

BONES.

} BONE (SlernUIII)
AI.M BONE
4TH LUMRAR VERTEBRA • HAUNCH' BONE t (pelvis) J Ul.NA
RADIUS.
METACARPUS' -\
PHALANGRS .•
THIGH BONK (femur)
KNEE CAl' (patella)
SHiN BONE (liLia)
ilROOCH BONE (fibula)
ARTERIES
1 J ht 'III ,,1.1,-.] d,)ts IllOW rt: I"Uuts tll'- lilt:' artt.:lu:, n: nUllliJt:rs ill lextOt:LlPI;:;--
FACIAl•• ('\1(0 illS. , AVIAN
A,,/I, AI.:V. ._. (I"I XIOII). hlAe.. RAnl,\I. /(·"AI. 1ft;). '. ".AN.
TARSUS
PHALA N GES
••••
• •
.
- •• - TE\ll-O'IAI.

FIRsrr AID TO THE INJURED·
ARRANGED ACCORDING TO TH']; REVISED SYLLABl':i OF TIlE FIRST AID COURSE OF TilE
T . JOB;\' AS BY J :\f.A . ) :\J.H.) F.R.C . ..,.,
Honorary Assoclat.· t'/ tlu Order 0./ St. lohn. I/onorar), Lift .lfelJl/>,·r oj; allli Lecturer alld FxaJllilI(J /f', lite Issocia/ion.
\\'ilh a CIIAI'TER on ;0 Slrclcher Transport," revise,] from that originally written by Sir JOH:>: Furu.EY. A-nie-I,t o//ustice 0/ til<' Order f!/' St. lolm, in accon.lancc with the ,\rmy . lretcher Exercises. Also a <.. H ,\ PTER the Fifth Lecture, for Females only), by E. :\IAcDoWEL COSGRAVE, \l.D., V.R.C.P.l., A-'IIi:I,t o/Grace o/tlu Order 0./ St. lolllt, H01lora,y Lift .lJembcr of, a n d Lt!cturer and Examiner fo flu AssociatIon.
FIFTEENTH EDITIO N , 6 3 0 ,00 0 to 680,000.
(This Edition is silJli/a>- to Ille d,"i'cl/ll" twd/tll, tltirfewtlt &> /ourtunth.)
Price in Clo lh, IS. n<:t: by post. ,_. 2d. In :\\orocco, 2S. 6d.; by POSt, 2,. Sd. TO BE ORTAl:-lEO AT
T. JO IlN' :-; GA T E, LO X DO X , E . C. \V.H . & L. C . SO,noo-g to.
Ii ,
I[
®rrmb of tDt' ®r'trrr of tDt l!1o.spttal
of S t. .3Jobn of in l1Ellglnn'tr.
S ovzulg n anb -:patron of Orbu.
Hi s Mos t Graciolls Majesty Kin g George V.
(!;ranb -:pr lo:- .
Field M al"sbal His Royal Highness the Duke of Connaught, K.G.
SUb--:PrlOL
T 11) Right Bon b le . the Viscount Knutsford . G.C M. G.
Y-lalhff of tgle .
Fie ld Ma rsh al His Royal Highness the Duke of Connau g ht, K.G.
Chanallor-Colonel HI'llfIEWI .1110:\1 .1., K.C . .\I.G., S<,crel(lJ) •. General-Colonel ir HEIWERT C. PERROTT, 13t., c.n. FRESIIFIELD, LL.D.
Almoner-The Rev. Canon DUCKWORTII , C.V.O., D n. Registrar-Major-Gener:)} the Lonl K.C. \".0. (;emalo::ist--Sir ALFRED SCOT I ScoTr-G.\TT\·, C.Y.O. (Ganer).
Director of th e Ambulance lJ.par{lIlenL-The ' l ost Hon. the of BHEADALI3ANE, K.G.
Librarian-Lieut.-Col. RICHAltD HOLI3ECIlE.
Secrela ,y-\VILLIAM R EDWAROS, Esq., A.C.A.
Chairmalt 0/ the Srilislt Ophthalmic frosfilal, juusalelll-The Rig ht Hon. the Earl of Plymolllh, C.B.
Chit,! Scoclo , y oj I;'c AlJlbulanct Departmutl-Coloncl Sir HERBERT C. PI """ IT HI., C. D.

Asslstant Offlcu 5 .
ASSlslanl Director 0/ lite A JJlbu/allct! DIt/,olll/en! Llcut.·Cu\ul1C"1 ."it
RICIIARD C . Bt., c.1. E.
Assista n t Receiz.er-Gcltt'rol-I',I>IYlN H. r""I·
Assislant Llbrana n -C\,RII. J·-::'4·
!lOlt. Secretary 0/ the 8rilislt (Jj>/ttilallllic 1I0sj>'-tal, jel umhmColonel T. H. HENDLEY, C.l.E.
Assistant HOltolary SeC/etar)' (.lor Scot/and) 0/ tlte B,ilislt Oplalmlmir lIospilalJel1lSalelll J. I [ORl\ES I"I;I'ENSO=', Esq. (['niconl PlIrSIIJ,·,wt.) <tounc\1.
The Cou!lCil con,i,ls of the Suu-Prior, PI e,i<ient ex "Ifhio, the Exe<:t1til't! Onicels, and the following
. ir JOH1'\ FURt n. C. B. .\lajor-Gcneral j. C. ]) .-\1.10:-;, H..A.
The Right Hon. the Earl of RAt';· f"URI.V, G.C.l\l.G.
Col. C. W. HOWI>J.ER, C.H.
Sir JAJIIES DIC":, K.C.B., i\l.R C.P.I., R.N
Colonel Sir CIIARLES I\£. WATSON, K C.i'lLG., C.B, R.E. ir DVCE DUCKI\ ()RTII, Hl., LL.D., :'II.D.
Inspe c tor-General HI' 1.c.,l{AI 1
Sir RICIIARO 1'<)11 I! I, lk, K,C.V. O., :'Il.lJ
ED.\Il!SD OWEt', E,q., LL.lJ., F.R.C.S.
Lieut..Colonel Sir I<ICIIAIW C. fEMI'l.E, Bt., C.l.I>..
\YILLIAM D. JAMES, J..sq., C.\'.O.
The Right Hon. the Lord :-\01 TIlCOTE, G.C.l\l.G., G.C.l.E .. C.n.
The- Right Hon. the Earl of lh "S' 1\,'I{'JL'GII, C.\·.O c.n . :-\1",,15, :'Il.lJ ., R.:\.
The Chapter COlbhts of Ihe hlll.:(lllo; of Jlhllee :11\ SlIb-Prelate, ti,' ,'/I'C ; lhe Exectlti,e OniCO:h; the sclcL(ed \\ "mh"r, of C JUllLil ; and the iollo" in::: Offlclatlng
'lheRcv.C.,nonSII['PI'ARI>,C. \.O \).1). lIl- l> -" lhe H.el. P.\UI \\. \\·VI ,.
A 5 'J{ o f a n b tsqula .s . S i r \ V TA\I.I>II, The Ri!!;ht Hon. the! uf ;\1.1) K.P.
I'he RI:;ht Hon Lord CI.\l:1J C,lonel T. H Hr-:t'DLE\, C.I.F
II A \111. ru;>;. j h .. II L'II. J Am-s :\oTer. Srv IRT rhe Ri!.dll HOll Larl C.IWD(>R. \b,ter of Gm)".
II \!'so;>; \'·I'FSllI'IFl.n, !':,q. C. B. C . .\l.l;. Cll. Sir Clement .\1. Ro)"(h, C.Il. Lieut.-ColUllel IVOR PHll.Il'l·",
It.-Col. En\lo:-:n;\\' WI I.Sul" , C.G., D.S.O., i'Ll'. U.S.O., R \.:'Il.C. C"lunel r. ST. CI AIll Lt. .Col. 'ir Ll'FS K:-:O\\11S , I:t, :'II.Y.O ,n...,.!!. c.Y.O. EOII"I>: DA\lb, ""Lj. The ]{il!hl Ir on. the Lord Ill S- HE:-:r'Y ""1'. JOIl:, H ()I'F. J,.,q. IJl1 IWl:f.11 , K.C.\ -.O. II 2
H.R.H. Prince CIIlliST1AN tH' SCHLESWIG-Hol.STEIN, K.C.
H.:\!. Kl"G HAAKO:-; OF :'\ORII'\\", K.C., G.c. B., G.C \ .0.
H .H. Plince i\l.I!ERr tW !-oLlfl
II 1(, - H 0 l.!) r I, iI', C.C.Il., (;.C. \T.O.
1I S.H. The Duke of TECK, G C.V 0, C.1\LG, H., .H. Prince I-In 'CIS 01' TLCK, K C.V.O., D-5.0.
Rear-_\dmiral H.S.H. Prillce LOLl!) (w BAT'I ENBERG, C.C.B., K.C.l\I.G.
H.S. H. Prince GEORGE "I TEC", C.C. \T.O., D.S.O.
H.R.ll. Prince ARTIIUf{ OF CUN"AUGIIT, K.G .
Sir JOH'I FURLKY, C . B. (If OIL. Bniliff).
The Rt. Hon. Lord G.C :\I.G.
Sir N. DICK-LAUDEI{, 13t.
?l l ajor Sir ARCIlII!ALI) LA\lIl, Bt.
Col. Sir H C. l'EIWOTJ, Bt.. C.B.
The Rl. H OIl. Earl FERIo-.RS.
Col. .ir J. CILDEA, K.C.\'.O., C.B.
HENf{Y JOHN LOFTUS, E C]
Colonel BETHEL MARTIN DAII ES.
Gen. Sir CIIAULES \\'AI<REI', G.C.:\l.C., K C.B., R.E.
l\laj.-Gen. J AllES C DALTO ,"'. R.A. Col. AVUIER GOULD HU ;o;TE"\\·ESTO;o;, D.S.O., R.h..
Colonel The Rt. Hon . Lord \VII. l.IAM CECIL, C. V.O.
EDWIN FRESIIFJELD, Esq., LL.D. (Hon. Ba i Lrff).
His Grace the Duke of FIFE, leT.
The Rt. Hon. Lord BRASSEY,G.C.H.
The Rt. Hon. Viscount TOll':\'

The 1<1. Hon Viscount K;o;UTSVOIlD, t; C.i\I.G. (Suo·Prim).
R. :'I I Ic l .EA;O; ]\ [ AcLEAN, E'q.
A. I' (;. LEVESClN (:011 I£R, EsC]
Lieut-Col. F.A. H EVG:\
Col. Sir C. :\ \ UI{I{A Y,C. B.
The Rt. l i on the Ea,l of RAN. FURLY, G.C.i\J. G.
The Rt. lIon Lortl SANDHURST. G.C.S.I., C.C.l. b:. Sir HE'IRY ,\ . BLAKE, G.C,j\LG.
The Rt. Hon. the Earl of l\II;.ATH, K .1'.
A . FI{ASER, The Rt. Hon. Lord j\\OSI ,,,.
The j\lost Hon. the :'Ilarquess of DREADALBANE, K.C.
His Grace the Duke of PUR 11."""1>, K.G., G . C.V.O . F . -1\I. the Rt. I [on. the l arl ROIlERTS, K .(;., K.l' ,Y.(".,etc. ROBER r BI{UVE"FI I c.,\f{ 1'1",1""1., F.R.C.S. (!fOil. COJlIJJlnlld.r) HAY FlIHII;.", -"."1.,
F.R.C.S.
Colonel C. \V. Boll' ()I EI{, C.I:. (flolL. CommaILJer).
Lieut.-Col. A. C. YATE. :'bjor-General ASTI.EY I,
The Rt. Hon the Earl of PI Y· C.B.
Ihe Rt. Hon. the Earl 0f .:A:-:D\\ rCH, K.C.V.O.
The Rr. Hon. the Lord :\ORTII. COTE, .. G.C.J.I-<:., C.B.
The Rt. HOll. the Earl of EI I ESE. HA:\su:oI FHESIIFIl'L1), .i\L\.
fbe Rt. Hon. Viscount BRACh.LE\', 1\1.V.O.
F -1\1. t he Rt. Hon. Viscou nt KITKHA"rOU\I. (;.C.ll., 0.:'11., G.C.:'II.G., (;,C. l. E. following ar¢ Sub-lJr¢latu :
Th" Lord Bish op of SALlSll\'R\" . I Tile Ili,hop of (;IIIRAI.T\R. Th e in JERUSALEM. The Hi,hop of DUl'EOIN
The Dishop ORMSBY. (Primate ''.I New Zea/an d )
B EING T U E DE P ARTl'>r KNT OF QJirttnb 19tiot2 of iD e ®rbet ot lbe of 'st. ]lobn of 31ctlH5alem iu QI;nnIanb . lJatron.
HIS MOST GRA CIOU S MI\JESTY KING GEORGE V. IIEAIl .\:\D I'ATR<)" OF Till': ORIlER.)
F IELD MARSHAL HI S ROYAL HIGHNESS TH E DUK E OF CO NNAUGHT . K. G. «, I{ANIl I'llIOR Of TilE ORIlER. <!:¢ntt"al t .u .cutiVIl. <!:ommlttll.ll. . Consi>ling exclusi\'ely of "[embers and ,\ssoLiates of the Order.
/)1I 'uior 0/ tl:e AIII!'"/ftl/C/! /h/,nrtJJU:lLt ('OLd til COIJIIIII!turhe ]\Iost Hon. lhe :'Ilarqlless of llrlEAIlAI B.\ T, KG.
A,\-sistnllt Director alld I),"j>uty C/ltlillllilll-Lieul.·Culonel . ir l 'ILIIAllD C. l'nll 'I f'. Ht C.l.E.
Dt/,utl'-Cltalllllnll Sir FURI.!'\,. C. R (Life :'IIember of the Committee 1I01l01lS (. all.Hi). s
j\[ajor.Gener:!1 J C. l) '\II"C;;o;: l' .. \.
Colonel C. \\ 111m Ill.1 R. C. h
Lieut.-Colonel \. C \'.\ rEo [he Rev. T. \\'. \\·OOIl. \\',\ '\ D"o .·
Major G. E. i\r·\1 _ Colonel ir J. \\' . OTTlEY. K . C.l.E., R.I·.. ,
Inspector-General 1l;:I.GRA\E NI,,;o;IS, :'1. I)
GEOI1GE FnWLKR, 1<_sq.
Surgeon-:'ILtj<?r (y. H. "LD.
GEORGE S. !:i,I L1STOS, r, C]., :'II. R.C.S .
Lieut.-Colonel C. J. TRDIIlI E, C.;\I.C., L R.C P
Colonel Sir CI.E\II' :'II. ROYI)S, C. n.
aptain J. \\ '. :\(l"(T BOWEll .•
H\IwJ.1l HOlIT(lS 1<.sq .• 1\1.\.0.
Ellm.;sll O\\E", ,. sq., LL.D. , F.R.C
cSt
<t llo n tr ol (!ommlttu -co lltillutd.
I.ord CLAUD
Sir J Oli N L. Bt.
The Hon . Sir JOHN A. COCI,IlURN, .. :\1.D.
Sir A RTHUR C ONAN D OYl.E , J\l . [).
The Right lion. J. L. WIlARTON, P.C
Surgeon. General Sir Al.FREIl KE O(;Il. !Z.C .B. , F . R . C.S .E. & I.
VDNEV \V . M ALKIN, E-q.
Lieut.·Colonel Sir JA\lES R A CLARK, Bt.. C .B., F.R.C.S.E. ir FRANKLIN, K .C. r.F·. .
JOH:'l • GRIFFITIlS, Fsq., l\LR .C.S.
Lieut.-Colonel JOHN AR'iAtl.l· [ ONES. :\I. D.
S ir \\'Il.L1AM 1'1I0\t}\5 1,E\\'IS. i:t., !z.C \ ' 0.
The Hon. A.
The Right Hon. the Earl of II ESSlIOROUG lI, C. \ '.O., C B.
Lieut.-Colonel GEORGE E. TIl ISS. F.R.C.S.I.
Colonel JAMES C ,\NTl.IP, F. R.C.S.
Colontl'1'. H. HENDl.EY. C .l.I...
J. ;\tOR(;AN, Esq, C.Y.O., F.R.C.:: .
Surgeon.i\1ajor l;. A. H l,;rr"".
lIrgeon·General ir CIIARLES :'I[CDONOU<;II CUFFL k .C.B., F.l<.C.S .E.
Depllt),-lnspeClOr.General :'II. COITES, .\\.])., R.:\'.
FRANCIS R. CASSIlJI, Esq., :'II 1> .
•.\. THEODORE BRAI'D. Fsq., ;\1. Il. J. ASTLEY 131.0:-'.·\\1, E"<1., F ... J'RANCI'; N. EI LIS, E.q :\[ajor E. W EST-.'nIEs. :'II.D. \\ E . AUDl.ANIl, Esq ,
Ex·O./Jici(l ,1/cml'crs 01 C(lJIlllli/{'·,·.
C olonel Sir HERoERT C. 1'1 RROTT, Bt., L.ll. (Secretal), (,eneral of the Order).
I:.LJII·IN FRESHFlEl.D, Esq., LL.D. (Receil er-General o f the The Right Hon. the Earl of PI nwu'l If, C. B. (Ch;tinnan, Brili,h Oph t halmic H ospital) .
Colunel Sir 1l1<:1-UlERT C. l ' EI<RO ' 1 1' , 111. c n. of the Orderl. .... of a n O :A c countant.
WJLLlr\;\1 R . ElIW ,\Rll S, bq., \. c. \ (S ecretary 0/ the Ultt er l
\\'1 I. l.l A\t H :\ \ 1I1{(, (')UPOill!clldellt. IIt""lld j' ralts/,o rt COl } .,).

REV IS ED 1908.
FIRST AID TO THE INJURED . SYLLABUS OF INSTRUCTIO
FIRST LECTURE,
A. Principle s of Aid .
E. A brief De sc ription o f the Human Skeleton .lnd of th e Muscles.
C. Fractures-Causes, \'a ri eties, signs and - ymp tollls.
D. Treatm ent of Fractures-General Rul e:'>.
E. The Triangular Bandage and its application .
SECO:--lU LECTURE.
A. Treatment of Fractures (co ntinued) . Details o f treatment.
B. Dislocation s, prains , Strains-Sign -, sympto ms and treatment.
C. The Hearl and Blood Ye s. els. The Ci l cul a tio n of th e Blood. "
D. an ' ] wounds. CenerJ. 1 rule s fur t reatmen t .
E, T he T riangular Bandage and its ,' ppli c,Lli ':1.
R S FI!RE NCF. X o . :,8. 1908
THIRD LECTU RE.
A . Hremorrhage and wounds ( continued). Details u( treatm ent.
B. Internal Hremorrhage-Signs, symptoms and a rr est.
C. Hremorrhage from Special Regions. -S igns , symptoms and arrest.
D. Bruis.es, Bur? Bites and Stings, Frost-bite.
E. Forelgn boche,; JI1 the Eye, ose and Ear.
F. The Triangular Bandage and its application.
FOURTH LECTURE.
A. The N ervou System.
B. The Organs and M echanis m of Respiration-Artificial Respiration.
C. Insensibili ty .
D. Poi coning.
FIFTH LECTURE (for :'Irale:. only).
.A. Improvised methods of lifting and carrying the sick or lI1Jure d.
B. Meth ods of lifting and car rying the sick o r injured on stretchers.
C. The conveyance of s uch by rail or in country carts.
FIFTH LECTURE ( for Females only).
A. P reparation for reception of accident cases.
B. Means of lifting and carrying.
C. Preparation of bed.
D . Removing the c lot hes.
E. Preparations for surgeon.

9
NOTE I.-The subject of poisons should be treated in a general manner; the common poisons cla ssified, and only the ir general symptoms, effects and treatment taught.
NOTE n.-The last half-hour of each lecture should be devoted to practical work, such as the application of bandages and splints, lifting and carrying wounded on stretchers.
NOTE IlL-Th e re c:;hould be an interval of a week between each lecture. A candidate for examination must attend at least four out of the fiye lectures.
NOTE IV.-Male classes must passin that ystem ofstretche1 exercise most ' uitable for the locality.
NOTE V.-As little time ac:; possible is to be spent on in · struction in anatomical and physiological details. Lecturers and examiners are particularly reque sted to remember that it is II First Aid" that has to be taught and tested, and not anatomy and phy sio logy.
AIixed classes 0/ men and women are Oil no a CCOUll: permitted.
PUPILS U;-';DER SIXTEEN YEARS OF AGE 0 LV ATTEND THE" JUN IOR" C0URSE (SECTION A, SYLLABUS 40 ).
Lecturers instructin g- a First Aid clasG, and Local Secretarle5, can obtain further particulars on application to the Chief Secretary for .. Paper R.eference No. 80."
No Lecturer may cXu1Jline Ilis OWIl Class for Certificat es .
C f-L\PTf!:R II.
The Human Skeleton. Skull, spine, rib alit! breast· bone, upper limbs (collar-bone, shoulder-blade, annbone, hones of the forearm, carpus, metacarpus, pha!angesl. peh' is, lo\\er limbs (thigh -bone, knee::ap, lar. us, metalarsus, phalange

Special Fractures. Cranium, lower jaw, spine, ribs, IJrcast-bone, collar, bone, sh ou ld er-blade, arm-bop!.! or b ,) llc ... close to the elbow jJint, forearm, ern hed hand,
:0
C H.\PTER 1. Page PrincipIes of First Aid 17 Explanatory 20 Questions on Chapter 2 I
SUMMARY OF CONTENT.
.. I 22 Joints .. 31 Muscle:;. \ -oluntaryantl ill\'oluntary 32 Fractures. nuietie<;, igns
lnpl0111<; 33 Apparatus for treatment of Fractures ... 36 General Rules to be observed in the treatment of Fractures 4[
thigh-bone,
crushed foot 43 Dislocatjons 62 Sprains 64 Sprains and Ruptured Muscles ", 65 O'lest:ons on Chapter 66 1 I CHAPTER III. Pag; Circulation of the Blood. Organs; general (sys temic ) and pulmonary circulations 70 Hcemorrhage or Bleeding. Arterial, venous, capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage ". / 76 Course of the Main Arteries and Pressure Points , Aorta, arteries of the head and neck, of the upper liml>s, of the lower limbs 79 Venous Hcemorrhage and Varicose Veins 93Wounds with Venous Hcemorrhage 94 Capillary Hcemorrhage 9 5 Internal Hcemorrhage 95 Hcemorrhage from Special Regions 96 Questions on Chapter 99 ., CHAPTER lY, Miscellaneous Injuries. Bruises, burns and scalds, bites of snakes and rabid animals and wounos by poi oned weapons, stings of plants
ls, frost bite, needle embedded
embedded in the skin, injuries
joints,
the eye,
wall
abdomen, injuries to the organs wilhitl the abdomen and peh'i; 102 Questions on Chapter ". . .. 1I5 CHAPTER V. The Nervous System. Cereb ro-spinal , sympathetic ... II7 The Respiratory System llS Artificial Respiration. Schafer's, Silvester's, H oward', combined with Silvester's, Laborde's and Marshall Hall's methol;:' . , ' 1=1
and £)
knee-cap, leg,
and anima
undrr the kin, fish hook
10
foreign body in
ear passage and nose, wound in the front
of the
I2
Insensib ility . general rules for treatment, concussion of the brain, compression of the brain, apoplexy, epilepsy, hysleria, shock, fainting and collapse, HlOstroke !"tnd heat-stroke, cOlwulsions in chi ldren, asphyxia
Electric Shock and Effects of Lightnin g
Questions on Chapter
CHAPTER \'I.
Poi soning. General rules for treatment,
Q u esti ons on Chapter
CHAPl'LR YII.
Bandaging. Bandagu; for th e scalp , forehead, de., shoulder, hip, hanel, foot, chest, back, knee, L'lbo\\, fingers and toes. _.
CHAPTER VIII.
Methods of Carryin g . Four, two, and three handed seats, fireman's lift, fore and aft method, imprO\'ised stretchers, to cross a ditch or wall , to load or unload a wagon ..
IX.
S tretcher Transpo rt. Stretch e rs, stretcher excrcis s, litters
CHAPTER X.
Th e F ifth Lecture (for Females only ). PreparatilJn fo r reception of accident ca es, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparat ion for surgeon

Skeleton showing position of main arteries
Skull and vertebral column
Vertebra ...
Bones of the left upper limb
Bones of the right lower limb
Sboulder Joint
Ankle ...
Rectus 1\1 uscle
Triangular bandage spread out and folded
Luge arm sling "
Small arm sling
Reef knot
Gra nny knot ...
Loop knot
Bandage for fracture - lower jaw
Bandages fror simple fracture of ribs
St. John sling '"
Band 1ges for fracture of both collar bones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint ... . ..
Treatment of fracture of forearm
Treatment of crushed hand... ... . ..
Treatment of fracture of thigh bone ' "
Treatment of fracture of thigh bone (woman)
Fracture of knee cap ... . ..
Treatment of fracture of knee cap ...
Treatment of fracture of leg (man and woman)
Treatment of crushed foot... ... . ..
D iagram of the heart, lungs and air passages
... Questions on Chapter 128 142 145 ISS 160 197 206 13 LI ST OF ILLUu TRATIONS.
. . . ... . . . .
. .. . . . . . .
... . ..
...
... ... ..
Par' jrontispiece 24 24 27 29 3 1 3 1 32 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 71
Oiagram of the clfculation of the blood
Digital pressure on carotid artery ..
Digital preosure on facial artery .. .
Digital pressure on temporal artery
Digital pressure on occipital artery ...
Pad and bandage to arrest hremorrhage from temple
Ring pad
Digital pressure on subclayian artery
Pad and bandages to apply pressure on axi llary artery ...
Digital pressure on brachial artery (two methods) ."
Flexion at elbow
'Digital pressure on radial and ul nar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen
The lungs and bronchial tubes
Schafer's method of artificial respiration
Silvester's method of artificial respiration
Silvester's and Howard 's methods of artifici .,d respiration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage for the hand
Band age for the foot
Bandage for the chest
Band age for [he knee
Bandage for the e lbow
Grip for four-handed seat ...
Lifting by two-handed seat. ..
Grips for two- handed seats ...
Carrying by two-handed seat

Grip for three-banded seat ...
Supporting patient ...
Fore and aft method of carrying
Carrying on improviscd seat
Improvised stretcher
Furley stretchers
Stretcher exercise, No.!." Fall in "
Ditto, ready to lift patient
Ditto, lifting patient. ..
Ditto, placing stretcher
Ditto, preparing to low e r patient. ..
Ditto "Lower"
Ditto: No. II. Ready to lift patient
Ditto, patient lifted .. .
Ditto, No. IV. First positio n
Ditto, second position
Diagrams illustrating Army stretcher drill
Ditto
Bcd cradle
Lnprovised bed cradles
.
...
... ... ... ... . ..
...
.... ..
.
..
. .. ... ...
. .. . .. .. .
...
... . ..
...
. .
... ... ... ... ... . ..
Pa:-e 73 81 81 82 82 83 84 85 86 87 87 90 9 1 9 2 112 II9 122 124 12 5 155 156 156 157 157 158 159 159 160 161 162 163 IS
...
Pqr 164 165 167 168 168 17 2 175176 177 17 8 179 180 182 183 188 189 19 1 194 203 203, 204
PREFACE.
AT the request of the Central Executive Committee
I have revised the manual written by myself in 1901 as the official handbook of the St. John Association.
Throughout the revision an endeavour has been made to the study of FIrst Aid to the Injured by dra\\'lng up a number of general rules for the of accidents and sudden illness, and by the omISSIOn of all detail \\'hich is not absolutely necessary to enable the student to acquire an intellisent of the subject.
.
I w1sh to expr ess my thanks to Professor E. A. :,chaJer for furnishing instructions for performing a met?o? of artificial respiration, to Dr. L. M. F. for many valuable suggestions, and to the Med1cal Members of the Central Executive Committee, especially G. H. Darwin, M.D. and Dr. F. R. Cass1dl, for perusing the proof sheets and for a number of useful additions to the work .
I cannot omit also to offer my best acknowledgments to Mr. ,V. R. Edwards, the Accountant and of the S.J.A.A., for his i 1valuable co-opera t1 on.
JAMES CANTLIE.
FIRST AID TO THE INJURED.
CHAPTER 1.
The St. John Ambulance Association has now completed thirty years of its existence, and during that period hundreds of thousands of men and women have been taught at its classes, in all parts of the world, how to help their injured neighbours.
First Aid to the Injured is a special branch of practical medicine and surgery, by a knowledge of which trained persons are enabled to afford skilled assistance in cases of accident and sudden illness. The instruction begins and ends with First Aid, and the subject is taught simply but thoroughly and exhaustively. fhe duty of the ambulance pupils ends where the doctor' , commences, and there ought to be no overlapping or clashing of duty or interests.
PRINCIPLE OF FIR T AID.
I. The First ... 'Lid student should be-
(a) Observant, that he may note the causes and signs* of injury.
( b) Tactful, that he may without thoughtless questions learn the symptomst and historyt of the case.
--------------- -----------
• Signs are what may be perceiYed.
t Symptoms are what the patient can tell you.
t History means the circumstances attending the accicient or luddcn illness.
(c) Resourceful , that he may use to the best advantage whatever is at hand to prevent further damage and to assist Nature's efforts to repair the mischief already done.
(d) Explicit, that he may give clear instructions to the patient or the bystanders how best to assist him.
(e) Discriminating, that he may decid e which of several injuries presses most for treatment by himself, and what can best be left for the patient or the bystanders to do.
2. Remove the cause of iniury or danger whenever possible. .
c 3. Severe must receive the first attention, no matter what are the other injuries.
4· Air. - patient must be in a position in whIch breathmg IS possible; the air passages must be free from obstruction; if breathing has ceased prompt measures must be taken to restore it.
S· restful position of the body will assist the vItal functlOns; support of the injured part will help to prevent further damage, and is essential in the case of fractures of limbs.
Warmth. -After every accident keep the patIent warm so as to prevent the fall of temperature below the normal point.
7· When the skin is broken the wound

19
should be promptly covered with.a clean dressing. Should the \yound be pOlsoned, IS most important immediately to prevent the pOIson permeating the S) stem. .
8. Poisons S\\ allowed be got nd of, or when that is inexpedient. neutrahsed.
9. The best means of transport must be studied and provision made for proper care when the pat'ient is -brought to shelter. .
ro. Removal of should not be taken off unnecessarily, but _ when. It IS needful to remove them, the following rules \\'111 be found of service in serious cases :- .
COAT: RemO\'e from the sound sIde first, and, if necessary, slit up the seam of the sleeve on the injured side.
SHIRT A D VEST: lit down the front and remove as the coat.
TROUSERS: lit up the outer seam.
BOOT: Slit the back seam and undo the laces.
SOCK: Cut off.
II Stimulants. - It is incorrect to suppose that alcohol is the only form of stimulant, and far .too frequent use of spirits is. to restore a patIent after an accident often WIth senous results; the safest rule, therefore, is' to defer the of Cl:lcohol until the arrival of a doctor. " 'hen the patIent IS able to swallow, strong tea or coffee, or milk, as hot as can
18
zo be drunk, or a small quantity of sal volatile in water may be given. Smelling salts may be held to the nose. Sprinkling the face with cold and hot wate r alternately, warmth applied to the pit of the stomach and over the heart, and vigorous friction of the lim bs upwards have a stimulating effect.
12. Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an apparently slight injury is accom. pani ed by grave danger and may actually cause loss of life. When sending for a doctor, state the nature of the casE', and remem ber that written parti culars are safer than a verbal message.
It is necessary that something should be known of th e structure .of the body (elementary anat<:>my), and of the functIons of some of the more Important organs and systems (elementary physiology). A short descripti on of the necessary anatomical and physiopoints is therefore given as the several subjects are dIscussed. For purposes of description the human body is. supposed to be erect, with the arms hanging by the sIde and the palms of the hands directed forwards. Th e" middle lin e " of the body runs vertically from the top of the head to a point between the feet
QUESTIONS ON CHAPTER I
What is First Aid to the injured ?...
What qualities should the Fir t Aid student possess?
'What are signs?
'What are symptoms?
\Vhat is the history of a case?
What is often the first thing to do in an accident ?
What result of injury must re cei \'e the first attention? ...
What three things are absolutely necessary to an injured

What steps musl be
be) ond the actual treatment of injuries?
Should clothing always be remo\'ed?
How would you remove clothing \\ hen necessary?
Explain the use and abuse of stimulants ...
What must the First Aid sludent nol do ?
What is elementary anatomy?
What is elementary physiology? . ..
For purposes of description how is the human body supposed to be plr.cen?
21
. The num erals indicate the pages wh e1e the answers may be found.
..
PAC K 17 r7, 18 17 17 17 18 18 person? .. ' .. , ... ... ... Whal must be done when the skin is broken? How must poisoning be treated? '" ... 18 ... 18, 19 19
laken
What is the middle line of the body? 19 r9 19 19,20 20 20 20 20 20

CHAPTER II.
FRACTURES, DISLOCATIONS, SPRAINS AND STRAINS.
THE SKELETON.
The human body is moulded upon a bony framework (the skeleton) which serves-
I. - To give shape and firmness to the body.
2.- To afford attachment to the muscles.
3·-To protect important organs, as in the skull, chest, and abdomen.
THE
SKULL.
The Bones of the Skull are arranged in t\\ 0 groups, those of the brain case or cranium, and those of the face.
The Boundaries of the Cranium are the vault or dome, the rounded portion forming the top of the head; the front or brow; the back of the head, where the greatest extent of brain exists, and where therefore the cranium is widest and deepest; the sides or temples. The base of the cranium is hidden from view by the bones of the face and of the vertebral column; in it are numerous perforations for the passage of blood vessels and nerves; through the largest opf!1ing the brain and spinal cord are continuous.
The Bones of the Face with the exception of .)
the lower jaw are firmly jointed together, so movement between them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the bones of the cranium a nd of the face conjointly. The mouth cavity is forn:ed between the upper and lower jaws, the bemg the bony of the which separates It from the nasal cavIty above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions term inating on either side at the joint between lower jaw an? the base of the cranium, sItuated Jlnmedlately in front of the ear.
The an o- Ie of the jaw indicJ.tes the junction of the b horizontal and the vertical p ortIOns.
THE SPINE, OR VERTEBRAL
The Vertebral Column (Fig. 1) is composed of bones called vertebrce, each of which consists ofI.-A body or bony mass in front.
2.-Process Es projecting backwards, which enclose a canal for the spinal cord - the spinal canal.
3. - Two transverse twelve pairs of which support the nbs.
=2
FIG. I.
Co ...
SKULL AND VERTEBRAL COLUMN.
Showing left ril:s and portion of breut bone. The right ribs are removed.
SPINOUS P ROCESS.

Bonv OF VI!RTEBRA.
FIG. "'2A.
••• SPINOUS ; , PROCI!SS SURJI'ACES SUPPORTING HEADS 01'" RIBS.
FIG. ZB,
4·-A pinous process. The spinous processes of the vertebrce can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
The Vertebrce, 33 in all, are grouped into regions, in each of which they are known by numbers, counting downward :-
I.-In the n eck 7 Cervical vertebrce. The fir st vertebra, lite atias, forms a joint \\ ith the base of the skull, at which the nodding movement of the head takes place; the second, tlte a,r/s, by the joint het\reen it and the atlas, allows of the side-to- ide movements of the head.
2.-1n the back 12 Dorsal yertebrre.
3.-111 [he loin 5 Lumbar \'ertebrce.
4·-The rump-bone, or acrum, consist of 5 'acral \'ertebrce united in adults as a solid ma-s.
5·-Th e tail-bone or Coccyx, consists of 4 vertebrre joined together to form a single group.
Bet\\ ee n the bodies of the Yertebrre, in the upper thre€ regions, are interposed thick piece of cartilage (gristle), which, \\hile they bind the bone together, allo\\' of free moyement to the column as a \\ hole, and help to break the shock of any sudden force applied to the spme (for example, when falling from
25
a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Rib s consist of tweh'e pairs of curved bones ex tending from the dorsal vertebrre to the front of the body, and are known by numbers-first, sec ond, etc., commencing from above. The ribs are not bony throughout their entire length, out at a short distance f rom the front the bony material ends, and cartilage t akes its place. The upper seven pairs, named the true ribs, are attached by their cartIlages. to t h e Breast-bone (sternum), a dagger-shaped bone with the point downwards, just over the pit of the st omach. The lower five pairs are termed the false ribs, as their ca r tilages fall short of the middle line. The eleventh and twelfth pairs are termed the floating ribs, as their ends are free in front. The ribs enclose the chest, and serve to protect the lungs, h eart, liver, stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder - bones are the Collar-bon e (dav iclt ) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the nec k a s a narrow curved rod about the thickness of a fi nge r. I ts in ner end rests on the upper part of th e

FIG. 3A.
BO:-<ES OF THE LEFT UPPEP.. LD/B.
FIG. 3B.
HOWl G THE POSITION OF THE RADIUS AND ULNA "'HE);' TH& ;rHUMB IS T U RNED INWARDS.
Co mpare Fig. 3A, in which the thumb is turned outwards.
26
OF C O L l. AR
PART
BONE
L DER
B ONK •• ...• ( H L' MERUS ) { U I.NA 0 1' RA lJ IU S --+t-!'-\
SHOU
BLADE (SCHULA )
breast-bone, and its outer end joins with the shoulderblad e.
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints \\ ith the collar-bone and the bone of the arm .
The bone of the Arm (Izumerus) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the U ln a on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their relatiye position with every turn of the hand (Figs. 3A and 3 n).
The Hand is composed of-
r.- The bones of the wrist, or carpus, eight in number, arranaed in two ro\\ s of four.
2.-The metacarpus (the framework of the palm ): five bones which form the knuckles and support the bones of the fingers.
3·-The phalanges, or finger-bones, three in each finger, and two in the thumb.
THE PELVIS AND Lo\\ ER LIMBS.
The Pelvis. - The large basin-lIke mass of bone attached to the lower part of the spme is composed of the two h a u n c h -bones and the sacrum. The haunch bo nes mee t in front (at the pubes) in the middle line, o nly a small piece of cartilage intervening, but behind, the sacrum is placed between them. The' pelvis

FIG,4.
Ho' I OF THE RIGHT
LO\\'ER LI:,;B, "IW\\', J'\(; JOJ:\'f \n I'll '1'£11:: PSL\'IS .\1' THE IIr!' . 2<)
28
PELVIS,
THIGH BOtiE (FEMUR).
K:-IEE CAl' (P ATELLA )
llROOClI 130NE (FIBUl.A).
111101 BONK (TIBIA), TARSUS.
30
sup p o rts the abdomen and its contents, and provides t he d eep sockets for the thigh-bones-the hip joints.
T he Thigh-bone (femur) reaches from the hip
t o the k n ee joint. Its shaft is stout, rounded, and a r ched fOT\yards; the upper end presents a rounded head, supported on a neck \\ hich projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base UP\\ ards in front of the knee joint immediately beneath the skin.
The bones of t he L eg are the Shin-bone (t/bia) and the Brooch-bone (jibula). The Sh in- bo ne extends from the knee to the ankle, in coth of \\ hich jo ints it plays an important part; its sharp edge, tile shin, can be felt im mediately beneath the skin of the fr o nt of the leg. The Brooch·b o ne lies on the outer side of the tibia. It does not enter into the for m ation of the knee joint, but its 10\\ er end forms the outer boundary of the ankle joint.
The Foot is composed of--
I.-The tarsus, a group of se\ en Irregular bones at the instep. The largest IS tbe heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.- The metatarsl/s, the five long bones in front of the tarsus \\ hich support the toes.
3.-The phalanges, or toe-bones, two in the hig toe, and three in each of tIle other toes.
3 1 JOINTS.
A Joint is formed at the junction o f two or mor e bones. In moveable joints silch as the hip, kne e , elbow, etc., the surfaces of the bones are covered by cartilage, which lessens friction and the shock of :"

FI G 5. Compare Fig. 4, Page 29.
fall.. joint is clear, rather sticky flUid, the Jomt oIl, or S),Il()Vta, enclosed within a capsule. Tymg the bones to;ether, but allowing of movement, a number of bands or lz"o-amenls.
To e'Cpbin the form€.lJion of limb joints, the
FIG. 6. LEFT ANKLE.FIG. 7.
S110WI'JG RECTUS
E OF THIGH, W ITH ARTERY , V E IN A N
32
{allowing examples are give n :-
The Shoulder, a balland-socket joint, co n sists of a shallow socket on the outer angle of the s;lOulder-blade, and of the head of the arm-bone. (Fig. 5). Owing to ti,e shallowness of the socb-' t the arm-bone is very prolle to escape from its socket ( dislocate).
The Ankle , a hinge joint, is formed at the ju n ction of three bones, the shin-bone above and on the inner side, the broochbone on the outer side, a n d the ankle bone belo\V. (Fig. 6).
T HE MUSCLES.
The Muscles of the body are classified in to t wo groups- volunta ry and i nvoluntary.

33
Th e Voluntary muscles are met with in the limbs the head and neck, and the surface of th e Their ends are attached to different b o n es, and as they pass from one to anothtr they cros s a joint, and, being endowed \\ ith the power of contraction and relaxation, cause the movements of th e body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the the nerves entering them bnng them under the direct control of the brai nand spi nal corel.
The Involuntary muscles are met wIth in th e walls of the stomach and intestines, in the ai r passages, and in most of the organs and blood-v€ssels, also, in a special form, m the heart. They are not under the mftUEnce of the WIll, continue their \\ ork during the hours of sleep j then functIOns are regubted by a SE parate set of nerve s (see Sympathetic ),stem, page I 18).
FRACTURE AKD THEIR TREATME NT .
When a bone breaks a Fract ure is said to occ ur.
CAUSES OF FRACTURE.
I. Direct Violence., \ 'hen from a seve re blow, i mpact of a bullet, crush of a wheel, etc. , a bone br eaks at the where the force is a p p lied the fracture is ter m ed d i re c t. c
A RT RR Y T ISSU Il PA T E LL A TEN DON O R LI G AM I!:NT 01'" PA TELL A
DIAGRAM
MUSCL
D NE RV E.

2. Indirect Violence. -\Vhen the bone breaks at som e d istanc e from th e spo t where the forc e is applied the fracture is term e d ind irect. Alighting on th e feet a n d fractu ring t h e thigh - bo ne or the bones of th e leg, or falling on the hand and ore:lking th e radiu s or the collar-bone, a re examples.
3. Muscular Action. - Th e knee-cap and the arm -bone are occasionally broken by a violent contrac tion of the muscles attached to them.
VARIETIES OF FRACTURES.
F ractures are classified accordi n g to the conditio n of the tissues adjacent to the bone as fo ll o ws :-
1. Simple. - The bone is brok e n with but slight injury to the surrounding parts. .
2. Compound.-The bone is broken and the a nd tissues are punctured or torn, thus allowmg disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude t hrough the skin, or (for example, when a bone is brok en b y a bullet) the wound may lead down to the frac t ur e .
3. Complicated. - The bone is broken and in addition th er e is an injury to some internal organ (for e xample, the brain, spinal cord, lung, etc.) or to some important blood-vessel or nerve.
A fracture may be compound or complicated as t he im me diate result of the injury; or a hacl ure, 35
originally simple, may be converted into a compo u nd or cO:11plicated fracture-
(a) By careless movemellt on the part of th e patient.
(b) By carelessness or ignorance on the part of one rendering first aid.
p 2ci:ll offractures may be clas lfied according to the injury to the bone Itself as .fo11o\\s:- .
1. Com!l1 i nuted . - The bone IS broken mto several pieces.
2. Green-stick. -In children, owing to the softer state of the bony tissues, a bone may bend and crack without breakin6 completely across.
3. Impacted. - The broken ends of the bone are drn'en one into the other.
G.s:--rER.\L IG':>:S A':>:D \\ HICH MAY BE PRJ. E;>;T .
(A fracture of the fem ur, humeruc:, or both bones of the fore.1.rm or leg, affords most complete example).
1. Pa i n at or ne:u the seat of fracture.
2. Loss of Power in the limb.
3. Swelling about the seat of Swel.ling frequently renders it difficult to percel\'e other sIgns of fracture, and care must be. not to mistake a fracture for a less senous mJury.
4. Deformity of the limb.-The lim b aSS Ullle s a n
34
unnaturdl posltlon and is mis-shapen at the seat of fracture. The contra ting muscles rnay cause the broken ends of the bone to override, thereby producing shortening.
5. Irregularity of the bone.-If the bOlle is close to the skin the fracture may be felt, and if compound it may be seen.
6. Unnatural Mobility. -Movement may be made o u t at the seat of fracture.
7. Crepitus , or bony grating, may be felt or heard whe n the broken ends move one upon the other.
Tile last two s(!{llS slwlIld only be /J..J' a dorioI'.
Several of the abm 'e signs are absent in green-stick and impacted fractures .
In addition to the signs and symptoms the patient or the bystanders may be able to gi\'e the history of the injury, and mark.s on the clothing or skin should be noted, as they may en'e to locate the fra turf'. The snap of the bone may have been heard or felt.
ApPARATUS FOR TRE"\Tl\IE;'\T OF FRACTURES.
Splints and bandages for First Aid frequently haye to be improvised,
A Splint may be improvised from a walking tick, umbre lla, billiard cue, broom or brush handle, policeman 's t r uncheon, rifle, folded coat, piece of \\ ood, caTdboard, paper firmly folded, a rolled -up map, or, in fact, anytlz/71g that is firm and 10llg ellollglz to keep

the jo/nts immed/ately above alld below the fractured bone at rest. \ Vhen the above appliances are r: ot available, the upper limb, jf fractured may be to the trunk, and in all cases a fractured lower 11mb should be bandaged to its fellow. .
Bandages may be improVIsed from belts, straps, braces, neckties, or any pIece of lInen, calico, string or cord that comes to hand. , .
Esmarch 's Triangular Bandages 8) are made by cutting a pIece of ,lInen or ,cahco about forty inches square diagon,dly II1to t\\ 0
The broad bandage is made by hnngIng pOInt down to the base (Fig. 9), and then foldll1g into two (Fig. 10).. '
The narrow bandag e IS made by foldIng the broad bandage once (Fig. I J). , ,
Th e medium ba n da ge is by the point down to the bJ. e and then ll1to three. (Fig. 12). ThIS bandage may be ll1stead of ,the broad or the narrow bandage \\ hen It is better SUIted to the proportions of the patient. .
It is sometimes adVIsable to ha.h'e the sIze of the bandage by brinaing the t\\O ends before folding it into the broad, narrow, or medlllm bandage.
\Vhen not in use, the triangubr bandage should be folded narrow ' the two end hould be turned to the centre, and the bandage then folded four, r educing it to a packet about lI1ches by ll1ches .
37
-

39
Large arm-sling (Fig . J 3).-Spread out a b andage, put one end over the on the sou nd side, pass it r ou n d the neck so that it appears over the shou lder of the injured side, and let the other end hang down in front of the chest; carry the point behin d the clb')':1 of the injured limb, and bend the forearm
I3.
I4. over the middle of the bandage ; then carry the second end up to the first and tie them; bring the point forward, and secure \\ ith two pins to the front of the bandage.
Small arm -slin g (Fig. 14).-Place one end of a
FIG. 10. BROAu BANDAGE. FIG. It . NARROW BANDAGE. FIG. 12.-1H}!; UUl'JElJ LINES SIlOW THE FOLDS OF THE MEOW7-r BA:\DA G E. FIG. FIG.broad bandage over the shoulder on the sound side pass it round the neck so that it appears over of the injured side; place the forearm over the mIddle of the bandage; then bring the second end up to the first and tie them. This sling is used in cases of humerus, and occasionally \\ hen the sllJ1g \You Id be too conspicuous. Slmgs may be improvised in many simple \\'a)s, such

as. pinning the to the clothing, turning up the tall of the coat, passll1g the hand inside the buttoned coat or waistcoat, etc.
R eef Knots (Fig. IS) are to be used. Avoid granny knots (Fig. ] 6).
GENERAL RULES TO BE OBSERVED I THE T R E ATMENT OF FRACTURES.
The object of First A id Treatment of Fract u r es is to guard against further mischief, and especially to prevent a Imple fracLure from becoming compound or complicated. To attain this end :-
1. Attend to t he fr a ctu re on t h e spot. No matter how cro\\ ded the thoroughfare, or how short the distance to a more cOI1\'enient or comfortable pia e, no attempt must be made to move the patIent until the limb has been rendered as immovable as possible by splints or other restraining apparatus .
2. S t eady a nd s upp ort the inj u r ed lim b at once, so that its further movement on the part of ither the patient or the bystander IS prevented.
3. S t ra igh t e n t h e lim b w it h g reat care, and If shortenmg is observed in the case of a fracture of a bone of the 10\\ er lim b pull upon the foot until the limb regains a more normal length. 'Vhen th e shape of the limb is improved, on no account let go until it is secured in position by splints, otherWIse there is great danger of the fracture becoming compound or complicated.
4. Apply splints (when practicable) and bandages as follo\\ S :-
(0) The splints must be firm, and long enou gh to keep the joints imme d ia tel y a bo ve an d
40
FIG. I5.-REEF KNOT. FIG. I6.-GRANNY KNOT.
42
below the fractured bone at rest. They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The bandage s must be appli ed firmly, but not so ti ghtl y as to con strict the circul a tion of blo od in th e limb. ·When the pa ti ent is in the r e cumb ent positi on doubl e th e bandage over a sp lint t o pass it un de r the trunk or low er lim b. As a ge ne ral rul e :-
For th e tnmk th e broad ban dage should be u sed. Pass it once round th e trunk and fasten it by tying the ends, or with two or three safety pins on the sid e opposite t o th e fr ac ture , but if to secure a splint for a broke n thi g h, over the splint.
For the arm or for tarm the n a rr ow ban d age should be u se d. Pass it twic e round the limb, and tie the e nds over the out er splint.
For the thig h or leg th e narrow or medium bandage may be used. It is fr e qu e ntly convenient to double the banda ge at the centre, pass it under the limb, bring the loop over the limb, pass both ends of th e bandage through it in opposite dIrections, and tie them over the outer splint (Fig. 17).
In applying bandages near a fracture the upper one should be first.
5. When hcemorrhage accompanies a fracture it mu st be a t te nd e d to firs t, and the woun d cove red by a clea n dr essing.

FIG. J7.
6. No attemp t must be made to remove a patient suffering from a fracture of the sp i ne, pelvis , or thigh, except in a recumbent p03ition , preferably UpO!l stretcher.
7. In every case of fracture it is necessary to cover the patient to keep him warm, and so le sse n th e effects of t he SHOC K of th e accide n t.
8. In all doubtful cases, treat as a fra ctur e.
SPEC I AL FRACTURES.
Fracture of the CraniiIm. -A fracture of t he u ppe r pa rt is usua ll y cau ed by di rec t viole nce-for e '\ amp le, a b low o n the head . A frac tur e of the ba e is caused by in direc t viole nce, throush a fa ll on th e
43
44
head, a fall on the feet or lower part of the spine, or a severe blow on the lower jaw. If tlte lIPPe?' part is fradllred, the signs are swelling, irregularity, a.nd frequently insen ibility, either immediate or coming on gradually. If tIl e base is fradllred in-
sensibility may come on jmmediately, blood or a c1ear fluid may issue from the ear channel, blood may escape from the nose, or it may pass do\\' n to the stomach, v\hence it may be vomited; the fracture may imoh'e the orbit, causing a blood-shot eye.
TREATJ\IEKT.
Injury to the brain is the great danger attending a fracture of the cranium. For treatment see "Concussion and Compression of the Brain," pag es 131, 132.
YIG. lIS.

Fracture of the Lower ]aw. -Pain, : . ss of power (inability to speak and to move the jaw freely), i rr egula rity of the teeth, crepitus and bleeding from t he g u m a r e the usual signs and symptom s.
45 TREAT:\lE;\TT
1.- Place the palm of the hand below the injured bone and press it gently against the upper jaw.
z. -Apply the centre of a narrow bandage under the chi n , carry one end over the h ead, cross the ends at the angle of the jaw, carry the long end across the chin, and tie the ends on the side (Fig. 18).
Fracture of the Spine .-The vertebral column may be broken either by dHect or indirect violence. Falling from a height on the back across a bar or upon an uneven surface is an example of direct fracture, and a fall on the head, ca using a b.rokcn neck, is an example of ll1direct yiolence. .'Vhat is common ly regarded as a broken back of a fracture of one r..H more of the yertebrre with dIS placement of the fragments, whereby the spinal cord .1I1d the nerves ISSUll1g from it may be torn, causing complete or partial paral} IS of the below the fracture. Pain IS pre em at the seat of ll1Jury.
I.-Prevent all moyernent on the part of the patient.
2.-Cover the patient warmly.
3.-To remove th e patient, place him on a stretcher or shutter as follo\\'s :-
(a) Turn up the collar of his coat: roll up a stick or umbrella \11 each ide of the coat
so that the ends are level with the top of hIS ; pas a br xld bandage or bandkerchief under the head and secure it to the sticks. If no coat is worn or doubt as to its strength and length pass a of bandages under the patient to serve ll1stead of, or in addition to, the coat.
(b) A bearer on each side grasps the HIlled coat \\'ith his .hands well apart; a third grasps the clothing on both sIdes on a level with the hips; a fourth bearer takes charae of the legs.
(c) On the word being given, all lift together and carry the patient by short side paces oyer the stretcher and carefully lower him on to it. If a (]fth bearer is available the should be passed under the patient Instead of carrying him over it.
4·-0n arrival at shelter nothin a further is to be tAe arrival of a doctor, except to gIve the patIent water, tea, etc., if he is conscious.
Fr,actured Ribs. - The ribs usually fractured are the SIxth, seventh, eighth, and ninth and aenerally the fracture is midway between the and the spine. The fracture may be caused by indirect violence, driving the fractured ends of the bone outwards, or by violence. driving the fractured ends of the bone Inwards and so:netimes injuring the

47 lungs or other internal organ. ,If the lower. ri,bs on the right side are broken, tbe lIver may be mJured; and a fracture of the lower left ribs may wound the spleen. Evidence of the fracture is afforded by pain; especially on attempting to take a deep breath, and by short and shallow breathing. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hcemorrhage (see page 95) may occur.
(a) TT , Then the fracture is i/ot complicated by an z'njury to an internal organ :-
I.-Apply two broad b::mdages round FIG. 19. the sufficiently firmly to afford comfort, with the centre of the first immediately above and that of the second immediately below the fracture. The lower bandage should overlap the upper to half its

ext e n t. The knots are to be tied rather the front on the opposite side of the body. Another good plan IS to apply a strong towel, folded about eight inches wide, tightly round the chest, securing it \\ ith three orfour safety pins.
2.-Place the arm on the injured side ina large sling. (Fig. 19).
(b) T["hen all z'lllt'rlla! OJKC7Jl is z'lljured-
I.-Do not apply bandages round the chest.
2 .-Lay the patient do\\ 11, inclined a little to\\ ards the injured ide.
3·-Loosen the clothing, giye ice to suck, and place an ice bag oyer the seat of injury. Treat a for internal hrem orrh age (see page 95).
4.-Place the arm on the injured side in a large slin.s.
Fracture of the Breast -bone (slerllllm).-
'Vhen this fracture can be felt or is suspected undo all tight clothing and keep the patient quiet in an easy position until the arrival of a doctor.
FRACTURE OF THE BO'IE OF THE UPPER LIMB.
Fracture of the Collar -bone (daz1lde).-This fracture is frequently caused by a hll on the hand nr shoulder.-Tbe arm on the injured side is partially 49
he lp less, and the patient usually supports it at the elbow with his hand, and inclines his head towardsthe injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lower The general signs and symptoms of fracture ar mostly present.
TREATMENT.
l.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and fOUl Inches across in the armpit.
3·-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it iIi a " St. John /I sling, made as fo 110\\'s :_
(a) Lay an unfolded bandage across the chest over the injured limb \\ ith one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fig. 20).
(b) Pass the lower end of the bandage under the injured limb, across the back, and tie the ends some\\ hat loosely in the hollow in fro n t of the sound shoulder.
(c) Fold the point over the eloow of the injured limb and secure it by one or t wo pins (Figs. 2I and 22).
21.

Cuody bandage omitted to show details of Sling.)
4.-Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
s.-No\r tighten the When both collar - bones are broken keep the
5houlders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by the bandages (Figs. 23A and 23B ) .
Fracture of th e Shou lder-b lade (scapula) .Apply the centre of a broad ban dage in the armpit of
FIG.51
FIG. 23 A.
FIG. 23 B.
th e injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24)·
Fracture of the Arm

FIG. 24.
(humerus).- The bone may be broken :-(a) Close up to the shoulder; (b) near the middle of the shaft; (c) close to the elbow.
All the general signs and symptoms of fracture are usually present.
TREATMENT.
When the Fracture is close to tlze Shoulder-
I.-Apply a broad bandage with its centre above the middle of the arm round the limb and body, tying it on the opposite side.
2.-Support the forearm by a small arm sling
When the Fracture is ?lear the Jl/iddle 0/ tht Sha.ft-
I.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back cUso. The front splint
must on no account be so long as to press upon the blood-vessels at the elbow join t.
3. - ecure the splints by above and below the fracture. If spll11ts are not available, secure the arm to the side by two broad bandages.
4.-Support the forearm by a small arm sling. (.Fig. 25).
Fractures involving the elbow joint, whether of the aTm or forearm, are attended ",ith so much swelli n g, and it is so di fficult to ascertain the exact nature of the injury, that when the accident occ ur s indoors the limb sho uld be laid upon a pillow in the most co mfortable position; ice or cold \yater dressings should be applied to the injured par.l, but no treatment should be atte:11pted pendm.g the arnval of a doctor
FIG. 25.
J;Vhen tlze accident occurs out of doors -
1.-Take two pieces of thin flat wood, one long enough to reach from the armpit to below the elbow, the other long enough to reach from above the elbow to the finger tips; tie t.hem together to form rig.ht angle. (FibP'. 26).
2.-Apply the anFIG 26. gular sp:int so made on the inner side of the flexed limb.
3.-Secure by bandages above and below the fracture.
4.-Support the limb hy S!. large arm sling.
5·-0n arrival ::.t hOILe remove the splint, and treat the :Djury as it had occurred indoors.
Fracture of the Forearm. -\Vhen bdh bones (the Radius and Ulna) are broken, the general sic;ns an d symptoms of fracture are usually present. one of the bones only is broken the signs and sympto ms are as a rnle pain, loss of power, swelling, an d irregularity. An impacted fracture of the R adius
just above the wrist is a common result o f a fall on the hand .
TREATMENT.
This is the same, whether the fracture is of one bone or of both.
I.-Bend the forearm at right angles to the arm,

FIG. 27. FIG . 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sides from the elbow to the fingers.
3·-A pply bandages, embracing both splints, immediately abm'e and below the fracture and round the hand (Fig. 27).
4.-Apply a large arm-sling.
Crushed hand (fracture of the bones of the arpus, metacarpus , or fingers).
TREATMENT.
I.-Apply a carefully padded splint to the front of the hand, reaching from well above the wrist to beyond the tips of the fingers .
54
55
2.-To secure the splint apply a narrow bandage crossed in the mannel of the figure 8 to the wrist and hand ( F ig. 28) .
3.-Apply a large arm-sling.
Fracture of the P e lvis. - ,\Vhen, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to th e lower limbs, but the p:ltient is unable to stand or even to Illoye the lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being \\ ounded.
TRK\ DIE:-,rT.
I.-Lay the patient in \\hate\'er posltlOn IS found to give the greate t ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tigh t enough to support the parts, but not so tight as to press the broken bone further il1\\·ards.
3.-To remove the patient place him on a stretcher, a<;ting on the same principle as that described under " Fractur e of th e pine II (see page 45).
FRACTURE OF THE BO?\ES OF THE LOWER LIMB.
Fracture of the Thig h-bone (femur).- The thigh bon e may be broken at its neck, anywhere in the shaft, or close to the knee. A [raLture at the
57
neck is likely to occur in old people from very slight and is often diffi c ult to distinguish from a severe bruise of the hip, but it may be assurr.ed that when, after an injury near the hip joint, tile patient cannot, when lying on the back, raise the heel from the ground, the bone is broken. All the general slgns and symptoms of fracture are usually present, and a prominent sign is the position of the foot,

which as a rule lies on its outer side. Shortening may from to three inches.
TREATMENT.
I.-Steady the limb by holding the ankle and fo ot.
2.-Gently draw down the foot and it into line with its fellow. 'When two or three 9.SSlstants are at hand, it is one pcrs ::m's duty to hold the foot in position until the splints are secured.
3.-A pply a splint on the outer side from the ar mpit to beyond the foot.
58
4·-A pply a splint on the inner side from the top of the thigh (the fork) to the knee. .
5·-Secure the splints by bandages as follows :(a) Round the chest just b elow the arm pits, (b) round the pelvis on a level with th e hip joints, (c) above

59
Wh e n the fo) t slips in the attc.npt to prevent a fall the mus cles in th e front of the thi gh act with such forc e as to snap the knee-cap in two (Fig. 3 I).
Pain, loss of pJwer (the limb will be quite helpless), and irregularity (a gap may be felt between the b roken fr-1.6ments of bone) accompany this injury.
TREAT:'I[ENT.
I.-L'ly the patient on his back, rai se well and
FIG. 30.
the fracture, (d) below tbe fracture, (e) round the leg, (f) round both ankles and feet and tied below the feet, (g) a broad bandage round both knees (Fig . 29).
\V hen ingle-handed, or" hen the patient lS a woman, it is expt!'dient, after extension d the limb, to tie the feet together, di pense with the inner splint, and pass the bandrlgcs round both limbs (Fig. 30 ).
Fracture of the Knee-cap (patella).-Thc knee-cap nay be
FIG. 3 I • broken by falling on t} e knee (direct violence), but more frequently it is broken by muscular action , as follows :_
supp ort the head and shoulders, 5traighten and raise th e limb.
2.-Apply a splint alon a the back of the limb, from the buttock to beyond the heel.
3.- Apply a narrow bandage with its centre imme-
60 diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. To ensure firmness apply a second bandage in a similar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5.-·Support the fo ot well off the ground by a pillow, roll of clothing, etc., or if none of these are at band by resting it on its fellow (Fig. 32).
6.-Apply an ice bag or a cold \\ ater dressing over the fracture.
Fracture of the Leg (tibia and fibula ).- One or both of the bones may be broken. -VVhen both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches abO\'e its lower end is frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATl\'!ENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond
61
foot. If only one splint is available place it on the outer side.
4.- ecure the splints by bandages (a) above, (b) below the fracture, (c) immediately above the knee,

33.
34·
(d) round both ankles, (e) a broad bandage round both knees (Fig. 33).
\Vhen single-handed, or \\ hen the patient is a
FIG. FIGwoman, after extending the limb tie both feet together, dispense \\ ith the inner splint, and pass the bandagfs round both limbs (Fig. 34). 'Vhen no splint is available tying the legs, ankles: and knees together is of great service.
Crushed Foot (fracture of the tarsus, and toes).-This accident is cOlrmonly caused by the passage of a heavy \\elght oYer the fcot, and may be recognised by s\\"elhng, and loss of PO\\ er.
TREATJ\IE T.
tr.e boot

FIG. 35.
(see page 19).
2.-Apply a \\" 11padd ed splmt to the sole of the foot, rcaching flOm the heel to tOES .
3·-Apply a bandage aftEr the n . anncr (f the figure 8 (Fig . .3 5).
4·-Su pport the foot in a slIghtly raIsed position.
DbLOCATION
.
A dislocation is the di placement of one or more of the bones at a joint.
The joints most frequently dislocated are those of the shoulder, elbow, thumb, fingers, and lo\\er ja\\'.
SIGNS AND SYMPTOMS OF DISLOCATION.
1. -'- Pain of a severe sickening character at or near the joint.
2. - Loss of power in the limb.
3. -Numbness of the parts below the seat of dislocati on.
4. - Swelling about and below joint.
S. - Fixity of the jomt.-The. lImb cannot be moved at the jOlllt by either the patIent or others.
6. - Deformity of the limb.-The limb an unnatural position, and IS mis-shapen at the ]omt.
No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival:-
(a) JVhell tile accident o{mrs out oj . Support the limb 111 whate\'er p.Osltl.on most ease to the patient, bearIng m mmd the neces - ity of lessening the effects of jolting d urmg tran port.
(b) lJ"/lfll tile pat/ellt z's /IldoorsI.-RemO\'e the clothll1g from the limb.
2.-Pb.ce the patient on a couch or bed.
3.-Rest th 2 11mb on plllo\\s in the most comfortable POSlllOl1.
4.-Apply cold (Ice or cold water) dressings to the jomt.
s.-\Vhen cold ceases to give comfort apply
62
warmth (flannels or to\\"els wrung out of hot water).
6.- Treat shock (see page 135).
PRAIN" .
When, by a sudden wrench or t\\ ist, the ligamenf s and the parts around a joint are stretched and torn the joint is said to be sprained. "Going over" the ankle is a common example.
IG:\'S AND
I.-Pain at the joint after a tWIst or wrench.
2.-Inability to use the joint.
3.-S\\'elling and discoloration.
TREAT;\fE:\,T OF SPRAI:\'ED A;';-KLE.
When out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing it on the front of the ankle and carrying it round and round the ankle, where it IS to be firmly tied.
2.-'Wet the bandage after applicaton; it is thereby tightened.
After l'eadtiJlg sltdter-
I.-Remove the boot and stocking (see page 19).
2.-Place the limb in the most comfortable position; usually that is well raised.
3.-Apply ice or cold water dressings to the joint as long as they relieve pain.
4.- 'Yhen cold falls to give comfort, apply hot fomentations.
\\'hen other joints are sprained, treat them as If dislocated.
When in doubt as to the nature of the injury, treat as a fmcture.
AXD RUPTURED CLE .
'Vhen, during severe exertion, muscles or tendor s are over-stretched they are said to be strained, if th( y arc actually torn they are descnbed as ruptured.
IG:'\S A ,\,D
1.- :\ sudd e n sharp pain.
::!.-\rhen the of a limb are strained they may swell and cause eyere cramp.
3.-Further exertion is difficult or impossible; for eX.lmple, if the stram has occurred in the back the patient may be unable to stand upright.
I.-Place the patient in the most comfortable posItion, and afford support to the injured part.
2.-Apply hot water bottles 01 hot fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injur}' of a totally different nature . (see page 114). D
QUESTIONS ON CHAPTER II.
The nume1'als £lldica te til e pages where the allswers may be jOlmd.
\\'hat is the skeleton, and what purpo. es are sen'e d by it?
IJ ow are the bones o f the skull arranged?
\\' hat are the b oundaries of the cranium?
Describe the bones o f the face
Describe the low e r jaw
\Yhat is the angle of the jaw?
" ' hat othe r names has the back-bone? .. ,
\Vhat is a vertebra ? ...
How many vertebra! are there in the spine?
What are the regi ons of the spine, and h ow many vertebrre are there in each? ..
How is the spine endowed ith free movement?
\"hat is a rib?
H o w many pairs of ri bs are there?
\Vhat is the breast-bone? .. ,
\ Vhat are the bones o f the upper Ii mbs ? .. .
What is the pelvis? ...
What is the hip joint?
\Vhat are the bones of the lower lim bs? .. ,
What is a joint?
Describe a moveable joint '"
Describe the shoulder joint
Describe the ankle j oint
How are muscles classified?
Describe voluntary muscles
Describe involuntary muscles
\Vhat is a fracture?
\Yhat are the

\\-he re dlee; a bone break when direct violence is the Call. e of frac t ure ? ... Wh ere d oes a bune Ineak when i ndirect yiolence is the c:tuse of fra ct ure?
I [ ow maya fracture be causccl hy l11u;,cular action? In
\\ hat i:s a simple fractur e ? ...
\\'Int is a compound fracture?
What i a complicated fracture?
h.ll is a comminuted fracture?
m in a case of fracture... J)' 3')
What fractures alTord the lllO:st complete cxample of the signs amI symptoms? ... ...... .
In making up your mind whether a fracture had occurred or n lil , \1 hat points slnuld you take into considera· tion beyond the . igns and symptoms?
\\'hat apparatus may be necessary [or the treatment of 15 fraclure ? 30 Hnw may splints be impro\'ised ? ... ... 3 5 , ::,7 ] low may bandages be impru\'isecl? ... 37
Describe Esmarch's tri1.ngular bandage 37,38 (Fig. S)
In what \\aysmay the triangular bandage be folded for use? 37
lI ow many kinds of arm-slings are there, and what are they called? ......... 39, 4 0 , 49
\ \ -hat knot is to be tied, and what knot avoided? 40
\\'hat is the object of first aititreatment of fractures? 41
Give the general rul es for the treatment of fractures 41
lI u\\' should be applied? ... ... 41 ,42
IT )\\' hould bandages be applied? . .p, 43
\Yha l may can e a fractnre cf the upper part of the claniul11 ? 43 C2
66
PAGE
22 22 22 22, 23 23 23 23 23 25
...
causes of frl.c!>u.r.?, 25 25 26 26 26 26 to 28 2 30 ;0 3 1 31 32 32 32 33 33 33 ·_·33,34
J'ALE 33 34 34
\\ hat two ways may fractures
cl::tssifiecl ?
34, 35
...
be
..
\\
\\ hal is
fracture? \\'hal i an impact...:d fracture? . :a e the general igns and symptom that may be 34 34 35 35 35 pre
a green-:Slick
'e
\Vhat may cause a fracture of the base of the cranium? 43, 44
\\' hat are the signs of fracture of th e upper part of the cranium? ...... 44
What are the signs of fracture of the base of the cranium? 44
What is the treatment for frac t ure of the crarnum ? 44
\Vha t are the signs of fracture of the lower jaw? 44
How maya fractured spine be caused ? ... 45
"Vhat is comm o nly regard ed as a broken back? . . . 45
What are the sympt oms of a fra ctured _pine? 45
H ow may ribs be fractured? 46
How maya fracture of ribs be complicated? 47
State the signs and symptoms of a simple and of a complicated fracture or ribs 47
\Vh at is a frequent cau e of fra ctured collar-bone? 48
\\That a re the signs and symptoms of fractured colIarI)one?
At points may the bone o f the arm be broken? ... 52
Are the general signs and symptoms of a fracture always present in a broken fo rearm ? ... 54
State the cause of a common fracture of the rarlius 55
How would you rec ognise a fra ctur e of the pelvis? 56
At what points may the thigh-bone be broken? ... 57
\Vha t are the signs and symptoms of fracture of the thigh-bone? 57
\Vhat are the causes of fracture of the knee-cap? ... 58, 59
What are the signs and symptoms of fracture of the kneecap? 59
Ar e the general signs and symptoms always present in a fracture of the leg?
What mistake may easily be mad e when the fibula is broken near its lower end?
What is a dislocati on?
State the signs and symptoms of dislocation

a prained an kle
64 tate the treatment of other sprains .. , 63, 65 When not sure whether the injury is a sprain or Iraclure
treat
First Aid tudent should practise improvi!->ing material, folding bandages, tyIng knots, making slings, and the t r eatment of the following injuries.
Improvising splints ...
Improvising bandages
Folding bandages
Large arm sling
Snull arm sling
Reef and granny knots
Knot for applying splint to lower limb
Fractures - Lower jaw, 44. c pine, 45, 46. Ribs (. ill1ple and complicated fractures), 4610 4· Breastbone, 48. Collar-bone, 48 to 51. Both collarbones, 51. Arm, close up to shoulder, 52. Arm, near mIddle of shaft, 52. Arm or forearm when the elbow is in\'olved, 53. f'orearm, 55· Crushed hand, 55,56. Pelvis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single-handed), 58. Kneecap, 59,60. Leg (man), 60, 61. Leg (woman, o r
man when single-handed), 62. Crushed foot, 62 .
and
... 63, 64
PAG!!:
... ... ... ... ... ..,
... 48 , 49
60
60
62
63 Gg PAG E tate
treatment of dislocation. . .
Wha t is a sprain? ... .., ... ...
\Vh at are the sign
64 tate t
treatment
may
o
65 tate the signs
65
65
the
63
64
s and symptoms of a sprain?
h e
of
...
h ow would you
it? 65 Ibw
muscles be strained
r ruptured?
and symptoms of strains
Sute the treatment of strains
36, 37 37 37 39
doors
Sprained ankle 64 Strains and ruptured muscles 65
D islocations-Out of
indoors
CHAPTER III.
THE ORGANS OF CIRCULATION.
THE organs concerned in the circulation of th 2 blood are the Heart, the Arteries, the Veins , and th r Capillaries.
The Heart is situated in the chest behind th-= bre:lst -bone and rib cartilages, between the lungs and immediately above the diaphrJ.gm; it lies obliquely with a quarter of its bulk to the right and the remaining three-quarters to the left of the middle lin e of the b ody . Its beat may be felt just below and to the inner side of the left nipple. The heart has bur cavities, two on either side of a central partition. The two upper cavities are named the right and left auricles, the two lower the right and left ventricles.
Arteries are vess-=ls which convey blood from the heart. Veins carry blood to the heart. Capillaries connect the arteries and veins.
In general (systemic ) circulation arterial blood 1S driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are giYen off to all parts of the body. These divide and sub-divide, and become so small as to assume microscopic dimensions, when they are term ed capillaries.

L. Larynx (voice box); T. Trachea (wind-pipe); R.L. Right Lung; L.L. Left Lung (the lungs are d,rawn to expose the heart and hlood :ressels) ; .R . A. Right Auncle ; L.A. Left Auri cle; R.V. Right Ventncle; Left tricle; P .A. Pulmonary Artery; Ao. Aorta; S. \ . C. Supenor vena cava (the large vein carrying blo<"?d from the upper part of the body to the heart); LV.C. Infenor vena ca....a (the large vein carn-ing hlood from the lower part of the body the The four pulmonary veins cannot be shown lD the diagram .
In the capillaries an interc hange of gases and fluids takes place, whereby the nourishment and maintenance of the tissues and organs of the body are provided for, and the blood becomes dark and impure.
Venous blood passes from the capi llaries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with valves at frequent interv.:tls, whi ch prevent the backward fl ow of the blood.
The pulmonary system of blood vessels is in carrying the blood through the lungs. From the right auricle the blood passes to the right v entricle, and is thence carried to the lungs, where it is purified b y contact with air, and be comes scarlet in colour; it is then conveyed t o the left auricle of the heart and p:tsses into the left ventr;icle, th us completing the circulation.
The heart contracts in adults at an average rate of seventy-two times a minute, but the rate varies, increasing as the PJsition is changed from the lying to the sitting or to the standing position; hence the importance of ad.iusting the patient's position in cases of hcemorrhage . At every contraction of the left ventricle blood is forced into the arteries, causing the pulse, which may be felt wherever the finger can pe

ExplallatiolZ. - In the middJe o f t hc diagram i· the heart \, it h \ its fuur chambers. A bo\'e the l< heart is shuwn the lung (pul. monary) circulatiun. The lmHr part repres ents the genual (sys· tenlic) circulation. \ con. taiJllllg impure (\,c ncll) lJIc.od a l c ., ho\,. n Llack, \\ hile [huse cunta ining pure (arte rial) bluod a re shown \\hile. Tl:e cGnntcting repres ent the c3lillaries. The arrows 5ho \\ the dlltCtlOD of lhl flu\\ of blood.
placed on an artery as it passes over a bone. In ilie vems no pulse is to be found.
Hremorrhage, or IS of three kinds :r. ArccIial. 2 . Venous. 3. Cap illary.
72
73 • i
fIG. 3i.
DrAGRA"-1 THE eIRCULATlO:--< OF THE BLOOD.
ART ERIAL
I. - Blood from an artery is scarlet. .
2. - If the wounded artery is near Sk111 the blood spurts out in jets corresp ondmg to the pulsation of the heart.
3. - The pressure point (see below) is on th e heart side of the wound.
ARR E T OF ARTERIAL H ...
Arterial hremorrhage is, when practi able, to be by pressure, position of the body, and t ior' of the blee di ng part.
Pre;:,sure may be :-
L-Digital -that is , applie d with the thumb or fingers, and may be (a) on the wound; ( b) at a spot called the pressure point . The pressure p')ints are indicated by numbered dots on the frontispiece .
2 .- By a pad and bandage (a) on the wound; (b) on the pressure IJ\JJl1t.
3 .- By flexion.
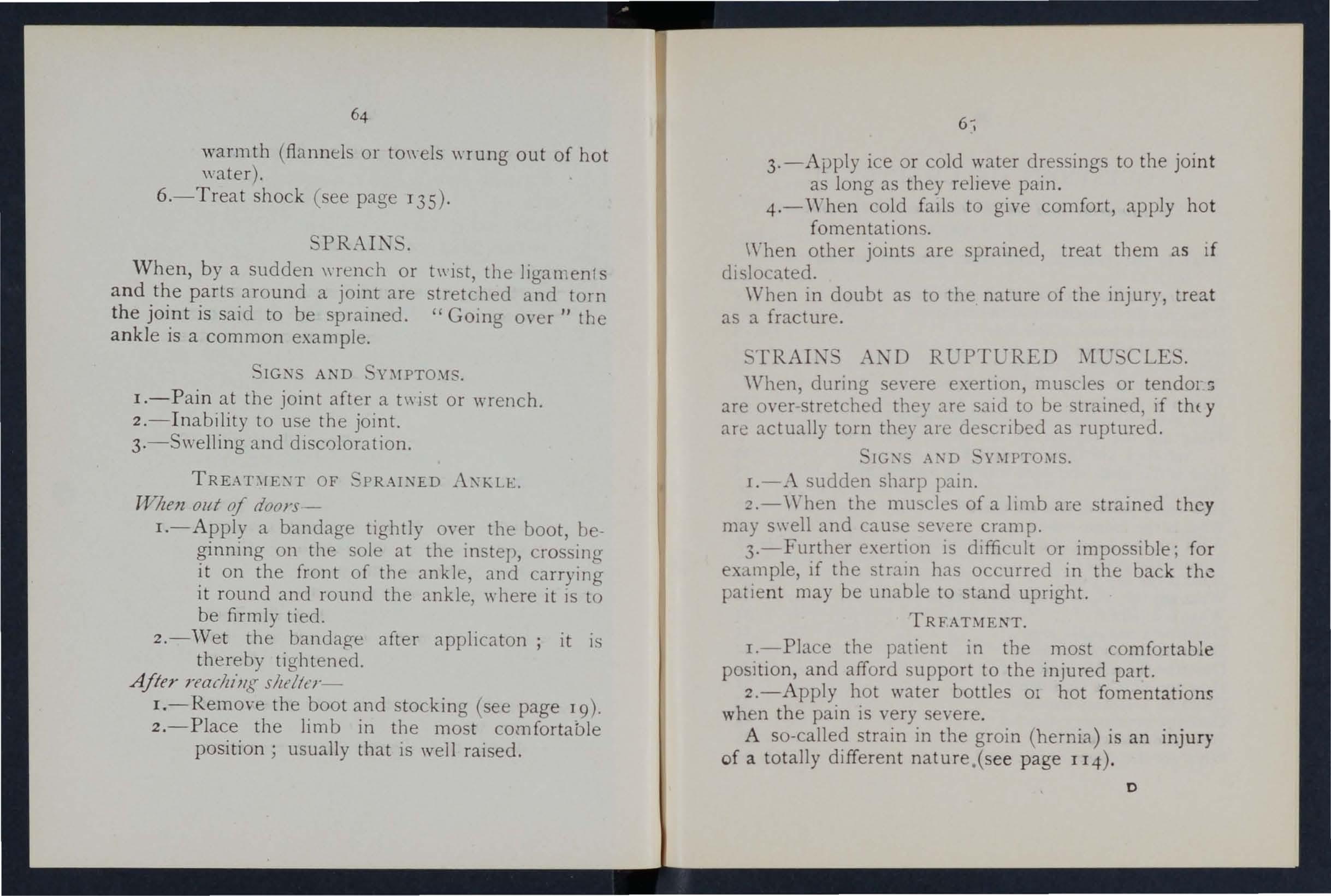
To apply a pad and bandage to the wound ) place a pi ece of lint or linen or a clean. chi ef folded into a hard pad, o n the bleedmg POl11t, and secure it by a bandage tightly tie.c rou.nd the injured part. To fold the handkerchi e f, bnng th e four corn ers t o th e cent re, and the process cntil a h ard pad is formed. The smooth surface is

75
placed on the \\ ound, and, to I rc\'em tbe pad tWIn unfc..luing-, the puckered surface may be stitched or fixed by a safety pin. A hard substance, such as a stone may be enclosed in the centre of the pad.
A may consist of a pad to be place d on the pressure point, a strap, cord, or baJ/dage to enCircle the lim b and pad, and a tl;r;/Lten/J/g armn/?twen/, such ns a stit k or other cf t\\ isting the band to tighten It.
To and apply a tcurniq u(t :-
I.-Apply a firm pad en tre pressure [oint.
2.-Encircle tbe lin,b hy a nnrro\\ b[!ndage \\lth Its centre oyer the pad.
3.- Tie the ends of the bnndage in a half knot on the opprsite side to the pad.
4..-Lay the t\\isting stick en tr.e half knot, and oyer it tie a r d knot.
).-Twi t the stick to tighten the bandage, thereby press:ng the pad ur n the artery, ::md arresting tr.e flo\\' of blood.
G.-Lock the stick in position hy the ends of the bandage already applied or by another h::ll1d age passed round the stick nnd limb
T he pad of th e tour11lquet r.lust be accurate ly plRc:ed upon the pressure point 0 as completely t ,:ompress the art ry; othen\ ise arterial bloed \\ ill be allowed to pass along the limb, and the yeins, being 'om pressed bv the tourniquet, \\ ill not a11O\ the
74
b loo d to return th rouJh the n to t:le he.lrt, and the res ul t will be dangervu and co n gestion .
Sho u ld a sUltable p .:td n ot be at h:md, a k n ot may b" m ade ill the cen tre of the b.mJage, a n d 'v"hen av.:ti lable, a stolle, cork, etc ., e n closed in it to give it firmness and bulk. . ee that the bulO'inO' a n d n ot t he fht side of the knot i ne"{t the skin.o 0
An elast ic bandage pJ.sseJ tightly rou n d the Ii nb, il1111eJiJ.tely above the selt of arterial h<:el11orringe, wIll bleeJinJ. The sImplest prevucll
f orm of thls bJ.IlJage is a strip of elastic webbin(Y t wenty-five to thirty inches 10nO' and two inches with a pIece of tape se.m at 0 e.lcb en 1. An b e l t or br.:tce \V.ill serve the Stme purpose. Except whe n pIrt of a hmb IS torn off, it IS not ad vi Ible to u se an cord or bandage if other applratus can be h1.d, as It cuts off all circulation in the limb.
Flexion COll ists of the application of a pad on t he p ressure point at the knee or elbow joi n t, flexing t h e lt mb to make pre sure , and securinO' the limb in t ht! fl exed positio n b y a ba n dage cro o sed like the fi g ur e 8.
G :L N ERAL RULE FOR TREAT:\IE'H OF A \ VOU\'T) ACCOMPAl'.IED BY ARTERIAL H.'E:'IIOin.HAGE.
1. SLOp b leeding.
II . P revent injurious germs [rom getting into the wounJ.

77
To attaill these nds :--
1. Place the pat ient in a suitable position t b earing in mind that the blood escapes WIth less fo r ce when the patient sits, and is sti ll more checked when he lies down.
2. Elevate the bleeding part, as thereby less blood finds its" ay into it.
3. Expose the wound, remoying whatever clothing is necessary. (ee Rule 8, a.)
4. Apply digital pressure.
(a) If the wound IS small on the leed1l1g (b) If the wound is large o n the pressure pomt next to the wound on the heart s1de. The neartst pl essure point is chosen m order to avoid c.uttlng off the circulatIon as much of the part as possible, but sometm:t.s it is necessar) to apply pre UTe sull nearer to the heart.
S. Remo ve foreign bod ie s, such as broken bits of cloth1l1g, hair, etc., seen in the \\ound; co not search for foreign bodie you cannot see.
6. Cover t he wo und with a clea n and firm absorbent dressi n g. .A hard dry pad of bor:lcic gauze or is to be preferred, but abs o rbent cott .n. \\'001, lint, or gauze, or a clean piece of 11l1cn ""111 answer the purpose. hould a n y doubt be entu tained as to the cleanliness of the dressmg, a clean piece of unprinted paper. such as the insIde of ar.
envelope, should be placed next the '\"GUile! before a p p lying the pad. (Compare pages 75 and 76.)
7. Bandage tightly over th e pad unless ;-
(a) Foreign bodies are su ' pected to be left unseen in the woulld.
(b) There is danger of causing injury to a fr.lcture. In these cases a lIght dressin.; only 'hould be applied .
8. Apply a pad and bandage or fle x io n on the pressure p oi nt (see Rule 4, b ), but o nly in the following cases ;-
(a) As a temporary measure while the wound is being exposed, examined and co,·ered.
(b) As a more permanent measure ,,,hen bleeding cannoL be stopped by the pad and bandage on the wound, or "hen, in accord met: \\ ith Rule 7, the tight band,lge h,b not been applied.
9. Afford support to the injured pa r t.
,Vhen part of a ltmb has been torn olI or the \\ ound is l acerated (for example by the cla\\' of an anImal or b y machine r y) hcr;morrhage frequently does not come on at once, but as there is a danger uf seyerc h c.emorrhage later, mea n s for its arre ·t should be appl ied to the limb, but not tightened unles necessary.

THF COl:R':;j' OF THE .\RTr: RlES, AND THE .\RREST OF H "E:\[ORR}HCl ', .
(Tnt: numher.;, of the prlssure points refer to thos e ()ll tilt' Frontispiece.)
TIII;- !,\RGF .'\RTFRIT:'-; 'WITHI,\ 'Ii'lL CIIE_T A:\D
The Aorta. 1::' the central or trunk artery of the bod). Commencing at the left ventricle it forms an arch helm'lll the upper part of th hreast-bonc. From the arch are gi,-en off the larue branches which c-"1.rry the blood to either sid of the head and neck and to the upper limbs. The Aorta passe down on the left of the spine to just below the nayel, \\ here It dl\ ides into two grc:lt branches (the iliacs)
D o n ot disturb a clot of blood formed oyer a \\ ound. No attempt should be made to cleanse a wound except with sterilised \\ater (that i - pre\,lou::,J) boiled 79 and allowed t) cool), and exreriencL , especia ll y in recent has shown that those \\ounds \\ h ic h we r e proyisionalh tre1tecl with a dry elr ssing a n d sl1hse'J.l1ently dressed by a surgeon \\ith proper app liances did he tuc.lents p,acti :ng arrest of arteria l hremorrhaae should feel the pu I e to see when the CUlT ·nt of in the artery ha been stopped, and should then immediately reb\: the pre . me made on the artcn. II: thl- \\'ay th.e Importance of the 8ccuratc application ot prl':--,>ure \\"Ill be rcaliseu, and the amOllnt of force nccc sary \\'ill he ascertained .
80 which convev the blood to the organs in the pelvis an d to the lo'wer limbs.
'Wounds of these arteries are one cause of internal bremorthag e, (see page 96).
ART ERfES OF THE HEAD AND NECK.
The Carotid Arteries (right and left) Je:1.\'e the upper p :Ht of the chest and pass up on ei ther side of the wi n dpipe and, just belo\v the level of the a n; le of tlte lower jJ.w, divide into the Intern J.l and External Carotid Art erIes. The Internal Carotid Artery ascends deeply in the n eck, and enters the cL1nium to supply the brain \\'ith blooe The External Carotid Artery gn'es off a number of branches; to th e front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the Occipital; the artery itself IS continued upwards in front of the ear, 'where it changes its nJ.l1le to the Temp'lral, a nd supplIes th e s calp in th e neighbourhood of the temples.
When a Carotid Artery is wounded, as in the case of a cut thro at, apply the thumb of one hand on the artery at pressure point I, pressi n g backwards agai nst th e backbone and taking care to avoid the ·\ mdpipe . I t may also be ne ces5a ry to pressure wi th th e other thumb J.bov e the v\ ound for two r nsons: (a) To arrest the fl o'.\' of blood from the main (jugular) vein in the neck, which runs

alonO'sicle of tbe carotiel :'dlery and is usually "'oundwd : t same time; (v) To check the flo\\' of from the upper e n d of the carotid artery it,se lf, \\'h1Ch .s ofte n considerable o\\ing to communlcatJon 1 et\\ec.: n the branches of this artery and those of its
idlv w. Di gital pressure must be m,aint::lI ned, by Ttlays of assisL:lIlts if n eces 'a ry, untIl the doctor :nri\'es (Fig. 38), . . The Facial Artery crosses the lowe r JaW 111 a hollo\\' t,,'o fingers' hreadth in front of the angle, <1n'd se nds branche::: to the Chlll, hps, cheek, and
Sr
FIG , 38.
FIG. 39.
outs ide of the n ose. Hrem orrhage from wounds o f the fac e below the level of the eye is to be arrested by:-
(a ) D igital pressure on pressure poi n t 2 (Fig. 39) ,
(b ) or G rasping the lips or cheek on both sides of the \\"ound by the finger inside -and the t hum b outside the mouth or v/ce versa.

. 40 . FIG.
The Temporal A rt e ry may be felt pulsating in front of the upper part of the ear. Hremorrhage from the region i)f the temple may be arrested by pressure applied at pressure point 3 (Fig. 40).
The Occipital Artery supplies branches to the
83
regIon of the scalp from the ear to the back of the head. Hremorrhage from this region may be arrested by digital pressure on pressure point 4, four fingers' breadth behInd the ear (FIg. 41). This point is difficult to find, and it is usually ufficient to apply pressul e im mediately below the wound.
Hcemorrha g e fro m the F o rehea d or anyw he re in the S cal p may be arrested by appl) ing a small firm pad on the bleeding point and securing it by a narrow bandage \\ ith Its centre laid on the pad, the ends carried round the held in the dIrection most cOl1\enient, and tied tightly O\'er the pad (Fig. 42) .
When a \\ ound of the torehead or scalp is assoCIated with a fracture, the FIG. 4 2 best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fingers; pass the other end of tIle bandage through the rin a thus formed and continue to pass it through and until the whole of the bandage is used and a r:ng as sho\\l1 in Fig. 43 is formed.
82
7IG
4I.
ARTERIES OF THE UPPER LIMBS.
The Subclavian Artery passes from a point be hind the inner end of the collar-bone across the fir r ib to the armpit.

FIG. 43. FIG. 44.
To apply digital pres UJ e ;-
I.-Bare the neck and upper part of the chest
2.-Place the patient's arm against the body ( as to depress the shoulder, and ca use him [l mcline his head towards the injured sid_
3·-Take your stand opposite the shoulder.
-i.- Using the left hand for the right artery, allll zl/ce versa, grasp the neck low duwn, placIn? the fingels behind the shoulder and th thumb immediately above the centre of th, collar-bone in the hollow between U"'! muscles attached to the bone (press Uf point 5).
85 the thumh deeply dO\\Il\\arcl s and backwards agatn<,t the first rih, \\ hi h i ben ath th collar-bone at this spot (FIg. -t-t).
The Axillary Artery , which is a continuation ( f the subcla\ ian, keeps close to the shoulder joint. i'nd can be felt pulsating when the fingers are deeply pre. sed into the armpit. Digital pressure is dIfficl Jlt to apply to this artery.
To apply a pad 11.1ndage ;-
l .- rlacc a hard pad the of a billiar d ball in the annpit (pre ure point 6).
z -Apply the centre of a narrow bandage on th e pad; ross the FI G. 45. bandage on . the shoulder; pull the ends tight ::md tle :llem und er the o ppos ite armpit, takll1g tare t hat the pad does not slip.
3.-F1ex the forearm and tie the limb tightly to the trunk with a oroal o 'l ndage, applied on a level \\ ith the elbo\\ (Fig -1-5) ·
The Brachial Artery is a continuation of the Axillary, and runs down the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The inner seam of the coat above the elbow roughly indicates its course.
Digital or instrumental pressure may be applied at or near pressure point 7.

FIG. 47.
To apply digital pressure extend the limb at right to the body, palm of the hand upwards. Stll1d ')ehlnn limb, and pass the fingers under the b:lck
87
of the arm over the seam of the coat or the groove on the inside of the biceps muscle. Press the pulps (not the tips) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47). A slight turn of the hand DS it grasps the arm will better ensure compresslOn of the artery.
The Brachial artery may be compressed at the
FIG. 49.
FIG. 48. elbow (pressure point 8) by fl exion. The pad may be a folded handkerchIef with a small stone or a cork \\,[:lpped up in it, but \\ hen no pad is ayailable the coat sleeve rolled or gathered up will serve instead 'Fig. 48).
86
88
, Just the elbow the Brachial artery dIvides mto the RadIal and Ulnar arteries which run alon cy the front of the forearm on the out'er and i::ner respectively . The pressure points (9 and 10) art: about one inch above the wnst and about half all inch from the outer and inner sides of foream where the arteries may be felt puls a tilw Branche:; of arteries join to form the Arches Ir the hand. The arteries run along 0n either sld f of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and 10 by the thumb c (Fig. 4-9 ) or as follows :- '
I.-Cut the cork of a quart or pint bottle in tW ( ' length wise.
2.-Lay the rounded s ide of one half on the Radial, and of the other half on the 1Jlnar artery.
3·-Secure them by a tight bandage.
To arrest hcemorrhage from the palm of the hand :-
I.-Apply a firm pad, and make the patient grasp it firmly. .
2.-Spread out a triangular bandage, turn up the base about four inches, lay the back of the patient's ha.nd on the centre of the bandage, fold the pomt over the knuckles and wrist pass the two ends fOund the \\"rist, make
89
patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the point (A) down to the knuckles and fasten with a pin at B (Fig. 50 ).
3·-E1e\,ate the forearm and supfJort it with a " St. John" sling (s e e page 49).
Arterial hcemorrhage from the fingers may be arrested by alJplying a small pad o n th e \\ ound, and securing
it firmly "lth a strip of t.l p e , linen or plaster.
ART E RIES O F THE Lo\\ ER LIMBS.
The Femoral Artery,
FIC. 50.
a c on tin ua ti o n of the iliac, e nt t' rs the thigh in the c e ntre of the fold of the
gro in, \\ her e it may be fe lt pulsatin g immediately b elo w th e skin . The cour e of the artery may be indicated by a line dra\\n fr o m the centre of the groin to the inner sIde of the back part of the knee. After traversing two-thirds of this line the femoral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressur e point II) as follows ;-
I.-Lay the pat ient on hIS back.

2.-Kneel beside the patient.
3.-To find the groin, raise the foot high so as lv flex the thigh; the fold in the clothing at the top of the thigh will indicate the groin
4.-Place the thumbs one on the other upon the pressure point, grasping the thigh with the hands (Fig. 5 I).
5.-Press firmly against the brim of the pelvis.
As there is ill)mediate danger of death it is important not to ,yaste time in removin g the trousers.
'When the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been
FIG. 51. devised for compression at this point, and relays of assistants should be employed to keep up the pressure until the doctor arrives ; each fresh assistant places his thumbs ove r those of his predecessor, who slips his away from beneath, and thus gushes of blood are prevcnt =d durin g the change.
Application of a tourniquet to the Femoral artery (pressure point 12) :-
When practising compression of this artery, it is a
90
g ood plan to draw a chalk line from the centre of thlt groin to the inner side of the back of the kn e place the pad of the tourniquet on this line as hlg up as the bandage can be applied . The pad shoul d be the size of a lawn te nnis ball (Fig. 52).
Pressure may be applied to the Popliteal arter Dy flexion at the knee (pressure point the pad shouJo

FIG. 53.
be the size of a lawn tennis bal1, or if no pad 1 available the trouser leg may be rolled or gathered up to serve instead. It is not necessary to take off the clothing (Fig. 53).
Just below and behind the knee joint the PoplIteal artery divides into the Anterior (front) Postenor (bac k) Tibial arteries.
The Posterior Tibial Artery passes down the.
93
back of the leg to the inner side of the ankle . I t is at first deeply placed between the musclEs of the calf, but it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the inner side of the ankle. It enters the sole as the Plantar Arteries, which run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery, on leaymg the Popliteal, at once pas es fon\ ard beh\ efn the leg bones, and, deeply placed amongst the musclE:s, runs down the leg to the centre of the front of the ankle. This artery is continued as the Dorsal Artery of the Foot, which, pa sing fon\ ard OYEr the tarsus, dips down to the s Ie bet" een the first and sfccnd metatarsal bones. Here it forms \\ith the Plantar arteries what is known as the Plantar Arch. At the ankle (pressure points 14 and 15) pressure may be applied by the fingers or by pads and bandages.
VEN OUS
I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3. - It issues from the side of the wound further from the heart.
4. - In the case of a wound of a varicose vein it flows also from th e side of the wound nearer to the heart, especially if the patient is kept standing.

Varicose Ve i ns .-The veins of the leg are speci::tlly apt to becom:! varicose. A varicose vein is dihteJ , winding, and with bead-like (varicose ). pr ojections alonO' its course . A vein becomes vancose f rom several 0 causes, such as long standing or tight garters. The first effect is to throw extra work upon the valves, and the bead-like pro jections are. caused by blo ::d accu!l1uhtll16 in the behll1d the valves . I n time the vein becomes so dIlated that the valves can no longer span it.
RULES FOR OF A 'VOUND I\CCO:vIP.UIED BY H.J!L\IORRHAGE.
I. - Place t h e patient in a sui t able position , beannz in mind th:lt the blood escapes with when the patient sits and is still more checked a s he lies down.
2. - Elevate the part, as thereby less blood finds its way into it.
3·- Expos e th e wound, remO\'ing "hatever clothin.:; is necessary.
4 .- Remove any constrictions, such as the collar or garters, from the side of the wound ..
5. - A pply digital pressure on the \yound untll you can apply a pad and tight bandage. If that does stop the bleeding, make pressure near the wound on the side away from the heart. In the case of a wound of a varicose vein it may also be necessary to 95
apply a pad and bandage to the vein imme d iate ly above the wound, espeCIally if the limb cannot be maintained in an elevated position.
6. - Treat the wound as directed by Rules 5,6 and 7, stated on pages 77 and 78.
7. - Afford support to the injured part.
CAPILL\RY HIE:\IORRHAGE.
I. - The blood is r e d .
2. - It flows briskly in a cont inuous stream , or may merely ooz e fr o m t he wound.
3. - It wells up from all parts o f t he wound . A slight amount of pressure "ill suffice to arrest capillary hcemorrhage.
INTERNAL HIE:\IORRHAGE.
'Vounds of the blood vessels within the trunk c:::tuse hc:emorrhage into the cavity of the che t or of the abdomen.
A. D nIPTmrs OF INTERNAL HIE:\IORRHAGE.
I.-Rapid loss of giddiness and especially when the upright position is assumed.
2.-Pallor of the face and lips.
3.-Breathing hurned and laboured, and accompanied by ya\\ l11ng and sighing.
4·-The pulse fails, ::tnd may altogether disappear at the wri t.
94
5.-The p3.tient throws his arms tugs at the clothina round the neck, and calls for aIr.
6.-FinallY the patient may become totally unconscious.
TREATHE?'i'T.
I.-Keep the patient 111 a recumbent position.
2.-Undo all tight clothll1g about the neck.
3.-Provide for free circulation of air; fan the patient . .
4.-Sprinkle cold water on the face; hold smellmg salts to the nostrIls; avoid other forms of stim ulants, at all events until the h<emorrhage has been controlled.
s.-Giv e ice to suck or cold water to drink; if the seat of the hcemorrhage is known, apply an ice bag over the region.
6.-Should the patient be reduced to a state of collapse, raise the feet and bandage the limbs fir mIl' from the toes to the hips and from the fingers to the shoulders .
HlEMORRHAGE FROM THE NOSE (NOSTRILS).
I.-Place the patient in a sitting position in a current of air before an open \\ indo"v, with the head th r own slightly back and the hands raised above the head.
2.- Un do all tight clothing around the neck and chest.
3.-A p pl y cold (ice, a cold sponge or bunch of

C7
keys) over the nose and also the spll1e at the level of the collar; place the feet in hot "'ateI'.
4 .-Cause the patient to keep the rr.outh ope n, and so avoid breathing through the nose.
Blood issuin g from the mouth may come from the tongue, the gums, the socket of a tooth after extraction, the throat, the lung", or the stomach
HlEMORRHAGE THE To ' GUE, THE GU MS, THE SOCKET OF A TOOTH, OR 1 HE THROA T
T .-G Ive ice to suck or cold \\ ater to hold in the mouth. If this IS not successful gl\ 'e \\ ater as hot as can be borne to hold in the mouth.
2.-If necessary make pressure on the carotid arterIes.
3.-If bleeding from the front part of the to:1gue IS excessive compress the part by a pIece of clean 11l1t held between the fing e r and thumb.
4.-If the bleedJllg tre ocket of a tooth) plug the socket wIth a piece of clean lint or cotton wool; over this place a small cork or other sut-stan c e of suitable size, and instruct the patient to bite on it
HJE:\IORRHAGE FROM THE LU;\Gs.
Blood f rom the lungs is coughed up and is scarle t fr othy in appea ran c e.
Treat a s fo r In te rn a l H cem orrha ge (see pag e 95 )' E
HJE;\[ORRHAGE FRO:\[ THE STmI ACH .
Blood from the stomach is vomited; It is o f a dark c olour a n d has the appearance of coffee grounds; it m ay be mixed with food. ,
T reat as for Internal H,emorrhage ,see page 95), except that nothing is to be giYen by the mouth.
Blood issuing from the Ear Channel, \\ hich generally indicates a fracture ?f. the base of the cranium, must be wiped away as It Issues; no attempt is to be made to pI ug the ear.
QU EST I ONS ON CHAPTER III.
The ll ulIl erais i Jl dirate Ihe pages where the auswei s may be fouJld.
organs a r e concerned in the circulation of the blood?
How many times a minute does the heart contract on the average?
is the effect of the patient's position on the rate at which the heart contracts?
would you know a case of arterial ha:-morrhage
what way should arlerial ue controlled?
is meant by" presure p oint"
Why is accuracy necessary in placing the pad of a tourniquet?
'-Vhen mayan elastic bandage be used instead of a tourniquet?
is flexion?
ta te th e general rules for treatment of a wound accompanie d by arterial ha:-morrhage ... 77, 78
If part of a li mb had been torn off, but there was nd mu ch bleed i ng, how would you act?
Sh ould b lood clots be disturbed ?..
I s it wise fo r a n unskilled person to attempt to cleanse a wound? . .. . 78, 79 Wha t is th e ao na? . . .
99
PAG K 'What
70 Describe
heart '" 7q T
body
70 to 72
72 Vhat
72 What is the pulse? ... 72 How
73 How
... 74 In
74 \\That
? 74 How
74 What
75
76
76
...
the
race the circulation of the blood through the
and lungs
many kinds of are there?
?
may pres ure be applied?
is a tourniquet?
n
What
78
70
79
roo
De cribe the arteries of the hend and neck 80
'''hy is it sometimes necess;tcy LO compress the carotid artery b.)th b elow and above the wound? ... 80, 8r
\Vhat is a ring pad, ancl what is it use? 4
Describe the art e ri es of the upper lim bs 84 to 89
Describe the arteries of the lower limbs... 89 to 93
How would you know a case of yenou - ? 93
" 'hat is a yarico e yein? ... ... ... ... 94
lI ow maya yein become y:uicose? ... ... ... 94-
SLate the general rules for treatment of a wound accompanied by yenous hXl11.Jrrhage 94, 95
lIow would you know a case of capillary hzemorrhage ? 9S
lIow would you stop capillary hxmorrhuge? ... . 95
"That is internal hxmorrhage? ... .. ... ... 95
\\'hat VI'ould lead you to suspect internal hxmorrlll.,e? 95, 96
State the treatment for internal hXll1orrhage? .,. 96
How would you arrest from the nose? ... 9 6 , 97
" 'here may blood i.suing from the m outh come [rom?.. 97
H?,," would you treat bleeding from the gums or throat? 97
" hat el e would you do if the tongue \\ ere bleeding?. 97
And if the bleeding \\ ere from the socket of the tuoth ? 97
H ow \\ ould you distinguish bet ween bleeJing fr0111 the lung and from the stomach ?.. .. . .., ... 97
And what would be the difTerence in the treatment? .. , 97
Of what i bleeding from the ear channel generally a sign? 98
The Student should practise placing supposed patienh in a proper position [or the arre·t of h::emorrhage ( ee page 72, 77 and 94), folding firm pads (74 anti 15 ), tying hard knots in bandages to form a t·.)nrnique[ (76), and the application of pressure at all the pressure point shown in the frontispiece, at vanous points on the forehead and scalp, and on the palm of the hand. Pres ure should be digital, by pad and bandage, or flexion, as directed i!l the text.

l'rc sure points- lan.liel arler) 8a. Facial, 82. Temporal. ? ()cripiLal 'uhclayian, 84·
Axillary, 85. Brachial (by pad and lmndage, pres.sure heing made against the humerus and 'by fleXIon at the ellJ()\\), l{adial an(l Ulnar. '67·
ITxmorrhage fr0111 the [urehcad or calp ...
J f:emurrhage fr0111 the palm of the h[t1Hl.. ..
Y (,l1llUS hxmon hage from a Yaricu;.e or other \ Lin
Fcmoral at thc groin, 90. Fcmoral in the thinh 92. J>uplitca1. 92. "\lltLrial and posterior arteric". 03. Sol 7 to 9 ···93,94
PAGE
101 PAGE

CHAPTER IV. BRUISES.
A blow anywhere on the surface of the b?dy cause ex tensi ve hcemorrhage beneath the skIn, \\'lthout breakino- it-a" black eye " is an instance. The injury is by discoloration and swelling.
TREATMENT.
Apply ice or cold water dressings. A piece of lint soak ed in extract of witch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is caused-
(a) By dry heat, such as fire or a piece o,f hot ir?n.
(b) By a rail, wire o r dynamo charged Wlth a hIgh pressur e electric current. " ,
(c) By a corrosive acid, such as 011 of
(d) By a corrosi\'e alka:i, such as caustic soda, ammoni a, or quick lim e.
(e) By fri ction, caused, for e,amr1e, by contact with a revolvi ng wheel. (Brush burn.)
A scald is caused by moist heat, such as boiling wat e r, hot oi l or tar. "
The e ffect may be a mere reddening of the .skm ; blisters may be formed; or even the deeper t issues I03
of the body may be charred and blackened. The clothin g may adhere to the burnt skin, and its removal is impossible without further detriment to the injured part. The great danger is Shock.
TRE ,\T:\fE;-';T.
I. - Carefully remove the clothing over the injured part. If sluck to the skin, the adherent clothino- mu t be cut around with scissors, soaked WIth oil, and left to come a\\ay subsequently.
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear pieces of lint or linen \\ ith oil, or vaseline, bnoline, or cold cre::tm; a st1l::tll quantity of boracic powder added to these \\ III he of benefit. The inside of a raw potato scrJ.ped out and spread on lint makes a soothing appllCJtion. \Vhen the injured surface is extensive do not co\'er It with one large sheet of lint, but \\'ith stripe:; about the breadth of the hand; this is advisable as they fit better on the part, and durino- subsequent dre sll1gs one strip can be removed at a tune, and a fresh dressing applied before tIle ad· jacent strip is taken off, The shock to the system is thereby less than if the whole of the burnt surface were I'aid bare to the air by the removal of all the dreSSings at one time . \V hen co\'ered by the oily dresslllg em'elop the part in cotton \\ 001 or a plece of fLlllnel and apply a ba n dage.
102
104
'When the face is burnt, cut a mask out of lint or lmen leavin a holes for the eyes, nose, and mouth , Dip ;h1s in oil or smear it \\ith vaseline and apply it to the face and cover it with cotton wool, leaving openings to correspond "ith the hoI s in the mask.
'When possible place the injured part at the temperature of the body (98 degrees) untIl sUItable dressings can be prepared. A dessert-spoonful of baking soda added to a basinful of the \,arm water make a soothing lotion.
'As it is important not to leave the part exposed to the air, it is the duty of the bystanders to prepare the dressings while the clothing is being removed.
4. - Treat Shock. -This is particularly necessary III the case of every burn or scald of any considerable extent (see page 135) ' Be very npprehensiYe of danger 111 the case of even slight burns of the neck. .
S. - If the burn is caused by a acid bathe the part with a weak alkahne lotio'n, such as washi ng soda, so?a (bicarbonate of soda), magnesia, or slaked hme 111 "arm water befo r e applying the dressings. .
6. - If the burn is caused by a corrOSIve alkali bathe the part with a weak acid lotion , s uch lemon juice or vinegal diluted with an eq u al qu an tity of water. Caut£on.-Before usi ng water brus h off a ny lime that r e mains on the part.

105
7. - When a woman ' s dress catches fire -
(
a) Lay the woman flat on the floor a t on c e, so that the flames are uppermost; that IS to say, if the front of the dress is on fi re lay her on her back, and if the back of th dress is burning, place her face do\\'nward s. The reason for this is that flames asce nd so that if the upri gh t position IS assumed, 'the flames "ill quickly :-each an rJ burn the body, neck, anu face; or if the woman flnmes undermost, they will, If unextmgUlsh ed , pass o\-er and burn the lim bs and set lire to the rest of the dress.
,b) As so on :1.S the \\'oman is laId flnt, smother the names with anvthin cr at hand such as a rug, coat, blanket: or table coye;; if made wet so much the better.
(
c) A woman rend erinr; assi, tance should hold a rug or blank et in front of herself when approaching the flam es . 9
(
d) I.f a woman's dress catches fire \\'hen nobody IS by, she should lie fiat, flames uppe r most} smother flames \\ith anything handy, an d c all for aSSIstance, or crawl to the bell- pu ll and ring; on no account should sh e rus h into the open air.
Th e use of fire guards would Od:>vent man '! c alamll ies
BI TES OF SNAKES AND R ABID ANIMALS , AND WOUNDS BY POISONED ·WEAPONS.
Hydrophobia is caused by the bite of an animal, such as a dog, cat, fox, wolf, or deer suffering from rabies. The special poisons introduced into wounds caused by yenomous snakes and poisoned \yeapons cause immediate danger to life.
TREADIENT.
1. - Immediately place a const riction betwe en the wound and the heart so as to pr eyent the venous blood from carrying the poison through the body. If, fo r example, a finger is bitten it bc encircled on the side of the wound tc 'Lhe "neart, with the finger and thumb, ar:.d as soon as possible a ligature (a string, piece of tape, or strip of handkerchief) should be placed tightly round the root of the finger. Compression with the finger and thumb must not be relaxed until the ligature has been applied. Additional ligatures may, with adyantage, be applied at intervals up the limb.
2. - Encourage bleeding for a time :-
(a) By bathing the wound with warm water.
( b) By keeping the injured limb low; the upper limb should be allowed to hang down, and in the case of the lower limb the patient should be seated with the foot on the g ro und.

IC7
3. - Cauterise the wound , if it is quite impossible to obtain the services of a doctor.
T his is best done by burning with a fluid caustic, suc h a s ca us tic potash, pure carbolic acid, or nitric acid, o r if th ese a r e not at hand, with a red hot wire or a fusee.
T he u sual solid caustic is insufficient, as it does not reach the botto:n of the wound, where the poison is .
T o ensure the caustic reaching the bottom of the wound, it should be applied on a piece of wood , such as a match cut to a point. \Vhen the caustic been thoroughly applied, but not till then, the lIgatures may be removed.
4. - Cover the wound, afte r a while, with a clean dressing.
s. - Afford support to the injured part.
6 - Treat shock if it occurs (see page 135).
7. - ln the case of a bite by a venomous rub in powdered permanganate of potash and Inject under the skin in the neighbourhood of the wound a solution of permanganate of potash.
ST I NGS OF P LANTS AND AN I MALS.
These give rise to serious inconvenience. a n d In some cases grave symptoms develop. -
TREATME TT.
I , - Extract the sting if left in.
2.- Mop the part freely with dilute ammonia
I06
o r spirits. A paste of bicarbonate 01 soda sal volatile is an efficient application. A solullon of washing soda or potash or the application of the blue bag will relieve pain.
3. - Treat c ollaps e if it occurs (see page 135)·
FRO T BITE.
During exposure to se\'e re cold, parts of the bo?y, u sually the feet, fingers, nos e, or ears, lose sensatIOn
a n d become first \\ axy \\ hite and afterwards congested and of a purple appearance. As sensation is l ost in the part, it is often only by the remarks of bystanders that the frost-bitten person is made aware of his condition.
I. - Do no t bring th e patient into a 'foom until, by fri tion of the band or by rubbmg wIth soft snow sensation and circulation in th e affected
p ar ts are Neglect of this precaution may lead to death of the of the frost-bitt en part.
2. - When circulation is r esto r ed , keep the patient in a room at a t emperature of 60 degree".
NEEDLE EMBEDDED UNDER THE SKIN.
\Vhen a needle breaks off after penetrating the skin and disappears, take the pati e nt to a doctor at once. If the wound is near a joint, ke ep the limb at rcst on splint.

10)
FIS[{ -HOOK L THE SKIN,
Do not attempt to withdraw the fish-hook by the way it went in, but cut off the dres ing of the hook, so that only the metal is left, and then force the point ol1\\'ards through the skm untIl the hook can pulled out .
INJURIE TO JOI TT .
WhU1 a JOInt is injured by a bullet, stab, or othe» cause-
I. - Wrap the part in cotton wool.
2. - Afford rest and support to the injured limb; if the upper limb, in a t1e'\ed posItion by a sling if the 10\\' er limb, in a straight po<;JtIon by a splint.
BODY L T THE EYE.
I. - Prevent the patient rubbing the eye, t)'lI1g do\\ n a chIld's hanc1 ' If nec es ary.
2. - Pull down the lower eyelid, \\-hen, if th ... foreign body IS seen, it can readily be removed wIth a camel's hair brush, or \\ Ith the corner of a handker chief twirled up and wetted.
3. - W hen the foreign body is beneath the upper ey elid lift the lId fo[\\ ard, pu h up the lower lid beneath it and let 0-0. The hair of the lower lid brushes the inner surface of the upper one, and may dislodgE. the body. hould the first attempt be unsuccessful, repeat it several times if necessary. If
108
II O
the foreign body is not dislodged call the services of a d octor as soon as possible . When, however skilled help cannot be had , proceed as follows
(a) Seat the patient so as to face the light, an d stand behind him, st ea dying his head against your chest. .
(
b) Place a small rod, such as a match or bodkin, on the upper eyelid, half-a n-inch aboye the edge, pressing it backwards as far as f ossib le .
(c) Pull the upper eye-lashes up\\ards oyer the rod, and thereby evert the eyelid.
(d) Remove the foreign cody.
4. - When a piece of steel is e m be dd e d in the eyeball a little olive or castor oil c n the eyeball after pulling down the lower eyelid, close the lIds, apply a soft pad of cotton \\ 001 and [ecure it by a bandage tied sufficiently firmly to keep the eyeball steady; take the patient to a doctor.
5. - When quick-lime is in the eye brush away as much of it as possible; bathe the eye "ith vinegar and \\"arm water, and treat s for a riece of steel embedded in the eyeball.
F O RE I G N BODY I N THE EAR PASSAGE.
A,s a rule n:ake no attempt to treat a patient with &. fo r eIgn body In the ear if the services of a doctor can po ssibly be had! any attempts to remove the foreign bo d y may lead to fatal consequences. If a child

III
cannot be induced to keep the fingers from the ear$ tie his hands down or cover up the ear. If an insect IS in the ear-passage, fill the ear with olive oil, when the insect will float and may be removed. Never sy ringe or probe the ear.
FOREIGN BODY IN THE NO E.
Induce sneezing by pepp er or snuff. Cause the pat1ent to blow his nose violently after closing the nostril. There is no immediate danger from a foreign body in th e nose .
THE ABDOMEN.
The abdomen is bounded above by the diaphragm; bel ow by the pelvis; behind by the lumbar vertebrce; and in front and at th e sides by muscular walls. (Fig. 54 .)
THE ORGANS GF THE ABDo:'IlEN.
The Stomach lies immediately below the" pIt of the sto:m1.ch " just below the breast-bone.
Th e L iver lies in the upper part of the abdomen, where it is mostly covered by the ri ght lower ribs.
Th e Sple e n lies beneath the ribs at upper part of the left side of the abdomen.
Th e Int estines occupy the greater part of the cavit y of the abdomen.
The Ki d n e ys lie at the back, in the region of the loin.
The Bladder lies In the pelvis.
FIG . 54.
'WOUND IN THE FRONT \VALL OF THE ABDO !EN .
Wh en the £ntestl'nes 01 otller organs protrude throug h the wou n d, whether vertical or transverse, ben d th e kn ees, raise the shoulders, and apply lint, a t o\\ el, or co t t o n wool wrapped in soft li n en, a n d k eep the

iI3
pati e nt war m u ntil the doctor arrives. \ Vhen there IS n o p rot ru slOn of organs, if tile 7.i..Ioltlld is verHcal, lay t h e pat ie n t flat on the back 'with the 10\\ er limbs straigh t ; if the wound lS transverse , bend the knee!: a n d r aise the shoulders.
I NJURIES TO THE ORGAXS \VITHIN THE AB D OMEN PELVIS.
Injuries of the Stomach are attended by extreme collapse and sometimes by vomiting of da rk blood like coffee-grounds. For treatment seE " from tomach /I (page 98 ).
InJunes of the LIver, Spleen and Intestines may be caused by a blow, a stab or a bullet; the liver or spleen may be injured by a fracture of the lower ribs. The igns and ymptoms are those of mterr:al hremorrhage accompanied by pain and swellmg at the seat of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, al.so by a crush, stab or bullet. Blood may escape with the urine, and the re may be pai- 1 and s\\'ellinO' oyer the injured k idney. b
The Bladder may be injured by a fracture of the pelvis. The signs and symptoms are either inabilIty to pass water, or if a little is pas-sed it is tinged with bl o od .
lI 2
TREATMENT OF INJURY TO THE KID EYS OR BLADDER.
:1:.- Keep the patient quiet until the doctor arrives.
2. - Apply hot fomentations over the painful or injured part.
Rupture (hernia) consists of a protrusion of an internal organ, usually the bowel, through the muscular wall of the abdomen, most frequently at the groin. Should a sudden swelling accompanied by pain and sickness take place in that region
I.-Send for a doctor instantly.
2.-Lay the patient down with the buttocks raised.
3.-Apply ice or cold ,yater dressings to the affected part.

QUESTION ON CHAPTER IV.
Til : Iwmera!s z'ndi'm'e the pages wllere tile answers may be found.
is a bruise?
How would you treat a bruise?
lIow maya burn be cau ed? 102 How is a scald caused? 102 \Vhat is the great danger of a burn or scald? ... 103
State the general treatment for burns and scalds r03, '104
J I)w would you treat a burn caused by a corrosiYe acid?
How would you treat a burn causecl by a Corro ive alkali? r 04
\\,h1.t steps should be taken when a woman's dress catches fire? ... roS
State the general rules for treatment of by poisonous bites or weapons ... ... 106, 107 \Vhat special treatment is required for the bite of a venomous snake?
107 IJow you treat a sting? 107, 108 State the sIgns, symptoms and treatment of frost-bite ... 108 W.).lld you attempt to rem ove a needle embedded under the skin?
Il)w would you extract a fish hook em bedded in the skin?
Slate the tre3.tmcnt ::: ::: ::: late the general rul es for ren10ving a foreign body from the eye... ...... ... ... r09 , IIO
\V hJ.t would you do if a piece of .;teel were embedded in t he eve ball?
Ant! quick-lime is in the eye?
lIow would you try to remove an insect from the ear
passage? .. III
114
PAGE
102
What
102
..
, ... 104
... ... ... .,. ...
.. , ... ... ... ... . ..
108
IIO rIO
u6
Would you try to H'1110Ye any other form of fo reign body from the ear passage? ...
. 1 10 I II
How would you a foreign body from the nose? 'I I J tate the boundaries of the abdomen and its contents I [J
State the treatment for wounds of the abdomen 112 I 13
How may injuries to the liver, spleen and intestines be ' caused?
l IJ
What is the diA'erence treatment of injuries to the stomach and of lnJunes to the liver spleen and intestines?
State the treatment of injuries to the kidneys or bladder
State the treatment of hernia ... " . 11 4

CHAPTER V.
THE NERVOU Y. TEM.
T\\ 0 systems of nerves, the Cerebro-spinal and the Sympathetic, regulate the movements and functions of the body.
The Cerebro-sp inal System is made up of the Brain, the pinal Cord and Neryes, and through its agency sensations are received and the will causes the action of the voluntary muscles. For example, when a part is injured a sen ation of pain is conveyed to the brain by the nerye, thus affording an indication of the seat of injury or a warning of a possible danger of further damage. On attention being dire ted to the injury. an attempt is instantly made to ease the pain or to moye the injured part from danger.
The Brain is ituated within the cranium, and is divided in the middle lllle, 0 that, with the exception of some connectll1g bands, the right and left sides are separate.
The Spinal Cord i the long cord of nen'ous matter lying wi th III the spinal canal (ee Vertebral Column, page 23). It leaves the brain through an opening in the ba -e of the cranium and extends to the upper lumbar , -ertebrre .
... ... . .
... ... ... ... .....
. .. .. ...
.
...'
11 7

The Nerves proceed from tbe train and spina cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissues of the body. When a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed .
The Sympathetic System extends as a nervous chain on each side of the front of the spinal column along its entire length, and sends branches to all the organs of the chest and abdomen to control the mvoluntary muscles, and thereby regulate the vital functions. This system is not under the control of the \\'ill, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air reaches the lungs by \yay of the nmtrils (or mouth), the throat, the wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it e nters the \\ ind-pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, however, the yalyc falls to act, that should solids or fluids be given by the mouth, they may enter the wind-pipe and cause asphyxia. The wind-pipe extends to two inches below the top of the breast-bone, where it divides into the right and left bronchial tube. Each bronchial tube enters a lung a n d divides into small and still smaller tubes, until
II 8
FIG. 55. THE LUN '}S AND BRONCHIAL TUBES.
A . Trachea, or Wind -pipe. B. Left Bronchus. C. RigM Bronchus. D. maller Bronchial Tubes.
12J
the ultimate recesses of the luna-the air cells or air sn8ces-ar e reached. 0
fhe Lungs, Right and Left, occupy tl1e g r eater of the chest; they lie immediately within the nbs, and practically wherever a rib is felt whether front,. back or sides, there IS lung beneath. Each lun.g is enveloped in a fine (the pleura ) wh ich allm:'s It to move \Vlthm the chest during breathmg without friction.
or breathing, consists of two acts, InsplratlOn, an expansion of the chest durin<Y
W,hICh air .is drawn into the lungs, and Exp'iration: a contrac tIOn of the chest, during \\ hich air lea vee; the lungs. A pause follow') the act of expiration . In. health fifteen to eighteen breaths arc tak e n per mInute, at each inspiration about 20 to 30 cubic Il1ches of alr e nt er the lungs, and a similar quantity is at each expiration.
Th e exp3..nsion and contraction of the chest are effected. partly by the muscl es of respiration attached to the nbs, but chiefly by the Diaphragm the larrre arched muscular partition \\ hi ch separates' the ch:St from the abdomen . In inspiration, \\hich is chiefly a act, the ribs are raised, and the a r ch of the dIaphra gm falls and becomes flattened thus in· the capaCIty of the chest and the aI : to en ter. In expiratio n , a n act performed almost without e ff ort , the ribs fall and the arch of the

diaphragm nses; this lessens the capacity of the ches t and forc es air out. The mechanism of respna tIOn IS somewh at like that of ordi nary household bellows, but \\ itbout a valve ; the may be com pared to the boards of the bellows, whi le the diaphragm corr esponds to the leather, the air passages bei n g equivalent to the nozzle.
As the blood depends upon the air for its punficatlon and the oxygen necessary to maintain life, inte rference with breathing very soon may produce a dangerous state called asphyxia, examples of whi ch are afforded by drowning, suffocation, choking, etc.
ARTI fICIAL RE PIRATION.
PR OFESSOR CH't\FER ' S lETROD.
I. - Waste no time in loosening or in removing clothing.
2. - Lay the patient in a prone position (i.e., back upwards) with his bead turned to one side, so as to keep his nos e and mouth away from the gro und . No pad is to be placed und er the patient, nor need the t ongu e be drawn out, as it ,,,ill fall naturally.
3. - Kneel at one side facing the patient's head, and place the palms of your hands on his lowest ribs, one at each side, the thumbs nearly t ouching one another in the small of the back. Leaning your body forward, slo\\ ly apply firm but
121
not violent pressure strajght downwards upon the back and lower part of the chest, thus drivi n g air out a nd producing expiration (Fig. 56). D raw back

1 2 3
yo ur body somewhat more rapid ly a nd relax th e p ress u re, but do not remove your hands; this produ ces inspi ration (Fig. 57).
4 . · - Alternate these movements , by a rhyth mic s waying backwards and forwards of your body, twelve t o fi fteen times a minute, persevering unti l respiratio n is r estor e d, or a doctor pronounces life to be extinct
DR . ILVESTER ' S }'IETHOD.
I . Adjust the patient's position. -Without wasting a moment place the patient on his back on a flat surface, inclined if possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women. Raise and support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades.
2 . Maintain a free entrance of air into the windpipe. -Cleanse the lips and nostri ls; open and wipe the mouth; an assistant In ust draw forward the patient 's tongue as far as possible, and keep it in that positio n.
3. - Imitate the movements of breathing. Induce IJlspl>·atloJl.-Kne el at a co nvenient di st anc e be h ind the patient 's head, and, grasping his forearms just below the elbow, draw the arm s
122
FIG. 57. INSPIRATION
FIG. 58. INSPIRATION.

FTG. 59. EXPIRATION.
upwards, outwards, and towards you, with a swetpmg movement, making the elbows touch the ground
FIG. 61. EXPIRATION.
(FIg . 58). The cavity of the chest is thus enlarged i and air 1S drawn into the lungs.
12-1
1 2 5
Induce expzration.-Bring the patient's flexed arms slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (Fig. 59). By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and perseverin gly about fifteen times a minute.
'Vhen a sufficient number of assi5tants are present, Howard's method may be combined with Silvester's, as follows :-
The additiO.nal assistant kneels astride the patient's hips with the balls of the thumbs resting on eIther side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Usin g his knees as a pivot, he presses forward on his hands. Then suddenly, with a final push, he springs back and remains erect on his kne es while he slowly (ounts I, 2, 3. These motions are to be repeated to correspond with those being performed by Silvester's method, pressure on the chest being made simultaneously by those performing the t\\'o methods (Figs. 60 and 6 I).
LABORDE's METHOD.
\Vhen from any cause the above methods cannot be carried out, Laborde's method of artificial respiration should be tried. It is especially useful in suffocated children and when the ribs are broken.

The patient is placed on his back or side; the mouth cleared; the tongue is seized- using a handkerchief or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede into the mouth. Th ese movements should be repeated about fifteen tim es a minute.
Artificial respi ration must be continued until breathing is established, or until a doctor arrives.
'Vh en natural breathing com mences, regulate the artificial respiration to correspond with it. Success may result even after two hours' time.
Excite respiration. - 'Vh ilst artificial respiration is being applied, other useful steps may be employed, such as applying smelling salts or snuff to the nostrils J and flicking the chest with a damp towel.
Induce circulation and \\-armth after natuml breathing has been restored. "'rap the patient in dry blankets or other cO\'erino-, and rub the limbs energetically towards the heart. Promote warmth by hot flannels, hot-water bottles, or hot bricks ,(wrapped in flannel) applied to the feet, to the limbs and body.
'When the po\\'er of swallowing has returned give hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go t o sleep Large poultices or fomentations applied to the
126
I 2 7
front and back of the chest will serve to assIst breathing .
Watch the patient carefully for some time to see that the breathin g does n ot fail; should any signs of failure appear, at on ce begin artificial respiration IN IBILITY.
Unconsciousness or Insensibility may arise as follows :-
Injury to the Head. - C oncussion and Compression of the brai n.
Disease of the Brain. -r\po plexy , Ep1l epsy: Hysteria.
Various Causes. -Shock, Fainting (Syncope), Collaps e, Alcoholic a nd ot h er poisoning, Sunstroke and Heat-strok e , Infanti le COIwulsions, Asphyxia .
GENERAL RULE FOR TREATMENT OF IN E J ' IBILITY.
I. - If a person appears about to lose consciousness, prev ent him from fallin g, and lay him gently down.
2. - i '\ rre:st rtcemorrh _-..:, when apparent; atten Jjlg tv mir:or injuri r · '-; less importa nt than treating the unconscious
3.-Lay the patient in the position in which breathing is most easy-esually this will be on the back, or inclined to one side. As a general rule

f. l;...,e h ead 8n<.1 shoulc1ers slz;E;ltllj the face is and keep the head low "hen the face is p8lc.
4. - Undo all tight clothing round the neck, chest and waist, unfastening tl'c traCES and t< p button of the trousers in men, and the corsets in women, the object bei ng to reline pressure on tbe air passages, lun gs, heart and abdonlinal organs. Bt: sm-;e that there is no ob trut tion to the air p8ssages by the tongue or by a foreIgn body in the throat. Th e pos"dJilily of false teeth otqlUcting lreatbing must be ( umluered.
5. - Provide for a sufficiEncy of fresh air hy ( doors amI "indo\\ s, amI by keeping back a (ro\\ (1.
6. - When breathing cannot be discerne d apply artificial respiration.
7. - 0btain a doctor 's help as soon as possible.
8. - Un.Jess unavo idabie, never leave the patient until you have placed h'm in charg e of a responsible pe rson .
9. - Give no food or flu ids whatever by the mouth while the patient is insensible.
10. - Should the spine or an important bone of the upper or of the lower limb be fractured, It must "teadied anc1 maintained at rest as s on as pos. ible. the iousnf'ss be prolonged, thl! pati ent may be remOl t'd m a recumbent p o ition 11'
128
to shelter, provi ded that the broke n bone is adeq uately supported.
II.-When the patient is in a state of consuppJrt his head, and after wrapping a pIece of wood or any other hard material in a 'handkerchi ef, hold it in his to prevent biting of th e ton.gue. Do forcibly restrain his limbs; prevent him from hurtmg himself by dragging hirD away from a of such as machinery, a wall, or fireplace ; lJght pieces of furniture should be pushed out of the way.
to consciousness water may be given to dnnk . . If the pulse is fe e ble give warm tea or provided hcemorrhage, internal or external, IS not A desire to sleep should be except 111 cas es of opium poisoning, a. COn:1ltlO 1 that may generally be recognised by the hIst ory of the case, and alsJ by the pupils of the bh,ck openings in the grey, blue or brown lrls ) m111utely contracted (pin-head pupils).
. - I t not be assumed that a person IS Insensible as the result of drink merely because the breath smells of alcohol' frequently people are feeling ill they take or' are given '>tIm ulants, after which they may become from the drink, but from the cause mduc.ed them to take it, for example, insensibility commg on, effects of poisoning, etc. Even if

13 1
drink is believed to De the actual cause of insensibility, it must be bOI ne mind that the patient is in a very dangerous state, and he must be treated for Ccllapse by being cov.ered up and kept \\'arm . The above general rules \\ ill enable first aid to be rendered efficiently in most cases of insensibillty, although the exact form from \\ hich the patient is suffering is unkno\\'n.
CONCUS ION OF THE BRAIN.
[he patient may be stunned by a bIo\\' or fall on the head, or by a fall on the feet or 10\\ er part of the spine. He may qui ckly regain consciousness, or insensibility, more or less complete, may be prolonged.
TREATi\l E' T.
I . - Apply the general rules for the treatment of InsensibIlity
2. - Be very apprehensive of danger in all cases of injury to the head. The patient may be stunned, and after a short interval may reconf some degree of consciousness, or even the brain may apparently have escaped injury; yet in both instances there is a grave risk that a structure within the cranium has been and that a serious st:.tte of insensibility may develop later. (See Fracture of \he Cranium, page 43') A cautio n should therefore be given to a patient who has lost consciousness eve n
130

[3 2 for only a moment after nt1 injury to the he::td not to r es ume physical or mental activity \\"ithout t he consent of a doctor.
CO:\IPRE.' 'ION OF THE BRAIN, APOPLEXY .
Compressio n of the Brain may result from the same cau se as produce Concus ion; in fact, C ompression is frequen:l y preceded by Concussion .
Apoplexy usu::tlly occurs in elderly people, and no of injury ::tre necess::trily present .
In both conditions the face is flu ·hed ; the breathing s[trtorolls; one side of the body lllay be l:lOre limp than the other: and the pupil of one C) e may be larger than th::tt of the other; the temperature of the body IS ge nenlly r::tised.
I. - App ly the general rules for treatment of In sensibilit,·
2. - Pro'mote warmth in the lower part of the body by the ::tppltcatlon of hot \\<lLer bottle to the abdomen and lo\\er limbs. C1rc must 1 (. tJken not to burn the patie n t \\ ith the bottles, ,,11 ich should be \\ rapped In -lbnnel, and their heat tested \\ ith the elbo\v.
EPILEP Y.
Epilepsy may occur in persons of any age, but usually occurs in young adults . The patient ta Us to I " J.)
the g round, sc,metimes with . a sC'l. eam, a n d passes Into a state of convulsion, thro\\ Illg hIS limbs abo ut. The treatment is acconling to the G ne ral R ules especially Rule I I.
BY TERIC.:"I.L FIT (BY . TER IAl \)iD
The patient, usually a young gnl, in conse qucr.c e of mental excitement, suddenly loses comma nd nt her feelinas and actions. . .he subsldes on a co uch or in comfortable posItion, throws herself about, grinding her teeth, clenching her fists, shak1l1g her hair loose; she cl utches at anyone or anythll1g ne :H her, kicks, cries and laughs alternately The eyeballs may be turned upwards, and the eyehds opened and shut rapidly. At times froth appears aT. the lips, and otrLel irregul :n 3ymptvms may develop
TRFAT:\fFxT.
I.-Avoid sympathy with the patient, and speak. firmly to her.
2.-Threaten her \\·ith a cold" ater do uche, and if she p ersists in her "tit," sprinkle her wi th cold water.
3.-Appiy a mustard leaf at the back of the neck, Medical treatment is necessary to cure the condl < tion of mind and hody which gives rise to hyster ic a l att ac ks.
SHOCK, FAINTING (SYNCOPE), COLLAPSE. CAUSES.
I. - -Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated \younds, and severe crush are some of the more frequent physical causes of shock ,
2.-Fright, anticipation of injury, and sudden bad news, or sometimes sudden removal of fear and anxiety after prolonged suspense, produce shock or fainting.
3 - ome poisons cause shock, \"hile others, such as alcohol, so depress the nervous system that collapse ensues.
4.-Hremorrhage or heart weakn ess , a close or crowded room, tight clothing, fatigue, or \\ ant of food may bring on fainting or collapse.
SIGNS AND SnlPTOl\lS.
The general condition of shock may be by extreme pallor, a feeling of cold, clammy skm, feebl e pulse, and shallow breathin g accompanied, If hremorrhage has been severe, by ya\\ ning and sighing. The term "collapse" 5igniiies , a Ye:y ' serious condition in which the life of the .pauent js In the greatest danger; the tern perature of the body falls below the normal, and one great object of treatment is to prevent it sinking to a point at which lIfe is Imp0ssible. An attendant danger of the condition of

135
collapse is the liability to sudden relapse after a temporary Improvement, and the utmost care and watchfulness must therefore be exercised to maintain the heat of the body and to guard against failur@ of the heart and lungs.
TR EAT:o.IEXT
.
I. - Remove the Cause by arresting hremoro rhage, attending to injuries, loosening all tight cloth · ing, especially about the chest and abdomen remov · ing from a close or crowded room, using words, etc,
2. - Lay the patient on the back with the low. the lower lim bs; \\ the patient IS m bed thls IS best done by raising the foot of th e bedstead.
3. - P rovide for a free circulation of fresh air.
4:. - l ,f hcemorrhage has been severe and the patIent IS collapsed, firmly bandage the lim bs from the toes to the hips, alld from the fingers to the armpits.
5. - To stimulate the action of the heart sal volatile and water may be gIven if the ]:atient ' can swallow, or smelling salts may be held to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of ture below nor,mal point. To accomplish this cover the patIent WIth extra clothing, or by placing
r ugs or blankets o v er hI m; ge t him to bed in a wa rm but well-ventila te d r oo m as soo n as possible. Apply warmth to th e fe et a n d t o th e pit of the storr. a ch by hot water bottl es or hot fl an n els . (Test th e h eat of these with th e elbo w befo re a pply in g th em .) If th e patient c a n s \vallow, give hot d ri n ks , s u c h . a s . tea or coffee. I t is well to add su ga r, as It aIds In r aIsin g t he t emperature of the body .
7. - If breathing cannot be discerned, app ly artificia l r esp iratIon.
8. - If want of nourishment has bee n th e ca u se o f faintin g or collapse, give food spari n gly a t fi rst.
SUN S TROK E A 1D HEAT -STROKE .
\Vhen expose d to great heat, as in the stok e- h ole of a steamer, especially in t he tropics, or t o th e r ays of the sun durin g a ma rch in ve ry h ot weath e r w h e n heavily burd e n ed , p ersons may d evelo p s ic kn ess, faintness, gid di n ess, a n d dIffic u lty i n breat h in g . Th e patient comp lai ns of t hirst, t h e ski n bec om es a nd burnin g , the face v e r y flu s h ed, t he p ul se q UI c k and bounding. A v e ry high te m pe rat ur e , s te rtorous (sn o rmg) breathin g , a nd insensibi lity may e n s u e.
T REATMENT .
I. - Undo all t ight clothing.
2.-Remove the patlent t o a cool, shJ.dy spot
137
).-":trlp the patient to the waist.
-t .-Lay the patient do\\n, with tlle head and trunk well raised.
5.-Procure as free a circulation as possible of fresh all', and fan the patient vigorously.
6.-.\pply ice bags or cold water freely to the hearl, neck, and . pine, and maintain this treatment until the "\ mptoms subside.
return to consciousness, the patient may h:wc water to drink.

or 5tOl1l:1ch troubles arc the commonest ('::tuses of this ::ulment.
Src;,>.'.
:'pasm of the of the limhs and trunk, blueness uf the flce, more or Ie s complete, and occasionally squinting, su. p nc1.ecl ItSplralIOn, and froth at the mouth are the pr01llll1ent sll)ns.
TRE .\T\IJ '{T.
I.-SU pport the child 111 a warm bath slightly abo\e the tempemture of the boely (98 d grees), so that the water reach '5 to the middle of the trunk.
2.- Place a sponge dippell in cold water on the top of t:1C head.
[N
13 8
ASPHYXIA.
''''hen, owing to want of air, the blooa 1S not supplied with oxygen the patient becomes insensible, and is said to be asphyxiated. This condition may be brought about as follows: -
I. Obstruction of t h e air passage s .
(a) By DROWNING.
(b) By OUTSlDE: Strangulation, hanging, smothering.
(c) By A FORElGN BODY IN THE THROAT; Choking.
(d) By S VELLING OF THE Tl SUE OF THE THROAT: Infhll1111atlOn, scald of the throat, poisoning by a corrosive.
II . Inhaling pois onou s gases. By coal gas (as used in the house), producer, or water, gas, smoke, fumes from a charcoal or coke fire, sewer gas, limekiln gas, carbonic acid gas.
III. Pressure o n the cQe s t, as when crushed by sand or debris, or by a crowd.
IV. Nervous a ffe ction s, as the result of narcotic and certain other poisons, collapse, electric shock, or stroke by lightning.
GEI\ERAL TREA.TMENT.
In all cases of Asphyxia attempts must be made to remove the cause, or to fl m ::)Ve the patient from t h e caus e. When this has been done artificia l

respiration m u st be applied , taking care that tn.e air passages are not obs tructed, ar:u. that there lS abunda nce of fr sh air.
mO'v\NIKG.
Persons comp! tely immersed in \\ ater or fifteen minut s have been restored by means. Therefore, if the body is recovered wlthm a reasonable time, absence of of is not to deter immediate attempts to restore ::mlmatl0D:'
The first thing to do when the b ely IS :s to ge t rid of the '" at r froth obstructmg. the . alI. passages, and th n artIfiCially. to rEstore This is best accomplJshed tIther by proceedl11g at once to p rf orm arttfi ial respIratIon by r's m thod or as follows ;-
I. -AS quickly as pos ible l oosen th e clothing, and clear the mouth and the back o f the throat.
2 .-Turn the patient face downwards, with a pad below the chest, and with the forehead upon the nght forearm.
3.-,\Vhilst in this pos1tlOn apply pressure. by the hands to the patient's back over the lower nbs, and keep the pressure up for three . ' .
4.- Turn the patI e nt on the rIght SIde, mallltallllllg that position al 0 for three seconds.
5.- Repeat these m o vements alternately as long as troth and \\ater issue from the mouth.
139
These op e ra tions (Marshall Hall 's method ) 111 the l1lselves tend t o p r omote respiration, uut ',\ hen the air pas ag e are clear of froth and water 'l lvester 's metbod of artificial respiration may ue used oy ils elf or \\ith Howard 's method in conjunctlOn.
" Tbil e uerforming tbese operations send someone to th e nearest house to procur e blanket s and dry clothing, hot water bottles, etc., and to fet ch a doctor.
SI' RANGULATiON.
Cut and remove the band constrictmg the throat. Apply artificial respiration.
HANGING.
Do not wait for a policeman: grasp the ] 0\\ er Ii m bs and raise the body to take the t en ion off the rope; cut the rope, free the neck; apply ar tifici al rCSplratlOll .
SMOTHERING.
Remov e whateyer is smothering the patient: apply artificial respiration . CHOKING.
Open the mouth, forcibly if need be; pass the f orefinger right to the back of th e throat and attempt to dislodge the foreign body; if yomitin g H;SUlt , so much the better. If unsuccessful, thump the back hard whilst the head is bent fOf\\ald. .l\.ppl) artificial r es piration.

S ,\ E LLL\ (; OF 1 HE TIS. UES OF THE '.tHR OAT.
'Whether th e s we lling is caused by inflam matlOq b y s\\a ll owlI1g vcry hot ,Yater, as not infre u cntly hap pc ns to children attemptlllg- to d r ink from the spout of a kettle, or by the effe ,t uf a cu rr os iv e pofson, th e trmlJllellt IS as follows :-
1.-. \. ppl\', a piece of flannel or cl ot h, wrung uut u t yery hot watcr, to the front o f the neck 1 fro,11 the chin to the top )f the brc:1.st-bo n e.
2.-, et patient before the fire.
3.-Glye Ice .t(} slick if it call be had; if n o t, gIve cold \\ater tn drInk.
4.-CIve animal or ver;etablc oil, a dessertspoonfut at a tllnc, to soothe the scalded thro a t and ease the pa In.
. 5·-If breathing has ceaseu apply artificial resplra tl()l1.
TIV • \T OKE OR GJ\SES.
L -"R..f:.mm'e the patient II1to thc frr"h air. R fO:'e
.!l1tE'nr:g- a huilcling full of smoke tIe a handk t'f( hlef, \\ et if ['(}:)sIble, ronnel thc head 0 as t cover th : nO:'.e and mouth . It is well to I1IOYC 10\\ ly , kp · low, or en:n c ra\\lmg, "hilst in a ronm full of makein search ot a suffoca ted perso n. Every OppOl tunit y of lettmg It1 fr esh aIr by opening doors or wmdo\.\ ·s shou !Ll be seized.
qr
2.-Appl y artificial respiration. .
3 - I n th e case of producer or water gas, mhalatlOD f oXYlSen wi ll a lso be necessary.
ELECTRIC HOCK.
Electric cuuent is cOlweyed by a cable, \\ ire, rail, or bar, called the "Positive," and to the ource of supply by another cable, 'Wlre, rali, or bar, called the" Negatiye," or through the eal:th. In the case of an electric railway, the current IS generally conveyed by an insulated. rail the rail, ret u rr.s t brough the LlInmng ratls or an ll1sulated called t he fourth rail, 3.Lcl in the case of an electriC t!"amway it is frequently conveyed by an overhead conuctor or trolley wire, and returned through the run· l1mg rails. . .. "
Through conlact Wlth a "pOSitive the shock may be so severe as to cause insensibility, and the sufferer \ ' lJI be unable to extricate himself, and must be l iberated with all possible speed. As it is genendly Impossib le or inexpedient to S\\ itch off the current :;ome other method must u s ually be adopted; but recautions nlust be taken or else the per o n lOa assistance will himself receive a shock. To liberate the fron; contact-
I. - Insulate yourself from the e:. rth by ma on a n " or " non-conductor," that is, a oOd y whic h resists the current. Amongst such bodie s

143 are indiarubber, dry glass, ury bm.. ks, dry silk, dry cloth, dry wood and dry hay or straw.
2. - Protect your hands from contact with the sufferer or the elect ri c medium by covering them "'lith an insulator. Althoul',h indiarubber is probably the best insulator, do ;10t waste time in running for indiarubbcr glo\'es, but U' dry articles of clothind ; an indiaruuber tobacco pouch or cap, or folded ne\\ spaper, \\ ould serve to protect the hands 111 an emerg n y. If no means of insulating the hanus are at haml an attempt may be made to drag the sufferer away by means of a loop of dry rope or a crooked stick; an umbrella IS not safe because the metal rib would act as conciuctors* of electricity, ,and it 1S not infrequently the case that the" stick" of the umbrella is a metal tube.
3.- Pu ll t h e suffe r er away fro m conta ct. Care should be taken to avoid tou hing \\ it h naked hands the sufferer's hands, wet clothing, or boots if the soles are nailed. The armpits should be avoided as perspiration usually makes th e clothing damp there.
\Vhen the sufferer is removed from conLact-
I.-App ly t h e ge neral treatm e nt for insen -
.' ..\ conductor i· a body through which electricity readily passes. Amongs t such bodies are copper, bras, iron, moisture and one's CWI1 body.
142
14-1-
ibility ( lo o sen clothing, procure free cIrculatIOn of air and place in a recumbent position).
2.-Dip a towel in cold water an d attem.pt f'tQ aro u se him by sharply flicking the bce and chest.
. 3.- Commence artifi ci a l re spi ration If 0 he·J methods fail to restore animatIOn. c. Laborde's /I method (see p:tge 126) has been found to be very s u.cce'1sful
4 . -Treat b urn s if there are any (see pages r03, X04)
EFFECTS OF LICHT 'Jt\G.
A struck by lightning is us-ua ll) more OJ !p"s depnved of consciousness. The treatment IS c;ame as that for electric shock, e-.;cept, of courc;e, that the instructions for lemOYllW Lhe patIent from contact with the electric medlti"m dQ not ap p ly .
QUE 01\ CHAPTER Y.
The 111llllcra/s inciicate the pages 'where tilC all
lIW)' i'e fouJld.
\\That are the two systems of ner.es?
In what system of artificial r eo piration is the patient
IA
hat system is he wiled alternately on his side and face
\-Vould you ex:{mi')e the pati ent to see if any bunes
\ Yhat wrong opini .n mil)' IJC fOlmed when the patient smells of
145
SWCJS
rAG;;
I I 7 Of what is
cere bro·spi,lal S) made up? ... I 17 What is the spinal cord? 117 \\'hat are nerves like? I I Explain the system lIS Explain the respiratory system I I to 120 Explain the
of r espiration 12u How are the eXFw-;ion anti contraction of the chest effected? 120 to 121
the
acts
upwards? ... 121 In
... 123, 126 In
.. 127
laid back
what systems is he laid on his back?
\0\ hat system is he laid on his back or side? .
downwards? .. 139. 140 How long should artificial respiration be persc\'ered \\ ilh? 12 7 What is exciting respiration? 12 7 " ' hat is inducing circulation? .. 12 7, 128 'Why is it nece sary to wat ch the patient? 128 J low may insensii,ility ... ... 128 Slate the yarious forms of insensibili y 128 State the general rules for treatment of in ensibility 12 to 13 1
were broken? ... 12 9
\\
drink? 13 0 Is collapse
conditi(;>ll.r 1JI is concussion of the b,ain? ...... 13 1 State the rules fo r treatment of Cunc u sion 13 1 , 13 2
from drink a seriuu,>
\Vh at danger accompanies injury to the head? ...
\Vh at caution should be gi\'en to a pati ent who has lost consciousne s, even for a moment, after an injury to the head?
\Vha t are the causes of compre: sion of the bra in?
In what aged people dOfs apop lexy usually occur?
'What a r e the signs and symptom:; of compressi o n and apoplexy?
State the rules for tr eatment of the e conditions ...
\Yhat dange r is there in applying hot water tottles to insensible person, and what precautions should be
taken ? ... J 32
Describe a Case of epilepsy 132, 133
\Yh at specia l care must be taken in treating a case of epi lepsy? 130, 132
Descri be a hysterical fit I 3
How would you treat a hystelical fit? ...
\Y hat are the commonest physical causes of shock?
\\That may produce shock 01 fainting?
What conditions do certain poisons bring about?
What may bring about fainling or col'apse? 134
How would yuu recognise the general condition of sheck? 134
\ Vhat specia l precaution must be taken in the case of collapse? 135
State the treatment for shock, fainting (syncope) at cI collapse ... 135, 136
\Vhat is the effect of sugar on the temperature of the body?
\\' hat are the causes of sunst roke and heat-stroke?
State the treatment for sunstroke and heat-stroke
\Vh at are the causes of convu lsions in children?
\Vh at are the igns of convulsions in children?
, tate the treatment for convul ions in children .. .
State fully the causes of asphyxia ...

What two things have to be d one in al cases 0 8 13 2r asphyxia?
What two things' must be seen to before It 15 possIble for artificial re spiration to do any good? :.. . 13S
Is artificial respirati on likely to do any good If the passages are obstructed, o r if there is not abundance of fre sh air?
Wha t is the first thing to do in a case of drowning?
By what mayarlific!al r espiration be perfo r med without takl11g any prevIOus steps ?
\"hat ste ps must be before proceeding wIth Silvester's method?
What should be done while artificial re spIratIOn IS bemg performed ?
State the treatment for strangulation
State the treatment for hanging
State the t reatm ent for smothering
tate the treatment for
How may a swelling of the tissues of the th roat be cause d?
tate the treatment for swelling o f the ti sue of the
the treatment for suffocation by smoke or ga
How would you liberate a sufferer from contact wllh an electric medium?
14
, 14 3
;\That would you do when the su ffe re r was remo\'ed from contact?
ha would you do in the case of a ligh tning stroke
146
I' .\( I'; 13 1 13 2 13 2 13 2 13 2 13 2
1" , .,., 134 134
134
.
.
.
13 6 136 13 6 , 137 137 l.. 17 137 138 147
... ... ... ....
. ' ''. 13 ::!
... .. . .., . .. ..
. ... .
...
...
.. : ....
...
.:..
.. , . .. . ..
... ... ... ... . ..
I141 throat... ... ... ... ... ... 141 tate
es 141, 142 H ow
... ... ..... 142
is electricity conveyed?
.. . ... ..
2
,. .. > • •
Cl-l ArU: R VI.
POI ONING.
P oiso ns may be classifieu according to their treat· ment u nder t\\ 0 beads :-
1.-Those which do n ot stain the mouth , and in the treatment of which an e metic is to be given. An'ongst these are :-
(a) Arsenic, Phosphorus (cc nta;ncu in rat 'pOIson and lucifer matcr.esl, Tartar en: euc anu Corrosi"e ublJmatc, \\hich cause a metallic taste in the mouth und a burning pain in the mouth, throat and stOll ach.
(b) Strychnine, Prussic Acid, Belladonna (deadly nicrhtshade plant) 8nd seyeral other vaneties of plants, such (1S laburnum seeds, etc.; these give rise to connIlsions, delirium, failure of respiration and .
(
c) Poisonous meat, fish and fungi (often IVIStaken for mushrooms). ic ion of these poi::ons should be directed to ca::cs \\ here se\'eral persons \\ho haye partaken of the same food develop similar signs and symptoms.
(d ) Alcohol, which .may cau e cc:llaps e. .
(e) O pium and It s pre paratIOns,

L audan U :11, P aregori , Chlorodyne, Sy rup 'J f Poppies anJ various soothing drinks a nd cordial::,; these cause a tendency t o go t o sleep, \\hich continues until sleep bec?me s deep an:i breathll1g sterotorus ; the pupIls o f the eyes bCCO :l1C minutely contracted ',Pll1head pupils).
2. - Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. These a r e of two cLl ses :.
(a) Acids, such as itric Acid (Aqua fortiS), Su lphuric AciJ (011 of Yitriol), HydrochlorJc or Muriatic, ./l.cid ( ' pints of Salt), strong Carbultc Acid (P henol), Oxalic Acid which is contained in oxalate of potash, salts of orrel, salts uf lemon and som e polt hin6 pa'ite .
( b) A lkalis, such as Cau tlc Ca u sti c S o da auJ A mmonia.
SUM:'IARY Of L\JPlE FOR THE TREATME0." 1 m' ONI:-IC.
1. - Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali,
148
-140
ISO
promptly give an emetic-that is, make the patient vomit as follows :- .
(a) Tickle the back of the throat wIth the finger or with a feather.
(b) Mustard- a dessert-spoonful in a tumblerful of luke-vvarm water.
(c) Salt-a table-spoonful· in a tumblerful of luke-warm water.
(d) Ip ecadtanha Wine-for a young child, a teaspoonful repeated at intervals of fifteen minutes.
3.-1n all cases when the patient is not insensible, give Milk, Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, o.r Vegetable Oil (except in phosphorus and Olive Salad and Cod-lIver 011, or OIl such as that in sardines are prEserved, may be mineral machine oils and paraffin are unSUItable. Oil is soothing, and is therefore especially useful in poisoning by Acids, Alkalis and such as Arsenic and Corrosive Sublimate. Demulcent dnnks, such as barley water or thin gruel, act in the same manner, and are free from danger in cases of phosphorus poisoning.
These may be given either before or after the emetic if the poison calls for one. .
Strong Tea acts as a neutraliser of many pOIsons,

and is always safe. A handful of tea should be thrown into a kettle and boiled.
4·-If the lips and mouth are stained or burned give no emetic, but-
(a) If an is known to be the poison give an AlkalI at once. First wash the mouth out with lime water or other alkaline mIXture? such as soda, chalk, whiting, or magllesia or wall plaster in water, and afterwards let the patient sip a little of it. Soda and are not to be given in the case of pOlsonmg by oxalic acid.
(b) If .a strong. Alkali is known to be the poison gIve an aCId at once. First wash the mouth freely with lemon juice or vinegar diluted Wlth an equal qua.ntity of water and afterwards let the patient sip a little it In both cases give oil (Rule 3). 0
5·-When a person has swallowed poison and to go to sleep, keep him awake by hIm about and slapping his face, neck and WIth wet towel. Strong black coffee may be gIven to .drmk. Slapping the soles of the feet may also be tned.
6.-If throat is so swollen as to threaten obstructlon to air passage, apply hot or poultlc«:s to the front of the neck and give frequent S1pS of cold drinks.
lSI

7. - Apply artificial respiration if breathing cannot be discerned.
8. - Treat shock and collapse.
9. - Preserve any vomited matter food jlr . other substance, suspected of pc:nson. not \\ ash yessels which may have contamed the pOlson, and carefully guard them.
Certain poisons require special treatment, an d a f ew of the commoner of these are mentioned belm\' with their treatment.
CARBOLIC ACID.
The odour of the breath will aid in the detection of . this tbe lips and moulh are usually '5tatne d whIte, and several nervous s) mptoms come 011.
TH.E \T:\lE\,T.
1.- GiYe milk, to a pint of \\ hich half an ounce of Epsom Salts has been added.
2. - Treat accorJing to tbe general rules.
PRUS IC ACID.
.Th.e action of this poison is extremely rapid. staggering, insensibility accompanied by pantmg respiration, profound collapse and possibly convulsions are the general signs, and in addition a smell of bitter almonds is often present.
I.-Place the patient in the open air. IS3
2.-Da.sh cold water on the head and sptne contll1uously.
3.-Apply artificial respiration.
4.-Hold s'1lelling salts to the nostrils.
5. -Treat shock and collapse. (ee page 135·)
POISOXOUS ?\IEAT, FISH AXD FUXGI.
.Tbe signs an? symptoms are vomiting and purging (dlarrhrea), COlIC, headache, great \"eaknes, raised temperature and a quick pulse.
TREATMEXT.
I. -Give an emetic.
2. - \Vh en the emetic has acted, gi \'e castor oil.
3 -Treat collapse. (ee page 135')
STR \"CHX'INE.
The signs and sympt011S are a feelin a of suffocation features, and convublOllS. The patiel1t rests hIS head an d feet, and the body is archea.
TREATMENT.
1. -Give an emetic.
2. - Apply artificial respiration .
ALCOHOL.
I.-Give an emetic If the patient can swallow.
2. -Treat collapse by keeping the patient warm) etc. (See page 135 )
152
QUE TIO ON CHAPTER VI.
The llumerals i7ldi,-ate the page, where tlte allSW{) S may be found.
Under what two heads may poisons be classified?
\Yhat are the ymptoms of poisoning by arsenic?
\Vh at other poisons give ri e to the same. ymptom '"
\Vhat poisons give ri e to Jcliriu111, failure of re piration and collapse? ... ..
If several people who hac! partaken of the ame fo ocl developed similar signs ancl symptoms, by \I hat would you su peci they had been poison ed? . 148
\Vhat condition may result from poi oning by alcohol? 148
\\That are the effects of such poisons as opium ?.. qS, 149
\\' hat t\\'o classes of poison burn or stain the mouth? 149
\Vould you giyc an emetic for such poi ons? 149
Name some of the principal acids J 49 ame some of the principal alkalis 149
State the general rules fLl r the treatment of poisoning ... .., 149 to 152
State the best methods o f making a per on vomit 150
How would you treat a ca e of acid poisoning? ... 151
How would you treat a case of poisoning by an alkali? 151
State the signs, symptoms and treatment of carbolic acid poisoning .,' 15 2
State the signs, symptoms and treatment of poisoning by Prussic Acid 152, J 53
State the sIgns, symptoms and treatment l f poisoning by poisonous food .,.
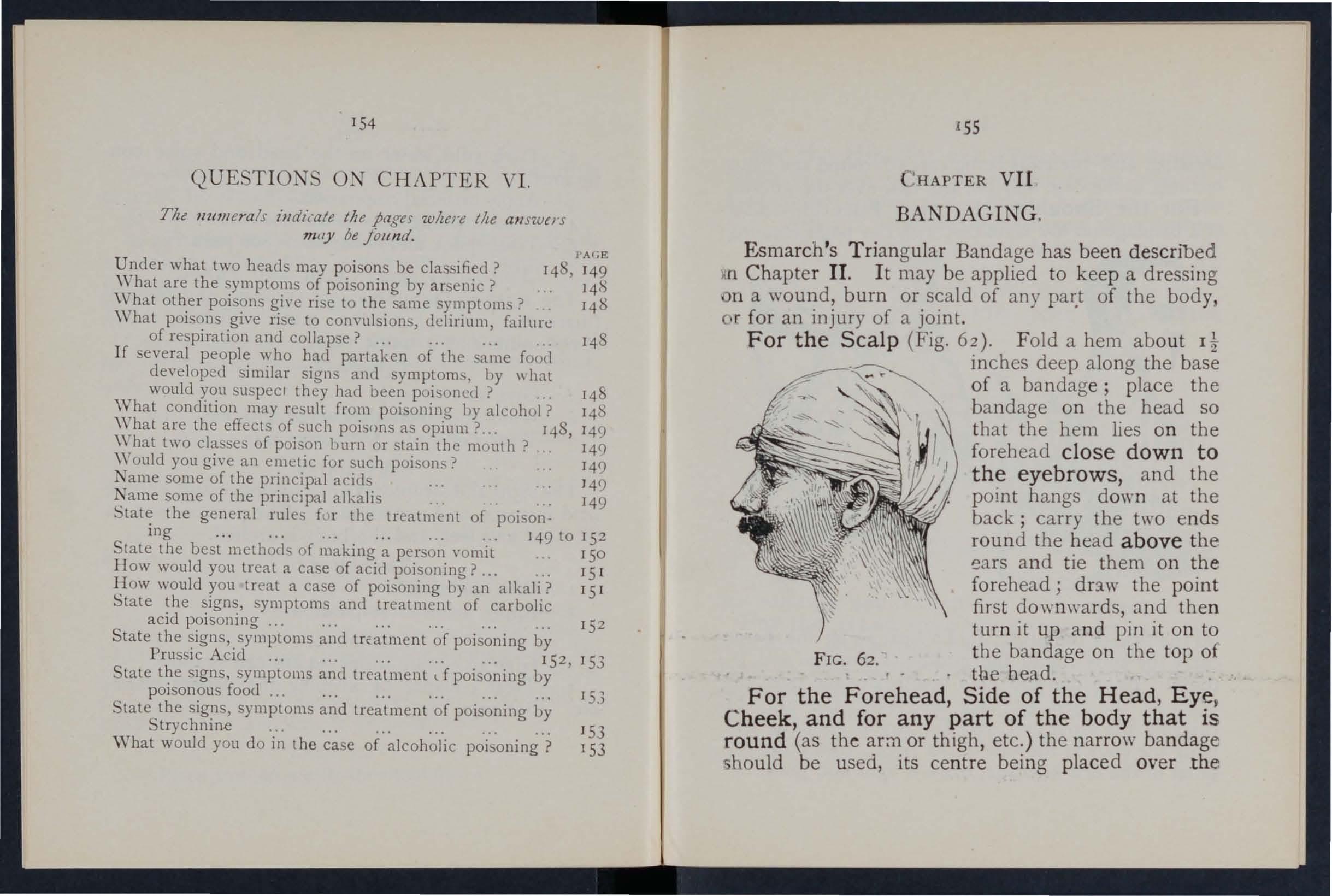
:HAPTER VII
BANDAGING,
Esmarch 's Tri angular Bandage has been descr ibed lIrl Chapter II. It may be applied to keep a dressing n a \vound, burn or scald of any of the body r.r for an injury of a joint.
For the Scalp (Fig. 62). Fold a hem abo u t It
FIG. 62. inches deep along the base of a bandage; place the bandage on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down at the back; carry the two ends round the head above the ears and tie them on the forehead; dr:lw the point first downwards, and then turn it up a nd pin it on to the ba ndage on the top of the head.
For the Side of the Head
State the sign, symptoms and treatment of poisoning by Strychnine J 53
What would you do in the case of alcoholic poisoning? 153 153
, Eye, Cheek and for any part of the body that is round '(as the ar:n or thigh, etc. ) the narro\\· bandage hould be used, its centre being placed over the
154
I'AGE
dressmg, a n d the ends bei n g carned round thf' h i'.!' or limb, as the case may be, and tied over th ";.10])1).
For the Shoulder (Flg. 63). Plac t A 0 f a bandage on the shoulder, \\ith the pomt T'..i.nmn;!
'op the side of the neck; a hem a!ong th I)a c arry the ends round the 111ludle of the arm a d r '" them. Place one end of a broad bandage 0 ei th" point of the first bandage and sling the a ff b v carrymg the other end over the sound shou . der and tying the ends at the side of the turn dO'wn the point of the first bandage, draw It tlght and , llll t . IS7
For the Hip (Fig. 64). Tie a narrow bandage I ound the body above the haunch bones, the knot on the injured side. Fold a hem accordmg to the site of the patient alollg the base of a second bandage; place its entre over the dress1ng, carry the \'\\: enus round the thigh and tie them; thcn l..ury the point up under the

FIG. 63 . FIG.
FIG. 65. FIG. 66. hrst bandage, turn it do\\n over the knot and pin it.
For the Hand \\hen the finger are extended
}:<, ::' 5 1 • Fold a hem along the base of a bandage; - "he wnst on the hem \\ ith the fingers towards ' np, _ "'mt , then br ins the point oyer the \uist, pass . -. d ::; round the \\ rist, cross alld tie then); ..r n g'h P pomt O\'er t11e knot and pin It to the .. u n dage on the hanJ.
8
For the Foot (Fi g. 66). Place the foot on the centre of the bandage with the toes towards th e point; draw up the point over the instep, brin g the ends forward and cross them ; now pass the ends round

FI G. 67a.
the in step and t ie th e m. Draw the poin t fo rw a rd and pin it to th e ba nd age on the in step .
For the Front of the Chest (Figs. 67a a nd
67 b). Place the middle of th e ba nd age ov e r the dressing with the point o ve r th e should e r on th e same 'ide; carry the ends round the waist and t ie them j
159
th e n draw the point ove r the sh o ul der and tie it t o one of the e n ds .
For the Back. T he ba n dage is applied as the foregoi ng, except that it is begun at the bac k .
For the Knee. Fold a narro\\" hem along the base of a bandage; lay the point on the thigh and the mIddle of the base just below the knee-cap; cross the ends first behind the knee , then over the thitrh and tie them. Dring the point down and pin it to the base (FIg . 68) .
For the Elbow. Fold a FIG. G'. narrow hem along the base o f a bandage; lay the point on the back of the arm and the middle of the base on the back o f the forearm; cross the e n ds first in front o f the elb ow, the n ov er t h e arm and tie the m, d raw dow n and pin p oint (FIg. 69).
For the Fingers and Toes 'Hap
a st rip of calico or linen round and round the part; split the fref" end, a n d secure it ro un d t he '\"fist or FIG. 69.
15
CHAPTER YIII.
METHODS OF CARRYING
THE FOUR-HANDED EAT.
This seat is used when the patient can assIst th bearers and use his arms.
1.-T\\·o bearers face each other behind the patIent and grasp their left forearm with then right hand an

FIG. 70.
each other'::; right fv i-earm '\' .tb their left 70 ), and stoop do\\'n.
2.-The patient sits on the hands and places one a rin round the neck of each bearer.
3.-The bearers rise together and step off, the bearer on the right hand side of the patient with the right foot, and the left-hand bearer with the left foot.
THE Two-HA DED EAT.
This seat may be used to carry a helpless patient.
FIG. 71.
I.-Two bearers face each other and stoop, one on each side of the patient. Each bearer passes his forearm nearest to the patient's head under his back just G
L
161
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig. 7 I), and clasp their hands by one of the methods shown in Figs. 72 and 73. A handkerchief should be held in the hands if the first grip is used.

2.-The bearers rise together and step off, the right-hand bearer ,,·ith the right foot, and the left -hanrl bearer with the left foot (Fig. 74)·
THE THREE-HANDED SEAT.
This seat is useful for carrying a patient and supporting either of his lower limbs, when he is able to use his upper limbs.
1,-Two bearers face each other behind the patient. For supporting the left 11mb the bearer to the patient's right grasps his own left wrist with his right hand, 9.nd the other bearer's right wrist with his left hand. The bearer to the left grasps the first bearer's right wrist with his right hand (Fig . 75). This leaves his
FIG. 72. FIG. 73.163

left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting "right" for" left" and" left" for " right." The bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3·-The bearers rise together and step off, the FIG. 75. right-hand bearer with the right foot, and the leftband bearer with the left foot.
THE FIREMAN'S LIFT.
(To be attempted only by a strong man.)
Turn the patient face downwards; place yourself at his head, stoop down, slightly raise his head and FIG . 76.
164
shoulders and take hold of him close under his armpits, locking your hands on his back. Raise his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head rests on your left shoulder. Throw his left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your shoulders. Rise to an upright position; hold the patient's left wrist with your left hand and leave your right hand free.
Assistance may be given to an in jured person by supporting him in the manner shown in Fig. 76.
The plan of carr)'t"Jlg the jatz"ent by the arms and legs wz"th the face downwards, commonly called the "frogs' marcll, " must ne'l'er be used, as death may ensue from tlzz"s treatment.
blPRO\'ISED STRETCHERS.
A stretcher may be improvised as follows :-
1.-Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The patient sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a longer stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 79).

THE FORE AND AFT METHOD.
Thi plan of carrying is us efu l when space does not permit of a hand seat.
166
FIG. 77.

H19
2 .-MaKe holes in the bottom corners of one or two sacks and pass stout poles through them.
3.- 'pread out a large piece of carpet, sack ing, ca r paulin, or a strong blanket, and roll two stout poles u p in the sides. Two bearers tand on each side and grasp tl:e middle of the pole with one halld , and near the end with the other. They walk side\\'ays .
4.-A hurdle, broad piece of wood, orhutter may be used as a stretcher ; some stra\\", hay or cloth ing -s h ould be placed on it, and cO\-en.::d with a piece of sto u t cloth or sacking; the latter i u eful in taki n g t he patient off the stret her.
Always test an improvised stretcher use.
Stretchers must be carried, and the patient placed on them, as laid down in the ,e -'tretcher Exercises ."
As a general rule carry the patient feet foremost.
T h e exceptions are :-
(a) When going up hill with a patient \\ hose lo wer limbs are not injured.
(b) \ Vhen going do\\ n hill \\"irh a patient who se lower limbs are injured.
Avoid lifting the stretcher oyer ditches or walls , b ut where t h ese can not be avoided the tretcher m u st be la rr ied in the following ways :-
To CROSS A D ITCH.
In c rossin g a ditch, the stretcher hould be low ered wi t h its foot o n e pace from the edge of the ditch
," \ FIG . 79.
170
Nos. I and 2*' bearers then descend. The stretcher, with the patient upon it: is afterwards advanced, Nos. I and 2 in the ditch supporting the front end vhile its other end restes on the edge of the ground above. No. 3 now descends. All the Nos . now carry the stretcher to the opposite side, and the foo of the stretcher is made to rest on the edge of the ground, while the head is supported by No. 3 in the ditch. No. I climbs out, No. 2 remaining in thl ditch to assist NO.3. The stretcher is lifted forward on the ground above, and rests there while Nos. 2 and 3 climb up.
To CROS S A 'VALL.
The stretcher is lo""ered with the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the walL No. I then climbs over the ,yall and tak:s hold of the foot of the stretcher, ,,,hile Nos. 2 and 3 support the head; the stretcher is then carried forward till the head rests on the wall; No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
• These numbers are explained later in the detailed "Stretcher Exercises."

171
To LOAD A 'VAGON.
The stretcher is lo\\'ered with the foot one pace from the end of the wagon. N os. I and 2 take hold of the foot of the stretcher, No. 3 the head. The stretcher is then raised and carried forward till the front wheels rest on the floor of the wagon. No. I then jumps into the wagon, while No.2 goes to the head of the stretcher and helps NO.3. The stretcher is then pushed slowly into the wagon. If the tailboard cannot be sh ut, the stretcher must be lashed firml y to the sides of the \\ agon.
To UNLOAD A ,,7AGOX.
Nos. 2 and 3 take hold of the head of the stretcher, ""hile No. I gets into the wagon; the stretcher is then gradually drawn out till the foot-wheels rest on the edge of the wagon. No. I jumps out of the wagon, and with No. 2 takes hold of the foot of the stretcher, No. 3 supporting the head. The stretcher is now aently dra \\'n away one pace and lo,"ered. With four bearers Nos. I and 2 would lift the foot of the stretcher, while Nos. 3 and 4 lift the head. This applies to crossing a ditch or wall. as well as to loading ana unloading a wagon.
CHAPTER IX.
STRETCHER TRANSPORT.
The "FurIey " Stretchers (Model 1899) are of three patterns, viz "Ordinary,"" Telescopic-handled," and "Police ./I In general principle they are alike, the co mponent parts being designated the po les,

Fig. 80.-0RDINARY STRETCHER - CLOSED.
Fig. 8I.-TELESCOPIC-HANDLED STRETCHER-OPEN.
handles, traverse bars, foot \\heels, bed, pillow sack and slings.
The Ordinary Stretcher (Fi g. 80), is 7 feet 9 inches m length, and I foot TO inches wide. The bed is 6 feet in length, and the handles Jot inches. The height is Sf inches. At the head of th e stretcher is a canvas overlay (the pillow sack) which can be filled with 3traw, hay, clothing, etc., to form a pillow. The jointed traverse bars are provided with joints.
173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) is very similar, but the handles can be slid underneath the pol es , thus reducing the len gth to 6 feet. This arrangement is of great value when working in confined spaces, or when a patient has to be taken up or down a narrow staircase with sharp turns. The Police stretcher is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory patient.
\Vh en closed, the poles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly folded on the top of the poles and held in position by the slings" hich are bid along the canvas, and secured y a strap, placed transversely at the end of each sling, being passed through the large loop of the other, and round the poles and bed.
In closing a stretcher care should be taken to raise the centre of the canvas \\ hen pushing in the traverse bar, as it is otherwise liable to get caught.
To prepare, or open a stretcher, unbuckle the transverse straps of each sling j remm-e the slings from the stretcher; separate the poles; take hold of each traverse bar and draw it fo[\\ ard. The sli ngs will then be folded to half their length, one being laid neatly over the handles at each end of the stretcher.
As a general rul e, the stretcher \\ ill be prepared by NJs. I a nd 3 bearers in Exercises I., II., and III. ;
II : .f!!!!!!i:B!! -..--s =r
174
and by No. 2 in Exercise I\r. These bearers will, ho\\,ever, jf required, assist the other bearers in attending to the patient's injuries.
Note.- The various movements detailed in the following Exercises should be carried out steadily, the bearers \vorking in unison, hurrying being carefully avoided, and every attention being paid to the bearer who gives the words of command.
STRETCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised in 1904 to accord with the drills adopted by the Royal Army Medical Corr)6 :-
EXERCISE No. I.
FOR FOUR BEARERS.
1.-The In structor selects the bearers and num bers them-I, 2, 3, 4 at his discretion. Should one man be taller and stronger than the others, he should be styled NO.3, as he will haye to bear the heavier part of the All orders will be given by NO.4.
2. -" Fall in."-N os. I, 2, and 3 take positiorl on the left side of and facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, NO.3 at the patient's shoulders. At the same
*. !3earers however, be taught to take any of the named In the following Exercises, whether that of No. I , 2, 3, or 4 beare r.
175
tIme No. 4 places the prepared stretcher on the ground by the right side of the patient abc-ut two
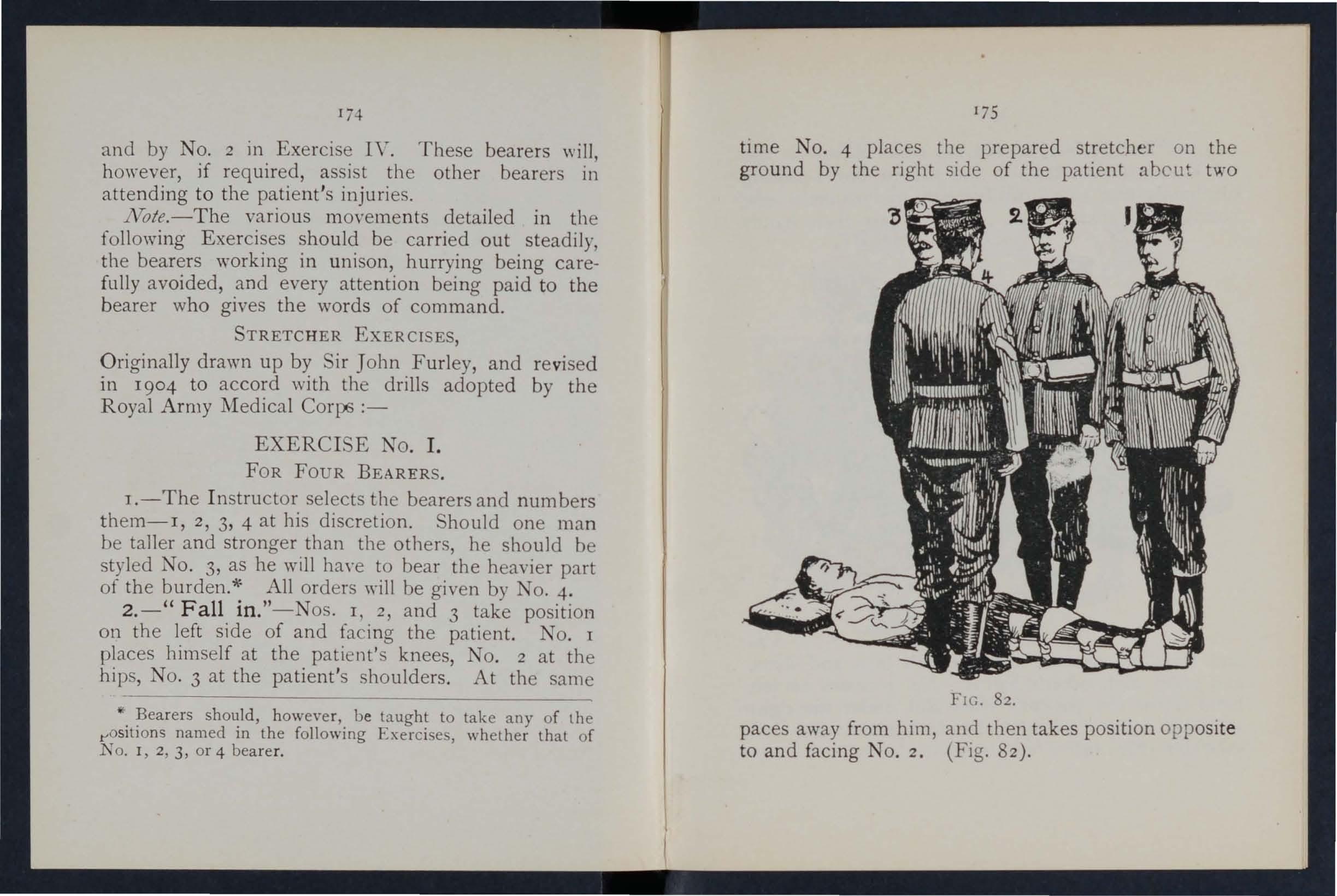
FIG. 82.
paces away from him, and then takes position opposIt e to and facing NO.2. (Fig. 82).
3·-" R ·eady. "-The bearers kneel down on the knee 8nd take hold of the patient, No. I passing hIs and fore-arms beneath the patient ' s legs , hands wIde apart. Nos. 2 and 4 pass their hands

FIG. 83 . and forearms beneath the patient 's hips and loins and grasp each other's hands. No. 3 passes his hand across the patient's chest and under the riaht shoulder, and his right hand ben eath the left shoulder (Fig 83).
177
4. - " Lift. "- O n the word "Lift," the bearers raise the patient gently and fest him on the knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as he
Flc. f4· is securely rested, NO.4 di engag es bands with 1'\0. runs round by the head of the st retcher and place It unuer the patIent, close to the other bearers' feet ,
176
that the pillo w is immediately under th,., patIent s head (Fig. 85 ) ; he then kneels down loc k s his hands with those of No.2 (F i<Y. 86).
5 "L "Th b/:)' . - ower. . - e place the patIent OH the stretcher (FIg. 87), dIsengage their hands, and then stand up.

FIG. 85.
6.-" Stand to Stretcher."-No. I goes to the foot of t he his back to the patient; N o. 3 to head wIth hIs face to the patient ; Nos. 2 a nd 4 remam on each side of the stretche r.
7·-" Ready. "-Nos . I and 3 place the shngs (If u sed) over their sho ulders , stoop down, and slIp the
T79
loops of the slings on to the handles of the stretcher, which they then grasp . , . As soon as all is right the word IS gIven :-
8. - "Lift Stretcher. "-Nos. I and 3 bearers raise .Lhe stretcher steadily together and stand up.
NO/I1.-1 os, 2 and 4 will now adjust the slings ?n the shoulders of Nos. 1 and 3, taking care that each I? well belo\\' the level of the collar and lies m the holln\\' of the shoulder in front. Th ey w111 also l engthen or shorten the slings, r.egarc1 to the patient's injuries and the relatlve helght of the bearers.
FIG 86.
9. - " March ."- move off :-NoTSi. 2, and -+ stepping off \\lth theIr left foot, and No . .:>
178
with his r ight foot ( F ig. 87) . T he step should be a short one of twenty inches, and taken with bent knees ,md no sprIng from the fore part of the foot. 10. - " Halt. "- The bearers remain steady.

FIG. 87.
II. - " Lower Stretcher. "-The bearers place the stretcher gently on the ground, slip the loops of t h e slings off the handles of the stretcher the slings from the shoulders, and then up .
181
12.- " Unload Stretcher - Ready." - T h e beare r s p repare to take the patIent off the as at O rders 2 and 3.
13. - " Lift. "-The bearers the as a t Order 4 (Fig. 86); NO.4, in thIS case, dlse.ngages hands from No.2, removes the stretcher (FIg . 8 5" and resumes his former position. If necessary, the bearers will then steadily rise together, and carefully carry the patient Lo the bed, or ?ther place to which it has been arranged to com'ey hll11.
14. - "Lower. "·-The patient is carefully lowered
EXERCI
E No. II . FOR THREE BEARERS.
I.-Number the bearers I, 2, 3.
All orders will be given by No.2, who will look after the injured part of the patient's body or limbs, to see that no bandages or splints become displaced , and also that J o. I bearer, in lifting or carrying the stretcher, does not touch the patient 's feet .
2 .-" Place the Stretcher. "-No. 3 places the stretcher in a line with the patient 's body, the foot of the stretcher being close to his head.
3.-" Fall In. "-No: I on the le ft side of the patient in a lIne \\,Ith hIS knees, No .2 on the left side just below the patient 's shoulders, and No . . at the right side, and faces NO . 2.
180
4. -" Ready." -All kneel on the left knee. No. l' places his hands, well apart, underneath the 100yer limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of injury.
2 and 3 grasp each other 's hands under the houlders and thighs of the patient (Fig . 88).

FIG. 88.
Lift."- Tl:e bearers rise together, keeping the patIent In a honzontal position (Fig. 89).
6.'.' March. "-All take short side-paces, carrying the patIent over the stretcher until his head is imme· diately above the pillow.
7.-" Halt. "- The bearers remain steady.
8. -" Lower."-The bearers stoop down, gently place the patient on the stretcher, disengage their hands, and then stand up.
FTC. Rq.
9.-"Fall In. "-No. I places himself at the foor of the stretcher with his back to the patient, No.2 places himself at the left side of the patient, and No. 3 at the head, with his face towards the patient.
I 2
1 84
10. - " Ready. "-Nos. I and 3 pkce the slings (if us ed) over t h eir shou lders , stoop down, and slip the lo ops of the slings on to the han d les of the st retcher, wh ich they then grasp.
As soon as all is right the word is given-
II .-" Lift Stretcher. "-Nos. I and 3 bearers raise the stretcher steadily together and stand up . No. 2 will now adjust the slings on the shoulders of lOS. I and 3, taking care that each is 'Nell below the le\'el of the collar, and lies accurately in the hollow of the shoulder in front. IIe will also lengthen or shorten the slings, haying regard to the patient's injuries and the relative heights of the bearers.
12. - " March. "- Nos . I and 2 step off with the left foot, and No. 3 with the right. The step should be a short one of 20 inches, and taken with bent kn ees, and no spring from the fore part of the foot .
13. - " Halt. "-The bearers remain steady.
14.- " Lower Stretcher. "-The bearers place the stretcber gently on the ground, slip the loops of the slings off the handles of the stretcher, remove the slings from. the shoulders, and then stand up.
IS. - " Unload Stretcher - Ready. " - The bear e rs prepare to take the patient off the stretcher, as a t Orders 3 and 4 (Fig. 88).
16. - " L ift. "-The bearers raise the patient, as at Or der S. alld carry him by short SIde steps, clear of the stretche r , t o the b ed, or other place to WhlCb it bas b een arra nged to convey him (Fig. 8 9)·

18 5
17. - " Lower."-The patient is carefu lly lowered.
EXERCI E No. III.
WHEN ONLY THREE BEARERS ARE AVAILABLE A D THE TRETCHER CA. NOT BE PLACED AS IN EXERCISE II.
I.-The Instructor numbers the bearers-I, 2, 3· All orders will be given by NO.2.
2 .-" Place the S t retche r."-No. I taking the foot of the stretcher, and NO.3 the head, place it on the ground by the side of the patient, and as close to him as practIcable.
3.-" F all I n."-The three bearers take the same positions on one side of the patient, as laid down in Exercise No. 1.
4.-" R eady."-Nos. I, 2, and 3 kneel down on the left knee, placing themselves as close to the patient as they conveniently can, and then take hold of him as directed in Exercise No. 1.
S. -" Lift. "-Nos. I, 2, and 3 raise the patient as dIrected in Exercise No. I, and then move in a kneeling position up to the stretcher.
6.-" Lower. "-The bearers bend forward, carefully lower the patient on to the stretcher, and disengage hands.
7. - " Stand to Stretcher."-All the bearers up; No. goes to the foot, No. 2 remains In posItIOn at the sIde, and 1 o. 3 goes to the head 0\ the stretcher.
8.-" I and 3 place the slings (if used) over their shoulders, stoop down, anri slip the loops of the slings on to the handl es of the stretcher which they then grasp. '
.9.-" Lift Stretcher." -Nos. I and 3 bearers raIse the steadily together and stand up.
No.2 WIll no\y adjust the slings on the shoulders of TOS. I and 3. taking care that each is well below the level or the colla.r, and lies accurately in the hollow of the m. front. IIe will also lengthen or shorten the regard to the patient's injuries and the relatIve heIghts of the bearers.
10. -" March."-Nos. I and 2 step off with the left foot, and NO.3 with the right, The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
11. - " Halt." -The bearers remain steady.
12.-" Lower Stretcher." -The bearers place the gently on the ground, slip the loops of the sl.mgs off the handles of the stretcher, remO'le the slIngs from the shoulders and then stand up "U I ' .
13.-- . noad Stretcher-Ready." - No. T places hl!llself. on the left side of the patient, and in a lme wIth hIS knees, No. 2 on the left side just below the patient's shoulders, and NO.3 at the right
187
side, and faces NO.2. All kneel on the left knee. No. I places his well apart, underneath the lower limbs, always taking care, in case of a to have one hand on each side of the seat of mJury. Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient. .
14.-" Lift ." - The bearers rise togethe.r. to theIr feet, keeping the patient in a horizontal pOSItIOn, and carry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
15 .-«( Lower." - The patient is carefully lowered.
EXERCI E No. IV.
FOR U E IN "MIN ES AND NARROW CUTTINGS \,"HERE T\\"o MEN 01 LYCAN BE E GAGED.
Nos. I and 2 will carefully place the stretcher in a Ime with the injured man's body, the foot of the stretcher being, if possible,* close to his head.
No. I straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the hee l of No.2; he then stoops down, passes the left hand under the patient's thighs and
• It is not advisable to be too particular as to the head or foot of a stretcher in a mine, as it would probably be quite impossible to reverse it.
186
the right hand across and under the patient's calves. NO.2 places his feet one 011 each side of the patient between his body and arms, the toe of each foot as near the armpits as possible. He then stoops down and passes hIS hands between the sides of the chest and the arms underneath the shoulders, and locks

FIG. 90.
the fingers (Fig. 90). If the patient's arn-:;s are umnjured he n1.1y put them round the neck of No.2, and by this means greatly assist him in lifting.
189
\Vhen both are ready, No. I will give the order "Lift and move forward." The patient is then to be slowly lifted, just sufficient to allow his body to clear the stretcher. Both bearers will slowly and gradually move the patient forward, NO.2 by very short steps. No. I by bending his body forward as much as he .can wit/lOut moving his feet (Fig. 9 I). No. I now gIves the order" Halt" whereupon NO.2 remains steady, and No. I advances his right foot to his left, and
91.
again advances his left foot till the toe touches the heel of NO.2. No. I then gives the order " Advance," when the patient will again be moved forward. These movements are to be repeated untIl
188
2
FIG.
the patient is over the stretcher, when he is to be gently lowered.
The following Stretcher Exercise is adapted by permission from the R oyal Army Medical C orps Ianual, 1908.
All orders ,,,ill be given by .No. 4.
1. "Fall in." - ix bearers fall ill behind each other.
2. "Number." -The bearers number from front to rear.
3. "No·3 Bearer, right (or left) turn - supply stretcher-quick 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower fool wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place . He turns to the front, and, passing the lower e nd forward, places th e stretcher on the ground to the right of the squad, \\ heels to the right, front end of the poles in line with th e toes of No. l. and rises.
4. "Stand to Stretcher." -No. 1 places himself with his toes in line with the front ends of the poles. No. 3 with his heels in line with the rear ends 01 the poles, close to and touching the stretcher with

93. FIG. 94.
1\ 0 u \ 13 []] 1\\ :.?'; " I m ,'. '5'1.3 ". 1'1 tdJ ,I. / , " , I , , 4- : I 1,' ; ,/ ". : :?Y / , .. ...
FIG. 95· , .': 4. , .. , .. -.. 2 : ; ;
FIG.
his right foot. lOS. 2, 4, 5 amI 6 take up their positions one pace hehind and covering off the bearer in front of th em (Fig . 92 ).
S. "Lift Stretcher. " -. os. I and 3 stoop, grasp both handles of the poles with the right hand, rise together holding the stretcher at the full extent of the arm, wheels to the right.
6. "Collect Wounded ·- Advance. " - The squad douhles by the shorte t route the patient, and halts without further \\ord of command one pace from the head of and in a line \\-ith the patient (Fig.93).
7. cc Lower Stretcher. "-No . 1 :111d 3 stoop, place the stretcher quietly on the ground, and rise smart ly together.
8. cc Prepare Stretcher. "-Nos. I and 3 turn to the right, kneel on the left knee, unhuckle the tran " erse straps, and place the slings on the ground beside them, separate the poles, and straighten the traverse. .
T'lL'o. On the word two each takes a slll1g, dou bles it on itself, slips the loop thus formed on the near handle, and places the free ends over the oppo ite handle, buckle uppermost. They then rise and turn to their left together.
'While the stretcher is being prepared by Nos. I and 3, the disengaged bearers will advance and render to the patient such assistance as may be required (Fig. 94).

193
lllc necessary assistance having betn rendered, NO.4 "ill give the command-
9. "Load Stretcher. " - The bearers place thems elves as follo\\s:- IOS. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; I and 4 at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the whole kneeling on the left knee. Nos. I and 4 pass their hands beneath the patient's knees, 2 and 5 beneath the hip, 3 and 6 beneath the . houlders, care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. 95)'
10. "Lift." -The \,hole \\'ill carefully 11ft the patient on to the knees of TO .. I, 2 and 3.
_ T'lC'o. Nos. -t, 5 and 6 will then ell engage rise; Nos. 4 and 6 ' tep back one pace. Xo. 5 turns to his left, to the stretcher, takes hold of and raises it, left hanc1 acros, the near pole resting on the left hip; carryll1g the stretcher, he returns to his place between -t and 6, and places it beneath the patient.
TlzTCC. Nos. -t and 6 tep forward one pace, and together \\lth o. 5 kne 1 do\\ n on the left knee, and prepare to assist in lowering the patient (Fig. 96).
II. (( Lower. "-The patient is lowered slowly and ge ntly on to the centre of the canvas (special care being taken of the injured part).
Two. The bearers disengage, ri e; Nos. I, 2, 3 and 6 turn to the left j Nos. 4 and 5 to the right .= 11
194-
No. -I- 1 bees himself three paces in front of the s tretcher. No.6, having collected the kit and arms of the patient) places himself three paces in rear of t he stretcher, Nos . 2 and 5 opposi te the centre of the stretcher. The whole are now r eady to lift stretcher and move off (Fig. 97) .

Fig. 97.
Fig. 98.
195
12. "Lift Stretcher. "-.I. os. I :lOll 3 Stoop, grasp the doubled sling mid\\'ay betweel: the poles with the fo r efinger and thumb of the nght hanel , sweep it o ff the handles, rise, holding the sling at the full extent of the arm, buckle to the front, a side pace to the front between. h:ll:dle , and place the sling over the houlders dlndmg It equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollo\\' of lhe shoulders in front. In the event of the slings requiring to be adjuste?, either as regards length or for the greater comfort ?f tbe bearers, No. -+ will detaIl a bearer to carry thIS out, the length of the slings being adjusted, when necessary, by means of the buckles,
Two. Nos. I and 3 stoop, slip the loops o\'er the handles, commencing \\ ith the left, and gra p the handles firmly.
Tlzree. 'os. I and 3 rise slo\dy together, 3 conforming closely to the movements of No. 1.
13. "Advance. "-Nos. I, 2, 4, 5 and 6 step off \\ith the left foot, No. 3 with the right, stepping short , knees bent, feet raised as little as po.ssible.
14. "Halt. " - The whole halt.
IS. " Unload Stretcher. "- The bearers place themse lves in the same position at the stretcber as d esc r ibed for Loading (Order C)) .
16. "Lift. " -As described for Loading (Order 10), H2
o

196 except that the tretcher is carried forward three paces cl ear of the patient 's feet.
17. "Lower." - The patient is gently lowered to the g round. The bearers disengaae rise ' Nos I 2 and 3 turn to the left, 4, 5 a n d b 6 'to right, the whole step off to their places at the stretcher, as at Order "Stand to 'tretcher " (Fig. 98) .
The Ashford Litter is made up of either of the Furley stretchers mentioned on pages J 7 2 and 173 a whee led under-carriage and a waterproof hood apron, or, if preferred, a light wet -resisting canvas cover. The stretcher is kept in position on the under-carriage by the fo ot-wheels, ,,,hich fit into slots in the sides Gf the under-carriage, and it can be removed at pleasure. under-carriage is fitted with a cranked axle, whIch allows the bearers to pass with the stretcher between the wheels instead of lifting it o,'er them. At both ends are two legs which may be turned up as when \\heeling the lItter. The hood and apron fit sockets screwed to the stretcher. In wheeling the care be taken to keep the patient in a honzontal posItIOn , Should it be nece Sal'\, two bCc:uds can easily lift the litter and patient. '
The Litter, introduced in 1904, IS used 111 a SImIlar manner. and one model of it is fitted with pneumatic tyres, which add immensely to t h e c omfort of the patient and to the ease of propulsion . 197
CHAPTER X.
(Bez'llg the Fzfth Lecture for Females ollly, z'1l ac(ordance with SyllalJUs 58.)
BY E. MACDo\\ELL COSGRAYE, ::11. D., F.R.C.P.I.FOR OF ACClDEXT CASES.
ne\\s of an accident comes, preparations should at once be made so as to have everything ready before the injured person is brought in. Of course the pre parations needful \\'ill vary according to the nature and e\:tent of the injury, but the following are the chief things which may have to be done.
) CHOICE ,\XD OF Rom!.
A room must be chosen. In a bad case this should be one easily reached, as it is dIfficult to carry an injured person through narnw passages and up-stairs Dnle s there is some such reason against it the injured person's own room is best.
The way to the room must be cleared, projectmg furniture and loose mats in the hall or in lobbIes should be removed. If the injured person is carned on a door, shutter, or stretcher, t\\'o strong chairs should be placed ready to support it wherever [he bearers would be likely to require rest.
Useless furniture should be removed from the bedroom. The bed should be drawn out from the wall
I)
so that b)th sides can be approached, and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much collapse several hot bottles and hot blankets may be required j CO\'E:r the hot bottles with flannel.
If the injury is very se\'ere, if mud-stained clothes have to be removed, or if extensive dressings have to be applied, it may be necessary to have another bed, a couch or a table placed near the bed to lay the sufferer on in the first instance. This should be so arranged that soiling may do no harm j old sheets, waterpoof materials, thin oilcloths, or even ne\\ spaper, may be used as a protection.
LIFTING AND CARRYING.
If present at the place where the accident occurred, it will be necessary to see that the patient is carefully lifted after proper "First Aid JJ has been rendered.
The following rules should be remembered :- Select the proper number of persons to assist, and do not let them lift the patient until they thoroughly understand how they are to do it.
For ordinary cases, \\ here the injured person has to be lifted a very short distance, three helpers are sufficient. Two (\\'ho should be as far as possible of equal height) are to bear the "'eight, the third is to support and take charge of the injured part. This is

199
b st done by a person \\·ho has been through a " First .\id" course. If the injured person lS l11senslble, another helper shoulJ support his head.
The lifters one at eacb side, should kneel on one knee, and their hands under the patient's back at t le lower part of tbe shoulder blades, and under the h1ps, clasping each his right 111. tbe otber 's I'he injured patient should, If practIcable, place hIS ,Hms round the necks of the bearers.
The third helper should attend to seat of If tbis is a fractured limb, he should support It by placmg tbe palms of hIS hands uncler .the limb, above and one below the of the ll1Jury, gras].lll1g It firmly but avoiding unnecessary pressure.
The helpers should remain thus until order " Lift /I is given, and then they should all lift .10\\ I? and steadIly, avoiding jars, attempts to change pOSItion of hands, etc.
H the injured person is to be. placed on a or shutter, this should be prevIously placed WIth the bottom end at his head; the bearers should the:l moye, one at each side of it, until the is o\'er It. The word" Lower JJ should then be glVen, and the lIljured person should then be lo\\'ly lowered. A pillO\\' or folded-up coat should be ready, and as the suffere r IS lowered this should be pia ed und er his head.*
• Full di-cctions arc gi"en in Chapter IX
OF CAR R YI NG
B e si des a str e t cher , a n d subs tit u tes suc h a s a ga te, a shutt er, or a doo r, oth er m ean s o f carrying can b e improvised.
In sl ight inj ur ies, where the injured person is unab le to wal k , two bearers can carry him by fo r ming a fo ur ha n ded , three-handed, or two-handed seat.
A four-handed seat is formed as described o n page I60 .
A three -handed seat is made as described on page I62 . The two-handed seat is made as described on page I6I.
A single helper can lift by supporting with one arm the two knees, and with the other the back . The arms must be passed well under before commencing to lift.
A single helper can give support by putting his arm round the waist, grasping the hip and placing the ll1j ur ed person's arm round his own neck, holding th e h and with his 0\\ n hand (Fig. 76, page I65).
A capital stretcher can be improvised out of a s t r ong sheet and hm I' room handles or other sho rt p oles. Each side of the sheet is wound up on a broo m handl e unti l there is just room for a person to lie betw een , T his requires four bearers, two at eac h sid e, to prevent the sheet slippi n g .

20 1 CARRYB\G UP STAIRS.
I n carrying a stretcher up stairs the head should go first, and an extra he lper should assist at the lowe r end, so as to raise it and keep the stretcher nearly horizontal.
The t\\·o three, or four-handed seat may be used fo r carrying up stairs; or a strong chair, the patien t being carried up backwards . In the latter case one helper should walk after the chair and to support.. it, and to prevent the injured person slIpping out.
LIFTING INTO BED
If the b e d i narrow and there is ro o m the str e tcher should be placed on the floor \\ ith the head close to the foot of the bed. The injur e d person should then be lift e d m'er the foot and plac e d on the bed If the bed is too \\ ide to admit of this, the stretcher should be placed beside it, and t\\ 0 h e lpers should stand at the far side o f the st r etcher. O n e helpe r passes one arm beneath the shoulders and o n e the middle of the back, the other helper p lacmg hIS under the 10\\'er part of the back and under the T he injured person is t h en lifted, a n other helpe r pulls a\\ay the stretcher, and a f te r a single o rw a r d t he burde n is placed on the bed .
200
OF B ED.
A iir:n mattress, n o t a feathe r bed, should be electeJ. If there is much injury, or if dressi n gs hJ.YC to b e applied, a draw-s heet ought to be placed on the bed. It should be of [our or more tllickncsses. extend across the bed, and reach from the middle of the p:1tient's blck Lo the knees. A pie c of water ?roof heeting or of thin oil-cloth should be placed un leI' the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean part drawn smooth ly under the patient.
In fra ct ure of the leg or thigh, sprained ankle and some cases, a "cradle IJ (Fig. 99) hould be :mproYised. The Llse of a " cradle " i. to support the ned-clothes and keep them from pressing on the limb . . A band-bO',: (Fig. r oo), three-legged stool (Fig. TOT), or hoop sa\\ 11 across and the two hal\'es secured togethe r ( Fig. I02 \ may be used. .A corkscrew passed through the bed-clothes, with it point guarded by a cork, and tied by string to the bed or a nail in the ",.- a ll, \\ ill relieye the pressure of the bod-cbthes effec tually.
RE:\IOVING THE CLOTHI'.S .
In taking clothes off an injur ed p2rson a few ru les should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury ,

99.
lOt.
202
2 0 3 =--=----____ _ -----::::::::...=---=- - - -
FIG.
FIG.
In removing a coat, etc., in a case of fractured arm the uninjured arm should be drawn out first.
In putting on a coat or shirt the injured arm should be put in first.
In burns and scalds nothing should ever be dragged off. A sharp pair of scissors should be used, and everything not adhering should be cut away. If .anything adhere it should be left until medical aid

FI G . 102.
can be obtained. The clothing adhering may, with advantage, be soaked with oil. To remove the trousers from a severely injured limb, the outsl'de seam should be ripped up.
PREP_\RATIO TS FOR SURGEON.
As soon as the injured person has been attended to, preparation should be made for the surgeon's visit.
20 5
Thepreparations needful will depend upon the nature of the case. The follo\\"ing hints may be of use :A fire in the room helps ventilation, even in summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot-bath does well. The basins should be placed on a table, covered wi th a clean \\" hi te cloth; a large to\\ el makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be \\ ithin easy reach. The foot-b3.th should be' under the table or dose at hand.
In the case of a burn, absorbent :.otton wool, soft cloths, old linen, oil, and baking soda, should be ready, and materials should be torn up for bandages. In the case of hremorrhage, plenty of water should be boiled and allo\\ ed to cool, and pads of absorbent cotton wool should be baked in a tin box in the O\-en, and at least two basins should be ready.
In the case of a person rescued from drowning the ;heets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flanntl or handkerchiefs may be required.
204
F or fo mentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large towel.
"When summoning a medical man to all accident let him know by a written message what kind of case he is required to treat, so that he may bring whatever is needful. By this means valuable timemay be saved. p
QUESTIONS ON CHAPTER X.
.The nume r als i lldicat e th e p ages w h ere t he all swers may be found.
What points woul d you con sider when choosin g a sick PAGa room? 197
How would y ou clea r the way to the sick room ? 197
vVhat means of r es ting would you provide for those carrying a patient o n a stretch e r? 197
How w ould you pl a ce and arrange a b ed for an accid e nt case? 197, 198
Are h ot b ottl es ne ce ssary, an d how w ould you prepa re them? . . 198
'Vhat is often ne cessary to lay th e su ffer er on in th e first instance? .. '" 198
How would you prote c t this from ge tting soiled? 198
How would you se e to the proper lifting and ca rrying of an injured p ers on? 198, 199
\\"hat substitutes for a regul a r stret c her can you sugge st? 200
How is the four -handed sea t made? ... .. . r60, 161
For what cases is this seat useful ?... 160
How is the three-handed seat made? 162, 164

20,/
Fo r what cases is this sea t use ful ?,"
I lo w is the two- h a nde d seat made?
Fo r what cases is this sea t use ful ?.. ,
H ow ca n a si ng le he lpe r lift ?
H o w ca n a sin gle h e lpe r give SUppO IL?
H ow wou ld you im pro\'ise a st r etcher?
H ow many bear ers are requ ired for this st retcher?
H o w should a stretcher be carried upstairs?
H o w would you carry a patient upstairs on a chair? ..
Ho w would you lift a patient from a stretcher to a }" 1 ')
How should a bed be prepared for an per on ? .
How should a draw sheet be made?
\Yh a t wou ld you place under the dra\\ sheet? ,.
\ Vhat should be done with the soiled part of a dl.1\\ sheet?
\V ha t is the use of a ., cradle')? .. ,
I n what ways ma) a cradk be imprO\' ised ?
How would you remove a coat o r shirt in the case of 3. fractured arl11? '.'
How would you put on a coat or shirt if the arm wert:! injured? .. ,
I n the case of a bad burn, what \\ ould you do with cloLhing lhat adhered to the paLient ?
How \\ ould you remove tronser rrom a se\"'erd)' injured limb?
\\' b at preparations would you make fo r the surgeon ' ", visit?
\Vhat would YOll gel ready in the case of a burn?
And what in the case of hremo rr hage ?
And what in the cas e of a person rescued fr om d rowning?
Wh at wo uld yo u get r eady for making po ul tice s ? '
A nd for fom entation s ?
\Y ha t sort of a message wou ld you sen d t o sum mon a do ct or? ",
206
P A r ll 102 161, 162 16r
200 r6s 20C 20C ::01 20} 201 :0:;.,> 202 202 ::CO] 204 205 205 20 5 20 5 20 5 206
INDEX .
Abdomen Page III wound of 112
Acc/dent case, preparation for 197
Acid s poisoning by 149, 151
Air, always necessary... 18
Alcohol, caution as to smell of 130
Alcohol, poisoning by 134, 153
Alkalis, poisoning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30, 32
" sprained... 64
Anterior tibial artery 93
Aorta 79
Apoplexy 132
Apparently drowned, to restore... 139
Arm, bone of 2
II fracture of 52
Arm-slings 39, 49
Arsenic, poisoning by .. I4S

Artery, brachiaL .. " carotid dorsal of foot " facial femoral ... iliac occipital plantar ... p op liteal radial subclavian tibial temporal " ulnar
Artifici a l respirati on 121 , 129 , Asphyxia Alla Auri c le s ... Axillary artery Axis
Bites of rabi:i animals 106
Bladder ... II I, II3
Brachial artery .. , 86 Brain 117 compression of 13 2 " concussion of 13 1
Breast-bone 26 " fracture of 48
Broad bandage ... 37
Broken bones, see Fracture.
Bronchial tubes... . .. lIS
Brooch-bone 30
Bruises 102
Burns 102
Capillaries ...
Capillary h::emorrhage
5 25
Back, bandage fUl 159 Backbone 23
II practbing arrest of 79
" signs of 74
Arterial hremorrhage, " Arteri es arrest of 74
Artery , axillary ...
" course o f main 70 79 85
Bandage, to apply 42 to folel 37 " to improvise... 37
Bandaging 155 Bed, lifting into. .. 201 " preparation of 202
Belladonna, poisoning by 148
means of upstairs
160 , 200 201 25 117 25 82 Cerebro-spinal syst em Cen'ical verte brre Cheek, bleeding from Chest, for Chlorodyne, poisoning by Choking ... IS:::> 149 140
208
I'fTge 86 80 93 81 89 79 2 93 02 8 4 93 82 g8 136, 138 138
70
25
209 Page
...
Carotid
... "
from 3 1 15 2 80 o 28 Carpus
Carrying,
Par-' Circulation
blood,
.
induce
Clavicle
" fracture of 48 Clothes, rem oyal
19, 202 Coccyx 25 Collapse .. . 138 Collar-bone 26 " fracture of... 48 Comminuted fracture 35 Complicated fracture .. , 34 Compound fracture . . . 34 Compression of the 13? Concussion of the braw 131 Conductor 143 Convulsions in children 137 Cradle, bed 202 Cranium ... 22 " fracture o f 43 Crepitus... 36 Crushed hand 55 foot 62 Diaphragm 120 Digital pressure..
74 Direct yiolence
Dislocation
Capsule
70 , 72 95 Carbolic acid, by
arteries
h::emorrhage
... . ..
Cartilage
cf the
organs of ... .
. 7c Circulation of the blood, to
.. 12"
26
of
.
.. 33
62 Ditch, to cross with stretcher J 69 Dorsal artery of foot 93 vertebra: " 2S
Page
Dress, woman 's, on fire . .. 105
Drowning 139
Ear·channel, blood issuing from ... ...
Ear-passage, foreign body in Elbow, bandage for " joint, fracture inIIO 159 volving
Electric ...
Emetic 148, Epilepsy."
Ssmarch's 53 J.t2 149, ISO 13 2 bandage triangular
Expiration .. . '"
External carolid arlen' ...
Eye, bandage for ' foreign body in
Face, bones of Facial artery
Fainting
Femoral artery " "digilal pressure at groin ... ...
Femoral artery, tourniquet for
Femur fracture of " .... fracture
Fingers, bandage for fracture of 37 120 80
109 90 30 56 30 60 159 55 210
Fireman's lift
First aid, meaning of " student Fi h-hook. embedJeu
FlexlOn . . . at elbo\\ " at knee ...
Food, poisoning by Foot, bandage for bones of .. . " crushed ..
Forearm, bunes of " fracture of .
Forehead, bandage for. " ha:!l11orrhage frOIll
Foreign body in the carpassa;e ... in the eye " "in the pose
Four-handed seat
Fracture, apparatu fur treatmcr;' of causes of dcfiniti on of general rul es for treatmcnt invoh' ing elbow joint of arm ... of breast- bone of carpus of collar -
of

Page
Fracture of forearm 54 of knee-cap 5g of leg... 6e' of lower ja w ... 44 of metacarpu 55
o f metatarsus .. 62
o f pelvis 56 of ribs . .. 46 of spine 45 of tarsus 62 of thigh- b ::me.. 56 of toes.. 62 signs and symptoms of 35 " yarieties of 34
Frost-bite 108
Fungi, poisoning by 153
General circulation 70 Granny knot 40 Green- tick fracture 35, 36 Gums, h;emorrhage from 97
H::emorrhage, a rterial ... 74 capillary... :>_ from gum s 97 from head and neck 80 from lower limbs ... 89 from lungs 97 from nose 96 from stomach 98 211
Hremorrhage from throa t 97 from tongue 97 from tooth socket... 97 from upp e r limbs... 84 internal ... 95 kinds
, bandage for 155
to... 128, 131 " side of, bandage for 155
7C ., rate of contraction of 72 Ileat-stroke r 3E Hernia 11..1
Hip, bandage for 157
History, meaning of I 'j Howard's method of artificial respiiation
H\1merus " fracture of Hydrophobia II)' terical fits Iliac arteries
ISS
bone
cranium of finger 110 109 1 I r 160 36 33 33 41 53 52 48 55 43 5S
of ... 73 " venous 93 Hand, bandage for 157 " bones of ... 28 Hanging ... 140 Haunch-bones ... 28
arteries
80
II eadand neck,
of
Head
injury
Heart
Impacted fracture Indirect violence Insensibility 12t 2 52 106 79 35, 36 34 ... 128
In sensibility, g ene ral rules for treatment 128
Inspirati on 120
Inst ep 30
Insulat or... . .. 142
Internal carotid artery
Intern al hremorrhage 95
Intes tines, injury of JI 3
In )'oluntary muscles 33
Jaw , angle of 23
" lower 23
" "fracture of 44
J oint, definition of 3 I
" injuries to... 109
Jugul ar vei n 80
Kidneys ... I I I
" injury of 113
Knee, bandage for 159
Knee-cap 30
" fracture of 58
Knot for bandage of lower limb... . . . 42
Knots, r eef and granny 40
Laborde's method of artificia l r espiration ... 126
L aburnum seeds, poisoning by... ... . .. 148
L acerated wound 78
Large arm-s ling ... 39
Lau danum, poisoning by 149
Leg, bones of ... . .. 30 21:2
Leg, fracture of Lifting and carrying " into bed
Ligaments . Lightning of Limbs, 10\\ er " uPI er .
Lime in the eye
Lip!', bleeding from Litters
Liver " injury of Lower limbs ...
Lu mbar vert e brre
Lungs hremorrhage
Marshall II all's method of artificial respiration
Medium ..
Metacarpus .. fract ure of ... " fracture of ... Middle line of body
Mouth, blood issuing fr om
Mu sc les " ruptured l\1 uscular action Narrow bandage
Needle, embedded Nerves

Nervous system
Nose, foreign body in h remorrhage from
Occipital artery ...
Opium, p oisoning by
Pad, ring ... " to fold
Palm, hremorrhage from Palmar arches ...
Paregoric, poisoning by Patella fracture of " fracture of Phalanges of foot " of hand
Phosphorus, poisoning by 148,
Physiology (elementary)
Plantar arch
" artery
Plants, various, poi oning by ... Pleura
Poi son e d we a p 0 n s, wounds by
Poisoning
Popliteal artery ...
Posterior ti bial artery
Potash, cau stic, poisoning by...
Princip les of
Prussic acid, poisoning by
Pubes .. .
Pulmonary circulation .. .
Pulse
Pupils of eyes
RaIJid animals, bites of. .. Radial artery
Radius " fracture of Reef knot
Respiration artificial 12I, 129, 116, " to excite
Respiratory system
Rest, necessity for Ribs " fracture of ...
Room, choice and
Pare 60 ... 198 ... 201 26, 31 144 28 26 110 82 196 III I 13 28 25 1 20 from 97
140 37 28 55 30 62 20 97 3 2 65 34 37 108 lIS
... Pare 117 III 96 213 83 74 88 88 149 30 58 28 56 30 28 150 20 93 93 106 148 9 2 9 2 Par· Pressure, digital. .. " point ...
...
First aid
Questions
Chapter I. II. III. IV. V . ., \,I. X.
on
pre-
of 74 74 17 15 2 28 72 72 13° 21 66 99 liS 145 154 206 106 88 28 54 40 120 13 8 1 2 7 JI8 18 26 46 197
paration
Pace
Rupture (hernia) 114
Ruptured muscles 65
Sacral yerLebrre ... acrum ... 25. 28
Scalds
Seal p, bandage for " h<emorrhage from . capula ...
" fracture of chafer's method of artificial respiration
Seat, four-handed three-handed
" two·handed
Shin- bone ... 161 hock
" electric
Shoulder, uandage for ...
" blade ... " flacture of bones .. . " joint .. .
Sick room, choice and preparation of. ..
Signs, meaning of .
Silvester's method of arlJ' ficial respiration
Simple fracture ... keleton ...
Skull
" fracture of
Slings, arm 43 39, 40, 49
Small arm sling .. Smothering
Snake bites
Soda, can tic, poi::.oning by pleen " injury of ... pinal canal cord ,. fracture of
Spirit of alt, by
Splint, angnlar
Splint. rule for apply ing " to prains
Sternum . . . " fracture of
Stimulants
Stings of plants animals
Stomach ... ant! h<emorrhage frum " injury of .. Strains
Strangulation
Stretcher exercise .. \1ll1y -o. I.

21 5
['.tire
Stretchers, lO ca rry 169 " to improvise 166
Strychnine, poisoning by 153
Subclavian artery
Suffocation 141
Sunstroke 136
Surgeon' yisit, preparation for 204
Syllabus of instruction . .. 7
Sympathetic system I IS
Symptoms, meaning of 17 'yncope ... 134. 'ynovia . . . 31
Systemic circulation 70
Tar<;us 30
Temporal ar t ery. 02
Thigh-bone 30 " fracture of. . 56
Three-handed seat 162
Throat, h::emorrhage fr0111 97
" sw.elling of tissues of .. 141 TIbia 30 " fracture of 60
Toe, bandage for 159
Tongue, hremorrhage from 97
Tooth socket, hremorrhage from 97
T ourniquet 75
Transverse wound of abdomen 113
T\yo -handed seat 161
Ulna " fracture of ..
Ulnar artery
Unconsciousness
Upper limbs
Varicose veins
Veins
Ve'1ous blood " hremorrhage
Ventricles
Vertebra .,.
Vertebr::e ...
Vertebral column
VerUcal wound of abdomen
Vitriol, burn by ...
Voluntary muscles
\Yagon, to loael or unload
\Vall, to cross with S1retcher \\'ar111th, necessity for " to promote \\'ind-pipe
\Voman's dress on fire
Wounds by poisoned weapons " accompanied by arterial hremorrhage . . . "rounds accompanied by venous hremorrhage
\Vounds, lacerated
Wri -t
102 155
51 121
3 26
160 162
30 134 142 156 28 51 26 32 197 17
22
12 3 34 22
214
-.},
?
r o. II. No. If I. " ., No. IV. Stretchel's, Furley Pn.ee 39 140 106 149 I I I 113 :13 117 23 45 149 54 Ie7 III 113 65 140 190 174 181 18 5 18 7 172
94 70 72 93 70 23 25 23 II3 10Z 33 170 18 11.7 118 105 106
5t. 30bn Bt1\bllJance BaBociRtion.
GENERAL PRICE LIST . INTRODUCTION .
Thi Price List, which is subject to revision frum time to time, has been compiled with a view to assist members of the Association and others in the purchase of the necessary equipment for corps and divisions of the Brigade, ambulance stations, classes and first aid and nursing work generally.
A complete and reliable Ambulance Equipment is an actual necessity, and experience has proved that employers of labour and others interested in the district readily subscribe for the purchase of such appliances. Collecting cards, stating the purposes for which subscriptions are required, will be supplied gratuitously on application to the Head Office of the Association, where also any information with regard to its work can be obtained.
Stores of the value of lOS or upwards \\ill be . ent carriage paid to any part of the United Kingdom.
Owing to fluctuations in market prices it is impossible tll gua rantee that the quotations herein can be adhered to.
Quotations will be furni shed for articles rel at ing to Ambulan ce Nursing and IIygiene, not mentioned in this list.
O rde rs and correspondence should be addressed to the St. J ohn Ambulance Association, St. John s Gate, Clerkenwell , L ondon, E.C.
"Remittances should be made payable to the St. John Ambua nce Assoc iation, and c rossed "London County and ·Westminste r Bank , Lothbury."
HORSE AMBU L ANCE CARRIAGES & \VAGONS.

Registered deign 418,030.
\ nUl11uer of imp rO\·ed designs for Ambulance Carriages have reccntly heen perfected, and scve,al specimen can usually be seen at St. John's Gate, varying from a light vehicle to be elra\\ n by two men or by a pony, co ting with india-rubber l)re,; to wheels £32 IO:;., to a large single o r pair-horse \\ agon capablc of accommodating threc patients in a recumbent Pl:ilion and an attenda nt in ;de. A fully illustrated price lit \\ ill hc sent 0:1 :1pplication.
M- M- n 0 o·
e. g- g- ... 5' M- g- >-3
t:j 0 8 ::1. c:; ::r ::r
g. 5:?-' ::rrlQ &p.. 3.
(I) _. vC'tl
- g- p..;r :;:
g- .... g- ;:;- 8- g:'<.. a.
;: en ;: n P> 3. ::
(l) (t) Pl (l) -';:S p.l B::=: 5!2. b c.. t ::J"",...;...>::J r.P>p>n:n"" t:j
P> ] ;:,... g. $I> g ::r;;J
o c.. ::r $I> :::: :::' S Pl (b M" en &\0 ;r] 5.ua s...;r 8
:: b if 0 CT' p.. P> 8-
>yj ;;. c CT' g- ;:l.g 8 :::. '§.'< ;. en P>(b'< :;: c <3 en {; g :: ;r g c; g ;;; 0 11 .... ::?-,... A;3] ;r ." n,... 0 '" >-3 ::J $I> 0 3

PRICES OF THE IMPROV E D
ASHFORD LITTER, 1899 MODEL
Iron Tyres to Wheek
Without Wilh
'Wilh Cover or With Cover or With Hood and Hood and Cover. Hood and Hood and Cover. Apron. Apron . Apron. Apron.
Under -ca.rriage (no
Litter complete with
with Telescopic
Ditto with Police Stretchert
• Prices quoted for Litter wilh Ordinary Stretcher include Wide Webbing Slings but no Chest Strap. Leathel, instead of Webbing Slings, 55. 6d. extra; Chest S trap, IS. 6d. extra. If sup· plied without any Slings, 45. allowed.
t Prices quoted for Lllter with Telescopic.handled Stretcher include Wide Webbing Slings and Strap. Leather, instead of Webbing Slings, 55. 6d. extra. If supplied without any Sling-;, 4S. allowed; and if without Chest Strap, IS. 6d. allowed.
t Prices quoted for Litter with Police Stretcher include Wide Webbing Slings and Leather Straps for securing a refractory patient. Leather, instead of Webbing Slings, 5S • 6d. extra. Hood and Apron, complete (state pattern of Stretcher) ... £2 10 0
Extra Sockets and Studs, 'per set ." 0 I 6
Waterproof Sheet (washable) to be laid on the stretche r bed... 0 10 6
Crates (returnable) charged 4S. 6d. for each Litter.
!!
§
0
7' I
0 d PO' 3. c..
[] ,.... ::
n
S
> (Jl :J: "'!l 0 " t"4 " (Jl With
1ndia RubherTyresto Wheel s
Without
£ s. d. £ s d. I. s. J. £ s. d. £ 5. d. £, s. J.
810 0 9 5 OIl 0 o II IS 012 10 01 4 5 0
Ordinary Stretcher* - II 2 6 12 17 6 - 14 7 616 2 6
handled Stretchert - I I 10 o 13 5 0 - 14 IS 016 10 a
- 12 2 6 13 17 6 - [5 7 617 2 6
Wah
Stretcher)
I)illO
w :ii r. :r: C V> ...; :f. :-,'
s PRICE LIST.
THE "REA =EDW ARDS " LI TTER .

THE LITTER, with \\ ooden wheels, showing meth od of loading; also first aid box fitled to axle.
The und e r-carri age or wheeled portion of this Litter is of an enlirely new design, and is adapted to carry either of "Furley" or "Cl eme lso n" Pattern Stretchers in preCIs ely the same manner as the "Ashford" Liller. It is fitted either. bicycle wheels and extra strong pneumatic o r. WIth I!ght strong wooden wheels, eithe r with sol!d IndIa-rubber or Iron lyres. Owing to the reduction in the h e ight of lhe wheels it i s easy t o lift a loaded st r etche r
uver them, and the cranked ha .· , therefore, Leen replaced by a straight one of tubular steel.
C l{EA-l'.[)\\" AJ{[ S·, LITTER. filleu \\ ith pneumatic tyn:d w111:els, sho\\ing the Stretcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden, and the hubs are so arranged that the wheels can be removed from the axle without disturbing the bearings. In place of thc fuur legs made to raise as handles. two flx.ccl legs filled with small india-rubber \\ heels or rollers afC placed al the foot end, while a. combincd leg and handle fitted \\ith a cro sbar and capalJle uf being raised or lowered i'i used at the end. \\"h en raised as a handle It may be locked In one of twn positions, and \\ hen lo wered it is loched in a n:rtical position. The achantage' claimed for this arrangement arc Ul"l' and rapidity of manipulation and
t
RICE LIST. 6

7 I' IUCI:: LIST.
t!le fac.ility afforded uy the two fixed legs for raISing the lmcr, If necessary, on to the pavement. Th e question o f balance has been carefully studied, and the stretcher is shifted forward so that the middle of it is inches in front of the axle, a perfect balance when the stretcher is loaded and in a horizontal position being thus obtained, and consequent ly there is no weight on the hands of thc per'ion propelling the litter.
The pneumatic tyred wheels are strongly recommended in ca e where the small amount of care necessary to keep them inflated can be given, a the comfort to the patient and ca. c !? propulsion are increased. beyond :1.11 comparison II ith any Iltter. yet produced. It \\Ill ue noted t hat the prices are con Iderably lower than those of the "J\. hford ' Litter, and the following are gi"en as eX:1.ll1ple, uut 0\\ ing to the \'ast number of combinations that can ue made with the different stretchers and con:rings, it is imp'ssible II it hin rea onab le limits to set out quotations for the II hole c)f uut the'e may lJe calculated by adding together the prIces of the under·carriage. stretcher selected, and hout! ;ll1d apron or cover, see pages 4 and S to I I.
SPECIMEN PRICES.
Under·carnage only, either with pneumatic tyred cycle wheels or solid rubber tyred wooden wheel, £10.
Litter complete with ordinary stretcher (no slings or chest strap) a nd hood and apron, £q 3s. 6d.
Ditto with Telescopic lIandled tretcher (with chet strap) and hood and apron, £14 I IS.
H Ilith iron tyred II heels price are £2 less. The lowest priced liLLer complete i· fitted with iron tyred lI·heels. ordinary stretcher (no slings or che t strap) and coyer. Price £10 8. cd. lJ:1.nd lnakl' , which acts automatically IIhen the litter is at re l. £1 ros. ,rh en ordering state II hich wheel:; arc required. PRICE LIST. THE " CLEMETSON" STRETCHER.
" CLE:'IIETSOX" STRETCHER, with back raied, also showing extending leg.
On this stretcher the patient can be mOI'ed as desired, from the recumbent to the sitting position. There is no complicated mechani 111 to get out of order, and the adjustment depends simply on the balance of the patient's body. The stretcher will fit either the" Ashford" or the "Rea-Edwards" Unde!'Carriage. Price £3 3s. ; with extending legs, £4 3s.
Hood and Apron, £2 I5s.
ADJUSTABLE LEGS FOR STRETCHERS .
Primarily these legs, \\ hich are independent of and add:jonal to the ordinary foot wheels, are intended to facilitate the carriage of a stretcher in a railway compartment, in which case two on one side would be lowered and adjustec by a telescopic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the adjus table legs on the other side would rest on the floor. The four legs may be used to raise the stIetcher as required. \Vhen not in use they are folded up immediately under the poles of the stretcher.
Price per set or four, /, I.
FIRST AID BOX
,
To be carried below the axle of the" Rea-Edwards" Lilter, from which it is easily detachable.
Contents :-Set of Splinls, 12 Triangular Bandages, 12 Roller Bandages, 2 i-ll). packets each Cotton Wool and Boric L int, Adhesive Plaster, Pair of Scis ors, Knife. 2 oz. each Olive Oil, Tinct. Eucalyptuf B.P.C., Sal Yolatile, and Spirits Ether Comp., Graduated :'IIeasure Glass, Kidneyshaped Dressing Basin, 6 Tampons for washing wounds, Tourniqu et Pins, Safety Pins, Needles, Thread and Tape. l'rice £2.
" FURLEY" STRETCHERS WITH LATEST IMPROVEMENTS, 1899 MODELS
.

ORO! ARY STRETCHER-<:LOSED.
The impro\'ements in all patterns of the "FurIe " . r8 99 Model, are numerous. The comfort to patlen,t IS Increa ed; t!'c stretcher is stronger, nlore rig!d, and lighter, it. folds up more closely, and its handles "-Ie more comfortaDle tf) hold and afford greater protectior '0 he hands of the bt:<Lrers in pa ing through narrow do"', or passages. -'hould it be necessary to reduce t'l .wIdth of l": loaded stretcher order, fIr example, to carr') _. IOta. a railway carr age, thIS can be done, either when it restI ng on the .grou nd or supporl ed by the bearers with U' tr<?uble and wllhout the. slighte't jar to the patie'nt. Th pnce of the streIcher. IS lowered. All minor points ha\been most carefully considered, and the stretchers al. confidently recommendeu as th roughly efficient in way.
These strekt1ers a re adapted for use alone or as pa.rt Dt th " Ashford" " R Ed d" L' ·e or \.e!l.-· war sItter, and the cover, hOlld ahnd !l'pron, a!my rug, and water. roof described m t is hst are SUllable for use with them.
9 PRICE LIST.
PRICK LIST. 10

PRICES OF THE H FUR LEY " STRETCHERS, WITH THE LATEST IMPROVEMENTS (1899 MODELS ).
N B.-The p r ices of the Standard Models are shown in heavy type.
sri ou Webbing Webbing Leather Leathel W'th t IWith Wide \ With Wide I With \ With Chgs Slings Slings Slings Slings anrl St es (no Chest and Chest (no Chest Webbing rap. Strap). Strap. Strap). ChestStrap
Ordinary Slrelcher, for General I
and Brigade use, taking the place of both the olel ordinary and military patterns
Telescopic· handled Stretcher for workinginconfined
Police Stretcher, very strong, with Ash Poles, anrl provided \\
Leather Straps to secure a refractory palient-
with Wide Webbing Slings
" "Leather Slings
Slings , Wide Webbing
Do. Leather
(or if purchased with the Stretcher instead of Webbing Slings, 5/ 6 extra)
Cover (awning) for Stretcher (when ordering please state pattern of
Stretcher)
Superior Hood and Apron (see illustration, page 3)
Spare Bed for Stretcher
Army Rug to cover Patient on Stretcher ...
Pillow for Stretcher, stuffed hair ... .,.
Chest Strap
s. d.
f, s. d. [. s. d. 1:£ s. d. I £ s.
······1 I r
61 1 17 6 1 I 19 0 12 3 0 \ 2 4
f,
I
3
I 19 6 2 3 6 2 5 0 2 9 0 2 10 d. 6 6 'oj ;:<) n t:l r' d. 6
spaces
ith
:£ R.
17 0 0
3 3
per pair 0 4
per pair 0 9
6
y 'P 0 ....., '"0 r 0 C' r (") U. p:;- ('1\ ('1\ ;:: n . (") ('1\ (1) ('1\ (")0' § "'" S· < -_.(") 5-('1) 2 (b -. '.F.e. - i?, N (') ('):3 '"0 -e. .. g rt -, p;g n g. P' 5§'2 : If ::l -'- 0- C ::. : tI -c YI g .; 0\...., ;::: fL8:7 ::r11:(;' $» n'r.. :l -. .., ,.. ." f. 8 :; n::::::;;::;::." 0 13-;[ :;. ("" ::; Z C') c. :;;: ::l _.::>l (", n =- ;l> ::: "0 y.err::::: 2 b:l /c. n' til 8 :? 1:'U\ -'p Y'" ;:i 0', f ;::-··2 ("') :l ;I) r ::- r: (1) sr:r:-l s 1". C ; :' =-'-< ::;-' - t.l (b --' :: :;: 0 ,....,.. !'I' ;::"::J 0 5 1--1 0 r- 2"-" (/) = ::3 I.J\· (t) Y) (") 0\ $» ." (t '< U IS 0 2 10 0 086 066 o 7 o "7 :to ): 6 =: t!j c: r. < z>?:;:: >- '-' r' >-on co O::Y, r' <: :;;:>t!j D e ""1:1 o C/'J t!j :;; t= ;. "7 t:j .J :.'/' :: ..., ('Tl 6 6 'oj !:<:: t': tv: :-l ;:;
" LOWMOOR JACKET."
For use in mines, ships' hold, eLc., to secu re a patient on a stretcher (see illustration), which can then be placed in an upright pC'sition. Price £1 5s.
WATER BOTTLE.

Copper tinned, with carrying strap .
Price l OS. od.
Enamelled Iron \VaL er Bottle, Cloth covered, with Strap, 55.
LAMP
.
This is fitted with a socket, by which to fix it to a Li tte r, or it can he convenientl y carried by hand, or attached to a belt or the clothing .
Price complete, 5<;· 6d. ,.
Dressing Basin, kidney shaped, made of enamelled iron.
Price I . 3d.
Ambulance Station Plate, Enamelled Iron, 3s. 6d. each . Stretcher Depot Plate , Enamelled Iron, 35. 6d. each.
Carrying Sheet for carrying patients up and down stai rs or otherwise about a hou e. Designed by J. c. Derham, E sq ., Blackpool, and Mrs. Alfred Paine, Bedford. The sheet is fitted with rope handles and detachable bamboo poles, and may be placed on a st retcher without disturbing the patient.
Price complete, ISS.
13 PRICE
LIST
LARGE HAMPER FOR AMBULANCE
STATION AND RAILWAY PURPOSES.

THE
I Set of Cane Splints.
I Elastic Band Tourniquet.
, lb. Carbolic l Cotton Wool ... In Tin ... JCases.
I pair I Knife.
12 Surgeon' Needles.
, lb. Boric Lint
I Roll Adhe::;ive Plaster.
20 Roller Bandages, a sorted.
I doz. Triangular Bandages.
3 Pieces Tape.
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda..
4 oz. of Olive Oil.
4 oz. Spirit Ether Compo
i lb. Tin Powdered Boric Acid.
4 oz. Tincture Eucalyptus B.P.C.
I pair Pean's Forceps.
I packet each afety and Plain Pins.
()Z. CarboliS<!d Chinese Twist.
oz . . ·ilkworm Gut.
I reel each Black and \\-hite Sewing Thre'ld.
I Kidney-shaped Basin. topper Loosener.
I Graduated Measure.
I cake 20 per cen Carbolic Soap.
I Nail Brush .
3 Empty 8 oz . Bottles.
Price complete, £4
LIST.
PRICE
PRICE LIST. r 6
SMALL AMBULANCE HAMPER.
\Yith waterproof cover and strap, for u e in factories, collierie , station, and large wurks, a well as for parochial and domestic use.

CC:":TA1,\I:\G
et plints, 1 Elastic Tuurniquel. 3 Tampons, for '.\'asuing wounds. 2 Packets Lint. 4 Roller BlOdages (wide and narrow). 4 Triangular Bandages.
Wool... ... } In Tin Cases. Bone \Vool ... .. .
Spool of Adhesive PIa ter.
Knife, Scissors. Thread, Tape, Needles, and Pins.
\Yeight complete, lbs. Length, 1ft. 6 in. Depth, C; in . Width, 7 in. Price £ 1 lIS. 6d.
PRICE LIST.
SURGICAL HA VERSAC.
lMPROVE D PATTERN, fitted with a tin, so arranged that any article can be taken out without disturbing the rest of contents.
Contents: T Set of Splints, 6 Triangular Bandages, 6 Rollel Bandages (.vide and narrow), Cotton \Vool, Boric Lint, in tin cases, I Roll Adhesive Plaster, 1 Pair Scissors, I Knife, 2 oz.
Olive Oil, 2 oz. Tinct. Eucalyptus B.P.C., 2 oz. Sal Volatile. 2 oz. Spirits Ether Comp.. I Graduated Glass Measure. I Elastic Band Tourniquet, Pins, and Thread. Price £1 I IS. 6d.
White Linen Ration Haversacs, I S. gd. each.
17 PRICE LlST.
FIRST AID COMPRESSED KIT .
The box is made of wo)d cO\'cred with damp· resisting material, and is fitted \\ith a lock ancl key. It contains a number of practical ambulance appliances arranged so that any article can be withdrawn or replaced without disturbing the remainder. Being fitted with a handle it i portable, and the lid, when let down, can be used as a table. All bandages ancl d r e sings are compressed. ize - Length 16,i in . ; width in. ; height 8 in. without handle.
Contenls: 4 Triangular Bandage•. 6 Roller Bandages, 4 First Aid Dressings, 6 Small Packets of COlton " rool, 0 mall Packets of Boric Lint, I Elastic Band Tourniquet, I Glass, I tin Lox containing a Roll of Pia ter, Boric Lint Patches, Sci"sors and Pins, tray containing 3 boltie'i Cal Volatile, Tincture of Eucalyptus and Oli ve Oil) ami a Dredger of Boric Acid, 1 set of improved Splints, with angle piece, g Splint Straps (sufficient for a fractu red thigh) .
Price £1 I IS. 6d. Each a rt icle is priced separ ately (se e I ndex).
FIRST RID

Size ·n hy 3i II}' 1+ inches. 'uitable for the pocket. TS.
,Y' Tlian&,ular 2. Fir:.t Aid Dressing. 3. Cutton \\ oul. 4· fwo Splllll trap. 5 Adhe_i\'e Plaster 6 Perll1angallutl uf ]'llta ... h. 7. Lanoline. . Boric Lint Palches. o. "'afl t y and l'l:1in Pin!:.. each h . uti. B}' Post I::i. d. Per <lvz. I;', 6J . caniage ]lnirl. '--I 1'.\IC\'l'J' .\l{TII'LES.
1 1).
1 4<1. each ur 3/9 doz.
2 zd. ., 2/0
.3 J(f. " lod. "
4 2d . pc:' trap or I 9 ..
5 1<1. per bu.\. llr Icd .. , '\0 . 6 Id. per box or wd. p-. r duz .
7, I per tin or 1/4 ,_ Hl. per IXl.cket or Iod.
9 Id. [od . .\"'1 kss LI e tlIl/L' n "llplJlicd at <lozen ..
19 PRIer:; UST.
eeMP.lJNION.
21

Pl<.ll.':l!: LIST.
FIRST AID BOX FOR "ASHFORD" LITTER OR AMBULANCE STATION.
This is primarily designed to be placed on the" Ashford " Litter (rg99 Modell, but it is further adapted to be hung up on it w·,ll. A detachable le... ther handle is also fitted for pllq)OSE.5.
Fer contents see next page.
CO TE 'TS OF FIR. T A ID BOX. (lllu,nated on prt:viou" pag",)
Set of Wooden Splints; ) I<:l:tstic Baml Tourniquet; Carbolic Wool, Bonc Lint, in tin cases; TRoll Adhe"ive Plaster; 17 Roller Bandages, as.orted; 6 Triangular Bandages; 3 Pieces of Tape; I Pair Scissors;
1 Knifl! ; T Kidney·,haped Ba,in; ) Graduated Measure; 7 oz. Olive Oil; 2 oz. Tinct. Eucalyptus B. P.C. 2 oz. Sal Volatile; 2 0Z. Spirits Ether
Compo ; 8 0 % Carron Oil; Pins, Safety Pins, Needle", Thread.
PRICE CO:'IPLETE £2 lOS.
POUCH FITTINGS,
specially selected for the 't. John Ambulance Brigade, consi ting of :-
2 Triangular Bandages, one of \\ hich i sealed up in waxed paper. The other may be u ed fur practice, but sho uld be kept as clean as possible.
2 Bandages (3 in. ancl I in.).
Packet of Cyanide Gauze (1 yd. compressed ).
I Pair Scissors.
6 Safety Pins.
Small Bottle of strong Smelling Salts.
Piece of strong Cane, for tightening improvised Tourniquets. Price, 25. d. each. 6 doz. or more, 2S. 7d. each .
Padcts of Syanide Gauze (I yd. compressed). Price per doz, 2S. d.
Small Bollles strong Smelling alts. Price per doz., 5s. 6d.
SAFETY PINS.
All fasten or unfasten on either side.
Facile TO. S 600 llr .' 602 per 3 doz.
" ,,' 60 3 "
Duchess Duplex, To. 2 . . per doz.
" Assorted
Special Blanket Safety Pins, 3 in. in.
PRICE LIST. 22
s. d. o 6 o o 2 o 3 I 0 I 0
Tourniquet ,
Tourniquet, F ield
Splints, \ Voode n , per set, 2/6 ; I.. :lilt: , pL:! scl
G really impr oved \ Vooden Splinlc;, with groO\'cel joints and angle piece, strongly recommended
Tow, fo r splint padding .,. . .. per Ill.
First Field Dressing- (Army I{egulatiun Pattern),
Plice ... cach
9
] aconette, 44 inches", ide per yard 2 3
Tow, Carbolized or Styptic . per I h. 0 9
Wound Pad.-A pad of collon wuul an(1 gaul.e, to \\ hich a bandage is allached. The of the pa<l coming in contact w it h t he wound is nol touched hy the hand of lhe per<son applying the p.1U. Price 4d. each.
First Aid Dressing, consi<sting of a small compressed packet of boric lint, a compressed roller handagt'. :In<l a s:lfet)' pin. Price 2d. each.
Dredger, contain i ng horic acid pO\\Clt'I". h. -+<1.
Glass , 2d .
Knife with strong b lade each 9'\. : per dol..
Pair of Scissors l':lch IS. : pCI' doz.
Splint Straps, \ Vebbing, and Per F'et uf 12 ya rds of strong 2·inch \\'ebbing and 15 Budle. 25. 6d.
T hese make very compact Strn.ps for in the Puuch. T he \ Vebbing sh ould be cut to meet local requirements.
Bu c kl es only, I S. 3d. pe r clozen . W ebb ing only, I S 3d. per dozen yards.
It is unn ecessary to se w the Bucklec; The pikes <should be p assed t hr ough t h e webhing. a nd the short ed of th e webbing sh ou ld li e ollt. wa rds.
I R C E LIST.
Leiceste r Adhc,i,L' 1";1 ter on Cambric, in .tilh "f 1 prd, 6 inches \\I UI.: Gel.
T he Leiceo,ler . \ dhe..,iyp·
Ribbons, in tin l)()\.e-;, 6 yards long. inch \\-ide r illch wiele

National Rubber .\dhe.,iye Plaster (. \ nti eplic), on spools.
5 )<1". 10 yds.
inch \\ ioe C)I.\. h. IS. I,. 6d.
2 Is. 9t1. 2s. 3d.
Ditto in card l)l)x, ill. \\ i<k, long lin 1 3 5 " 5 "
OURT Pl.A'iJ'RR, TRICOLOR Sil.e, 9'1. : :'-lediu/11, Sd. ; .'m:1l1. 3d .
6d. d. rd . 3d • 3d. 6<1. 9el •
?' - J
PRICK LhT.
s. tI. I 6 6 2 6 4 6 o 6
0
NURSES' WALLETS.
ORDINARY PAOLOCK SUAI'IJ:.
\ Vithoul instruments, 4S. 3d.
Fitted complete , contatning Spring Dressing Forceps, . 'patula, Probe, 2 pairs Scissors (round and sharp pointed), Clinical Thermometer, and Knife.
Advanced price lOs.
T. JOllN'S PATTlu{N, a .. illustrated, out improved I)), the 3.dditiolt of flaps to prutcct the j'1Strul11ents.
\ Vithout instrumenls , 7S. 9t1.
Fitted completc, containing Spling Dressing Forceps, Artery Forceps (also useful for dn.:ssing), Spatula, Probe, Director with .car Scoop, 2 p["irs Scissors (round and sharp pointcd),
Clinica l Thermometer (minute, round), Knife, Pencil, and Safety Pins.
Price £r Is.

ROLLER BANDAGES in AssorlInent.
I ::lSIt pac III uJIltaills 6 I),lllclagl: a'i fullows: -
Fill' Cn y ( alico per packet o
Plaill Triangular Bandagell, L,tch (Special qU0talions for large quantities.) . .
UilLu COJllpres'>cd (thlnllCf quality), each 4d. ; per doz. 35. 9d .
IIIuslrated Triangular 1l<tIHlage5 (after Esmarch) showing 25 applications of the Triangular Bandage, with printed insLrucLions
PRH I'. t rST
I'R U"'J.
BANDAGES . (6 yards 1(Jllg.) 26 Or UIl J Ille C;rf'y Beq quality, Superior WC)v.: ( If 0, CJ' Whitt-, with Wlrile Open Grey. SliP' rlfJr While \Vo "f:lI Wove Opell \\ ')\ c. COlli pressed. d. d d. d. " . pl'r dl)l J 9 ;1 Il. I III. 0 9 0 2 0 3 I Ill. 3 2 6 6 2 ill. 3 G 3 0 I 9 ill. I K 2 0 3 G 2 3 3 in. 2 0 2 6 4 0 2 9 4 ill. 3 G 4 6 3 9 -; ill. 4 G
ROLLER
G yards l<lflg - fHlC (j illch, 1WI) 3 illch, olle I inch; 4 yards IOllg
s. d.
-tWI) 2 1 , illch
each per doz. o 6
6
...
4
PRICE LIST.
.I\.OLLER. BANDAGE MACHiNE
.

D e:;ign ed by Dr. A. C. Tunstall.
Price 2s. 6<1.
Forc eps , sprinl5 dressing, full size o r sma ll as I . ; bow dres"ing, 5 in. locked joint I S. 6 d.; Pean' Artery , in. lo cked joint, I S. 3d. ,SClssors, round-po inteil, IE'.; sharp-pointed, for delicatl work, 3d.; small round-p.ointed blades, locked joint , or 5 In., I S. 6d.; rOl:nd-po mt ed curved blades, locked Jomt, I S 6d.; curved blade, locked joint. f IS. 9d. locked Jomt allows the b lad es to ue taken apan or cl ea nmg.
9d. 6d. D ire ctor , with E ar S c oop , IS. 9 l l. Kn?ie , very t hm, . Ivory hand.le, two b lades, h. 9d. Nursmg Chart, deSIgned by MISS Ind erwick, each . Temperature eac h.
CLINICAL THERMOMETERS .
Reduced Pri ces.
RF:olaund. Ordinary, I S. ; minute, IS. 3d.; half-minule. I.. 6<1. t. Strongly r ecomme nded as they will not r oll. Ordinary, I S 6d. ; .rapid (s pecially selected and resel\'Ld for the Assocl atw n ), \\ Ith \'ery open scal e, 35.
CLINICAL THERMOMETERS -(·Ol/llIIlIed.)
With M ag n ifyi ng L ens. Price, o rdin a ry , I S. 6cl . ; minute, I . 9(1.; ha lf-minute. 25. 3 ci . -j . B.- \[i llule and half-minute instruments "ill only register ill the time stated under favourahl e circumstance!'.. No I ab/!il)1 is lakenforbreal.·a/:c 0/ Thermomelers ill tral/s it.
BATH THERMOMETERS.
Til 1h. Forbes' specification. Japanned with zinc scale , 2-;. 3t l. ; Clinical Thermometer size. in case, IS. 6<1. L\ 0 /t'abdi(J' IS taken /01' I>real.·ag. 0./ j/iCrlllolllelers ill trallsit.
COTTON WOOL .
Plain, I oz., 2(1.; 2 oz, 3d. ; .4 07.., 4<1.:! lb., 7d.; I lb., I S. ; small packet (Comprec;sed), Id. Medicat ed, Bor::tcic. i lb., 6d. ; I Ih., IS. 6d.; Carbolic, .pe r 11>., IS. ' d.; .\lemIJrnt h. per lh., IS. 6<1 .; DOllble Cyanide , per 11,., 2 6<1.
LINT .
Plain, I oz. , 2(1. . .., lIZ., 3d. : 4 oz., 6tl. ; lu., lOd. ; I lb .• 6<1.
Boracic, 4 oz., 6(1. : I 11>., Is. 6<1. ; "quare foot packet, 2d. ; ,-mall packet (Com pre "'ed). I d.
GAUZES .
The"e are <;l1pplied in 6 ya rd length ... , width al,out 36 inches s. d.
Ulll11edicated wbite
Alcmbroth
DlHlllle pnide
GAUZE TISSUE.
A laye r of aU50ruent cotlnn wool between two sheets of gaule, good quality, per lb., I S. 6d.
0 10 I 0 2 2
per length
I'RICE LIST.
TEXT BOOKS, &c.
"FIRST Am TO I:\JuRP'n." By James Cantlie, ?If.B., F . R.C.S. The Tc\.t Book of the First ,\icl Course. IS.; by post, B. 2(1. "CATECHISM OF FIRST AID." Compiled from Dr. Cantlie'" Manual. By J. Brown, L.R.C.P., L.RG.., and J. Carvell, M.R.C.S., L.S.A. Price 6<1. ; by post 7d. "HINTS AND HELPS FOR TUR5ING AND IfYGIE.'U;. '
By E. MacDowell Cosgra\'e, M.D , illustrated, on the ilpplication of the roller bandage, by h.. J. CollJe, M.D. The allthorise(l Te\.t Book for the Course. rs. ; by post Is. 2d.
"CATECHIS;\I ON Ifo\m NUR (based on Dr. Cosgra\'e's Text Book). By J. Brown, L R.S:.P., L.R.C.S., and J. M. Carvell, i\I R.eS., L.S.A. Pnce 6cl. ; by post, 7d. lIYGlENE." By rohn F. J. Sykes, D.Se. (Puhiic Health), 1. D., &c. lilustrateci. The authorised Text Book for the Home IIygiene Course. IS.; hy post, I.. 2(1. " QUESTIONS ANn uro;-.l .\MBULA 'CE \VORK." By Tohn \V. Martin, ?lLD., ancl John F.R.C.S. Ed. '15.; oy post, IS. Id. "QUESTIO SAND ,\"'iWERS UPO:\ NURSI:\G." By }t)hn \\'. i\1.D. IS. 6(1. ; by post, IS. Bd. Am 1'0 l'IIE INJURED (Six .\mi>ulance Lecture)." By Pl'ofessor Frcclerich Esmarch. Translated from the German by I r. R. II. Princess Christian. 2S.: hy post, 25. 2d. " ELEl\lENTARY DA AND SURGICAL ') By Waller Pye, F.R.C.S. 2<;; by po t, 2 2U.
DR. G. H. DARWIN'S" FIRST ..\II)S," being a card to hang up, giving treatment of \'ariOllS accidents. 2cI.; by post, 5d.
• • To RESTORE THE ApPARENTLY DROWNED,' printed in large Type with two Diagrams. Unmounted, each: by post, 3d. Mounted, with red border, and varnished to hang up, 6d. ; post free, packed, IS.

PRICE LIST.
TEXT BOOKS, &c. -(COlltillued).
"lIo\\' TO ACT WHEN CLOTHI TAKES FIRE." By J. E. II. ?lfackinlay, M.R.C.S. Unmounted, 2d.; by po ·t, 3d. on card and varni. hed, 4d.; by post, packed, 7d " FIRST AID PRINCIPLES." Cards or concise directions for waistcoat pocket, ld. each; 4d. per dol.. Special quotations for large quap 1ities.
" J'J<:CI:\lEN EXAMINATION PAPERS, Fir!>t Aid, Nursing and Hygiene Courses." 3d.; by post 4d.
S\IALL ANATOi\fICAL DIAGRAM. Showing thc human skele. ton, main arteries, and points where pressure should be applied to arrest bleeding. 2d.; by post, 3 d . DIRECTIONS AS TO THIO: RESTORATION OF PERSONS SUFFERING FRO\! ELECTRIC SHOCK. Large print, poster size . 3d . each; by post, 4d. ; or 2S. 6d. per dozen.
Alor: :\fE;\IOTRE. On cardboard, in linen ·lined envelope, fo r the pocket. By the late ' urgeon·l\fajor P. Shepherd. Containing useful hints for First Aid to the J njurccI. 3d.; 1)), P:)st 4d.
GENPRAL NOTES ON FIRST AID TO BE REN;, ::RIW 11'\ CASES OF POIO;-.llNG. By :\Iilnes lIey, M.R.C .. ' ., L.R.C.P. l'rice 2<1. ; by post, 3d. , ..\\IllLTLA1'\CE TABLErs." By 'ydney Partridge, :\1. D. Price IS. ; by post, rs. rd.
NUl ES ON MILITARY. ANI1ATIO,. By Lt.·Colonel H. P. G. Elkington, R.A. M. C. Price 6d. ; b)' post 7(\. .. 1':\lER(;ENCY BOOK," for instantaneous reference, giving cuncise instructions; to hang on wall. Size about one foot Price 2S. 6d. ; by post, 3s . .\ J[lS TO FOR FIRST AID S1UDENTS. Revised to datt:o Additiunal IllustratIOns. By L. ;\1. Frank Christian , M. B. C.l\r., Edin. 6". per copy; by post, 7d. RULRS FOR CORPS AND DIVISIONS, .'t. John Ambulanc e Brigade. 2d. per copv.
jV
TEXT BOOKS, &c. (,o n lil/lled) .
A History of the Order of the Hospital of St. John of Jerusalem. By the late Rev . W. K. R. BEDFORD. .-\ .. and Li eut.·Culo ne l R. II. lIOLBECJ[E. Price 5s ; hy P',l 5S. 4d .
The Knights Hospitaller s in Scotland and t heir P ri ory at Torphichen. By GEORGI? THOMAS D., L. B. Price 2 s. 6d . , post fl ee, 2S. Sel. Registers . Class Attendance, 2..;. 6d. Cenilicak s , .p;. (d. Case Report, IS.
St. John Amb u lan ce Brigade Cash Book , M inute Book and Occurrence Book. Set of three. 7s. 6d. Receipt Book, 6d. .
Large Physiological D iagrams. Fur Lecturers' use. Cum · prising: The lIuman Skeleton, the l\lu cular, . \rlnial ard Venous System. , the Heart and Circulation uf the H],,, ,d. Simple Fracture, Compound Fracture, Dislocations. l'ri , \: per set of six, ISS. These may be hired for a C,HIP·\: of "First Aill" lectures, given under the auspices of t h\: As ociation, for a fee of 5s., or \Iith the addition of Tourniquet, and plain Triangular Bandage:". for a fee of l Os.
Boxes of Stationery for the use of Sl c rctarie :'lilt others connected wilh the .\ssucialion, co ntaining L\I el\L sheets of high·clas paper, suitably headed, and t\\ eht envelopes bearing toe device of the Association. Price 6d, by post 9d. Twice that (luantity, price IS., by po t 3d. Medallions, issued only in accordance \\ ith paper No. 62, t, be had on application. Coinage Bronze, 2S. ; Silnr, 7s. 6<.1 : Gold, £2 lOS ; including engraying name anti number IJII back "clvet ·lined case, Labels, to be placcdabove for each sub",equentyear\ examination, issued only in accordance \\ ith paper 62. Coin· .lg e Bronze, 6d . ; Silver, IS. 6d.; Gold, 12S. 6d.

A r m Badges, \1 ilh the deyicc. under the a uthority of the Central Executi\'e Committee, ha\'ing been fir t apprOl'ed by H. R . H. the Grand Prior as the sole official and recognised Badge of the Associati on and Brigade.
N. 8.- This design is jrotcctui.
TO. I, for the use of individual certificated pupils- s. d.
In G e rman S ilver, Large ize...
hole
In Electro Plate, Large Size mall ize ditto
Small. 'ize for button hole
In Enamel [ur button hole " brooch
In Cloth and Silk ...
In Cloth and Silver (Registered Number, 3522)
I n Cloth and Worsted
Small Celluloid Badge, for button hole or brooch
\ Yhite Satin Armlet, with woven Badge
Black Silk Armlet, with printed Barlge .. N .B.-Tltuc Bndgrs nrt' 11(>110 /or worn as d.-corn/im
31 PRICE LIST.
P r ice s mu c h Re duced in many cases..
0 71 mall Size ditto 0 6 Small ize for button
0 6
o o 9 o 9 c 3 o 9 2 0 o 6 o o o 2 6
33 PRICE LIST.
BADGES.

Xo. 2.
O. 2, for members of the t. John. bulance Brigade, having the name of the Corps or DIYISlOn annexed on :1 labe l, or.ly issued in quantities-
In Ge rman Sil\'er, fir t doz., £1; subsequent dozs., 12S.
In Electro Plate, first doz., £ 1 J 2S. ; subsequent dclZs., £14 s.
I n Cloth and ilk, per doz., J 23.
I n Cloth and Sih'er, per doz., £1 lOs.
All the aboyc may lIe lI'orn by member of the l. John A mbulance Bri"ade, not \\cHing unirorm.
BRIGADE UNIFORM E ADGES,
etc.
Officers. Cap Badge ( R eg. No . Collar Badges ( " Pouch Badge ( Sergeants . ap Badge ( " Collar Badges ( 101) 103) 3,657) 102) 104) each per pair each per pair
Corporals and Privates .
Cap Baoge (Reg. No. 102) ... each
o \'e rcoat Badge ( " 1,5 82 ).. "
Shoulder Titles, S.J.A. B., with numeral, pe r pair
Shoulder . ' traps, fitted with title and numeral
Lady Offi cers of Nu rsin g D i v isions.
Superilll endent's Cloak Badge (Reg. o. 3,65 8)
Superintendent's Arm Badge ( " 3.659)
Other Nursing Officer's Cloak Badge (" 3·555)
Other l'\ursing Officer's Ann Badge (" 3,65 6 )
Nu r sing S iste rs . I'm Badge ( 3 522 ) " Cloak Badge ( " 3·5 21 )
Hono ra ry Surg eon's
Medalli on B a d ge (pattern D) ..
N ursi n g B ad ge (pattem E)
(pattern A)
Sati n B a d ge lo r Sister's Pin Cushion
Bu g ler's Bad ge .. , .j. 0 Bugler 's Cord
Hono r ary S ec retary's B
Wh istle and Chain
rivate's B r own Waist B e lt a nd Pouch "
White Pipi n g, per packet of yards, enough fo r 3 pair of trouer (packet cannot be broken) 2 Lace , per yard II 0 Black , 0 (, \ Cap Band gel1t:rally runs about 24 inches.)
Silver Wire Cross (pattern B) . S upe ri nte nd e nt 's \\,ire
r
'ta
a d ge .. 34 s d. 0 8 3 2 6 0 6 0 101 0 6 0 6 0 6 3 4 6 3 9 4 0 3 3 :: 0 2 3 0 8 0 8 0 0 0 3 0 1 0
each 2 0 P
7 8
BUTTONS FOR THE UNIFORM OF TH E ST. JOHN AMBULANCE BRIGADE.
I ss u ed only for th e use of Officers and M emhe rs of Co rps ano Divisions \\'earing the prc<;clib ec1 uniform.
Electro Plate, large small cap
Ge rm an Sih'er, la rg e small cap

ELECTROTYPES OF THE ST . JOHN AMBULANCE DEVICE
I O. I. For Cards, .\:C . ... ,,2. For Note Paper . Small Circulan" .xc.
"J' For lluano and Foolsc.lp Letter ·
paper, C irculars, &c.
4. For Small Pusters...
,, 5. For Large
Prints of the abo \'e Electrot ypes ( I to 3\ appear
following page. NO.4 is shown on p:tge 32. Th e diamltcr uf 3A is 3 in., anci of 5B \\ ithollt scroll.
35
PRICK LIST.
s. d.
Black 11
small per duz. 4 2 2 0 0 () 0 0
0m , large
. 0 0 0 5l u 4 Series \. Il.
for fllr Ungade use. use. , d. , d. o 0 o 3
0 3
()
() 3 0 Complete Series 3 5 6
Posters...
011
PRICE LIST. ELECTR.O
YPES. 1\ 0. I A. X I> . 2 A. 1\ ,. 3 .\. For prices see page 35. 'I NO.3 B. ·u. 2 B. No . I B.
tilL
T
Flags bearing As oc ialilln de\ice-I2 (eet by 6 feeL 5 feeL by 3

6
[2 6 Brigade 4 fl. q in. Ill' 3 fl. o [2 0
SWAGGER STICKS
for the use of Officers and Membe rs the St. John Ambulan c e B r igade .
Ebonised Canes, German Sih'er MounLs bearing the Brigade Device.
PRICR Is. EACH.
Officers' :'pecial Canes with Sterling Sih el'
PRICE 7s. EACH.
All Orders for the foregoin g Stores should be -; iven t o the Local Secretary, or to the Stores Department ,
St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E .C.
1'ldC/·. 1.1:-'1.
UNIFORMS FOR AMBULANCE UNITS OF THE S.J.A.B.
These may be obtained direcL from lIehbert and ClI., .35. Belhnal G r een Road, L Tdephone No. 909, Lon· dun \\ all. Telegraphic Address: ., Otherwise, London."
CIlIEF SURGIW:--f AND HONORARY SURGEON.
(Badges
andl'ouch: Black Morocco (Bltclge extra)
Sli \'er em IJfuilierecl (Badge c>,lra)
CO.lt (lhdge extra)
SUPT. OF DI\'ISION A);J) AMBULA:-.ICE OFFICERS.
Crus '-belt, 'White Patent Leather and Black :\forocco PUlich (B llige extra) ... Furage Cap (Badge extra)
37
L d.
feet
o
/, s. d. Tunic
extra'... 4 4 0 T\\o-inch Braid, side seams 5 0
0 0
Fllr.tgL
ap
l; IlI\ t:s ... l;real ('Ilat (Badges extra) 3 7 6 9/6 and 0 15 6 0-+6 4 -+ 0 Cl1l1el SUP'!. .\:\/) (YJ 111'..1{ UIlIILF OFFICERTUI,ie (Hadges extra) ... o I'allul
(Badges extm) Fat igue Iacket (RIdges ext raj 3 3 0 2 10 6 Two-inch :'IIohair Braid down side eams Crv-.s I> -It, White Patent Leather
5 o l'ouch
extra)
0 r 4 () }'vrage
9/6 an,i 0 15 () l:lu\L's 0 4 6 Leggings 0 6 C;real
-+
l'ro..,s-helt
(
(Badge extra)
.lacket
and l3Iack
(Badge
.
Cap (Badge CAtm)
4- 0
l'atrol Jacket (Badge.., eXlr,I) 2 6 6 Trollsers: Two-inch
down side seam 5 0
l\Iohair Braid
c;
Leggings
, ... Greal
o q 6 9/ 6
0 15 6 o 6 o 6 4 o
lm'e ...
..
Coat (Badges extra)
and
LIST.
:\IESS Dlmss FOR OFr-ICI'R.
Jacket (Badges extra)
\ Tcst .. . 1ST CLASS SERGEANT.
Patrol fackel (Badges extra) ...
Cheno-n, 4 lJar-, .-ilvl'l, 3" 4d ., \Vorsted
Trousers
Forage Cap (Badge exLra) .
Cross-belt and Pouch (lh<1:;e c,l ra\
Buckskin (; loves
Collon
Leggings
Creal Coal Chen,)l1 and Uallge extra)
CORPORALS, AND l' A1'.'k ANil
PaLrol Jacket, Black T:1.1'al1 e,t r:l )
Trousers, Black TarLan
Forage Cap (Badge c:-..lra)
\\'aist-belt and l'oueh
GreaL Coat I(hevrun \\here requir e d and Badge extra)
t;IO\e5 \per pair) (per pair)
C!1e\T0I1 , 31iar", :-iih'e r,2" 6el., \\ \lIsted
t.·orprJral's 2 IS. 'd . C YCLIS lS - SU PERIN
Patrol Jacket (Badges e'lra)
Cap (Badge e:-..tra)
Breeches; l; rey Serge
Cross Hell and Pouch (Badge extra)
Gloves
Gaiters oJ
Hose ...
GreaL CGal (Badges ext ra)

Jacket (Badges extra)
Cap (Badge extra)
Breeches: Grey Serge Belt ,
Gloyes (per pair)
Gaite rs (per pair)
UNIFORM
Tiles e may be obtained from l\I essrs. E. & R. Garrould, ISO to 160, Edgware Road, Hyde Park, \V.
5320 and 5321 Paddington, and 3751 Mayfair. Telegrams: .c Garrlll1ld. London."
Cloak (Badge extra)
Bonnet
Dre.. , made to M easure (Badge extra)
Collars '"
Cuffs
Cap: ctr Sister Dora ., Apron
61 and
I 8 and 2s. 6d.
Carriage paid on all orders over ten shillings in \·alue.
II All Badges to be obtained from St. John's Gate.
H the Corps or Diyision is out of London, measurements to be supplied to contractors free of charge.
PRICE
39
1
.f, 3 3 [ 1:) 2 3 0 I 0 0 II 0 -l0 -l0 13 FII E. 0 11 0 () 0 .2 0 6 0 13 0 0 0 -l0 I 0 0 2 LO I 3 0 12 0 II 0 -l0 -t 0 4 4 4d. 6 0 6 -+ 0 <) 0 () 0 0 () 6 0 S tJ 0 0 6 0 0 II 6 6 0 PRICI:. LIsT. 40 CYCLISTS-RA T-;K A;-.II) FILl:. £ " d.
..
Carriage out uf
l xtra o 19 0 2 0 12 0 10 () 4 0 -l-
Londun
UNITS OF THES.J.A.B . 6 0 0 6 6 6
FOR NURSING
..... . ..
.. ... . ..
... . ..
£ d. o o 10 9 I 13 6 and £2 2S. o 2 3
dozen. o 2
o 0
o
blf
3" "
Dressing
INDEX TO PRICE LIST,

(Horse Ambulance) \Vater Roule' \Vaterproof
Whistl e anu Chain Wool (Cotton) Wound Pad
Hampers
Station
Bandage
... Basin,
Bed,
"
Books ... Bottles
rAGE 15 to 17 14 32 to 34 27 26 12 Buttons .. . ... ... . .. Carriages
Ambulance) Carrying Sheet Cash Book .. . 12 29 to 3T '3 35 2 T4 3 1 28 Cotton \V 001 ... ... ... Cover for Stretcher or Litter Diagrams, Large 1t "Small 30
(Boric Acid) 23 Dressing Basin '4
Tackle 12 Electroty-pes.. ...35, 36 Emergency Book 30 First
Box .. ... 9, 21
22 "
2 0
Flags 37
27
... ... 28
... ... ..,
Hood
4 Instruments
23 Knife , 23 Labels .. . .., 31
. 34 Lamp .. , .. ,
. .. .., 28
Nur.;;es'
Pillow Pla;,ters
Roller Ban
I\Iacllllle Rug I'AGP: 5 lO 7 13 23 3 3' 27 Rules
30 Safety
22 Scissors
Ambulance
..
Plate ,
Rol\i{lg Machine Bandag..s
Equipoise
Camp
(Water)
(Horse
Dredger
Drowning
Aid
,
Companion..
" "Compressed Kit T9 First Field Dressings
Forceps
Gauzes , 28 Gauze Tissue
Hampers (Ambulance) 15 to '7 Haversacs
18
and .\ pt'on for Litter..
(various) Jaconette ,...
Lace for Caps, &c
Ii Lint
Litter (Ashford) 3, 4 Lown10or Jac ket Measure Glass Medallions :'>Itnute
r\ursing Charh Occurrence Dook
." Pouch Fittings Receipt Book Registers
dage
for or \m b llian ce Brigade
Pill S
23, 27 Sling., Slretcher II Splint Padding 23 Splint Straps .. , 23 Splints..... 23 Stationery. 31 lretcher Depot Plate '4 Stretchers ... ... 8 to It " Adjustable Legs for 9 Swagger Stick.. 37 Temper"ture Ch:ut 27 Text Books .. , 29 to 31 Thermometers .. 27, 28 Tourniquets . 23 Tow, carbolized 23 "plain 23 Uniform Sundries 34 Uniforms ... to 40 \Vagons

