AS COMPANIONS TO THIS BOOK" A CATECHISM ON FIRST AlD."
BY J. M. CARVELL, M.R.C.S., L.S.A .Price 6d. post free.

"PROBLEMS
IN FIRST AlD."
BY L. M. FRANK CHRISTIAN, M.B., AND W. R. EDWARDS, A.C.A.Price 6d. post free.
FIRSY[ AID TO TIlE INJURED
ARRANGED ACCORDING TO THE REVISED Sl'LLABUS OF THE FIRST AIV COURSE OF THE ST. ASSOCIATIOX.
BY JAMES CANTLIE, ;\;.A., :.\f.B.,
f(w'sld 0/ Craa 0/ the Order '1./ St. J<1ll1l. l-loIlOla)y Lije Jfcmo.:l' O/, alt" Lectlerer all,t E,raJl/ilh" to, tilt: A ssociatiOIl.
a on, "Slr<:lcher Tra..nsport," reviset! from thaI tlly Wl'llte':l by Sn 1- VllLEY, c.n., o/Iustlce 0/ the: Order 01 St. ]Oll.", III accordance wilh lhe Army Stretcher Exercises. .\,1;0 a C" \1'I'J"R (iJellli,; Fiflh L:clure, for F'em.des only), by E. L COSGI<.\ \'£, M.n., V.R.C.P.I., 0/ (,race 0/ tlu Order 0/ St . .John, //"ltura»), Life ,){emoer 0/, alld L,'ctrerel illl.! EX,lillino' to, tllr: ASSOclatiOll.
TWENTIETH EDITION. 880,000 to 930.000.
(Tllis':cil,tIOIL is similar to the in wlticll "difiClIl lIlallY 01 the tllus" atlons iCel ere-drawn; otlUl WISt! Lt diffi'n bitt lif tie /i-ulll t1lol ell!vt!lt!lt 10 tilt! "."lelllcclttIL ed"iolls)
Price in Cloth, IS. nct i by post, IS In Morocco, 25. 6d.; by post, 25. 8J. TO BE OBTAINED AT ST.
JOIlN'S GATE, CLERKEN\\"ELL, LONDuX, E.C.
W. H. & L. C. 50 ,000-Io/r9 I2 .
,We <PraHl> IPrior}] of U1)e of tbe 1boapitaL of 5t. 3-c bn of 3 cnlsalem in JEllglalll>.
SOVEREIGN IIl·:AO AND PATRON: IllS MAJES1 Y KING GEORGE V.
GRAND PRIOR: II. R. II. The DUKE OF CONNAUGHT, K.G.
SUD-PRIOR: The VISCOUNT KNUTSI' ORD, G .C. :M .G.
EXECUTIVE OFFICERS:
PRELATE.-IIis Grace The Archbishop of York.
CHAKCELLOR. -Col. Sir Herbert Jekyll, K C.M.G.
SKCR.ETARY-GENERAL.-Col. Sir llerbert C. Pe.rott, Bt., C.B.
Rl<.CEIvER-GENERAL.-Edwin Freshfield, LL.D.
DIRECTOR OF THE AMBULAKCE DEPART.\lEKT.-Thc Earl of PI) mouth, C. B.
CIIAIRMAN OF TilE BRITISH OPIlTIIALl\llC IIOSPITAL, JERUSALEM.-Col. Sir Charles M. \\'atson, ICC l\I.G., C. B.
ALMONER.-Sir Dyce Duckworth, Bt., M.D., LL.D.
LIBRARIAN.-Liellt.-Col. Richard Holbeche.
REGISTl{AR.-The Earl of Ranfllrly, G.C.M.G.
GENEALOGIST.-Sir Alfred Scull Scott-GaUy, K.C. v.o. (Carter).
ASSISTANT FXKCUTlVE OFFICERS:
A SSISTANT Rl..CEIvER-GENERAL.-Edwin Ii. I resbfichl. ASSISTANT DIRli.CTOR OF THE Al\lBULANCE DErAKT:llENT.-
1 ieut. -CoL Sir Richard C. Temple, TIt., C. I.E. HONORARY SECRETARY OF TilE BFITlSlI 01'1ITHAUlIC IIQSl'ITAL, JERUSALEM.-Col. Thomas II. llendley, C.LE. ASSISTANT [lONORARY SECRETARY (FOR OF TIlE BlUTlSll OPHTHAUflC I JOSPITAL, ] ERUSALE:ll.-] v!ll1 IIUll1e Ste, enson (Ullicorn F1lrJuivall/).
LIBRARIAN.-Cyril L'a,'enport.
SECRETARY. \\'i'liam R. Edwards, A.C.A.

THE COUNCIL:
The CounCIl or the Sub· Prior . of the F.xf"clltin • EMBERS; n clles, ru>d the following
SIr J. Furley, C.B. MaJor·Gen. J. C. Dalton Inspector. General B. . c.Y.O., M.D., R.N. Tinnis, E: H. Freshl,eld. • Llt!ut..Cot. Sir R. C. Tem I· B C.t.E. P , t., SIr R. D. Powell, Bt. t M.D. K.C.\'.o ••
The Bisnop of Southwark Inspecto "-General Sir J.' N. Dick K.C.B. J R.N. ' ¥h Owen, LL.D., F.R.C.S. C ,e i,ordHClauJ Ha lIilton, M.P. O. • Hendley C.l.lt.
Th THE CIIAPTER'
e Chnpt r consists of the Kn'<Th .• the r_},ecutive Offi I", ts of J LJstlce and c: bPI
Selected Offi , eu .\Lemb . rs of
The Rey Ca Sh nOD C.v.O.,D.D I The R
And the foll owing Selected'. ev. T. C. El -don. Maj. G. E. W. Ma'et Kn'ghtsdGraee a, d Esquires I
L Sir J. W. Ottley. ·K.C.l E. lRh' A._.G bho,s. M.D. _ ord A verSlUne e V IScoun E h Sir C. M. Royd;, .. ..M.G. C. B. G.c.Y.o.
<J. Gen. THe Lord Che)'les F. H. Cook, C.I E. K.C.V.O more, E. Dawes.
J. A. .m s, M V.O. W. H St. John H ,.., e {;hS GrIffiths, M R.C.S Col. w. G. C r cr p • e Lod Merthyr, K K. \\7 .. M ':rray (Carnar;: 'o1l PurTh Sll.'l'ant Extra })dinar)' )
e fllowing are the K ' '. HIS :-'fAJESTY KING GEO OF JUSTrCE: RGE Y S . H.R.H. THE DUKE 0 C . ., .:JVerelg' Head Patron. P' ONNAUGHT K G G
THE VISCOUNT KNunFORD G C'M' ., rand PrIor.
H. R. Prince Christi:::n of S hI ' .' . .G., Sub Prior. H "Ig-Hobtein, X.G. C es- HIS J\.bjesty The Kin ·", of N HH Albert of Schleswig_ H.S.H. Pc nee Alexander ot!f"a k·
H H 0 G C B., G.C v.o . D.S.O. <:c , The Duk of Teck. G C v 0 H.R H.Pn lceAr,b " r ofeon h 1 <;.M.G. . ..• , Io.:.G. nau\; t,
A t.mlral H.S. H Pein L' Sir J hn Furl Battellber : G ce nu s of Bail 0) e . C.B. (Hororary
K.c M.G. R'N .C.B., G.c.v.o., Sir T. rio k L , . . i\l j. Sir A.. Bt.
THE OF JUSTICE - continued.
C 1. S'r H C. Perrott, Bt., C.B.
Col. S r J. Gildea, K.C.V.O., C.B.
H. J Loftus .
Co K 1\1. Da wes.
Gen. Sir C. 'Narren, G.C.M G., K.C.B., R.E.
1Iaj.-Gen. J. C. Dalton.
Co A. G. - Weston of Hunterston, C.B., D.S 0 ., R.E
Co. The Lord Wilham Cecil, c.v.o .
E. F'reshfie d, LL.D_ (HonoLlry Baihff.)
The Earl Brassey, G.C.B. Tl,t! Viscount Templetown.
R. :-'1. :\IacLean.
A. F. G. Leveson Gower.
C·I F. A. H. Lambert.
Col. Sir C. W. 1\Iurray, C.Il.
The Earl of Ranfurly, 'j he L ord Sandhurst,G .C.S.l .,G.C. [. E.
S r H. A. Bake, G.C.M.G.
The Earl of 1\leat,), K.P.
A. E . Fraser.
The Lord Mostyn. T he :\Iarquess of Breadalhane, K.G.
The Duke of Portlanu, K.G. F.·l\I. The Earl R oLerts, K.G., R.A.
R. H. Carter, F.R.C.S. (Honorary Comma der).

N. H. Forbes, F.R.C.S., EDIN.
Col. C. W. 13. Bow cler, C.II. (H onorary Commander).
Lieut.·Col. A. C. Yate.
l\laj.-G n. A. F. Terry.
The Earl of Plymo l:h, C.B.
The Earl of Sandwich , K:.C.V.O.
The Earl of Ellesmere (Commander, Ellesmere Comma ·1dery).
E . H. Freshfield.
The Viscou nt Drackley M v.o .
F.-:\1. The Viscount Kitchener of Khartmm, K.P., R.E.
Sir R. C. Temple, Bt., C.I.E.
Sir A. S. Scott-Gatty, K.C.V.O.
Col. Sir H. Jek) 11, K.C.M.G.
H.E. Loru Islington vf Is!in ton,
D.S o.
Col. Sir J. R. A. Clark, Bt.. C.B.
Sir R. Harvey.
H.E. Sir G. S. Clalke, G.C.M.G., G.C.I.E.
Li - ut.-Col. J. W. Wray.
Sir W. W Portal, 13t.
The Earl ,. f :\Imto, K.G.
The Duke of Somer et.
Sir D. Dlickworth, Bt. LL.D. , M.D. H. E . B lUlton,
The follow:ng are th SUB,PRELATES:
Th e Bishop in ]t!rusa' em and the I The Bi hop 'l r Gibraltar. East. The Prilllate of New Zealand. The D sh p Ormsby. The Bishop of Southwark.
Ube (l;rnllt) of trbe ®rt)et of tbe 1bospital of St. 3-01)11 of 3-erllsn[cm in JEnglnlltl.
AMBULANCE DEPAl, T:\lENT.
UI)e St. 50bn :ambulance :associatfon.
rATRON:
IllS ThIAJESTY KING GI'ORGE V., Soyereign Head and Patron of the OHler.
rRESIDENT:
II.R.II. THE DUKE OF CO,\Nl\UGllT, K.C., Grand I'rior uf the Order.
CENTRAL EXECUTl VIi.: COl\DllTTEE: Consisting ex lusi\'ely of McmlJcrs and IIonorary Assucia'cs of the Order.
DIRECTOR OF 1 III'; A"IDULANCE DEI'ART;\IF:\T A[,;D CIIAIlDI,\:-< OF COl\DII1 ·nE.-The Earl of r ;Y l1wutll, C.B.
ASSISTANT DIRLCTO R AND Dld'U '! Y v!. Sir Richard C. Ternrle, Bt., C.LE
DEPUTY CHAIl MAN.-Sir John FuJley, C.B., Life Member of the COI1' mitlee, HOlloris C.IUSI1. :
11:1j. Gen. J. C. Dahon. Lit!UI.-Col A. C. Yate.
Col. S)' J. R. A Cia k, B. , C.Il., H. E. I'o .d ton, \'.0.
Th t! Rev. T. C. EI d,,". The Rev. H. D.
In <i B. Ninnis, c.v.o. , 1I1. D ., F:.N.
Maj. G H. Da win,
Col. G. S. Ell ,C.B. M.1l c.s.
C, l. C. J. Tri l ble, L.R .c.r. E.
Capt. Si J. W. 10tt.Bo\\er, C.\ .0
E. Ow(n LL.T". F.Il.C.S.
The L urd Clal1d Halll It , n, M.P.
Sir J. L. Lal' gman, Bt.
CETfRAL EXECUTIVE COc.lMfTTEE-f'">nlinucd.
S. W. Malkin.
C. CO'lon, F.R.C.P.E., M.R .C.S.
Surg.·l;en. SIr B. FJan:-:lin, K.C.I.E., 1-:.H.I'.
C. H. Poll mer.
Admiral Sir F. G. D. BeJ rorJ, G.C.B. G.C.1>I.G.
Lieut.-Co!' G. E. Til iss, F.R.C.S.I. '
Co'. T. H. Hendley, C I.E.
]. H. Morga " C.Y.O. F.R.C.S.
S ,l rg. Liellt.-Col. S.r W. R. C I.E., M.D.
Col. H. R. Mends. '
Lieut.-Col. A. D. Aclanu_
F.<!i:., Col. 1<:. D. Brown-Synge-Hutchinsan.
Sir James Porter, K.C.B., M.U., K.H.P., It.M.
J. A. Bluxam, F.ll.C.S.
Lieut.-Col. Sir R. W. Inglis.
.Maj. P. G. Shewell.
T. H. Woobton.
F. l\. Ellis.
W. E •. \udland, M.R.C.S.
A. 11. Johnst0n, M.R C.S.
EX-OFFICIO MEMBERS OF COMI>UTTEE:
The Secretary-General of the Order.
The Receiver-General of the Order.
T_ e Chairman, Briti,h Ophthalmic Hospital.
CHIEF SECRETARY :
Col Sic H. C. Perrott, Bt.,c.B.(Secretary-General of the Order).
DIRl!:CTOR OF STORES AND ACCOUNTANT:
W. R. Edwards, A.C.A. (Secretary of the Order).
STOREKEEPER:
W. II. Morgan (Superintendent, Inmlid Transp r L Corps).
SECRETARY:
D. G. Monteith.
TERRITORIAL BRANCH.
CONTROLLER-IN-CHI EF:
Lieut. -Col. Sir l{. C. Temple, BL, C I.&,
ASSISTANT SECRETARY:
P. G.

FIRST AID TO THE INJURED SYLLABUS OF INSTRUCTION .
FIRST LECTURE.
A. Principles of First Aid.
B. A brief Description uf the Human Skeleton and of ( e 'Muscles.
C. Fractures-Causes, Yarieties, signs ann symptoms
D. Treatment of Fractures - General Rules.
E. The Triangular Bandage anJ its application. SECO" n LECTURE.
A. Treatment of Fractures (continued). Details of trez. Iment.
B. Disloc:ltions, Sprains, symptoms imQ
C. The Heart and Blood Vessels. The Circulation of t Blood.
D. II;emorrhage ann wounds. General rules for treatment.
E rhe Tnangular Bandage and its
8
TUIRD LECTURE.
A and w o unds (continued). Details of tr eatme nt.
Internal symptoms and arrest.
L. I-lGemorrhage from SpecIal Regions.-Sin-ns s t an d <l rrest. '" , ymp oms
Scalds, Bites and Stings, Frost.bite.
E. bodies Il1 the Eye, Nose and Ear.
F. The Tnangular Bandage and its application.
FOURTH LECTURE..
A. The Nervous Syste m.
B . Organs and Mechanism of Respirati o n-Artific' 1 R C5jll ratlc,7". la
C. Insensibili ty.
D.

FrFTH LECTURE (for Males only) .
• .A. Improvised me1hods of liftin a and carrying the si k IllJ Ired . b C or
H. Meth ods of lifling and c arrying the sick or inJ'ured on str etche rs.
C. The conveyance of such by rail or in country carts.
FIFTH LECTURE (for F emales only).
A. recep tion of accident cases.
B. Means of hfLIng and carrying.
C. Preparation of bed.
D. Removing the clothes.
E. Preparations for surgeo n. 9
NOTE 1.-The suhject of p()isons shou ld be treatcd in a general manner; the com1110n poisons classified, and only their general symptoms, effects and treatment taught.
NOTE II .-The last half·hour of each lecture should be de\'oted to practical work, such as the npp'icat ion of bandages ar d spli(,ts, lifting and carr) ing wounded on stretchers.
OTE. III. -There .,hould be an interv"l of a week between each lecture. A candidate for examination mllst attend at hast fuur out o f the five lectures.
NOTE IV.-:-Ial e classes must passin that system of stretcher exercise most suitable [or the locality .
N orE V. -As lillIe time a<; po 'sible is to be spent o n instruction in anatomical and ],hysiological dClails. Lectuters and examiners are particularly ref[ uesll d to remember th l.t it is " 1, irst Aid" thal has to be taughl anu lesteu, and not analomy ancl physiology.
jllixed classc:s oj lIlel/ IlIzd WJIJlell are 011 itO account jerllldled.
rl'l'll S SIXTFEN YEARS OF AGE CA:-< ONLY ATTE:-<D TilE c , JU:--IIOR" CvURSE (SEC["O:--r A, SYLLABUS 40).
Lecturers instructing a First Aid class, and Local Secretarie5, can obtain further particulars on application to the Chief Secretl'.ry for "Paper Reference No 80"
No Lecturer may examine his OWIZ Class for Certificates.
CHAPTER I.
of First Aid
Explanatory
Questions on Chapter
CHAPTER II.
The Human Skull, spine, ribs and breastbone, upper lImus (collar-bone, shoulder-blade. armbone, bones of. the carpus, metac a rpus, ph alanges), pelvls, lower limbs (thigh -bone, kneecap, tarsus, metatarsus, phalanges) ... . ..
Joints ...
Muscles. Voluntary and involuntary ...
Fractures. Causes, varieties, signs and ptO:11S
Appa!'atus for treatment of Fractures
General Rules to be observed in Fractures ... '"
Special Fractures. Cranium, lower br easL-b one, coll a r-b one, shoulder -blade or bones c.lose .to the elb ow j uint, cru s@.c d . pelvIs, th Ig h .b one, kn ee-cap, leg, c rushed foot
DlslocatlOns
Sprains Sprains and

of the Main Arteries and Pressure Points . Aorta, arteries of the head and neck, of the uppe r limbs, of the
1\'.
Miscellaneous Injuries . Bruises, burns and scalds, hites of snakes and rabid animal and w0und - by poisoned weapons, stings of plants and .animals, frost bite, needle emb edded unde r the skin, fi h hook embedded in the skin, injuries to joints, fo reig n b ody in the eye, ear passage and nose , \-\'Ollnd in the front wall of the abdomen, injuries to the organs
CHAPTER -V.
The Nervous System. Ce rebro-spinal, sympathelic. .. II ; The Respiratory System I IS
Artificial Respiration. Schafe r' s,. ih'ester's, Howa rd 's combin ed wi th Sil veste r's , L 3.bo rde·s and H a ll 's method s . ..
Insensibility. Causes, general rules for treatment concus ion of the brain, compression of the brain apop:exy, epilepsy, hysteria, shock, fainting and EUnstroke and heat -stroke) convulsions in children, asphyxia ...
Electric Shock and Effects of Lightning
Questions on Chapter ... ... . ..
CHAPTER VI.
Poisoning. General rules for trealmen t, special pois Dns
Questions on Chapter ... .. . ... ... ...
CHAPTER VII.
Bandaging. for the scalp, forehead, etc., shoulder, hlP, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. FOl' r, two, and three. handed seats, fireman 's lift, for.e and aft method, improvised stretchers, to cross a dnch or wall, to load or unload a wagon ..
CHAPTER IX.
Stret.cher Transport. Stretchers, stretcher exercises, Inters ... . ..
CHAPTER X.
The Fifth (fo: Females only). Preparati on f?r receptlOn of and preparatlOn of a hfllng amI carrylOg. preparat ion of bed, rcmovlllg the clothes, preparation for surge on ...
Questions on Chapter

Skeleton showing position of main nrteriui.
Skull and vertebral column
Vertebra of the left upper lim h-
Bones of the right lower lim b
Shoulder J oint
Ankle .,.
Rectus -:\1 uscle
Triangular bandage out and folded
Large arm sling
Small arm sling
Reef knot
Granny knot" .
Loop knot
Bandage for fracture of lower jaw " ,
Bandages for simple fracture of ribs
St. John sling
Band 1ges for fracture of b oth collar bones
Bandage for fracture of sh ollld er blad e
Treatment of of arm
Angular splint
Treatment of fracture of forearm
TreatmfUt of crushed hand ...
Treatment of fracture of thigh bone
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap ... 1
Treatment of fracture of leg (ma n and W0tlL.1.n)
Treatment of crushed foot .,
Diagram of the heart, lungs and air pa<;"sages
.
Diagram of the circulation of the blood
Digital pressure on carotid artery .. .
Digital pre:sure on facial artery .. .
DigiLal pressure on Lemporal artery
Digital pres ure on occipital artery
Pad and bandage to arrest hremon hage from temple
Ring pad
Digital pressure on suLclayian artery
Pad and bandages to apply pressure on axillary artery ...
Digital pressure on brachial artery (two methods)
Flexi on at elLow ...
Digital pressure on radial and ulnar arteries
Pad and bandage to arreSL hremorrhage from palm
Digital pressure on femoral artery ...
Tourniquet on femoral artery
Flexion at knee
Orgai1s of the chest and abdomen ...
The lungs aud bronchial tubes
Schafer's method of artificial respiration ...
Silvester's method of altificial respiration
Silvester's and Howard's me.hJds of artificiJ.l respiratiun combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage [or the hand
Bandage [or the foot
Baud age for the chest
Baudage fur the knee
Bandage for the elbow
Grip for four-handed seat
LifLing by two-handed seat .. .
Glips for two-handed seats .. .

Grip for three-handed seat .. .
Supporting patient ... .. .
Fore and aft method of carrying
Carrying on improvised seat
Ilmprovised stretcher ...
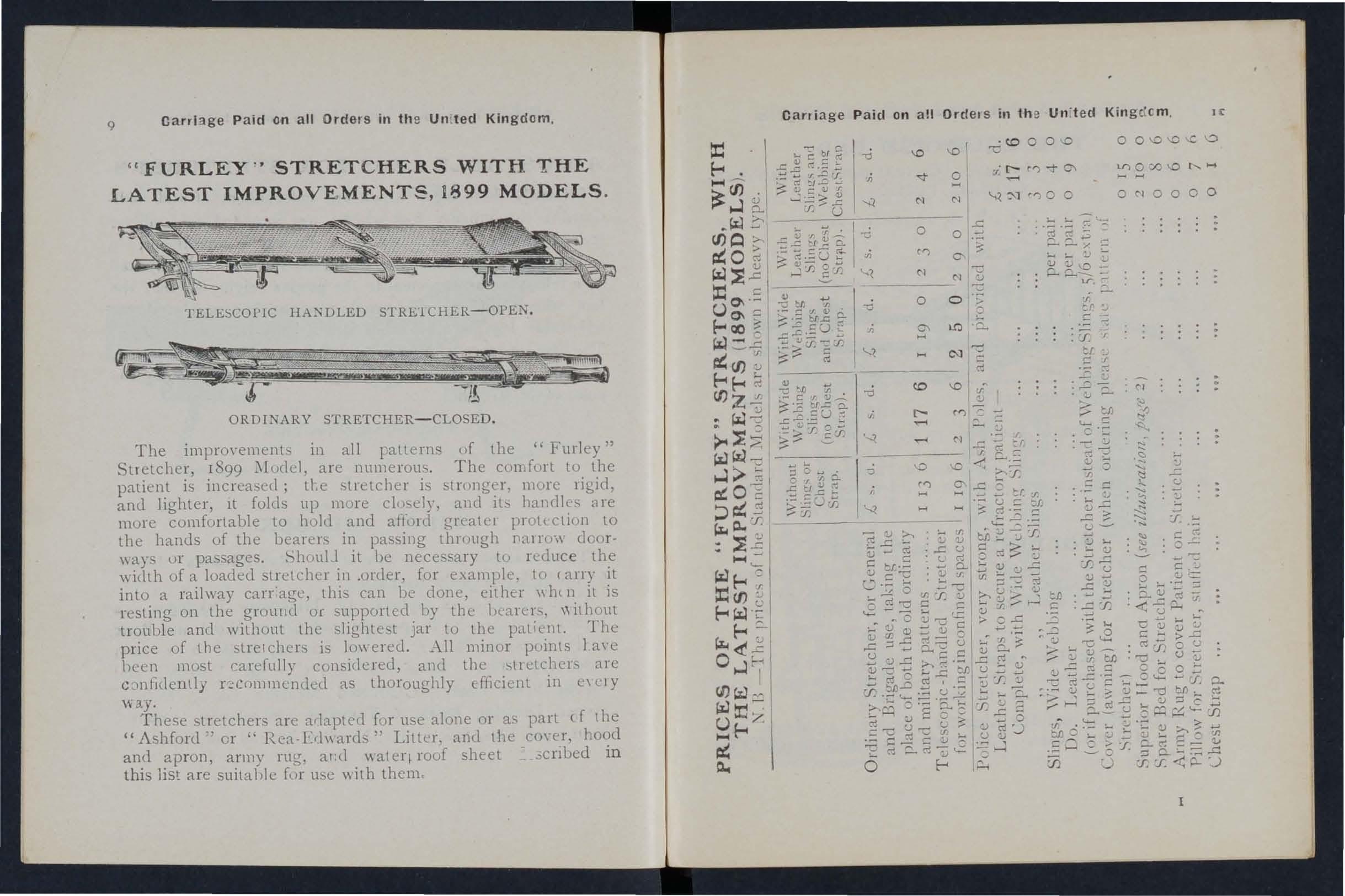
Fu rJey stretchers
Carrying by tW(J-handed seat 15
exercise, No. 1. " Fall in "
. DItto, ready to lirt patient
D Itto, lifting patient ...
DItto, placing stretcher ... . ..
DItto, preparing to lower patient. ..
DItto, " Lower"
Ditto, No. II. Ready to lift patient
DItto, patient lifted ... . ..
Ditto, No. IV. First position
: Itt!), second position ... ... . ..
DIagrams illustrating Army stretcher drill
DItto .. .
ltir:d cradle IrnpT0YIsed bed cradles
PREFACE.
AT the request of the Central Executive Committee
I have the manual written by myself in 1901, as the officIal handbook of the St. John Ambulance Association.
Throughout the revision an endeavour has 'been made to simplify the study of FIrst Aid to the Injured by drawing up a number of general rules for the of accidents and sudden illness, and by the omISSIOn of all detail \\ hich is not atsolutely necessary to E:nable the student to acquire an intelligent knowledge of the subject.
I wish to express my thanks to Professor E. A. Schafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. M. F. for many valuable suggestions, and to the MedIcal Members of the Central Executive Committee, especially Surgeon-Major G. H. Darwin, M.D. and Dr. F. R. Cassidi, for perusing the proof sheets and for a number of useful additions to the \york.
I cannot omit also to offer my best acknowledgments to Mr. 'V. R. Edwalds, the Accountant and Storekeeper of the S.J.A.A., for his invaluable co-opera ti on.
JAMES CANTLIE.

FIRST AID TO THE INJURED.
CHAPTER 1.
Th-.; St. John Ambulance Association has n,ow completed thirty years of its existence, and d unng that period hundreds of thousands ?f men and women have been taught at its classes, 111 parts of the world hmv to help their injured Fi;st Aid to the Injured is a speClal branch of practical medicine and surgery, by a kno\\ of which trained persons are enabled to afford assistance in cases of accident and ,Illness. The instruction begins and ends with First Ald, and the subject is t::tught simply but thoroughly exhaustively. The duty of the ambulance pupIls ends where the doctor's commences, and the,re ought to be no oyerlapping or clashing of duty or 111terests.
PRINCIPLES OF FIRST AID.
I The First Aid student should be-
. (a) Observant, that he may note the causes and signs* of injury.
(b) Tactful, that he may without questions learn the symptomst and hlStoryt of the case.
* Signs are what may be p e rcei\'ed.
t Symptoms are what the patient can tell you. .
t History means the circumstances altendmg the acclClent or suddrn illness.
(
c) Resourceful, t hat h e may us e to t h e best adva n tage whatever is at h a nd t o p revent fur ther ,da mage a nd t o assist N a ture 's efforts
d t o th e m ischi ef a lre,ad y d on e.
( ) th a t h e may g Ive cl ear inst ructIons to t he patie n t or the bys ta n ders how bes t to assist him ,
(e) that h e may d ecide which of se,'eral injurIes presses most for trea tment by himself, and ,,\'hat can best b e left for the patient or the bystanders to do, h 2. Remove, the cause of injury or danger w enever possIble,
3· hcemorrhage must rece ive the .attentIon, no matter what are th e oth lilJunes. er
h4·hAbir. - ,!,he, patient must be in a position in W IC reathl11'"T IS p 'bl h . fr f b":> OSSI e; t e aIr passages must be ee rom 0 struction; if breathing has ceased prompt m easures must be taken to restore it.
th 5· restful position of tbe body will assist h VIta unctIOns; support of the injured part WIll tl: p to p revent further. damage, and is essential in .e case of fractures of lImbs,
Warmth.-After e,'ery accident kee the patI en t warm so as to. preyent the fall of belo w the nor mal pOlllt.
7· When the skin is broken the wound

19
should be promptly covered wilh a clean dressing. Sho ul d the \\ oUlld be poisoned, IS mos t im portant immediately to I TCYCnt the pOIscn perl1,eating the s) stel1l . ,
8. Poisons S\\ alJo\\'ec1 should be got rId of, o r when that is inexpedient, neutralised .
9. The best means of .transport mL1st Le studied, and provision n ade 10r proper care wben the patient is brought to sheller.
10. Removal of Clothing. -Clothes should not ue take n off unnecessari ly, but WhUl it is needful to remove them, the following rules will be found of service in serious cases :-
COAT: Remove from the sound side fjrst, ano, if necessary, slit up the seam of the sleeye on the injured side .
SHIRT A D VE T: Slit down the front and remO\'e as the coat.
TROUSERS: lit up the outer seam.
BOOT: Slit the brrck seam and unclo the laces.
SOCK: Cut off.
II. Stimulants. -It is incorrect to suppose that alcohol is the only form of stimulant, and far too frequent use of spirits is made to restore a patit.nt after an accident, often with serious results; the safest ru le therefore is to Jefer the adminIstration d alcohol until the of a doctor, When the patient is able to s\\ allow, strong tea or cc ·ffee, or milk, as hot as ca n
be drunk, or a small quantity of sal volatile in water may be given. Smelling salts may be held to the nos€:. Sprinkling the face with cold and hot water alternate ly, warmth applied to the pit of the and oyer the heart, and vigorous friction of the limbs upwards have a stimulating effect.
I2. Throughout his work · the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an app:uently slight injury is accompanied by grave danger and may actually cause loss of life. \Vhen sending for a doctor, state the nature of the case, and remem ber that written particulars are safer than a verbal message.
It is necessary that something should be knO\yn of the structure of the body (elementary anatomy), and of the functions of some of the more important organs and systems (elementary physiology) A short descripti on of the necessary anatomical and physiological points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms batlging by the side and the palms of the hands directed forwards. The" middle line" of the body runs vertically from the top of the head to a point between the feet.

QUESTIONS ON CHAPTER
The llumer-als

ClI APTI ' R II.
FRACTURES, DISLOCATIONS, SPRAINS AND STRAINS.
THE SKELETON.
The human body is moulded up ::m a bony framework (the skeleton; which
1. - To gi"e sl l ape and firmness to the body.
2.- To afford allachment to tIle musc1es.
3.-To protect important organs, as in the skull, chest, and abdomen.
THE SKULL.
Th:! Bones of the Skull are arranged in t\·:o groups, those of the brain case or cranium , and thos e of the face.
The Boundaries of the Cranium are the vault or dome, the rounded portion forming the top of the head; the front or brow; the back of the head, where the greatest extent of brain exists, and \\ here therefore the cranium is \\"idest and deepest; the sides or temples. The base of the cranium is hidden from view by the bones of the face and of the vertebral column; in it are numerous perforations for the passage of blood vessels and nerves; through the largest opening the brain and spinal cord are continuous.
T h e Bones of t he F a ce with the exception of 23
the lower jaw are firmly jointed together, so that movement between them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face conjointly. The mouth cavity is formed between the upper and lower ja \\"5, the p::tlate being the bony roof of the mouth which sep:trates it fro:11 the nasal cavity above.
T he Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions terminating on either sid e at the joint between the lower jaw and the b:1se of the cranium, situated immediately in front of the ear.
The angle of the jaw indicates the junction of the norizontal and the vertical p 8rtions.
THE BACK-BONE, SPINE, OR VERTEBRAL
T h e Ve rteb r al Co lumn (Fig. 1) is composed of boneS called vertebne, each of \\hi ch consists of-
r .-A body 0r bony mass in front.
2. - Process : s projecting backwards, which enclose a canal for the spinal cord - the spinal canal.
3.-Two transverse processes, twelve pairs of ,,'hich supp " rt the ri bs.
FIG. 2A.

PRllCESS.
SPJI'OUS ;: ,'. '\ PROCESS.
SURFACES SUPPORTING HEA DS OF RJllS.
FIG. 2B.
SKULL AND VERTEBRAL COLU:\lN.
Showing left ribs and portion of breast bone. The right ribs are removed.
4 . - A spinous process. The spinous processes of the vertebrre can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
The Vertebrce , in all, are grouped into regions, in each of which they are known by numbers, counting dowD\\"llrd :-
1. -In the neck 7 Cervical vertebrre . The first vertebra, tile atlas, forms a joint with the base of the skull, at which the noddi ng movement of the head takes place; the seconJ, tile ax/s, by the joint between it and the atlas, allows of the side-to-side movements of the head.
2.-In the back 12 Dorsal vertebrre.
3. -In the loin 5 Lumbar vertebrre.
4.-The rump-bone, or Sacrum, consists of 5 Sacral united in adults as a solid mass.
S. -The tail-bone, or Coccyx, consists of 4 vertebrre joined together to form a single group.
Between the bodies of the vertebrre, in the upper three regions, are interposed thick pieces of cartilage (gristle), which, while they bind the bones together, allow of free movement to the column as a whole, and l1elp to break the shock of any sudden force a pplied to the spine (for example, when falling from
BOllY OF VERTEBRA.height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of twelve pairs of curved bones from the dorsal vertebrre to the front of the body, and are known by numbers-first, seccnd, etc., eo mmencing from above. The ribs are not Lony fthro ughout their entire length, but at a sr.ort distance ffro m the front the bony material ends, and cartilage its place. The upper senn pairs, named ribs, are attached by their cartllages to 3reast-bone (sternum), a dagger-shaped bene with the point downwards, just 0\ er t}le I it of the
The lower five pairs are tErn Ed tI-:e false ri bs, as their cartilages fall short of the n icdle line
The eleventh and t\\'e1fth pairs are termed the float :ng ribs, as their ends are free in front. The ribs the chest, and serve to protect the lungs) heart, liver, stomach, spleen, etc.
THE U PI'ER L1J\rBs.
The Shoulder - bones are the Collar-bone (clavicle) and the Shoulder-blade (scapula).
The Collar-bone can be felt on eithe r slde beneath the skin at the lower and front part of the Illeck as a narrow curved rod about the thickness of a !finger. Its inner end rests on the upper part of the
PAHT OF COLLAR DOl\E
SIIOULDER
BLADE (SorULA)
Botm (II U;IIERU')

BONES {ULNA OF R.-HJlUS --+HH
WRIST (CARPUS) :'II ETAC.-\Rl'US
P',ALANGES
FIG, 3A.
BONES OF TllE LEFT UPPER LDID.
RADIU5
FIG. 3B.
SIl()\\'lNG THE POS1T10N or TilE RADIUS AND ULNA
TYllEK THE TlIU:-rB IS TUR:\,]';D INWARDS.
Compare Fig. 3A, in which the thumb is turned outwards.
b reast-bone , and its outer end j()iIlS with the shoulde rblade.
The Shoulder-blade lies at the upper .:111 ...1 outer part of the back of the chest, and forllls joints \\ ith the collar-bone and the bone of the arm.
The bone of t he Arm (humerus) reaches fr o m the shoulder to tbe elbow.
In the Forearm are byo bones, the R adius on the outer, or thumb side, and the Ul na on the inl1l r, or little finger side. B oth bones reach fr0111 the elbow to tbe wrist, and th ey change th eir rebti ye p osition with every turn cf the hand (Figs. 3A and 3 B).
The Hand is composed of-
l.- The b on es of the wrist, or carpus, t in number, arranged in two rows of four.
2.-The metacarjJlts (the framework of the pali11) ; five bones which form the knuck:es and support the bones of the fingers.
3·- T be tilalallges, or finger-b o nes, three in each finger, and two in the thum b.
T HE PELVIS AND LOWER LIl\rEs.
T h e Pelvis. - T he large basin-like mass of bone a ttac hed to the lower part of the spine is composed of t he two haunch-bones and the sacrum . The haunchbo nes meet in front (at the pubes) in the middle line, o n ly a small piece of cartilage intervening, but be:l1 'n d, the sacrum is placed between them . The pelvis

4.
Bo"I:.S OF THE RIGHT LOWER LIMB, SHOW· ING JOINT WITH THE PELVIS AT THE HIP.
30 supports the abdorncn and its contents, and prm ides the deep sockets for the tbigh-bones-the hip joints.
The Thigh-b0ne (fi71lur) reaches from the hip to the knee joint. Its shaft is stout, rounded, and arched forwards; the upper end presents a rounded head, supported on a neck which projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying \..-ith its base upwards in front of the knee joint immedIately beneath the skin.
The bones of the Leg are the Shin-bone (ttoia) and the Brooch·bone (jibula). The Shin-bone extends from the knee to the ankle, in both of VI hieh joints it plays an important part; its sharp edge, (I.e shin, can be felt immediately beneath the skin of the front of the Jeg. The Brooch-bone lies on the outer side of the tibia. It does not enter into the formation of the knee joint, but its lo,,;er end forms the outer boundary of the ankle joint.
The Foot is composed of-
1.-The tarsus, a group of seven irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.- The metatarsus, the five long bones in front of the tarsus which support the toes.
3·-The phalanges, or toe-bones, two in the big toe, and th ree in each of the other toes.
31 JOINTS.
A Joint is formed at the junction of two. or more bones. In moveable joints such as the hlP, knee, @lbow, etc., the snrfaces of the bones are covered by cartilage, which lessens friction and the shock of a

LEFT A]'\KLE.
Compare Fig. 4, Page 29·
FIG. 5.
fall. Lubricating the joint is a clear, rather. fluid, the "joint oil," or sJlJlovt'a, enclosed wl!hll1 a capsule. Tying the bones together, allowlDS; of movet1lent are a number of bands or ltgam ents. To explain the formation of limb joints, the
'FIG. 6.TENDON NERVE
ARTERY

l\IUSCULAR TISSUE
PATELLA
TENDON OR LIGAMENT OF PATELLA
FIG 7.
DIAGRAM SHOWING RECTUS
MUSCLE OF THIGII, WITH !\RTERY, VEL.'/" AND NERVE
J 2
fo llO\ying examples are g i ve n :-
T he She ulder, a a n d -sock e t join t, of a sh a ll ow socket en the outer ang le of sho ul der-blade, and of tl 'e head of the arm-bore (Fig. 5) . 0" ing to the shallowness of the socl et t he anl1-;"oi"; is very prone to esc2.pe fl" m its socket ( dislocate).
The Ankle, a hi n ge joint, is fOi'l11!: d at the jUllCof tbree bones , tbr:! above and on t he inner side, the brocchb one on the outer side, and the ankle-bone below (Fig. 6).
T HE MU SCL ES.
The Muscles of body are ciassified into L\\O groups-v 0 1zt1t1ary an d z'tlvolu 7l tar), .
33
The Vo luntary muscles 3.re met with in the limbs the head and neck, and the surface of the Their ends are atta'ched to different bones, and as they pass from one to anotbt.r they cross a joint, and, being endowed with the power of contrac· tion and relaxatIOll, cause the mo\'e n,ents of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels trayerse and supply the muscles, and the neryes entering them bring them under the direct control of the brain and spinal cord.
The In vo l unt a r y muscl e s are met with in the \Valls of the stonlach and intestines, in the :-cir passages, and in most of th.e organs and blood-vessels, also, in a speCial form, m the. heart. They are not under the influence of the wIll, continue their \\ork during the bOUlS of sleep; tbur functions are regulated by a separate set of neryes (see Sympathetic System, page II S).
FRACTURES A TD THEIR TREATi\IE TT.
\\'hen a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE.
I . D i rect Violence.-\Vhen from a severe blow, impact of a bu l1et, crush of a ,,,heel, etc., a bone breaks at t he " ,here the force is appJied the fracture is termed d irec t. c
Indirect Violence. - 'When the bone breaks at some distance from the spot where the force is applied the fr<1cture. is termed indirect. Allghting on the feet and fractunng the thigh- bone or the bones of the leg, or falling on the hand and breaking the TJ.di us or the collar-bone, are examples .
3. Muscular Action.-The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them.
V_-\RIETIES OF FRACTURES.
Fractures are classified according to the condition of the tissues adjacent to the bone as follows :-
I. Simple.-The bone is broken wIth Gut slight injury to the surrounding parts.
2. Campound.-The bone is broken and the skin and tissues are punctured or torn, thus allowin'T disease-producing germs to obtain entrance to seat of fracture. The fractured ends may protrude through the skin, or (for example, when a bone is broken by a bullet) the wound may lead down to the fracture.
3. Complicated. - The bone is broken and in addition there is an mjury to some internal organ (for the bram, spmal cord, lung, etc.) or to some Important blood-vessel or nerve.
A .fracture may be compound or complicated as the Immedi ate result of the injury j or a fracture

35
originally simple, may be converted int o a compound or complicated fracture-
(a) By careless movement on the part of the patient.
(b) By carelessness or ignonmce on the part cf one rendering first aid.
Special varieties of fr:lctures may be classified according to the injury to the bone itself as follows :-
I. Comminuted. - The bone is broken into several pieces.
2. Green-stick. -In chilc1ren, owing to the softer state of the bony tiss1.H' s, a bone may and cf:lck \\ ithout breaking completely across.
3. Impacted.-The Groken ends of the bone are driven one into the other.
SIGNS AND SYMPTOMS \\ H I CH J\IAY BE PRESE. T.
. (A fracture of the femur, humerns, or both bones ot the forearm or leg, affords the most complete example ,'.
I. Pain at or near the seat of fracture.
2. Loss of Power in the limo.
3. Swelling t,he seat of fracture. Swelling frequently renders It dIfficult to perceive other si fT ll3 of fracture, and care must therefore be taken to mistake a fracture for a less serious injury.
4. Deformity of the limb.-The lim b assumes an
po ilIon, :lnd is at lhe L.lt of The contr:lcling muscle may all:-,C lhe end' of the bone to oYerrick, lhereh) pro jUC1l1g Shorlenin o·.
S. Irregularity of the bone. - If the bone is cIa. e w the skin the fr,lctme may be felt, and jf compound 't ma\' be seen.
6. -Unnatural Mobility.-lIoH' l11L'nl mny be made out :It the seat of fracture.
7. Crepitus, or bon) grating, may be fell or heard when the broken end - lllOYC one upon the otll r.
The last l'ic'o siLO/tid olll!' /1(' SOl" /11/11' iT dodoJ -... .,.'\. eyeral of lhe abo\'e slgns nre in gl el' ll-stick and 1l11pacted fra tun::';.
In to the signs and symptoms the patient or may be able to gi\'e the of he 1I1Jury, and mnrl-..3 on the clothing or skin should be noted, as they may scn'e to locate the fra ct Ul'f! The snap of the bone may haye uccn heard or felt.
ApPARATU - FOR TRE.\..T:\fEKT OF FR,\..CTURI
Splints and bandages for First Aid frequenth ha\-e to be imprO\-isecl, .
A Splint may be improvised from a walkillfr tick umbrelb, billiard cue, broom or brush handle,'='police' man's truncheon, rifle, folded coat, piece of \\ ood, cardboard paper firmly folded, a rolled-up map, or, m fact, aJ(l'llllJlg lilat lJ firlll and 101lg' ellol/gll to Awl
37
Ilu joints immed/ate{l' above alld below tile fractured bOJle at nsf. When the above appliances are no available, the upper limb, jf fractured, may be tie to the trunk, and in all cases a fractured lower lim should be bandaged to its fellow.
Bandages may he improvIsed from hanclkerchief5 belts, straps, bra es, neckties, or any piece of linen -alIco, string or cord that comes to hanel.
Esmarch's Triangular Bandages (Fig. 0) are made by cutting a plcce of linen or calico about forty inches s(l1.1are dw.gonally into t\\ 0 picces.
The broad bandage is made by bringing th point down to the base (Fig. 9), and then foldinr mto t\\ 0 (Fig. 10).
The narrow bandage is made by folding th broad landage once (FiJ. II).
The medium ba:ndage is made by bringing thtpomt down to the base, and then folding into three (FIg. 12). This bandage may be used instead of th broad or the narrow bandage when it is better suite to the proportions of the patient.
It is sometimes advisable to halve the size of the bandage by uringing the t\\ 0 ends together befor folding it into the broad, narrow, or medium bandage
\Vhen not in use, the triangular bandage should be folded narrow; the two ends should be turned t the centre, and the bandage then folded into fom reducmg it to a packet about 6! inches by inches.
PO NT

39
Large arm-sling ( Fig. 13). -Spreacl out a bandage, put one end over the shoulder on the sound sid e, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang dovvn in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm
FIG. 9. ONCE FOLDED .
FIG. 10 BROAD BANDAGE. eo
FIG. II. NARR.OW BANDAGE.
FIG. 12. '- THE DOTTED LINES SHOW THE FOlL S OF THE BAl\[)AGE.
FIG. r3. FIG. 14. over the middle of the then carry the second end up to the first and tie them; bring the point forward, and secure with two pins to the front of the bandage.
Small arm-sling (Fig. q).-Place one end of a
bro ad b a nd age ov er th e shoul de r . on th e sound sid e, pass it roun d th e n ec k so tha t It a pp ea rs ove r t he shoulder of the injured side; pla ce the for ea rm oY er the middle of the ba ndage; then brin g the sf con d end up to the first, and tie them. This shn.g is u sed in cases of fr act ur ed hu me r u s, and occasIOnally \\ he n t he la rge sling woul d b e t oo c on sp ic uo us.
Slings may be improvised in ma ny simple ways , s uch

as p inning the sl ee ve to the clothing, turnin g up th e tail of the coat, pa ssing the hand insi de the b utt on e d c oa t or waist coa t, etc .
Reef Knots (F ig. IS ) a re to be used. A voi d granny kn ots (Fig. 16) .
The object of First Aid Fractures is to guard against further mIschi ef, especially to prevent a si mple fracture from becomIng compound or complicated . To attain th is end :-
1. Attend to the fracture on the spot. :\0 matter how cr owded the t horoughfare, or how short the distance to a rnore cOlwenit:nt or comfortable place , no attempt m ust be made to mo:' e the pati ent until the limb has been rendered as lmmovable as possIble by splints or othe r restrai n in.s apparat us.
2 . Steady and support the injured limb at once so that its furthe r movement on the part of the pati ent or the bystande r is preyented .
3. Straighten the limb with gre a t care, and if shorteninU" is obse rved in the case of a fracture of a bone of tile lowe r limb, pull upon the f,::o t u ntil the limb regain s a mo re n or mal length . W hen tbe sba pe of the Ii mb is im prm'ed, on no accoun t let until it is secured in position by splints , other\Ylse there is great danger of the fra c ture becoming com, pound or complicated .
4. Apply splints (when practicable) and bandages as follo\\ S :-
(a ) The splints must be firm, and long enough to keep the joints immediately above and
FIG. I5.-R EEF K NOT. FIG. I6. - GRAN NY Kr'oT.42
below the fractured bone at rest They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The b:m.dages must be applied firmly, but not so tlghtly as to constrict the circulation ?f blood in the limb. \tVhen the patient is In the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule:-
.F'or the trunk the broad bandage should be used . Pass it once round the trunk and fasten it by tying the ends, or y\ith two or three safety pins on the side opposite to the frac! ure but jf to secure a splint for a broken thigh,' over the splint.
For tIle arm or forearm the narrow bandage should be used. Pass it twice round the limb, and tie the ends over the outer splint.
For the thigh or leg the narrow or medium bandJ.ge may be used. 1t 13 frequently convenient tu double the bandage at the cent::c, P.:l.SS it under the limb, bring the loop over the liob, p:::.ss both ends of the cando age through it ia opposite directions, and tie them over t:.c £plillt (Fig. 17).
In applying bandages near a the upper one should be hecured first.
43
S. When hcemorrhage accompanies a fracture it must be attooded to nlst, and the \,"ound covered by a clean dressing.

FIG . 17.
6. No attempt must be made to remove a patient suffering from a fracture of the spine, pelvis, or thigh, except in a recumbent position, preferably upon a stretcher.
7. In every case of fracture it is necessary to cover the patient to keep him warm, and so lessen the effects of the SHOCK of the accident.
8. In all doubtful cases, treat as a fracture.
SPECIAL FRACTURES.
Fracture of the Cranium.
-A fracture of the t1 pper part is usually caused by direct yiolence- for xample, a blow on the head. A fracture of the base is caused by indirect violence, through a fall on the
44
head, a fall on the fept or lower part of the spine, (H a severe blow on the lower jaw. If the lIppn part Z"S fractured, the signs are swelling, irregularity, and frequently insensil ility, either immediate or coming on gradually. If the base Z"S fractured insensibility may come on j l1mediately, blood or a dear fluid may issue [rom the ear channel, hlood may escape from the nose, or it may pass down to the stomach, \\ hence it may be vomitcd; the fracture may involve the orbit, C::LUSing a blood-shot eye.

In jury to the brain is the great danger attend· FIG. 18. ing a fracture of the cranium. For treatment see "Concussion and Compression of the Brain," pages 131, 132.
Fracture of the Lower Jaw.-Pain, loss of power (inability to speak and to move the jaw [reeLy), irregularity of the teeth, crepitus and bleeding frum the gum are the usual signs and symptoms.
45
TRL\DILNT.
1.- Place the palm of the hand below the injured bone and press it gently against the upper jaw.
2.-ALJply the centre of a narrow bandage under the chin, carry one end over the head, cross the ends at the angle of the jaw, carry the long end across the chin, and tie the ends on the side (Fig. 18).
Fracture of the Spine.- The vertebral column may be broken either by direct or indirect violence. Falling from a height on the back across a har or upon an uneven surface is an example of direct fracture, and a fall on the head, causing a broken neck, is an example of indirect violence. 'What is commonly regardeJ as a broken back consists of a fracture of one or more of the vertebrc:e \\ ith displacement of the fragments, \\ hereby the spinal cord and the nerves issuing from it may be torn, causing complete or partial paralysis of the parts below the fracture. Pain is present at the seat of injury.
TREA
I. - Prevent all movement on the part of the patient.
2.-Cover the patient warnily.
3.-To remO\·e the patient, place him on a stretche1 or shutter as follO\\"s :-
(a) Turn up the collar of his coat j roll up a stick or umbrella in each side of the coat
46
so that the ends are level with the top of his head; pass a br )ad bandage or handkerchief under the head and secure it to the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
(b) A bea rer on each side grasps th e HIlled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes charge of the legs.
(c) On the word being given, all lift together and carry the patient by short side paces over the stretcher and carefully lower him on to it. If a fifth bearer is available the stretcher should be passed under the patient instead of carrying him over it.
4.-0n arrival at shelter nothing further is to be attempted until the arrival of a doctor, except to give the patient water, tea, etc., if he is conscious.
Fractured
Ribs.- The ribs usu ally fractured are t he sixth, seventh, eighth, and ninth, and generally the fracture is midway between the breast-bone and the spine. The fracture may be caused by indirect violence) driving the fractured ends of tht bone out wards, or by direct violence, driving the fractured ends of the bone inwards and sometimes injuring the

lungs or other internal organ. If the lower ribs on the right SIde are broken, the liver may be injured and a fracture of the lower left ribs may wound spleer:. Evidence of the fracture is afforded by pain9 especlally on attempting to take a deep breath, and by short and shallow breathing. If tIle lun gs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hcemorrhage page 95) may occur.
TREAT.i\lEl\T.
(a) Tll,ell tlll'j;adllre is not complzt:ated by an injury to an z"7tlc'nzal OJ'.::, all :-
T.-Apply two broad bandages round FIG. 19. the chest sufficiently firmly to afford comfort, with the centre of the {jrst immediately above and that of the second immediately below the fracture. The lower bandage should overlap the upper to half its
48
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong towel, folded about eight inches wide, tightly round the chest, securing it with three or four safety pins.
2. -Place the arm on the injured side in a large sling. (Fig. 19)'
(b) TVhen an z'nternal organ z's z'njured-
I.-Do not apply bandages round the chest.
2.-Lay the patient down, inclined a little towards the injured side.
3.-Loosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Treat as for internal hremorrhage (see page 95).
4.-Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (stertzum).-
"When this fracture can be felt or is suspected undo all tight clothing, and keep the patient quiet in an easy position until the arrival d a doctor.
FRACTURE OF THE BONES OF THE UPPER LIMB
Fracture of the Collar-bone (davlde).-This fracture is frequently caused by a fall on the hand or shoulder.-The arm on the injured side is partially
49
helpless, and the patient usually supports it at the elbow \\'ith his hand, and inclines his head to\\'ards the injured side. The fractured ends can generally 1> 2 felt to oyerlap, the outer fragment being the lower. 'fhe general signs and symptol1ls of fracture are mostly present.

I.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about byo inches thick and four inches across in the armpit.
3.-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a "St. John" sling, made as fo\1O\\'s:-
(a) Lay an unfolded bandage across the chest over the injured limb \\ith one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fig. 20).
(1/) the end of the bandage under the ll1Jured 11mb, across the back, and tie the ends some\\'bat loosely in the hollow in front of the sound shoulder.
(c) F?ld tbe point the elbow of tb e injured limb and secure It by one or two pins (Figs. 21 and 22).
FIe n. (Body handage omitt ed to show details of Sling.)
4--Tightly secure the injured limb to the side by ::I broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5.-Now tighten the sling.
'When both collar-bones are broken keep the

shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by Lhe b,1.ndages. (Figs. 23A and 238).
Fracture of the Shoulder-blade (rmplt!a).-
,c'\ pply the centre of a broad ban d age in the armpit of
52
the injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24)·
Fracture of
the Arm (hume7lts). - The bone may be broken :-(a) Close up to the shoulder; (b) near thE' middle of the shaft; (c) close FIG 24· to the elbo\\'.
All the general signs and symptoms of fracture are usually present.
TREATMENT.
TVhen the Fracture z's close to the Sholtlder-
I.-Apply a broad bandage \\'ith its centre above the middle of the arm round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
TVlzen tlte Fracture z's mar tlze Mzddle oj tIe Shaft-
I.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder [0 the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
must on no account be so long as to press upon the blood-vessels at the elbow joint.
3.-Secure the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad bandages.
4.--S11Pport the forearm by a small arm sling. (Fig. 25).
Fractures in volving the elbow joint, \\ bether of the arm or forearm, are attended \\ ith so much S\\ elling, and it is so difficult to ascertain the exact nature of the injury, that when the accident occurs indoors the limb should be laid upon a pillO\Y in the most comfortable position; ice or cold \\ ater dressings be applied to the injured part, but no further treatment should be a.1 tempted pending the arrival of a doctor.
FIG. 25.
54
TVhen the accidmt occ?trs out of doors-
r. Take two pieces of thin flat wood, one I j ng enough to reach from the armpit to below the elbow, the other long enough to reach I. from above the elbow to the finger tips; tie them together to form a right angle. (Fig . ==- 26).
2.--Apply the angular splint so made FIG . 26. on the inner side of the flexed limb.
3.-Secure hy bandages above and below the fracture.
4·- Support the limb by a large arm sling.
5.- On arrival at home remove the splint, and treat the injury as if it had occurred indoors .
Fracture of the Forear m . - \iVhen both bones
Radius and Ulna) are broken, the general signs an d symptoms of fracture are usually present. When one of the bones only is broken the signs and symptoms are as a rule pain, loss of power, s\yelling, and irregularity. An impacted fracture of the Radius
55
just above the wrist is a common result of a fall on the hand .
TREATMENT.
This is the same, whether the fracture is of one bone or of both.
1.- Bend the forearm at right angles to the arm ,

FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the bocy.
2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers .
3.-Apply bandages, embracing both splints, immediately above and belo\\' the fracture and round the hand (Fig. 27).
4.-Apply a large arm-sling.
Crushed Hand (fracture of the boners of the carpus, metacarpus, or fingers).
TREATMENT.
I.-Apply a carefully padded splint to the front of the hand, reaching frol11 well above the wrist to beyond the tips of the fingers .
56
2.-T? secure the splint apply a narrow bandage c ro ssed In the man n el of the figure 8 to the wrist and hand ( F ig. 28).
3.-Apply a large arm-sling.
Fracture of the Pelvis .-'Vhen, after a severe !nj ury iI: the neighbourhood of the haunch-bone, there IS sIgn of damage to the 10\\'er limbs, but the patIent is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The and organs, especially the bladder J wIthm the pelvis are in danger of being \\"ounded.
TREATME T.
I.-Lay the patient in \vhatever posItlOn IS found to give the greatest ease, and flex or straigh ten the lower limbs as the patient desires.
2.-Apply a broad bandage round tl1e hips tight e n ough to support the parts, but not so tight as to p ress the broken bone further inwards.
3.-To remove the patient place him on a stretcher, ac ting on the same principle as that described under " F racture of the Spine /I (see page 45).
FR ACTURE OF THE BONES OF THE LOWER LIMB.
Fracture of the Thigh-bone (femur).- Th e thigh bone may be broken at its neck, anywhere in the shaft, or close to the knee. A fracture at the
57
is to occur in Old peop1e very slight lDJury, IS often .dlfficult to dIstinguish from a severe brUIse of the hlP, but it may be assumed that when, after an near the hip joint, the patient cannot, when lylllg on the back, raise the heel from ground, the bone is broken. All the general SIgns and sYI?ptom . of fracture are usually present and a promment sign is the po ition of the foot,

FIG. 29.
which, as a rule, lies on its outer side . Shortening may vary from one-half to three inches.
TREAT)fENT.
I.-Steady the lim b by holding the ankle and foot.
2.-Gently draw down the foot and brin c' it into line with its fello\\'. When two or three are at hand, it is one person's duty to hold the foot in position until the splints are secured.
3.-Apply a splint on the outer side frem the armpit to be) ond the fl)ot.
4·-A pply a splint on the inner side from the top of the thigh (the fork) to the knee.
5·-Secure the splints by bandages as follows :(a) Round the chest just below the armpits, (b) round the pelvis on a leyel with the hip joints, (c) abm-e the fracture, (d) below the fracture, (e) round the leg, (I) round both ankles and feet, and tied below tlle feet, (g) a broad bandage round both knees ( Fig. 2».

FIG. 30.
'When single-handed, or ,\ hen the patient is a woman, it is expedient, aft e r extension of the 1i111 b, to tie the feet together, dispense \\ ith the inner splin r , and pass the bandages round both limbs (Fig. 3 0 ).
Fr.: cture of the Knee-car (patella) -The knee-cap may be
FIG. 31. broken hy falling on the knee (direct violence), but f1lore frequently it is broken by muscular action, as follows;-
59
'Vhen the foot slips in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee-cap in two (Fig. 3 [).
Pain, loss of p::>wer (the limb will be quite helpless), and irregularity (a gap may be felt between the broken fragments of bone) accompany this injury.
TREA 'L\IE T.
l..-Lay the patient on his back, raise ,yell and
FIG. 32.
Support the head and .,houlders, straighten and raise the limb.
2.-Apply a splint along the back of the limb, reaching from the buttock to beyond the heel.
3·-A pply a narrow bandage with its centre imme-
diately above the knee-c:.1p, cross the ends behind over the splint, and tie in front below the broken bone. To ensure firmness apply a second bandage in a similar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5·- Support the foot \\ ell off the ground by a pillow, roll of clothing, etc., or jf none of these are at hand by resting it on its fello\\ (Fig. 32).
6 .-Apply an ice bag or a cold \\ ater dressing oyer the f ractu reo
Fracture of the Leg (tiNa and jibztla).-One or both of the bones may be broken. \Vhen both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches abm'e its lower end is frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond th e 61
foot. If only one sp1ll1t is ayailable place it on the outer side.
4·-Sec ure the by b.andages (a) abm'e, (b) below the (() lmmedlately abo\'e tbe knee,

3J.
. 34.
(d) round both ankles, (e) -a broad bandage round both knees (Fig. 33).
'Vhen single-handed, or \\"hen the patient is a
fz , woman, after extending the limb tie both feet together, dispense with the inner .splint, an 1 p:tss the round both limbs (Fig . 34). 'Vhen no spll11t IS available tying the legs, ankles, and knees together is of great service.
C rushed Foo t (fracture of the tarsus, metatarsus and toes) .-This accident is commonly caused by the p:tssage of a heavy weight over the foot, and m:ty be recognised by pain, swelling, and loss of power.
TREAT..\JE\,T.
T.-Remove the boot (see page 19).
2.-Apply a wellpadded splint to the sole of the foot, reachingfrom the heel to the toes.
3. -Apply a FIG. 35. crossed after the manner of the figure 8 (Fig. 35).
4.-Support the foot in a slightly raised p osition.
DISLOCATIO_ S.
A dislocation is the displacement of one or more of the bones at a joi n t.
The joints most frequently dislocated are tl:ose of the shoulder, elb .:)\v, thumb, fingers, and lower pw.

SIGNS AND SYMPTO.\-!S OF DISLOCATION.
1 ..- Pain of a severe sickening character a t or near the Jo :nt.
2. - Loss of powe r in the limb.
3· - Numbness of the parts b elow seat of dlslocation.
4.- S welling about and below the joint.
S.- Fix ity of the joint.-The linib cannot be moved at the joint by either the pJ.tient or others.
6.- Deformity of the limb.-The limb assume s an llnm.tural pOsition, and is mis ·shapen at the joint.
TREATMENT.
No attempt be .made by anyone except a doctor to reduce a dlslocatIOn. Pending his arrival :_
(a) TVhen the aCCIdent Occurs out of doorsSupport the limb in whatever position gives most ease .to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) TVhen the pat/ent £s £Jldoors-
I.-Remove the clothing from the limb.
2.-Place the patient on a couch or bed.
3·-R est the limb on pillo\\ s in the most comfortable position.
4·-A pply cold (ice or cold water) dressinas to the joint.
0
5·-When cold ceases to give comfort apply
warmth (flannels or to\\"els wrung out of hot water).
6.-Treat shock (see page I35)·
SPRAINS.
When, by a sudden wrench or and the parls around a joint are the joint is said to be sprained. ankle is a common example.
SIGNS AND

t\\ ist, the ligaments stretched and torn "Going over" the
I.-Pain at the joint after a twist or wrench.
2.-Inability to use the joint.
3.-Swelling and discoloration.
OF SPRAINED ANKLE.
T,f/hen out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing it on the front of the ankle, and carrying it round and round the ankle, where it is to be firmly tied.
2.-Wet the bandage after applicaton; it is thereby tightened.
After readzi17g sltelter-
I.-Remove the boot and stocking (see page I9)·
2.-Place the limb in the most comfortable position j usually that is well raised.
3..- Apply ice or cold \yater dressings to the joint as long as they relieve pain. v
4.--When cold fails to give comfort, apply hot fomen tations.
\Vhen other ioints are sprained, treat tbem as if dislocated.
. When in doubt as to the nature of the injury, trc::tt as a fracture.
PRAIN AND RUPTURED MU 'CLES.
When durino severe exertion, muscles or tend o ns are they are said to be strained, if they are actually torn they are described as ruptured.
SIGNS A D SV:\IPTOi\lS.
J .-A sudden sharp pain.
2.-\Vhen the muscles of a limb are strained they may s\yell and cause severe cramp.
3. - Further exertion is difficult or .impossibl e ; for example, if tbe strain bas occurred 111 the back the patient may be unable to stand upright.
I.-I'lace the patient in the most comfortable position, and afford support to the injured part. .
2.- Apply hot \yater bottles or hot fomentatloIlS '."ben the pain is very severe.
A so-called strain in the groin (hernia) is an injury tJf a totally different nature (see page II 4)· o
QUESTIONS ON CHAPTER II.
The numerals ind£cate the pages where tIle answers may be .found.
"Vhat is the skeleton, and what purposes are served by it?.. '"
How are the bones of the skull arranged?
\Vhat are the boundaries of the cranium?
Describe the bones of the face
Describe the lower jaw ...
What is the angle of the jaw? ...
"Vhat other names has the back-bone?
What is a vertebra?..
How many vertebne are there in the spine?
"Vbat are the regions of the spine and h ow many verte bree are there in each?.. '
How is the spine endowed with free movement?
What is a rib?
How many pairs of ;i'bs are' 't'h er e ?"
What is the breast-bone?
What are the bones of the upper limbs?
What is the pelvis? '"

Where does a b
How maya fra cture be caused hy muscular action?
In what two ways may fractures be classified? ...
\Vhat is a simple fractur e? ..
"Vhat is a compound fracture? \Vhat is a complicated fracture?
is a comminuted
What fractures afford the most complete example of the signs and symptoms?
In making up your mind whether a fracture had occurred or not, what points should you take into consideration beyond the signs and symptoms?
apparatus may be necessary for the treatment of
'"
What is the hip joint? '"
What are the bones of the lower lim bs ? '"
What is a joint? '"
Descr!be a moveable joint .. .
Descz:be the shoulder joint
Descnbe the ankle joint ...
How are muscles classified
Describe voluntary muscles
Describe involuntary muscles
\Vhat is a fracture?
\Vhat are the causes of fracture?
(Fig. 8)
In what ways may the triangular bandage be folded for use?
How many kinds of a rm -slings are there, and what are they called?
"Vhat knot is to be tied, and what knot avoided? 40 \Vhat is the object of first aid treatment of fractures? 4I
the general rules for the treatment of fractures 4I
lIow should splints be applied? ... ... 4I, 42
How sho uld bandages be applied?
\Vhat may cause a fracture of the upper part of the cranium?
42, 43
What may cause a fra cture of the base of the cranium? 43· H
'What the signs of fracture of the upper part of the cramum?
What are the signs of fracture of the base of .the cranium?

44
, ... ... 44
What is the treatment for fracture of the cranium? <14
'What are the signs of fracture of the lower jaw? 44
How maya fractured spine be caused? ...... 45
What is commonly regarded as a broken back? ... 45
What are the symptoms of a fractured spine? 45
How may ribs be fractured? ... ... 46
How maya fracture of ribs be complicated? 47
State the signs and symptoms of a simple and of a complicated fracture of ribs '" ... ... 47
What is a frequent cause of fractured collar-bone? .. , 48
What are the signs and symptoms of fractured colla rbone?
48, 49
At what points may the bone of the arm be broken? ... 52
Are the general signs and sympt oms of a fracture always present in a broken forearm?
When not sure whether the injury is a sprain or fract ure h ow would you treat
First Students should practise improvising material, foldmg bandages, tying knots, making slings, and the treatment of the following injuri es.
Improvising splints
Improvising bandages
F ulding bandages
54
State the cause of a common fracture of the radius 55
How would you rec ognise a fracture of the pelvis? 56
At what points may the thigh-bone be broken? ... 57
\Vh at are the signs and symptoms of fracture of the thigh-bone?
57
What are the causes of fracture of the knee-cap? ... 58, 59
What are the signs and symptoms of fracture of the kneecap? '"
Are the general signs and symptoms always present in a fracture of the leg?
What mistake may easily be made when the fibula is broken near its lower end?..
What is a dislocation?
59
Fractures -Lower jaw, 44. Spine, 45, 46 . Ribs (simple and complicated fractures), 46 to 48. Breastbone, 48. Collar-bone, 48 to 51. Both collar· bones, 51. Arm, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm when the elbow is involved, 53. Forearm, 55. Crushed hand, 55, 56. Pelvis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single-handed), 58. Kneecap, 59,60.. Leg (man), 60, 61. Leg (woman, or man when smgle-handed), 62. Crushed foot 62, Dislocations-Out of doors :lnd ind oors ' ... 63 , 64
CH APTER III.
THE ORGANS OF CIRCULATION.
THE organs concerned in the circulati on of the blood are the Heart, the Arteries, the Veins, and the Capillaries.
The Heart is situated in the chest behind the breast-bone and rib cartilages, between the lun gs and immediately above the diaphragm; it lies obliquely with a quarter of its bulk to the right and the remaining three-quarters to the left of the middle line of the body. Its beat may be felt just b elow and to the inner side of the left nipple. The heart has four cavities, two on either side of a central partition. The two upper cavities are named the right and left auricles, . the two lower the right and left ventricles.
Arteri es are vessels which convey blood from the heart. Veins carry blood to the heart. C api llaries connect the arteries and veins.
In the general (systemic) circulation arterial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all parts of the body. Th ese divide and sub-divide, and become so small as to assume microscopic dimensions, whe n they are termed capillaries.

L. Larynx (voice box); T. Tr'1chea (wi!1d I ipe) ; R.L. Right Lung; L.L L.·ft Lung (the lungs are (1I:1wn back to expose the heart and hlood vessels): R.A. Right uricle; L.A. Left Auricle; R.V . Right Ventricle; L V Left Ventricle; P.A. Pulmonary Artery; Ao. A orta; S . V C Superior vena cava (the large vein carrying blood from ih up pe r part of the body to the heart); I. V.C. Inferior vena cava (the large vein carrying blood from the low e r part of the body to the hea rt) . Th e four pulmonary veins cannot be shown in th e diagram.
72 ,
In the capillaries an interchange of gases and fluicls takes place, whereby the nobrishment and maintenance of the tissues and organs of the body are provided for, and the blood becomes dark and impure.
Venous blood pass es from the capillaries to the veins, which conv ey it towards the he:ut, getting larger and larger as they proceed by being joined by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided v·lith valves at frequent intervals, which prevent the backward fl ow of the blood.
The pulmonary system of blood vessels is concerned in carrying the blood through the lungs. From the right auricle the blood passes to the right ventricle, and is thence carried to the lungs, where it is purified by contact with and becomes sca-rlet in colour; it is then conveyed to the left auricle of the heart and pass es into the left ventricle, thus completing the circulation.
' The heart contracts in adults at an average rate of seventy- two times a minute, but the rate varies, increasing as the position is changed from the lying to the sitting or- to the standing position; hence the importance of adjusting the patient's position in cases of hcemorrhage. At every contraction of the left ventricle blood is forced into the arteries, causing the pulse, which may be felt wherever the finger can tole

EX/J 'anat/oll.-In the middle of the diagram is the heart wi t h its (our chamber!'. Abo,-e the heart i shown the lung (pulmonary) circulat ion . Th e lowe r part represents the general (sytemic) ci rcul ation. Vessels containing impure (yenous) bloud a re shown black, while those containing pure (arterial) blood are sho wn white. Th e connecting ," essels rep resent the capillari es. The a lTO" "S sho w the direction of the flow of blood.
placed on a n artery as it passes over a bone. In the veins no pulse is to be found.
HADIORRHAGE.
Hzemorrhage, or bleeding, is of three kinds :1. Arterial. 2. Venous. 3. Capillary.
FIG. 37.AR TERIAL HIEMORRHAGE.
, I.-Blood from an artery is scarlet. .
2. - If the wounded artery is near skm the blood spurts out in jets correspondmg to the pulsation of the heart.
3. - The pressure point (see below) is on the heart side of the wound.
ARREST OF ARTERIAL HIEMORRHAGE.
Arterial hcemorrhage is, when practicable, to be arrested by pressure, position of the body, and elevation of the bleeding part. .
Pressure may be :-
I.-Digital-that is, app lied with the thumb or fmo'ers and may be (a) on the wound ; (btat spot called the pressure point. The pressure points are mdlcated by numbered dots on the front-.Lsplece .
2.--Bya pad and b3.ndage (a) on the wound; (b) on the pressure pomt.
3. - By flexion.
To apply a pad and bandage to the wound, place a piece of lint or linen or a clean . chief folded into a hard pad, on the bleedmg pomt, and secure it by a bandage tightly tie.d the injured part. To fold the handkerchief, bnng the four corners to the centre, and repeat the until a hard pad is formed. The smooth surface IS

75
placed on the wound, and, to prevent the pad from unfolding, the puckered surface may be stitched or fixed by a safety pin. A hard substance, such as a stone, may be enclosed in the centre of the pad.
A Tourniquet may consist of a fad to be placed on the pressure point, a strap, cord, or bandage to encircle the lim b and pad, and a arrange?JZmt, such as a stic k or other means of t\\isting the band to tighten it.
To improvise and apply a tourniquet :-
I.-Apply a firm pad on the pressure point.
2.-Encircle the limb by a narro\\' bandage with its centre over the pad.
3.-Ti e the ends of the bandage in a balf Knot on tbe opposite side to the pad.
4.-Lay the h\isting stick on the half knot, and oyer it tie a reef knot.
5·-Twist tbe stick to tighten the bandage, thereby pressing the pad uron the artery, and arresting the flo\\- of blood.
6.-Lock the stick in position by tbe ends of tbe bandage already applied, or by another bandage passed round the stick and limb.
The pad of the tourniquet must be accurately placed upon the pressure point so as compl etely to compress the artery; otherwise arterial blood ",ill be allowed to pass along the limb, and tbe veins, being compressed by the tourniquet, will not allow the
blood to return through them to the hectrt, and the.. result \\' ill be dangerous swelling and congestion. a suitable pad not be at hand, a knot may be made in the centre of the bandage, and when available, a stone, cork, etc., enclosed in it to give it ilrlllness and bulle See tha.t the bulging and not the flat side of the knot is next the skin .
An elastic bandage [Jassed tightly round the limb, immediately above the seat of arterial hcemor· rhaae, ,,·ill arrest bleeding. The simplest prepared of thi\\ bandage is a str!p of elast.ic ,yebb!ng.
L\yenty·five to· thirty inches long and two Jnches with a piece of tape sewn at each end. An elastIC belt or brace will sen'e the same purpose. Except when part of a limb is Lorn off, it is not aclvisabl e to use an elastic cord or bandage if other a ppar::tL us can be had, as it cuts off all circulation in the limb.
Flexion consists of the application of a pad on th e pressure point at the kne e or elbo.,,· joint, the limb to make pressure, and seCurIng the lImb ll1 the ft exer! position by a bandage crossed I ike the flgure 8.
Gl£:,\ERAL Run.s FQR TREAnIEN r OF A WOUND "\CCG:\lPANIED BY ARTERIAL H M \LORR H"\GE.
r. Stop bleeding.
11. Prevent inj urious germs from getting into the wound .

'17
To attain these ends :--
I. Place the patient in a suitable position, bearing in mind that the blood escapes with less force the patient sits, and is still more checked when be lies down.
2. Elevate the bleeding part, as thereby lesS1 blood finds Its \\·ay into it.
3. Expose the wound, removing whatever clothing is necessary. (See Rule 8, a.)
4. Apply digital pressure. ..
(a) If the wound IS small on the bleeomg spot: (b) If the wound is laro-e on the pressure pomt , n ext to the wound/:) on the heart side. The nearest pressure point is chosen in order to avoid cutting off the circulation from as much of the part as possible, but sometimes it is necessary to apply pressure still nearer to the heart.
5. Remove foreign bodies, as broken glass, bits of clothmg, haIr, etc., seen 111 the \yound: do not search for foreign bodies you cannot see. .
6. Cover the wound with a clean and flrt? absorbent dressing. A hard dry pad of boraCIC gauze or lint is to be preferred, but. absorber:t wool, lint, or gauze, or a clean pIece of 1men WIll answer the purpose. Should any doubt be tained as to the cleanliness of the dressing, a clean piece of unprinted paper, such as the inside of an

78 envelope, should be placed next the wo und before applying the pad. (Compare pages 75 and 76.)
7· Bandage tightly over the pad unless :-
(a) Foreign bodies are s u spected to be left unseen in the wound.
(v) There is danger of causing injury to a fracture. I n these c ases a light dressing only shou ld be applied.
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4, b ), but only in the following cases: -
(a ) As a temporary measure while the wound is be ing exposed, examined and covered.
(b) As a more permanent measure when bleeding cannot be stopped by the pad and bandage on the wound, or when, in accordance with Rule 7, the tight bandage has not been applied.
9· Afford support to the injured part .
"1:J.en part of a limb has been torn off or the wound is lacerated (for example by the claw of an animal or by machinery) heemorrhage frequently do es not come on at once, but as there is a danger of severe hcemorrhage later, means for its arrest should be applied to the limb, but not tightened unless necessary. Do not disturb a clot of blood formed over a wound . No attempt should be mace to cleanse a wound except with sterilised water (that is previously boiled 79
and allowed to cool), and experience, especially in recent wars, has shown that those wounds \\ hich were provisionally treated with a dry dr ess ing and subsequently dressed by a surgeon \\ ith proper appliances did best.
practising arrest of arterial hcemorrhage should feel the pulse t o see when the current of blood in the artery has been stopped, and should then immediately relax th e pressure made on the artery. In this way the importan ce of the accurate application of pressure will be realis ed, and the amount of force necessary will be ascerLained.
THE COURSE OF THE MAIN ARTlmTES, AND THE ARRE T OF H.iE:\IOR RIIAGK
( The numbers of the pressure points refer to those on the Frontispi ece .)
THE LARGE ARTERIES "WITHIN TH E CHEST AND ABDOMEN.
T he Aorta is the central or trunk artery of the body. Commencing at the left ventricle it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branches which carry the blood to either side of the head and neck and to the upper limbs. The Aorta passes down on t he left of the spi ne to just below the navel, wh e re it d ivides into two great branches (the iliacs )
which convey the blood to the organs In the pelvIs and to the lower limbs.
Wounds of these arteries are one cause of internal hcemorrhage ' (see page 96).
ARTERIE S OF THE HEAD AND NECK.
The Carotid Arteries (right and left) leave the upper part of the chest and pass up on either side of the windpipe and, just below the level of the angle of the lower jaw, dIvide into the Internal and External Carotid Arteries. The Internal Carotid Artery ascends deeply in the neck, and enters the cral1lum to supply the brain with blood. The External Carotid Artery gives off a number of branches; to the front the of the tongue (Lingual), the artery to the .face (FacIal); to the back the OccipItal; artery Itself IS contInued upwards in front of the ea r, It changes its name to the Temporal, and supplIes the scalp in the n eighbourhood of the temples. .
When a Carotid Artery is wounded, as in the case of a cut throat, a pply the thumb of one hand on the .artery at pr essure point I, pressIng the backbone and taking care to aVOld the wIndpipe. It may also be necessary to apply pressure with the other thumb above the wound for two reasons: (a) To arrest'the flow of blood from the main (juguLar) vein in the neck, which runs
Sr of the carotid artery and is usually wounded at the same time; (b) To check the flow of blood from the upper end of the carotid artery \\"bich is often considerable owing to commUl1lCatIOn between the branch es of this art ery and those of its

fe iiow. Di gital pr es sure must be by relays of assi stants if n ecessary, untIl th e d octor arrives (Fig. :) 8). . ' .
The Facial Artery crosses the low er ]a W In a sli a- ht hollow two fin a-e rs ' br eadth in fr ont of th e angle, and sends t o the chin, lips, ch eek, and
82
outside of the nose . Hremorrhage from wounds of the face below the level of the eye is to be arrested by ;-
(a) Digital pressure on pressure point 2 (Fig. 39), or
(b) Grasping the lips or cheek on both sides of the wound by the finger inside and the thumb outside the mouth or viC.! vers a.

40.
FIG. 41.
The Temporal Arte ry may be felt pulsating in front of the upper part of the ear. Hremorrhage from the region of the temple may be arrested b¥ pressure applied at pressure point 3 (Fig. 40).
The Occipital Artery supplies branches to the
83
region of the scalp from behind the ear to the back of the h ead. Hremorrhage from this rEgion may be arrested by digital pressure on pressure point 4, four fingers ' breadth behind the ear (Fig. 4 I ).. This point is difficult to find, and it is usually suffiCIent to apply pressure immediately below the \\'ound. fr om the Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the bleedingpoint and securing it by a narrow bandage with its centre laid on the pad, the ends carried round the head in the direction most convenient. and tied tightly over the pad (Fig. 42) . When a wound of the for e head or scalp is associated with a fracture, the FIG . 4 2 . best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fingers; pass the other end of the bandage through the ring thus formed and continue to pass it through and through until the whole of the bandage is used and a ring as shown in Fig. 43 is formed.
FIG.ARTERIES OF THE UPPEk Lll\lBS
The Subclavian Art e ry passes from a point behind the end of the collar-bone across the first rib to the armpit.

FIG. 43· FIG. 44.
To apply digital pressure:-
I.-Bare the n eck and upper part of the chest.
2.-Place the patient's arm against the body so as to depress the shoulder, and cause him to incl1l1e his head towards the injured side.
3. - Take your stand opposite the shoulder.
4. - the left hand for the right artery, and vue versa, grasp neck low down, placing the fingers behmd the shoulder and the thumb immediately above the centre of the collar-hone in the hollow between the attached to the bone (pressure pomt 5).
s.-Press the thumb deeply downwards and hackwards agaillst the first rib, which is beneath the collar bone at this spot (Fig. 44)·
T he Axillary A rte ry, which is a continuation of the subclavian, keeps close to the shoulder and can be felt pulsating when the fmgers are deeply pressed into the armpit. Digital pressure is dJlficuli: to apply to this artery.
To apply a pad and bandage: -
I. -Place a hard pad the size of a billiard ball in the armpit (pr essure point 6).
2 -Apply the centre of a narrow bandage on tIle pad i cross the bandage on FiG. 45. the shoulder; rull t11e ends tight and tie them under the opposite armpit, laking care that the pad does not slip.
3. -Flex the forearm and tie the limb tightly to the trunk ",ith a broad bandage, applied on a level with the elbow (Fig. -1-5)·
Brachial Artery is a continuation of the and runs down the arm on the inner side of the bIceps muscle, gradually passing forward until it the middle of the front of the elbow. The of the coat sleeve above the elbow rou a hly mdlcates Its course.
0
Digital or instrumen tal pressure may be applied at or near pressure point 7.

FIG. 47.
To apply digital pressure extend the limb at riaht to body, palm of the hand upwards. St:nd behmd the 11mb, and pass the fingers under the back
of the arm over the seam of the coot or the groove on the inside of the biceps muscle. Press the pulps (not the tips) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47). A slight turn of the hand outwards as it grasps the arm will better ensure compression of the artery .
The Brachial artery may be compressed at the
elbow (pressure point 8) by flexion. The pad may be a folded handkerchief with a small stone or a cork wrapped up in it, but when no pad is available the coat sleeve rolled or gathered up will serve instead (Fig. 4'8).
88
. Just below. the elbow the Brachial artery divides Into the RadIal and Ulna r arteries, which run along the of the forearm on the outer and inner sides respectIvely.. The press ure points (9 and 10) are one mch above the wrist and about half an Inch from the outer and inner sides of the forearm where the arteries may be felt pulsatin a . of these arteries join to form the A rch es in the hand. The arteries run along on either side o f the fingers to the tip.
may be applied to the R adial and Uln ar art.e nes at pressure points 9 and 10, by the thumbs (FIg. 49) o r as fo llows :-
I.-Cut the cork of a quart or pint bottl e in tw o length wise.
.
2.-Lay rounded side of one half o n the RadIal, and of the other half on the U ln a r artery.
3·-Secure them by a ti g ht bandage.
To arrest h::em orr hage from the palm of the hand:-
I.-Apply . a firm pad, and the pat ient grasp It firmly.
'Z .-Spread out a trian.gular bandage, turn up the a?out four mches, lay the ba c k of the patIent s ha.nd on the centre of the banda ge, fold the POInt over the knu c kles a nd wri st the two ends round the \\"fist, make

89
patient pull on the point of the bandage, cross the ends over the fingers twice and tie th em as firmly as possible. Bring the po!nt (A) down to the knuckles a nd fasten \\"lth
a pin at B (Fig. 50)'
3.-Elevate the forearm and support it with a " t. J ohn " sling (see page 49)·
Arterial hremorrhage from the fingers may be by applying a small pad on th e and it firmly wIth a strIP of tape, linen or plaster.
... R TERIES OF THE Lo \ E R LIl\IBS.
The Femoral Artery, a continuation of the iliac,
FIG. 50. enters the thigh in the centre of the fold of the groin, where it may be felt pulsating immediately below the skin . The course of the artery may be indicated by a line drawn from the centre of the g roin to the inner side of the back part of the knee. After traversing two-thirds of this line, the femoral artery passes behind thci:high bone to the back of the knee joint as the Popliteal artery.
Diaital pressure may be applied to the Femoral arter; at the groin (pressure point II) as follows :-
I . -Lay the patient on his back.
2.-Kneel beside the patient.
3·-To find the groin, raise the foot high so as to flex the thigh; the fold in the clothing at the top of the thigh will indicate the groin.
4·-Place the thumbs one on the other upon the pressure point, grasping the thigh with the hands (.Fig 51).
5·-Press firmly against the brim of the pelvis.
As there is immediate danger of death it is important not to waste time in removing the trousers.
'Vhen the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been FIG. SI. devised for compression at this point, and relays of assistants should be employed to keep up the pressure until the doctor arrives; each fresh assistant places his thum bs over those of his predecessor, \vho slips his away from beneath, and thus gushes of blood are prevented during the change.
Application of a tourniquet to the Femoral artery (pressure point 12) :-
When practising compression of this artery, It is a

S2
9 2
goo,d plan to draw a ch8.lk l ine from the centre of the groll1 to the inner side of the back of the kn ee ' place the pad of the tourni quet on this lin e as high up as th,e band age can be applied, T he pad should be the SIze of a lawn tennis .ball (Fig. 52). may be applied to the Popliteal artery by fl exIOn at the knee (pressu re point 13); the pa d

FIG . 53.
be the size of a law n tennis ball, or if no pad IS avmLtble trouser leg may be rolled or gathered up to It is not n ecessary to take off the clothll1g (FIg . 53'.
. Just beh ind knee joint the Popliteal at tery dIvIdes ll1to the Antenor (front) a n d Posterior (back) Tibial arteries.
The Posterior Tibial Artery passes down the
93
Ixtck of the leg to the i nn er side of the ank le. IL is at nest deeply placed between the muscles of the calf: but it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the inner side of the ankle. It enters the sole as the Plantar Arteries, which run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery, on leaving the Popliteal, at once passes fOl'\\'ard between the leg bones, and, deeply placed amongst the muscles, runs down the leu to the centre of the front of the ankle. This artery;:' is continued as the Dorsal Artery of the Foot, which, passing forward over the t8.rSllS, dips down to the sole between the first and second metatarsal bones. Here it forms \\ ith the Plantar arteries what is known as the Plantar Arch. At the ankle (pressure points 14 and IS) pressure may be applied by the fingers or by pads alHl bandages.
VEL OUS HfE:\lORRHAGE.
. I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3. - It issues from the side of the wound further from the heart .
4.- In the case of a wound of a varicose vein it Hows also from the side of the wound nearer to the heart, especially if the p:ttient is kept standing.
Varicose Veins . -The veins of the leg are specially apt to become varicose . , A var,icose vein is dilated , winding, and with bead-lIke (vancose) projections along its course . A vein becomes varicose from several causes, such as long standing or tight garters. The first effect is to throw extra work upon the valves, and the bead-like projections are caused by the blood accumulating in the behind the valves. In time the vein becomes so dllated that the valves can no longer span it.
GENERAL RULES FOR TREATMENT OF A 'WOUND ACC01'VIPANlED BY VEN OUS HJEr.IORRHAGE.
I.-,Plac e t he patient in a su itable position, bearing in mind that the blood escapes with less force when the patient sits and is still more checked as he lies down.
2.-Elevate t h e part, as thereby less blood finds its way into it.
3. - Expose t h e w ound, removing whatev e r clothing is necessary. ,
4.- Remove any cons tricti ons, such as the collar or garters, from the heart side of the wound.
S. - Apply digital pressure on the wound until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure nedr the \\ ound on the side away from the heart. In the case of a wound of a varicose vein it may also be necessary to

apply a pad and bandage to the vein immediately above the wound, especially if the limb cannot be maintained in an elevated position.
6.--Treat the wound as directed by Rules 5, 6 and 7, stated on pages 77 and 78.
7·- Afford support to the injured part.
CAPILLARY
r .- T he blood is red.
2.- It fl ows briskly in a continuous stream, or may me rely ooze from the wound.
3. - It wells up from all parts of the wound.
A sl igh t amount of pressure \rill suffice to arrest capillary
HIEMORRHAGE.
'W o unds of the blood vessels within the trunk cause into the cavity of the chest or of the abdom e n.
SIGNS AND SYMPTOMS OF INTERNAL HJE;\IORRHAGE.
I loss of strength, giddiness and faint n ess espeCIally when the upright position is as sumed. '
2.-Pallor of the face and lips.
3.- Brea thing hurried and laboured and ac c ompanied by yawning and sighing. '
4·- pulse fails, and may altogether disappear at the wnst.
5.-The patient thro\\"s his arms tu gs at the clothing round the neck, and calls for an.
6.-Finally the patient may become totally uncon· scious.
TREATMENT.
I.-Keep the patient in a recumbent position.
2.- Undo all tight clothing about the 3.-Provide for free circulation of aIr; fan the p:ltient. . .
4.-S prinkl e cold wat er on the face; hO.ld sllle1l1l1g salts to the nostrils; avoid other forms of stImulants, at all events until the hcemorrhage has been c,antrol.led.
5.- Giv e ic e to suck or .cold water to drink If seat of the hcemorrhage IS known, apply an Ice bat:> over the re
6.-Shouldgion.the patient be reduced to. a state of collapse, raise the feet and bandage the lImbs firmly from the toes to the hips and from th e fingers to the shoulders.
HiEi\IORRHAGE THE NO SE (NOSTRILS).
I.-Place the patient in a sitting position in a current of air befor e an open window, with the head thrown slightly back and the hands rais ed ahoye the head.
2.- Undo all tight clothing around the n eck and chest.
3. - A pply cold (ice, a cold sponge or bunch of

97
over the nose and also thc spine the level of the collar; place the fee t in hot water.
4.-.Cause the patient to keep the mouth open, and so avoId breathing through the nose.
Blood issuing from the mouth may come from the tongue, th e gums, the socket of a tooth after extraction, tbc thlOat, the lungs, or tbe stomach.
HiE [ORRHAGE FROl\r THE TO!'\GUE, THE GUMS, THE SOCKET OF A TOOTH, OR THE THROAT.
y .-G lve ice to suck or cold \\'ater to hold in the mouth. If this is not successful gi \'e water as hot as can be borne to hold in th e mouth.
2.- If n ecessary make pressure on the carotid al tcries.
}.-If. bleedltlg from the front parl of the tongue IS excessIve compress t he part by a piece of clean lint h eld beh\een th e finger and thumh.
4.- If the bleedlllg is' from the socket of a toolh plug the socket with a piece of clean jint or \\ 001; over this plac e a small cork or other su bstance nf suitable size, and instruct the pallent to bite on it.
HlE"\I ORRHAGE FROi\r THE LUNG S.
Blood from the lungs is coughed up and is scarlet an i frothy in appearance.
Treat as for Internal Hcemorrhage (see page 95)·
HJEMORRHAGE FROM THE STOMACH.
Blood from the stomach is vomited; it is of a dark colour and has the appearance of coffee grounds j it may be mixed with food.
Treat as for Internal Hcemorrhage (see page 95), except that nothing is to be given by the mouth.
Blood issuing from the Ear Channel, which generally indicates a fracture of the base of the cranium, must be wiped away as it issues j no attempt is to be made to pI ug the ear.

QUESTIONS ON CHAPTER III.
Tlte nUl7ura!s indicate the pages wlw'e the answers may be found.
What organs a r e concerned in the circulation of the
blood? ...
Describe the heart . . .
Trace the circulation of the blood through the body and lungs 70 to 72
How many times a minute does the heart contract on the average? 72 \Vhat is the effect of the patient's po ition on the rate at which the heart contracts? 72
is the pulse? ... 72 How many kinds of hremorrhage are there? 73 How would you know a case of arterial hremorrhage ? ...
In what way should arterial hremorrhage be controlled?
is meant by " pressure point" ?
may pressure be applied?
What is a tourniquet? 75 \Vhy is accuracy necessary in placing the pad of a tourniquet? 75 'When mayan elastic bandage be used instead of a tourniquet? 76 What is flexion?
76
State the general rules for treatment of a wound accompanied by arterial hremorrhage ... 77, 78
If part of a limn had been torn off, but there was not much bleeding, how would you act?
78 Should blood clots be di turbed ?... . . 78
Is it wise for an unskilled person to attempt to cleanse a wound? '" '" 78, 79 What is the aorta? ... . 79 11:2
roo
Describe the arteries of the head and neck 80
\Vhy is it sometimes necessary to compress the carotid artery both below ancl aboye the wound? '" So, 81
\Vhat is a ring pad, and \\ hat is its use ? ... 84
Describe the arteries of the upper limbs. .. 84 to 89
Describe the arteries of the lower limbs .. . '" 89 to 93
How Y?U know a case of venous hremon-hage? 93
What IS a Yancose vein? ... ... ... '" 94
How maya veill beccme varicose? '. , '.. ... 9-l
State the general rules for treatment of a wound accompanied by yenous brcl11orrhagc? ..., .. 94, 95
How would you ].;no\\' a case of capillary b::emorrhage? 95
How would you stop capillary hrcmorrhage?.. . ., 95
'What is internal h::el11orrhage ? .,. ,.. .,' '.. 95
\Vhat would lead you to suspect internal h::emorrhage? 95, 9 6
State the treatment for internal h::e1110rrhage? ... 9 6
How would you arrest hremorrhage from the nose? ' .. 96, 97
\Vhere may blood is uing from the mouth come from ?.. 97
How would you treat bleeding fr0111 the gums or throat? 97
\Vhat else would you do if the longue \\ere bleeding?.. '97
And if the bleeding were frol11 the socket of the tooth? 97
How would you distinguish between bleeding from the lungs and from the stomach? ... '" '" .. , 97
And what would be the difference in the treatment? .. 97
Of what i bleeding fr o m the ear channel generally a sign? 98
The Student sbould. practise placing supposed patients 111 a proper posItIOn for the arrest of hremorrhage (<;ee pages 72 , 77 and 94), folding firm pads (74 and 75), tying hard knots in bandages to form ii tourniquet and the application of pressure at all the pressure pOInts shown 111 the frontispiece, a.t various points on the forehead and scalp, and on the palm of the hand. Pressure should be digital, by pad and banda.ge, or flexion, as directed in the text.

101
Pre sure points-Carotid artery, 80. Fac.ial, 82. Temporal, 82. Occipital , 83. SubclaVIan, 84·
Axillary, 85. Brachial. (by pad and bandage, pressure being made agamst the humerus and by flexion at t1leelbov.),86. Ulnar,.87. Femoral at the groin, 90. Femoral m .the 9 2 . Popliteal, 92. Anterial and posterIor TIbIal
arteries, 93·
Hremorrhage from the forehead or scalp , ..
II::emorrhage from the palm of hand.. , .:.
Venous h::emorrhage from a "ancose or other \ em , ., 84
87 to 89 ,,, 93, 94
C HAPTER IV.
BR U IS E S.
A bl ow a nyw h ere on the sur face of th e bo d y may ca u se h Gel110rrhage beneath the skin, withIt-a" b lack eye II is an in stance. The ll1]ury IS accompanied by discolo ration and swelling.
TREATMENT.
ice or cold dressings. A piece of lint soaked 111 extract of wItch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is
(a) By dry such as fire or a piece of hot iron.
(b) By a WIre or dynamo charged with a high pressure electrIc current.
(c) By a corrosive acid, such as oil of vitriol.
(d) a corrosive alkali, such as caustic soda a111l110111a, or quicklime. '
,(e) By ca u sed, for example, by contact with a wheel. (Brush burn.)
A scald !S caused by moist heat, such as boiling water, hot oIl or tar.
The effect may be a mere reddening of the skin' blIsters may be formed i or even the deeper

of the bod y may be ch arre d and , The clothing may adhere to the burnt and Its is impossible without furth er detn me nt to the Injured part . Th e g reat d an ge r is Shoc k.
T REATMENT .
I. - Carefully remove the over the injured part. If stuck to t he, sk m , . the adherent cl oth ing m u st b e c u t arou nd WIth SCIssors, soaked wi th oil, and left to c ome away subsequently.
2. - Do not break blisters.
3. - Immediately cover up or smear pieces of Imt or 1men WIth OIl? or vasehne, lanoline, or cold cream; a small quantIty of boraCIC powder added to these WIll be of be n efit. The inside of a raw potato scraped out and spread on lint makes a soothing applIcation. "When the injured surface is extensive do not cover it with one large sheet of hnt, but with strips about the breadth of the hand j this is advisable as they fit better on the part, and during subsequent dressmgs, one strip can be removed at a time, and a fresh dressmg applIed before the jacent strip is taken off. The shock to the system IS t hereby less than if th e whole of the burnt surface we re laid bare to the air by the r emoval of all the dressings _ at o n e time. 'When covered by oily d ressing envelop the part in cotton \\'001 or a p Iece of fl ann el a n d apply a b a n dage.

104
When the face is burnt, cut a mask o ut of lint or linen, leaving holes fo r the ey es, nose and mouth. Dip this in oil or smear it with vaseline and apply it to the face and cover it with cotton wool, leaving openings to corr esp o nd with the holes in the mask.
When possible place the injured part in water at the temperature of the body (98 Jeg rees) until suitable dressings can be prepClred. A dessert spoonful of baking soda added to a pint of the warm water will make a soothin g lo tion.
As it is important not to leave the part exposed [0 the air, it ' is the duty of the bysta n ders t o prepare t h e dr essings wh ile the clothing is being remov e d .
4·- Treat Shock. - This IS particularly ne c e ssary In the case o f every burn or scald o f a n y co n siderable ext e nt (see page 135) Be very ajJpr e he n siv e of dange r in th e case of even sli g ht burns of the neck .
5·-If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as wa shing soda. baking soda ( bicarbo n ate o f soda ) , magn esia, or sbked lime in warm wate r befo re a pplyi n g the dressings.
6.- If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion , suc h as lemon juice or vinegar diluted with a n e qual q ua nt ity of water. Cautz"on.-Before using wateI brush off a n y lime that remai n s o n the part . 105
7 - \.Vhen a woman's dress catches fire -
. (a) Lay the woman fl a t on the floor at once., so that t he flames are upp e rmost ; tha t IS to say if the front of the dress is on fi r e lay he; on her back, and if the back o f the dress is burnin g, place her face dow n wards. The reason for this is that flames ascend, so that if the upri ght position is assumed, the fl a nl es will quickly reach and burn the body, neck, and face; or if the lies WIth the fl a mes und e rmost, they WIll, if unextinguished, pass o\'er and burn the limbs and set fire to the rest of the dress,
(b ) As as the woman is laid flat, smother th e flames with an ything at hand, as a ru g, coat, blanket, or table cover; lf made wet so much the better.
(c ) A woman rend e rin g assistance should hold a ru O" or blanket in front of herself when b approachin g the fl a m es.
(d) If a woman's dress catches fire when nobody is by, she should lie flat, uppermost, smother the flames \\'ith anythmg handy, and call fo r assistance, or crawl to the bell-pull an d rin g ; on n o a ccount should sh e rush into the open a ir.
The use of fire guards would preven t m a n} calamities.
BITES OF SNAKES A ND RABID AN AND 'WOUND S BY POI SO ED ·WEAPONS.
Hydrophobia is caused by the bi te of an animal, such as a dog, cat, fox, \\"olf, or deer suffe ring from rabies. The special poisons introduced into wounds camed by yenomous snakes and poisoned \yeapons cause immediate danger to life .
TREADIENT.
I.-Immediately place a constriction between the wound and the heart so as to prevent the venous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircled on the side of the wound nearest to the heart, with the finger and thum b, and as soon as possible a ligature (a string, piece of tape, or strip of handkerchief) should be placed tightly round the root of the finger. Compression "ith the finger and thumb must not be relaxed until the ligature has been applied. Additional ligatures may, with adYantage, be applied at intervals up the lim b.
2 . - Encourage bleeding for a time :-
(
a) By bathing th e wound with warm water.
(b) By keeping the injured limb low; the upper limb should be allowed to hang down, and in the case of the lo\\"er limb the patient should be seated " 'ith th e foot on the grou nd.

3.-Cauterise the wound, if it is quite impossible to obtain the services of a doctor . This is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or if these are not at hand, with ared hot wire or a fusee. The usual solid caustic is insufficient, as it does not reach the bottom of the wound, where the poison is.
To ensure the caustic reaching the bottom of the \\ ol1l1d, it should be applied on a piece of wood, such as a match cut to a point. ' Vhen the caustic has been thoroughly applied , but not till then, the ligatures may be removed.
4. - Cover the wound, after a while, with a clean dressing.
S. - Afford support to the injured part.
6.- Treat shock if it occurs (see page 135).
7.-In the case of a bite by a venomous snake, rub in powdered permanganate of potash and inject under the skin in the neighbourhood of the wound a solution of permanganate of potash .
STINGS OF PLANTS AND AN I MALS.
These give rise to serious inconvenience, and III some cases grave sym ptoms develop.
TREATMENT.
I. - Extract the sting if left in.
2. - Mop the part freely with dilute ammonia
or spirits. A paste of bicarbonate of soda and sal volatile is an efficient application . A solution o f washing so?a O! potash or the application of th e blu e bag WIll relIeve pain.
3. - Treat collapse if it occurs (see page I35 )·
FR O ST BITE.
D uring exposure to severe cold, parts of the body, usually the feet , fingers , nose, or ears, lose sensation a n d become first \yaxy \\ hite and aftel'\\"ards c ongested and of a purple appearance. As sensation is lost in part, it is often only by the remarks of bystanders that the frost-bitten perso n is made aware of his condition . £ TT .
I. - Do not bring the patient into a warm r<?om un til, by frict!on of the hand or by r ubbing wIth soft snmv, sensatIOn and circulation in the affected parts are restored. Neglect of this precau tio n may lead to death of the of the frost-bittcn part. circulation is restored , keep the pat Ient 111 a room at a temperature of 60 degrees.
NE E D LE El\ l BE D DE D U NDER TH E SKIN
a need le breaks off after penetrating th e skin an d dIsappears, take the patient to a doctor at once. If the woun d is near a joint, k eep th e limb at rest on a splint.
!OJ
FI;:;H-HOOK IX THE SK I N.
Do not attempt to withdraw th e fish -hook by the way it went in, but cut off the dressing of the hook, SJ that only the metal is left) and then force the point ol1\yards through th e skin untIl the hook can be pulled out.
I NJURIE TO JOL TS.
When a joint is injureJ by a bullet, stab, or othe r cause-
I. - Wrap the part in cotton wool.
2. - AfTord rest and support to the injured limb; if the upper limh, in a fte'\ed jJosition by a sling; if the lower limb , in a str<li6ht position by a splint .
BODY I:\T THE EYE .
I. - Prevent t he patien t rubbing the eye, tying dO\\' n a child 's hands if necessa ry .
2. - Pull down the lower eyelid, \\'hen, if the foreign body is seen, it can readily be remm-ed with a camel 's hair brush, or \\ ith fIe corner of i1 handkerchief twirled up and we tted.
3. - W he n the fore ign body is beneath the upper ey elid lift the lid fOI\\arcl, push up the 10\yer lid beneath it and let go_ The hair of the lower lid brushes the inner surface of the upper one, and may dislodge. the body. hould the fir. t attempt be u nsuccessful, repeat it seycral times if necessary . If
lIO
the foreign body is not dislodged call the services of a doctor as soon as possible. When however skilled help cannot be had, proceed follows
(a) Seat the patient so as to face the light, and stand behind him, steadying his again st your chest.
(b) Place a small rod, such as a match or bodkin; on the upper eyelid, half-an-inch above the edge, pressing it backwards as far as p ossible.
(c) Pull the upper eye-lashes upwards over the rod, and th ereby evert the eyelid.
(d ) Remove the foreign body.
4.-When a piece of steel is embedded in the eyeball drop a little olive or castor oil on th e after pullin g down the lower eyelid, cl ose th e lIds, apply a soft pa d of co tton wool and secure it by a bandage tied sufficiently firmly to keep the eyeball steady j ta ke the pa tient to a do c tor.
5.-When qu.ick-lime is in the eye brush a:",ay as much of It as possi hle ; bathe the eye with vmegar and warm water, and treat as for a piece of steel embedded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
A.s a rule n:ake no attempt to treat a patient with a foreIgn body m the ear if the .services of a doctor can possibly be had j any attempts to remove the forei an body may lead to fatal consequences. If a child

III
cannot be induced to keep the fin gers fr o m the ear, tie his hands do\vn or cove r up the ea r. If an insec t is in the ear-pas sage, fill the ear with olive oil, wh en the insect will flo a t and may be removed. Nev er syringe or prob e the ear.
FOREIGN BODY IN THE NO E.
In d uce sn eez ing- by pe pp er or sn uff. Ca use t he pat ie nt to bl ow h is nose violen tly after closin g th e un affected nost ril. T he re is no imme dia te da n ge r fr o m a foreign body in the nose .
TH E AB DOMEN.
Th e a b dome n is bo un ded abo ve by the diaph rao·m ; b elow by t h e pelvis ; beh in d by the lu mbar j in front a n d at the sides by muscu lar \yall s. (Fig. S-t .)
T HE O RGA TS OF THE ABDO:\TE .
The Stomach lies immediately belDlY the" pit of the stomach /I just below the breast-bone .
The Liver lies in the upper part of the abdomen, where it is mostly covered by the right lower ribs .
The Spleen lies beneath the ribs at the u pper part of the left side of the abdomen. Intestines occupy the greate r part of the c av ity of the abdome n.
The Kidneys lie at t he bac k, in t he region of the loin. '-
The Bladder li es in th e pe lvis.
FIG. 54.
'VOUND L THE FRo:,\T 'VALL OF THE ABDO;\IEN. When the z'ntestines or ollzer organs protrude through the wound whether vertical or transverse, bend the knees, the shoulders, and apply lint, a to\\"el, or cotton wool wrapped in soft linen, and keep the

113
patient warm until the arrives. is no protrusion of organs, if the u:ound lS VI- lay the patient flat on the back wIth the lower hmbs straiaht· tif tlze wound is /ramverse, bend the 1:) , and raise the shoulders.
TO THE THE ABDOMEN PELVIS.
Inj uries of the Stomach are attended by extreme collapse and sometimes by vomiting of dark blood like coffee-grounds. For treatment see " Hremorrhage from the Stomach" (page 98). .
Injuries of the Liver, Spleen and Intestmes may be caused by a blow, a stab or a buIIet; the liver or spleen may be injured by a fracture of the lower ribs. .The Signs and Symptoms are those of internal hremorrhage accompanied by pain an? swelling at the seat of injury, and the treatment ISas for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a crush, blow, sub or bullet. Blood may escape with the urine, and there may be pain and swelling over the injured kidney.
The Bladder may be injured by a fracture of the pelvis. The signs and symptoms are inabil.ity to pass water, or if a little is passed it is tmged WIth blood.
TREATMENT OF INJURY TO THE KIDNEYS OR RLADDER.
Keep the patient quiet until the docto r arnves.
2.-Apply hot fomentations ov er the painful or inj ured part.
Rupture (h e rnia) consists of a protrusion of an interna l organ, usu ally th e bo we l, through the l1lUSwall of the abdomen, most fr eq uently at t he gr?ll1. a sudden swelling accompanied by pam a nd sIckness tak e place in that regio n
I.-Send for a doctor instantly.
2.-Lay th e patient down with the buttocks raised.
3·- Apply ice or cold water dressings to the affec ted part.
QUESTIONS ON CHAPTER IV.

State the tr eatment for injuries to joints '.
the genera l rules fo r removing a foreign body from the
-hat would you do if a piece ot steel were em bedded In the eye ball
And when quick-lime is in the eye?
H
would you try to remove an insect from the ear passage?,
n6
Would you try to remove any olher form of foreign body from the ear passage? ... .,. ... ... IIO,
How would you remove a foreign body from the nose?
State the boundaries of the abdomen and its contents?
State the treatment for wounds of the abdomen 112
How may injuries to the liver, spleen and intestines be ' caused?
What is the difference between treatment of injuries to st?mach and of injuries to the liver, spleen and 1ntestines ?
CSta' e the treatment of injuries to the kidneys or bladder
State the treatment of hernia

T\\ 0 systems of nerves, the Cerebro-spinal and the Sympathetic, regulate the movements a nd functions of the body
The Cerebro-spinal System is made up of the Br<l.Il1, the Spinal Cord a nd Nerves, and through its agency sensatiolls are received and the \,ill causes the action of the \'oluntary muscles. For example, when a part is injured a sensation of p:lin is conveyed to the brain by the n erve, thus affordi ng an indicatio n of the seat of injury, or a warning of a po . sibie danger of further damage. On attention being directed to Lhe injury, an attempt is instantly made to ease the pain or to move the injured part from danger.
The Brain is siLuated \\ithin the cranium, and is divitled in the middle line, so that, \\ ith the exception of sone conne cting bands, the right and left sides are separate.
The Spinal Cord is Lhe long cord of n ervou s m l.tter lying within the spinal canal (see Vertebral Column, page 23)' It leaves the brain through an opening in the base of the cranium and extends the upp er IU '11bar verteblGe.
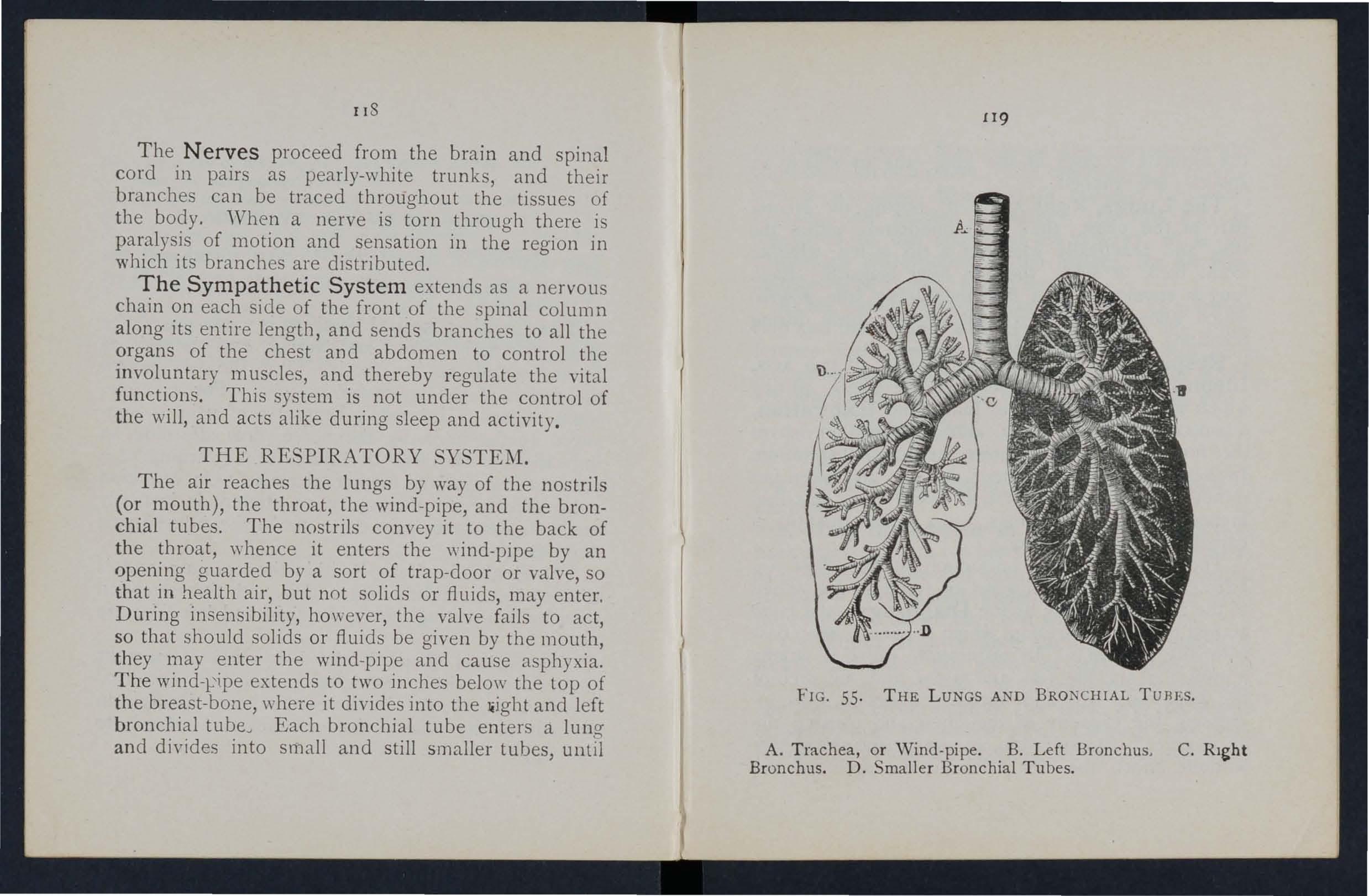
The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissues of the body. 'Vhen a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nervous chain on each side of the front of the spinal column along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary muscles, and thereby regulate the vital functions . This system is not under the control of the will, and acts alike during sleep and activity ,
THE RESP I RATORY SYSTEM,
The air reaches the lungs by way of the nostrils (or mouth), the throat, the wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind-pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they may enter the wind-pipe and cause asphyxia. The wind-ripe extends to two inches below the top of the breast-bone, where it divides into the Jiight and left bronchial tubeJ Each bronchial tube enters a lung and divides into small and still smaller tubes, until
the ultimate recesses of the lung-the air cells or air spaces-are reached.
The Lungs, Right and L ,: ft, occupy the greater part of the chest; they lie immediately within the ribs, and practically wherever a rib is felt, whether front, back or sides, there is lung beneath. Each lung is enveloped in a fine membran (the plmra) which allows it to move within the chest during bre::lthing without friction.
Respiration, or breathing, consists of two acts, Inspiration, an expansion of the chest, during which air is drawn into the lungs, and Exp iration , a contraction of the cl1est, during \yhich air lec:n ·es the lungs. A pause follows the act of expira tion. In health fifteen to eighteen breaths are taken per minute, and at each inspiration about 20 to 30 cubic inches of air enter the lun gs, and a similar is expelled at each expiration.
The explnsion and contraction of the cllest <lIe effected partly by tIle mu scles of respiratJon att;!ched to the ribs, but chiefly by the Dia p hrag m , the brge arched muscular partition which separates th e chest from the abdomen. In inspirati o n, \\ hich is chiefly a musc1.11ar act, the ribs are rais ed, and the arch of the diaphragm falls and becom es flattened, thus increasing the capaciLy of the cbest and causing the air to enter. In expiration, an act performed almost without effort, the ribs fali and the arch of the
12 1
diaph ragm rises; t his lessens t he capacity 0f thrchest and forces air out. The m echanism of resplfation is somewhat like that of ordinary household bellows but without a valve; the ribs may be to the boards of the bellows, wh.ile the diaph ragm corresponds to the leather, the au passa ve s bein a equivalent to the nozzle.
o As the °blood depends upon the air for its purification and the oxygen necessary to maintain life, interfere nce with breathing very soon may produce a dangerous state called asphyxia, examples. of which are afforded by drowning, su ffocation, c hokmg, et c.
ART I FICIAL RESP IR AT IO N .
PROFESSOR SCHAFER ' S METHOD .
I. - Make no attempt to loosen o r remove clothing.
2. - Lay the patient in a prone positio.n (i .e., back upwards) with his head turned to one Side , so as to keep his nose and mo u th away from the gro un d . No pad is to be placed under the patient , nor need the be d rawn out, as it will fal l n aturally .
3. -.Kneel at o ne side facing the patient'.s head "and place the pa lms of your hands on hiS loins, "one at each side, the thumbs nearly touching one anothe r in the small of the back , a nd the fingers p:-;:tending over the lowest ribs. Leaning your body fon\ ard, let ItS ,,·eight press straight downwards upon the
loins and lower part of the back, thus compressing the abdomen against the ground and driving air out of the chest. This produces expiration (Fig 56\. Draw back

4.-Alternate these movements, by a rhythmic swaying backwards and forwards of your body, twelve to fifteen times a minute, persevering until respiration is restored, or a doctor pronounces life to be extinct.
DR. SILVESTER'S METHOD.
I. Adjust the patient's position.-Without wasting a moment place the patient on his back on a flat surface, inclined if possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women. Raise and support the shoulders on a small, firm cushion or folded article of dress placed under tIle shoulder-blades.
2. Maintain a free entrance of air into the windpipe.-Cleanse the lips and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position.
3.-Imitate the movements of breathing. Induce Inspiratiolt.-Kneel at a convenient distance behind the patient's head, and, grasping his (orearms just below the elbow, draw the arms
FIG. 57. INSPIRATION. 123 your body somewhat more rapidly and relax the pressure, but do ,pot remove your hands; this pro· duces inspiration (Fig. 57).
12-1-

FIG 58. INSPIRATION.
FIG. 59. EXPIRATION.
12 5
upwards, outwards) and towards you, \\"ith a sweeping movement) making the elbows touch the ground
FIG. 61. EXPIRATION.
(Fig. 58). The cavity of the chest is thus enlarged, and air is drawn into the lungs.
Induce exptratt'o1Z .-Bring the patient's flexed arms slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (FIg. 59). By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and perseveringly about fifteen times a minute.
When a sufficient number of assistants are present, Howard's method may be combined with Silvester's, as follows :-
The additional assistant kneels astride the patient's hips with the balls of the thumbs resting on either side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Using his knees - as a pivot, he presses forward on his hands. Then suddenly, with a final push, he springs back and remains erect on his knees while he slowly counts I, 2, 3. These motions are to be repeated to correspond • with those being performed by Silvester's method, pressure on the chest being made simultaneously by those performing the two methods (Figs. 60 and 61).
LABORDE'S METHOD.
When from any cause the above methods cannot be carried out, Laborde's method of artificial respiration should be tried. It is especially useful in suffocated children and when the ribs are broken.

127-
The patient is placed on his back or side; the cleared; the. tongue is seized-using a handkerchIef or somethmg to prevent it slipping from the fingers-the lower jaw depressed; the tongue is. pulled forward and held for two seconds in that position, then allowed to recede into the mouth should be repeated about times a mll1ute.
Artificial respiration must be continued until breathing is established, or until a doctor arrives. "\Vhen natural breathing commences re o' ulate the artificial respiration to correspond wit11 it Success may result even after two homs' time.
. 'Vhilst artificial respiration IS b ell1g other. us eful steps may be employed, such as applYll1g sm ellll1g ' W snuff to the nostrils and flicking the chest "ith a dump towel. ' circulation and warmth after natural breat_hll1g has been resto.red. 'Vrap the patient in dry or other covenng, and rub the limbs energe tIcally towards the heart. Promote warmth by hot flannels, hot-.water bottles, or hot bricks (wrapped in fl,-;nnel) applied to the feet, the limbs and body. "hen the po\yer of swallomncr has returned crive hot tea or coffee, or meat The patient should be kept in. bed and encouracred to go to sleep. Large poultIces or fomentations applied to the
front and ba ck of th e chest will serve to asslst breathing. . Watch the patie nt carefully for some lim e to st:e that the breathing docs not fail; should any signs of failure appear, at on ce begi n artificial respiration.
INSE " IBILITY.
U n cons ci ousne ss o r I n s ensib ili ty may arise as follo\\'s :-
Injury to t he H ead . - Concussion and Compression of the brain.
D is e as e of the Brain . - Apopl exy , Epilepsy, H\ steria . 'Vari ous Causes .·-Shoc k, Fainting (Syncope), Collapse, Alcoholic and other poisoning, Sunstroke and H eat-st rok e, Infanti le COl1nilsions, Asphy:-.:ia.
RULE S FOR TREAT11ENT OF I TSEN,· I BILITY.
L-- If a person appears about to lose consciousness, prevent him from b ll ing, and by hIm gently dOI\ n.
2. - Arrest when app:nent; at· tending to minor injUries is less ilrlportant than tr eati ng the unco nscious state.
3 . - Lay the patient in the position in wh ic h breathing is most easy- usually Ihis will be un the back, or inclin ed to olle side. As a general rulf

12 9
raise the head an d shoulders sliglzlly when the fac e is fl ushed, and keep the head low \\ hen the face is pale .
4. - Undo all tight clothing round the neck , chest and waist, unfastening tl,e braces and top b utton of the tro users in men, and the corsets in \,:omen, the object being to relieye pressure on the a ir passages, lungs, heart and abdominal organs. Be sur.e that there is no obstruction to the air pc.ssages by t he tongue or by a foreign body in the throat. The possibility of false teeth obstructing breathing Il1ust be considered.
s. - Provide for a sufficiency of fresh air by opening donrs and windows, and by keeping bac k. a crowd.
6.- When breathing cannot be discerned apply artificial resp i ration .
7.- 0btain a doctor's help as soon as possible.
8.- UnJess unavoidable , never leave the patient until you have placed him in charge of a responsible person.
9. - Give no food or fluids whatever by the mouth while the patient is insensible .
10. - Should the spine or an important bone of the upper or of the lower limb be fractured, it must steadied and maintained at rest as soon as possible. Should the u nconsciousness be prolonged, th e patient may be removed in a recumbent position

to shelt er , p rovid ed that the broken bone is adeq uat ely support ed. ., .
lI.-When the patient IS In a state of ,convulsion , s u p po r t h is head, an d v:rapp m g a piece of wood or a n y othe r h ard matena l m ,ha n dkerchief h old it in h is mo uth t o bl lmg of the tona'ue . D o not forcibly restrai n h i,s h m?s; prevent from hurtin; himself by pUll!!lg hIm away from a so ur ce of danger, as machmery, a wall, o r fireplace ; l ight pieces,. of furniture shou ld be pushed ou t of the way.
12.-0n return to consciousness may be given to drink. If the pulse is feeb l,e v.,arm tea or coffee, provided eIther ll1ternal or externa l, is not present. A deslre t? sleep, be encouraged, e:cept in cases of pOlSOnll1 b , a condition t hat may generally be by the history of t h e case, and also by the pupIls of the eyes ( the b lack openings in g,rey, blue bro\\n iris) bei n g minu tely contracreL.l (pm-head pupJls ) . ..'
13. - 1t must not be assumed a person is insensible as the result of dnnk merely because the breath smells of alcohol; freque,ntly whe n people are fee ling ill tl:ey take or are given alc oholic stimu la n ts, afte r whlch they may become in sens ible" not from the d r ink, but from the cause tha t them to take it, for example , in se n sib ility coming o n, effec1.s of p oisoni ng, etc. E ve n if 13 1
drmk is beli eved to be the actual cause of insensibility, it must be borne in mind that the patient is in a ve ry dang erous state, and he must be treated for Collapse by being covere d up and kept warm.
The above ge neral rul es will enable first aid to te rendered effi ciently in most cases of insensibility, although the exact form from which the patient is suffering is unknown.
CONCUSSION OF THE BRAIN.
The patient may be stunned by a blow or fall on the head, or by a fall on the feet or lower part of the spine. He may quickly regain consciousness, or insensibility, more or less complete, may be prolonge d .
TREATMENT.
I. -Apply the general rules for the treatment of Insensibility.
2.-Be very apprehensive of danger in all cases of injury to the head. The patient may be stunned, and after a short interval may recover some degree of consciousness, or even the brain rna l a p parently have escaped injury; yet in both instance'\; th ere is a grave risk that a structure within the cranium has J been injured, and that a se rious state of insensibility may develop later (See Fracture of the Cranium, page 43). A caution shou ld therefore be given to a patient who has lost consc iousn ess even r. 2
£3 2
for only a moment after an injury to the head not to resume physical or mental activity without the consent of a doctor.
COMPRESSION OF THE APOPLEXY.
Compression of the Brain may result from the same causes as produce Concussion; in fact, Compression is frequently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no signs of injury are necessarily present.
In both conditions the face is flushed; the breathing stertorous; one side of the body may be more limp than the other, and the pupil of one eye may be larger than that of the other; the temperature of the body is generally raised.
TREATMENT.
I.-Apply the general rules for treatment of Insensibility.
2.-Promote warmth in the lower part of the body by the applicc:tion of hot \Yater bottles to the abdomen and lower limbs. Care must be taken not to burn the patient with the bottles, which should be \\"fa pped in flannel, and their heat tested with the elbow.
EPILEPSY.
Epilepsy may occur in persons of any age, but usually occurs in young adults. The patient falls to

the grou nd, sometimes with a scream, and passes into a state of convulsion, throwing his limbs about.
The treatment is according to the General Rules, especi::tlly Rule 11.
HYSTERICAL FITS (HYSTERIA).
AND Y:\IPTO:\J.
The patient, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and actions. he subsides on a couch or in some comfortable position, throws herself about, grinding her teeth, clenchi n g her fists, shaking her hair loose; she clutches at anyone or anything n e:H her, kicks, cries and laughs alternately. The eyeballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears at th e lips, and other irreguhr symptoms may develop.
TR EAT'lIE:--1T.
I.-Avoid sympathy with the patient: and speak firmly to her.
2.-Threaten her with a cold water douche, and if she persists In her" fit," sprinkle her with cold water.
3.-Apply a mustard leaf at the back of the neck. Medical treatment is necessary to cure the condition of mind and body which gives rise to hysterical attack s.

SHOCK, FAINTING (SYNCOPE), COLLAPSE.
CAUSES.
l.--Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated 'wounds, and severe crush are some of the more frequent physicaJ causes of shock.
2.-Fright, anticipation of injury, and sudden bad news! or sometimes sudden removal of fear and anxiety after prolonged .suspense, produce shock or fainting.
3·-Some pOl sons cause shock, ,\,hile others, such as alcohol, so depress the nervous system that collapse ensues.
4·-Hremorrhage or heart weakness, a close Ot crowded room, tight clothing! fati g ue, or want uf food may bring on fainting or collapse.
SIGNS AND SYMPTOMS.
The general condition of shock may be recognised Dy extreme pallor, a feeling of cold, clammy skin , feeble pulse, and shallow breathing accompanied, If hremorrhage has been severe, by yawning and sighing. The term "collapse" signifies aver) serious condition in which the life of the patient is in the greatest danger; the temperatur e of the body falls below the normal, and one great object of treatmenl is to prevent it sinking to a point at which life is impossible. An attendant danger of the conditlcn of 135
collapse is the liability to sudden relapse after a temporary improvement, and the utmost care and watchfulness must therefore be exercised to maintain the heat of the body and to guard against fail ure of the heart and lun gs .
T R EA DIE NT.
I.-Remove the cause by arresting hremorrllage, attending to injuries, loosening all tight clothing especially about the chest and abdomell, removing from a close or cro\\ded room, using encouraging words, etc.
2. --- Lay the patient on the back, with the head low. Raise the lower limbs; when the patient IS in bed this is best done by raising the foot of tbe bedstead.
3.-Provide for a free circulation of fresh air.
4.-If hcemorrhage has been severe and the patient is collapsed, Jirmly bandage the limbs from the toes to the hips, and from the fingers to the armpits.
5.-To stimulate the action of the heart, sal ,volatile and water may be giyen if the patient can swallow, or smelling salts may be held to th e nostrils.
6.-It is of the utmost importance to use every means of preventing a fall of temperature below the normal point. - To accomplish thIS cover the patient with extra clothing, or by placing
I3 6
rugs or blanket5 over him; get him to bed in a warm but well-ventilated room as soon as possible. Apply warmth to the feet and to the pit of the stomach by hot water bottles or hot flannels. (Test the heat of these with the elbow before applymg them .) If the patient can swallow, give hot drinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the temperature of the body.
7·- If breathing cannot be discerned, apply artificial respiration.
B.-If want of nourishment has been the cause of fainting or collapse, give food sparingly at first.
SUNSTROKE AND
When exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weather when heavily burdened, persons may develop sickness, faintn ess, giddiness, and difficulty in breathing. The patient compbins of thirst, the skin becomes dry and burning, the face very flushed, the pulse quick and boundin g. A very high temperature, stertorous (snoring) breathing, and insensibility may ensue.
TREATMENT.
I. - Undo all tight clothing.
2.-Remove the patient to a cool, shady spot.

137
3.-Strip the patient to the waist.
4.-Lay the patient down, with the head and trunk well raised.
5.-Procure as free a circulation as possible of fresh air, and fan the patient vigorously.
6.-Apply ice bags or cold water freely to the neck, and spine, and maintain this treatment unttl the symptoms subside.
7.-0n return to consciousness, the patient may haye water to drink.
CONVUL IONS IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
SIGNS.
pasm of the muscles of the limbs and trunk, blueness of the face, insensibility, more or less complete, and occasionally squinting, suspend.ed respiration, and froth at the mouth are the promment signs.
TREATMENT.
I.-Support the child in a warm bath slightly aboye the temperatllle of the body (98 degrees), so that the water reaches to the middle of the trunk.
2.-Place a sponge dipped in cold water on the top of the head.
ASPHYXIA.
When, o wing to want of air, the blood is not supplied with oxygen the patient becomes insensi ble, and is said to be asphyxiated. This condition may be brought about as follows :.-
1. Obstruction of the air passages.
(a) By DROWNING.
(b) By FRQ;\1 OUTSIDE: Strangulation, hangll1g, smothering.
(c) By A FORE[GN BODY I J THE THROAT: Choking.
(d) By OF THE TISSUES OF THE TH.ROAT: Inflam matlOn, scald of the throat, pOIsoning by a corrosIve.
II. Inhaling poisonous gases. By coal gas (as used in the house), producer, or water, gas, smoke, from a charcoal or coke fire, sewer gas, limekiln gas, carbonic acid gas .
III. Pressure on the clJest, as when crushed by or debris, or by a crowd.
IV. Nervous affections, as the result of nar cotic and certain other poisons, collapse, electric shock or stroke by lightning. '
GENERAL TREATIIIE T.
In all cases of Asphyxia attempts must be l1lade to remove the cause, or to rem ::)Ve the patient from the cause. ·When this has been done artificia)

respiration must be applied, taking care that the air passages are not obstructed, and that there is abundance of fresh air.
DROWNING.
Persons completely immersed in water for eve n ten or fifteen minutes have been restored by artificial means. Th erefore, if the body is recovered within a reasonable time, absence of signs of life is not to del er immediate attempts to restore animation.
The first thing to do when the body is recovered is to get rid of the vvater and froth obstructing the air passages, and then artificially to restore breathing. Thls is best accomplished either by proceeding at once to perform artificial respiration by Schafer's method, or as follows :-
I.-As quickly as possible loosen the clothing, and clear the mouth and the back of the throat.
2.-Turn the patient face downwards, with a pad below the chest, and with the forehead upon the right forearm.
3.-Whilst in this position apply pressure by the hands to the patient's back oyer the lower ribs, and keep the pressure up for three seconds.
4.-Turn the patient on the right side) maintaining that position also for tbree seconds.
s.-Repeat these movements alternately as long 8.:3 froth and \yater issu.e from the mouth .
These operations ( Iarshall Hall's method) in themselves tend to promote respiration, but ,,,hen the <lir passages are clear of froth and water Silvester's method of artificial respiration may be used by itself or with Howard's method in conjunction.
While performing these operations send someone to the nearest house to procure blankets and dry clothing, hot water bottles, etc., and to fetch a doctor.
STRANGULATION.
Cut and remove the band constricting the throat. Apply artificial respiration.
HANGING.
Do not wait for a policeman: grasp the lower limbs and raise the body to tak e the tension off the rope; cut the rope, free the neck; apply artificial respiration,
SMOTHERING.
Remove whatever is smothering the patient: apply artificial respiration.
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to the back of the throat and attempt to dislodge the foreign body; if vomiting results, so much the better. If unsuccessful, thump the back hard \\ hilst the head is bent forward. Apply artificial respiration.

SNELLING OF THE TISSUES OF THE THROAT.
Whether the sw elling is caused by inflammation by swallowing very hot water, as not infrequently happens to children attem pting to drink from the sp out of a kettle, or by the effect of a corrosi,'e poison, the treatment is as follo\\'s :-
I.-Ap ply a sp onge, piece of fl lI1ncl or other cloth, wrung of very hot water, to the front of the neck. from the chin to the top of the breast-bone. the patient before the fire.
3.-Give Ice to suck if it can be ' had; if not, give cold water to drink.
4.-Give animal or vegetable oil, a dessertspoon fuJ at a time, to soothe the scalded throat and ease the pain.
5.- If breathing has ceased apply artificial respiration .
SUFFOCATION BY S:\IOKE OR GASES.
I.-Remove the patient into the fresh air. Before ent ering a building full or smoke tie a handkerchief wet if possible, round the head so as to cover nose and mouth. It is well to move slowly, keeping low, or even crawling, \\'hilst in a room full of smoke in sear,ch of a pers on. Every opportunity of lett mg m fresh air by openin G' doors or windows should be seized.
0
2.-Apply artificial resp iration.
3 - In the case of produc er or water gas, inhalation of oxygen will also be necessary.
ELECTRIC SHOCK.
E lectric c urrent is conveyed by a cable, " 'ire, rail, or bar, called the "Positive," and r eturns to the source of supply by another cable, ,,,ire, rail, or bar, called the" Negative, " or through the earth . In the case of an electric railway, the current is gene rally conveyed by an . insulated rail cal;led tbe third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an electri c tr amway it is frequently conveyed by an oyerhead conductor o r troll ey wire, and returned through tbe running rails.
Through contact \\"ith a "positive II the shock may be so severe as to cause insensibilrty, and the sufferer will be unable to extncate himself, and must be liberated with all possib le speed. As it is generr.1ly impossible or inexpedient to switch off the current some other method must usually be adopted; but precautions must be taken or else the person rendering assistance will himself receive a shock.
To liberate the sufferer from contact-
I. - Insulate yourself from the earth by standing on an "insulator" or (( n on-conductor," that is, a body which resists the current. Amongst such bodiE'S

are indiarubber, dry gla8S, dry bricks, dry silk, dry cloth, dry wood and dry bay or straw.
2.-Protect your hands from contact the sufferer or the electric medium by covenng them with an insulator. Altbough indiarubber is probably tbe best insulator, do not waste in running for indiarubber gloves, but use dry artIcle s of clotbing; an indiarubber tobacco pouch or cap, or folded newspaper, would serve to hands in an emergency. If no means of msulatll1g th e bands are at band an attempt may be made to drag the sufferer away by means of a loop of dry rope or a crooked stick; an umbrella is not safe because. metal ribs would act as conductors*' of electrICIty, and it is not infrequently the case that the" stick " of th e umbrella is a metal tube.
3.-Pull the sufferer away fr?m should be tak en to avoid touchll1g WIth naked lmnds the sufferer 's hands, wet clothin g, or boots if the soles are nailed. The armpits should be avoide d as perspiration usually makes the clothing damp there.
\Vhen the sufferer is remo,'ed from contact -
I.-Apply the general treatment for insen-
A concluclor is a body through which p'lsses. Amongst such bodies are copper, bn.>.ss, Iron, mOIstu re and one's own body.
144 sibility (loosen clothing, procure fr ee circulation of air and place in a recumbent positio n ).
2. - Dip a towel in cold water and attempt to arouse him by sharply flicking the face and chest.
3. - Commence artificial respiration jf othe·r meth'ods fail to restore animation. "Laborde's " method (see page I26) has been found to be very successful.
4. - Treat burns if there are any (see pages r03 , I 04-).
EFFECTS OF LIGHTNING
.
A pe rson struck by lightning is us-ually mor·e or less deprived of consciousness. The treatment is t he same as that for electric shock, except, of course, that the instructions for the patient from contact with the electric medium do n ot apply.

145
Q UEST IO NS ON CHAPTER V.
T he numerals t"nd£cate the pages where the an S7Ue
may be found.
What are the two systems of nerves?
Of what is the cerebra-spinal system made up? ...
What is the spinal cord?
are nerves like?
are the expansion and contraction of
In what system is he rolled alternately on his side and face downwards?
long should artificial respiration be perse\"ered \\ith?
you examine the patient to see if any bones
\Vhal wrong opinion may be formed when the patient smells
Is collapse from drink a serious condition?
is
\Vhat danger accompanies injury to the hear! ?
What caution should be given to a patient who has lost consciousness, even for a moment, after an injury to the head? ,,' ,.. '"
What are the causes of compre -sion of the brain?
lin what aged people does apoplexy usually occur?
What are the signs and symptoms of compressi on and apoplexy?
State the rules for treatment of these conditions. _.
What dangE'r is there in applying hot water hottles to insensible persons, and what precautions should be
taken?
Describe a case of epilepsy 132, 133
What special care must be taken in treating a case of epilepsy?
Describe a hysterical fit
How would you treat a hysteric al fit?
What are the commonest physical causes of shock?
What may produce shock 01 fainting?
What conditions d o certain poisons brbg about?
What may bring about faint ing or collapse?
How would you recognise the general condition of shock?
What special precaution must be taken in the case of collapse?
State the treatment for shock, fainting (syncope) a'd
collapse .. ,
What is the effect of sugar on the temperature of the body?
What are the causes of sunstroke and heat-stroke?
tate the treatment for sunstroke and heat-stroke
What are the causes of convulsions in children?
What are the signs of convulsions in children? . .
State the treatment for convulsions in children " .
State fully the causes of asphyxia

Is artificial respirati on likely to do any good if the air passages are obst ructed, or if there is not abundance of fresh air?
is the first thing to do in a case of drowning?
what method may artificial respiratio n be performed without taking any previous steps ? ...
steps must be taken before proceecling with Silveste r's method?
should be clone while artificial respiration is being performed?
would you liberate a suffe rer from contact with an electric medium?
2 ,
at would you do when the sufferer was rem oved fr ol11 contact?
Whatwoulcl you do in the case of a lightning stroke? ... 14.4
CHAPTER VI. POISONING.
Poisons may be classified according to their treatment under two heads :-
1.- Those which do not stain the mouth, and in the treatment of which an emetic is to be given. Amongst these are :-
(a) Arsenic, Phosphorus (con tained in rat poison and lucifer matches), Tartar emetic and Corrosive Sublimate, \\hich cause a metallic taste in the mouth and a burning pain in the mouth, throat and stomach.
(b) Strychnine, Prussic Acid, Belladonna (deadly nightshade plant) and seyeral other vaneties of plants, such as laburnum seeds, etc.; these give rise to convulsions, delirium, failure of respiration and collapse.
(c) Poisonous meat, fish and fungi (often mistaken for mushrooms). Suspicion of these poisons should be directed to cases where several persons who have partaken of the same food develop similar signs and symptoms.
(d) Alcohol, which may cause collapse.
(e) Opium and its preparations, Morphia,

149
Laudanum, Paregoric, Chlorodyne, Syrup of Poppies and various soothing drinks and cordials; these cause a tendency to go to sleep, which continues until sleep deep and breathing stertorous; the puplls,of the eyes become minutely contracted (pInhead pupils),
2.-Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. These are of two classes :- .
(a) Acids, such as Nitric Acid (Aqua fortis), Sulphuric Acid (Oil of Vitriol), Hydrochloric, or Muriatic, Acid (Spirits of Salt), strong Carbolic Acid (Phenol), Oxalic Acid, which is contained in oxalate of potash, salts of sorrel, salts of lemon and some polishing pastes.
(b) Alkalies, such as Caustic Potash, Caustic Soda and Am monia.
SUMMAR Y OF SIMPLE DIRECTIONS FOR THE TREATMENT OF POISONING.
I.-Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali.
promptly give an emetic -th a t is, nlake th e patient vomit as follows :-
(a) Tickle tlze back of the tllroat with the finaer or with a feather.
0
(0) J1
15 1
an d is always safe. A hand f ul of tea sho uld be t hrow n into a kett le a n d boiled ,
4.-If the lips and mouth are stained or burned give no emetic, but-
( a ) If an Acid is known to be the poison give an Alkali at once. First wash the mouth out freely with lime water or other alkaline mixture, such as soda, chalk, whiting, or magnesia or wall plaster in water, and afterwards let the patient sip a little of it. Soda and potash are not to be given in the case of poisoning by oxalic acid.
( b) If a strong Alkali is known to be the poison give an acid at once, First wash the mouth out freely with lemon juice or vinegar diluted with an quantity of water, and afterwards let the patient sip a little of it.
In both cases give oil (Rule 3)'
5.-Wh e n a perso n has swallo wed poiso n and t hreatens t o go t o s leep , keep him awake by walking him about and slapping his face, neck and chest with a wet towel. Strong black coffee may be given to drink" Slapping the soles of the feet may also be tried.
6.-If the throat is so swollen as co threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
,.-Apply artificial respiration if breathing cannot be discerned .
8.-Treat shock and collapse.
9. - Preserve any vomited matter, food , Dr . other substance , suspected of being the pOlson. Do not \"ash vessels which may have con· tained the poison, and carefully guard them.
Certain poisons require special treatment, and a few of the com moner of these are mentioned below with their treatment.
CA R BOLlC ACID.
The odour of the br eath will aid in the detection of this poison; the lips and mouth are usually stained and several nervouS symptoms come on.
TR EA TMENT.
1.- Give milk, to a pint of \vhich half an ounce of Epsom Salts has been added.
2.- Treat according to the general rules.
PRUSS IC ACID .
The action of this poison is extreme ly rapid. Giddiness, staggering, insensibility accompanied by panting respiration, profound collapse and possibly c onvulsions are the general signs, and in addition a of bitter almonds is often present.
TREATMENT.
l.- Place the patient in the ®pen air.

2.-D3.sh cold water 0 th h d n e ea and spine co n· tinuously.
3·-Apply artificial respirati on.
4·-Hold smelling salts to the nostrils.
5·-Treat shock and collapse. (See page 135.)
MEAT, FISH Ai D FUNGI.
SIgns and symptoms are vomitin a and purging larr rea), colic, headache, great we:kness rai<;ed temperature and a quick pulse. ,-
. TREATl\l ENT .
I. - GIve an emetic.
z - \V,hen the emetic has acted, give castor oil.
3-Treat colJapse. (See page I35.)
STRYCHNINE
The signs and sympt f' J'
1 . 'd r oms are a ee Ing of suffocation IVI leatures and con l' Th ' h' h d' vu slons. e patIent rests on IS ea and feet, and the body is arched.
.
I.-Give an emetic.
z .-Apply artificial respiration.
ALCOHOL.
I.-Give an emetic if the patient can swallow .
2. - Treat collapse by keepina the patient etc. (See page 135,) I:> v. arm,
QUESTIONS ON CHAPTER VI.
Th( 1Zumerals illdicate the pagu when the answe1'S may be found.
Under what two heads may poisons be classified?
What are the symptoms of poisoning by arsenic?
What other poisons give rise to the same symptoms?
PAG. 148, 149 14 E
What poisons give rise to convulsions, delirium, failure of respiration and collapse? ...
H several people who had partaken of the same food developed similar signs and symptoms, by what would you suspec! they had been poisoned? .. 148
':.;"-!hat condition may result from poisoning by all (lh.)1 ? 148
What are the effects of such poisons as opium?.. 148, 149
vVhat two classes of poison burn or stain the mouth? . . . 149
\Vould you give an emetic for such poisons? 149
Name some of the principal acids 149
Name some of the principal alkalis 149
State the general rules fur the treatment of poisoning 149 to 15 2
State the best methods of making a person vomit ISO
How would you treat a case of acid poisoning? ... 151
How would you treat a case of poisoning by an alkali? 151
State the signs, symptoms and treatment of carbolic acid poisoning ...
State the signs, symptoms and treatment of poisoning by Prussic Acid 15 2 , -I53
State the signs, symptoms and treatment 0f poisoning by poisonous food... ... ... ... ... ...
State the signs, symptoms and treatment of poisoning b)
153 Strychnine 153
What would you do in the case of alcoholic poisoning? 153

155 CHAPTER VII. BANDAGING.
Esmarch's Triangular Bandage has been described in Chapter II. It may be applIed to keep a dressing on a wound, burn or scald of any part of the body, or for an injury of a joint.
For the Scalp (Fig. 62). Fold a hem about dinches deep along the of a bandage; place the bandage on tlle head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down at the back; carry the two ends round the head above the ears and tie them on the forehead; dYa\\' the point first dO\\'l1\\ ards, and then turn it up and pin it on to the bandage on the top of the head.
FIG. 62.
For
the Forehead, Side the Head, Eye, Cheek, and for any part of the body that is round (as the arm or thigh, etc.), the narrow bandage should be used, its centre being placed over the
15 6
dr essing) and the ends being carried round the head or limb, 8S th e C:lse may be, and tied over the wound.
For the Shoulder (Fig. 63)· Plac e the centre of a bandage on the sho ulder, \vith the ooint funning

157
For the Hip (Fig 64). Tie a narrow bandage round the body above the haunch bones, with the knot on the injured side . Fold a hem accordino- to the size of the patient along the base of a second bandage; place its centre over the dressing, carry the ends round the thigh and tie them; then carry the point up under the
FIG. 64.
up the side of the neck; fold a hem along the base; carry the ends round the middle of the arm and tie them. Place one end of a broad bandage oyer the point of the first bandage and sling the arm by carrying the other end over the sound shoulder and tying the ends at the side of the neck; turn down the point of the first bandage, draw it tight pin it.
FIG. 65. FIG. 66. first bandage, tum it down over the knot and pin it.
For the Hand when the fingers are extended (Fig. 65). F?ld a hem along the base of a bandage; place the \\'l'lst on the hem \\'ith the fino-ers towards the point; then bring the. point over thOe \\'fist, pass the ends round the \\"l'lst, cro s and tie them' bring the point oyer the knot and pin it to bandage on the hand.
ISS
For the Foot (Fig. 66). Place the foot on the centre of the bandage with the toes towards the point; draw up the ·point over the instep, pass the ends round the ankle and cross them in front j now pass the en ds round the instep and tie th em . Draw the

FIG. 67a.
FIG. 67b.
point forward and pin it to the bandage on the ins tep.
For the Front of the Chest (Figs. 67a an d 67b). Place the middle of the bandage over the dressing with the point over the shoulder on the same side; carry the ends round the waist and tie them;
159
toen draw the point over the shou ld er and tie it to one c,f the end s. . F the Back. The bandage IS apphed as the foregoing, except that it is begun at the back.
For the Knee. Fold a narrow hem along the base of a bandage; by the point 011 the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then over the thigh and tie them. Bring the point down and pin it to the base (Fig. 68).
FI G . 68.
For the Elbow. Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and the middle of the base on the back of the forearm j cross the ends first in front of the elbow then over the arm and tie them in front ' (Fig. 69).
For the Fingers and Toes wrap a strip of calico or linen round and round the part; split the freeend, and secure it round the wrist or ankle . FIG. 69
C I-fAPTER VIII.
METHODS OF CARRYIKG.
TH E FOUR - HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
I.-Two bearers face each other behind the patient and grasp th ei r left forea rm with their right hands and

FIG. 70 each other's right forearm with their left hands (Fig. 70), and stoop down.
2.- The patient sits on the hands and places one arm round the neck of each bearer.
16r
3.-The bearers rise together and step ofC the bearer on the right hand side of the patient with the right foot, and the left hand bearer with the left foot.
THE T\\'o-HANDED SEAT.
This seat may be used to carry a helpless patient.
FIG. 71.
J.---: Two bearers face each other and stoop, one on each sIde of the patient. Each bearer passes his forearm nearest to the patient's head under his back just co
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig. 7I), and clasp their hands by one of the methods shown in Figs. 72 and 73. A handkerchi ef should be held in the hands if the first grip is used.

FIG. 72. FIG. 73.
2.-The bearers rise together and step off, the right-hand bearer with the right foot, and the left-hand bearer with the left foot (Fig. 74).
THE THREE-HANDED SEAT.
This seat is useful for carrying a patient and supporting either of his lo\yer limbs, when he is able to use his upper limbs.
1.-Two bearers face each other behind the patient. For supporting the left limb the bearer to the patiEnt's right grasps his own left wrist \\ ith his right hand, and the other bearer's right wrist with his left hand. The bearer to the left grasps the first bearer's right wrist with his right hand (Fig. 75). This leaves his
74.

left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting" right /I for" left " and" left /I for "right. " TI1 bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3· - The bearers rise tot.rether and step off) the FIl;. 75right-hand bearer ,, "ith the right fOOL, the leftbearer with the left foot.
THE FIRE.:\fAN'S LIFT
(To be attempted only by a strong man).
Turn the patient face do\\ n wards; place yourself at his head, stoop do\\ n, slightly raise his head and fIG 76.
shoulders and take hold of him close under his armpits, locking your hands on his back. Raise bis body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head rests on your left shoulder. Thro\V his left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your shoulders. Rise to an upright position; hold the patient's left wrist with your left hand and leave your right hand free.
Assistance may be given to an injured person by supporting him in the manner shown in Fig. 76.
The plan of carrying tlte padent by the arms and legs 'if/jill tile face downwards, commollly called tile" frogs' marc/'l, " must never be used, as death may ensue from tlzis treatment.
hIPROVISED STRETCHERS.
A scretcher may be improvised as follows :-
1.-Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The pati.ent sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a longer stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 79).

THE FORE A ND AFT METHOD.
This plan of carrying is useful when space doe::; not permit of a hand seat.
FIG. 78 .

FIG. 79.
2.-Make holes in the bottom corners of one 0( two sacks and pass stout poles through them.
3.-S pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides. Two bearers stand on each side and grasp the middle of the pole with one halJd, and near the end \\'ith the other. They walk sideways.
4.- A hurdle, broad piece of wood, or shutter may be used as a stretcher; some straw, hay, or clothing should be placed on it, and covered \\ ith a piece cf stout cloth or sacking; the latter is useful in taking the patient off the stretcher.
Al wa ys test an im prm'ised stretcher before use.
Stretchers must be carried, and the patient placed on them, as laid down in the "Stretcher Exercises."
As a general rule carry the patient feet foremost.
The exceptions are :-
(a) When going up hill with a patient y;hose lowel limbs are not injured.
(b) 'When going do\yn hill with a patient whose lower limbs are injured.
Avoid lifting the stretcher oyer ditches or walls, but where these cannot be ayoided the stretcher must be carried in the following ways :--
To CROSS A DITCH.
In crossing a ditch, the stretcher should be lowered with its foot one pace from the edge of the ditch.
Nos. I and 2* bearers then descend. The stretcher, ith the patient upon it, is afterwards advanced, Nos. I and 2 in the ditch supporting the front end while its other end rests on the edge of the ground above . No. 3 now descends. All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by No. 3 in the ditch. No. I climbs out, No. 2 remaining in the ditch to assist NO.3. The stretcher is lifted forward on the ground above, and rests there \"hile Nos. 2 and 3 climb up.
To CROSS A WALL.
The stretcher is lowered with the foot about one pace from the wall. N os. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the ,vall. No. I then climbs over the wall and takes hold of the foot of the stretcher, while Nos. 2 and 3 support the !-lead; the stretcher is then carried forward till the rests on the wall, No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
• These numbers are explained later in the detailed "Stretcher Exercises."

I7 1
To LOAD A ,-rAGON.
Th e stretcher is lowered with the foot one pace from the end of the 'wagon. Nos. I and 2 take hold of the foot of the stretcher, No. 3 the head., The stretcher is then raised and carried forward tIll the front wheels rest on the floor of the wagon. No. I then jumps into the wagon, while IO. 2 goes to the head of the str etcher and helps TO. 3. The is then pushed slowly into the wagon. If the tallboard cannot be sh ut, the stretcher 111 ust be lashed fir1111y to the sides of the "agon.
To UNLO.\D A 'V AGON.
Nos. 2 and 3 take hold of the head of the while No. I gets into the wagon; the stretcher IS then uradually drawn out tjJ\, the foot-wheels rest on the ebdge of the wagon. No. I jumps out of the wagon, and with No.2 ,tak es hold of the foot .of the stretcher, NO.3 supportmg the head. The stretcher is now gently dra\\n away one pace an? lowered: \Vith four bearers TOS. I and 2 "ould 11ft the fOOL of the sLretchcr, while os. 3 and 4 lift the head. This applies to crossing a ditch or \\ all, as well a 3 to loading and unloading a wagon.
CHAPTER IX.
STRETCHER TRANSPORT.
The Stret,chers (Model 1899) are cf thr ee patterns, VIZ ,Ie OrdInary,"" Telescopic-handled I) and "Police." In general principle they are the component parts being designated the poles:

FIG. S a.-ORDINARY TRETCHER-CLOSED.
FIG. 8I,-TELESCOPIc-HANDLED STRETCHER - OPEK, handles, traverse bars, fo o t wheels, bed , pillow sack and slIngs.
. The Ordinary Stretcher (Fig. 80) is 7 feet 9 in.ches 111 len.gth, and I foot 10 inches wide. The bed is 6
In . and the handl es inches The h eight IS 54 lI1ches. At th e head of the stretcher is a overlay (the pillow sack) which can be filled wIth hay, clothing, etc., to form a pillow. The ]oll1ted traverse bars are provided with joints.
1 '1 3
for ope nin g or closin g the stretche r. The Telescopicll and led pattern (Fig . 81) is very similar , but the handles can be slid underneath the poles, thus red ucing tIle length to 6 feet. This arrangement is of g reat ,-alue when working in confined spaces, or when a patient has to be taken up or down a narrow staircase with sharp turns. The Police stretcher is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a r efractory patie llt.
When closed, tbe poles of the stretcher lie close togel her, the tra,'erse bars being bent inwards, the canvas bed neatly folded on the top of the poles and beld in position by the slings \\'h ich are laid along the canvas, and secured by a strap, pbced transversely a t the end of each ling, beJl1g pa sed through tbe large loop of the other, and round the poles and bed. .
In closing a stretcher care should be taken to rmse the centre of the canvas when pushing in the trai'erse bar, as it is othen, ise li::-,ble to get caught. ,
To prepare, or open a stretcher, unbuc.kle tl,le tr:?,!1Sverse straps of each sling ; r emove the slmgs hom the stretche r; t separate tbe poles; take bolel of each trayerse bartland dra\\' it forward. The slin gs ",ill then be folded to half their length, one bein8' laid neatly over the handles at each end, of the tretcher.
As a aenera l rule, th e stretcher \\'111 be prepared Ly as. I 3 bearers in Exercises 1., 11., and Ill.;
174
and by No. 2 in Exercise IV. These bearers will, however, if req uired, assist the other bearers in attending to the patient's in juries.
Note. - The various movements detaIled III the following Exercises should be carried out steadily, the bearers working in unison, hurrying being carefully avoided, and every attention being paid to the bearer who gives the words of command.
STRETCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised in 19 0 4 to accord with the drills adopted by the Royal Army Medical Corps :_
EXERCISE No . 1.
FOR FOUR BEARERS.
1.-The Instructor selects the bearers and numbers them-I, 2, 3, 4 at his discretion. Should one man be taller and stron,;er than the others, he should be styled No. 3, as he will have to bear the heavier part of the burden. * All orders will be given by NO.4.
2. -" Fall in." - os. I, 2, and 3 take position on the left side of and facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, NO·3 at the patient's shoulders. At the same
" Bearers should, hflwever, be taught to take any of the p vsitions named in the following Exercises, whether that of No. I, 2, 3, or 4 beare r.

175
time No. 4 places the prepared stretcher on the ground by the right side of the patient about two he. 82.
paces away from him, then takes position opposite to and facing NO.2. (FIg. 82).
3· -" Ready. "-The bearers kneel down on the knee and take hold of the patient, No. I passing hIS hands a nd for e-a rms benenth th e patient 's le a s h a nds wide apart. Nos . 2 and 4 pass their

FIG. 83. and forearms be!1eath the patient's hips and loins, and grasp each othe r' s hands. NO.3 passes his left hand across the patient's chest and under the riaht shoulder, a nd his right hand beneath the left shoulder (Fig. 83) .
4. - "Lift." -On the word ". Lift ," the bearers raise the patient ge ntl y and rest h1l11 on the knees of N os . I, 2, and 3 bearers (Fig . 8-/.) ; as soo n as he is sec ur ely rested, NO.4 disengages hands with N o. runs round by the head of the stretcher and places lt und er the patient, close to the other bearers' feet,
being careful that the pillow is immediately under the patient 's head (Fig. 85); he then kneels down and locks his han ds with those of No.2 (Fig. 86).
5·- " Lower."-The bearers p lace the patient on the stretcher (Fig. 87), disengage their hands, and then stand up.

FIG . 85.
6.- " Stand to Stretcher. I!-No. I goes to the foot of the stretcher, with his back to the patient; No. 3 to the head with his face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7.- " Ready. "-Nos. I and 3 place the slings (if used) over their shoulders, stoop do\\"n, and slip the
179
loops of the slings on to the handles of the stretcher, \\' hich they then grasp. . .
As soon as all is right the word IS given :- .
8 .-" Lift Stretcher."-Nos . I and 3 bearers raise the stretcher steadily together and stand up.
Note.-N os. 2 and 4 will now adjust the slings ?n the shoulders of Nos. 1 and 3, taking care that each I? well below the level of the collar and lies \hc hollow of the shoulder in front.. They 'dv1 athso 1 r h mg regal' to e lengthen or shorten t le s mgs, . h f th patient's injuries and the relatl v'" helg ts 0 e bearers.
FIG. 86.
9.-" move off :-Nos. I, 2, and 4 stepping off with their left foot, and No. 3
wi th his fIght foot (Fig. 87). The step should be a short one of t\\'enty inches, and taken with bent knees and no spring from the fore part of the foot 10.- " Halt. "-Tbe bearers remain steady. .

FIG. 87.
II. - "Lower Stretcher. "-The bearers place the gently on the ground, slip the loops of the sl.lOgs off the handles of the stretcher, remove the slIngs from the shoulders, and then stand up.
IS r
12. -" Unload Stretcher - Ready." - The bearers prepare to take th e patient. off the stretcher, as at Or ders 2 and 3. -
13.-" Lift. "-Tlle bearers raise the patient as at Order 4 (Fig . 86); NO .4 , in this case, disengages hands from No . 2, removes the stretcher (Fig. 85), alld resumes his former position. If necessary, the bearers will then steadily rise together, and carefully carry the patient to the bed, or Dther place to wlli ch it has been arranged to convey him.
14. - "Lower. "-The patient is carefully
EXERCI E TO. I I.
FOR THREE BEARERS.
I.-Number the bearers I, 2, 3.
All orders will be given by o. 2 , ",ho will look after the injured part of the patient's body or limbs, to see that no bandages or splints become displaced, and also that No . I bearer, in liftin g or carrying the stretcher, does not touch the patient 's feet .
2 .- " Place the Stretcher. "-No. 3 pla ces the stretciler in a line with the patient 's body, the foot of the stretche r be ing close to his head.
3.- " Fall In."-No. I places himself on the left ;:iide of the patient in a line with his knees, TO . 2 on the left side just below the patient 's shoulders, and NO. 3 a t th e r igh t side, and fa ces No.2.
. 4. -" Ready. "-All kneel on the left knee . No. t places his hands, well apart, underneath the lo\\-er limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of inj my. Nos. 2 and 3 grasp each other's hands under the shoulders and th ighs of the pa tien t (Fig. 88).

The rise together, keeping the patIent 111 a hOrIzontal posltlOn (Fig. 89).
6. -'.' March. "-All take shor t side-paces, carrying the patIent over the stretcher until his head is immediately above the pillow.
183
7. -'( Halt."- The bearers remain steady. 8.-" Lower. "-The bearers stoop _down, place the patient on the stretcher, dIsengage theIr hands, and then stand up_
9. -" Fall In."-No- I places himself the /oot of the stretcher with his back to the patIent, NO.2 places himself at the left side of the patient, and NO.3 at the head, with his face towards the pat.ent.
10. - " Ready. "-Nos. I and 3 place the slings (if used) over their sho ulders, stoop down, and slip the loops of the slings on to the handles of the stretcher, which they then grasp .
As soon as all i. right the word is given-
II.-" Lift Stretcher." - Ios . I and 3 bearers raise the stretcher steadily together and stand up.
TO 2 \\ ill now adjust the slings on the shoulders of Nos. I and 3. taking care that each is well below the Y level of the collar, and lies accurately in the hollow of the shoulde r in front. IIe will also length en or shorten the slings, having regard to the patient's injuri es and the relatiye heights of the bearers . .
12. -" March."- Nos . I and 2 step off with the left foot, and No . 3 with the right. The step sho uld be a short one of 20 inclles, and taken with bent knees, and no spring from the fore part of the foot . 13.-" Halt. "--The bearers remain steady.
14·-" Lower Stretcher."--The bearers pJace the stretcher gently on the ground , slip the loops of the slings off the handles of the stretcher, remove the slings from the shoulders, and tllen stand up.
IS· - " Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, as at Ord ers 3 and 4 (Fig. 88) .
16. -" Lift."- The bearers raise the patient, as at Order 5, and carry him by short side steps, clear of th e stretcher, to the bed, or other place to whIch it h:l.s been arranged to convey him (Fig. 89) .

185
17.-" Lower." - Tl,c patient is carefully lo\\·ered .
EXERCISE No . III.
WHE ONLY THREE EAR .,
B ERS t.RE AVAILABLE
THE STRETCHILR CA l NOT BE PLACED AS L EXERCISE II.
I.-The Instructor numbers T the bearers - I, 2, .s. All orders will be given by NO.2.
2 - " Place the S tretcher."- o. I takll1g the f t' of the streLcher and No. 3 the head, place it on
0 10 d by the s1c1e of the patient, a nd as close to t1e groLln him as pracLicable.
.
"F 11 I "-The three bearers take the s<ll1:e 3: -:- a of the patient, as laid down 111 pOSitIOns 011 Exercise No. 1.
. "R d "-Nos. I 2, and 3 kneel down on 4 _. ea y. 'I I se to the the' left knee, pbcing ves as c 0 holJ
. tl ey convenient1y can, and then take patient as 1 . . I of him as directed 111 Exerclse o. . .
-"L·ft"..--:Nos. 1,2, and 3 raIse the patient as 5· 1. . I nd then move in a eli rected 111 ExerCise o. ,a kneeling position up to the stretcher. .
6
" L "--The hearers bend forward, car.e. - ower. hand dlS- fully lower the patient on to the stretc eT, engage hands.
, .- " Stand to Stretcher. "-All the bearers up; No. goes to the foot, No. 2 remains in pOSItIO n at the sIde, and No . 3 goes to the head of the stretcher. ...
8. - " I and 3 place the slings (if used) over shoulders, stoop down, anti slip the loops of the slIngs on to the handles of the stretcher whIch they then grasp. '
.9. -" Li.ft I and 3 bearers raIse the stIetcher steadIly together and stand No.2 will adjust the slings on the shoulders N 1 and 3, takll1g that each is well below the the col\a.r, and Ites accurately in the hollow of the 111. front. lIe will also lengthen or shorten the regard to the patient's injuries and the relatIve heIghts of the bearers.
10. -" M h " N . arc . -. os. I and 2 step off WIth the left foot, and NO.3 WIth the right. The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot II. - " Halt. "-The bearers remain steady. .
12. - " Lower Stretcher."-The bearers place gently on the ground, slip the loops of t e slmgs off the handles of the stretcher remove the from the shoulders, and then up.
13. --. Unload Stretcher - Ready."-No. I places hI!llSelf. on the left side of the patient, and in a lme WIth h.ls knees, No . 2 on the left side 'ust be low the patIent's shoulders, and No. 3 at the r[gh t

187
side, and faces NO.2. All kneel on the left k nee. No. I places his hands, 'Nell apart, underneath tbe lower limbs, always taking care, in case of a fracture, to have one han:! on each side of the seat of injury . Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
14.-" Lift ."- The bearers rise together to their feet, keeping the patient in a horizontal position, and carry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him. IS .-" Lower."-The patient is carefully lowered.
EXERCISE No. IV.
FOR USE IN MINES AL\'D NARROW CUTTlXGS \\ HERE T\\ 0 1lEN O:;\lLY CAN BE ENGAGED.
Nos. I and 2 \"ill carefully place the stretcher in a line with the injured man's body, the foot of the stretcher being, if possible,* close to his head.
No. I straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, passes the left hand under the patient's thighs and
• It is not advisable to be too particular as to the head or foot of a stretcher in a mine, as it would probably be quite impossible to reverse it.
188
the right hand.across and under the patient's calves.
2 plac.es hIS feet one on each side of the patient be L\\'een hIS body and arms, the toe of each foot as near the armpits as possible. He then stoops down and passes hIs hands between the sides of the chest and the arms und c ln eat h the shoulders, and locks

(Fig. 9 0 ) . If the pati ent 's arms are uninmay put them r?und the neck of No.2, and by thIs means greatly assIst him in lifting.
189
When both are ready, No. I will give the order " Lift and move forward. " The is then to be slowly lifted just sufficient to allow hIs body to clear the stretcher. 'Both bearers will slowly and gradually move the patient forward, NO.2 hy very short steps, N o. I by bending his body forward as much as he 'Without movz'ng Ids feet (Fig. 9 T). I O. I . no\\' gIves the ord e r" Halt, " whereupon No. 2 steady, and No. I advances his right foot to hIS left, and FIC. 91.
again advances his left foot till the toe touches the heel of No.2 . No. I the order " Adva n ce," when the patient \\'111 agall1 be forward . These movements are to be repeated untIl

the patient is over the stretcher, when he is to be gently lowered.
The follO\ying Stretcher Exercise is adapted by permis ion from the Royal Army Medical Corps l\Ian ual, I 908 .
All orders will be given by NO . 4.
1. "Fall in. "- ix bearers fall 111 behind each o:her.
2 . " Numb e r. "-The bearers number from front to rear.
3· " No·3 Bearer, ri g ht (or left ) turn - supp ly stretcher- quick march. "-No. 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lo\yer fOOL wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place. He turns to the front, and, passing the lower end forward, places the stretcher on the ground to the right of the squad, wheels to the right, front end of the poles in line with the toes of No. I and rises.
4· "Stand to Stretcher. "-No. I places him- self with his toes in line with the front ends of the poles . No . 3 with his heels in line with the rear ends of the poles, close to and touching the stretcher with

19 2 his. foot. Nos .. 2, 4, 5 and 6 take up their posItIOns one pace behmd and covering off the be In fro n t of them (Fig . 9 2 \. arer
"L'f
S· 1 t Stretcher. " -N.o s. I and 3 stoop, grasp both handles of the poles WIth the right hand rise together holdin g the stretcher at the full of the arm, whe els to the right.
6. "Collect Wounded - Advance." - The squad by th e shortest route to the patient, and h a lts wIthout fLl1:th er .word. of command one pace from head of and In a lm e wIth the patient (Fig.93) .
7· Lower Stretcher. " - N os. I and 3 stoop place the stretcher quietly on th e ground and smartly together. '
8. Stretcher. " - Nos . I and 3 turn to the fight, kneel on the left kn ee, unbu ckle the straps, and place th e slings on th e ground beSIde th em, separate the poles, and straight e n the traverses .
. On word two each tak es a sling, dou bles It on Itse lf, slIps the loop thus formed on the near handle, and places the free e nds over the opposite buckle upp ermost. Th ey th en ris e and turn to theIr left together.
"While the s.tretche r is b eing prepared by N os . I and 3, the dIs e ngaged b earers will advance and to patient su ch assistance as may be r eqUIred (FIg. 94) . 193
The necessary assistance having been rendered, NO.4 will give the command-
9. "Load Stretcher." - The bearers pbce themselves as follo\\s :-Nos. I, 2 and 3 on the Jeft, Nos. 4, 5 and 6 on the righ( of the patient; lOS. I and 4 at the knees, 2 and 5 at the hIpS, 3 and 6 at the shoulders the r. hole kneeling on the left knee. , I Nos. I and 4 pass their hands beneath the patient s knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the bear:rs being detailed for this purpose l.Fig. 95)·
10. "Lift.)'-The "hole \\ill carefully lift the patient on to the kne( s of Nos r, 2 and 3·
Two. Nos. 4, 5 and 6 will then disengage, rise; Nos. 4 and 6 step back one pace. No. 5 turns to his left, doubles to the stretcher, takes hold of and raises it left hand across, the near pole resting on the left hip; carrying the stretcher, he returns to place between -+ and 6, and places it beneath the patIent.
Tlzree. Nos 4 and 6 step for\\'ard one pace, and together with NO.5 kneel do\\'n on the left knee, and prepare to assist in 10\\ eri ng the patient (Fig. 96).
II "Lower."- The patient is lowered slowly and gently on to the centre of the canvas (special care being taken of the injured part).
Two. The bearers disengage, rise; Nos. r, 2, 3 and 6 turn to the left; TOS. -t and 5 to the right; H
No. 4 places himself three paces in front of the st.retcher. . No.6, haying collected the kit and arms of the patIent, places himself three paces in rear of the stretcher, Nos. 2. and 5 opposite the centre of the stretcher. The \Vhole are no\V ready to lift stretcher and mo\'e off (Fig. 97).

97
98.
195
12. "Lift Stretcher. "-Nos. I and 3 stoop, grasp the doubled sling midway between the poles with the forefinger and thumb of the right hand, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between the handles, and place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollow of the shoulders in front. In the event of the slings requiring to be adjusted, either as regards length or for the greater comfort of the bearers, NO.4 vyill detail a bearer to carry this out, the length of the slings being adjusted, when necessary! by means of the buckles.
Two. Nos. I and 3 stoop, slip the loops oyer the handles, commencing \\ith the left, and grasp the handles firmly.
Three. Nos. I and 3 rise slo\\'ly together, No. 3 conforming closely to the mo\"ements of N"o. I.
13. "Advance."-Nos. I, 2, 4, 5 and 6 step off with the left foot, NO.3 with the right, stepping short, knees bent, feet raised as little as possible.
14. "Halt." - The whole halt.
IS. "Unload Stretcher. "- The bearers place lthemselves in the same position at the stretcher ·described for Loading (Order <)).
"Lift."-As described for Loading (Order 10), H'l
196 except that the stretcher is carried forward three paces clear of the patient's feet.
I7. " Lowe r ." -The patient is genfly lowered to the grounc The bearers disengage, rise; Nos. I, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whole step off to their places at the stretcher, as at Order "Stand to Stretcher II (Fig. 98).
The Ash fo rd Litter is made up of either of the Furley stretchers mentioned on pages J72 and 173, a wheeled and a waterproof hood and apron, or, If preferred, a light wet-resisting canvas cover. The stretcher is kept in position on the under-ol.Iriage by the foot-wheels, which fit into slots in the sides Qf the under-carriage, and it can be removed at pleasure. The under-carriage is fitted v.-ith a cranked axle which allows the bearers to pass with the stretche; between the wheels instead of lifting it m'er them. At both ends are two legs which may be turned up as when wheeling the litter. The hood and apron fit mto sockets screwed to the stretcher. In wheelinO' the litter, care should be taken to keep the patient a horizontal P?siti?n. it be necessary, two bearers can easIly 11ft the htter and patient.
. The L itter, introduced in 1904, IS used m a SimIlar manner. and one model of it is fitted with pneumatic .tyres, which add immensely to the comfort of the patIent and to the ease of propulsion.

197
CHAPTER X.
(Being flu Fifth Ltdure for Females only, z'n accordana with Syllabus 58.)
BY E. :'vIACDOWELL COSGRAVE, :\I.D., F.R C . P.I.PREPARATION FOR RECEPTION OF ACCIDENT CASES.
WHEN news of an accident comes, preparations should once be made so as to have everything ready before the injured person is. brought in. course the preparations needful \\ III vary according the nature and extent of the injury, but the follOWing are the chief things which may have to be done.
CHOICE AND PREPARATION OF Rom.!.
A room must be chosen. In a bad case this should be one easily reached, as it is difficult to carry.an injured person through narrow passages Unless there is some such reas on agamst It, the Injured person's own room is best.
The way to the room must be cleared, furniture and loose mats in the hall or 111 lobbies should be removed. If the in jured person is carried on a door shutter or stretcher, two strong chairs should be 'placed ;eady to support it wherever the bearers ,,"ould be likely to require rest.
Useless furniture should be removed from the bedroom. TL: bed should be drawn out from the \Vall
so bJth sides can be approached and the clothe!t turned back to one side to their full'length. A hot bottle should be got ready. If there is much collapse several hot bottles and hot blankets may be required ' con::r the hot bottles with fbnnel.
If th e injury is very severe, if mud-stained clothes have to, be r,emoved, or if extensive dressings have t{1 be apphed, It may necessary to have another bed a couch or, a table near the bed to lay sufferer on 111 the first I11stance. This should be so arranged that soiling may do no harm· old sheets waterp oo f materials, thin oJ!cloths, or 'even news paper, may be us ed as a protection.
LIFTING AND CARRYING.
If,pres ent at the place where the accident occurred it WIll , be necessary to see that the patient is care fully lifted after proper "First Aid" has been rendered.
The following rules should be remembered :- Select the proper number. of persons to assist, and do not let them 11ft the patIent until they thoroughly underhow they are to do it.
For cases, \"here the injured person has to be, li,ted a very short distance, three helpers are Two (\"ho should be as far as possible of equal height) are to bear the ".eight, the third is to' s upport and take charge of the injured part This 1

199
done by a person who has been through a " First Aid" course. If the injured person is insensIble, another helper should support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient's back at the lower part of the shoulder blades, and under the hips, clasping each his right hand in the other's left. The injured patient should, if practicable, place his arms round the necks of the bearers.
The third helper should nttend to the seat of injury; if this is a fractured limb, he should support it by placing the palms of his hands under the limb, one above and one below the seat of the injury, grasping it firmly but avoiding unnecessary pressure.
The helpers should remain thus until the order " Lift" is given, and then they should all lift slo\\'ly and steadily, avoiding jars, attempts to change position of hands, etc.
H the injured person is to be placed on a stretcher or shutter, this should be previously placed with the bottom end at his head; the bearers should then move, one at each side of it, until the patient is over it. The word" Lower" should then be given, and the injured person should then be slowly lowered. A pillow or folded-up coat should be ready, and as the sufferer is lowered this should be placed under his head.'*'
• Full directions are given in Cl:apter IX.
2CO
MEANS OF CARRYING.
Besides a stretcher, and substitutes such as a gate, or a door, other means of carrying can be 1m proVlsed.
In slight injuries, where the injured person is unable to walk, two bearers can carry him by forming a fourhanded, three-handed, or two-handed seat.
A four-handed seat is formed as described on page 160.
A three.handed seat is made as described on page 162 .
The two -handed seat is made as described on page 161.

20J UP STAIRS.
Ir1 carrying a stretcher up stairs the head sbould go first, and an extra l:elper should assist 8t the lmycr end, so as to raise It and keep the stretcber nearly borilOntal.
The hY(l tbree or four-11anded seat may he used for carr) ing up or a strong chair, the patient bein cT carried IIp In the laUer case cne should ,yalk after the chair and l:elp to support it, and to prevent the in.inred person sh pP1l1g out.
LIFTlXG IXTO BI,n.
A single helper can lift by supporting with one arm the two knees, and with the other the back. The arms must be passed well under before COlll'llencinO" to lift.
b
A single helper can give support by puttinO" his arm round the waist, grasping the hip and the injured person's arm round his own neck, holdinO" t h e hand .with his own hand (Fig. 76, page 16 5) .
If the bed is narro\\' and there IS room the stretcll'''r should be placed on the floor \ itb the head close to the foot of the bed. The injured person should then be lifted oyer the foot and placed on the bed. If the bed is too \\ iell' to admit of this, the stretcher
b
A capItal stretcher can be improvised out of a st r ong sheet and two broom handles or other short poles. Each SIde of the sheet is ,,,,ound up on a broom ha n dle until there is just room for a person to lie be tween. T his requires four bearers, two at eac h side, to p revent the sheet slipping.
SllOU I( I be placed beside it, and b\ 0 belpers should stand at the far side of the stretcher One helper passes one arm beneath the shoulders and one the middle of the back, the other helper placmg hIS under the lo\yer part of the back and under the knees. The injured person is then lifted,. another helper pulls a\Yay the stretcher, and after a smgle step forward the burden is placed on the bed.

PREPARATION OF BED.
A firm mattress, not a feather bed, shoulJ be selected. If there is much injury, or if dressings hwe to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed un ler the draw-sheet. As the draw-sheet becomes soiled, the soiled portioa should be rolled and a clean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and s:>me other cases, a "cradle 1/ (Fig. 99) should be l:np rovised. The use of a " cradle II is to support the bed-clothes and keep them from pressing on the limb.
A b.:ll1d-box (Fig. 100), three-legged stool (Fig. 101), or hoop S:1\\ n across and the two halves s:?cured tOJether (Fig. 102:' nuy be us ed . A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
RE.\IOVH\G THE CLOTHES.
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
In removing a coat, etc., in a case of fractured arm the unll1jured ann should be drawn out first.
In putting on a coat or shirt the injured arm should be put in first.
In burns and sc.alds should ever be dragged off. A. sharp pair of sCissors should be used, and not a.dhering should be cut away. If anything adheres It should be left until medical aid

FIG. 102.
can be obtained. The clothing adherin6" may, with be soaked with oil. To remove the trous-:-rs from a severely injured limb the outside se::t.m should be ripped up. '
PREPARATIONS FOR SURGEO:-,r.
As so?n as the injured perSOll has been attended to, preparatIOn should be made for the surgeon's VISIt.
205
Thepreparations needful will depend upon the nature of the case. The follo\\ mg hll1ts may be of use :-
A fire in the room helps ventilation, even in summer. There should be plenty of ,Yater, hot, cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot bath does well. The basins shoultl be placed on a table, covered \\"ith a clean \\ hlte cloth; a large towel makes a suitable cloth; the to\\els, folded up, should be placed on the same table, and the hot an d cold water should. be within easy reach. The foot-bath should be under. the table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths, old ljnen, oil, and baking soda, should be ready, and materials should be torn up for bandages.
In the case of hremorrhage, plenty of \\ater should be boiled and allowed to cool, and pads of absorbent cotton wool should be baked in a tin box in the oven, and at least two basins should be ready.
In the case of a person rescued from drowning the sheets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
For fomentation, have boiling water flannel a I{itc hen roller, and two sticks, or a large tow el. '
'When summoning a medical man to a ll . accident always let him know by a \\Titte n message what kind of case is required to so that he may bring whatever IS needful. By tIllS me a ns valuable time may be saved.
QUESTIONS ON CHAPTER X.
The I/ZlllIerals illd/ca/e the pages where the allsw(J s ilia) ' be foul/d.
Wh:1.t points would y ou consider when choosing a room?...

... 197
How would you clear the way to the sick 100m? 197
What me.ans of would you provide fur th ose carryIng a patIent on a stretcher?.. . ... '" 197
How would you place and Rrrang e a bed fur un accident case?
'" 197, 198
Are hot bottles necessary, and how would you prepare them?..
\Yha.t is often necessary to lay the sutTerer on in the first mstance?
193
'" '" 198
How would you protect this from getting soi led? ... 19 8
How w?u}d you see to the proper lifting and carrying of an Injured person?
... 198 199
'Vhat.subs titutes for a regular stretcher can you sUGgest? ':<00
How IS the seat m ade? 160, 161
For what cases IS thIS seat ustful ?.. ICO
How is the three-handed seat made? 162)
207
For what cases is this seat useful? ..
H ow is the two-handed seat made ?
For what cases is this seat usefu l ? ..
How can a single helpe r lift? PAGE 16z 161 , 162 161
How can a single helper giye SUppOlt?
H ow would you ill1proyise a str etc h e r?
How many beare rs are requ ired for this stretcher?
I l ow should a stretche r be carried upstairs?
H ow would you carry a patient upstairs on a chair?
How would you lift a patient from a stretcher to a hed?
How should a hed be prepared for an injured person? ...
How draw sheet be made?
\Vhat would you place under the draw sheet? .. ,
What should be done with the soiled part of a d raw sheet?
'Vhat is the use of a " cradle "? ...
In what ways maya cradle be imprO\-iscd ?
How would you rem ove a coat or shirt in case of a fractured arm? ...
How would you put on a coat or shi rt if the arm were injured? ...
In the case of a bad bm n, what would you do Wilh clothing that adhered to t he patient?
H ow would you rem ove trousers from a severely injured limb? .. ,
\Vhat preparations would you make for the surg eo n's risit ? ".
'''hat would you get ready in the case of a burn?
And what in the case of hcemorrhage ?
And what in the case ofa per (In rescued from drowning?
\Vhat would you get r eady for making p oul tices?
A nd for fomentations?
\Vhat sort of a message wou ld you send tft summon a doctor? ...
DEX. ,}".:{( III wound of ... lI2
case, prep,uatl HI for 107 p'Clisoning' 149 I5l
All', ab ... I')
Alcohol caution a" Le smell of ... ... 130
Alcol:ol, by 134, 153
AlkalIs, pOIsOI:llng by 149, 151
AIl11l10111a, pOIsoning by 149
Anatomy (elementary) ... 20
Ankle 30 , 32 " sprained... 64
Anterior tibial artery 93
Aorta ... ... 79
Apoplexy 132
Apparently drowned, to restore, ..
Ann, bone of ... " fracture of Arm-slings .. , 13') 52 39. 49 148
Anl:l,}. hrach ..t1 ... carotid ... ciJrsal of foot facial ... femural iliac ... occipital plantar p')pliLeal radial ti Ilial temporal " ulnar ...
ArLificial respiration
A<;phyxia
Atla
Auricles ::: 121, 12), 136,
Axillary arLery
Axis .:.
Bites of rabid animals 106
Bladder ... II I, II3
Brachial artery .,. 86
Brain II7
COll1pression of 13 2 " concussion of 13 1
Breast- bone zll " fracture of 4 S
Broad bandage .. , 37
Bruken bones, see Fracture
Blonchial tuLes ... I IS
Bw)ch-bone
,7 2 95
Carbolic acid, poisoning by Carotid arteries ... " hremorrhage
Circulation of the blood, organs of Circulation of the blood, to induce Cla\'icle " fracLure of Clothes, removal of I), Coccyx Collapse ...
Arsen.ic, poisoning by Artenal h<emorrhaae of 74 practising arrest of 79 74 70 79 85 signs of " course of main ...
Back, bandage fOl
Backl)one
Bandage, to app'ly " to fold " to improvise:::
Bandaging .. . . ..
Artery, axillary ...
Bed, lifting into .. . " preparation of ... Belladonna, poisoning by
Ptl ,'e
Dress, woman's, on fire ... Ic;5
Drowning 139
Ear·channel, bl ootl issuing from
Ear-passage, foreign bocly in
Elbow, bandage for joint, fracture in110 159 voh'ing
Electric shock
Emetic
Epilepsy ...
Esmarch's 53 1.-12 148, 149, 150 triangular bandage
Expiration ... . ..
External carotid arte ry ...
Eye, bandage fo r
" foreign body in
Face, bones of Facial artery
Fainting ...
Femoral artery " "digital pressure at groin ... . ..
Femoral artery, tourniquet for Femur fracture of " fracture of Fingers, bandage fo r " fracture of 13 2
Fireman's lift
First aid, meanin;; uf " student
Fish-hook, embcddt d
Flexion at elbow " at knee ...
Food, poisoning 1:)'
Foot, bandage for bones uf ' "
" cru shed
Forearm, bones of " fracl ure of .. .
Forehead, bandage fo r .. .
" hrelTIorrhage from Foreign Gody in the earpassage ... " in the eye .. "in the nose
Four -'nanded seat
Fracture, apparatus fo r trcatmer,t of '" " " causes of .•. definitio n of ... general rul es for treatment invohring elbow joint of arm ... of breast-bone of carpus of collar - bone - of cranium of finger

Fm cture of forea rm o f knee·cap of leg .. , . 54 5S 60 " of lower jaw ... 0f metacarpus o f metatar ·us of pelvis of rib .. . of spine of tarsus of thigh-bone ... of toes .. signs and symptoms of ...
varieties of
Fungi, poisoning by 153
circulation 70 Granny knot 40 Green-stick fraclure ::'5, 36 G UlllS, h<:emorrhage from 97 lI::ennrrhage, arterial... 74 capillary... 95 from gums 97 fwm head " and neck 80 frum lower li mbs ... 89 from lungs 97 from no e 96 from stomach 98
bandage for 155 injury Lo... 128, 13 1 " side of, Gandage for ISS Healt 70 rate of contraction of 72 136 Hernia 114 Hip, bandage .for 157 History, meamng of . 17 Howard's method of artIficial respiration 126 Humerus 28
212
Page
CnsensiLility, general rules fortreatmellt 128
In spi ration 120
Inst ep :)0
In sulator... 142
Internal carotid artery fo
Int ernal 95
Inte stines, injury of 113
Involuntary muscles 33
Jaw, angle of " lower " "fracture Gf
J oint, definition of " injuries to ...
Jugular vein 2) 23 44 3 1 109 So
Kidneys ... I I I " injury of 113
Knee, bandage for 159
Knee-cap ')0 " fract ure of 58
Knot for bandage of lower lim b 42
Knots, reef and granny 40
Laborde's metllod of artificial respiration 126
Laburnum seeds, poisoning by... 148
Lacerat ed wound 78
Large arm-sling 39
Lau danum, poisoning by 149
Leg, bones of 30
Leg, fracture of
Lifting and carrying " into bcd
Ligaments
Lightning, effccL of Limbs, 10\\ er " up, er
Lime in the cye
Lip<, bleeding fn m
Litters
Liver " injury of Lo\\er limbs
Lum bar "erte 1)] ::e
Lungs hremorrbagc
Marshall ITall's metlJe tl of artificial re!'piral io n
Medium bandage 1\J etacarpus
fract ure of " fracture of ...
Middle line of bGdy
Mouth, blood issl.ing from 1\1 uscJes " ruptured
Muscular action .. .
Narrow bandage
Needle,

Nervous system... ) 17
Nose, foreign body in ... ) II hremorrhage frolll 96
Occi pital artery... 82
Opium, poisoning by 148
Pad, ring... 83 " to fold 74-
Palm. hXlllorrhage from 8
Palmar arches .. , 88
Paregoric, poisoning by 149
Patella 30 fracture of 58 28 " fracture of 56
Phalanges of foot 30 ,. of hand 28
Phosphorus, poisoning by 148, 150
Physiology (elemental'}) 20
Plantar arch 93 " artery 93
Plants, various, poisoning by... '48
Pleura 120
Poi son e d w e a p 0 n s, wounds by 106
Poisoning 148
Popliteal artery ... 92
Posterior tibial artery 91
Potash, caustic, poisoning by... 149
Pupils of eyes 13
Questions on Chapter 1. 21 II. 66 III. 99 IV. lIS V. 145 VI. 154 X. 206
Rabid animals, bites of. .. IOE
Radial artery
Radius' .. , '2 " fracture of 54 Reef knot 4l
Respiration I2C aliificial 1'1, 129, 136, " to excite 127
Respiratory syslem lIS
Rest, necessity for 18
Ribs 26 " fracture of... 4
Room, choice and preparation of 191
F4J;e
Rupture (hernia) 114
Ruptured muscles 65
;S::..cral verte .. '
acrum ... 25 25, 28
Scalds
Scalp, bandage for " hremorrhage from Scapula... ...
" fracture of Schafer's method of artificial respiration
Seat, four-handed " three-handed " two handed Shin-bone
Shock " electric
Shoulder, bandage for ... " blade ...
" f:asture of " bones .. . " joint .. .
,"i ck room, choice and preFaralion of. ..
igns, meaning of "'ilvester's method of artificial respiration
Simple fracture ...
Ske leton ..
Skull " fracture of Slings, arm 22 43 39· 40 ,
Small arm sling ...
Smothering
Snake bites
Soda, caustic, poisoning Fagt 39 by 149
Spleen II)
" injury of... II
Spinal canal...
" cord 23,117
Spine 23
" fracture of ... 4
Spirits of salt, poisoning by ... 149
Splint, angular ... 54
Splints, rules for apply. ing to improvise
Sternum ...
" fracture of Stimulants
Stings of plants and animals
Stomach ...
" hremorrhage from
" injury of .. .
Strains .. .
Strangulation .. .
Stretcher exercise, Army No. 1. No. II
No. III.
" "No. IV.
Stretchers, Furley

Falre
Stretchers, to carry I6j
" to improvise 166
Strychnine, by 153
Subclavian artery
Suffocation 141
Sunstroke 136
Surgeon's visit, prepara· tion for 204
Syllabus of instruction... 7
Sympathetic system 118
Symptoms, meaning of ... 17
Syncope ... r 34
Synovia ... 31
Systemic circulation 70
Tarsus 3°
Temporal artery. 82
Thigh-bone 30
" fracture of ... 56
Three-handed seat 162
Throat, hremorrhage from 97
" swelling of tissues of... 141
Tibia 30
" fracture of 60
Toes, bandJ.ge for 159
Tongue, h::emorrhatie from 97
Tooth socket, h:l!mor97
T uurniq uet 75
Transverse wound of abdomen 113
Two-ha.nded seat 161
Ulna " [facture of ..
Ulnar artery
Unconsciousness
Upper limbs
Varicose veins
Veins
Venous blood " hremorrhage
Ventricles
Vertebra . . .
Vertebr:l! .. .
Vertebral column
Vertical wound of abtlomen
Vitriol, burn by ...
Voluntary muscles
\Vagon, to load or unload
\Vall, to cross with stretcher '"
\Yarmth, necessity for " to promote Wind-pipe
\Yoman's dress on fire \ \' ounds by weapons " accompanied by arterial hre:110rrhage ... accompanied by venous hremorrhage
\\' ounds, lacerated
\\' rist