

BONES.

SEVENTH)
CL': llVI CAL \" V EJ{ l'Ell llA J
C()l.l,AI'} HONE (cl:\\'ic1e) RIU6 - -
AI/\i BONK(hUlllerus)
-iI"H LUMIIAR VeRTltBllA. (pelvis) 5 ULNA RAUIUSCARPUS
THIGH B ONE (femur)
KNH:H: CAl' (patella) SHiN HONE (tiIJia)
nt>OOCH HONE(fibula)
ARTERIES.
Tile !lumbered dotll show IN'essure pomts for the arteries_ Compare numbers ill text. - - OCCIPITAl" - TKJotl'OIlAL,
FACIAl..
CAROTInS. SUBCLAVIAN, - AXILLARY_
BRACHIAL (Digit,,) or Tourniquet), AORTA. ___ BRACHIAL (FJexiou). -' h.UC.
POPI.l1'EAL (Flexion).
•• ANTERIOR TIBIAL.
• - - POSTERIOR TIBIAL_
PIlALANGJJ:S '
AS COMPANIONS TO THIS BOOK-
"
A CATECHISM ON FIRST AlD."
BY j. M. CARVELL, M.R.C.S., L.S.A.Price 6d. post free.

"PROBLEMS
IN FIRST AID."
BY L. M. FRANK CHRISTIAN, M.B., AND W. R. EDWARDS, A.C.A.Price 6d. post free.
FIRsrr AID TO THE INJURED
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE ST.
JOHN AMBULANCE ASSOCIATION.
BY JAMES CANTLIE,M.A., M.B., F.R.C.S., Knight of Grace of the Order of St. Jol"". Honorary L'Je Me-mber of, and Lecturer and Examiner to, the Association.
a on Stretcher Transport," revised from that originally wntte',l by SIr JOHN FURLEY, C.B., Knight of J'4stice of the O,-del' of St. John, 10 accordance with the Army Stretcher Exercises. Also a CHAPTER (being the Fifth Lecture for Females only). by E. MACDoWEL COSGRAVE. M.D., F.R.C.P.I.. Ktu'ght of Grace of the Order of St. John. Honorary Life Metnber of, and Lectltrer and Examiner to, the AssociatiOIl.
TWENTY-FIFTH EDITION. 1,190,000 to 1,240,000 is similar to et'ghteenth, iTt which edition many of the tltust ratIOns were re-dra-um; otherwise it differs bitt little frOIlt the eleventh to the seventeellth editiolls.)
Price in Cloth, is. post free.
LONDON:
THE ST. JOHN AMBULANCE ASSOCIATION, ST. JOHN'S GATE, CLERKENWELL, E.C.
W. II. & L. C. 50,000, 9/1914.
UlJe u;rantl .}Prlor).? of \tbe @rt'el' of tlJe 1fJospftal (If St. JolJn of Jerusalem In JEnglanb.
SOVEREIGN HEAD AND PATRON: HIS MOST GRACIOUS MAJESTY THE KING.
GRAND PRIOR: H.R.H. THE DUKE OF CONNAUGHT, K.G.
SUB-PRIOR:
BAILIFF OF EGLE: H.R.H. THE DUKE CONNAUGHT, K.G.
EXECUTIVE OFFICERS:
PRELATE.-The Archbishop of York.
CHANCELLOR.-Col. Sir Herbert Jekyll, K.C.M.G.
SECRETARy-GENERAL.-Col. Sir Herbert C. Perrott, Bt., C.B.
RECEIVER-GENERAL.-Edwin Freshfield, LL.D.
DIR ECTOR OF THE AMBULANCE DEPARTMENT.-The Earl of Plymouth, P.C., C. B.
OF THE BRITISH OPHTHALMIC HOSPITAL, J E RUSALElIf.-Col. Sir Charles M. Watson, K.C.II1.G., C.B.
ALlIIONER.-Sir D yce Duckworth, Bt., M.D., F.R.C.P., LL.D.
LIBR ARIAN .-A. Edmund FI-as er.
RE GISTRAR.-The Earl of R anfurly, p.c., G.C.M.G.
GENEALOGIST.-Sir Alfred Scott Scott-GaUy, K.C.V.O. (Garter).
ASSISTANT EXECUTIVE OFFICERS:
ASSISTANT REC EIVER-GENE RAL.-Edwin H. Freshfield.
ASSISTANT DIRECTOR OF THE AlIIBULANCE DEPARTlIIENT.Lieut.-Col. Sir Ri c hard C. Tempie, Bt., C.I.E.
HO NORARY SECRETARY OF THE BRITISH OPHTHALMIC HOSPITAL, JER USALEM.-Col. Thomas H. Hendley, C.I.E., M.R.C.S.
ASSISTANT HONORARY SECRETARY (FOR SCOTLAND) OF THB BRITISlI O PHTHALl\Il C" HOSPITAL, JERUSALEM.-Jobn Horne Stevenson (Unicoru Pllrsuivanl)_
ASSISTANT LIBRARIAN.-
SECRETARY.-\Villiam R. Edwards, A.C.A.
ASSISTANT SECRETARY.-Duncan G. Monteith.

THE CHAPTER-GENERAL:
The Chapter-General consists of the Grand Prior. the Sub-Prior! other Knights of Justice, the Prelate and the de Jltre, the Officiating Chaplains; all members of Counc!l; nl)t m?re than ten Knights of Grace and not more than SIX ES<.julres apPolllted by lhe Grand Prior.
KNIGHTS OF J USTICE:
HIS 1\10ST GRAC[oUS l\IAJESTY TIlE KING (Sovereign Head and Patron).
FIELO-MARSHAL H.R.H. TilE DUKE OF CO:-lNAUGIIT, K G. , K.T., re.p .. P.C , Etc. (Grand Prior).
GENERAL H.R.H. PRINCE CHRISTIAN OF SCIILESWIG-HOLSfEIN, ICG .. P.C., G.C.V.O.
H.H. PRINCE ALBERT OF SCHLE WIG-IIOLSTEIN, G.C.B., G.C.V.O.
COLONEL H.H. THE DUKE OF TECK, G.C.B ., G.C.\·.O., C.M.G.
AomRAL !-I.S.H. PRINCE LOUIS OF BATTENBERG, G.C.B .. G.C.V.O. , K.C.M.G.. R.N.
H.1\I. HAAKON VII., KING OF NORWAY, K.G • G.C.B., G.C.v.O.
M .\ JOR H.S.H. PRINCE ALEXANDER OF TECK. G.C.B., G.C.V.O., n.s.?
l\IAJOR n.R.H. PRINCE ARTHUR OFCONNAUGHT, K.G., K.T., P.C , G.C.I.. D. H.II. PRINCE ALEXANDER OF BATTENBERG, G.C. v.o.
Sir Jobn Furley, C.B. (Honorary The Earl of Mealh, K. P.. P.C. Bailiff). A. E. Fraser.
Sir T. N. Dick-Lauder, Bt. The Lord 1\10 tyn .
Maj. Sir A. Lamb, I:H. The Marquess of Breadalbane.
Col. Sir H. C. Perrott, Bt.. C.B . K.G., P.C.
Col. Sir J. Gildea, K.C.V.O., C.B. The Duke of Portland, K.G., P.C. H. J. Loftus. y. Qt Field - Marshal The Earl Col. B. 1\1. Dawes. Roberts, K.G., K.P., Etc. Gen. SirC.vYarren, G.C.M.G., K.C.B., R. B. Carter, F.R.C.S. (Honorary R.E. Commander).
Maj.-Gen. J. C. Dalton. Col. C. " T. B. BowdleI', c.s. Brig.-Gen. A. G. IIunte r-'Yeston ( H onorary Commander). of IIunlerslon, C.B.. D.S.O., R.E, Lieut.-Col. A. C. Yate. Col. The Lord 'Yilliam Cec il, c. v.o. l\Iai.-Gen. A. F. Terry. E. Freshfield, LL.D. (Honorary The Earl of Plymouth, P.C., C.II. Bailiff). The Earl of Sandwich, ICC. v.o. The Earl BrasseJr, G.C. B. The Earl of (ComThe Viscount Templetown, m ande r, Ellesmere Commandery ' , R. M. l\lacLean. E. H. Freshfield, A. F. G, Leveson Gower. The Viscount Brackley. M. v.o. Col. F. A. II. Lambert. Field-l\larshal The Earl Kitchener Col. Sir C. VY l\Iurray, C.B. of Khartoum, ICP.
The Earl of Ranfurly, P.C., G.C.M.G. Lieut.-Col. Sir R. C. Temple, Bt.• The Lord Sandhurst, P.C.• G.C.S.I.. C.LE.
G.C.I.E. Sir A. S. Scott-Gally, K.C. \' .0. Sir II. A. l3lake, G.C.M G. Col. Sir H. J ekyll, K.C.M.G.
KNIGHTS OF' JUSTICE.-continued.
The LOI'd Islington of Islington, Sir \-V. \-V. Portal, Bt. P.C., G.C.M.G., D.S.O. The Duke of Somerset.
Col. Sir J. R. A. Clark, Bt., C.B., Sir D. Duckworth, Bt., M.D., F.R.C.S.E. H. E. Boulton, c.v.o.
Sir R. Harvey. TheViscount Esher,G.c.B ., G.C.V.0.
Col. The Lord Sydenham, G.C.S.I., C?1. Sir C. 1\1. Royd!':, C.B. [G.C.B. G.C.M.G., G.C.I.E. F!eld-Marshal The Lord Nicholson, Lieut.-Col. J. \V. 'Vray. LIeut.-Col The Lord Herbert Scott, PRELATE: D.S.O.
The Archbishop of York.
SUB-PRELATES:
The Bishop in Jerusalem and the I The Primate of New Zealand . Ea.st. The Bishop of Southwark. The BIshop Ormsby. The Bishop of Gibraltar.
OFFICIATING CHAPLAINS:
The Rev. Canon Sir E. Sheppard, IThe Rev. T. C. Elsdon. K.C.V.O., D.O.
KNIGHTS OF GRACE APPOINTED BY THE GRAND PRIOR:
Major. G. E. W. Malet. I The Lord Merthyr, K.C. v.o. Col. SI.r J. 'V. Ottley, K.C. I.E ., R.E. R. A. Gibbons, M.D.
The VIscount Alverstone, G.C.M.G. Lt.-Col. F. W. Pixley, F.S.A.
J. A. M.V.O. Sir W. H. St. J. Hope, LlTT.D. J. S. Gnffiths, III.R.C.S. F. H. Cook, C.I.E.
• . ESQUIRES APPOINTED BY TIlE GRAND PRIOR: B. Ham.Iton, C.IIf.G. I Col. W. G. Carter. E. Dawes. K. 'V. Murray, (Portcullis Pursu ivant).
THE COUNCIL:
The Council consists of the Grand Prior, the Sub-Prior, the Executive Officers of the Order, the Commanders of existing Commanderies and not than. fifteen members of the Grades of Knight of KnIght of Grace and Esquire appointed by the Grand MEIlfBERS APPOINTED
Sir J. Furley, C.B.
Major-Gen. J. C. Dalton. E. H. Freshfield.
Lieut.-Col. Sir R. C. Temple, Bt , C.I.E.
Th e Bishop of Southwark.
I nspector-General Sir J. N. Dick, K.C.B., R.N.
BY THE GRAND PRIOR:
Inspector-General B. Ninnis,c. V.O., IIf.D., R.N.
Sir R. D. Powell, Bt., ICC. \'.0., IIf.D.
E. Owen, F.R.C.S., LL.D.
The Lord Claud Hamilton, M.P.
Col. T. H. Hendley, C.I.E.,M.R.C.S.

Ube of Ube Or tbe 1bospltal of St. Jobn or Jerusalem in AMBULANCE DEPARTMENT. Ube St. lobn Btllbulance :associatton.
PATRON:
HIS MAJESTY THE KING, Sovereign Head and Patron of the Order.
PRESIDENT:
H.R.H. THE DUKE OF CONNAUGHT, K.G., Grand Prior of the Order.
CENTRAL EXECUTIVE COMMITTEE:
Consisting exclusively of Members and Honorary Associates of the Order.
DIRECTOR OF THE AMBULANCE DEPARTMENT AND CHAIRMAN OF COMMITTEE.-The Earl of Plymouth, P.C., C.B.
ASSISTANT DIRECTOR AND DEPUTY CHAIRMAN.-Lieut.-Col.
Sir Richard C. Temple, Bt., C.I.E.
DEPUTY CHAIRMAN.-Sir John Furley, C.B., Life Member of the Committee, Honoris Causa.
MEMBERS:
Maj.-Gen. J. C. Dalton.
Col. Sir J. R. A. Clark, Bt., C.B., F.R.C.S.E.
Col. The Lord Sydenham, G.C.S.I., G.C.l'<1.G., G.C.I.E, H. E. Boulton, C.v.O.
Lieut.-Col. The Lord Herbert Scott, D.S.O.
The Rev. T. C. Elsdon.
Inspector-General B. Ninnis. C.V.O.. 1\1.0., R.N.
Maj. G. H. Darwin, M.D.
Col. G. S. Elliston, C.B., M.R.C.S.
Col. C. J. Trimble, C.M.G., L.R.C.P.E.
Capt. Sir J. W. Nott-Bower, c. V.o.
E. Owen, F. R.C.S., LL. D.
The Lord Claud Hamilton, M.P.
Sir J. L. Langman. B t.
S. \-V. Malkin.
C. Cotton, F.R.C.P.E., M.R.C.S.
CENTRAL EXECUTIVE COMMITTEE-Conlinued.
Surg.-Gen. Sir B. Franklin, ICC.I.E., K.H.P.
C. B. Palmer.
Lieut.-Col. G. E. Twiss, F.R.C.S.I.
Col. T. H. Hendley. C.I.E .• lVI.R.C.S.
J. H. Morgan. C.V.O .. F.R.C.S.
CO!. Sir Trevredyn 'Vynn e. K.C.S.I.. ICC.I.E .
Brig.-Gen. H. R. Mends.
Lieut.-Col. A. D. Acland.
]I .4]" Col. E. D. Brown-Synge-Hutchinson.
Surg -Gen. Sir J. Porter ICC.B .• lVI.D" LL.D., ICll .P., R.N.
J. A. Bloxam. F.R.C.S.
Li eut.-Col. Sir R. 'V. Inglis.
l\Iaj. P. G. Shewell.
The Viscount Acheson.
T. H. Woolston.
F. N. Ellis.
\V. E. Alldland. M.R.C.S.
A. H. Johnston. !\T.R.C.S.
EX-OFFICIO MElIH3ERS OF COMMITTEE.
The Secretary-General of the Order.
The Receiver-General of the Order.
The Chairman. British Ophthalmic Hospilal.
CHIEF SECRETARY:
Col. Sir H. C. Perrott, Bt., C.B. (Secl-etal-y-Gencral of the Order).
DIRECTOR OF STORES AND ACCO UNTANT :
\Y. R. Edwards, A.C.A. (Secretary of the Order).
STOREKEEPER:
\V. H. Morgan (Superintendent, Invalid Transport Corps).
ASSISTANT SECRETARY:
D. G. Monteith (Assistant Secretary of the Order).
TERRITORIAL BRANCH.
CONTROLLER-IN-CHIEF:
Lieut.-Col. Sir R. C. Temple, Bt., c. I. E.
LADY COMMANDANT-IN-CHIEF OF ST. JOHN \VOMEN'S V.A. DETACHMENTS:
Lady Pen-ott.
SECRETARY:
P. G. Darvil-Smith.
REVISED 1908.

REI'ERENClt No. 5/1. 1908•
FIRST AID TO THE INJURED.
SYLLABUS OF INSTRUCTION.
FIR.ST LECTURlL
A. Princirles of First Aid.
B. A brie Description of the Human Skeleton and of Muscles.
C. Fractures-Causes, varieties, signs and symptoms..
D. Treatment of Fractures-General Rules.
E. The Triangular Bandage and its application.
SECOND LECTURll.
A. Treatment of Fractures (continued). Details of treat· ment.
B. DisloQtions, Sprains, Strains-Signs, symptoms and treatment.
C. The heart and Blood Vessels. The Circulation of the Blood.
D. Hremorrhage and wounds. General rules for treatment.
E. The Triangular Bandage and its application.
8
THIRD LECTURE.
A. Hremorrhage and wounds (continued). Details o f treatment.
B. Internal Hremorrhage-Signs, symptoms and arrest.
C. Hremorrhage from Special Regions. -Signs, symptoms and arrest.
D. Bruises, Burns and Scalds, Bites and Stings, Frost-bite.
E. Foreign bodies in the Eye, Nose and Ear.
F. The Triangular Bandage and its application.
FOURTH LECTURE.
A. The Nervous System.
B. The Organs and Mechanism of Respirati on -Ar:ificial Respiration.
C. Insensibility.
D. Poisoning.
FIFTH LECTURE (for Males only).
A. Improvised methods of lifting and carrying the sick or injured.
B. Methods of lifting and carrying the sick or injured on stretchers.
C. The conveyance of such by rail or in country carts.
FIFTH LECTURE (for Females only).
A. Preparation for reception of accident
B. Means of lifting and carrying.
C. Preparation of bed.
D. Removing the clothes.
E,

NOTE I.-The subject of poisons should be treated in a general manner; the common poisons classified, and only their general symptoms, effects and treatment taught.
NOTE H.-The last half-hour of each lecture should be devoted to practical work, such as the application of bandages and splirlts, lifting and carrying wounded on stretchers.
NOTE IlL-There should be an interval of a week between each lecture. A candidate for examination must attend tU least fuur out of the five lectures.
NOTE IV.-Male classes must pass in that system of stretcher exercise most suitable for the locality.
NOTE V.-As little time as possible is to be spent Oil instruction in anatomical and physiological details. Lecturers and examiners are particularly requested to remember that it is " First Aid" that has to be taught and tested, and not anatomy and phy siology.
ll.fixed classes o/mell and women are on no account pC1'mitted.
PUPILS UNDER SIXTEEN YEARS OF AGE CAN ONLY ATTEND THE" JUNIOR" C0URSE (SECTION A, SYLLABUS 40).
Lecturers Instructing a First Aid class, and Local Secretarie.. can obtain further particulars on application to the Chief Secretary for .. Paper Reference No. 80."
No Lecturer may examine his own Class (or Certificates.
SUMMARY OF CONTENTS.
Principles of First Aid
Explanatory on Chapter CHAPTER I.
CHAPTER II.
Ttle Human Skeleton. Skull, spine, ribs and breastbone, upper limbs (collar-bone, shoulder-blade, armbone, bones of the forearm, carpus, metacarpus phalanges), pelvis, lower limbs (thigh-bone, cap, tarsus, metatarsus, phalanges)
Muscles. Voluntary and involuntary
Fractures. Causes, varieties, signs and Apparatus for treatment of Fractures
General Rules
be observed in the treatment of Fractures
Special Fractures. Cranium, lower jaw, spine, ribs, breast-bone, colhr-bone, shoulder-blade, arm-bone or bones close to the elbow joint, forearm crushed hand, pelvis, thigh-bone, knee·cap, leg, cru'shed foot

Miscellaneous Injuries. Bruises, burns and scalds, bites of snakes and rabid animals and wounds by poisoned weapons, stings of plants and animals, frost bite, needle embedded under the skin, fish hook embedded in the skin, injuries to joints, foreign !body in the eye, ear passage and nose, wound in the front wall of the abdomen, injuries to the organ!> within the abd
Schafer's, Silvester's, Howard's combined with Silvester's, Laborde's and Marshall Hall's methods...
10
._
...
to
Sprains Sprains and Ruptured Muscles .. Questions on Chapter Pagt 17 20 2I 22 3 1 3 2 33 36 41 43 62 64 65 66 II CHAPTER III. Page Circulation of the Blood. Organs; general (systemic) and pulmonary circulations 70 Hcemorrhage or Bleeding. Arterial, venous, capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage ... 76 Course of the Main Arteries and Pressure Points. Ao rta, arteries of the head and neck, of the upper limbs, of the lower limbs 79 Venous Hcemorrhage and Varicose Veins 93 Wounds with Venoils Hcemorrhage 94 Capillary Hcemorrhage 95 Internal Hcemorrhage 95 Hcemorrhage from Special Regions 96 Questions on Chapter 99 CHAPTER IV.
102 Questions on Chapter I I 5 CHAPTER V. The Nervous System. Cerebro-spinal, sympathetic ... 117 The Respiratory System 118 Artificial
121
Dislocations
omen and pelvis
Respiration.
Insensibility. Causes, general rul es for treatment, concussion of the brain, compression of the brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, sunstroke and heat-stroke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPTER VI.
Poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes . ..
CHAPTER VIII.
Methods of Carrying. Four, two, a nd three. handed seats, fireman's lift, fore and aft method, improvised stretchers, to cross a ditch or wall, to load or unload a wagon ...
CRAPTER IX.
Stretcher Transport. Stretchers, stretcher exercises, litters
CHAPTER X.
The Fifth Lecture (for Females only). Preparation for reception of accident cases, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparation for surgeon ...
Questions on Chapter

Skeleton showlng position of main arteries
Skull and vertebral column
Vertebra
Bones of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle ...
Rectus Muscle
Triangular bandage spread out and folded
Large arm sling
Small arm sling
Reef knot
Granny knot
Bandage for fracture of lower jaw
Bandages for simple fracture of ribs
St. John sling
Bandages for fracture of both coUar bones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint
Treatment of fracture of forearm
Treatment of crushed hand ...
Treatment of fracture of thigh bone ...
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap ...
Treatment of fracture of leg (man and wuman)
Treatment of crushed foot ... 9f beart1 lungs and air passages
12
Page 128 142 J45 155 197 206 LIST OF ILLUSTRATIONS.
.. . ... .. . . ..
... Loop
.., ... .. .
knot...
.. .
... ... .., ...
. ..
...
Pare frontispiece 24 27 29 3 I 3 1 32 38 39 39 40 40 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 71.
Diagram of the cir-ulation of the blood
Digital pressure on carotid artery",
Digital pressure on facial artery '"
Digital pressure on temporal artery
Digital pressure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad ,., .. , .. , .. , ... ..,
Digital pressure on subclavian artery
Pad and bandages to apply pressure on axillary artery" ,
Digital pressure on brachial artery (two methods)
Flexion at elbow
Digital pressure on radial and ulnar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery." ,., ,.'
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen .. ,
The lungs and bronchial tubes
Schafer's method of artificial respiration ...
Silvester's method of artificial respiration '" , ,'
Silvester's and Howard's meth ods of artificial respiration combined ... ... ... .., .. , ...
Bandage for the head
Bandage for the shoulder
Bandage for the hip. ,.
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the el bow
Grip for four-handed seat
Lifting by two-handed seat. "
Grips for two-handed seats,., by two-handed seat

Grip for three-banded seat, ..
Supporting patient ... "',
Fore and aft method of carrymg
Carrying on improvised seat
Improvised stretcher '"
Furley stretchers '"
Stretcher exercise , No. I. \' Fall in "
Ditto, ready to lift patient
Ditto, lifting patient .. ,
Ditto, placing stretcher .... ...
Ditto, preparing to lower patlent."
Ditto, "Lower" "
Ditto, No. II. Ready to hft patIent
Ditto, patient ,, ' . ':'
Ditto, No. IV. FIrst p OSItIOn
Ditt o, second position ". '" , '"
Diagrams illustrating Army stretcher drill
Ditto ...
Bed cradle
Improvised bed cradles
14
12 5 155 156 156 157 157 158 159 159 160 161 162 161
Page 164 165 1 6 7 168 168 li 2 175 17 6 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
PREFACE.
AT the request of the Central Executive Committee
I have revised the manual written by myself in 1901, as the official handbook of the St. John Ambulance Association.
Throughout the revision an endeavour has been made to simplify the study of First Aid to the Injured by drawing up a number of general rules for the treatment of accidents and Sudden illness, and by the omission of all detail which is not absolutely necessary to enable the student to acquire an intelligent knowledge of the subject.
I wish to express my thanks to ·Professor E. A. Schafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. M. F. Christian for many valuable suggestions, and to the Medical Members of the Central Executive Committee, especially Surgeon-Major G. H. Darwin, M.D. and Dr. F. R. Cassidi, for perusing the proof sheets and for a number of useful additions to the work.
I cannot omit also to offer my best acknowledgments to Mr. W. R. Edwards, the Accountant and Storekeeper of the S.J.A.A., for his invaluable .co-operation.
JAMES

FIRST AID TO THE INJURED#
CHAPTER I.
The St. John Ambulan.ce has n.ow completed thirty years of lts eXlstence, and dunng that period hundreds of thousands ?f men artd women have been taught at its classes, In of the world how to help their injured f Fi;st Aid to the Injured is a specIal branch 0 practical medicine and surgery, by a 01 which trained persons are enabled to afford assistance in cases of accident an? ?llness, The instruction begins and ends wlth Flrst Ald, and the subject is bught simply but thoroughly ar:- d exhaustively. The duty of the ambulance puplls ends where the doctor's commences, and the.re ought to be no overlapping or clashing of duty or Interests.
PRINCIPLES OF FIRST AID.
I The First Aid student should be-
o (a) Observant, that. may note the causes and signs* of Injury.
(b) Tactful, that he may without questions learn the symptomst and hIS toryt of the case.
• Signs are what may be perceived.
t Symptoms are what the patient can tell you. .
t History means the circumstances attendmg the aCCIdent 0% suddtn illness.
(C) Resourceful, that h e may us e to the best advantage "whatever is at hand to prevent furth er damage and to Nature's efforts to repair the mischief already done.
(d) that he may give clear instructions to the patient or the bystanders how best to assist him.
(e) Discriminating, that he may decide which of several injuries presses most for treatment by hims elf, and what can best be left for the patient or the bystanders to do.
2. Remove the cause of injury or dano-er whenever possib le. . b
3. Severe must receive the .attention, no matter what are the other lllJunes.
4. Air.. patient m ust be in a position in which breathmg IS. possi.ble; the air passages must be fr ee from obstructIon; If breathing has ceased prompt measur es must be taken to restore it.
5. restful position of the body will assist th e VItal functIOns; support of th e injur ed part will h el p to prevent further damage , and is essential in th e case of fr ac tures of li mbs.
Warmth.-After every accident k ee p the pat ient warm so as to preven t the fall of temperature below the norm al point.
7. When the skin is broken the wound

19
should be promptly covered with a clean absorbent dressing. Should the wound be pois oned , is most important immediately to prevent the pOlson permeating the system.
8. Poisons swallowed should be got rid of, or when that is inexpedient, n eutralised.
9. The best means of transport must be studied, and provision made for proper care when the patient is brought to sheller.
10: Removal of Clothing.-Clothes should not be taken off unnecessarily, but when it is needful to remove them, the following rules will be found of service in serious cases :-
COAT: Remove from the sound side first, and, if necessary, slit up the seam of the sleeve on the injured side.
SHIRT AND VEST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: Slit the back seam and undo the laces.
SOCK: Cut off.
II. Stimulants.-It is incorrect to suppose that alcohol is the only form of stimulant, and far too frequent use of spirits is made to restore a patient after an accident, often with serious results; the safest rule, therefore, is to defer the ad minH:itration of alcohol until the arrival of a doctor. \Vhen the patient is able to swallow, strong tea or coffee, or milk, as hot as CCln
18
be drunk, or a. small quantity of sal volatile in water may be Smelling salts may be held to the nose. Sprinkling the face with cold and hot water alternately, warmth applied to the pit of the stomach and over the heart, and vigorous friction of the limbs up wards have a stimulating effect.
12. Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an apparently slight injury is accompanied by grave danger and may actually cause loss of life. Whelil sending for a doctor, state the nature of the case, and remember that written particulars are safer than a verbal message.
It is necessary that something should be known of the structure of the body (elementary anatomy), and of the functions of some of the more important organs and systems (elementary physiology). A short description of the necessary anatomical and physiological points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms hanging by the side and the palms of the hands directed forwards. The" middle line" of the body runs vertically from the top of the head to a point between the feet.

The numerals indicate the pages whe r e t he ans we rs may be found.
What is First Aid to the injured? ..
What qualities should the First Aid student possess?
" ' hat are signs?
What are symptoms? ...
What is the history of a case?
What is often the first thing to do in an accident?
What result of injury must receive the first attention?
What steps must be taken beyond the actual treatment of injuries?
clothing always be remove d
would you remove clothing when necessary?
10
21 QUESTIONS ON CHAPTER I.
. . .
. . .
three things are absolutely necessary to an injured PAGE 17 17 , I S 17 17 17 18 18 18 person? ... ... ... .. . . .. What must be done when the skin is broken? . . . 18, 19 How must poisoning be treated? ... ... ... ... 19
... .. . . . . Should
? How
Explain the use
... What must the First Aid student not do ? What is elementary anatomy? 19 19 19 .. . 19, 2 0 20 20 20 What is elementary physiology? ... For purposes of description how is the human body supposed to be placed? What is the middle line of the body? 20 20
What
and abuse of stimulants

CHAPTER II.
FRACTURES, DISLOCATIONS, SPRAINS AND STRAINS.
THE SKELETON.
The human body is moulded upon a bony framework (the skeleton) which serves-
1. - To give shape and firmness to the body.
2.-To afford attachment to the muscles.
3·-To protect important organs, as in the skull, chest, and abdomen.
THE
SKULL.
The Bones of the Skull are arranged in two groups, those of the brain case or cranium, and those of the face.
The Boundaries of the Cranium are the vault -or dome, the rounded portion forming the top of the head ; the front or brow j the back of the head, where the greatest extent of brain exists, and where therefore the cranium is widest and deepest; the sides or temples.( The base of the cranium is hidden from view by the bones of the face and of the vertebral column -; in it are numerous perforations for the passage of blood vessels and nerves j through the largest opening the brain and spinal cord are continuous.
The Bones of the Face with the exception of 23
the lower jaw are firmly jointed togethe r, so movement betwe en them is impossible. The ca vItIes of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face conjointly. The mouth cavity is forn:ed between the upper and lower jaws, the palate bemg the bony ro.of of the mouth which separates it from the nasal cavIty above.
The Lower Jaw consists of:-
(a) A horizontal portion in \vhich are the sock ets for the teeth.
(b) Vertical portions term inating on. either side at the joint between the lower Jaw and the base of the cranium, situ a ted immediately in front of the ear.
The angle of the jlW indicates the junction of the horizontal and the vertical portions.
THE BACK-BONE, SPINE, OR VERTEBRAL COLUMN.
The Vertebral Column (Fig. 1) is compos ed of bones called vertebrre, each of which consists of-
I.-A body or bony mass in front.
2.-Processes projecting backwards, which enclose a canal for the spinal cord - ::-:e spinal canal.
3.-Two transverse twelve pairs of which support the nbs.
22
SKULL AND VER'J:' EBRAL COLU:'IN.
lett ribs and portion of weast bont:. The right ribs are rcmoveti.
SPINOUS PROCESS.
'fRANSVKRS& PaOCKSSas. ,'" : ..

BODY OF VKRTEBRA.
FIG. 2A.
TRANSVKRS B PROCESS.
SPINOUS PROCIi:SS•
SURFAC)l:S SUPPORTING M EADS OF RIBS.
4.-A spinous process. The spinous processes of the vertebrre can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
The 33 in all, are grouped in to re. gions, in each of which they are known by numbers, counting downwards :-
I.-In the neck 7 C ervical vertebrre. The first verte bra, the atlas , forms a joint with the b ase of the skull, at which t he no dding movement of the head takes place; the second , tlxe axis, by the joint between it and the atlas, allo ws of the side-to-s ide movements of the head.
2.-1n the back 12 Dorsal vertebrre.
3.-In the loin 5 Lumb ar vertebrre.
4.-The rump-bone, or Sacrum, consists of S Sacral vertebrre united in adults as a sol id mass.
5.-The tail-bone, or Coccyx, consists of 4 ver· tebrre joined together to form a singl e group.
Between the bodies of the vertebrre, in the upper three regions, are interposed thick pieces of cartilage (gristle), which, while they bind the bones together, a1Iow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for exa mpl e, when falling from
. . I •
FIG.
25
a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of twelve pairs of curved bones extending from the dorsal vertebrce to the front of the body, and are known by numbers-first, second, etc., commencing from above. The ribs are not bony throughout their entire length, but at a short distance from the front the bony material ends, and cartilage takes its place. The upper seven pail s, named the true ribs, are attached by their cartilages to the Breast-bone (sternum), a dagger-shaped bone with the point dowl1Vvards, just over the pit of the stomach. The lower five pairs are termed the false ribs, as their cartilages fall short of the middle line. The eleventh and twelfth pairs are termed the floating ribs, as their ends are free in front. The ribs enclose the chest and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder-bones are the Collar-bone (clavicle) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thickness of a finger. Its inner end rests on the upper part of the

313.
SHOWING THE POSITION OF THE RADIUS AND ULNA WHEN THE THUMB TURNED INWARDS.
Compare Fig. 3A, in which the thumb is turned outwards.
PART OF COLLAl< BONE SHOULDER BLADK (SCAPULA) ARM BONE BONES {ULNA OF FOREARM RADIUS --1'HH FIG. 3A. BONES OF THE LEFT UPPER LIMB. FIG.breast-bone, and its outer end joins with the shoulderblade.
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints with the collar-bone and the bone of the arm.
The bone of the Arm (humerus) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their relative position with every turn of the hand (Figs. 3A and 3B).
The Hand is composed of-
l.-The bones of the wrist, or carpus, eight in number, arranged in two rows of four.
2.-The tJzttacarpus (the framework of the palm) ; five bones which form the knuckles and support the bones of the fingers.
3.-The phalangtS, or finger-bones, three in each finger, and two in the thumb.
THE PELVIS AND LOWER LIMBS.
The Pelvis.-The large basin-like mass of bone attached to the lower part of the spine is composed of the two haunch-bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed between them. The pelvis

4.
BONES OF THE RIGHT LOWER LIMB, SHOWING JOINT WITH THE PELViS AT THE HIP.
28
FIG.
__ THIGH B ON E (F RMUK).
KNEE CAP ( PATELLA).
30 supports the abdomen and its contents, an d provides th e deep sockets for the thigh-bones-the hip JOInts.
The Thigh-bone (femur) reaches from the h lp t o the knee joint. Its shaft is stout, rounded, and arched forwards; the upper end presents a round ed head, supported on a neck which projects in wards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base upvyards in front of the knee joint immediately beneath the skin.
Th e bones of the Leg are the Shin-bone (tibia) and the Brooch-bone (jibula). The Shin-bone extends {rom the knee to the ankle, in both of which joints it plays an important part; its sharp edge, the shin, can be felt immediately beneath the skin of the front of the leg. The Brooch-bone lies on the outer side of the tibia. It does not enter into the formation of the knee joint, but its lower end forms the outer boundary of the ankle joint.
The Foot is composed of-
I.-The tarsus, a group of seven irregular bone! at the instep. The large st is t he heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.-The metatarsus, the five long bones in front of the tarsus which support the toes.
3.-The phalangtS, or toe-bon es, two in the big toe. and three in each of the other toes.
31 JOINTS.
A Joint is formed at the junction of two or more bones. In moveable joints such as the hip knee etc., t?e surfaces of the bones are b; cartIlage, whIch lessens friction and the shock of a

fal!. joint is clear, rather sticky flUId, the Jomt oIl, or sy"ovza, enclosed within a capsule . Tymg the bones together, but allowing of movem ent, a number of bands or ligaments. To explaIn the formation of limb joints, the
FI G 6. LEFT ANhLE. FI G 5. Compare Fig. 4, Page 29.M USCULAR TISSUE

T E NDO)! OR LIGAMENT
O F PATELLA
FIG . 7.
DIA GRAM SH OWlr-;G RECTU S MUSCLE OF THIGH, WITH ARTERY, VEIN AND NERVE.
following examples are given :-
The Shoulder, a balland-socket joint, consists of a shallow socket on the outer angle of the shoulder-blade, and of the head of the arm-bone (Fig. 5). Ov\ing to the shallowness of th e socket the arm-bone is very prone to escape from its socket (dislocate).
The Ankle, a hinge joint, is formed at the junction of three bones, the shin-bone above and on the inner side, the broochbone on the outer side, and the ankle-bon e below (Fig. 6).
THE MUSCLES.
The Muscles of the body are classifi ed into two groups-v 0 luntary and involun tar)'.
The Voluntary muscles are met with in the limbs, the head and neck, and the surface of the trunk. Their ends are attaLhed to different bones, and as they pass from one to another they cross a joint, and, being endowed with the power of contraction and relaxation, cause the movements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the nerves entering them bring them under the direct control of the brain and spinal cord.
The Involuntary muscles are met with in the walls of the stomach and intestines, in the air passages, and in most of the internal organs and blood-vessels, also, in a spe cial form, in the heart. They are not under the influence of the will, but continue their ,york during the hours of sleep j th ei r functions are regulated by a separate se t of nerv es (see Sympathetic System, page lI8).
FRACTURES AND THEIR TREATMENT.
\Vhen a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE.
I. Direct Violence.-When from a severe blow, impact of a bullet, crush of a wheel, etc., a bone breaks at the where the force is appJied the fracture is termed direct. o
32
NERVE
rltNDON
ARTERY
33
2. Indirect Violence.- 'Vh en the bone breaks at some distance from the spot \\ here the force is applied the fracture is termed indirect. Alighting on the feet and fracturing the thigh-bone or the bones of the leg, or faDing on the hand and breaking the . radius or the collar-bone, are examples.
3. Muscular Action. - The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them.
VARIETIES OF FRACTURES.
Fractures are classified according to the condition of the tissues adjacent to the bone as follows :-
I. Simple. - The bone is broken with but slight injury to the surrounding parts.
2. Compound.-The bone is broken and the skin and tissues are punctured or torn, thus allowing disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude through the skin, or (for example, when a bone is broken by a bullet) the wound may lead down to the fractur e.
3. Complicated.-The bone is broken and in addition there is an injury to some internal organ (for example, the brain, spinal cord, lung, etc.) or to some important blood -vessel or nerve.
A fracture may be compound or complicated as the immediate result of the injury; or a fracture,

originally. simple, may be converted into a compound or complIcated fracture-
(a) By careless movement on the part of the patient.
(0) By carelessness or ignorance on the part of one rendering first aid.
. Special of fractures may be classified accordmg to the In J:uy to the bone itself as follows :_
I. COt?mmuted. - The bone is broken into several pIeces.
2. Green-stick.-Irl children, owing to the softer of the bony tissues, a bone may bend and crack wIthout breaking completely across.
;3. Impa.cted.-The broken ends of the bone are driven one mto the other.
GENERAL SIGNS AND SYMPTOMS WHICH MAY BlI: PRESENT.
(A fracture of the femur, humerus, or both bones of the forearm or leg, affords the most complete example).
I. Pain at or near the seat of fracture.
2. Loss of Power in the lim b.
3· Swelling about the seat of fracture. Swelling frfequentl y renders it difficult to perceive other signs a and care must therefore be taken not to mIstake a for a. less serious injury.
4· Deformlty of the hmb.-The limb aSSumes at'
34
35

unnatural position, and is mis-shapen at the seat of . fracture. The contracting muscles may cause the broken ends of the bone to override, thereby producing shortening.
5. Irregularity of the bone.-If the 1S close to the skin the fracture may be felt , and 1f compound it may be seen.
6. Unnatural Mobility.-Movement may be made out at the seat of fracture.
7. Crepitus, or bony grating, may be felt or heard when the broken ends move one upon the other:
The last two sz"gns should only be sough! by a Several of the above signs are absent 111 green-stIck and impacted fractures.
. In addition to the signs and symptoms the patIent or the bystanders may be able to the of the injury, and marks on the clothmg or skm should be noted, as they may serve to locate the fracture. The snap of the bone may have been heard or felt.
ApPARATUS FOR TREATlI[ENT OF FRACTURES.
Splints and bandages for First Aid frequentlY have to be improvIsed.
. .
A Splint may be improvised from a walkmg st1.ck, umbrella, billiard cue, broom or brush polIceman's truncheon, rifle, folded coat, p1ece of wood, cardboard, paper firmly folded, a rolled-up map, or, in fact, anything that is firm and long enough to keep
the jO/itts z'mmediately above and below the fractured at rest. vVhen the above appliances are not available, the limb, if fractured, may be tied to the trunk, and 111 all cases a fractured lower limb should be bandaged to its fellow.
Bandages may be iIi1provised from handkerchi efs bel.ts, straps, braces, neckties, or any piece of linen: calico , stnng or cord that comes to hand.
BCl:ndages (Fig. 8) are made. by cuttmg a of lmen or calico about forty mches square diagonally into two pieces. broad bandage is made by bringing the pomt to the base (Fig. 9), and then folding mto two (Fig. 10).
The narrow bandage is made by folding the broad banda&e once (Fig. I I).
medium bandage is made by bringing the down to . the base, and then folding il.tO three. \L 10 , 12). ThIS bandage may be used instead of the broad or the bandage when it is better suited to proportIons of the patient.
It IS sometimes advisable to halve the size of the ?y bringing the two ends together before It the broad, narrow, or medium bandage. f Vhen not 111 use, the triangular bandage should be olded narrow; the two ends should be turned to the and the bandage then folded into four reducmg It to a packet about 6t inches by 3t- inches:
36
.
37
FIG. 10. BROAD BANDAGE.

12.-THE
FIG. II. NARROW BANDAGE.
Large arm-sling ( Fig . 13).-Spread out a bandage, put one end over the shoulder on the sound side f pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang down in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm
13. FIG. 14.
Over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure with two pins to the front of the bandage.
Small arm-sling (Fig. 14).-Place one end of a
FIG. DOTTED · LINES SHOW TilE FOLDS OF THE MEDIUM BANDAGE.39
FIG.
broad bandage over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side; place the forearm over the middle of the bandage; then bring the second end up to the first, and tie them. This slin.g is used in cases of fractured humerus, and occasIOnally when the large sling would be too conspicu?us. Slings may be improvised in many SImple ways, such

as pinning the to the turning up the tail of the coat, passmg the hand mSIde the buttoned coat or waistcoat, etc.
Reef Knots (Fig. IS) are to be used. Avoid granny knots (Fig. 16).
G E NERAL RULES TO BE OBSERVED IN THE TREATMENT OF FRACTURES.
The object of First Aid Treatment of Fractures is to gl'ard against further mischief, anc especially to prevent a simple fracture from becoming compound or complicated. To attain this end :-
I. Attend to the fracture on the spot. No matter how crowded the thoroughfare, or how short th e distance to a more convenient or comfortable pla ce , no attempt must be made to move the patient until the limb has been rendered as immovable as possible by splints or other restraining apparatus.
2. Steady and support the injured limb at o nce, so that its further movement on the part of either the patient or the bystander is prevented.
3. Straighten the limb with great care, and if shortening is observed in the case of a fracture of a bone of the lower limb, pull upon the foot until the limb regains a more normal length. W'hen the shape of the limb is improved, on no account let go until it is secured in position by splints, otherwise there is great danger of the fracture becoming compound or complicated.
4. Apply splints (when practicable) and bandages as follows:-
(a) The splints must be firm, and long enough to keep the joints imm ediately above and
40
FIG. IS.-REEF KNOT. FIG. 16.- GRANNY KNOT.
below the fractured bone at rest. They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
<I) The bandages must be applied firmly , but not so tightly as to constrict the circul.ltion of blood in the limb. When the pati e nt is in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule ;-
For the trunk the broad bandage should be used. Pass it once round the trunk and fasten it by tying the ends, or with two or three safety pins on the side opposite to the fracture, but if to secure a splint for a broken thigh, over the splint.
For tlze arm or forearm the narrow bandage should be used. Pass it twice round the lim b, and tie the ends over the outer splint.
F or the thigh or leg the n:::urow or medium bandage may be used. It is frequently convenient to double the bandage at the centre, pass it under the limb, bring the loop over the limb, pass both ends of the bandage through it in opposite directions, and tie them over the outer splint (Fig. 17).
applying bandages near a fracture the upper one should be secured first.
S· When accompanies a frae ture It must ?e to first, and the wound covered by a. Clean dressmg.

FIG. 17.
6. No attempt must be made to remove a ,Patient suffering from a fracture of the spme, pelvis, or thigh, except in a recumbent position, preferably upon a stretcher.
7. In every case of fracture it is necessary to cover the patient to keep him warm, and so lessen the effects of the SHOCK of the accident .
8. In all doubtful cases, treat as a fracture.
SPECIAL FRACTURES.
Fracture of the Cranium.-A fracture of the upper part is usually caused by direct violence-for a blow on the head. A fracture of the base J caused by indirect violence, through a fall on
'
43
44
head a fall on the feet or lower part of th e sp in '? , or a' severe blow on the lower jaw. If t he upter part z's fractured, the are and frequently ins enSIbIlity, eIther. lmmed mte .or comin g on g radually. If Ilz e base zs fractu red Insensibil ity may come on
FI G. I S. imm edi a tely, blood or a clear fluid may iss·ue from the ear ch anne l) blood may escap e fr om the nose, or it may pass down to the stoma ch , whence it may be vom ited; the fracture m :1. j involve the orbit, causing a blood-shot eye.
TR E AT ME TT.
In jury to the brain IS the great danger attendin g a fractur e of the cranium. For treatm ent see " Con cussion a nd
Compression of t h e Bra in," pag es 13 1 , 13 2 .
Fracture of the Lower J aw.-Pain, loss of power (in ability to speak and move the freely), irreg ula rity of the tee th, crepItus and bl ee dmg fr om the gum are the usu al sig ns and symptoms.

45 TREA TIIIENT.
I.-Place the palm of the hand below the injured bon e and press it gently against the upper jaw.
2.-AlJply the centre of a narrow bandage under t he chin, carry one end over the head, cross the ends at the an gle of the ja w, carry the long end across the chi n, and tie the ends on the side (Fig. 13).
Fracture of the Spine.- The vertebral column may be broken either by direct or indirect violen ce. Fa ll ing from a h eight on the back across a har or up on an uneven surface is an example of direct fra cture, and a fall on the head, causing a broken neck, is an example of indir ect violence. What is co mmonly regarded as a broken back consists of a fra cture of one or more of the vertebrce with displacement of the fragm ents, whereby the spinal cord a nd the nerves issuing from it may be torn, causing co mplete or partial paralysis of the parts below the frac ture. Pain is present at the seat of injury.
TREATMENT.
I. Prevent all movement on the part of the patient.
2.-Cover the patient warmly.
3· - To remove the patient, place him on a stretcher or shutter as follows :-
(a) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
so that the ends are level with the top of his bead; pass a broad bandage or handkerchief under the head and secure it to the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
(b) A bearer on each side grasps the rolled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes charge of the le gs.
(c) On the word being given, all lift together and carry the patient by short side paces over the stretcher and carefully lower him on to it. If a fifth bearer is available the stretcher should be passed under the patient instead of carrying him over it.
4.-0n arrival at shelter nothing further is to be attempted until the arrival of a doctor, except to give the patient water, tea, etc., if he is conscious.
Fractured Ribs.- The ribs usually fractured are the sixth, seventh; eighth, and ninth, and generally the fractur e is midway between the breast-bone and the spine. The fracture may be caused by indirect violence, driving the fractured ends of the bone outwards, or by direct violence, driving the fractured ends of the bone inwards and sometimes injuring the

fungs or other internal organ. If the lower ribs 001 the right side are broken, the liver may be injured y and a fracture of the lower left ribs may wound the spleen. Evidence of the fmcture is afforded by pain! especially on attempting to take a deep breatl"'lj and by short and shallow breathing. If the lun gs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hremorrhage (see page 95) may occur.
TREATME TT.
(a) TT?ze7t tIle fracture is not complicated by an i llju 'ry to an internal organ :-
r .-Apply two broad bandages round FIG. 19. the chest sufficiently firmly to afford comfort, with the centre of the flrst above and that of the second immediately below the fr acture. The lower bandage should overlap the upper to half its
46
47
extent. The knots are to be tied rather tothe front on the opposite side of the body. Another good plan is to apply a strong towel, folded about eight inches wide, tightly round the chest, securing it with three or four safety pins.
2.-Place the arm on the injured side in a large sling , (Fig. 19)'
(b) Wizen an internal organ is z'njzwed-
J .-Do not apply bandages round the chest.
2.- Lay the patient down, inclined a little towards. the injured side
3.-Loosen the clothing, give ice to and place an ice bag over the seat of Injury. Treat as for internal hremorrhage (see page 95).
4.-Place the arm on the injured side in a large slIng ,
Fracture of the Breast-bone (stel'num).When this fracture can be felt or is suspected undo all tight clothing, and keep the patient quiet in an easy position until the arrival of a doctor.
FRACTURE OF THE BONES OF THE UPPER LlMB.
Fracture of the Collar-bone (cla vicle ).- This fracture is frequently caused by a fall on the hand or shoulder.-The arm on the injured side is partially

49
helpless, and the patient usually supports it at the elbow with his hand, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lower. The general signs and symptoms of fracture are mostly present.
TREATMENT.
I.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3.-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a " St. John" sling, made as fo 110ws :
(a) Lay an unfolded bandage across the chest'over the injured limb with one end on the uninjured and t,he point beyond! the elbow on the lllJured slde. (Fig. 20"
(b) the end of the bandage under the lllJured 11mb, across the back, and tie the ends somewhat loosely in the hollow in front of the sound shoulder.
(c) F?Id the point the elbow of the injured 11mb and secure It by one or two pins (Figs. 21 and 22).
4.-Tightly secure the injured limb to the side by It broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
5.-Now tighten the sling. When both collar-boBes are broken keep the

Fw 2(.
FIG. 22.
(Bod y bandage omitted to show details of Sling.)
FIG. 23A. FIG. 23B. shoulders back by narrow bandages tied round each cum, close to the shoulder, passed across the over the opposite arm and tied together in front. Th e forearms should be raised and supported by the bandages. (Figs. 23A and 23B).
Fracture
of the Shoulder-blade (sca}zt la ).Apply the centre of a broad bandage in the armpit of
50
51
52
injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24)·Fracture of the Arm (humerus). - The bone may be broken :-(a) Close up to the shoulder; (b) near the middle of the shaft; (c) close FIG. 24· to the elbow.
All the general signs and symptoms of fracture arc usually present.
TREATMENT.
When. the Fracture Z:s close to the Shoulder-
I.-Apply a broad bandage with its centre above the middle of the ann round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
When the Fracture £s near the M£ddle of the Skaft-
I.-Bend the forearm at a right angle to the arm.
.2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
must on no account be so long as to p ress upon the bl oo.d-ves sels at the elbow joi nt. 3·-Secure the splmts by bandages above and bel?w the fractur e. If splints are not avallabl e secure the arm to the side by two broad band ages.
4.-Support the for earm by a small arm sling. (Fig. 25).
Fractures involving the elbow joint, "h ether of the arm or forearm, are attend ed with so much swelling, and it \s so difficult to asce rta in the exact natu! e of the injury, that w;1en the accident occurs i-ndoors the j ; mb should be laid upon a pillow in the most comfortable po.·ition; ice or . ,-old water dressings should be applI ed to the injured part, but no further treatment should be attempted pending the arrival of a doctor.
FIG. 25.
H/7zen the accidmt occurs out oj doors-
1.- Take two pieces
FiG. 26 of thin flat \':l)OC, onp. lUl1g enougb to rear.h from the armpit tv below the tbe other long enough to reach from above the elbow to the finger tips; tie them together to form a right angle. (Fig. 26).
2.-Apply the angular splint so made on the inner side of the fl exed limb.
s.-Secure by bandages above and below the fracture.
4·-Support the limb by a large arm sling.
5.-0n arrival at horne remove the splint, and treat the injury as if it had occurred indoors.
Fracture of the Forearm. --When b oth bones (the Radius and Ulna) are broken, the gen e ral signs and symptoms of fracture are usually present. When one of the bones only is broken the si gns and symptoms are as a rule pain, loss of power, s\\'elling , and irregularity. An impacted fracture of the Radius

just above the wrist is a common result of a fall on the hand.
TREATMENT.
This is the same, whether the fracture is of one bone or of both.
1.- Bend the forearm at right angles to the arm,
FIG. 27.
FIG. 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sides from the elbows to the fingers. .
3·-A pply bandages, embracing both splints, immediately above and below the fracture and round the hand (Fig. 27).
4,-Apply a large arm-sling.
Crushed Hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREATMENT.
I.-Apply a carefully padded splint to the front of the hand, reaching from well above the wrist to beyond the tips of the fingers.
51
55
, I . i., l
2.-To secure the splint apply a narrow <:rossed in the manner of the figure 8 to the wnst and hand (Fig. 28).
3.-A pply a large arm-sling.
Fracture of the Pelvis.-When, after a severe injury in the neighbourhood of the there is no sign of damage to the lower limbs, but patient is unable to or even to. move the lower limbs without great dlfficulty and pam, a fracture of the pelvis may be assumed to have occurred. The blood-vessels and organs, especially .the bladder, within the pelvis are in danger of bemg wounded.
TREATMENT.
I.-Lay the patient in whatever is found to give the greatest flex or straIghten lower limbs as the patlent deSIres. . '
2.-Apply a broad bandage round the .hIpS tight enough to support the parts, not so tIght as to press the broken bone further inwards.
To remove the patient place him on stretcher, on the same principle as that descnbed under "Fracture.of the Spine II (see page 45).
FRACTURE OF THE BONES OF THE LOWER LIMB.
Fracture of the Thigh-bone teigh bone may be broken at its neck, anywhere m the shaft, or close to the knee. A fracture at the 57
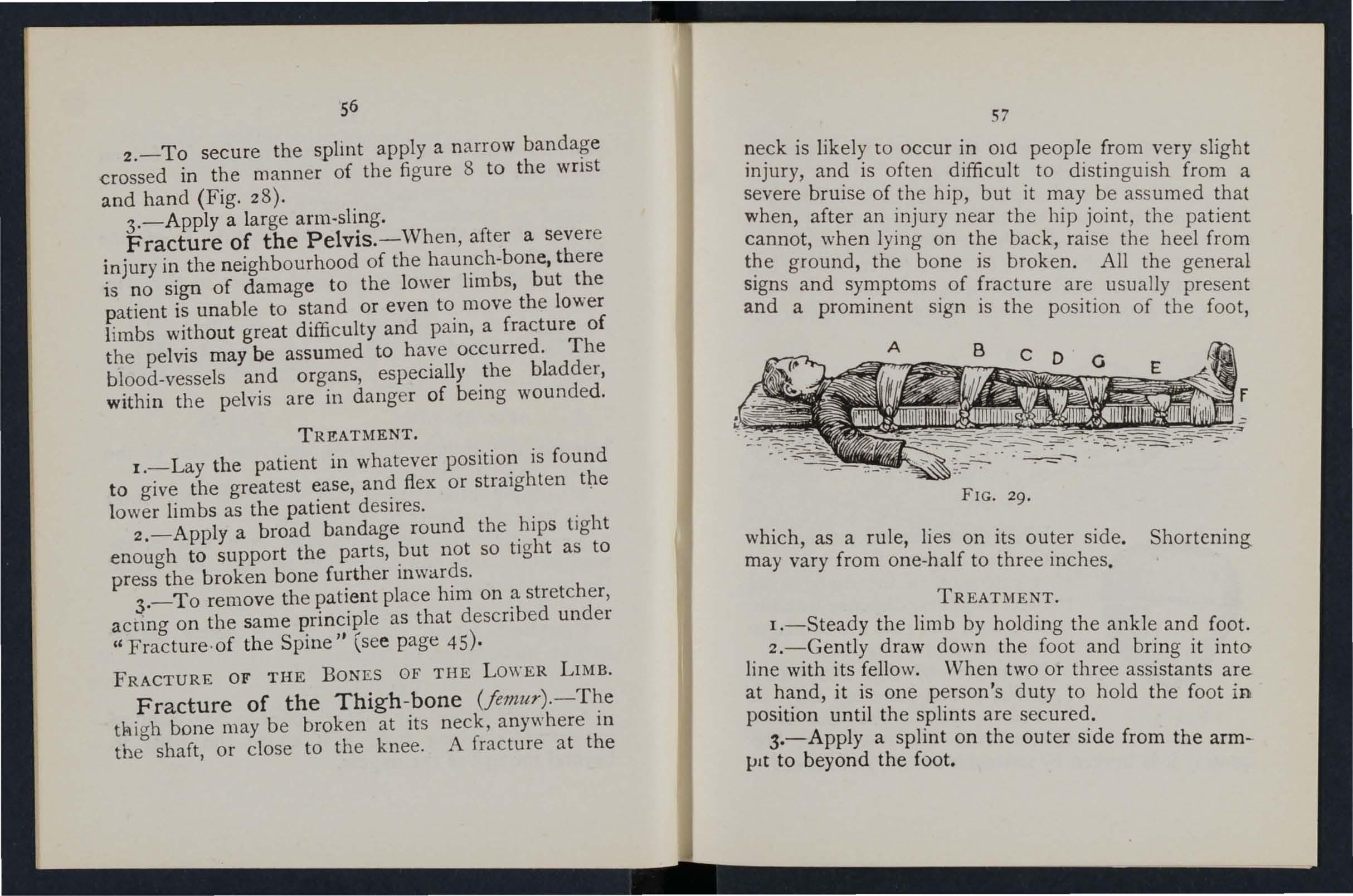
neck is likely to occur in ow people from very slight injury, and is often difficult to distinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patient cannot, when lying on the back, raise the heel from the ground, the bone is broken. All the general signs and symptoms of fracture are usually present and a prominent sign is the position of the foot,
29.
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Gently draw down the foot and bring it into line with its fellow. When two or three assistants are at hand, it is one person's duty to hold the foot in position until the splints are secured.
S.-Apply a splint on the ou ter side from the armlJlt to beyond the foot.
56
FIG.
58
4.-Apply a splint on the inner side from the top of the thigh (the fork) to the knee.
S.-Secure the splints by bandages as follows :(a) Round the chest just below the armpits, (b) round the pelvis on a level with the hip joints, (c) above the fracture, (d) below the fracture, (e) round the leg, (f) round both ankles and feet, and tied below the feet, (g) a broad bandage round both knees ( Fig. 29).

FIG. 30.
When single-handed, or when the patient is a woman, it is expedient, after extension of the lim b, to tie the feet together, dispense with the inner splint, and pass the bandage£ round both limbs (Fig. 30).
Fracture of the Knee-cap (patella).-The knee-cap may be FIG. 3I. broken by falling on the knee (direct violence), but more fre.quently it is broken by muscular action, as follows:-
59
When the slips in the attempt to prevent a fan the muscles III the front of the thigh act with such force. as to snap the knee-cap in two (Fig. 3 I) . .
Pam, loss of power (the limb will be quite helpless), and irregularity (a gap may be felt between the broken fragments of bone) accompany this injury.
TREATMENT.
I.-Lay the· patient on his back, raise well and
FIG. 32.
support the head and shoulders straighten and raise the limb. '
2.-Apply a splint along the back of the limb reaching from the buttock to beyond the heel. '
3·-Applya narrow bandage with its centre imme-
60
.diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone . . To ensure firmness apply a second bandage in a similar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5.-.Su pport the foot well off the ground by a -pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 3 2 ).
6.-Apply an ice bag or a cold water dressing over the fracture.
Fracture of the Leg (tibia and fibula).-One .or both of the bones may be broken. When both bones are broken all the general signs of fracture are usually present, but when one bone only is broken -deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end is frequently mistaken for a sprain and sometimes fot .a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
61
foot. If only one splint is available place it on the outer side.
4.-Secure the splints by bandages (a) above (b) below the fracture, (c) immediately above the knee,

FIG. 33.
FIG. 34.
(d) round both ankles, (e)" a broad bandage round both knees (Fig. 33).When single-handed, or when the patient is a..
-woman, after extending the limb tie both feet together, .dispense with the inner splint, and pass the ban?ages round both limbs (Fig. 34). 'Vhen no splmt is .available tying the legs, ankles, and knees together is of great service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).-This accident is commonly caused by the passage of a heavy weight over the foot, and may be recognised by pain, swelling, and loss of power.
TREATMENT.
I.-Remove the boot (see page 19).
2.-Apply a wellpadded splint to the sole of the foot, reachingfrom the heel to the toes.
3.-Apply a bandage FIG. 35· crossed after the manner of the figure 8 (Fig. 35).
4·-Support the foot in a slightly raised position.
DISLOCATIONS.
A dislocation is the displacement of one or more of the bones at a joint.
The joints most frequently dislocated are those <>f the shoulder, elbow, thumb, fingers, and lower jaw.

SIGNS AND SYMPTOMS OF DISLOCATION.
1.- Pain of a severe sickening character at or near the joint.
2.-Loss of power in the limb.
3· -Numbness of the parts below the seat of dislocation.
4.-Swelling about and below the joint.
S.-Fixity of the joint.-The limb cannot be moved at the joint by either the patient or others.
6.-Deformity of the limb.-The limb assume!! an unnatural position, and is mis ·shapen at the joint.
TREATMENT.
No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival :_
(a) When the accident occurs out o.f doorsSupport the limb in whatever position gives most ease to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) When the paHent is indoors-
I.-Remove the clothing from the limb.
2.-Place the patient on a couch or bed.
3·-R est the limb on pillows in the most comfortable position.
4·-Apply cold (ice or cold water) dressings to the joint.
S·-When cold ceases to give comfort apply
warmth (fl a nnels or towels wrung out of hot wa ter).
6.-Treat shock (see page 135).
SPRAINS.
When, by a sudden wrench or t wist, the ligaments and the parts around a joint are stretched and torn the joint is said to be sprained. "Going over" the ankle is a common exam pIe.
SIGNS AND SYMPTOM S.
I.-Pain at the joint after a twist or wrench.
2.-Inability to use the joint.
3.-Swelling and discoloration.
TREATMENT OF SPRAINED ANKLE.
When out of doors-
I.-Apply a bandage tightly the boot, ginning on the sole at the mste p, it on the front of the ankle, and carryll1 g it round and round the ankl e, where it is to be firmly tied.
2.-vVet the bandage after application; it is thereby tightened.
,After reaching sltelter-
1.-Remove the boot and stocking (see page 19)'
2.-Place the limb in the most comfortable position;, u sually that is well raised.

65
3·- A pply ice or cold water dressings to the as long as they relieve pain.
4·-, Vhen cold fails to give comfort, apply hot fomentations .
When other joints are sprained, treat them as if dislocated.
When in doubt as to the nature of the injury, treat as a f racture .
STRAINS AND RUPTURED MUSCLE .
,Vhen, during severe exertion, muscles or tendons are over-s t retched they are said to be strained, if th ey are actually torn they are described as ruptured.
A:\,D SYl\IPTOMS.
I.-A s udden sharp pain .
2.- When the muscles of a limb are strained they may swell and cause severe cramp .
3·- Further exertion is difficult or impossible ; fl lr example, if the s train has occurred in the back the patien t may be unable to stand uprigh t.
TREATMENT.
I.- Pl ace th e pa tient in the most comfortalJle pOsit ion , and afford support to the injured part.
2.-App ly ho t water bottles or hot fomentations when t he pain is very severe .
A so-called strain in the groin (hernia) is an injury of a to tally different nature (see page I q). D
64
QUESTIONS ON CHAPTER II.
Tilt numerals t"ndicat e the pages where the answers lIlay be found.
What is the skeleton, and what purposes are served by it?
How are the bones of the skull arranged?
\\-hat are the b oundaries of the cranium?
Describe the bones of the face
Describe the lower jaw
\\'hat is the angle of the jaw? ...
\\'h at othe r names has the back-bone?
\\'hal is a ve rteb ra
How many vertebne are there in thc spine?
What are the regions of the spine, and how many ve rte bra! are there in eac h?
H ow is the spin e endowed with free movement?
"-hat is a rib?
How many pairs of ribs are thCle ?
What is the breast-bone?
\Yha t are the bones of the upper limbs?
What is the pelvis?
What is t he hip joint?
\Vhat are the bones of the lower lIm bs?
What is a joint?
Describe a moveable joint ...
Describe the shoulder joint
De sc ri be the ankle joint ...
How are m'.!scles classified t;
Describe voluntary muscles
Describe involuntary muscles
\Vhat is a fracture?
'What are the causes of fracture?

Where does a bone break when direct violence is the
does a bone b reak w!1cn indirect vi olence is the cause of
How maya fracture be caused hy muscular action?
In what two ways may fractures be cia sified ?
What is a simp le fracture? ...
What is a compound fracture?
State the general signs and symptoms that may be present in a case of
What fractur es afford the most complete example of the signs and sy mptoms?
In making up your mind whether a fraclure had occ urred or not, what points should you take into consideration beyond the signs and symptoms?
cause a fracture of the upper part of the
66
PAGK
... ... .., ... ...
... 22 22 22 22, 23 23 23 23 23 25
?..
25 25 26 26
..
.. .
...
...
..
,
.. , .... ...
..
,
...
.. 26 26 to 28 28 30 ')0 31 31 32 32 32 33 33 33 ···33, 34 PAGlI
cause of fracture? 33
fracture?
Where
What
fracture? \Vhat is a
fracture? What is a green-stick fracture? \Vhat is an impacted fracture? 34 34 ... 34-, 35 34 3 34 3]' 35 35
... 35, 36
.. .
is a complicated
comminuted
fracture
\Vhat
35 fractur es? 36 How may splints be impro\"ised ? _.. ... 35, 37 How may bandages be improvised? 37 Describe Esmarch's triRngular bandage 37 , 38 lFiti. 8) In
use? 37 How
39, 40 , 49 What knot is to be tied,
avoided? 40 What is
41 J ive
fractures 4 1 How
... ... 41, 42 How
-- 42, 43 \Vhat
43
apparatus may be necessary for the treatment of
what ways may the tri angular bandage be folded for
many kinds of arm-slings are there, and what are they called?
and what knot
the object of first aid treatment of fracture
the general rule s for the treatment of
should splints be applied?
should bandages be applied?
may
c.ranium?
What may cause a fracture of the base of the cranium? 43, 44
\\'hat are the signs of fracture of the upper part of the cranium?
" That are the signs of fracture of the base of the cranium?
\Vhat is the treatment for fracture of the craniulll ?
What are the signs of of the lower jaw?
lIow maya fractured spme be caused?..
\ \'bat is commonly regarded as a broken back?
What are the symptoms of a fractured spine ?
How may ribs be fractured ?
How maya fracture of ribs be compl,icated?
State the signs and symptoms of a simple and of a complicated fracture of ribs
\Vhat is a frequent cause of fractured collar-bone? ...
'Vhat are the signs and symptoms of fractured collarbone?
At what points may the b one of the arm be broken? 52
Are the general signs and symptoms of a fracture always present in a broken forearm?
State the cause of a common fracture of the rad:us
IIow would you recognise a fracture of the pelvIs?
At what points may the thigh-bone be broken?
\Yhat are the signs and symptoms of
thiah -bone
\Yhat the causes of fracture of the knee-cap? .. . 58, 59
\ Vhat are the signs and symptoms of fracture of the kneecap?
Are the general signs and symptoms always present m a fracture of the leg?
\ Yhat mistake may ea sily be made when the liGula IS broke n near its lower end?
\Yhat is a di slocation?
Students should practise improvi ing mat e ria l, foldll1g bandages, tying knots, making slings, and the treatment of the following injuries.
Fractures - Lower jaw, 44. Spine, 45, 46 . Ribs (simple and complicated fractures), 46 to 48. Breastbone, 48. Collar-b one, 48 to 5I. Both collarbones, 5I. Arm, close up to shoulder, 52. Arm, near m.1d9le of shaft, 52. Arm or forearm when the elbow IS mvol.ved, 53. Forearm, 55 . Crushed hand, 55, 56. PelVIS, 56. (man), 57, 58. Thigh (woman, or man when sll1gle-handed), 58. Kneecap, 59, 60. Leg (man), 60, 61. Leg (woman or . when single-handed), 62. Crushed foot, 6d.
DlslocallOns-Out of doors and indoors 6' 64 Sprained an kle
.. . .. .) 64
68 PAGE
... ... . .. . ..
.. ,
... ... . ..
.,.
..,
.. ,
.. ,
.. . 44 44 44 44 45 45 45 46 47
... ... ... .., ... . ., .. .
48, 49
. .. .
..
.,'- ...
.. ,
fracture of
54 55 56 57 57
... .. . ... ... ...
the
?
.. . .
... .., .. ,
.
."
... State the signs and symptoms of disl ocation 59 Go (.0 62 6] S PAGE tate the treatment of dislocation... ... 63 What is a sprain? ... ... ... ... 64 \Vhat are the signs and symptoms of a sprain r 64 State the treatment of a sprained ankle ... 64 State the treatment of other ... . ... ... 63, 65 \Vhen not sure whether the m Jury IS a spram or [ ract ure how would you treat it? 65 H ')w may muscles be strained or ruptured? 65 State the signs and symptoms of strains 65 Stftte the treatment of strains 65
.. . Improvi -ing Folding bandages Large arm sling .. . Sl1ull arm sling .. . Reef and granny ... 36, 37 3 7 37 39 .. . 39,40 40 42 Knot for applying splint to lower
First
Improvising sp'ints
limb
St rains
ruptured mu scles
..
and
65
CHAPTER III.
THE ORGANS OF CIRCULATION.
THE organs concerned in the circulation of the blood are the Heart, the Arteries, the Veins, and the Capillaries.
The Heart is situated in the chest behind the breast-bone and rib cartilages, between the lungs and immediately above the diaphragm; it lies obliquely with a quarter of its bulk to the right and the remaining three-quarters to the left of the middle line of the body. Its beat may be felt just below and to the inner side of the left nipple. The heart has four cavities, two on either side of a central partition. The two upper cavities are named the right and left auricles, the two 10\\ er the right and left ventricles.
Arteries are vessels which convey blood from the heart. V tins carry blood to the heart. Capillaries connect the arteries and veins.
In the general (systemic) circulation arterial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all parts of the body. .' These divide and sub-divide, and become so small as to assume microscopic dimensions, \\ hen they are termed capillaries.

.L. Larynx (voice box); T. Trachea (wind-pipe): R.L. Right Lung; L.L L e ft Lung (the lungs are drawn bJ.ck to expose the heart and hlooc1 vessels); R.A. Right Auricle; L:A. Left Auricle; R.V. Right Ventricle; LV . Left Yentncle; r.A. Pulmonary Artery; Ao. Aorta; S. V.C. lIpe rio r vena cava (the large vein carrying blood from th e up pe r part of body t.o the heart); LV.C. Inferior vena cava (the large vem carrymg blood from the lower part of the body to th e The four pulmonary veins cannot be shown in th e diagram.
FIG. 31).72
In the capilIaries an interchange of gases and fluids takes place, whereby the nourishment and maintenance of the tissues and organs of the body are provided for, and the blood becomes dark and impure.
Venous blood passes from the capillaries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by neighbouring veins until they finally, as tw o large vesse ls, reach the right auricle of the heart. The veins, especially in the limbs, are provided with valves at frequent intervals, which prevent the backward fl ow of the blood.
The pulmonary system of blood vessels is concern ed in carrying the blood through the lungs. From the right auricle the blood passes to the righ t ventricle, and is thence carried to the lungs, where it is purifieJ by contact with air, :md becomes scarlet in colour; it is then conveyed to the left auricle of the heart and pass e:> into the left ventricle, thus completing the circulation.
The heart contracts in adults at an average rate of seventy-two times a minute, but the rate varies, incre:tsing as the position is changed from the lying to the sitting or to the standing position; hence the importance of adjusting the patient's position in cases of hc:emorrhage. At every contraction of the left ventricle blood is forced into the arteries, causing the pulse, which may be felt wherever the finger can tle

Exp'analiolt.-In the miJdle of the diagram is the heart \\ ilh its four chambers. Above the heart is shown the lung (pulmonary) circulation. The lower part represents the general (systemic) circulation. Vessels con · taining impure (venous) blo od are shown black, while those containing pure (arlelial) bl ood are shown white. The conn ec t· ing vessels represent tlTe capil. laries. The arrows show the direction of the flow of blo ou .
placed on an artery as it passes over a bone. In the veins no pulse is to be found.
HiEMORRHAG E.
Hc:emorrhage, or bleeding, is of three kinds :I. Arterial. 2. Venous. 3. Capillary.
FIG. 37.73
DIAG RAM OF THE CIRCULATION OF THE BLOOD.
ARTERIAL HJEMORRHAGE.
L Blood from an artery is scarlet. .
2: - If the wounded artery is near t.he skm the blood spurts out in jets correspondmg to the pulsation of the heart. .
3. - The pressure point (see below, 1S on the heart side of the wound.
ARREST OF ARTERIAL HJEMORRHAGE.
Arterial hcemorrhage is, when practicable, to be arrested by pressure, posltion of the body, and elevation of the bleeding part.
Pressure may be :- . .
I. - Digital-that is, applIed wIth the thumb or finaers and may be (a) on the wound; (b)bat spot called pressure point. The pressure points are mdlcated by numbered dots on the frontisplece .
2. --By a pad and b l ndage (a ) on the wound; (I)) on the pressure pomt.
3. - By flexion.
To apply a pad and bandage to the wound, place a piece of lint or lin en or a clean chief folded into a hard pad, on the bJeedmg POll1t, and secure it bv a bandage tightly tie.d rou.nd th e injured part. To fold the handkerchi ef, bnng the four corners to the centre, and repeat the un til a hard pad is formed. The smoolh surface IS
placed on the wound, and, to prevel1t the pad from unfolding, the puckered surfase may be stitched or fixed by a safety pin. A hard substance, such as a stone, may be enclosed in the centre of the pad.
A Tourniquet may consist of a pad to be placed on the pressure point, a strap, cord, or bandag( to encircle the limb and pad, and a tighfming arrangemen t, such as a stick or other means of twisting the Land to tighten it.
To improvise and apply a tourniquet:- -
I.-Apply a firm pad on the pressure point.
2.-Encircle the limb by a narrow bandage with its centre over the pad.
Tie the ends of the bandage in a half on the opposite side to the pad .
s:.
4·-Lay the bdsting stick on the half knot, and over it tie a reef knot.
5·-Twist the stick to ti ghten the bandage, thereby pressing the pad uron the artery, and arresting the flow of blood.
G.-Lock the stick in position by the ends of the bandage already applied, or by another bandage passed round the stick and limb.
The pa d of the tourniqu et must be accurately placed upon the pressure point so as compl etely to compress the artery; otherwise arterial blood \"ill be allowed to pass along the limb, and the veins, being compressed by the tourniqu et, \\ ill not allow the
74
blood to re turn through them to the heut, and the result will be dangerous swelling and con.sestion.
Should a suitable pad not be at hand, a knot ffii1y be made in the centre of the banJage, and when available, a stone, cork, etc., enclosed in it to give it firmness and bulk. See that the bulging and not the fiJ,t side of the knot is next the skin.
An elastic bandage passed tightly round the limb, im!11ediately above the seat of arterial hremorrhage, will arrest bleeding, The simplest prepared form of this bandage is a strip of elastic webbing, twenty-five to thirty inches long and two inches wide, wi th a piece of tape Se \\:1 at each end, An ebstic b elt or brace will serve the S3.me purpose. Except when p3.rt of a limb is torn off, it is 'not advis.lble to use an elastic cord or bandage if other apparatus can be had, as it cuts off all circulation in the limb.
Flexion consists of the application of a pad on the pressur e point at the knee or elbow joint, fL:xing the limb to make pressure, and securing the limb in the fl exed position by a b:lndage crossed like the figure 8. 6
RULES FG:lR TREATMENT OF A WOUND BY ARTERIAL HiE.\IORRHAGE.
I, Stop bleeding.
II. Prevent injurious germs from getting into the wvund.

To attain these ends :-
1. Place the patient in a suitable position, bearing in milld that the blood escapes with less force " 'hen the patient sits, and is still more checked when he lies down.
2. Elevate the bleeding part, as thereby less blood finds its \yay into it.
3. Expose the wound, remoying whatever clothing is necessary. (See Rule 8, a.)
4. Apply digital pressure.
(a) If the wound is small on the bleeding spot. (b) If the wound is large on the pressure point n e xt to the wound on the heart side. The nearEst pressure point is chosen in ord er to a\-oid cutting off the circulation from as much of the part as possible, but sometime s it is necessary to apply pressure still nearer to the heart.
5. Remove foreign bodies, such as broken glass , bits of clothing, hair, etc., seen in the \\'ound; do not search for foreign bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boracic gauze or lint is to be preferred, but absorbent cotton wool, lint, or gauze, or a clean piece of linen will answer the purpose. Should any doubt be entertained a.s to the cleanliness of the dressing, a clean piece of unprinted paper, such as the inside of an
77
78 envelope, should be placed next the wound before a.pplying the pad .. (Compare pages 75 and 76.) .
7. Bandage bghtly over the pad unless .-
(a) Foreign bodies are suspected to be left unseen in the wound.
(b) There is danger of in jury to a lracture. In these cases a light dressl11g only should be applied. .
8. Apply a pad and bandage or flexlOn the pressure point (see Rule 4, b), but only 1ll the following cases:-
(a) As a temporary while the wound is being exposed, exammed and covered. .
(b) As a more permanent measure v,·hen bleedmg cannot be stopped by the pad and on the wound, or when, in accordance wIth Rule 7, the tight bandage has not been applied.
9. Afford support to the injured part. ,\Vhen part of a limb has been torn off or the .wound is lacerated (for example by the claw of an ammal or by machinery) hremorrhage frequently does not come on at once, but as there is a danger of severe hremorrhage later, means for its arrest should be applied to the limb, but not tightened unless r.ecessary. Do not disturb a clot of blood formed over a wound. No attempt should be made to clear:se a except \\'ith sterilised \\aler (that is pre\'lously boiled

and allowed to evol) , and experience, especially in recent wars, has shown that those wounds \\'hich were provisionally treated with a dry dressing and subsequently dressed by a surgeon with proper appliances did best.
Students pmctlsll1g arrest of arterial hremorrhage should feel the pulse to see when the current of blood in the artery has been stopped, and should then immediately relax the pressure made on the artery. In this way the importance of tIle accurate application of pressure will be realised, and the amount of force necessary will be ascertained.
THE COURSE OF THE ARTERIES, A TD THE ARREST OF HJE iHORRHAGE.
(The numbers of the pressure points refer to those on the Frontispiece.)
THE LARGE ARTERIES "'!THIN THE: CHEST A D ArmO;\IEN.
The Aorta is the central or trunk artery of the body. Commencing at the left ventricle it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branches which carry the blood to either side of the head and neck and to the upper limbs. The Aorta passes down On the left of the spine to just below the navel, where it divides into two great branches (the iliacs)
79
which convey the blood to the organs in the pelvis and to the lower limbs.
\Vounds of these arteries are one cause of internal hzemorrhage (s ee page 96).
ARTERIES OF THE HEAD AND NECK.
The Carotid Arteries (right and left) leave the upper part of the chest and pass up on either side of the windpipe a n d , just below the level of the a ngle o f the lo\\'er jaw, divide into the I nternal and External Carotid A rteries. The Internal Carotid Artery ascends deeply in the neck, and enters the cranium to supply the brain with blood . The External Carotid Artery gives off a number of branches; ,to the front the artery of the tongue (Lingual), the artery to the {:lce (Facial) ; to the back the Occipital; the artery itself is continued upwards in f ront of the ear, \\ here it changes its name to the Temporal, and supplies the scalp in the n eighbourhood of the temples.
When a Carotid Artery i·s wound e d, as in the case of a cut throat, apply the thumb of one hand on the artery at pressure point I, pressing backwards against the backbone and taking care to avoid the windpipe. It may also be nec essary to apply pressure with the other thumb abov e the \yound for two reasons : ( a) To arrest"the flo w of blood from the main (ju gular) Vein in the neck , which runs
8r
alongside of the carotid artery and is usually wounded at the same time; (b) To check the flo\y of blood from the upper end of the carotid artery itself, \yhich is often considerable owing to communication between the branches of this artery and those of its

FIG. 38. FIG, 39, feliow. Digital pressure must be by relays of assistants if necessary, untIl the doctor arrives (F ig. 38). . , The Facial Artery crosses the lower j8.w m a sli ght hollow t\\'o tina-ers' breadth in fr ont of the angle) and sends to the chin, lips, cheek, and
80
outside of the nose. Hremorrhage from wounds of the face below the level of the eye is to be arrested by :-
(a) Digital pressure on pressure point 2 (Fig. 39), or
(b) Grasping the lips or ch eek on both sides of the wound. by the finger inside and the thumb outside the mouth or vicd versa.

40.
FIG 41.
The Temporal Artery may be felt in front of the upper part of the ear. Hremorrhage from the region of the temple may be arrested by pressure applied at pressure point 3 (Fig. 40).
The Occipital Artery supplies branches to the
region of the scalp from behind the ear to the back of the Hcemorrhage from this rEgion may be arrested by digital pressure on pressure point 4, four fingers' breadth behind the ear (Fig. 4 T). This point is difficult to find, and it is usually sufficient to apply pressure immediately below the \\ ound. from the Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the bleeding point and securing it by a narrow bandage with its centre laid on the pad, the ends carried round the head in the direction most con\lenient, and tied tightly over the pad (Fig. 42).
When a wound of the forehead or seal p is associated with a fracture, the best plan is to apply a ring
FIG. 42. pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fingers; pass the other end of the bandage through the ring thus formed and continue to pass it through and through until the whole of the bandag<.: is used and a ring as shown in Fig. 43 is formed.
82
FIG.
ARTERIES OF THE UPPER LI:\IBS.
The Subclav ia n Ar te ry passes from a point behind the inner end of the collar-bone across the first rib to the armpit.

FIG. 43. FIG. 44.
To apply digital pressure:-
I.-Bare the neck and upper part of the chest.
2.-Place the patient's arm against the body so as to depress the shoulder, and cause him to incline his head towards the in jured side .
3. - Take your stand opposite the shou lder.
4.- U sing the left hand for the righ t artery, and vl'ce versa, grasp the n eck low down, p lacing the fingers behind the shoulder and the thumb immediately aboye the cent re of the collar-bo ne in the hollow bet ween the muscles attached to the bone ( pressure point 5) .
5.--Press the thumb deeply do\ynwards and backwards against the first rib, which is be?-eath the coll::tr bone at this spot (Fig. 44)
The Axlliary Arte ry , which is a continuation of the subclavian, keeps close to the shoulder joint and can. be felt pu Isating when the fingers are deepl; pressed 111to the armpit. Di g ital pressure is difficult to apply to this ::trtery.
To apply a p::td and band::tge: -
I. ·-Pbce a hard pad the size of a billiard ball in the · armpit (pressure point 6).
2. Apply the centre of a narrow bandage on. the pad; cross the bandage on FiG. 45, the shoulder; pull the ends tight and tie the .n under the opposite armpit, takin g are that the pad does not slip.
3 . - Fie .x the and tie the limb tightly to the trunk \\,Ith a broad bandage, applied on a le\'el with the elbow (Fig. 45).
The Brachial Artery is a continuation of the Axillary, and runs do,,\ n the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The inner seam of the coat sleeve above the elbow roughly indicates its course.
Digital or instrumental pressure lTI:ly be applied at or near pressure point 7.

FIG. 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back
of the arm over the seam of the coot or the groove on the inside of the biceps muscle. Press the pulps (not the tips) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47). A slight turn of the hand outwards as it grasps the arm will better ensure compression of the artery.
The Bracrual artery may be com pressed at the
FIG. 49.
elbow (pressure point 8) by flexion. The pad may be a folded handkerchief "'lith a snu11 stone or a cork wrapped up in it, but when no pad is available the coat sleeve rolled or gathered up will serve instead (Fig. 48).
86
Just below the elbow the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 and 10) are about one inch above the wrist and about half an inch from the outer and inner sides of the forearm, where the arteries may be felt pulsating. Branches of these arteries join to form the Palmar Arches in the hand. The arteries run along on either side of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and la, by the thumbs (Fig. 49) or as follows :-
I.-Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one half on the Radial, :lnd of the other half on the Ulnar artery.
3.-Secure them by a tight bandage.
To arrest hcemorrhage from the palm of the hand:-
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, turn up the base about four inches, lay the back of the patient's hand on the centre of the bandage, fold the point over the knuckles and wrist, pass the two ends round the \Hist, make the

patient pull on the puint of the bandage, cross the ends over the fi',gers twice and tie them as firmly as possible. Bring the point (.\) down to the knuckles and fasten with a pin at B (Fig. So).
3·-Elevate the forearm and support it \\"ith a "St. John" sling (see page 49).
Arterial hcemorrhage from the fingers may be arrested by applying a small pad on the wound, and securing it firmly with a strip of tape, linen or plaster.
OF THE Lo ·,\ ER LIMBS.
The Femoral Artery, a continuation of the iliac, FIG. 50. enters the thigh in the centre of the fold of the groin, where. it be felt pulsating immediately bel?w the skir:. 1 he course of the artery may be mdlcated by a lll1e drawn from the centre of the groin to the inner side of the back part of the knee. After traversing of this line, the femoral artery p:1sses behmd the tlllgh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressure point I I) as follows ;_ 1. -Lay the patient on his back.

2.-Kneel beside the patient.
3.-To find the groin, raise the foot high so as to flex the thigh; the fold in the clothing at the top of the thigh will indicate the groin .
4.-Place the thumbs one on the other upon the pressure point, grasping the thigh ,yith the hands (FIg 5 I).
5.-Press firmly against the brim of the pelvis.
As there is immediate danger of death it is important not to ,mste time in removing the trousers .
\Vhell the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been
FIG 51. devised for compression at this point, and relays of assistants should be employed to keep up the pressure until the doctor arrives; each fresh assistant places his thum bs over those of his predecessor, who slips his away from beneath, and thus gushes of blood are prevented during the change.
App li cation of a tourniquet to the Femoral artery (pressure point 12) :-
'When practising compression o f this artery, It is a
90
9I
9 2
good plan to draw a chalk line from the centre of the groin to the inner side the back. of. the place the pad of the tourmque t o n thIS lll1e as hIgh up as the ban dage can applied.. T he pad should be the size of a law n tenms ball (FIg. 52).
Pressure may be applied to the Popliteal arte r y by flexion at the knee (pressure point 13); the pad

FIG . 53.
should be the size' of a law n tennis ball, or if no po.. d is available the t ro user leg may be rolled or gathered up to serve in stead . I t is n ot n ecessa r y to take off the cl othing (Fig. 5 3). . . .
Just below and behind knee Jomt the artery divides into the AnterIor (front) a n d Postenor (back) Tibial arteries . The Posterior Tibial Artery passes down the 93
bJck of the leg to the inn er side of the ankle . I t is at fi r.st deeply placed between the muscles of th e calf, ?ut It appr oaches the surface as it proceeds , so that It can be felt pulsating b ehind the laro'e bone at the inn e r side of the ankle. It enters the sole as th e Plantar Arteries, which run forward amon ers t the ill uscles to supply the foot and toes . 0
The Anterior T ibial A r tery , on leaviner the P L)p liteal, at once p::lsses forward between leer I> mes, and, deeply placed amongst the muscles, down the leg to the centre of the ffont of the ankle. This artery is continued as the Dorsal Artery of Foot, whicll, passing forward oYer the tarsus, d!ps down to the sole between the first and second metatarsal bones . Here it forms with the Planta r arteries what is known as the Pla nt ar Arch. At the ankle points 14 and IS) pressure may be applied by the fingers or b y pads and bandages.
VENOUS II iE.\IORRHAGE.
I .- B loo d from a vei n is dark red.
2 .- It fl ows in a slow continuous stream
3·-It is sues from t h e side of the woun'd furthe r fr o m the hea r t.
4·- In the case of a wound of a varicos e veL1 it fl o ws also from the side of the wound nearer to the heart , especially if the patient is kept standing.
Varicose Veins.- Th e " eins of the leg are specially apt to become varicose. A varicose Hin is dilated) winding, and "ith bead-like (varicose) 1 rojections along its course. A vein becomes varicose from sereral causes, such as long standing o r tight garters. The first effect is to throw extra \york u po n the valves, and the bead-like are caused by the blood accumulating in the pockets behind the va lves. In time th e vein becomes so dibted that the valves can no long er span it.
GI<:NERAL RULES FOR TREATMENT OF A AccmIPANIED BY VENOUS H1E;\IORRHA GE
1.- Place the patient in a suitable position, bearing in mind that the blood escapes \\ ith less fo rce when the patient sits and is still more check ed as he lies down.
2.-Elevate the part, as thereby less blood fin d s its way into it. " .
3.-Expose the wound, removing whatever clothing is n ecessa.ry.
4. - Remove any constrictions, su ch as the c ollar or garters, from the heart side of the wound.
5. - Apply digital pressure on the wound until you can apply a pad and tight bandage. If that do e s not stop the bleeding, make pressure near the \\'oun d on the side away from the heart. In the case of a wo und of a varicose ve in it may also be n eces sary to

9 3
apply a pad and bandage to th e vein immediately above the wound, especial ly if the limb cannot be maintained in an elevated position.
6.-Treat the wound as directed by Rules 5,6 and 7, stated on pages 77 and 78.
7.-,Afford support to the injured part.
CAPILLAR y HIE:-I ORR H AGE.
1.-The blood is red.
2. -- It flows briskly in a continuous stream or may merely ooze from the wound. ' wells up from all parts of the wound.
/ \. sl!gh t amount of pressure \"ill suffi ce to arrest capillary IN TERNAL H ..IE:\IORRHAGE.
\Vou nds of the blo od vessels within the trunk cause heemorrhage into the cavity of the chest or o f the a.bdomen .
SYi\lPTmIS OF IN TERNAL H r'E \lOR R HAGE.
L--:-Rapid loss of giddiness and fai n t n ess, especially when the uprtght position is assllmed.
2.- Pallor of the face a nd lips. hurried. and laboured, and aCCOffipat1led by yawnll1g and SIghing.
4·- pulse f.1ils, and may altogether disappear at the WrISt.
94
5.-The patient thro\\ s his ar ms a b o ut) tug s at tlle clothing round the neck, and calls for air.
6.-Finally the patient may b ecom e totally unconscious.
TREATMENT.
I.-Keep the patient in a recumbent position.
2.- Undo all tight clothing about the neck.
3.- Provide for free circulation of air; fan the patient.
4 -Sprinkle cold water on the face; hold smellll1g salts to the nostrils; avoid other forms of stimulants, at all events until the hcel110rrhage has been controll ed .
5.- Give ice to suck or cold water to drink; if the seat of the hcemorrhage is kno\YD, apply an ice bag over the region.
6.-Should the patient be reduced to a slate of collapse, raise the fee t and bandage the limbs firmly from the to es to the hips and from the fingers to the shoulders.
H}E:\IORRHAGE FROM THE NOSE (NOSTRILS).
I.-Place the patic.nt in a sitting positi on in a current of air before an open window, with the head thro\yn slightly back and the hands raised above the head.
2.- Undo all tight clothing around the neck and chest.
3.- Apply cold (, ice, a cold sponge or bunch of

97
keys) over th e nos e and also the sp ine at the level of the collar; place t he feet in hot water.
4·-Cause the patient to keep the mouth ope n and so avoid breathing through the nose . '
Blood issuing from the mouth may come from the tongue, the g ums, the socket of a tO otl1 after extr.'l.ction, the throat, the lungs, or the stomach.
FROM THE TON GUE , THE GUJ\ ; S, THE SOCKET OF A TOOTH, OR THE THROAT.
T .-Give ice to suck or cold water to hold in the mouth. If this is not successful give water as hot as can be borne to hold in the mouth.
n ecessary make pr ess ure on the carotid artenes.
. 3·-If . bleeding from the front part of the ton gue exceSSlYe compr ess the part by a piece of cl ea n lmt held between th e fing er and thumb.
4·-If the bleeding 1S from the socket of a tooth plug the soc ket with a pi ece of clean lint or wool; over this place a small cork or other substance of suitable size, and instruct the patient to bite on it.
H}El\'fORRHAGE FROM THE LUNGS.
Blood from the lungs is coughed up and is scarlet and frothy in appearance.
Treat as for Internal Hcemorrhage (see page 95).
F.
96
.
H1EillORRHAGE FRO:'.! THE STOMACH.
Blood from the stomach is vomited; it is of a colour and has the appear:mce of coffee grounds j It may be mixed with food.
Treat as for Internal (see page 95), except that nothing is to be gl\-en by the mouth. .
Blood issuing from the Ear Channel, whIch generaily indIcates a fracture ?f. the base of the cranium, must be wiped away as It Issues; no attempt is to be made to plug the ea.r.
QUESTIONS ON CHAPTER III.
Tht numerals indicate the pages where flu anSWdrl may be found.
organs are concerned in the circulation of the blood?
the heart '"
the circulation of the blood through the body and lungs
many Limes a minute does the heart contract on the average?
'Vhat is the effe ct of the patient'S position on the rate at which the heart contracts?

In what way should arterial h8.:morrbage be controlled?
is meant by " pressure point"
is accuracy necessary in placing the pad of II. tourniquet?
,Vhen mayan elastic bandage be used instead of a tourniquet?
is flexion?
State the general rules for treatment of a wound accompanied by arterial hrcmorrhnge ... 77, 78
If part of a lim b had been lorn ofT, but there was not much bleeding, how would you act?
Should blood clots be disturbed ?..
Is it wise for an unskilled person to attempt to clearrse a wound?
is the aorta?
93
99
P4GJI "'bat
... 70 Describe
70
70
72 lIow
7l
72 What
pulse? ... 72 IIow
73 !low
... 74
74 ,\'hat
74 IIow may pressure
74 Wbat is a tourniquet? 75
Trace
to
is the
many kinds of hremorrhage are there?
would you know a case uf artelial ha.morrhage?
?
be applied?
Why
75
76 \Yhat
... 76
78
78
... .
\Yhat
.. -
.. 78, 79
79
100
D escrib e the arteries of the head and neck

80
\Vhy is it sometimes necessary to compress the carotid artery both below and above the wound? .. , 80, 8r
What is a ring pad, an.l what is its use? ... .., 84
Describe the arteries of the upper limbs .. , 84 to 89
Describe the arteries of the lower lim bs .. , 89 to 93
H, )w would you know _ case of :7enous hremorrhage? 93
\Vhat is a varicose ... • ••• 9-1-
How maya vein becc me varicose? ... ... ... 9+
State the general rules for treatmen t of a wound accompanied by venous bre:::norrhage? ... ... ... 94, 95
How would you know a case of capillary hremorrhage ? 95
How would you stop capillary hremorrhage ? 95
\Vhat is internal hremorrhage ? .. , ... .., ... 95
What would lead you to suspect internal hremorrhage 1 95, 96
State the treatment for internal hremorrhage? ... 96
How would you arrest hremorrhage from the nose? ... 96, 97
\Vhere may blood issuir,g from the mouth come fr om ?.. 97
How woult.! you treat bleeding from gums or 97
What else would you do if the tongue were bleedmg ? ... 97
And if the bleedin rr were from the socket of the tooth? 97
How would you clislingLlish between bleeding from the lun gs and from the stomach ?.. 97
And what would be the difference in the treatment? 97
Of what is bleedinG from tht; ear channel generally a sign 1 98
The Student practise placing supposed patients . in a proper posilion for the arrest of hremorrhage (see pages 72, 77 and.94), folding firm pads and 75 ), tying hard knots III bandages to form a tourmquet . (7 6 ), and the application of pressure at all pres .ure points shown in the frcntispiece, at vanous pomt, on the forehead and scalp, and on the palm of the hand. Pressure shouk, be digital, by pad and bandage, or flexion, as directed in the text
101
points - Carotid artery, 8:1. Facial, 82. Temporal, 82. Occipital, 83. Subclavian, 84.
Axillary, 85. Brachial (by pad and band age , pressure being made again-;t the humerus a nd by fl exion at the elbow), 86. Radial and Ulnar, 87.
Fem ora l at the groin, 90. Femoral in the thirrh, 92. Popliteal, 92. Anterial and posterior Ti bial arteries, 93.
Haemorrhage from the forehead or scalp ...
Haemorrhage from the palm of the ha nd... ...
Venous hremorrhage from a varicose or other vein
PAGE
PAGB
CHAPTER IV. BRUISES.
A blow anywhere on the surface of the body may cause extensive beneath the skin, without breaking it-a" black eye" is an instance. The injury is accomp:mied by discoloration and swelling .
TREATMENT.
Apply ice or cold water dressings. A piece of lint soaked in extract of witch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is ca!lsed-
(a) By dry heat, such as fire or a piece hot ir?n.
(b) By a rail, wire or dynamo charged wIth a hIgh pressure electric current.
(c) By a corrosive acid, such as oil of vitriol.
(d) By a corrosive alkali, such as caustic soda, ammonia; or quicklime.
(e) By friction, caused, for exam pIe, by contact with a revolvinO' wheel. (Brush burn,)
A scald is ;aused by moist beat, such as boiling water, hot oil or tar.
The effect may be a mere reddening of the skin; blisters may be formed; or even the deeper tissues

103
of the body may be charred and blackened. The clothing may adhere to the burnt skin, and its removal Is impossible without further detriment to the injured part. The great danger is Shock.
TREATMENT.
I.-Carefully remove the clothing over the injured part. If stuck to the skin, the adherent clothing must be cut around with scissors! soaked with oil, and left to come away subsequently.
2.- Do not break blisters.
3.-Immediately cover up the part. Soak or smear pieces of lint or linen with oil, or vaseline, lanoline, or cold cream; a small quantity of boracic powder added to these will be of benefit. The inside of a raw potato scraped out and spread C?n lint makes a soothing application. 'When the injured surface is extensive do not cover it \yith one large sheet of lint, but with strips about the breadth of the hand; this is advisable as they fit better on the part, and during subsequent dressings one strip can be removed at a time, and a fresh dressing applied before the adjacent strip is taken off. The shock to the system is thereby les!! '.than if the whole of the burnt surface were laid bare to the air by the removal of all the dressings at one time. "When covered by oily dressing envelop the part in cotton wool or a plece of flannel and apply a bandage.
102
104
'Vhen the face is burnt, cut a mask out of lint or linen, leaving holes for the eyes, nose and mouth. Dip this in oi l or smear it with vaseline and apply it to the face and cover it with cott on wool, leaving openings to correspond with the holes in the mask.
'Vhen possible place the injured part in water at the temperature of t he body (9 8 degrees) until suitable dressings can be prepar ed . A dessert spoonful of baking soda added to a basinful of th e warm water will make a soothing lotion.
As it is important not to leave the part exposed to the air, it is the l uty of the bystand e rs to prepare the dressings while the clothing is being removed.
4. - Treat Shock.- This is pa rticularly nec essary in the case of every burn or scald of any c ons iderable extent (see page 135)' Be very apprehensive of danger in the case of even slight burns of the neck.
5.-If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bi ca r bonate of soda ), magnesia, o r slaked lime in warm water before applying the dressings.
6.-If the burn is caused by a corrosive alka'i, bathe the part with a weak acid lotion, such as lemon juice or vinegar diluted with an equal quantity of water. Cazdt·oJl.-Before using water brush off any lime that remains on the part.

7.-When a woman's dress catches fire-
(a) Lay the woman fbt on the floor at once., so that the flames are uppermost; that IS to say, if the front of the dress is on fire lay her on her back, and if the back of the dress is burning, place her face do\\ n\\ards. The reason for this is that flames ascend, so that if the upright position is assumed, the flames will quickly reach and burn the body, neck, and face; or if the lies With the fllmes undermost, they \\"111, if unextinguished, pass over and burn th e limbs and set fire to the rest of the dress.
(b) As as the woman is laid flat, smother t he flames with anything a t hand, sllch as a rug, coat, blanket, or table c over; if mad e \Yet so much the better.
(c) A woman rendering assistance should hold a ru O' or blanket i n front of herself ,,-ben approaching the flames.
(d) If a woman's dress catches fire wh en nobody is by, she should lie fl at, flames uppermost, sm othe r the flames with anything handy, and ca ll fo r assistance, or crawl to the bell-pu ll and ring; on no account should she rush into the open air.
The of fire guards ,yould prevent ma ny calamities.
rC7
BITES OF SNAKES AND RABID ANI11ALS,
A:\D \VOUNDS BY POISONED 'WEAPONS.
Hydrophobia is caused by the bite of an animal, such as a dog, cat, fox, \\ olf, or deer sufferin; frpm rabies. The special poisons introduced into wounds camed by yenomous snakes and poisoned \\ eapcns cause immediate danger to life.
r.-Immediatelyplace a constriction between the wound and the heart so as to prevent the venous blood from carrying the poison through the body. If, for example, a :finger is bitten it should be encircled on the side of the wound nearest to the heart, with the :finger and thumb, and as soon as lJossible a ligature (a string, piece of tape, or strip of handkerchief) should be placed tightly round tile root of the fing er. Compression \\"ith the finger and thumb must not be relaxed until the ligature has been applied. Additional ligatures may, with adYantage, be applied at intervals up the limb.
2. - Encourage bleeding for a time:-
( a) By bathing the wound with warm water.
( b) By keeping the injured limb low; the upper limb should be allowed to hang down, ,and in the case of the lo\\'er limb the patie ' t should be seated ,;\"ith the foot 04: tne ground.
"-
3.-Cauterise the wound, if it is quite impossible to obtain the services of a doctor , This is best don e by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or if these are not at hand, with a red-hot wire or a fusee.
The usual solid ea ustic is in sufficient, as it do es not r ea ch the bottom of the wound, where the poison is.
To ensure the caustic reaching the bottom of the \\'olll1d, it should be applied on a piece of wood: such as a match cut to a point. 'When the caustic has been th orou ghly applied, but not till then, the li ;,;, atures may be remov eu.
4.-Cover the wound, after a while, with a clean drtssing.
S. -Affo rd support to the injured part.
6.- Treat shock if It occurs (s ee page 135 ).
7.-In the case of a. bite by a venomous s ... ake, ru b in powd ered p ermanganate of potash a nd inj ect under the skin in the neighbourhood of the wound a solution of p e rmanganate of potash.
STINGS OF PLANTS AND ANDIALS.
These give rise to serious inconvenience, and in some cases grave symptoms develop.
TREAT:\1ENT.
I.-Extract the sting if left in.
2. - l\1op the part freely with dilute ammonia
106
108 or spirits. A paste of bicarbonate of soda and sal volatile is an efficient application. A solution of washing soda or potash or the application of the blue bag wi ll relieve pain.
3.-Treat collapse if it occurs (see page 135)·
FROST BITE.
During exposure to severe cold, parts of the body, usu ally the feet, fingers, nose, or ears, lose sensation and become first 'waxy white and afterwards congested and of a purple appearance. As sensation is lost in the part, it is often only by the remarks of hystanders that the frost-bitten person is made aware of his condition.
TREATMENT.
I. - Do not bring the patient into a warm room until , by friction of the hand by rub bing with soft snow, sensation and circulation in the affected parts are restored. N eglect of this precaution may lead to death of the of the frost-bitten part.
2. - When circulation is restored, keep the patient in a room at a temperature C?f 60 degrees.
NEEDLE EMBEDDED UNDER THE SKIN
'When a n ee dle breaks off after penetrating the skin and disappears, take th e patient to a doctor at once. If the wound is near a joint, keep the limb at rest on splint.

109
FISH-HOOK EMBEDDED IN THE SKIN.
Do not attempt to withdraw the fish-hook by the way it went in, but cut off the dressing of the hook, so that only the metal is left, and then force the point onwards through the skin unti l the hook c an be pulled out.
INJURIES TO JOINTS.
\Vhen a joint is injured by a bullet, stab, or other cause-
r - Wrap the part in cotton wool.
2: - Afford rest and support to the injured limb' if the upper limb, in a flexed position by a sling s If the 'lo wer limb, in a straight position by a splint.
FOREIGN BODY IN THE EYE.
I.-Prevent the patient rubbing the eye, tying down a child's hands if n ecessary.
2.-Pull down the lower eyelid, when, if the foreign body is seen, it can readily be removed with a camel's hair brush, or with the corner of a handker· chief twirled up and wetted.
3. - When the foreign body is beneath the upper eyelid lift the lid forward, push up the lid beneath it and let go . The hair of the lo'wer hd brushes the inner surface of the upper one, and may dislodge the body. Should the first attempt be unsuccessful, repeat it several times if necessary. If
the foreign body is not dislodged call the services of a doctor as soon as possilJle. When, however, skilled help cannot be had, proceed as follows ;-
(a) Seat the patient so as to face the light, and stand behind him, steadying his against your chest.
(b) Place a small rod, such as a match or bodkin, on the upper eyelid, half-an-inch above the edge, pressing it back wards as far as p ossi ble.
(c) Pull the upper eye-lashes upv.ards over the rod, and thereby evert the eyelid.
(d) Remove the for eign body.
4·-When a piece of steel is embedded in the eyeball drop a little olive or castor oil on the eyeball after pulling down the 10'wer eyelid, close the lids, apply a soft pad of cotton wool and it by a bandage tied sufficiently fir mIl' to keep the eyeball steady; tak e the patient to a doctor.
5·-When quick-lime is in the eye brush away as much of it as possib.Je ; bathe the eye \\ith vinegar and warm water, and treat as for a piece of steel embedded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
As a rule make no attempt to treat a patient with a foreign body in the ear if the .services of a doctor can possibly be had; any attempts to remove the forei gn body ulay lead to fatal consequences. If a child

III
cannot be induced to keep the fingers from th.e ear, tie his hands do\vn or cover up the .ear. . If a? lJ1sect is in the ear-passage, 611 the ear wIth olIve 011, the insect will float and may be removed. N evet syringe or probe the ear .
FOREIG N BODY IN THE NO E.
Induce sneezing by pepper or snuff. the patient to blow his nose v!olently. after unaffected nostril. There IS no ImmedIate danger from a foreign boJy in the nose.
THE ABDO)'IEN.
The abdomen is bounded above by the diaphragm; below by the pelvis; behind by the lumbar vertebrre· and in front and at the sides by muscular \valls. (FIg. 54·)
THE ORGANS OF THE ABDQ:\[EN.
The Stomach lies immediately below the" pit of the stomach" just below the breast-bone.
The Liver lies in the upper pa:t of the ab?omen, where it is mostly covered by the 10\\ er nbs.
The Spleen lies beneath the nbs at the upper part of the left side of the abdomen. .
The Intestines occupy the greater part of the cavity of the abdomen . . .
The Kidneys lie at the back, 111 the regIOn of the loin.
The Bladder lies in the pelvis.
110
FIG. 54. 'WOUND IN THE FRONT WALL OF THE ABDOMEN.
When the z'ntestines or other organs protrude through the wound, whether vertical or transverse, bend the raise the shoulders, and apply lint, a to'v\'el, or cotton wool wrapped in soft linen, and keep the

p:::.tient warm until the arrives. is no protrusion of organs, if tlte zs lay the patient fiat on the back wlth the lower 11m bs str3.ight; if tile w ound is transverse, l-end the knees anJ
I;{. URIES TO THE \VITHIN THE ABDOMEN AND PELVIS.
Injuries of the Stomach are attended by extreme collapse and sometimes by yomiting of d :uk blood like coffee-grounds. For treatment see " 1-L:emorrhage from the Stomach" (page 98).
Injuries of the Liver, Spleen and Intestines may be caused by a blow, a stab or a buliet; the li ver or spleen may be injured by a fracture of the lower ribs. The Signs and Symptoms are those of internal accompanied by pain and swelling at the seat of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a cru h, blow, stab or bullet. Blood may escape with the urine, and there may be pain and swelling over the injured kidney.
The Bladder may be injured by a fracture of the pelvis. The signs and symptoms are either inability to pass water, or if a little is passed it is tinged with blood.
II3
OF IN JURY TO THE KIDNEYS OR BLADDI:R.
I.-Keep the patient quiet until the doctor arrives.
2.-Apply hot fomentations over the painful or injured part... .
Rupture (herma) consIsts of a protrusIon of an internal organ, usually the bowel, through the muscular wall of the abdomen, most fr equently at the groin. Should a sudden by pain and sickness take place m that reglOl1
I -Send for a doctor instantly.
2:-Lay the patient down with the raised.
3.-A pply ice or cold water dressll1gs to the affected part.
QUESTIONS ON CHAPTER IV.
Tlte Jlumerals illdim ie the pages where the allswerJ may be lOllI/d.
is a bluise ?
would you treat a bruise?
maya burn be causeJ
a scald
\Yhat is the great danger of a burn or scald?
State the general treatment for burns and scalds
would you treat a burn caused by a corrosi\'e acid?
would you lreat a burn caused by a corro sive alkali?
st eps should be taken \\ hen a woman's dress catches fire?
State the general rules for treatment of wounds caused by poisonous biLes or weapons... 106, 107 What special treatment is required for the bite of a venom ous snake?
How would you treat a sting?
ro8 State the signs, symptoms and treatment o f fro st-bite...
you attempt to remove a needle embedJeu under the skin?..
How would you extract a fish hook embeC:ded in the ..kin?

r09
State the trea tment for injuries to joints ... 109
State the gen eral rules [or removing a foreign body [rom the eye...
r09, !IO
What would you Jo if a piece of steel were embedd ed in the eye ball?
And when quick-lime is in the eye? IIO
How woulu you try to remolle an insect from the ear passage ?.••
II4
PAGE:
102
ro2 IIow
? 102 IIow
103
How
104 [low
104-
............ lOS
What
How
is
caused? I02
103, 104
'Nhat
... ... ... ... ... 107
... ...
108 \Vould
...... 108
......
107,
... ... ...
...
...
......
I IO
[
r
I
\Y ould you l ry to rem ove any othe r form of foreign b od y from the ea r passage? ... ... ... ... 110
How would you re.move a for eign body fr om the nose? .
Stale the bo und anes of the al d omen and its content s ?
Slate the trcatment for wounds of the abdomen 112
How may in juries to the liver, spleen and be ' caus ed ?
\Vh at is the diffe r en ce between t reatment of injuries to !he st ?ma ch and of injurie s to the liver , spleen and mtestID es ?
S tate the treatment of injuri es to the kidneys or Gl adder
State the treatment of hernia

CHAPTER V.
THE NERVOUS SYSTEM.
Two systems of nerv es, the Cerebro-spinal and the Sympathetic, regulate the movements an d functions o f the body.
The Cerebro-spinal System is mad e up of the Brain, the Spinal C ord and Nerves, and through us agency sensations are received and the will causes the action of the voluntary muscles. F or example, 'when a part is injured a sensation of pa in is conveyed to the brain by the nerve, thus affording an indication of the seat of injury, or a warni n g of a p ossible danger of further damage. On attention b ein g directed to the injury, an attempt is instantly made to ease the pain or to move the injured part from danger.
The Brain is situ ated within the cranium, and i.s divided in the middle line, so that, with th e excep tion of some conn ecting bands, the right and left sides are separate.
The Spinal Cord is the long cord of nervous matter lying \vithin the spinal canal (see V ertebral Column, page 23). It leaves the brain through an opening in the base of the cranium and extends to the upper lumbar vertebr::e.
II6
... ... ... .•. ... .•. .. .
... ... ... ... ... . . .
PAGE III III III 113 113 I 13 114 114

The Nerves proceed from the brain and spinal cord in pairs as pearly-\\'bite trunks, and their branches can be traced tbroughout tbe tissues of the body. "When a nerve is torn through there is paralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nervous chain on each side of the front of the spinal column along its entire length, and sends branrh es to all the organs of the chest and abdomen to control tbe involuntary muscles, and thereby regulate the vital functions. This system is not under the control of the \\ ill) and acts alike during sleep and actiYity.
THE RESPIRATORY SYSTE;'I.
The air reaches the lUllgs by way of the nostrils (or mouth), the throat, the wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters tke \yind pipe by an opening guarded by a sort of trap-door or valve, so that in health air, but nf"lt solids or fluids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they may enter the wind-pipe and cause asphyxia. The wind-ripe extends to two inches below the top of the breast-bo:1e, wbere it divides into the right and left b i onchial tube. Each bronchial tube enters a lung and divides into.;' small and still smaller tubes, until
II8
119
FIG. 55. TIn: LU,"IGS AND BRONCHIAL TU BES.
A. Tr:l chea, or Wind.pipe. B. Left Bronchus. C. Rlght Bronchus. D. Smaller Bronchial Tubes.

the ultimate recesses of the lung-th e air cells or all spaces-are re ached.
The Lungs, Right and l:eft, occupy part of the chest; they lie wIthm the ribs and practically wherever a rIb IS felt, whether back or sides, there is lung beneath . Each luna is enveloped in a fine membrane (the pleu ra) allows it to move within the chest during breathing without friction.
Respiration, or breathing, consists of two Inspiration, an expansion of the chest,. du.rm g which air is drawn into the lungs, and EXpiratIOn, a contraction of the chest, during \\ hich air l eaves the lungs. A pause follows the act of expiration. In health fifteen to eighteen breaths are taken minute , and at each inspiration about 20 to 30 cybl.c inches of ai r enter the lungs, and a similar quan tit y IS expelled at each expiration.
The expansion and contraction of. chest are effected partly by the muscl es of respIratJOn attached to the ribs, but chiefly by the Diaphra.gm, the large arched muscular partition which separates c?est fram the abdomen. In inspiration, which IS chiefly a muscular ac4 the ribs are rais ed, and the arch.of the diaphragm falls and b ecomes flattened, mcreasing the capacity of the chest and causing the air to enter. In expirati o n, an act performed almost w ithout effort, the ribs fall and the arch of the r ::r
di ap hragm ris es ; this lessens t he c apacity o f the chest and forces air out. The mechanism of respirati on is somewhat like th a t of ordinary household bellows but without a valve; the ri bs may be to the boards of the bellO\\"s, \Vh.ile the diaphragm corresponds t o the leather, the all' passarres beina equivalent to the nozzle.
b As the blood depends upon the air for its pUl"ification and the oxygen n ecessary to maintain life, interfere nce with breathing very soon may prod uce a dan aerous state called asphyxia, examples of which arc by drowning, suffocation, etc.
ARTIFICIAL RESPIRATION.
PROFESSOR SCHt\'FER ' S METHOD.
I. - IVIake no attempt to loosen or remoYe cl othing . . . . .
2.- Lay the patient in a prone poslbol! (l .e., ba ck upwards) with his head turned. to one Side, so as to keep his nose and mouth away the ground . No pad is to be placed t.he patIent, nor need th e ton <Yue be drawn out, as It WIll fall naturally.
3.-Kneel at one s id e facing the patien t's h ea d, and place the p::t1ms of your h:1l1ds on .hlS loins one at each side, the thu rn bs ne:nl y on in the small of the back, nnel the e over the lo\\"es t ribs. L eaning)'l ur body forlVard , let its weight press do\\" I l\\"8. rds upon the
120
loins and palt of the back, thus compressing the abdomen the ground and driving air out of the chest. Thls produces expiration (Fig 56). Draw back

FIG. 57. bSPIRATION.
1 2 3 your body somewhat more rapidly and relax the pressure, but do not remove your hands; this produces inspiration (Fig. 57)·
4.-Alternate these movements, by a rhythmic swaying backwards and forwards of your body, twelve to fifteen times a minute, persevering until respiration IS restored, or a doctor pronounces life to be extinct.
DR. SILVESTER'S METHOD.
I. Adjust the patient's position.-\Vithout Wlsting a moment place the patient on his back on a fiat surface, inclined if possible from the feet upwards. Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women. Raise and support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades.
2. Ivlaintain a free entrance of air into the windpipe.-Cleanse the lips and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position.
3.-Imitate the movements of breathing. Induce IllSpiration.-Kneel at a convenient dIstance behind the patient's head, and, grasping his forearms just below the elbo\y, draw the arms
122
FIG. 58. INSPIRATION.

FIG. 59. EXPIRATION.
12 5
upwards, outwards, and towards you, with a s \\'eeping movement, making the elbows touch th e ground
F l '- 60. IN SP IRATION.
(Fig. 58). The cavity of the chest is thus enlarged" and air is dra" 'n into the lungs.
124
Induce expzration.-TIring the patient's flexed arms sl ow ly forward, downwards and inwards, press the a rms and elbows firmly on the chest on either side of the breast-bone (Fig. 59). By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and perseveringly about fifteen times a minute.
When a sufficient number of assistants are present, Howard's method may be combined with Silvester's, as follows :-
The additional assistant kneels astride the pati ent 's hips with the balls of the thumbs resting on elther side of the pit of the stomach, and the fin gers grasping the adjacent parts of the chest. Using his knees as a pivot, he presses forward on his hands. Then suddenly , with a final push, he springs back and remains erect on bis Imees while he slowly counts I, Z, 3. These motions are to be repeated to correspond • with those being performed- by Silvester's method, pressure on the chest being made simulby those performing the two methods (FIgS. 60 and 6 I).
LABORDE's METHOD.
When from any cause the above methods cannot be carried out, Labo1'de's method of artificial respiration should be tried. It is especially useful in suffocated children and when tpe ribs are broken.

1 2 7
The patient IS placed On his back or side j the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede into the mouth. These movements should be repeated about fifteen times a minute.
Artificial respirati on must be continued until breathing is established, or until a doctor arrives.
" Then natural breathing commences, r egulate the artificial respiration to correspond with it. Success may result even after two hours' tim e.
Excite respiration. - 'Whilst artificial re spiration is being applied, other useful steps may be employed, such as applying smelling salts or snuff to the nostrils, and flicking the chest \\ith a damp towel.
Induce circulation and warmth after natural breathing has been restored . ,Vrap the patient in dry blankets or other covering, and rub the limbs energetically towards the heart. Promote warmth by hot flannels, hot-.water bottles, or hot bricks (wrapped in flannel\ applJed to the feet, to the limbs and body.
\Yhen the power of swallowing has return ed give hot tea or coffee, or meat extract. The patient 3hould be kept in bed and encourao-ed to 0-0 to sleep. Large poultices or applied to the
126
I23
front 8.l1d b;:lck of the chest ,yill serve to assist breathing . Watch the patient carefully for some time to see the breath ing does not fail; should any signs of faIlure appear, at once begin artificial respiration.
I TY.
U nconsciousne s or Insensibility may arise as fo11o\\"s :-
I njury to the Head.-C oncussio n and Compression of the brain.
of the Brain .-Apoplexy, Epilepsy, Hyst ena .
Var ious F ainting (Syncope), Coll apse, AlcoholIc and othe r poisoni ng, Sunstroke and Heat-stroke, Infantile Conntlsions, Asphyxia.
GE. ERAL RULES FOR OF INSE
:-')IB ILITY.
a person appears abou t to lose ccnsClOusness, prevent him from falling , and by him gently down,
2. :-Arrest Hcemorrhage when apparent ; attendl.ng to min or injuries is less important th an tr eatmg the unconscious state .
3. - patient in the p ositio n in wh ich breath1l1g 1S most easy-usually this will be on the ba ck , or incl ined to one side. As a general rule

rais e th e hea o a nd shoulders sligld/y when the f8.ce ts flushed, and ke ep the heau low when the face is pale.
4. - Undo all tight clothing round the neck, chest and waist, unfastening the braces a nd top button of the trous ers in men, and the cors ets in women) the object being to reli eve pressure on th e air passages, lun gs , heart and abdominal organs. Be sure th at there is no obstructi on to the air passages by the tongue or by a foreign body in the thro at. Th e possibility of false teeth obstructing breathing must be considered.
s. - Provide for a sufficiency of fresh air by op ening do ors and windows, and by keep ing back a crowd.
6. - When breathing cannot be discerned apply artificial respiration.
7. -- 0btain a doctor's help as soon as possible.
8. - Unless unavoidable, never leave the patient until you have placed him in charg e of a responsible person.
9. - Give no food or fluids whatever by the mouth while the patient is insensible.
rO. - Should the spine or an important bone of the upper or of the lower limb be fractured it must be steadied and maintain ed at rest as soon Should the unc on sciousness be pro! o ng", d, the patI en t may be removed in a recum bent po itio n ..
13 0 to s!1elter, prov ided that the broken bone is adequately Sllilported.
lI.-When the patient is in a state of convulsion, support hi3 head, and after wrapping a piece of wood or any other hard material in a handkerchief, hold it in his mouth t o prevent biting of the t0l16ue. Do not for cibly restrain his limbs; pre\'ent hIm from hurting himself by pulling him awa.y from a source of danger, such as machinery, a wall, or fireplace ; li ght pieces of furn iture should be pushed out o f t he way. '
12. -On return to consciousness \yater may be given to drink. If the pulse is feeble give warm tea or coffee, proviJed hremorrhage, either internal or is n ot presellt. A d esire to sleep should be en ouraged, e::cept i n C.lses of opium poisoning, a cvndltion that may generally be r ecog n ised by the hisLOry of th e and also by the pupils of the eyes (the black openings in the grey, blue or brov'\1 ir is) being minutely cuntrdctec.i (pin-head pupils).
13.-It must not be assumed that a person is insensible as the result of drink merely because the breath smells of alcohol; frequently wben peop le are fee ling ill they take or are given alcoholic .?timulants, after whic:: they may become insensible; not fr om t he drink, but from th e cause that induced th em to take it, for example, insensib !lity coming on, of p oiso ning, etc. Even if

13 1
drink is believed to be the actual cause of insen si bility, it must be borne in mind that the patient is in a very dangerous state, and he must be treateJ for Collapse by being covered up and kept
The above general rules will enable aId be rendered efficiently in most cases of although the exact form from which the patIe nt IS suffering is unknown.
CONCUSSION OF THE
. The patient may be stunn ed by a blow or £:111 on the head, or by a fall on the feet or lower part of t.he spi ne. He may quickly regain consciousn ess, or 111sensibility, more or less complete, may be prolonged.
TREA Tl\lEI T T .
I. - Apply the general rules for the treatment of Ins ensIbiljt y.
2.- Be ve r y apprehensive of in all cases of injury to the head. TJ1e p.ltlcnt may be stunned, and after a short interval may some dearee of consciousn ess, or even the bra.m m ay apparently have escaped injury; yet in bCJth there is a grave ri sk that a structure \\'.hl11n lhe cranium has been injur ed , and that a senous stale of insensibility may develop later. (See Fracture of the Cranium, page 43 ). A caution should the refor e be given to a patient who has lost consciou s.1CSS even
13 2
for only a moment after an injury to the head not to resume physical or mental activity without the consent of a doctor.
CO.:\lPRESSION OF THE BRAIN, APOPLEXY.
Compression of the Brain may result from the same causes as produce Concussion; in fact, Compression is frequen :ly preceded by Concussion.
Apoplexy usually occurs in elderly people, and no sitns of injury are necessarily present.
In both conditions the fac e is flushed; the brea.thing st;ertorous; one side of the boJy :nay be more limp than the other, and the pupil of one eye rna y be larger than that of the other j the tem pera ture of the body is generally raised.
1. - Apply the general rules for treatment of I ns,:nsibility.
2. - Promote warmth in the lower part of the body by the application of hot "vater bottles to the abdomen and lower limbs. Care must be taken not to burn the patient with the bottles, which sflould be wrapped in fl .1l1nel, and their heat tested 'with the elbow.
EFILEP.3Y.
Epilepsy may occur in persons of any age, but usually occurs in young adults. 1'1e patiellt falls to

133
the ground, sometimes with. a and passes into a state of convulsion, throwing hIS hmbs abo ut. The treatm ent is according to the General Rules, especially Rule I I.
HYSTERICAL FITS (HYSTERIA). AND
The patient, usually a young girl, in cons equenc e of mental excitement, suddenly loses command of her feelinas and actions. She subsides on a couch or in comfortable position, throws he rsel f about, grinding her teeth, clenching her fists, her hair loos e ; she clutches at anyone or anyth1l1g near her, kicks, cries and laughs alternately. T.he eyeballs may be turned up\yards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregular symptoms may devel op .
c.1\ T.
I -·-Avoid sympathy with the patient, and speak firmly to her.
2.-Threal en her with a cold water and if she persists in her" fit," sprinkle her wIth cold water.
•
3.-A pp!y a mustard leaf at the back of the neck ..
Medical treatment is necessary to cure the tion o f mind and body which gives rise to hystencal attacks.
SHOCK, FAINTING (SYNCOPE), COLLAPSE.
CAUSES.
I.-I njury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and severe crush are some of the more frequent physical causes of shock.
2. - Fright, anticipation of injury, and sudden bad ne\\"s, or sometimes sudden removal of fear and anxiety after prolonged su spense , produce shock or fainting.
3·-Some poisons cau se shock, while otbers, such as alcohol, so depress the nervous system that collapse ensues.
4·-Hcemorrllage or heart weakness, a close or crowded room, tight clothiug, fatigue, or want of food may bring on fainting or collapse.
SIGXS AXD SV':\fPTO:\lS.
The general condition o.f shock may be recognised by extreme pallor, a feelIng of cold, clammy skin, fe eble pulse, and shallo\\' br eathing accompanied, has been severe, by yawning and slghll1g. The term "collapse" signifies a very scri0us condition in which the life of the patient is in the greatest danger; the temperature of the body falls belmy the normal, and one great 'ob ject of treatment is to prevent it sinking to a point at which life is imp Issible . An attendant danger of the condition of

!3 S
:olbnse is the liability to sud len relarse after R temporary improvement, and the C:1re and watchfulness must therefore be exerCised to mamtain the h eat of the body and to guard against failure of the heart and lungs.
I.-Remove the cause by arresting hcemorrhage , attending to injuries, loosening all tight clothing especially about the chest and a?domen, rem.oving from a close or era\\ ded room, usmg encouraging words, etc.
.
2.-Lay the patient on the back, wlth head low. Raise the lower limbs; \yhen the patIent is in bed this is best done by raising the foo t of the bedstead.
3.-Provide for a free circulation of fresh air.
Lt.-If ha:morrhage has been and the pat'i ent is collapsed, firmly bandage the lImbs from. the toes to the hips, and from the fingers to the armpIts.
5.-To stimulate the .o f the sal volatile and water Illay be gIven If the patIent c.8n s\\'allo w , or smelling salts may be h eld to the nostnla,
6. - It is of the utmost importance to use every means of preventing a fall of te l:nperature below the normal point. - To ac com pltsh th lS cover the patient with extra clothing, or by pbring
134
136
ru;?;s or blankets over him j get him to bed in a warm bue well-ventilated rOO .11 as soon as possible. Apply \\'armt h to the fe et and to the pit of the stomach by hot water bottles or hot flannels. (Test the heat of these with the elbow before applymg them.) If the p ,ltie nt can swallo ·.\" give hot drinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the temperature of the body.
7·- If breathing cannot be discerned, apply artificial respiration.
8.-If want of nourishment has been the cause of Llinting or collapse, give fool sparin;l)' at first.
SUN::;TROKE AND HEAT-STROK'E.
'Vhen exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weather \\hen heavily burdened, persons may develop sickness, faintness, giddiness, and difficulty in breathing. ' The patient complains of thirst, the skin becomes dry and burning, the face yery flush ed, the pulse quick and buunding. A very high temperature, stertorous (snorin 6) b reathing, and insensibIlity may ensue.
TREATMENT.
I.-Undo all tight clothing.
z.-Remove the patient to a co ol, shady spot.

137
3.-Str ip the patient to the waist.
4.-Lay the patient down, with the head and trunk well raised.
s·-Procure as fre e a circulation as possible vf fresh air, and fan the patient vigorously.
6.-Ap ply ice bags or cold water freely to the head, neck, and spine, and maintain this treatment until the symptoms subside.
,.-0n return to consciousness, the patient may have water to drink .
IN CHILDR EN.
Teething or stomach troubles are the commonest causes of this ailment.
SIG.TS.
Spasm of the muscles of the limbs and trunk, blueness of the face, insensibility, more or less complete, and occasionally squinting, suspended respiration, and froth at the mouth are the prominent signs.
TREATME H.
I.-Support the child in a warm bath slightly above the temperature of the body (9 8 degrees), so that the water reaches to the middle of the trunk.
2.-Pl ac e a sponge dipped jn colJ water on the t op of the hpad.
ASPI-IYXIA.
'''hen, owing to want of air, tbe blood is not supplied wi h oxygen the patient becomes insensibl e, and is said to be asphyxiated. This conditiun may Le brought about as follows :-
I. Obstruction of the air passages.
(a) By DRO ,\' NIXG.
(b) By PRESSURE FRO:'.I OUTSIDE: Stranguiati on, hanging, smotherin6 ·
(c) By A FOREIGN BODY THE THROAT: Choking.
(d) By OF THE TISSUES OF THE
tI THROAT: Infl ammation, scald of the throat, poisoning by a corrojve.
II. Inhaling poisonous gases. By coal gas (:lS used in the house), produc er, or water, gas, smoke, fumes from a charcoal or coke fire, sewer gas, limekiln gas, carbonic acid gas.
III. Pressure on the chest, as when crush ed by sand or debris, or by a crowd.
IV. N erVOllS affections, as the result of narcotic and certain other poisons, collapse, electric shock, or stroke by lightning.
GEN ERAL TREATl\IENT.
In all cases of Asphyxia attem l,ts must be made to remove the cause, or to rel1lO\'e the patient fro 11 the cause. \V hen this Ins been done artificial

7;9
must be applied, taking care that the all" passages are not obstructed, and that there is abundance of fresh air.
DRO\\ NING.
Persons completely immersed in water for even ten or fifteen minutes baye been restored by artificial means. Therefore, if the body is recovered within a reasonable time, absence of signs of Me is not to de' cr imm ediate attempts to restore animation.
The first thing to do when the body is recovered is to get rid of the "water and fr ot h obstructing the air passages, and tbcn artiflCially to restore breathing. Thls is best accomplished either by proceeding at once to perform artificial respiration by Schilfer's method, or as follows :-
I.-As quickly as possible loosen the clothing, and clear the mouth and the back of the throat.
2.-Turn the patient face downwards, with a pad below the chest, and with the forehead upon the right fore arm.
3.-\Vhil st in this position apply pressure by the hands to the patient's back over the 10\\'e r ribs, and keep the pressure up for three seconds.
4.-Turn the patient on the right side) rru..intaining that po?ition also for three second::;. .
5.-Repeat these moyements alternately as long fr oth and water issue from the m.outh.
These operations Hall's method) in themselves tend to promote respiration, but when the air passages are clear of froth and \-vater Silvester's method of artificial r esp iration may be used by itsdf or with Howard's method in conjunction.
While performing these operations send some one to the nearest house to procure blankets and dry cl othing, hot water bottles , etc., and to fetch a doctor.
STRANG ULATlON.
Cut and remove the band constricting the throat. Ap ply artificial respiration .
HANGING.
Do n ot wait for a policeman: g rasp the lower lim bs an d raise the body to take the tensi on off the rope; cut the rope, free the neck. Apply artificial respiration .
SMOTHERING.
Remove whatever is smothering the patient Apply art i (lclal respirati on.
;. CHOKING.
Open the mouth, fo rcib ly if n eed be; pass the for efinge r right to the back of the throat and attempt to dislodge the foreig n body; if vomiting results, so much the b etter. If unsuccessful, thump th e back bard whilst the head is bent fOl ward. Apply artificial r espi ration.

OF THE TISSUES OF THE THROAT.
,¥he the r the swelling is caused by inflammation by swallowing, very hot water, as not infrequently happens to children attempting to drink from the sp out of a kett,le, or by the effect of a corrosive poison r the treatmeJlt IS as fo11o\\'s :-
I.-Ap ply a sponge, piece of flannel or othe r cl oth ,,'rung out of very hot water, to the front of the neck: from the chin to the top o f the breast-bone.
2.-Set the patient before the fire .
3.-Give ice to suck if it can be had' if not rri\'e cold water to drink. " b
4,--:-Give animal or ve,;etable oil, a dessertspoonful at a tune, to soothe the scalded throat and ease the pain.
5.- If brf8.thing has ce3.sed apply artificial respiration.
SUFFOCATION l3Y SMOKE OR GASES.
I.-Remov e the patient into the fresh air. Before entering a building full of smoke tie a handkerchief wet if possible, round the head so as to cover nose and mouth . It is well to move slowly, keeping low, or even crawling, ,,,bilst in a ro om full of sm oke in sear,ch 0: a person. Every opportunity of lettmg m fresh air by opening doors or ,yindows should be seize d.
140
2.-Apply artificial respiration
3.-1n the case of producer or \\'ater gas, inhalation of oxygen will also be necessary.
ELECTRIC SHOCK.
Electric current is com'eyed by a cable, ",ire, rail, or bar, called the "PositiYe," and returns to the source of supply by another cable, ",ire, rail, or bar, called the" Negative," or through the earth. In the case of an electric railvyay, th e current is generally conveyed by an insulated rail the third rail, and returns through the running rails or an insulated rail called the fourth rail, and in the case of an electric tram \vay it is frequently conveyed by an oyerhead conductor or trolley wire, and returned through the running rails.
Through contact \\'ith a " positi,-e " the shock may be so severe as to cause insensibilIty, and the sufferer \\'ill be unable to extncate himself, and must be liberat ed with all possible speed. As it is gener:;;1)' impossible or inexpedient to switch off the some other method must usually be adopted; but precautions must be taken or else the person rendering assistance \"ill himself reccive a shock.
To liberate the sufferer from contact-
I. - Insulate yourself from the earth by standing on an " insulator" or " n o n-cond uctor," that is, a body \\'hich resists the current. Amongst such bodies

I43
are indi arubb c r, dry dry bricks, dry silk, dry cloth, dry wood and dry hay or straw.
2. - Protect your hands from contact with the sufferer or the electric medium by coytring them with an insulator. Although indiarubber is probably the best insulator, do not waste time in running for indiaru bber gloves, but use dry articles of clothing j an indiarubber tobacco pouch or cap, or folded newspap er, would serve to protect the hands 111 an emergency. If no means of insubting the hands are at hand an attempt may be made to dm6' the sufferer away by means of a loop of dry rope or a crooked stick; an umbrella is not safe because the metal ribs would act as conductors* of electricity, and it is not infrequently the case that the" stick" of the umbrella is a metal tube.
3.- Pull the sufferer away from contact. C:ue should be taken to avoid touching with naked hands the sufferer's bands, wet clothing, or boots lf the soles are nailed. The armpits should be a"oided as perspiration usually makes the clothing damp there.
\Vhen the sufferer is removed from contact -
I.-Apply the general treatment for insen-
.... A c onducto r is a b ldy through which electricity read ily pa<;ses. Am ongst sLlch budies are c 'pper, bra ss , iron, 1l1 uisture and one's own bvc1y.
144 sibility (loosen clothing, procure f ree circuhtion o f air and p lace in a recumbent position).
2. - Dip a towel in cold water a nd att empt to arouse him by sharply flicking the face and chest.
3·-Commence artific ial r espirat ion if other methods fail to restore animation. "Laborde 's II method (see page 126) has been found to be very s uccessful.
4. - Treat bu r ns if there are any (see pages 103, 1 0 4).
E FFECTS OF LIGHTNING
.
A p erson s truck by li ght n ing is u s-ually more or less deprived of consc iousness . The treatment is the same as that for electric shock, except, of course, t hat the instructions for remO\'inp- the patient from contact with the electric mediu"'m do l.ot app ly.

145
QUESTIONS ON CHAPTER V.
T ltlJ numerals indicate the pages where the answer s may be found.
'What are the two systems of nerYes? ... . ..
Of what is the cere bro·spinal system made up ? ...
What is the spinal cord? \\' ha' are nen'es like ?
Explain the sympathetic system
n I\hat system is he laid on his bad: or side ..
In \Ihat system is he rolled alternately on hIS sIde and face downwards?
long should artificial respiration bL perseyercd wilh?
State the aeneral rules for treatment of insensibility
\ Vould examine the patient to see if any bones were
" That wrong opinion may be formed when the patient smells of drink?
s collapse from drink a serious conJition ?
\ Yh.lt is concussion of lhe bl ain ?
PAG!!: 117 117 117 I IS lI8
Ex plain the respiratory syst em E'.plain the acts of respiration I IS to 120 120 lIow are the expan ion and contraction of the chest effected? .. . ... ...... 120 to 1 21 I n \\
laid back upwards? .. , ... . .. I n
on
121 123, I 26 1 2 7
hat system of artificial respimtion is the patient
II hat systems is he laid
his back?
I
:
... ... ... ... 139,
How
12 7 \ \
1 2 7 What is inducing circulation? ...... 12 7, 128 \ \'hy
128 IIow
... J:!8 Slate
128
I40
hat is exciting respiration?
is it necessary to watch the patient?
may insensilJility arise?
the various forms of insensibili'y
128
13
to
I
." ... . .. 1 2 9
130 I
13 1
... 13 1 Slate
rules
treatment
concussion I3I , 13 2
...
lhe
for
of
'''hat dang-er accompanies injury to the head? . ..
\"hat caution should be given to a patient has consciousness, even for a moment, after an injury to the head?
'Yhat are the causes of compre sion of the brain?
In what ag d people does apoplexy usually OCClll ?
\Yhat are the signs and symptoms of compression ar.<l ap oplexy?
State the rules for treatment of these conditions ...
'Yh '1.t dangpr is there in applying hot water l'ott les to insensible persons, and \\hat precautions shr.uJd I- e taken?

''1hat two things ll1ust be seen to Lcfore It IS pn slule for artificial respiration to do any good?
artificial respiration likely to do any good If the
passa6es are obstructed, or if there is not
Describe a case of epilepsy 132, 133
\Yhat special care must be taken in trea ting a case of 13 2 epilepsy ? 130, 132
Describe a hysterical fit 133
lIow would you treat a hysterical fit? 133
"That are the comm onest physical causes (If shod: ?
"'hat may produce shock or fainting?
"'hat condilions do certain p,)isons bring ahout?
'Yhat may hring about fainting or col'apse?
JIow wou 'd yun recognise the general eondi ' ion of shrJck?
\\'hat special precaution must be taken in the ca"e of collapse?
State the treatment for shock, faintli1g (!'yncope) a d collapse ... 135 , 136 is the of sugar on the tempe rature of the body?
'Vhat are the causes of sunstroke and heat-stroke?
State the treatment for sunstroke and heat-struke
"'hat are the causes of cOlwulsions in chi1dren?
\Yhat are the signs of convulsions in chi ldren ? .. .
State the treatment for convulsions in childn:. n .. .
State fully the causes of
should be done while artillcial respiration is ueing perfurmed?
How would you liberate a suITerer from c ,mtacL WI,h an electric medium?
\\'hal w ould you do when th-:: sufferer was remo\'cd from c ontact?
\Yhat would you do ill the ca.;c of a lightning strvke ?..
13 1 13 2 13 2 13 2 I3 2 13 2
134 134 134 134 134 135
... 13 6 .)/ 137 1)7 137 138 I I..J7 PAGE "Vhat
cases of asphyxia? . _. ... ... ..... .... 13 3 , 139
.... . 139 Is
air
... ... ... 13 9 \"I1\t i::; the first thing to dJ in a of drowning?.. 139 By what method mayartillcial re pi ration be performed without taking any preyiou steps? 13 9 What
must be
Silvester's methvd? 139 What
... ... ... 140 Slate the treatmenl for strangulation 140 State the treatment for hanging 140 tate the treatment for smothering qo S la te the treatment for choking 140 IIow may a swelling of the tissues of the thr0al be caused? ... ... ... ... ... 141 Slate lh' ueatmen t for s\\e
of the tissues of the throat ... ... I4 I State the treatment fur suff )c8.tion by or gases 14 I, Lj.2 1
... ... .... ... Lj.2
.. , ......
143
asphyxia
two thi ngs have to be 'd Jne in all
abund:tnce of fresh air?
steps
taken before proceeding with
Iling
[ow is electricity com'cy c u?
14 2 ,
Lj.3
1,4
CHAPTER VI.
POISOI II G .
Poisons may be classified ::lccording to their tr eatment under t wo heads :-
1.-Those which do not stain the mouth, and in the treatmE;nt of which an emetic is to be given. Amongst these are: -
(a) Arsenic, Phosphorus (c ontaineu in rat poison and lu cife r matches), Tartar emetic and Corrosi ve Subhmate, \\"hich cause a metallic taste in the mouth a nd a burning pain in the mouth, throat and stomach.
(b) Strychnine, Prussic Acid, Belladonna (aeadly ni ghtshade plant) a n d seyeral other nmeti es of plants, such as laburnum seeds, etc .; these give rise to convulsio ns, delirium, failure of respiration a nd collapse.
(c) Poisonous mea t, fish and fungi (ofte n mistaken for mushrooms). Suspicion of these poisons should be directed to cases \\ here several perso ns \\"ho have partaken of the same food develop similar signs and symptoms.
(d ) Alcohol, which may cause colla pse .
(e) Opium and its preparations, Morphia,

149
L ::ludanul1l, .P.:negoric, Chloro dy ne, Syrup of Pop pies and various so oth ing drinks and cordials; these ca use a tendency to go to sleep, which con ti nues until sl eep de ep and breathing stertorous; the puplls. of the ey es become mi nutely contracted (pmh ead pupils).
2.-Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. These are of :- .
(a) Acids, such as Nltnc ACld fortls), Sulphuric Acid (Oil of VitrIol), Hydrochloric, or Muriatic, Acid (Spirits of Salt), strong Carbolic Acid (Phenol), Oxalic Acid, which is contained in oxalate of potash, sa lts of sorrel, salts of lemon and some polishing pastes.
(b ) Aikalies, such as C::lustic Potash, C a ustic Soda and Ammonia.
Sl,; :\I?IIARY OF SIl\IPLE D I REC TIONS FOR T HE
TREAT:\IEX T OF P01SONli\G.
I. - Send for a doctor at once, stating what has occurred and if possible the name of the poison .
2 . - Except when the lips and mouth are st ai ned or burned by an acid or alkali,
ISO
promptly give an emetic-that is, make the patient vomit as follows :-
(a) Tickle tIle vf the tltroat with the finger or with a feather.
(b) lV.!ustard-a dessert-spoonful in a tUl1lblelful of luke-warm watu.
(c) Salt-a table-spoonful in a of luke-warm water.
(el) Ipecacuanha "YVim- for a young child, a teaspoonful repeated at intervals of fifteen minutes.
3.-In all cases when the patient is not insensible, give Milk, Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, Animal or Vegetable Oil (except in phosphorus poisoning), and Tea.
Olive, Salad, and Cod-liver oil, or oil such as that in which sardines are preserved, may be given; mineral machine oils and paraffin are unsuitable. Oil is soothing, and is therefore especially useful in poisoning by Acids, Alkalies and such substances as Arsenic and Corrosive Sublimate. Demulcent drinks, such as barley water or thin gruel, act in the same manner, and are free from danger in ca"es of phosphorus poisoning.
These may be given either before or after the emetic if the poison calls for one.
Strong Tea acts as a neutraliser of many poisons,

anI is always sJJe. A handful of tea should be thrown into a kettle and boiled. .
4.-If the lips and. mou!h are stamed or burned give no emetic, bu\..- .
(a) If an Acid is known to be the pOlson glve an Alkali at once. FIrst wash the mouth out freely with lime water or other mixture, such as soda, chalk, \\'hltmg, or malT Ilesi:1 or \Yall plasler in \\'ater, and after\va;ds let the patient sip a lillIe of it. Soda and potash are not to be given in the case of poisoning by oxalic acid. " .
(b) If a strona Alkali is known to be the pOlson give an at once. Firs.t :vash the I?outh l'ut freely with lemon JUIce or vll1egar diluted with an equal quantity of\vater, and afterwards let the patient sip a little of it.
In both cases give oil (Rule 3)' .
S. -When a person has pOlson and threatens to go to sleep, keep him awake by walking him about and slapping his face, neck and chest ,;vith a wet tovvel. StroDg black coffee may be gi ven to drink o Slapping the soles of the feet may also be tried.
6. - If the throat is so swollen as to threaten o ')struction to air passage, apply fbnnels or to the ?f the nec" and give frequent S1pS of cold dnnKs.
15 2
,.-Apply artificial.respiration if breathing cannot be discerned.
8.-Treat shock and collapse.
9.-Preserve any vomited matter, food, or other substance, suspected of being the poison. Do not \\"ash vessels which may have contained the poison, and carefully guard them.
Certain poisons require special treatment, and a few of the commoner of these are mentioned below \vith their treatment.
CARBOLIC ACID.
The odour of the breath will aid in the detection of this poison; the lips and mouth are usually stained white, and several ner\'ous symptoms come on.
TREATl\IE\lT• •
1.- Give milk, to a pint of \\ hich half an ounce of Epsom Salts has been added.
2.- Treat according to the general rules.
PRUSSIC ACID.
The actio:l of this poison is extremely rapid. Giddiness, staggering, insensibility accompanied. by panting respiration, profound collapse and posslhly convulsions are the general signs, and in addition a mlell of bitter almonds is often present.
I.-Place the patient in tr-,e op en .lir.

2. - D.lsh cold water on the head and spine contll1ucusly.
3·-A pply artificial respin.tion.
4·-H old sllelling salts to the nostrils.
5·-Treat shock and collapse. (See page I35.)
POISONOUS l\IEAT, FISH AND signs an? sym ptoms are vomiting and purging ( d ..lrrhcea), colic, headach e, gr eat weakness raised te :npe : ature and a quick pulse. '
I. - G ive an emetic.
2 - 'Vhen the emetic has acted, give castor oil.
3 --Treat collapse. (See page I35.)
STRYCH:\,INE.
' . !he signs and sympto .l1S. are a feeling of suffocation, ll .vld feJ.tures, and convulSIOns. The patient rests on ill:') head 1nd fee t, and th e body is arched.
TR EAnIEI'{T.
1. - Gi,-e an emetic.
2. - .\ pp ly artificial respiration.
ALCOHOL.
1. - G ive an emetic if the patient can swallow .
2. - Treat collapse by k eeping the patient \\"arm etc. (See page 135.)
fS3
QUESTIONS ON CHAPTER YI
TIlt llZtlll(.rais i1ldicate the pages where QlISwen nUl)1 be j'olt Jld.
Under what two heads may p oisons be classified?
Wbat are the symptoms of p oisoning by arsenic?
\Yhat other poisons give rise to the same symptoms?
I4 3 , I4 9 qS 14 3
'What poisons give rise to convulsi ons, delirium, failure of respiration and collapse? .. ' .. 148
If several people who had partaken of the same ie. d developed similar signs and symptoms, by what would you su spe ct they had poisoned? ... 148
""nat condition may result from pois oning by alcoh ol ? 143
'Vhat are the effects of such poisons as op ium?.. 148, J 49
What two classes of poison burn or stain the mou th ? . .. 149
Would you give an emetic for such po isons ? 149
Name some of the principal acids J49
N:o.me some of the principal alkalis 149
State the general rules for the treatment of p,)ison!ng ... '49 to 15 2
State the best me thods o f making a person vomit ISO
How wou1d you treat a case of acid poisoning? ... 15 1
H ow would you treat a case of poisoning by an alka'i? 15 1
State the signs, symp tom s and treatment of carbolic acid poisoning ...
State the sign!!, symptoms and lreatment of poisoning by Prussic Acid 15 2 , 153
State the signs, symptoms and t r ealmen t .J poisoning by poison ous fo od ... ... ... ... .. , .. , 153
State t he sig-ns, sympt oms and treatment of p ois'ming by Strychnine
What would you do in the case of alcoholic p',isoning ? 153 153

155 CHAPTER VII.
BANDAGINC
. Esmarch's Triangular Bandage has been described In Chapter II. It may be appli ed to keep a dressing on a wound, burn or scald of any part of the body, or for an in jury of a joi nt.
For the Scalp (Fig. 62). Fold a hem about d · inches deep along the of a bandage ; place the bandage on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs dO\\'n at the back; carry the two ends round the head above the ears and ti e them on the forehead ; draw the point first do\\,nwards, and then turn it up and pin it on to FIG. 62. the bandage on the top of the head.
For the Forehead, Side .of the Head, Eye, Cheek, and for any part of the body that is round (as the arm or thigh, etc.), the narrow bandage should be used, its centre being phced over the
;54
PAGE
I '/1 % III

63. """'=:::-===-
FIG. 64. up the side of the neck; fold a hem along the base; carry the ends round the middle of the arm and tie them. Place one end of a broad bandage over the point of the fi-rst bandage and sling tIle arm by carrying the other end over the sound shoulder and tying the ends at the side of the neck; turn down the point of the first bandage, draw it tight and pin it.
157
For the Hip (Fig 64). Tie a narrow bandage round the above the haunch bones, with the knot on the ll1Jured side. Fold a hem accordinG' to the size of the patient along the base of a second bandage; place its centre over the dressing, carry the en d s round the thigh and tie them; th e n carry the point up under the
FIG. 65. FIG. 66. first bandage, turn it down over the knot and pin it. the Hand when the fingers are extended (Fig. 65). F?ld a hem along the base of a bandage; place wnst on. the hem with the fingers towards the pomt ; then bnng the. point over the 'wrist, pass th ,: ends the wnst, cross and tie them j brIng the POll1t oyer the knot and pin it to the b;:l.l1dage on the hand.
For the Foot (Fig. 66). Place the foot on .the centre of the bandage with the toes towards the POll1t ; draw up the point over the instep, pass the ends round the ankle and cross them in front; now pass the ends round the instep and tie them. Draw the
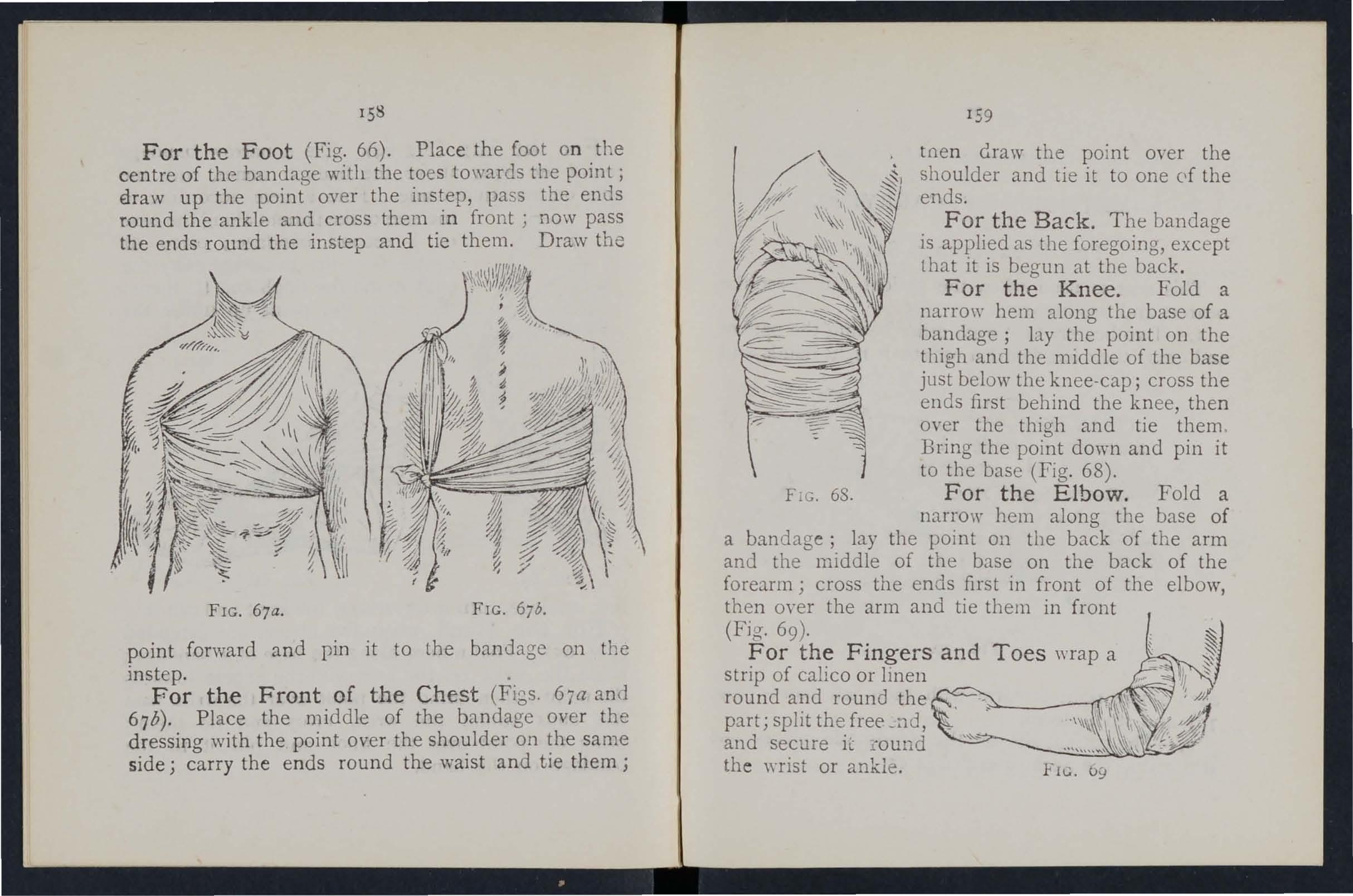
FIG. 67a.
FIG. 67b. point forward and pin it to the bandage on the .
For the Front of the Chest (FiGs. 67a and 67 b). Place the middle of the bandage over the dressina with the point over the shoulder on the same side j cbarry the ends round the waist and tie them; I59
tnen draw the point over the shoulder and tie it to one of the ends.
F or the Back. The bandage is applied as the foregoing, except that it is begun at the back.
For the Knee. Fold a narrow hem along the base of a bandage; by the point on the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then over the thigh and tie them . Bring the point down and pin it to the base (Fig. 68).
F IG. 68. For the Elbow. Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and the middle of the base on the back of the forearm; cross the ends first in front of the elbow, then over the arm and tie them in front (Fig. 69)' . and Toes wrap a strip of calIco or lmen I" -,.. 1; " round and round the _ !.,a, " \\ and secure lL """"""the \\'fist or ankle. FIG. b9
158
CHAPTER VIII.
11ETHODS OF CARRYING.
THE SEAT.
This seat is used wben the patient can assist the bearers and use his arms. .
I.-Two bearers fa ce eacb other the patil nt and grasp their left foreJ.rm with then" nght hands and

FIG. 70. each other's right forearm with their left hands (Fig. 70 ), and stooP. "
2,-Tbe patIent SIts on llands r..uci places one arm round tbe neck of each Dearer.
161
3,-The bearers rise together and step off, h _ bearer on the right hand side of the patient with th fc rIght foot, and the left hand bearer with the left foo t
THE Two-HANDED SEAT.
This seat may be used to carry a helpless patiento
FIG. 71.
1,-:Two bearers race each other and stoop, one 0 each sIde of the patient. Each bearer passes his forearm nearest to the patient's head unEier his back jusli
160
<fA
below the shoulders, and, if possible, takes hold of his. clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs t Fig. 7 I), and clasp their hands by one of th e methods sho\\n in Figs. 72 and 73. A handkerchief should be h e ld in the hands if th e first grip is u sed.

FI G. 72. FIG. 73.
2.- The bearers rise toge ther and step off, the right-hand bearer with the right foot, and the left -hand bearer with the l..;ft fOJt (Fig. 74i'
THE THR.b-E-HAXDED SEAT.
This seat is use ful for carrying a patient and supporting either of his lo\yer limbs, when he is abl e to use his upper limbs.
I.-T\\ 0 bearers face each other behind the patient.
For supporting the le ft limb the bearer to the patit.nt's right grasps his own left wrist \\ ith his rig ht hand, and the othe r bearer's ri ght \\ rist with his left hand.
The bearer to the left grasps the bearer's right wrist \\ ith his right hand (FIg. 75). This IllS
162

left band free to support tbe patient's left leg. For the patient's right lmrer limb follow the same directions, substituting" right" for" left " and" left" for "right." The bearers stoop down.
2.-The patient places one arm round the neck of c3.ch bearer and sits on their hands.
3. - The bea rers rise together and step off) the FI G, 75.
bearer ,\,ith the right foot, and tLe lefthand bearer with the left foot.
THE FIRE..'IAN'S LIFT.
(To be attempted only by a strong man).
Turn the r atient face dOlI n wards; place yourself at 11:5 head, stoop do\\'n, slightly raise his head and
164
shoulders and take hold of him close under his arm pits, locking your hands on his back. Raise his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head rests on your left shoulder. ThrOlv his left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your shoulders . Rise to an upright position; hold the patient's left \\Tist with) our left hand and leave yoUl rIght hand free.
Assistance may be giYen to an injured perso n bi supporting him in the manner shown in Fig. 76.
The plan of carryz'llg tlte patient by tlze arms and leg5 witlz tlze fcJce dO'lt'Jt7.vards, commonly called tlze "frogs! marclz," mllst never be used, as death ma)1 ensue jrOff'l thz's treatmelli.
bIPROVISED STRETCHERS.
A scretcher may be improvised as follo\\'s ;-
1.-Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The patient sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a longel stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 79)

77.
THE FORE AFT
This plan of carryin cr is useful when space does not permit of a band
166
FIG.
FIG. 78.

FIG. 79.
Ie)
2.-2'1ake holes in the bottom c orners of 0:1e or two sacks and pass stout poles through them.
3.-S pread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides. 'Two bearers stand on each side and grasp the middle of the pole with one haud, and ncar the end with the other. They walk side\\'ays.
4.- A hurdle, broad piece of wood, or shutter may be used 2..S a stretcher ; some straw, hay, or cloth ing should be placed on it, and covered " 'jth a piece c f stout cloth or sacking; the latter is useful in taking lhe patient off the stretcher.
Always t es t an improvised stretcher before use. Stretchers must be carried, and the patient pla ce d on them, as laid down in the "Stretcher Exercises."
As a general rule carry the patient feet foremost. The exceptions are :-
(a) When going up hill with a patient whose lower limbs are not injured.
(b) 'When going do\\n hIll with a patient whose lower limbs are injured.
Avoid lifting the stretcher oyer ditches or walls, but where these canno t be avoided the stretcher must be carried in the following \\'ays :--
To CROSS A DITCH.
In crossing a ditch, the stretcher should be lowel-e d with its foot one pace from the edge of the ditch.
T68
Nos. I and 2# bearers then desc end. T he stretcher, with the patie n t upon it, is afterwards advanced, Nos . I a n d 2 in the ditch supporting the front eml whIle its other end rests on the edge of the ground above. No . 3 now descends . All the Nos. now cury the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edcre of the ground, while the head is supported by 3 in the diten. No. I climbs out, No . 2 renJamlllg in the dItch to assist NO . 3. The stretcher is lifted forward on the ground above, and rests there \\ htle N os . 2 and 3 climb up.
To CROSS A ' VALL.
The stretcher is lo\\ ere d with the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO .3 of the head; the stretcher is raised tlll the foot IS placed on the wall. No. I then clImbs over the wall and takes hold of the foot of the stretcher, while Nos . 2 and 3 support the head; the st retcher is then carried forward tIll the head rests on the 'vvall, No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the h ea d of the stretcher, which is then slo\\"ly J ifted off the wall on to the ground and the b earers take their usual places.
• These numbers are explained lale( in the dela.led "Strelcher Exercises."

I; I
To LOAD A
The stretcher is lo\\"er ed \\ ith the foot one pace from the end of the wagon. Nos. I and 2 take hold vf the foot of the stretch e r, K o. 3 the he3.d. The stretche r is then raised LInd carried fOT\y ard till the front \\ heels rest on the floor of the \ya gon . No. I then jumps into the \Y::tgon , \\ hile NO.2 c..goes to the head of the stretcher and helps NO.3· The stre tch er is then pushed slowly into the wagon. If the t ailboard cannot be shut, the stretcher must be lashed firnlly to the sides of the wagon.
To UNLOAD A 'V AGON.
Nos. 2 and 3 take hold of the head of the stretcher, \yhile No. I gets into the wagon; the str etc her is then gradually dra\\n out till the f?ot-\\,heels rest on the edge of the wagon. No. I Jumps out of the wagon, and with No.2 takes hold of the foot of the stretcher, No. 3 SD pporting the head. The stretcher is now gently drawn a\\ay one pace and lo\\" ered.
"\Vith four bearers Nos. I and 2 would lift the foot of the stretcher, \\hile Nos. 3 and 4 lift the head. This applies to crossing a ditch or wall, as v;ell as to loading and unloading a \YDogon.
170
CHAPTER IX.
STRETCHER TRAN SPORT.
The "Furley" Stretchers (l\lodel 1899) are of three patterns, viz," Ordinary,"" Telescopic-handled," and "Police." In ge neral principle they are alike, the component parts being designated the poles,

FIG. t'O .-ORDIN.\RY STRETC HER -CLOSED .
FIG. 8I. -TELESCOPIC-HANDLED STRETCHER - O PE:-I . handles, traverse bars, foot wheels, bed, pillo\\' sack and shngs.
The Ordinary Stretcher (Fig. 80) is 7 feet 9 inch es in length, and r foot r 0 inches wid e. The bed is 6 feet in length, and the handles roi inches . The h eigh t is si inch es . At the head of the stretcher is a overlay (the pillow sack) which can be filled wIth . hay, clothing, etc., to form a pillow. The JOInted tray erse bars are provided with joints,
173
for opening or closing the stretche r. Th e T elescopichandled pattern lFig. 8r) is very similar, but the handles ca n be slid underneath the poles, tbus reducin G' the length to 6 feet. This arrangement is of greaf value when working in confined spaces, or when a patient to be taken up or. down a staircase sharp turns. The Police stretcher IS similar to the Ordinary p::tttern, but is more slrong ly made, and has, in addition, straps for securing a refractory patient . .
\V he n closed, tbe poles of tbe stretcher lIe close together the tr averse bars being bent imyards, the cam'as bed neatly folded on the top of the poles and held in position by the slings which are laid along the canvas, and secured by a strap, phced transversely at the end of each sling, bell1g passed tllrough the large loop of the other, and round thE; poles and bed. .
In closing a stretcher care should be tak en to raise the cen tr e of the canvas when pushing in the trayerse bar, as it is othen\ise liable to get caugh t.
To prepare, or open a stretcher, unbuckle the tr a nsverse straps of each sling; remo'\'e the slings from the stretcher ; separate the poles ; take bold ?f tra' erse bar and draw it forward. The slmgs \\ill then be folded to balf thei r length , one b eing laid neatly over the handles at each end of the stretcher.
As a general rule, the stretcher will be prep:ued I y Nos. I and 3 bearers in Exerci se s 1., 11., and Ill.;
and by No. 2 in Exerc.ise IV. Th ese belrcrs wilt, however , if required, assist the other In attending to the patient 's injuries.
Note. - The various movements detail ed In the following Exercises should be carried out steadily, the bearers working in unison, hurrying being carefully avoided, and every attention bem;; paid to the beare r who gives the words of comm a nd.
STRETCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised in 1904 to accord with the drills adopted by the Royal Army Medical Corps ;-
EXERCISE No 1.
FOR FOUR BEARE.RS .
I.-The Instructor selects the beare rs and numbers them-I, 2,3,4 at his discretion. Should one man be taller and stronger titan the others, he should b e styled No. 3, as he will have to bear the heavier part of the burden. * All orders \vill be given by NO.4.
2.-" F all in. "- Nos. I, 2, and 3 take position on 'the left side of and facing the patient. No. I places himself at the pati e nt's knees, No. 2 at the hips, No. 3 at the p:l.lient's shoulders. At the same
• Bearers should, h0wever, be taught to take any of the pusitions named in the following Exercises, \\ hether th<lt of Nv. I, 2, 3, or 4
175
ti me No . 4 p1aces the prepared stretche r on the gr ound by the right side of the patien t about two

FIG. 82.
p:l.c es away from hil11, an? then takes position oppo site t o and facing NO.2. (FIg. 82).
174
•
176
3· -" Ready."-The bearers kneel down on the knee and take hold of the patient, No. I passing hIS hand.s and fore-arms beneath the patient's legs, hands wIde apart. Nos. 2 and 4 pass their hands

FIG. 83. , and forearms be!leath the patient's hips and loins and grasp each other's hands. NO.3 passes his leff hand across the pati e nt's chest and und er tbe rio-ht shoulder, and his right hand beneath the left shoulder (Fig. 83).
177
4.-"Lift."-On the word "Lift," the bearers raise the patient gently and rest him on the knees of N os . I, 2, and 3 bearers (Fi g. 84) ; as soon as he
is securely rested, NO.4 disengages hands with No.2, runs round by the head of the stretcher and places it under the patient, close to the other bearers' feet,
I78
being ca reful that the pillo\\' is immediately under the patie n t's head (Fig . 85); he then k neels down and loc k s hi s ha n ds wi th those of NO . 2 (FiG". 86).
5·- " Lower."-The bearers place the patient on stre tcher ( F ig. 87), disengage their hands, and tl1en stand up . FIG 85.
6. - " Stand to Stretcher. "-No. I goes to the foot of the stre tcher, with his back to the patient; NO·3 t o th e h ead \Vith his face to the patient; Nos . 2 and 4 remai n on each side of the stretcher.
7·-" I and 3 place the slings (if u sed) over t h ei r shou lders, stoop down , and slip the
Ii9
loops of the slin.;s on to the handles of the stretcher, \\ hich they then grasp, . . As soon as all is right the \\ ord lS gl\'en :-
8 .-"Lift S tretc her."-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
Notc.-Xos . 2 and 4 will now adjusl lhe slings the shoulders of J\" as. I and 3, taking care that each well below the level of the collar and lies III the hollow of the sh0ulder in front. They will also lengthen or slDrten the lings, r.egard to the p,ltient's injuries anJ the relallve heights of the bearers.

I-IG. 86.
9.-" M arch. "-The bearers move off :-Nos. I, 2, and 4 stepping off with their left foot, and NO·3
with his right foot (Fig. 87). The step should be a short one of twenty inches, and taken with b ent knees and no spring from the fore part of the foot. ro.-" Halt."-The bearers remain steady.

FIG. 87.
IIo-" Lower Stretcher."-The bearers place the gently on the ground, slip the loops of the slmgs off the handles of the stretcher remove the slings from the shoulders, and then stand up.
12. -'! Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, as at Ord ers 2 and 3·
13.-" Lift."-The bearers raise the patient as at O rder 4 (Fig. 86); NO.4, in this case, disengages b ::m ds from No.2, removes the stretcher (Fig. 85), and resumes his former position. If necessary, the will then steadily rise together, and carefully carry the patient Lo the bed, or Dther place to which it has been arranged to convey him.
14.-"Lower."--The patient is carefully lowered.
EXERCISE
No. II.
F OR THREE BEARERS.
1.- Number the bearers I, 2, 3·
All orders will be given by No.2, who will look after the injured part of the patient's body or limbs, to see that no b andages or splints become displaced, and also that No. I bearer, in lifting or carrying the stretcher, does not touch the patient's feet.
2.-" Place the Stretcher."-No. 3 places the stretch e r in a line with the patient's body, the foot of th e str etcher being close to his head.
3.-" Fall In."-No. I places himself on the left ;;ide of the patient in a line with his knees, No.2 on the left side just below the patient's shoulders) and NO.3 "t the ri ght side, and faces No.2.
180
4.-" Ready."-All kn eel on the left No. t places his hands,. \VeIl underneath the 10\\ er );imbs, always takIng care, ll1 case of a to have one hand on each side of the seat of Injury. Hos. 2 and 3 grasp each under the shoulders and thighs of the patIent (FIg. 88 ).
5. -" L i ft. "-The bearers rise together, keepillg . a patient in a horizontal position (Fig. 89). , 6. -" March ."-All take short side-pac es, the patient oyer the stretcher until his head is imme diately above the pillow. 183
7.-" Halt. "-The bearers remain steady. 8 .-" Lower. "-The bearers stoop down, gently place the patient on the stretcher , disengage their hands, and then stand up.

9. -" Fall In. "-No. I places himself at the foo t ')f the stretcher with his back to the patient, NO.2 places himself at the left side of the patient, and NO,3 at the head, with his face towards the pat:ent.
2 lif' o I -:;:=:'.-_-' - 17 - - -.. -, .
10.-" Ready."-Nos . .I and 3 place the slings (i f used) over their shoulders, stoop down, and slip th e loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given-
11.-" Lift Stretcher."-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now adjust the slings on the shoulders of N os, I and 3, taking care that each is well below the level of the collar, and lies accurately in the h ollow of the sh ould er in fr ont. He will also lengthe n or sh orten ·the slings, having regard to the pati ent 's injuries and the relative heights of the bearers.
12.-" March."- Nos. I and 2 step off with the left foot, and NO.3 with the right. The step sh o uld be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
13.-" Halt."-The bearers rem ai n stead y.
14.-" Lower Stretcher."-The bearers place the stretcher gently on the ground, slip the loo ps of the slings off the handles of the stretcher, rem ov e the slings from the shoulders, and then stand up.
IS. - " Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretch e r, as at Orders 3 and 4 (Fig. 88).
16.-" Lift."- The bearers raise the patient, as at Order 5, and carry him by short side steps, clear of the stretcher, to the bed, or other place to whIch it has been arranged to convey him (Fig. 89).

17.-" Lower."- Th e patient is carefully lowered .
EXERCISE No. III.
\VHEN ONLY TH REE B EA R E RS ARE AVAILA BLE AND THE STR E TCH ER CANN OT BE PLACED AS EXERCISE II.
I.-Th e In struct or nu mbers the bearerS-I, 2, 3· All orders will be given by NO.2.
2. -" Place the Stretcher."-No. I taking th e fJo t of t he stretcher, and NO.3 the head, place it on the ground by th e side of the patie nt, and as close to him as practi.cable.
3. - " Fall In."-The thre e bearers take the same p03itions on on e siJe of the patient, as laid down in Ex erci se No. 1.
4.-" Ready." -Nos. I, 2 , and 3 kneel down on the left knee, pbcing themselves a s close to the p atien t as th ey com' en icntly can, and then take hold of him as dir ected in Exercise No. 1.
S. -" Lift."-Nos. I, 2, and 3 raise the patient as dir ected in Exercise No. I, and th en move in a kn ee ling posit ion up to th e stretcher.
6. -" Lower."-The bearers bend forwa rd, caref ully lowe r the pati ent on to the stretche r, and diseng:1ge hands.
184
7. - " Stand to Stretcher. "-All the bearers stand up; No. I goes to the foot, No. 2 remains JI1 position at the side, and No. 3 goes to the head of the stretcher.
8 "R . "N d I . . - eaay. - oc:;. I an 3 p ace the sImas (if u sed) over their shoulders, stoop down, anrl sIp the loops of the slings on to the handles of the stretcher which they then grasp. '
.9·-" Lift Stretcher. " -Nos. I and 3 bearers raise }he st:etcher s.teadily t?gcther and stand up.
No.2 WIll no\y adjust the slIngs on the shoulders of T O <;. I and 3 taklng care that each is well below the level I)f the collar, and lies accurately in the hollow of the inJront. He will also lengthen or shorten the sllng.s, ha\'lng regard to the pa tie nt 's injuries and the relative heights of the bearers .
IO. - " March. "-Nos. I and 2 step off with the left foot, and 1 o. 3 with the right The step should be a short one of 20 inches, and taken with bent knees, and n o spring from the fore part of the foot .
n. - " Halt. "-The bearers remain steady.
I2. - " Lower Stretcher. " -The bearers place the stretcher gently on the around slip the loons of the slings off the handles the 'stretcher the slings from the shoulders and then sta:1d up
I3· Un load - Ready." - No: I places on the left side of the patient, and in a lme wIth h.ls knees, No. 2 on the left side just belo\\' the patIent's shoulders, and NO.3 at the right

187
5ide, and faces NO.2. All kneel on the left knee No. I places his hands, \yell apart, underneath the lower limbs, abays taking care, in case of a fracture, to have one han:l on each side of the seat of injury . Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
I4.-" Lift." - The bearers rise together to theiI keeping the patient in a horizontal position, and nrry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
IS .-" Lowtr."- The patient is carefully lowered.
EXERCISE No. IV.
fOR USE IN MIXES AXD NARROW CUTTINGS \\ HERE' Tllo ME.'f OXL Y CAN BE ENG.-\GED .
Nos. I and 2 will carefully place the stretcher in a Lne \\'ith the injured man's body, the foot of the stretcher being, if possible,*' close to his head. No. I straddles across the patient's legs, placing his . right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, asses the left hand under the patient's thighs an d
• It is not advisable to be too particular as to the head foot of a stretcher in a mine, as it would probably be Impossible to reverse it,
186
188
the right hand across and und e r the patient's calves. No.2 places his feet one on each side of the pati ent between his body and arms, the toe of each foot as near the armpits as possible. He then dO\\'n and passes his hands between the sid es of the chest and the arms underneath the should ers, and locks FI G . 90.

the fingers (Fig. 90). If the patient's arms are uninjure d he may put them round the neck of No.2, and by· this means greatly assist him in lifting.
189
When both are ready, No. I will give the order " Lift and move forward.' The patient is then to be slowly lifted, just sufficient to allow his body to clear the stretcher. Both b.earers will slowly and gradually move the patient forward, NO.2 by very short steps, No. I by bending his body forward as much as he can 1vithout moving hz's feet (Fig. 9T ). No. I no\\' gives the order" Halt," whereupon No.2 remains steady, and No. I advanc es his ri ght foot to his left, and
FIG. 91.
a gain advances his le ft fo ot till the toe touch es the h ee l of NO.2. No. I then gives the order " Adva::ce," \"he n the patient ""ill aga in be moved fon \ ard. These movements are to be rep eated until
the patient is O\'er the stretchcr, when he is to be gently lo\yered.
T Ile follo\yi ng Stretcher Exercise is adapted by permissio n from the Royal Army Medical Corps ual, 1905.
All orders \\'ill be gi"cl1 by N O. 4.
I. "Fall in." -Six bearers fall 111 beh ind ea ch othe r.
2. "Number."-The bearers number from front t o rear.
3. (( NO·3 Bearer, righ t (or left) turn-supply stretcher- quick march." - TO . 3 bearer \\' ill march to the stretcher, stoo p, lay hold of it and place it on his right shoulder at the sl ope, holding it by the lo wer foot wheels, wheels to the front. As soon :15 the b ea rer is provided with a stretcher, he will tu rn about and rej oin his squad in quick time, halting .as he arrives in his place. He turns to the front, an d , passing the lower end forward, places the stretcher on the ground to the ri ght of the squad, "heels to the ri g ht, front end of the poles in line 'with the toes of No. I and rises.
4. "Stand to I places himself with his toes in line with the front ends of the poles. NO.3 with his heels in line with the rear ends of the poles, cluse to tuu c hing tLe stretcher with

FIG·Y2.
m m'G m m.
FIG. 93.
FIG·94.
95.
190
[J rn (!J rn @]
i
19 1 ml\ : \\ I .' \\'. , ,', r ,I \m[] 'j '. i\ \ 'I " L?j ,', , , I I' I rn I' I 3 " /:,' , r.-' I , 4 ' 17' • :•. .Y j ...--" / ' :5:/ ' ,·..··"'7
:'mJ m @J 1 J . .1 , 1 .. :"< ;: 0 , ;.. .' \ \ \\ FIG.
I 41 o -.. ,. Z • 5: • t... __ J 1 • r : ; "\O'l FI,G. 96'

his foot. Nos., 2, 4, 5 and 6 take up their posItIOns one pace behmd and covering off the bearer In front of them (Fig. 9 2 1. "L'f S S· 1 t tretcher." -N,os. I and 3 stoop, grasp both handles of the poles wIth the right hand rise together holding the stretcher at the full of the arm, wheels to the right.
6. "Collect Wounded - Advance." - The squad doubles by tre shortest route to the patient and halts without fur.ther .word. of command one from head of and 10 a lme wIth the patient (Fig.93).
7· Lower Stretcher." - N os. 1 and 3 stoop place the stretcher quietly on the ground, and smartly together.
8. Stretcher." - Nos. I and 3 turn to the rIght, kneel on the left knee, unbu ckle the straps, and place the slings on the ground besIde them, separate the poles, and straight e n the traverses.
. Two. On the word two each takes a slinO' dou bles It on itself, slips the loop thus formed onO'the near handle, and places the free ends over the opposite buckle uppermost. They then rise and turn to then left together.
\Vhile the is being ,prepared by Nos. I and 3, the dIsengaged bearers will advance and to patient such assistance as may be requued (FIg. 94).
The necessary assistance having been rendered, NO.4 will give the command-
9. "Load Stretcher." - The place themselves as follows :-Nos. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; Nos. I and 4 at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the whole kneeling on the left knee. Nos. I and 4 pass their hands beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. 95).
10. "Lift."- The whole will carefully lift the patient on to the knees of Nos. I, 2 and 3.
Two. Nos. 4, 5 and 6 will then disengage, rise j Nos. 4 and 6 step back one pace. No. 5 turns to his left, doubles to the stretcher, takes hold of and raises it, left hand across, the near pole resting on the left hip; carrying the stretcher, he returns to his place between 4 and 6, and places it beneath the patient.
Three. Nos . 4 and 6 step forward one pace, and together with No. 5 kneel down on the left knee, and prepare to assist in lowering the patient (Fig. 96).
II '( Lower."- The patient is lowered slowly and gently on to the centre of the canvas (special care being taken of the injured part).
Two. The bearers disengage, rise; Nos. I, 2, 3 and 6 turn to the left; Nos. 4 and 5 to the right; H
192
193
No. 4 places himself three paces in front of the stretcher. No.6, having collected the kit and arms of the patient, places himself three paces in rear of the stretcher, Nos. 2 and 5 opposite the centre of the stretcher. The whole are now ready to lift stretcher and move off (Fig. 97).

FIG . 97 FIG, 98.
195
12. "Lift Stretcher. " -K os . I and 3 stoop, g rasp the doubled sling midway the poles \\'i-th the forefing er and thumb of the rIght hanel, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between the handles, and place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed, !:i0 that they lie well below the collar of the coat beb 1l1d and in the hollow of the shoulders in front. In the event of the slings req uiring to be adjusted, either as regards length or for the greater comfort ?f bearers, NO.4 will detail a bearer to carry thIS out , the length of the slings being adjusted, when neces!:i ary , by means of the buckles.
Two. Nos. I and 3 stoop, slip the loops over the handles, commencing with the left, and grasp the handles firmly.
TllTet. Nos. I and 3 rise slowly together, No. 3 conforming closely to the movements of o. I.
13. "Advance."-Nos . I, 2, 4, 5 and 6 step off \\'ith the left foot, NO,3 with the right, stepping sh Olt , knees bent, fe e t raised as little as possible.
14. "Halt."-The whole halt.
IS. "Unload Stretcher."- The bearers place themselves in the same position at the stretcher as described for Loading (Order 9).
16. "Lift."-As described for Loading (Order 10), lIZ
194
. I
196 except that the stretcher is carried forward three paces clear of the patient's feet.
17. "Lower. " -The patient is gently lo we red to the ground The bearers disengage, rise; N os. I, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whole step off to their places at the stretcher, as at Order "Stand to Stretcher" (Fig. 98).
The Ashford Litter is made up of either of the Furley stretchers mentioned on pages 172 and 173, a wheeled under-carriage and a waterproof hood and apron, or, if preferred, a light wet-resisting canvas cover. The stretcher is kept in position on the under-carriage by the foot-wheels, which fit into slots in the sides Gf the under-carriage, and it can be removed at pleasure. The under-carriage is fitted with a cranked axle, which allows the bearers to pass with the stretcher between the wheels instead of lifting it over them. At both ends are two legs which may be turned up as handles when wheeling the litter. The hood and apron fit into sockets screwed to the stretcher. In wheeling the litter, care should be taken to keep the patient in a horizontal position. Should it be necessary, two bearers can easily lift the litter and patient.
Rea-Edwards Litter, introduced in I9 0 4, is used in a similar manner. and one model of it is fitted with pneumatic tyres, which add immensely to the comfort of the patient and to the ease of propulsion.,

197
CHAPTER X.
(Being the Ftfth Lectu1'e for Females only, z'JZ accordaNce zvdlz Syllabus 58.)
BY E. :.\IACDo\YELL COSGRAVE, M.D., F.R.C . P.I.PREPARATION FOR RECEPTION OF ACClDE TT CASES.
\ VHEN news of an accident comes, preI?arations should at once be made so as to have .everythmg ready before the injured person is brought m. <?f course the pret · s needful will vary accordmg to the nature para IOn , h and extent of the injury, but the following are t e chief things which may have to be done.
CHOICE
AND PREPARATION OF ROOM.
A must be chosen. In a bad case this should room . d'ffi I t be one easily reached, as it IS I cu t 0 carry.an ' . d throuah narrow passages and up-stans. m Jure per;:, b , 1 Unless there is some reason agamst It, t le mjured person's own room IS best. . .
The way to the room must be cleared, furniture and loose mats in. hall or ]l! should be removed . If the Injured ]5
d or shutter or stretcher, two strong chalIs on a 0" . h th should be placed ready to support It w erever e bearers would be likely to reqUIre rest.
Useless furniture should be removed from the room. The bed should be drawn out from the" all
so that both sides can be approached , and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much collapse several hot bottles and ,hot blankets may be required; cover the hot bottles WIth flannel.
If the injury is very severe, if mud-stained clothes have to be removed, or if extensive dressings have to be applied, it may be necessary to have another bed, a couch or, a table near the bed to lay the sufferer on ll1 tbe first ll1stance. This should be fOO arranged that soiling may do no harm; old sheets, waterpoof materials, thin oilcloths, or even ne\yspaper, may be used as a protection.
LIFTH;G AND CARRYING .
If present at the place where the accident occurreJ it will , be necessary to see that the patient, is fully lJfted after proper "First Aid" has been render ed,
The following rules should be remembered ;- Select the proper number of persons to assist and do not let them lift the patient until they tho'roughly l1r'ierstand how th ey are to do it.
For ordina ry cases, where the injured person has to be, lift ed a very short distance, three helpers are s T\yo (\\'ho should be as far as possible of equal heIght) are to bear the weight, the third is to su pport and take charge of the injured part. This is

hest done by a person who has been a "First l\id II course. If the injured person IS msensible anothe r helper should su pport his head,
The lifters, one at each side, should on on e knee, and pass their h a nds und er the patient s back at the lower part of the sh ou lde r-blades , and under the hips, clasping each his ri gh t in, the other's lef,L, The injured patient should, If practIcable, place hI S ar ms round the n ecks of th e bearers . , ,
The third helper should a ttend to the seat of ; if this is a fractured limb, he should support It by placing the palms of his hands ,the limb, above and one below the sea t of the ll1Jury, graspll1g it firmly but avoiding unnecessary pressm:e. _
The helpers should remain thus untIl order " Lift" is given, and then they should all 11ft slo\\'ly and stea dil y, avoiding jars, attempts to change POSItion of hands, etc.
H the injured person is to be. placed on a or shutter, this should be prevIOusly pl aced WIth the bottom end at his head; the bearers should th en move one at each side of it, until the patient is over it. The word" Lo wer" should then be given, th e injured person should then be slowly lowered A pillow or folded-up coat should be ready, and as the sufferer is lowered this should be placed und er his head:l(-
• Full directi ons are given in Chapter IX.
198
199
lIIEANS OF CARRYING.
Besides a stretcher, and substitutes such as a gate, or a door, other means of carrying can be ImprovIsed.
In slight injuries, where the injured person is unable to walk, two bearers can carry him by forming a four· handed, three-handed, or two-handed seat.
A four-handed seat is formed as described on page 160.
A three-handed seat is made as described on page 162.
The two-handed seat is made as described on page I6r.
A single helper can lift by supporting with one arm the two knees, and with the other the 'back. The arms must be passed well under before cornrnencing to lift.
A single helper. can support by putting his round the waIst, graspmg the hip and placing the Injured arm round his own neck, holding the hand .wIth hlS own hand (Fig. 76, page 165).
A capItal stretcher can be improvised out of a strong sheet and two broom handles or other short poles. Each side of the sheet is wound up on a broom handle until th ere is just room for a person to lie b.etween. This requires four bearers, two at each SIde, to prevent the sh eet slipping.

201 CARRYING UP STAIRS.
In carrying a stretcher up stairs the head should go first, and an extra helper should assist at the lower end, so as to raise it and keep the stretcher nearly horizontal.
The two, three, or four-handed seat may be used for carrying up stairs; or a strong chair, the patient being carried up backwards. In the latter case one helper should walk after the chair and help to support it, and to prevent the injured person slipping out.
LIFTING INTO BED.
If the bed is narrow and there is room the stretcher should be placed on the floor with the head close to the foot of the bed. The injured person should then be lifted over the foot and placed on the bed. If the bed is too wide to admit of this, thte stretcher should be placed beside it, and two helpers should stand at the far side of the stretcher. One helper passes one arm beneath the shoulders and one beneath the middle of the back, the other helper placing his under the lower part of the back and under the knees. The injured person is then lifted, another helper pulls away the stretcher, and after a single step forward the burden is placed on the bed.
200

PREPARATl0N 0F BED.
A firm mattress, not a feather bed, should be selected. If there is much injury, or if dressings h ave to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed under the draw-sheet. As the draw-sheet beco mes soiled, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " cradle " is to support the bed-clothes and keep them from pressing on the li mb.
A band-box (Fig. 100), three-legged stool (Fig. lor), or hoop sawn across and the two halves secur ed t ogether (Fig. IOl), may be used. A corkscrew passed through the bed-clothes, with its point gua rded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REM0VI N G THE CL0THES.
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury. 2 0 3
FIG . 99· FIG. 100 FIG . 10I.In removing a coat, etc.,in a case of fractured arm the uninjured arm should be drawn out first.
In on a coat or shirt the injured arm should be put m first.
In burns and nothing should ever be dragged off. A. sharp palr of scissors should be used, and everyt.hmg not a?hering should be cut away. If anythmg adheres It should be left until medical aid

FlG. 102.
can be obtained. The clothing adhering may with advantage, be soaked with oil. To the trousers from a severely inj ured limb the outside seam should be ripped up. '
PREPARATIONS FOR SURGEON.
As so?n as the injured person has been attended to, preparatIOn should be made for the surgeon's visit. " ,
20 5
Thepreparations needful will depend upon the natur6 of the case. The foUowmg hints may be of use:-
A fire in the room helps ventilation, even in summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot-bath does well. The basins should be placed on a table, covered with a clean white cloth; a large towel makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be within easy reach. The foot-bath should be under the table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths, old linen, oil, and baking soda, should be ready, and materials should be torn up for bandages.
In the case of hremorrhage, plenty of water should be boiled and allowed to cool, and pads of absorbent cotton wool should be baked in a tin box in the oven, and at least two basins should be ready.
In the case of a person rescued from drowning the sheets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, 1inseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
204
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large towel.
\Vhen summoning a medical man to an accident always let him know by a written message what kind of case he is required to treat, so that he may bring whatever is needful. By tbis means valuable time may be sayed.
QUESTIONS ON CHAPTER X.
The Uti merals indicate tht pages where the amwct'l may be found.
\Yhat points would you consider when choosing a sick PAGE room? ... 19 7
Ii ow would you clear the way to the sick room? 197
What means of resting would you provide for those carrying a patient on a stretcher? ... ... ... 197
lIow would you place and arrange a bed for an accident case? ... 197, 198
Arc hot bottles necessary, and how would you prepare them? ...
... '" ... .. I9 8
',"hat is often necessary to lay the sufferer on in the first instance? ...... 198
II ow would you protect this from getting soiled? ... 198
lIow would you see to the proper lifting and carrying of an injured person? ... ... ... ... 198 199
',"hat suhstitutes [or a regular stretcher can you suggest? '200
How is the four-handed seat made? r60 161
For what cases is this seat useful ?.. ' 1 ('0
How is the three-handed seat made? 162, r 6..*
For what cases is this seat useful? ...
How is the two-handed seat made?
For what cases is this seat useful? ..
How can a single helper ? "'?
How can a single helper glve suppolL.
How would you improvise a stretcher? ... . ..
How many bearers are for this

PAG;!' 16.:: 161, 162 161
How should a stretcher be carned upstairs? .. : ...
How would you carry a patient upstairs on a chaIr? .. ,
How would you lift a patient from a Bt.re.tcher to a bed?
How should a bed be prepared for an lDJured person? .. ,
How sheuld a draw sheet be made? ...
'What would you place under the draw sheet?
What should be done with the soiled part of a draw sheet?..
What is the use of a " craule " ? . ?
In what ways maya cradle be lmpro.vlsed .
How would you remove a coat or shut lD the case of a fractured arm?
How would you put on a coat or shlrt If the arm were injured?
In the case of a bad burn, what you do wlth clothing that adhered to Lhe patlent . . .
How would you remove trousers from a severely Injured limb?...
preparations would you make for the surgeon
visit?..
What would you get ready m the case of a burn.
't'
And what in the case of hremorrhage? ... .... ...
And what in the case ofa person froJ?
What would you get ready for makmg poultlces .
And for ? .,. . .. ... . ..
"What sort of a message would you send to summon a doctor? ...
206
... ...
207
. .
. ..
... . .. . .. . .
...
... .., .. , ... ... ... ....
... ... .., ... ... .,.
s
... .... ... ... .
200 165 200 200 201 201 201 202 202 202 202 20...! 20:! 20.) 20..1 204 204 205 205 2 0 5 2 0 5 20 5 206
208 INDEX.

Abdomen
Page III wound of 112
Accident case, preparation for 197
Acids, poisoning by 149, 15 r
Air, always necessary ... 18
Alcohol, caution as to smell of 130
Alcohol, poisoning by 134, 153
Alkalis, poisoning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary)... 20
Ankle 30,32 " sprained... 64
Anterior tibial artery 93
Aorta 79
Apoplexy 132
Apparently drowned, to restore... 139
Arm, bone of 28 " fracture of 52
Arm-slings 39, 49
Arsenic, poisoning by ... 148
Arterial hremorrhage, arrest of 74 " practising arrest of 79 " " signs of 74
Artery, brachial. .. " " carotid dorsal of foot " facial femoral ... iliac occipital plantar ... popliteal radial " su belavian " tibial " temporal " ulnar
Artificial respiration
Asphyxia
Atlas 121, 129,
Auricles ...
Axillary artery
Axis
Back, bandage for 159
Backbone 23
Bandage, to apply 42 " to fold ... 37 " to improvise... 37
Bandaging 155
Page
Bites of rabid animals .. , 106
Bladder ... II r, 113
Brachial artery ... 86
Brain 117 compression of 13 2 " concussion of 13 1
Breast- bone 26 " fracture of 48
Broad bandage ... 37
Broken bones, see Fractw 'e _
Bronchial tubes... II8
Brooch-bone 30 Bruises 102 Burns 102
Circulation of the blood, organs of Circulation of the blood, to induce
Page
Clavicle " fracture of 1 0
Clothes, removal ot Coccyx
Collapse ...
Collar-bone 19, 202 25
" fracture of ...
Comminuted fracture
Complicated fracture ...
Compound fracture
Compression of the brain
Concussion of the brain
Capillary hremorrhage
Capillaries ... 70,7 2 95 31
Capsule ... Carbolic acid, poisoning by... ..
Carotid arteries 15 2 80 from" hremorrhage
Carpus... ...
Cerebro-spmal system
Cervical verte brre
Carrying, means of " uDstairs Cartilage So 28 160, 200 201 25 117 25 82
Conductor
Convulsions in children Cradle, bed Cranium ... " fracture of Crepitus ... Crushed hand foot
Diaphragm 12Q.. Digital pressure... 74
Direct violence... 33
Dislocation 6z-
Arteries ( . " course 0, mam ... 70 79 85
Bed, lifting into... 201 " preparation of 202
Artery, axillary .n
Belladonna, poisoning by 148
Cheek, bleeding from Chest, bandage for Chlorodyne, poisoning by Choking ... 158 149 140
Ditch, to cross with stretcher 169
Dorsal artery of foot 93 vertebrre... 25.
Pag 6 86 80 93 81 89 79 82 93 9 2 88 84 93 82 88 136, 138 138 25 70 85 25
134 26 48 35 34 34 13 2 131 143 137 202 22 43 36 55 62
210 Pag l!
Dress, woman's, on fire ... 105
Drowning 139
Ear-chann el, 1)lood issuing from
Ear -passage , foreign bod y in
Dbow, bandage for joint, fra ct ure involving 98 110 159 53
Electric shock
E metic
EpiJe-psy ...
Esma rch's 14 2 148, 149, ISO 13 2 bandage
Expiration triangular
External caro t id artery ...
Eye, bandage for foreign body in
Face, bones of Fa cial artery
Fainting ...
Fe moral artery
" " digital presSllre at groin ...
Femoral artery, tourniquet for
Femur fracture of " fracture of Fingers, bandage fo r fracture of 37 120 80 155 109 22 8 1 134 89 89 90 30 56 30 60 159 55
Fireman's lift
First aid, meaning of " student
Fish-hook, embedded Flexion _. at elb uw " at knee ... Ii
15 3 J Food, poisoning b y
Foot, band age for bones of . .. " crushed ... 15 8 30 62
Forearm, bones of " fracture of Forehead, bandage for ... " hremorrhage frol11
Foreign body in the earpassage in the eye " "in the nose
Four -'nanc1ed seat Fra cture, apparatus for treatment of causes of d e finiti on of general rulLs for treatment inVOlvin g elb ow
of arm ...
of breast-bone
of carpus
of coll ar - bone
of cranium 4 3 55 of finger

Zil of forearm Page 54 58 60 " " " of knee-cap ofl eg ... of lowe r jaw ... of meta carp us of metatarsus ... of pelvis of ribs ... of spine of ta rsus of thigh -bone .. . of toes .. signs and symptoms of . . . 44 55 62 56 46 45 62 56 62 " varieties of 35 34 108 F rost·bite !<'ungi, p oisoning by 153
General circulation 70 Granny 40 3reen-stick fraclure 35, 36 Gums, hremorrhage from 97
Hremorrhage , arterial.. 74 " capillary... 95 from gums 97 from h ead and neck 80 from lowe r limbs ., . 89 from lu ngs 97 from nose 96 from stomach 98 ... ae....
Hremorrhage from t hroa t 91 from tongu e 97 from tooth socket . .. 9 7 from upper limbs .. 84 internal.. 95 kinds of ._. 73 " venous 93 Hand, bandage for 157 " bones of ... 28 Hanging . .. 1 4 0 I1aunch- bones 28
Head and neck, arteries of 80 Head bandage for 155 " injury to .. , 1 28, 13 1 " side of, bandage for 155 Heart ... 70 " rate of contraction of 7'1. Heat-stroke 136 Hernia 114 Hip, bandage ror 157 Hist ory, meamng of 17 Howard's method of arli ficial respiration 126 Humerus 28 " fraclure of 52 H yd ropho bia 106 Hysterical fits 133
Iliac arteries Impacted fracture Indirect violence I n sensibility
20 109 76 87
28 54 83 83 110 109 III 160 36 33 33 4 1
53
48
join t
52
55
4g
Pag-I
insensibility, general rules for treatment... . .. 128
Inspiration 120
Instep 30
Insulator... . . . . .. 142
Internal carotid artery . .. 80
Internal hremorrhage ... 95
Intestines, injury of 113
Involuntary muscles 33
Jaw, angle of 23 " lower 23 " "fracture of 44
Joint, definition of 3 1 " injuries to... 109
Jugular vein 80
Kidneys .. . I I I " injury of 113
Knee, bandage for 159
Knee-cap 30 " fracture of 58
Knot for bandage of lower lim b ... ' " 42
Knots, reef and granny 40
Laborde's !:iethod of artificial respiration '"
Laburnum seeds, poisoning by... . ..
Lacerated wound
Large arm-sling :::
Laudanum, poisoning by
Leg, bones of ... 126 30
Ligaments ...
Lightning, effects of Limbs, lower '" " upr er Lime in the eye
Lips, bleeding from Litters ... . .. Liver " injury of 82 196 III 113
Lower limbs ...
Lumbar \'ert ebn:e Lungs hremo rrhage 28 25 120 from 97
Marshall Hall's method of artificial respiration
Iedium bandage '"
Metacarpus .. . fract ure of . . . " fractur e of ...
Middle line of body
Mouth, blood issuing from Mu scles " ruptur ed 1\1 uscular action ... Tarrow

Nervous system...
Nose, foreign body in 111 hremorrhage from 96
Occipital artery... 82
Opium, poisoning by 148
Pad, ring .. . " to fold
Palm, hremorrhage from Palmar arches ...
Paregoric, poisoning by Patella fracture of " fracture of Phalanges of foot " of hand
Phosphorus, poisoning by 148,
Physiology (elementary) Plantar arch " artery
Plants, various, poisoning by ... Pleura
Poi son e d we a p 0 n s, wounds by Poisoning
Popliteal artery ...
Posterior tibial artery
Potash, caustic, poisoning by ...
Rabid animals, bites of...
" fracture of 54
knot 40
Respiration artificial 121, 129, " to excite
Respiratory system
Rest, necessity for Ribs " fracture of ... Room, choice and paration of
212
Pag-I! 60 .. . 198 ... 201 26,3 1 I4-/28 26 I IO
Leg, fracture of Lifting and carrying " into bed
bandage Needle, embedded Nerves J40 37 28 55 30 62 20 37 108 IIS 213 Pag-e
117
83 74 88 88 149 30 58 28 56 30 28 150 20 93 93 148 120 149 Pap. Pressure, digitaL. 74. " point ... 74 Principles of First aid 17 Prussic
poisoning by 15Z Pubes 28 Pulmonary circulation ... 72 Pulse 72 -Pupils of eyes 130 Questions on Chapter I. 21 66 99 II. III. IV. V. VI. 115 145 154 X. 206
acid,
106
88
Radial artery
Radius 28
Reef
136, 138 1 2 7 uS IS 26 4(r pre-
Pag il
Rupture (hernia) 114
Ruptured muscles 65
Sacral verte br<e . . .
Sacrum ...
Scalds 25 25, 28 102
Scalp, bandage for " h.emorrhage from Scap ula ... " fracture of Schafer's method of artificial respiration
Sea.t, four-handed three-hand e d " two -hand ed
Shin-bone
Shock " electric
Shoulder, bandage for ..blade ... " frac ture of bones ... " j oint. ..
Sick room, choice and prepralion of. _.
Signs, meaning of Sil vester's meth od of anificial respiration
Simple fracture ...
Skeleton ... Skull
., fracture of
SitllgS. arm 39,40 ,49
Small arm sling ...
Smotherin g
Snake bites
Soda, caustic, poisoning by
Splee n .,
S pinal canal
" fra c tur e of Spirits of salt, poisoning by
Splint, angular .. _ ...
Splints, rul es for applying " to im provise
Sprains
Stern....m ... " fracture of
Stimulants
S tings of plan ts and anima!.s
Stomach ... " hremorrhage from " inj ury of ...
Strains
Strangulation
Stretcher exercise, Army No. I. No. II. No. III . " " No. IV. Stretchers,

St retchers, to ca rry 169 " to improvise 166
Stry chn ine, poisoning by 153
Subclavian artery
Suffocation 141
Sunstroke 136
Surgeon's visit, prepa ration for 204-
SyllabUS of instruction... 7
Sympathetic system 118
Symptoms, meaning of ... 17
Syncope ... 134
Synovia 31
Systemic circulation 70
Tarsus 30
Temporal artery... 82
Thigh-bone ... ... 30 " fracture of ... 56 Three-handed seat 162
Throat, hremorrhage from 97 " swelling of tissues of. . . 141
Tibia 30 " fracture of 60
Toes, bandage for 159
Tongue, hremorrhage from 97
Tooth socket, bremorrhage from 97 Tourniquet 75
Transverse wound of abdomen 113 Two-handed seat 161
'Wagon, to load or unload 171 'Vall, to cross with stretcher 170 'Yannth, necessity for I S " to promote 127 Wind-pip e 118 ' ''oman's dress on fire lOS ' Vonnds by poisoned weapons 106 " accompanied by arterial hremorrhage ... 76 'Vounds accompanied bv venous bremorrhage 94 ' Vounds, lacerated 78 Wrist 23
155 83 26 51 121 160 162 161 30 134 142 15 6 28 51 26 3 2 19 7 17 1 2 3 34 22 22 43
214
Page 39 140 I OD Lt9 I I I II3
injury of...
23 23, II 7
cord
2J 45 149 54 107 III 98 11 3 65 140 190 17-1181 18 5 ' 187 172. 21 5
Furley
Page Ulna 28 " fracture of... 54 Ulnar artery 88 Unconsciousness 128 Upper limbs 26 Varicose veins 94 Veins 70 Venous blood 72 "hremorrhage 93 Ventricles 70 Vertebra ... 23 Vertebrre... 25 Vertebral column 23 Vertica l wound of abdomen 11 3 Vitriol,
by ... 102 Voluntary muscles 33
burn
Ube $t. Jobn Bntbn!ance tiosociatioll.
GENERAL PRICE LIST.
A complete and reliable Ambulance Equipment is an actual necessity, and experience has proved that employers of labour and others interested in the d istrict readily subscribe for the purchase of such appliances. Collecting cards, slating the purposes for which subscriptions are required, will be sup' plied to approved persons gratuitously on application. to the Head Office of the Association, where also any info rmati on with regard to its work can be obtained.
All stores will be sent carriage paid to any part of the United Kingdom. Returns may be sent carriage forward. If carriage is prepaid it will be allowed.
Owing to fluctuations in market prices it is imposs ible to guarantee that the quotations herein can be adhered to.
Quotations will be furni shed for Ambulance Carriages and other articles relating to Ambulance, Nursing and Hygien e, not mentioned in this list.
Orders and correspondence should be addressed to the St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E.C.
Remittance s should be made payable to the St. John Ambulance Association, and crossed "London Coun ty and vVest· minster Bank, Lothbury."

The "Ashford" Litter (1899 model) consists of a two· wheeled under-carriage fitted with ellip tical springs, and either
o f th e ,. Furley " stretchers, with a cover so arranged on a jointed frame that it can be folded up inside the stretcher, o r with a hood and apron (as shown above). The undercarriage, having a cranked axle, the b earers can pass between the wheels with the stretcher, and thus avoid lifting it over them . vVhen travelling, the legs oJ the und er-carriage are raised, and thus form the handles by which to prope l it.
Should it be necessa ry to p ass ove r rough ground, two bearers can easily lift the litter and patient. Th e" Clemetson :> stretcher can be used instead of the" Furley" pattern .
Carriage Paid on all Orders in the United Kingdom. 2 " ASHFORD" LITTER.rRICES OF THE IMPROVED ASHFORD LITTER, 1899 MODEL. _ w With Iron Tyres to Wheels. 'With IndiaRubberTyresto \Vh eels
Under-carriage (no
T e lescopi c
with Police

With Cover or With Hood and f;J Without Cover or Hood and Apron. With Hood and Cover. Apron. Without I With
Hood and co.ver. Apron, as 3, Apron.
* Prices quoted for Litter with Ordinary Stretcher include \'\Tid e Webbing Slings but no Chebt c:: S trap. Leather, instead of W ebbing Slings, 5S. 6d. extra; Chest Strap, IS. 6d. extra If sup- ::I plied without any Slings, 4S. allowed
t Prices quoted for Litter with Telescopic·bandled Stretcber include \Vide \'\Tebbing Slings and Co Chest Strap. Leather, instead of \Vebbing Slings, 5S. 6d. extra. If supplied without any Slings, " 4S. allowed; and if without Chest Strap, [s. 6d. allowed. :;.
t Prices quoted for Litter with Police Stretcher include Wide " Tebbing Slings and Leather tJQ Straps for securing a refractory patient. Leather, instead of Webbing Slings, 5S. 6d extra g. Hood and Apron, complete (" Furley" pattern Stretcher) £2 10 0 .3 Do. do. do. (" Clenlf'tson " Stretcher) 2 IS a Wa terp roof Sheet (washable) to be laid on the stretcher bed . .. 0 JO 6 Crates (returnable) charged 4S. 6d. for cach Liller. """'"'ft
Fg
____ ;:, s d. ;; s. d. ;:, :s. d, ;:, s. d (I>
0
iJ Stretcher)
8 10 0 9 0 II 0 0 II IS 0 12 IO 0 14 0 a: Litter complete with 0 Ordinary Stretcher* 11 2 6 12 17 6 14 7 616 2 6 Dittowith
= handled Stretched I [ IO 0 13 5 0 14 IS 016 10 0
Stretcher! ... 12 2 6 13 17 6 IS 7 6 17 2 9 ;;; Do. with 'Clemetson ' ;5' Stretcher '" 14 8 0 17 13 0
'"
Ditto
:11!}.;'
_. (1J (1J n ::r' ::r' .:l...!!' CL,< n rt> -. no '"t:J-. ciQ' 5. S-:; g Oi' ;; n (;'< ;:; .; _ ., '< :t:ln :' g: 0 g- -:. CL ji)' 0 0-3 :ll... n'l» Ol!!.CD g- r:;' § (;U;3 Q !!. g
III
\I>
5.! -'
CD_.
11Q t:lttl ::r'ilo ' CLM o 0 ...... ::;: CLl':I _.t::I o r.n ITQ :: III -'"' II> '"' o t;z;I u e ::;. o 0 K 0 ::t>;:; ;+0 ::r o b (b I" :n ..< u (;CIl::r o tI1 tI1 M t=' > t;1 (fJ 'l ., ii " ii o :s o :i ... ;r CD c:: :!. roe [ tI1 u ? ? ...
n
ii" 8· CIl
n
<:
n 0 n t::I _ en V'J (1Q :_. co (). CJ) I'll tIl::l. ..... !s.. \.1.;»:: -t 5' S- in
in' <lUQ Po. (It !!.;:; :=. n 01 n -"c,... C."'"t r:::: ::I-..J n 0 a,....
s· o·;;;" H-)
Ca rr iage Paid on a l l Order s in t h e Uni ted Kingaom.
ove r t hem, and the cranked a xle has, therefore, been replaced by a straight on e constructed of tubula r steel.

UREA -ED WARDS" LITTER, fitt ed with pneumatic tyred wheels, sh owing the " Cl emetson" Str etcher.
Ball bearLt'lgs are fitt ed to t he wh eels, bot h cycle pattern and wooden , and the hubs are so a rran g ed tha t the wheels can be removed from the axle w ithout disturbing the bearings. In place of th e fo ur legs made to raise as hand les, two fixed legs fi tted wi th small ind ia -rubber wheels or rollers are pla ced a t the foot end, while a c ombined leg a nd handl e fitte d wit h a c ross bar and ca pable of being raised or lowered is used at th e head e nd.< When raised as a handle it ma y be locked in one of two positions, a nd w he n lowered it is loc ked in a vertical position. Th e ad vantages claimed fo r t his arran gem ent are simp licity, ease a nd rapidity of manipulation anJ
Ca rriage Pai d on a ll Or derS i n th e U ni ted Kingdom
the facility afforded by the t IVO fixed legs for the litter, if necessary, on to the p2;vement. The questIOn balance has been care fully studIed, and the stretcher IS shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is loaded and in a horizontal position being thus obtained, and consequently there is no weight on the hands of the person propelling the litter. .
The pneumatic tyred wheels are strongly recommended In cases where the small amount of care necessary to keep them inflated can be given, as the comfort to the pat.ient ease in propulsion are inc reased beyond all comparIson any litter yet produced. It will be noted that the pnces are considerably lower than those of the Litter, and the fo ll owing are given as examples, but owmg. to the vast number of combinations that can be made wIth the different srretchers and cove rings, it is impossible within reasonable limits to set out quotations for the whole of them, but these may be calculated by adding together the prices of the under-carriage, stretche r selected , and hood and apron or cover, see pages 4 to 10
SPECIMEN PRICES.
Unde r -ca rriage only, eithe r with pneumatic tyred cycle whee ls or solid rubbe r ty red woode n wh eels, £IO; Litte r complete with st ret ch er (no slI ngs or ch est strap) and hood and ap ron, as Ill ustrated, £ 14 3.s. 6d .
Ditto with T elescop ic Hand led Stretche r (WIth chest strap) and hood and a pron, £ 14 I I S . .
Ditto with " Clemetson " St retche r and ventllated hood and apron, £1 5 18s. .
If with iron ty red wheels pnces a re £2 less.
lIand brake, which acts automatically when the litter is at rest, ext ra £ 1 lOS
' Vhen ordering please stat e which wheels a r e required.
Carriage Paid on all Orders in the United Kingdom . THE" CLEMET50N" STR.ETCHER.

" STRETCHER, with Lack raised, also sho\\ ing exte nding legs.
On thi s stretch e r the patient can ue moyed as desired, from the recumbent to the ::,itling posili on . Th ere is no complicated mechanism to get out of orde r, and the adjustment depentl s simply on the Lalance of the patient's body. The stretcher will fit eilher the ;: or the" Rea-Edwards" Under· Carriag e. Pri ce £3 3s. j with extending legs , £ 4 3".
IIoml amI i ... pron, Ventilated, £2 15::,.
Canlage Paid on all Orde .s il1 the United Kingdom.
ADJUSTABLE LEGS FOR STRETCHERS.
Primarily these legs, whi ch are indep ende nt of and ndditional to the ordinal y foot wheels, are intended to facilita te the carriage of a stretcher in a rai l way c o mpa rtm ent , i n which case two on one side would be 10,Y eltd and adjusted by a telescopic arrangement to the proper height, so th at th e foot wheels on one side would rest on the seat, and th e adjustable legs on the other side would rest on the floor. The four legs may be used to raise the stretc he r as required. \Vhen not in use they are folded up imm ecJiate ly un der the poles of the itr etcher.
Price per set of four, £ r.
FIRST AID BOX.
To be c a rried below the axle of the" Rea -EJwards " Lilter, from which it is easily detachaule.
Contents :-Set of Splints, 12 Triangular Bandages, 12 Roller Bandages, 2 i lb. packets each Cotton Wool and Boric Lint, Adhesive Plaster, Pair of Scissors, Knife, 2 oz. ea ch O live Oil. Tinct. Iotline B.P.C., Sal Volatile, and Spirits Ether Comp., Graduated Measure Glass, Kidneyshaped Dressing Basin, 6 Tampons fo r ;\' J5hing wounds, Tourniquet Pins, Safety Pins, N ee dl es, Threatl and T ap e.
Price £2.
Carriage Paid Con all Orders in the United Klngoom.
" FURLEY" STRETCHERS WITH THE
LATEST IMPROVEMENTS, 1899 MODELS.

ORDINARY STRETCHER--CLOSED.
The im provements in all patterns of the "Furley" Stretcher, 1899 Model, are numerous. The comfort to the patient is increased; the stretcher is stronger, more rigid, and lighter, it folds up more closely, and its handles are more comfortable to hold and afford greater protection to th e hands of the bearers in passing through narrow doorways or passages. Should it be necessary to reduce the width of a loaded stretcher in order, for example, to carry it into a railway carriage, this can be done, either when it is resting on the ground or supported by the bearers, without trouble and without the slightest jar to the patient. The price of the stretchers is lowered. All minor points have heen most carefully considered, and the stretchers are confidently recommended as thoroughly efficient in every way.
These stretchers are adapted for use alone or as part of the " Ashford" or "Rea-Edwards" Litter, and the cover, hood and apron, army rug, and waterproof sheet desclibed in this list are sui ta'ble for use with them.
Paid
all Orders In the United
..cCOOOIO 10
Carriage
on
Kingdom.
II Carriage Paid oa an Order. In the United Klnjdom.
"LOWMOOR JACKET."
For use in mines, ships' holds, etc., to secure a patient on a stretcher (see illustration), which can then be placed in an upright position. Price £1 5s.

WATER BOTTLE.
Copper tinned, with carrying strap .
Price lOS.
Carriage Paid on all OrCfers in th e United Kingdom . I:>
LAMP.
This is fitted with a socket , by which to fix it to a Litter, or it can be conveniently carrie d by hand, or attached to a bel t or the clothing.
Price complete, 5s. cd.
Dressing Basin , kidney shll(Jc,J, made of enamelled iron.
PriceLarge size , IS. 3d . Small II I01d.
Ambulance Station Plate, Enamelled Iron, 35. 6cl. each. Stretc.her Depot Plate, Enamelled'Iron, 3s. 6d. each . Carrymg Sheet for carrying patients up and down stain or otherwise about a hou se. Desi gned by the late J. C. Derham, Esq., B1ackpool, and Mrs. Alfred Paine, Bedford. The sheet is fitted with rope handles and detachable bamboo poles, and may be placed on a stretcher without di sturbin l the lJatient. Price complete, ISS.
13 carriage Paid on all Orders in th e United Kingdom.
REGULATION POUCH FITTINGS
for the St . John Ambulance Brigade, consisting of: -
I Triangular Bandage, sealed up i n waxed paper.
2 Grey Calico R o ller Bandages ( 2 in. and I in .).
I Packet of Surge on 's Lint.
I P a cket of Absorbent Cotton Wool.
I Pair Sciss ors .
6 Safety Pins.
I Box of 3 Phials" Vaporole " Iodine Tinc ture.
I Piece of Strong Cane, for tightening improvised Tourn iquets.
List Price, 2S. 8d. each; 6 doz. or more, 2S 7cl . each.
Box of 3 Phials" Vap orole" Iodine Tincture, packed for post , each I od.; per doz , 8s. cd.
SAFETY PINS.
All fasten or unfasten on either side. s. d .
Faci le No. S 600 or S 602 per 3 doz. 0 6
" "S 603 ... ,,0 8
Duchess Duplex, No . 2... per d oz. 0 2 " "Assorted 0 3
Special Blanket Safety Pins, 3 in. 0 in. 6
Pocket Cork Line and D r ag, with 80 feet of line, in case; for recovering a drowning person from the water . Price complete, with instructions for use, 6s. 6d.
Pocket Reel and Ice Line for use in ice accidents, with 80 feet of line in case. Price complete, with inslructions for use, 6s. 6d .
Carriage Paid on all Or ders in the United Kin gd om 14
LARGE HAMPER FOR AMBULANCE STATION AND ..RAILW . ....Y PURPOSES.

For cont ents see next pag e.
IS Oarrlage PaId Oft all Orders In the United KIngdom.

THE HAMPER CONTAINS
I Set of Cane Splints.
I St. John Tourniquet.
i lb. Carbolic ... LIn Tin ... JCases. Cotton "Vool
! lb. Boric Lint
I Roll Adhesive Plaster.
20 Roller Bandages, assorted.
I doz. Triangular Bandages.
3 pieces Tape.
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda..
4 o%. of Olive Oil.
40&' Spirit Ether Compo
i lb. Tin Powdered Boric Acid.
4 oz. Tincture Iodine.
I pair Pean's Forceps.
I pair Scissors.
Carrlag' Paid OR all Order. In the United KIngdom. 16 SMALL AMBULANCE HAMPER.
With waterproof cover and strap, for use in factories, collieries, stations, and large works, IU well as for parochial and domestic use.
I Knife.
12 Surgeon's Ne edles .
I packet each Safely and Plain Pins.
oz. Carbolised Chinese Twist.
O%:. Silkworm Gut.
I reel each Black and '''hile
Sewing Thread .
I Kidney-shaped Basin.
I Stopper Loos ener.
1 Graduated Measure.
1 cake 20 per c ent. Carbolic Soap.
I Nail Brush.
3 Empty 8 oz. Bottl es.
3 Saucers.
3 Camel Hair Brushe s.
Price complete, £4
CONTAINING
Set Splints, 1 St. John Tourniquet. 3 Tampons, for washing wounds. 2 Packets Lint. 4 Roller Bandages (wide and narrow). 4 Triangular Bandages.
Wool ... ... } In Tin Cases. Bone Wool... .. .
Sp ool of Adhesive Plaster.
Knife, Scissors , Thread, Tape, N eedl es, and Pins.
Weight complete, lbs.
Length, 1ft. 6 in. Depth, 5 in. Width , 7 in. Price £1 I IS. 6d.
17
Carriage Paid on all Ordera In the United Kingdom.
SURGICAL HAVERSAC.

hn- k0VED PATTERN, fitted with a tin, so arranged t hat any article can be taken out with out distur ll.ing the rest of the contents. Size, I ft. 3 in . , by 9 in., by i lL
Conten ts: I Set of Splints, 6 Triangular Bancb.ges, 6 Roller Bandages (wi de an d narrow), Cott on Wool, Boric Lint, in tin cases, I Roll Adhesive Plaster, 1 Pair Scissors, 1 Knife, 2 oz. Ol ive Oil, 2 Tinct. Iodine, 2 oz. Sal Volatile, 2 Spirit Et her Comp., I Graduated Glass Measu re, I St. John T ourniqu et, Pins, Ne edles and Thread, 3 Saucers, 3 Camel H ai r Brushes. Price £1 lIS. 6d. White Ration Haversacs, I S 9d. each .
Carriage Paid on all Orders in the Un i ted Kingdom.
FIRST AID COMPRESSED KIT.
box is. of. wood covered with damp· resisting matenal, and IS hlted wlth a lock and key . It contains a ntll?1ber of praetie.al ambulance appliances arranged so that any artlcle can be wlthdrawn or replaced without disturbinO" the r.emainder. Being filled with a handle it is portable, and the lId, let down, can be used as a table . All bandages and dressll1gsare compressed. Size-Length , 16! in.; width, in.; height, 8 in., without handle .
COI:tents: 4 Triangular Bandages, 6 Roller Bandages, 4 First AiJ. DreSSings, 6 Small Packets of Cotton \Vool 6 Small Packets of Boric Lint I St. John I Mea yre Glass,' I tin Lox containing a Roll of Plaster, Patches, I tray containing 3 Volaule,. Tincture of .and Ohve Od) ane! a Dredger of Boric ACId , I set of ImIJroved Sphnts, WIth angle piece, 8 Splint Straps (sufficient [or a fractured thIgh), 2 Saucers, 3 Camel Hair Brushes . Price £1 I IS. 6d.
Clln'lage Paid Oft an Ord III Unfte4t KIn.,do

FIRST RID
(DRESSINGS AND BANDAGES COMPRESSED).
51. :lebn R$$«IiJIICII. Pri /'" 6d SI. jC!Jft'$ 6ale. • C/trktnwm. £!Jlu/on, E.e. fly Post Is. 8 d.
Size, by 3a by Ii inches. Suitable for the pocket.
CONTENTS.
1. Triangular Bandage. 2. First Aid Dressing. 3. Cotton Wool. 4. Two Splint Slraps. 5. Adhesive Plaster. 6. PerIDanganate of Potash. 7. Lanoline. 8. Boric Lint Patches. 9. Safety and Plain Pins.
Price, each IS. 6d. Packed for Post IS 8d. Per doz. 17s. 6d.
SEP ARA TE ARTICLES.
No.
1 4d. each or 3/9 per doz.
2 2d. 2/0"
3 Id. " "Iod. " "
4 2d. per strap or 1/9" " No. 6 Id. per box or IOd. per doz..
Sid. per box or lod. " "
7 I per tin or 1/4 " "
8 Id. per packet or IOd.
9 Id." " Iod."
Not less than one dozen supplied a.t dozen prices.
Carri<'ge Paid on all Orders in the United Kingdom .
FIRST AID BOX FOR USE IN MINES.
CONTENTS. 20
Set of I mproved Woode n Splints j St. John Tourniquet; Cotton Wool j Lint I
12 Compressed Roller assorted j 6 Tri a ngular Bandages in waxed paper Adhesive Plaster I Pair Scissors j Spatula j Graduated Measure j
2 oz. Sal Volatile; 2 QL Spiri t Ether Comp. j 8 0&. Boracic
B oz. Tinct. Iodine j 3 Saucers j 3 Camel Hair Brushes; Pilla; Safety Pins. ( , PaICE COMPLETE, £2 los. "
This First Aid Equipment is also very suitable for use in factories and other large works, and can be fitted for carrying on the" Ashford " Lilter.
21 Carriage Paid on all Orders In the United Kingdom.
SMALL FIRST AID OUTFIT.
Wh en cl osed can be carried by a Strap-handle.
Dim ensions-9! by 7! by inches.

CO NT EN TS: :a Tria ngu la r B a ndages, I St. John Tourniquet, 8 S olint
S traps (for securing Splints in lieu of Bandages), :a oz. Cotton Wool, x Pair of Scissors, " x-in. Roller Bandages, :I :I-in. Roller Randages,
I 2 -0 Z. Bottle Sal Volatile, I :I-OZ. Bottle Tincture Iodin e B.P C , • oz. Plain Lint, I :a-oz. Measure G lass, :I China Saucers, and 2 Ca mel Hair Brushes to be used when ap plying Tincture of Iodine.
Price:
\\Tooden Box, covered with Damp Resisting Material, ISS.
Stout Cardboard Box, Cloth Covered, lOS. 6d.
Carriage Paid .n all Order. In the United Kln&,dom.
The St. John Tourniquet, as supplied to the Admiralt y with directions for use (Sp ecial quotations for large quantities. )
Splints, Wooden, per set, 2/6; Cane ... ._per set
Greatly improved Wooden Splints, with grooved joints an d a ngle piece, strongly recommended .-
Tow, fo r splint padd ing ... .. .per lb.
First Field Dressing (Army Pattern)
J aconette, 44 inche s wide per yard
Tow, Carbolized or Styptic ... ...per lb.
First Aid Dressing, consisting of a small compressed packe t of boric lint, a compressed roller bandage, an d a sa fe ty pin
Knife with stron g blade each 9d . ; per doz. 85.
Pair of Scissor s each IS. ; per doz. lOS.
Small Bottles str ong Smelling Salts, per doz., 55. 6d.
Splint Straps, Webbin g, and suitable Buckles. Per set of lZ yards of strong 2-inch \Vebbing and IS Buckles, 2S. 6d.
T hese make very c ompact Straps for carrying in the Pouch.
T he Webbin g should be cut to meet local requirements.
Buckles on ly, IS. 3d. per doze n.
\ Vebbing only, IS. 3d. per doze n yards.
It is unnecessary to se w th e Buckles. T h e spikes sh ou ld be passed through the webhing, and th e sh ort end of th e webbing shou ld lie outwards.
-
a • .. d. o 9 7 6 4 , o , o , 2 J o 9 o 2 Dredger, containi ng boric acid powder 4 Measure Glass .. . 0 2
23 Carriage Paid on all Ordera In the UnIted Kingdom , PLASTERS.
L eiceste r A d hesive Plaster on Cambric, in tins of i yard, 6 inches wide 6d.

N at ion al Rubb er Adhesive
Pl a ste r (Ant ise ptic)
o n spo ols.
S yd s. 10 yds . i nc h wide 9d . IS. od.
I S. od. IS. 6d .
The Leicester Adhesive R ibbons, in tin boxes, 6 yard s long.
2 I S. 9d . 2 S. 3d . ! inch wi de I wide
Ditt o in card bo x, in. wid e, i yds . 10n.'I- '" lin I 1 ,,. 2 J; S & 5 COURT PL ASTER , T RI COLOR
Large Size, 9d. ; Medium , Sd . ; Small , 3d.
Canlage Paid Oft all Ordera In the United Kingdom . 24
NURSES' WALLETS.
ORDINARY PADLOCK SHA P E.
Without instruments, 4s. 3d.
Fitted complete, containing Spring Dressing Forceps, Spat ul a , Probe, 2 pairs Scissors (round and sharp poi nted), Clinical Thermometer, and Knife .
Price 105
ST. JOHN'S PATTERN, as illustrated, but improved by the addition of flaps to protect the instruments.
Without instruments, 7s. 9d.
Fi tted complete, con taining Spring
Dressing Forceps, Artery Forceps (also useful for dressing) , Spatula, Probe, Direc to r wi th
Ear Scoop, 2 pairs Sciss ors (round and sharp pointed) , C linical Thermometer (minut e, round), Knife, Pencil, and Safe ty Pins.
Price 185
6d. 8d. Id. 3d
3d . 6d
9d •
.
.
·s
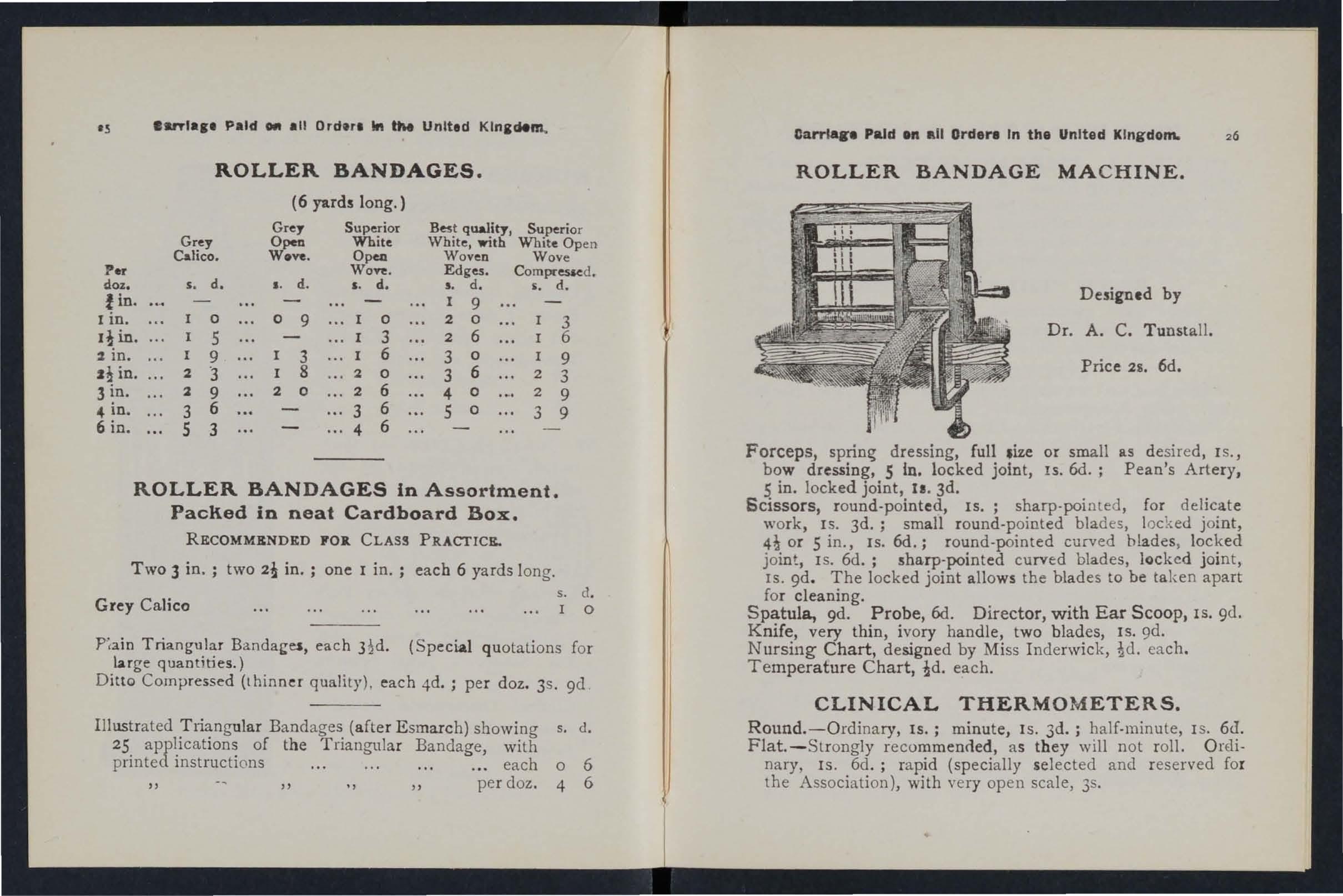
Per doz.
fin.
I in.
I! in.
2 in.
J! in.
3 in.
4 in.
6 in.
.tnta,_ Paid 011 all Ordara In tM United Klnidem.
ROLLER BANDAGES.
(6 yards long.)
Grey Superior Best quality, Superior
Grey Open White White, with White Open Calico. Wove. Open Woven Wove Won:. Edges. Com(l£essed.
ROLLER BANDAGES in Assortment.
Paclied in neat Cardboard Box.
RECOMMENDED FOIt. CLASS PRACI'ICE.
Two 3 in. ; two 2! in. ; one I in.; each 6 yards long.
Grey Calico
Piain Triangular Bandai;es, each (Special quotalions for luge quantities.)
Ditto Compressed (thinner quality), each 4d. ; per doz. 3s. gd .
Illustrated Triangular Bandages (after Esmarch) showing s. d. 25 applications of the Triangular Bandage, with printed instructi ons ... each 0 6 " per doz. 4 6
Carriage Paid Oil All Orders In the United Kingdom.
ROLLER BANDAGE MACHINE.
Price 25. 6d.
Forceps, dressing, full .ize or small as desired , IS., bow dressing, 5 in. locked joint, Is. 6d.; Pean's Artery, 5 in. locked joint, II. 3d.
Scissors, round-pointed, IS.; sharp-pointed, for delicate work, IS. 3d.; small round-point ed blades, loc ked joint, or 5 in., Is. 6d.; round-pointed curved blades, locked joint, IS. 6d.; sharp-pointed curved blades, locked joint, IS. gd. The locked joint allows the blades to be taken apart for cleaning.
Spatula, 9d. Probe,6d. Director, with Ear Scoop, IS. 9d. Knife, very thin, ivory handle, two blades, IS. 9d. Nursing Chart, designed by Miss Inderwic k, each. Temperature Chart, each.
CLINICAL THERMOMETERS.
Round.-Ordinary, IS.; minute, Is. 3d. ; half-minute, I S. 6c1. Flat.-Strongly recommended, a s they will not roll . O relinary, IS . 6d.; ra pid (specially select ed and reserved for the Association), with very open scale, 35.
s. d. I. d. s. d. s. d. i. d. I 9 a 0 9 a 2 0 3 5 3 2 6 6 9 3 6 3 0 9 2 "3 8 2 0 3 6 2 3 l 9 2 0 2 6 4 0 2 9 3 6 3 6 5 0 3 9 S 3
4 6
s. d. I 0
Designed by
Dr. A. C. Tunstall.
Carriage Paid (In all Orders In the United Kingdom.
CLINICAL THERMOMETERS- (collthl/led).
With Magnifying Lens. Price, ordinary, I S. 6d.; minute, IS. 9d. ; half-minute, 2S. 3d.
N.B .-Minute and half-minute instruments will on ly register in the time stated under favourable circumstances.
No liability is taken for breakage o.f Thermometers in t1'allSit.
BATH THERMOMETERS.
To Dr. Forbes' specification . Japanned with zinc scale, 2S. 3d. ; Clin ical Thermometer size, in case, IS. 6d.
No liability is taken for b1'eakag'e o.f Tlzermomete1'S in transit.
COTTON WOOL.
Plain, I oz., 2d. ; 2 oz ., 3d. ; 4 oz., 4d. ; lb., 7d.; I lb., small packet (Compressed), Id.
Medicated, Boracic, lib., 6d.; I lb. , IS. 6d.; Carbolic, per lb., I S. 8d.; Alembroth, per lb., IS. 6d.; Double Cyanide, per lb., 2S. 6d.
LINT.
Plain, I oz., 2d. ; 2 oz., 3d. ; 4 oz., 6d. ; lb., IOd. ; I lb., IS. 6d.
Boracic, 4 oz., 6d. ; I lb., IS. 6d. ; square foot p3.cket, 2d. ; small packet (Compressed), rd.
GAUZES.
The se are supplied in 6 yard lengths, width about 36 inches.
Unmedicated white
Alembroth
Double Cyanide
Boracic
Packets of Cyanide doz., 2S. 8d.

Gau·ze ( r yd.
GAUZE TISSUE.
A laye r of absorbent cotton wool between two sheets of gauze, good quality, per lb., I S. 6d.
Carriage Paid on all Orders in the United I<ingdom.
TEXT BOOKS, C3C.
"First Aid to the Injured." By James Cantlie, M.B., F. R. C. S. The authorised Text Book of the First Aid Course. IS.
"A Catechism of First A id." Compiled from Dr. Cantlie's By J. M. Carvell, M.R.C.S., L.S.A. 6d.
" Problems in First Aid. " A companion to t he authorised Text Book of the St. John Ambulance Association" First Aid to the Injured." By L. M. F. Christian, M.B., C.il-f., Ed., and W. R. Edwards, A . C.A. 6J .
"Hints and Helps fo r Home Nursing and Hygiene." By E. MacDowell Cosgra\'C' , M.D., illustrated.' with on the application of the roller bandage, by SIr R. J. CollIe, M. D. The authorised Text Book for the Nursing Course. IS.
" A Catechism of Home Nursing" (based on Dr. Cosgrave's Text Book). By J. Brown, L.R.C.P., L.R.C.S., and J. :-1. Carvell, :-LR.C.S., L.S.A. 6d.
" Home Hygiene." By John F. J. Sykes, D . Sc. (Public Health), M. D . , &c. Illustrated. The authorised Text. Book for the Home Hygiene Course. IS.
II A Catechism of Home Hygiene" (based on Dr. Sykes' Text Book) . By J. 1\1. Carvell, M.R. C. S. , L.S.A. 6d.
" Questions and Answers upon Ambulance Work." By John W. Martin, l\1.D., and John Martin, F.R.C.S., Ed. IS. ·
/I Questions and Answers upon Nursing." By John \ • Martin, M .D. IS. 6d.
/I First Aid to jthe Injured" (Six Ambula,nce Lectures). By Professor Frederich Esmarch. Translated from the Ge rman by H.R.H. Princess Christian. 2S.
"Elementary Bandaging and Surgical Dressing. " By Walter Pye, F.R.C.S. 2S.
s. d.
0 10 o 2 2
per length
per
carriage Paid on all Orders In the United Kingdom.
TEXT BOOKS,
"To Restore the Apparently Drowned," printe d in large T ype with two Diagrams . 2d.
Dr.. <:7. H. Darwin' s Aids t." being a card t o hang up, giVing t r eatment of vanous accidents. 2d.; packed for p ost, 4d .
" Manual of Drill and Camping for the St. John Ambulance Brigade." 5d.
" Manual for John Volu ntary Aid Detachmen ts." By L ieut.-Col. G . E. T wiss , P .A . M.C. (Retired Pay) . 6d.
H How to Act w h en Clothing takes Fire." By J. E. H. Mackinlay , M.R . C. S. 2d.
"First Aid Principles . " Cards of concise directions for waistcoat pocket, each; 4d. per doz. Special quotations for la rge quantit ies.
" Specimen Examination Papers, First Aid, ursing anel Hygiene Courses." 3d .
Small Anatomical Diagram . Showing the human skeleton main arteli es, and points where pressure should be applied to arrest bleeding. 2d .
Directions as to the Restoration of Persons suffering from Electric Shock. Large print, poster size. 3d . each; or 2S. 6d . pe r dozen.
General otes on First Aid to be Rendered in Cases o f P01soOlng. By Milnes Hey, M.A . , M. R . C . S. , L.R.C . P . 2d.
Notes. on Military Sanitation. By Lieut.-Col. II. P. G. Elkmgton , R . A . M. C. 6d.
B.ook," for instantaneous re ference, giving conc ise mst ructlOns ; to hang on wal l. Size about one foot squa re. 2S. 6d. ; packed fo r post, 2S. 8d .

carriage Paid on all Orders in the United Kingdom. 30 TEXT BOOKS,
Aids to Memory for First Aid Students. Revise d to date . Addit ional I1I ust rations . By L. M . Frank Ch ristian , M . B., C.M ., Edin. 6d.
General Regulations for the St. John Ambulance Brigade, 19 1 3. 3d .
Rules for Corps and Divisions, St. John Ambulanc e Brigade. 2d . A History of the Order of the Hospital of St. John of Jerusalem. By the late Rev . W. K. R . Bedford, M.A. , and Lieut.-Colonel R. H. Holbeche . 5s . Registers. Class Attendance, 2S. 6d . Certificates, 4S. 6d . Case Repo rt, IS.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three, 7s. 6d . Receipt Book, 6d.
Large Physiological Diagrams (N ew Series) . For L ecturers' use . T he Human Skeleton, show ing the main arte ries and pressure points . The General A natomy of the Body. The Systemic and Pulmonary Circulat ion of the Blood. Sect ion T hrough Middle Line of H ead and N eck, sh owing the To ngue in two p ositions in r elation to the Trac h ea , and Sc hafe r 's method of Artificial Res piration (Expi ration and I ns piration ). Dislocations. Price . p e r set of five 15s. These may be hi red for a course of "First Aid" l ec tures, given unele r the a uspices of the Assoc iation, fo r a fee of 5s., or the addItion of Sp lints , T ourni quet, and 30 plain Tnangular Bandages, for a fee of lOS .
Boxes of Stationery for the use of Class Sec retaries and others connected with the Association , contain ing t welve sheets of high-class paper, suitably headed, and twelve envelopes bearing the device of the Association. 6d . T wice that quantity , IS.
Arm Badges, with the device, issued under the authority of the Central Executive Committee, having been first approved by H. R. H. the Grand Prior as the sole official and recognised Badge of the Association and Brigade.
N.B.-TMs desips is
SERIES A.-For the use of individual certificated pupilsNo.
I. In German Silver,
2.
3.

9. In Cloth and
10. In Cloth and Silver (Registered Number, 3522)
I 1. In Cloth and Cotton
12. Small Cenuloid for button hole or brooch
13· White Satin Armlet, with woven Badge 21 ,
7i N.S.-TkSl Sadres art Mt t. 6, worn as decorations.
all Orders
SERIES B.-For members of the St. John Ambulance Brigade, not wearing uniform, having the name of the Corps or Division annexed on a label, only issued in quantities-No. 15. In German Silver, 2 ins. in diameter, first doz., £1 ; subsequent dozs., 12S.
16. In Electro Plate, 2 " first doz . , £1 125. ; su bs equent dozs., £1 4s.
" 17. In and Silk, 2 per doz., I
18. In Cloth and Silver, 2 per doz., £1 101.
V.B -These cadg es a r e 11 0t t o be worn as
31 BADGES·
!.. d.
Size 2 in. dia. 0 71-
Large
Small Size ditto ...... Ii 0 6
Small Size for button hole ... 0 6
In Electro Plate, Large Size 2 0
Smali Size ditto... It 0 9
Small Size for button hole 0 9
In Enamel for button hole 1 0
" brooch 3
Ii" 0
4·
5·
6.
7.
8.
Silk
9
2 0
2"
... ... 1 t 0 6
...
... ... ... ... i" 0 2
0
.
Dan-lags Paid on
in the United Kingdom. 3-
U Carriage Paid on all Orders in the United Kingdom.
BRIGADE UNIFORM BADGES, etc. s. d.
Officers. Cap Badge (Reg. No. " CoUar Badges ( " Pouch Badge ( lOr ) 10 3) 3,657)
Sergeants, Corporals and Privates. per pair
Cap Badge (Reg. No. 102) ...
Collar Badges ( " 104) ._ per pair
Overcoat Badge ( " 1,582) ...
Shoulder Titles, S.J.A.B., with numeral, per pair
Shoulder Straps, fitted with title and numeral per rai r
Reserve Badge for all ranks per pair
Lady Officers of Nursing Divisions.
Lady District Supt., Arm, 45. 9d. ; Cloak
Lady Supt., Arm, 4S. 3d. ; Cloak ...
Lady DiVIsional Supt., Arm, 3s. 9d. ; Cloak
Nursing Officer, Arm, 3s. 3d. ; Cloak
White Box Cloth Backs, for Badges... per pair
Nursing Sisters. Arm Badge (Reg. No. 3,522) Cloak Badge ( " 3,521)
District Numeral [or Nursing Divisions...
Black Silk Armlet for Arm Badge, for all ranks ...
Honorary Surgeon's Crosses (pattern B) per pair
Superintendent's Stars (pattern A) per pair
Medallion Badge (pattern D) ...
Nursing Badge (pattern E)
Satin Badge for Nursing Sister's Pin Cushion
BUi"ler's Badge 45. Bugler's Cord

Paid on all Orders in tile United
Bandsman's Wings per pair
Bandsman's Cross Belt and Pouch for music
Signaller'S Badge ... Signaller, IS.; Instruct or
Drummer's Badge
Div. Secretary and Sergeant's Badge
Whistle and Chain
Private' s Brown Waist Belt and Pouch
White Piping, per packet of yards, enough for 3 pairs of trousers (packets cann ot be broken)
Lace , per yard, Silver, lOS. ; Black
St. John Voluntary Aid Detachments.
UNIFORM BUTTONS.
Isslled only for the use of Offic ers and Members wearing the prescribed uniform.
St. John Ambulance Brigade.
German Silver, No. I (large ) No. 2 (medium) ... No. 3 (small, for caps) NO.4 (large) NO.5 (medium) ... " No. 6 (small, for caps)
St. John Voluntary Aid Detachments.
German
N
single double
o 8 3 2 6 o 6 o ro b o 6o 6 3 o 3 5 6 5 0 4 6 4 0 o 3 2 0 2 3 o 3 o 5 o 4 o 6 o 6 o I o 3 o 3 0 Cc::.rriage
Kingdom.
34 s. d. 2 6 12 6 3 0 5 0 o 2 (l 7 8 2 o Cap Badge ... 6d. Officers' Stars ... per pair 1 4 Belt Furniture ... 6
per doz. s. d. a 6 o 4 o 3 3 0 6 ()
Silver,
o. 7 (larg e) per doz. 0 6 No.8 (medium) 0 4 NO.9 (small) ,,0 3
3S Carriage Paid on all Orders in the United Kingdom. ELECTROTYPES.

OF THE ST. JOHN AMBULANCE DEVICE.
Ube GranO I)rtonl of 1tlie of tbe tlospttal ot f,it. Jobn ot 3erusalem In £ngllln.,.
ttbe St. 30,," amDlllllnce tlsGo.cilltton. No. I All.
For Note Paper, Small
For Quarto and Foolscap Letter-paper, Circulars, &c. ...
Prints of the above Electrotypes (I to 3) Series A and B, and (I) Series AH and BH, '-ppear on page 3S. No. 4A is shown on page 3 I. The diameter of SA and SB is zu inc hes .
I BH.
N ::>. I A. K o. 2 A. N O.3 A.
No. lB. No. z B. NO.3 B.
•
DEPARTMENT
No.
No. CarrIage
For Assoc iation use. Series Series For Brigad e use Series S eries A. AH. B. BII. s. d. s. d. s. d. s . d. I. For Cards, Tickets, &c. 3 3 3 3 2.
Circulars,
3 3 3 3 3·
3 7 3 7 4·
Small
6 S· For Large Posters 9 9 Complete Series 6 0 3 9 4 9 3 9
UIX Granb I)rlorll ot 1tbe of tbe 1\)osl>lIal of St. Job" of Jerusalem In
,H48ULANCE
ttbe st. lobn tlmblllllllce
Paid on all Orders in the United Kingdom. 36 ELECTROTYPES
&c.
For
Posters
£ s. d. Flags bearing Association device-Iz feet by 6 feet 7 6 S feet by 3 feet o 12 6 Brigade 4 ft. 1 in. by 3 ft. o 12 0
37 Carrlqe Paid on all Orders In the United Kingdom.
SW AGGER STICKS
for the use of Officers and Members of the St. John Ambulance Brigade.
E bonised Canes, Gennan Silver M ounts bearing the Brigade Device.
PRICK IS KAC H.
Officen' Special Canes, with Sterling Silver Mounts.
PR I CR 7s . EACH.

BEARER'S DR.ESSING CASE .
PRI CR 12s. 6d.
All Orders for the Stores should be g iven to t he Lo cal Secretary, or sent direct to
The St. John Ambulance Associ a tion, St. John's Gate, ClerkenweIi, Lond o n , E .C.
Contractors ' List. Carriage out of London Extra.
PRICE LIST.
UNIFORMS FOR AMBULANCE UNITS OF THE S.J.A.B.
These may be obtained from HAZEL & Co . (sole propl;etor, D. Hazel, for many years associated with the laLe firm of Hebbert & Co., Ltd., as Director), Clothing and Equipment Manufacturers, 65, East Road, City Road, London, E. C. ; and aL 6, '!ork Place, Leeds; 69, Piccadilly, ManchesLer; and 8+, MIller Street, Glasgow. Telephone: 5678 London 'Vall. Telegrams: "Hazelism, London." vVhere two prices are given for an article they are for first and second qualities .
All Badg-es, and carriage outs£de London area, extra. MeasU1'ements to be suppl£ed free of charge.
CORPS SURGEON AND DIVISIONAL SURGEON.
Tunic, Superfine Black CloLh ... ...
Trousers, Superfine Black Doeskin (if Silver Lace Stripe, extra) ...
Cross Belt and Pouch, Plain, 20/- ; Silver Embroidered .. . Gloves
Great Coat, Grey Cloth ...
Divisional Surgeon
DISTRICT SUPERINTENDENTS
Tunic, Superfine Black Cloth ...
Patrol Jacket, Super-fine Black Cloth ...
Tro users, Supe rfine Black Doeskin
Cross Be lt and Pouch
Gloves, 4/6; Leggings, 8/6
Great Coat, Grey Cloth
Cap-District Superintendent
and Corps Office
... .. .
Cap-Corps Su rgeon £ 1 17 6 and ;£ . d. 3 15 0 2 6 3 7 6 0 4 6 376 6 0
I 9 0" 0 17 0 AND CORPS OFFICERS .
.
..
.. . £ 1 1 2 6
r I 1 0 0 " 3 15 0 2 10 0 2 6 o 13 6 3 7 6 I 0 o 18 0
J' Dontraotor. ' Lilt. Carrlag. Paid .n all Drapery Cood-.
DIVISIONAL SUPKllINTKN DKNTS AND
Pat rol Jacket, Superfine Black Cloth
Trousers, Superfine Black D oeskin
Cross Belt and Pouch
Gloves, 4/6; Leggings, 8/6
G reat Coat, Grey Clot h
F atigue J a cke t , Black Vicuna Serg e ....
" Trousers, Black Vicuna
Cap-Divisional Superintendent £ I 4 0 and " Ambulance Officer ._ 0 15 6
FIRST CLASS SERG EAN T S.
P at rol Jacket, Superfine Black Cloth ...
Ch evrons, Four Bars, Silver
T rousers, Superfi n e Black Doeskin
Cross Belt and Pouch
Cap, 2/ 9 ; Gloves, Buckskin, 4/6; Gloves, Cot ton, 8d.
Leggin gs, Black or Brown Leather . .. ...
'Vat er B ottle and Ca rrier
H aversack, White Duck
Great Coat, Dark Grey Melton
SERGEANTS, CORPORALS AND PRIVATES.
Patrol Jacket , Black Tartan
Chevrons, Silver .. .
T rousers, Bla ck Tartan
\Vaist B elt and Pouch, Brown Lea ther
Cap, 2/9; Gloves, Cotton, 8d,
L eggin gs, Black Leather ... . ..
Wate r Bottle and Carrier, 3(9; H a versack, White Duck
Great Coa t , D ar k G rey Me lt on 16/- and D R AB SERGE UNIFOR MS.
Jacke t, D rab Mixtu re S erge
T rousers
Cap Great Coat, 'Drab 16/ 6 and

I NDEX TO PR I CE LI ST.
(For General Ind ex pages 208-215).
\ mb ulance Hampers .. Station Plate ... .,.
Bandage Roll ing l\Iachinc
Bandages
Basin, Dressing Hearer's Case Belt and Pou ch
Books...
Boltles (Water)
Buttons ...
Carrying Sheet
COLton W ool...
Cover for Stretcher or Litter
Diagrams, Large lJ Small ...
Dredger (BOI ic Acid)
Dressing Basin 10
Drowning Tackle 13
Electrotypes ... ... 35, 36
Emergency Book 29 Aid Box .. , .. . 8, 20, 2I JJ JJ Companioll.. 19 JJ "COlllpressed l';:it 18 First Field Dre:.sings ... 22 36 Forceps 26 (;auzes ... 27 Gauze Tissue
27 Hampers (Ambulance) ]4 to]6 Haversacs
. ... 17 Hood and Apron for LitLer ... 3 ) Ilstr uments (various) 26
AMBULANCE OFP'ICEltS. ;; s d.. 2 6 6 2 6 o 13 6
per Bar
3 7 15 o 16 o 14 o 9 I 18 o 3 o 19 o 10 o o 4 3 o I o 16 6 o o o o 6 4 6 6 3 9 6 o o II 0 o 0 10 09 6 066 o 4 o I o 14 o o 9 8 o 2 o 19 3 6 o 9 o o 6
PAGR ]4 to 16 3I to 34 26 25 ]3 37 .,. 33 28 to 30 I2
Cash Book ...
J acone tte Knife ... ... Lace for Caps , &c. Lamp Lint ... ... Liner (Ashford) 26 33 12 2, 3 Litter (Rea-Ed wards) Lowlll oor Jacke t i\leasure Glass l\linute Book Nurses' "Walle ts ursing Char ts Occurrence Book Pillow Plasters.. . .. Pouch Fittings Receipt Book Registers ... ... Roller Bandage l\lachine Rug ., ... ... PAGl': ... 4 LO 6 II 22 30 2 { 26 30 1 0 23 13 30 30 26 10 Rules for COl ps or Di visions St. John AlltiJulance I3rigade Safety Pin s 29 13 22, 26 Scissors ... ... Slings (Stretcher) Smelling Salts .. . 10 Splint Padding 22 JJ Straps ... 22 Splints 22 Stationery 30 Stretcher Depot PlaLe 12 Stretchers ... ... i to 10 " Adjustable for Swagger Stick ... Temperature Ch:ut Text Books Thermometers .., Tourniquet Tow (carbolized) JJ (plain) ... Uniform Sundries Uniforms \Vater ... \Vaterproof Sheet Whi s tl e and Chain W hite Piping .. . \\'001 (Cotton) .. . 37 26 28 to 30 26, 2 7 2 2 22 33 38 to 39 II 33 33
... ..,
...


