff er is removed from contact--
I .-Apply the general treatment for
• A conductor is a through which readily passes. , Amongst such bodies are copper, brass, 1r0n, moi stu re and one s own body.
142
IH sibility (loosen clothing, procure free circulation of air and place in a recumbent position).
2. - Dip a towel in cold water and attempt to arouse him by sharply flicking the face and chest.
3. - Commence artificial respiration if othe·r methods fail to restore animation. "Laborde's" method ( see page 1 26) has been found to be very successful.
4. - Treat burns if there are any (see pa.ges 10 3, 1°4)·
EFFECTS OF LIGHT ING.
A person struck by lightning: is us-ually more or less deprived of consciousness. The treatment IS the same as tha.t for electric shock, except, of course, that the instructions for removin the patient from contact with the electric medium do not apply.
QUESTION Or CHAPTER V.
Tile numerals indicate th e 'lvlure tile answers may be found.
'''h at are the two system . of neryes? ... ..
Of what is the cere bro-spinal sy ·tem made up?
What is the spinal cord?

In what system of artificial respiration is the patient laiel
what ystem is he laid on
back or side?
what ystem i he rolled alternately on hiS side and face
Would you ex:tmi:1e the patient to see if any bones were broken?
wrong opinion may be formed when the
Is collapse from drink a seriou condition?
What i concu ion of the brain?
145
...
\Vh at are nerves like? I';\CE 117 117 117 118 II8 Explain .he sympathetic system Explain the respiratory system Explain the acts of r espiration I I to 120 120 How are
expQ.nsi on
the chest effected? ." ... ... 120 to 121
the
and contraction of
upwards? ... . .. In
on hi
.. , In
": !21 123. 126 127 h
downward ? ... ... 139. 140 How long should artificial respiration be persevered with? 127 What i exciting respiration? 12 7 \Yh at i inducing circulation? 12 7. 128 \Vhy is it nece sary to watch the patient? 128 I row may insensil)ility ari..,e? ." 128 'ta te the yariou forms of insensibility 128 the general rules for treatment of insensibility 12 to 13 1
bac·k
what ystem is he laid
back?
hi
... . " \Yhat
smells of drink? 129 130 13 1 13 1
patient
.. , ... State the rul es for treatment of concussion 131, 13 2
What danger accompanies injury to the head?
What caution should be given to a patient who has ].ost consciousness, even for a moment, after an injury to the head?
What are the , causes of compre.sion of the brain?
In what aged people does apoplexy usually occu r?
What are the signs and symptoms of compression and apoplexy?
State the rules for treatment of these conditions ...
What danger is there in applying hot water bottles to insensible persons, and what precautions should be taken? ... 132
Describe a Case of epilepsy 132, 133
What special care must be taken in treating a case of epilepsy? 130,
Describe a hysterical fit
How would you treat a hysterical fit ?
What are the commonest physical causes of shock?
What may produce shock or fainting?
What conditions do certain poisons bring about?
What may bring about fainling or colJapse?
How would you recognise the general condition of shock?
'What special precaution must be taken in the case of collapse?
State the treatment for shock, fainting (syncope) and collapse ... 135, 136
What is the effect of sugar on the temperature of the body?
\Vhat are the causes of sunstroke and heat·stroke ?
State the treatment for and heat ·stroke
\Vhat are the caus es of convulsions in children?
What are the signs of convulsi in children? .. .
State the treatment for convulsions in children .. .
State fully the causes of asphyxia ...

What two things have to be d one In all cases of asphyxia?
What two things must be seen to before It IS possible for artificial respirat ion to do any good? :.. . Is artificial respiration likely to d o any good If the pas ages are obstructed, or if th e re is not abundance of fre sh air?
What is the first thing to do in a drownIng?
By what method may a rti fic!al respJratlOn be performed without taking any prevIous ste ps?
"'hat ste ps must be take:: before proceedmg with ilvester's method?
\Vhat should be done while artificial re spnatlOn IS bemg perform ed ?
Stat e the treatment for strangulation
S'tate the treatment for hanging
State the treatment for smothering
tate the treatment for ...
How may a swelling of the tissues of the throat be caused?
State the treatmen t for swelling of the tIssues of the throat
for suffocation by smoke or
How would you liberate a suffe rer from contact wIth an electric medium?
What would you do when the sufferer was rem oved from contact?
What would you do in the case of a hghtmng stroke?
PAGR 13 1 13 2 13 2 13 2 13 2 13 2
13 2 133 133 134 134 134 134 134 135
136 136 136, 137 137 137 137 13 3 147 P G»
.. . ... ... ':'. "'. 13 8 , 139
... .., ... ... :.. ...
... : .. .,.
... ... ':'. . .
... ... ...
... ... ... ... .... ... . ..
.. , ... ... ... ... . .. 139 139 139 139 139 141 State the treatment
gases 141. 142 H ow is electricity conveyed? ... ... ..... .. 14 2
.. ,
14
."
2 , 143
.. .. ... . .: .
CH APTER VI.
PO I SON I NG.
Poisons may be classified according to their treatm ent under two heads :-
I.-Those which do not stain the mouth and in the treatment of which an emetic is be given. Amongst these are :-
(a) Arsenic, Phosphorus (contained in rat poison and lucifer matche), Tartar emetic and Corrosive ublimate, \\ hich cause a metallic tas te in the mouth and a burning pain in the mouth, throat and stomach.
(b) Strychnine, Prussic Acid, Belladonna (deadly nightshade plant) and several other vaneties of plants, such as laburnum seeds, etc.; these g ive rise to convulsions, deliriulll, failure of respiration and collapse.
(c) Poisonous meat, fish and fungi (often mistaken for mushrooms). Suspicion of these poisons should be directed to cases \\ her e several persons who have partaken of th e same food develop similar signs and symptoms.
(d) Alcohol, which may cause collapse.
(e) Opium and its preparations, Morphia,

149
L audanum, P aregoric, Chlorodyne, yrup :>f Poppies and various soothing drinks a nd cordials; these cause a tendency to go to sleep, which continues until sleep becom es deep and breathing sterotorus ; the pupils of the eyes become minutely contracted (pinhead pupil ).
Those which burn or stain the mouth, and In the treatment of which no emetic is to be given, These are of t\\·o classes :-
(a) Ac ids, such a 1 itric Acid (A.qua fortis) r Sul phuric Acid (Oil of Vitriol), Hydrochloric, or Acid ( pirits of al t), strong Carbolic Acid (Phenol), Oxalic Acid y which is contained in oxalate of potash , salts of orrel, sa lts of lemon and som e pO'lishing pa te .
(b) A lkalis, such a Caustic Potash, Caustic Soda and Ammonia.
Smv[l\IARY OF DIPLE DIRECTIONS FOR THE TREAT:'IIENT OF P r.lj
I. - Send for a doctor at once, s t ating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali,

150
promptly give an emetic- that is, make the patient vomit as follows : -
(a ) Tz'ckle tile back of the th?'oat with t he fi nger or with a feather.
(
b) Mustard- a dessert-spoonful in a tumblerful of luke-warm water.
(c) Salt-a table-spoonful in a tumblerful of luke-warm \Yater.
(
d) Hi'm-for a youn a child a teaspoonful repeated at of 'fifteen minutes .
3. - In all cases when the patient is not insensible, give Milk , Raw Eggs beaten up with milk or water, Cream and Flour beaten together, An imal or Vegetable Oil (except In poison ing ), and Tea.
. Oln·.e, alad, and Cod-liver oil, or oil such as that m. which sar?illes. are preserved, may be given j mmeral mach Ine ods and paraffin are unsuitable. is .soothing, and is therefore especially useful in p OIsonmg by Acids, Alkalis and such substances as A rsenic and Corrosive Sublimate. Demulcent drinks, s uch as barley ,yater or thin g ruel, act in the same manner, and are free from danger in cases of phosp horus poisoning.
These may be given either before or after the emetic if the poison calls for one.
Strong Tea acts as a neutraliser of many pOIsons, 151
a n d is always safe. A handful of tea should be t hrow n in to a kettle and boiled.
4. - If the lips and mouth are stained or burned give no emetic, but -
( a) If an Acid is known to be the poison give a n Alkali at once . First wash the mouth out freely with lime water or other alkaline mixture, such as soda, chalk, whiting, or magll es ia or wall plaster in water, and afterwards let the patient sip a little of it. Soda and potash are not to be given in the case of poisoning by oxalic acid.
(b) If a strong Alkali IS known to be the poison give an acid at once. First wa. h the mouth out freely with lemon juice or vinegar diluted with an equal quantity of water, and afterwards let the patient sip a little of it.
I n both cases give oil (Rule 3)'
5. - When a person has swallowed poison and to go to sleep , keep him awake by him about and slapping his face, neck a nd chest wlth a wet towel. Strona black coffee may b e given to drink . Slappin a the of t he feet ma y also be tried. b
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7·- A pply .artificial respiration if breath ing cannot be dIscerned.
8. - Treat shock and collapse.
9·- Preserve any vomited matter food
J>r . other substance, suspected of P?lson . not wash vessels which may have contamed the pOlson, and carefully guard them.
Certain poisons require special treatment, and a few of the com moner of these are mentioned below with their treatment.
CARBOLIC ACID.
The odour of the breath will aid in the detection of this poison; the lips and mouth are usually stained white, and several nervous symptoms come on.
1.- Give milk, to a pint of \\ hich half an ounce of Epsom alts has b een added.
2.- Treat according to the general rules.
PRUSSIC ACID.
The action of this poison is extremely rapid. Giddiness, staggering, insensibility accompanied by panting respiration, profound collapse and possibly convulsions are the general signs, and in addition a smell of bitter almonds is often present.
TREAT::\IE:\TT.
I.-Place the patient in the open air.

153
2.-Dash cold water on the head and spme contmuously.
3.-Apply artificial re pimtion.
4.-Hold sl1elling salts to the nostrils.
5.-Treat shock and collapse. (ee page 135.)
POISO:\TOUS IEAT, FISH A);,D FU;';'GI.
The signs and symptoms are vomiting and purging (diarrhrea), colic, headache, great weakness, raised temperature and a quick pulse.
TREATMENT.
1.-Give an emetic.
2.-\Vhen the emetic has acted, give castor oil.
3 -Treat collapse. (ee page 135.)
TRYCHNINE.
. !he signs and symptom are a feeling of suffocation, lIVId features, and convulsions. The patient rests on his head and feet, and the body is arched.
TR
I.-Give an emetic.
2.-Apply artificial respiration.
ALCOHOL.
I.-Give an emetic if the patient can swallow.
2.- Treat collap e by keeping the patient \\'arm, etc. (See page 135 .)
152
QUESTIONS ON CHAPTER VI.
The num erals iudicale the jages wiw'e tite answers mq be found .
Un der what two heads may poisons be classified?

CH APTER VII. BANDAGING.
What other poi ons give rise to the same symptoms?
\Vh at are the symptoms of poisoning by arsenic? PAGE 148, I49 148 14 8
What poisons give rise to convulsions, delirium, failure of respiration and co\lap e? ...
If several people who had partaken of the same fooC: developed similar signs and symptoms, by \\ hat you suspect they had been poisoned ? 148
What condition may result from poisoning by alcohol? 148
What a re the effects of such poisons as opium ?... 148, 149
'What two classes of poison burn or stain the mouth? ... 149
\V ould you give an emetic for such poison ? 149
Nam e some of the principal acids 149
Name some of the principal alkalis 149
State the general rules for the treatment of poisoning 149 to I5 2
Stat e the best methods of making a person vomit
How would you treat a case of acid poisoning? ...
H ow would you treat a case of poisoning by an alkali?
State the signs, symptoms and treatmenl of carbolic acid poisoning ...
State the signs, symptoms and t re atment of poi oning by
State the signs, symptoms and treatment uf poisoning by p oisonous
State
WhAt would you d o in the case of alcoholic poisoning? 15 3
Esmarch's Tri angular Bandage has been described m Chapter II. It may be applied to keep a dressing on a wound, burn or scald of any part of the body, or for an injury of a joint .
For the Scalp (Fig.
62). F old a hem abo ut I i inches deep along the base of a bandage; place the bandage on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down at the back; carry the two ends round the head above the ,=ars and tie them on the forehead; dr:lw the point first downwards, and the n turn it up and pin it on to FIG. 62. the bandage on the top of the head .
For the Forehead, Side of the Head
, Eye, Cheek, and for any part of the body that is round (as the arm or thigh, etc .) the narrow bandage should be used, its centre being placed over the
!54
Acid 152 ,153
150 151 151 15 2 Prussic
.. .
food
signs, symptoms an d treatment
153 Strychnine 153
the
of poisoning by
15& dressing, and the ends being carried round the head o r limb, as the case may be, and tied over the wound. For the Shoulder (Fig. 63)' P lace 'entr f a bandage on the shoulder, \\ ith the pOID J:unnmg

FIG. 63 . FIG. 64-. up the side of the neck; fold a hem along the base; carry the ends round the middle of the arm and tIe them. Place one end of a broad bandage over the point of the first bandage and sling the arm by carrying the other end over the sound shou l der a d tying the ends at the side of the neck; turn dO 'wn tnrpoi nt of the first bandage, draw it tight and pm J •
157
For the Hip (Fig. 64). Tie a narrow bandage round the body above the haunch bones with the knot on the injured side. Fold a hem to the size of the patient alollg the base of a second bandage; place its centre over the dressing, carry the e n ds round the thigh and tie them; then carry the point up under the
FIG. 65. FIG. 66. first bandage, turn it down over the knot and pin it.
.For the Hand when the fingers are extended (FIg 05) , Fold a hem along the base of a bandacre . la h' h b ) P c e wnst on .t e hem with the fingers towards the pomt; then brIng point O\'er the \\'rist, pass the ends the wnst, cross and tie them; bnng he pomt oyer the knot and pin it to the andage on the hand.
For the Foot (Fig. 66). Place the foot on the centre of the with the toes towards the point; draw up the pomt over the instep, bring the ends fOIward and cross them; now pass the ends round

FIG. 67a. FIG. 6jb.
the instep and tie th em. Draw the point forward and pin it to the bandage on the instep.
For the Front of the Chest (Figs. 67 a and 67 b). Place the middle of the bandacre over the dressing with the point over the shoulder the same side j carry the ends round the waist and tie them j
159
then draw the point over the shoulder and tie it to one of the ends .
For the Back. The bandacre is appli.ed as the foregoing, except that It IS begun at the back.
For the Knee. Fold a narrow hem along the base of a ba.ndage i lay the point on the thIgh and the mIddle of the base just below the knee-cap; cross the ends first behind the knee then over the thigh and tie 'them. Drin cr the point down and pin it to the base (Fig. 68).
For the Elbow. Fold a FIG. 6 . narrow hem along the base of a bandage; lay tbe pomt on the back of the arm and the middle of rhe base on the back of the forearm j cross the e n ds first in front of the elbow, then m·er the arm and tie them (Fig. 69).
the and Toes \\ rap a stnp of calIco or lll1tn round and round the pal t; split the free end, secure it round the wrist or ankle.
FTG. 69.
15 8
CHAPTER VIII.
METHOD OF CARRYING
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
1.-Two bearers face each other behind the patIent and grasp their left forearm with their right hands and

FIG. 70.
other's right forearm with their left hands (FIg 70), and stoop down.
2.-The patient sits on the hands and place one arm round the neck of each bearer.
3·-The bearers rise together and step off, the bearer On the right hand sIde of the patient \\ith the right foot, and the left-hand bearer wIth the left foot.
THE L\T.
ThJS seat may be used to carry t:!. helpless patient
FIG. 7I.
1.-Two bearers face each other and stoop, one on each side of the patient. Each belIer passes his forearm nearest to the patient's head under his back just G
160
161
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig. 7I), and clasp their hands by one of the methods shown in Figs. 7 2 and 73. A handkerchief should be held in the hands if the first grip is used.

2.-The bearers rise together and step off, the right-hand bearer with the right foot, and the left-hand bearer with the left foot (Fig. 74).
THE THREE-HA TDED EAT.
This seat is useful for carrying a patient and supporting either of his lower limbs, wh en he is able to use his upper limbs.
I.-Two bearers fac e each other behind the patient. For supporting the left 11mb the bearer to the patient's right grasps his own left wrist with his right hand, and the other bearer's right wrist with his left hand. The bearer to the left grasps the fir t bearer' right wrist with his right hand (Fig 75). This leayes his
162
FIG. 72. FIG. 73.
FIG. 74.
G l'
ldt hand free to upport the patient 's left leg . For the patient's righl lo"Yer limb follow the same directions, substituting "right" for" left " and" left" for " right." The bearers stoop dm\'n.
2,-The patient places one ;nm round the neck of each bearer and sit on their bands.
3,-The bearers rise to 'Tethe r and step off, the

right -hand bearer wilh the right foot, and the left· Gand bearer ,,,ith the left foot.
THE FIRE:\L\N'S LIFT.
(To be attempted only by a strong man.)
Turn the patient face do\\ nward : place yourself at his head, stoop do\\'n, slightly raise his head and
164
FIG. 75.
166
snoulders and take hold o f him clos e under his armpits, locking your hands on hIS bac k. Rai se his body and rest it on your left knee; shift yo ur a rms and, taking him round his wa ist, lift him un til his head rests on your left should e r. Thro\\" b is left a r m over yo ur h ead, stoo p d own a nd pl ace yo ur left a rm betw ee n his thi ghs, le tting h is body fa ll across your should ers. Ris e to a n u p ri gh t position ; hold t b e pati ent's left wri st wi th yo ur left h and a n d lea ve yo ur ri ght h an d fr ee.
Ass ista n ce m ay be gi ve n t o a n in jured person by suppor ting hi m in th e m a nn er sho wn in F ig . 76 .
Th e plalZ of can:l li71l[ the jatt"mt the arms alld It:r;s w i tlt the f a ce dO'Z(lJlwards, called the "frogs' m a r ch," mltst never be used, as deatlt may ellSltf from this t reatment.
bI PROVISED STRETCHER ._
.
A str etch er may be imp r ov ised as follows:-
I. - Turn th e sleev es o f a coat insi d e out; pass t \Y o stron g poles thr ou g b tb em; button t he co a t. T he pati ent sits on th e b a ck of th e coat a nd rests agai nst the back of the front bearer (Fig. 78 ). If a longer stretcher is - req uired two or three coats mu st be treated in the same manner. The pol es may b e k ept apart by strips of wood lashed to th e pol e s at both ends of the bed formed by the coats (Fi g. 79).

FIG. 77.
THE F O RE AND AFT METHOD.
This plan of ca rr yin g is useful when space does not permit of a hand seat.
167
FIG. 79.

2.- :\lake holes in the bottom corners of o n e cr two sack and pass. tout poles through them.
3.- S pread out a l.:i.rge piece of carpet, sacking , tarpaulm, or a strong blanket, and r oll two stout poles up in the sides . T\\'o bearers stand on each side and grasp t:-:e middle of the pole \yith one halld, and ncar the end \\ ith the other. They walk side\\ ays .
4 .-A hurdle, broad piece of wood, or shutter may be uc,l:U as a trctcher; some straw, hay, or clothing should be placed on it, and covered \yith a piece o f stout cloth or sacking; the latter is useful in taki n g th e patient off the stretcher.
Always test a n improyised stretcher before use.
Stretchers must be carried, a n d the patient placed on them , as laid dO\\'ll in the" tretcher Exercises. /I
As a general rule carry the patient feet foremos t.
T he exceptions are :-
(a) , \'hen going up hill with a patie n t whose lo wer limbs are not injured.
(b) " Then gomg do\\ 11 hill \\ ith a patient who se lower limbs are injured .
Avoid lIftmg the stretcher oyer ditches or \\"alls , b u t " 'here these can n ot he avoided the stretche r m u st be rarr ied in th e follo\\ i n g ways :-
T o CROSS A D ITCH .
In c r os s in g a d itch the stretcher should be low ered wit h its foot one pace from the edge of t he ditch
16
9
Nos. I and bearers then descend. The stretcher, 'vyith the patient upon it, is afterwards advanced, N os. I and 2 in the ditch supporting the front end while its other end rests on the edge of the ground above. No . 3 now descends. All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by 3 the ditch . No . I climbs out, No . 2 renJamll1g 111 the ditch to assist NO . 3. The stretcher is lifted forward on the ground above, and rests there while Nos . 2 and 3 climb up.
To
CROSS
A 'VALL .
The stretcher is lowered with the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the wall. No. I then climbs over the \Yall and hold of the foot of the stretcher, while Nos. 2 and 3 support the head' the stretcher is then carried forward till the head'rests on the wall, No . I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
• These numbers are explained later in the detailed "Stretcher Exercises."

17 1
T o LOAD A ' VAGON.
The stretcher is lowered with the foot one pace from the end of the wagon. N os . I and 2 take hold of the foot of the stretcher, No. 3 the head .. The stretcher is then rai ed and carried forward tIll the front wheels rest on the floor of th e wagon. No. I th en jumps into the ,,'agon, ",hile No, 2 goes to the head of the stretcher and helps NO.3. The is then pushed slowly into the wagon. If the tallboard cannot be sh ut, the stretcher 111 Ilst be lashed fi r111l y to the sides of the \\ agon,
To U 1 LO,\ D A 'VAGON.
Nos. 2 and 3 take hold of the head of the whlle No. I gets into the wagon; the stretcher IS then gradually drawn out till the foot-wheels rest on the edge of the wagon. No. I jumps out Of. the wagon, and with No.2 .takes hold of the, foot 01 the stretcher, o. 3 support111g the head. 1 he stretcher is now gently dra\\ n a\\"ay one pace lowered.
'Vith four bearers Nos. I and Z ,,'ould lIft the foot of the stretcher, \\hile Nos. 3 and 4 lift the head. This applies to cro sing a ditch or \\ all. as well as to loading ano unloading a wagon.
170
CHAPTER IX.
STRETCHER TRANSPORT.
The ( Model 1899) are of three patterns, VIZ., "Ordl11ary " "Telescopic-handled ,. and "Police. " In general principle they are the c omponent parts being desi gnate d the poles,

Fig. 80. -0 RDINARY STRETCHER-CLOSED.
Fig. 8r.-TELESCOPIC·HA;-';DLED TRETCHFR-OPEN.
handles, jointed trayerse bars, foot \\'heds, bed, pillo\\ sack and slings.
The Ordinary Stretcher (Fig. 80), is 7 feet 9 inches 1Il length , and I foot TO inches wide. Th e bed is 6 feet in length, and the handles 10.; inches. Th height is S-f inches. At the head of the stretcher is a c,:nvas oyerlay (the pillo\\' sack) which can be filled wIth hay, clothing, etc., to form a pillow
The ]oll1ted tra\'erse bars are prm'ided with joints.
tor opening or the ::.tretcher. The Telescoplch.mdled pattern S I) IS ,'ery similar, but the handles can be slid underneath the poles, thus reduclI1g the to 6 feet . This arrangement is of great value \\ h >n \\"orking in confined sp:(ces, or when a p:ltient has to he taken up or do\\ n a narrow stalrC:lse 'nth sharp turns. The Police stretcher is similar to the Ordin:lry pattern, but is more strongly mad, and has, in audition, straps for securIng a refrac tory patient.
'When losed, the poles of the stretcher lie close together, the bars being bent in\\ards, the can\'as bed neatly folded on the top of the poles and held in position by the slings \\ hich are laid along the cam as, and secured by a strap, placed transversely at the end of each sling being pa sed through the large loop of the other, and round the poles and bed.
In c.losin o a stretcher care should be taken to raise the centre of the canvas when pushing in the traverse bar, as it is other",ise liable to get caught.
To prepare, or open a stretcher, unbuckle the transverse straps of each sling; remO'.'e the slings from the stretcher; separate the poles; take hold of each traverse bar and dl::tw it fOf\\ard. The slings \\,111 then be folded to half their length, one being laid neatly 0'. er the handles at each end of the str tcher.
.\ ::t general rule the stretcher \\ III be prepared by N -.>s. I and 3 be::trcrs in Exerci es I., II., and III.;
174 and by No. 2 in Exercise IV. Th ese bearers will, however, if required, assist th e other bearers in attending to th e patient's injuries.
Note.- The various movements detailed in the followin g Exercises should be carried out steadily, th e bearers working in uni son, hurrying being carefully avoided, and every attention being paid to the _:":-lrcr \\"ho gives the words of command.
STRETCHER EXERCISES,
O riginally dra,Yn up by ir John rurley, and revised in I 904 to accord \\'ith the drills adopted by the Roy al Army ::\Iedical Corps :-
EXERCI E No. I.
FOR FOUR BEARERS .
1. - The Instructor selects the bearers and numbers th em-I, 2, 3, 4- at his discretion . hould one man be taller and stronger than the others, he should be s:yled 1-0. 3, as he will have to bear the heayier part of the burden.*' All orders will be gi,'en by No. -1.
2.-" Fall in." -Nos . I, 2, and 3 take position on the left side of and facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, N O.3 at the patient's shoulders. At the same
• B ea re rs should, however, be taught to take any of the positi ons named in the following Exercises, whether that of No. I, 2,3, or 4 bearer.

175
time No. 4 places the prepared stretcher on the ground by the ri ght side of the patient about two 82.
paces away from him, and then takes position opposite to and facing NO.2. (Fig. 82).
3.- " R ,eady. " - The bearers kn ee l down on the kne e and tak e hold of th e patient, No. I p:lssing hIS hands and forc-:lrms beneath the patient's leer s hands wide apart. N os . 2 and 4 pass th ei r

FIG. 83 . and forearms ben eath [he p:ltient's hips and loms and grasp each a tht-r's hand . No. 3 passes h is hand across the p:ltient's ch est :lnd under the ri a ht shoulder, and his hand beneath the le ft shoulder (Fig 8'))
In
4 . - " Lift. "-On th e word " .Lift," the bearers. raise the patient gently and rest hIm on th e knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as he
FIG. 84·
IS ecurely rested , NO.4 disengages hands with No. runs round by the he:ld of the stretcher and places It mder the patient, close to the other bearers' feet.
17
6
178
being careful that th e pillow is imm ed iately under the patient's head (Fi g. 85); he th en kneels down and locks his hands with those of No.2 (Fig. 86 ).
5.-" Lower." - The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and then stand up.

FI G. 85.
6.-" Stand to Stretcher."-No. I goes to the foot of the v.:ith his back to the patient; No. 3 to the head wIth hIS face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7·-" Ready."-Nos. I and 3 place the slings (if used) over theIr shoulders, stoop down, and slip the
179
loops of the slings on to the handles of the stretcher, \\'hich they then grasp. . .
As soon as all is ri gh t the word IS gIv en :-
8.-"Lift Stretcher. "-No? I a nd 3 b ea rers raise the stretcher steadily together and stand up.
Not e.- os . 2 and 4 will no\\' adjust the slings t he shoulders of N os. I and j, taking care that each IS well below the level of the collar and lies accurately in the hollow of the in front. They \\ ill also lengthen or shorten the slings, to the patient's injuries and the rel al1\'e heIghts of the bearers.
FIG 86.
9.-" March."- Th e bearers move off :-N()s I , 2, and 4 stepping off with their left foot. and NO . 3
with hIS right foot 87) . The step should be a short one of t\\:enty mches, and taken with bent kn ees and no spnng from the fore part of the foot 10.-" Halt."- The bearers remain steady:

FIG . 8 7.
11.-" Lower Stretcher."-The b earers place he gently on the ground , slip the loops of th e sl.m gs off the handles of th e stretcher, remov th e slIngs from the shoulders, and then stand up.
181
I2. - " Unload Stretcher - Ready." - The be are rs prepare to take the patient off the stretcher, as at Ord ers 2 and 3.
I3.- " Lift." -The bearers raise the patient as at Or der 4 (Fig. 86); NO.4, in this case, disengages hands from N o.2, removes the stretcher ( F ig . 85" and resumes his former position . If necessary, t he bearers will then steadily rise together, and carefully clrry the patient to th e bed, or other place to which it has been arranged to cOlwey him.
I4.-"Lower. "-The patient is car efully lowered
EXERCI E No. II.
FOR THREE BEARERS.
I.-Number the bearers I, 2, 3.
All orders will be si ,- en by No.2, ,,·ho will look after the injured part of the patient's body or limbs, to ee that no band ages or splints become dispbced. and also that TO . I bearer, in liftina or carrying the stretcher, does not touch the patient's feet.
2. - " Place the Stretcher. "-No. 3 places the stretcher in a line with the patient's body, the foot of the stretcher being close to his head.
3. -" Fall In." - TO. I places himself on the left side of the patient in a lin e "ith his knees, No.2 on th e left side ju st below the patient 's shoulders , and No. at the ri ght side, and faces Xo. 2.
180
182
4.-"Ready." -All kneel on the left knee. No. I places his hands, well apart , underneath the lower limbs, always taking care, in case of a fractu re, to have one hand on each side of the seat of injury. N os. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient (Fig. 88).
1

FIG. 88.
5.-" Lift."- The bearers rise together, keeping the patient in a horizontal position (Fig. 89).
6.-" March." -All take short side-paces, carrying the patient over the stretcher until his head is immediately above the pillow.
183
7. -" Halt."-The bearers remail1 steady.
8. - " Lower." - The bearers stoop down, gently place the patient on the stretcher, disengage their hands, and then stand up.
FIG. Rq.
9.-"Fall In. "-No. I places himself at the foot of the stretcher with his hack to the patient, No. 2 places himc:;elf at the le ft ide of the patient and No. 3 at the head, \vith his face towards the patIent.
I 4-
10.-" Ready." -Nos . I and 3 place the slings (if us ed) over their shoulders , stoop down, and slip the lo ops of the slings on to the han d les of the stretche r, which they then grasp.
As soon as all is right the word is gi\'en-
II. - " Lift Stretcher."-Nos . I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now udJu t the lings on the shoulders o f Nos. I and 3. taking care thut each is \\ ell below the le\'el of the collar, and lies accurately in the hollow of the shoulder in front. IIe will also lengthen or short en the slings, ha\'ing regard to the patient's injuries and the relati\'e heights of the bearers .
12. - " March."-N os. I and 2 step off with the left foot, and No. 3 with the right. The step should be a short one of 20 inches, and taken \,ith bent kn ees , and no spring from the fore part of the foot.
13. - " Halt."-Th e bearers remain steady.
14. - " Lower Stretcher." -The bearers place the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher, remove the slings from the shoulders, and then stand up.
IS. - " Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, as at Or de rs 3 and 4 (Fig . 88),
16.-" Lift."- The bearers raise the patient, as at Ord er 5. all d carry him by short slde steps, clear the stretcher, to the bed, or other place to whIch It has been arranged to convey him (Fig. 89).

18 5
I7.-" Lower."- The patient lS carefully lowere d.
EXERCI E No. III.
WHEN ONLY THREE BF<2ARERS ARE AVAILABLE AND THE TRETCHER C.\:\,XOT BE PLACED AS IN EXERCISE II.
I.-The In tructor numb ers the bearers-I, 2, 3. All orders will be gi \'cn by NO.2.
2. -" Place the Stretcher. "-No. I taking the foot of the stretcher, and 1 o. 3 the head, place it on the ground by the side of the patient, and as close to him as practicable.
3.-" Fall In." -The three hearers take the same positions on one side of the patient, as laid down in Exerclse o. 1.
4. -" Ready. " - TOS. I 2, and 3 kneel down on the left knee, pbcll1 r them eh'es as close to the patient as they com'cniently can, and then take hold of him as directed in Exercise Xo. 1.
5. -" Lift. "-Nos. I, 2, and 3 mise the patient as directed in Exercise :t\o. I, and then move in a kneeling position up to the stretcher.
6.-" Lower. "-The hearer bend forward, carefully lower the patient on to the stretcher, and disengage hands.
7.- " Stand to Stretcher."-All the bearers stand up; No. I goes to the foot, No. 2 remains 111 position at the side, and No. 3 goes to the head of the stretcher.
8. - " Ready."-Nos. I and 3 place the slings (if used) over their shoulders, stoop down, anrl slip the loops of the slings on to the handles of the s tretcher which they then grasp. '
9. -" Lift Stretcher. "-_ os. I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now adjust the slings on the shoulders of Nos. I and 3. taking care that each is well below the leyel of the collar, and lies accurately in the hollow of the shoulder in front. He will al 0 lengt h en or sho rten the slings, having regard to the patient's injuries and the relative heights of the bearers.
10. - " March ."-Nos. I and 2 step off with the left foot, and No. 3 with the right The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
11. - " Halt."-The bearers remain steady.
12. - " Lower Stretcher. "-The bearers place the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher remove the sli ngs from the shoulders, and then up.
13. --" Unload Stretcher - Ready. "-No. I places hi!'l1self. o n the left side of the patient, and in a lme wi t h h.IS knees, No. 2 on the left side just bel ow th e pati en t's sh oulders, a n d N O.3 at the r ight

side, and faces NO.2. All kneel on the left knee. No. I places his hane's, \Yell apart, underneath the lower limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of injury. Nos. 2 and 3 gra P each other's hands under the shoulders and thighs of the patient.
14.-" Lift." - The bearers rise together to their feet, keeping the patient in a horizontal position, and carry him by short . ide clear of the stretcher, to the bed, or other pbcc to which it has been alT1.nged to convey him.
15·-" Lower." - The p:1tient is carefully lowered.
EXERCISE IY.
FOR USE 1:-" AXD TARRO\\- CUTTIXGS \\ HERE
T \ 0 ::\h." O,LY C\X DE E;\'GAG£D.
1\05. I and 2 \\"111 carefully place tbe stretcher in a 1ll1 e \\itb the injured man's body) the foot of the stretcher bCJI1rY, if possible,* dose to his head.
o. I stradJles acro-,s the patient's legs, placing his ricrht foot, with the toe turned outwards, a little below the knees and with the toe of the left foot dose to the heel of TO. 2; he then stoops down, passes the left hand under the patient's thighs and
• It is not advisable to be too particular as the head or foot of a stretcher in a mine, as it would prob\l.bly be quite imp(')ssible to reverse it.
186
I ' , the right hand. across and unuer the patient's calves, No. 2 hIS feet one 011 each sIde of the patient between hIS body and arms, the toe of each foot as near the armpits as pos ibJe. He then stoops down and passes hIs hands between the sides of the chest and the arms underneath the shoulders, and locks

FIG. 90.
the fingers (Fig . 90) . If the patient's arnlS are unin jured he may put them round the neck of TO. 2, and by this means greatly assist him in lifting.
I I)
'When both are ready, No. I will give order "Lift and move forward ." The patient IS then to be slowly lifted just sufficient to allow his body to clear the stretcher. 'Both bearers will slowly and gradually move the patient forward, ' TO. 2 by very short steps. No. I by bending his body forward as rnuch as he ,can witllOltl moviJ/g llis feet (Fig. 9 I). TO. I. now gIves the order " Halt " "'hereupon 1 TO, 2 remams steady, and o. 1 ad,'ances his right foot to his left, and
IG . 91.
again ad,'anccs his left fov till the toe touches the heel of ::';-0. 2. No. I then the order " Ad v ance ," when the patient will again be forward. These mO\'cments are to be repeated until
2
F
the patient is over the stretcher, when he is to be gently lowered.
The following Stretcher Exercise is adapted by permission from the Royal Army C orps l\Ianual, 1908.
All orders will be give n by N o. -to
1. "Fall in."' ix bearers fall In behind each other.
2. "Number."- The bearers number from front to rear.
3· "No·3 Bearer, right (or left ) turn - supply stretcher - quick march."-?\o. " bcarer will march to the stretcher, stuop, lay hold of it and place it on his right shoul ler at the slope, holding it by the lower fool wheels, wheels to the front. As soun as the bearer is provided \\ ith a stretcher, he will turn about and rejoin his squad in quick tIme, halting as he arrives in his place. He turns to the front, and, passing the low er end forward, places the stretcher on the ground to the right of the squad, \\ heels to the right, front end of the poles in line \\ ith the toes of No. i and rises.
4. "Stand to Stretcher."-?\o. 1 places himself with his toes in line with the front ends of the poles. No. 3 with his heels in line with the rear ends of the poles, close to and touching the stretcher with

95.
FIG·92
FIG. 93.
FIG. 94.
FIG 96.
m rn C!J rn @J
i m
m G @J @J
19 1 / rnJ @J @J .' , ,\' . ' m, '.'. ., 1 \ ""'i'O I \ " I , ' I : •. -' I 1\ 0 U \ \ '. \ '\ '. I' \.' .•. " 't I.?.i /'
I' I " I rn I I I' 3 ,I. I .': .,. , /,1 , r .. , 2 : 'of, ,1 ' • "'.1 j " : " I ,_ •• , /1 , ''\O'l : 5 : 1 ' I..... I tl /1 "if' ,'/ , /'
FIG.
his. foot . N os . 2, 4, 5 and 6 take up their posltlO ns one pace behind and covering off the bearer in front them (Fig. 92'. -
5· "L1ft Stretcher. " - N0S. I and 3 stoop, grasp both handles. of the poles \\ ith the right hand, rise together holdll1g the stretcher at the full extent of the arm, wheels to the rwht.
6 " I:) . Collect Wounded - Advance ." - The squad by the shortest route to the patient, halt \\·lthout further \\"orJ of command one pLlce trom the head of and in £lIme with the patient (Fig . 9").
7· "Lower Stretc.her. " - as . I and 3 place the stretcher qUIetly on the ground, and rise smartly together
8. S t retcher. " - O. I and 3 turn to the nght, kneel on the left knee, unbuckle the straps, and place the slin.;s on the around beSIde them, separate the poles, and straighten the traverses.
T'i.oo. On the \Yord two each takes a slin(r doubles it on itself, slips the loop thus formed ont:>'the near handle, and places the free ends over the opposite handle, buckle uppermost. They then rise and turn t o their left together.
' Vhile the s.tretcher is being prepared by Nos. I and 3, the dIsengaged bearers "'ill advance and r ender to the patient such assistance as may be required (Fig. 94) .

I93
The as 'istanct; ha\·jng been rendered, o. 4 "ill give the command-
9. "Load Stretcher. " - The bearers pIa e thcmselve . as fo11o\\s J, 2 and 3 n tIle left, i\os. 4, 5 and 6 on the right of the patient· Nos. I and 4 at the knees, 2 and 5 at tIle hips, 3 and 6 at the . houlders, the whole kneeling on the left knee. Nos. I and 4 pa s their hands beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. 95).
10. « Lift. "-The "hole \"ill carefully lift the patient on to the knc'. of Kos. 1,2 and 3'-
Two. No . ..J. 5 and 6 will then disengage, rise; ;\()S . ..J. and 6 step back one pace. o. 5 turns to his left, doubles to the "tretcher, takes hold of and raist:s it, left hane! acros:-- the near pole re'>tlng on the left hip' carrying stretcher, he returns tu his place bet\\llll..J. and 6, and pbc·s it the patient.
TI1N('. 1\os . ..J. and 6 ,>lep fUf\\arc1 one pace, and together \\ Ith • 5 kneel do\\ n on the left knee, and prepal'l.' to assist in lowering the patient (Fig. 96).
II. (( Lower. "- The patient is lowered slowly <lnd lyon to the entre of the cam-as (pecial rare I>ein! taken of the injurec1 part).
1;t'o. The bearers rise; Nos. I, 2, 3 and 6 turn to the left j Ko . ..J. and 5 to the right; H
No. 4 places himself thr ee paces in fr ont o f the stretcher. No.6, having collected the kit and arms of the patient, places himself three paces in rear o f the stretcher, Nos. 2 and 5 opposite the centre of the stretcher. The \yhole are now ready to lift stretch er and move off (Fig . 97).

Fig. 97 Fig. 98 .
195
12. "Lift Stretcher. " -N os. I and 3 stoop, grasp the doubled sling midway the poles ,,·ith the forefinger and thumb of the nght band, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between hal:dles, and place the sling over the shoulders dIvIding It equally, buckle to the right. The slings should be placed . so that they lie well belm\' the collar of the coat behmd and in the hollo\\' of the shoulders in front. In the event of the slings requiring to be adjusted, either as r egards length or for the greater comfort ?f the bearers, NO.4 \\ ill detail a bearer to carry thiS out, th e length of the slings being adju ted, when necessary, by means of the buckles.
Two. os. I and 3 stoop, slip the loops oyer the handles, commencing \\ ith the left, and grasp the han dles firmly.
Three. os. I and 3 rise slo\\'I)' together, No. 3 c onforming closely to the movements of No. 1.
13. "Advance. "- N os. I, 2, 4, 5 and step off \\'ith the left foot, TO. 3 with the right, steppltlg short, kn ees bent, feet raised as little as possible.
14. "Halt. " -The whole halt.
IS. "Unload Stretcher. " -The bearers place themselves in the same position at the stretcher as d escribed for Loading (Or der 9).
16. "Lift. " -As described for Loading (Ord er 10), HZ
194
o
196
except tha t th e st r etche r is ca rri ed fOflya r d t hree paces clear of th e pa t ient 's fee t.
17· "Lower. ,. - T he pati e nt is gently lowered to the ground. T he beare r s dise ngage, rise; os. I, 2 and 3 turn t o the left, 4 , 5 a n d 6 to the right, and the wh ole step off to their places at t he stretcher, as at Order " tand to 'tretcber II (Fig. 9 8) .
The Ashford Litter is made up of either of the Furl ey stre t che rs mentio n ed o n pages I]2 and 173, a wheele d und er-carriage a nd a waterproof hood and aproll, o r, i f p referred, a light we t-r esisting ca n vas co yer.
The str e tch er is kept in position on the under-carriage by th e fo o t-wheels, which fit into slot in the sides Gf t he und er-carriage, and it can be removed at pleasure.
The un der-carriage is fitted with a cranked axle, w h ich allows the bearers to pass with the tretcher the wheel instead of lifting it O\'er them.
A t both en d s are two legs which may be turned up as h andles when \\ heeling the lItter. The hood and apron fi t mto so ckets screwed to the stretcher. In ,,'heelin er th e litter , care should be taken to keep the patient a h o ri zontal position . bould it be necessary, t \\'0 beare r s ca n easily lift the litter and patient.
The Rea-Edwards Litter, introduced in 19 0 4,
IS use d in a similar manner. and one model of it is fit t e d with pneumatic tyres, which add immen ely to t h e c omfort of the patient and to the ease of propulsion.

197
CHAPTER X .
(Beillg t he Ftfth Led u re for Females ollly, z";z acco r da nce wdll 5),llal' lfs 58.)
BY E. \ ELL CO GRAVE, :-'LD., F.R.C.P .I.FOR RECEPTlOX OF ACCIDE.XT CASES.
ne\\s of an accident comes, preparatIons sh ould at on e be made so as to hase .eyerythlllg be for e 1 .. ed person is brouullt 111. Of COlllse the pre- t 1e ll1Jur l' h . needful \\ ill vary accorc 1I1g to t e na ture pardatl t of the inJ'ur\' but the iollo\\'ing are the a.n ex n _ , chi f thin<ys whIch may ha\'e to be done.
CHOICE A:\D PREPAR,\TlO. OF RomI.
1\ ·t be chosen In a bad case this shoul d .l rool11 nUL .' __ be one eclsily reached, ,1S It IS clIthcult to carry.an injured per 011 throuuh narD'" passages ar: d Unless there is some reasol1 agamst It) the iniurl'd person ' 0\\,11 room IS best. .
'Tl 'a)' to the room must be cleared, 1e "L . the hall or m lobbIes furniLure and loose mats m ., should be remov-cd. If the tnjurecl person IS 011 a door, shutter, or stretcher, t\\'? strong chaIrs should be placed ready to u,Pport It \\hereve r the bearer. \\ ould be Ekel y to req Ulre rest. h b d
Useless furniture should be removed from tee 11 The bed should be drawl1 out from the wa r oom.
so that both sides be approached, and the clothes turned back to one sIde to their full lenerth A h t bottle should be got ready . If there is colla several hot bottles and hot blankets may be . COVE:r the hot bottles with flannel. '
h If the injury is very if mud-stained clothes ave to. be r.emoved, or If extensive dressings have to be applIed, It may be necessary to have another bed a couch or. a table placed near the bed to by sufferer on In the first instance. This should b that may do no harm; old sh:etSs O water poof materIals thin Ollcloths . ' • , or e"en news paper, may be used as a protection.
LIFTING AND CAR RYING.
. Ifyresent at the place where the accident occurred It wIll be necessary to see that t'ne t· . ' f II l ·f pa lent IS careu y I ted after proper "First Aid /J 1 b rendered. 1:lS een
The following rules should be remembered:- elect the proper num ber. of persons to assist, and do not let them 11ft the patIent until they thoroughly understand how they are to do it.
For .ordinary cases, "here the injured person has to be. lIfted a very short distance, three helpers are Two (\\·ho should be as far as po SIble of equal heIght) are to bear the weierht the th Od . db' Ir IS to support an take charge of the injured part. This is

199
best done by a person who has been through a " FIrst .Aid /J course. If the injured person is insensIble, another helper should support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient's back at the lower part of the shoulder-blades, and under the hips, clasping each his right hand in the other's
The injured patient should, if practicable, place hIS arms round the necks of the bearers.
The third helper should attend to the seat of injury; If this is a fractured limb, he should support it by placing the palms of his hands under the limb, one above and one below the seat of the injury, grasping it firmly but avoiding unnecessary pressure.
The helpers should remain thus until the order " Lift" is given, and then they should all lift slowly and steadily , avoiding jars, attempts to change position of hands, etc .
H the injured person is to be placed on a stretcher or shutte r, this should be previously placed with the bottom e nd at his head; the bearers should then move, one at each side of it, until the patient is over it. The word" Low er " should then be given, and the injured person should then be slowly lowered. A pillow or folded-up coat should be ready, and as the suffere r is lowered this should be placed under his head.*
• Full di rect ions are given in Chapter IX.
198
MEANS OF
.B esides a stretcher, and substitutes such as a gate, a shu tter, or a door, other means of arrying can be im provised .
I n slight injuries, where the injured person is unable to walk, two bearers can carry him by forming a fourh a n ded, thrpe-handed, or two-handed seat.
A four-handed seat is formed as described on p age 160
A three -handed seat is made as described on p age 162.
The two-handed seat is made as de cribed aD page 161.
A single helper can lift by supporting with one arm t he two knees, and with the other the back. The arms must be passed well under beLre commencing to lift.
A single helper can give support by putting his arm round the waist, grasping the hip and placing the mjured person's arm round his own n eck, holding t he hand with his own hand (Fig. 76, p.lge 165).
A capital stretcher can be improvis ed ru t of a strong sheet and two broom handles or other short (Joles. Each ide of the sheet is \\ound up on a broom handle until there is just 1'00111 for a person to lie hetween . This req ui res four bearer, t\\O at each si d e, to prevent the sheet slipping.

201 C,\RRYI);,G UP TAlRS .
In carrying a tretcher up stairs the head should go first, and an extra helper should a. sist at the lower end, a as to raise it and keep the stretcher nearly horizontal.
The t\\ 0, three, or four-handed seat may be used for carr) ing up stairs; or a strong chair, the patient being carried up backwards. In the latter case one h Iper hould \yalk after the chair and help to support it, and to prevent th e injured person slipping out.
LI FTIN 7 I)1TO BED.
If the bed is narro", and there is room th e stretcher should be placed on the floor \\ ith the head close to the foot of the bed. The injured per on should then be lifted oyer the foot ::tnc1 placed on the bed. If the hed is too \\ ide to admit of this, the stretche r should he placed heside it, and h\'o helpers should stand at the far Side of the stretcher. One helper pa se one arm beneath the shoulders and one the midJIt.: of the hack, the other helper placmg hi under the lo\\-er part of the back and under th The injured person is then lifted, another helper pull a\\"ay the tretcher, and after a single stet forward the burden is placed on the bed.
200

PR EPARATIO OF BED.
A firm mattress, not a feather bed, should be selected. If there is much injury, or if dre sings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of t he patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed un ler the draw-sheet. As the draw-sheet becomes soil ed, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fracture of the le g or thigh, sprained ankle and som e other cases, a "cradle" (Fig. 99) should be improvis ed . The use of a " cradle 'I is to support the bed -clothes and keep them from pressing on the lim b.
A band-box (Fig. I 00), three-legged stool (Fig. 10 T), or hoop S:l \\ n across and the two hah'es secured together ( Fig. 102, may be used. A cork crew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, \\·ill relie\'e the pressure of the bed-clothes effectually.
RE:\IO\,ING THE CLOTHI£S.
In t aking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
202
20
---
3
FIG. lO T
In removing a coat, etc .. in a case of fractured arm the arm should be drawn out first.
In on a coat or shirt the injured arm F-hould be put In first.
In burns and scalds nothing should eyer be dragCTed off. A. sharp pair of scissors should be used, not a.dhering should be cut away. If anything adheres It should be left uHtil medical aid

FIG. 102.
can be obtained. The clothing adhering ma\', with advantage, be soaked with oil. To the trousers from a seyerely injured limb, the olltszde seam should be ripped up.
PREPAR,\TIO:\S FOR URGEO",".
As so?n as the in jured person has been attended to preparatIon should be made for the surgeon 's visit.
20 5
The preparations needful \\'ill depend upon the nature of the case. The following hints may be of use:-
A fire in the room helps ventilation, even in summer. There should be plenty of water, hot) cold, and also boiling, also several basins, plenty of clean to\\ el and soap. There should be somethin6 to empty water into; a foot-bath does well. The basins should be placed on a table, covered \\ ith a clean \\ hite cloth' a large to\\ el makes a sUItable cloth; the towels, folded up, Ilould be placed on the same table, and the hot and cold water should be \\ ithin e::tsy reach. The foot-b3.th sho'.lld De under the table or dose at h::tnd.
In the case of a hum, absorbent .:. otton \\'001, soft cloth, old llllen, oil, and soda, should be re.ldy, and ll1:l.l e rials should be torn up for bandages
In the case I)f bremorrhage, plenty of water should be boiled and allo\\ ed to cool, and pads of absorbent cotton \\'001 should be baked in a tin bo\: in the and at lea t t,,'o ba . 1ll should be rc ad,' .
In the case of a llerson rescued fron; drowning the ;heets should be taken off the bed, plenty of blankets should be heated before the fire, and <;ev ral h(}( bottles should be ready,
If poultices are likely to be required boiling water, lll1seed meal, mustard, a loaf of stale bread, a small baSin, a large spoon, s\\ eet oil, and tow, flannel Or handkerchIefs may be required.
204
. For fomentation, have boiling water, fl an nel, a kltchen roller, and two sticks, or a large towel.
When summoning a medical man to all accident al ways let h.i m by a written message what kind of case IS reqUIred to treat, so that h e may bring whatever IS ne e dful. By this means valuable time may be saved.
QU ESTIONS ON CHAPTER X.
Tlte mtmera ls indicate tlte pages where the answers may be found.
Wh . PACK at pomts would you consider when choosing a sick room?
How would you clear the way to the sick' '?'
What me,ans of would you provide for those carrymg a patient on a stretcher? '" '" ".
How would you place and arrange a bed for an accident 197 197 case? ". .,. '" ... '" '" 197, 198
Are h ot necessary, and how would you prepare them.
'Wha,t is often necessary to lay the sutlere; 'on in"the mstance? ". ... ,.. . ..
How would you protect this from gelling soiled'?' ...
How w<;m!d you see to the proper lifting and carrying of an m]u,red person? '" .. ... .. . 198, 199
"What, substitutes for a regular stretcher can you suggest? 200
How IS the four-handed seat made? 160 161
For w.hat cases is this seat useful?" ' 160
How 15 the three-handed seat made? 162, 164

207
For what cases is this seat u eful?.,
How is the two-handed seat made?
For what cases is this seat usefu l ? ,.
How can a single helper lift?
How can a single helper give sup pall ?
How would you improvise a stretcher?
How many bearers are required for this stretcher?
How should a stretcher be carried upstairs?
How would you carry a patient upstairs on a chair?
How would you lift a patient from a stretcher to a bed?
How should a bed be prepared for an injured person? ,
How should a draw sheet be made?
\Vhat would you place under the draw sheet? ,"
What shou ld be done with the soiled part of a draw sheet?
'Vhat is the use of a C( cradle"? '"
In what ways maya cradle be improvised?
How would you rem ove a coat o r shirl in the case of a fractured arm? ",
H ow would you pul on a coat o r shirt if the arm were injured? ".
In the case of a bad burn, what would you do with clothing that adhered to the patient?
How would you remove trousers from a severely injured limb?
\Vhal preparations would you make for the surgeon's visit?
What would you get ready in the case of a burn?
And what in the case of h::emorrhage ?
And what in the case of a person res cued from drowning? . "
'''hat would you get ready for making poultices? '
A nd for fomentations?
What sort of a message would you send t . summon a doct or? .. ,
206
... ... ...
... ... ... ...
.
PACK 161, 162 161
200 165 20C 20C 20 1 201 201 202 202 202 202 202 202 204 204 204 204 205 205 205 205 205 206
I D EX.
Abdomen
" wound of 112 case, preparatlOn for 197 poisoning' 'by 149', 15 1
AIr, a lway necessary ...
Alc ohol, caution as to smell of ... '" 13 0
Alc ol:ol, p<;>i oning by 134,153
AlkalI s, 'pOIsoning by 149, 151
Ammoma, poisoning by 149
Anat om y (e lem enta l)') ... 20
Ankl e ... '" 30, 3 2
" spra ined. .. 64
Anteri o r tibial a rt ery 93
Aorta 79
Apoplexy 13 2
Appa r ent ly drowned, to restore ...
Arm, bone of '" 139 2
" fracture of 52
Arm · lings ... 39, 49
Arsenic, poisoning by 14
Arteri a l hcemorrhaae
" Art eries of 7-J. practising arrest of 7q " signs of 7-J.
Art e ry, axillaI)' ...
" couce of main ... 70 79 5
Artery, brachial. .. carotid dorsal of foot fa cial femoral ... iliac occipital plantar poplillal ra dial ,' u bcla \'ian tibial tempulal " ulna! '"
A phyxia
Atlas ... Auricl es ... Axillary arte ry Axis ..
Hack. handage fur BacklJOne
Bandage, to apI;I) " to fold " to i m pro\ i l:
Bandaging ..
Bed, lifting into... .. " preparation of . Belladonna, poioning by

Bites of rabd ammals 106
Blad cer ... 11 I, 113
Brachial artery ... 86
Brain 1 17 corn pres ion of 13 2 " concussion of 13 1
Brea t-bone 26 " fracture o f 4
Broad bandage ... 37
Broken bones, see Fractllrt'.
208
Artifi c ia l r espirat ion I ".Ft" 6 So 93 9 79 '2 93 02 8' -J. 93 2 121, 129, 136, I3 13 25
70 5 25 I5 9 23 42 37 37 155 20I 202 148 209
Brooch -bone 30 Brui ses Burn s 102 102 Capillaries Capillary hremorrhage Cap ule ... 70,7 2 95 Carb olic acid, poisoning by Carotid art erie ... J' hremorrhage 31 15 2 80 fr om 0 Carpus 28 Carrying,
"upstairs 201 Cartilage 25 Cerehro-spinal
117 Cen-ic a l vertebr::e 25 Cheek,
Chest,
Chlorodyne , poisoning
Choking .. ..
Pag' Circulation
blood,
rgans
7( Circula ion
f the blood, to induce Clavicle 26 " fracture o f 48 Clothes, rem o \'al o f 19, 202 Coccyx 25 Collapse ... 13 Collar-bone 26 " fraclur e of... 4 Comminuted fracture 35 Complicated fracture 34 Compound fracture ... 34 Compre . sion of the brain 132 Concussion of the brain 131 Conductor 143 COl1\'ulsions in children 137 Cradle, bed 202 Cranium ... 22 " fracture of 43 Crepitu ... 36 Cm hed hand 55 foo t 62 Diaphragm 120 Digital presure... 74 Direct \-iolence .. 33 Dislocation 62 Ditch. to cros", wi th tretche r 169 Dor al artery of foot 93 vertebrre... 25
Bronchial tubes... I I
means of 160 , 200
system
bleeding from b2
bandage for 1
U)' 149
140
of the
o
of
o
210 Page
Dress, woman's, on fire . .. 105
Drowning 139
Ear·channel, blood issuing from
Ear-passage, foreign body in
Elb ow , bandage for joint, fracture involving 110 159 53
Electric shock
Emetic
Epilepsy ...
Esmarch's 14 2 148, 149, 150 13 2 bandage
Expiration triangular
External carotid arterv . ..
Eye, bandage for ' foreign body in 37 120 80 155 109
Face, bones of 22
Facial artery 81
Fainting ... 134
Femoral artery 89 " "digi tal pressure at groin ... 89
Femoral artery, tourniquet for 90
Femur 30 fracture of 56 30 " fracture of 60
Fingers, bandage for 159 fracture of 55
Fireman's lift
First aid, meaning of " student
Fi h-hook, embedded
Flexion ... at elbow " at knee ...
Food, poi oning by Foot, bandage for bones of ... " crushed
Forearm, bones of " fracture of Forehead, bandage for. .. " hremorrhage from
Foreign body in the earpassas-e .-in the eye " "in the nose
Four-handed seat
Fracture, apparatus for treatment of cau es of definition of " general rules for treatment involving el bow joint of arm ... of breast- bone of carpus of collar - bone of cranium of finger

Frac{ure of forearm " of knee-cap of leg ... of lower jaw ... of metacarpus of meta.tarsus ... of pelvis o f ribs ... of pine of tar u of thigh-bone ... of toes _.
sign ancl symptoms of " '-arieties of fi'rost-bite
Fungi, poi. on ing by
orrhage , arterial ...
capillary... =u from gums 97 from head and neck 0 from lower limbs ... 89 from lungs 97 from nose 96 from stomach 98
Pal{t 164 17 20 10 9 76 87 9 2 153 15 8 30 62 28 54 83 83 110 109 I I I 160 36 33 33 41
Pal{t 54 58 6C' 44 55 62 56 46 45 62 56 62 35 34 108 153 General circulation 70 Granny knot 40 Green-stick fracture 35, 36 Gums,
97 21 I H::em
Pal{e
97
97
97
om upper
84
95 kinds of 73 " ven ous 93 Hand, bandage for 157 " bones of ... 2 Hanging... 140 Haunch-bones 28 Headancl neck, arteries of 8e Head banclage for 155 injury to ... 128, 131 " side of, bandage fo r 155 Heart 70 ., rate of contraction of 72 Heat-stroke 136 Hernia 114 Hip,
157
126
" fracture
52 IIydrophobia 106 IIyst erical fits 133 Iliac arteries Impacted fracture Indirect violence Insensi bility 79 35, 36 12
h::emorrhage from
74
Hremorrhage from throat
from tongue
from tooth socket...
fr
limb
internal
bandage for
History, meaning of ... 17 Howard's method of artificial respi,ation
Humerus 28
of
Insensibi lity, general rules for treatment 128
In piration 120
Instep
Insulator ", 142
Internal carotid artery .. ,
Internal h remorrhage 95
Intestine, injury of 113
In-roluntary muscle.; 33
taw, angle of 2 I
" lower 23
" " fracture d 44
oint, definition of 3 1
" injuries to .. , I09
ugular \'ein So
-\:idneys .. , II 1
" injury of 113
Knee, bandage for J 59
Knee-cap 30 " fracture of 5
Knot for bandage of lower lim b 42
Knots, reef and granny 4 0
Laborde's method o f artificial respiration 126
Laburnum seeds, poisoning by .. , 1.+
Lacerat ed wound 7'<
Large arm-sling 39
Laudanum, poisoning by 149
Leg, bones o f 30 2111
Leg, fracture (If
Lifting and carrying " into bed
Ligaments
Lightning, effect,.. of Limbs, 10\\ er "
Lime in the eye
Lip-, bleeding from
Litters
Ll\'er injury of LO\\lrjil1)hs
Lumllar \'enehrre
Lungs hxmorrhage
:'\1a1'5ha11 TIall's method ,) f artificial re!'pirallon 140 :,\Iedium L&dag:- 37 :,\letacarpus 2 fracture of , 55 " fracture of .. :,\Iiddle line of body :,\1 outh, blood i uing from :,\Iu cles " ru ptured :,\ItL cular action ,
Narrow bandage 37
Needle, embedded ro8
Nerves lIB

Nervous system ", I 17
Nose, foreign body in .. , I II " hremorrhage from 96
Oc cip ital artery",
Opium, poisoning by
Pad, ring " 3 " to fold .. , 74
Palm, hremorrhage from P almar arche
Paregoric, poisoning by 149 Patella 30 fracture of 5 2 " fracture of 56
Phalanges of foot 30 " of hand 2
Pho phoru , poisoning bv qS,150
Phy iology (elementary) ::'0
Plantar arch 03 " artery 93
PI:l11ts, \'arious , poisoning by .. , 1..1
Pleura 120
Poi s n n d w cap 0 n s, wounds by 106
Poisoning 14
Popliteal artery ... 02
Po terior ti bial artery 92
Potash, cau tic, poisoning by,.. 149
Rahid animals, bites of.,
Radial artery 8, Radius fracture of 54 Reef knot 4c Respiration 12C artificial 121, 129, " to excite
Re . piratory sy-tem
Rest, nece ity for Ribs
PaJ:'e 60 .. , 198 .. , 201 26, 31 144 28 26 110 82 196 III I 13 28 25 1::'0 from 97
30 62 20 97 3 2 65 34
213 Page
Pag. Pressure, dIgital .. , 74 point ... 74 of First aid 17 Pru sic acid, poisoning by 15 2 Pubes 2 Pulmonary circulation 72 Pul e 72 Pupils of eyes 130 Questions on Chapter I. 2, " II, III. IV. V, VI. X. 66 99 II5 145 154 20e
lOt
fracture
Room,
n6, rr II 20 4 6 pre-
"
of .. ,
choice and paralion of
Rupture (hernia) 114
Ruptured muscles 65
acral \'erte brre ... 25 acrum ... cald 25. 28 102
Scalp, bandage for , , hremorrhage ISS from 83 capula ... ... , fracture of ...
Schafer's meth od of artificial respirati on
Seat, four-handed three-handed " two-handed hin-bone
hock
" elect ric ... .. . houlder, IJandage for .. . " blade ... ,. fracture of bones .. . " joint .. .
Sick room, choice and preparation of. ..
Sign , meani ng of .:.
Sih-ester's method of artIficial respir2tion
Simple fracture ... 'keleton ... kull
" fracture of
Slings, arm 39, 4'),
Small arm sling ... Smothering
Snake
by
Splint, angular ' "
Splints, rules for apply ing to improyi e
Sternum ... " fracture of
Stimulants
Stings of plants and animals
Stomach ... hremorrhage from ,. injury of ...
Strains
Strangulation
Stretcher exercise, Army
Stretchers, to carry 169 " to improvise 166
Strychnine, poisoning by 153 Subclavian artery
Suffocation 141
Sunstroke 136
Surgeon' \'ibit, preparation for 204 yllabus of instruction... 7 ympathetic system ... 1 18 ymptoms, meaning of... 17 yncope ... 134 ynoyia ... 31 'ystemic circulation 70
Tarsus 30
Temporal artery. 82
Thigh-bone... 30
fracture of... 56 Three-handed seat 162
h::emorrhage from 97 " swell ing of tissues of... 141 Tibia 30 " fracture of 60
Toes, bandage for 159 Tongue, hremorrhage &om 97 T ooth socket, hremorrhage from 97 T ourniq uet 75
Tran verse wound of abdomen 113 Two-handed seat 161
'.Yagon, to load or unload 171 'lYall, to crabS with stretcher 170 \\'armth, nece sit)' for ,8 " to promote 127
118 \Y oman's dress on firt ..
ounds hy poisoned
hy
Pag-t:
26 51 121 160 162 161 30 134 142 15 6 28 51 26 32 197 17 12 3 34 22 22 43
49 214
bite Pagt: 39 140 106
oning
149
" injury of ...
canal cord " fracture of III .. 1 13 23 23, I I 7 23 45
poi oning
Soda, caustic, poi
by
pleen
pinal
.'pirits o f .salt,
1\0. 1. 1\0. II. TO. III. " ., ITO. IV. Stretchers, Furley 149 54 107 1 J 1 98 113 65 14 0 190 '7-1I I 18 5 I 7 172 21 5 Pare
"
Throat,
Pag-e Ulna 28 " fracture of... 54 Ulnar artery 88 Unconsciousness 128 Upper lim bs 26 Varicose veins 94 Veins 70 Venous blood 72 "hremorrhage 93 Ventricles 70 Vertebra ... 23 Vertcbrre... 25 Vertebral column 23 Vertical wound of abdomen 113 Vitriol, burn by... 102 Voluntary muscles 33
\Y ounds, lacerated 78 Wri t 28
Wind-pipe
105 \V
weapon 106 " accompanied by arterial hremorrhage ... 76 \Vound accompanied
\'enous hremorrhage 94
HORSE AMBULANCE CARRIAGES « WAGONS.
st. 30bn B111bl1[ance Bssociation.
GENERAL PRICE LIST.
INTR.ODUCTION.
This Price List, which is subject to revi ion from time to time, has been compiled \1 ith a view to assist members of the Association and others in the purchase of the neces ary equipment for corps and divisions of the Brigade, ambulance stations, classes and fi rst aid and nursing work generally .
.A complete and reliable Ambulance Equipment is an actual necessity, and experience has proved that employers of labour and others intere ted in the district readily subscribe for the purchase of such appliances. Collecting cards, stating the purposes for which subscriptions are required, \lill be supplied gratuitously on application to the Head Office of the As>'ociation, \\ here also any information with regard to it work can be obtained.
tores of the value of lOS. or upll"arus will be sent carriage p a i d to any pan of the United Kingdom.
Olring to fluctuations in market prices it is impossil)1e t< guarantee that the quotations herein can be adhered to.
Quotations will he furnished for articles relating to c\.llJhu lance Nursing and IIygiene, not mentioned in this list.
Orders ancl correspondence "hould be aclclre. sed to the St. John .Ambulance Association, St. John's Gate, lerkenwell, London, E . C.
RemittanceR should be made payable LO the t. John Am buance Asociation, and crossed "Lonclon County rmd "'estmin ter Dank, Lothbury."

Registered design 4 18,030.
A numbe r of improved designs for Am bulance Carriages have rece ntly been perfected, and several specimens ca:1 usually be seen at t. John'.; Gate, varying from a light vehicle to be drawn by two men or by a pony, co ting with india-rubbe r tyres to wheels £ 32 lOS., to a large single or pair-hor e wagon c:lpable of accommodating three patients in a recumbent p0sition and an attendant inside _ .A fully illutrated prict' li st will be sent on application ,
n 0 5'

a 5' n (l) ;:;: 0 a g.g':i
;. ... g.", g
With Iron Tyres to Wheels. l WllhlntliaRubberTyresto\Vheels
Withollt Cover or Hood alltl Apron. With Cover. Wilh Hood and Apron. Without CO\'er or Hood and Apron. With Cover With Hood and Apron.
U nrler-carriage (no Stretcher)... "'18 10 0/9 5 Liller complete \\ith
Dittu with Teiesc()pic handled Slretcherl' I II I 10
Ditto "ilh Police
Prices quoteu for Litter with Ortlillary SlI etcher include \Vid e \V ebbing Slings but no Chest Str::tp. Leathet, of Webbing Slings, 5s 6d. extra ; Chest S trap, IS. 6U extra. If supplied without any Slings, allowed
t Prices quoteu for Liller with Telescopic.handled Stretcher include \Vid e \"ebbing Slings anu Strap Leather, in'lt!ad or Wehhing ss 6d. extra If supplied without any Sling'i, allowed; and if without Chest Strap, IS. 6t1. allowed
t Prices qllott!tI for Litter with Police Stretcher include Wide \Vebbin g Slings and Leather Straps for securing a refractory patient. Leather, insteau of Webbing Slings, 5'" 6d. extra lIood and Apron, complete (state pattern of Strelcher) £2 10 0
Extra Sockets and Studs, per set 0 1 6
Waterproo f Sheet (washaole) to oe laiJ on the stretcher bed... 0 10 6
Crates (returnable) charged 45. 6d. fo r each Litter.
;.
-.::;:,-<!
..,]
p..
o
::
>-::j::lO
::l"d :::... ::r'<::r rb '" _. rb '" rb rb '" "'::r::l.., '< s:::
Ul
:: ::r
]
;:: ::..0.,.... A;3] Pi!f' rb () n- 0 '" _. Ul >-l ::l '" 0 B Ul :3 0 d _. 3. 0. '" !! r-:: 5 n 0 7- 9 (/) o t"'1 1-4 .., .., tr! PRICES OF THE IMPROVED ASHFORD LITTER. 1899 MODEL
::l 0 3 .., (; ::r ::r n rb So. · p.. rb rb rb • -< ::l <Ul::r", '" >-::j::J > i?" 0. ::3 0 r; CY g- ,.... ::rcrq 8-;.'<.. g a
Ul ;. '" S. :: 3. rb 0' rb Pi II
'" Ul rb ::r rb >< rb
& Ul ::r rb -;- s: ::' s '" Cb '" Ul 2.;::';, \0 & & rb 3
if 0 n- so.", =: 8-
::rrb<s:::n"Orb s::: "" c7,....
ci Ul 0 !!!.
g
g :!.::J ;:,; 0
rb::J ::l-;--
J,
J, s. u.
Stretcher" I I 2 01 II 0 o I I I 15 0112 10 0114 5 616 2 6 61 12 17 14 7 o 6
ai. I
I
Ordinary
o
IS 0116 10 o
01 13 5
[4
Stretcheri I 12 2 61 13 I? 6 [5 7 6117 2 6
w "= ;<l n trl t'"' U; ;l ..,.
PRICE LIST.
THE "REA=EDW ARDS" LITTER .

' HR "REA-E DWARDS " LITTER, wilh wooden wheels, showi ng method of loading; also first aid box filled to axle.
Th e und e r·carri aae or wheeled portion of this Litter is of ..n entirely new d;sign, and is adapted to carry of :he "Furley" o r "Clemetson" PalLern tretchers 111 prethe same manner a" the "Ashford" Litter. It js 1lted e it h er with bicyc le wh eels and extra strong pneuma.t lc 'yres, o r with light but strong wheels, :o lid in dia·rubber o r iron tyres. OW111g to the reductIO n 111 I e height of th e wheels it is easy to lift a loaded stretche r
over them, and the cranked axle has, the refu re, been replac ed by a straight one cunst ruc ted of tubular steeL
" REA-EI>\L\KUS" Llt'l l<:R. hlled \I ilh pneumatic tyred sho\\ ing- t h· .. Clcmetsnn .. :-;: relcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden . and the hubs are so the wheels can be removed froQ the axle without disturbing the bearings. In place of l hL f':lll' leg to raise as hill1Jles, two fixed legs filled wllh slllall wheels or roll ers are placed at the foot end, wh'le a combined lea and handle filled with a crossbar capable of being rai"ed or is used at th: heac! end . \\' hen ra ised a" a handle It mar be locked In one of t\\ 0 PJ ilion", and \I'hen it is locked in a \'eni cal pusition. The alh antages. fur. this ::rrangemenl are simplicity, ca can.] rapldl y uf l1uI1lpulatl)J1 and
PRICE UST. 6
the facility afforded by the two fixed legs for raising the litter, if necessary, on to the pavement. The queqion of balance has been carefully studied, and the stretcher is shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is in a horizontal position being thus obtained, and consequently there is no weight on the hand of the per on prope IIi ng the litter.
The pneumatic tyred wheels are strongly recommended in cases where the mall amount of care necessary to keep them inflated can be giYen the comfort to the patient and ease in propulsion are increased beyond all comparison with any litter yet produced. It will be noted that the prices are considerably lower than those of the "Ashford" Litter, and the following are given as examples, hut owing to the vast number of combinations that can be made with the different stretchers and coverings, it i impll . sible within reasonable limits to set out quotations for the whule of them, but these may be calculated by adding together the prices of the under-carriage, tretcher selected, and hood and apron or coyer, see pages 4 and 8 to I I.
SPECIMEN PRICES .
Under-carnage only, either with pneumatic tyred cycle wheels or solid rubber tyred wooden wheel, £10.
Litter complete with ordinary stretcher (no slings or chest strap) and hood and apron, £14 3s. 6d.
Ditto with Telescopic Handled Stretcher (with chest strap) and hood and apron, £r4 IIS.
H with iron tyred wheels prices are £2 Ie .
The lowe t priced liller complete is fitted with iron tyreel wooden wheels. ordinary stretcher (no slings or chest strap) and coyer. Price £ fa 8s. 6d.
Hanel brake, which acts automatically when the litter is at rest, extra ir 105.
When ordering please state which wheels are required.

On thi stretcher the patient can be mo\' en as de ired, from reCU111 bent to the sitting position. There is no complicated mechanism to get out of order, and the adjustment depends simply on the balance of the patient's body. The stretcher will fit either the" A hford " or the "Rea-Edward " Under-
Carriage. Price £3 3s. ; with extending legs, £4 J. Hood and Apron, Yentilated, £2 ISS.
7 PRICE LIST.
PRICE LIST. 8 THE "
CLEMETSON" STRETCHER.
" l} STRETCHER, with back rai ed, al a showing extending legs.
9 PRICE LIST.
ADJUSTABLE LEGS FOR STRETCHERS .
Primarily these legs, which are independent of and :-dditional to the ordinary foot wheels, are intended to facilItate the carriage of a stretche r in a railway compartment, in which ca e two on one side would be lowered and adjusted by a telescopic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the a ljustable legs on the other . ide would reo t on the floor. The four legs may be used to raise the stI etcher as ref] uired. \ Vhen not in use they are folded up immediately under the poles of the stretcher.
Price per set of four, .£ l.
FIRST AID BOX .
To he fixed helow the axle of the c. Rea-Edwards" Liller.
This is intended to he kept permanently attached to U1e litter, and is not designed to hang in a station or to he ,arried by hand.
Contents :-Set of Splints, 12 Triangular BandngL's, 12 Roller Bandages, 2{-lb. packets each Collon 'Wool and BOllC Lint, Adhesive I'laster, Pair of nrs, Knife. 2 oz. each Olive Oil, TiIH't. Eucalyptus B.P.C., Sal Yolatik and Ether Comp., Graduated ure Glass, }:;:iclneyshaped Dressing Basin, 6 Tampons for washing wuunds, T ourniquet Pins, afety Pin", Teeclles, Thread and Tape . I'rice £2.
" FURLEY" STRETCHERS WITH THE LATEST IMPROVEMENTS, 1899 MODELS.
 STRETCHF.R-CLOSElJ.
STRETCHF.R-CLOSElJ.
The impro\cments in all patterns of the "Furley' tfetcher, 1899 :'>lodel, are numerous. The comfort to the' patient i5 increased; the stretcher is stronger, more rigid and lighter, folds up more closely, and its handles ar more comfortaule to hold and afford greater protection tc ,he hands of the bearer' in passing through narrow dom or passages. it be necessary to reduce the \>\ Idlh of a loaded stretcher in order, for example, to carry lt into a railway carrIage, this can be done, either \\hen it is re"ting on the ground or supported by the bearer, wlthout trouhle and without the slightest jar to the patient. The price of tl,e tfetchers is lowered. All minor points have heen most carefully considered, and the stretchers are contidently recommended as thoroughly efficient in every way.
The e trek,1ers are adapted for use alone or as part of the " Ahford " or "Rea,-Edwards" Litter, and the cover, hood and apron, army rug, and watewroof sheet described in this list are suitahle for use with them.
10
'1'IN4t'W '/' - •• ;--
TELESCOPIC
LIST.

PRICE LIST. 17-
THE EQUIPOISE BED.
iNVALUABLE FOR INVALIDS, AND THE GENERAL PUBLIC .
Th e movement of the llcu to any posJlllln is so easIly effected that the person lying on it can regulatc the moyement of the bed to any angle without assistance. It can be locked in seven (Erferent positiuns. Price from £5 ISS. 6d
FOLDING CAMP BED.
Thi s can be folded in a "ery small compass and can be readily set up to form a cumfortable ucd. Price, £1 55.; case for same, when folded, filled \\ith carrying strap, 55. 6d.
Pocke t Cork Line and Drag , \\ ith 80 feet ot line, In case; for recovering a c1ro\\ ning per on from the water. Price ccmplete, with instructions for use, 6s. 6d.
Pocket Reel and Ice Line for use in ice accidents, wIth o feet of linc in case. Price complete, ",ith instructions fo'l use, 65 6d.
"" 2 N N 0 -= 0 .C\ , ;:; N N
PRICE
\0 \,Q I
r3 PRICE LIST.
" LOWMOOR JACKET ."
For use in mines, hip' hold, elc ., lo secu r e a patient on '1. stretche r (see illustration), \I hich can lh en be placed in an upright p 0 sition . Price £1 5s.
WATER BOTTLE .

Copper tinned, with carrying strap . Price lOS. I)d.
Enamelled Iron \Yalel Botlle, Cloth cO\'ered, \\ i h trap, 55.
Dressing Basin, J..idnl) ·11 1]1L 1. madv of cnall1l:llcJ iron. Priel' I s. 3d. LAMP.
This i,; filted with a !-ockeL, hy which l!J fix it to a Litter, or it can be cOI1\'eniently carried by hand, or attached to ::t hell or the clnthing.
Pril'e complctc, 5 . 6d.
Ambul ance Station Plate , Enamelled Ir on , 35. 6t1 . each .
Stretcher D epot Plate , Enamcl1t:d Iron, 3s. 6el . tach .
Carrying Sheet fdr GHryiTlt:! pallL'I1!S up and d,)wn stai rs (,r ')lhl'l"\\ise alHhll huu,;c. by J. C. Derham, Esq., Hlackp"lll, ,lnd :\Irs..\lfrec1 Paine, Bedford. The sheet is titled \\ it h rope hauc11t:s and detachable bamboo poles, and may be placed on a . tretcher withuut disturbing the patient. I'ric.: c o m plett.!. 15,.;·
PRICE LIST .
LARGE HAMPER FOR AMBULANCE
STATION AND RAILWAY PURPOSES
.

For contents see next page.
1 Set of Cane Splints.
I Elastic Band T ourniquet.
lb. Boric Lint ...
lb. Carbolic I Cotton 'Wool ... l len Tin J ases .
I Roll Adhesiye Plaster.
20 Roller Bandages, a sorted.
I doz . Tl:iangular Bandages.
3 Pieces Tape.
-+ oz. Sal Volatile .
4 oz. Bicarl)onate of Soda.
-+ oz. of Olive Oil.
4 oz . Spirit Ether Compo
i I b. Tin Po\\-dered Boric Acid.
-+ oz. Tincture Eucalyptus B.P.C.
I pair Pean's Forceps.
I pair Scissor:>.
1 Knife.
12 urgeon's Needles.
I packet each Safety ano Plain Pins.
oz. Carbolised Chinese Twist.
oz. Silkworm Gut.
1 reel each Blackand \YhiteSewing Thread.
1 Kidney-shaped Basin.
1 ,'topper Loosener.
I Graduated
1 cake 20 per cent Carbolic; oap,
1 Nail Brush.
3 Empty 8 oz. Bottks.
Pri ce complete, £4
PRICE LIST. T HE CONTAINS
(7 PRICE LIST.
SMALL AMBULANCE HAMPER.
\\'lth waterproof coyer and strap, for use in factories oliJeries, stations, and wo r ks, as we l l as for p:1.n chial
3n (1 d"mestic use.

CC:\IAI:--I:\ ( ,
'et Splints. I Elastic !ourniquet. 3 Tampons, fO.r wash ng wounds. 2 Packet LInt. 4 Roller Bandages (wIele all r 1a rrow). 4 Triangular Bandages.
Cotton \\ 001 , 1 In Tin Cases
Boric \\'uul I
Spool of Aclhes \ ' e Plaster.
Knife, Scissors. Thread, Tape, Xeedles, and \Veight complete, Ibs.
L.engltl, 1 f 6 in . Depth, 5 in. Width, 7 in. Price l
PRICE LIST.
SURGICAL H A VERSAC.
h 1PROVED PATTER);, fitted wit h a tin, so arranged that ali; dftic.le can be taken out withouL disturbing the rest of tbl ':on t ts.
'Jntents: I Set of SplintR, 6 Triangular Bandages, 6 Rolle 8a nctages (wide and Larrow), olton \Vool, Boric Lint, in b , .. ses, I Roll Adhesive PIa. ter, I Pair Sci sors, I Knife, 2.0Zo
')hvc Oil, 2 oz. Tinct. Eucalyptu;; B. P.C . . 2 oz. Sal VolatJle. .! oz. Spirits Ether Comp., I Graduated :\Ieasure. I Elastic Band T o urniquet, Pins, Needles and Thread.
Price £1 I IS. 6cl. 'White Linen Ration Have rsac3, IS. gd. each.
., FIRST RID' eeMPlINICN*
(DRESSINGS AND BANDAGES CXJMPRFSSED)
" JOhn HmlJulan(t R5SCCliJ(/On, Price Is. 6d. $1, :/OlJll'$ fiatt. • B) Post Is. "d. Cltrtenwell. ComioP-, €."
FIRST AID COMPRESSED KIT.
The h)x is made of wo)(l cm'ereel \rith damp·n:. i ling maLLrial, and is tilteel Wilh a lock and kt:)'. It contains :i: numher of praclical ambulance appliances '1rrallged so that ally a.rticle can be wilhelm\\ Il or replaced wilhnut dislurbing the cemainder. Being fitted with a handle il is portahle, and he Jid, when let down, can he used as a l'1I-le . .\11 bandage" and dressings are compres ee1. Size - Length r6_t in. ; width in. ; height > in . without handle.
Cuntents: 4 Triangular Bandage-. 6 Roller Bantla"es, 4 Fir,t ,\ id
6 Small Pack.:ts of COllon \\'001. 6 mall PackclS of Boril. Lim, 1 l3and Tourniquet, I i\[ea,ure Glass, I lin Lox containing a H"ll of Plaster, Boric Lint Patches, • amI Pins, T tray containing 3 hottle, (Sal Volatile, Tincture of Eucalyptus and Olive Oil) and a of Boric Acid, I of improved Splints, with angle piece, g • I'lint (or a thigh) .
Prjce £1 lIS . 6d . E8.ch article is priced separately (see Index).

1. Triangular Bal1lbgc. 2 FirL Aid 3. Cotton \\'uul. 4. 1'\\0 plinL Straps. 5 Aclhesl\'e 6. Perf l )utasI1. 7. La, nolinc. . Bonc Lmt J'a\ches. manganale 0 • 9. SafelY and Plain Pins.
Price, each IS. 6e1. By Post IS. Per doz. 175 . 6d. caniage paid.
.1 "'0
J 4cl. Lach
2 2d. or 3/9 per doz . " 2/0 " rod. TO.
6 rd. per box or lad. per doz.
7 per tin or 1/4 "
3 rd.
4 2cl.
5 rd. rd. per p:lcket o r rod. " l d. rod, " per trap o r J 9., " 9 per box or lad. " " .
N ot less than one dozen supplied at dozen pnces,
19 PRICE LIST.
LIST.

FIRST AID BOX FOR "ASHFORD" LITTER OR AMBULANCE STATION.
.T his is primarily desi gned (0 he pbced on the "AshrfH"CI" LItt er (r899 :\lodel), but it is further adapted to he hun::; llj) on a. w1.ll. A detachable le"ther handle is al.-o fitlt·l for carrymg purposeE'.
Fo r contents £ee next
PRIl.E LIST.
CONTE. 'TS OF FIRST A ID BOX . lllll';lratcll ell pr.,,-i ,Lh page.)
Set _,f \\'o..<1en "pliots; I El"'lie Baml Tourniquet j Carbolic W ool, Lint, in .in cases; 1 Roll "\dhesi,-e P1:J.stEr; 12 Roller
Cls'<;nell 6 rriangular Bal1d:u?;es; 3 I'iect!s of Tape; I Pair Scissors;
1 ; 1 Kl<lney.shaped ; I (;raduated j 2 oz. Olive Oil ;
2 01. Tinct. LllcaiYPllls n.p.c.; 2 oz. Sal Volatile 2 l)Z. Spirits Eth er Compo ; L oz. Carron Oil j Pin" • afcty Pins, Needles, Thread
PR1CE CO:l[PLETE £2 lOS.
POUCH FITTINGS,
specially selecteJ for the :-it. John Ambulance Brigade , consiting of:-
2 Triangular Bandages, one uf \\ hich is sealed up in waxed paper. The other may he used for practice, but should he kept as clean as posslhle.
2 Bandages (J in. a\ld 1 in. ).
Packet of Cyanide Gauze (1 y<1 . compressed).
I Pair Scissors.
6 Safety Pins.
I Small Bottle of strong Smelling Salts.
I Piece of strong Cane, for lightening impro\'isecl Tourniquets.
PricL, 25. d . each. 6 doz . or more, :!S. 7d. each.
Packet-; of C)anicle (r yd . compre.,sed). rrice per d lL. ,2". ScI.
Small llllllles strong . :tIts. Price per doz., 5s. 6u.
SAFETY PINS.
\ 11 fa<;(ln or unfasten on either side.
Facile :\' 0. 600 "r (i02 ptr 3 do,,;.
. , 60 3
Duches<; Durk ,. :\' ,_ :! .. r er doL. . ., • \ ... 1'1, ,I Special Blanke Fins 3 i,) . 3 l in.
21 PRICE
s. d. 0 6 0 0 2 0 3 I 0 I 6
Tourniquet, Ela tic
Tourniquet, Field PRICE LIST .
Splints, \Y ooden, per set, 2/6; Cane '" ... perset ·exeatl), improyed \Y ooden Splints, with groo\'ed joinLs and ang le piece, strongly recommended
Tow, for sp lin t padding ... . .. per lb.

4 6 o 6
First F iel d Dressing (Army H. egulation Pat tern), Price ... each 0 9
J aconette, 4-+ inches \\ ide per yard 2 3
Tow, Carbo lize d or Styptic ... per lb. 0 9
Wound Pad.-A pad of cotton wo o l and g:1.Uze, to \\ hich a bandage is attached. The of the pad coming in contact with the w o und is not touched hy the hane! uf the person app lyi ng the Price 4(1. each.
First Aid Dressing, consi ting or a small com pre sed packet or boric lint, a compressed roller lJandage, and a . akty pin. Pri ce :!d. each.
D redge r, containing boric acid powder, IS. 4d. Glass , 2d .
Kni fe with strong hladc each 9el. ; per doz. '-.
Pair of Scis s ors each IS. ; per dnz.
Splif't Straps, Webbing, and suitable Buckles. Per "et of 12 yards or strong 2·inch \Y ehbing and 15 Duckles, 25. 6<1.
These make very compact Straps for carrying in the P Olich. 'The \V eblJing should be cut to meet loc al requirements.
Buckles on ly, IS. 3(1. per dozen . 'W ebbing only, I S. 3d. per dozen yards.
It is unnecessary to sew the Buckles T he spikes should be -passed th rough the webhing, and the short end of th e \\ ebbing .should lie ol1twD. rcls.
PLASTE.RS.
I .. ' ,\ D St Dalmas & Co. "\I anufactufcc1 by . •. e .. . . ,\d hesi\'e Plas ter 1m CalH1Jric. 111 tlJ1 of yard, 6 in cht.· \\ ide 6d .
The Leic este r Adhesiv
Ribbons, in tin boxe,,> 6
yar Is lung.
inch \\ide I inch wide
:\'at i)na l R uhhcr . (.\.nLiscptiC), on "pools. 5 yck inch wiue 9(1. I S. 2 " " IS . 9d. 10 yds. 1.. IS. 6d . 2S. 3d.
Ditto in cal'll box, in . wide, yc1s. long ... tin I I 3 5
Large t ' 5 . , OURT PLASTER, TRICOLOR . ' ize, 9U. ; s d. ; Small, 3d .
6<1. btl. Id. 3d. 3d • 6d. 9eL
s d. I 6 6 2 7 6
25 PRICE LIST.
NURSES' WALLETS
.
O R DI NARY PA D L OCK S HAPE.
\ Yitho ut ins tr uments, 4S . 3d.
Fitted complete , contaIning Spring D ressing Forceps , Spatu!.., Probe, 2 pairs Scissors (roUJ.(i and sharp pointed), Clinical ane! Knife .
Adyanced price lOS
ST . JOHN'S PATTER:\, as illns· -trated, but improyed hy the addition of flaps to protect the i'lstruments .
\ Yithout instruments, 7s. 9ll.
itted complete, containing pring Dre!)sing Forceps, Artery For· ceps (also useful for dressing), Spatula, Probe, Director II ith .2ar Scoop, 2 pairs Sci 5tl i S (round and sharp pointed), Clinical Thermometer (minute·, round), Knife, Pencil, alld Safety Pins.
Price £I Is.

ROLLER BANDAGES in Assor t ment .
Eas:h packet contains 6 hanclagcc; as follows :-
6 yanls lung-one 6 inc'l, tl\O 3 inch, one
inch; 4 yards long-tIm inch.
Fine Grey nlico per packet
Plain Triangular Bandages, each (,'pecial quotalions for large quantities.)
Dillu Compressed (thinner quality). each 4d. : per doz. 3s . 90 .
Triangular Banclages (after !:.march) showing 25 applicalJOlb of the Bandage, \\ ith printe.l instructions each 0 (, per
PRICE LIST. ROLLER BANDAGES. (6 yards long. ) 26 Open \\ u\e Grey. Fine Grey Calico, or Superior \\'hite Opt!n ·Wo\e. Best quality, S uperior W hite, wi t h White Open \ Voven Wove d. s. d. s. d. s d. in. pe r doz. I in. I in. 2 in. in. 3 in. 4 in. 6 in. 0 ·9 3 2 0 0 3 6 2 0 2 6 3 6 4 6 I 9 2 0 2 6 3 0 3 6 2 4 0 2 4 6 3
3 6 9 3 9 9
d.
o
I
dOl. 4 6
ROLLER BANDAGE M A CHIN E.

De igned by Dr. A . C. Tun tall. Price 2S. 6d.
NURS ING INSTRUMENTS.
Bow D ressing Forceps) full size, Is . 3d. ; small, extra W\!11 finished, IS. 6d.
Scisso rs, round-pointed, IS 3el. ; sharp-p0inte(1, for delicate work. IS 3d . ; small round-pointed, blades take apart for cleaning. IS. 9el
Spatula, IS . 2el. Probe , gel. Director, with Ear Scoop , IS. gd_ Artery F o rc e p s , 25. -td . Knife , ve ry thin, ivory handle, two bladps, JS 9el.
Nurs ing C hart, hy I nelerwick, each . Temperatu re C hart, 1d . each.
CLINICAL THERMOMETERS
. Reduced P rices .
Ro u nd . O rdinary, I S. j minute, IS . 3el . j half-minute, I S. 6el. Flat. trongly recommended as they will not r oll. Ordina r y, I S. 6d . ; rapid (spec ially. elected and rese r ved for the A ssociat ion) , w i th ve ry open scale, 3s.
PRICE LIST. 28
CLINICAL THERMOMETERS - (ro lltil1l1 ed.)
W it h Mag n ifyi ng L e n s. Price , o rdina ry , I S. Gd.; minute ,
I S. gel.; half-minute, 2S: 3d. . .
N B.- M inute and ha l f-mmute lI1strumenls will only r egiste r in the time stated unde r favourabl e ci rcumstances.
N o Imbifity is take n for breakage oj Thermo m eters £Il tra/lsit .
BATH THERMOMETERS.
To Dr. Forbes' specification . Japanned with zinc scale, 25. 3(1. ; Clinical Thermometer size . in ca'>e, I:. 6d: . 1\'0 liability is take n /01' breaka,!:,'t; of TherlJlolllehrs III trallszt.
COTTON W O O L.
Pl a in, I oz . , 2d . ; 2 02 ,3d . ; 4 oz., 4d. ; lb., 7d.; I lb., IS. ; snull packet (Compn:<;secl), reI. . .
M edi cat ed, Boracic, ! lb., 6el.; I lh., IS. 6d. j Carbolic, ,Per lb., IS. d.; Alembroth, per lb., I . 6d .; Double Cyalllde, per lb., 2. 6el.
LINT.
P l ai n , I oz. , 2el . . 2 oz., 3d. j 4 oz., Gel . ; lb . , IOel. ; I lb., I. Gel .
B o r acic, 407 , Gel. : I lb., IS. 6tl. j square fool 2d. j small packet (Compressed), HI.
G AU Z E S .
These are supplied in 6 yard length", \\'idth 36 inches s. d .
Unmeclicn.ted white
Alemb r oth
Doubl\! Cyan ide
Boracic
GAUZE TISSUE.
per length 0 10 o 2 2
A laye r of absorbent cotton wool bet ween two sheets o f gauze, good qual i ty, per lb. , I S. 6d .
27 PRICE
LIST .
I'RICE LIST .
TEXT BOOKS , &
c.
(, FIRST AID TO THF: IKJuRFo." By James 'antlie, :\I.B., F.R.C.S. The authorised Text Book of the First ..\icl Cour e. IS. by I'>. 2cl. OF FIR:T .AI n." Compiled from Dr. Cantlie' :\Ianual. By J. Brown, L.R.C.P., L.JZ '."., and J. :'II. Carvell, :'II. R. C. S . , L. S. A. Price 6d. ; hy post 7d. "HIKTS A:-;'D fIELPS FOR IIO\[E II \'(,I E:--IE. "
By E. D., illustrated, with chaptcr on the appiI call on . of the roller bandage, by R J. Collie, :'II.D. The authOr! cd Text Book for the Cour c. Is. ; hy post IS. 2d.
"Ho:\m By John F. J. Sykes, D.Sc (Public Health), :'I1.D., &c. Illustrated. The authoriscd Te:-.t Book for the IIome Hygiene Course. L.; by po';t, h. 2<1 " CATECHIS\[ Ho IE (based on Dr. Cosgr<\\e's Text Book). By J. Brown. L.R.C.P., L.R.C.S., and J. " M. Carvell, M.R.C.S., L.S.A. Price 6d. ; by pust, 7cl.
AKswERs UPO:--l A:lIBL'U?-<CE "·ORK." By John W. ilIartm, M.D., and John .'Ilanin, F.r .C.S. Ed IS. ; by post, IS. Id.
AI'.n:;\\'ERS UPO . By john 'Yo :'Ianin, :'ltD. 15 6d.; by p l.t. Is. Sd. "FIRST AID TO IHE I'J URED (Six c\.mbulance Lectures)."
By Professor Frederich ESl11arch. Translated from the German by H. R. n. Princess Chri<;tian. 2S.; by po<,[, 2<.;. :,(\. " BA. "DAGI:--IC A?-<]) 'URGICAL DRESSI:-<G."
Walter Pye, F.R.C. <-; 2S; hy post, 2S. 2d. ' DH 9-. H . ., l'>RST AI.ns," being a card to hang up, " treatment of Y'lrIOU<; accl,ients. ::!cl.; by post, 5(1. To h.E.s rORE . THE .i\ PPARE;-'; fLY printed in large Type WIth two Unmounted, 2cl. each; by PDst. 3d. ;\Iour,t ed. \\Ilh red border, and varnished to hang up, 60. ; post free, packed, IS.

PRICE LIST.
TEXT &c.- (continued}.
"lIow TO ACT WHE LOTI£I;-o;r; 1AKES FIRE." By J. E. H. Mackinlay, M.R.C.S. Unmounted, 2cl.; by post, 3d Mounted on card and varnished, 4cl.; by post, packed. 7d .
"FIRST AID PRINCIPLES." Cards of concise direction for \\ ]Jocket, each; 4d. per dOL:. pecial quotations f<lr large quantities .
EXA;\IINATlON PAPERS, Fir t Aid, N"ursing and Hygiene Cour es." 3d. j by post 4d. ANATO:\llCAL DIAGRA:\l. 'ho\\ ing the human skele· ton, main arterie • and points where pressure should be applied to arrest bleeding. 2c1.; by post, 3d
DIRECTIONS AS TO THE OF PERSOI\S SUFFERING I RO\! ELECTRIC SHOCK. Large print, poster size. 3d. each; by post, 4d. ; or 2S. 6d. per dozen.
AI DE :'IIE\IOIRE. On cardboard, in linen·lined enyclope, for the P JckeL. By the late ,urgeon.:'lajor P. ,hepherd. useful hints for First Aid to the Tnjured 3d .; hy PI)st 4(l.
C 1,:-'; l'"RAL NOTES 0"" FIRST;\.m 10 BE RE:--iIlERED IN ASES OF POlso:>n 'G. By :'Iilnes lIey, :'I1.A., :'II.R.C. '. , L.R.C.P. Price 2(1. : by po. t, 3d.
, . \:lIll UI ANCE TAln Id·S." By. ydneyPartridge, Price IS. ; by post. IS. Id.
:\IHES :'IIII ITARY SAKIT.\TIO:--i. Dy Lt.·Colonel II. P. G. Elkington, R.c\..:'1. C. Price 6d. ; hy post 7d.
., BOOK," for in tantaneous reference, conci e instructions; to hang on wall. ize about one flO: sfluare. Price 25. 6el. ; by pust, 3::.·
'\IIlS Tn l\IUIORY FOR FIIL"I \11) • Rc\"i,;cd to d:llL. .\clc1itiUJl1.l I1lu tfallon;,. By L. :'L. Frank :'II. B.C. :'IL, Edin. 6,1. l)pr Cllp),' hy p'):',!, 7(1. PULFS FoR CnRI'S l)IYI'iIO,'i, St. John .\mbulance Brigadc. 2J. per CllP).
/
3 1 PRICE LIST.
TEXT BOOKS, &c. - (con tin ued) .
A History of the Order of the Hospital of St. John of Jerusalem. By the Rev. \ V. K . R. BEDFORIJ, ?lLA., Genealogist of the Oruer, and Lieut.-C o lonel }Z. II.
HOLBECHE, Librarian of the Order In one \'01., Demy vo., 230 pp. Profusely illu lrated Price 5s ; by p u t 5s. -+d.
Th e Kn ights Hospitall ers i n S c otland and th eir P riory at To r phichen. By GEORGR THo:\[AS BEATSON, :'11.0., L'.B. \Yith 15 page . of illustrations. Price 2S. 6d., bounll in cluth; post free, 2S. St.!.
R egi st e r s . Class .\ttendance, 25. 6d. Certificate,;, ,",s o cd. Case Report, IS.
Large P h ys iological D iagrams . For Lecturer' use. o m ·
The Human '-kelelon the :'Ilu5cular, .-\ncri:tl ant.!
Venous, ystem,;, the Heart and Circulation of the I;l uo d, Simple Fracture, Compound Fracture, Dislocatio ns, Price per set of six, 15s. These may be hired fo r a CI)l1r<; c of c, Aid" lectures given under the auspices uf lhe AssoclatlOn, for a fee of 5s., or with the audition uf Tourniquet, an.d plain Triangular Bandages, for a. fee of lOS.
Boxes of S t abo ner y for the u e of CIa s Sc:crLlari<.:s 8n ,1 others connected with the Association, containing twch'e sheets of high-class paper, suitably headed, and t\\ eln.. envelopes bearing the de\' icc of the Associatiun. Price 6d., by po;;t 9d. Twice that quantity, price IS., by p ost IS. 3d. Medalltons, issued in accordance with special regulalions, fu r which see leaAet 62, to he had on applicatilJl1: o.inage Br?l1ze, 2S. ; Slh' er, 7S. 6d.; Gold, £2 lOS. ; ll1cludlDg name and number on back. ;'Ioroccu \ LlyetIi ned case, 2S.
Labels , to be placedabo\'e :'ledallions for each subsequent year's issued in accordance with regulations, as per paper 62 . Bronze, 6d. ; Silve r , I S. 6d. ; Gold) 12S 6d.

with the dc\'ice, issued under the authority of th e Central Executive uml1lillec, haying been first appr oyed by H.R.II. the GranJ Prior as the sole official and rec ognised Badge of the Associatiun and Brigade. 1 B. - This desl:F{Il is jrotec ted XO. I, fo r the nse of individual certificated pupils-
"'i / e
0 9 In Enamel for ImtL o ll h o le 0 ,. hru nc h In ('I,)th and Silk In Clu t h and Sih'<.: r (Registered Xumber, 3522) In Cloth and \\" o rstcd
Small Celluloid Badge. for hUlto n h ole or lJw och \\ hite Salin Armlet, \\ ith \\'()\en Badge
Black Silk Arml e t, with printerl RHlge .. N,S.-
Pr ices much Reduced Xo. '.)2 i n many cases. A rm B a d ges,
d. I n German Silver, Large Size... 0 7 Size dillo 0 6 SI111.11 •' ize for button h o le 0 6 I n Electro Plate, Large Size 0 ditt o 0 9 Sn1'l.1I
S.
for bullon hole
I", 'S , B a ';, 's 1"(. Jl( ," l,) Itt· .... 'o r).' a s d(.·co '1 "((!'( liS I 0 2 0 0 0 0 3 9 0 6 2 71 6
7
PRI CE LIST.
BADGES.

1 O 2.
No, 2, for members of the St. John Am bulaIlce Brigade, having the name of the Corps or Division annexed on a lab el , only issued in quantities-
In German Silver, first doz., £1; subsequent dozs., 12S (0 Electro Plate, first doz., £1 12S.; subsequent dozs. £14s.
Cloth and Silk, per doz., J 25.
In Cloth and Silver, per doz., £1 105.
A U t he above may b e worn by members of the t. John Ambulance Brigade, not wearing uniform, and the German Sil ver and Electro Plated may be worn as the Arm Badge ,fo' a.ll ranks on the Brigade Uniform.
BRIGADE UNIFORM BADGES, etc.
Officers . Collar Badges (Reg. No. 3,5 2 4) " l'uuch ( " 3,657) per pair each
Sergeants. Ca.p Badge ( 3 520 ) " Arm Badge ( ,,3,5 2 3) "
Fatigue Cap Badge for Officers and Sergeants (Reg. No. 3,55 8 ) ...
Corporals and Privates.
Cap Badge (Reg. No. 3,5 21 ) .. .
Ann Badge ( " 3 542) .. .
O"ercoal Badge ( " 1. 582 ) .. . each
Field Service Cap Badge for a.1I ranks
Lady Officers of Nursing Divisions.
Superinlendenl's Cloak Badge (Reg. N o. 3,65 8)
Sup e rintendent's Arm Badge ( " 3.659 )
Other :\ursing Officer's Cloak Badg e ( " 3,555)
Other l\lIr"ing Officer's .\rm Badge (,' 3,65 6 )
Nursing Sisters. L\rm Badge ( " 3,5 22 ) ,. Cloak Badge ( " 3.5 21 )
Honorary Surgeon's Sih'er \\"ire Cross (pattern B) ...
Superintendent's ih'er \Yire , tar (pattern A)
Medallion Badge (paltern D) ... ... . .
Nursing Badge (pattern E) .. .
Satin Badge ror Nursing ,'isler'. Pin Cushirn
Bu gler's Badge ... 4 0 Bugler ' s Cord
Honora.ry Secretary's Badge .. .
Whistl e and Chain each
Field Service Cap. complele... ...
Private's Brown Waist Belt and Pouch "
White Piping, per packet of 7 yards, enough fur 3 1Ylirs lIf lrouser" (packets cannot he broken)
Lace -';11' er pLl' yard gllrk ... , . \ C'lP Band generally runs ahr,ut 2-+ inches.)
13 PRICE LIST.
34 s . d. 3 0 2 6 6 0 2 0 3 9 2 3 2 3 0 6 0 8 4 6 3 9 4 0 3 3 2 0 2 3 0 0 8 0 I 0 8 o :; 0 I 0 2 0 3 9 7 8 I 2 II 0 0
BUTTONS FOR THE UNIFORM OF THE ST. JOHN AMBULANCE BRIGADE.
!:'sued only for the u e of Officers and Members of Corps and Di"isions wearing the prescribed uniform . Electro Plate, large small German Silyer, large small
Black

ELECTR O TYPES OF THE ST . J OHN AMBULAN C E DEVICE.
eries \. Series D. for for .\ swcwtion llri.t::ade use. lise.
No. I. For Cards, Ticl,et, &.c . ...
2 For Kote Paper. Small Circulars, <Xc . ,,3 . For Quarto and Foolscap Lelterpaper, c·c.
4. For mall PosteL .. ,,5. For Large Posters
Complete e r ies
Prints of the above Electrotypes (I to 3) appear on the following page. NO·4 is shown on page 32 . The of 3A i 3 in., and of 5R with out scroll.
ELECTROTYPES.
35
PRICE LLT.
I
rn I large smu ll per doz. S. .1. 4 0 2 0 o S1 o o 6 o 4
[o
s. d . s. d . I 0 I 0 I 0 3 I 0 :3 6 9 3 0 5 5 6
PR
ICE LIST.
No. I A. r\u. 2 A 1\ u . 3 -'L
'0
3 B. No.2 l3.
For prices .ee page 35·
.
e may be obtained di rect from :'\lessrs. II ebbe
and Co., 35. Beth nal Green E. T elephone o
gog , London \\·all. T e legraph ic Address: "Otherwise, London."

SWAGGER STICKS
for the use of Officers and Members of the St. John Ambulance Brigade.
Ebonised Canes, German Sih'er :,lounts beaTIng the Brigade Device . PRICE IS. EACH.
AI1 Orders for the foregoing Stores should be given to (he Local Secretary, or to the Stores Department.
St. John Ambulance Association, St. John's Gate. Clerkenwel1, London, E.C.
Cru';s helt, \Y hite P:l.lenl Leather and Black '\Inrocco Pouch (Badge extra) ...
Forage Cap anu Cover Field Cap
PRICE
£ s. d bearing A ssociation de\'ice - 12 feet hy 6 feel 7 6 5 feet by 3 feet o 12 6 Brigade 4 ft. I in. by 3 ft. 0 12 II
LIST.
PRICE LIST.
Th
rt
CHIEF A. D II o:\,oR AR Y SURGEON. .£ s. d Tu nic (Badges ext ral ... 4 4 0 Tr ousers ; Two-inch '\l oha ir Braid, side seams I 5 0 Cross-belt and Pouch: Black Morocco I 0 0 " ,,-'ilver emuroidered 3 7 6 Forage Cap an d Cove r I 9 6 Field Cap 0 12 6 Glo"es .. , 0 4 6 Great Coat (Badges extra) 4 4 0 C][iEF SUPT. /\ :\'lJ OTIll!:R 'llIEF O FFICERS T unic (Badges ext ra ). . . 4 4 0 Patrol Jacket (Badges extra) 3 3 0 Fatigue Jacket (Badges extra) ... ... 2 10 6 T rou ers: Two-inch .\Iohair Braid down side seams 5 0 C ros -belt, \\'hile Patent Leather and Black Morocco Pouch (Badge extra).. 0 14 6 Forage Cap and Cm-er I 5 6 Fielu Cap (Badge extra) 0 10 0 Glu\-es ... 0 4 6 Leggings .,. ... 0 8 6 Great Coat (Badges extra) ... 4 4 0 • UPT. OF DIVISION OTHI£R OE'FICERS. Tacket (Badges cxu") ... .. . ... 2 6 6 Trousers: Two-inch '\loh:1.Ir Braid down side seam 5 0
UNIFORMS.
es
.
... ... . .. Gre:1t C03.t (Badges extra) o 14 6 5 6 o 10 0 o 6 o 6 4 4 o
G\'l\'ei;
39 PRICE LIST
MESS DRESS FOR OFFICPR.
J acket (Badges extra)
V est ...

1ST CLASS SERGEANT.
P at rol Jacket (Badges extra)
Chenon,4 bars, ih'cr, 3s 6d., "\Yorsted Trousers
Forage Cap (Badge extra) ... . ..
Cross-belt and Pouch (Badge extra)
Field Cap (Badge e>..tra)
Buckskin Gloves
Cotton .,
Leggings ... ... . ...
Great Coat (Chevron and Bat.!ge extra)
SERGEAXTS, CORPORALS, AXD RAXK AND Patrol Jacket, Black Tanan (Badges extra)
T rousers, Black Tartan
Forage ('ap (Badge extra) .
Cover for Cap
\ \'aist- bell and Pouch
Fielt.! Cap (Badge extra)
Great Coat (Badge extra)
Gloves (per pair)
Leggings (per pair) ...
Sergeant's Chenon, 3 bars SJ!ver,2' 6d., "\\'o rsted
Corporal's 2 IS . d.
Pat rol Jacket (Badges extra)
Cap (Badge extra) ...
Breeches: Grey .'e rge
Shoulder Belt and Pouch
Gloves
GaIters
H ose ' "
Great Coat
PRICE LI.5T.
CYCLISTS-RANK A:\O FILE
Jacket (Badges extra)
Cap (Badge extra)
Breeches: Grey Serge ... ....huulc1er Bell
(:; loves (per pair)
(per pair)
All Badges to be obtained I))" the Corps or Div1 ion from t. John's Gate .
If the Corps or D;\'ision is out of London) measurements tc!"If supplied to contractor. free of charge.
Carriage Ollt of London extra
£, d . 33 6 I 8 0 2 r, 0 -II 0 0 10 9 () II 0 0 2 S 0 4 6 0 0 0 3 6 o 13 6 I'll E. 0 II 0 0 C) 6 0 3 -I0 0 f) b () 0 2 o 13 6 0 0 S 0 3 6 0 I 0 0 0 S 2 )f) 0 3 b 0 12 0 0 10 6 0 4 6 0 4 6 0 4 6 4 4 G
Ca iters
£ 0 0 0 0 0 0 40 s. d. 19 6 2 .:: 12 0 10 I) 4 6 4 U
INDEX TO PRICE LI T

l' U.E
Ambulance Hamper,; 15 10 '7 ... Station Plale 32 to
Bantbge Rolling :'Iachine ... 27 Bandagf's 20 Basin, Dressing q Bed, Equipoise 12 " Camp 12 Books 29 to 3'
BOllles (Water) 13 Buttons 35
Carriages .-\mbulance)
Carrying Sheet 14 COllon \Vool .,. ... ... 28
Cover for Stretcher or Litter
Diagrams, Large il " Small ... 30
Dredger (Bolic Acid) 23 Dressing Basin 14
Drowning Tackle 12 Electrot);'pes.. 35. 36 Emergency Book 30 Fir'st Aid Box ... ... 9, 21, :l2 " "Companion.. 20 " "Compressed Kit H/ First Field Dressings... 23 Flags 37 Gauzes 28
Gauze Tissue ... 28 (Ambulance) 15 to ]7 H aversacs ., ]8 Hood and A pron for Litter... 4 Jaconette 23 Knife ... 23 Labels .. , ... 3 Lace for Caps, &c. 34 Lamp 14 Lint .,. ... 28 Litter (Ashford) 3, 4
Litter (Rea.Edwards) .,. 5 to 7
Lowmaor J al.ket \lea,ure C;lass ... .:'Iledallions ... urses' \\'allets ursing Charts " Pillow ... Plasters ... Fittings h.eg"ters Roller Bandage .:'Ilachine Rug.. . .. Rules for Corps or DiYisions John Ambulance Brigade
Stretcher plint Padding 73 Splint Straps ... 23 plints
Stationery ... 3 1 tretcher Depot Plate 14 Stretchers .. , ... 8 to 1 r " Adjustable Legs for 9 wagger tick 37 Temperature Chart 27 Text Books 29 to 3 1 Thermometers ... . . 27,28 Tourniquets 23 Tow, cnrbolized 23 "plain ... 23 Uniform Sundries 34 l'niforms .,. 38 to 40 Wagons (Horse Arnbulanc·) 2 \\·ater 13 \Vaterproof Sheet Whistle and Chain \\"001 (Cotton) .. \V ound P::u\
Safety Pins ... ... .. Scis.ors ... PAGE 13 23 3 t 25 27 ':'.7 3 1
Slings,
23

