I/r

I/r
_ 1,\1 n"'1E(I "1II\t 1 us)
4TH LU\IIHR \ ' lc R fEHRA
llAU 'U'/ Bt'N'- 5 (t'"h'j,,)
UI.,' A
l{AO'US -
THIGH BPNE (femur)
KNEE CAP (patella)
SHi" BONE (liIJia)
B'WOCH (tibula)
1\1 E " A'I/\
ARR.\.NGED TO THE SYLLABUS OF 'J lie: lIRST AID COURSE OF T. ) OII X
J.,:\ ,IES C.\:'\TLIE, ;\1.:\" ;\f.B., F.R.C.::).,
flOIIOJfll"J' As ,rooah r/ th,' Order I)f St. johll. J //Jno' fl ' Y I.I/i: .Ilclllb,'r of. alld /.cc/llrcr all,; }, talllinc)' t", ti,,: ./SS,,,i, l ·/OIl ,
"'ilh a CIIAI'TFR on" Strdl..her Tran,port," rel'iseli from that origin.lIl} \\' 'inen by Si, )"11" Ft: ,F'·. A'"il[itt ol'}u:;!'cc 0/ I;' .. Orda if SI . jo/w. in ac<:on.lance with the ,\rl11), tretcher Exercises. A1,0 a CHAPTER the fifth Lecture, for Fell! des 0111\,), by E. ;\L,cll,,\\'FL COSGRA\'E, M.D., F.R.C.P.I., (! <if tlu Ortie> if St. jolllJ, J!ollt1l'a'J' LljC .J/onb. r o/, alt'; La'iura ,i'ld Ex,tlllinN t{l, !ht: .-iSj'oclati{lll.
FOU R'IEl! NTH EDITION, 580,000 to 6'30,000
(TllI's Ed t :, n IS SIII/I,ar to the d''<'Clltll. fwd/lil and tit:,
Prie,o ill Cl0th, IS. net: I,), po,t, g. 2J.
In ;\1 0J\)CCO, 25. 6d.; by post, 2S. Su.
TO IIF AT
. T. CLERKEX\\ ELL, u')XDOX. LC.
\\' H. &. L. C. 5",'>00 2,1<:',
'l})dor2 of tbe ®r'tler of tbc of .st. mobn of ]crusalem in ,$aocrcigtt Ultlr fl.ltrO'It O'f tlJC ®rbcr.
His Most Gracious Majesty King Edward VI!., K.G. 'pri.o r.
His Royal Highness the Prince of Wales, K.G. YJrior.
Th 3 Most Honble . the Marquess of Linlithgow , K. T. of Field Marshal
His Royal Highness the Duke of Connaught, K.G.
<!:H.cntibr (0iu.crl"!:i.
Cllalleellol-The Right lion. the \ 'iscount G C::'II
Sccrctary.General-Colond Sir HERIlERT JFK\l.I, J.....C.:'Il G., T".H:. E,C\., LL.D.
Alm,mer--The Rev. Canon DucKworHfl, c.Y.O., D.D.
Reoistrar-l\Iajor.Gen"ralthe LorJ Cfll'YI.F SMORF, K.C V.O. ·-Sir AI.FRI<:D SCOTT SCOTT·G \TTY, C.V.O . (Ganer).
Dace/or 0/ the Ambulance De/'aI·tmCllt-The l\l ost Han. the ?llarquess of BRE\!)-\I.Il.-\i\E. K.G.
Librarian-Lieut.·Col. HICHAIW HOT IlECIlE.
S!cretary-Colonci Sir HERBERT C. PL·.RROTT, nt., C .n. Clzairman 0/ tite Slitisit Ophtlzalllllr flostita" jel11sa/t;m The Right Hon.the Earl ofPlyntollth, C.II.
C ltie/ Secreta r y 0./ tlte A IIll'u l rwa neta' tmw! C olonel Sir H FRBERT C. PERROTT, Ht., C. U.
@Xt.Clttib'e @ffi.cms.
Asslstallt Din!ctoy 0/ the A ",bit/alice Departmellt-Lieut.-Colonel Si r RICHARD CARNAC TEMPI E, Bt., C.LE.
Assistant H. I· Rl:.SllFIELD, Esq. '-/SS/Slaltl L/inall"" CYRIl.
ASSIStOld Sec yaal), and .-iccoltllla"t-WIl.LlA\I R. Esq., A.C _\. Hot/ 0/ tlte SUl/slt (iP/zI/Ia!III1C !lostu"I , jCJu;'aLcm-
Colon,,1 T. H. Ih:-;f)u:v, C.I.E.
Assislrl1Lt 11(llIoJaJ)' (1'01' .)col/rlJl.l1 0./ lIte RJ'J'lislL Orlzl/laimic .:.; /lospilal,jeJ usaicm- J. HUR!,; t;;STE\E:-;SO.', E'lJ. (Ullicorn {'uysui,'ant ) tGlJc Il' ollllcil.
Th" Coulll il consisls of the Sub- Plior. as Pre,id"nl ex,o'/Jicio, the om, :e", anJ the following !Hrtllllrrs.
Sir JOll"! FURII(Y, C.B ]\[ajor-t;cneral J. C. I>At TO., R.A.
The Right HOIl. t!te Earl of RA;\FliRI v, t;.C..'>l.l;.
Col. C. W . Ilo\\'I'U'll, c.n .
Sir J A E S I) I C K, K. C . D • , :\I.R.C.l'I., R.N.
Colonel Sir Cll.\I{l.t·'i \f. " 'A1S0N, KC.\I.G, c.n ., R.r:.:.
Sir DyC!': VUCK\\'OI{ I'It, Bt., LL.D., ,\Ul.
Ins p e c t 0 r-C en era I B I. (, R \ \. E :'1.1>., R.::-I.
-;ir Rlul \I:t> IIOL";LrS POWELL, lIt. K.C.\'.O., :'I\'V.
The Hun.lh" Fall ofLHH '.'1 . 1 rnlUl'll OWE"!, E'lj., LL.D., F.R.C.S
Lieut.-Colc,ne! Sir C, TE'11'1 h, nr., C.l.t:. "'ILLlA "1 I). JA'LE<';. I· sq C.\'.O.
The lI nn. the LorJ 'UlaHCOTE, G.(,.\\.(;., C.C. l. r., c. n.
The Right Iloll. the Earl uf BESSI3UROUGlI, C.\·.O , C.B. [he <cgaph r.
The ..ts of Ihe Knight" of Justice anJ St!!J.Pn::btes de jure; the the ,\1 embers of Coun tl ; allrlthe followincr @lli[l(lllnq "
The Rev. Canon SlIIPPAIW, C. V.O., D.D., J)ean of the lhap"ls Royal)
The H"v. PAUl. \\'. \\"VAll, ANU
HrprrSCldntiur Hnirrhts of (Grarr nnb Esqlurrs.
Sir I J be> , Right H un ,the \ -iscoull t L\YL/1R, k .C.B., .'>I.D. E.llALKI FY, ?II. \ .0
The RtI{ltt H on. Lord CLAUD Colon,,1 T. H. Tlt-"lll C.LE.. H ·\\111 '1 be H on J.\\tI-S J\1e L t.:E-; • 1
The Right Hon. Earl C,\WDOR GRAV, of vIa)'.
T ' U\\IN HAI'SON I· t.:ESIIFIElll, R>;q. c. B. HA\11110N, E-'1., c.,\[ G. Lt.-Col. \1. WIl.SON, C.B., Lieut.-Colenel l\'oR PII II.I PI'S C :'11.(;., D.S.O., R.A.,\1.C. D.S.O., M.P. .,
Lt.·Cnl. Sir LEES BL, Colonel CHARLES F . ST. CLAIR
C.V.O. A:-;STRUTHER. \I.V.O . , D.S.O .
The Ron. the Lord Dr·s DAWES, F'q . K.C.\'.O. HE"RY ST . JOHN HOPE, E q. Th" Rlgln Hon. the Earl of K.P. B2
{!;'he fol ' ohling are th ittnights of ]usitce:
H.R.H. Prince CIiRISTrnN OF SClil ESWlt.- H OI.STE IN, K.G., G.C.B.
11.;\1. KI NG OF 'IORWAY, K.G., G.C. R., G.C V.O.
fT. H . Prince AI IlEI<T OF "CHI.I':S\I I - HOI 5 TEl N, G.C.D., G.C.V.O.
H .S. H. The Duke of TECK, C; CV 0 , C;\I.G .
H .S. H. Prince FRll'CIS OF TFC". I) <;.0
Rear-.\.dmiral H S H Prince L ouIs OF HITTF"HFRI;, G.C.B., K.C \I.G., R N.
H.S. H Prince AI.I·" ,I:-':DF.R Gl':nRl.,E OF TFCI-:. (;,C.\',O" D.S.O.
H,R,H. PRI"CE OF CON. "AUr,HT, K (; . G.C.V.O.
Lieut.-Col TRI':VENEN HDl.1·,,,1\, C 13.
Sir JOHN FURLEV, C. B (Hon. /lnil(T)
The Ri2ht Hon. Lord <: .C \1 (;
Sir 'I'll .I,IS NORTH DICK-LAUDER, Ht.
::\fajor Sir ARCHIBAI.D L.O\\IB, fit. Col. C;ir III.'RIWRT C. PEIWUTT, fit. C.11
The Hight HOll Farl FFRIWRS, 01. Sir J. (;11 IIF I, K.C \'.0., C.n. HENRV JOH N L ewl us. Esq.
Colonel BETHEL ,\ 1 ,IRT IN I),\\\T,S. Gen, Sir CHARI.ES WARIH- :-':, G,C.l\LG ., K C.B" R.E. ::\Iaj or General J AMES CECIl. DALTON, R.A.
Col. GOUl.D HUNTER\VESTON, D.C:,O., R,E.
Colonel The l<ight Hon. Lord CECIL, C,V .O.
EDWIN FRESIIF1ELD, Esq., LL.D. (Honorary Commander ).
Lord Bishop of <:;ALlSBURY.
Th e Bishop in f ERUSALEM
The Di5hop OrmSBY .
H is Grace li,t: Duke o f FIFF, K ,T.
rhe R I, H on. L01 d BII ,ISSI-:, G.C.B .
The H.iglll li on. \ i'CllUl1l
I'(J\\'" ' I he:: Ric:11l 11 011 Earl A;\IIIFRST. '1 he Right II Oil. \ ',,-count K l'lITS1-(11<11, G C.\I.(;. firm. Dnili/J) . H, 1\1 t 1.1·...\1'.
\, II'IIl,rl I, CllESII.\lIl LE\,E(;Il\\ !',IL 1
IIe::lIt Lull' ,\,IIII', .. Culonel CII,IRI.ES " 'Y"IlI/.HI ::\ILJRII,\\'. C.ll.
The Riehl Il ull Ibe Ead of FLt;lI. (;.C.\l.l;.
The [{Ight 11 <111 I ()lei S,\NDHURST.
G.C.S,I, (;.C.1.1;'.
Sir HI"ln ,\1I'rIlUR bLAKE, G.C::\l.l,.
The Rl. Hon tht! I,arl of 1.1EATH , K..P
A. I'_D\1L'ND Esq,
The l'ighl Ilon l onl \InsTI'N
The ::\Iost Hon. the \larllue,s of I"I', "'.(,. Ris (;, ace the 1)ukt! of P()RTI.AND, KG .• (;.C.\' O. Fielu-:\Iar,hal the Hon. the Earl ROBERTS, K.G , K.P., }".I!:' .• etc.
ROPERT BRUDE, 'FLL CARTER, E"q .,
F R C.S.
NORlI1AN H ... v FOR BES, 1.sq.,
F R. C. S,
Colonel C . \V C .D.
Li"ut.-Col. A. C. \ ,11 E.
l\lajor-General ASTI.FY F. TFRIIV.
Tb e Right Hon The Earl of l'I.V. C.B.
The Rl. HOIl. The Farl !If LATHOM.
The Right Hon. The Earl of SAI':D' WICH, K.C.V O
The Right Hon. The Lord ORTHCOTE. G . c.1\I.G .. G.C .I.E.• C.B.
Qi:1)£ folloming are the r": \ The of CIRR,\t.TAR . Th e Hishop of DUi\EIlIN.
( Przmate 0/ NoW Zealalld.)
B[;;I:-1G T il le \.\lJlUL ,\-';CE OF'
tlhiotg of tDe @rbet 01 the 31'1ospital of eSt. ]oDlI of ]ctllsalrm tn QE;nglanb-. 1 atron.
HIS MOST GRACIOU';; MAJESTY KING EDWARD VII, KG. (SUI FlU 1(.:-1 II ,'" ""l' I'A II{ 1:-' OF Ok,'FR .) rSll:Irnt.
HIS ROYAL HIGHNE S THE PRINCE OF WALES, K .G. (",I INIl 11:1 )1' 01' liE ORIlc.i{,) l"rnlrill Errrut iur \[omnlltlrr.
eXLhhi\'t:ll' uf \It'IIl,,<:rs and of the Order.
Du'ecto' 01 II:,' .-1l11t1ll/,(JI<I' /I,/"v (II«'J/! 'llll C/;"inl/,Vl ,'I COIliJ/lit!Ec'-
1 he :'IIos[ 11)11 Ihe \I.lI<jdL" of II Iltn Il,·1 I 1\1 'I', K (,
A \S/,<!,lll! {)i"'(:'" nll'/ n,'pull' C/lclh III,VI - 1.1Ilt·Co lone] :-ir h.ILilll{ll C. 1'''\11'1.1', Ht., l' I.L.
[)'/'JllI',( kr''''',H/ ir }>lI" I' URI 1'1', C. B, (I.ife \[L'I1Iber or II ! C r,l_ tllilee IloNo'I;' L,l,(,1 I).
.1/ (III S. :\ I.dor r C I), I r., . R.,\. C", l1el C \\' -1\UII 'l.I'" C.I;. ] 1t'1I1 -l'oh)nel ,\. C \ I nr.
I I, 1'<:\,. r \\' \\ lOll, \\ 1"111" 1) '\0". ]""'1. ;\1, I' \;. I, \\ I' IJII I\! :\1 II h r. (olull 1.." J \\, Unll'I'. K.C.I F., E,F. 1"'1 Coil 1\'1'. :-;" ,1<;, \1.1).,1'.(-; I;; '\\' (;, II. 1) 11<11'1'. \I.n. ('!'''III;h'' J·.I 0'. F"I-> \I.I{ 11 lIt·( ,,1,,1,..1 C. J. F. c.:'IU;., L.R.C.P. (,,,1 ,11,,1 :'ill' l't.E\IF!\ r \1 I-tlll )S, C.1l. l"I-".lIII J. \\'. :\")1 r 1;""1 I H ,\III)U' Hoc l''-'':'' , \1.\ .0. Ullh:-l, !o"sq., I.L.D, le.R.c.s.
Qtentra: I qJ';omm itt ce- - colltinued.
Th e Lord CLAUD HA i\II LTON.
A d miral A LF RED J OHN C HATFIELD, C n.
Si r J OHN L Bt.
Th e H o n Si r J ,)l IN A . C.)CKBVRN, K .C. M .G., M . D .
Sir A RT HUR C O.'lA N D OYI.E, 11.D.
Th e Ri g ht n on . J. L . W IlARI'O'i, P .C.
Surgeon. General Sir A I.FR IW K EO(.;H, K .C . n., F. R .C .S IT. & 1.
SY DNEY \V. :'Il.\LKIN, E-q .
Li e u t.-Colone l .-ir J .\\IES R. A. CLARK, Bl., C. B , F R.C. E
Surgeon·General Sir BI!:"J ·\\11:-: FRANKLl'i, K .C. 1. I£.
J OIl'i GRIFFI rllS, Esq., :'I L R.C.S.
Lieut. Colonel })lI" AR"AI 1.1' JO'lES, i\1 D.
Sir \ VII.LlA\1 1'110\[ \S LEWIS, Ilt., K .C. V.O.
T he Hnn_ i'HI/\I\S A.
The Rie;ht H o n. The Earl pf Ih:'SIIOROIJr.H, CV.O . , C 13.
Lleut.·Col.lIlell:g"RGE E TWISS, Colonel J C \" 11.11', F R.C.:'.
Colonel T H. HENDLEV, C. l.E<.. .
Surgeoll.\bjor (;. A. HUTTO".
Surgeon·General Sir CH \llLI!:S i\ l cDONOVGIl CUFFE, K C B , V R.C S I':.
Deputy· i lhpec tor G e neral :'II. COATES, :'oLD., R.:--I.
F. R. C\"SII>I, I':,,{o, \ 1 Il.
A. THEOO .)IIE n"A'I>. .. :'of. n .
J. ASI'LEY 111.<>" \\1, E"I, F H.C.S. FilA "CIS _ . EI LIS, E. Q
l\ l ajor E. \\'E"T Snn-:s, \ f. D . \ VIl.LlA\1 A UlJl.\'Il, E,q, \f RC S. J . ;'Ifo!!L \" , I£sq " C. \ ' , 0, I , R . C.S. Ex·Olli e/,' ,lft'IIIPtrs ,if COlllllllfh',:.
Sir HERBERT JEKYLl., K. ' 1\I.G " R E. (Secretary General ot lhe Orderl
E DWIN FRESIII' IELD, Esq. , LL.D. of tiL Ortler).
T he Ri!!;ht Hun. I'he Klil of PLY.\I<lV fl1, C. ll. (Ch.lIr11nn, Brit is17 Opluhalmic Hu'pi tal).
([hirf .%r rrr t il T!)
C o lonel S ir HERflEPT C. PI'..RR0l'f, 13l., C B. (Se;rela ry of the Onler)
D trrcL or of .%to rr5 an'tJ 'f{r rotlntan f •
Wf LLl,\. \[ R. EIJ\\'ARDS, E-.q., A.C A.
(A ss'stant Secre ta r)' and ..J.CCOltlltall t 0/ !Iu: Orde r} .
\V ILLIAM H ENRY I\fnJl(; \ '1, Esq. ( 'upt: r i n ten i e n t, !,walid r,·(f. ll sj>ort Corps )
REVI SED
F'I R ST AID TO THE INJURED.
SYLLAB U S O F IN
A. Principles of Fir. t .\lt1.
B. ..:\ IJlid De"criptilln o f the IT uman keletun and of the M uscles.
FracturL's CausL's, ' -:Hidies, and symptoms .
D. Treatllient uf Fractures - GenL'ral Rults.
E. T he Triangular lhndage and its application. LECTURE.
. \ . Treatment o f Fracturls (continued). Deta ils o f t r ea tm en t.
B . Dis locations, Sprains, Strains-Signs, symptoms a nd t rea tm ent.
C. T he H emt a nd Blood \ 'esse ls . T he Ci rculat i o n of the Bl o()d_
D. H re mo rrh age a n 1 woun ds. Gene ral r ul es for tre atment
E. T he Triangul a r Ba ndage an d its a pplic at io n,
TllTRD LECTL1RE.
A. anLl \\ (continued). Details 0' treatment.
B. Internal ILemorrhage Signs. arrest.
C. from Special Regions. SI rns, symptoms and arrest. . l' I .
D. Bruises, Burne; and Scalds, Bites and • rost- )lte.
E. Foreign bodie,.; in the Eye, a':1<1. },a:.
F. The Trianguhr Ihndage and Its applicatIOn.
FOURTl! LECTl'RE.
A. The N en'ous System.
B. The Organ'i and Mechanism of Respirat ion -Artificial Respiration.
C. Insensibility.
D.
FIFTl! LECTL'RE (for :orale::; only).
A. Improvised methods of lifting and carrying the sick o r tnjured. .' k .. r1
B. ;\fethods of lifting and CHI)'ll1g the SIC - or Injure on 5t retchers.
C. The cOl1\'eyallce of such I»), rail or in count r y carts.
FIFTII LeCtURE ([o r Females 0nl)" .
A. Preparation f )r reception ?f acciLlent cases.
B. M eans of lifting and rar ryl11g .
C. Preparatiun of bed.
D. Removing the c lolhes.
E. P repa rations for surgeon . !)
NOTE 1.-The bject of p()isons should be treated in a general manner; the common poison- classitied, and only the ir general symptoms, effects and treatment taught.
II.-The last h.llf-hour of each lecture should be devoted to practical work, such as the . pp ication of bandage s and spliltts, lifting and carr),ing wounded on stretchers
XOTE IIT.-There "hould be an interval ofa week betwee n each lecture .\ candidate for examination must attend at least four Olt of the fi\'e lt ctures
OTE cbsses IllllSt pass in that y:tem of stretcher exercise most SUitable fur the locality
V.-I\S lime as possible is to be spent on instruction in anatomict.1 and l,hysiological details. Leci ure rs and examiners are particularly reqaest( <l to rememlJl.r dInt it is Ie First Aid" that has to be taught and tested, and not anatom y and physiology.
JJixtd '/,ISSLS 0)' lltell alld 'W,)JIlell are Oil no aaOltllt pt,ymitted.
PUPILS U:-;DER SIXTKE!'I YEARS OF AGE O"LY ATTEND
TIlE c· JU!'IIOR" CI..lURSE (SeCTI O!'l A, :YLLABUS 40),
Lecture r s in a First Aid c'ass and Local Secretarie.!l, can obtain further particulars on application to the Chief Secretary for •• P a per Reference No. 80."
No Ledurer 111<1)1 i'X7JII!'lle his own Class),,,r Crrtificates
CH.\ PTE R 1.
Principles of First Aid
Explanatory
Questions on Chapter
C HAPTER II.
The Human Skeleton. S kull, spine, ribs and breastbon e, upper li mbs (colla r-b on e, shoulder-blade, armbone, bones of the forearm, carpus , metacarpus, phal anges), p elvis, lowe r lim bs (th igh-bone , kneecap , tarsus, metatarsus, phalanges) ... . ..
Joints ...
Muscles. Volu nta ry and involuntary
Fractures. Causes, variet ies, signs and £ymptoms
Apparatus for treatment of Fractures ...
General Rules to be observed in the treatment of Fractures
Special Fractures. Cran iu m, lowe r jaw, spine, ri bs, breast- b one, collar- bone, shoulde r -b lade , arm -bon e or b ones cl ose to th e elb ow j Jint, forearm, crushed ha nd, pelvis, thi gh -bone, k nee-ca p, leg, crushed foot
Dislocations
Sprains
Sprains and Ruptured Muscles ... on Chapter
C H APTE R III.
Circulation of the Blood. Organs; general (systemic) a nd pulmona ry circulations
Hcemorrhage or Bleeding. Arterial, venous, capillary
Arterial Hcemorrhage. Principl es of arrest
Wounds with Arterial Hcemorrhage ... '
Course of the Main Arteries and Pressure Points. Aorta, a rteries of the head and neck, of the upper limbs, of the lower limLs
Venous Hcemorrhage and Varicose Veins
Wounds with Venous Hcemorr hage
Capillary Hcemorrhage
Internal Hcemorrhage
Hcemorrhage from Special Regions
Questions on Chapter
C HAPTER I V.
Miscellaneous Injuries. Bruises, bums and scalds, hites of snakes and rabid an imals and wound,., by poisoned weapons, sti ngs of plants and animals, fros t bite , needle embedded under the skin, fish hook embedded in the skin, injuries to joints, fo reign b ody in the eye, ear passage and nose, wound in the front wall of the abdomen, injuries ta th e organs wi th in th e abdomen and pe l\'i; . ..
Questions on Chapter
CHAPTER V.
The Nervous System. Cereb ro-spinal, sympath etic ...
The Respiratory System
Artificial Respiration. Schafe r's, Silveste r"s. H oward's combined wi t h Sil vester's, L abo rd e's and Ma rsh3I! Hall's methods ...
[2
Insensib1l1ty. Cause s, general rul es for treatment, concus "ion of the brain, compression of the brain, apoplexy, epilepsy, hyste ri a , shock, fainting and collapse, unstroke and heat-strJke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPTER VI.
poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for the s calp , forehead , etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three hande(' seats, fireman's lift, fore and aft method, impro\;sl-'d stretchers, to cross a ditch or wall, to load or unload a wagon ..
CHAPTER IX.
Stretcher Transport. Stretchers, stretcher exerci ses, litters
CHAPTER X.
The Fifth Lecture (for Females only). Pr epa rat ion fo r reception of accident cases, choice and preparation of a room, lifting and carrying, preparat ion of bed, removing the clothes, preparation for surgeon ...
Questions on Chapter
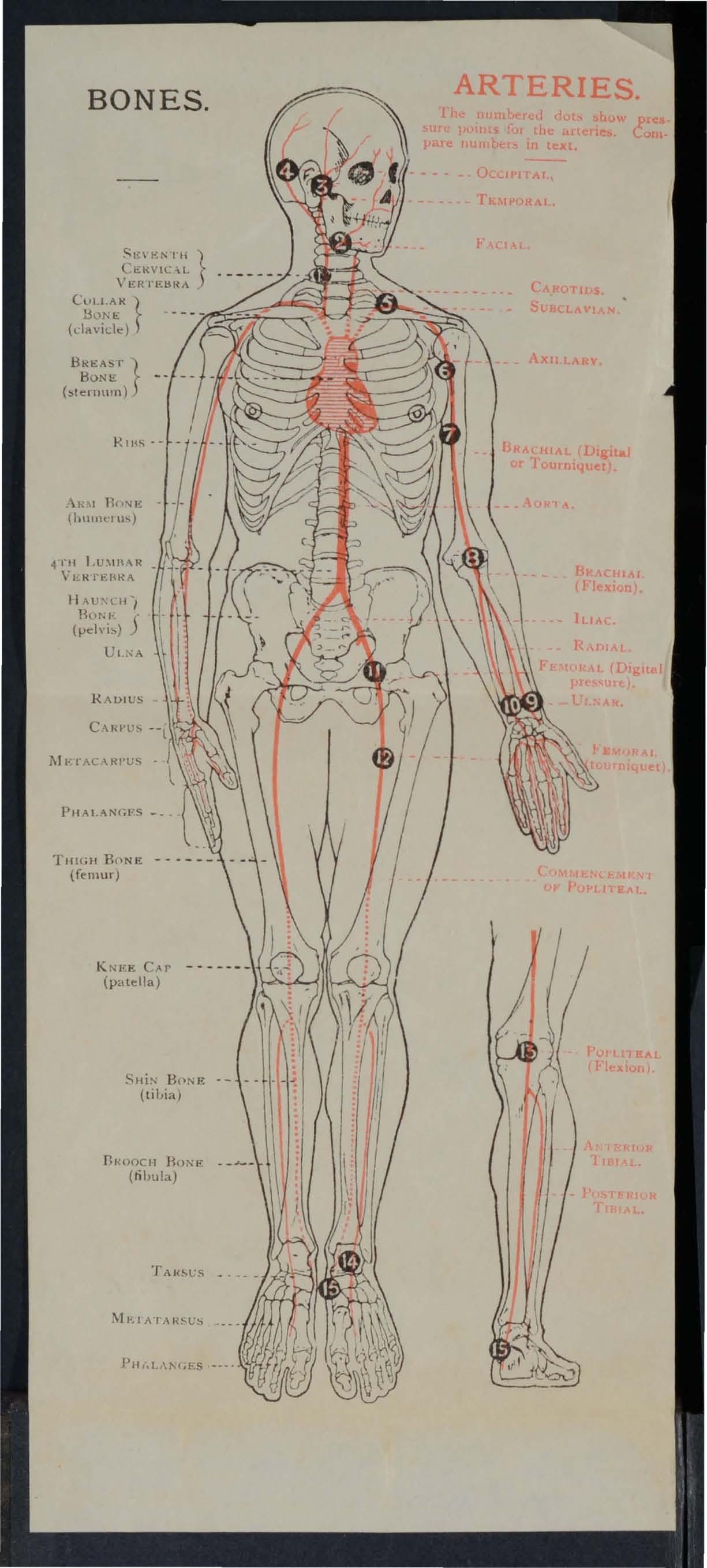
Skeleton showing position of main arteries
Skull and vertebral column
Vertebra
Bones of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle ...
Rectus i\Iuscle ... . . .
Triangular bandage spread out and folded
Large arm sling .. ... "
Small arm sling
Reef knot
Gr:ilnny knot
Loop knot .
Bandage for fracture of lower jaw . .
Bandages fur simple fracture of rib:;
St. John sling ... ..
Band ges for fracture of both collar bone:;
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint ...
Treatment uf fracture of forearm
Treatmt nt of crushed hand. .. . " .. .
Treatment of fmcl ure of thigh bone .. .
Treatment of fracture of thigh bonL (\\"oman)
Fracture of knee cap ... ." . ""
Treatplent of fracture of knee cap . . ,
Treatment of fracture of leg (man and w0man)
Treatment of crushed foot... .
Diagram of the heart, lungs and ail pa ages
Diagram of the circulation of the blood
Digital pressure on carotid artery '"
Digital on facial artery '"
Digital pressure on temporal artery
Digital pres-ure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad
Digital pressure on subclavian artery
Pad and bandage5 to apply pressure on axillary artery ..
Digital pressure on brachial artery (two methods)
Flexion at elbow
Digital pressure on radial and ulnar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on fem ora l artery ..
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen,.,
The lungs and bronchial tubes
Schafer's method of a rtificial respirati on ...
Silvester's method of artificial respiration
Silvester's and Howard's methods of artifici I respiration com bi ned
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage for the hand
Band age for the foot
Bandage for the chest
Bandage for the knee
Bandage for the el bow
Grip for fou r-handed seat
Lifting by two-handed seat."
Grips for two-handed seats .. ,
Carrying by two-handed seat
Grip for three-banded seat",
Supporting patient ... ...,
Fore and aft method of carrylOg
Carrying on improvised seat
Impro\'ised stretcher .,'
Furley stretchers
Stretcher exercise, Ko. I. " Fall in ..
Ditto, ready to lift patient
Ditto, lifting patient. ..
Ditto, placing stretcher ,."
Ditto, preparing to lower patICnt.
Ditto "Lower"
Ditto: No, II. Ready to lift patient
Ditto, patient lifted.. ...
Ditto, No, IV, First pl)siliun
Ditto second position .. , , . . .
Diag;ams illustrating Army stretcher drill
Ditt o ".
Bed cradle
lmpro\'ised bed cradles
PREFACE.
AT the request of the Central Executive Committee
I have revised the manual ,,,ritten by myself in 19 01 as the official handbook of the St. John Association.
Throughout the revision an endeavour bas been made to simplify the study of First Aid to the Injured by dra\\ing up a number of general rules for the of accidents and sudden illness, and by the omISSion of all detai l \\ hich is not atsolutely necessary to enable the student to acquire an intelligent kno\\ ledge of the subject.
I \\ ish to expre s my thanks to Professor E. A . Schafer for fUl:nis.hing for performing a method of artIflclal respiration, to Dr.' L. M. F. for many val uable suggestions, and to the MedIcal Members of the Central Executive Comm ittee, especially Surgeon-Major G. H. Darwin, M.D. a nd Dr. F. R. Cassidi, for p erusing the proof sheets a n d for a number of usefu l additions to the work.
I cannot omit also to offer my best ackno\\'ledgments to Mr. ,\V. R. Edwards, the Accountant and Storekeeper of the S.J.A.A., for his i .valuable co-operati on .
C A NTLIE
The t. John Ambulance Association has now completed thirty years of its existence, and during that period hundreds of thousands of men and women have been taught at its classes, in all parts of the world, how to help their injured neighbours.
F irst Ai d to t h e I njure d is a special branch of practical medicine and surgery, by a kno\\ ledge of which trained persons are enabled to afford skilled assistance in cases of accident and sudden illness. The instruction begins and ends with First Aid, and the subject is taught simply but thoroughly and exhaustively. The duty of the ambulance pupils ends where the doctor's commences, and there ought to be no overlapping or clashing of duty or interests.
1. The First .... IJ student should be-
(a) Obse r vant, that he may note the causes and signs * of in j ury.
(b) Tactful , that he may without thoughtless questions learn the symptoms t and h istory t of the case . --------- --------------------
• Signs are what may be perceived.
t Symptoms are what the patient can tell you.
t History means the circumstances attending the accirlent or sudden
(c) Resourceful, that he may use to the bes t advantage \\ hatever is at hand to prevent further damage and to assist Nature 's efforts to repair the mischief already done .
(d) Explicit, that he may give clear instructions to the patient or the bystanders how best to assist him.
(e) Discriminati n g, tbat he may decide \\ hich of several injuri es presses most for treatment by hims e lf, and \\ hat can best be left for the patient or the bystanders to do.
2. Remove the cause of injury or danger whenever possible.
3· Severe hcemorrhag e must rec e ive t he first attention , no matter what are the ot her injuries.
4· Air. - ,!,he. patient must be in a position in which breathlll 6 IS possible; the air passages must be free from obstruction; if breathing has ceased prompt m easures must be taken to restore it.
S· restful position of the body will assist the vItal functIOns; support of the injured part \\ ill h elp to prevent further damage, and is essential in t he case of fractures of limbs.
Warmth. -After every accident keep the pati ent warm so as to prevent the fall of temperatur e belo w the normal point.
7· When the skin is broken the wound
19
should be promptly covered wilh a clean absorbe nt dressi ng . Should the \\ OUlld be poisoned, it is mos't important immediately to preyent the poiso n permeating the S) stem.
8. Poisons s\\allowed should be got rid of, o r when that is lIlexpedlcnt. neutralised.
9. The b e st means of must Le studied, and provi ion n ade for pruper care when the patlent is brought to sheller.
ro . Removal of Clothing. - Clothes should not be taken off unnecessarily, but wht n it is ll( edful to remove them, the following ruies "ill be found of service in serious cases :-
COAT: Ren oye from tbe so und side first, and, if nece sar)" slit up the seam of the slee \'e on the injured side .
SHIRT A;\'D VI<: T : lit down the front and remove as the coat.
TROUSERS: lit lip the outer seam.
BOOT: lit the back seam and undo the laces.
SOCK: Cut off.
II. Stimulants. -It is incorrect to suppose tha t alcohol is the only form of stimulant, <lnd far to o f req uent use of spirits is made to restore a patient after an accident, often with serious re ults; the safes t rule, therefore, is to defer the administration of alcoho l until the arrival of a doctor. \Vhen the patient is able to s\\'allow, strong tea or c(·ffee o r milk, as hot as c a n
xo
be d r u nk, or a small quantity of sal volatile in water m ay be given. Smelling salts may be held to the n ose. Sprinkling t he face with cold and hot watel alternately, warmth applied to the pit of the stomach a nd oyer the heart, and vigorous friction of the limbs u pwards have a stimulating effect.
12. Throughout his work th e First Aid student must on no accoun t tak e upo n h imself the duties and responsibilities of a Medica l man. At times an apparently slight injury is accomp anied by graye danger and may actually cause loss of life. "When se nding for a doctor, state the nature of the cast': and remem ber that \\Titten particu lars are safer than a verbal message.
It is necessary that something should be known of t he structure of the body (elementary anatomy), and of the functions of some of the more important organs and systems (tlementary pbysiology). A short description of the necessary anatomical and physiologIcal puints is therefore glVen as the several subjects are discussed . For purposes of description the human budy is supposed to be erect, \\ ith the arms hanging by the side and the palms (If the hands directed forwards. TIle" middle line" of the body runs vertlcall) from the top of the head to a point between the feet
Tlze nU1I!u'a!s 2l1dz"cate tlu jar.:es wlil1e tlu answers 11 ay be jOlflld.
\Yhat is First Aid to the injurld?
\\hat qualities sh ould the }jrst Aid student
\\'hat are signs?
\\'hat are synlptoms? .
\\'hat is the history ofa \\'hat is often the first thing to dL) in
How must poisoning be tTl attd
\\ hat step ... must be laJ,.en be)ord the actual treatment of inJuries?
Should clothing always be ren]('\'eo?
How would yuu remove clothing \\ hen nece ar)?
Explain the use and abu<.;e (If slil11ulal ts ..
What must the First Aid student not dv ?
\\' hat is elementary analOl11) ?
\\'hat is elementar) physiology?
Fo r of deserip'i d n how is the hUll all I
supposed to be pI. ce' I
CHAPTER II.
F RACTURES, DISLOCATIONS, SPRAINS AND STRAINS.
THE SKELETON.
The human body is moulded upon a bony framework (the skeleton) which serves-
I. - To give shape and firmness to the body.
2.-To afford attachment to the 111usc1es.
3 · - To protect important organs, as in the skull, chest, and abdomen.
SKULL.
The Bones of the Skull are arranged in two groups, those of the brain case or cranium, and those of the face.
The Boundaries of the Cranium are the vault or dome, the rounded portion forming the top of the h ead; the front or brow; the back of the head, where the greatest extent of brain exists, and where therefore the cranium is widest and deepest; the sides or temples. The base of the cranIUm is hidden from view by the bones of the face and of the vertebral column; in it are numerous perforations for the passage of blood vessels and nerves; through the largest opening t he brain and spinal cord are continuous.
The Bones of the Face with the exceptIOn of
the lower jaw are firmlx to;ether, so movement between them IS ImpossIble. The ca vlt!es of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face conjointly. The mouth cavity is between the upper and lower jaws, the pal<l:te bemg the bony ro.of of the which separates It from the nasal cavity above.
The Lower Jaw consists of:-
( a) A horizontal portion in which are the sockets for the teeth.
(f) Vertical portions terminating on either side at the joint between the lower ja \V an? the base of the cranium, situated immedIately in front of the ear.
The an crle of the j1w indicates the junction of the horizontal the \ ertical portions .
The Vertebral Column (Fig. 1) is composed of bones called vertebrre, each of which consists ofl.-A body or bony mass in front.
2.-Process s projecting backwards, which enclose a canal for the spinal cord - the spinal canal.
3.-Two tranS\'erse twel\-e pairs of which supp o rt the nbs.
S KULL A ND VERTEBRAL COLUl\IN
Showin g left ril-s and portion of breast bon e. The right riLs ar e r emoved.
SPINOUS PROCI!.SS.
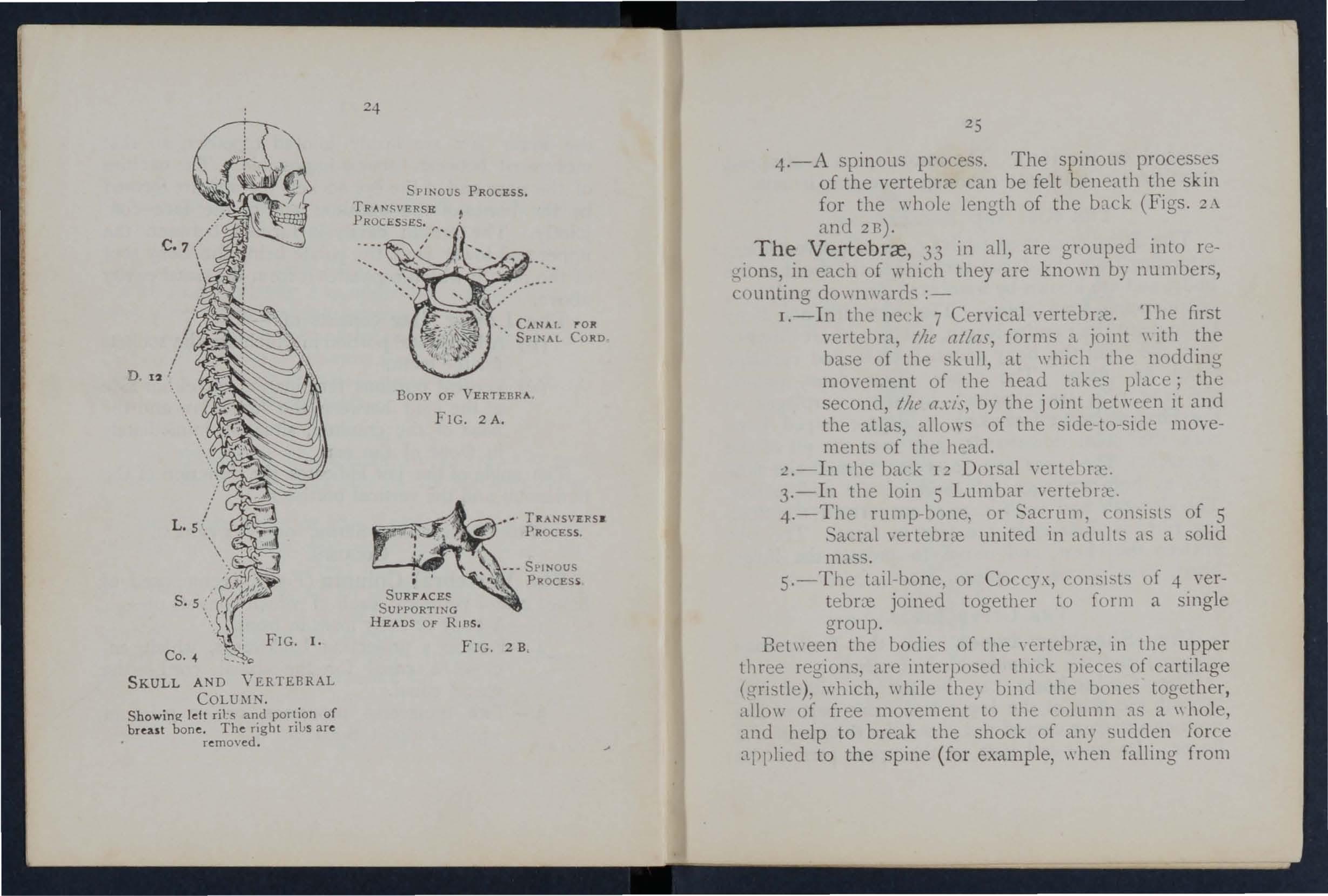
OF VERTEBRA
FIG. 2 A.
SU RFACI!.S SUPPORTING HE A DS OF RIB S.
FIG. 2 B
4.-A spinoLls process. The spinous processes of the vertebrrc can be felt beneath the skin for the \\ length of the b:1ck (Figs. 2.\ amI2n).
Th e Vertebrce , 33 in all, are grouped into r egions, in each of which they are known by nUI11bers, counting downwards :-
I.-In the neck 7 Cervical vertebr::-e. The fir t vertebra, tile atlas, forms a joint \\ ith the base of the skull, at \\ bich the nodding movement of the head takes place; the second, tile by the joint bet\\ cen it and the atlas, al10\\"s of the side to -s ide movements of the head.
:? .-In the back 12 Dorsal ycrtel>ra.:.
3.-1n the loin 5 Lumbar
4.- The rump-bo lle, or .... acrum, c()nsist of 5 acral"ertebrrc united in adults a a solid mass .
5.-The tail-bone. or Cocey" con..,i..,ts l>f -I- vertebr:-e joined together to form a single group.
Bet\\ een the bodies of the' crlehr:l;, in the upper three region, are interposed thick pieces of cartilage (gristle), which, \\hile they bind the bones together, <lllo\\ of free mO\'ement to the column as a \\hole, and help to break the shock of any sudden force applied to the spine ( fo r example, when falling from
a height on the feet). The \\ hole spine is strapped together by ligaments reaching its entire length.
THE RIBS A D BREAST-BO 'E.
The Ribs consist of tweh e pairs of curved bones ext ending from the dorsal vertebrce to tbe front of the body, and are known by scccnd, etc., commencing from above. TIle ribs are not Leny throughout their entire length, but at a s1.('1't distance from the front the bony material ends, and cartill1ge takes its place. The upper seven I airs, named the true ribs, are attached by their Gntllages to the Breast-bone (sternum), a dagger-sl1aped h ne with the point do\\ n\\'ards, just 0\ e1' tl.e 1 it of tIle stom ach . The Io\\er fi\e pairs are tern ed h.]se r ibs, as their cartilages fall short of tbe n iddJe line. The eleventh and t\\ elfth pairs are termed tl e floatmg rib s, as their ends are free in front. 1 Le ribs enclose the chest, and scn'e to protect the lungs, heart, liver, stomach, spleen, etc .
THE UPPER Lll\JBS.
The Shoulder - bones are the Collar-bone (davie/e) and the Shoulder-blade (scap?lla).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thi ckness of a finger. Its inn er end rests on the upper part of the PART OF COLLAR
\[)E ( C \PL' I ) ,\Il\t BONE ( 11 ERUS)
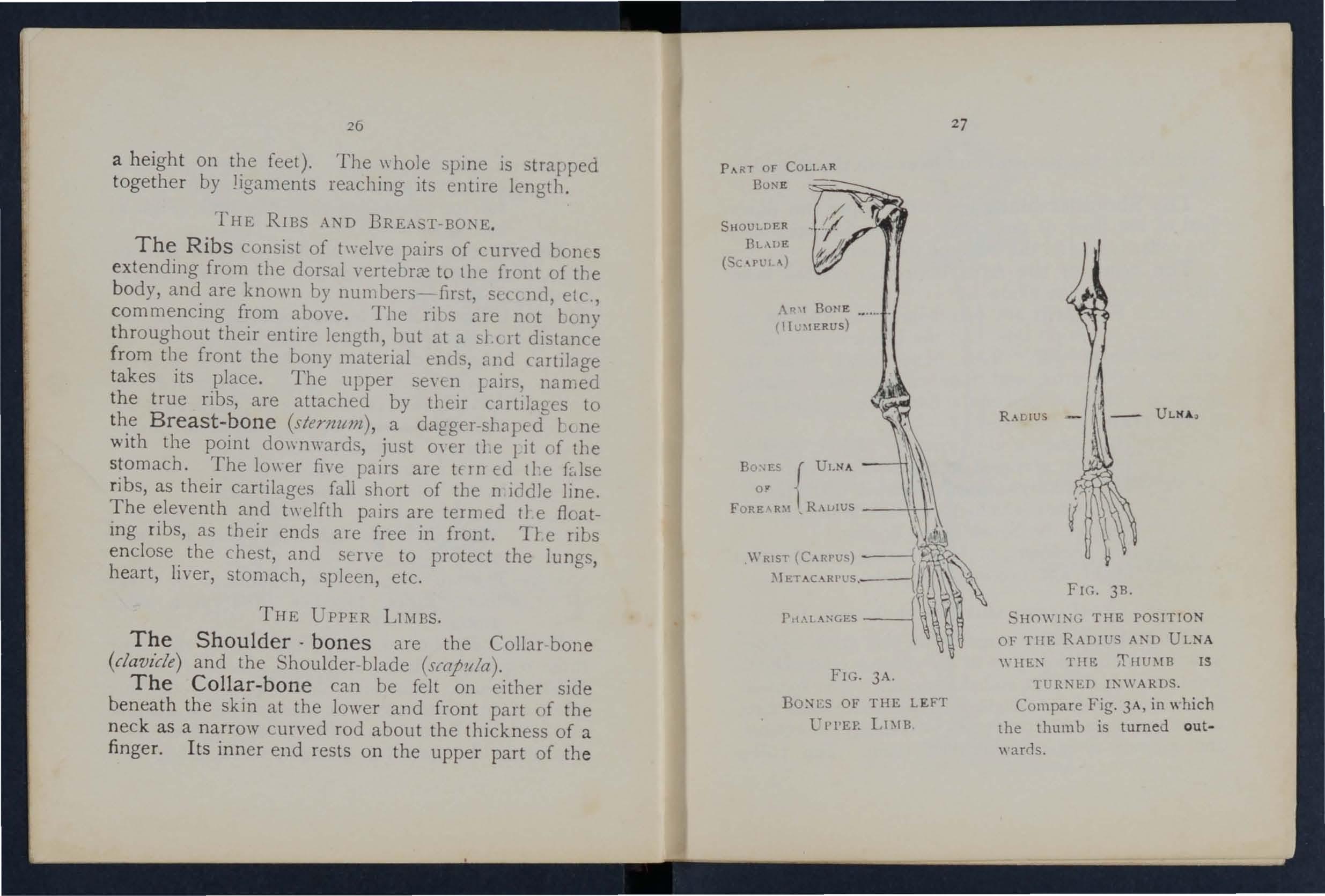
{ UI.NA or , R.\lJIUS --++-i-I
R.UIUS
FIG. 3A.
BO:-'ES OF THE LEFT
l'l'l'EP. LD[B
FH-;. 3B.
SHO\\'ING THE POSITION OF THE RADIUS AND ULNA
TilE: IS
Tl'R:\ED INWARDS . Compare Fig. 3A, in which the thumb is turned outwards.
2
b r east-bone, and its outer end joi n s with the shouldcrb la d e .
The Shoulder-blade lies at the upper and outer pa r t of the back of the chest, and forms joints \\ lth the collar-bone and the bone of the arm.
The bone of the Arm (lwmerlls) reachls from the shoulder to the elba\\'.
I n the Forearm are two bones. the Rad ius un outer, or thumb side, and the Ul n a on the mner, or little finger side. Both bLnes reach from the e lbow to thLe wrist, and t11ey change their n:latiyc positiun \\ ith e"ery turn of the hand (Flgs. 31\ and 31\).
The Hand is composed of-
I -The bones uf the \\ rist, or ((1I}/(S. eigbt in numb er, in tllO ro\\s (f lour.
.., The 111c/thWjWS (the franle\\ ork l fthe palm) : fire bones which form the knuckles and support the bones of the fingers.
3.- The plwiaJlges, or fll1ger -bo nes, three in (ach finger, and byo in the thumb .
THE PELVIS 1\I'\D LO\I ER LDIDS.
The P e lvis. - The large b8sin 11 ke mass uf I Olll' attached to the 10\\ er pa rt the spllle is composul of the two ;1aunch-bones and the sacrum The !launch bones meet in front (at the pubes) in the middle line, only a small piece of cartibge intervening, but behllld. the S,lcrum is placed bet\\ een them. The peh is
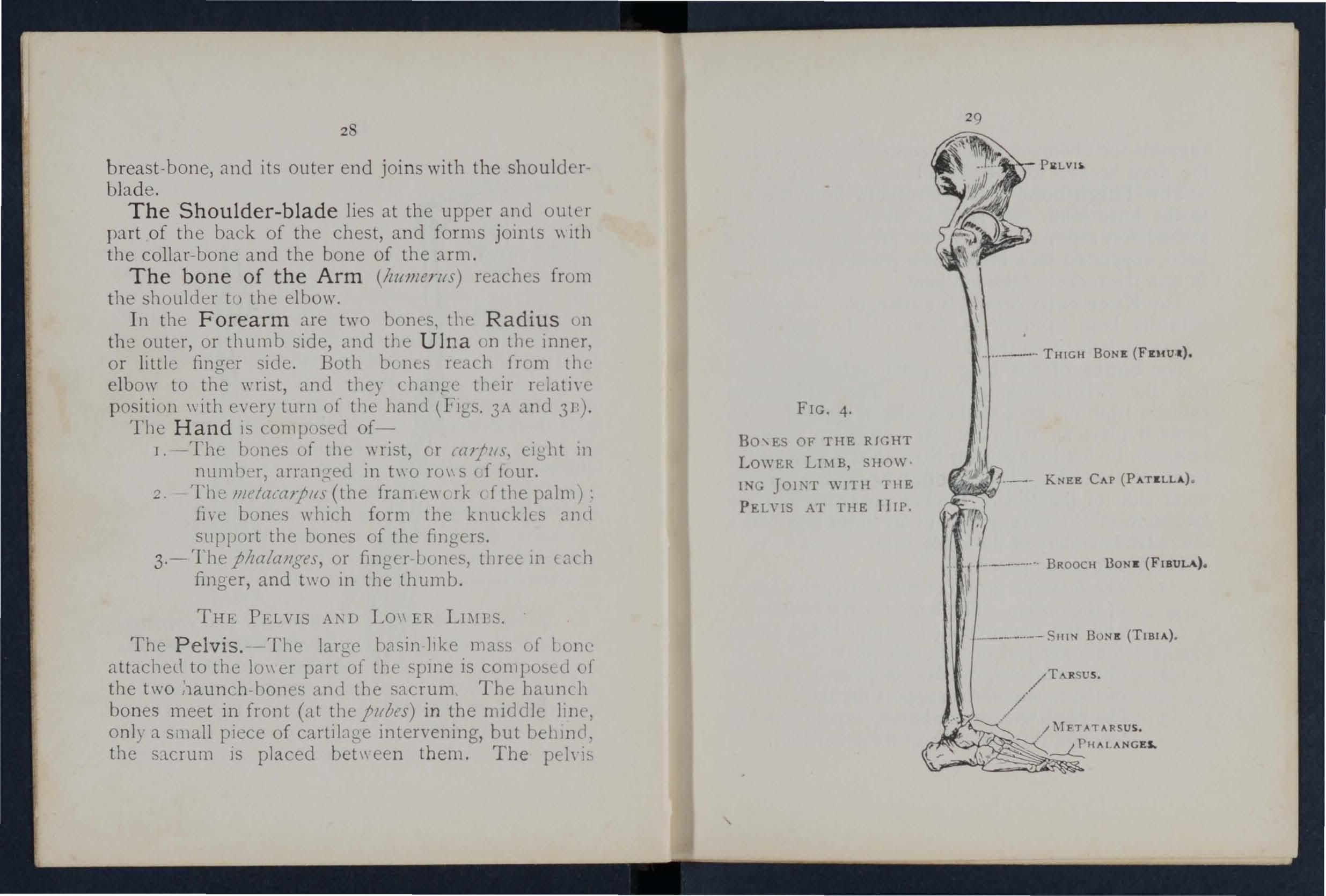
FIG. 4.
BO'ES OF THE RIGHT LOWER LDIB, SHOW· ING J01:-;T WITH 111E PEL\'IS AT THE flIP.
30 supports the abdomen and its contents, and pro\'ides the deep sockets for the thigh-bones-the hip joints.
The Thigh-bone (fe1ll1lr) reaches from t1 e hip to the knee joint. Its shaft is stout, rounded, and arched for" ards; tIl e upper end presents a TOtmdcd head, supported on a neck \\ hich projects il1\\ ards, to fit into the socket of the l1ip joint.
The Knee-cap (fatella) is a trian g ular Lone l) ing \\ith its base in front of the knce joint imme diately b(neath the skin.
The bones of the Leg are the Sbin-lor:e (//bia) and the Brooch ·cone (jibula). Tbe Shin-bone extends from the knee to the ankle, in loth of \\ hich jo ints it plays an important rart; its sharp ed f, e, tile shin, can be felt immediately beneath tbe Shin of the front of the leg. The Brooch·bone lies en the out er side of the tibi,1. It does not enter into tbe form ation of the knee joint, but its 10\\([ end fom ,s the out er boundary of the ankle joint.
The Foot is composed of--
I.-The tarsus, a group of se\(; n nre g ular b o nes at the instep. The largest is tl e heel-bone, and the uppermost (tbe ankl e-bone) forms the lO'vyer part of the ankle joint.
2 ,-The metatarsl{s, the five long bones in front of the tarsus \\ hich support the toes.
3. - The phalanges, or toe-bones, two in the hig t OE', and three in each of the other toes.
3 r JOINTS.
A Joint is formed at the junction of two or more bones. In moveable joi nts such as the hip, knee, etc., surfaces of the bones are covered by cartIlag e, which lesse ns friction and the shock of a
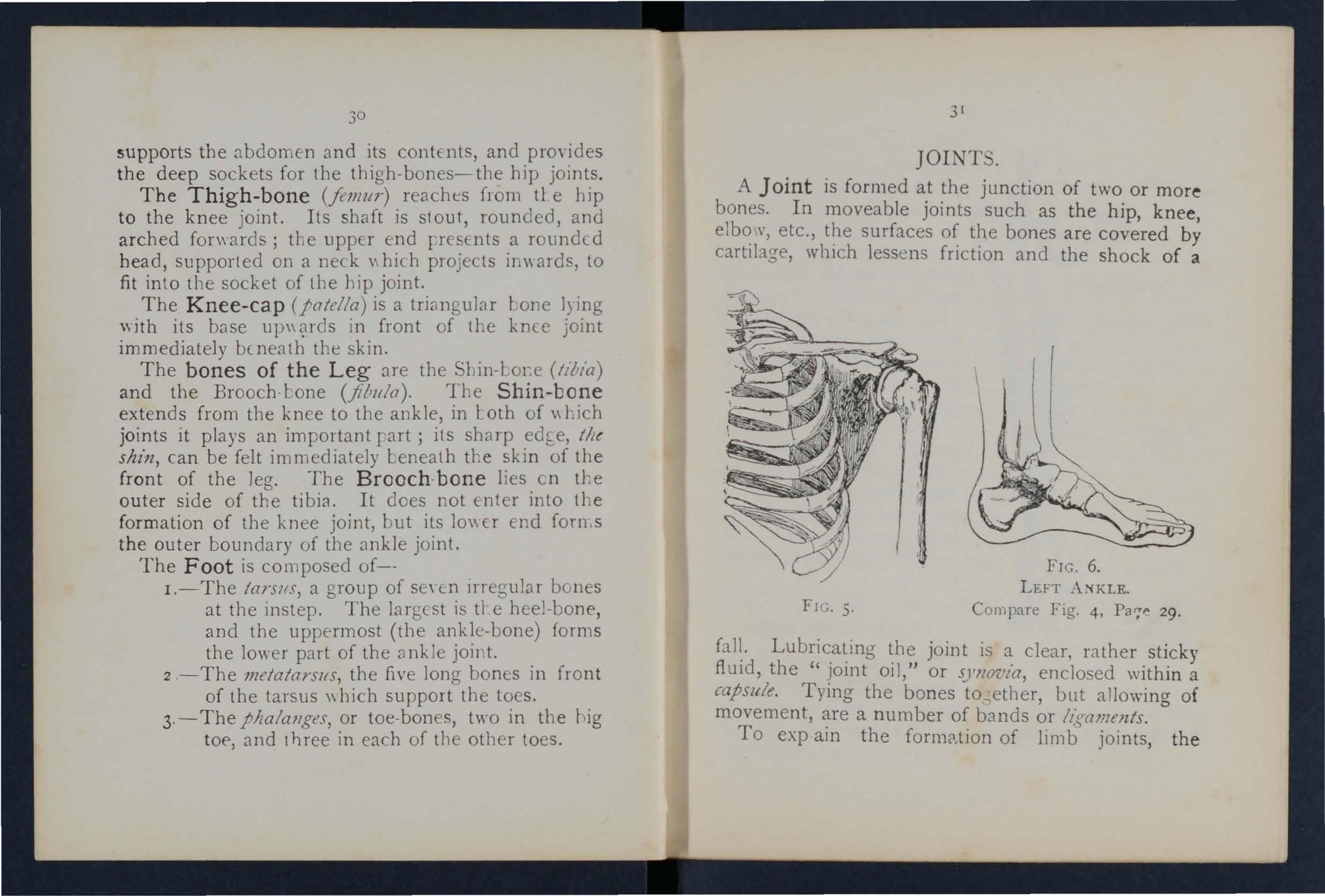
joint is clear, r a ther sticky fluId, the Jomt oIl, or S),Jl OVta, enclo se d ",ithin a capsule. Tymg the bones to ,.; ether, but allowing of movement, a number of bands or lz:saments .
To exp am the formC1.tion of limb joints, the
FI C. 6. L E FT .\:iKLE. FI G. 5. Compare Fi g. 4, Pa,;,1" 29.MUSCULAJ! TISSUE
PATELLA
TINDON OR LIGAMENT OF PATELLA
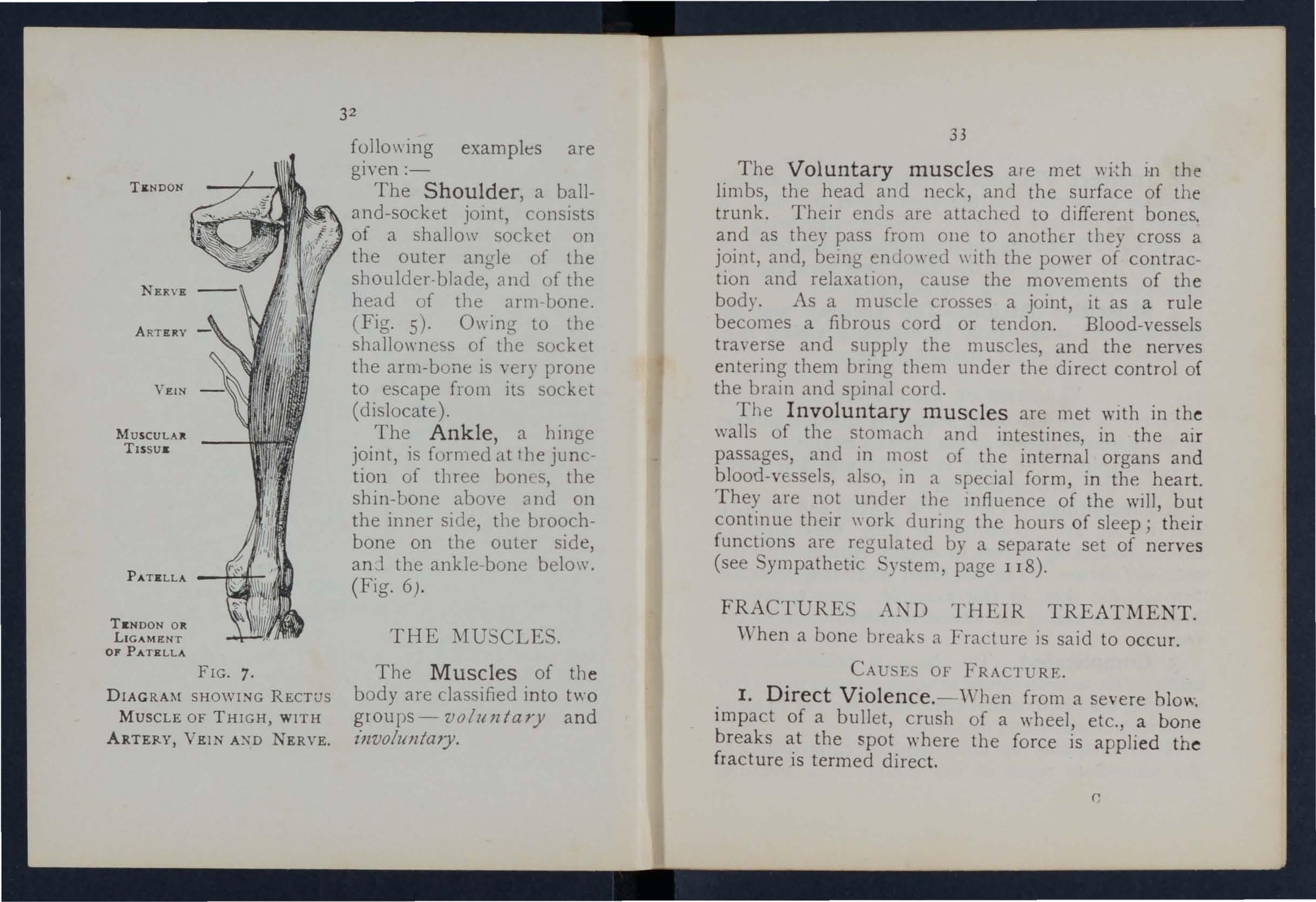
FIG. 7.
DIAGRAM SHOWING RECTUS
MUSCLE OF THIGH, WITH ARTERY, VEIN NERVE.
32
fOllO\\ ing examples are given :-
The Shoulder, a balland-socket joint, consists of a shallo\V socket on the outer angle of the shoulder-blade, and of the head of the arm -bone. (Fig. 5). Ow ing to the shallowness of the socket the arm-bone is very prone to escape from its socket (dislocate) .
The Ankle , a hinge joint, is formed at 1he junction of three bones, the shin-bone abo\'e 3 ncl 011 the inner side, the broochbone on the outer side, anj the ankle-bone belo\\'. (Fig. 6).
The Muscles of the body are classified into two groups - voluntary and in voluJl taJy.
33
The Voluntary muscles ale met m the lim bs, the head and neck, and the surface of the trunk. Their ends are attached to different bones. and as they pass from olle to another they cross a joint, and, being enu o wed with the power of contraction and relaxation, cause the mO\'ements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the nerves entering them bring them under the direct control of the brain and spinal cord.
The Involuntary muscles are met WIth in th e walls of the stomach and intestines, in the ai r passages, and in most of the internal organs and blood-vessels, also, in a special form, in the heart. They are not under tIle mfluence of the will, but their" ork dunng the hours of sleep; their functIons are regulated by a separate set of nerves (see ympathetic System, page 118).
When a bone breaks a Fracture is said to occur.
CAU E OF FRACTURE.
I. Direct Violence. - "\\'hen from a severe hlow impact of a bullet, crush of a wheel, etc., a breaks at the spot 'tV here the force is applied the fracture is termed direct.
2. Indirect Viol e nce. - \ \ Then the bone br c,lks at som e dista n ce from the spot \\ here the fm c e IS appl ied the fracture is term e d indirect. . \ lightin g on the feet and fractu r in g the thigh - hone or the bon es of the leg, or falling on the hand and breaking the radiu s or the colla r -bone, are examples.
3. Muscular Action. - The knee-cap and th e arm- bone are occasionally broken by a violent co ntract ion of the muscles attached to them .
VAR 1U ' IES OF FRACTURES.
Fr actures are clas s ified a c cor d ing to the condi t io n of th e tissues adjacent t o the bone as fol1o\\s ;-
1. S im pl e . - Th e bon e is broken with but sligh t in j ury t o t he surr o undin ,; pa rts .
2. Compound. - The bone is broken and th e s k in an d tissues are p un c tured or t o rn, thus all o\\ in g d isease-produ c ing g e rms to obtain e ntrance to th e seat o f fracture . T he fractured end s may protrud e t h rough th e skin , or ( for example, \\ h e n a b o n e is broken by a bull e t) t h e wou n u may le ad down to the fr acture.
3. Complicated. - Th e bone is broken and in ad dition th e re is a ll injury to som e int e rnal or:;all (fo: e 'mmple, the brain, s pinal coru, lung, e tc.) or t o o me imp ortant blo o u -v e ssel or nerve.
A fractur e .may be c o mpound or complicat e d as t he immediate resu lt of the injury; or a fracture,
simple , 111 1:- he cO ll yerte\.1 in to a' c om poun J
P I' CQ.11p li cated frLlc t urc -
(a) ny c:1r eless Illon:me ll t o n the p:nt of th e patie n t. (/)) By C lre le,,;s lh:-;S or o n the p a rt of
o n = fir:;t :lid .
)·(·ial \'.trt oifr:lctll r l:''> mLl' lit..: cbs<,tfied aC('o r d-
t,) thL injun to t l1l IhJtle It:->eii it" folio\'s;-
I. Comminuted. - T ht..: hone is Illoken in to St:\ Lr II pie, e.,.
2. Green- 3 tick. [ n chIldren , 0\\ [ I) t he soft er
st III 01 the 1) 0 ,1\ lISSU JS. :1 I)(lne 111:1 \ ' a n 1 cra ck
\\ itho I '- U llp lctely acro ss.'
3· 1m ,).3.cted. T he 1)/( )h'n ends of the hone ar e d r!\ e,l \l];L 1I1'U th . () t her.
\1. :-;'l. '> \\]1 • \ \\ H ICll .\ J.\ \" BE 1' RI "I '\ I
(. \ (r,lcture ()f the knllll. h1ll11erll , or hoth bo n es of t h ( hrl:arm or c.rrords tIll' must (om plete l'\..l lip' L ).
I. Pain ,H or Ill'lr t h·, -',\ll ll( (r.lctu re . 2 . L033 o f Po wer ill lil11l).
3· Swelling :11> )ut till' :->C:lt 01 frac t u r e. S wel lin g ]1 'IlL!.' rendl':-' Il dit"lit'lllt to perce l\ e oth " r ut 1r,lctllrc:, an I C.lre l1lLhl therefore he taken n ot to 111 1J..'..: :1 [r.lc lLIre (()r a "enUl!' Il1jun.
4· Deformity of t ht..: limb. - rile limb a,::'Slllilt: S a n
unnatural position, and is mis-shapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to override, thereby producing shortening.
5. Irregularity of the bone.-If the ?one IS close t the skin the fracture may be felt, and If compound it may be seen.
6. Unnatural Mobility. -Movement may be made out at the seat of fraclure.
7. Crepitus, or bony grating, may be felt or heard when the broken ends move one upon the other.
The last two signs should on!), be sough! by a Several of the above signs are absent m green -stick and impacted fractures.
. In addition to the signs and symptoms the patient or the bystanders may be able to the of the injury, and marks on the clothmg or skll1 should be noted, as they may serve to locate the fracture The snap of the bone mav nave been heard or felt.
ApPARATUS FOR 'IREATMENT OF FRACTURES.
Splints and banda.ges for First Aid frequently have to be improvised.
. .
A Splint may be improvised from a walkmg stl.ck, umbrella, billiarcl cue, broom or brush polIce man's truncheon, rifle, folded coat, piece of wood . cardboard, paper firmly folded, a rolled-up map, or , m fact, anytht"1tg that is firm and 10nK enough to keep
?J7
the joints above and below the fractured bone at rest. When the above appliances are not available, the upper limb, If fractured, may be tied to the trunk, and in all cases a fractured lower limb sh o uld be bandaged to its fellow.
Bandages may be improvised from handkerchiefs, bel ts, straps, braces, neckti es, or any piece of calico, string or cord that comes to hand.
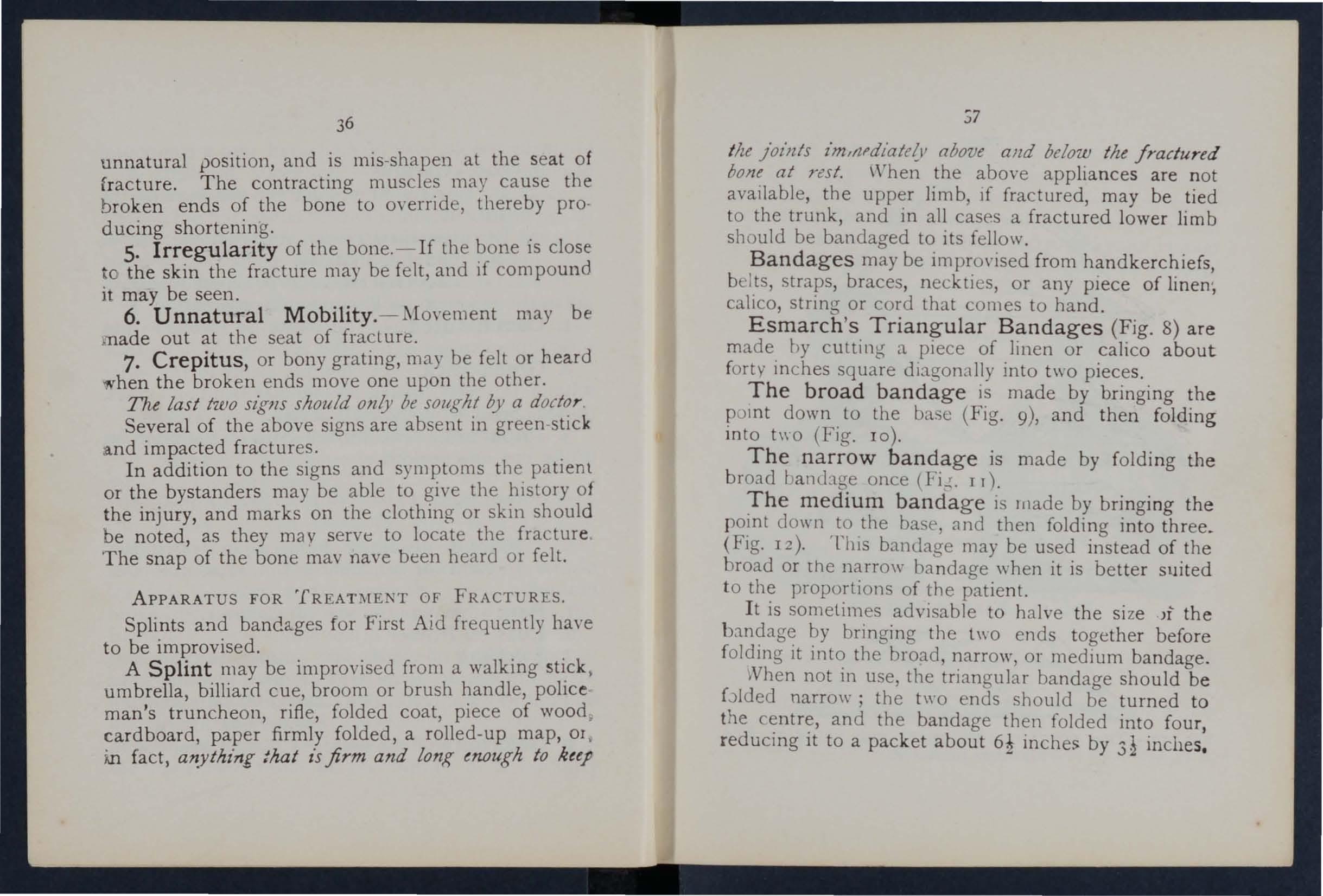
Esmarch's Triangular Bandages (Fig. 8) are made by cutting a piece of linen or calico about forty in ches square dlagon <ll1y into two pieces.
The broad bandage is made by bringing the po mt down to the b< sc (Fig. 9), and then folding into h\ 0 (Fig. 10).
The narrow bandage is made by folding the broad I al1lhge once (Fi..!;. I r).
The medium bandage is lllade by bringing the point clown to the bas e , and then folding into three_ (Fig. 12). ThiS bandage may be used instead of the broad or the narrow bandage when it is better suited to the proportions of the patient.
It is sometimes advisable to halve the size J1 the bandage by bringing the t\\O ends together before folding it into the broad, narrow, or medium bandage.
Nhen not in use, the triangular bandage should be bIded narro\\'; the two ends should be turned to the centre, and the bandage then folded into four, red ucing it to a packet about 6! inches by 3 inches.
FI G. 12.-T Hlt DOTTRD LlNES SHOW THE FOLDS OF Tlla l\IEDlur.r BA:-'DACE.
3)
Large arm-slin g (FJg. J 3).- pread out a bandage, put one end over the shoulder on the sound side, rXlSS it round the neck so that it appears over the shoulder of the injured side, the other end hang clo,,-n in front of the chest; carry the point behind the of the injured limb, and bend the forearm
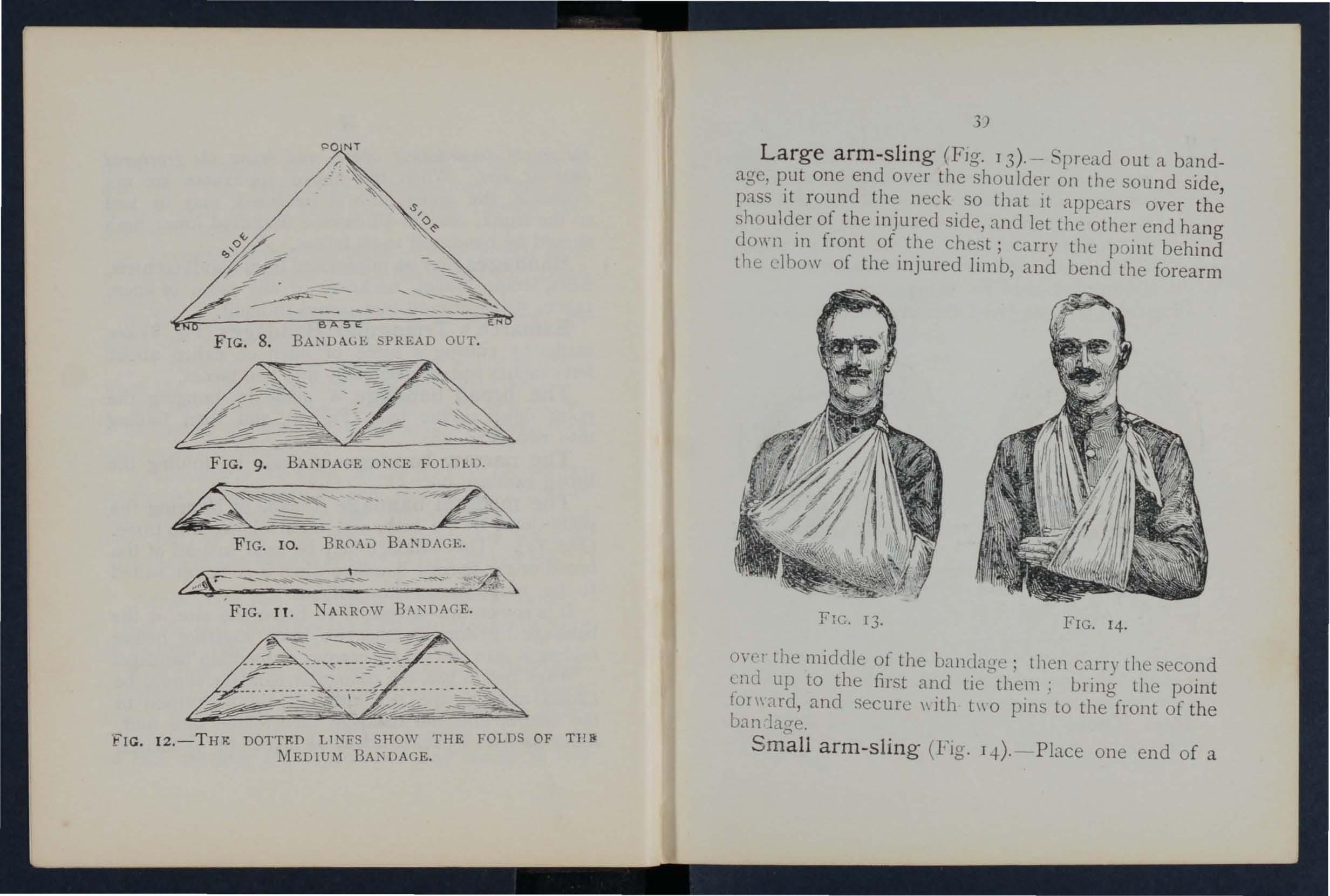
I4. on'l the middle of the uandage; then carry the second end up to the first and tic them: bring the point Cor\\'ard, and secure with t\\O pins to the front of the ban
Sma ll arm-s li n g (Fig. Lj.).-Place one end of a
FIC. I3. FIG.broad bandage over the shoulder on the sound side, pass it round the n eck so that it appears over the shoulder of the injured side; place the forearm oyer the middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in cases of fractured humerus, and occasionally \\ hen the large sling "ou ld be too conspicuous . Slings may be improvised in many simple \\ ays, such
as pinning the sleeve to the clothing, turning up the tail of the coat, passing the hand inside the buttoned coat or waistcoat, etc.
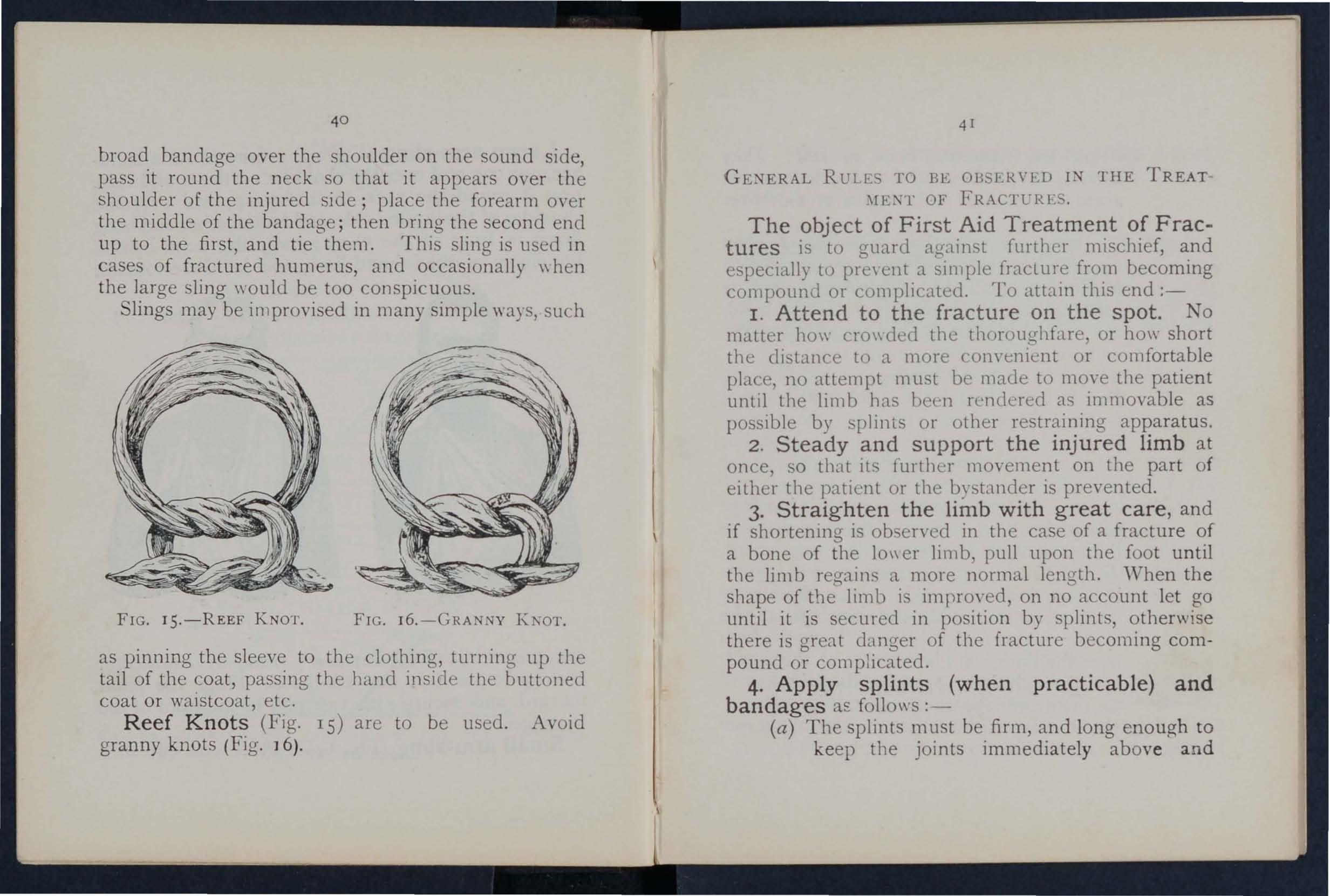
Reef Knots (Fig. IS) are to be used. Avoid granny knots (Fi g. J 6).
GE, ERAL RULE TO BE OBSERVED IN THE TREAT \11<'.1\1' OF FRAC1TRES.
The object of First Aid Treatment of Fractures is to guard against further m1schief, and especially to pre"cnt a sit1lple fracture from becoming compound or complicated. To attain this end :-
I. Attend to the fracture on the spot. No matter ho\\ cro\\ eled the thoroughfare, or ho\\" short the elisL1I1ce to a more convel1lent or comfortable place, no attempt must be made to move the patient until the limb has heen rendered as immovable as possible by splints or other restraining apparatus.
2. Steady and support the injured limb at once, so that Its further movement on the part of either the IXltlcnt or the bystander is prevented .
3. Straighten the limb with great care, and if shortenll1g is ob en'ed in the case of a fracture of a bone of the 10\\ er limb, pull upon the foot until the limb regains a more normal length. "When the shape of the limb i imrroYed, on no account let go until it is secured in position by splints, otherwise there is great danger of the fracture becoming compound or complicated.
4. Apply splints (when practicable) and bandages as follows :-
(a) The splints must be firm, and long enough to keep the joints immediately above and
the fractured bone at rest They should, If practicable, be padded to fit accurately to the limb and be applied mer the clothing .
(b) The bandages must be applied firmly, but not so as to constrIct the circulatIOn of blood' in the limb. \"hen the patient IS in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a rule:-
For the tnmk the broad baLndage should be used. Pass it once round the trunk and L.l.slen It by tying the ends, or with two or three safety pins on the side opposite to the fro. lUI e, but if to secure a splint for a broken thIgh, oyer the splint.
F or the arlit or j()narm lhe narrow Landage should be used. Pass it twice round the limb, and tie the ends oYer the outer :,pI1l1t.
F or the or leg the narrow or medium bandage may be used. It i. frequelltly convenient to double the bandage at the centre, pass it under the lim b, bring the loop over the limb, pass botb ends of the I andage through it in opposite dIrec t ions, and ti e them over the outer splint (Fig. Ii)·
I n apply in g bandages near a fra cture the upper on e 3hould be i ecure d fir st.
5. When hcemorrhage accomlJanies a tu r e it must be attended to first , and th e wou n d covered by a clean dressing.
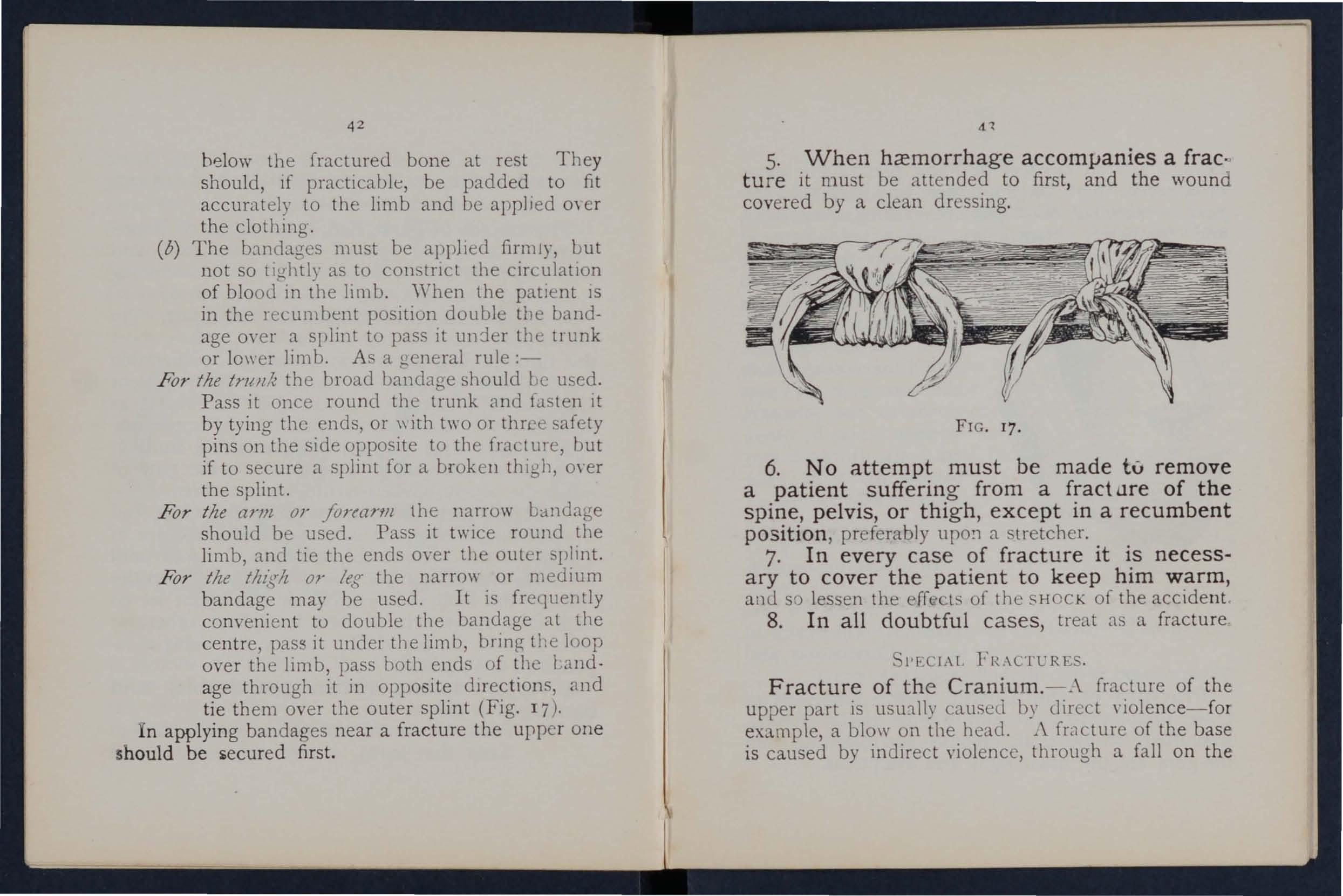
FIG. 17.
6. No attempt must be made tv remove a patient sufferin g from a [ract LIre of the spine, pelvis, or thigh , except in a recumbent position , preferably UpO!1 a stretcher.
7. In every case of fracture it is necessary to cover the pat ient to keep him warm, and so les en the err l. of the SHOCK of the accide n t.
8. In all doubtful c ase s, treat as a fracture
l>r·. CIA[' FR.\CTURES .
Fracture of t h e Cran ium. -.\ fracture of the upper part is usu:111)' causeli by direct yiolence- for example, a blow on the head. i\ fracture of the base is caused by indirect yiolencc, through n. fall o n the
44
head, a fall on the f et or lower part of the spine, or a blo\\' on the lower jaw. Jf Ille upper jart tS fractured, the signs are S\\ ellin a , irregularity, and frequently insensibility, either im mediate or coming on gradually. Jf tile base l'S fractured in-
FIG. lR. sensibility may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass down to the stomach, \\ hence it may be yom ited; the fracture may im'olve the orbit, causing a blood-shot eye.
TRFATl\fENT.
Injury to the brain is the great danger attending a fracture of the cranium. For treatment see "Concussion and Compression of the Brain," pages 131, 132.
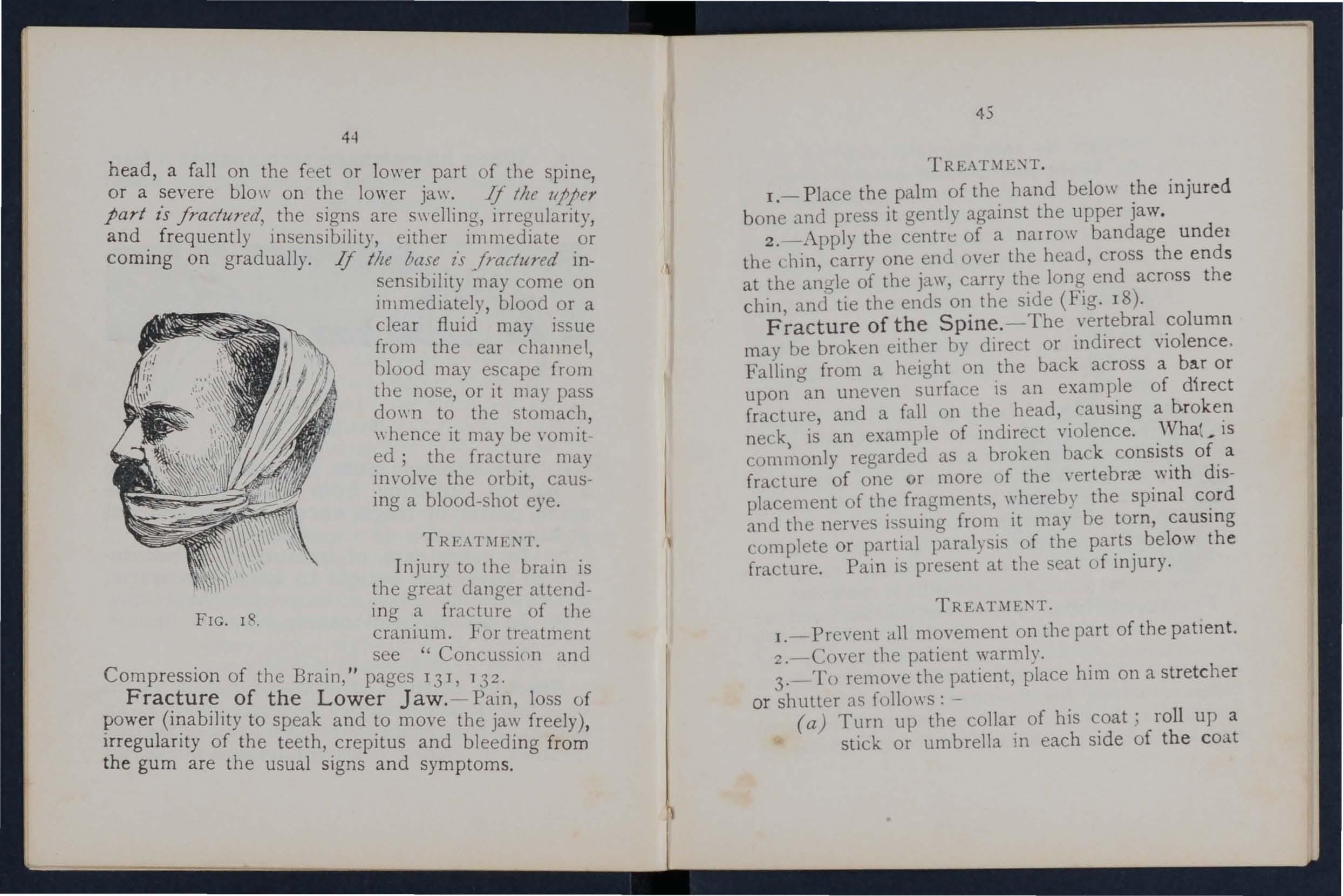
Fracture of the Lower Jaw.- Pain, loss of power (ir:ability to speak and to move the jaw freely), lrregulanty of the teeth, crepitus and bleeding from the gum are the usual signs and symptoms.
45
1.- Place the palm of the hand below the injured bone and press it genUy against the upper jaw.
2.-Apply the centre of a narrow bandage undet the chin, carry one enu over the head, cross the ends at the anU'le of the jaw, carry the long end across the chin anS'tie the ends on the side (Fig. 18).
of the Spine.-The vertebral column may be broken either hy direc.t or indirect violence. Falling from a height on the back across a ba.r or upon an uneven surface is an example of direct fracture and a fall on the head, causing a b.roken neck) an example of indirect violence. .'Vhat _ is commonly regarded as a broken hack of. a fracture of one or more of the yertebrce WIth dISplacement of the fragments, whereby the spinal cc: rd and the nerves from it may be torn, causmg complete or partial paralysis of the below the fracture. Pain IS present at the eat of Injury. 'T.
I.-Prevent all movement on the part of the patient.
2.-Cover the patient warmly.
3.-To remove the patient, place him on a stretcher or shutter as follo\\'s : -
(a) Turn up the of his c.oat; roll up a stick or umbrella In each Side of the coat
46
so that the e nds are level with the top l)( hIs head; pass a broad bandage or handkerchief under the head and secure it to the sticks. If no coat is worn, or doubt as to its trength and length exists, pass a 11 umber of bandages under the patient to serve in tead 0(, or in addition to, the coat.
(b) A ben rer on each side grasps the ndled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes charge of the legs.
(() On the word being given, all lift together and carry the patient by short side paces over the stretcher and carefully lower him on to it. If a fifth benrer is avallable the stretcher hould be passed under the patient instead of carrying him over it.
4·-0n arrival at shelter nothing further is to be attempted until the arrival of a doctor, except to give the patient water, tea, etc., if he is conscious.
Fractured Ribs. - The ribs usually fractured are the sixth, seventh, eighth, and ninth, and generally the fracture is midway between the breast-bone and the spine. The fracture may be caused by indirect ',iolence, driving the fractured ends of the bone c,utwards, or by direct violence, driving the fractured ends of the bone inwards and sometimes injuring the
47
n If the lower nbs on lungs. or o,ther In'er may be injured, the rIght Side are 10 1 " left ribs may wound the d f ture of the 0\\ el db' a rac . f tl fracture is afforde y pam , spleen. E\,luence 0 1e t a deep breath, and by especially on atte rl1pt1l1g 0 < < short and shallo\\'
'.., If the lun rr s are 111- 111):,. ::> I jured blood, frothy an bricrht red may be cou ,rhe d up and expecIf the liYer or spleen is wounded internal htcll10rrhagc (sec page 95) may L)Ccur.
TRE,\T\fF,\T. (a) TTk" the/rae/lire is /lId (olllpllmittl by all ., tfl lUI /Jltt'J'lla! l11JlflY
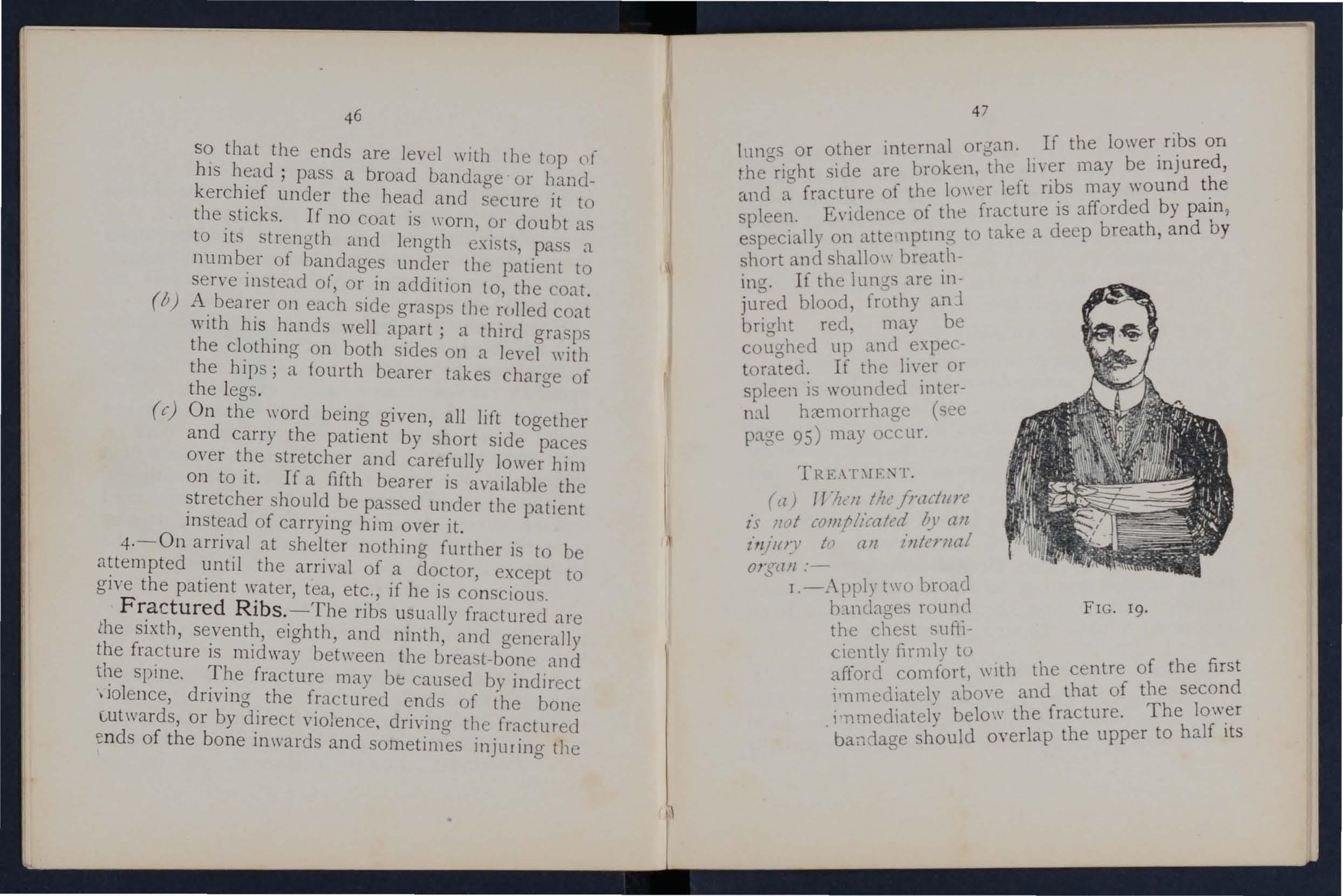
On;ll/l :" r.-.\pply t,,·o broad h:ll1Lbge. FIG. 19. the chest SUtil-
cicntly I1r1111), to 1 1 entre of the first f - I 11 fort \'lt1 t1e c d a 10r L .COt '. d that of the secon irnmcdlately abo\ e an f t The lower i·nmedi8.tely belo\\,. th1e to half its balldage should 0\ er ap
z
48
extent. The knots are to be tied rather to the front on the opposite side of the body. An other good plan IS to apply a strong towel, fo lded about eight inches wide, tightly round t he chest, securi ng it \\ ith three or four safety pins.
.- P lace the arm on the injured side In a lar ge sling. (Fig. I9).
(b) TrlzeJl all interllalorgan z·s /Jljured-
I.-Do not apply bandages round the chest.
1.-Lay t he patient do\\ n, inclined a little to\\ ard s the injured side.
3·-Loosen the clothing, gi,'e ice to suck, and place an ice bag over the seat of injury. Treat as for internal hcemorrhage (see page 95).
4 · - Plac e the arm on the injured side m a large sling.
F racture of the Breast-bone (slerllIlJll).-
Vhen this fracture can be felt or is suspected undo all tight clothing, and keep the patient quiet in an easy positIon until the arrival d a doctor.
FRACTURE OF TIrE BOXES OF THE UrPFR LIMB.
Fracture o f t he Co ll ar -b one (da'Z.'/de).-This fracture is frequently caused hy a fall on the hand o r sho ulde r. - The arm on the in jurec side is partially
49
helpless, and the patient u::>ually supportS It at thE: e lbow wIth his hand, and inclines hIS head the injured side. The fracturfd ends can generally be felt to overlap, the outer fragment being the lower The general signs anJ SYlllptOlllS of fracture ate mos tly present.
I.-Remove the coat (see page 19), and as mud more of the clothing as is expedient.
2.-Pla.ce a pad about two inches thick and four inches across in the armpit.
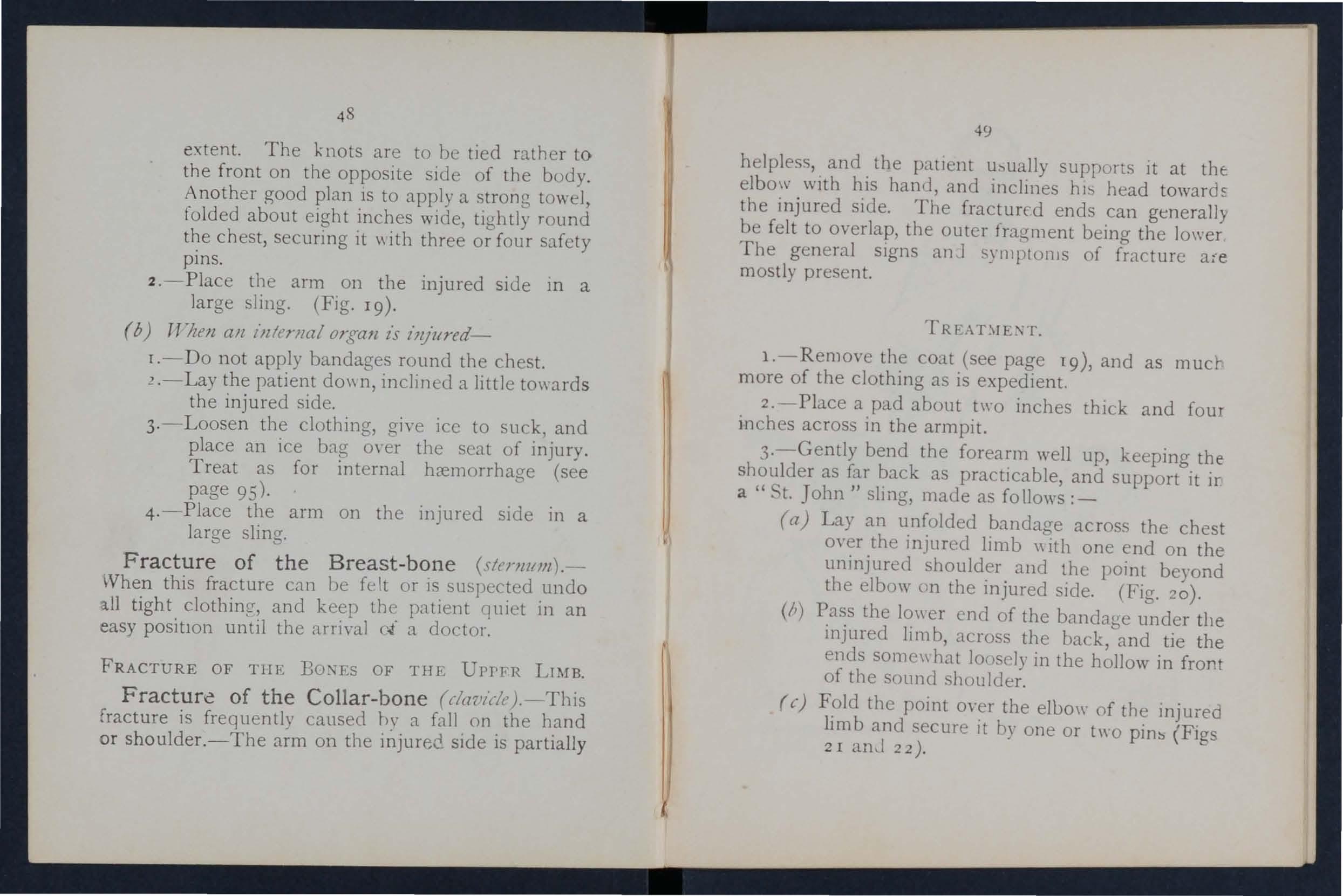
3·-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it ir a" t. John" slmg, made as fo llows :_
(a) Lay an unfolded b:ll1dage across the chest over the injured limb \\ith one end on the uninjured ·shoulder and the point beyond the elbow tJn the injured side. (Fig. 20).
(II) Pass the 10\\ er end of the bancbtre under the injured limb, across the back,oand tie the ends some\\ hat loosely in the hollow in front of the sound shoulder.
(c) Fold the point over the eloo\\ of the mjured lim b and secure it by one or l\\0 (Figs 2 I 22).
4·-Ti3htly secure the injurer! limb to the side by a broad bal1llat;e passed rounu the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5·- No\\ tighten the sling
W hen both collar - bones are broken keep the
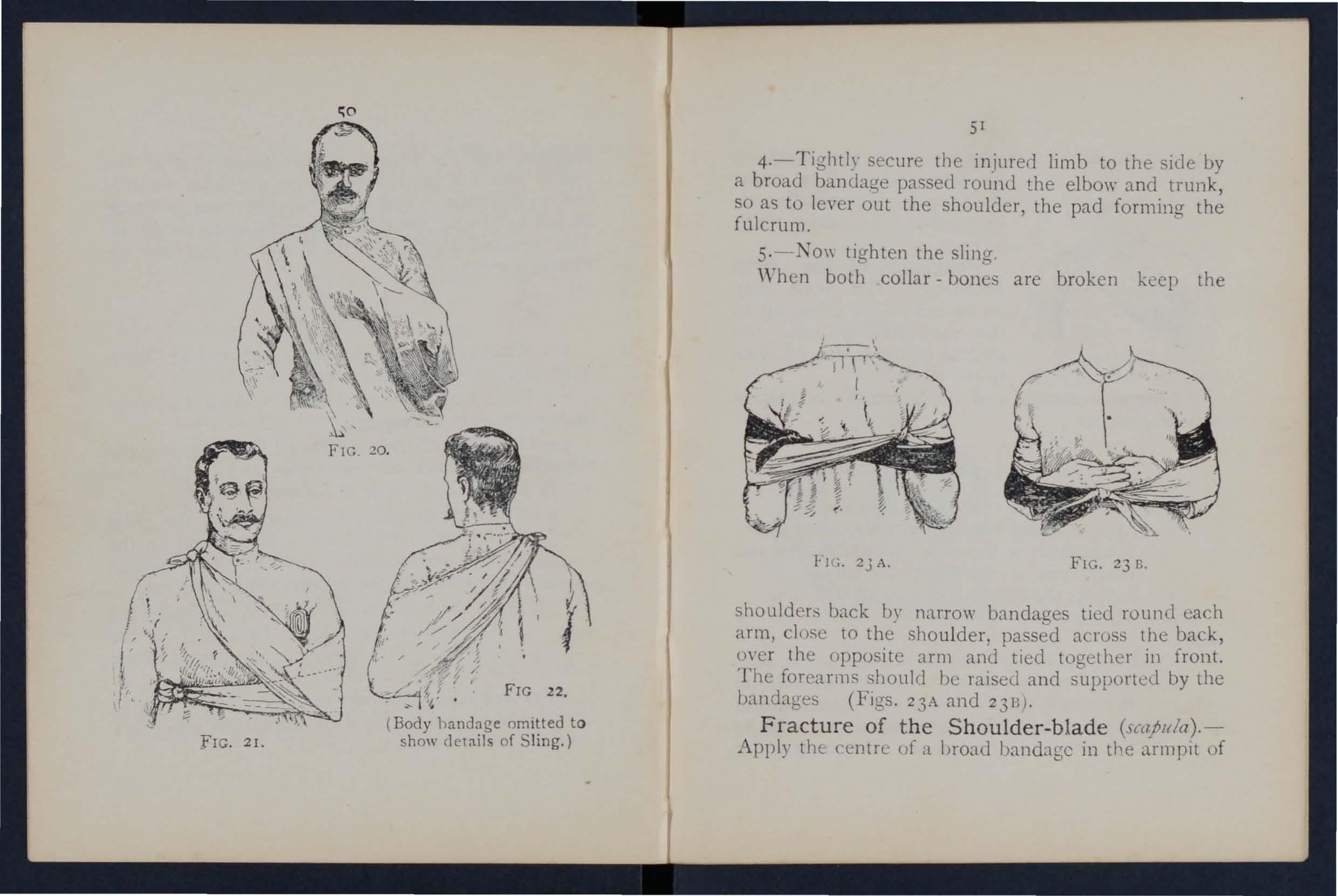
(Body handage omitted t o show details of S ling.)
shoulder:, back by narrow bandages tied round each arm, c lose to the shou l der, passed across the back, over the opposite arm and tied together ill front. The forearms should be rai ed and supported by the bandages (FIgs . 23A and 2313) .
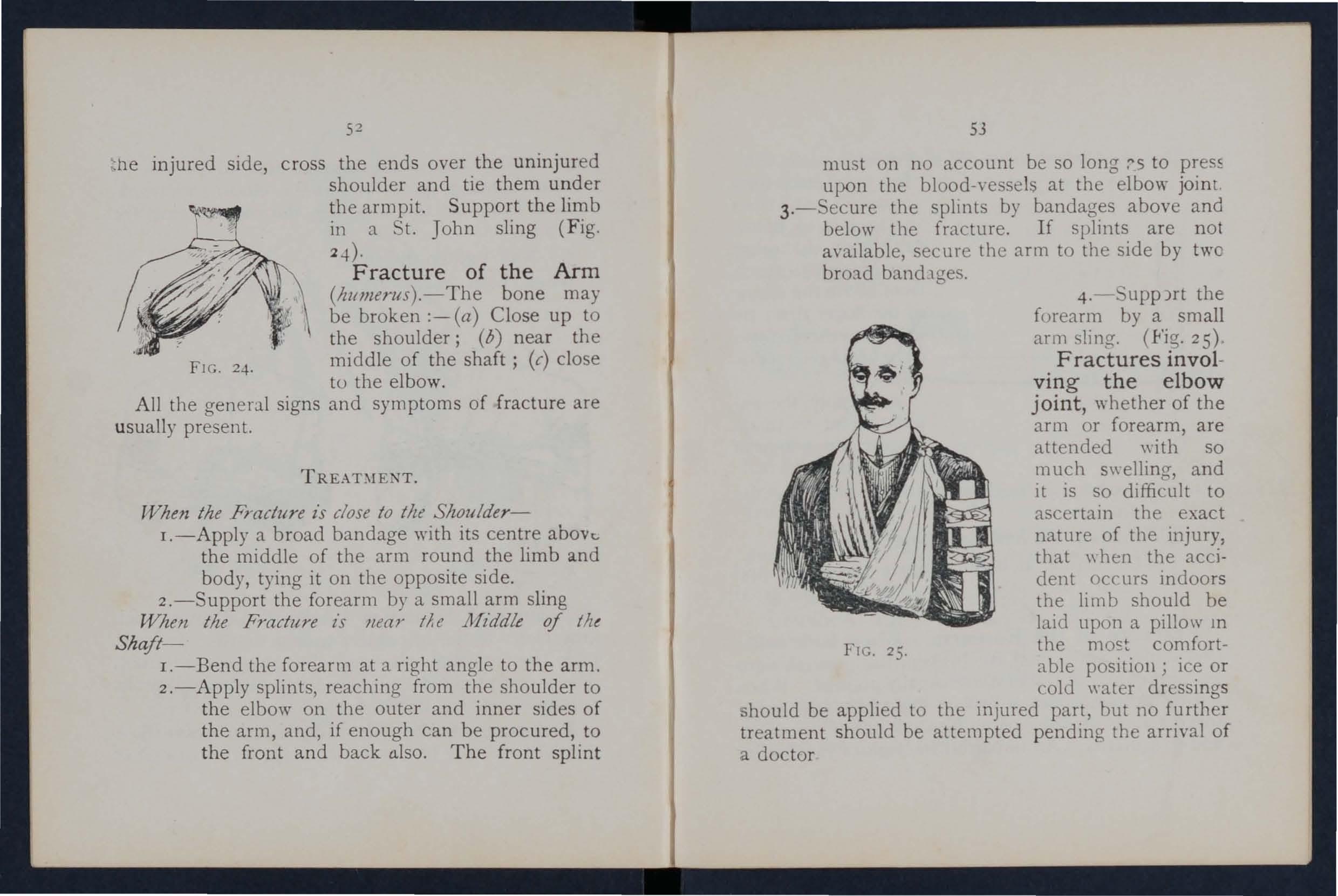
Fra cture o f t he Sh o ulder-b lad e
Apply the: centn: uf a broad bandage in the armpit of
fIG. 2I.injured side, cross the ends over the uninjured shoulder and tie them under
FIG. 2-1-. the armpit. Support the limb in a t. John sling (Fig. :q).
Arm (hltmerus).- The bone may be broken :- (a) Close up to the shoulder; (b) near the middle of the shaft; (c) close to the elbow.
All the general signs and symptoms of fracture are usuall y present.
TREAT:llENT.
When the Fracture is close to tile Shoulder-
I.-Apply a broad bandage with its centre above. the middle of the arm round the limb and body, tying it on the opposite side.
2.-Support the forearm by a small arm sling Wizen tlze Fracture z's near tAe JJfzddle of tht Shaft-
I.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back £.llso. The front splint
53
must on no account be so long :'5 to press upon the blood-ve sels at the elbow joint
3. - ecure the spltnts by bandages above and below the f mcture. If splints are not available, secure the arm to the side by two bro:ld bandlges.
4.- upp)rt the forearm by a small arm sling. (.Fig. 25)'
Fractures involving the elbow joint, whether of the arm or forearm, are attended wi th so much s\\ elling, and it is so difficult to ascertain the exact nature of the injury: that \\ hen the accident occurs indoors the Ii m b should be laid upon a pillow 111 the moc:t comfortable positioll; ice or cold \yater dressings should be applied to the injured part, but no further treatment should be attempted pending the arrival of a doctor
FIG. 25.
54
TTllen til e accidellt ormrs Ollt oj doors-
I.-Take t\\'o pieces of thin flat \\ ood, one long enough to reach frum the armpit to below the elbo\\', the other long enough to reach from above the elbow to the finger ti ps; tie them together to form a right angle. (Fit'. 6) '2
FrG 26.
3.- "'ecure by bandages fracture .
" Apply tlle angular sp'int 0 made on the I11ner side of the flexed limb. above and below the
4·- upport the limb by a large arm sling.
5·-0n arrival a.t !lome remO\'e the splint and treat the IIlJury as if it had occurred indoors.
Fracture o f the Forearm. - ,\Then both bOIl ES (the Radius and Clna) are broken, the general . I!!;n.:; and symptoms of are usually present. one of the bones only IS the signs and symptom". are as. a rille loss of power, and IrregularIty. An Impacted fracture of the Radius
55
Just abO\'e the wrist is a common result of :l fall a ll the hand.
ThIs IS the same, \\ b e ther the fracture is of one or of both.
I.-Bend the forearm at right angles to the arms
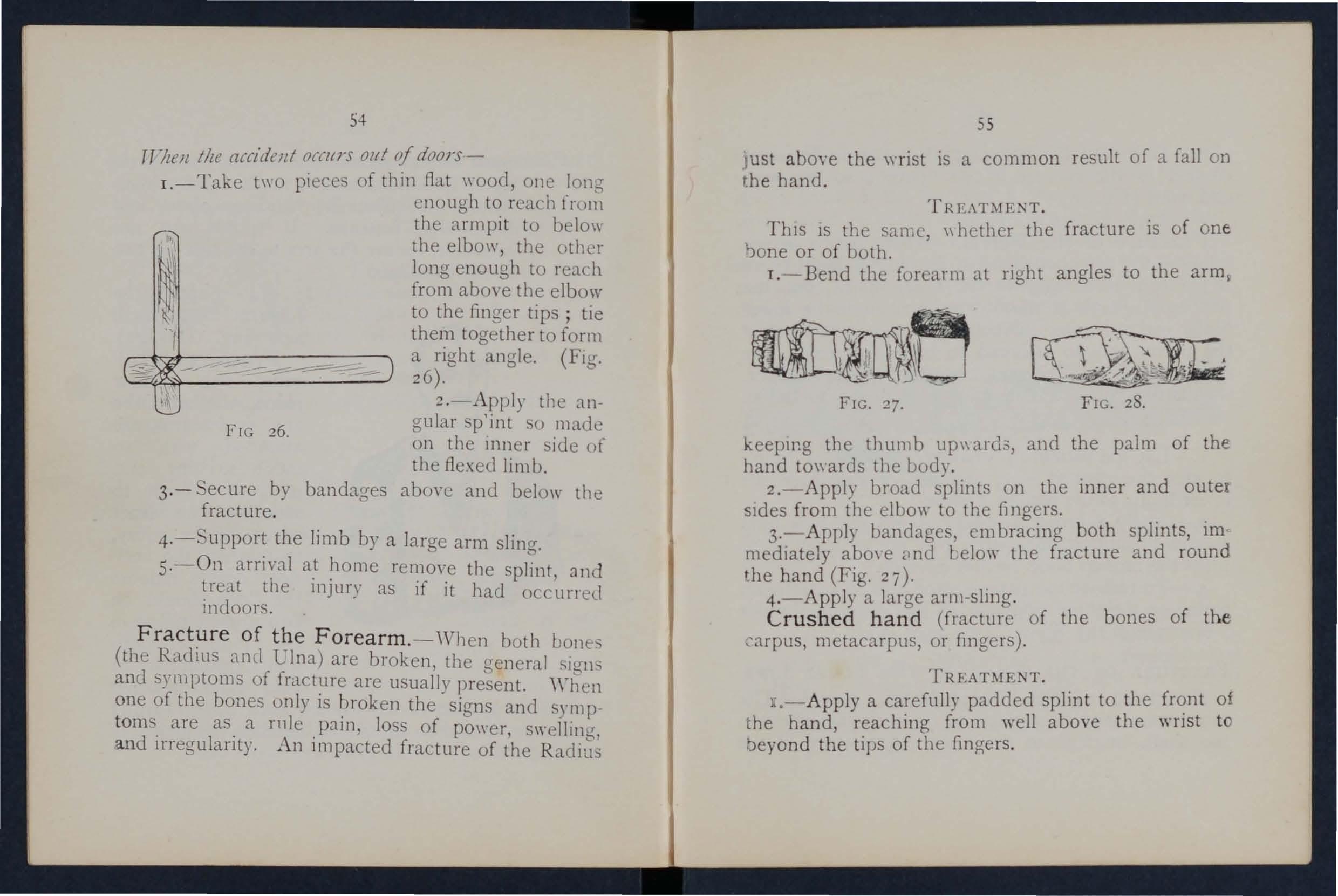
FIG. 27. FIG, 28.
keepIng the thumb up\\ard.3, and the palm of the hand to\\ards the body.
2.-Apply broad s'plints on the mner and outer SIdes from the elba\\' to the ongers.
3.-A pply bandages, em bracing both splints, im mediately abo\ e ,md Lela\\' the fracture and round the hand (Fig. 27).
4 .-Apply a large arll1-sling. Crushed hand (fracture of the bones of the ::- arpus, metacarpus, or ongers) .
TT .
L-Apply a carefully padded splint to the front a the hand, reaching from well above the wrist t beyond the tips of the ongers.
56
2.--To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 28).
3. -Apply a large arm-sling.
Fracture of the Pelvis.-\Vhen, after a severe mjury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the patient is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture ot the pelvis may be assumed to have occurred. The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
TREATME TT.
I.-Lay the patient in whatever position is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further inwards.
3·-To remove the patient place him on a stretcher, acting on the same principle as that described under (( Fracture of the Spine" (see page 45).
FRACTURE 0F THE BONES OF THE LOWER LIMB,
Fracture of the Thigh-bone (femur).- The thigh bone may be broken at its neck, anywhere in shaft. or close to the knee. A fracture at the 57
neck is likely to occur in old people from very sligh t ;njury, and is often difficult to distinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patien t cannot, when lying on the back, raise tbe heel from the ground, the bone is broken. All the generc.l signs and symptoms of fracture are usually present, and a prominent sign is the position of the foot,
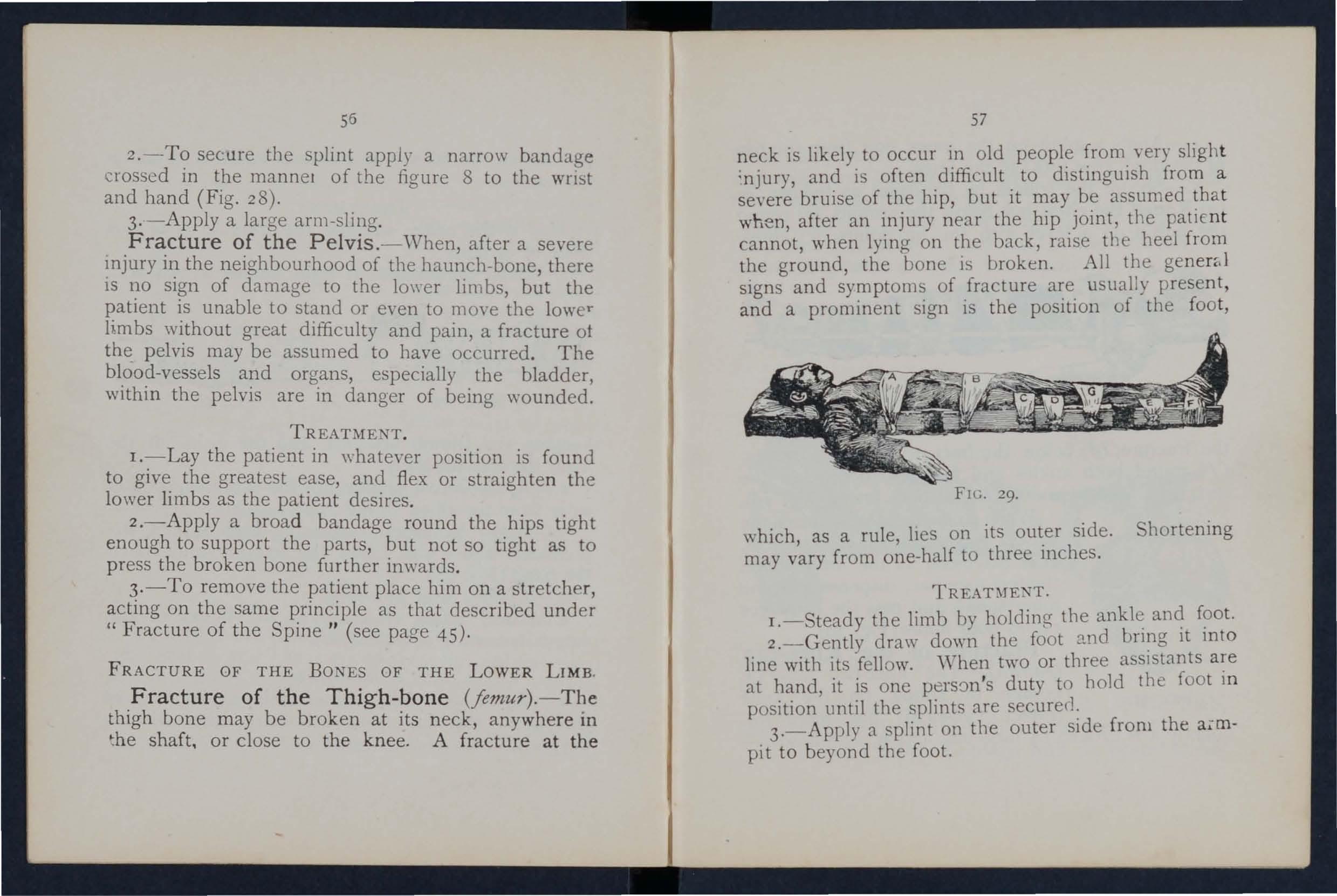
29.
vhich as a rule lIes on its outer side. Shortening may v'ary from to three inches.
TREAT:\fEXT.
I.-Steady the limb by the f?ot.
2.-Gently draw down the foot 2.nd It mto line with its fellow. "Then two or three assIstants a:e at hand, it is one duty to hold the foOt m position until the splints are secured:
3.- Apply a splint on the outer SIde from the a.mpi t to beyond the foot.
FIG.4 -Apply a splint on the inner side from the to p of t he thigh (the fork) to Ole knee .
5·- Secure the sp li nts by bandages as follows :(a) R ou n d tIle chest just below the arm pi t, (/I) round th e pe lvis o n a le \'el \\ ith the hip joints, (c\ above
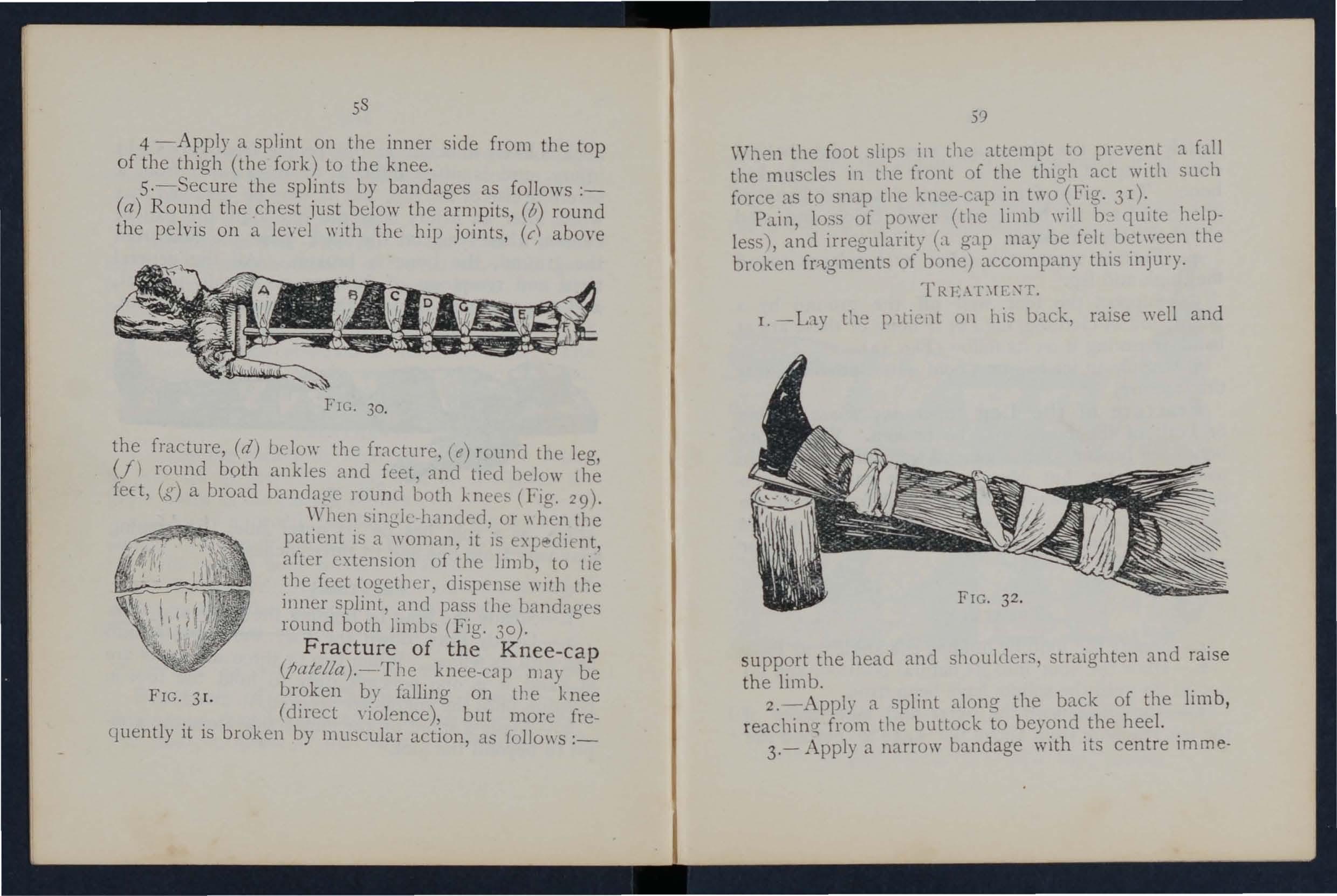
FIG. 30.
the fracture, (d) beluw tbe frncture, (e) rOllnd the leg, (fl rollnd both ankles and feet. and tied belo\\' the feet, (g) a broad bandage round l)oth J..nCLs (Fig. 29).
""Vhen <,ingk-hnnded . or \\ hen the patient is a woman, it IS l\p client, after extension of tIle limb, to tie the feet together, dispense \\ jIb the inner splint, and pass the bandages ronnd both limbs (Fig. 30 ).
(patella).-·The knee-cap may be F broken b)! falline- on tl'e knee IG. 3 I. <.J (direct violence), but more frequent ly it is broken by muscular action, as {ollo\\s : _ 5')
When the foot slips in the attempt to a fall the muscles 111 the fcont of the thigh act with such force as to snap the knec-Cil.p in two (Fig. 3 T )'.
Pcl.ll1, 10. s ot pO\\'l.;r (the limb will_ C"]Lllte helpless!, and irregularity Cl. gap ma.y be kIt the broken fr"l.gments of bone) accompany thiS l11Jury.
TRE.\T\r[\T
1. - Lt.y the p ltie,lt on his back, raise \yell and support the head and shoulders, straighten and raise the limb. .
2.-Apply a. splint along the back of the lim b, r eaching from the buttock to bey?nd .the hee l. .
3.- Apply a narrow bandage WIth Its centre lmme-
diately above the knee-cap, cross the ends behi nd. over the splint, and tie in front below the broken bone. To ensure firmness apply a second bandage in a similar way, but commenced bela\\" and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5·- upport the foot \Yell off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig-. 32).
6. -App ly an ice bag or a cold \\ ater dressing ove r the fr acture .
Fracture of the Leg (tibia alld fibllla).-One or both of the bones may be broken. When both bones are broken all the general signs of fracture are usually present, but \\'hen one bone only is broken deformity is not always notic eable. A fracture of the fibula three or four inches abO\'e its lower end frequently mistaken for a sprain and sometimes for a di slocation of the ankle.
ENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its na.tural position, and do not let go until the splints have been fixed.
3. -Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
61
((J()t. If only one splint is available place it on the outer ide.
-J..-.'t:cure the splints b)' bandages (a) above, (b) helow the fracture, (c) immediately above the knee,
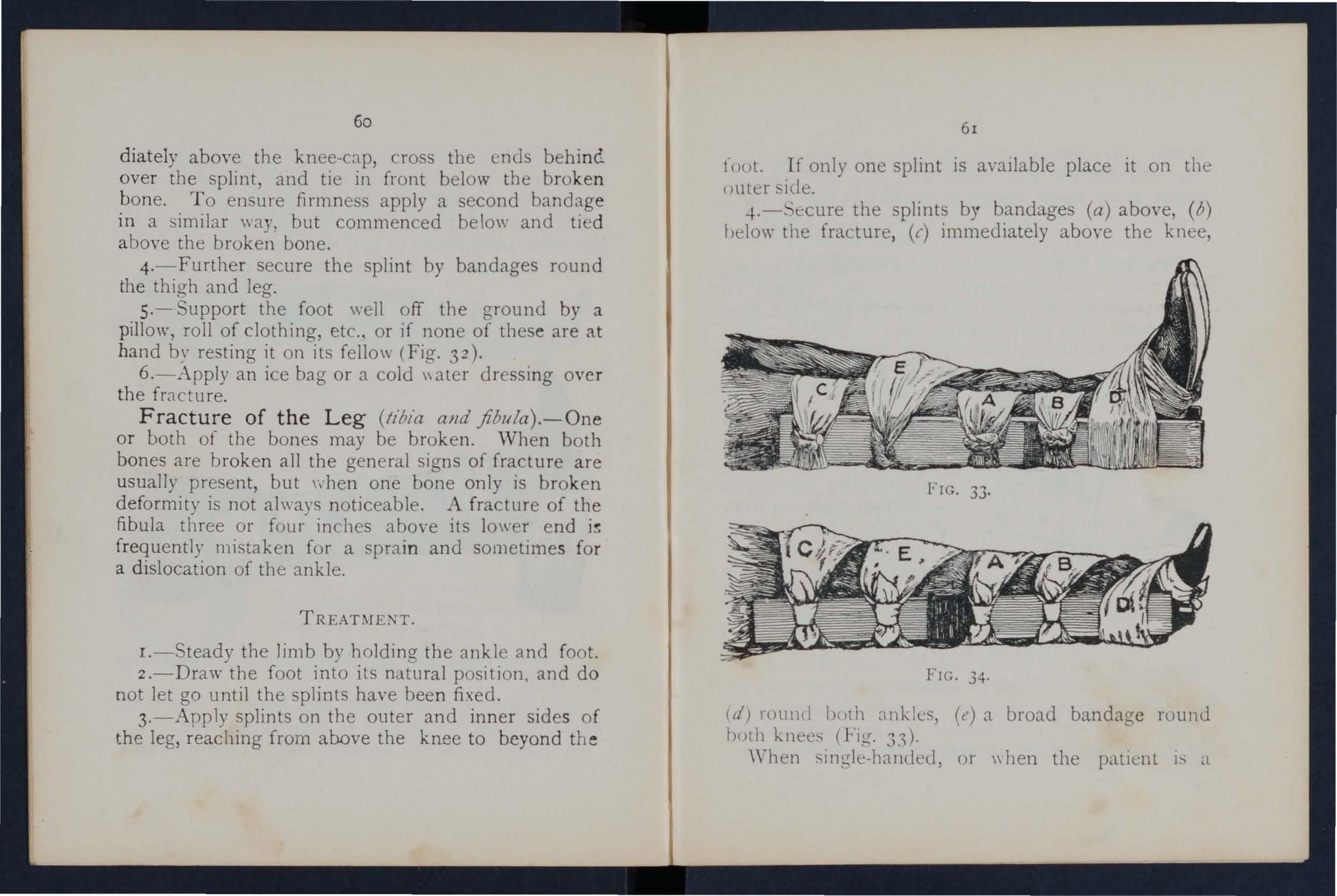
FIG. 34.
(d) roulld \)oth onklc . , (t') a broad bandage round huth knees (Fig. 33)' \Vhen . ingle-handeu, or \\ hen the patient is a
02
w o m a n, ,tft
e r e xt e n di n g the limb tie both feet together, d i pe n se II i[h t he inner ,-pl1l1 t , and p,l..;S the S
r o un d bo t h limbs (FIb ' 34 · \\' 11<:11 110 IS a vailable t} ing the leg", anJ, and kllllS together is of crr ea.t Se n let:' .
Crushed Foot (fracture of the tal!::.us, 1l1l' tatJrsus
a n d t oes) . - ThIS aecl(k'l1t is con mo n l) c:ws<.:!d by t he p as age OLl hLLl \ y \'elght on:1 lile [(.Jot: and 111,1 )' be hy pain SII ell lll g, and of J,OIl er.
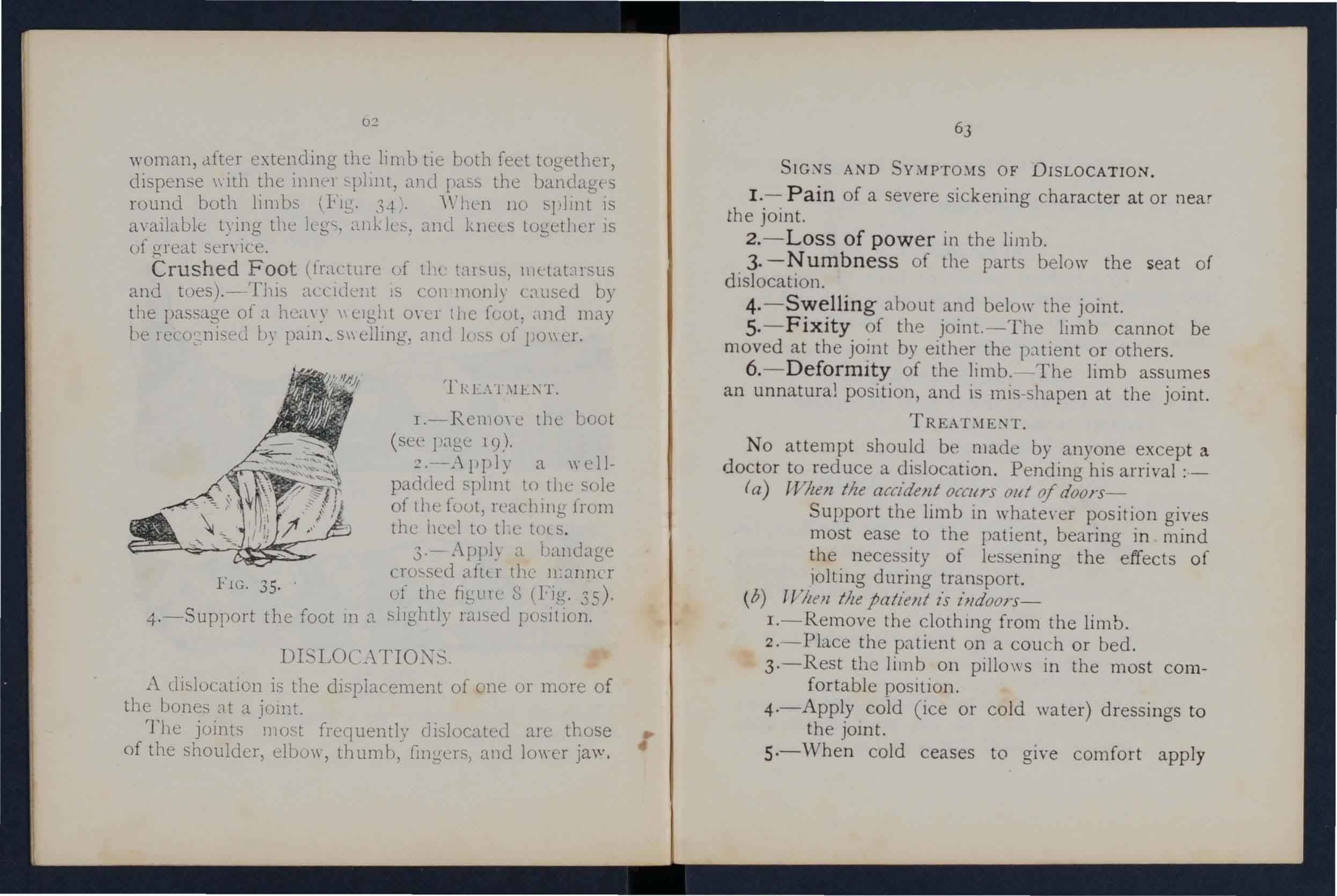
TIU:.\T:\ I L :-\ T .
I. - R cmo \ c t he boo t ( see l'age 1<)).
a \\ ellp added splm t to th<: sole of the fout, rl'achi ll g 1rum the heel to t1.c tUlS .
3·- A pply a bandage
cJu"sed dfl Ll" the 11.:1n11L r FI c . 35· . uf t he figtllC g (FIg. 35 ) '
4 . - Su ppo rt t he f oot 111 a sl Ightly !"abed pO!:li t lO n .
DI'LOCAT I OXS.
..\ dislocation is the dispiacement of one or more o f t he bones at a jOll1t.
T he j oints most frequent ly disloc[tled are of t he shoulder, elbulr, t humb, and lo \\' e r ja\V,
SI GNS AND OF D ISLO CAT IO N.
1. - Pain of a severe sickening characte r a t or near the joint.
2. - Loss of power in the limb.
3· -Numbness o f th e parts b e lo w the s eat o f dislocation.
4·- Swelling a b o Llt and b e !O\\- t h e joint.
S.- Fixity of th e jo int. - T he li mb cannot be moved at th e joint by eith e r th e pa t ie nt or others.
6. - Deformity of th e limb. Th e limb assume s a n unnatural po s ition, and is ml s-s hap e n at the j o int.
N o attempt sh o uld bE' mad e by any o ne excep t a doc t or to reduce a dis location . P e ndin g his arrival :_
(a) TVlten tile accident oCOIrs out of d oo J's -
Support th e limb in wh a te\-er position gives most eas e to [h e patient, bearing i n mind the necess ity of Ie se ning the effects of iolting durin g transport.
( b) ll lleJl tile patient /s l'"doo rs-
I. - Remove th e clothlll g from the limb .
2 .·-Pla.ce the p[ttient on a cou c h or bed .
3·- Rest th e limb on pillo \IS in the most co mfortable posItIOn .
4 ·-A pply cold ( ice or cold water) dressi n g s t o the JOInt.
s·- \ Vhe n cold ceases to give comfort app ly
warmth (flannels or towels wrung out of hot ,,·ater).
6.-Treat shock (see page 135).
·When, by a sudden wrench or t",ist, the ligaments and the parts around a joint are stretched and torn the joint is said to be sprall1ed. "Going over" the ankle is a common example.
SIC SAND Y:\[PTO:\fS.
I.-Pain at the joint after a t",ist or wrench.
2. - Inability to use the joint.
3. - welling and discoloration.
TREAT;\IEXT OF AXKLE..
Jf7zcJ/ 011 1 of doors -
I.-Apply a bandage tightly oyer the boot, beginning on the sole at the instep, it on the front of the ankle, and carryIng it round and round the ankle, where it is to be firmly tied.
z.-\Vet the bandag-e after applicaton; it is thereby tightened.
Aflt-r 1'eariziJlg slleller-
I.-Remoye the boot and stocking (see page 19).
2.-Place the limb in the most comfortable position j usually that is we1l raised.
3. -Apply i e or cold water drc ·sings to th e joint as long as they relIeve pain,
-I.-When cold falls to giYe comfort, apply hot fomentatIons.
\\ ' hen other JOInts are sprained, treat them as if (!J.)located.
When in doubt as to the nature of the It1jury, treat as a fraclur e.
\Vhen, dUring se\·ere e,ertion, muscles or tendons are over-stretl hed they are said to be strained, if they are actually torn they arc described as ruptured.
[c'\s A:-.iD L\[PTO:'lIS. sudden sharp pain.
2.-\\'hen the mucles of a limb are strained they may swell and cause seYere cramp.
3·-Further e , ertio n is difficult or impossible; for e,ample, if the strain has occurred in the back the r :ltient may be unable to stand upright.
J.-PLt.ce the patient in the most comfortable po ition, and affurd support to the injured part,
z.-Apply hot water bottles 01 hot fomentations when th e pain is \·ery se"ere.
A so-called train in the groin (hernia) is an injury of a totally dIfferent nature ( ee page 114),
o
The numerals iud/'rate the pages where tile all s'Wers 1IIay be /ouJ/d.
What is the skeleton, and \\ hat pllrp o. cs arc se r\"ld by it?
lIow are the bones of the sl,ull arranged?
\Vhat are the bonndaries of the cranium?
Describe the bones of the face
Describe the lower jaw
What is the angle of the jaw? ...
What other names has the back-Lone?
\Yhat is a vertebra?..
How many \'erlebrre are there in the spine?
\Vhat are the regions of the spine, and how many vertehr::c are there in each ? ..
lIow is the spine endowed with free movement?
What is a ri b ? ..
How many pairs of ribs are (hue?
What is the breast-bone?
\Vhat are the bones of the upper limbs ?
What is the pelvis?
What is the hip joint?
'Vhat are the bones of the lower llm bs? .. ,
What is a joint?
Describe a moveable joint . ..
D escribe the shoulder joint
Describe the ankle joint
ITow are muscles classified?
Describe voluntary muscles
Describe involuntary n"lScJcs
What is a fracture? ...
What are the causes of fracture?
r low maya fracture be cau -eel by mu . cular action?
In what two ways may fractures be cla sified? ...
What is a simple fracture ?...
\Vhat is a c o mp ound fracture?
\\' hat is a c o mplicated fracture?
a c omminuted fracture?
In making up your mind whether a fracture had occurred or not, what points should you take into consideration beyond the igns and ymptoms?
apparatu may be necessary for the treatm e nt of
E march' tri r1.l1g11lar bandage
(Fig. 8) In what way. may the triangular bandage b e folded for u e?
II"w many kinds of arm-sling - arc there, and what are they called?
knot is to be tied, and what knot avoided?
What is the object of fir t aid treatment of fractures? 4I
the general rules fur the treatment of fractures 4I ([ow should splints be applied? ... . .. 41, 42
should bandages be applied? '" 42, 43
\Yhat may cause a fracture of the upper part of the cranium?
\-Vhat may cause a fracture of the base of the cranium ? 43, 44
\Vhat are the signs of fracture of the upper part of the cranium?
What are the signs o f 'of of the cranium? ... .., ...
\Vhat is the treatment for fracture of the cranium?
\Vhat are the signs of fracture of the lower ja \\ ?
How maya fractured spine be caused? ...
\Vhat is commonly regarded as a brohn !Jacl, ? ...
\Vhat are the symptoms of a fractured. pille? ..
How may ribs be fractured?
How maya fracture of rib s be compl.icated? .. ..
State the signs and symptoms of a SImple and of a cumplicated fractur e or ribs ...
\Vhat is a frequent cause of fractured collar-hone? ..
\Vhat are the signs and symptoms of fractured c"llarhone?
At what poillts may the bone of the arm be broken? .. 52
Are the general signs and symptoms of a fracture always present in a hroken forearm?
State the cause of a common fracture of the rad.ltls
How would you recognise a fracture of the pelns?
At what points may the thigh-bone be broken?
\Vhat are the signs and symptoms of fracture of the
thigh-bone?
\Vhat are the causes of fracture of the knee-cap? 58,
'What are the signs and symptoms of fracture of the kneecap?
Are the general signs and sym ptoms always present m a fracture of the leg?
\Vhat mistake may easily be made when the fibula IS broken near its lower end?
What is a dislocati on?
the
First Aid Students ::.houlcl practise imprO\ ising material, folding bandages, tying knots, making slings, and the treatment of the following injuries.
Impru\"i .ing splint
Im p rovising bandages
Folding bandages
Large arm sling
m til arm sling
Red and granny knots
Knot for appl),ing splint to lower limb
Fracture Lower jaw, 44. . pine, 45. 46. Ribs (Sililple and cnmplicated fractures), 46tu ..J.t'. Breastbone, 4 '. Collar-bone, 48 to 51. Both collarbones, Sf. Arm, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm \I hen the elbow is in\-oh-ccl, 53. Forearm, 55. Crushed hand, 55, 56. Pehis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single-handed), 5. Kneecap, 59 , 60. Leg (man), 60, 61. Leg (woman, or
man \\ hen single-handed), 62. Crushed foot, 62.
Disl ocations-Out of doors and induors .. 63, 04 Spraineci. ankle
Strains and ruptured muscles 65
CHAPTER III.
THE organs concerned in the circulation of the blood are the Heart, the Arteries, the Veins, and the Capillaries .
The Heart is situated in the chest behind the bre:\st -bo ne and rib cartilages, between the lungs and immediately above the diaphw_gm; it lies obliquely with a quarter of its bulk to the right and th e remaining three-quarters to the left of the middle lin e of the body. Its beat may be felt just below and to the inner side of the left nipple. The heart has four cavitie , two on either side of a central partiti on. The two upper cavities are named the right and left auricles, the two lower the right and left ventricles.
Arteries are vessels which convey blood from the heart. Veins carry blood to the heart. Capillaries connect the arteries and veins.
In the general (systemic ) circulation arterial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all parts of the body. These divide and sub-divide, and become so small as to assume microscopic dimensions, when they are termed capillaries.
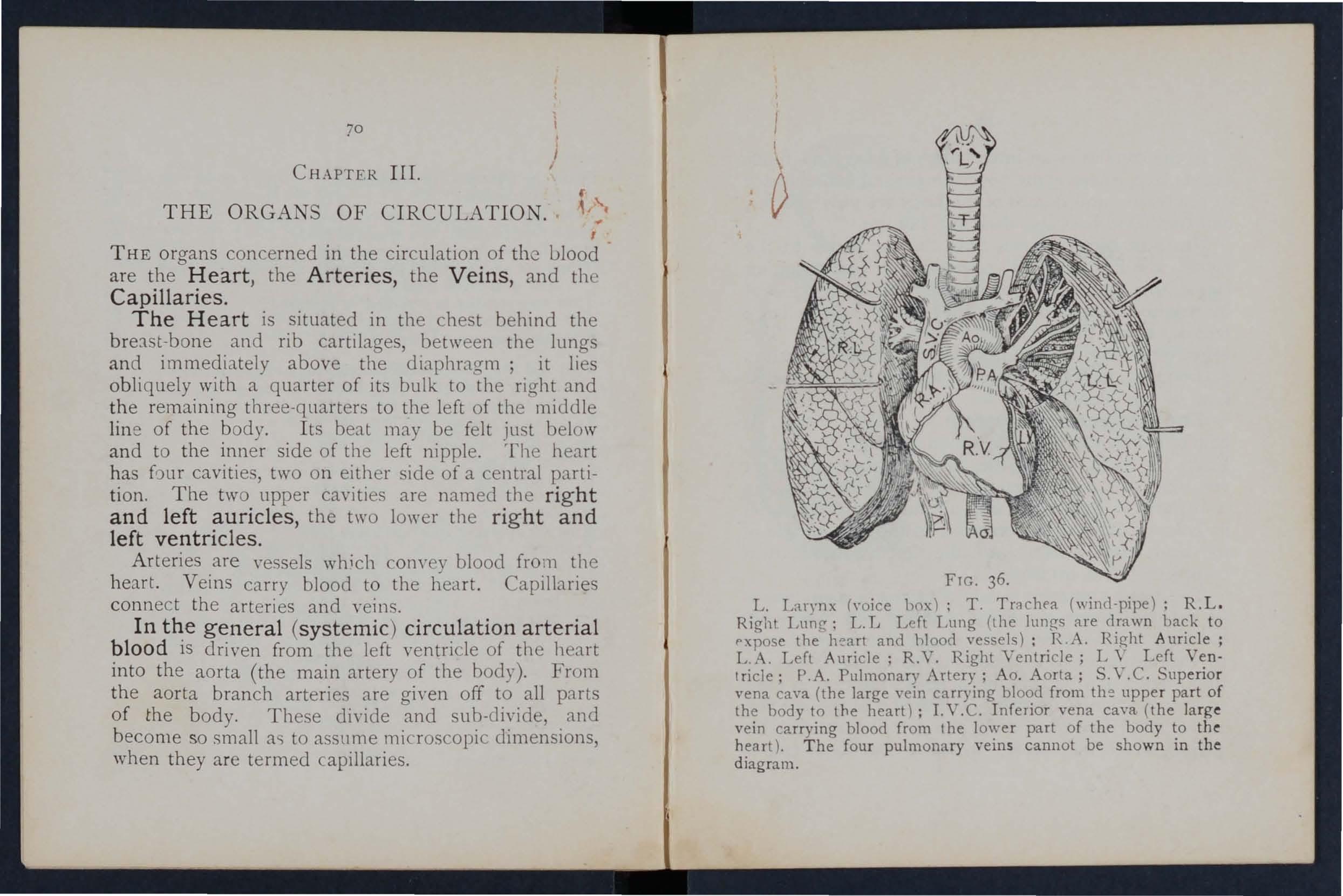
L. L:uynx ('·oice hox); T. (wind-pipe); R.L. Right Lung; L. L Left Lung (the lungs are drawn back to pxpose the' h!:'art and 11lood vessels); R.A. Right Auricle; L.A. Left Auricle; R.V. Right Ventricle; L \' Left Ventricle; P.A. Pulmonary Artery; Ao. Aorta; S.V.C. Superior vena cava (the large vein carrying blood from upper part of the body to the heart); LV.C. Inferior vena cava (the large vein carrying blood from the lower part of the body to the heart). The four pulmonary veins cannot be shown in the diagram.
I n the capillaries an interchange of gases and fluids takes place, wherehy the nourishment and mall1tenance of the tissues and organs of the body are provided for , and the blood becomes dark and impure.
Venous blood passes from the capdhries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with valves at frequent intervals, which prevent the backward flow of the blood.
The pu lmonary s yste m of blood vessels is concerned in carrying the blood through the lungs. From the right auricle the blood passes to the right ventricle, and is thence carried to the lung, where it is p u rified by contact with air, and becomes scarlet in colour; it is then conveyed to the left auricle of the heart and p:lsses into the left Yentr,icle, thus completing the circuhtion.
The heart contracts in adLllts at an average rate of !3eventy-two times a minute, but the rate varies, increasing as the is changed from the lying to the sitting or to the standing position; hence the importance of ad,iusting the patient's position in cases o f hcemorrhage . At every contraction of the left ventricle blood is forced into the arteries, causing the pulse, which may be felt wherever the finger can
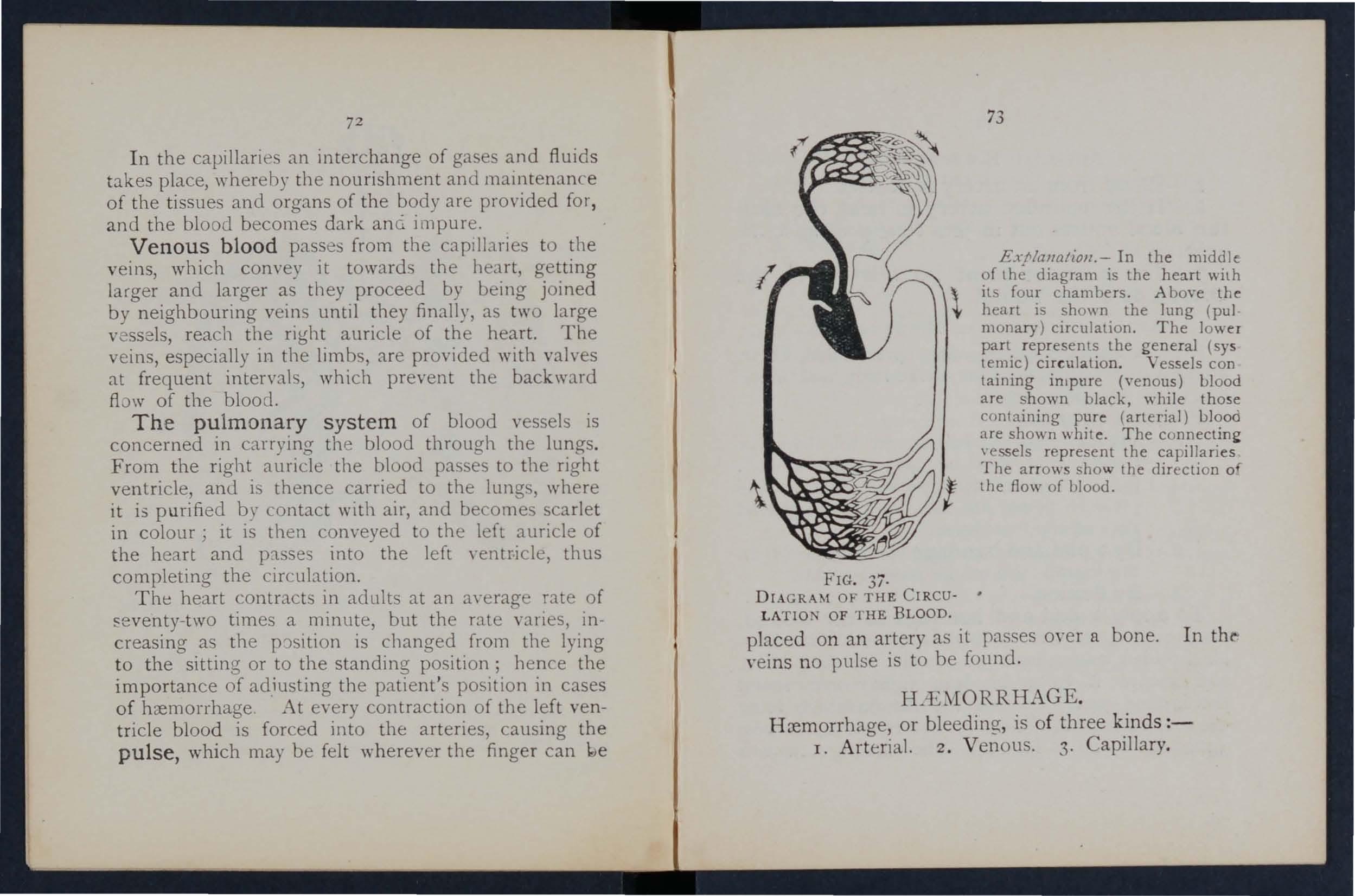
ExNaJlatioJl.- In the middle of diagram is the heart \\ilh , its four chambers. .Above the l- heart is shown the lung (pul monary) circulation. The lower part represents the general (sys temic) cir culation . Vessels con taining in'pure (venous) Llood are shown black, while those containing pure (arterial) blood are shown white. The represent the capillaries [he arrows show the direction 0 the flow of blood.
3i .
DIAGRAM OF THE CIRCU- • L ATlON OF THE BLOOD.
place d on a n artery as it passes oyer a bone. I n thl" yeins no pulse is to be found.
E.
H ::emorrhage, or bleeding, is of three k in ds:-
I. A rterial. 2 . V enous. 3. Capillary.
ART ER[AL
I. - Blood from an artery is scarlet.
2. - lf the wounded artery is near the skin the blood spurts out in jets corresponding to the pulsation of the heart.
3.-The pressure point (see below) is on the heart side of the wound.
ARR EST OF . \. RTLRL\L
Art e r la l hremorrhage is, wh en practicable, to be arr ested by pressure, position of the body, and eleyation of bleeding- part, Pressure m3.Y be : -
I. - Digital -that is, applied \\ith the thumb or fi n..(er, and may he (a) on the wound; ( b) at a spot called the pressure point T he pressure p oints are indicated or numbered dots on the frontispiece, .
2. - By a pad and bandage (tourniquet) (a) on the wound; (0) on the prcssur'-' point.
3 . - By flexion.
To apply a pad and bandage to the wound, a piece of lint or linen or a clean handkerchief folded into a hard pad, on the uleeding point, and secure it by a bandag-e t ight")' tied round the injured part. To fold the handkerchief, bring th e four corners to the cent re, and the process unt il a hard pad is formed. The s m oo th surface is
75
placed on the wound, and, to 1 reyent the I ad fr e m unfulding, the puckered surface may be stitched or rixed by a safety pin. "\ hard substance, such as 1 ..,tone may be enclosed in the centre of the pad .
A Tou rniquet may consist of a pad to be place d 0n the pressure point, a slrap, mrci, or /Jallciage to encircle the limb and pad, and a tt;£;!tlmilll[ meill, such as a stie k or other lyeanS of t\\ isting the to tighten it.
To improvise and apply a tourniquet :-
1.-- Apply a firm pad on the pres ure roint.
2 _- Encircle the Jil1' b by a narrow ndage \\ ith its centre mer the paJ .
3,- Tie the ends of the br.ndage in a half knot on the oPJlC'site side to the pad,
to-Lay the t\\ isting stick en the half k not, and m -cr it tie a r(cf knot.
).-T\\ist the t:ck to til.hten the handage, therehy pres,.' ng tl'e p8d uron the artery, and 81Tcsting tIe Ao\\ of blood.
6.-Lock the stick in po, it 'on by the ends of the 81ready applied, or by another bandage passed round the s1 ick lim h.
The pad of the tourlllquet must be accurateh t)IRr.ed upon the pressure point as completely to ompress the art ry; otben\ise arterial bloed \\ill be lllowed to pass along the limb, and the Yeins, being 'umpressed by the tourniquet, \\ ill not allow th e
blood to return through them to the heart and the result will be dangeruus swelling and congedtion.
Should a suitable p ad not be at hand, a knot ma y be .made in the centr e of the bandage, and when avaIlable, a stone, cork, etc ., enclosed in it to give it and bulk. See that the bulging anel not the flat Side of the knot is next the skin.
. An . bandage passed tightly round the 11mb, 11llI:nedlately abo\'(; the seal of arterial hcemorrhage, WIll .arrest bleeding. Th e simplest prepared form of thIS IS a strip of elastic webbing, to thIrty Il1ches long and two inches wide, With a pIece of tape se\\'n at each end . An elastic belt or brace \\:i ll the same purpose. Except when part o.f a limb IS torn off, it is not advisable to use an corel or bandage if other apparatus can be had, It cuts off all circulatIOn in the limb.
FlexlOn of the application of a pad on t he pressure pomt at the knee or elbow joint, flexing t he lImb to make pressure, and securin CT the limb in t he fle xed posi tion by a bandage like the figure 8.
GENERAL RUL ES FOR OF A 'VOu. D ACC OMPANfED BY ARTERL\L H1E:JIORRHAGE.
I. Stop bleeding.
II. Prevent injur io us germs from getting into the wound.
77
To attain the se ends :
1. Place the patient in a suitable position, bearing in mind that th e blood escapes v"ith less force wh en the patient sits, and is still more checked when he lies down.
2. Elevate the bleeding part, as thereby less blood finds its \\ay into it.
3. Expose the wound, removing whatever clothing is nec es ar)'. (ee Rule 8, a.)
4. Apply digital pressure.
(a) If the wound IS sm all on the bleeding spot.
(b) If the wound is large on the pressure point next to the wound on the heart side. The nearest pre. sure point is chosen in order to avoid utting off the circulation from as much of the part as possible, but sometimes it is necessary to apply pressure still nearer to tbe heart.
S. Remove foreign bodies, sucb as broken glass , bits of clothlllg, hair, etc., seen in the \\ound; do not search for foreign bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boracic gauze or lint is to be preferred, but absorbent cotton wool, lint, or gauze, or a clean piece of linen WIll answer the purpose . hOllld any doubt be entertained as to the cleanline s of the dressing, a clean piece of unprinted paper. such as the inside of an
enyelope) should be pbced next the wOLllld bdore applying the pad. (Compare pages 75 ::1.I1cl 7 6 .)
7. Bandage tightly ove r th .e pad unl ess:-
(a) Foreign bodies are suspected to uc left unSeen in the wound.
(b) There is danger of cilusing injury Lo a fr,lcture. In these cases a light dressing only should be applied.
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4, b )) but only in the following cases :-
(a) As a temporary measure while the \\ ound is being exposed, examined and cO\'t;rcd.
(b) As a more permanent measure when bleeding cannot be stopped by the pad and bandage on the \\ ound, or when. in arcord ,lIlcc \\ itb Rule 7, the tight bandage has not been applJed.
9. Afford support to the injured part.
When p::nt of a limb has been torn off or the \\ oLlnd is lacerated (for example by the cIa\\' of an animal or by machinery) hc:emorrhage frequently does not come on at once, but as there is a danger of se\ 'ere h:emorrhage laLer, me::ms for its arrest should bc applied to the limb, but not tightened unless neces:,ary. Do not disturb a clot of blooJ formed O\'er a \\ ound. No attempt should be made to cleans e a "ouml except \\'ith sterilised \\ater (that is pre\'iously bolled
i9
and allowed to cool), and experience, especially in recent wars, has sho\\ n th3t those wounds \\ hich \\'ere pro\'isionally tre<1ted \\ith a dry dressing and suhsequently dressed by a surgeon \\ith proper applitlnces did best.
tudents pr[lcLising arrest of arterial hren'orrhage should feel the pulse to see \\ hen the cur"pnt of blood in the artery has heen stGPred, and hould then immediately rcla\: tbe pres ure made on the artery. In this way the importance of the accurate application of pressure will be re[llised, and the ::lmounl of force nece sary \\ ill be [lscert<1 ined.
THE COURSE OF THE i\hlX ARTFRIFS, AJ\'D ARRE.Sr OF lL'E:\IORRHAGE.
(The numhers of the pressure points refer to tho:e on the Fronlispiece.)
THE LARGE \RTE.RJES '\-ITHI'i THE CHEST AJ\'D • \llDO:\fl·: :-\.
The Aorta is the central or trunk allery of the body. Commencing at tbe left \'entricle it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branche s \\ hich carry the blood to either side of tIle llead and neck and to the upper lim bs. The Aorta passes down on the left of the spine to just below the na\-el J where it divides into two great branches (the iliacs)
which con \'ey the blood to the organs in the pelvi s and to the lower limbs.
\Vounds of these arteries are one cause of internal h remorrhage (see page 96).
The Carotid Arteries (right a n d left) leave the u pper part of the chest and pass up on either side of t he wi n dpipe and, just below the level of the angle of t h e lower jaw, divide into the Internal a n d External Carotid Arteries. The Internal Carotid Arte ry ascends deeply in the neck, and enters the cr:1nium to supply the brain with blood The External Carotid Artery gIves off a number of branches; to the front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the Occipital; the a rtery itself is continued upwards in front of the ear, where it changes its name to the Temporal, and supplies the scalp in the neIghbourhood of the temples.
When a Carotid Art e ry is wounded , as in th e case of a cut throat, apply the thumb of one h and on the artery at pressure point I, pressing backwards against the backbone and taking care to avoid the It may also be neces.sary to apply pressure with the other th un, b abo\'e the \\ ound for t\\·o re:lsons: (a) To arrest the flo\\ of blood from t he maiI'l. (jugular) vein in the neck, which runs
Sr
alongside of the carotid artery and is usually \\ ounded at the same time; (b) To check the flow of blood from the upper end of the carotid artery Itself, \\ hich is often considerable 0\\ ing to com m unicatio n between the branches of this artery and those of its
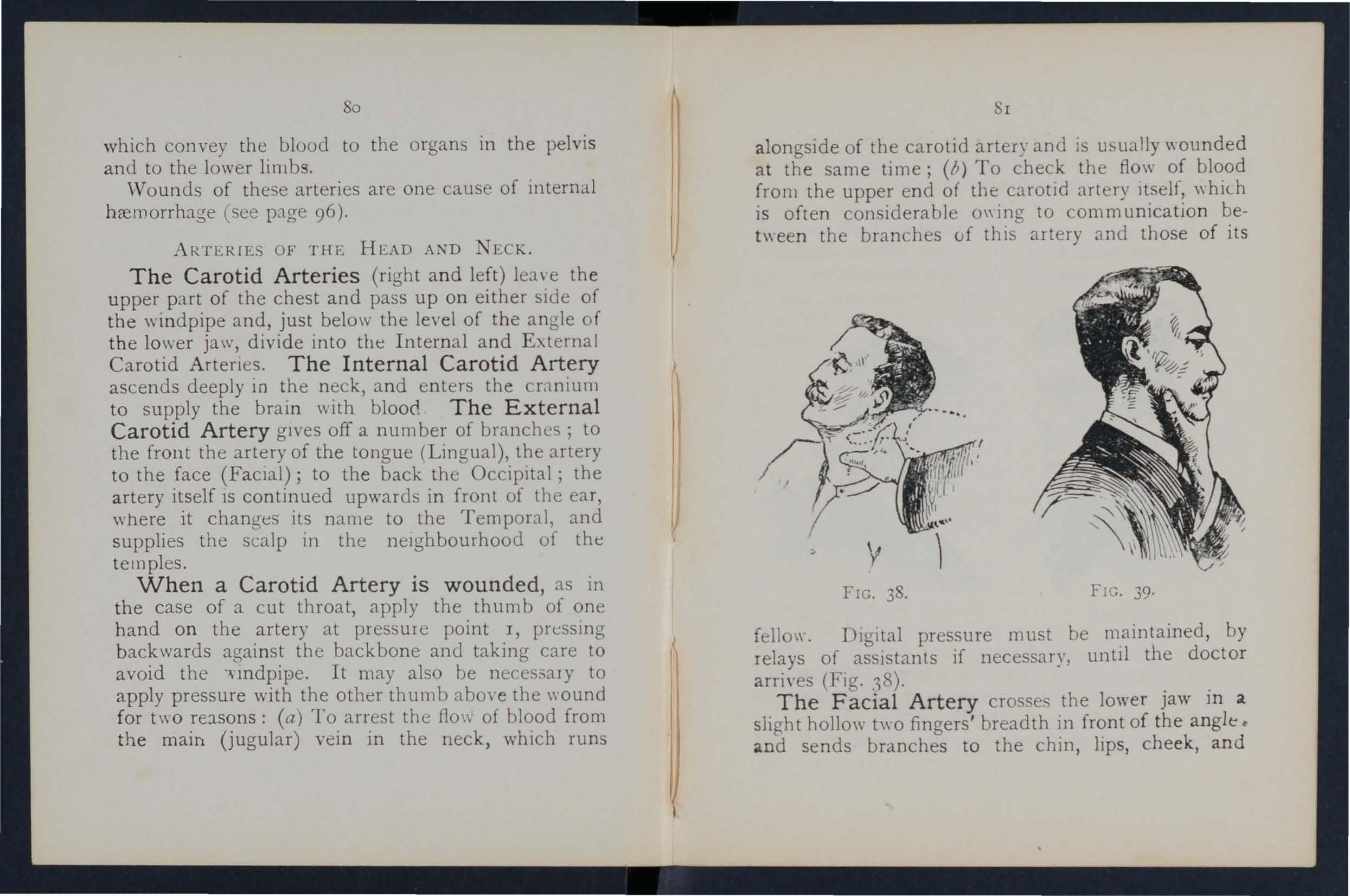
fello\\". Digital pressure must be m.aintained, by relays of assistants if necessary, untIl the doctor arri\'es (Fig. 38). . .
T h e Faci al Art e ry crosse the lower jaW 111 a slight hollo\\' two fingers' breadth in front of the angle. and sends branches to the chin, lips , che ek, and
outside of the nose. Hremorrhage from wounds of the fac e below the level of the eye is to be arrested by:-
(a) Digital pressure on point 2 (Fig. 39),
(b ) or Graspin g the lips or cheek on both sides of the \\'ound by the finger inside -and the thumb outside the mouth or vice versa .
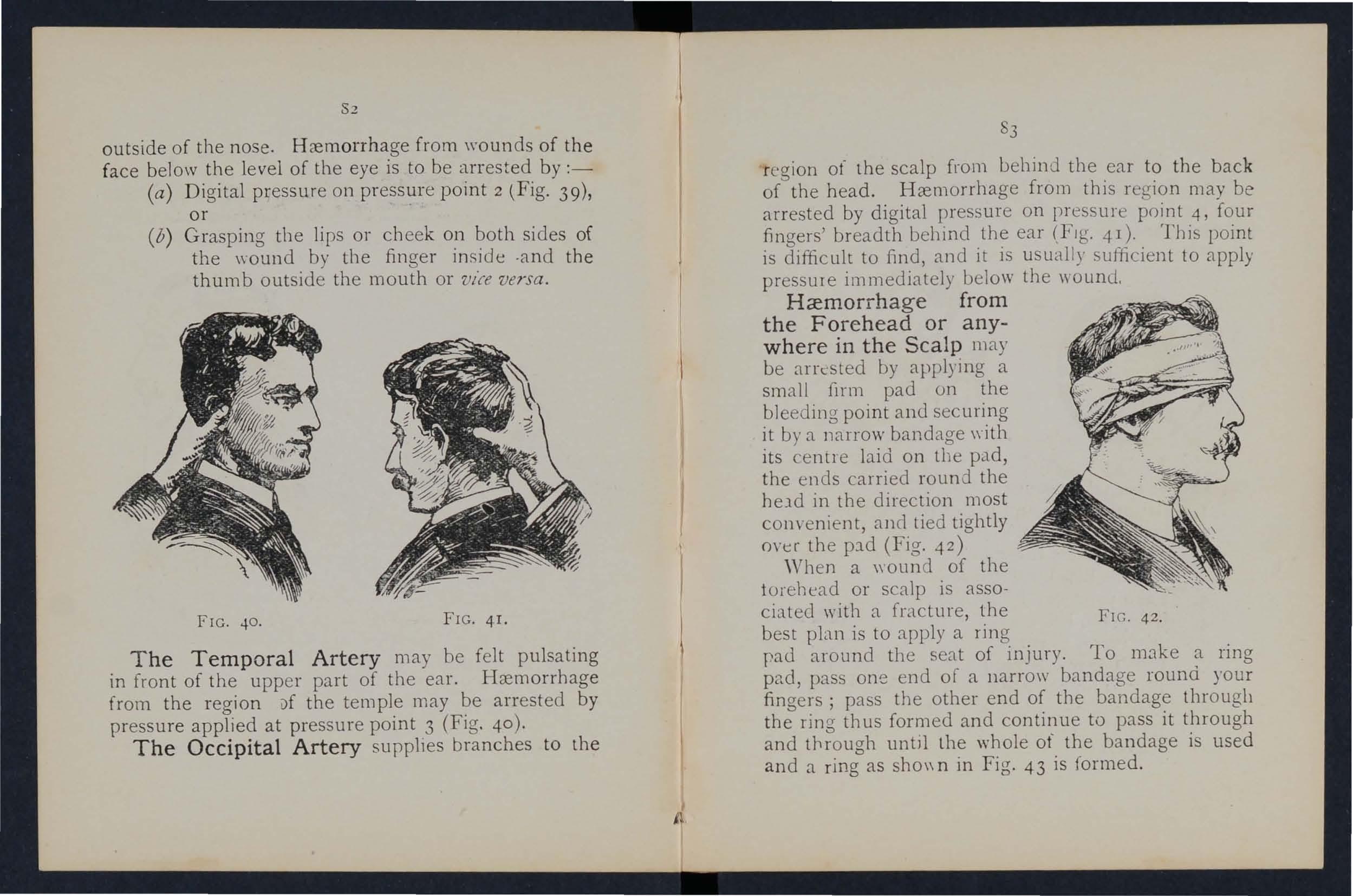
The Temporal Artery may be felt pulsating in front of the upp er part of the ear. Hremorrhage from the region l)f the temple may be arrested by pressure applied at pressure point 3 (Fig. 40 ).
The Occipital Artery supplies branches to the
83
re g Ion ot' the scalp from behind the ear to the back of the head. Hrem orrhage from this region may be arrested by digital pressure on pressure point 4, four fingers' breadth behind the ear (FIg. 41). This point is difficult to find, and it is usually sufficient to apply pressure immediately below the wound.
Ha:morrhage from the Forehead or anywhere in the Scalp may be arrested by applying a small firlll pad on the bleeding point and securi ng it by a narrow bandage \yith its ce ntr e laid on tbe pad, the ends carried round the held in the direction most convenient, and tied tightly OYer the p:ld (Fig. 42)
When a wound of the torehead or scalp is associated with a fracture, the FIG. 42 . best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narr ow bandage round your fingers; pass the other end of the bandage through the ring thus formed and continue to pass it through and through until the whole of the bandage is used and a ring as sho\\ n in Fig. 43 is formed.
FIG. 40. FIG. 4 I.ARTERIE OF THE UPPER LDfBS.
The Subclavian Artery passes frorn a point beh in d the inner end of the collar-bone across the first r ib t o the armpit.
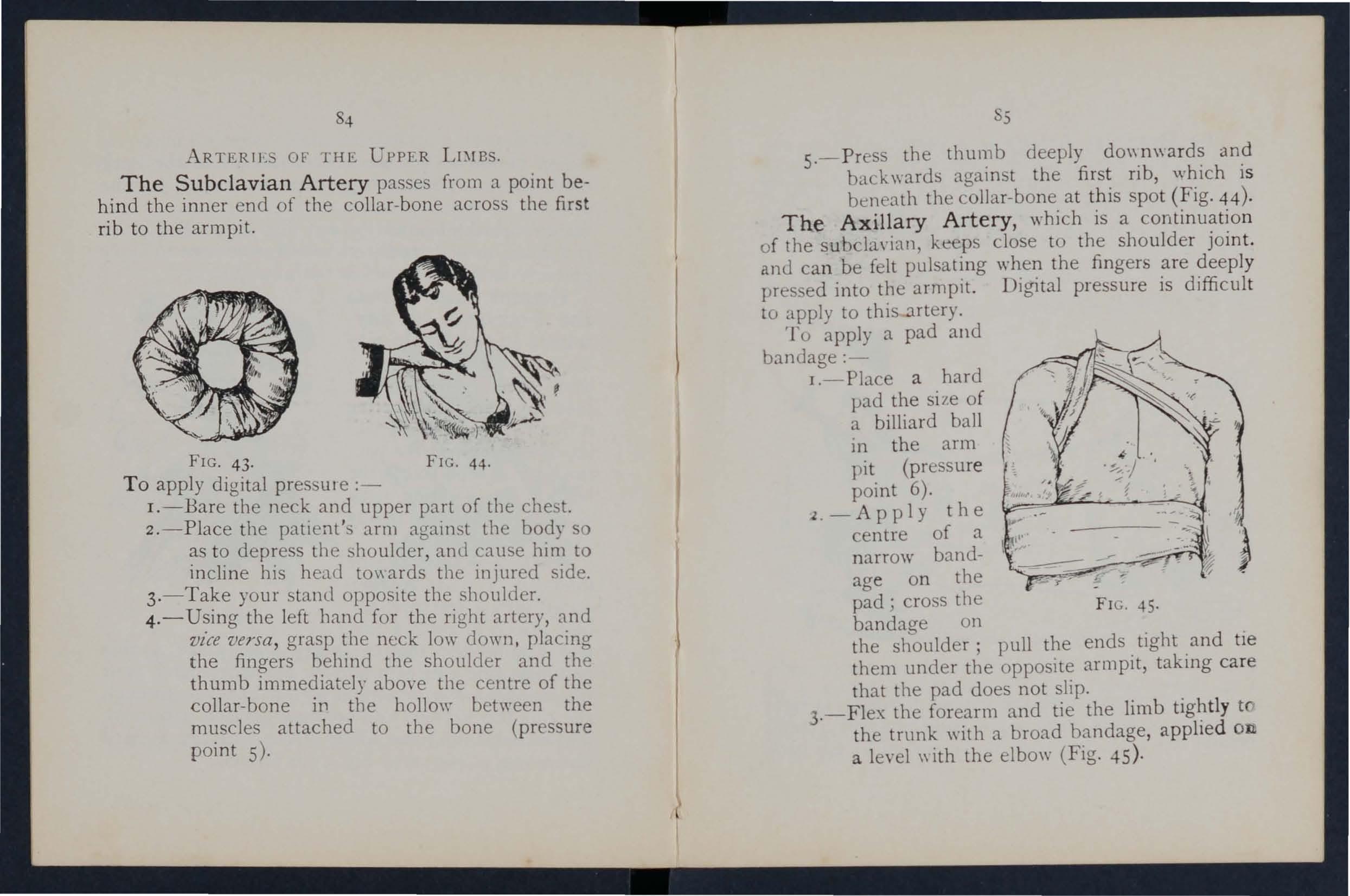
FIG. 4 3. FIG. 44·
To apply digital pres ule :-
I.-Bare the neck and upper part of the chest.
2.-Place the patient's arm against the body so as to depress the shoulder, and cause him to incline his head to\\ ards the injured side.
3.- Take your stand opposite the shoulder.
4. - Using the left band for the right artery, and vz"ce versa, grasp the neck low down. pIa ing the fingers behind the shoulder and the thumb immediately above the centre of the collar-bone in the hollow between the muscles attached to the bone (pressure point 5).
5
s. - Press the thumb deeply an? back\\"ards against the first nb, whIch IS ben ath the collar-bone at this spot (Fig . 44)·
The Axillary Artery, which is a o f the subcla\·ia n, keeps close to the shoulder ]Oll1 t. antl can be felt pulsating when the fingers are deeply pressed into the armpit. Digital pressure is difficul t to apply to this artery.
To a pply a pad and banuage:-
J .- Place a hard pad the si ze of a billiard ball 111 the arm pit (pressure point 6).
l.-Apply the centre of a narrow bandage on the pad; cro s the FI G. 45. bandaae on the shboulder; pull the ends. tight .and tIe them under the opposite armpIt, takll1g care that the pad does not slip.
3.-Flex the forearm and tie the limb tfI the trunk with a broad bandage, applIe d OIL a level \\ ith the elbow (Fig. 45)·
The Brachial A rtery is a continuation of the Axillary, and runs dOl\'n the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the midJle of the front of the elbo\\'. The inner seam of the coat abo\'e the elbo\\' roughly indicates its course.
Digital or instrumental pressure may be applied at or near pressure point 7.
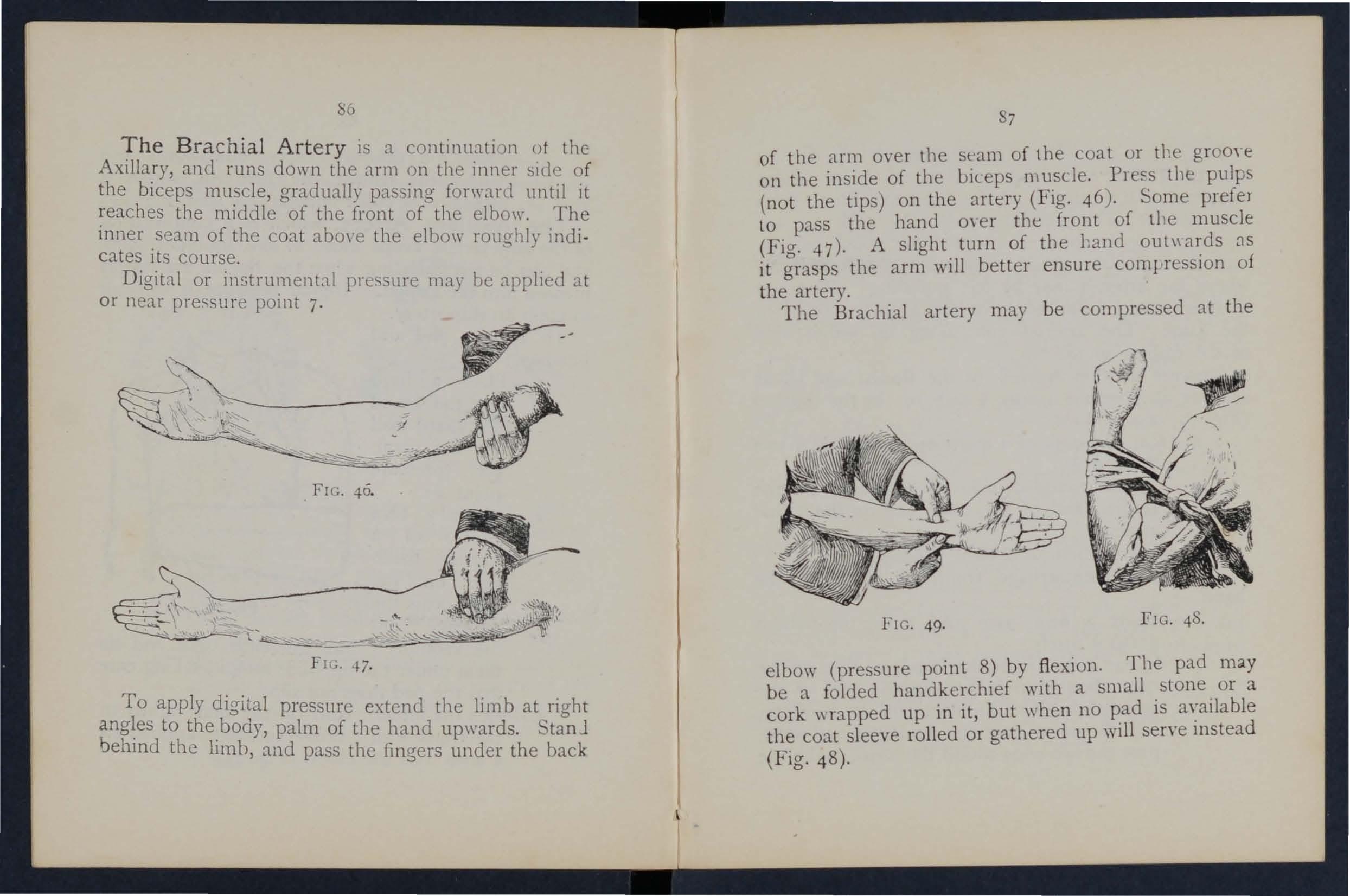
FIG. 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. StanJ behind the limh, and pass the fingers under the back
of the arm over the seam of the Loat or the grooye on the inside of the biceps mu.scle. PIes,S tIle pulps (not the tips) on the artery (FIg. 46). Some prete) to pass the hand 0\ er the front of the muscle (Fig ...n). A slight. turn of tbe hand as it grasps the arm WIll better ensure com I,1 eSSlOn of the artery.
The Brachial artery may be compressed at the
FIG. 49.
elbow (pressure point 8) by fl exion. Tbe pad may be a folded handkerchief with a small. stone. or a cork wrapped up in it, but when no p.ad IS a\?ilable the coat sleeve rolled or gathered up WIll serve mstead (Fig. 48).
ss
. Just below. the elbow the Brachial artery divides mto the RadIal and Ulnar arteries, which run along the front of the forearm on the outer and ir.ner sides respectively. The pressure points (9 and 10) are one inch above the \\"fist and about half an Ineh from the outer and inner sides of .he forearm where the arteries may be felt pulsatin u of these arteries join to form the Arehes in the hand. The arteries run along 0n either side of the fingers to the tip.
a Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and 10, by the thumbs (Fig. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3·-Secure them by a tight bandage.
To arrest hremorrhage from the palm of the hand:-
I.-Apply a Rrm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, turn up the four inches, lay the back of the patlent s ha.nd on the centre of the bandage, fold the POInt over the knuckles and wrist pass the two ends round the wrist, make
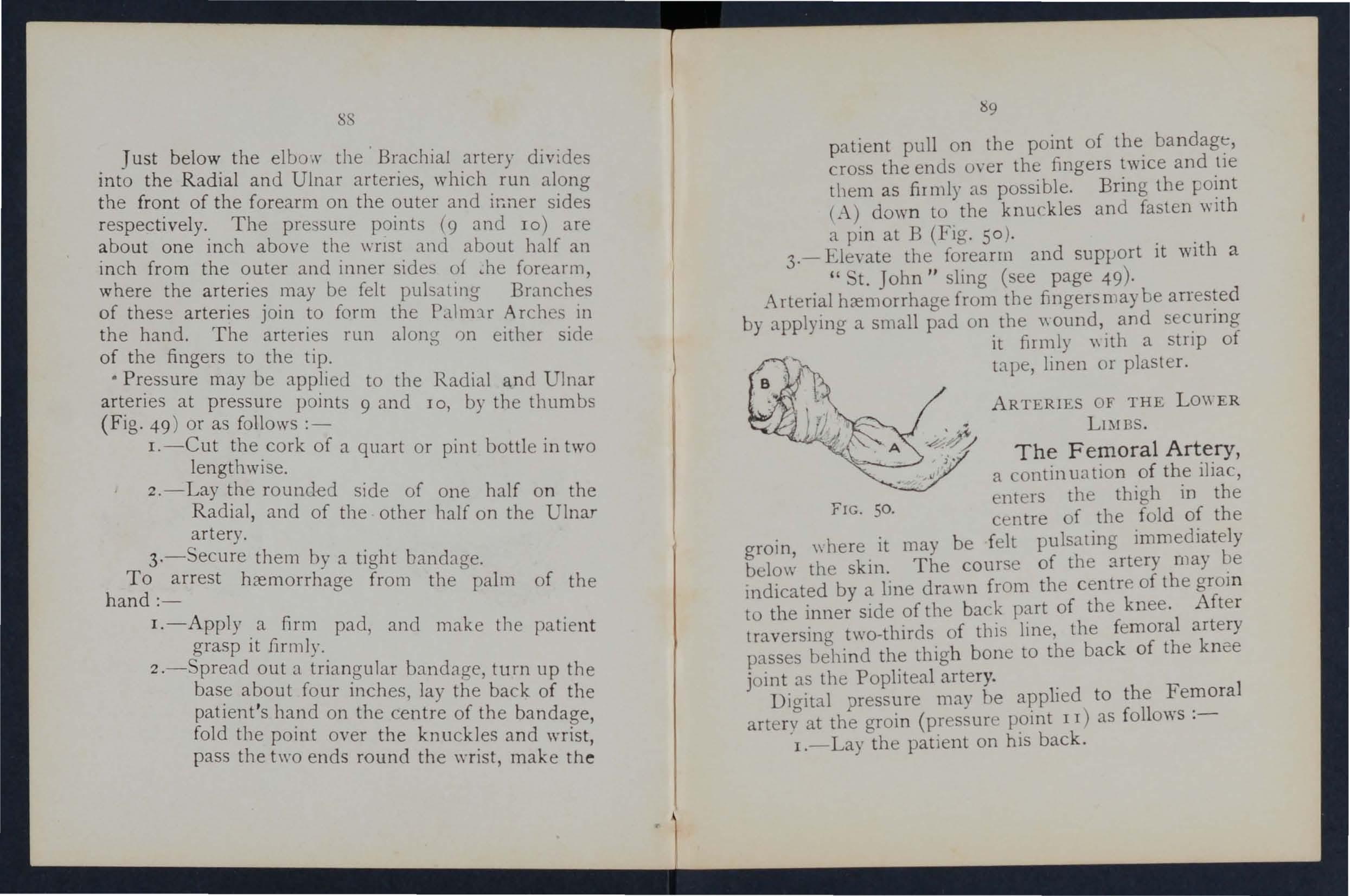
patient pull on the point of the bandage, cro s the enus over the fingers twice and tie tbem as firmly as possible. Bring the Foint (A.) down to the knuckles and fasten with a pin at B (FIg. 50).
3.- Elevate the forearm and SuplJort it with a " St. John" sling (see page 49)·
Arterial hcemorrhage from the fingers may be arrested by applying a small pad on the \\ ound, and s curing it filmly \\ Ith a strip of tape, linen or plaster.
AR TERIES OF THE LO\\ ER LIMBS.
The Femoral Artery, a contin ua tion of the iliac, enters the thigh in the centre of the fold of the grom, \\ here it may be felt pulsating immediately below the skin. The course of the :utery may be l11dicated by a line dra\\ n from the centre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the femoral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
FIG. So.
Digital pressure may he applied to the Femoral artery at the groin (pressure point II) as follows :-
I.-Lay the patient on his back.
2 -Kneel beside the patient.
3· -To find the groin, raise the foot high so as to Rex the thigh; the fold in the clothing at the top of the thigh will indicate the groin.
4· - Place the thumbs one on the other upon the pressure point, grasping the thigh with the hands (FIg: 51).
5.-Press firmly against the brim of the pelvis.
As there is ill)mediate danger of death it is im· portant not to" aste time in removing the trousers.
'Vh en the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been
FIG. 51. devised for compression at this point, :md relays of assistants should be employecl to keep up the pressure until the doctor arrives; each fresh assistant places his thumbs over those of his predecessor, \\'ho slips his away from beneath, and thus gushes of blood are prevented during the change .
Application of a tourniquet to the Femora] artery (pressure point 12) :When practising compression of this artery, It IS a
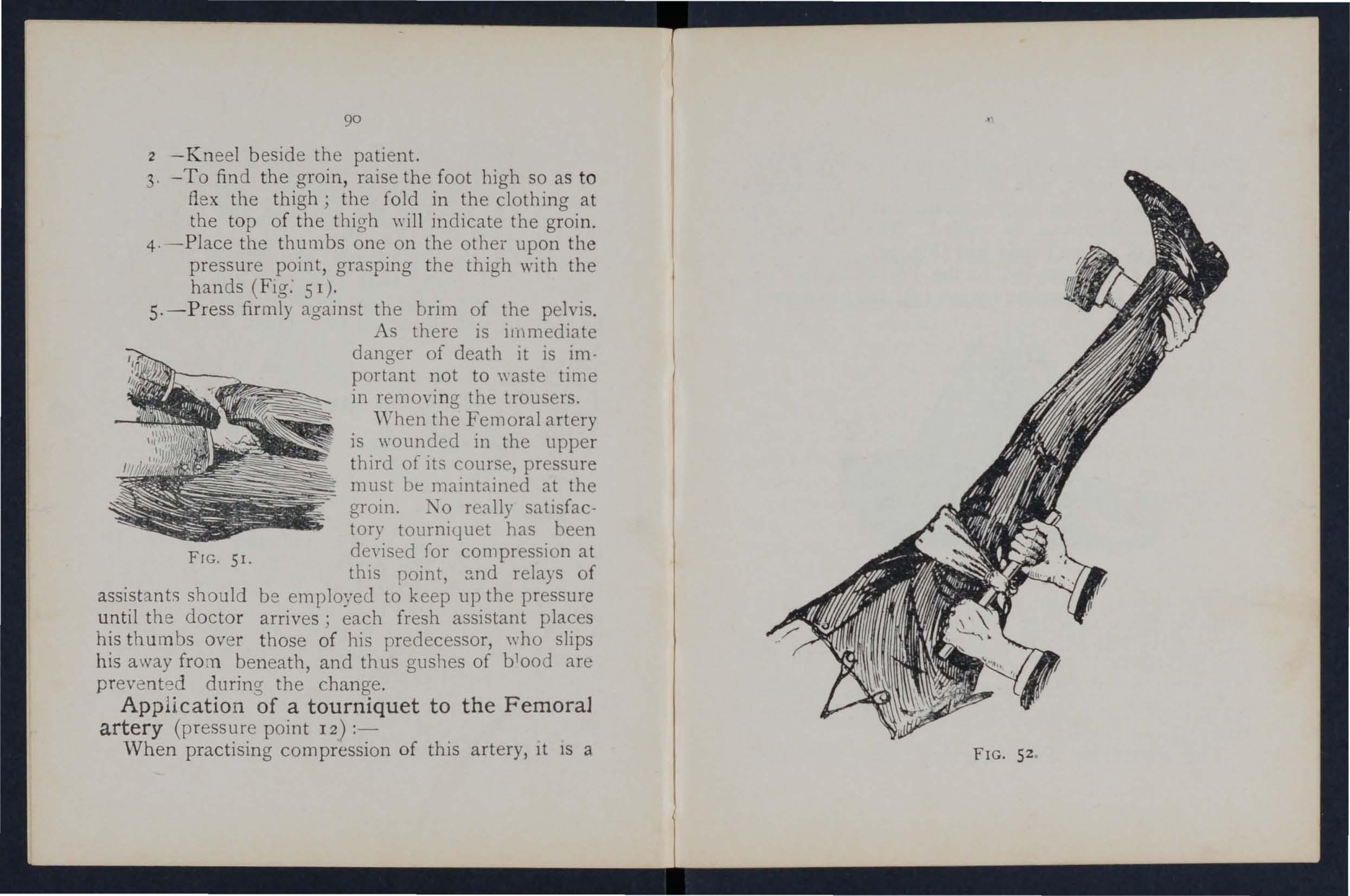
52
92
good plan to draw a chalk line from the centre of th(' groin to the inner side of the back of the kr.ee . place the pad of the tourniquet on this line as high up as the bandage can be applied. The pad should be the size of a lawn tennis ball (Fig. 52).
Pressure may be applied to the Popliteal artery by tlexion at the knee (pressure point 13); the pad should
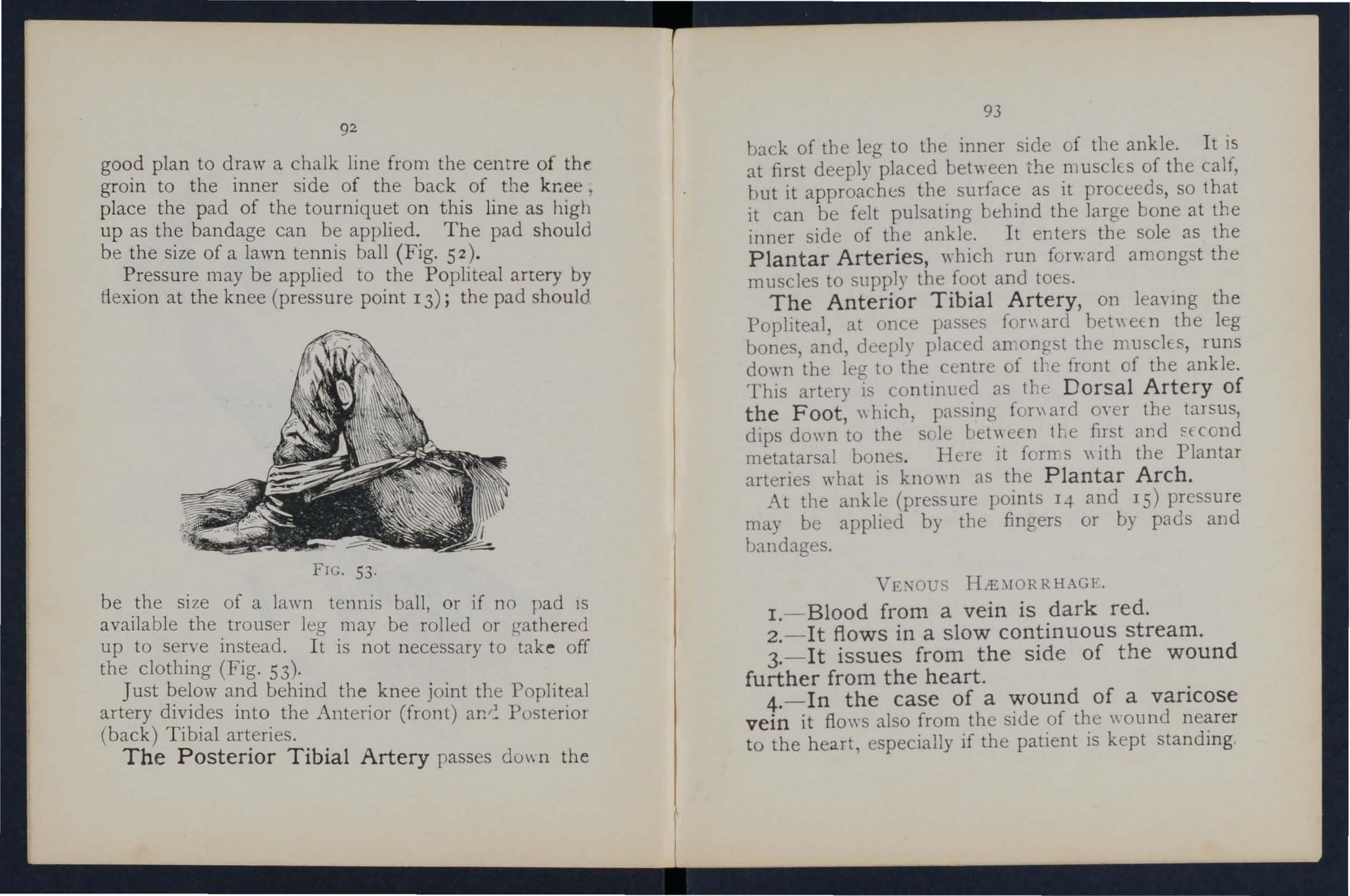
FIC. 53 .
be the si ze of a lawn tennis ball, or if no pad 1S available the trous e r leg may be rolled or!.;athered up to serve instead. It is not necessary to take off the clothing (Fig. 53).
Just below and behind the knee joint th e Popliteal artery divides into the Anterior (front) Posterior (back) Tibial arteries.
The Posterior Tibial Artery passes do\\ n the
93
back of the leg to the inner side of the ankle. It is at first deeply placed between the musclEs of the calf, but it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the inner side of the ankle. It enters the sole as the Plantar Arteries, "hich run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery, on leaymg the Popliteal, at once pas es f n\ ard bet" eE. n the leg bones, and, deeply placed an1 0 ngst the muscles, runs down the leg to the centre of tl'e front of the ankle. This artery is continued as the Dorsal Artery of the Foot, \\ hich, passing fon\ aId oyer the tarsus, dips do\\ n to the sole bet:, cen tte fi.lst and ffcond metatarsal bones. Here It \\ lth the Plantar arteries what is k11o" 11 as the Plantar Arch.
At the ankle (pressure points 14 and IS) pressure may be applied by the fingers or by pads and bandages.
I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3.-It issues from the side of the wound further from the heart. .
4.- In the case of a of a vancose vein it flows also from the sIde of the \\ ound to the heart, especially if the patient is kept stand mg .
Varlco3e Ve i ns .-The veins of the leg are speci :ll ly apt to varicose. A varicose vein is dibteJ, winding, a n d with bead-like (varicose ) projections along its course. A vein becomes varicose from several causes, such as long standing or tight garters. The first effect is to throw extra work upon the valves, and the bead-like projections are caused by the b loJd accumulatll1g in the pockets behind the valves . I n time the vein becomes so dilated that the vah'es can no longer span it.
GE:\ERAL RULES FOR OF A
J\CCO'\IP .\ \TIED BY H.tE \ IORRH,\GE.
I. - PlaCe the patient in a suitable position, bear1nJ in 111 ind that t he bloo i escapes wi th forc \\'hen the patient sits and is still more checked a s he lies do .\"n.
2. - Elevate the part, as thereby less blood finds its way into it.
3. - Expose the wound, rel110ying \\ hat eycr clothi n:2: is nece:;sary.
4·- Remove any constrictions, such as i.he collar or f rom the he "ul side of the \\ ound.
5. - A pply digital pressure on the wound until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure near the "ound on the side away from the heart I n the case of a wound of a varicose vein it may also be necessary to
95
a ppl y a pad and ba n dage to the yein immediate ly above th e wound, especially if the limb cannot be maintained in an elevated position.
6. - Treat the wound as directed by Rules S, 6 and 7, stated on pages 77
7. - Afford support to the lnJured part.
CAP1LLAR'{ H .'E.\lORRHAGE.
1. - The blood is red.
2. - It flows bri s kly in a continuous stream, or may merely ooze from the wound .
3. - It wells up from all parts of the wound. A slight amount of pres ure \\ dl uffice to arrest capillary hremorrhage.
I:\TER I .tIL
oW ounds of the blood vessels \\ ithin the trunk ca u se bremorrhage into the cayity of the che:,t or of the abdomen .
SIG, s A l D OF HiE.\IORRHAGE.
I. -Rapid loss of strength, giddiness and faintm:ss, especially \\ hen the upright P?sition is assumed.
2. -Pallor of the fa e and lIps .
3.-Breathing hurned and laboured, and accompanied by ya\\ ning and sighing.
4.-The pulse fails, and may altogether dIsappear at the wrist.
s.-Tile plticnt throl\':; his arms about, tugs ilt the cluthing round the neck, and calls fur air.
.6.-Finally the patient may become totally unconSCIOUS.
TRK\T\[I;, .\T.
I.-Keep the p:ltient in a recumbent position.
2.-Undo all tight clothing about the neck.
3. - Prm'ide for fre e circulation of air; hn the patienL.
4.-Sprinkle cold water on the face; hold smelling slIts tCl the n ostrils; avoid other forms of sti'nubnts, at all events until the hremorrhage has been controlled.
s.-Give ice to suck or cold water to drink; if the seat of the hremorrhage is known, apply an ice bag over the region.
6.-Should the patient be reduced to a state of collapse, rais e the feet and bandage the limbs fil1111." from the toes to the hips and from the fingers t the shoulders.
H.K\lORRHAGE FRO:Jr THE NOSE (NOSTRILS).
I.-Plac e the patient in a sitting position in a current of air before an open \\ indo"" \\ ith the head thro\\'!1 slightly back and the hands raised above the head.
2.-Undo all tight clothing around the neck and chest.
3.-Apply cold (ice, a cold sponge or bunch of
97
keys) oyer the nose and also the spme at the level of the collar; place the feet in hot \\ ater.
.f.-Cause the patient to keep the mouth open, and so a\'oid breathing through the nose.
Blood issuing from the mouth may come from the tOll O" Ue, the gums, the socket of a tooth after extraction, the throat, the lungs, or the stomach
FRO",! THF TONGUE, THE GUMS. THE 'OO-:FT OF A TOOTH, OR THE THROAT.
r .-Glve Ice to suck or cold \Yater to hold in the mouth, If thiS IS not successful gl\'C ,yater as hot as can be borne to hold in the mouth.
2.-If necessary make pressure on the carotid arterIes.
3.-If bleeding from the front part of the tongue IS excessIve compress the part by a piece of clean llJ1t held hetween the finger and thumb.
4.-If the bleedmg is from the socket of a tooth, plug the so ket with a piece of clean lint or cotton \\"001; over this place a small cork or other substance of suitable size, and instruct the patIent to bite on it
THE. LU:"G .
Blood from the lungs IS coughed up and is scarlet 'C.nn frothy in appearance.
Treat as for Internal Hcemorrhage (see page 95) ' £
H .'E\ IORR H AGI£ FRO;'l [ THE TO:\ f AC H.
Bl ooJ from the stomach is vomited; 1t 1S o f a dar k colou r an d has the appea r a n ce of coffee grounds; it ma y be mixed with food.
T rea t as for I nte l nal H;emorrklge (SCC page 95), e xcept that nothlllg is to be giYen by the mouth .
Blood issuing from the Ear Channel, \\' hich ge nerally indicates a. fracture of thc base of the c ra n ium , m u st be \\'ipeu a\\'ay as It issues; no attempt is to be made to plug the ear.
99
Tile lI UlJl t la l S i"diratc tltt! fag'es where the aIISUle!S lila), be found.
W hat organs are cuncerned in the circulatiun of the
olood?
many times a minute doe the heart contract on the average?
hat is the etTect of the patient's positilln on the rate at which the
ow many kind ' of hremorrhage are there?
Wby i accuracy necessary in placing the pad of a tourniquet ? '-Vh en mayan elatic bandage be used i nSlcad o f a tourniquet?
State t he gene ral rules for treatment of a II ollnel accom· pan ie d oy arterial '" 77, 78
If part of a li mb had oeen torn off, Imt there "as nd u:uch bleed i ng, ho \\ would )'0l1 act?
Sh o u ld bl ood c lots be eli tmbed ?... ... '"
Is i t wi e fo r a n unshilled per on to a ltempt to cleanse a wound? .
100
Describe the arteries of the head and neck . 80
vVhy is it sometimes necessary LO compress the carotId a r tery both below and above the wound? .. , 80, 8 I
vVhat is a ring pad, and what j its use? 84
Describe the arteries of the upper lim b 84 to 89
Describe the arteries of the lower limbs... 89 lO 93
How would you know a ca-;e of yenou h:.emorrhage? .. 93
\ Vhat is a varico e vein? 94
How maya vein become varico e? ... ... .. 94
tate the general rule for lreatment of a wound accumpanied by venous h:.el1'·... ... .. 94. 95
How v'Quld you k now a case of capillary hremon hag\: ? 95
How would you stop capillary h:.emorrhage ? 9S
What is internal h:.emorrhage? ... ... . . ... 95
Nh at would lead you to suspect internal hXl11orrhage? 95, 96
State the t r eatment for internal h:.emorrhage? . . 96
How would you arrest h<.t:morrhage from the nose? .. 9 6 , 9 7
\Vhe re may blood issuing from the mouth come from? ., 97
How would you treat bleeding from the gum or throat? 97
What else w ould you do if the tongue were bleeding?,. 97
And if the bleeding were from the socket the tooth? 97
How would you distinguish between bleed1l1g fml11 the l ungs and from the stomach ?,.. 97
And what would be the difference in the treatmel1l ? 97
.of what is bleeding from the ear channel generally:1. ? 9
t he Student should praclise placing supposed patIents i n a proper position for the a,rrest of h:.emorrhage (see pages 72, 77 and 94), foldmg firm pads (74: and 7 5 ), tying hard knots in bandages to form a t·.)url1Jquet 76 ), andlhe application of pre.ssure at all the press.nre f'oint!. shown in the frontIspIece, at \'anOUS pOInts :m the forehead and scalp, and on the palm of the nand . Pressure should be digital, by pad an o r flexion, as directed in the text
PreSque pomL -CarotiJ artery, 80. Facial, 82 .
Temporal, 82. Occipital 83. Subclayian, 84. Axillary, 85. Brachial (by pad and bandage, pressure being made against the humerus and by flexion at the elbow) 86. Radial and Ulnar, 87. Femoral at the groin, 90. Femoral in the thigh, 9 2 l'opliteal, 92. Anterial ancl poterior Tibial arteries, 93.
Hremorrhage from the forehead or scalp ...
Hremorrhage from the palm of the hand.. . ..
Venous hremorrhage from a \'arico e or other vein
87 to 89 .. 9.1 ' 94
CHAPTER IV. BRUISES.
A blow anywhere on the surface of the body may cause extensIve heemorrhage beneath th e skin, \\ ithout breakmg it-a" black eye" is an instance. The injury is accompanied by discoloration and S\\ elling .
TR L\'nfI:.NT
Apply ice or cold \Yater dressings . A piece of lint soaked in ex tr act of \\ itch hnel may be p laced on the affected part.
. \1\'D ..
A burn is caused--
(a) By dry heat, such as ore or a piece of hot iro n.
(b) By a raIl, wire or d) namo charged with a high pressure electric current.
(c) By a corrosive acid, such as oil of vitriol.
(d) By a corrosive alkali, such as caustic soda , ammoni a, or quicklime.
(
e) By friction, caused, for example, by contact with a Tf·volving wheel. (Brush burn.)
A scald is caused by moist heat, such as boili ng \\'::Iter, hot oil or tar.
Th e effect may be a mere reddening of the skin; blist e rs may be formed; or even the deeper t issues r03
of the body may be charred and blackened . The clothing may adhere to the burnt skin, and its removal is impossible without further detriment to the injured
The great danger is hock.
TR F-\T\f1' '-T.
. .I. - Carefully remove the clothing over the Injured part. If to thp skin, the adherent cl o thin:; mu ·t be rut around \\'Ith SCIssors, soaked WIth 011, and le ft to come a\\ay subsequently.
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear pieces of lint or linen \\ith oil or vaseline hnoline, or cold cream; a small quantity of p 8 \\'d er added to the -e \\ ill be of be n efit. The inside of a raw potato scrap ed out and spread on I lilt makes a soothing appltcation. "'hen the injured is do not cover It \\ith one large shee t of 11l1t, but \\ Ith strips about the breadth of the hand' this . I advisable as they fil better on the part, :ll1d suhsequent dre sIngs one strip can be remo ved at a tIme, and a fresh dres ing appli e d before the adjacent strip is taken off. The shock to the system IS thereby less tl,an if the whole of the burnt surface were laid bare to the air by the removal of all the dressings at o ne time. \Vh en covered by th e ody dressing em"elop the part in cotton \\'00 1 o r a piece of A.wnel and apply a bandage.
'When the face is burnt, cut a mask out of lint or linen, leaving holes for the e) es, nose, and mouth. Dip this in oil or smear it ,\ ith vaseline and apply it to the face and cover it with cotton wool, leaving openmgs to correspond "ith the holes in the mask.
\Vh en po sible place the injured part in ,yater at the temperature of the body (98 degrees) until uitable dressings can be prepared. A des ert-spoonful of baking soda added to a oa. inful of the" arm \\ ater will make a soothing lotion .
As it is important not to leave the part cxposeJ to the air, it is the duty of the bystanders to prepare the dressings while the clothing is being removed.
4. - Treat Shock. -This is particularly necessary In the case of eyery burn or scald of any t oniderable extent (see page 135)' Be very apprehensive of danger In the case of even slight burns of the neck.
5. - If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bHaroonate of soda), magnesia, or slaked lime in "arm \\ ater before applying the dressings.
6. - If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion, su ch as lemon juice or vinegal diluted wirh all equal quantity of water. Caut£on.-Before using water brush o ff any lime that remains on the part .
7. - When a woman's dress catches fire -
(a) Lay the" oman fiat on the floor at once, so that the names are uppermost; that is to say, if the front of the dress is on fire lay her on her back, and if the back of the dress i.., burning, place her face do\\' nwards. The reason for this is that names ascend, so that if the upright position is assumed, the flames "ill quickly reach and burn the body, neck, and face; or if the woman lies WIth the flames undermost, they will, if unextinguished, pass o\'er and burn the limbs, and set fire to the rest of the dress.
(b) As soon as the woman is laid flat, smother the Aames with anything at hand, such as a rug coat, blanket, or table co\'er; if made wet so much the better.
(c) A \yoman rendering assistance should hold a rug or blanket in front of herself when approaching the flam es.
(
d) If a woman's dress catches fire when nobody is by, she should lie flat, flames uppermost, smother the flames ,yith anything handy, and call for assistance, or cra\d to the bell-pull and ring; on no account should she rush into the open air.
The use of fire guards would prevent many : alamities.
BI TES O F SNAKE AND R AB ID A 'UrAL , AN D ,rO U ND S BY P OI O NED 'WEAPONS.
Hy d rophobia is caused by the b i te of an animal , such as a dog, cat, fox, \\ olf, or deer suffering from rabies. The special poisons introduced into" ounds camed by yenOI11OUS snakes and poisoned \\ eapons cause immediate danger to life.
1. - Immediatelyplace a constriction betwe en the wound and the heart so as to pre\ ent the venous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircled on the side of the \\"01..l11d nearest to the heart, with the finger and thum b, and as soon as possible a ligature (a string, piece of tape, or stnp of handkerchief) should be placed tightly round the root of lhe finger. Compression with the finger and thumb must not be relaxed until the ligature has been applted. Additional ligatures may, with adyantage, be applied at intervals up the lim b.
2. - Encou r age bleed in g for a t ime :-
(a) By bathing the wound with \\ arm \\ ater.
(b) By keeping the injured limb low: the upper limb should be allowed to hang do\\n, and in the case of the lo\\'er limb the patient srnuld be seated \\ ith the foot on the ground.
3. - Cauterise th e wound, if it is quite impossible to obtain the services of a doctor. T his is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or if these are not at hanu, \\ ith a red hot ",ire or a fusee .
The usual solid caustic is insufficient, as it does not reach the bottom of the \\ ound, where the poison is.
To ensure the caustic reaching the bottom of the wound, it should be applied on a piece of wood, such as a match cut to a point. ,Vhen the caustic has been thoroughly applied, but not till then, the ligcltures may be removed.
4. - Cover the wound , after a while, \yith a clean dres3ing,
5. - Afford support to the injured part.
6 - Treat shock if it occurs (see page I35) .
7. - In the case of a bite by a venomous snake, rub in powdered permanganate of potash and inject under the skin in the neighbourhood of the wound a solution of permanganate of potash .
These give rise to serious inconvenience, and 1U some cases grave symptoms develop.
I,- Extract the sting if left in.
2.- Mop the part freely with dilute ammonia
100 or spirits. A paste of bicarbonate of soJa and saJ vobtlle is an efficient application. A solution of 'ashmg soda or potash or the application of the blue bag \yill relieve pain.
Z.- Treat collapse if it occurs (. ee page 135)·
During exposure to se\ ere cold, parts of the bod)', usually the feet, fingers, nose, or ears, 10 e sensation a n d become first \\ ax)' \\ hite and aften\ards congested and of a purple appearance. As sensation is lost in the part, it is often only by the remarks of bystanders that the frost-bitten person is made aware of his condItion .
I. - Do not bring the patient into a warm oom until, by frict!on of the band or by rubbing ,vIth soft snow, sensatlon and circulation in the afferted parts are restored . Neglect of this precaution may lead t o death of the ti:::sues of the frost-bitten part. circulation is restored, keep the 8)a,tlent 111 a room at a temperature of 60 degrees.
a needle breaks off :1fter penetrating the skin .nd dIsappears, take the patient to a doctor at once. If the wound is near a joint, keep the limb at rest on a splint.
Do not attempt to withdraw the fish -hook by th way it went in, but cut off the dressing of the hook. so that only the metal is left, and then force the point Ol1\\'ards through the sk111 untIl the hook can be pulled out.
'Vhen a joint is injured by a bull e t, stab, or othet cause-
I. - Wrap the part in cotton wool. . rest. and support to the injure d ; If the lllnb, in a flexed position by a sling n If the lower 11mb, in a straight position by a splint.
I. - Prevent the patient rubbing the eye tying do\\ n a child's hands if ne c e sar),.
2..- Pull the lower eyelid, ",hen, if th .. lor e lgn body IS seen, it can readily be removed with a camel's hair brush, or \\ith th e corner of a handkerchId twirl e d up and wett (1.
3. - Wh en the foreign body is beneath the upper eyelid lift the lid fon\ arc\, up the lower lid beneath it and let go. Th e hair of the lower lid brushes th e inner surface of the upp e r one, and may dislodge the body. -' hould the first attempt be unsl1('C'essful, repeat it seyeral times if necessary. If
!lO
the foreign body is not dislodged call the se n -ices of a doc t or as soon as possible. When, however skilled help cannot be had, proceed as follows
(a) "':cat the patient so as to face the light, an d stalld behind him, steadying bis head agains t your chest.
(
b) Place a small rod, such as a match or bodkins on the upper eyelid, half-an-inch abm e the edge, pressing it back ,yards as far as }- ossi ble
(c) Pull the upper e)C-lasllE:s up"ards mer the rod, and thereby eyert the eyelid .
(d) Remm-e the foreign cody .
4. - When a piece of steel is (mb(dded in the eyeball d-::-op a little olive or castor oil n the eyeball after pulling down the 10" er eyelid, the lids, apply a soft pad of cotton ,\ 001 and it by a bandage tied sufficiently fir mIl' to keep tbe f) cball take the patient to a doctor.
5. - When quick-lime is in the eye brush away as much of it as possible; bathe the eye ,\jth vinegar and warm \\ater, and treat as for a piece of steel embedded in the eyeball.
As a rule make no attempt to treat a patient with d fo r eign body in the ear if the services of a doctor can possibly be had: any attempts to remm-e the foreign body may lead to fatal consequences . If a child
III
cannot be induced to keep the fingers froill the ear, tie his hands do\\-n or cover up the ear . If an insect 1.S in the ear-pl.ssl.ge, fill the ear \\"ith olive oil, when the insect will float anu may be removed. Neyer -yringe or probe the ear.
Induce sneezing by pepper or snuff. Cause the: patient to blo\\' his nose after closing the nostril. There is no immediate danger from a foreign body in the nose.
The abdomen is bounJeu aboye by the diaphragm « belo\\' by the pelvis; hehind by the lumbar ,ertebrc:e' and In front anu at the siues by muscular ,,-alls. (Fig. 54·)
The Stomach lie immediately belo\\' the" pit of t he stomach " ju t belo\\ the breast-bone .
The Liver lies in the upper part of the abdomen, where it is 1110 tly coyered by the right lo\\er ribs.
The Spleen lies beneath the ribs at th':! upper part of the left siue of the abdomen.
The Intestines occupy the greater part of thecavit\· of the abdo nell.
The Kidneys lie at the back, in thG region of the loin.
The Bladder lies in the pelvis.
LARGE. INT[STINe
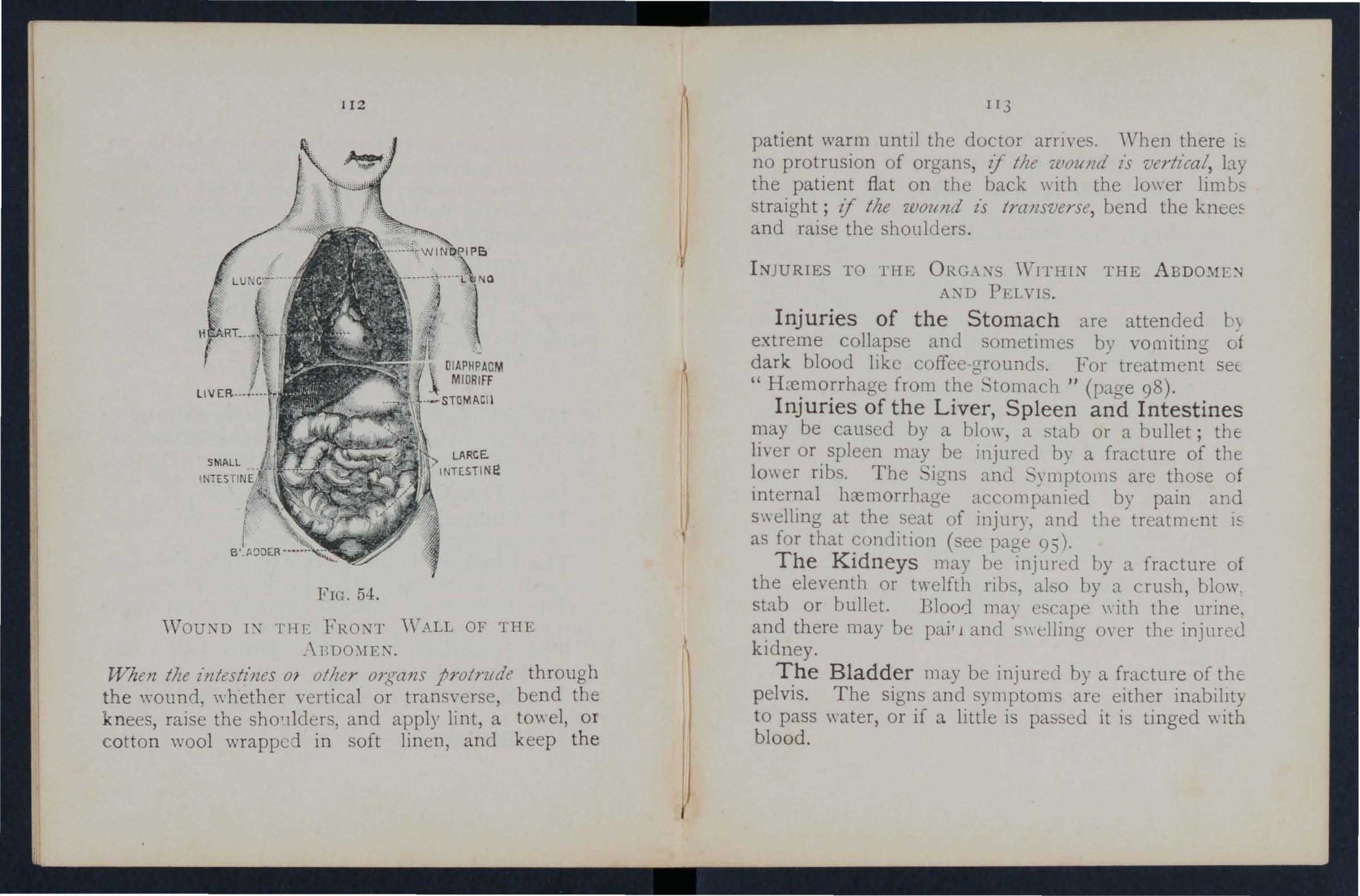
FIG. 54.
'YoUi'm IX ['HE FRONT '\'ALL OF THE _\BDO:\IE:"l'.
When tlze z"Jltesthzes 01 other Olgans protrude through the ,,"ound, \,"hether vertical or transYerse, bend the knees, raise the sho,llders, and apply lint, a to\\ el, or cotton wool wrapped in soft linen, and keep the
patient warm until the doctor arnves. 'Vhen there no protrusion of organs, if tlle 'wolllld is vertical, by the patient fiat on the back \\ lth the 10\\ er lim straight; if the wound zs tramverse, bend the and raise the shoulders .
TO l'HE ORG.\" 'YITHli'l" THE AXD PELYI .
Injuries of the Stomach are attended b\ extreme collapse and sometimes by vomitmg of dark blood lIke coffee grounds. For treatment sec " H:-e.ffio;rhage from t?e "'tomach " (page 9 8 ).
InJunes of the LIver, Spleen and Intestines may be caused by a blow a stab or a bullet; thE: liver or. spleen may be injured by a fracture of the lower nbs. The 'igns and 'ymptoJl1s are those of Internal h::emorrhage accompanied by pain and s\\ ellmg at the seat of injury, and the treatment as for that (sec page 95).
The Kldneys may be injured by a fracture of the eleventh or twelfth nbs abo by a cru h blow stab or bullet. Bloor] m::1/ escape \\ith the' urine, a?d there may be pair 1 and S\\ elling o,' cr the injur e u kIdney.
The Bladder may be injured by a fracture of thE: pelvis. The signs and symptoms are either inablllt) to pass \Yater, or if a little is pas-sed it is tinged with blood.
I I-!-
OF I:-;J"cRY TO THE KlDXEYS OR BLADDER.
I. - Keep th e pat ie nt quie t until the ,loctor arrives.
2. - Apply hot fom e nt ations over the painful or injured part.
Rupture (hernia) consists of a protrusion of an mternal organ, usually the bo\yeJ, through the muscular wall of the abdomen, most frequently at the groin. 'houlJ a sudden s\\elling accompanied by pain and sickness take place in that region
I.-Send for a doctor instantly.
2.-Lay the patient down \\'itb the bUllocks raised.
3.-Apply ice or cold water dressings to the affect ed part. I 15
Th Jlumerals ilZ.i/(lZ't: 1/1<1 p.1ges where tile answers
would yOll treat a burn caused by a corrosive acid?
,., would you \ reat a burn caused by a corrusi\'e al kali
taken when a woman's dress catches
H)w
when quick-lime is in the eye?
lIow \\ ould you try to rel1lo\'e an insect from the ear passage?
W ould yuu t ry to H'1110ye any othe r fo r m of fo reign body from the ear passage? ... ... ... ... 11 0, I II
How wOlild you remove a foreign body from t h e nose ? I I J
State the boundaries of the abdomen and its contents I I I
State the treatment for wounds of the abdomen 1 12, 113
How may injuries to the spleen and intestines oe caused? ... II J
Vhat is the diffe rence het ween treatment of in juries tc the stomach and of injuries to the live r , spleen and in testines ? . . . . 1 13 the treatment of injuries to the kidneys or bladder 1 q
;tate the t r eatment of h ernia I I4 II 7
Two systems of nerves, the Cerebro-spinal and thl' Sympathetic , regulate the movements and function' of the body
The Cerebro-spinal System is made up of th,' Brain, the pinal Cord and and through it, age n cy sensations are received and the will cause" the action of the voluntary muscles. For examplt when a part is injured a sensation of pain is con veyed to the brain by the nen"e, thus affording aT Indicatio n of the seat of injury, or a warning of " possible da nger of further damage . O n at t enti01 being directed to the itljury, an attempt is instanth made to ease the pam or to moye the injured from danger .
The Brain is situated \\ ithin the cranium, and IS divided in t he middle line, so that, \\ ith the exceptior: of some conne cting bands , the right and left side an' separate.
The Spinal Cord is the long cord of nen"ou" matter lying within the spll1al canal (see Vertebra Column, page 23). I t lea,-es the brain through ar ')penmg in the base of th e cranium and [0 the uppe r lumbar verteblGe.
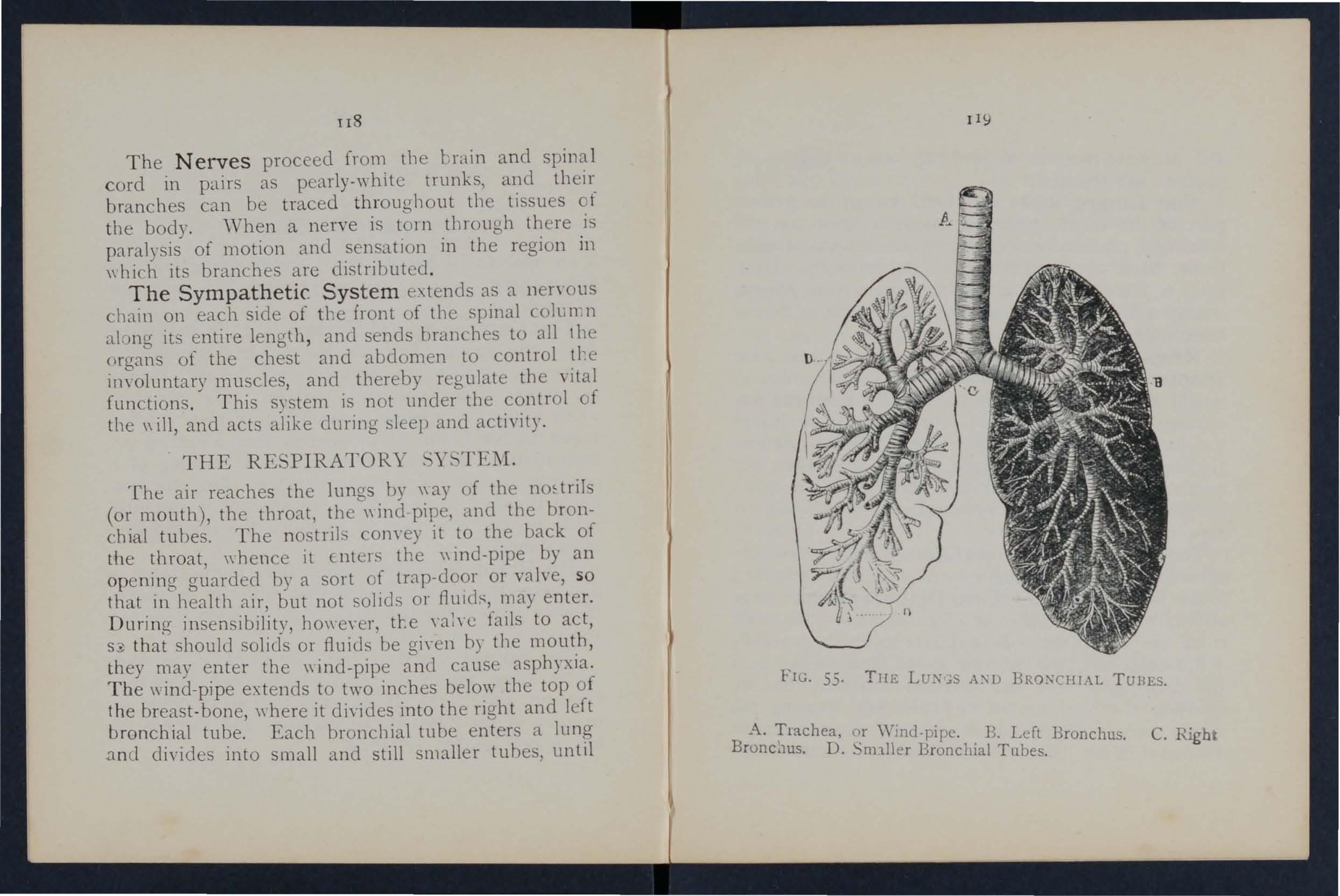
The Nerves proceed from tIle brain and spinal cord in pairs as pearly-\yhite trunks, and their branches can be traced throllghout the tissues of the body. 'When a nerve is tOln through there is paralysis of motion and sensation in the region in \\ hich its branches are distributed .
The Sympathetic Sys te m e\tends as a neryous chain on each SIde of tIle front of the spinal coll.t1. n along its e ntire length, and sends branches to all I he organs of the chest and abdomen to control tl'e ir1Yoluntary muscles, and tbereby regulate the "ital functions. This system is not llllder the control f the \\ ill, and acts alike during sleep and actiyity.
The air reaches the lungs by \\ay of the nmtriIs (or mouth), the throat, the \\ ind -pipe, and the bronchial tubes. The nostrils cOlwey it to the back of the throat, \\ hence it Enters the \\ ind-pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but not solids or may e nt er. Durin g insen ibility, hO\\'e \,er, tl:e \'ah e falls to act, S3 that should solids or fluids be gi\'en by the mouth, they may enter the \\ind-pipe and ca use asphyxia. The \\ ind-pipe extends to two inches below the top of the breast-bone, "here it di"ides into the right and left bronchial tube. Each bronchial tube enters a lung a nd divides into small and still smaller tunes, until
55. TH E LU:\;5 A\"O BRO\"CHlAL TU BES. A. Trachea, "'mel.pipe. B. Lefl Bronchus. C. Right Bronc.1us. D. Snnller Bronchial Tnbes.the ultimate recesses of the lung-the air cells or aIr spaces-are reached.
The Lungs, Ri ght and Left, occupy the greater part of th e chest; they lie immedJately withm the !"ibs, and practically wherever a rib is felt, whether fr ont, back or sides, there is lung beneath. Each lunO" is enveloped in a fine membrane (the pleura) allows Jt to move withm the chest during breathll1g without friction.
Respiration, or breathing, consists of two acts, Inspiration, an expansion of the chest, during whIch air is drawn into the lungs, and Expiration, a contraction of the chest, during which air leaves the lungs. A pJ.use follows the act of expiration. In health fifteen to eighteen breaths are taken per minute, and at each inspiration about 20 to 30 cubic inches of air enter the lungs, and a similar quantity is expelled at each expiration.
The expansion and contraction of the chest are effec ted partly by the rnuscl es of respiration attached to the ribs, but chiefly hy the Diaphragm, the large arched muscular partition" hich separates the chest from the abd01l1 en. In inspHation, which is chIefly (l. muscular act, the ribs are raised, and tl1P arch of the diaphragm falls and becomes flattened, thus increasing thE' capacity of the chest and causing the air to enter. In expiration, an act performed almost without effort, the ribs fall and the arch of the
121
diaphragm rises; this lessens the capacity of the chest and forces air out. The mechanism of respiratIOn IS somewhat like that of ordi nary household bellows, but \, ithout a valve; the rib5 may be compared to the boards of the bello\\s, .,hile the diaphragm corresponds to the leather, the air passages bemg equivalent to the nozzle.
As the blood depends upon the air for its purification and the oxygen necessary to maintain life, interference with breathing very soon may produce a dangerous state called asphyxia, examples of which are afforded by dro\\'nmg, suffocation, choking, etc.
PROFES OR ,'C H:\FER'S J\fI... THOD,
I. - Waste no time in loosening or in removing clothing .
2.-Lay the patient in a prone position (i.e., back upwards) \\'ith his head turned to one sJde, so as to k eep his nose and mouth a\\'ay from the grou nd. No pad is to be placed under the patient, nor need the tongue be dra\\n out, as it ,,·ill bll naturally.
3. - Kneel at one side facing the patient's head, and place the palms of your hands on his lowest ribs, one at each sIde, th e thumbs nearly touching one another 111 the small of the back. Leaning your body forward, slo\\ 1)' apply firm but
not violent pressure strajght dowl1wards upon the b.ck and lower part of the chest, thus driving air out and producing expiration (Fig . 56). Draw back
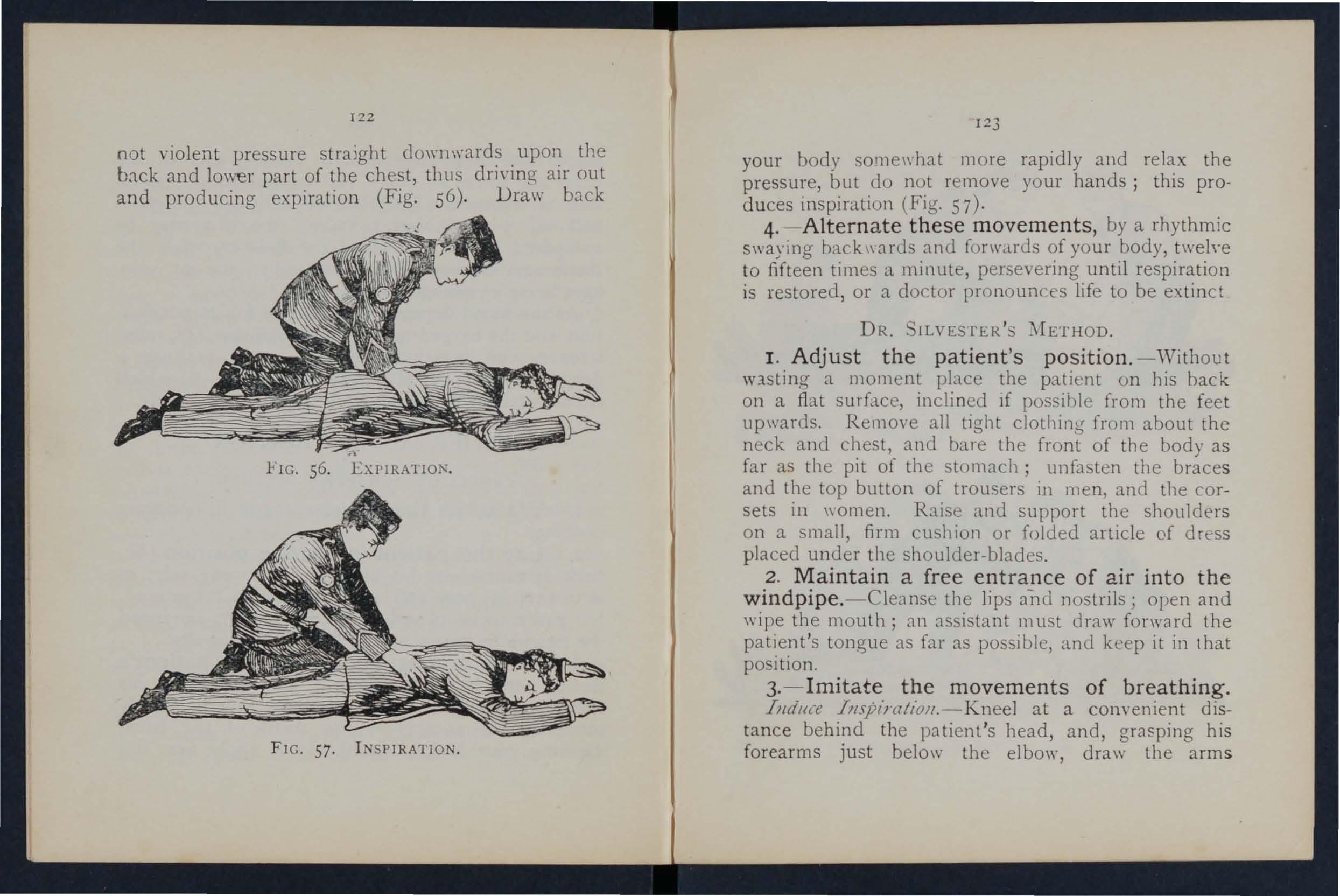
FIG. 56. EXPIRATION.
FIG. 57. I NSPIRATION.
1 2 3
your body sOlllewhat more rapidly and relax the pressure, but do not remove your hands; this prod u ces inspiration (Fig. 57) ·
4. - Altern a te these movements, by a rhythmic swaying back\\ards and forwards of your body, twelve to fifteen times a minute, persevering until respiration is restored, or a doctor pronoun ces life to be extinct
DR. ILVESTER'S
I. Adjust the patient's pos it ion. -'\Vithout Wlsting a moment place the patient on 11is back on a fiat surface, inclined If possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in \\ omen. Rais e Clnd support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades.
2 . Maintain a fre e en t r a nce of air into t h e windpipe. -Cleanse the lips and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position.
3. - Imi t ate the movements of breathing. Illdu{e Impt'l'at/oJl.-Kneel at a convenient distance behind the patient 's bead, and, grasping his forearms just below the el bow , draw the arm s
FIG. 58. INSPIRA'lION.
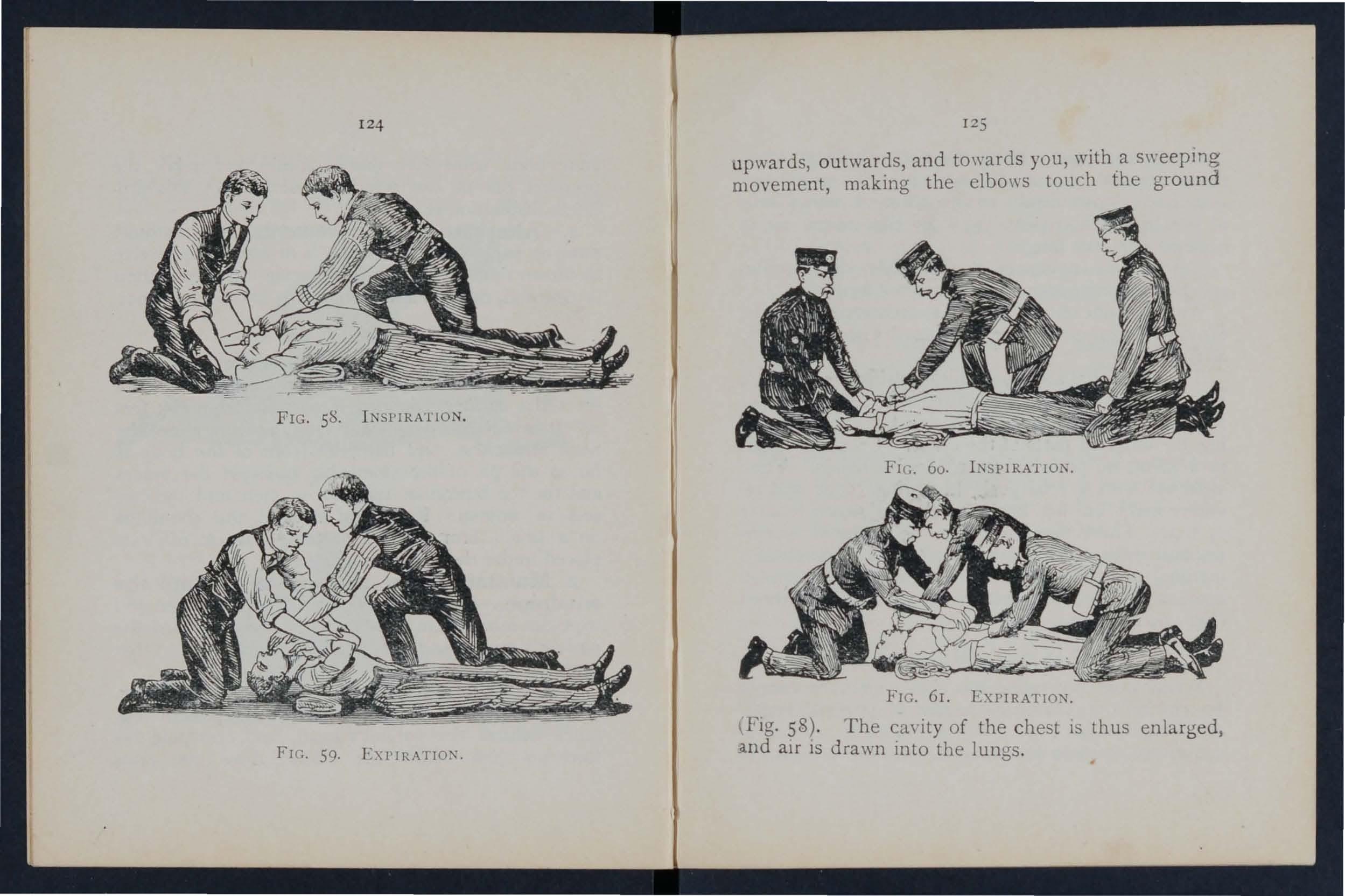
FIc. 59.
1 2 5 upwards, outwards, and to\\'ards you, with a s\\'eepmg movement, making the elbows touch the ground
FIG. 61. EXPIRA1
' Fig. 58). The ca,'ityof the ch est IS thus enlarged, .and aIr IS drawn into the lungs .
Illduce exptratiolZ.-Bring the patient 's flexed arms slowly forward, downwards and inwards, press the a rms and elbows firmly on the chest on either side of the breast-bone (Fig 59) . By this means air is expelled from the lungs .
Repeat these movements alternately, deliberately, and perseveringly about fifteen times a minute.
\\'hen a sufficient number of assistants are present, JIO\\ ard 's method may be combined \\ ith ih'ester 's, as follo\\'s :-
The additional assistant kneels astride the patient 's hips \\·ith the balls of the thumbs restin3 on elther siue of the pit of the stomach, and the fingers grasping the adjacent parts of the chest . Using his knees as a pivot, he presses forward on his hand, Then slIdden£v, \\'ith a final push, he springs back and remains erect on his knees \\'hile he slo\\ ly counts
I, 2, 3. These motions are to be repeated to co rrespond with th 05 e being perfor rned by ilvester's method, pressure on the chest being made simultaneously by those performing the t\\ 0 methods (Figs. 60 and 6 r) .
LABORDE'S METHOD.
When from any cause the above methods cannot be carried out, Laborde's method of artificial respiration should be tried. It is especially usef u l in suffocated children and when the ribs are broken.
T;1e patient is placed on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to pre\'ent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for t\\O seconds in that position, then allo\\ed to recede into the mouth. The e movements :hould be repeated about fifteen times a minute.
Artlficiai respiration must be continued umil breathing IS established, or until a doctor arrives. '\\-hen 11cltural breathing commences, regulate the artificia.l respiration to correspond with It. uccess may resul t even aCtt;r t\\'o hours' time.
Excite respiration.- \\'bilst artincial respiration is bt;ing applied, uth e r u!:>eful steps may be employed, sllch as applying smelling salts or snuff to the nostrils, and fllckin;j the chest \\ ith a dam} tmrel.
Induce circulation and warmth after natural brcathl11g has b e en restured. " -rap the patient in dry blankets or oth e r co\'erin o' , anti rub the limbs energdically to\\arJs the hearf, Promote \\"armth by hot flannels, hot-\\at er bottles, or hot bricks ,('napped in ft1l1ncl) applieJ to the fed, to the limbs and body. ,rhen the po\\cr of 5\\".1110\\ ing has returned give hot tea or coffee, or meat extract. The patienr should be kept in beel and encouraged to go tv sleep. Large pOUllH... cs or fomentations applieJ to the
front and back of the chest ,yill sen'e to assist breathing. , Watch the patient carefully for some to see that the breath ing does n?t fa.I .any. sIgns of failure appear, at once beglt1 art1l10al respiratIOn.
IN ' Ei-CIBILITY.
Unconsciousness or Insensibility may arise as follo ws :-
Injury to the Head. -Concussion and Compression of the brain. .
Disease of the Brain. -Apoplexy, Hysteria. . .
Various Causes. - hock, Famtl11g (Syncope)) Collapse, Alcoholic and other poisoning, un:troke and Heat-stroke, Infantile Conyulsions, Asphyxia.
GENERAL RULE' FOR OF IN 'El ·IBILITY.
I.- If a person appears abou.t to lose sciousness, prevent hi'll from fallIng, and lay hIm gently down.
2. - Arrest Hc:emorrhage when. apparent; attending to minor injuries is less Important than tr eating the unconscious state. ... .
3.-Lay the patient in the poslt1<?n which breathing is most easy-usually thIS WIll be on the ba ck , or inclined to one side. As a general rule
raise the head and ,,,hen the face IS flushed, and keep the head 10\\ \\ hen the face IS pale .
4·- Undo all tight clothing round the neck, chest and waist, unfastening the brJces and top button of the trousers in men, and the corsets m women, the obje t being to relieve pressure on the air passages, lung, heart and abdominal organs. Be sur.t that there is no obstruction to the aIr passages by the tongue or b) a foreign bod} in tIle throat. The pOSSibility of false teeth obstructIng breathIng must be conSidered.
5·- Provide for a sufficiency of fresh air by doors <mu "JJ1do\\'s, and by ke ping bade a cro\\d.
6. - When breathing cannot be discerned apply artificial respiration.
7·- 0btain a doctor 's help as soon as possible.
8: - U nJess unavoidable, never leave the patient until you have placed him in charge of a responsible person.
9·- Give no food or fluids whatever by the mouth while the patient is insensible.
lO. - Should the spine or an important bone uf the upper or of the lower limb be fractured, it must be steadied and maintained at rest as soon as possible. Should the unconsciousness be prolonged, the patient may be removed in a recu mbent posItion
13° to sh elte r , p rovided that the broken bone is adeq uately su ppo rted.
II. - When the patient is in a state of convulsion, support his head, and after wrapping a p iece of wo od or any other hard materIal in a handk e rc hief, hold it in his mouth to prevent biting of t he tongue. Do not forcibly restrain his limbs; prevent him from hurting himself by dragging him a\\ay f ro m a source of danger, such as machin e ry, a wall, or fi repla c e; light pieces of furniture should be pushed o ut of the way.
12.- 0n return to consciousnes s water may be given to dri n k. If th e pulse is fe,:ble g ive warm te::t or coffee, provided hzemorrhage, internal I)r extern::tl, is not present. A deSire to sleep should encouraged, except in cases of opium poisoning, .1 condition that may generally be recognised by the I, istory of the case, and alS8 by the pupils of the eyes (the black openings in the grey, blue or brown ir is) bei n g minutely contracted (pin-head pupils).
13. - It must not be assu med that a person is insensible as th e r e sult of drink merely because t h e breath sm e ll s o f a lcoh ol; frequently when people are feeling ill they tuke or are given Ct lcoholic <;timulants, after which thE-Y may become t'lsensible J1Clt from the drink, but from the cause , . Lut induced them to take it, for example, ltlsens\ · bili t y coming on, effects of poisoning, etc, Even 1 t
13 1
drink is be1Je\'ed to De the actual cau e of insensibility, It must be Dome in mind that the patient is in a "ery dang e rous state and he must be treated for Collapse being cmered up and kept \\arm.
The abo\'e general rules \\ill enab le first aid to be rendered efficiently in 1110st cases of Itlsensibility, although the exact form from \\ hich tIle patient is suffering is unknown.
rh e patient may be stunned by a blo\\ or fall on the head, or by a fallon th e feet or lo\\er palt of the spine. He may C} uie k ly regain cOllsciousnts, or inensibility, more or less complete, may be prolonged.
'flU _\T'I1L:\T .
I. - Ap p ly t h e general rules for the treatment of In. cnstbilit\,
2. - B e v e'ry apprehensive o f dange r in all cases o f inj u ry to the hea d . The patient may be stunned, and afler a short inleryal may recover some degree of consciousness, or e \'en th e Gram ma\ app1rently have escared injury; yet in both instance-s there is a gra,-e ri k that a structure \\ ithin the craniul11 has been in:ured, and that a serious state of insensibility may de\'e10p later ('ee Fracture of the Cranium, page 4-3 .) A caution should therefore be gi,-en to a patient \\'ho has lost consciousness even
for only J. moment after an injury to head not to res u me physical or mental actiyity wIthout the const"nt of a doctor.
C01IPRE OF THE HR.\ll , APOPLEXY.
Compression of t he Brain from the same causes as produce ConcusslOn; 111 fact, Compression is freq uentl)' by on llssion.
Apoplexy usually occu:s 111 elderly people, and no sIgns of injury are necessanly present.
In both conditions the face fI ushed; the breathing stertorous; one side of the may be m o re limp than the other, and the pupll ot one eye may be larger than that of the the temperature of the body is generally ralsed.
TREAT:'IENT.
I. - Apply the general rules for treatment of lnsensi bi lit y.
2. - Promote warmth in the low e r p a r t of t he body by the application of hot \\ ater bottles to the abdomen and lower limbs. Care must be taken not to burn the patient \\ith the .bottles, which "'hould be \Happed in flannel, and theIr heat tested w)th the elbow.
r Amlepsy rna)' occur in persons of any age, but usually occurs in young adults. The patient falls to
the ground, sometimes with a scream, and .nto a state of convulsion, thro\\' ing his limbs about. ThL treatment is according to the General Rules, especially Rule I I.
SIG:\'S .\:'\D Y:\IPTO:\!.
The patient, usually a young girl, in of mental e"citcl11ent, suddenly loses command of her feelings and actions. he subsides on a couch or in some comfortable position, throws herself about, grinding her teeth, clenching her fIsts, shakll1g her hair loose; she clutches at anyone or anythll1g near her, kicks, cries and laughs alternately The eyeballs may be turned upwards, and the eyelIds opened and shut rapidly. At times froth appears at the lips, and othei' irregubl symptoms may develop
TREAT;'[l':'-'T.
I.-Avoid sympathy with the patient, and spea firmly to her.
2.-Threaten her with a cold water douche, and if she persists in her C( fit, II sprinkle her with cold water.
.1.-Apply a mustard leaf at the back of the neck
Iedical treatment is nece sary to cure the condition of mind and body which gives rise to hystencal attacks.
[34
C .-\l'SE .
1. - I njury 111 the region of the abdomen, extensive wounds and burns, fractures, lacerated \\ ounds, and severe crush are some of the more frequent physical causes of shock.
2.-Fright , anticipation of injury, and sudden bad ne\\s , or sometimes sudden removal of fear and anxi ty after prolonged suspense, produce shock or faintmg.
3.-Some poisons cal.l. e shock \\ hile others, such as alcohol, so depress the nen'ous system that colbpse ensues.
-t .-Hremorrhage or heart \\ eaknt.ss, a close or crowded room, tight clothing. fatigue, or \\ Jnt of food may bring o n famting or colbp::e.
IG:\'S .L\:\D SnIPTO:'IlS.
The general condItion of shock may be by ext reme pallor, a feeling of cold, clammy Sklll, feeble pulse, and shallow breatblllg :lccompanied, If hremorrhage has been severe, by )'a\\ ning and si ghing. The term 'collapse" :3igniiies a wry seriou2 condition in \\ hich the lIfe of the [Xl' ient IS in t he greatest danger; the temperature of the body fa1!:; b e low the normal, and one great object of treatment is to prevent it sinking to a point at \\ hich lIfe is im possible . A n attendant danger of the condition cf
135
collapse is the liability t o sudden relapse afte r a temporary Improvement, and the utmost care and watchfulne ss must therefore be exercised to mai n tain the heat of the body and to guard against failu re of the heart and lungs.
I. - Remove the Cause by arresting hremo rrhage, attending to injuries, loosening all tight clo t h ing, especially about the chest and abdomen, remov ing from a close or cro\\ ded room, using encouragi n g words, etc.
2. - Lay the patient on the back, with the head low. Raise the lo\\'er limbs; "hen the pati en t is in bed this is best done by raising the foot of t he bed tead.
3.- Provide for a free circulation of fresh air.
4. - If has been severe and the patient is collapsed, firmly bandage the limbs from the toes to the hips, and from the fingers to the armpit s . To stimulate the action of the heart, sal volatIle and \\ ater may be gIven if the j:'atient can swallow, or smalling salts may be held to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of temperature below the normal poi n t. To accomplish t hi s cove r t he pa t ient wi t h ext ra clo t h ing, or by p lac in g
13 6
rugs or blankets over hi 111 • ge t hi m to bed in a warm but well-ventilated room as soon as possIble. Apply warmth to the feet and to the pit of the stomach bv hot water bottles or hot flannels . (Test the heat o;f with the elbow before applying them.) If the p atIent can s\vallow) give hot drinks, such as milk, .or coffee. It is "'ell to add sugar, as it aids in raJsll1g the temperature of the body.
7- -:- If cannot be discerned , apply artlficul respIratIon.
8. - If want of nourishmen t has been the cause of fainting or collapse, giye food sparingly at first.
\ Vhen exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the during a march in very hot weather ",hen persons may deyelop sickness, glddll1ess, and difficulty in breathing. The complall1s of thirst, the skin becomes dry and burnll1.g, the face flushed, the pulse quick and ?o u ndll1g. A very hIgh temperature, stertorous (snor· Il1g) breathing, and insensibility may ensue.
1. -Undo all tight clothing. the patient to a cool, shady spot .
137
3.-Strip the patient to the \\alst.
-t.-Lay the patient do\\n, with the head and trunk well raIsed.
5.-Procure as free a circulation as possible of fresh air, and fan the patlcnt yigorously.
6.-Apply ice bags or cold \\ater freely to the head, neck, and spine, and maintain this treatment until the symptoms subside.
7.-0n return to consciousness, the patient m:1V haye \Yater to drink.
Teething or stomach troubles are the commone<;T causes of this ailment.
IGX.
pJsm of the muscles of the limbs and trunk: blueness of the facc, insensibility, more or less com plete, and occac;ionally squinting, suspended respira tion, and froth at the mouth Jre the prominent signs
T.-Support the child III a \\arm bath sllghtl) above the tf-· mperJture of the boely (98 degrees, sr that the \Ya.ter reaches to the middle of the trunk.
2.- Place :l. sponge dIpped 111 cold \\ ater on the top of the head.
13 8
A PHYX I A.
\V hen , owing to want of air, the blood IS not s upp lied with oxygen the patient becomes insensible, and is said to be asphyxiated. This condition may be brought about as follows: -
I. Obstruction of the air passages.
(a) By DROW\'Ii'\G.
(b) By PRESSURE FRO:\[ OU rSlDE :'trangubtIOn, hanging, smothering.
(c) By A FOR E[G.\' BODY L\, THI<: THROXf: hoking.
(d) By s.\ ELLl.\'G OF THE TIS UES OF THE THRO.\f: InflammatIOn, scald of the throat, poisoning by a COrrOSI\'e.
II. Inhaling poisonous gases . By coal gas ( as used in the house), producer, or water, ga . , smoke, f umes from a charcoal or coke fire, e\\'er gas, lImek iln gas, carbonic acid gas.
III. Pressure on the chest, as when crusheu by sand or debri . , or by a ero\\ d.
IV. Nervous affec t ions , as the result of narcotic a n d certain other poisons, collapse, electric shock, or stroke by lightning.
GE;'I[LRAL TRE\T\IE:-':T.
I n all cases of As ph yx ia aHem pts 111 ust be made to remove the cause, or to rem::>ye the patient from the \Vhen (laS been done artificial I39
r es piration must be applied, taking care that th.e air passages are not obstructed, ant! that the r e 15 abunda n ce of fresh air.
rersons completely imnlersed in \\ ater for or fifteen minutes been restored by artifiCIal means. Therefore, if the body is recovered Within a rea on able time, absence of signs of life is not to d ete r IITlmediate attempts to restore .
The first thJl1O' to do \\ hen the boely IS recovered IS to £!;et rid of the b \\ ater and froth obStruCtlllg the ai r p.:1s'-;ages, and then ;1rtificially. to r store This is best accomplI. hed eIther by proceedlllg at once to perform artin ial respJratlOn by Schafel's method, or follows :- .
I.-As quickly a possible loosen the clothll1g, an d clear the mouth and the back of the throat.
2.- Turn the patIent face dm\'nwards, with a pad below the chest, and with the forehead upon the nght forearm.
3.-\\ "hilst in this pOSitIOn apply pre sure. by the hands to the patient 's back oyer the 10\\ er nbs, a n ci k eep the pressure up for three second.s . . ' .
4.-Turn the patient on the right Side, mamtamm; that position also for three seconds.
5.- Re peat the e movements aiternately a s lon g lroth and water issue from the mouth .
These operations (:IIarshall Hall's method) in themselves tend to promote respiration, but \\ .hen lh,e air passages are clear of froth and waler llvcster s method of artificial respiration may be used by Itself or \\ith Howard's method in conjunctlOn.
vVhlle performing these operations send someone to the nearest hOllse to procure blanket s and dry clothing, hot water bottles, etc., and to fetch a doctor.
Cut and remove the band constricting the thr oa t. Apply artificial respiration.
Do not ",ait for a policeman: grasp the lower limbs and raise the body to take the tension off the rope; Cllt the rope, free the neck; apply artificial respiratloll.
:'.JOTHERl};G.
Remove whatever is smothering tl1f patient: apply artificial respiration.
CHOKU\G.
Open the mouth, forcibly if need be; pass the forefinger right to the back of t.he and attempt to dislodge the foreign body; If vomltll1g results, so much the better. If unsuccessful, thump the back hard 'whilst the head is bent fOf\\ard. Apply artificial respiratIOn.
141
'Whether the swelling is caused by infl1.mmation b\, s\\"allo\ying vcry hot \\ater, as not infrequently h;ppens to children attempting to drink. from. the spout of a kettle, or by the effect of a corrOSl\'e pOlson, th e treatmellt is as fo11o\\s :-
I.-Appl), a sponge, piece of flannel or other cloth, ",run O" out of "ery hot water, to the front of the neck, fro 11 chin to the top of the breast-bone.
:!.-. et the patient before the fire.
3·-Gi\·e Ice to suck if it can be had; if not, gIve cold \yater to drink.
..j..-Gi\·e animal or vegetable oil, a dessertspoonful at a tIme, to soothe the scalded throat and ease the pain
5·-If breathing has ceased apply artificial respiration
SL:FFOCA.TlO:-\ BY \JOKE OR GASES.
I. -Rel110\·e the patient into the fresh air. Before ent ering a building full of smoke tie a handkerchief, \yet if possible, round the head so as to cover the nose and mouth. It IS ,Yell to nJO\'e slo\\ ly, keeping low or e\'en era\\ lin a , \\ hilst in a room full of smoke in s'earch of a person. Eyeryopportunlty of letting 111 fresh air by opening doors or windows should be seized.
1.+2
t .-App ly artificial respiration.
3.-1n the case of p roducer or \\'ater gas , in halation . f oxyge n \\"111 a Iso be necessary .
E lectric current is conveyed by a cable, \\ ire, rail, ') r b ar, called the "Positive," and returns to the so urce of supply by [mother cable, \\ire, rail, or bar, called the " Negative," or through the earth. In the case of an electric railway, the current is generally conveyed by an insulated rail called the third rail, and re turn s through the running rails or an insulated rail ca ll ed the fourth rail, and in the case of an e1ectnc tmmway it is frequently conveyed by an oyerhead con? r trolley wire, and returned through the runnm g ralls .
Through contact \\ ith a " positiye " the shock may be so severe as to cause insensibility, and the sufferer will be unable to extnca te himself, and 111 ust be with poss!ble speed. As it is generD lIy m p osslble or mexpedlent to switch off the CUrrUl[ wme other method mu t usually be atloIJted; but preca u tions must be taken or else the person renderin g assistance will himself receiYe a shock.
To liberate the sufferer from contact-
I.-Insulate yourself from the earth by stand· Ing on a n (C insulator" or " non-conductor" that is a which resists the current , Amongst bodies
Indiarubber, dry gllss, dry briCks, dry :,Ilk, dry cloth, elry \\ ood and dry h:1Y or straw,
2, - Protect y ou r h ands fr o m contact with t h e s uffere r or th e ele ct ri c me d i u m 1)\· em erin rr the 11 \'. nh :111 1I1suhtor. • I I1lklrubbcr probahly t he best l11::iubtor, do not waste time in rUllnind for llllkl.rub1>er glo\ c', but use ell'\' articles of clothII1J ; al1 indiaru0ber tobacco pOlIch or cap, or fol ckd n el\'spaper, would sen e to protect the hands IJ1 an e;llergenC\ If 110 mean of 1t15Ulatlll r the hands are at ha;l 1 an aLlempt may be lnade to 0 drag thc sufferer a\\ay by means of a loop of dry rope or a crooh.cd stick: an umhrella is not safe becaus ;:! the meLd nbs \rould act as conductors* of electricit\, , . - -, and It IS not l11tre I lIently the case that the' stick IJ of the umbrella IS a meled tube
3, - Pull the su ffer er awa y f r om contact. C,l.l'c should he to:1\ oid tOU( hl11<T \\ Ilh naked han Is the suffLrcr's hands, \Y e t clothing: or boots if the soles arc 11<l.llcd. The :Hl1lpits should be avoided a."; perspiration usually make the clothing damp t Ilcrc.
\\'hen the sufferer is removed from contact--
I. - Apply the general treatment for insen-
" . \ conclUClOr i., a b :)(ly through which electricity readily r"- ses. Among t hodic !i are c )pper, bra s, iron, mois ure :11'0 o'le's o\\'n hod) .
I.t4
(loosen clothing, procure tree ClfcuJation of -air and place in a recumbent position).
2. - Dip a towel in cold water and attempt : 0 arouse him by sharply flicking the b.ce and chest.
3. - Commence artificial respiration if other nethods fail to restore animation. "La horde 's 11 n ethod (see page I26) has been foup.d to be very , uccessf u1.
4. - Treat burns If there are any (see pages I03, 0 0 4).
EFFECT OF LIGHTNl?--G.
.A person struck by lightninr. is us-ually more or ess deprived of consciousness. The treatment 1S ' he same as that for electric shock, e\c( pt, of ::ourse, that the instructions for remO\ Lhe patIe nt from contact \\ ith the electric do 10t apply.
Tile 1lltlJhra/s indi(al<' Ih< where the allsweu 1Ilc7), be fouJld.
\\'h al :ue the two systems of nen'es ? ...
Of what is the cere bm.spinal system made up?
\\'hal is the spinal corel ?
\Vhat are nen'es like?
Explam lhe system
Explain the respiratory system
Explain the acts of respiratiun
How are the exp:w -ion and contraction of the chest effected? . 120 to 121
In \\ hat system of artificial re . pi ration is the patient laid back upwards? ... ..
In \\ hat systems is he laicl on his back?
In II hat system is he laid on his hack or ide? ... 1). 1\ hat system is he rolled alternately on his side allll
face downwards?
How long shoulll artificial respiration be persenreel \I
\\'hal is exciting respiration? I27
\\'hat is inducing circulal1on? ...
\\'hy is il neces ary to watch lhe patient? I2S
J [uw may insensiilility arise?
State the "alious forms of insensibility 12 '
State the general rul(!s for treatment of insensibility 12 ' to 13 1
Would you eX:lmi-e the patient to see if any bunes \\e re broken? ...
\"hat wrong opini,)n may he formed when the pa{ient smells of drink?
I s collapse from drink a serious condition?
\\'hat is concussion of the brain? ...
State the rul es for t realment of concu.sion
'v hat danger accompanie . injury to the heari?
What caution should he giycn to a ratient who has lost consciousness, even for a moment, after an injmy to the head?
What are the causes of compre·sion of the brain?
'i'n. what aged pe?ple dot s apoplexy llsually occur ? are the sIgns and symptoms of compr ession and apoplexy? '"
'"
tate the rules for treatment of these c o nditi ons. .. ..
Vrhat dangpr is there in applying hot water 10llles to insensible persons, and what precautions should be
taken?
... 13
l('\ escribe a Case of epilepsy J 32, J 33
!II. hat special care must be taken in treating a case of epilepsy? .. . 1.30, 132
Describe a hysterical fit 133
How would you treat a hy terical fit? ... ... 133
That are the commonest physical causes of shock? 134
Vhat may produce shock 01 fainting? ... ... 134
'1,-\That conditions do certain poisons bring about? 134
What may bring about fainting or collapse? ... ... 134
How would yuu recognise the general condition of shock? 134
¥hat special precaution must be taken in the case of collapse?
"'tate the trealment for shock, faintlllg (syllcope) and i35 collapse ... ... ... '" .. , ... 135, 13 6
,Yhat is the effect of on the temperature of the body?
'What are the causes of sUllstroke and heat ·stroke ?
... . .. 13 136
tate the treatment for and heat·stroke
\Vhat are the causes of convulsions in children? 13 6 , 137
What are the sign of com' ulsi ' ns in children? .. .
':;tate fully the causes of asphyxia ... 137 137 137 138-
tate the treatment fJr convulsions in children .. .
"V hJ. t two things have to be done 111 all cases 01 asphyxiJ. ? . 131=0· f
What two things must be seen to before it i3 possible tor artificial respirati'J n to do any good? ..
Is artificial respiration likeiy to do any gooJ if the !:'..ir pa ·sa.ges are obstruckd, or if there is nut abundance of fresh air?
\VhJ.t is the first thing to du in a case of drowning?
By what method may artificial respiration be performed without taking any previous steps? ...
What steps must be before proceeding with Silvester's method?
What should be done while artificial respiration is being performed?
State the treatment for strangulation
tate the treatment for hanging ...
State the treatment [oc s mothering
tate the treatment for
How may a swelling of the ti s ues of the throat be caused? ...
tate the treatmen t for swelling of the tissues of the
tate the tr.eatment for suffocati o n by smoke or gases 141, 142
How is electricity conveyeJ ?
How would you liberate a sufferer from c ontact with an electric medium? . . 14 2 , 143
Nhat would you rio when the sufferer was re mo\' ed from .: ontact • . .
')I\> ha WOlud yuu do !D r,he case of a lightning strok e
CH A PTER VI.
POlO 1IKG.
P oisons may be cln.ssified according to their ment under two heads :I.-Those which do not stain the mouth, and in the treatment of which an emetic is to be given. Amongst these are:-
(a) Arsenic, Phosphorus (containeu in rat poison a nd lucifer matches), Tartar emetic and CorrosiYe ub h mate, \\ hich cause a metallic tas te in the mouth and a burning pain in the mouth, throat and stomach .
(b) St rych n ine, Prussic Acid, Belladonna (ueadly nightshade plant) nnd seyeral otber vnneties of plants, such a. laburnum seeds, etc.; these give rise to conyulsions, delinum, failure of respiration and collapse.
(c) P oisonolls meat, fish and fungi (often mistaken for IT1UShrool1ls). ,'uspicion of these poisons should be directed to cases \\ here se,'eral persons \\bo haye partaken of the same food develop similar sIgns and symptoms.
(d) Alcohol, which may cause collapse .
(e) Opium and its preparations, Morphia.
140
L audanum, Paregoric, Chlorodyne, )rup of Poppies and yarious soothing drinks and cordiab; these cause a tendency to go to sleep, whi h continues until sleep becomes deep nnd breathing sterotorllS ; the pupils of the eyes become minutely contracted ,plllhead pupil ).
2. - Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. Theseareoft\\oclas. e:- .
(a) Acids , such ,1S Acid (. \ qua fortiS), ' u lphuric Acid (O il of Yitriol), Hydroch loriC, or :\ I uriatic, .Acid (Spirits of 'alt), st r on g Carbolic AC id (P henol), Oxalic Acid, which is contained in oxalate of potash, sa l ts of sorrel, alts of lemon and ome polishing pastes.
(b) A lkali, such as Caustic P otash, Caustic S oda and Ammonia.
U:'I[l\fARY Or' DIPLE DIRECTIOI\ FOR THE TRr_. \T\[r. \'1' OF PQlSO:\I:\G.
I. - Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali,
150
promptly give a n e metic - that is, m a ke tr.e pal ier.t vomit as follows :-
(a) Tzdde bark of tile tll l'Oat .,yith the finger o r 'with a fea tb e r.
(
b ) JJ1ilsta r d - a dessert-sp o o nful in a tum blerful of I u k e- \y a rm wa ter.
(c) Sa l t-a table-spoonful in a tumbl e rful of luk e-wa rm wate r.
(d) Trine- fo r a yo u ng c h ild, a teasp o onfu l rr peated at inte rn tl s of fifteen minu tes.
3. - In all cases when t h e pati ent is not insensible, give Milk , Raw E ggs b e a t en up with milk or water, Cr eam and Flou r beaten up together, An imal or Ve get ab le Oil (exc e pt in phosphorus poisonin g), a n d Tea.
Oli ve, a lad, a n d C o d-liyer oil , or oil s u ch as that III whi c h sa r d in es a r e p r ese ry ed, may b e given ; min e ra l ll wc h in e oi ls a n d pa ra ffin are un s uitabl e .
Oil is so othin g, a n d is t he r efo r e especia lly us e ful in roisonin g by Ac ids, Alk a lis a n d s u ch s u bs ta n c es a s Ars enic and C o rro s iv e Subli mate. D e mulc e nt dri n ks, :> uch a s barley wa t e r or thin g ru e l, ac t in the same mann e r, and a r e fr ee fr o m dan ge r i n c ases of phos ! horus poi soning .
Thes e m ay b e give n e ith e r b e fo r e or after the e metic if th e p o ison calls fo r o n e .
Stron g T ea acts as a n e ut ra lis e r of many pOIso n s,
and is alwa ys A ha n d f u l o f tea sho uld be thrown into a k ettle a n d boiled .
4. - If t he lips and mou t h a re stain e d or burned give no em et ic, but -
(a) If a n Acid is k now n to be t h e poiso n give a n Alkal i at o n ce . F irs t wash t he mo u th, out fr eely with lillie \\ater o r othe r al k aline mixture, such as soda, chalk, whi ting, or maglle ia o r wall plaster in \\ater, and afte rwards let the patient sip a little of it. Soda and potash are not to be given in the case o f pOisoning by oxalic acid.
(b) If a stro ng Alka li IS know n to be th e poiso n give an acid at once . F irst \\ash the mouth out free ly with lemon juice or vinega r diluted with an equal qU:1ntity of water , and afterwotrds let the patient sip a little of it.
In b o th cases give oil (Rule 3).
S. - Wh en a person has swallowed poison an d to go to sleep, keep him awake by hlln about and slapping his face, n eck a n d ch es t WI th a wet towel. Str ong black co ffee may be g iv en to d rin k . Slapping the soles of t he feet may als o b e tr ied.
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the nec k and give frequent sips of cold drinks.
7. - Apply a rtificial resp irat ion if breat hing c annot be discerned.
8. - Treat shock a nd collapse.
9.- Pr eserve any v om ite d mat ter , food , -.Dr other substance , su s pe ct ed of be ing th e poison. Do not wash vessels ,,-hich may have conl:ained the poison, and carefully guard them.
Certain poisons require special treatl!1ent, and a few of the commoner of these are mentlOned below with their treatment
CARBOLIC ACID.
The odour of the breath will aid in the detection iJf this poison; the lips and mouth are usually ,;;tained white, and several nen-ous s) mptoms come 011.
TRE,\T:\JE'iT_
1.- Give milk, to a pint of \\ hich half an ounce of Epsom Salts has been added.
2.- Treat according to the general rules.
PRUSSIC ACID.
The action of this poison is extremely rapid. Giddiness staaaerina insensibilit), accompanied by , bb 0' 'b panting respiration, profound. collapse .and ly convulsions are the general signs, and 111 addltlOn a smell of bitter almonds is often present.
TRFAT::\[ExT.
I.-Place the patient in the open air.
153
2.-Dash cold wate r on the head and spine continuously.
3.-Apply artificial respiration. .
4.-Hold sllelling salts to the nostnls.
s.-Treat shock and collapse. (ee page 135·)
POISONOUS 1L\T, FISH AND Fu TGl.
The signs and symptoms are vomiting and (diarrho:a), colic, headache, great weakness, raIsed tempe.ature and a quick pulse.
TREAT}lENT.
1. -Give an emetic.
2 - \Vhen the emetic has acted, give castor oil.
3 -Treat collapse. (See page 135·)
TRYCHNINE.
The signs and symptoms are a feeling of. suffocation, livid features, and convulsIons. The patIent rests on hi he:Hl 3.nd feet, and the body is arched.
TREAT::\JE 'T.
1. - Give an emetic.
2.-Apply artificial respiration.
ALCOHOL.
I.-Give an emetic if the patient can swallow.
2. - Treat collapse by keeping the patient wa r m, etc. (See page 135 )
TIle! 11l1l)/e1'a!s iud/mie the pages w!zere tlte nJ . S7.0frJ 17111)' be found .
Under what two heads may poisons be classified?
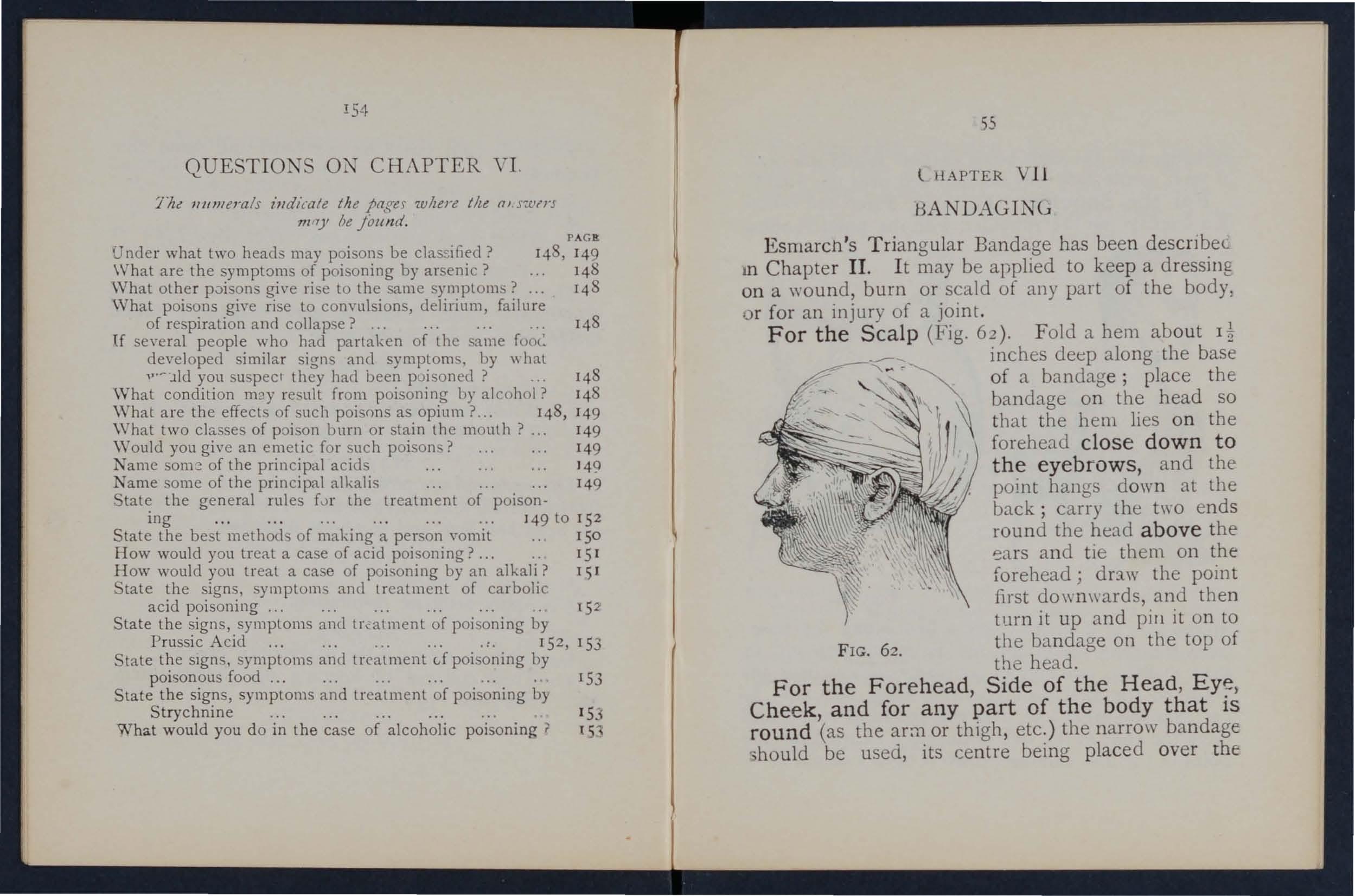
\Vhat other p0isons give ri e to the same symptoms?
What are the symptoms of poisoning by arsenic? PAGa 148 , 149 148 14 8
What poisons give rise to convulsions, delirium, failure of respiration and collapse? ...
U several people who had partaken of the same foot: developed similar signs and symptoms, by \\hat "'- 'lld you suspec 1 they had been p oisoned? 148
What condition m::!y result from poisoning by alcohol? 148
\Vhat are the effects of such poisons as opium ?... 148, 149
\Vhat two classes of poi on burn or stain the mouth? ... 149
\Yould you give an emetic for such poi ons? 149
Name of the principal acids ... ' 49
Name some of the principal alkalis 149
. tate the general rules fvr the treatment of poisoning ...
... '49 to 15 2
State the best methods of making a person vomit 150
How would you treat a case of acid poisoning?... .. 151
How would you treat a case of poisoning by an alkali? lSI tate the signs, symptoms and treatment of carbolic acid poisoning... .......... 152
State the signs, symptoms and tr.:-atment of poi son ing by Prussic Acid ...
152,153
State the sIgns, symptoms and treatment d poisoning by poisonous food
. 153
State the signs, symptoms and treatment of poisoning by Strychnine
153
What would you do in the case of alcoholic poisoning? l5
Esrnarch 's Triangular Bandage has been descnbeL III Chapter II . I t may be applied to keep a dressing on a wound, burn or scald of any part of the body, or for an injury of a joint.
For the Sc a lp (Fig. 62). Folo a hem about It
FIG. 62. inches deep along the base of a bandage; place the bandage on the head so that the hem lies o n the forehead clos e down to t he eyeb r ows, and the point hangs down at the back; carry the two ends round the head above the and tie them on the forehead; df3.w the point first downwards, and then turn it up and pill it on to the bandage on the top of the head.
, Chee k , and fo r any part of the body that is round (as the arm or thigh, etc.) the narrow bandage ';hould be used, its centre being placed over the
150 and the ends being carried round rht" h,d<1 .)r limb as the case may b d' d For 'th S e, an tIe over tile '1:;(.JIIPd. e houlder (Fig. 63)' Place tn-, ; efJtre 0f a bandage on the shoulder, with the pomt r'rIning
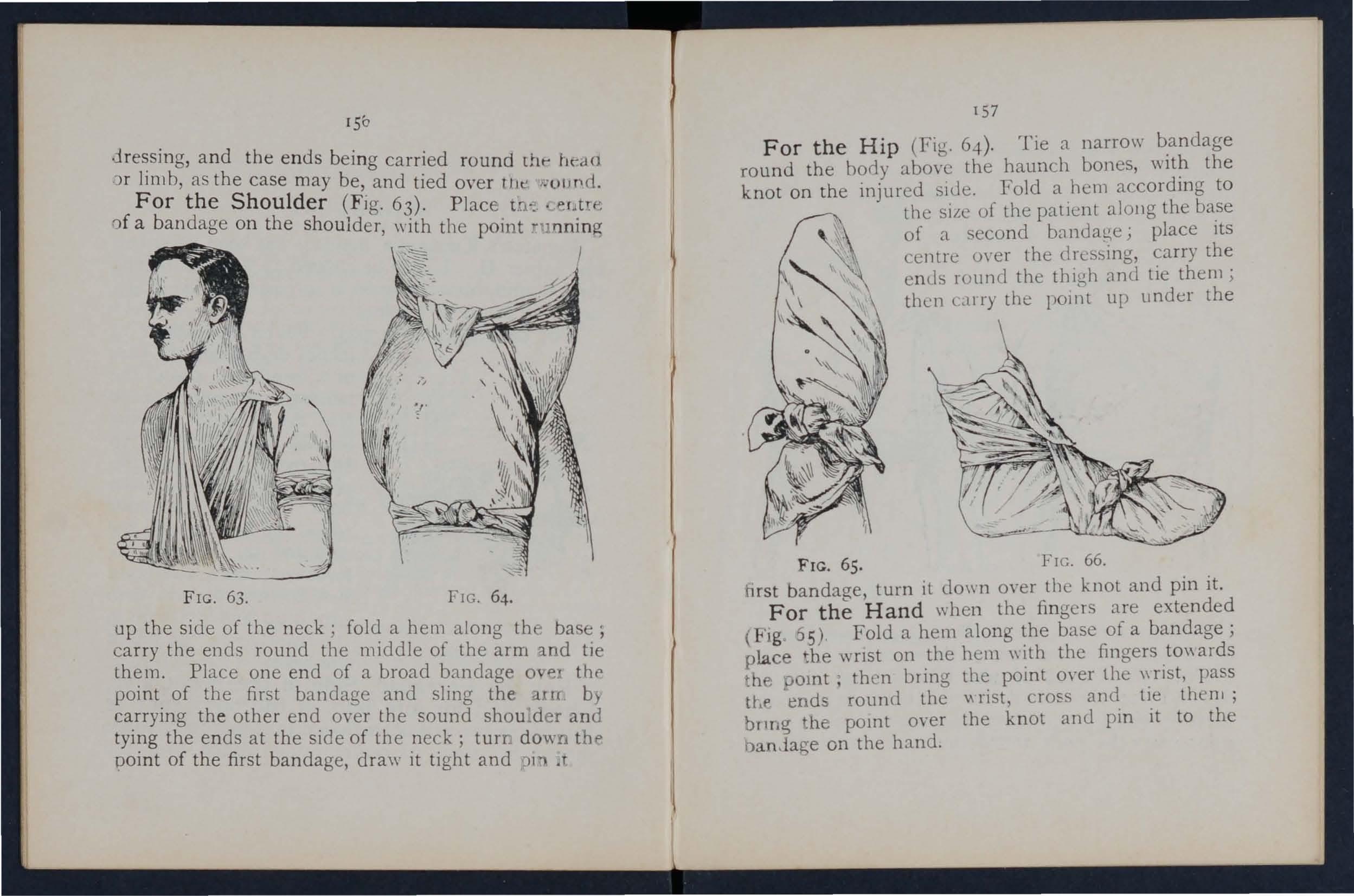
FIG. 63.
FIG. 64. up the side of the neck; fold a hem along th base' carry the ends round the middle of the arm and Place one end of a broad bandage 0 e thf' p01l1t. of the first bandage and sling the auc b} ca.rrymg the other end over the sound shou . der and the ends at the side of the neck; turr dO\w.i tht> pomt of the first bandage, draw it tight and "11 .t
157
For the Hip (Fig. 64). Tie a narrow bandage round the body above the haunch bones, with the knot on the injured side. Fold a hem according to the siLc of the patient along the base of a second brl11dat!;e; place its cen tre oyer the cl ressing, carry the ends rollnd the thigh and tie them ; then carry the point up under the
FIG. 65.
FIG. 66. hrst bandage, turn it down oyer the knot and pin it. For the Hand when the fingers are extended (Fig :lS) . Fold a hem along the base of a bandage; place the WrIst on the hem \\ ith the fingers to\\ ards t h , omt; then bring the point over the \\ rist, pass tt-Lf' end rounel. the rist, cros and tie thenl; bnng he pomt over the knot and pin it to the banJage on the hand.
For the Foot (Fig. 66) . Place the foot on the centre of the bandnge with the toes towards th e point; draw up the point over the instep, bring the e nd s fO[\\'a rd and cross them; now pass the ends round
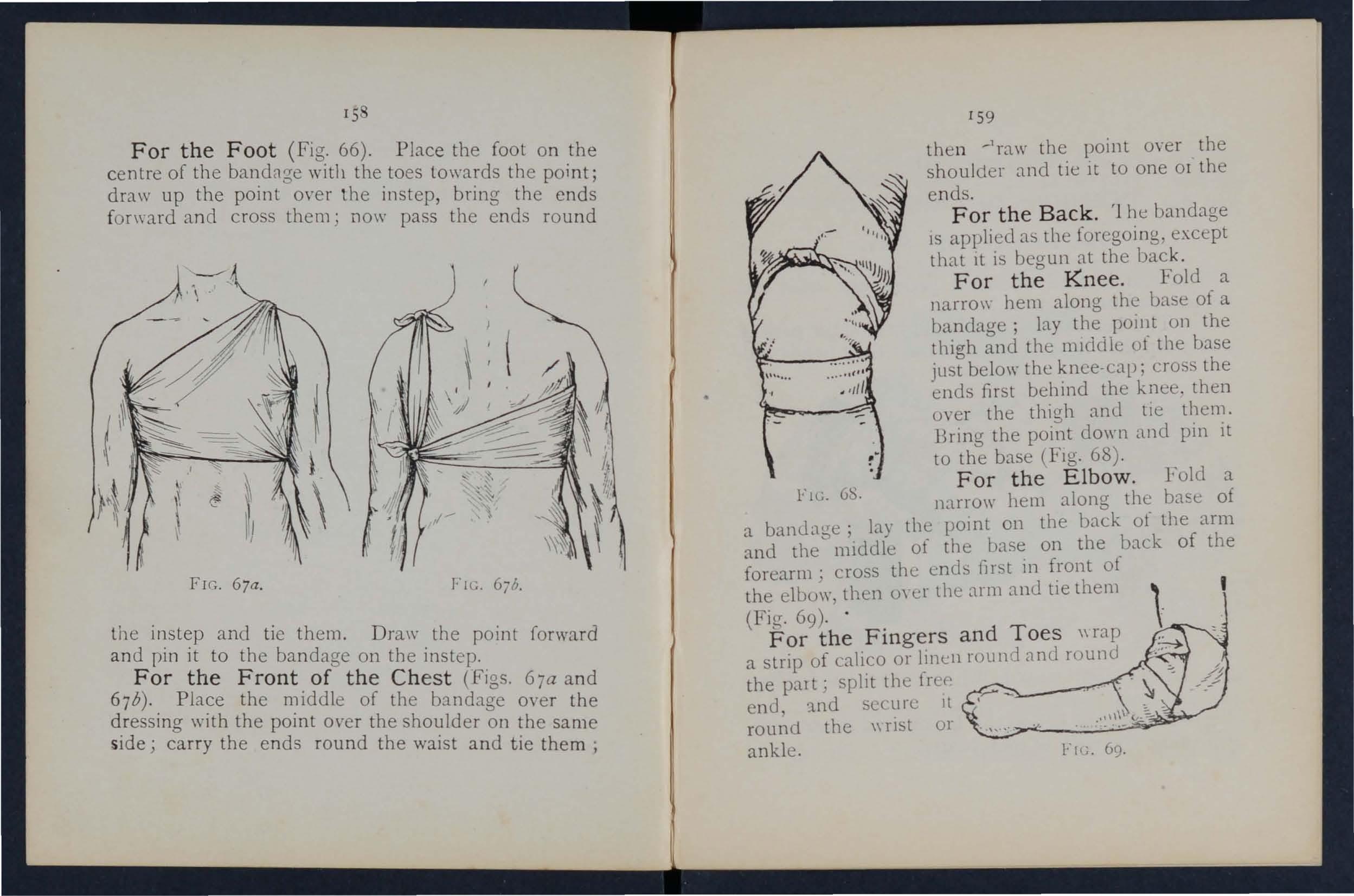
67b.
the instep and tie them. Draw the point forward an d pin it to the bandage on the instep.
For the Front of the Chest (Figs. 67a and 67b). Place the middle of the bandage over the dressing with the point o\'er the shoulder on the same side; carry the e n ds round the waist and tie them;
159 then the point over the shoulder and tie it to one or the e nd s.
For the Back. '1 he bandage IS applied as the foregoing. except that It is begun at the back.
For the Knee. Fold a narro\\" hem along th e base of a bandage; lay the POJilt on the thigh and the l11lddie of the base just belo\\" the knee-cap; cross the ends first behind the knee . then oyer the thigh amI ti e Bring the point down and pm It to the base (FIg. 68) .
For the Elbow. Fold a F Il;. 6S. narro\\' hem along the base of a lay the pomt on the back of the arm and the middle of the base on the ,back of the forearm; crosS the ends first in f:-ont ot the elbo\\', then m oer the arm anu tie them (Fig. 69)· .
For the Fingers and Toes \\rap a strip of calico or linen rounri nnd round the part; split the [rc(' .. end, ::tnd secure It round the \\ fist or ankle.
1"1,-'; 69·
CHAPT.c.R VIII.
This seat is used when the patient can aSSIst th bearers and use his arms.
1.-T\\ 0 bearers face each other behind the patIent and grasp their left forearm with their right hand and
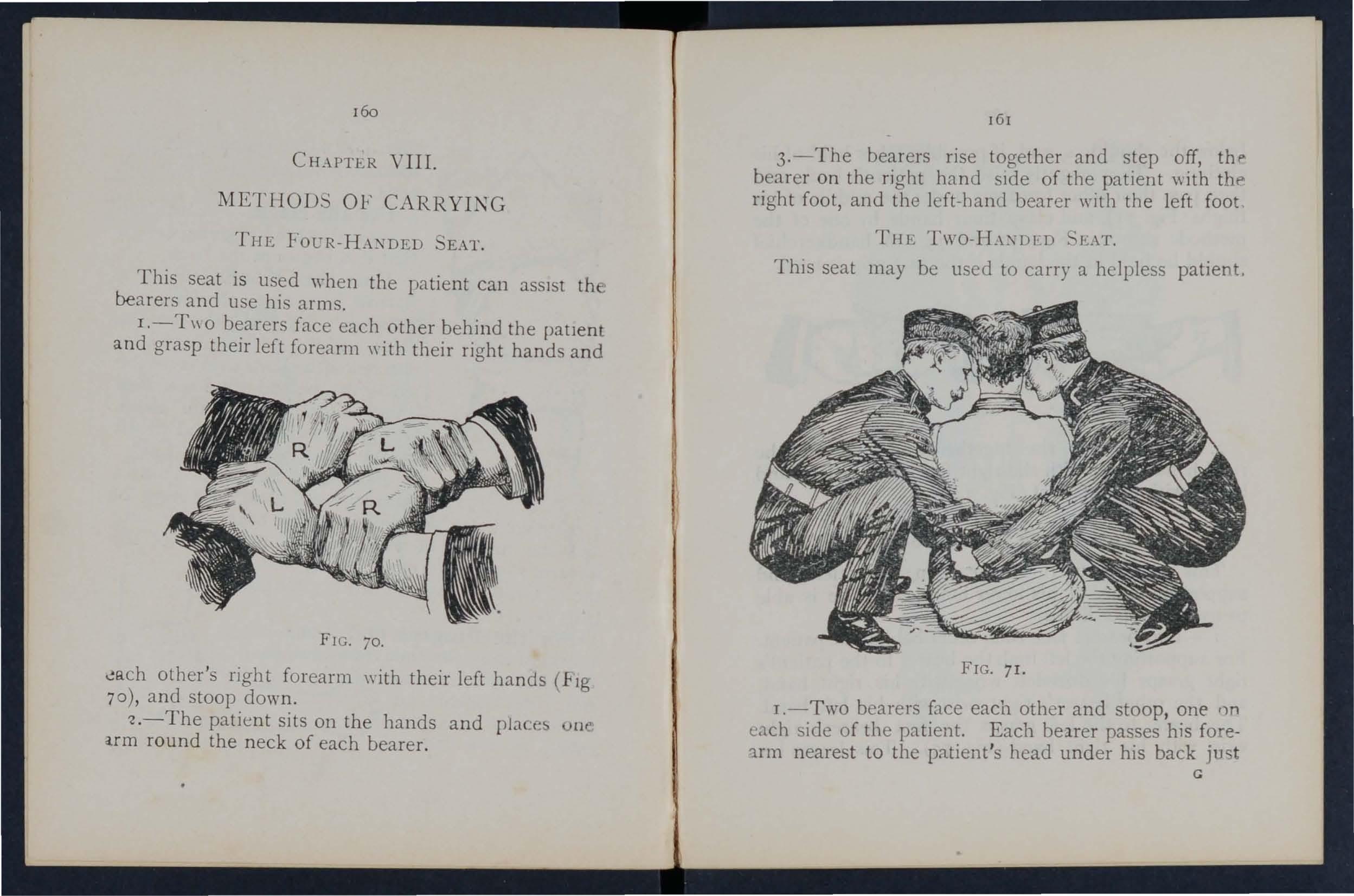
FIG. 70.
';!9.ch other's right forearm with their left hands (hg 70 ), and stoop down.
'2.- The patient sits on the hands and placc5 arm round the neck of each bearer.
161
3.-The bearers rise together and step off, thp. bearer on the right hand sIde of the patient with thf'> right foot, and the left-hand bearer with the left foot
THE , L\T.
This seat may be used to carry a helpless patient.
FIG. 71.
1.-Two bearers face each other and stoop, one r)n t.ach side of the patient. Each belrer passes his fore'lrm nearest to the patient's head under his back ju t G
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of hi s thighs ( Fig. 7 I), and clasp their hands by one of the methods shown in Figs. 72 and 73. A handkerchief should be held in the hands if the first grip is used.
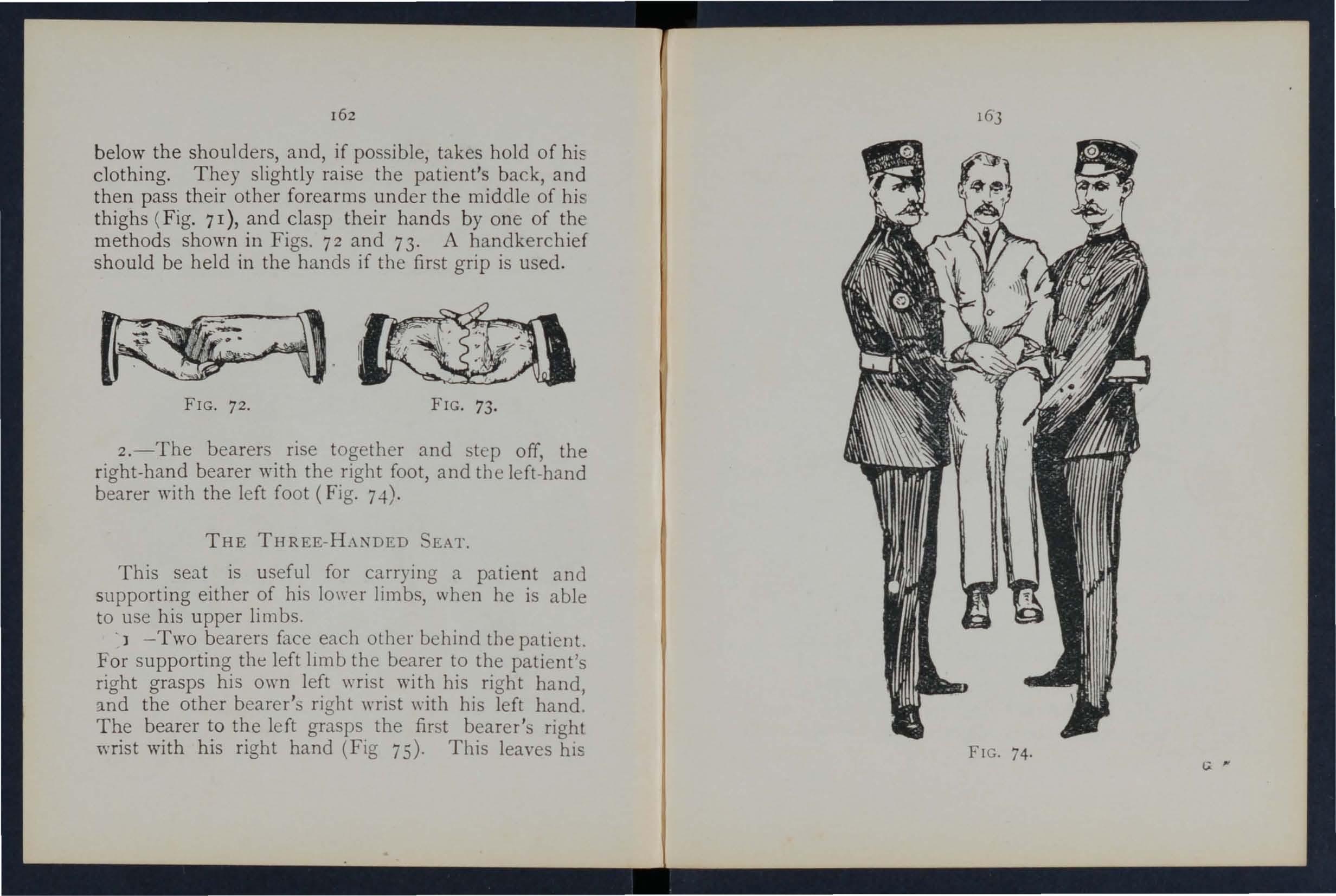
2.-The bearers rise together and step off, the right-hand bearer with the right foot, and the left-hand bearer with the left foot (Fig. 7.f).
THE THREE-H.\NDED SEAT.
This seat is us eful for carrying a patient and supporting either of his lower limbs, when he is able to use his upper limbs .
. ] -Two b earers face each other behind the patient. For supporting the left 11mb the bearer to the patient's right grasps his own left wrist 'with his right hand, the other bearer's right wrist with his left hand.
The bearer to the left grasps the first bearer's right wrist with his right hand (Fig 75). This leaves hIS
[eft hand free to support the pct:icnt's left leg. For the patient's right lower limb follow the same directions, substituting "right" for" left" and" left 1/ for " right." The bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3.-The bearer. rise together and step off, the
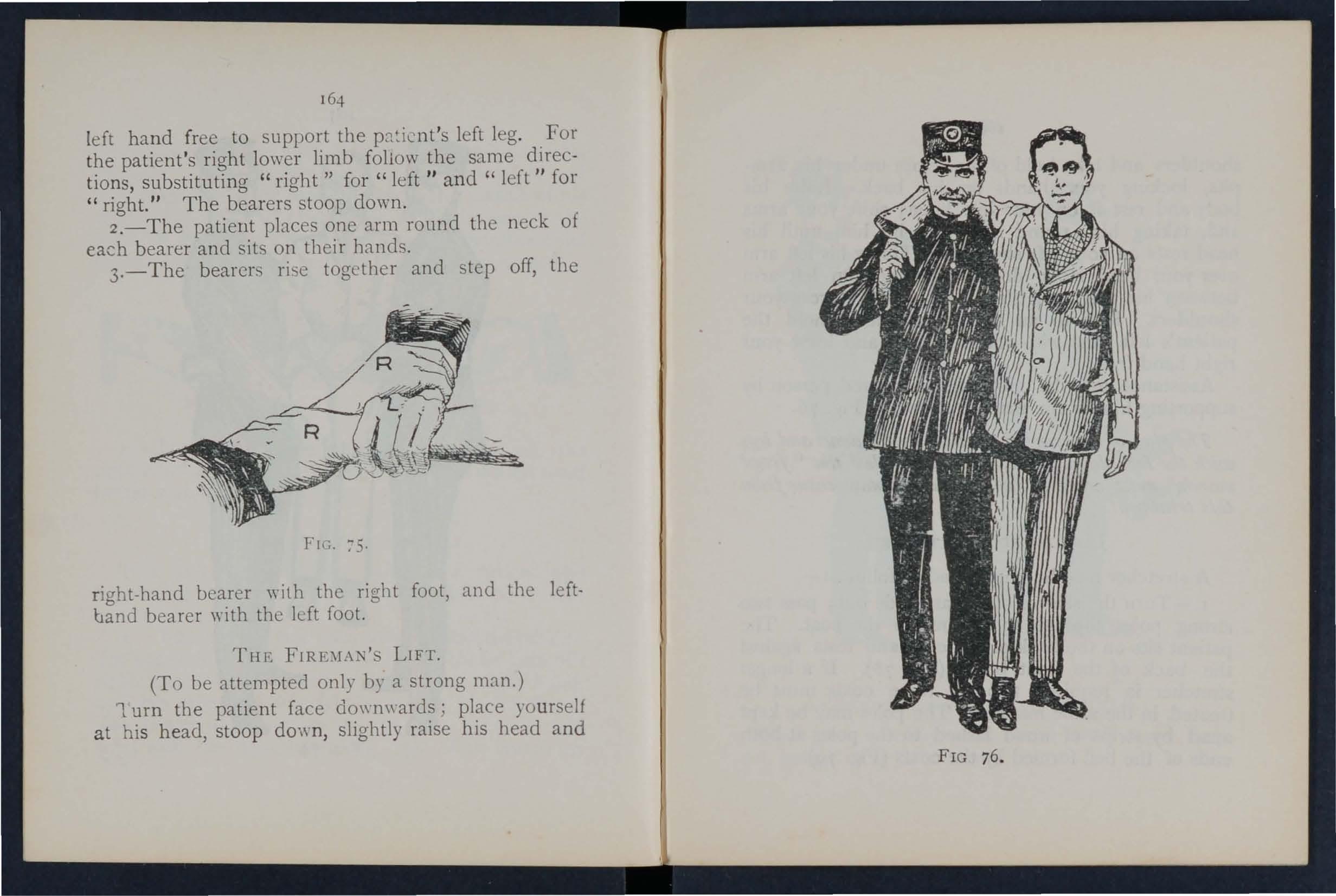
Fl\;. 75.
right-hand bearer ,,·ith the right foot, and the leftband bearer with the left foot.
THP: FIRE:\IAN'S LIFT.
(To be attempted only by a strong man.)
1 urn the patient face downwards; place yourself at his head, stoop dO'\\,n, slightly raise his head and
166
shoulders and take hold of him close under his armpits, locking your hand s on h1S back. Raise his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head rests on your left shoulder. Throw his left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your 5houlders. Rise to an upright position; hold the patient's left ",rist with your left hand and leave your right hand free.
Assistance may be give n t o an injur ed person by supporting him in the manner shown in Fig. 76.
Tlze plalZ of can')'z'llg the patz'eJlt by the arms and legs wz'tlz the face doze.l7lwards, called the" frogs ' marclz," must never be lIsed, as death may ensue from thz's treatment.
hIPROVlSED STRETCHERS.
A stretcher may be improvised as f01l0\\"s :-
1.-Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The patient sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a longer stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of wood lash ed to the poles at both ends of the bed formed by the coats (Fig. 79).
167
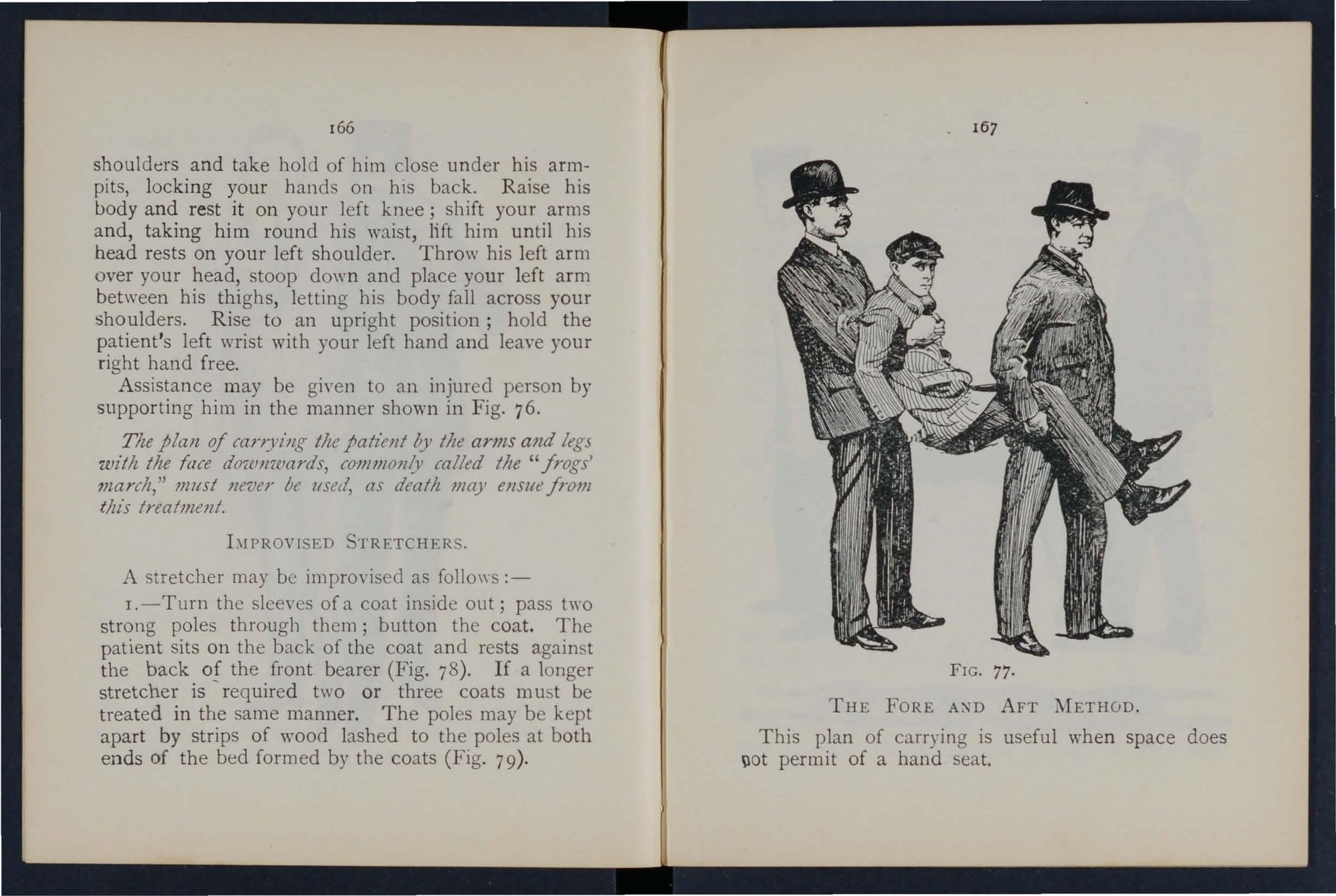
THE FORE AND AFT METHOD.
This plan of carrying is us eful when space does \lot permit of a hand seat.
FIG. 77.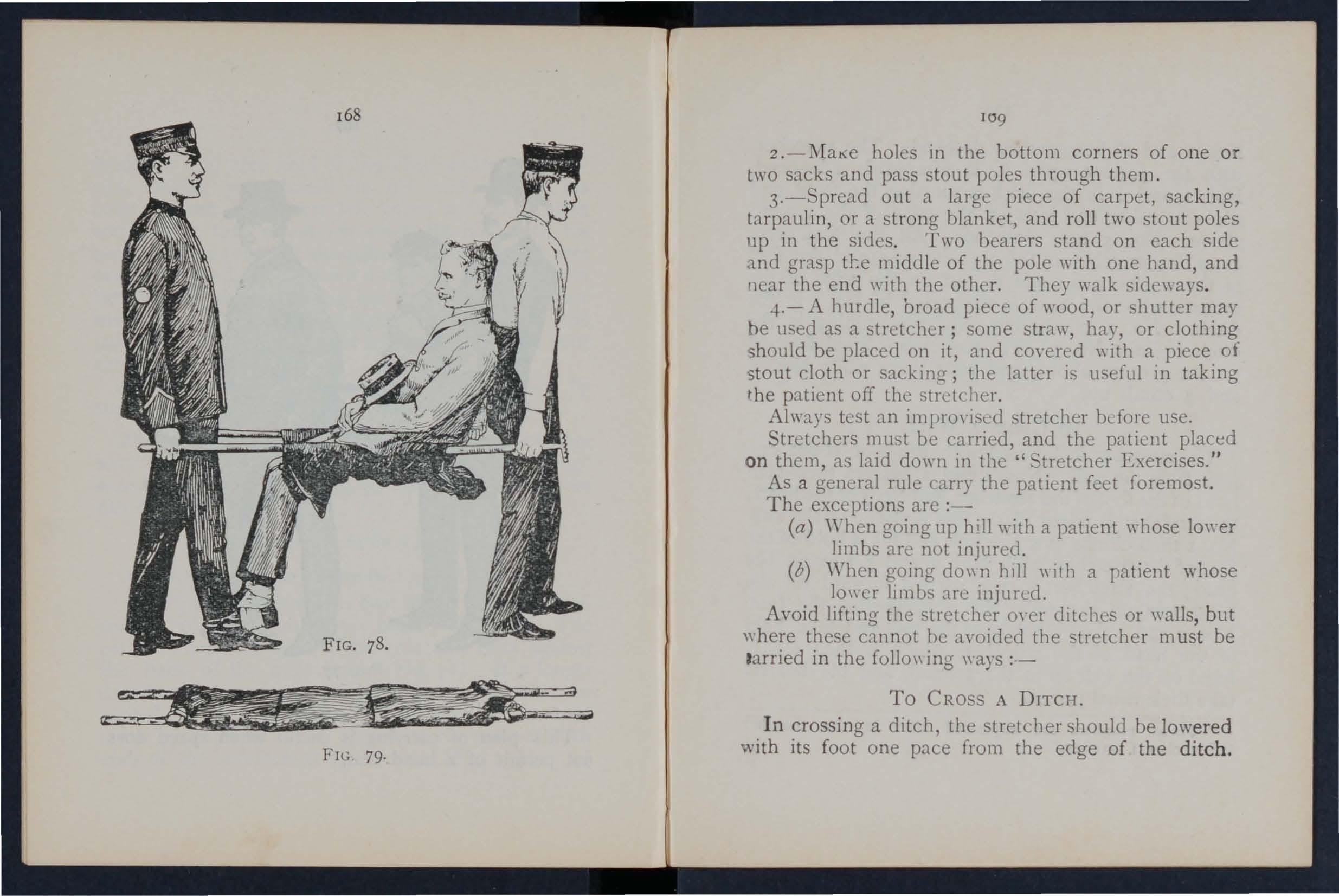
2 holes in the bottom corners of one or two sacks and pass stout poles through them.
3.- pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides. Two bearers stand on each side and grasp tl:e middle of the pole with one halld, and near the end with the other. They \\'alk sjde\\ays.
4.-A hurdle, broad piece of wood, or . hutter may he used as a stretcher; some str::I.\\', hay, or clothing should be placed on it, and covered \\ith a piece of -stout doth or sacking; the latter is useful in taking the patient off the stretcher.
Always test an improyised stretcher blfore use.
Stretchers must be carried, and the patient placed on them, as laid down in the 'c tretcher Exercises."
As a general rule carry the patient feet foremost.
The exceptions are :-
(a) When going up hill with a patient whose lo\\'er limbs arc not injured.
(b) " Then going do\\ n hill \\ ith a patient whose 10\\'c r lim bs are injured.
Avoid lifting the stretcher oyer ditches or \\alls, but "here these cannot be avoided the stretcher must be tarried in the follo\\ ing \\ ays :--
In crossing a ditch, the stretcher should be lowered with its foot one pace from the edge of the ditch.
170
Nos. I and bearers then descend. The stretcher. with the patient upon it, is aftenyards advanced , Nos. I and 2 in the ditch supporting the front enc while its other end rest') on the edge of the ground above. No. 3 now descends. All the Nos. nO\'carry the stretcher to the opposite side, and the foo' of the stretcher is made to rest on the edge of the ground, while the head is supported by NO·3 in th e ditch. No. I climbs out, No. 2 remaining in the ditch to assist NO.3. The stretcher is lifted fonyard on the ground above, and rests there while Nos. 2 and 3 climb up.
To CRO SS A 'VALL.
The stretcher is lowered with the foot about onE pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO·3 of the head; the stretcher is raised till the foot is placed on the wall No. I then climbs over the \yall and tak.:!s hold of the foot of the stretcher, while Nos. 2 and 3 support the head; the stretcher is then carri ed forward till the head rests on the wall; No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
.. These numbers are explained later in the deta.iled II Stretcher Exercises."
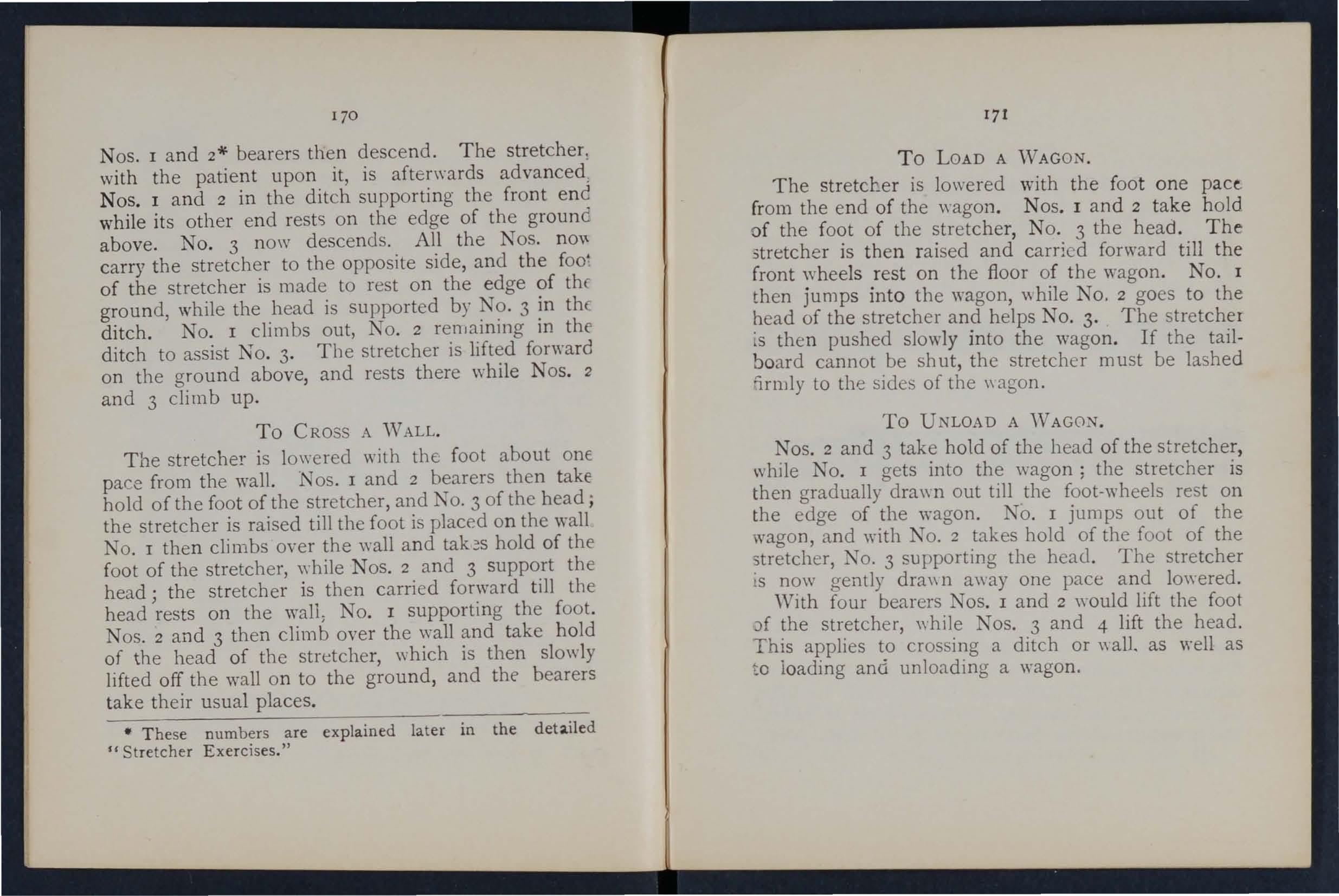
171
The stretcher is lowered with the foot one pact. from the end of the wagon. Nos. I and 2 take hold of the foot of the stretcher, No. 3 the head. The .stretcher is then raised and carri ed forward till the front wheels rest on the floor of the wagon. No. I then jumps into the wagon, "hile No.2 goes to the head of the stretcher and helps NO.3. The stretche r 's then pushed slowly into the wagon. If the tailbo ard cannot be shut , the stretcher must be lashed li.rmly to the sides of the \\ agon .
Nos. 2 and 3 take hold of the head of the stretcher while No. I gets into the wagon; the stretcher then gradually drawn out till the foot-wheels rest on the edge of the wagon. No. I jumps out of the wagon, and \yith NO.2 takes hold of the foot of the stretcher, No, 3 su pporting the head. The stretcher is now gently dra\\l1 away one pace and lo\yered. With four bearers Nos. I and 2 would lift the foot 0f the stretcher, \yhile Nos. 3 and 4 lift the head. This applies to crossing a ditch or "all. as well as to loading and unloading a wagon.
CHAPT ER IX .
STRETCHER TRA TSP ORT.
The "FurIey " Stretchers ( Model 1899) are of three patterns, viz "Ordinary," "Telescopic-handled,' and "Police ." In general principle they are alike. the component parts being designated the poles,
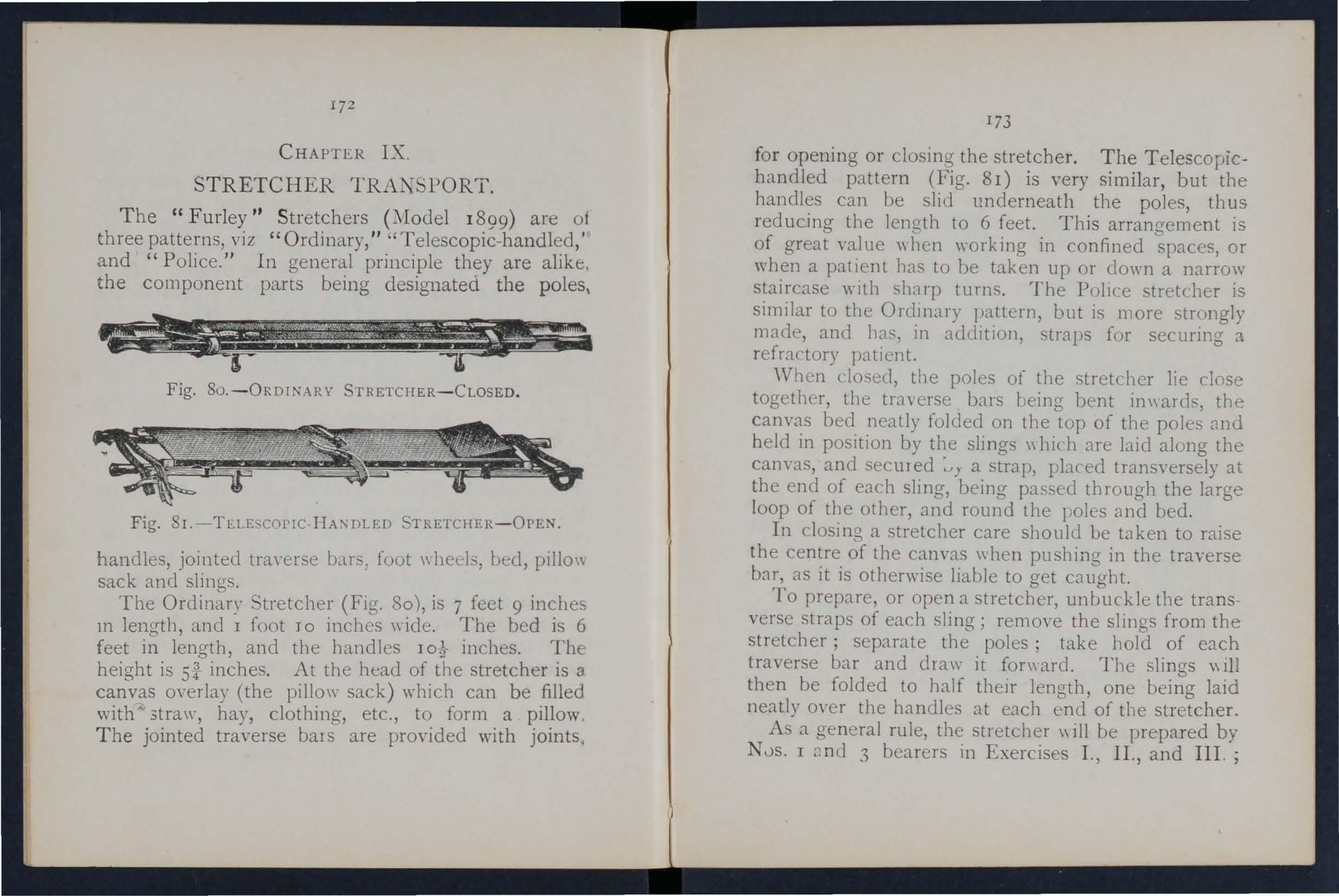
Fig. SO. - ORDINARY STRETCHER-CLOSED.
Fig. 8I.-TE.LESCOPIC·HA:'\DLED STRETCHER -OPEN . handles, jointed tra,'erse bars, foot wheeb, bed, pillo\\ sack and slings.
The Ordinary tretcher (Fig. 30), is 7 feet 9 inches 111 length, and I foot TO inches \ride. The bed is 6 feet in length, and the handles IO} inches. The height is Sf inches. At the head of the stretcher is a canvas m-erlay (the pillo\\' sack) which can be filled with" 3tra\\', hay, clothing, etc., to form a pillow The jointed traverse bals are provided with joints,
173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) is very similar, but the handles can be slid underneath the pol es, thus reducing the length to 6 feet. This arrangement is of great value when working in confined spaces, or when a patient llas to be taken up or clown a narrow staircase wIth sklrp turns. The Pollee stretcher is similar to the Ordll1ary pattern, but is more strongly made, and has, in addition, straps for securing a refractory patient.
'V hen closed, the poles of the stretcher lie close together, the erse . bars being bent il1\\ ards, the canvas bed neatly folded on the top of the poles and held in position by the slings \\ bich are laid along the cam-as, and secured a strap, pl.:tced transversely at the end of each sling, being passed through the large loop of the other, and round the 1 oles and bed.
In closing a stretcher care should be taken to raise the centre of the canvas \\ hen pushing in the traverse bar, as it is otherwise liable to get caught.
To prepare, or open a stretcher, unbuckle the transverse straps of each sling; remo,-e the slings from the stretcher; separate the poles; take hold of each traverse bar and dJ aw it fon\ ard. The slings \\ ill then be folded to half then' length, one being laid neatly over the handles at each end of the stretcher.
As a general rule, the stretcher \\ ill be prepared by NJs. I nnd 3 bearers 111 Exercises I., II., and III. ;
174and by No. 2 in Exercise IV. These bearers will, however, if required, assist the other bearers in atte ndin g to the patient 's injuries.
Note.- The various movements detailed in th e following Exercises should be carried out steadily, the bearers working in un ison, hurrying being carefully avoided, and e\'ery attention being paid to the bear e r who gives the words of command.
Ori ainally drawn up by ir John Furley, and revised in to accord ",ith the drills adopted by the Royal Army Medical Corps :-
EXERCISE No. 1.
FOR FOUR BE-\RERS.
1. -The In structor selects the bearers and numb e rs them-I, 2, 3, -+ at hi s discretion. ,hould o n e man be taller and stronger than the others, he should be styled 1 o . 3, as he will haye to bear the heavier part of the burden.'" All orders will be gi\'en by NO.4 .
2 . - " Fall in." -Nos . I, 2, and 3 take position on th e left side of and facing the patient. TO . I places hims elf at the patient's knees, No. 2 at th e hips, No. 3 at the patient's shoulders. At the same
'" Bearers should, howeyer, be taught to take any of the positions named in the following whether that of No. I, 2,3, or 4 beare r.
175
time No. 4 places the prepared stretcher on the ground by the right side of the patient :l2C'ut two
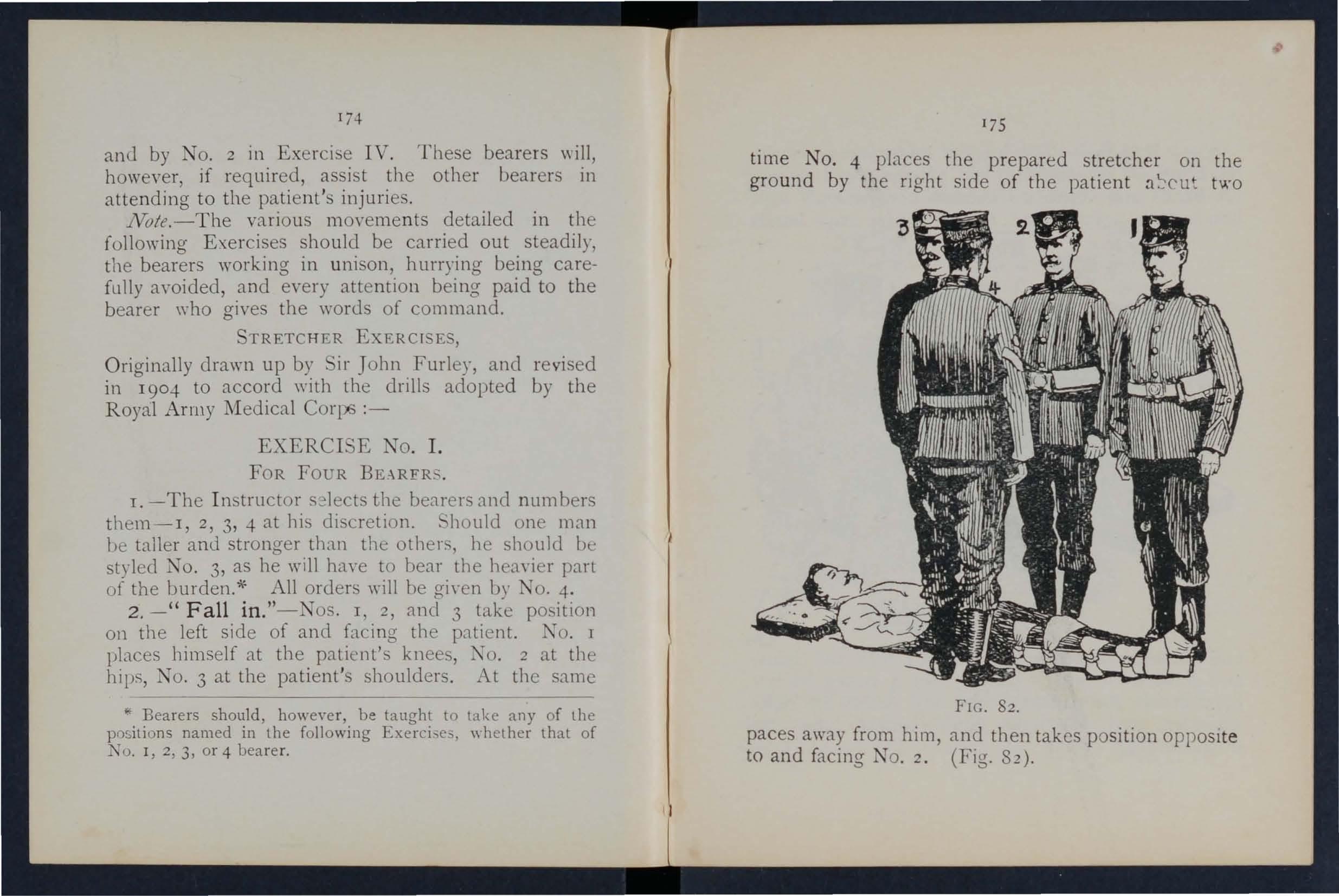
FIG. 82.
paces away from him, and then takes position opposi te to and facing NO.2 . (Fig. 82).
3.-" R e ady. "-Tbe bearers kneel down on the le.ft knee and take hold of the patient, No. I passing hiS and fore-arms beneath the patient's legs, hands wide apart. Nos. 2 and 4 pass their hands
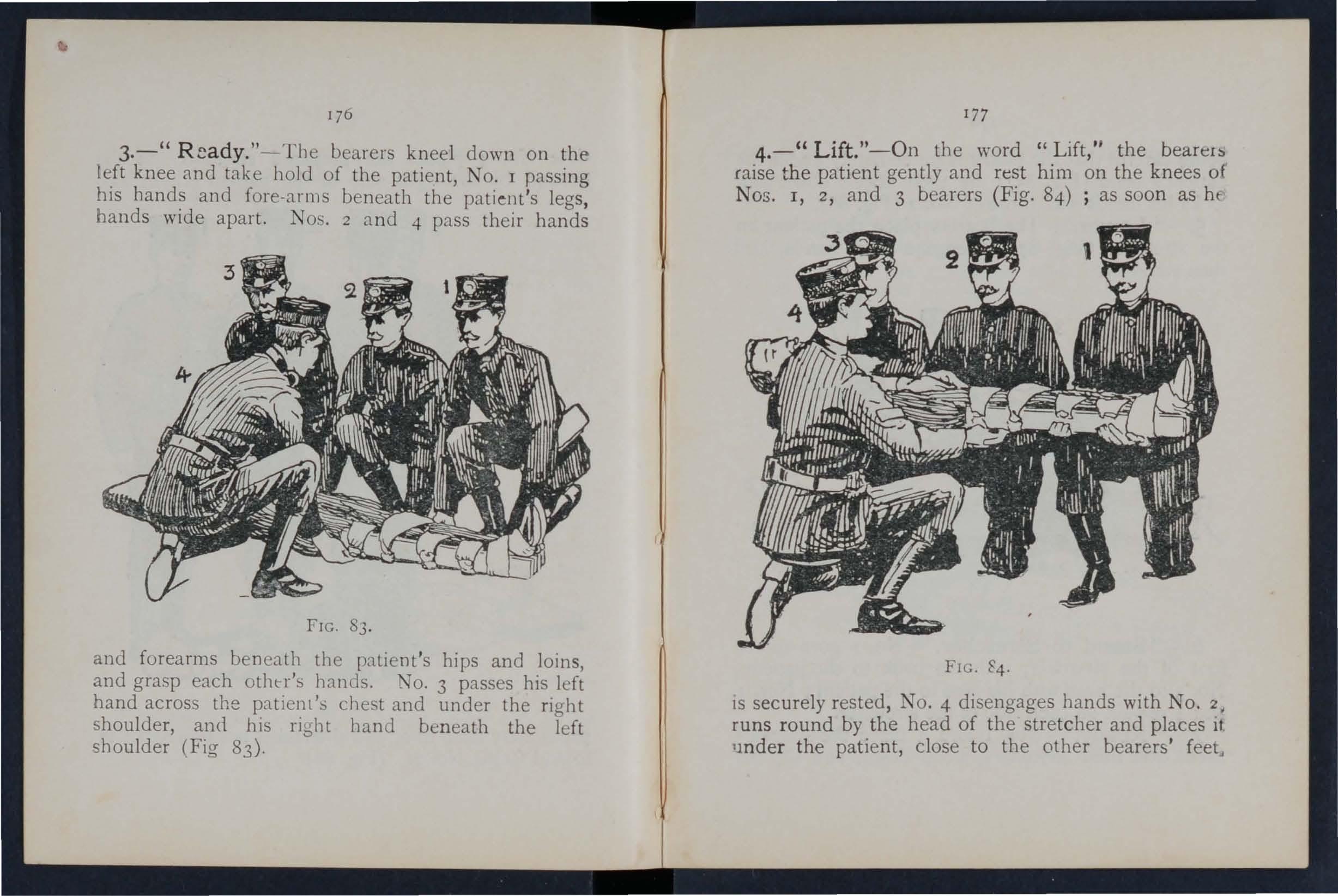
FIG. 83. and forearms beneath the patient's hi ps and loins, and grasp each otht"r's hands. No. 3 passes his left hand across the p::ttienl's chest and under the right shoulder, and his right band beneath the left shoulder (Fig 83).
177
4.-" Lift. "-On the word "Lift," the bearer:, raise the patient gently and rest him on the knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as hf"
FIG. 84.
IS securely rested, NO.4 disengages hands with No. runs round by the head of the stretcher and places if lmder the patient, close to the other bearers'
178
being careful that the pillow is imm ediately under the patient's head 85); he then kneels down ancl locks his hands with those of No.2 (Fig. 86).
5.-" Lower."- The bearers place the patient on he stretcher (Fig. 87), disengage their hands, awl hen stand up.
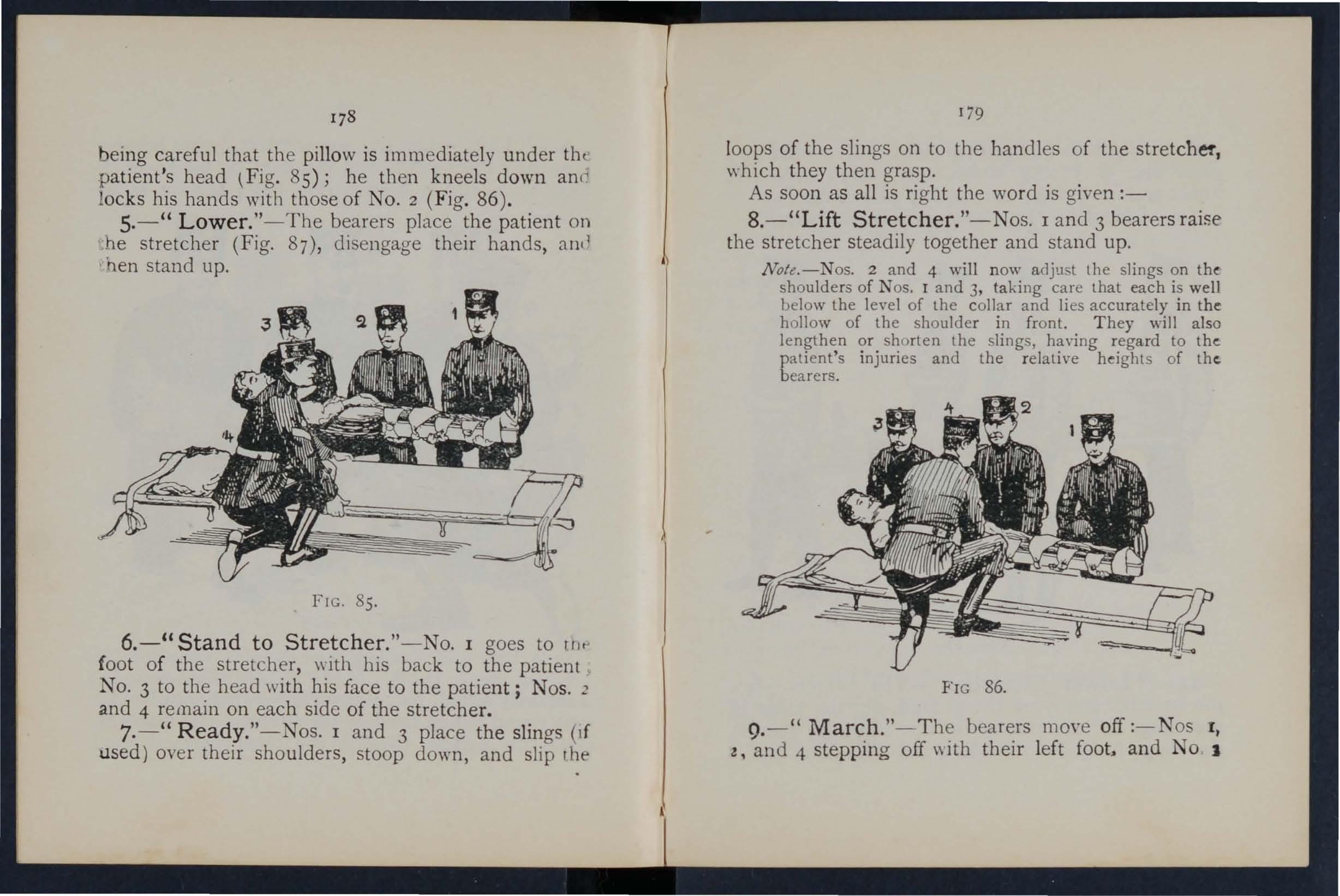
FIG. 85.
6.-" Stand to Stretcher."-No. I goes to rllt' foot of the stretcher, with his back to the patient NO·3 to the head with his face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7.-" Ready."-Nos. I and 3 place the slings (I f used) over their shoulders, stoop down, and slip rhe
179
loops of the slings on to the handles of the which they then grasp.
As soon as all is right the word is given :-
8.-"Lift Stretcher."-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
Note.-Nos. 2 and 4 will n ow adjust the slings on shoulders of Nos. 1 and 3, taking care that each is well below the level of the collar and lies accurately in the h ollow of the shoulder in front. Th ey will also lengthen or shorten the slings, having regard to the patient's injuries and the relati ve heights of the. bearers.
FIG 86.
9.-" March." - The bearers moye off :-Nos I, z, and 4 stepping off \\ ith their left and No I
wIth his right foot (Fig. 87). The step sho uld be a short one of twenty inches, and taken with bent knees and no spring from the fore parl of the foot. Io. -" Halt. "- The b earers remain steady.
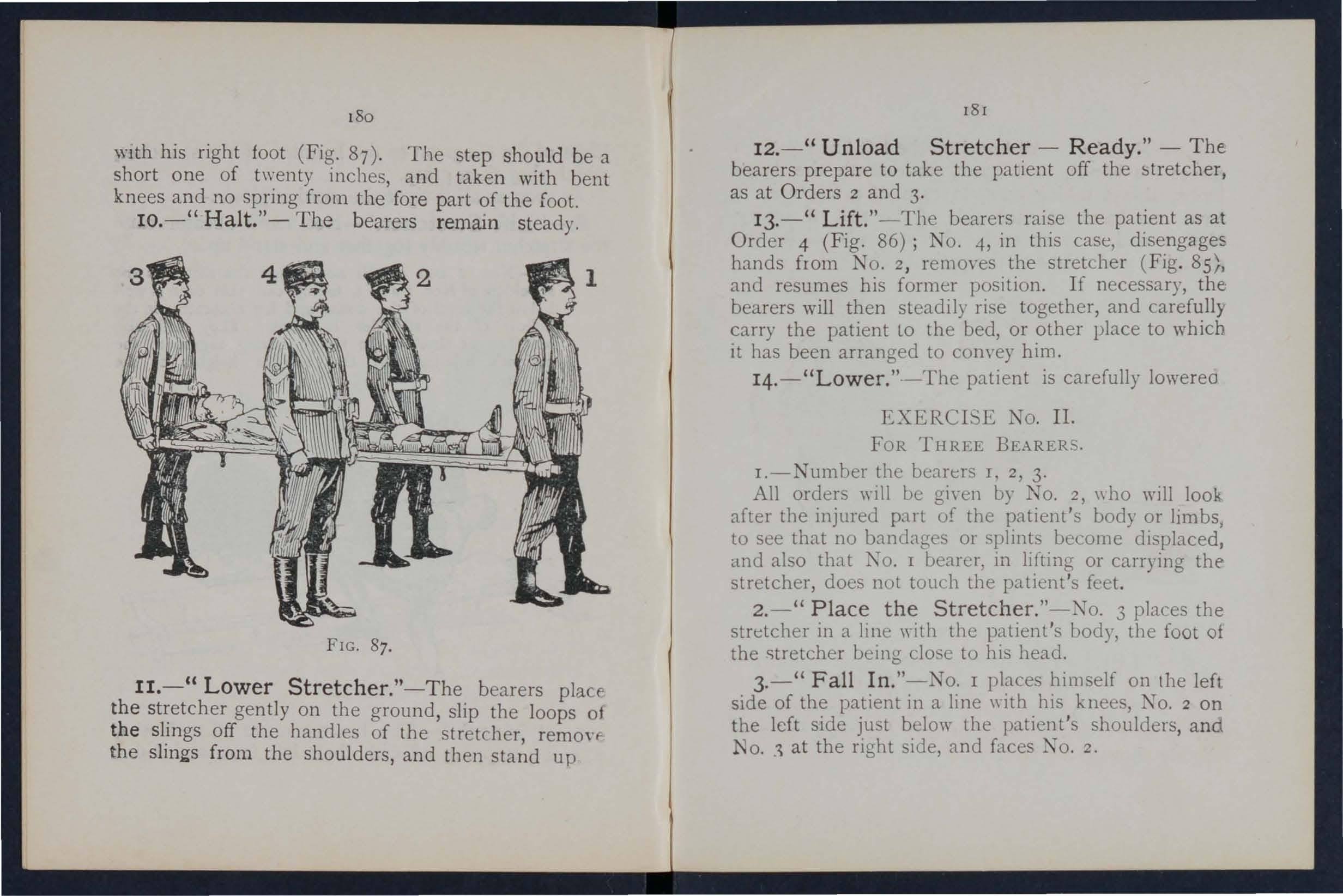
FIG. 87.
II.- " Lower Stretcher."-The bearers placf'
t he gently on the ground, slip the loops of the slmgs off the handles of the stretcher remonc t h e sling s fro m the shoulders, and then up
12.- " Unload Stretcher - Ready." - The. bearers prepare to take the patient off the as at Orders 2 and 3.
13. - " Lift. "-The bearers raise the patient as at Order 4 (Fig. 86); NO.4, in this case, disengages hands from No.2 , remO\'es the stretc.her (Fig. 85/1 and resumes his former position. If necessary, the: bearers will then steadily rise together, and carefully carry the patient to the bed, or other place to which it has been arranged to convey him.
14.-" Lowe r." -The patient is carefully lowerea
EXERCI 'E No. II.
FOR THREE BEARERS.
I.-Number the benrers I, 2, 3.
All orders wi II be given by 1 O. 2, \\ ho will look after the injured pnrt of the patient's body or limbs, to see that no bnncbges or splints become displaced, and also thnt 1\0. I bearer, 111 lifting or carrying thestretcher, does not touc.h the feet.
2.-" Place the Stretcher."- TO. 3 places the stretcher in a line \yith the patient's body, the foot of the stretcher being close to his head.
3.-" Fall In ."-No. I places himself on the left side of the patient in a line \\ith his knee, TO. 2 on the left side ju t below the patien t's shoulders, and N o. . at the right side, and faces o. 2.
4.-"Ready." -All kneel on the left knee. No. I places his hands, well apart, underneath the 10\\ er jimbs, always taking care, in case of a fracture, to have one hand on each side of the seat of injury. Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient (Fig. 88).
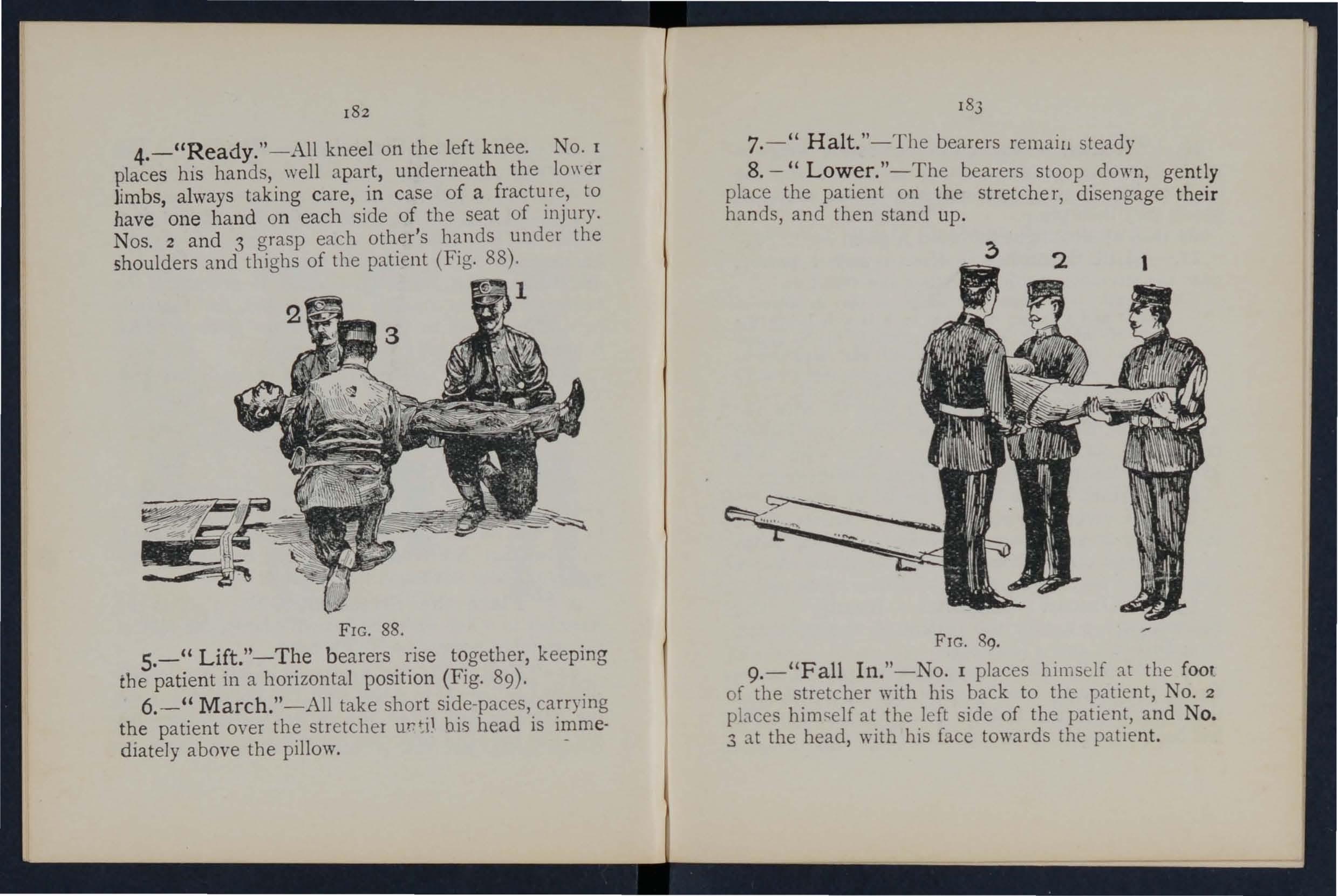
FIG. 88.
5.-" Lift."-The bearers rise together, keeping the patient in a horizontal position (Fig. 89)·
6.-" March."-A ll take short side-paces, carrying the patient over the stretcher bis head is immediately above the pillow.
7. -" Halt."-T he bearers remaill steady
8. -" Low.er."-The bearers stoop down, gently place the patient on the stretcher, disengage their hands, and then stand up.
FIG. 89.
9.-"Fall In."-No. I places hims elf at tbe fOOl of tbe stretcher with bis back to the patient, No.2 places himself at the le ft side of tbe patient, and No. 3 at the head, with his face towards the patient.
10.-" Ready." -Nos . I and 3 place the slings (if used) over their shoulders , stoop down, and slip the loo ps of the slings on to the handles of the stretcher, whi ch they then grasp.
As soon as all is right the word is given-
!I. - " Lift Stretcher."- Jos. I and 3 bearers raise the stret cher steadily together and stand up.
No. 2 will now adjust the slings o n the shoulders of Nos. I and 3, taking care that each is well below the le\'e l of the collar, and lies accurately in the hollow of the shou lder in front. IIe "ill also lengthen or shorten the slings, haying regard to the patient's injuries and the relative heights of the bearers.
12. - " March." - Nos. I and 2 step off with th e left foot, and No. 3 with the right. The step should be a short one of 20 inches, and taken "ith bent knees, and no spring from the fore part of the foot.
13. - " Halt. "--The bearers remal11 steady .
14. - " Lower Stretcher." --The bearers place the stretcher gently on the ground, slIp the loops of the slings off the handles of the stretcher, remm-e the slings from the shoulders, and then stand up.
IS. -" Unload Stretcher - Ready." - The bear ers prepare to take the patient off the stretcher, as at Orders 3 and 4 (Fig. 88).
16.-" Lift."- The bearers raise the patient, as at Order 5, alld carry him by short SIde steps, clear of the stretcher, to the bed, or other place to whIch it has been arranged to convey him (Fig. 89).
17.-" Lower ."-The patient IS carefully lowered.
EXER 't'E No. III.
WHEN ONL \' TH REE Bl:!,ARLR ,\RE AVAILABLE AND THE C \:":'WT BE PLACED AS IN E\ERCISE II.
r.-The II1'>tructor numb-rs the bearers-I, 2, 3 "\11 orders \\ ill be given by TO. 2.
2.-" Place the Stretcher."-Xo. I Ltkmg the foot of the stretcher, and 3 the head, place it on the ground by the side of the p:l.tient, and as close to him as practicable.
3. -" Fall In ." -The three bearers t:l.ke the same pO"iltions 011 on ' 'SIde of the patient, as laid dO\\ n in Exercise TO. 1.
4. - " Ready. "-i\05 I, 2, ancl 3 kneel down on the left kllee, plaCIl1,!; themseh-es as close to the p:l.tient as the)' COl1\'l'nil'ntly can, and then take hold of him as directed in EXerci::;e :\0.1.
5.-" Lift." -N05. I, 2, and 3 rai::;e the patient as directed in E"ercise TO. I, an I then 11100-e in a kneding position up to the stretcher.
6. _" Lower. "-The bearers bend forward, carefully lower the patient on to the stretcher, and dis engage hands.
7.-" Stand to Stretcher. "-All the bearers stand up; No. I goes to the foot, No. 2 remains III position at the side, and No. 3 goes to the head the stretcher.
8.- " Ready. "-Nos. I and 3 place the slinrrs (if used) over their shoulders, stoop down, anli sl p the loops of the slings on to the handles of the stretcher, which they then grasp.
.9.-" Lift Stret ch e r. "-Nos. I and :; bearers raIse the stretcher steadily together and stanu up.
No.2 will now adjust the slings on the shoulders of os. I and 3. taking care that each is well beluw the lenl of the collar, and li es accurately in the hollow of the shoulder in front. lIe will also lengthen or shorten the slings, having regard to the patient's illjun-:s and the relative heights of the bearers.
10. -" Mar c h."-N os . I and 2 step off with the left foot, and NO,3 with the right , The ::,tep shou ld be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
11.-" Halt. "-The bearers remain steady .
12. -" Lowe r S tretch e r."-The bearers phlce the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher remove the slings from the shoulders, and then st:1;1d up.
Unload Stretcher- Read y." - 1 places on the left side of the pati ent, and in a lme wIth his knees, No. 2 on the left side just below t he patie n t's shoulders, and NO.3 at the right
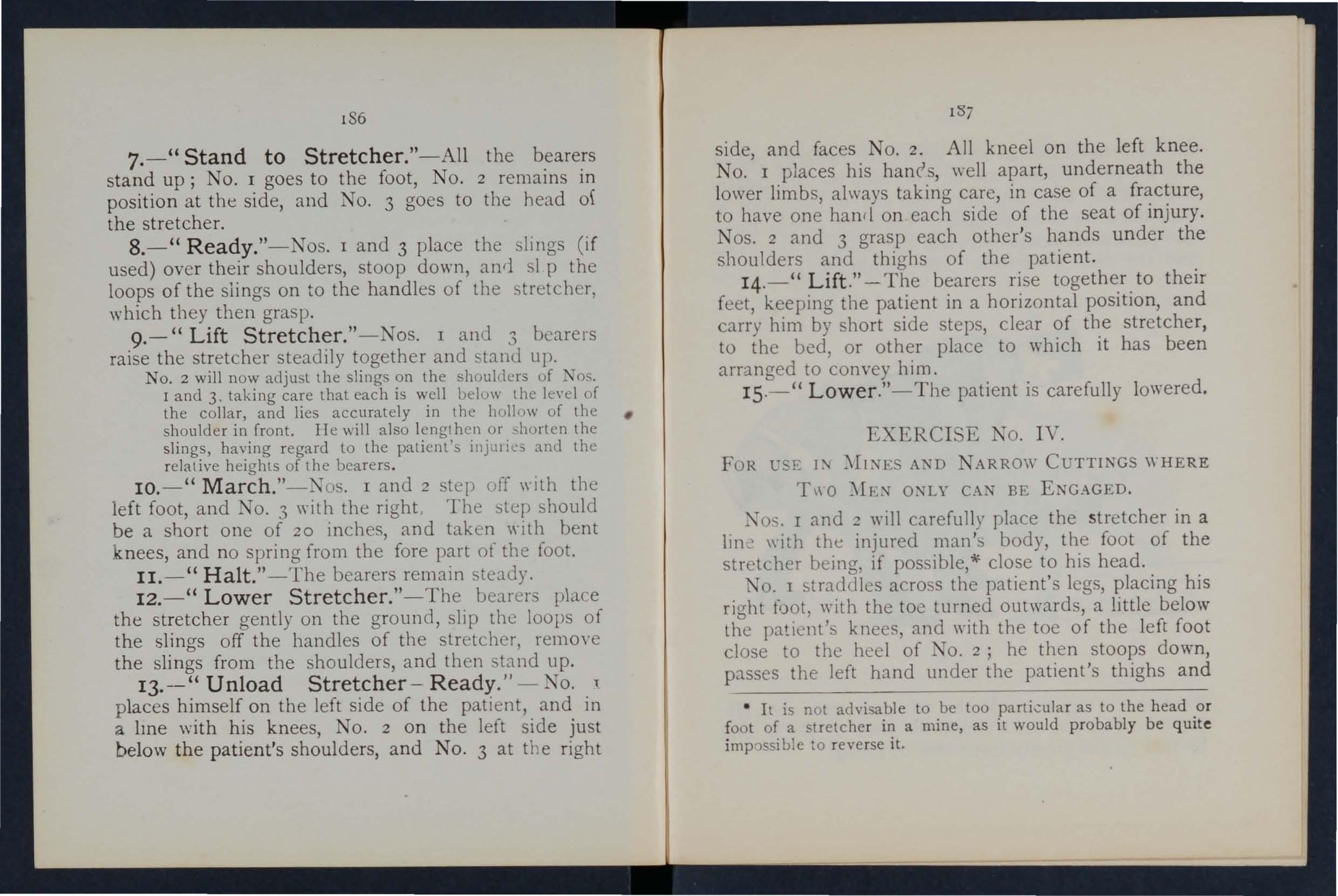
side, and faces NO.2. All kneel on the left knee. No. I places his hanrs, well apart, underneath the lower limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of injury. Nos. 2 and 3 grasp each other's hands under the shoulders and thi ghs of the patient.
14.-" L ift." - The bearers rise together to their feet, keeping the patient in a horizontal position, and C:1rry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
15.- " Lower."- The patient is carefully lowered.
FOR lJ_E 1:-' )'II:-.r ES A. D NARROW CUTTlNGS \\ HERE
T,\ 0 )'b,N O:-.rLY CAN BE ENGAGED.
Nos. I and 2 ",ill carefully place the stretc her in a 1ll1 c \\ ith the injured 111:1n':, body, the foot of the stretcher being, if possible,';;' close to his head.
TO. I straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, passes the left hand under the patient's thighs and
• I t is not advisable to be too particular as to the head or fo ot of a stretche r in a mine, as it would probably be quite imp CJssible to reverse it.
I
t he right hand across and under the patient 's calves . NO.2 places his feet one 011 each side of the patient be t wee n his body and arms, the toe of each foot as nea r the armpits as possible. He then Sl{)OpS dovm and passes his hands between the sides of the chest and the arms underneal h the shoulders, and locks
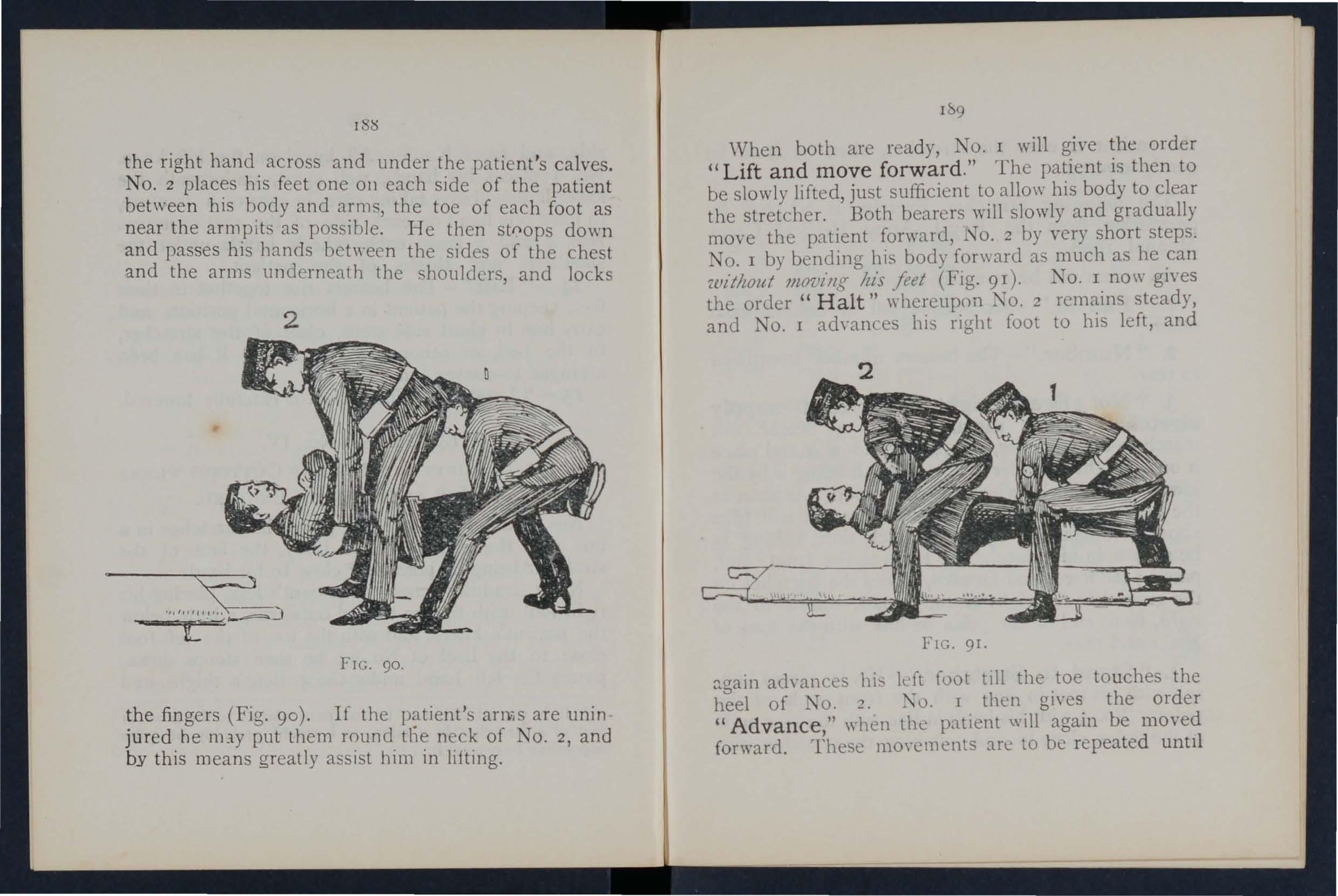
FIG. 90.
the fin gers (Fig . 90). If the arniS are unin jure d h e nny put them round the neck of No.2, and by th is means greatly assist him in lifting.
I 9
\Vhen both are ready, No. I will give order " Lift and move forward ." The patient IS then to be slowly lifted, just sufficient t? allo\\" his body to clear the stretcher. Both bearers wIll slowly and gradually move the patient forward, NO.2 by very short steps. No. I by bending his body fo[\\ard as much as he 'lillilLOut JIL07)illg ltis feet (Fig. 91). No. I no\\" gIves the order" Halt" whereupon No. 2 steady, and No. I ad\'anles his righ t foot to hIS left, and
FIG. 91.
::1.gain aJ\"anccs his kft foot till the .toe touches" the heel of NO.2. ?\o. I then gIves. the Older " Advance ," wh en the patient \.\ III agam be moved forward. Thest.: mO\"Cl1lcnts are to be repeated untll
the patient is over th e str etcher, \\' hen he is to be gentl y lo we red.
T he foll ow in g Stretcher Exercise is adapted by permission from the R oyal Army C orps 1908.
All orde rs will be given by No. -t-.
1. (( Fall in. "- 'ix bearers fall III behind each other.
2. (( Number. "-The bearers number from front to r ear.
3. "No·3 Bearer, right (or left ) turn supply stretcher- quick march. "-No. 3 bearer will march to the stretcher, stoop, lay hold uf it and place it on his right shoulder at the slope, holdlllg It by the lower foot wheels, wheels to the front. soon as the bearer is provided with a stretcher, he wIll turn about and rejoin his squad in quick time, halting as he arr ives in his place. He turns to the front, and, passing the lower end forward, places the stretcher on the ground to the right of the squad, \\heels to the right, fro n t end of the poles in line \\ ith the toes of No . [ a n d rises.
4. (( Stand to Stretcher. "-No. I places himself with his toes in line with the front ends of the pol es . No. 3 with his heels in line \vith the rear ends of the po les, cl ose to and tOUChing the stretcher wit h
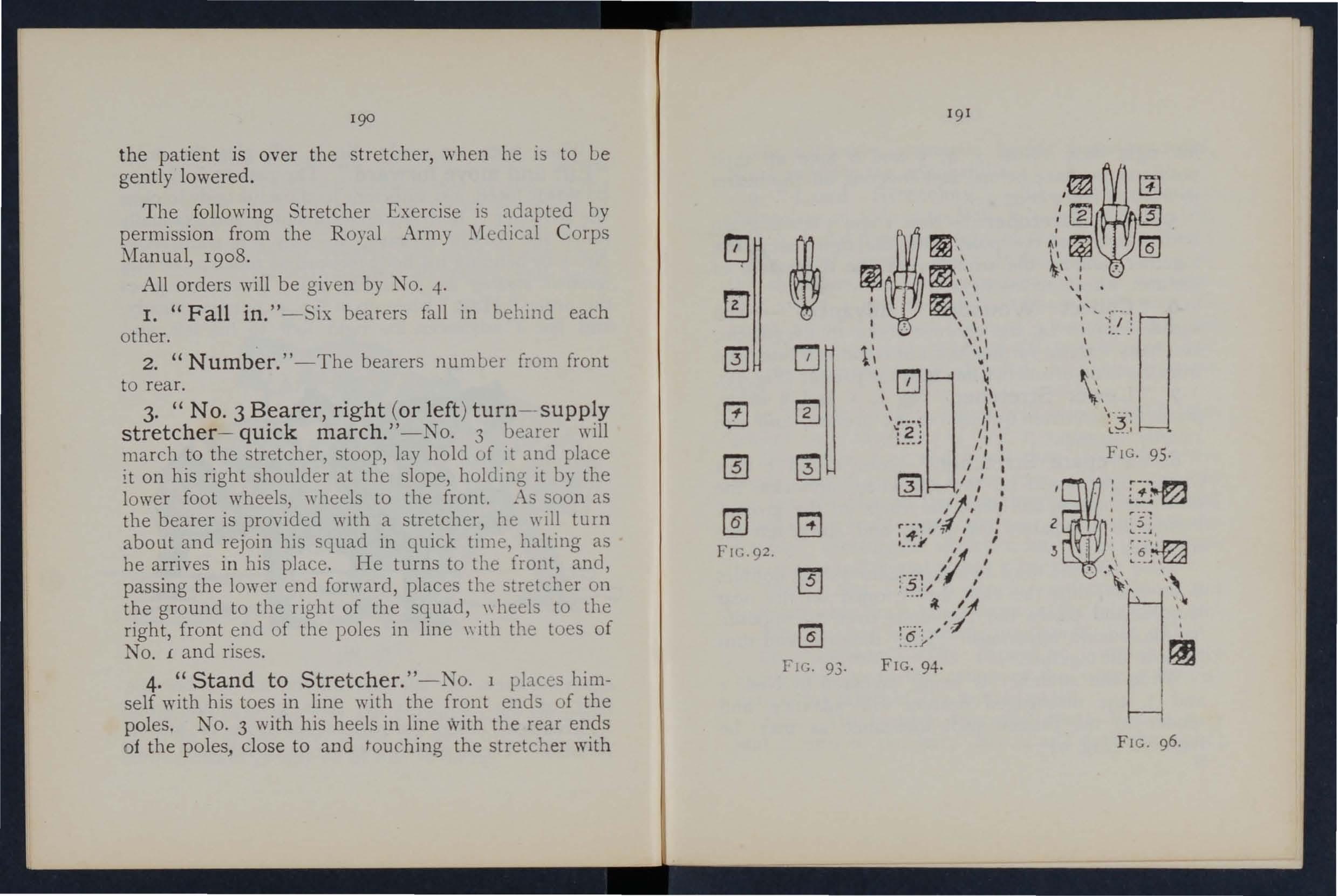
r[(:;. 93.
FIG. 94.
FIG. 96.
his . foot. 1 0.. 2 4, 5 and 6 take up their posltlO n s one pace behind and cO\'ering off the bearer i n fro n t of them (Fig. 92 \.
s. "Lift Stretcher. " - 1 .os. 1 and 3 stoop, grasp both handles of the poles \\'lth the rItTht hand rise together holding the stretcher at the 'f-ull exter;t of the arm, wheels to the rwht.
6. "Collect - Advance. " - The squad by the hOrlest route to the patient, and halts without further \yonl of com mallLl one pace from the head of and in a line with the patient (FI CT. 9 '1).
7. "Lower Stretc.h e r. " -N "s. 1 and 3 place the stretcher qUietly on the grollllLl, and rise martly together
8. S t r etcher. " - 0". I and 3 turn to the nght, kneel on the left knee, unhuckle the strap<;, and pbce tIle slin.;s on the ground beSide them, separate the poles, and traighten the traverses.
Two . On the \\ oru t\yO each takes a slina doubles it on itself, slips the loop thus /" )rmeu onb'the near handle , and places the free ends O\'er the opposite handle, buckle uppermost. They then rise anu turn to their left together.
\Vhile the stretcher is being prepared by Nos. I and 3, the disengageu bearers \\111 advance and render to the patient such assistance as may be required (Fig. (4).
The necessar} assistance baying becn rendered, NO.4 \\ill give tbe command9. "Load Stretcher. " - The bearers place themsehes as fo11o\\s :-Nos. J, 2 and 3 on tIle left,
TOS. 4, 5 and 6 on the right of the patient; lOS. I and 4- at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the whole kneeling on the left knee.
TOS. I and 4 pass their hands beneath the patient's knees, 2 and 5 beneath the hip.) 3 and 6 beneath the shoulder", care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. (5).
10. " Lift. "-The \\hole will carefully lift the patient on to the knees of Tas. J, 2 ancl 3·
Two. Nos. -i, 5 and 6 will then dic:;engage, rise; Nos. -+ and 6 step back one pace. i\ o. 5 turns to hiS left, douhlcs to tbe stretcher tahes bold of and r<lise:, it, left hand acruss, the near pole resting on the left hip; carrying the stretcher he returns to his place bet\\ eLl) -+ and 6, and plnces it beneath the patient.
TIIl'ce. Nos. -+ and 6 st p fOf\\ard one pace, and together \\Ith NO.5 kneel dO\\l1 on the lert knee, and prepare to assist in lowering the patient (Fig. 9 6 ).
II. (( Lower. "-Th patient is lo\\ered slowly and gently on to the centre of the canvas (special care bein..!' taken of the injured part).
1z(lo. The bearers disengage, rise; Nos. I, 2, 3 and 6 turn to the left; Nos . 4 and 5 to the right; H
No. 4 places himself three pac es in fr o nt of the stretcher. No.6, havin g coll ec te d the kit a nd a rms of the patient, places him se lf three pa c es in r ear of the stretch e r, N os. 2 a nd 5 o pp os it e th e c e ntre of the stretcher. Th e wh ole a re n o \\' read y to lift stretcher and moy e off (Fi g . 97).
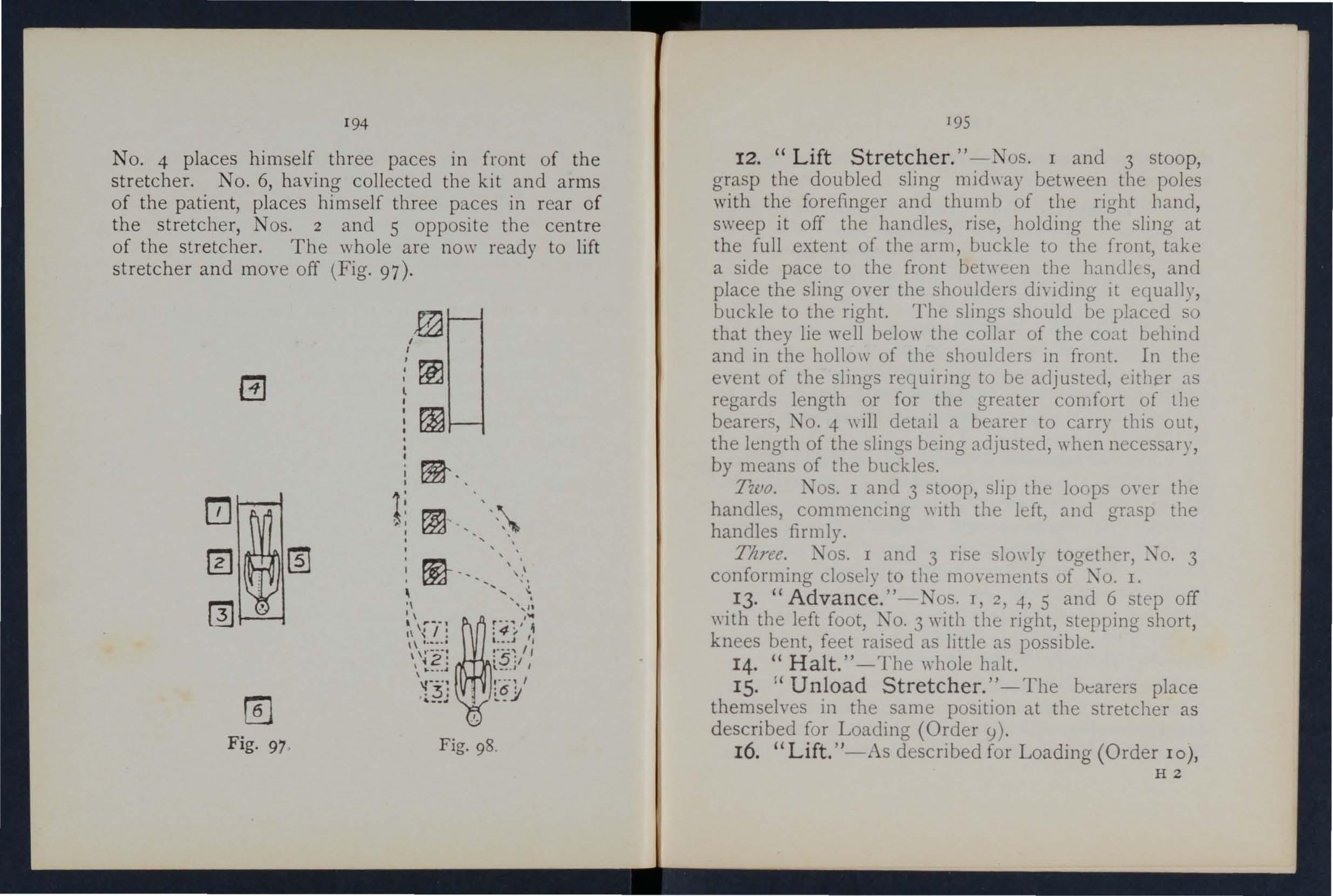
Fig. 97 , Fig. 98.
195
12. "Lift Stretcher. " -Nos . I a n d 3 s too p, g ras p th e doub led sling midway be tween the poles with th e fo refinger and th u mb of th e right hand , s\\'eep it off the h andles , rise , ho lding the sling at th e f ull extent of the arm, buckle to the front, take a side pace to the front between the handlE's, and place the sling over the shoulders dividing it equally, buck le to the right. The slll1gs should be placed so that they lie \Yell below the collar of the COclt behind and in the hollo\\ of the should e rs in front. In the event of the slings requIring to be adjustecl, either as regards le ngth or for the greater comfort of the bearers, o . -+ \\i ll detaIl a bearer to carry this out, t he length of the slings being adjusted, when necessary, by means of the buckles.
T'wo. Nos. I and 3 stoop, slip the loops oy e r the handles, commencing \\ ith the left, and gra p the hand les firmly.
Three. Nos. I and 3 rise slo\\'ly together, 4 TO. 3 conforming closely to the mo,'ements of I.
13· "Advance. "-Nos. I, ::!, 4, 5 and 6 st e p off \\ ith the left foot, .I. o. 3 with the right, stepping short , knees bent, feet raised as little as po.ssible.
14. "Halt. " -The whole halt.
IS. " Unload Stretcher. " - The bearers place th emselves in the same position at the stretcher as d esc ribed for Loading (Order SI) .
16. "Lift. "-As described for L oa ding (O rde r 10), HZ
I96
except that the stretcher is carried forward three paces clear of the patient's feet.
17- "Lower."- The patient is gently lowered to the ground. The bearers disengage, rise; Nos. I, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whole step off to their phces at the stretcher, as at Order " 'tand to ' tretcber 1/ (Fig. 98).
The Ashford Litt er is made up of either of the Furley stretchers mentioned on pages J 7 2 and 173, a wheeled under-carriage and a waterproof hood and apro n , or, if preferred, a light wet-resisting canvas cover. The stretcher is kept in position on the und er-ca rriage by the foot-wheels, which fit into slots in the sides Gf the under-carriage, and it can be removed at pleasure. The under-carriage is fitted with a cranked a'\le, which allows the bearers to pass with the stretcher the wheels instead of lifting it over them. At both ends are two legs which may be turned up as handles when \\ heeling the litter. The hood and apron fit into sockets screwed to the stretcher. In wheeling the litter, care should be taken to keep the patient in a horizontal position . Should it b e necessary, two blcu,;rs can easily lift the litter and patient.
The Rea-Edwards Litt er, introduced in 1904, is used in a similar m:ll1ner. and one model of it is fitted with pneumatic tyres, \\ hich add immensely to t he comfort of the patient and to the ease of propulsion.
197
CHAPTER X.
(Bez'llg the FtjlJl Lecture for Females oJ/I.)', ill accordance 'with ... 58.)
BY E. :\IACDO,\ELL CO GRAYE, ?II.D., F.R.C.P.I.PREP,\.RATIOX FOR R ECEPTIOX OF ACCIDLXT CASE
\YHI<.N ne\\ s of an accident comes, preparations should at once be made so as to have e\'er)thingready before the injured person is brourrllt in. Of course the preparations needful \\ ill vary according to the nature and extent of the injury, but the following are the chief things ,,'hich lllay have to be done.
CHOICE ,\.XD PREP,\RATIO:\" OF ROOM.
.A room mllst be chosen. In a bad case this should be one easily reach ed, as it is difficult to carry an injured person through narn\\' passages and up-stairs Unless there is some sucb reason against it the injureL! person's own room is best.
The way to the room must be cleared, projectmg furniture and loose mats in the hall or in lobbIes shoulL! be removed. If the injured person is carri.e d on a door, shutter, or stretcher, t\\ 0 strong chairs should be placed ready to support it \\ helever the bearers would be likely to require rest.
Useless furniture should be remO\'ed from the bed room. The bed should be dra\\-n out from the wall
so that both sides can be approached, and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much several hot bottles and hot blankets may be requIred; cover the hot bottles with flanne1.
If the injury is ,-e(y severe, if mud-stained clothes have to be removed, or if extensiye dressings have to be applied, it may be necessary to have another bed, a couch or a table placed near the bed to lay the sufferer on in the first instance. This should be so arranged that soiling may do no harm; old sheets, waterpoof materials, thin oilcl?ths, or eyen ne\\ s paper, may be used as a protectIon.
LIFTI0.'G AND CARRYI0.'G.
If present at the place where the ,accide:lt it will be necessary to see that toe patIent IS carefully lif[ed after proper "First Aid" has been rendered.
The following rules should be remembered :- Select the proper number of persons to assist, and do not let them lift the patient until they thoroughly understand how they axe to do it.
For ordinary cases, "here the injured person has to be lifted a very short distance, three helpers are sufficient. Two (\\'ho should be as far as possIble of equal height) are to bear the weight, the third is to support and take charge of the injured part. This is
199
best done by a person who has been through a "First Aid " course. If the injured person is insensIble, another helper should support his head.
The lifters, one at each side, should kneel on one k nee, and pass their hands under the patient's back at the lower part of the shoulder blades, and under the hips, clasping each his right hand 111 the otber's left. The injured patient should, jf practicable, place his arms round the necks of the bearers.
helper should attend to the seJt of injury; If thIS IS a fractured limb, lle should support it by plac111g the palms of his hands under the limb, one above and one below the seat of the injun' crraspina it firmly but a\'oidinlT unnecessary pressure:' b b
The helpers should remain thus until the order " Lift" is giyen and then tIley should all lift slo\\ ly and steJdily, avoidll1g jars, attempts to change position of bands, etc.
H the injured person is to be placed on a stretcher or shutter, this should be previously placed with the bottom end at Ris head; the bearers should then moye, one at each side of it, until the patient is oyer it. The word cc Lo\\ er" should then be aiyen and the 111 jured person should then be slowly 'A pillo,v or folded-up coat should be ready, and as the sufferer is lowered this should be placed hi head.*
• Full directions are gi\'cn in Cl ' apter IX.
B esides a stretcher, and substitutes such as J. gate, shutter, or a door, other means of carrying can be improvised.
In slight injuries, where the injured person is unable to ,Yalk, two bearers can carry him by forming a four handed, three-handed, or two-handed seat.
A four-handed seat is formed as described 0[\ "xlge 160.
A three-handed seat is made as described on page 162.
The two -handed seat is made a described or page 161.
A single helper can lift by supporting with one am the two knees, and with the other the back. Th arms must be passed well under before commencing to lift.
A single helper (,8.n give support by putting his arm round the waist, grasping the hip and pbcing the mjured person's arm round his ow'h neck holding the hand with his own hand (Fi6' 76 , page 16 5).
A capital stretcher can be improvised out of a strong sheet and two br )om llandles or other short poles. Each side of the she"t is wounn up on a broOl? handle until tllere is just room fur a person to lie between This requires four bearers, t\\O at each side, to prevent the sheet slipping.
In carrying a stretcher up stairs th e bead should go first, and an extra helper should assist at the lower end, so as to raise it and keep the stretcher nearly horizontal.
The two, three, or four-handed seat may be used for carrying up stairs; or a strong cbair, the patient being carried up backwards. In the btter case one helper should walk after the chair and help to support It, and to prevent the injured person slipping out.
If the bed is n8.rrow and there IS room the stretcher should be placed on the floor \\ ith the head close to the foot of the bed. The injured person should then be lifted oyer the foot and pJaC'((l on tbe bed If the hed is too \dde to admit of this, the stretcher should be pbced beside it, and t\\O helpers should st:l.nd at the far side of the stretcher. One helper pas_ e. one arm beneath the s,houlders and one beneath the middle of the back, the other helper placing hIS unn.::r the lo\\er part of the back and under the The injured person is then lifted, anothe! helpe r pulls away the stretcher, and after a single forward the burden is placed on the bed.
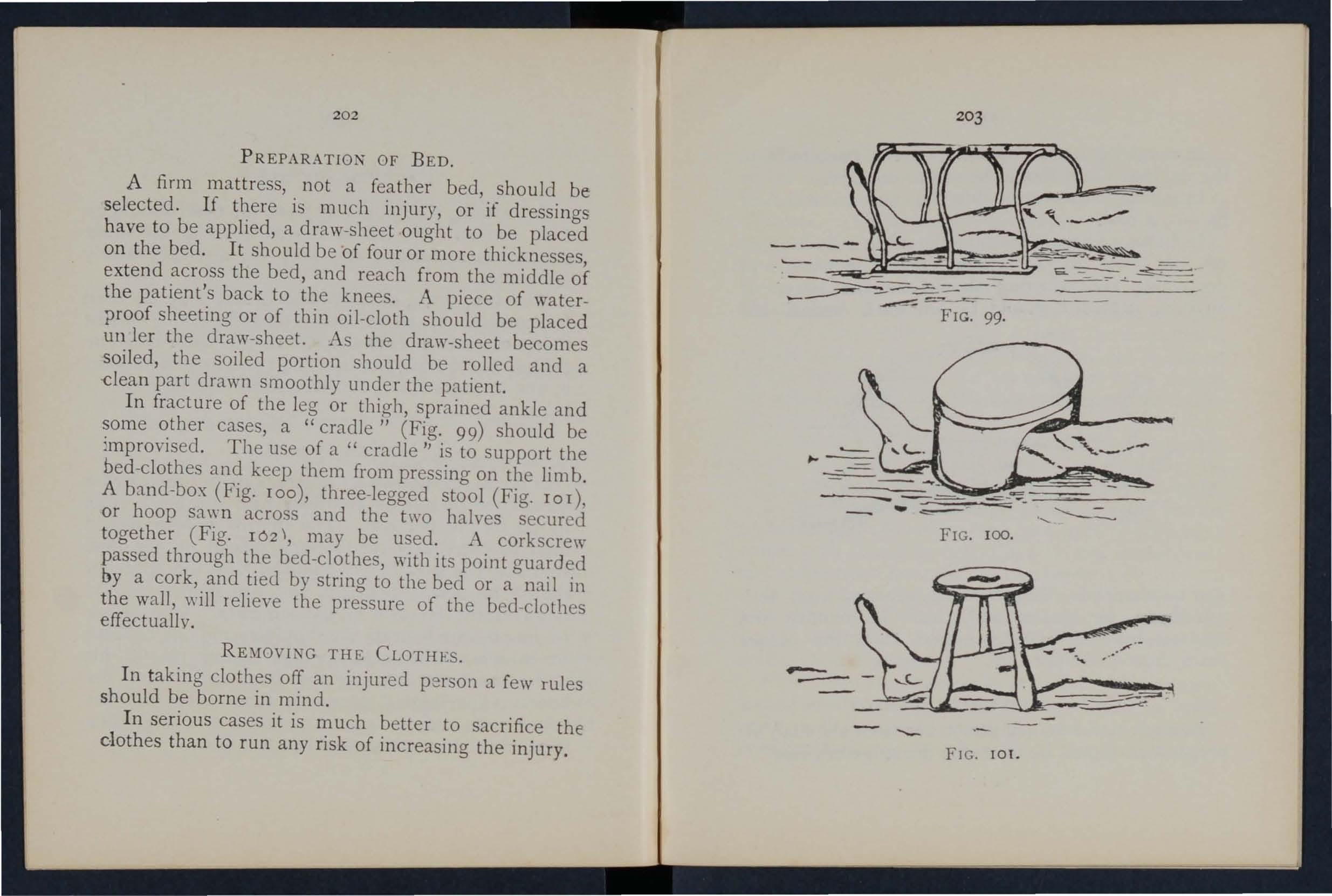
PREPARATIO • OF BED.
A firm mattress, not a feather bed, should be selected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed un ler the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a dean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be The use of a " cradle " is to Support the bed-clothes and keep them from pressing on the limb.
A band-box (Fig. roo), three-legged stool (Fig. ror), or hoop sa \\"n across and the two halves secured together (Fig. r02" may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed -clothes effectually.
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the dothes than to run any risk of increasing the injury,
In removing a coat, etc .. in a case of fractured arm t he uninjured arm sho ul d be drawn out first.
In putting 0l. a coat or shirt the injured arm should be put in first.
In burns and scalds nothing should ever be dragged off. A sharp pair of scissors should be used, and everything not adhering should be cut away. It anything adheres it should be left uti.til medical aid
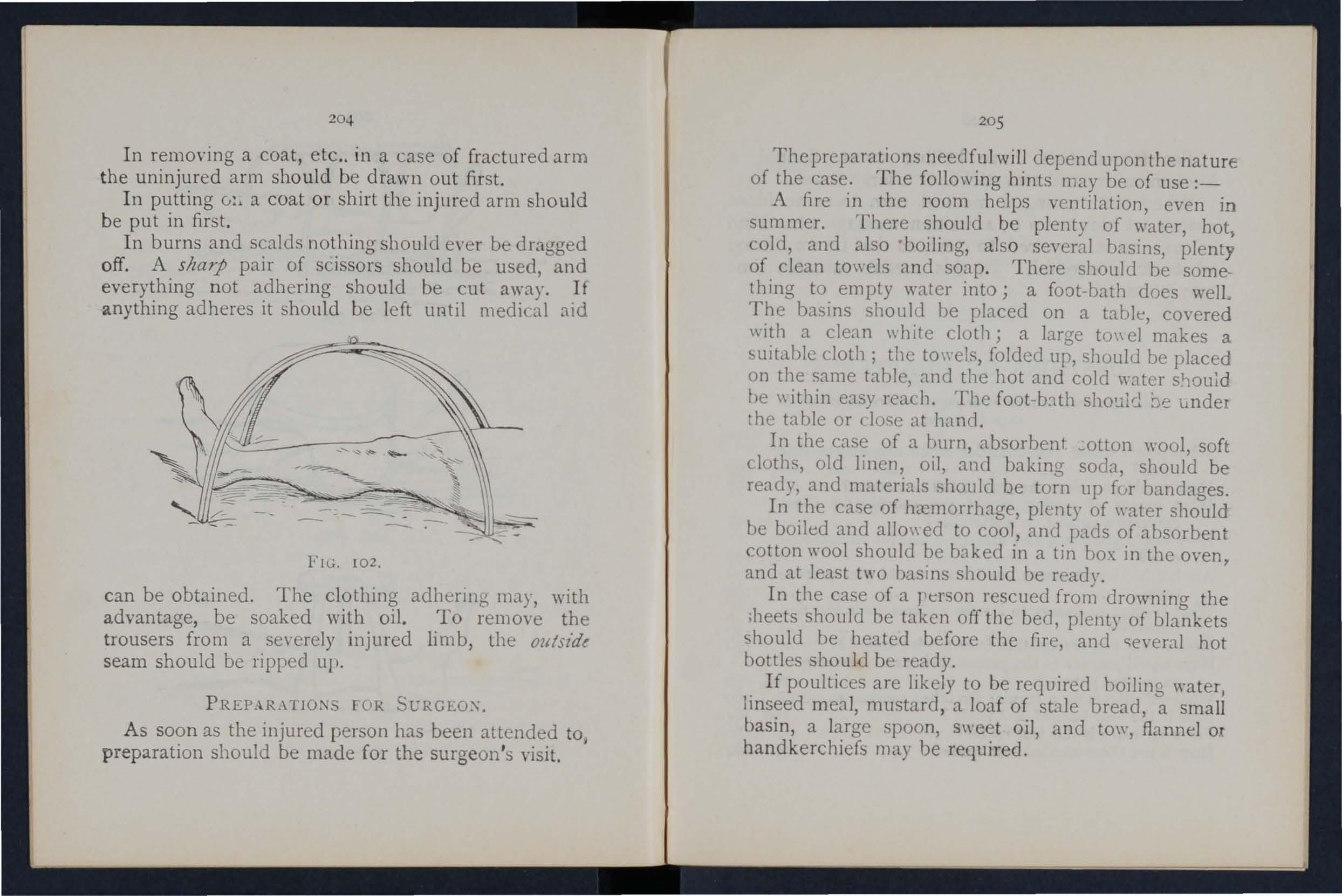
FIG. 102.
can be obtain ed . The clothin g adhering may, with advantage, be soaked with oil. To remove the trousers from a severely injured limb, th e outszde seam should be ripped up.
PREP_-\.RAllOr-.s FOR SURGEOX.
As soon as the injured person has been attended to; preparation should be made for the surgeon's visit.
20 5
The preparations needful will depend upon the nature of the case. The fo11o\\ ing hints may be of use :_
A fire in the room helps ventilation, even in sum mer. There should be plenty of water, hot, cold, and also boiling, also sev eral basins, plenty of clean towels and soap. There should be something to empty water into; a foot -bath does well. The basins shou ld be placed on a table, covered with a clean \\ h ite cloth; a large towel makes a suitable cloth; the towels, folded up, sllould be placed on the same table, and the hot and cold water be \\ithin easy reach. The foot -b:1 th be unde he table or dose at
In the case of a burn, absorbent wool, soft cloths, old linen, oil, and baking sod::!, should be ready, and materials should be torn up fur bandages.
In the case of hremorrhage, plenty of \yater should be boiled and allo\\ eel to coo), and pads of absorbent cotton wool shoulu be baked in a tin box in the oven, and at least two basll1s should be ready.
In the case of a person rescued from drowning the ,heets should be taken off the bed, plenty of blankets should be heated before the fire, and c;everal hot bottles hould b ready.
If poultices are likely to be required boiling water) linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, s\\'eet oil, and tow, flannel ox handkerchiefs may be required.
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large tmyel. When summoning a medical man to all accident always let him know by a written message what kind of case he is required to treat, so that he may bring whatever is needful. By this means valuable time may be saved.
The numerals i l1dicate the pages where the allswo S may be foulld.
What points would you consider when choosing a sick room? ...
How would you clear the way to the sick room?
What means of r esting would you provide for those carrying a patient on a stretcher? ... ... ."
How would you place and arrange a bed for an accident case? 197,
Are hot bottles necessary, and how would you prepare them?
\Vhat is often necessary to lay the sufferer on in the first instance?
How would you protect this from getting soiled?
How would you see to the proper lifting and carrying of
PAGK: an injured person? ". ... ... ... 198, 199
'What substitutes for a regular stretcher can you suggest? 200
How is the four-handed seat made? 160, 161
For what cases is this seat ustful ?... 160
Bow is the three-handed seat made? 162, 164
207
For what cases is this seat useful?
lIow is the two-handed seat made'?'
For what cases is this seat useful? ...
How can a single helper lift? '"
How can a single helper give suppott ?
How would you improvise a stretcher? '" ...
How many bearers are required for this stretcher?
How should a stretche r be carried upstairs? ...
How would you c.arry a patient upstairs 0.: '1 chair?
How would you lIft a patient from a stretcher tc a bed?
How should a bed be prepared for an injured person ;>
How shculd a draw sheet be made? ...
What would you place under the draw ...
\Vhat should be Jone with the suiled part or"a draw sheet?
\Vh at is the use of a " cradle" ?
In what ways maya cradle be
How would you remuve a coat ur shirt in the case of a fractured ar,lI? ... . ..
How would you put on a coal or shirt if the arm were injured? ... '" ... ... '"
In the case of a bad burn, what would you do with clothing [hat adhered to the patient? ..
How you remove trousers frum a severely injured 11mb. '" '" '" '" '"
What would you make [or the , VISIt. ... ... '" ...
\Vhat would you get rcady in the case burn';'
And what in the case of h[l?morrhaae? ... .
And w hat in the case of a person from .
\Vhat would you get ready for makina poultices? .
And for fomentations? I:>
What sort of a message \\ send" to a doctor?
208
IN DEX.

Abd omen
Pag-e III wound of 112
Acci'd ent case, preparation for 197
A cid , poisoning by 149, 15 [
Air, always necessary", 18
Alc ohol, caution as to smell of 130
Alcohol, poisoning by 1 34, 153
Alkalis, poioning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30 ,3 2
" sprained .. , 64
Anteriur tibial artery 93
Aorta 79
Apoplexy 13 2
Apparently dro\\ ned, to restore '.,
Ann, bone of fracture of
A;;u- lings
Arsenic, poisoning I)),
A rterial 139 28 52 39, 49 148 arrest of 74
" practising arrest of 79
" signs of 74
Arteries 70
" course of main 79
Artery, axillary .. 85
Artery, brachial. .. carotid ... dorsal of fout facial femoral ... iliac occipital plantar puplitlal radial subclavian til;ial temporal " ulnar
Arlificial rcspirat ion 121, 129,
Asphyxia
Alias
Alllicles ...
Axillary artery
AAis
Rack. bandage fur 159
Backl)one 23
Bandage, to apply 42 to fold 37 " to .. 37
Bandaging 155
Ikcl, lifting into... 201 " preparation of 202
Belladonna, poisoning b) 148
Bites of rabU anllnals 106
Blad":er 111,113
Brachial artery ... 86
Brain 117 compression of 13 2 " concussiun of 13 1
Breast-bone 26 " fracture of 48
Broad bandage , 37
Broken bone, sa rrac/llu.
Bronchial tuLes... .. II
Brooch-bone 30
Bruises 102
Burns 102
209
of the blood, 7e o rgans of Circulation of the blood, to induce Clayicle "
of Clothes, remoyal cf Coccyx
Capillaries 70, 72 95 3 1
Capillary hn:n1onhage ( 'apsule
acid, poi"vning II)" l'.uutid rtltt:ril's .. , " fr (lm
Carpu-; Carrying. I11ean ... of 160. 200 upstairs
artery of foot 9 yertebr::e .. , 2)
2 10 Page
D r ess, woman's, on fire .. . 105
Dr o wning 139
Ear ·c hannel , blood issuing from Ea r-passage, foreign body in Elbow, bandage for joint, fracture in98 110 159 volving
Electric shock
Emetic
Epilepsy . . ,
Esmarch's 53 14 2 148 , 149, ISO 13 2 bandage
Expiration lliangular
External carotid arterv
Eye, bandage fur ' foreign body in
Face, bones of
Facial artery
Fainting .. .
Femoral artery
" "digilal pressure at groin .. .
Femoral artery, tourniquet fur
Femur fracture ()f
" fracture of
Fingers, bandage for fracture of 37 120 80 ISS 109 22 81 134 89 89 90 30 56 30 60 159 55
Fireman's lift
First aid, meani ng of " sludent
Fi h-hook, embedded
FlexIOn ... at elbow
" at knee ...
Food, poisoning by Foot, bandage for bones uf
" crushed
Forearm, bones of " fracture of ...
Forehead, bandagc for ...
" h::elllorrhage from Foreign body in thc earpassabe ... in the eye " "in the nose
Four-handed seat
Fract ure, apparatus for treatmCl.t of causes of definilion of " general rules for treatment involving el bow joint of arm ... of breast-bone of carpus of collar - bane of cranium of finger
Page
F ractur e of forearm 54 of knee ·cap 58 of leg ... 6c of lower jaw .. , 44 of metacarpus 55 of metatarsus ... 62 of pelvis 56 d ribs... 46 of spine 45 o f lars us 62 of thigh-bone... 56 of toes. 62 signs and symptoms of 35 varieties of 34 108
Fungi, p oisoning by 153
General circulation 70 Granny knot 40 Green-stick fracture 35, 36 Gums, h::emorrhage from 97 f 'Lemo rrhage, arterial... 74 capillary... from gumc; 97 f(Om head and neck 80 from lower limbs ... S9 from lungs 97 from nose 96 from stomach 98
Hremorrhage from throat 9 7 from tongue 97 from tooth socket '" 97 from upper limbs... 84 internal ... 9S kinds of... 73
neck,arteriesof
Head bandage fur ISS injury to... 128, 131 " side of, bandage for ISS Heart 70 ., rate of contraction of 72 Heat-stroke 13E Hernia 114
IIip, bandage for 157 History, meaning of Ii Howard's method of artificial respi;ation I2t H";!n-=!'us
" fracture of 5:;: Hydrophobia 10E IIy terical fits 133
rage
Insensibi:ity, geneLll rules for treatment 128
Inspiration 120
Instep 30
Insulator... 142
Internal carotid artery fo
[nternal hLel110rrhage 95
Intestines, injury of II 3
In-roluntary muscle; 33
Jaw, angle of 2)
" lower 23
" "fracture uf 44
Joint, definition of 31
" injuries to... 109
Jugular vein 80
Kidneys I I I
" injury of 1 r 3
Knee, bandage for 15 9
Knee-cap 30
" fracture of 5
Knot for bandage of lower limb 42
Knots, reef and granny 40
Laborde's method of artificial respiration 126
Laburnum seeds, po;soning by... .. 148
Lacerated wound 7X
Large arm-sling 39
Laudanum, poisoning by J49
Leg, bones of 30
Leg, fract ure u{
Lifting and carrying " into bed
Ligaments
Lightning, effect ... of Limbs, 10\\ er
" uP . er
Lime in the eye
Lip', bleedlllg fn III
Litters
Liver " injury of Lower limbs
Lum bar "erte bILe Lungs hremorrhage
:-'Tarshall TTall's method of artificial re<.piratilln
1IrdiUl11 J..:;nd8ge ;,T et acarpus ., fracture of ;,Ietatarsus
" fracture of .. ;,Jiddle line of body }\fouth, blood is uing from ;\[ uscle. " ruptured ;,[uscular action ...
I'\arrow bandage eeelle, embedded
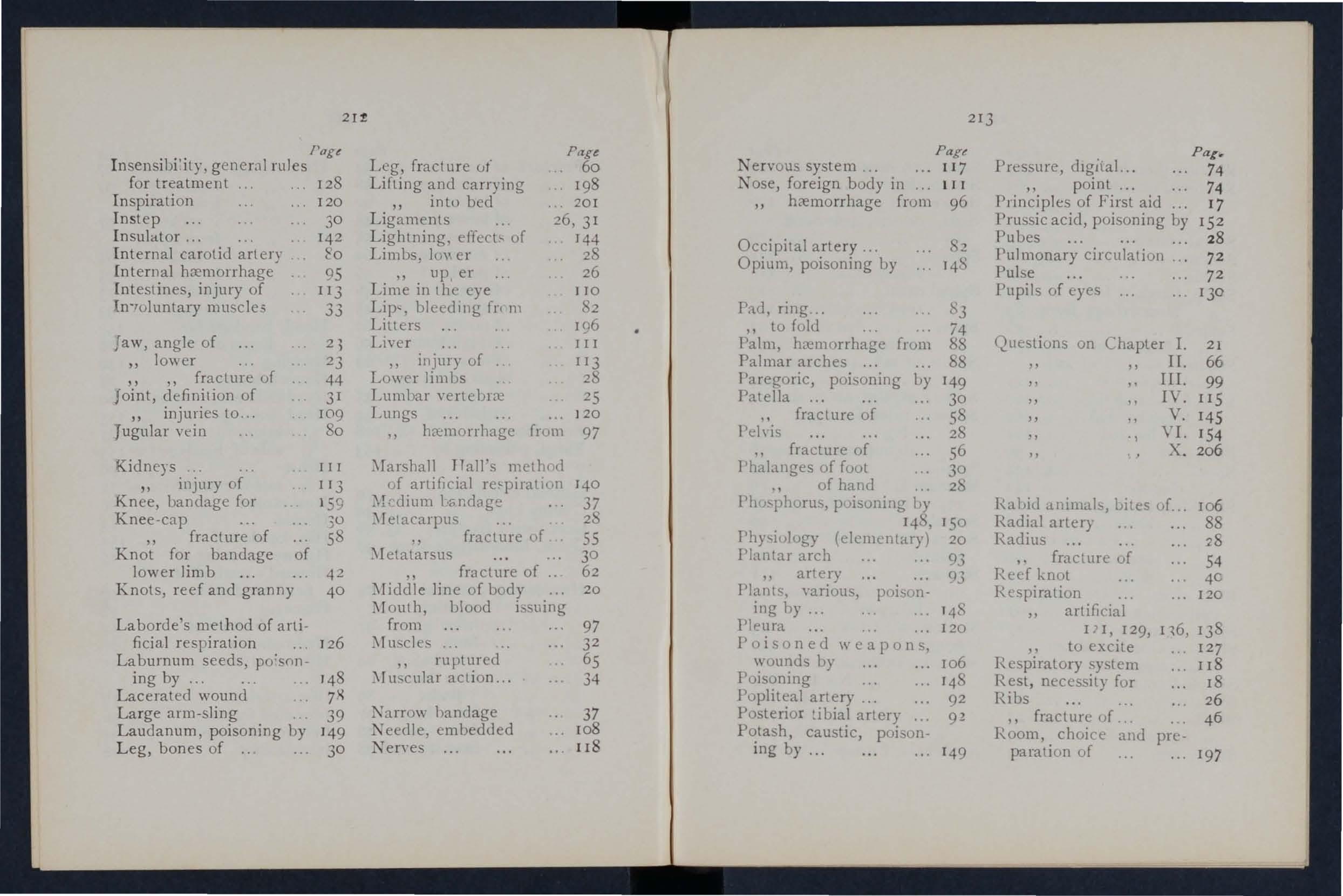
Nervous system ...
Nose, foreign body in h.-elllorrhage frum
Occipital artery ...
Opium, poisoning by
Pad, ring ... " to fold
Palm, hLemorrhage frum
Palmar arches ...
Paregoric, poisoning by Patella fracture of l'd\'is fracture of Phalanges of fuot ., of hand
Phu:-phurus, p'Jisoning hy 14S, Physiulugy (elementary)
Plantar arch " artery
Plants, "ariou'>, poisoning by ... Pleura
Poi son e d w cap 0 n s, wounds by
Poisoning
Popliteal artery .. .
Posterior artery
Potash, caustic, poisoning by...
Pressure, dIgital. .. " point
Principles of First aid
Prussic acid, poisoning by Pubes
Pulmonary circulation
Pulse
Pupils of eyes Questions on Chapter
animals, bites of. .. Radial artery
Radius fracture of Reef knot
Respiration artificial Ill, 129, 116, " to excite
Respiratory system
Rest, necessity fur Ribs " fracture uf ..
choice and preparation uf
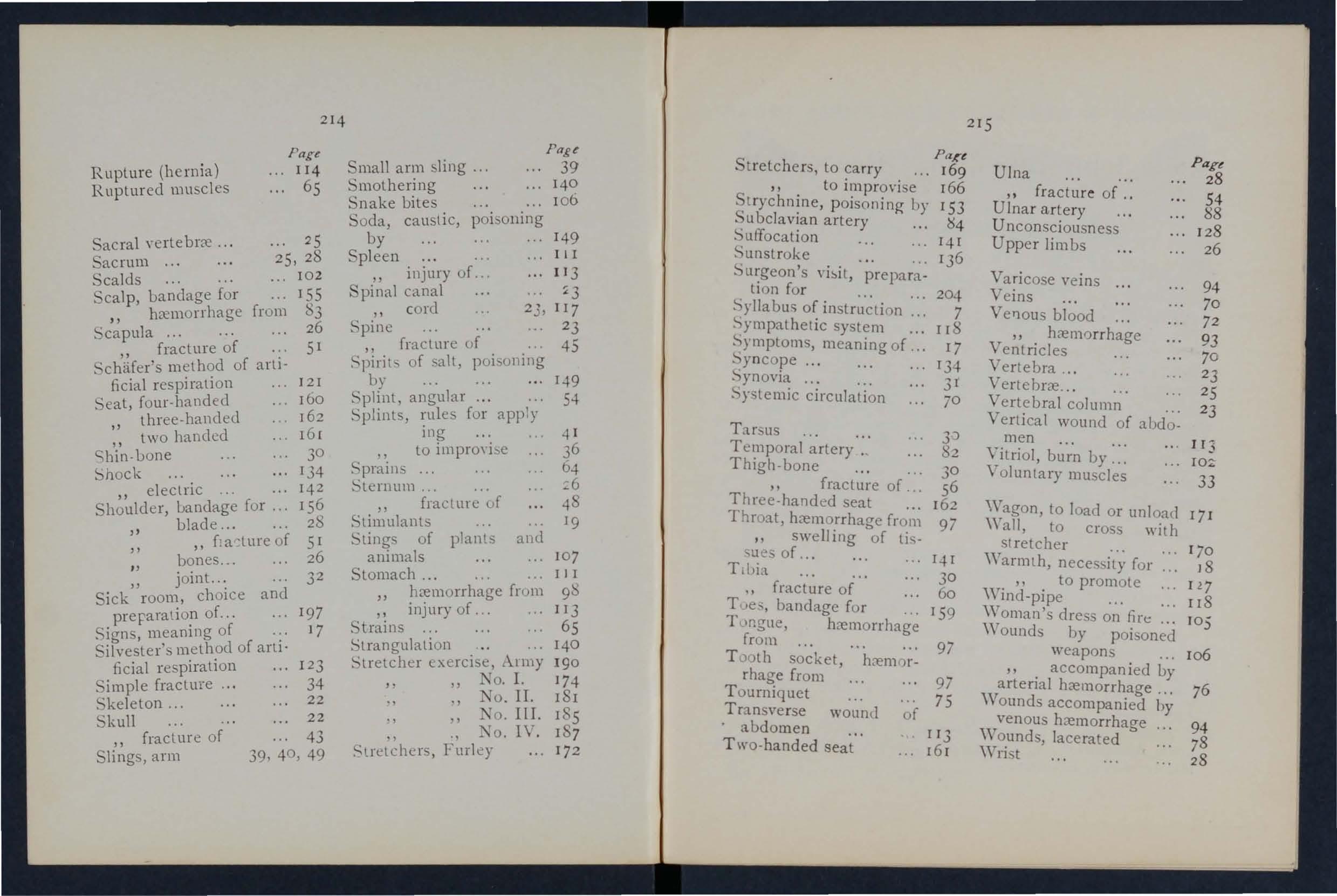
Rupture (hernia)
Ruptured muscles Page 1I4 65 214
Smothering
Snake bites
Sacral yerte brre ... acrum ...
Scalds... ... ... 25 25, 28 102 calp, uandage for hremorrhage ... 155 from 83 fracture of . ' chlfer's of artIficial respnal10n .. ,
Seat, four-handed three-handed " two handed h'i'n-uone
Shock . electnc ...
uandage for .. . blade...
" " [; a ·'ture of 5 I bones .. . 26 joint .. .
Sick" rooll:, choice and preraratlO? of... ... 197
Signs meaDlng of .:. 17 . meth.od of arl!o ficial respiratIOn 1 2 3 3 2
Simple fracture ...
Skeleton... 22
Skull ... ... 43 " fracture of
Slings, arm 39, 40, 49 Small ann sling ...
Soda, caustic, poisoning by 149
Spleen.:....
InJury of... II3 canal :t 3 " cord 23,117
Spine ...... 23 fracture of 45 of salt, by ... 149
Splint angular... 1. 54
Splints, rules [or app') ing to impro\'ie
Sternum ... ... " fractme of Stimulants
Slings of plants and animals
Stomach ... ... . .. " from " injury of ...
Strains
Strangulation . " .. .
Stretcher exerCIse, A.rmy No. 1. TO . II.
Stretchers, to carry 169 " to improvise 166 t rychnine, poisoning by 153 .'ubclavian artery
Suffocation r -+ I
Sunslroke 13 6
Surgeon's visit, preparation for 2 0 4 of instruction ... 7 system ... 118 meaning of 17 yncope ... 1343 1 circulation 70 Tarsus 3'::>
Temporal artery. 82 Thigh-bone 30 " fracture of... 56 Three-hand ed seat 162 Throat, h::emorrhage from 97 " swell ing of li..,ues of... 141 Ttl)i .\ 30 ., fracture of 60 bandage for 159 T Ingll , h::emorrhage from 97 T )o lh socket, h::emorrhage from 97 Tourniq uet 75
wount! of abdomen 113
cles
to load or unload 17 J "'all, to cros with
necesily for J8
by arterial h::emorrhage ... 76 ,Vounds accompanied by venous h::emorrhage 94
Thi Price List, which is subjecl to revision from time to time, has been compiled with a view to assist I11Lmhers of the Association and others in the purchase of the necessary equipment for corps and divisions of the Brigade, ambulance stations, classes and first aid and nursing" ork generally.
A complete and reliable Ambulance Equipment is an aClual necessity, and experience has proved that employers of labour and others interested in the district readily suhscribe for the purchase of such appliances. Col:ecting cards, stating the purposes for which subscriptions are requin:c1, "ill be . upplied gratuitously on to t 1.1e I I c.ad Office uf
As 'ociation, where also any 1I1furmatlUn w1lh regard to 1lS work can be obtained.
Stores of the value of lOS. or upwards \lill l)e sent carriage paid to a ny part of the United Kingdom.
Owi ng to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhered to.
Quotations will he furnished for articles relating to Amhulance Nursing and l1ygiene, not mentioned in this list.
Orders and correspondence should he addre<;secl to the "I. John A mbulance Association, St. John's Gate, ClerkeJ1\\ell, London, E.C.
Remittances should be made payable to the l. John Am buance Association, and crossed "London County and \\' estmi nste r Bank, Lothbury."
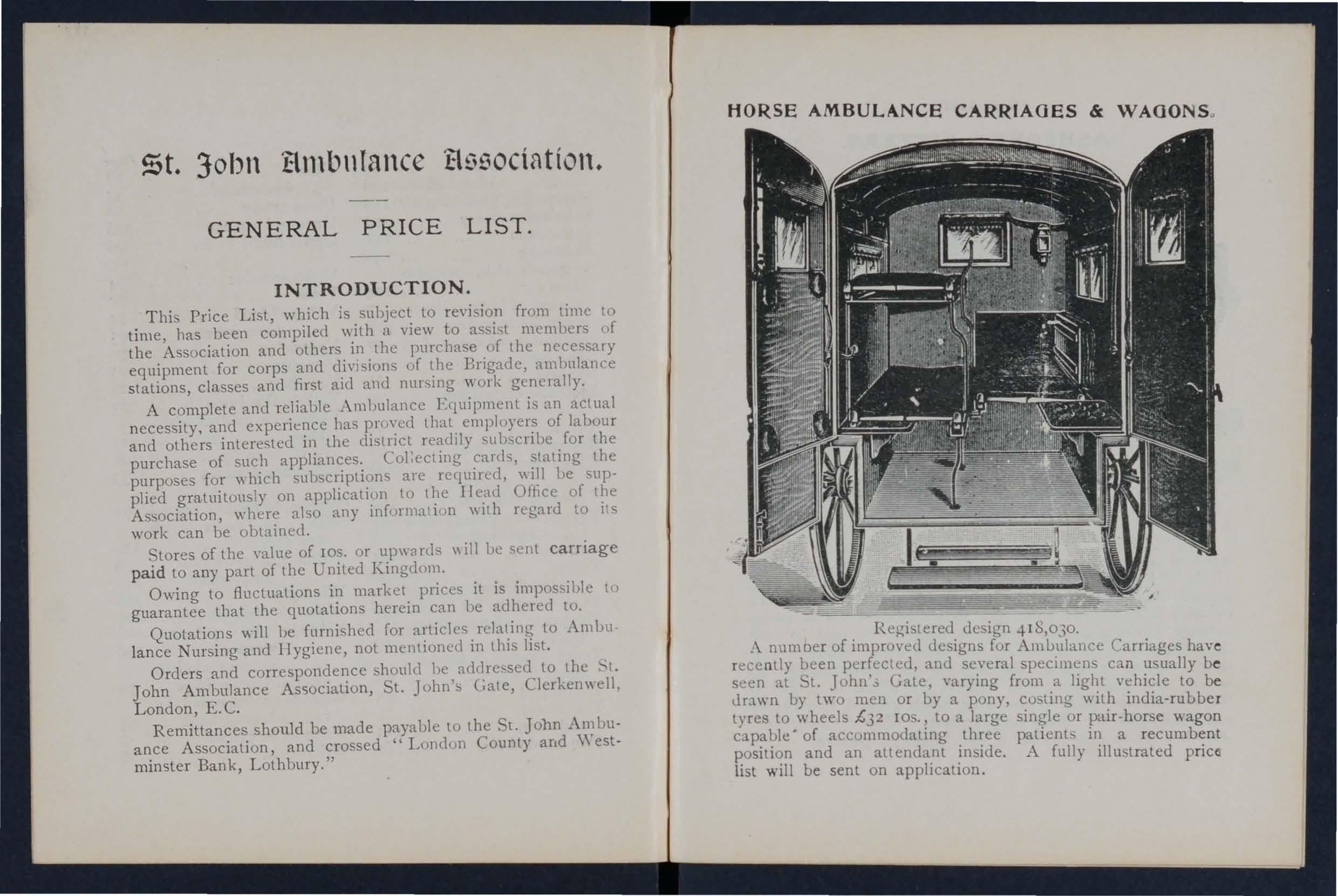
Registered design 418,030.
.\ nUl110er of improved designs for Ambulance Carriages hav e rece ntly been perfected, and several specimens can usually be seen at Sl. John',; Gate, varying from a light vehicle to be JrJ.wn by two men or by a pony, co ting with india-rubbe r tyres to wheels £32 10 . , to a large single or pair-horse wagon capable' of accommodating three patients in a recumb e nt position and an attendant inside. A fully illu:;trated price. list will be sent on application.
n 0""""0 ::e if if e! .. 5' :' if t:l 0 B ::l' ::e ;:; ;:;r ;:;r g. (l) 5:?-' ;::rJQ;: (l) 2.. (l) ('tI Cb ::
if ::::
r- ==' 0 (b 0' ?f ...,. g- ;::;- ;:;r(fq 8. ;''<u 2 2.. ;. (fl ;. I" (flu 2. .;
o ro pl "'""""'1(1) (t) """: ::s _0,.- p.:l s:: r. ::J ...,. ...,. B ::J ,. P> n ::n fll ."0..... no f1> 1;; ::J ?f.0 0-::;-
o 5. (fl ;:;r (l) u" }; s;l .....,:;! ::.$' ::' 9 P' (b" P' r- (J) s: \0 ;:;r"O ni ::l (1Q ::l ;:;r Ul O-;:;r _ :: (1;' 0 u s: P> ;:;-: g, >-rj::lg
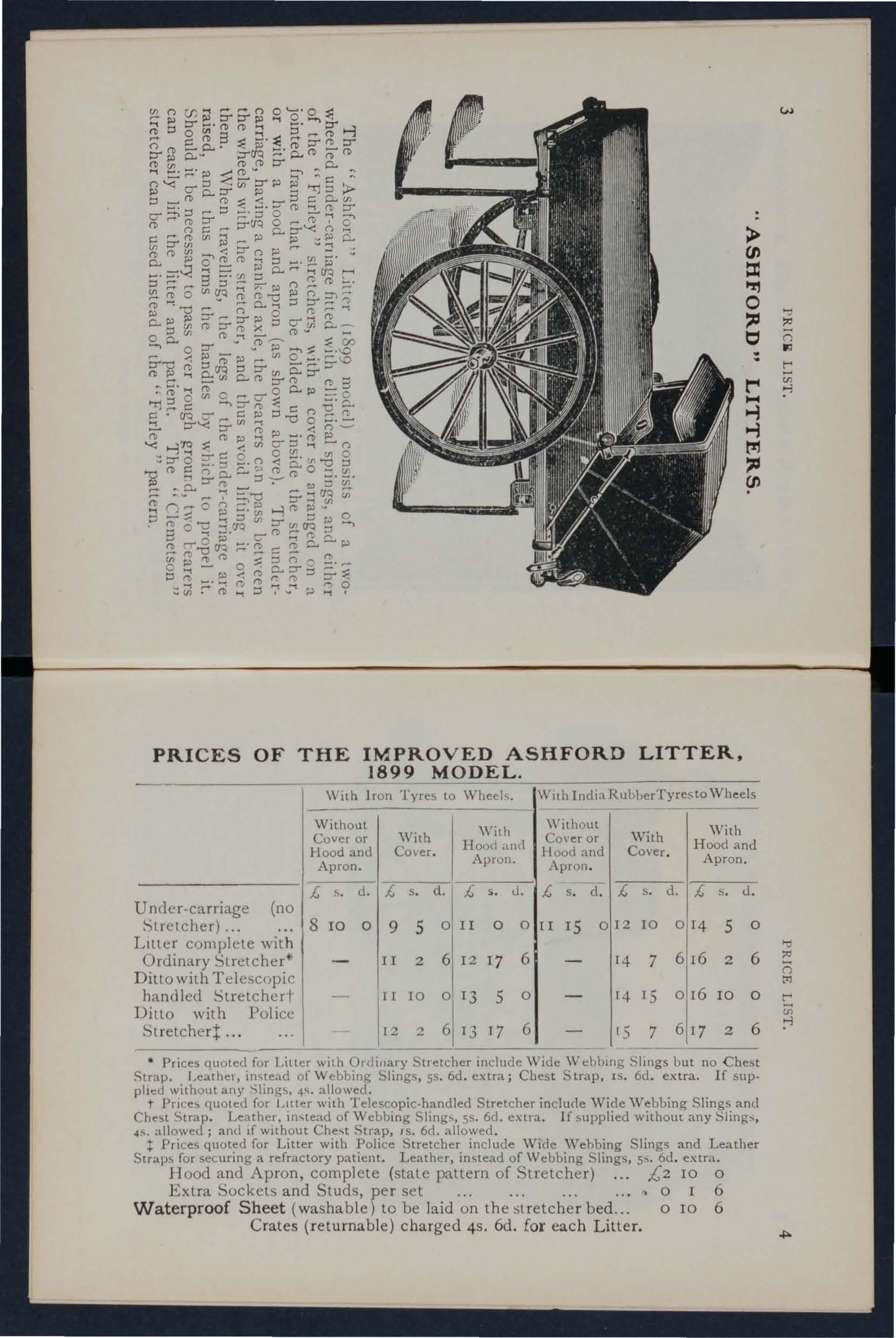
189 9
With Iron Tyres to Wheels. IWllh IndiaRuhberTyresto \Vhcels WithoLlt Cover or Hood and Apron. With Cover. With Hood and Apron.
U ncler·carriage (no
Liller complete with Ordinary Stretcher*
Ditto with Telescopic handled Stretched-
Ditto with Police Stretchert...
Prices quoted for Litler with Ordinary Stretcher include \\ ide \\T cbblllg Slings but no Chest Strap. Leathel, in'tead of Webbing Slings, 55. 6d. extra; Chest S lrap. IS. 6d. extra. If sup· piled wilhout any Slings. 4S. allowed.
t for Liller with Telescopic·handled Stretcher include \Vide \Vebbing Slings and Strap. Leather, IOslead of Webbing Slings, 5S. 6d. extra. If supplied without any Slings, 4S. allowed; and If wIthout Chest Strap, 15. 6d. allowed.
t Prices quoted for Litter with Police Stretcher include Wide '''ebbing Slings and Leather Straps for securing a refractory patient. Leather, instead of Webbing Slings, 6d. extra. Hood and Apron, complete (state pattern of Stretcher) £2 10 0
Extra Sockets and Studs, per set 0 I 6
Waterproof Sheet (washable) to be laid on the stretcher bed... 0 IO 6
Crates (returnable) charged 4s. 6d. for each L itte r.
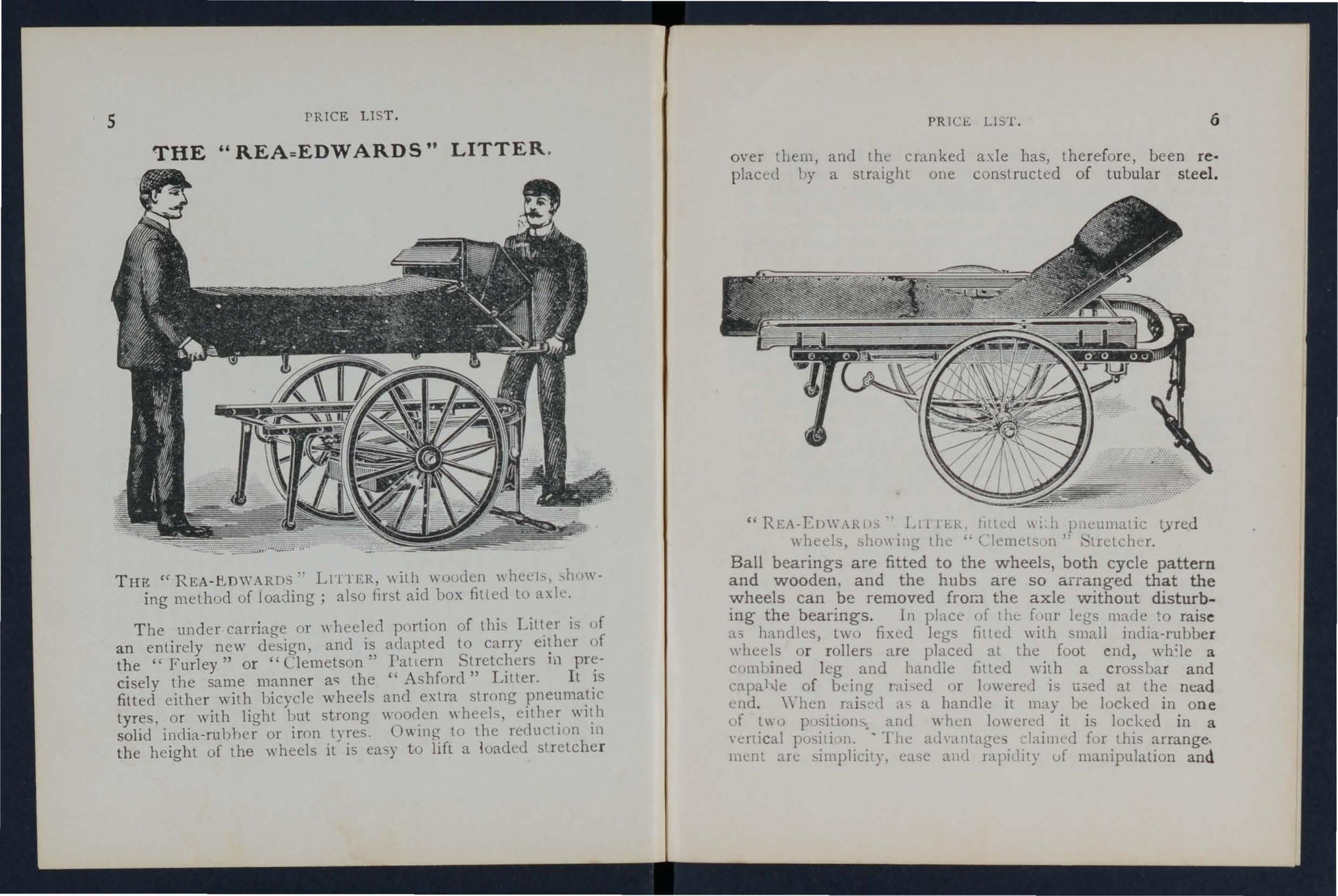
THE rc REA - ./:!,DWARDS·· LIlll£R, \\ ith \\ Duden wheels. "howing method of loading; also first aid box filled to a\1c.
The under carriage or \\ heeled portion of this is of an entirely new design, and is acLlpted to carry of the "Furley" or "Clemetson" Pall ern 111 cisely the same manner as the "Ashford" LIller. It:5 fitted eithe r with bicycle wheels and extra strong tyres. o r with light but strong wheels, solid india-rubher or iron tyres. Ov.lI1g to the reduCIlnn In the height of the wheels it is ea y to lift a loaded stretche r
PRICE LIS 1. 6
ove: them, and the cranked a\le has, therefore, been reo placl:d by a straight one constructed of tubular steel.
"REA-ED\\'.\Rlh" Lt '11 ER. hllLl! \\: h pnLlllnaIic tyred whcds. shc)\\ illg tIlL .. Clemels'JI1" 'tfetcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden. and the hubs are so arranged that the wheels can be removed froI7l the axle without disturbing the bearings. In phce of the [uur legs made to raise h handles, lWll fixed legs filled \dIh small india-rubber wheels or rollers are placed at the fool end, whqe a cfll11lJined leg and handle Jllled with a crossbar and capahle of IJLing rai,,,eo or )c}\\'ereo is li.;ed at the nead end , \\'hen raised ::t-.; a handle it may be locked in one o f t\\ 0 pt)sition, and wh..:n lowered it is locked in a \'ertical position. - The ath',tlltages [ur this arrange. mull .,re simplicity. l:L1se alld rapidllY uf manipulation and
the facility afforded by the two fixed leg for raising the litter if necessary, on to the pavement. The que»tion of baladce has been carefully studied, and the stretcher is shifted forward so that the 111iddle of it is several inches in front of the axle, a perfect balance when the stretcher is in a horizontal po ition being thus obtained, and consequently there is no weight on the hands of the person propt IIi ng the litter.
The pneumatic tyred wheels are strongly recommended in cases where the small amount of care necessary to keep them inflated can be given, as the comfort to the pat.ient :lI:d case in propulsion are increased. beyond all companson any litter yet produced. It Wlll be noted that the p,l'Ices. are considerably lower than those of the ".\shfurd ' Lltter, and the following are given as examples, but o\\ing to the vast number of combinations thal can be made \I ith the different stretchers and coverings, it is imp ssible within reasonable limits to set out quotations for the whule of them, but these may be calculated by adding together the prices of the under-carriage, stretcher selected, and houu and apron or cOYer, see pages 4 and 8 to 11.
Under-carriage only, either with pneumatic tyrell cycle wheels or solid rubber tyred wooden wheels, £10.
Litter complete ",ith ordinary stretcher (no slings or chest strap) and hood and apron, iLl- 3S. 6d. .
Ditto with Telescopic lIandled Stretcher (\\Ith chest strap) and hood and apron, £14 I IS.
H with iron tyred wheels prices are £2 less.
The lowest priced litter complete is fitled with iron lyred wooden wheels, OIclinary stretcher (no slings or chest strap) and cover. Price £ 10 8s. (d.
Hand brake, which acts automatically \\ hen the litter is at rp-st, extra £r 105.
When ordering please state which wheels are required.
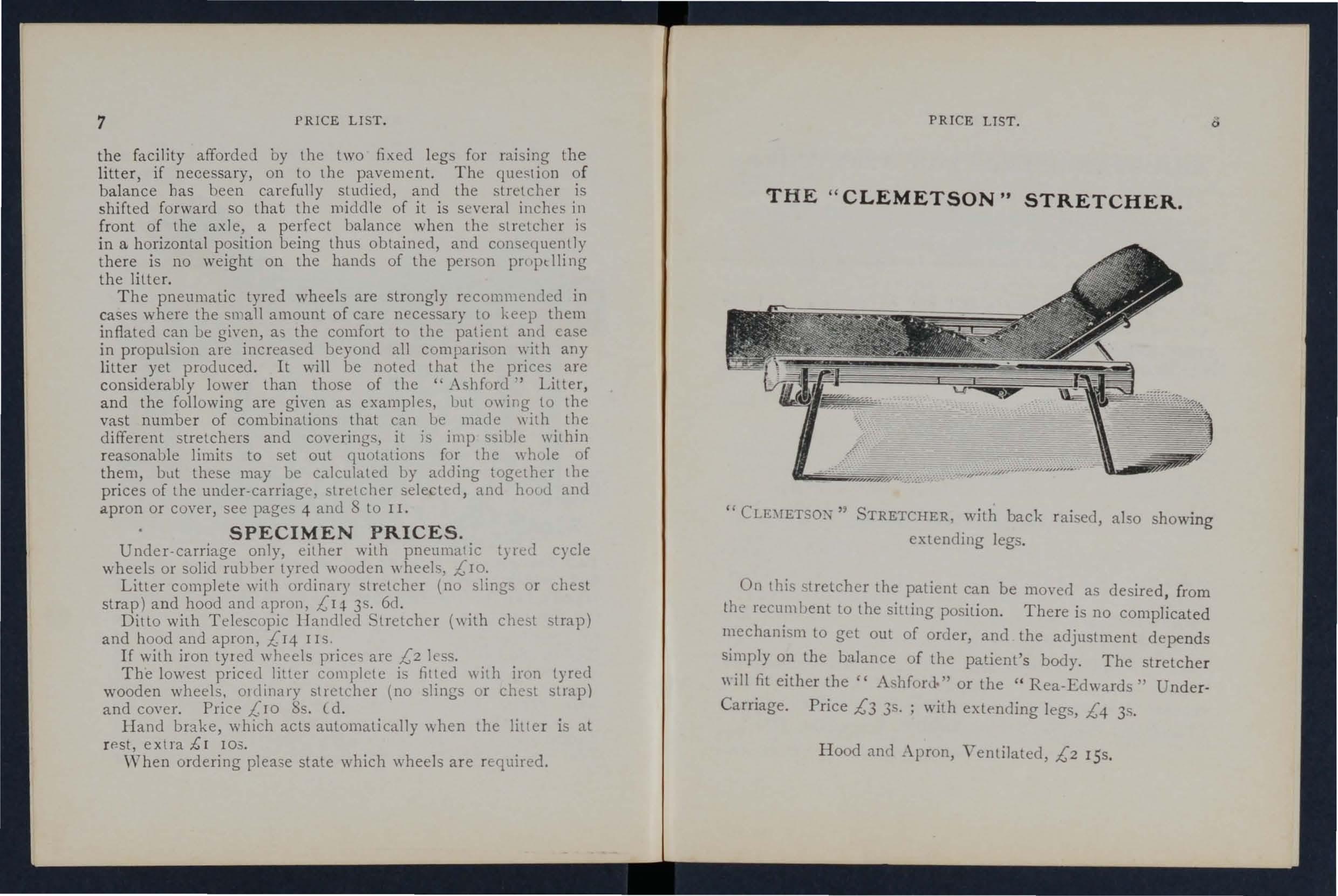
" STRETCHER, with back raised, also showing extending legs.
On this stretcher the patient can be moved as desired, from tht> recumbent to the sitting position. There is no complicated mechanism to get out of order, and the adjustment depends simply on the balance of the patient's body. The stretcher will fit either the" AshrorJ" or the" Rea-Edward!;" UnderCarriage, Price £3 3s. ; with legs, £4 3s.
Hood and _\pron, Ventilated, £2 I5s.
PRICI'.
. I . I pendent of anll add!-
Primarily these legs, \\ hIe 1 a re m.l e. I' \ t facilitate t'onal to the ordinary foot \\ heels, ale !I1tel1l Cl 0 .
1 • f stt'etcher in a railway compartment, 111 th e carna<Te 0 .. l' t d
<>. I ' \\ ould he lowered and a< JllS e whi ch case two on one Sj{ t; • I the by a teleocopic arrangement to the proper height, so t the
• t 'heels on one side \\ ollid rest on the SLat, aLl 100 \\ 1 Id' t on the floor. d' tile le<Ts on the other Sl( e wou I es . a Jusa) 0 h t tcher as rCCJllHed.
Th e four leas may be llSe(\ to raise t e S Ie
.0 till')' arc fulded up immediately un(kr the When not!l1 use , pol es of the stretcher.
Pric e per set of fOll r £ r.
, d 1 I the a:-..le of the c. Rea-Edwards" litter, To be canle )e ow < from which it is easily c1etacbal)le.
S f S lints 12 Trian<Tlllar Halldagec;, 12 Contents :-. et 0 • p . , 0 \Y 11 Forie Roller Bandages, 21-lb. packets cach Cot tun. ,00 an ! ) h . f " s h .nlfe " 07. cae Lint .t\rlhesi\-e Pay 0 • CIS. or., , - 'I ' d "D P C c:,al \ olatl e, an 01 ' Oil Tinct. Eucalyptu<' '), . ., , . . lYe , \f. Class h.ldney- S irits Ethe r Com]1 , , GJadnatecl - easure ),' . 1 P . B' 6 Tampons for \\aShlOg \\oune 5, shaped Dress1I1g as 111 , T
T . t p'ns S'lfd)" Nceclks, Thread and ape. ourmque I " l'ri'ce £2.
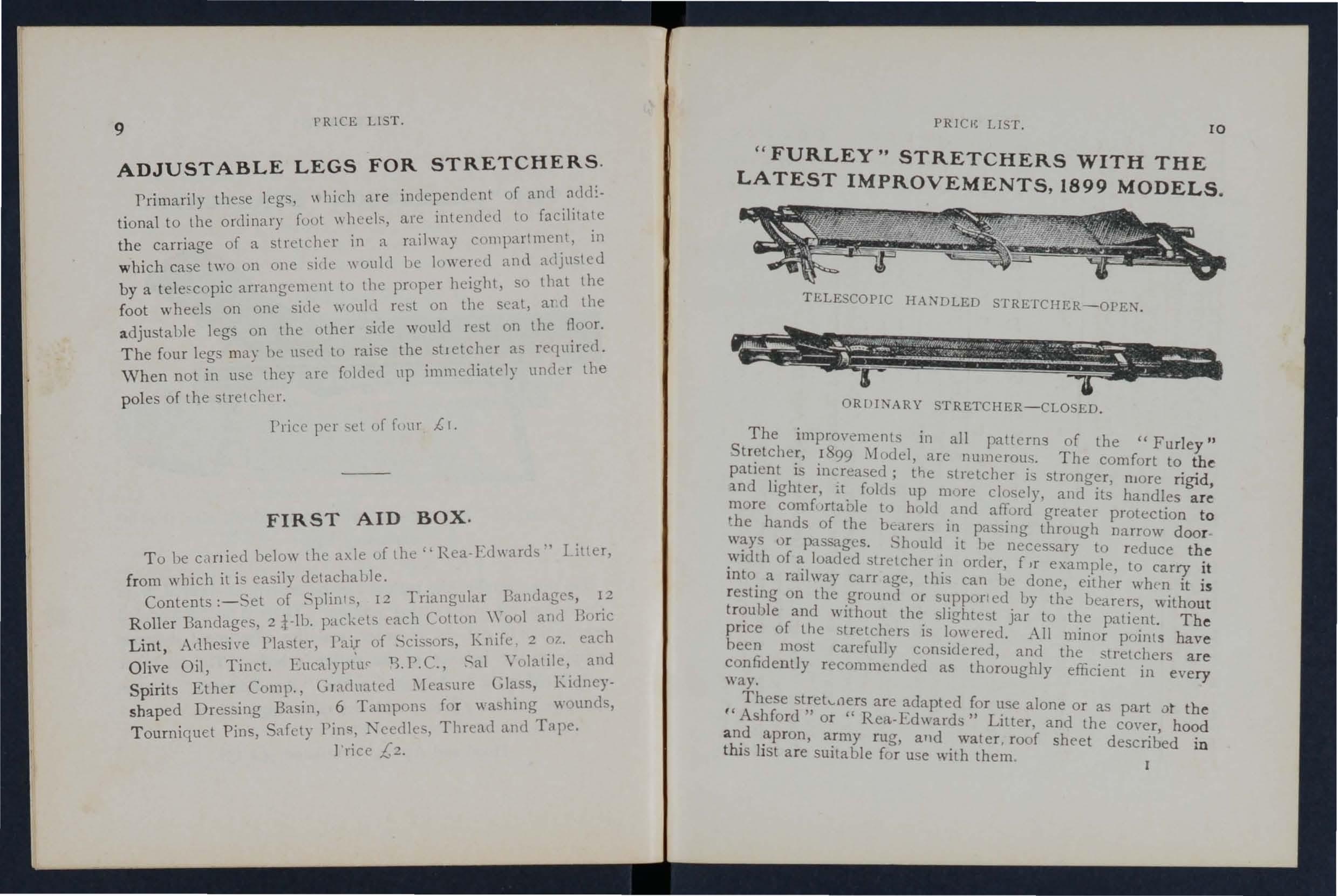
TELESCOPIC HANDLED STRETCHER-OPEN.
ORflDIARY STRETCHER-CLOSED.
The improvements in all patterns of the "Furley " St retcher, 1899 l\lodel, are numerous. The comfort to the patient is increased; the stretcher is stronger, nlOre rigid, and lighter, it folds up mure closely, and its handles are more comfurtable to hold and affurd greater protection to the hands of the ucilrers in passing through narrow door ways or passages. Should it be necessary to reduce the width of a loaded stretcher in order, fIr example, to carry it into a railway carr age, thi - can ue done, either when it is resting on the ground or supporl ed by the bearers, witho ut trouble and without the slightest jar to the patient. The price of the stretchers is lowered. All minor points have been most carefully considered, and the stretchers are confidently recommended as thoroughly efficient in eve ry way.
These strekners are adapted for use alone or as part 0t the I C Ashford" or "Rea-Edwards" Litter, and the co\-er, hood a nd apron, army rug, and water. roof sheet described in thi s list are suitable for use with them
PRICES OF THE "FURLEY" STRETCHERS. WITH THE LATEST IMPROVEMENTS (1899 MODELS ).
N.B.-The prices of the Standard Models are shown in heavy type. ( Without Slings or Chest
Strap.
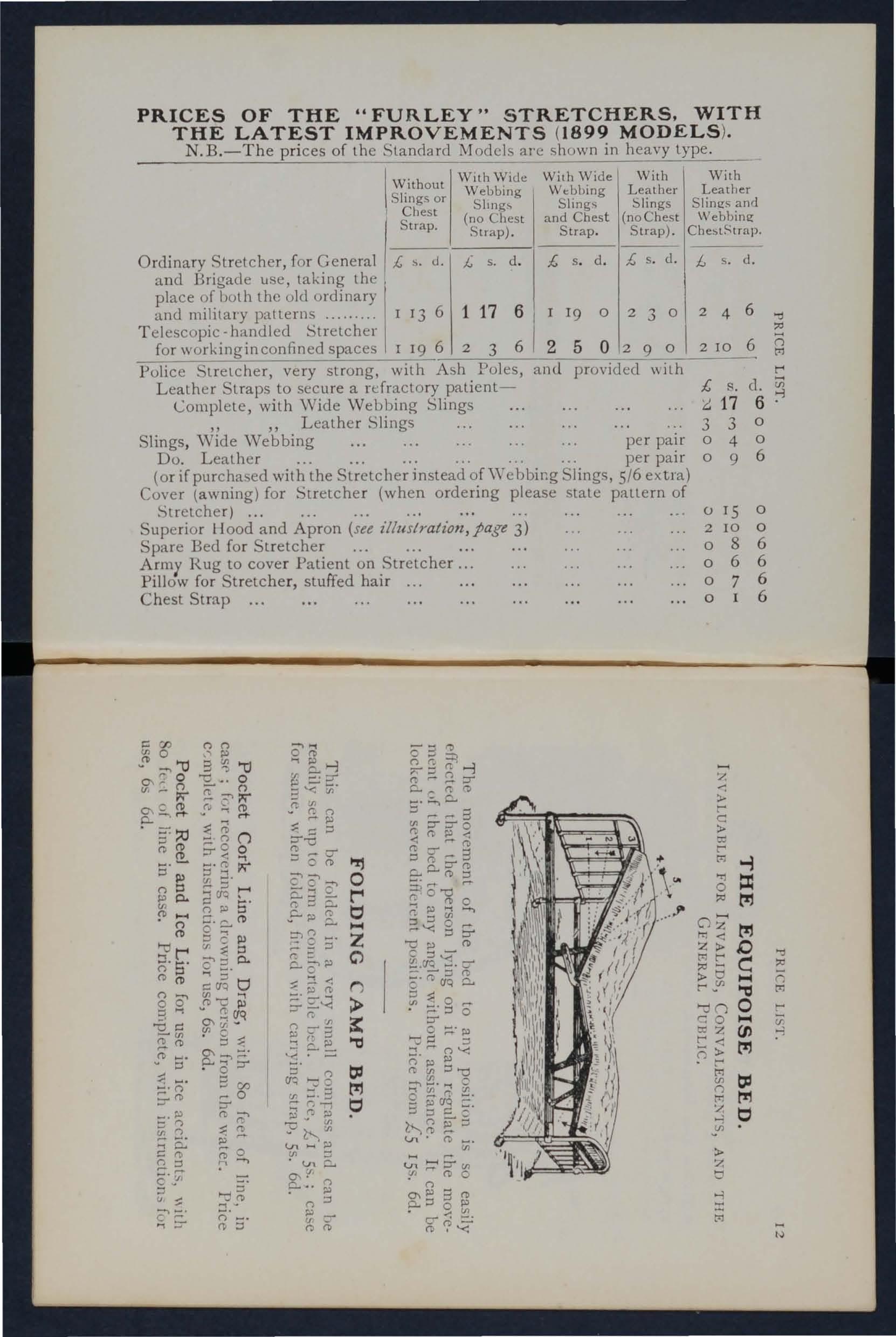
WithWlc.1e Webbing (no Chest Strap).
With Wide With I With Wt:bbing Leather Leather Slings !::>Iings Slings and and Chest (no Chest Webbing Strap Strap). Che5tStrap.
IOrdinary Stretcher, for General ;; s.
and Brigade use, taking the place of both the old ordinary and military patterns 1
Telescopic -handled Stretcher for workinginconfined spaces
Police Stretcher, very strong, with Ash Poles, and provided
Leather Straps to secure a refractory patient-
Complete, with \Vide
Slings , Wide Webbing
Do. Leather
(or if purchased with the Stretcher instead ofWebbir.g Slings, 5/6 extra)
Cover (awning) for Stretcher (when ordering please state pattern of Stretcher) ...
Superior Hood and Apron (see illustration, page 3)
Spare Bed for Stretcher
Army Rug to cover Patient on Stretcher ...
Pillow for St retche r, stuffed hair
Chest Strap
For use in mines, ships' holds, elc., to secure a patient on a stretcher (see illuslralion), which can then be placed in an upright p('\sition . rrice £r 5--.
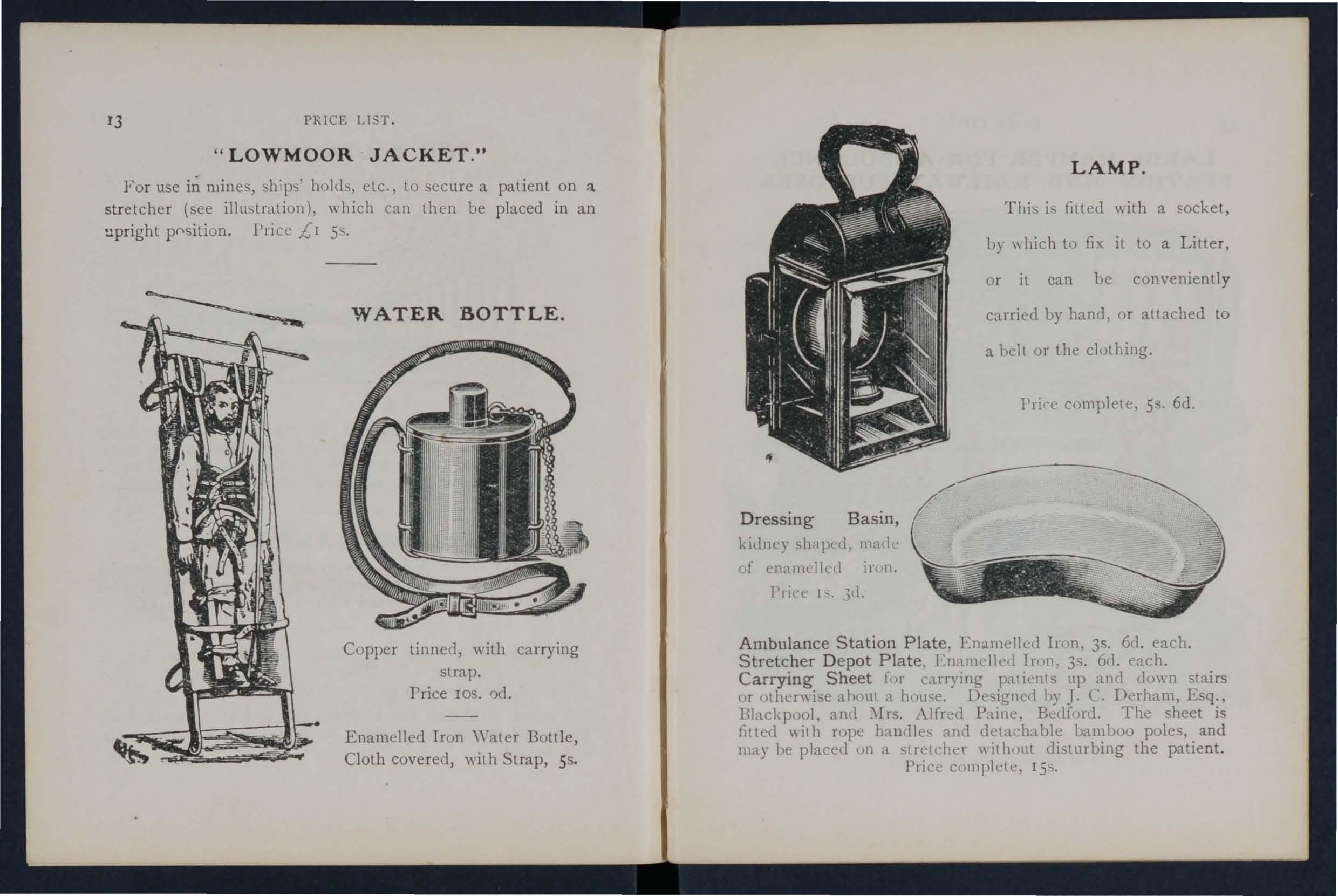
Copper tinned, with carrying strap. rrice 105. ')d.
Enamelled Iron \Vater Bottle, Cloth covered, with Strap, 55.
This i' filled wilh a socket, by \\ hich to fix il to a Litter, or il can be conveniently carried by hand, Qr attached to a hell or the clothing.
Pri cc complete, 5s. 6d.
Dressing Basin, kltll1l') sh lpt:d. lllad uf enan1Lllcd irnn.
I'rice I ' . 3d.
Ambulance Station Plate. Enamelled Iron. 35. 6d. each. Stretcher Depot Plate. Enamelled 1nm. 35. 6d. each.
Carrying Sheet for can) ing patients up and dmYl1 stairs or otherwise ahnlll a house. Designccl hy J. . Derham, Esq., Blackpool, al1(1 \Irs. Alfre<1 Paine. Bedford. The sheet is filted ,\jth rope hawlles and detachable bamboo poles, and may be placed on a stretcher withoul uistllrbing the patient. Price c,)mplcte. 15<;.
1 Set of Cane Splints.
1 Elastic Band Tourniquet.
; lb. Carbolic '\ Cotton Wool ... lIn Tin JCases . lb. Boric Lint ..
1 Roll Plaster.
20 Roller Bandages, assorted.
1 doz. Triangular Bandages.
3 Pieces Tape.
-t oz. Sal Volatile.
4 oz. Bicarbonate of Soda,.
4 oz. of Olive Oil.
4 oz. Spirit Ether Compo
i lb. Tin PO\\ clereo Boric Acid.
-+ oz. Tincture Eucalyptus B.P.C.
1 pair Pean's Forceps.
I pair I Knife. 12 Surgeon's Needles,
I packet each Safd}' ann Pbin Pins.
oz. Carbo'ised Chinese Twist.
oz. Silkworm Gut.
I reel each Black a'1d \\'hite
Sewing Thread.
Kidney-shaped Ba Ill, I Stopper Loosener.
I Graduated :\Ieasure.
I cake 20 per cent Carb:.>li Soap.
I Nail Brush.
3 Empty 8 oz. Bouks,
Price complete, £4
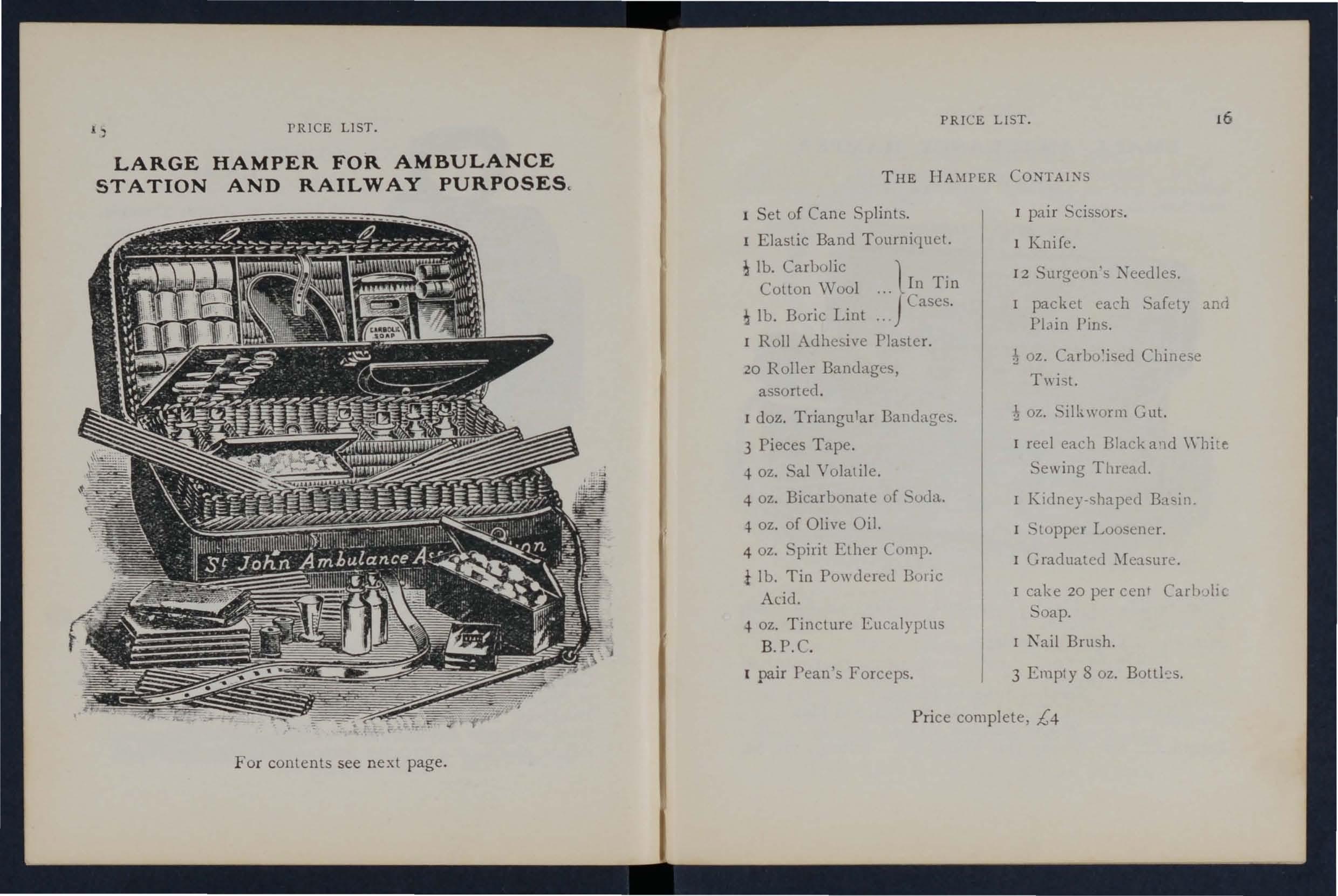
For contents see next page.
With waterproof cover and strap, for use in factories, colli eries, stations, and larhe works, as well as for parochial a.nd domestic use .
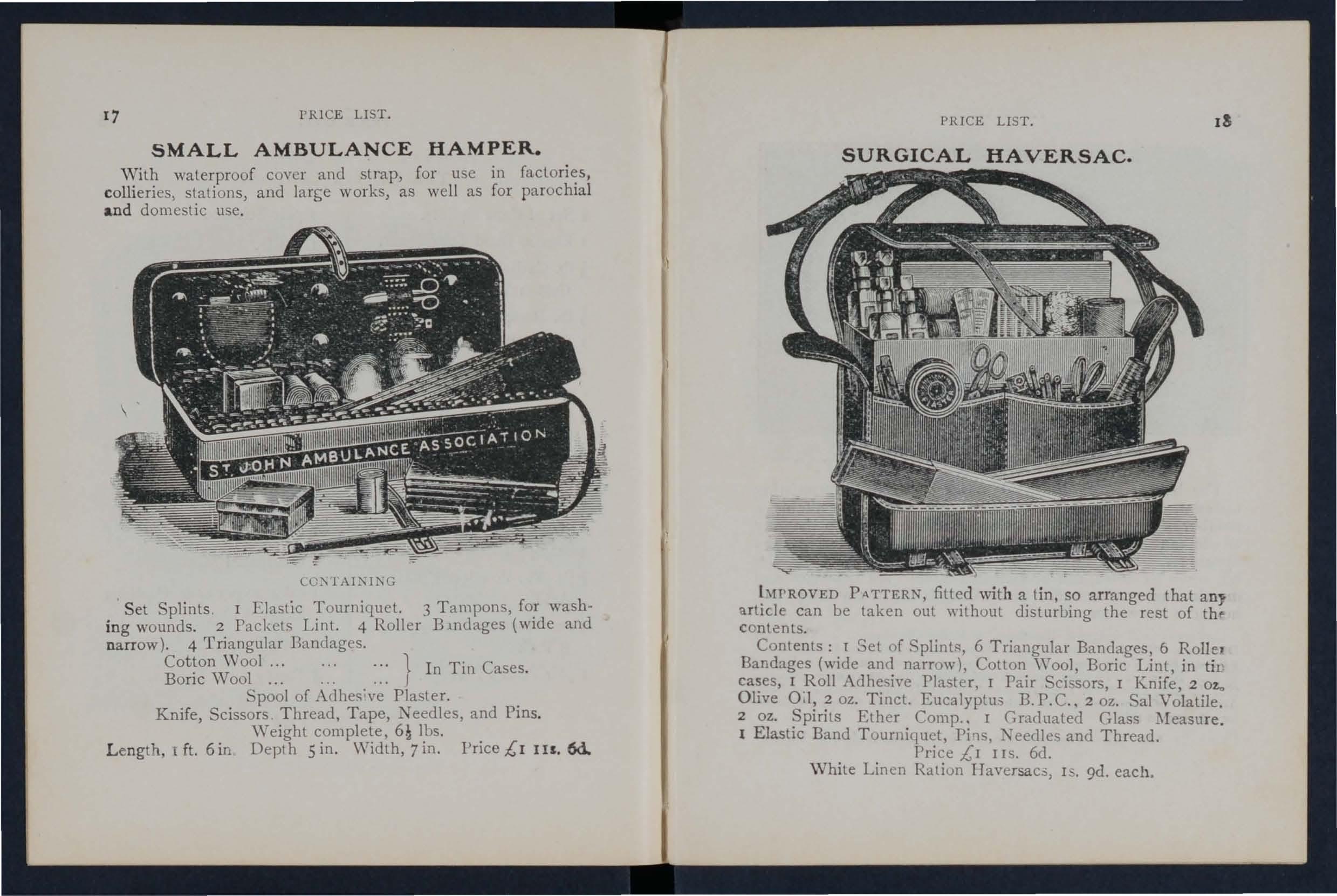
LO:\lAIl\Il\G
S et Splints. I Elastic Tourniquet. 3 Tampons, fO.r washing wounds. 2 Packets Lint. 4 Roller Bmdages (wIde and narrow). 4 Triangular Bandages.
Cotton Wool... ... 1 In Tin Cases. Boric Wool .. . .. . J
Spool of Adhes;ve Plaster. . Knife, Scissors Thread, Tape, eedles, and Pms.
Weight complete, 6§ lbs.
Length . 1 ft. 6 in Depth 5 in. Width, 7 in. Price £1 IU 6d.
hl1'ROVED PATTERN, filted with a tin. so arranged that any artiGle can be taken out without dislurbing the rest of thf' contents.
Contents: I Sel of SplintR, 6 Triangular Bandages, 6 Rolle, Bandages (wide and narrow), Cotlon 'Vool, Boric Lint, in tit cases, 1 Roll Adhesi,-e PIa ter, I Pair Scissors, I Knife, 2 02." Olive 0;1, 2 oz. Tinct. Eucalyptus B. P.C .. 2 oz. Sal Volatile.
2 oz. Spirits Ether Comp.. I Graduated Glass I Elastic Band Tourniquet, Pi'1s, and Thread. Price £1 JIs. 6d. \Vhite Linen Ration Haversac5, IS. 9d. each.
(JJRESSlNGS AND BANDAGES COMPRESSED).
Sf.. jC/1lJ RmIJlJlan(t R$S(K/i1(/on. Price Is. 6d.
51. jO/Jn'$ (ialt, B), Post ,.;; 8d CUrktfJU-OfIl. rondon. E.e. ' . •
fhl: box is of "nod cm'creel \\ i' h clamp· resisting n1.ltl'riaL and is fitted \\ilh a lock and key. It cOlltains a number of practical amhulance appliances arranged so that any article can he \\ithdra\\n or replaced "ilhOlll di..,lurbing the remainder. Being filted \\ilh a handle it is pnrlahle. and the lid, when let clown, can be a<; a t'lhle. All IX1.Ildages and dressing-sare compressed. Site-Length 16:1 in.; in.; height in. without handle.
Cvntenls: 4 Trian,!?;ular Band:lge<. 6 Roller 4 First Aid Dre"sing<;, 6 Small Packeh of Cvll,)ll \\ 0<11. 6 Small Pa ckch of Boric Lint.
I Band Tourniquet, Glas<, I tin Lox cOnlaining a Roll of Plaster, BOflc Lint Patches, Sci,-;ors ami Pins, T tray cOnlaining 3 hottles (Sal Volatile, Tincture of and Olive Oil) ancl a Dredger of Boric Acid, I of improved Splints, with angte piece, g Splint Straps (sufficient fvr a fractured thigh).
Price £1 I IS. 6d. Each article is priced separately (su Ind ex).
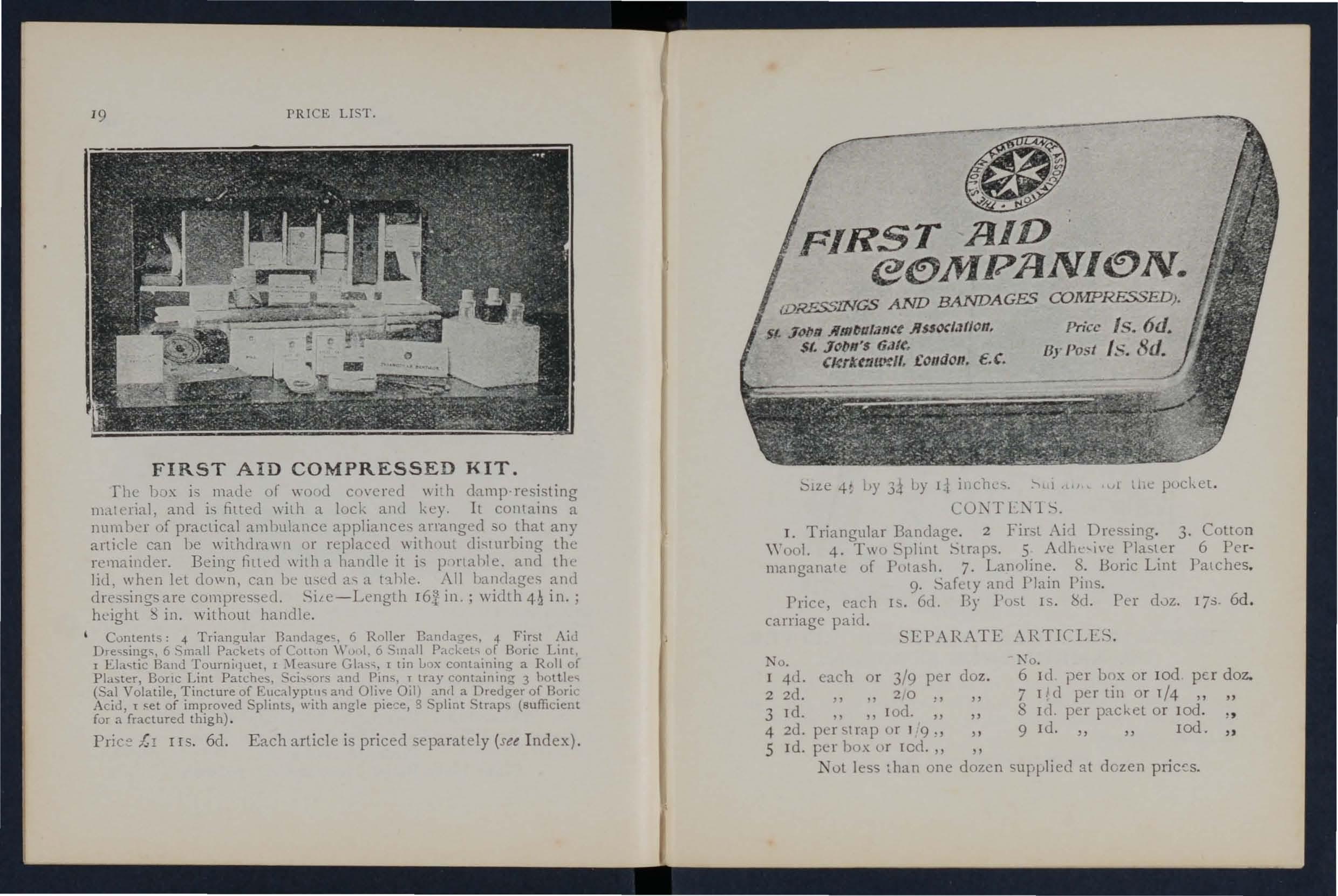
::'Il.e I,)' 3j by 1.1 illC.11L'>. "i , ,.v ! d,e pucket.
CO:\ T L:\,1 S.
1. Triangular Bandage. 2 First ,\i'l Dressing. 3. Colton \Y oul. 4. T\\() :-,phnt !->lraps. 5 AdLe'-I\'e T'la<,ter 6 Permanganal e of Putash. 7. Lan()line. S. Boric Lint Patches.
9. SafelY and Plain Pins.
Price, each IS. 6<1. By l'u!>L IS. btl. Per d0Z. 17:;· 6d . carriage paid.
EPARATE ARTICLES .
No.
I 4{1.
2 2d.
3 Td.
4 2d.
5 Id. each or 3/9 per doz. ., 2 , 0 " Ioel. pcrSlmp ur 119., per l>r lcd. "
No.
6 III per box or lOd per doz.
7 1 d per lin or I/4 "
S 1<1. per p:l.cket or lod.
9 ld. lOd. "
Not less ,han one dozen suplJlied at dozen
PRICE LIST.
FIRST AID BOX FOR "ASHFORD" LITTER OR AMBULANCE STATION.
This is oril'fl'H>ly clesir-ned to be placed on the" Ashford ., Litter 'nell. bu' It is fur'her arhpled to he lip on a will. A le'1ther handle is <1,150 fitted for carrying puq)O cs.
Fer contents cee next page .
PRICE LIST.
CO TENTS OF FIRST AID BOX. (Illustrated 011 previouq page.)
Set of Wooden "plints; I Ela,lic Band Tourniquet; Carbolic W oo)) Boric Lint, in lin cases; I R,)l1 Adhe,ive Plaster: 12 Roller Bandages, as<orted; 6 Triangular Bandae;es; 3 Pieces 01 Tape; J Pair Scissors; 1 Knife ; 1 Kidney.,haped Ba,in; I Graduated l\Ieasure; 2 oz. Olive Oil; 2 oz. Tinct. EucalYPlus n. P.e. ; 2 oz. Sal Volatile; 2 0Z. Spirits Etb er Compo ; 8 oz. Carron Oil; Pins, Safety Pins, :-ieedle", Thread.
PRJ( E £2 lOS.
..,pecially selectcd for the Sl. Juhn AmlJulance Brigade, con<,isting of:-
2 Triangular Bandages, onc of \\ hich is sealed up in waxed paper. The otht.:r may he for practice, but should be kept as clean as P()sstl lie.
2 Bandages 13 ill. alit! I in. \.
Packet of Cyanide Gauze (r yd. conlpre·secl) .
I Pair Scissors.
6 Safety Pins .
I Small Bottle of strong Smelling Salts.
I Piece of strong Cane , fll[ lIghtening impn)\ ised T,)urniquets.
Price, 2s. cac h. 6 doz. or more. 2s. 7ll. each.
l'adeh of C)anide Gauze (I yd. compressed) . Price per cloz, 2S. <l.
Small Buule-.; strong '-imclling "ails. Price per ch)/.. 5. 6d.
_\11 filsten or unfastLn on either side. Facile XI) .. 600 Ilr (;02 per 3 duz.
" .. S 003
Duchess Duplex. :-\0. 2 per doz.
" \ ".'I)rll'd
Special Blankct Pins, 3 in. in.
Tourniquet, E lastic
Tourniquet, F ie ld PR
LI ST .
Splints, \\Tooden, per 2/6 ; Cane ... ... per sc t
Greatly improycd \ "oodcn " ith grooved joinlS and angle piece, strongly recommended
Tow , for splint padding ... . .. per lb.
F irs t Field Dressing (A rmy R egulalion Pattcrn),
Jac o n ette, 44 inches wide per )ard 2 3
Tow, Carbolized or Styptic ... per II,. 0 9
Wou nd Pad . - A pad of C1tton wool and gauzc, to "hich a bandage is attached. The ourface of the pad coming in contact w ith the wound i'> not touched by the hand of the person applying the p td. Price 4t1. lach.
F irst A id Dre s s ing , con<;isting uf a smail comprcssed packet of boric lint, a compressed roller bandage, and a S8.fdy pin. l'rice 2d. each.
Dredger, containing boric acid PJ\\"lll'r, Is. 4(1.
Measure Glass , 2d.
with strong blade C1ch 91. : per doz. S:;.
P air of S c is s ors each IS : per d()z. IO.,.
S plint Str aps , \ Yehhing, and suilahle Per of 12 yards of stro!lg 2-inch Webbing and IS Dudles, 25. Gd.
Thcse J11:1ke very compact Strap,> for carrying- in the Pouch. The \\'ebbing should lle cut to meet local requi reme nts.
Buckles only, IS 3d. per dozen.
' \'ebbing only, IS. 3e1. pcr dozen yards.
It is unnecessary to sew the Buckles The spikc,> shou ld be passed thruugh the webbing, and the shun cnd of th e \\ ebbing shoalcl lie PR CE LIST.
Leiccster Adh('si\'e Plaster on Cambric, in.tin ... uf !, pl"l, 6 inches 111-1..: 6,1.
National RuhLer Aclhe:-.il'c Pla"LLr t_\ntlscplic), on spools.
5 ) tl-;. 10 ytls. inch \I ide SIt!· I '. I". I 6d. ()II. 3d.
H.ibbulh. in lin [, 6 yard::; long. inch \I ide I inch \\ id..:
Dilto in carcl \)ox, in. \\ itle,{ yds. long ... lin I 1 3 5 ;{I ., ) " COCRT PLASrER, TRICOLOR. Large Size, 9<1. ; 5d. ; 3d . r)l. c l. ! i. 3d. 3d . 61. I)<l.
PRIC.I£ LIST.
ORDINARY PADLOCK SHAPE.
\Vithout instruments, 4S. 3d .
L,ted complete, containing Spring Dressing Forcep , Spatula, Probe, 2 pairs Scissors (round and sharp pointed), Clinical and Knife.
Advanced price lOS.
ST. JOHN'S PATTERN, as illustrated, but il11prvved I,y the addItion of Baps to protect the i'1SlrLll11ents.
\Vithout instruments, 7s. 9d.
Filted complete, containing , pring Dressing Forceps, Artery Forceps (also useful for dressing), Spatula, Probe, Director with .Gar Scoop, 2 pairs Scissors (round and sharp pointed), Clinical Therl110me!t:r {minute, (vund), Knife, Pencil, and Safety Pins.
Price £r IS.
packet contains 6 as follows :6 yards long-one 6 inch, two 3 inch, one I inch; 4 yards long-two inch.
}. ine Grey Calico
1'I.lin Triangular Bandage, each quotations for large Cluantities.)
Dittu Compressed (thinner quality). each
;
Illustrated Triangular Bandages (after Esmarch) showing 25 applications of the Triangular with printed instructions
35. 9d .
rRICE LIST.
R.OLLER. BANDAGE MACHINE.
Dr. .\.. C.
Price 2", 6.\.
Force p s, dressing, full size or small as dl'''ll'ul, Is, ; bow dres-ing. 5 in. joint, IS. 6d,; Pean's ,Artuy. 5 in. locked juint, IS. 3(1.
S c isso r s , round-pointerl, If:.; sharp-pointed, fur lklicate work, IS. 3d.; small round-pointed hlades. Inc\.;L'd join:. 4lor 5 in., Is. 6d.; ruunel-pointed CUl'\'ed Illudes, IllcLtd joint, IS. 6c1.; s11'1rp·pointed ('UlYed blades, lucked juint. IS. 9d . The locked joi nt allo\\' the blades to he taken apart for cleaning.
Spat u la , 9(1. Prob e,6d. Director, wit h E ar Sc oo p, IS. <;.1. Kni fe, very thin, i,'ory hanclle, t\\O blades, Is. 9(1. Nursing Char t , designed by inder",ick, each. Temperatu r e Chart, u1.ch.
CLINICAL THERMOMETERS .
ReJuced Prices.
Round. Ordinary, IS. ; minute, IS. 3ll.; half-minute, I,.;. 6.1. Flat. Strongly recommended as they will not roll. Ordi· nary, I S. 6d. ; rapid (specially stlectul and rc"er\'LJ fur the Association), with "ery open scale. 35.
CLINICAL THERMOMETERS -(· onti ll lled.)
With Magnifying Lens . Price, ordinary, IS. 6d.; minute , Is. 9<1.; half-minute, 2S 3d.
N B.-Minute and half·minute in'.>tlUll1ents \\ill only regi5ter in the t i me stated under favourabl e circumstances. /\'0 /.ab/!ity l'S taken jor breakage of T/ul'711omelcrs in trallSr't .
Tu Dr. Forbes' specification. Japanned \lith zinc scale, 2S. 3d. ; Clinical Thennu111elcr size. in ca"e, h. 6d. 1\0 liability is la/;:ell for breakage q/ 7herlll0lllelers ill 11'aJlszt.
Pl ai n , I oz., 2d. ; 2 oz ,3d. ; 4 oz., 4(1. ; 1Ib., 7d.; I 11')., IS.; small packet Iel.
M,'dicatzd, Buracic, t lb., 6c1. ; I 11) , IS. 6d.; Carbolic, per 11>., IS. Set; AlemlJl'uth, per lb., b 6d.; Duuble Cyanide , per lb., 2s. 6J.
L I N T .
Plain, I oz., 2d .. ., oz., 3d. ; 4 liZ., 6<1. ; ill)., lod. ; I lb .. h.6d.
Boracic, 4 oz., 6cl. : r 11)., IS. 6t1. ; fuot packet, 2<1. ; sl11111 packt.:l Td,
The:;e arc supplied in 6 ya1d \\idth al)out 36 inches s. d.
l nl11cclicated wbite
\IUll broth
I>uublc Cyanide
}',(lIacic
GAUZE T I SSUE. per length 0 10 o 2 2
.\ layer of absorbent cotton \\'001 between two sheets of guod quality, per lb., Is. 6d.
i'RICE LIST.
"FIRST AID TO '1' II Ii: INJURED . " By .lame Cantlie, l\1.B., F. R.C.S. The authorised Te\.t Book of the Aid Course. IS.; by post, Is. 2(l. "CATECHIS)1 OF FIRST AI n." ('Llmpikd from Dr. Cantlie'..; :'IIanual. By J. Bro\\I1, L. R.C. P., L R '.S., and J. Carvell, 1\1. P.. C.. , L. S .•\ . Price 6d. ; by posl 7c1· "HINTS AND HELPS FOR Ilo\u;; A?\,D !fYCIE;\g." By E. MacDowell Cosgra\'e, , illustrated, \\ith chaptlr on the ::lpplication of the roller bandage, by R J. Collie. M.D. The authorised 1'o.::\.t Eo ;)k for the CourSL. IS. ; by post Is. 2ll. O:--l IIo)m NURSJr-<G ., (IJased on Dr. Cosgra\"(:"·..; Text Book). By J. Brown, L R.C]>., L R.eS., and J. M. Can'ell, R.C.S., L.S .. \. Price 6d. ; IJY post, 7(1. HVGIENE." By Jllhn F. J. Sykes, D.Sc. (Pulllie Health), &c. 1Iluslrated. The authorised Te\.l Book for the IIome ITygiene Cour<;e. h.; by post, IS. 2'1. "QUESTIONS AND UI'O',' .\\!IlLTI\','CL \\·ORK." By John \Y. ilIartin, and John I· .R.C. ... hI. IS. ; by post, IS. rd. ,. QUESTIO:;S A"D .\:\'iWERS lll' ( )'\ " ny Juhn \\' . Martin, 1. D. 1.. 6d. ; or post, h. Sd. "FIRST AID TO TIlE INJURED (Six ArnlJUbnce Lecture )." By Professor Frederich Tran"laled from tilL' German by II.R.II. Prillcess Christian. 2,.;.; by post, 2s. 2<1. BA"lHGI,,(; .\:--il) SL'I·";IC,U ])Rb";SI:-;(;." \ValLer Pye, F. R.C.S. 2,.;; Ily p ,-;t. 2,.;. 2(1. DR. G. n. DARWl:;'S" FIRSi' . \10::>," being a card to hang up, gl\'ing treatment of v.ui()us acci lent · . 2<1.; 1)\ ]>,)..,t, 5<1· ,. To RICsrORE TIlE ApPARE L TLY DRO\\:-;Icl>," print e d i n large Type \\ith two Diagrams. Unmounted, 2d. each j by post, 3d. .Mour,ted, with red bonier, and \'arnished to hall g up, 6d. ; post free, pac keel, Is.
FRIeL LbT.
T EXT BOOKS, &c. -(Colltillued).
<. Ilo\v :1'0 ACT WHE'i CLOTHING TAKES FrRE." By J. E. H. ;"facklI1lay, M.R.C.S. U:nll1()unted, 2cl.; hy post, 3(1. . on card and varmshed, 4d.; by post, packed, 7d . 'l'IRST Am PRr;o..;cIPIES." Carels of concise directions for \\ai..,tcoat each; 4d. per doz. Special quotations for larg-e q uapiltles.
(. C;Pf'CDIE'I PAPERS, First Aiel, ?\u["ing and '. II ygiene Courses." 3d.; lJY post 4d.
S\lALL Showing the human skele· ton, main arteries, and points where pressure shOUld be applied to arrest bleeding. 2d.; by post, 3c1.
DIRECflONS AS TO THI; RESTORATiON OF PERSO:;S SUFFfRIKG
FRO\! ELECTRIC SnocK. Large print, puster size. 3d . each; oy post, 4(1. ; or 2S. 6c1. per dozen.
.\IDE On cardboard, in linen·lined envelope, for the By .the late urge?n.ilfajor P. hepherd. useful hll1ts for FIrst AId to the Jnjurul 3 d .; by P)st 4<1.
CE:-1FRAl 'OTES O?\' rrRsT AID TO BE I:; CASF:S OF By '\Iilnes IIey, '\L\., .\I.R.C.S., L.F.. C.P. Pnce 2<1. ; by P )st, 3<1.
c' \ TABI E'1"S." By Sydney Partridge, :\f. D. Price ro;;. ; hy post, IS. rd.
• ON :\IILlTARY By Lt.·Culonel H. P. G. R.A. :\1.C. 6d. ; hy post id.
., B?OK," for instantaneous reference, givingconnse JI1strllctlOns; to hang on \\all. Size about one foot qu:ue. Price 2S. 6<1. ; by po!'.t, 3s.
\ InS TO 1\1 fOR AID S'l U[)E?\'TS. Reyi:;ed to dale. Additional IllustratIOns. By L. :\1. Frank rhristian ?l1.B.C. ;"L, Edin. 61. ppr copy: by po l. ill.
FoR CORPS A,\,[) DJ\' JSIO?\,S, ."t. John Ambulance Bngade. :!d. per cUP:.
TEXT BOOKS, &c. ((o il /i I/li ed).
A History of the Order of the Hospital of St. John of Jerusalem. By the late R e v. W. K. R. BEDFORD, M A . . and Lieut.-Colonel R . II. 11 0LBECltE Price 5s ; by post 5s . 4d .
The Knights Hospitallers in Scotland and their Prior y at Torphichen. By GEORGF. :\LD., C.B. Price 2S. 6d., post flce, 2S. Sd.
Registers. Class \ tlentlance, 2S . 6d. Ccrtificates, 4S. (d. Case Report, I S
St. John Ambulance Brigade Cash Book , Mi nute Book and Occurrence Book. Set of three, 7s. 6d. Receipt Book, 6d.
Large Physiological Diagrams. For Lecturcrs' use. Cumpri ing : The lIum an Ske leton, the :'[lIscular, Artuial al (1 Venous Systems, the Heart alHI C irculation of the moud. Simple Fracture, Compound Fracture, Dislocations. Price per set of si x, I5 s These may be hired fur a Cllurse o f " First Aid" lectures, given under the auspices uf the -\ sc;ociation, for a fee of 5s., or \I ith the addition of Tourniquet, and plain Triangular Bandages, for a fee of lOS.
Boxes of S t ationery for the use of Class Secretaries ::lId others connected with the Association, containing t\\ Lh'e sheets of high-class paper, suitably hC:1.eled, and t\\"elye envelopes bearing the cleyice of the Assuciation. Price trl, hy p ost 9d. Twice that quantity, ptice I S., lJ)" 1'o:;t If'. 3d.
Medallions, issucd only in accordance "ith paper :1\'0. 62, tn he had on application . Cuinage Bronze, 2S.; Siln:r, 7s. 6el. : Gold, £2 lOS.; inclueling engra\-ing name and numbe r nn back. M o r occo yelvet-lined case, 2S.
Labels, to be placeelabo\"e :'[ eelallions for each sub;::eCJuentyear's examin ation, issued on ly in accordance \\ith paPLf 62. Coin_l ge Bronze, 6d. ; Sih-er} IS. 6d.; Gold, 12 S. 6d.
Arm Badges, "il h the de\ icc, iosuecl uncler the authurity of the Central Executi\'e ()111mittec, haying \)een nr"t appron:d by IJ. R. n. lhe Grand Prior as the sole official and recognised Badge of the Association and Brigade. liT B. - Tit is desl:I:Jl is p,·otected
K O. I. for the use of indi\idual certificated pl1pils-
In German Silver, Large Size
Small Size ditto
Small SiJ:e for \mllnn h()le
In Electro Plate , Large Size
Small Size dItto
Small SiJ:c for bl1tlon hule
In Enamel for bllttlln hole
" hr,,,)ch
I n Cluth and ..
In Cloth and. ihrer (Registered Number, 3522)
In Cloth and Worsted
mall Celluloid Badge, fur button hole or urooch
" 'hite Salin Armlet, ,,-ith woven Badge
Black ilk Armlet, with printed Bange.
N.I::.-Tllt;·St BadJ,"Y{'s -tri.· ll t / ( ) I'L' 'j(l()J"Jl
PRICE LIST. BADGES.
Xo. 2.
No.2, fur members o f the St. John .\111IJlllance Brigadc.
having the name of the Corps or Division annexed on a label, o(. ly issued in quantities-
In Ge rm an Silvcr, first doz., £1 : subsequent dozs., 125
In Electro Plate, d07 ., £ 1 J2 S. · sulJsequent OOZS., £r 4S.
I n Cloth and. ilk, per doz., J 2-.
I n C loth and Sih-er, per duz., £ I lOS.
All the above may he worn by membc.:rs uf the.: t. J()hn
Ambul ance not we:uing uniform. and the German Silver and Electro Plated may he worn as tbe .\rm Badge fur all ranks on the Brigade Uniform.
LI ST .
etc.
Officers. Co ll ar Haclges (Reg. N o. 3,524) " Pouch B.HIge ( " 3,657\ per pair each
Sergeants. Cap Badge ( ;) 3520\ ., AIl11 Badge ( ., 3.523) "
Fatigue Cap Badge fur Officers and. Sergeants (l'eg. 1\'0.3.558)
Corporals and Privates.
( ap Baclge (Peg . No. 3,5':1) (ach
.Ann Badge ( 3,542)
Overcoat Badge ( " r 582) . .
Field Service Cap Badge for all ranks .,
Lady Officers of Nursing Divisions.
Superintendent's C!clak Badge (Reg . No. 3,658)
Superintendent's Arm Badge ( ., 3.6;q)
Other Iursing Officer's Cloak Badge I., 3,555)
Other ll rsing Officer's Arm Badge ( ., 3,656)
Nursing Sisters. Arm Badge ( 3.522) ,. Cloak Badge ( " 3521)
Honora ry Surg:eon's Silver \\ire Cross (pattern B) ...
Superintendent' s Sih'er \\"ire Star (pattern A)
Medallion Badge (patlern D) ...
Nursing Badg e (pattern E)
Satin Badge fo r Sister's Pin Cushic n
Bu? ler's Badge 4 0 Bugler' s Cord
Honorary Secretary' s Badge ...
Whistl e and Chain each
Field Service Cap , complete... ...
Private ' s Brown Waist Belt and Pouch .. "
White Piping, per packet of 7:\ yards, enough rur 3
pailS ( f trullser" (packets cannot be ])ro1-('n)
Lace, !-'il\'er pLl' yard
Dlack , (A Cap Band. gcnerally runs about 24 inches. )
BUTTONS FOR THE UNIFORM OF THE ST. JOHN AMBULANCE BRIGADE .
I ssued only [or the use of Officers and Members of Corps :1I:(] Di\-isions wearing the presclibec1 uniform.
Eleclro Plate, large small
German Sih'er, large small
Black Horn, large small
ELECTROTYPES OF T HE S T . J OHN AMBULANCE DEV I C E .
No.1. For Cards, Ticket", &c. ...
2 . For :t\ote Paper . Small Circulars, &c . ,,3 . Fo r Quarto and Foolscap Letterpaper, Circular,:, &c. ... '" ,,4. For Small 1\ sler" . ..
5 For Large Posters .. Complete Series
Prints of the above Electrotypes (I 10 fo llowing page. o. 4 i.s on r: tm· '>2 3 Ais3il1 'lnd •• fcH "II1.,\\l l h>l,· Seri<'cs \. 1:. for fill .\S!'-(lClalion
For prices see page 35 . No . I B.
These may be obtained direct from ;\Iessl';' . IIebbe
and Co., .35. Bethnal
Rr)ac1, E. Te lephone No. 909 , London \Yal1. Telegraphic "\ddress: "Otherwise, London." CalEF SUI{GIW:-;
for the use of Officers and Members 0 - t he St. John Ambulance Brigade.
E bon ised Canes, German Sil\,er Mount uearil.1,! the Brigade Dc\'ice.
.\11 Orders for the for egoin g Stores should be g ive n t o the Local Secretary , or to th e Stores Depart me nt
st. John Ambulan c e As sociation, St. John ' s Gate . Clerkenwell, London , E .C.
Cross-Lc:lt, \\'hile Patent Leather and Black
Morocco Pouch (Bulge extra)
39
MESS DRESS FOR OFFIC R.
Jacket (Badges extra)
Vest
1ST CLASS SERGEANT.
Patrol Ja"ket (Badges extra)
Chevron, 4 lJafs, Silver, 3s 6d., Trousers
Forage Cap (Bange extra) ...
Cross-belt and Pouch (Badge extra)
Field Cap (Badge extra)
Buckskin Gloves
Cotton
Leggings
Great Coat (Chenon and Badge extra)
SJj,RGI!:ANTS, CO}{PORAI.S. Al D RA 'K ANI>
Patrol Jackel. Black Tarlan (Badges extra)
Trollsers, Black Tartan
Forage Cap Badge extra} ...
Cover for Cap
\\'aist-bt'll al,d Pouch
Field C::tp (B:lclge extra)
Greal Clla l (Badge extra)
Gloves (per pair)
Leggings \ per pair) ...
Sergeant 's Chen'on, 3 bars, Sih'er,2s. 6d., \\'orsted
Corporal's 2",. IS. 8<1. \\'CLISTS-SUl'ERI TEN DENT.
Patrol Jacket (Badges extra)
Cap extra) ...
Breeches: Grey Serge
Shoulder Belt and Pouch
Gloves
Gaiters
Hose ...
Greal Coat
Carriage out of London extra.
These may Le obtained fn m :c. & R. Garrould ISO to 160, Edgware Road, I1yde Park, W. '
Telephone!': 5320 and 5321 Paddington, and 3751 Mayfair. Telegrams: "Garrould, London."
Cloak (Badge extra) Bonnet
Dress, made to extra) Collars.. ... ... ... Cuffs
Cap. Dura ., Apron
and o I 8 and 25.6d .
Carriage paid on all orders oyer ten in valu€'.
Al! to I.;e obtained [rom 't. John's Gate.
H the Corp or Di\,ision is out of London, measurements to be supplied to cuntractors free of charge.
Ambulance Hampers . Station Plate .. , ..
]hndage Rolling l\bchinc
Bandagf's
Ba,ilt, Dressing Bed, Equipoise " BooksCamp .. ...
B,)ttles (Water) r ,\G E 15 to 17 q 32 to 27 26 q \ ... 17 12
Button,..
Carriages (Horse Ambulance)
Carrylllg Sheet
Cash Book ...
Colton \\' 001... ." .. ,
Co\'er for Stretcher or Litter
Diagrnms, Large " Small
Drellger (Bonc Acid)
Dres<;ing Ba,in
Drownll1g Tackle
Electrotypes
Emergency Book
First Aid Hox.. ... 1I 30 23 ... 35. 36 30 9, 21) '22 II Companion " "Compressed Kit lq Field Dressings .. 21
FI:Igs 37
Forceps 27
Gauzes .. 28
GauLe Tissue .., 28
Hamper' (Ambulance) 15 to 17
Haversacs IS
Hood and pron for Litter 4 Instruments (various) 27
Jacondte 23
Knife ... 23
Labels... .., 3'
Lace for Cap" &c 34 Lamp... ... q Lint ... ... 28
Litter (,\sbfonJ) 3· 4
Litter(Re:l.I dwanl-) 5 to 7
LO\\,Ill0or Jack<!l 1., j\1 ea,ure GIaS'i 2) i\1"dallions ,I ;\llllute Houk .. )1
2:; N ttr,in;!; Charts '7
Occurrence Book
Hand:lge ;\Iachine 27
Rug .. ... .. ... Rules for Corp" or ])ivi,iOIl'i 't. J- .ltn \mbulan ce Brigade ,0
Saf ty PII1S ."
Scissors 23, 27
IllIg', Stretcher
Splint Padding 23
Splint Straps 23 "iplints .. 23
Statiunery ...... 3 1
Stretcher Depot Plate 14
Stretchers ... ... 3 to 1 t .. Adjustable Leg<; f,'r 9
Swagger Stick.. 37
Temperature Ch:ut 27
Text Books ... 29 to 31
Thermometers.. .. 27,28
Tourniquets .. 23 Tow, carbolized 23 "plain. 23 Uniform 34 Uniforms .. ... ,8 to ..0 W agon, (Horst: .\mbulance) \" ater . 1.3 \\'aterproof Sheet 4 Whistle ami Chain 34 Wool (Cotton) 28 \Y ound Pad 23 R