BONES.

SF.VI;:WI'H} CEIIVICAL VEwnLURA - - -COLI.AII} (davide)
AXil I AUY " h 'A;,"'AI (lh';:I1<\ or ] ournl'lllt'I). _ .A.Ok I'A.
BONE ' -
4T1t LUMIlAR VI<Wn;BI1AHAUNCH) BONg 5 ' , ULNA RADIUS -
I\JETACAHI'US • -_"
THIGH BONE (femur)
KNEll: CAP (patella)
SHiN BONK (tihia)
IlIWOCH BONE (fibllla) TARSUS
Ml!:TATARSUS , PIIAI ANGES
ARTERJES.
Tilt" '1un Ie (t JII\V •• t' 1 It-' tit". ( Lr( I III hn 11 [e\1 - - OCll"1 rAI TnMPORAT , 1< \ 1-\ ('"..\1(01'11 oS III \\ 1.\
)f'I'III"'"
'I·r", III 1111 IS '{l )1< JIII\I••
_ __ HI, 'l'j AI ( "1"'>10111. 1 lAC. R lIquel) M. r 01' POI'L1TEAI •
("I,
AS A COMPANION TO THIS BOOK-
"A CATECHISM OF FIRST AlD."
BY j. M. CARVELL. M . R .C.S .• L.S.A.Price 6d. net; by post, 7 d.
FIRsrr AID TO THE INJURED ·
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE
ST. JOHN AMBULANCE ASSOCIATION.
BY
JAMES CANTLIE, M.A., F .R .C .S. , Knigltt 0/ Grace 0/ tlte Order 0/ St . Jolm. HOllo"ary Life llIember 0./, ami Lecturer a1td Examiner to, the Association.
With a CHAPTER on "Stretcher Transport," revised from that originally written by Sir JOHN FURLEY. C.B., Knig-Itt o//ustlce 0/ the Order 0/ St . John, in accordance with the Army Stretcher Exercises. Also a CHAPTER (being the Fifth Lecture, for Females only), by E. MAcDoWEL COSGRAVE, M.D., F.R.C.P.I., o/Grace o/tlte Orde,. 0/ St Jolw , Honorary Lijc lllember of, and L.:cturer an.d Examiner to, tlte Association.
EIGHTEENTH EDITION, 780,000 to 830,000
(In tit is Edition m any o/tlu illustra'ions have been re·drawn; otlr.erwisl it diffirs but little/rom the elt!vcnth to tlt e seventuJttlt edztiolts.)

Price in Cloth, IS. net; by post, IS. 2d. In Morocco, 25. 6d.; by post, 25. Sd. TO BE OBTAINED AT
ST . JOHN' S GATE, CLERKENWELL, LONDON, E .C.
W. H . & L. C. SO, OOO- O!lqtT
l!Lu t
6ranlJ of tbe ®rl:rer of tbe J110spttal
of cSt. .3Jobn of lentsalem in QEnglanl:r.
5 0vu¢lgn lJatron of tl,¢ Orb¢r.
His Most Gracious Majesty King George V. lJr\or.
Field ·Marshal His ROYRl Highness th e Duke of Connaught, K.G.
5ub-lJr\or.
The Ri g ht Honble. the Vi scount Knutsford , G C M.G. of tg\¢.
Field·Marshal His Ro yal Hi g hn ess the Duke of Connau g ht, K.G.
-"-£>.¢cutlv¢ 0fflc¢rs .
P r elate -His Grace the A RCI!BISHOP OF YORK .
Clt a 1zcell or- C olonel Sir HERBERT J EKYLL, K.C .1\I. G., R.E.
Sec re t ary·Gene>'aZ-Colonel Sir H ERBERT C. PERROTT, Bt. , C.B.
Rece iver· Gene1-al-EDWIN FRESHFrELD, Esq., LL.D
A Lmon er-
Registr ar-Major·General T he Lord CHEVLESMORR, K.C.V.O .
Ge>lea logist-Sir ALFRED SCOTT SCOTT·GATTY, K.C .V.O. (Garter).
Direc t or o/, tlze Ambulance Dcpm-tJJlent-The. Most Hon the l\larqu ess of BREADALBANE, K.G .
Librarian -Lieut. · Colonel R ICHARD HOLBECHE .
S ecreta ry-\Vu.LlAM R. EDWARDS, Esq., A .C.A .
Chair m an 0/ the British O/>!ttltabnic Hospital j eru salem-The R ight H on . the Earl of PLYMOUTH, C.B . '
Chie/' S ec,'e t ary o/, tlte A mbulan ce Dep a rtm ent- C olonel S ir HERBE RT C.
P ERROTT, B t , C B.

::t\ss lstant tx¢cutlv¢ Offlcus .
ASSIstant Di1'lIctor oj' the Ambulance Department-Lie ut.·Colonel Sir R. C. BL, Assistant H. FRESHFIELD , Esq . .r/.sslslant Lib'1l,irL11-C. V \VENPORT, HOIl. Secrelflr), (Jf tile Bntislt UplltlL/llmic Hospital , j erusalemColonel T. H . HENDLEY, C .I. E., 1. 1\1.S · Assista'lt HOlLolary Secretary (jor Scotlaltd) of fhe British Op htha lmic . Hospital, jenesalem-J. II. STEVENSON, Esq. (U1LiCOY1l (!:ounc\l.
The Council consists of the Sub.Prior, as Preside.nt ex.o!ficio , the Executive Officers, and the following m ¢mb¢rs.
Sir J . FURLEY, C.B.
Major·General J. C DALTON, R.A
The Earl of RAKFURI.Y, G .C.1\I.G. Col. C. w. B BOWllLER, C.B.
Lieut.·Colonel Sir R. C. TEMPl.E, Et., C.LE .
Sir J . DICK, K. C .B ., M. R . C.P. L, R .N .
Colonel S ir C 1\1. \VATSON, K.C.M.G., C.B., R .E.
Sir D. DUCKWORTH, B t., L L.D., 1\LD.
I nspector·Gen e ral B. NI NNIS, M.D., R.N.
Sir R. D POWELL, Bt., K C V.O., 11 D.
CoL Sir C . M . ROYDs, C.B . . E . OWEN, Esq., LL.D., F.R .C.S. W D J -'MES, Esq., C.V.O
The Earl of BESSBOROUGH, C. V.O. , C.B.
The Chapter consists of the Knights of Justice and Sub·Prelates d e f u r e; the Execu tive Officers; the selected Members of Council; and th e
Officiating
Th e Rev. Canon SHEPPARD, C.V.O., D. D (Sub· Dean of the Chapels Royal), The Rev . P. \V. \VYATT, AND ::t\s lKnlgl,ts of tsquiru.
Surgeon·Ge neral S ir \V TAYLOR, Colonel IT H. HENDLEY, C.LE , K.C.B. , M D. 1.1\1.
The Lord CLAUD HAMILTON, The Viscoun t ESHER, G. C.B., M.P. G C V.O
Lt ·Col. E 1\ L WIl.SON. C.B , C. E. HAWLTON, E-q., C.;\I.G. C.M.G., D.S .O ., R.A.:\f.C . Lt.·Col. 1. PHILIPPS. D.S.O., M .P. L t. ·Col. Sir L . Bt. , Colonel C. F. ST. CLAII,I.\ NSTRU. C V O THER, 1\LV O., D.S.O
The Lord DliSBOROUGH, K .C .V.O. E . DAWES, Esq .
Tht: Earl of KILMOREY, K.P. W M. H . ST . J . HOPE, E'q .
Following of '3
H.R.H. Prince CHRISTIAN OF SCHLESWIG-HOLSTEIN, K.G.
H.H Prince ALBERT OF SCHLESWIG-HOLSTEIN, G.C.B.
H.H. Th e Duke of TECK, G.C.B., G.C. V.O .
Vice-Admiral H.S.H. Prin ce LOUIS OF BATTENBERG, G.C.B.
H.M. KING HAAK ON OF NORWAY, K.G.
H.S.H . PrinceALEXANDEROFTECK
G.C.B., G.C.V.O., D.S.O
H.R.H. Prince ARTHUR OF CONNAUGHT, K.G.
Sir J. FURLEV, C.B. (Hon. Btliliff)
The Lord STANilIORE, G.C.M . G.
Sir T. DICK LAUDEH, Bt.
Major S ir A. Bt.
The Earl FERReRs.
Col. Sir H. C. PEImOTT, Bt., C.B.
Col. Sir J. GILDEA, K.C.V.O , C.B.
H. J. L OFTUS, Esq.
Colonel B. M. DAWES.
Gen. Sir C. WARREN, G.C.M G., K C.B., R.E.
Maj.- Gen . J.C. DALTON, R.A.
Col. A. G . HUNTER-WESTON, C.B., D.S.O., R.E.
Colonel The Lord WILLIAM CECIL, C.V.O.
E. FRESHFlELD, Esq., LL.D. (H01t. Bailiff)·
The Duke of FIFE, K .G.
The Earl BRASSEY, G .C. B.
The TEMPLETOWN.
The Visco un t K NUTS FORD, G.C.M.G. (Sub-Prior).
R. M. MACLEAN, Esq.
A. F. G LEVESON GOWER, Esq.
Lieut. -Col. F. A. H. LAMB ERT.
Col. Sir C. W. MURRAY, C.B.
Following
The Bishop in JERUSALEM.
The Bishop ORMSBY.
The Bishop of GIBRALTAR. I
The Earl of RANFURLY, G.C.M.G.
The L ord SANDHURST. G.C.S.I., G.C.I.E.
Sir H. A. BLAKE, G.C .M.G.
The Earl of MEATH, K.P.
A. E. FRASER, Esq.
The Lord MOSTYN.
The Marquess of BREADAI.BANE, K,G.
The Duke of PORTLAND, K.G.
F .- M. The Earl ROBERTS, K.G., lJ.qr
R. BRUDENELL CARTER, Esq., F.R.C.S. (Hon. Commander).
N_ H. FORRES, Esq ., F.R.C.S. Ed.
Colonel C. W. B. BOWDLER, C.B (Ho.t. Comma1tder) .
Lieut.-Col. A. C. VA TE.
Major-General A. F. TERRY.
The Earl of PLYMOUTH, C. B.
The Earl OfSANDW ICll, K.C.V.O.
The Earl of ELLESMERE.
E. H. FRESIFIELD, Esq.
The Viscount BR ACKl.EY, M.V.O .
F.-M. The Viscuunt KITCHENER OF KHARTOUM, K.P.
Lt.-Col. Sir R. C. TEMPLE, Bt., C.I.E.
Sir A. S. SCOTT-GATTY, K.C.V.O. (Garter).
Colonel Sir H. JEKYLL, K .C. M.G., R.E.
H.E. the Lord I SLINGTON OF I SLINGTON, K.C.M.G., D.S.O.
Col. Sir J. R. A. CLARK, Bt., C . B., F.R.C.S. E.
Sir R. HARVEY
H. E. Sir G. S. CLARKE, G.C.M.G., G.C.I.E.
Lt.-Col. J. W. WRAY.

The Bishop of DUNEDIN. ( Primate 0./ New ZCtlla t£d.)
The Bishop of SOUTHWARK
BEING THE AlI1BGLA CE OF' QJiX'ltub- of tbe ®rber of tlJe of .st. ]obn of JlerlH,alem in Qtnglanb-. lJatron.
HIS MOST GRACIOUS MAJESTY KING GEORGE V. (SOVEREIGN BEAU AND PATRON OF THE ORDER.)
FIELD -MARSHAL HIS ROYAL HlGHNESS THE DUKE OF CONNAUGHT, K.G. (GRAND PRIOR THE ORDER.)
(tommlttu..
Consisting exclusively of Members and of the Order.
Dwt:Cior or the Ambultlnce Depart1llCltt and Chairma1t 0./ Committ eeThe Marquess of BREt\DALBANE, K.G.
ASSIstant Director and Deputy Clzairmat£-Lieut.-Colonel Sir R. C. TEMPLE, Bt., C.l.E.
DepuLJ/-Cltalyman-Sir J. FURLEY, C.B. (Life Member of the CommI ttee Honoris Causd) . fifembers.
lIIajor-General J. C. DALTON, R.A.
Colonel C. W. B. BOWDLER, C. B.
Lieut.-Colonel A C YATE
Colonel Sir ]. R. A. CLARK, Bt., C.B ., F.R.C.S.E.
Th e Rev . T. C. ELSDON.
\V. DIXON, Esq .
I1Iajor G. E W. 1\ [ t\LET
Colonel S ir J. W. OTTLEY, K.C.1. E., R.E.
Inspector-General B. NINNIS, I1I.D., R ..
G. FOWLER, Esq.
Surgeon-Major G. H DARWIN, IIL D
Colonel G. S. ELI.ISTON, C.B., I\I.R.C.S., R.A. I.C. (T.)
Lieut.·Colonel C. ]. C.M.G., L.R.C.P .
Colonel Sir C. I\L ROVIlS, C. B.
Captain ir]. \V. NOTT-R o WER , H. BOULTON, Esq ., IILV.O .
E. OWEN, Esq. , LL. I) ., F. R.C.S .
The Lord CI.AUD M.P .
<r:¢ntr-al tXltcuU,,1t <r:ommlttu -colltillued.
Sir J. L. LANGMAN, Bt.
The Han. Sir J. A. COCKBURN, K.C.M.G., M.D.
Sir A. CONAN DOYLE, M.D.
The Right Hon. J. L. WHARTON, P.C.
Surgeon-General Sir A. KEOGH, K.C.B., F.R.C.S.E. & 1.
S. \V. MALKIN,
Surgeon-General Sir B. FRANKLIN, K.C.1.E.
J
.. S. GRIFFITHS, Esq., M.R.C.S.
Lieut.-Colonel J. A. J ONES, M.D.
The Lord MERTHYR, K.C.V.O.
The Viscount HYTHE.
C. B. PALMER, Esq.
The Earl of BESSBOROUGII. C.V.O., C.B.
Lieut.-Colonel G. E. TWIss, F.R.C.S.I., R.A.I\I.C.
Colonel/.. CANTLIE, F.R.C.S., R.A.l\l.C. (T.)
Colonel r. H. HENDLEY, C.LE., 1.M. S.
R. A. GIBBONS, Esq., M.D.
]. H. MORGAN, Esq., C.V.O., F.R.C.S.
Surgeon-Major G. A. HUTTON.
Surgeon-General Sir C. McD. CUFFE K C B F.R.C.S.E.
F. R. CASSIDI, Esq., M.D. , ... ,
A. T. BRAND, Esq., M.D.
]. A. BLOXAM, Esq. , F.R.C.S.
F. N. ELLIS, Esq.
Major E. WEST-SYMES, M.D., R.A.M.C. (T.)
\V. E. AUDL AND , Esq., M.R.C.S.
Ex-Officio Members 0/ Committee.
Secretary General of the Order; th e Receiver G"ene ral of the Order; the Chairman, British Ophthalmic
<r:l,lltf Sltcrdarl'.
Colon el Sir HEKBERT C. PERROTT, BI., C. H.
-l>trltctor of Storlts :2\ccOulttant.
WILLIAM R. EDWARDS, Esq., A.C.A.
S tou!\ltltp¢r.
WILLIAM H. MORGAN, Esq.
:2\sslstant Sltcrdarl'.
DUNCAN G MONTEITll, Esq.
TERRITORIAL BRANCH.
<r:ontrollltr in <r:l,lltf.
Lieut.·Colonel Sir R. C. flt., C. LE.
:Assistant S¢crdarl'.
P. G. DAllVIL,SMITH. Ksq.
R ltVISEO 1 8,

REFERENCE No. 58. ---1908-.
FIRST AID TO THE INJURED SYLLABUS OF INSTRUCTION
.
FIRST LECTURE.
Principles of First Aid.
B. A brief Description of the Human Skeleton and of th Muscles.
C. Fractures-Causes, varieties, signs and symptoms.
D . Treatment of Fractures-General Rules.
E. The Triangular Bandage and its application.
SECOND LECTURE.
A. Treatment of Fractures (continued). Details of treat· ment.
B. Dislocations, Sprains, Strains-Signs, sympto ms and
C. The Heart and Blood Vessels. The Ci rculati on of thil'! Blood. \-
D. H;-emorrhage and wounds. General rules for treatment,
E The Tnangular Bandage and its a pplication.
8
THIRD LECTURE.
A. Hremorrhage and wounds (continued). Details of treatment.
B. Internal Hremorrhage-Signs, symptoms and arrest.
C. Hremorrhage from Special Regions.-Signs, symptoms and arrest. .
D. Bruises, Bums and Scalds, Bites and Stings, Frost-bite.
E. Foreign bodies in the Eye, N?se and .
F. The Triangular Bandage and Its applIcatIOn.
FOURTH LECTURE.
A. The Nervous System.
B. The Organs and Mechanism of Respirati on-Artificial Respiration.
C. Insensibility.
D. Poisoning.
FIFTH LECTURE (for Males only).
A. Improvised methods of lifting and carrying the sick or injured.
B. Methods of lifting and carrying the sick or injured on stretchers.
C. The conveyance of such by rail or in country carts.
FIFTH LECTURE (for Females only).
A. Preparati on for reception of accident cases.
B. Means of lifting and carrying.
C. Preparation of bed.
D. Removing the clothes.
E. Preparations for surgeon. 9
NOTE I.-The subject of poisons should be treated in a g e neral manner; the common poisons classified, and only thei r general symptoms, effects and treatment taught.
NOTE n.-The last half-hour of each lecture should be to work, such as the application of bandages and sphnts, lIftIng and carrying wounded on stretchers.
NOTE HI.-There c;hould be an interv<1.1 of a week between each lecture. A ca.ndidate for examination must attend at least four out of the five lectures.
NO!E IV.-:\!ale classes must pa.ss in that system of stretcher exerCise most sUlta.hle for the locality.
NO!E V,.-As time as possible is to be spent on instructIOn In analol1l1cal and physi ological details. Lecturers and examiners are particularly reque 'led to remember that it is " First Aid" that has to be taught and tested and not anatomy and physiology. '
j).Iixed classes 0/ men and women are on 1Z0 account pe7:m itted
PUPILS UNDER SIXTEEN YEARS OF AGE CAN 0 LY ATTEND THE" JUNIOR" 00URSE (SECT ION A, SYLLABUS 40).

Lecturers instructing a First Aid class, and Local Secretaries, can obtain further particulars on application to the Chief Secretary for" Paper Reference No. 80."
No Lectzenr may examine his own Class /01" Cer tifica tes.
OF COKTENTS .
CHAPTER I.
Principles of First Aid
Explanatory
Questions on Chapter
CHAPTER II.
The Human Skeleton. Skull, spine, and bone upper limbs (collar-bone, shouldel-blade, aIl11bone: bones of the carp?s, phalanges), pelvis, lower lun bs (thIgh-bone , kneecap, tarsus, metatarsus, phalanges ) ... ...
Joints .,
Muscles. Voluntary and involuntary
Fractures. Causes, varieties, signs and £ymptollls
Apparatus for treatment of Fractures ...
General Rules to be observed in the treatment of Fractures .. ,
Special Fractures. Cranium, lower jaw, Till,S, breast-bone, coll:1.r-b one, aI1l:-ll01:e or bones close to the elbow J lInt, forearm, cll1shed hand, pelvis, thigh-b one , knee-cap, leg, crushed fOOL
Dislocations
Sprains ."

CHAPTER III.
Circulation of the Blood_ Organs; general (systemic) and pulmonary circulations
Hcemorrhage or Bleeding. Arterial, venous, capillary
Arterial Hcemorrhage. Principles of arrest
Wounds with Arterial Hcemorrhage
Course of the Main Arteries and Pressure Points .
Aorta, arteries of the head and neck, of the upper limbs, of the lower liml)s
Venous Hcemorrhage and Varicose Veins
Wounds with Venous Hcemorrhage
Capillary Hcemorrhage
Internal Hcemorrhage
Hcemorrhage from Special Regions
Questions on Chapter
CHAPTER IV.
Miscellaneous Injuries. Bruises, burns and scalds, hites of snakes and rabid animals and w0unds by poisoned weapons, stings of plants and animals, frost bite, needle embedded under the skin, fish hook embedded in the skin, injuries to joints, foreign body in the eye, ear passage and nose. wound in the front wall of the abdomen, injurie to the organs within the abdomen and pelvis
Questions on Chapter . . . . ..
CHAPTER V.
The Nervous System. Cerebro-spinal, sympathetic ...
The Respiratory System
Artificial Respiration. Schafer'S, ilvester's, Howard's combined with Silvester's, Laborde's and Marshall Hall's methods
10
... .,.
... .. Sprains
Ruptured Muscles Questions on Chapter 17 20 2 1 22 3 1 32 33 36 41 43 62 64 65 66 II
and
. .. Page 70 73 74 76 79 93 94 95 95 96 99 I02 !I5 117 lI8 I2I
Insensibility. Causes, general rules for treatment, concussion of the brain, compression of lhe brain, apoplexy , epilepsy , hyst eria, shock, fainling and collapse, sunstroke and heal-stroke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPTER VI.
Poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for lhe scalp, fo re head, elc., shoulder, hip , hand, foot, chest, back, knee, elbow , fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three. handed sealS, fireman's lift, fore and aft method, improvised stretchers, to cross a dilch or wall, to load or unload a wagon ..
CHAPTER IX.
Stretcher Transport. Stretchers, stretcher exercises, li lte rs
CHAPTER X.
The Fifth Lecture (for Females only). Preparation for reception of accident cases, choice and preparation of a room, lifling and carrying, preparalion of bed, removing lhe clolhes, preparalion for surgeon ...
Questions on Chapter

LIST OF ILLU TRATIO
Skeleton showing position of main arteries
Skull and verte bral column '" ...
Vertebra ...
Bone!5 of the left upper lim b
Bones of lhe right lower limb
Shoulder Joint
Ankle . . .
Rectus Muscle .
Triangular bandage spread out and folded
Large arm sling
Small a rm sling
Reef knot
Granny knot ...
Loop knot
Bandage for fracture of lower jaw .. .
Bandages for simple fracture of ribs
St. John sling
Band1ges for fracture of both collar bones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
An gular splint '" ... ..
Treatment of fracture of foreanll . . .
Treatment of crushed hand... ... . ..
Treatment of fractu re of thigh bone '"
Treatment of fracture of thigh bone (woman)
Fracture of knee cap ... '"
Treatment of fracture of knee cap ...
Treatment of fracture or leg (man and w0man)
Treatment of crushed foot ...
Diagram of th e heart, lungs and air passages
I2
Page 128 I4 2 145 155 I60 197 206 I3
. . . ...
. .. ... .. . .. .
.
..
.. .
... ...
'"
. . . . ..
S. Par e fr011tispl'ece 24 27 29 3 1 3 1 32 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 71
Diagram of the of the blood
Digital pressure on car?tld artery .. .
Digital pressure on facIal artery .. .
DigItal pressure on temporal artery
Digital pressure on occipital artery ... ...
Pad and bandage to arrest hzemor1 nage from temple
Ring pad ... ... :.. .. .
Digital pressure on subclaVian artery .
Pad and bandages to apply pressure on axillary artery .. .
Digital pressure on brachial artery (two methods) .. .
Flexion at elbow
Digital pressure on radial and ulnar arteries ...
Pad and bandage to arrest hzemorrhage from palm
Digi tal pressure on femoral artery .. .
Tourniquel on femoral artery .. .
Flexion at knee
Organs of the chest and abdomen .. .
The lungs and bronchial tubes .. .
Schafer's method of artificial respiration ...
Silvester's method of al ti Gcial respiration ... . ..
Silvester's and Howard's methods of artificial respiration combined
Bandage for the bead
Bandage for the shoulder
Bandage [or the hip . ..
Band age for the hand
Band age for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
(;rip for four-handed seat ...
Lifting by two-handed seal. ..
Clips for two-banded seats ...
Carrying hy two-handed seat

rip for three-banded seat ...
Supporting patient ...
Fore and aft method of carrying
Carrying on improvised seat
Improvised stretcher
Furley stretchers
, tretcher exercise, No. 1. . , Fall in"
Ditto, ready to lift patient itto, lifting patient ... itto, placing stretcher itto, preparing to lower patient. ..
Ditto "Lower"
Ditto: No. II. Ready to lift patient
Ditto, patient lifted ...
Ditto, No. IV. First position
Ditto, second position
lagrams illustrating Army stretcher drill itto .. ed cradle (mproVlsed bed cradles
14
/'flt't 73 8I 81 82 82 83 84 85 86 87 87 89 90 9 1 9 2 II2 I I9 122 124 12 5 ISS 15 6 156 157 157 158 159 go 161 162 163 IS
Pare 1 64 165 167 168 168 172 175 176 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
PREFACE.
AT the request of the Central Executive I have revised the manual written by myself m 1901, as the official handbook of the St. John Ambulance Association.
Throughout the revision an . ende.avour has .been made to simplify the study of FIrst AId to the Injured by drawing up a number of general rules for the treatment of accidents and sudden Illness, and by the omission of all detail \\'hich is not absolutely necessary to enable the student to acquire an intelligent knowledge of the subject.
I wish to express my thanks to Professor A. Schafer for furnishing instructions for performmg a method of artificial respiration, to Dr. L. M. F. Christian for many valuable suggestions, and to the Medical Members of the Central Executive Committee, especially Surgeon-Major G. H . Darwin, M.D . and Dr. F. R. Cassidi, for perusing the proof sheets a nd for a number of useful additions to the \\"ork .
I cannot omit also to offer my best acknowledgments to Mr. W. R . Ed\\ards, the Accountant and Storekeeper of the S.J.A.A., for hIs invaluable co-operatio n.
JAMES CA TLIE .
F IR S T A I D T O THE I NJURED.
CHAPTER 1.
The St. John Ambulance Association has now completed thirty years of its existence, and during that period hundreds of thousands of men and \yomen have been taught at its classes, in all parts of the world, how to help their injured neigbbours.
Fi r st Aid to the Inj ured is a special branch of practical medicine and surgery, by a kno\dedge of wbich trained persons are enabled to afford skilled assistance in cases of accident and sudd n illness. The instruction begins and ends with First Aid, and the subject is taught simply but thoroughly and exhaustively. The duty of the ambulance pupils ends where the doctor's commences, and there ought to be no overlapping or clashing of duty or interests.
PRINCIPLES OF FIR T AID.
I. The First Aid student should be-
(a) Observant, that he may note the ca uses and sig ns* of injury.
(b) Tactful, that he may without thoughtless questions learn the symptomst and history t of the case.
* Signs are what may be perceived.
t Symptoms are what the patient can tell you.
t History means the circumstances attending the accident or sUrldrn illness.
(c) Resourceful, that he, may use to th e b est advantage whatever IS at hand to preve nt further damage and to assist Nature 's efforts to repair the mischief alre,ady done. ,
(d) Explicit, that he may gIve clear inst ructions to the patie nt or the bystanders how best to assist hi m ,
(e) Discriminating, that he may decide which of several injuries presses most for treatment by himself, and \\'hat can best b e left for the patient or the bystanders to do .
2. Remove the cause of injury or danger wh enever possible ,
3. Severe must receive the first attention, no matter what are the other injuries. , , '
4. Air. - The patient must be in a pOSItIOn In which breathing is possible; the air passages must be free from obstruction; if breathing has ceased promp t m easures must be taken to restore it.
S. Rest. -A restful position of the body will the vital functions; support of the injured par t WIll h elp to preven t further damage , a n d is esse ntial in t he case of fractures of limbs.
6. Warmth. -After every accident keep the pa ti ent warm so as t o prevent the fall of tempe rature below th e nor mal poin t.
7. When the skin is broken the wound

19
should be promptly covered with a clean absorbent dressing, Should the \\ oUlld be poisoned, it is 1110S't important immediately to preyent the poison permeating the system.
8. Poisons s\\'allowed should be got rid of, or when that is inexpedient, neutralised.
9. The best means of transport must be studied, and provision made for proper care when the patient is brought to sheller.
10. Removal of Clothing. -Clothes should not be taken off unnecessarily, but \yhen it is n edful to remove them, the following rules \\'ill be found of service in serious cases :-
COAT: Remove from the sound side first, and, if necessary, slit up the seam of the sleeve on the injured side.
SHIRT A D VE T : lit do\\'n the front and remove as the coat .
TROUSERS: Slit lip the outer seam.
BOOT: Slit the ba k seam and undo the laces ,
SOCK: Cut off.
II. Stimulants.-I t is incorrect to suppo. e that alcohol is the only form of slim u lant, and far too freq u en t use of spirits is made to restore a patient after an accident, often with serious results; the safesr ru le, therefore, is to defer the admi n istration of al ohol u nt il the arrival of a doctor. 'When the patient is able to s\\'allo\\', strong tea or coffee, or milk , as bot as can
18
2 0
be drunk, or a small quantity of sal vol a tile in wat er may be giv en. Smelling salts may be held to the nos e. prinkling the face with c old and hot wate r alterna tely, warmth applied to th e pit of the stomach and over the heart, and vigorous friction of the limb s u pwards have a stimulating effect.
12. Throughout his work the First Aid stude nt must on no account take upon himself the duties and responsibilities of a Medical man. At tim es an apparently slight injury is accompani e d by grave danger a n d may actually cause loss of life. When sending for a doctor, state the n ature of the case, and remember that wr itten partic ulars ar e safer than a verbal message.
I t is n ecessary that something should be known of t he structure of the body (el e mentary anatomy), and of t he functions o f some of the more importan t organs and sy stems (elementary physiology) A shor t d escription of the necessary anatomical and physiological points is therefore give n as the several subjec ts are discussed . For purposes of description the human body is supposed to be erect, with the arms hangi n g by the sid e and the palms of the hands directed forw:uds . The" middle li n e " of the body runs verticall y fr om the top of the head to a point between the fee t.

QUESTIONS ON CHAPTER I .
The n u m er als in d icate th e pages whe1e th e an swers 1llay be fou1ld.
What is F irst Aid to the inju r ed ?.. . .. .
Wha t should the First Aid student
What a re sIgns? . ..
Wha t ar e symptoms? ... . ..
What is t h e history of a case? .
W h at is often first thing to do in an ? .. .
\Vh at result of IDJury must r eceive the first attentio n ?
W ha t t hr ee things are absolutely necessary to an
Wh at must be done when the skin is How m ust poisoning b e treat ed?
W hat .must be taken beyond' the treatment of IDJunes?
Sh ould clothing always be removed? . ..
H ow you remove clothing when ExplaIn t h e use and abu se of stimulants ..
W ha t m ust the First Aid student not do ?
W hat elementary anatomy? .. ..
Wh a t IS elementa ry physiology? . . .
Fo r purposes of descripti on h ow is th e human body supposed to be p lacer!? . ..
W hat is the middle line of the bod y ?
21
. . .. .
..
PAGa 17 17, 18 17 17 17 18 18 p e rson ? ... ... .. . ...
18 . .. 18, 19
.. . .. . .
..
19 19 19 19 19, 20 20 20 2 0 20 20

CHAPTER II.
FRACTURES, DISLOCATIONS, SPRAINS AND STRAINS.
THE SKELETON.
The human body is moulded upon a bony framework (the skeleton) which serves-
1.- To give shape and firmness to the body.
2.- To afford attachment to the muscles.
3.-To protect important organs, as in the skull, chest, and abdomen.
THE
SKULL.
The Bones of the Skull are arranged in two groups, those of the brain case or cranium, and those of the face.
The Boundaries of the Cranium are the vault or dome, the rounded portion forming the top of the head' the front or brow; the back of the head, the greatest extent of brain exists, and ,w here therefore the cranium is widest and deepest; the sIdes or temples. The base of the cranium is hidden from view by the bones of the face and?f the vertebral column; m it are numerous perforatIOns for the passage, of blood vessels and nerves; through the largest openmg the brain and spinal cord are continuous.
The Bones of the Face with the exceptlon of 23
the lower jaw are firmly jointed together, so that movement between them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face conjointly. The mouth cavity is formed between the upper and lower jaws, the palate being the bony roof of the mouth which separates it from the nasal cavity above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions term inating on either side at the joint between the lower jaw and the base of the cranium, situated immediately in front of the ear.
The angle of the jaw indicates the junction of the norizontal and the vertical portions.
THE BACK-BONE, SPINE, OR VERTEBRAL COLUMN.
The Vertebral Column (Fig. ]) is composed of bones called vertebrre, each of which consists ofI.-A body or bony mass in front.
2.-Processes projecting backwards, which enclose a canal for the spinal cord - the spinal canal.
3·--Tw? transverse processes, twelve pairs of WhlCh support the ribs.
Z2
FIG. I.
Co. 4
SKULL AND VERTEBRAL
COLUl\1 . Showing left ribs and portion of breast bone The right ribs are removed .
SPINOUS PROCESS.

CANAL FOR SPINAL CORll.
BODY OF VERTEBllA.
FIG. 2 A.
SURFACES SUPPORTING HEADS OF RIBS.
FIG 2B.
TRANSVERSE PROCESS.
SPINOUS PROCESS.
4.-A spinous process. The spinous processes of the vertebrre can be felt beneath the skin for the whole length of the back (Figs . 2A and 2B).
The Vertebrce, 33 in all, are grouped into regions, in each of which they are known by numbers, counting downwards :-
I.-In the neck 7 Cervical vertebrre. The first vertebra, tIle atlas, forms a joint with the base of the skull, at which the nodding movement of the head takes place; the second, tlze axis, by the joint between it and the atlas, allows of the side-to-side movements of the head.
2.-1n the back 12 Dorsal vertebrre.
3·-1n the loin 5 Lumbar vertebrre.
4·- The rump-bone, or Sacrum, consists of 5 Sacral vertebrre united in adults as a olid mass.
5·- The tail-bone, or Coccyx, consist of -t vertebrre joined together to form a single group.
Between the bodies of the vertebrre, in the upper three regions, are interposed thick pieces of cartilage (gristle), which, while they bind the bones together, allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, when falling from
C· 7 D.12
24
l height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of t\\'elve pairs of curved bones -extending from the dorsal vertebrc:e to the front of the body, and are known by numbers-first, second, etc., <comme ncing from above. The ribs are not bony their entire length, but at a short distance the front the bony material ends, and cartilage takes its place. The upper seven pairs, named t he true ribs, are attached by their cartilages to t he Breast-bone (sternum), a dagger-shaped cone with the point downwards, just over the pit of the stomach. The lower five pairs are terrr ed the false ribs, as their cartilages fall short of the middle line . The eleventh and twelfth pairs are termed the floating ribs, as th eir ends are free in front. The ribs :enclose the chest, and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder - bones are the Collar-bone (dav£cle) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thickness of a finger. Its inner end rests on the upper part of the

BONES {Ul.NA OF RAlJlUS __
WRIST - -{ l\IETACARPUS _--{n
PHALANGES_ r·.
FIG. 3A.
BONES OF THE LEFT UPPER LDID.
JR.
SHOWING TITE POSITION OF THE RADIUS AND ULNA
WIlEN THE TIl UnrB IS TURNED INWARDS.
Compare Fig. 3A, in which the thumb is turneJ outwards.
26
PART OF COLLAR D ONE
AR'!
SHOULDER BLADE (SCAPULA)
RADIUS UI . NA .
FIG.
breast-bone, and its outer end joins with the shoulderblade.
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints with the collar-bone and the bone of the arm.
The bone of the Arm (humerus) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both b ones reach from the elbow to the wrist, and they change their r elative position with every turn of the hand (Figs. 3 A and 3 B ).
The Hand is composed of-
I.-The bones of the wrist, or cmilts, eight in number, arranged in two ro\\ s of four.
2.-The metacarpus (the framework of the palm) ; five bones which form the knuckles and support the bones of the fingers.
3.-The phalanges, or finger-bones, three in each finger, and two in the thumb.
THE PELVIS AND LOWER LIMBS.
The Pelvis. - The large basin-like mass of bone attached to the lower part of the spme is composed of the two haunch-bones and the sacrum. The haunch bones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed between them. The· pelvis
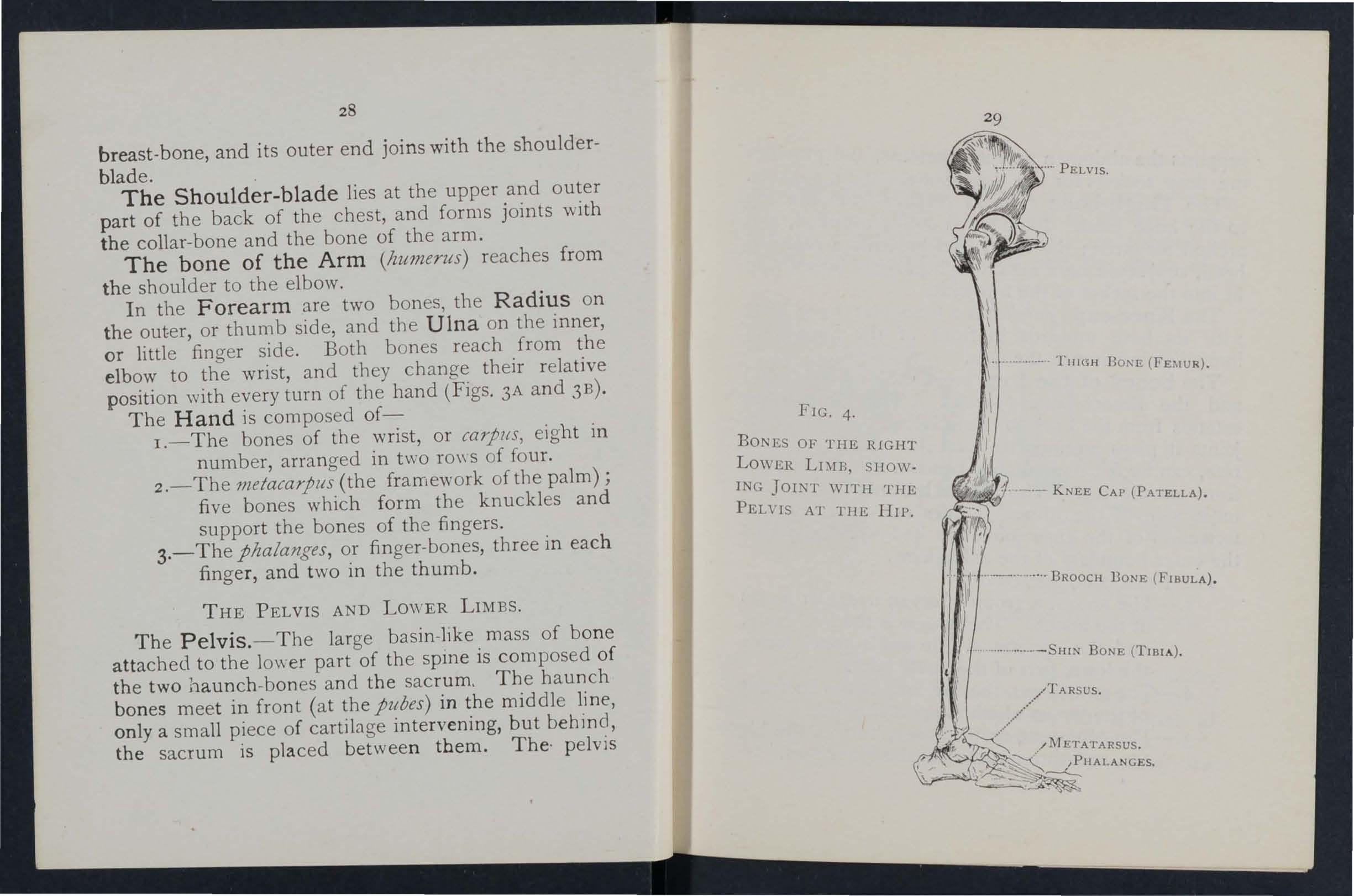
FIG. 4.
BONES OF THE RIGHT LOWER LIMB, snowING JOI;\T WITH THE PELns AT T1IE IIII'.
28
\" THIGH D O!'>E
_.- KNEE CAP (PATELLA).
supports the abdomen and its contents, and provides tbe deep sockets for tbe thigh-bones-tbe bip joints.
The Thigh-bone (lemur) reacbes from the bip to tbe knee joint. Its sbaft is stout, rounded, and arched forwards; the upp er end presents a rounded bead, supported on a neck \\hich projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying \\ ith its base up" ards in front of the knee joint immediately beneath tbe skin.
The bones of the Leg are the Shin-hone (tib/a) and the Brooch-bone (fibula). The Shin-bone extends from tbe knee to the ankle, in hotb of ,,!1ich joints it plays an important part; its sbarp edge, tile slt/Il, can be felt immediately beneath tbe skin of the front of tbe leg. The Brooch-bone lies on the outer siJe of the tibia. It does not enter into the form ation of the knee joint, but its lower end forms the outer boundary of the ankle joint.
The Foot is composed of--
1.- The tarsus, a group of seven irregular bones at the instep. The largest is tbe heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.-The metatarsus, the five long bones in front of the tarsus \\ hich support the toes.
3.- The plzalanges, or toe-bones, two in the big toe, and three in each of the other toes.
3r JOIi'\TS.
A Joint is formed at the J'unctl'011 of t b I wo or more n moveable joints such as the hip knee e etc., t?e smfaces of the bones are b' cartIlage, whIch lessens friction and the shock of

5. Compa re Fig. 4, Page 29. fall. Lubricatil Cf th .. , fluid the ". ,10 , e J01l1l IS a clear, rather sticky , JOlt1t 011", . capsllie T' h' 01 SJ1JZOVza, enclosed within a moven; ent :lt1g t e bbones together, but allo\\"inrr of To ' ,re a nUI11 er of bands or 1':faJlleJlts. ., expb1l1 the [ormation of l' b . , 1m JOll1ls, the
'FIG. 6. LEFT ANKLE. FIG.MUSCULAR TISSUE

TEN DO N OR LIGAMENT OF PATELLA
FIG 7·
J2 foHowing examples :lre given :-
The Sh ould e r , a and-socket joint, conslstS of a shallow socket on the outer angle of tlle shoulder-blade, and of the head of the arm-bone (Fig. 5). 0\\ ing to the shallo\\ nesS of the socket the arm-bone is very prone to escape from its socket
33
The Voluntary muscles are met with in the limbs, the head and neck, and the surface of t h e trunk. Their ends are atta"ched to different bones, and as they pass from one to another they cross a joint, and, being endowed with the power of contraction and relaxatlOn, cause the movements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon . Blood-vessels traverse and supply the muscles, and the nerves entering them bring them under the direct control of the brain and spinal cord.
T H E MUSCLES
.
T he Muscles of the body are classified into tw o groups--vo!ltntary and z'nvolu1l ta ry .
D I AGRA M SHOWING RECTUS MUSCLE OF THIGH, WITH ARTERY, VEIN A ND N ERVE. (dislocate). . The Ankle , a joint, is formed at the Junction of three bones, the shin-bone above and on the inner side, the bone on the outer slde, and the ankle-bone below (Fig . 6).
The Involuntary muscles are met with in the walls of the stomach and intestines, in the air passages, and in most of the internal organs and blood-vessels, also, in a special form, in the heart. They are not under the influence of the will, bu t continue their \york during the hours of sleep; their functions are regulated by a separate set of nerves (see Sympathetic System, page II 8).
FRACTURES AND THEIR TREATlVIENT.
"When a bo ne breaks a Fracture is said to occur.
CA USES OF FRACTURE.
I. Direct Violence. - \ Vhen from a severe blo w impact of a bullet, crush of a wheel, etc ., a breaks at the where the force is applied the fracture is termed direct. o
rENDON NERVE

Indirect Violence. - vVhen the bone at some distance from the spot. where the 15 applied the fracture is termed mdrrect. AlIghtmg on th e fee t a nd fracturing the thIgh-bone o r the of the leg, or falling on the hand and breakmg th e radi us or the collar-bone, are examples . .
3. Muscular Action. - The knee-cal? and the arm-bone are occasionally broken by a vIOlent contraction of th e muscles attached to them.
VARIETIES OF F RACTURES.
Fractures are classified according to the co nditi on of th e ti ss ues adjacent to the bone as follows:- .
1. Simple. - The bone is broken wIth but slIght injury to the surrounding parts. .
2. Compound. - The bone is broken and the and tissues are punctured or t?rn, thus allowmo disease-producing germs to obtam entrance to th e seat of fractur e. Th e fractured ends may protrud.e through the skin, or (for example, when a bone ]S broken by a bullet) the wound may lea d down to the fr acture. .
3. Complicated. ---:- The bone i.s brok en. and m addition there is an mJury to some mternal OIgan (for example, th e bram, sp mal cord, lung, etc.) or to some irnoortant blood -vessel or nerv e. .
A fracture may be compound or complIcated as the immediate result of the injury; or a fracture 35
originally simple, may be converted into a compou nd or complicated fracture-
(
a) By careless movement on the part of the patient .
(b) By carelessness or ignora.nc e on the part of one rendering first aid .
Special yarieties of fractures may be classified accor ding to the injury to the bone itself as follows : _
I. Comminuted. - The bone is broken into several pieces .
2. Green-stick. - In children, owing to the softe r state of the bony tissues, a bone may bend and crack without breaking completely across .
3· Impacted. -The broken ends of the bone are dnven one into the other.
GE:-I'ERAL IGNS A D WHICH l\IAY BE PRESENT.
(A fracture of the femur, humerus, or both bones of the forearm or leg, affords the most complete example ).
1. Pain at or n ear th e seat of fracture.
2. Loss of Power in the limb .
3· Swelling about the seat of fracture. welling frequently renders it difficult to perceive other signs of fracture, and care must therefore be taken not to mistake a fract ure for a less serious injury.
4· Deformity of the limb.-The limb assumes an
34
36
unn at ural p osition, and is mis-shapen at the seat of fr acture. T he contracting muscles may cause the brok en ends of the bone to override, thereby producing shorte ning . .
S. Irregularity of the bone.- If the lS close to the skin the fracture may be felt, and If compound it may be seen.
6. Unnatural Mobility. -Movement may be m ade o u t at the seat of fracture .
7. Crepitus, or bony grating, may be felt or heard wh e n t he broken ends move one upon the other.
T he las t two s£<Tns should only be souglzt by a doctor.
Several of the signs are absent in green-stick an d impacted fractures.
,
In addition to the siO'ns a n d symptoms the patlent or the bystanders may bbe able to the ?istory of the in jury, and mark:s on the clothll1g or skin should be n oted, as they may serve to locate the fracture. T he snap of the bone may have been heard or felt.
ApPARATUS FOR T REATMENT OF FRACTURES.
Spli nts a n d bandages for First Aid frequently have to be improvised. , ,
A Splint may be improvised from a walklll g stl,ck, u mbrella, billiard cue, broom or brush polIceman 's truncheon, rifle, folded coat, plece of \\'ood, cardboard, paper firmly folded, a rolled -up map, or, i.n fact, anything tltaf is firm and long enouglz to keep

37
the joints £mmediate/y above and below the fractured at rest. ' Vhen the above applian ces are nOl avallable, the upper limb, if fractured, may be ti e d to the tr unk, and in all cases a fractured lower li mb should be bandaged to its fellow.
Bandages may be improvised from handkerchiefs bel,ts, straps, braces, neckti es, or any piece of line n: calIco, stnng or cord that comes to hand.
Esmarch 's , Triangular (Fig. 8) a r e made, by c u tting a plece of linen or cali co abou t forty Inches square diagonally into two pieces,
!,he broad bandage made by bnngi ng t h e pOint down, to the base (Flg . 9), and then fo lding In to two (Flg , 10). .
The narrow bandage is made by foldinO' t he broad ba ndage once (Fig, It). b
!,he medium bandage is made by bringi ng the po!nt down ,the base, and then folding into three . (Flg, 12) . 1h1s bandage may be used instead of the broad or the narrow bandage when it is bet ter suited to th<: proportions of the patient.
I t IS some times advisab le to h alve the size of the ?y br in gi ng the two ends toge ther befo re foldIng It the broad, narrow, or medium ba n dage.
Whe n no t In u se, the triangular bandage sh o ul d be folded narrow ; the two en ds should be t urned to the and the bandage folded into fou r, redUCIng It to a pac k et a bout In ches by inch es.
FIG. 8. BA. DAGE SPREAD OUT.

FIG. y. BANDAGE 0 ' CE FOLDED .
FIG . 10 BROAD BANDAGE.
FIG. II. N ARROW B A NDAGE.
FIG. 1 2. - THE DOTTED LINES SHOW THE FOLDS OF THE ;,{EDIUM BANDAGE.
Larg e arm -slin g (Fig. 13). - Spread out a ban dage, put one end over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, an d let the other end hang dO\\'n in front of the chest; carry the point behi n d the eloow of the injured limb, a n d bend the forearm
1 3. FIG. 14.
ove r the middle of the bandage; then carry the seco nd end up to the first and tie them; bring the poi nt forward, and secure with two pins to the front of the bandage.
Small arm -sling (Fig. I-+).-Place one end of a
--=::. / ":SE
0"'// .-
................
---."",-=-=---'---- ... --':---
39
FIG.
broad ban dage over the shoulder on the so und side, pass it round the n ec k so that it a p pears over the shoulder of the injured side; place the for earm over the middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in cases of fractur ed humerus, and occasionally when the large sling would be too conspicuous. Slings may be improvised in many simple ways, s uch

as pinning the sleeve to the clothing, turnin g up th e tail of the coat, passing the hand inside the buttoned coat or waistCJ)at, etc.
Reef Knots (Fig. IS) are to be used. Av oi d granny knots (Fig. 16).
GE ERAL RULES T O BE OBSERVED IN THE TREAT;\IE T OF FRACTURES.
The object of First Aid Treatment of FracIS to guard against further mischief, and espeCIally to a simple fracture from becomin a compound or complicated. To attain this end:- b
1. Attend to the fracture on the spot. 0 how crowded the thoroughfare, or how short the dIstance to a more convenient or comfortable no attem pt must be made to mo,'e the patient the ltmb has been rendered as immovable as possIble by splints or other restrainin::b apparatus.
2. Steady and support the injured limb at so its further movement on the part of eIther the patient or the bystander is prevented.
. 3· the limb with great care and If shortel1lng IS observed in the case of a of a of lower limb, pull upon the foot until the 11mb regal11S a more normal len C7 th. ·When the shape. of. the Ii mb is. im on account let go untIl .It IS secured 111 posItion by splints, otherwise there IS great danger of the fracture becomin a om . pou nd or complicated.
4· Apply splints (when practicable) and bandages as follows:-
(a ) The splints be.tirm, and long enough to keep the ]omLs Imm edia tely above and
FIG. 15.-REEF KNOT. FIG. 16.-GRANNY KNOT.below the fractured bone at rest. They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The bandages must be applied firmly, but not so tightly as to constrict the circulation of blood in the limb. 'When the patient is in the recumb ent position double the bandage over a splint to pass it und e r the trunk or lower lim b. As a general rul e :-
For the trunk the broad bandage should be used. Pass it once round the trunk and fasten it by tying the ends, or with two or three safety pins on the side opposite to the fracture, but if to secure a splint for a broken thigh, over the splint.
For the ann or fonarm the narrow bandage should be used. Pass it twice round the limb, and tie the ends over the outer splint.
For the thigh or leg the narrow or medi urn bandage may be used. It is frequently convenient to double the bandage at the centre, pass it under the limb, bring the loop over the limb, pass both ends of the bandage through it in opposite directions, and tie them over the outer splint (Fig. 17)·
In applying bandages near a fracture the upper one jhould be 5;ecured first.
S· .When hcemorrhage accompanres a fractUre It must be attellded to n lst, and the wound cm'ered by a clean dressing.

r7.
6. !'10 attemp.t must be made to remove a pattent from a fracture of the pelvIs, or th1gh, except in a recumbent posItIon, preferably upon a stretcher.
7· In every case of fracture it is necessary to cover the patient to keep him warm and so lessen the effects of the SHOCK of tIle a ccident'
8. In all doubtful cases, treat as a fracture. .
SPECIAL FR ACTURES.
Fracture of the Cranium. -A fracture of the upp er part is usually caused by direct yjolence-for a bI?w the head. A fracture of the base lS caused by ll1chrect violence, through a falJ on the
43
FIG.

head a fall on the feet or lower part of the spine, or a' severe blow on the lower ja w: If tlte upJ?er part £s fractured, the are and frequently either. Immediate .or coming on gradually. If tlze .zs fractured 111senslblhty may come on
FIG. 18. immediately, blood or a clear fluid may issue from the ear chan!1el, hlood may escape from the nose, or it may pass dovyn to the stomach, whence it may be Yomited; the fracture may involve the orbit, causing a blood-shot eye.
TREATMENT.
Injury to the brain is the great danger attending a fracture of the cranium. For treatment see "Concussion and Compression of the Brain ," pages 13 1 , 13 2 :
Fracture of the Lower J loss of power (inability to speak and to move the Ja:v freel.y) , irregularity of the teeth, crepitus and bl eedtng frum the gum are the usu al sig ns and symptoms. 45
I.-Place the palm of the band belo\\" the injured bone and press it gently against the upper jaw.
2.-AlJply the centre of a narrow bandage under the chin, carry one end over the head, cross tbe ends at the angle of tbe ja \\, carry the long end across the chin, and tie the ends on the side (Fig. 18).
Fracture of the Spine.- The vert e bral column may be broken either by direct or indirect violence. Falling from a beight on the back across a har or upon an uneven surface is an example of direct fracture, and a fall on the bead, causll1g a broken neck, is an example of indirect violence. " ' hat is commonly regarded as a broken back consi ts of a fracture of one or more of the vertebne with displacement of the fragments, whereby the spinal cord and the nerves issuing from it may be torn. causing complete or partial paral), is of the parts below the fracture. Pain is present at the seat of injury.
TR EAT IE T.
1. - Prevent all movement on the part of the patient.
2.-Cover the patient warmly.
3·-To remove the patient, place him on a stretcher or shutter as follows :-
(a) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
44
so that the ends are level with the top of his head; pass a broad bandage or kerchief under the head and secure It to the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
(b) A bea rer on each side grasps th e wiled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes charge of the legs.
,
(c) On the word being given, all 11ft together and carry the patient by short side over the stretcher and carefully lower hIm on to it. If a fifth bearer is available the stretcher should be passed under the patient instead of carrying him over it.
4.- 0n arrival at shelter nothing further is to be attempted until the arrival 0f ,a dO,ctor, to give the patient water, tea, etc ., If he IS conscIous.
Fractured Ribs. - The ribs usu ally fractured are the sixth, seventh, eighth, and ninth, and generally the fracture is midway between th e breast-bo,ne ,and the spine. The fracture may be caused by mdJrect violence, driving the of the bone outwards, or by direct vIOlence, dnv,mg tl:e ends of the bone inwards and sometImes InjUrIng the

47
lungs or other internal organ. If the lower ribs on the right sIde are broken, the liver may be injured, and a fracture of the lower left ribs may wound the spleen. Evidence of the fmcture is afforded by pain, especially on attempting to take a deep breath, a nd by short and shallow breathjng. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hcemorrh<Jge (see page 95) may occur.
TREATl\IENT.
( a) Tr j,en .fractllre is !lot cOlllplll:ated b)' an injury 10 an z'nterJlal organ :-
r . - Apply two broad bandages round FIG. 19. the chest sufficiently firmly to afford comfort, with the centre of the {jrst immediately above and that of the second - immediately below the fracture. The lower bandage should overlap the upper to half its
46
48
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to a s.trong towel, folded about eight inches wide, ti ghtly round the chest, securing it with three or four safety pins . . . .
2.-Place the arm on the mJured Side in a large sling. (Fig. 19)·
(b) When an z"nler1lal organ Z"S z"njured-
I.-Do not apply bandages round the chest.
2.-Lay the patient down, inclined a littl e tovvards the injured side.
3. -Loosen the clothing, give ice to .and place an ice bag over the seat of mJury. Treat as for internal hcemorrhage (see page 95).
4 .-Place the arm on the injured side in a large sling.
Fracture of th e Breast -bone (sternum).When this fracture can be felt or is suspected undo a ll tight clothing, and patient quiet in an easy position until the arnval ot a doctor.
FRACTURE OF THE BONES OF THE UPPER LIMB.
Fracture of the Collar-bone (clavzde).-Thi s f ract ur e is frequently caused by a fall. on. the h.and or sh oulder.-The arm on t he in jur ed Side IS partia ll y

49
helpless, . and. the patient usually supports it at the elbow With hiS hand, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lower. The general signs and sympt0111S of fracture are mostly prest;nt.
TREATMENT.
I.-Remove coat (see page 19), and as much more of the clothlllg as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3·-Gently bend the forearm well up, keeping the shoulder as far back as practicable and Support it in a " St. John" sling, made as fo : _
(aJ Lay an unfolded bandage across the chest .the injured limb with one end on the un1l1Jured and point beyond the elbow on the 1l1Jured slde. (Fig. 20).
(b) the end of the bandage under the 1l1Jured lImb, across the back, and tie the ends somewhat loosely in the hollow in fro nt of the sound shoulder.
( c) F?ld the point the elbow of the injured lImb and secure It by one or two pins (Figs. 21 a n d 22).
FIG 2 1. } IG 22. -
(Body bandage omi.lled to show details of SlIng.)
4·-Tightly secure the injured limb to the side by a broad bandage pas ed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5·-N o w ti ghten the sling.
\Vhen both collar-bones are broken keep the

shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by the ban dages. (Figs. 23 A an d 23 B).
Fracture of the Shoulder-blade (uajJ1l/a)._
Apply the centre of a broad bandage in the armpit of
50
51
4
FI G . 23A.
FlG. 23B.
5::
the injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24)·
Fracture of the Arm (humerus). - The bone may be broken :- (a) Close up to the shoulder; (b) near thE> middle of the shaft; (c) close FIG 24· to the elbow .
All the general signs and symptoms of fracture are usu ally present.
TREATMENT.
TVheJt tlze Fracture Z"S close to the Shoulder-
I.-Apply a broad bandage \Yith its centre above the middle of the arm round the limb and body, tying it on tbe opposite side.
2.--Support the forearm by a small arm sling.
Wizen tlze Fracture Z"S mar the Middle of tlte Shaft -
I.-Bend the forearm at a rigbt angle to the arm.
2.-Apply splints, reacbing from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint
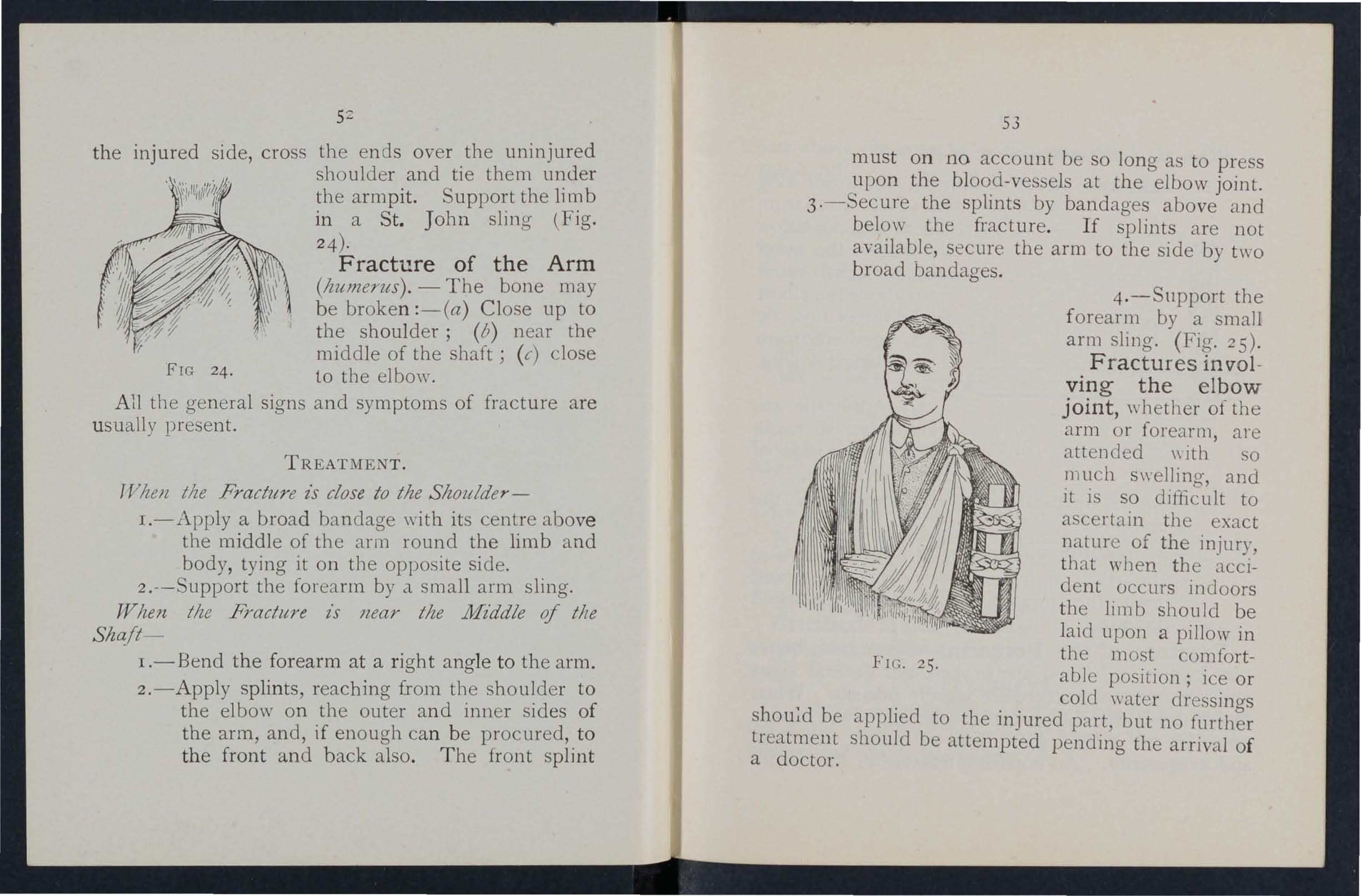
53
must on no account be so long as to press upon the blood-vessels at the elbow joint.
3·-Secure the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad bandages.
4.-Snpport the forearm by a small arm sling. (Fig . 25).
Fractures involving the elbow joint, whether of the arm or forenrm, are attended \\ ith so much swellin O', and it is so dIfficult to ascertain the exact natur e of the injury, that when tbe accident occurs indoors the limb should be laid upon a pillow in tbe most comfortabl e position; ice or cold wat er clre sinO's be applied to the injured part, but no treatment should be attempted pending the arrival of a doctor.
FIG. 25.
54
Wizen the accz'dent occurs out of doors -
Take t wo pieces of thin flat wood, one long enough to reach from the armpit to below the elbow, the other long enough to reach from above the elbow to the finger tips; tie them together to form a right angle. (Fig. 26) . 2.-Apply the angular splint so made F IG. 26. o n the inner side of the flexed limb.
3.-Secure by bandages above and below the fracture .
4.- Support the limb by a large arm sling .
s .-On arrival at home remove the splint, and treat the injury as if it had occurred indoors .
Fracture of the Forearm.-\iVhen both bones (the Radius and Ulna) are broken, the general signs and symptoms of fracture are usually present. When one of the bones only is broken the signs and symptoms are as a rule pain, loss of power, swelling, and irregularity . An impacted fracture of the Radius
55
just above the wrist is a the hand. common result of a fall on
TREATi\1Ei\'"T
b
This is the same, ",bether one or of both. fracture is of one
1 . - Bend the forearm at right angles to u tbe arm, , 1

FIC. 27· FIG. 28. keeping the thumb upwards and hand towards the body. ' tbe palm of the
. 2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers .
3·:- A pply bandage, embracing both ]" . mediately above and b I sp I11tS ]mthe hand (Fig. 27 ). e ow the fracture and round
4.- A pply a large arm-slinoCrushed Hand of the bones of the carpus, metacarpus, or fin.gers) .
T REATMENT
I I.-Apply a carefully padded splint to th f b t 1e lland, frOI11 \VeIl above th e of eyo nd the t ipS of the fino-ers e WIlSt to I:> •
•. V i-I
2.-To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 28).
3.-A pplya large arm-sling.
Fracture of the Pelvis. - vVhen, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the patient is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
TREATMENT.
I.-Lay the patient in whatever position is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further inwards.
3.-To remove the patient place him on a stretcher, acting on the same principle as that described under "Fracture of the Spine 1/ (see page 45)·
FRACTURE OF THE BONES OF THE LOWER LIMB.
Fracture of the Thigh-bone (femur).- The thigh bone may be broken at its neck, anywhere in the shaft, or close to the knee. A fracture at the

57
neck is likely to occur in a injury, and is often very slight severe bruise of the hi b . 0 dlstlllgUlsh from a wh f . p, ut It may be as umed th t en, a ter an llljury near the hi J ..' a cannot, when l"in o' on tl b k J }Olllt, the patIent the CYIound Db .1e b ac , false the heel from • to , one IS roken \11 h sIgns and symptoms of f _ . r t e general a d lacture are usuall n a prominent sivn is the .' . y pre ent o pOSItIOn of the foot, .FIG. 29, which as a 1 l' , " c ru e, les on lls outer side. may vary from one-half to three inches. Shortening
TREATMENT.
I. -Steady the limb b h ld' , draw l?g the f?ot. lllle wlth Its fello\\T \\1] oat and brmg It 1l1to . 1cn two or t] . . at hand, it is one perso " d 11eea slstants are position until the Spll'11t - n uty to hold the foot in . ::, ale secured .
. 3·-Apply a splll1t on tbe 0 L". d f pIt to beyond the foot. u el Sl e rem the arm-
58
4.- A pply a splint on the inner side from the top of the thigh (the fork) to the knee .
s.-Secure the splints by bandages follows :(a) Round the chest below (b) round the pelvis on a leyel wIth the hlp ]omts, (c) above the fracture (d) below the fracture, (e) round the leg, (f) round both ankles and feet, and tied below the feet, (g) a broad bandage round both knees ( Fig. 29) ·

FIG. 30.
"\iVh en single-handed, or when the patient is a woman, it is expedient, after extension of the lim b, to tie the feet together, dispense with the inner splint, and pass the bandages round both limbs (Fig. 30)'
Fracture of the Knee -cap (patella).-The knee-cap may be FIG. 3I. broken by falling on the knee (direct violence), but more frequently it is broken by muscular action, as follows:-
59
'When the slips in the attempt to prevent a fall the muscles 111 the front of the thigh act with such force. as to snap the knee-cap in two (Fig. 3 r).
Pall1, of po:ver (the limb will be quite helpless), and IrregularIty (a gap may be felt between the broken fragments of bone) accompany this injury.
I.-Lay the patient on his back, raise well and
FIG. 32.
support the head and shoulders,. straighten and raise the limb .
2.-ApDly a splint along the back of the limb reaching from the buttock to beyond the he el. '
3·-A pply a narrow bandage with its centre imme-
60 diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. To ensure firmness apply a second bandage in a similar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5.-.Su pport the foot well off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 3 2 ).
6.-Apply an ice bag or a cold water dr essing over the f ractu reo
Fracture of the Leg (tibia and jibula).-One or both of the bones may be broken. When both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end is frequently mIstaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
61
foot. If only one splint is availal ' le . outer side. u place It on the
4·- E: cure the splints b b d below the fracture (c)' y d · an ages (a) abov e, (b) , llTIme lately above th k e nee,

(d) round both ankles (e)'·.) b' both knees (F'a ',.,) , a road bandage round lb' J,) • 'Vhen single-handed , or when the patient is a
o
. % ___-:::---::-o---,--_.:::::="'-
FIG. 33.
(-2
d' g the lim b tie both feet together, woman, 111 s )lint and P1SS the b1ndages dispense with 1 1 34')< ,Vhen no splint is d b th hm s -qg . . . rou!l I o. the leas ankles and knees together IS avallab e tymg 0 , ,
of great (fracture of the tarsus, metatarsus
Crus ) Tl's accident is commonly c.aused by and toes.- 11 < h f t nd may ssaae of a heavy weight over t e 00, a tb he pa 0. d bv pain swelling, and loss of power. e recogl1lse J
TREAT JENT.
I -Remove the boot (see' page 19)'
2.-Apply a wcllpadded splint to. the sole of the foot, reachlngfrol11 , the heel to the toes.
3.-A pplya bandage crossed after the manner FIG. 35· of the figure 8 35).
4.-Su pport the foot in a slightly raised pOSItIOn.
DISLOCATIONS.
A dislocation is the displacement of one or more of the .at a joint. f. tly dislocated are those The Jomts most requen . of the shoulder, elbow, thumb, fingers, and lower Jaw.

SIGNS AND SYMPTOMS OF DISLOCATION.
I.- Pain of a severe sickening character at or near the joint.
2.-Loss of power in the limb.
3· -Numbness of the parts below the geat of dislocation.
4·-S welling about and below the joint.
s.-Fixity of the joint.-The limb cannot be moved at the joint by either the patient or others.
6.-Deformity of the limb.-The limb assumes an unnatural position, and is mis-shapen at the joint.
TREATMENT.
No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival :_
(a) When the accident Occurs out o.f doorsSupport the limb in whatever position gives most ease to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) J;Vhen the patient t5 z"Jldoors-
I.-Remove the clothing from the limb.
2.-Place the patient on a couch or bed.
3·-R est the limb on pillows in the most comfortable position.
4·-A pply cold (ice or cold water) dressings to the joint.
S·-When cold ceases to give comfort apply
warmth (flannels or to'vYels wrung out of hot water).
6.-Treat shock (see page 135)· SPRAINS.
When, by a sudden \\'r.er:ch or and the parts around a )Olr:t are the joint is said to be spramed. ankle is a common example.
twist, the ligaments stretched and torn "Going over" the
SIGNS AND SYMPTOMS.
I.-Pain at the joint after a twist or wrench.
2.-Inability to use the 3.-Swelling and discoloratIOn.
TREATMENT OF SPRAINED ANKLE.
When out of doors- .
I.-Apply a bandage tIghtly the boot, ?eginning on the sole at the mst ep, it on the front of the ankle, and it round and round the ankle, where It IS to be firmly ti ed . . it
2.-vVet the bandage after applIcaton; IS thereby tightened.
After 1'mdzz'ng sltelter- . )
I.-Remove the boot and stockll1g (see page 19 .
2.-Place the limb in the most. comfortable position; usually that is well raised.

3· -Apply ice or cold water dressings to the joint as long as th ey relieve pain.
4·-When cold falls to give comfort, apply hot fomentations.
When other joints are sprained treat them as if dislocated. '
When in doubt as to the nature of the injury, treat as a fracture.
STRAINS AND RUPTURED MUSCLES.
When, during severe exertion , muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured.
SIGNS AND SYMPTOMS.
I.-A sudden sharp pain .
2.-\Vhen the muscles of a limb are strained they may swell and cause severe exert!on is difficult or impossible; for example, If the stram has occurred in the back the patient may be unable to stand upright.
TRFATl\IENT.
I.-Place the patient in the most comfortable position, and afford suppor t to the injured part.
2.-Apply hot water bottles 01 hot fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 114).
64
QUESTIONS ON CHAPTER II.
Tile numerals indicate tile pages where tile allswerS may be found.
\Vhat is the skeleton, and what purposes are servcd by it?
... ... ... ';'"
II ow are the bones of the skull arran.ged;
\\"hat are the boundaries of the cral1!um .
Describe the bones of the face ... . ..
Descri be the lo\\er jaw ...
\Vhat is the angle of the jaw?
\\'hat other names has the back-bone?
\Vh al is a ycrtebra?

Where does
TI ow maya fracture be caused hy muscnlar action?
In what two ways may fractures be classified? ...
\Vhat i a simple fracture ?...
\Vha t is a compound fracture?
\Vhat is a complicated fracture?
\Vhat is a comminuted fracture?
\Vha t is a green-stick
"'?
lIow many yertebrre are there In tl-:e spl!1e.
\Vhat are the regions of the spl!1e, and how many vertebra! are there in each? .. ... .,.
Irow is the '-pine endowed ",ith free movement?
\Vh at i _ a rii> . :..;, .
How many paIrs of n IJs at ethel e .
What is the breast-bune? .. .," . ) .
\\'hat are the bones of the upper 11ml)s. , .
\\"h at i the peh'is? ..
What is the hip juint ? .. , . . ?
" 'hat are the bones of the lower 11m us ..
\Vh at is a joint? .. .,. .. .
Describe a moveable JOInt .. .
Describe the shoulder joint
Describe the ankle joint ...
How are mu 'cles cIa 'ified?
Describ e voluntary muscles
Describe inv oluntary muscles
\ \'hat is a fracture? ...
\Vh at are the cau"es of fracture?
fractures afford the most cOl1lplete example of the signs and symptoms? ... '"
In making up your mind whether a fracture had occnrred or not, what point should you take into considera. tion beyond the sign and symptoms?
\Vhat apparatus may be ncces. ary for the treatment of fractures? 36
Tr ow may splint be improYised ? ... ... 36, -:'7 II ow may bandages be improvised? 37
Describe E. march's bandage . .. 37,3 (Fig. 8)
In what ways may the tnangular bandage be folded for 11 c? 37
I Tow many kinds of arm- ling are there, and what are they called? ... 39, 40, 49
\Vhat knot is to be tied , and what knot avoided? 40
What is the object of Ilr t aid treatment of fractures? 4I
Gi\'c the general rul e for the treatment of fractures 4I
TI ow should splints be applied? '" 41, 42
fT ow sho uld bandages be applied? , 4 2 , 43
What may cause a fractllre of the upper part of the cranium? 43 2
66
PACE
...
... 22 22 22 . . 22, 23 23 23 2J 25
.... ... .
25 25 26 26 26 26 to 28 28 30 )0 3 1 3 1 3 2 32 32 33 33 33 . .. 33, 34
bone
when direct \'iolence is the cause of fract ure ? .. , .,' ... ,., PAGK \Vh ere cloe a bone break whc:n indirect yiolence is the cause of fracture? ..... ... 33
a
break
fracture? \Vh at is an impacted fracture? 34 34 ... 3-1-. 35 34 34 34 35 35 35 State the general signs and symptom' that may be present in a case of fracture ... ... . .. 35, 36 \Vhat
35
What may c?.use a fr:lcture of the base of the cranium? , 43 14
\Vh at are the signs of fracture of th e upper part of thc cm.niul11? ." ... ." ... ..,
\\'lut :In.: the signs of fracture of the hl'C uf t 11;; cmnium? ... .. , . .. .... ... ?
\Vbat is the treatment for fracture of the •
\Vhat are the signs of fracture of the lower j<\" ?
II f)W maya fractured spine be cau ed? ... .?'"
\\ hat is commonly regarded as a broken ....
\Yhat are the symptoms of a fractured SpilL.
How may ribs \: e fractured? , How maya fracture of ribs be compl.lcatcd?
State the signs and of a sImple and of a C011\plicated fracture or nbs .. , ...
\Vhat is a frequent cause of fractured collar-hunt, ? ....
\Vhat are the signs and symptoms of fr:lctLllul culhl1I ?
At the of arm .
Are the rreneral sirrns and sympt()ms of a fractulc ,11\\.1}s in a foreorm ?
State the cause of a common fracture of the rac1.llIs
How would you recognise a fracture of the pehIs?
At what points may the thigh-bone be broken? : .. 5-1-
\Vhat are the signs and symptoms of fractUle of the
\Vhat are the causes of fracture of t he knee-cap?
\Vhat are the signs and symptoms of fracture of the kneecap?
Are the general signs and symptoms always present m fracture of the leg?
\Vhat mistake may easily be made when the fibula is broken near its lower end?
\Vhat is a dislocation? ... :.. : .. State the signs and symptoms of dIsl ocatIOn

State the treatment of other sprains ... 63, 65
When not sure whether the injury is a sprain or fracture how
First Aid Students should practise improvising material, folding bandages, tying knots, making slings, and the treatment of the following injuri es.
Improvising splints ...
Improvising bandages
Folding bandages
Large arm sling
Small arm sling
Reef and granny knots
Knot for applying splint to lower limb
Fractures - Lower jaw, 44. Spine, 45, 46. Ribs (Sililple and complicated fraclures), 46 to 48. Breastbone, 48. Collar-bone, 48 to 51. Both collarbones, 51. Arm, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm when the elbow is involved, 53. Forearm, 55. Crushed hand, 55, 56. Pelvis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single-handed), 58. Kneecap, 59, 60. Leg (man), 60, 61. Leg (woman, or
man when single-handed), 62. Crushed foot 62.
Dislocations-Out of doors and indoors ' ... 63, 04
Strains and ruptured muscles ("
68
-14 45 -1-5 45 -i 6 +7 +7 .,l:l
..·4,
. 49
... 52
.. , . .
h ' h b ... ... 57 t Ig - one r ." S
... 5 , 59
... .., ... .. ..
..
."
,
..
,
59 60 60 62 63 PAGE State the treatment of dislocation... 63 What is a sprain? 64 What are
signs
64
64
the
and symptoms of a sprain?
State the treatment of a sprained ankle ...
65 H'JW may muscles be strained or ruptured? 65 State the signs and symptoms of strains 65 State the treatment of strains 65
would you treat it?
36, 37 37 37 39 39,40 40 ,p
Sprained ankle .. ...
64
CH.WTER III.
THE ORGAN OF C I RCULAT IO N .
THE organs concerned in the circuhtion of the blood are the Heart, the Arte ri es, the V e i ns, and the Capillaries.
The Heart is ituateJ in the chest behind the breast-bone and rib cartilages, bet\\'een the lungs and immediately above the diaphragm; it lies obliquely with a quarter of its bulk to the right and the remaining three-qualters to the left of the middle line of the body. lts be}t rnay be felt just below and to the inner side of the left nipple . The beart has four cavities, two on either side of a central parl1tion. The t\\'o upper cavities are nameu 1he ri g ht a n d left auricl es, the t\\"o 10\\ er the right and left ventricles.
Arteries are vessels which convey blood from the heart. Veins carry blood to the beart. Capillaries connect the arteries and veins.
In the general (systemic ) circulation arteria l blood is driven from the left "Ventricle of the heart into the aorta (the main artery of the body). Flom the ao r ta branch arteries are given off to all parts of the body. These divide and sub-divide, and become so small as to assume microscopic dimension s, \\'ben they a re ter med capillaries ,

3 (' ,
L. Lar)' I1,( (\' oice ])0')' T T J (. P'I I " ' raC1ea \\'JIlt/'plpe)' ]{l Jllng; L.1J Ltft Lung (the lungs are c1ra\\1l llack' l;; IPse the hea.rt and hlood vesscls) : R.A, Auricle' J:i\. Left AUrIcle; R.\'. Rinhl Vcntricle' I \; I cft \' . lrIcle; I'.A. Pulmonary Arter;' Ao, Amla: ; V c J S \ena C1.Vil (the 1 'cr - " ...... ' < '. upellur tl I d ' ,:u",e Hill C,lll) 109 hlood from the up"cr p'lrt of )0 Y t.() tnc heart); LY.C. Inferior \'ena cant \Ihe 'Iarcre j)lo?cl from the er part of thc hody to' the I ' 1e OUt pulmona.ry \ lIns cannol he shown i'1 the ( lagral11,
70
In the capillaries an interchange of gases and fluids takes place, whereby the nourishment and maintenance of the tissues and organs of the body are provided for, and the bl ood becomes dark and impure.
Venous blood passes from the capillaries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with valves at fr equent intervals, which prevent the backwa rd flow of the blood.
The pulmonary system of blood vessels is concerned in carrying th e blood through the lungs. From the right auricle the blood passes to the right ventricle, and is thence carried to the lungs, where it is purified b y contact with air, and becomes scarlet in colour; it is then conveyed to the left auricle of the heart and passes into the left ventr.icle, thus completing the circulation.
The heart contracts in adults at an average rate of .;eventy-two times a minute, but the rate varies, increasing as the position is changed from the lying to the sitting or to the standing position; hence the importance of adjusting the patient's position in cases of hcemorrhage. At every contraction of the left ventricle blood is forced into the arteries, causing the pulse, which may be felt wherever the finger can he
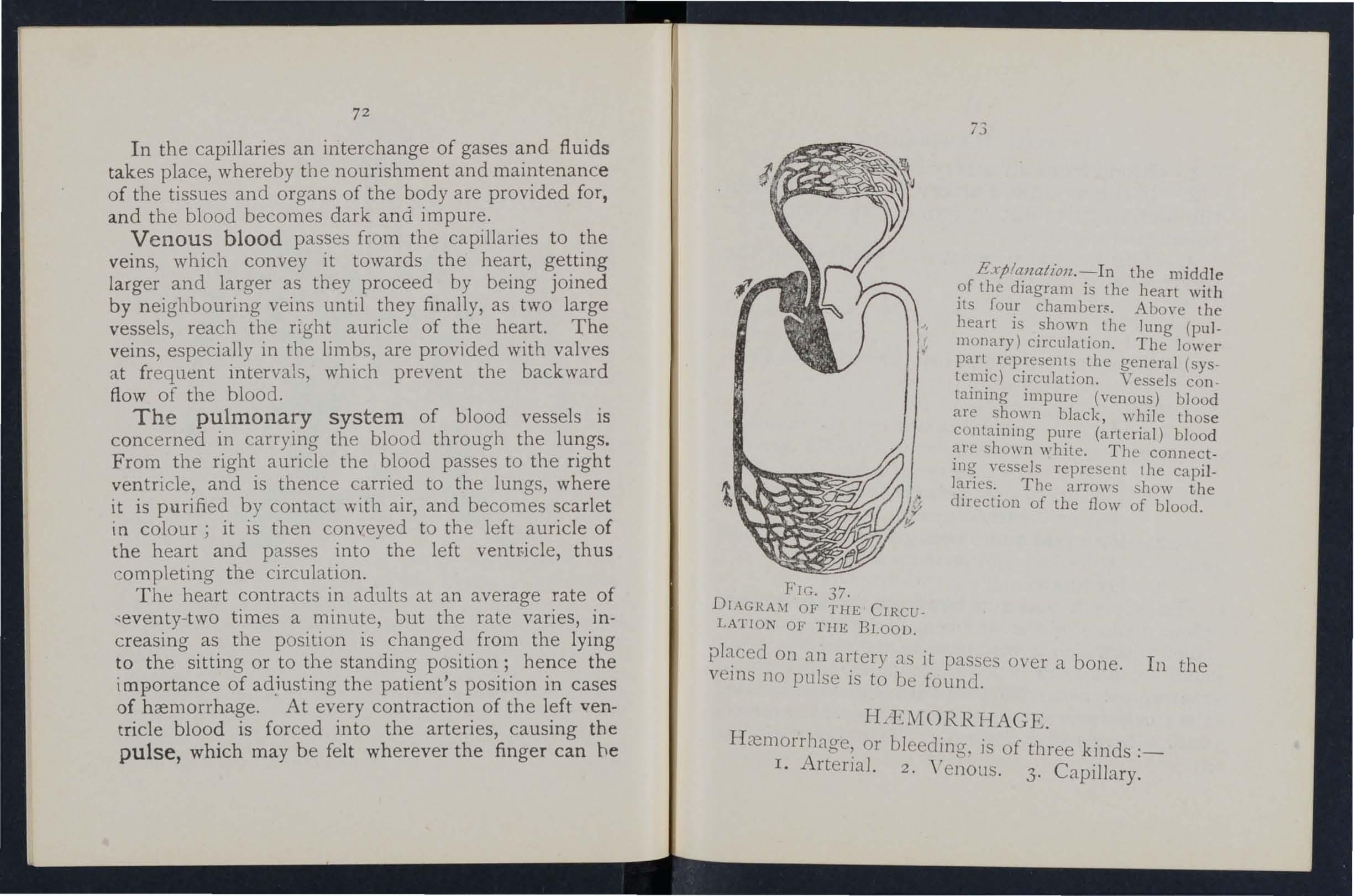
EXjJla1la tio71 .-In the middle ?f the diagram is the heart with Its four chambers. Above the heart i shown the lung (pu lmonary) circulation. The lower parL. the general (systemIc) CIrCUlatlOn. Vessels co ntaining impure (venous) blood are black, while those conta1111l1g pure (arterial) blood show n white. The connectvessels represent the capil-
The arrows show the dJrectlOn of the flow of blood.
FIr.. 37.
DrAGRAi\( OF TIfE CIRCULATION OF TIlE BLOOD.
On an al:tery as it passes oyer a bone. In the ve1l1S no pulse IS to be found. or ble ding, is of three kinds ;_ r. Artenal. 2. VenoLlS . 3. Capillary.
i3
ARTERIAL HlElI10RRHAGE .
I. - Blood from an artery is scarlet. .
2. - If the wounded artery is near skm . the blood spurts out i n jets correspondmg to the p u lsation of the heart. .
3. - The pre::;sure po i nt (see below) 1S o n t he h e art s i de o f t he w o und.
ARREST OF ARTERIAL
Arterial hremorrhase is, when practicable, to be arrested by pressure, posItion of the body, and elevation of the bleeding part.
P ressure may be :-
I.- Digital-that is, applied with the thumb or finaers, and may be (a) 011 the ,,"ound; (btat a spot called the pressure point. The pressure points are mdicated by numbered dots on the frontispIece.
2. - Bya p ad and b3 n d a ge (a) on the wound: (II) on the pressure pomt.
3.- By flexion.
To a pp ly a pad a n d bandage t o t h e w o un d , place a piece of lint or linen or a clean. chief folded into a hard pad, on thc bleedmg pomt, and secure it bv a bal1J 1ge tightly tied round the injured paTt.' To fold the handl-erchief, bring t he four corners to the cent re, and repeat the process un t il a hard pad is formco. T he smooth surface is

75
pbccd. on t1'1e wound, to preyent the pad frO:'1 1 unfoldmg, tIle puckered surface may be stitchf'd o r fixed by a safety pin . A hard substance, su h ::s a stone, may . be enclosed in the centre of the pad.
A may consist of a lad to be pbccd on .the press.ure point, a strap, cord, or balld(we to enCIrcle the 11m b .:J.nd pad, :J.nd a 1.'zent, such as a stIck or ether of t\\ istina th" LlIld to tighten it. b
To improvise an d apply a tourn i quet :a firm pad on the pressure point.
2.-Enclrcle the limb by a narrow bandaae \\'ith its centre over the pad . b Tie the ends of the bandage in a half knot the opposite side to the pad.
4·-La y the t\\'isting stick on the half knot and over it tie a reef knot. '
5·-T wist the stick to tighten the band[l["e, tllereby tIle p:J.d uron the [l n d arrestmg the flow of blood.
6.-Lock the stick in position by the ends of t he bandage already applied, or by another band age passed rou n d the stick and limb. TIle p:J.d of t he must be accurately placed u pon t he pressure pomt so as completely to comp ress the artery; othe r wise arteri[ll blood ,\'i11 be allowed to pass [I long tIle lim b, and tIle veins, being c om pressed by the tourniq ue,t, will not allow th e
74
olood to return through them to the heart, and the result will be dangerous swelling and congestion.
Should a suitable pad not be at hand, a knot may be made in the centre of the bandage, and when available, a stone, cork, etc ., enclosed in it to give it firmness and bulk. See that the bulging and not the flat side of the knot is next the skin.
An elastic bandage passed tigh tly round the limb, immediately above the seat of arterial heemorrhage, will arrest bleeding. The simplest form of this bandage is a strip of elastic webbIng, twenty-five to thirty inches long and two inches wide, with a piece of tape sewn at each encl. An elastic belt or brace will serve the same purpose. Except when p:lIt of a limb is torn off, it is not advisable to use an elastic cord or bandage if other apparatus can be had, as it cuts off all circulation in the limb.
Flexion consists of the application of a pad on the pressure point at the knee or elbow joint, flexing the limb to make pressure, and the limb in the flexed position by a bandage crossed like the figure 8.
RULES FOR OF A ACCOMPANIED BY ARTERIAL H ..iEi\lORRHAGE.
1. Stop bleeJinp-.
[1. Prevent injurious germs from getting into th e \yound.

To attain these ends :-
I. Place the patient in a suitable position, bearing m mind that the blood escapes with less force when the patient sits, and is still more checked when he lies down.
2. Elevate the bleeding part, as thereby less blood finds Its way into it.
3. Expose the wound, removing whatever clothing IS necessary. (See Rule 8, a.)
4. Apply digital pressure.
(a) If the wound IS small on the bleeding spot.
(b) If the wound is large on the point next to the wound on the heart SIde. The nearest pressure point is chosen in order to avoid cutting off the circulation from as much of the part as possilJle, but sometimes it is necessary to apply pressure still nearer to the heart.
S. Remove foreign bodies, such as broken glass , bits of clothmg, half, etc., seen in the wound; do not search for foreir;n bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boracic gauze or lint is to be preferred, but absorbent cotton wool, lint, or gauze, or a clean piece of linen will a nswer the purpose. Should any doubt be enterl.lIned as to the cleanliness of the dressing, a clean piece of unprinted paper, such as the inside of an
76
77
envelope, should be placed next the wound before applying the pad . (Compare pages 75 and 76.)
7. Bandage tightly over the pad unless :-
(a) bodies are suspected to be left unseen in the wound.
(b) There is dange.r of injury to a fracture. In these cases a lIght dressll1g only should be applied. . .
8. Apply a pad and bandage or flexlOn the pressure point (see Rule 4, b ), but only m the following cases :- .
,a) As a temporary measure while the w0und IS being exposed, exam1l1ed and covered. .
(b) As a more permanent measure when blee llllg cannot be stopped by the pad and on the wound, or whell, in accordance WIt h Rule 7, the tight bandage has not been applied.
o. Afford support to the injured part. \\'hen part of a limb has been torn off or the .wound is lacerated (for example by the claw of an a111ma1 or by machinery) h<emorrhage frequently does r:ot come 0;1 at once, but as there is a dang1t ot later, mcans for its arrest !ihould be .1pplied to the limb , but not tightened unl ess necessary. Do 11 Jt disturb a clot of blood formed over a wound.
1"0 att(!mpt should be made to cleanse C1 (' "('ept \\ith sterilised wat er (th:lt is previously bOIled

and allowed to coo]'). and experience, especially in recent wars, has shown that tho e wounds \\"hlch were provisionally treated with a dry and subsequently dressed by a sur;eon \\ ith proper appli:1I1 c cs; dld best.
Students p.-actising arrest of arterial h:t:'1lorrhag . feel the pulse to see when the current of blood th e. artery has been stopped, and should then lmme.dIately rel.ax the pressure made on the artery_ In thIS way the Importanc e of the accurate application of pressure ",111 be realised, and the amount of necessary ",ill be
THE COURSE OF THE MAl;\' ARTERIE , A7\'D THE. ARRE T OF H.IE:'IIORRHAGfS.
(The numbers of the pressure points refer to thos .)n the Frontispiece.)
THE LARGE ARTERIES \VITHI J THE CHEST AN AHDO:'lIE7\'.
1 is centlal or trunk artery of the: l)ouy. '-.,ul11l1lencmg at the left ventricle it forms an arch behind the upper p:ut of the the arch are gIven off the large branches \\'h1ch carry the blood to eIther side of the head and neck and to the upper lllnbs. The Aorta passes down on the left of the spine to just below the navel where it di"idcs into two great branches (th c iliaes'
79
which convey the blood to the organs m the pelvIs and to the lower limbs.
vVounds of these arteries are one cause of internal hcemorrhage (see page 96).
/ ART ERIES OF THE HEAD AND NECK.
The Carotid Arteries (right and left) leave the upper part of the chest and pass up on either sIde of the wi n dpIpe and, just below the level of the angle of the lower jaw, divide mto the Internal an? External Carotid Arteries. The Internal Carotid Artery ascends deeply in the neck, and enters the cranIum to supply the bram WIth blood. The External Carotid Artery gives off a number of branches; to the front the artery of the tongue (Lingual), the arte ry to the face (Facial); to the back the OCClpltal; the artery itself is continued upwards in front of the ear, where It changes its name to the Temporal, and supplies the scalp in the neighbourhood of the templ es . . .
When a Carotid Artery l'S wounded, as m the case of a cut throat, apply the thumb of one hand on the artery at pressure point I, pressmg backwards against the backbone and taking care to avoid the winclpipe. It may also be necessary to apply pressure with the other above the wound for two reasons: (a) To arrest the flo\\' of blood from the main (jugular) vein in the neck, which rUDS
alongside of th.e carotid artery and lS usuany,younded at the same tIme ; (b) To check the fiow of blood the uppe!' end of the carotid artery itself, "llich lS often conSIderable owing to com munication between the branches of this artery and those of its

FIG. 38. FIG. 39.
fellow. Digit1:,.J pressure must be maintained, by relays of assistants if necessary, until the doctor arriycs (Fig.
The Facial Artery crosses the lower jaw in a slight hollow two fingers' breadth in front of the angle, and sends branches to the chin, lips, cheek, and
81
o u tside of the nOSe . Hremo rr bage from \\"ou n cls of th e face below t he level of the eye is to be arrested by :-
(a) Di gital pressure o n p ressure poi n t 2 ( Fig. 39),
o r
(b) Grasping the li ps or cheek o r: sid es of th,:: \\"ound by the finger m Slde and th t>mmb outsIde the mouth o r 7.'/C: 7. 'ersa.

FrG. 41.
The Temp Jr al Artery may be felt pulsating in front of the upper part of the ear. H cemorrb age from the region of the templ: may ?e arrested by pressure applied at pressure pomt.3 (FIg . 4 0 ) . The Occipital Artery supplJes branches to the "
region of the scalp from behind the ear to the back of the head. Hremorrhage from this rEgion may be arrested by digital pressure on pressure point -1-, 'four breadth behind the ear (Fig . 41). Tbis point IS dIfficult to fin.d, and it is usually sufllcient to apply pressure lmmedlately below the \\oune!. f r om the For e head or anywhere in the Scalp may be arrested by appl) a small firm pac! on the blecdingpoillt :1l1d securing it by a narro\\ b.lI1cbge \\ ith its centre laid on the pad, the enc.ls ('an"ied round the head in the direction most cO\wenient. and tied tighll) over the pad (Fig. 42).
'When a \\ound of the I forehead or scalp is as:-,)ciated with a frn.cture, the best plan is to apply a FIG. 42. pad ,around the seat of Injury. To make a ring pao, pass one end of a narrow bancla(Te round fingers; pass the other end of the bandage through the 1'IIlg thus far.med and continue to pass it through a n d through until the \\ hole of the bandaO'L i used a n d a ring as shown in Fig. -1-3 is formed.
ARTl .: RIIL OF THE "CPPER LL'lIB
The Subclavia n Art e ry passes from a point behind the i-nner end of the collar-bone across the first rib to the armpit.

FIG. 43. FIG. 44·
To apply digital pressure :-
I .-Bare the neck and upper part of the chest.
2.- P lace the patient's arm against the body so as to depress the shoulder, and cause him to inclme his head towards the injured side.
3.- T ake your stand opposite the. shoulder.
4.-U sing the left hand for the nght artery. vice versa, grasp the neck low down, placmg the fingers behind the shoulder and the thumb immediately abo\'e the centre of the collar-bone in the hollow between the muscles attached to the bone (pressure point 5)·
s·-Press the deeply do\\ n\\"ards [l.nd backwards agamst the first rib, wbich is the collar bone at this spot (Fig. 44).
The Ax Illary A rt e ry, \\'llich is a continuation of the subclanCln, keeps close to the 110 1·1 .. d -' U l er J0111 t,. can. be telt pu Isat.ing wl:e.n the fingers are deeply ptessed ll1to t?e armpit. Digltal pressure is difficult to apply to thIS artery.
To apply a pad and bandage: -
r. --Place a bard p:ld the size of a billiard ball in the arm pit (pressure point 6).
2 . - Apply the centre of a narro IV b:ll1 dage on the pad; ross the bandage on Fie. 45. the shoulder; pull tl?e ends tigbt and tie them under the OppOSite armpit, taking care that the pad does not slip.
3· - the forearm and tie the limb tightly to tile trunk \\,lth a hroad handage, applied on a level With the elbow (Fig. 45).
SCi
The Brachial Arte ry is a continuation of the Axillary, and rune; do\\ n the arm on the inner the biceps muscle, gradually passing forward until It reaches the middle of tbe front of the elbow. The inner seam of tbl:: COlt sleev abm'e the elbo\\' roughly indicates its course,
Digital or instrumental pressure may be applied at or near pressure point 7,

FIC, ;;6.
FlG. 47,
To apply digital pressure extend the limb at ; ight a.ngles to the body, pal m of the hand upwards. tand behind the limb, and pass the fingers under the back
of the arm over the seam of the coat or the aroove 011 the of the biceps muscle. Press thee> pulps (not the tipS) on the artery (FJO'. -+6). 'o:'!le prefer to pass the hand over the front of the muscle 47)· A slight turn of the hand out\\'ards as It grasps the arm will better ensure compression of the artery .
The Brachial artery may he compressed at tlle
FIG. 49.
elbow (pressure point 8), by The pad may be a folded handkelchlef \\'Ith a small stone or a cork wrapped up in it, but when no pad is i1vailable the coat sleeve roll ed or gat h ered up \\'i ll e r ve instead (Fig. 48).
87
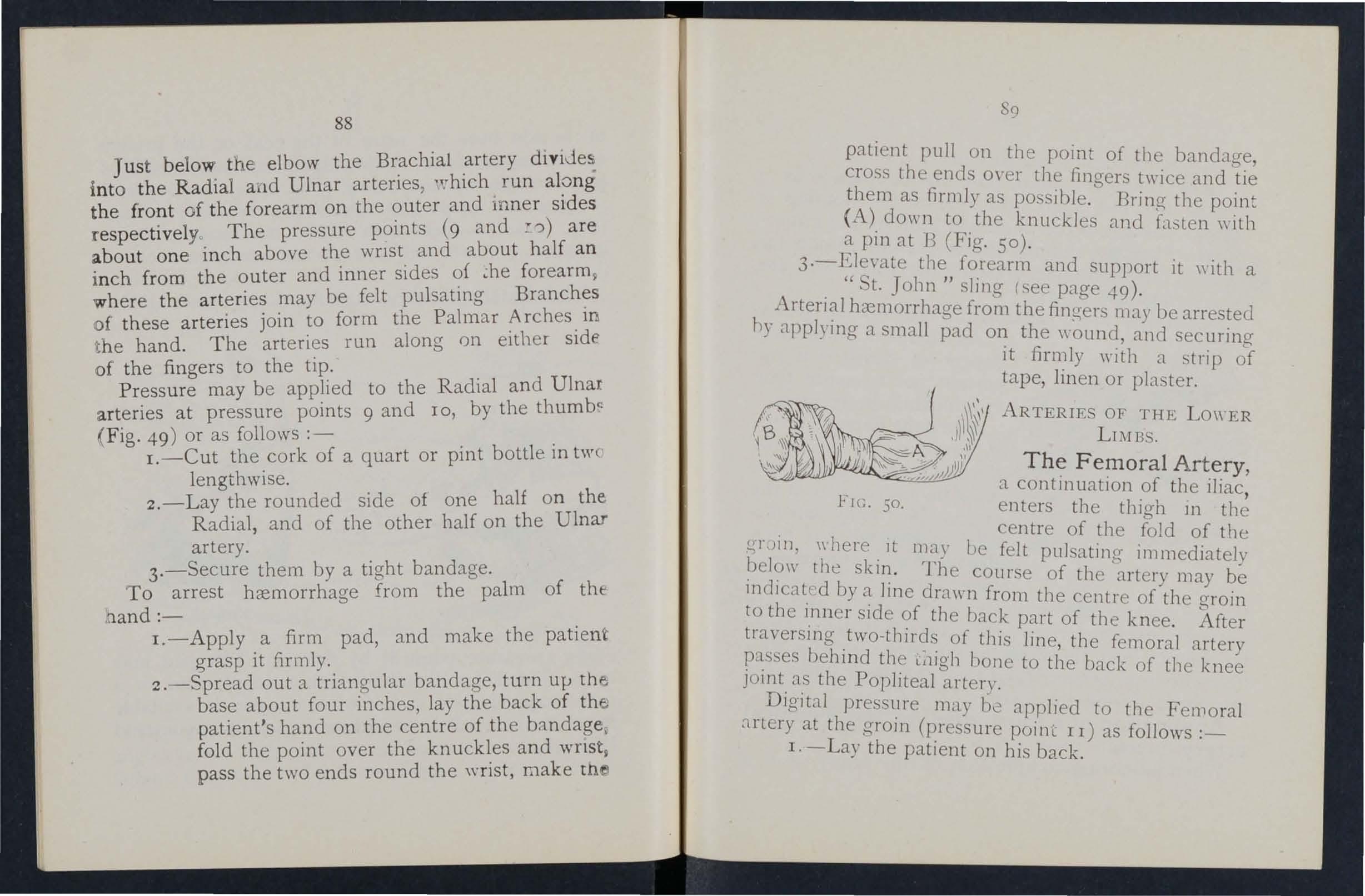
88
Just below the elbow the Brachial artery dlvlJeSi into the Radial and Ulnar arteries, 'vhich run along the front of the forearm on the outer and inner sides respectivelyo The pressure points (9 and :;')) are about one inch above the wnst and about half an inch from the outer and inner sides of forearm 9 where the arteries may be felt pulsating Branches of these arteries join to form the Palmar Arches in t he hand. The arteries run along on either side of the fingers to the tip.
Pressure may b e applied to the Radial and Ulnar arteries at pressure points 9 and 10, by the thumb.: ( Fig. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in tW ( lengthwise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3.-Secure them by a ti ght bandage.
To arrest hremorrhage from the palm of thenand:-
I.-Apply a firm pad, and make the patien grasp it firmly.
2.-Spread out a trian gu lar bandage, turn ulJ the base about four inches, lay the back of th e patient's hand on the centre of the bandage , fold the point over the kn uckles and wnst9 pass the two ends round the wrist, make th s<)
patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as. firmly as possible. Bring tIle point (A), do\\ n to the knuckles and fasten with a pm at 13 (Fig, 50).
fO,rearm and support it with a , St. John slJl1g (see page 4-9).
h hremorrhage from the fingers may be arrested ) applymg a small pad on the ,,'ound, and securin a it firmly with a strip of tape, lin en or pIa teL
AR TERlES OF THE LOWER LIl\I BS,
The F e!lloral Artery, , a contll1uatlOn of th e iliac 1:< Ie h' G , , J ' enters t e thlgh 111 the (rrJil1 where lt I centre of the fold of the 'b"'e10 '1 l' may Je felt pulsating- immediately \V tle S(Il1 The co f ] L - '1' b' urse a t le a rt ery may be y line drawn from the centre of the Laroin o e l,nner slde of the back part of the knee b traversmg ,two-thirds of this lin e, the femor;] behmd lll igh bone to the back of kn y ]01l1t, a,s the Poplrteal artery, ee
Dlgltal pressure may])\; applied to tIle F 1 :1rter t th '( el110 ra , y aLe arOlt1 pressure poi ilL I I) as follows :_ I. - ay the patIent on his back.
90
2.-Kn eel beside th e patient.
3.-To find th e groin, rais e the foo t high so as to fl ex th e thi g h; the fold in th e clothing at Lhe top of th e thio-h will indicate th e g roin.
4.-Pbce th e thumbs one on th e other upon the pressure pomt, g raspin g the thi gh "ith th e h a nd s (Fig 51).
s. - Press firmly against the brim of the p elvi .
As th ere is immediate danger of dea th it is important not to "aste tirne
111 r emov in g the tr ousers .
Wh e n the Femoral artery is wounded in th e upp er third of its course, pressure must be maintained the groin. No really satisfactor\, tourniquet has been
FlG 51. devised for compression :-:t tbis point, and relays of assistants shoulll be employed t o kcep up tIle pressure until the doctor arri,'es; each fresh assistant places his thumbs over those of bis predecessor, who slips his a\\ 8)' from beneath, and thus gushes of blood arc prc\'cntecl during the change,
Application of a tourniquet to the Femoral artery (pressure point J 2) : -
"\V ben practising com of this artery, it is a

52
91
FIG.
92
good plan to d raw a chalk line from the cen,tre ff the (Troin to the inner side of the back, of, tne old f the tourniquet on thIs line as hloh place t le pa 0 r d The pad should up as the ban dage can be app Ie -:. be the size of a lawn tennis ball (FIg. 52) ,. 1 t Pressure may be applied to the by flexion at the knee (pressure POlllt 13 ) , tepa

FIG,53 ·
1 Id b e the size of a lawn tennis ball, or if no padd S lOU 1 . lled or (Tathere . '1 ble the trouser leO' may )C 10 b 15 aVaI a . t d I t not necessary to take off up to serve 111S. ea , the clothing (FIg , 53)" d h k 'oint the Popliteal Just below and beb 111 t e nee J p' . artery di\'ldes ll1to .the Anterior (front) and ostenOl
(back) Tibial ar t.en eST ' 'bial Arte ry passes dO\\'n the The Postenor 1
93
b.1ck uf tbe Ie,.; to the inn er Side of the ankle. It at Ilist deeph' p'L.lced between the muscles of the calf, but it appruaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the side of the :1nk le . It enters the sole as the Plantar Arteries, which run forward amongst the muscl es to supply the foot ::1.lld toes .
T he An terior Tibial A r te ry, on leaving the Popliteal, at once passes forward between the leg bones, and, deeply placed amongst the muscles. runs dO lI n the leg to the centre of the front of the ankle . ThIS artery is continued as the D o r sal Art e ry of th e Fo o t, which, passing fOl'\\'ard over the tarsus, dips down to the sole between the first and second m eta tarsal bones. Here it forms with the Plantar arteries what is known as the P lantar A rch. At the ankle (pressure points 14 and IS) pressure may be applied by th e Ilngers or by pads and bandages.
\ YENOUS
I. -Blo o d fr o m a vein is dark l-e d .
2. - It fl o ws in a slo w c o n tinu ous s t rea m,
3·- It issues from t he side of t h e woun d fur t h e r fr om t he hea r t.
4·-In th e cas e o f a wou n d of a varicos e vei n it flows als) frOI1l the side of the wound nearer to the heart, if the p1tient is kept standing.
Varico3e Vein3. -The vcins of the leg specially apt to become varicose. A \'a rico:>e \'ein is dibted, \\"inding, and \\ith bead-like (\-aricose) pro iections along its course. A vein beco mes varicos e from seycral .....causes, SUd1 as long standing or tight garters. The first effect is to throw ext ra \\ ork upon the vah cs, and the bead-like are caused by the blood accull1ulatll1g in the pockets behind th . \'alvcs In time the yein b ecomes so dilated that the \-alv es can no span it.
GIi;i':ERAL Ruu,> FOR OF r\ \\'Cl1.:i':D
ACCO:'lII'.'\:-\ll!.D I)Y
1. - Place the patient in a suitable position, hearing in mind the blood escapes \\'ith less force when the patH'l1l <;Its and is sull chec ked as he lies do\\·n.
2. - Elevate the part, as thereby less blood finds its \Yay into it
3. - Expose the wound, removing \\ h:llC\Tr clothing is necessary.
4. - Remove any constrictions, such as the collar or garters, from the heart side of the wound.
5. - Apply digital pressure on the \youncl until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure near the \\ouad on the side a\\-ay frorn the heart. In the case of a \VoUlHl of a varicose vein it may () Iso be n CC'P5sary to

95
a pad and bandage to the vein immediatel e the \:'o und, espt:ctally if the limr cannot mall1tamed 111 an elevated position.
6. - Treat the wound as directed by Rules 5, 6 and 7, stated on pages 77 and 78.
7·- Afford support to the injured part.
C:\l'lLL\l\\'
1. - The blood is red.
2. - It flows briskly in a continuous stream or may merely ooze from the wound. '
3·- It wells up from all parts of the wound slIght amount of pre sure "ill suffice to arr . capIllary bxmorrhage. < est
IXTERNAL HADlORRH,\GE.
. \\ Tounds of the .blood yessels \\ ithin the trunk CJ.use lI1to tbe ca\"ity of tbe chest or f the abdomen. 0
SIG:\TS -\ , D -'Y.\IPTO.\J OF I;:-HER:\TAL
I. - Rapid loss of giddines and faintnessespeCIally \\'hen the upright po ition is assumed. '
2.-Pallor ?f the fa e and lips.
3:-Breathmg hurned and laboured and ae' pan led by ya\\ nin (T and sio-hino- ' L com., v \'""'I bO
4·- pulse fails, and may altoo-e ther eli appe at the WrISt. b aT
5.-The patient thro ws his arms about, tugs at the clothing round the neck, and calls for air.
6.-Finally the patient may become totally unconsci ous.
TREATi\IENT.
I.-Keep the patient in a recum bent position.
2.-Undo all tight clothing about the neck.
3.-Provide for free circulation of air; fan the patient.
4.-Sprinkle cold water on the face; hold smelling salts to th e nostrils; avoid other forms of stimulants, at all events until the h cem orrhage has been controlled.
5.- Give ice to suck or cold water to drink; if the seat of the hcemorrhage is known, apply an ice bag over the r egion.
6.-Should the patient be reduced to a state of c ollapse, raise the feet and bandage the lim bs firm ly fr om the toes to the hips and from the fingers to the
H A!:?IORRHAGE FRo:-.r THE NOSE (NOSTRJLS).
I.-Place the patient in a sitting position in a current of a ir b efore a n open window, with the h ead throV'm slightly back and the hands rais e d above tb e b ead.
2.- Undo all tigbt clothing around the neck and ch est.
3. - Apply cold (ice , a cold sponge or bunch o f
97
keys) over the no e and als h the collar' place th t' .0 ht e plne at the level of , e eet m ot \\ at r.
4·-Cause tIle patlent t k h so avoid breathing mouth open, a nd
Blood issuing from th fr om the tongue the cr e mouth Ill.ay come after extraction the tlhe ocket of a tooth , a, e unfTs, or the stomach.
HJEMORRH '\GE F . THE To 'G'UE THE G THE OCKET OF T , . A OOTH, OR THE THRO i \T.
r. -Gl\·e ice to suck Jd mouth. If th . ' or co. \\ater to hold in the lS le:; not success! ul cr ' ca n be borne to h ld' I b H e water as hot as o 111 t lC mouth.
2.-If necessary mak . arteries. . < e pI essure on the caroti d
3·-If bleedll1g from the f· IS excessIve com pres th lont part of the tongue lint held bet'vveen th s fi e part by a piece of clea n
4.-If th bI d e nger and thumb. e ee Illg IS from th 1 plug the socket \"ith' a " . e soc ,et of a tooth , \\'001; over this la pJece at clean llllt or c o tton of s u itable size hcork or other substanc e , I uct t e pat1ent to bite on it.
H}E,r O RRHAGF FRO;\[ THE LU;\'GS from the lungs IS coughed anG frotll ), 111 appearance. up and 1S scarlet
Treat as for Int ernal Hccmorrhage (see page 95).
If
96
HIE:\lORRHAGE FROM THE STO IACH.
. 'ted' it is of a dark
Blood from the stomach IS vomt , _ d _ it colour and has the appearance of coffee gloun s, , be mixed with food. , ') maT} t for Intern a l Hcernorrhage \see page 95 , rea as . b h outh h 'to be e n-en y t em. except that not mg IS t> ,
Blood issuing
gene.rally a ed as it issues; attempt cramum, mu _ is to be made to plug lhe ear.

99
QUESTIONS 0_ CHAPTER III.
The 17UlIltrars indicate the pagu where the ailS"".]! S may be fOUl/d,
vVhat organs are concerned in the circulation of the blood? '"
Describe the heart .. ,
Trace the circulation of the blood thruugh the bcd)' and lungs 70 to 72
IIow many times a minute does the heart contract on the average?
\\'hal is the effect of the patient's position on the rate at which the heart contracts?
\"hat is the pulse? ,,'
IIow many kinds of hremorrhage are there?
Bow would you know a case of arterial hXlllorrhage ? ..
In WhaL way should arterial hxmorrhage be controlLLd?
\Vhat is meant by " pressure point"?
IIow may pressure be applied?
\VhaL is a tourniquet?
Why is accuracy necessary in placing the pad of a tourniquet?
\Vhen mayan elastic bandagc ue used instead of a tourniquct?
What is flexion?
State th e general rules for treatment of a 1Y0und accompanied by arterial hxmorrhage ... 77, 78
If part of a limo had been torn off, uut there was not much bleeding, how would YOll act?
hould blood clots be disturbed ?.. , ,
Is it wise for an unskilled person to attempt to cleanse a wound? ... ... '" 78, 79
What is the aorta? ." •• , ' 79
98
PAGE ,0 70
72 72 72 73 7474 74 74 75 75
E2
roo
Describe the arteries of the head and neck

80
\Vhy is it sometimes necessary to compress the carotid artery both below and above the wound? ... So, 8r
What is a nng pad, and whaL is its use? ... 84
Describe the arteries of the upper limbs ... 84 to 89
Describe the arteries of the lower limbs... 89 to 93
How would you know a case of yenous ha!1110rrhage? 93
\Vhat is a varicose vein? 9+
IIo\\ maya vein beccme yaricose ? 9+
State the general rules for treaLment of a wound accumpanied by venuus hremorrhage? ... 94, 95
How would you know a case of capillary hremorrhage? 95
How would you stop capillary hxmorrhage ? 95
'What is internal hremorrhage? 95
\Vhat would lead you LO suspect internal hremorrhage? 95, 96
SLaLe the treatment for internal hremorrhage? ... 96
How would you arrest hremorrhage from the nose? 96, 97
\Vhere may blood issuing from the mouth come from?. 97
How \-\'ould you treat bleeding from the gums or throat? 97
What else would you do if the tongue were bleeding?.. 97
And if the lJleeding were from the socket of the touth? 97
How \\ ould you distinguish between lJleeding from the lungs and from the stomach? .. , 97
And what would be the difference in the treaLment? ... 97
Of what is bleeding from the ear channel generally a sign? 98
The Student should practise placing supposed patients in a proper posiLion for the arrest of hremorrhage (see pages 72, 77 and 94), folding firm pads (74 and 75), tying hard knots in bandages to form a tourniquet (76 ), and the application of pressure aL all the pressure points shown in the frontispiece, at various points on the forehead and scalp, and on the palm of the hand. I'ressure should be digital, by pad and bandage, or flexion, as directed in the text.
101
Pressure points - Carotid arter' 8 F' Te:11poral, 82. Occipital )8'" °S- 82. AxIllar)- 85 B I' I J' ubcla\Jan 84 , . rac lla (by pa d d I 'd . pressure heing made against the h an Jan age, flexion at the elbow) 86 . '{ d' I umerus and by Femoral at the rain' . 1 a la Ulnar, 87.
92 - Po lileal ,90 Femoral In the thigh, arterie' P9" 1 9· Antenai and posterior Tibial " .).
IIremorrhage from the forehead or scal )
IIremorrhage from the pal f 1 hI... .. .
Venous h -h 111 0 le and. .. .. . remon age fram a van case or other vein .. 84 87 to 89 .. ·93. 94
PAGE
P A G Jr
CHAPTER IV . BRUISES.
A blow anywhere on the surface of the b?dy n:ay tause extensIve hcemorrhage beneath the skm, wIthDut breakmg it-a" black eye" is a_n instance. !he mjury is accompanied by discoloratlOn and swellIng.
TREATMENT
Apply ice or cold dressings. A piece of Imt soaked in extract of \\,]tch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is caused- .
I a) By dry heat, such as fire or a piece of hot Ir?n.
(b) By a raIl, wire or dynamo charged WIth a high pressure electric curren.t .... .
(c) By a corrosive aCId, as 011 of \
(d) By a corrosi\-e alkali, such as caustIc soda. ammonia, or quicklime.
(e) By friction, caused, for e\ample, by contact 'Ith a revolving wheel. (Brush burn.) . A scald is caused by moist heat, such as bOl11l1f.!. water hot oil or tar. effect may be a mere redden1ng of the .skm ; blisters may be formed; or even the deeper tIssue

r03
of the body may be charred and blackened. The clothing may adhere to the burnt skin, and its remov al is impossible without further detnm ent to the injured part. The great danger is Shock.
TR EATME T.
I. - Carefully remove the clothing over the injured part. If stuck to the skin, the adherent clothing must be cut around with scissors, soaked with oil, and left to come away subsequently.
2. - Do not break blisters.
3. - Imm ediately cover up the part. Soak or smear pieces of 11l1t or lmen ",ith oil, or vaseline, lanoline, or cold cream; a small quantity of boracIc powder added to these \\ III be of benefit. The of a ra\V potato scraped out and spread on llllt l11Jkes a soothing apphcation. ,\Vhen the in jured surhce is extensive do not cover It with one large - heet of 11l1t, but with strips about the breadth of the hand; thIs IS advisable as they fit better on the part, and during subsequent dressll1gs one strip can be removed at a time, and a fresh dressing applied before tIle adjacent strip is taken off. The s110ck to the system is thereby less than if the whole of the burnt surface were laid bare to the air by the removal of all the dressings at one time. "When coYered by the oIly dressing envelop the part in cotton \\ 001 or a piece of flannel and a pply a bandage.
102
\Vhen the face 1S bur nt, cut a mask out of lint or Imen, leaving holes for the eyes, nose and month. Dip t!11S in oil or smear it w1th vaseline and apply it to the face and cover it with cotton wool, leaving openings to correspond with the holes in the mask.
\Vhen possible place the injured part in water at the temperature of the body (98 degrees) until suitable dressings can be prepared. A dessert spoonful of baking soda added to a pint of the warm water will hlake a soothing lotion.
As it is important not to leave the part exposed to the air, it is the duty of the bystanders to prepaI;e the dressings while the clothing is being removed.
4. - Treat Shock. - This lS particularly necessary in the case of every burn or scald of any considerable extent (see page 135). Be very apprehensive of danger 111 the case of even slight burns of the neck.
S.-If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion , such as washing soda. baking soda (bicarbonate of soda), magnesia, or slaked lime in warm water before applying the dressings .
6.- If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion, sm h as lemon juice or vinegar diluted \\ ith an equal quantity of \\ ater. Cautz'o71.-Before using \\ ater brush off any lime that remains on the part.

ro5
7·-When a woman 's dress catches fire -
( a) Lay the woman fllt on the floor at once, so that ,the flames are uppermost; that is to say, If the front of the dress is on fire Jay her o? her .back, and if the back 'of the d;'ess IS burnmg, place her face dowl1\\ ards. 1 he for this is that flames ascend so that If the upright po ition is assumed 'the flames will quickly reach and hum' the neck, anll b ,ce ; or if the woman flames undermost, they will, 1! unextll1gLllshed, pa. s over and burn the l1111 bs, and set nre to the rest of the dress,
(b ) As soon as tl-:e \\'Ol11an is laid flat, smother flames \\"Ith anything at hand, such a a rug, coat, bbnket, or table cm-er; if made \\et so much the better.
( l) A \\ oman r endering assistance should hold a rug or in front of herself when the flam e .
(d ) I.f a woman's dress catches fire when nobody IS by, she should 1ie fbt, fl ames uppermost, smother flames \\ ith anything hand\" and call fO,r ass1stance, or crawl to the beil-pull and nng; on no account should she rush mto the open
Th e use of nre guards would prevent many calamilles.
104
BITES OF SNAKES AND RABID ANIMALS p AND WOUNDS BY POISONED WEAPONS .
Hydrophobia is caused by the lJite of an such as a dog, cat, fox, wo lf, or deer suf!ering from rabies. The special poisons introduced mto wounds caused by venomous snakes and poisoned weapons ca us e immediate danger to life.
TREA Ti\IENT
-1.- Immediately place a constriction between the wound and the heart so as to prevent the ve nous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircled on the side of th e wound nearest to the with the a nd thumb, ar.d as as possIble a hgatur e (a string, piece tape, or stnp of handkerc hi ef) should be placed tIghtly round the root of the fi nge r. Compression with the finger and thumb not be relaxed until the ligature has been Additional ligatures may, with advantage, be applI ed at mt erv als up the limb.
2. - Encourage b leeding for a time :-
(a) By bathing th e w!th warm water.
(b} By keeping the mJured 11mb low ; the upper limb should be allowed to han g down, and in th e case of the lower limb the patient should be seated with the foot on the ground.

3.-Cauterise the wound, if it is quite impossible to obtain the services of a doctor. This is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, o r 1f these are not at hand, with a red hot wire or a fu see. The usual solid caustic is insufficient, as it does no t reach the bottom of the wound, where the poison is To ensure the caustic reaching the bottom of the wound, it should be applied on a piec e of wood such as a match cut to a point. "When the causti has been thoroughly applied, but not till then, the ligatures may be removed.
4. - Cover the wound, after a while, with a cleardressing.
S·- Afford support to the injured part.
6. - Treat shock if it occurs (see page 135).
7· - 1n the case of a bite by a venomou s snake, rub in powdered permanganate of potash and mject under the skin in the n eighbourhood of the wound a solution of pe rm anganate of potash .
STINGS OF PLANTS AND ANIMALS
.
These give rise to serious inconvenience, and 10 some cases grave symptoms d evelop.
TR EATMENT .
t , - Extract the stin g if left in. the part freely w ith dilute ammon ia
106
or spirits. A paste of bicarbo.nate of soda sal volatile is an efficient apphcatlOn. A solutlO n of wash ing soda or potash or the application of the blue bag will relieve pam.
3. - Treat collapse if it occurs (see page 135 )·
F RO ST BI TE.
D uring exposure to severe cold, parts of the bo?y, usually the feet, fingers , or ears, lose sensation an d become first \\axy white an d afterwards. gested and of a purple appearance . As sensatlOn ]s lost in the part, it is often on ly by remarks of bystanders that the frost-bitten person ]s made aware of his condition.
TREADIENT.
I. - Do not bring the patient into a room ua til, by friction of th e by rubbmg with soft snow, sensation and c ircula.tlOn 111 the. affected parts are restored . Neglect of thIS pre.cautlOn may lead to death of the of the frost-hltten part.
2. - When circulation is restored , keep the patient in a room at a of 60 degrees .
NE E D LE EYIBED DED UNDER TH E SKI N
\ Vhen a needle breaks off after penetrating the skm an d disappears, tak e the patient to a d?ctor at once. If the wo u nd is near a joint, k eep the 11mb at rest on a splint.

I09
F ISH-H OOK EMBEDDED IN T HE SKIN.
D o not attempt to WIthdraw the fish-hook by the way it went in, but cut off the dressing of the hoo k, so that only the metal is left, and then force the point onwards through the skin until the ho.ok can be p ulled out.
INJUR I ES TO JO I NTS.
When a joint is injured by a bullet, stab, or other canse-
I. - Wrap the part in cotton wool.
2. - Afford rest and support to the injured limb ; if the upper limb, in a flexed position by a sling ; if the lower limb, in a straight position by a splmt.
FO REIGN BODY IN THE EY E .
I. - Prevent th e patient rubbin g the eye, tying down a child's hands if necessary.
2.- Pull down the lower eyelid, when, if the fo reign body is seen, it can readily be remoyed with a came l's hair brush, or with the corner of a handkerchief twirled up and wetted.
3. - When the foreign body is beneath the upper eyelid lift the lid forward, push up the lower lid be neath it a n d let go . The hair of the 10'wer lid brushes the inner surface of the upper one, and may d islodge the body. hould the first attempt be u ns uccessful, repeat it seyeral times if necessary. If
108
th e fo reign body is not dislodge d call the services of a doctor as soon as possible. When , how ever, sk illed help cannot be h ad , proceed as follows :-
(a) Seat the patient so as to face tIl e lig1lt, and stand behind him, steadying his head against your cbest.
(b) Plac e a small rod, such as a match o r bodkin, on the upper eyelid, half-an-inch aboye the edge, pressing it backwards as far as p o sible.
(c) Pull the upp er eye-lashes upwards over the rod, and thereby evert the eyelid.
(d) R emove th e foreign body.
4.-When a piece of steel is embedded in the eyeball drop a litt1 e olive or castor oil on th e eyeball after pulling dO\m the lower eyelid, close tbe lids, apply a soft pad of cotton wool and £ecure it by a bandage tied sufficiently fir 1111)' to keep the eyebal1 steady: take the patient to a doctor.
5. - When quick-lime is in the eye brush <1\\ ay as much of it as possib.le ; bathe the eye \\ ith vinegar and warm water, and treat as for a piece of steel embedded in the eyebal l.
FOREIGN BODY IN THE EAR
As a rule make no attempt to treat a patient with a foreign body in the ear if the .services of a doctor can possibly be had; any attempts to r emove the foreign body may lead to fatal consequences. If a child

III
cannot be induced to keep the fingers from the tie his hands down or cover up the ear. If an insect is in the ear-passage, fill the ear with olive oil, when the insect will float and may be removed , Neve R' or probe the ear.
FOREIG N BODY IN THE NOSE.
Induce sneezing by pepper or snuff. Cause th" pat1ent to blow his nose violently after closing h unaffec ted nostril. There is no immediate dangeR' from a foreign body in the nose.
THE ABDO:\i(EN.
The abdomen is bounded above by the diaphrag rr. below by the pelvis; behind by the lum bar vertebrce; ana In front and at the sides by muscular walls. (Fig 54 )
TH E ORGANS OF THE ABDmrEN.
The Stomach lies immediately below the "Pit ... t 'the stomach t lies below the breast-bone.
The Liver just in the upper part of the where it is mostly covered by the right lower ribs .
The Spleen lies beneath the ribs at th0 upper part of the left side of the abdomen.
The Intestines occupy the greater part of the' cav ity of the 3.bdomen.
The Kidneys lie at the back, in the region of tht>o 10m.
T h e Blad d er lies ln the pelvis.
110
FTG · 54·
WOUND L'\ THE FRONT \VALL OF THE
Wizen the z"ntestill es or ot/ler organs protrude tllIough the \\ ound, whether vertical or bend knees raise the shoulders, and apply IJl1t, a towel, 101 wool wralJped in soft linen, and keep t 1e

1I3
patient warm untIl the doctor arrives. 'When there IS no protrusion of organs, if tlze wound is 7. Jcdz'cal, lay the patient flat on the back 'with the 10\\ er Ii m bs straight; if th e wmozd is transverse, bend the knees and raise the shoulders.
I J URIES T0 THE ORGA . ·S ,VITHIN THE ABD0:.\IE. AND PELVIS.
Inj u ri es of the Stomach are attended by extreme collapse and sometimes by vomiting of dark blood like coffee-grounds . For treatment see " from the Stomach 1/ (page 98).
Inj uries of the Liver, Spleen and In t est ines may be caused by a blow, a stab or a bullet; the liver or spleen may be injured by a fractur e of the lower ribs. The igns and ymptoms are those of internal hcemorrhage accompanied by pain and swelling at the seat of injury, and the treatm ent is as for that condition ( ee page 95).
Th e Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a crush, blow, stab or bullet. Blood may escape " 'ith the urine, and there may be pain and swelling over the injured kidney.
Th e Bladder may be injured by a fracture of the p elvis. The signs and symptoms are either inability to pass water, or if a little is passed it is tinged \\ ith blood.
112
Il4
TREATMENT OF IN JURY TO THE KID NEYS OR BLADDER.
1.- Keep the patient quiet until the doctor arrives.
2. - Apply hot fomentations over the painful or injured part. . Rupture (hernia) consists of a protruslOn of an mternal organ, usually the bowel, through the c ular wall of the abdomen, most fr equently .at th e groin. Should a sudd en by pain and sickness take place In that region , I.-Send for a doctor instantly.
2.-Lay th e patient down with the ralsed.
3.-Apply ice or cold water dr ess mgs to the affected part.
QUE TIONS ON CHAPTER IV.
TIle nUlJ/ erals i n dicate the pages 'When th e answers lila)' be ),o lf11 d .
\Yh at is a bruise ? II

State general treatment for burns and scalds I03. 10-1
J l ow w ould )'on treat a hurn caused I)), a C01Tosil'c acid? .
Ir OI\' would you ,reat a burn cansed by a cOl)'Llsi\'c alkali? 104 ',\' hal steps shou ld taken \\ hen a \Ioman's dress catches fi r e? . . ... lOS
State the general rul es fo r treatment of w ounds can.ed by poisonous hiles or weap ons 106. 107 ,Yhat special treatment i required for th e bite of ;, venomous snake? ..
TLm \vould you treat a sLing? ... 107. 10, ;;Iate the signs, symptom!:> and treatment of frost,bite ... lob \\'odd you attempt to r emo\'e a needie embedded under the skin? '. ...... .. lOS
110\\ would you extract a fish hook emhddecl in the skin? ... I09
Stat c the treatment [l.r injuries to joints... ... ... I09
State the general r ules [or rcm o\'ing n [oreii;n bocly from the eye... ............ I09, IIO
\\'hat would you do if a picce ot sleel \\'Cre cmhecltktl in the eye 1)3.1\ ? 110
An rl when quick, lim e is i n the eye? I lO
lI ow w ould you try to r emO\'C an insect from the La!' passage ?... I I (
i 15
PAGE
treat
c;e? 102'
0 \\ \\ ou ld you
a l lrui
he camerl ? r02
ed? lO2
I l ow maya burn
JI ow is ascald CUI
r03
\\'h:1.t i., the great c1:1.nger of a burn or scald?
104
h . [. of foreign lJOrly
\You ld you try to remove any ot el onn 1 ro. I r I [ro111 the ear passage? .. :. b' d ? II 1
How would youd its contents? 111
Slale the boun anes 0 [h bdomen II2, Il3
State the intestines be
How may ll1JulIes 0, .. ". II3 caused? ", ". "t f injuries to \i\·hat is the differendce spleen and the stomach an 0 Injun ... II3
. intestines? "f'..::' to the 114
Slate the treatment 0 lllJUI.les ... t 14
Slale the lreatment of hernIa .. , ... .. ,

CHAPTER V.
THE NERVOU SYSTE L
Two systems of nerves, the Cerebro-spinal and the Sympathetic, regulate the movements and functions of the body.
The Cerebro-spinal System is made up of the Brain, the Spinal Cord and Nerves, and through its agency sensations are received and the will causes the action of the voluntary muscles. For example when a part IS injured a sensation of pain is conveyed to the brain by the nerve, thus affording an indication of the seat of injury, or a warning of a possible danger of further damage. On attention being directed to the in jury, an attempt is instantly made to ease the pain or to move the injured part from danger.
The Brain is situated within the cranium, and IS divided in the middle line, so that, with the exception of wme connecting bands, the right and left sides are separate.
The Spinal Cord is the long cord of nervous matter lying within the spinal canal (see Vertebral Column, page 23). It leaves the brain through an opening in the base of the cranium and extends to the upper lumbar vertebr:e.
TI6 PAGE
lI 7

II8
The Nerves proceed from the train and cord in pairs as pearly-white trunks, and their branches can be traced throu ghout the tissues of the body. Vvhen a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nerYOUS chain on each side of tLe front of the spinal COlll IT n along its entire length, and sends branches to all the ")rgans of the chest and abdomen to control tl:e nvoluntary muscles, and thereby regulate the vital unctions. This system is not under the control Gf he \\ ill, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air reaches the lungs by \Yay of the (or mouth), the throat, the \\ ind-pipe, and the bronchial tubes. Th e nostrils convey it to the back of the throat, whence it enters the \\ ind-pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, however, the valve fails to act, that should solids or fluids be given by the mouth, they may enter the wind-pipe and cause asphyxia. The \-\'ind-pipe extends to two inches below the top of the breast-bone, where it divides into the right and left bronchial tube. Each bronchial tube enters a lung and divides into small and still smaller tubes, until
II9 F1G. 55. THE LUNGS A D DROKCllIAI. TUllES. A. Tr:t::he3., or \Vind-pi e B L Bronchus D ' II. B p. . . eft Bronchus . . n11. el rOl1chml Tllbes.th e ultimate recesses of the lung-the air cells or ai r spaces-are reached.
The Lungs, Right and Left, occupy the greater part of the chest; they lie immediately \\itbin tbe nbs. and practically wherever a rib is felt, wbetber front, back or sides, there IS lung beneath. Each lung is enveloped in a fine membrane (tbe plmra) \\'blch a110\\"5 It to moye \yitilln the chest during breathing \ylthOUl frictIon.
Respiration , or breathing, consi'lts of two acts, Inspiration , an expansion of the chest, during which air is drawn into the lungs, and Expiration , a contraction of the chest, during \\ hich an leaves the lungs. A pause follows the act of expiration. In health fifteen to eighteen brenths are taken per mInute, and at each inspiration about 20 to 30 cubic inches of air enter the lungs, and a similar quantity IS e"pelled at each expiration.
The expansion and contraction of the chest a1 e effected partly by th muscles of respiratlOn aW\ched to the ribs, but chieny by the Diaphragm, the large a rrh ed muscular partition \vhich separates the chest from the abdomen. In inspiration, which is chieRy a muscular act, the nbs are raised, and th e ::11'ch of the diaphragm falls and becomes fbttened, thus 111creasing the capaciLy of the cbest and causing the air to enter. In e\.piration, an act performed almost wIthout effort. the ribs fall and the arch of the

121
diaphragm rises;. thi lessens the capacity of tbe c.hest forces aIr The mechanism of respirat10n IS somewhat like that of ordinary household bellows, but without a valve; the ribs may be c?mpared to the board of the bellows, while the to the leather, the air pass, a:;,es belt1g eqUIvalent to the nozzle.
. A tbe blood depends upon the air for its purificatIOn a.nd oxygen. necessar) to mainta.in life interferen e wlth brea t hLl1g \'er)' soon may procluce a state aspby\:ia, examples of which ale afforded by drownLl1g, suffocation chokinCT etc , :;".
ARTIFICL\L RE PIRATIOl-J.
PROFESSOR ,--'CH METHOD .
I. -:- Make no attempt to loosen or remO\'e clothmg.
2',- Lay the flatient in a prone position (t' .c., back upwards) wllh hIS head tulned to one side so as to hI ' nose and mouth away from the No pad IS to be placed under the patient neeci tbe be drawn out, as it will fall
3.- Kneel at one side facing the patient's and place p:tlm. · of your hancJ on his lOIllS, one each 'Ide, the thumbs nearly touchin()' ol:e an?ther ID, the small of ba.ck, and the 10\\ est nbs. Leaning your bod\' fOr\\ard, let Its weIght press straIght do\\ u\\ards upon the
120
1 22
loins and lower par t of t h e back , th u s compressi n g the abdomen against th e ground a n d d riving air out of the chest. T his produces expiration (Fig 56). Draw back

FIG. 57. bSPIRATION.
1 2 3
your body somewhat more rapid ly and relax the p ressure, but do not remove yo ur hands ; th is du ces in spiration (Fig. 57).
4. - A1ternate these movements, by a rhyth mic swaying backwards and forwards of your body, t welve t o fifteen times a minute, persevering until respiration is restored , or a doctor pronounces life to be extinct
DR. SILVESTER ' S METHOD.
I . Adjust the patient's positi on .' Vithou wasting a moment place the patient on his back on a flat surface, inclined if possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the cor sets in women. Raise and support the shoulders on a small, firm cush ion or folded article of dress placed under the shoulder-blades.
2. Maintain a free entrance of air into the windpipe.-Cleanse the lips and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position.
3.-Imitate. movements of breathing.
Induce IllSpzJ'atlOll.-KneeJ at a convenient distance behind the patient's head, and, grasping his forearms just below the elbow, draw the armS'
FlG. 58. I SPIRATION.

F[G. 59. EXI'IRATIOl'<.
12 5
upwards, outwards, and towards YOll, with a sweeping movement, making the elbows touch the ground
61. LXPIRATlO.
(Fig. 58). The cavity of tIle chest is thus enlarged, and air is drawn into the lungs.
FlG.Induce expzration .-Bring t h e flexed ar ms slowly fonvard downwards and ll1wards, press the arms and firmly on the chest on either side of the breast-bone (Fig . 59) . By this means air is expelled from the lungs .
Repeat these movements .deliberately, and perseveringly about fifteen a mmute.
\Vhen a sufficient ,",umber of assistants are present, HO\Yard 's method may be combined with Silvester's, as fo11O\\"s ;-
The additional assistant kneels astride the patient's hips 'vvith the balls of the thumbs restin[j on either side of the pit of the stomach, and the fingers graspmg the adjacent parts of the chest . .Using his knees as a pivot, he presses forward on his hands. Then suddenly, with a final push, he springs back and remains erect on his knees while he slo\:\'ly counts I, 2, 3. These motions are to be to correspond with th ose being perfor med by met hod, pressure on the chest being made Slm ultaneously by those performi ng the h,·o methods ( F igs . 60 and 61).
LA BORDE ' S M ETHO D.
'Wh en from any cause th e ab ove m ethods cannot be carri ed out, L aborde's meth od of ar tifi cial respiration sho ul d be tried . It is especially u seful in children and wh en the ribs are broken.
T he patient is placed on his back 0 : sid e ; the mo uth cleared; the tongue is seized- u sing a handkerc h ief or something to prevent it slipping from th e fingers-the lower jaw depressed ; the tongue pulled forward and held for two seconds in th at position, then allowed to recede into the mouth, T hese movements should be repeated about fiftee n times a minute.
Artificial respiration must be continued until breathing is established, or until a doctor arrives.
'When natural breathing com menees, regulate the artificial respiration to correspond with it. SUCCCSg may resull even after two hours' time .
Exc ite resp irat ion . - 'Whilst artificial respiratIon is being applied, other useful steps may be employed, such as applying smelling salts or snuff to the nostrils, and flicking the chest with a damp to\yel.
In duc e ci rc ulation and warmth after natural breathing has b een restore:d. \Yrap the patient in dry blankets or other covering, and rub the limbs energetically towards the heart. Promote warmth by hot flannels, hot-.water bottl es, or hot bricks ,(wrapped In flannel) applIed to the feet, to the limbs and body ' VheD the power of swallowing has returne d give hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep. Large poullices or fomentations applied to the
126
1
2 7
front and back of the chest will serve to assist breathing.
Wat ch th e p atie n t carefully for some Lnne to see that the breathing does not fail; should any slgns of failure appear, at once begin artificial respiration.
IN EN IBILITY.
U nc o n sciousn e ss o r Insensibi lity may arise as follows :-
Injury to the Head. -Concussion and Compression of the brain.
Di s ease o f the Brain.-A.popJe,<y, Epilepsy, Hysteria.
Va rio u s Causes.-Shock, Fainting (Syncope), Collapse, Alcobolic and other poisoning, Sunstroke and Heat-stroke, Infantile Conyulsions, Asphyxia
GEiERAL RULE' FOR TREATMENT OF IN 'ENSIBILITY.
:'. -If a pers o n app e a r s about to lose co nscio u sness, prevent him frOlT! falling, and lay him gently Ju\Vn,
2.-Arrest when apparent; attending to minor injuries is less important than treating the unconscious state.
3.- Lay the patient in the positio n in wh ic h breath ing is most easy-usually this will be on the back, or inclined to one side. As a general rule

129 ,
raise the head and shoulders sliglztly when the face is fl ushed, and keep the head lo\\' when the face is pale.
4.- Undo all tight clothing round the neck chest and waist, unfastening the braces and top button of the trousers in men, and the corsets in women, the object being to relieve pressure on the air passages, lungs, heart and abdominal organs . Be sur.e that there is no obstruction to the air passages by the tongue or by a foreign body in the throat. The possibility of false teeth obstructing breathing must be considered .
S. - Provide for a sufficiency of fresh air by opening don!"s and windows, and by keeping back a crowd .
6. - When breathing cannot be apply artificial r e spiration.
7·- 0btain a doc t or's help as soon as possible.
8.- UnJess unavoidable, never leave the patient until you have placed him in charge of a responsible person.
9·- Give no food or fluids whatever by the mouth while the patient is insensible.
lo. - Should the spine or an important bone of the upper or of the lower limb be fractured, it must steadied and maintained at rest as soon as possible. Should the unconsciousness be pro longed, th e patient may be removed in a recumbent position
128
to shelter , p r o v ided t ha t th e broke n bone is adeq u ately suppor t e d. .. .
II.-When the pabent 1S m a state of .convulsion , support his head, and ' :'rappll1g a piece of wood o r any other hard materIal 111 .handkerchief hold it in his mouth to prevent bltll1g of the tona'ue. Do not forcibly restrain his limbs; prevent from hurting himself by him away from a source of danger, such as machll1 ery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way.. ..
12.-0n return to co n SClOusne s s nw) be Diven to drink. If the pulse is fe e bl.e "arm tea b or coffee, provided h<emorrh? ,Q,e, eIther ll1ternal or external, is n ot present. A deSIre t? sleep. sbn.uld be encouraged, except in cases of pCJJsotllng, a condition tkLt may generally be by the hisLOry of the caS2, and also by the pu plls of the eyes (the black openi ngs in g.rey, bl LIe or bro\\ n iris) bein(T minutely C,)J1tracteli (pll1-head pupIls). tf
13.-It mu st n ot be assumed a person is ins en s ib le a s the re s ult of dnnk merely b ec ause th e breath s mell s of alc oh ol i freCjuc.ntly when people arc fceling ill tll ey take or are glyen alcoholic sLmulants, after which they may become insens ible, not frol11 the drink, but from the cause that induced them to tLlke it, for example, insenslhdity (,,)111 i I1 6 on, effech::; of pJisoning, etc. E,'e n if

1
drink is belie,'e d to be the actual cause of III ensibilitv, it must be borne in mind that the patient IS in a dangerous state, and he must be treated for Collapse by being cm'ered up and kept" arm.
The above general rules will enable first aid to be rendered efficiently in most case of insen'ibility, although the exact form from which the patient IS suffering is unknown.
CONCU SIOl OF THE BRAE.
The patient may be stunned by a blow or fall on the head, or by a fall on the feet or lower part of the spine. He may quickly regain consciousness, or insensibility, more or less complete, may be prolonged.
TREAT:'IIE IT.
1. - Apply the general rules for the treatment of Insensibility.
2.- Be very apprehensive of danger in all cases of injury to the head. The pJti e nt may be stunned, and after a short interval may recover some degree of consciollsness, or even the brain may apparently haye es aped injury ; yet in both instances there is a grave risk that a structure \\ ithin the cralllum bas been injured, and that a serious tate of insen ibility may develop later (See Fracture of the Crani um, page 43 ) . A caution should therefore be giYen to a patient \\'bo has lost consciousness even I) 2
130
I3
for only a moment after an injury to the head not to resume physical or mental activity without the consent of a doctor.
COMPRESSION OF THE APOPLEXY.
Compression of the Brain may result from the same causes as produce Concussion; in fact, Compression is frequently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no signs of injury are necessarily present..
In both conditions the face IS flushed; the breathing stertorous; one side of the may be more limp than the other: and the pupIl of one eye may be larger than that of the the ture of the body is generally raIsed.
TR EA DIENT.
I.-Apply the general rules for treatment of Insensibility.
2. - Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be taken not to burn the patient v;ith the bottles, which should be \\ rapped in flannel, and their heat tested with the elbow.
EPILEPSY.
Epilepsy may occur in . persons of any age, but usually occurs in young adults. The patIent falls to

I33
th e gro und, sometimes with a scream, and passes into a state of convulsion, thro\\'ing his limbs about . The treatment is according to the General Rules, especially Rule I I.
HYSTERICAL FITS (HYSTERIA).
SIG:'-lS .\.1 TD "- Y
The patient; usually a young girl, in consequence of mental excitement, suddenly loses command of h er feelin ers and actions. he subsides on a couch or in comforta ble position, throws h erself about, grindi ng her teeth, clenching h er fists, shal-ing her hair loose; she clutches at anyone or anything her, kicks, cries and laughs alternately. The eyeballs may be turned upwards, and the eyelids op ened and shut rapidly. At times froth appears at th e lips, and other irreguhr sym ptoms may develop.
I.-Avoid .sympathy \\ ith the patient: and speak firmly to her.
2.-Threaten her with a cold water douche, and if she persists In her" fit," sprinkle her \\'ith cold waLer.
.i·-Apply a mustard leaf at the back of tbe neck. Medical tr ecltrnent is necessary to cure the condition of mind and body ",hich gives rise to hysterical atta.cks.
SHOCK, FAINTING (SYNCOPE), COLLAPSE.
CAUSES.
I.--Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and severe crush are some of the more frequent physical causes of shock.
2.-Fright, anticipation of injury, and sudden bad news, or sometimes sudden removal of fear and anxiety after prolonged produce shock or fainting.
3. -Some pOlsons cause shock, ",hile others, such as alcohol, so depress the nervous system that collapse ensues.
4.-Hremorrhage or heart weakness, a close or cro wd ed room, tight clothing, fatigue, or want of food may bring on fainting or collapse.
SIGNS A D SnfPTQ;\Is.
The general condition of shock may be recognised by extreme pallor, a feeling of cold, clammy skin, feeble pulse, and shallow breathmg accompanied, I.f hremorrhage has been severe. by yav1ning and sIghing. The term "collapse" signifies a very serious condition in wh ich the life of the patient is in the greatest danger; the tem perature of the body falls below the normal, and one great object of treatment is to prevent it sinki n g to a point at which life is i mpossible. An attendant danger of the condition of

collapse is the liability to sudden relap e after a lemporary improvement, and the utmost care and watchfulness must therefore be exercised to maintain the heat of the body and to guard against failure of the heart and lungs.
TREAT:\lE:\T.
I.-Remove the cause by arrestill" to injuries, loosening all tight clothespeCIally about the chest and abdomcll, remoy111g from a close or crowded room, using encouraging word, etc.
2.--Lay the patient on the back with the low. the lower limbs; the patient IS 111 bed thIS IS best done by raising the foot of the bedsteau.
3.-Provide for a free circulation of fresh air.
4.-If hcemorrhage has been severe and the patient is collapsed, firmly handage the limbs from the toes to the hips, anu from the fingers to the artllpits . To stimulate the action of the heart, sal volatde and water may be given if the patient CC1n S\\ allo\\", or smelling aILS may be held to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of temperature below the norl1181 point To accomplish this cover the patient witb extra clothing, or by placll1g
134
135
ru gs or blan kets over him; get him to bed in a war m bu t well-ve n tilated room as soon as possible, Apply warmth to the feet and to the pit of the stomach by h o t wate r bottles or hot flannels. (Test the heat of these with the elb ow before applyll1g them. ) If t he p atient can swallow, glve hot dri nks, such as milk, tea or coffee. J t is well to add sugar, as it aids ir raising the temperature of the body.
7. - If breathing cannot be discerned, apply artificial respiration.
8. - If want of nourishment has been the cause of fainting or colbpse, give food sparii1gly at first .
SUN3TROKE A D HEAT- TROK'E.
'When exposed to great heat, as in the stoke-hole of a steamer, especially 111 the tropics, or to the rays of the sun during a march in very hot 'weather ,,,hen heavily burdened, persons may develop slckness) faintness, giddiness, and difficulty in breathing . The patient complains of thirst, the skin becomes dry and burning, the face very flushed, the pulse quick and bounding. A very high temperature, stertorous (snoring ) breathing, and insensibility may ensue.
TREATMENT .
1. - Undo all tight clothing ,
2 . - Remove the patient to a cool, shady spo t.

137
3.-Strip the patient to the ,\·aist. the patient do\\'n, with the head and trunk vye ll ralsed.
. 5.-Procure as free a circulation as possible of fresh alr, and fan t!1e patient vigorously.
6.-Apply lCe bags or cold \\ater freely to the head neck, and spine, and maintain this treatment untii the sym ptoms su bside.
7.-0n return to consciousness, the patient may ha.\'e water to drink.
CO VULSIONS IN CH I LDREN.
Teelhmg or stomach troubles are the C0:11mOnest auses of this ailment.
IGNS .
pasm of the muscles of the lim bs and trunk blueness of the face, insensibility, more or Ie plete, and occasionnlly squinting, susp nded re piratlon, and froth at the 11loulh are the prominent sIgns.
TREATi\lENT.
1.- upport the child in a \\'arm rath sliallL ly above the tcmperatur of the b ody (98 degrees), so that the \', aLer reaches Lo the middle of the trunk.
2.-Place a sponge dipped in cold \yater on the top of the head.
135
!.i 8 ASPHYXIA.
'Vhen, owing to want of air, the blood is not supplied with oxygen the pati en t becomes insensible, 2.nd is said to be asphyxiated . This condition may be brought about as [0110\\ S : -
I. Obstruction of the air passages.
(a) By DROWNING.
(b) By PRESSURE FROM OUTSIDE: Strangulation, hanging, smothering.
(() By.'I. BODY IN THE THROAT: Choking.
(el) By S \,ELLll'\G OF THE TISSUES OF THE THRO.-'l.T: Infb.mmatloll, scald of the throat, poisoning by a corrosIve.
II. Inhaling poisonous gases. By coal gas (as used in tbe house), producer, or water, gas, smoke, fumes from a charcoal or coke fire, se\\ er £!;::lS, limekiln gas, carbonic acid gas.
III. Pressure on the chest, as wben crushed by sand or de bris, or by a crowd .
IV. Nervous affections, as the res ult o[ narcotic and certain other poisons, collapse, electric shock, or by lightni1l8·
GE:\ TRE,\·nm;\lT.
In all cases of .\sl_byxia attempts must be made to remove the cause, or to rem:)Ve the pltient from the cause. 'When thi :, has been dOl1l"! artificia)

139
respiration must be applied, taking care that the [llr passages are not obstructed , and that there is ubundar!ce of fresh air.
DRO\\' ' I I-G .
P ersons completely imnl.ersed in water for even te1\ or fifteen minutes have been restored by artificial means. Therefore, if the body is rec0i'ered \\'llhin a rea onable time, absence of signs of life is not to de' immedi ate attempts to r estore animation .
The first thing to do when the body is recovered is to get rid of the ,,·uter and froth obstructing the :J.ir and then artificially to restore breathing. ThIS is best accornplishe 1 eithe r by proceeding at once to perform artificial r espiratio n by 'chMer 's or as follows :-
I.-As quickly as possible loosen the clothing, and c1e].r the mouth and the back of the throat.
Z.- Turn the patIent face downwards, with a pad below the chest, and with the forehead upon the rIght for ea rm.
3.-,\Yhilst in this position opply pressure by the h a nds to the patient 's back over the 10\\'er rIb , and kcep the pressure up for three seconds .
4.-Turn the ]Jaticnt on the right side) maintaining that position also [or three seco nds.
s.-Repeat these movements alternately as lon a 8.S froth and \\ater iss ue from the mouth. b
140
These operations (Marshall method) in 'themselves tend to promote respIration, but "'.hen th,e air passages are clear of and water SIlvester s method of artificial respiratIOn may be used by itself or with Howard's method in conjunction.
While performing th ese operations send someone to the nearest house to procure blankets and dry clothing, hot water bottles, etc., and to fetch a doctor.
TRANGULATlON.
Cut and remove the band constricting the throat. Apply artificial respiration.
HANGING.
Do not "\'ait for a policeman: the lower limbs and raise the body to take the tenSIOn off the. rope; cut the rope, free the neck; apply artificial reSpIratIOll.
MOTHERI TG.
Remove \\hatever is smothering the patient: apply artificial respiration.
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to the back of t?e and attempt to dislodge the foreign body; If VOlTIltmg results, so much the better. If unsuccessful, thump the hard whilst the head is bent forward. Apply artIfiCIal respiration.

141
SWELLING OF THE TISSUES OF THE THROAT.
Whether the swelling is caused by inflammation by swallowing. very hot as not. infrequently happens to chIldren attemptmg to dnnk. from. the spout of a kettle, or by the effect of a corrOSIve pOlson, the treatment is as follows :-
I.-Apply a sponge, piece of flannel or other cloth, wrung out of very hot water, to the front of the neclc. g from the chin to the top of the breast-bone .
2.-Set the patient before the fire.
3.-Give ice to suck if it can be had; if not, gIve cold water to drink.
4.-Give animal or vegetable oil, a dessertspoonful at a time, to soothe the scalded throat and ease the pam.
5.-If breathing has ceased apply artificial respira< tion.
SUFFOCATION BY SMOKE OR GASES
I.-Remove the patient into the fresh air. Before a building full of smoke tie a handkerchief, wet if possible, round the head so as to cover the nose and mouth. It is well to move slowly, keeping low, or even crawling, whilst in a room full of smoke in search of a suffocated person. Every opportunity of letting in fresh air by opening doors or window! should be seized.
2.-Apply artificial respiration.
3·-1n the case of producer or \':a ter r::s, inllab.tio n of oxygen will also be necessary. '-
ELECTRIC SHOCK.
Electric current is conveyed by a cable \\"ire rai l or bar, called the "Positive," and retu:ns source of supply by another cable, \-vire, rail, or bar, called the ,e egative," or through the earth. In the case of an electric railway, the current is generally conveyed by an insulated rail the third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an elec tric tramway it is fr eq uently conveyed by an overhead conductor or trolley \\-Jr e, and r eturned through th e running rails.
Throu gh contact with a " positive" the shock may be so severe as to cause ins ensibility, aml the sufferer will be unable to ex trIcat e himself, and must be liberated with all possible spee d. As it is generre,1]y impossible or in exped ient to switch off the current some other m e thod must usually be adopted; but prtcautions must be laken or else the person r ende ring assistance will himself receiv e a shock.
To liberate the sufferer frolll contact-
I.- Insulate yourself £room th e e arth by standing on "ins.ulator" or " non-cond ucto r," th at is, a. body \\"hlch resists the current. AmOngst such DGuit::

I43
are incliarubber, dry glass, dry bricks, dry silk, dry cloth, dry wood and dry hay or straw.
2.- Protect your hands from contact w ith the sufferer or the electric medium by covtrins th e m with an insulator. Although indiarubber is probably the best insulator, do not waste time in running for indiarubber gloves, but use dry articles of clothing; an indiarubber tobacco pouch or cap, or folded newspaper, would serve to protect the hands in an emergency . If no means of insubting the hands are at hanu an attempt may be made to drag the sufferer away by means of a loop of dry rope or a crooked stick; an umbr ella is not safe because the metal ribs would act as conductors* of electriritv, :1nd it is not infrequently the case that the" stick" of the umbrella is a metal tube.
3.- P ull the sufferer a way from contact. Care should be taken to avoid touching with naked :lands the sufferer's baneI-;, wet clothing, or boots if the so les are nailed. The armpits should be aVOided as perspiration usually makes the clothing camp there.
\Vhen the sufferer is removed frolll contact -
I. - Apply the g eneral treatment for inse n-
.j;. A conductor is a body through which electricity readily passes. Amongst such bodies are copper, brass, iron, moisture '1nd one's own body.
144
sibility (loosen clothing, procure free circulation of air and place in a recumbent position).
2. - Dip a towel in cold water and attempt to arouse him by sharply flicking the face and chest.
3. - Commence artificial respiration if other m ethods fail to restore animation. "Laborde's" method (see page 126) has been found to be very su ccessful.
4.-Treat burns if there are any (see pages 10 3, t:04)·
EFFECTS OF LIGHT?\I ' G.
A person struck by li ght ning is us-ually more or less deprived of consciousness. The tr ea tment is the same as that for electric shock, except, of course, that the instructions for the patient from con tact with the electric medium do not apply.

145
QUESTIONS ON CHAPTER V.
Tile nllmerals indicate the pages where tile answers ma}1 be found.
vVh at are the two systems of nerves? ... ' "
Of what is the cere bro-spinal system made up ? . ..
What is the spinal cord?
What are nen'es like ? ...
Explain the sympathetic system
Expla.in the respiratory system
Explam the acts of respiration
How are the exp::msion and contraction of the
effected?
In what system of artificial respiration is the patient laid back upwanb?
In what systems is he laid on his back?
In what system is he laid on his hack or side?
In what system is he rolled alternately on his side and face downwards?
TIoW" long should artificial respiration be perscnred \\ith?
'What is exciting respiration? I27
'What is inducing circulation? ...... I27, 12
'Why is it necessary to watch the patient? !low may insensiiJility arise?
State the various forms of insensibility
State the generall11les for treatment of insensibility I28 to I "I
Would you examine the patient to sec if any bones \\ere J broken?..
'''hat wrong opinion may be (ormed \\ hen the patient smells of drin k ? ... ...
Is collapse from drink a serious condition?
\Vhat is concussion uf the brain?
PAGE 117 117 11 7 JIg II 118 to 120 120
...
... ... '" ... . .. 120 to 121
chest
... ... ... ... ... ... 121
... ... 123, 1 26
.. .
7
I 2
... ... ... ... 139, 140
127
... ...... 128
... ...
128
........ 129
...
... . .. 1:)0 13 1 13 1 State
for treatment of concus::;ion 13 1 , , 3 2
lhe rules
What danger accompanies injury to the head?
What caution should be given to a patient who has lost consciousness, even for a moment, afte r an injury to the head?
What are the causes of compre<sion of the brain?
Un what aged people does apoplexy usually occur?
"'bat are the signs and symptoms of compression and apoplexy?
"tate the rules for treatmenl of these conditions ...
"\IVhat dangf'r is there in applying hot water bottles to insensible persons, and what precautions should be
uescribe a case of epilepsy 13 2 , 133
Yvhat special care must be taken in treating a case of epilepsy? 130, 13 2
Describe a hysterical fit 133
How would you treat a hysterical fit?
What are the comn1flneSl physical causes of shock?
What may produce shock 01 fainting?
What conditions do certain poisons bring about?
What may bring about fainling or collapse? ...
How would yuu recognise the general condition of shock?
What special precaution must be taken in the case of collapse?
State the treatment for shock, faintmg (syncope) ard
collapse .. , ... 135, 136
Wh;)t is the effect of sugar on the temperature of the body ?
What are the causes of sunst roke and heat-stroke?
State the treatment for sunstroke and heat-stroke
vVhat are the causes of convulsions in children?
What are the sign of convul ions in children? .. .
State the treatment for convulsions in
State fully the
of asphyxia

What two things have to be done in all cases of
What two things mu sl be seen to before it is possible for artificial respirati on to do any good?
Is artificial respirati on likely to do any good if the air passages are obstructed, or jf the re is not abundance of fresh air?
What is the first thing to do in a case of drowning-?
[39 By what method may artificial respiration be performed without taking any previous steps ?
What steps must be taken before proceeding wit h
should be done while artificial respiration is performed?
How may a swelling of the tissues of the throat be caused?
State the treatmen t for swelling of the tissues of the throat [41
State the treatment for sllff"cation by smoke or gases q [, [42 How is electricity conveyed? £42
How would you liberate a sufferer from contact with an electric medium? 14 2 , [43 What would you do when the sufferer was removed from contact?
What would yon rio in the case of a lightning stroke?
l'AGE 13 1 13 2 13 2 13 2 13 2 13 2 taken? ... 13 2
. ..
133 134 134 134 134 134 135
... ... ... ... .., ...
children
... 136 136 137 137 07 137 138 PAGa
... 138, 139
causes
asphyxia?
... ...
139
... ...
... ... ... 139
... ... ... ... ... 139 'What
[40 State
140 State
[40 State the treatment for smothering 140 State
140
...
[39
...
Silvester's method?
the treatment for strangulation
the treatment for hanging
the treatment for choking
...
I4J
143
144
...
1-1-8

CHAPTER VI.
POISONI G.
Poisons may be classified accordin:>; to their treatment under t\\ 0 heads :-
I. - Those which do not s t a in t he mou th, and in the treat m e nt of w h ich a n emetic is to be g iv en . Amongst these are :-
(a) Phosphorus (containell in rat poison and lucife r matches), Tartar emetic ::md
Corrosive Su bhmate, \\ hich cause a metallic taste in the mouth and a burning pain in the mouth, throat and stomach .
(b) Strychnine, Prussic Acid, Belladonna (deadly nightshade plant) and several other vaneties of plants, such as laburnum seeds, etc . ; these give rise to cOlwulslOns, delirium, failure of respiration and coll<lpse .
(
c) Poisonolls meat, fish and fungi (often mistaken for mushrooms). Suspicion of these poisons should be directed to cases ,\ he r e several persons who have partaken of the same food develop simila.r signs and symptom s.
(d) Alcohol, which may cause cullapse.
(e) Opium and its preparations, Morphia,
149
Laudanum, Paregoric, Chlorodyne, Syr u p of Poppies and various soothing drinks an d cordials; . these cause a tendency to go to sleep, whlch continues until sleep becomes. deep and breathing stertorous; the pupils of the eyes become minu tel}' contracted (l;inhC'.1(1 pupIls).
2 .-Those which burn or stain the mouth and in t he tr e atment of which no emetic is b e given . These are of two classes :-
(a) Acids, as Titric Acid (Aqua fortis), A cid (Oil of Vit riol), HydrochlOrIC, or Muriatic, Acid (Spirits of Salt)}
S:a rbolic Acid (Phenol) . OXCllic Acid, whIch IS contained in oxalate of potash, salts of sorrel, salts of lemon and some polishing pastes .
(l)) Alkalies, such as Caustic Potash, Caustic Soda and Ammonia.
SU\Il\IARY OF SIMPLE DIRECTIOl'\S FOR TIlE TREATMENT OF
I. -Send fo r a doctor at once, s tating wh at ha s occurred and if poss ible t he name of th e pois on.
2. - Except wh e n the lips and mou t h are stained or bu rne d by a n aci d or alkali "
ISO
promptly give an emetic- that is, make the patient vomit as follows :-
(a) 71:ckle t lze back of tIle titroat with the finger or WJth a feather.
(b) jlfusta rd- a dessl'rt-spoonful in a tumblerful of luk e-warm water.
(c) Salt-a table-spoonful in a tumblerful of luk e-warm \Yater.
(d) Ip ecaCZlanila TVine - for a young cll ild, a teaspoonful repeated at inten'als of fifteen minutes,
3.- 1n all cases when the patient is not insensible, give Milk , Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, Animal or Vegetable Oil (e xcept in phosphorus poisoning), and Tea.
Oliv e, Sabd, and Cod-liyer oil, or oIl :,uch as th a t in. which .are preserved, may be give n; mmeral machme oIls and pa raffin are ull:'llitable . Oil is sootb ing, and is therefore especially useful in poisoni n g by Acids, Alkalies and such substances as Arsenic and Corros ive ·ll b limate. D emulc ent drinks such as barley waler o r thin gr u el, act in the mann er, and are free from danger in cases of phosphorus poisoning . may be gi yen either before or after the emetic if the poi. on calls for one.
Strong T(:::tacts as a neutraliser of many poisons,

lSI
and is always safe. A handful of tea should be thrown into a k ettl e and boiled .
4.-If the lips and mouth are stained or burned give no emetic, but-
( a) If a n Acid is known to be th e poison give an Alkali at o nce . First wash the mouth out freely with lime water or other alkaline mixture, s u ch as soda, chalk, whiting, or magtlesia or wall plaster in water, and afterwards let the patient sip a little of it. "'oda and potash arc not to be gi';en in the case of poisoning by oxalic aCJd.
( b) If a strond L\lkali IS known to be the poison g Iv e an acid at once. First wash the mouth out freely ,,·ith lemon juice or vinegar diluted \\ lth an eClllC11 q llantity of water, and afterwards let the patient sip a little of it.
I n both cases give oil (Rule 3)'
5. - When a person has swallowed poison and to go to sleep, l:.:eep him awake by walkmg h1l11 about and sb.pping his face, nee k o.nd chest with a wet towel. Strong black coffee may be given to drink. Slapping the soles of the feet may also be tried.
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7. - A pply artificial respiration if breathing cannot be discerned .
8. - Treat shock and collapse.
9. - Preserve any vomit ed matte r, food , or other substance, suspe cted of bei ng the poison. Do not wash vessels which may have contained the poison, and carefully guard them.
Certain poiso ns require special treatment, and a few of the commoner of these are mentioned below with their treatment.
CARBOLIC ACID .
The odour of the breath "vill aid in the detection of this poison; the lips and mouth are usually whi1:e, and several nervouS symptoms come on.
TREATMENT.
1.- Give milk, to a pint of whIch half an ounce of Epsom Salts has been added.
2.- Treat according to the general rules.
PRUSSIC ACID.
The action of this poison is extremely rapid. Giddiness, staggering, insensibility accompanied , by panting respiration, profound collapse .and con vulsions are the general signs, and 111 addltlOn a smell of bitter almonds is often present.
TREATMENT .

.
I . - Place the patient in the ®pen air. 153
2.- Dash cold water on the head and spine cone tmuously.
3.-Apply artificial respiration.
4.-Hold sllelling salts to the nostrils.
5.-Treat shock and collapse. (See page 135 ·)
POISO OUS MEAT, FISH AND FUNGI.
,The signs an? symptoms are vomiting and purging (dlarrhc:ea), colIc, great weakness, raised temperature and a qUlck pulse.
TREATl\lE l T.
I.-Give an emetic,
2.-When the emetic has acted, give castor oil.
3·-Treat collapse. (See page 135.)
STRYCHNI E
. !he signs and symptoms are a feeling of suffocatlOn\ features, and convulsions. The patient rests on hIS head and feet, and the body is arched.
TREATMENT.
I.-Give an emetic.
2.-Apply artificial respiration.
ALCOHOL.
I.-Give an emetic if the patient can swallow.
2. - Treat collapse by keeping the patient warm g etc. (See page 135.)
152
QUEST I ONS ON CHAPTER VI.
Tlu numerals illdicate die pages wizen tlte a n swe1'S m ay be found .
Under what two head may poisons be classified?
\Yhat are the S)'lllPLul1lS of puisoning by arsenic?
"Vhat other poisons give rise to the same symptoms?
I'A(;& 148, 149 148 14 8
\Yhat poisons give rise to convulsion, delirium, failure of respiration and collapse? ...
If several pcople who had partaken of the same food developed similar signs and sympLoms, by \\ hat would you suspeci they had been poisoned ?
';..:":!hat condition may result from poisoning by alcohol?
\Vhat are the effects of such poisons as opium?.. q8,
\Yhat two classes of poison burn or stain the mouth? ...
\\'ould you give an emetic for such poisons?
Name some of the principal acids
Name some of the principal alkalis
State the general rules fJr the treatment of poison, ing
State the best methocls of making a person vomit
How would you treat a case of acid poisoning? ...
How would you treat a case of poisoning by an alkali?
State the signs, symptoms and treatment of carbolic acid poisoning ...
State the signs, symptoms and treatmcnt of poisoning by Prussic Acid 152,
State the sIgns, symptoms and treatment d poisoning by poisonous food ...
State the signs, symptoms and treatment of poi oning by Strychnine
W hat would you do in the ca

BANDAG I I G .
. Esma.rcb's Triangu lar Bandage has been d escribed 111 Chapter II . I t may be a pplied to keep a. dressing on a \\ burn or. of any part of the body, or for an 1I1Jury of a J01l1t.
For the Scalp (Fig. 62) . Fold a hem about dinches deep along the base of a bandage; place the bandage on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down :It the back; carry the t\\O ends round the head abo ve the ears and tie them on the forehead ; draw the pOint first do\\ !1\\,;:uds, and then turn it up and pin it on to
FIG. 62 . the banda.ge on the top of tIle head.
Fo
r
the Forehead, Side of the Head,
Eye, Cheek , and for any part of the body that is round (as the arm or thigh, etc.), the narrow bandao-e shou Id be used, its centre being placed over the
154
149 to 15 2
. . . . .. . . . . . . . ..
e of alcoholic poisoni ng? 150 151 151 15 2 153 153 153 153 ISS
CHAPTER VII.
dressing) and the ends being carried round the head or limb, as the case may be, and tied over the wound.
For the Shoulder (Fig . 63)· P lace the centre of a bandage on the shoulder, with the ooint running

15 7
. For the Hip (Fig 64) . T ie a narrow bandage lound the body above the haunch bones, with the knot on the injured side . Fold a hem accordinO" to the size of the patient along the base of a second ba n dage; place its centre over the dressing, carry the ends round the thiO"h and tie them· then carry the up under
FIG. 65· FIG. 66. first bandage, tu rn it down over the knot an d pin it. the Hand when the fingers are exte n ded ( } Ig. 65)· F?ld a hem along the base of a bandage ; p lacc wnst on, the hem with the fingers towards the pomt ; then brIng the point over the \\ rist pass ends the wrist, cross and tie bnng the POll1t Oycr the knot and pin it to the bandage on the bane1.
156
\
IS
For the Foot (Fig. 66). Place the foot on the centre of the bandage with the toes towards the point; draw up the point over the instep, pass the ends round the ankle and cross them in front; now pass the ends round the instep and tie them. Draw the

FIG. 6Tb.
point forward and pin it to thc bandage on the instep .
F or the Fron t o f t he Ches t (Figs. 67 Cl and 67 b). Place the middle of the bandagc O\'er the dressing with the point ovcr the shoulder on the same side; carry the ends round the \,yaist and tie them;
159
toen draw the point over the shoulder and tie it to one elf the ends.
. the Back. The bandage IS as the foregoing, except that It IS begun at the back .
For the Kne e . Fold a narrow heL11 along the ba e of a bandage; lay the point 011 the and the mIddle of the base Just below the knee-cap; cro s the ends first behind the knee, then the thigh and tie them. Lnng the {,oint clown and p1t1 it to the base (Fig. '68).
FIG. 68.
For the Elbow. Fold a narrow llcm along tllC base of a bandage;. by the POlllt on the back of the arm and the middle of the bn e on the back of the forcarm; cross the ends first in front of the elbow then oycr the arm and llc them in front ' (Fig. 69).
or Fingers and Toes \\ ra p a SUlp of calICO or linen round nnd round the pnrt; split the freeencJ " and secure it rouna the \\ rist or nnk1c.
.' ff(¥! " i
CHAPTER VIII .
METHOD OF CARRYING.
THE FOUR - HANDED SEAT.
This seat is used when the patient can assi. t the b earers and use his arms .
1.-Two bearers face each other behind the patient and grasp their left forearm with th eir ri ght hands and

FIG. 70 . each other's right forearm with their left bands (Fig. 70), and stoop dow n.
2.- Tbe patient sits on the hands and placts one arm round the neck of each bearer.
r 6r
3.-The bearers rise together and step off, the bearer on the right hand side of the patient with the right foot, and th e left hand bearer with the left foot.
Tn E T\\"o-HANDED SEAT.
This seat may be used to carry a helpless patient.
FIG. 71.
I. - Two bearers fare each ol11er and stoop, one on each side of the patient. Each bearer passes hi forearm near est to the patient's head under his back just G
r60
IS:!
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient 's back, and then pass tbeir other forearms under the middle of his thighs (Fig . 71), and clasp their hands by one of the methods sho\\'n in Figs. 72 and 73. A handk e rchief should be held in the hands if the first grip is useu.

F1G. 72.
F1C. 73.
2.-The bearers rise together and step off, th e right-hand bearer with the right fOOL, and the left-hand bearer with the left foot (Fig. 7-1-)'
THE THR}!-E-HANDED SEAT.
This seat is useful for carrying a pntient and supporting either of his lo\\er limbs, when he is able to use h is upp er Ii ll1 hs .
1.-Two bearers face each other behind the patient. For supporting the left limb the bea rer to the patient's right grasps his own left wrist \\ ith his right hand, and the other bearer's right wrist with his left hand. Tlle bearer to the left grasps the first bearer's right wrist with his right hand (Fig. 7 SI' This leaves his
164
left hand free to support the patient's left leg. For the patient's right lower linib follow the same directions, substituting" right" for" left" and" left" for "right.'· The bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3. - The bearers rise together and step off, the FIG. 75. right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE 's L1FT.
(To be attempted only by a strong man).
Turn the patient face down wards; place yourse lf at his head, stoop down, slightly raise his head and
165

FIG 76.
shoulders an::! take hold of him close under his armpits, locking your hands on hIS uack. H.2.ise his body and rest it on your left knee; shifL your arms and, taking him round his waist, lift him until his head rests on your left shoulder. Thro\\' bis left arm over your head, stoop down and place your left arm bet\\'een his thighs , letting his body fall across your shoulder:;. Rise to an upright position; bold the patient's left \\"fist with your left hand and lea,-e your right hand free . ..:-\.ssistance may be given to an injured person by supporting him in the manner shown in Fig . 76.
Til e plalZ of carrying- tlte jatient lry tlte arms a/ld legs the face dO'ZVJlZvartis, aJII/IlLOil[l' called tlte "frogs' marclt, " must never be /lsed, as deatlz JIlay ellSItl! from tltis treatmellt.
blPROVISED STRETCHERS.
A scretcher may be irnprovi 'e d as follo\\'s :-
r.-TLHn the sleeves of a coat irlside out; pass two strong poles through them; button the coat. The patient sits on the back of Lhl! coat and against the back of the front bearer (Fig. 78). If <:l longer stretcher is required two or three coats 111 ust be treated in the same manner. The poles may be kept :tpart by strips of wood lashed to the poles aL both ·;nds of the bed formed by the coats (Fig . 79)·

FIG. 7i.
THE FORE AFT 1\IETHOD.
This plan of carrying is useful when space does not permIt of a hand seat.
166
FIG. 78 .

FIG. 79.
169
2.-Make holes in the bottom corners of one 0. two sacks and pass stout poles through them.
3.-S pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides. Two bearers stand on each side and grasp the middle of the pole with one hand, and near the end with the other. They walk side" a ys.
+-A l:urdle, broad piece of wood, or shutter may be used as a stretcher; some stra\y, hay, or clothing should be placed on it, and coyered "ith a piece of stout cloth or sacking; the latter is u eful in taking the patient off the stretcher.
Always test an im prOi-ised stretcher before use. Stretchers must be carried, and the patient placed on them, as laid down in the "Stretcher Exercises."
As a general rule carry the patient feet foremost. The exceptions are :-
(a) ·When going up hill with a patient ",'hose lo\yeJ limbs are not injured.
(b) ·When going do\\ n hill witb a patient whose lower limbs are injured.
Avoid lifting the stretcher oyer ditches or \\alls, but where these cannot be avoided the stretcher 111 ust be carried in the follo\\ ing \Yays :--
To CROSS A DlTCH.
In crossing a ditch, the stretcher should be lowered with its foot one pace from the edge of the ditch.
168
I70
Nos. I and bearers then descend. The stretcher, with the patient upon it, is aftenyards advanced, Nos. I and 2 in the ditch supporting the front enJ while its other end rests on the edge of the ground above. No. 3 now descends. All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by No. 3 in the ditch. No. I climbs out, No. 2 remaining in the ditch to assist 1'0 3. The stretcher is lifted fOr\yard on the ground above, and rests there \yhile N os . and 3 climb up.
To CROSS A ,VALL.
The stretcher is 10\\'ered with the fool about one pace from the wall. 10S . I and 2 bearers then take hold of the foot of the stretcher, and No. 3 of the head; the stretcher is raised till the fool is placed on the wall. No. I then climbs over the \Y3.11 and takes hold of the foot of the stretcher, \vhile Nos . 2 and 3 support the the stretcher is then carried forward till the '-lead rests on the wall, No. I supporting the foot. Nos. 2 and 3 then climb over the \\"all and take hold of the head stretcher, which is then slowly lifted off the wall on to the ground , and the bearers take their usual places.
.. These num bers are explained laler in the detailed "Stretcher Exerc.ises."

To LOAD A
Th e stretcher is lower ed \yith the foot one p::.ce from the end of the wagon. IOS . I and 2 take hold of the of the No. 3 the head. The stretcher IS then raI sed and carried fOr\yard till the front :yheels .rest on the floor of the wagon. No. I then Jumps mto the \yagon, \\ hile TO . 2 goes to the of the stretcher and helps 1\0. 3. The stretcher IS then pushed slowly into the wagon. If the tailboard cannot be sh ut, the stretcher 111 ust be lashed firmly to the sides of the \\agon.
To UNLO"\.D A ,VAGON.
Nos. 2 and 3 take hold of the head of the stretcher 1 '1 N' , \\' 11 e o. I gets mto the wagon; the stretcher is then gradually dra\\n out till the foot-wheels rest on the edge of the wagon. -'- TO . I jumps out of the ,,'agon, and with TO. takes hold of the foot of the ?tretchcr, _"'0. 3 SUppOI ting the head. The stretcher IS ))?'" gently dra\\ 11 3.\\ ay one pace and 10\\'ered. \\ Jth four bearers TOS I and 2 \\'ould lift the foot ?! the stretcher, while Nos. 3 and 4 lift the head. I hIS t,o cros ing a ditch or wall, as "rell as to loadmg anu unloadinb a
CHAPTER IX.
STRETCHER
TRA I.-PORT.
The "Furley" Stretchers (Model 1899) are of three patterns, viz.," Ordinary," "Telescopic-bandIed," and" Police." In general principle they are alike, the component parts being designated the poles,

SO.-ORDINARY
FIG. 81. -TELESCO PIC-HANDLED STRETCHER- OPEN.
handles, jointed traverse bars, foot wheels, bed, pillo\\" sack and slings.
The Ordinary Stretcher (Fig. 80) is 7 feet 9 inches in length, and I foot 10 inches wide. The bed is 6 feet in length, and the handles 10k inches. The heigh t is si inches . At the head of the stretcher is a canvas overlay (the pillow sack) which can be filled with stra'.\·, hay, clothing, etc., to form a pillow. The jointed traverse bars are provided with joints,
173
for open ina or closing the stretcher. The Telescopichandled patt rn 8I} is very simiIar, but the hanJles can be slId underneath the poles, reducing the length to 6 feet. This arrangement is of great value when working in confined spaces, or when a patient has to be taken up or down a narrow staircase with sharp turns. The Police stretcher is si milar to the Ordinary pattern, but is more strongly made, and has, in addItion, straps for securing a refractory patient.
'Vh en closed, the poles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly folded on the top of the poles and held in position by the slings which are laid along the canvas, and ecured by a strap, placed transyerselyat the end of each sling, bell1g passed through the large loop of the other, and round the pole and bed.
In closing a stretcher care should be taken to raise the centre of the canvas when pushing in the trayerse bar, as it is othen' ise liable to get caught.
To prepare, or open a stretcher, unbuckle the transverse straps of each sling; remoYe the slings from the stretcher; separate the poles; take bold of each tra\' erse bar and draw it forward. The slings \\ ill tben be folded to half their length, one being laid neatly over the handles at each end of the stretcher.
As a general rule, the stretcher will be prepared by I and 3 bearers in Exercises 1., 11., and III.;
FIG.174
8.nd by No. 2 in Exerclse IV. These be1rers will, however, If required, assist the other becucrs In attending to the patient's injuries.
Note. - The various movements detaded 111 the following Exercises should be carried out stead]ly, the bearers working in unison, hurrying being carefully avoided, and every attention paid to the bearer who gives the words of command.
STRETCHER EXERCISES,
Origim.lly drawn up by 'ir John Furley) and revised in I90-l- to accord with the drills adopted by the Royal Army Medical Corps :--
EXERCISE No. 1.
FOR FOUR BEARERS.
1.-The Instructor selects the bearers and numbers them- I, 2 , 3, 4 at his discretion. 'hould one man be taller and stronger than the others, he should be styled No. 3, as he will have to bear the heavier part uf the burden. * All orders will be given by 1 O. 4.
2. - " Fall in." - os. I, 2, and 3 take position on the left side of facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, No. 3 at the j)8.ticnt's shoulders . At the S8.me
,. Bearers should, lH'wever, be taught to take any of the P)Silions named in the fullowing Exercises, whether that of N o. J, 2, 3, or 4 IJearer.
175
ti (TIe No. 4 places the prepared stretcher on the ground liy the right side of the p8.tient about two

y](;. b2.
p8.ces a",n), frorn him, nnd. then t8.ke pO-5ition Opposlte to nnd bcing NO.2. (Fig. 82).
3.-" R eady. "-The bearers kneel down on the knee and take hold of the patient, o. I passing hIS hands and fore-arms beneath the patient's leas hands wide apart. Nos. 2 and 4 pass their

FIG. ti3. and forearms be!1eath the patient's bips and loins, and grasp each other's hands. No. 3 passes his left hand across the patient's chest and und e r the right shoulder, and his right hand beneath the left shoulder (Fig. 83).
1';7
4. -" Lift." -On the word "Lift," the bearers raise the patient gently and rest him on the knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as he
is ecurely rested, .J: o. 4 disengages hands with No.2, runs round by the head of the stretcher and places it under the patient, close to the other bearers' feet,
176
being carefu1 thDt the pillo\\' is immediately under the patient's ll ead (Fig . 85); he then kneels do\\n and locks his hands with those of o . 2 (Fi g , 86),
5,- " Lower."-The bearers place the prttient on the stretcher (Fig. 87), disengage their hands, and stand up. FIG, 85.
6, -" Stand to Stretcher. "-No, I goes to tbe foot of the stretcher, \\ith his bacl' to the patient; No. :3 to the head \\'] th his face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7. -" Ready."'-l os . I and 3 place the slings (if used) over their shoulders, stoop down, and slip the
I/9
loops of the s1ll1gs on to the handles of the stretcher, \\ hich they then grasp,
.:\.s soon as all is right the \\ ord is given :-
8. - "Lift Stretcher."-.l 0 . I and 3 bearers raise the stretcher steadily together Dnd . tand up.
iVo/e.-Nos. 2 and 4- \\ill now adjust the slings the shoulders of Nos. I and 3, taking care that each I. ' well below the [e\'e[ of the collar and acCnrakl): 111 lhe hollow of the ,houlder ill front. They wIll also lengthen or sh')rlen the slings, r.cg.lrtl LO the patient's injuries anc! the relatl\'''' helgllls of the i1earerc;,

11(;. U!.
9.-" March."-The bearer move off:- os. I, 2, and ..j. steppll1g off \\ ith their left foot, and 1 o. 3
liS
•
with his nght foot (Fig. 87). The step should be a short one of twenty inches, and taken with bent knees and no spring from the fore part of the foot.
10.-" Halt."-The bearers remain steady.

FIG. 87.
II. -" Lower Stretcher."-The bearers place the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher remove the slings from the shoulders, and then stand up.
12.-" Unload Stretcher - Ready." - The bearers prepare to take the patient -off the stretcher} as at Orders 2 and 3·
13.-" Lift."-The bearers raise tl1e pati en t as at Order 4 (Fig. 86); NO.4, in this case, disengages hands from No.2, removes the stretcher (Fig. 85), and resumes his former position. If necessary, the bearers will then steadily rise together, and carefully carry the patient Lo the bed, or other place to \rhich it bas been arranged to convey him.
14.-"Lower." - The patient is carefully lowered..
EXERC I SE No. II.
FOR THREE BE:\RERS.
I.-Number the bearers I, 2, 3·
All orders will be given by No.2, who ,yill look after the injured part of the patienes body or limbs to see that no bandnges or splints become displaced: and als o that No. I bearer, in lifting or carryin rr the stretcher, does not touch the patient's feet. 1:)
2.-" Place the Stretcher."-No. 3 places the stretci1er in a line with the patient's body, the fool of the stretcher being close to his b ea d.
3.-" Fall In."-No. I places himself on the left side of the patient in a line with his knees, No.2 on the left side just below the patient's shoulders and NO.3 at the right side, and faces No.2. '
180
181
4.-" Ready."-A11 kneel on the left knee. No. I places his hands, \\ ell apart, underneath the 10\\ er limbs, always taking Glre, in case of a fracture, to have one hand on each side of the seat of injury. Nos. 2 and 3 grasp each other's hands under the shoulders and th ighs of the patien t (Fig. 88).

Lift. bearers rise together, keepIng the patIent 111 a hOrizontal position (Fig. 89).
6. -'.' March . :'-.\11 take sllort side-paces, carrying the patient over the stretcher until hIs head is immediately above the pillo\\" .
7.-" Halt."-The bearers remain steady.
8.-" L owe r."-The bearers stooP. down, gently place the patient on the stretcher, dIsengage theIr hands, and then stand up.
9. - " Fall In. "-No.. I places himself foot of the stretcher \\'lth his back to the patlel,t. No . l)laces himself at side of the [Xlll ;: nr. ai)Q N o. -1 at the head, wIth hIS face towards the patient
I84
10.- " Ready."-Nos. I and 3 place the slings (if used) over their shoulders, stoop down, and slip the loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given-
II. - " Lift Stretcher."-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
No . 2 will now adjust the slings on the shoulders of N as. I and 3, taking care that each is well below the level of the collar, and lies accurately in the hollow of the shoulder in front. He will also lengthen or shorten the slings, having regard to the patient's injuries and the relative heights of the bearers.
12.- " March."- os . I and 2 step off with the left foot, and No. 3 with the right. The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
13. - " Halt."--The bearers remain steady .
14.-" Lower Stretcher."-The bearers place the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher, remove the slings from the shoulders, and then stand up.
IS. - " Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, as at Orders 3 and 4 (Fig . 88) .
16.-" Lift."-The bearers raise the patient, as at Order 5, and carry him by short side steps, clear of the stretcher, to the bed, or other place to whIch it has been arranged to convey him (Fig. 89).

185
17.-" Lower."-The patient IS carefully lowered.
EXERCI E No. III.
WHEN ONLY THREE BEARERS ARE AVAILABLE AND THE STRETCHER
BE PLACED AS IN II.
r.-The Instructor numbers the bearers-I, 2, 3 All orders will be given by NO.2.
2. -" Place the Stretcher."-No. I taking th foot of the stretcher, and NO.3 the head, place it on the ground by the side of the patient, and as close to> him as practi.cable.
3. -" Fall In."-The three bearers take the same posItions on one side of the patient, as laid down i Exercise No. 1.
4. - " Ready. "-Nos. I, 2, and 3 kneel down 0 the left knee, placing themselves as close to the patient as they conve niently can, and then take hold of him as di rected in Exercise No. 1.
S. - " Lift."-Nos. I, 2, and 3 raise the patient as dIrected in Exercise No. I, and then move in a kneeling position up to the stretcher.
6, - " Lower."-The bearers bend forward, care· fully lower the patient on to the stretcher. and dl . ngage hands.
1::'6
7. - " Stand to Stretche r."-All the stand up; No. I goes to the foot, No. 2 remains 1 posltion at"the side, and No. 3 goes to the head the stretcher.
8. - " Ready. "-Nos. I and 3 place the slings (If used) over their shoulders, stoop down, ant} slip the oops of the slings on to the handles of the stretcher, which they then grasp.
9. -" Lift Stretcher."-Nos. I and 3 bearers aise the stretcher steadily together and stand up.
No.2 will now adjust the slings on the shoulders of Nos. I and 3. taking care that each is well below the level of the collar, and lies accurately in the hollow of the shoulder in front. He wilJ also lengthen or shorten the slings, having regard to the patient's injuri es and the relative heights of the bearers.
10.- " March. "-Nos. I and 2 step off with the ' eft foot, and No. 3 with the right The step should e a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
1 1. - " Halt."-The bearers remain steady.
12.-" Low er Stretch er."-The bearers p1ace [c he stretcher gently on the ground, slip the loops of t he slings off the handles of the stretcher, remo"e t he slings from the shoulders, and then stand up.
13. --" U nload Stre tcher - Ready." - No. I hlmself on the left side of the patient, and in lme with hI knees No. 2 on the left side just the patlent' houlders. and No. 3 at the nght

IS7
side, and faces No. 2. kneel on the left knee. No. I places his hands, well apart, underneath the b\\"er limbs, al\\'ays taking care, in case of a fracture, to have one han:1 on each side of the seat of injury. N os. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
14.-" Lift ." - The bearers rise together to their feet, keeping the patient in a horizontal positlOn, and carry him by short ide steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
15·-" Lower."- The patient is carefully lowered.
EXERCISE No. IV.
FOR USE I:\, :JhXE A;'I;'D NARRo\\" CUTTL" GS "HERE T,\ 0 T\IEN O::-l"LY CA::-I" BE ENGAGED.
Nos. I and 2 "'ill carefully place the stretcher in a Iltle with the injured man's body, the fool of the stretcher being, if possible,"" close to his head.
o. I straddles a ross the patient's legs, placing his right foot, with th e to e turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of 1 o. 2; he then stoops down, passes the left hand under the patient's thi ghs and
• It is not ad\'isable to he too particular as to th e head or foo t of a stretcher in a mine, as it would probably be quite impossible to rev e rse it.
188
the right hand across and under the patient's calves . No.2 places his feet one on each side of the patient between his body and arms, the toe of each foot as n ear the armpits as possible . He then stoops down and passes his hands between the sides of the chest and the arms underneath the shoulders, and locks
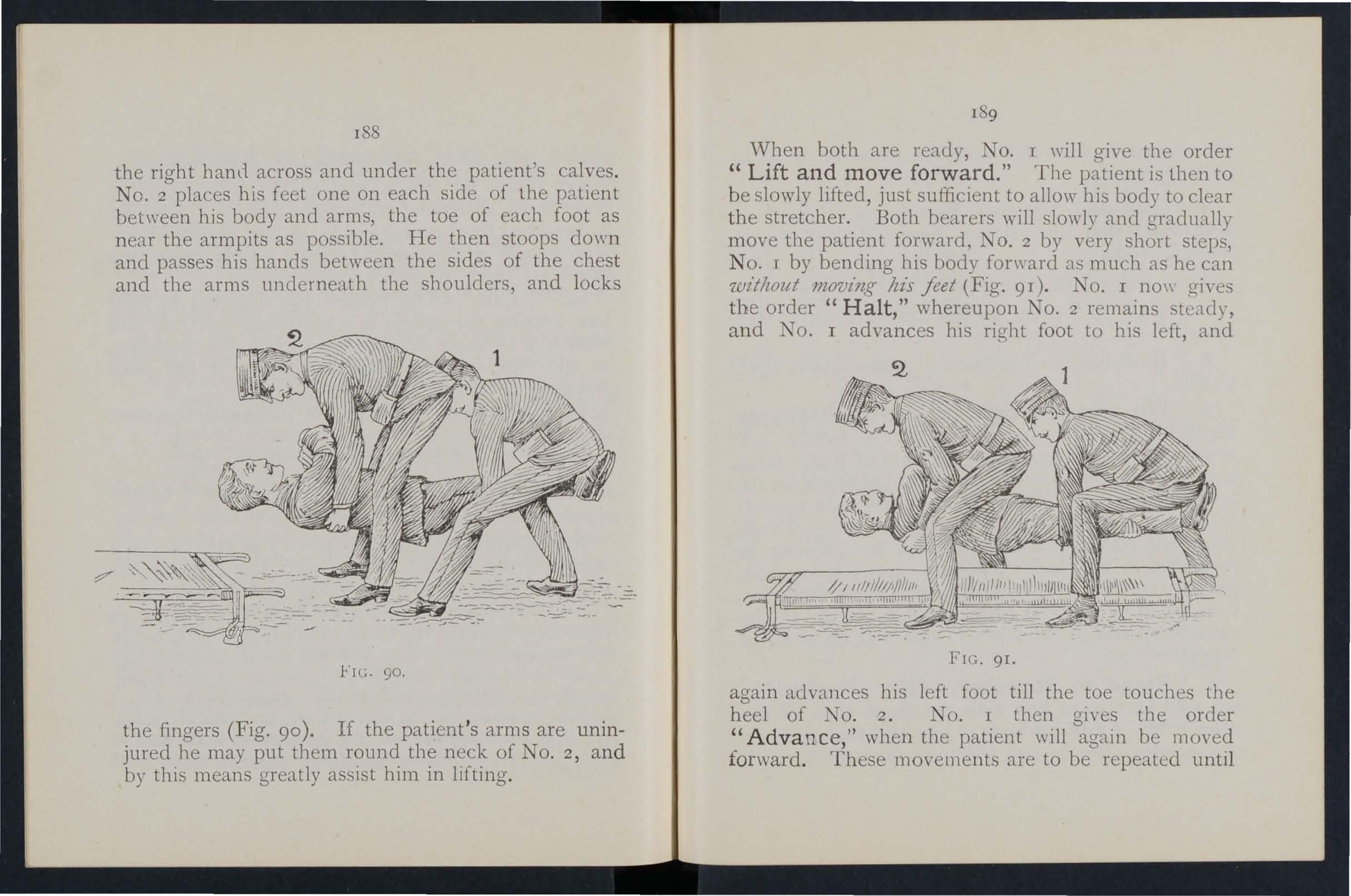
the fingers (F ig. 90). If the patient 's arm s are uninj ured he may put them round the neck of No .2, a nd by this means greatly assIst him in lift ing.
189
\Vhen both are ready, 1 o. I will give the order " Lift and move forward. " The patient is then to b e slowly lifted, just sufficient to allow his body to clear the stretcher. Both bearers will slowly ancl gradually move the patient forward, NO . 2 by very short step, N o. I by bending his body forward as much as he can 'lvz"tlwut movz'ng Ius .feet (Fig. 91) . No. I no\\- gi,'es t he order " Halt," whereupon No.2 remains steady, a n d IO I advances his right foot to his left, and
FIG. 91.
agai n adva nces his left foot till the toe to uches the h eel of NO . 2. No . I then gi yes the order "Advance," when the patient \\'ill again be moved for ward. T h ese mo \'ell1e n ts are to be repeated unti l
. -c----

the patiell t is over the stretcher, when he is to be gently lowered .
The follO\\"ing St retcher Exercise is adapted hy permission from the Royal Army Medical COr[ . .:'II anual, I908.
All orders ,,,ill be given by o. 4.
r. " Fall in. "- 'ix bearers fall 111 behind e2.cb other.
2. "N urn ber. "-Th e bearers n umber from fron t to rear.
3· " No·3 Bearer, ri g ht (or left) t urn -- supply s tretcher- q u ick march ."-No. 3 bearer ,,,ill march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower foot wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place . He turns to the front, and, passing the lower end forward, places tlle stretcher on the ground to the right of the squad, wheels to the right, fro n t end of the poles in line with the toes of No . I a n d r ises .
4· "Stand to Stretche r. " -No. I places himself with h is toes in line with the fron t ends of the poles . NO ·3 with his hee ls in line with the rear ends of the po les , close to and touching the stretcher with
190

19 2 his right foot. Nos. 2, 4, 5 and 6 take up their positions one pace behind and covering off the bearer in front of them (Fig. 9 2 ).
S. "Lift Stretcher." - os. I and 3 stoop, grasp both handles of the poles with the right hand, rise together holding the· stretcher at the full extent of the arm, wheels to the right.
6. "Collect - Advance." - The squad doubles by the shortest route to the patient, and halts without further \Yord of command one pace from the head of and in a line with the patient (Fig·93)·
7. "Lower Stretcher."-I as. 1 and 3 stoop, place the stretcher quietly on the ground, and rise smartly together.
8. "Prepare Stretcher." - Nos. I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps, and place the slings on the ground beside them, separate the poles, and straighten the traverses.
Two. On the word two each takes a sling, doubles it on itself, slips the loop thus formed on the near handle, and places the free ends over the opposite handle, buckle uppermost. They then rise and turn to their left together.
\ Vhile the stretcher is being prepared by Nos . I and 3, the disengaged bearers \\'ill advance and render to the patient such assistance as may be required (Fig. 94)· 193
The necess3.ry assistance having been rendered, NO.4 will give the command-
9. "Load Stretcher. II - The bear ers place themselves as follows I, 2 and 3 on the left, Nos. 4, 5 and 6 on the fl ght of the patient; Nos. I and 4 at the kn ees, 2 and 5 at the hips , 3 and 6 at the shoulders, the ..,... hole kn ee ling on the left knee. Nos. I and 4 pass their hands ben ea th the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being tak e n of the injured part, one of. the oeJ.crs being d etai led for this purpose (FIg. 95).
1.0. "Lift."- The 'whole will carefully lift the p:ltJent on to the knees of Nos . I, 2 and 3.
Two. N os. 4,5 and 6 will th e n disen o-age rise' N b , ) os. 4 and 6 step back one pace. No. 5 turns to his left, doubl es to th e stretcher takes hold of and raises. it, left across, th e nea; pole resting on the left hlp; carrymg th e stretcher, he returns to his place between 4 and 6, and places it beneath the pati ent.
Three. .N os. 4 and 6 step forward one pace, and together wIth NO.5 kn eel down on the left kne e, and prepare to assist in lo wering the patient (Fig. 96).
II. "Lower."- Th e pati ent is lowered slowly and ge?tly on to the centre of the canvas (special care bemg taken of th e injured part).
Tw.J. The bearers dIsengage, rise; Nos . J, 2, 3 and 6 turn to the left; Nos. 4 and 5 to the right; H
No. 4 places himself three paces In front of the stretcher. o. 6, having collected the kit and arms of the patient, places himself three paces in rear of the stretcher, Nos. 2 and 5 opposite the centre of the stretcher. The whole are no\\' ready to lift .stretcher and move off (Fig. 97).

97.
FIG. 98.
195
12. "Lift Stretcher." -N os . I and 3 stoop, the doubled sling midway between the poles wIth forefinger and thumb of the right hand, sweep 1t off the handles, rise, holding the sling at the full extent of the arm, buckle to the front take a side pace to the front between the handles' and place the sling over the shoulders dividing it buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollow of the shoulders in front. In the event of the slings requiring to be adjusted, either as regards length or for the greater comfort of the bearers, NO.4 will detail a bearer to carry this out, the length of the slings being adjusted, when by means of the buckles.
Two. Nos. I and 3 stoop, slip the loops over the handles, commencing with the left, and grasp the handles firmly.
Three. Nos. I and 3 rise slowly together, No. 3 conforming closely to the movements of No. 1.
.13. "Advance."- Nos. I, 2, 4, 5 and 6 step off WIth the left foot, NO,3 with the right, stepping short» knees bent, feet rais ed as little as possible.
14. "Halt." -The whole halt.
IS. "U n .load Stretcher." - The bearers place themselves In the same position at the stretcher a des cribed for Loading (Order 9).
16. "Lift/'-As described for Loading (Order- 10), HZ
194
FIG.
196 except that the stretcher is carried forward three paces clear of the patient's feet.
17. "Lower. "-The patient is gently lowered to the grouncl The bearers disengage, rise; Nos. 1, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whole step off to their places at the stretcher, as at Order " tand to Stretcher" (Fig. 98).
T he Ashfo rd L itter is made up of either of the Furley stretchers mentioned on pages 17 2 and 17 3, a wheeled under-carriage and a waterproof hood and a.pron, or, if preferred, a light wet-resisting canvas cover. The stretcher is kept in position on the under,c1.rriage by the foot-wheels, which fit into slots in the sides Gf the under-carriage, and it can be removed at pleasure. The under-carriage is fitted with a cranked axle, which allows the bearers to P:lSS with the stretcher between the wheels instead of lifting it O\'er them. At both ends are two legs which may be turned up as handles when wheeling the litter. The hood and apron fit into sockets scre\ved to the stretcher. In wheeling the litter, care should be taken to keep the patient in a horizontal position. Should it be necessary, two bearers can easily lift the litter and patient.
The Rea-Edwards Litter, introduced in 1904, is used in a similar manner. and one model of it is fitted with pneumatic tyres, which add immensely to the comfort of the patient and to the ease of propulsion.

197
CHAPTER X.
(BeiJl(>' tlt e PI/til Lectlf7'C for Females olll)" z>z accordance 'l.f}itlz S)'llabu s 58.)
EY E. MACDOXEl.L COSGRAVE, M.D., F.R.C.P .I.PREPARATIO:\ FOR RECEPTIO I OF ACClDE:\T CASE, \VHE T ne\\'s of an accident comes, preparations should at once be made so as to have everything ready before th e injured person is brou gh t in. Of course the prepara tions needful \\ ill vary according to the nature and extent of the injury, but the following are the chief things which may hm'e to be done.
CHOICE A D PREPARATION OF RomI.
A room must be chosen. In a bad case thi hould be one easily reached, as it is difficult to arry an ll1jured person through narrow passages up, stair, Unless there is some such rcas on agall1st It , the lt1jured person 's own room is best.
'The way to the room must be cleared, projecting furniture and loose mats in the hall or in lobbies should be removed. If the injured person is carried on a door, shutter, or stretcher, two strong chairs should be placed ready to support it wh erever the bearers ,,'ould be likely to require rest.
Useles furniture should be removed from the bedroom. The bed should be drawn out from the \\all
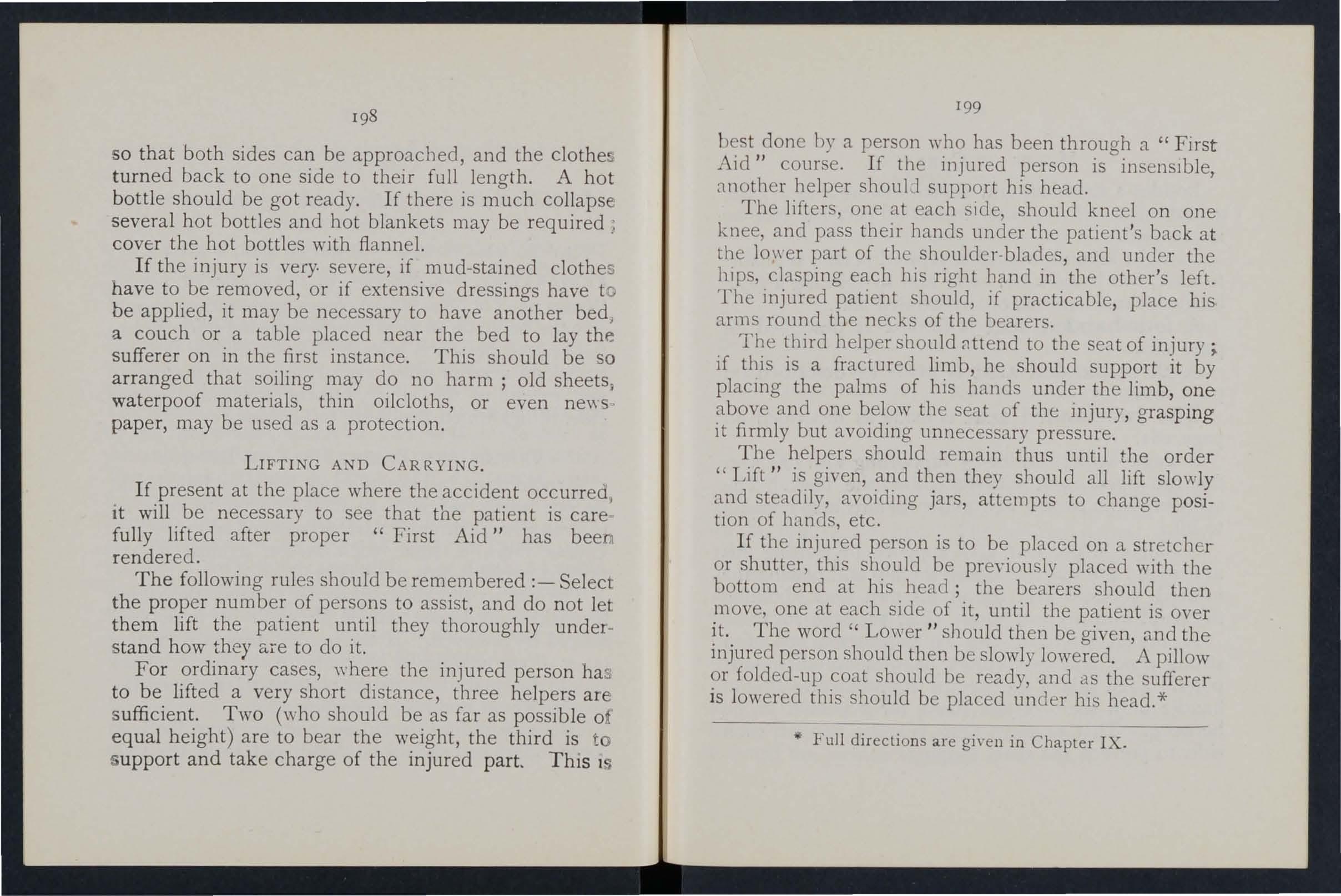
I98
so that both sides can be approached, and the clothe turned back to one side to their full length. A hot bottle should be got ready. If there is much collaps several hot bottles and hot blankets may be required ) cover the hot bottles with flannel.
If th e injury is very. severe, if mud-stained clothes have to be removed, or if extensive dressings have to be applied, it may be necessary to have another bed ) a couch or a table placed near the bed to lay the sufferer on in the first instance. This should be so arranged that soiling may do no harm ; old sheets J waterpoof materials, thin oilcloths, or even new " paper, may be used as a protection.
LIFT! G AND CAR RYING.
If present at the place where the accident occurreo , it will be n ecessary to see that the patient is care fully lifted after proper "First Aid" has bee rendered.
The following rules should be remembered:- Select the proper number of persons to assist, and do not let them lift the patient until they thoroughly understand how they Ci.l"e to do it.
For ordinary cases, where the injured person has to be lifted a very short distance, three helpers are sufficient. Two (who should be as far as possible of equal height) are to bear the weight, the third is to up port and take charge of the injured part. This 1 199
best done by a person who has been through a "First Aid /I course. If the injured person is insenslble t helper shouLl support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under tIle patient's back at the lower part of the shoulder-blades, and under the hips, clasping each his right band in the other's left.
The injured patient should, if practicable, place his. arms round the necks of the bearers.
The third helper should 8ttend to the of injury; if this is a fractured limb, he should support it by placing the palms of his hands under the limb, one above and one below the seat of the injury, grasping it firmly but avoiding unnecessary pressure.
The helpers should remain thus until the order " Lift" is given, and then they should all lift slowly and steadily, avoiding jars, attempts to change position of bands, etc.
H the injured person is to be placed on a stretcher or shutter, this should be preyiously placed with the bottom end at his head; the bearers should then move, one at each side of it, until the patient is over it. The word" Lower" sllould then be given, and the injured person should then be slowl y lowered. A pillow or folded-up coat should be ready, and as the sufferer is lowered this should be placed under his head. *
<if Full directions are gi\-en in Chapter IX-
MEANS OF CARRYING .
Besi d es a stretcher, and substitutes such as a gate, a sh ut ter, or a door , other means of carrying can be improvised .
I n slight injuries , where the injured person is unable to walk, two bearers can carry him by forming a fourhanded, three-handed, or two-handed seat.
A four-handed seat is formed as described on page 160.
A three.handed seat is made as described on page 162 . The two-handed seat is made as described on page 16 r.
A single helper can lift by supporting with one arm the two knees, and with the other the back. The arms must be passed well under before cOID 1nencing to Ii ft.
A single helper can give support by putting his arm round the waist, grasping the hip and placing the injured person's arm round his own neck, holding t h e hand with his own hand (Fig. 76, page 165).
A capital stretcher can be improvised out of a strong sheet and two broom handles or other short poles. Each side of the sheet is wound up on a broom handle until there is just room for a person to lie between . This requires four bearers, two at each side, to prevent the sheet sli pping .

CARRYING UP TAJRS.
In carrying a stretcher up stairs the head should go first, and an extra helper should assist at the lo"wer end, so as to raise it and keep the stretcher nearh' horizontal. -
The two, three, or four-handed seat may be used fOl: carryir:g up stairs; or a strong chair, the pati ent bemg earned up backwards. In the btter ca e cne should walk after the chair and help to support It, and to prevent the in.iured person slipping out.
LIFTING INTO BED.
If the bed is narrow and there J. room the stretcher should be placed 011 the floor "ith the hea d close to the foot of the bed. The injured person should then be lifted o\'er the foot and placed on the bed. If the bed is too ",ide to admit of this, the stretcher should be pbced beside it, and two belpers should stand at the far side of the stretcher. One helper passes one arm beneath the shoulders and one beneath the middle of the back, the other helper placing his under the lower part of the back and under the knees. The injured person is then lifted, another help 2r pulls aW:lY the stretcher, and after a single step forward the burden is placed on the bed.
200

PREPARATION OF BED.
A firm mattress, not a feather bed, should be selected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should b e of four or more thicknesses, extend across the bed, and reach from the middle of th e patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed un cler the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fracture of the leg or thi gh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " crad le " is to support the bed -clothes and keep them from pressing on the lim b.
A band-box (Fig. 100 ), three-legged stool (Fig. 101), or hoop sawn across and the two halves secured together ( Fig. 102), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REMOVING THE CLOTHES.
I n taking clothes off an injured person a few rules should be borne 111 mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
202
203
FlG IOO.
FlG. IO[,
In removing a coat, etc., in a case of fractured arm the unmjured arm should b e drawn out first.
In putting on a coat or shirt the injured arm should be put in first.
In burns and scalds nothing should ever be dragged off. A sharp pair of scissors should be used, and everything not adhering should be cut away. If anything adhere3 it should be left until medical aid

FIG. 102.
can be obtained. The clo!hing adhering may, \\ lth advantage, be soaked \\ ith oil. To remove the trousers from a severely injured lim b, the ollts/dl! seam should be ripped up.
PR EP,\ RATIO:-iS FOR SURG1... O:.r.
As soon as the injured pl:rson Ius been attended to, preparation should be made for the surgeon's \,1 It.
20 5
Thepreparations needful ,,·ill depend upon the nature of the case. The follo\\ ll1g hll1ts may be of useA fire in the room helps ventIlatlOn, even in 'Summer. There should be plenty of wat er, 110t cold, and also boiling, also several basll1s, of clean to\\ els and soap . There should be something to empty water into; a foot bath does well. The basins should be placed on a table cm'ered with a clean \\'hlte cloth: a large towel' make a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be \\'ithin easy reach. The foot-bath should be under the table or close at hand.
In the case of a burn, absorbent cotton wool soft cloth , old linen, oil, and baking soda, should be r cady, and materials should be torn up for bandages.
In case of hremorrhage, plenty of \\'ater should be bolled and allo\\'ed to cool, and pads of absorbent cotton wool should be baked in a tin box in the oven, and at least two basll1 should be ready.
In the case of a person rescued from drowninO' the sheets should be taken off the bed, plenty of should be heated b efo re the fire, and several hot bottl es should be ready.
" If poultices are likely to be required . boiling wat e r, meal, mustard, a loaf of stale bread, a small basll1, a spoon, s\\'eet oil, and tow, flannel or handkerchIefs may be required.
204
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large towel.
'When summoning a medical man to all accident always let him know by a 'written message what kind of case he is required to treat, so that he may bring whatever is needful. By tbis means valuable time may be saved.
QUESTIONS ON CHAPTER X.
The 1ntme1'a/s indicate tlze pages whe1'e the al1swe1' S may be fouNd.
What points would you consider when choosing a sick
room?

197
How would you clear the way to the sick room? 197
What means of re sting would you provide for those carrying a patient on a stretcher? 197
How would you place and arrange a bed for an accident case? 197, 198
Are bot bottles necessary, and how would you prepare them? 198
What is often necessary to lay the sufferer on in the firsl instance? 198
Mow would you protect this from getting soiled? 198
How would you see to the proper lifting and carrying of an injured person?
... 198, 199
'What substitutes for a regular stretcher can you suggest? 200
!How is the four-handed seat made? ... ... 160, r61
For what cases is this seat useful ?... 160
How is the three-handed seat made? 162, 164
207
For what cases is this seat useful? ...
How is the two-handed seat made?
For what cases is this seat useful? ...
H ow can a single helper lift ?
How can a single helper gIve support?
How would you improvise a stretcher? ...
How many bearers are required for I his stretcher?
How should a stretcher be carried upstairs? .. ,
How would you carry a patient upstairs on a chair? . . .
How would you lift a patient from a stretcher to a bed?
How should a bed be prepared for an injured person? .. .
How sh6uld a draw sheet he made? .. . ... .. .
vVhat would you place under the draw sheet?
What should be done with the soiled part of a draw sheet?
'''hal is the use of a " cradle "? ... .. .
In what ways maya c radl e be improvIsed?
How would you remove a coat or shirt in the case of a fractured arm?
IIow would you put on a coat or shirt if the arm were injured? ... . '" ...
In the case of a bad bl!rn, what would you do with clothing that adhered to the patient? ... . ..
How would you remove trousers from a severely injured limb?...
\Vhal preparations would you make for the surgeon's risit?
'Vhat would you get ready in the case of a burn? ..
And what in the case of hzemorrhage ? . .. .. ..
And what in the case ofa per on resclled from drowning?
\Vhat would you get ready for making poultices?
And for fomentations? ... . . . ... ..
'iVhat sort of a message would you send tt> summon a doctor?
206
PAGE
PAGE 162 161, 162 161
... .
. ... .. .. .
.. . .. . . . .
... ... ... ... ... ...
... ... .. .. ... ... .. .
.
... 200 165 200 200 201 201 201 ::02 202 202 202 202 202 204 204 204 205 205 205 205 20 5 206 206
208 INDEX.

Abdomen wound of
Accident case, preparaPage III 112 tion for 197
Acids, poisoning by 149, 151
Air, always nece sary ... 18
Alcohol, caution as to smell of 13 0
Alcohol, poisoning by 134,153
Alkalis, poi. oning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30 , 32 " sprained... 64
Anterior tibial artery 93
Aorta 79
Apoplexy 13 2
Apparently drowned, to restore ...
Ann, bone of " fracture of Ann- ling'>
Arsenic, poisoning by
Arterial hremorrhage, 139 28 arre t of 74 practi ing arrest of 79 signs of 74
Arlerie " course of main 70 79 85 rtery, axillary ...
Arttry, brachial. .. " carotid ... dorsal of fool facial femoral iliac occipital plantar .. , popliteal radial subclavian tibial temporal " ulnar
Artificial re:piration 121, 129, 136,
Asphyxia
Atlas
Auricles ...
Axillary artery
Axis
Back, bandage (or 159
Backbone 23
Bandage, to apply 42 to fold 37 " to improvise... 37
Bandaging ... I S5
Bed, lifting into... ZOI " preparation of 202
Belladonna, poisoning by 148
Bites of rabid animals 106
Bladder ... II I, 113
Brachial artery ... 86
Brain I I 7 cornpre sion of 132 " concussion of 131
Brea t- bone 26 ,. fracture of 48
Broad bandage ... 37
Broken bones, see Fracture.
Bronchial tubes... II8
Brooch-bone 30
Bruises 102
Burns 102
Capillaries al-.illary hremorrhage
Capsule ... 70,7 2 95
Carbolic acid, poisoning by Carotid arterie 3 1 80 z8 (rom" <;arpus
Carrying, means of 160, zoo " upstairs
Cartilage
Cerebro-spinal ystem
Cervical verte brre Cheek, bleeding from Chest, bandage for Chlorodyne, poisoning by Choking ... 201 25 117 25 149 140
Circulation of the blood, organs of 70 Circulation of the blood, to induce 127 Cla,-icle ... 26 " fracture of 43
Clothes, remoyal of I), Z02 Coccyx 25
Ditch, Lo cross with tretcher 169 Dor al artery of foot 93 verte brre... 25
Pa,t;!! 86 80 93 SI 89 79 82 93 92 88 84 93 82 88
209
Page
Page
Collap e... 134Collar-bone z6 " fracture of '" 4 Comminuted fracture 35 Complicated fracture 3+ Compound fracture 34Compression of the brain 132 Concussion of the brain I 3 I ConducLOr 143 Convulsions
children 137 Cradle,
ZV2 Cranium
..,., " fracture
43 Crepitu
36 Crushed
55 foot 62 Diaphragm 120 Digital
74 Direct
Dislocation
in
bed
.. ,
of
'
hand
pres ure...
,:iolence ... 3
62
Dress, woman ' s, on fire ... 1 05
Drowning 139
Ea r·channel, blood issuing from
Ear-passage, foreign body in 110
210

Fireman's li[t
First aid, meaning of " student
Fish-hook, embedded
Flexion ... at elbow " at knee ...
Electric shock
Emetic
Elbow, bandage for '" 159 joint, fracture involving 53 J 4 2 148, 149, ISO
Epilepsy ...
Esmarch's bandage
Expiration t riangular
External carotid artery ...
Eye, bandage for foreign body in 13 2 37 120 80 155 109
Face, bones of 22
Facial artery 81
Fainting... 134
Femoral artery " "digital pres· sure at groin ... 89
Femoral arte ry, tourniquet for 90
Femur 30
" fracture of 56
Fibula 30 " fracture of 60
Fingers, bandage [or 159 fracture of 55
Food, poisoning by Foot, bandage [or bones of ... " crushed
Forearm, bones of " fracture of Forehead, bandage [or ... " hcemorrhage frOI11
Foreign body in the ar... in the eye " "in the nose
Four-'nanded seat ...
Fracture, apparalus for treatment of ... cau es of def-inition of '" general rules for treatment involving elbow joint of arm . . . of breast-bone of carpus of collar - bone of cranium of finger
:u 33
Fracture of forearm of knee-cap of leg ... Page 54 58 60 of lower jaw ... of metacarpus of metatarsus ... of pelvis of rib ... of spine of tarsus of thigh-bone ... of toes .. signs and symptoms of 44 55 62 56 46 45 62 56 62 " varieties of 35 34 108 F rost-bite Fungi, poisoning by 153 General circulation 70 Granny knot 40 Green-stick fracture 35, 36 Gums, hcel110rrhage from 97 Hoemorrhage, arterial 74 capillary... 95 from gums 97 from head and neck 80 from lower limbs ... 89 from lungs 97 from nose 96 from stomach 98 21 1 Page
Hoemorrhage from throat 9 7 from tongue 97 from tooth socket... 97 from upper limbs 84 internal 95 kinds of 73 " venous 93 Hand, bandage for 157 " bones of ... 28 Hanging... 140 IIaunch-bones ... 28 IIeadand neck, arteries of 80 Head bandage for 155 injury to... 128, 131 " side of, bandage for 155 Heart 70 ., rate of contraction of 72 Heat- troke 136 Hernia 114 Hip, bandage for 157 History, meaning of 17 Howard's method of artificial respiration 126 Humerus 28 " fracture of 52 Hydrophobia 106 Hysterical fits 133 Iliac arteries Impacted fracture Indirect violence Insensibility 79 35, 36 34 ... 128
Page 164 17 20 109 76 D7 9 2 153 1St> 30 62 28 54 83 83 110 J09 III 16:J 36
Face
In sensibility, general rules for lreatmell t 128
Inspiration 120
Jnstep 30
Jnsulator . 142
Internal carotid artery
Int ernal h::emorrhage 95
Intestines, injury of 113
Involuntary muscle.; 33
Jaw, angle of 2)
" lower 23
" "fracture of ... 44
Joint, definition of 31 " injuries to... 109
Jugular vein 80
Kidneys II 1 " injury of 1 13
Knee, uandage for 15 9
Knee-cap 30 " fracture of 58
Knot for uandage of lower lim b 42
Knots, re ef and granny 40
Laborde's method o[ artificial respiration 126
Laburnum seeds, poisoningby.. . 1 48
Lacerated wound 78
Large arm-sling 39
Laudanum, poisoning by 149
Leg, bones of 30 212
Leg, fracture of Lifting and carrying " into Led Ligaments
Lightning, effects of Limbs, 10\\ er
" upf er
Lime in the eye bleeding from
Litters
Liver " injury of Lower limbs
Lumuar \'ertebne
Lungs h::emorrhage
l\Jarshall 11 all's method of artificial respiration Medium uandage 140 37
l\J etacarpus
" frac t ure of ..
Metatarsus
" fracture of .. l\liddle line of uody
Mouth, ulood issuing fr om
Muscles " ruptured
Muscular action ...
bandage 'N eedle, embedded erves

Nen'ous system ...
Nose, foreign body in h::emorrhage from
Occipital artery
Opium, poi oning by
Pad, ring ... " to fold
Palm, h::emorrhage [rom Palmar arches
Pareg-oric, poi oning by Patella fracture of " fracture of Phalanges of foot " of hand
Phosphorus, puisoning hy 14S, Physiology (elementary)
Plantar arch " artery
Plants, ,-arious, poi oning by ... Pleura
Poi son e d we a p 0 n s, wounds by Poisonill£; Popliteal anery ...
Posterior tibial artery
caustic, poisoning by... '"
Pres ure, digital .. . " point .. .
Principle of First aid
I, 129, to excite
Rc piralory"ystc11l
Rest, necessity for Ribs , , fract lire of ... Room. choice and paration of
60 198 :201 26, 31 144 2:::26 11 0 196 III 113 28 25 120 from 97
Tarrow
2 ) 55 30 62 20 97 32 65 34 37 108 lI8
Potash,
... Pag-e II7 III 96 S.; 74 8S 88 149 30 58 2S 56 30 28 21 3
Prussic acid, poioning by Pubes Pag-e 74 74 17 15 2 2 Pulmonary circulation ... Pul. e 72 72 Pupils of eyes 13° Questions on eha pter I. 2 I II. 66 III. 99 IV. II5 V. 145 VI. 154 X. 206 RalJid animals, bites of... ra6 Radial artery 88 Radius fracture of 54 Reef knot 40 Respiration I::O artificial
I:>
I36, I3' I27 IIS 1 ::6 46 preI97
214
Pag-I!
Rupture (hernia) 114
Ruptured muscles 65
Sacral verte brre .. ,
Sacrum ... 25 25, 28 calds
Scalp, bandage for " h<rmorrhage from capula ... . ..
" fracture of r chafer's method of artificial respiration
eat, four-handed three-handed two-handed hin-b.one
Shock " electric bandage for ... blade ... " fracture of " bones .. . joint .. . ick" room, choice and preparati on of. ..
Signs, meaning of .
Silvester's method of artIficial respiration
imple fracture .. . ...
Skull " fracture of

26 3 2 197 17 123 34 22
Slings, arm 22 43 39, 4 0 , 49
Small arm sling ...
Smothering
Snake bites
Soda, caustic, poisoning by Pagt 39 140 106 149
Spleen " injury of. . .
Spinal canal cord
" fracture of I (I ,,, II3 23 23, II 7 23 45
Spirits of salt, poisoning by
Splint, angular Splints, rules for apply. ing to improvise
Sternum .. . " fracture of
Stimulants
Stings of plants and animals
Stomach ... hremorrhage fr om ,. injury of.. .
Strains
Strangulation
Stretcher exercise, Army No. 1. No. II No. III. " .,
Furley
PaJre
Stretchers, to ca rry 169 " to impro\'ise 166
Strychnine, poisoning by 153 ubclavian artery
Suffocation '" 141
Sunstroke " 136
Surgeon's visit, preparation for 204
Syllabus of in truction ., . 7
Sympathetic system 118
Symptoms, meaning of ". 17
Syncope ,.. ... '" 134
Synovia 31
Systemic circulation 70
Tar:>us
Temporal artery ..
Thigh-bone " fracture of ... Three-handed seat
Throat, hremorrhage from " swelling of tissues of .. , Tibia " fracture of Toes, bandage for Tongue, hremorrhag e from
Ulna " fract ure of ' .
Ulnar artery
U nconsciollsness
Upper limbs
Varicose veins
Veins
Venous blood " hremorrhage
Ventricles
Vertebra ...
Vertebrre, ..
Vertebral column
Vertical wound of ahllomen
Vitriol, burn by".
Transverse wound of 1:l_bdomen
Two-handed seat 113 161
\Vall, to cross with stretcher '" I 7c \Varmth, neces i't'y for IS " to promote 127
Wind-pip e '.. II8 \Voman's dress on fire 105 Wounds by poisoned weapon 106 ,. accompan ied by arterial hremorrhage ." 76 \Vounds accompanied hy venous hremorrhage 94
lacerat ed 78
102 ISS 83 26 51 121 160 162 161 30 134 142 156
28 51
I07 III 98 113 65 140 190 174 18r 18 5 187 172
o. IV. Stretchers,
Tooth ocket, hremor3':) 82 30 56 162 97 30 60 159 97 rhage
97 T
75
from
ourniquet
Voluntary mu c1es Pa "',' ;8 54 88 128 26 94 70 72 93 70 23 25 23 1I3 102 33 \Yagon
to load or unload 171
,
Wrist
\Vounds,
28
H()RSE AMBULANCE CARRIAGES & WAGONS.
st. 30bn ti1nbllIance tlBBociatioll .
GENERAL PRICE LIST. INTRODUCTION.
Thi s Pr ice List, which ;s subject to reyision from time tv time, has been compiled with a yiew to assist memhers of the Association and others in the purchase of the necessary equipment for corps and divisions of the Brigade, amlJUlance stations, classes and first aid and nursing work generally.
A complete and reliable Ambulance Eq !lipment is an actual necessity, and experience has proved that employers of labour and others int erested in the district readily subscribe for the purchase of such appliances . Collecting cards, the purposes for which subscriptions are required, "ill be supplied gratuitously on application to the Il ead Office of the Association, where also any information with regard to its work can be obtained.
Stores of the value of lOS. or uplnlrds \, ill l)e sent carriage paid to any part of the United Kingdom.
Owing to fluctuations in market prices it is impossilJle to guarantee that the quotations herein can be adhereu t o.
Quotations will be furni shed for articles 1 e:ating to An,blllance Nursing and Hygiene, not mentioned in this list.
Orders and correspondence should be to the Sl. John Amlmlance Association, S1. John's Gale, Clerkenwell, London, E.C.
Remittances should be made payable to the Sr. John Ambulance Association, and crossed "London COLlnty and \\' estminster Bank, L othbury."

Registered desig-n 4I8,030.
A number of improved designs for Ambulance Carriag-es have recent ly been per,fected, and can usually he seen at St. J ohn s Gate, varymg from a light '-chicle to be drawn by two men or by a pony, costing with india-rubber tyres to wheels £32 IO ., to a la rge single or pair-horse wagon capable of accommodating three :ratients in a recumbent position and an attendant in side . A fully illustrated price list will be sent on application.
rt n 0 o' s.,::E E. "" c+ [ a;:l g 3. ::E JJ' r; co
;:r' I" § >-rj:J
'< 0. ::E §.
t:S S;;:l ;.;:l g n 8.
"'" ;r 8. ..... jig' t-<
3. _ e; g =. rJ> 0. "" co ;:::.
;:;.'< ::l ;:l ::: ". I" n :n ro ....
'" 1l ;r :::. g- g g' ji1 0.-::;;:L r; ...
£, c. 9 ir r;:' -,..... &\0
&"d Ii 5.(fQ ::l ;:r' ;:r' co :3 co r;rJ> p,co b P,1";:;:0
:: (3 rJ> g' <: to: n Jg cT ,... e. ;:l "d
5. ;:r''<;r I" 6-;:;' - 8 to: C3 5: 'E
:: ;r g o' g. co I» ;:;. 0-' :l:::r" (b -" • ,..... too-: UQ en :: p.. ,- ';"::';"g ;r Pi 0 n;; 0 5' rJ> "'"' ;:l r; C j .U:< u CO :::;- 3. p, :>l c£ rh ;:::. g 0
g; .... CO :J I

Under-carriage (no Stretcher)
Litter c.omplete with Ordinary Stretcher'"
Dittowith T elescopic handled Stretchert
With I ron Tyres to Wheels. IWith IndiaRubberTyresto Wh pel,
Dilto with Police Slretchert vVith o.tt I \Vith With out I . I With Hxod and 111,\'od and Apron. pron. Apron. pron.
• Prices quoted for Litter with Ordinary Stretcher include Wid e Webbin g Slings but no Che,t Strap. Leather, of W ebbing Slings, 5S. 6d. extra; Chest Strap. IS. 6d. extra. If supplied without any Slings, 4'. allowed.
t Prices quoted for Litter with Tt:!escopic -handled Stretdter include \Vide Webbing Slings and Ch"st Strap. Leather, instead of 'Vebbing Slings, 5S. 6d. extra. If supplied without any Sling,;, 4 S allowed; and if without Chest Strap, IS. 6d. allowed .
t Prices quoted for Litter with Police Stretcher include \Vide Webbing Slings and Leatber Straps for securing a refractory patient. Leather, instead of W ebbing Slings, 5<. 6d. extra Hood and Apron, complete (stale pattern of Stretcher) £2 10 0
Extra Sock ets and Studs, per set 0 I 6 Vvaterproo£. S h eet (washable) to Le lail! on bed... 0 10 6
Crates (returnable) charged 4S. 6d. for each Liller.
•
E L . -----;----> (J) o t:; t"4 1-1 tt1 Cf>
PRICES OF THE IMPROVED AS H FORD LITTER, 1899 MOD
.- .£ s. d. .£ s d. .£ tI. .£ s d. .£ s. d .£ s. d. 8 10 0 I 9 5 0 I I 0 0 III IS 0 12 TO + 4 0 (I 2 6, 12 17 6 14 7 6.16 2 6 1 I 10 01 13 0 12 2 6 13 I7 6 14 15 0lI6 10 0 )15 7 61r7 2 6
w ." :oJ n [Xl (fl :-l "0 :oJ n [Xl t (fl ;!
THE " REA =EDW ARDS " LITTER .

THE" REA-EDWARDS" LITTER, with wooden wheels, showing of loading; also first aid box fitted to axle.
T he under-carriage or wheeled portion of this Liu:r is of an entirely new design, and is adapted to carry cI,ther of the "Furley" or " Clemetson" Pattern Stretch,ers l1l cisely the same manner as the "Ashford" LItter. It?s fitted either with bicycle wheels and extra strong lyres, or .vith light but strong wooden wheels, elthe: solid india-rubber or iron tyres. Owing to the reductlOn m the height of the wheels it is easy to lift a loaded stretcher
PRICE LfST .
over them, and the cranked a'\le has, therefore, been replaced by a lraight one con tructed of tulluhn steel.
" REA-En\\' \RD S " LITTER, fittet! with pneumatic tyred wheels, showing the" Clpl11ct on" Stretcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden, and the hubs are so arranged that the wheels can be removed from the axle without disturbing the bearings. In placc ''If t he; four legs made :0 raise as handlcs, two fixed legs fiLLed \\iLh small inc1m-l'uhber whecls or rollers are placed al the foot elid, \\hil c a combined lcg and handle fitLed with a cros!'.bar ar.d capable of bLing rai"eu or lowered is u eel al the head end \\-hen raised as a h:wdle iL may be locked in onl; of two positions, and when 100\''t:red it is luckul in :l ,erlicai po ilion. The ad\'anlages claimed for this arrang.::'ment are implicity, e'1.<;e and rapidity of manipulation a!:J
5 PRICE
LIST.
the facility afforded oy the two fixed legs for raising the litter, if necessary, on to the pavement. The question of balance has been carefully studied, and the stretcher is shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is loaded and in a horizontal position being thus obtained, and consequently there is no weight on the hands of the person propelli ng the Ii tter.
The pneumatic tyred wheels are strongly recommended in cases where the small amount of care necessary lo keep them inflated can be given, as the comfort to the patient and ease in propulsion are increased beyond all comparison with any litter yet produced. It will be noted that the prices are considerably lower than those of the "Ashford" Lilter, and the following are given as examples, but owing to the vast number of combinations that can be made with the different stretchers and coverings, it is impossible within reasonable limits to set out quotations for the whole of them, but these may be calculated by adding together the prices of the under-carriage, stretcher selected, and hood and apron or cover, see pages 4 and 8 to I I.
SPECIMEN PRICES .
Under-carriage only, either with pneumatic tyred cycle wheels or solid rubber tyred wooden wheels, £10.
Litter complete with ordinary stretcher (no slings or chest strap) and hood and apron, £q 3s. 6d.
Di tto with Telescopic Handled tretcher (with chest strap) and hood and apron, £14 lIS.
H with iron tyred wheels prices are £2 less.
The lowest priced litter complete is fitted with iron tyred wooden wheels. ordinary stretcher (no slings or chest strap) and cover. Price £10 8s. 6d.
Hand brake, which acts automati cally when the lilter is ?J rest, extra £[ lOS.
'Vhen ordering please state which wheels are required
THE
STRETCHER .

" CLEMETSON" STRETCHER, with 1.ac k . U raised, also showing extending legs.
On this stretcher the patient can be moved as desired, from the recumbe nt to the sitting position. There is no complicated 111 to get out of o rde r, and the adjustment depends Simply on the balance of the patient's body. The stretcher will fit either the .C Ashford" or the" Rea-Ed\\ard " Unde r -
Ca rriage. Price £3 3S. ; with extending legs, £4 3s.
Hood and pron, Ventilated, £2 ISS.
7 PRICE LIST.
PRICE LIST. 8
" CLEMETSON"
9
ADJUSTABLE LEGS FOR STRETCHERS .
Primarily these legs, hich are independent of and . tional to the ordinary foot wheels, are intended to fdclhta:e the carriage of a stretcher in a railway 10 which case two on one side would be lowered and by a telescopic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the adjustable legs on the other side would rest on the The four legs may be used to raise the stretcher as req lllred_ \Vhen not in use they are folded up immediately under the poles of the stretcher.
Price per set of four, £r.
FIRST AID BOX .
To be carried below the axle of the" Rea-Edwards" Litter, from which it is easily detachable.
Contents :- Set of Splints, 12 Triangular Bandages, 1.2 Roller Bandages, 2 -lb. packets each Cotton \Yool and Bonc Lint, Adhesive Plaster, Pair of Scissors, Knife, 2 ?z. each Olive Oil, Tinct. Eucalyptus B.P.C., Sal and Spirits Ether Comp., G laduated Measure h..ldneyDressing 6 Tampons for washlOg wounds, Tourniquet Pins, Safety Pins, Needles, Thread and Tape. I rice £2.
" FURLEY" STRETCHERS WITH THE L ATEST IMPROVEMENTS, 1899 MODELS .

TV;LESCOPIC HANDLED STRETCHER-OPEN.
ORDINARY STRETCHER-CLOSED.
The improvements in all patterns of the "Furley" Stretcher, r899 Model, are numerous. The comfort to the palient is increased; the stretcher is stronger, more rigid, and lighter, it folds up more closely, and its handle are more comfortable to hold and afford greater protection to the hands of the bearers in passing through narrow doorways or passages. Should it be necessary to reduce the widlh of a loaded stretcher in order, for example to carry it into a railway carriage, this can be done, either when it is re,ting on the ground or upported by the bearer, without trouble and without the slightest jar to the patient. The price uf the stretchert; is lowered. All minor points have heen most carefully considered, and the stretcher are confidently recommended as thoroughly efficient in every way.
These stretchers are for use alone or a part of the " Ashford" or "Rea-Edward " Litter, and the cover, hood anti apron, army rug, arid waterproof sheet described in this list are suitable for use with them.
PRICE LIST.
PRICE LIST. 10

t-l
PRICES OF THE "FUR LEY" STRETCHERS, WITH
:: THE LATEST
IMPROVEMENTS (1899 MODELS
N.B.-The pr ices of the Standard :Models are shown in heavy type.
).
--Without With Wide With Wide With With Slings or Webbing Webbing Leather Leatber Cbest Slings Slings Slings and Strap. (no Chest and Chest (no Chest Webbinl?; Strap). Strap. Strap). CheslStrap.
Ordinary Stretcher , for Genera l £, s. d. /, s, d.' £ ,.
and Brigade use, taking the place of both the old ordinary and military patterns 1 13 6 1 17 6
- handled Stretcher I 19 61 2 for workingin confined spaces 3
l'o lice Stretcher, very strong, with Ash Poles, and provided with Leather Straps to secure a refractory patient-
Complete, with ,\Vide W
Slings , Wide " Tebb
Do. Leather
(or if purchased with the Stretcher instead of Webbing Slings, 5/6 extra)
Cover (awning) for Stretcher (when ordering please state pattern of Stretcher)
Superior H ood and Apron (see illuslratiolt,page 3)
Spare Bed for Stretcher
Army Rug to cover Patient on Stretcher ...
Pillow for Stretcher, stun'ed hair
Chest Strap
s d. £ s. d.
I
0 2 3 0 2 4 6
0 2 9 0 2 10 6
d. {,
I
19
6 I 2 5
£ s. d. t-'
ebbing Slings 2 17 6
r Slings 3 3 0
" "Leathe
per pair 0 4 0
ing
per pair 0 9 6
"" (fl 0 -. "'0 (1) 0 0'Ir.(,) (fln;.;--' (1) 5' III (') ::l (1) . (') (1) ;::r. (") ::l (11 (1) (') -. o 0 9 I'-'( (') ...... ::l , ::;-,(11 ;:l (') -.0.. C (11 (') ::l ::; ...., ::r' (') (') l") p.J :3 "'0 -s .. g n ....., ;.;n Cl> ;.;;:; t""" S' (p g 2 III c _. tJ :no (0 "0 III • !1>(J'q -< 0 300 o , fl> ;5 r'-0 (11....., C1> ;j ...., P' ",o..f-j (11 I/) (1) (') rT P ;:j ::l'-o" o (1) 2-' 0 ;..,- 0' 1-1 n:3 0: ' -,.(') 1-1 5' Z " §. Ci > &5 ::; 'j (fl ;j tfj ;:; e; . - 1:"-, (fI lJl H P ::; Vl 0.. O'I!.. (') (') ::l e;o" (11 (l) o3fl> rDr-,..-:::::r' ==' rt-.- S I/) ::>::>0 (11 C1> P' < """(1) o o..o..(1I;:l 5:i .- "0 ,...,. (1) 0 (ll 0 ;:!.'< g ;:. "0 (11 o ::ly ...:. u - -':i o· (llcrq 0.. 0 J) 0::> o ,...,. P' '-j ::l ..., .- (') '< ::;'P' E ,1> 1/) "0 x. (') ii>;j v"') (1) t.n.. ('t) Y;' ..... .(') 0'IP'3fl> Cl> , '< o IS o 2 10 0
o o ..... ';;-: t-' C t:l t-' i:'l :3 := ?' t!j C'lZ t:!j <: l6) Z {O t: C 1-1 >-on 0 (; t: t!j ()t-' l'1 l'1 t!j z t) " t;:i' 6 (j '" ?' n t:<; (/) ;J ;;;
086 066
PRICE LIST.
"LOWMOOR JACKET."
For use in mines, ships' holds, etc., to secure a patient on a stretcher (see illustration), which can then be placed in an upright position. Price £r 5s.
WATER BOTTLE .

Copper tinned, with carrying strap.
Price lOS.
Enamelled Iron \-Vater Bottle, Cloth covered, with Strap 'ind Carrier, 45. 2cl
LAMP.
This is filted with a sockel, by \I hich lo fix it lo a Litler, or it can be conycniently carried by hand, or attached to a belt or the clothing.
Price complete, 5s. 6d.
Dressing Basin , kidney shaped, made of enamelled iron.
Price IS. 3d.
Ambulance Station Plate , Enamelled Iron, 3<;. 6d. each . Stretcher Depot Plate, Enamelled Iron, 3s. 6d. each.
Carrying Sheet for carrying patients up and clown stairs or otherwise ahout a house. Designed by J. C. Derham, Esq., Hlackpool, and Mrs. Alfred Paine, Bedford. The sheet is filled with rope handles and detachable hamboo poles, and Ulay be placed on a stretcher without disturbing the patient.
Price complele, 15 .
13 PRICE LIST.
LARGE HAMPER FOR AMBULANCE
STATION AND RAILWAY PURPOSES .

For contents see next page.
TH E DAM PER CONTAINS
I Set of Cane, plints.
I Elastic Band T ournique t.
} lb. Carbolic "\ Cotton \Yool LIn Tin . ..... J Cases. lb. Boric Lint
I Roll Adhesive Plaster.
20 Roller Bandages, asso rt ed .
T doz . Tria ngular Bandages.
3 Pieces T ape .
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda.
4 oz. of Olive Oil.
4 oz. Spirit Ether Compo
i l b. Tin Powdered Boric Acid.
4 oz. Tincture Eucalyptus B.P.C.
I pair Pean's Forceps.
I pair Scissors.
1 Knife.
12 Surgeon's Needles.
T packet each Safety and Plain Pins.
1 oz. Ca rbolised Chinese Twi st. oz. c.;ilkworm Gut.
I ree l eac h Black and vVhi tc Sewing Thread.
I Kidney-shaped Basin. topper Loosener.
1 Graduated Measure.
I cake 20 per cent. Ca r bolic Soap.
I N ai l Brush.
3 Empty 8 oz. Bottles.
Pric e complete, £4
PRICE LlST.
PRICE LIST. 16
PRICE LIST. 18 SURGICAL HA VERSAC .
SMALL AMBULANCE HAMPER .
'With waterproof cover and strap, for use in collieries, stations, and large works, as well as for parochIal and domestic use.
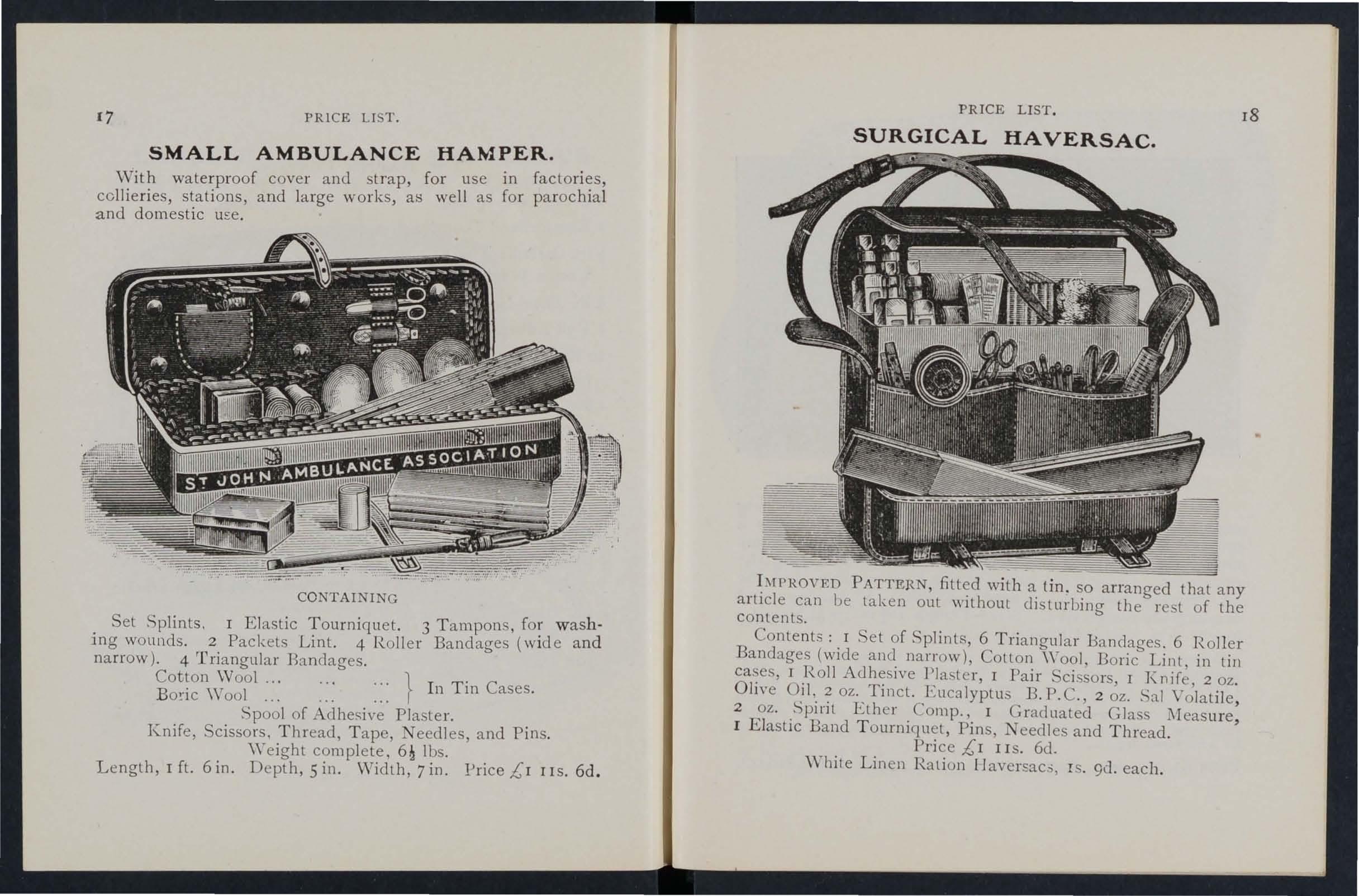
CONTAINING
Set Splints. I Elastic Tourniquet. 3 Tampons, washjng wounds. 2 Packets Lint. 4 Roller Bandages (w Id e and narrow). 4 rrriangl1lar Bandages.
Cotton Wool ... \Yool 1In Tin Cases.
Spool of Adhesive Plaster. . Knife, Scissors, Thread, Tape, eedles, and PiI1s.
Weight complete, Ibs.
Length, 1ft. 6 in. Depth,s in. vVidth, 7 in. !Jrice £1 I IS. 6d.
IMPROVED PATTERN, fitted with a tin. so arranged that any article can be taken out without di turbing the re t of the Content.
Contents: 1 Set of Splints, 6 Triangular Bandages. 6 Roller Bandages (wide and narrow), Cotton \Yool, Boric Lint, in till cases, I Roll Adhesive Plaster, I Pair Scissors, 1 J\:nife, 2 oz. Olive Oil. 2 oz. Tinct. Eucalyptus B.P.C., 2 oz. Sal Volatile, 2 oz. Spirit Ether Comp., 1 Graduated Glass Measure, I Elastic Band T ourniquet, Pins, eedles and Thread. Price £1 lIS. 6cl. \Vhite Linen Ration Il avcrsac;;, IS. 9d. each.
17 PRICE
LIST.
FIRST AID COMPRESSED KIT.
Th e box is made of wood covered with damp· resisting material, and is fitted with a lock and key. It contains a num ber of practical ambulance appliances. arrange? so t.hat any article can be withdrawn or replaced wIthout dIsturbing the remainder. Being fitted wil h a handle it is portable, and the lid when let down, can be used as a tahle . All bandages and compressed. Size -Length 161 in.; width in. ; height cl in. without handle.
Contents: 4 Triangular Bandages, 6 Roller Bandages, 4 Fi:st Dressings, 6 Small Packets of Cotton Wool, 6 Sn:,all Bonc Lint, :r Band Tourniquet, I Measure Glas', lln Lox contal.ntng a Roll of Plaster, Boric Lint Patches, Scissors and Pins, I tray contalnll1g 3 ( Sal Volatile, Tincture of Eucalyptus and Olive Oil) an0 a Dredger of B?rLC Acid, of improved Splints, with angle piece, 8 Splint Straps (sufficient for a fractured thigh).
Price £1 I IS. 6d. Each article is pri ced separately ( see I ndex ).
FIRST ,RID
eeMPRNI(f)lV.
mRESSINGS AND BANDAGES COMPRESSED).
SJ. Rlllblllan(t R$$tXlallon, Price Is. 6d. $t JObn 's 6alt, I 8 Ckrktnwtll, Coni/on. E.C. [J)' Post s. · d.

Size 4! by 31 by Ii inches. Suitable for the pocket.
CO L TE TS.
1. Triangular Bandage. 2. First Aid I?ressing. 3. \Vool. 4. Two ' plint Straps. 5· Adheslye PIa ter. 6 . Permangallate of Potash. 7. Lanoline. 8. Boric Lint Patches. 9. Safety and Plain Pins.
Price, each IS. 6d. By Post IS. 9d. Per doz. 17,:,· 6u. carriage paid . SEPAR,\.TE ARTICLE
No.
I 4(1. each or 3/9 per doz.
2 2d. ,,2/0
3 rd. "rod."
4 2d. per strap or 1/9 "
5 rd. per box or rod. " "
No.
6 Ill. per b ox or rod. per d,)Z.
7 per tin or 1/4 "
8 leI. per packet or rod.
9 rd. lod.
Not less than one dozen supplied at dozen prices.
19 PRICl<: LIST.
FIRST AID BOX FOR "ASHFORD" LITTER. OR AMBULANCE
STATION
.
'fhis is primarily d esigned to be placed on the "Ashford" Li tte r (1899 Mod el), but it is further adapte,d to be fi hUd,g t P on a wall. A detachable lea th er handl e IS also lte, Gr qrrying purposes .
F c r cont ents 5ee ne xt page.

l'RICE LIST. 22
CONTENT, OF FIRST AID BOX . (Jllu,trated on page.)
Sel of Wooden Splints; I Eia,tic Band Tourniquet; Carbolic Wool, Boric Lint, in tin cases; I Roll Adhesive Piaster; 12 Roller Ban<iages, ;H<orted; 6 Triangular Bandages; 3 Pieces of Tape; 1 Pair cissors; I Knife; t Kidn ey-shaped Basin; I Graduated Measure; 2 oz. OliYe Oil; 2 oz. Tinct EucalYPlus H. p.e.; 2 oz al Volatile; 2 0Z. Spirit Ether
Comp.; 8 oz. Carron Oil; Pins, Safely Pins, Needles, Thread.
PRICE COMPLETE £2 IOS.
POUCH FITTINGS,
specially selected for the St. John AmbuJaLCC Bi igade, consisting of :-..
2 Triangular Bandages, one of which is sealed up in \nlxed paper. The other may be used for praclice, but should be kept as clean as possible.
2 Roller B andages (3 in. and I in. ).
Packet o f Cyanide Gauze (r yd. compressed).
I Pair Scissors.
6 Safety Pins.
Small Bottle of strong Smelling Salts.
Piece of strong Cane, for tightening improvised Tourniquets.
Price, 2S. Sd. each. 6 doz. or more. 2S. 7e1. each.
Packets of Cyanide Gauze (r yd. compressed). Price per doz" 2S. Sci.
Smal l Bottles strong Smelling Salts. Price per doz., 6d.
S AFET Y PINS.
All fasten or unfasten on either sick.
Facile No. S 600 or S 602 per 3 doz.
" "S 603
Duchcss Duplex, No.2 ... per rio".
A sso rted
Special i{anket Safcly l'ins, 3 in.
21 PRICE LIST
il s , d. 0 6 0 R () 2 0 .') 0 6
PR:CE LIST.
Tourniquet, E lastic
Tourniquet, Field
Splints, \Vooden, per set, 2/6 ; Cane... . . ,per set
Greatly improved Wooden Splints, with grooved joints and angle piece, strongly recomm endec1
Tow, for splint padding ... ...per lb.

4 6 o 6
First Field Dressing (Army Regulation Pattern), Price ... each 0 9
Jaconette, 44 inches wide per yard 2 3
Tow, Carbolized or Styptic ... per lb. 0 9
Wound Pad.-A pad of cotton wool and gauze, to which a bandage is attached. The !;urface of the pad coming in contact with the wound is not touched by the hand of the person app lyi ng the p::td. Price 4d. each .
First Aid Dressing, consisting of a small compressed packet of boric lint, a compressed roller bandage, and a safety pin .
Price 2d. each.
Dredger, containing boric acid powder, IS. 4d .
Measure Glass, 2d.
Knife with strong blade each 9d . ; per doz. 8s,
Pair of Scissors each IS. ; per doz. lOS.
Splint Straps, \V ebbing, and suitable Buckles. Per set of 12 yards of strong 2-inch Webbing and 15 Buck les, 2S. 6d. These make very compact St raps fo r carryin g in the Pouch. The Webbing should be cut to meet lo cal requirements. Buckles on ly, IS. 3d. per dozen.
Webbing only, I S. 3d. per dozen yards.
It is unnecessary to sew the Buckles. Th e spikes should be passed th rough the webbing, and the short end of the webbing, shou ld lie olltwards.
PRICE LIST. PLASTERS.
Leic.ester Adhesive Plaster on Cambric, in tins of ,l; yard, 6 mches wide ... .. . ... ... ...... 6d.
The L eicester Adhesive
Ribbons, in tin boxes, 6 yards long.
N ational Rubber Adhesive Plaster (Antiseptic) on spools.
5 yd . IO yd . i inch wide 9 d . I S. od . I S. od . I S. 6cl . 2 IS. 9cl. 2S . 3d . inch wiele
I inch wide
Ditto in box, in. wide, !/. yds. long ... tm I ;) 3 s 1 " s " COURT l )LASTER , TRI COLOR Large Size, 9d. ; Medium, Sd. ; Small, 3d.
.
.
23
s. d. I 6 6 2 7 6
6d. 8el. rd. 3d. 3d
6d. 9d
PRICE LIST.
NURSES' WALLETS .
ORDINARY PADLOCK
\YiLh o ut in strum enLs, 4<;· 3d.
Fitted compleLe, containin g Spring Dressing Fo rceps, Spatula, Probe, 2 pair Sc isso rs (round and sharp pointed), Clinical Thermometer, a nd Knife.
Price lOS.

ST . J OlIN'S PATTER:\, as illustrated, but impro\'ed by the addit ion of flaps to protect the instruments.
\\'i thout in st rum ents, 7s. 9d .
Filled complete, containing Spring Dressing Forceps, Artery Forceps (a lsc useful fo r dressing), Spatu la, Probe, Director with Ear Scoop, 2 I a irs .cissors (round and sha rp pointed),
Clinical Th ermometer (m inute : round), Knife, Pencil, and Pins.
Price £ I I S.
Plain Triangular Bandages, eac h (Special quotations for la rge quantities . )
DiHo Com pressed (thinn e r quality), each 4d. ; per doz. 3s. 9d.
Illustrated Bandages. (afte r E march) showing 25. of th e Tna ngular Bandage, with printed mstruct lOns ...
PRICE LIST. 26 ROLLER BANDAGES. (6 yards long. ) Open W ove Grey. Fine Grey Calico, or Superior \Vhite Open \Vove. [jest qual it y, Superior 'White, with White O pen \\'oven \V ove Edges. Compressed . d. d . 5. d s. <I. in. per doz. I in. I in. 2 in. in. 3 in. 4 in. 6 in. 0 9 3 I:) 2 2 0 2 3 4 9 0 2 0 .3 2 6 6 3 0 0 3 6 2 6 4 0 2 6 4 6 3 6 ROLLER
Each packet contains 6 bandages as follows :3 6 9 3 9 9 6 yard long- one 6 in ch, two 3 inch, one I inch : 4 yards long-two 21 inch. s. d. Fine Grey Calico per packet 0
BANDAGES in Asso r tment.
each per d Ol. o 4 6 6
PRICE LIST.
ROLLER BANDAGE MACHINE.

De igned by Dr. A. C. Tunstall.
Price 25. 6d.
Forceps, dressing, f ull size or small as desired, IS. ; bow d ressi ng, 5 in. locked joint, I S. 6d . ; Pean s Artery, 5 in . locked joint, IS . 3d .
Scissors, round-pointed, IS.; sharp-pointed, fo r delicate work, I S. 3d. ; small r ound-pointed blades, locked joint, or 5 in . , I S. 6d.; round-pointed curved hlades, locked joint, IS. 6d.; sha rp-pointed curved blades, locked joint, IS 9d . The locked joi nt allows the blades to be taken apar t for cleaning.
Spatula, 9d . Probe ,6d. Director, with Ear Scoop, IS. 9d.
Knife , very thin, ivory handle, two blades, I S. 9d. Nursing Chart, designed by Miss I nderwick, each . Temperature Chart, !i-d . each.
CLINICAL THERMOMETERS.
Round. O rdinary, IS. ; minute, I S. 3d . ; half-minute, I . 6d.
Flat . Strongly recommended as they will not roll. Ordinary, IS. 6d. ; rapid (specially splected and reserved for the Association), with very open scale, 3s.
PRICE LIST.
CLINICAL THERMOMETERS -(continlled}.
W ith Magnify in g L ens. Price, ordinary, IS. 6d.; minute, IS. 9d. ; half-minute, 2S. 3d.
N.B .-Minute and half-minute instruments will only register in the time stated under favourable circumstances. No llabi!£ty is taken for breakage of Thermometers in b·aIlSl't.
BATH THERMOMETERS.
To Dr. Forbes' specification. Japanned with zinc scale, 2S. 3d. ; Clinical Thermometer size . in case, IS. 6d. iVo liability is taken for breakcz,E!'e of Tlzerlllolllete7's ill trails/!.
COTTON WOOL.
P lain, I oz., 2d. ; 2 oz., 3d. ; 4 oz., 4d. ; lb., 7d.; I lb., IS.; small packet (Compre sed), Iel.
M ed icated , Boracic, :! lb ., 6d. ; I lb., IS. 6d.; Carbolic, per lb., IS. Sd.; Alembroth, per lb ., 15 6el.; Double Cyanide, per lb., 25. 6el.
L INT.
Plain, I oz., 2d. ; 2 oz., 3d. ; 4 oz. , 6d. ; lb., lad. ; I lb., IS. 6el.
B or acic, 4 oz., 6d. ; I lb., IS. 6el. ; square foot packet, 2d. ; small packet (Compressed), Id .
GAUZES.
These are supplied in 6 yard lengths, width ahout 36 i'1ches. s. d
Unmedicated white
Alembr'oth
Double Cyan ide
Boracic
per length a ro a 2 2
GAUZE
TISSUE.
A layer of absorbent cotton wool uet ween two sheets of gauze, good quality, per lb., IS. 6el .
29 PRICE LIST.
TEXT BOOKS, &c.
"FIR.ST AID TO TIlE INJURED." By James Cantlie, M.B., f. . R. C. S. The authorised Text Book of the I<irst Aid Course. IS.; by post , IS. 2d.
"A CATECHISM OF FIRST AID." Compiled frol11 Dr.Cantlie's Manual. By J. I. Carvell, l\1.R C.S., L.S . A. Price 6d.; by post 7d .
"JIINTS AND HELPS FOR HOME URSING AND HYGIENE." By E. MacDowell Cosgrave, 1\1. D , illustrated, with on the application of the roller bandage, by R. J . Colhe, M.D. The authorised Text Book for the Nursing Course . IS. ; hy post IS. 2d. .
" A CATECHISM OF II O:-'IE URSING" (based on Dr. Co,;grave s Text Book) . By J. Brown L.R.c.P., L.R.C.S., and J. M . Carvell, M.R.C.S., L.S .A. Price6d . ; by post, 7d . " HOME lIYGIENE." By John F. J. Sykes, D . Sc. (Public Health), M . D., &c. I llustrated. The authorised Text Book for the IIome Hygiene Course. IS.; by post, IS. 2d.
" A CATECHISM OF IIOME HYGTENB:" (hased on Dr. Sykes' Text Book). By J. M. Carvel l, I RC.S., L.S.A. Price 6d. ; by post 7d.
"QUESTIO S ANSWB:RS UPON \V?RK':'
John \V. MartIn, M . D., and John Martll1, F.h.. C.S. Ed. I . ; by post, IS. Icl
"QUESTIONS A, 1) Al\S\\·ERS UPON NURSING." By John \V. :Martin M.D. IS. 6el . ; by post, IS. 8el. "FIRST 'AIO TO TIlE INJURED (Six Ambulance Lectures)."
By Professor Frederich Esmarch. Trnnslated from the German by H. R. II. Princess Christian. 2S.; by post, 2S. 2d . " BANDAG[l\G AND SURGICAL DRESSING." By Walter Pyc, F . R.C . S. 2S; l)y post, 2S. 2J." .
"To RESTORE THE ApPARENTLY DROWNED, printed in large Type with two Diagrams. Unmounted, 2d. each; by post, 3d . Mour.ted, with red Lorder, and varnished to up, 6d. ; post free, packed, IS .
PRICE LI T.
TEXT BOOKS. &c.- (continuea,.
DR. G. H. DAR"'!. 's "FIRST AIDS," being a card to hang up, giving treatment of various acciJents. 2d.; by post,
"MANUAL FOR '1'. JOHN AMBULANCE COi\IPANIES. By Lieut.-Col. G. E . TWIss, R.A.M.C. (Retired Pay). Pric;; 6d.; by post 7d.
"now TO ACT W[fE . CLOTIUNG TAKES FIRE." By J. E. II. l\Iackinlay, 1\I.R.. S. Unmounted, 2d.; by post, 3d.
Mounted on card and varnished, 4d.; by post, packed, 7cl.
"FIRST AID PRINCIPLES . " Cards of concise directions for wai tcoat pocket, eaeh; 4d. per doz. Special for large quantities. '..
"SPECDIEN EXt'I[NATION PAPERS, FIrst Aid, 1 llrs1l1g and IIygiene Courses." 3d. ; by po t 4d.
SlIIALL ANATOi\IlCAL DIAG1{Ai\L Showing the human skeleton, main arteries, and point where pressure should Le applied to arrest bleeding. 2d.; by po t, 3d .
DIRECTIONS AS TO TIm RESTORATION OF PERSONS SUFFER I G FROM ELECTRIC SIIOCK. Large prinl, poster size. 3d . eaeh ; by post, 4d. ; or 25. 6d. per dozen.
GENIl:RAL NOTES FIRST All) TO BE RENDERED I ' ASEs Of<'
POISO. I G. By Milnes Hey, M.A., M.R.C.S. , L.R.C.P. Price 2d. ; by post, 3d.
" Ai\IBULANCE TABLETS." By 'ydney Partridge, 1\1. D. Price IS. ; by post, IS. Id.
NOTES ON MILITARY SANITATION. By Lt.-Colonel II. P. G. Elkington, R.A. M. . Price 6d. ; by post 7c1.
"E IERGENCY BOOK," for in tantaneous refe rence, giving concise instructions; to hang on wall. Size about one foot square . Price 2S. 6el. ; by post, 3s.
AIDS TO MEMORY FOR FIRST AIn S 'I UDEKTS. Rc\"i3ed lo date . Additional IllustratIons. By L. 1\I. Frank Christian, M.B., C.M., Edin. 6J . pe r copy; by post, 7c1.
Ruu:s FOR CORPS AND DIVISIONS, L. John Ambulance Brigade. 2d. per copy.
31 PRICE LIST.
TEXT BOOKS, C3c. -(continuedl.
A History of the Order of the Hospital of St. John of Jerusalem. By the lat e Rev . W. K . R. BEDFORD, M.A., and Lieut.-Colonel R . H. II OLBECHE . Price 5s , ; by post 5s . 4d .
The Knights Hospitallers in Scotland and their Priory at Torphichen. By GEORGI<: THOMAS BEATSON, M.D., C.B.
Price 2S. 6d., post rIce, 2S. 8d.
Registers . Class Attendance, 2S. 6d. 4s. 6d. Case Report, IS.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three, 7S. 6d. Receipt Book, 6d.
Large Physiological Diagrams. For Lecturers' use. Comprising: Th e Human Skeleton, the Muscular, Arteria l and Venous Systems, the IIeart and Circulation of the Blood, Simple Fracture, ompound Fracture, Dislocations. Price per set of six, I5s. These may be hired for a course of "First Aid" lectures, given under the auspices of the Association, for a fee of 5s., or with the addition of Splints , Tourniquet, and plain Triangular Bandages, for a fee of lOS.
Boxes of Stationery for the use of Class Secretaries and othe r s connected with the Association, containing twelve of high-class paper, suitably headed, and twelve envelopes bearing the device of the Association. Price fid., by post 9d. Twice that quantity, price IS., by post I S. 3d. Medallions, issued only in accordance with paper No. 62. to be hael on app li cation. Coinage Bronze, 2S.; Silve r, 7s. 6el. ; Gold, £2 lOS.; including engraving name and number on back. ,\Lorocco velvet-lined case, '\ Labels, to be placed above Medallions for each subseq nent year's examination, issued only in accordance with paper No. 62. Coi nage Bronze, 6d. ; Silver, I S. 6d.; Gold, 12S. 6d.

Arm Badges, with the device, issued und er the a uth
of the Central Ex ecutive Comm ittee, having been first approved by H.R.H. the Grand Prior as the sole official and recognised Badge of the AssociatiQJl and Brigade . N. B.- TILis design is protected.
o. For the use 'of individual pupils- s. d .
Small Celluloid Badge, for button h ole or brooch
. White Satin Armlet, with woven Badge
32
ority
N
I. In German Silver, Large Size ... .. . .. 0 71 2. Small Size ditto 0 6 3. Small Size for button hole 0 6 4. In Electro L a rge Size 0 5. Small Size ditto 0 9 6. Small Size fo r button h ole 0 9 7. In Enamel for button h ole 0 8. " brooc h 3 9. In Cloth and Silk... 0 9 1 0 . In Cloth and Silver
Num :.h; r, 3522) 2 0 I
In Cloth
0 6 Ii.
0 2 13
0 14.
(Registered
I.
and \Vorst ed
Black Silk Arml et, with printed Badge 0 6 N.B.-Th ese Badges are 1Iot to be worn as decoratioll s.
33 BADGES. PRICE LIST.

For members of the St. John Am bu lanc e Brigade, having the name of the Corps o r Division ann..;xed on a label, oIlly issued in quantilies-
1 o. IS . In German Silver, fi rst d oz ., £1; subsequ e nt doz ., 12S
16. In Electro Plate, first d oz., £ 1 12S.; subsequent :lozs., £ I 4s.
17. In C loth and Silk, per d oz., J2S.
" 18. In C loth and Silver, per doz., £ r lOS.
All the above may be worn by members of the St. John
Am bulance Briaade, not we1fin g uniform.
Fo r o f St. J ohn Ambulance Companies-Cap
Bad2e in German Silver, 6d.
BRIGADE UNIFORM
Officers. Cap Badge (Reg. No. lOr) each 0 8
Colla r Badges ( I03) per pair 3 " POllch Badge ( ? ' 3,657) each 2 6
Sergeants , Corporals and Pnvates.
Cap Badge (Reg. N o. I02) ... each
Collar Badges \ " 104) pe r pai r
Overcoat Badge( " 1,582) ... ... eac.h
Shoulder Titles, '.J.A.B., with numeral, per paIr
Should er Straps, fitted with title and numeral ...
Lady Officers of Nursing Divisions.
Superintendent's Cloak Badge (Reg. No. 3,658)
ri ntendent's A r m Badge ( " 3.659) Other Nursing Orficer's Cloak Badge (" 3,555) Othe r Nursing Officer's Arm Badge ( " 3,656) \ Vhite Box Backs, for Badges ... per pair
Nursing Sisters . Arm Badge (Reg. o. 3 .522) ,. Cloak Badge ( " 3,521)
Black Silk Armlet for Arm Badge, Superintendent
Other mem bers
Honorary Surgeon's Crosses (pattern B ) per pair
Superintendent's Sta rs (pattern A)
Medallion Badge (pattern D ) ...
Nursing Badge (paLtern E) ..,
Satin Badge for ursing Sister's Pin Cushion
Bu g ler's Badge ... 4 0 Bugler's Cord
Secretary's Bad ge .. .
Whistle and Chain ... each :!
Brown Waist Belt and Pouch " 8
White Piping, per packet of 7i yards, enough for 3 pairs of trouser (packets cannot be broken) 2 L .'lce, per ya rd, Sih'er , lIS. ; Black 0
PRICE LIST.
34
BADGES, etc. s. d.
Supe
Honorary
0 6 0 0 6 0 6 3 4 6 3 9 4 0 3 3 0 3 2 0 2 3 0 0 3 0 6 0 6 0 0 3 0 3 0 I 0
0
Private's
BUTTONS FOR THE UNIFORM OF THE ST. JOHN AMBULANCE BRIGADE.
Issued only for the use o f Office rs and Members of Corps and Divisions wearing the prescribed uniform.
German S il ve r, No. I (large)
No.2 (merlium) ... ,.
No. 3 (small , for C:1ps)
Electro Plate, NO.4 (large)
NO.5 (medi um)
No. 6 (small, for cap'l)
Bu.ttons the Uniform of the Companies as per Nos. I to 3

ELECTROTYPES OF THE ST. JOHN AMBULANCE DEVICE.
N o.1. For Cards, Ticket s, &c
2. For Note Paper, Small Circulars, &c.
,,3 . For Quarto and Foolscap Leller-
paper, Circulars, &c.
4· For Small Posters...
,,5· For Large
Prints of the above Electrotypes (1 to 3\ appea r on the following page. No. 4A is shown on page 32. The diameter of SA is 3 in., and of 5B without scroll.
35
PRICR LIST.
St. per doz. s. d. o 6 0 4 0 3 3 0 J 6 I 6 J"hn Ambulanc (
Series A B for for Association Brigade use s d. 1 0 1 0 use. s. d. I 0 3
0 3
6
9 3 0 Complete Series 3 5 6
Posters...
PRICE LIST. ELECTROTYPES. No. I A. 3 A. For prices see pag-e 35. ;; NO.3 B. No.2 B. No. I R

37
Flags PRICE LIST. £ s. d.
PRICE LIST.
bearing Association device - 12 feet by 6 feet 6
5 feet by 3 feet o 12 6
Brigacle 4 ft. 11in. by 3 ft. o 12 0
SWAGGER STICKS
for the use of Officers and M embers of th e
St. John Ambulance Brigade.
Ebonised Canes, German Silver Tounts bearing the Brigade Devicc.
PRICE IS. EACH.
O fficers' Special Canes, with Ste rling Silver Mounts.
PRICE 7s. EACH.
BEARER'S DRESSING CASE.
PRICE 12S. 6d.
A II Orders for the foregoing Stores should be given to th e Local Secretary, or to the Stores Department,
St. John Ambulan ce Association, St. John's Gate, ClerkenweIl, London, E .C.
UNIFORMS FOR AMBULANCE UNITS OF THE S.J.A.B.
The,<: - may be obtained from Hazel & Co. (sole partner, D. IIatel. for many years associated with Hebbert & Co., Ltd., as Director), Clothing and Equipment Manufacturers, 65, East Road, City Road, London, E.C., and at 6, York Place, Leeds, and 8, Cadogan Street, Glasgow. Telephone: 4390 London \Vall. Telegrams:" IIazeli m, London."
All Badges and cm'riage outside London area exba. lI£easurtments 10 be supplied free of charge.
CHIEF A D IIONORARY SURGEO S.
Tunic, Superfine Black Cloth ...
Trousers, Superfine Black Doeskin (if Silver Lace Stripe, extra)
Cross Belt and Pouch, Plain, 20/-; Silver Embroidered
Cap
Gloves
Great Coat, Grey Cloth
DISTRICT AND COHPS SUPERINTENDRI TS.
DIVISIONAL SUPERINTENDE TS AND AMBULANCE OFFICERS
1St Quality. 2nd Quality. £, s. d. d 4 4 0 3 I7 6 5 o 3 7 6 o 15 6 04 6 440 o 0 9 0 o 3 6 3 10 0
Tunic, Superfine Black Cloth ... 4 4 0 3 T7 6 Patrol Jacket, Superfine Black Cloth ... 3 3 0 2 I7 6 Trousers, Superfine Black Doeskin I 0 Cross Belt and Pouch o 13 6 Cap o IS 6 0 9 0 Gloves 0 4 6 0 3 6 L eggings ... 0 g 6 0 6 6 GreaL Coat, Grey Cloth 4 4 0 3 10 0
Patrol Jackets, Superfine Black Cloth 2 6 6 I 17 6 Trousers, Superfine Black Cloth J 2 6 o 15 0 Cross Belt and Pouch ... 0 13 6
DIVISIONAL SUPERINTENDENTS AND AMRULANCE OFFICERS -contiJlued.

Great Coat, Grey Cloth
Jacket, Black Vicuna
Fatigue Trousers, Black VIcuna
FIRST CLASS SERGEANTS
Patrol Jacket, Superfine Black Cloth
Four Bars, Silver
Patrol Jacket
Chevrons, Silver, Three Bars, 2/6 " " T wo Ba rs, 1/15
Trouse rs
\Vaist Belt and Pouch
Cap
Gloves. COllon
L eggings, Black L
Bottl e ann Carner
ave rsa ck, WhiL e Duck
Coat,
UNIFORM FOR NURSING UNITS
Serge Cloak (Badge extra)
Special 'Waterpro of Serge, extra
Serge Dress, to measure
Do., Cheaper quality, in 'White
CaJ riag-e paid on all drap e?JI O?·ders. Self-measurement forms sent free Otl request.
T elegrams: "Everything, London ." Telephone: vVestern One (60 lines) .
39 PRICE LIST.
2nd Quality. 1St Quality. £ s. tl. £ s. d. Cap o IS 6 0 9 0 0 4 6 0 3 6 Gloves 0 8 6 0 5 b
... ... . ..
Leggings
4 0 0 3 10 0
... r IS 0
Serge
o 16 0 o 12 6
Serge
... I 18 6 Chevrons,
... . . . 0 3 6 Trousers,
0 0 15 0 Cross
0 10 6 . 0 9 6 Cap 0 2 9 0 4 6 0 3 6 Gloves 0 0 8 Cotton Gloves .. . ... . .. Leggings,
or
L ea ther 0 4 0 0 3 6 \\'ale r
and Carner 0 3 6 H ave rsack , 'White Duck ... 0 I 6 Gleat
Mellon o IS 0 o 13 6 SERGEANTS,
AND P R I V A rES.
Superfine Black CIOlh
Belt and Pouch
Black
Br?wn
Hottle
Coat, Dark Grey
CORPORALS,
. . . ..
...
...
II
... Great
D ark Grey, Mellon o II o 09 6 066 029 008 04 0 o 3 6 o I 6 o IS 0 o 10 o 8 o o 3 o 13 3 9 9 6 6 PRICE LIST.
eat h:r \ V ale r
OF THE S.J . A.B.
Better quality do. £ s. d. o 19 I I 026 7 6 I 10 0 Cotton Dresses, complete to measure 0 9 4 Cotte n Dress L ength s, 8 yards 0 3 10 B on net ... 0 9 6 Do. , for lady officers 0 J 0 6 Collars ... Si d. each; per doz. 0 5 6 Cuffs to maLch 6id . p er pair; per d oz . pairs 0 6 6 Cap, "Sister Dora" ... 8 id . each; per doz. 0 8 6
tucked ends 3id. per pair; per doz. 0 3 3 Nurses ' Sleeves, elastic band and button at wrist per pair 0 Stiff Linen Belt . . . 4id . each; per doz. 0 4 3 Nurse's All-Linen Apron, in white ... each 0 3 6
each IS. II
0 2
Cambric Strings for above,
Union,
and

INDEX TO PRICE LIST.
Ambulance Hampers ... Station Plate
Bandage Rolling 1Inchinc
Bandagps Basin, Dressing
Bearers Case Bed, Equipoise " Camp Books
Dottles (Water)
Buttons
Carriages (Horse Ambulance)
Carrying Sheet
Cash Book
Cotton Wool Cover for Stretcher or Litter
Diagrams, Large " Small
Dredger (BOlIC Acid)
Dressing Basin
Drowning Tackle
Klectroty-pes ... Emergency Book Aid Hox .,. " Companion
Fir5t Field Dressings ...
Forceps
Gau7es ... Gauze Tissue
Hamper, (.-\.mbulance)
J Iaversacs
B ]-lnou and 'pTOn for Lillcr llbtrllmcnb (variou,) T i'-lllf.-: Labels l.ace for Cap"', &.c
.. , . ..,
P,\GE 15 to 17 14 32 to 34 27 26 14 37 12 12 29 to 3T '3 35
.. " Kit
... ... 14 3 28 II 31 30 23 14 12 35, 36 30 9, 21,22 1'1 23 37 27 28 28
15 to 17
... .. .
J.nmp Lilll ...
4 27 23 '23 3 1 34 14 28 PAGE Litter(Rea.Ec\wnrc\s)
LO 7 Lowmoor Jacket 13 i\Jeasure Glass... 23 Medallions 3' l\linute Book 31 ur,es' \Vallets 25 ursing Charts 27 Occurrence Dook 3 1 Pillow... II Pla!:>ters . 24 Pouch Fittings Receipt Book 3 1 Registers .. , ... 3 1 Roller Bandage Machine 27 Rug .. ... ." Rules for Corps or Jobn Ambulancc Brigade :;0 Safety Pins 2'2 Scissors... 23, 27
Splint Padding 2, plint Straps ... 23 ' plints ... 23
3 1
14
... ." 8 to 1 T
Legs
37 Temperature
29
27,
23 Tow,
23 " plain 23
34
\\'''terproof Sheet ami Chain 34 Wool (Cnnon) ... 25 Wound Pad 23
Lllter
···5
Slings, Stretcher
Stationery......
Stretcher Depot Plate
Stretchers
,. Adjustable
for 9 Swagger Stick...
Ch:ut '27 Text Books
to 3 t Thermometers... ..,
2e
carbolized
U nifoTm Sundries
Uniforms 38 to 40 \Vagons ( H orse Ambulance) \\1 :lter Rottles 13