BONES.

The numbered sbl)w pres s ro: pomt, for fhl" arlerie'i Com• •ue in lor'.
•• OCCIPITAl. -. TSIifPORAI..
FACIAL.
SEVENTIi} CERVICAL VERTEBRA
CAROTIf\S. COLLAR} (clavicle) ::-..... "- SUJlCLAVIAN.
HONE BREAST} (sternum)
ARM BONE " · (humerus)
4TII LUMIlAR. VERTEBRA HAUNCH)
BONE 5" " ULNA
PHAI.Ar; G ES__ "
THIGH BONE (femur)
AXILLARV. __ • BRACHIAL (FlulOn).
- IL.IAC.
• RADIAL. tONAL (DiRilnl 'ORAl IQuel). r ..-ul'llrFAI••
KNEE CAP (patella)
SHiN BONE (tibia)
BROOCH BONE (fibula)
MI!:TATARSUS
PHALANGES
ARTERIES.
TAllSUS _ _
___ _
•
.---."'0,," '''mA lI
AS COMPANIONS TO THIS BOOK-

AID."
BY J. M. CARVELL, M.R.C.S., L.S.A.Price 6d. post free.
"PROBLEMS
IN FIRST AID."
BY L. M. FRANK CHRISTIAN, M.B., W. R. EDWARDS, A.C.A.Price 6d. post free.
AID THE INJURED
ARRANGED ACCORDING TO THE REVISfCD SYLLABUS OF THE FIRST AID COURSE OF TIlE
ST'. JOIIN ASSOCIATI01.
BY
JAMES CANTLIE,M.A ., l\I.B., F.R .C. S., 0/ Grace 0/ tite Order 0/ St. jolm.
IJollOlary Li.Je j1/l1mb,:r 0/, altd Lecturer altd Examiner to, tlte A ssociatio?l
With a CHAPTER on" Slrelcher Tran'porl," revised 110m that originally \wilten by Si. JOIir-: FURLEY, C.B., 0/ justlcc 0/ tlze Order 0/51. joitn, in accordance with the Army tretcher Exercise. AI,o a CII .\PTER (being lhe Firth L ecture, ror Females only), by E. .\lAC 00\\ COSGRAVE, M.D., F.R.C.I'.I., 0/ Grace 0/ tIlt: Order 0/ St. jolm, HOllorary LZ/rJ Illember 0./, flil.l Lt'ctureJ llnd ExaJJlllter to, tite ";'ss(}clation.
TWENTY·FIRST EDITION, 930,000 to 980,000.
(TIlls L'dltiOlt is similar 10 tite ei
In spector - G eneral B. Ninnis, C.V.D., M,D., R.N Sir P. D. POlI'e l, St., K.C.".O., D. Owen, LL.D., F.R.C.S. I he Lord ClauJ Hamilton :\1 P Co'. T. H. H<:!ndley . C IE: . .•
THE CHAPTER:
Th e Chnpter consists of th K . I f J . the I . ecutiv" OfJj'-e s: 0 ami dc jIUe ; 'electeJ Officiat:ng Chaplains :ected of COUllCt! j the following
The Re,·.Canon Shepp tr<.l, C,v.O.,D.D. I The Rev. T. C. Ebdon. Anu the foll owing Selected of Gmce and Esquires:
Maj. G. E. W. I\lalet 1'1 V' C I. ' ir J \V Ottl " _ 1e hcounl Esher G.C.B., G.C.V 0
The Lo d' A ,'ers, H. Hamilt on, C.)l.';. Col. Sir C. 1\1. vi II. C.,)ok, C.l E.
J. A. • • E . John H ope.
r S. GriffiLhs, R.C.S. \V: fhe Lord i\l<:!rthyr 1" C ,. . G. Calter.
R. A. Gibbons M v.o. K. \V I\Ilrmy (Carll(l}7'OIL PilI" , ' • sUI.'ant ExtraJrdiJlarJ')'
The following are the K NIGHTS OF JUSTICE' HIS 1lAJESTY KING GEORGE V S' . ., overelgn Head and Patron.
H.R.H. THE DUKE OF CO;.l;.lAUGHT, K .G., Grand Prior. !HE VISCOUI-<T KNUTSFOIW, G.C.l\I.G., Sub.P r:or.
H. Prince C hristi a n of Schlesn ti"lg;IIolstein, leG. I Albert of SchleswigH ol, tem G C B G C v 0
If.H. The D'uke ·G:c.v.o , ,
A 'miral H.S.IT. Prince L ou's o f Battenberg, G.C.B ., G.c.v.o, 1(.C R.N.
The Kin e!: of H.S.H. Pl'IflCe Alexand er of Teck G.C.V.0., D.S.O. ' Il'ofConnau<;ht,
Sir Furle y, C.B. (Holloral''' Latl.fT). -
Sir T. . Dick Lauder Bt l\l" j. Sir A. Lamb, Bt.· .
THE KNIGHTS OF JlJS'flCE- continued.
CuI S'r H C. Perrott, TIt., C.Il. N. H. Forhes, F.R C.S., EPI·:
Col. S,r J. Gilde3, K.C.\'.O., C.B. Col. C . W. B. BO\ldler, C.B . H. J L oftus. (Honor:1ry Command"r),
CoJ. B M. Lieut.-Col. A. C. Vatf'.
Gen , Sir C. Warren, G. K.C.B., :Maj. Gen . A. F. Terry. R.E, The Earl \ f Plymouth, c."..
Maj.-Gen. J . C . Dalton. R •.\ The Earl of Sanclwich. K.L.\·.n.
Col. A . G . Hunt r - \ \'",Ion of The Earl of Ellesmere (Com ,'ander, HUllterston, C.B ., D.S 0., R.t' . Ellesmere Commander \).
Col. The Lord Willi:1111 Cecil, c.v.n. E. H. Freshfidd.E . F'reshfieU, LL.D_ (Honor ,r)' The Viscoll t Brackley, :.1. \'.0. Bailiff). F.-? T. The Viscount Kit< hener of The Earl Brassey , G.C .H. Khartoum, K.l' ., R.E .
The Viscou t Templetown. Lieut. - Col. Sir R. C. Temple, Bt ., R . 1\1. MacLean . C.LF: .
A. F. G. Lev,son Gower Sir ,\. S. C;C<1ll-G.llty, K.c.\·.n.
Col F . A. H. Lamhert. Col. S:r II J"k) II,
Co 1. S'r C. W . 1\IlITray. C II. H .E. Lord ],Iin::;ton uf Is ·ngt.,n,
The Earl of Ranfurly, G.C.;lI.G . K.C.:lI.G ., D.S o .
TheLordSandhurst,G.c.s.I. .G.c I.E. Col. Sir J. R. A. Clark, Rt. C.l'.
Sir H . A. flIake, G.c. :ll.(i. Sir R. Han·ey.
The Earl of l\l eath, K.!'. H . I<: . Sir G. S . Clarke, G.C.:'I.G . ,
A . E. Frase]'. c.;.c.!. E,
The Lord i\Iostyn Lie\1I.-Col. J. W. Wray
The Marquess of Breadalh:1ne, K.G Sir \\T \Y. 1'0rtal, Bt
The Duke of Portland, K.G. The E:1rl 0f :'\frnt'l, K.G 1J. I!l'. , F .-M. The Earl Rol ens, The Duke of Somerset. K.G R.A . Sir D. D ckwortb, HI. !.l.• P., R. B. C lrter, F.R.C.S. (Hono r:1ry H. E B,)lliton, :lI.V O. Commander) .
The fcl low:ng are the Sun-PREL.\TES :
T he Bishop in ]ernoalem anti the \ The B ishop of Gihralt:11' E:1'-t. The P rima te of .J ew Ze:1l:lIld .
The Bishop OrJllsby . The Bishop of Sou thwark.

UIJe of t::1)c 0rtler of tIJ e 'ibospital of St. 3-olm of 3- erusalem in JEnglalltl.
AMBULAKCE DEPART:\lENT .
"[be St. John :ambulance :association.
PATRON :
Il l S ThIAJ ES T Y 1';' L G G I:ORGE Y.,
Sm-ere ign Head and Patron of the Order.
PRESIDENT:
11.1{.lI. TlfE DUKE OF CO;\, NAUG HT, K .G. , Gr:l.l1d P rio r of the O rde r.
CE'TRA L EXECUT I VE COM!I1ITTEE :
Consisting exclusivel y o f M e m be rs and H ono rary A"sociales o f t he Ord er.
DIRECTOR OF T II EA:\IBU LANCE D EPART:lI ENT A1'ID C llA iJU IA:'< OF CO;\IM lTTEE. - T he Earl o f P iymo u th, c. B.
ASS1STA:\T DIRECTOR AND DEPUTY C JI AIR1\IA .- L ieut.-Co l.
I' ic h a r d C . T emple, Bl. , C.L E.
DEPUTY C HAIRl\IA N -Sir Jo hn Furley, C B , L ife ?\Iemlle r o f the Com m ittee , H Ollon's Cfl l{ Stl. :,\ 1
M aj. Gen. J. C. n dtoll.
L ieul. -Col. A C. \':1tt'.
Co l. Sir J. R . A. Cia k, Ht. . C. B.. F.R.C.S.E .
H . E . Boulton,
T h::: Rev . T . C. Elsdon .
The Rev. H. D . J\ l ncl1:1mara.
I nspector-Genera l B. c.v.o., R,N.
Maj . G. H. Darwin ,
Col. G. S. Elliston. C.11. c.s.
Col. C. J . Trimble, , L.I"C.I'.E.
Capt. Si r J . W . Notl-B,)"er, C.\' .l'.
E Owen, LL D F 1l C.S
Tne Lord Claud IL1milton, Sir J. L. Langma n, l3t
CENTRAL EXECUTIVE CO;\Ii\rI TTRE-continllcd.
S W. I alkin .
C. COllon, F.R C.P E., il1.R C.S
Surg.-Gen. S , B. Fran kl in, ".C.I.E., K.B.I'.
C. B. Palmer.
Admira l Sir F. G. D. B ·Mor I, G C.B., C.C.M G.
Li eul.·Col. G. E . T\,iss, F.R C.S.I .
Col. T. H. Hendl ey, C.I.E.
]. H. l\f orgrln, C.V.O. F.R.C.S.
Surg. Lieut.·Col. SrI' W. H. Cruoke·Lawless, C I.E , M,;::.
Col. H. R \[ ends.
Lieu l ·Col. A. n. Aclantl. lU[L, Col. Ii:. D.
S Irg Gen. Sir ] lIl1cS Porl"r. K C.B , 1:.I1.f'., R N
]. A. Bluxalll, V.R .C.S .
Lieut.·Col. Sir R. W. I nglis. l\laj. P. G. Shewell.
T. H. Woolst0l1. F N. Ellis.
W. E . Audl"nri, A . .I L. ] vhns loll, ill ILC.S.
EX·OFFICIO OF
The Secretary·Gencral of tht: OJ(Jer.
The R "ceiver·Gtneral of the Order.
The Cilairman, Briti-h Opht'mllllic H ospilal.
CH IEF SECR J£TARY :
Col. Sir II . C. Perroll, Hl ,C.H. (Secrctary-General of the Order}.
OF STORRS A'ID ACCOUKTANT: "V. R. Edwards, A. C.A. (Scc retary of the Onler).
STOREKEEPER:
W. II. M organ (Supe rint endc nt, Inv<llid Co rps).
A 'iSISTANT SrrCRETARY:
D. G. M o nl eil h.
TERR ITORIAL BR .-\N C II.
CO:-<TROLLER-IN-ClIIEF:
Lieut.-Co l. Sir R. C. Temple, Bt., C. I.E.
ASSISTANT SECRETARY:
P. G. Darvil-Smilh.
REVISED 1908.

REFERE ' CE No. 58. 1908•
F IRST AID TO THE INJURED.
SY LLABUS OF I N STRUCTIO N.
FIRST LECTURE.
A. Prin c iples of First Aid.
E. A brief Desc ripli o n o f the IIuman Skeleton and of the M usc les.
C. Fractures-Causes, varieties, signs and symptoms.
D. Treatment o f Fractures-General Rules.
E. The Triangular Bandage antI its application.
D LECTU RE.
A. Treatment of Fractures (continued). Details of treatm e nt.
B . Disloqtions, Sprains, Strains-S igns, symptoms and treatment.
C. The Heart and Blood Vessels. The Ci rculalion of the Blood.
D . IIrem orrhage ann wounds. General ru les fo r treatment.
E. T he Triangu la r Bandage and its applicatio n.
8
THIR D LECTURE.
A. TJ:e morrhage and w ounds (continued). D etai ls o f treatment.
B. Interna l Hremorrhage-Signs , symptoms ::l.nd arrest.
C. Ilremorrhage from Special symptoms and a rrest.
D . Bruises, Bums and Scalds, Bite'S and Stings, Frost-bite.
E. Forei gn bod ies in the Eye, Nose and Ear.
F. The Triangula r Bandage and its application.
FOURTH LECTURB.
A. The Nervous System .
n. The Organs and l\lechanism of Respirati on -Artifi cial R espirati c.;-,.
C. Insensibili ty.
D. Poisoning.
FIFTH LECTURE (for 11ales only).
A. Improvised methods of lifting and carrying the sick or injured.
B. Methods of lifting and c J rrying the sick or inj ured on stretchers.
C. The conveyance of such by rail or in country carts.
FJFTH L ECTURE (for Females only) .
A. Preparati on for reception of accident cases.
B. Means of lifting and carrying.
C. Preparation of uecl .
D. Rem oving the cl othes.
E. Preparations for surgeon . 9
NOTE I.-The subject of poisons should be treated in a manner; the common poisons classified, and only their general symptoms, effects and treatment taught.
on: 11.-T he last half-hour of each lecture should be de\-oted to practical work, uch as the a pp' ication of bandages and lifting and carrying wounded on stretchers.
KOTE IlL-There ,>hould be an interv,11 of a week between each lecture. A candidate for examination must attend at least fuur out of the five lectures.
OTE IV.-l\Iale classes must pass in that system of stretcher exercise most suitable for the locality
NOTE V.-As little time a possible is to be spent on instruction in anatomical and }Ihysiological details . Lecturers and exal1i iners are particularly r equested to remember that it is " First Aid" that has to be taught and tested, and not anatomy and phy:;iology.
.illixed classes of //len and wOlllen are on no account term it led.

PUPILS U ' DER YEARS OF AGE CAN ONLY ATTEND THE (\ JUNIOR" CuURSE (SECTIOi'i A, SYLLAB US 40).
Lecturers instructing a First Aid class, and Local can obtain further particulars on application to the Chid Secretary for "Paper Reference No . 80."
No Lecturer may exallline his OW/l Class for Certiji..ales .
The Human Skeleton. Skull, spine, ribs and breastbone, upper limbs (collar-bone, shoulder-blade, armbone, bones of Lhe forearm, carpus, mel acarpus, phalanges), pelvis, lower limbs (thigh-bone, kneecap, tarsus, metatarsus, phalanges)

Cranium, lower jaw, spine, breast-bone, colhr-bone, shou lder-hlacle, a rl11-!Jope or bones
forea
Miscellaneous Injuries . Bruises, burns and scalds, hites of snakes and rabid animals and wound; by poisoned weapons, stings of plants and animals, frost bite, needle embedded under the skin, fish hook embedded in the skin, injuries to joints, foreign body in the eye, ear passage and nose, wound in the front wall of the
injuries to the organs within
10 SUMM ARY OF CrrAvn:R I. Page of First Aid 17 Explanatory 20 Questions on Chapter 21 CH,\PTER II.
... ... 22 Joints ... 31 Muscles. Voluntary and involuntary 32 Fractures. Cause" varieties, signs and !:ympLol11s 33 Apparatus for treatment of Fractures ... 36 General Rules to be observed in the treatment of Fractures 4I Special Fractures.
close
-ca p,
crushed
43 Dislocations 62 Sprains 64 Sprains and Ruptured Muscles ... 65 Questions on Chapter 66 II CHAPT E R III . Page Circulation of the Blood. Organs; general (system ic) and pulmonary circulations 70 Hcemorrhage or Bleeding. Arterial, venous, capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage . .. 76 Course of the Main Arteries
Pressure Points . Aorta, arteries of
head and neck, of the upper limbs, of the lowe r limus 79 Venous Hcemorrhage and Varicose Veins 93 Wounds with Venous Hcemorrhage 94 Capillary Hcemorrhage 95 Internal Hcemorrhage 95 Hcemorrhage from Special Regions 96 Questions on Chapter 99 CHAPT ER IV.
the abdomen and pelvis r02 Questions on Chapter ... ... 115 CHAPTER V. The Nervous System. Cerebro-spinal, sympathetic ... II1 The Respiratory System I IS Artificial Respiration.
combined with Silvester's,
Hall's methods ... IU
to the elbow j ,int,
rm, crushed hand, pelvis, thigh-bone, knee
leg,
fooL
and
the
abdomen,
Schafer's, Silvester's, Howard's
Laborde's and Marshall
Insensibility. Causes, general rules treatment, cus 'ion of the brain, compressIon of bralll, apoplexy, epilepsy, hysteria, shock, collapse, , un str oke and heat·stroke, convulsIOns In childr en, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPT ER VI.
Poisoning. Ge neral rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip , hand, foot, chest, back, knee, elbow, (j ngers and toes __ .
CHAPTER VIII.
Methods of Carrying. Four, two, a nd th r.ee.han.dell scats, fireman's lift, fore ancl aft method, ImproVised stretche rs, to cross a ditch or wall, to load or unload a wagon ..
CH.\l' 1 ER IX.
Stretcher Transport. St retche rs, stretcher exercis"s, litters
CHAPTER X.
The Fifth Lecture (for Females only ). Preparation for recept ion of accident cases, choice and prepara · tion of a room, lifting and ca rryin g, preparation of bed, removing the cl ot hes, preparation for surgeon ...
Questions on Chapter

13
LIST OF ILLUSTRATIONS
.
Skeleton showing position of main arteries
Skull and vertebral column
Vertebra
Bone3 of the left upper limb
Bones of the right lower lim b
Shoulder J oint
Ankle ...
Rectus :'Iuscle
Triangular ba ndage spread out and folded
Large arm sling
Small a rm sling
Reef knot
Gra.nny knot
Loop knot
Bandage for fracture of lower jaw
Bandages for simple fracture of ribs
St. John sling
for fracture of both collar bones
Bandage for fracture of shoulder blade
Treatment of fra....·ure of a rm
Angul a r splint
Treatm ent of fracture of forearm
Treatment of crushed hand ...
Treatment of fracture of thigh bone ...
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap
Treatment of fracture of leg (man and wuman)
Treatment of crushed foot ...
Diagra m of the heart, lungs and air
12
l'ag-e [28 q.2 q. 5 IS S ICO 197
...
.. . ... . ..
...
... . .. ... ...
Pare fr ontispiece 2-424 27 29 3 1 3 1 3 2 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 71
Diagram of the cir-ulation of the blo()o
Digital pressure on carotid artery .. .
Digital pre ·sure on facial ultery .. .
Digital pressure on temporal artery
Digital pres ure on occipital artery ... . ..
Pad and bandage to arrest hremorrhage from tfmp1c
Ring pad
Digital pressure on subclavian artery .. . ...
Pad and bandages to apply pressure on axillary artC'r.\
Digital pressure on brachial artery (two method<;)
Flexion at elbow
Digital pressure on radial and ulnar arteries ...
Pad and bandage to arrest hrel110rrhage from palm
Digital pressure on femoral artery ..
T ourniquet on femoral a rt e ry
Flexi on at kllee
Organs of the chest and abdomen ...
The lungs and bronchial tubes
Schafer's me thod of artificial respirat ion ...
Silvester's meth od of altificial re spi rati on
Silve"ter's and Howard's mehxls ofartific i I respiration combined
Bandage for the hea rl
Bandage fo r the sholh'der
Bandage for the hip ...
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
G rip for four- handed seat
Lifting by two-hand ed seal. ..
Grips for two-banded seats ...
Carrying by two ·handed sea t

Grip for three -handed seat .. .
Supporting patient ... . ...
Fore and aft method of carryIng
Carrying on improvised seat
Improvised stretcher .. .
Furley stretchers .. .
Stretcher exercise, No. 1." Fall in"
Ditto, ready to lift patient
Ditto, lifting patient. ..
Ditto, placing stretcher .... . ..
Ditto, preparing to lower patle nt. . .
Ditto, "Lower"
Ditto, No. II. Ready to lift patient
Ditto, patient lifted... . .:.
Ditto, No. IV. First pOSItIOn
Ditto second position .. . ... . ..
Diag;ams illustrating Army stretcher drill
Ditto ...
Bed cradle
Improvised bed cradles
Fa.</! 73 8f 8r 82 2 12 5 ISS 15 6 156 157 157 15 8 159 159 160 I6r r62 163 15
Farl 1 64 165 1 67 168 168 171175 176 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
AT the request of the Central Executive Committee
I h ave revised the manual writlen by myself in I9 01 , as the official handbook of the St. John Ambulance Association.
Throughout the revision an endeavour has been made to simplify the study of First Aid to the Injured by drawing up a number of general rules for the treatment of accidents and sudden illness, and by tIle omission of all detail \\"hich is not absolutely necessary to enable the student to acquire an intelligent knowledge of the subject.
I wish to express my thanks to Professor E. A. Schafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. }\1. F. Christian for many valuable suggestions, and to the Medical Members of the Central Executive Committee, especially Surgeon-Major G. H. Darwin, M.D. and Dr. F. R. Cassidi, for perusing the proof sheets and for a number of useful additions to the \\ ork.
I cannot omit also to offer my best ackno\\ ledgments to Mr. ,V. R. Edwards, the Accountant and torekeeper of the S.J.A.A., for his invaluable co-operation.
JAM ES CANTLIE.
FIRST AID TO THE INJURED.
CHAPTER 1.
Th-J St. John Ambulance Association has now completed thirty years of its existence, and dunng that period hundreds of thousands .of men and women have been taught at its classes, 111 parts of the world how to help their injured neIghbours.
Fi;st Aid to the Injured is a special branch of practical medicine and surgery, by a kno\\ of which trained persons are enabled to afford .skllled assistance in cases of accident and sudden Illness. The instruction begins and ends with First Aid, and the subject is taught simply but thoroughly exhaustively. The duty of the ambulance pllpIls ends where the doctor's commences, and there ought to be no overlapping or clashing of duty or interests.
PRINCIPLES OF FIR T AID.
1. The First Aid student should be-
(a) Observant, that he may note the causes and sio-ns* of injury.
(b) Tactful, that he may without questions learn the symptomst and hlStoryt of the case.
* Signs are what may be pcrcciYed. _
t Symptoms are what the patient can tell you. .
t History means the circumstances attendmg the aCCH1ent or illness.

(c) Resourceful, that he may use to the best advantage whatever is at hand to preyent further damage and to assist N:lture's efforts to repair the mischief already done.
(d) Explicit, that he may give clear instructions to the patient or the bystanders how best to assist him.
(e) D iscriminat ing, that he may decide which of several injuries presses most for treatment by himself, and ",hat can best be left for the patient or the bystanders to do.
2. R e move the cause of injury or danger whenever possible .
3· Severe hcemorrh a g e must rec e ive the fir s t attention , no mat ter what are the other inj uri es.
4. Air. - The patient must be in a posllJon in which breathing is possible; the air passages must be free from obstruction ; if breathing has ceased prompt measures must be taken to restore it.
5· Rest. ?,""""A restful position of the body will assist the vital functions; support of the injured part will help to prevent furthe r damage, and is essential in the case of fractures of li m bs ,
6. Warmth. -After every acciden t keep the pltient wa r m so as to prevent the fall of temperature b-=low the norn-tal point.
7· When the skin is broken the wound 19
should be promptly covered wilh,a clean dressing. Should tbe \yound be pOIsoned, IS most important immediately to prE.yent the pOIson pernieating the S) stem. "
8. Poisons S\\ allowed be get lId of, or when that is inexpedi( nt, neutralIsed.
9. The best of must , be studied, and prOYI 'lOn made tor pIoper care \\ ben the patient is brought to shelter.
ro. Removal of should no t be taken off unnecessarily, but whln It IS needful to remove them, the following rules will be found of service in serious cases :- ,
COAT: Remove from the sound SIde first, anc1, if necessary, slit up the seam of the sleeye on the injured side.
SHIRT VEST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: Slit the back scam and undo the laces.
SOCK: Cut off.
II S t im ulants .-It is incorrect to suppose that alcohol is the only form of stimulant, far ,too frequent use of spirits is to restore a patIent after an accident, often .."ith ,rEsul,1S; the safest rule, therefore, is to defer the adm1l1lSlratlOr: f until the arrival of a doctor. When t.he patIent IS able to swallow, strong tea or coffee, or mIlk, as hot as cc:n
18
%0
be drunk, or a small quantity of sal vo la tile in water ma y be given . Smelling salts may be held to the nose. Sprinkling the fac e with cold and hot water a lternately, warmth applied to the pit of the stoma.-=:h a.nd over the h eart, and vi gorous friction of the limbs up wards have a s timulating effect.
12. Throughout his work the First Aid stUdent must on no account take upon himself the duties and responsibilities of a Medical man. At times an a pparently slight injury is accompanie d by grave danger and may actually cause loss of life. 'When sending for a doctor, state the nature of the case, and remember that written particulars are safe r than a verbal message.
It is ne cessary that something should be known of the structure of the body (elementary anatomy), and of the functions of some of the more important organs a nd systems (elementary physiology) A short descripti on of the necessary anatomical and physiologica l points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms banging by tbe sid e and tbe palms of the hands directed forwards. The" middle line II of the body runs vertically fro m th e top of the head to a point between tbe feet.

Q UESTIONS ON C HA PT E
T he 1111111erals i lJdicale Ille rages wl,oe I IIe alls'Wtys 1l.ay be )01111£1.
What is F irst Aid lo the injured ?.. ... "') qualities hould the First Aid studull .
What are signs? .. .
\\' hat are symptoms? .. . ..
What is the history of a case? .:. .... ';>
What is often the fi rst thing lo 111 an :\ccldent.. ;> .. , . t 'e th e fi rst
\\'hal of injury m us r ecel\ '. . . d
\Vhat three things a re absolulely necessary lo an IS person?
'Vhat must ue done ,,,hen the
I low must poisoning be treated? .. . 1. d th aclual lreatment
\Vhat sl eps must be taken ue) 011 e of injuries? ... . "';>
Should clothing alway be rem o\ ed. ... ..")
IIow would. you remove hen !
Explain t h e use arJd ahuse of stlmulal ts ... . ..
W hat must the Fi;'st Aid tudent not du ?
\Vhat is ele mentalY anatomy?
, Vha t is e le m entalY p hysiology? .... . I the hun'a n cody
F or purposes of desc riptIOn 10W IS supposed t o be p la ced? .. .
Wha t is th e mi ddle li ne of the b ody ?
I.
R
rllenllOn
17 17, IS r7 17 17 IS IS
....
... .. . . .. . . U' I ;>'" I S J 9
l'lll 10
..., 19
,cn .
19 19 19 . " 19, 20 :0 20 :0
20 20

CHAPTER II.
FRACTURES, DISLOCATIONS, SPRAINS AND STRAI S.
THE SKELETO T.
Th e h u ma n body is moulded upon a bony frame\york (the skeleton) ,,·h ich serves-
I. - To gi"e shape and firmness to the body.
2. - To afford attacllment to the llluscles.
3·-To protect important organs, as in the skull, chest, and abdomen.
THE SKULL.
T he B o ne s of the Sku ll are arranged in hro groups, those of the brain case or cranium. and those of the face. '
Th e B o undarie s o f the Cranium are the "ault or dome, the rounded portion forming the top of the h ead ; the front or brow; the back of the head \\ here the greatest extent of brain exists, and therefore the cranium is \\ idest and deep est; the sides or temples. The base of the cranium is hidden from vie\\' by the bones of the face and of the vertebral column' in it are numerous perforations for the passage of blood and. nerves; through the largest opening the bram and spll1al cord are continuous.
T he Bon e s of th e F a ce with the exception of 23
the lower jaw are firmly jointed. together, so movement between them is impossIble.. The ca vltles of the nose and of the eye sockets (orbIts) are formed by the bones of the cranium and of the face conjointly. The mouth cavity is forn:ed between the upper and lower jaws, the bemg the bony roof of the mouth which separates It from the nasal cavIty above.
Th e Lower Jaw consists
(a) A horizontal portion in which are the sock et s for the teeth. .
(b) Vertical portions terminating on. either Sid\! at the joint between the lower )a\\' an? the base of the cranium, situated ImmedIately in front of the ear.
The an rr le of the jaw indicates the junction of the horizontal the \'ertical portions.
THE BACK-BONE, PINE, OR VERTEBRAL
Th e Vertebral Co lumn (Fig" J ) is of bones called vertebrce, each of whIch consIsts of-
I.-A body or bony mass in front . ;..
2.-Process :: s projecting whIch enclose a c.:lI1al for the sp1l1al cord - the spinal canal.
3.-Two tranS\'e rse proce ses, twelve pairs of which supp ort the ribs.
22
SKULL AND VERTEBRAL COLU:\1N.
left ribs and portion of breast bone. The right ribs are removed .
SPINOUS PROCESS.
TRM;SVERSE
PRUCIiSSES : I r_

CANAL FOR SPINAL CORD Bony OF VERTEllHA.
FIG. 2A.
SPINOUS ! : '" PROCESS.
SURFACES - \ SUPPORTING HE DS OF RIDS.
FIG. 2 B.
4 . - A spi n ous process. The spinous processes of the vertebrre ca n be felt beneath the skin for the \\"hole length of the back (Figs. 2 A and 2B) .
Th e Vertebrc:e, 3:) in all, are grouped into regions, in each of which they are known by number, counti ng dowl1\\"{\rd :-
I.-In the neck 7 Cervical vertebrce . The first vertebra, tlze atlas, forms a joint \yith the base of the skull, at which the nodding movement of the head takes place j the second, tIle ax/s, by the joint between it and the atlas, allows of the side-to-side movements of the head .
2.-1n the back 12 Dorsal vertebrre.
3.-1n the loin 5 Lumbar vertebrre.
4.-The rump-bone, or Sacrum, consists of 5 Sacral vertebrre united in adults as a solid mass.
5.-The tail-bone, or Coccyx, consi ts of -l- vertebrce joined together to form a single group .
Between the bodies of the vertebrre, in the upper three regions, are interposed thick pieces of cartilage (gristle), \vhich, while they bind the bones together. allow of free movement to the column as a whole, and help to break the shock of any sudden forct" applied to the spine (fo r example, \vhen falling from
'V _ ..--..
..
a height on the feet ). The whole spine is strapped together by ligaments reaching its entire length.
THE R!BS AND BREAST-BONE.
The R ibs consist of t\\-eIYe pairs of curved bones extending from the dorsal vertebrce to the fr on t of the body, and are known by num bers- first, second, etc., com rnencing from above. The ribs are not bony throughout their entire length, but at a short distance from the front the bony material ends, and cartilage takes its place. The upper seven r;airs, named the true ribs, are attached by their cartilages to the Breast-bon e (sternum), a dagger-shaped tcne ""ith the point downwards, just over the pit of the stomach. The lo.rer five pairs are terrred the false ribs, as their cartilages fall short of the n-ie'dle line.
The eleventh and t\\ elfth pairs are terID€d fieating ribs, as their ends are free in frent. Tl:e rits enclose the chest, and serve to protect the lungs, heart, liver , stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder - bones are the Collar-bone (davt"de) and the Shou lder-blade (scapula) .
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thickness of a finger. I ts in n er end rests on the upper part of the
SIIOULOER
BLADE (SCAPULA)
ARM Bome (HUMERU , )

5
nONES {ULNA OF RAIJlus ---++-'H
WRIST (CARPUS) I\IETACARPUS
PHALANGES
FIG. 3ABONES OF THE LEFT UPPER LDIB.
FIG. 3'13.
SHOWING THE POSITION OF TIlE RADIUS AND ULNA WHEN 1'1{& TIIUMB IS TUR 'l':D INWARD S.
Compare Fig. 3A, in which the thumb is turned out · wards.
26
27
RAOfU
breast-bone, and its outer end joills with the shoulderblade.
The Shoulder-blade lies at th e upp er and outer p:ut of the back of the chest, and forms joints \yith the collar-bone and the bone of the arm.
The bone of the Arm (Imm erus) reaches from the shoulder to the elbow.
In the Forearm are two bon es , the Radius on t he outer, or thumb side, and the Ulna on the inner, or little finger side. Both bon es reach from th e el bo w to the wrist, and th ey change th eir relative posi tion with every turn of the hand (Figs. 3A and 3B ).
The Hand is compose d of-
I.-The b ones of the wrist, or carpus, eight in number, arrange d in two rows of four.
2 .-The metacarpus (the framework of the palm) ; five bones \oyhich form the knuckles and support the bones of the fingers.
3·-The plzalanges , or finger-b ones, three in each finger, and two in the thumb.
THE PELVIS AND LOWER LurBs.
The Pelvis.-The large basin-like mass of bone attached to the lower part of the spine is composed of the two haunch -bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of ca rtilage intervening, but behind, the sacrum is placed between them. The pelvis

BOI'ES OF THE RIGHT LOWER LIMB, SHOW· JOI NT WITH THE PELVIS AT THE III P .
FIG. 4...._._.......
.,_
___ .•. _
_ .-
TIIlGH BONE (FEMUR).
KNEE CA P (PATELLA).
BROOCH 130:-lE (FI BU LA).
S HIN BONE (T IBIA).
IETATARSUS.
suppor ts the abdomen and its contents, and provides the deep sockets for the thigh-bones-the hip joints .
The Thigh-bone (femur) reaches from tf e hip the knee joint. It s shaft is stout, rounded, and forwards; the upper end presents a rounded head, supported on a neck "hich projects inwards, to fit into the socket of the hip joint.
TIle Knee-cap (faldla) is a bone lying \\ ith its base up" ards in front of tbe knee joint immediately bE neatb tIle skin.
The bones of the Leg are the Sbin-bone (tzha) and the Brooch -bone (fibula). The Shin-bone extends from tlle knee to tbe ank le, in both of \\ hich joints it plays an important part; its sharp edge, t!'e shill, can be felt immediately beneath the skin of tr.e front of the leg. The Brooch -bon e lies on tbe outer siJe of the tibia. It does not enter into tbe formation of the knee joint, but its lower end forms the outer boundary of the ankle joint.
The Foot is composed of--
I.- The tarsus, a group of se';en irregular bones at the instep. The largest is e heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.- The meta/anus, the five long bones in front of the tarsus" hich support the toes.
3·-The phalanges, or toe-bones, two in tbe big toe, and three in each of the otber toes.
JOINTS.
A Joint is formed at the junction of two . or more bones. In moveable joints such as the hlP, knee, elbow, etc., the sl1ffaces of the bones are covered by cartilaae which lessens friction and the shock of a b ,

Compare Fig. 4, Page 29·
fall. Lubricating the joint is a clear, rather. stjcky fluid, the "joint oil," or synovia, enclosed a capsule. Tying the bones together, but allowll1!?; of movel1lent are a number of bands or ligaments.
To expiain the formation of limb joints, the
31
FIG 6.
LE FT ANKLE.
FIG. 5.
P A TELLA
TENDON OR LIGA;,IENT OF PATELLA

following examples ar e given :-
The Shoulder, a balland-socket joint, consist s of a shallow sock t on the outer angle of th e slloulder-blade, and of th e head of the arm-bon e (Fig. 5). 0.\\ ing to th e shallowness of the sock et the arm-bon is very pron e to escape frr m its socket (dislocate).
The Ankle, a hinge joint, is formed at the junction of tIl ree bones, the shin-bone above and on th e inner side, the broochbone on the outer side, and the ankle-bone below (Fig. 6).
THE MUSCLES.
oJ> FIG. 7· The Muscles of tbe DIAGRA:VI SHOWING RECTUS body are classified into t\\'o !\IUSCLE OF TH IGH , WITH groups-v 0 lutttary and MTERY, VEIN AND NERVE. involuntary.
The Voluntary muscles are met with in the limbs, the head and neck, and the surface of the trunk. Their ends are atta·ched to different bon es , and as they pass from one to another they cross a joint, and, being endowed ,,\ith the power of contraction and relaxation, cause the mo\'ements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the neryes entering them bring them under the direct control of the brain and spinal cord.
The Involuntary muscles are met \vith in the walls of the stomach and intestines, in the 2.ir passages, and in most of the internal organs and blood-vessels, also, in a special form, in the heart. They are not under the influence of the will but tbeir \\ ork during the hours of sleep; 'their functIons are regulated by a scparate set of nerves (see Sympathetic System, page II 8) .
FRACTURES A JD THEIR TREATMENT.
When a bone breaks a Fract ure is said to occur.
CAUSES OF FRACTURE
.
. I. Direct Violence.-When from a severe blow, tmpact of a bullet, crush of a wbeel, etc., a bone breaks at tbe ",here the force is aIJPJied the fracture is termed direct. o
IENDOK NERVE
J2
33

Indirect V iolence. - '\Then the bone breaks at some distance from the spot where the force is applied the fracture is termed indirect. Allghting on the feet and fracturing the thigh-bone or the bones of the leg, or falling on the hand and breaking the ladius or the collar-bone, are examples,
3. Muscular Action.-The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them.
VARIETIES OF FRACTURES.
Fractures are classified according to the condition of the tissues adjacent to the bone as follows :-
I . Simple. -The bone is broken wIth but slight injury to the surrounding parts.
2 . Compound. -The bone is bl -,ken and the skin and tissues are punctured or torn, th us allowll1g disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude through the skin, or (for example, \Vhen a bone is broken by a bullet) the wound may lead down to the fracture.
3. Comp li cated.- The bone is broken and in addition there is an mjury to some internal organ (for example, the bram, spmal cord, lung, etc) or to some important blood-vessel or nerve.
A fracture may be compound c r complicated as the immediate result of the injury j or a fracture 35
originally simple, may be converted into a compound or complicated fracture-
(a) By careless movement on the part of the patient.
(b) By carelessness or ignorance on the part of one rendering first aid.
Special varieties of fractures may be classified according to the injury to the bone itself as follows :-
I. Comminuted. - The bone is broken into several pieces.
2. Green-stick.-In children, owing to the softer state of the bony tissues, a bone may bend and crack without breaking completely across.
3· !mpacted.-The broken ends of the bone are dnven one into the other.
SIGNS AND SYlIIPTOMS WHICH MAYBE PRES ENT
(A fracture of the femur, humerus, or both bones of the forearm or leg, affords the most complete example).
I. Pain at or near the seat of fracture.
2. Loss of Power in the lim b.
3· Swelling about the seat of fracture. Swelling frequently renders it difficult to perceive other si gns of fracture, and care must therefore be taken not to mistake a fracture for a less serious injury.
4· Deformity of the limb.-The limb assumes an
34
unnatural position, and is mis-shapen at the seat of fracture . The contracting muscles may cause the broken ends of the bone to override, thereby produ cing shorten ing.
S. Irregularit y of the bone . - If the bone is close to the skin the fracture may be felt, and if compound t may be seen.
6 . Unnatural Mobility. -Movem ent may be made out at the seat of fracture.
7. Crepi tus, or bony grating, may be felt or heard when the broken ends move one upon the other.
The last two signs should only be souglzt by a doctor
Several of the above signs are absent in green-stick and impacted fractures .
In addition to the signs and symptoms the patient or the bystanders may be able to give the history of the injury, and marks on the clothing or skin should be noted, as they may serve to locate the fracture The snap of the bone may have been heard or felt.
ApPARATUS FOR T REATMENT OF FRACTURES.
Splints and bandages for First Aid frequently ha\"e to be improvised.
A Spli nt may be i mprovised from a walking stick u mbre lla, billiard cue, broom or brush handle, police man 's truncheon , rifle, fo lded coat, piece of \yood, cardboard, paper firmly folded, a rolled-up map, or, in fact, anything that is firm and long enough to k eel

37
the joints z'mmedia tely above and below the fractured bone at rest. 'When the above appliances are not available, the upper limb, if fractured, may be to the trunk, and in all cases a fract ured lower lImt sh ould be bandaaed to its fellow.
Bandage s be improvised from belts, straps, braces, neckties, or any pIece of lmen, calico , string or cord that comes to hand . .
E smarch's Tria n o-ular Bandages (FIg. 8) are made by cutting a piece of linen or .calico about fort" inches squa re diagonally into two . .
T h e broad bandage is made by bnngmg point down to th e base (Fig . 9), an d then fo ldm into two (Fig . 10) . .
T he na r row bandage is made by fold mg the broad ba ndage once (Fi,j. I I).
T he medium bandag e is made by bri nging the point down to the base, and then folding into three. (Fig. r 2). This bandage may be used instead of .the broad or th e na rr ow bandage when it is better SUI ted to the proportions of the patient. .
It is sometimes advisab le to halve the sIze of the bandage by bringing the t \\'0 ends together before folding it into the broad, narrow, or mediu m bandage.
\Vhen not in use, the triangular bandage shou ld be folded narrow; the two ends should be turned to the centre, and the bandage then folded four. reducing it to a packet about inches by mchcs v
36
FIG. 10 BROAD B A ND AGE.

FIG. II. NARROW BANDAGE.
12. - THE DOTTED LINES SHOW THE FOLDS OF THE MEDIUM BANDA GE.
Large arm-sling (Fig. I3).-Spread out a bandage, put one end over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang do wn in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm
FIG. 13. FIG. 14. over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure tv,"O pins to the front of the bandage.
Small arm-sling (Fig. I4).-Place one end of a
--=--
A · ..
39
FIG.
broad bandage over the shoulder on the so und side, pas'. it round the neck so th a t it appears over the shoulder of the injured side; place the fore arm over the middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in cases of fractured humerus, and occasionally \\·hen the large sling would be too conspicuous.
Slings may be improvised in many simple ways, such

IS.-REEF KNOT. FIG. I6.-GRAN NY Kl\OT.
as pinning the sleeve to the clothing, turning up the tail of the coat, passing the hand insi de th e buttoned coat or waistcoat , etc.
Reef Knots (Fig. IS) are to be used. Avoid granny knots (Fig. 16).
GE:"ERAL RULES TO BE OBSERVED IN THE TREATMENT OF FRACTURES.
The object of First Aid Fractures is to guard against further mIschIef, especially to prevent a simple fractur.e fro.m becommg compound or complicated. To attam thIs end ;-
I. Attend to the fracture on the spot. No matter how crowded the thorou ghfare, or how short the distance to a more convenient or place, no attempt must be made to the patient until the limb has been rendered as Immovabl e as possib le by splints or other restrainin 6 apparatus.
2. Steady and support the injured limb at once, so that its further movemer:t on the part of either the patient or the bystander IS prevented.
3. Straighten the li1?b with great care, and if shortening is observed m the case of a fractur e a bone of the lower limb, pull upon the foot untIl the limb regains a more n ormal length . When the shape of the Ii mb is im proved, on no .ac count let until it is secured in position by splmts, ?the[\\'lse there is great danger of the fracture becommg compound or complicated. .
4. Apply splints (when practicable) and bandages as follo\\'s ;-
(a) The splints must be firm, a?d long enough to keep the joints imm edIa tely above and
FIG.41
below the fractured bone at rest They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The ban,dages must be applied firmly, but not so tIghtly as to constrict the circulation ?f blood in the lim b. \Vhen the patient is m the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a ge neral rule:-
For the trunk the broad bandage should be used. Pass it once round the trunk and fasten it by tying the ends, or with two or three safety pins on the side opposite to the fract ure but if to se,cure a splint for n. broken thigh,' o\'cr the splmt.
For the arm or .forearm th e narrow bandage should be used. Pass it twice round the limb, and tic the ends over the outer splint.
For the thigh or leg the narrow or medium bandJ.ge may be used. It;:, frequently convenient to double the bandage at centre, PQSS it under the limb, bring the loop over the limb, PQSS bot:1 ends cf the band· age through it in opposite di.ections, and tie them over the o12ter r:J1i].t (Fig. 17).
In applying banda.ges near a fracL:r :- the upper one be secured first.
5. When hcemorrhage accompanies a fracture it must be attended to fi l st, and the \yound oOm'ered by a clean dressing.

6. No attempt must be made to remove a patient suffering from a fracture of the spine, pelvis, or thigh, except m a recumbent position, preferably upon a stretcher. . .
7. In every case of fracture it necessary to cover the patient to keep h1m warm, and so lessen the effects of the SHOCK of the accident.
8. In all doubtful cases, treat as a fracture.
SPECIAL FRACTURES .
Fracture of the Cranium. -A fracture of the upper part is usu ally caused by direct violence-for example, a blow on the head. A fracture of the base is caused by indirect violence, through a fall on the
42
43
head, a fall on the feet or lower part of the spine, or a blow on the lo\\er ja\V. If the ZIpfel' part zs fractured, the si gns are sw elling, irregularity, and frequently insensibility, either immediate or coming on grad U,:j lly. If the base is fractured insensibility may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape fr om the nose, or it may pass down to the stomach, \\ hence it may be vomited ; the fracture may involve the orbit, causing a blood-shot eye.
TREAT.:.\IENT.
Injury to the brain is the great danger attendFIG. 18. ing a fracture of the cranium. For treatment see "Concussion and Compression of the Brain," pages 131, 132. p.Fracture of the Lower Jaw.-Pain, loss of power (inability to speak and to move the jaw freeL) '), irregularity of the teeth, crepitus and bleeding frum the gum are the usu al signs and sympt om s.

TREAT:'I EN T,
I.-Place the p:llm of the hand below the injured bone and press it gently against the upper jaw.
2.-Apply the centre of a narrow bandage under the chin, carry one end ov er the head, cross the ends at the angle of the ja \V , carry the long end across the chin, and tie the ends on the side (Fi g. IS).
Fracture of the Spine.- The vertebral column may be broken either by direct or indirect violence. Falling from a height on the back across a har or upon an uneven surface is an example of direct fracture, and a fall on the head, causing a broken neck, is an example of indirec t violence. " That is commonly r ega rd e d as a broken back consists of a fracture of one or more of the vertebrce " 'ith displacement of the fragm ents, whereby the spinal cord and the nerves issuing from it may be torn, causing complete or partial paralysis of the parts below the 1racture. Pain is present at the seat of injury.
TREATl\lENT.
1. Prevent all movement on the part of the patient.
2.-Cover the patient warmly.
3.-To remoye the patient, phce him on a stretcher or shutter as fullows ;-
(a ) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
44
4 6
SO that the ends are level with the to]) of hIS ; pass a broad bandage or handkerchJef under the head and secure it tC, the sticks. If no coat is worn or doubt as to its strength and length pass a of bandages under the patient to serve mstead of, or in addition to, the coat.
(b) A. on each side grasps the [Cllled coat wIth his .hands well apart; a third grasps the clothmg on both sIdes on a level with the hips; a fourth bearer takes charrre of the legs. t>
(c) On the word beil1.g given, all lift together and carry the patIent by short side paces over t?e stretcher and carefully lower him on to It. If a fifth be<lrer is available the be p.assed under the patient mstead of carrymg hIm over it.
4·-0n arrival at shelter nothing further is to be tHe arrival of a doctor, except to glve the pati en t water, tea, etc., if he is conscious.
Fr.actured Ribs.- The ribs usually fractured are the slxth, seventh, eighth, and ninth and generally the is midway between the breast-b'One and spme. !?e fracture may bE:: caused by indirect VIOlence, dnvmg the fractured ends of thb bone outwards, or by d.irect violence, driving the fractured ends of the bone mwards and sometimes injuring the

lungs or other internal organ. If the lower ribs on the right SIde are broken, the liver may be injured, and a fracture of the lo\yer left ribs may \yound the spleen. Evidence of the fmcture is afforded by pain, especially on attempting to take a deep breath, and by short and shallow breathmg. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hremorrhage (s(!e page 95) may occur.
TREATMENT.
( a) TTiZe1l t ll Pfracture is not complicated by an £njury to an internal oJ'.::,an :-
J. - - Apply two broad bandages round FIG. the chest sufficiently firmly to afford comfort, with the centre of the flrst immediately above and that of the second immediately below the fracture. The lower bandage should overlap the upper to half its
47
48
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong towel, folded about eight inches wide, tightly round the chest, securing it with three or four safet y pins.
2. -Place the arm on the injured side in a large sling. (Fig. 19).
(b) TVhen an z"nlernal organ is z"lljured-
I.-Do not apply bandages round the chest.
2.-Lay the patient down, inclined a little towards the injured side.
3. --Loosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Treat as for internal hcemorrhage (see page 95).
4.-Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (sternum).-
When this fracture can be felt or is suspected undo all tight clothing, and keep the patient quiet in an easy position until the arrival of a doctor.
FRACTURE OF THE BONES OF THE UPPER
LIMB
Fracture of the Collar-bone (davzde ).-ThIS fracture is frequently caused by a fall on the hand or shoulder.-The arm on the injured side is partially
49
helpless, and the patient usually supports it at the elbow with his hand and inclines his head towar ds the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lo\\ er. The general signs and symptoms of fracture are mostly present.

I.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about t\\'o inches thick and four inches across in the armpit.
3.-Gently bend the forearm well up, keepin g tbe shou lder as far back as practicahle, and support it in a "St. John" sling, made as follows:-
(a) Lay an unfolded bandage across the chest over the injured Ii 111 b \\ ith one end on t be uninjured shoulder and the point beyc ncl the elbow en the injured side. (Fig. 20).
(b) Pass the JO\\'er end of the bandage under tl :e injured limb, arross the back, and tie the ends some" hat loose ly in the holl ow in front of the sound shoulder.
(c) Fold the point over the elbow of thE' injured limb and secure it by O!1e or t\YO pins (F i;;s. 2I and 22).
FIG H.

FIG. 22. r
(Body bandage omitted to show details of Sling.)
5f
+-'ri ghtly secure the injured limb to the side by .1 broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming th e fulcrum .
5·-Now tighten the slin g. When both collar-bones are broken keep : h
FIG. 23A. FIG. 23B.
sho ulders back by n arrow bandages ti ed roun d each arm , close to the shoulder, passed across th e back, over the opposite arm and ti ed together in front. The forearms should be raised and supl-lorted by the ba ndages. (Figs. 23A and 23B).
Fracture
of the Shoulder-blade ('(mpltla).Apply the centre of a broad bandage in tbe armpi t of
50
the injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24)·
Fracture of the Arm (hume7'lts). - The bone may be broken :-(a) Close up to the shoulder; (b) near the F middle of the shaft; (c) close IG 24· to the elbo\\'.
All the general signs and symptoms of fracture are usually present.
':fREAT l\IE NT.
T;f/helZ the Fracture is close to the Shoulder-
I.-Apply a broad bandage with its centre above the middle of the arm round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
TVhen tlze Fracture is mar the Mz'ddle of H7e Shaft-
1.- Bend the forearm at a right angle to the arm.
2. -Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the ann, and, if enough can be procured, to the front and back also. The front splint

must on no account be so long as to press upon the blood-vessels at the elbow joint.
3.- ecure the splint. hy bandages above and below the fracture. If splints are not available, secure the arm to the side by t\\ 0 broad bandages.
4.-S11PPort the forearm by a small arm sling. (Fig. 25).
Fractures involving the elbow joint, \\bether of the arm or forearm, ar<; attended \\ ith so much s\\ elling, c: nd it is so difficull to ascertain the exact nature of the injury, that when the accident occurs indoors the limb should be laid upon a pillow in the most comfortable position; i e or cold \\ater dressings should be applied to the injured part, but no funh er treatment should be attem pted pending the arri\':11 of a doctor.
FIG. 25.
52
53
ITVlzen tile accidenl OCClI rs out 0./ d oors-
i. Take two pieces of thin flat \Vood, one long enough to reach from the to below II',. the elbow, the other lond enough to rea ch from ahm'e the elbo\\'
:X;I to the finger tips; tie '/ them toget h er to form a right angle. (Fig. , 26) .
2 -Apply th E: angulctr splint so rnud e FIG. 26 on th e inner side of the fl exed limb.
3.-Secure by bandages above a nd below the fracture.
4 .. - Support the limb by a large arm sling.
S. - On arrival at home rem ove the splint, an ti treat the injury as if it had occurred indoors.
Fracture of the Forearm. - ,Vh en both bon es (the Radi us and Ulna) are broken, the general signs and symptoms of fracture are usually present. ,\Then one of the bon es only is broken the signs and symptoms are as a rule painl loss of power, s\\ elling, and irregularity. An impacted fracture of the Radius
just above the '\'fist is a common result of a fall OIT the hand.
TREATMENT.
This is the same, whether the fracture is of one bone or of both.
I.-Bend the forearm at right angles to the arm, .

FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sid es from the elbo\\ s to the fingers.
3.-Apply bandages, embracing both splints, immediately above and below the fracture and round the hand (Fig. 27) .
4.-Apply a large arm -sling.
Crushed Hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREAT:'I1E T.
I.-Apply a carefully padded splint to the front of the hand, reaching from \VeIl above the wrist to beyond the tips of the fingers.
54
55
2.-To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. z8).
3.-Apply a large arm-sling.
Fracture of the Pelvis. - Wh en, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the p:ltient is unable to stand or even to move the 10\\ er limbs \\ ithout great difficulty and pain, a fracture of the pelvis may be assumed to haye occurred. The blood-vessels and organs, especially the bladder, \\ ithin the pelvis are in danger of being wounded.

I. -Lay the patient in \VIlateyer position is found to give the greatest case, and flex or straighten the 10,\ er lim bs as the pa tien t desires.
2.-Applya broad bandage round the hips tight enougil :0 the parts, but not so tight as to press the broken bone turther inwards.
3.-To remove the patient place him on a stretcher, acting on the same principle as that described under " Fracture of the Spine" (see page 45).
FRACnJRE OF THE BONES OF THE LOWER LIlIIB.
Fracture of the Thigh-bone (femur).- The thigh bone may be broken at its neck, anywhere in the shaft, or close to the knee. A fracture at the
is to occur i.n Old people from very slight ll1Jury, and IS often dIfficult to dIstinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patien t cannot, when lying on the back, raise the heel from the ground , the bone is broken. All the aeneral signs and symptoms of fracture are usually present and a prominent sign is the position of the foot,
29.
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREAT:\lENT.
I.-Steady the limb by holding the ankle and foot.
2.-Gently draw down the foot and brin n' it into line with its fellow. When two or three assis&nts are at hand, it is one person'::; duty to hold the foot in positio n until the splints are secured.
3·-Apply a splint on the outer side from the armpit to beyond tbe foot.
57
F
FIG.
4.-Apply a splint on the inner side from the top of the thigh (the fork) to the knee.
s.-Secure the splints by bandages as follows :(a) Round the chest just below the armpits, (b) round the pelvis on a level with the hip joints, (c) above the fracture, (d) below the fracture, (e) round the leg, (I) round both ankles and feet, and tied below the feet, (g) a broad bandage round both knees ( Fig. 29).

FIG. 30.
When single-handed, or when the patient is a woman, it is expedient, after extension of the limb, to tie the feet together, dispense \\'ith the inner splint, and pass the bandages round both limbs (Fig. 30).
Fr2cture of the Knee-cap (patella) -The knee-cap may be FIG. 31. broken by falling on the knee (direct violence), but more frequently it is broken by muscular action, as follows:59
'Vhen the foot slips in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee -cap in t wo (Fig. 3 I).
Pain, loss of po\yer (the limb will be quite helpless), and irregularity (a gap may be felt between the broken fragments of bone) accompa ny this injury.
TREAT:\lENT.
l.-Lay the patient on his back, raise ,yell and FIG. 32.
support the head and shoulders, straighten and raise the limb. .
2.-Apply a splint along the back of the limb, reaching from the buttock to beyond the heel.
3·-Applya narrow bandage with its centre imme-
58
diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. To ensure firmn ess app ly a second bandage in a similar way, but commenced below and tied ab ove the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
S.-·Support the foot well off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 3 2 ).
6.-Apply an ice bag or a cold \\ater dr es sing over the fracture.
Fracture of the Leg (tibia and jibula).-One or both of the bones may be broken. When both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not ahyays noticeable. A fracture of the fibula three or four inches above its lower end is frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the 6I
fo ot. If only one splint is available place it on the outer side.
4.-Secure the splints by bandages (a) above, (b) below the fractur e, (c) immediately above the knee,

FIG. 33.
FIG 34.
(d) round both ankles, (e) -a broad bandage round both knees (Fig. 33)·
'When single-handed, or when the patient is a
60
D
woman, after extending the limb tie both feet together, dispens e with the inner splint, anj P1SS the banjages ro und both limbs (Fig. 34). ,Vhen no splint is ava ilable tying the legs, ank les, and knees together is of g r eat ser vice.
Crushed Foot (fracture of the tarslls, metatarsus and toes).-This accident is commonly caused by the passage of a heavy \\'ei!Sht over the foot, and may be recognised by p:tin, swellin6, ;]nJ loss of power.
TREADTE:\ r.
I. -Remove the boot (see page 19).
2.-Apply a wellpadded spli n t to the sole of the foot, reachi ng from the heel to the toes.
3· -Apply a bandage FIG. 35· crossed after the manner of the figure 8 (F ig . 35).
4·-Su pport the foot in a sliglltly raised position.
DISLOCATIONS.
A dislocation is the displacemen t of one or mor e o f th e bones at a joi nt.
The joints m ost fr equent ly dislocated are those of the shoulder, elbow, thumb, fingers, and lower jaw.

SIGNS AND SYMPTOMS OF DISLOCATION .
1 .- Pain of a severe sickening character at or near (he jomt.
2. - Loss of power in the limb.
3. - Numbness of the parts b elow seat of dislocation.
4.-Swelling about ar:d below joint.
s .- Fix ity of the jomt.-The. lllnb cannot be moved at the joint by either the patIent others.
6.- Deform ity of the limb. - The 11mb an unn:ltural position, and is mis -shapen at the Jomt.
TREATMENT .
No attempt should be made by .anyo.ne :l. doctor to reduce a dislocation . Pendmg hIS arnval :--
(a) TVhm tile (lccident occurs 011 t of doors -:- . . Su p port the limb in whatever p,osltl.on gl:,es most ease to the patient, beanng m mmu the nec essity of lessening the effects o f jolting during transport.
(b) TVhm the jatt'ent z's z'ndoors- .
I.-Remove the clothing from the 11mb.
2.--P lace the patient on a couch or bed.
3.-Rest the limb on pillO\.... s in the most comfortable position.
4.- A pply cold ( ice or cold water) '::ressings to the joint.
5.-,Vhen cold ceases to give comfort apply
warmth (flannels or towels wrung out of hot water).
6.-Treat shock (see page 135).
SPRAINS.
'Vhen, by a sudden wrench or twist, the ligaments and the parts around a joint are stretched and torn the joint is said to be sprained. "Going over 1/ the ankle is a common example.
SIGNS AND SYMPTOMS.
I.-Pain at the joint after a t\\'i st or wrench.
2.-Inability to use the joint.
3·-Swelling and discoloration.
TREAT J'vTENT OF SPRAINED ANKLE.
When out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing it on the front of the ankle, and carrying it round and round the ankle, where is to be firmly tied.
2.-vVet the bandage after applicaton; it is thereby tightened.
After readzing slle!ter-
I.-Remove the boot and stocking (see page I9).
2.-Place the limb in the most comfortable position; usually that is well raised.
3. -.\pply ice or cold water to the joint t1S long as they reliev e pam.
4. - When cold fails to giYe comfort, apply hot fom e n ta tions. .
",V nen other join ts are sprLlined, treLlt them as If dislocated.
When in doubt as to the na.ture of the injury, treat as a fracture.
TRAIL S AND RUPTURED
Wben, during severe exertion, muscles. or arc ove r-s tretched they are said to be strall1ed, 1t they are actually torn they are described as ruptured.
Al D Y:'IIPTO:'llS.
J . - A sudden sharp pain. .
2.-When the mu-cles of a limb are stra1l1ed they may swell and cram p.. . .
3.-Further exertion is difficult or .lmposs1ble; tor example, if the strain has 111 the back the patie nt may be unable to stand uprlght.
I. - Place the patient in the most comfortable position, and afford support to the injured part . .
2. - Apply hot water bottles or hot fom entatlo11s when the pain is very severe . .., .
: \ so-calleJ strain in the groin (hern1a) 1S an 1l1Jury of a totally different nature (.-,;ee page 114). D
64
65
QUESTIONS ON CHAPTER II.
The nume1'als £1'ld£cate tIle pages whe1'e the answers may be foul/d.
\Vhat is the skeleton, and what purposes are served by it? ,,' ," .. ' ", ".
How are the bones of the skull arranged?
\Yhat are the boundaries of the cranium?
Describe the bones of the face
Describe the lower jaw
What is the angle of the jaw? ,.,
\Yhat other names has the back-bone?
What is a yerte bra?,.
How many vertebrre are there in the spine?
\Yhat are the regions of the spine, and how many
Yerte brre are there in each? ..
How is the spine endowed with free movement?
What is a rib?
How many pairs of ribs are the] e ?
What is the breast-bone? ...
\Yha are the bones of the upper limbs? ."
What is the pelvis? ...
\ \'hat is the hip joint? ". .... .,.
\Yhat are the bones of the lower 11m bs ? , ..
What is a joint?
Describe a moveable joint ...
Describe the shoulder joint
Describe the ankle joint . ..
How are muscles classified
Describe voluntary muscles
Describe involuntary muscles
\\' hat is a fracture? ., .
\Yhat a re the causes of fracture?

\Yhere does a b one break when direct vi olence is the cause of fractur e?
Where does a bone break whc:n indirect violence is the cause of fractur e?
How maya frac ture be caused by muscular action?
In what two ways may fractur es be classified?
What is a simple fracture? .. ,
\Yhat is a compound fracture?
\ Yhat is a complicated fracture?
is a comminuted
the general signs and symptoms that may be present in a case of
at fractures afford the most complete example of the signs and symptoms?
In making up your mind whether a fracture had occurred or not, what points should you take into considera· tion beyond the signs and symptoms?
apparatus may be necessary for the treatment of fractures?
what ways may the triangular bandage be folded fur use?
many kinds of arm-slings are there, and what are they called?
at is the object of first aid treatment of fractures?
the general rul es fo r the treatment of fra ctures ...
may cause a frac tme of the upper part of the cranium?
66
PAGK
22 22 22 22,23 23 23 23 23 25
25 25 26 26 26
26 to 28 28 30 ')0 3 I 3 1 32 32 32 33 33 33 ... 33, 34 PAG!!
33
\Vhat
What is a green-stick fracture? \Yhat is an impacted fracture? 34 34 , .. 3-+, 35 34 343-+ 35 35 35
... ... 35. 36 \Vh
'.. ... ... ... . ..
35 'What
"..., 36 How may
? . .. .. . 36, 37 How may bandages be improvised? ... 37 Describe
37
38
In
37
. . ... ... ... .., 39,
49 What
... 40 \Vh
4I ]ive
41 How
IIow
bandages be applied? , .. 4 2
43
43 02
fracture?
State
fracture
splints be improyised
Esmarch's triangular bandage...
,
(Fig. 8)
How
40,
knot is to be tied, and what knot avoided?
should splints be applied? ". 41, 42
sho uld
,
\Vhat
What may cause a fracture of the base of the cranium? 43, 44
What are the signs of fracture of the upper part of the cranium?
What are the signs of fracture of the base of the cranium?
What is the treatment for fracture of the cranium? 44
What are the signs of fracture of the lower jaw? 44
H olV maya fractured spine be caused?
What is commonly regard ed as a broken back?
What are the symptoms of a fractured spine?
How may ribs be fractured?
How maya fracture of ribs be complicated? 47
State the signs and symptoms of a simple and of a complicated fracture of ribs -
What is a frequent cause of fractured collar-bone? ... 48
What are the signs and symptoms of fractured collarbone?
.. 48, 49
At what points may the bone of the arm be broken? ... S2
Are the general signs and symptoms of a fracture always present in a broken forearm? ... '" 54
State the cause of a common fracture of the radius 55
How would you recognise a fracture of the pelvis? 56
At what points may the thigh -bone be broken? ... S7
What are the signs and symptoms of fracture of the thigh-bone?
What are the causes of fracture of the knee-cap? ... 58, S9 What are the signs and symptoms of fracture of the kneecap?
Are the general signs and symptoms always present in a fracture of the leg?
What mistake may easily be made when the fibula i8 broken near its lower end?

When not sure whether the injury is a sprain
First Aid Students should practise improvising material, folding bandages, tying knots, making slings, and the treatment of the following injuries.
Improvising splints
Improvising bandages
Folding bandages
applying splint to lower limb
Fractures - Lower jaw, 44. Spine, 45, 46. Ribs (simple and complicated fractures), 46 to 48. Breastbone, 48. Collar-bone, 48 to 51. Both collarbones, 51. Arm, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm when the elbow is involved, 53. Forearm, 55. Crushed hand. 55. 56. Pelvis, 56. Thigh (man), 57, 58. Thigh (woman, or man when single -handed), 58. Kneecap, 59. 60. Leg (man), 60, 61. Leg (woman, or man when single-handed), 62. Crushed foot, 62, Dislocations-Out of doors and indoors
. 63. 64
68 PAGSI
... ... .., . .. ...
... 44
... ...
... 44
.. . .. .
45
. .. 45
45
... .. .
46
... ......
47
... ... ... ... ... . . . .
... ... ... ... ... ... 57
... ... ... ... ...
... ... ... ... .•. 60
60 What
... . . . .. . 62 State
signs
63 69 PAGB State the treatment of disl ocation... 63 What is a sprain? . . . . .. ... .... 64 What are the signs and symptoms of a spram? 64 State the of a sprained an kle ... ... 64 State the treatment of other sprains . .. .. . . .. 63 , 65
or [racl ure how would you treat it? 65 How may muscl.-s be strained or rup tured? 65 State the signs and symptoms of strains 65 State the treatment of strains 65
59
is a dislocation?
the
and symptoms of dislocation
...
Large arm sling Small arm sling Reef and granny knots ... 36, 37 37 37 39 .. . 39,40 40 42 Knot
for
..
Sprained ankle .. 64 Stwns a,nd ruptured muscles 65
CH APTE R III.
THE ORGANS OF CIRCULATION.
T HE organs conc erned in the circulati on of the blood are the Heart, the Arteries, the Veins, and the Capillaries.
The Heart is situated in the chest behind the breast- bone and rib cartilages, between the lungs a nd imm edi a tely above the diaphragm; it lies o bliq uely with a quarter of its bulk to the right and t he rem aining three-quarters to the left of the middle lin e of the body. Its beat may be felt just b elow an d to the inn er side of the left nipple. The heart has fo ur cavities, two on either side of a central partiti on. The two u pper cavities are named the right and left auricles, the two lower the right and left ventricles.
Arteri es are vessels which convey blood from the h ea rt. Veins carry blood to the heart. Capillaries co nn ec t the arteri es and veins.
In the general (systemic) circulation arterial blood is driven from the left ve ntri cl e of the heart int o the aorta (the main artery of the body). From t he aorta branch arteries are given off to all parts of th e body. These divide and sub-divide, and become so small as to assume microscopic dimensions, wh en they are termed capillaries.

L. Laryn x (voice box); T. Trachea (windpipe); R:L. Right Lung; L.L L ... ft Lung (the lungs are c1.lawn to expose the heart and hl ood vess els) ; . R.A . Rl ghl unc_Ie; L.A. Left Aur icle ' R. V . Right Vent n cle ; L L eFt \ l:ntricle; P.A. Pulmona ry Arle ry ; An. A orta ; S. \ .C . Supenor '"ena cava (t h c large vein ca rrying blood from th up :·e r part of the body to th e h earl) ; L V .C. I nfe rior vena cava (the vein ca rry ing hlood f rom the lowe r part of th e body t e heart). The four pul mona ry ve ins ca nnot be shown In th e d iagra m.
70
FI G 3" ·
In the capill a ri es an int erchange of gases and fluics ta kes place, where by th e nourishment and maintenan ce of th e tissues and orga ns of the body are provided for, and the blood becomes dark and impure.
Venous blood pass es from the capillaries to the veins, which convey it towards the heart, getting la rger and larger as they proceed by being joined by n eighb ouring veins until they finally, as two large vess els, reach the right auricle of the heart. The veins, especially in the limbs, are provid ed with valves at fre quent intervals, which prevent the backward fl ow of the blood.
The pulmonary system of blood vessels is con ce rn ed in carrying the blood through the lungs. Fro m the ri g ht auricle the blood passes to the right ventricl e, and is thence carried to the lungs, where it is p urified by contact with air, and becomes scarlet in colo ur j it is then conveyed to the left auricle of the heart and pass es into the left ventricle, thus co mpleting the circulation.
'The heart contracts in adults at an average rate of seven ty- two times a minute, but the rate varies, increasing as the position is changed from the lying to the sitting or to the standing position; hence the imp ortance of adjusting the patient's position in cases of hremorrhage. At every contraction of the left ven- r tri cl e blood is forced into the arteries, causing the pulse, which nuy be felt wherever the finger can I.e
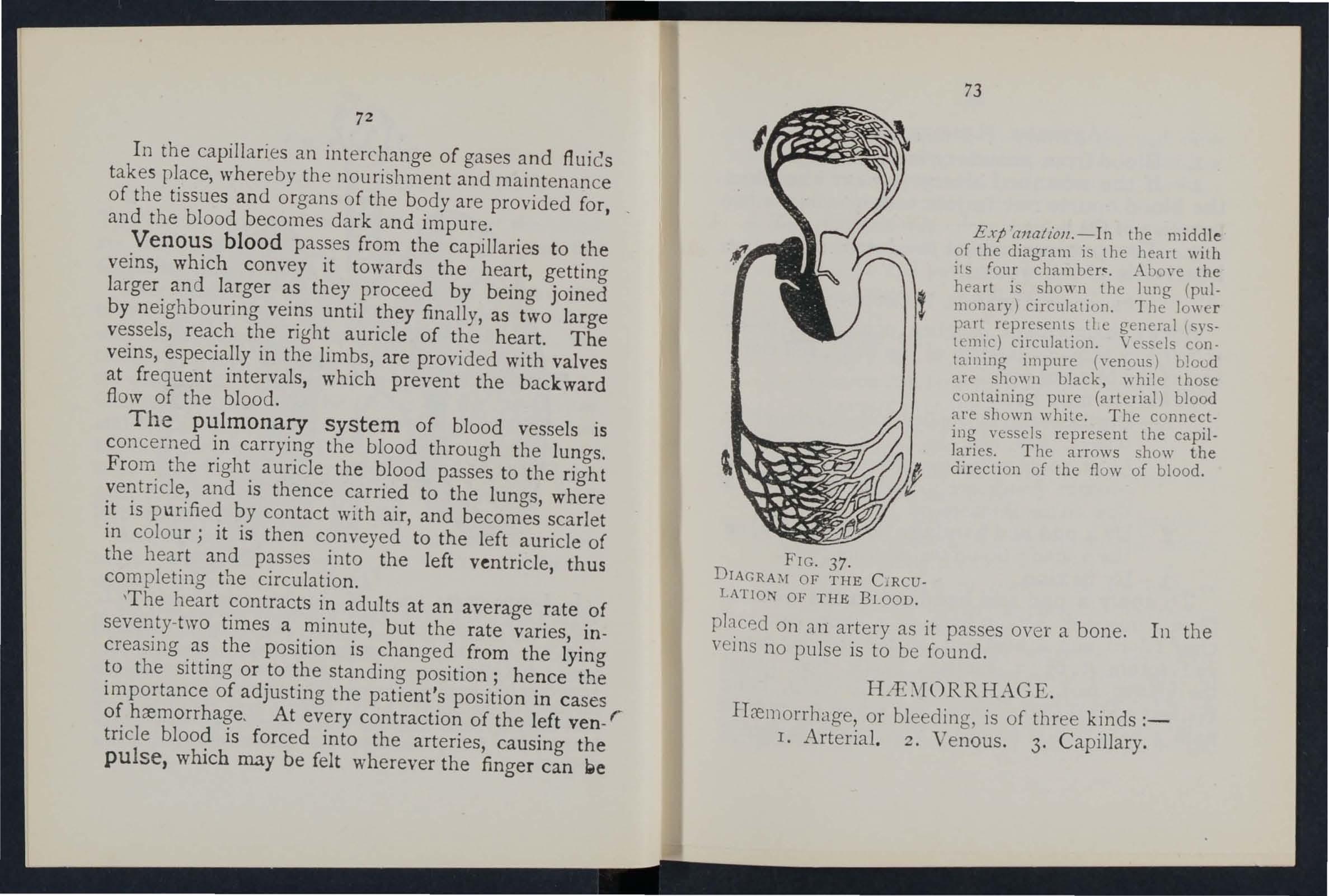
Exp 'anal/oll.- I n the middle of the diagram is the heart "ith its {our Abo\'e the heart is shown the lung (pulmonary) circulation. The lowe r part rep resents LLe general (systemic) circulation. Yessels containing impure (venous) Llood are shown black, while those containing pure (artelial) blood a r e shown while. The connecting vessels rep r esent the capillaries. The arrows how the di r ection of the flow of blood.
placed On a n a rt ery as it passes over a b on e. I n the vei ns no pulse is to be foun d.
R AGE
.
ITcemorrhage, or bleedi ng, is of th ree k.inds :r. Arteri al. 2 . Ven ous. 3. CapI ll ary.
72
73
FIG. 37. DIAGRAM OF THE C RCULATION OF THE BLOOD
ART ERIAL
. I. - Blood from an artery is scarlet. .
2. - If the wounded artery is near t.he skm the blood spurts out in jets correspondmg to the p ulsation of the heart. .
3. - The pressure point (see below ) 1S o n the heart ·side of the wound.
ARREST OF ARTERIAL HJEMORRHAGE .
Arterial hcemorrhage is, when practicable, to be arrested by pressure, posItio n of t he body , and elevation of the bleeding part .
Pressure may b e:- . .
I. - Digital-that is, applIed wIth the thumb or fi no-ers and may be ( a) on the wound j ( btat spot called pressure point. The pressure points are IndIcated by n umbered dots on the
2. -- By a pad a n d b 3n dag e (a ) on the wound; (b) on the pressure POInt.
3 - B y fl exion .
To 'apply a p a d an d bandage to t he woun d, place a piece of lint or linen or a clean . chief folded into a hard pad, on the bleedll1g POll1t, and secure it by a bandage tightly rou.nd the inju red part. To fold t he handkercmef, brIng the four corners to the centre, and rep ea t the until a hard pad is formed . T he smooth surtace IS

placed on the wound, and, to prevent the pad from unfolding, t he pucke red surfa:e may be stitched or fixed by a safety pi n . A hard substance, su 11 a stone, maybe enclosed in the cen tre of the pad. -
A Tourniquet may consist of a pad to be placed on the pressure point, a strap, cord, or bandage to encircle the lim b and pad, and a tz/: htmt"ng arrall/{e-
117Olt, such as a stic.k or other means of twisting the band to tighten it.
T o improvise and a p ply a tourniquet :-
I. - Apply a firm pad on the pressure point.
2.-Encircle the limb by a narro\\' bandage with its centre over the pad.
:;.-Tie the ends of the bandage in a llalf Knot on the opposite side to the pad .
4·-La y the t\\'isting stick on the half knot, and oYer it tie a reef knot.
5·-Twist the stick to tighten the banda re, thereby pressing the pad uron the artery, and arresting the flo\\" of blood .
6.-Lock the stick in position by the ends of tbe bandage already applied, or by anoth er bandage passed rou n d the stick and limb.
The pad of the tournique t mus t be accurately placed upon the press ure point so as completely to Compress tIle artery ; ot henrise arteria l blood" ill be allo wed to pass along tIle lirn b, and the veins, being compressed b-y the tourni q uet, \\ ill no t allow the
74
75
blood to return through thern to the and th e: result will be dangerous swelling and congestion. Should a suitable pad not be at hand, a knot may be made in the centre of the bandage, and when avaibble, a stone, cork, etc., enclosed in it to give it firmness and bulk. See that the bulging and not the side of the knot is next the skin.
An elastic bandage passed tightly round the limb, immediately above the seat of arterial hremor[hage, will arrest bleeding. The simplest prepared form of bandage is a strip of elastic webbing, twenty· five to thirty inches long and two inches wide, with a piece of tape sewn at each end. An elastic belt or brace will serve the s::tme purpose. Except when p,ut of a limb is torn off, it is not advisable to use an elastic cord or bandage if other a pp::trat us can be had, as it cuts off all circulation in the limb.
F lex ion consists of the application of a pad on the pressure point at the knee or elbo\\' joint, fl exing the limb to make pressure, and securing the limb in the flexed position by a bandage crossed like the figure 8.
GE:-\ERAL RULES FQR TREATMENT OF A 'WOUND ACCO;\IPANlED BY ARTERIAL HiEl\lORRHAGE.
1. Stop bleeding .
II. Prevent injurious germs from getting into the wound.

To attain these ends ;--
1. , ,the patient in a suitable position, bearIng 111 mllld that the blood escapes with less force \"hen the patient sits, and is still more checked \"hen he lies down.
2. Elevate t h e bl eed ing part , as thereby less blood finds its ,,'ay into it.
3- Expose th e w ound, removing whateye: clothing is necessary . (ee Rule 8, a.)
4. App ly d igital pressure.
(a) If the wound is small on the bleeding spot.
(b) If the wound is large on tile pressure point next to tile wound on the heart side. The nearest pressure point is chosen in order to avoid cutting off the circulation flom as much of the part as possible, but sometimes it is necessary to apply pressure still nearer to the heart.
,5. Remove fore ign bodies, such as broken gla s, blls of clothing, hair, etc., seen in the " 'ound; ( 0 not search for foreign bodies you cannot see.
6. Cover the wound with a cle an and fir m abs or be nt dressing. A hard dry pad of boracic gauze or lint is to be preferred, but absorbent cotton wool, lint, or gauze, or a clean piece of linen answer the purpose. Should any doubt be enter· tained as to the cleanliness of the dressino- a clean piece of unprinted paper, such as the inside of an
77
envelope, should be placed next tbe wound before .-applying the pad. (Compare pages 75 and 76 .)
7. Bandage tightly over the pad unless :-
(a ) Foreign bodies are suspected to be left unseen in the wound.
(/I) There is danger of causing injury to a fracture. In these cases a light dressing only should be applied.
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4, b ), but only in the following cases:-
(a) As a temporary measure while the wound is being exposed, examined and co\·ered.
(b) As a more permanent measure \\hen bleeding cannot be stopped by the pad and bandage on the wound, or when, in accordance with Rule 7, the tight bandage has not been applied.
9. Afford support to the injured part.
When part of a limb has been torn off or the wound is lacerated (for example by the claw of an animal or by machinery) hremorrhage frequently does not come on at once, but as there is a danger of severe hremorrhage later, means for its arrest should be applied to the lim b, but not tightened unl ess r.ecessary. Do not disturb a clot of blood formed o\'er a wound. No attempt should be mace to cleanse a wound exc ept \",ith sterilised v\'ater (that is previously boiled

and allowed to coon, and experience, especially in recent wars, has shown that those wounds which were provisionally tre:1ted with a dry dressing and subdressed by a surgeon with proper appliances did best.
Studenb practising arrest of arterial hremorrhage should feel the pulse to see when the current of blood in the artery has been stopped, and should then immediately relax the pressure made on the artery . In this way the importance of the accurate application of pressure will be realised, and the amount of force neccssJ.ry will be ascertained.
THE COURSE OF THE MAIN A RTf<:RTES, AND THE ARREST OF HJEMORRHA(;B:.
(The numbers of the pressure points refer to those on the Frontispiece.)
THE LARGE ARTERIES 'VlTHIN THE CHEST Al\D ABDOMEN.
The Aorta is the central or trunk artery of the body. Commencing at the left ventricle it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branches which carry the blood to either side of the heau and neck and to the upper limbs. The Aorta passes down on the left of the spine to just below the navel, where it divides into two great branches (the iliacs)
79
-which convey the blood to the organs in the pelvis and to the lower limbs.
·Wounds of these arteries are one cause of internal hremorrhage (see page 96).
ARTERIES OF THE HEAD AKD NECK.
The Carotid Arteries (right and left) leave the upper part of the chest and pass up on either side of the windpipe and, just below the level of the angle of the lower jaw, dIvide into the Internal and External Carotid Arteries. The Internal Carotid Artery ascends deeply in the neck, and enters the cramum to supply the brain wIth blood. The External Carotid Artery gives off a number of branches; to the front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the OccipItal; the artery itself is continued upwards in front of the ear, where it changes its name to the Temporal, and supplies the scalp in the neighbourhood of the temples . \.
When a Carotid Artery is wounded, as in the case of a cut throat, apply the thumb of one hand on the artery at pressure point I, pressing backwards against the backbone and taking care to avoid the windpipe. It may also be n ecessary to apply pressure with the other thumb above the wound for two reasons: (a) To arrest'the flow of blood from the main (jugular) vein in the neck, which runs
8I
alongside of the carotid artery and is usually wounded at the same time j (b) To check the flow of blood from the upper end of the carotid artery itself, \"hich is often considerable owing to communication between the branch es of this artery and those of its

fe llow. Digital pressure must be by relays of assistants if necessary, untIl the doctor arrives (Fig . :;8). . .
The Facial Artery crosses the lower Jaw In a slight hol1ow two fingers' breadth in front of the angle, and sends branches to the chin, lips, cheek, and
80
FIG. 39·
outside of the nose. Hcemorrhage from wo un ds of the face below the level of th e eye is to be arrested by :-
(a) Digital pressure on pressure point 2 ( Pig . 39), or
(b) Graspi ng the lips or cheek on both sid es of the wound by the finger inside and the thumb outside th e mouth or v/c ] ver f a.

FIG. 40.
FIG 41.
The Temporal Artery may be felt pulsating in front of the upp er part of the ear. Hrem orrhage from the regio n of the tern pIe may be arrested by pressure applied at pressure point 3 (Fig. 40).
The Occipital Artery suppli es branches to the
regio n of the scalp from behind the ear to the back of the head. Hcemorrhage from this rEgion may be arrested by digital pressure on pressure point 4, four fingers' breadth behind th e ear (Fig. 41). This point is difficult to find , and it is usually sufficient to apply pressure imm ediately below the \\'ound . from
the Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the bleedingpoint and securing it by a narrow bandage with its centre laid on the pad, the ends carried round the head in the directio n most co nvenient, and tied tightly over the pad (Fig. 42).
When a wound of the for ehead or scalp is associate d with a fracture, the best. plan is to apply a ring
FIG. 42.
pad arou nd the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fi ngers; pass the other end of the bandage through the ring thus formed and continue to pass it through and through until the whole of the bandage is used and a ring as shown in Fig . 43 is formed.
82
ARTERIES OF THE UPPER LDI BS.
The Subclavian Artery passes from a poin t behind the inner end of the collar-bone across the first rib to the armpit.

FIG. 43· Flc. 4..J.
To apply digital pressure :-
J .-Bare the neck and upper part of the chest.
2 -Place the patient's arm against the body so as to depress the shoulder, and cause him (0 incline his head towards the injured side.
3. - Take your stand opposite the shoulder.
4- -Using the left hand for the right artery, and v/ce versa, grasp the neck low down, placing the fingers behind the shoulder and the thumb immediately aboye the centre of the collar-bone jn the hollow between the muscles attached to the bon e (press ur e point 5).
5.-Press the thumb deeply dO\\'nw8.fds and back wards against the first rib, which is benea th the collar bone at this spot (Fig. 44).
T he Axi llary Artery , which is a contin uati on of the subclavian, keeps close to the shoulder joint, and can be felt pu lsating when the fingers are deeply pressed into the armpit. Di g ital pressure is difficult to apply to this artery. .
To apply a pad and bandage: - (.1 "-. .1':'" \.,,"; 1j1 "', a billiard ball ,.. in the arm- -;: .. ( .
2. mnow band- \ age on th e -:;- ,
pid ; cross the ba ndage on FiG. 45. the shoulder; pull the ends tight and tie them und er the opposite armpit, takin g care that the pad does not slip.
3· - Flex the for ea rm alld tie the limb ti ght ly to the trunk with a broad bandage, applied on a level with the elbow (F ig. 45 ) .
The Brach ial Artery is a continuation of the A xillary, and runs down the arm on the inner side of t he biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The inner seam of the coat sleeve above the elbo\\' roughly indicates its course.
Digital or instrumental pressure m:!.y be applied at or near pressure point 7.

FIG. 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back g7
of the a: 111. over the seam of the coot or the groove on the of the biceps muscle. Press the pulps (not the tIpS) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47) . A slight turn of the hand outwards as it grasps the arm will better ensure compression of the artery.
The Brachial artery may be compressed at the
49.
FIG. 48.
elbow (pressure point 8) by flexion. The pad may be a folded handkerchief with a small stone or a cork wrapped up in it, but when no pad is available the coat sleeve rolled or gathered up will serve instead (Fig. 4 8).
86
FIG.
Just below the elbow the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 and 10) are about one inch above the wrist and about half an inch from the outer and inner sides of the forearm, where the arteries may be felt pulsating. Branches of these arteries join to form the Palmar Arches in the hand. The arteries run along on either side of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure pointS.9 and 10, by the thumbs (Fig. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3·-Secure them by a tight band..lge.
To arrest hremorrhage from the palm of the hand:-
I.-Apply a firm pad, and the patient gras p it firmly.
2.-Sp read out a triangular bandage, turn up the base about four inches, lay the back of the - patient's h an d on the centre of the bandage, fold the point over the knuckles a nd wrist, pass the two ends round the "'fist, make the

89
patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the point (A) down to the knuckles and fasten with a pin at B (Fig. 50).
3·-Elevate the forearm and support it with a "St. J ohn " sling (see page 49).
Arterial hremorrhage from the fingers may be arrested by applying a small p8d on the wound, and securing it firmly with a strip of tape, linen or plaster.
ARTERIES OF THE LOWER LIMBS.
The Femoral Artery, a continuation of the iliac, FIG. 50. enters the thigh in the centre of the fold of the g-roin, where it may be felt pulsating immediately below the skin. The course of the artery may be indicated by a line drawn from the centre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the femoral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may b e applied to the Femoral artery at the groin (pressure point I r) as follows :-
I . -Lay the patient on his back.
88

2.-Kneel beside the patient.
3.-To find the groin, raise the foot high so as to fl ex the thi gh; the fold in the clothing at the to p of the thigh will indicate the groi n.
4.-Place the thumbs one on the other upon the pressure point, grasping the thigh v,ith the hands (Fig 5 I).
5.-Press firmly against the brim of the pelvis.
As there is immediate danger of death it is important not to waste time in removing the trousers.
\V hell the Femoral artery is wounded in the upper lhird of its course, pressure must be maintained at the groin. No really SJti 'factory tourniquet has been FIG. 51. devised for compression ?t this point, and relays of assistants sho uld be employed to keep up the pressure until the doctor arrives; each fr esh assistant places his thumbs over those of his predecessor, who slips his away from beneath, and thus gushes of blood are prevented during the change. ..
Application of a tourniquet to the Femoral artery (pressure point J 2) :-
\Vh en practising compression of this artery, It is a
90
91
FIG. 52
good plan to draw a chalk line from the centre of the groin to the inner side of the back of. the place the pad of the tourniquet on this lIne as hIgh up as the bandage can be. applied.. The pad should be the size of a la'vvn tenl1ls ball (FIg. 52). .... Pressure may be applied to the artery by fl exion at the knee (pressure POll1t 13); the pad

FIG. 53.
should be the size of a lawn tennis ball, or if no pad is available the trouser leg may be rolled or gathered up to serve instead. It is not to take off the clothing (Fig . 53\ . . .
_ Just below and behind knee Jomt the artery divides into the Antenor (front) and Postenor (back) Tibial arteries.
The Posterior Tibial Artery passes down the 93
back of the leg to the inner side of the ankle. It is at fi{st deeply placed between the muscles of the calf, but it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the inner side of the ankle. It enters the sole as the Plantar Arteries, which run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery, on leaving the Popliteal, at once passes forward between the leg bones, and, deeply placed amongst the muscles, runs down the leg to the centre of the front of the ankle. This artery is continued as the Dorsal Artery of the Foot, which, passing forward over the tarsus, dips down to the sole between the first and second metatarsal bones. Here it forms with the Plantar arteries wha.t is known as the Plantar Arch. At the ankle (pressure points 14 and 15) pressure may be applied by the fingers or by pads and bandages.
HIE\lORRHAGE.
I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3· -- It issues from the side of the wound further from the heart.
4·- In the case of a wound of a varicose vein it flo\\'s also from the side of the wound near e r to the heart, especially if the pati e nt is kept standinJ.
92
Varicose Veins. -The veins of the leg are specJally apt to become varicose. A varicose vein is dilated, winding, and with bead-like (varicose ). projections along its course. A vein becomes vancos e from several causes, such as long standing or tight garters. The first effect is to throw extra work upon the valves, and the bead-like projections are caused by the blood accumulating in the pockets behind th e valves In time the vell1 becomes so dilated that th e valves can no longer span it.
GI£ TERAL RULES FOR TREATMENT OF A WOUND
ACCOMPANI ED BY VENOUS HIEMORRHAGE .
1.- Place the patient in a suitable position, bearing in mind that the blood esca pes \\ ith less force when the patient and is still more checked as he lies down.
2.-Elevate the part, as th ereby less blood finds its way into it.
3.-Expose the wound, removing whatever clothing is n ecessary.
4. - Remove any constrictions, such as the collar or garters, from the heart side of the wou nd.
5.-A pply digital pressure on wound until you can apply a pad and tIght bandage. • If that does not stop the bleeding, make pressur e near th e \\ ounJ on the side away from the heart. In the case of a wound of a varicose vein it may also be nec essa ry to

arp1y a pad and bandage to the vein imm ed iately above the wound, especially if the limb cannot be ll1aintained in an elevated position.
6.--Treat the wound as dir ec ted by Rul es 5, 6 al1Ll 7, stated on pages 77 and 78.
7. ·-Afford support to the injured part.
C.\PILLARY H IE;\ IORRHAGE.
1.-The blood is red.
2. -- It flows briskly in a continuous stream, or may merely ooze from the wound.
3.-It wells up from all parts of the wound.
/\. slight amount of pressure will suffice to arrest capillary
IN TERNAL H.,l£:\lORRHAGE.
Wounds of the blood vessels within the trunk ('ause hcemo rrha ge into the cavity of the chest or of the abdomen .
SIGXS AXD OF IN TERN AL I-flE:\JORRHAGE.
I.-Rapid loss of strength, giddiness and faintness, especially when the upright position is assumed.
2.- Pallor of th e face and lips.
3·-Breathing hurri e d and laboured, and accompanied by yawning and sighing.
4·-Tl:e pulse fails, and may altogether disappear at the WrlSt.
94
95

5.-The patient throws his arms about) tu gs at tbe clothing round the neck, and calls for air.
6.-Finally the patient may become totally uncon· scious.
TREATMENT.
I.-Keep the patient in a recumbent position.
2.-Undo all tight clothing about the n eck .
3.-Provide for free circulation of air; fan the p:ltient. .
4.-Sprinkle cold water on the face j hold smelltng salts to the nostrils; avoid other forms of stimulants, at all events until the hremorrhage has been controlled.
s.-Give ice to suck or cold water to drink if the seat of the hremorrhage is known, apply an Ice bag over the region.
6.-Should the patient be reduced to a state of collapse, raise the feet and bandage the limbs firmly from the toes to the hips and from the fingers to the shoulders.
HJEMORRHAGE FROTh! THE NOSE (NOSTRILS).
I.-Place the patient in a sitting position in a current of air before an open window, witb the head thrown slightly back and the hands raised above the head .
2. - Undo all tight clothing around the neck and chest.
3.-Apply cold (ice, a cold sponge or Luncl-- of 97
over the nose and also the spine at the le\'el of the collar; place the feet in hot \\ater.
4.-Cause the patient to keep tbe mouth open, and so avoid breathing through the nose.
Blood issuing from the mouth may come from the tongue, the gums, the socket of a tooth after extraction, tl-.e throat, the lungs, or the st omach .
HJEMORRHAGE FRO]\[ THE TONGUE, THE THE SOCKET OF A TOOTH, OR THE THR OAT
y.-Give ice to suck or cold \Yater to hold in the mouth. If this is not successful give \Yater as hot as can be borne to hold ill the mouth.
2.-If necessary make pressure on the carotid arteries.
3.-If bleeding from the front part of the tongue is excessive compress the part by a piece of clean lint held between the finger and thumb.
4·-If the bleeding is from the socket of a tooth 9 plug the socket with a piece of clean lint or cotton \\'001; over this place a small cork or other substance of suitable size, and instruct the patient to bite on it,
HJE\lORRHAGE FRO?l! THE LUNGS.
Blood from the lungs is coughed up and is scarlet f rothy in appearance. .
Treat as for Internal Hremorrhage (see page 95)' E
H JEM ORRH AGR FR OM THE ST0MACH.
Blood from the st omac h is vomited; it is of a dark and has the appea ra nce of coffee grounds i it may be mixed with food.
Treat as for Inte rn al H re morrhage (see page 95 ), except that not h ing is to be gi ven by the mou th.
Blood issuing from the Ear Channel, which generally in d Icates a fracture of the base of th e <:raniu m, must be wiped a way as it issues; no attempt is to be made to plu g the ear.

QUEST I ONS ON CHAPTER III.
The 111tllltrais z'ndicate tlte p 7ges where tile ans'wers may be fouila.
\Yhat organs are concerned in the circulation of the
blood?
Trace the circulation of the blood tbrough the body and lungs 70 to 7z
How many times a minute does the hEart contract on the average? 71-
What is the effect of the patient's position on the rate at which the heart contracts?
many kinds of hcemorrhage are there?
How would you know a case of arterial h::emorrhage? ...
In what way should arterial hremorrhage be controlleu?
What is meant by " pressure puiIJt " ?
Why is accuracy necessary in placing the pad of a tourniq uet ? 75
When mayan elastic bandage be used instead of a tourniquet?
76 What is flexion?
76
State the general rules for treatment of a wound accom, panied by arterial hcemorrhage '" 77, 78
If part of a lim i:> had been torn off, out the re was not much bleeding, how would you act? 78
Should blood clots be disturbed ?.. ... . 78
I it wise for an unskilled person to attempt to clean5e a wound?
78, 79
What is the aorta ? ... Itt 79
99
PAGS
... 70 Descri
... 70
be the heart
72 What is the pulse? ... 72 How
73
74
74 itow
74
74
may pressure be applied?
\\' hat is a tourniquet? 7:
..
. ... ...
E2
Describe the arteries of the head and neck 80
Why is it sometimes necessary to compress the carotid artery both below and above the wound? . .. 80, 81
What is a ring pad, and what is its use? ... 84
Describe the arteries of the upper limbs ... 84 to 89
Describe the arteries of the luwer limbs ... 89 to 93
How would you know a case of venous hzemorrhage? 93
What is a varicose vein ?
How maya vein becc me varicose? . . . ... ... 9-+
State the general rules for treatment of a wound accompanied by venous hzem orrhage? ... ... . .. 94, 95
How would you know a case of capillary hzemorrhage? 95
How would you stop capillary hcem orrhage ? 95
What is internal hzem orrhage? ... ... ... '" 95
What would lead you to suspect internal hzemorrhage? 95, 96
State the treatment for internal hremorrhage? ... 96
How would you arrest hzel110rrhage from the nose? . .. 96, 97
Where may blood issuing from the mouth come from ?.. 97
How would you treat bleeding fr0111 the gums or throat? 97
What else would you do if the tongue were bleeding? ... 97
And if the bleedin a were from the socket of the tooth? 97
How would you distingui sh between bleeding fr om the lungs and from the stomach? ... ... ... 97
And what would be the difference in the treatment? 97
Of what is bleeding from the ear generally a s.ign? 98
The Student should practise placmg supposed patients in a proper position for the arrest of hzemorrhage (se e pages 72, 77 and 94), folding firm pads (74; and 75), tying hard knots in bandages to form a tourniquet (76), and the application of pressure at all points shown in the frontispiece, at vanous pomts on the forehead and scalp, and on the palm of the hand. Pressure should be digital, by pad and bandage, or flexion, as directed in the text.

101
Pressure points - Carotid artery, 80. Facial, 82 .
Temporal, 82. Occipital , 83. Subclavian, 84
Axillary, 85. Brachial (by pad and bandage, pressure being made against the humerus and by flexion at the elbow), 86. Radial and Ulnar, 87. Femoral at the groin, 90. Femoral in the thigh, 92 • Popliteal, 92. Anterial and posterior Tibia arteries, 93.
Hzemorrhage from the forehead or scalp ...
Hzemorrhage from the palm of the hand ..
Venous hzemorrhage from a varicose or other vein
100 PAGK
84 87
089 .. . 93, 94 •
Clf APTER IV.
BRUISES.
A blow anywhere on the surface of the b?dy ca use extensive hGemorrhage beneath the skIn, wIthout breaking it-a" bbck eye" is a? instance. ,!,he injury is accompanied by discoloration and swellIng.
TREATMENT.
Apply ice or cold water dressings. A piece of lint so ::tked in extract of witch hazel may be placed on the a.ffected part.
BURNS AND SCALDS.
A burn is -
(a) By dry heat, such as fire or a pi ece hot ir?n.
(b) By a rail, wire or dynamo charged with a high press ure electric .. ,
(c) By a corrosive aCid, as 011 of vltno,l.
(d) By a alkalI, such as caustic soda, am monia , or quicklIme.
(e) By friction, caused, for example, by contact with a revolving wheel. (Brus h burn,) ..
A scald is caused by moist heat, such as bOlllllg wate r hot oil or tar.
effect may be a mere reddening of the .skin ; i:>li sters may be formed j or even the deeper tissues
103
of the body may be charred and blackened. Th e ciothing may adhere to the burnt skin, and its remm'ai is impossible without further detnment to the injured part. The great danger is Shock.
TR EATMENT
I.-Carefully remove the clothing over the injured part. If stuck to the skin, the adh erent clothing must be cut around with scissors, soaked with oil, and left to come away subsequently.
2.-Do not break blisters.
3.-Imm ediately cover up the part. Soak or smear pieces of lmt or lInen with oil, or vaselm e, lanolIne, or cold cream; a small quantity of bora CIC powder added to these \\'111 be of benefit. The inside of a raw potato scraped out and spread on lint makes a soothing applIcation. 'When the injured sur face is extensive do not cove r it with one large sheet of lmt, but with strips about the breadth of the hand; this is advisable as they fit better on the part, and during subsequent dressmgs one strip can be remo\'ed at a time, and a fresh dressing applied before the adjacent strip is taken off. The shock to the system IS thereby less than if the whole of the burnt surface were laid bare to the air by the removal of all the dressings . at one time. 'Vh e n covered by th e oily dressing envelop the part in cotton wool or a piece of flannel and apply a bandage.
102
\Yhen the face is burnt, cut a mask out of lint or linen, leaving holes for the eyes, nose and mouth. Dip this in oil or smear it with vaseline and apply it to the face and cover it with cotton wool leavin a openings to correspond \",ith the holes' in mask.
'Vhen possible place the injured part in water at the temperature of the body (98 degrees) until suitable dres.sings can be prepared. A dessert spoonful of soda added to a pint of the warm \vat er \\'111 make a soothing lotion.
As it is important not to leave the part exposed to the air.' it is the duty of the bysta nders to prepare the dressmgs while the clothing is being removed.
. 4.-Treat Shock.- This is parti cu la rly necessary 111 the case or every burn or scald of any considerable extent (see page 135). Be very apprehensive of dan ae r in the case of even slight burns of the ne ck. 0 the burn is caused by a corrosive aCid,... bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bicarb om.te of soda ), magn es ia, or slaked lime in warm \\ ater b efore applying the dressin g s.
6.----:-lf the burn is caused by a corrosi v e alkalt, bathe the part with a weak acid lotion such le mon juice or vinegar diluted with an equai quantlLy of \yat er. Ca1tlz"u1Z.-Before u . ing \\al er brush off any lime that remains on the part.

7. -When a woman's dress catches fire-
(a) Lay the woman fht on the floor at once, so that .the flames are uppermost; that is to say, If the front of the dress is on fire lay her on her back, and if the back of the d;ess is burning, place her face dO\ynwar d s.
1 he reason for this is that flames ascend 50 that if the upright position is assumed 'the flames will quickly reach and burn' the body, neck, and bce; or if the wom a n th: flames undermost, they will, If unextmgUlshecl, pass over and burn the lim bs, and set fire to the rest of the dress.
(b) As soon as the woman is laid flat smother the flames with anything at hand,' such as a rug, coat, blanket, or table cover; if made wet so much the better.
(c) A woman rendering assistance should hold a rug or blanket in front of herself when approaching the flames.
(d) I.f a woman's dress catches fire when nobody IS by, she should lie flat, flames uppermost smother the flames with anything handy and call fO.r assistance, or crawl to the rIng; on no account should she rush mto the open air.
Th: . use of fire guards would prevent m&nJ calamltles.
104
II roS
BITES
OF SNAKES AND RABID ANIi\IALS, AND \VOUNDS BY POISONED ·WEAPONS.
Hydrophobia is caused by tbe bite of an animal, such as a dog, cat, fox, \\'olf, or deer suf!ering from rabies. The special poisons introduced Il1to wounds caused by venomous snakes and poisoned \\ eCJ pons cause immediate danger to life.
TREATME T.
I.-Immediatelyplace a constriction between the wound and the heart so as to prevent the venous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircled on the side of the wound nearest to the heart, witb the finger and thumb, and as as possible a. ligature (a string, piece of tape, or stnp of handkerchief) should be placed tightly round the root of the finger. Compressio,n with finger and thumb not be rel axed untIl the hgature has been applIed. Additional ligatures may, with advantage, be applied at intervals up the limb.
2. - Encourage bleeding for a time:-
( a) By bathing the wound with warm water.
(b) By keeping the injured limb low; the upper limb should be allowed to hang down, and in the case of the lower limb the patient should be seated with the foat on the ground.

3.-Cauterise the wound, if it is quite impossible to obtain the services of a doctor This is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or If these are not at hand, with ared hot wire or a fusee.
The usual solid ca ustic is insufficient, as it does not reach the bottom of the wound, where the poison is.
To ensure the caustIc reaching the bottom of the v-ound, It should be applied on a piece of wood, such as a match cut to a point. \Vhen the caustic has been thoroughly applied , but not till then, the ligatures may be removed.
4.-Cover the wound, after a while, with a clean dressing.
5· - Afford support to the injured part.
6.- Treat shock if it occurs (see page 135)
7·-In the case of a bite by a venomous rub in powdered permanganate of potash and inject under the skin in the neighbourhood of the wound a solution of permanga.nate of potash.
STINGS OF PLANTS AND ANIMALS.
These give rise to serious inconvenience, and In some cases grave symptoms deveiop.
TREAD1ENT.
I.-Extract the sting if left in.
2. - Mop the part freely with dilute ammonia
Ic6
or spirits. A paste of bicarbonate of soda and sal volatile is an efficient application. A solution of washing soda or potash or the application of the blue bag will relieve pain.
3.-Treat collapse if it occurs (see page 135)·
FROST BITE.
During exposure to severe cold, parts of the body, usually the feet, fingers, nose, or ears, lose sensation and become first \\axy ,,\-hite and afterwards congested and of a purple appearance. As sensation is lost in the part, it is often only by the remarks of bystanders that the frost-bitten person is made aware of his condition.
TREATMENT.
I.-Do not bring the patient into a warm room until, by friction of the hand or by rubbing with soft snow, sensation and circulation in the affected parts are restored. Neglect of this precaution may lead to death of the ti:::sues of the frost-bitten part.
2. - When circulation is restored, keep the patient in a room at a temperature of 60 degrees.
NEEDLE EMBEDDED UNDER THE SKIN
-When a needle breaks off after penetrating the skin and disappears, take the patient to a doctor at once. If the wound is near a joint, keep the limb at rest on a splint.

10)
FISH-HOOK E.\rIBEDDED IN THE S1:.IN.
Do not attempt to withdraw the fish -hook by the way it went in, but cut off the dressing of the hook, so that only the metal is left, and then force the point onwards through the skin until the hook can be pulled out.
INJURIES TO JOINTS.
'Vhen a join t is in jureJ by a bullet, stab, or other canse-
I.-Wrap the part in cotton wool.
2.-Afford rest and support to the injured limb; if the limb, in a fl exe d position by a sli ng ; If the lower limb, in a stui6ht position by a splint.
FOREIGN BODY I I THE EYE.
I. - Prevent the patient rubbing the eye, tying down a child's hands if necessary.
2. - Pull down the lower eyelid, ",hen, if the foreign body is seen, it can readily be remm- ed \\"ith 3. camel 's haif brush, or with the corner of c.l. handkerchief twirled up and wett ed .
3. - When the foreign body is beneath the upper lift the lid for\Vard, push up the lower lid beneath it and let go . The hair of the lower lid the inner surface of the upper one, and may dIslodge the body. Should th e lirst attempt be unsuccessful, repeat it several times if necessary. If
108
the foreign body is not dislodged cali the services of a doctor as soon as possible . W hen, however, skilled help cannot be had, proceed as follows :-
(a) Seat the patient so as to face the light, and stand behind him, steadying his head against your chest.
(b) Place a small rod, such as a match or bodkin, on the upper eyelid, half-an-inch above the edge, pressing it backwards as far as p ossible .
(c) Pull the upper eye-lashes up\\ards over the rod, and thereby eyert the eyelid .
(d) Remove the foreign body.
4.-When a piece of steel is embedded in the eyeball drop a little olive or castor oil o n the eyeball after pulling down tIl e lo,yer eyelid, close the lids, apply a soft pad of cotton \\001 and !:ecure it by a bandage tied sufficiently firmly to keep the eyeball steady; tllke the patient to a ecclor.
s.-When quick-lime is in the eye brush away as much of it as possihle ; bathe the eye \\ ilh vinegar and warm water, and treat as for a piece of steel embedded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
As a rule make no attempt to treat a patient viith a foreign body in the ear if the services of a doctor can possibly be had; any attempts to r emO\'e the forei ,?n body may lead to fatal consequences . If a child

cannot be ind uced to keep the fingers from the ear> tie his hands down or cover up the ear. If an insect is in the ear-passage, fill the ear '\'yith olive oil, when the insect will float and may be removed. Never syringe or probe the ear.
FOREIGN BODY IN THE NOSE.
Induce sneezing by pepper or snuff. Cause the patient to blow his nose violently after closing the una.ffected nostril. There is no immediate danger from a foreign body in the nose.
THE ABDO)'1EN.
The abdomen is bounded above by the diaphrao-m ; below by the pelvis; behind by the lumbar vertebrGej in front and at the sides by muscular walls. (Fig. 54.)
THE ORGANS OF THE ABDOMEN.
The Stomach lies immediately below the" pit of the stomach " just below the breast-bone .
The Liver lies in the upper part of the abdomen p where it is mostly covered by the right lower ribs.
The Spleen lies beneath the ribs at the up pe r part of the left side of the abdomen.
1;'he Intestines occupy the greater part of the cavlty of the abdomen.
The Kidneys lie at the back, in the region of the loin.
The Bladder lies in the pelvis.
ITO
III
FIG . 54·
'VOUND 1:-1 THE WALL OF THE ABDOMEN
Wizen the z'ntestines or otlter organs protrude through the wou n d, whether vertical or transverse, bend the knees, raise the shoulders, and apply lint, a towel, or cotton wool wrapped in soft linen, and keep the

II3
patient warm until the doctor arrives. 'When there is no protrusion of organs, if the wound z's vcortical, lay the patient fi .lt on the back with the lower limbs straJgh t; if tlze wound z's transverse, bend the knees and raise the shoulders .
INJURIES TO THE ORGANS \V1TH1N THE ABDOMEN A; D PELVIS.
I nju r ies of the Stomach are attended by extreme collapse and sometimes by vomiting of dark blood like coffee-grounds. For treatment see " Hremorrhage from the Stomach" (page 98).
Inj uries of the
Liver, Spleen and Intestines
may be caused by a blow, a stab or a buliet; the liver or spleen may be injured by a fracture of the lower ribs. The Signs and Symptoms are those of internal hremorrhage accompanied by pain and swelling at the seat of injury, and the treatment is as for that condition (see page 95).
The K idneys may be injured by a fracture of the eleventh or twelfth ribs, also by a crush, blO\v , stab or bullet. Blood may escape with the urine, and there may be pain and swelling over the injured kidney.
'I
T he Bladder may be injured by a fracture of the pelvis. The signs and symptoms are either inability to pass water, or if a little is passed it is tinged with blood.
TREATMENT OF INJURY TO THE OR BLADDER.
Keep the patient quiet until the doctor arrIves.
2.-Apply hot foment3.tions over the pain'ful or injured part.
Rupture (hernia) consists of a protrusion of an internal organ, usually the bowel, through the DlUSwall of the abdomen, most fr equently at the gr?m. a sudden swelling accompanied by pam and SIckness take place in that region
I.-Send for a doctor instantly.
2.-Lay the patient down with the buttocks raised.
3.-Apply ice or cold water dressings to the affected part.

QUESTIONS ON CHAPTER IV.
II4
lIS
The numerals indicate the pages where tlu answers may be found. PAG8 'Yhat is a bruise ? 102 Ilow would you treat a bruise? 102 How maya burn be caused? 102 How is a scald caused? 102 \Vhat is the great danger of a burn or scald? 103 State the general treatment for burns and scalds 103, 104 How would you treat a burn caused by a corrosive acid? 104 How would you treat a burn caused by a corrosive alkali? 104 vVhat steps should be taken when a woman's dress catches fire? lOS State the general rules for treatment of wounds caused by poisonous bites or weapons 106, 107 What special treatment is required for the bite of a venomous snake? 107 How would you treat a sting? ... 107, 108 State the signs, symptoms and treatment of frost-bite ... 108 \VonJd you attempt to remove a needle em bedded under the skin? " . ... 108 How would you extract a fish hook em bedded in the skin? 109 State the treatment for injuries to joints ... 109 State the general rules for removing a foreign body from the eye... ... ... 10 9, IIO \Vhat would you do if a piece of steel were em bedded in the eyeball? 110 And when quick-lime is in the eye? 110 How would you try to rem ,)ve an insect from the ear passage? ... I II
Would you try to remove any other form of foreign body from the ear passage? ... .., ... '" 1 10, III
How would you rem ove a foreign body from the nose? I I I
State the boundaries of the al)domen and its contents? III
State the treatment for wounds of the abdomen 112, 113
How may injuries to the liver, spleen and intestines be caused? ... ...... .•. ... .- 113
What is the difference between treatment of injuries to the stomach and of injuries to the liver, spleen and intestines? ... ... ... ... 113
State the treatment of injuries to the kidneys or bladder 114
State the treatment of hernia .•. .., .•. .., 114

CHAPTER V.
THE NERVOUS SYSTEM.
Two systems of nerves, the Cerebro-spinal and the Sympathetic, regulate the movements and functions of the body.
The Cerebro-spinal System is made up of the Brain, the Spinal Cord and Nerves, and through its agency sensations are received and the will causes the aclion of the voluntary muscles. For example, when a part is injured a sensation of pain is conveyed to the brain by the nerve, thus affording an indicati o n of the seat of injury, or a warning of a possible danger of further damage. On attention being directed t.o the injury, an attempt is instantly made to ease the pain or to move the injured part fr om danAer.
Th e Brain is situated within the cranium, and is divided in the middle line, s that, with th e exceptio n of some connecting bands, the right and left sides are
Th e Spinal Cord is the long cord of nerv o us mDtler lying \\ilhin the spinal canal (see V e rtebral Column) page 23) . It leaves the brain throu g h an opening in the base of the cranium and extends to the upper lumbar vertebrre.
II6 PAC.
117

IIS
The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissues of the body. 'When a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nervous chain on each side of the front of the spinal column along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary muscles, and thereby regulate the "ital functions. This system is not under the control of the will, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air reaches the lungs by way of the nostrils (or mouth), the throat, the wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind -pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but nr'lt solids or fluids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they may en ter the wind-pipe and cause asphyxia. The wind-ripe extends to two inches below the top of the breast-bone, 'vvhere it divides into the liight and left bronchial tube_ Each bronchial tube enters a lung and divides into small and still smaller tubes, until
LI 9
rIG. 55- THE LUNGS AND BRONCHIAL TUBES.
A . Tr::tchea, or Wind-pipe. B. Left Bronchus. C. Ri gh t Bronchus. D. Smaller Bronchial Tubes.
the ultimate recesses of the lung-the air cells or air spaces-are reached.
The Lungs, Right and occupy th e g reater part of the chest; they lie immediately \yithin the ribs, and practically wherever a rib is felt, whether front, back or sides, there is lung beneath . Each lung is enveloped in a fine membrane (the pleura) which allows it to move within the chest during breathing without friction.
Respiration, or breathing, consists of two acts, lnspiration, an expansion of the chest, during which air is drawn into the lungs, and Expiration, a contraction of the chest, during which air leaves the lungs. A pause follO\"s the act of expiration. In health fifteen to eighteen breaths are tak en per minute, and at each inspiration about 20 to 30 cubic inches of air enter the lun gs, and a similar quantity is expelled at each expiration.
The expansion and contract ion of the chest are effected partly by the muscles of res piration attached to the ribs, but chiefly by the Diaphragm, th e la rge arched muscular partition which separates th e chest from the abdomen. In inspiration, \vhich is chiefly a muscular act, the ribs are rais d, and tile arch of the diaphragm falls and b eco mes flattened, thus increasing the capacity of the chest and causing the air to enter.... In expiration, an act performed almost without effort, the ribs fall and the arch of the

diaphragm rises; this lessens the capacity of the chest and forces air out. The mechanism of respiration is somewhat like that of ordinary household bellows but without a valve; the ribs may be to the boards of the bellows, wh!le the diaphragm corresponds to the leather, the air passages being equivalent to the nozzle.
As the blood depends upon the air for its purification and the oxygen necessary to maintain life, interference with breathing very soon may produce a dangerous state called asphyxia, examples. of which are afforded by drowning, suffocation, chokmg, etc.
ARTIFICIAL RESPIRATION.
PROFESSOR SCHAFER'S METHOD.
I.-Make no attempt to loosen or remove clothing.
2.-Lay the p-atient in a prone position (t'.e., back upwards) with his head turned to one side, so as to keep his nose and mouth away from the ground. No pad is to be placed under the patient, nor need the tonaue be drawn out, as it will fall naturally.
3.-Kncel at one side facing the patient's head, . and place the palms of your hands on .his loins, one at each side, the thumbs nearly touchmg one another in the small of the back, and the fingers extending over the lowest ribs. Leaning your body forw ard, let its weight press straight downwards upon the
120
121

loins and part of the back, thus compressing the abdomen the ground and driving a ir out of the chest. ThIs produces expiration (Fig 56). Draw back
FIG. 57. INSPIRATION. l 23
your body somewhat more rapidly and relax the pressure, but do not remove your hands; this produces inspiration (Fig. 57)·
4.-Alternate these movements, by a rhythmi c s\\'aying back\\'ards and forwards of your body, twelve to fifteen tim es a minute, persevering untii respiration IS restored, or a doctor pronounces life to be extinct.
DR. SILVESTER'S METHOD.
I. Adjust the patient's position. -\Vithout 'nsting a moment place the patient on his back on a flat surface, inclined if possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as fa.r as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women. Raise and support the shoulders on 3. small, firm cushion or folded article of dress placed under the shoulder-blades .
2. Maintain a free entrance of air into the windpipe. -Clea ns e the lips and nostrils; open and wipe the mouth; an assistant must draw forward tbe patient's tongue as far as possible, and keep it in that position.
3. - Imitate the movements of breathing. Induce Illspiratt'on.-Kneel at a convenient distance behind the patient's head, and, grasping his for earm s just below the elbow, draw the anns
122
FIG. 58. INSPIRATION.
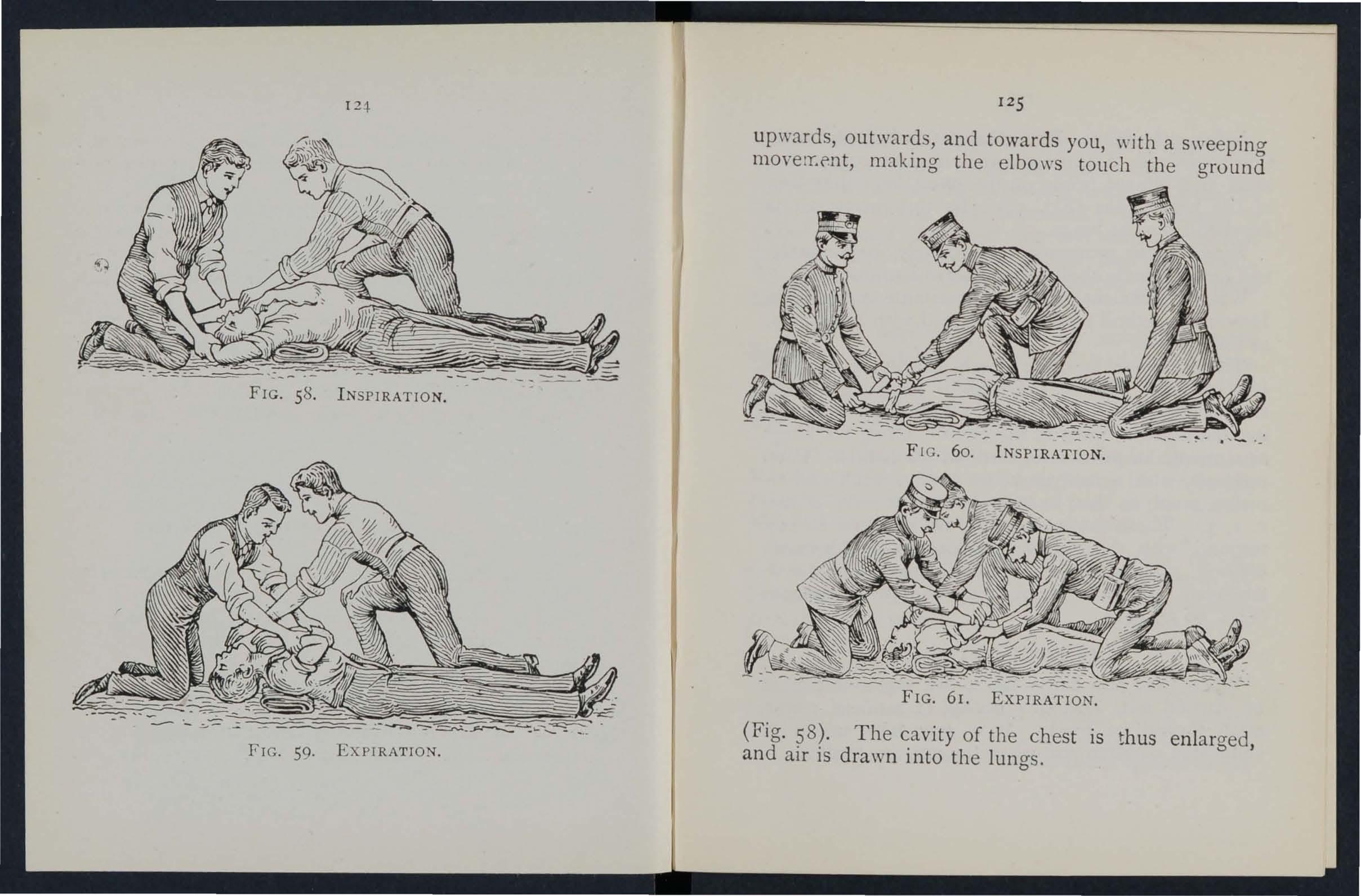
FIG. 59. EXPIRATION.
upwards, outwards, and towards you, with a swee ping mOVe lY.f'nt, mJ.king the elbows touch the ground
FI G. 60. INSPIRATION.
FIG. 61. EXPIRATION.
(Fig. 58). The cavity of the chest is thus enlarged, and air is drawn into the lungs.
12 :1-
125
Induce expz raHon.-Bring the patient's flexed arms slmvly forward, downwards and ill\\"ards, press arms and elbows firmly on the chest on either Slue of the breast-bone (Fig. 59). By this means air is expelled from the lun gs . , Repeat these movements alternately, dehberately, a nd perseverin gly about fifteen times a When a sufficient number of assistants are present, Howard's method may be combined \\"ith Silvester's, as follo\\'s ;-
The additional assistant kneels astride the patient's hips with the balls of the thumbs resting on either side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Using his knees as a pivot, he presses forward on his hands. Then suddenly, \\'ith a final push, he springs back and r emains erect on his knees while he slowly counts I, 2, 3. These motions are to be repeated to correspond • 'with those being perfor med by Silvester's method, pressure on the chest bein g made simulta n eously by those performing the t\\'O methods (Figs. 60 and 61).
LABORDE'S METHOD.
'Vhen from any cause the above methods cannot be carried out, Laborde's metlzod of artificial respiration should be tried. It is especially useful in suffocated children and when tpe ribs are broken.

I 2 7
The patient is placed on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for t\\'o seconds in that position, then allm\'ed to recede mto the mouth. These movements should be repeated about fifteen times a minute.
Artificial respiration must be continued until breathing is established, or until a doctor arrives. When natural breathing commences, regulate the artificial respiration to correspond with it. Success may result even after two hOllis' time.
Excite respiration.-
'Vhilst artificial respiration is being applied, other useful steps may be employed, such as applying smelling salte ()r snuff to the nostrils and flicking the chest with a dump towel. '
Induce circulation and warmth after natural breathing has been restored. \Vrap the patient in dry blankets or other covering, and rub the limbs energetically towards the heart. Promote \yarmth by hot fbnnels, hot-,water bottles, or hot bricks (wrapped in flannel) applied to the feet, to the lim bs and body. When the power of swallowing has returned gi\Te hot tea or coffee, or meat extract. The should be kept in. bed and encouraged to go to sleep. Large poultices or fomentations applied to the
126
front and back of the chest will serve to assist breathing. . Watch the patient carefully for some time to see that the breathing does not fail; should any signs of failure appear, at once begin artificial respiration.
INSEN SIBILITY.
Unconsciousness or Insensibility may arise a! follows :-
Injury to the Head. -Concussion and Compression of the brain.
Disease of the Brain. -Apoplexy, Epileps y, Hysteria.
Various Causes. -Shock, Fainting (Syncope), Collapse, Alcoholic and other poisoning, Sunstroke and Heat-stroke, Infantile Convulsions, Asphyxia.
GENERAL RULES FOR TREATMENT OF IN
SENSIBILITY.
t. -- If a person appears about to lose consciousness, prevent him from falling, and by him gently down.
2. - Arrest Hcemorrhage when apparent; attending to minor injuries is less important than treating the unconscious state.
3.- L ay the patient in the position in which breathing is most easy-usually this will be on the back, or inclined to one side. As a general rule

raise the head and shoulders sligldly when the face is flushed, and keep the head low \\ hen the face is pale.
4.- Undo all tight clothing round the neck, chest and waist, unfastening trle braces and top button of the trousers in men, and the corsets in women, the object being to relieve pressure on the air passnges, lungs, heart and abdominal organs. Be sur.e that there is no obstruction to the air pz.ssages by the tongue or by a foreign body in the throat. The possibility of false teeth oestructing breathin a must be considered. b
5.- Provide for a sufficiency of fresh air by opening donrs and windows, and by kef ping back. a crowd.
6. - When breathing cannot be disct:rned apply artificial respiration.
7.-0btain a doctor's help as soon as possible.
8 .. - UnJess unavoidable, never leave the patIent until you have placed him in charge of a responsible person.
9. - Give no food or fluids whatever by the mouth while the patient is insensible.
10.-Should the spine or an important bone the upper or of the lower limb be fractured, It must steadied and maintained at rest as soon as possible. Should the unconsciousness be prolonged, the patient may be removed in a recumbent position "
128
! 1:::9
to si1elter, provided that the broken bone is adequately supported.
!I. - When the paUent is in a state of convulsion, suppo r t his head, and after wrappin g a piece of wood or any other hard material in a handkerchief, hold it in his mouth to prevent biting of the tongue. Do not forcibly restrain his limbs; prevent him from hurting him se lf by pulling hill1 away from a source of danger, such as machinery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way.
12.-0n return to consciousness ,,-ate r may be given to drink. If the pulse is feeble E:,ive warm tea or coffee, provided either internal or externa l, is n ot prese llt. A desire to sleep should be en':ouraged , e::cept ill C<1ses of opium poisoning, a condition that may generally be recognised by the history of tlte case, and also by the pupils of lhe eyes (the black openings in the grey, blue or brown iri .) being c(mtrclcteci (pin-head pupils) .
13.-It must not be assumed that a person is insensible as the result of drink merely because the breath smells of alcohol; frequently when people are feeling ill they take or are given alcoholic stimulants, after which they may become insens ible, not from the drink, but from the cause t hat induced them to L1.ke it, for example, insensibIlity coming on, effects of poisoning, etc . Even if

drink is believed to be th e actual cau se of insensi bility, it must be borne ill mind that the patient i 111 a ve ry dang e-rous state, and he must be tr eatt.J for Collapse by being coyered up and kept "arm.
The above genera l ru!t:.:s \\'111 enable first aid to be rendered efficiently in mo s t cases of insensibilit_-, although the exact form from which the pati ent IS suffering is unknown.
' ION OF THE BRAIN .
The patient may be stunned by a blow or fallon the head, or by a fa:l on the feet or low er part of the He may quickly regain con ciousness, or insensibility , more or less complete, may be prolonged.
TREA'D1EN r.
1. - Apply the general rules for the tre::ttm C:1t of Insensibi lity.
2.- Be very apprehensive of danger in all cases of injury to the head. The p.ltient may be stunneri, and after a sbort inten-al may r(conr some degree of consciousness, or even the brain may apparently have escaped injury; yet in both instan ces there is a grave ri -k that a structure within the cra nium has been injured, and that a serious state o f may develop later. Cee Fracture d the Cranium, page A caution should ther efore be given to a patien t \\'ho has lost consciousness cyen
D 2
130
for only a after an injury to the head not to resume physIcal or mental activity without the consent of a doctor.
COYIPRESSION OF THE APOPLEXY.
Compression of the Brain may result from the same. as produce Concussion; in fact, Com preSSIOn IS frequently preceded by Concussion.
. usually occurs in elderly people, and no SIgns of ll1Jury are necessarily present.
In .both conditions the face is flushed; the breathl!1g stertorous; one side of the body may be more lImp than the other, and the pupil of one eye may be larger than that of the other; the tempera, ture of the body is generally raised.
TREATMENT.
I.-Apply the general rules for treatment of Insen sibility.
2.-Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be t3.ken not to burn the patient with the bottles, which be wrapped in flannel, and their heat tested WIth the elbow.
EPILEPSY.
Epilepsy occur in persons of any age, but Usually occurs In young adults. The patient falls to

the rr round, sometimes with a scream, and passes into a st:te of convulsion, throwing his limbs about. The treatment is according to the General Rules, especiaHy Rule I I.
HYSTERICAL FITS (HY STERIA).
SIGNS AND
The pati ent, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and actions. She subsides on a couch or in some comfortable positi(m, throws herself about, grinding her teeth, clenching her fists, shak!ng her hair loose; she cl utches at anyone or anythmg nelr her, kicks, cries and laughs alternately. The eyeballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregular symptoms may develop.
TR EA Tl'IfENT.
I.-Avoid sympathy with the patient: and speak firmly to her.
2.-Threat en her with a cold water douche, and if she persists 111 her "fit, 1/ sprinkle her with cold water.
a mustard leaf at the back of the neck.
Medical treatment is necessary to cure the condition of mind and body which gives rise to hysterical attacks.
132
133
SHOCK, FAINTING (SYNC OPE), COLLAPSE.

l.- -Injury in the region of the abdomen, extensIve wounds and burns, fractures, lacerated wounds, and evere are some of the more frequ ent physicaJ r auses of shock-
2.-Fright , anticipation of injury, and sudden bad ,1ews. or sometimes sudden removal of fear and an xiet after prolonged produce shock or fainting.
3 -Some pOl sons cause shock, ,,,h ile others, suc h a alcohol, so depress the nervous system that col ,a pse ensues.
4.-Hremorrhage or heart weakness, a close 01 cro wded room, tight clothing! fatigue, or want of may bnng on fainting or collapse.
SIGNS AND SYMPTOMS.
The general condition of shock may be recognised by extreme pallor, a feeling of cold, clammy skin , feeble pulse, a n d shallow breathing accompanied, hremorrhage h as been severe, by yawning and SIghi ng. The term "collapse" signifies aver, <6erious condition in which the life of the pat ient is in t he greatest danger; the tern perature of the body , e low the normal, and one great object of treatmen t IS t o prevent it sinking to a point at whic h life is mpossible , An attendant danger of the condition of 135
collapse is the liability to sudden relapse aft er a. tempo:ary improvem ent, and the utm ost care and watchtulness must th e r fore be exercisEd to maintain the hea t of the body and to guard against fa ilure of the heart and lun gs .
TRF.AnIENT
I.-Remove the cause by arrestin a hrem o r:hage, to injuries, loosening all tight clo t hmg especially about the chest and abdomen rem oving from a close or cro\\ ded room usin g words, etc. '
2. Lay the . patient on the back, with the low. Ra:se the lovver limbs; when the patient IS 111 bed th1S 1S best done by raising the foot o f the bedstead .
.3.-Provide for a free circulation of fres h aIr.
4. - If hcemorrhage has been severe and the patient is collapsed, firmly bandage the limb s from the toes to the hips, and from the fingers to the armpit s .
5. - To stimulate the action of the heart :::.a l volatile and water may be given jf the patient' c n swallow, or smelling salts may be held to the
6. - It is of the utmost importance to use every means of preventing a fall of tempe rature below the normal point. - To accomplish tLJS cover the pati ent with extra clothing, or hy pb c.ng
rugs or blankets over him j get him to bed in a warm but well-ventilated roo .n as soon as possible. Apply warmth to the fe et and to the pit of the stomach by hot water bottles or hot flannels. (Test the heat of the?e with the elbow before appl'jll1g them.) If the patient can swallow, give hot drinks, such as milk, coffee. It is well to add sugar, as it aids in ralsmg the temperature of the body. cannot be discerned, apply artificial resplratlOn.
8. - If want of nourishment has been the cause of fainting or collapse, give food sparingly at first.
SUNSTROKE AND HEAT-STROK'E.
"When exposed to great heat, as in the stoke-hole of a steamer, in the tropics, or to the rays of the dUring a march in very hot weather when persons may develop sickn ess, fal1-:tness, gldd1!less, and difficulty in breathing. Th e patle?t complall1s of thirst, the skin becomes dry and burnm.g, the face very flushed, the pulse quick and .. A very te.mperature, stertorous (snormg) breathmg, and msenslbllity may ensue.
TREATrlIENT.
I. - Undo all ti ght clothing.
2 - - R emo\'e the patient to a coul, shady spot. 137
3.-Stri p the patient to the waist.
4.-La y the patient down, wiLh the head and trunl well raised ....
s.-Procure as free a circulation as possible of fresh ' air, and fan the patient vigorously.
6.-Apply ice bags or cold water freely to the head, neck, and spine, and maintain this treatment until the symptoms subside.
7.-0n return to consciousness, the patient may have water to drink.
IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.

Spasm of the mllscles of the limbs and trunk r blueness of the face, insensibility, more or less comand occasionally squinting, suspended 1espiration, and froth at the mouth are the prominent signs.
TREATMENT.
I.-Support the child in a warm bath slightly above the temperatu12 of the body (98 degrees), so that the water reaches to the midule of the trunk.
2.-Place a sponge dipped in cold water on the top of the Lead.
136
n8
ASPHYXL\.
\Vhen, o wing to want of air, the blood is not supplied with oxygen the patient becomes insensibl e, and is said to be asphyxiated . This condition may be brought about as follows: -
1. Obst ruction of the air passages.
(a) By
(
b) By PRESSURE FRml OUTSIDE : Stra ng ulati on, hanging, smotherin g.
(c) By A BODY IN THE THROAT: Ch oking.
(d) By S OF THE TISSUES OF THE
THROAT : I nfL:ul1matlOn, scald of the throat, poisoning by a corrosIve .
II. Inhaling poisonous gases. By coal gas (as us ed in the house ) , producer, or water, ga s, smok e, fumes from a charcoal or coke fire, se\\'er gas, limekiln gas, car bonic acid gas .
III. Pressure on the ci].est, as wh e n cru shed by sand or d ebris, or by a crowd .
IV . Nervous affections, as the result of narcotic a nd certain olher poisons , collapse, electric sh ock , or stroke by lightninr;.
G E(\'IT.RAL TREAT:\IEN T .
I n all cases or Asphyx ia atte mpts must be rnade to r e move th e cau se, or lo rcm :)Ve the p1ti e nt fr o m th e caLIse . \V :l en th is has been do ne artificiaJ

respiration must be applied, taking care th at the an passages ar e not obstructed , a n d that there 1S abundance of fresh air.
D Ro\YN I N G.
P ersons com pletely immersed in water for or fift een mi n u tes have b ee n restored by arufi.cl a l means. Therefore, if the body is w1thll1 a reasonable time, absence of signs of life 1S not to de' d immediate attempts to restore .
T he firs t thing to do when the body IS 1S to get rid of th e \yater and froth obstructmg the . cu r pass:.1ges, and t hen artificially to r estore Tll1S is best acc o rnplisil ed by proceedmg aL once to p erform artificial respiratio n by Schafer's m ethod, or as follows ;- . 'l
I. -As q u ickly as possible loosen the clOllllng, an ... the mouth and the back of the throat.
2.-Turn the patient face downwards, with a pad below th e chest, and \\'ith the forehead upo n the nght for earm.
3.-\\,hilst in t h is positio n apply press u re. by the hands to the patie nt's back ove r the 10\\'er nbs, aNd ke ep th e pressure u p for tllree s:con d.s . .' .
4.- T um the patient on th e nght SI d e, mamtammg tbat posi t ion also for three seconds.
5.-Re peat these movements a ltern ately as long as froth \\ater issue from the mo uth.
129
These operations (Marshall Hall's method) in themsel\-es tend to promote respiration, but when the air passages are clear of froth and water Silvester's method of artificial respiration may be used by itself or with Howard's method in conjunction. While performing these operations send someone to the nearest house to procure blqnkets and dry clothing, hot water bottles, etc., and to fetch a doctor.
STRANGULATIO -.
Cut and remove the band constricting the throat. Apply artificial respiration.
HA ' GING.
Do not wait for a policeman: grasp the lower limbs and raise the body to take the tension off the rope; cut the rope, free the neck. Apply artificial respiration.
S.\IOTHERING.
R emove whatever is smothering the patient Apply arliflcml respiration.
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to the back of the throat and attem pt to dislodge the foreign body; if vomiting results, so much the better. If unsuccessfLlI, thump the back hard whilst the head is bent fOlward. Apply artificial respiration.

SWELLING OF THE TISSUES OF THE THkOAT.
'Whether the swelling is caused by inflammation by swallowing very hot water, as not infrequently happens to children attempting to drink from the spout of a kettle, or by the effect of a corrosive poison. the treatment is as follows :-
I.-Apply a sponge, piece of fbnnel or other cloth. wrung out o.f very hot water, to the front of the neck, from the chm to the top of the bTeast-bone.
2.-Sa.t the patient before the fire.
s.-Give ice to suck if it can be had; if not give cold water to drink. '
4.-Give animal or vegetable oil, a dessertspoonfuJ at a time, to soothe the scalded throat and ease the pain .
. S.-If breathing has ceased apply artificial respiratIOn.
SUFFOCATION BY SMOKE OR GASES.
I.-Remove the patient into the fresh air. Before entering a building full of smoke tie a handkerchief wet if possible, round the head so as to cover nose and mouth. It is well to move slowly, keeping ;ow, or even cra\vling, whilst in a room full of smoke m of a suffocated person. Every opportunity of lettmg in fresh air by opening doors or windows should be seized.
2.-Apply artificial respiration
3 - In the case of producer or \\'ate r gas, inhalation of oxygen WIll also be necessary.
ELECTRIC SUOCK.
Electric current is conveyed by a cable, wire, rai l, or bar, called the "Positive," and returns to the source of supply by another cable, wire, rail, or bar , called the " Negative," or through the earth. In the case of an electric railway, the current is generally conveyed by an insulated rail the third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an electric tram way it is freq uentl)' conveyed by all O\'erhead conductor o r trolley wire, and r eturned through tbe running rails.
Through contact \\ ith a "positi\'e " the shock may be so severe as to cause insensibilIty, and the sufferer will be unable to extncate himself, and must be liberated with all possible speed. A,!> it is gener;-.1I y impossible or inexpedient to s witch off the current some other method must usually be adopted; but precautions must be taken or else the person rendering assistance \\'ill himself receive a sbcck.
To liberate the sufferer from contact-
I.-Insulate yourself £i 'om the earth by standing on a n '(i nsulator " or" n on-conductor," that is, a body 'vv hi ch resists the current. Amongst s uch bodies

are inJiarubber, dry glass, dry dry silk, dry cloth, dry wood and dry 113.Y or straw.
2. - Protect your hands from contact w ith the sufferer or the electric medium by coverins them with an insulator. Although indiarubber is probably the best insulator, do not waste in running for indiarubber gloves, but use dry artIcles of clothing; an indiarubber tobac co pouch or cap, or folded newspap er, \\'ould serve to protect the hands in an emergency . If no means of insulating the hands are at hand an attempt may be made to drag the sufferer away by means of a loop of dry rope or a crooked stick; an u m bre]Ja is n ot safe because the metal ri bs would act as co nd uctors *' of electricity, and it is not infrequently the case that the" stick" of the um bre]Ja is a metal tube.
3. - Pull the sufferer away from contact. Care should be taken to avoid touching with naked hands the sufferer's hands, wet clothing, or boots if the soles are nailed. The armpits should be aVOIded as perspiration usually makes the clothing damp th ere .
\Vhen the sufferer is r emoved from contact -
I.-Apply the general treatment for ins en-
A conducto r is a body through whi ch passes. Am mgst such uodies are cupper, brass, Hon, ll1ulsLure and one's own body.
J44
-sibility (loosen clothing, procure free circ ulatio n of air and p lace in a recumbent position).
2. - Dip Ci: towel in cold water and attempt to arouse him by sharply flicking the face and chest . artificial respirat ion if other methods fall to restore animation. "Laborde's " method (see page 126) has been found to be very s uccessf ul.
4. - Treat burns if there are any (see pages r03 , ,104) .
EFFECTS OF LiGHTNING .
A struck by is us-ually more o r less deprIved of consciousness . The treatment is the same a s that .ror shock, except, of that the ll1structlons for lemovin a the patient from contact with t he electric d o not apply.
QUEST IO NS ON CHAPTER V.
The numerals indicate the pages wllere the answer s may be found.
V;hat are the two systems of nerv es ? ... . ..
Of what is the cere bro-spinal system made up ? ...
What is the spinal cord?
What are nerves like? ..
Explain the sympa!hetic system
E xpla in the respiratory system
Explain thp acts of respirati on
How are the exp:msion and contracti on of the
effected?
what system of artificial respiration is
back upwards?
In what systems is he laid on his back?
In what system is he laid on his back or side?
In \\ hat system is he rolled alternately on his side and face downwards?

you examine the patient to see if any bones
'hal wrong opinion may be formed when the patient
smells of drink?
Is collapse from drink a serious condition? \Yhlt is concussion of the brain?
14 5
PAGII rr7 117 II7 Il8 lI8
,
Il8 to 120 120
chest
... ... ...... 120 to 121 I n
patient laid 121 123, 126 127
.. , ... .. .
the
. , .
... .., 139,140 IT ow long should artificial respiration be p ersevered wilh? 1 2 7 \\ hat is exciting respi' ation ? 127 \ \-hat is inducing circulation? 1 2 7, 128 Why is it necessary to watch the patient? 128 How may insensiuility arise? 128 State the various forms of insensibility 128 Slate the general rules for treatment of insensibility 128 to 13 1 Would
were 1 2 9
... "
130
broken?
...
e the rules for treatm ent of concussion 13 1 13 1 131 , 13 2
Slat
\\'hat danger accompanies injury Lo the head?
'Vhat caution should be given to a patient who has lost consciousness, even for a moment, after an injury to the head? ...
'Vhat are the causes of compre sion of the brain?
In what ag d people dOfS apoplexy usually occur?
\\That are the signs and symptom.:; of compression and apoplexy? ...
State the rul es for treatment of these conditions ...
'Vh tt dangpr is there in applying hot water l' ottles to insensible persons, ancl what precautions should lJe taken?

b d in all cases of What two things have to e one ... 138, 139 asphyxia. ? .. , b ... to 'j't' is possible for What two thll1gs e seen an ood? ... .., I39 artificial respiration to do y g d if the air - .' likely to do any goo Is artificial respiration d 'f there is not abundance passages ll:re obstructe ,or 1 ........ . of fresh aIr?... .... of drovvning?
What is the first thll1g to .dfio be performed By what may artl. te s?
Describe a case of epilepsy 13 2 , 133
\\That special care must be taken in treating a case of 1 , > .)epilepsy? 130, 13 2
Descri be a hystel ical fit
How would you treat a hysterical fit? '"
\\That are Ihe comm ,nest physical causes of shock?
" 'hat may produce shock or fainting?
'Vhat conditions do certain poisons bring about?
What may hring about fainting or col'apse?
How wou'd yuu recognise the general condition of shock? 134
\\That special precaution must be taken in the case of collapse?
State the treatment for shock, fainting (synClJPc) a ' d collapse 135, 13 6
\Vhat is the effo.:ct of suga r on the tempernturc of the body?
\Vhat are the causes of sunstroke and heat-stroke?
State the treatment for sunstroke and heat-stroke
\Vhat are the causes of convulsions in children?
\\'hat are the signs of convulsions in children? '"
State the treatment for in d,ddr, n '" tate fully the cau es of a.
without tak1l1g any pLeVlOU\S f p e proceedina with \\'hat steps mu l be taken ear . respiration is being performed? ... ... . ...
State the treatment for State the treatment for hangmg. . ..
State the treatment for Slate the treatment for choking ... , of the lhruat be llow may a swelling of the tissues ... '.'
I [ow is electricit? conveyed ? wilh an How would you 1.lbemte a su ... 14 2 , 143 electric medIum? h h" from \\"bat would you do w en t e su .... .. c onlacdt? d':' the slroke ? \\"hat waul you
13 1 13 2 13 2 13 2 I3 2 13 2
J 1 .)) 133 134 134
134 134
135
13 6, 13
1 36 137 137 1)7 I37 13 8 PAGK
6
..
.
... ... . ..
139 139 139 139 141
.. , ...
... f of
S l the treat men t for swel mg 0 - 141 ta e . ... .., throat ... .., .. ·· ..b smol"e
ga es
142 State the treatment for suffocatIon y .. , ... 14 2
143 144
ca used?
I'
the
or
14I,
a m

CHAPTER VI. POISONING.
Poisons may be classified according to their treatment under two heads :-
I.-Those which do not stain the mouth and in the treatment of which an emetic is be given. Amongst these are :-
(a) Arsenic, (contained in rat poison and lucifer matches), Tartar emetic and Corrosive SublImate, \\hich cause a metallic taste in the mouth and a burning pain in the mouth, throat and stomach.
(b) St:ychnine, Prussic Acid, Bellad onna (deadly nIghtshade plant) and several other varieties of plants, such as laburnum seeds, etc.; these give rise to convulsi ons, delirium failure of respiration and collapse. '
(c) Poisonous meat, fish and fungi (often mistaken for mushrooms). Suspicion of these poisons should be directed to cases where several persons who have partaken of the same food develop similar signs and symptoms.
(d) Alcohol, which may cause collapse.
(e) Opium and its preparations, Morphia, 149
Laudanum, Paregoric, Syrup of Poppies and various soothIng dnnks and cordials - these cause a tendency to go to sl eep, which continues until sleep bec<;>mes de ep and breathing stertorous; the pupils. of the eyes become minutely contracted (pmhea d pupils). .
2.-Those which burn or stam the and in the treatment of which no emehc is to l; e given. These are of :- .
(a) Acids, s':lch as. ACId fortIs), SulphUrIC ACId (011 of Hydrochloric, or Muriatic, Acid (Spmts <;>f Sal.t), stronO" Carbolic Acid (Phenol), OxalIc ACId, which is contained in oxalate of potash, salts of sorrel, salts of lemon and some polishing pastes. .
(b) Alkalies, such as CaustIC Potash, Caustic Soda and Ammonia.
SUMMARY OF SIMPLE DIRECTIONS FOR THE TREATMENT OF POlSONING.
I.-Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2. - Except when the lips and mouth are stained or burned by an acid or alkali.
J 50
promptly give an emetic - that is, make t he patient vomit as follows :-
(,a) Tickle tlze back oJ t he I/lroat wllh tht Jinger or with a feather.
(
b) lI.fltstard- a dessert-spoonful in a tunlblerful of luke-warm wat er.
(
c) Salt-a table-spoonful in a tumblerful of luke-warm water.
(d) Ipecamallila Irine- for a young child, a teaspoonful repeated at inlel "aIs of fifteen minutes.
3·- 1n all cases when the patie nt is not insensible, give Milk , Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, Animal or Vegetable Oil (excep t in phosphorus poisoning), and Tea.
Olive, Salad, and Cod-liver oil, or oil such as that in \\ hich sardines are preserved, may be gi,-en; mineral machine oils and paraffin are unsuitable. Oil is soothing, and is therefore especially useful I II poisoning by Acids, Alkalies and such substances ;,s Arsenic and Corrosive Sublimate. Demulcent drinb, such as barley water or thin gruel, act in the san le manner, and are free [:0111 danger in cases of phos. phorus poisoning.
may be given either before or after the emetic if the poison calls for one .
Strong T ea acts as a neutraliser of many poisons}

15 1
and is always s .lfe. A of tea should be thrown into a kettle and boiled. .
4.- If the lips and. mouth are stamed or burned give no emetic, but. .
(a) If an Acid is kno\Vn be the pOison g ive an Alkali at once. FIrst wash the mouth freely \,·;tll lime water or other .Gl:lkalme mixture, such as soda,. chalk, whltmg, or macYllesia or \vall plaster 111 water, afterwa;ds let the patient sip a little It. Soda and potash are not to be. given 111 the case of poisoning by oxalic aCid. .
(II) If <1. strong Alkali is kl1o\\'.n to be the pOIson give an acid at once. Flrs.t the out freely with lemon or vll1egar diluted with an equal quantIty of ar:d afterwards let the patient sip a httle of It.
In both CJ.SeS gi\-e oil (Rule 3)' .
5. - When a person has pOlson and threatens to go to sleel?, hlm awake by walking hIm about and slappll1g hIS bce, n eck and chest with a wet towel. Strong black coffee may be given to drink. Slapping the soles of the feet may also be tried.
6.-If the throat is so swollen as to threaten obstruct ion to the a ir passage, apply hot flannels or poultices to the of the neck and give frequent sips of cold drinks.
7. - Apply artificial respiration if brea th in g cannot be discerned.
8. - Treat shock and collapse.
9. - Preserve any vomited matter , food ) or other substance, suspected of be ing th e poison. Do not 'wash vessels which may have COD-· tained the poison , and carefully guard them.
Certain poisons require special and a fe\V of the commoner of these are mentIoned below with their treatment.
CARBOLIC ACID .
The odour of the breath will aid in the detection of this poison ; the lips and mouth are usually staine d white, and several nerVOLlS symptoms come on.
1.- Give milk , to a pint of which half an ounce of Epsom Salts has been added.
2 . - Treat according to the general rul es.
PRUSS1C ACID.
The action of this poison is extremely. rapid. Giddiness, stagge"'ing, insens ibility accom pa nIed. 12y panting respiration, profound. collapse .and conv ulsio ns a re the general SIgns, a n d Il1 addItlOn smell of bitter almonds is often present .
TREATMENT .
I.-Place the patient in the ®pen air.

2.-D.1sh cold water o n the hea d and spine con· t inucu ly.
3.- A pply artificial respiration.
4. - H old s 'nelling salts to the no strils.
s.-Treat shock and collapse. (See page 135·)
POISONOUS MEAT, FISH AND F UNGI.
The signs and symptoms are vomiting and (tliarrhce.1), colic, headache, great weakness, raIsed te:l1 percJure and a quick pulse.
TREATMENT.
1. -Gi ve an emetic.
2. - \Vhen the emetic has acted, give castor oil.
3 collapse. (See page 135·)
STRYCHNINE.
The signs and symptoms are a feeling of suffocatio n, livid features, and convulsions . T he patient rests on his head :ll1d feet , and the body is arched.
TREATl\IENT.
1. - Give an emetic.
2. - Apply artificial respiration.
ALCOHOL.
1.- Give an emetic if the patient can swallow.
2. - Treat collapse by keeping the patie n t \\'arm, etc. (See page 135 .)
152
!55
QUESTIONS ON CHAPTER VI.
The 1lumerals indicate the pages where Ille anSW(l-S muy be found.

CHAPTER YII.
What are the symptoms of poisoning by arsenic?
What other poisons give rise to the same symptoms?
Under what two heads may poisons be classified? PAC.. 148, 149 148 148
What poisons give rise to convulsions, delirium, failure of respiration and collapse? ...
If several people who had partaken of the same food developed similar signs and symptoms, by what would you suspec 1 they had been poisoned ? 148 condition may result from poisoning by alcoh ol ? 148
What are the effects of sllch poisons as opium?.. q8, 149
\Vhat two classes of poison burn or stain the mouth? .. . 149
Would you give an emetic for such poisons? 149
Name some of the principal acids 149
Name some of the principal alkalis 149
State the general rules fur the treatment ing of poison-
State the best methods of making a person vomit
How would you treat a case of acid poisoning? ...
How would you treat a case of poisoning by an alkali?
State the signs, symptoms and treatment of carbolic acid poisoning ... 149 to 152 ISO ISl ISl
State the signs, symptoms and treatment of poisoning by Prussic Acid 15 2 ,153
State the sIgns, symptoms and treatment f poisoning by poisonous food ...
State the signs, symptoms and treatment of poisoning b} Strychnine
"What would you do in the case
Esmarch's Trian 'Y u 1ar Bandage has been in Chapter II. It be applied to keep a dressll1g on a wound, burn or scald of any part of the body, or for an injury of a joint. 1 For the Scalp (Fig. 62). Fold a hem about inches deep along the base of a bandage; place the on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down at the back; carry the two ends round the bead above the ears and tie them on the forehead ; draw the point first dO\\'l1\yards, and then turn it up and pin it on to the bandage on the top of
FIG. 62. the head.
For the Forehead, Side
,of
the Head,
Cheek and for any part of the body that 1S round '(as the arm or thigh, etc.),. the narrow bandage should be used, its centre beIng placed over the
154
.. .
alcoholic poisoning? 153 153 153
of
dressing) and the ends being carried round the head or limb, as the case may be, and tied over the wound.
For the Shoulder (Fig. 63). Place the centre of a bandage on the shoulder, \\'ith the ooint running
up the side of the neck; fold a hem along the base; carry the ends round the middle of the arm and tie them. Place one end of a broad bandage over the point of the first bandage and sling the arm by carrying the other end over the sound shoulder and tying the ends at the side of the neck; turn down the point of the first bandage, draw it tight and pin it. 157
For the Hip (Fig 64). Tie a narrow bandage round the body above the haunch bones, the knot on the injured side. Fold a hem accordmg to the size of the patient along the base of a second bandage; place its centre over the dressing, carry the ends round the thigh and tie them; then carry the point up under the

64.
65.
66. first bandaae turn it down over the knot and pin it.
For thO e ' Hand when the fingers are extended (Fig. 65). Fold a hem along the base of a bandage; place the wrist on the hem with the fingers towards the point; then bring the point over the wrist, pass the ends ro und the wrist, cross and tie them; bring the point oyer the knot and pin it to the bandage on the hand.
156
FIG.
FIG.
FIG.
For the Foot (Fig. 66). Place the foot on the centre of the banda ge with the toes to\yards the point; draw up the point over the instep, pass the ends round the ankle and cross them in front; now pass the ends round the instep and tie them. Dra w the

FIG. 67a.
point forward and pm it to the bandage on the instep.
For the Front of the Chest (Figs . 67a and 67b). Place the middle of the bandage over the dressing with the point over the shoulder on the same side; carry the ends round the waist and tie ; 159
t oen draw the point oyer the shoulder and tie it t o one o f the ends.
For the Back. The bandage is app li ed as the foregoing, except that it is begun at the back.
For the Knee. Fold a 'narrow hem along the base of a bandage; lay the point on the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then over the thigh and tie them. Bring the point d own and pin it to the base (Fig . 68).
FiG. 6S. For the Elbow. Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and the middle of the base on the back of the forearm; cross the e nds first in front of th e elbow, then oyer the arm and tie them in front (Fig. 69) .
For the Fingers and Toes \\fap a strip of calico or linen round and round the part; split the fr eee nd, and secure it round the wrist or ankle.
FIG. 69
CHAPTER VIII.
:\fETHODS OF CARRYING.
THE FOUR -HAND ED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
I,- Two face each other behind the patient and grasp their left forearm with their right hands and

70.
each other's right forearm with their left ba!1ds (Fig. 70), and stoop down.
2 . - The patient sits on the bands and places one arm round the neck of each bearer. 161
3.-Tbe bearers rise together and step off, the bearer on the right hand side of the patient with the right foot, and the left hand bearer with the left foot
THE Two-HANDED SEAT.
This seat may be used to ca rry a helpless pJ.tient.
7I.
T.- Two bearers fa ce each other and stoop, one on each side of the patient. Each bearer passes his forearm nearest to the patient's bead under his back jus t a
160
FIG.
FIG.
helm\" the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig. 7 I), and clasp their hands by one of th e methods shown in Figs. 72 and 73. A handkerchi ef should be held in the hands if the first grip is used.

FIG. 72. FIG. 73.
2.-The bearers rise together and step off, the right-hand bearer with the right foot; and the left-hand bearer with the left fovt (Fig. 74).
THE THREE-HANDED SEAT.
This seat is us efu l for carrying a patient and supporting either of his lo\\'er limbs, \\'hen he is able to u se his upper lim ns.
1.-Two bearers face each other behind the patient. For supporting the left limb th e bearer to the patiEnt's right grasps his own left wrist '" ith his ri ght hand, md the other bearer's right wrist with his left hand. The bearer to the left grasps the first bearer's righ t wrist with his right hand (Fig. 75). leaves his
162

left hand free to support the patienes left leg. For patient's right lower limb follow the same directions, substit uting" right" for" left" and" left " for Ie right." The bearers stoop down.
2.- The patient places one arm round the ne ck of each bearer and sits on their hands.
3. - The bearers rise together and step off) the FIG, 75.
ri ght-hanJ bearer with the right foot, and the 1efthand bearer with the left foot.
THE: FIRE..\IAN'S LIFT.
(To be attempted only by a strong man).
Turn the ratient face do\\ n \\'ards; place yourself It hiS head, stoop do\\'n, slightly raise his head and flG 76.
164
shoulders and take hold of him close under his armpits, locking your hands on hIS back. Raise his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head res ts on your left shoulder. Throw his left arm over your head, stoop down and place your left arm bet\\"een his thighs, letting his body fall across your shoul ders . Rise to an upright position; hold the p:.ttie nt's left wrist with your left hand and leave your n ;;h t han d free.
Assista nce ni.ay be given to an injured person by supporting him in the manner shown in Fig. 76.
Th e plalZ of carrying tlte patient by the arms and legs witlz tIle face downwards, common£v called tlte "frogs' marclz," must never be used, as deatlz may ensue from tltis treatment.
blPROVISED STRETCHERS.
A stretcher may be improvised as follows:-
I ,-Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The pat; ent sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a longer stretcher is required two or three coats must be treated in the same n13.nner. The poles may be kept apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 79).

77.
THE FORE AND AFT J\IETHOD
.
This plan of carrying is useful when space does not permit of a hand seat.
166
FIG.
FIG. 78.

FIG. 79.
2.-Make holes in the bottom corners of one or two sacks and pass stout poles through them.
3.-S pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides. Two bearers stand on each side and grasp the middle of the pole with one halld, and near the end with the other. They walk side\yays.
4.- A r..urdle, broad piece of wood, or shutter may be used as a stretcher; some straw, hay, or clothing should be placed on it, and covered \\ ith a piece cf stout cloth or sacking; the latter is useful in taking the patient off the stretcher.
Always test an imprO\'ised stretcher before use. Stretchers must be carried, and the patient placed on them, as laid down in the ,( Stretcher Exercises."
As a general rule carry the patient feet foremost. The exceptions are :-
(a) When going up hill with a patient y;ho e 10\\ e! limbs are not injured.
(b) 'When going do\\ n hll1 \\'ith a ratient \Yf:OSf lower limbs are injured.
Avoid lifting the stretcher over ditches or walls, but where these cannot be avoided the stretcher must be carried in the following ways :--
To CROSS A DITCH.
In crossing a ditch, the stretcher should be lowered with its foot one pace from the edge of the ditch.
169
Nos. I and bearers then descend. The stretcher, with the patient upon it, is afterwards advanced, Nos. I and 2 in the ditch supporting the front end while its other end rests on the edge of the ground above. No. 3 now descends. All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by No. 3 in the ditch. No. I climbs out, No. 2 remaining in the dl tch to assist NO.3. The stretcher is lifted forward on the ground above, and rests there while Nos. '7 and 3 climb up.
To CROSS A WALL.
The stretcher is lowered with the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the wall. No. I then climbs over the wall and takes hold of the foot of the stretcher, while Nos. 2 and 3 support the !'lead; the stretcher is then carried forward till the rests on the wall, No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
• These numbers are explained later in the detailed "Stretcher Exercises."

171
To LOAD A \\rAGON •
The stretcher is lowered with the foot one pace from the end of the wagon . Nos. I and 2 hold of the foot of the stretcher, No. 3 the head .. The stretcher is then raised and carried forward tIll the front wheels rest on the floor of the wagon. No. I then jumps into the wagon, \\ hile No.2 goes to the head of the stretcher and helps NO.3. The is then pushed slowly into the wago n. If the tallboard cannot be shut, the stretcher must be lashed firmly to the sides of the wagon.
To UNLOAD A "\V AGON.
Nos. 2 and 3 take hold of the head of the stretch e:-, while No. I gets into the wagon; the stretcher IS then gradually drawn out till the foot-wheels re t on the edge of the wagon. No. I jumps out of the IVaO'on and with No. 2 takes hold of the foot of the NO.3 supporting the head. The stretcher is now gently dra\\ n away one pace 'Vith four bearers Nos. I and 2 \\'ould lIft the of the stretch er , while Nos. 3 and 4 lift the head. This applies to crossing a ditch or wall, as well as to loading and unloading a wagon .
170
CHAPTER IX.
STRETCHER TRANSPORT.
The "Furley 1/ Stretcbers (Model 1899) are of three patterns, viz ," Ordim.ry,"" Telescopic-handled," and "Police. " In general principle they are alike, the component parts being designated the poles,

FIG. EO. -ORDIN ARY TRETCHER-CLOSED.
FIG. 81. - TELESCOPIC-HANDLED STRETCHER - OPEN. handles, traverse bars, foot wbeels, bed, pillo\\' sack and slIngs.
. The Ordinary Stretcher (Fig. 80) is 7 feet 9 ioch es 111 length, and r foot ro inches wide. The bed is 6 fe et in length, and the handles inches The heigbt is si inches. At the head of the stretcher is a canvas overlay (the pillow sack) which can be filled with .3t.raw, hay, clothing, etc., to form a pillow. The ]oll1ted traverse bars are provided with joints, 173
for opening or closing the stretcher. The Telescopichandled pattern 8r} is "ery simibr, but the handles can be sl1d underneath the poles, thU:3 reducina the length to 6 feet. This arrangement is of value when working in confined spll.ces, or when a patient has to be taken up or. down a staircase wit'-l sharp turns . The PolIce stretcher IS similar to the Ordinary p:tttern, but is more made, and has, in addition, straps for secunng a refractory patiel1t.
When closed, the poles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly folded 011 the top of the poles and held in position by the slings wbich are laid along the canV::lS , and secured by a strnp, pbced transycrsdy at the end of each sling, bemg passed through tbe large loop of the other, and round the poles and bed. ' .
In closin 'Y a stretcher care sbould be taken to the centre ;f the canvas when pushing in the tra.\"erse bar, as it is othen' ise liable to get caught.
To preparL', or open a st retcher, unbuc.kle the transverse straps of each sling; remo\"e tbe sll11gs from the stretcher; separate the poles; t::lke bolJ each tmrerse bar and draw it forward. The sll11gs \\ then be folded to h::llf their length, one beIng laId neatly over the handles at each end. of the stretcher.
As a general rule, stretcbe:- \\,111 be prepared Nos. I and 3 bearers 111 ExerCIse 1., II., and Ill.,
and by No. 2 in Exerc.ise IV. These belrers will, however, if required, assist the other bearers in attending to the pati e nt's injuries.
Note. - The various movements detailed m the following Exercises should be carried out steadily, the bearers working in unison, hurryin g being carefully avoi d ed , and every attentio n beinb paid to the bearer who gives the words of command.
S TRETCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised ,n 1904 to accord with the drills adopted by the Royal Army Medical Corps :-
EXERCISE No . I.
FOR BEARER S.
1.-The Instructor selects th e beare rs and numbers them -I, 2, 3, 4 at his discretion. Should one man be taller and stronJer than the others, he should be styled No 3, as he will have to bear th e heavier part of the burden." All orders will be given by NO.4.
2. -" Fall in." - Nos. I, 2, and 3 take position on the left side of and facing the patient No. I places himself at the patient's knees, No. 2 at the hips, NO ,3 at the p:1.ti e nt's shoulders. At the same
• Bearers should, h0w e vcr, be taught to take any of the pvsi! ions named in the following Exercises, whether that of N o. I, 2, 3, or 4 bearer.
175
time No. 4 places the prepared stretcher on the ground by the right side of the patient about two

82.
paces away fr om him, then takes position opposite to anc1 facing NO.2. (FIg. 82).
174
3· -" Re ady. "-The bearers kneel down on the knee and take hold of the patient, No. I passing hIS hand.s and fore-arms beneath the patient 's legs, hands wide apart. Nos. 2 and 4 pass their hands

FI G 83 . and for ea rms be!1cath the patient's hips and loins, and grasp each other's hanus. NO . 3 passes his left hand across the patient's chest and und er the riaht should er, and his right hand benea th the left shoulder (Fig;. 83).
177
4.-" Lift. "-O n the word ". Lift, " the bearers raise the patient gently and rest hIm on the knees of Nos. I, 2, and 3 bearers (Fig. 84) ; as soon as he
is securely rested, NO.4 disengages hands with No. runs round by the head of the stretcher and places It und er the patient, close to the other bearers' feet,
176
being careful that the pillow is immediately under the patient's head (Fig. 85); he then kneels dow n and locks his hands with those of No.2 (Fi g. 86).
5.-" Lower."-The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and then stand u p.

FIG. 85.
6.-"Stand to Stretcher. "-No . I goes to the foot of the stretcher, with his back to the patient; NO.3 to the h ead with his face to the patient ; Nos. 2 and 4 remain on each side of the stretcher.
7.-" Ready."-N os . I an d 3 place the slings (if used) over their shoulders, stoop do\\ n, and slip th e
179
loops of the slin6s on to the handles of the stretcher, which they then grasp. . .
As soon as all is right the word IS given :- .
8. -" Lift Stretcher."-Nos. I and 3 bearers raIse the stretcher steadily together and stand up.
Note.-N os. 2 and 4 will now adjust the slings the shoulders of Nos. I and 3, taking care that each l? well below the level of the C011ar and lies ill the hollow of the shoulder in front. They wdl also lengthen or shorten the slings, having r.egctrd t? patient's injuries and the relativ" helghts 0 t e bearers.
FIG. 86.
9. -" March."- move off :- Nos. I, 2, and 4 stepping off wIt h th eir left foot, and No. 3
I7 8
with his rIght foot (Fig. 87) . The step should be a short one of twenty inches, and taken with bent knees and no spring from the fore part of the foot. 10. - " Halt."- The bearers remain ·steady.

FIG. 87.
II. - "Lower Stretcher." -The bearers place the gently on the ground, slip the loops of the slmgs off the handles of the stretcher remove the slings from the shoulders, and then stand up.
13r
1:2._11 Unloa d Stretcher - Ready." - The bearers prepare to take the patIent off the stretcher, as at Orders 2 and 3. •
13.-" Lift,"- Th e bearers raise the patient as at Order 4 (Fig . 86) ; NO.4, in this case, disengages h:ll1ds from No.2, removes the stretcher (Fig. 85), <1nd resumes his former position. If necessary, the uearers will then steadily rise together, and carefully carry the patient to the bed, or bther place to wbich it has been arranged to cOlwey bim.
14.-"Lower."--The patient is carefully lowered.
EXERCI
E No. II.
FOR THREE BEARERS.
1.- Tumber th e bearers I, 2, 3.
All orders will be given by No.2, \\"ho will look after the injured part of the patient's body or limbs, to see that no bandages or splints become displaced, and also that No . I bearer, in lifting or carrying tbe stretcher, does not touch the patient 's feet.
2. -" Place the Stretcher."-No. 3 places the stretD1er in a line with the patient 's body, the foot of the stretcher being close to his head.
3. -" Fall In.It-No. I places himself on the left ::iide of the patient in a line with his knees, No.2 on the left side just below the patient 's shoulders, and :Po. 3 "t the right side, and faces No.2.
180
4.-" Ready."-All kneel on the left kn ee. No. t places his hands, well apart, underneath the 10\\'e r limbs, always tak ing care, in case of a fracture, to have one hand Oll each side of the seat of injury. Nos. 2 and 3 grasp each other 's hands under the shoulders and thi ghs of the patient (Fig. 88).

5. -" Lift."-- The bearers rise together, keeping the patient in a h orizontal position (Fi g . 8S).
6.-" March. "- All take short side-paces, carrying the patient over the stretcher until his head is immediately above the pillow. 183
7. - " Halt. " - The bearers remain steady.
8. -" Lower."-The bearers stoop down, gently place the patient on the stretcher, disengage their hands, and then stand up.
9. -" Fall In. "-No. I places himself at the foot of the stretcher with his back to the patient, No.2 places himself at the left side of the patient, and NO,3 at the head, with his face to\yards the pat ient.
182
IO. - " Ready. "- Nos . I and 3 place the slirgs (i f us ed) over their shoulders, stoop down, and sllp the loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given-
11.- " Lift Stretcher."-Nos. I and 3 bearers raise the stretche r steadily together and stand up.
No. 2 will now adjust the slings on the shoulders of 3 N os. I and 3, taking care that each is well below the level of the collar, and lies accurately in the hullo .." of the shoulder in fr ont. He will also lengthen Cor shorten the slings, having regard to the palient's injuries and the relative heights of the bearers. ,
I2. -" March."- Nos. I and 2 step off with the left foot, and NO.3 with the right. The step shoulcl be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of th e foot.
13.-" Halt."-The bearers remain steady.
14·-" Lower Stretcher."-The bearers place the stretcher ge ntly on the ground, slip the loops of the slings off the handles of the stretcher, remove t he slings from the shoulders, and th en stand up.
IS· - " Unload Stretcher - Ready." - The beare rs prepare to take the patient off the stretche r, as at O rde rs 3 and 4 (Fig. 88) .
16. - " Lift." - The bearers raise the patient, as ;] t Or der 5, and carry him by short side steps, clear d the stretcher, to the bed, or other place to y"hl Ch it has been arranged to convey him (Fig. 89).

185
17.-" Lower."- TL e patient is carefully lowered.
EXERCISE No. III.
WH EN ONLY THREE BEARERS ARE AVAILABLE AND THE TRETCHER CANNOT BE PLACED AS IN EXERCISE II.
I.-Th e Instructor numb ers th e bearers -I, 2, 3·
All orders will be given by NO.2.
2 -" Place the Stretcher."-No. I taking the foot· of the stretcher, and NO . 3 tl:e head, place jt o n the ground by the side of the patient, and as close to him as practicable.
3. -" Fall In."-The three ?earers the saIr: e positions on one side of the patient, as Llld down m Exercise No. I.
4. -" Ready." -Nos. I, 2, and 3 kneel down on the left knee, placing as close to the patient as they can, and then take hold of him as directed in ExerCise o. I.
5. -" Lift."-..:Nos. I, 2, and 3 raIse the as directed in Exercise No. I, and then move m a kneeling position up to the stretcher.
6.-" Lower."-Thc hearers bend forward, fully lower the patient on to the stretcher, and dl Sengage hands.
184
,.-" Stand to Stretcher."-All the bearers stand up; No. I goes to the foot, No. 2 remains In position at the side, and No. 3 goes to the head of the stretcher.
8.-" Ready."-No s. I· and 3 place the slings (if used) over their shoulders, stoop down, anrl sl p the loops of the slings on to the handles of the stretcher which they then grasp. '
,9.-" Lift Stretcher." -Nos. I and 3 bearers raIse the st:etcher steadily together and stand up.
No.2 will now adjust the slings on the shoulders uf Nos. I and 3. taking care that each is well below the level of the collar, and lies accurately in the hollow of the in. front. lIe will also lengthen or shorten the shngs, havIng regard to the patient's injuries and the relative heights of the bearers.
10. - " March."-Nos. I and 2 step off with the left foot, and NO.3 with the right The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
n. - " Halt." - The bearers remain steady.
12. - " Lower Stretcher." - The bearers place the gently on the ground, slip the loops of the c;lmgs off the handles of the stretcher remo,'e th e slings from the shoulders, and then up.
Unload Stretcher - Ready."- No. I hl!l1self on the left side of the patient, and in a lll1e wIth h.is No. 2 on the left side just below the patIent s shoulders, and No. 3 at the right

ide, and faces NO.2. All kneel on the left knee. No. I places his hands, \,yell apart, underneath the lower limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
14.-" Lift." - The bearers rise together to their feet, keeping the patient in a horizontal position, and carry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
15·-" Lower."- The patient is carefully lowered.
EXERCISE
No. IV.
FOR "C"SE IN MINES Al D NARROW CUTTINGS \\"HERE TIro MEN ONLY CAN BE ENGAGED.
Nos. I and 2 will carefully place the stretcher in a lIne " 'i th the injured man's body, the foot of the stretcher being, if possible, * close to his head.
No. I straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, passes the left hand under the patient's thighs and
• It is not advisable to be too particular as to the head or !oot a stretcher in a mine, a.s it would probably be quite Imposs!l:lle to reverse it.
186
187
188
the right hand across and under the patient's calves . N o . 2 places his feet one on each side of the patient between his body and arms, the toe of each foot as near the armpits as possible . He then stoo:--s down and passes his hands between the sides of the ches t and the arms un del neath the shoulders, and locks

FIG. 90 .
th e fingers (Fig. 90 ). If the patient 's arms are uninhe may put them round the neck of No.2 , an d this means greatly assist him in lifti ng .
189
\iVhen both are read y, No . I will gi,'e the order " Lift and move forward. " The patient is then to be slowly lifted, just sufficient to allow his body to clear the stretcher. Both bea rers will slmrly and gradually move the patient forward, NO . 2 by very short steps, No. I by be n ding his body forward as much as he can 7.N·tllOlIt movz'ng Ius feet (Fig. 9 J) . TO. I now cri,'es the order " Halt," whereupon No.2 remains st;ady, a n d No. I advances his right foot to his left , and
FIG. 9I.
again ad,'ances his left foot till the toe touches the heel of NO.2 . No. I then gives the order "Adva :1 c e, " when the patient will again be moyed fo rward . These moveme n ts are to be repeated until

the patient is over the stretcher, when he is to be gently lowered.
The following Stretcher Exercise is adapted by permission from the Royal Army Medical Corps Manual, 1908.
All orders will be given by NO·4·
I. "Fall in." -Six bearers fall 111 behind each
2. "Number."-The bearers number from front to rear.
3. "No.3 Bearer, right (or left) turn-supply stretcher-quick march."-N o. 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower foot wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place . He turns to the front, and, passing the lower end forward, places the stretcher on the ground to the ri ght of the squad, \\ heels to the right, front end of the poles in line with the toes of No. I and rises.
4. ,( Stand to Stretcher."-No. I places himself with his toes in line with the front ends of the poles. NO.3 with his heels in line with the rear encls of the poles, close to and touching the stretcher with
190
ID 1]] 0 rn @] ;.F IG, !;2. 8i m @ ' G m m Flc, 93. 19 1 ,m,,'rnJ 5 @] ' W\ ,T ; m,\'. ,. I " 0 I, '" I , ' \ ' ; ..... 1I ,I \ \ \ I " \ '. " !', \ •... 'I I, L?j ,II ' I I FiG. 95. I I I rn I' I ! "-'H2J .3 ,I. • , :4. /:,' t -4 r.",\ I Z >1 , 'f : : 6':' , I •• _.,,' I :5:/ ' L.... I ' .t' FIG. 94· 96'
hi s right foot. Nos. 2, 4, 5 and. 6 take up their positions one pace behind and covenng off the bearer in front of them (Fig. 92).
5. "Lift Stretcher. " -N os. I and 3 stoop, both handles of the poles with the right hand, rIse together holding the stretcher at the full extent of the arm, wheels to the right.
6. " Collect Wounde d - Advance ." - .The squad doubles by the shortest route to the patIent, and halts without further word of command one pace from the head of and in a line with the patient (Fig·93)·
7. "Lower Stretche r." -N os. I and 3 place the stretcher quietly on the ground, and rIse smartly together.
8. "Prepare Stretcher. " - Nos. I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps, and place the slings on tl:-e ground beside them, separate the poles, and straIghten the traverses.
Two. On the word two each takes a sling, doubles it on itself, slips the loop thus formed on the handle, and places the free ends over opposIte handle, buckle uppermost. They then rIse and turn to their left together.
'While the stretcher is being prepared by Nos. I and 3 the disenaaged bearers will advance and , b b render to the patient such aSSIstance as may e required (Fig. 94).

193
The necessJ.ry assistance haying been rendered, NO.4 will give the command-
9. "Load Stretcher." - The bearers place themselves as follows :-Nos. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; Nos. I and .f at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the \", hole kneeling on the left knee. Nos. I and 4 pass their hands beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the beacrs being detailed for this purpose (Fig. 95).
10. " Li ft."- The whole will carefully lift the patient on to the knees of Nos, I, 2 and 3.
Two. Nos. 4, 5 and 6 will then disengage, rise j Nos. 4 and 6 step back one pace. No. 5 turns to his left, doubles to the stretcher, takes hold of and raises it, left hand across, the near pole resting on the left hip; carrying the stretcher, he returns to his place between 4 and 6, and places it beneath the patient.
Tlzree. Nos . .f and 6 step forward one pace, and together with NO.5 kneel do\Vn on the left knee, and prepare to assist in lowering the patient (Fig. 96).
II. " Lo we r."- The patient is lowered slowly and gently on to the centre of the canvas (special care being taken of the injured part).
Two. The bearers dIsengage, rise ; Nos. J, 2, 3 a n d 6 turn to the left; Nos. 4 and 5 to the right; H
19 2
No. 4 places himself three paces in front of the stretcher. No. 6 having collected the kit and arms of the patient, places himself three paces in rear of the stretcher, Nos . 2 and 5 opposite the centre of the stretcher. The whole are now ready to Ii! t stretcher and move off (Fig. 97).

195
12 . " Lift Stretcher. " -N os. I and 3 stooPI grasp the doubled sling midway between the poles with the forefinger and thumb of the right hand, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between the handles, and place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed 'so that they lie well below the collar of. the coat behind and in the hollow of the shoulders 111 front. In the event of the slings requiring to be adjusted, either as regards length or for the greater comfort of the bearers, NO.4 will detail a bearer to carry this out, the length of the slings being adjusted, when necessary, by means of the buckles.
Two. Nos. I and 3 stoop, slip the loops over the handles, commencing with the left, and grasp the handles firm ly.
Three. Nos. I and 3 rise slmdy together, No. 3 conforming closely to the movements of No.1.
13. " A d vance."-Nos. I, 2, 4, 5 and 6 step off with the left foot, No. 3 with the right, stepping short.) knees bent, feet raised as little as possible.
14. " Halt ." - The whole halt.
15. "U nlo a d Str etch er." - The bearers place 1hemselves in the same position at the stretcher as .d.escribed for Loading (Order 9).
16. "Lift."-As described for Loading (Order- 10)1 HZ
194
::0 ;rE I I FI
FIG.
e 97
98.

I96
except that the stretcher is carried forward three paces clear of the patient's feet.
17. "Lower." - The patient is genti y low ered to the grounc The bearers disengage, ri se ; N os . I, 2 and 3 turn to the left, 4, 5 and 6 to the ri ght , and the whole step off to their places at the stretcher, as at Order "Stand to Stretcher" (Fig. 98).
The Ashford Litter is made up of either of the Furley stretchers mentioned on pages J 72 and 173, a wheeled under-carriage and a waterproof hood and apron, or, if preferred, a light wet-resisting canvas cover. The stretcher is kept in position on th e under-carriage by the foot-wheels, which fit into slots in th e sides Gf the under-carriage, and it can be removed at pleasure. The under-carriage is fitted with a cranked axle, \vhich allows the bearers to pass with the stretcher between the wheels instead of lifting it m-er them. At both end s a re two legs which may be turned up as handles when wheeling the litter. The hood and apron fit into sockets screwed to the stretcher. In wheeling th e litter, care should be takell to keep the patient in a horizontal position. Should it be necessary, two bearers can easily lift the litter and patient.
The Rea-Edwards Litter, introduced in I904, is used in a similar manner. and one model of it is fitted with pneumatic tyr es, which add immensely to the comfort of the patient and to the ease of propulsion. I97
CHAPTER X.
(Being the .F/jill L ecture for Females only, z'it accordance witll Syllal1lls 58.)
BY E. :'IIACDO .\ELL COSGRAVE, F.R . C.P.I.PREPARATION FOR RECKPTION OF ACClDE::'\T CASE
"\\-HEN ne\\ s of an accident comes, prepara tion shoulcJ. at once be made so as to have everything ready before the injured person is brought in. Of course the preparations needful \\ill vary according to the nature and exten t of the injury, but the following are the chief things wbicb may have to be done.
CHOICE AXD PREPARATION
OF
A room must be chosen. In a bad case this should be one easily reached, as it is difficult to carry an injured person through n::urow passages and up-stairs. Unless there is some such rC[lson against it, the It1jured person's own room is b st.
The way to the room mu t be cleared, projecting furniture and loose mats in tbe hall or in lobbi es should be remm-ed. If the injured person is carried on a door, shutter, or stretcher, two strong chairs shou ld b e placed ready to support it wherever the bearers ,,"ould be lik ely to require rest.
Useless furniture should be r emo yed fr om the bedr oom . The bed should be drawn out from the \Yall
so that both sides can be approached, and the clothes turned back to one side to their full lengrh. A hot bottle should be got ready. If there is much collap se several hot bottles and hot blankets be requIr ed; cover the hot bottles with flannel.
If th e injury is very severe, if mud-stained clothes have to be removed, or if extensive dressings have to be applied, it may be necessary to have another bed, a couch or a table plac ed near th e bed to lay the sufferer on in tbe first insta nce. This should be so arranged that soiling may do no harm; olel sheets, wat erpoof materials, thin oilcloths, or even nc\\ spaper, may be us ed as a protection.
LIFTI:\ G AND CARRYING .
If present at the place where the accident occurred, it will be necessary to see that the patient is carefully lif[c d after proper "First Aid" has been
The follO\\-ing rules should be remelTI b ereel :- Select the proper nUI11 ber of persons to assist, anel do not let them lift the patient until they thoroughly understand how they are to do it.
For ordinary cases, \\ here the injured person has to be lifted a very short distance, three h elp ers are 1\\"0 (\\ ho should be as far as possible of equal height) are to bear the wei ght, th e third is to support and take charge of the injured part. This is

hest done by a person who has been through a " FIrst Aid" course. If the injured person is insensIble, another helper should support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient's back at the 10\\ er part of the shoulder-blades, and und er the hips, clasping each his right hand in the other's left.
The injured patient should, if practicable, place his arms round the n ec ks of the bearers .
The third helpE"· should attend to the seat of injury; if tllis is a fractured limb, he should support it by placing the palms of his hands und er the limb, one above and one below tIl e sea t of the injury, grasping it fi rmly but avoiding unnecessary pressure.
The helpers should remain thus until the order ,. Lift" is given, and tben they sbould all lift slo\\ ly and steadily, ayoiding jars, attempts to change position of bands, etc.
H the injured person is to be placed on i1. stretcher or shutter, tbis should be preyi ously placed with tbe b ottom end at his head; the bearers sbould then move, one at each side of it, until tbe patient is 0\ er it. The word "Lower" should then be given, and the injured person should tben be slowly lowered. A pillow or folded-up coat sbould be ready, and as tbe sufferer is lowered this should be placed under his head. *
* Full dileclions are gi\'cn in Cl a.per IX.
199

.1IEANS OF CARR YIXG.
Besides a stretcher, and substitutes such as a gate, a shutter, or a door, other means of carrying can be improvised. .
In slight injuries, where the injured person IS unable to walk, byo bearers can carry him by forming a fourhanded three-handed, or two-handed seat.
A seat is formed as described on page 160.
A three-handed seat is made as described on page 162.
The two-handed seat is made as described on page 16I.
A sino-Ie helper can lift by supporting with one arm the two b knees, and with the other the back. The arms must be passed well under before cOlTP llcncing to lift.
A single helper can give SUPPOl:t by his arm round the waist, grasping tl:e hlp and placltlg injured person's arm round hIs own neck, holdll1g the hand with his own hand (Fig. 76, page 165).
A capital stretcher can be improvised out of a strong sheet and two broom handles or other short poles. Each side of the sheet is wound up on a broOl:n handle until there is just room for a person to he between. This requires four bearers, two at each side, to prevent the sheet slipping.
201 '> CARRYING UP STAIRS
.
In carrying a stretcher up stairs the. head should go Drst, and an extra helper should assIst at the lower end, so as to raise it and keep the stretcher nearly horizontal.
The two three or four-handed seat may be used , , . 1 . for carrying up stairs; or a strong chair, t 1e patI ent hein rr carried up backwards. In the latter case cne should walk after the chair and l:elp to support il, and to the injured person shppll1g out.
LIFT! TG INTO BED.
If the bed is narrow and there is room the stretcher be placed on the floor \\'ith the head close to the foot of the bed. The injured person should then be lifted over the foot and placed on the bed. If the bed is to o \"ide to admit of this, the stretcher should be placed beside it, and two helpers should stand at the far side of the stretcher. On e helper passes one arm beneath the shoulders and one the middle of the back, the other helper plaell1g hIS under the lower part of the. back .J1Dder the knees. The injured person IS then lIftea, another helper pulls away the stretcher, and after a single step f )[ward the burden is placed on the bed.
200

PREPARATIOK OF BED.
A firm mattress, not a feather bed, should be selected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placeu on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of wa terproof sheeting or of thin oil-cloth should be placed un ler the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean part drawn smo othly under the patient.
In fracture of the leg or thigh, sprained clt1kle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " cradle 1/ is to support the bed-clothes and keep them from pressing on the Ii m b.
A band-box (Fig. 100), three-legged stool (Fig. 101)/ or hoop sawn across and the two halves secured together (Fig. 102 ), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REMOVING THE CLOTHES.
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
201
203
FIG. 99·
FIG 100.
FIG. 101.
In removing a coat, etc., in a case of fractured arm the uninjured arm should be drawn out first.
In putting on a coat or shirt the injured arm shoulJ be put in first.
In burns and scalds nothing should ever be dragged off. A slzarp pair of scissors should be used, and everything not adhering should be cut away. If anything adheres it should be left until medical aiel

FIG. 102.
can be obtained. The clothing adhering may, with advantage, be soaked with oil. To remov e the trousers from a severely injured limb, the outside seam should be ripped up.
PREPARATIONS FOR SURGEON.
As soon as the injured persoll has been attended to, preparation should be made for the surgeon's visit.
205
Thepreparations needful will depend upon the nature of the case. The follOWIng hints may be of use ;A fire in the room helps vent ilation, even in summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot bath does well. The basins should be placed on a table, covered with a clean ,yhite cloth; a large towel makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be within easy reac h. The foot-bath should be under th e table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths, old l;nen, oil, and baking soda, should be r eady, and materials should be torn lJP for bandages.
In the case of hremorrhage, plenty of water should be boiled and allowed to cool, and pads of absorbent cotton wool should be baked in a tin box in the oven, and at least two basins should be ready.
In the case of a person rescued from drowning the sh eets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
204
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large towel.
When summoning a medlcal man to all accident always let him know by a written message what kind of case he is reqUlred to treat, so that he may bring whatever is needful. By this means valuable time may be saved.
QUE TIONS 0 CHAPTER X.
Tile II1tlllera/s iud/cate the pages wllere the allSwt1'$ ilia), be fOU 11 d.
What points would you consid er when choosing a sick
room?
197
How would you clear the way to the sick room? 197
What means of resting would ynu provide for those carrying a patient on a stretcher? ...... 197
How would you place and arrange a bed for an accident case? ... 197, 198
Are hot bottles necessary, and how would you prepare them?...
.. 198
'What is often necessary to lay the sufferer on in the first instan ce?
... 198
How would you protect this from gelling soiled? ... 198
How would you see to the proper lifLing and carrying of an injured person?
'" 198, 199
vVhat substitutes for a regular stretcher can you suggest? ::00
How is the four-handed seat made? 160, 161
For what cases is this seat ustful ?.. 160
How is the three-handed seat made? 162, 164
207
For what cases is this seat useful? ..
How is the two-handed seat made?
For what cases is this seat useful? ..
How can a single helper lift? ... PAGE 162 161, 162161
lIow can a single help er give SUppOlt?
How would you improvise a stretcher? ... . ..
How many bearers are req uired for this stretcher?
How should a stretcher be carried upstairs? '"
How would you carry a patient upstairs on a chair?
lIow would you lift a patient from a stretcher to a bed?
How should a bed be prepared for an injured person? ...
How sheuld a draw sheet be made?
What would you place under the draw ::: ...
What should be done with the soiled part of a draw sheet?...
vVhat is the use of a " cradle "?
In what ways maya cradle be improvised?
How would you rem ove a coat or shirt in the case of a fractur ed arm?
How would you put on a coat or shirt if the arm were injured?
In the case of a bad burn, what would you do with clothing that adhered to the patient? ...
How would you remove trousers from a severely injured limb?...
vVhat preparations would you make for the surgeon's risit?
\Vhat would you get ready in the case of a burn? .. .
And what the case of hzemorrhage ? ... ... .. . what In the case ora person from drowning?
\\ hat would you get ready for makmg poultices?
And for fomentations?
\Vhat sort of a message would you send tt) summon a doctor? ...
206
PAGE
......
... ... ... ... ...
...
... . ...
...
. .
... '" ...
... . ..
... ..
... ...
... ... ...
... .
... '"
..
... ... .. . ... ... ...
...
........ .
. . . . . . . .. . .
200 165 200 200 201 201 201 202 202 202 202 202 202 204 204 204 204 205 205 205 20 5 20 5 206 206
208 I NDEX .
Abdomen Page 11 I wound of 112
Accident case, preparation for 197
Acids, poisoning by I49, 151
Air, always necessary... 18
Alcohol, caution as to smell of 13 0
Alcohol, poisoning by 134, 153
Alkalis, poisoning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30, 32 " sprained.. . 64
Anterior tibial artery 93
Aorta 79
Apoplexy 13 2
Apparently drowned, to restore .. .
Ann, bone of " fracture of Ann-slings
Arsenic, poisoning by Arterial hGemorrhage, 139 28 52 39,49 148 arrest of 74 " "
Arteries pracli ing arrest of signs of " course of main ...
Artery, axillary . .. 79 74 70 79 85
Artery, brachIal. .. " " carotid dorsal of foot facial femoral ... iliac occipital plantar ... popliteal radia.l subclavian tilJial temporal " ulnar
Artificial respiration 121, 129, Asphyxia Atlas
Auricles ...
Axillary artery Axis
Back, bandage for BacklJone
Bandage, to apply to fold 13 6, " to improvise ...
Bandaging
Bed, lifting into .. . " preparation of Belladonna, poisoning by 159 23 42 37 37
Page
Bites of rabid animals 106
Bladder . .. II I, 113
Brachial artery ... 86
Brain I 17 compression of 13 2 " concussion of 13 1
Breast-bone 26 " fracture of 48
Broad bandage . . . 37
Broken bones, see Fracture.
Bronchial tubes... 118
Brooch-bone 30
Bruises 102
Burns 102
Capillaries
CafJillary hremorrhage
Capsule . . . 70, 72 95
Circulation of the blood, organs of Circulation of the blood, to induce Clavicle ... " fract me of
Clothes, removal of 19, 202 25 Coccyx
Collapse ... Collar-bone ... 13-1:6 " fracture of ...
Comminuted fracture
Complicated fracture
Compound fracture
Compression of the brain
Concus ion of the brain
Conductor

Carbolic acid, poisoning by Carotid arteries ... from" hGell10rrhage 31 15 2 80 80 28
Convulsions in chiltlren Cradle, bed
Carpus ... . ..
Carrying, means of 160, 200 " upstairs
Cart ilage
Ce rebro-spinal system
Cervical vertebrre
Ditch, to cross with stretcher 169 Dorsal artery of foot 93 verte brre... 25
155 201 202 148
Chlorodyne,
. .
Cheek, bleeding from Chest, bandage for
poisoning by Choking
. 201 25 1 I 7 25 82 149 140
Cranium
. " fracture of Crepitus ... Crushed hand foot 48 35 3-l 3413 2 131 '-1-3 137 202 22 43 36 55 62 Diaphragm 120 Digital pressure... 74 Direct violence... 33 Dislocation
..
62
Dress, woman's, on fire." 105
Drowning 139
Ear-channel, blood issuing from
Ear-passage, foreign body in

Fireman's lift
First aid, meaning of " student
Fish-hook, embedded
Electric shock
Emetic
Epilepsy ...
Elbow, bandage for " joint, fracture in98 110 159 volving 53 J4 2 148, 149, 150 13 2
ESl1larch's bandage
Expiration triangular
External carotid artery ...
Eye, bandage f"r foreign body in
Face, bones of
Facial artery
Fainting .. .
Femoral artery " "digilal pressure at groin ...
Femoral artery, tourniquet for
Femur " fracture of
Fibula " fracture of
Fingers, lJanc1age for " fracture of 37
Flexion ... at elbow " at knee ...
Food, poisoning by
Foot, bandage for Lones of ... " crushed
Forearm, bones of " fract ure of .. .
Forehead, bandage for .. . " h;emorrhage from
Foreign lJody in the earpassn.ge ." in the eye " "in the nose
Four-'nanded seat
Fracture, apparatus for treatment of ... causes of " " definition of ... general rules for treatment involving el bow joint of arm ... of breast-bone of carpus of collar - bone of cranium of finger
Fracture of forearm of knee-cap of leg ... 54 58 60 of lower jaw ... of metacarpus o f metatarsus .. . of pelvis of ribs ... of spine of tarsus of thigh-bone ... of toes .. signs and symptoms of
62 56 46
62 56 62 " varieties of 35 34 108 Frost-bite Fungi, poisoning by 153 General circulation 70 Granny knot 4 0 Green-stick fracture 35, 36 Gums, hremorrhage from 97 Hremorrhage, arterial ... 74 capillary... 95 from gums 97 from head " and neck 80 from lower limbs ... 89 from lungs 97 from nose 96 from stomach 98 Pag. IIremorrhage from throat 97 fr om tongue 97 fr om tooth socket... 97 fr om upper limbs... 84 internal 95 kinds of 73 " venous 93 Hand, bandage for 157 " bones of ... 28 Hanging... 140 Haunch-bones ... 28
Headand neck, arteries of 80 Head bandage for ISS injury to... 128, 131 " side of, bandage for 155 Heart 70 ., rate of contraction of 72 Ileat-stroke 136 Hernia 114 Hip, bandage for 157 History, meaning of 17 Iloward's method of artificial respiration 126 Humerus 28 " fracture of 52 Ilydrophobia 106 Hysterical fits 133 Iliac arteries Impacted fracture Indirect violence Insensi bility 79 35, 36 34 128
210 Page
120 80 ISS 109 22 8r 13189 90 30 56 30 60 159 55
110 109 1 II 160 36 33 33 53 52 48 55 48 43 55
211 Page
44 55
45
{ 'b'" 1 J Page nSenSl lilt)', genera ru es fur treatment 128
Inspiration 120
Instep 30
Insulator .. : 142
Internal carotid artery
Internal hremorrhage 95
Intestines, injury of 1 13
Involuntary muscle.; 33
Jaw, angle of " lower " "fracture of
Joint, definition of " injuries to .. ,
Jugular vein
Kidneys
" injury of Knee, bandage for Knee-cap " fracture of
Knot for bandage of lower limb
Knots, reef and granny
Laborde's method of artificial respiration
Laburnum seeds, poisoning by .. ,
Lacerated wound
Large ar!ll·sling
Laudanum, poisoning by
Leg, bones of , , '

Leg, fracture of Lirting and carrying " into bed
Ligaments
Lightning, effects of Limbs, lower "
Lime in the eye bleeding from Litters
Liver " injury of Lower limbs
Lumuar verteurre Lungs
Hall's
Page
Nervous system... II7
Nose, foreign body in I I I hremorrhage from 96
Occipital artery... 82
Opium, poisoning by 148
Pad, ring ... " to fold
Palm, hremorrhage from Palmar a,rches ... 83
Paregoric, poisoning by 149
Patella fracture of " fracture of Phalanges of foot " of hand
Phosphorus, poisoning by 148,
Physiology (elementary)
Plantar arch " artery
Plants, Yarious, poisoning by ... Pleura
Poi son e d we a po n s, wounds by Poisoning
Popliteal artery ...
Posterior tibial artery
Potash, caustic, poisoning by ... 30 58 28 56 30 28 150 20 93
Pressure, digital. " point ...
Principles of First aid
Prussic acid, poisoning by Pubes
Pul monary circulation
Pulse
Pupils of eyes
Rabid animals, bites of...
Radial artery
Radius " fracture of Reef knot
Respiration artificial I, 129, 136, " to excite
Respiratory system
Rest, necessity for Ribs " fracture of ... Room, choice and preparation of
... 2) 23 44 3 1 J09 80 III I J 3 159 30 58 42 40 126 212
hremorrhage Pa.!Ce 60 ... 198 ::01 26, 31 144 28 26 J 10 82 196 III II} 28 25 120 from 97 Marshall
l\f
bandage 11 elacarpus 14C 37 28 fracture of ... 55 30 67 2(.
... Middle line
from Muscles " ruptured 1\1 uscular action ... N arrow bandage Needle, embedded Nerves 97 3 2 65 34 37 108 118
method of artificial respiration
edium
" fracture of
of body l\I outh, blood issuing
74 88 88
2 1 3
93
Questions
1. II. III. IV. V. VI. X.
on Chapter
l'ac-t 74 74 J7 152 28 72 72 13° 21 66 99 lIS 145 154 206 106 88 28 54 40 120 13 8 1 2 7 II8 18 26 46 197
Rupture (hernia) 114
Ruptured muscles 65
214

Sa.cral verte brre .. '
Sacrum ...
Scalds
Scalp, bandage for " hremorrhage from :25 25, 28 102 155 83 26
Scapula .. , ...
" fracture of Schafer's method of artificial respiration
Seat, four-handed three-handed
" two ·handed
Shin-bone
Shock " electric ... ..,
Shoulder, bandage for ... " blade ... " fracture of bones ...
" joint..:
Sick room, chOlce and preparation of. ..
Signs, meaning of .
Silvester's method of artIficial respiration
Simple fracture .. .
Skeleton .. ... .
Skull
43 " fracture of Slings, arm 39, 40 , 49
Small arm sling ...
Smothering
Snake bites
Soda, caustic, poisoning by
Spleen
" injury of. ..
Spinal canal cord 23,
" fracture of
Spirits of salt, poisoning by
Splint, angular ...
Splints, rules for apply ing to improyise
Sternum ... " fracture of Stimulants
Stings of plants and animals
Stomach ... hremorrhage from " injury of ...
Strains
Strangulation
Stretcher exercise, Army No. I. No. II No. III. " "No. IV. Stretchers, Furler
Pa£,e
Stretchers, to carry 16:;) " to i 111 provise 166
Strychnine, poisoning by 153
Subclavian artery g4
Suffocation 141
Sunstroke 136
Surgeon's visit, preparation for 204
Syllabus of instruction... 7
Sympathetic system 118
Symptoms, meaning of ... 17
Syncope ... 134 31
Systemic circulation 70
Tarsus 30
Temporal artery .., 82
Thigh- bone 30 " fracture of... 56
Three-handed seat 162
Throat, hremorrhage from 97 " swelling of tissues of... 141
Tibia 30 " fracture of 60
Toes, bandage for 159
Tongue, hremorrhage hom 97
Tooth socket, hremorrhage from 97
Tourniquet 75
Transverse wound of abdomen 113
Two-handed -eat ... 161
Ulna " fracture of ..
Ulnar artery
Unconsci ousness
Upper limbs
Varicose veins
Veins
Venous blood " hremorrhage
Ventricles
Vertebra .. .
Vertebrre .. .
Vertebral column
Vertical wound of abdomen
Vitriol, burn by ... Voluntary muscles
'Wagon, to load or unload \Vall, to cross with stretcher . ..
\Varmth, necessity for " to promote
Wind-pipe
"Noman's dress on fire W L"lnds by poisoned weapons accompanied by a... uial hremorrhage ...
'Vounds accompanied by venous hremorrhage
\Vounds, lacerated Wrist
51 121 160 162 161 30 134 142 15 6 28 51 26 3 2 197 17 123 34 22 22
Pag. 39 140 106 149 III I13 23 IIi 23 45 149 54 lOi I II 98 II 65 140 190 174 181 18S 18 7 172.
Pagt! 28 5-+ 88 128 26 94 io 72 93 70 23 25 23 113 102 33 171 170 18 12 7 118 105 106
st. 30hn tllllblllRllce BBBoci
ntiotlf
GENERAL PRICE LIS T.
A complete and reliable Ambulance Equipmcnt is an actual necessity, and experience has proved that employers of labour and others interested in the district readily subscribe for the purchase of such appliances. Collecting cards, stating the purposes fur which subscriptions are required, "ill ue supplied to approved persons gratuitously on application to the II tad Office of the Association, where also any information with regard to i ts work can ue obtained .
All stores will be sent carriage paid to any part of the U nited Kingdom . Returns may IJe sent carriacre forward. If carriage is prepaid it will lJe allowed . ::>
Owing to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhercd to.
will ?e furnished for Amhulance Carriages anu other art.lcles .to Ambulance, Nursing and Ilygiene, not mentIOned 111 thIS list.
Orders and c orrespondence should be addressed to the St. John Ambulance Association, St. John's Gate, C lerkenwell, London, E. C.
Rem ittances should lJe made payable to the St . John Amlmlance Association, and crossed "London County and '" estminster Bank, Lothbury."

The "Ashford" Liller (1899 model) consists of a t\\Owheeled under-caniage fitted with ellilJtical oplings, and either of the "Furley" stretchers, with a coyer so' arranged on a jointed frame that it can be folded up inside the 'stretcher, or with a !;oocl ttnu apron (as sho\\ n abon). The undercarriage, having a cranked axle, the bearers can pass hetween the wheels with the stretcher, and thus avoid lifting, It oyer them. 'When travelling, the legs of the under-carriage are raised, and thus form the handles hy vyhich to pro pel it. Should it be necessary to pass oyer rough ground, l\\0 I earers can easily lift the litter and paLIent. The" Clemetso n " stretcher can be used instead of the" Fnrley" pattern
Carri ag e Paid on a ll Or d ers ill th e Un ited Kin gdom " ASHFORD" L ITT ERS.PR I CES OF THE IMPROVED AS H FORD LITT E R. 1899 MODEL
With I ron Tyres to Wheels. IWith I ndia Wheels
Without I Cover or With Hood and I Cover Apron.
Under-carriage (no Stretcher) . .. . . . I 8 10
Litler complete with Ordinary Stretcher*
Dittowith Telescopic handled Stretchert
Ditto with Police Stretcher!

With Hood and Apron.
Without Cover or Hood and Apron. With Cover. With Hood and Apron.
• Prices quoted fo r Litter with Ordillary Stretcher include 'Vide Webbing Slings but no Chest Strap. Leather, instead of Webbing Slings, 5S. 6d. extra; Chest Strap, 6tl. extra. If sup· p lied withou t any Slings, 4S' allowed.
t Prices quoted for Litter with Telescopic·handled Stretcher inclune 'Vide Webbing Slings and Chest Strap Leather, instead of Webbing Slings, 55. 6d. extra. l!"\'upplied without any Slings, 45. allowed; and if without Chest Strap, rs. 6d. allowed
:t Prices quoted for Litter with Police Stretcher include Wide Webbing Slings and Leather Straps for securing a r efractory patient. Leather, imtead of \Vebbing Slings, 5'. 6d. extra. Hood and Apron, complete (state pattern of Stretcher) £2 10 0 Extra Sockets and Studs, per set
W a t erp r oof Sheet (washable) tc be laid on the stretcher bed...
C ra tes (returnable) charged 4S. 6d . for each Litte r.
.£ s. d.I];7.d.1 .£ s. d.
... 019 5 II 2 I I 10 I2 2 0 1 I I 0 6! 12 17 0 1 13 5 61 13 17 0 112 10 0II4 5 6 I6 2 o o t!l 15 14 7 6 6 o 14 15 0116 10 o 6 115 7 6117 2 6
0 6
0 1 0 6
&. g' 2· ;::r 0. 3.3- C1> j 0 (!, n; ::=..0-: j ;;0(;; [Jq r-(Xl ::r:> o ' := o iii I7Q "C III c: o :l o tl II> S· ;;: c Co '" 5' I7Q Po ? o iii' (JQ ;- g: :: :: ;; 8. c::i :: 0. r;3' :::r-' -' n (U CIQ o.t"t:l o 0 I" c: o :l 2: 5 QJg. C1> CJ'J ::J Ul rJ -. :3 -. _.,.... ,- (t) _.""'" 0 :::r" en rf) ;:l ::r (Il C1> :l C1> S <"' C1> (i) ,....,...J -('0 C1> _::r -Ul ('0 o g ;::-:C1Q ==' x r- o· $I> ;. 0 """'" 2C1>Cii"d 0. _ - :l r' n ;>:> -. (b ri (b(fq J) =:--0 !i ;;; '-:: r. .- n ::s ('t'I g _.;:: (b ;:; g ... a ....... ;:r _. 2. r-"Q 0-: (ji' .... ;:l 9-:t:l ::l V' [JQ :: r' il'(Il >-1 o (Xl [.3 r-::;: :'!:J p:::r o 0 x 0 0. :::J")C1> (!l c. (!l (f) y9 ;=; > C/) o a. II> 5' ; C :l ;::;: Q. '" :;' 3 ?,, '
Carriage Paid on all Orders in the Un tted Kingdcm.
oyer them, anrl the cranked axle has, therefore, been replace I by a straight one constructed of tubular s·oel.

" REA-EDWARDS" filled with pneumatic tired wheels, showing the " Clemetson " Stretcher.
Ball b earings are fitted to the wheels, both cycle pattern and wooden, and the hubs are so arranged that the wheels can be removed from the axle without disturbing t he bearings. In place of the four legs made to raise a:; handles, twv fixed legs filted with slllall indIa-ruuue r or roUers arc placed at the foot end, while a coml)lned leg and hanule fitted wilh a crossbar ancl capaule of be ing raised or lowered is used at the head end. \Vhen raised as a handle it may he locked in olle of two position, and when lowered it is locked in a vertical position. The a(lIr antages claimed for this arrangement are simplicity, ease and rapidity of manipulation and
Carriage Paid on all Orders in the Un ited Kingdom
the facility afforded by the two fixed legs for raisin.g the litter if necessary on to the pavement. The que lIOn of has been' carefully studied, and the is shifted for wa rd so that the middle of it is several inches in froIrt of I he axle, a perfect balance when the stretcher is loaded and in a. horizontal position being thus obtained, and con seq lien II y there is no weight on the hands of the person propelling the litt er. .
The pneumatic tyred wheels are strongly rec ommenu ed JJ1 cases where the small amount of care necessary to keep them inflated can ue gi\'en, as the comfort to the pat,ient ease in propulsion are increaseu. beyond all compariso n any litter yet produceu_ It wIll be noted that the prices are consideral)ly lower than th ose of the Litter, and the following are gi\'en as examples, but O\\JJ1g. to the vast number of combinations that can be made \I Ith the different stretchers and coverings, it is i mpossiule within reasonahle limits to set out quotations for the whole of them, but these may be calculated by adding together the prices of the under-carriage, stretcher selected , and hooJ and apron or cover, see pages 4 and 8 to 10.
SPECIMEN PRICES.
Under-carriage only, either with pneumatic tyred cycle \\ heels or solid ruuber tyred wooden whe els, £10.
Littcr complete with ordinary stretcher (no slings or chest strap) and hood and apron, £14 3s. 6d. .
Ditto with Telescopic IIandled Stretcher (With chest strap) and hood and apron, £ 14 1 IS.
H "vith iron tyred wheels prices are '£2 less. . .
Th e lowest priced iiLL er c omplete IS fiLLed WIth Iron tyrecl wooden wheels, ordinary stretcher (no slings or chest stralJ) and cover. Price £10 8s. 6d_
Hand brake, which a cts automatically when the litter is at r est, extra £1 lOS.
\Vh en ordering please state which wheels are required.
'i Carriage Paid on all Orders in the United Kingdom . THE " CLEMETSON" STRETCHER.

"CLE:lIETSO:'\" STRETCHER, with back rai ed, also shulling extending legs.
On this stretcher the patient can be moved as desired, from the recumbent to the silting posilion. The re is no complicated mechanism to get out of orde r, and the adjustment depends simply on the balance of the patient's body. The stretcher wiH fit either the" AshforJ" or the" Rea-Edwards" Under. Carriage. Price £3 3S. ; with legs, £4 3s.
Hood and Apron, Ventilated, £2 15s.
Canlage Paid on a ll Or de r s in th e Un ited Ki n gdom. s
ADJUSTABLE LE GS FOR S TR ETC HE RS
.
Primarily these legs, II hich are inc1epen dent of and :1dd itionalto the ordinary foot wheels, are intended to f.lcili ta'e the carriage of a stretcher in a railw::ty compartm ent, in which case two on one side would be lowered al1<.l adjusted by a tele,copic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the adjustaule legs on the other side would rest on the Aoor. The four legs may be used to rai.,e the stretcher as reCJllircd . \Vhen not in use they are folded up immediately under lhe poles of the stretcher-
Price per set of four, £ 1.
FIRST AID BOX.
T o be carried uelow the axle of the" Rea-Edwards ,. from which it is easily detachable .
Contents :-Set of Splints, 12 Triangular Bandages, 12 Roller Bandages, 2 i lb. packets each Cotton \Vool and Bali: Lint_ Adhesive Plaster, Pai r of Scissors, Knife, 2 oz. each Olive Oil , Tin c t. Eucalyptus B.P.C., Sal Volatile, and Spi rits Ethe r Comp., GJaduated Measure Gla_s , Kic1ney£haped Dressing Basin , 6 T ampons fo r washing wound ;, T ourniquet Pins , Safety I ins, Needles, Thread and Tape.
1 rice £2 .

PRICES OF THE "FURLEY" STRETCHERS, WITH THE LATEST IMPROVEMENTS (1899 MOD E LS ). t\. B.-T he prices of the Standard :\Iodelc; are shown in heavy tY!x_'.__ With Wide With Wide With With Without Slin::", or Chest Strap Slings Slim;' Slings Slint:!' an I Webbing I W "hhing Leather Leather (no Chest and (no Chest WtbbinC! Strap). _ Str:1p).
O rdinn.ry Stretcher, for General [, ,. II. (, s. d. d. 1[' s d ami Brigade use, taki ng the place of both the olel ordinary and military patterns I r 3 6 1 17 6 I 19
T elescopic· handled Stretcher for workinginconfined spaces I H) 6 2 3 (, 2 5
2 () 0 Stretcher, very strong, with Ash POk5, an(l pw\·i.]ed with Leath er Straps to secure a refra cto lY patientComplete, with 'Yide Webbing Slings " "Leather Slings
Sl ings , \ Vide vYebbing per pair Do. L eather per pair (or if purchased with the Stretcher instead of We bbing SI ings, 5/6 extra)
Cover (awning) for Stretcher (when ordering please state p<l.llern of Stretcher) ...
Superior Hood and Apron (see illustration, page 2)
Spare Bed for Stretcher
Army Rug to cover Patient on Stretcher
Pillow for Stretcher, stuffed hair Chest Strap
ro
(I):::s<'""O 0-
(f) ::r-
::$ 'D
en OJ -. r"'1'"('t) 0 rt: o '"" l" u 0" l" ::l (f) ::l (b 0- 0 (I) ...,. ::r-l" (I) (f) () '""0 '" 0 p:> (')
(I)
o"u 0 (I)
o
<:
::l o·
(b
(I)
g
-.<
n (0
-
§ g (') (0 ;: ,..,. \0 3
9
r-- 0:
0 ::3 g ...,.
if. 0
U; () vi ;. 0 g- 5..§ ;: _, ; i ;ii i· ; r- Q =u ni jq.: p' g g. [ :. g ::r-::l > .., 0- S () 0-,<: (f) f' ::l CL 0 r- g &CfQ w ::r-(b l"..,"" l" '""....., D. 0 ,.- :r ;::.' () ;.. go a -. _ d 9 _, (J §, (t) Y. ::: 0 0.. (3 r; :l 8 8. (t) en 0.. 0' 0 §. g-....., g- ;. g ::l !>l era: ro 0 .po. rD o d Z :;d -< Ul :;d t<l () t<l i () t-' t<l t<l t-' Bl () o >u G ;; t; r-" t=l d Ul '"' () t<l :;d I o '"d t<l r > Me "a 0"",, <:= trlttj i("",, (f) :.'" CD \01-4 0= t"'tzj (J)
r- : [- g. i; (b 0 c..Ul c;? (f) 0 '"1
'"" u t-rJ l" c..c U'J -<
3.
:: 0'
,.-
-<
...,.
O-::r-
5· 8.
::; :;' ;.:;
g 0 (I) c.. c.;:; .....,
S 50 & (/) ro n
o(l)cn col"()('Jqr-::r-
5 -, Pl g ¢ ;; g
;. r- 0] U'J _.
:E
, 8
E.
t:
c.,
i
(f) u.
0 2 3 0
0
/., s. d. 2 4 6 2 10 6 ;; <1. 2 17 6 3 3 0 0 4 0 0 9 6 o IS 0 2 JO 0 0 8 6 0 6 6 0 7 () 0 I G .l) t:'J ;;;. IIQ C!l "0 s:u () :s o n rtJ c: (!) c. " ; . aq c. o .:J C') w· {JQ C!l " III ii o :s o ;. c: ;; Q. " ; ' I1Q g. ?
Carri J ge Pa i d c'n all Ordels in th e Un !te d K ingdom.
TH E EQUIPO IS E B ED.
I NVALUABLE FOR INVALIDS, CO:-i\'ALESCE -TS, A:\l) TilE GE ERAL PUBLIC.

The movement of the bed to any pOSItIOn is so easily effected that the person lying on it can regulate the muYcment of the bed to any angle without assistance. It can be locked in seven different positions. Price from £5 I5s. 6d.
FOLDING CAMP BED.
This can be folded in a very mall compass and can be readily set up to furm a comfortable bed. Price, £r case for same , when fulded, fitted with carrying strap, 55. 6d.
Pocket Cork Line and Drag, with 80 feet l, - line, in case' j for recovering a drowning person from the water. Price c')mplete, with instructions fu r use, 6s. 6cJ.
Pocket Reel and Ice L ine for use in ice accicJ(;nts, with a feet of line in case, Price complete, with instructions for use, 6s _ 6d .
\:arrlage Paid on all Ordel S in the United Kingdom. 12 " LOWMOOR JACKET ."
Fo r use in nlines, ships' holds, etc., to secure a ratient on a stretcher (see illustration), which can then be placed in an upr ight position. Price £r Ss.
WATER. BOTTLE.
Copper tinned, with carrying strap . Price lOS.
Enamelled I ron \Vater BOUle, Cloth co\'ereci, with Strap 'ind Carrier. Price 48. zd .
13

Carriage Paid on all Ordels in the Un i te d Ki ng d om .
Dressing Basin , kidney sh'lped, made of enamelled iron.
Price IS. 3d. LAMP.
This is fitted \\ith a socket, by \\ hich to fix il to a Lilter, or it can be cOl1\'cnicntly carried by hand, or attached to a uelt or the clothing.:
Price complete, S'l. Cd.
C arti a ge Paid on all Orders in the Un lted Kin g dom
L ARGE HAMPER FOR AMBULANCE ST A TI O N AND RAILWAY PURPOSES.
Ambulance Station Plate, Enamellcd Iron, 6d . each.
Stretc.her Depot Plate , Ellamelled Iron, 3s. 6d. cach. Carrymg Sheet for carrying patients up and down stairs or otherwise ahoLll a house. Dcs!gned by J. C. De rham, Esq., Blackpool , and l\Irs. Alfred Pame, Bedford The sheet is filled with rope handles and dctachable bamboo poles, and may be placed on a without disturbing the patient. Pnce complete, ISS
Fur contcnts see next page.
15 Carriage Paid on all Orders in thl! United kingdom. T ilE CONTAINS
I ,,{ "plints.
I Elastic Band Tourniquet.

l b. Boric Lint ..
Ih. Carholic I Cotton Wool Lrn T in JCases.
I Roll Adhesi \'e Plaster.
2 0 Ro)ler Bandages, assorted.
I do7.. Triangular Bandages.
3 pieces Tape .
4 oz. Sal Volatile .
4 oz. Bicarbonate of Soda.
4 oz. of Oli\'e Oil.
4 oz. Spirit Ether Compo
i lb . Tin Powdered Boric Ariel.
4 oz. Tincture I od in e.
I pair Pean's Furceps.
I pair Scissors.
I Kni fe .
1 2 Surgeon's Needles.
I packet each Safety and Plain Pins.
1 oz. Carbolised Chinese Twist.
oz. Silkworm Gut.
I reel each Black and " 11ite
Sewing T hread.
I Kidney-shaped Dasin.
I Stopper Loosener.
Graduated Measure.
I cake 20 per cent. Carboli c Soap.
I 1\'ail Brush.
3 Empty 8 oz. Bottles.
3 Sauce rs.
3 Cam 1 Hair Brushes.
Price complete, £ 4
Ca rri :l ga Paid on all in the Un ited King d c;m . 16
SMALL AMBULANCE HAMPER.
\\-ilh waterproof cO\-er and strap, for use in factories, collieries, :>t1.lions, and large \\'orks, al:l well as for parochial anu domestic use.
CC:\TAl!'\l!'\G
Set Splints I Elastic Tourniquet. 3 Tampons, for washing wounus. 2 Packets Lint. 4 Roller Bandages (wide anci narrow). 4 Triangular Bandages.
Cotton \Vool ... } I T' C Wool ... n 111 ases .
Spool of /Aclhesive PIa ter.
Knif-=, cissors. Thread, Tape, eedles, and Pin . 'Weight complete, Ihs.
Length, 1ft. 6 in . Depth 5 in . Width, 7 in. Price £1 I IS . 6d .
17

Carriage Paid on a ll O rde i s in th e Un ited I{ing dom.
SURGICAL HAVERSAC .
bfPROVED filled with a tin. so arranged that any arLicle can be taken ouL \\ iLhuut dislurbing the rest of the contents.
Contents: I . 'el of SplintR, 6 Triangular Bandages. 6 Paller Bandages (wide and narrow), CoLLon Wo')l, Buric Lint, in till cases, I Roll Adhesive Pia tel', I Pair Sciss()rs, I Knife, 201.. Olive Oil, 2 oz. Tillct. Iodine, 20t. Sal Vol::ttile, 2 fJl.. :-)pilit Ether Comp., I Gr.'tclLl1.ted Glass l\Ieasure, I Ela -tic Dand T ourniquet, Pins, • eec1les ancl Thread, 3 Saucers, 3 Camel Hair Brushes. Price £1 I IS. 6(1. \Vhite Linen Ralion TfaYersac3, I S. 9(\. each .
Cartiags PaId on all Orders in the Un ited Kingdom 18
FIR.ST AID COMPRESSED KIT.
The box ie; made of wont! C()\'ered \yith clamp-resisting material, and i" fitted \\ ilh a lock and key. It contains a numher of practical amhulance appliances arranged so that any article can be withdrawn or replaced \\'ithout di turbing the remainuer. Being hlleci \\ilh a handle il is portable, and the lid, \"hen let d()wn, can Ix: used a:-; a t'lhle . All handages ami dressings are Sil.e-Length 161 in.; width in. ; height in. without handle.
Contents: 4 Handnge<, 6 Roller Bandages, 4 First Aid Dressing;;, 6 Small Packet. of Cotton \\'001, 6 ,1I1all Packets of Boric Lint, r 1<:lastic Band Tourniquet, r :\leasure Glass, t lin IJOX containing a Roll of Plaster, Boric Lint Patches, Scissors and Pins, 1 tray containing 3 (Sal Volatile, Tincture of I odine and Olive Oil) anri a Dredger of Boric Acid, t et of impro\'ed Splints, \I·ith angle piece, g Splint Straps (sufficient for a fractured thigh), 2 Saucers, 3 Camel Hair Brushes.
Pric e £1 lIS. 6d.
19
Carriage Paid en all ardels in the Un ited Kingdem .

FIRST '.RID '.i/ " ."
dJRJ?3SINGS AND BAI"rvAGES cowJikrID).
SL .70/)11 RmlJuli111ct RS5«MfJl)i1,
51• .John's 6iilt.
Cttrk<nwtll, £cn{foo, e.'.
Size by 3! by Ii inches. Suitable for the pocket. CONTENTS .
I. Triangular Bandage. 2. First Aiel Dressing. 3 Cotton Wool. 4 . Two Splint trapc;. 5· Adbesiye Pla tel' 6 Pcrman gallate of Potash. 7. Lanoline. 8. Boric Lint Patches.
9. Safety and Pl ain Pins.
I ric e , each I S. 6d. Packed for Post r s. 8d. Per (1m. 17s. 61.
SEPARATE ARTICLES.
No.
I 4d. each or 3/9 per doz.
2 2el. " 2/0
3 Id. " " Jod. "
4 2el. per strap or 1/9"
5 rd. per box or IOel. " "
6 1d. per box or JOel per doz.
7 per tin or 1/4 "
8 Itl. per packet or 10(1.
9 lei. JOd
Not less than one dozen supplied at d c zen plic(s.
Carri?ge Paid (In all Orders in tha Un i ted Kingdom.
FIRST AID BOX FOR USE IN MINES .
Set of Improved \VofAlen ; Ebslic Hand Tourniqupt; Co llon \\' 001 ; Li nt; 12 Compressed Roller as<oned; 6 1', iangula, Bandages in waxed paper; Pair Spamb; Graduated i\le:lsure; 2 07. Sal \ 'ola tile; 2 oz. Spirit Ether Comp.; 8 oz. Boracic Ya,tline; 801. 1 inct. Iodine; 3 Saucers; 3 Camel 1-1 air Brushes; Pins; Safety Pins.
PRICE COI\[PLlCTE £2 105.
A somewhat similar hox can be supplied for carrying on the" Ashford" Lilter, or for hanging up in a faclory.
eeMP.lI.NI@J.V.,
al

Carriage Paid on all Orders In the Unlted Kingdom.
POUCH FITTINGS,
speciaJly selected for the St. J ohn Ambulance Brigade, con sisting of ;-
2 Triangular Bandages, one of which is sealed up in waxed paper. T he other may be used [or practice, but should be kept as clean as possible.
2 Roller Bandages U in. and I in.).
Packet of Cyanide Gauze (I yd. compressed).
Pair Scissors.
6 Safety Pins.
I Small Bottle of strong Smelling Salts.
Piece of strong Cane, for tightening improvi sed T ourn iquets.
Price, 2S. 8d. each . 6 doz. or more, 2S. 7<.1. each.
Packets of Cyanide Gauze (I yd . compre sed), pe r doz. , 2S. 8d.
Small Bottles strong Smelling Salts, per doz., 55. 6d.
SAFETY PINS.
All fasten or unfasten on either side .
Facile No. S 600 or S 602 " S 603 ...
Duchess Duplex, N o.2 ... " A ssorted
Special Blanke t Safety Pins, 3 in. " " in.
Carria ge Paid on all Orders in the Un i ted Kingdom.
The St. john Tou rniq uet , "ith d irections. use (.... pLcial (IUOlalions for htlge quantllles )
Tourniquet, Field
Splints, \Yooden, pcr set, 2/6 ; Cane .. per
Creatl), \\'ooden Splints, wilh groo\'ed joints and angle piece, strons!y recommended ... . ..
T ow, for splint padding... . .. per lb .
First Field Dressing (Army Pallern)
Jaconette, 44 inches \\ ide
Tow, Carbolized or Styptic per yard .. .pe r lb.
First Aid Dressing, of a small compressed packel of boric lint, a comp ressed roller bandage, alld a sarety pin
Dredger, containing boric acid powder
M eas ure Glass .. .
Knife \\ ith strung blade
Pair of Scissors o e.1c h 9d. ; per doz. ':'. each IS. ; per doz. lOs.
Splint Straps, Webl.Jin g, and suitable Budles. Per set of l2 ya rds of st rong 2-inch Webbing and IS Bucl-les, 25. 6d.
These .nak e ve ry compact Str3.ps [or in the Pouch. Th e Wel.Jbing hould be cut Lo mcellocal reql1lremenLs.
Ducklcs only, IS. 3d . per dozen.
\ Vebbing only, I S. 3(1. per dozen yards .
It is llnnece sal')' Lo sew the Duckles. Th e spikes "honld.be through the webbing, and the short end of the webLlIng :,hould lie OltL wanls .
3 doz.
" s. d. o 6 o 8 o 2 o 3 o 6
per
per doz.
set
22 S d. 0 9 2 6 7 6 4 6 0 6 0 9 2 3 0 9 o 2 4
carriage Paid en all Orders In the Un ited Kingccm .
PLASTERS.
Leiceste r Adhesive Plaste r on Call1lJric, in tins of yarel, 6 inches wide 6d.

N ational Rubber Adhesive Plaster (Antiseptic) on spools.
5 yds. 10 yds. inch wide 9d . I ad. IS. ad . IS. 6d.
The Leicester Adhesi\'e
Ribbons, in tin b ,nes, 6 yards long. inch wide 6(1.
2 IS. 9d . 2S . 3d . I inch wide
Dillo in card box, in. w ide, yds. long ... lin I t 3 l-, 5 5
COURT PLASTER, TRICOLOR. Large Size, 9c1. ; Medium, 5<'1. ; Sm::tll, 3d . 8d. rd. 3<1. 3<1. 6d. 9d•
C a rriage Paid on all Orders in the United Kingdom .
N U R SE S' W AL LETS.
ORJ)!)i:\RY PADLOCK SHArI!:.
\Vilhout instrulllents, 4S . 3(1.
Filled complete, contall1ing Spring
Dressing Forceps, Spatula, Probe, 2 pairs Scissors (round and sharp pointed), Clinical Thermometer, am1 Knife.
Price lOS.
ST. JOII="'S PATTER)<, as illus tratel1, but improved hy the addition of flaps to protect the Instruments. \\'ithout in truments, 7s. 9(1.
Filled complete, containing Spring
Dressing Forceps, Artery Forceps (also useful for dressing), Spatula, Probe, Director with Ear Scoop, 2 pairs Scissors (round and sharp pointed), Clinical Thermometer (minute, round), Knife, Penci l, and Safety Pins.
Price 18s.
Carri age P aid en all Order s in th e Un i t ed King d om
ROLLER BANDAG ES.
(6 yards long. )
Calico, or Sllper:or \Vhite Open Wove.

ROLLER BA N DAGE S in Assor1 m ent.
Packed in neat Ca r dbo ard B o x .
RECOJ,L\IEl\DED FeR CLASS PRACI ICE
Two 3 in . ; two in. ; one I in. ; each 6 y:ncls long. Grey Calico
Plain Triangular each (Special <rlOtations fur large quantities.)
Dillo Compressed (Lhinner quality), each 4(1. ; per doz . 35. 9 J . (after Esmarch) show ing 25. of the Tnangular Bandage, with p rI nted lI1st ru ctlOns .. . each per doz . s. d o 6 4 6
Carri age Paid on a ll Orders in the Un i ted K ing dom R.OLLER BANDAGE MACHINE.
Forceps, spri nt; dressing, full size or small as desired, IS.; bow dressing, 5 in. locked joint, Is. 6d . ; Pean's Artery, 5 in. locked joint, IS.3e1.
Scissors, round-pointed, IS.; sharp-pointed, for delicate work, I S. 3d.; small round-pointed blades locked joint or 5 in . , I S. 6el.; curved 'blades, locked j()1I1t, IS. 6el . ; curved blades, locked jlJint, IS 9d • The locked JOlDt allows the blades to be taken apart for clean ing. .
Spatula, 9d. Probe, 6d. Director, w ith Ear Scoop IS. 9d . Knife , ve ry thin, ivory handle, two blades, I S.9d. ' Nursing Chart, designed by Miss I neler\\'ick, each. Temperature Chart, each
CLINICAL THERMOMETERS.
Round. Ordinary, IS. ; minute, IS. 3d.; half-minute, IS. 6d. Flat. Strongly recommended a-they will not roll. Ordinary, I S. 6d. ; rapid (speciaily Rt.lectcd and reserved for the Associativn) , with very open scale, 3..
Open
Gre:y
Rest
Superior \\'hite,
\\hite Open \ \'QI-en \\" o,'e s. d. s. d. Ed ...:es. Compre,sec1. t1. s. d.
I in . q i n. 2 in. in. 3 in. 4 in . 6 in . 0 9 3 2 0 0 3 6 2 0 2 6 3 6 4 6 9 2 0 3 2 6 6 3 0 9 3 () 2 3 4 0 2 9 4 6 3 9
\\'O\'e Grey.
qualiry,
with
!J in. per duz.
s.
o
d.
Designed by
Dr. A. C. Tunstall.
Price 25. 6d.
carriage Paid on all Orders in the Un !te d I(ingtlom.
CLINICAL THERMOMETERS
-(rolltinlled).
With Magnifying Lens. Price, ordinary, I S. 6el.; minute, IS. 9d. ; half-minut e , 2S. 3d . . . N .13 .-Minute and half-minute in strum ents wlil only regIste r in the time stated under favourahl e circumstances: . No liability is takenforbrealla,;'Ye of Thermom eters lit tral/slt.
BATH THERMOMETERS.
T o Dr. Forbes' specification. with zin c scale, 2S. 3d . ; Clinical Therm omete r SIze, 111 case, IS. . /\'0 liability is ta ken fOY breakage of Thermollleters til t ramzt.
COTTON WOOL.
Plain, I oz., 2d. ; 2 oz., 3d. ; 4 oz., 4d. ; lb., 7(1.; I lb., IS.; small packet (Compressed), Id. '. .
Medicat ed, Boracic, !Ib., 6d.; I lb . , I S. 6(\.; Cal\Jollc,,Pe r lb. , I S. 8d. ; Alembroth, per lb., IS. 6ll.; DuulJle Cyal1lde , per llJ., 25 . 6el.
LINT.
Pl ai n, I oz., 2U. ; 2 oz., 3d. ; 4 oz. , 6el. ; 1 lb., Iod . ; I lb., IS. 6d . fit d' Borac ic, 4 oz. , 6d. ; I lb., IS. 6el. ; square vot p::tc;:e , 2 . , Sl11J.1l packet (Comp ressed), Id. GAUZES.
These are suppli ed in 6 yard lengths, width alJOut 36 in ches. s. d .
Unmedi cated white
Al embr oth
D ouble Cyanide Boracic GAUZE TISSUE. per length 0 10
A layer of absorbent cotlon wool between two sheets of gauze, good quality, per lb., IS. 6d.

Carriage Paid on all Orders in the United Kingdom.
TEXT BOOKS, 0C.
"First Aid to the Injured." By James Cantlie, M.B., F. R. C. S. Th e au th ori ed T exL Book vf the First Aid Course. I S.
"A Catechism of First Aid." Com pil ed from Dr. Cantlie's Manual. By J. 1\1. Ca rvdl, r-l. R C.S ., L.S.A. 6d_
"Problems in F irs t Aid." By L. \1 . Frank Chri [ian, M.B., and \V . l{. Edwards, A.C.A. 61.
"Hints and Helps for Home Nursing and Hygiene." By E. l\'facDowell Cosgrave, illu-;tralcd. with chapter on the flpplicat ion of the roller bandage , by Sir R. J. Collie, M.D. Th e author ised T ext Book furthe Nursing Cou rse. IS.
•• A Catechism of Home Nursing IJ (based on Dr. Cosgra \-e' s Text Book). By J. Brown, L R. C.P ., L.R.C.S., and J. M. Carvell, J\I.R.C.S., L. S.A . 6d.
II Home Hygiene." By J ohn F. J. Syke, D.Sc. (Public IIealth ), M.D., &c. lliustratecl. The authorised Text Book for the IIome IIygiene Course. IS.
II A Catechism of Home Hygiene" (based on Dr. Sykes' T ex t Book). By J. ;'1. Ca rv el l, l\L R C ' ., L. .A. 6d.
II Questions and Answers upon Ambulan ce Work." By John W. Martin, M.D., and John Martin, F.R.C.S. Ed. I S.
"Questions and Answers upon Nursing. " By John \V. Marlin, M.D. I s. 6e1.
II First Aid to the Injured " (Six Ambulance Lectures) . By Professor Frederich Esmarch. [rom the German by ILR.lf. Princess Ch ri stian. 2S.
(' Elementary Bandaging and Surgical Dressing." By \Valter Pye: F.R.C.S. 2S.
I 0 2 2
Carriage Paid on all Orders in the United I<ingdom.
TEXT BOOKS, &c.-( co l1t1"l/u ed).
<l To Restore the Apparently Drowned," printed in large Type with two Diagrams. 2d.
Dr. G. H. Darwin 's" First Aids," being a card 10 hang up, giv ing treatment uf \'arious acciJents. 2d.; pilcked fur post ,4d .
" Manual of Drill and Camping for the St. John Ambulance Brigade." 5c1.
"Manual for St. John Ambulance Companies.$) Dy Lieut.-Col. G. E. Til iss, R.:\.?lLC. (Retired Pay). 6d.
"How to Act when Clothing takes Fire." ny J. E. II. ;'Iackinlay, 1\1.1\.C.::>. 2d.
"First Aid Principles ." Cards of cuncise clirectiuns fl,r waistcoat puckel, each; 4d. per doz. Special for large quant ities.
" Specimen Examinati.on Papers, First Aid, Nursing and Ii ygiene Cour cs." 3d.
Small Anatomical Diagram. Sholling the human skeleton. main arteries, and puints where pressure houlcl be applied to arrest bleeding. 2d.
Directions as to the Restoration of Persons sufferin g from Electric Shock. Large plint, poster sileo 3d. each; or 25. 6d. per dozen .
General Notes on First Aid to be Rendered in Cases of Poisoning. By l\lilnes Hey, M.A., ;'I.R. C.S. , L. R.C. 1). 2d.
"Ambulance Tablets. " By Sydney .\1. D. IS.
Notes on Military Sanitation. By Lieut. -Cu I. II. P. G. Elkington, R.A. M.C. 6el.

Carriage Paid on all Orde· s In the United Kingdom.
TEXT BOOKS, &c. -(Co lltillll ed).
"Emergency Book," for instantaneous reference, gJl;lng concise inst ru ctions; to hang on wall. Size about one [OO[ square . 2S. 6d. ; packed for post, 25. Bel.
Aids to Memory for First Aid Students. tu date . Additional Illustrations. By L. .\1. Frank Christian, .\I. B., C.nI., Edin. 6d.
Rules for Corps and Divisions, St. John Ambulance Brigade. 2d.
A History of the Order of the Hospital . of St. John of Jerusalem. By the late Rev. ·W. K. R. Bedf(»)'(l, :'\1.A., and Lieut.-Colonel 1,(. II. IIolbeche. 55.
Registers. Class .Attendance, 2S. 6ll. Ce rtificates, 45. 6cl. Case Report, IS.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set o[ three, 7s. 6d. Receipt Book, 6d.
Large Physiological Diagrams. For use . Cumpri ing: The lIuman Skeleton, the Muscular, Arterial and Venous Systems, the Heart and Circulation of the Bloud, Simple Fracture, Compound Fracture, Dislocations. Price per set of six, 15. These may be hired fur a course of "First Aid" lecture.;, given under. the auspices of the Association, for a fee of 55., or with the addilion of Splints, Tourniquet, and plain Triangular Bandages, for a fee of las.
Boxes of Stationery for the use of Class Secretaries and others connected with the Association, containing twelve sheets of high-class paper, suitably headed, and envelopes bearing the de\;ce of the Association. 6d. T\\ ice that quantity, IS.
Ca r riage Paid on all Orders In th e Un ited Kingdom 3'

Arm Badges, with the d.evice, issu.ed under. the authority of the Central Executive Committee, havmg l)een flrst approved by II. R. II. the Grand as the s?le ofiicial and recoCTnisecl Badge of the ASSOCiatIOn and Bngac1e.
" N. B.- Tltis design is protected.
No. For the use of indiyiclual certificated pupils-
I. I n German S ilver, Large Size ...
2. Small Size ditto
3. Size for button hole
4. I n Electro Plate , Large Size
5. Small Size ditto
S. Small Size for button hole
7. In Enamel for button hole
8. brooch
9 . In ( oth and Silk ...
10. In Cloth and Silver (Registered Numbe r , 35 22 ) 2 0
I I. In Cloth and \Vorsted 0 6
12. Small Celluloid Badge, fo r button hole or brooch 0 2
IJ. White Satin A rmlet, with woven BaJge 0 N.B.- These Badges are 1101 to be 7.('0]"11 as decM·aliolls.
For members of the St. John Ambulance BriO'acle having the !lame the or Division annexed a'label, only Issued In ([Uantill esNt). 15 h Ge r man Siker, first doz., £1; subsequent clOZ5., 12S.
16. I n Electro Plate, flrst doz., £ 1 125.; subsequent c1ozs ., £1 4S.
" J 7. In'Cloth and Silk, per doz., 125.
JS. In Cloth and Silver, per doz., £ 1 105.
All the abo\'e may be worn by members of the St. Ambulance Brioude, not wearing uniform .
s . d. o o
o 6 o o
o 9 o o
6
9
3 ')
13 carriage Paid on all Orders in the United Kingdom.
BRIGADE UNIFORM BADGES. etc. s. d.
Officers. Cap Badge (Reg. No. 101)
Collar Badges ( '" I03) per pair I 3
" Pouch Badge ( ,,3,657) 2 6
-S ergeants, Corporals and Privates.
Cap Badge (Reg. No. 102) .. .
Collar Badges ( 104) per pair
Overcoat Badge ( " 1, 582 ) .. .
Shoulder Titles, S.J.A.B., with numeral, per p air
Shoulder Straps, filled with title and numeral ...... p er pair
Lady Officers of Nursing Divisions.
Superinte nd ent's Cloak Badge (R eg. N o. 3,65 8)
Supe rin tendent's Arm Badge ( " 3,659)
Other Nursing Officer's Cloak Badge (" 3,555)
Other Nursing Officer's Arm Badge (" 3,65 6 )
White Box Clolh Backs, fo r Badges ... per pair
Nursing Sisters. Arm Badge (Reg. N o . 3,5 22
" C loak Badg\ ( " 3,5 21 )
Black Silk Armlet for Arm Badge, Superintend ent
Other members
Honorary Surgeon's Crosses (pallern B) per pair
Superintendent's Stars (pallern A) ... pe r pair
Medallion Badge (pallern D) ...
Nursing Badge (patte rn E)... ... ...
Satin Badge for Nursing Sister's Pin Cushion
Bugler's Badge ... 4S. Bugler'S Cord
Div. Secretary and Sergeant's Badge
and Chain
s Brown Waist Belt and Pouch
White Piping, pe r packet of yards, enough for 3 pairs of trousers (packets cannot be broken)
Lace, per yard , Silver , II S. ; Black

Carriage Paid on all Orders in the United Kingdom.
BUTTONS FOR THE UNIFORM OF THE ST. JOHN AMBULANCE BRIGADE.
Issued only f? r. t.he use of.Officers and ::'.If'mbers of Corps an-J DIvIsIOns wearIng the presclibed uniform .
German Sil\'e r , Xo. I (large) Xo. 2 (meriium)
No. 3 (small, for caps)
Electro Plate, No. 4 (large)
NO.5 (medium) ... No.6 (small, for cap") " I
ELECTROTYPES OF THE ST. JOH N AMBULANCE DEVICE.
1. For Cards, Tickets, &c. I
For 1 ote Paper, Small Circulars, &c. . ..
For Quarto and Foolscap Leller-papcr, Cir&c . .. .
For Small Posters
For Large Posters
Prinls of the auove Eleclrotypes (r to 3) Series A an I B, and (I) Series All and BI.I, appear on page 35. K o. -1_\ j. shown on page 31. Th e dIameter of SA and 5B is iI.ches.
0 8
)
... ... ... ... ...
0 6 0 I Ol 0 6 0 6 3 4 6 3 9 4 0 3 3 0 3 2 0 2 3 0 0 3 0 6 0 6 0 I 0 3 0 3 0 0 Whistle
... ...... 2 0 Private'
... 7 8
2
0
per doz. < d. o 6 o
"
..> I o ..> o b t> No.
For l1se. Series Series For Driga.l . Series S "'rics \. AH. B HH. s. d. s. d . s . d . s. d.
0 I 0 I 0 0 2. 3· 4· 5·
Se ri cs o o I 6 o o 3 o I 9 I 9 o 3 53 3 0 4 0 3 0
Complete
35 Carriage Paid on all Orders in the United Kingdon.. ELECTR.OTYPES.

No. I A.
NO.3 A.
, Ubc <!lranO of it&e ot tbe tJospttal of St. 30bn of 3crusalcm In £nglantl.
Ilbc St. 301m tlmi)ulilllce B650.ciiltioll.
No. I A lI.
No. )
No.2 B.
No, 3 B.
nbe Grall!) Jl)rIOr\? of ot tbe lbospltal of Sf. 30bn of 3erusalem In J£nglanb.
$(, John Bmbulilnce 18rigai)e.
No. I. lHr.
Contractors' C!arrlage out of Lcnt:on extra.
Flags bearIng
SWAGGER STICKS
for the use of Officers and Members the St. John Ambulance Brigade.
Ehonised Cane. German. ilver l\Iounts bearing lhe Brigade Device.
IS, EACH.
Pa cked [or Post, IS. 2d.
Oft1cers' Special Canes, \\'jlh Sterling Sih'c r ;\Iounts.
75 EACH.
Packed [or Pust 7':5. 2d.
BEARER'S DRESSING CASE.
PI{ICE 125 6d,
All Orders for the foregoing Stores should be given to the Local Secretary, or sent direct to
The St. John Ambulance Association, St. John's Gate, Clerke nwell, London, E.C.
Ass nr iali on c1e\'ice - I 2 feel by 6 feet 5 feel by 3 feet ;( d. 6 o [2 6 " Brigade 4 fl. q in. l)y 3 ft. 0 I 2 0
37
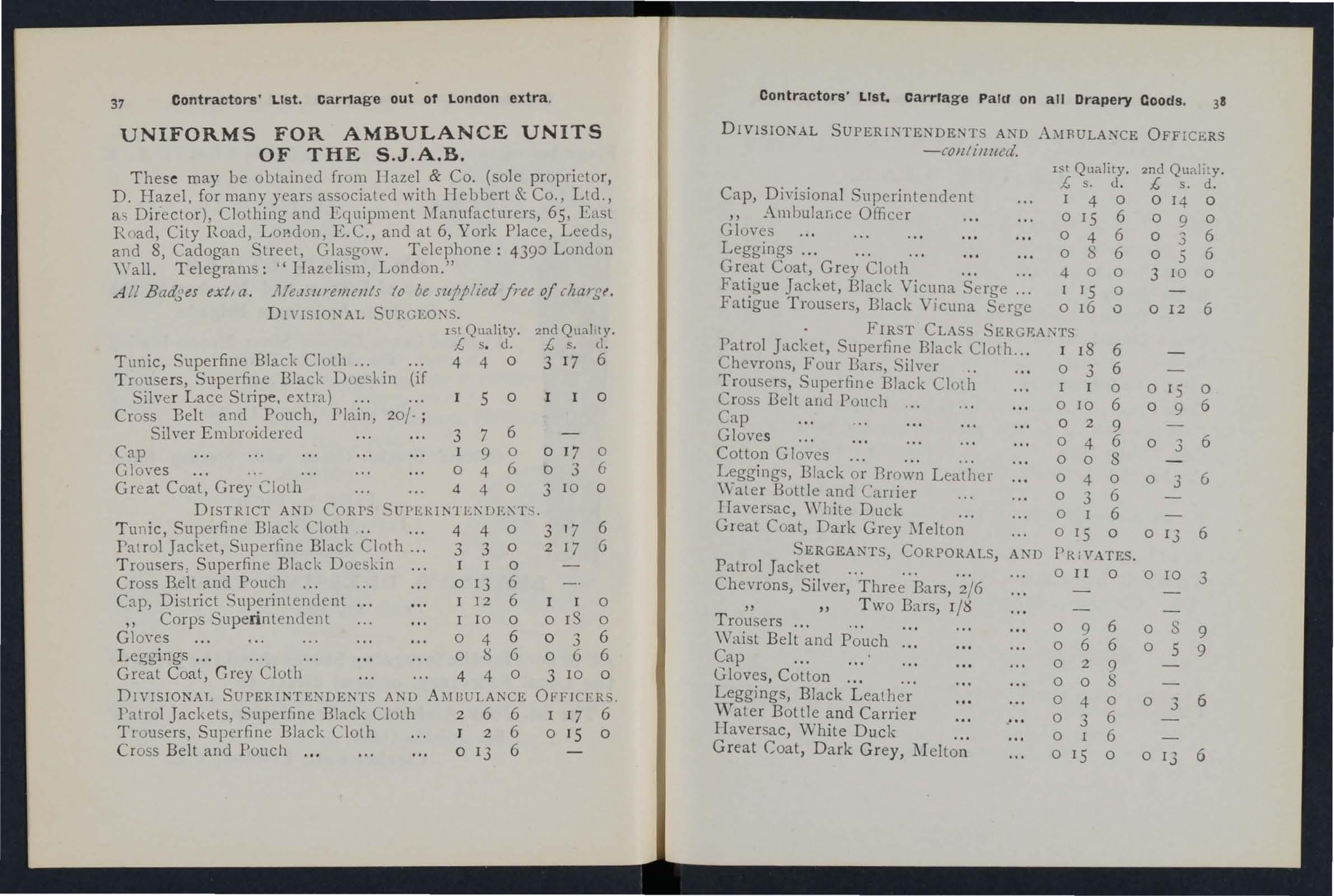
Contractors' List. Carriage out of loneton extra.
UNIFORMS FOR AMBULANCE UNITS OF THE S.J.A.B.
These may be obtained [rom Ilazel & Co. (sole propri etor, D. Hazel, for many years associated with IIebbert & Co., Ltd., as Director), Clothing and Equipment ]\Ianufacturers, 65, East Road, City Road, L oadon, E.C., and at 6, York Place, Leeds, and 8, Cadogan Street, Glasgow. Telephone: 439::> London
'Yall. Telegrams: ,e IIaz eli<..m, London."
.till Badges extl a. lI.1e,lsurell7ents 10 be wpplied free of charge.
DI\'ISIO:-<AL SURGEO:\'S.
Tunic, Superfine Black Cloth ...
Tronse rs, Superfine Black Doesl,in (if Silver Lace Stripe, extra)
Cross Belt and Pouch, Pl a in, 20;';
Embwiderec1
Coat, Grey Cloth
Tu nic, Superfine Black Cloth
Jacket, Superfine Black Cloth
T rousers: Superfin e Black
Silver, Three Bars,
" "Two Bars, 1/'6 Trousers ... ...
Waist Belt and Pouch Cap
Gloves , Cotton...
Leggings, Black L eather
Water Bottle and Carrier IIaversac, White Duck
1St Quality. 2nd QualIty. £, s. d. £, s. d.
4 4 0 3 17 6 5 o o
Silver
3 7 6 Cap I 9 0 0 17 0 Gloves 0 4 6 0 3 6 Great
4 4 0 3 10 0
UPER1l\1
.. 4 4 0 3' 7 6
3 3 0 2
6
DrSTRICT A D CORPS
Patrol
...
I7
Doeskin 0 Cross Belt and Pouch .. , 0 13 6 Cap, Distlict Superintendent I 12 6 I 0 " Corps Superin tendent I 10 0 0 IS 0 Gl oyes 0 4 6 0 3 6 ... 0 g 6 0 6 6 Great Coat, Grey Cloth 4 4 0 3 10 0 DIV1SIONATJ SUPERINTENDENTS AND Al\fU ULANCE OFFICFRS. l'atrol Jackets, Superfine Black Cloth 2 6 6 I 17 6 Trousers, Superfine Black Cloth J 2 6 0 15 0 Cross Belt and Pouch ... 0 13 6 Contractors' liSt. CarrIage PalCl on all Drapery Coods. 38 DIVISIONAL SUPERINTE. DENTS AND A:-'IRULA:-<CE OFFI CERS -COil! illlled. 1St Quality £, s. tl. Cap, Di\'isional Superintendent 4 0 " Ambulalice Officer 0 IS 6 Gloves 0 4 6 Leggings ... ... ... ... 0 8 6 Great Coat, Grey Cloth ... 4 0 0 Fatig u e Jacket, Black Vicuna Serge... I ISO Fatigue Trousers, Black Vicuna Serge 0 16 0 FIRST CLASS SERGRA:'<TS Patrol Jacket, Superfine Black Cloth... I 18 6 Chevrons, Four Bar', Silver .. ... 0 3 6 Trouse rs, Superfine Black Cloth I 0 Cross Belt and Pouch... .. . 0 10 6 Cap 0 2 9 Glove s 0 4 6 Cotton Gloves ... ... ... 0 0 8 Legg ings, Black or Brown Leather 0 4 0 '\-ater Bottle and Canie r 0 3 6 IIaversac, \V bite Duck ' " 0 I 6 Gleat Coat, Dark Grey 0 IS 0 SERGEAXTS, CORPORALS AND PRiVATES. Patrol Jacket ... ... ...' 0 II 0 Chevrons,
2/6
...
...
...
Gr ey,
o 9 6 o 6 6 o 2 9 008 040 03 6 o I o 15 6 o 2nd Quality. £, s. d. o o I4 090 6 6 o .3 S o 3 IO 0 o 12 6 o IS 0 09 6 o 3 6 o 3 6 o 13 6 o ro 3 o S 9 059 o 3 6 o 13 6
Great Coat, Dark
:Mellon
39

Oontrac!ors' List. Carriage Paid on all Drapery Coods.
UNIFORM FOR NURSING OF THE S.J.A.B. UNITS
Serge Cloak (Badge extra)
Special \Vaterproof Serge, exlra
Serge Dress, to m eas ure
Better quality do.
C otton Dresses, complete to measure
Cotten Dress L engt hs 8 yards
Bonnet ...
Do., for lady officers
Collars each; p er d oz.
Cuffs to match per pa ir; per d oz. pairs
Cap, "Sister D ora " . .. 8!rl. each; per doz.
Cambric Stri ngs for above, tucked ends per pair; per doz.
Nurses' Sleeves, elastic band and butlon at wrist . per paIr
S tiff Lin en Belt ... each; per doz.
Nurse's An ·L inen Apron, in white ... each
Do., Ch eape r qualily, in \Y hile
nio n,
and
S et/-measurem ent jonns sent free 01l l'equest
U}\ 'On 40iT'\S .lTD LONDON· S W
ru L Managing DIrector.
T e1egrams: If Every th ing Harrocs, London " 'l elephOlle: Western One ( 80 lines) . l;-;r DEX
TO PRICE
LI ST . P\GR
Amblliance Hampers.. 1{ to 16 Station Plate 13
Badges ... .. ... 31 to 33
Bandage Rolling l\Iachine 26
Ibnd agf>s ... ...
Casin, Dressing
Bearers Dres<;ing l.led (Equipoise) " (Camp) ... II Bel, and Pouch ... 33 23 to 30
Dottles (Water) BLlttons... ... 31
Carrying Sheet Cash Book .. , Cotton \\'001 Co\'er for Stretcher or Litt!.!r Diagrams, Large " Small
Dredger (Boric Acid) 10
Dressing Basin 13
Drowning Tackle 11
Electrotypes ... .. 34, 35
Emergency Book 29 Aid Box ... ... 8, 20, 21 " .. Companion.. 19 " "Compressed Kit 18 First Field Dressings.. 22
Flag, 36 Force ps 26
27 Gauze Tissue
27 Hampers (Ambula nce) 1.1 to 16 Haversacs 17 Hood and A pron for Litler.. 3 1nstruments (various) 26 Tacondte Knife... Lace for Caps, &c. Lamp
each I
f. s. d. o 19 II 026 7 6 IO 0 094 o 3 IO o 9 o 10 o 5 o 6 o 8 o 3 o o 4 o 3 o 2 6 6 6 6 6 3 3 6
U
1
S.
Lint 33 13 27 Litter (A"hford) " (Rea·Edwards) Lowmoor Jacke t AI easure Glass... Minute Book ... Xurses' " 'allets K ur5ing Charts Occurrence Book Pillow ... Plasters. Pouch Fittings Book .. . ... ... l{oller Eandage illachine PAGS 2, 3 4 to 6 12 23 21 l":"u6" .. ... .., ,. , RLlles for Corp, or Divisions .-\mbulance 29 SafelY PinS ... ... .., 21 Scissors... ... ... 22, 26 lings (Stretch er) Splint Padding " Straps 22 Splints... ...... 22 Stationery...... 30 Stretcher Depot Plate 13 Stretchers 7 to 10 " Adjustable for 8 Swagger Stick ... 36 Temperature Cb:u-t 26 Text Books ... 28 to 30 Thermometers... .., 26, 27 Tourniquets ... 2 :1 To\\' (carbolized) 22 " (plain) ... Uniform Sundries Uniforms \\'ater ... \Vaterproof hee t Whistle and Chain White Piping Wool (Cotton) 33 37 to 39 12 3 33 31
Gauzes
......